User login
An emerging enterovirus strain known as coxsackievirus A6 is associated with cases of severe hand, foot, and mouth disease with a more extensive and varied exanthem than usual, according to data from a review of recent cases.
As a result, some coxsackievirus A6 (CVA6) cases have been confused with bullous impetigo, eczema herpeticum vasculitis, and primary immunobullous diseases, Dr. Vikash Oza of the University of California, San Francisco, reported at the annual meeting of the American Academy of Dermatology.

The Centers for Disease Control and Prevention reported a CVA6 outbreak in March 2012, during which several states reported cases of hand, foot, and mouth disease (HFMD) with atypical cutaneous features. Dr. Oza and his colleagues reviewed 80 cases from seven academic centers and identified five distinct morphologies associated with the outbreak:
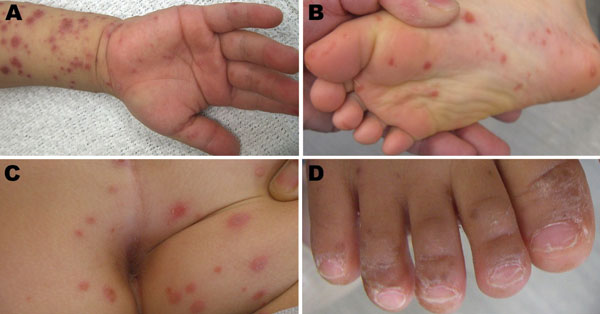
• Widespread vesiculobullous and erosive exanthema involving more than 10% of the body surface area. Some level of this condition was seen in nearly every patient, Dr. Oza said, noting that vesicles occurred on the face and trunk, and were much more widespread than with classic HFMD. Patients also had a marked predilection for perioral involvement, which led to an initial diagnosis of bullous impetigo in a number of cases, and some had "quite impressive development of bulli." These bulli occurred mainly in children under age 1, and "often evoked differentials that included primary immunobullous disorders."
• Eczema herpeticum–like eruption in atopic dermatitis patients. Dr. Oza and his colleagues termed this condition, seen in 55% of cases in the series, "eczema coxsackiuma." This eruption likely reflected the fact that cases were pulled from pediatric dermatology clinics where atopic dermatitis rates are high, he noted. The clinical morphology closely mirrors that of eczema herpeticum, with abrupt development of hollow ulcerations on areas of atopic dermatitis. Of note, none of the patients with this morphology developed serious systemic illness, unlike patients with eczema herpeticum, who may develop serious systemic sequelae, he said.
• Gianotti-Crosti–like eruption. This papular eruption on the face and extremities occurred in more than a third of patients, Dr. Oza said.
• Petechial/purpuric eruption. This eruption on acral surfaces was seen in 17% of the cases – mainly in older children, and often evoked a differential diagnosis including vasculitis or stocking-glove purpura.
• Delayed onychomadesis and palm and sole desquamation. In a subset of patients followed after their illnesses resolved, cases of onychomadesis were noted between 3 and 8 weeks after resolution, and cases of palm and sole desquamation were noted within 3 weeks after resolution.
No serious systemic complications, such as the meningoencephalitis, myocarditis, or pneumonitis seen with other enterovirus strains, were observed in these cases, but the findings underscore a need for awareness about CVA6 and the potentially severe cases of HFMD that may be associated with outbreaks, Dr. Oza said.
In the past 5 years, the number of reported cases has increased, beginning in Finland in 2008, with more recent reports from China and Japan, he added.
Patients in this study were children with a median age of 1.5 years who were treated at one of seven academic dermatology centers between July 2011 and June 2012. Of the 80 cases identified, 17 had polymerase chain reaction (PCR) confirmation of the disease, and 63 met predefined clinical criteria for inclusion.
Although the low median age is typical for HFMD, the case series spanned a range of ages, including adolescents and older teens, which likely reflects a lack of acquired immunity to this novel viral pathogen, Dr. Oza noted.
