User login
Doug Brunk is a San Diego-based award-winning reporter who began covering health care in 1991. Before joining the company, he wrote for the health sciences division of Columbia University and was an associate editor at Contemporary Long Term Care magazine when it won a Jesse H. Neal Award. His work has been syndicated by the Los Angeles Times and he is the author of two books related to the University of Kentucky Wildcats men's basketball program. Doug has a master’s degree in magazine journalism from the S.I. Newhouse School of Public Communications at Syracuse University. Follow him on Twitter @dougbrunk.
Managing blunt abdominal trauma in children tricky business
SAN DIEGO – In the clinical experience of Dr. Julia Grabowski, managing blunt abdominal trauma injuries in children can be tricky business because of the wide variation in development between infants and adolescents.
Such differences "affect both the care of the injured child and injury prevention efforts," she said at the University of California San Diego Critical Care Summer Session. Anatomic considerations in the management of pediatric abdominal trauma include the close proximity of multiple organs, "which can affect their overall injury patterns," said Dr. Grabowski, a pediatric surgeon at Rady Children’s Hospital in San Diego. "In addition, their solid organs are larger compared with the rest of their abdomen. They generally have less body fat, less connective tissue, and less muscle mass, and their bony skeleton is incompletely ossified."

Compared with adults, the rib cage in children "is higher and much more pliable, so rib fractures are quite uncommon in the pediatric population," she said. "If you do see a child who has a rib fracture, that’s a trigger to think they had a much worse trauma than you originally expected."
Blunt injuries account for about 90% of all injuries and deaths in children, Dr. Grabowski said. In blunt abdominal trauma, the most common mechanism of action is a fall, followed by motor vehicle collisions, pedestrian versus auto accidents, bicycle accidents, and assaults. The most commonly injured organs are the spleen and liver, followed distantly by the kidney, small bowel, and pancreas.
Diagnostic evaluation of blunt abdominal trauma includes C-spine imaging for those in whom you suspect C-spine trauma, chest x-rays, anterior-posterior x-ray of the pelvis as necessary, and a computed tomography scan, "which is really the workhorse of evaluation for blunt abdominal trauma," she said. Lab studies may include CBC, liver function tests, amylase, lipase, and blood type and cross.
Another option is Focused Assessment With Sonography for Trauma (the FAST scan). According to Dr. Grabowski, recent research has demonstrated that FAST has a low sensitivity and is inappropriate for use in hemodynamically stable children, but that it may be useful in unstable patients.
For splenic and hepatic injuries, grade and clinical exam dictates the need for PICU admission, frequency of vital signs, hematocrit and hemoglobin testing, diet, and activity. The American Pediatric Surgical Association published guidelines for the management of hemodynamically stable children with isolated spleen or liver injury (J. Pediatr. Surg. 2000; 35:164-9).
"Most children are in the hospital 1 day longer than their grade of injury, and they’re out of any activity for 2 weeks longer than their grade of injury," said Dr. Grabowski. Splenic injuries from to sports competition "are quite common, especially around football and hockey seasons," as are those caused by motor vehicle accidents and accidents from all-terrain vehicles. Common complaints include abdominal pain/tenderness, shoulder pain, nausea and vomiting, and anemia. CT scan is 98% sensitive in identifying the injury.
"Over time we have found that splenic salvage can be achieved in greater than 90% of children with blunt splenic injury, even up to a grade IV or V injury," she said. "Management of splenic injury should be based on physiologic parameters, rather than on a grading of the spleen injury or the presence of ‘blush’ on a CT scan. When an operation is required it’s usually for hemodynamic stability or for ongoing transfusion requirements."
For patients who undergo splenectomy, incidence of overwhelming post-splenectomy sepsis is thought to be about 0.8%, and the risk is greatest in the first 2 years. "Even though it’s such a low incidence, overwhelming post-splenectomy sepsis has a very high mortality, up to 50%," she said. "It’s important to educate the patients and the parents that if they develop a fever, it’s important to come to the hospital as soon as possible for evaluation."
Next, Dr. Grabowski discussed hepatic injuries, which involve the right lobe of the liver in 60%-78% of cases. Children with hepatic injuries commonly present with abdominal pain/tenderness and 56%-100% have associated injuries, most commonly involving the brain. Shock occurs in fewer than 10% of patients who present with a liver injury, while an aspartate aminotransferase/alanine aminotransferase (AST/ALT) level of greater than 250 units/L suggests liver injury.
Nonoperative treatment is successful about 90% of the time. This requires hemodynamic stability and absence of peritoneal signs. "Head injury is not a contraindication for nonoperative management," she said. "We have less experience with, and less studies looking at, angioembolization for hepatic injuries, but since we’ve had such good success with splenic injuries, we think it’s going to be helpful for hepatic injuries as well."
Operative treatment is indicated in cases of persistent bleeding, hemodynamic instability, or to rule out a missed injury.
Dr. Grabowski pointed out that there is little value in routine follow-up imaging studies after splenic or hepatic injury. The American Pediatric Surgical Association guidelines recommend a return to normal activities after a period of 2 weeks plus the grade of injury. "Normal activity is considered returning to school and walking," she said. "It’s not return to sports competition like football or wrestling. We usually say if your spleen gets injured during the football season, you can return to play the following season."
Bowel injuries comprise just 15% of intra-abdominal injuries in children, "but there is a high mortality, about 25%, and they’re easily missed on initial exam," Dr. Grabowski said. Clinical examination remains the most important diagnostic tool in the awake patient because only 60% of radiographic studies will be diagnostic. "It’s a difficult diagnosis to make, and delays occur in about 10% of cases," she said. "But many good studies have shown that children who have a delayed diagnosis of bowel injury did not have a worse outcome."
Seat belt injures also are common because most children are too large for car seats and too small for an adult seat belt system. "So they either don’t wear the cross-chest harness or they wear it inappropriately," Dr. Grabowski said. "Children also have a higher center of gravity, an immaturity and lack of structural integrity of their bony pelvis, and in most cases they have a relative paucity of abdominal musculature. Because they’re wearing their seat belt wrong they have a tendency to get injured by their seat belt more often than adults do."
An estimated 50%-70% of seat belt injuries are associated with a chance fracture, or a rupture of the posterior spinal ligament, or wedge, most commonly at L1 and L3. Those particular injuries "are very often associated with a bowel injury, so there’s a high index of suspicion in those children," she said. Indications for exploration in children who present with seat belt injuries include hemodynamic instability, pneumoperitoneum, peritonitis, bladder rupture, abdominal tenderness with free fluid in pelvis on CT without solid organ injury, if they worsen on exam, if they spike a fever, or if their labs become abnormal.
Dr. Grabowski advises clinicians to think nonaccidental trauma if children present with no history or explanation for injury, if the history is incompatible with the type or degree of injury, if a sibling is blamed for the injury, if caregivers give conflicting histories when interviewed separately, or if the history is not credible. "Health care providers are mandated reporters of nonaccidental trauma," she said, noting than an estimated 1 million children are victims of abuse each year.
Dr. Grabowski said that she had no relevant financial conflicts to make.
SAN DIEGO – In the clinical experience of Dr. Julia Grabowski, managing blunt abdominal trauma injuries in children can be tricky business because of the wide variation in development between infants and adolescents.
Such differences "affect both the care of the injured child and injury prevention efforts," she said at the University of California San Diego Critical Care Summer Session. Anatomic considerations in the management of pediatric abdominal trauma include the close proximity of multiple organs, "which can affect their overall injury patterns," said Dr. Grabowski, a pediatric surgeon at Rady Children’s Hospital in San Diego. "In addition, their solid organs are larger compared with the rest of their abdomen. They generally have less body fat, less connective tissue, and less muscle mass, and their bony skeleton is incompletely ossified."
Compared with adults, the rib cage in children "is higher and much more pliable, so rib fractures are quite uncommon in the pediatric population," she said. "If you do see a child who has a rib fracture, that’s a trigger to think they had a much worse trauma than you originally expected."
Blunt injuries account for about 90% of all injuries and deaths in children, Dr. Grabowski said. In blunt abdominal trauma, the most common mechanism of action is a fall, followed by motor vehicle collisions, pedestrian versus auto accidents, bicycle accidents, and assaults. The most commonly injured organs are the spleen and liver, followed distantly by the kidney, small bowel, and pancreas.
Diagnostic evaluation of blunt abdominal trauma includes C-spine imaging for those in whom you suspect C-spine trauma, chest x-rays, anterior-posterior x-ray of the pelvis as necessary, and a computed tomography scan, "which is really the workhorse of evaluation for blunt abdominal trauma," she said. Lab studies may include CBC, liver function tests, amylase, lipase, and blood type and cross.
Another option is Focused Assessment With Sonography for Trauma (the FAST scan). According to Dr. Grabowski, recent research has demonstrated that FAST has a low sensitivity and is inappropriate for use in hemodynamically stable children, but that it may be useful in unstable patients.
For splenic and hepatic injuries, grade and clinical exam dictates the need for PICU admission, frequency of vital signs, hematocrit and hemoglobin testing, diet, and activity. The American Pediatric Surgical Association published guidelines for the management of hemodynamically stable children with isolated spleen or liver injury (J. Pediatr. Surg. 2000; 35:164-9).
"Most children are in the hospital 1 day longer than their grade of injury, and they’re out of any activity for 2 weeks longer than their grade of injury," said Dr. Grabowski. Splenic injuries from to sports competition "are quite common, especially around football and hockey seasons," as are those caused by motor vehicle accidents and accidents from all-terrain vehicles. Common complaints include abdominal pain/tenderness, shoulder pain, nausea and vomiting, and anemia. CT scan is 98% sensitive in identifying the injury.
"Over time we have found that splenic salvage can be achieved in greater than 90% of children with blunt splenic injury, even up to a grade IV or V injury," she said. "Management of splenic injury should be based on physiologic parameters, rather than on a grading of the spleen injury or the presence of ‘blush’ on a CT scan. When an operation is required it’s usually for hemodynamic stability or for ongoing transfusion requirements."
For patients who undergo splenectomy, incidence of overwhelming post-splenectomy sepsis is thought to be about 0.8%, and the risk is greatest in the first 2 years. "Even though it’s such a low incidence, overwhelming post-splenectomy sepsis has a very high mortality, up to 50%," she said. "It’s important to educate the patients and the parents that if they develop a fever, it’s important to come to the hospital as soon as possible for evaluation."
Next, Dr. Grabowski discussed hepatic injuries, which involve the right lobe of the liver in 60%-78% of cases. Children with hepatic injuries commonly present with abdominal pain/tenderness and 56%-100% have associated injuries, most commonly involving the brain. Shock occurs in fewer than 10% of patients who present with a liver injury, while an aspartate aminotransferase/alanine aminotransferase (AST/ALT) level of greater than 250 units/L suggests liver injury.
Nonoperative treatment is successful about 90% of the time. This requires hemodynamic stability and absence of peritoneal signs. "Head injury is not a contraindication for nonoperative management," she said. "We have less experience with, and less studies looking at, angioembolization for hepatic injuries, but since we’ve had such good success with splenic injuries, we think it’s going to be helpful for hepatic injuries as well."
Operative treatment is indicated in cases of persistent bleeding, hemodynamic instability, or to rule out a missed injury.
Dr. Grabowski pointed out that there is little value in routine follow-up imaging studies after splenic or hepatic injury. The American Pediatric Surgical Association guidelines recommend a return to normal activities after a period of 2 weeks plus the grade of injury. "Normal activity is considered returning to school and walking," she said. "It’s not return to sports competition like football or wrestling. We usually say if your spleen gets injured during the football season, you can return to play the following season."
Bowel injuries comprise just 15% of intra-abdominal injuries in children, "but there is a high mortality, about 25%, and they’re easily missed on initial exam," Dr. Grabowski said. Clinical examination remains the most important diagnostic tool in the awake patient because only 60% of radiographic studies will be diagnostic. "It’s a difficult diagnosis to make, and delays occur in about 10% of cases," she said. "But many good studies have shown that children who have a delayed diagnosis of bowel injury did not have a worse outcome."
Seat belt injures also are common because most children are too large for car seats and too small for an adult seat belt system. "So they either don’t wear the cross-chest harness or they wear it inappropriately," Dr. Grabowski said. "Children also have a higher center of gravity, an immaturity and lack of structural integrity of their bony pelvis, and in most cases they have a relative paucity of abdominal musculature. Because they’re wearing their seat belt wrong they have a tendency to get injured by their seat belt more often than adults do."
An estimated 50%-70% of seat belt injuries are associated with a chance fracture, or a rupture of the posterior spinal ligament, or wedge, most commonly at L1 and L3. Those particular injuries "are very often associated with a bowel injury, so there’s a high index of suspicion in those children," she said. Indications for exploration in children who present with seat belt injuries include hemodynamic instability, pneumoperitoneum, peritonitis, bladder rupture, abdominal tenderness with free fluid in pelvis on CT without solid organ injury, if they worsen on exam, if they spike a fever, or if their labs become abnormal.
Dr. Grabowski advises clinicians to think nonaccidental trauma if children present with no history or explanation for injury, if the history is incompatible with the type or degree of injury, if a sibling is blamed for the injury, if caregivers give conflicting histories when interviewed separately, or if the history is not credible. "Health care providers are mandated reporters of nonaccidental trauma," she said, noting than an estimated 1 million children are victims of abuse each year.
Dr. Grabowski said that she had no relevant financial conflicts to make.
SAN DIEGO – In the clinical experience of Dr. Julia Grabowski, managing blunt abdominal trauma injuries in children can be tricky business because of the wide variation in development between infants and adolescents.
Such differences "affect both the care of the injured child and injury prevention efforts," she said at the University of California San Diego Critical Care Summer Session. Anatomic considerations in the management of pediatric abdominal trauma include the close proximity of multiple organs, "which can affect their overall injury patterns," said Dr. Grabowski, a pediatric surgeon at Rady Children’s Hospital in San Diego. "In addition, their solid organs are larger compared with the rest of their abdomen. They generally have less body fat, less connective tissue, and less muscle mass, and their bony skeleton is incompletely ossified."
Compared with adults, the rib cage in children "is higher and much more pliable, so rib fractures are quite uncommon in the pediatric population," she said. "If you do see a child who has a rib fracture, that’s a trigger to think they had a much worse trauma than you originally expected."
Blunt injuries account for about 90% of all injuries and deaths in children, Dr. Grabowski said. In blunt abdominal trauma, the most common mechanism of action is a fall, followed by motor vehicle collisions, pedestrian versus auto accidents, bicycle accidents, and assaults. The most commonly injured organs are the spleen and liver, followed distantly by the kidney, small bowel, and pancreas.
Diagnostic evaluation of blunt abdominal trauma includes C-spine imaging for those in whom you suspect C-spine trauma, chest x-rays, anterior-posterior x-ray of the pelvis as necessary, and a computed tomography scan, "which is really the workhorse of evaluation for blunt abdominal trauma," she said. Lab studies may include CBC, liver function tests, amylase, lipase, and blood type and cross.
Another option is Focused Assessment With Sonography for Trauma (the FAST scan). According to Dr. Grabowski, recent research has demonstrated that FAST has a low sensitivity and is inappropriate for use in hemodynamically stable children, but that it may be useful in unstable patients.
For splenic and hepatic injuries, grade and clinical exam dictates the need for PICU admission, frequency of vital signs, hematocrit and hemoglobin testing, diet, and activity. The American Pediatric Surgical Association published guidelines for the management of hemodynamically stable children with isolated spleen or liver injury (J. Pediatr. Surg. 2000; 35:164-9).
