User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Proposed scoring system predicts renal artery stenosis in CAG patients
A proposed scoring system based in part on the extent of carotid intima-media thickness and carotid atherosclerotic plaque on carotid ultrasonography may help predict significant renal artery stenosis in patients undergoing coronary angiography, a study suggests.
Of 641 consecutive coronary angiography (CAG) patients, 60 had significant renal artery stenosis (RAS). A number of factors were found to be independent predictors of RAS, including significant coronary artery disease (odds ratio, 5.6), unilateral carotid atherosclerotic plaque (OR, 2.6), bilateral carotid atherosclerotic plaque (OR, 4.9), stage 3 or greater chronic kidney disease (OR, 4.8), use of four or more antihypertensive medications (OR, 4.8), carotid intima-media thickness (OR, 2.3), age of 67 years or older (OR, 2.3), and body mass index less than 22 kg/m2 (OR, 2.4), reported Dr. Yonggu Lee of Hanyang University Guri Hospital, Republic of Korea.
The report was published online in BMC Nephrology.
A scoring system developed based on these predictors had 83.3% sensitivity and 81.6% specificity for predicting significant renal artery stenosis, the investigators said (BMC Nephrology 2014 April 14 [doi:10.1186/1471-2369-15-60].
"The proposed model for predicting significant RAS ... may be a useful tool for deciding whether a definite diagnostic procedure is needed at the time of CAG," the investigators concluded.
The investigators reported having no disclosures.
A proposed scoring system based in part on the extent of carotid intima-media thickness and carotid atherosclerotic plaque on carotid ultrasonography may help predict significant renal artery stenosis in patients undergoing coronary angiography, a study suggests.
Of 641 consecutive coronary angiography (CAG) patients, 60 had significant renal artery stenosis (RAS). A number of factors were found to be independent predictors of RAS, including significant coronary artery disease (odds ratio, 5.6), unilateral carotid atherosclerotic plaque (OR, 2.6), bilateral carotid atherosclerotic plaque (OR, 4.9), stage 3 or greater chronic kidney disease (OR, 4.8), use of four or more antihypertensive medications (OR, 4.8), carotid intima-media thickness (OR, 2.3), age of 67 years or older (OR, 2.3), and body mass index less than 22 kg/m2 (OR, 2.4), reported Dr. Yonggu Lee of Hanyang University Guri Hospital, Republic of Korea.
The report was published online in BMC Nephrology.
A scoring system developed based on these predictors had 83.3% sensitivity and 81.6% specificity for predicting significant renal artery stenosis, the investigators said (BMC Nephrology 2014 April 14 [doi:10.1186/1471-2369-15-60].
"The proposed model for predicting significant RAS ... may be a useful tool for deciding whether a definite diagnostic procedure is needed at the time of CAG," the investigators concluded.
The investigators reported having no disclosures.
A proposed scoring system based in part on the extent of carotid intima-media thickness and carotid atherosclerotic plaque on carotid ultrasonography may help predict significant renal artery stenosis in patients undergoing coronary angiography, a study suggests.
Of 641 consecutive coronary angiography (CAG) patients, 60 had significant renal artery stenosis (RAS). A number of factors were found to be independent predictors of RAS, including significant coronary artery disease (odds ratio, 5.6), unilateral carotid atherosclerotic plaque (OR, 2.6), bilateral carotid atherosclerotic plaque (OR, 4.9), stage 3 or greater chronic kidney disease (OR, 4.8), use of four or more antihypertensive medications (OR, 4.8), carotid intima-media thickness (OR, 2.3), age of 67 years or older (OR, 2.3), and body mass index less than 22 kg/m2 (OR, 2.4), reported Dr. Yonggu Lee of Hanyang University Guri Hospital, Republic of Korea.
The report was published online in BMC Nephrology.
A scoring system developed based on these predictors had 83.3% sensitivity and 81.6% specificity for predicting significant renal artery stenosis, the investigators said (BMC Nephrology 2014 April 14 [doi:10.1186/1471-2369-15-60].
"The proposed model for predicting significant RAS ... may be a useful tool for deciding whether a definite diagnostic procedure is needed at the time of CAG," the investigators concluded.
The investigators reported having no disclosures.
FROM BMC NEPHROLOGY
Key clinical point: A model for predicting significant renal artery stenosis may be useful in deciding whether a diagnostic procedure is needed at the time of coronary angiography.
Major finding: A proposed scoring system for RAS had 83.3% sensitivity and 81.6% specificity in patients undergoing CAG.
Data source: A prospective study of 641 consecutive patients.
Disclosures: The investigators reported having no disclosures.
ED utility of pediatric febrile UTI guidelines questioned
ORLANDO – The proportion of infants and young children who had voiding cystourethrograms after an emergency department visit for an initial febrile urinary tract infection decreased by more than 50% after the 2011 American Academy of Pediatrics guidelines advised a VCUG only if indicated by sonographic findings, based on a review of cases.
However, ultrasound findings and voiding cystourethrogram (VCUG) positivity were not correlated in the series of patients studied, Dr. Andrew J. Kirsch reported at the annual meeting of the American Urological Association.
The findings raise concerns that cases of vesicoureteral reflux are being missed and call into question whether the AAP recommendation to use sonographic findings as the determinant for obtaining additional imaging should be uniformly applied after an initial febrile UTI in children aged 2 months to 2 years, said Dr. Kirsch, a pediatric urologist with Children’s Healthcare of Atlanta. Those presenting to the ED may be more ill and may be more likely to have underlying vesicoureteral reflux or an anatomic abnormality.
While most clinicians agree with the majority of action statements in the AAP guidelines, the diagnostic imaging recommendations are widely debated. Several recent studies have demonstrated a lack of correlation between renal and bladder ultrasound results and VCUG positivity. Further, the recommendation to limit VCUGs was based on studies that showed no benefit with antibiotic prophylaxis in children with vesicoureteral reflux. Recent large, randomized controlled trials, however, have shown benefits of diagnosing and treating vesicoureteral reflux, he said.
For the case review study reported by Dr. Kirsch, two cohorts were evaluated at urgent care centers and EDs in a pediatric health care system during the 6-month periods before and after the guidelines were implemented. Children with a history of vesicoureteral reflux or VCUG, prior febrile urinary tract infection, or undocumented urine culture of afebrile UTIs were excluded from the analysis.
Of 178 children aged 2 months to 2 years who were seen in the ED between January and June 2012 for initial febrile UTIs, 31% underwent VCUG. Between January and June 2011 – before the updated Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months was released – 72% of 172 children in that age group had a VCUG, Dr. Kirsch said during a press briefing at the meeting.
The earlier and later cohorts were similar. They did not differ with respect to admissions for febrile UTI; 27% and 24% of patients in the cohorts, respectively, required hospitalization. The percentage of positive VCUGs also was similar in the cohorts at 36% and 38%, respectively. The mean maximum vesicoureteral reflux grade was similar at 2.9 and 2.5, respectively.
The number of renal and bladder ultrasounds obtained decreased by 17% in 2012 as compared to 2011; ultrasounds were obtained in 58% of patients in the later cohort, compared with 76% of those in the earlier cohort.
There was no association between abnormal renal and bladder ultrasound and VCUG positivity (P = .116), he noted.
About 60% of children diagnosed with vesicoureteral reflux in both cohorts were found to have moderate to severe reflux. A trend toward detection of higher-grade vesicoureteral reflux prior to guideline publication also raises concern that higher grade reflux – which has been associated with an increased risk of recurrent febrile UTIs and renal scarring – is being missed, he said.
Whether foregoing routine VCUG following initial febrile UTI as recommended by the AAP guidelines will result in increased morbidity from undiagnosed vesicoureteral reflux, or whether the guidelines should apply to all patients in the emergency setting, requires careful reevaluation, he concluded.
Dr. Kirsch reported having no disclosures.
ORLANDO – The proportion of infants and young children who had voiding cystourethrograms after an emergency department visit for an initial febrile urinary tract infection decreased by more than 50% after the 2011 American Academy of Pediatrics guidelines advised a VCUG only if indicated by sonographic findings, based on a review of cases.
However, ultrasound findings and voiding cystourethrogram (VCUG) positivity were not correlated in the series of patients studied, Dr. Andrew J. Kirsch reported at the annual meeting of the American Urological Association.
The findings raise concerns that cases of vesicoureteral reflux are being missed and call into question whether the AAP recommendation to use sonographic findings as the determinant for obtaining additional imaging should be uniformly applied after an initial febrile UTI in children aged 2 months to 2 years, said Dr. Kirsch, a pediatric urologist with Children’s Healthcare of Atlanta. Those presenting to the ED may be more ill and may be more likely to have underlying vesicoureteral reflux or an anatomic abnormality.
While most clinicians agree with the majority of action statements in the AAP guidelines, the diagnostic imaging recommendations are widely debated. Several recent studies have demonstrated a lack of correlation between renal and bladder ultrasound results and VCUG positivity. Further, the recommendation to limit VCUGs was based on studies that showed no benefit with antibiotic prophylaxis in children with vesicoureteral reflux. Recent large, randomized controlled trials, however, have shown benefits of diagnosing and treating vesicoureteral reflux, he said.
For the case review study reported by Dr. Kirsch, two cohorts were evaluated at urgent care centers and EDs in a pediatric health care system during the 6-month periods before and after the guidelines were implemented. Children with a history of vesicoureteral reflux or VCUG, prior febrile urinary tract infection, or undocumented urine culture of afebrile UTIs were excluded from the analysis.
Of 178 children aged 2 months to 2 years who were seen in the ED between January and June 2012 for initial febrile UTIs, 31% underwent VCUG. Between January and June 2011 – before the updated Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months was released – 72% of 172 children in that age group had a VCUG, Dr. Kirsch said during a press briefing at the meeting.
The earlier and later cohorts were similar. They did not differ with respect to admissions for febrile UTI; 27% and 24% of patients in the cohorts, respectively, required hospitalization. The percentage of positive VCUGs also was similar in the cohorts at 36% and 38%, respectively. The mean maximum vesicoureteral reflux grade was similar at 2.9 and 2.5, respectively.
The number of renal and bladder ultrasounds obtained decreased by 17% in 2012 as compared to 2011; ultrasounds were obtained in 58% of patients in the later cohort, compared with 76% of those in the earlier cohort.
There was no association between abnormal renal and bladder ultrasound and VCUG positivity (P = .116), he noted.
About 60% of children diagnosed with vesicoureteral reflux in both cohorts were found to have moderate to severe reflux. A trend toward detection of higher-grade vesicoureteral reflux prior to guideline publication also raises concern that higher grade reflux – which has been associated with an increased risk of recurrent febrile UTIs and renal scarring – is being missed, he said.
