User login
Official Newspaper of the American College of Surgeons
Drug manufacturers delayed reporting serious unexpected adverse events
Drug manufacturers did not report about 10% of serious and unexpected adverse events to the U.S. Food and Drug Administration within the required time period, investigators reported online in JAMA Internal Medicine.
Moreover, manufacturers were more likely to delay reporting serious and unexpected drug-related deaths than other AEs, said Paul Ma, Ph.D., of the University of Minnesota, Minneapolis, and his associates.

“As the FDA uses this information to update drug warnings, delays in reporting can have important public health consequences, particularly if manufacturers selectively delay reporting based on relevant patient outcomes,” the researchers said. “While increased enforcement may decrease violations, a simple alternative would be to recommend direct submission of reports to the FDA rather than via the manufacturer.”
Health providers and consumers can report adverse events to either drug manufacturers or the FDA under current regulations. Manufacturers have 15 days to forward reports of “expedited” events, defined as both unexpected (not included in the current FDA label) and serious (deaths, life-threatening drug reactions, new or prolonged inpatient hospitalizations, persistent or major disabilities, or birth defects). Although the extent to which drug manufacturers followed the 15-day requirement was unknown, there had been media reports of delays, the researchers noted (JAMA Intern. Med. 2015 July 27 [doi: 10.1001/jamainternmed.2015.3565]).
To better quantify the problem, Dr. Ma and his associates studied expedited AEs reported to the FDA Adverse Event Reporting System between 2004 and June 2014. Among 1.6 million reports, manufacturers failed to report 9.94% within the 15-day window, including more than 40,000 deaths. “Strikingly, AEs with patient death were more likely to be delayed,” added the investigators. “It is possible that manufacturers spend additional time in verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.”
Manufacturers reported about 90% of AEs that did not involve death on time, compared with 88% of those that did involve death. Furthermore, patient death remained linked to delayed reporting after accounting for multiple concurrent prescriptions; who reported the AE to the manufacturer; whether reported electronically or on paper; and the age, sex, and weight of patients.
“Further research is needed to better understand the mechanisms behind the manufacturers’ delayed reporting and the optimal regulatory policy toward mandatory disclosures of AEs,” the researchers concluded.
The Minnesota Accounting Research Center and the National Institute of Aging helped fund the research. The investigators disclosed no conflicts of interest.
“Our awareness of the potential adverse effects (AEs) of newly approved drugs and devices is limited. Premarket trials are often small and of limited duration, and the patients in clinical trials are healthier than unselected patients in routine clinical practice. Thus, the public and physicians rely on the U.S. Food and Drug Administration (FDA) Adverse Event Reporting System to inform us of unknown or unsuspected risks associated with use of drugs and devices.”
“Such reporting delays [as those found in the study] should never occur, as they mean that more patients are exposed to potentially avoidable serious harm, including death. However, no disciplinary actions have been taken when companies fail to submit reports to the FDA in the time frame required. Clearly, the lack of consequences contributes to a lack of deterrence for these illegal and dangerous delays.
“There is another enforcement tool that the FDA could begin to deploy immediately: suspending drug sales or withdrawing drug approval. Federal regulations give the FDA the power to withdraw drug approval ‘if an applicant fails to establish and maintain records and make [timely] reports [as] required under this section.’ One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer, as recommended by” Dr. Ma and his associates.
Dr. Rita F. Redberg is director of women’s cardiovascular services at the Philip R. Lee Institute for Health Policy Studies at the University of California, San Francisco. She reported no conflicts of interest. These comments were taken from her accompanying editorial (JAMA Intern. Med. 2015 July 27 [doi:10.1001/jamainternmed.2015.356]).
“Our awareness of the potential adverse effects (AEs) of newly approved drugs and devices is limited. Premarket trials are often small and of limited duration, and the patients in clinical trials are healthier than unselected patients in routine clinical practice. Thus, the public and physicians rely on the U.S. Food and Drug Administration (FDA) Adverse Event Reporting System to inform us of unknown or unsuspected risks associated with use of drugs and devices.”
“Such reporting delays [as those found in the study] should never occur, as they mean that more patients are exposed to potentially avoidable serious harm, including death. However, no disciplinary actions have been taken when companies fail to submit reports to the FDA in the time frame required. Clearly, the lack of consequences contributes to a lack of deterrence for these illegal and dangerous delays.
“There is another enforcement tool that the FDA could begin to deploy immediately: suspending drug sales or withdrawing drug approval. Federal regulations give the FDA the power to withdraw drug approval ‘if an applicant fails to establish and maintain records and make [timely] reports [as] required under this section.’ One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer, as recommended by” Dr. Ma and his associates.
Dr. Rita F. Redberg is director of women’s cardiovascular services at the Philip R. Lee Institute for Health Policy Studies at the University of California, San Francisco. She reported no conflicts of interest. These comments were taken from her accompanying editorial (JAMA Intern. Med. 2015 July 27 [doi:10.1001/jamainternmed.2015.356]).
“Our awareness of the potential adverse effects (AEs) of newly approved drugs and devices is limited. Premarket trials are often small and of limited duration, and the patients in clinical trials are healthier than unselected patients in routine clinical practice. Thus, the public and physicians rely on the U.S. Food and Drug Administration (FDA) Adverse Event Reporting System to inform us of unknown or unsuspected risks associated with use of drugs and devices.”
“Such reporting delays [as those found in the study] should never occur, as they mean that more patients are exposed to potentially avoidable serious harm, including death. However, no disciplinary actions have been taken when companies fail to submit reports to the FDA in the time frame required. Clearly, the lack of consequences contributes to a lack of deterrence for these illegal and dangerous delays.
“There is another enforcement tool that the FDA could begin to deploy immediately: suspending drug sales or withdrawing drug approval. Federal regulations give the FDA the power to withdraw drug approval ‘if an applicant fails to establish and maintain records and make [timely] reports [as] required under this section.’ One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer, as recommended by” Dr. Ma and his associates.
Dr. Rita F. Redberg is director of women’s cardiovascular services at the Philip R. Lee Institute for Health Policy Studies at the University of California, San Francisco. She reported no conflicts of interest. These comments were taken from her accompanying editorial (JAMA Intern. Med. 2015 July 27 [doi:10.1001/jamainternmed.2015.356]).
Drug manufacturers did not report about 10% of serious and unexpected adverse events to the U.S. Food and Drug Administration within the required time period, investigators reported online in JAMA Internal Medicine.
Moreover, manufacturers were more likely to delay reporting serious and unexpected drug-related deaths than other AEs, said Paul Ma, Ph.D., of the University of Minnesota, Minneapolis, and his associates.
“As the FDA uses this information to update drug warnings, delays in reporting can have important public health consequences, particularly if manufacturers selectively delay reporting based on relevant patient outcomes,” the researchers said. “While increased enforcement may decrease violations, a simple alternative would be to recommend direct submission of reports to the FDA rather than via the manufacturer.”
Health providers and consumers can report adverse events to either drug manufacturers or the FDA under current regulations. Manufacturers have 15 days to forward reports of “expedited” events, defined as both unexpected (not included in the current FDA label) and serious (deaths, life-threatening drug reactions, new or prolonged inpatient hospitalizations, persistent or major disabilities, or birth defects). Although the extent to which drug manufacturers followed the 15-day requirement was unknown, there had been media reports of delays, the researchers noted (JAMA Intern. Med. 2015 July 27 [doi: 10.1001/jamainternmed.2015.3565]).
To better quantify the problem, Dr. Ma and his associates studied expedited AEs reported to the FDA Adverse Event Reporting System between 2004 and June 2014. Among 1.6 million reports, manufacturers failed to report 9.94% within the 15-day window, including more than 40,000 deaths. “Strikingly, AEs with patient death were more likely to be delayed,” added the investigators. “It is possible that manufacturers spend additional time in verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.”
Manufacturers reported about 90% of AEs that did not involve death on time, compared with 88% of those that did involve death. Furthermore, patient death remained linked to delayed reporting after accounting for multiple concurrent prescriptions; who reported the AE to the manufacturer; whether reported electronically or on paper; and the age, sex, and weight of patients.
“Further research is needed to better understand the mechanisms behind the manufacturers’ delayed reporting and the optimal regulatory policy toward mandatory disclosures of AEs,” the researchers concluded.
The Minnesota Accounting Research Center and the National Institute of Aging helped fund the research. The investigators disclosed no conflicts of interest.
Drug manufacturers did not report about 10% of serious and unexpected adverse events to the U.S. Food and Drug Administration within the required time period, investigators reported online in JAMA Internal Medicine.
Moreover, manufacturers were more likely to delay reporting serious and unexpected drug-related deaths than other AEs, said Paul Ma, Ph.D., of the University of Minnesota, Minneapolis, and his associates.
“As the FDA uses this information to update drug warnings, delays in reporting can have important public health consequences, particularly if manufacturers selectively delay reporting based on relevant patient outcomes,” the researchers said. “While increased enforcement may decrease violations, a simple alternative would be to recommend direct submission of reports to the FDA rather than via the manufacturer.”
Health providers and consumers can report adverse events to either drug manufacturers or the FDA under current regulations. Manufacturers have 15 days to forward reports of “expedited” events, defined as both unexpected (not included in the current FDA label) and serious (deaths, life-threatening drug reactions, new or prolonged inpatient hospitalizations, persistent or major disabilities, or birth defects). Although the extent to which drug manufacturers followed the 15-day requirement was unknown, there had been media reports of delays, the researchers noted (JAMA Intern. Med. 2015 July 27 [doi: 10.1001/jamainternmed.2015.3565]).
To better quantify the problem, Dr. Ma and his associates studied expedited AEs reported to the FDA Adverse Event Reporting System between 2004 and June 2014. Among 1.6 million reports, manufacturers failed to report 9.94% within the 15-day window, including more than 40,000 deaths. “Strikingly, AEs with patient death were more likely to be delayed,” added the investigators. “It is possible that manufacturers spend additional time in verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.”
Manufacturers reported about 90% of AEs that did not involve death on time, compared with 88% of those that did involve death. Furthermore, patient death remained linked to delayed reporting after accounting for multiple concurrent prescriptions; who reported the AE to the manufacturer; whether reported electronically or on paper; and the age, sex, and weight of patients.
“Further research is needed to better understand the mechanisms behind the manufacturers’ delayed reporting and the optimal regulatory policy toward mandatory disclosures of AEs,” the researchers concluded.
The Minnesota Accounting Research Center and the National Institute of Aging helped fund the research. The investigators disclosed no conflicts of interest.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Drug manufacturers delayed reporting about 10% of serious unexpected adverse events to the FDA.
Major finding: Manufacturers broke the 15-day deadline for about 10% of such events, and those involving deaths were more likely to be delayed than others.
Data source: Analysis of 1.6 million serious and unexpected AEs reported to the FDA Adverse Event Reporting System between 2004 and June 2014.
Disclosures: The Minnesota Accounting Research Center and the National Institute of Aging helped fund the research. The investigators disclosed no conflicts of interest.

Value-based care poses new legal risks for doctors
The government’s push toward value-based care aims to fix a broken reimbursement system and improve quality of care for patients. But the new payment models also bring new legal risks for physicians, experts and anti-fraud officials warn.
