User login
Official Newspaper of the American College of Surgeons
AMA launches online tool to help address physician burnout
CHICAGO – The American Medical Association has launched an interactive tool to help physicians deal with burnout.
Dr. Steven Stack, who takes over as AMA president on June 9, said the organization wants “to the restore the joy to the practice of medicine. I think physicians feel besieged right now by an overburdened regulatory environment, too much paperwork, too much time doing clerical tasks that support the provision of care, and too little time actually interacting with patients.”

The “STEPS Forward” program gives physicians access to online modules to help them improve their practices. Currently, 16 modules are available addressing practice efficiency and patient care, patient health, physician health, and technology and innovation. Each module includes steps for implementation and case studies as well as downloadable tools, videos, and resources. CME credits are available for completed modules.
The modules were designed by physician teams, and all include real-world examples of how the processes that are displayed have been implemented.
We “recognize that in a complex world where everyone’s busy, giving someone a PDF outlining what to do does not get much traction,” AMA CEO Dr. James Madara said during a June 8 press conference at the annual meeting of the American Medical Association House of Delegates..
The AMA, in partnership with the Medical Group Management Association (MGMA), also are looking for solutions to add to the STEPS Forward program and plan to award several $10,000 prizes for those who propose the best solutions that help physicians adapt to the changing work environment. Entries are due Sept. 1. Dr. Madara said he hopes to give awards to at least five physicians and their practices for their ideas, but if more come in, AMA and MGMA will make more awards. He hopes those winners will be ready to be announced at MGMA’s annual meeting in October.
CHICAGO – The American Medical Association has launched an interactive tool to help physicians deal with burnout.
Dr. Steven Stack, who takes over as AMA president on June 9, said the organization wants “to the restore the joy to the practice of medicine. I think physicians feel besieged right now by an overburdened regulatory environment, too much paperwork, too much time doing clerical tasks that support the provision of care, and too little time actually interacting with patients.”
The “STEPS Forward” program gives physicians access to online modules to help them improve their practices. Currently, 16 modules are available addressing practice efficiency and patient care, patient health, physician health, and technology and innovation. Each module includes steps for implementation and case studies as well as downloadable tools, videos, and resources. CME credits are available for completed modules.
The modules were designed by physician teams, and all include real-world examples of how the processes that are displayed have been implemented.
We “recognize that in a complex world where everyone’s busy, giving someone a PDF outlining what to do does not get much traction,” AMA CEO Dr. James Madara said during a June 8 press conference at the annual meeting of the American Medical Association House of Delegates..
The AMA, in partnership with the Medical Group Management Association (MGMA), also are looking for solutions to add to the STEPS Forward program and plan to award several $10,000 prizes for those who propose the best solutions that help physicians adapt to the changing work environment. Entries are due Sept. 1. Dr. Madara said he hopes to give awards to at least five physicians and their practices for their ideas, but if more come in, AMA and MGMA will make more awards. He hopes those winners will be ready to be announced at MGMA’s annual meeting in October.
CHICAGO – The American Medical Association has launched an interactive tool to help physicians deal with burnout.
Dr. Steven Stack, who takes over as AMA president on June 9, said the organization wants “to the restore the joy to the practice of medicine. I think physicians feel besieged right now by an overburdened regulatory environment, too much paperwork, too much time doing clerical tasks that support the provision of care, and too little time actually interacting with patients.”
The “STEPS Forward” program gives physicians access to online modules to help them improve their practices. Currently, 16 modules are available addressing practice efficiency and patient care, patient health, physician health, and technology and innovation. Each module includes steps for implementation and case studies as well as downloadable tools, videos, and resources. CME credits are available for completed modules.
The modules were designed by physician teams, and all include real-world examples of how the processes that are displayed have been implemented.
We “recognize that in a complex world where everyone’s busy, giving someone a PDF outlining what to do does not get much traction,” AMA CEO Dr. James Madara said during a June 8 press conference at the annual meeting of the American Medical Association House of Delegates..
The AMA, in partnership with the Medical Group Management Association (MGMA), also are looking for solutions to add to the STEPS Forward program and plan to award several $10,000 prizes for those who propose the best solutions that help physicians adapt to the changing work environment. Entries are due Sept. 1. Dr. Madara said he hopes to give awards to at least five physicians and their practices for their ideas, but if more come in, AMA and MGMA will make more awards. He hopes those winners will be ready to be announced at MGMA’s annual meeting in October.
AT THE AMA HOD MEETING

Prostate cancer screening for men over 50 has declined
Subsequent to the 2012 U.S. Preventative Services Task Force recommendation discouraging prostate-specific antigen (PSA)-based screening, prostate cancer screening significantly declined among men age 50 years and older in the United States, according to a study published online in the Journal of Clinical Oncology.
Based on National Health Interview Surveys in 2005, 2010, and 2013, self-reported PSA-testing levels decreased most among men aged 50-59 years, from 33.2% in 2010 to 24.8% in 2013 (odds ratio, 0.66; P < .01). Declines from 2010 to 2013 were also observed among men aged 60-74 years (51.2%-43.6%; OR, 0.74; P < .01); and aged 75 and older (43.9%-37.1%, OR, 0.75; P = .03). Among men aged 40-49 years, the decline from 12.5% to 11.2% was not significant (Journ. Clin. Onc. 2015 June 8 [doi:10.1200/JCO.2015.61.6532]).
The declines may reflect increased adherence by physicians to USPSTF guidelines; nevertheless, in 2013 approximately one-third of men aged 65 or older who had high risk for 9-year mortality (about 1.4 million individuals) were screened.
“Persistently elevated screening rates among men with limited remaining life expectancies are troubling and merit further interventions,” wrote Dr. Michael Drazer of the University of Chicago Medical Center and colleagues. “These may include increasing awareness of initiatives such as Choosing Wisely recommendations from the American Society of Clinical Oncology and recommendations from the American Geriatrics Society,” they wrote.
If these efforts prove unsuccessful, reducing or eliminating reimbursements for screening and interventions may be considered, the authors suggest.
A multivariate model identified factors that predict which men over age 65 are likely to be screened, and these are men who went to college, were married, consumed alcohol, and received a colonoscopy in the last 10 years. They found no significant predictors in the patient population for declines in screening from 2010 to 2013.
Several studies support the use of extended screening intervals (every 2-3 years) for patients at low risk for prostate cancer. Annual screening of men aged 55-67 years has been estimated to result in a 50% overdiagnosis rate.
Drs. Drazer and Huo reported having no financial disclosures. Dr. Eggener reported having consulting or advisory roles with Myriad Genetics, Medivation, Janssen Pharmaceuticals, Genomic Health, OPKO Diagnostics, and MDxHealth.
Subsequent to the 2012 U.S. Preventative Services Task Force recommendation discouraging prostate-specific antigen (PSA)-based screening, prostate cancer screening significantly declined among men age 50 years and older in the United States, according to a study published online in the Journal of Clinical Oncology.
Based on National Health Interview Surveys in 2005, 2010, and 2013, self-reported PSA-testing levels decreased most among men aged 50-59 years, from 33.2% in 2010 to 24.8% in 2013 (odds ratio, 0.66; P < .01). Declines from 2010 to 2013 were also observed among men aged 60-74 years (51.2%-43.6%; OR, 0.74; P < .01); and aged 75 and older (43.9%-37.1%, OR, 0.75; P = .03). Among men aged 40-49 years, the decline from 12.5% to 11.2% was not significant (Journ. Clin. Onc. 2015 June 8 [doi:10.1200/JCO.2015.61.6532]).
The declines may reflect increased adherence by physicians to USPSTF guidelines; nevertheless, in 2013 approximately one-third of men aged 65 or older who had high risk for 9-year mortality (about 1.4 million individuals) were screened.
“Persistently elevated screening rates among men with limited remaining life expectancies are troubling and merit further interventions,” wrote Dr. Michael Drazer of the University of Chicago Medical Center and colleagues. “These may include increasing awareness of initiatives such as Choosing Wisely recommendations from the American Society of Clinical Oncology and recommendations from the American Geriatrics Society,” they wrote.
If these efforts prove unsuccessful, reducing or eliminating reimbursements for screening and interventions may be considered, the authors suggest.
A multivariate model identified factors that predict which men over age 65 are likely to be screened, and these are men who went to college, were married, consumed alcohol, and received a colonoscopy in the last 10 years. They found no significant predictors in the patient population for declines in screening from 2010 to 2013.
Several studies support the use of extended screening intervals (every 2-3 years) for patients at low risk for prostate cancer. Annual screening of men aged 55-67 years has been estimated to result in a 50% overdiagnosis rate.
Drs. Drazer and Huo reported having no financial disclosures. Dr. Eggener reported having consulting or advisory roles with Myriad Genetics, Medivation, Janssen Pharmaceuticals, Genomic Health, OPKO Diagnostics, and MDxHealth.
Subsequent to the 2012 U.S. Preventative Services Task Force recommendation discouraging prostate-specific antigen (PSA)-based screening, prostate cancer screening significantly declined among men age 50 years and older in the United States, according to a study published online in the Journal of Clinical Oncology.
Based on National Health Interview Surveys in 2005, 2010, and 2013, self-reported PSA-testing levels decreased most among men aged 50-59 years, from 33.2% in 2010 to 24.8% in 2013 (odds ratio, 0.66; P < .01). Declines from 2010 to 2013 were also observed among men aged 60-74 years (51.2%-43.6%; OR, 0.74; P < .01); and aged 75 and older (43.9%-37.1%, OR, 0.75; P = .03). Among men aged 40-49 years, the decline from 12.5% to 11.2% was not significant (Journ. Clin. Onc. 2015 June 8 [doi:10.1200/JCO.2015.61.6532]).
