User login
Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes
Lower extremity venous ulcerations impact the health, well-being, and associated costs of patient care. These ulcerations are associated with comorbidities such as diabetes mellitus and chronic venous insufficiency or may be related to trauma. Often, the standard of care fails to effectively and completely heal ulcers, causing them to become stalled, chronic, and require ≥ 1 month of treatment.
Healthy skin partial pressure of oxygen (PO2) approximates 100 mm Hg, but prolonged periods of poor blood perfusion from vascular damage can cause the PO2 within a wound bed to become as low as 10 mm Hg.1 Deprivation of oxygen impairs biological processes essential for bacterial control and growth factor activity, contributing to wound chronicity.2-5 Exposure to oxygen not only upregulates growth factors essential for maintaining a well-vascularized wound core, but also aids enzymatic reactions responsible for healing the skin that are sensitive to PO2 levels.3,6,7 These physiologic processes can be maximized by raising oxygen level concentrations by means of oxygen therapy.8
Hyperbaric oxygen therapy (HBOT) uses a pressurized system to deliver concentrated oxygen that is diffused in the lungs, resulting in increased blood oxygen levels for delivery to bodily tissues. Full chamber HBOT can accelerate the wound healing process. Some disadvantages of HBOT include its high cost, the possibility of oxygen toxicity, and travel time to facilities for daily therapy sessions that last an average of 1.5 hours and may continue for ≤ 60 sessions.7,9 Thus, alternatives to HBOT have been developed, including topical oxygen therapy (TOT), which uses portable bags or chambers that deliver concentrated oxygen applied directly over ulcers, allowing oxygen to diffuse directly into the injured tissue. Combined with the standard of care and regular debridement, TOT saturates the wound base and surrounding tissues with oxygen, thereby inducing growth factors that promote angiogenesis as well as upregulation of enzymatic reactions that create a reparative environment.6
In a study conducted in pigs, Fries et al induced full-thickness wounds that were allowed to heal by secondary intention. They demonstrated that wounds treated with TOT not only healed in fewer days but also revealed a higher presence of vascular endothelial growth factor, greater density of vascular structures, and more histologically mature healing tissues when compared with control wounds exposed to room air.2
The effectiveness of TOT in ulcer healing has been previously reported. Frykberg et al performed a multicenter randomized controlled trial (RCT) comparing TOT with sham therapy to determine the efficacy of TOT in diabetic foot ulcers (DFUs) that had previously failed treatment with the standard of care. The RCT demonstrated that wounds treated with TOT had a 4.5-fold greater likelihood of complete epithelialization within 12 weeks compared with the sham group.3 In a multicenter RCT, Al-Jalodi et al found that 56% of DFUs treated with TOT remained epithelialized at 12 months compared with 27% of ulcers treated with the standard of care alone. Al Jalodi et al argued that TOT may increase the durability of DFU closure.8 In addition, a small prospective cohort study biopsied 23 DFUs treated with TOT and noted increased cytokines and growth factors, as well as increased transcutaneous oxygen measurement perfusion after only 1 week of treatment compared with wounds treated with the standard of care.9
Yellin et al reported that patients with DFU treated with TOT had reduced hospital lengths of stay and a lower amputation rate compared with patients who did not receive TOT modality.10 Another study compared conventional compression dressings with TOT in managing 132 recalcitrant venous ulcers. In that study, Nataraj et al found that 76% of ulcers treated with TOT had completely healed at 12 weeks compared with 46% of those treated with compression only.11 Furthermore, numerous systematic reviews and meta-analyses have analyzed the efficacy of TOT, concluding that this modality not only improves healing among ulcers of varying severity when compared with the standard of care but also contributes to the durability of healed ulcers and thus helps improve patient quality of life by preventing recurrence.2,12-18
Intermittent cyclical compression topical oxygen therapy (cTOT) is a modality that provides concentrated oxygen at a rate of 10 L/min. cTOT cycles twice a minute and applies noncontact compression directly to ulcerations between 10 and 50 millibars (7.5-37.5 mm Hg). In a study of 8 patients with leg ulcers, transcutaneous oxygen tension was higher after treatment with intermittent pneumatic compression (42.7 mm Hg) when compared with baseline values. The authors postulated that intermittent compression decreased interstitial fluid volume and venous stasis, both of which lead to increased cutaneous oxygenation. The data suggested that removal of carbon dioxide from tissues and enhancement of cutaneous cyclical oxygenation promoted ulcer healing.19To the best of our knowledge, there are no published studies that have evaluated the efficacy of cTOT for traumatic injuries while also considering existing comorbidities such as diabetes mellitus and venous insufficiency in veterans. The aim of this study was to demonstrate the efficacy of cTOT in the setting of traumatic wounds that failed the standard of care and were complicated by venous insufficiency and diabetes mellitus. We hypothesized that cTOT enhances healing of trauma-induced venous leg wounds in patients with diabetes mellitus, achieving full epithelialization within 12 weeks after failing the standard of care.


B, controller. Source: Advanced Oxygen Therapy Inc. Reprinted with permission.
Methods
Institutional review board approval was granted prior to commencement of this single-center retrospective review at the Veterans Affairs Illiana Healthcare System (VAIHS) in Danville, Illinois. Electronic health records between May 1, 2016, and July 31, 2021, were examined to find patients treated with cTOT using the Advanced Oxygen Therapy Inc. Topical Wound Oxygen (TWO2) system (Figure). Data collected included demographics, follow-up, and outcomes.
