User login
Doctors Push Bill to Avert DXA Cuts
Without Congressional action, Medicare payments for dual-energy x-ray absorptiometry will be cut in about half at the beginning of 2012.
But a small, bipartisan group of lawmakers in the House and Senate is pushing to extend DXA payment rates, which were passed as part of the Affordable Care Act and are set to expire at the end of this year, through 2013. Under the ACA, Congress instructed officials at the Centers for Medicare and Medicaid Services to increase DXA payments to 70% of the rate paid by Medicare in 2006.
The Preservation of Access to Osteoporosis Testing for Medicare Beneficiaries Act of 2011 (H.R. 2020/S. 1096) was introduced at the end of May; it would keep the current DXA payment rate in place for 2 years.
Rep. Michael Burgess (R-Tex.), one of the bill’s sponsors, said that cutting DXA payments is shortsighted. "Osteoporosis and related bone diseases pose a public health issue of enormous proportions, affecting millions of Americans and costing billions of dollars," he said in a statement. "As a physician, I diagnosed and treated many patients during my 25 years of practicing medicine in Texas, and I saw firsthand the way osteoporosis affects patients and their families. The more we can do to promote and encourage education, awareness, and prevention, the better. Why Medicare will pay for a fracture, but not reimburse a reasonable amount for a scan that can prevent that fracture, is beyond me."
Medicare began cutting DXA payments in 2007, after Congress included bone densitometry among a group of high-cost imaging services that were slashed as part of the Deficit Reduction Act of 2005. Since then, physicians have been struggling to cover their costs as reimbursement steadily declined from around $148 per scan in 2006 to about $54 in 2010. Exacerbating the problem is that private insurers have largely followed Medicare’s lead, ratcheting down their reimbursements as well. The ACA brought DXA payments up to about $98.
Physicians’ organizations, including the American College of Rheumatology (ACR) and the American Association of Clinical Endocrinologists (AACE), are urging lawmakers to pass an extension of the current DXA payment rate
Dr. Timothy J. Laing, government affairs committee chair for the ACR and a rheumatologist at the University of Michigan, Ann Arbor, said that if the reimbursement for the test falls below current levels, it will become economically unsustainable for physicians to provide the test in their offices.
Patients still will be able to get a DXA scan in the hospital, but there are downsides to that limited access, Dr. Laing said. Patients are far more likely to get the test if it can be done at the time it’s recommended, he said, adding that providing DXA scans in the office also provides an opportunity for on-the-spot, in-depth counseling from a physician who is knowledgeable about both interpreting the test and treating osteoporosis.
Forcing patients to seek osteoporosis screening in the hospital also means higher Medicare copayments, and usually means longer waits to get the test, said Dr. R. Mack Harrell, secretary of the AACE and an endocrinologist in the South Florida area.
AACE officials are concerned that a drop in reimbursement for DXA will create access problems for Medicare patients, Dr. Harrell said. This is troubling, he said, because osteoporosis testing is a service that is touted by the CMS in its "Your Medicare Benefits" booklet as an important preventive service available under Medicare. "If Medicare is going to make this a priority item for retired people, they have to make it accessible," he said.
Already, many physicians have stopped offering DXA services because of fee cuts, Dr. Harrell said. The good news is that there are still a substantial number of office practices and outpatient centers that can afford to keep their DXA scanners operating at the current reimbursement levels. But Dr. Harrell cautioned that the current payment level is the break-even point for most physicians who are really "hanging on by their fingernails." If rates are cut again, it will become "fiscally impossible" to offer the service in the office, he said.
ACR’s Dr. Laing predicted that getting the legislation passed this year will be an uphill battle. The major issue is the cost of extending the current payment rate.
"Right now, Congress is deadlocked over the budget, so any bill that is introduced that adds costs to anything is going to be difficult." Conversely, Dr. Laing said he is encouraged because the bill has bipartisan support in both the House and Senate.
>
>
>
Without Congressional action, Medicare payments for dual-energy x-ray absorptiometry will be cut in about half at the beginning of 2012.
But a small, bipartisan group of lawmakers in the House and Senate is pushing to extend DXA payment rates, which were passed as part of the Affordable Care Act and are set to expire at the end of this year, through 2013. Under the ACA, Congress instructed officials at the Centers for Medicare and Medicaid Services to increase DXA payments to 70% of the rate paid by Medicare in 2006.
The Preservation of Access to Osteoporosis Testing for Medicare Beneficiaries Act of 2011 (H.R. 2020/S. 1096) was introduced at the end of May; it would keep the current DXA payment rate in place for 2 years.
Rep. Michael Burgess (R-Tex.), one of the bill’s sponsors, said that cutting DXA payments is shortsighted. "Osteoporosis and related bone diseases pose a public health issue of enormous proportions, affecting millions of Americans and costing billions of dollars," he said in a statement. "As a physician, I diagnosed and treated many patients during my 25 years of practicing medicine in Texas, and I saw firsthand the way osteoporosis affects patients and their families. The more we can do to promote and encourage education, awareness, and prevention, the better. Why Medicare will pay for a fracture, but not reimburse a reasonable amount for a scan that can prevent that fracture, is beyond me."
Medicare began cutting DXA payments in 2007, after Congress included bone densitometry among a group of high-cost imaging services that were slashed as part of the Deficit Reduction Act of 2005. Since then, physicians have been struggling to cover their costs as reimbursement steadily declined from around $148 per scan in 2006 to about $54 in 2010. Exacerbating the problem is that private insurers have largely followed Medicare’s lead, ratcheting down their reimbursements as well. The ACA brought DXA payments up to about $98.
Physicians’ organizations, including the American College of Rheumatology (ACR) and the American Association of Clinical Endocrinologists (AACE), are urging lawmakers to pass an extension of the current DXA payment rate
Dr. Timothy J. Laing, government affairs committee chair for the ACR and a rheumatologist at the University of Michigan, Ann Arbor, said that if the reimbursement for the test falls below current levels, it will become economically unsustainable for physicians to provide the test in their offices.
Patients still will be able to get a DXA scan in the hospital, but there are downsides to that limited access, Dr. Laing said. Patients are far more likely to get the test if it can be done at the time it’s recommended, he said, adding that providing DXA scans in the office also provides an opportunity for on-the-spot, in-depth counseling from a physician who is knowledgeable about both interpreting the test and treating osteoporosis.
Forcing patients to seek osteoporosis screening in the hospital also means higher Medicare copayments, and usually means longer waits to get the test, said Dr. R. Mack Harrell, secretary of the AACE and an endocrinologist in the South Florida area.
AACE officials are concerned that a drop in reimbursement for DXA will create access problems for Medicare patients, Dr. Harrell said. This is troubling, he said, because osteoporosis testing is a service that is touted by the CMS in its "Your Medicare Benefits" booklet as an important preventive service available under Medicare. "If Medicare is going to make this a priority item for retired people, they have to make it accessible," he said.
