User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Oncology Nursing Professionalism: Advocating and Developing Oncology Certified Nurses
Introduction: The Commission on Cancer (COC), the New Mexico VA Health Care System (NMVAHCS) accrediting body for cancer care, mandates 25% of nurses maintain oncology nurse certification (OCN) to validate competency. However, the NMVAHCS remains deficient: threatening facility ability to maintain accreditation. Per the Oncology Nursing Certification Corporation, Albuquerque maintains 160 OCNs. However, 50% have retired and the remaining 50% are over 52. Leaving approximately 40 OCN nurses in a population of 500,000. This problem was not only a NMVAHCS problem, but a community problem: affecting quality of oncology care.
Problem: Not only is certification required for COC accredited facilities, it represents validation of expertise and skill set. Validation serves to build trust of Veterans, enables superior clinical judgment, and contributes to improved outcomes. With the Choice Program, many Veterans can leave the VAHCS. Certification serves to build necessary confidence required to keep Veterans within the VAHCS.
Methods: Barriers prohibiting certification were identified through survey of oncology nurses. Nurses reported fear related to failure, study material costs, exam fees, lack of mentors, and lack of internal leadership encouragement and support as barriers of certification. Funding was sought to provide a review course for 40 nurses, study guides, reimbursement of course and exam fees and held June 2017 in Albuquerque, New Mexico. A second review course, held during the 2017 AVAHO meeting, was conducted for another 24 nurses. The courses aimed to build confidence and decrease barriers. Both exceeded capacity.
Results: As a result of the Albuquerque course, VISN 22 and non-VA nurses attended from several states. Each received
a 30% reduction in exam fees and were eligible for exam reimbursement after passing: 50% of attendees are now OCNs.
The AVAHO course, to date, has resulted in an additional 2 OCNs, 2 certification renewals, and an additional 5 are registered for the exam. Those not taking the exam cite lack of leadership support and encouragement as the main
barrier.
Implications: Certification validates care provided and builds Veterans trust: necessary with Choice. Facilities that retain a strong foundation of OCNs, mentor staff, and maintain leadership support remain more apt to produce and sustain certified nurses. Therefore, leadership buy-in remains essential.
Introduction: The Commission on Cancer (COC), the New Mexico VA Health Care System (NMVAHCS) accrediting body for cancer care, mandates 25% of nurses maintain oncology nurse certification (OCN) to validate competency. However, the NMVAHCS remains deficient: threatening facility ability to maintain accreditation. Per the Oncology Nursing Certification Corporation, Albuquerque maintains 160 OCNs. However, 50% have retired and the remaining 50% are over 52. Leaving approximately 40 OCN nurses in a population of 500,000. This problem was not only a NMVAHCS problem, but a community problem: affecting quality of oncology care.
Problem: Not only is certification required for COC accredited facilities, it represents validation of expertise and skill set. Validation serves to build trust of Veterans, enables superior clinical judgment, and contributes to improved outcomes. With the Choice Program, many Veterans can leave the VAHCS. Certification serves to build necessary confidence required to keep Veterans within the VAHCS.
Methods: Barriers prohibiting certification were identified through survey of oncology nurses. Nurses reported fear related to failure, study material costs, exam fees, lack of mentors, and lack of internal leadership encouragement and support as barriers of certification. Funding was sought to provide a review course for 40 nurses, study guides, reimbursement of course and exam fees and held June 2017 in Albuquerque, New Mexico. A second review course, held during the 2017 AVAHO meeting, was conducted for another 24 nurses. The courses aimed to build confidence and decrease barriers. Both exceeded capacity.
Results: As a result of the Albuquerque course, VISN 22 and non-VA nurses attended from several states. Each received
a 30% reduction in exam fees and were eligible for exam reimbursement after passing: 50% of attendees are now OCNs.
The AVAHO course, to date, has resulted in an additional 2 OCNs, 2 certification renewals, and an additional 5 are registered for the exam. Those not taking the exam cite lack of leadership support and encouragement as the main
barrier.
Implications: Certification validates care provided and builds Veterans trust: necessary with Choice. Facilities that retain a strong foundation of OCNs, mentor staff, and maintain leadership support remain more apt to produce and sustain certified nurses. Therefore, leadership buy-in remains essential.
Introduction: The Commission on Cancer (COC), the New Mexico VA Health Care System (NMVAHCS) accrediting body for cancer care, mandates 25% of nurses maintain oncology nurse certification (OCN) to validate competency. However, the NMVAHCS remains deficient: threatening facility ability to maintain accreditation. Per the Oncology Nursing Certification Corporation, Albuquerque maintains 160 OCNs. However, 50% have retired and the remaining 50% are over 52. Leaving approximately 40 OCN nurses in a population of 500,000. This problem was not only a NMVAHCS problem, but a community problem: affecting quality of oncology care.
Problem: Not only is certification required for COC accredited facilities, it represents validation of expertise and skill set. Validation serves to build trust of Veterans, enables superior clinical judgment, and contributes to improved outcomes. With the Choice Program, many Veterans can leave the VAHCS. Certification serves to build necessary confidence required to keep Veterans within the VAHCS.
Methods: Barriers prohibiting certification were identified through survey of oncology nurses. Nurses reported fear related to failure, study material costs, exam fees, lack of mentors, and lack of internal leadership encouragement and support as barriers of certification. Funding was sought to provide a review course for 40 nurses, study guides, reimbursement of course and exam fees and held June 2017 in Albuquerque, New Mexico. A second review course, held during the 2017 AVAHO meeting, was conducted for another 24 nurses. The courses aimed to build confidence and decrease barriers. Both exceeded capacity.
Results: As a result of the Albuquerque course, VISN 22 and non-VA nurses attended from several states. Each received
a 30% reduction in exam fees and were eligible for exam reimbursement after passing: 50% of attendees are now OCNs.
The AVAHO course, to date, has resulted in an additional 2 OCNs, 2 certification renewals, and an additional 5 are registered for the exam. Those not taking the exam cite lack of leadership support and encouragement as the main
barrier.