Inclusion criteria included patients who failed standard wound care for ≥ 4 weeks with venous insufficiency, trauma to the lower legs by means of iatrogenic injury, accidental injury, thermal injury/burn, or diabetes mellitus determined to be an active problem and a hemoglobin A1c (HbA1c) obtained within 3 months of wound treatment. The VAIHS standard of care was weekly visits to a wound care physician, physician assistant, or a nurse practitioner who performed sharp wound debridement and applied multilayer compression therapy. Patients with confirmed history of intermittent claudication, stroke, absent pedal pulses, abnormal blood pressure, deep vein thrombosis, pulmonary embolism, revascularization of the lower extremity, trauma fractures of the affected leg, phlebitis, pregnancy, coagulopathy, infection, or history of malignancy were excluded.
Patients who failed the standard of care for ≥ 4 weeks were enrolled in the cTOT program, after which they began weekly visits to an outpatient wound healing center where visits consisted of sharp wound debridement, wound measurement, and application of compressive dressing to the affected lower extremity. Following wound-healing center visits, the subjects received cTOT at home according to the manufacturer’s protocol, which consisted of ≤ 90-minute sessions, 5 to 7 times weekly. The wounds were measured from initial presentation to complete epithelialization, and the patients were followed for ≤ 27 months.
Results
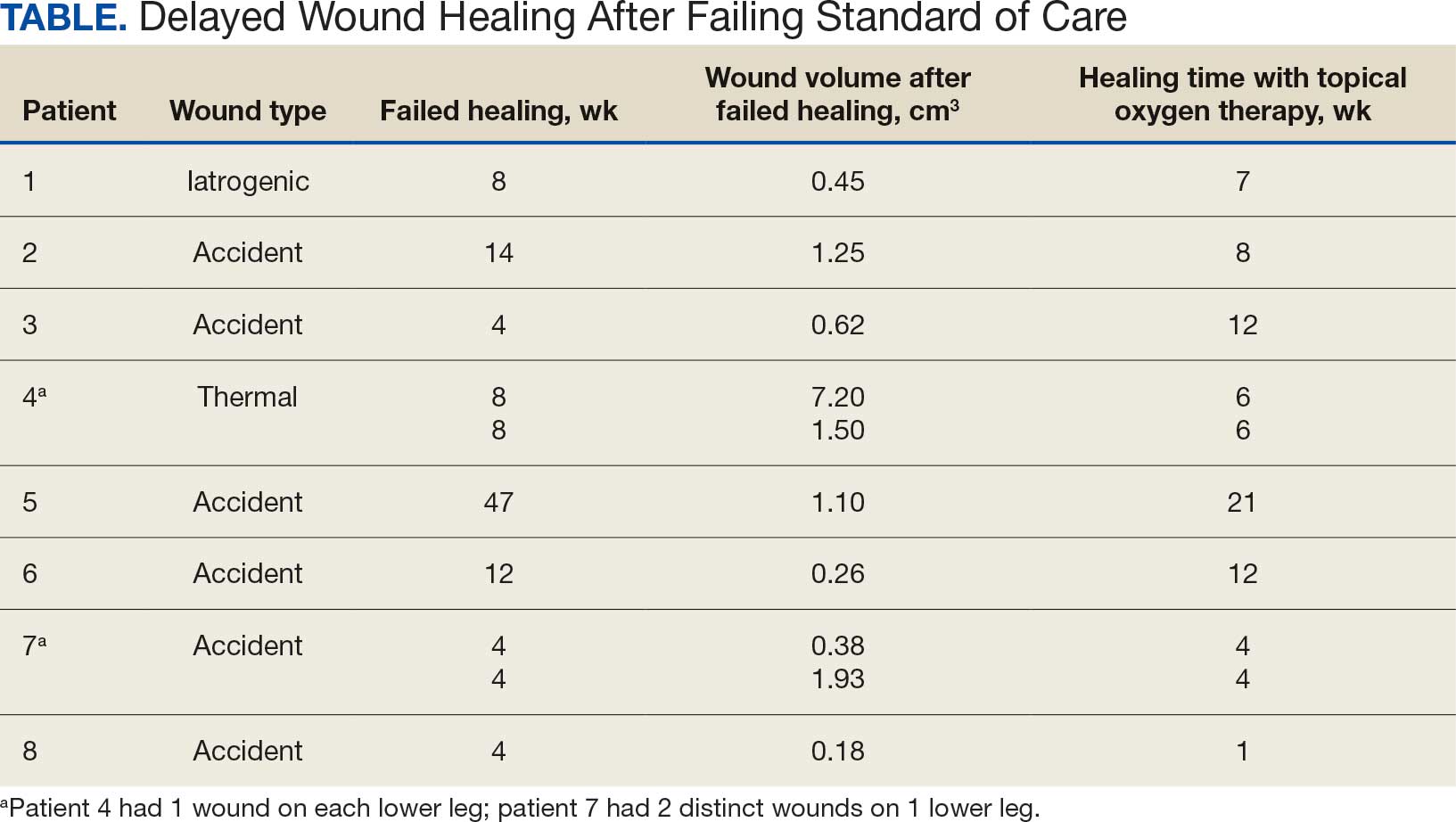
Sixty-nine patients underwent cTOT between May 1, 2016, and July 31, 2021, and 8 patients with 10 wounds met the inclusion criteria. The patients had a mean age of 76 years, BMI of 27, and HbA1c of 8.0%. All wounds completely healed following cTOT. Prior to the use of cTOT, the included patients had a mean 11.3 weeks of failed healing attempts when receiving standard of care therapy. Following cTOT implementation, the mean time to healing was 8.1 weeks (Table). One wound recurred after 10 weeks in a patient with uncontrolled diabetes mellitus. One patient died of causes unrelated to the wound and was excluded from follow-up. All other wounds remained closed and healed after a mean end follow-up period of 110 weeks through June 2023.
