User login
Steroid-Eluting Sinus Stent May Minimize Postop Events
CHICAGO – A bioabsorbable steroid-eluting stent preserved sinus patency following endoscopic sinus surgery in 50 patients with chronic rhinosinusitis in a prospective, multicenter study.

The stent was associated with low rates of polyp formation, inflammation, and adhesions, despite a challenging patient population and withholding of postoperative oral and topical steroids for 30 days, lead author Dr. Keith D. Forwith said at the Combined Otolaryngology Spring Meetings.
The results were consistent across different patient populations and consistent with the pilot study in 43 patients (Int. Forum Allergy Rhinol. 2011;1:23-32).
"I think with any kind of new technique or device, the ultimate thing is how the surgeon feels about it and his or her results," he said. "What I noticed most of all when we stopped doing the study is that I missed using this device. Patients I had used it in during the study had very clean results, very easy debridements. ... We’re very pleased with the results and think it’s a promising technology."

Study sponsor Intersect ENT Inc. has submitted the investigational stent for federal review and hopes to market the device within 6-9 months.
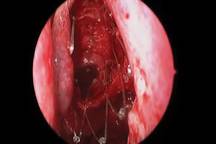
The springlike stent maintains patency by propping open the sinus cavity and releasing mometasone furoate into the sinus lining over 30 days before being resorbed. If approved, it could provide patients with an alternative to space-filling packing materials and silicone stents, and reduce the use of systemic steroids.
The current study involved 50 adults from seven centers with chronic rhinosinusitis for at least 8 consecutive weeks that was confirmed by CT scan (mean CT stage, 11.2). Antibiotics could be prescribed per physician standard of care, and saline irrigation was permitted postoperatively as needed. Polyps were present in 66% of patients, and 28% had undergone a prior sinus procedure. Their mean age was 44 years, and 52% were male.

Ethmoidectomy and maxillary antrostomy were performed in all 50 patients, with 28 also undergoing frontal sinusotomy and 31 sphenoidotomy. Stents were placed unilaterally in 10 patients and bilaterally in 40 patients. Device placement was successful in 100% of sinuses treated, and the implants were resorbed as predicted, Dr. Forwith said. At postoperative day 30, 15% of the material remained and 0.2% remained at day 60.
Endoscopic follow-up at 1 month revealed polypoid edema in 10% of patients, significant adhesion formation in 1%, and middle turbinate lateralization in only 4.4%, said Dr. Forwith, who is in private practice in Louisville, Ky.
When patients were asked about the procedure, their mean score on the 22-question Sino-Nasal Outcome Test improved significantly from baseline through 6 months. The same was true using the Rhinosinusitis Disability Index. "We were pretty pleased that our patients liked the results of the intervention," he said.
No clinically significant changes from baseline occurred in lens opacities or intraocular pressure, which was a theoretical concern given the close proximity of the device. The patients’ mean intraocular pressure was 15 mm Hg at baseline and 14.3 mm Hg at day 30.
One patient experienced headache with sinus pressure/irritation at day 21 that was determined to be related primarily to the surgery and was exacerbated in intensity by the presence of crust on the device. The device was removed and the event resolved without sequelae by day 28.
When asked during a discussion of the study whether the drug-eluting stent resulted in any systemic complications or adrenal corticol suppression, Dr. Forwith replied that they did not specifically look at adrenal suppression, but added that the 370-mcg dose of mometasone furoate is lower than the dose patients receive with most b.i.d. nasal spray administration.
Stent maker Intersect ENT provided funding, administrative support, and materials for the study. Dr. Forwith reported no conflicts of interest.
CHICAGO – A bioabsorbable steroid-eluting stent preserved sinus patency following endoscopic sinus surgery in 50 patients with chronic rhinosinusitis in a prospective, multicenter study.
The stent was associated with low rates of polyp formation, inflammation, and adhesions, despite a challenging patient population and withholding of postoperative oral and topical steroids for 30 days, lead author Dr. Keith D. Forwith said at the Combined Otolaryngology Spring Meetings.
The results were consistent across different patient populations and consistent with the pilot study in 43 patients (Int. Forum Allergy Rhinol. 2011;1:23-32).
"I think with any kind of new technique or device, the ultimate thing is how the surgeon feels about it and his or her results," he said. "What I noticed most of all when we stopped doing the study is that I missed using this device. Patients I had used it in during the study had very clean results, very easy debridements. ... We’re very pleased with the results and think it’s a promising technology."
Study sponsor Intersect ENT Inc. has submitted the investigational stent for federal review and hopes to market the device within 6-9 months.
The springlike stent maintains patency by propping open the sinus cavity and releasing mometasone furoate into the sinus lining over 30 days before being resorbed. If approved, it could provide patients with an alternative to space-filling packing materials and silicone stents, and reduce the use of systemic steroids.
The current study involved 50 adults from seven centers with chronic rhinosinusitis for at least 8 consecutive weeks that was confirmed by CT scan (mean CT stage, 11.2). Antibiotics could be prescribed per physician standard of care, and saline irrigation was permitted postoperatively as needed. Polyps were present in 66% of patients, and 28% had undergone a prior sinus procedure. Their mean age was 44 years, and 52% were male.
Ethmoidectomy and maxillary antrostomy were performed in all 50 patients, with 28 also undergoing frontal sinusotomy and 31 sphenoidotomy. Stents were placed unilaterally in 10 patients and bilaterally in 40 patients. Device placement was successful in 100% of sinuses treated, and the implants were resorbed as predicted, Dr. Forwith said. At postoperative day 30, 15% of the material remained and 0.2% remained at day 60.
Endoscopic follow-up at 1 month revealed polypoid edema in 10% of patients, significant adhesion formation in 1%, and middle turbinate lateralization in only 4.4%, said Dr. Forwith, who is in private practice in Louisville, Ky.
When patients were asked about the procedure, their mean score on the 22-question Sino-Nasal Outcome Test improved significantly from baseline through 6 months. The same was true using the Rhinosinusitis Disability Index. "We were pretty pleased that our patients liked the results of the intervention," he said.
No clinically significant changes from baseline occurred in lens opacities or intraocular pressure, which was a theoretical concern given the close proximity of the device. The patients’ mean intraocular pressure was 15 mm Hg at baseline and 14.3 mm Hg at day 30.
One patient experienced headache with sinus pressure/irritation at day 21 that was determined to be related primarily to the surgery and was exacerbated in intensity by the presence of crust on the device. The device was removed and the event resolved without sequelae by day 28.
When asked during a discussion of the study whether the drug-eluting stent resulted in any systemic complications or adrenal corticol suppression, Dr. Forwith replied that they did not specifically look at adrenal suppression, but added that the 370-mcg dose of mometasone furoate is lower than the dose patients receive with most b.i.d. nasal spray administration.
Stent maker Intersect ENT provided funding, administrative support, and materials for the study. Dr. Forwith reported no conflicts of interest.
CHICAGO – A bioabsorbable steroid-eluting stent preserved sinus patency following endoscopic sinus surgery in 50 patients with chronic rhinosinusitis in a prospective, multicenter study.
The stent was associated with low rates of polyp formation, inflammation, and adhesions, despite a challenging patient population and withholding of postoperative oral and topical steroids for 30 days, lead author Dr. Keith D. Forwith said at the Combined Otolaryngology Spring Meetings.
The results were consistent across different patient populations and consistent with the pilot study in 43 patients (Int. Forum Allergy Rhinol. 2011;1:23-32).
"I think with any kind of new technique or device, the ultimate thing is how the surgeon feels about it and his or her results," he said. "What I noticed most of all when we stopped doing the study is that I missed using this device. Patients I had used it in during the study had very clean results, very easy debridements. ... We’re very pleased with the results and think it’s a promising technology."
Study sponsor Intersect ENT Inc. has submitted the investigational stent for federal review and hopes to market the device within 6-9 months.
The springlike stent maintains patency by propping open the sinus cavity and releasing mometasone furoate into the sinus lining over 30 days before being resorbed. If approved, it could provide patients with an alternative to space-filling packing materials and silicone stents, and reduce the use of systemic steroids.
The current study involved 50 adults from seven centers with chronic rhinosinusitis for at least 8 consecutive weeks that was confirmed by CT scan (mean CT stage, 11.2). Antibiotics could be prescribed per physician standard of care, and saline irrigation was permitted postoperatively as needed. Polyps were present in 66% of patients, and 28% had undergone a prior sinus procedure. Their mean age was 44 years, and 52% were male.
Ethmoidectomy and maxillary antrostomy were performed in all 50 patients, with 28 also undergoing frontal sinusotomy and 31 sphenoidotomy. Stents were placed unilaterally in 10 patients and bilaterally in 40 patients. Device placement was successful in 100% of sinuses treated, and the implants were resorbed as predicted, Dr. Forwith said. At postoperative day 30, 15% of the material remained and 0.2% remained at day 60.
Endoscopic follow-up at 1 month revealed polypoid edema in 10% of patients, significant adhesion formation in 1%, and middle turbinate lateralization in only 4.4%, said Dr. Forwith, who is in private practice in Louisville, Ky.
When patients were asked about the procedure, their mean score on the 22-question Sino-Nasal Outcome Test improved significantly from baseline through 6 months. The same was true using the Rhinosinusitis Disability Index. "We were pretty pleased that our patients liked the results of the intervention," he said.
No clinically significant changes from baseline occurred in lens opacities or intraocular pressure, which was a theoretical concern given the close proximity of the device. The patients’ mean intraocular pressure was 15 mm Hg at baseline and 14.3 mm Hg at day 30.
One patient experienced headache with sinus pressure/irritation at day 21 that was determined to be related primarily to the surgery and was exacerbated in intensity by the presence of crust on the device. The device was removed and the event resolved without sequelae by day 28.
When asked during a discussion of the study whether the drug-eluting stent resulted in any systemic complications or adrenal corticol suppression, Dr. Forwith replied that they did not specifically look at adrenal suppression, but added that the 370-mcg dose of mometasone furoate is lower than the dose patients receive with most b.i.d. nasal spray administration.
Stent maker Intersect ENT provided funding, administrative support, and materials for the study. Dr. Forwith reported no conflicts of interest.
FROM THE COMBINED OTOLARYNGOLOGY SPRING MEETINGS
Major Finding: At 1 month follow-up, the occurrence of polypoid edema was 10%, significant adhesion formation 1%, and middle turbinate lateralization 4.4%.
Data Source: Prospective, multicenter study in 50 patients with chronic rhinosinusitis undergoing endoscopic sinus surgery.
Disclosures: Stent maker Intersect ENT provided funding, administrative support, and materials for the study. Dr. Forwith reported no conflicts of interest.
Everolimus Gets Nod for Pancreatic Neuroendocrine Tumors
The U.S. Food and Drug Administration has approved everolimus as the first new drug in roughly 30 years for the treatment of advanced pancreatic neuroendocrine tumors.
The move was widely anticipated following the unanimous vote last month by the FDA’s Oncologic Drugs Advisory Committee (ODAC) that the drug’s benefit outweighs its risks for this disease. Everolimus is marketed as Afinitor by Novartis, and fills a therapeutic void for this rare, slow-growing cancer.
"Patients with this cancer have few effective treatment options," Dr. Richard Pazdur, director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research, said in a statement. "Afinitor has demonstrated the ability to slow the growth and spread of neuroendocrine tumors of the pancreas."
Dr. Johanna Bendell, director of GI oncology research at the Sarah Cannon Research Institute in Nashville, said in an interview that for patients with advanced disease, the only approved therapies had been cytotoxic regimens that carry the potential for significant side effects with questionable benefit.