Already, many physicians have stopped offering DXA services because of fee cuts, Dr. Harrell said. The good news is that there are still a substantial number of office practices and outpatient centers that can afford to keep their DXA scanners operating at the current reimbursement levels. But Dr. Harrell cautioned that the current payment level is the break-even point for most physicians who are really "hanging on by their fingernails." If rates are cut again, it will become "fiscally impossible" to offer the service in the office, he said.
ACR’s Dr. Laing predicted that getting the legislation passed this year will be an uphill battle. The major issue is the cost of extending the current payment rate.
"Right now, Congress is deadlocked over the budget, so any bill that is introduced that adds costs to anything is going to be difficult." Conversely, Dr. Laing said he is encouraged because the bill has bipartisan support in both the House and Senate.
Without Congressional action, Medicare payments for dual-energy x-ray absorptiometry will be cut in about half at the beginning of 2012.
But a small, bipartisan group of lawmakers in the House and Senate is pushing to extend DXA payment rates, which were passed as part of the Affordable Care Act and are set to expire at the end of this year, through 2013. Under the ACA, Congress instructed officials at the Centers for Medicare and Medicaid Services to increase DXA payments to 70% of the rate paid by Medicare in 2006.
The Preservation of Access to Osteoporosis Testing for Medicare Beneficiaries Act of 2011 (H.R. 2020/S. 1096) was introduced at the end of May; it would keep the current DXA payment rate in place for 2 years.
Rep. Michael Burgess (R-Tex.), one of the bill’s sponsors, said that cutting DXA payments is shortsighted. "Osteoporosis and related bone diseases pose a public health issue of enormous proportions, affecting millions of Americans and costing billions of dollars," he said in a statement. "As a physician, I diagnosed and treated many patients during my 25 years of practicing medicine in Texas, and I saw firsthand the way osteoporosis affects patients and their families. The more we can do to promote and encourage education, awareness, and prevention, the better. Why Medicare will pay for a fracture, but not reimburse a reasonable amount for a scan that can prevent that fracture, is beyond me."
Medicare began cutting DXA payments in 2007, after Congress included bone densitometry among a group of high-cost imaging services that were slashed as part of the Deficit Reduction Act of 2005. Since then, physicians have been struggling to cover their costs as reimbursement steadily declined from around $148 per scan in 2006 to about $54 in 2010. Exacerbating the problem is that private insurers have largely followed Medicare’s lead, ratcheting down their reimbursements as well. The ACA brought DXA payments up to about $98.
Physicians’ organizations, including the American College of Rheumatology (ACR) and the American Association of Clinical Endocrinologists (AACE), are urging lawmakers to pass an extension of the current DXA payment rate
Dr. Timothy J. Laing, government affairs committee chair for the ACR and a rheumatologist at the University of Michigan, Ann Arbor, said that if the reimbursement for the test falls below current levels, it will become economically unsustainable for physicians to provide the test in their offices.
Patients still will be able to get a DXA scan in the hospital, but there are downsides to that limited access, Dr. Laing said. Patients are far more likely to get the test if it can be done at the time it’s recommended, he said, adding that providing DXA scans in the office also provides an opportunity for on-the-spot, in-depth counseling from a physician who is knowledgeable about both interpreting the test and treating osteoporosis.
Forcing patients to seek osteoporosis screening in the hospital also means higher Medicare copayments, and usually means longer waits to get the test, said Dr. R. Mack Harrell, secretary of the AACE and an endocrinologist in the South Florida area.
AACE officials are concerned that a drop in reimbursement for DXA will create access problems for Medicare patients, Dr. Harrell said. This is troubling, he said, because osteoporosis testing is a service that is touted by the CMS in its "Your Medicare Benefits" booklet as an important preventive service available under Medicare. "If Medicare is going to make this a priority item for retired people, they have to make it accessible," he said.
Already, many physicians have stopped offering DXA services because of fee cuts, Dr. Harrell said. The good news is that there are still a substantial number of office practices and outpatient centers that can afford to keep their DXA scanners operating at the current reimbursement levels. But Dr. Harrell cautioned that the current payment level is the break-even point for most physicians who are really "hanging on by their fingernails." If rates are cut again, it will become "fiscally impossible" to offer the service in the office, he said.
ACR’s Dr. Laing predicted that getting the legislation passed this year will be an uphill battle. The major issue is the cost of extending the current payment rate.
"Right now, Congress is deadlocked over the budget, so any bill that is introduced that adds costs to anything is going to be difficult." Conversely, Dr. Laing said he is encouraged because the bill has bipartisan support in both the House and Senate.
Leaders: Pediatric Hospitalist Tackles Interhospital Variation
Dr. Raj Srivastava is leading the effort to find answers to the most pressing questions on quality, cost-effectiveness, and patient safety in the care of hospitalized children. Dr. Srivastava, of the department of pediatrics at the University of Utah, Salt Lake City, chairs Pediatric Research in Inpatient Settings (PRIS), a hospitalist-run research network. This network is a joint project of the Society of Hospital Medicine (SHM), the American Academy of Pediatrics, and the Academic Pediatric Association.
Dr. Srivastava has won several teaching awards, and recently SHM bestowed upon him its 2011 Excellence in Research Award. In an interview with Hospitalist News, he shared his thoughts on future directions for PRIS and pediatric hospital medicine.
HN: PRIS is working to identify conditions that are prevalent, costly, and show high interhospital variation. Why is this important?
DR. SRIVASTAVA: Unlike hospitalists who take care of adults, where essentially only a handful of conditions account for the majority of the costs, it’s very different in pediatrics, where a number of conditions are very prevalent but not very costly. But the reverse also can be true in pediatrics.
We believe that by prioritizing these conditions using prevalence, cost, and variation, we will be able to create a roadmap for pediatric inpatient medicine. If you go after condition X as opposed to condition Y, this is the potential return on investment you might get, for example. And I don’t just mean in terms of money, but in terms of the effort expended.
HN: How will this information be used?
DR. SRIVASTAVA: First, we’re going to identify drill-down conditions after the initial prioritization project. These drill downs will make up the next year and a half of work for the PRIS network, where we will study why there’s interhospital variation. Ultimately, we want to understand if there’s overutilization of resources for a particular condition. If we find that to be the case, we think we have two potential avenues to pursue. If there’s no evidence, maybe that’s why there’s overutilization. It’s a case of not knowing what to do. So then we can perform comparative effectiveness research. If the evidence is known, but not followed, then that’s the perfect avenue for quality improvement interventions.
HN: You have won several teaching awards; what do you find most rewarding about working with medical students and residents?
DR. SRIVASTAVA: I love seeing patients, and I love working with students. One of the huge joys I get comes from working through complex issues or teaching points on patients. I enjoy working with the house staff and the students to figure out how to pose the right questions and use the literature to try to figure out to the best of our ability what we should do. I think that sort of lifelong learning skill is really fun.
HN: How do you think the implementation of the Affordable Care Act will affect pediatric hospitalists?