Implications: Certification validates care provided and builds Veterans trust: necessary with Choice. Facilities that retain a strong foundation of OCNs, mentor staff, and maintain leadership support remain more apt to produce and sustain certified nurses. Therefore, leadership buy-in remains essential.
Occurrence of Skeletal-Related Events in Multiple Myeloma and Prostate Cancer Patients Receiving Standard Versus Extended-Interval Zoledronic Acid
Background/Purpose: Dysregulation of osteoclast activity and uncontrolled bone resorption are hallmarks of multiple myeloma and metastatic prostate cancer, predisposing patients to net bone loss and pathologic fractures. Zoledronic acid, a bisphosphonate, induces osteoclast apoptosis and reduces bone resorption, reducing fracture risk, but the optimal dosing interval is the subject of current clinical debate. Historically, the standard dosing interval has been every 4 weeks, but recent research demonstrated no difference in the rate of skeletal-related events (SREs)—fracture, spinal compression, bone irradiation, or surgery—when zoledronic acid was dosed every 12 weeks. The primary objective of this study was to determine if extending the zoledronic acid dosing interval would increase the incidence of SREs in a Veteran population.
Methods: Retrospective observational analysis of multiple myeloma and prostate cancer patients who received zoledronic acid. Patients were stratified by zoledronic acid dosing interval (standard or extended). Baseline data, duration of treatment, type and incidence of SREs, and incidence of osteonecrosis of the jaw (ONJ) were determined for each group. Pearson’s chi-square test was used to determine statistical significance.
Results: One hundred twenty-three patients were eligible for inclusion based on prespecified criteria. No difference in the rate of SREs was found between the standard- and extended-interval dosing groups (30.6% vs 22.9%, P = 0.374). All instances of ONJ occurred in the standard-interval dosing group, but the difference in incidence between groups was not statistically significant (2.5% vs 0%, P = .347). Subgroup analysis did not reveal a difference between multiple myeloma and metastatic prostate cancer in the incidence of SREs (42.9% vs 14.3%, P = .172; and 28% vs 25%, P = .753, respectively) or ONJ (4.8% vs 0%, P = .451; and 2% vs 0%, P = .577, respectively).
Conclusions/Impliacations: Based on our results, extending the zoledronic acid dosing interval does not increase the incidence of SREs. Dosing zoledronic acid every three months offers a potential avenue to increase Veteran compliance and decrease the chance for adverse drug reactions without compromising therapeutic benefit.
Background/Purpose: Dysregulation of osteoclast activity and uncontrolled bone resorption are hallmarks of multiple myeloma and metastatic prostate cancer, predisposing patients to net bone loss and pathologic fractures. Zoledronic acid, a bisphosphonate, induces osteoclast apoptosis and reduces bone resorption, reducing fracture risk, but the optimal dosing interval is the subject of current clinical debate. Historically, the standard dosing interval has been every 4 weeks, but recent research demonstrated no difference in the rate of skeletal-related events (SREs)—fracture, spinal compression, bone irradiation, or surgery—when zoledronic acid was dosed every 12 weeks. The primary objective of this study was to determine if extending the zoledronic acid dosing interval would increase the incidence of SREs in a Veteran population.
Methods: Retrospective observational analysis of multiple myeloma and prostate cancer patients who received zoledronic acid. Patients were stratified by zoledronic acid dosing interval (standard or extended). Baseline data, duration of treatment, type and incidence of SREs, and incidence of osteonecrosis of the jaw (ONJ) were determined for each group. Pearson’s chi-square test was used to determine statistical significance.
Results: One hundred twenty-three patients were eligible for inclusion based on prespecified criteria. No difference in the rate of SREs was found between the standard- and extended-interval dosing groups (30.6% vs 22.9%, P = 0.374). All instances of ONJ occurred in the standard-interval dosing group, but the difference in incidence between groups was not statistically significant (2.5% vs 0%, P = .347). Subgroup analysis did not reveal a difference between multiple myeloma and metastatic prostate cancer in the incidence of SREs (42.9% vs 14.3%, P = .172; and 28% vs 25%, P = .753, respectively) or ONJ (4.8% vs 0%, P = .451; and 2% vs 0%, P = .577, respectively).
Conclusions/Impliacations: Based on our results, extending the zoledronic acid dosing interval does not increase the incidence of SREs. Dosing zoledronic acid every three months offers a potential avenue to increase Veteran compliance and decrease the chance for adverse drug reactions without compromising therapeutic benefit.
Background/Purpose: Dysregulation of osteoclast activity and uncontrolled bone resorption are hallmarks of multiple myeloma and metastatic prostate cancer, predisposing patients to net bone loss and pathologic fractures. Zoledronic acid, a bisphosphonate, induces osteoclast apoptosis and reduces bone resorption, reducing fracture risk, but the optimal dosing interval is the subject of current clinical debate. Historically, the standard dosing interval has been every 4 weeks, but recent research demonstrated no difference in the rate of skeletal-related events (SREs)—fracture, spinal compression, bone irradiation, or surgery—when zoledronic acid was dosed every 12 weeks. The primary objective of this study was to determine if extending the zoledronic acid dosing interval would increase the incidence of SREs in a Veteran population.
Methods: Retrospective observational analysis of multiple myeloma and prostate cancer patients who received zoledronic acid. Patients were stratified by zoledronic acid dosing interval (standard or extended). Baseline data, duration of treatment, type and incidence of SREs, and incidence of osteonecrosis of the jaw (ONJ) were determined for each group. Pearson’s chi-square test was used to determine statistical significance.
Results: One hundred twenty-three patients were eligible for inclusion based on prespecified criteria. No difference in the rate of SREs was found between the standard- and extended-interval dosing groups (30.6% vs 22.9%, P = 0.374). All instances of ONJ occurred in the standard-interval dosing group, but the difference in incidence between groups was not statistically significant (2.5% vs 0%, P = .347). Subgroup analysis did not reveal a difference between multiple myeloma and metastatic prostate cancer in the incidence of SREs (42.9% vs 14.3%, P = .172; and 28% vs 25%, P = .753, respectively) or ONJ (4.8% vs 0%, P = .451; and 2% vs 0%, P = .577, respectively).