The declines may reflect increased adherence by physicians to USPSTF guidelines; nevertheless, in 2013 approximately one-third of men aged 65 or older who had high risk for 9-year mortality (about 1.4 million individuals) were screened.
“Persistently elevated screening rates among men with limited remaining life expectancies are troubling and merit further interventions,” wrote Dr. Michael Drazer of the University of Chicago Medical Center and colleagues. “These may include increasing awareness of initiatives such as Choosing Wisely recommendations from the American Society of Clinical Oncology and recommendations from the American Geriatrics Society,” they wrote.
If these efforts prove unsuccessful, reducing or eliminating reimbursements for screening and interventions may be considered, the authors suggest.
A multivariate model identified factors that predict which men over age 65 are likely to be screened, and these are men who went to college, were married, consumed alcohol, and received a colonoscopy in the last 10 years. They found no significant predictors in the patient population for declines in screening from 2010 to 2013.
Several studies support the use of extended screening intervals (every 2-3 years) for patients at low risk for prostate cancer. Annual screening of men aged 55-67 years has been estimated to result in a 50% overdiagnosis rate.
Drs. Drazer and Huo reported having no financial disclosures. Dr. Eggener reported having consulting or advisory roles with Myriad Genetics, Medivation, Janssen Pharmaceuticals, Genomic Health, OPKO Diagnostics, and MDxHealth.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Prostate cancer screening rates among men aged 50 years and older declined nationwide from 2010 to 2013.
Major finding: From 2010 to 2013 screening rates significantly declined among men aged 50-59 (33.2%-24.8%, P < .01); aged 60-74 (51.2%-43.6%, P < .01); and aged 75 and older (43.9%-37.1%, P = .03).
Data source: The National Health Interview Survey is a face-to-face, cross-sectional survey that included men ≥ 40 years who had seen a physician in the previous year, representing over 60,000,000 men.
Disclosures: Drs. Drazer and Huo reported having no financial disclosures. Dr. Eggener reported having consulting or advisory roles with Myriad Genetics, Medivation, Janssen Pharmaceuticals, Genomic Health, OPKO Diagnostics, and MDxHealth.
Bariatric surgery, lifestyle intervention had similar effects on hemoglobin A1c
BOSTON – Weight loss was greater with laparoscopic adjustable gastric banding than with an intensive lifestyle intervention among obese patients with type 2 diabetes in a randomized clinical trial, but the effects on diabetes control, cardiometabolic risk, and quality of life were comparable.
Weight loss in 18 patients randomized to undergo the bariatric surgery was an average of 13.5 lb at 12 months’ follow-up, compared with 8.5 lb in those randomized to the active component of the study: a 12-week lifestyle intervention (Weight Achievement and Intensive Treatment–the Why WAIT program), Dr. Osama Hamdy reported in a poster at the annual scientific sessions of the American Diabetes Association.
However, hemogobin A1c reduction was similar in the two groups at –1.2% vs. –1%, respectively. Further, improvements in blood pressure, triglycerides, and low-density lipoprotein levels did not differ between the groups, said Dr. Hamdy, medical director of the obesity clinical program, and director of the inpatient program at Joslin Diabetes Clinic, Harvard Medical School, Boston.
The risk of fatal coronary heart disease events also decreased in both groups, from 6.5% to 5.9% in the bariatric surgery group, and from 5.8% to 5.5% in the Why WAIT group; the difference between the groups was not statistically significant, he said.
Quality of life as assessed by the 36-item Short Form Survey’s physical and mental health summary measures changed only slightly from baseline in both groups, with no between-group differences. Similarly, scores on the Impact of Weight on Quality of Life and on Problem Areas in Diabetes improved significantly in both groups, but no between-group differences were seen.
“These findings suggest that the Why WAIT program and laparoscopic adjustable gastric banding have similar benefits for diabetes control, cardiometabolic risk, and quality of life parameters,” according to Dr. Hamdy, who noted that the findings may be useful for guiding obese patients with type 2 diabetes as they explore weight management options.
Dr. Hamdy reported that he has received research support and is an advisory panel member and author for Metagenics, that he is a consultant and author for Abbott Nutrition and Merck, and that he has received research support and is an author for Neurometrix.
BOSTON – Weight loss was greater with laparoscopic adjustable gastric banding than with an intensive lifestyle intervention among obese patients with type 2 diabetes in a randomized clinical trial, but the effects on diabetes control, cardiometabolic risk, and quality of life were comparable.
Weight loss in 18 patients randomized to undergo the bariatric surgery was an average of 13.5 lb at 12 months’ follow-up, compared with 8.5 lb in those randomized to the active component of the study: a 12-week lifestyle intervention (Weight Achievement and Intensive Treatment–the Why WAIT program), Dr. Osama Hamdy reported in a poster at the annual scientific sessions of the American Diabetes Association.
However, hemogobin A1c reduction was similar in the two groups at –1.2% vs. –1%, respectively. Further, improvements in blood pressure, triglycerides, and low-density lipoprotein levels did not differ between the groups, said Dr. Hamdy, medical director of the obesity clinical program, and director of the inpatient program at Joslin Diabetes Clinic, Harvard Medical School, Boston.
The risk of fatal coronary heart disease events also decreased in both groups, from 6.5% to 5.9% in the bariatric surgery group, and from 5.8% to 5.5% in the Why WAIT group; the difference between the groups was not statistically significant, he said.
Quality of life as assessed by the 36-item Short Form Survey’s physical and mental health summary measures changed only slightly from baseline in both groups, with no between-group differences. Similarly, scores on the Impact of Weight on Quality of Life and on Problem Areas in Diabetes improved significantly in both groups, but no between-group differences were seen.
“These findings suggest that the Why WAIT program and laparoscopic adjustable gastric banding have similar benefits for diabetes control, cardiometabolic risk, and quality of life parameters,” according to Dr. Hamdy, who noted that the findings may be useful for guiding obese patients with type 2 diabetes as they explore weight management options.
Dr. Hamdy reported that he has received research support and is an advisory panel member and author for Metagenics, that he is a consultant and author for Abbott Nutrition and Merck, and that he has received research support and is an author for Neurometrix.
BOSTON – Weight loss was greater with laparoscopic adjustable gastric banding than with an intensive lifestyle intervention among obese patients with type 2 diabetes in a randomized clinical trial, but the effects on diabetes control, cardiometabolic risk, and quality of life were comparable.
Weight loss in 18 patients randomized to undergo the bariatric surgery was an average of 13.5 lb at 12 months’ follow-up, compared with 8.5 lb in those randomized to the active component of the study: a 12-week lifestyle intervention (Weight Achievement and Intensive Treatment–the Why WAIT program), Dr. Osama Hamdy reported in a poster at the annual scientific sessions of the American Diabetes Association.
However, hemogobin A1c reduction was similar in the two groups at –1.2% vs. –1%, respectively. Further, improvements in blood pressure, triglycerides, and low-density lipoprotein levels did not differ between the groups, said Dr. Hamdy, medical director of the obesity clinical program, and director of the inpatient program at Joslin Diabetes Clinic, Harvard Medical School, Boston.
The risk of fatal coronary heart disease events also decreased in both groups, from 6.5% to 5.9% in the bariatric surgery group, and from 5.8% to 5.5% in the Why WAIT group; the difference between the groups was not statistically significant, he said.
Quality of life as assessed by the 36-item Short Form Survey’s physical and mental health summary measures changed only slightly from baseline in both groups, with no between-group differences. Similarly, scores on the Impact of Weight on Quality of Life and on Problem Areas in Diabetes improved significantly in both groups, but no between-group differences were seen.
“These findings suggest that the Why WAIT program and laparoscopic adjustable gastric banding have similar benefits for diabetes control, cardiometabolic risk, and quality of life parameters,” according to Dr. Hamdy, who noted that the findings may be useful for guiding obese patients with type 2 diabetes as they explore weight management options.
Dr. Hamdy reported that he has received research support and is an advisory panel member and author for Metagenics, that he is a consultant and author for Abbott Nutrition and Merck, and that he has received research support and is an author for Neurometrix.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: Weight loss was greater with bariatric surgery than with an intensive lifestyle intervention in obese patients with type 2 diabetes in a randomized trial, but the effects on diabetes control, cardiometabolic risk, and quality of life were comparable.
Major finding: Hemoglobin A1c reduction was similar at –1.2% vs. –1% in the gastric banding and lifestyle intervention groups, respectively.
Data source: A randomized clinical trial involving 40 patients.
Disclosures: Dr Hamdy reported that he has received research support and is an advisory panel member and author for Metagenics, that he is a consultant and author for Abbott Nutrition and Merck, and that he has received research support and is an author for Neurometrix.
AMA HOD: Delegates call for ICD-10 grace period
CHICAGO – With the ICD-10 transition looming, delegates to the annual meeting of the American Medical Association House of Delegates want their organization to advocate for giving some room to physicians to adjust.
A resolution submitted by the Alabama delegation calls on the AMA to push for a 2-year grace period during which physicians would not be penalized for errors, mistakes, and other system malfunctions, and payments would not be withheld due to coding errors.

