User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Diet linked to lower risk of death from breast cancer
A balanced, low-fat diet was associated with a lower risk of death from breast cancer in a large cohort of postmenopausal women who had no previous history of breast cancer.
Researchers studied nearly 49,000 postmenopausal women and found a 21% lower risk of death from breast cancer among women who followed the balanced, low-fat diet, compared with women who followed their normal diet.
This research is scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Rowan Chlebowski, MD, PhD, of the Los Angeles Biomedical Research Institute at Harbor–UCLA Medical Center in Torrance, Calif., discussed the research during a press briefing in advance of the meeting.
About the study
The research is part of the Woman’s Health Initiative (NCT00000611), which is focused on investigating methods for preventing heart disease, breast and colorectal cancer, and osteoporotic fractures in postmenopausal women.
This trial enrolled 48,835 postmenopausal women, ages 50-79 years, with no history of breast cancer and normal mammograms at enrollment. From 1993 to 1998, the women were randomized to the study diet (n = 19,541) or their normal diet (n = 29,294).
With the normal diet, fat accounted for 32% or more of subjects’ daily calories. With the study diet, the goal was to reduce fat consumption to 20% or less of caloric intake. The study diet also required at least one daily serving of vegetables, fruits, and grains.
Dr. Chlebowski said the study diet is similar to DASH (Dietary Approaches to Stop Hypertension), but is slightly more focused on lowering fat intake.
Diet adherence
Subjects followed the study diet for a median of 8.5 years, and the median cumulative follow-up was 19.6 years.
Dr. Chlebowski noted that most women on the study diet were not able to reduce their daily fat consumption to the 20% goal. They did reduce fat consumption to 24.5% overall, which increased to 29% at the end of the intervention.
In the study-diet group, there was an average weight loss of 3%, significantly different from that of the normal-diet group (P less than .001).
Dr. Chlebowski said the weight loss indicates that subjects did adhere to the study diet, at least in part, as there was no change in physical activity among study participants. Furthermore, the researchers have evidence after 1 year that suggests subjects were incorporating more fruits and vegetables into their diets.
Breast cancer and death
At a median follow-up of 19.6 years, there were 3,374 cases of breast cancer, 1,011 deaths, and 383 deaths attributed to breast cancer.
The risk of death from breast cancer was significantly lower in the study-diet group than in the normal-diet group. The hazard ratio was 0.79 (95% confidence interval, 0.64-0.97; P = .025).
The risk of death (from any cause) after breast cancer was significantly lower in the study diet group as well, with a hazard ratio of 0.85 (95% confidence interval, 0.74-0.96; P = .01).
“Adoption of a low-fat dietary pattern reduces the risk of death from breast cancer in postmenopausal women,” Dr. Chlebowski said. “To our review, this is the only study providing randomized clinical trial evidence that an intervention can reduce a woman’s risk of dying from breast cancer.”
Dr. Chlebowski noted that the researchers have blood samples from all subjects enrolled in this study. The researchers plan to analyze those samples to further explore how the study diet affected the women and determine which components of the diet account for which effects.
The National Institutes of Health funded the study. The researchers disclosed relationships with Novartis, Pfizer, Amgen, AstraZeneca, Immunomedics, Metastat, Bayer, and Genentech/Roche.
SOURCE: Chlebowski R. et al. ASCO 2019. Abstract 520.
A balanced, low-fat diet was associated with a lower risk of death from breast cancer in a large cohort of postmenopausal women who had no previous history of breast cancer.
Researchers studied nearly 49,000 postmenopausal women and found a 21% lower risk of death from breast cancer among women who followed the balanced, low-fat diet, compared with women who followed their normal diet.
This research is scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Rowan Chlebowski, MD, PhD, of the Los Angeles Biomedical Research Institute at Harbor–UCLA Medical Center in Torrance, Calif., discussed the research during a press briefing in advance of the meeting.
About the study
The research is part of the Woman’s Health Initiative (NCT00000611), which is focused on investigating methods for preventing heart disease, breast and colorectal cancer, and osteoporotic fractures in postmenopausal women.
This trial enrolled 48,835 postmenopausal women, ages 50-79 years, with no history of breast cancer and normal mammograms at enrollment. From 1993 to 1998, the women were randomized to the study diet (n = 19,541) or their normal diet (n = 29,294).
With the normal diet, fat accounted for 32% or more of subjects’ daily calories. With the study diet, the goal was to reduce fat consumption to 20% or less of caloric intake. The study diet also required at least one daily serving of vegetables, fruits, and grains.
Dr. Chlebowski said the study diet is similar to DASH (Dietary Approaches to Stop Hypertension), but is slightly more focused on lowering fat intake.
Diet adherence
Subjects followed the study diet for a median of 8.5 years, and the median cumulative follow-up was 19.6 years.
Dr. Chlebowski noted that most women on the study diet were not able to reduce their daily fat consumption to the 20% goal. They did reduce fat consumption to 24.5% overall, which increased to 29% at the end of the intervention.
In the study-diet group, there was an average weight loss of 3%, significantly different from that of the normal-diet group (P less than .001).
Dr. Chlebowski said the weight loss indicates that subjects did adhere to the study diet, at least in part, as there was no change in physical activity among study participants. Furthermore, the researchers have evidence after 1 year that suggests subjects were incorporating more fruits and vegetables into their diets.
Breast cancer and death
At a median follow-up of 19.6 years, there were 3,374 cases of breast cancer, 1,011 deaths, and 383 deaths attributed to breast cancer.
The risk of death from breast cancer was significantly lower in the study-diet group than in the normal-diet group. The hazard ratio was 0.79 (95% confidence interval, 0.64-0.97; P = .025).
The risk of death (from any cause) after breast cancer was significantly lower in the study diet group as well, with a hazard ratio of 0.85 (95% confidence interval, 0.74-0.96; P = .01).
“Adoption of a low-fat dietary pattern reduces the risk of death from breast cancer in postmenopausal women,” Dr. Chlebowski said. “To our review, this is the only study providing randomized clinical trial evidence that an intervention can reduce a woman’s risk of dying from breast cancer.”
Dr. Chlebowski noted that the researchers have blood samples from all subjects enrolled in this study. The researchers plan to analyze those samples to further explore how the study diet affected the women and determine which components of the diet account for which effects.
The National Institutes of Health funded the study. The researchers disclosed relationships with Novartis, Pfizer, Amgen, AstraZeneca, Immunomedics, Metastat, Bayer, and Genentech/Roche.
SOURCE: Chlebowski R. et al. ASCO 2019. Abstract 520.
A balanced, low-fat diet was associated with a lower risk of death from breast cancer in a large cohort of postmenopausal women who had no previous history of breast cancer.
Researchers studied nearly 49,000 postmenopausal women and found a 21% lower risk of death from breast cancer among women who followed the balanced, low-fat diet, compared with women who followed their normal diet.
This research is scheduled to be presented at the annual meeting of the American Society of Clinical Oncology.
Rowan Chlebowski, MD, PhD, of the Los Angeles Biomedical Research Institute at Harbor–UCLA Medical Center in Torrance, Calif., discussed the research during a press briefing in advance of the meeting.
About the study
The research is part of the Woman’s Health Initiative (NCT00000611), which is focused on investigating methods for preventing heart disease, breast and colorectal cancer, and osteoporotic fractures in postmenopausal women.
This trial enrolled 48,835 postmenopausal women, ages 50-79 years, with no history of breast cancer and normal mammograms at enrollment. From 1993 to 1998, the women were randomized to the study diet (n = 19,541) or their normal diet (n = 29,294).
With the normal diet, fat accounted for 32% or more of subjects’ daily calories. With the study diet, the goal was to reduce fat consumption to 20% or less of caloric intake. The study diet also required at least one daily serving of vegetables, fruits, and grains.
Dr. Chlebowski said the study diet is similar to DASH (Dietary Approaches to Stop Hypertension), but is slightly more focused on lowering fat intake.
Diet adherence
Subjects followed the study diet for a median of 8.5 years, and the median cumulative follow-up was 19.6 years.
Dr. Chlebowski noted that most women on the study diet were not able to reduce their daily fat consumption to the 20% goal. They did reduce fat consumption to 24.5% overall, which increased to 29% at the end of the intervention.
In the study-diet group, there was an average weight loss of 3%, significantly different from that of the normal-diet group (P less than .001).
Dr. Chlebowski said the weight loss indicates that subjects did adhere to the study diet, at least in part, as there was no change in physical activity among study participants. Furthermore, the researchers have evidence after 1 year that suggests subjects were incorporating more fruits and vegetables into their diets.
Breast cancer and death
At a median follow-up of 19.6 years, there were 3,374 cases of breast cancer, 1,011 deaths, and 383 deaths attributed to breast cancer.
The risk of death from breast cancer was significantly lower in the study-diet group than in the normal-diet group. The hazard ratio was 0.79 (95% confidence interval, 0.64-0.97; P = .025).
The risk of death (from any cause) after breast cancer was significantly lower in the study diet group as well, with a hazard ratio of 0.85 (95% confidence interval, 0.74-0.96; P = .01).
“Adoption of a low-fat dietary pattern reduces the risk of death from breast cancer in postmenopausal women,” Dr. Chlebowski said. “To our review, this is the only study providing randomized clinical trial evidence that an intervention can reduce a woman’s risk of dying from breast cancer.”
Dr. Chlebowski noted that the researchers have blood samples from all subjects enrolled in this study. The researchers plan to analyze those samples to further explore how the study diet affected the women and determine which components of the diet account for which effects.
The National Institutes of Health funded the study. The researchers disclosed relationships with Novartis, Pfizer, Amgen, AstraZeneca, Immunomedics, Metastat, Bayer, and Genentech/Roche.
SOURCE: Chlebowski R. et al. ASCO 2019. Abstract 520.
REPORTING FROM ASCO 2019
Key clinical point: Women who followed a balanced, low-fat diet had a lower risk of death from breast cancer compared with women who followed their normal diet.
Major finding: The risk of death from breast cancer was significantly lower in the study-diet group than in the normal-diet group (hazard ratio, 0.79, 95% confidence interval, 0.64-0.97; P = .025).
Study details: A cohort from the Women’s Health Initiative, which randomized 48,835 postmenopausal women to a low-fat diet or to their normal diet.
Disclosures: The National Institutes of Health funded the study. The researchers disclosed relationships with Novartis, Pfizer, Amgen, AstraZeneca, Immunomedics, Metastat, Bayer, and Genentech/Roche.
Source: Chlebowski R. et al. ASCO 2019. Abstract 520.
PET imaging at diagnosis improves oropharyngeal cancer outcomes
For patients with oropharyngeal squamous cell carcinoma (OPSCC), initial staging with PET is associated with better cancer-specific survival (CSS) than staging with other imaging modalities, based on a retrospective analysis of more than 1,700 patients.
PET was associated with a better 3-year overall survival rate than either MRI without PET or CT alone, reported lead author Rustain L. Morgan, MD, of the University of Colorado at Denver, Aurora, and colleagues.
“To our knowledge, there have been no prospective, randomized, controlled trials to date to evaluate the effect of different imaging modalities at the time of initial staging on cancer-specific survival,” the investigators wrote in Cancer. “A population-based data source such as the Surveillance, Epidemiology, and End Results [SEER]–Medicare database provides an excellent opportunity to compare the impact of imaging modality differences on survival in patients with OPSCC.”
Using SEER data, the investigators identified more than 3,704 patients with oropharyngeal cancer; following exclusions, 1,765 patients were involved in the final analysis based on various factors, including survival beyond 2 months after diagnosis and squamous cell carcinoma histology. A Cox proportional hazards model was used to assess relationships between the primary outcome and 3-year CSS rate and imaging, sex, age, region, race, and education.