"Most children are in the hospital 1 day longer than their grade of injury, and they’re out of any activity for 2 weeks longer than their grade of injury," said Dr. Grabowski. Splenic injuries from to sports competition "are quite common, especially around football and hockey seasons," as are those caused by motor vehicle accidents and accidents from all-terrain vehicles. Common complaints include abdominal pain/tenderness, shoulder pain, nausea and vomiting, and anemia. CT scan is 98% sensitive in identifying the injury.
"Over time we have found that splenic salvage can be achieved in greater than 90% of children with blunt splenic injury, even up to a grade IV or V injury," she said. "Management of splenic injury should be based on physiologic parameters, rather than on a grading of the spleen injury or the presence of ‘blush’ on a CT scan. When an operation is required it’s usually for hemodynamic stability or for ongoing transfusion requirements."
For patients who undergo splenectomy, incidence of overwhelming post-splenectomy sepsis is thought to be about 0.8%, and the risk is greatest in the first 2 years. "Even though it’s such a low incidence, overwhelming post-splenectomy sepsis has a very high mortality, up to 50%," she said. "It’s important to educate the patients and the parents that if they develop a fever, it’s important to come to the hospital as soon as possible for evaluation."
Next, Dr. Grabowski discussed hepatic injuries, which involve the right lobe of the liver in 60%-78% of cases. Children with hepatic injuries commonly present with abdominal pain/tenderness and 56%-100% have associated injuries, most commonly involving the brain. Shock occurs in fewer than 10% of patients who present with a liver injury, while an aspartate aminotransferase/alanine aminotransferase (AST/ALT) level of greater than 250 units/L suggests liver injury.
Nonoperative treatment is successful about 90% of the time. This requires hemodynamic stability and absence of peritoneal signs. "Head injury is not a contraindication for nonoperative management," she said. "We have less experience with, and less studies looking at, angioembolization for hepatic injuries, but since we’ve had such good success with splenic injuries, we think it’s going to be helpful for hepatic injuries as well."
Operative treatment is indicated in cases of persistent bleeding, hemodynamic instability, or to rule out a missed injury.
Dr. Grabowski pointed out that there is little value in routine follow-up imaging studies after splenic or hepatic injury. The American Pediatric Surgical Association guidelines recommend a return to normal activities after a period of 2 weeks plus the grade of injury. "Normal activity is considered returning to school and walking," she said. "It’s not return to sports competition like football or wrestling. We usually say if your spleen gets injured during the football season, you can return to play the following season."
Bowel injuries comprise just 15% of intra-abdominal injuries in children, "but there is a high mortality, about 25%, and they’re easily missed on initial exam," Dr. Grabowski said. Clinical examination remains the most important diagnostic tool in the awake patient because only 60% of radiographic studies will be diagnostic. "It’s a difficult diagnosis to make, and delays occur in about 10% of cases," she said. "But many good studies have shown that children who have a delayed diagnosis of bowel injury did not have a worse outcome."
Seat belt injures also are common because most children are too large for car seats and too small for an adult seat belt system. "So they either don’t wear the cross-chest harness or they wear it inappropriately," Dr. Grabowski said. "Children also have a higher center of gravity, an immaturity and lack of structural integrity of their bony pelvis, and in most cases they have a relative paucity of abdominal musculature. Because they’re wearing their seat belt wrong they have a tendency to get injured by their seat belt more often than adults do."
An estimated 50%-70% of seat belt injuries are associated with a chance fracture, or a rupture of the posterior spinal ligament, or wedge, most commonly at L1 and L3. Those particular injuries "are very often associated with a bowel injury, so there’s a high index of suspicion in those children," she said. Indications for exploration in children who present with seat belt injuries include hemodynamic instability, pneumoperitoneum, peritonitis, bladder rupture, abdominal tenderness with free fluid in pelvis on CT without solid organ injury, if they worsen on exam, if they spike a fever, or if their labs become abnormal.
Dr. Grabowski advises clinicians to think nonaccidental trauma if children present with no history or explanation for injury, if the history is incompatible with the type or degree of injury, if a sibling is blamed for the injury, if caregivers give conflicting histories when interviewed separately, or if the history is not credible. "Health care providers are mandated reporters of nonaccidental trauma," she said, noting than an estimated 1 million children are victims of abuse each year.
Dr. Grabowski said that she had no relevant financial conflicts to make.
EXPERT ANALYSIS AT THE UCSD CRITICAL CARE SUMMER SESSION

Critically ill obstetric patients: Delivering the right care
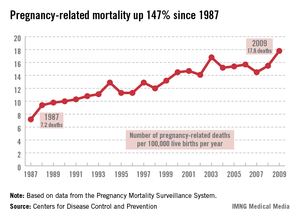
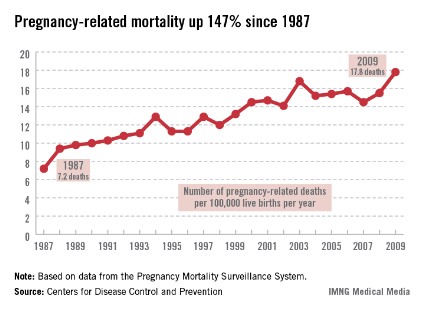
SAN DIEGO – Fewer than 1% of pregnant women present to the intensive care unit critically ill, but when they do, "there’s often significant morbidity and mortality," Dr. Kimberly S. Robbins said at the University of California, San Diego Critical Care Summer Session.
Dr. Robbins, an assistant professor in the UCSD department of anesthesiology, noted that the greatest physiologic changes of pregnancy affect the pulmonary and cardiovascular systems, and the most common conditions that land obstetric patients in the intensive care unit (ICU) are obstetric hemorrhage and complications of the hypertensive disorders of pregnancy.
"In general we consider pregnant patients to be potentially difficult airway patients, or difficult to intubate," she said. "That’s because pregnant patients are predisposed to edema and swollen airways." This patient population also has increased minute ventilation, "mostly because of an increase in tidal volume but also due to an increase in respiratory rate. They have increased oxygen demand, an increased metabolic rate because they are supplying oxygen to another being, and they have decreased functional residual capacity, which is the amount of volume that’s left in the lung after passive expiration."
From a cardiovascular standpoint, pregnant patients have an increased cardiac output both from an increased stroke volume and an increased heart rate. "During pregnancy the heart is shifted upward and to the left," Dr. Robbins added. "That impacts where you place your hands for CPR [cardiopulmonary resuscitation]. We also commonly see a decrease in systemic vascular resistance and diastolic blood pressure, as well as aortocaval compression. This means that the large gravid uterus can compress the great vessels. Not only does that impede venous return to the heart, but you can also get a decrease in the outflow of blood from the heart into the aorta."
Pregnant patients also experience a 45% increase in blood volume. This makes them relatively anemic "because there’s a relative increase in the plasma volume over the red cell volume," she explained. "Normal hemoglobin in a pregnant patient is around 11 or 12 g/dL."

Neurologically, pregnant patients can experience enhanced toxicity of local anesthetics used during cesarean section and during labor and delivery. Such complications "can land a person in the ICU," Dr. Robbins said. "Pregnant patients also have decreased anesthetic requirements. This is important as we’re titrating our sedatives or analgesics in the ICU. They also have distention of their epidural venous plexus. This makes it more likely that we may inadvertently inject local anesthetic into the vasculature and cause complications."
From a gastrointestinal standpoint, pregnant patients are considered full-stomach patients at all times, "even if they’ve had nothing by mouth," she said. "This is believed to occur after the first trimester, typically because of increased gastric pressure and decreased lower esophageal sphincter tone. During labor we see decreased gastric emptying, increased gastric volume, and decreased gastric pH levels."
Pregnancy also impacts renal function by increasing renal blood flow and glomerular filtration rate. In addition, it can cause decreased levels of creatinine and mild glucosuria and proteinuria. From an endocrine standpoint, pregnant patients have impaired glucose tolerance, increased sensitivity to insulin, and an increase in T3, T4, and thyroid size.
Dr. Robbins went on to discuss preeclampsia, a hypertensive disorder that causes 50,000-70,000 deaths worldwide per year. She characterized the condition as a triad of hypertension, proteinuria, and edema that usually occurs during a woman’s first pregnancy. Other factors include molar pregnancy, multiple gestation, and vascular endothelial disorders. General diagnostic criteria include at least 20 weeks gestation, new-onset hypertension (blood pressure of 140/90 mm Hg or 30/15 increase x2 at least 6 hours apart), proteinuria of greater than 0.3 g/day, and generalized edema or weight gain greater than 5 pounds/week.
Diagnostic criteria for severe preeclampsia include a systolic blood pressure of greater than 160 mm Hg or a diastolic blood pressure of greater than 110 mm Hg sustained, proteinuria of greater than 5 g/day, and signs of end organ dysfunction.
The pathophysiology of preeclampsia is unknown. "This is probably the greatest area of research in obstetrics and obstetric anesthesiology," Dr. Robbins said. "Some have postulated that it is a dysfunction of the maternal endothelium that develops because of abnormal formation of the placenta such that the placenta does not normally invade into the maternal vasculature. There are vasoactive substances that are released into the maternal circulation. That causes dysfunction of the maternal endothelium."
Patients with mild preeclampsia can be treated expectantly, but if the gestational age is greater than 37 weeks delivery should be considered. "The hallmark of treatment is prompt delivery of the fetus," she said.
For patients with severe preeclampsia, the focus is on improving placental perfusion through optimizing maternal cardiac output and peripheral vasodilation. "Most patients with pregnancy-induced hypertension are volume depleted and require careful volume repletion," she said. "Continuous fetal monitoring is also warranted."
In cases of severe preeclampsia, magnesium sulfate is the standard seizure prophylaxis. Dr. Robbins and her associates typically give a loading dose of 4-6 grams over 20 minutes, and then they run an infusion of 1-2 g/hr to keep the patient in a range of 4-8 mg/dL. "We can start to see toxicity such as loss of deep tendon reflexes at magnesium levels above 10 mg/dL," she said.
Hallmark agents for blood pressure control include hydralazine and labetalol. "You want to avoid rapid vasodilation and manage fluids in a goal-directed fashion," she said. "You may see these patients receiving steroids if their gestational age is less than 34 weeks. That’s to help with fetal lung maturity."
If preeclampsia progresses to seizures, magnesium therapy is the mainstay of treatment. "Once the patient is stabilized, she should undergo a neurologic evaluation and imaging to rule out other things such as stroke, hemorrhage, epilepsy, or a tumor," she said. "The highest risk of morbidity in this group of patients is from cerebrovascular events, including both ischemic and hemorrhagic events."
Patients with preeclampsia face an increased risk for HELLP syndrome, which stands for hemolysis, elevated liver enzymes, and low platelets. "The treatment here is delivery of the fetus and other supportive measures," Dr. Robbins said. Steroids have not been shown to be beneficial (Am. J. Obstet. Gynecol. 2005;193:1591-8). The clinical course of patients with HELLP syndrome "is fraught with complications, including liver hematoma rupture and renal failure, so you need to be prepared for that."
Dr. Robbins also discussed obstetric hemorrhage, which is the second-leading cause of pregnancy-related death in the United States and is the leading cause in developing countries. Hemorrhage is defined as losing greater than 500 mL of blood at vaginal delivery or greater than 1,000 mL after cesarean section. "Life-threatening hemorrhage can occur in the antepartum or postpartum period," she said. Antepartum hemorrhage is usually associated with placenta previa or abruption, while postpartum hemorrhage is most often associated with uterine atony. Risk factors for postpartum hemorrhage include preexisting anemia, obesity, fetal macrosomia, prior cesarean sections, and multiple gestations. "In these patients, disseminated intravascular coagulation may develop because of the dilutional effects of massive transfusion or some other underlying process," she said.
Treatment of obstetric hemorrhage includes volume resuscitation, correction of coagulopathy, maintaining adequate tissue perfusion, and controlling the source of blood loss. "Patients with uterine atony can be treated with uterine massage or with uterotonic drugs such as oxytocin, Methergine [methylergonovine], Hemabate [carboprost], and misoprostol," Dr. Robbins said. Surgical treatments such as uterine compression sutures or hysterectomy may be required.
Dr. Robbins said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Fewer than 1% of pregnant women present to the intensive care unit critically ill, but when they do, "there’s often significant morbidity and mortality," Dr. Kimberly S. Robbins said at the University of California, San Diego Critical Care Summer Session.
Dr. Robbins, an assistant professor in the UCSD department of anesthesiology, noted that the greatest physiologic changes of pregnancy affect the pulmonary and cardiovascular systems, and the most common conditions that land obstetric patients in the intensive care unit (ICU) are obstetric hemorrhage and complications of the hypertensive disorders of pregnancy.
"In general we consider pregnant patients to be potentially difficult airway patients, or difficult to intubate," she said. "That’s because pregnant patients are predisposed to edema and swollen airways." This patient population also has increased minute ventilation, "mostly because of an increase in tidal volume but also due to an increase in respiratory rate. They have increased oxygen demand, an increased metabolic rate because they are supplying oxygen to another being, and they have decreased functional residual capacity, which is the amount of volume that’s left in the lung after passive expiration."
From a cardiovascular standpoint, pregnant patients have an increased cardiac output both from an increased stroke volume and an increased heart rate. "During pregnancy the heart is shifted upward and to the left," Dr. Robbins added. "That impacts where you place your hands for CPR [cardiopulmonary resuscitation]. We also commonly see a decrease in systemic vascular resistance and diastolic blood pressure, as well as aortocaval compression. This means that the large gravid uterus can compress the great vessels. Not only does that impede venous return to the heart, but you can also get a decrease in the outflow of blood from the heart into the aorta."
Pregnant patients also experience a 45% increase in blood volume. This makes them relatively anemic "because there’s a relative increase in the plasma volume over the red cell volume," she explained. "Normal hemoglobin in a pregnant patient is around 11 or 12 g/dL."
Neurologically, pregnant patients can experience enhanced toxicity of local anesthetics used during cesarean section and during labor and delivery. Such complications "can land a person in the ICU," Dr. Robbins said. "Pregnant patients also have decreased anesthetic requirements. This is important as we’re titrating our sedatives or analgesics in the ICU. They also have distention of their epidural venous plexus. This makes it more likely that we may inadvertently inject local anesthetic into the vasculature and cause complications."
From a gastrointestinal standpoint, pregnant patients are considered full-stomach patients at all times, "even if they’ve had nothing by mouth," she said. "This is believed to occur after the first trimester, typically because of increased gastric pressure and decreased lower esophageal sphincter tone. During labor we see decreased gastric emptying, increased gastric volume, and decreased gastric pH levels."
Pregnancy also impacts renal function by increasing renal blood flow and glomerular filtration rate. In addition, it can cause decreased levels of creatinine and mild glucosuria and proteinuria. From an endocrine standpoint, pregnant patients have impaired glucose tolerance, increased sensitivity to insulin, and an increase in T3, T4, and thyroid size.
Dr. Robbins went on to discuss preeclampsia, a hypertensive disorder that causes 50,000-70,000 deaths worldwide per year. She characterized the condition as a triad of hypertension, proteinuria, and edema that usually occurs during a woman’s first pregnancy. Other factors include molar pregnancy, multiple gestation, and vascular endothelial disorders. General diagnostic criteria include at least 20 weeks gestation, new-onset hypertension (blood pressure of 140/90 mm Hg or 30/15 increase x2 at least 6 hours apart), proteinuria of greater than 0.3 g/day, and generalized edema or weight gain greater than 5 pounds/week.
Diagnostic criteria for severe preeclampsia include a systolic blood pressure of greater than 160 mm Hg or a diastolic blood pressure of greater than 110 mm Hg sustained, proteinuria of greater than 5 g/day, and signs of end organ dysfunction.