Conclusions/Impliacations: Based on our results, extending the zoledronic acid dosing interval does not increase the incidence of SREs. Dosing zoledronic acid every three months offers a potential avenue to increase Veteran compliance and decrease the chance for adverse drug reactions without compromising therapeutic benefit.
Use of Simulated Patients to Teach Goals of Care Conversations
Background: Understanding a patient’s expectations with treatment for their cancer is an important first step in caring for patients with cancer. Establishing goals of care allows providers to understand what their patients are willing to endure especially if they have a limited life expectancy. It provides a plan of care that is agreed upon by both the patient and provider. However, talking to patients about goals of care requires a skill set that many providers have not fully developed.
The use of simulated patients (SPs) has been shown to be an effective method to teach communication skills. However, many people feel intimidated when they are asked to work with SPs, especially if their conversations are viewed and critiqued by others. At the Pittsburgh VA we have developed a method that uses SPs to teach communication skills in a comfortable non-threatening environment for the learner. We tested this method with our Oncology providers.
Methods: Oncologists, nurses and social workers attended a meeting where they were asked to view a scenario where a patient and his family( SPs) were informed that the patient had progression of his cancer. In the first scenario the information was presented to SPs focusing on the cancer and treatment options. In the second scenario the same information was presented by an oncologist trained in palliative care focusing on the patient’s understanding of his disease and his goals of care. SPs were asked to contrast and comment on the different styles. The audience was then asked to provide comments and feedback.
Results: Twenty-two participants provided feedback. Twenty one of the participants agreed or strongly agreed that the simulation improved their knowledge and skill set and was done in a safe and comfortable learning environment.
Conclusions: Using SPs and allowing providers to contrast different styles of communicating the same set of information can be an effective and non-threatening teaching method of teaching communication skills. Longitudinal review of patient records will further help to determine the effectiveness of this method of training.
Background: Understanding a patient’s expectations with treatment for their cancer is an important first step in caring for patients with cancer. Establishing goals of care allows providers to understand what their patients are willing to endure especially if they have a limited life expectancy. It provides a plan of care that is agreed upon by both the patient and provider. However, talking to patients about goals of care requires a skill set that many providers have not fully developed.
The use of simulated patients (SPs) has been shown to be an effective method to teach communication skills. However, many people feel intimidated when they are asked to work with SPs, especially if their conversations are viewed and critiqued by others. At the Pittsburgh VA we have developed a method that uses SPs to teach communication skills in a comfortable non-threatening environment for the learner. We tested this method with our Oncology providers.
Methods: Oncologists, nurses and social workers attended a meeting where they were asked to view a scenario where a patient and his family( SPs) were informed that the patient had progression of his cancer. In the first scenario the information was presented to SPs focusing on the cancer and treatment options. In the second scenario the same information was presented by an oncologist trained in palliative care focusing on the patient’s understanding of his disease and his goals of care. SPs were asked to contrast and comment on the different styles. The audience was then asked to provide comments and feedback.
Results: Twenty-two participants provided feedback. Twenty one of the participants agreed or strongly agreed that the simulation improved their knowledge and skill set and was done in a safe and comfortable learning environment.
Conclusions: Using SPs and allowing providers to contrast different styles of communicating the same set of information can be an effective and non-threatening teaching method of teaching communication skills. Longitudinal review of patient records will further help to determine the effectiveness of this method of training.
Background: Understanding a patient’s expectations with treatment for their cancer is an important first step in caring for patients with cancer. Establishing goals of care allows providers to understand what their patients are willing to endure especially if they have a limited life expectancy. It provides a plan of care that is agreed upon by both the patient and provider. However, talking to patients about goals of care requires a skill set that many providers have not fully developed.
The use of simulated patients (SPs) has been shown to be an effective method to teach communication skills. However, many people feel intimidated when they are asked to work with SPs, especially if their conversations are viewed and critiqued by others. At the Pittsburgh VA we have developed a method that uses SPs to teach communication skills in a comfortable non-threatening environment for the learner. We tested this method with our Oncology providers.
Methods: Oncologists, nurses and social workers attended a meeting where they were asked to view a scenario where a patient and his family( SPs) were informed that the patient had progression of his cancer. In the first scenario the information was presented to SPs focusing on the cancer and treatment options. In the second scenario the same information was presented by an oncologist trained in palliative care focusing on the patient’s understanding of his disease and his goals of care. SPs were asked to contrast and comment on the different styles. The audience was then asked to provide comments and feedback.
Results: Twenty-two participants provided feedback. Twenty one of the participants agreed or strongly agreed that the simulation improved their knowledge and skill set and was done in a safe and comfortable learning environment.
Conclusions: Using SPs and allowing providers to contrast different styles of communicating the same set of information can be an effective and non-threatening teaching method of teaching communication skills. Longitudinal review of patient records will further help to determine the effectiveness of this method of training.
Model of Integrated Oncology- Palliative Care in an Outpatient Setting
Background: Early introduction of palliative care for oncology patients has demonstrated enhanced quality of life and satisfaction. We developed a model for integrating palliative care into outpatient oncology care.
Hypothesis: Optimal integration of oncology and palliative care requires palliative care clinician’s presence at initial, and many subsequent, patient encounters.
Objective: To implement and evaluate outpatient integrated oncology and palliative care.
Method: In January 2015, we implemented an integrated outpatient practice of oncology and palliative care with: Pre-clinic “huddle” among palliative care and oncology staff to identify patients in need of palliative care; shared palliative care-oncology appointments. Initial visit: New oncology patients are seen by an oncologist and palliative care physician together. Palliative care physician introduces palliative care and initiates advance care planning. Concurrent oncology-palliative care follow-up: High-risk patients (aggressive histology, progressing disease, etc) are followed by oncologist and palliative care physician. Palliative care physician facilitates goals of care discussions and addresses symptom management. End-of-life care: Hospice care remains a part of oncology care. Palliative care physician and oncology team co-manage all oncology patients enrolled in hospice care.
