User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Colorectal cancer risk elevated in anticoagulated AF patients with lower GI bleeding
A new study has found that patients with atrial fibrillation (AF) who take oral anticoagulants and then suffer from lower GI bleeding have a much higher risk of being diagnosed with colorectal cancer.
“Our data indicate that lower GI bleeding in these patients should not be dismissed as a mere consequence of anticoagulation treatment,” wrote Peter Vibe Rasmussen, MD, of the University of Copenhagen in Denmark and his coauthors, adding that “timely examination could potentially provide early detection of malignant colorectal lesions.” The study was published in the European Heart Journal.
To determine whether being treated with oral anticoagulants (OACs) and subsequently undergoing GI bleeding indicates colorectal cancer, the researchers examined data from 125,418 Danish AF patients gathered from a nationwide registry. Their median age was 73 years old, and 58% (n = 73,271) were males.
Over a 3-year follow-up period, 2,576 cases of lower GI bleeding were identified; 140 of those cases led to a diagnosis of colorectal cancer within a year. (95% confidence interval, 6.1-10.6%) in patients aged 76-80 and 3.7% (95% CI, 2.2-6.2%) in patients 65 years old or younger.
All age groups had a higher risk of colorectal cancer after bleeding, compared with patients without bleeding. Patients 65 or younger had a risk ratio of 24.2 (95% CI, 14.5-40.4) while patients over 85 had a risk ratio of 12.3 (95% CI, 7.9-19.0).
The authors acknowledged their study’s limitations, including a lack of information regarding certain risk factors, such as alcohol consumption, dietary habits, and obesity. In addition, they noted that the absolute risk of colorectal cancer in patients without bleeding is likely underdiagnosed, as “patients without GI bleeding are less likely to undergo diagnostic procedures.”
Two of the authors are employees at Bristol-Myers Squibb and Pfizer, respectively. Six additional authors reported receiving grants, speaker honoraria and consulting fees from various pharmaceutical companies. The remaining authors reported no conflicts of interest.
SOURCE: Rasmussen PV et al. Eur Heart J. 2020 Feb 7. doi: 10.1093/eurheartj/ehz964.
A new study has found that patients with atrial fibrillation (AF) who take oral anticoagulants and then suffer from lower GI bleeding have a much higher risk of being diagnosed with colorectal cancer.
“Our data indicate that lower GI bleeding in these patients should not be dismissed as a mere consequence of anticoagulation treatment,” wrote Peter Vibe Rasmussen, MD, of the University of Copenhagen in Denmark and his coauthors, adding that “timely examination could potentially provide early detection of malignant colorectal lesions.” The study was published in the European Heart Journal.
To determine whether being treated with oral anticoagulants (OACs) and subsequently undergoing GI bleeding indicates colorectal cancer, the researchers examined data from 125,418 Danish AF patients gathered from a nationwide registry. Their median age was 73 years old, and 58% (n = 73,271) were males.
Over a 3-year follow-up period, 2,576 cases of lower GI bleeding were identified; 140 of those cases led to a diagnosis of colorectal cancer within a year. (95% confidence interval, 6.1-10.6%) in patients aged 76-80 and 3.7% (95% CI, 2.2-6.2%) in patients 65 years old or younger.
All age groups had a higher risk of colorectal cancer after bleeding, compared with patients without bleeding. Patients 65 or younger had a risk ratio of 24.2 (95% CI, 14.5-40.4) while patients over 85 had a risk ratio of 12.3 (95% CI, 7.9-19.0).
The authors acknowledged their study’s limitations, including a lack of information regarding certain risk factors, such as alcohol consumption, dietary habits, and obesity. In addition, they noted that the absolute risk of colorectal cancer in patients without bleeding is likely underdiagnosed, as “patients without GI bleeding are less likely to undergo diagnostic procedures.”
Two of the authors are employees at Bristol-Myers Squibb and Pfizer, respectively. Six additional authors reported receiving grants, speaker honoraria and consulting fees from various pharmaceutical companies. The remaining authors reported no conflicts of interest.
SOURCE: Rasmussen PV et al. Eur Heart J. 2020 Feb 7. doi: 10.1093/eurheartj/ehz964.
A new study has found that patients with atrial fibrillation (AF) who take oral anticoagulants and then suffer from lower GI bleeding have a much higher risk of being diagnosed with colorectal cancer.
“Our data indicate that lower GI bleeding in these patients should not be dismissed as a mere consequence of anticoagulation treatment,” wrote Peter Vibe Rasmussen, MD, of the University of Copenhagen in Denmark and his coauthors, adding that “timely examination could potentially provide early detection of malignant colorectal lesions.” The study was published in the European Heart Journal.
To determine whether being treated with oral anticoagulants (OACs) and subsequently undergoing GI bleeding indicates colorectal cancer, the researchers examined data from 125,418 Danish AF patients gathered from a nationwide registry. Their median age was 73 years old, and 58% (n = 73,271) were males.
Over a 3-year follow-up period, 2,576 cases of lower GI bleeding were identified; 140 of those cases led to a diagnosis of colorectal cancer within a year. (95% confidence interval, 6.1-10.6%) in patients aged 76-80 and 3.7% (95% CI, 2.2-6.2%) in patients 65 years old or younger.
All age groups had a higher risk of colorectal cancer after bleeding, compared with patients without bleeding. Patients 65 or younger had a risk ratio of 24.2 (95% CI, 14.5-40.4) while patients over 85 had a risk ratio of 12.3 (95% CI, 7.9-19.0).
The authors acknowledged their study’s limitations, including a lack of information regarding certain risk factors, such as alcohol consumption, dietary habits, and obesity. In addition, they noted that the absolute risk of colorectal cancer in patients without bleeding is likely underdiagnosed, as “patients without GI bleeding are less likely to undergo diagnostic procedures.”
Two of the authors are employees at Bristol-Myers Squibb and Pfizer, respectively. Six additional authors reported receiving grants, speaker honoraria and consulting fees from various pharmaceutical companies. The remaining authors reported no conflicts of interest.
SOURCE: Rasmussen PV et al. Eur Heart J. 2020 Feb 7. doi: 10.1093/eurheartj/ehz964.
FROM the European Heart Journal
Myth busting: Sudden cardiac death in athletes
SNOWMASS, COLO. – Myths and misconceptions abound regarding the merits of universal incorporation of the resting 12-lead ECG into preparticipation cardiovascular screening of young athletes, Aaron L. Baggish, MD, declared at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.

Dr. Baggish, director of the Cardiovascular Performance Program at Massachusetts General Hospital and a cardiologist at Harvard Medical School, Boston, set out to pop the balloons of a handful of these widely floating myths. These are commonly held fictions: In an electronic poll at the outset of his talk, only one in five members of his large audience recognized all of the following boldface statements as false.
“Preparticipation cardiovascular screening (PPCVS) has been shown to reduce the incidence of sudden cardiac death (SCD) among young competitive athletes.”
FALSE. Not for PPCVS by history and physical examination alone, or with the addition of a screening 12-lead ECG. In Italy, where a cluster of high-profile sudden cardiac deaths led to passage of a 1982 national law mandating 12-lead ECG screening as part of the PPCVS, investigators presented studies purporting to demonstrate a subsequent reduction in the risk of SCD. But those studies were subsequently shown to be fraught with problems. And a high-quality study capable of convincingly demonstrating such a benefit would need to be prohibitively large and expensive. “Don’t hold your breath waiting for that to happen anytime soon,” advised Dr. Baggish, who is medical director for the Boston Marathon, as well as team cardiologist for Harvard University Athletics, the New England Patriots, the Boston Bruins, USRowing, and U.S. Soccer.
“Hypertrophic cardiomyopathy is the leading cause of sudden death among young competitive athletes.”
FALSE. A study of the National Collegiate Athletic Association (NCAA) comprehensive database, with 4.2 million athlete-years of follow-up, showed that the most common cause of SCD was autopsy-negative sudden unexplained death (SUD), accounting for 25% of cases. Hypertrophic cardiomyopathy was deemed the cause of 8% of the SCDs (Circulation. 2015 Jul 7;132[1]:10-9).
“The same thing has been shown in studies done in the United Kingdom and in Australia: . Over the next 10 years, I suspect that one of the most important areas that we’ll be looking into will be this SUD area, perhaps using molecular autopsy to make some headway there,” according to the cardiologist.
SCD is rare. In the NCAA study, the incidence was 1 in 53,703 athlete-years. In sobering contrast, accidents, suicide, and homicide accounted for 50% of all deaths in the collegiate athletes.
“When you think about what’s important in terms of educating young people to be safe, the history and physical exam and 12-lead ECG are nowhere near as important as talking with them about minimizing accident risk and staying away from guns,” Dr. Baggish commented.
“Contemporary ECG interpretation criteria designed specifically for use in young athletes have eliminated the problem of false-positive testing.”
FALSE. The story of adding ECG screening to the PPCVS is one of dramatically improved sensitivity over history and physical exam alone, but always at the cost of reduced specificity. In the Harvard Athlete Initiative Study, Dr. Baggish and coworkers reported that adding the 12-lead ECG resulted in a 17% false-positive rate (Ann Intern Med. 2010 Mar 2;152[5]:269-75). Similar findings were reported in independent studies at two other large universities.
“An ECG false-positive rate of 16%-20%? That’s big trouble. Remember, the conditions we’re looking for are uncommon, with a prevalence of maybe 1 in 500 at most. So if you’re flagging one-fifth or one-sixth of your athletes, the ECG is really not an appropriate tool for screening,” he commented.
Recognition of this limitation has led to development of refined, improved ECG criteria: most notably, the 2012 Seattle criteria, with an associated false-positive rate of 4%-8%, followed by the 2017 International Consensus Criteria (J Am Coll Cardiol. 2017 Feb 28;69[8]:1057-75), with a false-positive rate of 1%-2%. That’s a great improvement. Still, when Dr. Baggish, a marathoner himself, thinks about the roughly 32,000 Boston Marathon runners at the starting line each year, that false-positive rate would translate into 320-640 of those individuals being needlessly subjected to the not-insignificant time and expense of further testing, along with considerable anxiety for the runners and their families, and perhaps even inappropriate disqualification.
“Current ACC/AHA guidelines recommend against the use of the 12-lead ECG during the PPCVS.”
FALSE. Dr. Baggish was a coauthor of the current guidelines, which he described as “an open-door invitation to local decisions, with some important caveats” (Circulation. 2015 Dec 1;132[22]:e267-72).
The guidelines state that the minimum requirement and legal standard for PPCVS of young competitive athletes is a focused history and physical examination, such as the American College of Cardiology/American Heart Association 14-point screen, which consists of 10 elements addressing personal and family history and 4 focused on the physical examination, or the American Academy of Pediatrics Preparticipation Physical Evaluation. Further, while mandatory universal inclusion of the 12-lead ECG is not recommended – it’s rated Class III, meaning don’t do it – the guidelines state that screening programs are at liberty to choose the 12-lead ECG as an additional tool, “provided that close physician involvement and sufficient quality control can be achieved. If undertaken, such initiatives should recognize the known and anticipated limitations of the 12-lead ECG as a population screening test, including the expected frequency of false-positive and false-negative test results, as well as the cost required to support these initiatives over time.”
Dr. Baggish considers the ACC/AHA guidelines to be one of the two most important developments in the field of SCD during sports in recent years. The other is the NCAA-sponsored multidisciplinary Interassociation Consensus Statement on Cardiovascular Care of College Student-Athletes, which he also coauthored (J Am Coll Cardiol. 2016 Jun 28;67[25]:2981-95).
The report lays out the case for a much broader than traditional view of the PPCVS, with “goals that extend beyond detection of occult high-risk pathology.”
“The NCAA has done something very interesting,” Dr. Baggish explained. “It has said that, if we’re going to be screening, we should be thinking about screening with a much broader rationale. It’s not just about finding the needle-in-a-haystack hypertrophic cardiomyopathy or anomalous coronary arteries, it’s about engaging student-athletes at an early point in their collegiate career and trying to improve their health overall – and not just while they’re in college, but over their lifespan.”
He reported having no financial conflicts regarding his presentation.
SNOWMASS, COLO. – Myths and misconceptions abound regarding the merits of universal incorporation of the resting 12-lead ECG into preparticipation cardiovascular screening of young athletes, Aaron L. Baggish, MD, declared at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
Dr. Baggish, director of the Cardiovascular Performance Program at Massachusetts General Hospital and a cardiologist at Harvard Medical School, Boston, set out to pop the balloons of a handful of these widely floating myths. These are commonly held fictions: In an electronic poll at the outset of his talk, only one in five members of his large audience recognized all of the following boldface statements as false.
“Preparticipation cardiovascular screening (PPCVS) has been shown to reduce the incidence of sudden cardiac death (SCD) among young competitive athletes.”
FALSE. Not for PPCVS by history and physical examination alone, or with the addition of a screening 12-lead ECG. In Italy, where a cluster of high-profile sudden cardiac deaths led to passage of a 1982 national law mandating 12-lead ECG screening as part of the PPCVS, investigators presented studies purporting to demonstrate a subsequent reduction in the risk of SCD. But those studies were subsequently shown to be fraught with problems. And a high-quality study capable of convincingly demonstrating such a benefit would need to be prohibitively large and expensive. “Don’t hold your breath waiting for that to happen anytime soon,” advised Dr. Baggish, who is medical director for the Boston Marathon, as well as team cardiologist for Harvard University Athletics, the New England Patriots, the Boston Bruins, USRowing, and U.S. Soccer.
“Hypertrophic cardiomyopathy is the leading cause of sudden death among young competitive athletes.”
FALSE. A study of the National Collegiate Athletic Association (NCAA) comprehensive database, with 4.2 million athlete-years of follow-up, showed that the most common cause of SCD was autopsy-negative sudden unexplained death (SUD), accounting for 25% of cases. Hypertrophic cardiomyopathy was deemed the cause of 8% of the SCDs (Circulation. 2015 Jul 7;132[1]:10-9).
“The same thing has been shown in studies done in the United Kingdom and in Australia: . Over the next 10 years, I suspect that one of the most important areas that we’ll be looking into will be this SUD area, perhaps using molecular autopsy to make some headway there,” according to the cardiologist.
SCD is rare. In the NCAA study, the incidence was 1 in 53,703 athlete-years. In sobering contrast, accidents, suicide, and homicide accounted for 50% of all deaths in the collegiate athletes.
“When you think about what’s important in terms of educating young people to be safe, the history and physical exam and 12-lead ECG are nowhere near as important as talking with them about minimizing accident risk and staying away from guns,” Dr. Baggish commented.
“Contemporary ECG interpretation criteria designed specifically for use in young athletes have eliminated the problem of false-positive testing.”
FALSE. The story of adding ECG screening to the PPCVS is one of dramatically improved sensitivity over history and physical exam alone, but always at the cost of reduced specificity. In the Harvard Athlete Initiative Study, Dr. Baggish and coworkers reported that adding the 12-lead ECG resulted in a 17% false-positive rate (Ann Intern Med. 2010 Mar 2;152[5]:269-75). Similar findings were reported in independent studies at two other large universities.
“An ECG false-positive rate of 16%-20%? That’s big trouble. Remember, the conditions we’re looking for are uncommon, with a prevalence of maybe 1 in 500 at most. So if you’re flagging one-fifth or one-sixth of your athletes, the ECG is really not an appropriate tool for screening,” he commented.
Recognition of this limitation has led to development of refined, improved ECG criteria: most notably, the 2012 Seattle criteria, with an associated false-positive rate of 4%-8%, followed by the 2017 International Consensus Criteria (J Am Coll Cardiol. 2017 Feb 28;69[8]:1057-75), with a false-positive rate of 1%-2%. That’s a great improvement. Still, when Dr. Baggish, a marathoner himself, thinks about the roughly 32,000 Boston Marathon runners at the starting line each year, that false-positive rate would translate into 320-640 of those individuals being needlessly subjected to the not-insignificant time and expense of further testing, along with considerable anxiety for the runners and their families, and perhaps even inappropriate disqualification.
“Current ACC/AHA guidelines recommend against the use of the 12-lead ECG during the PPCVS.”
FALSE. Dr. Baggish was a coauthor of the current guidelines, which he described as “an open-door invitation to local decisions, with some important caveats” (Circulation. 2015 Dec 1;132[22]:e267-72).
The guidelines state that the minimum requirement and legal standard for PPCVS of young competitive athletes is a focused history and physical examination, such as the American College of Cardiology/American Heart Association 14-point screen, which consists of 10 elements addressing personal and family history and 4 focused on the physical examination, or the American Academy of Pediatrics Preparticipation Physical Evaluation. Further, while mandatory universal inclusion of the 12-lead ECG is not recommended – it’s rated Class III, meaning don’t do it – the guidelines state that screening programs are at liberty to choose the 12-lead ECG as an additional tool, “provided that close physician involvement and sufficient quality control can be achieved. If undertaken, such initiatives should recognize the known and anticipated limitations of the 12-lead ECG as a population screening test, including the expected frequency of false-positive and false-negative test results, as well as the cost required to support these initiatives over time.”
Dr. Baggish considers the ACC/AHA guidelines to be one of the two most important developments in the field of SCD during sports in recent years. The other is the NCAA-sponsored multidisciplinary Interassociation Consensus Statement on Cardiovascular Care of College Student-Athletes, which he also coauthored (J Am Coll Cardiol. 2016 Jun 28;67[25]:2981-95).
The report lays out the case for a much broader than traditional view of the PPCVS, with “goals that extend beyond detection of occult high-risk pathology.”
“The NCAA has done something very interesting,” Dr. Baggish explained. “It has said that, if we’re going to be screening, we should be thinking about screening with a much broader rationale. It’s not just about finding the needle-in-a-haystack hypertrophic cardiomyopathy or anomalous coronary arteries, it’s about engaging student-athletes at an early point in their collegiate career and trying to improve their health overall – and not just while they’re in college, but over their lifespan.”
He reported having no financial conflicts regarding his presentation.
SNOWMASS, COLO. – Myths and misconceptions abound regarding the merits of universal incorporation of the resting 12-lead ECG into preparticipation cardiovascular screening of young athletes, Aaron L. Baggish, MD, declared at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
Dr. Baggish, director of the Cardiovascular Performance Program at Massachusetts General Hospital and a cardiologist at Harvard Medical School, Boston, set out to pop the balloons of a handful of these widely floating myths. These are commonly held fictions: In an electronic poll at the outset of his talk, only one in five members of his large audience recognized all of the following boldface statements as false.
“Preparticipation cardiovascular screening (PPCVS) has been shown to reduce the incidence of sudden cardiac death (SCD) among young competitive athletes.”
