User login
Drug Resistance Triggers Lung Cancer Transformation
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - A small study provides compelling data that both the genotype and phenotype of non-small cell lung cancers can transform with acquired resistance to tyrosine kinase inhibitors.
Repeat tumor biopsies revealed that the histologic diagnosis of the tumor shifted from adenocarcinoma to small cell lung cancer (SCLC) in 14% of 37 consecutive patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) and acquired tyrosine kinase inhibitor (TKI) resistance, Dr. Lecia Sequist said at the Multidisciplinary Syposium on Thoracic Oncology.
The L858R mutation or E 19 deletion was retained in all cases. In one patient, an additional PIK3CA mutation was seen only when the tumor shifted to SCLC.
Although other groups have documented sporadictransformation, Dr. Sequist called the 14% transformation rate remarkable. “I think this points to a broader conceptual model of acquired resistance, and we need to think very carefully about doing more repeat biopsies in patients,” she said.
EGFR-mutant NSCLC is highly sensitive to EGFR TKI therapy, but acquired resistance develops at about 9-12 months due to T790M mutations in half of patients and MET amplification in 10% to 15%, said Dr. Sequist of Massachusetts General Hospital Cancer Center, Boston.
Although re-biopsy is not common practice, invited discussant Dr. Mark Socinski said it should be on the clinician's radar because it can alter the therapeutic course of refractory disease and arguably the clinical benefit.
“I think the message here is to consider re-biopsy more often in selected patients until we have a better understanding of this one disease we call non-small lung cancer that we realize is an incredibly heterogenous disease,” said Dr. Socinski, director of the thoracic oncology program at the Lineberger Comprehensive Cancer Center at the University of North Carolina-Chapel Hill.
Among the five patients whose cancer transformed, two maintained a slow, indolent course after SCLC transformation, while three had a change around the time of their biopsy to an explosive growth pattern more clinically reminiscent of SCLC, Dr. Sequist said. Four patients were treated with SCLC-like chemotherapy regimens, and three responded with marked partial responses.
Longitudinal data from fluorescent in situ hybridization analysis for MET and EGFR gene copy number suggest that the resistant tumor is distinct from the original tumor and that MET amplification lies in a distinct subpopulation of the cell and is selected out under pressure from TKI therapy, she said.
Multiple biopsies over time also identified a waxing and waning of genotypic and phenotypic findings in response to TKI therapy. This pattern was most pronounced in a case that transformed from EGFR TKI-sensitive adenocarcinoma to resistant SCLC while on erlotinib (Tarceva) for more than 1 year, switched back to TKI-sensitive adenocarcinoma following treatment with chemotherapy and radiation and a 9- to 10-month break from erlotinib, and then after a very successful, but short-lived re-response to erlotinib, shifted back to SCLC a second time upon clinical resistance.
“It's showing us that if you do repeat biopsies, it can direct patients towards clinical trials that they have a higher likelihood of benefiting from,” she said.
The population comprised 15 men and 22 women, median age 60 years. All had responded to either gefitinib (Iressa) or erlotinib, with a median of 18.4 months of initial EGFR TKI therapy. The majority (81%) remained on TKI at the time of repeat biopsy. Repeat biopsy showed T790m mutations in 49%, PIK3CA in 5%, MET amplification in 5%, and an unknown mechanism in 30%, reported Dr. Sequist.
Dr. Sequist and Dr. Socinski disclosed no relevant conflicts.
Nonsurgical Approaches to Perforation Are Rising
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
CHICAGO - Nonsurgical approaches are beginning to dominate the management of acute esophageal perforations.
An analysis of 81 consecutive acute esophageal perforation cases between June 1989 and March 2009 revealed that nonsurgical management jumped from 0% during the first 4 years of the study to 75% in the last 4 years.
The average length of stay declined significantly over the same period, from 26 days to 20 days , while complications trended downward, from 50% to 33%, Dr. Michal Hubka reported on behalf of lead author Dr. Madhan Kumar Kuppusamy and their colleagues at Virginia Mason Medical Center in Seattle.
In all, 33 patients were managed nonoperatively and 48 surgically. Primary repair was the most common surgical approach (34 cases). Nonsurgical treatments included endoscopic stenting (11 cases), drainage procedures including mediastinal drainage (13 cases), total parenteral nutrition (7 cases), Dobhoff feeding tube (5 cases), gastrostomy (5 cases), endoscopic repair with clips or glue (3 cases), and feeding jejunostomy (3 cases).
"Nonoperative treatment options are increasing and surgeons must be able to apply these techniques to improve outcomes,” Dr. Hubka said at the annual meeting of the Western Surgical Society.
Hybrid-type management was performed in 21% of patients and most often took the form of endoscopic stents or drainage at the time of open or thoracoscopic drainage or decortication.
The nonoperative group was less likely than the operative group to experience pneumonia (4 patients vs. 7 patients) and dysrhythmias (4 patients vs. 11 patients), but more likely to experience persistent leak at the 14th day (3 vs. 2), stent migration (3 vs. 0), sepsis (1 vs. 0), and renal failure (1 vs. 0), Dr. Hubka said. Deep vein thrombosis occurred in one patient in each group.
Two patients managed medically died vs. one treated surgically (6% vs. 2%), for an overall mortality rate of 3.7%. A historical comparison of nine other studies involving nonoperative management of esophageal perforations presented by Dr. Hubka showed mortality rates reaching a high of 24% between 1973 and 1993 and a low of 3.8% between 1990 and 2001.
One of those nine studies identified a stepwise increase in mortality as time from perforation to diagnosis increased, with 5% of 75 patients dying with an immediate diagnosis vs. 14% with a diagnosis within 24 hours and 44% if the diagnosis occurred after 24 hours (Eur. J. Cardiothorac. Surg. 2003;23:799-804).
In all, 57 patients in the current analysis were treated within 24 hours and 24 were treated after 24 hours. Length of stay was significantly shorter in the early-treatment group at 15.6 days vs. 29.4 days in the late-treatment group. In the early-treatment group, complications occurred in 20 and death in 1; in the late-treatment group, 11 had complications and 2 died, Dr. Hubka said.
"Time to diagnosis continues to be important; however, management in an experienced center facile with all current management techniques is the major issue affecting outcomes,” he said.
The percentage of cases referred to the tertiary referral center was 50% from 1989 to 1992 and 79% from 2005 to 2009. Referred patients were significantly more likely to be treated more than 24 hours after perforation.
The improvement in outcomes is likely related to increasing diversity of treatment techniques and management in specialty centers, Dr. Hubka said.
Invited discussant Dr. Jeffrey Peters from the University of Rochester (N.Y.) Medical Center, said, "What you heard was an increasing chorus of a paradigm change, if you will, that's sort of paradoxical to most of us - that someone with a hole in their esophagus does better if you don't operate on them. I still struggle trying not to do that when patients present in the emergency room with these issues.”
Still, he described the improvement in outcomes as true progress for patients. Dr. Peters noted that the etiology of acute perforations has changed over time, with most now iatrogenic, and thus the benefit of early treatment may not be as critical as in years past. He said referral to a tertiary center is important, but that the paper did not prove a causal effect.
Based on the findings, Dr. Peters asked when surgeons should operate, how the size of the injury and presence of underlying disease should be taken into account in treatment decisions, and when surgery should be considered if nonoperative therapy fails.
Dr. Hubka said patients with larger esophageal tears or injuries and moderate mediastinal pleural contamination who can tolerate surgery are the ones who proceed to the operating room. He suggested that the study's operative rate would likely have been higher if patients with perforations due to neoplasia or cancer had been included and that the presence of such underlying disease would surely push them toward operative management in clinical practice. Finally, if a patient becomes unstable or their level of contamination increases despite nonsurgical management, they would proceed to surgery and decontamination.
"A point of our study is that this management, whether it's endoscopic or operative, should be performed by surgeons because we have all the tools to manage all patients appropriately,” Dr. Hubka said.
The study authors and discussant said that they had no financial disclosures.
Streamlining Method Yields OR Savings
CHICAGO - Applying the Lean streamlining methodology across the entire surgical process significantly improved several operating room performance measures such as on-time starts and turnover time. At the same time, the operating margin in some ORs was increased by more than $45,000 per day, as demonstrated at the Mayo Clinic in Rochester, Minn.
“This was all during a period of increased growth and volume of cases," Dr. Robert Cima said at the annual meeting of the Western Surgical Association.
“What's even more important was that during this time when we had increased volume of cases, we actually had a decreased need for personnel because we were reducing the need for overtime staffing as well as the just the plain need for extra bodies," added Dr. Cima.
That translated into 37 fewer full-time surgical services employees, 50% fewer late shifts among certified registered nurse anesthetists, and an 18%-56% decrease in health care security services overtime.
The Lean and Six Sigma methodologies, popularized decades ago by companies like automobile maker Toyota as a way to eliminate wasteful steps and improve productivity, have typically been applied to a limited number of ORs or to specific operations.
The Mayo Clinic credits its success to applying the methodology across the entire surgical process and in all 88 of its main ORs performing both in- and outpatient procedures.
“Multiple areas of redundant or non-value-added steps were identified across the entire process flow that would not have been identified with a focus on specific steps," said Dr. Cima, a colorectal surgeon at the Mayo Clinic.
First, a multidisciplinary leadership team developed a map of the surgical process from the decision for surgery to leaving the OR. The team analyzed each step for personnel required, information process, and time expended. In all, 28 systems and 14 points of delay were identified, he said.
Next, multidisciplinary teams were formed and given 6 months to redesign systems around five essential work streams: minimizing unplanned surgical volume variation, streamlining the preoperative process, reducing nonoperative time, reducing redundant information collection, and engaging employees.
“Specific goals were set for each specialty," he said. “It was not 'one size fits all.'“
Each work stream was tweaked to standardize procedure descriptions, implement dedicated staggered surgery start times, and develop a first-case scheduling checklist to eliminate barriers to on-time OR starts.
When streamlining the preoperative process, Dr. Cima said, the most important thing is to start on time.
The hospital tried to get buy-in from employees by implementing OR briefings with the OR team, creating a communication council to effectively disseminate information through all levels of staff, and conducting a survey to identify major drivers of employee participation - many of which were not financial, Dr. Cima noted.
Some of the drivers included promotion of shared goals, encouragement of continuous professional growth, frequent recognition of individual employee contributions, and executive demonstration of values and commitment to the project.
Data collected before the intervention and 18 months afterward from the first three specialties tested showed that on-time starts increased from 50% to 80% for thoracic surgery, from 64% to 92% for gynecologic surgery, and from 60% to 92% for general/colorectal surgery.
The differences were all significant (P less than .05), he said.
The percentage of operations performed past 5 p.m. stayed relatively constant before and after intervention among thoracic surgeons at 34% vs. 36%, respectively. However, it decreased significantly for gynecologic surgeons (from 42% to 36%) and general/colorectal surgeons (from 37% to 31%) (P less than .05 for both).
The average nonoperative or turnover time was reduced by 10-15 minutes among the three specialties, or 25% for thoracic surgery, 43% for gynecologic surgery, and 32% for general/colorectal surgery, Dr. Cima said.
Staff overtime was reduced by an average of 17 minutes per month for thoracic surgery (16%), 19 minutes for gynecologic surgery (18%), and 46 minutes for general/colorectal surgery (53%).
The financial impact of these improvements was at times quite dramatic, he said.
For example, the financial margin increased 22% or $21,340 per OR/day for thoracic surgery, 16% or $24,570 per OR/day for gynecologic surgery, and 55% and $47,700 per OR/day for general/colorectal surgery.
“Some people say this is a Hawthorne effect . . . but this is sustainable and in some cases actually increases as the teams become more efficient," he said, noting that positive improvements have now been reported in nine separate specialties.
Invited discussant Dr. R. Stephen Smith called the project a “monumental effort," but questioned whether the methodology is applicable to the average worker in the average hospital.
“Surgeons and others who toil in the operating room are not analogous to Toyota assembly line workers in Japan," according to Dr. Smith, interim chair, department of surgery, Virginia Tech Carilion School of Medicine in Roanoke.
He also questioned how less affluent institutions could marshal the hospitalwide resources necessary to institute Lean/Six Sigma projects.
Dr. Cima responded that the project required very few resources, and that smaller institutions actually may be in a better position to implement Lean/Six Sigma because they are less constrained by bureaucracy.
Dr. Cima acknowledged that the hospital population may be unique in its commitment to the success of the overall institution, as opposed to individual productivity, but added that there are advantages for the employees to come together in smaller settings such as in ambulatory, outpatient surgical practices.
For example, surgeons may be able to return to the clinic earlier and see more cases if the surgical suite is run more efficiently.
“One of the efforts that has to be brought out to bring people together is to make sure everyone knows what they want out of it and what they are willing to give up," Dr. Cima said. “It is a collaborative effort."
During the discussion, Dr. Tyler Hughes, from Memorial Hospital in McPherson, Kan., asked whether institutions can survive if they don't push through these kinds of process improvements.
“I would submit that any institution that doesn't look at their processes - and not just a step, but the whole process - will not be able to survive the next 10-15 years," Dr. Cima responded.
“The government is clearly sending a signal that efficiency, value, and safety are the three main ways you're going to survive."