Whether foregoing routine VCUG following initial febrile UTI as recommended by the AAP guidelines will result in increased morbidity from undiagnosed vesicoureteral reflux, or whether the guidelines should apply to all patients in the emergency setting, requires careful reevaluation, he concluded.
Dr. Kirsch reported having no disclosures.
ORLANDO – The proportion of infants and young children who had voiding cystourethrograms after an emergency department visit for an initial febrile urinary tract infection decreased by more than 50% after the 2011 American Academy of Pediatrics guidelines advised a VCUG only if indicated by sonographic findings, based on a review of cases.
However, ultrasound findings and voiding cystourethrogram (VCUG) positivity were not correlated in the series of patients studied, Dr. Andrew J. Kirsch reported at the annual meeting of the American Urological Association.
The findings raise concerns that cases of vesicoureteral reflux are being missed and call into question whether the AAP recommendation to use sonographic findings as the determinant for obtaining additional imaging should be uniformly applied after an initial febrile UTI in children aged 2 months to 2 years, said Dr. Kirsch, a pediatric urologist with Children’s Healthcare of Atlanta. Those presenting to the ED may be more ill and may be more likely to have underlying vesicoureteral reflux or an anatomic abnormality.
While most clinicians agree with the majority of action statements in the AAP guidelines, the diagnostic imaging recommendations are widely debated. Several recent studies have demonstrated a lack of correlation between renal and bladder ultrasound results and VCUG positivity. Further, the recommendation to limit VCUGs was based on studies that showed no benefit with antibiotic prophylaxis in children with vesicoureteral reflux. Recent large, randomized controlled trials, however, have shown benefits of diagnosing and treating vesicoureteral reflux, he said.
For the case review study reported by Dr. Kirsch, two cohorts were evaluated at urgent care centers and EDs in a pediatric health care system during the 6-month periods before and after the guidelines were implemented. Children with a history of vesicoureteral reflux or VCUG, prior febrile urinary tract infection, or undocumented urine culture of afebrile UTIs were excluded from the analysis.
Of 178 children aged 2 months to 2 years who were seen in the ED between January and June 2012 for initial febrile UTIs, 31% underwent VCUG. Between January and June 2011 – before the updated Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months was released – 72% of 172 children in that age group had a VCUG, Dr. Kirsch said during a press briefing at the meeting.
The earlier and later cohorts were similar. They did not differ with respect to admissions for febrile UTI; 27% and 24% of patients in the cohorts, respectively, required hospitalization. The percentage of positive VCUGs also was similar in the cohorts at 36% and 38%, respectively. The mean maximum vesicoureteral reflux grade was similar at 2.9 and 2.5, respectively.
The number of renal and bladder ultrasounds obtained decreased by 17% in 2012 as compared to 2011; ultrasounds were obtained in 58% of patients in the later cohort, compared with 76% of those in the earlier cohort.
There was no association between abnormal renal and bladder ultrasound and VCUG positivity (P = .116), he noted.
About 60% of children diagnosed with vesicoureteral reflux in both cohorts were found to have moderate to severe reflux. A trend toward detection of higher-grade vesicoureteral reflux prior to guideline publication also raises concern that higher grade reflux – which has been associated with an increased risk of recurrent febrile UTIs and renal scarring – is being missed, he said.
Whether foregoing routine VCUG following initial febrile UTI as recommended by the AAP guidelines will result in increased morbidity from undiagnosed vesicoureteral reflux, or whether the guidelines should apply to all patients in the emergency setting, requires careful reevaluation, he concluded.
Dr. Kirsch reported having no disclosures.
AT THE AUA ANNUAL MEETING
Major finding: VCUGs obtained declined by more than 50%.
Data source: A study comparing ED practices in 350 infants and children before and after AAP guideline implementation.
Disclosures: Dr. Kirsch reported having no disclosures.
Vascular reconstruction may have a role in pancreatic adenocarcinoma resection
BOSTON – In skilled hands, various vascular reconstructive methods used during pancreatic resections for adenocarcinoma result in early survival rates that are comparable to those in patients who undergo resection without vascular reconstruction, according to a retrospective review of cases.
This is important because up to 25% of cases in high-volume centers are borderline for resection using pancreaticoduodenectomy (Whipple procedure) because of vascular involvement. Resection is the only curative option for the disease, Dr. Michael D. Sgroi said at a meeting hosted by the Society for Vascular Surgery.
Of 270 Whipple procedures and total pancreatectomy procedures performed from January 2003 to February 2013 at a single institution, 147 were for pancreatic adenocarcinoma that involved the surrounding vasculature (T3 lesions); 60 of these involved vascular reconstructions (including 49 venous and 11 arterial reconstructions) and 87 were Whipple procedures without reconstruction, The venous reconstructions included 37 primary repairs, four reconstructions with CryoVein, three repairs using an autologous vein patch, three autologous saphenous reconstructions, and two portacaval shunts. The arterial reconstructions included seven hepatic artery reconstructions, and four were superior mesenteric artery reconstructions.
All were performed by the vascular surgery service, said Dr. Sgroi of the department of surgery, University of California, Irvine Medical Center, Orange.
Overall survival was greater than 18 months in the vascular reconstruction group, with no statistically significant difference seen between the various types of procedures or compared with the Whipple-only group. One perioperative death occurred (1.7%), and survival at 1 year for all reconstructions was 70.3% – a rate similar to the 72.6% survival among patients with T3 lesions who did not undergo vascular reconstruction.
Survival in the two groups remained similar at 3 years, but a survival advantage among those in the Whipple-only group emerged by year 4 and was statistically significant by year 5, Dr. Sgroi said.
No factors were found to be significantly associated with outcome, but there was a trend toward significance for positive lymph nodes and positive margins as predictors of survival. Positive margins were present in 22% of patients in the vascular reconstruction group, compared with only 11% of those in the Whipple-only group, he noted.
"Pancreatic adenocarcinoma is one of the most deadly neoplasms, with 1- and 5-year survival rates for all stages being 25% and 5%, respectively," he said, noting that resection is associated with high rates of morbidity.
Currently the only curative option for this disease is a margin-negative resection, but because most cases are not detected until they are in later stages, only about 20% of patients undergo resection, he said.
"As the morbidity and mortality rates have declined postoperatively following Whipple operations, the National Comprehensive Cancer Network guidelines have also changed to now consider borderline resectable or stage 2 tumors for resection. These are tumors that have portal vein, superior mesenteric vein, or confluence involvement as well as arterial involvement of less than 180 degrees of the common hepatic or right hepatic artery," he explained, adding that "in general, superior mesenteric artery or celiac access involvement is a contraindication to surgery, and these cases now account for about 25% of all Whipples performed in high-volume institutions."
The various approaches to reconstruction that can be performed have been used with acceptable patency rates and outcomes, and multiple single-institution reviews have demonstrated that both venous and arterial resections performed concomitantly with Whipple procedures have equivalent morbidity and mortality rates to Whipple performed without reconstruction.
"A flaw of these studies has always been that their sample size is small, diminishing the power of the study," Dr. Sgroi noted.
Further complicating the issue are two recent manuscripts demonstrating significantly increased morbidity and mortality with vascular reconstruction, while a review of the National Surgical Quality Improvement Program database showed that when vascular surgeons are involved, outcomes are comparable with and without reconstruction – with the exception of increased blood loss and time in the operating room with vascular reconstruction.
The findings of the current study support the latter finding.
Notably, with the advances in chemotherapy agents it is now protocol that all patients at the University of California, Irvine receive neoadjuvant chemotherapy, and survival was improved in those who received both vascular reconstruction and neoadjuvant chemotherapy, compared with those who received vascular reconstruction without neoadjuvant chemotherapy.
"We believe that experience matters with this operation and that there is a learning curve," he said.
An example involves the need for packed red blood cells. The average number of units of packed red blood cells given with each case declined over time, and now less than one unit is used per case, he noted.
"Pancreatic adenocarcinoma is a dismal disease with poor long-term survival. Performing a Whipple on T3 lesions with vascular invasion will allow for an increased amount of surgical resections, and it is possible to achieve equivalent survival outcomes, compared with patients who receive a Whipple only," he said, adding that further study is needed to determine if any of the multiple vascular reconstruction options is superior to the others.
"It is our recommendation that a multidisciplinary team with surgeons experienced with vascular reconstruction perform these operations, and that, if possible, these patients be referred to a high-volume institution for the best outcome," he concluded.
Dr. Sgroi reported having no disclosures.
BOSTON – In skilled hands, various vascular reconstructive methods used during pancreatic resections for adenocarcinoma result in early survival rates that are comparable to those in patients who undergo resection without vascular reconstruction, according to a retrospective review of cases.
This is important because up to 25% of cases in high-volume centers are borderline for resection using pancreaticoduodenectomy (Whipple procedure) because of vascular involvement. Resection is the only curative option for the disease, Dr. Michael D. Sgroi said at a meeting hosted by the Society for Vascular Surgery.
Of 270 Whipple procedures and total pancreatectomy procedures performed from January 2003 to February 2013 at a single institution, 147 were for pancreatic adenocarcinoma that involved the surrounding vasculature (T3 lesions); 60 of these involved vascular reconstructions (including 49 venous and 11 arterial reconstructions) and 87 were Whipple procedures without reconstruction, The venous reconstructions included 37 primary repairs, four reconstructions with CryoVein, three repairs using an autologous vein patch, three autologous saphenous reconstructions, and two portacaval shunts. The arterial reconstructions included seven hepatic artery reconstructions, and four were superior mesenteric artery reconstructions.
All were performed by the vascular surgery service, said Dr. Sgroi of the department of surgery, University of California, Irvine Medical Center, Orange.
Overall survival was greater than 18 months in the vascular reconstruction group, with no statistically significant difference seen between the various types of procedures or compared with the Whipple-only group. One perioperative death occurred (1.7%), and survival at 1 year for all reconstructions was 70.3% – a rate similar to the 72.6% survival among patients with T3 lesions who did not undergo vascular reconstruction.
Survival in the two groups remained similar at 3 years, but a survival advantage among those in the Whipple-only group emerged by year 4 and was statistically significant by year 5, Dr. Sgroi said.
No factors were found to be significantly associated with outcome, but there was a trend toward significance for positive lymph nodes and positive margins as predictors of survival. Positive margins were present in 22% of patients in the vascular reconstruction group, compared with only 11% of those in the Whipple-only group, he noted.
"Pancreatic adenocarcinoma is one of the most deadly neoplasms, with 1- and 5-year survival rates for all stages being 25% and 5%, respectively," he said, noting that resection is associated with high rates of morbidity.