“Novel payment methodologies may present new program integrity vulnerabilities,” Dr. Shantanu Agrawal, director of the Center for Program Integrity at the Centers for Medicare & Medicaid Services, said at a recent American Bar Association meeting. “As they assume financial risk, providers are also assuming program integrity risk. Without adequate controls, provider-run systems may be relatively vulnerable.”

The Department of Health and Human Services plans to have 30% of Medicare payments in value-based payment structures by the end of 2016, and 50% by the end of 2018. The transition will be driven through investments in alternative payment models such as Accountable Care Organizations (ACOs), advanced primary care medical home models, bundled payments models, and integrated care demonstrations for Medicare and Medicaid patients.
At the end of 2014, value-based payments represented 20% of Medicare fee-for-service payments to providers, according to CMS data. The rate was fueled by government programs such as the Medicare Shared Savings Program (MSSP), Pioneer ACOs, the Bundled Payments for Care Improvement Initiative, and the Comprehensive Primary Care Initiative. Meanwhile, HHS is encouraging private payers, marketplace plans, Medicare Advantage plans, and state Medicaid programs to move in the same value-based direction.
With so many new regulations, mandates, and programs coming down the pipeline, physicians are likely not thinking about the legal dangers that may arise with alternative payment structures, said Mark S. Kopson, a health law attorney in Bloomfield Hills, Mich., and chair of the American Health Lawyers Association’s Payers, Plans and Managed Care Practice Group.

Fee-for-service models can involve claims “about excess treatments and unnecessary services to drive up reimbursement,” Mr. Kopson said in an interview. “When you get into these [value-based] types of programs, it’s the exact opposite. The real threat is the withholding of necessary care in order to reduce expenses and therefore drive up those margins for the providers.”
To avoid such claims, physicians should ensure that their charts include the reasoning behind treatment decisions and a thorough record of why certain treatments were chosen and diagnoses were made, Mr. Kopson advised.
“Going forward, your charting better be completely accurate and detailed so that you don’t leave room for the government to make an argument that you should have provided this or that additional treatment,” he said.
Inaccurate reporting of enrollment data or financial information within new payment models could also land doctors in legal trouble, according to CMS officials.
Problematic reports, enrollee data, or other information physicians are required to submit to the government could be considered falsification and lead to False Claims Act violations.
“Providers are responsible for the information reported and should ensure that the appropriate checks and balances are in place that verify data is reported timely and accurately,” Tony A. Salters, a CMS spokesman, said in an interview. “For some models, providers must attest to the accuracy of this data. [To] report inaccurately could result in violations of federal laws.”
Physician-run payment models, such as doctor-led ACOs, may also draw legal scrutiny if physicians fail to prevent bad behavior by de facto partners. Physicians must ensure that all costs claimed by subcontractors, other providers, and suppliers who are paid from or authorized by the provider-run system, have been validated, Mr. Salters said.
“Doctors need to be aware that other entities who become new partners should hold themselves to the same high standards,” he said. “Providers should have basic financial mechanisms in place, with more sophisticated systems requiring more sophisticated methods,” to ensure validation.
CMS officials recommend doctors conduct independent audits of their accounts, manual validation of record system accuracy, and periodic verification of subcontractor claims to confirm the accuracy of claims and costs within new payment models.
These are “all routine steps that practitioners can take in their own offices but which are even more important when the doctor assumes responsibility for a larger scope of services,” Mr. Salters said.
Gaps in documentation surrounding bundled payments can be another legal land mine, Mr. Kopson noted. Adequate records of the care spectrum are essential to prevent accusations that care was not provided during a single episode of care, or over a specific period of time.
“You have to capture and document all the services you are delivering, and have accurate tracking in place for the entire continuum of care,” Mr. Kopson said.
CMS recommends that physicians establish a strong compliance program to assist with anti-fraud controls of new payment systems. When creating or updating a compliance program, government officials said providers should consider the unique characteristics of the model in which they participate.
On Twitter @legal_med
The government’s push toward value-based care aims to fix a broken reimbursement system and improve quality of care for patients. But the new payment models also bring new legal risks for physicians, experts and anti-fraud officials warn.
“Novel payment methodologies may present new program integrity vulnerabilities,” Dr. Shantanu Agrawal, director of the Center for Program Integrity at the Centers for Medicare & Medicaid Services, said at a recent American Bar Association meeting. “As they assume financial risk, providers are also assuming program integrity risk. Without adequate controls, provider-run systems may be relatively vulnerable.”
The Department of Health and Human Services plans to have 30% of Medicare payments in value-based payment structures by the end of 2016, and 50% by the end of 2018. The transition will be driven through investments in alternative payment models such as Accountable Care Organizations (ACOs), advanced primary care medical home models, bundled payments models, and integrated care demonstrations for Medicare and Medicaid patients.
At the end of 2014, value-based payments represented 20% of Medicare fee-for-service payments to providers, according to CMS data. The rate was fueled by government programs such as the Medicare Shared Savings Program (MSSP), Pioneer ACOs, the Bundled Payments for Care Improvement Initiative, and the Comprehensive Primary Care Initiative. Meanwhile, HHS is encouraging private payers, marketplace plans, Medicare Advantage plans, and state Medicaid programs to move in the same value-based direction.
With so many new regulations, mandates, and programs coming down the pipeline, physicians are likely not thinking about the legal dangers that may arise with alternative payment structures, said Mark S. Kopson, a health law attorney in Bloomfield Hills, Mich., and chair of the American Health Lawyers Association’s Payers, Plans and Managed Care Practice Group.
Fee-for-service models can involve claims “about excess treatments and unnecessary services to drive up reimbursement,” Mr. Kopson said in an interview. “When you get into these [value-based] types of programs, it’s the exact opposite. The real threat is the withholding of necessary care in order to reduce expenses and therefore drive up those margins for the providers.”
To avoid such claims, physicians should ensure that their charts include the reasoning behind treatment decisions and a thorough record of why certain treatments were chosen and diagnoses were made, Mr. Kopson advised.
“Going forward, your charting better be completely accurate and detailed so that you don’t leave room for the government to make an argument that you should have provided this or that additional treatment,” he said.
Inaccurate reporting of enrollment data or financial information within new payment models could also land doctors in legal trouble, according to CMS officials.
Problematic reports, enrollee data, or other information physicians are required to submit to the government could be considered falsification and lead to False Claims Act violations.
“Providers are responsible for the information reported and should ensure that the appropriate checks and balances are in place that verify data is reported timely and accurately,” Tony A. Salters, a CMS spokesman, said in an interview. “For some models, providers must attest to the accuracy of this data. [To] report inaccurately could result in violations of federal laws.”
Physician-run payment models, such as doctor-led ACOs, may also draw legal scrutiny if physicians fail to prevent bad behavior by de facto partners. Physicians must ensure that all costs claimed by subcontractors, other providers, and suppliers who are paid from or authorized by the provider-run system, have been validated, Mr. Salters said.
“Doctors need to be aware that other entities who become new partners should hold themselves to the same high standards,” he said. “Providers should have basic financial mechanisms in place, with more sophisticated systems requiring more sophisticated methods,” to ensure validation.
CMS officials recommend doctors conduct independent audits of their accounts, manual validation of record system accuracy, and periodic verification of subcontractor claims to confirm the accuracy of claims and costs within new payment models.
These are “all routine steps that practitioners can take in their own offices but which are even more important when the doctor assumes responsibility for a larger scope of services,” Mr. Salters said.
Gaps in documentation surrounding bundled payments can be another legal land mine, Mr. Kopson noted. Adequate records of the care spectrum are essential to prevent accusations that care was not provided during a single episode of care, or over a specific period of time.
“You have to capture and document all the services you are delivering, and have accurate tracking in place for the entire continuum of care,” Mr. Kopson said.
CMS recommends that physicians establish a strong compliance program to assist with anti-fraud controls of new payment systems. When creating or updating a compliance program, government officials said providers should consider the unique characteristics of the model in which they participate.
On Twitter @legal_med
The government’s push toward value-based care aims to fix a broken reimbursement system and improve quality of care for patients. But the new payment models also bring new legal risks for physicians, experts and anti-fraud officials warn.
“Novel payment methodologies may present new program integrity vulnerabilities,” Dr. Shantanu Agrawal, director of the Center for Program Integrity at the Centers for Medicare & Medicaid Services, said at a recent American Bar Association meeting. “As they assume financial risk, providers are also assuming program integrity risk. Without adequate controls, provider-run systems may be relatively vulnerable.”
The Department of Health and Human Services plans to have 30% of Medicare payments in value-based payment structures by the end of 2016, and 50% by the end of 2018. The transition will be driven through investments in alternative payment models such as Accountable Care Organizations (ACOs), advanced primary care medical home models, bundled payments models, and integrated care demonstrations for Medicare and Medicaid patients.
At the end of 2014, value-based payments represented 20% of Medicare fee-for-service payments to providers, according to CMS data. The rate was fueled by government programs such as the Medicare Shared Savings Program (MSSP), Pioneer ACOs, the Bundled Payments for Care Improvement Initiative, and the Comprehensive Primary Care Initiative. Meanwhile, HHS is encouraging private payers, marketplace plans, Medicare Advantage plans, and state Medicaid programs to move in the same value-based direction.
With so many new regulations, mandates, and programs coming down the pipeline, physicians are likely not thinking about the legal dangers that may arise with alternative payment structures, said Mark S. Kopson, a health law attorney in Bloomfield Hills, Mich., and chair of the American Health Lawyers Association’s Payers, Plans and Managed Care Practice Group.
Fee-for-service models can involve claims “about excess treatments and unnecessary services to drive up reimbursement,” Mr. Kopson said in an interview. “When you get into these [value-based] types of programs, it’s the exact opposite. The real threat is the withholding of necessary care in order to reduce expenses and therefore drive up those margins for the providers.”
To avoid such claims, physicians should ensure that their charts include the reasoning behind treatment decisions and a thorough record of why certain treatments were chosen and diagnoses were made, Mr. Kopson advised.
“Going forward, your charting better be completely accurate and detailed so that you don’t leave room for the government to make an argument that you should have provided this or that additional treatment,” he said.
Inaccurate reporting of enrollment data or financial information within new payment models could also land doctors in legal trouble, according to CMS officials.
Problematic reports, enrollee data, or other information physicians are required to submit to the government could be considered falsification and lead to False Claims Act violations.
“Providers are responsible for the information reported and should ensure that the appropriate checks and balances are in place that verify data is reported timely and accurately,” Tony A. Salters, a CMS spokesman, said in an interview. “For some models, providers must attest to the accuracy of this data. [To] report inaccurately could result in violations of federal laws.”
Physician-run payment models, such as doctor-led ACOs, may also draw legal scrutiny if physicians fail to prevent bad behavior by de facto partners. Physicians must ensure that all costs claimed by subcontractors, other providers, and suppliers who are paid from or authorized by the provider-run system, have been validated, Mr. Salters said.
“Doctors need to be aware that other entities who become new partners should hold themselves to the same high standards,” he said. “Providers should have basic financial mechanisms in place, with more sophisticated systems requiring more sophisticated methods,” to ensure validation.