Dr. W. Jeff Terry, chairman of the Alabama delegation, noted that, despite the AMA’s policies and efforts against ICD-10, the government stands firm on its Oct. 1 implementation date.
“I truly believe that we have just not educated Congress well enough as to the issues of the consequences of ICD-10,” Dr. Terry said.
“We – as our AMA, me, and all of you – just haven’t done our job well enough. … I want to stress here today what our AMA message should be from out of this meeting. Even though the American Medical Association is firm in its view that the switch to ICD-10 is a mistake, we also recognized that there are other groups that are fighting to maintain the Oct. 1 implementation date. In order to maintain patients’ access to care and protect physicians’ practices, we offer a compromise solution that will allow ICD-10 to be implemented as planned on Oct. 1, and at same time, protect physicians from suffering financial consequences as a result of coding errors and mistakes for a 2-year period,” he said.
He called for the AMA to put in motion a letter-writing campaign to advocate for the grace period. “This should be our number-one priority, at least from now until Oct. 1, when it won’t matter.”
Dr. Wanda Filer, delegate from the American Academy of Family Physicians, echoed Dr. Terry.
“At this point, we believe that the adoption of ICD-10 is inevitable and, recognizing that advocacy resources are finite, we would like to encourage our AMA to work with CMS to prepare for this and ensure a soft landing for all physicians and patients … rather than a hard start,” said Dr. Filer, who is also AAFP president-elect.
Delegates suggested that the organization focus on how ICD-10 requirements could affect small practices and their patients. They called on the AMA to track data on rejected claims, payment delays resulting from coding errors, and the impact on patient volume.
Reference Committee B, which addresses matters of federal legislation, considered a number of other issues, almost without dissent. One exception was a resolution advocating for background checks on all gun sales, which met with some resistance as being onerous for certain people in specific situations.
Resolutions will be voted on by the full House of Delegates June 8-10.
CHICAGO – With the ICD-10 transition looming, delegates to the annual meeting of the American Medical Association House of Delegates want their organization to advocate for giving some room to physicians to adjust.
A resolution submitted by the Alabama delegation calls on the AMA to push for a 2-year grace period during which physicians would not be penalized for errors, mistakes, and other system malfunctions, and payments would not be withheld due to coding errors.
Dr. W. Jeff Terry, chairman of the Alabama delegation, noted that, despite the AMA’s policies and efforts against ICD-10, the government stands firm on its Oct. 1 implementation date.
“I truly believe that we have just not educated Congress well enough as to the issues of the consequences of ICD-10,” Dr. Terry said.
“We – as our AMA, me, and all of you – just haven’t done our job well enough. … I want to stress here today what our AMA message should be from out of this meeting. Even though the American Medical Association is firm in its view that the switch to ICD-10 is a mistake, we also recognized that there are other groups that are fighting to maintain the Oct. 1 implementation date. In order to maintain patients’ access to care and protect physicians’ practices, we offer a compromise solution that will allow ICD-10 to be implemented as planned on Oct. 1, and at same time, protect physicians from suffering financial consequences as a result of coding errors and mistakes for a 2-year period,” he said.
He called for the AMA to put in motion a letter-writing campaign to advocate for the grace period. “This should be our number-one priority, at least from now until Oct. 1, when it won’t matter.”
Dr. Wanda Filer, delegate from the American Academy of Family Physicians, echoed Dr. Terry.
“At this point, we believe that the adoption of ICD-10 is inevitable and, recognizing that advocacy resources are finite, we would like to encourage our AMA to work with CMS to prepare for this and ensure a soft landing for all physicians and patients … rather than a hard start,” said Dr. Filer, who is also AAFP president-elect.
Delegates suggested that the organization focus on how ICD-10 requirements could affect small practices and their patients. They called on the AMA to track data on rejected claims, payment delays resulting from coding errors, and the impact on patient volume.
Reference Committee B, which addresses matters of federal legislation, considered a number of other issues, almost without dissent. One exception was a resolution advocating for background checks on all gun sales, which met with some resistance as being onerous for certain people in specific situations.
Resolutions will be voted on by the full House of Delegates June 8-10.
CHICAGO – With the ICD-10 transition looming, delegates to the annual meeting of the American Medical Association House of Delegates want their organization to advocate for giving some room to physicians to adjust.
A resolution submitted by the Alabama delegation calls on the AMA to push for a 2-year grace period during which physicians would not be penalized for errors, mistakes, and other system malfunctions, and payments would not be withheld due to coding errors.
Dr. W. Jeff Terry, chairman of the Alabama delegation, noted that, despite the AMA’s policies and efforts against ICD-10, the government stands firm on its Oct. 1 implementation date.
“I truly believe that we have just not educated Congress well enough as to the issues of the consequences of ICD-10,” Dr. Terry said.
“We – as our AMA, me, and all of you – just haven’t done our job well enough. … I want to stress here today what our AMA message should be from out of this meeting. Even though the American Medical Association is firm in its view that the switch to ICD-10 is a mistake, we also recognized that there are other groups that are fighting to maintain the Oct. 1 implementation date. In order to maintain patients’ access to care and protect physicians’ practices, we offer a compromise solution that will allow ICD-10 to be implemented as planned on Oct. 1, and at same time, protect physicians from suffering financial consequences as a result of coding errors and mistakes for a 2-year period,” he said.
He called for the AMA to put in motion a letter-writing campaign to advocate for the grace period. “This should be our number-one priority, at least from now until Oct. 1, when it won’t matter.”
Dr. Wanda Filer, delegate from the American Academy of Family Physicians, echoed Dr. Terry.
“At this point, we believe that the adoption of ICD-10 is inevitable and, recognizing that advocacy resources are finite, we would like to encourage our AMA to work with CMS to prepare for this and ensure a soft landing for all physicians and patients … rather than a hard start,” said Dr. Filer, who is also AAFP president-elect.
Delegates suggested that the organization focus on how ICD-10 requirements could affect small practices and their patients. They called on the AMA to track data on rejected claims, payment delays resulting from coding errors, and the impact on patient volume.
Reference Committee B, which addresses matters of federal legislation, considered a number of other issues, almost without dissent. One exception was a resolution advocating for background checks on all gun sales, which met with some resistance as being onerous for certain people in specific situations.
Resolutions will be voted on by the full House of Delegates June 8-10.
AT THE AMA HOD MEETING

User errors are top reason for EHR-related malpractice claims
User error, such as incorrect data input, contributes to the majority of medical malpractice claims that involve electronic health records.
Of 97 EHR-related malpractice claims that closed from January 2007 to June 2014, 64% involved user errors, while 42% related to system factors, according to an analysis from national medical liability insurer The Doctors Company. (Numbers do not add up to 100% because some claims contained more than one contributing factor.)

The most common user errors included incorrect information in the EHR (16%), hybrid health records/EHR conversion (15%), and problems regarding prepopulating/copy and pasting (13%). Less common user factors involved training/education, EHR alert issue or fatigue, and workarounds, according to the report.
EHR-related malpractice claims appear to be on the rise, said Dr. David B. Troxel, medical director for The Doctors Company. Of the 97 EHR-related claims, 26 claims closed in the first half of 2014, compared with 28 claims that closed in 2013, 22 that closed in 2012, 19 that closed in 2011, and 2 that closed between 2007 and 2010.
“Electronic health records provide benefits but also create risks that can contribute to medical malpractice claims,” Dr. Troxel said in an interview. “Their widespread use is too recent to tell whether the benefits will outweigh the risks and result in a decrease in adverse patient events. In the meantime, I believe we will see an increase in claims over the next few years in which EHRs are a contributing factor.”
Of system-related EHR claims, 10% involved system design failures. Electronic systems/technology failures contributed to 9% of cases, and 7% involved a lack of EHR alert or alarm/decision support. Other system-related claims were attributed to inappropriate data routing, insufficient scope/area for documentation, and fragmentation.
In one such case examined, a plaintiff claimed the lack of a medication risk alert led to the death of a dialysis patient. The patient was transferred to a skilled nursing facility with an active hospital transfer order for enoxaparin. A physician evaluated the patient upon admission but made no comment about the enoxaparin order. During the first dialysis treatment, there was active bleeding at the fistula site, but a nurse did not inform the physician. During the second dialysis treatment, there was uncontrolled bleeding from the fistula, and the patient later died.
As for practice area, internal medicine subspecialists – including cardiologists, hospitalists, oncologists, and gastroenterologists – were the most likely to see EHR-related claims at 20%. Primary care physicians – family physicians and general internists – faced claims in 16% of cases, while ob.gyns. were accused in 15% of cases. Other cases involved claims against surgeons (14%), nurses (7%), radiologists (5%), anesthesiologists, (4%), general surgeons (4%), pediatricians (2%), emergency medicine physicians (2%), psychiatrists (2%), orthopedists (2%), and pathologists (1%). Other claims were against nonphysician providers.
Among all EHR-related claims, the top allegations made were diagnosis failure and medication error, including allegedly ordering the wrong medication, prescribing an incorrect dosage, or improper medication management.
User error, such as incorrect data input, contributes to the majority of medical malpractice claims that involve electronic health records.
Of 97 EHR-related malpractice claims that closed from January 2007 to June 2014, 64% involved user errors, while 42% related to system factors, according to an analysis from national medical liability insurer The Doctors Company. (Numbers do not add up to 100% because some claims contained more than one contributing factor.)