FALSE. Not for PPCVS by history and physical examination alone, or with the addition of a screening 12-lead ECG. In Italy, where a cluster of high-profile sudden cardiac deaths led to passage of a 1982 national law mandating 12-lead ECG screening as part of the PPCVS, investigators presented studies purporting to demonstrate a subsequent reduction in the risk of SCD. But those studies were subsequently shown to be fraught with problems. And a high-quality study capable of convincingly demonstrating such a benefit would need to be prohibitively large and expensive. “Don’t hold your breath waiting for that to happen anytime soon,” advised Dr. Baggish, who is medical director for the Boston Marathon, as well as team cardiologist for Harvard University Athletics, the New England Patriots, the Boston Bruins, USRowing, and U.S. Soccer.
“Hypertrophic cardiomyopathy is the leading cause of sudden death among young competitive athletes.”
FALSE. A study of the National Collegiate Athletic Association (NCAA) comprehensive database, with 4.2 million athlete-years of follow-up, showed that the most common cause of SCD was autopsy-negative sudden unexplained death (SUD), accounting for 25% of cases. Hypertrophic cardiomyopathy was deemed the cause of 8% of the SCDs (Circulation. 2015 Jul 7;132[1]:10-9).
“The same thing has been shown in studies done in the United Kingdom and in Australia: . Over the next 10 years, I suspect that one of the most important areas that we’ll be looking into will be this SUD area, perhaps using molecular autopsy to make some headway there,” according to the cardiologist.
SCD is rare. In the NCAA study, the incidence was 1 in 53,703 athlete-years. In sobering contrast, accidents, suicide, and homicide accounted for 50% of all deaths in the collegiate athletes.
“When you think about what’s important in terms of educating young people to be safe, the history and physical exam and 12-lead ECG are nowhere near as important as talking with them about minimizing accident risk and staying away from guns,” Dr. Baggish commented.
“Contemporary ECG interpretation criteria designed specifically for use in young athletes have eliminated the problem of false-positive testing.”
FALSE. The story of adding ECG screening to the PPCVS is one of dramatically improved sensitivity over history and physical exam alone, but always at the cost of reduced specificity. In the Harvard Athlete Initiative Study, Dr. Baggish and coworkers reported that adding the 12-lead ECG resulted in a 17% false-positive rate (Ann Intern Med. 2010 Mar 2;152[5]:269-75). Similar findings were reported in independent studies at two other large universities.
“An ECG false-positive rate of 16%-20%? That’s big trouble. Remember, the conditions we’re looking for are uncommon, with a prevalence of maybe 1 in 500 at most. So if you’re flagging one-fifth or one-sixth of your athletes, the ECG is really not an appropriate tool for screening,” he commented.
Recognition of this limitation has led to development of refined, improved ECG criteria: most notably, the 2012 Seattle criteria, with an associated false-positive rate of 4%-8%, followed by the 2017 International Consensus Criteria (J Am Coll Cardiol. 2017 Feb 28;69[8]:1057-75), with a false-positive rate of 1%-2%. That’s a great improvement. Still, when Dr. Baggish, a marathoner himself, thinks about the roughly 32,000 Boston Marathon runners at the starting line each year, that false-positive rate would translate into 320-640 of those individuals being needlessly subjected to the not-insignificant time and expense of further testing, along with considerable anxiety for the runners and their families, and perhaps even inappropriate disqualification.
“Current ACC/AHA guidelines recommend against the use of the 12-lead ECG during the PPCVS.”
FALSE. Dr. Baggish was a coauthor of the current guidelines, which he described as “an open-door invitation to local decisions, with some important caveats” (Circulation. 2015 Dec 1;132[22]:e267-72).
The guidelines state that the minimum requirement and legal standard for PPCVS of young competitive athletes is a focused history and physical examination, such as the American College of Cardiology/American Heart Association 14-point screen, which consists of 10 elements addressing personal and family history and 4 focused on the physical examination, or the American Academy of Pediatrics Preparticipation Physical Evaluation. Further, while mandatory universal inclusion of the 12-lead ECG is not recommended – it’s rated Class III, meaning don’t do it – the guidelines state that screening programs are at liberty to choose the 12-lead ECG as an additional tool, “provided that close physician involvement and sufficient quality control can be achieved. If undertaken, such initiatives should recognize the known and anticipated limitations of the 12-lead ECG as a population screening test, including the expected frequency of false-positive and false-negative test results, as well as the cost required to support these initiatives over time.”
Dr. Baggish considers the ACC/AHA guidelines to be one of the two most important developments in the field of SCD during sports in recent years. The other is the NCAA-sponsored multidisciplinary Interassociation Consensus Statement on Cardiovascular Care of College Student-Athletes, which he also coauthored (J Am Coll Cardiol. 2016 Jun 28;67[25]:2981-95).
The report lays out the case for a much broader than traditional view of the PPCVS, with “goals that extend beyond detection of occult high-risk pathology.”
“The NCAA has done something very interesting,” Dr. Baggish explained. “It has said that, if we’re going to be screening, we should be thinking about screening with a much broader rationale. It’s not just about finding the needle-in-a-haystack hypertrophic cardiomyopathy or anomalous coronary arteries, it’s about engaging student-athletes at an early point in their collegiate career and trying to improve their health overall – and not just while they’re in college, but over their lifespan.”
He reported having no financial conflicts regarding his presentation.
REPORTING FROM ACC SNOWMASS 2020
Remdesivir under study as treatment for novel coronavirus
“What they’re looking at is the effect of this drug -- either the drug plus standard of care versus standard of care alone,” Anthony S. Fauci, MD, reported Feb. 7 during a press briefing held by members of President Trump’s Coronavirus Task Force. “I think pretty soon we are going to get a definitive answer, whether one of these among several drugs works.”
Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases, added that several organizations and individual investigators are developing vaccines for 2019-nCoV. In one such effort, the National Institutes of Health is working with Moderna Inc. to develop a vaccine built on a messenger RNA platform. “One of the first steps is to successfully get that [novel coronavirus] gene and insert it into the messenger RNA platform successfully and allow it to express proteins,” Dr. Fauci explained. “We’ve succeeded in that. The next [step] is to put it in a mouse animal model to induce immunogenicity, and to get the company to make [gold nanoparticle] products. All of those have been successfully implemented. There have been no glitches so far. If that continues, we will be in Phase 1 trials in people within the next two-and-a-half months.”
In another development on the same day, Robert R. Redfield, MD, director of the Centers for Disease Control and Prevention, announced that Heath & Human Services issued an interim final rule to amend foreign quarantine regulations in the wake of the public health threat posed by the 2019-nCoV. “This will enable CDC to collect certain contact information data regarding airline passengers and crew when they arrive from other countries. . .and may be exposed to communicable disease,” Dr. Redfield said. “This action is part of our multi-layered approach to the U.S. response and demonstrates our commitment to take all necessary actions to protect the American people.”
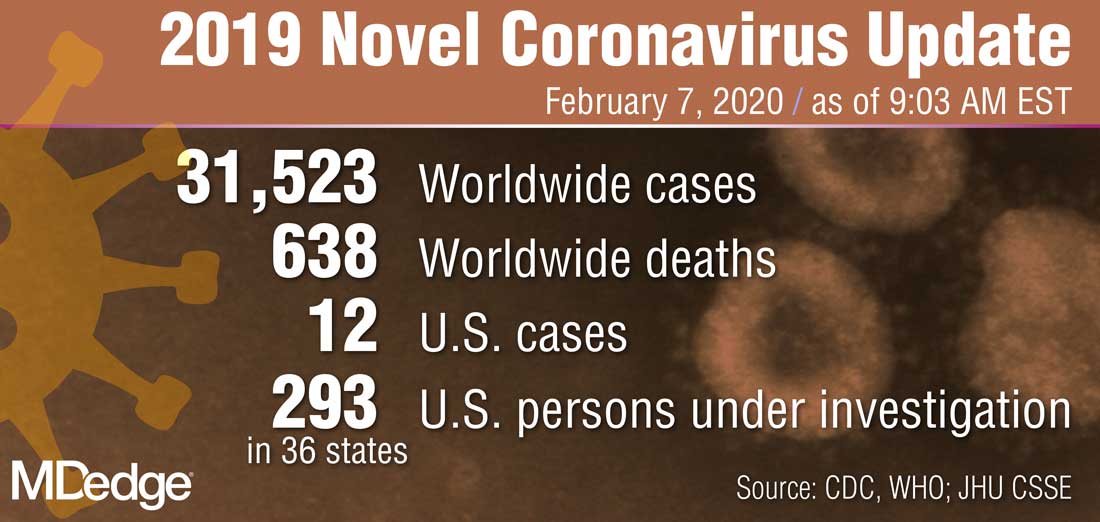
According to Alex Azar, secretary of Health and Human Services, and chair of President Trump’s Coronavirus Task Force, there are 12 confirmed cases of the novel coronavirus in the United States, including two cases of transmission to people who had not recently been in China. “Although the virus represents a potentially very serious public health threat, and we expect to continue seeing more cases here, the immediate risk to the American public is low at this time,” Mr. Azar said. “We are working as quickly as possible on the many unanswered questions about this virus. That includes exactly how it spreads, how deadly it is, whether it’s commonly transmitted by patients who are not yet displaying symptoms, and other issues.”
“What they’re looking at is the effect of this drug -- either the drug plus standard of care versus standard of care alone,” Anthony S. Fauci, MD, reported Feb. 7 during a press briefing held by members of President Trump’s Coronavirus Task Force. “I think pretty soon we are going to get a definitive answer, whether one of these among several drugs works.”
Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases, added that several organizations and individual investigators are developing vaccines for 2019-nCoV. In one such effort, the National Institutes of Health is working with Moderna Inc. to develop a vaccine built on a messenger RNA platform. “One of the first steps is to successfully get that [novel coronavirus] gene and insert it into the messenger RNA platform successfully and allow it to express proteins,” Dr. Fauci explained. “We’ve succeeded in that. The next [step] is to put it in a mouse animal model to induce immunogenicity, and to get the company to make [gold nanoparticle] products. All of those have been successfully implemented. There have been no glitches so far. If that continues, we will be in Phase 1 trials in people within the next two-and-a-half months.”
In another development on the same day, Robert R. Redfield, MD, director of the Centers for Disease Control and Prevention, announced that Heath & Human Services issued an interim final rule to amend foreign quarantine regulations in the wake of the public health threat posed by the 2019-nCoV. “This will enable CDC to collect certain contact information data regarding airline passengers and crew when they arrive from other countries. . .and may be exposed to communicable disease,” Dr. Redfield said. “This action is part of our multi-layered approach to the U.S. response and demonstrates our commitment to take all necessary actions to protect the American people.”
According to Alex Azar, secretary of Health and Human Services, and chair of President Trump’s Coronavirus Task Force, there are 12 confirmed cases of the novel coronavirus in the United States, including two cases of transmission to people who had not recently been in China. “Although the virus represents a potentially very serious public health threat, and we expect to continue seeing more cases here, the immediate risk to the American public is low at this time,” Mr. Azar said. “We are working as quickly as possible on the many unanswered questions about this virus. That includes exactly how it spreads, how deadly it is, whether it’s commonly transmitted by patients who are not yet displaying symptoms, and other issues.”
“What they’re looking at is the effect of this drug -- either the drug plus standard of care versus standard of care alone,” Anthony S. Fauci, MD, reported Feb. 7 during a press briefing held by members of President Trump’s Coronavirus Task Force. “I think pretty soon we are going to get a definitive answer, whether one of these among several drugs works.”
Dr. Fauci, director of the National Institute of Allergy and Infectious Diseases, added that several organizations and individual investigators are developing vaccines for 2019-nCoV. In one such effort, the National Institutes of Health is working with Moderna Inc. to develop a vaccine built on a messenger RNA platform. “One of the first steps is to successfully get that [novel coronavirus] gene and insert it into the messenger RNA platform successfully and allow it to express proteins,” Dr. Fauci explained. “We’ve succeeded in that. The next [step] is to put it in a mouse animal model to induce immunogenicity, and to get the company to make [gold nanoparticle] products. All of those have been successfully implemented. There have been no glitches so far. If that continues, we will be in Phase 1 trials in people within the next two-and-a-half months.”
In another development on the same day, Robert R. Redfield, MD, director of the Centers for Disease Control and Prevention, announced that Heath & Human Services issued an interim final rule to amend foreign quarantine regulations in the wake of the public health threat posed by the 2019-nCoV. “This will enable CDC to collect certain contact information data regarding airline passengers and crew when they arrive from other countries. . .and may be exposed to communicable disease,” Dr. Redfield said. “This action is part of our multi-layered approach to the U.S. response and demonstrates our commitment to take all necessary actions to protect the American people.”
According to Alex Azar, secretary of Health and Human Services, and chair of President Trump’s Coronavirus Task Force, there are 12 confirmed cases of the novel coronavirus in the United States, including two cases of transmission to people who had not recently been in China. “Although the virus represents a potentially very serious public health threat, and we expect to continue seeing more cases here, the immediate risk to the American public is low at this time,” Mr. Azar said. “We are working as quickly as possible on the many unanswered questions about this virus. That includes exactly how it spreads, how deadly it is, whether it’s commonly transmitted by patients who are not yet displaying symptoms, and other issues.”
IBD quality initiative slashes ED utilization
AUSTIN, TEX. – A quality improvement initiative aimed at patients with inflammatory bowel disease (IBD) has reduced emergency department visits and hospitalizations by 20% or more and slashed opioid use by half, according to study results presented at the Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.

After 15 months, the quality improvement program saw emergency department visit rates decline from 18% to 14%, a 22% relative decrease, Gil Y. Melmed, MD, of Cedars-Sinai Medical Center, Los Angeles, said. Additionally, the study documented a similar decrease in the rate of hospitalization, declining from 14% to 11%, while opioid utilization rates declined from 8% to 4%. “We also found decreases in special-cause variation in other measures of interest, including CT scan utilization as well as corticosteroid use, which was reduced 29% during the course of the program,” he said.
The quality initiative was conducted through the Crohn’s & Colitis Foundation as an outgrowth of its IBD Qorus quality improvement program. The 15-month study involved 20,392 patient visits at 15 academic and 11 private/community practices from January 2018 to April 2019. “This specific project within Qorus is focused specifically around the concept of improving access during times of urgent care need,” Dr. Melmed told this news organization. The goal was to identify practice changes that can drive improvement.
The intervention consisted of 19 different strategies, called a “Change Package,” and participating sites could choose to test and implement one or more of them, Dr. Melmed said. Some examples included designating urgent care slots in the clinic schedule, installing a nurse hotline, a weekly “huddle” to review high-risk patients, and patient education on using urgent care.
One of the drivers of the program was to provide immediate care improvement to patients, Dr. Melmed said in the interview. “As opposed to investments into the cure of IBD that we need, but which can take years to develop, this research has immediate, practical applicability for patients today,” he said.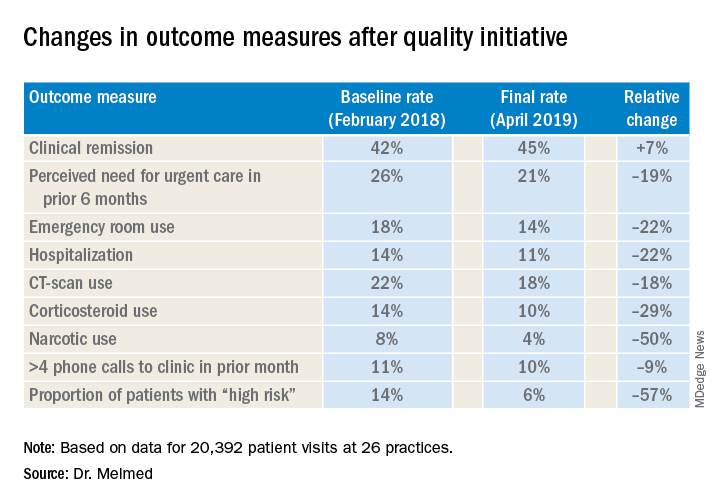
“The fact that we were able to demonstrate reduction in emergency room utilization and hospitalization, steroid use, and narcotic use has really energized the work that we were doing. We can now show that very-low-cost process changes at a site level lead to robust improvement in patient outcomes. These changes are potentially implementable in any practice setting,” Dr. Melmed said in the interview.
After Dr. Melmed’s presentation, Maria T. Abreu, MD, director of the Crohn’s and Colitis Center at the University of Miami, asked about the cost of the interventions. Dr. Melmed said the costs were nominal, such as paying for a new phone line for a patient hotline. “But overall the cost really involved in the program was the time that it took to review the high-risk list on a weekly basis with the team, and that is essentially a 15-minute huddle,” he said.
Later, Dr. Abreu said in an interview that the program was “a terrific example of how measuring outcomes and sharing ideas can make huge impacts in the lives of patients.” She added, “An enormous amount of money is spent on clinical trials of expensive biologics which have revolutionized treatment, yet the humanistic aspects of our care have just as great of an impact. In this study, each center focused on ways they could lower ER visits and hospitalizations. One size did not fit all, yet they could learn from each other. The very platform they used to conduct the study is a model for all of us.”
Corey A. Siegel, MD, of the Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and Dr. Melmed's coprincipal investigator on Qorus, said the quality initiative now includes 49 GI practices across the country with plans to grow to 60 by the end of the year. "We have created this 'collaboratory' for providers from actross the country to work togetherr to learn how to best deliver high-qulaity care for patients with IBD," he said.
Another feature of the quality initiative allowed participating sites to see how they compared with others anonymously, Dr. Melmed said. “Using the data, we called out high-performing sites to teach the rest of us what they were doing that enabled them to improve, so that all of us could learn from their successes,” he said.
The researchers are aiming to evaluate costs and identify the most successful interventions, with the plan to present the latter at Digestive Disease Week® 2020 and use them to develop a toolkit practices can use. “Ultimately,” said Dr. Melmed, “this is scalable.”
Dr. Melmed disclosed financial relationships with AbbVie, Boehringer-Ingelheim, Celgene, Jannsen, GSK, Medtronic, Pfizer, Samsung Bioepis, Takeda, and Techlab; IBD Qorus receives support from Abbvie, AMAG, Helmsley Charitable Trust, Janssen, Nephoroceuticals, Pfizer, Takeda, and UCB.
SOURCE: Melmed GT et al. Crohn’s & Colitis Congress 2020, Session 28.
AUSTIN, TEX. – A quality improvement initiative aimed at patients with inflammatory bowel disease (IBD) has reduced emergency department visits and hospitalizations by 20% or more and slashed opioid use by half, according to study results presented at the Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
After 15 months, the quality improvement program saw emergency department visit rates decline from 18% to 14%, a 22% relative decrease, Gil Y. Melmed, MD, of Cedars-Sinai Medical Center, Los Angeles, said. Additionally, the study documented a similar decrease in the rate of hospitalization, declining from 14% to 11%, while opioid utilization rates declined from 8% to 4%. “We also found decreases in special-cause variation in other measures of interest, including CT scan utilization as well as corticosteroid use, which was reduced 29% during the course of the program,” he said.