CMS officials recommend doctors conduct independent audits of their accounts, manual validation of record system accuracy, and periodic verification of subcontractor claims to confirm the accuracy of claims and costs within new payment models.
These are “all routine steps that practitioners can take in their own offices but which are even more important when the doctor assumes responsibility for a larger scope of services,” Mr. Salters said.
Gaps in documentation surrounding bundled payments can be another legal land mine, Mr. Kopson noted. Adequate records of the care spectrum are essential to prevent accusations that care was not provided during a single episode of care, or over a specific period of time.
“You have to capture and document all the services you are delivering, and have accurate tracking in place for the entire continuum of care,” Mr. Kopson said.
CMS recommends that physicians establish a strong compliance program to assist with anti-fraud controls of new payment systems. When creating or updating a compliance program, government officials said providers should consider the unique characteristics of the model in which they participate.
On Twitter @legal_med

Similar outcomes for salvage vs. planned surgery after chemoradiotherapy in esophageal cancer
For patients with esophageal cancer, salvage surgery after definitive chemoradiotherapy had similar mortality and morbidity rates, and similar survival outcomes, to the combination of neoadjuvant chemoradiation and planned surgery, according to a study published online in the Journal of Clinical Oncology.
Definitive chemoradiotherapy (dCRT) is an alternative to highly invasive surgical resection, which carries a significant rate of morbidity and mortality; however, recent data indicate that 50% of patients with complete response to dCRT experience tumor recurrence.

“Our study demonstrated a similar survival and recurrence pattern for the SALV [salvage surgery after definitive chemoradiotherapy] and NCRS [neoadjuvant chemoradiation and planned surgery] groups, potentially validating an approach of dCRT with reserved SALV for persistent or recurrent disease. Importantly, there were no differences in oncologic safety of surgery, including extent of nodal dissection, between the SALV and NCRS groups,” wrote Dr. Sheraz Markar, a clinical research fellow from Imperial College, London, and colleagues (Journ. Clin. Onc. 2015 July 20 [doi:10.1200/JCO.2014.59.9092]).
The retrospective study compared 308 patients with esophageal cancer who underwent SALV with 540 patients who received NCRS at European centers from 2000 to 2010. After a median follow up of 54 months, the SALV and NCRS groups had similar rates of 3-year overall survival (43.3% vs. 40.1% ) and disease-free survival (39.2% vs. 32.8%). The two groups also had similar rates tumor recurrence: overall (46.8% vs. 47.9%), locoregional (18.8% vs. 15.9%), distant (24.3% vs. 28.1%) and mixed (13.0% vs. 13.5%).
The SALV and NCRS groups had similar rates of in-hospital mortality (8.4% vs. 9.3%) and morbidity (63.6% vs. 58.9%), but SALV patients had significantly more complications from anastomotic leak (17.2% vs. 10.7%) and surgical site infection (18.5% vs. 12.2%).
Subset analysis of the SALV group showed that patients who received a total radiation dose ≥ 55 Gy (compared with SALV patients who received a lower dose) had significantly increased in-hospital mortality (27.8% vs. 4.3%; P < .001), overall morbidity (75.9% vs. 61%; P = .039), anastomotic leak (27.8% vs. 15%; P = .023), surgical site infection (29.6% vs. 16.1%; P = .02), and pulmonary complications (55.6% vs. 40.2%; P = .038).
“Currently, there is no evidence in terms of locoregional control or survival benefit to support a high total radiation dose (> 50 Gy) in patients receiving dCRT,” according to the researchers, who noted that the findings suggest, “an upper threshold of 50 Gy should be used in these patients to optimize the benefits of dCRT without compromising the safety of SALV, if required.”
Patients who underwent SALV at high-volume centers had significantly lower rates of in-hospital mortality (6.3% vs. 16.2%; P = .009) and overall morbidity (58.8% vs. 80.9%; P = .001) compared with procedures done at low-volume centers.
Compared with recurrent disease, patients with persistent disease after dCRT had poorer long-term prognoses, suggesting a more aggressive tumor biology. Early identification of CRT-resistant tumors to allow early surgical treatment is an important area for future investigation, the investigators said.
For patients with esophageal cancer, salvage surgery after definitive chemoradiotherapy had similar mortality and morbidity rates, and similar survival outcomes, to the combination of neoadjuvant chemoradiation and planned surgery, according to a study published online in the Journal of Clinical Oncology.
Definitive chemoradiotherapy (dCRT) is an alternative to highly invasive surgical resection, which carries a significant rate of morbidity and mortality; however, recent data indicate that 50% of patients with complete response to dCRT experience tumor recurrence.
“Our study demonstrated a similar survival and recurrence pattern for the SALV [salvage surgery after definitive chemoradiotherapy] and NCRS [neoadjuvant chemoradiation and planned surgery] groups, potentially validating an approach of dCRT with reserved SALV for persistent or recurrent disease. Importantly, there were no differences in oncologic safety of surgery, including extent of nodal dissection, between the SALV and NCRS groups,” wrote Dr. Sheraz Markar, a clinical research fellow from Imperial College, London, and colleagues (Journ. Clin. Onc. 2015 July 20 [doi:10.1200/JCO.2014.59.9092]).
The retrospective study compared 308 patients with esophageal cancer who underwent SALV with 540 patients who received NCRS at European centers from 2000 to 2010. After a median follow up of 54 months, the SALV and NCRS groups had similar rates of 3-year overall survival (43.3% vs. 40.1% ) and disease-free survival (39.2% vs. 32.8%). The two groups also had similar rates tumor recurrence: overall (46.8% vs. 47.9%), locoregional (18.8% vs. 15.9%), distant (24.3% vs. 28.1%) and mixed (13.0% vs. 13.5%).
The SALV and NCRS groups had similar rates of in-hospital mortality (8.4% vs. 9.3%) and morbidity (63.6% vs. 58.9%), but SALV patients had significantly more complications from anastomotic leak (17.2% vs. 10.7%) and surgical site infection (18.5% vs. 12.2%).
Subset analysis of the SALV group showed that patients who received a total radiation dose ≥ 55 Gy (compared with SALV patients who received a lower dose) had significantly increased in-hospital mortality (27.8% vs. 4.3%; P < .001), overall morbidity (75.9% vs. 61%; P = .039), anastomotic leak (27.8% vs. 15%; P = .023), surgical site infection (29.6% vs. 16.1%; P = .02), and pulmonary complications (55.6% vs. 40.2%; P = .038).
“Currently, there is no evidence in terms of locoregional control or survival benefit to support a high total radiation dose (> 50 Gy) in patients receiving dCRT,” according to the researchers, who noted that the findings suggest, “an upper threshold of 50 Gy should be used in these patients to optimize the benefits of dCRT without compromising the safety of SALV, if required.”
Patients who underwent SALV at high-volume centers had significantly lower rates of in-hospital mortality (6.3% vs. 16.2%; P = .009) and overall morbidity (58.8% vs. 80.9%; P = .001) compared with procedures done at low-volume centers.
Compared with recurrent disease, patients with persistent disease after dCRT had poorer long-term prognoses, suggesting a more aggressive tumor biology. Early identification of CRT-resistant tumors to allow early surgical treatment is an important area for future investigation, the investigators said.
For patients with esophageal cancer, salvage surgery after definitive chemoradiotherapy had similar mortality and morbidity rates, and similar survival outcomes, to the combination of neoadjuvant chemoradiation and planned surgery, according to a study published online in the Journal of Clinical Oncology.
Definitive chemoradiotherapy (dCRT) is an alternative to highly invasive surgical resection, which carries a significant rate of morbidity and mortality; however, recent data indicate that 50% of patients with complete response to dCRT experience tumor recurrence.
“Our study demonstrated a similar survival and recurrence pattern for the SALV [salvage surgery after definitive chemoradiotherapy] and NCRS [neoadjuvant chemoradiation and planned surgery] groups, potentially validating an approach of dCRT with reserved SALV for persistent or recurrent disease. Importantly, there were no differences in oncologic safety of surgery, including extent of nodal dissection, between the SALV and NCRS groups,” wrote Dr. Sheraz Markar, a clinical research fellow from Imperial College, London, and colleagues (Journ. Clin. Onc. 2015 July 20 [doi:10.1200/JCO.2014.59.9092]).
The retrospective study compared 308 patients with esophageal cancer who underwent SALV with 540 patients who received NCRS at European centers from 2000 to 2010. After a median follow up of 54 months, the SALV and NCRS groups had similar rates of 3-year overall survival (43.3% vs. 40.1% ) and disease-free survival (39.2% vs. 32.8%). The two groups also had similar rates tumor recurrence: overall (46.8% vs. 47.9%), locoregional (18.8% vs. 15.9%), distant (24.3% vs. 28.1%) and mixed (13.0% vs. 13.5%).
The SALV and NCRS groups had similar rates of in-hospital mortality (8.4% vs. 9.3%) and morbidity (63.6% vs. 58.9%), but SALV patients had significantly more complications from anastomotic leak (17.2% vs. 10.7%) and surgical site infection (18.5% vs. 12.2%).
Subset analysis of the SALV group showed that patients who received a total radiation dose ≥ 55 Gy (compared with SALV patients who received a lower dose) had significantly increased in-hospital mortality (27.8% vs. 4.3%; P < .001), overall morbidity (75.9% vs. 61%; P = .039), anastomotic leak (27.8% vs. 15%; P = .023), surgical site infection (29.6% vs. 16.1%; P = .02), and pulmonary complications (55.6% vs. 40.2%; P = .038).
“Currently, there is no evidence in terms of locoregional control or survival benefit to support a high total radiation dose (> 50 Gy) in patients receiving dCRT,” according to the researchers, who noted that the findings suggest, “an upper threshold of 50 Gy should be used in these patients to optimize the benefits of dCRT without compromising the safety of SALV, if required.”
Patients who underwent SALV at high-volume centers had significantly lower rates of in-hospital mortality (6.3% vs. 16.2%; P = .009) and overall morbidity (58.8% vs. 80.9%; P = .001) compared with procedures done at low-volume centers.
Compared with recurrent disease, patients with persistent disease after dCRT had poorer long-term prognoses, suggesting a more aggressive tumor biology. Early identification of CRT-resistant tumors to allow early surgical treatment is an important area for future investigation, the investigators said.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: As management for esophageal cancer, salvage esophagectomy after definitive chemoradiotherapy (SALV) produced similar outcomes to the combination of neoadjuvant chemoradiation and planned surgery (NCRS).
Major finding: The SALV and NCRS groups had similar rates of 3-year overall survival (43.3% vs. 40.1% ) and disease-free survival (39.2% vs. 32.8%), tumor recurrence (46.8% vs. 47.9%), and in-hospital mortality (8.4% vs. 9.3%) and morbidity (63.6% vs. 58.9%).
Data source: Retrospective analysis of 848 patients (308 SALV, 540 NCRS) who underwent surgical resection for esophageal cancer in French-speaking European centers from 2000 to 2010.
Disclosures: Dr. Markar reported having no disclosures. Two of his coauthors reported ties to industry.

Combined ablation–mitral surgery safe for atrial fib
NEW YORK – Patients with both mitral valve regurgitation and atrial fibrillation who undergo concurrent mitral valve surgery and surgical ablation are more than twice as likely to be free of AF a year after surgery than are their counterparts who have mitral valve surgery alone, according to results of a randomized trial.