Discussion
Traumatic wounds are commonly seen in the emergency department (ED), accounting for 5.4% of all ED visits.20-22 According to the National Hospital Ambulatory Medical Care Survey, 14.6% of 117 million ED visits in 2007 involved lower-extremity wounds, costing the health care system > $25 billion annually.23 Kulkarni et al reported that 44% of patients experienced leg ulcerations secondary to trauma.24 Traumatic wounds that lack epithelialization > 4 weeks are categorized as chronic, placing a large social and financial impact on patient health and well-being.
This case series supports the benefits of cTOT and demonstrates improved wound-closure rates with sustained healing compared with standard care alone, corroborating findings reported by the American Diabetes Association (ADA).23 The ADA cited high-quality RCTs and systematic reviews supporting the healing benefits of cTOT for chronic DFUs through the upregulation of essential growth factors.24
The current literature offers many examples of the healing benefits of TOT for arterial ulcerations. Benefits include faster healing with longer lasting reparative ulcer tissue, prevention of amputation and improved quality of life. However, there is a lack of literature on the use of cTOT for venous stasis traumatic wounds, which prompted this study. Our case series presents evidence that cTOT enhances healing of trauma-induced venous leg wounds in male veterans with diabetes mellitus within 12 weeks after failure of the standard of care. Other risk factors that were recorded but not included in our analysis included tobacco use, chronic kidney disease, chronic obstructive pulmonary disease, use of cellular-based tissue/collagen products, and neuropathy.
This case series provides evidence that cTOT can be a beneficial and cost-effective treatment. Economic considerations are derived from retrospective cohort analyses and a published decision-analytic Markov model representing modeled estimates and need to be interpreted in that context rather than as findings from prospective comparative cost analyses healing.25,26
The authors did not conduct an independent health economic evaluation as part of this review. Wound recurrence, hospitalizations and lower extremity amputations represent major cost drivers in chronic wound care. In addition, repeat ED admissions, surgical intervention, rehabilitation, prosthetics, and long-term disability contribute to economic burden and negative psychosocial and quality of life impacts on patients and caregivers. The reductions in hospitalization (≤ 88%) and amputation (≤ 73%) observed in real-world TWO2 cohorts suggest significant potential downstream cost savings. A recent Markov model analysis suggested that TWO2 may be cost-favorable compared with standard care, with modeled estimates indicating lower total 2-year costs and improved quality-adjusted life years. These projections are based on modeling assumptions and require confirmation through prospective economic evaluations comparing TWO2 directly with negative pressure wound therapy, HBOT, and skin substitutes across longer time horizons.
Limitations
The findings of this case series were small and lacked statistical power with only 8 male patients. Literature gaps also exist regarding the specific effects of TOT on traumatic wounds. This review was limited by its single-center location.
Conclusions
This case series suggests that cTOT may be an effective adjuvant therapy in managing trauma-induced venous leg wounds and supports consideration of early implementation for expedited epithelialization. However, further studies with larger sample sizes are required.
Tawfick WA, Sultan S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc Endovascular Surg. 2013:30-37. doi:10.1177/1538574412467684
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005:172-181. doi:10.1016/j.mrfmmm.2005.02.023
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TWO2 study. Diabetes Care. 2020:616-624. doi:10.2337/dc19-0476
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Al-Jalodi O, Kupcella M, Breisinger K, et al. A multicenter clinical trial evaluating the durability of diabetic foot ulcer healing in ulcers treated with topical oxygen and standard of care versus standard of care alone 1 year post healing. Int Wound J. 2022:1838-1842. doi:10.1111/iwj.13789
Carter MJ, Frykberg RG, Oropallo A, et al. Efficacy of topical wound oxygen therapy in healing chronic diabetic foot ulcers: systematic review and meta-analysis. Adv Wound Care (New Rochelle). 2023;12:177-186. doi:10.1089/wound.2022.0041
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022:657-665. doi:10.1089/wound.2021.0118
Nataraj M, Maiya AG, Karkada G, et al. Application of topical oxygen therapy in healing dynamics of diabetic foot ulcers: a systematic review. Rev Diabet Stud. 2019:74-82. doi:10.1900/RDS.2019.15.74
Thanigaimani S, Singh T, Golledge J. Topical oxygen therapy for diabetes-related foot ulcers: a systematic review and meta-analysis. Diabet Med. 2021:e14585. doi:10.1111/dme.14585
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Oropallo AR, Serena TE, Armstrong DG, et al. Molecular biomarkers of oxygen therapy in patients with diabetic foot ulcers. Biomolecules. 2021:925. doi:10.3390/biom11070925
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Kahle B, Hermanns HJ, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl Int. 2011:231-237. doi:10.3238/arztebl.2011.0231
Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on hyperbaric oxygen therapy: applications, mechanisms, and translational opportunities. Medicina (Kaunas). 2021:864. doi:10.3390/medicina57090864
Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy and micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018:363-374. doi:10.1111/iwj.12873
Chen AH, Frangos SG, Kilaru S, et al. Intermittent pneumatic compression devices: physiologic mechanisms of action. Eur J Vasc Endovasc Surg. 2001:383-392. doi:10.1053/ejvs.2001.1348
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the emergency department: position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016:30. doi:10.1186/s13017-016-0084-3
Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017:599-610. doi:10.1007/s12325-017-0478-y
Kamal S, Sehgal A, Shahi P, et al. Topical oxygen therapy in acute traumatic musculoskeletal wounds of the foot and ankle. J Wound Care. 2023:92-97. doi:10.12968/jowc.2023.32.2.92
Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012:284-290. doi:10.1007/s11999-011-1982-z
Kulkarni SR, Gohel MS, Whyman MR, et al. Significance of limb trauma as an initiating factor in chronic leg ulceration. Phlebology. 2008:130-136.