DR. SRIVASTAVA: I think the potential for pediatric hospitalists could be similar to adult hospitalists in the sense of our being relied on to provide efficient care, streamline care, and study systems of care. The Accountable Care Organizations called for in the law are probably going to be utilized first in the adult world. I think if you were to look at pediatric ACOs, you would target the chronically ill pediatric patient (the 5% of kids that account for 50% of your costs). With the PRIS analysis of specific pediatric conditions, we will also have some cost data from hospitals that could aid with bundled payments. For example, we could provide very specific complication data based on many admissions for a condition, and this could be used by stakeholders to work with policy makers to determine the appropriate bundled payment for that condition.
Dr. Raj Srivastava is leading the effort to find answers to the most pressing questions on quality, cost-effectiveness, and patient safety in the care of hospitalized children. Dr. Srivastava, of the department of pediatrics at the University of Utah, Salt Lake City, chairs Pediatric Research in Inpatient Settings (PRIS), a hospitalist-run research network. This network is a joint project of the Society of Hospital Medicine (SHM), the American Academy of Pediatrics, and the Academic Pediatric Association.
Dr. Srivastava has won several teaching awards, and recently SHM bestowed upon him its 2011 Excellence in Research Award. In an interview with Hospitalist News, he shared his thoughts on future directions for PRIS and pediatric hospital medicine.
HN: PRIS is working to identify conditions that are prevalent, costly, and show high interhospital variation. Why is this important?
DR. SRIVASTAVA: Unlike hospitalists who take care of adults, where essentially only a handful of conditions account for the majority of the costs, it’s very different in pediatrics, where a number of conditions are very prevalent but not very costly. But the reverse also can be true in pediatrics.
We believe that by prioritizing these conditions using prevalence, cost, and variation, we will be able to create a roadmap for pediatric inpatient medicine. If you go after condition X as opposed to condition Y, this is the potential return on investment you might get, for example. And I don’t just mean in terms of money, but in terms of the effort expended.
HN: How will this information be used?
DR. SRIVASTAVA: First, we’re going to identify drill-down conditions after the initial prioritization project. These drill downs will make up the next year and a half of work for the PRIS network, where we will study why there’s interhospital variation. Ultimately, we want to understand if there’s overutilization of resources for a particular condition. If we find that to be the case, we think we have two potential avenues to pursue. If there’s no evidence, maybe that’s why there’s overutilization. It’s a case of not knowing what to do. So then we can perform comparative effectiveness research. If the evidence is known, but not followed, then that’s the perfect avenue for quality improvement interventions.
HN: You have won several teaching awards; what do you find most rewarding about working with medical students and residents?
DR. SRIVASTAVA: I love seeing patients, and I love working with students. One of the huge joys I get comes from working through complex issues or teaching points on patients. I enjoy working with the house staff and the students to figure out how to pose the right questions and use the literature to try to figure out to the best of our ability what we should do. I think that sort of lifelong learning skill is really fun.
HN: How do you think the implementation of the Affordable Care Act will affect pediatric hospitalists?
DR. SRIVASTAVA: I think the potential for pediatric hospitalists could be similar to adult hospitalists in the sense of our being relied on to provide efficient care, streamline care, and study systems of care. The Accountable Care Organizations called for in the law are probably going to be utilized first in the adult world. I think if you were to look at pediatric ACOs, you would target the chronically ill pediatric patient (the 5% of kids that account for 50% of your costs). With the PRIS analysis of specific pediatric conditions, we will also have some cost data from hospitals that could aid with bundled payments. For example, we could provide very specific complication data based on many admissions for a condition, and this could be used by stakeholders to work with policy makers to determine the appropriate bundled payment for that condition.
Dr. Raj Srivastava is leading the effort to find answers to the most pressing questions on quality, cost-effectiveness, and patient safety in the care of hospitalized children. Dr. Srivastava, of the department of pediatrics at the University of Utah, Salt Lake City, chairs Pediatric Research in Inpatient Settings (PRIS), a hospitalist-run research network. This network is a joint project of the Society of Hospital Medicine (SHM), the American Academy of Pediatrics, and the Academic Pediatric Association.
Dr. Srivastava has won several teaching awards, and recently SHM bestowed upon him its 2011 Excellence in Research Award. In an interview with Hospitalist News, he shared his thoughts on future directions for PRIS and pediatric hospital medicine.
HN: PRIS is working to identify conditions that are prevalent, costly, and show high interhospital variation. Why is this important?
DR. SRIVASTAVA: Unlike hospitalists who take care of adults, where essentially only a handful of conditions account for the majority of the costs, it’s very different in pediatrics, where a number of conditions are very prevalent but not very costly. But the reverse also can be true in pediatrics.
We believe that by prioritizing these conditions using prevalence, cost, and variation, we will be able to create a roadmap for pediatric inpatient medicine. If you go after condition X as opposed to condition Y, this is the potential return on investment you might get, for example. And I don’t just mean in terms of money, but in terms of the effort expended.
HN: How will this information be used?
DR. SRIVASTAVA: First, we’re going to identify drill-down conditions after the initial prioritization project. These drill downs will make up the next year and a half of work for the PRIS network, where we will study why there’s interhospital variation. Ultimately, we want to understand if there’s overutilization of resources for a particular condition. If we find that to be the case, we think we have two potential avenues to pursue. If there’s no evidence, maybe that’s why there’s overutilization. It’s a case of not knowing what to do. So then we can perform comparative effectiveness research. If the evidence is known, but not followed, then that’s the perfect avenue for quality improvement interventions.
HN: You have won several teaching awards; what do you find most rewarding about working with medical students and residents?
DR. SRIVASTAVA: I love seeing patients, and I love working with students. One of the huge joys I get comes from working through complex issues or teaching points on patients. I enjoy working with the house staff and the students to figure out how to pose the right questions and use the literature to try to figure out to the best of our ability what we should do. I think that sort of lifelong learning skill is really fun.
HN: How do you think the implementation of the Affordable Care Act will affect pediatric hospitalists?
DR. SRIVASTAVA: I think the potential for pediatric hospitalists could be similar to adult hospitalists in the sense of our being relied on to provide efficient care, streamline care, and study systems of care. The Accountable Care Organizations called for in the law are probably going to be utilized first in the adult world. I think if you were to look at pediatric ACOs, you would target the chronically ill pediatric patient (the 5% of kids that account for 50% of your costs). With the PRIS analysis of specific pediatric conditions, we will also have some cost data from hospitals that could aid with bundled payments. For example, we could provide very specific complication data based on many admissions for a condition, and this could be used by stakeholders to work with policy makers to determine the appropriate bundled payment for that condition.