The study was supported by the Mayo Clinic, department of surgery. Dr. Cima and Dr. Smith reported no conflicts of interest.
CHICAGO - Applying the Lean streamlining methodology across the entire surgical process significantly improved several operating room performance measures such as on-time starts and turnover time. At the same time, the operating margin in some ORs was increased by more than $45,000 per day, as demonstrated at the Mayo Clinic in Rochester, Minn.
“This was all during a period of increased growth and volume of cases," Dr. Robert Cima said at the annual meeting of the Western Surgical Association.
“What's even more important was that during this time when we had increased volume of cases, we actually had a decreased need for personnel because we were reducing the need for overtime staffing as well as the just the plain need for extra bodies," added Dr. Cima.
That translated into 37 fewer full-time surgical services employees, 50% fewer late shifts among certified registered nurse anesthetists, and an 18%-56% decrease in health care security services overtime.
The Lean and Six Sigma methodologies, popularized decades ago by companies like automobile maker Toyota as a way to eliminate wasteful steps and improve productivity, have typically been applied to a limited number of ORs or to specific operations.
The Mayo Clinic credits its success to applying the methodology across the entire surgical process and in all 88 of its main ORs performing both in- and outpatient procedures.
“Multiple areas of redundant or non-value-added steps were identified across the entire process flow that would not have been identified with a focus on specific steps," said Dr. Cima, a colorectal surgeon at the Mayo Clinic.
First, a multidisciplinary leadership team developed a map of the surgical process from the decision for surgery to leaving the OR. The team analyzed each step for personnel required, information process, and time expended. In all, 28 systems and 14 points of delay were identified, he said.
Next, multidisciplinary teams were formed and given 6 months to redesign systems around five essential work streams: minimizing unplanned surgical volume variation, streamlining the preoperative process, reducing nonoperative time, reducing redundant information collection, and engaging employees.
“Specific goals were set for each specialty," he said. “It was not 'one size fits all.'“
Each work stream was tweaked to standardize procedure descriptions, implement dedicated staggered surgery start times, and develop a first-case scheduling checklist to eliminate barriers to on-time OR starts.
When streamlining the preoperative process, Dr. Cima said, the most important thing is to start on time.
The hospital tried to get buy-in from employees by implementing OR briefings with the OR team, creating a communication council to effectively disseminate information through all levels of staff, and conducting a survey to identify major drivers of employee participation - many of which were not financial, Dr. Cima noted.
Some of the drivers included promotion of shared goals, encouragement of continuous professional growth, frequent recognition of individual employee contributions, and executive demonstration of values and commitment to the project.
Data collected before the intervention and 18 months afterward from the first three specialties tested showed that on-time starts increased from 50% to 80% for thoracic surgery, from 64% to 92% for gynecologic surgery, and from 60% to 92% for general/colorectal surgery.
The differences were all significant (P less than .05), he said.
The percentage of operations performed past 5 p.m. stayed relatively constant before and after intervention among thoracic surgeons at 34% vs. 36%, respectively. However, it decreased significantly for gynecologic surgeons (from 42% to 36%) and general/colorectal surgeons (from 37% to 31%) (P less than .05 for both).
The average nonoperative or turnover time was reduced by 10-15 minutes among the three specialties, or 25% for thoracic surgery, 43% for gynecologic surgery, and 32% for general/colorectal surgery, Dr. Cima said.
Staff overtime was reduced by an average of 17 minutes per month for thoracic surgery (16%), 19 minutes for gynecologic surgery (18%), and 46 minutes for general/colorectal surgery (53%).
The financial impact of these improvements was at times quite dramatic, he said.
For example, the financial margin increased 22% or $21,340 per OR/day for thoracic surgery, 16% or $24,570 per OR/day for gynecologic surgery, and 55% and $47,700 per OR/day for general/colorectal surgery.
“Some people say this is a Hawthorne effect . . . but this is sustainable and in some cases actually increases as the teams become more efficient," he said, noting that positive improvements have now been reported in nine separate specialties.
Invited discussant Dr. R. Stephen Smith called the project a “monumental effort," but questioned whether the methodology is applicable to the average worker in the average hospital.
“Surgeons and others who toil in the operating room are not analogous to Toyota assembly line workers in Japan," according to Dr. Smith, interim chair, department of surgery, Virginia Tech Carilion School of Medicine in Roanoke.
He also questioned how less affluent institutions could marshal the hospitalwide resources necessary to institute Lean/Six Sigma projects.
Dr. Cima responded that the project required very few resources, and that smaller institutions actually may be in a better position to implement Lean/Six Sigma because they are less constrained by bureaucracy.
Dr. Cima acknowledged that the hospital population may be unique in its commitment to the success of the overall institution, as opposed to individual productivity, but added that there are advantages for the employees to come together in smaller settings such as in ambulatory, outpatient surgical practices.
For example, surgeons may be able to return to the clinic earlier and see more cases if the surgical suite is run more efficiently.
“One of the efforts that has to be brought out to bring people together is to make sure everyone knows what they want out of it and what they are willing to give up," Dr. Cima said. “It is a collaborative effort."
During the discussion, Dr. Tyler Hughes, from Memorial Hospital in McPherson, Kan., asked whether institutions can survive if they don't push through these kinds of process improvements.
“I would submit that any institution that doesn't look at their processes - and not just a step, but the whole process - will not be able to survive the next 10-15 years," Dr. Cima responded.
“The government is clearly sending a signal that efficiency, value, and safety are the three main ways you're going to survive."
The study was supported by the Mayo Clinic, department of surgery. Dr. Cima and Dr. Smith reported no conflicts of interest.
CHICAGO - Applying the Lean streamlining methodology across the entire surgical process significantly improved several operating room performance measures such as on-time starts and turnover time. At the same time, the operating margin in some ORs was increased by more than $45,000 per day, as demonstrated at the Mayo Clinic in Rochester, Minn.
“This was all during a period of increased growth and volume of cases," Dr. Robert Cima said at the annual meeting of the Western Surgical Association.
“What's even more important was that during this time when we had increased volume of cases, we actually had a decreased need for personnel because we were reducing the need for overtime staffing as well as the just the plain need for extra bodies," added Dr. Cima.
That translated into 37 fewer full-time surgical services employees, 50% fewer late shifts among certified registered nurse anesthetists, and an 18%-56% decrease in health care security services overtime.
The Lean and Six Sigma methodologies, popularized decades ago by companies like automobile maker Toyota as a way to eliminate wasteful steps and improve productivity, have typically been applied to a limited number of ORs or to specific operations.
The Mayo Clinic credits its success to applying the methodology across the entire surgical process and in all 88 of its main ORs performing both in- and outpatient procedures.
“Multiple areas of redundant or non-value-added steps were identified across the entire process flow that would not have been identified with a focus on specific steps," said Dr. Cima, a colorectal surgeon at the Mayo Clinic.
First, a multidisciplinary leadership team developed a map of the surgical process from the decision for surgery to leaving the OR. The team analyzed each step for personnel required, information process, and time expended. In all, 28 systems and 14 points of delay were identified, he said.
Next, multidisciplinary teams were formed and given 6 months to redesign systems around five essential work streams: minimizing unplanned surgical volume variation, streamlining the preoperative process, reducing nonoperative time, reducing redundant information collection, and engaging employees.
“Specific goals were set for each specialty," he said. “It was not 'one size fits all.'“
Each work stream was tweaked to standardize procedure descriptions, implement dedicated staggered surgery start times, and develop a first-case scheduling checklist to eliminate barriers to on-time OR starts.
When streamlining the preoperative process, Dr. Cima said, the most important thing is to start on time.
The hospital tried to get buy-in from employees by implementing OR briefings with the OR team, creating a communication council to effectively disseminate information through all levels of staff, and conducting a survey to identify major drivers of employee participation - many of which were not financial, Dr. Cima noted.
Some of the drivers included promotion of shared goals, encouragement of continuous professional growth, frequent recognition of individual employee contributions, and executive demonstration of values and commitment to the project.
Data collected before the intervention and 18 months afterward from the first three specialties tested showed that on-time starts increased from 50% to 80% for thoracic surgery, from 64% to 92% for gynecologic surgery, and from 60% to 92% for general/colorectal surgery.
The differences were all significant (P less than .05), he said.
The percentage of operations performed past 5 p.m. stayed relatively constant before and after intervention among thoracic surgeons at 34% vs. 36%, respectively. However, it decreased significantly for gynecologic surgeons (from 42% to 36%) and general/colorectal surgeons (from 37% to 31%) (P less than .05 for both).
The average nonoperative or turnover time was reduced by 10-15 minutes among the three specialties, or 25% for thoracic surgery, 43% for gynecologic surgery, and 32% for general/colorectal surgery, Dr. Cima said.
Staff overtime was reduced by an average of 17 minutes per month for thoracic surgery (16%), 19 minutes for gynecologic surgery (18%), and 46 minutes for general/colorectal surgery (53%).
The financial impact of these improvements was at times quite dramatic, he said.
For example, the financial margin increased 22% or $21,340 per OR/day for thoracic surgery, 16% or $24,570 per OR/day for gynecologic surgery, and 55% and $47,700 per OR/day for general/colorectal surgery.
“Some people say this is a Hawthorne effect . . . but this is sustainable and in some cases actually increases as the teams become more efficient," he said, noting that positive improvements have now been reported in nine separate specialties.
Invited discussant Dr. R. Stephen Smith called the project a “monumental effort," but questioned whether the methodology is applicable to the average worker in the average hospital.
“Surgeons and others who toil in the operating room are not analogous to Toyota assembly line workers in Japan," according to Dr. Smith, interim chair, department of surgery, Virginia Tech Carilion School of Medicine in Roanoke.
He also questioned how less affluent institutions could marshal the hospitalwide resources necessary to institute Lean/Six Sigma projects.
Dr. Cima responded that the project required very few resources, and that smaller institutions actually may be in a better position to implement Lean/Six Sigma because they are less constrained by bureaucracy.
Dr. Cima acknowledged that the hospital population may be unique in its commitment to the success of the overall institution, as opposed to individual productivity, but added that there are advantages for the employees to come together in smaller settings such as in ambulatory, outpatient surgical practices.
For example, surgeons may be able to return to the clinic earlier and see more cases if the surgical suite is run more efficiently.
“One of the efforts that has to be brought out to bring people together is to make sure everyone knows what they want out of it and what they are willing to give up," Dr. Cima said. “It is a collaborative effort."
During the discussion, Dr. Tyler Hughes, from Memorial Hospital in McPherson, Kan., asked whether institutions can survive if they don't push through these kinds of process improvements.
“I would submit that any institution that doesn't look at their processes - and not just a step, but the whole process - will not be able to survive the next 10-15 years," Dr. Cima responded.
“The government is clearly sending a signal that efficiency, value, and safety are the three main ways you're going to survive."
The study was supported by the Mayo Clinic, department of surgery. Dr. Cima and Dr. Smith reported no conflicts of interest.
Robotic Hysterectomy Patients: Older, Thinner
Major Finding: Women having robotic total hysterectomy were older (mean, 51 vs. 44 years), had a lower BMI (27.4 vs. 29.8), and had a lower uterine weight (144 vs. 204 g) than did women who had a laparoscopic total hysterectomy.
Data Source: Retrospective chart review of 380 women who underwent either robotic or laparoscopic total hysterectomy for benign indications.
Disclosures: The researchers received support from the Florida Hospital Continuing Medical Education. Dr. Colimon disclosed no relevant conflicts of interest.
CHICAGO – Surgeons tended to select women who were significantly older and thinner and who had a smaller uterine size for robotic total hysterectomy in a retrospective analysis of 380 women.
Women who underwent robotic total hysterectomy averaged 51 years of age, compared with 44 years among women who underwent laparoscopic total hysterectomy. They had a body mass index of 27.4 vs. 29.8 kg/m
Charts were reviewed for information regarding pain levels and analgesic use among 162 women who underwent robotic total hysterectomy and 218 women who had laparoscopic total hysterectomy at three urban teaching hospitals in the Southeast in 2008-2009. All surgeries were performed by gynecologists or gynecologic oncologists for benign indications.
Women undergoing laparoscopic hysterectomy were significantly more likely to stay in the hospital longer than were those undergoing the robotic-assisted approach, said Dr. Colimon of the Florida Hospital in Orlando. Average length of stay was 1.2 days vs. 0.7 days, respectively.
Pain levels were similar in the two groups, but the incidence of patient-controlled analgesia was significantly higher in the laparoscopic group. This finding may be because the laparoscopic group had a longer hospital stay or surgeon preference, Dr. Colimon suggested.
Major Finding: Women having robotic total hysterectomy were older (mean, 51 vs. 44 years), had a lower BMI (27.4 vs. 29.8), and had a lower uterine weight (144 vs. 204 g) than did women who had a laparoscopic total hysterectomy.
Data Source: Retrospective chart review of 380 women who underwent either robotic or laparoscopic total hysterectomy for benign indications.
Disclosures: The researchers received support from the Florida Hospital Continuing Medical Education. Dr. Colimon disclosed no relevant conflicts of interest.
CHICAGO – Surgeons tended to select women who were significantly older and thinner and who had a smaller uterine size for robotic total hysterectomy in a retrospective analysis of 380 women.