Kerr M, Wild D, Edmonds M, et al. Cost effectiveness of topical wound oxygen therapy for chronic diabetic foot ulcers. J Diabetes Complications. 2025;39:109016. doi:10.1016/j.jdiacomp.2025.109016.
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022;11:657-665. doi:10.1089/wound.2021.0118
Lower extremity venous ulcerations impact the health, well-being, and associated costs of patient care. These ulcerations are associated with comorbidities such as diabetes mellitus and chronic venous insufficiency or may be related to trauma. Often, the standard of care fails to effectively and completely heal ulcers, causing them to become stalled, chronic, and require ≥ 1 month of treatment.
Healthy skin partial pressure of oxygen (PO2) approximates 100 mm Hg, but prolonged periods of poor blood perfusion from vascular damage can cause the PO2 within a wound bed to become as low as 10 mm Hg.1 Deprivation of oxygen impairs biological processes essential for bacterial control and growth factor activity, contributing to wound chronicity.2-5 Exposure to oxygen not only upregulates growth factors essential for maintaining a well-vascularized wound core, but also aids enzymatic reactions responsible for healing the skin that are sensitive to PO2 levels.3,6,7 These physiologic processes can be maximized by raising oxygen level concentrations by means of oxygen therapy.8
Hyperbaric oxygen therapy (HBOT) uses a pressurized system to deliver concentrated oxygen that is diffused in the lungs, resulting in increased blood oxygen levels for delivery to bodily tissues. Full chamber HBOT can accelerate the wound healing process. Some disadvantages of HBOT include its high cost, the possibility of oxygen toxicity, and travel time to facilities for daily therapy sessions that last an average of 1.5 hours and may continue for ≤ 60 sessions.7,9 Thus, alternatives to HBOT have been developed, including topical oxygen therapy (TOT), which uses portable bags or chambers that deliver concentrated oxygen applied directly over ulcers, allowing oxygen to diffuse directly into the injured tissue. Combined with the standard of care and regular debridement, TOT saturates the wound base and surrounding tissues with oxygen, thereby inducing growth factors that promote angiogenesis as well as upregulation of enzymatic reactions that create a reparative environment.6
In a study conducted in pigs, Fries et al induced full-thickness wounds that were allowed to heal by secondary intention. They demonstrated that wounds treated with TOT not only healed in fewer days but also revealed a higher presence of vascular endothelial growth factor, greater density of vascular structures, and more histologically mature healing tissues when compared with control wounds exposed to room air.2
The effectiveness of TOT in ulcer healing has been previously reported. Frykberg et al performed a multicenter randomized controlled trial (RCT) comparing TOT with sham therapy to determine the efficacy of TOT in diabetic foot ulcers (DFUs) that had previously failed treatment with the standard of care. The RCT demonstrated that wounds treated with TOT had a 4.5-fold greater likelihood of complete epithelialization within 12 weeks compared with the sham group.3 In a multicenter RCT, Al-Jalodi et al found that 56% of DFUs treated with TOT remained epithelialized at 12 months compared with 27% of ulcers treated with the standard of care alone. Al Jalodi et al argued that TOT may increase the durability of DFU closure.8 In addition, a small prospective cohort study biopsied 23 DFUs treated with TOT and noted increased cytokines and growth factors, as well as increased transcutaneous oxygen measurement perfusion after only 1 week of treatment compared with wounds treated with the standard of care.9
Yellin et al reported that patients with DFU treated with TOT had reduced hospital lengths of stay and a lower amputation rate compared with patients who did not receive TOT modality.10 Another study compared conventional compression dressings with TOT in managing 132 recalcitrant venous ulcers. In that study, Nataraj et al found that 76% of ulcers treated with TOT had completely healed at 12 weeks compared with 46% of those treated with compression only.11 Furthermore, numerous systematic reviews and meta-analyses have analyzed the efficacy of TOT, concluding that this modality not only improves healing among ulcers of varying severity when compared with the standard of care but also contributes to the durability of healed ulcers and thus helps improve patient quality of life by preventing recurrence.2,12-18
Intermittent cyclical compression topical oxygen therapy (cTOT) is a modality that provides concentrated oxygen at a rate of 10 L/min. cTOT cycles twice a minute and applies noncontact compression directly to ulcerations between 10 and 50 millibars (7.5-37.5 mm Hg). In a study of 8 patients with leg ulcers, transcutaneous oxygen tension was higher after treatment with intermittent pneumatic compression (42.7 mm Hg) when compared with baseline values. The authors postulated that intermittent compression decreased interstitial fluid volume and venous stasis, both of which lead to increased cutaneous oxygenation. The data suggested that removal of carbon dioxide from tissues and enhancement of cutaneous cyclical oxygenation promoted ulcer healing.19To the best of our knowledge, there are no published studies that have evaluated the efficacy of cTOT for traumatic injuries while also considering existing comorbidities such as diabetes mellitus and venous insufficiency in veterans. The aim of this study was to demonstrate the efficacy of cTOT in the setting of traumatic wounds that failed the standard of care and were complicated by venous insufficiency and diabetes mellitus. We hypothesized that cTOT enhances healing of trauma-induced venous leg wounds in patients with diabetes mellitus, achieving full epithelialization within 12 weeks after failing the standard of care.
B, controller. Source: Advanced Oxygen Therapy Inc. Reprinted with permission.