The pathophysiology of preeclampsia is unknown. "This is probably the greatest area of research in obstetrics and obstetric anesthesiology," Dr. Robbins said. "Some have postulated that it is a dysfunction of the maternal endothelium that develops because of abnormal formation of the placenta such that the placenta does not normally invade into the maternal vasculature. There are vasoactive substances that are released into the maternal circulation. That causes dysfunction of the maternal endothelium."
Patients with mild preeclampsia can be treated expectantly, but if the gestational age is greater than 37 weeks delivery should be considered. "The hallmark of treatment is prompt delivery of the fetus," she said.
For patients with severe preeclampsia, the focus is on improving placental perfusion through optimizing maternal cardiac output and peripheral vasodilation. "Most patients with pregnancy-induced hypertension are volume depleted and require careful volume repletion," she said. "Continuous fetal monitoring is also warranted."
In cases of severe preeclampsia, magnesium sulfate is the standard seizure prophylaxis. Dr. Robbins and her associates typically give a loading dose of 4-6 grams over 20 minutes, and then they run an infusion of 1-2 g/hr to keep the patient in a range of 4-8 mg/dL. "We can start to see toxicity such as loss of deep tendon reflexes at magnesium levels above 10 mg/dL," she said.
Hallmark agents for blood pressure control include hydralazine and labetalol. "You want to avoid rapid vasodilation and manage fluids in a goal-directed fashion," she said. "You may see these patients receiving steroids if their gestational age is less than 34 weeks. That’s to help with fetal lung maturity."
If preeclampsia progresses to seizures, magnesium therapy is the mainstay of treatment. "Once the patient is stabilized, she should undergo a neurologic evaluation and imaging to rule out other things such as stroke, hemorrhage, epilepsy, or a tumor," she said. "The highest risk of morbidity in this group of patients is from cerebrovascular events, including both ischemic and hemorrhagic events."
Patients with preeclampsia face an increased risk for HELLP syndrome, which stands for hemolysis, elevated liver enzymes, and low platelets. "The treatment here is delivery of the fetus and other supportive measures," Dr. Robbins said. Steroids have not been shown to be beneficial (Am. J. Obstet. Gynecol. 2005;193:1591-8). The clinical course of patients with HELLP syndrome "is fraught with complications, including liver hematoma rupture and renal failure, so you need to be prepared for that."
Dr. Robbins also discussed obstetric hemorrhage, which is the second-leading cause of pregnancy-related death in the United States and is the leading cause in developing countries. Hemorrhage is defined as losing greater than 500 mL of blood at vaginal delivery or greater than 1,000 mL after cesarean section. "Life-threatening hemorrhage can occur in the antepartum or postpartum period," she said. Antepartum hemorrhage is usually associated with placenta previa or abruption, while postpartum hemorrhage is most often associated with uterine atony. Risk factors for postpartum hemorrhage include preexisting anemia, obesity, fetal macrosomia, prior cesarean sections, and multiple gestations. "In these patients, disseminated intravascular coagulation may develop because of the dilutional effects of massive transfusion or some other underlying process," she said.
Treatment of obstetric hemorrhage includes volume resuscitation, correction of coagulopathy, maintaining adequate tissue perfusion, and controlling the source of blood loss. "Patients with uterine atony can be treated with uterine massage or with uterotonic drugs such as oxytocin, Methergine [methylergonovine], Hemabate [carboprost], and misoprostol," Dr. Robbins said. Surgical treatments such as uterine compression sutures or hysterectomy may be required.
Dr. Robbins said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Fewer than 1% of pregnant women present to the intensive care unit critically ill, but when they do, "there’s often significant morbidity and mortality," Dr. Kimberly S. Robbins said at the University of California, San Diego Critical Care Summer Session.
Dr. Robbins, an assistant professor in the UCSD department of anesthesiology, noted that the greatest physiologic changes of pregnancy affect the pulmonary and cardiovascular systems, and the most common conditions that land obstetric patients in the intensive care unit (ICU) are obstetric hemorrhage and complications of the hypertensive disorders of pregnancy.
"In general we consider pregnant patients to be potentially difficult airway patients, or difficult to intubate," she said. "That’s because pregnant patients are predisposed to edema and swollen airways." This patient population also has increased minute ventilation, "mostly because of an increase in tidal volume but also due to an increase in respiratory rate. They have increased oxygen demand, an increased metabolic rate because they are supplying oxygen to another being, and they have decreased functional residual capacity, which is the amount of volume that’s left in the lung after passive expiration."
From a cardiovascular standpoint, pregnant patients have an increased cardiac output both from an increased stroke volume and an increased heart rate. "During pregnancy the heart is shifted upward and to the left," Dr. Robbins added. "That impacts where you place your hands for CPR [cardiopulmonary resuscitation]. We also commonly see a decrease in systemic vascular resistance and diastolic blood pressure, as well as aortocaval compression. This means that the large gravid uterus can compress the great vessels. Not only does that impede venous return to the heart, but you can also get a decrease in the outflow of blood from the heart into the aorta."
Pregnant patients also experience a 45% increase in blood volume. This makes them relatively anemic "because there’s a relative increase in the plasma volume over the red cell volume," she explained. "Normal hemoglobin in a pregnant patient is around 11 or 12 g/dL."
Neurologically, pregnant patients can experience enhanced toxicity of local anesthetics used during cesarean section and during labor and delivery. Such complications "can land a person in the ICU," Dr. Robbins said. "Pregnant patients also have decreased anesthetic requirements. This is important as we’re titrating our sedatives or analgesics in the ICU. They also have distention of their epidural venous plexus. This makes it more likely that we may inadvertently inject local anesthetic into the vasculature and cause complications."
From a gastrointestinal standpoint, pregnant patients are considered full-stomach patients at all times, "even if they’ve had nothing by mouth," she said. "This is believed to occur after the first trimester, typically because of increased gastric pressure and decreased lower esophageal sphincter tone. During labor we see decreased gastric emptying, increased gastric volume, and decreased gastric pH levels."
Pregnancy also impacts renal function by increasing renal blood flow and glomerular filtration rate. In addition, it can cause decreased levels of creatinine and mild glucosuria and proteinuria. From an endocrine standpoint, pregnant patients have impaired glucose tolerance, increased sensitivity to insulin, and an increase in T3, T4, and thyroid size.
Dr. Robbins went on to discuss preeclampsia, a hypertensive disorder that causes 50,000-70,000 deaths worldwide per year. She characterized the condition as a triad of hypertension, proteinuria, and edema that usually occurs during a woman’s first pregnancy. Other factors include molar pregnancy, multiple gestation, and vascular endothelial disorders. General diagnostic criteria include at least 20 weeks gestation, new-onset hypertension (blood pressure of 140/90 mm Hg or 30/15 increase x2 at least 6 hours apart), proteinuria of greater than 0.3 g/day, and generalized edema or weight gain greater than 5 pounds/week.
Diagnostic criteria for severe preeclampsia include a systolic blood pressure of greater than 160 mm Hg or a diastolic blood pressure of greater than 110 mm Hg sustained, proteinuria of greater than 5 g/day, and signs of end organ dysfunction.
The pathophysiology of preeclampsia is unknown. "This is probably the greatest area of research in obstetrics and obstetric anesthesiology," Dr. Robbins said. "Some have postulated that it is a dysfunction of the maternal endothelium that develops because of abnormal formation of the placenta such that the placenta does not normally invade into the maternal vasculature. There are vasoactive substances that are released into the maternal circulation. That causes dysfunction of the maternal endothelium."
Patients with mild preeclampsia can be treated expectantly, but if the gestational age is greater than 37 weeks delivery should be considered. "The hallmark of treatment is prompt delivery of the fetus," she said.
For patients with severe preeclampsia, the focus is on improving placental perfusion through optimizing maternal cardiac output and peripheral vasodilation. "Most patients with pregnancy-induced hypertension are volume depleted and require careful volume repletion," she said. "Continuous fetal monitoring is also warranted."
In cases of severe preeclampsia, magnesium sulfate is the standard seizure prophylaxis. Dr. Robbins and her associates typically give a loading dose of 4-6 grams over 20 minutes, and then they run an infusion of 1-2 g/hr to keep the patient in a range of 4-8 mg/dL. "We can start to see toxicity such as loss of deep tendon reflexes at magnesium levels above 10 mg/dL," she said.
Hallmark agents for blood pressure control include hydralazine and labetalol. "You want to avoid rapid vasodilation and manage fluids in a goal-directed fashion," she said. "You may see these patients receiving steroids if their gestational age is less than 34 weeks. That’s to help with fetal lung maturity."
If preeclampsia progresses to seizures, magnesium therapy is the mainstay of treatment. "Once the patient is stabilized, she should undergo a neurologic evaluation and imaging to rule out other things such as stroke, hemorrhage, epilepsy, or a tumor," she said. "The highest risk of morbidity in this group of patients is from cerebrovascular events, including both ischemic and hemorrhagic events."
Patients with preeclampsia face an increased risk for HELLP syndrome, which stands for hemolysis, elevated liver enzymes, and low platelets. "The treatment here is delivery of the fetus and other supportive measures," Dr. Robbins said. Steroids have not been shown to be beneficial (Am. J. Obstet. Gynecol. 2005;193:1591-8). The clinical course of patients with HELLP syndrome "is fraught with complications, including liver hematoma rupture and renal failure, so you need to be prepared for that."
Dr. Robbins also discussed obstetric hemorrhage, which is the second-leading cause of pregnancy-related death in the United States and is the leading cause in developing countries. Hemorrhage is defined as losing greater than 500 mL of blood at vaginal delivery or greater than 1,000 mL after cesarean section. "Life-threatening hemorrhage can occur in the antepartum or postpartum period," she said. Antepartum hemorrhage is usually associated with placenta previa or abruption, while postpartum hemorrhage is most often associated with uterine atony. Risk factors for postpartum hemorrhage include preexisting anemia, obesity, fetal macrosomia, prior cesarean sections, and multiple gestations. "In these patients, disseminated intravascular coagulation may develop because of the dilutional effects of massive transfusion or some other underlying process," she said.
Treatment of obstetric hemorrhage includes volume resuscitation, correction of coagulopathy, maintaining adequate tissue perfusion, and controlling the source of blood loss. "Patients with uterine atony can be treated with uterine massage or with uterotonic drugs such as oxytocin, Methergine [methylergonovine], Hemabate [carboprost], and misoprostol," Dr. Robbins said. Surgical treatments such as uterine compression sutures or hysterectomy may be required.
Dr. Robbins said that she had no relevant financial conflicts to disclose.
EXPERT ANALYSIS AT THE UCSD CRITICAL CARE SUMMER SESSION
Collaborative quality improvement projects work, expert maintains
SAN DIEGO – In the opinion of Dr. Wayne J. English, it doesn’t take much for collaborative quality improvement projects to demonstrate a return on investment.
At the national conference of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), he discussed his experience as a member of the Michigan Bariatric Surgery Collaborative (MBSC), a clinical outcomes registry and quality improvement program funded by Blue Cross Blue Shield of Michigan (BCBS) "Hospitals across the state are collecting, sharing, and analyzing data, then designing and implementing changes to improve patient care, and it’s working," said Dr. English, medical director of bariatric surgery at the Bariatric and Metabolic Institute at Marquette (Mich.) General Hospital.

In 1997, a group of five hospitals in Michigan joined with Blue Cross Blue Shield of Michigan Foundation and Blue Care Network to collaborate on the study of variation in angiography procedures and treatment. Recommendations from the group’s analysis "contributed to dramatic decreases in coronary emergency bypass surgeries and other complications," Dr. English said. "The initiative also saved an estimated $102 million in statewide health costs over 3 years." Since then, 11 more initiatives have [been] launched to address many of the most common and costly areas of surgical and medical care in Michigan. These included cardiac imaging, vascular intervention, cardiothoracic surgery, trauma, general surgery, breast cancer, surgical outcomes, hospital medicine, knee/hip replacement, radiation oncology, and bariatric surgery.
Speaking in the context of his experience with the MBSC, Dr. English said that much of the success comes from the three-part approach to each initiative. First, funding from BCBS "enables hospitals to work in collaborative environment," he said. "BCBS provides resources for data collection and analysis along with administrative oversight."
Second, a separate coordinating center serves as a data warehouse, conducts data audits, performs data analyses, and generates comparative performance reports.
Third, participating hospitals "work together by sharing data and best practices to improve patient care throughout the state of Michigan," he said.
The MBSC collects data on perioperative care and outcomes, late outcomes, structure and process of care, technical quality, subjective aspects of quality, and cost. "There are site visits that occur on a regular basis," he said. "There are usually two surgeons and two nurses that go along on a site visit. We share ideas during those visits; these are collegial events."
The primary focus is the registry data. "We look at variation in practice and determine best evidence. We meet three times a year to analyze risk- and reliability-adjusted data, develop quality improvement projects and, ultimately, best practices," Dr. English said. Currently, the collaborative comprises 39 sites, 76 surgeons, and data on more than 40,000 patients. Approximately 6,500 patients are added into the database each year.
Notable outcomes from MBSC projects to date, he said, include a 24% decrease in complication rates from 2007 to 2009, a 35% decrease in readmission rates decreased from 2007 to 2009, and a 35% decreased in ED visits from 2007 to 2010. "The decline in ED visits alone resulted in overall savings for BCBS of Michigan of $4.7 million and an overall savings for statewide plans of $14.6 million," Dr. English said.
One of the first initiatives launched by the MBSC involved a quality improvement effort to reduce the rate of pulmonary embolism, which accounts for almost half of all deaths after bariatric surgery. Standard approaches to prophylaxis include early ambulation, compression stockings/devices, and anticoagulation.
"When we surveyed surgeons in the state of Michigan, we found that there was tremendous variation in how medical chemoprophylaxis was implemented," Dr. English noted. "Many surgeons were using low-molecular-weight heparin and/or unfractionated heparin to varying degrees preoperatively, postoperatively and post discharge, while some used none at all. So the collaborative data determined statistically significant patient risk factors and developed a VTE risk calculator to stratify the baseline risk for VTE. Once surgeons started participating and utilizing risk-stratified treatment guidelines, we started to see a downward trend on the rates of thromboembolic events."
A parallel initiative evaluated the impact of placing inferior vena cava (IVC) filters during bariatric surgery. The value of IVC filters as a prophylaxis in bariatric surgery patients "is unclear, but their use has been growing rapidly since the availability of removable filters," Dr. English said. "According to data from the collaborative, there was wide variability in utilization from never to almost 40% of patients receiving IVC filters."
After analyzing outcomes data from the MBSC, it was discovered that complication rates were significantly higher in patients who had IVC filters placed during bariatric surgery, compared with those who did not. "In fact, over half of deaths and permanent disability were directly attributable to the filter itself," he said. "Once provided with the initial data feedback, many surgeons started decreasing the use of IVC filters during bariatric surgery. Now, fewer than 2% use them."
MBSC data also showed that costs were about $13,000 less per case to perform gastric bypass procedures without the use of IVC filters. "As a result of this one quality improvement project, an estimated $1.3 million was saved over the course of 1 year while all Michigan payers saved an estimated $2.6 million over the course of 1 year," Dr. English said. "That savings is more than enough to cover the cost of operating MBSC each year."
Dr. English disclosed that he serves as a consultant for ReShape Medical.
SAN DIEGO – In the opinion of Dr. Wayne J. English, it doesn’t take much for collaborative quality improvement projects to demonstrate a return on investment.
