User login
Monthly transfusions may prevent stroke recurrence in SCD

Credit: St Jude Children’s
Research Hospital
Monthly blood transfusions can reduce the risk of silent or overt stroke among children with sickle cell disease (SCD) who previously had a silent stroke, according to a study published in The New England Journal of Medicine.
Children with evidence of silent cerebral infarcts who received monthly blood transfusions for 3 years had a 58% lower risk of suffering repeat silent or overt
strokes than children who did not receive transfusions.
In fact, researchers said the actual benefit of transfusion therapy may be even higher, as 15% of the children who were assigned to receive transfusions either did not receive them or only received them for a brief period.
“The results of our study show that blood transfusions can play a critical role in preventing this insidious and potentially devastating condition,” said study author James F. Casella, MD, of the Johns Hopkins Children’s Center in Baltimore, Maryland.
“They also highlight the importance of intervening early to preclude ongoing or further brain injury among these youngsters. Most importantly, our findings suggest a much-needed treatment option for clinicians and families of children with sickle cell disease who have had silent strokes.”
Previous studies have suggested that blood transfusions may help prevent stroke in patients with SCD by increasing the number of normal red blood cells and decreasing the likelihood of blocked blood vessels.
But Dr Casella and his colleagues wanted to determine if monthly blood transfusions would help prevent stroke in children with SCD who had evidence of a previous silent cerebral infarct, as well as whether the benefits of transfusion outweigh the risks.
The researchers analyzed 196 children, ages 5 to 15 years, who were diagnosed with SCD and had infarct-like lesions on their MRI scans. The children were randomized to an observation arm or to receive blood transfusions every month for 3 years.
Six percent (6/99) of children who received regular transfusions suffered another silent or overt stroke. One of the patients had a stroke, and 5 had new or enlarged silent cerebral infarcts.
In comparison, 14% (14/97) of children in the observation arm experienced a silent or overt stroke. Seven had a stroke, and 7 had new or enlarged silent cerebral infarcts.
So children who did not receive transfusions were more than twice as likely as their peers to have repeat strokes.
Children who did not receive transfusions were also more likely to suffer a range of other SCD-related problems, such as episodes of extreme pain. There were 295 pain episodes among children who did not receive transfusions and 126 episodes among transfused patients.
An unexpected result, according to the researchers, was that intelligence measures were not different between the 2 treatment arms. Previous studies suggested that silent strokes are associated with a 5-point reduction in IQ. The researchers said they plan to explore this finding further.
Nevertheless, this study provides “clear evidence” that transfusions can decrease the progression of silent strokes in children with SCD, said study author Michael R. DeBaun, MD, of Vanderbilt University in Nashville, Tennessee.
“These results suggest that children who have this disease should be screened early for silent strokes, at least by the time they begin elementary school, to help them manage the disease and to ensure minimal impact on school performance,” he added.
Dr DeBaun and his colleagues said children with SCD should have a surveillance MRI, preferably without sedation, at a young age. Most children with SCD who are at risk for a silent stroke will have one by age 6 years.
The researchers also noted that healthcare providers should discuss treatment options with families to determine if transfusion therapy is appropriate, as there is a risk of transfusion reactions and iron overload.
The decision to transfuse should be made by factoring in each child’s overall health, medical history, and the ability to take time from school for monthly procedures.
The researchers said further study is needed to identify which children with a history of silent strokes are at greatest risk for recurrence so transfusion therapy can be targeted to them.
An editorial related to this study also calls for additional research to determine if the findings can be translated to clinical practice. ![]()
Credit: St Jude Children’s
Research Hospital
Monthly blood transfusions can reduce the risk of silent or overt stroke among children with sickle cell disease (SCD) who previously had a silent stroke, according to a study published in The New England Journal of Medicine.
Children with evidence of silent cerebral infarcts who received monthly blood transfusions for 3 years had a 58% lower risk of suffering repeat silent or overt
strokes than children who did not receive transfusions.
In fact, researchers said the actual benefit of transfusion therapy may be even higher, as 15% of the children who were assigned to receive transfusions either did not receive them or only received them for a brief period.
“The results of our study show that blood transfusions can play a critical role in preventing this insidious and potentially devastating condition,” said study author James F. Casella, MD, of the Johns Hopkins Children’s Center in Baltimore, Maryland.
“They also highlight the importance of intervening early to preclude ongoing or further brain injury among these youngsters. Most importantly, our findings suggest a much-needed treatment option for clinicians and families of children with sickle cell disease who have had silent strokes.”
Previous studies have suggested that blood transfusions may help prevent stroke in patients with SCD by increasing the number of normal red blood cells and decreasing the likelihood of blocked blood vessels.
But Dr Casella and his colleagues wanted to determine if monthly blood transfusions would help prevent stroke in children with SCD who had evidence of a previous silent cerebral infarct, as well as whether the benefits of transfusion outweigh the risks.
The researchers analyzed 196 children, ages 5 to 15 years, who were diagnosed with SCD and had infarct-like lesions on their MRI scans. The children were randomized to an observation arm or to receive blood transfusions every month for 3 years.
Six percent (6/99) of children who received regular transfusions suffered another silent or overt stroke. One of the patients had a stroke, and 5 had new or enlarged silent cerebral infarcts.
In comparison, 14% (14/97) of children in the observation arm experienced a silent or overt stroke. Seven had a stroke, and 7 had new or enlarged silent cerebral infarcts.
So children who did not receive transfusions were more than twice as likely as their peers to have repeat strokes.
Children who did not receive transfusions were also more likely to suffer a range of other SCD-related problems, such as episodes of extreme pain. There were 295 pain episodes among children who did not receive transfusions and 126 episodes among transfused patients.
An unexpected result, according to the researchers, was that intelligence measures were not different between the 2 treatment arms. Previous studies suggested that silent strokes are associated with a 5-point reduction in IQ. The researchers said they plan to explore this finding further.
Nevertheless, this study provides “clear evidence” that transfusions can decrease the progression of silent strokes in children with SCD, said study author Michael R. DeBaun, MD, of Vanderbilt University in Nashville, Tennessee.
“These results suggest that children who have this disease should be screened early for silent strokes, at least by the time they begin elementary school, to help them manage the disease and to ensure minimal impact on school performance,” he added.
Dr DeBaun and his colleagues said children with SCD should have a surveillance MRI, preferably without sedation, at a young age. Most children with SCD who are at risk for a silent stroke will have one by age 6 years.
The researchers also noted that healthcare providers should discuss treatment options with families to determine if transfusion therapy is appropriate, as there is a risk of transfusion reactions and iron overload.
The decision to transfuse should be made by factoring in each child’s overall health, medical history, and the ability to take time from school for monthly procedures.
The researchers said further study is needed to identify which children with a history of silent strokes are at greatest risk for recurrence so transfusion therapy can be targeted to them.
An editorial related to this study also calls for additional research to determine if the findings can be translated to clinical practice. ![]()
Credit: St Jude Children’s
Research Hospital
Monthly blood transfusions can reduce the risk of silent or overt stroke among children with sickle cell disease (SCD) who previously had a silent stroke, according to a study published in The New England Journal of Medicine.
Children with evidence of silent cerebral infarcts who received monthly blood transfusions for 3 years had a 58% lower risk of suffering repeat silent or overt
strokes than children who did not receive transfusions.
In fact, researchers said the actual benefit of transfusion therapy may be even higher, as 15% of the children who were assigned to receive transfusions either did not receive them or only received them for a brief period.
“The results of our study show that blood transfusions can play a critical role in preventing this insidious and potentially devastating condition,” said study author James F. Casella, MD, of the Johns Hopkins Children’s Center in Baltimore, Maryland.
“They also highlight the importance of intervening early to preclude ongoing or further brain injury among these youngsters. Most importantly, our findings suggest a much-needed treatment option for clinicians and families of children with sickle cell disease who have had silent strokes.”
Previous studies have suggested that blood transfusions may help prevent stroke in patients with SCD by increasing the number of normal red blood cells and decreasing the likelihood of blocked blood vessels.
But Dr Casella and his colleagues wanted to determine if monthly blood transfusions would help prevent stroke in children with SCD who had evidence of a previous silent cerebral infarct, as well as whether the benefits of transfusion outweigh the risks.
The researchers analyzed 196 children, ages 5 to 15 years, who were diagnosed with SCD and had infarct-like lesions on their MRI scans. The children were randomized to an observation arm or to receive blood transfusions every month for 3 years.
Six percent (6/99) of children who received regular transfusions suffered another silent or overt stroke. One of the patients had a stroke, and 5 had new or enlarged silent cerebral infarcts.
In comparison, 14% (14/97) of children in the observation arm experienced a silent or overt stroke. Seven had a stroke, and 7 had new or enlarged silent cerebral infarcts.
So children who did not receive transfusions were more than twice as likely as their peers to have repeat strokes.
Children who did not receive transfusions were also more likely to suffer a range of other SCD-related problems, such as episodes of extreme pain. There were 295 pain episodes among children who did not receive transfusions and 126 episodes among transfused patients.
An unexpected result, according to the researchers, was that intelligence measures were not different between the 2 treatment arms. Previous studies suggested that silent strokes are associated with a 5-point reduction in IQ. The researchers said they plan to explore this finding further.
Nevertheless, this study provides “clear evidence” that transfusions can decrease the progression of silent strokes in children with SCD, said study author Michael R. DeBaun, MD, of Vanderbilt University in Nashville, Tennessee.
“These results suggest that children who have this disease should be screened early for silent strokes, at least by the time they begin elementary school, to help them manage the disease and to ensure minimal impact on school performance,” he added.