Currently the only curative option for this disease is a margin-negative resection, but because most cases are not detected until they are in later stages, only about 20% of patients undergo resection, he said.
"As the morbidity and mortality rates have declined postoperatively following Whipple operations, the National Comprehensive Cancer Network guidelines have also changed to now consider borderline resectable or stage 2 tumors for resection. These are tumors that have portal vein, superior mesenteric vein, or confluence involvement as well as arterial involvement of less than 180 degrees of the common hepatic or right hepatic artery," he explained, adding that "in general, superior mesenteric artery or celiac access involvement is a contraindication to surgery, and these cases now account for about 25% of all Whipples performed in high-volume institutions."
The various approaches to reconstruction that can be performed have been used with acceptable patency rates and outcomes, and multiple single-institution reviews have demonstrated that both venous and arterial resections performed concomitantly with Whipple procedures have equivalent morbidity and mortality rates to Whipple performed without reconstruction.
"A flaw of these studies has always been that their sample size is small, diminishing the power of the study," Dr. Sgroi noted.
Further complicating the issue are two recent manuscripts demonstrating significantly increased morbidity and mortality with vascular reconstruction, while a review of the National Surgical Quality Improvement Program database showed that when vascular surgeons are involved, outcomes are comparable with and without reconstruction – with the exception of increased blood loss and time in the operating room with vascular reconstruction.
The findings of the current study support the latter finding.
Notably, with the advances in chemotherapy agents it is now protocol that all patients at the University of California, Irvine receive neoadjuvant chemotherapy, and survival was improved in those who received both vascular reconstruction and neoadjuvant chemotherapy, compared with those who received vascular reconstruction without neoadjuvant chemotherapy.
"We believe that experience matters with this operation and that there is a learning curve," he said.
An example involves the need for packed red blood cells. The average number of units of packed red blood cells given with each case declined over time, and now less than one unit is used per case, he noted.
"Pancreatic adenocarcinoma is a dismal disease with poor long-term survival. Performing a Whipple on T3 lesions with vascular invasion will allow for an increased amount of surgical resections, and it is possible to achieve equivalent survival outcomes, compared with patients who receive a Whipple only," he said, adding that further study is needed to determine if any of the multiple vascular reconstruction options is superior to the others.
"It is our recommendation that a multidisciplinary team with surgeons experienced with vascular reconstruction perform these operations, and that, if possible, these patients be referred to a high-volume institution for the best outcome," he concluded.
Dr. Sgroi reported having no disclosures.
BOSTON – In skilled hands, various vascular reconstructive methods used during pancreatic resections for adenocarcinoma result in early survival rates that are comparable to those in patients who undergo resection without vascular reconstruction, according to a retrospective review of cases.
This is important because up to 25% of cases in high-volume centers are borderline for resection using pancreaticoduodenectomy (Whipple procedure) because of vascular involvement. Resection is the only curative option for the disease, Dr. Michael D. Sgroi said at a meeting hosted by the Society for Vascular Surgery.
Of 270 Whipple procedures and total pancreatectomy procedures performed from January 2003 to February 2013 at a single institution, 147 were for pancreatic adenocarcinoma that involved the surrounding vasculature (T3 lesions); 60 of these involved vascular reconstructions (including 49 venous and 11 arterial reconstructions) and 87 were Whipple procedures without reconstruction, The venous reconstructions included 37 primary repairs, four reconstructions with CryoVein, three repairs using an autologous vein patch, three autologous saphenous reconstructions, and two portacaval shunts. The arterial reconstructions included seven hepatic artery reconstructions, and four were superior mesenteric artery reconstructions.
All were performed by the vascular surgery service, said Dr. Sgroi of the department of surgery, University of California, Irvine Medical Center, Orange.
Overall survival was greater than 18 months in the vascular reconstruction group, with no statistically significant difference seen between the various types of procedures or compared with the Whipple-only group. One perioperative death occurred (1.7%), and survival at 1 year for all reconstructions was 70.3% – a rate similar to the 72.6% survival among patients with T3 lesions who did not undergo vascular reconstruction.
Survival in the two groups remained similar at 3 years, but a survival advantage among those in the Whipple-only group emerged by year 4 and was statistically significant by year 5, Dr. Sgroi said.
No factors were found to be significantly associated with outcome, but there was a trend toward significance for positive lymph nodes and positive margins as predictors of survival. Positive margins were present in 22% of patients in the vascular reconstruction group, compared with only 11% of those in the Whipple-only group, he noted.
"Pancreatic adenocarcinoma is one of the most deadly neoplasms, with 1- and 5-year survival rates for all stages being 25% and 5%, respectively," he said, noting that resection is associated with high rates of morbidity.
Currently the only curative option for this disease is a margin-negative resection, but because most cases are not detected until they are in later stages, only about 20% of patients undergo resection, he said.
"As the morbidity and mortality rates have declined postoperatively following Whipple operations, the National Comprehensive Cancer Network guidelines have also changed to now consider borderline resectable or stage 2 tumors for resection. These are tumors that have portal vein, superior mesenteric vein, or confluence involvement as well as arterial involvement of less than 180 degrees of the common hepatic or right hepatic artery," he explained, adding that "in general, superior mesenteric artery or celiac access involvement is a contraindication to surgery, and these cases now account for about 25% of all Whipples performed in high-volume institutions."
The various approaches to reconstruction that can be performed have been used with acceptable patency rates and outcomes, and multiple single-institution reviews have demonstrated that both venous and arterial resections performed concomitantly with Whipple procedures have equivalent morbidity and mortality rates to Whipple performed without reconstruction.
"A flaw of these studies has always been that their sample size is small, diminishing the power of the study," Dr. Sgroi noted.
Further complicating the issue are two recent manuscripts demonstrating significantly increased morbidity and mortality with vascular reconstruction, while a review of the National Surgical Quality Improvement Program database showed that when vascular surgeons are involved, outcomes are comparable with and without reconstruction – with the exception of increased blood loss and time in the operating room with vascular reconstruction.
The findings of the current study support the latter finding.
Notably, with the advances in chemotherapy agents it is now protocol that all patients at the University of California, Irvine receive neoadjuvant chemotherapy, and survival was improved in those who received both vascular reconstruction and neoadjuvant chemotherapy, compared with those who received vascular reconstruction without neoadjuvant chemotherapy.
"We believe that experience matters with this operation and that there is a learning curve," he said.
An example involves the need for packed red blood cells. The average number of units of packed red blood cells given with each case declined over time, and now less than one unit is used per case, he noted.
"Pancreatic adenocarcinoma is a dismal disease with poor long-term survival. Performing a Whipple on T3 lesions with vascular invasion will allow for an increased amount of surgical resections, and it is possible to achieve equivalent survival outcomes, compared with patients who receive a Whipple only," he said, adding that further study is needed to determine if any of the multiple vascular reconstruction options is superior to the others.
"It is our recommendation that a multidisciplinary team with surgeons experienced with vascular reconstruction perform these operations, and that, if possible, these patients be referred to a high-volume institution for the best outcome," he concluded.
Dr. Sgroi reported having no disclosures.
AT THE 2014 VASCULAR ANNUAL MEETING
Key clinical point: Performing a Whipple on borderline T3 lesions with vascular invasion may allow for an increased amount of surgical resections.
Major finding: One-year survival was 70.3% with Whipple plus reconstruction and 72.6% with a Whipple-only procedure, but a survival advantage among those in the Whipple-only group emerged by year 4 and was statistically significant by year 5.
Data source: A retrospective review of 147 cases.
Disclosures: Dr. Sgroi reported having no disclosures.
Adding rapid trichomonas test to the sexually transmitted infection panel boosts rapid treatment
ATLANTA – Adding a rapid Trichomonas vaginalis test to the adolescent sexually transmitted infection laboratory regimen facilitated on-site diagnosis and treatment at an urban medical center emergency department.
The OSOM rapid trichomonas test provided point of care testing results in 10 minutes, with a sensitivity of 83% and specificity of 99%, Dr. Heather Territo reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention. The prevalence of Trichomonas vaginalis approaches 25% in inner-city adolescents. Prior studies have demonstrated an association between Trichomonas vaginalis and cervical neoplasia, enhanced HIV transmission, and pregnancy complications.

After routine Trichomonas vaginalis testing was implemented at the Women’s and Children’s Hospital of Buffalo, N.Y., in November 2011, 212 females aged 13-20 years were tested in the following year; 13.6% tested positive by rapid test and 15.5% by nucleic acid amplification test (NAAT). In the year before routine testing was implemented, 31 of 234 patients were tested, based on a retrospective chart review. Treatment was administered to 24% and to 7% of patients during the respective study periods, said Dr. Territo of the hospital’s division of emergency medicine.
Additionally, two positive results were found in 20 males tested.
In the emergency department, Trichomonas vaginalis is often diagnosed on the basis of clinical findings; the positive predictive value of this approach is less than 50%. Direct microscopy of vaginal secretions has a sensitivity of about 60%-70%.
The rapid test and the NAAT test results were concordant in 178 of 188 cases (94.6%). Ten of the 33 positive NAAT tests (30%) were negative on the rapid test.
Dr. Territo reported having no relevant financial disclosures.
ATLANTA – Adding a rapid Trichomonas vaginalis test to the adolescent sexually transmitted infection laboratory regimen facilitated on-site diagnosis and treatment at an urban medical center emergency department.
The OSOM rapid trichomonas test provided point of care testing results in 10 minutes, with a sensitivity of 83% and specificity of 99%, Dr. Heather Territo reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention. The prevalence of Trichomonas vaginalis approaches 25% in inner-city adolescents. Prior studies have demonstrated an association between Trichomonas vaginalis and cervical neoplasia, enhanced HIV transmission, and pregnancy complications.
After routine Trichomonas vaginalis testing was implemented at the Women’s and Children’s Hospital of Buffalo, N.Y., in November 2011, 212 females aged 13-20 years were tested in the following year; 13.6% tested positive by rapid test and 15.5% by nucleic acid amplification test (NAAT). In the year before routine testing was implemented, 31 of 234 patients were tested, based on a retrospective chart review. Treatment was administered to 24% and to 7% of patients during the respective study periods, said Dr. Territo of the hospital’s division of emergency medicine.
Additionally, two positive results were found in 20 males tested.
In the emergency department, Trichomonas vaginalis is often diagnosed on the basis of clinical findings; the positive predictive value of this approach is less than 50%. Direct microscopy of vaginal secretions has a sensitivity of about 60%-70%.
The rapid test and the NAAT test results were concordant in 178 of 188 cases (94.6%). Ten of the 33 positive NAAT tests (30%) were negative on the rapid test.