Results: Increase in palliative care consults from oncology clinics: After this intervention, there is a 10-fold increase in number of palliative care consultation requests from oncology clinics from fiscal year 2014 to 2017. Increase in percentage of inpatients deaths with prior palliative care consultation: Since the implementation of this model, there is an increase in the percentage of inpatient deaths with prior palliative care consultations; from 75% in fiscal year 2014 to 97% in fiscal year 2017.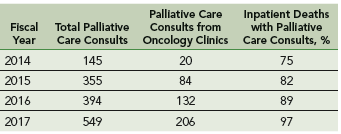
Challenges/Limitations: Single clinic setting, with one oncologist and palliative care physician, palliative care staffing, clinic space, administrative support.
Conclusions: Studies are needed to show impact of palliative care integration on acute care utilization, hospice care accession and satisfaction with care. There is a need to explore improved training and structures for both oncology and palliative care teams.
Background: Early introduction of palliative care for oncology patients has demonstrated enhanced quality of life and satisfaction. We developed a model for integrating palliative care into outpatient oncology care.
Hypothesis: Optimal integration of oncology and palliative care requires palliative care clinician’s presence at initial, and many subsequent, patient encounters.
Objective: To implement and evaluate outpatient integrated oncology and palliative care.
Method: In January 2015, we implemented an integrated outpatient practice of oncology and palliative care with: Pre-clinic “huddle” among palliative care and oncology staff to identify patients in need of palliative care; shared palliative care-oncology appointments. Initial visit: New oncology patients are seen by an oncologist and palliative care physician together. Palliative care physician introduces palliative care and initiates advance care planning. Concurrent oncology-palliative care follow-up: High-risk patients (aggressive histology, progressing disease, etc) are followed by oncologist and palliative care physician. Palliative care physician facilitates goals of care discussions and addresses symptom management. End-of-life care: Hospice care remains a part of oncology care. Palliative care physician and oncology team co-manage all oncology patients enrolled in hospice care.
Results: Increase in palliative care consults from oncology clinics: After this intervention, there is a 10-fold increase in number of palliative care consultation requests from oncology clinics from fiscal year 2014 to 2017. Increase in percentage of inpatients deaths with prior palliative care consultation: Since the implementation of this model, there is an increase in the percentage of inpatient deaths with prior palliative care consultations; from 75% in fiscal year 2014 to 97% in fiscal year 2017.
Challenges/Limitations: Single clinic setting, with one oncologist and palliative care physician, palliative care staffing, clinic space, administrative support.
Conclusions: Studies are needed to show impact of palliative care integration on acute care utilization, hospice care accession and satisfaction with care. There is a need to explore improved training and structures for both oncology and palliative care teams.
Background: Early introduction of palliative care for oncology patients has demonstrated enhanced quality of life and satisfaction. We developed a model for integrating palliative care into outpatient oncology care.
Hypothesis: Optimal integration of oncology and palliative care requires palliative care clinician’s presence at initial, and many subsequent, patient encounters.
Objective: To implement and evaluate outpatient integrated oncology and palliative care.
Method: In January 2015, we implemented an integrated outpatient practice of oncology and palliative care with: Pre-clinic “huddle” among palliative care and oncology staff to identify patients in need of palliative care; shared palliative care-oncology appointments. Initial visit: New oncology patients are seen by an oncologist and palliative care physician together. Palliative care physician introduces palliative care and initiates advance care planning. Concurrent oncology-palliative care follow-up: High-risk patients (aggressive histology, progressing disease, etc) are followed by oncologist and palliative care physician. Palliative care physician facilitates goals of care discussions and addresses symptom management. End-of-life care: Hospice care remains a part of oncology care. Palliative care physician and oncology team co-manage all oncology patients enrolled in hospice care.
Results: Increase in palliative care consults from oncology clinics: After this intervention, there is a 10-fold increase in number of palliative care consultation requests from oncology clinics from fiscal year 2014 to 2017. Increase in percentage of inpatients deaths with prior palliative care consultation: Since the implementation of this model, there is an increase in the percentage of inpatient deaths with prior palliative care consultations; from 75% in fiscal year 2014 to 97% in fiscal year 2017.
Challenges/Limitations: Single clinic setting, with one oncologist and palliative care physician, palliative care staffing, clinic space, administrative support.
Conclusions: Studies are needed to show impact of palliative care integration on acute care utilization, hospice care accession and satisfaction with care. There is a need to explore improved training and structures for both oncology and palliative care teams.
Rapid Onset of Severe Transaminitis in a Patient With Non-Small Cell Lung Cancer Receiving 480-mg Nivolumab
Background: This case describes severe transaminitis resulting 21 days after administration of the first dose of nivolumab 480 mg for non-small cell lung cancer (NSCLC) adenocarcinoma. The patient was an 81-year-old male whose disease had progressed after 3 cycles of carboplatin/pemetrexed. Molecular tumor marker testing did not reveal any actionable mutations prior to treatment.
Case Report: The patient initially presented with headaches, worsening shortness of breath and Grade 4 transaminitis (AST/ALT > 10x ULN). During hospitalization, he was treated with PO prednisone and IV methylprednisolone with a decrease in transaminases. Due to ongoing psychoses and worsening myopathies, the steroid doses were reduced. On day 14 of hospitalization, mycophenolate mofetil (MMF) 500 mg PO BID was initiated due to steroid refractory transaminitis. The patient was put on infection prophylaxis with sulfamethoxazole/trimethoprim and fluconazole at the time of MMF initiation. Valacyclovir was initiated when MMF was increased to 1,000 mg PO BID after three days without a response to lower doses. Ultimately the patient expired from cardiac failure 18 days after
hospitalization.
Discussion: Nivolumab recently received US Food and Drug Administration approval for every 4-week dosing based on pharmacokinetic data. Without clinical evidence, it was concluded that this increased dosing would not differ in safety or efficacy from previously approved doses, despite steady-state peak and average time concentrations predicted to be higher than the every 2-week dosing regimen. Both the National Comprehensive Cancer Network and American Society of Clinical Oncology recommend initiation of MMF for steroid refractory irAE transaminitis. These recommendations are based on case reports in patients receiving ipilimumab or nivolumab. The specific dosing and timing of initiation is not well elucidated. Additionally, there are case reports of use of antithymocyte globulin for management of irAEs.