“About a quarter to a half of our your patients coming for mitral valve surgery also have AF,” Dr. A. Marc Gillinov said at the 2015 Mitral Valve Conclave sponsored by the American Association for Thoracic Surgery. “A great mitral valve repair is your first priority, but you also want to treat the AF.” Currently, cardiac surgeons perform concurrent mitral valve surgery and surgical ablation about 60% of the time in patients eligible for both procedures, he said.

The American College of Cardiology/American Health Association Guidelines state that surgical ablation in patients with AF having cardiac surgery for other indications is “reasonable” – “not very strong language,” he noted, and the level of evidence for concurrent procedures is C.
That led the Cardiothoracic Surgical Trials Network to pursue the clinical trial. The investigators randomized 260 patients with persistent or long-standing persistent atrial fibrillation who needed mitral valve surgery to also undergo either surgical ablation (133) or no ablation (127). The primary endpoint was freedom from AF at both 6 months and 12 months as assessed by 3-day Holter monitoring.
Almost two-thirds (63%) of patients in the ablation group were free from atrial fibrillation at both 6 and 12 months, compared with 29% of those who had mitral valve surgery only, a highly significant difference. Dr. Gillinov described the trial population as “tougher patients” with persistent AF whose average age was around 70 years, and most had organic mitral valve regurgitation.
Results were similar whether the patients underwent pulmonary vein isolation or biatrial maze procedure (61% and 66%, respectively). One-year mortality was 6.8% in the ablation group and 8.7% in the control group, reported Dr. Gillinov, who is surgical director of the Center for Atrial Fibrillation at Cleveland Clinic.
The trial found no significant differences between the ablation and nonablation groups in major cardiac or cerebrovascular adverse events, overall serious adverse events, or hospital readmissions. The results were published prior to the Dr. Gillinov’s presentation (N. Engl. J. Med. 2015;372:1399-409).
These results debunk findings from a survey a few years ago that found cardiac surgeons avoided doing surgical ablation during mitral valve surgery because it makes the operation too complex, requires longer pump times, and raises the risk of surgery, said Dr. Gillinov. “Does ablation improve rhythm control? Yes. Does ablation increase risk? No. Does ablation improve clinical outcomes? It probably does,” he said.
The trial had some limitations, Dr. Gillinov said. Its endpoint was not a clinical outcome, although looking at stroke risk or mortality would have required thousands of patients. Also, 20% of patients did not have follow-up with the 3-day Holter test. However, previous studies have shown a strong association between surgical ablation and a reduced risk of stroke. When Dr. Jolanda Kluin of Utrecht (the Netherlands) University asked if a patient would be better off with AF or a pacemaker, Dr. Gillinov replied, “I think it’s better to have an AV sequential rhythm, but the truth is no one can answer that question without clinical data.”
The bottom line is, “if you have a patient who’s having mitral valve surgery who also has AF, do an ablation,” he said.
The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
NEW YORK – Patients with both mitral valve regurgitation and atrial fibrillation who undergo concurrent mitral valve surgery and surgical ablation are more than twice as likely to be free of AF a year after surgery than are their counterparts who have mitral valve surgery alone, according to results of a randomized trial.
“About a quarter to a half of our your patients coming for mitral valve surgery also have AF,” Dr. A. Marc Gillinov said at the 2015 Mitral Valve Conclave sponsored by the American Association for Thoracic Surgery. “A great mitral valve repair is your first priority, but you also want to treat the AF.” Currently, cardiac surgeons perform concurrent mitral valve surgery and surgical ablation about 60% of the time in patients eligible for both procedures, he said.
The American College of Cardiology/American Health Association Guidelines state that surgical ablation in patients with AF having cardiac surgery for other indications is “reasonable” – “not very strong language,” he noted, and the level of evidence for concurrent procedures is C.
That led the Cardiothoracic Surgical Trials Network to pursue the clinical trial. The investigators randomized 260 patients with persistent or long-standing persistent atrial fibrillation who needed mitral valve surgery to also undergo either surgical ablation (133) or no ablation (127). The primary endpoint was freedom from AF at both 6 months and 12 months as assessed by 3-day Holter monitoring.
Almost two-thirds (63%) of patients in the ablation group were free from atrial fibrillation at both 6 and 12 months, compared with 29% of those who had mitral valve surgery only, a highly significant difference. Dr. Gillinov described the trial population as “tougher patients” with persistent AF whose average age was around 70 years, and most had organic mitral valve regurgitation.
Results were similar whether the patients underwent pulmonary vein isolation or biatrial maze procedure (61% and 66%, respectively). One-year mortality was 6.8% in the ablation group and 8.7% in the control group, reported Dr. Gillinov, who is surgical director of the Center for Atrial Fibrillation at Cleveland Clinic.
The trial found no significant differences between the ablation and nonablation groups in major cardiac or cerebrovascular adverse events, overall serious adverse events, or hospital readmissions. The results were published prior to the Dr. Gillinov’s presentation (N. Engl. J. Med. 2015;372:1399-409).
These results debunk findings from a survey a few years ago that found cardiac surgeons avoided doing surgical ablation during mitral valve surgery because it makes the operation too complex, requires longer pump times, and raises the risk of surgery, said Dr. Gillinov. “Does ablation improve rhythm control? Yes. Does ablation increase risk? No. Does ablation improve clinical outcomes? It probably does,” he said.
The trial had some limitations, Dr. Gillinov said. Its endpoint was not a clinical outcome, although looking at stroke risk or mortality would have required thousands of patients. Also, 20% of patients did not have follow-up with the 3-day Holter test. However, previous studies have shown a strong association between surgical ablation and a reduced risk of stroke. When Dr. Jolanda Kluin of Utrecht (the Netherlands) University asked if a patient would be better off with AF or a pacemaker, Dr. Gillinov replied, “I think it’s better to have an AV sequential rhythm, but the truth is no one can answer that question without clinical data.”
The bottom line is, “if you have a patient who’s having mitral valve surgery who also has AF, do an ablation,” he said.
The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
NEW YORK – Patients with both mitral valve regurgitation and atrial fibrillation who undergo concurrent mitral valve surgery and surgical ablation are more than twice as likely to be free of AF a year after surgery than are their counterparts who have mitral valve surgery alone, according to results of a randomized trial.
“About a quarter to a half of our your patients coming for mitral valve surgery also have AF,” Dr. A. Marc Gillinov said at the 2015 Mitral Valve Conclave sponsored by the American Association for Thoracic Surgery. “A great mitral valve repair is your first priority, but you also want to treat the AF.” Currently, cardiac surgeons perform concurrent mitral valve surgery and surgical ablation about 60% of the time in patients eligible for both procedures, he said.
The American College of Cardiology/American Health Association Guidelines state that surgical ablation in patients with AF having cardiac surgery for other indications is “reasonable” – “not very strong language,” he noted, and the level of evidence for concurrent procedures is C.
That led the Cardiothoracic Surgical Trials Network to pursue the clinical trial. The investigators randomized 260 patients with persistent or long-standing persistent atrial fibrillation who needed mitral valve surgery to also undergo either surgical ablation (133) or no ablation (127). The primary endpoint was freedom from AF at both 6 months and 12 months as assessed by 3-day Holter monitoring.
Almost two-thirds (63%) of patients in the ablation group were free from atrial fibrillation at both 6 and 12 months, compared with 29% of those who had mitral valve surgery only, a highly significant difference. Dr. Gillinov described the trial population as “tougher patients” with persistent AF whose average age was around 70 years, and most had organic mitral valve regurgitation.
Results were similar whether the patients underwent pulmonary vein isolation or biatrial maze procedure (61% and 66%, respectively). One-year mortality was 6.8% in the ablation group and 8.7% in the control group, reported Dr. Gillinov, who is surgical director of the Center for Atrial Fibrillation at Cleveland Clinic.
The trial found no significant differences between the ablation and nonablation groups in major cardiac or cerebrovascular adverse events, overall serious adverse events, or hospital readmissions. The results were published prior to the Dr. Gillinov’s presentation (N. Engl. J. Med. 2015;372:1399-409).
These results debunk findings from a survey a few years ago that found cardiac surgeons avoided doing surgical ablation during mitral valve surgery because it makes the operation too complex, requires longer pump times, and raises the risk of surgery, said Dr. Gillinov. “Does ablation improve rhythm control? Yes. Does ablation increase risk? No. Does ablation improve clinical outcomes? It probably does,” he said.
The trial had some limitations, Dr. Gillinov said. Its endpoint was not a clinical outcome, although looking at stroke risk or mortality would have required thousands of patients. Also, 20% of patients did not have follow-up with the 3-day Holter test. However, previous studies have shown a strong association between surgical ablation and a reduced risk of stroke. When Dr. Jolanda Kluin of Utrecht (the Netherlands) University asked if a patient would be better off with AF or a pacemaker, Dr. Gillinov replied, “I think it’s better to have an AV sequential rhythm, but the truth is no one can answer that question without clinical data.”
The bottom line is, “if you have a patient who’s having mitral valve surgery who also has AF, do an ablation,” he said.
The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
AT THE 2015 MITRAL VALVE CONCLAVE
Key clinical point: Patients with atrial fibrillation who have mitral valve surgery would benefit from surgical ablation at the same time.
Major finding: People with AF who had surgical ablation along with mitral valve surgery were more than twice as likely to be free of AF afterwards than were those who had mitral valve surgery only (63.2% vs. 29.4%).
Data source: A clinical trial in 260 patients with AF undergoing mitral valve surgery that randomized 127 to mitral valve surgery alone and 133 to mitral valve surgery with surgical ablation.
Disclosures: The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
ProPublica releases surgeon complication rates based on Medicare data
The investigative journalism website ProPublica has released a “Surgeon Scorecard” to help patients research surgeons’ complication rates for elective operations, the organization announced July 13.
Based on an analysis of Medicare data, the database contains death and complication rates for about 17,000 surgeons performing one of eight elective procedures, including knee and hip replacement, lumbar spinal fusion, and prostate removal, among others. ProPublica used 5 years of Medicare data to compare surgeon performance, adjusting for factors such as patients’ age, health, and hospital quality.
Eleven percent of doctors accounted for about 25% of the complications, and hundreds of surgeons had rates double or even triple the national average, the report found. About 756 doctors who performed 50 or more operations in the time period did not record any complications, and about 1,423 surgeons had only one complication.
The results suggest that although rates were relatively low overall, ranging from 2% to 4%, “the typical surgeon’s rate can and should be significantly lower,” the authors said.
“Recent studies estimate that at least 200,000 patients a year die in hospitals from preventable errors and complications related to their care, which would make patient harm the nation’s third-leading cause of death.”
The analysis also shows that while choosing a “good” hospital is important, “it is much more important to pick the right surgeon” for an elective surgery, the report said.
View the Surgeon Scorecard and the related ProPublica story here.
The investigative journalism website ProPublica has released a “Surgeon Scorecard” to help patients research surgeons’ complication rates for elective operations, the organization announced July 13.