Results showed that most patients had PET imaging upon diagnosis (83.3%), while fewer had CT alone (11.4%) or MRI without PET (5.2%). Several underlying trends were found: Patients in the West were more likely to undergo PET than patients in the Midwest, South, or East; patients younger than 75 years were more likely to have PET than older patients; and men were more likely to be staged with PET than women. The 3-year CSS was longest for patients who underwent PET (56.8%), followed by MRI without PET (50.1%) and CT alone (47.3%). Controlling for treatment and stage of disease, multivariate analysis also suggested that PET is associated with better CSS; patients staged with MRI without PET had a hazard ratio of 1.748 (P = .0036) and those imaged with CT alone had an HR of 1.337 (P = .0491). Although the Cox proportional hazards model for overall survival revealed numerical trends, these lacked statistical significance for MRI without PET (HR, 1.365; P =.0683) and CT alone (HR, 1.213; P = .114).
“The current study demonstrated a significant difference in CSS based on initial imaging,” the investigators wrote. “These findings are consistent with a prior study that reported that PET imaging can improve the staging of patients with head and neck cancers, particularly as it relates to radiotherapy planning.
“The data from the current study suggest the need for further prospective research to evaluate whether CT or MRI should be considered adequate for the initial staging of patients with OPSCC,” the investigators concluded.
The study was funded by the University of Colorado Cancer Center. One coauthor reported relationships with the American Heart Association and the National Heart, Lung, and Blood Institute.
SOURCE: Morgan RL et al. Cancer. 2019 May 1. doi:10.1002/cncr.32148.
For patients with oropharyngeal squamous cell carcinoma (OPSCC), initial staging with PET is associated with better cancer-specific survival (CSS) than staging with other imaging modalities, based on a retrospective analysis of more than 1,700 patients.
PET was associated with a better 3-year overall survival rate than either MRI without PET or CT alone, reported lead author Rustain L. Morgan, MD, of the University of Colorado at Denver, Aurora, and colleagues.
“To our knowledge, there have been no prospective, randomized, controlled trials to date to evaluate the effect of different imaging modalities at the time of initial staging on cancer-specific survival,” the investigators wrote in Cancer. “A population-based data source such as the Surveillance, Epidemiology, and End Results [SEER]–Medicare database provides an excellent opportunity to compare the impact of imaging modality differences on survival in patients with OPSCC.”
Using SEER data, the investigators identified more than 3,704 patients with oropharyngeal cancer; following exclusions, 1,765 patients were involved in the final analysis based on various factors, including survival beyond 2 months after diagnosis and squamous cell carcinoma histology. A Cox proportional hazards model was used to assess relationships between the primary outcome and 3-year CSS rate and imaging, sex, age, region, race, and education.
Results showed that most patients had PET imaging upon diagnosis (83.3%), while fewer had CT alone (11.4%) or MRI without PET (5.2%). Several underlying trends were found: Patients in the West were more likely to undergo PET than patients in the Midwest, South, or East; patients younger than 75 years were more likely to have PET than older patients; and men were more likely to be staged with PET than women. The 3-year CSS was longest for patients who underwent PET (56.8%), followed by MRI without PET (50.1%) and CT alone (47.3%). Controlling for treatment and stage of disease, multivariate analysis also suggested that PET is associated with better CSS; patients staged with MRI without PET had a hazard ratio of 1.748 (P = .0036) and those imaged with CT alone had an HR of 1.337 (P = .0491). Although the Cox proportional hazards model for overall survival revealed numerical trends, these lacked statistical significance for MRI without PET (HR, 1.365; P =.0683) and CT alone (HR, 1.213; P = .114).
“The current study demonstrated a significant difference in CSS based on initial imaging,” the investigators wrote. “These findings are consistent with a prior study that reported that PET imaging can improve the staging of patients with head and neck cancers, particularly as it relates to radiotherapy planning.
“The data from the current study suggest the need for further prospective research to evaluate whether CT or MRI should be considered adequate for the initial staging of patients with OPSCC,” the investigators concluded.
The study was funded by the University of Colorado Cancer Center. One coauthor reported relationships with the American Heart Association and the National Heart, Lung, and Blood Institute.
SOURCE: Morgan RL et al. Cancer. 2019 May 1. doi:10.1002/cncr.32148.
For patients with oropharyngeal squamous cell carcinoma (OPSCC), initial staging with PET is associated with better cancer-specific survival (CSS) than staging with other imaging modalities, based on a retrospective analysis of more than 1,700 patients.
PET was associated with a better 3-year overall survival rate than either MRI without PET or CT alone, reported lead author Rustain L. Morgan, MD, of the University of Colorado at Denver, Aurora, and colleagues.
“To our knowledge, there have been no prospective, randomized, controlled trials to date to evaluate the effect of different imaging modalities at the time of initial staging on cancer-specific survival,” the investigators wrote in Cancer. “A population-based data source such as the Surveillance, Epidemiology, and End Results [SEER]–Medicare database provides an excellent opportunity to compare the impact of imaging modality differences on survival in patients with OPSCC.”
Using SEER data, the investigators identified more than 3,704 patients with oropharyngeal cancer; following exclusions, 1,765 patients were involved in the final analysis based on various factors, including survival beyond 2 months after diagnosis and squamous cell carcinoma histology. A Cox proportional hazards model was used to assess relationships between the primary outcome and 3-year CSS rate and imaging, sex, age, region, race, and education.
Results showed that most patients had PET imaging upon diagnosis (83.3%), while fewer had CT alone (11.4%) or MRI without PET (5.2%). Several underlying trends were found: Patients in the West were more likely to undergo PET than patients in the Midwest, South, or East; patients younger than 75 years were more likely to have PET than older patients; and men were more likely to be staged with PET than women. The 3-year CSS was longest for patients who underwent PET (56.8%), followed by MRI without PET (50.1%) and CT alone (47.3%). Controlling for treatment and stage of disease, multivariate analysis also suggested that PET is associated with better CSS; patients staged with MRI without PET had a hazard ratio of 1.748 (P = .0036) and those imaged with CT alone had an HR of 1.337 (P = .0491). Although the Cox proportional hazards model for overall survival revealed numerical trends, these lacked statistical significance for MRI without PET (HR, 1.365; P =.0683) and CT alone (HR, 1.213; P = .114).
“The current study demonstrated a significant difference in CSS based on initial imaging,” the investigators wrote. “These findings are consistent with a prior study that reported that PET imaging can improve the staging of patients with head and neck cancers, particularly as it relates to radiotherapy planning.
“The data from the current study suggest the need for further prospective research to evaluate whether CT or MRI should be considered adequate for the initial staging of patients with OPSCC,” the investigators concluded.
The study was funded by the University of Colorado Cancer Center. One coauthor reported relationships with the American Heart Association and the National Heart, Lung, and Blood Institute.
SOURCE: Morgan RL et al. Cancer. 2019 May 1. doi:10.1002/cncr.32148.
FROM CANCER
Key clinical point: For patients with oropharyngeal cancer, initial staging with PET imaging is associated with better cancer-specific survival than staging with other imaging modalities.
Major finding: Patients who underwent PET at diagnosis had a 3-year overall survival rate of 56.8%, compared with those who had MRI without PET (50.1%) or CT alone (47.3%).
Study details: A retrospective analysis of 1,765 patients with oropharyngeal cancer who had imaging performed at diagnosis.
Disclosures: The study was funded by the University of Colorado Cancer Center. One coauthor reported relationships with the American Heart Association and the National Heart, Lung, and Blood Institute.
Source: Morgan RL et al. Cancer. 2019 May 1. doi:10.1002/cncr.32148.
FDA approves venetoclax/obinutuzumab combo for CLL
The Food and Drug Administration has approved the combination of venetoclax (Venclexta) plus obinutuzumab (Gazyva) for patients with previously untreated chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma.

The approval provides a chemotherapy-free, fixed duration treatment. The FDA based the approval on the results of the phase 3 CLL14 trial, which will be presented at the 2019 annual meeting of the American Society of Clinical Oncology.
Researchers randomized 432 patients to either a 12-month duration of venetoclax with a 6-month duration of obinutuzumab or to a 6-month duration of obinutuzumab plus chlorambucil and another 6-month duration of chlorambucil.
The newly approved combination reduced the risk of disease progression or death (progression-free survival as assessed by an independent review committee) by 67%, compared with obinutuzumab/chlorambucil (hazard ratio, 0.33; P less than .0001).
Venetoclax/obinutuzumab also had a higher rate of minimal residual disease negativity in bone marrow and peripheral blood, compared to the other combination, according to Genentech.
The most common adverse reactions of any grade reported for venetoclax/obinutuzumab were neutropenia, diarrhea, fatigue, nausea, anemia, and upper respiratory tract infection.
The Food and Drug Administration has approved the combination of venetoclax (Venclexta) plus obinutuzumab (Gazyva) for patients with previously untreated chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma.
The approval provides a chemotherapy-free, fixed duration treatment. The FDA based the approval on the results of the phase 3 CLL14 trial, which will be presented at the 2019 annual meeting of the American Society of Clinical Oncology.
Researchers randomized 432 patients to either a 12-month duration of venetoclax with a 6-month duration of obinutuzumab or to a 6-month duration of obinutuzumab plus chlorambucil and another 6-month duration of chlorambucil.
The newly approved combination reduced the risk of disease progression or death (progression-free survival as assessed by an independent review committee) by 67%, compared with obinutuzumab/chlorambucil (hazard ratio, 0.33; P less than .0001).
Venetoclax/obinutuzumab also had a higher rate of minimal residual disease negativity in bone marrow and peripheral blood, compared to the other combination, according to Genentech.
The most common adverse reactions of any grade reported for venetoclax/obinutuzumab were neutropenia, diarrhea, fatigue, nausea, anemia, and upper respiratory tract infection.
The Food and Drug Administration has approved the combination of venetoclax (Venclexta) plus obinutuzumab (Gazyva) for patients with previously untreated chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma.
The approval provides a chemotherapy-free, fixed duration treatment. The FDA based the approval on the results of the phase 3 CLL14 trial, which will be presented at the 2019 annual meeting of the American Society of Clinical Oncology.
Researchers randomized 432 patients to either a 12-month duration of venetoclax with a 6-month duration of obinutuzumab or to a 6-month duration of obinutuzumab plus chlorambucil and another 6-month duration of chlorambucil.
The newly approved combination reduced the risk of disease progression or death (progression-free survival as assessed by an independent review committee) by 67%, compared with obinutuzumab/chlorambucil (hazard ratio, 0.33; P less than .0001).
Venetoclax/obinutuzumab also had a higher rate of minimal residual disease negativity in bone marrow and peripheral blood, compared to the other combination, according to Genentech.
The most common adverse reactions of any grade reported for venetoclax/obinutuzumab were neutropenia, diarrhea, fatigue, nausea, anemia, and upper respiratory tract infection.
Subclinical hypothyroidism may be associated with increased cancer risks
LOS ANGELES – There is no consistent evidence to suggest that subclinical hypothyroidism is linked to an increased risk of incident breast, prostate, or colon cancer. The condition, however, may be linked to an increased risk of thyroid malignancy and to an increased risk of overall cancer mortality.
These findings come from the first systematic review to examine the effect of subclinical hypothyroidism on the risk of incident cancer and cancer mortality.
“Subclinical hypothyroidism is very prevalent,” lead study author Oriana Yu, MD, MSc, said in an interview at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists. “It affects up to 10% of people, yet at this time we are uncertain as to whether or not [we should] treat them. Most studies have focused on cardiovascular outcomes, because we know that thyroid hormone is very important in lipid metabolism.”