Women who underwent robotic total hysterectomy averaged 51 years of age, compared with 44 years among women who underwent laparoscopic total hysterectomy. They had a body mass index of 27.4 vs. 29.8 kg/m
Charts were reviewed for information regarding pain levels and analgesic use among 162 women who underwent robotic total hysterectomy and 218 women who had laparoscopic total hysterectomy at three urban teaching hospitals in the Southeast in 2008-2009. All surgeries were performed by gynecologists or gynecologic oncologists for benign indications.
Women undergoing laparoscopic hysterectomy were significantly more likely to stay in the hospital longer than were those undergoing the robotic-assisted approach, said Dr. Colimon of the Florida Hospital in Orlando. Average length of stay was 1.2 days vs. 0.7 days, respectively.
Pain levels were similar in the two groups, but the incidence of patient-controlled analgesia was significantly higher in the laparoscopic group. This finding may be because the laparoscopic group had a longer hospital stay or surgeon preference, Dr. Colimon suggested.
Major Finding: Women having robotic total hysterectomy were older (mean, 51 vs. 44 years), had a lower BMI (27.4 vs. 29.8), and had a lower uterine weight (144 vs. 204 g) than did women who had a laparoscopic total hysterectomy.
Data Source: Retrospective chart review of 380 women who underwent either robotic or laparoscopic total hysterectomy for benign indications.
Disclosures: The researchers received support from the Florida Hospital Continuing Medical Education. Dr. Colimon disclosed no relevant conflicts of interest.
CHICAGO – Surgeons tended to select women who were significantly older and thinner and who had a smaller uterine size for robotic total hysterectomy in a retrospective analysis of 380 women.
Women who underwent robotic total hysterectomy averaged 51 years of age, compared with 44 years among women who underwent laparoscopic total hysterectomy. They had a body mass index of 27.4 vs. 29.8 kg/m
Charts were reviewed for information regarding pain levels and analgesic use among 162 women who underwent robotic total hysterectomy and 218 women who had laparoscopic total hysterectomy at three urban teaching hospitals in the Southeast in 2008-2009. All surgeries were performed by gynecologists or gynecologic oncologists for benign indications.
Women undergoing laparoscopic hysterectomy were significantly more likely to stay in the hospital longer than were those undergoing the robotic-assisted approach, said Dr. Colimon of the Florida Hospital in Orlando. Average length of stay was 1.2 days vs. 0.7 days, respectively.
Pain levels were similar in the two groups, but the incidence of patient-controlled analgesia was significantly higher in the laparoscopic group. This finding may be because the laparoscopic group had a longer hospital stay or surgeon preference, Dr. Colimon suggested.
From the Annual Meeting of the International Pelvic Pain Society
CMS Tweaks Hospital Sedation Policy, Again
The Centers for Medicare and Medicaid Services has revised its recently updated anesthesia guidelines, following complaints the policy was unworkable.
Hospitals are now directed to develop their own internal policies concerning what is anesthesia versus analgesia, which leaves open the option of using different guidelines in different clinical departments. The revisions also provide greater flexibility regarding pre- and postanesthesia evaluations, while particularly problematic references to propofol and labor epidural anesthesia were dropped entirely.
Following the December 2009 release of the updated interpretive guidelines for hospital anesthesia services, practitioners called for clarifications regarding the distinction between anesthesia and analgesia, suggesting that some of the examples didn’t fall clearly on one side or the other of the anesthesia/analgesia spectrum. The use of propofol (Diprivan) during screening colonoscopy was cited as an example of deep sedation, which meant it could only be delivered by providers trained in general anesthesia.
"The examples caused a lot of consternation," acknowledged Marilyn Dahl, director of the Centers for Medicare and Medicaid Services (CMS) survey and certification division of acute care services. "What the current guidelines say is that we are going to leave it up to the hospital, relying on nationally recognized guidelines, to decide which things fall on the anesthesia side of the continuum."
The guidelines retain the six broad categories of anesthesia and analgesia, but acknowledge that the level of sedation for a particular medication may vary on the basis of such factors as dosage and route and timing of administration. Thus, it’s possible for the same drug to be used for general anesthesia in the operating room and for sedation in the emergency department (ED) or a procedure room. In what could be considered a mea culpa, the CMS stressed that "for some medications there is no bright line that distinguishes when their pharmacological properties bring about the physiologic transition from the analgesic to the anesthetic effects."
Under the current guidelines, hospital policies should address whether specific clinical situations involve anesthesia versus analgesia, and specify the qualifications for each category of practitioner who administers analgesia and their supervision requirements. Federal regulations regarding who may administer anesthesia continue to apply for procedures that require anesthesia.
Hospital policies must be based on nationally recognized guidelines, even though the CMS recognizes that the issuing organizations "may not always fully agree with each other." A hospital could use the American College of Emergency Physicians (ACEP) guidelines in its ED and follow those of the American Society of Anesthesiologists (ASA) for its surgical services.
"There’s more flexibility in terms of a hospital deciding what type of personnel need to be present and involved depending on what type of sedation is used," Ms. Dahl said.
ACEP’s federal affairs director Barbara Tomar agreed that the current revisions provide hospitals with greater flexibility than the 2009 update, which she said was overly restrictive in its interpretation of federal regulations.
"If there is some controversy or disagreement between anesthesiologists and the emergency department, this will provide some clarification and additional evidence that the guidelines developed by the emergency physicians are more than adequate for use in the emergency department," Ms. Tomar said. "We have no qualms about the anesthesiology guidelines being used for surgical services. That’s their bailiwick."
ACEP, jointly with the Emergency Nurses Association and American Academy of Emergency Medicine, wrote to the CMS in March 2010 expressing concern over what constituted anesthesia, particularly with regard to propofol. The college noted that ED physicians are trained to provide resuscitation should propofol administration accidentally result in deep sedation, and that propofol administration by emergency nurses in the presence of an emergency physician complies with current Joint Commission standards.
Propofol is no longer cited as an example of deep sedation, and there is a particular reference in the guidelines to the "unique environment" in the ED, as well as acknowledgment that emergency physicians have "very specific skill sets" that allow them to provide patient rescue and "all levels of analgesia/sedation and anesthesia (moderate to deep to general)."
The failure to specifically address the issue of propofol leaves unfinished business, said sedation expert Dr. John Vargo, a member of the governing board of the American Society for Gastrointestinal Endoscopy (ASGE) and acting chair of the gastroenterology and hepatology department at the Cleveland Clinic.
"The endoscopy society has been collecting evidence-based data over the past 15 years on endoscopist-directed propofol sedation, and frankly, there is no evidence on the other side showing that monitored anesthesia care is safer, more effective, or better tolerated than endoscopist-directed propofol sedation," he said.
Dr. Vargo said he hoped that hospitals would use the evidence available in order to craft an appropriate anesthesia policy regarding propofol and other types of procedural sedation. He also observed that an evidence-based position paper on non-anesthesiologist administration of propofol for GI endoscopy was recently jointly published by the ASGE, American Association for the Study of Liver Disease, American College of Gastroenterology, and American Gastroenterological Association (Gastrointest. Endosc. 2009;70:1053-9).
Dr. Douglas K. Rex, a vocal opponent of the CMS’s position on propofol and director of endoscopy at Indiana University Hospital, Indianapolis, said the CMS guidelines still state that deep sedation is the domain of anesthesia specialists, a concept for which there is virtually no evidence and plenty of evidence that the policy is wrong and unnecessary.
"CMS’s handling of this process has been tragic," he said. "They stuck their noses in an issue they did not and still do not understand."
Dr. Alexander A. Hannenberg, ASA immediate past-president and associate chair of anesthesia at Newton-Wellesley Hospital in Newton, Mass., said the ASA met with CMS officials in April 2010 to contest its position that a labor epidural was not considered anesthesia, and therefore could be administered without physician supervision by certified registered nurse anesthetists (CRNAs).
Dr. Hannenberg said the CMS appeared not to understand the physiology of epidural pain relief, and that epidurals for labor, just as those used as anesthesia for surgery, produce a sympathetic block, or block the nerves that control circulation. He went on to say that the CMS’s previous position appeared to lower the standard of care for laboring women.
"I think they appreciated the physiology lesson, and went back and realized that the distinction was not as crisp or clear as they had originally thought, and removed the language that said it’s different and that the requirement for physician supervision is therefore different," he said.
CRNAs can still administer anesthesia if the hospital is located in one of 16 states that have elected to opt out of the CRNA physician supervision requirement. Ms. Dahl noted, however, that in theory, the updated guidance does not preclude a hospital in a non-opt-out state from choosing to make a determination that labor epidurals are not anesthesia, if it could point to support in nationally recognized guidelines when doing so, and as long as this would not be in violation of the state’s scope of practice law.
Dr. Hannenberg said the ASA also sought changes to the CMS pre- and postanesthesia evaluations. Preanesthesia evaluation must be completed within 48 hours prior to surgery or a procedure requiring anesthesia services, but the CMS clarified that some elements may be performed before then, as long as they are reviewed and appropriately updated within the 48-hour time frame. Dr. Hannenberg said the new wording recognizes that tests are often performed before the 48-hour time frame, and that it is standard of care for all elements of a case to be reassessed by anesthesiologists immediately before anesthesia administration.
The postanesthesia evaluation previously had to be completed before discharge, but may now be completed within 48 hours after a patient is moved to another inpatient location within the hospital or is discharged. This flexibility allows for a more complete evaluation of a patient because some things, such as adverse events, may not be fully knowable until after a patient is sent home, he said.
Ms. Dahl, Dr. Hannenberg, and Dr. Vargo reported no conflicts of interest. Dr. Rex reported consulting and advisory arrangements with American BioOptics, Avantis Medical Systems, CheckCap, Epigenomics, Given Imaging, and SoftScope. He receives grant support from Braintree Laboratories and Given Imaging, and a salary as well as speaking and teaching fees from Olympus America.
The Centers for Medicare and Medicaid Services has revised its recently updated anesthesia guidelines, following complaints the policy was unworkable.
Hospitals are now directed to develop their own internal policies concerning what is anesthesia versus analgesia, which leaves open the option of using different guidelines in different clinical departments. The revisions also provide greater flexibility regarding pre- and postanesthesia evaluations, while particularly problematic references to propofol and labor epidural anesthesia were dropped entirely.
Following the December 2009 release of the updated interpretive guidelines for hospital anesthesia services, practitioners called for clarifications regarding the distinction between anesthesia and analgesia, suggesting that some of the examples didn’t fall clearly on one side or the other of the anesthesia/analgesia spectrum. The use of propofol (Diprivan) during screening colonoscopy was cited as an example of deep sedation, which meant it could only be delivered by providers trained in general anesthesia.
"The examples caused a lot of consternation," acknowledged Marilyn Dahl, director of the Centers for Medicare and Medicaid Services (CMS) survey and certification division of acute care services. "What the current guidelines say is that we are going to leave it up to the hospital, relying on nationally recognized guidelines, to decide which things fall on the anesthesia side of the continuum."
The guidelines retain the six broad categories of anesthesia and analgesia, but acknowledge that the level of sedation for a particular medication may vary on the basis of such factors as dosage and route and timing of administration. Thus, it’s possible for the same drug to be used for general anesthesia in the operating room and for sedation in the emergency department (ED) or a procedure room. In what could be considered a mea culpa, the CMS stressed that "for some medications there is no bright line that distinguishes when their pharmacological properties bring about the physiologic transition from the analgesic to the anesthetic effects."
Under the current guidelines, hospital policies should address whether specific clinical situations involve anesthesia versus analgesia, and specify the qualifications for each category of practitioner who administers analgesia and their supervision requirements. Federal regulations regarding who may administer anesthesia continue to apply for procedures that require anesthesia.
Hospital policies must be based on nationally recognized guidelines, even though the CMS recognizes that the issuing organizations "may not always fully agree with each other." A hospital could use the American College of Emergency Physicians (ACEP) guidelines in its ED and follow those of the American Society of Anesthesiologists (ASA) for its surgical services.
"There’s more flexibility in terms of a hospital deciding what type of personnel need to be present and involved depending on what type of sedation is used," Ms. Dahl said.
ACEP’s federal affairs director Barbara Tomar agreed that the current revisions provide hospitals with greater flexibility than the 2009 update, which she said was overly restrictive in its interpretation of federal regulations.
"If there is some controversy or disagreement between anesthesiologists and the emergency department, this will provide some clarification and additional evidence that the guidelines developed by the emergency physicians are more than adequate for use in the emergency department," Ms. Tomar said. "We have no qualms about the anesthesiology guidelines being used for surgical services. That’s their bailiwick."
ACEP, jointly with the Emergency Nurses Association and American Academy of Emergency Medicine, wrote to the CMS in March 2010 expressing concern over what constituted anesthesia, particularly with regard to propofol. The college noted that ED physicians are trained to provide resuscitation should propofol administration accidentally result in deep sedation, and that propofol administration by emergency nurses in the presence of an emergency physician complies with current Joint Commission standards.
Propofol is no longer cited as an example of deep sedation, and there is a particular reference in the guidelines to the "unique environment" in the ED, as well as acknowledgment that emergency physicians have "very specific skill sets" that allow them to provide patient rescue and "all levels of analgesia/sedation and anesthesia (moderate to deep to general)."