Methods
Institutional review board approval was granted prior to commencement of this single-center retrospective review at the Veterans Affairs Illiana Healthcare System (VAIHS) in Danville, Illinois. Electronic health records between May 1, 2016, and July 31, 2021, were examined to find patients treated with cTOT using the Advanced Oxygen Therapy Inc. Topical Wound Oxygen (TWO2) system (Figure). Data collected included demographics, follow-up, and outcomes.
Inclusion criteria included patients who failed standard wound care for ≥ 4 weeks with venous insufficiency, trauma to the lower legs by means of iatrogenic injury, accidental injury, thermal injury/burn, or diabetes mellitus determined to be an active problem and a hemoglobin A1c (HbA1c) obtained within 3 months of wound treatment. The VAIHS standard of care was weekly visits to a wound care physician, physician assistant, or a nurse practitioner who performed sharp wound debridement and applied multilayer compression therapy. Patients with confirmed history of intermittent claudication, stroke, absent pedal pulses, abnormal blood pressure, deep vein thrombosis, pulmonary embolism, revascularization of the lower extremity, trauma fractures of the affected leg, phlebitis, pregnancy, coagulopathy, infection, or history of malignancy were excluded.
Patients who failed the standard of care for ≥ 4 weeks were enrolled in the cTOT program, after which they began weekly visits to an outpatient wound healing center where visits consisted of sharp wound debridement, wound measurement, and application of compressive dressing to the affected lower extremity. Following wound-healing center visits, the subjects received cTOT at home according to the manufacturer’s protocol, which consisted of ≤ 90-minute sessions, 5 to 7 times weekly. The wounds were measured from initial presentation to complete epithelialization, and the patients were followed for ≤ 27 months.
Results
Sixty-nine patients underwent cTOT between May 1, 2016, and July 31, 2021, and 8 patients with 10 wounds met the inclusion criteria. The patients had a mean age of 76 years, BMI of 27, and HbA1c of 8.0%. All wounds completely healed following cTOT. Prior to the use of cTOT, the included patients had a mean 11.3 weeks of failed healing attempts when receiving standard of care therapy. Following cTOT implementation, the mean time to healing was 8.1 weeks (Table). One wound recurred after 10 weeks in a patient with uncontrolled diabetes mellitus. One patient died of causes unrelated to the wound and was excluded from follow-up. All other wounds remained closed and healed after a mean end follow-up period of 110 weeks through June 2023.
Discussion
Traumatic wounds are commonly seen in the emergency department (ED), accounting for 5.4% of all ED visits.20-22 According to the National Hospital Ambulatory Medical Care Survey, 14.6% of 117 million ED visits in 2007 involved lower-extremity wounds, costing the health care system > $25 billion annually.23 Kulkarni et al reported that 44% of patients experienced leg ulcerations secondary to trauma.24 Traumatic wounds that lack epithelialization > 4 weeks are categorized as chronic, placing a large social and financial impact on patient health and well-being.
This case series supports the benefits of cTOT and demonstrates improved wound-closure rates with sustained healing compared with standard care alone, corroborating findings reported by the American Diabetes Association (ADA).23 The ADA cited high-quality RCTs and systematic reviews supporting the healing benefits of cTOT for chronic DFUs through the upregulation of essential growth factors.24
The current literature offers many examples of the healing benefits of TOT for arterial ulcerations. Benefits include faster healing with longer lasting reparative ulcer tissue, prevention of amputation and improved quality of life. However, there is a lack of literature on the use of cTOT for venous stasis traumatic wounds, which prompted this study. Our case series presents evidence that cTOT enhances healing of trauma-induced venous leg wounds in male veterans with diabetes mellitus within 12 weeks after failure of the standard of care. Other risk factors that were recorded but not included in our analysis included tobacco use, chronic kidney disease, chronic obstructive pulmonary disease, use of cellular-based tissue/collagen products, and neuropathy.
This case series provides evidence that cTOT can be a beneficial and cost-effective treatment. Economic considerations are derived from retrospective cohort analyses and a published decision-analytic Markov model representing modeled estimates and need to be interpreted in that context rather than as findings from prospective comparative cost analyses healing.25,26
The authors did not conduct an independent health economic evaluation as part of this review. Wound recurrence, hospitalizations and lower extremity amputations represent major cost drivers in chronic wound care. In addition, repeat ED admissions, surgical intervention, rehabilitation, prosthetics, and long-term disability contribute to economic burden and negative psychosocial and quality of life impacts on patients and caregivers. The reductions in hospitalization (≤ 88%) and amputation (≤ 73%) observed in real-world TWO2 cohorts suggest significant potential downstream cost savings. A recent Markov model analysis suggested that TWO2 may be cost-favorable compared with standard care, with modeled estimates indicating lower total 2-year costs and improved quality-adjusted life years. These projections are based on modeling assumptions and require confirmation through prospective economic evaluations comparing TWO2 directly with negative pressure wound therapy, HBOT, and skin substitutes across longer time horizons.
Limitations
The findings of this case series were small and lacked statistical power with only 8 male patients. Literature gaps also exist regarding the specific effects of TOT on traumatic wounds. This review was limited by its single-center location.
Conclusions
This case series suggests that cTOT may be an effective adjuvant therapy in managing trauma-induced venous leg wounds and supports consideration of early implementation for expedited epithelialization. However, further studies with larger sample sizes are required.
Lower extremity venous ulcerations impact the health, well-being, and associated costs of patient care. These ulcerations are associated with comorbidities such as diabetes mellitus and chronic venous insufficiency or may be related to trauma. Often, the standard of care fails to effectively and completely heal ulcers, causing them to become stalled, chronic, and require ≥ 1 month of treatment.