Conclusions: Administration of 480-mg nivolumab may lead to more rapid onset of severe transaminitis. Administration of this dosing should be delayed until a patient demonstrates tolerability to the 240-mg dosing. High-dose steroids, in combination with MMF may provide more rapid clinical improvement. All patients on increased doses of immunosuppressive agents should receive opportunistic infection prophylaxis.
Background: This case describes severe transaminitis resulting 21 days after administration of the first dose of nivolumab 480 mg for non-small cell lung cancer (NSCLC) adenocarcinoma. The patient was an 81-year-old male whose disease had progressed after 3 cycles of carboplatin/pemetrexed. Molecular tumor marker testing did not reveal any actionable mutations prior to treatment.
Case Report: The patient initially presented with headaches, worsening shortness of breath and Grade 4 transaminitis (AST/ALT > 10x ULN). During hospitalization, he was treated with PO prednisone and IV methylprednisolone with a decrease in transaminases. Due to ongoing psychoses and worsening myopathies, the steroid doses were reduced. On day 14 of hospitalization, mycophenolate mofetil (MMF) 500 mg PO BID was initiated due to steroid refractory transaminitis. The patient was put on infection prophylaxis with sulfamethoxazole/trimethoprim and fluconazole at the time of MMF initiation. Valacyclovir was initiated when MMF was increased to 1,000 mg PO BID after three days without a response to lower doses. Ultimately the patient expired from cardiac failure 18 days after
hospitalization.
Discussion: Nivolumab recently received US Food and Drug Administration approval for every 4-week dosing based on pharmacokinetic data. Without clinical evidence, it was concluded that this increased dosing would not differ in safety or efficacy from previously approved doses, despite steady-state peak and average time concentrations predicted to be higher than the every 2-week dosing regimen. Both the National Comprehensive Cancer Network and American Society of Clinical Oncology recommend initiation of MMF for steroid refractory irAE transaminitis. These recommendations are based on case reports in patients receiving ipilimumab or nivolumab. The specific dosing and timing of initiation is not well elucidated. Additionally, there are case reports of use of antithymocyte globulin for management of irAEs.
Conclusions: Administration of 480-mg nivolumab may lead to more rapid onset of severe transaminitis. Administration of this dosing should be delayed until a patient demonstrates tolerability to the 240-mg dosing. High-dose steroids, in combination with MMF may provide more rapid clinical improvement. All patients on increased doses of immunosuppressive agents should receive opportunistic infection prophylaxis.
Background: This case describes severe transaminitis resulting 21 days after administration of the first dose of nivolumab 480 mg for non-small cell lung cancer (NSCLC) adenocarcinoma. The patient was an 81-year-old male whose disease had progressed after 3 cycles of carboplatin/pemetrexed. Molecular tumor marker testing did not reveal any actionable mutations prior to treatment.
Case Report: The patient initially presented with headaches, worsening shortness of breath and Grade 4 transaminitis (AST/ALT > 10x ULN). During hospitalization, he was treated with PO prednisone and IV methylprednisolone with a decrease in transaminases. Due to ongoing psychoses and worsening myopathies, the steroid doses were reduced. On day 14 of hospitalization, mycophenolate mofetil (MMF) 500 mg PO BID was initiated due to steroid refractory transaminitis. The patient was put on infection prophylaxis with sulfamethoxazole/trimethoprim and fluconazole at the time of MMF initiation. Valacyclovir was initiated when MMF was increased to 1,000 mg PO BID after three days without a response to lower doses. Ultimately the patient expired from cardiac failure 18 days after
hospitalization.
Discussion: Nivolumab recently received US Food and Drug Administration approval for every 4-week dosing based on pharmacokinetic data. Without clinical evidence, it was concluded that this increased dosing would not differ in safety or efficacy from previously approved doses, despite steady-state peak and average time concentrations predicted to be higher than the every 2-week dosing regimen. Both the National Comprehensive Cancer Network and American Society of Clinical Oncology recommend initiation of MMF for steroid refractory irAE transaminitis. These recommendations are based on case reports in patients receiving ipilimumab or nivolumab. The specific dosing and timing of initiation is not well elucidated. Additionally, there are case reports of use of antithymocyte globulin for management of irAEs.
Conclusions: Administration of 480-mg nivolumab may lead to more rapid onset of severe transaminitis. Administration of this dosing should be delayed until a patient demonstrates tolerability to the 240-mg dosing. High-dose steroids, in combination with MMF may provide more rapid clinical improvement. All patients on increased doses of immunosuppressive agents should receive opportunistic infection prophylaxis.
Use of Mobile Messaging System for Self-Management of Chemotherapy Symptoms in Patients With Advanced Cancer
Purpose/Rationale: Our Minneapolis VA Healthcare System (MVAHCS) team developed a self-management symptom program using the existing Annie Mobile Messaging System platform that was designed to be userfriendly for Veterans. We are currently determining which patients with advanced cancer might benefit most from the system. Here we describe early results from this program.
Background: Symptom monitoring programs using electronic communications platforms in patients with advanced solid tumors undergoing routine outpatient chemotherapy has resulted in benefits such as improved quality of life, improved survival, and reduced Emergency Room (ER) usage.
Methods: We created a symptom management protocol in conjunction with the Annie Program Team. Patients are sent text messages twice daily Monday through Friday, and they are asked to rate the following symptoms with a severity scale of 0-4 (absent, mild, moderate, severe, or disabling): Nausea/vomiting, mouth sores, fatigue, trouble breathing, appetite, constipation, diarrhea, numbness/tingling, and pain. In addition, patients are asked whether they have had a fever or not. Based on the patient response, the patient receives an automated, corresponding text back. The text may provide positive affirmation that they are doing well, give them education, refer them to an educational hyperlink, ask them to call a direct number to the clinic, or report directly to the ER.