The quality initiative was conducted through the Crohn’s & Colitis Foundation as an outgrowth of its IBD Qorus quality improvement program. The 15-month study involved 20,392 patient visits at 15 academic and 11 private/community practices from January 2018 to April 2019. “This specific project within Qorus is focused specifically around the concept of improving access during times of urgent care need,” Dr. Melmed told this news organization. The goal was to identify practice changes that can drive improvement.
The intervention consisted of 19 different strategies, called a “Change Package,” and participating sites could choose to test and implement one or more of them, Dr. Melmed said. Some examples included designating urgent care slots in the clinic schedule, installing a nurse hotline, a weekly “huddle” to review high-risk patients, and patient education on using urgent care.
One of the drivers of the program was to provide immediate care improvement to patients, Dr. Melmed said in the interview. “As opposed to investments into the cure of IBD that we need, but which can take years to develop, this research has immediate, practical applicability for patients today,” he said.
“The fact that we were able to demonstrate reduction in emergency room utilization and hospitalization, steroid use, and narcotic use has really energized the work that we were doing. We can now show that very-low-cost process changes at a site level lead to robust improvement in patient outcomes. These changes are potentially implementable in any practice setting,” Dr. Melmed said in the interview.
After Dr. Melmed’s presentation, Maria T. Abreu, MD, director of the Crohn’s and Colitis Center at the University of Miami, asked about the cost of the interventions. Dr. Melmed said the costs were nominal, such as paying for a new phone line for a patient hotline. “But overall the cost really involved in the program was the time that it took to review the high-risk list on a weekly basis with the team, and that is essentially a 15-minute huddle,” he said.
Later, Dr. Abreu said in an interview that the program was “a terrific example of how measuring outcomes and sharing ideas can make huge impacts in the lives of patients.” She added, “An enormous amount of money is spent on clinical trials of expensive biologics which have revolutionized treatment, yet the humanistic aspects of our care have just as great of an impact. In this study, each center focused on ways they could lower ER visits and hospitalizations. One size did not fit all, yet they could learn from each other. The very platform they used to conduct the study is a model for all of us.”
Corey A. Siegel, MD, of the Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and Dr. Melmed's coprincipal investigator on Qorus, said the quality initiative now includes 49 GI practices across the country with plans to grow to 60 by the end of the year. "We have created this 'collaboratory' for providers from actross the country to work togetherr to learn how to best deliver high-qulaity care for patients with IBD," he said.
Another feature of the quality initiative allowed participating sites to see how they compared with others anonymously, Dr. Melmed said. “Using the data, we called out high-performing sites to teach the rest of us what they were doing that enabled them to improve, so that all of us could learn from their successes,” he said.
The researchers are aiming to evaluate costs and identify the most successful interventions, with the plan to present the latter at Digestive Disease Week® 2020 and use them to develop a toolkit practices can use. “Ultimately,” said Dr. Melmed, “this is scalable.”
Dr. Melmed disclosed financial relationships with AbbVie, Boehringer-Ingelheim, Celgene, Jannsen, GSK, Medtronic, Pfizer, Samsung Bioepis, Takeda, and Techlab; IBD Qorus receives support from Abbvie, AMAG, Helmsley Charitable Trust, Janssen, Nephoroceuticals, Pfizer, Takeda, and UCB.
SOURCE: Melmed GT et al. Crohn’s & Colitis Congress 2020, Session 28.
AUSTIN, TEX. – A quality improvement initiative aimed at patients with inflammatory bowel disease (IBD) has reduced emergency department visits and hospitalizations by 20% or more and slashed opioid use by half, according to study results presented at the Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
After 15 months, the quality improvement program saw emergency department visit rates decline from 18% to 14%, a 22% relative decrease, Gil Y. Melmed, MD, of Cedars-Sinai Medical Center, Los Angeles, said. Additionally, the study documented a similar decrease in the rate of hospitalization, declining from 14% to 11%, while opioid utilization rates declined from 8% to 4%. “We also found decreases in special-cause variation in other measures of interest, including CT scan utilization as well as corticosteroid use, which was reduced 29% during the course of the program,” he said.
The quality initiative was conducted through the Crohn’s & Colitis Foundation as an outgrowth of its IBD Qorus quality improvement program. The 15-month study involved 20,392 patient visits at 15 academic and 11 private/community practices from January 2018 to April 2019. “This specific project within Qorus is focused specifically around the concept of improving access during times of urgent care need,” Dr. Melmed told this news organization. The goal was to identify practice changes that can drive improvement.
The intervention consisted of 19 different strategies, called a “Change Package,” and participating sites could choose to test and implement one or more of them, Dr. Melmed said. Some examples included designating urgent care slots in the clinic schedule, installing a nurse hotline, a weekly “huddle” to review high-risk patients, and patient education on using urgent care.
One of the drivers of the program was to provide immediate care improvement to patients, Dr. Melmed said in the interview. “As opposed to investments into the cure of IBD that we need, but which can take years to develop, this research has immediate, practical applicability for patients today,” he said.
“The fact that we were able to demonstrate reduction in emergency room utilization and hospitalization, steroid use, and narcotic use has really energized the work that we were doing. We can now show that very-low-cost process changes at a site level lead to robust improvement in patient outcomes. These changes are potentially implementable in any practice setting,” Dr. Melmed said in the interview.
After Dr. Melmed’s presentation, Maria T. Abreu, MD, director of the Crohn’s and Colitis Center at the University of Miami, asked about the cost of the interventions. Dr. Melmed said the costs were nominal, such as paying for a new phone line for a patient hotline. “But overall the cost really involved in the program was the time that it took to review the high-risk list on a weekly basis with the team, and that is essentially a 15-minute huddle,” he said.
Later, Dr. Abreu said in an interview that the program was “a terrific example of how measuring outcomes and sharing ideas can make huge impacts in the lives of patients.” She added, “An enormous amount of money is spent on clinical trials of expensive biologics which have revolutionized treatment, yet the humanistic aspects of our care have just as great of an impact. In this study, each center focused on ways they could lower ER visits and hospitalizations. One size did not fit all, yet they could learn from each other. The very platform they used to conduct the study is a model for all of us.”
Corey A. Siegel, MD, of the Dartmouth-Hitchcock Medical Center, Lebanon, N.H., and Dr. Melmed's coprincipal investigator on Qorus, said the quality initiative now includes 49 GI practices across the country with plans to grow to 60 by the end of the year. "We have created this 'collaboratory' for providers from actross the country to work togetherr to learn how to best deliver high-qulaity care for patients with IBD," he said.
Another feature of the quality initiative allowed participating sites to see how they compared with others anonymously, Dr. Melmed said. “Using the data, we called out high-performing sites to teach the rest of us what they were doing that enabled them to improve, so that all of us could learn from their successes,” he said.
The researchers are aiming to evaluate costs and identify the most successful interventions, with the plan to present the latter at Digestive Disease Week® 2020 and use them to develop a toolkit practices can use. “Ultimately,” said Dr. Melmed, “this is scalable.”
Dr. Melmed disclosed financial relationships with AbbVie, Boehringer-Ingelheim, Celgene, Jannsen, GSK, Medtronic, Pfizer, Samsung Bioepis, Takeda, and Techlab; IBD Qorus receives support from Abbvie, AMAG, Helmsley Charitable Trust, Janssen, Nephoroceuticals, Pfizer, Takeda, and UCB.
SOURCE: Melmed GT et al. Crohn’s & Colitis Congress 2020, Session 28.
REPORTING FROM CROHN’S & COLITIS CONGRESS
Cardiac arrest: Targeted temperature management a game changer
SNOWMASS, COLO. – Targeted temperature management maintained at 32-36 degrees Celsius is now a strong class I recommendation for all comatose patients who experience return of spontaneous circulation after out-of-hospital cardiac arrest, including those with nonshockable rhythms, Erin A. Bohula, MD, PhD, said at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.

“Our practice is that ,” said Dr. Bohula, a cardiologist and critical care specialist at Brigham and Women’s Hospital and Harvard Medical School, Boston.
The current ACC/AHA guidelines declare: “There are essentially no patients for whom temperature control somewhere in the range between 32 degrees C [89.6 F) and 36 degrees C [96.8 F] is contraindicated.” The writing committee cited “recent clinical trial data enrolling patients with all rhythms, the rarity of adverse effects in trials, the high neurologic morbidity and mortality without any specific interventions, and the preponderance of data suggesting that temperature is an important variable for neurologic recovery” (Circulation. 2015 Nov 3;132[18 Suppl 2]:S465-82).
“That’s a pretty strong statement,” Dr. Bohula observed.
The current guidelines, which date back to 2015, give a class I, level of evidence B recommendation for targeted temperature management (TTM) in patients who are comatose with return of spontaneous circulation (ROSC) after out-of-hospital cardiac arrest involving ventricular fibrillation or pulseless ventricular fibrillation. The bedside definition of comatose is lack of meaningful response to verbal commands to squeeze hands, blink, or move toes.
The current recommendation for TTM in patients resuscitated from out-of-hospital cardiac arrest with a nonshockable rhythm is class I, level of evidence C, meaning it’s based on expert consensus. However, that recommendation is now out of date and due for a level-of-evidence upgrade in light of the recent results of the French HYPERION trial, an open-label randomized trial of 584 patients resuscitated from cardiac arrest with a nonshockable rhythm. Although 90-day mortality was similarly high in the TTM and targeted normothermia groups, the rate of favorable neurologic outcome as assessed by a Cerebral Performance Category scale score of 1 or 2 was 10.2% in the TTM group, significantly better than the 5.7% rate in controls (N Engl J Med. 2019 Dec 12;381[24]:2327-37).
The 2010, ACC/AHA guidelines recommended a TTM range of 32-34 degrees C, but on the basis of subsequent persuasive randomized trial data, that range was broadened to 32-36 degrees C in the 2015 guidelines, with a class IB recommendation. Maintenance of TTM for at least 24 hours has a IIa, level of evidence C recommendation in the current guidelines.
The guidelines emphasize that specific features may favor selection of one temperature for TTM over another. For example, patients with seizures or cerebral edema might be better off with TTM at a lower temperature, while a higher temperature may be best for those with bleeding or severe bradycardia. At Brigham and Women’s Hospital, the default temperature is 33 degrees C. However, TTM with a goal of 36 degrees C is seriously considered in patients with recent head trauma, major surgery within the past 2 weeks, refractory hypotension, severe sepsis, pregnancy, or high bleeding risk. Rewarming is done at a rate of 0.25 degrees C per hour, with sedation maintained until the patient has been returned to 98.6 degrees F, according to Dr. Bohula.
Based on several negative studies of TTM using rapid infusion of chilled fluids in the ambulance en route to the hospital, the guidelines rate that practice class IIIA, meaning don’t do it. Avoidance of a systolic blood pressure below 90 mm Hg and a mean arterial pressure of less than 65 mm Hg gets a class IIb level of evidence C recommendation to lessen the risk of cerebral hypoxia.
TTM a major breakthrough
Prior to the introduction of TTM, comatose patients with ROSC after out-of-hospital cardiac arrest had a dreadful prognosis, with survival rates of 1%-10% in registry studies. In contrast, the survival rate in the landmark TTM clinical trials was 50%-60%. And while that’s a dramatic improvement, ROSC after cardiac arrest remains a high-mortality condition. Dr. Bohula was first author of a report by the Critical Care Cardiology Trials Network, composed of 16 tertiary cardiac intensive care units in the United States and Canada. Cardiac arrest was the primary indication for 8.7% of 3,049 consecutive admissions, and its 38% mortality rate was the highest of all cardiac critical care indications (JAMA Cardiol. 2019 Jul 24;4[9]:928-35).
TTM was developed in response to a recognition that two-thirds of deaths in patients who make it to the hospital after out-of-hospital cardiac arrest are neurologic – the result of brain anoxia – rather than being due to the myocardial ischemia that may have initially brought them to medical attention.
“Time is brain cells, the same way we think of time as cardiac muscle,” Dr. Bohula observed.
The main idea behind therapeutic hypothermia is that it lowers the cerebral metabolic rate of oxygen to reduce the consequences of ongoing anoxia. The brain doesn’t require as much perfusion when cooled.
TTM has other beneficial neurologic effects as well: It reduces cerebral blood volume via autoregulation, decreases intracranial pressure, and blunts the inflammatory response involved in the postcardiac arrest syndrome. In addition, TTM has anticonvulsant properties, an important effect because seizures and/or myoclonus occur in up to 15% of adults who achieve ROSC after cardiac arrest – and in even more of those who are comatose after doing so. And seizures increase the brain’s metabolic rate threefold, resulting in more cerebral ischemic injury, she explained.
Seizure activity can be difficult to distinguish from shivering in a patient on TTM. For this reason Dr. Bohula recommends putting patients on continuous EEG monitoring from the time of admission, as is the routine practice at the Brigham.
She reported serving as a consultant to Daiichi Sankyo, Servier, Lexicon, Kowa, Merck, Novartis, Novo Nordisk, and the National Institutes of Health. In addition, she generates institutional research grants provided by a half-dozen pharmaceutical companies.
SNOWMASS, COLO. – Targeted temperature management maintained at 32-36 degrees Celsius is now a strong class I recommendation for all comatose patients who experience return of spontaneous circulation after out-of-hospital cardiac arrest, including those with nonshockable rhythms, Erin A. Bohula, MD, PhD, said at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“Our practice is that ,” said Dr. Bohula, a cardiologist and critical care specialist at Brigham and Women’s Hospital and Harvard Medical School, Boston.
The current ACC/AHA guidelines declare: “There are essentially no patients for whom temperature control somewhere in the range between 32 degrees C [89.6 F) and 36 degrees C [96.8 F] is contraindicated.” The writing committee cited “recent clinical trial data enrolling patients with all rhythms, the rarity of adverse effects in trials, the high neurologic morbidity and mortality without any specific interventions, and the preponderance of data suggesting that temperature is an important variable for neurologic recovery” (Circulation. 2015 Nov 3;132[18 Suppl 2]:S465-82).
“That’s a pretty strong statement,” Dr. Bohula observed.
The current guidelines, which date back to 2015, give a class I, level of evidence B recommendation for targeted temperature management (TTM) in patients who are comatose with return of spontaneous circulation (ROSC) after out-of-hospital cardiac arrest involving ventricular fibrillation or pulseless ventricular fibrillation. The bedside definition of comatose is lack of meaningful response to verbal commands to squeeze hands, blink, or move toes.
The current recommendation for TTM in patients resuscitated from out-of-hospital cardiac arrest with a nonshockable rhythm is class I, level of evidence C, meaning it’s based on expert consensus. However, that recommendation is now out of date and due for a level-of-evidence upgrade in light of the recent results of the French HYPERION trial, an open-label randomized trial of 584 patients resuscitated from cardiac arrest with a nonshockable rhythm. Although 90-day mortality was similarly high in the TTM and targeted normothermia groups, the rate of favorable neurologic outcome as assessed by a Cerebral Performance Category scale score of 1 or 2 was 10.2% in the TTM group, significantly better than the 5.7% rate in controls (N Engl J Med. 2019 Dec 12;381[24]:2327-37).
The 2010, ACC/AHA guidelines recommended a TTM range of 32-34 degrees C, but on the basis of subsequent persuasive randomized trial data, that range was broadened to 32-36 degrees C in the 2015 guidelines, with a class IB recommendation. Maintenance of TTM for at least 24 hours has a IIa, level of evidence C recommendation in the current guidelines.
The guidelines emphasize that specific features may favor selection of one temperature for TTM over another. For example, patients with seizures or cerebral edema might be better off with TTM at a lower temperature, while a higher temperature may be best for those with bleeding or severe bradycardia. At Brigham and Women’s Hospital, the default temperature is 33 degrees C. However, TTM with a goal of 36 degrees C is seriously considered in patients with recent head trauma, major surgery within the past 2 weeks, refractory hypotension, severe sepsis, pregnancy, or high bleeding risk. Rewarming is done at a rate of 0.25 degrees C per hour, with sedation maintained until the patient has been returned to 98.6 degrees F, according to Dr. Bohula.
Based on several negative studies of TTM using rapid infusion of chilled fluids in the ambulance en route to the hospital, the guidelines rate that practice class IIIA, meaning don’t do it. Avoidance of a systolic blood pressure below 90 mm Hg and a mean arterial pressure of less than 65 mm Hg gets a class IIb level of evidence C recommendation to lessen the risk of cerebral hypoxia.
TTM a major breakthrough
Prior to the introduction of TTM, comatose patients with ROSC after out-of-hospital cardiac arrest had a dreadful prognosis, with survival rates of 1%-10% in registry studies. In contrast, the survival rate in the landmark TTM clinical trials was 50%-60%. And while that’s a dramatic improvement, ROSC after cardiac arrest remains a high-mortality condition. Dr. Bohula was first author of a report by the Critical Care Cardiology Trials Network, composed of 16 tertiary cardiac intensive care units in the United States and Canada. Cardiac arrest was the primary indication for 8.7% of 3,049 consecutive admissions, and its 38% mortality rate was the highest of all cardiac critical care indications (JAMA Cardiol. 2019 Jul 24;4[9]:928-35).
TTM was developed in response to a recognition that two-thirds of deaths in patients who make it to the hospital after out-of-hospital cardiac arrest are neurologic – the result of brain anoxia – rather than being due to the myocardial ischemia that may have initially brought them to medical attention.
“Time is brain cells, the same way we think of time as cardiac muscle,” Dr. Bohula observed.
The main idea behind therapeutic hypothermia is that it lowers the cerebral metabolic rate of oxygen to reduce the consequences of ongoing anoxia. The brain doesn’t require as much perfusion when cooled.
TTM has other beneficial neurologic effects as well: It reduces cerebral blood volume via autoregulation, decreases intracranial pressure, and blunts the inflammatory response involved in the postcardiac arrest syndrome. In addition, TTM has anticonvulsant properties, an important effect because seizures and/or myoclonus occur in up to 15% of adults who achieve ROSC after cardiac arrest – and in even more of those who are comatose after doing so. And seizures increase the brain’s metabolic rate threefold, resulting in more cerebral ischemic injury, she explained.
Seizure activity can be difficult to distinguish from shivering in a patient on TTM. For this reason Dr. Bohula recommends putting patients on continuous EEG monitoring from the time of admission, as is the routine practice at the Brigham.