Dr. Territo reported having no relevant financial disclosures.
ATLANTA – Adding a rapid Trichomonas vaginalis test to the adolescent sexually transmitted infection laboratory regimen facilitated on-site diagnosis and treatment at an urban medical center emergency department.
The OSOM rapid trichomonas test provided point of care testing results in 10 minutes, with a sensitivity of 83% and specificity of 99%, Dr. Heather Territo reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention. The prevalence of Trichomonas vaginalis approaches 25% in inner-city adolescents. Prior studies have demonstrated an association between Trichomonas vaginalis and cervical neoplasia, enhanced HIV transmission, and pregnancy complications.
After routine Trichomonas vaginalis testing was implemented at the Women’s and Children’s Hospital of Buffalo, N.Y., in November 2011, 212 females aged 13-20 years were tested in the following year; 13.6% tested positive by rapid test and 15.5% by nucleic acid amplification test (NAAT). In the year before routine testing was implemented, 31 of 234 patients were tested, based on a retrospective chart review. Treatment was administered to 24% and to 7% of patients during the respective study periods, said Dr. Territo of the hospital’s division of emergency medicine.
Additionally, two positive results were found in 20 males tested.
In the emergency department, Trichomonas vaginalis is often diagnosed on the basis of clinical findings; the positive predictive value of this approach is less than 50%. Direct microscopy of vaginal secretions has a sensitivity of about 60%-70%.
The rapid test and the NAAT test results were concordant in 178 of 188 cases (94.6%). Ten of the 33 positive NAAT tests (30%) were negative on the rapid test.
Dr. Territo reported having no relevant financial disclosures.
AT THE 2014 STD PREVENTION CONFERENCE
Key clinical point: A positive rapid trichomonas vaginalis test allows immediate treatment in the ED.
Major finding: Treatment was administered to 24% vs. 7% of patients before and after implementing routine testing.
Data source: A retrospective review of 234 patients, and a prospective evaluation of 212 patients.
Disclosures: Dr. Territo reported having no disclosures.
Flaxseeds may protect against urinary incontinence in women
ORLANDO – Lignan-type phytoestrogens, but not isoflavone-type phytoestrogens, were associated with a decreased risk for incontinence symptoms in women, based on findings from a large prospective population-based cohort study.
Lignan-type phytoestrogens are found in a wide variety of plant-based foods including flaxseeds, sesame seeds, legumes, whole grains, fruits, and vegetables. Isoflavone-type phytoestrogens are found primarily in soybeans and soy-based products.
The study is the first to demonstrate an association between urinary phytoestrogen levels and urinary symptoms, according to the study’s author, Dr. Evgeniy I. Kreydin of Massachusetts General Hospital, Boston. Prospective studies are warranted to investigate the mechanism for this relationship, he added.
Increasing concentrations of the lignan phytoestrogens enterolactone and enterodiol were associated with significantly decreased likelihood of urge incontinence, bother from incontinence, and effect of urinary incontinence on daily living in 4,104 women who participated in the NHANES (National Health and Nutrition Examination Survey) between 2000 and 2010. Increasing concentrations of enterolactone were also associated with significantly decreased likelihood of "other incontinence," Dr. Kreydin reported during an "outstanding posters" session at the annual meeting of the American Urological Association.
Odds ratios for urinary symptoms per unit change in urinary enterodiol and enterolactone concentrations, respectively, were 0.43, 0.49, 0.32, and 0.14, and 0.47, 0.32, 0.30. The odds ratio per unit change was 0.24 for urge incontinence, other incontinence, incontinence bother, and incontinence effect on daily activities, Dr. Kreydin said.
Alternatively, none of the isoflavone-type phytoestrogens was associated with decreased urinary symptoms in this study. In fact, one isoflavone-type phytoestrogen – genistein – was associated with an increased likelihood of incontinence bother (odds ratio, 2.45).
Study subjects completed a urinary function and quality of life questionnaire and underwent measurement of urinary phytoestrogen levels. Urinary symptoms were assessed after adjusting for age, race, smoking status, body mass index, diabetes, parity, and menopausal status – factors known to affect lower urinary tract symptoms in women.
Dr. Kreydin reported having no relevant financial disclosures.
ORLANDO – Lignan-type phytoestrogens, but not isoflavone-type phytoestrogens, were associated with a decreased risk for incontinence symptoms in women, based on findings from a large prospective population-based cohort study.
Lignan-type phytoestrogens are found in a wide variety of plant-based foods including flaxseeds, sesame seeds, legumes, whole grains, fruits, and vegetables. Isoflavone-type phytoestrogens are found primarily in soybeans and soy-based products.
The study is the first to demonstrate an association between urinary phytoestrogen levels and urinary symptoms, according to the study’s author, Dr. Evgeniy I. Kreydin of Massachusetts General Hospital, Boston. Prospective studies are warranted to investigate the mechanism for this relationship, he added.
Increasing concentrations of the lignan phytoestrogens enterolactone and enterodiol were associated with significantly decreased likelihood of urge incontinence, bother from incontinence, and effect of urinary incontinence on daily living in 4,104 women who participated in the NHANES (National Health and Nutrition Examination Survey) between 2000 and 2010. Increasing concentrations of enterolactone were also associated with significantly decreased likelihood of "other incontinence," Dr. Kreydin reported during an "outstanding posters" session at the annual meeting of the American Urological Association.
Odds ratios for urinary symptoms per unit change in urinary enterodiol and enterolactone concentrations, respectively, were 0.43, 0.49, 0.32, and 0.14, and 0.47, 0.32, 0.30. The odds ratio per unit change was 0.24 for urge incontinence, other incontinence, incontinence bother, and incontinence effect on daily activities, Dr. Kreydin said.
Alternatively, none of the isoflavone-type phytoestrogens was associated with decreased urinary symptoms in this study. In fact, one isoflavone-type phytoestrogen – genistein – was associated with an increased likelihood of incontinence bother (odds ratio, 2.45).
Study subjects completed a urinary function and quality of life questionnaire and underwent measurement of urinary phytoestrogen levels. Urinary symptoms were assessed after adjusting for age, race, smoking status, body mass index, diabetes, parity, and menopausal status – factors known to affect lower urinary tract symptoms in women.
Dr. Kreydin reported having no relevant financial disclosures.
ORLANDO – Lignan-type phytoestrogens, but not isoflavone-type phytoestrogens, were associated with a decreased risk for incontinence symptoms in women, based on findings from a large prospective population-based cohort study.
Lignan-type phytoestrogens are found in a wide variety of plant-based foods including flaxseeds, sesame seeds, legumes, whole grains, fruits, and vegetables. Isoflavone-type phytoestrogens are found primarily in soybeans and soy-based products.
The study is the first to demonstrate an association between urinary phytoestrogen levels and urinary symptoms, according to the study’s author, Dr. Evgeniy I. Kreydin of Massachusetts General Hospital, Boston. Prospective studies are warranted to investigate the mechanism for this relationship, he added.
Increasing concentrations of the lignan phytoestrogens enterolactone and enterodiol were associated with significantly decreased likelihood of urge incontinence, bother from incontinence, and effect of urinary incontinence on daily living in 4,104 women who participated in the NHANES (National Health and Nutrition Examination Survey) between 2000 and 2010. Increasing concentrations of enterolactone were also associated with significantly decreased likelihood of "other incontinence," Dr. Kreydin reported during an "outstanding posters" session at the annual meeting of the American Urological Association.
Odds ratios for urinary symptoms per unit change in urinary enterodiol and enterolactone concentrations, respectively, were 0.43, 0.49, 0.32, and 0.14, and 0.47, 0.32, 0.30. The odds ratio per unit change was 0.24 for urge incontinence, other incontinence, incontinence bother, and incontinence effect on daily activities, Dr. Kreydin said.
Alternatively, none of the isoflavone-type phytoestrogens was associated with decreased urinary symptoms in this study. In fact, one isoflavone-type phytoestrogen – genistein – was associated with an increased likelihood of incontinence bother (odds ratio, 2.45).
Study subjects completed a urinary function and quality of life questionnaire and underwent measurement of urinary phytoestrogen levels. Urinary symptoms were assessed after adjusting for age, race, smoking status, body mass index, diabetes, parity, and menopausal status – factors known to affect lower urinary tract symptoms in women.
Dr. Kreydin reported having no relevant financial disclosures.
AT AUA ANNUAL MEETING
Key clinical finding: A lignan-rich diet might protect women against urinary incontinence.
Major finding: Odds ratios for urinary symptoms per unit change in urinary enterodiol and enterolactone concentrations, respectively: 0.43, 0.49, 0.32, and 0.14, and 0.47, 0.32, 0.30, and 0.24 for urge incontinence, other incontinence, incontinence bother, and incontinence effect on daily activities.
Data source: An analysis of data from 4,104 NHANES participants.
Disclosures: Dr. Kreydin reported having no disclosures.
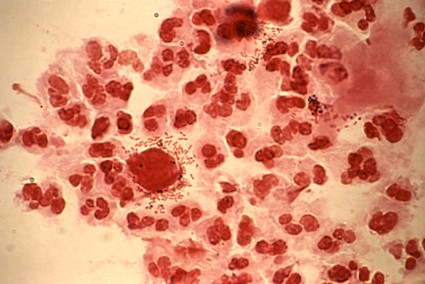
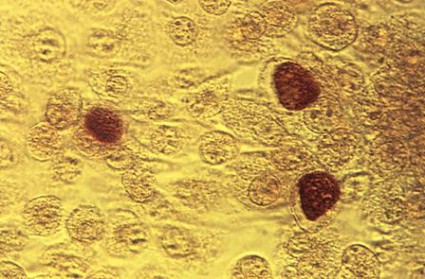
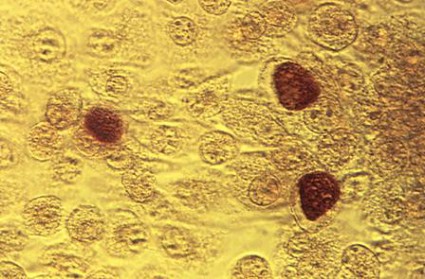
Chlamydia Prevalence is High, Many Infections Go Undiagnosed
ATLANTA – An estimated 1 in 15 sexually active adolescent girls has a chlamydial infection, and many of these infections go undiagnosed, according to an analysis of National Health and Nutrition Examination Survey data.
According to 2007-2012 NHANES data, the overall prevalence of chlamydia among sexually active adolescents and adults aged 14-39 years is 1.7%, suggesting that there are 1.8 million infections nationally, Elizabeth Torrone, Ph.D., reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.

However, only 1.4 million infections are reported annually, according to information from the CDC, suggests that approximately 400,000 infections go undetected each year.
