User login
Official Newspaper of the American College of Surgeons
SVS: Stroke reduction outweighs bleeding risk of dual antiplatelet therapy in CEA
CHICAGO – Don’t automatically discontinue dual antiplatelet therapy for carotid endarterectomy because the neuroprotective effects may outweigh the bleeding risks, researchers concluded after a review of more than 28,000 patients who underwent the procedure during 2003-2014.
They found in the study that the 7,059 patients on perioperative dual antiplatelet therapy with clopidogrel (Plavix) and aspirin had about a 40% reduction in transient ischemic attacks (TIAs), strokes, and stroke-related deaths when compared with the 21,624 patients on aspirin alone.
The investigators found on multivariate analysis that bleeding bad enough for a return trip to the operating room was more common in their dual antiplatelet group (odds ratio, 1.73; P < .01), but they felt the neuroprotective effect was probably worth the “slightly increased bleeding risk.” Earlier research suggests that about half of vascular surgeons will discontinue clopidogrel a week or so before carotid endarterectomy (CEA) because of bleeding risks (Eur. J. Vasc. Endovasc. Surg. 2009;38:402-7).
“Although dual therapy increases perioperative bleeding, it confers an overall benefit by reducing stroke and death. Patients taking dual therapy at the time of CEA should continue treatment preoperatively. This study also suggests that initiating dual therapy is beneficial for asymptomatic patients,” lead investigator Dr. Douglas Jones of the New York Presbyterian Hospital in New York said at the meeting hosted by the Society for Vascular Surgery.
The team used the Society for Vascular Surgery’s (SVS) Vascular Quality Initiative database. Patients were about 70 years old on average and about 60% were men. Dual-therapy patients had more coronary artery disease, congestive heart failure, chronic obstructive pulmonary disease, and diabetes.
On multivariate analysis to control for those differences, dual therapy was protective against TIA or stroke (OR, 0.60; P < .01); ipsilateral TIA or stroke (OR, 0.68; P = .05); stroke (OR, 0.62; P = .04); and stroke death (OR, 0.65; P = .03). It did not protect against myocardial infarction.
“More than 95% of patients received heparin for these cases,” said Dr. Jones, noting that protamine-reversal after the case “had the greatest protective effect” against major bleeding, which is consistent with previous reports. Protamine reversal reduced it by more than 50% (OR, 0.44; P < .01).
The results, for the most part, were similar on propensity matching of 4,548 patients on dual therapy to 4,548 on aspirin alone, all of whom had CEA after 2010. Dual-therapy patients were about twice as likely to return to the operating room for bleeding (1.3% vs. 0.7%), but also had fewer thrombotic complications (for instance, stroke 0.6% vs. 1.0% in the aspirin cohort).
Asymptomatic patients on dual therapy were again about twice as likely to return to surgery for major bleeding, but half as likely to have a stroke. Bleeding was more common in symptomatic dual therapy patients, as well, but for reasons that aren’t clear, a trend toward fewer thrombotic events in symptomatic patients on propensity matching did not reach statistical significance. “The protective effect was greatest among asymptomatic patients,” Dr. Jones said.
Patients on dual therapy were also more likely to have a drain placed, but drain placement did not protect against reoperation for bleeding (OR, 1.06; P = .75).
Dr. Jones has no disclosures. Other investigators disclosed consulting fees from Medtronic, Volcano, Bard, and AnGes.
CHICAGO – Don’t automatically discontinue dual antiplatelet therapy for carotid endarterectomy because the neuroprotective effects may outweigh the bleeding risks, researchers concluded after a review of more than 28,000 patients who underwent the procedure during 2003-2014.
They found in the study that the 7,059 patients on perioperative dual antiplatelet therapy with clopidogrel (Plavix) and aspirin had about a 40% reduction in transient ischemic attacks (TIAs), strokes, and stroke-related deaths when compared with the 21,624 patients on aspirin alone.
The investigators found on multivariate analysis that bleeding bad enough for a return trip to the operating room was more common in their dual antiplatelet group (odds ratio, 1.73; P < .01), but they felt the neuroprotective effect was probably worth the “slightly increased bleeding risk.” Earlier research suggests that about half of vascular surgeons will discontinue clopidogrel a week or so before carotid endarterectomy (CEA) because of bleeding risks (Eur. J. Vasc. Endovasc. Surg. 2009;38:402-7).
“Although dual therapy increases perioperative bleeding, it confers an overall benefit by reducing stroke and death. Patients taking dual therapy at the time of CEA should continue treatment preoperatively. This study also suggests that initiating dual therapy is beneficial for asymptomatic patients,” lead investigator Dr. Douglas Jones of the New York Presbyterian Hospital in New York said at the meeting hosted by the Society for Vascular Surgery.
The team used the Society for Vascular Surgery’s (SVS) Vascular Quality Initiative database. Patients were about 70 years old on average and about 60% were men. Dual-therapy patients had more coronary artery disease, congestive heart failure, chronic obstructive pulmonary disease, and diabetes.
On multivariate analysis to control for those differences, dual therapy was protective against TIA or stroke (OR, 0.60; P < .01); ipsilateral TIA or stroke (OR, 0.68; P = .05); stroke (OR, 0.62; P = .04); and stroke death (OR, 0.65; P = .03). It did not protect against myocardial infarction.
“More than 95% of patients received heparin for these cases,” said Dr. Jones, noting that protamine-reversal after the case “had the greatest protective effect” against major bleeding, which is consistent with previous reports. Protamine reversal reduced it by more than 50% (OR, 0.44; P < .01).
The results, for the most part, were similar on propensity matching of 4,548 patients on dual therapy to 4,548 on aspirin alone, all of whom had CEA after 2010. Dual-therapy patients were about twice as likely to return to the operating room for bleeding (1.3% vs. 0.7%), but also had fewer thrombotic complications (for instance, stroke 0.6% vs. 1.0% in the aspirin cohort).
Asymptomatic patients on dual therapy were again about twice as likely to return to surgery for major bleeding, but half as likely to have a stroke. Bleeding was more common in symptomatic dual therapy patients, as well, but for reasons that aren’t clear, a trend toward fewer thrombotic events in symptomatic patients on propensity matching did not reach statistical significance. “The protective effect was greatest among asymptomatic patients,” Dr. Jones said.
Patients on dual therapy were also more likely to have a drain placed, but drain placement did not protect against reoperation for bleeding (OR, 1.06; P = .75).
Dr. Jones has no disclosures. Other investigators disclosed consulting fees from Medtronic, Volcano, Bard, and AnGes.
CHICAGO – Don’t automatically discontinue dual antiplatelet therapy for carotid endarterectomy because the neuroprotective effects may outweigh the bleeding risks, researchers concluded after a review of more than 28,000 patients who underwent the procedure during 2003-2014.
They found in the study that the 7,059 patients on perioperative dual antiplatelet therapy with clopidogrel (Plavix) and aspirin had about a 40% reduction in transient ischemic attacks (TIAs), strokes, and stroke-related deaths when compared with the 21,624 patients on aspirin alone.
The investigators found on multivariate analysis that bleeding bad enough for a return trip to the operating room was more common in their dual antiplatelet group (odds ratio, 1.73; P < .01), but they felt the neuroprotective effect was probably worth the “slightly increased bleeding risk.” Earlier research suggests that about half of vascular surgeons will discontinue clopidogrel a week or so before carotid endarterectomy (CEA) because of bleeding risks (Eur. J. Vasc. Endovasc. Surg. 2009;38:402-7).
“Although dual therapy increases perioperative bleeding, it confers an overall benefit by reducing stroke and death. Patients taking dual therapy at the time of CEA should continue treatment preoperatively. This study also suggests that initiating dual therapy is beneficial for asymptomatic patients,” lead investigator Dr. Douglas Jones of the New York Presbyterian Hospital in New York said at the meeting hosted by the Society for Vascular Surgery.
The team used the Society for Vascular Surgery’s (SVS) Vascular Quality Initiative database. Patients were about 70 years old on average and about 60% were men. Dual-therapy patients had more coronary artery disease, congestive heart failure, chronic obstructive pulmonary disease, and diabetes.
On multivariate analysis to control for those differences, dual therapy was protective against TIA or stroke (OR, 0.60; P < .01); ipsilateral TIA or stroke (OR, 0.68; P = .05); stroke (OR, 0.62; P = .04); and stroke death (OR, 0.65; P = .03). It did not protect against myocardial infarction.
“More than 95% of patients received heparin for these cases,” said Dr. Jones, noting that protamine-reversal after the case “had the greatest protective effect” against major bleeding, which is consistent with previous reports. Protamine reversal reduced it by more than 50% (OR, 0.44; P < .01).
The results, for the most part, were similar on propensity matching of 4,548 patients on dual therapy to 4,548 on aspirin alone, all of whom had CEA after 2010. Dual-therapy patients were about twice as likely to return to the operating room for bleeding (1.3% vs. 0.7%), but also had fewer thrombotic complications (for instance, stroke 0.6% vs. 1.0% in the aspirin cohort).
Asymptomatic patients on dual therapy were again about twice as likely to return to surgery for major bleeding, but half as likely to have a stroke. Bleeding was more common in symptomatic dual therapy patients, as well, but for reasons that aren’t clear, a trend toward fewer thrombotic events in symptomatic patients on propensity matching did not reach statistical significance. “The protective effect was greatest among asymptomatic patients,” Dr. Jones said.
Patients on dual therapy were also more likely to have a drain placed, but drain placement did not protect against reoperation for bleeding (OR, 1.06; P = .75).
Dr. Jones has no disclosures. Other investigators disclosed consulting fees from Medtronic, Volcano, Bard, and AnGes.
AT THE 2015 VASCULAR ANNUAL MEETING
Key clinical point: Strokes are less likely after CEA if patients are on perioperative clopidogrel and aspirin.
Major finding: On multivariate analysis, dual therapy was protective against TIA or stroke (OR, 0.60; P < .01); ipsilateral TIA or stroke (OR, 0.68; P = .05); stroke (OR, 0.62, P = .04); and stroke death (OR, 0.65; P = .03).
Data source: Review of more than 28,000 carotid endarterectomy patients
Disclosures: The presenter has no disclosures. Other investigators disclosed consulting fees from Medtronic, Volcano, Bard, and AnGes.
SVS: Choose endarterectomy over stenting for complex carotid lesions
CHICAGO – Carotid endarterectomy is safer than stenting when lesions have greater complexity based on length, location, and presence of sequential lesions, according to a subanalysis of the CREST study.
Previous studies have shown that carotid artery stenting (CAS) is also risky in patients with type 3 aortic arches; atherosclerotic aortic arches; internal carotid artery tortuosity; circumferential calcification; and ulcerated lesions.
Taken together, “we can now begin to populate a list of conditions that are high risk for carotid artery stenting. For patients with these factors, we would strongly recommend that carotid endarterectomy be employed rather than carotid artery stenting,” said CREST (Carotid Revascularization Endarterectomy versus Stent Trial) investigator Dr. Wesley Moore, professor and chief, emeritus, of the division of vascular surgery at the University of California, Los Angeles.

“However, in the absence of these higher risk characteristics, carotid artery stenting should yield results equivalent to carotid endarterectomy,” he said at a meeting hosted by the Society for Vascular Surgery.
CREST demonstrated that carotid artery stenting carries about twice the risk of stroke and death (4.4%) as carotid endarterectomy (2.3%); the investigators revisited their subjects’ preop angiograms to see if lesion characteristics were to blame in a subanalysis of the trial results.
In CREST, 438 patients had angiograms before carotid endarterectomies (CEA), about a third of the total number of CEA patients, while preop angiograms were done in all of the 1,262 CAS patients. There were no statistically significant differences in age, gender, stenosis symptoms, smoking history, arrhythmias, and left ventricular hypertrophy between CEA and CAS patients.
For lesions longer than 12.85 mm – the median length in CREST – the combined outcome of strokes and death occurred in 1.9% of CEA and 6.1% of CAS patients (CAS odds ratio, 3.45; 95% confidence interval, 1.21-9.83). For sequential lesions, strokes and death occurred in 0.7% of CEA and 5.8% of CAS patients (CAS OR, 9.21; 95% CI, 1.23-68.94).