"This approval is an important step forward in the treatment of patients with PNET [pancreatic neuroendocrine tumors] who formerly had limited treatment options," she said. "We hope to see a second agent approved for these patients in the near future."
Indeed, it’s possible that patients with PNET may have an additional option in the coming months. At the same April 12 advisory meeting in which everolimus received unanimous support, ODAC voted 8-2 in favor of Pfizer’s sunitinib malate (Sutent) for treating patients with unresectable PNET. Some reservations were expressed over the magnitude of the drug’s effect on progression-free survival in a key trial that was terminated early because of significant benefits in the sunitinib arm compared with a placebo.
Pfizer continues to work closely with the FDA to finalize its review of Sutent’s supplemental new drug application for PNET in an effort to continue to advance treatment for this disease.
"What we can say at this time is that a decision from the FDA is expected by mid-year," Christopher Loder, Pfizer head of U.S. media relations, said in an interview.
Fewer than 1,000 new cases of PNET are estimated to occur in the United States each year. The FDA announcement specifies that everolimus is indicated for patients with progressive tumors "that cannot be removed by surgery or that have spread to other parts of the body (metastatic)."
Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, was approved on the strength of the phase III RADIANT-3 trial in 410 patients with advanced low- or intermediate grade PNET. Everolimus 10 mg per day plus best supportive care provided a median gain of 6.4 months of progression-free survival when compared with best supportive care alone (11 months vs. 4.6 months). This translated into a significant 65% reduction in the risk of progression compared with placebo.
"Everolimus should be considered the standard of care for patients with [advanced pancreatic] neuroendocrine tumors," Dr. James C. Yao, with the University of Texas M.D. Anderson Cancer Center in Houston, said when presenting the RADIANT-3 findings at last year’s European Society for Medical Oncology meeting in Milan.
In the RADIANT-3 trial, 62% of patient on everolimus had a grade 3/4 adverse event, compared with 40% of those on placebo. Pneumonitis, opportunistic infections, and renal failure were among the significant adverse events associated with everolimus therapy. The most commonly reported side effects included inflammation of the mouth, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever and headache.
Importantly, ODAC members cautioned that everolimus and sunitinib shouldn’t automatically be given to all patients with PNET, noting the often indolent nature of the cancer and that the treatments appear to have a more favorable risk-benefit profile in patients with aggressive disease.
Panelists recommended that more work be done to identify the subset of patients with the disease who can benefit most from treatment with everolimus. They also recommended that it not be used to treat patients with carcinoid tumors because it has not been shown to be effective and may be harmful in this population.
Several ODAC panelists also pointed out that sunitinib’s labeling should indicate that most patients in the phase III pivotal trial had metastatic disease and that sunitinib should not be used to treat patients with indolent forms of the disease.
Dr. Bendell pointed out that that benefits from everolimus and sunitinib were comparable. When the data were unblinded from the phase III sunitinib trial, the significant improvement in progression-free survival for patients had a hazard ratio of 0.418. The phase III everolimus vs. placebo study also showed a significant improvement in progression-free survival, (HR, 0.34).
"There is really no known specific benefit over sunitinib or vice versa, as noted in the PFS data," she said. "The hazard ratios were the same."
Other currently available treatment options for patients with PNET include interferon, somatostatin analogs, metabolic radiotherapy, and chemotherapy.
Everolimus was approved in the United States in 2009 for treating advanced renal cell carcinoma, and in 2010 for subependymal giant cell astrocytoma. It is also known by the trade name Zortress and is used in some adults to prevent organ rejection after kidney transplantation.
* This article was updated with additional information on 5/7/2011.
The U.S. Food and Drug Administration has approved everolimus as the first new drug in roughly 30 years for the treatment of advanced pancreatic neuroendocrine tumors.
The move was widely anticipated following the unanimous vote last month by the FDA’s Oncologic Drugs Advisory Committee (ODAC) that the drug’s benefit outweighs its risks for this disease. Everolimus is marketed as Afinitor by Novartis, and fills a therapeutic void for this rare, slow-growing cancer.
"Patients with this cancer have few effective treatment options," Dr. Richard Pazdur, director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research, said in a statement. "Afinitor has demonstrated the ability to slow the growth and spread of neuroendocrine tumors of the pancreas."
Dr. Johanna Bendell, director of GI oncology research at the Sarah Cannon Research Institute in Nashville, said in an interview that for patients with advanced disease, the only approved therapies had been cytotoxic regimens that carry the potential for significant side effects with questionable benefit.
"This approval is an important step forward in the treatment of patients with PNET [pancreatic neuroendocrine tumors] who formerly had limited treatment options," she said. "We hope to see a second agent approved for these patients in the near future."
Indeed, it’s possible that patients with PNET may have an additional option in the coming months. At the same April 12 advisory meeting in which everolimus received unanimous support, ODAC voted 8-2 in favor of Pfizer’s sunitinib malate (Sutent) for treating patients with unresectable PNET. Some reservations were expressed over the magnitude of the drug’s effect on progression-free survival in a key trial that was terminated early because of significant benefits in the sunitinib arm compared with a placebo.
Pfizer continues to work closely with the FDA to finalize its review of Sutent’s supplemental new drug application for PNET in an effort to continue to advance treatment for this disease.
"What we can say at this time is that a decision from the FDA is expected by mid-year," Christopher Loder, Pfizer head of U.S. media relations, said in an interview.
Fewer than 1,000 new cases of PNET are estimated to occur in the United States each year. The FDA announcement specifies that everolimus is indicated for patients with progressive tumors "that cannot be removed by surgery or that have spread to other parts of the body (metastatic)."
Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, was approved on the strength of the phase III RADIANT-3 trial in 410 patients with advanced low- or intermediate grade PNET. Everolimus 10 mg per day plus best supportive care provided a median gain of 6.4 months of progression-free survival when compared with best supportive care alone (11 months vs. 4.6 months). This translated into a significant 65% reduction in the risk of progression compared with placebo.
"Everolimus should be considered the standard of care for patients with [advanced pancreatic] neuroendocrine tumors," Dr. James C. Yao, with the University of Texas M.D. Anderson Cancer Center in Houston, said when presenting the RADIANT-3 findings at last year’s European Society for Medical Oncology meeting in Milan.
In the RADIANT-3 trial, 62% of patient on everolimus had a grade 3/4 adverse event, compared with 40% of those on placebo. Pneumonitis, opportunistic infections, and renal failure were among the significant adverse events associated with everolimus therapy. The most commonly reported side effects included inflammation of the mouth, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever and headache.
Importantly, ODAC members cautioned that everolimus and sunitinib shouldn’t automatically be given to all patients with PNET, noting the often indolent nature of the cancer and that the treatments appear to have a more favorable risk-benefit profile in patients with aggressive disease.
Panelists recommended that more work be done to identify the subset of patients with the disease who can benefit most from treatment with everolimus. They also recommended that it not be used to treat patients with carcinoid tumors because it has not been shown to be effective and may be harmful in this population.
Several ODAC panelists also pointed out that sunitinib’s labeling should indicate that most patients in the phase III pivotal trial had metastatic disease and that sunitinib should not be used to treat patients with indolent forms of the disease.
Dr. Bendell pointed out that that benefits from everolimus and sunitinib were comparable. When the data were unblinded from the phase III sunitinib trial, the significant improvement in progression-free survival for patients had a hazard ratio of 0.418. The phase III everolimus vs. placebo study also showed a significant improvement in progression-free survival, (HR, 0.34).
"There is really no known specific benefit over sunitinib or vice versa, as noted in the PFS data," she said. "The hazard ratios were the same."
Other currently available treatment options for patients with PNET include interferon, somatostatin analogs, metabolic radiotherapy, and chemotherapy.
Everolimus was approved in the United States in 2009 for treating advanced renal cell carcinoma, and in 2010 for subependymal giant cell astrocytoma. It is also known by the trade name Zortress and is used in some adults to prevent organ rejection after kidney transplantation.
* This article was updated with additional information on 5/7/2011.
The U.S. Food and Drug Administration has approved everolimus as the first new drug in roughly 30 years for the treatment of advanced pancreatic neuroendocrine tumors.
The move was widely anticipated following the unanimous vote last month by the FDA’s Oncologic Drugs Advisory Committee (ODAC) that the drug’s benefit outweighs its risks for this disease. Everolimus is marketed as Afinitor by Novartis, and fills a therapeutic void for this rare, slow-growing cancer.
"Patients with this cancer have few effective treatment options," Dr. Richard Pazdur, director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research, said in a statement. "Afinitor has demonstrated the ability to slow the growth and spread of neuroendocrine tumors of the pancreas."
Dr. Johanna Bendell, director of GI oncology research at the Sarah Cannon Research Institute in Nashville, said in an interview that for patients with advanced disease, the only approved therapies had been cytotoxic regimens that carry the potential for significant side effects with questionable benefit.
"This approval is an important step forward in the treatment of patients with PNET [pancreatic neuroendocrine tumors] who formerly had limited treatment options," she said. "We hope to see a second agent approved for these patients in the near future."
Indeed, it’s possible that patients with PNET may have an additional option in the coming months. At the same April 12 advisory meeting in which everolimus received unanimous support, ODAC voted 8-2 in favor of Pfizer’s sunitinib malate (Sutent) for treating patients with unresectable PNET. Some reservations were expressed over the magnitude of the drug’s effect on progression-free survival in a key trial that was terminated early because of significant benefits in the sunitinib arm compared with a placebo.
Pfizer continues to work closely with the FDA to finalize its review of Sutent’s supplemental new drug application for PNET in an effort to continue to advance treatment for this disease.
"What we can say at this time is that a decision from the FDA is expected by mid-year," Christopher Loder, Pfizer head of U.S. media relations, said in an interview.
Fewer than 1,000 new cases of PNET are estimated to occur in the United States each year. The FDA announcement specifies that everolimus is indicated for patients with progressive tumors "that cannot be removed by surgery or that have spread to other parts of the body (metastatic)."
Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, was approved on the strength of the phase III RADIANT-3 trial in 410 patients with advanced low- or intermediate grade PNET. Everolimus 10 mg per day plus best supportive care provided a median gain of 6.4 months of progression-free survival when compared with best supportive care alone (11 months vs. 4.6 months). This translated into a significant 65% reduction in the risk of progression compared with placebo.
"Everolimus should be considered the standard of care for patients with [advanced pancreatic] neuroendocrine tumors," Dr. James C. Yao, with the University of Texas M.D. Anderson Cancer Center in Houston, said when presenting the RADIANT-3 findings at last year’s European Society for Medical Oncology meeting in Milan.
In the RADIANT-3 trial, 62% of patient on everolimus had a grade 3/4 adverse event, compared with 40% of those on placebo. Pneumonitis, opportunistic infections, and renal failure were among the significant adverse events associated with everolimus therapy. The most commonly reported side effects included inflammation of the mouth, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever and headache.
Importantly, ODAC members cautioned that everolimus and sunitinib shouldn’t automatically be given to all patients with PNET, noting the often indolent nature of the cancer and that the treatments appear to have a more favorable risk-benefit profile in patients with aggressive disease.
Panelists recommended that more work be done to identify the subset of patients with the disease who can benefit most from treatment with everolimus. They also recommended that it not be used to treat patients with carcinoid tumors because it has not been shown to be effective and may be harmful in this population.
Several ODAC panelists also pointed out that sunitinib’s labeling should indicate that most patients in the phase III pivotal trial had metastatic disease and that sunitinib should not be used to treat patients with indolent forms of the disease.