Adolescent girls – and particularly adolescent non-Hispanic black girls – are at highest risk, according to Dr. Torrone.
The estimated overall prevalence among adolescent girls aged 14-19 years in this study was 6.4%. The estimated prevalence among white girls in this age group was 3.2%, and among black girls in this age group it was 18.6%, reported Dr. Torrone of the division of STD prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention at the CDC, Atlanta.
The overall prevalence was 1.4% among males, 2.0% among females, 2.4% among persons aged 14-19 years, 2.9% among those aged 20-24 years, 1.1% among those aged 25-39 years, 2.3% among Mexican Americans, 5.2% among non-Hispanic blacks, and 0.8% among whites.
Having multiple sex partners in the past year was associated with increased prevalence: 3.2% for those with two or more partners, compared with 1.4% among those with one or no partner.
NHANES respondents included in this analysis were 8,330 adolescents and adults aged 14-39 years between 2007 and 2012 who were tested for C. trachomatis using the Gen-Probe Aptima test. Prevalence estimates were based on demographics and self-reported sexual activity measured through audio, computer-assessed self-interviews.
Estimates were weighted to be nationally representative and to account for oversampling and nonresponse, and the number of infections in the population was estimated by multiplying census estimates by weighted prevalence, Dr. Torrone explained.
Chlamydia is the most commonly reported infection in the United States, and annual screening is currently recommended for all sexually active females under age 25 years, she noted.
Since the findings of this study likely represent an underestimate of the true burden of disease because the estimates do not account for nongenital infection and infections in nonsampled populations where prevalence may be higher (such as incarcerated individuals), they highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women and underscore the importance of adhering to the screening recommendations.
"Health care providers should screen all sexually active young females annually and ensure that all sex partners of patients diagnosed with chlamydia are treated appropriately," Dr. Torrone concluded.
Dr. Torrone reported having no disclosures.
ATLANTA – An estimated 1 in 15 sexually active adolescent girls has a chlamydial infection, and many of these infections go undiagnosed, according to an analysis of National Health and Nutrition Examination Survey data.
According to 2007-2012 NHANES data, the overall prevalence of chlamydia among sexually active adolescents and adults aged 14-39 years is 1.7%, suggesting that there are 1.8 million infections nationally, Elizabeth Torrone, Ph.D., reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
However, only 1.4 million infections are reported annually, according to information from the CDC, suggests that approximately 400,000 infections go undetected each year.
Adolescent girls – and particularly adolescent non-Hispanic black girls – are at highest risk, according to Dr. Torrone.
The estimated overall prevalence among adolescent girls aged 14-19 years in this study was 6.4%. The estimated prevalence among white girls in this age group was 3.2%, and among black girls in this age group it was 18.6%, reported Dr. Torrone of the division of STD prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention at the CDC, Atlanta.
The overall prevalence was 1.4% among males, 2.0% among females, 2.4% among persons aged 14-19 years, 2.9% among those aged 20-24 years, 1.1% among those aged 25-39 years, 2.3% among Mexican Americans, 5.2% among non-Hispanic blacks, and 0.8% among whites.
Having multiple sex partners in the past year was associated with increased prevalence: 3.2% for those with two or more partners, compared with 1.4% among those with one or no partner.
NHANES respondents included in this analysis were 8,330 adolescents and adults aged 14-39 years between 2007 and 2012 who were tested for C. trachomatis using the Gen-Probe Aptima test. Prevalence estimates were based on demographics and self-reported sexual activity measured through audio, computer-assessed self-interviews.
Estimates were weighted to be nationally representative and to account for oversampling and nonresponse, and the number of infections in the population was estimated by multiplying census estimates by weighted prevalence, Dr. Torrone explained.
Chlamydia is the most commonly reported infection in the United States, and annual screening is currently recommended for all sexually active females under age 25 years, she noted.
Since the findings of this study likely represent an underestimate of the true burden of disease because the estimates do not account for nongenital infection and infections in nonsampled populations where prevalence may be higher (such as incarcerated individuals), they highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women and underscore the importance of adhering to the screening recommendations.
"Health care providers should screen all sexually active young females annually and ensure that all sex partners of patients diagnosed with chlamydia are treated appropriately," Dr. Torrone concluded.
Dr. Torrone reported having no disclosures.
ATLANTA – An estimated 1 in 15 sexually active adolescent girls has a chlamydial infection, and many of these infections go undiagnosed, according to an analysis of National Health and Nutrition Examination Survey data.
According to 2007-2012 NHANES data, the overall prevalence of chlamydia among sexually active adolescents and adults aged 14-39 years is 1.7%, suggesting that there are 1.8 million infections nationally, Elizabeth Torrone, Ph.D., reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
However, only 1.4 million infections are reported annually, according to information from the CDC, suggests that approximately 400,000 infections go undetected each year.
Adolescent girls – and particularly adolescent non-Hispanic black girls – are at highest risk, according to Dr. Torrone.
The estimated overall prevalence among adolescent girls aged 14-19 years in this study was 6.4%. The estimated prevalence among white girls in this age group was 3.2%, and among black girls in this age group it was 18.6%, reported Dr. Torrone of the division of STD prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention at the CDC, Atlanta.
The overall prevalence was 1.4% among males, 2.0% among females, 2.4% among persons aged 14-19 years, 2.9% among those aged 20-24 years, 1.1% among those aged 25-39 years, 2.3% among Mexican Americans, 5.2% among non-Hispanic blacks, and 0.8% among whites.
Having multiple sex partners in the past year was associated with increased prevalence: 3.2% for those with two or more partners, compared with 1.4% among those with one or no partner.
NHANES respondents included in this analysis were 8,330 adolescents and adults aged 14-39 years between 2007 and 2012 who were tested for C. trachomatis using the Gen-Probe Aptima test. Prevalence estimates were based on demographics and self-reported sexual activity measured through audio, computer-assessed self-interviews.
Estimates were weighted to be nationally representative and to account for oversampling and nonresponse, and the number of infections in the population was estimated by multiplying census estimates by weighted prevalence, Dr. Torrone explained.
Chlamydia is the most commonly reported infection in the United States, and annual screening is currently recommended for all sexually active females under age 25 years, she noted.
Since the findings of this study likely represent an underestimate of the true burden of disease because the estimates do not account for nongenital infection and infections in nonsampled populations where prevalence may be higher (such as incarcerated individuals), they highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women and underscore the importance of adhering to the screening recommendations.
"Health care providers should screen all sexually active young females annually and ensure that all sex partners of patients diagnosed with chlamydia are treated appropriately," Dr. Torrone concluded.
Dr. Torrone reported having no disclosures.
AT THE 2014 STD PREVENTION CONFERENCE
Chlamydia prevalence is high, many infections go undiagnosed
ATLANTA – An estimated 1 in 15 sexually active adolescent girls has a chlamydial infection, and many of these infections go undiagnosed, according to an analysis of National Health and Nutrition Examination Survey data.
According to 2007-2012 NHANES data, the overall prevalence of chlamydia among sexually active adolescents and adults aged 14-39 years is 1.7%, suggesting that there are 1.8 million infections nationally, Elizabeth Torrone, Ph.D., reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
However, only 1.4 million infections are reported annually, according to information from the CDC, suggests that approximately 400,000 infections go undetected each year.
Adolescent girls – and particularly adolescent non-Hispanic black girls – are at highest risk, according to Dr. Torrone.
The estimated overall prevalence among adolescent girls aged 14-19 years in this study was 6.4%. The estimated prevalence among white girls in this age group was 3.2%, and among black girls in this age group it was 18.6%, reported Dr. Torrone of the division of STD prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention at the CDC, Atlanta.
The overall prevalence was 1.4% among males, 2.0% among females, 2.4% among persons aged 14-19 years, 2.9% among those aged 20-24 years, 1.1% among those aged 25-39 years, 2.3% among Mexican Americans, 5.2% among non-Hispanic blacks, and 0.8% among whites.
Having multiple sex partners in the past year was associated with increased prevalence: 3.2% for those with two or more partners, compared with 1.4% among those with one or no partner.
NHANES respondents included in this analysis were 8,330 adolescents and adults aged 14-39 years between 2007 and 2012 who were tested for C. trachomatis using the Gen-Probe Aptima test. Prevalence estimates were based on demographics and self-reported sexual activity measured through audio, computer-assessed self-interviews.
Estimates were weighted to be nationally representative and to account for oversampling and nonresponse, and the number of infections in the population was estimated by multiplying census estimates by weighted prevalence, Dr. Torrone explained.
Chlamydia is the most commonly reported infection in the United States, and annual screening is currently recommended for all sexually active females under age 25 years, she noted.
Since the findings of this study likely represent an underestimate of the true burden of disease because the estimates do not account for nongenital infection and infections in nonsampled populations where prevalence may be higher (such as incarcerated individuals), they highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women and underscore the importance of adhering to the screening recommendations.
"Health care providers should screen all sexually active young females annually and ensure that all sex partners of patients diagnosed with chlamydia are treated appropriately," Dr. Torrone concluded.
Dr. Torrone reported having no disclosures.
ATLANTA – An estimated 1 in 15 sexually active adolescent girls has a chlamydial infection, and many of these infections go undiagnosed, according to an analysis of National Health and Nutrition Examination Survey data.
According to 2007-2012 NHANES data, the overall prevalence of chlamydia among sexually active adolescents and adults aged 14-39 years is 1.7%, suggesting that there are 1.8 million infections nationally, Elizabeth Torrone, Ph.D., reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
However, only 1.4 million infections are reported annually, according to information from the CDC, suggests that approximately 400,000 infections go undetected each year.
Adolescent girls – and particularly adolescent non-Hispanic black girls – are at highest risk, according to Dr. Torrone.
The estimated overall prevalence among adolescent girls aged 14-19 years in this study was 6.4%. The estimated prevalence among white girls in this age group was 3.2%, and among black girls in this age group it was 18.6%, reported Dr. Torrone of the division of STD prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention at the CDC, Atlanta.
The overall prevalence was 1.4% among males, 2.0% among females, 2.4% among persons aged 14-19 years, 2.9% among those aged 20-24 years, 1.1% among those aged 25-39 years, 2.3% among Mexican Americans, 5.2% among non-Hispanic blacks, and 0.8% among whites.
Having multiple sex partners in the past year was associated with increased prevalence: 3.2% for those with two or more partners, compared with 1.4% among those with one or no partner.
NHANES respondents included in this analysis were 8,330 adolescents and adults aged 14-39 years between 2007 and 2012 who were tested for C. trachomatis using the Gen-Probe Aptima test. Prevalence estimates were based on demographics and self-reported sexual activity measured through audio, computer-assessed self-interviews.