Dr DeBaun and his colleagues said children with SCD should have a surveillance MRI, preferably without sedation, at a young age. Most children with SCD who are at risk for a silent stroke will have one by age 6 years.
The researchers also noted that healthcare providers should discuss treatment options with families to determine if transfusion therapy is appropriate, as there is a risk of transfusion reactions and iron overload.
The decision to transfuse should be made by factoring in each child’s overall health, medical history, and the ability to take time from school for monthly procedures.
The researchers said further study is needed to identify which children with a history of silent strokes are at greatest risk for recurrence so transfusion therapy can be targeted to them.
An editorial related to this study also calls for additional research to determine if the findings can be translated to clinical practice. ![]()
NICE supports lenalidomide for MDS

The UK’s National Institute for Health and Care Excellence (NICE) has issued a final draft guidance recommending lenalidomide (Revlimid) as an option for treating myelodysplastic syndromes (MDS) characterized by 5q deletion.
Lenalidomide is approved in the European Union to treat transfusion-dependent anemia caused by low- or intermediate-1 risk MDS characterized by 5q deletion when other therapeutic options are insufficient or inadequate.
However, the main treatment option for this patient population in the UK is best supportive care, which involves regular red blood cell transfusions.
In earlier draft guidances, NICE did not support lenalidomide use in MDS patients with 5q deletion. Although data suggested the drug is effective for these patients, a NICE advisory committee was not convinced the drug provided a survival benefit.
But now, the committee has concluded that lenalidomide is a clinically effective treatment for these patients because it is associated with a statistically significant improvement in transfusion independence and health-related quality of life compared with placebo.
Furthermore, the committee said it is plausible that lenalidomide can indirectly improve overall survival by improving transfusion independence.
“The committee heard from clinical experts that lenalidomide is an effective therapy,” said Sir Andrew Dillon, NICE chief executive.
“Celgene–who market lenalidomide–worked with us to provide enough evidence to make it possible for us to recommend it for this group of people. Celgene provided a revised analysis and further information on their proposal for a reduction in the cost of the drug to the NHS [National Health Service].”
This patient access scheme involves the NHS paying for lenalidomide treatment for up to 26 monthly cycles. And Celgene will provide the drug free of charge for those people who receive more than 26 monthly cycles.
Lenalidomide is available in 21-day packs of 10 mg and 5 mg capsules at net prices of £3780 and £3570, respectively. The cost of a 28-day cycle of treatment with 10 mg of lenalidomide (excluding value-added tax) is £3780.
The committee noted that the incremental cost-effectiveness ratio for lenalidomide compared with best supportive care is uncertain because the proportion of people who might need treatment beyond 26 cycles is uncertain.
However, the committee accepted that a commitment from Celgene to publish data on the proportion of people receiving treatment beyond 26 cycles would provide reassurance that lenalidomide is a cost-effective use of NHS resources in MDS patients with 5q deletion.
NICE’s final draft guidance is now with consultees, who have the opportunity to appeal against it. Until NICE issues a final guidance, NHS bodies should make decisions locally on the funding of specific treatments. ![]()
The UK’s National Institute for Health and Care Excellence (NICE) has issued a final draft guidance recommending lenalidomide (Revlimid) as an option for treating myelodysplastic syndromes (MDS) characterized by 5q deletion.
Lenalidomide is approved in the European Union to treat transfusion-dependent anemia caused by low- or intermediate-1 risk MDS characterized by 5q deletion when other therapeutic options are insufficient or inadequate.
However, the main treatment option for this patient population in the UK is best supportive care, which involves regular red blood cell transfusions.
In earlier draft guidances, NICE did not support lenalidomide use in MDS patients with 5q deletion. Although data suggested the drug is effective for these patients, a NICE advisory committee was not convinced the drug provided a survival benefit.
But now, the committee has concluded that lenalidomide is a clinically effective treatment for these patients because it is associated with a statistically significant improvement in transfusion independence and health-related quality of life compared with placebo.
Furthermore, the committee said it is plausible that lenalidomide can indirectly improve overall survival by improving transfusion independence.
“The committee heard from clinical experts that lenalidomide is an effective therapy,” said Sir Andrew Dillon, NICE chief executive.
“Celgene–who market lenalidomide–worked with us to provide enough evidence to make it possible for us to recommend it for this group of people. Celgene provided a revised analysis and further information on their proposal for a reduction in the cost of the drug to the NHS [National Health Service].”
This patient access scheme involves the NHS paying for lenalidomide treatment for up to 26 monthly cycles. And Celgene will provide the drug free of charge for those people who receive more than 26 monthly cycles.
Lenalidomide is available in 21-day packs of 10 mg and 5 mg capsules at net prices of £3780 and £3570, respectively. The cost of a 28-day cycle of treatment with 10 mg of lenalidomide (excluding value-added tax) is £3780.
The committee noted that the incremental cost-effectiveness ratio for lenalidomide compared with best supportive care is uncertain because the proportion of people who might need treatment beyond 26 cycles is uncertain.
However, the committee accepted that a commitment from Celgene to publish data on the proportion of people receiving treatment beyond 26 cycles would provide reassurance that lenalidomide is a cost-effective use of NHS resources in MDS patients with 5q deletion.
NICE’s final draft guidance is now with consultees, who have the opportunity to appeal against it. Until NICE issues a final guidance, NHS bodies should make decisions locally on the funding of specific treatments. ![]()
The UK’s National Institute for Health and Care Excellence (NICE) has issued a final draft guidance recommending lenalidomide (Revlimid) as an option for treating myelodysplastic syndromes (MDS) characterized by 5q deletion.
Lenalidomide is approved in the European Union to treat transfusion-dependent anemia caused by low- or intermediate-1 risk MDS characterized by 5q deletion when other therapeutic options are insufficient or inadequate.
However, the main treatment option for this patient population in the UK is best supportive care, which involves regular red blood cell transfusions.
In earlier draft guidances, NICE did not support lenalidomide use in MDS patients with 5q deletion. Although data suggested the drug is effective for these patients, a NICE advisory committee was not convinced the drug provided a survival benefit.
But now, the committee has concluded that lenalidomide is a clinically effective treatment for these patients because it is associated with a statistically significant improvement in transfusion independence and health-related quality of life compared with placebo.
Furthermore, the committee said it is plausible that lenalidomide can indirectly improve overall survival by improving transfusion independence.
“The committee heard from clinical experts that lenalidomide is an effective therapy,” said Sir Andrew Dillon, NICE chief executive.
“Celgene–who market lenalidomide–worked with us to provide enough evidence to make it possible for us to recommend it for this group of people. Celgene provided a revised analysis and further information on their proposal for a reduction in the cost of the drug to the NHS [National Health Service].”
This patient access scheme involves the NHS paying for lenalidomide treatment for up to 26 monthly cycles. And Celgene will provide the drug free of charge for those people who receive more than 26 monthly cycles.
Lenalidomide is available in 21-day packs of 10 mg and 5 mg capsules at net prices of £3780 and £3570, respectively. The cost of a 28-day cycle of treatment with 10 mg of lenalidomide (excluding value-added tax) is £3780.
The committee noted that the incremental cost-effectiveness ratio for lenalidomide compared with best supportive care is uncertain because the proportion of people who might need treatment beyond 26 cycles is uncertain.
However, the committee accepted that a commitment from Celgene to publish data on the proportion of people receiving treatment beyond 26 cycles would provide reassurance that lenalidomide is a cost-effective use of NHS resources in MDS patients with 5q deletion.
NICE’s final draft guidance is now with consultees, who have the opportunity to appeal against it. Until NICE issues a final guidance, NHS bodies should make decisions locally on the funding of specific treatments. ![]()
SCID may be more common than we thought

Credit: Vera Kratochvil
Severe combined immunodeficiency (SCID) may be nearly twice as common as we thought, new research suggests.
The study is the first combined analysis of more than 3 million infants screened for SCID in 10 US states and the Navajo Nation.
The results suggest SCID may affect as many as 1 in 58,000 infants. Previous estimates had indicated that 1 in 100,000 infants may be born with SCID.
This study and a related editorial were published in JAMA.
Jennifer Puck, MD, of the University of California, San Francisco, and her colleagues analyzed infants from 10 states and the Navajo Nation who were born from January 2008 through July 2013 and were screened for SCID.
The screening detected 52 cases of SCID among the 3,030,083 newborns, suggesting the disorder may affect roughly 1 in 58,000 infants.
The incidence of SCID was not significantly different in any state program, but it was higher in the Navajo Nation, where an ancestral trait is known to confer a higher risk of the disease.
Of the 52 infants who had SCID, 49 received therapies such as hematopoietic stem cell transplants, enzyme replacement therapy, and/or gene therapy. Three infants died before receiving treatment, and 4 children died after transplant, but the other 45 treated infants survived.
Of those 52 cases of SCID identified by newborn screening, 9 were considered “leaky SCID.” These infants had an incomplete mutation in a typical SCID gene, retaining small amounts of immune function that can actually be detrimental because the poorly regulated cells can attack the child’s own tissues.
“We’re finding that leaky SCID is more common than previously thought,” Dr Puck said. “Before screening, we’d typically not make the diagnosis for several months or even years, but because of newborn screening, they are being treated before they get into any trouble.”
The screening test detects more than a dozen genetic causes of SCID, in addition to other conditions with significantly low T cells. The researchers discovered that population-based testing uncovers a broader range of the underlying genetic causes for SCID than previously known.
For example, X-linked SCID, a form of the disorder caused by mutations in a gene on the X chromosome and affecting only males, was previously thought to account for half of SCID cases. But this study showed that only 19% of SCID infants had X-linked disease with a corresponding increase in other gene defects.