She reported serving as a consultant to Daiichi Sankyo, Servier, Lexicon, Kowa, Merck, Novartis, Novo Nordisk, and the National Institutes of Health. In addition, she generates institutional research grants provided by a half-dozen pharmaceutical companies.
SNOWMASS, COLO. – Targeted temperature management maintained at 32-36 degrees Celsius is now a strong class I recommendation for all comatose patients who experience return of spontaneous circulation after out-of-hospital cardiac arrest, including those with nonshockable rhythms, Erin A. Bohula, MD, PhD, said at the annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
“Our practice is that ,” said Dr. Bohula, a cardiologist and critical care specialist at Brigham and Women’s Hospital and Harvard Medical School, Boston.
The current ACC/AHA guidelines declare: “There are essentially no patients for whom temperature control somewhere in the range between 32 degrees C [89.6 F) and 36 degrees C [96.8 F] is contraindicated.” The writing committee cited “recent clinical trial data enrolling patients with all rhythms, the rarity of adverse effects in trials, the high neurologic morbidity and mortality without any specific interventions, and the preponderance of data suggesting that temperature is an important variable for neurologic recovery” (Circulation. 2015 Nov 3;132[18 Suppl 2]:S465-82).
“That’s a pretty strong statement,” Dr. Bohula observed.
The current guidelines, which date back to 2015, give a class I, level of evidence B recommendation for targeted temperature management (TTM) in patients who are comatose with return of spontaneous circulation (ROSC) after out-of-hospital cardiac arrest involving ventricular fibrillation or pulseless ventricular fibrillation. The bedside definition of comatose is lack of meaningful response to verbal commands to squeeze hands, blink, or move toes.
The current recommendation for TTM in patients resuscitated from out-of-hospital cardiac arrest with a nonshockable rhythm is class I, level of evidence C, meaning it’s based on expert consensus. However, that recommendation is now out of date and due for a level-of-evidence upgrade in light of the recent results of the French HYPERION trial, an open-label randomized trial of 584 patients resuscitated from cardiac arrest with a nonshockable rhythm. Although 90-day mortality was similarly high in the TTM and targeted normothermia groups, the rate of favorable neurologic outcome as assessed by a Cerebral Performance Category scale score of 1 or 2 was 10.2% in the TTM group, significantly better than the 5.7% rate in controls (N Engl J Med. 2019 Dec 12;381[24]:2327-37).
The 2010, ACC/AHA guidelines recommended a TTM range of 32-34 degrees C, but on the basis of subsequent persuasive randomized trial data, that range was broadened to 32-36 degrees C in the 2015 guidelines, with a class IB recommendation. Maintenance of TTM for at least 24 hours has a IIa, level of evidence C recommendation in the current guidelines.
The guidelines emphasize that specific features may favor selection of one temperature for TTM over another. For example, patients with seizures or cerebral edema might be better off with TTM at a lower temperature, while a higher temperature may be best for those with bleeding or severe bradycardia. At Brigham and Women’s Hospital, the default temperature is 33 degrees C. However, TTM with a goal of 36 degrees C is seriously considered in patients with recent head trauma, major surgery within the past 2 weeks, refractory hypotension, severe sepsis, pregnancy, or high bleeding risk. Rewarming is done at a rate of 0.25 degrees C per hour, with sedation maintained until the patient has been returned to 98.6 degrees F, according to Dr. Bohula.
Based on several negative studies of TTM using rapid infusion of chilled fluids in the ambulance en route to the hospital, the guidelines rate that practice class IIIA, meaning don’t do it. Avoidance of a systolic blood pressure below 90 mm Hg and a mean arterial pressure of less than 65 mm Hg gets a class IIb level of evidence C recommendation to lessen the risk of cerebral hypoxia.
TTM a major breakthrough
Prior to the introduction of TTM, comatose patients with ROSC after out-of-hospital cardiac arrest had a dreadful prognosis, with survival rates of 1%-10% in registry studies. In contrast, the survival rate in the landmark TTM clinical trials was 50%-60%. And while that’s a dramatic improvement, ROSC after cardiac arrest remains a high-mortality condition. Dr. Bohula was first author of a report by the Critical Care Cardiology Trials Network, composed of 16 tertiary cardiac intensive care units in the United States and Canada. Cardiac arrest was the primary indication for 8.7% of 3,049 consecutive admissions, and its 38% mortality rate was the highest of all cardiac critical care indications (JAMA Cardiol. 2019 Jul 24;4[9]:928-35).
TTM was developed in response to a recognition that two-thirds of deaths in patients who make it to the hospital after out-of-hospital cardiac arrest are neurologic – the result of brain anoxia – rather than being due to the myocardial ischemia that may have initially brought them to medical attention.
“Time is brain cells, the same way we think of time as cardiac muscle,” Dr. Bohula observed.
The main idea behind therapeutic hypothermia is that it lowers the cerebral metabolic rate of oxygen to reduce the consequences of ongoing anoxia. The brain doesn’t require as much perfusion when cooled.
TTM has other beneficial neurologic effects as well: It reduces cerebral blood volume via autoregulation, decreases intracranial pressure, and blunts the inflammatory response involved in the postcardiac arrest syndrome. In addition, TTM has anticonvulsant properties, an important effect because seizures and/or myoclonus occur in up to 15% of adults who achieve ROSC after cardiac arrest – and in even more of those who are comatose after doing so. And seizures increase the brain’s metabolic rate threefold, resulting in more cerebral ischemic injury, she explained.
Seizure activity can be difficult to distinguish from shivering in a patient on TTM. For this reason Dr. Bohula recommends putting patients on continuous EEG monitoring from the time of admission, as is the routine practice at the Brigham.
She reported serving as a consultant to Daiichi Sankyo, Servier, Lexicon, Kowa, Merck, Novartis, Novo Nordisk, and the National Institutes of Health. In addition, she generates institutional research grants provided by a half-dozen pharmaceutical companies.
EXPERT ANALYSIS FROM ACC SNOWMASS 2020
The 2019 novel coronavirus: Case review IDs clinical characteristics
A group of physicians in Wuhan, China, who are treating patients with the 2019 novel coronavirus have gone the extra mile to share their clinical experiences with colleagues around the world.

Nanshan Chen, MD, of Jinyintan Hospital, Wuhan, and his team conducted a retrospective study on 99 cases and, in very short order, published their initial findings in the Lancet online on Jan. 29. These findings could guide action in other cases and help clinicians all over the world create treatment plans for patients of the 2019-nCoV.
The findings show that and characteristics of those with fatal infections align with the MuLBSTA score – an early warning model for predicting viral pneumonia–related mortality, according to a case review.
Of 99 patients who presented with 2019-nCoV pneumonia at Jinyintan Hospital between Jan. 1 and Jan. 20, 67 were men, the mean age was 55.5 years, and 50 patients had chronic diseases.
“All the data of included cases have been shared with [the World Health Organization]. The study was approved by Jinyintan Hospital Ethics Committee and written informed consent was obtained from patients involved before enrollment when data were collected retrospectively,” the researchers noted.
Nearly half of the patients (49%) lived or worked near a specific seafood market, suggesting disease clustering.
Clinical manifestations affecting the majority of patients included fever and cough in 83% and 82% of patients, respectively. Other symptoms included shortness of breath in 31%, muscle aches in 11%, confusion in 9%, headache in 8%, sore throat in 5%, and rhinorrhea, chest pain, diarrhea, and nausea and vomiting in 1%-4% of patients, the investigators found.
Imaging showed bilateral pneumonia in 75% of cases, multiple mottling and ground-glass opacity in 14%, and pneumothorax in 1%. Organ function damage was present in a third of patients at admission: 17% had acute respiratory distress syndrome (ARDS) – including 11 patients who worsened quickly and died of multiple organ failure. Eight percent had acute respiratory injury, 3% had acute renal injury, 4% had septic shock, and 1% had ventilator-associated pneumonia, they said, noting that all cases were confirmed by real-time polymerase chain reaction.
A notable laboratory finding was reduced absolute lymphocyte counts in most patients, the investigators said.
All patients were treated in isolation and 76% received antiviral treatment with oseltamivir, ganciclovir, lopinavir, or ritonavir for 3-14 days (median, 3 days). Most patients also received antibiotic treatment, including a single antibiotic in 25% of cases and combination therapy in 45%, with most antibiotics used to cover “common pathogens and some atypical pathogens,” they said, adding that “when secondary bacterial infection occurred, medication was administered according to the results of bacterial culture and drug sensitivity.”
Cephalosporins, quinolones, carbapenems, tigecycline against methicillin-resistant Staphylococcus aureus, linezolid, and antifungal drugs were used, and duration ranged from 3 to 17 days (median, 5 days).
Nineteen patients also received steroid treatments.
As of Jan. 25, 31 patients had been discharged and 57 remained hospitalized. Of the 11 who died, the first 2 were a 61-year-old man and a 69-year-old man, each diagnosed with severe pneumonia and ARDS. The first experienced sudden cardiac arrest and died on admission day 11, and the second died of severe pneumonia, septic shock, and respiratory failure on admission day 9. Neither had underlying disease, but both had a long history of smoking, the investigators noted.
“The deaths of these two patients were consistent with the MuLBSTA score,” they wrote, explaining that the scoring system takes into account multilobular infiltration, lymphopenia, bacterial coinfection, smoking history, hypertension, and age.
Eight of the nine other patients who died had lymphopenia, seven had bilateral pneumonia, five were over age 60 years, three had hypertension, and one was a heavy smoker, they added.
Most coronavirus infections cause mild symptoms and have good prognosis, but some patients with the 2019-nCoV, which was identified Jan. 7 following the development of several cases of pneumonia of unknown etiology in Wuhan, develop fatal disease. The paucity of data regarding epidemiology and clinical features of pneumonia associated with 2019-nCoV prompted the current retrospective study at the center where the first cases were admitted, the investigators explained.
They noted that the sequence of 2019-nCoV “is relatively different from the six other coronavirus subtypes, including the highly pathogenic severe acute respiratory syndrome (SARS)-CoV and Middle East Respiratory Syndrome (MERS)-CoV, as well as the human coronaviruses (HCoV)-OC43, -229E, -NL63, and -HKU1 that induce mild upper respiratory disease, but can be classified as a betacoronavirus with evidence of human-to-human transmission.
Mortality associated with SARS-CoV and MERS-CoV have been reported as more than 10% and more than 35%, respectively; at data cutoff for the current study, mortality among the 99 included cases was 11%, which is similar to that in another recent 2019-nCoV report, they said.
The finding of greater risk among older men also has been seen with SARS-CoV and MERS-CoV, and the high rate among individuals with chronic diseases, mainly cerebrovascular disease, cardiovascular disease, and diabetes, also has been reported with MERS-CoV, they added.
“Our results suggest that 2019-nCoV is more likely to infect older adult males with chronic comorbidities as a result of the weaker immune functions of these patients,” they wrote.
Coinfection with bacteria and fungi occurred in some patients, particularly those with severe illness, and cultures most often showed A. baumannii, K. pneumoniae, A. flavus, C. glabrata, and C. albicans, and the findings of reduced absolute lymphocyte values in most patients suggests that “2019-nCoV might mainly act on lymphocytes, especially T lymphocytes, as does SARS-CoV,” they noted.
Given the rapid progression with ARDS and septic shock in some patients in this review, “early identification and timely treatment of critical cases is of crucial importance,” they said.
“Use of intravenous immunoglobulin is recommended to enhance the ability of anti-infection for severely ill patients, and steroids (methylprednisolone 1-2 mg/kg per day) are recommended for patients with ARDS, for as short a duration of treatment as possible,” they added.
Further, since some studies suggest that a substantial decrease in lymphocyte count indicates consumption of many immune cells by coronavirus, thereby inhibiting cellular immune function, damage to T lymphocytes might be “an important factor leading to exacerbations of patients,” they wrote, adding that “[t]he low absolute value of lymphocytes could be used as a reference index in the diagnosis of new coronavirus infections in the clinic.”
The MuLBSTA score also should be investigated to determine its applicability for predicting mortality risk in patients with 2019-nCoV infection, they added.
The current study is limited by its small sample size; additional studies are needed to include “as many patients as possible in Wuhan, in other cities in China, and even in other countries to get a more comprehensive understanding of 2019-nCoV,” they said.
The National Key R&D Program of China funded the study. The authors reported having no conflicts of interest.
SOURCE: Chen N et al. Lancet. 2020 Jan 29. doi: 10.1016/S0140-6736(20)30211-7.
A group of physicians in Wuhan, China, who are treating patients with the 2019 novel coronavirus have gone the extra mile to share their clinical experiences with colleagues around the world.
Nanshan Chen, MD, of Jinyintan Hospital, Wuhan, and his team conducted a retrospective study on 99 cases and, in very short order, published their initial findings in the Lancet online on Jan. 29. These findings could guide action in other cases and help clinicians all over the world create treatment plans for patients of the 2019-nCoV.
The findings show that and characteristics of those with fatal infections align with the MuLBSTA score – an early warning model for predicting viral pneumonia–related mortality, according to a case review.
Of 99 patients who presented with 2019-nCoV pneumonia at Jinyintan Hospital between Jan. 1 and Jan. 20, 67 were men, the mean age was 55.5 years, and 50 patients had chronic diseases.
“All the data of included cases have been shared with [the World Health Organization]. The study was approved by Jinyintan Hospital Ethics Committee and written informed consent was obtained from patients involved before enrollment when data were collected retrospectively,” the researchers noted.
Nearly half of the patients (49%) lived or worked near a specific seafood market, suggesting disease clustering.
Clinical manifestations affecting the majority of patients included fever and cough in 83% and 82% of patients, respectively. Other symptoms included shortness of breath in 31%, muscle aches in 11%, confusion in 9%, headache in 8%, sore throat in 5%, and rhinorrhea, chest pain, diarrhea, and nausea and vomiting in 1%-4% of patients, the investigators found.
Imaging showed bilateral pneumonia in 75% of cases, multiple mottling and ground-glass opacity in 14%, and pneumothorax in 1%. Organ function damage was present in a third of patients at admission: 17% had acute respiratory distress syndrome (ARDS) – including 11 patients who worsened quickly and died of multiple organ failure. Eight percent had acute respiratory injury, 3% had acute renal injury, 4% had septic shock, and 1% had ventilator-associated pneumonia, they said, noting that all cases were confirmed by real-time polymerase chain reaction.
A notable laboratory finding was reduced absolute lymphocyte counts in most patients, the investigators said.
All patients were treated in isolation and 76% received antiviral treatment with oseltamivir, ganciclovir, lopinavir, or ritonavir for 3-14 days (median, 3 days). Most patients also received antibiotic treatment, including a single antibiotic in 25% of cases and combination therapy in 45%, with most antibiotics used to cover “common pathogens and some atypical pathogens,” they said, adding that “when secondary bacterial infection occurred, medication was administered according to the results of bacterial culture and drug sensitivity.”
Cephalosporins, quinolones, carbapenems, tigecycline against methicillin-resistant Staphylococcus aureus, linezolid, and antifungal drugs were used, and duration ranged from 3 to 17 days (median, 5 days).
Nineteen patients also received steroid treatments.
As of Jan. 25, 31 patients had been discharged and 57 remained hospitalized. Of the 11 who died, the first 2 were a 61-year-old man and a 69-year-old man, each diagnosed with severe pneumonia and ARDS. The first experienced sudden cardiac arrest and died on admission day 11, and the second died of severe pneumonia, septic shock, and respiratory failure on admission day 9. Neither had underlying disease, but both had a long history of smoking, the investigators noted.
“The deaths of these two patients were consistent with the MuLBSTA score,” they wrote, explaining that the scoring system takes into account multilobular infiltration, lymphopenia, bacterial coinfection, smoking history, hypertension, and age.
Eight of the nine other patients who died had lymphopenia, seven had bilateral pneumonia, five were over age 60 years, three had hypertension, and one was a heavy smoker, they added.
Most coronavirus infections cause mild symptoms and have good prognosis, but some patients with the 2019-nCoV, which was identified Jan. 7 following the development of several cases of pneumonia of unknown etiology in Wuhan, develop fatal disease. The paucity of data regarding epidemiology and clinical features of pneumonia associated with 2019-nCoV prompted the current retrospective study at the center where the first cases were admitted, the investigators explained.
They noted that the sequence of 2019-nCoV “is relatively different from the six other coronavirus subtypes, including the highly pathogenic severe acute respiratory syndrome (SARS)-CoV and Middle East Respiratory Syndrome (MERS)-CoV, as well as the human coronaviruses (HCoV)-OC43, -229E, -NL63, and -HKU1 that induce mild upper respiratory disease, but can be classified as a betacoronavirus with evidence of human-to-human transmission.
Mortality associated with SARS-CoV and MERS-CoV have been reported as more than 10% and more than 35%, respectively; at data cutoff for the current study, mortality among the 99 included cases was 11%, which is similar to that in another recent 2019-nCoV report, they said.
The finding of greater risk among older men also has been seen with SARS-CoV and MERS-CoV, and the high rate among individuals with chronic diseases, mainly cerebrovascular disease, cardiovascular disease, and diabetes, also has been reported with MERS-CoV, they added.
“Our results suggest that 2019-nCoV is more likely to infect older adult males with chronic comorbidities as a result of the weaker immune functions of these patients,” they wrote.
Coinfection with bacteria and fungi occurred in some patients, particularly those with severe illness, and cultures most often showed A. baumannii, K. pneumoniae, A. flavus, C. glabrata, and C. albicans, and the findings of reduced absolute lymphocyte values in most patients suggests that “2019-nCoV might mainly act on lymphocytes, especially T lymphocytes, as does SARS-CoV,” they noted.
Given the rapid progression with ARDS and septic shock in some patients in this review, “early identification and timely treatment of critical cases is of crucial importance,” they said.
“Use of intravenous immunoglobulin is recommended to enhance the ability of anti-infection for severely ill patients, and steroids (methylprednisolone 1-2 mg/kg per day) are recommended for patients with ARDS, for as short a duration of treatment as possible,” they added.
Further, since some studies suggest that a substantial decrease in lymphocyte count indicates consumption of many immune cells by coronavirus, thereby inhibiting cellular immune function, damage to T lymphocytes might be “an important factor leading to exacerbations of patients,” they wrote, adding that “[t]he low absolute value of lymphocytes could be used as a reference index in the diagnosis of new coronavirus infections in the clinic.”
The MuLBSTA score also should be investigated to determine its applicability for predicting mortality risk in patients with 2019-nCoV infection, they added.
The current study is limited by its small sample size; additional studies are needed to include “as many patients as possible in Wuhan, in other cities in China, and even in other countries to get a more comprehensive understanding of 2019-nCoV,” they said.
The National Key R&D Program of China funded the study. The authors reported having no conflicts of interest.