At the national conference of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), he discussed his experience as a member of the Michigan Bariatric Surgery Collaborative (MBSC), a clinical outcomes registry and quality improvement program funded by Blue Cross Blue Shield of Michigan (BCBS) "Hospitals across the state are collecting, sharing, and analyzing data, then designing and implementing changes to improve patient care, and it’s working," said Dr. English, medical director of bariatric surgery at the Bariatric and Metabolic Institute at Marquette (Mich.) General Hospital.
In 1997, a group of five hospitals in Michigan joined with Blue Cross Blue Shield of Michigan Foundation and Blue Care Network to collaborate on the study of variation in angiography procedures and treatment. Recommendations from the group’s analysis "contributed to dramatic decreases in coronary emergency bypass surgeries and other complications," Dr. English said. "The initiative also saved an estimated $102 million in statewide health costs over 3 years." Since then, 11 more initiatives have [been] launched to address many of the most common and costly areas of surgical and medical care in Michigan. These included cardiac imaging, vascular intervention, cardiothoracic surgery, trauma, general surgery, breast cancer, surgical outcomes, hospital medicine, knee/hip replacement, radiation oncology, and bariatric surgery.
Speaking in the context of his experience with the MBSC, Dr. English said that much of the success comes from the three-part approach to each initiative. First, funding from BCBS "enables hospitals to work in collaborative environment," he said. "BCBS provides resources for data collection and analysis along with administrative oversight."
Second, a separate coordinating center serves as a data warehouse, conducts data audits, performs data analyses, and generates comparative performance reports.
Third, participating hospitals "work together by sharing data and best practices to improve patient care throughout the state of Michigan," he said.
The MBSC collects data on perioperative care and outcomes, late outcomes, structure and process of care, technical quality, subjective aspects of quality, and cost. "There are site visits that occur on a regular basis," he said. "There are usually two surgeons and two nurses that go along on a site visit. We share ideas during those visits; these are collegial events."
The primary focus is the registry data. "We look at variation in practice and determine best evidence. We meet three times a year to analyze risk- and reliability-adjusted data, develop quality improvement projects and, ultimately, best practices," Dr. English said. Currently, the collaborative comprises 39 sites, 76 surgeons, and data on more than 40,000 patients. Approximately 6,500 patients are added into the database each year.
Notable outcomes from MBSC projects to date, he said, include a 24% decrease in complication rates from 2007 to 2009, a 35% decrease in readmission rates decreased from 2007 to 2009, and a 35% decreased in ED visits from 2007 to 2010. "The decline in ED visits alone resulted in overall savings for BCBS of Michigan of $4.7 million and an overall savings for statewide plans of $14.6 million," Dr. English said.
One of the first initiatives launched by the MBSC involved a quality improvement effort to reduce the rate of pulmonary embolism, which accounts for almost half of all deaths after bariatric surgery. Standard approaches to prophylaxis include early ambulation, compression stockings/devices, and anticoagulation.
"When we surveyed surgeons in the state of Michigan, we found that there was tremendous variation in how medical chemoprophylaxis was implemented," Dr. English noted. "Many surgeons were using low-molecular-weight heparin and/or unfractionated heparin to varying degrees preoperatively, postoperatively and post discharge, while some used none at all. So the collaborative data determined statistically significant patient risk factors and developed a VTE risk calculator to stratify the baseline risk for VTE. Once surgeons started participating and utilizing risk-stratified treatment guidelines, we started to see a downward trend on the rates of thromboembolic events."
A parallel initiative evaluated the impact of placing inferior vena cava (IVC) filters during bariatric surgery. The value of IVC filters as a prophylaxis in bariatric surgery patients "is unclear, but their use has been growing rapidly since the availability of removable filters," Dr. English said. "According to data from the collaborative, there was wide variability in utilization from never to almost 40% of patients receiving IVC filters."
After analyzing outcomes data from the MBSC, it was discovered that complication rates were significantly higher in patients who had IVC filters placed during bariatric surgery, compared with those who did not. "In fact, over half of deaths and permanent disability were directly attributable to the filter itself," he said. "Once provided with the initial data feedback, many surgeons started decreasing the use of IVC filters during bariatric surgery. Now, fewer than 2% use them."
MBSC data also showed that costs were about $13,000 less per case to perform gastric bypass procedures without the use of IVC filters. "As a result of this one quality improvement project, an estimated $1.3 million was saved over the course of 1 year while all Michigan payers saved an estimated $2.6 million over the course of 1 year," Dr. English said. "That savings is more than enough to cover the cost of operating MBSC each year."
Dr. English disclosed that he serves as a consultant for ReShape Medical.
SAN DIEGO – In the opinion of Dr. Wayne J. English, it doesn’t take much for collaborative quality improvement projects to demonstrate a return on investment.
At the national conference of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), he discussed his experience as a member of the Michigan Bariatric Surgery Collaborative (MBSC), a clinical outcomes registry and quality improvement program funded by Blue Cross Blue Shield of Michigan (BCBS) "Hospitals across the state are collecting, sharing, and analyzing data, then designing and implementing changes to improve patient care, and it’s working," said Dr. English, medical director of bariatric surgery at the Bariatric and Metabolic Institute at Marquette (Mich.) General Hospital.
In 1997, a group of five hospitals in Michigan joined with Blue Cross Blue Shield of Michigan Foundation and Blue Care Network to collaborate on the study of variation in angiography procedures and treatment. Recommendations from the group’s analysis "contributed to dramatic decreases in coronary emergency bypass surgeries and other complications," Dr. English said. "The initiative also saved an estimated $102 million in statewide health costs over 3 years." Since then, 11 more initiatives have [been] launched to address many of the most common and costly areas of surgical and medical care in Michigan. These included cardiac imaging, vascular intervention, cardiothoracic surgery, trauma, general surgery, breast cancer, surgical outcomes, hospital medicine, knee/hip replacement, radiation oncology, and bariatric surgery.
Speaking in the context of his experience with the MBSC, Dr. English said that much of the success comes from the three-part approach to each initiative. First, funding from BCBS "enables hospitals to work in collaborative environment," he said. "BCBS provides resources for data collection and analysis along with administrative oversight."
Second, a separate coordinating center serves as a data warehouse, conducts data audits, performs data analyses, and generates comparative performance reports.
Third, participating hospitals "work together by sharing data and best practices to improve patient care throughout the state of Michigan," he said.
The MBSC collects data on perioperative care and outcomes, late outcomes, structure and process of care, technical quality, subjective aspects of quality, and cost. "There are site visits that occur on a regular basis," he said. "There are usually two surgeons and two nurses that go along on a site visit. We share ideas during those visits; these are collegial events."
The primary focus is the registry data. "We look at variation in practice and determine best evidence. We meet three times a year to analyze risk- and reliability-adjusted data, develop quality improvement projects and, ultimately, best practices," Dr. English said. Currently, the collaborative comprises 39 sites, 76 surgeons, and data on more than 40,000 patients. Approximately 6,500 patients are added into the database each year.
Notable outcomes from MBSC projects to date, he said, include a 24% decrease in complication rates from 2007 to 2009, a 35% decrease in readmission rates decreased from 2007 to 2009, and a 35% decreased in ED visits from 2007 to 2010. "The decline in ED visits alone resulted in overall savings for BCBS of Michigan of $4.7 million and an overall savings for statewide plans of $14.6 million," Dr. English said.
One of the first initiatives launched by the MBSC involved a quality improvement effort to reduce the rate of pulmonary embolism, which accounts for almost half of all deaths after bariatric surgery. Standard approaches to prophylaxis include early ambulation, compression stockings/devices, and anticoagulation.
"When we surveyed surgeons in the state of Michigan, we found that there was tremendous variation in how medical chemoprophylaxis was implemented," Dr. English noted. "Many surgeons were using low-molecular-weight heparin and/or unfractionated heparin to varying degrees preoperatively, postoperatively and post discharge, while some used none at all. So the collaborative data determined statistically significant patient risk factors and developed a VTE risk calculator to stratify the baseline risk for VTE. Once surgeons started participating and utilizing risk-stratified treatment guidelines, we started to see a downward trend on the rates of thromboembolic events."
A parallel initiative evaluated the impact of placing inferior vena cava (IVC) filters during bariatric surgery. The value of IVC filters as a prophylaxis in bariatric surgery patients "is unclear, but their use has been growing rapidly since the availability of removable filters," Dr. English said. "According to data from the collaborative, there was wide variability in utilization from never to almost 40% of patients receiving IVC filters."
After analyzing outcomes data from the MBSC, it was discovered that complication rates were significantly higher in patients who had IVC filters placed during bariatric surgery, compared with those who did not. "In fact, over half of deaths and permanent disability were directly attributable to the filter itself," he said. "Once provided with the initial data feedback, many surgeons started decreasing the use of IVC filters during bariatric surgery. Now, fewer than 2% use them."
MBSC data also showed that costs were about $13,000 less per case to perform gastric bypass procedures without the use of IVC filters. "As a result of this one quality improvement project, an estimated $1.3 million was saved over the course of 1 year while all Michigan payers saved an estimated $2.6 million over the course of 1 year," Dr. English said. "That savings is more than enough to cover the cost of operating MBSC each year."
Dr. English disclosed that he serves as a consultant for ReShape Medical.
EXPERT ANALYSIS AT THE ACS NSQIP NATIONAL CONFERENCE

Splenectomy mortality risk similar for malignant and benign disease
SAN DIEGO – The overall 30-day morbidity rate following surgery for elective splenectomy for hematologic disorders is 13.6% while the overall 30-day mortality rate is 1.6%, results from an analysis of national data demonstrated.
While the morbidity rate was significantly higher for patients with malignant versus benign disease (19.6% vs. 11.9%, respectively), the mortality rate was similar between the two patient groups, Mary Belding-Schmitt reported at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
"There are limited data regarding complications and mortality following elective splenectomy, especially for malignant disease," said Ms. Belding-Schmitt, a staff nurse in the division of surgical oncology and endocrine surgery in the department of surgery at University of Iowa Hospitals and Clinics. "Most of the published studies are from single institution series and focus on primary splenic diseases. More recent data report a wide range of complications and mortality across different diseases treated with splenectomy."

In an effort to evaluate complications and mortality following elective splenectomy for benign and malignant hematologic disorders, she and her associates searched the ACS NSQIP database for patients who underwent elective splenectomy procedures from 2006 to 2011. Benign disease was defined as hemolytic anemia or thrombocytopenia, while malignant disease was defined as leukemia or lymphoma. The researchers excluded cases of nonelective splenectomy or splenectomy combined with another procedure. Perioperative clinicopathologic variables and operative complications were analyzed and compared between patients treated for benign and malignant hematologic disease.
Of the 4,859 splenectomy procedures identified from the data set, 1,762 cases met criteria for analysis. Of these, 1,379 operations were for benign conditions while 383 were for malignant conditions. Of the benign indications for splenectomy, most (73.5%) were for thrombocytopenia, 11.7% were for hemolytic anemia, and the remainder were for other conditions. Of the malignant indications for splenectomy, most (83.6%) were for lymphoma and 16.4% were for leukemia.
Patients with benign disease tended to be younger (a mean of 50 vs. 61 years, respectively), were more commonly female (58% vs. 43%), tended to be diabetic (15% vs. 12%), had a higher body mass index (a mean of 29.7 kg/m2 vs. 27.3 kg/m2), received preoperative steroids (60% vs. 13%), and underwent significantly more laparoscopic procedures (82% vs. 39%; P less than .0001).
Ms. Belding-Schmitt reported that the rate of overall complications was significantly higher for patients with malignant vs. benign disease (19.6% vs. 11.9%, respectively; P = .0002), but there was no significant difference between the two groups in overall mortality (2.1% vs. 1.5%; P = .37). She characterized the 2.1% mortality rate as being similar to that following pancreatectomy in high-volume centers.
Patients with malignant disease tended to have a higher rate of infection complications (16% vs. 9%; P = .0002) and a longer median hospital length of stay (5 vs. 3 days; P = .0005).
Ms. Belding-Schmitt said that a multivariable analysis is underway to determine specific variables which account for significant morbidity and mortality from splenectomy for hematologic disorders. She said she had no relevant financial disclosures.
SAN DIEGO – The overall 30-day morbidity rate following surgery for elective splenectomy for hematologic disorders is 13.6% while the overall 30-day mortality rate is 1.6%, results from an analysis of national data demonstrated.
While the morbidity rate was significantly higher for patients with malignant versus benign disease (19.6% vs. 11.9%, respectively), the mortality rate was similar between the two patient groups, Mary Belding-Schmitt reported at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
"There are limited data regarding complications and mortality following elective splenectomy, especially for malignant disease," said Ms. Belding-Schmitt, a staff nurse in the division of surgical oncology and endocrine surgery in the department of surgery at University of Iowa Hospitals and Clinics. "Most of the published studies are from single institution series and focus on primary splenic diseases. More recent data report a wide range of complications and mortality across different diseases treated with splenectomy."
In an effort to evaluate complications and mortality following elective splenectomy for benign and malignant hematologic disorders, she and her associates searched the ACS NSQIP database for patients who underwent elective splenectomy procedures from 2006 to 2011. Benign disease was defined as hemolytic anemia or thrombocytopenia, while malignant disease was defined as leukemia or lymphoma. The researchers excluded cases of nonelective splenectomy or splenectomy combined with another procedure. Perioperative clinicopathologic variables and operative complications were analyzed and compared between patients treated for benign and malignant hematologic disease.
Of the 4,859 splenectomy procedures identified from the data set, 1,762 cases met criteria for analysis. Of these, 1,379 operations were for benign conditions while 383 were for malignant conditions. Of the benign indications for splenectomy, most (73.5%) were for thrombocytopenia, 11.7% were for hemolytic anemia, and the remainder were for other conditions. Of the malignant indications for splenectomy, most (83.6%) were for lymphoma and 16.4% were for leukemia.
Patients with benign disease tended to be younger (a mean of 50 vs. 61 years, respectively), were more commonly female (58% vs. 43%), tended to be diabetic (15% vs. 12%), had a higher body mass index (a mean of 29.7 kg/m2 vs. 27.3 kg/m2), received preoperative steroids (60% vs. 13%), and underwent significantly more laparoscopic procedures (82% vs. 39%; P less than .0001).
Ms. Belding-Schmitt reported that the rate of overall complications was significantly higher for patients with malignant vs. benign disease (19.6% vs. 11.9%, respectively; P = .0002), but there was no significant difference between the two groups in overall mortality (2.1% vs. 1.5%; P = .37). She characterized the 2.1% mortality rate as being similar to that following pancreatectomy in high-volume centers.
Patients with malignant disease tended to have a higher rate of infection complications (16% vs. 9%; P = .0002) and a longer median hospital length of stay (5 vs. 3 days; P = .0005).
Ms. Belding-Schmitt said that a multivariable analysis is underway to determine specific variables which account for significant morbidity and mortality from splenectomy for hematologic disorders. She said she had no relevant financial disclosures.
SAN DIEGO – The overall 30-day morbidity rate following surgery for elective splenectomy for hematologic disorders is 13.6% while the overall 30-day mortality rate is 1.6%, results from an analysis of national data demonstrated.
While the morbidity rate was significantly higher for patients with malignant versus benign disease (19.6% vs. 11.9%, respectively), the mortality rate was similar between the two patient groups, Mary Belding-Schmitt reported at the American College of Surgeons/National Surgical Quality Improvement Program National Conference.
"There are limited data regarding complications and mortality following elective splenectomy, especially for malignant disease," said Ms. Belding-Schmitt, a staff nurse in the division of surgical oncology and endocrine surgery in the department of surgery at University of Iowa Hospitals and Clinics. "Most of the published studies are from single institution series and focus on primary splenic diseases. More recent data report a wide range of complications and mortality across different diseases treated with splenectomy."