Dr. Bendell pointed out that that benefits from everolimus and sunitinib were comparable. When the data were unblinded from the phase III sunitinib trial, the significant improvement in progression-free survival for patients had a hazard ratio of 0.418. The phase III everolimus vs. placebo study also showed a significant improvement in progression-free survival, (HR, 0.34).
"There is really no known specific benefit over sunitinib or vice versa, as noted in the PFS data," she said. "The hazard ratios were the same."
Other currently available treatment options for patients with PNET include interferon, somatostatin analogs, metabolic radiotherapy, and chemotherapy.
Everolimus was approved in the United States in 2009 for treating advanced renal cell carcinoma, and in 2010 for subependymal giant cell astrocytoma. It is also known by the trade name Zortress and is used in some adults to prevent organ rejection after kidney transplantation.
* This article was updated with additional information on 5/7/2011.
FROM THE FOOD AND DRUG ADMINISTRATION
Everolimus Gets Nod for Pancreatic Neuroendocrine Tumors
The U.S. Food and Drug Administration has approved everolimus as the first new drug in roughly 30 years for the treatment of advanced pancreatic neuroendocrine tumors.
The move was widely anticipated following the unanimous vote last month by the FDA’s Oncologic Drugs Advisory Committee (ODAC) that the drug’s benefit outweighs its risks for this disease. Everolimus is marketed as Afinitor by Novartis, and fills a therapeutic void for this rare, slow-growing cancer.
"Patients with this cancer have few effective treatment options," Dr. Richard Pazdur, director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research, said in a statement. "Afinitor has demonstrated the ability to slow the growth and spread of neuroendocrine tumors of the pancreas."
Dr. Johanna Bendell, director of GI oncology research at the Sarah Cannon Research Institute in Nashville, said in an interview that for patients with advanced disease, the only approved therapies had been cytotoxic regimens that carry the potential for significant side effects with questionable benefit.
"This approval is an important step forward in the treatment of patients with PNET [pancreatic neuroendocrine tumors] who formerly had limited treatment options," she said. "We hope to see a second agent approved for these patients in the near future."
Indeed, it’s possible that patients with PNET may have an additional option in the coming months. At the same April 12 advisory meeting in which everolimus received unanimous support, ODAC voted 8-2 in favor of Pfizer’s sunitinib malate (Sutent) for treating patients with unresectable PNET. Some reservations were expressed over the magnitude of the drug’s effect on progression-free survival in a key trial that was terminated early because of significant benefits in the sunitinib arm compared with a placebo.
Pfizer continues to work closely with the FDA to finalize its review of Sutent’s supplemental new drug application for PNET in an effort to continue to advance treatment for this disease.
"What we can say at this time is that a decision from the FDA is expected by mid-year," Christopher Loder, Pfizer head of U.S. media relations, said in an interview.
Fewer than 1,000 new cases of PNET are estimated to occur in the United States each year. The FDA announcement specifies that everolimus is indicated for patients with progressive tumors "that cannot be removed by surgery or that have spread to other parts of the body (metastatic)."
Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, was approved on the strength of the phase III RADIANT-3 trial in 410 patients with advanced low- or intermediate grade PNET. Everolimus 10 mg per day plus best supportive care provided a median gain of 6.4 months of progression-free survival when compared with best supportive care alone (11 months vs. 4.6 months). This translated into a significant 65% reduction in the risk of progression compared with placebo.
"Everolimus should be considered the standard of care for patients with [advanced pancreatic] neuroendocrine tumors," Dr. James C. Yao, with the University of Texas M.D. Anderson Cancer Center in Houston, said when presenting the RADIANT-3 findings at last year’s European Society for Medical Oncology meeting in Milan.
In the RADIANT-3 trial, 62% of patient on everolimus had a grade 3/4 adverse event, compared with 40% of those on placebo. Pneumonitis, opportunistic infections, and renal failure were among the significant adverse events associated with everolimus therapy. The most commonly reported side effects included inflammation of the mouth, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever and headache.
Importantly, ODAC members cautioned that everolimus and sunitinib shouldn’t automatically be given to all patients with PNET, noting the often indolent nature of the cancer and that the treatments appear to have a more favorable risk-benefit profile in patients with aggressive disease.
Panelists recommended that more work be done to identify the subset of patients with the disease who can benefit most from treatment with everolimus. They also recommended that it not be used to treat patients with carcinoid tumors because it has not been shown to be effective and may be harmful in this population.
Several ODAC panelists also pointed out that sunitinib’s labeling should indicate that most patients in the phase III pivotal trial had metastatic disease and that sunitinib should not be used to treat patients with indolent forms of the disease.
Dr. Bendell pointed out that that benefits from everolimus and sunitinib were comparable. When the data were unblinded from the phase III sunitinib trial, the significant improvement in progression-free survival for patients had a hazard ratio of 0.418. The phase III everolimus vs. placebo study also showed a significant improvement in progression-free survival, (HR, 0.34).
"There is really no known specific benefit over sunitinib or vice versa, as noted in the PFS data," she said. "The hazard ratios were the same."
Other currently available treatment options for patients with PNET include interferon, somatostatin analogs, metabolic radiotherapy, and chemotherapy.
Everolimus was approved in the United States in 2009 for treating advanced renal cell carcinoma, and in 2010 for subependymal giant cell astrocytoma. It is also known by the trade name Zortress and is used in some adults to prevent organ rejection after kidney transplantation.
* This article was updated with additional information on 5/7/2011.
The U.S. Food and Drug Administration has approved everolimus as the first new drug in roughly 30 years for the treatment of advanced pancreatic neuroendocrine tumors.
The move was widely anticipated following the unanimous vote last month by the FDA’s Oncologic Drugs Advisory Committee (ODAC) that the drug’s benefit outweighs its risks for this disease. Everolimus is marketed as Afinitor by Novartis, and fills a therapeutic void for this rare, slow-growing cancer.
"Patients with this cancer have few effective treatment options," Dr. Richard Pazdur, director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research, said in a statement. "Afinitor has demonstrated the ability to slow the growth and spread of neuroendocrine tumors of the pancreas."
Dr. Johanna Bendell, director of GI oncology research at the Sarah Cannon Research Institute in Nashville, said in an interview that for patients with advanced disease, the only approved therapies had been cytotoxic regimens that carry the potential for significant side effects with questionable benefit.
"This approval is an important step forward in the treatment of patients with PNET [pancreatic neuroendocrine tumors] who formerly had limited treatment options," she said. "We hope to see a second agent approved for these patients in the near future."
Indeed, it’s possible that patients with PNET may have an additional option in the coming months. At the same April 12 advisory meeting in which everolimus received unanimous support, ODAC voted 8-2 in favor of Pfizer’s sunitinib malate (Sutent) for treating patients with unresectable PNET. Some reservations were expressed over the magnitude of the drug’s effect on progression-free survival in a key trial that was terminated early because of significant benefits in the sunitinib arm compared with a placebo.
Pfizer continues to work closely with the FDA to finalize its review of Sutent’s supplemental new drug application for PNET in an effort to continue to advance treatment for this disease.
"What we can say at this time is that a decision from the FDA is expected by mid-year," Christopher Loder, Pfizer head of U.S. media relations, said in an interview.
Fewer than 1,000 new cases of PNET are estimated to occur in the United States each year. The FDA announcement specifies that everolimus is indicated for patients with progressive tumors "that cannot be removed by surgery or that have spread to other parts of the body (metastatic)."
Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, was approved on the strength of the phase III RADIANT-3 trial in 410 patients with advanced low- or intermediate grade PNET. Everolimus 10 mg per day plus best supportive care provided a median gain of 6.4 months of progression-free survival when compared with best supportive care alone (11 months vs. 4.6 months). This translated into a significant 65% reduction in the risk of progression compared with placebo.
"Everolimus should be considered the standard of care for patients with [advanced pancreatic] neuroendocrine tumors," Dr. James C. Yao, with the University of Texas M.D. Anderson Cancer Center in Houston, said when presenting the RADIANT-3 findings at last year’s European Society for Medical Oncology meeting in Milan.
In the RADIANT-3 trial, 62% of patient on everolimus had a grade 3/4 adverse event, compared with 40% of those on placebo. Pneumonitis, opportunistic infections, and renal failure were among the significant adverse events associated with everolimus therapy. The most commonly reported side effects included inflammation of the mouth, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever and headache.
Importantly, ODAC members cautioned that everolimus and sunitinib shouldn’t automatically be given to all patients with PNET, noting the often indolent nature of the cancer and that the treatments appear to have a more favorable risk-benefit profile in patients with aggressive disease.
Panelists recommended that more work be done to identify the subset of patients with the disease who can benefit most from treatment with everolimus. They also recommended that it not be used to treat patients with carcinoid tumors because it has not been shown to be effective and may be harmful in this population.
Several ODAC panelists also pointed out that sunitinib’s labeling should indicate that most patients in the phase III pivotal trial had metastatic disease and that sunitinib should not be used to treat patients with indolent forms of the disease.
Dr. Bendell pointed out that that benefits from everolimus and sunitinib were comparable. When the data were unblinded from the phase III sunitinib trial, the significant improvement in progression-free survival for patients had a hazard ratio of 0.418. The phase III everolimus vs. placebo study also showed a significant improvement in progression-free survival, (HR, 0.34).
"There is really no known specific benefit over sunitinib or vice versa, as noted in the PFS data," she said. "The hazard ratios were the same."
Other currently available treatment options for patients with PNET include interferon, somatostatin analogs, metabolic radiotherapy, and chemotherapy.
Everolimus was approved in the United States in 2009 for treating advanced renal cell carcinoma, and in 2010 for subependymal giant cell astrocytoma. It is also known by the trade name Zortress and is used in some adults to prevent organ rejection after kidney transplantation.
* This article was updated with additional information on 5/7/2011.
The U.S. Food and Drug Administration has approved everolimus as the first new drug in roughly 30 years for the treatment of advanced pancreatic neuroendocrine tumors.
The move was widely anticipated following the unanimous vote last month by the FDA’s Oncologic Drugs Advisory Committee (ODAC) that the drug’s benefit outweighs its risks for this disease. Everolimus is marketed as Afinitor by Novartis, and fills a therapeutic void for this rare, slow-growing cancer.
"Patients with this cancer have few effective treatment options," Dr. Richard Pazdur, director of the Office of Oncology Drug Products in the FDA’s Center for Drug Evaluation and Research, said in a statement. "Afinitor has demonstrated the ability to slow the growth and spread of neuroendocrine tumors of the pancreas."
Dr. Johanna Bendell, director of GI oncology research at the Sarah Cannon Research Institute in Nashville, said in an interview that for patients with advanced disease, the only approved therapies had been cytotoxic regimens that carry the potential for significant side effects with questionable benefit.
"This approval is an important step forward in the treatment of patients with PNET [pancreatic neuroendocrine tumors] who formerly had limited treatment options," she said. "We hope to see a second agent approved for these patients in the near future."
Indeed, it’s possible that patients with PNET may have an additional option in the coming months. At the same April 12 advisory meeting in which everolimus received unanimous support, ODAC voted 8-2 in favor of Pfizer’s sunitinib malate (Sutent) for treating patients with unresectable PNET. Some reservations were expressed over the magnitude of the drug’s effect on progression-free survival in a key trial that was terminated early because of significant benefits in the sunitinib arm compared with a placebo.
Pfizer continues to work closely with the FDA to finalize its review of Sutent’s supplemental new drug application for PNET in an effort to continue to advance treatment for this disease.