Healthy skin partial pressure of oxygen (PO2) approximates 100 mm Hg, but prolonged periods of poor blood perfusion from vascular damage can cause the PO2 within a wound bed to become as low as 10 mm Hg.1 Deprivation of oxygen impairs biological processes essential for bacterial control and growth factor activity, contributing to wound chronicity.2-5 Exposure to oxygen not only upregulates growth factors essential for maintaining a well-vascularized wound core, but also aids enzymatic reactions responsible for healing the skin that are sensitive to PO2 levels.3,6,7 These physiologic processes can be maximized by raising oxygen level concentrations by means of oxygen therapy.8
Hyperbaric oxygen therapy (HBOT) uses a pressurized system to deliver concentrated oxygen that is diffused in the lungs, resulting in increased blood oxygen levels for delivery to bodily tissues. Full chamber HBOT can accelerate the wound healing process. Some disadvantages of HBOT include its high cost, the possibility of oxygen toxicity, and travel time to facilities for daily therapy sessions that last an average of 1.5 hours and may continue for ≤ 60 sessions.7,9 Thus, alternatives to HBOT have been developed, including topical oxygen therapy (TOT), which uses portable bags or chambers that deliver concentrated oxygen applied directly over ulcers, allowing oxygen to diffuse directly into the injured tissue. Combined with the standard of care and regular debridement, TOT saturates the wound base and surrounding tissues with oxygen, thereby inducing growth factors that promote angiogenesis as well as upregulation of enzymatic reactions that create a reparative environment.6
In a study conducted in pigs, Fries et al induced full-thickness wounds that were allowed to heal by secondary intention. They demonstrated that wounds treated with TOT not only healed in fewer days but also revealed a higher presence of vascular endothelial growth factor, greater density of vascular structures, and more histologically mature healing tissues when compared with control wounds exposed to room air.2
The effectiveness of TOT in ulcer healing has been previously reported. Frykberg et al performed a multicenter randomized controlled trial (RCT) comparing TOT with sham therapy to determine the efficacy of TOT in diabetic foot ulcers (DFUs) that had previously failed treatment with the standard of care. The RCT demonstrated that wounds treated with TOT had a 4.5-fold greater likelihood of complete epithelialization within 12 weeks compared with the sham group.3 In a multicenter RCT, Al-Jalodi et al found that 56% of DFUs treated with TOT remained epithelialized at 12 months compared with 27% of ulcers treated with the standard of care alone. Al Jalodi et al argued that TOT may increase the durability of DFU closure.8 In addition, a small prospective cohort study biopsied 23 DFUs treated with TOT and noted increased cytokines and growth factors, as well as increased transcutaneous oxygen measurement perfusion after only 1 week of treatment compared with wounds treated with the standard of care.9
Yellin et al reported that patients with DFU treated with TOT had reduced hospital lengths of stay and a lower amputation rate compared with patients who did not receive TOT modality.10 Another study compared conventional compression dressings with TOT in managing 132 recalcitrant venous ulcers. In that study, Nataraj et al found that 76% of ulcers treated with TOT had completely healed at 12 weeks compared with 46% of those treated with compression only.11 Furthermore, numerous systematic reviews and meta-analyses have analyzed the efficacy of TOT, concluding that this modality not only improves healing among ulcers of varying severity when compared with the standard of care but also contributes to the durability of healed ulcers and thus helps improve patient quality of life by preventing recurrence.2,12-18
Intermittent cyclical compression topical oxygen therapy (cTOT) is a modality that provides concentrated oxygen at a rate of 10 L/min. cTOT cycles twice a minute and applies noncontact compression directly to ulcerations between 10 and 50 millibars (7.5-37.5 mm Hg). In a study of 8 patients with leg ulcers, transcutaneous oxygen tension was higher after treatment with intermittent pneumatic compression (42.7 mm Hg) when compared with baseline values. The authors postulated that intermittent compression decreased interstitial fluid volume and venous stasis, both of which lead to increased cutaneous oxygenation. The data suggested that removal of carbon dioxide from tissues and enhancement of cutaneous cyclical oxygenation promoted ulcer healing.19To the best of our knowledge, there are no published studies that have evaluated the efficacy of cTOT for traumatic injuries while also considering existing comorbidities such as diabetes mellitus and venous insufficiency in veterans. The aim of this study was to demonstrate the efficacy of cTOT in the setting of traumatic wounds that failed the standard of care and were complicated by venous insufficiency and diabetes mellitus. We hypothesized that cTOT enhances healing of trauma-induced venous leg wounds in patients with diabetes mellitus, achieving full epithelialization within 12 weeks after failing the standard of care.
B, controller. Source: Advanced Oxygen Therapy Inc. Reprinted with permission.
Methods
Institutional review board approval was granted prior to commencement of this single-center retrospective review at the Veterans Affairs Illiana Healthcare System (VAIHS) in Danville, Illinois. Electronic health records between May 1, 2016, and July 31, 2021, were examined to find patients treated with cTOT using the Advanced Oxygen Therapy Inc. Topical Wound Oxygen (TWO2) system (Figure). Data collected included demographics, follow-up, and outcomes.
Inclusion criteria included patients who failed standard wound care for ≥ 4 weeks with venous insufficiency, trauma to the lower legs by means of iatrogenic injury, accidental injury, thermal injury/burn, or diabetes mellitus determined to be an active problem and a hemoglobin A1c (HbA1c) obtained within 3 months of wound treatment. The VAIHS standard of care was weekly visits to a wound care physician, physician assistant, or a nurse practitioner who performed sharp wound debridement and applied multilayer compression therapy. Patients with confirmed history of intermittent claudication, stroke, absent pedal pulses, abnormal blood pressure, deep vein thrombosis, pulmonary embolism, revascularization of the lower extremity, trauma fractures of the affected leg, phlebitis, pregnancy, coagulopathy, infection, or history of malignancy were excluded.