Results: We have currently enrolled 5 patients in the program through screening new patient consults or those referred for chemotherapy education. There have not been any calls to the clinic or visits to the ER to date. Initial evaluation of the program via survey found no technology challenges and patients have been very positive about the program, including ease of use, appreciation of messages that validated when they were doing well, empowerment of self-management, and utilization of the texting advice.
Conclusions: Development and introduction of the MVAHCS Mobile Messaging System for Self-Management of Chemotherapy Symptoms has been completed. Early evaluation has not revealed any major concerns. We will continue to introduce this technology to patients undergoing chemotherapy and will further assess the feasibility and efficacy of this novel VA program.
Purpose/Rationale: Our Minneapolis VA Healthcare System (MVAHCS) team developed a self-management symptom program using the existing Annie Mobile Messaging System platform that was designed to be userfriendly for Veterans. We are currently determining which patients with advanced cancer might benefit most from the system. Here we describe early results from this program.
Background: Symptom monitoring programs using electronic communications platforms in patients with advanced solid tumors undergoing routine outpatient chemotherapy has resulted in benefits such as improved quality of life, improved survival, and reduced Emergency Room (ER) usage.
Methods: We created a symptom management protocol in conjunction with the Annie Program Team. Patients are sent text messages twice daily Monday through Friday, and they are asked to rate the following symptoms with a severity scale of 0-4 (absent, mild, moderate, severe, or disabling): Nausea/vomiting, mouth sores, fatigue, trouble breathing, appetite, constipation, diarrhea, numbness/tingling, and pain. In addition, patients are asked whether they have had a fever or not. Based on the patient response, the patient receives an automated, corresponding text back. The text may provide positive affirmation that they are doing well, give them education, refer them to an educational hyperlink, ask them to call a direct number to the clinic, or report directly to the ER.
Results: We have currently enrolled 5 patients in the program through screening new patient consults or those referred for chemotherapy education. There have not been any calls to the clinic or visits to the ER to date. Initial evaluation of the program via survey found no technology challenges and patients have been very positive about the program, including ease of use, appreciation of messages that validated when they were doing well, empowerment of self-management, and utilization of the texting advice.
Conclusions: Development and introduction of the MVAHCS Mobile Messaging System for Self-Management of Chemotherapy Symptoms has been completed. Early evaluation has not revealed any major concerns. We will continue to introduce this technology to patients undergoing chemotherapy and will further assess the feasibility and efficacy of this novel VA program.
Purpose/Rationale: Our Minneapolis VA Healthcare System (MVAHCS) team developed a self-management symptom program using the existing Annie Mobile Messaging System platform that was designed to be userfriendly for Veterans. We are currently determining which patients with advanced cancer might benefit most from the system. Here we describe early results from this program.
Background: Symptom monitoring programs using electronic communications platforms in patients with advanced solid tumors undergoing routine outpatient chemotherapy has resulted in benefits such as improved quality of life, improved survival, and reduced Emergency Room (ER) usage.
Methods: We created a symptom management protocol in conjunction with the Annie Program Team. Patients are sent text messages twice daily Monday through Friday, and they are asked to rate the following symptoms with a severity scale of 0-4 (absent, mild, moderate, severe, or disabling): Nausea/vomiting, mouth sores, fatigue, trouble breathing, appetite, constipation, diarrhea, numbness/tingling, and pain. In addition, patients are asked whether they have had a fever or not. Based on the patient response, the patient receives an automated, corresponding text back. The text may provide positive affirmation that they are doing well, give them education, refer them to an educational hyperlink, ask them to call a direct number to the clinic, or report directly to the ER.
Results: We have currently enrolled 5 patients in the program through screening new patient consults or those referred for chemotherapy education. There have not been any calls to the clinic or visits to the ER to date. Initial evaluation of the program via survey found no technology challenges and patients have been very positive about the program, including ease of use, appreciation of messages that validated when they were doing well, empowerment of self-management, and utilization of the texting advice.
Conclusions: Development and introduction of the MVAHCS Mobile Messaging System for Self-Management of Chemotherapy Symptoms has been completed. Early evaluation has not revealed any major concerns. We will continue to introduce this technology to patients undergoing chemotherapy and will further assess the feasibility and efficacy of this novel VA program.
First-Line Pembrolizumab Therapy in a Cisplatin-Ineligible Patient With Plasmacytoid Urothelial Carcinoma: A Case Report
Background: Plasmacytoid urothelial carcinoma (PUC) is a rare but aggressive variant of transitional cell carcinoma. In patients with unresectable disease, the most commonly used treatment is combination chemotherapy with methotrexate, vinblastine, doxorubicin and cisplatin (MVAC) or gemcitabine and cisplatin (GC). However, many patients with urothelial carcinoma are cisplatin-ineligible due to renal dysfunction, poor performance status or other comorbidities. We report a case of a cisplatin-ineligible veteran with metastatic PUC who was treated with pembrolizumab.
Case Report: A 71-year-old male veteran with 30 packyear smoking history, schizoaffective disorder and type 2 diabetes found to have multiple right-sided lung nodules and perihilar lymphadenopathy after presenting with atypical chest pain. Staging CT abdomen and pelvis showed bilateral adrenal masses and a large soft tissue mass in the right iliac fossa. Subsequent biopsy of the soft tissue mass had pathology consistent with PUC. As the patient was cisplatin-ineligible due to poor performance status and multiple medical comorbidities, the decision was made to treat with pembrolizumab 2 mg per kg IV every 3 weeks. Repeat CT chest, abdomen and pelvis showed partial response at 3 months and stable disease at 6 months.
Discussion: The KEYNOTE-052 study found that firstline pembrolizumab in cisplatin-ineligible patients with urothelial cancer resulted in complete or partial response in 24% of patients with few adverse effects. However, it is unclear if patients with plasmacytoid variant were included. To our knowledge, this is the first case report of a patient with metastatic PUC not only treated with pembrolizumab but shown to have clinical response.