The findings demonstrate the evolving role of viral pathogens in dermatologic illness, and should alert physicians to the fact that CVA6-related disease can closely mimic other dermatologic conditions in children, he said.
In addition, the data suggest that enterovirus PCR testing is the best approach for identifying CVA6, said Dr. Oza. It is important to send samples in suspected cases, but it remains prudent to continue testing for other more common causes of vesicular eruptions in children as well, he said.
Dr. Oza had no financial conflicts to disclose.
An emerging enterovirus strain known as coxsackievirus A6 is associated with cases of severe hand, foot, and mouth disease with a more extensive and varied exanthem than usual, according to data from a review of recent cases.
As a result, some coxsackievirus A6 (CVA6) cases have been confused with bullous impetigo, eczema herpeticum vasculitis, and primary immunobullous diseases, Dr. Vikash Oza of the University of California, San Francisco, reported at the annual meeting of the American Academy of Dermatology.
The Centers for Disease Control and Prevention reported a CVA6 outbreak in March 2012, during which several states reported cases of hand, foot, and mouth disease (HFMD) with atypical cutaneous features. Dr. Oza and his colleagues reviewed 80 cases from seven academic centers and identified five distinct morphologies associated with the outbreak:
• Widespread vesiculobullous and erosive exanthema involving more than 10% of the body surface area. Some level of this condition was seen in nearly every patient, Dr. Oza said, noting that vesicles occurred on the face and trunk, and were much more widespread than with classic HFMD. Patients also had a marked predilection for perioral involvement, which led to an initial diagnosis of bullous impetigo in a number of cases, and some had "quite impressive development of bulli." These bulli occurred mainly in children under age 1, and "often evoked differentials that included primary immunobullous disorders."
• Eczema herpeticum–like eruption in atopic dermatitis patients. Dr. Oza and his colleagues termed this condition, seen in 55% of cases in the series, "eczema coxsackiuma." This eruption likely reflected the fact that cases were pulled from pediatric dermatology clinics where atopic dermatitis rates are high, he noted. The clinical morphology closely mirrors that of eczema herpeticum, with abrupt development of hollow ulcerations on areas of atopic dermatitis. Of note, none of the patients with this morphology developed serious systemic illness, unlike patients with eczema herpeticum, who may develop serious systemic sequelae, he said.
• Gianotti-Crosti–like eruption. This papular eruption on the face and extremities occurred in more than a third of patients, Dr. Oza said.
• Petechial/purpuric eruption. This eruption on acral surfaces was seen in 17% of the cases – mainly in older children, and often evoked a differential diagnosis including vasculitis or stocking-glove purpura.
• Delayed onychomadesis and palm and sole desquamation. In a subset of patients followed after their illnesses resolved, cases of onychomadesis were noted between 3 and 8 weeks after resolution, and cases of palm and sole desquamation were noted within 3 weeks after resolution.
No serious systemic complications, such as the meningoencephalitis, myocarditis, or pneumonitis seen with other enterovirus strains, were observed in these cases, but the findings underscore a need for awareness about CVA6 and the potentially severe cases of HFMD that may be associated with outbreaks, Dr. Oza said.
In the past 5 years, the number of reported cases has increased, beginning in Finland in 2008, with more recent reports from China and Japan, he added.
Patients in this study were children with a median age of 1.5 years who were treated at one of seven academic dermatology centers between July 2011 and June 2012. Of the 80 cases identified, 17 had polymerase chain reaction (PCR) confirmation of the disease, and 63 met predefined clinical criteria for inclusion.
Although the low median age is typical for HFMD, the case series spanned a range of ages, including adolescents and older teens, which likely reflects a lack of acquired immunity to this novel viral pathogen, Dr. Oza noted.
The findings demonstrate the evolving role of viral pathogens in dermatologic illness, and should alert physicians to the fact that CVA6-related disease can closely mimic other dermatologic conditions in children, he said.