Dr. Yu, an endocrinologist at McGill University, Montreal, and her colleagues searched the Ovid MEDLINE database for articles published from the date of its inception until Nov. 13, 2017, and combined words related to thyroid function and cancer in their search. They limited the analysis to randomized clinical trials and cohort and case-control studies in which the thyroid dysfunction chronologically preceded the cancer incidence or mortality by at least one year.
Of the 180 records screened, 51 full-text articles were assessed for eligibility. Of those, nine met the criteria for systematic review – seven related to cancer risk and two to cancer mortality. The studies were deemed to be of good to medium quality, but six of the nine were cohort studies, the rest case-control studies. “We had hoped to do a systematic review and meta-analysis, but there was high heterogeneity in the studies, especially in terms of different risk measures and outcomes reported,” Dr. Yu said. “As a result, we were not able to perform a meta-analysis.”
The researchers found that the studies had inconsistent findings when it came to the impact of subclinical hypothyroidism on the risk of breast, prostate, and colon cancer. For example, one prospective cohort study of 2,738 patients found no association between subclinical hypothyroidism and the risk of breast cancer (odds ratio, 1.9; 95% confidence interval, 0.8-4.9; Thyroid. 2005;15[11]:1253-9). Women with breast cancer, however, were more likely to have thyroid autoantibodies.
Meanwhile, a case-control study of 1,201 men found that those with elevated TSH levels had a decreased risk of prostate cancer (OR, 0.71; 95% CI, 0.47-1.06; PLoS One. 2012 Oct 30. doi: 10.1371/journal.pone.0047730). “That was a bit surprising to us,” Dr. Yu said. In addition, a nested case-control study of 103,044 patients found that subclinical hypothyroidism was linked to an increased risk for colon cancer (OR, 1.16; 95% CI, 1.08-1.24; J Natl Cancer Inst. 2015 Apr 8. doi: 10.1093/jnci/djv084).
Of the two studies that focused on cancer mortality, one retrospective cohort analysis of 4,735 patients showed that treatment of subclinical hypothyroidism was associated with a decreased risk of cancer mortality in those aged 40-70 years (hazard ratio, 0.59; 95% CI, 0.21-0.99; Arch Intern Med. 2012;172[10]:811-7). The other study, a retrospective cohort analysis of 115,746 patients, found that subclinical hypothyroidism was associated with an increased risk of cancer mortality (relative risk, 1.51; 95% CI, 1.06-2.15; PLoS One. 2015 Apr 1. doi: 10.1371/journal.pone.0122955).
“We need to interpret the cancer-related mortality findings with caution,” Dr. Yu said. “There’s concern about whether patients who are treated might be [generally] healthier or were less frail, compared with those who were not treated. Although these studies adjusted for a number of confounders, it may be difficult to measure and adjust for [those two] factors. That might explain the findings in the two studies on cancer-related mortality.”
Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
LOS ANGELES – There is no consistent evidence to suggest that subclinical hypothyroidism is linked to an increased risk of incident breast, prostate, or colon cancer. The condition, however, may be linked to an increased risk of thyroid malignancy and to an increased risk of overall cancer mortality.
These findings come from the first systematic review to examine the effect of subclinical hypothyroidism on the risk of incident cancer and cancer mortality.
“Subclinical hypothyroidism is very prevalent,” lead study author Oriana Yu, MD, MSc, said in an interview at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists. “It affects up to 10% of people, yet at this time we are uncertain as to whether or not [we should] treat them. Most studies have focused on cardiovascular outcomes, because we know that thyroid hormone is very important in lipid metabolism.”
Dr. Yu, an endocrinologist at McGill University, Montreal, and her colleagues searched the Ovid MEDLINE database for articles published from the date of its inception until Nov. 13, 2017, and combined words related to thyroid function and cancer in their search. They limited the analysis to randomized clinical trials and cohort and case-control studies in which the thyroid dysfunction chronologically preceded the cancer incidence or mortality by at least one year.
Of the 180 records screened, 51 full-text articles were assessed for eligibility. Of those, nine met the criteria for systematic review – seven related to cancer risk and two to cancer mortality. The studies were deemed to be of good to medium quality, but six of the nine were cohort studies, the rest case-control studies. “We had hoped to do a systematic review and meta-analysis, but there was high heterogeneity in the studies, especially in terms of different risk measures and outcomes reported,” Dr. Yu said. “As a result, we were not able to perform a meta-analysis.”
The researchers found that the studies had inconsistent findings when it came to the impact of subclinical hypothyroidism on the risk of breast, prostate, and colon cancer. For example, one prospective cohort study of 2,738 patients found no association between subclinical hypothyroidism and the risk of breast cancer (odds ratio, 1.9; 95% confidence interval, 0.8-4.9; Thyroid. 2005;15[11]:1253-9). Women with breast cancer, however, were more likely to have thyroid autoantibodies.
Meanwhile, a case-control study of 1,201 men found that those with elevated TSH levels had a decreased risk of prostate cancer (OR, 0.71; 95% CI, 0.47-1.06; PLoS One. 2012 Oct 30. doi: 10.1371/journal.pone.0047730). “That was a bit surprising to us,” Dr. Yu said. In addition, a nested case-control study of 103,044 patients found that subclinical hypothyroidism was linked to an increased risk for colon cancer (OR, 1.16; 95% CI, 1.08-1.24; J Natl Cancer Inst. 2015 Apr 8. doi: 10.1093/jnci/djv084).
Of the two studies that focused on cancer mortality, one retrospective cohort analysis of 4,735 patients showed that treatment of subclinical hypothyroidism was associated with a decreased risk of cancer mortality in those aged 40-70 years (hazard ratio, 0.59; 95% CI, 0.21-0.99; Arch Intern Med. 2012;172[10]:811-7). The other study, a retrospective cohort analysis of 115,746 patients, found that subclinical hypothyroidism was associated with an increased risk of cancer mortality (relative risk, 1.51; 95% CI, 1.06-2.15; PLoS One. 2015 Apr 1. doi: 10.1371/journal.pone.0122955).
“We need to interpret the cancer-related mortality findings with caution,” Dr. Yu said. “There’s concern about whether patients who are treated might be [generally] healthier or were less frail, compared with those who were not treated. Although these studies adjusted for a number of confounders, it may be difficult to measure and adjust for [those two] factors. That might explain the findings in the two studies on cancer-related mortality.”
Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
LOS ANGELES – There is no consistent evidence to suggest that subclinical hypothyroidism is linked to an increased risk of incident breast, prostate, or colon cancer. The condition, however, may be linked to an increased risk of thyroid malignancy and to an increased risk of overall cancer mortality.
These findings come from the first systematic review to examine the effect of subclinical hypothyroidism on the risk of incident cancer and cancer mortality.
“Subclinical hypothyroidism is very prevalent,” lead study author Oriana Yu, MD, MSc, said in an interview at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists. “It affects up to 10% of people, yet at this time we are uncertain as to whether or not [we should] treat them. Most studies have focused on cardiovascular outcomes, because we know that thyroid hormone is very important in lipid metabolism.”
Dr. Yu, an endocrinologist at McGill University, Montreal, and her colleagues searched the Ovid MEDLINE database for articles published from the date of its inception until Nov. 13, 2017, and combined words related to thyroid function and cancer in their search. They limited the analysis to randomized clinical trials and cohort and case-control studies in which the thyroid dysfunction chronologically preceded the cancer incidence or mortality by at least one year.
Of the 180 records screened, 51 full-text articles were assessed for eligibility. Of those, nine met the criteria for systematic review – seven related to cancer risk and two to cancer mortality. The studies were deemed to be of good to medium quality, but six of the nine were cohort studies, the rest case-control studies. “We had hoped to do a systematic review and meta-analysis, but there was high heterogeneity in the studies, especially in terms of different risk measures and outcomes reported,” Dr. Yu said. “As a result, we were not able to perform a meta-analysis.”
The researchers found that the studies had inconsistent findings when it came to the impact of subclinical hypothyroidism on the risk of breast, prostate, and colon cancer. For example, one prospective cohort study of 2,738 patients found no association between subclinical hypothyroidism and the risk of breast cancer (odds ratio, 1.9; 95% confidence interval, 0.8-4.9; Thyroid. 2005;15[11]:1253-9). Women with breast cancer, however, were more likely to have thyroid autoantibodies.
Meanwhile, a case-control study of 1,201 men found that those with elevated TSH levels had a decreased risk of prostate cancer (OR, 0.71; 95% CI, 0.47-1.06; PLoS One. 2012 Oct 30. doi: 10.1371/journal.pone.0047730). “That was a bit surprising to us,” Dr. Yu said. In addition, a nested case-control study of 103,044 patients found that subclinical hypothyroidism was linked to an increased risk for colon cancer (OR, 1.16; 95% CI, 1.08-1.24; J Natl Cancer Inst. 2015 Apr 8. doi: 10.1093/jnci/djv084).
Of the two studies that focused on cancer mortality, one retrospective cohort analysis of 4,735 patients showed that treatment of subclinical hypothyroidism was associated with a decreased risk of cancer mortality in those aged 40-70 years (hazard ratio, 0.59; 95% CI, 0.21-0.99; Arch Intern Med. 2012;172[10]:811-7). The other study, a retrospective cohort analysis of 115,746 patients, found that subclinical hypothyroidism was associated with an increased risk of cancer mortality (relative risk, 1.51; 95% CI, 1.06-2.15; PLoS One. 2015 Apr 1. doi: 10.1371/journal.pone.0122955).
“We need to interpret the cancer-related mortality findings with caution,” Dr. Yu said. “There’s concern about whether patients who are treated might be [generally] healthier or were less frail, compared with those who were not treated. Although these studies adjusted for a number of confounders, it may be difficult to measure and adjust for [those two] factors. That might explain the findings in the two studies on cancer-related mortality.”
Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
REPORTING FROM AACE 2019
Key clinical point: Further studies are needed to assess the association between untreated subclinical hypothyroidism and the risks of different types of cancer.
Major finding:
Study details: A systematic review of nine studies.
Disclosures: Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
Ultrasound offers advantages for long-term lymph node surveillance in high-grade SCC patients
BALTIMORE – Ultrasound can be a very effective way to track early nodal metastasis in patients with high-stage cutaneous squamous cell carcinomas, and at a fraction of the cost of other imaging modalities.

The technique shows not only abnormal variations in the shape of nodes, but changes in the core and outer density, and vascular patterns, Emily Ruiz, MD, said at the annual meeting of the American College of Mohs Surgery. And over a 2-year surveillance period, this costs thousands less than radiation-based imaging.
Dr. Ruiz, director of the High-Risk Skin Cancer Clinic at Dana-Farber/Brigham and Women’s Cancer Center, Boston, said the standard imaging technique at that center used to be serial CT scans performed at diagnosis and every 6 months thereafter, for 2 years. But recently, the protocol changed: Ultrasound is now the preferred technique.
“The big problem with CT in this earlier disease, is that it can only identify the nodes that are enlarged, and doesn’t tell us anything about the etiology. Ultrasound, on the other hand, looks at a number of different features of the node.”
Tracking high-risk squamous cell carcinoma patients is a must, she said. “About 4% of people diagnosed with high-risk SCC will develop nodal metastases, and 1.5% of those will die from disease-specific death,” most often from locoregional disease. “So it’s critical to identify nodal diseases early as possible. Earlier identification leads to better outcomes.” Ultrasound simply provides more information about nodal metastasis, Dr. Ruiz added.