"What we can say at this time is that a decision from the FDA is expected by mid-year," Christopher Loder, Pfizer head of U.S. media relations, said in an interview.
Fewer than 1,000 new cases of PNET are estimated to occur in the United States each year. The FDA announcement specifies that everolimus is indicated for patients with progressive tumors "that cannot be removed by surgery or that have spread to other parts of the body (metastatic)."
Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, was approved on the strength of the phase III RADIANT-3 trial in 410 patients with advanced low- or intermediate grade PNET. Everolimus 10 mg per day plus best supportive care provided a median gain of 6.4 months of progression-free survival when compared with best supportive care alone (11 months vs. 4.6 months). This translated into a significant 65% reduction in the risk of progression compared with placebo.
"Everolimus should be considered the standard of care for patients with [advanced pancreatic] neuroendocrine tumors," Dr. James C. Yao, with the University of Texas M.D. Anderson Cancer Center in Houston, said when presenting the RADIANT-3 findings at last year’s European Society for Medical Oncology meeting in Milan.
In the RADIANT-3 trial, 62% of patient on everolimus had a grade 3/4 adverse event, compared with 40% of those on placebo. Pneumonitis, opportunistic infections, and renal failure were among the significant adverse events associated with everolimus therapy. The most commonly reported side effects included inflammation of the mouth, rash, diarrhea, fatigue, edema, abdominal pain, nausea, fever and headache.
Importantly, ODAC members cautioned that everolimus and sunitinib shouldn’t automatically be given to all patients with PNET, noting the often indolent nature of the cancer and that the treatments appear to have a more favorable risk-benefit profile in patients with aggressive disease.
Panelists recommended that more work be done to identify the subset of patients with the disease who can benefit most from treatment with everolimus. They also recommended that it not be used to treat patients with carcinoid tumors because it has not been shown to be effective and may be harmful in this population.
Several ODAC panelists also pointed out that sunitinib’s labeling should indicate that most patients in the phase III pivotal trial had metastatic disease and that sunitinib should not be used to treat patients with indolent forms of the disease.
Dr. Bendell pointed out that that benefits from everolimus and sunitinib were comparable. When the data were unblinded from the phase III sunitinib trial, the significant improvement in progression-free survival for patients had a hazard ratio of 0.418. The phase III everolimus vs. placebo study also showed a significant improvement in progression-free survival, (HR, 0.34).
"There is really no known specific benefit over sunitinib or vice versa, as noted in the PFS data," she said. "The hazard ratios were the same."
Other currently available treatment options for patients with PNET include interferon, somatostatin analogs, metabolic radiotherapy, and chemotherapy.
Everolimus was approved in the United States in 2009 for treating advanced renal cell carcinoma, and in 2010 for subependymal giant cell astrocytoma. It is also known by the trade name Zortress and is used in some adults to prevent organ rejection after kidney transplantation.
* This article was updated with additional information on 5/7/2011.
FROM THE FOOD AND DRUG ADMINISTRATION
Preoperative Hyponatremia Points to Dismal Outcomes After Cardiac Surgery
NEW ORLEANS – Preoperative hyponatremia was common in patients undergoing cardiac surgery and associated with a dramatic increase in the risk of death and surgical complications in a large retrospective analysis.
Of the 4,370 patients who underwent cardiac surgery between 2002 and 2009 at the Ohio State Medical Center in Columbus, 931 (21%) had hyponatremia, defined as serum sodium less than 135 mEq/L on at least one of three sodium tests obtained before surgery.

In unadjusted analysis, hyponatremic patients had significantly higher rates than did those without hyponatremia of early mortality (9% vs. 4%), late mortality (24% vs. 15.6%), longer mean hospital length of stay (12.6 days vs. 8.2 days), and operative complications (13% vs. 7%), Dr. Juan Crestanello and his colleagues reported in a poster at the annual meeting of the American College of Cardiology.
This isn’t all that surprising since hyponatremic patients were sicker at baseline, but the poor outcomes remained, even after adjustment for a slew of baseline clinical and operative variables.
In multivariable logistic regression analysis, preoperative hyponatremia was independently associated with a 31% increase in overall mortality, a 52% increase in early mortality, and a 56% increase in late mortality, said Dr. Crestanello, a thoracic surgeon at the medical center.
Hyponatremia also significantly increased the risk of operative complications by 30%, pulmonary complications by 73%, renal failure requiring dialysis by 64%, and hospital length of stay by 26%. Infectious and neurologic complications were not independently associated with preoperative hyponatremia.
"Hyponatremia identifies a group of patients at higher risk for cardiac surgery," Dr. Crestanello said in an interview. "It constitutes another tool to risk-stratify these patients and will help surgeons advise patients of their risk associated with surgery."
At baseline, patients with hyponatremia had a significantly lower mean ejection fraction than did patients without hyponatremia (39% vs. 46%), higher mean pulmonary artery pressure (32 mmHg vs. 28 mmHg), and higher incidence of comorbidities, including diabetes (47% vs. 34%), chronic obstructive pulmonary disease (24.5% vs. 18%), and history of a previous MI (44.5% vs. 35.6%).
Hyponatremic patients also had significantly higher New York Heart Association functional class, higher surgical risk as predicted by the European System for Cardiac Operative Risk Evaluation (19% vs. 9%) and underwent more complex surgical procedures including coronary artery bypass surgery with valve replacement and ventricular-assist device placement.
Their mean age was 62 years, 66.5% were male, and the mean sodium level was 134 mEq/L.
Sodium levels are one of the most common laboratory values measured and are routinely obtained preoperatively.
"In spite of being widely available, they are often overlooked," Dr. Crestanello said.
Data on other factors that may have influenced serum sodium like medications, glucose levels, and fluid use were not accounted for in the study because of its retrospective nature, he noted.
When asked to speculate on the mechanism behind the association between hyponatremia and poor outcomes, Dr. Crestanello said they are not well understood. "Obviously, hyponatremia is a marker for high-risk patients, but at the same time it is likely that it has pathophysiological effects on its own ... hyponatremia is also associated with changes in the neurohormonal milieu that, by itself, can have deleterious effects."
The analysis was based on data from electronic medical records, the Society of Thoracic Surgery database, and Social Security Death Index. Mean follow-up was 2.2 years.
The authors plan to analyze the effects that correcting preoperative hyponatremia has on outcomes of cardiac surgery. The current study was supported by a grant from Biogen Inc.
NEW ORLEANS – Preoperative hyponatremia was common in patients undergoing cardiac surgery and associated with a dramatic increase in the risk of death and surgical complications in a large retrospective analysis.
Of the 4,370 patients who underwent cardiac surgery between 2002 and 2009 at the Ohio State Medical Center in Columbus, 931 (21%) had hyponatremia, defined as serum sodium less than 135 mEq/L on at least one of three sodium tests obtained before surgery.
In unadjusted analysis, hyponatremic patients had significantly higher rates than did those without hyponatremia of early mortality (9% vs. 4%), late mortality (24% vs. 15.6%), longer mean hospital length of stay (12.6 days vs. 8.2 days), and operative complications (13% vs. 7%), Dr. Juan Crestanello and his colleagues reported in a poster at the annual meeting of the American College of Cardiology.
This isn’t all that surprising since hyponatremic patients were sicker at baseline, but the poor outcomes remained, even after adjustment for a slew of baseline clinical and operative variables.
In multivariable logistic regression analysis, preoperative hyponatremia was independently associated with a 31% increase in overall mortality, a 52% increase in early mortality, and a 56% increase in late mortality, said Dr. Crestanello, a thoracic surgeon at the medical center.
Hyponatremia also significantly increased the risk of operative complications by 30%, pulmonary complications by 73%, renal failure requiring dialysis by 64%, and hospital length of stay by 26%. Infectious and neurologic complications were not independently associated with preoperative hyponatremia.
"Hyponatremia identifies a group of patients at higher risk for cardiac surgery," Dr. Crestanello said in an interview. "It constitutes another tool to risk-stratify these patients and will help surgeons advise patients of their risk associated with surgery."
At baseline, patients with hyponatremia had a significantly lower mean ejection fraction than did patients without hyponatremia (39% vs. 46%), higher mean pulmonary artery pressure (32 mmHg vs. 28 mmHg), and higher incidence of comorbidities, including diabetes (47% vs. 34%), chronic obstructive pulmonary disease (24.5% vs. 18%), and history of a previous MI (44.5% vs. 35.6%).
Hyponatremic patients also had significantly higher New York Heart Association functional class, higher surgical risk as predicted by the European System for Cardiac Operative Risk Evaluation (19% vs. 9%) and underwent more complex surgical procedures including coronary artery bypass surgery with valve replacement and ventricular-assist device placement.
Their mean age was 62 years, 66.5% were male, and the mean sodium level was 134 mEq/L.
Sodium levels are one of the most common laboratory values measured and are routinely obtained preoperatively.
"In spite of being widely available, they are often overlooked," Dr. Crestanello said.
Data on other factors that may have influenced serum sodium like medications, glucose levels, and fluid use were not accounted for in the study because of its retrospective nature, he noted.
When asked to speculate on the mechanism behind the association between hyponatremia and poor outcomes, Dr. Crestanello said they are not well understood. "Obviously, hyponatremia is a marker for high-risk patients, but at the same time it is likely that it has pathophysiological effects on its own ... hyponatremia is also associated with changes in the neurohormonal milieu that, by itself, can have deleterious effects."
The analysis was based on data from electronic medical records, the Society of Thoracic Surgery database, and Social Security Death Index. Mean follow-up was 2.2 years.
The authors plan to analyze the effects that correcting preoperative hyponatremia has on outcomes of cardiac surgery. The current study was supported by a grant from Biogen Inc.
NEW ORLEANS – Preoperative hyponatremia was common in patients undergoing cardiac surgery and associated with a dramatic increase in the risk of death and surgical complications in a large retrospective analysis.
Of the 4,370 patients who underwent cardiac surgery between 2002 and 2009 at the Ohio State Medical Center in Columbus, 931 (21%) had hyponatremia, defined as serum sodium less than 135 mEq/L on at least one of three sodium tests obtained before surgery.
In unadjusted analysis, hyponatremic patients had significantly higher rates than did those without hyponatremia of early mortality (9% vs. 4%), late mortality (24% vs. 15.6%), longer mean hospital length of stay (12.6 days vs. 8.2 days), and operative complications (13% vs. 7%), Dr. Juan Crestanello and his colleagues reported in a poster at the annual meeting of the American College of Cardiology.
This isn’t all that surprising since hyponatremic patients were sicker at baseline, but the poor outcomes remained, even after adjustment for a slew of baseline clinical and operative variables.
In multivariable logistic regression analysis, preoperative hyponatremia was independently associated with a 31% increase in overall mortality, a 52% increase in early mortality, and a 56% increase in late mortality, said Dr. Crestanello, a thoracic surgeon at the medical center.
Hyponatremia also significantly increased the risk of operative complications by 30%, pulmonary complications by 73%, renal failure requiring dialysis by 64%, and hospital length of stay by 26%. Infectious and neurologic complications were not independently associated with preoperative hyponatremia.
"Hyponatremia identifies a group of patients at higher risk for cardiac surgery," Dr. Crestanello said in an interview. "It constitutes another tool to risk-stratify these patients and will help surgeons advise patients of their risk associated with surgery."
At baseline, patients with hyponatremia had a significantly lower mean ejection fraction than did patients without hyponatremia (39% vs. 46%), higher mean pulmonary artery pressure (32 mmHg vs. 28 mmHg), and higher incidence of comorbidities, including diabetes (47% vs. 34%), chronic obstructive pulmonary disease (24.5% vs. 18%), and history of a previous MI (44.5% vs. 35.6%).