Estimates were weighted to be nationally representative and to account for oversampling and nonresponse, and the number of infections in the population was estimated by multiplying census estimates by weighted prevalence, Dr. Torrone explained.
Chlamydia is the most commonly reported infection in the United States, and annual screening is currently recommended for all sexually active females under age 25 years, she noted.
Since the findings of this study likely represent an underestimate of the true burden of disease because the estimates do not account for nongenital infection and infections in nonsampled populations where prevalence may be higher (such as incarcerated individuals), they highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women and underscore the importance of adhering to the screening recommendations.
"Health care providers should screen all sexually active young females annually and ensure that all sex partners of patients diagnosed with chlamydia are treated appropriately," Dr. Torrone concluded.
Dr. Torrone reported having no disclosures.
ATLANTA – An estimated 1 in 15 sexually active adolescent girls has a chlamydial infection, and many of these infections go undiagnosed, according to an analysis of National Health and Nutrition Examination Survey data.
According to 2007-2012 NHANES data, the overall prevalence of chlamydia among sexually active adolescents and adults aged 14-39 years is 1.7%, suggesting that there are 1.8 million infections nationally, Elizabeth Torrone, Ph.D., reported in a poster at a conference on STD prevention sponsored by the Centers for Disease Control and Prevention.
However, only 1.4 million infections are reported annually, according to information from the CDC, suggests that approximately 400,000 infections go undetected each year.
Adolescent girls – and particularly adolescent non-Hispanic black girls – are at highest risk, according to Dr. Torrone.
The estimated overall prevalence among adolescent girls aged 14-19 years in this study was 6.4%. The estimated prevalence among white girls in this age group was 3.2%, and among black girls in this age group it was 18.6%, reported Dr. Torrone of the division of STD prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention at the CDC, Atlanta.
The overall prevalence was 1.4% among males, 2.0% among females, 2.4% among persons aged 14-19 years, 2.9% among those aged 20-24 years, 1.1% among those aged 25-39 years, 2.3% among Mexican Americans, 5.2% among non-Hispanic blacks, and 0.8% among whites.
Having multiple sex partners in the past year was associated with increased prevalence: 3.2% for those with two or more partners, compared with 1.4% among those with one or no partner.
NHANES respondents included in this analysis were 8,330 adolescents and adults aged 14-39 years between 2007 and 2012 who were tested for C. trachomatis using the Gen-Probe Aptima test. Prevalence estimates were based on demographics and self-reported sexual activity measured through audio, computer-assessed self-interviews.
Estimates were weighted to be nationally representative and to account for oversampling and nonresponse, and the number of infections in the population was estimated by multiplying census estimates by weighted prevalence, Dr. Torrone explained.
Chlamydia is the most commonly reported infection in the United States, and annual screening is currently recommended for all sexually active females under age 25 years, she noted.
Since the findings of this study likely represent an underestimate of the true burden of disease because the estimates do not account for nongenital infection and infections in nonsampled populations where prevalence may be higher (such as incarcerated individuals), they highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women and underscore the importance of adhering to the screening recommendations.
"Health care providers should screen all sexually active young females annually and ensure that all sex partners of patients diagnosed with chlamydia are treated appropriately," Dr. Torrone concluded.
Dr. Torrone reported having no disclosures.
AT THE 2014 STD PREVENTION CONFERENCE
Key clinical point: These findings highlight a need for targeted interventions to reduce the impact of chlamydia among young African American women, and they underscore the importance of adhering to the screening recommendations.
Major finding: Estimated chlamydia prevalence among all girls, white girls, and black girls aged 14-19 years is 6.4%, 3.2%, and 18.6%, respectively.
Data source: Analysis of data from 8,330 NHANES participants from 2007 to 2012.
Disclosures: Dr. Torrone reported having no disclosures.
Azithromycin benefits older pneumonia inpatients
Treating pneumonia with azithromycin is linked to lower risk of death but a slightly higher risk of myocardial infarction in older patients, according to a large retrospective cohort study.
Although azithromycin is recommended in combination with macrolides for the first-line treatment of patients hospitalized with pneumonia, recent research suggests that azithromycin is associated with an increased risk of cardiovascular events.

However, the current findings suggest that although the drug is associated with a slight increase in the risk of myocardial infarction (number needed to harm equals 144), it is not associated with "any cardiac event," cardiac arrhythmia, or heart failure, and that the reduction in 90-day mortality risk (number needed to treat of 21) is large enough to provide an overall net benefit.
Dr. Eric M. Mortensen of the Veterans Affairs North Texas Health Care system, Dallas, and his colleagues reported their findings on treating pneumonia with azithromycin in JAMA.
In the current study, 90-day mortality in 31,863 patients aged 65 years and older who were exposed to azithromycin was significantly lower than in an equal number of propensity-matched controls who were not exposed (17.4% vs. 22.3%; odds ratio, 0.73).
The risk of myocardial infarction, however, was significantly increased in the azithromycin group (5.1% vs. 4.4%; OR, 1.17), the investigators reported.
Azithromycin use was defined as patients’ receipt of at least one dose of azithromycin during the first 48 hours after admission.
Study subjects were a mean age of 77.8 years in the national Department of Veterans Affairs administrative database who were hospitalized with pneumonia between 2002 and 2012 (JAMA 2014 June 4 [doi: 10.1001/jama.2014.4304]). Most patients (98%) were male.
The study hada relativelysmall number of few female subjects and relied "upon ICD-9 diagnosis of cardiovascular events rather than clinical information, which particularly may affect the diagnosis of heart failure." However, researchers said, treating physicians were likely to have believed that the patients in the study indeed had pneumonia and did not show any bias toward azithromycin.
Dr. W. Michael Alberts, FCCP, comments: Azithromycin is a widely used (perhaps too widely) and effective (it’s hard to be too effective) antibiotic commonly used in patients with respiratory illnesses. Recent reports, however, have called the safety of this medication into question. The results of this very large study may ease the practitioner’s anxiety, at least when treating patients hospitalized with pneumonia.
For a slight increased risk of heart attack, use of azithromycin provides a significantly lower risk of death. As long as the drug is used for the appropriate indication, I’ll take that deal in most situations.
Dr. W. Michael Alberts, FCCP, comments: Azithromycin is a widely used (perhaps too widely) and effective (it’s hard to be too effective) antibiotic commonly used in patients with respiratory illnesses. Recent reports, however, have called the safety of this medication into question. The results of this very large study may ease the practitioner’s anxiety, at least when treating patients hospitalized with pneumonia.
For a slight increased risk of heart attack, use of azithromycin provides a significantly lower risk of death. As long as the drug is used for the appropriate indication, I’ll take that deal in most situations.
Dr. W. Michael Alberts, FCCP, comments: Azithromycin is a widely used (perhaps too widely) and effective (it’s hard to be too effective) antibiotic commonly used in patients with respiratory illnesses. Recent reports, however, have called the safety of this medication into question. The results of this very large study may ease the practitioner’s anxiety, at least when treating patients hospitalized with pneumonia.
For a slight increased risk of heart attack, use of azithromycin provides a significantly lower risk of death. As long as the drug is used for the appropriate indication, I’ll take that deal in most situations.
Treating pneumonia with azithromycin is linked to lower risk of death but a slightly higher risk of myocardial infarction in older patients, according to a large retrospective cohort study.
Although azithromycin is recommended in combination with macrolides for the first-line treatment of patients hospitalized with pneumonia, recent research suggests that azithromycin is associated with an increased risk of cardiovascular events.
However, the current findings suggest that although the drug is associated with a slight increase in the risk of myocardial infarction (number needed to harm equals 144), it is not associated with "any cardiac event," cardiac arrhythmia, or heart failure, and that the reduction in 90-day mortality risk (number needed to treat of 21) is large enough to provide an overall net benefit.
Dr. Eric M. Mortensen of the Veterans Affairs North Texas Health Care system, Dallas, and his colleagues reported their findings on treating pneumonia with azithromycin in JAMA.
In the current study, 90-day mortality in 31,863 patients aged 65 years and older who were exposed to azithromycin was significantly lower than in an equal number of propensity-matched controls who were not exposed (17.4% vs. 22.3%; odds ratio, 0.73).
The risk of myocardial infarction, however, was significantly increased in the azithromycin group (5.1% vs. 4.4%; OR, 1.17), the investigators reported.
Azithromycin use was defined as patients’ receipt of at least one dose of azithromycin during the first 48 hours after admission.
Study subjects were a mean age of 77.8 years in the national Department of Veterans Affairs administrative database who were hospitalized with pneumonia between 2002 and 2012 (JAMA 2014 June 4 [doi: 10.1001/jama.2014.4304]). Most patients (98%) were male.
The study hada relativelysmall number of few female subjects and relied "upon ICD-9 diagnosis of cardiovascular events rather than clinical information, which particularly may affect the diagnosis of heart failure." However, researchers said, treating physicians were likely to have believed that the patients in the study indeed had pneumonia and did not show any bias toward azithromycin.
Treating pneumonia with azithromycin is linked to lower risk of death but a slightly higher risk of myocardial infarction in older patients, according to a large retrospective cohort study.
Although azithromycin is recommended in combination with macrolides for the first-line treatment of patients hospitalized with pneumonia, recent research suggests that azithromycin is associated with an increased risk of cardiovascular events.
However, the current findings suggest that although the drug is associated with a slight increase in the risk of myocardial infarction (number needed to harm equals 144), it is not associated with "any cardiac event," cardiac arrhythmia, or heart failure, and that the reduction in 90-day mortality risk (number needed to treat of 21) is large enough to provide an overall net benefit.
Dr. Eric M. Mortensen of the Veterans Affairs North Texas Health Care system, Dallas, and his colleagues reported their findings on treating pneumonia with azithromycin in JAMA.
In the current study, 90-day mortality in 31,863 patients aged 65 years and older who were exposed to azithromycin was significantly lower than in an equal number of propensity-matched controls who were not exposed (17.4% vs. 22.3%; odds ratio, 0.73).
The risk of myocardial infarction, however, was significantly increased in the azithromycin group (5.1% vs. 4.4%; OR, 1.17), the investigators reported.
Azithromycin use was defined as patients’ receipt of at least one dose of azithromycin during the first 48 hours after admission.
Study subjects were a mean age of 77.8 years in the national Department of Veterans Affairs administrative database who were hospitalized with pneumonia between 2002 and 2012 (JAMA 2014 June 4 [doi: 10.1001/jama.2014.4304]). Most patients (98%) were male.