“The first thing we look at is the general architecture of the node. Resting and reactive nodes have a hypoechoic hilus and a hyperechoic cortex. As they become infiltrated with tumor, the hilus becomes more hyperechoic, and areas of metastasis stand out as much more hyperechoic than the surrounding node.”
Another tip-off is overall shape. If the ratio of the long axis to short axis diameter is less than 2, the lymph node is more likely to be malignant, she said.
“One more important factor that can’t be seen on CT is the node’s vascular pattern. Both resting and reactive nodes tend to have a centralized vascular pattern in the hilus. With tumor infiltration you start to see an asymmetrical vascularization as the nodes are replaced by tumor. The perfusion becomes much more peripheral.”

Cost is another consideration, Dr. Ruiz said. Five CT scans conducted over the recommended 2 years of follow-up will run about $5,000. Five scans with magnetic resonance imaging come in at about $6,500. PET CT is, of course, the most expensive, racking up a national average cost of $28,500 for five scans.
Ultrasound is amazingly inexpensive, Dr. Ruiz said. The national average cost of one scan is around $180, bringing the 2-year cost of five surveillance scans to $900.
Finally, clinicians and patients should consider the potential impact of repeated radiation exposure. “This can really add up over the follow-up period. Because there’s a 10-year latency period for these cancers, this might not be an issue for our older patients, but it really is something to consider in younger ones. “
However, she acknowledged that it’s not a completely rosy picture.
“Ultrasound is very user dependent, but we do think that by putting this in the hands of dermatologists with special training, we can solve this issue. In Europe, ultrasound’s very high sensitivity and specificity, combined with clinical exams, really improves disease detection.”
Unfortunately, at this point, anyone who wants to learn the technique has to go to Europe. “I trained in Germany, where I took a standard 3-day course, did 250 supervised scans, and completed an exam. I realize that’s unrealistic for most people,” she said. But a training protocol is being developed at Brigham and Women’s, under the auspices of the institution’s imaging experts, who felt that 3 days and 250 supervised scans was excessive. The Brigham and Women’s program comprises 8 hours of didactic training and at least 30 supervised scans with at least three abnormalities correctly identified, and will be put into place soon, Dr. Ruiz said.
The biggest obstacle to large-scale adoption of this protocol is data – there are not a lot, at least now.
“We are working on that, too. In conjunction with the Skin Cancer Foundation, we’re launching a prospective study. We want to recruit 80 patients with T2B/T3 cutaneous SCCs. They get both and ultrasound and a CT scan at diagnosis and every 6 months for 2 years,” she said.
BALTIMORE – Ultrasound can be a very effective way to track early nodal metastasis in patients with high-stage cutaneous squamous cell carcinomas, and at a fraction of the cost of other imaging modalities.
The technique shows not only abnormal variations in the shape of nodes, but changes in the core and outer density, and vascular patterns, Emily Ruiz, MD, said at the annual meeting of the American College of Mohs Surgery. And over a 2-year surveillance period, this costs thousands less than radiation-based imaging.
Dr. Ruiz, director of the High-Risk Skin Cancer Clinic at Dana-Farber/Brigham and Women’s Cancer Center, Boston, said the standard imaging technique at that center used to be serial CT scans performed at diagnosis and every 6 months thereafter, for 2 years. But recently, the protocol changed: Ultrasound is now the preferred technique.
“The big problem with CT in this earlier disease, is that it can only identify the nodes that are enlarged, and doesn’t tell us anything about the etiology. Ultrasound, on the other hand, looks at a number of different features of the node.”
Tracking high-risk squamous cell carcinoma patients is a must, she said. “About 4% of people diagnosed with high-risk SCC will develop nodal metastases, and 1.5% of those will die from disease-specific death,” most often from locoregional disease. “So it’s critical to identify nodal diseases early as possible. Earlier identification leads to better outcomes.” Ultrasound simply provides more information about nodal metastasis, Dr. Ruiz added.
“The first thing we look at is the general architecture of the node. Resting and reactive nodes have a hypoechoic hilus and a hyperechoic cortex. As they become infiltrated with tumor, the hilus becomes more hyperechoic, and areas of metastasis stand out as much more hyperechoic than the surrounding node.”
Another tip-off is overall shape. If the ratio of the long axis to short axis diameter is less than 2, the lymph node is more likely to be malignant, she said.
“One more important factor that can’t be seen on CT is the node’s vascular pattern. Both resting and reactive nodes tend to have a centralized vascular pattern in the hilus. With tumor infiltration you start to see an asymmetrical vascularization as the nodes are replaced by tumor. The perfusion becomes much more peripheral.”
Cost is another consideration, Dr. Ruiz said. Five CT scans conducted over the recommended 2 years of follow-up will run about $5,000. Five scans with magnetic resonance imaging come in at about $6,500. PET CT is, of course, the most expensive, racking up a national average cost of $28,500 for five scans.
Ultrasound is amazingly inexpensive, Dr. Ruiz said. The national average cost of one scan is around $180, bringing the 2-year cost of five surveillance scans to $900.
Finally, clinicians and patients should consider the potential impact of repeated radiation exposure. “This can really add up over the follow-up period. Because there’s a 10-year latency period for these cancers, this might not be an issue for our older patients, but it really is something to consider in younger ones. “
However, she acknowledged that it’s not a completely rosy picture.
“Ultrasound is very user dependent, but we do think that by putting this in the hands of dermatologists with special training, we can solve this issue. In Europe, ultrasound’s very high sensitivity and specificity, combined with clinical exams, really improves disease detection.”
Unfortunately, at this point, anyone who wants to learn the technique has to go to Europe. “I trained in Germany, where I took a standard 3-day course, did 250 supervised scans, and completed an exam. I realize that’s unrealistic for most people,” she said. But a training protocol is being developed at Brigham and Women’s, under the auspices of the institution’s imaging experts, who felt that 3 days and 250 supervised scans was excessive. The Brigham and Women’s program comprises 8 hours of didactic training and at least 30 supervised scans with at least three abnormalities correctly identified, and will be put into place soon, Dr. Ruiz said.
The biggest obstacle to large-scale adoption of this protocol is data – there are not a lot, at least now.
“We are working on that, too. In conjunction with the Skin Cancer Foundation, we’re launching a prospective study. We want to recruit 80 patients with T2B/T3 cutaneous SCCs. They get both and ultrasound and a CT scan at diagnosis and every 6 months for 2 years,” she said.
BALTIMORE – Ultrasound can be a very effective way to track early nodal metastasis in patients with high-stage cutaneous squamous cell carcinomas, and at a fraction of the cost of other imaging modalities.
The technique shows not only abnormal variations in the shape of nodes, but changes in the core and outer density, and vascular patterns, Emily Ruiz, MD, said at the annual meeting of the American College of Mohs Surgery. And over a 2-year surveillance period, this costs thousands less than radiation-based imaging.
Dr. Ruiz, director of the High-Risk Skin Cancer Clinic at Dana-Farber/Brigham and Women’s Cancer Center, Boston, said the standard imaging technique at that center used to be serial CT scans performed at diagnosis and every 6 months thereafter, for 2 years. But recently, the protocol changed: Ultrasound is now the preferred technique.
“The big problem with CT in this earlier disease, is that it can only identify the nodes that are enlarged, and doesn’t tell us anything about the etiology. Ultrasound, on the other hand, looks at a number of different features of the node.”
Tracking high-risk squamous cell carcinoma patients is a must, she said. “About 4% of people diagnosed with high-risk SCC will develop nodal metastases, and 1.5% of those will die from disease-specific death,” most often from locoregional disease. “So it’s critical to identify nodal diseases early as possible. Earlier identification leads to better outcomes.” Ultrasound simply provides more information about nodal metastasis, Dr. Ruiz added.
“The first thing we look at is the general architecture of the node. Resting and reactive nodes have a hypoechoic hilus and a hyperechoic cortex. As they become infiltrated with tumor, the hilus becomes more hyperechoic, and areas of metastasis stand out as much more hyperechoic than the surrounding node.”
Another tip-off is overall shape. If the ratio of the long axis to short axis diameter is less than 2, the lymph node is more likely to be malignant, she said.
“One more important factor that can’t be seen on CT is the node’s vascular pattern. Both resting and reactive nodes tend to have a centralized vascular pattern in the hilus. With tumor infiltration you start to see an asymmetrical vascularization as the nodes are replaced by tumor. The perfusion becomes much more peripheral.”
Cost is another consideration, Dr. Ruiz said. Five CT scans conducted over the recommended 2 years of follow-up will run about $5,000. Five scans with magnetic resonance imaging come in at about $6,500. PET CT is, of course, the most expensive, racking up a national average cost of $28,500 for five scans.
Ultrasound is amazingly inexpensive, Dr. Ruiz said. The national average cost of one scan is around $180, bringing the 2-year cost of five surveillance scans to $900.
Finally, clinicians and patients should consider the potential impact of repeated radiation exposure. “This can really add up over the follow-up period. Because there’s a 10-year latency period for these cancers, this might not be an issue for our older patients, but it really is something to consider in younger ones. “
However, she acknowledged that it’s not a completely rosy picture.
“Ultrasound is very user dependent, but we do think that by putting this in the hands of dermatologists with special training, we can solve this issue. In Europe, ultrasound’s very high sensitivity and specificity, combined with clinical exams, really improves disease detection.”
Unfortunately, at this point, anyone who wants to learn the technique has to go to Europe. “I trained in Germany, where I took a standard 3-day course, did 250 supervised scans, and completed an exam. I realize that’s unrealistic for most people,” she said. But a training protocol is being developed at Brigham and Women’s, under the auspices of the institution’s imaging experts, who felt that 3 days and 250 supervised scans was excessive. The Brigham and Women’s program comprises 8 hours of didactic training and at least 30 supervised scans with at least three abnormalities correctly identified, and will be put into place soon, Dr. Ruiz said.
The biggest obstacle to large-scale adoption of this protocol is data – there are not a lot, at least now.
“We are working on that, too. In conjunction with the Skin Cancer Foundation, we’re launching a prospective study. We want to recruit 80 patients with T2B/T3 cutaneous SCCs. They get both and ultrasound and a CT scan at diagnosis and every 6 months for 2 years,” she said.
EXPERT ANALYSIS FROM the ACMS Annual Meeting
Neoadjuvant removal of DCIS helps identify HER2+ nonsurgical trial candidates
Breast cancer patients with HER2-positive disease are more likely to be nonsurgical candidates for clinical trials after neoadjuvant systemic therapy if they have eradicated both invasive and ductal carcinoma in situ (DCIS) disease, according to research presented in a recent webcast from the annual meeting of the American Society of Breast Surgeons.
While there is a high rate of pathologic complete response (pCR) in HER2-postive breast cancer after neoadjuvant systemic therapy, it is difficult to determine which patients have achieved pCR because standard imaging generates a high rate of false negatives, noted Susie Sun, MD, from the University of Texas MD Anderson Cancer Center, Houston.
“Although radiological imaging such as mammograms, ultrasounds, and MRIs have been shown to be unreliable in identifying patients with pCR, we have previously determined that patients with clinically significant residual disease can be accurately identified using a combination of multimodality imaging and image-guided, vacuum-assisted biopsy to the tumor bed,” Dr. Sun said in her presentation.
In the Multicenter Trial for Eliminating Breast Cancer Surgery in Exceptional Responders With Neoadjuvant Systemic Therapy, Dr. Sun and colleagues enrolled 280 patients with T1-T2, N0-N1 HER2-positive breast cancer who had undergone HER2-targeted therapy, followed by surgical resection and axillary surgery. The researchers studied both the effects of neoadjuvant therapy patients with pCR and the clinicopathologic characteristics of residual disease to determine how patients with pCR differed from those with residual disease.