With long, sequential lesions distal to the carotid bulb, stroke and death occurred in 6.3% of CAS patients but no CEA patients, giving an “infinite odds ratio in favor of CEA,” Dr. Moore said.
Two-thirds of all the patients in CREST had lesion risk factors for CAS, which might help explain the original findings.
CREST also found that stenting was riskier in older people and women, but it seems likely now that age and gender were surrogates for adverse lesion characteristics.
“The fact of the matter is that older patients have more complex lesions, so age tended to be a surrogate for lesion complexity. If I have an 80-year-old with a short, isolated lesion, I don’t think the fact that they are 80 represents higher risk. I think the lesion being short puts them in the same low risk [category] as other favorable CAS characteristics. I think that’s also true for gender,” Dr. Moore said.
Angiograms almost always underestimate the length of carotid lesions. CT and MRI do a better job, but “ultrasound may be even better than those two,” he noted.
CREST was funded by the National Institutes of Health and Abbott Vascular Solutions. Dr. Moore has no disclosures. Other authors reported relationships with Abbott, Medtronic, Boston Scientific, and other companies.
CHICAGO – Carotid endarterectomy is safer than stenting when lesions have greater complexity based on length, location, and presence of sequential lesions, according to a subanalysis of the CREST study.
Previous studies have shown that carotid artery stenting (CAS) is also risky in patients with type 3 aortic arches; atherosclerotic aortic arches; internal carotid artery tortuosity; circumferential calcification; and ulcerated lesions.
Taken together, “we can now begin to populate a list of conditions that are high risk for carotid artery stenting. For patients with these factors, we would strongly recommend that carotid endarterectomy be employed rather than carotid artery stenting,” said CREST (Carotid Revascularization Endarterectomy versus Stent Trial) investigator Dr. Wesley Moore, professor and chief, emeritus, of the division of vascular surgery at the University of California, Los Angeles.
“However, in the absence of these higher risk characteristics, carotid artery stenting should yield results equivalent to carotid endarterectomy,” he said at a meeting hosted by the Society for Vascular Surgery.
CREST demonstrated that carotid artery stenting carries about twice the risk of stroke and death (4.4%) as carotid endarterectomy (2.3%); the investigators revisited their subjects’ preop angiograms to see if lesion characteristics were to blame in a subanalysis of the trial results.
In CREST, 438 patients had angiograms before carotid endarterectomies (CEA), about a third of the total number of CEA patients, while preop angiograms were done in all of the 1,262 CAS patients. There were no statistically significant differences in age, gender, stenosis symptoms, smoking history, arrhythmias, and left ventricular hypertrophy between CEA and CAS patients.
For lesions longer than 12.85 mm – the median length in CREST – the combined outcome of strokes and death occurred in 1.9% of CEA and 6.1% of CAS patients (CAS odds ratio, 3.45; 95% confidence interval, 1.21-9.83). For sequential lesions, strokes and death occurred in 0.7% of CEA and 5.8% of CAS patients (CAS OR, 9.21; 95% CI, 1.23-68.94).
With long, sequential lesions distal to the carotid bulb, stroke and death occurred in 6.3% of CAS patients but no CEA patients, giving an “infinite odds ratio in favor of CEA,” Dr. Moore said.
Two-thirds of all the patients in CREST had lesion risk factors for CAS, which might help explain the original findings.
CREST also found that stenting was riskier in older people and women, but it seems likely now that age and gender were surrogates for adverse lesion characteristics.
“The fact of the matter is that older patients have more complex lesions, so age tended to be a surrogate for lesion complexity. If I have an 80-year-old with a short, isolated lesion, I don’t think the fact that they are 80 represents higher risk. I think the lesion being short puts them in the same low risk [category] as other favorable CAS characteristics. I think that’s also true for gender,” Dr. Moore said.
Angiograms almost always underestimate the length of carotid lesions. CT and MRI do a better job, but “ultrasound may be even better than those two,” he noted.
CREST was funded by the National Institutes of Health and Abbott Vascular Solutions. Dr. Moore has no disclosures. Other authors reported relationships with Abbott, Medtronic, Boston Scientific, and other companies.
CHICAGO – Carotid endarterectomy is safer than stenting when lesions have greater complexity based on length, location, and presence of sequential lesions, according to a subanalysis of the CREST study.
Previous studies have shown that carotid artery stenting (CAS) is also risky in patients with type 3 aortic arches; atherosclerotic aortic arches; internal carotid artery tortuosity; circumferential calcification; and ulcerated lesions.
Taken together, “we can now begin to populate a list of conditions that are high risk for carotid artery stenting. For patients with these factors, we would strongly recommend that carotid endarterectomy be employed rather than carotid artery stenting,” said CREST (Carotid Revascularization Endarterectomy versus Stent Trial) investigator Dr. Wesley Moore, professor and chief, emeritus, of the division of vascular surgery at the University of California, Los Angeles.
“However, in the absence of these higher risk characteristics, carotid artery stenting should yield results equivalent to carotid endarterectomy,” he said at a meeting hosted by the Society for Vascular Surgery.
CREST demonstrated that carotid artery stenting carries about twice the risk of stroke and death (4.4%) as carotid endarterectomy (2.3%); the investigators revisited their subjects’ preop angiograms to see if lesion characteristics were to blame in a subanalysis of the trial results.
In CREST, 438 patients had angiograms before carotid endarterectomies (CEA), about a third of the total number of CEA patients, while preop angiograms were done in all of the 1,262 CAS patients. There were no statistically significant differences in age, gender, stenosis symptoms, smoking history, arrhythmias, and left ventricular hypertrophy between CEA and CAS patients.
For lesions longer than 12.85 mm – the median length in CREST – the combined outcome of strokes and death occurred in 1.9% of CEA and 6.1% of CAS patients (CAS odds ratio, 3.45; 95% confidence interval, 1.21-9.83). For sequential lesions, strokes and death occurred in 0.7% of CEA and 5.8% of CAS patients (CAS OR, 9.21; 95% CI, 1.23-68.94).
With long, sequential lesions distal to the carotid bulb, stroke and death occurred in 6.3% of CAS patients but no CEA patients, giving an “infinite odds ratio in favor of CEA,” Dr. Moore said.
Two-thirds of all the patients in CREST had lesion risk factors for CAS, which might help explain the original findings.
CREST also found that stenting was riskier in older people and women, but it seems likely now that age and gender were surrogates for adverse lesion characteristics.
“The fact of the matter is that older patients have more complex lesions, so age tended to be a surrogate for lesion complexity. If I have an 80-year-old with a short, isolated lesion, I don’t think the fact that they are 80 represents higher risk. I think the lesion being short puts them in the same low risk [category] as other favorable CAS characteristics. I think that’s also true for gender,” Dr. Moore said.
Angiograms almost always underestimate the length of carotid lesions. CT and MRI do a better job, but “ultrasound may be even better than those two,” he noted.
CREST was funded by the National Institutes of Health and Abbott Vascular Solutions. Dr. Moore has no disclosures. Other authors reported relationships with Abbott, Medtronic, Boston Scientific, and other companies.
AT THE 2015 VASCULAR ANNUAL MEETING
Key clinical point: Carotid endarterectomy had a lower rate of the combined outcome of stroke or death in patients with greater lesion complexity, which may be a better marker than age or gender for determining the best treatment modality.
Major finding: For lesions longer than 12.85 mm, the combined outcome of strokes and death occurred in 1.9% of carotid endarterectomy patients and 6.1% of carotid stent patients (CAS OR, 3.45; 95% CI, 1.21-9.83). Subsanalysis of the CREST study
Data source: Subsanalysis of the CREST study
Disclosures: CREST was funded by the National Institutes of Health and Abbott Vascular Solutions. The presenter has no disclosures. Other authors reported relationships with Abbott, Medtronic, Boston Scientific, and other companies.

EUROPCR: New technology shows early promise for transcatheter tricuspid valve repair
PARIS – Early highly preliminary results from the first-in-human study of percutaneous repair of a failing tricuspid valve indicate that the transcatheter procedure appears safe, durable, and effective – at least through the first 6 months.
“Even though the one-grade reduction of tricuspid regurgitation on color Doppler flow imaging is modest, the impact in terms of clinical improvement seems very encouraging and warrants pursuing this innovative technique,” Dr. Jean-Michel Juliard said in presenting the early findings at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

The three-country, prospective, single-arm study is aimed at winning European regulatory approval for 4tech Cardio’s TriCinch System. The study includes 24 patients with severe functional tricuspid regurgitation. Dr. Juliard, a cardiologist at Bichat Hospital in Paris, presented 6-month follow-up data on two patients and 3-month follow-up for a third.
First, a bit about the procedure. It’s conducted under general anesthesia and relies upon transesophageal and intracardiac echocardiographic guidance. The objectives are to reduce the effective cross-sectional valve area by diminishing the septo-lateral dimension of the tricuspid annulus diameter, restore tricuspid valve leaflet coaptation, and relieve symptoms.
The 4tech delivery system consists of two parts. To begin, a guidewire is placed in the right coronary artery, a 24-French sheath is introduced via the right femoral vein, and an exchange guidewire is positioned in the right ventricular apex. The first part of the delivery system is then inserted in order to place an anchor on the tricuspid valve annulus in the vicinity of the antero-posterior commissure.
“This is probably the most difficult part of the whole procedure,” according to Dr. Juliard. “It is done using intracoronary and transesophageal echo guidance.”
Once the anchor is well positioned, the second part of the system is advanced, locked into the first part, and tension is applied under echocardiographic control in order to implant a nitinol self-expanding stent in the inferior vena cava. As soon as traction is applied, the tricuspid regurgitation decreases. Once the correction process is completed, the TriCinch delivery system and venous introducers are removed. For study purposes, dosing of diuretics remained unchanged post procedure.
In the first 6 months, the tricuspid septo-lateral distance improved from 52 to 42 mm in one patient and from 45 to 40 mm in another. A third patient had improvement from 43 to 34 mm at 3 months of follow-up.
In terms of clinical improvement, two patients went from New York Heart Association functional class III to class II, and another went from class III to class I. Six-minute walk distance increased from a baseline of 320 m to 367 m at 6 months of follow-up in one patient and from 400 m to 750 m in another, with a 3-month improvement from 160 to 280 m in the third patient.
Serial imaging studies showed device stability over time, with no migration and no stent thrombosis.
In response to an audience question, Dr. Juliard conceded that at this early stage in the development of the procedure, the placebo effect can’t be ruled out as a possible explanation for the observed strong clinical improvement despite what he conceded was “very modest” reduction in tricuspid regurgitation. Time will tell.
“I hope it is not a placebo effect, but as we maintain the same dose of diuretics, it does seem that the patients feel better,” he added.
The rationale for developing a transcatheter solution to functional tricuspid regurgitation, especially one that’s compatible with concomitant transcatheter mitral valve procedures, as the TriCinch System is intended to be, lies in the wealth of evidence that tricuspid regurgitation is associated with increased mortality, substantial morbidity, and severely impaired quality of life due to the need for repeated hospitalizations. Surgery for patients with tricuspid regurgitation is often extremely high risk because affected patients typically have right ventricular dysfunction, pulmonary hypertension, and/or previous valve surgery.
The ongoing study is funded by 4tech Cardio. Dr. Juliard reported having no financial conflicts.
PARIS – Early highly preliminary results from the first-in-human study of percutaneous repair of a failing tricuspid valve indicate that the transcatheter procedure appears safe, durable, and effective – at least through the first 6 months.
“Even though the one-grade reduction of tricuspid regurgitation on color Doppler flow imaging is modest, the impact in terms of clinical improvement seems very encouraging and warrants pursuing this innovative technique,” Dr. Jean-Michel Juliard said in presenting the early findings at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The three-country, prospective, single-arm study is aimed at winning European regulatory approval for 4tech Cardio’s TriCinch System. The study includes 24 patients with severe functional tricuspid regurgitation. Dr. Juliard, a cardiologist at Bichat Hospital in Paris, presented 6-month follow-up data on two patients and 3-month follow-up for a third.