The failure to specifically address the issue of propofol leaves unfinished business, said sedation expert Dr. John Vargo, a member of the governing board of the American Society for Gastrointestinal Endoscopy (ASGE) and acting chair of the gastroenterology and hepatology department at the Cleveland Clinic.
"The endoscopy society has been collecting evidence-based data over the past 15 years on endoscopist-directed propofol sedation, and frankly, there is no evidence on the other side showing that monitored anesthesia care is safer, more effective, or better tolerated than endoscopist-directed propofol sedation," he said.
Dr. Vargo said he hoped that hospitals would use the evidence available in order to craft an appropriate anesthesia policy regarding propofol and other types of procedural sedation. He also observed that an evidence-based position paper on non-anesthesiologist administration of propofol for GI endoscopy was recently jointly published by the ASGE, American Association for the Study of Liver Disease, American College of Gastroenterology, and American Gastroenterological Association (Gastrointest. Endosc. 2009;70:1053-9).
Dr. Douglas K. Rex, a vocal opponent of the CMS’s position on propofol and director of endoscopy at Indiana University Hospital, Indianapolis, said the CMS guidelines still state that deep sedation is the domain of anesthesia specialists, a concept for which there is virtually no evidence and plenty of evidence that the policy is wrong and unnecessary.
"CMS’s handling of this process has been tragic," he said. "They stuck their noses in an issue they did not and still do not understand."
Dr. Alexander A. Hannenberg, ASA immediate past-president and associate chair of anesthesia at Newton-Wellesley Hospital in Newton, Mass., said the ASA met with CMS officials in April 2010 to contest its position that a labor epidural was not considered anesthesia, and therefore could be administered without physician supervision by certified registered nurse anesthetists (CRNAs).
Dr. Hannenberg said the CMS appeared not to understand the physiology of epidural pain relief, and that epidurals for labor, just as those used as anesthesia for surgery, produce a sympathetic block, or block the nerves that control circulation. He went on to say that the CMS’s previous position appeared to lower the standard of care for laboring women.
"I think they appreciated the physiology lesson, and went back and realized that the distinction was not as crisp or clear as they had originally thought, and removed the language that said it’s different and that the requirement for physician supervision is therefore different," he said.
CRNAs can still administer anesthesia if the hospital is located in one of 16 states that have elected to opt out of the CRNA physician supervision requirement. Ms. Dahl noted, however, that in theory, the updated guidance does not preclude a hospital in a non-opt-out state from choosing to make a determination that labor epidurals are not anesthesia, if it could point to support in nationally recognized guidelines when doing so, and as long as this would not be in violation of the state’s scope of practice law.
Dr. Hannenberg said the ASA also sought changes to the CMS pre- and postanesthesia evaluations. Preanesthesia evaluation must be completed within 48 hours prior to surgery or a procedure requiring anesthesia services, but the CMS clarified that some elements may be performed before then, as long as they are reviewed and appropriately updated within the 48-hour time frame. Dr. Hannenberg said the new wording recognizes that tests are often performed before the 48-hour time frame, and that it is standard of care for all elements of a case to be reassessed by anesthesiologists immediately before anesthesia administration.
The postanesthesia evaluation previously had to be completed before discharge, but may now be completed within 48 hours after a patient is moved to another inpatient location within the hospital or is discharged. This flexibility allows for a more complete evaluation of a patient because some things, such as adverse events, may not be fully knowable until after a patient is sent home, he said.
Ms. Dahl, Dr. Hannenberg, and Dr. Vargo reported no conflicts of interest. Dr. Rex reported consulting and advisory arrangements with American BioOptics, Avantis Medical Systems, CheckCap, Epigenomics, Given Imaging, and SoftScope. He receives grant support from Braintree Laboratories and Given Imaging, and a salary as well as speaking and teaching fees from Olympus America.
The Centers for Medicare and Medicaid Services has revised its recently updated anesthesia guidelines, following complaints the policy was unworkable.
Hospitals are now directed to develop their own internal policies concerning what is anesthesia versus analgesia, which leaves open the option of using different guidelines in different clinical departments. The revisions also provide greater flexibility regarding pre- and postanesthesia evaluations, while particularly problematic references to propofol and labor epidural anesthesia were dropped entirely.
Following the December 2009 release of the updated interpretive guidelines for hospital anesthesia services, practitioners called for clarifications regarding the distinction between anesthesia and analgesia, suggesting that some of the examples didn’t fall clearly on one side or the other of the anesthesia/analgesia spectrum. The use of propofol (Diprivan) during screening colonoscopy was cited as an example of deep sedation, which meant it could only be delivered by providers trained in general anesthesia.
"The examples caused a lot of consternation," acknowledged Marilyn Dahl, director of the Centers for Medicare and Medicaid Services (CMS) survey and certification division of acute care services. "What the current guidelines say is that we are going to leave it up to the hospital, relying on nationally recognized guidelines, to decide which things fall on the anesthesia side of the continuum."
The guidelines retain the six broad categories of anesthesia and analgesia, but acknowledge that the level of sedation for a particular medication may vary on the basis of such factors as dosage and route and timing of administration. Thus, it’s possible for the same drug to be used for general anesthesia in the operating room and for sedation in the emergency department (ED) or a procedure room. In what could be considered a mea culpa, the CMS stressed that "for some medications there is no bright line that distinguishes when their pharmacological properties bring about the physiologic transition from the analgesic to the anesthetic effects."
Under the current guidelines, hospital policies should address whether specific clinical situations involve anesthesia versus analgesia, and specify the qualifications for each category of practitioner who administers analgesia and their supervision requirements. Federal regulations regarding who may administer anesthesia continue to apply for procedures that require anesthesia.
Hospital policies must be based on nationally recognized guidelines, even though the CMS recognizes that the issuing organizations "may not always fully agree with each other." A hospital could use the American College of Emergency Physicians (ACEP) guidelines in its ED and follow those of the American Society of Anesthesiologists (ASA) for its surgical services.
"There’s more flexibility in terms of a hospital deciding what type of personnel need to be present and involved depending on what type of sedation is used," Ms. Dahl said.
ACEP’s federal affairs director Barbara Tomar agreed that the current revisions provide hospitals with greater flexibility than the 2009 update, which she said was overly restrictive in its interpretation of federal regulations.
"If there is some controversy or disagreement between anesthesiologists and the emergency department, this will provide some clarification and additional evidence that the guidelines developed by the emergency physicians are more than adequate for use in the emergency department," Ms. Tomar said. "We have no qualms about the anesthesiology guidelines being used for surgical services. That’s their bailiwick."
ACEP, jointly with the Emergency Nurses Association and American Academy of Emergency Medicine, wrote to the CMS in March 2010 expressing concern over what constituted anesthesia, particularly with regard to propofol. The college noted that ED physicians are trained to provide resuscitation should propofol administration accidentally result in deep sedation, and that propofol administration by emergency nurses in the presence of an emergency physician complies with current Joint Commission standards.
Propofol is no longer cited as an example of deep sedation, and there is a particular reference in the guidelines to the "unique environment" in the ED, as well as acknowledgment that emergency physicians have "very specific skill sets" that allow them to provide patient rescue and "all levels of analgesia/sedation and anesthesia (moderate to deep to general)."
The failure to specifically address the issue of propofol leaves unfinished business, said sedation expert Dr. John Vargo, a member of the governing board of the American Society for Gastrointestinal Endoscopy (ASGE) and acting chair of the gastroenterology and hepatology department at the Cleveland Clinic.
"The endoscopy society has been collecting evidence-based data over the past 15 years on endoscopist-directed propofol sedation, and frankly, there is no evidence on the other side showing that monitored anesthesia care is safer, more effective, or better tolerated than endoscopist-directed propofol sedation," he said.
Dr. Vargo said he hoped that hospitals would use the evidence available in order to craft an appropriate anesthesia policy regarding propofol and other types of procedural sedation. He also observed that an evidence-based position paper on non-anesthesiologist administration of propofol for GI endoscopy was recently jointly published by the ASGE, American Association for the Study of Liver Disease, American College of Gastroenterology, and American Gastroenterological Association (Gastrointest. Endosc. 2009;70:1053-9).
Dr. Douglas K. Rex, a vocal opponent of the CMS’s position on propofol and director of endoscopy at Indiana University Hospital, Indianapolis, said the CMS guidelines still state that deep sedation is the domain of anesthesia specialists, a concept for which there is virtually no evidence and plenty of evidence that the policy is wrong and unnecessary.
"CMS’s handling of this process has been tragic," he said. "They stuck their noses in an issue they did not and still do not understand."
Dr. Alexander A. Hannenberg, ASA immediate past-president and associate chair of anesthesia at Newton-Wellesley Hospital in Newton, Mass., said the ASA met with CMS officials in April 2010 to contest its position that a labor epidural was not considered anesthesia, and therefore could be administered without physician supervision by certified registered nurse anesthetists (CRNAs).
Dr. Hannenberg said the CMS appeared not to understand the physiology of epidural pain relief, and that epidurals for labor, just as those used as anesthesia for surgery, produce a sympathetic block, or block the nerves that control circulation. He went on to say that the CMS’s previous position appeared to lower the standard of care for laboring women.
"I think they appreciated the physiology lesson, and went back and realized that the distinction was not as crisp or clear as they had originally thought, and removed the language that said it’s different and that the requirement for physician supervision is therefore different," he said.
CRNAs can still administer anesthesia if the hospital is located in one of 16 states that have elected to opt out of the CRNA physician supervision requirement. Ms. Dahl noted, however, that in theory, the updated guidance does not preclude a hospital in a non-opt-out state from choosing to make a determination that labor epidurals are not anesthesia, if it could point to support in nationally recognized guidelines when doing so, and as long as this would not be in violation of the state’s scope of practice law.
Dr. Hannenberg said the ASA also sought changes to the CMS pre- and postanesthesia evaluations. Preanesthesia evaluation must be completed within 48 hours prior to surgery or a procedure requiring anesthesia services, but the CMS clarified that some elements may be performed before then, as long as they are reviewed and appropriately updated within the 48-hour time frame. Dr. Hannenberg said the new wording recognizes that tests are often performed before the 48-hour time frame, and that it is standard of care for all elements of a case to be reassessed by anesthesiologists immediately before anesthesia administration.
The postanesthesia evaluation previously had to be completed before discharge, but may now be completed within 48 hours after a patient is moved to another inpatient location within the hospital or is discharged. This flexibility allows for a more complete evaluation of a patient because some things, such as adverse events, may not be fully knowable until after a patient is sent home, he said.
Ms. Dahl, Dr. Hannenberg, and Dr. Vargo reported no conflicts of interest. Dr. Rex reported consulting and advisory arrangements with American BioOptics, Avantis Medical Systems, CheckCap, Epigenomics, Given Imaging, and SoftScope. He receives grant support from Braintree Laboratories and Given Imaging, and a salary as well as speaking and teaching fees from Olympus America.
CMS Tweaks Hospital Sedation Policy, Again
The Centers for Medicare and Medicaid Services has revised its recently updated anesthesia guidelines, following complaints the policy was unworkable.
Hospitals are now directed to develop their own internal policies concerning what is anesthesia versus analgesia, which leaves open the option of using different guidelines in different clinical departments. The revisions also provide greater flexibility regarding pre- and postanesthesia evaluations, while particularly problematic references to propofol and labor epidural anesthesia were dropped entirely.
Following the December 2009 release of the updated interpretive guidelines for hospital anesthesia services, practitioners called for clarifications regarding the distinction between anesthesia and analgesia, suggesting that some of the examples didn’t fall clearly on one side or the other of the anesthesia/analgesia spectrum. The use of propofol (Diprivan) during screening colonoscopy was cited as an example of deep sedation, which meant it could only be delivered by providers trained in general anesthesia.
"The examples caused a lot of consternation," acknowledged Marilyn Dahl, director of the Centers for Medicare and Medicaid Services (CMS) survey and certification division of acute care services. "What the current guidelines say is that we are going to leave it up to the hospital, relying on nationally recognized guidelines, to decide which things fall on the anesthesia side of the continuum."
The guidelines retain the six broad categories of anesthesia and analgesia, but acknowledge that the level of sedation for a particular medication may vary on the basis of such factors as dosage and route and timing of administration. Thus, it’s possible for the same drug to be used for general anesthesia in the operating room and for sedation in the emergency department (ED) or a procedure room. In what could be considered a mea culpa, the CMS stressed that "for some medications there is no bright line that distinguishes when their pharmacological properties bring about the physiologic transition from the analgesic to the anesthetic effects."
Under the current guidelines, hospital policies should address whether specific clinical situations involve anesthesia versus analgesia, and specify the qualifications for each category of practitioner who administers analgesia and their supervision requirements. Federal regulations regarding who may administer anesthesia continue to apply for procedures that require anesthesia.
Hospital policies must be based on nationally recognized guidelines, even though the CMS recognizes that the issuing organizations "may not always fully agree with each other." A hospital could use the American College of Emergency Physicians (ACEP) guidelines in its ED and follow those of the American Society of Anesthesiologists (ASA) for its surgical services.
"There’s more flexibility in terms of a hospital deciding what type of personnel need to be present and involved depending on what type of sedation is used," Ms. Dahl said.