SOURCE: Chen N et al. Lancet. 2020 Jan 29. doi: 10.1016/S0140-6736(20)30211-7.
A group of physicians in Wuhan, China, who are treating patients with the 2019 novel coronavirus have gone the extra mile to share their clinical experiences with colleagues around the world.
Nanshan Chen, MD, of Jinyintan Hospital, Wuhan, and his team conducted a retrospective study on 99 cases and, in very short order, published their initial findings in the Lancet online on Jan. 29. These findings could guide action in other cases and help clinicians all over the world create treatment plans for patients of the 2019-nCoV.
The findings show that and characteristics of those with fatal infections align with the MuLBSTA score – an early warning model for predicting viral pneumonia–related mortality, according to a case review.
Of 99 patients who presented with 2019-nCoV pneumonia at Jinyintan Hospital between Jan. 1 and Jan. 20, 67 were men, the mean age was 55.5 years, and 50 patients had chronic diseases.
“All the data of included cases have been shared with [the World Health Organization]. The study was approved by Jinyintan Hospital Ethics Committee and written informed consent was obtained from patients involved before enrollment when data were collected retrospectively,” the researchers noted.
Nearly half of the patients (49%) lived or worked near a specific seafood market, suggesting disease clustering.
Clinical manifestations affecting the majority of patients included fever and cough in 83% and 82% of patients, respectively. Other symptoms included shortness of breath in 31%, muscle aches in 11%, confusion in 9%, headache in 8%, sore throat in 5%, and rhinorrhea, chest pain, diarrhea, and nausea and vomiting in 1%-4% of patients, the investigators found.
Imaging showed bilateral pneumonia in 75% of cases, multiple mottling and ground-glass opacity in 14%, and pneumothorax in 1%. Organ function damage was present in a third of patients at admission: 17% had acute respiratory distress syndrome (ARDS) – including 11 patients who worsened quickly and died of multiple organ failure. Eight percent had acute respiratory injury, 3% had acute renal injury, 4% had septic shock, and 1% had ventilator-associated pneumonia, they said, noting that all cases were confirmed by real-time polymerase chain reaction.
A notable laboratory finding was reduced absolute lymphocyte counts in most patients, the investigators said.
All patients were treated in isolation and 76% received antiviral treatment with oseltamivir, ganciclovir, lopinavir, or ritonavir for 3-14 days (median, 3 days). Most patients also received antibiotic treatment, including a single antibiotic in 25% of cases and combination therapy in 45%, with most antibiotics used to cover “common pathogens and some atypical pathogens,” they said, adding that “when secondary bacterial infection occurred, medication was administered according to the results of bacterial culture and drug sensitivity.”
Cephalosporins, quinolones, carbapenems, tigecycline against methicillin-resistant Staphylococcus aureus, linezolid, and antifungal drugs were used, and duration ranged from 3 to 17 days (median, 5 days).
Nineteen patients also received steroid treatments.
As of Jan. 25, 31 patients had been discharged and 57 remained hospitalized. Of the 11 who died, the first 2 were a 61-year-old man and a 69-year-old man, each diagnosed with severe pneumonia and ARDS. The first experienced sudden cardiac arrest and died on admission day 11, and the second died of severe pneumonia, septic shock, and respiratory failure on admission day 9. Neither had underlying disease, but both had a long history of smoking, the investigators noted.
“The deaths of these two patients were consistent with the MuLBSTA score,” they wrote, explaining that the scoring system takes into account multilobular infiltration, lymphopenia, bacterial coinfection, smoking history, hypertension, and age.
Eight of the nine other patients who died had lymphopenia, seven had bilateral pneumonia, five were over age 60 years, three had hypertension, and one was a heavy smoker, they added.
Most coronavirus infections cause mild symptoms and have good prognosis, but some patients with the 2019-nCoV, which was identified Jan. 7 following the development of several cases of pneumonia of unknown etiology in Wuhan, develop fatal disease. The paucity of data regarding epidemiology and clinical features of pneumonia associated with 2019-nCoV prompted the current retrospective study at the center where the first cases were admitted, the investigators explained.
They noted that the sequence of 2019-nCoV “is relatively different from the six other coronavirus subtypes, including the highly pathogenic severe acute respiratory syndrome (SARS)-CoV and Middle East Respiratory Syndrome (MERS)-CoV, as well as the human coronaviruses (HCoV)-OC43, -229E, -NL63, and -HKU1 that induce mild upper respiratory disease, but can be classified as a betacoronavirus with evidence of human-to-human transmission.
Mortality associated with SARS-CoV and MERS-CoV have been reported as more than 10% and more than 35%, respectively; at data cutoff for the current study, mortality among the 99 included cases was 11%, which is similar to that in another recent 2019-nCoV report, they said.
The finding of greater risk among older men also has been seen with SARS-CoV and MERS-CoV, and the high rate among individuals with chronic diseases, mainly cerebrovascular disease, cardiovascular disease, and diabetes, also has been reported with MERS-CoV, they added.
“Our results suggest that 2019-nCoV is more likely to infect older adult males with chronic comorbidities as a result of the weaker immune functions of these patients,” they wrote.
Coinfection with bacteria and fungi occurred in some patients, particularly those with severe illness, and cultures most often showed A. baumannii, K. pneumoniae, A. flavus, C. glabrata, and C. albicans, and the findings of reduced absolute lymphocyte values in most patients suggests that “2019-nCoV might mainly act on lymphocytes, especially T lymphocytes, as does SARS-CoV,” they noted.
Given the rapid progression with ARDS and septic shock in some patients in this review, “early identification and timely treatment of critical cases is of crucial importance,” they said.
“Use of intravenous immunoglobulin is recommended to enhance the ability of anti-infection for severely ill patients, and steroids (methylprednisolone 1-2 mg/kg per day) are recommended for patients with ARDS, for as short a duration of treatment as possible,” they added.
Further, since some studies suggest that a substantial decrease in lymphocyte count indicates consumption of many immune cells by coronavirus, thereby inhibiting cellular immune function, damage to T lymphocytes might be “an important factor leading to exacerbations of patients,” they wrote, adding that “[t]he low absolute value of lymphocytes could be used as a reference index in the diagnosis of new coronavirus infections in the clinic.”
The MuLBSTA score also should be investigated to determine its applicability for predicting mortality risk in patients with 2019-nCoV infection, they added.
The current study is limited by its small sample size; additional studies are needed to include “as many patients as possible in Wuhan, in other cities in China, and even in other countries to get a more comprehensive understanding of 2019-nCoV,” they said.
The National Key R&D Program of China funded the study. The authors reported having no conflicts of interest.
SOURCE: Chen N et al. Lancet. 2020 Jan 29. doi: 10.1016/S0140-6736(20)30211-7.
FROM THE LANCET
NASH ‘an epidemic of the 21st century’
LOS ANGELES – The way Christos S. Mantzoros, MD, DSc, PhD, sees it, nonalcoholic steatohepatitis (NASH) is an epidemic of the 21st century that can trigger a cascade of reactions.

“If more than 5.8% of fat is in the liver, we call it nonalcoholic fatty liver disease [NAFLD],” Dr. Mantzoros, professor of medicine at Harvard Medical School, Boston, and Boston University, explained at the World Congress on Insulin Resistance, Diabetes, and Cardiovascular Disease. “If inflammation develops to remove the fat, we call it NASH. If this progresses to decompensated reaction and fibrosis and cirrhosis, then we call it nonalcoholic steatohepatitis with fibrosis. That can lead to liver cirrhosis, hepatocellular carcinoma, and liver failure.”
The underlying problem stems from the rise in obesity prevalence, according to Dr. Mantzoros, who is also chief of endocrinology at the Boston Veterans Affairs Healthcare System. For 75%-80% of individuals with metabolically unhealthy obesity, the storage space in their adipose tissue is exceeded. “Fat is deposited into muscle, causing insulin resistance, and into the liver,” he explained. “If it’s more than 5.8%, it causes NAFLD. Most of us don’t realize that most of the patients with diabetes we have in our clinics also have nonalcoholic fatty liver disease. That’s because we don’t have an easy diagnostic tool or an easy treatment. It’s an unmet clinical need.” (There are currently no drugs approved for the treatment of NASH or NAFLD. Current recommended first-line treatment is weight loss through diet and exercise and control of diabetes, if it is present.)
“Assuming the rate of increase in cost due to NAFLD parallels the growth in obesity, the 10-year projection for direct cost is $1.005 trillion,” said Dr. Mantzoros, who is also editor in chief of the journal Metabolism. “Obesity, NAFLD, and insulin resistance are each independently associated with a twofold risk for diabetes. If all three are present, there is a 14-fold risk for diabetes. Insulin resistance promotes an increase in free fatty acid traffic to the liver, which can trigger hepatic lipotoxicity. Hyperinsulinemia enhances free fatty acid uptake and activates de novo lipogenesis. Hyperglycemia can also activate de novo lipogenesis.”
About 85 million Americans have NAFLD, he continued. Most (80%) are cases of steatosis, but 20% have NASH. Of those, 20% develop advanced fibrosis, which leads to liver failure and transplantation or death. A study of data from the National Health and Nutrition Examination Survey found that (odds ratio, 18.20), followed by a body mass index of 30 kg/m2 or greater (OR, 9.10), hypertension (OR, 1.20), and age (OR, 1.08; Ailment Pharmacol Ther. 2017;46:974-80). “Most of the patients who come to our clinics with diabetes have nonalcoholic fatty liver disease – 75%-80% in our clinics, and about 10% have advanced fibrosis,” Dr. Mantzoros said. “Most of them go undiagnosed.”
Patients with type 2 diabetes and NAFLD progress faster to fibrosis and end-stage liver disease, compared with those who do not have diabetes. One study of 108 patients with biopsy-proven NALFD showed that 84% of those with fibrosis progression had type 2 diabetes (J Hepatol. 2015;62:1148-55). Other findings have shown that patients with type 2 diabetes are at increased risk of chronic NAFLD and hepatocellular carcinoma (Gastroenterol. 2001;126:460-8). “We are doing more liver transplantations because of NAFLD and NASH than because of hepatitis C,” Dr. Mantzoros said. “What we need to keep in mind is that, although liver morbidity and mortality is important, this is a component of the cardiometabolic syndrome. So, people have all the risk factors for cardiovascular disease. Because CVD is much more common, people with NAFLD suffer from and die from CVD. The more advanced the NAFLD, the higher the risk of death from cardiovascular disease.”
Multiple risk factors can help identify patients with advanced fibrosis because of NASH, he continued, including having features of the metabolic syndrome, being over 50 years of age, being Hispanic, having high levels of ALT/AST, low platelets, and having low albumin. “These are frequent tests that we can find in the EMR,” Dr. Mantzoros said. “The problem with ALT is that, in many stages of the disease, ALT goes up. But after a certain stage of the disease, when most of the liver is controlled by fibrosis and cirrhosis, most of the hepatocytes are dead and don’t secrete ALT, so ALT in end-stage renal disease goes up.”
Recent guidelines recognize the association between diabetes, NAFLD, and NASH, and call for increased vigilance and screening tests. According to guidelines from the American Association for the Study of Liver Diseases, the Fibrosis-4 Index or the NAFLD Fibrosis Score are clinically useful tools for identifying NAFLD in patients with higher likelihood of having bridging fibrosis or cirrhosis (Hepatology. 2018;67[1]:328-57). Vibration-controlled transient elastography or MRI are clinically useful tools for identifying advanced fibrosis in patients with NAFLD, whereas clinical decision aids, such as Fibrosis-4, NAFLD Fibrosis Score, or vibration-controlled transient elastography, can be used to identify patients at low or high risk for advanced fibrosis.
“If we have a patient with suspected NAFLD, we need to rule out alcohol use, we need to confirm NAFLD, and we need to risk stratify, and classify as low, intermediate, or high risk,” Dr. Mantzoros said. Most of his patients who meet criteria for high-risk NASH do not elect to undergo a liver biopsy. “I don’t blame them for that,” he said. “There is a 0.1 per 1,000 mortality risk, even in the best hands. If 80 million people who have fatty liver were to undergo a liver biopsy, we would have 16,000 deaths every year just because of that. We would not tolerate that.”
Recently, Dr. Mantzoros and colleagues published a proof-of-concept study that proposes novel models using lipids, hormones, and glycans that can diagnose the presence of NASH, NAFLD, or healthy status with high accuracy (Metabolism. 2019 Nov 8. doi: 10.1016/j.metabol.2019.154005). “We are now working with companies to validate it and expand it, not only as a diagnostic marker, but as a prognostic marker, and to try to commercialize it in the future,” he said.
Current pharmacotherapies are limited to patients with biopsy-confirmed NASH and fibrosis. Pioglitazone is a first-line, off-label pharmacologic treatment, while vitamin E may be used in patients with biopsy-confirmed NASH without diabetes. Metformin, glucagonlike peptide–1 receptor agonists, and sodium-glucose transporter 2 inhibitors are either not recommended or have insufficient evidence to recommend their use. More than 60 phase 2 trials are planned or ongoing, Dr. Mantzoros added, with phase trials underway for cenicriviroc, elafibranor, obeticholic acid, and selonsertib.
The role of lifestyle management is also important. “The Mediterranean diet has the best evidence, along with exercise, to improve early stages of NAFLD,” he said. “Weight loss is very important. If the patient loses 10% of their weight or more, there is NASH resolution 90% of the time. With less weight loss, we have less resolution. The problem is that only 10% of patients or less can sustain a more than 90% weight loss over a year.”
Dr. Mantzoros reported being a shareholder of Coherus BioSciences and Pangea Therapeutics, having served as an adviser to Coherus, Novo Nordisk, and Genfit and having received research grants through his institution from Coherus, Eisai, and Novo Nordisk.
LOS ANGELES – The way Christos S. Mantzoros, MD, DSc, PhD, sees it, nonalcoholic steatohepatitis (NASH) is an epidemic of the 21st century that can trigger a cascade of reactions.
“If more than 5.8% of fat is in the liver, we call it nonalcoholic fatty liver disease [NAFLD],” Dr. Mantzoros, professor of medicine at Harvard Medical School, Boston, and Boston University, explained at the World Congress on Insulin Resistance, Diabetes, and Cardiovascular Disease. “If inflammation develops to remove the fat, we call it NASH. If this progresses to decompensated reaction and fibrosis and cirrhosis, then we call it nonalcoholic steatohepatitis with fibrosis. That can lead to liver cirrhosis, hepatocellular carcinoma, and liver failure.”
The underlying problem stems from the rise in obesity prevalence, according to Dr. Mantzoros, who is also chief of endocrinology at the Boston Veterans Affairs Healthcare System. For 75%-80% of individuals with metabolically unhealthy obesity, the storage space in their adipose tissue is exceeded. “Fat is deposited into muscle, causing insulin resistance, and into the liver,” he explained. “If it’s more than 5.8%, it causes NAFLD. Most of us don’t realize that most of the patients with diabetes we have in our clinics also have nonalcoholic fatty liver disease. That’s because we don’t have an easy diagnostic tool or an easy treatment. It’s an unmet clinical need.” (There are currently no drugs approved for the treatment of NASH or NAFLD. Current recommended first-line treatment is weight loss through diet and exercise and control of diabetes, if it is present.)
“Assuming the rate of increase in cost due to NAFLD parallels the growth in obesity, the 10-year projection for direct cost is $1.005 trillion,” said Dr. Mantzoros, who is also editor in chief of the journal Metabolism. “Obesity, NAFLD, and insulin resistance are each independently associated with a twofold risk for diabetes. If all three are present, there is a 14-fold risk for diabetes. Insulin resistance promotes an increase in free fatty acid traffic to the liver, which can trigger hepatic lipotoxicity. Hyperinsulinemia enhances free fatty acid uptake and activates de novo lipogenesis. Hyperglycemia can also activate de novo lipogenesis.”
About 85 million Americans have NAFLD, he continued. Most (80%) are cases of steatosis, but 20% have NASH. Of those, 20% develop advanced fibrosis, which leads to liver failure and transplantation or death. A study of data from the National Health and Nutrition Examination Survey found that (odds ratio, 18.20), followed by a body mass index of 30 kg/m2 or greater (OR, 9.10), hypertension (OR, 1.20), and age (OR, 1.08; Ailment Pharmacol Ther. 2017;46:974-80). “Most of the patients who come to our clinics with diabetes have nonalcoholic fatty liver disease – 75%-80% in our clinics, and about 10% have advanced fibrosis,” Dr. Mantzoros said. “Most of them go undiagnosed.”
Patients with type 2 diabetes and NAFLD progress faster to fibrosis and end-stage liver disease, compared with those who do not have diabetes. One study of 108 patients with biopsy-proven NALFD showed that 84% of those with fibrosis progression had type 2 diabetes (J Hepatol. 2015;62:1148-55). Other findings have shown that patients with type 2 diabetes are at increased risk of chronic NAFLD and hepatocellular carcinoma (Gastroenterol. 2001;126:460-8). “We are doing more liver transplantations because of NAFLD and NASH than because of hepatitis C,” Dr. Mantzoros said. “What we need to keep in mind is that, although liver morbidity and mortality is important, this is a component of the cardiometabolic syndrome. So, people have all the risk factors for cardiovascular disease. Because CVD is much more common, people with NAFLD suffer from and die from CVD. The more advanced the NAFLD, the higher the risk of death from cardiovascular disease.”
Multiple risk factors can help identify patients with advanced fibrosis because of NASH, he continued, including having features of the metabolic syndrome, being over 50 years of age, being Hispanic, having high levels of ALT/AST, low platelets, and having low albumin. “These are frequent tests that we can find in the EMR,” Dr. Mantzoros said. “The problem with ALT is that, in many stages of the disease, ALT goes up. But after a certain stage of the disease, when most of the liver is controlled by fibrosis and cirrhosis, most of the hepatocytes are dead and don’t secrete ALT, so ALT in end-stage renal disease goes up.”
Recent guidelines recognize the association between diabetes, NAFLD, and NASH, and call for increased vigilance and screening tests. According to guidelines from the American Association for the Study of Liver Diseases, the Fibrosis-4 Index or the NAFLD Fibrosis Score are clinically useful tools for identifying NAFLD in patients with higher likelihood of having bridging fibrosis or cirrhosis (Hepatology. 2018;67[1]:328-57). Vibration-controlled transient elastography or MRI are clinically useful tools for identifying advanced fibrosis in patients with NAFLD, whereas clinical decision aids, such as Fibrosis-4, NAFLD Fibrosis Score, or vibration-controlled transient elastography, can be used to identify patients at low or high risk for advanced fibrosis.