First, a bit about the procedure. It’s conducted under general anesthesia and relies upon transesophageal and intracardiac echocardiographic guidance. The objectives are to reduce the effective cross-sectional valve area by diminishing the septo-lateral dimension of the tricuspid annulus diameter, restore tricuspid valve leaflet coaptation, and relieve symptoms.
The 4tech delivery system consists of two parts. To begin, a guidewire is placed in the right coronary artery, a 24-French sheath is introduced via the right femoral vein, and an exchange guidewire is positioned in the right ventricular apex. The first part of the delivery system is then inserted in order to place an anchor on the tricuspid valve annulus in the vicinity of the antero-posterior commissure.
“This is probably the most difficult part of the whole procedure,” according to Dr. Juliard. “It is done using intracoronary and transesophageal echo guidance.”
Once the anchor is well positioned, the second part of the system is advanced, locked into the first part, and tension is applied under echocardiographic control in order to implant a nitinol self-expanding stent in the inferior vena cava. As soon as traction is applied, the tricuspid regurgitation decreases. Once the correction process is completed, the TriCinch delivery system and venous introducers are removed. For study purposes, dosing of diuretics remained unchanged post procedure.
In the first 6 months, the tricuspid septo-lateral distance improved from 52 to 42 mm in one patient and from 45 to 40 mm in another. A third patient had improvement from 43 to 34 mm at 3 months of follow-up.
In terms of clinical improvement, two patients went from New York Heart Association functional class III to class II, and another went from class III to class I. Six-minute walk distance increased from a baseline of 320 m to 367 m at 6 months of follow-up in one patient and from 400 m to 750 m in another, with a 3-month improvement from 160 to 280 m in the third patient.
Serial imaging studies showed device stability over time, with no migration and no stent thrombosis.
In response to an audience question, Dr. Juliard conceded that at this early stage in the development of the procedure, the placebo effect can’t be ruled out as a possible explanation for the observed strong clinical improvement despite what he conceded was “very modest” reduction in tricuspid regurgitation. Time will tell.
“I hope it is not a placebo effect, but as we maintain the same dose of diuretics, it does seem that the patients feel better,” he added.
The rationale for developing a transcatheter solution to functional tricuspid regurgitation, especially one that’s compatible with concomitant transcatheter mitral valve procedures, as the TriCinch System is intended to be, lies in the wealth of evidence that tricuspid regurgitation is associated with increased mortality, substantial morbidity, and severely impaired quality of life due to the need for repeated hospitalizations. Surgery for patients with tricuspid regurgitation is often extremely high risk because affected patients typically have right ventricular dysfunction, pulmonary hypertension, and/or previous valve surgery.
The ongoing study is funded by 4tech Cardio. Dr. Juliard reported having no financial conflicts.
PARIS – Early highly preliminary results from the first-in-human study of percutaneous repair of a failing tricuspid valve indicate that the transcatheter procedure appears safe, durable, and effective – at least through the first 6 months.
“Even though the one-grade reduction of tricuspid regurgitation on color Doppler flow imaging is modest, the impact in terms of clinical improvement seems very encouraging and warrants pursuing this innovative technique,” Dr. Jean-Michel Juliard said in presenting the early findings at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The three-country, prospective, single-arm study is aimed at winning European regulatory approval for 4tech Cardio’s TriCinch System. The study includes 24 patients with severe functional tricuspid regurgitation. Dr. Juliard, a cardiologist at Bichat Hospital in Paris, presented 6-month follow-up data on two patients and 3-month follow-up for a third.
First, a bit about the procedure. It’s conducted under general anesthesia and relies upon transesophageal and intracardiac echocardiographic guidance. The objectives are to reduce the effective cross-sectional valve area by diminishing the septo-lateral dimension of the tricuspid annulus diameter, restore tricuspid valve leaflet coaptation, and relieve symptoms.
The 4tech delivery system consists of two parts. To begin, a guidewire is placed in the right coronary artery, a 24-French sheath is introduced via the right femoral vein, and an exchange guidewire is positioned in the right ventricular apex. The first part of the delivery system is then inserted in order to place an anchor on the tricuspid valve annulus in the vicinity of the antero-posterior commissure.
“This is probably the most difficult part of the whole procedure,” according to Dr. Juliard. “It is done using intracoronary and transesophageal echo guidance.”
Once the anchor is well positioned, the second part of the system is advanced, locked into the first part, and tension is applied under echocardiographic control in order to implant a nitinol self-expanding stent in the inferior vena cava. As soon as traction is applied, the tricuspid regurgitation decreases. Once the correction process is completed, the TriCinch delivery system and venous introducers are removed. For study purposes, dosing of diuretics remained unchanged post procedure.
In the first 6 months, the tricuspid septo-lateral distance improved from 52 to 42 mm in one patient and from 45 to 40 mm in another. A third patient had improvement from 43 to 34 mm at 3 months of follow-up.
In terms of clinical improvement, two patients went from New York Heart Association functional class III to class II, and another went from class III to class I. Six-minute walk distance increased from a baseline of 320 m to 367 m at 6 months of follow-up in one patient and from 400 m to 750 m in another, with a 3-month improvement from 160 to 280 m in the third patient.
Serial imaging studies showed device stability over time, with no migration and no stent thrombosis.
In response to an audience question, Dr. Juliard conceded that at this early stage in the development of the procedure, the placebo effect can’t be ruled out as a possible explanation for the observed strong clinical improvement despite what he conceded was “very modest” reduction in tricuspid regurgitation. Time will tell.
“I hope it is not a placebo effect, but as we maintain the same dose of diuretics, it does seem that the patients feel better,” he added.
The rationale for developing a transcatheter solution to functional tricuspid regurgitation, especially one that’s compatible with concomitant transcatheter mitral valve procedures, as the TriCinch System is intended to be, lies in the wealth of evidence that tricuspid regurgitation is associated with increased mortality, substantial morbidity, and severely impaired quality of life due to the need for repeated hospitalizations. Surgery for patients with tricuspid regurgitation is often extremely high risk because affected patients typically have right ventricular dysfunction, pulmonary hypertension, and/or previous valve surgery.
The ongoing study is funded by 4tech Cardio. Dr. Juliard reported having no financial conflicts.
AT EUROPCR 2015
Key clinical point: A novel technology for transcatheter repair of a failing tricuspid valve shows early promise of safety and efficacy.
Major finding: At 3-6 months of follow-up, the first three participants in a first-in-human study of percutaneous tricuspid valve repair show substantial clinical benefits.
Data source: This is a prospective, three-center, nonrandomized, single-arm study of a novel percutaneous therapy in 24 patients with severe functional tricuspid regurgitation.
Disclosures: This ongoing study is funded by 4tech Cardio. The presenter reported having no financial conflicts.

Moderate THST was most effective at treating thyroid cancer
Moderate thyroid hormone suppression therapy (THST) is associated with the best outcomes for patients with all stages of thyroid cancer, according to a prospective analysis of a multi-institutional registry published in the Journal of Clinical Endocrinology & Metabolism.
The researchers examined the outcomes of initial treatment for 4,941 patients with differentiated thyroid cancer (DTC), according to registry data from the National Thyroid Cancer Treatment Cooperative Study Group. The treatments included total/near total thyroidectomy (T/NTT), postoperative radioactive iodine-131 (131I), and THST. The median duration between treatment and follow-up for a patient was 6 years, with follow-up information available for all but 94 (1.9%) of the patients in the cohort.
Overall improvement was noted in stage III patients who received 131I (risk ratio, 0.66; P = .04) and stage IV patients who received both T/NTT and 131I (RR, 0.66; P = .049). In all stages, moderate THST was associated with significantly improved overall survival (RR stages I-IV: 0.13, 0.09, 0.13, and 0.33, respectively) and disease-free survival (DFS) (RR stages I-III: 0.52, 0.40, and 0.18, respectively); no additional survival benefit was achieved with more aggressive THST, even when distant metastatic disease was diagnosed during follow-up.
Lower initial stage and moderate THST were independent predictors of improved overall survival during follow-up years 1-3.
Consistent with previous research, this study also showed that T/NTT followed by 131I is associated with benefit in high-risk, but not low-risk patients.
“We report for the first time, in multivariate analysis of primary treatments for DTC, across all stages, only THST was associated with both improved stage-adjusted OS and DFS,” noted Dr. Aubrey A. Carhill and his colleagues.
“This analysis of the larger, more mature registry database extends and refines earlier observations regarding the impact of initial therapies on patient outcomes and further justifies the need for prospective, long-term, controlled studies,” the researchers noted.
Read the full study in the Journal of Clinical Endocrinology & Metabolism (doi:10.1210/JC.2015-1346).
Moderate thyroid hormone suppression therapy (THST) is associated with the best outcomes for patients with all stages of thyroid cancer, according to a prospective analysis of a multi-institutional registry published in the Journal of Clinical Endocrinology & Metabolism.
The researchers examined the outcomes of initial treatment for 4,941 patients with differentiated thyroid cancer (DTC), according to registry data from the National Thyroid Cancer Treatment Cooperative Study Group. The treatments included total/near total thyroidectomy (T/NTT), postoperative radioactive iodine-131 (131I), and THST. The median duration between treatment and follow-up for a patient was 6 years, with follow-up information available for all but 94 (1.9%) of the patients in the cohort.
Overall improvement was noted in stage III patients who received 131I (risk ratio, 0.66; P = .04) and stage IV patients who received both T/NTT and 131I (RR, 0.66; P = .049). In all stages, moderate THST was associated with significantly improved overall survival (RR stages I-IV: 0.13, 0.09, 0.13, and 0.33, respectively) and disease-free survival (DFS) (RR stages I-III: 0.52, 0.40, and 0.18, respectively); no additional survival benefit was achieved with more aggressive THST, even when distant metastatic disease was diagnosed during follow-up.
Lower initial stage and moderate THST were independent predictors of improved overall survival during follow-up years 1-3.
Consistent with previous research, this study also showed that T/NTT followed by 131I is associated with benefit in high-risk, but not low-risk patients.
“We report for the first time, in multivariate analysis of primary treatments for DTC, across all stages, only THST was associated with both improved stage-adjusted OS and DFS,” noted Dr. Aubrey A. Carhill and his colleagues.
“This analysis of the larger, more mature registry database extends and refines earlier observations regarding the impact of initial therapies on patient outcomes and further justifies the need for prospective, long-term, controlled studies,” the researchers noted.
Read the full study in the Journal of Clinical Endocrinology & Metabolism (doi:10.1210/JC.2015-1346).
Moderate thyroid hormone suppression therapy (THST) is associated with the best outcomes for patients with all stages of thyroid cancer, according to a prospective analysis of a multi-institutional registry published in the Journal of Clinical Endocrinology & Metabolism.
The researchers examined the outcomes of initial treatment for 4,941 patients with differentiated thyroid cancer (DTC), according to registry data from the National Thyroid Cancer Treatment Cooperative Study Group. The treatments included total/near total thyroidectomy (T/NTT), postoperative radioactive iodine-131 (131I), and THST. The median duration between treatment and follow-up for a patient was 6 years, with follow-up information available for all but 94 (1.9%) of the patients in the cohort.
Overall improvement was noted in stage III patients who received 131I (risk ratio, 0.66; P = .04) and stage IV patients who received both T/NTT and 131I (RR, 0.66; P = .049). In all stages, moderate THST was associated with significantly improved overall survival (RR stages I-IV: 0.13, 0.09, 0.13, and 0.33, respectively) and disease-free survival (DFS) (RR stages I-III: 0.52, 0.40, and 0.18, respectively); no additional survival benefit was achieved with more aggressive THST, even when distant metastatic disease was diagnosed during follow-up.
Lower initial stage and moderate THST were independent predictors of improved overall survival during follow-up years 1-3.
Consistent with previous research, this study also showed that T/NTT followed by 131I is associated with benefit in high-risk, but not low-risk patients.