ACEP’s federal affairs director Barbara Tomar agreed that the current revisions provide hospitals with greater flexibility than the 2009 update, which she said was overly restrictive in its interpretation of federal regulations.
"If there is some controversy or disagreement between anesthesiologists and the emergency department, this will provide some clarification and additional evidence that the guidelines developed by the emergency physicians are more than adequate for use in the emergency department," Ms. Tomar said. "We have no qualms about the anesthesiology guidelines being used for surgical services. That’s their bailiwick."
ACEP, jointly with the Emergency Nurses Association and American Academy of Emergency Medicine, wrote to the CMS in March 2010 expressing concern over what constituted anesthesia, particularly with regard to propofol. The college noted that ED physicians are trained to provide resuscitation should propofol administration accidentally result in deep sedation, and that propofol administration by emergency nurses in the presence of an emergency physician complies with current Joint Commission standards.
Propofol is no longer cited as an example of deep sedation, and there is a particular reference in the guidelines to the "unique environment" in the ED, as well as acknowledgment that emergency physicians have "very specific skill sets" that allow them to provide patient rescue and "all levels of analgesia/sedation and anesthesia (moderate to deep to general)."
The failure to specifically address the issue of propofol leaves unfinished business, said sedation expert Dr. John Vargo, a member of the governing board of the American Society for Gastrointestinal Endoscopy (ASGE) and acting chair of the gastroenterology and hepatology department at the Cleveland Clinic.
"The endoscopy society has been collecting evidence-based data over the past 15 years on endoscopist-directed propofol sedation, and frankly, there is no evidence on the other side showing that monitored anesthesia care is safer, more effective, or better tolerated than endoscopist-directed propofol sedation," he said.
Dr. Vargo said he hoped that hospitals would use the evidence available in order to craft an appropriate anesthesia policy regarding propofol and other types of procedural sedation. He also observed that an evidence-based position paper on non-anesthesiologist administration of propofol for GI endoscopy was recently jointly published by the ASGE, American Association for the Study of Liver Disease, American College of Gastroenterology, and American Gastroenterological Association (Gastrointest. Endosc. 2009;70:1053-9).
Dr. Douglas K. Rex, a vocal opponent of the CMS’s position on propofol and director of endoscopy at Indiana University Hospital, Indianapolis, said the CMS guidelines still state that deep sedation is the domain of anesthesia specialists, a concept for which there is virtually no evidence and plenty of evidence that the policy is wrong and unnecessary.
"CMS’s handling of this process has been tragic," he said. "They stuck their noses in an issue they did not and still do not understand."
Dr. Alexander A. Hannenberg, ASA immediate past-president and associate chair of anesthesia at Newton-Wellesley Hospital in Newton, Mass., said the ASA met with CMS officials in April 2010 to contest its position that a labor epidural was not considered anesthesia, and therefore could be administered without physician supervision by certified registered nurse anesthetists (CRNAs).
Dr. Hannenberg said the CMS appeared not to understand the physiology of epidural pain relief, and that epidurals for labor, just as those used as anesthesia for surgery, produce a sympathetic block, or block the nerves that control circulation. He went on to say that the CMS’s previous position appeared to lower the standard of care for laboring women.
"I think they appreciated the physiology lesson, and went back and realized that the distinction was not as crisp or clear as they had originally thought, and removed the language that said it’s different and that the requirement for physician supervision is therefore different," he said.
CRNAs can still administer anesthesia if the hospital is located in one of 16 states that have elected to opt out of the CRNA physician supervision requirement. Ms. Dahl noted, however, that in theory, the updated guidance does not preclude a hospital in a non-opt-out state from choosing to make a determination that labor epidurals are not anesthesia, if it could point to support in nationally recognized guidelines when doing so, and as long as this would not be in violation of the state’s scope of practice law.
Dr. Hannenberg said the ASA also sought changes to the CMS pre- and postanesthesia evaluations. Preanesthesia evaluation must be completed within 48 hours prior to surgery or a procedure requiring anesthesia services, but the CMS clarified that some elements may be performed before then, as long as they are reviewed and appropriately updated within the 48-hour time frame. Dr. Hannenberg said the new wording recognizes that tests are often performed before the 48-hour time frame, and that it is standard of care for all elements of a case to be reassessed by anesthesiologists immediately before anesthesia administration.
The postanesthesia evaluation previously had to be completed before discharge, but may now be completed within 48 hours after a patient is moved to another inpatient location within the hospital or is discharged. This flexibility allows for a more complete evaluation of a patient because some things, such as adverse events, may not be fully knowable until after a patient is sent home, he said.
Ms. Dahl, Dr. Hannenberg, and Dr. Vargo reported no conflicts of interest. Dr. Rex reported consulting and advisory arrangements with American BioOptics, Avantis Medical Systems, CheckCap, Epigenomics, Given Imaging, and SoftScope. He receives grant support from Braintree Laboratories and Given Imaging, and a salary as well as speaking and teaching fees from Olympus America.
The Centers for Medicare and Medicaid Services has revised its recently updated anesthesia guidelines, following complaints the policy was unworkable.
Hospitals are now directed to develop their own internal policies concerning what is anesthesia versus analgesia, which leaves open the option of using different guidelines in different clinical departments. The revisions also provide greater flexibility regarding pre- and postanesthesia evaluations, while particularly problematic references to propofol and labor epidural anesthesia were dropped entirely.
Following the December 2009 release of the updated interpretive guidelines for hospital anesthesia services, practitioners called for clarifications regarding the distinction between anesthesia and analgesia, suggesting that some of the examples didn’t fall clearly on one side or the other of the anesthesia/analgesia spectrum. The use of propofol (Diprivan) during screening colonoscopy was cited as an example of deep sedation, which meant it could only be delivered by providers trained in general anesthesia.
"The examples caused a lot of consternation," acknowledged Marilyn Dahl, director of the Centers for Medicare and Medicaid Services (CMS) survey and certification division of acute care services. "What the current guidelines say is that we are going to leave it up to the hospital, relying on nationally recognized guidelines, to decide which things fall on the anesthesia side of the continuum."
The guidelines retain the six broad categories of anesthesia and analgesia, but acknowledge that the level of sedation for a particular medication may vary on the basis of such factors as dosage and route and timing of administration. Thus, it’s possible for the same drug to be used for general anesthesia in the operating room and for sedation in the emergency department (ED) or a procedure room. In what could be considered a mea culpa, the CMS stressed that "for some medications there is no bright line that distinguishes when their pharmacological properties bring about the physiologic transition from the analgesic to the anesthetic effects."
Under the current guidelines, hospital policies should address whether specific clinical situations involve anesthesia versus analgesia, and specify the qualifications for each category of practitioner who administers analgesia and their supervision requirements. Federal regulations regarding who may administer anesthesia continue to apply for procedures that require anesthesia.
Hospital policies must be based on nationally recognized guidelines, even though the CMS recognizes that the issuing organizations "may not always fully agree with each other." A hospital could use the American College of Emergency Physicians (ACEP) guidelines in its ED and follow those of the American Society of Anesthesiologists (ASA) for its surgical services.
"There’s more flexibility in terms of a hospital deciding what type of personnel need to be present and involved depending on what type of sedation is used," Ms. Dahl said.
ACEP’s federal affairs director Barbara Tomar agreed that the current revisions provide hospitals with greater flexibility than the 2009 update, which she said was overly restrictive in its interpretation of federal regulations.
"If there is some controversy or disagreement between anesthesiologists and the emergency department, this will provide some clarification and additional evidence that the guidelines developed by the emergency physicians are more than adequate for use in the emergency department," Ms. Tomar said. "We have no qualms about the anesthesiology guidelines being used for surgical services. That’s their bailiwick."
ACEP, jointly with the Emergency Nurses Association and American Academy of Emergency Medicine, wrote to the CMS in March 2010 expressing concern over what constituted anesthesia, particularly with regard to propofol. The college noted that ED physicians are trained to provide resuscitation should propofol administration accidentally result in deep sedation, and that propofol administration by emergency nurses in the presence of an emergency physician complies with current Joint Commission standards.
Propofol is no longer cited as an example of deep sedation, and there is a particular reference in the guidelines to the "unique environment" in the ED, as well as acknowledgment that emergency physicians have "very specific skill sets" that allow them to provide patient rescue and "all levels of analgesia/sedation and anesthesia (moderate to deep to general)."
The failure to specifically address the issue of propofol leaves unfinished business, said sedation expert Dr. John Vargo, a member of the governing board of the American Society for Gastrointestinal Endoscopy (ASGE) and acting chair of the gastroenterology and hepatology department at the Cleveland Clinic.
"The endoscopy society has been collecting evidence-based data over the past 15 years on endoscopist-directed propofol sedation, and frankly, there is no evidence on the other side showing that monitored anesthesia care is safer, more effective, or better tolerated than endoscopist-directed propofol sedation," he said.
Dr. Vargo said he hoped that hospitals would use the evidence available in order to craft an appropriate anesthesia policy regarding propofol and other types of procedural sedation. He also observed that an evidence-based position paper on non-anesthesiologist administration of propofol for GI endoscopy was recently jointly published by the ASGE, American Association for the Study of Liver Disease, American College of Gastroenterology, and American Gastroenterological Association (Gastrointest. Endosc. 2009;70:1053-9).
Dr. Douglas K. Rex, a vocal opponent of the CMS’s position on propofol and director of endoscopy at Indiana University Hospital, Indianapolis, said the CMS guidelines still state that deep sedation is the domain of anesthesia specialists, a concept for which there is virtually no evidence and plenty of evidence that the policy is wrong and unnecessary.
"CMS’s handling of this process has been tragic," he said. "They stuck their noses in an issue they did not and still do not understand."
Dr. Alexander A. Hannenberg, ASA immediate past-president and associate chair of anesthesia at Newton-Wellesley Hospital in Newton, Mass., said the ASA met with CMS officials in April 2010 to contest its position that a labor epidural was not considered anesthesia, and therefore could be administered without physician supervision by certified registered nurse anesthetists (CRNAs).
Dr. Hannenberg said the CMS appeared not to understand the physiology of epidural pain relief, and that epidurals for labor, just as those used as anesthesia for surgery, produce a sympathetic block, or block the nerves that control circulation. He went on to say that the CMS’s previous position appeared to lower the standard of care for laboring women.
"I think they appreciated the physiology lesson, and went back and realized that the distinction was not as crisp or clear as they had originally thought, and removed the language that said it’s different and that the requirement for physician supervision is therefore different," he said.
CRNAs can still administer anesthesia if the hospital is located in one of 16 states that have elected to opt out of the CRNA physician supervision requirement. Ms. Dahl noted, however, that in theory, the updated guidance does not preclude a hospital in a non-opt-out state from choosing to make a determination that labor epidurals are not anesthesia, if it could point to support in nationally recognized guidelines when doing so, and as long as this would not be in violation of the state’s scope of practice law.
Dr. Hannenberg said the ASA also sought changes to the CMS pre- and postanesthesia evaluations. Preanesthesia evaluation must be completed within 48 hours prior to surgery or a procedure requiring anesthesia services, but the CMS clarified that some elements may be performed before then, as long as they are reviewed and appropriately updated within the 48-hour time frame. Dr. Hannenberg said the new wording recognizes that tests are often performed before the 48-hour time frame, and that it is standard of care for all elements of a case to be reassessed by anesthesiologists immediately before anesthesia administration.
The postanesthesia evaluation previously had to be completed before discharge, but may now be completed within 48 hours after a patient is moved to another inpatient location within the hospital or is discharged. This flexibility allows for a more complete evaluation of a patient because some things, such as adverse events, may not be fully knowable until after a patient is sent home, he said.
Ms. Dahl, Dr. Hannenberg, and Dr. Vargo reported no conflicts of interest. Dr. Rex reported consulting and advisory arrangements with American BioOptics, Avantis Medical Systems, CheckCap, Epigenomics, Given Imaging, and SoftScope. He receives grant support from Braintree Laboratories and Given Imaging, and a salary as well as speaking and teaching fees from Olympus America.
The Centers for Medicare and Medicaid Services has revised its recently updated anesthesia guidelines, following complaints the policy was unworkable.
Hospitals are now directed to develop their own internal policies concerning what is anesthesia versus analgesia, which leaves open the option of using different guidelines in different clinical departments. The revisions also provide greater flexibility regarding pre- and postanesthesia evaluations, while particularly problematic references to propofol and labor epidural anesthesia were dropped entirely.
Following the December 2009 release of the updated interpretive guidelines for hospital anesthesia services, practitioners called for clarifications regarding the distinction between anesthesia and analgesia, suggesting that some of the examples didn’t fall clearly on one side or the other of the anesthesia/analgesia spectrum. The use of propofol (Diprivan) during screening colonoscopy was cited as an example of deep sedation, which meant it could only be delivered by providers trained in general anesthesia.
"The examples caused a lot of consternation," acknowledged Marilyn Dahl, director of the Centers for Medicare and Medicaid Services (CMS) survey and certification division of acute care services. "What the current guidelines say is that we are going to leave it up to the hospital, relying on nationally recognized guidelines, to decide which things fall on the anesthesia side of the continuum."