The most common user errors included incorrect information in the EHR (16%), hybrid health records/EHR conversion (15%), and problems regarding prepopulating/copy and pasting (13%). Less common user factors involved training/education, EHR alert issue or fatigue, and workarounds, according to the report.
EHR-related malpractice claims appear to be on the rise, said Dr. David B. Troxel, medical director for The Doctors Company. Of the 97 EHR-related claims, 26 claims closed in the first half of 2014, compared with 28 claims that closed in 2013, 22 that closed in 2012, 19 that closed in 2011, and 2 that closed between 2007 and 2010.
“Electronic health records provide benefits but also create risks that can contribute to medical malpractice claims,” Dr. Troxel said in an interview. “Their widespread use is too recent to tell whether the benefits will outweigh the risks and result in a decrease in adverse patient events. In the meantime, I believe we will see an increase in claims over the next few years in which EHRs are a contributing factor.”
Of system-related EHR claims, 10% involved system design failures. Electronic systems/technology failures contributed to 9% of cases, and 7% involved a lack of EHR alert or alarm/decision support. Other system-related claims were attributed to inappropriate data routing, insufficient scope/area for documentation, and fragmentation.
In one such case examined, a plaintiff claimed the lack of a medication risk alert led to the death of a dialysis patient. The patient was transferred to a skilled nursing facility with an active hospital transfer order for enoxaparin. A physician evaluated the patient upon admission but made no comment about the enoxaparin order. During the first dialysis treatment, there was active bleeding at the fistula site, but a nurse did not inform the physician. During the second dialysis treatment, there was uncontrolled bleeding from the fistula, and the patient later died.
As for practice area, internal medicine subspecialists – including cardiologists, hospitalists, oncologists, and gastroenterologists – were the most likely to see EHR-related claims at 20%. Primary care physicians – family physicians and general internists – faced claims in 16% of cases, while ob.gyns. were accused in 15% of cases. Other cases involved claims against surgeons (14%), nurses (7%), radiologists (5%), anesthesiologists, (4%), general surgeons (4%), pediatricians (2%), emergency medicine physicians (2%), psychiatrists (2%), orthopedists (2%), and pathologists (1%). Other claims were against nonphysician providers.
Among all EHR-related claims, the top allegations made were diagnosis failure and medication error, including allegedly ordering the wrong medication, prescribing an incorrect dosage, or improper medication management.
User error, such as incorrect data input, contributes to the majority of medical malpractice claims that involve electronic health records.
Of 97 EHR-related malpractice claims that closed from January 2007 to June 2014, 64% involved user errors, while 42% related to system factors, according to an analysis from national medical liability insurer The Doctors Company. (Numbers do not add up to 100% because some claims contained more than one contributing factor.)
The most common user errors included incorrect information in the EHR (16%), hybrid health records/EHR conversion (15%), and problems regarding prepopulating/copy and pasting (13%). Less common user factors involved training/education, EHR alert issue or fatigue, and workarounds, according to the report.
EHR-related malpractice claims appear to be on the rise, said Dr. David B. Troxel, medical director for The Doctors Company. Of the 97 EHR-related claims, 26 claims closed in the first half of 2014, compared with 28 claims that closed in 2013, 22 that closed in 2012, 19 that closed in 2011, and 2 that closed between 2007 and 2010.
“Electronic health records provide benefits but also create risks that can contribute to medical malpractice claims,” Dr. Troxel said in an interview. “Their widespread use is too recent to tell whether the benefits will outweigh the risks and result in a decrease in adverse patient events. In the meantime, I believe we will see an increase in claims over the next few years in which EHRs are a contributing factor.”
Of system-related EHR claims, 10% involved system design failures. Electronic systems/technology failures contributed to 9% of cases, and 7% involved a lack of EHR alert or alarm/decision support. Other system-related claims were attributed to inappropriate data routing, insufficient scope/area for documentation, and fragmentation.
In one such case examined, a plaintiff claimed the lack of a medication risk alert led to the death of a dialysis patient. The patient was transferred to a skilled nursing facility with an active hospital transfer order for enoxaparin. A physician evaluated the patient upon admission but made no comment about the enoxaparin order. During the first dialysis treatment, there was active bleeding at the fistula site, but a nurse did not inform the physician. During the second dialysis treatment, there was uncontrolled bleeding from the fistula, and the patient later died.
As for practice area, internal medicine subspecialists – including cardiologists, hospitalists, oncologists, and gastroenterologists – were the most likely to see EHR-related claims at 20%. Primary care physicians – family physicians and general internists – faced claims in 16% of cases, while ob.gyns. were accused in 15% of cases. Other cases involved claims against surgeons (14%), nurses (7%), radiologists (5%), anesthesiologists, (4%), general surgeons (4%), pediatricians (2%), emergency medicine physicians (2%), psychiatrists (2%), orthopedists (2%), and pathologists (1%). Other claims were against nonphysician providers.
Among all EHR-related claims, the top allegations made were diagnosis failure and medication error, including allegedly ordering the wrong medication, prescribing an incorrect dosage, or improper medication management.

ERAS protocol superior for postop cystectomy pain management
NEW ORLEANS – The enhanced recovery after surgery (ERAS) protocol resulted in significantly less opioid use for pain management for radical cystectomy patients, compared with traditional postop approaches, according to Dr. Hooman Djaladat.
“The whole idea behind the ERAS protocol was to diminish hospital stay and send the patients home sooner, with no increase in complications or readmission rates,” said Dr. Djaladat, associate professor of clinical urology at the University of Southern California, Los Angeles.

ERAS protocols are multimodal perioperative care pathways, the aim of which is early recovery after surgery by maintaining preoperative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counseling, optimization of nutrition, standardized analgesic and anesthetic regimens, and early mobilization.
Opioids have traditionally been the standard for pain management after radical cystectomy (RC) for bladder cancer, but opioid use is often accompanied by side effects such as respiratory depression, nausea, vomiting, confusion, and ileus – the leading cause of prolonged hospital stay.
Dr. Djaladat and his colleagues at USC compared the amount of opioid use, pain score, and postoperative ileus in consecutive ERAS and traditional postop RC patients at USC, and presented their findings in a poster at the annual meeting of the American Urological Association.
Study Methods
Dr. Djaladat and his colleagues retrospectively evaluated 205 open-RC patients, 124 of whom underwent pain management as outlined by ERAS protocol (May 2012 to December 2013) and 81 who underwent traditional pain management with opioids (February 2010 to September 2013); the two groups were matched according to patient demographics, and those with a history of opioid use prior to surgery were not included in the study.
Traditional pain management protocol relied primarily on intravenous and epidural opioids, with acetaminophen and ketorolac as supplements as needed. Patient-controlled analgesia also was used if necessary.
The ERAS protocol utilized predominantly acetaminophen and ketorolac started intraoperatively, supplemented by consistent use of local anesthetic through subfascial catheters. Opioids were used only for breakthrough pain.
All opioids used (oxycodone, hydromorphone, tramadol, hydrocodone, morphine, and fentanyl) were converted to intravenous morphine equivalents. Opioid use and pain scores were examined and compared up to postoperative day 4.
“Bottom line, a traditional pathway has been mostly opioid controlled, but ERAS protocol is mostly focused on nonopioid control,” said Dr. Djaladat. “We believe that opioids cause a lot of problems.”
Results
Length of hospital stay in the ERAS cohort was half that in the traditional cohort (4 days vs. 8 days, P < .0001). Additionally, mean morphine equivalent use in the ERAS group was about one-quarter of that observed in the traditional patients (4.9 mg/day vs. 20.87 mg/day, P < .0001).
Postoperative ileus was higher in the traditional group, compared with the ERAS group (22.2% vs. 7.3%, P < .0028). “One of the most important contributing factors to decreased ileus is less narcotic,” he said.
ERAS patients reported higher mean visual analogous (VAS) pain scores per day than traditional patients (3.1 vs. 1.14 on a 4-point scale, P < .0001). VAS scores are the modality by which patients’ pain is measured subjectively. However, Dr. Djaladat suggested in an interview that the statistically significant difference in VAS scores did not necessarily reflect a substantial difference in pain from a clinical perspective.
Dr. Djaladat and his colleagues observed that patients on ERAS protocol used significantly fewer opioid analgesics, which may have potentially contributed to decreased postoperative ileus and shorter lengths of hospital stay, he suggested. They affirm, however, that multi-institutional studies would aid in externally validating these results.
“We find that ERAS is sufficient to manage pain immediately and at the time of discharge, with less narcotic use, in patients who have just undergone radical cystectomy,” Dr. Djaladat reported.
Dr. Djaladat disclosed no relevant financial relationships.
NEW ORLEANS – The enhanced recovery after surgery (ERAS) protocol resulted in significantly less opioid use for pain management for radical cystectomy patients, compared with traditional postop approaches, according to Dr. Hooman Djaladat.
“The whole idea behind the ERAS protocol was to diminish hospital stay and send the patients home sooner, with no increase in complications or readmission rates,” said Dr. Djaladat, associate professor of clinical urology at the University of Southern California, Los Angeles.
ERAS protocols are multimodal perioperative care pathways, the aim of which is early recovery after surgery by maintaining preoperative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counseling, optimization of nutrition, standardized analgesic and anesthetic regimens, and early mobilization.
Opioids have traditionally been the standard for pain management after radical cystectomy (RC) for bladder cancer, but opioid use is often accompanied by side effects such as respiratory depression, nausea, vomiting, confusion, and ileus – the leading cause of prolonged hospital stay.