“We report for the first time, in multivariate analysis of primary treatments for DTC, across all stages, only THST was associated with both improved stage-adjusted OS and DFS,” noted Dr. Aubrey A. Carhill and his colleagues.
“This analysis of the larger, more mature registry database extends and refines earlier observations regarding the impact of initial therapies on patient outcomes and further justifies the need for prospective, long-term, controlled studies,” the researchers noted.
Read the full study in the Journal of Clinical Endocrinology & Metabolism (doi:10.1210/JC.2015-1346).
ZEUS: Second-generation DES with 30 days DAPT best in bleeding-risk patients
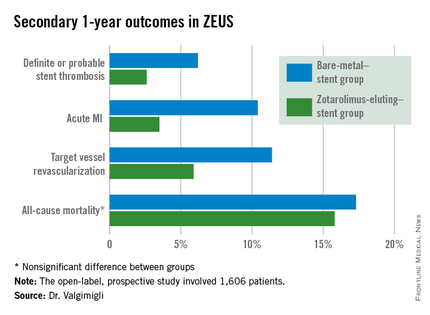
PARIS – The use of a second-generation zotarolimus-eluting coronary stent rather than a bare metal stent in conjunction with 30 days of dual antiplatelet therapy (DAPT) in patients deemed at high bleeding risk results in lower 1-year rates of major adverse cardiovascular events and stent thrombosis, according to a prespecified analysis of the ZEUS trial presented at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Asked if the ZEUS results mean it’s time to take bare-metal stents (BMS) out of the cupboard and get rid of them, the study presenter, Dr. Marco Valgimigli, replied “I did so already.”

ZEUS (Zotarolimus-Eluting Endeavor Sprint Stent in Uncertain DES Candidates Study) was an open-label, prospective study in which 1,606 patients undergoing urgent or emergent percutaneous coronary intervention were randomized to a thin-strut BMS or the zotarolimus-eluting Endeavor Sprint stent, a second-generation hydrophilic polymer-based device that, uniquely, elutes 100% of the drug within the first 2 weeks. All participants were placed on an intended 30-day regimen of DAPT. The study was conducted in four European countries, explained Dr. Valgimigli of Erasmus University in Rotterdam.
This prespecified analysis focused on the 828 patients with one or more factors placing them at high bleeding risk, since the use of a drug-eluting stent (DES) with a 30-day DAPT protocol hadn’t been adequately studied in that setting, the cardiologist noted.
High bleeding risk was defined by one or more of the following: age greater than 80, being on oral anticoagulation therapy, a prior bleeding event, need for corticosteroid or NSAID therapy, known anemia, or a bleeding diathesis; 47% of study participants had more than one of these criteria.
The primary study endpoint was the composite of all-cause mortality, acute MI, or target vessel revascularization through 1 year of follow-up. The rate was 29% in the BMS group, compared with 22.6% in the DES group, for a highly significant 26% relative risk reduction.
The zotarolimus-eluting stent group also fared significantly better in terms of stent thrombosis and the other prespecified secondary endpoints.
Asked how the ZEUS findings have affected his own clinical practice, Dr. Valgimigli replied, “My stent of choice in patients at high bleeding risk is a second-generation DES. Since there aren’t data showing a specific second-generation DES is preferable, basically whatever I have I implant.”
He sticks to the 30-day DAPT regimen featured in the ZEUS protocol except under specific circumstances, which were allowed under the protocol. One involves staged PCI procedures, in which case the 30 days of DAPT begins after the last stent is implanted, even though the patient has been on DAPT in the interim. The other circumstance where he goes beyond 30 days of DAPT in a patient on a second-generation DES is if an ischemic event occurs down the road: “That patient is put back on DAPT and left there,” he said.
In response to another question, Dr. Valgimigli said he doesn’t believe the lower stent thrombosis rate seen in the Endeavor Sprint group in ZEUS is unique to that stent.
“If you look at any BMS versus DES study, taking the first-generation DES out of the picture, it’s quite clear that the second-generation DES are much safer than a BMS,” according to the cardiologist.
The ZEUS study was sponsored by the University of Ferrara (Italy) and funded by Medtronic. Dr. Valgimigli serves as a consultant to and/or on speakers’ bureaus for Medtronic and more than half a dozen other pharmaceutical and medical devices companies.
PARIS – The use of a second-generation zotarolimus-eluting coronary stent rather than a bare metal stent in conjunction with 30 days of dual antiplatelet therapy (DAPT) in patients deemed at high bleeding risk results in lower 1-year rates of major adverse cardiovascular events and stent thrombosis, according to a prespecified analysis of the ZEUS trial presented at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Asked if the ZEUS results mean it’s time to take bare-metal stents (BMS) out of the cupboard and get rid of them, the study presenter, Dr. Marco Valgimigli, replied “I did so already.”
ZEUS (Zotarolimus-Eluting Endeavor Sprint Stent in Uncertain DES Candidates Study) was an open-label, prospective study in which 1,606 patients undergoing urgent or emergent percutaneous coronary intervention were randomized to a thin-strut BMS or the zotarolimus-eluting Endeavor Sprint stent, a second-generation hydrophilic polymer-based device that, uniquely, elutes 100% of the drug within the first 2 weeks. All participants were placed on an intended 30-day regimen of DAPT. The study was conducted in four European countries, explained Dr. Valgimigli of Erasmus University in Rotterdam.
This prespecified analysis focused on the 828 patients with one or more factors placing them at high bleeding risk, since the use of a drug-eluting stent (DES) with a 30-day DAPT protocol hadn’t been adequately studied in that setting, the cardiologist noted.
High bleeding risk was defined by one or more of the following: age greater than 80, being on oral anticoagulation therapy, a prior bleeding event, need for corticosteroid or NSAID therapy, known anemia, or a bleeding diathesis; 47% of study participants had more than one of these criteria.
The primary study endpoint was the composite of all-cause mortality, acute MI, or target vessel revascularization through 1 year of follow-up. The rate was 29% in the BMS group, compared with 22.6% in the DES group, for a highly significant 26% relative risk reduction.
The zotarolimus-eluting stent group also fared significantly better in terms of stent thrombosis and the other prespecified secondary endpoints.
Asked how the ZEUS findings have affected his own clinical practice, Dr. Valgimigli replied, “My stent of choice in patients at high bleeding risk is a second-generation DES. Since there aren’t data showing a specific second-generation DES is preferable, basically whatever I have I implant.”
He sticks to the 30-day DAPT regimen featured in the ZEUS protocol except under specific circumstances, which were allowed under the protocol. One involves staged PCI procedures, in which case the 30 days of DAPT begins after the last stent is implanted, even though the patient has been on DAPT in the interim. The other circumstance where he goes beyond 30 days of DAPT in a patient on a second-generation DES is if an ischemic event occurs down the road: “That patient is put back on DAPT and left there,” he said.
In response to another question, Dr. Valgimigli said he doesn’t believe the lower stent thrombosis rate seen in the Endeavor Sprint group in ZEUS is unique to that stent.
“If you look at any BMS versus DES study, taking the first-generation DES out of the picture, it’s quite clear that the second-generation DES are much safer than a BMS,” according to the cardiologist.
The ZEUS study was sponsored by the University of Ferrara (Italy) and funded by Medtronic. Dr. Valgimigli serves as a consultant to and/or on speakers’ bureaus for Medtronic and more than half a dozen other pharmaceutical and medical devices companies.
PARIS – The use of a second-generation zotarolimus-eluting coronary stent rather than a bare metal stent in conjunction with 30 days of dual antiplatelet therapy (DAPT) in patients deemed at high bleeding risk results in lower 1-year rates of major adverse cardiovascular events and stent thrombosis, according to a prespecified analysis of the ZEUS trial presented at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Asked if the ZEUS results mean it’s time to take bare-metal stents (BMS) out of the cupboard and get rid of them, the study presenter, Dr. Marco Valgimigli, replied “I did so already.”
ZEUS (Zotarolimus-Eluting Endeavor Sprint Stent in Uncertain DES Candidates Study) was an open-label, prospective study in which 1,606 patients undergoing urgent or emergent percutaneous coronary intervention were randomized to a thin-strut BMS or the zotarolimus-eluting Endeavor Sprint stent, a second-generation hydrophilic polymer-based device that, uniquely, elutes 100% of the drug within the first 2 weeks. All participants were placed on an intended 30-day regimen of DAPT. The study was conducted in four European countries, explained Dr. Valgimigli of Erasmus University in Rotterdam.
This prespecified analysis focused on the 828 patients with one or more factors placing them at high bleeding risk, since the use of a drug-eluting stent (DES) with a 30-day DAPT protocol hadn’t been adequately studied in that setting, the cardiologist noted.
High bleeding risk was defined by one or more of the following: age greater than 80, being on oral anticoagulation therapy, a prior bleeding event, need for corticosteroid or NSAID therapy, known anemia, or a bleeding diathesis; 47% of study participants had more than one of these criteria.
The primary study endpoint was the composite of all-cause mortality, acute MI, or target vessel revascularization through 1 year of follow-up. The rate was 29% in the BMS group, compared with 22.6% in the DES group, for a highly significant 26% relative risk reduction.
The zotarolimus-eluting stent group also fared significantly better in terms of stent thrombosis and the other prespecified secondary endpoints.
Asked how the ZEUS findings have affected his own clinical practice, Dr. Valgimigli replied, “My stent of choice in patients at high bleeding risk is a second-generation DES. Since there aren’t data showing a specific second-generation DES is preferable, basically whatever I have I implant.”
He sticks to the 30-day DAPT regimen featured in the ZEUS protocol except under specific circumstances, which were allowed under the protocol. One involves staged PCI procedures, in which case the 30 days of DAPT begins after the last stent is implanted, even though the patient has been on DAPT in the interim. The other circumstance where he goes beyond 30 days of DAPT in a patient on a second-generation DES is if an ischemic event occurs down the road: “That patient is put back on DAPT and left there,” he said.
In response to another question, Dr. Valgimigli said he doesn’t believe the lower stent thrombosis rate seen in the Endeavor Sprint group in ZEUS is unique to that stent.
“If you look at any BMS versus DES study, taking the first-generation DES out of the picture, it’s quite clear that the second-generation DES are much safer than a BMS,” according to the cardiologist.
The ZEUS study was sponsored by the University of Ferrara (Italy) and funded by Medtronic. Dr. Valgimigli serves as a consultant to and/or on speakers’ bureaus for Medtronic and more than half a dozen other pharmaceutical and medical devices companies.
AT EUROPCR 2015
Key clinical point: High bleeding risk patients fare significantly better with a second-generation drug-eluting stent and 30 days of dual antiplatelet therapy than with a bare-metal stent.
Major finding: The 1-year incidence of major adverse cardiovascular events was 29.6% in high bleeding risk patients who received a bare-metal stent and 22.6% in those who got a second-generation zotarolimus-eluting stent with 30 days of dual antiplatelet therapy.
Data source: This was a prespecified analysis of 828 high bleeding risk patients randomized to a bare-metal stent or a second-generation zotarolimus-eluting stent in conjunction with 30 days of DAPT and then followed prospectively for 1 year.
Disclosures: The ZEUS study was sponsored by the University of Ferrara (Italy) and funded by Medtronic. The presenter serves as a consultant and/or on speakers’ bureaus for Medtronic and more than half a dozen other pharmaceutical and medical devices companies.