The guidelines retain the six broad categories of anesthesia and analgesia, but acknowledge that the level of sedation for a particular medication may vary on the basis of such factors as dosage and route and timing of administration. Thus, it’s possible for the same drug to be used for general anesthesia in the operating room and for sedation in the emergency department (ED) or a procedure room. In what could be considered a mea culpa, the CMS stressed that "for some medications there is no bright line that distinguishes when their pharmacological properties bring about the physiologic transition from the analgesic to the anesthetic effects."
Under the current guidelines, hospital policies should address whether specific clinical situations involve anesthesia versus analgesia, and specify the qualifications for each category of practitioner who administers analgesia and their supervision requirements. Federal regulations regarding who may administer anesthesia continue to apply for procedures that require anesthesia.
Hospital policies must be based on nationally recognized guidelines, even though the CMS recognizes that the issuing organizations "may not always fully agree with each other." A hospital could use the American College of Emergency Physicians (ACEP) guidelines in its ED and follow those of the American Society of Anesthesiologists (ASA) for its surgical services.
"There’s more flexibility in terms of a hospital deciding what type of personnel need to be present and involved depending on what type of sedation is used," Ms. Dahl said.
ACEP’s federal affairs director Barbara Tomar agreed that the current revisions provide hospitals with greater flexibility than the 2009 update, which she said was overly restrictive in its interpretation of federal regulations.
"If there is some controversy or disagreement between anesthesiologists and the emergency department, this will provide some clarification and additional evidence that the guidelines developed by the emergency physicians are more than adequate for use in the emergency department," Ms. Tomar said. "We have no qualms about the anesthesiology guidelines being used for surgical services. That’s their bailiwick."
ACEP, jointly with the Emergency Nurses Association and American Academy of Emergency Medicine, wrote to the CMS in March 2010 expressing concern over what constituted anesthesia, particularly with regard to propofol. The college noted that ED physicians are trained to provide resuscitation should propofol administration accidentally result in deep sedation, and that propofol administration by emergency nurses in the presence of an emergency physician complies with current Joint Commission standards.
Propofol is no longer cited as an example of deep sedation, and there is a particular reference in the guidelines to the "unique environment" in the ED, as well as acknowledgment that emergency physicians have "very specific skill sets" that allow them to provide patient rescue and "all levels of analgesia/sedation and anesthesia (moderate to deep to general)."
The failure to specifically address the issue of propofol leaves unfinished business, said sedation expert Dr. John Vargo, a member of the governing board of the American Society for Gastrointestinal Endoscopy (ASGE) and acting chair of the gastroenterology and hepatology department at the Cleveland Clinic.
"The endoscopy society has been collecting evidence-based data over the past 15 years on endoscopist-directed propofol sedation, and frankly, there is no evidence on the other side showing that monitored anesthesia care is safer, more effective, or better tolerated than endoscopist-directed propofol sedation," he said.
Dr. Vargo said he hoped that hospitals would use the evidence available in order to craft an appropriate anesthesia policy regarding propofol and other types of procedural sedation. He also observed that an evidence-based position paper on non-anesthesiologist administration of propofol for GI endoscopy was recently jointly published by the ASGE, American Association for the Study of Liver Disease, American College of Gastroenterology, and American Gastroenterological Association (Gastrointest. Endosc. 2009;70:1053-9).
Dr. Douglas K. Rex, a vocal opponent of the CMS’s position on propofol and director of endoscopy at Indiana University Hospital, Indianapolis, said the CMS guidelines still state that deep sedation is the domain of anesthesia specialists, a concept for which there is virtually no evidence and plenty of evidence that the policy is wrong and unnecessary.
"CMS’s handling of this process has been tragic," he said. "They stuck their noses in an issue they did not and still do not understand."
Dr. Alexander A. Hannenberg, ASA immediate past-president and associate chair of anesthesia at Newton-Wellesley Hospital in Newton, Mass., said the ASA met with CMS officials in April 2010 to contest its position that a labor epidural was not considered anesthesia, and therefore could be administered without physician supervision by certified registered nurse anesthetists (CRNAs).
Dr. Hannenberg said the CMS appeared not to understand the physiology of epidural pain relief, and that epidurals for labor, just as those used as anesthesia for surgery, produce a sympathetic block, or block the nerves that control circulation. He went on to say that the CMS’s previous position appeared to lower the standard of care for laboring women.
"I think they appreciated the physiology lesson, and went back and realized that the distinction was not as crisp or clear as they had originally thought, and removed the language that said it’s different and that the requirement for physician supervision is therefore different," he said.
CRNAs can still administer anesthesia if the hospital is located in one of 16 states that have elected to opt out of the CRNA physician supervision requirement. Ms. Dahl noted, however, that in theory, the updated guidance does not preclude a hospital in a non-opt-out state from choosing to make a determination that labor epidurals are not anesthesia, if it could point to support in nationally recognized guidelines when doing so, and as long as this would not be in violation of the state’s scope of practice law.
Dr. Hannenberg said the ASA also sought changes to the CMS pre- and postanesthesia evaluations. Preanesthesia evaluation must be completed within 48 hours prior to surgery or a procedure requiring anesthesia services, but the CMS clarified that some elements may be performed before then, as long as they are reviewed and appropriately updated within the 48-hour time frame. Dr. Hannenberg said the new wording recognizes that tests are often performed before the 48-hour time frame, and that it is standard of care for all elements of a case to be reassessed by anesthesiologists immediately before anesthesia administration.
The postanesthesia evaluation previously had to be completed before discharge, but may now be completed within 48 hours after a patient is moved to another inpatient location within the hospital or is discharged. This flexibility allows for a more complete evaluation of a patient because some things, such as adverse events, may not be fully knowable until after a patient is sent home, he said.
Ms. Dahl, Dr. Hannenberg, and Dr. Vargo reported no conflicts of interest. Dr. Rex reported consulting and advisory arrangements with American BioOptics, Avantis Medical Systems, CheckCap, Epigenomics, Given Imaging, and SoftScope. He receives grant support from Braintree Laboratories and Given Imaging, and a salary as well as speaking and teaching fees from Olympus America.
Mesothelioma Watch: Is Erionite the New Asbestos?
CHICAGO – Exposure to erionite, a fibrous, cancer-causing mineral more lethal than asbestos, is becoming a public health hazard in the United States.

Erionite was originally thought to be a peculiarity of Turkey, but naturally occurring deposits have been identified throughout the western United States. A new study shows that concentrations of airborne erionite in Dunn County, N.D., equal or exceed those in Boyali, a Turkish village with a 6.25% mesothelioma-related mortality rate.
Moreover, the study found no significant difference in the physical characteristics or biological activity of erionite from North Dakota and that from Cappadocia, Turkey, where in some villages 50% of all deaths are due to mesothelioma. Turkish homes made of stone laced with erionite from nearby mountains have been tagged as "houses of death" by residents resettled with the help of the Turkish Ministry of Health and researchers.
"We have a unique opportunity to implement novel prevention and early detection programs in erionite-rich regions of the United States, similar to what has been done in Turkey," researcher Dr. Michele Carbone said at the Chicago Multidisciplinary Symposium in Thoracic Oncology, where he presented the new study.

Erionite-contaminated gravel has been used in North Dakota for 2-3 decades to pave more than 300 miles of roads, including school bus routes, parking lots, and other public areas. The North Dakota Department of Health became aware of the health problem in 2006, and the following year recommended discontinuing use of erionite-containing gravel for roads and testing for erionite prior to new or continued gravel mining. The recommendations slowed the use of erionite-containing gravel in North Dakota, but it continues to be shipped outside the state, said Dr. Carbone, director of the Cancer Research Center of Hawaii and professor and chair of pathology at the University of Hawaii, both in Honolulu.
After a baseball field with erionite-containing gravel was closed in 2008 in the tiny town of Killdeer, N.D., the Associated Press quoted a state legislator as telling state and federal officials they were making a "mountain out of a molehill with what little data you have" and that taxpayers were having a "tough time trying to swallow this." One resident said she used the bright white gravel on her flower beds, while an area rancher said concerns over erionite were "one of those sky-is-falling kinds of deals."
Part of the battle over public opinion may be due to timing. No increase in mesotheliomas has been observed in Dunn County, but we are just now approaching the latency period where cancers would begin to develop, Dr. Carbone said. "We are in the same situation we were in the United States in the ’20s and ’30s with asbestos, and hopefully we will not repeat the same mistakes when danger was ignored until many people died of mesothelioma," he said, pointing out that mesothelioma kills about 3,000 Americans each year.
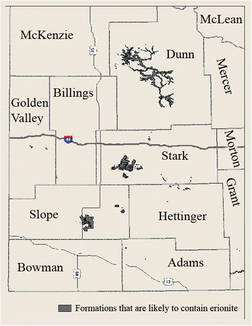
Dr. Carbone drew a parallel between Dunn County and Libby, Montana, where vermiculite containing asbestiform amphiboles were mined from 1920 to 1990 and given free of charge for insulation and to build driveways and ball fields. In 2004, researchers at the Center for Asbestos Related Disease in Libby identified accelerated loss of lung function in 94 of 123 miners, family members, and residents (Am. J. Med. 2004;46:219-25) and more recently reported on 11 new cases of mesothelioma in people with environmental exposure to contamination in the community, surrounding forest, and Kootenai river and railroad tracks used to haul the vermiculite (Am. J. Med. 2008; 51:877-80). The authors conclude that, "An epidemic of mesothelioma can likely be expected from this type of asbestos contamination over the next 20-plus years."
Despite prior identification of asbestos in the mine and illness among workers, the situation went unnoticed and unaddressed by health authorities for over a decade until a Seattle Times newspaper article appeared in November 1999, noted Dr. Aubrey K. Miller, a coresearcher and senior medical adviser with the National Institute of Environmental Health Sciences in Bethesda, Md.
"Thus, individuals in North Dakota should be concerned," he said in an interview. "Erionite is a very hazardous substance and we should not wait for disease to occur to start taking actions to protect public health. There is no excuse based on our current knowledge to play a wait-and-see game."
Lung screening was offered to Dunn County residents exposed to erionite, but only 34 residents, including gravel pit and road maintenance workers, enrolled in the study. A significant increase in interstitial changes above background prevalence was observed on high-resolution computed tomography in 17.6% of residents, compared with 1.5% for male urban transportation workers with low cumulative asbestos fiber exposure, Dr. Carbone said.
Transmission electron microscopy (TEM) revealed higher total concentrations of erionite fibers in air samples taken street-side in Dunn County (mean 0.108 structures per cubic centimeter [s/cc]) than from samples taken from the streets of five Turkish villages including Boyali (mean 0.00 s/cc), he said. Total TEM erionite concentrations were also higher indoors in Dunn County than in Boyali (mean 0.175 s/cc vs. 0.043 s/cc).
Research in Turkey has shown that increased industrialization significantly increases airborne particulates, an observation that is particularly worrisome since oil production activity has increased road traffic in Dunn County and development has grown in states such as Nevada where erionite deposits are far more common than in North Dakota.
Equally worrisome is that unlike asbestos, erionite has no current health benchmarks nor is it regulated by the U.S. Environmental Protection Agency or other agencies, Dr. Miller said. "The horse is out of the barn for some, but I think we can do a lot more to protect others," he said. "You can’t ban a natural substance, but I’d certainly like to see contaminated materials and disturbance of problem areas managed more effectively."
Dr. Carbone stressed the need to reduce erionite exposure, but is also working to isolate mesothelioma-susceptibility genes that might help to explain the pathogenesis of the disease and to identify high-risk patients for early treatment. The U.S. Early Detection Research Network, a branch of the National Cancer Institute, has funded a clinical trial that is prospectively evaluating osteopontin and mesothelin as early markers for the detection of mesothelioma. The 800-patient trial is expected to begin in 2011 and to be completed sometime in 2014, said Dr. Carbone, its coprincipal investigator together with thoracic surgeon Dr. Harvey I. Pass, professor and chief of the thoracic surgery division at New York University’s Langone Medical Center in New York City.
Dr. Carbone and his team are also looking to identify some point in the evolution of mesothelioma process that is vulnerable to intervention. Dr. Haining Yang, now also at the University of Hawaii Cancer Center, was the first author of a previous report that tumor necrois factor–alpha inhibits asbestos-induced cytotoxicity via a nuclear factor-kappa B-dependent mechanism that increases the percentage of human mesothelial cells that survive asbestos exposure, thus increasing the pool of asbestos-damaged cells susceptible to malignant transformation (Proc. Natl. Acad. Sci. USA. 2006;103:10397-402).
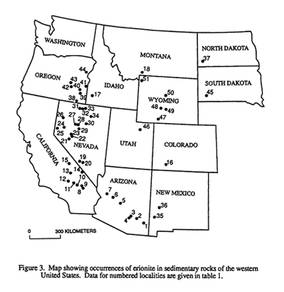
In tissue culture, North Dakota, Oregon, and Turkish erionite have been found to induce high-mobility group protein B1 (HMGB1) and TNF-alpha release from human mesothelial cells and macrophages, Dr. Yang et al also reported. When coupled with chronic inflammation of the peritoneum and pleura, HMGB1 and TNF-alpha release have been linked to malignant mesothelioma in mice and in humans (Proc. Natl. Acad. Sci. USA, 2010;107:12611-6).