Conclusions: Given our patient’s clinical response, pembrolizumab is a promising first-line agent for treating cisplatin-ineligible patients with metastatic PUC. Further evaluation is warranted to confirm the benefit of treatment with pembrolizumab in this patient population.
Background: Plasmacytoid urothelial carcinoma (PUC) is a rare but aggressive variant of transitional cell carcinoma. In patients with unresectable disease, the most commonly used treatment is combination chemotherapy with methotrexate, vinblastine, doxorubicin and cisplatin (MVAC) or gemcitabine and cisplatin (GC). However, many patients with urothelial carcinoma are cisplatin-ineligible due to renal dysfunction, poor performance status or other comorbidities. We report a case of a cisplatin-ineligible veteran with metastatic PUC who was treated with pembrolizumab.
Case Report: A 71-year-old male veteran with 30 packyear smoking history, schizoaffective disorder and type 2 diabetes found to have multiple right-sided lung nodules and perihilar lymphadenopathy after presenting with atypical chest pain. Staging CT abdomen and pelvis showed bilateral adrenal masses and a large soft tissue mass in the right iliac fossa. Subsequent biopsy of the soft tissue mass had pathology consistent with PUC. As the patient was cisplatin-ineligible due to poor performance status and multiple medical comorbidities, the decision was made to treat with pembrolizumab 2 mg per kg IV every 3 weeks. Repeat CT chest, abdomen and pelvis showed partial response at 3 months and stable disease at 6 months.
Discussion: The KEYNOTE-052 study found that firstline pembrolizumab in cisplatin-ineligible patients with urothelial cancer resulted in complete or partial response in 24% of patients with few adverse effects. However, it is unclear if patients with plasmacytoid variant were included. To our knowledge, this is the first case report of a patient with metastatic PUC not only treated with pembrolizumab but shown to have clinical response.
Conclusions: Given our patient’s clinical response, pembrolizumab is a promising first-line agent for treating cisplatin-ineligible patients with metastatic PUC. Further evaluation is warranted to confirm the benefit of treatment with pembrolizumab in this patient population.
Background: Plasmacytoid urothelial carcinoma (PUC) is a rare but aggressive variant of transitional cell carcinoma. In patients with unresectable disease, the most commonly used treatment is combination chemotherapy with methotrexate, vinblastine, doxorubicin and cisplatin (MVAC) or gemcitabine and cisplatin (GC). However, many patients with urothelial carcinoma are cisplatin-ineligible due to renal dysfunction, poor performance status or other comorbidities. We report a case of a cisplatin-ineligible veteran with metastatic PUC who was treated with pembrolizumab.
Case Report: A 71-year-old male veteran with 30 packyear smoking history, schizoaffective disorder and type 2 diabetes found to have multiple right-sided lung nodules and perihilar lymphadenopathy after presenting with atypical chest pain. Staging CT abdomen and pelvis showed bilateral adrenal masses and a large soft tissue mass in the right iliac fossa. Subsequent biopsy of the soft tissue mass had pathology consistent with PUC. As the patient was cisplatin-ineligible due to poor performance status and multiple medical comorbidities, the decision was made to treat with pembrolizumab 2 mg per kg IV every 3 weeks. Repeat CT chest, abdomen and pelvis showed partial response at 3 months and stable disease at 6 months.
Discussion: The KEYNOTE-052 study found that firstline pembrolizumab in cisplatin-ineligible patients with urothelial cancer resulted in complete or partial response in 24% of patients with few adverse effects. However, it is unclear if patients with plasmacytoid variant were included. To our knowledge, this is the first case report of a patient with metastatic PUC not only treated with pembrolizumab but shown to have clinical response.
Conclusions: Given our patient’s clinical response, pembrolizumab is a promising first-line agent for treating cisplatin-ineligible patients with metastatic PUC. Further evaluation is warranted to confirm the benefit of treatment with pembrolizumab in this patient population.
Outcomes similar for concurrent versus sequential treatment in HER2-positive breast cancers
Outcomes for women with operable HER2-positive breast cancer were similar whether they received standard combination chemotherapy with either concurrent or sequential paclitaxel/trastuzumab, long-term results of the phase 3, randomized American College of Surgeons Oncology Group Z1041 trial showed.
Among 280 women with HER-2 positive breast cancer followed for a median of 5.1 years, there were no significant differences in either pathological complete response rates (pCR), disease-free survival (DFS), or overall survival with either concurrent or sequential therapy, wrote Aman U. Buzdar, MD, from the University of Texas MD Anderson Cancer Center, Houston, and his colleagues.
“A previous publication of this study’s primary analysis reported that breast pCR in patients treated with paclitaxel and trastuzumab followed by FEC [fluorouracil, epirubicin, cyclophosphamide] and trastuzumab did not differ significantly from that of patients receiving FEC followed by paclitaxel and trastuzumab. We now report the findings concerning the secondary outcomes, that is, with a median follow-up of approximately 5 years, DFS is similar among the two treatment arms,” they wrote in JAMA Oncology.
The purpose of the current analysis was to evaluate long-term outcomes associated with the two treatment approaches.
In the trial, conducted at 36 centers in the continental United States and Puerto Rico, 280 women (median age, 50 years; range, 28-76 years) were treated with 500 mg/m2 of fluorouracil, 75 mg/m2 epirubicin, and 500 mg/m2 cyclophosphamide every 3 weeks for 12 weeks with concurrent weekly paclitaxel at 80 mg/m2 and trastuzumab at 2 mg/kg – after an initial dose of 4 mg/kg – or the same paclitaxel/trastuzumab combination delivered weekly for 12 weeks, followed by FEC every 3 weeks with weekly trastuzumab for 12 weeks.
Women who also had hormone receptor–positive disease received endocrine therapy. Radiotherapy was delivered at the discretion of the attending physician.
As noted, there were no differences in either DFS rates (adjusted hazard ratio, 1.02; P = .96) or overall survival rates (adjusted HR, 1.17; P = .73) between the trial arms.
The authors concluded that “concurrent administration of trastuzumab with FEC was not found to offer additional clinical benefit and is not warranted.”