After neoadjuvant systemic therapy, 55.4% of pCR invasive cancer was eradicated in patients, 37.5% of both pCR invasive and DCIS cancer was eradicated in patients, and 17.9% of patients had eradication of only residual DCIS. Compared with patients where DCIS was not identified at initial biopsy, DCIS identification was associated with a higher likelihood of residual disease (69% vs. 57%; P = .04). The researchers found patients having hormone receptor–positive/HER2-positive disease was associated with a higher rate of predictive residual disease (26.6%), compared with patients who had hormone receptor–negative/HER2-positive disease (49.2%; odds ratio, 2.7; 95% confidence interval, P less than .0001).
“For the currently occurring trial, evaluating the safety of eliminating surgery for patients who are exceptional responders to neoadjuvant systemic therapy, eradication of both the invasive and DCIS components are necessary because DCIS may serve as a nidus for carcinoma in the future,” said Dr. Sun.
The researchers also studied the effectiveness of multimodality imaging on identifying pathologic response. The multimodality imaging consisted of a mammogram and ultrasound for all patients, and approximately 13% of patients had MRI in addition to mammogram and ultrasound. The multimodality imaging response after neoadjuvant systemic therapy had a sensitivity of 97.1% and a negative predictive value of 70.6% for detecting residual disease in the breast and lymph nodes.
“[O]ur study found that multimodality imaging was not reliable in assessing for pathologic response within the breast or lymph nodes,” said Dr. Sun. “Therefore, imaging alone cannot be used to select patients for no surgery. This requires patients who have image-guided percutaneous biopsy to safely select patients for inclusion and elimination of surgery trial.”
In a discussion session, Dr. Sun clarified the combination of multimodality imaging and image-guided percutaneous biopsy was used to select HER2-positive patients for a clinical trial, and is not standard of practice to determine pCR at the University of Texas MD Anderson Cancer Center.
Dr. Sun reported no relevant financial disclosures.
Breast cancer patients with HER2-positive disease are more likely to be nonsurgical candidates for clinical trials after neoadjuvant systemic therapy if they have eradicated both invasive and ductal carcinoma in situ (DCIS) disease, according to research presented in a recent webcast from the annual meeting of the American Society of Breast Surgeons.
While there is a high rate of pathologic complete response (pCR) in HER2-postive breast cancer after neoadjuvant systemic therapy, it is difficult to determine which patients have achieved pCR because standard imaging generates a high rate of false negatives, noted Susie Sun, MD, from the University of Texas MD Anderson Cancer Center, Houston.
“Although radiological imaging such as mammograms, ultrasounds, and MRIs have been shown to be unreliable in identifying patients with pCR, we have previously determined that patients with clinically significant residual disease can be accurately identified using a combination of multimodality imaging and image-guided, vacuum-assisted biopsy to the tumor bed,” Dr. Sun said in her presentation.
In the Multicenter Trial for Eliminating Breast Cancer Surgery in Exceptional Responders With Neoadjuvant Systemic Therapy, Dr. Sun and colleagues enrolled 280 patients with T1-T2, N0-N1 HER2-positive breast cancer who had undergone HER2-targeted therapy, followed by surgical resection and axillary surgery. The researchers studied both the effects of neoadjuvant therapy patients with pCR and the clinicopathologic characteristics of residual disease to determine how patients with pCR differed from those with residual disease.
After neoadjuvant systemic therapy, 55.4% of pCR invasive cancer was eradicated in patients, 37.5% of both pCR invasive and DCIS cancer was eradicated in patients, and 17.9% of patients had eradication of only residual DCIS. Compared with patients where DCIS was not identified at initial biopsy, DCIS identification was associated with a higher likelihood of residual disease (69% vs. 57%; P = .04). The researchers found patients having hormone receptor–positive/HER2-positive disease was associated with a higher rate of predictive residual disease (26.6%), compared with patients who had hormone receptor–negative/HER2-positive disease (49.2%; odds ratio, 2.7; 95% confidence interval, P less than .0001).
“For the currently occurring trial, evaluating the safety of eliminating surgery for patients who are exceptional responders to neoadjuvant systemic therapy, eradication of both the invasive and DCIS components are necessary because DCIS may serve as a nidus for carcinoma in the future,” said Dr. Sun.
The researchers also studied the effectiveness of multimodality imaging on identifying pathologic response. The multimodality imaging consisted of a mammogram and ultrasound for all patients, and approximately 13% of patients had MRI in addition to mammogram and ultrasound. The multimodality imaging response after neoadjuvant systemic therapy had a sensitivity of 97.1% and a negative predictive value of 70.6% for detecting residual disease in the breast and lymph nodes.
“[O]ur study found that multimodality imaging was not reliable in assessing for pathologic response within the breast or lymph nodes,” said Dr. Sun. “Therefore, imaging alone cannot be used to select patients for no surgery. This requires patients who have image-guided percutaneous biopsy to safely select patients for inclusion and elimination of surgery trial.”
In a discussion session, Dr. Sun clarified the combination of multimodality imaging and image-guided percutaneous biopsy was used to select HER2-positive patients for a clinical trial, and is not standard of practice to determine pCR at the University of Texas MD Anderson Cancer Center.
Dr. Sun reported no relevant financial disclosures.
Breast cancer patients with HER2-positive disease are more likely to be nonsurgical candidates for clinical trials after neoadjuvant systemic therapy if they have eradicated both invasive and ductal carcinoma in situ (DCIS) disease, according to research presented in a recent webcast from the annual meeting of the American Society of Breast Surgeons.
While there is a high rate of pathologic complete response (pCR) in HER2-postive breast cancer after neoadjuvant systemic therapy, it is difficult to determine which patients have achieved pCR because standard imaging generates a high rate of false negatives, noted Susie Sun, MD, from the University of Texas MD Anderson Cancer Center, Houston.
“Although radiological imaging such as mammograms, ultrasounds, and MRIs have been shown to be unreliable in identifying patients with pCR, we have previously determined that patients with clinically significant residual disease can be accurately identified using a combination of multimodality imaging and image-guided, vacuum-assisted biopsy to the tumor bed,” Dr. Sun said in her presentation.
In the Multicenter Trial for Eliminating Breast Cancer Surgery in Exceptional Responders With Neoadjuvant Systemic Therapy, Dr. Sun and colleagues enrolled 280 patients with T1-T2, N0-N1 HER2-positive breast cancer who had undergone HER2-targeted therapy, followed by surgical resection and axillary surgery. The researchers studied both the effects of neoadjuvant therapy patients with pCR and the clinicopathologic characteristics of residual disease to determine how patients with pCR differed from those with residual disease.
After neoadjuvant systemic therapy, 55.4% of pCR invasive cancer was eradicated in patients, 37.5% of both pCR invasive and DCIS cancer was eradicated in patients, and 17.9% of patients had eradication of only residual DCIS. Compared with patients where DCIS was not identified at initial biopsy, DCIS identification was associated with a higher likelihood of residual disease (69% vs. 57%; P = .04). The researchers found patients having hormone receptor–positive/HER2-positive disease was associated with a higher rate of predictive residual disease (26.6%), compared with patients who had hormone receptor–negative/HER2-positive disease (49.2%; odds ratio, 2.7; 95% confidence interval, P less than .0001).
“For the currently occurring trial, evaluating the safety of eliminating surgery for patients who are exceptional responders to neoadjuvant systemic therapy, eradication of both the invasive and DCIS components are necessary because DCIS may serve as a nidus for carcinoma in the future,” said Dr. Sun.
The researchers also studied the effectiveness of multimodality imaging on identifying pathologic response. The multimodality imaging consisted of a mammogram and ultrasound for all patients, and approximately 13% of patients had MRI in addition to mammogram and ultrasound. The multimodality imaging response after neoadjuvant systemic therapy had a sensitivity of 97.1% and a negative predictive value of 70.6% for detecting residual disease in the breast and lymph nodes.
“[O]ur study found that multimodality imaging was not reliable in assessing for pathologic response within the breast or lymph nodes,” said Dr. Sun. “Therefore, imaging alone cannot be used to select patients for no surgery. This requires patients who have image-guided percutaneous biopsy to safely select patients for inclusion and elimination of surgery trial.”
In a discussion session, Dr. Sun clarified the combination of multimodality imaging and image-guided percutaneous biopsy was used to select HER2-positive patients for a clinical trial, and is not standard of practice to determine pCR at the University of Texas MD Anderson Cancer Center.
Dr. Sun reported no relevant financial disclosures.
FROM ASBS 2019
Researchers propose new risk groups for NK-AML
NEWPORT BEACH, CALIF. – New research suggests patients with normal karyotype acute myeloid leukemia (NK-AML) can be divided into four risk groups associated with overall survival.
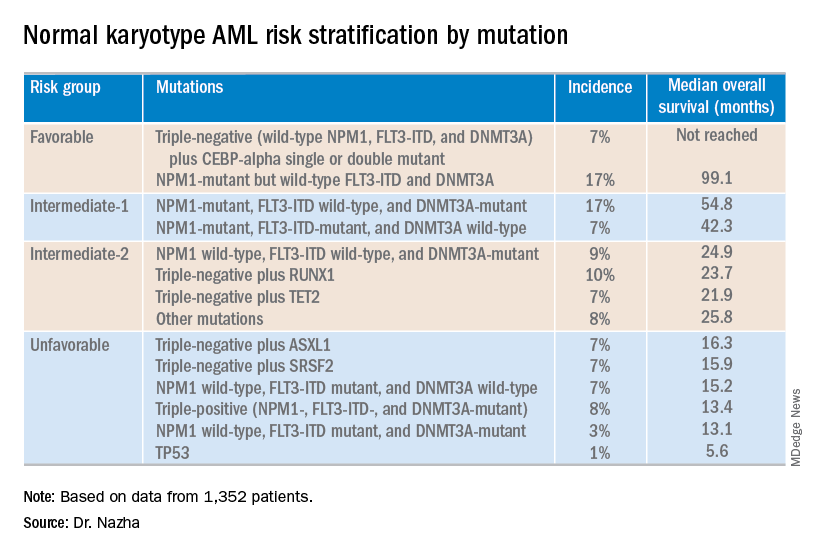
Investigators used machine learning algorithms to study the association between mutations and overall survival in 1,352 patients with NK-AML. The analysis revealed combinations of mutations that could be used to classify NK-AML patients into favorable, intermediate-1, intermediate-2, and unfavorable risk groups.
For example, patients who had NPM1 mutations but wild-type FLT3-ITD and DNMT3A, had a median overall survival of 99.1 months and could be classified as favorable risk. Conversely, patients who had NPM1, FLT3-ITD, and DNMT3A mutations, had a median overall survival of 13.4 months and could be classified as unfavorable risk.
Aziz Nazha, MD, of the Cleveland Clinic, and his colleagues conducted this research and presented the findings at the Acute Leukemia Forum of Hemedicus.
The investigators looked at genomic and clinical data from 1,352 patients with NK-AML. The patients were a median age of 55 years and had a median white blood cell count of 21.3 x 109/L, a median hemoglobin of 9.1 g/dL, and a median platelet count of 61 x 109/L. More than half of patients (57.3%) were male.
The patients were screened for 35 genes that are commonly mutated in AML and other myeloid malignancies. The investigators used machine learning algorithms, including random survival forest and recommender system algorithms, to study the association between mutations and overall survival in an “unbiased” way.
Dr. Nazha said there were a median of three mutations per patient sample, and “there are some competing interests between those mutations to impact the prognosis of the patient.”
The investigators used the mutations and their associations with overall survival to classify patients into the risk groups outlined in the table below.