Moreover, the proportion of SCID infants without a known genetic defect (15%) was higher than anticipated, indicating that widespread screening presents opportunities to discover previously unknown genes implicated in SCID.
“The whole point of newborn screening is to identify conditions that are treatable, and for which early treatment saves lives,” Dr Puck said. “The excellent outcomes of SCID infants across the country reported in this study prove that SCID is such a condition.” ![]()
Credit: Vera Kratochvil
Severe combined immunodeficiency (SCID) may be nearly twice as common as we thought, new research suggests.
The study is the first combined analysis of more than 3 million infants screened for SCID in 10 US states and the Navajo Nation.
The results suggest SCID may affect as many as 1 in 58,000 infants. Previous estimates had indicated that 1 in 100,000 infants may be born with SCID.
This study and a related editorial were published in JAMA.
Jennifer Puck, MD, of the University of California, San Francisco, and her colleagues analyzed infants from 10 states and the Navajo Nation who were born from January 2008 through July 2013 and were screened for SCID.
The screening detected 52 cases of SCID among the 3,030,083 newborns, suggesting the disorder may affect roughly 1 in 58,000 infants.
The incidence of SCID was not significantly different in any state program, but it was higher in the Navajo Nation, where an ancestral trait is known to confer a higher risk of the disease.
Of the 52 infants who had SCID, 49 received therapies such as hematopoietic stem cell transplants, enzyme replacement therapy, and/or gene therapy. Three infants died before receiving treatment, and 4 children died after transplant, but the other 45 treated infants survived.
Of those 52 cases of SCID identified by newborn screening, 9 were considered “leaky SCID.” These infants had an incomplete mutation in a typical SCID gene, retaining small amounts of immune function that can actually be detrimental because the poorly regulated cells can attack the child’s own tissues.
“We’re finding that leaky SCID is more common than previously thought,” Dr Puck said. “Before screening, we’d typically not make the diagnosis for several months or even years, but because of newborn screening, they are being treated before they get into any trouble.”
The screening test detects more than a dozen genetic causes of SCID, in addition to other conditions with significantly low T cells. The researchers discovered that population-based testing uncovers a broader range of the underlying genetic causes for SCID than previously known.
For example, X-linked SCID, a form of the disorder caused by mutations in a gene on the X chromosome and affecting only males, was previously thought to account for half of SCID cases. But this study showed that only 19% of SCID infants had X-linked disease with a corresponding increase in other gene defects.
Moreover, the proportion of SCID infants without a known genetic defect (15%) was higher than anticipated, indicating that widespread screening presents opportunities to discover previously unknown genes implicated in SCID.
“The whole point of newborn screening is to identify conditions that are treatable, and for which early treatment saves lives,” Dr Puck said. “The excellent outcomes of SCID infants across the country reported in this study prove that SCID is such a condition.” ![]()
Credit: Vera Kratochvil
Severe combined immunodeficiency (SCID) may be nearly twice as common as we thought, new research suggests.
The study is the first combined analysis of more than 3 million infants screened for SCID in 10 US states and the Navajo Nation.
The results suggest SCID may affect as many as 1 in 58,000 infants. Previous estimates had indicated that 1 in 100,000 infants may be born with SCID.
This study and a related editorial were published in JAMA.
Jennifer Puck, MD, of the University of California, San Francisco, and her colleagues analyzed infants from 10 states and the Navajo Nation who were born from January 2008 through July 2013 and were screened for SCID.
The screening detected 52 cases of SCID among the 3,030,083 newborns, suggesting the disorder may affect roughly 1 in 58,000 infants.
The incidence of SCID was not significantly different in any state program, but it was higher in the Navajo Nation, where an ancestral trait is known to confer a higher risk of the disease.
Of the 52 infants who had SCID, 49 received therapies such as hematopoietic stem cell transplants, enzyme replacement therapy, and/or gene therapy. Three infants died before receiving treatment, and 4 children died after transplant, but the other 45 treated infants survived.
Of those 52 cases of SCID identified by newborn screening, 9 were considered “leaky SCID.” These infants had an incomplete mutation in a typical SCID gene, retaining small amounts of immune function that can actually be detrimental because the poorly regulated cells can attack the child’s own tissues.
“We’re finding that leaky SCID is more common than previously thought,” Dr Puck said. “Before screening, we’d typically not make the diagnosis for several months or even years, but because of newborn screening, they are being treated before they get into any trouble.”
The screening test detects more than a dozen genetic causes of SCID, in addition to other conditions with significantly low T cells. The researchers discovered that population-based testing uncovers a broader range of the underlying genetic causes for SCID than previously known.
For example, X-linked SCID, a form of the disorder caused by mutations in a gene on the X chromosome and affecting only males, was previously thought to account for half of SCID cases. But this study showed that only 19% of SCID infants had X-linked disease with a corresponding increase in other gene defects.
Moreover, the proportion of SCID infants without a known genetic defect (15%) was higher than anticipated, indicating that widespread screening presents opportunities to discover previously unknown genes implicated in SCID.
“The whole point of newborn screening is to identify conditions that are treatable, and for which early treatment saves lives,” Dr Puck said. “The excellent outcomes of SCID infants across the country reported in this study prove that SCID is such a condition.” ![]()
Rise of new anticoagulants means higher costs

Credit: CDC
A new study suggests the use of novel oral anticoagulants (NOACs) has surpassed warfarin use in the last few years, but the cost burden for NOACs is much higher than that of warfarin.
By mid-2013, the NOACs dabigatran, rivaroxaban, and apixaban accounted for 62% of all new anticoagulant prescriptions included in the study, but this represented 98% of the total anticoagulant costs.
These findings and a related commentary appear in The American Journal of Medicine.
NOAC use on the rise
To better understand NOAC use, researchers analyzed medical and prescription claims data from the insurance company Aetna. They identified 6893 patients with atrial fibrillation (AF) who were prescribed an oral anticoagulant from 2010 to 2013.
During that time, 45,472 anticoagulant prescriptions were filled—26,253 (57.7%) for warfarin, 14,922 (32.8%) for dabigatran, 4241 (9.3%) for rivaroxaban, and 56 (0.1%) for apixaban.
The researchers noted that the US Food and Drug Administration (FDA) approved dabigatran for use in AF patients in October 2010. And by October 2011, patients were as likely to receive dabigatran as warfarin.
Rivaroxaban was FDA-approved for AF in November 2011, and, by June 2013, the drug had overtaken both warfarin and dabigatran. Apixaban use increased the least, as the drug gained FDA approval for AF in December 2012.
Though NOACs appeared to be on the rise overall, the researchers found NOAC use was significantly less likely for women, patients living in lower income areas, and patients with higher CHADS2, CHA2DS2-VASC, and HAS-BLED scores (P<0.001 for each variable).
The team said this finding is significant because, in the clinical trials supporting NOAC approvals, most patients had CHADS2/CHA2DS2-VASC scores in the higher ranges.
“The greatest absolute benefit from novel anticoagulants has been shown in clinical trials to be among patients at highest baseline risk for stroke or systemic embolization,” said lead investigator Niteesh K. Choudhry, MD, PhD, of Brigham and Women’s Hospital in Boston.
“[This] is at odds with our observation of [physicians selecting] seemingly lower-risk patients for these drugs. Such a finding may reflect provider conservatism for new drug adoption, particularly given longitudinal experience with warfarin.”
Higher costs
Dr Choudhry and his colleagues also found that NOACs confer high healthcare cost consequences. The data revealed that NOACs represented 98% of the total dollars spent on anticoagulants from 2010 to 2013.
Over the first 6 months, the average combined patient and insurer cost associated with starting a NOAC was $900 greater than the cost of starting warfarin.
“Average patient out-of-pocket and insurance spending was more than 5-fold and 15-fold higher, respectively, for novel anticoagulants as compared with warfarin,” Dr Choudhry said. “A 6-month difference in total costs of $900 in our cohort translates into billions of dollars at a national level.”
Taking their findings together, the researchers said this study suggests more information may be needed to fully understand the implications of rising NOAC prescriptions.
“These findings point to the need to conduct ongoing surveillance of the adoption of new agents into clinical practice,” Dr Choudhry said, “as well as the need for robust, real-world comparative-effectiveness analyses of these medications, to enable patients and providers to make informed decisions about their relative benefit, safety, and cost-effectiveness.” ![]()
Credit: CDC
A new study suggests the use of novel oral anticoagulants (NOACs) has surpassed warfarin use in the last few years, but the cost burden for NOACs is much higher than that of warfarin.
By mid-2013, the NOACs dabigatran, rivaroxaban, and apixaban accounted for 62% of all new anticoagulant prescriptions included in the study, but this represented 98% of the total anticoagulant costs.
These findings and a related commentary appear in The American Journal of Medicine.
NOAC use on the rise
To better understand NOAC use, researchers analyzed medical and prescription claims data from the insurance company Aetna. They identified 6893 patients with atrial fibrillation (AF) who were prescribed an oral anticoagulant from 2010 to 2013.
During that time, 45,472 anticoagulant prescriptions were filled—26,253 (57.7%) for warfarin, 14,922 (32.8%) for dabigatran, 4241 (9.3%) for rivaroxaban, and 56 (0.1%) for apixaban.
The researchers noted that the US Food and Drug Administration (FDA) approved dabigatran for use in AF patients in October 2010. And by October 2011, patients were as likely to receive dabigatran as warfarin.
Rivaroxaban was FDA-approved for AF in November 2011, and, by June 2013, the drug had overtaken both warfarin and dabigatran. Apixaban use increased the least, as the drug gained FDA approval for AF in December 2012.