Dr. Carbone called for a larger, more detailed epidemiologic survey of the health implications of erionite in North Dakota, as was performed for Libby, and said that it should include mine and road workers with direct exposure as well as adults and children with environmental exposure. This also should include correlative studies that exploit recent findings regarding biomarkers involved in fiber carcinogenesis, as is being done in Libby, he said.
The study was partially funded by a National Cancer Institute investigator grant. Dr. Carbone and Dr. Miller reported no conflicts of interest. Coauthors report funding from Rosetta Genomics, Celera, Soma Logic, and SourceMDX and a leadership role in the American College of Radiology Imaging Network.
CHICAGO – Exposure to erionite, a fibrous, cancer-causing mineral more lethal than asbestos, is becoming a public health hazard in the United States.
Erionite was originally thought to be a peculiarity of Turkey, but naturally occurring deposits have been identified throughout the western United States. A new study shows that concentrations of airborne erionite in Dunn County, N.D., equal or exceed those in Boyali, a Turkish village with a 6.25% mesothelioma-related mortality rate.
Moreover, the study found no significant difference in the physical characteristics or biological activity of erionite from North Dakota and that from Cappadocia, Turkey, where in some villages 50% of all deaths are due to mesothelioma. Turkish homes made of stone laced with erionite from nearby mountains have been tagged as "houses of death" by residents resettled with the help of the Turkish Ministry of Health and researchers.
"We have a unique opportunity to implement novel prevention and early detection programs in erionite-rich regions of the United States, similar to what has been done in Turkey," researcher Dr. Michele Carbone said at the Chicago Multidisciplinary Symposium in Thoracic Oncology, where he presented the new study.
Erionite-contaminated gravel has been used in North Dakota for 2-3 decades to pave more than 300 miles of roads, including school bus routes, parking lots, and other public areas. The North Dakota Department of Health became aware of the health problem in 2006, and the following year recommended discontinuing use of erionite-containing gravel for roads and testing for erionite prior to new or continued gravel mining. The recommendations slowed the use of erionite-containing gravel in North Dakota, but it continues to be shipped outside the state, said Dr. Carbone, director of the Cancer Research Center of Hawaii and professor and chair of pathology at the University of Hawaii, both in Honolulu.
After a baseball field with erionite-containing gravel was closed in 2008 in the tiny town of Killdeer, N.D., the Associated Press quoted a state legislator as telling state and federal officials they were making a "mountain out of a molehill with what little data you have" and that taxpayers were having a "tough time trying to swallow this." One resident said she used the bright white gravel on her flower beds, while an area rancher said concerns over erionite were "one of those sky-is-falling kinds of deals."
Part of the battle over public opinion may be due to timing. No increase in mesotheliomas has been observed in Dunn County, but we are just now approaching the latency period where cancers would begin to develop, Dr. Carbone said. "We are in the same situation we were in the United States in the ’20s and ’30s with asbestos, and hopefully we will not repeat the same mistakes when danger was ignored until many people died of mesothelioma," he said, pointing out that mesothelioma kills about 3,000 Americans each year.
Dr. Carbone drew a parallel between Dunn County and Libby, Montana, where vermiculite containing asbestiform amphiboles were mined from 1920 to 1990 and given free of charge for insulation and to build driveways and ball fields. In 2004, researchers at the Center for Asbestos Related Disease in Libby identified accelerated loss of lung function in 94 of 123 miners, family members, and residents (Am. J. Med. 2004;46:219-25) and more recently reported on 11 new cases of mesothelioma in people with environmental exposure to contamination in the community, surrounding forest, and Kootenai river and railroad tracks used to haul the vermiculite (Am. J. Med. 2008; 51:877-80). The authors conclude that, "An epidemic of mesothelioma can likely be expected from this type of asbestos contamination over the next 20-plus years."
Despite prior identification of asbestos in the mine and illness among workers, the situation went unnoticed and unaddressed by health authorities for over a decade until a Seattle Times newspaper article appeared in November 1999, noted Dr. Aubrey K. Miller, a coresearcher and senior medical adviser with the National Institute of Environmental Health Sciences in Bethesda, Md.
"Thus, individuals in North Dakota should be concerned," he said in an interview. "Erionite is a very hazardous substance and we should not wait for disease to occur to start taking actions to protect public health. There is no excuse based on our current knowledge to play a wait-and-see game."
Lung screening was offered to Dunn County residents exposed to erionite, but only 34 residents, including gravel pit and road maintenance workers, enrolled in the study. A significant increase in interstitial changes above background prevalence was observed on high-resolution computed tomography in 17.6% of residents, compared with 1.5% for male urban transportation workers with low cumulative asbestos fiber exposure, Dr. Carbone said.
Transmission electron microscopy (TEM) revealed higher total concentrations of erionite fibers in air samples taken street-side in Dunn County (mean 0.108 structures per cubic centimeter [s/cc]) than from samples taken from the streets of five Turkish villages including Boyali (mean 0.00 s/cc), he said. Total TEM erionite concentrations were also higher indoors in Dunn County than in Boyali (mean 0.175 s/cc vs. 0.043 s/cc).
Research in Turkey has shown that increased industrialization significantly increases airborne particulates, an observation that is particularly worrisome since oil production activity has increased road traffic in Dunn County and development has grown in states such as Nevada where erionite deposits are far more common than in North Dakota.
Equally worrisome is that unlike asbestos, erionite has no current health benchmarks nor is it regulated by the U.S. Environmental Protection Agency or other agencies, Dr. Miller said. "The horse is out of the barn for some, but I think we can do a lot more to protect others," he said. "You can’t ban a natural substance, but I’d certainly like to see contaminated materials and disturbance of problem areas managed more effectively."
Dr. Carbone stressed the need to reduce erionite exposure, but is also working to isolate mesothelioma-susceptibility genes that might help to explain the pathogenesis of the disease and to identify high-risk patients for early treatment. The U.S. Early Detection Research Network, a branch of the National Cancer Institute, has funded a clinical trial that is prospectively evaluating osteopontin and mesothelin as early markers for the detection of mesothelioma. The 800-patient trial is expected to begin in 2011 and to be completed sometime in 2014, said Dr. Carbone, its coprincipal investigator together with thoracic surgeon Dr. Harvey I. Pass, professor and chief of the thoracic surgery division at New York University’s Langone Medical Center in New York City.
Dr. Carbone and his team are also looking to identify some point in the evolution of mesothelioma process that is vulnerable to intervention. Dr. Haining Yang, now also at the University of Hawaii Cancer Center, was the first author of a previous report that tumor necrois factor–alpha inhibits asbestos-induced cytotoxicity via a nuclear factor-kappa B-dependent mechanism that increases the percentage of human mesothelial cells that survive asbestos exposure, thus increasing the pool of asbestos-damaged cells susceptible to malignant transformation (Proc. Natl. Acad. Sci. USA. 2006;103:10397-402).
In tissue culture, North Dakota, Oregon, and Turkish erionite have been found to induce high-mobility group protein B1 (HMGB1) and TNF-alpha release from human mesothelial cells and macrophages, Dr. Yang et al also reported. When coupled with chronic inflammation of the peritoneum and pleura, HMGB1 and TNF-alpha release have been linked to malignant mesothelioma in mice and in humans (Proc. Natl. Acad. Sci. USA, 2010;107:12611-6).
Dr. Carbone called for a larger, more detailed epidemiologic survey of the health implications of erionite in North Dakota, as was performed for Libby, and said that it should include mine and road workers with direct exposure as well as adults and children with environmental exposure. This also should include correlative studies that exploit recent findings regarding biomarkers involved in fiber carcinogenesis, as is being done in Libby, he said.
The study was partially funded by a National Cancer Institute investigator grant. Dr. Carbone and Dr. Miller reported no conflicts of interest. Coauthors report funding from Rosetta Genomics, Celera, Soma Logic, and SourceMDX and a leadership role in the American College of Radiology Imaging Network.
CHICAGO – Exposure to erionite, a fibrous, cancer-causing mineral more lethal than asbestos, is becoming a public health hazard in the United States.
Erionite was originally thought to be a peculiarity of Turkey, but naturally occurring deposits have been identified throughout the western United States. A new study shows that concentrations of airborne erionite in Dunn County, N.D., equal or exceed those in Boyali, a Turkish village with a 6.25% mesothelioma-related mortality rate.
Moreover, the study found no significant difference in the physical characteristics or biological activity of erionite from North Dakota and that from Cappadocia, Turkey, where in some villages 50% of all deaths are due to mesothelioma. Turkish homes made of stone laced with erionite from nearby mountains have been tagged as "houses of death" by residents resettled with the help of the Turkish Ministry of Health and researchers.
"We have a unique opportunity to implement novel prevention and early detection programs in erionite-rich regions of the United States, similar to what has been done in Turkey," researcher Dr. Michele Carbone said at the Chicago Multidisciplinary Symposium in Thoracic Oncology, where he presented the new study.
Erionite-contaminated gravel has been used in North Dakota for 2-3 decades to pave more than 300 miles of roads, including school bus routes, parking lots, and other public areas. The North Dakota Department of Health became aware of the health problem in 2006, and the following year recommended discontinuing use of erionite-containing gravel for roads and testing for erionite prior to new or continued gravel mining. The recommendations slowed the use of erionite-containing gravel in North Dakota, but it continues to be shipped outside the state, said Dr. Carbone, director of the Cancer Research Center of Hawaii and professor and chair of pathology at the University of Hawaii, both in Honolulu.
After a baseball field with erionite-containing gravel was closed in 2008 in the tiny town of Killdeer, N.D., the Associated Press quoted a state legislator as telling state and federal officials they were making a "mountain out of a molehill with what little data you have" and that taxpayers were having a "tough time trying to swallow this." One resident said she used the bright white gravel on her flower beds, while an area rancher said concerns over erionite were "one of those sky-is-falling kinds of deals."
Part of the battle over public opinion may be due to timing. No increase in mesotheliomas has been observed in Dunn County, but we are just now approaching the latency period where cancers would begin to develop, Dr. Carbone said. "We are in the same situation we were in the United States in the ’20s and ’30s with asbestos, and hopefully we will not repeat the same mistakes when danger was ignored until many people died of mesothelioma," he said, pointing out that mesothelioma kills about 3,000 Americans each year.
Dr. Carbone drew a parallel between Dunn County and Libby, Montana, where vermiculite containing asbestiform amphiboles were mined from 1920 to 1990 and given free of charge for insulation and to build driveways and ball fields. In 2004, researchers at the Center for Asbestos Related Disease in Libby identified accelerated loss of lung function in 94 of 123 miners, family members, and residents (Am. J. Med. 2004;46:219-25) and more recently reported on 11 new cases of mesothelioma in people with environmental exposure to contamination in the community, surrounding forest, and Kootenai river and railroad tracks used to haul the vermiculite (Am. J. Med. 2008; 51:877-80). The authors conclude that, "An epidemic of mesothelioma can likely be expected from this type of asbestos contamination over the next 20-plus years."
Despite prior identification of asbestos in the mine and illness among workers, the situation went unnoticed and unaddressed by health authorities for over a decade until a Seattle Times newspaper article appeared in November 1999, noted Dr. Aubrey K. Miller, a coresearcher and senior medical adviser with the National Institute of Environmental Health Sciences in Bethesda, Md.
"Thus, individuals in North Dakota should be concerned," he said in an interview. "Erionite is a very hazardous substance and we should not wait for disease to occur to start taking actions to protect public health. There is no excuse based on our current knowledge to play a wait-and-see game."
Lung screening was offered to Dunn County residents exposed to erionite, but only 34 residents, including gravel pit and road maintenance workers, enrolled in the study. A significant increase in interstitial changes above background prevalence was observed on high-resolution computed tomography in 17.6% of residents, compared with 1.5% for male urban transportation workers with low cumulative asbestos fiber exposure, Dr. Carbone said.
Transmission electron microscopy (TEM) revealed higher total concentrations of erionite fibers in air samples taken street-side in Dunn County (mean 0.108 structures per cubic centimeter [s/cc]) than from samples taken from the streets of five Turkish villages including Boyali (mean 0.00 s/cc), he said. Total TEM erionite concentrations were also higher indoors in Dunn County than in Boyali (mean 0.175 s/cc vs. 0.043 s/cc).
Research in Turkey has shown that increased industrialization significantly increases airborne particulates, an observation that is particularly worrisome since oil production activity has increased road traffic in Dunn County and development has grown in states such as Nevada where erionite deposits are far more common than in North Dakota.
Equally worrisome is that unlike asbestos, erionite has no current health benchmarks nor is it regulated by the U.S. Environmental Protection Agency or other agencies, Dr. Miller said. "The horse is out of the barn for some, but I think we can do a lot more to protect others," he said. "You can’t ban a natural substance, but I’d certainly like to see contaminated materials and disturbance of problem areas managed more effectively."
Dr. Carbone stressed the need to reduce erionite exposure, but is also working to isolate mesothelioma-susceptibility genes that might help to explain the pathogenesis of the disease and to identify high-risk patients for early treatment. The U.S. Early Detection Research Network, a branch of the National Cancer Institute, has funded a clinical trial that is prospectively evaluating osteopontin and mesothelin as early markers for the detection of mesothelioma. The 800-patient trial is expected to begin in 2011 and to be completed sometime in 2014, said Dr. Carbone, its coprincipal investigator together with thoracic surgeon Dr. Harvey I. Pass, professor and chief of the thoracic surgery division at New York University’s Langone Medical Center in New York City.