Patients who failed the standard of care for ≥ 4 weeks were enrolled in the cTOT program, after which they began weekly visits to an outpatient wound healing center where visits consisted of sharp wound debridement, wound measurement, and application of compressive dressing to the affected lower extremity. Following wound-healing center visits, the subjects received cTOT at home according to the manufacturer’s protocol, which consisted of ≤ 90-minute sessions, 5 to 7 times weekly. The wounds were measured from initial presentation to complete epithelialization, and the patients were followed for ≤ 27 months.
Results
Sixty-nine patients underwent cTOT between May 1, 2016, and July 31, 2021, and 8 patients with 10 wounds met the inclusion criteria. The patients had a mean age of 76 years, BMI of 27, and HbA1c of 8.0%. All wounds completely healed following cTOT. Prior to the use of cTOT, the included patients had a mean 11.3 weeks of failed healing attempts when receiving standard of care therapy. Following cTOT implementation, the mean time to healing was 8.1 weeks (Table). One wound recurred after 10 weeks in a patient with uncontrolled diabetes mellitus. One patient died of causes unrelated to the wound and was excluded from follow-up. All other wounds remained closed and healed after a mean end follow-up period of 110 weeks through June 2023.
Discussion
Traumatic wounds are commonly seen in the emergency department (ED), accounting for 5.4% of all ED visits.20-22 According to the National Hospital Ambulatory Medical Care Survey, 14.6% of 117 million ED visits in 2007 involved lower-extremity wounds, costing the health care system > $25 billion annually.23 Kulkarni et al reported that 44% of patients experienced leg ulcerations secondary to trauma.24 Traumatic wounds that lack epithelialization > 4 weeks are categorized as chronic, placing a large social and financial impact on patient health and well-being.
This case series supports the benefits of cTOT and demonstrates improved wound-closure rates with sustained healing compared with standard care alone, corroborating findings reported by the American Diabetes Association (ADA).23 The ADA cited high-quality RCTs and systematic reviews supporting the healing benefits of cTOT for chronic DFUs through the upregulation of essential growth factors.24
The current literature offers many examples of the healing benefits of TOT for arterial ulcerations. Benefits include faster healing with longer lasting reparative ulcer tissue, prevention of amputation and improved quality of life. However, there is a lack of literature on the use of cTOT for venous stasis traumatic wounds, which prompted this study. Our case series presents evidence that cTOT enhances healing of trauma-induced venous leg wounds in male veterans with diabetes mellitus within 12 weeks after failure of the standard of care. Other risk factors that were recorded but not included in our analysis included tobacco use, chronic kidney disease, chronic obstructive pulmonary disease, use of cellular-based tissue/collagen products, and neuropathy.
This case series provides evidence that cTOT can be a beneficial and cost-effective treatment. Economic considerations are derived from retrospective cohort analyses and a published decision-analytic Markov model representing modeled estimates and need to be interpreted in that context rather than as findings from prospective comparative cost analyses healing.25,26
The authors did not conduct an independent health economic evaluation as part of this review. Wound recurrence, hospitalizations and lower extremity amputations represent major cost drivers in chronic wound care. In addition, repeat ED admissions, surgical intervention, rehabilitation, prosthetics, and long-term disability contribute to economic burden and negative psychosocial and quality of life impacts on patients and caregivers. The reductions in hospitalization (≤ 88%) and amputation (≤ 73%) observed in real-world TWO2 cohorts suggest significant potential downstream cost savings. A recent Markov model analysis suggested that TWO2 may be cost-favorable compared with standard care, with modeled estimates indicating lower total 2-year costs and improved quality-adjusted life years. These projections are based on modeling assumptions and require confirmation through prospective economic evaluations comparing TWO2 directly with negative pressure wound therapy, HBOT, and skin substitutes across longer time horizons.
Limitations
The findings of this case series were small and lacked statistical power with only 8 male patients. Literature gaps also exist regarding the specific effects of TOT on traumatic wounds. This review was limited by its single-center location.
Conclusions
This case series suggests that cTOT may be an effective adjuvant therapy in managing trauma-induced venous leg wounds and supports consideration of early implementation for expedited epithelialization. However, further studies with larger sample sizes are required.
Tawfick WA, Sultan S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc Endovascular Surg. 2013:30-37. doi:10.1177/1538574412467684
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005:172-181. doi:10.1016/j.mrfmmm.2005.02.023
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TWO2 study. Diabetes Care. 2020:616-624. doi:10.2337/dc19-0476
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Al-Jalodi O, Kupcella M, Breisinger K, et al. A multicenter clinical trial evaluating the durability of diabetic foot ulcer healing in ulcers treated with topical oxygen and standard of care versus standard of care alone 1 year post healing. Int Wound J. 2022:1838-1842. doi:10.1111/iwj.13789
Carter MJ, Frykberg RG, Oropallo A, et al. Efficacy of topical wound oxygen therapy in healing chronic diabetic foot ulcers: systematic review and meta-analysis. Adv Wound Care (New Rochelle). 2023;12:177-186. doi:10.1089/wound.2022.0041
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022:657-665. doi:10.1089/wound.2021.0118
Nataraj M, Maiya AG, Karkada G, et al. Application of topical oxygen therapy in healing dynamics of diabetic foot ulcers: a systematic review. Rev Diabet Stud. 2019:74-82. doi:10.1900/RDS.2019.15.74
Thanigaimani S, Singh T, Golledge J. Topical oxygen therapy for diabetes-related foot ulcers: a systematic review and meta-analysis. Diabet Med. 2021:e14585. doi:10.1111/dme.14585
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Oropallo AR, Serena TE, Armstrong DG, et al. Molecular biomarkers of oxygen therapy in patients with diabetic foot ulcers. Biomolecules. 2021:925. doi:10.3390/biom11070925
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Kahle B, Hermanns HJ, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl Int. 2011:231-237. doi:10.3238/arztebl.2011.0231
Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on hyperbaric oxygen therapy: applications, mechanisms, and translational opportunities. Medicina (Kaunas). 2021:864. doi:10.3390/medicina57090864
Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy and micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018:363-374. doi:10.1111/iwj.12873
Chen AH, Frangos SG, Kilaru S, et al. Intermittent pneumatic compression devices: physiologic mechanisms of action. Eur J Vasc Endovasc Surg. 2001:383-392. doi:10.1053/ejvs.2001.1348
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the emergency department: position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016:30. doi:10.1186/s13017-016-0084-3
Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017:599-610. doi:10.1007/s12325-017-0478-y
Kamal S, Sehgal A, Shahi P, et al. Topical oxygen therapy in acute traumatic musculoskeletal wounds of the foot and ankle. J Wound Care. 2023:92-97. doi:10.12968/jowc.2023.32.2.92
Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012:284-290. doi:10.1007/s11999-011-1982-z
Kulkarni SR, Gohel MS, Whyman MR, et al. Significance of limb trauma as an initiating factor in chronic leg ulceration. Phlebology. 2008:130-136.