Hyponatremic patients also had significantly higher New York Heart Association functional class, higher surgical risk as predicted by the European System for Cardiac Operative Risk Evaluation (19% vs. 9%) and underwent more complex surgical procedures including coronary artery bypass surgery with valve replacement and ventricular-assist device placement.
Their mean age was 62 years, 66.5% were male, and the mean sodium level was 134 mEq/L.
Sodium levels are one of the most common laboratory values measured and are routinely obtained preoperatively.
"In spite of being widely available, they are often overlooked," Dr. Crestanello said.
Data on other factors that may have influenced serum sodium like medications, glucose levels, and fluid use were not accounted for in the study because of its retrospective nature, he noted.
When asked to speculate on the mechanism behind the association between hyponatremia and poor outcomes, Dr. Crestanello said they are not well understood. "Obviously, hyponatremia is a marker for high-risk patients, but at the same time it is likely that it has pathophysiological effects on its own ... hyponatremia is also associated with changes in the neurohormonal milieu that, by itself, can have deleterious effects."
The analysis was based on data from electronic medical records, the Society of Thoracic Surgery database, and Social Security Death Index. Mean follow-up was 2.2 years.
The authors plan to analyze the effects that correcting preoperative hyponatremia has on outcomes of cardiac surgery. The current study was supported by a grant from Biogen Inc.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Preoperative Hyponatremia Points to Dismal Outcomes After Cardiac Surgery
NEW ORLEANS – Preoperative hyponatremia was common in patients undergoing cardiac surgery and associated with a dramatic increased the risk of death and surgical complications in a large retrospective analysis.
Of the 4,370 patients who underwent cardiac surgery between 2002 and 2009 at the Ohio State Medical Center in Columbus, 931 (21%) had hyponatremia, defined as serum sodium less than 135 mEq/L on at least one of three sodium tests obtained before surgery.
In unadjusted analysis, hyponatremic patients had significantly higher rates than did those without hyponatremia of early mortality (9% vs. 4%), late mortality (24% vs. 15.6%), longer mean hospital length of stay (12.6 days vs. 8.2 days), and operative complications (13% vs. 7%), Dr. Juan Crestanello and his colleagues reported in a poster at the annual meeting of the American College of Cardiology.
This isn’t all that surprising since hyponatremic patients were sicker at baseline, but the poor outcomes remained, even after adjustment for a slew of baseline clinical and operative variables.
In multivariable logistic regression analysis, preoperative hyponatremia was independently associated with a 31% increase in overall mortality, a 52% increase in early mortality, and a 56% increase in late mortality, said Dr. Crestanello, a thoracic surgeon at the medical center.
Hyponatremia also significantly increased the risk of operative complications by 30%, pulmonary complications by 73%, renal failure requiring dialysis by 64%, and hospital length of stay by 26%. Infectious and neurologic complications were not independently associated with preoperative hyponatremia.
"Hyponatremia identifies a group of patients at higher risk for cardiac surgery," Dr. Crestanello said in an interview. "It constitutes another tool to risk-stratify these patients and will help surgeons advice patients of their risk associated with surgery."
At baseline, patients with hyponatremia had a significantly lower mean ejection fraction than did patients without hyponatremia (39% vs. 46%), higher mean pulmonary artery pressure (32 mmHg vs. 28 mmHg), and higher incidence of comorbidities, including diabetes (47% vs. 34%), chronic obstructive pulmonary disease (24.5% vs. 18%), and history of a previous MI (44.5% vs. 35.6%).
Hyponatremic patients also had significantly higher New York Heart Association functional class, higher surgical risk as predicted by the European System for Cardiac Operative Risk Evaluation (19% vs. 9%) and underwent more complex surgical procedures including coronary artery bypass surgery with valve replacement and ventricular-assist device placement.
Their mean age was 62 years, 66.5% were male, and the mean sodium level was 134 mEq/L.
Sodium levels are one of the most common laboratory values measured and are routinely obtained preoperatively.
"In spite of being widely available, they are often overlooked," Dr. Crestanello said.
Data on other factors that may have influenced serum sodium like medications, glucose levels, and fluid use were not accounted for in the study because of its retrospective nature, he noted.
When asked to speculate on the mechanism behind the association between hyponatremia and poor outcomes, Dr. Crestanello said they are not well understood. "Obviously, hyponatremia is a marker for high-risk patients, but at the same time it is likely that it has pathophysiological effects on its own ... hyponatremia is also associated with changes in the neurohormonal milieu that, by itself, can have deleterious effects."
The analysis was based on data from electronic medical records, the Society of Thoracic Surgery database, and Social Security Death Index. Mean follow-up was 2.2 years.
The authors plan to analyze the effects that correcting preoperative hyponatremia has on outcomes of cardiac surgery. The current study was supported by a grant from Biogen Inc.
NEW ORLEANS – Preoperative hyponatremia was common in patients undergoing cardiac surgery and associated with a dramatic increased the risk of death and surgical complications in a large retrospective analysis.
Of the 4,370 patients who underwent cardiac surgery between 2002 and 2009 at the Ohio State Medical Center in Columbus, 931 (21%) had hyponatremia, defined as serum sodium less than 135 mEq/L on at least one of three sodium tests obtained before surgery.
In unadjusted analysis, hyponatremic patients had significantly higher rates than did those without hyponatremia of early mortality (9% vs. 4%), late mortality (24% vs. 15.6%), longer mean hospital length of stay (12.6 days vs. 8.2 days), and operative complications (13% vs. 7%), Dr. Juan Crestanello and his colleagues reported in a poster at the annual meeting of the American College of Cardiology.
This isn’t all that surprising since hyponatremic patients were sicker at baseline, but the poor outcomes remained, even after adjustment for a slew of baseline clinical and operative variables.
In multivariable logistic regression analysis, preoperative hyponatremia was independently associated with a 31% increase in overall mortality, a 52% increase in early mortality, and a 56% increase in late mortality, said Dr. Crestanello, a thoracic surgeon at the medical center.
Hyponatremia also significantly increased the risk of operative complications by 30%, pulmonary complications by 73%, renal failure requiring dialysis by 64%, and hospital length of stay by 26%. Infectious and neurologic complications were not independently associated with preoperative hyponatremia.
"Hyponatremia identifies a group of patients at higher risk for cardiac surgery," Dr. Crestanello said in an interview. "It constitutes another tool to risk-stratify these patients and will help surgeons advice patients of their risk associated with surgery."
At baseline, patients with hyponatremia had a significantly lower mean ejection fraction than did patients without hyponatremia (39% vs. 46%), higher mean pulmonary artery pressure (32 mmHg vs. 28 mmHg), and higher incidence of comorbidities, including diabetes (47% vs. 34%), chronic obstructive pulmonary disease (24.5% vs. 18%), and history of a previous MI (44.5% vs. 35.6%).
Hyponatremic patients also had significantly higher New York Heart Association functional class, higher surgical risk as predicted by the European System for Cardiac Operative Risk Evaluation (19% vs. 9%) and underwent more complex surgical procedures including coronary artery bypass surgery with valve replacement and ventricular-assist device placement.
Their mean age was 62 years, 66.5% were male, and the mean sodium level was 134 mEq/L.
Sodium levels are one of the most common laboratory values measured and are routinely obtained preoperatively.
"In spite of being widely available, they are often overlooked," Dr. Crestanello said.
Data on other factors that may have influenced serum sodium like medications, glucose levels, and fluid use were not accounted for in the study because of its retrospective nature, he noted.
When asked to speculate on the mechanism behind the association between hyponatremia and poor outcomes, Dr. Crestanello said they are not well understood. "Obviously, hyponatremia is a marker for high-risk patients, but at the same time it is likely that it has pathophysiological effects on its own ... hyponatremia is also associated with changes in the neurohormonal milieu that, by itself, can have deleterious effects."
The analysis was based on data from electronic medical records, the Society of Thoracic Surgery database, and Social Security Death Index. Mean follow-up was 2.2 years.
The authors plan to analyze the effects that correcting preoperative hyponatremia has on outcomes of cardiac surgery. The current study was supported by a grant from Biogen Inc.
NEW ORLEANS – Preoperative hyponatremia was common in patients undergoing cardiac surgery and associated with a dramatic increased the risk of death and surgical complications in a large retrospective analysis.
Of the 4,370 patients who underwent cardiac surgery between 2002 and 2009 at the Ohio State Medical Center in Columbus, 931 (21%) had hyponatremia, defined as serum sodium less than 135 mEq/L on at least one of three sodium tests obtained before surgery.
In unadjusted analysis, hyponatremic patients had significantly higher rates than did those without hyponatremia of early mortality (9% vs. 4%), late mortality (24% vs. 15.6%), longer mean hospital length of stay (12.6 days vs. 8.2 days), and operative complications (13% vs. 7%), Dr. Juan Crestanello and his colleagues reported in a poster at the annual meeting of the American College of Cardiology.
This isn’t all that surprising since hyponatremic patients were sicker at baseline, but the poor outcomes remained, even after adjustment for a slew of baseline clinical and operative variables.
In multivariable logistic regression analysis, preoperative hyponatremia was independently associated with a 31% increase in overall mortality, a 52% increase in early mortality, and a 56% increase in late mortality, said Dr. Crestanello, a thoracic surgeon at the medical center.
Hyponatremia also significantly increased the risk of operative complications by 30%, pulmonary complications by 73%, renal failure requiring dialysis by 64%, and hospital length of stay by 26%. Infectious and neurologic complications were not independently associated with preoperative hyponatremia.
"Hyponatremia identifies a group of patients at higher risk for cardiac surgery," Dr. Crestanello said in an interview. "It constitutes another tool to risk-stratify these patients and will help surgeons advice patients of their risk associated with surgery."
At baseline, patients with hyponatremia had a significantly lower mean ejection fraction than did patients without hyponatremia (39% vs. 46%), higher mean pulmonary artery pressure (32 mmHg vs. 28 mmHg), and higher incidence of comorbidities, including diabetes (47% vs. 34%), chronic obstructive pulmonary disease (24.5% vs. 18%), and history of a previous MI (44.5% vs. 35.6%).
Hyponatremic patients also had significantly higher New York Heart Association functional class, higher surgical risk as predicted by the European System for Cardiac Operative Risk Evaluation (19% vs. 9%) and underwent more complex surgical procedures including coronary artery bypass surgery with valve replacement and ventricular-assist device placement.
Their mean age was 62 years, 66.5% were male, and the mean sodium level was 134 mEq/L.
Sodium levels are one of the most common laboratory values measured and are routinely obtained preoperatively.
"In spite of being widely available, they are often overlooked," Dr. Crestanello said.
Data on other factors that may have influenced serum sodium like medications, glucose levels, and fluid use were not accounted for in the study because of its retrospective nature, he noted.
When asked to speculate on the mechanism behind the association between hyponatremia and poor outcomes, Dr. Crestanello said they are not well understood. "Obviously, hyponatremia is a marker for high-risk patients, but at the same time it is likely that it has pathophysiological effects on its own ... hyponatremia is also associated with changes in the neurohormonal milieu that, by itself, can have deleterious effects."
The analysis was based on data from electronic medical records, the Society of Thoracic Surgery database, and Social Security Death Index. Mean follow-up was 2.2 years.
The authors plan to analyze the effects that correcting preoperative hyponatremia has on outcomes of cardiac surgery. The current study was supported by a grant from Biogen Inc.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: In adjusted analysis, preoperative hyponatremia was independently associated with a 52% increase in early mortality and a 56% increase in late mortality.