In an effort to evaluate complications and mortality following elective splenectomy for benign and malignant hematologic disorders, she and her associates searched the ACS NSQIP database for patients who underwent elective splenectomy procedures from 2006 to 2011. Benign disease was defined as hemolytic anemia or thrombocytopenia, while malignant disease was defined as leukemia or lymphoma. The researchers excluded cases of nonelective splenectomy or splenectomy combined with another procedure. Perioperative clinicopathologic variables and operative complications were analyzed and compared between patients treated for benign and malignant hematologic disease.
Of the 4,859 splenectomy procedures identified from the data set, 1,762 cases met criteria for analysis. Of these, 1,379 operations were for benign conditions while 383 were for malignant conditions. Of the benign indications for splenectomy, most (73.5%) were for thrombocytopenia, 11.7% were for hemolytic anemia, and the remainder were for other conditions. Of the malignant indications for splenectomy, most (83.6%) were for lymphoma and 16.4% were for leukemia.
Patients with benign disease tended to be younger (a mean of 50 vs. 61 years, respectively), were more commonly female (58% vs. 43%), tended to be diabetic (15% vs. 12%), had a higher body mass index (a mean of 29.7 kg/m2 vs. 27.3 kg/m2), received preoperative steroids (60% vs. 13%), and underwent significantly more laparoscopic procedures (82% vs. 39%; P less than .0001).
Ms. Belding-Schmitt reported that the rate of overall complications was significantly higher for patients with malignant vs. benign disease (19.6% vs. 11.9%, respectively; P = .0002), but there was no significant difference between the two groups in overall mortality (2.1% vs. 1.5%; P = .37). She characterized the 2.1% mortality rate as being similar to that following pancreatectomy in high-volume centers.
Patients with malignant disease tended to have a higher rate of infection complications (16% vs. 9%; P = .0002) and a longer median hospital length of stay (5 vs. 3 days; P = .0005).
Ms. Belding-Schmitt said that a multivariable analysis is underway to determine specific variables which account for significant morbidity and mortality from splenectomy for hematologic disorders. She said she had no relevant financial disclosures.
AT THE ACS NSQIP NATIONAL CONFERENCE
Major finding: Following elective splenectomy, the rate of overall complications was significantly higher for patients with malignant vs. benign disease (19.6% vs. 11.9%, respectively; P = .0002), but there was no significant difference between the two groups in overall mortality (2.1% vs. 1.5%; P = .37).
Data source: An analysis of 1,762 splenectomy procedures from the ACS NSQIP database that were performed from 2006 to 2011.
Disclosures: Ms. Belding-Schmitt said that she had no relevant financial conflicts to disclose.

CRTC1 polymorphisms affect BMI, novel study finds
Polymorphisms of the CREB-regulated transcription coactivator 1 gene contribute to the genetics of human obesity in psychiatric patients and in the general population, results from a novel study demonstrated.
Specifically, the CRTC1 nonsynonymous polymorphism rs3746266A>G was associated with body mass index in three independent psychiatric samples in which lower BMI values were measured in carriers of the G allele compared with noncarriers, while the protective effect of the T allele of rs6510997C>T (a proxy of rs3746266A>G) against fat accumulation also was observed in a large population-based sample.
"Psychiatric, psychological, sociodemographic, and behavioral factors, as well as heritability, have been shown to influence individual susceptibility to overweight or obesity, both in the general population and in psychiatric patients before and after treatment with potentially weight gain–inducing psychotropic drugs," researchers led by Eva Choong, Pharm.D., Ph.D., reported online Aug. 7 in JAMA Psychiatry. "Genome-wide association studies conducted to date only explain a small fraction of body mass index (BMI) heritability, and more obesity susceptibility genes remain to be discovered."
For the study, which is thought to be the first of its kind, researchers from two university hospitals and a private clinic in Switzerland evaluated the effect of three CRTC1 polymorphisms on BMI and/or fat mass in a cohort of 152 patients taking weight gain–inducing psychotropic drugs (sample 1). The CRTC1 variant that was significantly associated with BMI was then replicated in two independent psychiatric samples, which consisted of 174 patients in sample 2 and 118 patients in sample 3, and in two white population-based samples, which consisted of 5,338 patients in sample 4 and 123,865 patients in sample 5 (JAMA Psychiatry 2013 Aug. 7 [doi: 10.1001/jamapsychiatry.2013.187]).
The researchers found that in the three psychiatric samples, carriers of the CRTC1 rs3746266A>G allele had a lower BMI than did noncarriers (P = .001 in sample 1, P = .05 in sample 2, and P = .0003 in sample 3). In a combined analysis that excluded patients taking other weight gain–inducing drugs, G-allele carriers had a 1.81-kg/m2 lower BMI, compared with noncarriers (P less than .0001). The strongest association was seen in women age 45; in this subset of patients, G-allele carriers had a 3.87-kg/m2 lower BMI, compared with noncarriers (P less than .0001).
In the analysis of population-based samples, the T allele of rs651099C>T, which is a proxy of the G allele, was associated with lower BMI (P = .01 in sample 5) and fat mass (P = .03 in sample 4).
The investigators acknowledged several limitations of their study. For example, most patients were not drug naive and had already developed weight gain because of previous treatments. "It was therefore not possible to determine with certainty whether the strong association of CRTC1 genotypes with BMI and fat mass in psychiatric populations was due to the psychiatric illness and/or to the pharmacological treatment," they wrote. "Extensive hormonal measurements were not available for our samples, so the role of sex hormones on the association of CRTC1 variants with adiposity could not be explored."
In addition, the racial and ethnic makeup of the patients sampled means that the results are not generalizable.
Despite those limitations, Dr. Choong expressed optimism about where these results might lead. "Our results suggest that CRTC1 plays an important role in the high prevalence of overweight and obesity observed in psychiatric patients," she and her colleagues concluded. "Besides, CRTC1 could play a role in the genetics of obesity in the general population, thereby increasing our understanding of the multiple mechanisms influencing obesity.
"Finally, the strong associations of CRTC1 variants with adiposity in women younger than 45 years support further research on the interrelationship between adiposity and the reproductive function."
The study was funded in part by the Swiss National Research Foundation and by the National Center of Competence in Research, which is funded by the Swiss National Science Foundation. Dr. Choong had no disclosures; several of her colleagues disclosed that they have received grants or honoraria from numerous pharmaceutical companies.
Polymorphisms of the CREB-regulated transcription coactivator 1 gene contribute to the genetics of human obesity in psychiatric patients and in the general population, results from a novel study demonstrated.
Specifically, the CRTC1 nonsynonymous polymorphism rs3746266A>G was associated with body mass index in three independent psychiatric samples in which lower BMI values were measured in carriers of the G allele compared with noncarriers, while the protective effect of the T allele of rs6510997C>T (a proxy of rs3746266A>G) against fat accumulation also was observed in a large population-based sample.
"Psychiatric, psychological, sociodemographic, and behavioral factors, as well as heritability, have been shown to influence individual susceptibility to overweight or obesity, both in the general population and in psychiatric patients before and after treatment with potentially weight gain–inducing psychotropic drugs," researchers led by Eva Choong, Pharm.D., Ph.D., reported online Aug. 7 in JAMA Psychiatry. "Genome-wide association studies conducted to date only explain a small fraction of body mass index (BMI) heritability, and more obesity susceptibility genes remain to be discovered."
For the study, which is thought to be the first of its kind, researchers from two university hospitals and a private clinic in Switzerland evaluated the effect of three CRTC1 polymorphisms on BMI and/or fat mass in a cohort of 152 patients taking weight gain–inducing psychotropic drugs (sample 1). The CRTC1 variant that was significantly associated with BMI was then replicated in two independent psychiatric samples, which consisted of 174 patients in sample 2 and 118 patients in sample 3, and in two white population-based samples, which consisted of 5,338 patients in sample 4 and 123,865 patients in sample 5 (JAMA Psychiatry 2013 Aug. 7 [doi: 10.1001/jamapsychiatry.2013.187]).
The researchers found that in the three psychiatric samples, carriers of the CRTC1 rs3746266A>G allele had a lower BMI than did noncarriers (P = .001 in sample 1, P = .05 in sample 2, and P = .0003 in sample 3). In a combined analysis that excluded patients taking other weight gain–inducing drugs, G-allele carriers had a 1.81-kg/m2 lower BMI, compared with noncarriers (P less than .0001). The strongest association was seen in women age 45; in this subset of patients, G-allele carriers had a 3.87-kg/m2 lower BMI, compared with noncarriers (P less than .0001).
In the analysis of population-based samples, the T allele of rs651099C>T, which is a proxy of the G allele, was associated with lower BMI (P = .01 in sample 5) and fat mass (P = .03 in sample 4).
The investigators acknowledged several limitations of their study. For example, most patients were not drug naive and had already developed weight gain because of previous treatments. "It was therefore not possible to determine with certainty whether the strong association of CRTC1 genotypes with BMI and fat mass in psychiatric populations was due to the psychiatric illness and/or to the pharmacological treatment," they wrote. "Extensive hormonal measurements were not available for our samples, so the role of sex hormones on the association of CRTC1 variants with adiposity could not be explored."
In addition, the racial and ethnic makeup of the patients sampled means that the results are not generalizable.
Despite those limitations, Dr. Choong expressed optimism about where these results might lead. "Our results suggest that CRTC1 plays an important role in the high prevalence of overweight and obesity observed in psychiatric patients," she and her colleagues concluded. "Besides, CRTC1 could play a role in the genetics of obesity in the general population, thereby increasing our understanding of the multiple mechanisms influencing obesity.
"Finally, the strong associations of CRTC1 variants with adiposity in women younger than 45 years support further research on the interrelationship between adiposity and the reproductive function."
The study was funded in part by the Swiss National Research Foundation and by the National Center of Competence in Research, which is funded by the Swiss National Science Foundation. Dr. Choong had no disclosures; several of her colleagues disclosed that they have received grants or honoraria from numerous pharmaceutical companies.
Polymorphisms of the CREB-regulated transcription coactivator 1 gene contribute to the genetics of human obesity in psychiatric patients and in the general population, results from a novel study demonstrated.
Specifically, the CRTC1 nonsynonymous polymorphism rs3746266A>G was associated with body mass index in three independent psychiatric samples in which lower BMI values were measured in carriers of the G allele compared with noncarriers, while the protective effect of the T allele of rs6510997C>T (a proxy of rs3746266A>G) against fat accumulation also was observed in a large population-based sample.
"Psychiatric, psychological, sociodemographic, and behavioral factors, as well as heritability, have been shown to influence individual susceptibility to overweight or obesity, both in the general population and in psychiatric patients before and after treatment with potentially weight gain–inducing psychotropic drugs," researchers led by Eva Choong, Pharm.D., Ph.D., reported online Aug. 7 in JAMA Psychiatry. "Genome-wide association studies conducted to date only explain a small fraction of body mass index (BMI) heritability, and more obesity susceptibility genes remain to be discovered."
For the study, which is thought to be the first of its kind, researchers from two university hospitals and a private clinic in Switzerland evaluated the effect of three CRTC1 polymorphisms on BMI and/or fat mass in a cohort of 152 patients taking weight gain–inducing psychotropic drugs (sample 1). The CRTC1 variant that was significantly associated with BMI was then replicated in two independent psychiatric samples, which consisted of 174 patients in sample 2 and 118 patients in sample 3, and in two white population-based samples, which consisted of 5,338 patients in sample 4 and 123,865 patients in sample 5 (JAMA Psychiatry 2013 Aug. 7 [doi: 10.1001/jamapsychiatry.2013.187]).
The researchers found that in the three psychiatric samples, carriers of the CRTC1 rs3746266A>G allele had a lower BMI than did noncarriers (P = .001 in sample 1, P = .05 in sample 2, and P = .0003 in sample 3). In a combined analysis that excluded patients taking other weight gain–inducing drugs, G-allele carriers had a 1.81-kg/m2 lower BMI, compared with noncarriers (P less than .0001). The strongest association was seen in women age 45; in this subset of patients, G-allele carriers had a 3.87-kg/m2 lower BMI, compared with noncarriers (P less than .0001).
In the analysis of population-based samples, the T allele of rs651099C>T, which is a proxy of the G allele, was associated with lower BMI (P = .01 in sample 5) and fat mass (P = .03 in sample 4).
The investigators acknowledged several limitations of their study. For example, most patients were not drug naive and had already developed weight gain because of previous treatments. "It was therefore not possible to determine with certainty whether the strong association of CRTC1 genotypes with BMI and fat mass in psychiatric populations was due to the psychiatric illness and/or to the pharmacological treatment," they wrote. "Extensive hormonal measurements were not available for our samples, so the role of sex hormones on the association of CRTC1 variants with adiposity could not be explored."
In addition, the racial and ethnic makeup of the patients sampled means that the results are not generalizable.
Despite those limitations, Dr. Choong expressed optimism about where these results might lead. "Our results suggest that CRTC1 plays an important role in the high prevalence of overweight and obesity observed in psychiatric patients," she and her colleagues concluded. "Besides, CRTC1 could play a role in the genetics of obesity in the general population, thereby increasing our understanding of the multiple mechanisms influencing obesity.
"Finally, the strong associations of CRTC1 variants with adiposity in women younger than 45 years support further research on the interrelationship between adiposity and the reproductive function."
The study was funded in part by the Swiss National Research Foundation and by the National Center of Competence in Research, which is funded by the Swiss National Science Foundation. Dr. Choong had no disclosures; several of her colleagues disclosed that they have received grants or honoraria from numerous pharmaceutical companies.
FROM JAMA PSYCHIATRY
Major finding: In three samples of psychiatric patients, carriers of the CREB-regulated transcription coactivator 1 gene polymorphism rs3746266A>G allele had a lower BMI than did noncarriers (P = .001 in sample 1, P = .05 in sample 2, and P = .0003 in sample 3). In an analysis of two separate population-based samples, the T allele of rs651099C>T, which is a proxy of the G allele, was associated with lower BMI (P = .01 in sample 5) and fat mass (P = .03 in sample 4).
Data source: An analysis of five different samples of patients from two university hospitals and a private clinic in Switzerland.
Disclosures: The study was funded in part by the Swiss National Research Foundation and by the National Center of Competence in Research, which is funded by the Swiss National Science Foundation. Dr. Choong had no disclosures; several of her colleagues disclosed that they have received grants or honoraria from numerous pharmaceutical companies.
Postop pneumonia risk strong for subset of thoracic surgery patients
SAN DIEGO – For thoracic surgery patients, being on neoadjuvant chemotherapy, having chronic obstructive pulmonary disease, and a weight loss of greater than 10% were all associated with the development of postoperative pneumonia, results from a single-center study showed.
At the national conference of the American College of Surgeons/National Surgical Quality Improvement Program, Dr. Elisabeth Dexter noted that after the first ACS/NSQIP data harvest at the Roswell Park Cancer Institute in Buffalo, N.Y., the risk of postoperative pneumonia was found to be 4.4%, compared with a rate of 1.1% in all other NSQIP hospitals.
"Of particular note, the thoracic surgery service had a high incidence of 13.2%," said Dr. Dexter, an attending surgeon in the department of thoracic surgery at the Institute. "The high incidence of our postoperative pneumonia was likely [affected] by our thoracic surgery service because our thoracic surgery service had an increased percentage of the abstracted NSQIP data in our cohort, from 12% to 14%, compared with other NSQIP hospitals of similar academic size abstracting 2%. When we found this high postoperative pneumonia rate, we decided to query our NSQIP data and our tumor registry between July 1, 2011, and Oct. 8, 2012, to ask the question: Is there an increased incidence of postoperative pneumonia in thoracic surgery patients who received neoadjuvant chemotherapy compared with those who did not?"