Though NOACs appeared to be on the rise overall, the researchers found NOAC use was significantly less likely for women, patients living in lower income areas, and patients with higher CHADS2, CHA2DS2-VASC, and HAS-BLED scores (P<0.001 for each variable).
The team said this finding is significant because, in the clinical trials supporting NOAC approvals, most patients had CHADS2/CHA2DS2-VASC scores in the higher ranges.
“The greatest absolute benefit from novel anticoagulants has been shown in clinical trials to be among patients at highest baseline risk for stroke or systemic embolization,” said lead investigator Niteesh K. Choudhry, MD, PhD, of Brigham and Women’s Hospital in Boston.
“[This] is at odds with our observation of [physicians selecting] seemingly lower-risk patients for these drugs. Such a finding may reflect provider conservatism for new drug adoption, particularly given longitudinal experience with warfarin.”
Higher costs
Dr Choudhry and his colleagues also found that NOACs confer high healthcare cost consequences. The data revealed that NOACs represented 98% of the total dollars spent on anticoagulants from 2010 to 2013.
Over the first 6 months, the average combined patient and insurer cost associated with starting a NOAC was $900 greater than the cost of starting warfarin.
“Average patient out-of-pocket and insurance spending was more than 5-fold and 15-fold higher, respectively, for novel anticoagulants as compared with warfarin,” Dr Choudhry said. “A 6-month difference in total costs of $900 in our cohort translates into billions of dollars at a national level.”
Taking their findings together, the researchers said this study suggests more information may be needed to fully understand the implications of rising NOAC prescriptions.
“These findings point to the need to conduct ongoing surveillance of the adoption of new agents into clinical practice,” Dr Choudhry said, “as well as the need for robust, real-world comparative-effectiveness analyses of these medications, to enable patients and providers to make informed decisions about their relative benefit, safety, and cost-effectiveness.” ![]()
Credit: CDC
A new study suggests the use of novel oral anticoagulants (NOACs) has surpassed warfarin use in the last few years, but the cost burden for NOACs is much higher than that of warfarin.
By mid-2013, the NOACs dabigatran, rivaroxaban, and apixaban accounted for 62% of all new anticoagulant prescriptions included in the study, but this represented 98% of the total anticoagulant costs.
These findings and a related commentary appear in The American Journal of Medicine.
NOAC use on the rise
To better understand NOAC use, researchers analyzed medical and prescription claims data from the insurance company Aetna. They identified 6893 patients with atrial fibrillation (AF) who were prescribed an oral anticoagulant from 2010 to 2013.
During that time, 45,472 anticoagulant prescriptions were filled—26,253 (57.7%) for warfarin, 14,922 (32.8%) for dabigatran, 4241 (9.3%) for rivaroxaban, and 56 (0.1%) for apixaban.
The researchers noted that the US Food and Drug Administration (FDA) approved dabigatran for use in AF patients in October 2010. And by October 2011, patients were as likely to receive dabigatran as warfarin.
Rivaroxaban was FDA-approved for AF in November 2011, and, by June 2013, the drug had overtaken both warfarin and dabigatran. Apixaban use increased the least, as the drug gained FDA approval for AF in December 2012.
Though NOACs appeared to be on the rise overall, the researchers found NOAC use was significantly less likely for women, patients living in lower income areas, and patients with higher CHADS2, CHA2DS2-VASC, and HAS-BLED scores (P<0.001 for each variable).
The team said this finding is significant because, in the clinical trials supporting NOAC approvals, most patients had CHADS2/CHA2DS2-VASC scores in the higher ranges.
“The greatest absolute benefit from novel anticoagulants has been shown in clinical trials to be among patients at highest baseline risk for stroke or systemic embolization,” said lead investigator Niteesh K. Choudhry, MD, PhD, of Brigham and Women’s Hospital in Boston.
“[This] is at odds with our observation of [physicians selecting] seemingly lower-risk patients for these drugs. Such a finding may reflect provider conservatism for new drug adoption, particularly given longitudinal experience with warfarin.”
Higher costs
Dr Choudhry and his colleagues also found that NOACs confer high healthcare cost consequences. The data revealed that NOACs represented 98% of the total dollars spent on anticoagulants from 2010 to 2013.
Over the first 6 months, the average combined patient and insurer cost associated with starting a NOAC was $900 greater than the cost of starting warfarin.
“Average patient out-of-pocket and insurance spending was more than 5-fold and 15-fold higher, respectively, for novel anticoagulants as compared with warfarin,” Dr Choudhry said. “A 6-month difference in total costs of $900 in our cohort translates into billions of dollars at a national level.”
Taking their findings together, the researchers said this study suggests more information may be needed to fully understand the implications of rising NOAC prescriptions.
“These findings point to the need to conduct ongoing surveillance of the adoption of new agents into clinical practice,” Dr Choudhry said, “as well as the need for robust, real-world comparative-effectiveness analyses of these medications, to enable patients and providers to make informed decisions about their relative benefit, safety, and cost-effectiveness.” ![]()
Autologous NK cells can fight ALL

Credit: Bjorn Onfelt/Dan Davis
In vitro experiments suggest a patient’s own natural killer (NK) cells can be expanded and modified to fight acute lymphoblastic leukemia (ALL).
Researchers successfully expanded CD56+ cells isolated from the bone marrow and peripheral blood of ALL patients.
And these cells exhibited cytotoxicity against the patients’ own ALL cells. The effect was enhanced by the addition of IL-15 and a monoclonal antibody (mAb) targeting BAFF-R.
Hisham Abdel-Azim, MD, of Children’s Hospital Los Angeles, and his colleagues reported these results in Leukemia.
The researchers first used flow cytometry to detect CD56+ cells in bone marrow and peripheral blood samples from ALL patients. The team discovered these cells were detectable at diagnosis, post-induction, and relapse.
To expand the cells, the researchers cocultured them with artificial antigen-presenting K562 clone 9.mbIL-21 cells. The expanded CD56+ cells demonstrated allogeneic cytotoxicity against ALL cells, even in the absence of antibody.
The addition of a mAb targeting BAFF-R enhanced CD56+ cells’ cytotoxicity against ALL cells. The activity of these CD56+ cells was comparable to that of NK cells derived from healthy patients.
The researchers also compared CD56+CD3- cells to CD56+CD3+ cells and found the CD3- cells exhibited increased levels of activation in antibody-mediated cellular cytotoxicity reactions. The CD56+CD3+ cells were not stimulated by BAFF-R mAbs.
The team then tested the NK cells’ autologous cytotoxicity. And, as in previous experiments, the CD56+ cells from ALL samples demonstrated nonantibody-dependent cytotoxicity and enhanced cytotoxicity in the presence of BAFF-R mAbs.
Finally, the researchers decided to investigate whether the addition of IL-2 or IL-15 could further stimulate CD56+ cells’ cytotoxicity. And while they found that both cytokines did the job, IL-15 proved more successful.
“These results are very promising, with potential as a part of first-line therapy and also as a treatment for eliminating any remaining cancer cells . . . following standard chemotherapy,” Dr Abdel-Azim said. “We anticipate additional preclinical testing and then a clinical trial to evaluate the therapy in children with leukemia.” ![]()
Credit: Bjorn Onfelt/Dan Davis
In vitro experiments suggest a patient’s own natural killer (NK) cells can be expanded and modified to fight acute lymphoblastic leukemia (ALL).
Researchers successfully expanded CD56+ cells isolated from the bone marrow and peripheral blood of ALL patients.
And these cells exhibited cytotoxicity against the patients’ own ALL cells. The effect was enhanced by the addition of IL-15 and a monoclonal antibody (mAb) targeting BAFF-R.
Hisham Abdel-Azim, MD, of Children’s Hospital Los Angeles, and his colleagues reported these results in Leukemia.
The researchers first used flow cytometry to detect CD56+ cells in bone marrow and peripheral blood samples from ALL patients. The team discovered these cells were detectable at diagnosis, post-induction, and relapse.
To expand the cells, the researchers cocultured them with artificial antigen-presenting K562 clone 9.mbIL-21 cells. The expanded CD56+ cells demonstrated allogeneic cytotoxicity against ALL cells, even in the absence of antibody.
The addition of a mAb targeting BAFF-R enhanced CD56+ cells’ cytotoxicity against ALL cells. The activity of these CD56+ cells was comparable to that of NK cells derived from healthy patients.
The researchers also compared CD56+CD3- cells to CD56+CD3+ cells and found the CD3- cells exhibited increased levels of activation in antibody-mediated cellular cytotoxicity reactions. The CD56+CD3+ cells were not stimulated by BAFF-R mAbs.
The team then tested the NK cells’ autologous cytotoxicity. And, as in previous experiments, the CD56+ cells from ALL samples demonstrated nonantibody-dependent cytotoxicity and enhanced cytotoxicity in the presence of BAFF-R mAbs.
Finally, the researchers decided to investigate whether the addition of IL-2 or IL-15 could further stimulate CD56+ cells’ cytotoxicity. And while they found that both cytokines did the job, IL-15 proved more successful.
“These results are very promising, with potential as a part of first-line therapy and also as a treatment for eliminating any remaining cancer cells . . . following standard chemotherapy,” Dr Abdel-Azim said. “We anticipate additional preclinical testing and then a clinical trial to evaluate the therapy in children with leukemia.” ![]()
Credit: Bjorn Onfelt/Dan Davis
In vitro experiments suggest a patient’s own natural killer (NK) cells can be expanded and modified to fight acute lymphoblastic leukemia (ALL).
Researchers successfully expanded CD56+ cells isolated from the bone marrow and peripheral blood of ALL patients.