Data Source: Retrospective analysis of 4,370 patients undergoing cardiac surgery.
Disclosures: The analysis was supported by a research grant from Biogen Inc.
Surgeon Recruitment Plagues Rural Hospitals
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
Surgeon Recruitment Plagues Rural Hospitals
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
Surgeon Recruitment Plagues Rural Hospitals
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
DETROIT – Rural hospitals will need to devise unique strategies to enhance hiring and retention in the face of a looming shortage of almost 30,000 surgeons over the next 20 years.
“We think this shortage will result in competition between urban and rural hospitals, maybe perpetuating in bidding wars,” Dr. Thomas E. Williams Jr. said at the annual meeting of the Central Surgical Association.
“In a sense, this shortage could be a perfect storm; an imperative for both the urban and rural hospitals we see in America today.”
The researchers previously reported that an estimated 101,838 surgeons will need to be trained by 2030 to address a projected shortage in the United States of 29,138 surgeons in seven surgical specialties: obstetrics and gynecology, orthopedic surgery, general surgery, otolaryngology, urology, neurosurgery,
and thoracic surgery (Ann. Surg. 2009;250:590-7). I’ve searched and can’t find the print reference. Help?—EW The trick is to search by the article name in Google. I got abut 5 different versions that way./CNW»
The current analysis went one step further, focusing on the average recruitment needs for the seven specialties in rural vs. urban hospitals in light of the projected U.S. population of 364 million by 2030. The model assumed that there will be equal population growth in urban and rural areas; that rural hospitals will need to recruit obstetric/gynecologic, orthopedic, and general surgeons; and that the percentage of the population receiving care at urban and rural hospitals will remain constant, Dr. Williams explained.
Currently, the American Hospital Association estimates that there are 3,012 urban hospitals in the United States. serving 82% of the population or 253 million Americans, and 1,998 rural hospitals serving 18% or 56 million Americans.
Based on these assumptions, the total number of surgical hires over the next 19 years will be 83,507 for urban hospitals and 13,953 for rural hospitals. This means urban hospitals must hire and retain 4,175 surgeons per year or 27.7 surgeons per hospital, while rural hospitals will need to hire 698 surgeons per year or 7 surgeons per hospital, said Dr. Williams «not facs»of the department of surgery at Ohio State University in Columbus.
While the recruitment goals for urban hospitals might appear more daunting, rural hospitals are already facing a dramatic loss of general surgeons.
“In rural hospitals, general surgery is essential,” he said. “[General surgeons] account for 60% of the revenue. What’s happening now is that about 34% of general surgeons are notifying their administrators of retiring or leaving in 2 years. Thirty-three percent of rural hospitals are recruiting now.”
Factors that might make rural recruitment more difficult include professional and social isolation, cross coverage, insufficient training for the variety of procedures performed and pathologies encountered, and women’s preference for urban areas, he said.
Factors that positively influence rural recruitment include the chance to be a critical part of the community, independence, the wide spectrum of procedures, and hailing from a rural area.
One strategy that can tip a surgeon toward a rural hospital is doing a residency in a rural training program. The researchers estimate that half of general surgery residents who rotate through such a program will go on to practice in rural towns.
“It’s to the advantage of rural hospital administrators to establish rotations with medical schools in their hospitals, so they can have the opportunity to recruit some of the people that rotate through their rural hospitals,” Dr. Williams said.
Consideration of the needs of the surgeon’s family is another factor. Typical
ly, this will be a two-income family that values education and will need either good public schools or the means to pay for private schools. Most couples will also have educational debts, some as high as $400,000 for a two-physician couple. Thus, educational loan repayment could be a potential “trump card” for rural hospitals in the future, he said.
Rural hospitals are already throwing out the welcome mat. Most offer hiring incentives such as a relocation allowance; signing bonus; health, disability, and life insurance; and malpractice coverage. Educational loan forgiveness was offered by 38% of hospitals last year, up 7% from 2009, Dr. Williams said. Still, competition for new hires is fierce.
“In many general surgery programs in the United States, senior residents are receiving as many as 50 offers for employment today,” he said.
To illustrate the point, Dr. Williams showed a recent classified ad in the New England Journal of Medicine offering a starting base salary of $600,000 for an orthopedic surgeon in coastal Georgia plus a sign-on and relocation bonus, full benefits, and a high-yield bonus. This is nearly double the median starting salary of $370,000 for an orthopedic surgeon identified in a recent Cejka Executive Search survey, he pointed out.
Median starting salaries for the seven surgical specialties studied ranged from a low of $260,000 for a general surgeon to a high of $450,000 for a neurosurgeon in the Cejka survey.
Invited discussant Dr. Nathaniel Soper, «facs»chair of the department of surgery at Northwestern University in Chicago, said, “It may end up being ultimately that these bidding wars are good for general surgeons, but I think it’s not going to be good for the population we serve, as there is going to be a shortage unless something is done.”
Dr. Sober suggested that the basic problem is not so much the division between rural vs. urban, but the supply of surgeons, and asked what can be done to meet the estimated shortfall. He also questioned the model’s assumption that the population would remain equal in rural and urban areas.
Co-author and colleague Dr. Bhagwan Satiani replied that the analysis included a simplified version of the federal model used to calculate supply and demand, but added that every projection in the last 50-75 years has been wrong. “You have to look at this model and say, ‘This is the best we can do right now,” he said.
According to Dr. Satiani, one of the best ways to increase the rural surgeon supply is through a comprehensive medical school rural program (MSRP). “If you took 10 medical students out of the class and put them into the MSRP pro
gram, you could double the number of rural surgeons. That’s how important that is,” said Dr. Satiani, «facs»medical director of the vascular surgery laboratory and a professor of clinical surgery at Ohio State University.
A recently published report from the Physician Shortage Area Program (PSAP) at Jefferson Medical College in Philadelphia provides a similar calculation for rural physicians and reports that 79%-87% of graduates from the two MSRPs with long-range rural outcomes – the PSAP and University of Minnesota at Duluth – remained in rural practice for up to 20 years (Acad. Med. 2011;86:272). It also notes that the Affordable Care Act authorized a new Rural Physician Training Grants program to provide grants to medical schools to develop or expand MSRPs.
Only 25 of the roughly 250 medical schools have general surgery programs, and just 10% of these could be considered programs that attract rural surgeons, according to Dr. Satiani. “I think American surgery is going to have to give this a separate tract within residency programs.”
Audience member Dr. Mark Malangoni, «facs»associate executive director of the American Board of Surgery in Philadelphia, pointed out that in such rural areas as Wyoming, the closest medical school is more than 1,000 miles away in Washington state.
He suggested that one way to link rural hospitals and to counteract the professional isolation experienced by some rural physicians is through Web-based surgeon-to-surgeon consultations, an idea strongly supported by a recent survey of American College of Surgeons fellows.
If a new medical school were located in a rural area, Dr. Satiani said it could feed two to three nearby states, but not one of the new medical schools built in the last 5 years has been in truly rural areas.
Finally, several audience members suggested that efforts need to be made to eliminate the perception among residents that surgical specialists are somehow better than general surgeons.
“It’s the one-on-one thing that’s going to work with the residents, because all they see are these super-specialists,” Dr. Satiani said. “I think it has to come from the programs and the leadership; defining general surgery better, even going as far as changing the name, if that becomes an important issue.”
When asked in an interview what that new name might be, Dr. Satiani said the terms “master surgeon” and “omni surgeon” have been floated, with master surgeon more likely to resonate with the general public.
I have checked the following facts in my story: (Please initial each.)
The authors reported no conflicts of interest.
TAVR Usable in Older, High-Risk Patients
NEW ORLEANS Transcatheter aortic valve replacement was associated with the same survival rates at 1 year as was found in conventional surgery for older, high-risk patients who suffered from severe, symptomatic aortic stenosis, according to the results of the PARTNER trial.
All-cause mortality at 30 days favored the use of transcatheter aortic valve replacement (TAVR) at 3.4%, compared with 6.5% for open surgery, and was similar at 1 year (24% vs, 27%, respectively).
The difference at 1 year reached the trial's prespecified noninferiority margin with a P value of .001.
"We already learned from the previous cohort that TAVR is the standard of care for patients who can't tolerate surgery. So this [finding] opens up a new set of patients who may very well benefit as much with TAVR as with the gold standard surgery," coprincipal investigator Dr. Craig B. Smith said at the annual meeting of the American College of Cardiology.
However, The stroke rate with TAVR as seen in the industry-sponsored PARTNER (Placement of Aortic Transcatheter Valve) trial, turned out to be twice the rate for these patients as that observed with conventional surgical repair.
Stroke plus transient ischemic attack (TIA) rates were significantly more frequent with TAVR than surgery at both 30 days (5.5% vs. 2.4%) and 1 year (8.3% vs. 4.3%).
When only major strokes were compared, the difference was not significant between TAVR and convential surgery at 30 days (3.8% vs. 2.1%) or 1 year (5.1% vs. 2.4%), said Dr. Smith, chief of cardiothoracic surgery at New York Presbyterian Hospital/Columbia University Medical Center in New York City.
Notably, patients who un?derwent conventional surgery were significantly more likely than TAVR patients to experience major bleeding at 30 days (19.5% vs. 9.3%) and 1 year (26% vs. 15%), as well as new atrial fibrillation at both 30 days (16% vs. 8.6%) and 1 year (17% vs. 12%).
An examination of echocardiographic findings indicated a small hemodynamic benefit ocurred with TAVR vs. surgery at 1 year, but there was significantly increased paravalvular aortic reÂgurgitation at 30 days, 6 months, and 1 year.
"TAVR and AVR [aortic valve replacement] are both acceptable therapies in these high-risk patients; differing periprocedural hazards should influence case-based decision making," Dr. Smith said.
Dr. David Moliterno, chair of the intervention program (i2 Summit) at the meeting, told reporters that they were witnessing histoÂry in the making.
"This will probably be seen as one of the biggest steps in cardiovascular medicine, as far as intervention is concerned, potentially in our lifetime," said Dr. Moliterno, chief of cardiovascular medicine at the University of Kentucky, Lexington.
"If we look back to balloon angioÂplasty, the advent of stents and drug-eluting stents, this will be seen as the next major turning point."
Last year, the PARTNER trial investigators reported a 20% survival benefit at 1 year in a separate cohort of 358 inoperable patients with severe aortic stenosis who underwent transfemoral TAVR vs. standard therapy, including balloon aortic valvuloplasty (N. Engl. J. Med. 2010;363:1597-607). TAVR was associated with significantly more major vascular complications (16% vs. 1%) and a higher incidence of major strokes (5% vs. 1%).
The current portion of PARTNER randomly assigned 699 patients at 26 centers to surgery or TAVR. These patients were treated using the transfemoral approach in 492 cases and the transapical approach in 207.
Severe stenosis was defined as an aortic valve area of less than 0.8 cm2 and mean aortic valve gradient of more than 40 mm Hg or a peak aortic jet velocity of more than 4.0 m/second.
The patients in the trial had a New York Heart Association heart failure class II or greater, and they also had a predicted risk of operative mortality of at least 15% as determined by the site surgeon and cardiologist, coupled with a Society of Thoracic Surgery (STS) score of at least 10.
The mean age of the patients in the study was 83 years, and 94% of them were NYHA class III or IV. In all, 42 patients were not treated as assigned, Dr. Smith said.
All-cause mortality at 1 year was simÂilar for the transfemoral TAVR subgroup, at 22.2% and 26.4% for surgery, as well as for the transapical TAVR subgroup (29% vs. 28%, respectively).