Dr. Djaladat and his colleagues at USC compared the amount of opioid use, pain score, and postoperative ileus in consecutive ERAS and traditional postop RC patients at USC, and presented their findings in a poster at the annual meeting of the American Urological Association.
Study Methods
Dr. Djaladat and his colleagues retrospectively evaluated 205 open-RC patients, 124 of whom underwent pain management as outlined by ERAS protocol (May 2012 to December 2013) and 81 who underwent traditional pain management with opioids (February 2010 to September 2013); the two groups were matched according to patient demographics, and those with a history of opioid use prior to surgery were not included in the study.
Traditional pain management protocol relied primarily on intravenous and epidural opioids, with acetaminophen and ketorolac as supplements as needed. Patient-controlled analgesia also was used if necessary.
The ERAS protocol utilized predominantly acetaminophen and ketorolac started intraoperatively, supplemented by consistent use of local anesthetic through subfascial catheters. Opioids were used only for breakthrough pain.
All opioids used (oxycodone, hydromorphone, tramadol, hydrocodone, morphine, and fentanyl) were converted to intravenous morphine equivalents. Opioid use and pain scores were examined and compared up to postoperative day 4.
“Bottom line, a traditional pathway has been mostly opioid controlled, but ERAS protocol is mostly focused on nonopioid control,” said Dr. Djaladat. “We believe that opioids cause a lot of problems.”
Results
Length of hospital stay in the ERAS cohort was half that in the traditional cohort (4 days vs. 8 days, P < .0001). Additionally, mean morphine equivalent use in the ERAS group was about one-quarter of that observed in the traditional patients (4.9 mg/day vs. 20.87 mg/day, P < .0001).
Postoperative ileus was higher in the traditional group, compared with the ERAS group (22.2% vs. 7.3%, P < .0028). “One of the most important contributing factors to decreased ileus is less narcotic,” he said.
ERAS patients reported higher mean visual analogous (VAS) pain scores per day than traditional patients (3.1 vs. 1.14 on a 4-point scale, P < .0001). VAS scores are the modality by which patients’ pain is measured subjectively. However, Dr. Djaladat suggested in an interview that the statistically significant difference in VAS scores did not necessarily reflect a substantial difference in pain from a clinical perspective.
Dr. Djaladat and his colleagues observed that patients on ERAS protocol used significantly fewer opioid analgesics, which may have potentially contributed to decreased postoperative ileus and shorter lengths of hospital stay, he suggested. They affirm, however, that multi-institutional studies would aid in externally validating these results.
“We find that ERAS is sufficient to manage pain immediately and at the time of discharge, with less narcotic use, in patients who have just undergone radical cystectomy,” Dr. Djaladat reported.
Dr. Djaladat disclosed no relevant financial relationships.
NEW ORLEANS – The enhanced recovery after surgery (ERAS) protocol resulted in significantly less opioid use for pain management for radical cystectomy patients, compared with traditional postop approaches, according to Dr. Hooman Djaladat.
“The whole idea behind the ERAS protocol was to diminish hospital stay and send the patients home sooner, with no increase in complications or readmission rates,” said Dr. Djaladat, associate professor of clinical urology at the University of Southern California, Los Angeles.
ERAS protocols are multimodal perioperative care pathways, the aim of which is early recovery after surgery by maintaining preoperative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counseling, optimization of nutrition, standardized analgesic and anesthetic regimens, and early mobilization.
Opioids have traditionally been the standard for pain management after radical cystectomy (RC) for bladder cancer, but opioid use is often accompanied by side effects such as respiratory depression, nausea, vomiting, confusion, and ileus – the leading cause of prolonged hospital stay.
Dr. Djaladat and his colleagues at USC compared the amount of opioid use, pain score, and postoperative ileus in consecutive ERAS and traditional postop RC patients at USC, and presented their findings in a poster at the annual meeting of the American Urological Association.
Study Methods
Dr. Djaladat and his colleagues retrospectively evaluated 205 open-RC patients, 124 of whom underwent pain management as outlined by ERAS protocol (May 2012 to December 2013) and 81 who underwent traditional pain management with opioids (February 2010 to September 2013); the two groups were matched according to patient demographics, and those with a history of opioid use prior to surgery were not included in the study.
Traditional pain management protocol relied primarily on intravenous and epidural opioids, with acetaminophen and ketorolac as supplements as needed. Patient-controlled analgesia also was used if necessary.
The ERAS protocol utilized predominantly acetaminophen and ketorolac started intraoperatively, supplemented by consistent use of local anesthetic through subfascial catheters. Opioids were used only for breakthrough pain.
All opioids used (oxycodone, hydromorphone, tramadol, hydrocodone, morphine, and fentanyl) were converted to intravenous morphine equivalents. Opioid use and pain scores were examined and compared up to postoperative day 4.
“Bottom line, a traditional pathway has been mostly opioid controlled, but ERAS protocol is mostly focused on nonopioid control,” said Dr. Djaladat. “We believe that opioids cause a lot of problems.”
Results
Length of hospital stay in the ERAS cohort was half that in the traditional cohort (4 days vs. 8 days, P < .0001). Additionally, mean morphine equivalent use in the ERAS group was about one-quarter of that observed in the traditional patients (4.9 mg/day vs. 20.87 mg/day, P < .0001).
Postoperative ileus was higher in the traditional group, compared with the ERAS group (22.2% vs. 7.3%, P < .0028). “One of the most important contributing factors to decreased ileus is less narcotic,” he said.
ERAS patients reported higher mean visual analogous (VAS) pain scores per day than traditional patients (3.1 vs. 1.14 on a 4-point scale, P < .0001). VAS scores are the modality by which patients’ pain is measured subjectively. However, Dr. Djaladat suggested in an interview that the statistically significant difference in VAS scores did not necessarily reflect a substantial difference in pain from a clinical perspective.
Dr. Djaladat and his colleagues observed that patients on ERAS protocol used significantly fewer opioid analgesics, which may have potentially contributed to decreased postoperative ileus and shorter lengths of hospital stay, he suggested. They affirm, however, that multi-institutional studies would aid in externally validating these results.
“We find that ERAS is sufficient to manage pain immediately and at the time of discharge, with less narcotic use, in patients who have just undergone radical cystectomy,” Dr. Djaladat reported.
Dr. Djaladat disclosed no relevant financial relationships.
AT THE AUA ANNUAL MEETING
Key clinical point: Consider ERAS protocol for patients after radical cystectomy to reduce hospital stays and complications.
Major finding: Length of hospital stay in the ERAS cohort was half that in the traditional cohort (4 vs. 8 days). Mean morphine equivalent use in the ERAS group was about one-quarter of that observed in the traditional patients (4.9 vs. 20.87 mg/day).
Data source: Comparative study of 205 well matched, open radical cystectomy patients, 124 of whom underwent pain management as outlined by ERAS protocol and 81 who underwent traditional pain management with opioids.
Disclosures: Dr. Djaladat disclosed no relevant financial relationships.

ASCO: Research IDs new subtype of refractory prostate cancer
CHICAGO – Researchers have identified a new histologic subset of metastatic castration-resistant prostate cancer called intermediate atypical carcinoma.
“Despite being cytologically bland, this is an aggressive cancer with shortened survival similar to that seen with small-cell neuroendocrine cancer,” study author Dr. Eric J. Small said at the annual meeting of the American Society of Clinical Oncology.

Therapies targeting the androgen receptor (AR) like abiraterone and enzalutamide have revolutionized the treatment of metastatic castration-resistant prostate cancer (mCRPC), but resistance to these agents is near-universal and leads to progressive disease and death. At the same time, clinicians are seeing an increasing number of patients with small cell neuroendocrine prostate cancer (SCNC), Dr. Small, professor of medicine at the University of California, San Francisco, said.
As part of a larger project designed to understand the mechanisms of resistance to abiraterone (Zytiga) and enzalutamide (Xtandi) undertaken by the West Coast Prostate Cancer Dream Team, biopsies were performed of a metastatic site in about 160 eligible men with mCRPC.Most (58%) had a Gleason score of 8 or more at diagnosis; 40% had been treated with abiraterone, 10% with enzalutamide, and 17% with both.
Formalin-fixed paraffin-embedded tissue was collected for histologic evaluation by three independent pathologists. Fresh frozen tissue, which underwent laser capture microdissection, was used for genomic analysis.
As of May 1, 173 of 300 planned biopsies have been conducted. In the 160 samples evaluated to date, there was adequate tissue for analysis in 124, for a 78% biopsy success rate, he said.
Among the 124 evaluable biopsies, 35% were classified as pure adenocarcinoma and 13% as pure SCNC.
A novel subtype was identified in another 26% that “consisted of a pure population of cells that was distinct from adenocarcinoma and distinct from small cell neuroendocrine cancer. We have termed this group intermediate atypical carcinoma (IAC),” Dr. Small said.
The remaining quarter of biopsies was composed of mixed populations.
In addition to the independent review, a consensus meeting with two additional pathologists confirmed that this was a new, highly reproducible pathologic subclass, he said.
The researchers next sought to determine whether IAC is phenotypically distinct. A survival analysis was performed based on biopsy pathology and revealed that men who develop IAC have poor survival.
Indeed, survival with IAC (median 11.9 months) tracks with that of SCNC (median 6.6 months) and is distinct from adenocarcinoma, with a log-rank P value of .041, Dr. Small said. Further, when IAC and SCNC were grouped together, there was a dramatically different survival curve (median 8.9 months) than that seen with adenocarcinoma (P = .006).