The study was supported by grants to participating institutions from the National Cancer Institute. Dr. Buzdar reported no conflicts of interest. Three coauthors reported research support, consulting fees, travel support, and/or other relationships with multiple companies.
SOURCE: Buzdar AU et al. JAMA Oncol. 2018 Sept 6. doi: 10.1001/jamaoncol.2018.3691.
Outcomes for women with operable HER2-positive breast cancer were similar whether they received standard combination chemotherapy with either concurrent or sequential paclitaxel/trastuzumab, long-term results of the phase 3, randomized American College of Surgeons Oncology Group Z1041 trial showed.
Among 280 women with HER-2 positive breast cancer followed for a median of 5.1 years, there were no significant differences in either pathological complete response rates (pCR), disease-free survival (DFS), or overall survival with either concurrent or sequential therapy, wrote Aman U. Buzdar, MD, from the University of Texas MD Anderson Cancer Center, Houston, and his colleagues.
“A previous publication of this study’s primary analysis reported that breast pCR in patients treated with paclitaxel and trastuzumab followed by FEC [fluorouracil, epirubicin, cyclophosphamide] and trastuzumab did not differ significantly from that of patients receiving FEC followed by paclitaxel and trastuzumab. We now report the findings concerning the secondary outcomes, that is, with a median follow-up of approximately 5 years, DFS is similar among the two treatment arms,” they wrote in JAMA Oncology.
The purpose of the current analysis was to evaluate long-term outcomes associated with the two treatment approaches.
In the trial, conducted at 36 centers in the continental United States and Puerto Rico, 280 women (median age, 50 years; range, 28-76 years) were treated with 500 mg/m2 of fluorouracil, 75 mg/m2 epirubicin, and 500 mg/m2 cyclophosphamide every 3 weeks for 12 weeks with concurrent weekly paclitaxel at 80 mg/m2 and trastuzumab at 2 mg/kg – after an initial dose of 4 mg/kg – or the same paclitaxel/trastuzumab combination delivered weekly for 12 weeks, followed by FEC every 3 weeks with weekly trastuzumab for 12 weeks.
Women who also had hormone receptor–positive disease received endocrine therapy. Radiotherapy was delivered at the discretion of the attending physician.
As noted, there were no differences in either DFS rates (adjusted hazard ratio, 1.02; P = .96) or overall survival rates (adjusted HR, 1.17; P = .73) between the trial arms.
The authors concluded that “concurrent administration of trastuzumab with FEC was not found to offer additional clinical benefit and is not warranted.”
The study was supported by grants to participating institutions from the National Cancer Institute. Dr. Buzdar reported no conflicts of interest. Three coauthors reported research support, consulting fees, travel support, and/or other relationships with multiple companies.
SOURCE: Buzdar AU et al. JAMA Oncol. 2018 Sept 6. doi: 10.1001/jamaoncol.2018.3691.
Outcomes for women with operable HER2-positive breast cancer were similar whether they received standard combination chemotherapy with either concurrent or sequential paclitaxel/trastuzumab, long-term results of the phase 3, randomized American College of Surgeons Oncology Group Z1041 trial showed.
Among 280 women with HER-2 positive breast cancer followed for a median of 5.1 years, there were no significant differences in either pathological complete response rates (pCR), disease-free survival (DFS), or overall survival with either concurrent or sequential therapy, wrote Aman U. Buzdar, MD, from the University of Texas MD Anderson Cancer Center, Houston, and his colleagues.
“A previous publication of this study’s primary analysis reported that breast pCR in patients treated with paclitaxel and trastuzumab followed by FEC [fluorouracil, epirubicin, cyclophosphamide] and trastuzumab did not differ significantly from that of patients receiving FEC followed by paclitaxel and trastuzumab. We now report the findings concerning the secondary outcomes, that is, with a median follow-up of approximately 5 years, DFS is similar among the two treatment arms,” they wrote in JAMA Oncology.
The purpose of the current analysis was to evaluate long-term outcomes associated with the two treatment approaches.
In the trial, conducted at 36 centers in the continental United States and Puerto Rico, 280 women (median age, 50 years; range, 28-76 years) were treated with 500 mg/m2 of fluorouracil, 75 mg/m2 epirubicin, and 500 mg/m2 cyclophosphamide every 3 weeks for 12 weeks with concurrent weekly paclitaxel at 80 mg/m2 and trastuzumab at 2 mg/kg – after an initial dose of 4 mg/kg – or the same paclitaxel/trastuzumab combination delivered weekly for 12 weeks, followed by FEC every 3 weeks with weekly trastuzumab for 12 weeks.
Women who also had hormone receptor–positive disease received endocrine therapy. Radiotherapy was delivered at the discretion of the attending physician.
As noted, there were no differences in either DFS rates (adjusted hazard ratio, 1.02; P = .96) or overall survival rates (adjusted HR, 1.17; P = .73) between the trial arms.
The authors concluded that “concurrent administration of trastuzumab with FEC was not found to offer additional clinical benefit and is not warranted.”
The study was supported by grants to participating institutions from the National Cancer Institute. Dr. Buzdar reported no conflicts of interest. Three coauthors reported research support, consulting fees, travel support, and/or other relationships with multiple companies.
SOURCE: Buzdar AU et al. JAMA Oncol. 2018 Sept 6. doi: 10.1001/jamaoncol.2018.3691.
FROM JAMA ONCOLOGY
Key clinical point: Sequencing of chemotherapy, paclitaxel, and trastuzumab did not affect outcomes in women with HER2-positive breast cancers.
Major finding: There were no significant differences in disease-free survival or overall survival among treated with concurrent or sequential therapy.
Study details: A phase 3, randomized trial in 280 women with operable HER2-positive breast cancers.
Disclosures: The study was supported by grants to participating institutions from the National Cancer Institute. Dr. Buzdar reported no conflicts of interest. Three coauthors reported research support, consulting fees, travel support, and/or other relationships with multiple companies.
Source: Buzdar AU et al. JAMA Oncol. 2018 Sept 6. doi: 10.1001/jamaoncol.2018.3691.