A preliminary subgroup analysis sugÂgested that there may be a possible benefit found with TAVR in women and in patients without prior coronary artery bypass surgery, but Dr. Smith said that those results should be interÂpreted cautiously.
Overall, the TAVR mortality of 3.4% at 30 days was the lowest reported in any series, despite the use of an early-generation device and limited previous operator experience, he said, noting that nine of the participating centers had never performed TAVR before the trial.
Symptom improvement, including NYHA class and 6-minute walk distance, favored TAVR at 30 days and was similar to conventional surgery at 1 year, Dr. Moliterno said.
Coinvestigator Dr. Murat Tuzcu, vice chair of the department of cardiovascu?lar medicine at the Cleveland Clinic, stressed that the results were accomplished only through unprecedented teamwork among cardiologists, surgeons, and imaging experts, who conÂsulted on each case in the trial.
"I want to emphasize that if we fail to pay equal attention to what we have done in this trial after the device is approved, I don't think we will be able to replicate the same results," he said.
Several speakers at the press conference noted the balancing act that all clinicians will face regarding public demand for the new procedure.
Dr. Michael Crawford, chief of clinical cardiology at the University of California, San Francisco, observed that centers will face substantial up-front costs in the adoption of TAVR, including hybrid surgical/interventional suites, and that this will restrict initial uptake to high-volume centers of excellence.
The 3.4% mortality rate represents an “amazing effort, particularly in the use of the larger, first-generation device, said invited discussant Dr. Martyn Thomas, clinical director of cardiothoracic services at St. Thomas Hospital, London.
The delivery catheters used in PARTNER are sized at 22 and 24 French, which corresponds to an outside diamÂeter of 7-8 mm.
The size of catheters has been decreased down to 16-Fr in Europe, where more than 5,000 TAVR procedures have been done and where both the Edwards Lifesciences Corp.'s Sapien valve that was used in PARTNER and the Medtronic Inc.'s CoreValve are already approved for commercial use.
Recruitment began in February for the PARTNER II trial that is evaluating the smaller Edwards Sapien XT device and the later generation NovaFlex delivery system among inoperable patients with symptomatic severe aortic stenosis. The trial is expected to enroll 600 patients, and is targeted for primary completion in December 2011.
When asked whether the advent of newer, thinner devices will mean adoption in patients with lower risk, Dr. Smith replied that the adoption of TAVR will "march steadily down the risk categories."
Edwards Lifesciences sponsored the trial. Dr. Smith and his coauthors reported no conflicts of interest.
NEW ORLEANS Transcatheter aortic valve replacement was associated with the same survival rates at 1 year as was found in conventional surgery for older, high-risk patients who suffered from severe, symptomatic aortic stenosis, according to the results of the PARTNER trial.
All-cause mortality at 30 days favored the use of transcatheter aortic valve replacement (TAVR) at 3.4%, compared with 6.5% for open surgery, and was similar at 1 year (24% vs, 27%, respectively).
The difference at 1 year reached the trial's prespecified noninferiority margin with a P value of .001.
"We already learned from the previous cohort that TAVR is the standard of care for patients who can't tolerate surgery. So this [finding] opens up a new set of patients who may very well benefit as much with TAVR as with the gold standard surgery," coprincipal investigator Dr. Craig B. Smith said at the annual meeting of the American College of Cardiology.
However, The stroke rate with TAVR as seen in the industry-sponsored PARTNER (Placement of Aortic Transcatheter Valve) trial, turned out to be twice the rate for these patients as that observed with conventional surgical repair.
Stroke plus transient ischemic attack (TIA) rates were significantly more frequent with TAVR than surgery at both 30 days (5.5% vs. 2.4%) and 1 year (8.3% vs. 4.3%).
When only major strokes were compared, the difference was not significant between TAVR and convential surgery at 30 days (3.8% vs. 2.1%) or 1 year (5.1% vs. 2.4%), said Dr. Smith, chief of cardiothoracic surgery at New York Presbyterian Hospital/Columbia University Medical Center in New York City.
Notably, patients who un?derwent conventional surgery were significantly more likely than TAVR patients to experience major bleeding at 30 days (19.5% vs. 9.3%) and 1 year (26% vs. 15%), as well as new atrial fibrillation at both 30 days (16% vs. 8.6%) and 1 year (17% vs. 12%).
An examination of echocardiographic findings indicated a small hemodynamic benefit ocurred with TAVR vs. surgery at 1 year, but there was significantly increased paravalvular aortic reÂgurgitation at 30 days, 6 months, and 1 year.
"TAVR and AVR [aortic valve replacement] are both acceptable therapies in these high-risk patients; differing periprocedural hazards should influence case-based decision making," Dr. Smith said.
Dr. David Moliterno, chair of the intervention program (i2 Summit) at the meeting, told reporters that they were witnessing histoÂry in the making.
"This will probably be seen as one of the biggest steps in cardiovascular medicine, as far as intervention is concerned, potentially in our lifetime," said Dr. Moliterno, chief of cardiovascular medicine at the University of Kentucky, Lexington.
"If we look back to balloon angioÂplasty, the advent of stents and drug-eluting stents, this will be seen as the next major turning point."
Last year, the PARTNER trial investigators reported a 20% survival benefit at 1 year in a separate cohort of 358 inoperable patients with severe aortic stenosis who underwent transfemoral TAVR vs. standard therapy, including balloon aortic valvuloplasty (N. Engl. J. Med. 2010;363:1597-607). TAVR was associated with significantly more major vascular complications (16% vs. 1%) and a higher incidence of major strokes (5% vs. 1%).
The current portion of PARTNER randomly assigned 699 patients at 26 centers to surgery or TAVR. These patients were treated using the transfemoral approach in 492 cases and the transapical approach in 207.
Severe stenosis was defined as an aortic valve area of less than 0.8 cm2 and mean aortic valve gradient of more than 40 mm Hg or a peak aortic jet velocity of more than 4.0 m/second.
The patients in the trial had a New York Heart Association heart failure class II or greater, and they also had a predicted risk of operative mortality of at least 15% as determined by the site surgeon and cardiologist, coupled with a Society of Thoracic Surgery (STS) score of at least 10.
The mean age of the patients in the study was 83 years, and 94% of them were NYHA class III or IV. In all, 42 patients were not treated as assigned, Dr. Smith said.
All-cause mortality at 1 year was simÂilar for the transfemoral TAVR subgroup, at 22.2% and 26.4% for surgery, as well as for the transapical TAVR subgroup (29% vs. 28%, respectively).
A preliminary subgroup analysis sugÂgested that there may be a possible benefit found with TAVR in women and in patients without prior coronary artery bypass surgery, but Dr. Smith said that those results should be interÂpreted cautiously.
Overall, the TAVR mortality of 3.4% at 30 days was the lowest reported in any series, despite the use of an early-generation device and limited previous operator experience, he said, noting that nine of the participating centers had never performed TAVR before the trial.
Symptom improvement, including NYHA class and 6-minute walk distance, favored TAVR at 30 days and was similar to conventional surgery at 1 year, Dr. Moliterno said.
Coinvestigator Dr. Murat Tuzcu, vice chair of the department of cardiovascu?lar medicine at the Cleveland Clinic, stressed that the results were accomplished only through unprecedented teamwork among cardiologists, surgeons, and imaging experts, who conÂsulted on each case in the trial.
"I want to emphasize that if we fail to pay equal attention to what we have done in this trial after the device is approved, I don't think we will be able to replicate the same results," he said.
Several speakers at the press conference noted the balancing act that all clinicians will face regarding public demand for the new procedure.
Dr. Michael Crawford, chief of clinical cardiology at the University of California, San Francisco, observed that centers will face substantial up-front costs in the adoption of TAVR, including hybrid surgical/interventional suites, and that this will restrict initial uptake to high-volume centers of excellence.
The 3.4% mortality rate represents an “amazing effort, particularly in the use of the larger, first-generation device, said invited discussant Dr. Martyn Thomas, clinical director of cardiothoracic services at St. Thomas Hospital, London.
The delivery catheters used in PARTNER are sized at 22 and 24 French, which corresponds to an outside diamÂeter of 7-8 mm.
The size of catheters has been decreased down to 16-Fr in Europe, where more than 5,000 TAVR procedures have been done and where both the Edwards Lifesciences Corp.'s Sapien valve that was used in PARTNER and the Medtronic Inc.'s CoreValve are already approved for commercial use.
Recruitment began in February for the PARTNER II trial that is evaluating the smaller Edwards Sapien XT device and the later generation NovaFlex delivery system among inoperable patients with symptomatic severe aortic stenosis. The trial is expected to enroll 600 patients, and is targeted for primary completion in December 2011.
When asked whether the advent of newer, thinner devices will mean adoption in patients with lower risk, Dr. Smith replied that the adoption of TAVR will "march steadily down the risk categories."
Edwards Lifesciences sponsored the trial. Dr. Smith and his coauthors reported no conflicts of interest.
NEW ORLEANS Transcatheter aortic valve replacement was associated with the same survival rates at 1 year as was found in conventional surgery for older, high-risk patients who suffered from severe, symptomatic aortic stenosis, according to the results of the PARTNER trial.
All-cause mortality at 30 days favored the use of transcatheter aortic valve replacement (TAVR) at 3.4%, compared with 6.5% for open surgery, and was similar at 1 year (24% vs, 27%, respectively).
The difference at 1 year reached the trial's prespecified noninferiority margin with a P value of .001.
"We already learned from the previous cohort that TAVR is the standard of care for patients who can't tolerate surgery. So this [finding] opens up a new set of patients who may very well benefit as much with TAVR as with the gold standard surgery," coprincipal investigator Dr. Craig B. Smith said at the annual meeting of the American College of Cardiology.
However, The stroke rate with TAVR as seen in the industry-sponsored PARTNER (Placement of Aortic Transcatheter Valve) trial, turned out to be twice the rate for these patients as that observed with conventional surgical repair.
Stroke plus transient ischemic attack (TIA) rates were significantly more frequent with TAVR than surgery at both 30 days (5.5% vs. 2.4%) and 1 year (8.3% vs. 4.3%).
When only major strokes were compared, the difference was not significant between TAVR and convential surgery at 30 days (3.8% vs. 2.1%) or 1 year (5.1% vs. 2.4%), said Dr. Smith, chief of cardiothoracic surgery at New York Presbyterian Hospital/Columbia University Medical Center in New York City.
Notably, patients who un?derwent conventional surgery were significantly more likely than TAVR patients to experience major bleeding at 30 days (19.5% vs. 9.3%) and 1 year (26% vs. 15%), as well as new atrial fibrillation at both 30 days (16% vs. 8.6%) and 1 year (17% vs. 12%).
An examination of echocardiographic findings indicated a small hemodynamic benefit ocurred with TAVR vs. surgery at 1 year, but there was significantly increased paravalvular aortic reÂgurgitation at 30 days, 6 months, and 1 year.
"TAVR and AVR [aortic valve replacement] are both acceptable therapies in these high-risk patients; differing periprocedural hazards should influence case-based decision making," Dr. Smith said.
Dr. David Moliterno, chair of the intervention program (i2 Summit) at the meeting, told reporters that they were witnessing histoÂry in the making.
"This will probably be seen as one of the biggest steps in cardiovascular medicine, as far as intervention is concerned, potentially in our lifetime," said Dr. Moliterno, chief of cardiovascular medicine at the University of Kentucky, Lexington.