These findings can improve the risk stratification of NK-AML and may aid physicians in making treatment decisions, according to Dr. Nazha and his colleagues. To move this work forward, the investigators are attempting to develop a personalized model that can make predictions specific to an individual patient based on that patient’s mutation information.
Dr. Nazha reported having no financial disclosures relevant to this research. Other investigators reported relationships with the Munich Leukemia Laboratory.
The Acute Leukemia Forum is held by Hemedicus, which is owned by the same company as this news organization.
NEWPORT BEACH, CALIF. – New research suggests patients with normal karyotype acute myeloid leukemia (NK-AML) can be divided into four risk groups associated with overall survival.
Investigators used machine learning algorithms to study the association between mutations and overall survival in 1,352 patients with NK-AML. The analysis revealed combinations of mutations that could be used to classify NK-AML patients into favorable, intermediate-1, intermediate-2, and unfavorable risk groups.
For example, patients who had NPM1 mutations but wild-type FLT3-ITD and DNMT3A, had a median overall survival of 99.1 months and could be classified as favorable risk. Conversely, patients who had NPM1, FLT3-ITD, and DNMT3A mutations, had a median overall survival of 13.4 months and could be classified as unfavorable risk.
Aziz Nazha, MD, of the Cleveland Clinic, and his colleagues conducted this research and presented the findings at the Acute Leukemia Forum of Hemedicus.
The investigators looked at genomic and clinical data from 1,352 patients with NK-AML. The patients were a median age of 55 years and had a median white blood cell count of 21.3 x 109/L, a median hemoglobin of 9.1 g/dL, and a median platelet count of 61 x 109/L. More than half of patients (57.3%) were male.
The patients were screened for 35 genes that are commonly mutated in AML and other myeloid malignancies. The investigators used machine learning algorithms, including random survival forest and recommender system algorithms, to study the association between mutations and overall survival in an “unbiased” way.
Dr. Nazha said there were a median of three mutations per patient sample, and “there are some competing interests between those mutations to impact the prognosis of the patient.”
The investigators used the mutations and their associations with overall survival to classify patients into the risk groups outlined in the table below.
These findings can improve the risk stratification of NK-AML and may aid physicians in making treatment decisions, according to Dr. Nazha and his colleagues. To move this work forward, the investigators are attempting to develop a personalized model that can make predictions specific to an individual patient based on that patient’s mutation information.
Dr. Nazha reported having no financial disclosures relevant to this research. Other investigators reported relationships with the Munich Leukemia Laboratory.
The Acute Leukemia Forum is held by Hemedicus, which is owned by the same company as this news organization.
NEWPORT BEACH, CALIF. – New research suggests patients with normal karyotype acute myeloid leukemia (NK-AML) can be divided into four risk groups associated with overall survival.
Investigators used machine learning algorithms to study the association between mutations and overall survival in 1,352 patients with NK-AML. The analysis revealed combinations of mutations that could be used to classify NK-AML patients into favorable, intermediate-1, intermediate-2, and unfavorable risk groups.
For example, patients who had NPM1 mutations but wild-type FLT3-ITD and DNMT3A, had a median overall survival of 99.1 months and could be classified as favorable risk. Conversely, patients who had NPM1, FLT3-ITD, and DNMT3A mutations, had a median overall survival of 13.4 months and could be classified as unfavorable risk.
Aziz Nazha, MD, of the Cleveland Clinic, and his colleagues conducted this research and presented the findings at the Acute Leukemia Forum of Hemedicus.
The investigators looked at genomic and clinical data from 1,352 patients with NK-AML. The patients were a median age of 55 years and had a median white blood cell count of 21.3 x 109/L, a median hemoglobin of 9.1 g/dL, and a median platelet count of 61 x 109/L. More than half of patients (57.3%) were male.
The patients were screened for 35 genes that are commonly mutated in AML and other myeloid malignancies. The investigators used machine learning algorithms, including random survival forest and recommender system algorithms, to study the association between mutations and overall survival in an “unbiased” way.
Dr. Nazha said there were a median of three mutations per patient sample, and “there are some competing interests between those mutations to impact the prognosis of the patient.”
The investigators used the mutations and their associations with overall survival to classify patients into the risk groups outlined in the table below.
These findings can improve the risk stratification of NK-AML and may aid physicians in making treatment decisions, according to Dr. Nazha and his colleagues. To move this work forward, the investigators are attempting to develop a personalized model that can make predictions specific to an individual patient based on that patient’s mutation information.
Dr. Nazha reported having no financial disclosures relevant to this research. Other investigators reported relationships with the Munich Leukemia Laboratory.
The Acute Leukemia Forum is held by Hemedicus, which is owned by the same company as this news organization.
REPORTING FROM ALF 2019
Oropharynx cancer burden is shifting to older men
The burden of the U.S. oropharynx cancer epidemic is shifting toward older adults, finds a population-based cohort study spanning 23 years. As a result, the disease will likely become one predominantly affecting elderly white men over the next decade. In addition, projections suggest that the annual number of new cases will likely rise exponentially.
Historically, the incidence of oropharynx cancer rose rapidly among white men aged younger than 60 years because of human papillomavirus (HPV) infections (J Clin Oncol. 2011;29:4294-301). But given factors such as aging, possible changes in behavior, and vaccination, the current trajectory is unknown.
Investigators led by Joseph E. Tota, PhD, of the division of cancer epidemiology and genetics at the National Cancer Institute analyzed Surveillance, Epidemiology, and End Results registry data for 1992-2015 to ascertain whether the increases in oropharynx cancer have continued into recent birth cohorts and to forecast future burden across subgroups.
Results published in the Journal of Clinical Oncology showed that, among white men, oropharynx cancer incidence accelerated among those born during 1927-1939 (by 3.5% per 2-year birth cohort) and during 1939-1955 (by 5.3% per 2-year birth cohort), whereas the pace of increase moderated among those born during 1955-1969 (by 1.7% per 2-year birth cohort).
Given these trends, the investigators forecast that incidence will increase sharply between 2016 and 2029 among older white men aged 65-74 years (from 40.7 to 71.2 per 100,000) and 75-84 years (from 25.7 to 50.1 per 100,000), increase moderately among white men aged 55-64 years (from 40.3 to 52.0 per 100,000), and remain stable among white men aged 45-54 years (at roughly 18 per 100,000).
Taking population growth into account, Dr. Tota and colleagues project a 52% increase in annual number of cases in the United States (from 20,124 to 30,629 between 2016 and 2029), mainly driven by a 127% increase among older adults aged at least 65 years (from 7,976 to 18,072) and a 54% increase among white men (from 14,453 to 22,241). As of 2029, white men older than 65 years will account for approximately 44% of all cases.
“Our results suggest an ebbing of the oropharynx cancer epidemic in younger individuals, exaggeration of the epidemic in older individuals, and a continued exponential increase in the annual number of oropharynx cancers over the next decade,” Dr. Tota and coinvestigators summarized.
The findings have important implications regarding treatment of older patients with oropharynx cancer, they noted. “It is likely that the biology of HPV-positive tumors is similar in younger versus older patients; nonetheless, older patients have poorer survival outcomes because of competing comorbidities, treatment-associated acute and chronic toxicity with chemoradiation, or an inability to receive maximally effective therapies. … Thus, older patients with oropharynx cancer may have different risks and benefits when receiving deintensified regimens than younger patients. The emergence of immunotherapies, whose efficacy may be more age invariant than cytotoxic chemotherapies, could provide a promising treatment avenue for older patients with oropharynx cancer.”
Dr. Tota reported receiving travel, accommodations, and expenses from Merck. The study was supported by the Intramural Research Program of the National Institutes of Health/NCI.
SOURCE: Tota JE et al. J Clin Oncol. 2019 Apr 26. doi: 10.1200/JCO.19.00370.
The burden of the U.S. oropharynx cancer epidemic is shifting toward older adults, finds a population-based cohort study spanning 23 years. As a result, the disease will likely become one predominantly affecting elderly white men over the next decade. In addition, projections suggest that the annual number of new cases will likely rise exponentially.
Historically, the incidence of oropharynx cancer rose rapidly among white men aged younger than 60 years because of human papillomavirus (HPV) infections (J Clin Oncol. 2011;29:4294-301). But given factors such as aging, possible changes in behavior, and vaccination, the current trajectory is unknown.
Investigators led by Joseph E. Tota, PhD, of the division of cancer epidemiology and genetics at the National Cancer Institute analyzed Surveillance, Epidemiology, and End Results registry data for 1992-2015 to ascertain whether the increases in oropharynx cancer have continued into recent birth cohorts and to forecast future burden across subgroups.
Results published in the Journal of Clinical Oncology showed that, among white men, oropharynx cancer incidence accelerated among those born during 1927-1939 (by 3.5% per 2-year birth cohort) and during 1939-1955 (by 5.3% per 2-year birth cohort), whereas the pace of increase moderated among those born during 1955-1969 (by 1.7% per 2-year birth cohort).
Given these trends, the investigators forecast that incidence will increase sharply between 2016 and 2029 among older white men aged 65-74 years (from 40.7 to 71.2 per 100,000) and 75-84 years (from 25.7 to 50.1 per 100,000), increase moderately among white men aged 55-64 years (from 40.3 to 52.0 per 100,000), and remain stable among white men aged 45-54 years (at roughly 18 per 100,000).
Taking population growth into account, Dr. Tota and colleagues project a 52% increase in annual number of cases in the United States (from 20,124 to 30,629 between 2016 and 2029), mainly driven by a 127% increase among older adults aged at least 65 years (from 7,976 to 18,072) and a 54% increase among white men (from 14,453 to 22,241). As of 2029, white men older than 65 years will account for approximately 44% of all cases.
“Our results suggest an ebbing of the oropharynx cancer epidemic in younger individuals, exaggeration of the epidemic in older individuals, and a continued exponential increase in the annual number of oropharynx cancers over the next decade,” Dr. Tota and coinvestigators summarized.
The findings have important implications regarding treatment of older patients with oropharynx cancer, they noted. “It is likely that the biology of HPV-positive tumors is similar in younger versus older patients; nonetheless, older patients have poorer survival outcomes because of competing comorbidities, treatment-associated acute and chronic toxicity with chemoradiation, or an inability to receive maximally effective therapies. … Thus, older patients with oropharynx cancer may have different risks and benefits when receiving deintensified regimens than younger patients. The emergence of immunotherapies, whose efficacy may be more age invariant than cytotoxic chemotherapies, could provide a promising treatment avenue for older patients with oropharynx cancer.”
Dr. Tota reported receiving travel, accommodations, and expenses from Merck. The study was supported by the Intramural Research Program of the National Institutes of Health/NCI.
SOURCE: Tota JE et al. J Clin Oncol. 2019 Apr 26. doi: 10.1200/JCO.19.00370.
The burden of the U.S. oropharynx cancer epidemic is shifting toward older adults, finds a population-based cohort study spanning 23 years. As a result, the disease will likely become one predominantly affecting elderly white men over the next decade. In addition, projections suggest that the annual number of new cases will likely rise exponentially.
Historically, the incidence of oropharynx cancer rose rapidly among white men aged younger than 60 years because of human papillomavirus (HPV) infections (J Clin Oncol. 2011;29:4294-301). But given factors such as aging, possible changes in behavior, and vaccination, the current trajectory is unknown.
Investigators led by Joseph E. Tota, PhD, of the division of cancer epidemiology and genetics at the National Cancer Institute analyzed Surveillance, Epidemiology, and End Results registry data for 1992-2015 to ascertain whether the increases in oropharynx cancer have continued into recent birth cohorts and to forecast future burden across subgroups.