Study: Seeing Price Tag on Lab Tests Affects Ordering
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
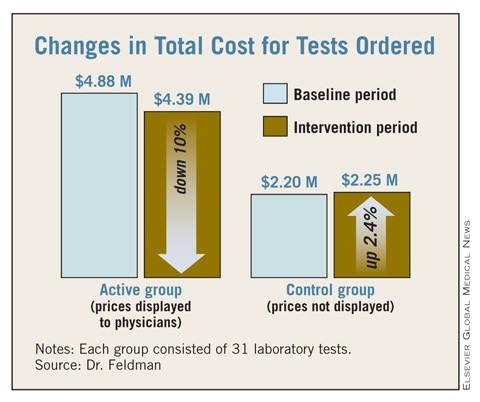
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: Displaying laboratory cost data for 6 months resulted in a savings of $15,692 per test, a 10% reduction from baseline. Control tests increased by about $1,718 per test.
Data Source: Laboratory cost data from Johns Hopkins Hospital in Baltimore, Md.
Disclosures: The authors reported no relevant financial disclosures.
Study: Seeing Price Tag on Lab Tests Affects Ordering
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: Displaying laboratory cost data for 6 months resulted in a savings of $15,692 per test, a 10% reduction from baseline. Control tests increased by about $1,718 per test.
Data Source: Laboratory cost data from Johns Hopkins Hospital in Baltimore, Md.
Disclosures: The authors reported no relevant financial disclosures.
Study: Seeing Price Tag on Lab Tests Affects Ordering
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: Displaying laboratory cost data for 6 months resulted in a savings of $15,692 per test, a 10% reduction from baseline. Control tests increased by about $1,718 per test.
Data Source: Laboratory cost data from Johns Hopkins Hospital in Baltimore, Md.
Disclosures: The authors reported no relevant financial disclosures.
Study: Seeing Price Tag on Lab Tests Affects Ordering
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
In invited commentary, Dr. Franklin A. Michota said
that “Dr. Leonard Feldman and his colleagues at Johns Hopkins
Hospital have recently
demonstrated that cost visibility for health care providers can decrease
resource utilization. They are cautious to limit their findings to several
specific laboratory tests; however, this simple approach has widespread
applicability beyond laboratory testing and has the potential for great cost
savings across the U.S.
health care system. But before we start putting visible price tags on all of
our hospital order sheets, products, and medications, we should review what we
really know about cost visibility and the risk for adverse consequences”
according to Dr. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic.
“Dr. Feldman readily
admits that patient outcomes were not reviewed in their preliminary study. It
certainly seems plausible that cost visibility reduced the ordering of
redundant and unnecessary laboratory tests. It is also plausible that necessary
and appropriate testing was omitted because of concerns over cost. We cannot
and should not look at a reduction in resource utilization with a smile on our
face without confirming at least a neutral effect on patient outcome” said Dr.
Michota.
“To that end, we must
also consider the spectrum of patient outcome and how we as individual
providers factor cost into medical decision making. There are many outcomes in
patient care, including patient satisfaction and comfort. Which outcomes should
matter the most? From which perspective do we apply our cost thresholds?
“I have often said
that I have yet to meet an American who isn’t willing to have an infinite
amount of money spent on them for the smallest improvement in outcome. How
should physicians weigh the various outcomes in balance with the visible cost?
One particular danger is the effect of physician experience on the benefit/cost
equation. Cost visibility puts the cost data right in front of the physician in
real time, yet there is no ‘equal display’ regarding the benefits. It stands to
reason that if the physician is unaware of the benefits due to lack of
experience, the medical decision making will be inappropriately weighted toward
the cost,” Dr. Michota said.
“Finally, there is
also an inherent injustice to applying cost-based decisions at the individual
patient level which is the basis of the cost-visibility approach. Most patients
are randomly assigned to hospitalists. Despite identical presentations, one
patient could receive less ‘care’ (such as testing, therapies, resources) because
his or her physician weighted the visible cost of care differently than did the
physician caring for the patient in the next bed. To avoid this conflict,
bioethicists recommend that cost-based decisions be made at the population, not
the individual level. Hospital formularies are a good example of this
technique. Cost visibility applied to individual patients without standardized
approaches on how to use the information consistently across all patients could
otherwise be considered unethical,” he said.
“Ultimately,
hospitalists should strive for value (quality/cost) in health care. As patient
advocates, we need to make sure that the quality is just as visible as the
cost,” according to Dr. Michota.
Dr. Franklin A. Michota, director of academic affairs in the department of
hospital medicine at the Cleveland Clinic. He declared no relevant financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: Displaying laboratory cost data for 6 months resulted in a savings of $15,692 per test, a 10% reduction from baseline. Control tests increased by about $1,718 per test.
Data Source: Laboratory cost data from Johns Hopkins Hospital in Baltimore, Md.
Disclosures: The authors reported no relevant financial disclosures.
Study: Seeing Price Tag on Lab Tests Affects Ordering
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
GRAPEVINE, TEX. – Policy makers are scrambling for ways to bring down health care spending, but what if it were as simple as telling physicians how much things cost?
A new study by investigators at Johns Hopkins Hospital in Baltimore, which looks at the impact of displaying cost data on laboratory tests, shows that physicians' behavior is affected by seeing the price of the tests they order.
To see how having cost data at the time of order entry would affect behavior, researchers at Johns Hopkins compiled a list of both the most frequently ordered and the most expensive laboratory tests in their hospital, based on 2007 data.
Costly tests were only included in the study if they were ordered at least 50 times during the year. The researchers then randomized the tests to be either active tests or concurrent controls. For active tests, the researchers displayed the price, based on 2008 Medicare allowable cost figures, on the hospital's computerized provider order entry (CPOE) system. For example, a blood gas was listed at $28.25 and a heme-8 lab was $9.37.
Results
During the 6-month intervention period from November 2009 to May 2010, there was a mean decrease of about $15,692 per test for the lab tests in which cost data was displayed in the CPOE, compared with a baseline period exactly 1 year earlier.
For all 31 of the active tests, there was a combined decrease of about $486,000, resulting in a 10% reduction among tests in which the costs were displayed. The active test costs dropped from $4,877,439 to $4,390,979. Among the group of 31 control tests, in which cost information was not listed on the CPOE, there was a mean increase of $1,718 per test. Overall, costs for the control group went up about $53,000 for all 31 tests.
The total number of tests ordered in the active group fell from 458,518 during the baseline period to 417,078 during the intervention. But in the control group, the number of tests rose from 142,196 to 149,455 during the study period.
Investigator Doesn't Find Results Surprising
Dr. Leonard Feldman, one of the study investigators and who is in the department of medicine at Johns Hopkins, said the results did not come as a surprise.
"I think many of us do recognize that a lot of these tests and imaging studies that are done are unnecessary," Dr. Feldman said during the annual meeting of the Society of Hospital Medicine.
Physicians order unnecessary tests for a number of reasons, he said, ranging from defensive medicine to patient expectations. But another reason is a lack of awareness of how much the tests cost, he said. "We, as doctors, have a limited understanding of diagnostic and nondrug therapeutic costs," Dr. Feldman said. "We just have no idea, mostly, how much things cost when we go to order them."