Dr. Dexter and her associates cross-referenced ACS/NSQIP data on 1,723 patients at the cancer center with the tumor registry. Of the 1,723 patients, 1,645 had no postoperative pneumonia while 78 did. Compared with the non-pneumonia patients, those who had pneumonia tended to be older (a mean of 67 vs. 60 years, respectively; odds ratio, 1.05; P less than .001), more likely to be male (59% vs. 37%; OR, 2.48; P less than .001), have chronic obstructive pulmonary disease (35% vs. 9%; OR, 5.08; P less than .001), be a smoker (36% vs. 24%; OR, 1.75; P = .021), and had lost more than 10% of body weight (10% vs. 2.5%; OR, 4.47; P less than .001).
On univariate analysis, postoperative pneumonia was associated with being on neoadjuvant chemotherapy (4.2% vs. 14%; OR, 3.75; P less than .001).
In addition, certain surgical subspecialties at the Institute had a high incidence of postoperative pneumonia, including thoracic surgery (46%), GI surgery (21%), and gynecology (12%).
When the researchers included the entire cohort of patients, those who were on neoadjuvant therapy had an increased incidence of postoperative pneumonia, compared with those who were not on neoadjuvant chemotherapy (P = .001). When thoracic surgery patients were excluded from the analysis, non-thoracic surgery patients who were on neoadjuvant chemotherapy had no increased incidence of postoperative pneumonia, compared with the patients who were not on neoadjuvant chemotherapy (P = .681). On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P= .001), having chronic obstructive pulmonary disease (P less than .0001), and having weight loss of greater than 10% (P = .004).
"Institutions with disproportionately busy complex thoracic surgery programs may have rates of postoperative pneumonia skewed higher than predicted by NSQIP models," Dr. Dexter concluded. "Optimization of nutritional status and COPD treatment in neoadjuvant chemotherapy patients may reduce postoperative pneumonia risk and incidence. Balance of oncologic benefit of neoadjuvant chemotherapy versus risk and morbidity of postoperative chemotherapy warrants future study in thoracic surgery patients."
Dr. Dexter said that she had no relevant financial conflicts to make.
SAN DIEGO – For thoracic surgery patients, being on neoadjuvant chemotherapy, having chronic obstructive pulmonary disease, and a weight loss of greater than 10% were all associated with the development of postoperative pneumonia, results from a single-center study showed.
At the national conference of the American College of Surgeons/National Surgical Quality Improvement Program, Dr. Elisabeth Dexter noted that after the first ACS/NSQIP data harvest at the Roswell Park Cancer Institute in Buffalo, N.Y., the risk of postoperative pneumonia was found to be 4.4%, compared with a rate of 1.1% in all other NSQIP hospitals.
"Of particular note, the thoracic surgery service had a high incidence of 13.2%," said Dr. Dexter, an attending surgeon in the department of thoracic surgery at the Institute. "The high incidence of our postoperative pneumonia was likely [affected] by our thoracic surgery service because our thoracic surgery service had an increased percentage of the abstracted NSQIP data in our cohort, from 12% to 14%, compared with other NSQIP hospitals of similar academic size abstracting 2%. When we found this high postoperative pneumonia rate, we decided to query our NSQIP data and our tumor registry between July 1, 2011, and Oct. 8, 2012, to ask the question: Is there an increased incidence of postoperative pneumonia in thoracic surgery patients who received neoadjuvant chemotherapy compared with those who did not?"
Dr. Dexter and her associates cross-referenced ACS/NSQIP data on 1,723 patients at the cancer center with the tumor registry. Of the 1,723 patients, 1,645 had no postoperative pneumonia while 78 did. Compared with the non-pneumonia patients, those who had pneumonia tended to be older (a mean of 67 vs. 60 years, respectively; odds ratio, 1.05; P less than .001), more likely to be male (59% vs. 37%; OR, 2.48; P less than .001), have chronic obstructive pulmonary disease (35% vs. 9%; OR, 5.08; P less than .001), be a smoker (36% vs. 24%; OR, 1.75; P = .021), and had lost more than 10% of body weight (10% vs. 2.5%; OR, 4.47; P less than .001).
On univariate analysis, postoperative pneumonia was associated with being on neoadjuvant chemotherapy (4.2% vs. 14%; OR, 3.75; P less than .001).
In addition, certain surgical subspecialties at the Institute had a high incidence of postoperative pneumonia, including thoracic surgery (46%), GI surgery (21%), and gynecology (12%).
When the researchers included the entire cohort of patients, those who were on neoadjuvant therapy had an increased incidence of postoperative pneumonia, compared with those who were not on neoadjuvant chemotherapy (P = .001). When thoracic surgery patients were excluded from the analysis, non-thoracic surgery patients who were on neoadjuvant chemotherapy had no increased incidence of postoperative pneumonia, compared with the patients who were not on neoadjuvant chemotherapy (P = .681). On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P= .001), having chronic obstructive pulmonary disease (P less than .0001), and having weight loss of greater than 10% (P = .004).
"Institutions with disproportionately busy complex thoracic surgery programs may have rates of postoperative pneumonia skewed higher than predicted by NSQIP models," Dr. Dexter concluded. "Optimization of nutritional status and COPD treatment in neoadjuvant chemotherapy patients may reduce postoperative pneumonia risk and incidence. Balance of oncologic benefit of neoadjuvant chemotherapy versus risk and morbidity of postoperative chemotherapy warrants future study in thoracic surgery patients."
Dr. Dexter said that she had no relevant financial conflicts to make.
SAN DIEGO – For thoracic surgery patients, being on neoadjuvant chemotherapy, having chronic obstructive pulmonary disease, and a weight loss of greater than 10% were all associated with the development of postoperative pneumonia, results from a single-center study showed.
At the national conference of the American College of Surgeons/National Surgical Quality Improvement Program, Dr. Elisabeth Dexter noted that after the first ACS/NSQIP data harvest at the Roswell Park Cancer Institute in Buffalo, N.Y., the risk of postoperative pneumonia was found to be 4.4%, compared with a rate of 1.1% in all other NSQIP hospitals.
"Of particular note, the thoracic surgery service had a high incidence of 13.2%," said Dr. Dexter, an attending surgeon in the department of thoracic surgery at the Institute. "The high incidence of our postoperative pneumonia was likely [affected] by our thoracic surgery service because our thoracic surgery service had an increased percentage of the abstracted NSQIP data in our cohort, from 12% to 14%, compared with other NSQIP hospitals of similar academic size abstracting 2%. When we found this high postoperative pneumonia rate, we decided to query our NSQIP data and our tumor registry between July 1, 2011, and Oct. 8, 2012, to ask the question: Is there an increased incidence of postoperative pneumonia in thoracic surgery patients who received neoadjuvant chemotherapy compared with those who did not?"
Dr. Dexter and her associates cross-referenced ACS/NSQIP data on 1,723 patients at the cancer center with the tumor registry. Of the 1,723 patients, 1,645 had no postoperative pneumonia while 78 did. Compared with the non-pneumonia patients, those who had pneumonia tended to be older (a mean of 67 vs. 60 years, respectively; odds ratio, 1.05; P less than .001), more likely to be male (59% vs. 37%; OR, 2.48; P less than .001), have chronic obstructive pulmonary disease (35% vs. 9%; OR, 5.08; P less than .001), be a smoker (36% vs. 24%; OR, 1.75; P = .021), and had lost more than 10% of body weight (10% vs. 2.5%; OR, 4.47; P less than .001).
On univariate analysis, postoperative pneumonia was associated with being on neoadjuvant chemotherapy (4.2% vs. 14%; OR, 3.75; P less than .001).
In addition, certain surgical subspecialties at the Institute had a high incidence of postoperative pneumonia, including thoracic surgery (46%), GI surgery (21%), and gynecology (12%).
When the researchers included the entire cohort of patients, those who were on neoadjuvant therapy had an increased incidence of postoperative pneumonia, compared with those who were not on neoadjuvant chemotherapy (P = .001). When thoracic surgery patients were excluded from the analysis, non-thoracic surgery patients who were on neoadjuvant chemotherapy had no increased incidence of postoperative pneumonia, compared with the patients who were not on neoadjuvant chemotherapy (P = .681). On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P= .001), having chronic obstructive pulmonary disease (P less than .0001), and having weight loss of greater than 10% (P = .004).
"Institutions with disproportionately busy complex thoracic surgery programs may have rates of postoperative pneumonia skewed higher than predicted by NSQIP models," Dr. Dexter concluded. "Optimization of nutritional status and COPD treatment in neoadjuvant chemotherapy patients may reduce postoperative pneumonia risk and incidence. Balance of oncologic benefit of neoadjuvant chemotherapy versus risk and morbidity of postoperative chemotherapy warrants future study in thoracic surgery patients."
Dr. Dexter said that she had no relevant financial conflicts to make.
AT THE ACS NSQIP NATIONAL CONFERENCE
Major finding: On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P = .001), having COPD (P less than .0001), and having weight loss of greater than 10% (P = .004).
Data source: A study of 1,723 patients who underwent surgery at Roswell Park Cancer Institute in Buffalo, N.Y. Of the postoperative pneumonia cases that developed, 46% were from the thoracic surgery service.
Disclosures: Dr. Dexter said that she had no relevant financial disclosures to make.

Preoperative screening program helped reduce 30-day mortality
SAN DIEGO – The implementation of an intensive preoperative screening and intervention process led to a significant decrease in 30-day mortality for general surgery and vascular procedures, results from a single-center study demonstrated.
In 2007, Carilion Roanoke (Va.) Memorial Hospital became a member of the American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP). "After receiving our first report, it became evident that surgical mortality at our institution was significantly higher than expected and significantly higher than the national average," Dr. Agathoklis Konstantinidis said at the ACS/NSQIP National Conference. "After further evaluation of this data, it became obvious that we were operating on people with several undiagnosed, untreated medical diseases such as diabetes, obstructive sleep apnea, hypertension, lung disease, and renal disease that all constituted significant preoperative risk factors."

In an effort to improve surgical mortality at the hospital, Dr. Konstantinidis and his associates implemented a strict preoperative screening and intervention program that began in January 2010. Since that time, every patient scheduled for surgery is required to undergo a preoperative screening appointment with a registered nurse who performs an extensive computer-based checklist of risk factors for heart disease, renal disease, abnormal EKG, sleep apnea, and pulmonary disease.
"If a problem is identified, the surgery is postponed until the issue is addressed, either by the primary care physician or by the surgeon who is directly involved in the care of the patient, and in close communication with other specialists, such as those in internal medicine, family practice, and endocrinology," explained Dr. Konstantinidis, who is a surgeon at the hospital.
Between July 2007 and December 2009 – prior to initiation of the preoperative screening and intervention program – the odds ratios for 30-day mortality in all cases were 1.40, 1.43, 1.58, and 1.56 in successive reporting periods. Beginning with the first report after implementation of the preoperative screening and intervention program, 30-day mortality in all cases progressively decreased in successive reporting periods (OR, 1.26, 1.19, 1.14, and 0.86, respectively), with similar reductions in both general surgery (OR, 0.92) and vascular surgery (OR, 0.92) for the last year.
"After the implementation of our new preoperative screening and intervention process, overall 30-day surgical mortality at our institution decreased from 3.5% to 1.9%, which is clinically and also statistically significant based on the P value (P = .007)," Dr. Konstantinidis said.
He went on to report that out of 5,866 patients who underwent screening in 2012 alone, 3,691 had undiagnosed obstructive sleep apnea, 2,361 had an abnormal preoperative EKG, 437 had undiagnosed diabetes, 192 had undiagnosed hypertension, and 167 had undiagnosed shortness of breath. "As a result of the screening intervention, surgery was canceled in 218 patients, and 147 were referred to cardiology specialists for further evaluation," he said.
Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
Carilion Roanoke (Va.) Memorial Hospital, American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP), Dr. Agathoklis Konstantinidis, ACS/NSQIP National Conference, diabetes, obstructive sleep apnea, hypertension, lung disease, renal disease, preoperative risk factors, improve surgical mortality,
SAN DIEGO – The implementation of an intensive preoperative screening and intervention process led to a significant decrease in 30-day mortality for general surgery and vascular procedures, results from a single-center study demonstrated.
In 2007, Carilion Roanoke (Va.) Memorial Hospital became a member of the American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP). "After receiving our first report, it became evident that surgical mortality at our institution was significantly higher than expected and significantly higher than the national average," Dr. Agathoklis Konstantinidis said at the ACS/NSQIP National Conference. "After further evaluation of this data, it became obvious that we were operating on people with several undiagnosed, untreated medical diseases such as diabetes, obstructive sleep apnea, hypertension, lung disease, and renal disease that all constituted significant preoperative risk factors."
In an effort to improve surgical mortality at the hospital, Dr. Konstantinidis and his associates implemented a strict preoperative screening and intervention program that began in January 2010. Since that time, every patient scheduled for surgery is required to undergo a preoperative screening appointment with a registered nurse who performs an extensive computer-based checklist of risk factors for heart disease, renal disease, abnormal EKG, sleep apnea, and pulmonary disease.
"If a problem is identified, the surgery is postponed until the issue is addressed, either by the primary care physician or by the surgeon who is directly involved in the care of the patient, and in close communication with other specialists, such as those in internal medicine, family practice, and endocrinology," explained Dr. Konstantinidis, who is a surgeon at the hospital.
Between July 2007 and December 2009 – prior to initiation of the preoperative screening and intervention program – the odds ratios for 30-day mortality in all cases were 1.40, 1.43, 1.58, and 1.56 in successive reporting periods. Beginning with the first report after implementation of the preoperative screening and intervention program, 30-day mortality in all cases progressively decreased in successive reporting periods (OR, 1.26, 1.19, 1.14, and 0.86, respectively), with similar reductions in both general surgery (OR, 0.92) and vascular surgery (OR, 0.92) for the last year.
"After the implementation of our new preoperative screening and intervention process, overall 30-day surgical mortality at our institution decreased from 3.5% to 1.9%, which is clinically and also statistically significant based on the P value (P = .007)," Dr. Konstantinidis said.
He went on to report that out of 5,866 patients who underwent screening in 2012 alone, 3,691 had undiagnosed obstructive sleep apnea, 2,361 had an abnormal preoperative EKG, 437 had undiagnosed diabetes, 192 had undiagnosed hypertension, and 167 had undiagnosed shortness of breath. "As a result of the screening intervention, surgery was canceled in 218 patients, and 147 were referred to cardiology specialists for further evaluation," he said.
Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
SAN DIEGO – The implementation of an intensive preoperative screening and intervention process led to a significant decrease in 30-day mortality for general surgery and vascular procedures, results from a single-center study demonstrated.
In 2007, Carilion Roanoke (Va.) Memorial Hospital became a member of the American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP). "After receiving our first report, it became evident that surgical mortality at our institution was significantly higher than expected and significantly higher than the national average," Dr. Agathoklis Konstantinidis said at the ACS/NSQIP National Conference. "After further evaluation of this data, it became obvious that we were operating on people with several undiagnosed, untreated medical diseases such as diabetes, obstructive sleep apnea, hypertension, lung disease, and renal disease that all constituted significant preoperative risk factors."