"If we look back to balloon angioÂplasty, the advent of stents and drug-eluting stents, this will be seen as the next major turning point."
Last year, the PARTNER trial investigators reported a 20% survival benefit at 1 year in a separate cohort of 358 inoperable patients with severe aortic stenosis who underwent transfemoral TAVR vs. standard therapy, including balloon aortic valvuloplasty (N. Engl. J. Med. 2010;363:1597-607). TAVR was associated with significantly more major vascular complications (16% vs. 1%) and a higher incidence of major strokes (5% vs. 1%).
The current portion of PARTNER randomly assigned 699 patients at 26 centers to surgery or TAVR. These patients were treated using the transfemoral approach in 492 cases and the transapical approach in 207.
Severe stenosis was defined as an aortic valve area of less than 0.8 cm2 and mean aortic valve gradient of more than 40 mm Hg or a peak aortic jet velocity of more than 4.0 m/second.
The patients in the trial had a New York Heart Association heart failure class II or greater, and they also had a predicted risk of operative mortality of at least 15% as determined by the site surgeon and cardiologist, coupled with a Society of Thoracic Surgery (STS) score of at least 10.
The mean age of the patients in the study was 83 years, and 94% of them were NYHA class III or IV. In all, 42 patients were not treated as assigned, Dr. Smith said.
All-cause mortality at 1 year was simÂilar for the transfemoral TAVR subgroup, at 22.2% and 26.4% for surgery, as well as for the transapical TAVR subgroup (29% vs. 28%, respectively).
A preliminary subgroup analysis sugÂgested that there may be a possible benefit found with TAVR in women and in patients without prior coronary artery bypass surgery, but Dr. Smith said that those results should be interÂpreted cautiously.
Overall, the TAVR mortality of 3.4% at 30 days was the lowest reported in any series, despite the use of an early-generation device and limited previous operator experience, he said, noting that nine of the participating centers had never performed TAVR before the trial.
Symptom improvement, including NYHA class and 6-minute walk distance, favored TAVR at 30 days and was similar to conventional surgery at 1 year, Dr. Moliterno said.
Coinvestigator Dr. Murat Tuzcu, vice chair of the department of cardiovascu?lar medicine at the Cleveland Clinic, stressed that the results were accomplished only through unprecedented teamwork among cardiologists, surgeons, and imaging experts, who conÂsulted on each case in the trial.
"I want to emphasize that if we fail to pay equal attention to what we have done in this trial after the device is approved, I don't think we will be able to replicate the same results," he said.
Several speakers at the press conference noted the balancing act that all clinicians will face regarding public demand for the new procedure.
Dr. Michael Crawford, chief of clinical cardiology at the University of California, San Francisco, observed that centers will face substantial up-front costs in the adoption of TAVR, including hybrid surgical/interventional suites, and that this will restrict initial uptake to high-volume centers of excellence.
The 3.4% mortality rate represents an “amazing effort, particularly in the use of the larger, first-generation device, said invited discussant Dr. Martyn Thomas, clinical director of cardiothoracic services at St. Thomas Hospital, London.
The delivery catheters used in PARTNER are sized at 22 and 24 French, which corresponds to an outside diamÂeter of 7-8 mm.
The size of catheters has been decreased down to 16-Fr in Europe, where more than 5,000 TAVR procedures have been done and where both the Edwards Lifesciences Corp.'s Sapien valve that was used in PARTNER and the Medtronic Inc.'s CoreValve are already approved for commercial use.
Recruitment began in February for the PARTNER II trial that is evaluating the smaller Edwards Sapien XT device and the later generation NovaFlex delivery system among inoperable patients with symptomatic severe aortic stenosis. The trial is expected to enroll 600 patients, and is targeted for primary completion in December 2011.
When asked whether the advent of newer, thinner devices will mean adoption in patients with lower risk, Dr. Smith replied that the adoption of TAVR will "march steadily down the risk categories."
Edwards Lifesciences sponsored the trial. Dr. Smith and his coauthors reported no conflicts of interest.
Transcatheter Valve Replacement Skips Sticker Shock
NEW ORLEANS – The cost of transcatheter aortic valve replacement among patients with inoperable severe aortic stenosis is in line with the cost of other accepted cardiovascular procedures, according to an economic analysis of the PARTNER trial.
The index hospitalization costs were higher with TAVR, but the reduction in subsequent hospitalizations, and the projected gain in survival, associated with the procedure yielded overall lifetime cost-effectiveness. “In this extremely high-risk population, an elderly population, the intervention is adding roughly 2 years of life, and that is the return on investment,” principal investigator Dr. Matthew Reynolds said at the meeting. The cost-effectiveness ratio “works out to just over $50,000 per life-year gained.”
Efficacy data for the same 358 inoperable patients, known as cohort B, showed a 20% survival benefit with TAVR at 1 year, compared with standard medical therapy, including balloon aortic valvuloplasty (N. Engl. J. Med. 2010; 363:1597-1607).
To determine the economic value of the procedure, Dr. Reynolds and his colleagues assessed lifetime incremental cost-effectiveness ratios (ICERs) and lifetime incremental costs per QALY using hospital billing data or MEDPAR when bills were unavailable. Costs from the last 6 months for surviving patients were used to project future costs beyond 12 months, while parametric survival models fit to the trial data were used to extrapolate patient-level life expectancy beyond the follow-up period.
The initial $78,540 price tag for TAVR includes $42,806 for procedural costs, based on an estimated cost of $30,000 for the investigational Edwards Sapien valve; $30,756 for nonprocedural expenses; and $4,978 for physician fees, said Dr. Reynolds, director of the Economics and Quality of Life Research Center at the Harvard Clinical Research Institute, Boston. Twelve-month follow-up costs were $23,372 higher for patients treated with standard medical therapy. This was a result of significantly more hospitalizations in the control group than in the TAVR group (2.15 vs. 1.02), mainly due to cardiovascular causes (1.7 vs. 0.50).
The estimated life expectancy was 3.1 years for TAVR patients and 1.2 years fortpatients treated with medical therapy, or a difference of 1.9 years. The lifetime incremental cost per patient was $79,837, and the lifetime incremental gain in life expectancy was 1.59 years. This translated into an ICER of $50,212 per life-year gained and $61,889 per QALY, he said.
On the basis of the data, TAVR in this older inoperable cohort falls very close to published cost-effectiveness estimates for implantable defibrillators and atrial fibrillation ablation, and is actually lower than current estimates for hemodialysis or percutaneous coronary intervention for stable coronary artery disease, Dr. Reynolds said.
Edwards Lifesciences provided grant support for the analysis.
NEW ORLEANS – The cost of transcatheter aortic valve replacement among patients with inoperable severe aortic stenosis is in line with the cost of other accepted cardiovascular procedures, according to an economic analysis of the PARTNER trial.
The index hospitalization costs were higher with TAVR, but the reduction in subsequent hospitalizations, and the projected gain in survival, associated with the procedure yielded overall lifetime cost-effectiveness. “In this extremely high-risk population, an elderly population, the intervention is adding roughly 2 years of life, and that is the return on investment,” principal investigator Dr. Matthew Reynolds said at the meeting. The cost-effectiveness ratio “works out to just over $50,000 per life-year gained.”
Efficacy data for the same 358 inoperable patients, known as cohort B, showed a 20% survival benefit with TAVR at 1 year, compared with standard medical therapy, including balloon aortic valvuloplasty (N. Engl. J. Med. 2010; 363:1597-1607).
To determine the economic value of the procedure, Dr. Reynolds and his colleagues assessed lifetime incremental cost-effectiveness ratios (ICERs) and lifetime incremental costs per QALY using hospital billing data or MEDPAR when bills were unavailable. Costs from the last 6 months for surviving patients were used to project future costs beyond 12 months, while parametric survival models fit to the trial data were used to extrapolate patient-level life expectancy beyond the follow-up period.
The initial $78,540 price tag for TAVR includes $42,806 for procedural costs, based on an estimated cost of $30,000 for the investigational Edwards Sapien valve; $30,756 for nonprocedural expenses; and $4,978 for physician fees, said Dr. Reynolds, director of the Economics and Quality of Life Research Center at the Harvard Clinical Research Institute, Boston. Twelve-month follow-up costs were $23,372 higher for patients treated with standard medical therapy. This was a result of significantly more hospitalizations in the control group than in the TAVR group (2.15 vs. 1.02), mainly due to cardiovascular causes (1.7 vs. 0.50).
The estimated life expectancy was 3.1 years for TAVR patients and 1.2 years fortpatients treated with medical therapy, or a difference of 1.9 years. The lifetime incremental cost per patient was $79,837, and the lifetime incremental gain in life expectancy was 1.59 years. This translated into an ICER of $50,212 per life-year gained and $61,889 per QALY, he said.
On the basis of the data, TAVR in this older inoperable cohort falls very close to published cost-effectiveness estimates for implantable defibrillators and atrial fibrillation ablation, and is actually lower than current estimates for hemodialysis or percutaneous coronary intervention for stable coronary artery disease, Dr. Reynolds said.
Edwards Lifesciences provided grant support for the analysis.
NEW ORLEANS – The cost of transcatheter aortic valve replacement among patients with inoperable severe aortic stenosis is in line with the cost of other accepted cardiovascular procedures, according to an economic analysis of the PARTNER trial.
The index hospitalization costs were higher with TAVR, but the reduction in subsequent hospitalizations, and the projected gain in survival, associated with the procedure yielded overall lifetime cost-effectiveness. “In this extremely high-risk population, an elderly population, the intervention is adding roughly 2 years of life, and that is the return on investment,” principal investigator Dr. Matthew Reynolds said at the meeting. The cost-effectiveness ratio “works out to just over $50,000 per life-year gained.”
Efficacy data for the same 358 inoperable patients, known as cohort B, showed a 20% survival benefit with TAVR at 1 year, compared with standard medical therapy, including balloon aortic valvuloplasty (N. Engl. J. Med. 2010; 363:1597-1607).
To determine the economic value of the procedure, Dr. Reynolds and his colleagues assessed lifetime incremental cost-effectiveness ratios (ICERs) and lifetime incremental costs per QALY using hospital billing data or MEDPAR when bills were unavailable. Costs from the last 6 months for surviving patients were used to project future costs beyond 12 months, while parametric survival models fit to the trial data were used to extrapolate patient-level life expectancy beyond the follow-up period.
The initial $78,540 price tag for TAVR includes $42,806 for procedural costs, based on an estimated cost of $30,000 for the investigational Edwards Sapien valve; $30,756 for nonprocedural expenses; and $4,978 for physician fees, said Dr. Reynolds, director of the Economics and Quality of Life Research Center at the Harvard Clinical Research Institute, Boston. Twelve-month follow-up costs were $23,372 higher for patients treated with standard medical therapy. This was a result of significantly more hospitalizations in the control group than in the TAVR group (2.15 vs. 1.02), mainly due to cardiovascular causes (1.7 vs. 0.50).
The estimated life expectancy was 3.1 years for TAVR patients and 1.2 years fortpatients treated with medical therapy, or a difference of 1.9 years. The lifetime incremental cost per patient was $79,837, and the lifetime incremental gain in life expectancy was 1.59 years. This translated into an ICER of $50,212 per life-year gained and $61,889 per QALY, he said.
On the basis of the data, TAVR in this older inoperable cohort falls very close to published cost-effectiveness estimates for implantable defibrillators and atrial fibrillation ablation, and is actually lower than current estimates for hemodialysis or percutaneous coronary intervention for stable coronary artery disease, Dr. Reynolds said.
Edwards Lifesciences provided grant support for the analysis.