Study Limitations
While the study appears to show a relatively simple and inexpensive way to reduce the ordering of tests, Dr. Feldman acknowledged that the study had some limitations. For example, the study looked at only costs and did not include data on how the change in orders might have affected patient outcomes. And the intervention period was only 6 months.
Dr. Feldman said more time would be needed to show whether physicians would begin to ignore the costs over time. Similarly, costs were only displayed for 31 tests during the study. It's unclear if displaying all laboratory test costs would have the same effect on behavior, Dr. Feldman said.
The authors reported no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: Displaying laboratory cost data for 6 months resulted in a savings of $15,692 per test, a 10% reduction from baseline. Control tests increased by about $1,718 per test.
Data Source: Laboratory cost data from Johns Hopkins Hospital in Baltimore, Md.
Disclosures: The authors reported no relevant financial disclosures.
HHS Requires Reviews of Big Insurance Hikes
Starting Sept. 1, health plans in the small group and individual markets that propose rate hikes of 10% or more must have their proposals vetted by either state or federal officials.
The mandatory review is a new requirement related to insurance premium review that has been released by the Health and Human Services Department and was required under the Affordable Care Act. The final regulation has been published in the Federal Register. The regulation does not apply to the large group insurance market or to small and individual plans that have “grandfather” status under the ACA.
Under the regulation, states will take the lead when it comes to reviewing rate increase proposals. Federal officials will step in only when states don't have the resources or the statutory authority to review rates. Currently, insurance commissioners have differing authority based on state law, with some having the power to reject rate increases before they go into effect and others possessing more limited review powers. Officials at HHS have encouraged states to beef up their oversight authority, and the agency has awarded about $44 million in grants to help with that process.
The final rule also includes a requirement that states give the public a chance to comment on proposed rate increases. And health plans are required to provide justification for their rate increases. HHS will post the outcome of all reviews on a rate increase of 10% or more at www.HealthCare.gov
The new regulation does not give new authority to deny rate increases. But Steve Larsen, director of the Center for Consumer Information and Insurance Oversight at HHS, said that the ability to thoroughly review proposed increases and question the underlying assumptions is enough.
“Review, in and of itself, is in fact very effective in helping to ferret out reasonable and unreasonable rate increases,” Mr. Larsen said at a press conference to announce the new regulation.
Elizabeth P. Sammis, Ph.D., acting Maryland Insurance Commissioner, agreed. Maryland has prior approval authority, allowing it to reject a premium increase if state officials conclude it is too high. But in practice, she said, that authority is rarely used. Typically, health plans voluntarily withdraw the higher rate increase after discussions with state officials. “We're confident that insurers everywhere are already thinking twice and checking their math before submitting large rate hikes,” HHS Secretary Kathleen Sebelius said. “This means millions of Americans will see savings to their own bottom lines.”
But America's Health Insurance Plans (AHIP) http://www.ahip.org/
“Focusing on health insurance premiums while ignoring underlying medical cost drivers will not make health care coverage more affordable for families and employers,” AHIP President and CEO Karen Ignagni said in a statement. “The public policy discussion needs to be enlarged to focus on the soaring cost of medical care that threatens our economic competitiveness, our public safety net, and the affordability of health care coverage.” She also criticized the 10% threshold for review, saying that creating a “de facto presumption of unreasonableness” can influence the evaluation of the proposed rate increase.
The regulation calls for the use of state-specific thresholds in Sept. 2012.
Starting Sept. 1, health plans in the small group and individual markets that propose rate hikes of 10% or more must have their proposals vetted by either state or federal officials.
The mandatory review is a new requirement related to insurance premium review that has been released by the Health and Human Services Department and was required under the Affordable Care Act. The final regulation has been published in the Federal Register. The regulation does not apply to the large group insurance market or to small and individual plans that have “grandfather” status under the ACA.
Under the regulation, states will take the lead when it comes to reviewing rate increase proposals. Federal officials will step in only when states don't have the resources or the statutory authority to review rates. Currently, insurance commissioners have differing authority based on state law, with some having the power to reject rate increases before they go into effect and others possessing more limited review powers. Officials at HHS have encouraged states to beef up their oversight authority, and the agency has awarded about $44 million in grants to help with that process.
The final rule also includes a requirement that states give the public a chance to comment on proposed rate increases. And health plans are required to provide justification for their rate increases. HHS will post the outcome of all reviews on a rate increase of 10% or more at www.HealthCare.gov
The new regulation does not give new authority to deny rate increases. But Steve Larsen, director of the Center for Consumer Information and Insurance Oversight at HHS, said that the ability to thoroughly review proposed increases and question the underlying assumptions is enough.
“Review, in and of itself, is in fact very effective in helping to ferret out reasonable and unreasonable rate increases,” Mr. Larsen said at a press conference to announce the new regulation.
Elizabeth P. Sammis, Ph.D., acting Maryland Insurance Commissioner, agreed. Maryland has prior approval authority, allowing it to reject a premium increase if state officials conclude it is too high. But in practice, she said, that authority is rarely used. Typically, health plans voluntarily withdraw the higher rate increase after discussions with state officials. “We're confident that insurers everywhere are already thinking twice and checking their math before submitting large rate hikes,” HHS Secretary Kathleen Sebelius said. “This means millions of Americans will see savings to their own bottom lines.”
But America's Health Insurance Plans (AHIP) http://www.ahip.org/
“Focusing on health insurance premiums while ignoring underlying medical cost drivers will not make health care coverage more affordable for families and employers,” AHIP President and CEO Karen Ignagni said in a statement. “The public policy discussion needs to be enlarged to focus on the soaring cost of medical care that threatens our economic competitiveness, our public safety net, and the affordability of health care coverage.” She also criticized the 10% threshold for review, saying that creating a “de facto presumption of unreasonableness” can influence the evaluation of the proposed rate increase.
The regulation calls for the use of state-specific thresholds in Sept. 2012.
Starting Sept. 1, health plans in the small group and individual markets that propose rate hikes of 10% or more must have their proposals vetted by either state or federal officials.
The mandatory review is a new requirement related to insurance premium review that has been released by the Health and Human Services Department and was required under the Affordable Care Act. The final regulation has been published in the Federal Register. The regulation does not apply to the large group insurance market or to small and individual plans that have “grandfather” status under the ACA.
Under the regulation, states will take the lead when it comes to reviewing rate increase proposals. Federal officials will step in only when states don't have the resources or the statutory authority to review rates. Currently, insurance commissioners have differing authority based on state law, with some having the power to reject rate increases before they go into effect and others possessing more limited review powers. Officials at HHS have encouraged states to beef up their oversight authority, and the agency has awarded about $44 million in grants to help with that process.
The final rule also includes a requirement that states give the public a chance to comment on proposed rate increases. And health plans are required to provide justification for their rate increases. HHS will post the outcome of all reviews on a rate increase of 10% or more at www.HealthCare.gov
The new regulation does not give new authority to deny rate increases. But Steve Larsen, director of the Center for Consumer Information and Insurance Oversight at HHS, said that the ability to thoroughly review proposed increases and question the underlying assumptions is enough.