“If we have a patient with suspected NAFLD, we need to rule out alcohol use, we need to confirm NAFLD, and we need to risk stratify, and classify as low, intermediate, or high risk,” Dr. Mantzoros said. Most of his patients who meet criteria for high-risk NASH do not elect to undergo a liver biopsy. “I don’t blame them for that,” he said. “There is a 0.1 per 1,000 mortality risk, even in the best hands. If 80 million people who have fatty liver were to undergo a liver biopsy, we would have 16,000 deaths every year just because of that. We would not tolerate that.”
Recently, Dr. Mantzoros and colleagues published a proof-of-concept study that proposes novel models using lipids, hormones, and glycans that can diagnose the presence of NASH, NAFLD, or healthy status with high accuracy (Metabolism. 2019 Nov 8. doi: 10.1016/j.metabol.2019.154005). “We are now working with companies to validate it and expand it, not only as a diagnostic marker, but as a prognostic marker, and to try to commercialize it in the future,” he said.
Current pharmacotherapies are limited to patients with biopsy-confirmed NASH and fibrosis. Pioglitazone is a first-line, off-label pharmacologic treatment, while vitamin E may be used in patients with biopsy-confirmed NASH without diabetes. Metformin, glucagonlike peptide–1 receptor agonists, and sodium-glucose transporter 2 inhibitors are either not recommended or have insufficient evidence to recommend their use. More than 60 phase 2 trials are planned or ongoing, Dr. Mantzoros added, with phase trials underway for cenicriviroc, elafibranor, obeticholic acid, and selonsertib.
The role of lifestyle management is also important. “The Mediterranean diet has the best evidence, along with exercise, to improve early stages of NAFLD,” he said. “Weight loss is very important. If the patient loses 10% of their weight or more, there is NASH resolution 90% of the time. With less weight loss, we have less resolution. The problem is that only 10% of patients or less can sustain a more than 90% weight loss over a year.”
Dr. Mantzoros reported being a shareholder of Coherus BioSciences and Pangea Therapeutics, having served as an adviser to Coherus, Novo Nordisk, and Genfit and having received research grants through his institution from Coherus, Eisai, and Novo Nordisk.
LOS ANGELES – The way Christos S. Mantzoros, MD, DSc, PhD, sees it, nonalcoholic steatohepatitis (NASH) is an epidemic of the 21st century that can trigger a cascade of reactions.
“If more than 5.8% of fat is in the liver, we call it nonalcoholic fatty liver disease [NAFLD],” Dr. Mantzoros, professor of medicine at Harvard Medical School, Boston, and Boston University, explained at the World Congress on Insulin Resistance, Diabetes, and Cardiovascular Disease. “If inflammation develops to remove the fat, we call it NASH. If this progresses to decompensated reaction and fibrosis and cirrhosis, then we call it nonalcoholic steatohepatitis with fibrosis. That can lead to liver cirrhosis, hepatocellular carcinoma, and liver failure.”
The underlying problem stems from the rise in obesity prevalence, according to Dr. Mantzoros, who is also chief of endocrinology at the Boston Veterans Affairs Healthcare System. For 75%-80% of individuals with metabolically unhealthy obesity, the storage space in their adipose tissue is exceeded. “Fat is deposited into muscle, causing insulin resistance, and into the liver,” he explained. “If it’s more than 5.8%, it causes NAFLD. Most of us don’t realize that most of the patients with diabetes we have in our clinics also have nonalcoholic fatty liver disease. That’s because we don’t have an easy diagnostic tool or an easy treatment. It’s an unmet clinical need.” (There are currently no drugs approved for the treatment of NASH or NAFLD. Current recommended first-line treatment is weight loss through diet and exercise and control of diabetes, if it is present.)
“Assuming the rate of increase in cost due to NAFLD parallels the growth in obesity, the 10-year projection for direct cost is $1.005 trillion,” said Dr. Mantzoros, who is also editor in chief of the journal Metabolism. “Obesity, NAFLD, and insulin resistance are each independently associated with a twofold risk for diabetes. If all three are present, there is a 14-fold risk for diabetes. Insulin resistance promotes an increase in free fatty acid traffic to the liver, which can trigger hepatic lipotoxicity. Hyperinsulinemia enhances free fatty acid uptake and activates de novo lipogenesis. Hyperglycemia can also activate de novo lipogenesis.”
About 85 million Americans have NAFLD, he continued. Most (80%) are cases of steatosis, but 20% have NASH. Of those, 20% develop advanced fibrosis, which leads to liver failure and transplantation or death. A study of data from the National Health and Nutrition Examination Survey found that (odds ratio, 18.20), followed by a body mass index of 30 kg/m2 or greater (OR, 9.10), hypertension (OR, 1.20), and age (OR, 1.08; Ailment Pharmacol Ther. 2017;46:974-80). “Most of the patients who come to our clinics with diabetes have nonalcoholic fatty liver disease – 75%-80% in our clinics, and about 10% have advanced fibrosis,” Dr. Mantzoros said. “Most of them go undiagnosed.”
Patients with type 2 diabetes and NAFLD progress faster to fibrosis and end-stage liver disease, compared with those who do not have diabetes. One study of 108 patients with biopsy-proven NALFD showed that 84% of those with fibrosis progression had type 2 diabetes (J Hepatol. 2015;62:1148-55). Other findings have shown that patients with type 2 diabetes are at increased risk of chronic NAFLD and hepatocellular carcinoma (Gastroenterol. 2001;126:460-8). “We are doing more liver transplantations because of NAFLD and NASH than because of hepatitis C,” Dr. Mantzoros said. “What we need to keep in mind is that, although liver morbidity and mortality is important, this is a component of the cardiometabolic syndrome. So, people have all the risk factors for cardiovascular disease. Because CVD is much more common, people with NAFLD suffer from and die from CVD. The more advanced the NAFLD, the higher the risk of death from cardiovascular disease.”
Multiple risk factors can help identify patients with advanced fibrosis because of NASH, he continued, including having features of the metabolic syndrome, being over 50 years of age, being Hispanic, having high levels of ALT/AST, low platelets, and having low albumin. “These are frequent tests that we can find in the EMR,” Dr. Mantzoros said. “The problem with ALT is that, in many stages of the disease, ALT goes up. But after a certain stage of the disease, when most of the liver is controlled by fibrosis and cirrhosis, most of the hepatocytes are dead and don’t secrete ALT, so ALT in end-stage renal disease goes up.”
Recent guidelines recognize the association between diabetes, NAFLD, and NASH, and call for increased vigilance and screening tests. According to guidelines from the American Association for the Study of Liver Diseases, the Fibrosis-4 Index or the NAFLD Fibrosis Score are clinically useful tools for identifying NAFLD in patients with higher likelihood of having bridging fibrosis or cirrhosis (Hepatology. 2018;67[1]:328-57). Vibration-controlled transient elastography or MRI are clinically useful tools for identifying advanced fibrosis in patients with NAFLD, whereas clinical decision aids, such as Fibrosis-4, NAFLD Fibrosis Score, or vibration-controlled transient elastography, can be used to identify patients at low or high risk for advanced fibrosis.
“If we have a patient with suspected NAFLD, we need to rule out alcohol use, we need to confirm NAFLD, and we need to risk stratify, and classify as low, intermediate, or high risk,” Dr. Mantzoros said. Most of his patients who meet criteria for high-risk NASH do not elect to undergo a liver biopsy. “I don’t blame them for that,” he said. “There is a 0.1 per 1,000 mortality risk, even in the best hands. If 80 million people who have fatty liver were to undergo a liver biopsy, we would have 16,000 deaths every year just because of that. We would not tolerate that.”
Recently, Dr. Mantzoros and colleagues published a proof-of-concept study that proposes novel models using lipids, hormones, and glycans that can diagnose the presence of NASH, NAFLD, or healthy status with high accuracy (Metabolism. 2019 Nov 8. doi: 10.1016/j.metabol.2019.154005). “We are now working with companies to validate it and expand it, not only as a diagnostic marker, but as a prognostic marker, and to try to commercialize it in the future,” he said.
Current pharmacotherapies are limited to patients with biopsy-confirmed NASH and fibrosis. Pioglitazone is a first-line, off-label pharmacologic treatment, while vitamin E may be used in patients with biopsy-confirmed NASH without diabetes. Metformin, glucagonlike peptide–1 receptor agonists, and sodium-glucose transporter 2 inhibitors are either not recommended or have insufficient evidence to recommend their use. More than 60 phase 2 trials are planned or ongoing, Dr. Mantzoros added, with phase trials underway for cenicriviroc, elafibranor, obeticholic acid, and selonsertib.
The role of lifestyle management is also important. “The Mediterranean diet has the best evidence, along with exercise, to improve early stages of NAFLD,” he said. “Weight loss is very important. If the patient loses 10% of their weight or more, there is NASH resolution 90% of the time. With less weight loss, we have less resolution. The problem is that only 10% of patients or less can sustain a more than 90% weight loss over a year.”
Dr. Mantzoros reported being a shareholder of Coherus BioSciences and Pangea Therapeutics, having served as an adviser to Coherus, Novo Nordisk, and Genfit and having received research grants through his institution from Coherus, Eisai, and Novo Nordisk.
EXPERT ANALYSIS FROM WCIRDC 2019
Avelumab maintenance in gastric cancer is down but maybe not out
SAN FRANCISCO – Maintenance therapy with avelumab does not prolong survival in patients with advanced gastric cancer relative to continued chemotherapy, results of the JAVELIN Gastric 100 trial suggest.

However, it may not be end of the line for avelumab in this setting, as the checkpoint inhibitor may benefit certain subgroups of patients, according to Markus H. Moehler, MD, PhD, of the Johannes Gutenberg-University Clinic in Mainz, Germany, who presented results from the trial at the symposium.
In the phase 3 trial, investigators enrolled 805 patients with untreated locally advanced or metastatic HER2-negative gastric or gastroesophageal junction cancer. All patients received first-line chemotherapy.
The 499 patients (62%) who did not experience progression were randomized to receive the anti– programmed death-ligand 1 (PD-L1) antibody avelumab (n = 249) or continued chemotherapy (n = 250). There were 6 patients in the avelumab arm and 12 in the chemotherapy arm who did not receive maintenance treatment, and 7 patients in the chemotherapy arm received best supportive care as maintenance.
Efficacy and safety
The minimum follow-up was 18 months. The median overall survival in the entire population was about the same for both treatment groups, 10.4 months with avelumab and 10.9 months with chemotherapy (P = .1779).
Findings were similar among the 12.3% of patients whose tumors were PD-L1 positive as defined by staining of at least 1% of tumor cells. The median overall survival in this group was 16.2 months with avelumab and 17.7 months with chemotherapy (P = .6352).
On exploratory analysis, results with avelumab were more favorable among the 64.3% of patients whose tumors were PD-L1 positive as defined by a combined positive score (CPS) of 1 or greater. The median overall survival in this group was 14.9 months with avelumab and 11.6 months with chemotherapy.
In subgroup analyses by other characteristics, avelumab appeared to have the edge among patients free of metastases at baseline. In this group, the median overall survival was 16.3 months with avelumab, compared with 10.7 months with chemotherapy (hazard ratio for death, 0.52).
Among all patients, the pattern comparing avelumab with chemotherapy was similar for median progression-free survival (3.2 months vs. 4.4 months) and objective response rate (13.3% vs. 14.4%). The median duration of response was not reached.
“JAVELIN Gastric 100 did not meet its primary objective of demonstrating superior overall survival with avelumab maintenance versus chemotherapy or best supportive care in gastric cancer, either in all randomized patients or in the PD-L1–positive population,” Dr. Moehler said. “However, avelumab maintenance showed clear clinical activity. Further studies are needed to identify patients who can derive benefit from checkpoint inhibitor therapy across the continuum of care with gastric and gastroesophageal junction cancer.”
The avelumab and chemotherapy groups had similar rates of any grade 3 or higher adverse events (54.3% vs. 53.8%), but the avelumab group had a lower rate of treatment-related grade 3 or higher adverse events (12.8% vs. 32.8%).
A ‘yin-yang’ pattern of survival
“Monotherapy checkpoint blockade with anti–programmed death-1 (PD-1) and anti–PD-L1 inhibitors has had relatively unimpressive results in gastroesophageal adenocarcinoma as a whole,” said invited discussant Daniel V. T. Catenacci, MD, of University of Chicago Medicine.
He added that the JAVELIN Gastric 100 survival analysis was noteworthy for the presence of a “yin-yang” pattern, whereby the avelumab curve during follow-up was lower than the chemotherapy curve initially but came out on top eventually.
The 12-month overall survival rate was 43.6% with avelumab and 45.3% with chemotherapy. The 24-month overall survival rates were 22.1% and 15.5%, respectively.
This type of pattern is seen in many similar gastroesophageal adenocarcinoma trials of checkpoint inhibitor monotherapy, even among patients selected for higher CPS, Dr. Catenacci noted.
“This tells us that standard chemotherapy is better in a large subgroup of patients and worse in a separate subgroup: those with MSI-high [microsatellite instability–high], and then MSS [microsatellite stable] with even higher PD-L1 scores like CPS greater than 50, low burden of disease (few metastatic sites), preserved performance status, EBV [Epstein-Barr virus] positivity, Asians within global studies compared with non-Asians, and other unknown factors,” Dr. Catenacci explained.
He commended the design of the JAVELIN Gastric 100 trial, whereby the 38% of patients having rapidly progressive disease were excluded, as this subset is known to fare poorly on checkpoint inhibitor monotherapy.
“This could be potentially a great way to select for those patients most likely to benefit,” Dr. Catenacci said. “Unfortunately, even despite that large fallout, the yin-yang curve was still observed in the intention-to-treat population (unselected by any biomarker). This tells us that, even among the most stable and best prognostic patients, checkpoint blockade is still inferior to standard chemotherapy in a large subgroup of patients.”
However, among patients with a CPS of at least 1, the overall survival curve was consistently higher with avelumab.
“So perhaps by excluding patients with rapid disease progression (about 40% of patients) and then those that are CPS 0 (about 33% more of the total), you can then safely switch to monotherapy checkpoint blockade to first do no harm, and also to do better than standard chemotherapy,” Dr. Catenacci proposed.
“However, we have to be careful, as this was an unplanned retrospective analysis and so should be confirmed prospectively. We might also argue that a higher CPS cut off of greater than or equal to 10 could enrich for the benefit observed. Future ongoing phase 3 studies may help to further increase our understanding of where and where not to implement checkpoint monotherapy or combination therapy with standard chemotherapy.”
The JAVELIN Gastric 100 trial was sponsored by EMD Serono and Merck KGaA, which market avelumab in collaboration with Pfizer. Dr. Moehler disclosed relationships with these companies and many others. Dr. Catenacci disclosed relationships with Merck and other companies.
The 2020 GI Cancers Symposium is sponsored by the American Gastroenterological Association, the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology.
SOURCE: Moehler MH et al. 2020 GI Cancers Symposium, Abstract 278.
SAN FRANCISCO – Maintenance therapy with avelumab does not prolong survival in patients with advanced gastric cancer relative to continued chemotherapy, results of the JAVELIN Gastric 100 trial suggest.
However, it may not be end of the line for avelumab in this setting, as the checkpoint inhibitor may benefit certain subgroups of patients, according to Markus H. Moehler, MD, PhD, of the Johannes Gutenberg-University Clinic in Mainz, Germany, who presented results from the trial at the symposium.
In the phase 3 trial, investigators enrolled 805 patients with untreated locally advanced or metastatic HER2-negative gastric or gastroesophageal junction cancer. All patients received first-line chemotherapy.
The 499 patients (62%) who did not experience progression were randomized to receive the anti– programmed death-ligand 1 (PD-L1) antibody avelumab (n = 249) or continued chemotherapy (n = 250). There were 6 patients in the avelumab arm and 12 in the chemotherapy arm who did not receive maintenance treatment, and 7 patients in the chemotherapy arm received best supportive care as maintenance.
Efficacy and safety
The minimum follow-up was 18 months. The median overall survival in the entire population was about the same for both treatment groups, 10.4 months with avelumab and 10.9 months with chemotherapy (P = .1779).
Findings were similar among the 12.3% of patients whose tumors were PD-L1 positive as defined by staining of at least 1% of tumor cells. The median overall survival in this group was 16.2 months with avelumab and 17.7 months with chemotherapy (P = .6352).
On exploratory analysis, results with avelumab were more favorable among the 64.3% of patients whose tumors were PD-L1 positive as defined by a combined positive score (CPS) of 1 or greater. The median overall survival in this group was 14.9 months with avelumab and 11.6 months with chemotherapy.
In subgroup analyses by other characteristics, avelumab appeared to have the edge among patients free of metastases at baseline. In this group, the median overall survival was 16.3 months with avelumab, compared with 10.7 months with chemotherapy (hazard ratio for death, 0.52).
Among all patients, the pattern comparing avelumab with chemotherapy was similar for median progression-free survival (3.2 months vs. 4.4 months) and objective response rate (13.3% vs. 14.4%). The median duration of response was not reached.
“JAVELIN Gastric 100 did not meet its primary objective of demonstrating superior overall survival with avelumab maintenance versus chemotherapy or best supportive care in gastric cancer, either in all randomized patients or in the PD-L1–positive population,” Dr. Moehler said. “However, avelumab maintenance showed clear clinical activity. Further studies are needed to identify patients who can derive benefit from checkpoint inhibitor therapy across the continuum of care with gastric and gastroesophageal junction cancer.”
The avelumab and chemotherapy groups had similar rates of any grade 3 or higher adverse events (54.3% vs. 53.8%), but the avelumab group had a lower rate of treatment-related grade 3 or higher adverse events (12.8% vs. 32.8%).
A ‘yin-yang’ pattern of survival
“Monotherapy checkpoint blockade with anti–programmed death-1 (PD-1) and anti–PD-L1 inhibitors has had relatively unimpressive results in gastroesophageal adenocarcinoma as a whole,” said invited discussant Daniel V. T. Catenacci, MD, of University of Chicago Medicine.
He added that the JAVELIN Gastric 100 survival analysis was noteworthy for the presence of a “yin-yang” pattern, whereby the avelumab curve during follow-up was lower than the chemotherapy curve initially but came out on top eventually.
The 12-month overall survival rate was 43.6% with avelumab and 45.3% with chemotherapy. The 24-month overall survival rates were 22.1% and 15.5%, respectively.
This type of pattern is seen in many similar gastroesophageal adenocarcinoma trials of checkpoint inhibitor monotherapy, even among patients selected for higher CPS, Dr. Catenacci noted.
“This tells us that standard chemotherapy is better in a large subgroup of patients and worse in a separate subgroup: those with MSI-high [microsatellite instability–high], and then MSS [microsatellite stable] with even higher PD-L1 scores like CPS greater than 50, low burden of disease (few metastatic sites), preserved performance status, EBV [Epstein-Barr virus] positivity, Asians within global studies compared with non-Asians, and other unknown factors,” Dr. Catenacci explained.