Elevated IL-6 linked to complications after major abdominal surgery
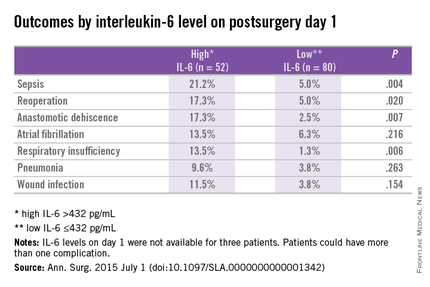
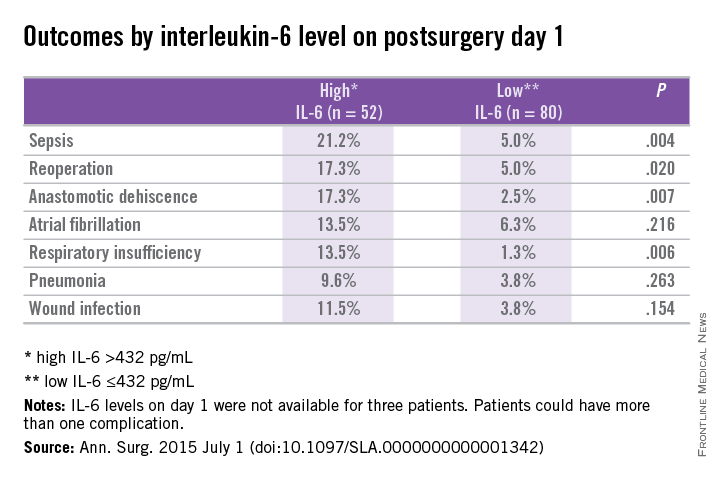
On postoperative day 1, elevated interleukin-6 level was associated with postoperative complications, according to a single-center cohort study of patients who had major abdominal surgery.
“Up to 28% of patients undergoing major abdominal surgery experience postoperative complications, including wound infection, sepsis, anastomotic dehiscence, pneumonia,cardiovascular or respiratory events, and mortality” but an accurate means of identifying those in the risk category would contribute the development of prevention stratetgies, the investigators wrote.
Previous studies of cardiothoracic surgery have supported an association of systemic inflammation to poor outcomes. Dr. Thijs Rettig and colleagues at St. Antonius Hospital, Nieuwegein, the Netherlands, sought to clarify if markers of inflammation and major abdominal surgery correlate with outcomes. Their results were published in the July issue of Annals of Surgery.
Researchers conducted a prospective cohort study at a single center using data obtained from the Myocardial Injury and Complications after major abdominal surgery (MICOLON) study. Participants in the MICOLON study were individuals aged 45 years or older who underwent elective major abdominal surgery. Other inclusion criteria included major cardiovascular (CV) risk factors, coronary artery disease, cerebrovascular accident, diabetes, renal insufficiency, atrial fibrillation, left ventricular dysfunction, aortic valve stenosis, or two minor CV risk factors.
Interleukin-6 (IL-6), tumor necrosis factor (TNF)-alpha, and C-reactive protein (CRP) levels were obtained at baseline and postoperative days 1, 3, and 7 in 137 patients. Systemic inflammatory response syndrome (SIRS) scores were calculated within 48 hours of surgery.
Primary endpoints were 30-day mortality, sepsis, pneumonia, wound infection, anastomotic dehiscence, reoperation, new-onset atrial fibrillation, respiratory insufficiency, congestive heart failure, and myocardial infarction. Data were also collected on length of stay and patients were followed up at 30 days postoperatively for further complications.
With a mean age of 68 years, 59% of patients were male and 30% (n = 40) had an ASA score of 3 or higher. Colorectal (50%), gastroesophageal (22%), and pancreatic (10%) surgery were the most common procedures performed. After excluding 2 patients from analysis for elevated baseline IL-6, 135 patients were analyzed.
At least one postoperative complication was observed in 29% (n = 39) of study subjects with a mean onset of 5 days after surgery. Use of preoperative steroids, aspirin, and statins were not associated with complications; however, blood loss and longer surgery duration where associated with worse outcomes.
In patients with and without complications, differences in IL-6 levels were observed at day 1 at 596 pg/mL vs. 303 pg/mL (P < .01), day 3 at 128 pg/mL vs. 69 pg/mL (P < .01), and day 7 at 76 pg/mL vs. 27 pg/mL (P = .02).
On day 1, CRP was similar in both groups (90 mg/L vs. 78 mg/L; P = .131), but on days 3 (223 mg/L vs. 131 mg/L; P < .001) and 7 (131 mg/L vs. 63 mg/L; P < .001) differences were observed.
Differences in TNF-alpha were observed between groups on day 7 (0.5 pg/mL vs. 0, P < .01). The two groups demonstrated similar leukocyte counts postoperatively.
Prediction for postoperative complications was associated with an IL-6 of 432 pg/mL at day 1, which was 70% specific and 64% sensitive, and had a positive predictive value (PPV) of 44% and negative predictive value (NPV) of 84%. A longer hospital stay of 12 days vs. 7 days (P < .001) was associated with high IL-6 (> 432 pg/mL) vs. a low IL-6 (< 432 pg/mL) at day 1.
Elevated IL-6 level on postoperative day 1 was independently associated with postoperative complications by multivariant regression analysis (AOR: 3.3; 95% confidence interval, 1.3-8.5; P < .02).
The researchers concluded that an increased IL-6 level on postoperative day 1 was associated with increased length of stay and threefold increased risk of complications after major abdominal surgery. They further continued, “It is plausible that early recognition of postoperative complications optimizes the chance of better outcome. One way to enhance early detection of complications is using inflammatory markers as predictors of outcome.”
The authors reported no conflicts of interest.
On postoperative day 1, elevated interleukin-6 level was associated with postoperative complications, according to a single-center cohort study of patients who had major abdominal surgery.
“Up to 28% of patients undergoing major abdominal surgery experience postoperative complications, including wound infection, sepsis, anastomotic dehiscence, pneumonia,cardiovascular or respiratory events, and mortality” but an accurate means of identifying those in the risk category would contribute the development of prevention stratetgies, the investigators wrote.
Previous studies of cardiothoracic surgery have supported an association of systemic inflammation to poor outcomes. Dr. Thijs Rettig and colleagues at St. Antonius Hospital, Nieuwegein, the Netherlands, sought to clarify if markers of inflammation and major abdominal surgery correlate with outcomes. Their results were published in the July issue of Annals of Surgery.
Researchers conducted a prospective cohort study at a single center using data obtained from the Myocardial Injury and Complications after major abdominal surgery (MICOLON) study. Participants in the MICOLON study were individuals aged 45 years or older who underwent elective major abdominal surgery. Other inclusion criteria included major cardiovascular (CV) risk factors, coronary artery disease, cerebrovascular accident, diabetes, renal insufficiency, atrial fibrillation, left ventricular dysfunction, aortic valve stenosis, or two minor CV risk factors.
Interleukin-6 (IL-6), tumor necrosis factor (TNF)-alpha, and C-reactive protein (CRP) levels were obtained at baseline and postoperative days 1, 3, and 7 in 137 patients. Systemic inflammatory response syndrome (SIRS) scores were calculated within 48 hours of surgery.
Primary endpoints were 30-day mortality, sepsis, pneumonia, wound infection, anastomotic dehiscence, reoperation, new-onset atrial fibrillation, respiratory insufficiency, congestive heart failure, and myocardial infarction. Data were also collected on length of stay and patients were followed up at 30 days postoperatively for further complications.
With a mean age of 68 years, 59% of patients were male and 30% (n = 40) had an ASA score of 3 or higher. Colorectal (50%), gastroesophageal (22%), and pancreatic (10%) surgery were the most common procedures performed. After excluding 2 patients from analysis for elevated baseline IL-6, 135 patients were analyzed.
At least one postoperative complication was observed in 29% (n = 39) of study subjects with a mean onset of 5 days after surgery. Use of preoperative steroids, aspirin, and statins were not associated with complications; however, blood loss and longer surgery duration where associated with worse outcomes.
In patients with and without complications, differences in IL-6 levels were observed at day 1 at 596 pg/mL vs. 303 pg/mL (P < .01), day 3 at 128 pg/mL vs. 69 pg/mL (P < .01), and day 7 at 76 pg/mL vs. 27 pg/mL (P = .02).
On day 1, CRP was similar in both groups (90 mg/L vs. 78 mg/L; P = .131), but on days 3 (223 mg/L vs. 131 mg/L; P < .001) and 7 (131 mg/L vs. 63 mg/L; P < .001) differences were observed.
Differences in TNF-alpha were observed between groups on day 7 (0.5 pg/mL vs. 0, P < .01). The two groups demonstrated similar leukocyte counts postoperatively.
Prediction for postoperative complications was associated with an IL-6 of 432 pg/mL at day 1, which was 70% specific and 64% sensitive, and had a positive predictive value (PPV) of 44% and negative predictive value (NPV) of 84%. A longer hospital stay of 12 days vs. 7 days (P < .001) was associated with high IL-6 (> 432 pg/mL) vs. a low IL-6 (< 432 pg/mL) at day 1.
Elevated IL-6 level on postoperative day 1 was independently associated with postoperative complications by multivariant regression analysis (AOR: 3.3; 95% confidence interval, 1.3-8.5; P < .02).
The researchers concluded that an increased IL-6 level on postoperative day 1 was associated with increased length of stay and threefold increased risk of complications after major abdominal surgery. They further continued, “It is plausible that early recognition of postoperative complications optimizes the chance of better outcome. One way to enhance early detection of complications is using inflammatory markers as predictors of outcome.”
The authors reported no conflicts of interest.
On postoperative day 1, elevated interleukin-6 level was associated with postoperative complications, according to a single-center cohort study of patients who had major abdominal surgery.
“Up to 28% of patients undergoing major abdominal surgery experience postoperative complications, including wound infection, sepsis, anastomotic dehiscence, pneumonia,cardiovascular or respiratory events, and mortality” but an accurate means of identifying those in the risk category would contribute the development of prevention stratetgies, the investigators wrote.
Previous studies of cardiothoracic surgery have supported an association of systemic inflammation to poor outcomes. Dr. Thijs Rettig and colleagues at St. Antonius Hospital, Nieuwegein, the Netherlands, sought to clarify if markers of inflammation and major abdominal surgery correlate with outcomes. Their results were published in the July issue of Annals of Surgery.
Researchers conducted a prospective cohort study at a single center using data obtained from the Myocardial Injury and Complications after major abdominal surgery (MICOLON) study. Participants in the MICOLON study were individuals aged 45 years or older who underwent elective major abdominal surgery. Other inclusion criteria included major cardiovascular (CV) risk factors, coronary artery disease, cerebrovascular accident, diabetes, renal insufficiency, atrial fibrillation, left ventricular dysfunction, aortic valve stenosis, or two minor CV risk factors.
Interleukin-6 (IL-6), tumor necrosis factor (TNF)-alpha, and C-reactive protein (CRP) levels were obtained at baseline and postoperative days 1, 3, and 7 in 137 patients. Systemic inflammatory response syndrome (SIRS) scores were calculated within 48 hours of surgery.
Primary endpoints were 30-day mortality, sepsis, pneumonia, wound infection, anastomotic dehiscence, reoperation, new-onset atrial fibrillation, respiratory insufficiency, congestive heart failure, and myocardial infarction. Data were also collected on length of stay and patients were followed up at 30 days postoperatively for further complications.
With a mean age of 68 years, 59% of patients were male and 30% (n = 40) had an ASA score of 3 or higher. Colorectal (50%), gastroesophageal (22%), and pancreatic (10%) surgery were the most common procedures performed. After excluding 2 patients from analysis for elevated baseline IL-6, 135 patients were analyzed.
At least one postoperative complication was observed in 29% (n = 39) of study subjects with a mean onset of 5 days after surgery. Use of preoperative steroids, aspirin, and statins were not associated with complications; however, blood loss and longer surgery duration where associated with worse outcomes.
In patients with and without complications, differences in IL-6 levels were observed at day 1 at 596 pg/mL vs. 303 pg/mL (P < .01), day 3 at 128 pg/mL vs. 69 pg/mL (P < .01), and day 7 at 76 pg/mL vs. 27 pg/mL (P = .02).
On day 1, CRP was similar in both groups (90 mg/L vs. 78 mg/L; P = .131), but on days 3 (223 mg/L vs. 131 mg/L; P < .001) and 7 (131 mg/L vs. 63 mg/L; P < .001) differences were observed.
Differences in TNF-alpha were observed between groups on day 7 (0.5 pg/mL vs. 0, P < .01). The two groups demonstrated similar leukocyte counts postoperatively.