The study hada relativelysmall number of few female subjects and relied "upon ICD-9 diagnosis of cardiovascular events rather than clinical information, which particularly may affect the diagnosis of heart failure." However, researchers said, treating physicians were likely to have believed that the patients in the study indeed had pneumonia and did not show any bias toward azithromycin.
Key clinical point: The benefit of azithromycin for elderly pneumonia patients outweighs MI risk.
Major finding: Ninety-day mortality in patients receiving azithromycin was 17.4% vs. 22.3% among controls.
Data source: A retrospective cohort study of 63,726 adults aged 65 years or older and hospitalized for pneumonia.
Disclosures: Support came from a National Institute of Nursing Research grant. Dr. Mortensen had no disclosures. Other researchers received grants from industry sources.

Midurethral sling study: At 5 years satisfaction remained high, though continence declined
ORLANDO – Success rates at 5 years were similar in women treated with a transobturator midurethral sling and women treated with a retropubic midurethral sling, but the transobturator patients were more likely to report an easing of symptoms, according to an extension of the Trial of Mid-Urethral Slings.
Overall satisfaction was similar in the two groups, Dr. Leslie M. Rickey reported during a Best Abstract session at the annual meeting of the American Urological Association.
Of 597 subjects in the Trial of Midurethral Slings (TOMUS), 404 participated in the extension phase (E-TOMUS). There was no significant difference in success rates – which declined over time – between those in the transobturator group and those in the retropubic group (43% vs. 51%). However, treatment success for retropubic midurethral slings was nearly 8% higher and did not meet equivalency criteria at 1 or 5 years, said Dr. Rickey, a urologist at Yale University, New Haven, Conn., who presented on behalf of Dr. Kimberly S. Kenton and the Urinary Incontinence Treatment Network.
Stress incontinence symptoms continued to increase over time in both groups but did not differ between the groups at 5 years; urge symptoms also increased over time but were reported significantly more often in the retropubic midurethral sling group.
"Overall urgency symptoms and sexual dysfunction, although still improved from baseline, did worsen over time," Dr. Rickey said, noting that they worsened significantly more overall in the retropubic group.
However, the proportion of patients who were completely or mostly satisfied remained similar in the groups (although it decreased from 92% and 93% to 80% and 85% in the groups, respectively, over time). Those in the transobturator group were almost twice as likely to report improvement in their urinary condition as measured by the Patient Global Impression of Improvement scale (odds ratio, 1.94), Dr. Rickey said.
With respect to adverse events, 10% of women overall experienced an adverse event (mainly urinary tract infections or mesh exposure) or serious adverse event; the rate did not differ between the groups. There were six serious adverse events requiring intervention, including one case of mesh erosion in each group and four urinary tract infections in the retropubic midurethral sling group.
"Importantly, there were seven new mesh exposures in years 3-5 after surgery," Dr. Rickey said, noting that three occurred in the retropubic midurethral sling group and four occurred in the transobturator midurethral sling group.
Women included in the extension phase were TOMUS participants who did not undergo surgical retreatment for stress urinary incontinence after the initial procedure. Participants completed annual in-person visits, including pelvic examination, symptom, mesh, and quality of life questionnaires.
Treatment success was defined as no retreatment for stress urinary incontinence, and no self-reported stress urinary incontinence symptoms using the Medical, Epidemiological, and Social Aspects of Aging questionnaire, she said.
"In conclusion, the 5-year continence rates did decline after either retropubic midurethral sling or transobturator sling, and did not meet prespecified criteria for equivalency. Satisfaction does remain high in both groups. In general, urinary symptoms and quality of life were more improved at 5 years after the transobturator approach, and mesh erosion rates remain low at 1.7%," she said.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. The authors reported having no disclosures.
ORLANDO – Success rates at 5 years were similar in women treated with a transobturator midurethral sling and women treated with a retropubic midurethral sling, but the transobturator patients were more likely to report an easing of symptoms, according to an extension of the Trial of Mid-Urethral Slings.
Overall satisfaction was similar in the two groups, Dr. Leslie M. Rickey reported during a Best Abstract session at the annual meeting of the American Urological Association.
Of 597 subjects in the Trial of Midurethral Slings (TOMUS), 404 participated in the extension phase (E-TOMUS). There was no significant difference in success rates – which declined over time – between those in the transobturator group and those in the retropubic group (43% vs. 51%). However, treatment success for retropubic midurethral slings was nearly 8% higher and did not meet equivalency criteria at 1 or 5 years, said Dr. Rickey, a urologist at Yale University, New Haven, Conn., who presented on behalf of Dr. Kimberly S. Kenton and the Urinary Incontinence Treatment Network.
Stress incontinence symptoms continued to increase over time in both groups but did not differ between the groups at 5 years; urge symptoms also increased over time but were reported significantly more often in the retropubic midurethral sling group.
"Overall urgency symptoms and sexual dysfunction, although still improved from baseline, did worsen over time," Dr. Rickey said, noting that they worsened significantly more overall in the retropubic group.
However, the proportion of patients who were completely or mostly satisfied remained similar in the groups (although it decreased from 92% and 93% to 80% and 85% in the groups, respectively, over time). Those in the transobturator group were almost twice as likely to report improvement in their urinary condition as measured by the Patient Global Impression of Improvement scale (odds ratio, 1.94), Dr. Rickey said.
With respect to adverse events, 10% of women overall experienced an adverse event (mainly urinary tract infections or mesh exposure) or serious adverse event; the rate did not differ between the groups. There were six serious adverse events requiring intervention, including one case of mesh erosion in each group and four urinary tract infections in the retropubic midurethral sling group.
"Importantly, there were seven new mesh exposures in years 3-5 after surgery," Dr. Rickey said, noting that three occurred in the retropubic midurethral sling group and four occurred in the transobturator midurethral sling group.
Women included in the extension phase were TOMUS participants who did not undergo surgical retreatment for stress urinary incontinence after the initial procedure. Participants completed annual in-person visits, including pelvic examination, symptom, mesh, and quality of life questionnaires.
Treatment success was defined as no retreatment for stress urinary incontinence, and no self-reported stress urinary incontinence symptoms using the Medical, Epidemiological, and Social Aspects of Aging questionnaire, she said.
"In conclusion, the 5-year continence rates did decline after either retropubic midurethral sling or transobturator sling, and did not meet prespecified criteria for equivalency. Satisfaction does remain high in both groups. In general, urinary symptoms and quality of life were more improved at 5 years after the transobturator approach, and mesh erosion rates remain low at 1.7%," she said.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. The authors reported having no disclosures.
ORLANDO – Success rates at 5 years were similar in women treated with a transobturator midurethral sling and women treated with a retropubic midurethral sling, but the transobturator patients were more likely to report an easing of symptoms, according to an extension of the Trial of Mid-Urethral Slings.
Overall satisfaction was similar in the two groups, Dr. Leslie M. Rickey reported during a Best Abstract session at the annual meeting of the American Urological Association.
Of 597 subjects in the Trial of Midurethral Slings (TOMUS), 404 participated in the extension phase (E-TOMUS). There was no significant difference in success rates – which declined over time – between those in the transobturator group and those in the retropubic group (43% vs. 51%). However, treatment success for retropubic midurethral slings was nearly 8% higher and did not meet equivalency criteria at 1 or 5 years, said Dr. Rickey, a urologist at Yale University, New Haven, Conn., who presented on behalf of Dr. Kimberly S. Kenton and the Urinary Incontinence Treatment Network.
Stress incontinence symptoms continued to increase over time in both groups but did not differ between the groups at 5 years; urge symptoms also increased over time but were reported significantly more often in the retropubic midurethral sling group.
"Overall urgency symptoms and sexual dysfunction, although still improved from baseline, did worsen over time," Dr. Rickey said, noting that they worsened significantly more overall in the retropubic group.
However, the proportion of patients who were completely or mostly satisfied remained similar in the groups (although it decreased from 92% and 93% to 80% and 85% in the groups, respectively, over time). Those in the transobturator group were almost twice as likely to report improvement in their urinary condition as measured by the Patient Global Impression of Improvement scale (odds ratio, 1.94), Dr. Rickey said.
With respect to adverse events, 10% of women overall experienced an adverse event (mainly urinary tract infections or mesh exposure) or serious adverse event; the rate did not differ between the groups. There were six serious adverse events requiring intervention, including one case of mesh erosion in each group and four urinary tract infections in the retropubic midurethral sling group.
"Importantly, there were seven new mesh exposures in years 3-5 after surgery," Dr. Rickey said, noting that three occurred in the retropubic midurethral sling group and four occurred in the transobturator midurethral sling group.
Women included in the extension phase were TOMUS participants who did not undergo surgical retreatment for stress urinary incontinence after the initial procedure. Participants completed annual in-person visits, including pelvic examination, symptom, mesh, and quality of life questionnaires.
Treatment success was defined as no retreatment for stress urinary incontinence, and no self-reported stress urinary incontinence symptoms using the Medical, Epidemiological, and Social Aspects of Aging questionnaire, she said.
"In conclusion, the 5-year continence rates did decline after either retropubic midurethral sling or transobturator sling, and did not meet prespecified criteria for equivalency. Satisfaction does remain high in both groups. In general, urinary symptoms and quality of life were more improved at 5 years after the transobturator approach, and mesh erosion rates remain low at 1.7%," she said.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. The authors reported having no disclosures.
AT THE AUA ANNUAL MEETING
Key clinical point: The benefits of midurethral slings persisted 5 years in the majority of women.
Major finding: Overall rates of satisfaction at 5 years were 79% and 85% with retropubic midurethral and transobturator midurethral slings, respectively.
Data source: Extended follow-up of 404 patients from the TOMUS trial (E-TOMUS).
Disclosures: This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. The authors reported having no disclosures.
PREVAIL: Enzalutamide benefits patients with visceral and nonvisceral disease
ORLANDO – Treatment with enzalutamide significantly improved survival and radiographic progression-free survival in men with chemotherapy-naive metastatic prostate cancer – including those with visceral disease – according to a subgroup analysis of the randomized, double-blind PREVAIL study.
Of 1,717 patients in the study, 204 had visceral disease at screening, including 130 with lung disease and 74 with lung disease and/or liver disease. Those without visceral disease had lower baseline median prostate-specific antigen levels (46.8 vs. 72.5 ng/mL), better performance status (68.9 vs. 61.8%), and less lymph node disease (49.8% vs. 57.8%), than those with visceral disease, but the two groups had similar rates of bone disease (83.7% and 80.4%), Dr. Christopher Evans reported during a late-breaking abstract session at the annual meeting of the American Urological Association.
"That patients with visceral disease were included in the study is very important, as other studies have excluded patients with visceral disease," Dr. Evans said.