In an effort to improve surgical mortality at the hospital, Dr. Konstantinidis and his associates implemented a strict preoperative screening and intervention program that began in January 2010. Since that time, every patient scheduled for surgery is required to undergo a preoperative screening appointment with a registered nurse who performs an extensive computer-based checklist of risk factors for heart disease, renal disease, abnormal EKG, sleep apnea, and pulmonary disease.
"If a problem is identified, the surgery is postponed until the issue is addressed, either by the primary care physician or by the surgeon who is directly involved in the care of the patient, and in close communication with other specialists, such as those in internal medicine, family practice, and endocrinology," explained Dr. Konstantinidis, who is a surgeon at the hospital.
Between July 2007 and December 2009 – prior to initiation of the preoperative screening and intervention program – the odds ratios for 30-day mortality in all cases were 1.40, 1.43, 1.58, and 1.56 in successive reporting periods. Beginning with the first report after implementation of the preoperative screening and intervention program, 30-day mortality in all cases progressively decreased in successive reporting periods (OR, 1.26, 1.19, 1.14, and 0.86, respectively), with similar reductions in both general surgery (OR, 0.92) and vascular surgery (OR, 0.92) for the last year.
"After the implementation of our new preoperative screening and intervention process, overall 30-day surgical mortality at our institution decreased from 3.5% to 1.9%, which is clinically and also statistically significant based on the P value (P = .007)," Dr. Konstantinidis said.
He went on to report that out of 5,866 patients who underwent screening in 2012 alone, 3,691 had undiagnosed obstructive sleep apnea, 2,361 had an abnormal preoperative EKG, 437 had undiagnosed diabetes, 192 had undiagnosed hypertension, and 167 had undiagnosed shortness of breath. "As a result of the screening intervention, surgery was canceled in 218 patients, and 147 were referred to cardiology specialists for further evaluation," he said.
Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
Carilion Roanoke (Va.) Memorial Hospital, American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP), Dr. Agathoklis Konstantinidis, ACS/NSQIP National Conference, diabetes, obstructive sleep apnea, hypertension, lung disease, renal disease, preoperative risk factors, improve surgical mortality,
Carilion Roanoke (Va.) Memorial Hospital, American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP), Dr. Agathoklis Konstantinidis, ACS/NSQIP National Conference, diabetes, obstructive sleep apnea, hypertension, lung disease, renal disease, preoperative risk factors, improve surgical mortality,
AT THE ACS NSQIP NATIONAL CONFERENCE
Major finding: After implementation of a new preoperative screening and intervention process, overall 30-day surgical mortality decreased from 3.5% to 1.9%, which reached clinical and statistical significance (P = .007).
Data source: A single-center study of patients who underwent general surgery and vascular surgery procedures between 2007 and 2011 at Carilion Roanoke (Va.) Memorial Hospital.
Disclosures: Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.

Depression more troublesome than mania for youth with bipolar disorder
Among youths with bipolar spectrum disorder, depressive symptoms more adversely affected their psychological functioning and quality of life than did manic symptoms, results from a small study showed.
"We hypothesized that the impact of bipolar depression in youth would be significant, but the lopsided nature of the results was more striking than expected," researchers led by Anna R. Van Meter reported online in the Journal of Affective Disorders. "Across numerous measures, depression was a significant predictor of negative outcomes, mania was not.
"This is not to say that mania is not impairing, our sample included only youth with bipolar disorder, so we cannot comment on the degree to which mania and/or depression caused problems for youth with bipolar disorder, relative to youth without mood disturbance. Still, at the very least, these findings suggest that the collective focus on mania, often it seems at the exclusion of depression, may be misguided."
For the study, Ms. Van Meter and her associates recruited 54 youths aged 7-13 years old who met DSM-IV-TR criteria for bipolar spectrum disorders from a clinic in a large Midwestern city (J. Affect. Dis. 2013 June 12 [doi:10.1016/j.jad.2013.05.039]).
They used regression analyses to evaluate clinician and parent reports of manic and depressive symptoms from numerous survey instruments in an effort to determine how each set of symptoms affected child functioning. Measures included the Washington University Schedule for Affective Disorders, the Children’s Global Assessment Scale, the Young Mania Rating Scale, and the Child Bipolar Depression Rating Scale.
The mean age of the 54 study participants was 9 years, 42% were female, and more than half (60%) were of white European descent. Diagnoses included bipolar disorder not otherwise specified (57%), bipolar I disorder (41%), and bipolar II disorder (2%).
Parent-rated child depression symptoms were associated with problem behaviors (P less than .05) and lower quality of life (P less than .001), while clinician-rated child depression was associated with greater psychiatric illness (P less than .05), lower child self-concept (P less than .001), lower quality of life (P less than .05), hopelessness (P less than .05), and suicidal ideation (P less than .05), reported Ms. Van Meter of the department of psychology at the University of North Carolina, Chapel Hill, and her associates.
At the same time, parent-rated mania was associated with better self-esteem (P less than 0.05) and physical well-being (P less than .05), while clinician-rated mania was associated with greater psychiatric illness (P less than .05) and physical well-being (P less than .05).
"Which specific aspects of bipolar depression cause decreased quality of life and through what mechanisms mania provides protection against functional impairment remain important areas for study," the researchers concluded. "In general, the identification of how different symptom constellations in pediatric bipolar disorder relate to functional impairment should be an important mission for our research agenda. Thus, this study introduces new questions to guide researchers in developing a more in-depth understanding of this complex disorder and raises awareness of the debilitating effects of bipolar depression in youth."
They acknowledged certain limitations of the study. One is that specific outcomes predicted by parent- and clinician-rated symptoms vary.
The study was supported by the National Institute of Mental Health. The researchers stated that they had no relevant financial conflicts to disclose.
Among youths with bipolar spectrum disorder, depressive symptoms more adversely affected their psychological functioning and quality of life than did manic symptoms, results from a small study showed.
"We hypothesized that the impact of bipolar depression in youth would be significant, but the lopsided nature of the results was more striking than expected," researchers led by Anna R. Van Meter reported online in the Journal of Affective Disorders. "Across numerous measures, depression was a significant predictor of negative outcomes, mania was not.
"This is not to say that mania is not impairing, our sample included only youth with bipolar disorder, so we cannot comment on the degree to which mania and/or depression caused problems for youth with bipolar disorder, relative to youth without mood disturbance. Still, at the very least, these findings suggest that the collective focus on mania, often it seems at the exclusion of depression, may be misguided."
For the study, Ms. Van Meter and her associates recruited 54 youths aged 7-13 years old who met DSM-IV-TR criteria for bipolar spectrum disorders from a clinic in a large Midwestern city (J. Affect. Dis. 2013 June 12 [doi:10.1016/j.jad.2013.05.039]).
They used regression analyses to evaluate clinician and parent reports of manic and depressive symptoms from numerous survey instruments in an effort to determine how each set of symptoms affected child functioning. Measures included the Washington University Schedule for Affective Disorders, the Children’s Global Assessment Scale, the Young Mania Rating Scale, and the Child Bipolar Depression Rating Scale.
The mean age of the 54 study participants was 9 years, 42% were female, and more than half (60%) were of white European descent. Diagnoses included bipolar disorder not otherwise specified (57%), bipolar I disorder (41%), and bipolar II disorder (2%).
Parent-rated child depression symptoms were associated with problem behaviors (P less than .05) and lower quality of life (P less than .001), while clinician-rated child depression was associated with greater psychiatric illness (P less than .05), lower child self-concept (P less than .001), lower quality of life (P less than .05), hopelessness (P less than .05), and suicidal ideation (P less than .05), reported Ms. Van Meter of the department of psychology at the University of North Carolina, Chapel Hill, and her associates.
At the same time, parent-rated mania was associated with better self-esteem (P less than 0.05) and physical well-being (P less than .05), while clinician-rated mania was associated with greater psychiatric illness (P less than .05) and physical well-being (P less than .05).
"Which specific aspects of bipolar depression cause decreased quality of life and through what mechanisms mania provides protection against functional impairment remain important areas for study," the researchers concluded. "In general, the identification of how different symptom constellations in pediatric bipolar disorder relate to functional impairment should be an important mission for our research agenda. Thus, this study introduces new questions to guide researchers in developing a more in-depth understanding of this complex disorder and raises awareness of the debilitating effects of bipolar depression in youth."
They acknowledged certain limitations of the study. One is that specific outcomes predicted by parent- and clinician-rated symptoms vary.
The study was supported by the National Institute of Mental Health. The researchers stated that they had no relevant financial conflicts to disclose.
Among youths with bipolar spectrum disorder, depressive symptoms more adversely affected their psychological functioning and quality of life than did manic symptoms, results from a small study showed.
"We hypothesized that the impact of bipolar depression in youth would be significant, but the lopsided nature of the results was more striking than expected," researchers led by Anna R. Van Meter reported online in the Journal of Affective Disorders. "Across numerous measures, depression was a significant predictor of negative outcomes, mania was not.
"This is not to say that mania is not impairing, our sample included only youth with bipolar disorder, so we cannot comment on the degree to which mania and/or depression caused problems for youth with bipolar disorder, relative to youth without mood disturbance. Still, at the very least, these findings suggest that the collective focus on mania, often it seems at the exclusion of depression, may be misguided."
For the study, Ms. Van Meter and her associates recruited 54 youths aged 7-13 years old who met DSM-IV-TR criteria for bipolar spectrum disorders from a clinic in a large Midwestern city (J. Affect. Dis. 2013 June 12 [doi:10.1016/j.jad.2013.05.039]).
They used regression analyses to evaluate clinician and parent reports of manic and depressive symptoms from numerous survey instruments in an effort to determine how each set of symptoms affected child functioning. Measures included the Washington University Schedule for Affective Disorders, the Children’s Global Assessment Scale, the Young Mania Rating Scale, and the Child Bipolar Depression Rating Scale.
The mean age of the 54 study participants was 9 years, 42% were female, and more than half (60%) were of white European descent. Diagnoses included bipolar disorder not otherwise specified (57%), bipolar I disorder (41%), and bipolar II disorder (2%).
Parent-rated child depression symptoms were associated with problem behaviors (P less than .05) and lower quality of life (P less than .001), while clinician-rated child depression was associated with greater psychiatric illness (P less than .05), lower child self-concept (P less than .001), lower quality of life (P less than .05), hopelessness (P less than .05), and suicidal ideation (P less than .05), reported Ms. Van Meter of the department of psychology at the University of North Carolina, Chapel Hill, and her associates.
At the same time, parent-rated mania was associated with better self-esteem (P less than 0.05) and physical well-being (P less than .05), while clinician-rated mania was associated with greater psychiatric illness (P less than .05) and physical well-being (P less than .05).
"Which specific aspects of bipolar depression cause decreased quality of life and through what mechanisms mania provides protection against functional impairment remain important areas for study," the researchers concluded. "In general, the identification of how different symptom constellations in pediatric bipolar disorder relate to functional impairment should be an important mission for our research agenda. Thus, this study introduces new questions to guide researchers in developing a more in-depth understanding of this complex disorder and raises awareness of the debilitating effects of bipolar depression in youth."
They acknowledged certain limitations of the study. One is that specific outcomes predicted by parent- and clinician-rated symptoms vary.
The study was supported by the National Institute of Mental Health. The researchers stated that they had no relevant financial conflicts to disclose.
FROM THE JOURNAL OF AFFECTIVE DISORDERS
Major finding: Among youth with bipolar disorder, parent-rated child depression symptoms were associated with problem behaviors (P less than .05) and lower quality of life (P less than .001), yet parent-rated mania was associated with better self-esteem and physical well-being (both P less than .05). At the same time, clinician-rated child depression was associated with greater psychiatric illness (P less than .05) and lower child self-concept (P less than 0.001), while clinician-rated mania was associated with greater psychiatric illness and physical well-being (both P less than 0.05).
Data source: A study of 54 youths aged 7-13 years old who met DSM-IV-TR criteria for bipolar spectrum disorders.
Disclosures: The study was supported by the National Institute of Mental Health. The researchers stated that they had no relevant financial conflicts to disclose.
TVS useful for diagnosis of adenomyosis and leiomyoma
SAN DIEGO – Transvaginal ultrasound is accurate, sensitive, and specific in the diagnosis of leiomyoma and coexisting adenomyosis and leiomyoma, results from a single-center study showed.
"Menorrhagia is a very common condition which female patients are suffering from many days of the month," Dr. Magdi Hanafi, FACS, said in an interview after the American College of Surgeons/National Surgical Quality Improvement Program National Conference, where the study was presented at a poster session.
"It interferes with their normal day-to-day life and work, and causes anemia and its subsequent complications. Two of the common causes of menorrhagia are adenomyosis and leiomyoma. These two conditions are frequently missed by some gynecologists – especially adenomyosis – clinically and on some occasions by pelvic ultrasound."
Dr. Hanafi, medical director of Gyn. and Fertility Specialists at Saint Joseph’s Hospital of Atlanta, retrospectively evaluated 163 women with a preoperative transvaginal ultrasound (TVS) diagnosis of adenomyosis, leiomyoma, and adenomyosis with coexisting leiomyoma. Of the 163 patients, 130 underwent hysterectomy and 33 symptomatic patients underwent myomectomy with excision of the surrounding myometrium, which presumably contained adenomyosis. Following surgery, hospital pathologists performed a histological examination and recorded the diagnosis.
The mean age of the patients was 44 years. Dr. Hanafi reported that 123 of the patients were positively diagnosed with adenomyosis via TVS. Among these, histopathologic confirmation of TVS diagnosis of adenomyosis was positive in 93 patients (76%) and negative in 30 (24%). The sensitivity, specificity, and accuracy of TVS in the diagnosis of adenomyosis were 85% (P less than .0001), 43% (P = .41), and 71%, respectively. "This demonstrates that TVS diagnosis of adenomyosis is sensitive, but not specific," he said.
Histopathologic data on leiomyoma was complete in 134 of the patients. Among these, histopathologic confirmation of TVS diagnosis of leiomyoma was positive in 133 patients (99%) and negative in 1 (1%). The sensitivity, specificity, and accuracy of TVS in the diagnosis of leiomyoma were 96% (P less than .0001), 96% (P less than .0001), and 96%, respectively.
"In other published studies in the diagnosis of adenomyosis, combined adenomyosis and leiomyoma was not mentioned," Dr. Hanafi commented. "This combination is more common than we ever thought before, and all gynecologists should think of this combined condition in menorrhagic patients in their differential diagnosis."
He concluded that office TVS "is a very valuable procedure in the diagnosis of adenomyosis, leiomyoma, or combined [adenomyosis and leiomyoma]. It is sensitive and accurate in the diagnosis of leiomyoma, adenomyosis, or [the combination], but not specific in the diagnosis of adenomyosis alone."
Dr. Hanafi said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Transvaginal ultrasound is accurate, sensitive, and specific in the diagnosis of leiomyoma and coexisting adenomyosis and leiomyoma, results from a single-center study showed.
"Menorrhagia is a very common condition which female patients are suffering from many days of the month," Dr. Magdi Hanafi, FACS, said in an interview after the American College of Surgeons/National Surgical Quality Improvement Program National Conference, where the study was presented at a poster session.
"It interferes with their normal day-to-day life and work, and causes anemia and its subsequent complications. Two of the common causes of menorrhagia are adenomyosis and leiomyoma. These two conditions are frequently missed by some gynecologists – especially adenomyosis – clinically and on some occasions by pelvic ultrasound."
Dr. Hanafi, medical director of Gyn. and Fertility Specialists at Saint Joseph’s Hospital of Atlanta, retrospectively evaluated 163 women with a preoperative transvaginal ultrasound (TVS) diagnosis of adenomyosis, leiomyoma, and adenomyosis with coexisting leiomyoma. Of the 163 patients, 130 underwent hysterectomy and 33 symptomatic patients underwent myomectomy with excision of the surrounding myometrium, which presumably contained adenomyosis. Following surgery, hospital pathologists performed a histological examination and recorded the diagnosis.