An analysis using microresected samples indicated that IAC is also genomically distinct, he said. Small cell nuclear clusters showed enrichment of neuronal and cell cycle elements and downregulation of androgen-receptor elements and the immune system.
Based on these findings, machine learning was used to develop a 50-gene signature, with 88.3% accuracy to distinguish small cell from non–small cell histology and 78.5% accuracy to distinguish small cell or IAC histology from adenocarcinoma. The test is not clinically available at this time, but is being used to identify new therapeutic targets.
“We are actively identifying the unique features of this subtype that can be targeted with therapy,” Dr. Small said in an interview. “There is a huge unmet need, since no one knows how to treat these patients, who comprise a significant portion of patients.”
Indeed, in the analysis, IAC represented a fourth of all metastatic castration-resistant biopsies and when combined with small cell neuroendocrine cancer accounted for 40% of all samples.
“This comprises the single largest group of abiraterone- and enzalutamide-refractory patients,” he concluded. “The increasing use of highly potent AR-targeted therapy may contribute to the increasing frequency of this entity, although that is conjecture at this point and certainly ascertainment bias may play a role.”
Discussant Dr. Scott Tomlins, a pathologist from the University of Michigan in Ann Arbor, said one of the study’s major findings is that collecting tissue for comprehensive molecular analysis is feasible in the context of a well-funded, team-based infrastructure, adding that this will likely have to be the way going forward. Despite limited sample numbers, there also appears to be a “strong signal” that gene expression signatures can discriminate various subtypes.
The study was funded by StandUpToCancer, the Prostate Cancer Foundation, and American Association for Cancer Research. Dr. Small reported having no disclosures.
On Twitter @pwendl
CHICAGO – Researchers have identified a new histologic subset of metastatic castration-resistant prostate cancer called intermediate atypical carcinoma.
“Despite being cytologically bland, this is an aggressive cancer with shortened survival similar to that seen with small-cell neuroendocrine cancer,” study author Dr. Eric J. Small said at the annual meeting of the American Society of Clinical Oncology.
Therapies targeting the androgen receptor (AR) like abiraterone and enzalutamide have revolutionized the treatment of metastatic castration-resistant prostate cancer (mCRPC), but resistance to these agents is near-universal and leads to progressive disease and death. At the same time, clinicians are seeing an increasing number of patients with small cell neuroendocrine prostate cancer (SCNC), Dr. Small, professor of medicine at the University of California, San Francisco, said.
As part of a larger project designed to understand the mechanisms of resistance to abiraterone (Zytiga) and enzalutamide (Xtandi) undertaken by the West Coast Prostate Cancer Dream Team, biopsies were performed of a metastatic site in about 160 eligible men with mCRPC.Most (58%) had a Gleason score of 8 or more at diagnosis; 40% had been treated with abiraterone, 10% with enzalutamide, and 17% with both.
Formalin-fixed paraffin-embedded tissue was collected for histologic evaluation by three independent pathologists. Fresh frozen tissue, which underwent laser capture microdissection, was used for genomic analysis.
As of May 1, 173 of 300 planned biopsies have been conducted. In the 160 samples evaluated to date, there was adequate tissue for analysis in 124, for a 78% biopsy success rate, he said.
Among the 124 evaluable biopsies, 35% were classified as pure adenocarcinoma and 13% as pure SCNC.
A novel subtype was identified in another 26% that “consisted of a pure population of cells that was distinct from adenocarcinoma and distinct from small cell neuroendocrine cancer. We have termed this group intermediate atypical carcinoma (IAC),” Dr. Small said.
The remaining quarter of biopsies was composed of mixed populations.
In addition to the independent review, a consensus meeting with two additional pathologists confirmed that this was a new, highly reproducible pathologic subclass, he said.
The researchers next sought to determine whether IAC is phenotypically distinct. A survival analysis was performed based on biopsy pathology and revealed that men who develop IAC have poor survival.
Indeed, survival with IAC (median 11.9 months) tracks with that of SCNC (median 6.6 months) and is distinct from adenocarcinoma, with a log-rank P value of .041, Dr. Small said. Further, when IAC and SCNC were grouped together, there was a dramatically different survival curve (median 8.9 months) than that seen with adenocarcinoma (P = .006).
An analysis using microresected samples indicated that IAC is also genomically distinct, he said. Small cell nuclear clusters showed enrichment of neuronal and cell cycle elements and downregulation of androgen-receptor elements and the immune system.
Based on these findings, machine learning was used to develop a 50-gene signature, with 88.3% accuracy to distinguish small cell from non–small cell histology and 78.5% accuracy to distinguish small cell or IAC histology from adenocarcinoma. The test is not clinically available at this time, but is being used to identify new therapeutic targets.
“We are actively identifying the unique features of this subtype that can be targeted with therapy,” Dr. Small said in an interview. “There is a huge unmet need, since no one knows how to treat these patients, who comprise a significant portion of patients.”
Indeed, in the analysis, IAC represented a fourth of all metastatic castration-resistant biopsies and when combined with small cell neuroendocrine cancer accounted for 40% of all samples.
“This comprises the single largest group of abiraterone- and enzalutamide-refractory patients,” he concluded. “The increasing use of highly potent AR-targeted therapy may contribute to the increasing frequency of this entity, although that is conjecture at this point and certainly ascertainment bias may play a role.”
Discussant Dr. Scott Tomlins, a pathologist from the University of Michigan in Ann Arbor, said one of the study’s major findings is that collecting tissue for comprehensive molecular analysis is feasible in the context of a well-funded, team-based infrastructure, adding that this will likely have to be the way going forward. Despite limited sample numbers, there also appears to be a “strong signal” that gene expression signatures can discriminate various subtypes.
The study was funded by StandUpToCancer, the Prostate Cancer Foundation, and American Association for Cancer Research. Dr. Small reported having no disclosures.
On Twitter @pwendl
CHICAGO – Researchers have identified a new histologic subset of metastatic castration-resistant prostate cancer called intermediate atypical carcinoma.
“Despite being cytologically bland, this is an aggressive cancer with shortened survival similar to that seen with small-cell neuroendocrine cancer,” study author Dr. Eric J. Small said at the annual meeting of the American Society of Clinical Oncology.
Therapies targeting the androgen receptor (AR) like abiraterone and enzalutamide have revolutionized the treatment of metastatic castration-resistant prostate cancer (mCRPC), but resistance to these agents is near-universal and leads to progressive disease and death. At the same time, clinicians are seeing an increasing number of patients with small cell neuroendocrine prostate cancer (SCNC), Dr. Small, professor of medicine at the University of California, San Francisco, said.
As part of a larger project designed to understand the mechanisms of resistance to abiraterone (Zytiga) and enzalutamide (Xtandi) undertaken by the West Coast Prostate Cancer Dream Team, biopsies were performed of a metastatic site in about 160 eligible men with mCRPC.Most (58%) had a Gleason score of 8 or more at diagnosis; 40% had been treated with abiraterone, 10% with enzalutamide, and 17% with both.
Formalin-fixed paraffin-embedded tissue was collected for histologic evaluation by three independent pathologists. Fresh frozen tissue, which underwent laser capture microdissection, was used for genomic analysis.
As of May 1, 173 of 300 planned biopsies have been conducted. In the 160 samples evaluated to date, there was adequate tissue for analysis in 124, for a 78% biopsy success rate, he said.
Among the 124 evaluable biopsies, 35% were classified as pure adenocarcinoma and 13% as pure SCNC.
A novel subtype was identified in another 26% that “consisted of a pure population of cells that was distinct from adenocarcinoma and distinct from small cell neuroendocrine cancer. We have termed this group intermediate atypical carcinoma (IAC),” Dr. Small said.
The remaining quarter of biopsies was composed of mixed populations.
In addition to the independent review, a consensus meeting with two additional pathologists confirmed that this was a new, highly reproducible pathologic subclass, he said.
The researchers next sought to determine whether IAC is phenotypically distinct. A survival analysis was performed based on biopsy pathology and revealed that men who develop IAC have poor survival.
Indeed, survival with IAC (median 11.9 months) tracks with that of SCNC (median 6.6 months) and is distinct from adenocarcinoma, with a log-rank P value of .041, Dr. Small said. Further, when IAC and SCNC were grouped together, there was a dramatically different survival curve (median 8.9 months) than that seen with adenocarcinoma (P = .006).
An analysis using microresected samples indicated that IAC is also genomically distinct, he said. Small cell nuclear clusters showed enrichment of neuronal and cell cycle elements and downregulation of androgen-receptor elements and the immune system.
Based on these findings, machine learning was used to develop a 50-gene signature, with 88.3% accuracy to distinguish small cell from non–small cell histology and 78.5% accuracy to distinguish small cell or IAC histology from adenocarcinoma. The test is not clinically available at this time, but is being used to identify new therapeutic targets.
“We are actively identifying the unique features of this subtype that can be targeted with therapy,” Dr. Small said in an interview. “There is a huge unmet need, since no one knows how to treat these patients, who comprise a significant portion of patients.”
Indeed, in the analysis, IAC represented a fourth of all metastatic castration-resistant biopsies and when combined with small cell neuroendocrine cancer accounted for 40% of all samples.