Kerr M, Wild D, Edmonds M, et al. Cost effectiveness of topical wound oxygen therapy for chronic diabetic foot ulcers. J Diabetes Complications. 2025;39:109016. doi:10.1016/j.jdiacomp.2025.109016.
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022;11:657-665. doi:10.1089/wound.2021.0118
Tawfick WA, Sultan S. Technical and clinical outcome of topical wound oxygen in comparison to conventional compression dressings in the management of refractory nonhealing venous ulcers. Vasc Endovascular Surg. 2013:30-37. doi:10.1177/1538574412467684
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005:172-181. doi:10.1016/j.mrfmmm.2005.02.023
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TWO2 study. Diabetes Care. 2020:616-624. doi:10.2337/dc19-0476
Sun XK, Li R, Yang XL, et al. Efficacy and safety of topical oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Int Wound J. 2022:2200-2209. doi:10.1111/iwj.13830
Al-Jalodi O, Kupcella M, Breisinger K, et al. A multicenter clinical trial evaluating the durability of diabetic foot ulcer healing in ulcers treated with topical oxygen and standard of care versus standard of care alone 1 year post healing. Int Wound J. 2022:1838-1842. doi:10.1111/iwj.13789
Carter MJ, Frykberg RG, Oropallo A, et al. Efficacy of topical wound oxygen therapy in healing chronic diabetic foot ulcers: systematic review and meta-analysis. Adv Wound Care (New Rochelle). 2023;12:177-186. doi:10.1089/wound.2022.0041
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022:657-665. doi:10.1089/wound.2021.0118
Nataraj M, Maiya AG, Karkada G, et al. Application of topical oxygen therapy in healing dynamics of diabetic foot ulcers: a systematic review. Rev Diabet Stud. 2019:74-82. doi:10.1900/RDS.2019.15.74
Thanigaimani S, Singh T, Golledge J. Topical oxygen therapy for diabetes-related foot ulcers: a systematic review and meta-analysis. Diabet Med. 2021:e14585. doi:10.1111/dme.14585
Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina (Kaunas). 2021:917. doi:10.3390/medicina57090917
Oropallo AR, Serena TE, Armstrong DG, et al. Molecular biomarkers of oxygen therapy in patients with diabetic foot ulcers. Biomolecules. 2021:925. doi:10.3390/biom11070925
Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020:1986-1995. doi:10.1111/iwj.13490
Kahle B, Hermanns HJ, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl Int. 2011:231-237. doi:10.3238/arztebl.2011.0231
Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on hyperbaric oxygen therapy: applications, mechanisms, and translational opportunities. Medicina (Kaunas). 2021:864. doi:10.3390/medicina57090864
Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy and micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018:363-374. doi:10.1111/iwj.12873
Chen AH, Frangos SG, Kilaru S, et al. Intermittent pneumatic compression devices: physiologic mechanisms of action. Eur J Vasc Endovasc Surg. 2001:383-392. doi:10.1053/ejvs.2001.1348
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the emergency department: position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016:30. doi:10.1186/s13017-016-0084-3
Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017:599-610. doi:10.1007/s12325-017-0478-y
Kamal S, Sehgal A, Shahi P, et al. Topical oxygen therapy in acute traumatic musculoskeletal wounds of the foot and ankle. J Wound Care. 2023:92-97. doi:10.12968/jowc.2023.32.2.92
Lambers K, Ootes D, Ring D. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin Orthop Relat Res. 2012:284-290. doi:10.1007/s11999-011-1982-z
Kulkarni SR, Gohel MS, Whyman MR, et al. Significance of limb trauma as an initiating factor in chronic leg ulceration. Phlebology. 2008:130-136.
Kerr M, Wild D, Edmonds M, et al. Cost effectiveness of topical wound oxygen therapy for chronic diabetic foot ulcers. J Diabetes Complications. 2025;39:109016. doi:10.1016/j.jdiacomp.2025.109016.
Yellin JI, Gaebler JA, Zhou FF, et al. Reduced hospitalizations and amputations in patients with diabetic foot ulcers treated with cyclical pressurized topical wound oxygen therapy: real-world outcomes. Adv Wound Care (New Rochelle). 2022;11:657-665. doi:10.1089/wound.2021.0118
Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes
Cyclical Topical Oxygen Therapy of Trauma-Induced Venous Leg Wounds in Patients With Diabetes