Based on an analysis of Medicare data, the database contains death and complication rates for about 17,000 surgeons performing one of eight elective procedures, including knee and hip replacement, lumbar spinal fusion, and prostate removal, among others. ProPublica used 5 years of Medicare data to compare surgeon performance, adjusting for factors such as patients’ age, health, and hospital quality.
Eleven percent of doctors accounted for about 25% of the complications, and hundreds of surgeons had rates double or even triple the national average, the report found. About 756 doctors who performed 50 or more operations in the time period did not record any complications, and about 1,423 surgeons had only one complication.
The results suggest that although rates were relatively low overall, ranging from 2% to 4%, “the typical surgeon’s rate can and should be significantly lower,” the authors said.
“Recent studies estimate that at least 200,000 patients a year die in hospitals from preventable errors and complications related to their care, which would make patient harm the nation’s third-leading cause of death.”
The analysis also shows that while choosing a “good” hospital is important, “it is much more important to pick the right surgeon” for an elective surgery, the report said.
View the Surgeon Scorecard and the related ProPublica story here.
The investigative journalism website ProPublica has released a “Surgeon Scorecard” to help patients research surgeons’ complication rates for elective operations, the organization announced July 13.
Based on an analysis of Medicare data, the database contains death and complication rates for about 17,000 surgeons performing one of eight elective procedures, including knee and hip replacement, lumbar spinal fusion, and prostate removal, among others. ProPublica used 5 years of Medicare data to compare surgeon performance, adjusting for factors such as patients’ age, health, and hospital quality.
Eleven percent of doctors accounted for about 25% of the complications, and hundreds of surgeons had rates double or even triple the national average, the report found. About 756 doctors who performed 50 or more operations in the time period did not record any complications, and about 1,423 surgeons had only one complication.
The results suggest that although rates were relatively low overall, ranging from 2% to 4%, “the typical surgeon’s rate can and should be significantly lower,” the authors said.
“Recent studies estimate that at least 200,000 patients a year die in hospitals from preventable errors and complications related to their care, which would make patient harm the nation’s third-leading cause of death.”
The analysis also shows that while choosing a “good” hospital is important, “it is much more important to pick the right surgeon” for an elective surgery, the report said.
View the Surgeon Scorecard and the related ProPublica story here.
Good news, bad news in the Medicare trustees report
As Medicare approaches its 50th anniversary next week, the federal program got some welcome financial news Wednesday: Its giant hospital trust fund will be solvent until 2030, and its long-term outlook has improved, according to a report from the program’s trustees.
But the report warned that several million Medicare beneficiaries could see their Medicare Part B monthly premiums skyrocket by 52% in January – from $104.90 to $159.30. Medicare Part B, which is paid for by a combination of federal funds and beneficiary premiums, generally covers physician and outpatient costs.

The huge rate hike is predicted because of a confluence of two factors: Medicare Part B costs increased more than expected last year, and Social Security is not expected to have a cost of living increase next year. By law, the cost of higher Medicare Part B premiums can’t be passed on to most Medicare beneficiaries when they don’t get a Social Security raise. As a result, the higher Medicare costs have to be covered by just 30% of Medicare beneficiaries. This includes the 2.8 million Medicare enrollees new to the program next year, 3.1 million Medicare beneficiaries with incomes higher than $85,000 a year, and 1.6 million Medicare beneficiaries who pay their premium directly instead of having it deducted from Social Security. An additional 9 million people affected by the higher rates are so called “dual eligibles” – those on Medicare and Medicaid. States pay the Medicare Part B premium for duals.
Medicare Part B premiums are set largely by a complicated formula written into law. The trustees’ predictions on premiums are typically close to the final rates that are announced each fall by the U.S. Department of Health & Human Services.
HHS Secretary Sylvia M. Burwell said she will examine her options and make a final decision on rates in October. “Seventy percent of enrollees in Part B will have no change in premiums,” she said at a briefing with other program trustees.
A senior government official, speaking only on background at a Treasury Department briefing on the report, said the projected premium increase in Part B is “atypical” and noted that outpatient health services were among those services that saw higher than expected costs last year. Another senior government official said Ms. Burwell has several “policy options” to lessen the premium increases but would not say what they are.
If the Social Security program determines in the next 2 months that a cost of living increase is needed for next year, that could diminish the premium hikes because they could be spread over millions more beneficiaries. But currently that is not expected.
Medicare advocacy groups expressed concern about the projected rate increase. Judith Stein, executive director of the Center for Medicare Advocacy, said she is concerned the predicted Medicare Part B premium hike signals that, for many, the program is becoming too expensive. She said the higher premiums will force more seniors to join Medicare Advantage, which offers lower costs but also restricts which providers they can use.
“I am concerned that people will start to rail against Medicare rather than love it, as they have for 50 years,” Ms. Stein said.
“We are pleased to see that 70% of people with Medicare are expected to have a stable Part B premium, and it is concerning to us that 30% could see an increase,” said Stacy Sanders, federal policy director at the Medicare Rights Center. “When the final premium amounts are released, we are committed to educating people about their Part B premium, and most importantly, about the potential availability of [programs] that can help with the cost of the Part B premium.”
The possible huge Medicare Part B premium increase overshadowed a generally positive report about the financial health of the Medicare Part A, which covers hospital costs.
The trustees report noted that the financial health of the program is being helped by factors such as an improved economy, while other factors such as more seniors in private Medicare Advantage are increasing costs. The government pays higher costs for those in Medicare Advantage, which is managed care.
While 2030 remained unchanged as the year that the program’s funds would be exhausted, the report said the program’s long-term outlook was improved. That improvement was largely due to assumptions that health costs will grow at a slower rate after 2050.
In 2014, Medicare provided health insurance coverage to 53.8 million people at a cost of $613 billion – roughly the GDP of Argentina. The average value of the Medicare benefit per enrollee was $12,432, about 2% higher than last year.
Medicare turns 50 on July 30 – eligible for its own AARP card – but it is increasingly feeling the strains of retiring baby boomers.
Medicare is adding 10,000 new beneficiaries a day as baby boomers reach age 65. The Obama administration is in the midst of overhauling the way Medicare pays doctors and hospitals to emphasize quality results over the sheer volume of procedures, tests and services. The HHS has set a goal of tying 30% of payments under traditional Medicare to new models of care by the end of 2016 and an increasing share thereafter.
The trustees report also cautioned that the Social Security Disability Insurance program, which covers 11 million people, is projected to become insolvent in the fourth quarter of 2016, unchanged from last year. President Barack Obama has proposed shifting funding from another Social Security trust fund to address the imbalance.
The projected trust fund insolvency doesn’t mean that Medicare is “running out of money.” Even in 2030, when the hospital trust fund is projected for exhaustion, incoming payroll taxes and other revenues will cover 86% of program costs.
The Medicare trustees are Ms. Burwell, Treasury Secretary and Managing Trustee Jacob Lew, Labor Secretary Thomas Perez, and Acting Social Security Commissioner Carolyn Colvin. Two other members are public representatives who are appointed by the president: Charles Blahous III and Robert Reischauer. CMS Acting Administrator Andy Slavitt is designated as secretary of the board.
Kaiser Health News is a nonprofit national health policy news service. KHN’s coverage of aging and long-term care issues is supported in part by a grant from The SCAN Foundation.
As Medicare approaches its 50th anniversary next week, the federal program got some welcome financial news Wednesday: Its giant hospital trust fund will be solvent until 2030, and its long-term outlook has improved, according to a report from the program’s trustees.
But the report warned that several million Medicare beneficiaries could see their Medicare Part B monthly premiums skyrocket by 52% in January – from $104.90 to $159.30. Medicare Part B, which is paid for by a combination of federal funds and beneficiary premiums, generally covers physician and outpatient costs.
The huge rate hike is predicted because of a confluence of two factors: Medicare Part B costs increased more than expected last year, and Social Security is not expected to have a cost of living increase next year. By law, the cost of higher Medicare Part B premiums can’t be passed on to most Medicare beneficiaries when they don’t get a Social Security raise. As a result, the higher Medicare costs have to be covered by just 30% of Medicare beneficiaries. This includes the 2.8 million Medicare enrollees new to the program next year, 3.1 million Medicare beneficiaries with incomes higher than $85,000 a year, and 1.6 million Medicare beneficiaries who pay their premium directly instead of having it deducted from Social Security. An additional 9 million people affected by the higher rates are so called “dual eligibles” – those on Medicare and Medicaid. States pay the Medicare Part B premium for duals.
Medicare Part B premiums are set largely by a complicated formula written into law. The trustees’ predictions on premiums are typically close to the final rates that are announced each fall by the U.S. Department of Health & Human Services.
HHS Secretary Sylvia M. Burwell said she will examine her options and make a final decision on rates in October. “Seventy percent of enrollees in Part B will have no change in premiums,” she said at a briefing with other program trustees.
A senior government official, speaking only on background at a Treasury Department briefing on the report, said the projected premium increase in Part B is “atypical” and noted that outpatient health services were among those services that saw higher than expected costs last year. Another senior government official said Ms. Burwell has several “policy options” to lessen the premium increases but would not say what they are.
If the Social Security program determines in the next 2 months that a cost of living increase is needed for next year, that could diminish the premium hikes because they could be spread over millions more beneficiaries. But currently that is not expected.
Medicare advocacy groups expressed concern about the projected rate increase. Judith Stein, executive director of the Center for Medicare Advocacy, said she is concerned the predicted Medicare Part B premium hike signals that, for many, the program is becoming too expensive. She said the higher premiums will force more seniors to join Medicare Advantage, which offers lower costs but also restricts which providers they can use.
“I am concerned that people will start to rail against Medicare rather than love it, as they have for 50 years,” Ms. Stein said.
“We are pleased to see that 70% of people with Medicare are expected to have a stable Part B premium, and it is concerning to us that 30% could see an increase,” said Stacy Sanders, federal policy director at the Medicare Rights Center. “When the final premium amounts are released, we are committed to educating people about their Part B premium, and most importantly, about the potential availability of [programs] that can help with the cost of the Part B premium.”
The possible huge Medicare Part B premium increase overshadowed a generally positive report about the financial health of the Medicare Part A, which covers hospital costs.
The trustees report noted that the financial health of the program is being helped by factors such as an improved economy, while other factors such as more seniors in private Medicare Advantage are increasing costs. The government pays higher costs for those in Medicare Advantage, which is managed care.
While 2030 remained unchanged as the year that the program’s funds would be exhausted, the report said the program’s long-term outlook was improved. That improvement was largely due to assumptions that health costs will grow at a slower rate after 2050.
In 2014, Medicare provided health insurance coverage to 53.8 million people at a cost of $613 billion – roughly the GDP of Argentina. The average value of the Medicare benefit per enrollee was $12,432, about 2% higher than last year.
Medicare turns 50 on July 30 – eligible for its own AARP card – but it is increasingly feeling the strains of retiring baby boomers.
Medicare is adding 10,000 new beneficiaries a day as baby boomers reach age 65. The Obama administration is in the midst of overhauling the way Medicare pays doctors and hospitals to emphasize quality results over the sheer volume of procedures, tests and services. The HHS has set a goal of tying 30% of payments under traditional Medicare to new models of care by the end of 2016 and an increasing share thereafter.