Dr. Carbone and his team are also looking to identify some point in the evolution of mesothelioma process that is vulnerable to intervention. Dr. Haining Yang, now also at the University of Hawaii Cancer Center, was the first author of a previous report that tumor necrois factor–alpha inhibits asbestos-induced cytotoxicity via a nuclear factor-kappa B-dependent mechanism that increases the percentage of human mesothelial cells that survive asbestos exposure, thus increasing the pool of asbestos-damaged cells susceptible to malignant transformation (Proc. Natl. Acad. Sci. USA. 2006;103:10397-402).
In tissue culture, North Dakota, Oregon, and Turkish erionite have been found to induce high-mobility group protein B1 (HMGB1) and TNF-alpha release from human mesothelial cells and macrophages, Dr. Yang et al also reported. When coupled with chronic inflammation of the peritoneum and pleura, HMGB1 and TNF-alpha release have been linked to malignant mesothelioma in mice and in humans (Proc. Natl. Acad. Sci. USA, 2010;107:12611-6).
Dr. Carbone called for a larger, more detailed epidemiologic survey of the health implications of erionite in North Dakota, as was performed for Libby, and said that it should include mine and road workers with direct exposure as well as adults and children with environmental exposure. This also should include correlative studies that exploit recent findings regarding biomarkers involved in fiber carcinogenesis, as is being done in Libby, he said.
The study was partially funded by a National Cancer Institute investigator grant. Dr. Carbone and Dr. Miller reported no conflicts of interest. Coauthors report funding from Rosetta Genomics, Celera, Soma Logic, and SourceMDX and a leadership role in the American College of Radiology Imaging Network.
FROM THE CHICAGO MULTIDISCIPLINARY SYMPOSIUM IN THORACIC ONCOLOGY
Major Finding: Concentrations of airborne erionite in a North Dakota county equal or exceed those in a Turkish village with a 6.25% mesothelioma-related mortality rate.
Data Source: A study examining air samples, erionite microchemistry and morphology, chest x-rays and CT, and other factors.
Disclosures: Partially funded by a National Cancer Institute investigator grant. Dr. Carbone and Dr. Miller reported no conflicts of interest. Coauthors report funding from Rosetta Genomics, Celera, Soma Logic, and SourceMDX and a leadership role in the American College of Radiology Imaging Network.
Microscopic Vascular Invasion May Be a Powerful Prognosticator in Early Lung Cancer
CHICAGO – New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size–based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non–small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm) and 11 T3 (greater than 7 cm) tumors.
Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant conflicts.
CHICAGO – New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size–based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non–small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm) and 11 T3 (greater than 7 cm) tumors.
Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant conflicts.
CHICAGO – New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size–based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non–small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm) and 11 T3 (greater than 7 cm) tumors.
Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant conflicts.
Microscopic Vascular Invasion May Be a Powerful Prognosticator in Early Lung Cancer
CHICAGO – New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size–based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non–small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm) and 11 T3 (greater than 7 cm) tumors.
Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant conflicts.
CHICAGO – New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size–based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non–small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm) and 11 T3 (greater than 7 cm) tumors.
Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant conflicts.
CHICAGO – New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size–based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non–small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm) and 11 T3 (greater than 7 cm) tumors.
Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant conflicts.
Major Finding: Five-year overall survival was 50% for patients with microscopic vascular invasion vs. 66% for those without MVI (P = .001).
Data Source: Retrospective analysis of 514 patients with early non–small cell lung cancer.
Disclosures: Dr. Ruffini, his coauthors, and Dr. Socinski disclosed no relevant financial conflicts.
Bevacizumab Maintenance Extends Lung Cancer Survival in Community Practice
CHICAGO – Bevacizumab maintenance after first-line chemotherapy for advanced non–small cell lung cancer was associated with longer overall survival in a retrospective study of 403 patients who were treated in outpatient community settings.
Median NSCLC disease progression was 10.3 months among patients who continued on bevacizumab (Avastin) until disease progression after they received first-line chemotherapy plus bevacizumab, compared with 6.5 months for those who discontinued the monoclonal antibody after chemotherapy.
Median overall survival reached 20.9 months vs. 10.2 months, respectively, Dr. Eric Nadler reported in a poster at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
Although it is standard practice in clinical trials to continue bevacizumab until disease progression, recent assessments of treatment patterns in the United States have shown that bevacizumab is often discontinued when chemotherapy ends. Price has been an issue, with the typical monthly cost of bevacizumab for advanced lung cancer placed at about $8,800 in 2006. Only 38% (or 154) of the 403 patients in the study received bevacizumab until disease progression.
The industry-sponsored study identified patients with nonsquamous NSCLC from an electronic health records system that contains data from 884 community-based oncologists in US Oncology Inc.–affiliated practices or clinics in 20 states.
Patients were treated from July 2006 through June 2008, with 31% located in the Southwest and 30% in the Southeast. In all, 37% of patients had private insurance, 57% were covered by Medicare, and 6% had some other payer.
The maintenance group tended to have better pre- and postchemotherapy performance status scores and a greater number of completed chemotherapy cycles (median, six vs. four). Overall, 56% of the maintenance group and 39% of the no-maintenance group received a second-line therapy.
To control for survivorship and selection bias, researchers excluded patients with disease progression or death within 30 days of chemotherapy completion; landmark analyses were conducted at 18, 21, and 26 weeks from initial treatment.
Among those who were alive and progression free at 18 weeks, bevacizumab monotherapy until disease progression was associated with a 46% reduced risk of death (hazard ratio, 0.54), reported Dr. Nadler of the Texas Oncology–Baylor Sammons Cancer Center in Dallas. The association between bevacizumab and longer residual overall survival persisted among patients who remained progression free and alive at 21 weeks (HR, 0.58) and 26 weeks (HR, 0.61).
Bevacizumab monotherapy was associated with longer progression-free survival at 18 weeks (HR, 0.73), but the association was no longer observed at 21 weeks (HR, 0.82) and 26 weeks (HR, 0.79).
Although the nonrandomized nature of the study precludes making any conclusions about causality, the authors concluded that the findings provide "significant insights into real-world patterns of care and associated outcomes and provide important evidence on which to base future comparative effectiveness research."
In a separate national survey of oncologists, Dr. Nadler and associates at Tufts University in Boston reported that 84% of oncologists say that patients’ out-of-pocket spending influences treatment recommendations, even though only 43% frequently or always discuss costs with patients. Among the 787 oncologists surveyed, 79% favored more comparative effectiveness research and 80% supported more cost-effectiveness data, but only 42% felt well prepared to interpret it (Health Aff. [Millwood] 2010;29:196-202).
Genentech supported the study. Dr. Nadler reported no conflicts of interest. Three coauthors reported employment with Genentech and ownership interest in Roche Holdings.
CHICAGO – Bevacizumab maintenance after first-line chemotherapy for advanced non–small cell lung cancer was associated with longer overall survival in a retrospective study of 403 patients who were treated in outpatient community settings.
Median NSCLC disease progression was 10.3 months among patients who continued on bevacizumab (Avastin) until disease progression after they received first-line chemotherapy plus bevacizumab, compared with 6.5 months for those who discontinued the monoclonal antibody after chemotherapy.
Median overall survival reached 20.9 months vs. 10.2 months, respectively, Dr. Eric Nadler reported in a poster at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
Although it is standard practice in clinical trials to continue bevacizumab until disease progression, recent assessments of treatment patterns in the United States have shown that bevacizumab is often discontinued when chemotherapy ends. Price has been an issue, with the typical monthly cost of bevacizumab for advanced lung cancer placed at about $8,800 in 2006. Only 38% (or 154) of the 403 patients in the study received bevacizumab until disease progression.
The industry-sponsored study identified patients with nonsquamous NSCLC from an electronic health records system that contains data from 884 community-based oncologists in US Oncology Inc.–affiliated practices or clinics in 20 states.
Patients were treated from July 2006 through June 2008, with 31% located in the Southwest and 30% in the Southeast. In all, 37% of patients had private insurance, 57% were covered by Medicare, and 6% had some other payer.
The maintenance group tended to have better pre- and postchemotherapy performance status scores and a greater number of completed chemotherapy cycles (median, six vs. four). Overall, 56% of the maintenance group and 39% of the no-maintenance group received a second-line therapy.
To control for survivorship and selection bias, researchers excluded patients with disease progression or death within 30 days of chemotherapy completion; landmark analyses were conducted at 18, 21, and 26 weeks from initial treatment.
Among those who were alive and progression free at 18 weeks, bevacizumab monotherapy until disease progression was associated with a 46% reduced risk of death (hazard ratio, 0.54), reported Dr. Nadler of the Texas Oncology–Baylor Sammons Cancer Center in Dallas. The association between bevacizumab and longer residual overall survival persisted among patients who remained progression free and alive at 21 weeks (HR, 0.58) and 26 weeks (HR, 0.61).
Bevacizumab monotherapy was associated with longer progression-free survival at 18 weeks (HR, 0.73), but the association was no longer observed at 21 weeks (HR, 0.82) and 26 weeks (HR, 0.79).
Although the nonrandomized nature of the study precludes making any conclusions about causality, the authors concluded that the findings provide "significant insights into real-world patterns of care and associated outcomes and provide important evidence on which to base future comparative effectiveness research."
In a separate national survey of oncologists, Dr. Nadler and associates at Tufts University in Boston reported that 84% of oncologists say that patients’ out-of-pocket spending influences treatment recommendations, even though only 43% frequently or always discuss costs with patients. Among the 787 oncologists surveyed, 79% favored more comparative effectiveness research and 80% supported more cost-effectiveness data, but only 42% felt well prepared to interpret it (Health Aff. [Millwood] 2010;29:196-202).
Genentech supported the study. Dr. Nadler reported no conflicts of interest. Three coauthors reported employment with Genentech and ownership interest in Roche Holdings.
CHICAGO – Bevacizumab maintenance after first-line chemotherapy for advanced non–small cell lung cancer was associated with longer overall survival in a retrospective study of 403 patients who were treated in outpatient community settings.
Median NSCLC disease progression was 10.3 months among patients who continued on bevacizumab (Avastin) until disease progression after they received first-line chemotherapy plus bevacizumab, compared with 6.5 months for those who discontinued the monoclonal antibody after chemotherapy.
Median overall survival reached 20.9 months vs. 10.2 months, respectively, Dr. Eric Nadler reported in a poster at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
Although it is standard practice in clinical trials to continue bevacizumab until disease progression, recent assessments of treatment patterns in the United States have shown that bevacizumab is often discontinued when chemotherapy ends. Price has been an issue, with the typical monthly cost of bevacizumab for advanced lung cancer placed at about $8,800 in 2006. Only 38% (or 154) of the 403 patients in the study received bevacizumab until disease progression.
The industry-sponsored study identified patients with nonsquamous NSCLC from an electronic health records system that contains data from 884 community-based oncologists in US Oncology Inc.–affiliated practices or clinics in 20 states.
Patients were treated from July 2006 through June 2008, with 31% located in the Southwest and 30% in the Southeast. In all, 37% of patients had private insurance, 57% were covered by Medicare, and 6% had some other payer.
The maintenance group tended to have better pre- and postchemotherapy performance status scores and a greater number of completed chemotherapy cycles (median, six vs. four). Overall, 56% of the maintenance group and 39% of the no-maintenance group received a second-line therapy.
To control for survivorship and selection bias, researchers excluded patients with disease progression or death within 30 days of chemotherapy completion; landmark analyses were conducted at 18, 21, and 26 weeks from initial treatment.
Among those who were alive and progression free at 18 weeks, bevacizumab monotherapy until disease progression was associated with a 46% reduced risk of death (hazard ratio, 0.54), reported Dr. Nadler of the Texas Oncology–Baylor Sammons Cancer Center in Dallas. The association between bevacizumab and longer residual overall survival persisted among patients who remained progression free and alive at 21 weeks (HR, 0.58) and 26 weeks (HR, 0.61).
Bevacizumab monotherapy was associated with longer progression-free survival at 18 weeks (HR, 0.73), but the association was no longer observed at 21 weeks (HR, 0.82) and 26 weeks (HR, 0.79).
Although the nonrandomized nature of the study precludes making any conclusions about causality, the authors concluded that the findings provide "significant insights into real-world patterns of care and associated outcomes and provide important evidence on which to base future comparative effectiveness research."
In a separate national survey of oncologists, Dr. Nadler and associates at Tufts University in Boston reported that 84% of oncologists say that patients’ out-of-pocket spending influences treatment recommendations, even though only 43% frequently or always discuss costs with patients. Among the 787 oncologists surveyed, 79% favored more comparative effectiveness research and 80% supported more cost-effectiveness data, but only 42% felt well prepared to interpret it (Health Aff. [Millwood] 2010;29:196-202).
Genentech supported the study. Dr. Nadler reported no conflicts of interest. Three coauthors reported employment with Genentech and ownership interest in Roche Holdings.