“Review, in and of itself, is in fact very effective in helping to ferret out reasonable and unreasonable rate increases,” Mr. Larsen said at a press conference to announce the new regulation.
Elizabeth P. Sammis, Ph.D., acting Maryland Insurance Commissioner, agreed. Maryland has prior approval authority, allowing it to reject a premium increase if state officials conclude it is too high. But in practice, she said, that authority is rarely used. Typically, health plans voluntarily withdraw the higher rate increase after discussions with state officials. “We're confident that insurers everywhere are already thinking twice and checking their math before submitting large rate hikes,” HHS Secretary Kathleen Sebelius said. “This means millions of Americans will see savings to their own bottom lines.”
But America's Health Insurance Plans (AHIP) http://www.ahip.org/
“Focusing on health insurance premiums while ignoring underlying medical cost drivers will not make health care coverage more affordable for families and employers,” AHIP President and CEO Karen Ignagni said in a statement. “The public policy discussion needs to be enlarged to focus on the soaring cost of medical care that threatens our economic competitiveness, our public safety net, and the affordability of health care coverage.” She also criticized the 10% threshold for review, saying that creating a “de facto presumption of unreasonableness” can influence the evaluation of the proposed rate increase.
The regulation calls for the use of state-specific thresholds in Sept. 2012.
From a Briefing by the Health and Human Services Department
CMS Finalizes Plan to Pay Hospitals for Quality
Starting in October 2012, about 1% of the payments that hospitals receive from Medicare will be calculated based on performance on clinical quality measures and patient satisfaction scores.
Details of the new initiative, known as the Hospital Inpatient Value-Based Purchasing program, were unveiled in a final rule released by the Centers for Medicare and Medicaid Services (CMS) on April 29. The initiative was mandated by Congress under the Affordable Care Act.
Under the program, CMS will take 1% of the payments that would otherwise go to hospitals under Medicare's Inpatient Prospective Payment System and put them in a fund to pay for care based on quality. In the first year, CMS estimates that about $850 million will be available through the fund. Medicare officials will score hospitals based on their performance on each of the measures compared with other hospitals and with how their performance has improved over time.
The program is the first step in shifting payments toward quality and away from volume, Dr. Donald Berwick, CMS administrator, said in a press conference.
“This is one of those areas where improvement of quality and reduction in cost go hand-in-hand,” Dr. Berwick said. “My feeling continues to be that the best way for us to arrive at sustainable costs for the health care system is precisely through the improvement of quality of care.”
Under the program, payments will be based on performance on 12 clinical process-of-care measures and a survey of patient satisfaction. Process-of-care indicators include measures such as the percentage of patients with myocardial infarction who are given fibrinolytic medication within 30 minutes of arrival at the hospital.
To evaluate patient satisfaction, a random sample of discharged patients will be surveyed about their perceptions, including physician and nurse communication, hospital staff responsiveness, pain management, discharge instructions, and hospital cleanliness. A complete list of the measures is available at http://www.healthcare.gov/news/factsheets/valuebasedpurchasing04292011b.html
The measures have been endorsed by such national panels as the National Quality Forum, and hospitals have already been reporting their performance on them through Medicare's Hospital Compare website. The measures are weighted so that 70% of the payment is based on the quality measures and 30% is based on patient evaluations.
Over time, CMS officials plan to add measures focused on patient outcomes, including prevention of hospital-acquired conditions. And measures will be phased out over time if hospitals achieve consistently high compliance scores, Dr. Berwick said.
The new value-based purchasing initiative is only one way that hospital payments will be tied to quality of care. Starting in 2013, Medicare will reduce payments to hospitals if they have excess 30-day readmissions for patients who suffer heart attacks, heart failure, and pneumonia. And in 2015, hospitals could see their payments cut if they have high rates of certain hospital-acquired conditions.
The final rule on hospital value-based purchasing will be published in the Federal Register in May and becomes final on July 1.
Starting in October 2012, about 1% of the payments that hospitals receive from Medicare will be calculated based on performance on clinical quality measures and patient satisfaction scores.
Details of the new initiative, known as the Hospital Inpatient Value-Based Purchasing program, were unveiled in a final rule released by the Centers for Medicare and Medicaid Services (CMS) on April 29. The initiative was mandated by Congress under the Affordable Care Act.
Under the program, CMS will take 1% of the payments that would otherwise go to hospitals under Medicare's Inpatient Prospective Payment System and put them in a fund to pay for care based on quality. In the first year, CMS estimates that about $850 million will be available through the fund. Medicare officials will score hospitals based on their performance on each of the measures compared with other hospitals and with how their performance has improved over time.
The program is the first step in shifting payments toward quality and away from volume, Dr. Donald Berwick, CMS administrator, said in a press conference.
“This is one of those areas where improvement of quality and reduction in cost go hand-in-hand,” Dr. Berwick said. “My feeling continues to be that the best way for us to arrive at sustainable costs for the health care system is precisely through the improvement of quality of care.”
Under the program, payments will be based on performance on 12 clinical process-of-care measures and a survey of patient satisfaction. Process-of-care indicators include measures such as the percentage of patients with myocardial infarction who are given fibrinolytic medication within 30 minutes of arrival at the hospital.
To evaluate patient satisfaction, a random sample of discharged patients will be surveyed about their perceptions, including physician and nurse communication, hospital staff responsiveness, pain management, discharge instructions, and hospital cleanliness. A complete list of the measures is available at http://www.healthcare.gov/news/factsheets/valuebasedpurchasing04292011b.html
The measures have been endorsed by such national panels as the National Quality Forum, and hospitals have already been reporting their performance on them through Medicare's Hospital Compare website. The measures are weighted so that 70% of the payment is based on the quality measures and 30% is based on patient evaluations.
Over time, CMS officials plan to add measures focused on patient outcomes, including prevention of hospital-acquired conditions. And measures will be phased out over time if hospitals achieve consistently high compliance scores, Dr. Berwick said.
The new value-based purchasing initiative is only one way that hospital payments will be tied to quality of care. Starting in 2013, Medicare will reduce payments to hospitals if they have excess 30-day readmissions for patients who suffer heart attacks, heart failure, and pneumonia. And in 2015, hospitals could see their payments cut if they have high rates of certain hospital-acquired conditions.
The final rule on hospital value-based purchasing will be published in the Federal Register in May and becomes final on July 1.
Starting in October 2012, about 1% of the payments that hospitals receive from Medicare will be calculated based on performance on clinical quality measures and patient satisfaction scores.
Details of the new initiative, known as the Hospital Inpatient Value-Based Purchasing program, were unveiled in a final rule released by the Centers for Medicare and Medicaid Services (CMS) on April 29. The initiative was mandated by Congress under the Affordable Care Act.