“This comprises the single largest group of abiraterone- and enzalutamide-refractory patients,” he concluded. “The increasing use of highly potent AR-targeted therapy may contribute to the increasing frequency of this entity, although that is conjecture at this point and certainly ascertainment bias may play a role.”
Discussant Dr. Scott Tomlins, a pathologist from the University of Michigan in Ann Arbor, said one of the study’s major findings is that collecting tissue for comprehensive molecular analysis is feasible in the context of a well-funded, team-based infrastructure, adding that this will likely have to be the way going forward. Despite limited sample numbers, there also appears to be a “strong signal” that gene expression signatures can discriminate various subtypes.
The study was funded by StandUpToCancer, the Prostate Cancer Foundation, and American Association for Cancer Research. Dr. Small reported having no disclosures.
On Twitter @pwendl
AT THE 2015 ASCO ANNUAL MEETING
Key clinical point: Researchers have identified an aggressive new histologic subset of metastatic castration-resistant prostate cancer.
Major finding: Of 124 evaluable biopsies, 35% were pure adenocarcinoma, 13% pure small cell neuroendocrine cancer, and 26% intermediate atypical carcinoma.
Data source: Pathologic and genomic analyses in men with metastatic castration-resistant prostate cancer.
Disclosures: The study was funded by StandUpToCancer, the Prostate Cancer Foundation, and American Association for Cancer Research. Dr. Small reported having no disclosures.

Report identifies hiring trends emerging after ACA implementation
Full implementation of the Affordable Care Act has brought change to the hiring needs of medical practices and the health care industry.
While staff turnover and the physician shortage remain the key problems, recruiting a new set of staff members has become the third biggest concern, according to a report from Health eCareers.
To keep in step with the ACA, practices might consider the following staff changes:
• Integrate technologists across the continuum of care.
• Hire more case management professionals.
• Keep hiring more educated nurses.
• Emphasize data.
Data from the Health eCareers’ 2015 Healthcare Recruiting Trends Survey Report came from 565 healthcare employers and recruiters, customers of Health eCareers, who were surveyed in late 2014 and early 2015.
For the full report, click here.
Full implementation of the Affordable Care Act has brought change to the hiring needs of medical practices and the health care industry.
While staff turnover and the physician shortage remain the key problems, recruiting a new set of staff members has become the third biggest concern, according to a report from Health eCareers.
To keep in step with the ACA, practices might consider the following staff changes:
• Integrate technologists across the continuum of care.
• Hire more case management professionals.
• Keep hiring more educated nurses.
• Emphasize data.
Data from the Health eCareers’ 2015 Healthcare Recruiting Trends Survey Report came from 565 healthcare employers and recruiters, customers of Health eCareers, who were surveyed in late 2014 and early 2015.
For the full report, click here.
Full implementation of the Affordable Care Act has brought change to the hiring needs of medical practices and the health care industry.
While staff turnover and the physician shortage remain the key problems, recruiting a new set of staff members has become the third biggest concern, according to a report from Health eCareers.
To keep in step with the ACA, practices might consider the following staff changes:
• Integrate technologists across the continuum of care.
• Hire more case management professionals.
• Keep hiring more educated nurses.
• Emphasize data.
Data from the Health eCareers’ 2015 Healthcare Recruiting Trends Survey Report came from 565 healthcare employers and recruiters, customers of Health eCareers, who were surveyed in late 2014 and early 2015.
For the full report, click here.
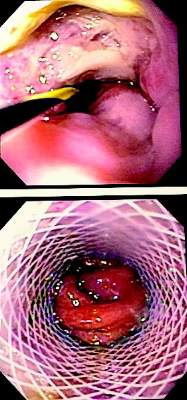
Stents better than surgery for esophagus tears?
While stent placement has proved to be safe and effective for acute esophageal perforation, a head-to-head comparison with surgical repair has never been reported, so a team of investigators performed a small, single-system analysis that compared stenting and surgery and found that while both are equally effective, esophageal stent placement resulted in lower costs and lower morbidity rates.
Investigators led by Dr. Richard Freeman of St. Vincent Hospital in Indianapolis published their results in the June issue of the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.01.066]). Their study evaluated only 60 patients who had either stent placement or an operation for acute intrathoracic esophageal perforation between 2009 and 2012 within Ascension Health, a national Catholic-based network of 36 regional health systems; but the authors noted that they had extracted their data from the national Premier Inc. database, which covers 20% of U.S. hospital discharges, and used propensity matching to generate similar stent and surgical groups. Dr. Freeman presented the results at the annual meeting of the American Association of Thoracic Surgery in Toronto, April 28-30.
Patients who received stents had intensive care unit stays about half that of the surgery group – an average of 2 vs. 4 days. Likewise, their total hospital stays were about half: 6 days vs. 11 days for the surgery group. Complication rates were comparable: postrepair leaks were reported in 17% of the stent group and 20% who had surgery. While reoperation rates were significantly lower in the stent group (3% vs. 13%), four patients (13%) of the stent group did have stent migration. Morbidity was significantly higher in the surgery group (43% vs. 17%). While postprocedure leak rates were similar, those who had surgery were more likely to have reoperation for persistent leaks, the authors said.
Further, stent recipients were able to take nutrition by mouth earlier after surgery and had lower rates of needing enteral feeding at discharge – 17% vs. 60% for the surgery group. Dr. Freeman and his team also analyzed costs between the two procedures and found that total costs, including inpatient and outpatient costs, averaged $142,000 for surgery vs. $91,000 for stenting.
Because the incidence of esophageal perforation is so low, Dr. Freeman and his coauthors reported that performing a randomized trial comparing esophageal stenting and surgery has been difficult. The off-label nature of stenting for esophageal perforation has also complicated funding of a prospective trial. The study authors said a prospective, randomized design would have been preferable to the propensity-matched approach.
Surgery for esophageal tear has been around for almost 70 years with many improvements in technique, anesthesia, and antimicrobial therapy, but with a need for prolonged inpatient and outpatient care along with a postoperative leak rate as high as 39% (Ann. Thorac. Surg. 2010;90:1669-73). “A persistent leak following operative repair may also result in the need for esophageal diversion and subsequent reconstruction with its associated significant morbidity and patient dissatisfaction,” Dr. Freeman and his coauthors said.
The authors acknowledged shortcomings of their study included not accounting for how different stents used in the stenting group and individual surgeons and facilities may have influenced outcomes. Other shortcomings were that cost calculations may not have accounted for inflation or costs outside the Ascension Health system and the uniqueness of the procedure itself. “Lastly, the fact that both treatment strategies employed for iatrogenic esophageal perforation are likely uncommon procedures at most treatment facilities implies that standardization, even at the local level, may be lacking,” the authors stated.
The authors reported having no financial disclosures.
“This paper addresses an important question for thoracic surgeons and the findings are promising,” Dr. Katie S. Nason of the University of Pittsburgh said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.02.028]). She also commended the study authors for using propensity matching to create comparable groups.
Document
|
Dr. Katie S. Nason |
However, the study did not address several patient factors that can influence a surgeon’s selection of an operation or stent placement, Dr. Nason said: injury size and location, other esophageal disorders patients might have, and the degree of contamination around the operative site. “It is premature to definitively interpret the higher rate of mortality, morbidity, cost, and length of stay with surgery as a direct result of treatment choice, when unmeasured differences in the patient’s perforation-associated condition are not accounted for in propensity-matching or outcomes analysis,” she said.
Nonetheless, she called the data “compelling” and that examination of other studies was warranted. Dr. Nason cited four other reports that arrived at similar conclusions (Ann. Surg. 2014;259:852-60; World J. Surg. 2013;37:1051-9; J. Am. Coll. Surg. 2014;218:768-74; World J. Surg. 2014;38:902-9). “Taken together with these prior studies, the data for management of iatrogenic perforation increasingly favor early intervention with esophageal stenting,” Dr. Nason said.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
“This paper addresses an important question for thoracic surgeons and the findings are promising,” Dr. Katie S. Nason of the University of Pittsburgh said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.02.028]). She also commended the study authors for using propensity matching to create comparable groups.
Document
|
Dr. Katie S. Nason |
However, the study did not address several patient factors that can influence a surgeon’s selection of an operation or stent placement, Dr. Nason said: injury size and location, other esophageal disorders patients might have, and the degree of contamination around the operative site. “It is premature to definitively interpret the higher rate of mortality, morbidity, cost, and length of stay with surgery as a direct result of treatment choice, when unmeasured differences in the patient’s perforation-associated condition are not accounted for in propensity-matching or outcomes analysis,” she said.
Nonetheless, she called the data “compelling” and that examination of other studies was warranted. Dr. Nason cited four other reports that arrived at similar conclusions (Ann. Surg. 2014;259:852-60; World J. Surg. 2013;37:1051-9; J. Am. Coll. Surg. 2014;218:768-74; World J. Surg. 2014;38:902-9). “Taken together with these prior studies, the data for management of iatrogenic perforation increasingly favor early intervention with esophageal stenting,” Dr. Nason said.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
“This paper addresses an important question for thoracic surgeons and the findings are promising,” Dr. Katie S. Nason of the University of Pittsburgh said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.02.028]). She also commended the study authors for using propensity matching to create comparable groups.
Document
|
Dr. Katie S. Nason |
However, the study did not address several patient factors that can influence a surgeon’s selection of an operation or stent placement, Dr. Nason said: injury size and location, other esophageal disorders patients might have, and the degree of contamination around the operative site. “It is premature to definitively interpret the higher rate of mortality, morbidity, cost, and length of stay with surgery as a direct result of treatment choice, when unmeasured differences in the patient’s perforation-associated condition are not accounted for in propensity-matching or outcomes analysis,” she said.