He commended the design of the JAVELIN Gastric 100 trial, whereby the 38% of patients having rapidly progressive disease were excluded, as this subset is known to fare poorly on checkpoint inhibitor monotherapy.
“This could be potentially a great way to select for those patients most likely to benefit,” Dr. Catenacci said. “Unfortunately, even despite that large fallout, the yin-yang curve was still observed in the intention-to-treat population (unselected by any biomarker). This tells us that, even among the most stable and best prognostic patients, checkpoint blockade is still inferior to standard chemotherapy in a large subgroup of patients.”
However, among patients with a CPS of at least 1, the overall survival curve was consistently higher with avelumab.
“So perhaps by excluding patients with rapid disease progression (about 40% of patients) and then those that are CPS 0 (about 33% more of the total), you can then safely switch to monotherapy checkpoint blockade to first do no harm, and also to do better than standard chemotherapy,” Dr. Catenacci proposed.
“However, we have to be careful, as this was an unplanned retrospective analysis and so should be confirmed prospectively. We might also argue that a higher CPS cut off of greater than or equal to 10 could enrich for the benefit observed. Future ongoing phase 3 studies may help to further increase our understanding of where and where not to implement checkpoint monotherapy or combination therapy with standard chemotherapy.”
The JAVELIN Gastric 100 trial was sponsored by EMD Serono and Merck KGaA, which market avelumab in collaboration with Pfizer. Dr. Moehler disclosed relationships with these companies and many others. Dr. Catenacci disclosed relationships with Merck and other companies.
The 2020 GI Cancers Symposium is sponsored by the American Gastroenterological Association, the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology.
SOURCE: Moehler MH et al. 2020 GI Cancers Symposium, Abstract 278.
SAN FRANCISCO – Maintenance therapy with avelumab does not prolong survival in patients with advanced gastric cancer relative to continued chemotherapy, results of the JAVELIN Gastric 100 trial suggest.
However, it may not be end of the line for avelumab in this setting, as the checkpoint inhibitor may benefit certain subgroups of patients, according to Markus H. Moehler, MD, PhD, of the Johannes Gutenberg-University Clinic in Mainz, Germany, who presented results from the trial at the symposium.
In the phase 3 trial, investigators enrolled 805 patients with untreated locally advanced or metastatic HER2-negative gastric or gastroesophageal junction cancer. All patients received first-line chemotherapy.
The 499 patients (62%) who did not experience progression were randomized to receive the anti– programmed death-ligand 1 (PD-L1) antibody avelumab (n = 249) or continued chemotherapy (n = 250). There were 6 patients in the avelumab arm and 12 in the chemotherapy arm who did not receive maintenance treatment, and 7 patients in the chemotherapy arm received best supportive care as maintenance.
Efficacy and safety
The minimum follow-up was 18 months. The median overall survival in the entire population was about the same for both treatment groups, 10.4 months with avelumab and 10.9 months with chemotherapy (P = .1779).
Findings were similar among the 12.3% of patients whose tumors were PD-L1 positive as defined by staining of at least 1% of tumor cells. The median overall survival in this group was 16.2 months with avelumab and 17.7 months with chemotherapy (P = .6352).
On exploratory analysis, results with avelumab were more favorable among the 64.3% of patients whose tumors were PD-L1 positive as defined by a combined positive score (CPS) of 1 or greater. The median overall survival in this group was 14.9 months with avelumab and 11.6 months with chemotherapy.
In subgroup analyses by other characteristics, avelumab appeared to have the edge among patients free of metastases at baseline. In this group, the median overall survival was 16.3 months with avelumab, compared with 10.7 months with chemotherapy (hazard ratio for death, 0.52).
Among all patients, the pattern comparing avelumab with chemotherapy was similar for median progression-free survival (3.2 months vs. 4.4 months) and objective response rate (13.3% vs. 14.4%). The median duration of response was not reached.
“JAVELIN Gastric 100 did not meet its primary objective of demonstrating superior overall survival with avelumab maintenance versus chemotherapy or best supportive care in gastric cancer, either in all randomized patients or in the PD-L1–positive population,” Dr. Moehler said. “However, avelumab maintenance showed clear clinical activity. Further studies are needed to identify patients who can derive benefit from checkpoint inhibitor therapy across the continuum of care with gastric and gastroesophageal junction cancer.”
The avelumab and chemotherapy groups had similar rates of any grade 3 or higher adverse events (54.3% vs. 53.8%), but the avelumab group had a lower rate of treatment-related grade 3 or higher adverse events (12.8% vs. 32.8%).
A ‘yin-yang’ pattern of survival
“Monotherapy checkpoint blockade with anti–programmed death-1 (PD-1) and anti–PD-L1 inhibitors has had relatively unimpressive results in gastroesophageal adenocarcinoma as a whole,” said invited discussant Daniel V. T. Catenacci, MD, of University of Chicago Medicine.
He added that the JAVELIN Gastric 100 survival analysis was noteworthy for the presence of a “yin-yang” pattern, whereby the avelumab curve during follow-up was lower than the chemotherapy curve initially but came out on top eventually.
The 12-month overall survival rate was 43.6% with avelumab and 45.3% with chemotherapy. The 24-month overall survival rates were 22.1% and 15.5%, respectively.
This type of pattern is seen in many similar gastroesophageal adenocarcinoma trials of checkpoint inhibitor monotherapy, even among patients selected for higher CPS, Dr. Catenacci noted.
“This tells us that standard chemotherapy is better in a large subgroup of patients and worse in a separate subgroup: those with MSI-high [microsatellite instability–high], and then MSS [microsatellite stable] with even higher PD-L1 scores like CPS greater than 50, low burden of disease (few metastatic sites), preserved performance status, EBV [Epstein-Barr virus] positivity, Asians within global studies compared with non-Asians, and other unknown factors,” Dr. Catenacci explained.
He commended the design of the JAVELIN Gastric 100 trial, whereby the 38% of patients having rapidly progressive disease were excluded, as this subset is known to fare poorly on checkpoint inhibitor monotherapy.
“This could be potentially a great way to select for those patients most likely to benefit,” Dr. Catenacci said. “Unfortunately, even despite that large fallout, the yin-yang curve was still observed in the intention-to-treat population (unselected by any biomarker). This tells us that, even among the most stable and best prognostic patients, checkpoint blockade is still inferior to standard chemotherapy in a large subgroup of patients.”
However, among patients with a CPS of at least 1, the overall survival curve was consistently higher with avelumab.
“So perhaps by excluding patients with rapid disease progression (about 40% of patients) and then those that are CPS 0 (about 33% more of the total), you can then safely switch to monotherapy checkpoint blockade to first do no harm, and also to do better than standard chemotherapy,” Dr. Catenacci proposed.
“However, we have to be careful, as this was an unplanned retrospective analysis and so should be confirmed prospectively. We might also argue that a higher CPS cut off of greater than or equal to 10 could enrich for the benefit observed. Future ongoing phase 3 studies may help to further increase our understanding of where and where not to implement checkpoint monotherapy or combination therapy with standard chemotherapy.”
The JAVELIN Gastric 100 trial was sponsored by EMD Serono and Merck KGaA, which market avelumab in collaboration with Pfizer. Dr. Moehler disclosed relationships with these companies and many others. Dr. Catenacci disclosed relationships with Merck and other companies.
The 2020 GI Cancers Symposium is sponsored by the American Gastroenterological Association, the American Society of Clinical Oncology, the American Society for Radiation Oncology, and the Society of Surgical Oncology.
SOURCE: Moehler MH et al. 2020 GI Cancers Symposium, Abstract 278.
REPORTING FROM THE 2020 GI CANCERS SYMPOSIUM
Novel coronavirus cases now at 11; entry ban and quarantine measures begin
, Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during a Centers for Disease Control and Prevention press briefing.
Four of the new cases are in California, and one in Massachusetts. Although four of the new cases have recent travel history to Wuhan, China, the epicenter of the 2019-nCoV outbreak, the fifth is a close household contact of one of the other California patients, said Dr. Messonnier. This last case is the second instance of person-to-person spread of 2019-nCoV in the United States.
“We expect to find additional cases of the novel coronavirus in the United States,” she said. “We expect to see more cases of person-to-person spread among close contacts. And we continue to expect this will happen given the explosive nature of this outbreak in China.”
As of the morning of Feb. 3, 167 persons under investigation, or PUIs, for possible 2019-nCoV have tested negative for the virus, and an additional 82 PUIs have testing pending – this latter figure includes some tests that are still in transit to the CDC, said Dr. Messonnier.
During the briefing, Dr. Messonnier emphasized both the aggressive nature of the U.S. public health response and the rationale for quick and assertive action. “The goal of our public health response is to protect and contain,” she said. “Strong measures now may blunt the impact of this virus on the United States.”
She cited the intensity of transmission in Hubei Province, the expansion of transmission to other provinces in China, the expansion of cases outside of China, and sporadic ongoing deaths from 2019-nCoV as drivers of the aggressive U.S. public health response.
A presidential proclamation is currently in place that bars U.S. entry to foreign nationals who have visited mainland China within the past 14 days; the ban does not apply to travelers from Hong Kong and Macao. Immediate family members of U.S. citizens and individuals who have U.S. permanent resident status are exempted from the entry ban and will be allowed entry into the United States.
However, explained Dr. Messonnier, those who have traveled to China recently and are permitted entry will be subject to screening. All passengers with such recent travel will be directed to one of 11 U.S. airports set up to perform additional screening.
As of Feb 3, the list of airports includes:
- San Francisco International Airport in California.
- Los Angeles International Airport in California.
- Hartsfield-Jackson Atlanta International Airport in Georgia.
- Daniel K. Inouye International Airport in Hawaii.
- O’Hare International Airport in Illinois.
- Detroit Metropolitan Airport in Michigan.
- Newark Liberty International Airport in New Jersey.
- John F. Kennedy International Airport in New York.
- Dallas/Fort Worth International Airport in Texas.
- Washington Dulles International Airport in Virginia.
- Seattle-Tacoma International Airport in Washington.
Travelers who have been to Hubei Province in the previous 14 days will have an additional health assessment at which they will be screened for fever, cough, or difficulty breathing. Any American citizens or exempt individuals who are symptomatic would then be transferred for further medical evaluation. Asymptomatic travelers in this category will be subject to a mandatory 14-day quarantine near their point of entry, rather than continuing on to their final destinations.
Dr. Messonnier emphasized that the mandatory 14-day quarantine is specifically for Americans or exempt individuals returning from Hubei Province, adding that the CDC is presently working with individual states to determine the exact venues for quarantine.
American citizens and exempt individuals returning from other parts of mainland China will be routed to one of the 11 airports and will also receive additional health screening. Symptomatic individuals in this travel category would be referred for further evaluation before being able to complete their itinerary.
Asymptomatic American citizens and exempt individuals who are returning from mainland China – but not Hubei Province – will be allowed to travel on to their final destinations, but will be asked to stay home as much as possible and to monitor their health during the 14 days after their return.
The U.S. Department of State is bringing back more Americans from Wuhan province this week, and these individuals will also be kept under federal quarantine for 14 days.
“There are likely to be confirmed infections among returning travelers,” said Dr. Messonnier. “It is important to note that this strategy is not meant to catch every single traveler returning from China with novel coronavirus; given the nature of this virus and how it’s spreading, that would be impossible, but working together we can catch the majority of them.
“The goal here is to slow the entry of this virus into the United States,” she said, adding that the nation’s health care and public health systems stand on high alert to detect the virus in community settings. In response to questioning from the press, Dr. Messonnier defended the stringent quarantine measures, noting that they are in line with those taken by some other nations, and with the aggressive action being taken by the Chinese government itself. “These actions are science based and aimed at protecting the health of all Americans,” she said.
The real-time reverse transcription polymerase chain reaction (rRT-PCR) assay that the CDC has developed detects 2019-nCoV in both respiratory and serum specimens. Dr. Messonnier reported that the CDC is today filing an emergency use authorization (EUA) application to the U.S. Food and Drug Administration to expedite access to the assay for public health laboratories across the country. “This will greatly enhance our capacity to test for this virus,” she said, noting that EUA approval may come as soon as the end of this week.
Although the CDC is poised to send an expert team to China, it’s still awaiting favorable results from the international negotiations currently underway. “This is a horrible situation in China,” said Dr. Messonnier. “Our presence on the ground in China would be a help to China. ... Science should trump everything else; that’s what we’re hoping – that the scientific expertise of the global community can be brought to bear on the incredibly complicated, difficult situation that our colleagues in China are dealing with.”
, Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during a Centers for Disease Control and Prevention press briefing.
Four of the new cases are in California, and one in Massachusetts. Although four of the new cases have recent travel history to Wuhan, China, the epicenter of the 2019-nCoV outbreak, the fifth is a close household contact of one of the other California patients, said Dr. Messonnier. This last case is the second instance of person-to-person spread of 2019-nCoV in the United States.
“We expect to find additional cases of the novel coronavirus in the United States,” she said. “We expect to see more cases of person-to-person spread among close contacts. And we continue to expect this will happen given the explosive nature of this outbreak in China.”
As of the morning of Feb. 3, 167 persons under investigation, or PUIs, for possible 2019-nCoV have tested negative for the virus, and an additional 82 PUIs have testing pending – this latter figure includes some tests that are still in transit to the CDC, said Dr. Messonnier.
During the briefing, Dr. Messonnier emphasized both the aggressive nature of the U.S. public health response and the rationale for quick and assertive action. “The goal of our public health response is to protect and contain,” she said. “Strong measures now may blunt the impact of this virus on the United States.”
She cited the intensity of transmission in Hubei Province, the expansion of transmission to other provinces in China, the expansion of cases outside of China, and sporadic ongoing deaths from 2019-nCoV as drivers of the aggressive U.S. public health response.
A presidential proclamation is currently in place that bars U.S. entry to foreign nationals who have visited mainland China within the past 14 days; the ban does not apply to travelers from Hong Kong and Macao. Immediate family members of U.S. citizens and individuals who have U.S. permanent resident status are exempted from the entry ban and will be allowed entry into the United States.
However, explained Dr. Messonnier, those who have traveled to China recently and are permitted entry will be subject to screening. All passengers with such recent travel will be directed to one of 11 U.S. airports set up to perform additional screening.
As of Feb 3, the list of airports includes:
- San Francisco International Airport in California.
- Los Angeles International Airport in California.
- Hartsfield-Jackson Atlanta International Airport in Georgia.
- Daniel K. Inouye International Airport in Hawaii.
- O’Hare International Airport in Illinois.
- Detroit Metropolitan Airport in Michigan.
- Newark Liberty International Airport in New Jersey.
- John F. Kennedy International Airport in New York.
- Dallas/Fort Worth International Airport in Texas.
- Washington Dulles International Airport in Virginia.
- Seattle-Tacoma International Airport in Washington.
Travelers who have been to Hubei Province in the previous 14 days will have an additional health assessment at which they will be screened for fever, cough, or difficulty breathing. Any American citizens or exempt individuals who are symptomatic would then be transferred for further medical evaluation. Asymptomatic travelers in this category will be subject to a mandatory 14-day quarantine near their point of entry, rather than continuing on to their final destinations.
Dr. Messonnier emphasized that the mandatory 14-day quarantine is specifically for Americans or exempt individuals returning from Hubei Province, adding that the CDC is presently working with individual states to determine the exact venues for quarantine.
American citizens and exempt individuals returning from other parts of mainland China will be routed to one of the 11 airports and will also receive additional health screening. Symptomatic individuals in this travel category would be referred for further evaluation before being able to complete their itinerary.
Asymptomatic American citizens and exempt individuals who are returning from mainland China – but not Hubei Province – will be allowed to travel on to their final destinations, but will be asked to stay home as much as possible and to monitor their health during the 14 days after their return.
The U.S. Department of State is bringing back more Americans from Wuhan province this week, and these individuals will also be kept under federal quarantine for 14 days.
“There are likely to be confirmed infections among returning travelers,” said Dr. Messonnier. “It is important to note that this strategy is not meant to catch every single traveler returning from China with novel coronavirus; given the nature of this virus and how it’s spreading, that would be impossible, but working together we can catch the majority of them.
“The goal here is to slow the entry of this virus into the United States,” she said, adding that the nation’s health care and public health systems stand on high alert to detect the virus in community settings. In response to questioning from the press, Dr. Messonnier defended the stringent quarantine measures, noting that they are in line with those taken by some other nations, and with the aggressive action being taken by the Chinese government itself. “These actions are science based and aimed at protecting the health of all Americans,” she said.
The real-time reverse transcription polymerase chain reaction (rRT-PCR) assay that the CDC has developed detects 2019-nCoV in both respiratory and serum specimens. Dr. Messonnier reported that the CDC is today filing an emergency use authorization (EUA) application to the U.S. Food and Drug Administration to expedite access to the assay for public health laboratories across the country. “This will greatly enhance our capacity to test for this virus,” she said, noting that EUA approval may come as soon as the end of this week.
Although the CDC is poised to send an expert team to China, it’s still awaiting favorable results from the international negotiations currently underway. “This is a horrible situation in China,” said Dr. Messonnier. “Our presence on the ground in China would be a help to China. ... Science should trump everything else; that’s what we’re hoping – that the scientific expertise of the global community can be brought to bear on the incredibly complicated, difficult situation that our colleagues in China are dealing with.”
, Nancy Messonnier, MD, director of the National Center for Immunization and Respiratory Diseases, said during a Centers for Disease Control and Prevention press briefing.
Four of the new cases are in California, and one in Massachusetts. Although four of the new cases have recent travel history to Wuhan, China, the epicenter of the 2019-nCoV outbreak, the fifth is a close household contact of one of the other California patients, said Dr. Messonnier. This last case is the second instance of person-to-person spread of 2019-nCoV in the United States.
“We expect to find additional cases of the novel coronavirus in the United States,” she said. “We expect to see more cases of person-to-person spread among close contacts. And we continue to expect this will happen given the explosive nature of this outbreak in China.”
As of the morning of Feb. 3, 167 persons under investigation, or PUIs, for possible 2019-nCoV have tested negative for the virus, and an additional 82 PUIs have testing pending – this latter figure includes some tests that are still in transit to the CDC, said Dr. Messonnier.
During the briefing, Dr. Messonnier emphasized both the aggressive nature of the U.S. public health response and the rationale for quick and assertive action. “The goal of our public health response is to protect and contain,” she said. “Strong measures now may blunt the impact of this virus on the United States.”
She cited the intensity of transmission in Hubei Province, the expansion of transmission to other provinces in China, the expansion of cases outside of China, and sporadic ongoing deaths from 2019-nCoV as drivers of the aggressive U.S. public health response.