Under the program, CMS will take 1% of the payments that would otherwise go to hospitals under Medicare's Inpatient Prospective Payment System and put them in a fund to pay for care based on quality. In the first year, CMS estimates that about $850 million will be available through the fund. Medicare officials will score hospitals based on their performance on each of the measures compared with other hospitals and with how their performance has improved over time.
The program is the first step in shifting payments toward quality and away from volume, Dr. Donald Berwick, CMS administrator, said in a press conference.
“This is one of those areas where improvement of quality and reduction in cost go hand-in-hand,” Dr. Berwick said. “My feeling continues to be that the best way for us to arrive at sustainable costs for the health care system is precisely through the improvement of quality of care.”
Under the program, payments will be based on performance on 12 clinical process-of-care measures and a survey of patient satisfaction. Process-of-care indicators include measures such as the percentage of patients with myocardial infarction who are given fibrinolytic medication within 30 minutes of arrival at the hospital.
To evaluate patient satisfaction, a random sample of discharged patients will be surveyed about their perceptions, including physician and nurse communication, hospital staff responsiveness, pain management, discharge instructions, and hospital cleanliness. A complete list of the measures is available at http://www.healthcare.gov/news/factsheets/valuebasedpurchasing04292011b.html
The measures have been endorsed by such national panels as the National Quality Forum, and hospitals have already been reporting their performance on them through Medicare's Hospital Compare website. The measures are weighted so that 70% of the payment is based on the quality measures and 30% is based on patient evaluations.
Over time, CMS officials plan to add measures focused on patient outcomes, including prevention of hospital-acquired conditions. And measures will be phased out over time if hospitals achieve consistently high compliance scores, Dr. Berwick said.
The new value-based purchasing initiative is only one way that hospital payments will be tied to quality of care. Starting in 2013, Medicare will reduce payments to hospitals if they have excess 30-day readmissions for patients who suffer heart attacks, heart failure, and pneumonia. And in 2015, hospitals could see their payments cut if they have high rates of certain hospital-acquired conditions.
The final rule on hospital value-based purchasing will be published in the Federal Register in May and becomes final on July 1.
Policy & Practice : Want more health reform news? Subscribe to our podcast – search 'Policy & Practice' in the iTunes store
Ob.Gyns. Begin to E-Prescribe
About a third of ob.gyns. are actively e-prescribing in their practices, according to a new report by the Surescripts e-prescribing network. That puts ob.gyns. in the middle of the electronic pack. Cardiologists are the top e-prescribers, with 49% of using the technology regularly. Close behind are family physicians (47%), internists (45%), gastroenterologists (38%), and pediatricians (36%). About 36% of all office-based physicians were e-prescribing in 2010, and 1 in 10 prescriptions was delivered electronically, up from 1 in 18 in 2008. E-prescribing is being driven primarily by federal legislation, including health care reform, according to Surescripts. Some 326 million prescriptions were routed electronically in 2010, compared with 190 million in 2009, a 72% increase.
Episiotomies Down, C-Sections Up
The use of episiotomies fell 60% between 1997 and 2008, but cesarean sections rose 72%, according to data released by the Agency for Healthcare Research and Quality. The percentage of births by cesarean section rose from 21% in 1997 to 33% a decade later. At the same time, the rate of repeat cesareans nearly doubled, from 8% to 14%. The AHRQ report, which is based on data on inpatient hospital stays in the United States, also found that cesarean sections were more common in privately insured patients than in those without insurance. The report also noted decreases in the use of episiotomies and forceps. The use of forceps in vaginal births dropped by a third, from 14% in 1997 to 10% in 2008. About 29% of vaginal births involved episiotomies in 1997, compared with 12% in 2008, a drop of about 60% in a decade.
State Defunds Planned Parenthood
Indiana Gov. Mitch Daniels (R) has signed legislation withholding state funds from any health care entity other than hospitals or ambulatory surgery centers that provides abortions or operates with an abortion provider. The new law effectively strips state funding from Planned Parenthood clinics in Indiana. The law also bars health plans from providing coverage for abortions except in cases of rape, incest, or the risk of substantial injury to the woman. Any woman seeking an abortion would have to view fetal ultrasound imaging unless she provides a written refusal. Planned Parenthood of Indiana is challenging the law in court.
Report Finds Reform Pro-Women
The growing number of women who lack adequate health care will be aided by provisions in the Affordable Care Act, according to a report from the Commonwealth Fund. After a random national survey of 1,362 men and 1,671 women aged 19–64 years, the group calculated that 27 million women were uninsured in 2010, 42 million women had trouble paying their medical bills during the past decade, and 45 million avoided getting health care because of the cost. One of the main reasons for access problems is that women in their reproductive years face insurance premiums that are 84% higher than those for men the same age, the report asserted. However, uninsured women will gain coverage through provisions of health reform, such as increased Medicaid eligibility, subsidized private insurance in state insurance exchanges, and a ban on insurance underwriting based on health or gender, according to the report.
Headaches Take a Toll
Headaches were the main cause of 3 million emergency department visits and 81,000 hospital stays in the United States, according to an analysis of 2008 data by the Agency for Healthcare Research and Quality. Those figures represented 2.4% of ED visits and 0.2% of hospitalizations, respectively. Migraines made up one-third of the headache emergencies and two-thirds of the hospital stays for headaches. The ED visits increased during the summer months, peaked in September, and were lowest during February and December. Three-fourths of the headache sufferers were women, who also were four times as likely to have migraines as men were.
CME-Funding Dilemma Persists
Although physicians and other medical professionals say they're concerned that commercial funding of continuing medical education might bias the information provided, most are not willing to pay more to offset or eliminate such funding, a study in the Archives of Internal Medicine showed. Researchers surveyed 770 physicians, nurses, nurse practitioners, and physician assistants at CME sessions and found that the vast majority – 88% – said that commercial support of CME introduces bias. However, only 15% would eliminate commercial support from CME activities and only 42% said they were willing to pay more in an effort to cut industry financial involvement. Most CME participants also significantly underestimated the amount of commercial funding for their courses, the authors wrote, adding that “the dilemma remains of how to provide quality CME either with alternate funding or at reduced cost.”
Ob.Gyns. Begin to E-Prescribe
About a third of ob.gyns. are actively e-prescribing in their practices, according to a new report by the Surescripts e-prescribing network. That puts ob.gyns. in the middle of the electronic pack. Cardiologists are the top e-prescribers, with 49% of using the technology regularly. Close behind are family physicians (47%), internists (45%), gastroenterologists (38%), and pediatricians (36%). About 36% of all office-based physicians were e-prescribing in 2010, and 1 in 10 prescriptions was delivered electronically, up from 1 in 18 in 2008. E-prescribing is being driven primarily by federal legislation, including health care reform, according to Surescripts. Some 326 million prescriptions were routed electronically in 2010, compared with 190 million in 2009, a 72% increase.