The trustees report also cautioned that the Social Security Disability Insurance program, which covers 11 million people, is projected to become insolvent in the fourth quarter of 2016, unchanged from last year. President Barack Obama has proposed shifting funding from another Social Security trust fund to address the imbalance.
The projected trust fund insolvency doesn’t mean that Medicare is “running out of money.” Even in 2030, when the hospital trust fund is projected for exhaustion, incoming payroll taxes and other revenues will cover 86% of program costs.
The Medicare trustees are Ms. Burwell, Treasury Secretary and Managing Trustee Jacob Lew, Labor Secretary Thomas Perez, and Acting Social Security Commissioner Carolyn Colvin. Two other members are public representatives who are appointed by the president: Charles Blahous III and Robert Reischauer. CMS Acting Administrator Andy Slavitt is designated as secretary of the board.
Kaiser Health News is a nonprofit national health policy news service. KHN’s coverage of aging and long-term care issues is supported in part by a grant from The SCAN Foundation.
As Medicare approaches its 50th anniversary next week, the federal program got some welcome financial news Wednesday: Its giant hospital trust fund will be solvent until 2030, and its long-term outlook has improved, according to a report from the program’s trustees.
But the report warned that several million Medicare beneficiaries could see their Medicare Part B monthly premiums skyrocket by 52% in January – from $104.90 to $159.30. Medicare Part B, which is paid for by a combination of federal funds and beneficiary premiums, generally covers physician and outpatient costs.
The huge rate hike is predicted because of a confluence of two factors: Medicare Part B costs increased more than expected last year, and Social Security is not expected to have a cost of living increase next year. By law, the cost of higher Medicare Part B premiums can’t be passed on to most Medicare beneficiaries when they don’t get a Social Security raise. As a result, the higher Medicare costs have to be covered by just 30% of Medicare beneficiaries. This includes the 2.8 million Medicare enrollees new to the program next year, 3.1 million Medicare beneficiaries with incomes higher than $85,000 a year, and 1.6 million Medicare beneficiaries who pay their premium directly instead of having it deducted from Social Security. An additional 9 million people affected by the higher rates are so called “dual eligibles” – those on Medicare and Medicaid. States pay the Medicare Part B premium for duals.
Medicare Part B premiums are set largely by a complicated formula written into law. The trustees’ predictions on premiums are typically close to the final rates that are announced each fall by the U.S. Department of Health & Human Services.
HHS Secretary Sylvia M. Burwell said she will examine her options and make a final decision on rates in October. “Seventy percent of enrollees in Part B will have no change in premiums,” she said at a briefing with other program trustees.
A senior government official, speaking only on background at a Treasury Department briefing on the report, said the projected premium increase in Part B is “atypical” and noted that outpatient health services were among those services that saw higher than expected costs last year. Another senior government official said Ms. Burwell has several “policy options” to lessen the premium increases but would not say what they are.
If the Social Security program determines in the next 2 months that a cost of living increase is needed for next year, that could diminish the premium hikes because they could be spread over millions more beneficiaries. But currently that is not expected.
Medicare advocacy groups expressed concern about the projected rate increase. Judith Stein, executive director of the Center for Medicare Advocacy, said she is concerned the predicted Medicare Part B premium hike signals that, for many, the program is becoming too expensive. She said the higher premiums will force more seniors to join Medicare Advantage, which offers lower costs but also restricts which providers they can use.
“I am concerned that people will start to rail against Medicare rather than love it, as they have for 50 years,” Ms. Stein said.
“We are pleased to see that 70% of people with Medicare are expected to have a stable Part B premium, and it is concerning to us that 30% could see an increase,” said Stacy Sanders, federal policy director at the Medicare Rights Center. “When the final premium amounts are released, we are committed to educating people about their Part B premium, and most importantly, about the potential availability of [programs] that can help with the cost of the Part B premium.”
The possible huge Medicare Part B premium increase overshadowed a generally positive report about the financial health of the Medicare Part A, which covers hospital costs.
The trustees report noted that the financial health of the program is being helped by factors such as an improved economy, while other factors such as more seniors in private Medicare Advantage are increasing costs. The government pays higher costs for those in Medicare Advantage, which is managed care.
While 2030 remained unchanged as the year that the program’s funds would be exhausted, the report said the program’s long-term outlook was improved. That improvement was largely due to assumptions that health costs will grow at a slower rate after 2050.
In 2014, Medicare provided health insurance coverage to 53.8 million people at a cost of $613 billion – roughly the GDP of Argentina. The average value of the Medicare benefit per enrollee was $12,432, about 2% higher than last year.
Medicare turns 50 on July 30 – eligible for its own AARP card – but it is increasingly feeling the strains of retiring baby boomers.
Medicare is adding 10,000 new beneficiaries a day as baby boomers reach age 65. The Obama administration is in the midst of overhauling the way Medicare pays doctors and hospitals to emphasize quality results over the sheer volume of procedures, tests and services. The HHS has set a goal of tying 30% of payments under traditional Medicare to new models of care by the end of 2016 and an increasing share thereafter.
The trustees report also cautioned that the Social Security Disability Insurance program, which covers 11 million people, is projected to become insolvent in the fourth quarter of 2016, unchanged from last year. President Barack Obama has proposed shifting funding from another Social Security trust fund to address the imbalance.
The projected trust fund insolvency doesn’t mean that Medicare is “running out of money.” Even in 2030, when the hospital trust fund is projected for exhaustion, incoming payroll taxes and other revenues will cover 86% of program costs.
The Medicare trustees are Ms. Burwell, Treasury Secretary and Managing Trustee Jacob Lew, Labor Secretary Thomas Perez, and Acting Social Security Commissioner Carolyn Colvin. Two other members are public representatives who are appointed by the president: Charles Blahous III and Robert Reischauer. CMS Acting Administrator Andy Slavitt is designated as secretary of the board.
Kaiser Health News is a nonprofit national health policy news service. KHN’s coverage of aging and long-term care issues is supported in part by a grant from The SCAN Foundation.

Fighting the myth of the superdoctor
I remember waking up with my left hand swollen, red, in excruciating pain, and difficult to move. For several months prior, I had been exhausted, achy, and stiff. As a relatively new mother attempting to manage the age-old balance of family life with the rigors of fellowship training, I attributed those physical changes to personal and professional circumstances.
Yet, that morning, faced with a new rather troubling symptom, I did what my husband had suggested numerous times before and finally visited a doctor. After an emergency evaluation and referral to a rheumatologist, my diagnosis was clear: I had mixed connective tissue disease.

I became frantic – not because of the pain I was experiencing but because I would miss an important Grand Rounds that all of the fellows were expected to attend. I had struggled to decide if I should see the doctor or deal with it and head to Grand Rounds. In retrospect, the decision should not have been that agonizing. Most people would not have hesitated about making a choice between risking their health or pleasing their superiors. However, I am not most people; I am a doctor, and we do not get sick.
This is the message heard throughout medical school and training. Often, the message is not overt but communicated in a manner that no trainee could question: Take care of yourself, but do not take time off. It is fine to be sick but not so sick that you are unable to work.
For example, many programs have systems in place in which in case of illness or emergency, a trainee can call and another trainee can take her place – no questions asked. Yet, almost as quickly as this policy is described, it is followed with the disclaimer: “No one ever uses it.”
Why does this happen? Trainees are not immune to illness, but the expectation is that work supersedes personal concerns.
Despite receiving much support during my own training, my experience was often tainted by the need to push through. How could I be comfortable assuming the role of patient when at work I would hear my colleagues say things like, “I went to rounds at the hospital while I had pneumonia,” and, “I had conjunctivitis, put a patch on my eye, and went to work,” and, “she worked while getting chemo several times a week.”
For us, it seems that to be sick and to continue working is a badge of honor.
The U.S. health care system is under stress like never before. Newly insured people are coming into the system by the millions amid a shortage of physicians in primary care (Healthcare 2013;1:8-11) and across many specialties, including my own of psychiatry.
Against this backdrop are the expectations for physicians to be superheroes. It seems as if our profession is unlike any other. We are supposed to be healers of others but not ourselves.
After I became sick, I checked the literature in an effort to find support and insight into how medicine supports its own. But I found that discussions about these kinds of issues don’t seem to be available.
It’s time to discuss why support seems to be limited in residency programs, and why physicians feel a need to hide their illnesses for fear of losing employment. Why do the cultural expectations of our profession make us feel like we are less of a physician because of our illnesses?
Medicine needs to change so that we are treated not as flawless perfectionists but as humans who dedicated ourselves to healing and saving lives.
Dr. Thomas is a psychiatrist living in Warwick, R.I.
I remember waking up with my left hand swollen, red, in excruciating pain, and difficult to move. For several months prior, I had been exhausted, achy, and stiff. As a relatively new mother attempting to manage the age-old balance of family life with the rigors of fellowship training, I attributed those physical changes to personal and professional circumstances.
Yet, that morning, faced with a new rather troubling symptom, I did what my husband had suggested numerous times before and finally visited a doctor. After an emergency evaluation and referral to a rheumatologist, my diagnosis was clear: I had mixed connective tissue disease.
I became frantic – not because of the pain I was experiencing but because I would miss an important Grand Rounds that all of the fellows were expected to attend. I had struggled to decide if I should see the doctor or deal with it and head to Grand Rounds. In retrospect, the decision should not have been that agonizing. Most people would not have hesitated about making a choice between risking their health or pleasing their superiors. However, I am not most people; I am a doctor, and we do not get sick.
This is the message heard throughout medical school and training. Often, the message is not overt but communicated in a manner that no trainee could question: Take care of yourself, but do not take time off. It is fine to be sick but not so sick that you are unable to work.
For example, many programs have systems in place in which in case of illness or emergency, a trainee can call and another trainee can take her place – no questions asked. Yet, almost as quickly as this policy is described, it is followed with the disclaimer: “No one ever uses it.”
Why does this happen? Trainees are not immune to illness, but the expectation is that work supersedes personal concerns.
Despite receiving much support during my own training, my experience was often tainted by the need to push through. How could I be comfortable assuming the role of patient when at work I would hear my colleagues say things like, “I went to rounds at the hospital while I had pneumonia,” and, “I had conjunctivitis, put a patch on my eye, and went to work,” and, “she worked while getting chemo several times a week.”
For us, it seems that to be sick and to continue working is a badge of honor.
The U.S. health care system is under stress like never before. Newly insured people are coming into the system by the millions amid a shortage of physicians in primary care (Healthcare 2013;1:8-11) and across many specialties, including my own of psychiatry.
Against this backdrop are the expectations for physicians to be superheroes. It seems as if our profession is unlike any other. We are supposed to be healers of others but not ourselves.
After I became sick, I checked the literature in an effort to find support and insight into how medicine supports its own. But I found that discussions about these kinds of issues don’t seem to be available.
It’s time to discuss why support seems to be limited in residency programs, and why physicians feel a need to hide their illnesses for fear of losing employment. Why do the cultural expectations of our profession make us feel like we are less of a physician because of our illnesses?
Medicine needs to change so that we are treated not as flawless perfectionists but as humans who dedicated ourselves to healing and saving lives.
Dr. Thomas is a psychiatrist living in Warwick, R.I.