Prediction for postoperative complications was associated with an IL-6 of 432 pg/mL at day 1, which was 70% specific and 64% sensitive, and had a positive predictive value (PPV) of 44% and negative predictive value (NPV) of 84%. A longer hospital stay of 12 days vs. 7 days (P < .001) was associated with high IL-6 (> 432 pg/mL) vs. a low IL-6 (< 432 pg/mL) at day 1.
Elevated IL-6 level on postoperative day 1 was independently associated with postoperative complications by multivariant regression analysis (AOR: 3.3; 95% confidence interval, 1.3-8.5; P < .02).
The researchers concluded that an increased IL-6 level on postoperative day 1 was associated with increased length of stay and threefold increased risk of complications after major abdominal surgery. They further continued, “It is plausible that early recognition of postoperative complications optimizes the chance of better outcome. One way to enhance early detection of complications is using inflammatory markers as predictors of outcome.”
The authors reported no conflicts of interest.
FROM ANNALS OF SURGERY
Key clinical point: Postoperative complications after major abdominal surgery are associated with elevated IL-6.
Major finding: Elevated IL-6 level on postoperative day 1 was independently associated with postoperative complications by multivariant regression analysis (P < .02).
Data source: Prospective cohort study at a single center using data from the Myocardial Injury and Postoperative Complications after major abdominal surgery (MICOLON) study.
Disclosures: The authors reported no conflicts of interest.
New guidelines focus on pediatric thyroid nodules and cancer
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
FROM THYROID
Senators query GAO on healthcare.gov scam report
Patient access or program integrity? The question of which need outweighs the other was the theme of a Senate Finance Committee hearing that discussed the erroneous approval of subsidies by healthcare.gov for fake patients.
An investigation by the Government Accountability Office (GAO) found the federal exchange approved 11 of 12 telephone and online applications for fictitious applicants and paid $30,000 in annual insurance credits for the fake patients over a 2-year period. Investigators provided fake documents to the government, including Social Security numbers and proof of income, but encountered no barriers to obtaining taxpayer-funded credits, according to the report released July 15.
The findings are troubling and do not speak well of the management of healthcare.gov, the protection of taxpayer dollars, or the experience of enrollees, Senate Finance Committee Chairman Orrin Hatch (R-Utah) said during a July 16 hearing.
“The GAO’s investigation exposes not only huge gaps in federal exchange program integrity, but also flaws in how the exchange and [Centers for Medicare & Medicaid Services] contractors treat Americans who are trying to file or correct legitimate applications,” Chairman Hatch said during his opening statement. “The fact that GAO encountered mind-boggling levels of incompetence and inefficiency at nearly every turn does not bode well for the experience of your average, honest enrollee.”
CMS officials did not testify at the hearing nor did they respond to requests for comment.
The GAO’s investigation covered the marketplace’s first open-enrollment period from Oct. 1, 2013 to March 31, 2014, as well as follow-on work through 2014 and 2015. As part of its “secret shopper” investigation, GAO created 18 fictitious identities to apply for premium subsidies through the federal exchange by telephone, online, and in-person. The fake applicants were able to get health insurance and subsidies with fictitious information in nearly all cases. For 7 of the 11 fictitious applicants, GAO intentionally did not submit all required documentation to the marketplace, but CMS did not cancel the subsidized coverage.
“While these subsidies, including those granted to GAO’s fictitious applicants, are paid to health care insurers, and not directly to enrolled consumers, they nevertheless represent a benefit to consumers and a cost to the government,” according to the report.
Among the report’s findings:
• Information transmitted to the IRS for 3 of 11 fictitious enrollees, such as coverage periods and subsidy amounts, was incorrect.
• The marketplace automatically reenrolled coverage for all 11 fictitious enrollees for 2015.
• CMS terminated coverage for 6 of the 11 enrollees in 2015, stating that the fictitious enrollees had not provided necessary documentation. On appeal, five were reinstated and awarded higher subsidies.
The GAO tests were designed to identify potential control weaknesses in the market enrollment process and to inform the agency’s ongoing audit of these controls, Seto J. Bagdoyan, GAO director of forensic audits and investigative service, said at the hearing. GAO plans to provide recommendations about control efforts in a forthcoming report.
“A program of this scope and scale is inherently at risk for errors, including in proper payment and fraudulent activities,” Mr. Bagdoyan testified. “Accordingly, it is essential there are effective enrollment controls in place to help narrow the window of opportunities for such risks.”
Mr. Bagoyan noted that in response to the findings, CMS stated that they had limited capacity to respond to attempts at fraud within enrollment, and that officials must balance consumers’ ability to access coverage with program integrity concerns.
Sen Ron Wyden (D-Ore.) stressed the importance of this balance in his opening statement. He largely criticized the report, noting the study analyzed only fictitious cases and none involved a real person who filed taxes or received medical care.
“Part of any smart, ferocious strategy against fraud, on one hand, is drawing a distinction between aggressively going after scammers, and on the other, not harming a law-abiding American who’s made an honest, often technical mistake,” said Sen. Wyden, ranking member of the Finance Committee. “A retiree nearing Medicare age shouldn’t get kicked to the curb because she accidentally submitted an incorrect document. A transgender American shouldn’t lose health coverage after a name change because some forms don’t match. I can’t imagine the Congress wants a system that nixes the health insurance coverage of Americans because of simple issues like those.”
In the GAO report, CMS officials stated that there have been no cases of actual fraudulent marketplace applications or documentation referred to the Justice Department or the U.S. Department of Health & Human Services’ Office of Inspector General. Following the findings, CMS officials said they plan to conduct an assessment of the marketplace’s eligibility determination process, including the application process, and consistency surrounding the resolution process.
“CMS places a strong emphasis on program integrity and builds program integrity features into all aspects of implementation of the law,” CMS officials stated in the report.
On Twitter @legal_med
Patient access or program integrity? The question of which need outweighs the other was the theme of a Senate Finance Committee hearing that discussed the erroneous approval of subsidies by healthcare.gov for fake patients.
An investigation by the Government Accountability Office (GAO) found the federal exchange approved 11 of 12 telephone and online applications for fictitious applicants and paid $30,000 in annual insurance credits for the fake patients over a 2-year period. Investigators provided fake documents to the government, including Social Security numbers and proof of income, but encountered no barriers to obtaining taxpayer-funded credits, according to the report released July 15.
The findings are troubling and do not speak well of the management of healthcare.gov, the protection of taxpayer dollars, or the experience of enrollees, Senate Finance Committee Chairman Orrin Hatch (R-Utah) said during a July 16 hearing.
“The GAO’s investigation exposes not only huge gaps in federal exchange program integrity, but also flaws in how the exchange and [Centers for Medicare & Medicaid Services] contractors treat Americans who are trying to file or correct legitimate applications,” Chairman Hatch said during his opening statement. “The fact that GAO encountered mind-boggling levels of incompetence and inefficiency at nearly every turn does not bode well for the experience of your average, honest enrollee.”
CMS officials did not testify at the hearing nor did they respond to requests for comment.
The GAO’s investigation covered the marketplace’s first open-enrollment period from Oct. 1, 2013 to March 31, 2014, as well as follow-on work through 2014 and 2015. As part of its “secret shopper” investigation, GAO created 18 fictitious identities to apply for premium subsidies through the federal exchange by telephone, online, and in-person. The fake applicants were able to get health insurance and subsidies with fictitious information in nearly all cases. For 7 of the 11 fictitious applicants, GAO intentionally did not submit all required documentation to the marketplace, but CMS did not cancel the subsidized coverage.
“While these subsidies, including those granted to GAO’s fictitious applicants, are paid to health care insurers, and not directly to enrolled consumers, they nevertheless represent a benefit to consumers and a cost to the government,” according to the report.
Among the report’s findings:
• Information transmitted to the IRS for 3 of 11 fictitious enrollees, such as coverage periods and subsidy amounts, was incorrect.
• The marketplace automatically reenrolled coverage for all 11 fictitious enrollees for 2015.
• CMS terminated coverage for 6 of the 11 enrollees in 2015, stating that the fictitious enrollees had not provided necessary documentation. On appeal, five were reinstated and awarded higher subsidies.
The GAO tests were designed to identify potential control weaknesses in the market enrollment process and to inform the agency’s ongoing audit of these controls, Seto J. Bagdoyan, GAO director of forensic audits and investigative service, said at the hearing. GAO plans to provide recommendations about control efforts in a forthcoming report.
“A program of this scope and scale is inherently at risk for errors, including in proper payment and fraudulent activities,” Mr. Bagdoyan testified. “Accordingly, it is essential there are effective enrollment controls in place to help narrow the window of opportunities for such risks.”
Mr. Bagoyan noted that in response to the findings, CMS stated that they had limited capacity to respond to attempts at fraud within enrollment, and that officials must balance consumers’ ability to access coverage with program integrity concerns.
Sen Ron Wyden (D-Ore.) stressed the importance of this balance in his opening statement. He largely criticized the report, noting the study analyzed only fictitious cases and none involved a real person who filed taxes or received medical care.
“Part of any smart, ferocious strategy against fraud, on one hand, is drawing a distinction between aggressively going after scammers, and on the other, not harming a law-abiding American who’s made an honest, often technical mistake,” said Sen. Wyden, ranking member of the Finance Committee. “A retiree nearing Medicare age shouldn’t get kicked to the curb because she accidentally submitted an incorrect document. A transgender American shouldn’t lose health coverage after a name change because some forms don’t match. I can’t imagine the Congress wants a system that nixes the health insurance coverage of Americans because of simple issues like those.”
In the GAO report, CMS officials stated that there have been no cases of actual fraudulent marketplace applications or documentation referred to the Justice Department or the U.S. Department of Health & Human Services’ Office of Inspector General. Following the findings, CMS officials said they plan to conduct an assessment of the marketplace’s eligibility determination process, including the application process, and consistency surrounding the resolution process.
“CMS places a strong emphasis on program integrity and builds program integrity features into all aspects of implementation of the law,” CMS officials stated in the report.
On Twitter @legal_med
Patient access or program integrity? The question of which need outweighs the other was the theme of a Senate Finance Committee hearing that discussed the erroneous approval of subsidies by healthcare.gov for fake patients.
An investigation by the Government Accountability Office (GAO) found the federal exchange approved 11 of 12 telephone and online applications for fictitious applicants and paid $30,000 in annual insurance credits for the fake patients over a 2-year period. Investigators provided fake documents to the government, including Social Security numbers and proof of income, but encountered no barriers to obtaining taxpayer-funded credits, according to the report released July 15.
The findings are troubling and do not speak well of the management of healthcare.gov, the protection of taxpayer dollars, or the experience of enrollees, Senate Finance Committee Chairman Orrin Hatch (R-Utah) said during a July 16 hearing.
“The GAO’s investigation exposes not only huge gaps in federal exchange program integrity, but also flaws in how the exchange and [Centers for Medicare & Medicaid Services] contractors treat Americans who are trying to file or correct legitimate applications,” Chairman Hatch said during his opening statement. “The fact that GAO encountered mind-boggling levels of incompetence and inefficiency at nearly every turn does not bode well for the experience of your average, honest enrollee.”
CMS officials did not testify at the hearing nor did they respond to requests for comment.
The GAO’s investigation covered the marketplace’s first open-enrollment period from Oct. 1, 2013 to March 31, 2014, as well as follow-on work through 2014 and 2015. As part of its “secret shopper” investigation, GAO created 18 fictitious identities to apply for premium subsidies through the federal exchange by telephone, online, and in-person. The fake applicants were able to get health insurance and subsidies with fictitious information in nearly all cases. For 7 of the 11 fictitious applicants, GAO intentionally did not submit all required documentation to the marketplace, but CMS did not cancel the subsidized coverage.
“While these subsidies, including those granted to GAO’s fictitious applicants, are paid to health care insurers, and not directly to enrolled consumers, they nevertheless represent a benefit to consumers and a cost to the government,” according to the report.
Among the report’s findings:
• Information transmitted to the IRS for 3 of 11 fictitious enrollees, such as coverage periods and subsidy amounts, was incorrect.