In addition, the data suggest that enterovirus PCR testing is the best approach for identifying CVA6, said Dr. Oza. It is important to send samples in suspected cases, but it remains prudent to continue testing for other more common causes of vesicular eruptions in children as well, he said.
Dr. Oza had no financial conflicts to disclose.
An emerging enterovirus strain known as coxsackievirus A6 is associated with cases of severe hand, foot, and mouth disease with a more extensive and varied exanthem than usual, according to data from a review of recent cases.
As a result, some coxsackievirus A6 (CVA6) cases have been confused with bullous impetigo, eczema herpeticum vasculitis, and primary immunobullous diseases, Dr. Vikash Oza of the University of California, San Francisco, reported at the annual meeting of the American Academy of Dermatology.
The Centers for Disease Control and Prevention reported a CVA6 outbreak in March 2012, during which several states reported cases of hand, foot, and mouth disease (HFMD) with atypical cutaneous features. Dr. Oza and his colleagues reviewed 80 cases from seven academic centers and identified five distinct morphologies associated with the outbreak:
• Widespread vesiculobullous and erosive exanthema involving more than 10% of the body surface area. Some level of this condition was seen in nearly every patient, Dr. Oza said, noting that vesicles occurred on the face and trunk, and were much more widespread than with classic HFMD. Patients also had a marked predilection for perioral involvement, which led to an initial diagnosis of bullous impetigo in a number of cases, and some had "quite impressive development of bulli." These bulli occurred mainly in children under age 1, and "often evoked differentials that included primary immunobullous disorders."
• Eczema herpeticum–like eruption in atopic dermatitis patients. Dr. Oza and his colleagues termed this condition, seen in 55% of cases in the series, "eczema coxsackiuma." This eruption likely reflected the fact that cases were pulled from pediatric dermatology clinics where atopic dermatitis rates are high, he noted. The clinical morphology closely mirrors that of eczema herpeticum, with abrupt development of hollow ulcerations on areas of atopic dermatitis. Of note, none of the patients with this morphology developed serious systemic illness, unlike patients with eczema herpeticum, who may develop serious systemic sequelae, he said.
• Gianotti-Crosti–like eruption. This papular eruption on the face and extremities occurred in more than a third of patients, Dr. Oza said.
• Petechial/purpuric eruption. This eruption on acral surfaces was seen in 17% of the cases – mainly in older children, and often evoked a differential diagnosis including vasculitis or stocking-glove purpura.
• Delayed onychomadesis and palm and sole desquamation. In a subset of patients followed after their illnesses resolved, cases of onychomadesis were noted between 3 and 8 weeks after resolution, and cases of palm and sole desquamation were noted within 3 weeks after resolution.
No serious systemic complications, such as the meningoencephalitis, myocarditis, or pneumonitis seen with other enterovirus strains, were observed in these cases, but the findings underscore a need for awareness about CVA6 and the potentially severe cases of HFMD that may be associated with outbreaks, Dr. Oza said.
In the past 5 years, the number of reported cases has increased, beginning in Finland in 2008, with more recent reports from China and Japan, he added.
Patients in this study were children with a median age of 1.5 years who were treated at one of seven academic dermatology centers between July 2011 and June 2012. Of the 80 cases identified, 17 had polymerase chain reaction (PCR) confirmation of the disease, and 63 met predefined clinical criteria for inclusion.
Although the low median age is typical for HFMD, the case series spanned a range of ages, including adolescents and older teens, which likely reflects a lack of acquired immunity to this novel viral pathogen, Dr. Oza noted.
The findings demonstrate the evolving role of viral pathogens in dermatologic illness, and should alert physicians to the fact that CVA6-related disease can closely mimic other dermatologic conditions in children, he said.
In addition, the data suggest that enterovirus PCR testing is the best approach for identifying CVA6, said Dr. Oza. It is important to send samples in suspected cases, but it remains prudent to continue testing for other more common causes of vesicular eruptions in children as well, he said.
Dr. Oza had no financial conflicts to disclose.
EXPERT ANALYSIS FROM THE AAD ANNUAL MEETING