I remember waking up with my left hand swollen, red, in excruciating pain, and difficult to move. For several months prior, I had been exhausted, achy, and stiff. As a relatively new mother attempting to manage the age-old balance of family life with the rigors of fellowship training, I attributed those physical changes to personal and professional circumstances.
Yet, that morning, faced with a new rather troubling symptom, I did what my husband had suggested numerous times before and finally visited a doctor. After an emergency evaluation and referral to a rheumatologist, my diagnosis was clear: I had mixed connective tissue disease.
I became frantic – not because of the pain I was experiencing but because I would miss an important Grand Rounds that all of the fellows were expected to attend. I had struggled to decide if I should see the doctor or deal with it and head to Grand Rounds. In retrospect, the decision should not have been that agonizing. Most people would not have hesitated about making a choice between risking their health or pleasing their superiors. However, I am not most people; I am a doctor, and we do not get sick.
This is the message heard throughout medical school and training. Often, the message is not overt but communicated in a manner that no trainee could question: Take care of yourself, but do not take time off. It is fine to be sick but not so sick that you are unable to work.
For example, many programs have systems in place in which in case of illness or emergency, a trainee can call and another trainee can take her place – no questions asked. Yet, almost as quickly as this policy is described, it is followed with the disclaimer: “No one ever uses it.”
Why does this happen? Trainees are not immune to illness, but the expectation is that work supersedes personal concerns.
Despite receiving much support during my own training, my experience was often tainted by the need to push through. How could I be comfortable assuming the role of patient when at work I would hear my colleagues say things like, “I went to rounds at the hospital while I had pneumonia,” and, “I had conjunctivitis, put a patch on my eye, and went to work,” and, “she worked while getting chemo several times a week.”
For us, it seems that to be sick and to continue working is a badge of honor.
The U.S. health care system is under stress like never before. Newly insured people are coming into the system by the millions amid a shortage of physicians in primary care (Healthcare 2013;1:8-11) and across many specialties, including my own of psychiatry.
Against this backdrop are the expectations for physicians to be superheroes. It seems as if our profession is unlike any other. We are supposed to be healers of others but not ourselves.
After I became sick, I checked the literature in an effort to find support and insight into how medicine supports its own. But I found that discussions about these kinds of issues don’t seem to be available.
It’s time to discuss why support seems to be limited in residency programs, and why physicians feel a need to hide their illnesses for fear of losing employment. Why do the cultural expectations of our profession make us feel like we are less of a physician because of our illnesses?
Medicine needs to change so that we are treated not as flawless perfectionists but as humans who dedicated ourselves to healing and saving lives.
Dr. Thomas is a psychiatrist living in Warwick, R.I.

Family medicine most in demand specialty during 2014-2015
For the ninth straight year, family medicine was the most recruited medical specialty, according to a new report from physician job placement firm Merritt Hawkins.
During 2014-2015, there were 734 search assignments performed for doctors in family medicine, nearly one-quarter of the 3,120 total searches conducted during the period from April 1, 2014, to March 31, 2015, according to the company’s 2015 Review of Physician and Advanced Practitioner Recruiting Incentives. No other specialty came close to this number of search requests.
Internal medicine, the other primary care specialty and a nine-year stalwart of the faraway second position, finished the year with 237 recruitments, Merritt Hawkins reported.
Psychiatry was the most recruited non–primary care specialty with 230 searches, falling just short of usurping internal medicine in second place. Other specialty categories with more than 100 recruitments in 2014-2015 were hospital medicine with 176, nurse practitioner with 143, ob.gyn. with 112, and orthopedic surgery with 106.
Demand for primary physicians, NPs, gynecologists, and physicians who work with chronic illness increased from the 2013-2014 period. “Implementation of population health management through integrated systems such as accountable care organizations is likely to keep demand strong for these types of clinicians,” Travis Singleton, senior vice president of Merritt Hawkins, said in a written statement.
Nearly all new employments were done by a hospital or other large employer, and only 5% of recruitment was conducted by private, independent practices, continuing the decline of private practice. Value-based incentives have decreased, with 23% of employers basing the bonus on value, compared with 39% 2 years ago, according to Merritt Hawkins.
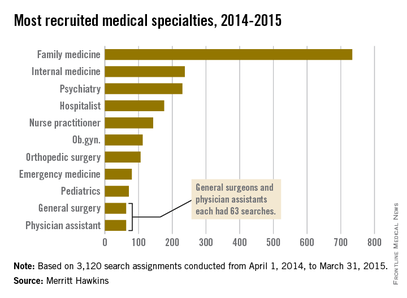
For the ninth straight year, family medicine was the most recruited medical specialty, according to a new report from physician job placement firm Merritt Hawkins.
During 2014-2015, there were 734 search assignments performed for doctors in family medicine, nearly one-quarter of the 3,120 total searches conducted during the period from April 1, 2014, to March 31, 2015, according to the company’s 2015 Review of Physician and Advanced Practitioner Recruiting Incentives. No other specialty came close to this number of search requests.
Internal medicine, the other primary care specialty and a nine-year stalwart of the faraway second position, finished the year with 237 recruitments, Merritt Hawkins reported.
Psychiatry was the most recruited non–primary care specialty with 230 searches, falling just short of usurping internal medicine in second place. Other specialty categories with more than 100 recruitments in 2014-2015 were hospital medicine with 176, nurse practitioner with 143, ob.gyn. with 112, and orthopedic surgery with 106.
Demand for primary physicians, NPs, gynecologists, and physicians who work with chronic illness increased from the 2013-2014 period. “Implementation of population health management through integrated systems such as accountable care organizations is likely to keep demand strong for these types of clinicians,” Travis Singleton, senior vice president of Merritt Hawkins, said in a written statement.
Nearly all new employments were done by a hospital or other large employer, and only 5% of recruitment was conducted by private, independent practices, continuing the decline of private practice. Value-based incentives have decreased, with 23% of employers basing the bonus on value, compared with 39% 2 years ago, according to Merritt Hawkins.
For the ninth straight year, family medicine was the most recruited medical specialty, according to a new report from physician job placement firm Merritt Hawkins.
During 2014-2015, there were 734 search assignments performed for doctors in family medicine, nearly one-quarter of the 3,120 total searches conducted during the period from April 1, 2014, to March 31, 2015, according to the company’s 2015 Review of Physician and Advanced Practitioner Recruiting Incentives. No other specialty came close to this number of search requests.
Internal medicine, the other primary care specialty and a nine-year stalwart of the faraway second position, finished the year with 237 recruitments, Merritt Hawkins reported.
Psychiatry was the most recruited non–primary care specialty with 230 searches, falling just short of usurping internal medicine in second place. Other specialty categories with more than 100 recruitments in 2014-2015 were hospital medicine with 176, nurse practitioner with 143, ob.gyn. with 112, and orthopedic surgery with 106.
Demand for primary physicians, NPs, gynecologists, and physicians who work with chronic illness increased from the 2013-2014 period. “Implementation of population health management through integrated systems such as accountable care organizations is likely to keep demand strong for these types of clinicians,” Travis Singleton, senior vice president of Merritt Hawkins, said in a written statement.
Nearly all new employments were done by a hospital or other large employer, and only 5% of recruitment was conducted by private, independent practices, continuing the decline of private practice. Value-based incentives have decreased, with 23% of employers basing the bonus on value, compared with 39% 2 years ago, according to Merritt Hawkins.
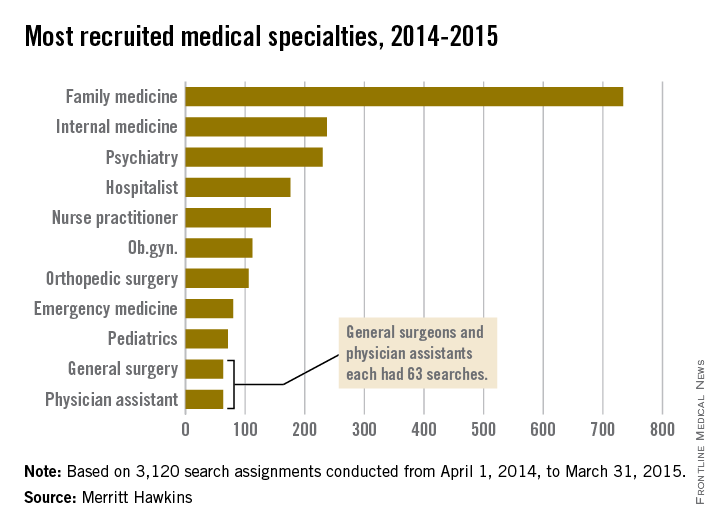
VIDEO: Postoperative cognitive decline hits women hardest
WASHINGTON – Postoperative cognitive decline, which occurs in roughly 20% of elderly patients who undergo major surgery, strikes older women with greater severity than it does similarly aged men, according to a retrospective analysis of data collected from 527 older Americans.
“We looked at the sex difference in postoperative cognitive decline and Alzheimer’s disease because of the sex difference in Alzheimer’s disease, where about two-thirds of patients are women,” Dr. Katie J. Schenning said in an interview during the Alzheimer’s Association International Conference 2015. “We know that a lot of the pathologic changes that happen to the brain after anesthesia and surgery are similar to the changes that happen in Alzheimer’s disease patients. But at this point that is all we can say about a link between the two. It is currently unknown whether there is a clear relationship between postoperative cognitive decline and Alzheimer’s disease,” said Dr. Schenning, an anesthesiologist at Oregon Health & Science University in Portland.
She and her associates studied data collected longitudinally from two cohorts, the Oregon Brain Aging Study and the Intelligent Systems for Assessment of Aging Changes. At baseline, the average age of the enrollees in the combined group was 83 years, and just under two-thirds were women. During follow-up, 182 of the participants underwent a total of 331 major surgeries, with some undergoing more than one surgery. The most common form of surgery was orthopedic, done in one-third of the patients, followed by general surgery, in a quarter.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The researchers running both studies collected data annually from participants using a battery of neuropsychological evaluations, brain MRIs, and information on their general health. Retrospective analysis of the data showed that following surgery, people showed evidence of statistically significant and clinically meaningful declines in several measures, compared with those who did not undergo surgery, including deficits measured by the Mini-Mental State Examination, instrumental activities of daily living, and logical memory delayed recall. The trajectory of these declines was significantly steeper in women following surgery, compared with men following surgery, Dr. Schenning reported in a poster at the meeting. In addition, the MRI scans showed ventricular enlargement in the postsurgical women but not in men, a change that is characteristic of neuropathology.
“Women who underwent surgery had a more rapid rate of decline in measures of cognition and function than women who did not have surgery, and it affected women in more categories than in men,” Dr. Schenning said.
The risk for postoperative cognitive decline “is one of the things that patients should take into consideration before undergoing elective surgery, especially if they are older or have pre-existing cognitive impairment,” Dr. Schenning suggested. The enhanced risk for postsurgical cognitive decline faced by older women and even the somewhat lesser risk that exists for older men “is certainly something that patients should discuss with their surgeon, anesthesiologist, and family members,” she said.
Dr. Schenning had no disclosures.
On Twitter @mitchelzoler
WASHINGTON – Postoperative cognitive decline, which occurs in roughly 20% of elderly patients who undergo major surgery, strikes older women with greater severity than it does similarly aged men, according to a retrospective analysis of data collected from 527 older Americans.