• The marketplace automatically reenrolled coverage for all 11 fictitious enrollees for 2015.
• CMS terminated coverage for 6 of the 11 enrollees in 2015, stating that the fictitious enrollees had not provided necessary documentation. On appeal, five were reinstated and awarded higher subsidies.
The GAO tests were designed to identify potential control weaknesses in the market enrollment process and to inform the agency’s ongoing audit of these controls, Seto J. Bagdoyan, GAO director of forensic audits and investigative service, said at the hearing. GAO plans to provide recommendations about control efforts in a forthcoming report.
“A program of this scope and scale is inherently at risk for errors, including in proper payment and fraudulent activities,” Mr. Bagdoyan testified. “Accordingly, it is essential there are effective enrollment controls in place to help narrow the window of opportunities for such risks.”
Mr. Bagoyan noted that in response to the findings, CMS stated that they had limited capacity to respond to attempts at fraud within enrollment, and that officials must balance consumers’ ability to access coverage with program integrity concerns.
Sen Ron Wyden (D-Ore.) stressed the importance of this balance in his opening statement. He largely criticized the report, noting the study analyzed only fictitious cases and none involved a real person who filed taxes or received medical care.
“Part of any smart, ferocious strategy against fraud, on one hand, is drawing a distinction between aggressively going after scammers, and on the other, not harming a law-abiding American who’s made an honest, often technical mistake,” said Sen. Wyden, ranking member of the Finance Committee. “A retiree nearing Medicare age shouldn’t get kicked to the curb because she accidentally submitted an incorrect document. A transgender American shouldn’t lose health coverage after a name change because some forms don’t match. I can’t imagine the Congress wants a system that nixes the health insurance coverage of Americans because of simple issues like those.”
In the GAO report, CMS officials stated that there have been no cases of actual fraudulent marketplace applications or documentation referred to the Justice Department or the U.S. Department of Health & Human Services’ Office of Inspector General. Following the findings, CMS officials said they plan to conduct an assessment of the marketplace’s eligibility determination process, including the application process, and consistency surrounding the resolution process.
“CMS places a strong emphasis on program integrity and builds program integrity features into all aspects of implementation of the law,” CMS officials stated in the report.
On Twitter @legal_med
To maintain independent practice, rethink structure, build partnerships
Sustaining an independent practice in today’s medical landscape isn’t easy, but it’s possible with the right care model, strong partnerships, and solid negotiation power.
There is no one-size-fits-all approach to maintaining independence, said David W. Hilgers, an Austin, Tex., health law attorney who specializes in advising independent practices and integrating systems.

“It depends on the market you’re in and the specialty you’re in,” Mr. Hilgers said in an interview. “It all comes down to how much leverage you can have, if you’re willing to consolidate to get that leverage, and if you’re willing to spend the money to have the technology that you need.”
It’s no secret that more physicians are becoming hospital and health system employees, in large part to escape a growing burden of government regulations and reimbursement woes. A 2015 physician survey by national staffing company Jackson Healthcare found the top reasons that doctors leave private practice include the high cost of maintaining a medical practice, reimbursement cuts, and a desire to focus on practicing medicine and patient care – rather than administrative hassles. Another study, released July 8 by the American Medical Association, found the share of physicians who worked directly for a hospital, or in practices that had at least some hospital ownership, increased from 29% in 2012 to 33% percent in 2014. The number of doctors who owned a practice fell from 53% to 51% during the same time period.
However, the AMA data show the majority of physicians (61%) were still in small practices of 10 or fewer physicians, and that practice size hardly changed between 2012 and 2014. Experts say the findings point to a strong desire by doctors to remain autonomous.
“There are benefits to being employed by a hospital or health care system as far as a steady income, but there’s also something very satisfying to physicians about controlling their own destiny,” said Heather F. Delgado, a Chicago health law attorney, who specializes in compliance and regulatory matters. Ms. Delgado and Mr. Hilgers recently spoke at an American Bar Association (ABA) conference about how physicians can sustain an independent practice.
To retain autonomy, physicians in smaller practices may want to consider changing their care delivery model to a less traditional structure, such as the concierge model, Mr. Hilgers advised. Primary care physicians may be more suited to this model than other specialties, he noted.
“For a very small practice, if you want to stay in practice, you need to look at concierge care and see if you can make that work,” Mr. Hilgers said in an interview. “If you’re in a larger town, you’re going to have a very difficult time remaining independent. If you’re in a small town, you may be able to continue because the insurance companies need you, but your income is going to be limited.”
Starting or joining an accountable care organization (ACO) is a good option for mid- to large-sized practices, Mr. Hilgers said. Doctors will want to analyze the type of technology they need to efficiently operate an ACO, he noted. Successful ACOs must possess an information technology infrastructure with specific competencies to support governance, operational, and clinical goals objectives. It also helps to have a stable patient base to bring to the ACO.
“If you’re in a larger practice, you need to expand your reach so that they can’t do without you,” Mr. Hilgers said in an interview. “The insurance plans have to have you. You need to perhaps [participate in] your own Medicare Advantage plan so that you are generating revenue from the federal government and insurers directly. You need to start looking at being more than just a medical group, but taking advantage of these alternative types of insurance plans.”

Consolidating with other physicians can also help secure a more stable place in the market, added attorney Albert D. Hutzler, a financial analyst at a health care valuation consulting firm in Delray, Fla. Adding more doctors can give a practice more leverage with insurance companies and better negotiating power to set rates. But once a practice grows, it’s vital to pay attention to ongoing recruitment, said Mr. Hutzler, who also spoke during the recent ABA meeting.
“A stable physician base is very important,” he said in an interview. “You need the ability to recruit others. That way if things don’t work out with somebody, you’ve got to have others in the pipeline.”
Physician-hospital partnerships – rather than employement relationships – also can provide strategies to stay independent, said Ms. Delgado. For example, doctors could opt for a clinically integrated system in which they maintain their office practice but become a preferred provider of a hospital. Other options include entering into a medical directorship or management services deal with a hospital or agreeing to staff a hospital clinic several days a week, she said.
“Maybe you enter into an agreement with a hospital that wouldn’t mean you are employed, but gives you a relationship with them so that you can work with them,” Ms. Delgado said in an interview. “That way, you are able to remain independent, but [are] able to get some benefits from the hospital.”

Doctors determined to retain their private practice must also be mindful of their collections efforts, Mr. Hutzler said. Most practices are going to have some debt on their books, he noted, but it should not grow out of control, nor should physicians constantly be borrowing against the practice. Additionally, practices should ensure their contracts with insurers are firm and that they are receiving payment as outlined in their agreements.
“You don’t want lose out in private practice just because you do an ineffective job collecting from payers,” Mr. Hutzler said in an interview. “You need a solid business office to make sure you’re getting everything you can out of your payer contracts.”
Whether it’s worth it to remain independent depends on the physician and his or her goals, Mr. Hutzler said.
“They both have their pros and cons,” he said. “You have to decide which set of risks that you want” to take on.
On Twitter @legal_med
Sustaining an independent practice in today’s medical landscape isn’t easy, but it’s possible with the right care model, strong partnerships, and solid negotiation power.
There is no one-size-fits-all approach to maintaining independence, said David W. Hilgers, an Austin, Tex., health law attorney who specializes in advising independent practices and integrating systems.
“It depends on the market you’re in and the specialty you’re in,” Mr. Hilgers said in an interview. “It all comes down to how much leverage you can have, if you’re willing to consolidate to get that leverage, and if you’re willing to spend the money to have the technology that you need.”
It’s no secret that more physicians are becoming hospital and health system employees, in large part to escape a growing burden of government regulations and reimbursement woes. A 2015 physician survey by national staffing company Jackson Healthcare found the top reasons that doctors leave private practice include the high cost of maintaining a medical practice, reimbursement cuts, and a desire to focus on practicing medicine and patient care – rather than administrative hassles. Another study, released July 8 by the American Medical Association, found the share of physicians who worked directly for a hospital, or in practices that had at least some hospital ownership, increased from 29% in 2012 to 33% percent in 2014. The number of doctors who owned a practice fell from 53% to 51% during the same time period.
However, the AMA data show the majority of physicians (61%) were still in small practices of 10 or fewer physicians, and that practice size hardly changed between 2012 and 2014. Experts say the findings point to a strong desire by doctors to remain autonomous.
“There are benefits to being employed by a hospital or health care system as far as a steady income, but there’s also something very satisfying to physicians about controlling their own destiny,” said Heather F. Delgado, a Chicago health law attorney, who specializes in compliance and regulatory matters. Ms. Delgado and Mr. Hilgers recently spoke at an American Bar Association (ABA) conference about how physicians can sustain an independent practice.
To retain autonomy, physicians in smaller practices may want to consider changing their care delivery model to a less traditional structure, such as the concierge model, Mr. Hilgers advised. Primary care physicians may be more suited to this model than other specialties, he noted.
“For a very small practice, if you want to stay in practice, you need to look at concierge care and see if you can make that work,” Mr. Hilgers said in an interview. “If you’re in a larger town, you’re going to have a very difficult time remaining independent. If you’re in a small town, you may be able to continue because the insurance companies need you, but your income is going to be limited.”
Starting or joining an accountable care organization (ACO) is a good option for mid- to large-sized practices, Mr. Hilgers said. Doctors will want to analyze the type of technology they need to efficiently operate an ACO, he noted. Successful ACOs must possess an information technology infrastructure with specific competencies to support governance, operational, and clinical goals objectives. It also helps to have a stable patient base to bring to the ACO.
“If you’re in a larger practice, you need to expand your reach so that they can’t do without you,” Mr. Hilgers said in an interview. “The insurance plans have to have you. You need to perhaps [participate in] your own Medicare Advantage plan so that you are generating revenue from the federal government and insurers directly. You need to start looking at being more than just a medical group, but taking advantage of these alternative types of insurance plans.”
Consolidating with other physicians can also help secure a more stable place in the market, added attorney Albert D. Hutzler, a financial analyst at a health care valuation consulting firm in Delray, Fla. Adding more doctors can give a practice more leverage with insurance companies and better negotiating power to set rates. But once a practice grows, it’s vital to pay attention to ongoing recruitment, said Mr. Hutzler, who also spoke during the recent ABA meeting.
“A stable physician base is very important,” he said in an interview. “You need the ability to recruit others. That way if things don’t work out with somebody, you’ve got to have others in the pipeline.”
Physician-hospital partnerships – rather than employement relationships – also can provide strategies to stay independent, said Ms. Delgado. For example, doctors could opt for a clinically integrated system in which they maintain their office practice but become a preferred provider of a hospital. Other options include entering into a medical directorship or management services deal with a hospital or agreeing to staff a hospital clinic several days a week, she said.
“Maybe you enter into an agreement with a hospital that wouldn’t mean you are employed, but gives you a relationship with them so that you can work with them,” Ms. Delgado said in an interview. “That way, you are able to remain independent, but [are] able to get some benefits from the hospital.”
Doctors determined to retain their private practice must also be mindful of their collections efforts, Mr. Hutzler said. Most practices are going to have some debt on their books, he noted, but it should not grow out of control, nor should physicians constantly be borrowing against the practice. Additionally, practices should ensure their contracts with insurers are firm and that they are receiving payment as outlined in their agreements.
“You don’t want lose out in private practice just because you do an ineffective job collecting from payers,” Mr. Hutzler said in an interview. “You need a solid business office to make sure you’re getting everything you can out of your payer contracts.”
Whether it’s worth it to remain independent depends on the physician and his or her goals, Mr. Hutzler said.
“They both have their pros and cons,” he said. “You have to decide which set of risks that you want” to take on.
On Twitter @legal_med
Sustaining an independent practice in today’s medical landscape isn’t easy, but it’s possible with the right care model, strong partnerships, and solid negotiation power.
There is no one-size-fits-all approach to maintaining independence, said David W. Hilgers, an Austin, Tex., health law attorney who specializes in advising independent practices and integrating systems.