Overall survival in the PREVAIL study, as reported at the American Society of Clinical Oncology Genitourinary Cancers Symposium in February and online June 1 in the New England Journal of Medicine (N. Engl. J. Med. 2014 June 1 [doi:10.1056/NEJMoa1405095]), was significantly better in patients who received enzalutamide, compared with those who received placebo (32.4 vs. 30.2 months; hazard ratio, 0.71). In the current subgroup analysis comparing those with and without visceral disease, overall survival in those with visceral disease was 27.8 months and 22.8 months in the treatment and placebo groups, respectively (hazard ratio, 0.82). In those without visceral disease, the median time to death was not yet reached, said Dr. Evans of the department of urology, University of California Davis Health System, Sacramento.
Median radiographic progression-free survival duration in those with visceral disease was not yet reached in the treatment group and was 3.6 months in the placebo group, and in those without visceral disease it was 14.1 vs. 4.0 months with treatment vs. placebo (hazard ratio, 0.18), he said.
Additionally, patients without visceral disease, who may be more likely to be seen in the urologist’s office, were much less likely to use a subsequent life-extending therapy (typically docetaxel) if they received enzalutamide treatment rather than placebo (40% vs. 70%), Dr. Evans noted.
In a post hoc analysis, the secondary endpoint of time to cytotoxic chemotherapy was 28 vs. 10.8 months overall in the treatment vs. placebo group (HR, 0.35), 22.6 vs. 6.6 months for treatment vs. placebo in those with visceral disease (HR, 0.30), and 28.4 vs. 11.6 months for treatment vs. placebo in those without visceral disease (HR, 0.36).
"These curves are similar again in the visceral and nonvisceral subgroups. However, if we look at the placebo subgroup in the intention-to-treat population, we can see that median time to initiation of chemotherapy is 12 months. This is similar in the nonvisceral sub group, but is 6.5 months in the visceral subgroup – again showing that these patients have worse disease burden," he said.
In the intention-to-treat population, there was an 18-month improvement overall in the time to initiation of chemotherapy, giving urologists an opportunity to get involved in the treatment of these patients, he added.
The PREVAIL study examined the impact of oral enzalutamide (160 mg/day, compared with placebo, in asymptomatic or mildly symptomatic chemotherapy-naive men with metastatic prostate cancer. The study, which was conducted at 207 centers in 22 countries between September 2010 and September 2012, was stopped at an interim analysis based on the significant survival benefits seen in the enzalutamide-treated patients. The current subgroup analysis demonstrates that although patients with visceral disease progressed more rapidly regardless of treatment allocation, the benefit of enzalutamide was consistent among patients with or without visceral disease.
Dr. Evans disclosed relationships with Amgen, Astellas, Medivation, Janssen, and Oncogenex, and investment interests in Medivation and Oncogenex.
ORLANDO – Treatment with enzalutamide significantly improved survival and radiographic progression-free survival in men with chemotherapy-naive metastatic prostate cancer – including those with visceral disease – according to a subgroup analysis of the randomized, double-blind PREVAIL study.
Of 1,717 patients in the study, 204 had visceral disease at screening, including 130 with lung disease and 74 with lung disease and/or liver disease. Those without visceral disease had lower baseline median prostate-specific antigen levels (46.8 vs. 72.5 ng/mL), better performance status (68.9 vs. 61.8%), and less lymph node disease (49.8% vs. 57.8%), than those with visceral disease, but the two groups had similar rates of bone disease (83.7% and 80.4%), Dr. Christopher Evans reported during a late-breaking abstract session at the annual meeting of the American Urological Association.
"That patients with visceral disease were included in the study is very important, as other studies have excluded patients with visceral disease," Dr. Evans said.
Overall survival in the PREVAIL study, as reported at the American Society of Clinical Oncology Genitourinary Cancers Symposium in February and online June 1 in the New England Journal of Medicine (N. Engl. J. Med. 2014 June 1 [doi:10.1056/NEJMoa1405095]), was significantly better in patients who received enzalutamide, compared with those who received placebo (32.4 vs. 30.2 months; hazard ratio, 0.71). In the current subgroup analysis comparing those with and without visceral disease, overall survival in those with visceral disease was 27.8 months and 22.8 months in the treatment and placebo groups, respectively (hazard ratio, 0.82). In those without visceral disease, the median time to death was not yet reached, said Dr. Evans of the department of urology, University of California Davis Health System, Sacramento.
Median radiographic progression-free survival duration in those with visceral disease was not yet reached in the treatment group and was 3.6 months in the placebo group, and in those without visceral disease it was 14.1 vs. 4.0 months with treatment vs. placebo (hazard ratio, 0.18), he said.
Additionally, patients without visceral disease, who may be more likely to be seen in the urologist’s office, were much less likely to use a subsequent life-extending therapy (typically docetaxel) if they received enzalutamide treatment rather than placebo (40% vs. 70%), Dr. Evans noted.
In a post hoc analysis, the secondary endpoint of time to cytotoxic chemotherapy was 28 vs. 10.8 months overall in the treatment vs. placebo group (HR, 0.35), 22.6 vs. 6.6 months for treatment vs. placebo in those with visceral disease (HR, 0.30), and 28.4 vs. 11.6 months for treatment vs. placebo in those without visceral disease (HR, 0.36).
"These curves are similar again in the visceral and nonvisceral subgroups. However, if we look at the placebo subgroup in the intention-to-treat population, we can see that median time to initiation of chemotherapy is 12 months. This is similar in the nonvisceral sub group, but is 6.5 months in the visceral subgroup – again showing that these patients have worse disease burden," he said.
In the intention-to-treat population, there was an 18-month improvement overall in the time to initiation of chemotherapy, giving urologists an opportunity to get involved in the treatment of these patients, he added.
The PREVAIL study examined the impact of oral enzalutamide (160 mg/day, compared with placebo, in asymptomatic or mildly symptomatic chemotherapy-naive men with metastatic prostate cancer. The study, which was conducted at 207 centers in 22 countries between September 2010 and September 2012, was stopped at an interim analysis based on the significant survival benefits seen in the enzalutamide-treated patients. The current subgroup analysis demonstrates that although patients with visceral disease progressed more rapidly regardless of treatment allocation, the benefit of enzalutamide was consistent among patients with or without visceral disease.
Dr. Evans disclosed relationships with Amgen, Astellas, Medivation, Janssen, and Oncogenex, and investment interests in Medivation and Oncogenex.
ORLANDO – Treatment with enzalutamide significantly improved survival and radiographic progression-free survival in men with chemotherapy-naive metastatic prostate cancer – including those with visceral disease – according to a subgroup analysis of the randomized, double-blind PREVAIL study.
Of 1,717 patients in the study, 204 had visceral disease at screening, including 130 with lung disease and 74 with lung disease and/or liver disease. Those without visceral disease had lower baseline median prostate-specific antigen levels (46.8 vs. 72.5 ng/mL), better performance status (68.9 vs. 61.8%), and less lymph node disease (49.8% vs. 57.8%), than those with visceral disease, but the two groups had similar rates of bone disease (83.7% and 80.4%), Dr. Christopher Evans reported during a late-breaking abstract session at the annual meeting of the American Urological Association.
"That patients with visceral disease were included in the study is very important, as other studies have excluded patients with visceral disease," Dr. Evans said.
Overall survival in the PREVAIL study, as reported at the American Society of Clinical Oncology Genitourinary Cancers Symposium in February and online June 1 in the New England Journal of Medicine (N. Engl. J. Med. 2014 June 1 [doi:10.1056/NEJMoa1405095]), was significantly better in patients who received enzalutamide, compared with those who received placebo (32.4 vs. 30.2 months; hazard ratio, 0.71). In the current subgroup analysis comparing those with and without visceral disease, overall survival in those with visceral disease was 27.8 months and 22.8 months in the treatment and placebo groups, respectively (hazard ratio, 0.82). In those without visceral disease, the median time to death was not yet reached, said Dr. Evans of the department of urology, University of California Davis Health System, Sacramento.
Median radiographic progression-free survival duration in those with visceral disease was not yet reached in the treatment group and was 3.6 months in the placebo group, and in those without visceral disease it was 14.1 vs. 4.0 months with treatment vs. placebo (hazard ratio, 0.18), he said.
Additionally, patients without visceral disease, who may be more likely to be seen in the urologist’s office, were much less likely to use a subsequent life-extending therapy (typically docetaxel) if they received enzalutamide treatment rather than placebo (40% vs. 70%), Dr. Evans noted.
In a post hoc analysis, the secondary endpoint of time to cytotoxic chemotherapy was 28 vs. 10.8 months overall in the treatment vs. placebo group (HR, 0.35), 22.6 vs. 6.6 months for treatment vs. placebo in those with visceral disease (HR, 0.30), and 28.4 vs. 11.6 months for treatment vs. placebo in those without visceral disease (HR, 0.36).
"These curves are similar again in the visceral and nonvisceral subgroups. However, if we look at the placebo subgroup in the intention-to-treat population, we can see that median time to initiation of chemotherapy is 12 months. This is similar in the nonvisceral sub group, but is 6.5 months in the visceral subgroup – again showing that these patients have worse disease burden," he said.
In the intention-to-treat population, there was an 18-month improvement overall in the time to initiation of chemotherapy, giving urologists an opportunity to get involved in the treatment of these patients, he added.
The PREVAIL study examined the impact of oral enzalutamide (160 mg/day, compared with placebo, in asymptomatic or mildly symptomatic chemotherapy-naive men with metastatic prostate cancer. The study, which was conducted at 207 centers in 22 countries between September 2010 and September 2012, was stopped at an interim analysis based on the significant survival benefits seen in the enzalutamide-treated patients. The current subgroup analysis demonstrates that although patients with visceral disease progressed more rapidly regardless of treatment allocation, the benefit of enzalutamide was consistent among patients with or without visceral disease.
Dr. Evans disclosed relationships with Amgen, Astellas, Medivation, Janssen, and Oncogenex, and investment interests in Medivation and Oncogenex.
AT THE AUA ANNUAL MEETING
Key clinical point: Treatment with enzalutamide significantly improved survival and radiographic progression-free survival in men with chemotherapy-naive metastatic prostate cancer, including those with visceral disease.
Major finding: Overall survival in those with visceral disease was 27.8 months and 22.8 months in the treatment and placebo groups, respectively (hazard ratio, 0.82).
Data source: A subgroup analysis of the 1,717 patients in the randomized PREVAIL trial.
Disclosures: Dr. Evans disclosed relationships with Amgen, Astellas, Medivation, Janssen, and Oncogenex (meeting participant or lecturer and/or scientific study or trial), and investment interests in Medivation and Oncogenex.