Results published in the Journal of Clinical Oncology showed that, among white men, oropharynx cancer incidence accelerated among those born during 1927-1939 (by 3.5% per 2-year birth cohort) and during 1939-1955 (by 5.3% per 2-year birth cohort), whereas the pace of increase moderated among those born during 1955-1969 (by 1.7% per 2-year birth cohort).
Given these trends, the investigators forecast that incidence will increase sharply between 2016 and 2029 among older white men aged 65-74 years (from 40.7 to 71.2 per 100,000) and 75-84 years (from 25.7 to 50.1 per 100,000), increase moderately among white men aged 55-64 years (from 40.3 to 52.0 per 100,000), and remain stable among white men aged 45-54 years (at roughly 18 per 100,000).
Taking population growth into account, Dr. Tota and colleagues project a 52% increase in annual number of cases in the United States (from 20,124 to 30,629 between 2016 and 2029), mainly driven by a 127% increase among older adults aged at least 65 years (from 7,976 to 18,072) and a 54% increase among white men (from 14,453 to 22,241). As of 2029, white men older than 65 years will account for approximately 44% of all cases.
“Our results suggest an ebbing of the oropharynx cancer epidemic in younger individuals, exaggeration of the epidemic in older individuals, and a continued exponential increase in the annual number of oropharynx cancers over the next decade,” Dr. Tota and coinvestigators summarized.
The findings have important implications regarding treatment of older patients with oropharynx cancer, they noted. “It is likely that the biology of HPV-positive tumors is similar in younger versus older patients; nonetheless, older patients have poorer survival outcomes because of competing comorbidities, treatment-associated acute and chronic toxicity with chemoradiation, or an inability to receive maximally effective therapies. … Thus, older patients with oropharynx cancer may have different risks and benefits when receiving deintensified regimens than younger patients. The emergence of immunotherapies, whose efficacy may be more age invariant than cytotoxic chemotherapies, could provide a promising treatment avenue for older patients with oropharynx cancer.”
Dr. Tota reported receiving travel, accommodations, and expenses from Merck. The study was supported by the Intramural Research Program of the National Institutes of Health/NCI.
SOURCE: Tota JE et al. J Clin Oncol. 2019 Apr 26. doi: 10.1200/JCO.19.00370.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
AGA Clinical Practice Update: Direct-acting antivirals and hepatocellular carcinoma
Achieving sustained virologic response to direct-acting antiviral therapy for chronic hepatitis C virus infection cuts lifetime hepatocellular carcinoma risk by approximately 70%, even when patients have baseline cirrhosis, experts wrote in Gastroenterology.

When used after curative-intent treatment for hepatocellular carcinoma, direct-acting antiviral (DAA) therapy also does not appear to make recurrent cancer more probable or more aggressive, wrote Amit G. Singal, MD, and associates in an American Gastroenterological Association clinical practice update. Studies that compared DAA therapy with either interferon-based therapy or no treatment have found “similar if not lower recurrence than the comparator groups,” they wrote. Rather, hepatocellular carcinoma is in itself highly recurrent: “While surgical resection and local ablative therapies are considered curative, [probability of] recurrence approaches 25%-35% within the first year, and 50%-60% within 2 years.”
Direct-acting antiviral therapy for chronic hepatitis C infection improves several aspects of liver health, but experts have debated whether and how these benefits affect the risk and behavior of hepatocellular carcinoma. To explore the issue, Dr. Singal, medical director of the liver tumor program and clinical chief of hepatology at UT Southwestern Medical Center in Dallas and associates reviewed published clinical trials, observational studies, and systematic reviews. Among 11 studies of more than 3,000 patients in five countries, sustained virologic response (SVR) to DAA therapy was associated with about a 70% reduction in the risk of liver cancer, even after adjustment for clinical and demographic variables. “The relative reduction is similar in patients with and without cirrhosis,” the experts wrote.
Since patients with fibrosis (F3) or cirrhosis are at highest risk for hepatocellular carcinoma, they should undergo baseline imaging and remain under indefinite post-SVR surveillance as long as they are eligible for potentially curative treatment, the practice update states. The experts recommended twice-yearly ultrasound, with or without serum alpha-fetoprotein, noting that current evidence supports neither shorter surveillance intervals nor alternative imaging modalities.
“The presence of active hepatocellular carcinoma is associated with a small but statistically significant decrease in SVR with DAA therapy,” the experts confirmed, based on the results of three studies. They recommended that, when possible, patients with hepatocellular carcinoma first receive curative-intent treatment, such as with liver resection or ablation. Direct-acting antiviral therapy can begin 4-6 months later, once there has been time to confirm response to hepatocellular carcinoma treatment.
For patients who are listed for liver transplantation, timing of DAA therapy “should be determined on a case-by-case basis with consideration of median wait times for the region, availability of HCV-positive organs, and degree of liver dysfunction,” they added. “For example, DAA therapy may be beneficial pretransplant for patients in regions with long wait times or limited hepatitis C virus–positive donor organ availability, whereas therapy may be delayed until posttransplant in regions with shorter wait times or a high proportion of hepatitis C virus–positive donor organs that would otherwise go unused.”
For patients with active intermediate or advanced liver cancer, it remains unclear whether DAA therapy is usually worth the costs and risks, they noted. This is because the likelihood of complete response is lower and the competing risk of death is higher than in patients with earlier-stage hepatocellular carcinoma. Pending further data, they recommend basing the decision on patients’ preferences, tumor burden, degree of liver dysfunction, and life expectancy. At their institutions, the researchers do not treat patients with DAA therapy unless their life expectancy exceeds 2 years.
The experts disclosed research funding from the National Cancer Institute, U.S. Veterans Administration, and the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Singal reported personal fees or research funding from AbbVie, Bayer, Bristol-Myers Squibb, Eisai, Exact Sciences, Exelixis, Gilead, Glycotest, Roche, and Wako Diagnostics. His coauthors disclosed ties to AbbVie, Allergan, Bristol-Myers Squibb, Conatus, Genfit, Gilead, Intercept, and Merck.
SOURCE: Singal AG et al. Gastroenterology. 2019 Mar 13. doi: 10.1053/j.gastro.2019.02.046.
Achieving sustained virologic response to direct-acting antiviral therapy for chronic hepatitis C virus infection cuts lifetime hepatocellular carcinoma risk by approximately 70%, even when patients have baseline cirrhosis, experts wrote in Gastroenterology.
When used after curative-intent treatment for hepatocellular carcinoma, direct-acting antiviral (DAA) therapy also does not appear to make recurrent cancer more probable or more aggressive, wrote Amit G. Singal, MD, and associates in an American Gastroenterological Association clinical practice update. Studies that compared DAA therapy with either interferon-based therapy or no treatment have found “similar if not lower recurrence than the comparator groups,” they wrote. Rather, hepatocellular carcinoma is in itself highly recurrent: “While surgical resection and local ablative therapies are considered curative, [probability of] recurrence approaches 25%-35% within the first year, and 50%-60% within 2 years.”
Direct-acting antiviral therapy for chronic hepatitis C infection improves several aspects of liver health, but experts have debated whether and how these benefits affect the risk and behavior of hepatocellular carcinoma. To explore the issue, Dr. Singal, medical director of the liver tumor program and clinical chief of hepatology at UT Southwestern Medical Center in Dallas and associates reviewed published clinical trials, observational studies, and systematic reviews. Among 11 studies of more than 3,000 patients in five countries, sustained virologic response (SVR) to DAA therapy was associated with about a 70% reduction in the risk of liver cancer, even after adjustment for clinical and demographic variables. “The relative reduction is similar in patients with and without cirrhosis,” the experts wrote.
Since patients with fibrosis (F3) or cirrhosis are at highest risk for hepatocellular carcinoma, they should undergo baseline imaging and remain under indefinite post-SVR surveillance as long as they are eligible for potentially curative treatment, the practice update states. The experts recommended twice-yearly ultrasound, with or without serum alpha-fetoprotein, noting that current evidence supports neither shorter surveillance intervals nor alternative imaging modalities.
“The presence of active hepatocellular carcinoma is associated with a small but statistically significant decrease in SVR with DAA therapy,” the experts confirmed, based on the results of three studies. They recommended that, when possible, patients with hepatocellular carcinoma first receive curative-intent treatment, such as with liver resection or ablation. Direct-acting antiviral therapy can begin 4-6 months later, once there has been time to confirm response to hepatocellular carcinoma treatment.
For patients who are listed for liver transplantation, timing of DAA therapy “should be determined on a case-by-case basis with consideration of median wait times for the region, availability of HCV-positive organs, and degree of liver dysfunction,” they added. “For example, DAA therapy may be beneficial pretransplant for patients in regions with long wait times or limited hepatitis C virus–positive donor organ availability, whereas therapy may be delayed until posttransplant in regions with shorter wait times or a high proportion of hepatitis C virus–positive donor organs that would otherwise go unused.”
For patients with active intermediate or advanced liver cancer, it remains unclear whether DAA therapy is usually worth the costs and risks, they noted. This is because the likelihood of complete response is lower and the competing risk of death is higher than in patients with earlier-stage hepatocellular carcinoma. Pending further data, they recommend basing the decision on patients’ preferences, tumor burden, degree of liver dysfunction, and life expectancy. At their institutions, the researchers do not treat patients with DAA therapy unless their life expectancy exceeds 2 years.
The experts disclosed research funding from the National Cancer Institute, U.S. Veterans Administration, and the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Singal reported personal fees or research funding from AbbVie, Bayer, Bristol-Myers Squibb, Eisai, Exact Sciences, Exelixis, Gilead, Glycotest, Roche, and Wako Diagnostics. His coauthors disclosed ties to AbbVie, Allergan, Bristol-Myers Squibb, Conatus, Genfit, Gilead, Intercept, and Merck.
SOURCE: Singal AG et al. Gastroenterology. 2019 Mar 13. doi: 10.1053/j.gastro.2019.02.046.
Achieving sustained virologic response to direct-acting antiviral therapy for chronic hepatitis C virus infection cuts lifetime hepatocellular carcinoma risk by approximately 70%, even when patients have baseline cirrhosis, experts wrote in Gastroenterology.
When used after curative-intent treatment for hepatocellular carcinoma, direct-acting antiviral (DAA) therapy also does not appear to make recurrent cancer more probable or more aggressive, wrote Amit G. Singal, MD, and associates in an American Gastroenterological Association clinical practice update. Studies that compared DAA therapy with either interferon-based therapy or no treatment have found “similar if not lower recurrence than the comparator groups,” they wrote. Rather, hepatocellular carcinoma is in itself highly recurrent: “While surgical resection and local ablative therapies are considered curative, [probability of] recurrence approaches 25%-35% within the first year, and 50%-60% within 2 years.”
Direct-acting antiviral therapy for chronic hepatitis C infection improves several aspects of liver health, but experts have debated whether and how these benefits affect the risk and behavior of hepatocellular carcinoma. To explore the issue, Dr. Singal, medical director of the liver tumor program and clinical chief of hepatology at UT Southwestern Medical Center in Dallas and associates reviewed published clinical trials, observational studies, and systematic reviews. Among 11 studies of more than 3,000 patients in five countries, sustained virologic response (SVR) to DAA therapy was associated with about a 70% reduction in the risk of liver cancer, even after adjustment for clinical and demographic variables. “The relative reduction is similar in patients with and without cirrhosis,” the experts wrote.
Since patients with fibrosis (F3) or cirrhosis are at highest risk for hepatocellular carcinoma, they should undergo baseline imaging and remain under indefinite post-SVR surveillance as long as they are eligible for potentially curative treatment, the practice update states. The experts recommended twice-yearly ultrasound, with or without serum alpha-fetoprotein, noting that current evidence supports neither shorter surveillance intervals nor alternative imaging modalities.