Episiotomies Down, C-Sections Up
The use of episiotomies fell 60% between 1997 and 2008, but cesarean sections rose 72%, according to data released by the Agency for Healthcare Research and Quality. The percentage of births by cesarean section rose from 21% in 1997 to 33% a decade later. At the same time, the rate of repeat cesareans nearly doubled, from 8% to 14%. The AHRQ report, which is based on data on inpatient hospital stays in the United States, also found that cesarean sections were more common in privately insured patients than in those without insurance. The report also noted decreases in the use of episiotomies and forceps. The use of forceps in vaginal births dropped by a third, from 14% in 1997 to 10% in 2008. About 29% of vaginal births involved episiotomies in 1997, compared with 12% in 2008, a drop of about 60% in a decade.
State Defunds Planned Parenthood
Indiana Gov. Mitch Daniels (R) has signed legislation withholding state funds from any health care entity other than hospitals or ambulatory surgery centers that provides abortions or operates with an abortion provider. The new law effectively strips state funding from Planned Parenthood clinics in Indiana. The law also bars health plans from providing coverage for abortions except in cases of rape, incest, or the risk of substantial injury to the woman. Any woman seeking an abortion would have to view fetal ultrasound imaging unless she provides a written refusal. Planned Parenthood of Indiana is challenging the law in court.
Report Finds Reform Pro-Women
The growing number of women who lack adequate health care will be aided by provisions in the Affordable Care Act, according to a report from the Commonwealth Fund. After a random national survey of 1,362 men and 1,671 women aged 19–64 years, the group calculated that 27 million women were uninsured in 2010, 42 million women had trouble paying their medical bills during the past decade, and 45 million avoided getting health care because of the cost. One of the main reasons for access problems is that women in their reproductive years face insurance premiums that are 84% higher than those for men the same age, the report asserted. However, uninsured women will gain coverage through provisions of health reform, such as increased Medicaid eligibility, subsidized private insurance in state insurance exchanges, and a ban on insurance underwriting based on health or gender, according to the report.
Headaches Take a Toll
Headaches were the main cause of 3 million emergency department visits and 81,000 hospital stays in the United States, according to an analysis of 2008 data by the Agency for Healthcare Research and Quality. Those figures represented 2.4% of ED visits and 0.2% of hospitalizations, respectively. Migraines made up one-third of the headache emergencies and two-thirds of the hospital stays for headaches. The ED visits increased during the summer months, peaked in September, and were lowest during February and December. Three-fourths of the headache sufferers were women, who also were four times as likely to have migraines as men were.
CME-Funding Dilemma Persists
Although physicians and other medical professionals say they're concerned that commercial funding of continuing medical education might bias the information provided, most are not willing to pay more to offset or eliminate such funding, a study in the Archives of Internal Medicine showed. Researchers surveyed 770 physicians, nurses, nurse practitioners, and physician assistants at CME sessions and found that the vast majority – 88% – said that commercial support of CME introduces bias. However, only 15% would eliminate commercial support from CME activities and only 42% said they were willing to pay more in an effort to cut industry financial involvement. Most CME participants also significantly underestimated the amount of commercial funding for their courses, the authors wrote, adding that “the dilemma remains of how to provide quality CME either with alternate funding or at reduced cost.”
Ob.Gyns. Begin to E-Prescribe
About a third of ob.gyns. are actively e-prescribing in their practices, according to a new report by the Surescripts e-prescribing network. That puts ob.gyns. in the middle of the electronic pack. Cardiologists are the top e-prescribers, with 49% of using the technology regularly. Close behind are family physicians (47%), internists (45%), gastroenterologists (38%), and pediatricians (36%). About 36% of all office-based physicians were e-prescribing in 2010, and 1 in 10 prescriptions was delivered electronically, up from 1 in 18 in 2008. E-prescribing is being driven primarily by federal legislation, including health care reform, according to Surescripts. Some 326 million prescriptions were routed electronically in 2010, compared with 190 million in 2009, a 72% increase.
Episiotomies Down, C-Sections Up
The use of episiotomies fell 60% between 1997 and 2008, but cesarean sections rose 72%, according to data released by the Agency for Healthcare Research and Quality. The percentage of births by cesarean section rose from 21% in 1997 to 33% a decade later. At the same time, the rate of repeat cesareans nearly doubled, from 8% to 14%. The AHRQ report, which is based on data on inpatient hospital stays in the United States, also found that cesarean sections were more common in privately insured patients than in those without insurance. The report also noted decreases in the use of episiotomies and forceps. The use of forceps in vaginal births dropped by a third, from 14% in 1997 to 10% in 2008. About 29% of vaginal births involved episiotomies in 1997, compared with 12% in 2008, a drop of about 60% in a decade.
State Defunds Planned Parenthood
Indiana Gov. Mitch Daniels (R) has signed legislation withholding state funds from any health care entity other than hospitals or ambulatory surgery centers that provides abortions or operates with an abortion provider. The new law effectively strips state funding from Planned Parenthood clinics in Indiana. The law also bars health plans from providing coverage for abortions except in cases of rape, incest, or the risk of substantial injury to the woman. Any woman seeking an abortion would have to view fetal ultrasound imaging unless she provides a written refusal. Planned Parenthood of Indiana is challenging the law in court.
Report Finds Reform Pro-Women
The growing number of women who lack adequate health care will be aided by provisions in the Affordable Care Act, according to a report from the Commonwealth Fund. After a random national survey of 1,362 men and 1,671 women aged 19–64 years, the group calculated that 27 million women were uninsured in 2010, 42 million women had trouble paying their medical bills during the past decade, and 45 million avoided getting health care because of the cost. One of the main reasons for access problems is that women in their reproductive years face insurance premiums that are 84% higher than those for men the same age, the report asserted. However, uninsured women will gain coverage through provisions of health reform, such as increased Medicaid eligibility, subsidized private insurance in state insurance exchanges, and a ban on insurance underwriting based on health or gender, according to the report.
Headaches Take a Toll
Headaches were the main cause of 3 million emergency department visits and 81,000 hospital stays in the United States, according to an analysis of 2008 data by the Agency for Healthcare Research and Quality. Those figures represented 2.4% of ED visits and 0.2% of hospitalizations, respectively. Migraines made up one-third of the headache emergencies and two-thirds of the hospital stays for headaches. The ED visits increased during the summer months, peaked in September, and were lowest during February and December. Three-fourths of the headache sufferers were women, who also were four times as likely to have migraines as men were.
CME-Funding Dilemma Persists
Although physicians and other medical professionals say they're concerned that commercial funding of continuing medical education might bias the information provided, most are not willing to pay more to offset or eliminate such funding, a study in the Archives of Internal Medicine showed. Researchers surveyed 770 physicians, nurses, nurse practitioners, and physician assistants at CME sessions and found that the vast majority – 88% – said that commercial support of CME introduces bias. However, only 15% would eliminate commercial support from CME activities and only 42% said they were willing to pay more in an effort to cut industry financial involvement. Most CME participants also significantly underestimated the amount of commercial funding for their courses, the authors wrote, adding that “the dilemma remains of how to provide quality CME either with alternate funding or at reduced cost.”