“We looked at the sex difference in postoperative cognitive decline and Alzheimer’s disease because of the sex difference in Alzheimer’s disease, where about two-thirds of patients are women,” Dr. Katie J. Schenning said in an interview during the Alzheimer’s Association International Conference 2015. “We know that a lot of the pathologic changes that happen to the brain after anesthesia and surgery are similar to the changes that happen in Alzheimer’s disease patients. But at this point that is all we can say about a link between the two. It is currently unknown whether there is a clear relationship between postoperative cognitive decline and Alzheimer’s disease,” said Dr. Schenning, an anesthesiologist at Oregon Health & Science University in Portland.
She and her associates studied data collected longitudinally from two cohorts, the Oregon Brain Aging Study and the Intelligent Systems for Assessment of Aging Changes. At baseline, the average age of the enrollees in the combined group was 83 years, and just under two-thirds were women. During follow-up, 182 of the participants underwent a total of 331 major surgeries, with some undergoing more than one surgery. The most common form of surgery was orthopedic, done in one-third of the patients, followed by general surgery, in a quarter.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The researchers running both studies collected data annually from participants using a battery of neuropsychological evaluations, brain MRIs, and information on their general health. Retrospective analysis of the data showed that following surgery, people showed evidence of statistically significant and clinically meaningful declines in several measures, compared with those who did not undergo surgery, including deficits measured by the Mini-Mental State Examination, instrumental activities of daily living, and logical memory delayed recall. The trajectory of these declines was significantly steeper in women following surgery, compared with men following surgery, Dr. Schenning reported in a poster at the meeting. In addition, the MRI scans showed ventricular enlargement in the postsurgical women but not in men, a change that is characteristic of neuropathology.
“Women who underwent surgery had a more rapid rate of decline in measures of cognition and function than women who did not have surgery, and it affected women in more categories than in men,” Dr. Schenning said.
The risk for postoperative cognitive decline “is one of the things that patients should take into consideration before undergoing elective surgery, especially if they are older or have pre-existing cognitive impairment,” Dr. Schenning suggested. The enhanced risk for postsurgical cognitive decline faced by older women and even the somewhat lesser risk that exists for older men “is certainly something that patients should discuss with their surgeon, anesthesiologist, and family members,” she said.
Dr. Schenning had no disclosures.
On Twitter @mitchelzoler
WASHINGTON – Postoperative cognitive decline, which occurs in roughly 20% of elderly patients who undergo major surgery, strikes older women with greater severity than it does similarly aged men, according to a retrospective analysis of data collected from 527 older Americans.
“We looked at the sex difference in postoperative cognitive decline and Alzheimer’s disease because of the sex difference in Alzheimer’s disease, where about two-thirds of patients are women,” Dr. Katie J. Schenning said in an interview during the Alzheimer’s Association International Conference 2015. “We know that a lot of the pathologic changes that happen to the brain after anesthesia and surgery are similar to the changes that happen in Alzheimer’s disease patients. But at this point that is all we can say about a link between the two. It is currently unknown whether there is a clear relationship between postoperative cognitive decline and Alzheimer’s disease,” said Dr. Schenning, an anesthesiologist at Oregon Health & Science University in Portland.
She and her associates studied data collected longitudinally from two cohorts, the Oregon Brain Aging Study and the Intelligent Systems for Assessment of Aging Changes. At baseline, the average age of the enrollees in the combined group was 83 years, and just under two-thirds were women. During follow-up, 182 of the participants underwent a total of 331 major surgeries, with some undergoing more than one surgery. The most common form of surgery was orthopedic, done in one-third of the patients, followed by general surgery, in a quarter.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The researchers running both studies collected data annually from participants using a battery of neuropsychological evaluations, brain MRIs, and information on their general health. Retrospective analysis of the data showed that following surgery, people showed evidence of statistically significant and clinically meaningful declines in several measures, compared with those who did not undergo surgery, including deficits measured by the Mini-Mental State Examination, instrumental activities of daily living, and logical memory delayed recall. The trajectory of these declines was significantly steeper in women following surgery, compared with men following surgery, Dr. Schenning reported in a poster at the meeting. In addition, the MRI scans showed ventricular enlargement in the postsurgical women but not in men, a change that is characteristic of neuropathology.
“Women who underwent surgery had a more rapid rate of decline in measures of cognition and function than women who did not have surgery, and it affected women in more categories than in men,” Dr. Schenning said.
The risk for postoperative cognitive decline “is one of the things that patients should take into consideration before undergoing elective surgery, especially if they are older or have pre-existing cognitive impairment,” Dr. Schenning suggested. The enhanced risk for postsurgical cognitive decline faced by older women and even the somewhat lesser risk that exists for older men “is certainly something that patients should discuss with their surgeon, anesthesiologist, and family members,” she said.
Dr. Schenning had no disclosures.
On Twitter @mitchelzoler
AT AAIC 2015

Pain, quality of life measures improve more in OA than RA after knee arthroplasty
Total knee arthroplasty provides osteoarthritis patients with greater improvement in pain and health-related quality of life than it does for rheumatoid arthritis patients, possibly relating to the lower pain and younger age of RA patients at the time of surgery, according to a study based on patients’ responses to semiannual questionnaires.
The study included 834 patients diagnosed with RA and 315 patients diagnosed with osteoarthritis (OA), who had a primary total knee arthroplasty (TKA) between Jan. 1, 1999, and June 30, 2012. The patients were probed on their demographic characteristics, disease duration, mental health, functional status, health-related quality of life (HRQoL), pain, and usage of pain medication. All study participants participated in at least three consecutive sampling intervals: a 6-month preoperative period, a 6-month immediate postoperative period, and a subsequent 6-month “recovery” period. Of the patients who underwent a TKA, 144 (11%) did not complete all three sampling intervals.

At baseline, compared with OA patients, RA patients had significantly less severe scores for measures of pain, lesser usage of pain medications, and significantly more severe scores for measures of disease activity.
After recovering from a TKA, the RA and OA patients improved in almost all outcome measures of pain, function, and HRQoL. The surgery had a larger beneficial effect in OA patients than in RA patients for all measures of pain and HRQoL indices, except for the RA disease activity index (RADAI)/total joint count. In contrast to the OA patients, RA patients showed greater improvements in joint involvement.
For both groups, all outcome measures of pain and function worsened a year before TKA and improved immediately after the surgery; however, the improvement leveled off in the 6-12 months after the procedure.
“After adjusting for preoperative variables, post TKA, a diagnosis of RA (vs. OA) (P = .03), income (P < .01), and anxiety (P = .03) were most useful in predicting the reduction in [visual analog scale] pain scores,” noted Dr. Anand Dusad of the Veterans Affairs Nebraska–Western Iowa Health Care System, Omaha, and his colleagues.
“In summary, using a large cohort of arthritis patients, we have shown that TKA is performed in patients with severe disease and leads to marked improvements in pain function and HRQoL,” according to the researchers.
Read the full study published online July 20 in Arthritis & Rheumatology (doi:10.1002/art.39221).
Total knee arthroplasty provides osteoarthritis patients with greater improvement in pain and health-related quality of life than it does for rheumatoid arthritis patients, possibly relating to the lower pain and younger age of RA patients at the time of surgery, according to a study based on patients’ responses to semiannual questionnaires.
The study included 834 patients diagnosed with RA and 315 patients diagnosed with osteoarthritis (OA), who had a primary total knee arthroplasty (TKA) between Jan. 1, 1999, and June 30, 2012. The patients were probed on their demographic characteristics, disease duration, mental health, functional status, health-related quality of life (HRQoL), pain, and usage of pain medication. All study participants participated in at least three consecutive sampling intervals: a 6-month preoperative period, a 6-month immediate postoperative period, and a subsequent 6-month “recovery” period. Of the patients who underwent a TKA, 144 (11%) did not complete all three sampling intervals.
At baseline, compared with OA patients, RA patients had significantly less severe scores for measures of pain, lesser usage of pain medications, and significantly more severe scores for measures of disease activity.
After recovering from a TKA, the RA and OA patients improved in almost all outcome measures of pain, function, and HRQoL. The surgery had a larger beneficial effect in OA patients than in RA patients for all measures of pain and HRQoL indices, except for the RA disease activity index (RADAI)/total joint count. In contrast to the OA patients, RA patients showed greater improvements in joint involvement.
For both groups, all outcome measures of pain and function worsened a year before TKA and improved immediately after the surgery; however, the improvement leveled off in the 6-12 months after the procedure.
“After adjusting for preoperative variables, post TKA, a diagnosis of RA (vs. OA) (P = .03), income (P < .01), and anxiety (P = .03) were most useful in predicting the reduction in [visual analog scale] pain scores,” noted Dr. Anand Dusad of the Veterans Affairs Nebraska–Western Iowa Health Care System, Omaha, and his colleagues.
“In summary, using a large cohort of arthritis patients, we have shown that TKA is performed in patients with severe disease and leads to marked improvements in pain function and HRQoL,” according to the researchers.
Read the full study published online July 20 in Arthritis & Rheumatology (doi:10.1002/art.39221).
Total knee arthroplasty provides osteoarthritis patients with greater improvement in pain and health-related quality of life than it does for rheumatoid arthritis patients, possibly relating to the lower pain and younger age of RA patients at the time of surgery, according to a study based on patients’ responses to semiannual questionnaires.
The study included 834 patients diagnosed with RA and 315 patients diagnosed with osteoarthritis (OA), who had a primary total knee arthroplasty (TKA) between Jan. 1, 1999, and June 30, 2012. The patients were probed on their demographic characteristics, disease duration, mental health, functional status, health-related quality of life (HRQoL), pain, and usage of pain medication. All study participants participated in at least three consecutive sampling intervals: a 6-month preoperative period, a 6-month immediate postoperative period, and a subsequent 6-month “recovery” period. Of the patients who underwent a TKA, 144 (11%) did not complete all three sampling intervals.
At baseline, compared with OA patients, RA patients had significantly less severe scores for measures of pain, lesser usage of pain medications, and significantly more severe scores for measures of disease activity.
After recovering from a TKA, the RA and OA patients improved in almost all outcome measures of pain, function, and HRQoL. The surgery had a larger beneficial effect in OA patients than in RA patients for all measures of pain and HRQoL indices, except for the RA disease activity index (RADAI)/total joint count. In contrast to the OA patients, RA patients showed greater improvements in joint involvement.
For both groups, all outcome measures of pain and function worsened a year before TKA and improved immediately after the surgery; however, the improvement leveled off in the 6-12 months after the procedure.
“After adjusting for preoperative variables, post TKA, a diagnosis of RA (vs. OA) (P = .03), income (P < .01), and anxiety (P = .03) were most useful in predicting the reduction in [visual analog scale] pain scores,” noted Dr. Anand Dusad of the Veterans Affairs Nebraska–Western Iowa Health Care System, Omaha, and his colleagues.
“In summary, using a large cohort of arthritis patients, we have shown that TKA is performed in patients with severe disease and leads to marked improvements in pain function and HRQoL,” according to the researchers.
Read the full study published online July 20 in Arthritis & Rheumatology (doi:10.1002/art.39221).
FROM ARTHRITIS & RHEUMATOLOGY