The mean age of the patients was 44 years. Dr. Hanafi reported that 123 of the patients were positively diagnosed with adenomyosis via TVS. Among these, histopathologic confirmation of TVS diagnosis of adenomyosis was positive in 93 patients (76%) and negative in 30 (24%). The sensitivity, specificity, and accuracy of TVS in the diagnosis of adenomyosis were 85% (P less than .0001), 43% (P = .41), and 71%, respectively. "This demonstrates that TVS diagnosis of adenomyosis is sensitive, but not specific," he said.
Histopathologic data on leiomyoma was complete in 134 of the patients. Among these, histopathologic confirmation of TVS diagnosis of leiomyoma was positive in 133 patients (99%) and negative in 1 (1%). The sensitivity, specificity, and accuracy of TVS in the diagnosis of leiomyoma were 96% (P less than .0001), 96% (P less than .0001), and 96%, respectively.
"In other published studies in the diagnosis of adenomyosis, combined adenomyosis and leiomyoma was not mentioned," Dr. Hanafi commented. "This combination is more common than we ever thought before, and all gynecologists should think of this combined condition in menorrhagic patients in their differential diagnosis."
He concluded that office TVS "is a very valuable procedure in the diagnosis of adenomyosis, leiomyoma, or combined [adenomyosis and leiomyoma]. It is sensitive and accurate in the diagnosis of leiomyoma, adenomyosis, or [the combination], but not specific in the diagnosis of adenomyosis alone."
Dr. Hanafi said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Transvaginal ultrasound is accurate, sensitive, and specific in the diagnosis of leiomyoma and coexisting adenomyosis and leiomyoma, results from a single-center study showed.
"Menorrhagia is a very common condition which female patients are suffering from many days of the month," Dr. Magdi Hanafi, FACS, said in an interview after the American College of Surgeons/National Surgical Quality Improvement Program National Conference, where the study was presented at a poster session.
"It interferes with their normal day-to-day life and work, and causes anemia and its subsequent complications. Two of the common causes of menorrhagia are adenomyosis and leiomyoma. These two conditions are frequently missed by some gynecologists – especially adenomyosis – clinically and on some occasions by pelvic ultrasound."
Dr. Hanafi, medical director of Gyn. and Fertility Specialists at Saint Joseph’s Hospital of Atlanta, retrospectively evaluated 163 women with a preoperative transvaginal ultrasound (TVS) diagnosis of adenomyosis, leiomyoma, and adenomyosis with coexisting leiomyoma. Of the 163 patients, 130 underwent hysterectomy and 33 symptomatic patients underwent myomectomy with excision of the surrounding myometrium, which presumably contained adenomyosis. Following surgery, hospital pathologists performed a histological examination and recorded the diagnosis.
The mean age of the patients was 44 years. Dr. Hanafi reported that 123 of the patients were positively diagnosed with adenomyosis via TVS. Among these, histopathologic confirmation of TVS diagnosis of adenomyosis was positive in 93 patients (76%) and negative in 30 (24%). The sensitivity, specificity, and accuracy of TVS in the diagnosis of adenomyosis were 85% (P less than .0001), 43% (P = .41), and 71%, respectively. "This demonstrates that TVS diagnosis of adenomyosis is sensitive, but not specific," he said.
Histopathologic data on leiomyoma was complete in 134 of the patients. Among these, histopathologic confirmation of TVS diagnosis of leiomyoma was positive in 133 patients (99%) and negative in 1 (1%). The sensitivity, specificity, and accuracy of TVS in the diagnosis of leiomyoma were 96% (P less than .0001), 96% (P less than .0001), and 96%, respectively.
"In other published studies in the diagnosis of adenomyosis, combined adenomyosis and leiomyoma was not mentioned," Dr. Hanafi commented. "This combination is more common than we ever thought before, and all gynecologists should think of this combined condition in menorrhagic patients in their differential diagnosis."
He concluded that office TVS "is a very valuable procedure in the diagnosis of adenomyosis, leiomyoma, or combined [adenomyosis and leiomyoma]. It is sensitive and accurate in the diagnosis of leiomyoma, adenomyosis, or [the combination], but not specific in the diagnosis of adenomyosis alone."
Dr. Hanafi said that he had no relevant financial conflicts to disclose.
AT THE ACS NSQIP NATIONAL CONFERENCE
Major finding: The sensitivity, specificity, and accuracy of transvaginal ultrasound in the diagnosis of adenomyosis were 85% (P less than .0001), 43% (P = .41), and 71%, respectively. At the same time, the sensitivity, specificity, and accuracy of TVS in the diagnosis of adenomyosis were 96% (P less than .0001), 96% (P less than .0001), and 96%, respectively.
Data source: A retrospective study of 163 female patients with a preoperative TVS diagnosis of adenomyosis, leiomyoma, and adenomyosis with coexisting leiomyoma.
Disclosures: Dr. Hanafi said that he had no relevant financial conflicts to disclose.
Coinfection with chronic hepatitis C and occult hepatitis B related to poor outcomes
Chronic hepatitis C patients who are coinfected with occult hepatitis B virus face a high risk of progression toward cirrhosis, the development of hepatocellular carcinoma, and lower survival, an observational study demonstrated.
To evaluate the clinical evolution of chronic hepatitis C (CHC) patients according to their occult hepatitis B virus infection (OBI) status, 326 hepatitis B surface antigen–negative CHC patients who had undergone needle liver biopsy in the liver unit at the University of Messina (Italy) between 1991 and 2000 were tested for OBI by analysis of liver biopsy DNA extracts. More than half of the patients (65%) were male, and their median age was 52 years, researchers led by Dr. Giovanni Squadrito and Dr. Giovanni Raimondo of the University of Messina reported in an article in press from the Journal of Hepatology (2013 June 10).
None of them had received any antiviral therapy before liver biopsy was performed, none was infected with HIV, and none had evidence of alcoholic or autoimmune liver disease.
Of the 326 patients, 128 (39%) were OBI positive while the remaining 198 were OBI negative. A total of 94 patients (37 OBI positive and 57 OBI negative) were followed for a median of 11 years. Among these 94 patients, 79 underwent anti-HCV treatments and 26 achieved a sustained virologic response that occurred independently of their OBI status.
The researchers reported that 18 of the 94 patients (19%) developed hepatocellular carcinoma (HCC). Of these, 13 were among the 37 who were OBI positive and 5 were among the 57 who were OBI negative, a difference that was statistically significant (P less than .01). Among the 76 patients who did not develop HCC, 15 (20%) developed advanced forms of cirrhosis. Of these, 8 were among the 24 who were OBI positive and 7 were among the 52 who were OBI negative, a difference that was statistically significant (P less than .05).
During the follow-up period, 18 patients died (19%) and 2 underwent liver transplantation (2%). Of the 18 deaths, 14 occurred among HCC patients and 4, among patients with clear worsening of liver disease. The researchers found that the cumulative survival rate was significantly shorter among OBI-positive patients compared with OBI-negative patients (P = .003), while liver-related deaths occurred significantly more frequently in OBI-positive patients than in OBI-negative patients (P less than .01). In addition, nonresponse to anti-HCV therapy was significantly associated with lower survival (P = .02).
"The pro-oncogenic role of OBI is not surprising, considering that HBV is a major causative agent of liver cancer worldwide and the potential mechanisms whereby overt HBV might induce tumor formation are mostly maintained in the occult status," the researchers wrote. "In addition, when patients who developed HCC were excluded from the analysis, OBI still appears to play a negative role in the CHC outcome since it was significantly associated with the progression toward the severe deterioration and decompensation of the liver disease. Although this association is in accordance with the results of many cross-sectional studies performed in different areas of the world, how OBI may favor (or accelerate) the progression toward cirrhosis of CHC patients is far from being clearly understood."
The investigators noted that there is evidence "both in humans and in animal models that intrahepatic persistence of occult hepadnavirus genomes may produce a very mild but constant liver necroinflammation, and recent reports have shown an association between phases of a rise in ALT levels and reappearance of circulating HBV DNA in patients with chronic hepatitis C and combined occult HBV infection, thus suggesting an active role of transient reactivation of HBV replication in liver cell injury."
The study was supported by grants from the Associazione Italiana per la Ricerca sul Cancro. The researchers said they had no relevant financial disclosures.
Chronic hepatitis C patients who are coinfected with occult hepatitis B virus face a high risk of progression toward cirrhosis, the development of hepatocellular carcinoma, and lower survival, an observational study demonstrated.
To evaluate the clinical evolution of chronic hepatitis C (CHC) patients according to their occult hepatitis B virus infection (OBI) status, 326 hepatitis B surface antigen–negative CHC patients who had undergone needle liver biopsy in the liver unit at the University of Messina (Italy) between 1991 and 2000 were tested for OBI by analysis of liver biopsy DNA extracts. More than half of the patients (65%) were male, and their median age was 52 years, researchers led by Dr. Giovanni Squadrito and Dr. Giovanni Raimondo of the University of Messina reported in an article in press from the Journal of Hepatology (2013 June 10).
None of them had received any antiviral therapy before liver biopsy was performed, none was infected with HIV, and none had evidence of alcoholic or autoimmune liver disease.
Of the 326 patients, 128 (39%) were OBI positive while the remaining 198 were OBI negative. A total of 94 patients (37 OBI positive and 57 OBI negative) were followed for a median of 11 years. Among these 94 patients, 79 underwent anti-HCV treatments and 26 achieved a sustained virologic response that occurred independently of their OBI status.
The researchers reported that 18 of the 94 patients (19%) developed hepatocellular carcinoma (HCC). Of these, 13 were among the 37 who were OBI positive and 5 were among the 57 who were OBI negative, a difference that was statistically significant (P less than .01). Among the 76 patients who did not develop HCC, 15 (20%) developed advanced forms of cirrhosis. Of these, 8 were among the 24 who were OBI positive and 7 were among the 52 who were OBI negative, a difference that was statistically significant (P less than .05).
During the follow-up period, 18 patients died (19%) and 2 underwent liver transplantation (2%). Of the 18 deaths, 14 occurred among HCC patients and 4, among patients with clear worsening of liver disease. The researchers found that the cumulative survival rate was significantly shorter among OBI-positive patients compared with OBI-negative patients (P = .003), while liver-related deaths occurred significantly more frequently in OBI-positive patients than in OBI-negative patients (P less than .01). In addition, nonresponse to anti-HCV therapy was significantly associated with lower survival (P = .02).
"The pro-oncogenic role of OBI is not surprising, considering that HBV is a major causative agent of liver cancer worldwide and the potential mechanisms whereby overt HBV might induce tumor formation are mostly maintained in the occult status," the researchers wrote. "In addition, when patients who developed HCC were excluded from the analysis, OBI still appears to play a negative role in the CHC outcome since it was significantly associated with the progression toward the severe deterioration and decompensation of the liver disease. Although this association is in accordance with the results of many cross-sectional studies performed in different areas of the world, how OBI may favor (or accelerate) the progression toward cirrhosis of CHC patients is far from being clearly understood."
The investigators noted that there is evidence "both in humans and in animal models that intrahepatic persistence of occult hepadnavirus genomes may produce a very mild but constant liver necroinflammation, and recent reports have shown an association between phases of a rise in ALT levels and reappearance of circulating HBV DNA in patients with chronic hepatitis C and combined occult HBV infection, thus suggesting an active role of transient reactivation of HBV replication in liver cell injury."
The study was supported by grants from the Associazione Italiana per la Ricerca sul Cancro. The researchers said they had no relevant financial disclosures.
Chronic hepatitis C patients who are coinfected with occult hepatitis B virus face a high risk of progression toward cirrhosis, the development of hepatocellular carcinoma, and lower survival, an observational study demonstrated.
To evaluate the clinical evolution of chronic hepatitis C (CHC) patients according to their occult hepatitis B virus infection (OBI) status, 326 hepatitis B surface antigen–negative CHC patients who had undergone needle liver biopsy in the liver unit at the University of Messina (Italy) between 1991 and 2000 were tested for OBI by analysis of liver biopsy DNA extracts. More than half of the patients (65%) were male, and their median age was 52 years, researchers led by Dr. Giovanni Squadrito and Dr. Giovanni Raimondo of the University of Messina reported in an article in press from the Journal of Hepatology (2013 June 10).
None of them had received any antiviral therapy before liver biopsy was performed, none was infected with HIV, and none had evidence of alcoholic or autoimmune liver disease.
Of the 326 patients, 128 (39%) were OBI positive while the remaining 198 were OBI negative. A total of 94 patients (37 OBI positive and 57 OBI negative) were followed for a median of 11 years. Among these 94 patients, 79 underwent anti-HCV treatments and 26 achieved a sustained virologic response that occurred independently of their OBI status.
The researchers reported that 18 of the 94 patients (19%) developed hepatocellular carcinoma (HCC). Of these, 13 were among the 37 who were OBI positive and 5 were among the 57 who were OBI negative, a difference that was statistically significant (P less than .01). Among the 76 patients who did not develop HCC, 15 (20%) developed advanced forms of cirrhosis. Of these, 8 were among the 24 who were OBI positive and 7 were among the 52 who were OBI negative, a difference that was statistically significant (P less than .05).
During the follow-up period, 18 patients died (19%) and 2 underwent liver transplantation (2%). Of the 18 deaths, 14 occurred among HCC patients and 4, among patients with clear worsening of liver disease. The researchers found that the cumulative survival rate was significantly shorter among OBI-positive patients compared with OBI-negative patients (P = .003), while liver-related deaths occurred significantly more frequently in OBI-positive patients than in OBI-negative patients (P less than .01). In addition, nonresponse to anti-HCV therapy was significantly associated with lower survival (P = .02).
"The pro-oncogenic role of OBI is not surprising, considering that HBV is a major causative agent of liver cancer worldwide and the potential mechanisms whereby overt HBV might induce tumor formation are mostly maintained in the occult status," the researchers wrote. "In addition, when patients who developed HCC were excluded from the analysis, OBI still appears to play a negative role in the CHC outcome since it was significantly associated with the progression toward the severe deterioration and decompensation of the liver disease. Although this association is in accordance with the results of many cross-sectional studies performed in different areas of the world, how OBI may favor (or accelerate) the progression toward cirrhosis of CHC patients is far from being clearly understood."
The investigators noted that there is evidence "both in humans and in animal models that intrahepatic persistence of occult hepadnavirus genomes may produce a very mild but constant liver necroinflammation, and recent reports have shown an association between phases of a rise in ALT levels and reappearance of circulating HBV DNA in patients with chronic hepatitis C and combined occult HBV infection, thus suggesting an active role of transient reactivation of HBV replication in liver cell injury."
The study was supported by grants from the Associazione Italiana per la Ricerca sul Cancro. The researchers said they had no relevant financial disclosures.
FROM THE JOURNAL OF HEPATOLOGY
Major finding: Among chronic hepatitis patients followed for a median of 11 years, 19% developed hepatocellular carcinoma. A significantly greater proportion of patients who were positive for occult hepatitis virus infection developed HCC compared with those who were occult hepatitis B negative (P value of less than .01).
Data source: An observational study of 326 hepatitis B surface antigen–negative chronic hepatitis patients who were tested for occult hepatitis B virus infection by the analysis of liver biopsy DNA extracts.
Disclosures: The study was supported by grants from the Associazione Italiana per la Ricerca sul Cancro. The researchers said they had no relevant financial disclosures.