And these cells exhibited cytotoxicity against the patients’ own ALL cells. The effect was enhanced by the addition of IL-15 and a monoclonal antibody (mAb) targeting BAFF-R.
Hisham Abdel-Azim, MD, of Children’s Hospital Los Angeles, and his colleagues reported these results in Leukemia.
The researchers first used flow cytometry to detect CD56+ cells in bone marrow and peripheral blood samples from ALL patients. The team discovered these cells were detectable at diagnosis, post-induction, and relapse.
To expand the cells, the researchers cocultured them with artificial antigen-presenting K562 clone 9.mbIL-21 cells. The expanded CD56+ cells demonstrated allogeneic cytotoxicity against ALL cells, even in the absence of antibody.
The addition of a mAb targeting BAFF-R enhanced CD56+ cells’ cytotoxicity against ALL cells. The activity of these CD56+ cells was comparable to that of NK cells derived from healthy patients.
The researchers also compared CD56+CD3- cells to CD56+CD3+ cells and found the CD3- cells exhibited increased levels of activation in antibody-mediated cellular cytotoxicity reactions. The CD56+CD3+ cells were not stimulated by BAFF-R mAbs.
The team then tested the NK cells’ autologous cytotoxicity. And, as in previous experiments, the CD56+ cells from ALL samples demonstrated nonantibody-dependent cytotoxicity and enhanced cytotoxicity in the presence of BAFF-R mAbs.
Finally, the researchers decided to investigate whether the addition of IL-2 or IL-15 could further stimulate CD56+ cells’ cytotoxicity. And while they found that both cytokines did the job, IL-15 proved more successful.
“These results are very promising, with potential as a part of first-line therapy and also as a treatment for eliminating any remaining cancer cells . . . following standard chemotherapy,” Dr Abdel-Azim said. “We anticipate additional preclinical testing and then a clinical trial to evaluate the therapy in children with leukemia.” ![]()
Combo offers better detection of invasive aspergillosis
Results of a retrospective study may have revealed the most accurate way to diagnose invasive aspergillosis (IA).
The fungal infection can be life-threatening, particularly for immunosuppressed patients, but it remains difficult to diagnose.
So researchers compared 3 tests used to diagnose IA and found the combination of nucleic acid sequence-based amplification (NASBA) and real-time quantitative PCR (qPCR) had a 100% positive predictive value.
The team reported this discovery in The Journal of Molecular Diagnostics.
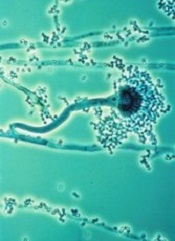
IA is caused by the fungus Aspergillus fumigatus, which is considered by many pathologists to be the world’s most harmful mold.
“Traditional diagnostic methods, such as culture and histopathology of infected tissues, often fail to detect Aspergillus,” said study investigator Yun Xia, PhD, of the First Affiliated Hospital of Chongqing Medical University in China.
With this in mind, he and his colleagues evaluated the diagnostic performance of 2 nucleic acid amplification assays—qPCR and NASBA—and 1 antigen-detection method—galactomannan enzyme-linked immunosorbent assay (GM-ELISA)—using blood samples from 80 patients at high risk of IA.
The researchers evaluated the tests alone and in combination. Of the 80 patients, 42.5% had proven or probable IA.
Tests showed that NASBA predicted IA with the highest sensitivity—76.47%, compared to 67.65% for qPCR and 52.94% for GM-ELISA. But qPCR offered the highest specificity—89.13%, compared to 80.43% for both NASBA and GM-ELISA.
NASBA had the highest negative predictive value—82.22%, compared to 78.85% for qPCR and 69.81% for GM-ELISA. And qPCR had the highest positive predictive value—82.14%, compared to 74.29% for NASBA and 66.67% for GM-ELISA.
NASBA and qPCR each had a high Youden index as well—0.5690 and 0.5678, respectively—compared to GM-ELISA—0.3337.
And combining the tests improved their accuracy. The combination of NASBA and qPCR led to 100% specificity and a 100% positive predictive value.
Dr Xia and his colleagues also noted that NASBA offers the advantages of rapid amplification (90 minutes) and simple operation with low instrument cost, compared with qPCR and GM-ELISA.
Finally, the team stressed that although GM-ELISA is widely and routinely used for aspergillosis diagnosis, this study indicates that it is inferior to both NASBA and qPCR. ![]()
Results of a retrospective study may have revealed the most accurate way to diagnose invasive aspergillosis (IA).
The fungal infection can be life-threatening, particularly for immunosuppressed patients, but it remains difficult to diagnose.
So researchers compared 3 tests used to diagnose IA and found the combination of nucleic acid sequence-based amplification (NASBA) and real-time quantitative PCR (qPCR) had a 100% positive predictive value.
The team reported this discovery in The Journal of Molecular Diagnostics.
IA is caused by the fungus Aspergillus fumigatus, which is considered by many pathologists to be the world’s most harmful mold.
“Traditional diagnostic methods, such as culture and histopathology of infected tissues, often fail to detect Aspergillus,” said study investigator Yun Xia, PhD, of the First Affiliated Hospital of Chongqing Medical University in China.
With this in mind, he and his colleagues evaluated the diagnostic performance of 2 nucleic acid amplification assays—qPCR and NASBA—and 1 antigen-detection method—galactomannan enzyme-linked immunosorbent assay (GM-ELISA)—using blood samples from 80 patients at high risk of IA.
The researchers evaluated the tests alone and in combination. Of the 80 patients, 42.5% had proven or probable IA.
Tests showed that NASBA predicted IA with the highest sensitivity—76.47%, compared to 67.65% for qPCR and 52.94% for GM-ELISA. But qPCR offered the highest specificity—89.13%, compared to 80.43% for both NASBA and GM-ELISA.
NASBA had the highest negative predictive value—82.22%, compared to 78.85% for qPCR and 69.81% for GM-ELISA. And qPCR had the highest positive predictive value—82.14%, compared to 74.29% for NASBA and 66.67% for GM-ELISA.
NASBA and qPCR each had a high Youden index as well—0.5690 and 0.5678, respectively—compared to GM-ELISA—0.3337.
And combining the tests improved their accuracy. The combination of NASBA and qPCR led to 100% specificity and a 100% positive predictive value.
Dr Xia and his colleagues also noted that NASBA offers the advantages of rapid amplification (90 minutes) and simple operation with low instrument cost, compared with qPCR and GM-ELISA.
Finally, the team stressed that although GM-ELISA is widely and routinely used for aspergillosis diagnosis, this study indicates that it is inferior to both NASBA and qPCR. ![]()
Results of a retrospective study may have revealed the most accurate way to diagnose invasive aspergillosis (IA).
The fungal infection can be life-threatening, particularly for immunosuppressed patients, but it remains difficult to diagnose.
So researchers compared 3 tests used to diagnose IA and found the combination of nucleic acid sequence-based amplification (NASBA) and real-time quantitative PCR (qPCR) had a 100% positive predictive value.
The team reported this discovery in The Journal of Molecular Diagnostics.
IA is caused by the fungus Aspergillus fumigatus, which is considered by many pathologists to be the world’s most harmful mold.
“Traditional diagnostic methods, such as culture and histopathology of infected tissues, often fail to detect Aspergillus,” said study investigator Yun Xia, PhD, of the First Affiliated Hospital of Chongqing Medical University in China.
With this in mind, he and his colleagues evaluated the diagnostic performance of 2 nucleic acid amplification assays—qPCR and NASBA—and 1 antigen-detection method—galactomannan enzyme-linked immunosorbent assay (GM-ELISA)—using blood samples from 80 patients at high risk of IA.
The researchers evaluated the tests alone and in combination. Of the 80 patients, 42.5% had proven or probable IA.
Tests showed that NASBA predicted IA with the highest sensitivity—76.47%, compared to 67.65% for qPCR and 52.94% for GM-ELISA. But qPCR offered the highest specificity—89.13%, compared to 80.43% for both NASBA and GM-ELISA.
NASBA had the highest negative predictive value—82.22%, compared to 78.85% for qPCR and 69.81% for GM-ELISA. And qPCR had the highest positive predictive value—82.14%, compared to 74.29% for NASBA and 66.67% for GM-ELISA.
NASBA and qPCR each had a high Youden index as well—0.5690 and 0.5678, respectively—compared to GM-ELISA—0.3337.
And combining the tests improved their accuracy. The combination of NASBA and qPCR led to 100% specificity and a 100% positive predictive value.
Dr Xia and his colleagues also noted that NASBA offers the advantages of rapid amplification (90 minutes) and simple operation with low instrument cost, compared with qPCR and GM-ELISA.
Finally, the team stressed that although GM-ELISA is widely and routinely used for aspergillosis diagnosis, this study indicates that it is inferior to both NASBA and qPCR. ![]()
Tool reveals how malaria parasites infect RBCs

an RBC; Credit: St Jude
Children’s Research Hospital
Researchers say laser optical tweezers have allowed them to study how Plasmodium falciparum interacts with red blood cells (RBCs) at the single-cell level.
The research has revealed new insights into malaria biology and may pave the way for more effective drugs or vaccines.
Julian Rayner, PhD, of the Wellcome Trust Sanger Institute in Cambridge, UK, and his colleagues described their use of laser optical tweezers in Biophysical Journal.
“Using laser tweezers to study red blood cell invasion gives us an unprecedented level of control over the whole process and will help us to understand this critical process at a level of detail that has not been possible before,” Dr Rayner said.
He and his colleagues noted that P falciparum merozoites usually leave one RBC and invade another in less than a minute. And the merozoites lose the ability to infect host cells within 2 or 3 minutes of release.