“It depends on the market you’re in and the specialty you’re in,” Mr. Hilgers said in an interview. “It all comes down to how much leverage you can have, if you’re willing to consolidate to get that leverage, and if you’re willing to spend the money to have the technology that you need.”
It’s no secret that more physicians are becoming hospital and health system employees, in large part to escape a growing burden of government regulations and reimbursement woes. A 2015 physician survey by national staffing company Jackson Healthcare found the top reasons that doctors leave private practice include the high cost of maintaining a medical practice, reimbursement cuts, and a desire to focus on practicing medicine and patient care – rather than administrative hassles. Another study, released July 8 by the American Medical Association, found the share of physicians who worked directly for a hospital, or in practices that had at least some hospital ownership, increased from 29% in 2012 to 33% percent in 2014. The number of doctors who owned a practice fell from 53% to 51% during the same time period.
However, the AMA data show the majority of physicians (61%) were still in small practices of 10 or fewer physicians, and that practice size hardly changed between 2012 and 2014. Experts say the findings point to a strong desire by doctors to remain autonomous.
“There are benefits to being employed by a hospital or health care system as far as a steady income, but there’s also something very satisfying to physicians about controlling their own destiny,” said Heather F. Delgado, a Chicago health law attorney, who specializes in compliance and regulatory matters. Ms. Delgado and Mr. Hilgers recently spoke at an American Bar Association (ABA) conference about how physicians can sustain an independent practice.
To retain autonomy, physicians in smaller practices may want to consider changing their care delivery model to a less traditional structure, such as the concierge model, Mr. Hilgers advised. Primary care physicians may be more suited to this model than other specialties, he noted.
“For a very small practice, if you want to stay in practice, you need to look at concierge care and see if you can make that work,” Mr. Hilgers said in an interview. “If you’re in a larger town, you’re going to have a very difficult time remaining independent. If you’re in a small town, you may be able to continue because the insurance companies need you, but your income is going to be limited.”
Starting or joining an accountable care organization (ACO) is a good option for mid- to large-sized practices, Mr. Hilgers said. Doctors will want to analyze the type of technology they need to efficiently operate an ACO, he noted. Successful ACOs must possess an information technology infrastructure with specific competencies to support governance, operational, and clinical goals objectives. It also helps to have a stable patient base to bring to the ACO.
“If you’re in a larger practice, you need to expand your reach so that they can’t do without you,” Mr. Hilgers said in an interview. “The insurance plans have to have you. You need to perhaps [participate in] your own Medicare Advantage plan so that you are generating revenue from the federal government and insurers directly. You need to start looking at being more than just a medical group, but taking advantage of these alternative types of insurance plans.”
Consolidating with other physicians can also help secure a more stable place in the market, added attorney Albert D. Hutzler, a financial analyst at a health care valuation consulting firm in Delray, Fla. Adding more doctors can give a practice more leverage with insurance companies and better negotiating power to set rates. But once a practice grows, it’s vital to pay attention to ongoing recruitment, said Mr. Hutzler, who also spoke during the recent ABA meeting.
“A stable physician base is very important,” he said in an interview. “You need the ability to recruit others. That way if things don’t work out with somebody, you’ve got to have others in the pipeline.”
Physician-hospital partnerships – rather than employement relationships – also can provide strategies to stay independent, said Ms. Delgado. For example, doctors could opt for a clinically integrated system in which they maintain their office practice but become a preferred provider of a hospital. Other options include entering into a medical directorship or management services deal with a hospital or agreeing to staff a hospital clinic several days a week, she said.
“Maybe you enter into an agreement with a hospital that wouldn’t mean you are employed, but gives you a relationship with them so that you can work with them,” Ms. Delgado said in an interview. “That way, you are able to remain independent, but [are] able to get some benefits from the hospital.”
Doctors determined to retain their private practice must also be mindful of their collections efforts, Mr. Hutzler said. Most practices are going to have some debt on their books, he noted, but it should not grow out of control, nor should physicians constantly be borrowing against the practice. Additionally, practices should ensure their contracts with insurers are firm and that they are receiving payment as outlined in their agreements.
“You don’t want lose out in private practice just because you do an ineffective job collecting from payers,” Mr. Hutzler said in an interview. “You need a solid business office to make sure you’re getting everything you can out of your payer contracts.”
Whether it’s worth it to remain independent depends on the physician and his or her goals, Mr. Hutzler said.
“They both have their pros and cons,” he said. “You have to decide which set of risks that you want” to take on.
On Twitter @legal_med

TEP inguinal hernia repairs have low incidence of chronic pain
Chronic pain after total extraperitoneal inguinal hernia repair occurs infrequently in patients, and findings from a study suggest that the means of mesh fixation, permanent or nonpermanant, is not linked to greater risk of this outcome.
Dr. Nihad Gutlic and colleagues from the Skåne University Hospital at University of Lund, Sweden, sought to compare total extraperitoneal inguinal hernia repair (TEP) done with permanent fixture (PF) of mesh vs. nonfixed (NF) or nonpermanent fixation (NPF) and the impact of the means of mesh fixation on chronic pain. Their results were published online in the July issue of Annals of Surgery.

Prospective data were obtained from the Swedish Hernia Registry (SHR) and participants completed the Inguinal Pain Questionnaire (IPQ) and the Short Form-36 (SF-36) to measure health-related quality of life to assess chronic pain. Chronic pain was defined as pain that persisted more than 3 months after surgery.
The study included men aged 30-75 years, consecutively registered in the SHR for TEP repair of a primary groin hernia during January 2005 and May 2009, and the questionnaire was send between February 2010 and May 2010. A minimum follow-up of 6 months was stipulated. The IPQ assessed pain with 19 questions regarding the pain modalities intensity, frequency, duration, influence on daily activities, and testicular pain. Questions concerned “pain right now” and “pain past week” respectively, and answers were given on a 7-grade scale from “no pain” to “pain that could not be ignored – prompt medical advice sought.” Patients were followed for up to 33 months.
A total of 1,110 respondents were analyzed: 325 patients in the PF group and 785 patients in the NPF group (281 with fibrin glue and 504 NF). The PF group had more medial hernias (P < .003) and larger defect sizes (P < .002). There were no differences in the rate of reoperation between the two groups (P < .735).
For the IPQ questionnaire, 7.7% (n = 85) of patients reported having “pain that could not be ignored” in the last week with no difference between the PF group and the NF/NPF groups (P < .462). Of those patients responding, 5.4% reported having “pain right now” (n = 59) with no difference between the two groups (P < .270).
The authors conclude, “that TEP, carried out on men for primary inguinal hernia, is associated with a low frequency of chronic postoperative pain. No difference was seen between permanent and nonpermanent fixation regarding chronic pain.”
The authors declared no conflicts of interest. The study was supported by the Lund (Sweden) University, Region Skåne Research and Development Funds, and the Bard Norden AB and Helge B. Wulffs Foundation.
Chronic pain after total extraperitoneal inguinal hernia repair occurs infrequently in patients, and findings from a study suggest that the means of mesh fixation, permanent or nonpermanant, is not linked to greater risk of this outcome.
Dr. Nihad Gutlic and colleagues from the Skåne University Hospital at University of Lund, Sweden, sought to compare total extraperitoneal inguinal hernia repair (TEP) done with permanent fixture (PF) of mesh vs. nonfixed (NF) or nonpermanent fixation (NPF) and the impact of the means of mesh fixation on chronic pain. Their results were published online in the July issue of Annals of Surgery.
Prospective data were obtained from the Swedish Hernia Registry (SHR) and participants completed the Inguinal Pain Questionnaire (IPQ) and the Short Form-36 (SF-36) to measure health-related quality of life to assess chronic pain. Chronic pain was defined as pain that persisted more than 3 months after surgery.
The study included men aged 30-75 years, consecutively registered in the SHR for TEP repair of a primary groin hernia during January 2005 and May 2009, and the questionnaire was send between February 2010 and May 2010. A minimum follow-up of 6 months was stipulated. The IPQ assessed pain with 19 questions regarding the pain modalities intensity, frequency, duration, influence on daily activities, and testicular pain. Questions concerned “pain right now” and “pain past week” respectively, and answers were given on a 7-grade scale from “no pain” to “pain that could not be ignored – prompt medical advice sought.” Patients were followed for up to 33 months.
A total of 1,110 respondents were analyzed: 325 patients in the PF group and 785 patients in the NPF group (281 with fibrin glue and 504 NF). The PF group had more medial hernias (P < .003) and larger defect sizes (P < .002). There were no differences in the rate of reoperation between the two groups (P < .735).
For the IPQ questionnaire, 7.7% (n = 85) of patients reported having “pain that could not be ignored” in the last week with no difference between the PF group and the NF/NPF groups (P < .462). Of those patients responding, 5.4% reported having “pain right now” (n = 59) with no difference between the two groups (P < .270).
The authors conclude, “that TEP, carried out on men for primary inguinal hernia, is associated with a low frequency of chronic postoperative pain. No difference was seen between permanent and nonpermanent fixation regarding chronic pain.”
The authors declared no conflicts of interest. The study was supported by the Lund (Sweden) University, Region Skåne Research and Development Funds, and the Bard Norden AB and Helge B. Wulffs Foundation.
Chronic pain after total extraperitoneal inguinal hernia repair occurs infrequently in patients, and findings from a study suggest that the means of mesh fixation, permanent or nonpermanant, is not linked to greater risk of this outcome.
Dr. Nihad Gutlic and colleagues from the Skåne University Hospital at University of Lund, Sweden, sought to compare total extraperitoneal inguinal hernia repair (TEP) done with permanent fixture (PF) of mesh vs. nonfixed (NF) or nonpermanent fixation (NPF) and the impact of the means of mesh fixation on chronic pain. Their results were published online in the July issue of Annals of Surgery.
Prospective data were obtained from the Swedish Hernia Registry (SHR) and participants completed the Inguinal Pain Questionnaire (IPQ) and the Short Form-36 (SF-36) to measure health-related quality of life to assess chronic pain. Chronic pain was defined as pain that persisted more than 3 months after surgery.
The study included men aged 30-75 years, consecutively registered in the SHR for TEP repair of a primary groin hernia during January 2005 and May 2009, and the questionnaire was send between February 2010 and May 2010. A minimum follow-up of 6 months was stipulated. The IPQ assessed pain with 19 questions regarding the pain modalities intensity, frequency, duration, influence on daily activities, and testicular pain. Questions concerned “pain right now” and “pain past week” respectively, and answers were given on a 7-grade scale from “no pain” to “pain that could not be ignored – prompt medical advice sought.” Patients were followed for up to 33 months.
A total of 1,110 respondents were analyzed: 325 patients in the PF group and 785 patients in the NPF group (281 with fibrin glue and 504 NF). The PF group had more medial hernias (P < .003) and larger defect sizes (P < .002). There were no differences in the rate of reoperation between the two groups (P < .735).
For the IPQ questionnaire, 7.7% (n = 85) of patients reported having “pain that could not be ignored” in the last week with no difference between the PF group and the NF/NPF groups (P < .462). Of those patients responding, 5.4% reported having “pain right now” (n = 59) with no difference between the two groups (P < .270).
The authors conclude, “that TEP, carried out on men for primary inguinal hernia, is associated with a low frequency of chronic postoperative pain. No difference was seen between permanent and nonpermanent fixation regarding chronic pain.”
The authors declared no conflicts of interest. The study was supported by the Lund (Sweden) University, Region Skåne Research and Development Funds, and the Bard Norden AB and Helge B. Wulffs Foundation.
FROM ANNALS OF SURGERY
Key clinical point: TEP inguinal hernia repair is associated with a low incidence of chronic pain.
Major finding: Utilizing the IPQ questionnaire, 7.7% of patients reported having “pain that could not be ignored” in the last week with no difference between the two groups (P < .462).
Data source: Prospective data obtained from the Swedish Hernia Registry, IPQ, and SF-36 questionnaires.
Disclosures: The authors declared no conflicts of interest. The study was supported by the Lund (Sweden) University, Region Skåne Research and Development Funds, and the Bard Norden AB and Helge B. Wulffs Foundation.