A presidential proclamation is currently in place that bars U.S. entry to foreign nationals who have visited mainland China within the past 14 days; the ban does not apply to travelers from Hong Kong and Macao. Immediate family members of U.S. citizens and individuals who have U.S. permanent resident status are exempted from the entry ban and will be allowed entry into the United States.
However, explained Dr. Messonnier, those who have traveled to China recently and are permitted entry will be subject to screening. All passengers with such recent travel will be directed to one of 11 U.S. airports set up to perform additional screening.
As of Feb 3, the list of airports includes:
- San Francisco International Airport in California.
- Los Angeles International Airport in California.
- Hartsfield-Jackson Atlanta International Airport in Georgia.
- Daniel K. Inouye International Airport in Hawaii.
- O’Hare International Airport in Illinois.
- Detroit Metropolitan Airport in Michigan.
- Newark Liberty International Airport in New Jersey.
- John F. Kennedy International Airport in New York.
- Dallas/Fort Worth International Airport in Texas.
- Washington Dulles International Airport in Virginia.
- Seattle-Tacoma International Airport in Washington.
Travelers who have been to Hubei Province in the previous 14 days will have an additional health assessment at which they will be screened for fever, cough, or difficulty breathing. Any American citizens or exempt individuals who are symptomatic would then be transferred for further medical evaluation. Asymptomatic travelers in this category will be subject to a mandatory 14-day quarantine near their point of entry, rather than continuing on to their final destinations.
Dr. Messonnier emphasized that the mandatory 14-day quarantine is specifically for Americans or exempt individuals returning from Hubei Province, adding that the CDC is presently working with individual states to determine the exact venues for quarantine.
American citizens and exempt individuals returning from other parts of mainland China will be routed to one of the 11 airports and will also receive additional health screening. Symptomatic individuals in this travel category would be referred for further evaluation before being able to complete their itinerary.
Asymptomatic American citizens and exempt individuals who are returning from mainland China – but not Hubei Province – will be allowed to travel on to their final destinations, but will be asked to stay home as much as possible and to monitor their health during the 14 days after their return.
The U.S. Department of State is bringing back more Americans from Wuhan province this week, and these individuals will also be kept under federal quarantine for 14 days.
“There are likely to be confirmed infections among returning travelers,” said Dr. Messonnier. “It is important to note that this strategy is not meant to catch every single traveler returning from China with novel coronavirus; given the nature of this virus and how it’s spreading, that would be impossible, but working together we can catch the majority of them.
“The goal here is to slow the entry of this virus into the United States,” she said, adding that the nation’s health care and public health systems stand on high alert to detect the virus in community settings. In response to questioning from the press, Dr. Messonnier defended the stringent quarantine measures, noting that they are in line with those taken by some other nations, and with the aggressive action being taken by the Chinese government itself. “These actions are science based and aimed at protecting the health of all Americans,” she said.
The real-time reverse transcription polymerase chain reaction (rRT-PCR) assay that the CDC has developed detects 2019-nCoV in both respiratory and serum specimens. Dr. Messonnier reported that the CDC is today filing an emergency use authorization (EUA) application to the U.S. Food and Drug Administration to expedite access to the assay for public health laboratories across the country. “This will greatly enhance our capacity to test for this virus,” she said, noting that EUA approval may come as soon as the end of this week.
Although the CDC is poised to send an expert team to China, it’s still awaiting favorable results from the international negotiations currently underway. “This is a horrible situation in China,” said Dr. Messonnier. “Our presence on the ground in China would be a help to China. ... Science should trump everything else; that’s what we’re hoping – that the scientific expertise of the global community can be brought to bear on the incredibly complicated, difficult situation that our colleagues in China are dealing with.”
FROM A CDC PRESS BRIEFING
Heart rhythm data from wearables confounds EP practice
NATIONAL HARBOR, MD. – or other warnings that flagged a possible cardiac arrhythmia.

While the clinical community has yet to reach an evidence-based consensus on how to deal with this information, or even asymptomatic arrhythmias identified by more standard means, the American public is voting with their wrists. People seem to like collecting and reviewing readouts on their heart rhythm and other vital data, and then they often take their numbers to a physician, especially when their device suggests a possible problem.
“The whole paradigm of ordering a test only if you intend to act on the result has been flipped. People now get what they want directly, and our job is to guide them” after the fact. “You need to teach people what’s actionable and what’s not,” Mintu P. Turakhia, MD, said at the annual International AF Symposium.
“We’re in a situation where the ability of a sensor to detect things is separate from access to the health care system. They are no longer coupled; they are disjointed. People can create their own ICU in their house just by shopping online, but what do we do with this information, whether it’s an irregular heart rhythm or their whole genome?” asked Dr. Turakhia, executive director of the Center for Digital Health at Stanford (Calif.) University and director of cardiac electrophysiology at the VA Palo Alto (Calif.) Health Care System.
“The main challenge is people without a diagnosis who get a notification. How much monitoring should you do until you can say it was a false positive? We don’t know what to do, so we monitor them. People are trying to figure this out.” Dr. Turakhia said. Some people who seek out electrophysiologists this way “may not even have a primary care physician,” he noted.
The potential implications of widespread monitoring for heartbeat irregularities in the general public began to surface in a study that Dr. Turakhia helped run that collected wearable data from nearly 420,000 Americans. Results from the Apple Heart Study showed that, during a median 117 days of monitoring with a smart watch, 2,161 people (0.5%) received a report of an irregular pulse, which led to further investigations that eventually diagnosed atrial fibrillation (AFib) in 153 people of the 450 who underwent follow-up assessment (N Engl J Med. 2019 Nov 14;381[20]:1909-17). These results “raise questions” about the large number of people who underwent follow-up testing who did not have arrhythmia, Dr. Turakhia noted.
“The dissemination of wearables has been quite dramatic, and electrophysiologists end up owning this,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director emeritus of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “I get a ton of calls from people whom I wish never bought a smart watch, and they say ‘I have atrial fibrillation. What do I do?’ ”
To document the growth of this trend, Dr. Turakhia cited results from a survey he collaborated on, run by Stanford and Rock Health, that found a 33% ownership rate among American adults of a wearable device capable of collecting health data, and a 42% rate of people who tracked their health data with a device, app, journal, or log. Both of these rates more than doubled what a similar survey found in 2015.
The cardiac electrophysiology community took a first step toward addressing one aspect of this evolving situation. In early 2020, the Heart Rhythm Society and the Consumer Technology Association jointly issued a guidance document targeted at consumers that walks them through the kinds of information their wearable devices might collect and how to approach this information. The main message: If you have questions or concerns about your data, consult a clinician. What remains in short supply is guidance to clinicians on what to do when they see these patients.

“Until recently, device-detected AFib was the sole purview of electrophysiologists using implanted rhythm-monitoring devices. Now mobile and other devices raise issues [of asymptomatic AFib] for a much broader population,” noted Daniel E. Singer, MD, professor of medicine and epidemiology at Harvard and Massachusetts General Hospital. “The world of device-detected AFib now includes watches.”
Researchers have tried for years to better understand the stroke risk faced by patients with asymptomatic or subclinical AFib that’s detected by an implanted device, as in the ASSERT study of nearly 2,600 patients followed for a median of 2.5 years that found an increased stroke risk when the duration of individual, subclinical AFib episodes surpassed 24 hours (Eur Heart J. 2017 May 1;38[17]:1339-44). More recently, a study of AFib duration collected by implanted cardiac devices in nearly 22,000 Americans showed a relationship between stroke risk and both the duration of AFib episodes and the underlying risk of a person for stroke as measured by their CHA2DS2-VAScscore (Circulation. 2019 Nov 12;140[20]:1639-46). Just under 30% of patients in the study were diagnosed with AFib at entry.
The implications of asymptomatic episodes of AFib have so far been largely studied in people with an implanted cardiac device, which may have limited applicability to wearable users. In addition, the field has not yet fully sorted out the relationships between the duration of individual AFib episodes and overall AFib burden, and a person’s stroke risk and the window of time when the potential stroke-preventing benefits of anticoagulation outweigh its bleeding risk.
The results of trials now in progress that are examining the safety and efficacy of medical interventions designed to avert strokes in patients with asymptomatic AFib “will bear on the use of anticoagulants in a large group of patients,” including people with AFib detected by a wearable, Dr. Singer predicted.
The Apple Heart Study was sponsored Apple. Dr. Turakhia has received funding from Apple, and he has received honoraria or research funding from several other companies. Dr. Ruskin has been a consultant or adviser to several companies, is a steering committee member for Pfizer, and holds equity or options in Portola, Element Science, NewPace, Gilead, and InfoBionic. Dr. Singer has been a consultant and adviser to Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, Merck, and Pfizer, and he has received research grants from Bristol-Myers Squibb.
NATIONAL HARBOR, MD. – or other warnings that flagged a possible cardiac arrhythmia.
While the clinical community has yet to reach an evidence-based consensus on how to deal with this information, or even asymptomatic arrhythmias identified by more standard means, the American public is voting with their wrists. People seem to like collecting and reviewing readouts on their heart rhythm and other vital data, and then they often take their numbers to a physician, especially when their device suggests a possible problem.
“The whole paradigm of ordering a test only if you intend to act on the result has been flipped. People now get what they want directly, and our job is to guide them” after the fact. “You need to teach people what’s actionable and what’s not,” Mintu P. Turakhia, MD, said at the annual International AF Symposium.
“We’re in a situation where the ability of a sensor to detect things is separate from access to the health care system. They are no longer coupled; they are disjointed. People can create their own ICU in their house just by shopping online, but what do we do with this information, whether it’s an irregular heart rhythm or their whole genome?” asked Dr. Turakhia, executive director of the Center for Digital Health at Stanford (Calif.) University and director of cardiac electrophysiology at the VA Palo Alto (Calif.) Health Care System.
“The main challenge is people without a diagnosis who get a notification. How much monitoring should you do until you can say it was a false positive? We don’t know what to do, so we monitor them. People are trying to figure this out.” Dr. Turakhia said. Some people who seek out electrophysiologists this way “may not even have a primary care physician,” he noted.
The potential implications of widespread monitoring for heartbeat irregularities in the general public began to surface in a study that Dr. Turakhia helped run that collected wearable data from nearly 420,000 Americans. Results from the Apple Heart Study showed that, during a median 117 days of monitoring with a smart watch, 2,161 people (0.5%) received a report of an irregular pulse, which led to further investigations that eventually diagnosed atrial fibrillation (AFib) in 153 people of the 450 who underwent follow-up assessment (N Engl J Med. 2019 Nov 14;381[20]:1909-17). These results “raise questions” about the large number of people who underwent follow-up testing who did not have arrhythmia, Dr. Turakhia noted.
“The dissemination of wearables has been quite dramatic, and electrophysiologists end up owning this,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director emeritus of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “I get a ton of calls from people whom I wish never bought a smart watch, and they say ‘I have atrial fibrillation. What do I do?’ ”
To document the growth of this trend, Dr. Turakhia cited results from a survey he collaborated on, run by Stanford and Rock Health, that found a 33% ownership rate among American adults of a wearable device capable of collecting health data, and a 42% rate of people who tracked their health data with a device, app, journal, or log. Both of these rates more than doubled what a similar survey found in 2015.
The cardiac electrophysiology community took a first step toward addressing one aspect of this evolving situation. In early 2020, the Heart Rhythm Society and the Consumer Technology Association jointly issued a guidance document targeted at consumers that walks them through the kinds of information their wearable devices might collect and how to approach this information. The main message: If you have questions or concerns about your data, consult a clinician. What remains in short supply is guidance to clinicians on what to do when they see these patients.
“Until recently, device-detected AFib was the sole purview of electrophysiologists using implanted rhythm-monitoring devices. Now mobile and other devices raise issues [of asymptomatic AFib] for a much broader population,” noted Daniel E. Singer, MD, professor of medicine and epidemiology at Harvard and Massachusetts General Hospital. “The world of device-detected AFib now includes watches.”
Researchers have tried for years to better understand the stroke risk faced by patients with asymptomatic or subclinical AFib that’s detected by an implanted device, as in the ASSERT study of nearly 2,600 patients followed for a median of 2.5 years that found an increased stroke risk when the duration of individual, subclinical AFib episodes surpassed 24 hours (Eur Heart J. 2017 May 1;38[17]:1339-44). More recently, a study of AFib duration collected by implanted cardiac devices in nearly 22,000 Americans showed a relationship between stroke risk and both the duration of AFib episodes and the underlying risk of a person for stroke as measured by their CHA2DS2-VAScscore (Circulation. 2019 Nov 12;140[20]:1639-46). Just under 30% of patients in the study were diagnosed with AFib at entry.
The implications of asymptomatic episodes of AFib have so far been largely studied in people with an implanted cardiac device, which may have limited applicability to wearable users. In addition, the field has not yet fully sorted out the relationships between the duration of individual AFib episodes and overall AFib burden, and a person’s stroke risk and the window of time when the potential stroke-preventing benefits of anticoagulation outweigh its bleeding risk.
The results of trials now in progress that are examining the safety and efficacy of medical interventions designed to avert strokes in patients with asymptomatic AFib “will bear on the use of anticoagulants in a large group of patients,” including people with AFib detected by a wearable, Dr. Singer predicted.
The Apple Heart Study was sponsored Apple. Dr. Turakhia has received funding from Apple, and he has received honoraria or research funding from several other companies. Dr. Ruskin has been a consultant or adviser to several companies, is a steering committee member for Pfizer, and holds equity or options in Portola, Element Science, NewPace, Gilead, and InfoBionic. Dr. Singer has been a consultant and adviser to Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, Merck, and Pfizer, and he has received research grants from Bristol-Myers Squibb.
NATIONAL HARBOR, MD. – or other warnings that flagged a possible cardiac arrhythmia.
While the clinical community has yet to reach an evidence-based consensus on how to deal with this information, or even asymptomatic arrhythmias identified by more standard means, the American public is voting with their wrists. People seem to like collecting and reviewing readouts on their heart rhythm and other vital data, and then they often take their numbers to a physician, especially when their device suggests a possible problem.
“The whole paradigm of ordering a test only if you intend to act on the result has been flipped. People now get what they want directly, and our job is to guide them” after the fact. “You need to teach people what’s actionable and what’s not,” Mintu P. Turakhia, MD, said at the annual International AF Symposium.
“We’re in a situation where the ability of a sensor to detect things is separate from access to the health care system. They are no longer coupled; they are disjointed. People can create their own ICU in their house just by shopping online, but what do we do with this information, whether it’s an irregular heart rhythm or their whole genome?” asked Dr. Turakhia, executive director of the Center for Digital Health at Stanford (Calif.) University and director of cardiac electrophysiology at the VA Palo Alto (Calif.) Health Care System.
“The main challenge is people without a diagnosis who get a notification. How much monitoring should you do until you can say it was a false positive? We don’t know what to do, so we monitor them. People are trying to figure this out.” Dr. Turakhia said. Some people who seek out electrophysiologists this way “may not even have a primary care physician,” he noted.
The potential implications of widespread monitoring for heartbeat irregularities in the general public began to surface in a study that Dr. Turakhia helped run that collected wearable data from nearly 420,000 Americans. Results from the Apple Heart Study showed that, during a median 117 days of monitoring with a smart watch, 2,161 people (0.5%) received a report of an irregular pulse, which led to further investigations that eventually diagnosed atrial fibrillation (AFib) in 153 people of the 450 who underwent follow-up assessment (N Engl J Med. 2019 Nov 14;381[20]:1909-17). These results “raise questions” about the large number of people who underwent follow-up testing who did not have arrhythmia, Dr. Turakhia noted.
“The dissemination of wearables has been quite dramatic, and electrophysiologists end up owning this,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director emeritus of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “I get a ton of calls from people whom I wish never bought a smart watch, and they say ‘I have atrial fibrillation. What do I do?’ ”
To document the growth of this trend, Dr. Turakhia cited results from a survey he collaborated on, run by Stanford and Rock Health, that found a 33% ownership rate among American adults of a wearable device capable of collecting health data, and a 42% rate of people who tracked their health data with a device, app, journal, or log. Both of these rates more than doubled what a similar survey found in 2015.
The cardiac electrophysiology community took a first step toward addressing one aspect of this evolving situation. In early 2020, the Heart Rhythm Society and the Consumer Technology Association jointly issued a guidance document targeted at consumers that walks them through the kinds of information their wearable devices might collect and how to approach this information. The main message: If you have questions or concerns about your data, consult a clinician. What remains in short supply is guidance to clinicians on what to do when they see these patients.
“Until recently, device-detected AFib was the sole purview of electrophysiologists using implanted rhythm-monitoring devices. Now mobile and other devices raise issues [of asymptomatic AFib] for a much broader population,” noted Daniel E. Singer, MD, professor of medicine and epidemiology at Harvard and Massachusetts General Hospital. “The world of device-detected AFib now includes watches.”
Researchers have tried for years to better understand the stroke risk faced by patients with asymptomatic or subclinical AFib that’s detected by an implanted device, as in the ASSERT study of nearly 2,600 patients followed for a median of 2.5 years that found an increased stroke risk when the duration of individual, subclinical AFib episodes surpassed 24 hours (Eur Heart J. 2017 May 1;38[17]:1339-44). More recently, a study of AFib duration collected by implanted cardiac devices in nearly 22,000 Americans showed a relationship between stroke risk and both the duration of AFib episodes and the underlying risk of a person for stroke as measured by their CHA2DS2-VAScscore (Circulation. 2019 Nov 12;140[20]:1639-46). Just under 30% of patients in the study were diagnosed with AFib at entry.
The implications of asymptomatic episodes of AFib have so far been largely studied in people with an implanted cardiac device, which may have limited applicability to wearable users. In addition, the field has not yet fully sorted out the relationships between the duration of individual AFib episodes and overall AFib burden, and a person’s stroke risk and the window of time when the potential stroke-preventing benefits of anticoagulation outweigh its bleeding risk.
The results of trials now in progress that are examining the safety and efficacy of medical interventions designed to avert strokes in patients with asymptomatic AFib “will bear on the use of anticoagulants in a large group of patients,” including people with AFib detected by a wearable, Dr. Singer predicted.
The Apple Heart Study was sponsored Apple. Dr. Turakhia has received funding from Apple, and he has received honoraria or research funding from several other companies. Dr. Ruskin has been a consultant or adviser to several companies, is a steering committee member for Pfizer, and holds equity or options in Portola, Element Science, NewPace, Gilead, and InfoBionic. Dr. Singer has been a consultant and adviser to Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, Merck, and Pfizer, and he has received research grants from Bristol-Myers Squibb.
REPORTING FROM THE AF SYMPOSIUM 2020