So the researchers used laser optical tweezers to study this transient event. The tweezers allow for precise control over the movements of cells by exerting extremely small forces with a highly focused laser beam.
The team used the tweezers to pick up individual merozoites that had just emerged from an RBC and deliver them to another RBC, demonstrating that the technique is suitable for studying the invasion process.
The researchers also used the tweezers to measure how strongly the merozoites adhere to RBCs. They discovered that attachment is probably mediated by multiple weak interactions, which could potentially be blocked by a combination of drugs or antibodies.
Finally, the team used the tweezers to shed light on how 3 different invasion-inhibiting drugs—heparin, cytochalasin D, and chymotrypsin—affect interactions between merozoites and RBCs.
The tweezers revealed that heparin blocks merozoite attachment to any surface, including glass slides. This suggests a receptor-independent mode of action, which contradicts the previously proposed mechanism.
Cytochalasin D, on the other hand, had no effect on attachment force, a finding that also contradicts previous thought.
And with chymotrypsin, the researchers observed 2 different effects. When merozoites adhered to chymotrypsin-treated RBCs, they did so with a reduction in the force of attachment that was similar to the effect the enzyme had on the overall efficiency of invasion.
However, merozoites that had been released more than 3 minutes previously were no longer able to adhere to chymotrypsin-treated RBCs. This suggests that chymotrypsin affects both the force of merozoite attachment and the time in which invasion can occur.
Taken together, these findings show that optical tweezers enable the study of malaria biology and drug mechanisms at the single-cell level.
“We now plan to apply this technology to dissect the process of invasion and understand what genes and proteins function at what step,” Dr Rayner said. “This will allow us to design better inhibitors or vaccines that block invasion by targeting multiple steps at the same time.” ![]()
an RBC; Credit: St Jude
Children’s Research Hospital
Researchers say laser optical tweezers have allowed them to study how Plasmodium falciparum interacts with red blood cells (RBCs) at the single-cell level.
The research has revealed new insights into malaria biology and may pave the way for more effective drugs or vaccines.
Julian Rayner, PhD, of the Wellcome Trust Sanger Institute in Cambridge, UK, and his colleagues described their use of laser optical tweezers in Biophysical Journal.
“Using laser tweezers to study red blood cell invasion gives us an unprecedented level of control over the whole process and will help us to understand this critical process at a level of detail that has not been possible before,” Dr Rayner said.
He and his colleagues noted that P falciparum merozoites usually leave one RBC and invade another in less than a minute. And the merozoites lose the ability to infect host cells within 2 or 3 minutes of release.
So the researchers used laser optical tweezers to study this transient event. The tweezers allow for precise control over the movements of cells by exerting extremely small forces with a highly focused laser beam.
The team used the tweezers to pick up individual merozoites that had just emerged from an RBC and deliver them to another RBC, demonstrating that the technique is suitable for studying the invasion process.
The researchers also used the tweezers to measure how strongly the merozoites adhere to RBCs. They discovered that attachment is probably mediated by multiple weak interactions, which could potentially be blocked by a combination of drugs or antibodies.
Finally, the team used the tweezers to shed light on how 3 different invasion-inhibiting drugs—heparin, cytochalasin D, and chymotrypsin—affect interactions between merozoites and RBCs.
The tweezers revealed that heparin blocks merozoite attachment to any surface, including glass slides. This suggests a receptor-independent mode of action, which contradicts the previously proposed mechanism.
Cytochalasin D, on the other hand, had no effect on attachment force, a finding that also contradicts previous thought.
And with chymotrypsin, the researchers observed 2 different effects. When merozoites adhered to chymotrypsin-treated RBCs, they did so with a reduction in the force of attachment that was similar to the effect the enzyme had on the overall efficiency of invasion.
However, merozoites that had been released more than 3 minutes previously were no longer able to adhere to chymotrypsin-treated RBCs. This suggests that chymotrypsin affects both the force of merozoite attachment and the time in which invasion can occur.
Taken together, these findings show that optical tweezers enable the study of malaria biology and drug mechanisms at the single-cell level.
“We now plan to apply this technology to dissect the process of invasion and understand what genes and proteins function at what step,” Dr Rayner said. “This will allow us to design better inhibitors or vaccines that block invasion by targeting multiple steps at the same time.” ![]()
an RBC; Credit: St Jude
Children’s Research Hospital
Researchers say laser optical tweezers have allowed them to study how Plasmodium falciparum interacts with red blood cells (RBCs) at the single-cell level.
The research has revealed new insights into malaria biology and may pave the way for more effective drugs or vaccines.
Julian Rayner, PhD, of the Wellcome Trust Sanger Institute in Cambridge, UK, and his colleagues described their use of laser optical tweezers in Biophysical Journal.
“Using laser tweezers to study red blood cell invasion gives us an unprecedented level of control over the whole process and will help us to understand this critical process at a level of detail that has not been possible before,” Dr Rayner said.
He and his colleagues noted that P falciparum merozoites usually leave one RBC and invade another in less than a minute. And the merozoites lose the ability to infect host cells within 2 or 3 minutes of release.
So the researchers used laser optical tweezers to study this transient event. The tweezers allow for precise control over the movements of cells by exerting extremely small forces with a highly focused laser beam.
The team used the tweezers to pick up individual merozoites that had just emerged from an RBC and deliver them to another RBC, demonstrating that the technique is suitable for studying the invasion process.
The researchers also used the tweezers to measure how strongly the merozoites adhere to RBCs. They discovered that attachment is probably mediated by multiple weak interactions, which could potentially be blocked by a combination of drugs or antibodies.
Finally, the team used the tweezers to shed light on how 3 different invasion-inhibiting drugs—heparin, cytochalasin D, and chymotrypsin—affect interactions between merozoites and RBCs.
The tweezers revealed that heparin blocks merozoite attachment to any surface, including glass slides. This suggests a receptor-independent mode of action, which contradicts the previously proposed mechanism.
Cytochalasin D, on the other hand, had no effect on attachment force, a finding that also contradicts previous thought.
And with chymotrypsin, the researchers observed 2 different effects. When merozoites adhered to chymotrypsin-treated RBCs, they did so with a reduction in the force of attachment that was similar to the effect the enzyme had on the overall efficiency of invasion.
However, merozoites that had been released more than 3 minutes previously were no longer able to adhere to chymotrypsin-treated RBCs. This suggests that chymotrypsin affects both the force of merozoite attachment and the time in which invasion can occur.
Taken together, these findings show that optical tweezers enable the study of malaria biology and drug mechanisms at the single-cell level.
“We now plan to apply this technology to dissect the process of invasion and understand what genes and proteins function at what step,” Dr Rayner said. “This will allow us to design better inhibitors or vaccines that block invasion by targeting multiple steps at the same time.”
DOJ closes investigation of PLATO trial

Credit: AstraZeneca
The US Department of Justice (DOJ) is closing its investigation of PLATO, a clinical trial of the antiplatelet agent ticagrelor (Brilinta), according to the drug’s developer, AstraZeneca.
The company also said the government is not planning any further action.
The DOJ began its investigation in October 2013, issuing a civil investigative demand requiring AstraZeneca to provide the department with documents and information related to the PLATO trial.
The trial compared ticagrelor to the antiplatelet agent clopidogrel in 18,624 patients with acute coronary syndromes (ACS), with or without ST-segment elevation.
The results suggested that ticagrelor significantly reduced the rate of myocardial infarction and death from any cause, although it did not decrease the risk of stroke. Ticagrelor did not increase the rate of overall bleeding, but it did increase the rate of bleeding not related to procedures.
These results led to ticagrelor’s approval in the US and more than 100 other countries. But members of the medical community questioned PLATO’s results, with some even suggesting the possibility of trial misconduct.
So the DOJ launched its investigation. The details of the inquiry are unclear, but AstraZeneca said it “focused on questions that have been raised previously in public about the trial.”
Many of those questions have been raised in the International Journal of Cardiology, in articles by Victor Serebruany, MD, PhD, of HeartDrug Research Laboratories in Towson, Maryland, and James DiNicolantonio, PharmD, of Wegmans Pharmacy in Ithaca, New York.
In the years since PLATO’s results were first published, Drs DiNicolantonio and Serebruany have pointed out differences between trial data published in the NEJM paper and FDA reviews of the data, noted the geographic discrepancies in results observed with ticagrelor, and raised questions about site monitoring, blinding practices, and patient deaths, among other issues.
PLATO investigators addressed these questions and allegations in an article of their own, which appeared in the International Journal of Cardiology in December 2013. The overall message was that PLATO’s results are valid.
“We have always had absolute confidence in the integrity of the PLATO trial, and we are proud of the important benefit [ticagrelor] offers to patients around the world suffering from acute coronary syndrome,” said Pascal Soriot, AstraZeneca’s Chief Executive Officer.
As for the future of ticagrelor, AstraZeneca recently announced the start of the SOCRATES trial, a study of the drug for patients with acute ischemic stroke or transient ischemic attack, and the THEMIS study in patients with type 2 diabetes and coronary atherosclerosis.
These studies form part of PARTHENON, a trial program involving more than 80,000 patients worldwide. The program also includes 2 trials that have recently completed recruitment—EUCLID, a study of patients with peripheral artery disease and PEGASUS, a study of ticagrelor for secondary prevention in patients with previous myocardial infarction.
AstraZeneca expects headline results from PEGASUS to be available in the first quarter of 2015.
Credit: AstraZeneca
The US Department of Justice (DOJ) is closing its investigation of PLATO, a clinical trial of the antiplatelet agent ticagrelor (Brilinta), according to the drug’s developer, AstraZeneca.
The company also said the government is not planning any further action.