“The presence of active hepatocellular carcinoma is associated with a small but statistically significant decrease in SVR with DAA therapy,” the experts confirmed, based on the results of three studies. They recommended that, when possible, patients with hepatocellular carcinoma first receive curative-intent treatment, such as with liver resection or ablation. Direct-acting antiviral therapy can begin 4-6 months later, once there has been time to confirm response to hepatocellular carcinoma treatment.
For patients who are listed for liver transplantation, timing of DAA therapy “should be determined on a case-by-case basis with consideration of median wait times for the region, availability of HCV-positive organs, and degree of liver dysfunction,” they added. “For example, DAA therapy may be beneficial pretransplant for patients in regions with long wait times or limited hepatitis C virus–positive donor organ availability, whereas therapy may be delayed until posttransplant in regions with shorter wait times or a high proportion of hepatitis C virus–positive donor organs that would otherwise go unused.”
For patients with active intermediate or advanced liver cancer, it remains unclear whether DAA therapy is usually worth the costs and risks, they noted. This is because the likelihood of complete response is lower and the competing risk of death is higher than in patients with earlier-stage hepatocellular carcinoma. Pending further data, they recommend basing the decision on patients’ preferences, tumor burden, degree of liver dysfunction, and life expectancy. At their institutions, the researchers do not treat patients with DAA therapy unless their life expectancy exceeds 2 years.
The experts disclosed research funding from the National Cancer Institute, U.S. Veterans Administration, and the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Singal reported personal fees or research funding from AbbVie, Bayer, Bristol-Myers Squibb, Eisai, Exact Sciences, Exelixis, Gilead, Glycotest, Roche, and Wako Diagnostics. His coauthors disclosed ties to AbbVie, Allergan, Bristol-Myers Squibb, Conatus, Genfit, Gilead, Intercept, and Merck.
SOURCE: Singal AG et al. Gastroenterology. 2019 Mar 13. doi: 10.1053/j.gastro.2019.02.046.
FROM GASTROENTEROLOGY
Bioimpedance spectroscopy may better identify lymphedema progression
Bioimpedance spectroscopy may better identify lymphedema progression in women at risk for breast cancer–related lymphedema over the traditionally used method of monitoring arm circumference with a tape measure, according to results from an interim analysis of the PREVENT trial presented in a recent webcast from the annual meeting of the American Society of Breast Surgeons.
“Despite advances in breast-conserving surgery, improved radiation protocol, the advent of sentinel [node] biopsies and recent improvement in chemotherapy regimens, breast cancer–related lymphedema ... remains a major source of morbidity and concern in this patient population,” Sheila Ridner, PhD, RN, FAAN, professor of nursing at the Vanderbilt University School of Nursing in Nashville, Tenn., said in her presentation. “Because it is thought that early identification of swelling in the limbs coupled with a compression intervention may reduce the risk of patients developing full-blown clinical lymphedema, clinicians are proposing to use a prospective surveillance model to follow breast cancer survivors post surgery in order to assess limbs in a routine fashion and perhaps instigate preventative mechanisms early.”
The larger randomized controlled Prevention of Lymphedema Following Locoregional Treatment for Breast Cancer (PREVENT) trial enrolled 1,201 patients, and 200 patients overall have completed the full protocol. The researchers plan to follow patients for 3 years after surgery. In this interim analysis, Dr. Ridner and colleagues analyzed data from 508 patients at eight sites in the United States and four sites in Sydney who had stage I through stage III or ductal carcinoma in situ (DCIS) breast cancer and underwent mastectomy, taxane-based chemotherapy, or an axillary treatment such as axillary radiation, axillary lymph node dissection, or sentinel lymph nose biopsy with more than 6 nodes.
The patients were randomized to be measured using either traditional tape measurement or bioimpedance spectroscopy (BIS). Patients were moved to a prevention intervention if there was a change in baseline volume of 5% or greater but less than 10% in the tape measure group and change from baseline L-Dex measurement of 6.5 or greater in the BIS group, which consisted of wearing an arm compression sleeve and chest gauntlet for 12 hours a day over 4 weeks. After surgery, the patients were followed up at 3 months, 6 months, 12 months, 18 months, and 24 months, with optional follow-up visits at 15 months and 21 months. Progression to full lymphedema was defined as a 10% or greater change in pretreatment baseline measurements in the tape measure group.
Of the 508 patients analyzed, 10 patients had already progressed to full lymphedema, leaving 498 patients available for the interim analysis. There were 68 patients in the tape measure group (28.5%) and 41 patients in the BIS group (15.8%) who received the prevention intervention, and 10 patients in the tape measure group (14.7%) and 2 patients in the BIS group (4.9%) eventually progressed to full lymphedema. In the BIS group, there was a 10% absolute reduction and 67% relative reduction in lymphedema progression, compared with the tape measure group.
“We believe that the 10% absolute reduction is clinically significant for this patient population,” said Dr. Ridner. “We also believe that our interim results may support the concept of posttreatment surveillance using BIS for early detection of subclinical lymphedema coupled with early intervention as our preliminary data suggest this does have clinical advantages to the patient.”
The study was funded by ImpediMed. Dr. Ridner reports being the principal investigator for ImpediMed and Tactile Medical through work agreements contracted between the companies and her institution.
Bioimpedance spectroscopy may better identify lymphedema progression in women at risk for breast cancer–related lymphedema over the traditionally used method of monitoring arm circumference with a tape measure, according to results from an interim analysis of the PREVENT trial presented in a recent webcast from the annual meeting of the American Society of Breast Surgeons.
“Despite advances in breast-conserving surgery, improved radiation protocol, the advent of sentinel [node] biopsies and recent improvement in chemotherapy regimens, breast cancer–related lymphedema ... remains a major source of morbidity and concern in this patient population,” Sheila Ridner, PhD, RN, FAAN, professor of nursing at the Vanderbilt University School of Nursing in Nashville, Tenn., said in her presentation. “Because it is thought that early identification of swelling in the limbs coupled with a compression intervention may reduce the risk of patients developing full-blown clinical lymphedema, clinicians are proposing to use a prospective surveillance model to follow breast cancer survivors post surgery in order to assess limbs in a routine fashion and perhaps instigate preventative mechanisms early.”
The larger randomized controlled Prevention of Lymphedema Following Locoregional Treatment for Breast Cancer (PREVENT) trial enrolled 1,201 patients, and 200 patients overall have completed the full protocol. The researchers plan to follow patients for 3 years after surgery. In this interim analysis, Dr. Ridner and colleagues analyzed data from 508 patients at eight sites in the United States and four sites in Sydney who had stage I through stage III or ductal carcinoma in situ (DCIS) breast cancer and underwent mastectomy, taxane-based chemotherapy, or an axillary treatment such as axillary radiation, axillary lymph node dissection, or sentinel lymph nose biopsy with more than 6 nodes.
The patients were randomized to be measured using either traditional tape measurement or bioimpedance spectroscopy (BIS). Patients were moved to a prevention intervention if there was a change in baseline volume of 5% or greater but less than 10% in the tape measure group and change from baseline L-Dex measurement of 6.5 or greater in the BIS group, which consisted of wearing an arm compression sleeve and chest gauntlet for 12 hours a day over 4 weeks. After surgery, the patients were followed up at 3 months, 6 months, 12 months, 18 months, and 24 months, with optional follow-up visits at 15 months and 21 months. Progression to full lymphedema was defined as a 10% or greater change in pretreatment baseline measurements in the tape measure group.
Of the 508 patients analyzed, 10 patients had already progressed to full lymphedema, leaving 498 patients available for the interim analysis. There were 68 patients in the tape measure group (28.5%) and 41 patients in the BIS group (15.8%) who received the prevention intervention, and 10 patients in the tape measure group (14.7%) and 2 patients in the BIS group (4.9%) eventually progressed to full lymphedema. In the BIS group, there was a 10% absolute reduction and 67% relative reduction in lymphedema progression, compared with the tape measure group.
“We believe that the 10% absolute reduction is clinically significant for this patient population,” said Dr. Ridner. “We also believe that our interim results may support the concept of posttreatment surveillance using BIS for early detection of subclinical lymphedema coupled with early intervention as our preliminary data suggest this does have clinical advantages to the patient.”
The study was funded by ImpediMed. Dr. Ridner reports being the principal investigator for ImpediMed and Tactile Medical through work agreements contracted between the companies and her institution.
Bioimpedance spectroscopy may better identify lymphedema progression in women at risk for breast cancer–related lymphedema over the traditionally used method of monitoring arm circumference with a tape measure, according to results from an interim analysis of the PREVENT trial presented in a recent webcast from the annual meeting of the American Society of Breast Surgeons.
“Despite advances in breast-conserving surgery, improved radiation protocol, the advent of sentinel [node] biopsies and recent improvement in chemotherapy regimens, breast cancer–related lymphedema ... remains a major source of morbidity and concern in this patient population,” Sheila Ridner, PhD, RN, FAAN, professor of nursing at the Vanderbilt University School of Nursing in Nashville, Tenn., said in her presentation. “Because it is thought that early identification of swelling in the limbs coupled with a compression intervention may reduce the risk of patients developing full-blown clinical lymphedema, clinicians are proposing to use a prospective surveillance model to follow breast cancer survivors post surgery in order to assess limbs in a routine fashion and perhaps instigate preventative mechanisms early.”
The larger randomized controlled Prevention of Lymphedema Following Locoregional Treatment for Breast Cancer (PREVENT) trial enrolled 1,201 patients, and 200 patients overall have completed the full protocol. The researchers plan to follow patients for 3 years after surgery. In this interim analysis, Dr. Ridner and colleagues analyzed data from 508 patients at eight sites in the United States and four sites in Sydney who had stage I through stage III or ductal carcinoma in situ (DCIS) breast cancer and underwent mastectomy, taxane-based chemotherapy, or an axillary treatment such as axillary radiation, axillary lymph node dissection, or sentinel lymph nose biopsy with more than 6 nodes.
The patients were randomized to be measured using either traditional tape measurement or bioimpedance spectroscopy (BIS). Patients were moved to a prevention intervention if there was a change in baseline volume of 5% or greater but less than 10% in the tape measure group and change from baseline L-Dex measurement of 6.5 or greater in the BIS group, which consisted of wearing an arm compression sleeve and chest gauntlet for 12 hours a day over 4 weeks. After surgery, the patients were followed up at 3 months, 6 months, 12 months, 18 months, and 24 months, with optional follow-up visits at 15 months and 21 months. Progression to full lymphedema was defined as a 10% or greater change in pretreatment baseline measurements in the tape measure group.
Of the 508 patients analyzed, 10 patients had already progressed to full lymphedema, leaving 498 patients available for the interim analysis. There were 68 patients in the tape measure group (28.5%) and 41 patients in the BIS group (15.8%) who received the prevention intervention, and 10 patients in the tape measure group (14.7%) and 2 patients in the BIS group (4.9%) eventually progressed to full lymphedema. In the BIS group, there was a 10% absolute reduction and 67% relative reduction in lymphedema progression, compared with the tape measure group.
“We believe that the 10% absolute reduction is clinically significant for this patient population,” said Dr. Ridner. “We also believe that our interim results may support the concept of posttreatment surveillance using BIS for early detection of subclinical lymphedema coupled with early intervention as our preliminary data suggest this does have clinical advantages to the patient.”
The study was funded by ImpediMed. Dr. Ridner reports being the principal investigator for ImpediMed and Tactile Medical through work agreements contracted between the companies and her institution.
REPORTING FROM ASBS 2019