Nonetheless, she called the data “compelling” and that examination of other studies was warranted. Dr. Nason cited four other reports that arrived at similar conclusions (Ann. Surg. 2014;259:852-60; World J. Surg. 2013;37:1051-9; J. Am. Coll. Surg. 2014;218:768-74; World J. Surg. 2014;38:902-9). “Taken together with these prior studies, the data for management of iatrogenic perforation increasingly favor early intervention with esophageal stenting,” Dr. Nason said.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
While stent placement has proved to be safe and effective for acute esophageal perforation, a head-to-head comparison with surgical repair has never been reported, so a team of investigators performed a small, single-system analysis that compared stenting and surgery and found that while both are equally effective, esophageal stent placement resulted in lower costs and lower morbidity rates.
Investigators led by Dr. Richard Freeman of St. Vincent Hospital in Indianapolis published their results in the June issue of the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.01.066]). Their study evaluated only 60 patients who had either stent placement or an operation for acute intrathoracic esophageal perforation between 2009 and 2012 within Ascension Health, a national Catholic-based network of 36 regional health systems; but the authors noted that they had extracted their data from the national Premier Inc. database, which covers 20% of U.S. hospital discharges, and used propensity matching to generate similar stent and surgical groups. Dr. Freeman presented the results at the annual meeting of the American Association of Thoracic Surgery in Toronto, April 28-30.
Patients who received stents had intensive care unit stays about half that of the surgery group – an average of 2 vs. 4 days. Likewise, their total hospital stays were about half: 6 days vs. 11 days for the surgery group. Complication rates were comparable: postrepair leaks were reported in 17% of the stent group and 20% who had surgery. While reoperation rates were significantly lower in the stent group (3% vs. 13%), four patients (13%) of the stent group did have stent migration. Morbidity was significantly higher in the surgery group (43% vs. 17%). While postprocedure leak rates were similar, those who had surgery were more likely to have reoperation for persistent leaks, the authors said.
Further, stent recipients were able to take nutrition by mouth earlier after surgery and had lower rates of needing enteral feeding at discharge – 17% vs. 60% for the surgery group. Dr. Freeman and his team also analyzed costs between the two procedures and found that total costs, including inpatient and outpatient costs, averaged $142,000 for surgery vs. $91,000 for stenting.
Because the incidence of esophageal perforation is so low, Dr. Freeman and his coauthors reported that performing a randomized trial comparing esophageal stenting and surgery has been difficult. The off-label nature of stenting for esophageal perforation has also complicated funding of a prospective trial. The study authors said a prospective, randomized design would have been preferable to the propensity-matched approach.
Surgery for esophageal tear has been around for almost 70 years with many improvements in technique, anesthesia, and antimicrobial therapy, but with a need for prolonged inpatient and outpatient care along with a postoperative leak rate as high as 39% (Ann. Thorac. Surg. 2010;90:1669-73). “A persistent leak following operative repair may also result in the need for esophageal diversion and subsequent reconstruction with its associated significant morbidity and patient dissatisfaction,” Dr. Freeman and his coauthors said.
The authors acknowledged shortcomings of their study included not accounting for how different stents used in the stenting group and individual surgeons and facilities may have influenced outcomes. Other shortcomings were that cost calculations may not have accounted for inflation or costs outside the Ascension Health system and the uniqueness of the procedure itself. “Lastly, the fact that both treatment strategies employed for iatrogenic esophageal perforation are likely uncommon procedures at most treatment facilities implies that standardization, even at the local level, may be lacking,” the authors stated.
The authors reported having no financial disclosures.
While stent placement has proved to be safe and effective for acute esophageal perforation, a head-to-head comparison with surgical repair has never been reported, so a team of investigators performed a small, single-system analysis that compared stenting and surgery and found that while both are equally effective, esophageal stent placement resulted in lower costs and lower morbidity rates.
Investigators led by Dr. Richard Freeman of St. Vincent Hospital in Indianapolis published their results in the June issue of the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.01.066]). Their study evaluated only 60 patients who had either stent placement or an operation for acute intrathoracic esophageal perforation between 2009 and 2012 within Ascension Health, a national Catholic-based network of 36 regional health systems; but the authors noted that they had extracted their data from the national Premier Inc. database, which covers 20% of U.S. hospital discharges, and used propensity matching to generate similar stent and surgical groups. Dr. Freeman presented the results at the annual meeting of the American Association of Thoracic Surgery in Toronto, April 28-30.
Patients who received stents had intensive care unit stays about half that of the surgery group – an average of 2 vs. 4 days. Likewise, their total hospital stays were about half: 6 days vs. 11 days for the surgery group. Complication rates were comparable: postrepair leaks were reported in 17% of the stent group and 20% who had surgery. While reoperation rates were significantly lower in the stent group (3% vs. 13%), four patients (13%) of the stent group did have stent migration. Morbidity was significantly higher in the surgery group (43% vs. 17%). While postprocedure leak rates were similar, those who had surgery were more likely to have reoperation for persistent leaks, the authors said.
Further, stent recipients were able to take nutrition by mouth earlier after surgery and had lower rates of needing enteral feeding at discharge – 17% vs. 60% for the surgery group. Dr. Freeman and his team also analyzed costs between the two procedures and found that total costs, including inpatient and outpatient costs, averaged $142,000 for surgery vs. $91,000 for stenting.
Because the incidence of esophageal perforation is so low, Dr. Freeman and his coauthors reported that performing a randomized trial comparing esophageal stenting and surgery has been difficult. The off-label nature of stenting for esophageal perforation has also complicated funding of a prospective trial. The study authors said a prospective, randomized design would have been preferable to the propensity-matched approach.
Surgery for esophageal tear has been around for almost 70 years with many improvements in technique, anesthesia, and antimicrobial therapy, but with a need for prolonged inpatient and outpatient care along with a postoperative leak rate as high as 39% (Ann. Thorac. Surg. 2010;90:1669-73). “A persistent leak following operative repair may also result in the need for esophageal diversion and subsequent reconstruction with its associated significant morbidity and patient dissatisfaction,” Dr. Freeman and his coauthors said.
The authors acknowledged shortcomings of their study included not accounting for how different stents used in the stenting group and individual surgeons and facilities may have influenced outcomes. Other shortcomings were that cost calculations may not have accounted for inflation or costs outside the Ascension Health system and the uniqueness of the procedure itself. “Lastly, the fact that both treatment strategies employed for iatrogenic esophageal perforation are likely uncommon procedures at most treatment facilities implies that standardization, even at the local level, may be lacking,” the authors stated.
The authors reported having no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Esophageal stent placement for the treatment of an acute esophageal tear seems to be as effective as surgery in propensity-matched patients.
Major finding: Morbidity scores were 43% for patients who had surgical repair vs. 17% for those who underwent stent placement for esophageal tear.
Data source: Retrospective analysis of 60 propensity-matched patients over a 4-year period at a single health system’s hospitals, as drawn from the Premiere national database.
Disclosures: The authors reported having no financial disclosures.
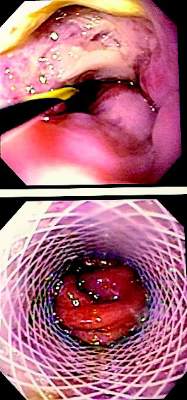
VIDEO: Dr. Walter M. Stadler gives take-home messages from ASCO 2015 GU sessions
CHICAGO – Dr. Walter M. Stadler provides his take on ASCO 2015 presentations and discussions around genitourinary research, including practice-changing results on the use of chemotherapy for treating prostate cancer and the timing of androgen suppression. He also addresses the disappointing results for using precision medicine to treat bladder cancer versus the encouraging results from immunotherapy for both bladder and renal cell cancer. Dr. Stadler is the Fred C. Buffett Professor of Medicine and Surgery; associate dean for clinical research; chief, section of hematology/oncology; and director, genitourinary program, University of Chicago. He had no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
lnikolaides@frontlinemedcom.com
On Twitter @nikolaideslaura
CHICAGO – Dr. Walter M. Stadler provides his take on ASCO 2015 presentations and discussions around genitourinary research, including practice-changing results on the use of chemotherapy for treating prostate cancer and the timing of androgen suppression. He also addresses the disappointing results for using precision medicine to treat bladder cancer versus the encouraging results from immunotherapy for both bladder and renal cell cancer. Dr. Stadler is the Fred C. Buffett Professor of Medicine and Surgery; associate dean for clinical research; chief, section of hematology/oncology; and director, genitourinary program, University of Chicago. He had no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
lnikolaides@frontlinemedcom.com
On Twitter @nikolaideslaura
CHICAGO – Dr. Walter M. Stadler provides his take on ASCO 2015 presentations and discussions around genitourinary research, including practice-changing results on the use of chemotherapy for treating prostate cancer and the timing of androgen suppression. He also addresses the disappointing results for using precision medicine to treat bladder cancer versus the encouraging results from immunotherapy for both bladder and renal cell cancer. Dr. Stadler is the Fred C. Buffett Professor of Medicine and Surgery; associate dean for clinical research; chief, section of hematology/oncology; and director, genitourinary program, University of Chicago. He had no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
lnikolaides@frontlinemedcom.com
On Twitter @nikolaideslaura
AT THE 2015 ASCO ANNUAL MEETING