The DOJ began its investigation in October 2013, issuing a civil investigative demand requiring AstraZeneca to provide the department with documents and information related to the PLATO trial.
The trial compared ticagrelor to the antiplatelet agent clopidogrel in 18,624 patients with acute coronary syndromes (ACS), with or without ST-segment elevation.
The results suggested that ticagrelor significantly reduced the rate of myocardial infarction and death from any cause, although it did not decrease the risk of stroke. Ticagrelor did not increase the rate of overall bleeding, but it did increase the rate of bleeding not related to procedures.
These results led to ticagrelor’s approval in the US and more than 100 other countries. But members of the medical community questioned PLATO’s results, with some even suggesting the possibility of trial misconduct.
So the DOJ launched its investigation. The details of the inquiry are unclear, but AstraZeneca said it “focused on questions that have been raised previously in public about the trial.”
Many of those questions have been raised in the International Journal of Cardiology, in articles by Victor Serebruany, MD, PhD, of HeartDrug Research Laboratories in Towson, Maryland, and James DiNicolantonio, PharmD, of Wegmans Pharmacy in Ithaca, New York.
In the years since PLATO’s results were first published, Drs DiNicolantonio and Serebruany have pointed out differences between trial data published in the NEJM paper and FDA reviews of the data, noted the geographic discrepancies in results observed with ticagrelor, and raised questions about site monitoring, blinding practices, and patient deaths, among other issues.
PLATO investigators addressed these questions and allegations in an article of their own, which appeared in the International Journal of Cardiology in December 2013. The overall message was that PLATO’s results are valid.
“We have always had absolute confidence in the integrity of the PLATO trial, and we are proud of the important benefit [ticagrelor] offers to patients around the world suffering from acute coronary syndrome,” said Pascal Soriot, AstraZeneca’s Chief Executive Officer.
As for the future of ticagrelor, AstraZeneca recently announced the start of the SOCRATES trial, a study of the drug for patients with acute ischemic stroke or transient ischemic attack, and the THEMIS study in patients with type 2 diabetes and coronary atherosclerosis.
These studies form part of PARTHENON, a trial program involving more than 80,000 patients worldwide. The program also includes 2 trials that have recently completed recruitment—EUCLID, a study of patients with peripheral artery disease and PEGASUS, a study of ticagrelor for secondary prevention in patients with previous myocardial infarction.
AstraZeneca expects headline results from PEGASUS to be available in the first quarter of 2015.
Credit: AstraZeneca
The US Department of Justice (DOJ) is closing its investigation of PLATO, a clinical trial of the antiplatelet agent ticagrelor (Brilinta), according to the drug’s developer, AstraZeneca.
The company also said the government is not planning any further action.
The DOJ began its investigation in October 2013, issuing a civil investigative demand requiring AstraZeneca to provide the department with documents and information related to the PLATO trial.
The trial compared ticagrelor to the antiplatelet agent clopidogrel in 18,624 patients with acute coronary syndromes (ACS), with or without ST-segment elevation.
The results suggested that ticagrelor significantly reduced the rate of myocardial infarction and death from any cause, although it did not decrease the risk of stroke. Ticagrelor did not increase the rate of overall bleeding, but it did increase the rate of bleeding not related to procedures.
These results led to ticagrelor’s approval in the US and more than 100 other countries. But members of the medical community questioned PLATO’s results, with some even suggesting the possibility of trial misconduct.
So the DOJ launched its investigation. The details of the inquiry are unclear, but AstraZeneca said it “focused on questions that have been raised previously in public about the trial.”
Many of those questions have been raised in the International Journal of Cardiology, in articles by Victor Serebruany, MD, PhD, of HeartDrug Research Laboratories in Towson, Maryland, and James DiNicolantonio, PharmD, of Wegmans Pharmacy in Ithaca, New York.
In the years since PLATO’s results were first published, Drs DiNicolantonio and Serebruany have pointed out differences between trial data published in the NEJM paper and FDA reviews of the data, noted the geographic discrepancies in results observed with ticagrelor, and raised questions about site monitoring, blinding practices, and patient deaths, among other issues.
PLATO investigators addressed these questions and allegations in an article of their own, which appeared in the International Journal of Cardiology in December 2013. The overall message was that PLATO’s results are valid.
“We have always had absolute confidence in the integrity of the PLATO trial, and we are proud of the important benefit [ticagrelor] offers to patients around the world suffering from acute coronary syndrome,” said Pascal Soriot, AstraZeneca’s Chief Executive Officer.
As for the future of ticagrelor, AstraZeneca recently announced the start of the SOCRATES trial, a study of the drug for patients with acute ischemic stroke or transient ischemic attack, and the THEMIS study in patients with type 2 diabetes and coronary atherosclerosis.
These studies form part of PARTHENON, a trial program involving more than 80,000 patients worldwide. The program also includes 2 trials that have recently completed recruitment—EUCLID, a study of patients with peripheral artery disease and PEGASUS, a study of ticagrelor for secondary prevention in patients with previous myocardial infarction.
AstraZeneca expects headline results from PEGASUS to be available in the first quarter of 2015.
Guidelines can predict infertility in child cancer survivors

patient and her father
Credit: Rhoda Baer
Guidelines developed almost 20 years ago can accurately predict infertility in girls with cancer, according to research published in The Lancet Oncology.
Researchers found the criteria in these guidelines can help healthcare professionals select which girls should be given the option of ovarian tissue cryopreservation.
The team noted that taking the initial samples of ovarian tissue involves a surgical technique that is still relatively experimental.
So it is crucial to accurately predict which patients are most likely to benefit from the procedure and when it can be safely performed.
The guidelines, known as the Edinburgh selection criteria, were instituted in 1996 to help healthcare professionals decide which girls should be given the option of cryopreservation, based on their age, type of cancer treatment, and their chance of cure.
Specifically, patients were required to meet the following criteria:
- Age younger than 35 years
- No previous chemotherapy or radiotherapy if 15 years or older at diagnosis, but mild, non-gonadotoxic chemotherapy was acceptable if a patient was younger than 15
- A realistic chance of surviving for 5 years
- A high risk of premature ovarian insufficiency (>50%)
- Informed consent (from parents and the patient, if possible)
- Negative serology results for HIV, syphilis, and hepatitis B
- Not pregnant and no existing children.
Testing the guidelines
To validate the selection criteria, W. Hamish B. Wallace, MD, of the Royal Hospital for Sick Children in Edinburgh, UK, and his colleagues analyzed 410 female cancer patients who were younger than 18 years at their time of diagnosis.
The patients were treated between January 1, 1996, and June 30, 2012, at the Edinburgh Children’s Cancer Centre, which serves the southeast region of Scotland.
In all, 34 patients (8%) met the Edinburgh selection criteria and were given the option of ovarian tissue cryopreservation before starting cancer treatment. Thirteen patients declined, 21 consented, and 20 had a successful procedure.
The researchers were able to assess ovarian function in 14 of the 20 patients with successful cryopreservation and 6 of the 13 patients who declined the procedure.
Of the 14 evaluable patients who underwent cryopreservation, 6 developed premature ovarian insufficiency at a median age of 13.4 years (range, 12.5–14.6), but 1 of these patients also had a natural pregnancy.
One patient each among the 6 evaluable patients who declined cryopreservation and the 141 evaluable patients who were not offered cryopreservation developed premature ovarian insufficiency.
So, overall, the probability of ovarian insufficiency was significantly higher for patients who met the Edinburgh selection criteria than for those who did not. The 15-year probability was 35% and 1%, respectively (P<0.0001).
The researchers said these results validate the use of the selection criteria, as they can accurately identify patients who will likely develop premature ovarian insufficiency.
“Advances in life-saving treatments mean that more and more young people with cancer are surviving the disease,” Dr Wallace said. “Here, we have an opportunity to help young women to have families of their own when they grow up, if they so choose.”
patient and her father
Credit: Rhoda Baer
Guidelines developed almost 20 years ago can accurately predict infertility in girls with cancer, according to research published in The Lancet Oncology.
Researchers found the criteria in these guidelines can help healthcare professionals select which girls should be given the option of ovarian tissue cryopreservation.
The team noted that taking the initial samples of ovarian tissue involves a surgical technique that is still relatively experimental.
So it is crucial to accurately predict which patients are most likely to benefit from the procedure and when it can be safely performed.
The guidelines, known as the Edinburgh selection criteria, were instituted in 1996 to help healthcare professionals decide which girls should be given the option of cryopreservation, based on their age, type of cancer treatment, and their chance of cure.
Specifically, patients were required to meet the following criteria:
- Age younger than 35 years
- No previous chemotherapy or radiotherapy if 15 years or older at diagnosis, but mild, non-gonadotoxic chemotherapy was acceptable if a patient was younger than 15
- A realistic chance of surviving for 5 years
- A high risk of premature ovarian insufficiency (>50%)
- Informed consent (from parents and the patient, if possible)
- Negative serology results for HIV, syphilis, and hepatitis B
- Not pregnant and no existing children.
Testing the guidelines
To validate the selection criteria, W. Hamish B. Wallace, MD, of the Royal Hospital for Sick Children in Edinburgh, UK, and his colleagues analyzed 410 female cancer patients who were younger than 18 years at their time of diagnosis.
The patients were treated between January 1, 1996, and June 30, 2012, at the Edinburgh Children’s Cancer Centre, which serves the southeast region of Scotland.
In all, 34 patients (8%) met the Edinburgh selection criteria and were given the option of ovarian tissue cryopreservation before starting cancer treatment. Thirteen patients declined, 21 consented, and 20 had a successful procedure.
The researchers were able to assess ovarian function in 14 of the 20 patients with successful cryopreservation and 6 of the 13 patients who declined the procedure.
Of the 14 evaluable patients who underwent cryopreservation, 6 developed premature ovarian insufficiency at a median age of 13.4 years (range, 12.5–14.6), but 1 of these patients also had a natural pregnancy.
One patient each among the 6 evaluable patients who declined cryopreservation and the 141 evaluable patients who were not offered cryopreservation developed premature ovarian insufficiency.
So, overall, the probability of ovarian insufficiency was significantly higher for patients who met the Edinburgh selection criteria than for those who did not. The 15-year probability was 35% and 1%, respectively (P<0.0001).
The researchers said these results validate the use of the selection criteria, as they can accurately identify patients who will likely develop premature ovarian insufficiency.
“Advances in life-saving treatments mean that more and more young people with cancer are surviving the disease,” Dr Wallace said. “Here, we have an opportunity to help young women to have families of their own when they grow up, if they so choose.”
patient and her father
Credit: Rhoda Baer
Guidelines developed almost 20 years ago can accurately predict infertility in girls with cancer, according to research published in The Lancet Oncology.
Researchers found the criteria in these guidelines can help healthcare professionals select which girls should be given the option of ovarian tissue cryopreservation.
The team noted that taking the initial samples of ovarian tissue involves a surgical technique that is still relatively experimental.
So it is crucial to accurately predict which patients are most likely to benefit from the procedure and when it can be safely performed.
The guidelines, known as the Edinburgh selection criteria, were instituted in 1996 to help healthcare professionals decide which girls should be given the option of cryopreservation, based on their age, type of cancer treatment, and their chance of cure.
Specifically, patients were required to meet the following criteria:
- Age younger than 35 years
- No previous chemotherapy or radiotherapy if 15 years or older at diagnosis, but mild, non-gonadotoxic chemotherapy was acceptable if a patient was younger than 15
- A realistic chance of surviving for 5 years
- A high risk of premature ovarian insufficiency (>50%)
- Informed consent (from parents and the patient, if possible)
- Negative serology results for HIV, syphilis, and hepatitis B
- Not pregnant and no existing children.
Testing the guidelines
To validate the selection criteria, W. Hamish B. Wallace, MD, of the Royal Hospital for Sick Children in Edinburgh, UK, and his colleagues analyzed 410 female cancer patients who were younger than 18 years at their time of diagnosis.
The patients were treated between January 1, 1996, and June 30, 2012, at the Edinburgh Children’s Cancer Centre, which serves the southeast region of Scotland.
In all, 34 patients (8%) met the Edinburgh selection criteria and were given the option of ovarian tissue cryopreservation before starting cancer treatment. Thirteen patients declined, 21 consented, and 20 had a successful procedure.
The researchers were able to assess ovarian function in 14 of the 20 patients with successful cryopreservation and 6 of the 13 patients who declined the procedure.
Of the 14 evaluable patients who underwent cryopreservation, 6 developed premature ovarian insufficiency at a median age of 13.4 years (range, 12.5–14.6), but 1 of these patients also had a natural pregnancy.
One patient each among the 6 evaluable patients who declined cryopreservation and the 141 evaluable patients who were not offered cryopreservation developed premature ovarian insufficiency.
So, overall, the probability of ovarian insufficiency was significantly higher for patients who met the Edinburgh selection criteria than for those who did not. The 15-year probability was 35% and 1%, respectively (P<0.0001).
The researchers said these results validate the use of the selection criteria, as they can accurately identify patients who will likely develop premature ovarian insufficiency.
“Advances in life-saving treatments mean that more and more young people with cancer are surviving the disease,” Dr Wallace said. “Here, we have an opportunity to help young women to have families of their own when they grow up, if they so choose.”
Team explains resistance to retinoic acid

Credit: Armin Kübelbeck
Preclinical experiments may have revealed why some cancer patients do not respond to retinoic acid.
Investigators found that a protein known as AEG-1 blocks the effects of retinoic acid in acute myeloid leukemia (AML) and liver cancer.
They also noted that AEG-1 is overexpressed in nearly every cancer type, so these findings could impact the care of countless cancer patients.
The team reported their findings in Cancer Research.
The group’s experiments revealed that AEG-1 binds to retinoid X receptors (RXR), which help regulate cell growth and development. RXR is typically activated by retinoic acid, but the overexpressed AEG-1 proteins found in cancer cells block these signals and help promote tumor growth.
“Our findings are the first to show that AEG-1 interacts with the retinoid X receptor,” said study author Devanand Sarkar, MBBS, PhD, of Virginia Commonwealth University Massey Cancer Center in Richmond.
Specifically, he and his colleagues found that AEG-1 protected hepatocellular carcinoma cells and AML cells from retinoid- and rexinoid-induced cell death.
But in nude mouse models, blocking the production of AEG-1 allowed all-trans retinoic acid to kill hepatocellular carcinoma cells.
The investigators therefore believe that targeting AEG-1 could sensitize AML patients and those with hepatocellular carcinoma to retinoid- and rexinoid-based therapies.
“This research has immediate clinical relevance, such that physicians could begin screening cancer patients for AEG-1 expression levels in order to determine whether retinoic acid should be prescribed,” Dr Sarkar added.
He and his colleagues have been studying AEG-1 for years. They were the first to create a mouse model demonstrating the role of AEG-1 in liver cancer, and they have been working to develop targeted therapies that block AEG-1 production.
The present study expanded their knowledge of the molecular interactions of AEG-1.
“We are continuing to test combination therapies involving AEG-1 inhibition and retinoic acid in animal models, and the initial results are promising,” Dr Sarkar said. “If we continue to see these results in more complex experiments, we hope to eventually propose a phase 1 clinical trial in patients with liver cancer.”
Credit: Armin Kübelbeck
Preclinical experiments may have revealed why some cancer patients do not respond to retinoic acid.
Investigators found that a protein known as AEG-1 blocks the effects of retinoic acid in acute myeloid leukemia (AML) and liver cancer.
They also noted that AEG-1 is overexpressed in nearly every cancer type, so these findings could impact the care of countless cancer patients.
The team reported their findings in Cancer Research.
The group’s experiments revealed that AEG-1 binds to retinoid X receptors (RXR), which help regulate cell growth and development. RXR is typically activated by retinoic acid, but the overexpressed AEG-1 proteins found in cancer cells block these signals and help promote tumor growth.
“Our findings are the first to show that AEG-1 interacts with the retinoid X receptor,” said study author Devanand Sarkar, MBBS, PhD, of Virginia Commonwealth University Massey Cancer Center in Richmond.
Specifically, he and his colleagues found that AEG-1 protected hepatocellular carcinoma cells and AML cells from retinoid- and rexinoid-induced cell death.
But in nude mouse models, blocking the production of AEG-1 allowed all-trans retinoic acid to kill hepatocellular carcinoma cells.
The investigators therefore believe that targeting AEG-1 could sensitize AML patients and those with hepatocellular carcinoma to retinoid- and rexinoid-based therapies.
“This research has immediate clinical relevance, such that physicians could begin screening cancer patients for AEG-1 expression levels in order to determine whether retinoic acid should be prescribed,” Dr Sarkar added.
He and his colleagues have been studying AEG-1 for years. They were the first to create a mouse model demonstrating the role of AEG-1 in liver cancer, and they have been working to develop targeted therapies that block AEG-1 production.
The present study expanded their knowledge of the molecular interactions of AEG-1.
“We are continuing to test combination therapies involving AEG-1 inhibition and retinoic acid in animal models, and the initial results are promising,” Dr Sarkar said. “If we continue to see these results in more complex experiments, we hope to eventually propose a phase 1 clinical trial in patients with liver cancer.”
Credit: Armin Kübelbeck
Preclinical experiments may have revealed why some cancer patients do not respond to retinoic acid.
Investigators found that a protein known as AEG-1 blocks the effects of retinoic acid in acute myeloid leukemia (AML) and liver cancer.
They also noted that AEG-1 is overexpressed in nearly every cancer type, so these findings could impact the care of countless cancer patients.
The team reported their findings in Cancer Research.
The group’s experiments revealed that AEG-1 binds to retinoid X receptors (RXR), which help regulate cell growth and development. RXR is typically activated by retinoic acid, but the overexpressed AEG-1 proteins found in cancer cells block these signals and help promote tumor growth.
“Our findings are the first to show that AEG-1 interacts with the retinoid X receptor,” said study author Devanand Sarkar, MBBS, PhD, of Virginia Commonwealth University Massey Cancer Center in Richmond.
Specifically, he and his colleagues found that AEG-1 protected hepatocellular carcinoma cells and AML cells from retinoid- and rexinoid-induced cell death.
But in nude mouse models, blocking the production of AEG-1 allowed all-trans retinoic acid to kill hepatocellular carcinoma cells.
The investigators therefore believe that targeting AEG-1 could sensitize AML patients and those with hepatocellular carcinoma to retinoid- and rexinoid-based therapies.
“This research has immediate clinical relevance, such that physicians could begin screening cancer patients for AEG-1 expression levels in order to determine whether retinoic acid should be prescribed,” Dr Sarkar added.
He and his colleagues have been studying AEG-1 for years. They were the first to create a mouse model demonstrating the role of AEG-1 in liver cancer, and they have been working to develop targeted therapies that block AEG-1 production.
The present study expanded their knowledge of the molecular interactions of AEG-1.
“We are continuing to test combination therapies involving AEG-1 inhibition and retinoic acid in animal models, and the initial results are promising,” Dr Sarkar said. “If we continue to see these results in more complex experiments, we hope to eventually propose a phase 1 clinical trial in patients with liver cancer.”