User login
Light-Brown Macule on the Upper Arm
Light-Brown Macule on the Upper Arm
THE DIAGNOSIS: Pigmented Bowen Disease
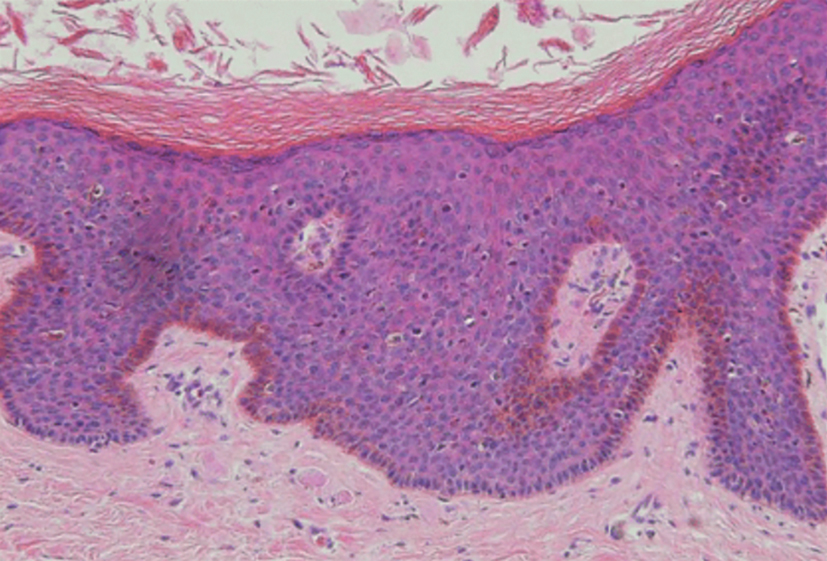
Histopathology revealed atypical keratinocytes throughout the entire thickness of a pigmented epidermis extending from the basal layer (Figure). Diffuse epidermal hyperpigmentation and melanophages in the papillary dermis were present. There was no dermal invasion or atypical melanocytic proliferation. On dermoscopy, this lesion had small brown globules, smudging, and an asymmetric nonspecific homogeneous pattern. Based on these features as well as the clinical findings, a diagnosis of pigmented Bowen disease (PBD), a rare subtype of squamous cell carcinoma in situ, was made. Complete removal of the lesion was achieved via the biopsy, and the patient was counselled regarding the malignant but noninvasive nature of the lesion. Appropriate follow-up was recommended to monitor for recurrence.
Our case presentation of PBD on the right upper arm in a female patient with a light skin tone is not classic, as PBD lesions usually manifest as well-demarcated scaly plaques on sun-protected sites in men with darker skin tones who are in the sixth to seventh decades of life.1
Dermoscopy of PBD in patients with lighter skin tones can present diagnostic challenges because characteristic clustered glomerular vessels may be faint or absent, particularly in small lesions such as this one. In such cases, PBD may instead demonstrate structureless brown pigmentation and irregular globules, patterns that overlap with pigmented actinic keratosis (PAK) and melanoma.3
Our case underscores the importance of maintaining a broad differential when evaluating small pigmented macules and reinforces biopsy as the diagnostic gold standard for PBD when dermoscopic findings are nonspecific.
- Mota AN, Piñeiro-Maceira J, Alves Mde F, et al. Pigmented Bowen’s disease. An Bras Dermatol. 2014;89:825-827. doi:10.1590 /abd1806-4841.20142725
- Lee JW, Hur J, Yeo KY, et al. A case of pigmented Bowen’s disease. Ann Dermatol. 2009;21:197-199. doi:10.5021/ad.2009.21.2.197
- Markowitz O. A Practical Guide to Dermoscopy. Philadelphia, PA: Wolters Kluwer; 2017.
- Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. doi:10.1111/jdv.12848
THE DIAGNOSIS: Pigmented Bowen Disease
Histopathology revealed atypical keratinocytes throughout the entire thickness of a pigmented epidermis extending from the basal layer (Figure). Diffuse epidermal hyperpigmentation and melanophages in the papillary dermis were present. There was no dermal invasion or atypical melanocytic proliferation. On dermoscopy, this lesion had small brown globules, smudging, and an asymmetric nonspecific homogeneous pattern. Based on these features as well as the clinical findings, a diagnosis of pigmented Bowen disease (PBD), a rare subtype of squamous cell carcinoma in situ, was made. Complete removal of the lesion was achieved via the biopsy, and the patient was counselled regarding the malignant but noninvasive nature of the lesion. Appropriate follow-up was recommended to monitor for recurrence.
Our case presentation of PBD on the right upper arm in a female patient with a light skin tone is not classic, as PBD lesions usually manifest as well-demarcated scaly plaques on sun-protected sites in men with darker skin tones who are in the sixth to seventh decades of life.1
Dermoscopy of PBD in patients with lighter skin tones can present diagnostic challenges because characteristic clustered glomerular vessels may be faint or absent, particularly in small lesions such as this one. In such cases, PBD may instead demonstrate structureless brown pigmentation and irregular globules, patterns that overlap with pigmented actinic keratosis (PAK) and melanoma.3
Our case underscores the importance of maintaining a broad differential when evaluating small pigmented macules and reinforces biopsy as the diagnostic gold standard for PBD when dermoscopic findings are nonspecific.
THE DIAGNOSIS: Pigmented Bowen Disease
Histopathology revealed atypical keratinocytes throughout the entire thickness of a pigmented epidermis extending from the basal layer (Figure). Diffuse epidermal hyperpigmentation and melanophages in the papillary dermis were present. There was no dermal invasion or atypical melanocytic proliferation. On dermoscopy, this lesion had small brown globules, smudging, and an asymmetric nonspecific homogeneous pattern. Based on these features as well as the clinical findings, a diagnosis of pigmented Bowen disease (PBD), a rare subtype of squamous cell carcinoma in situ, was made. Complete removal of the lesion was achieved via the biopsy, and the patient was counselled regarding the malignant but noninvasive nature of the lesion. Appropriate follow-up was recommended to monitor for recurrence.
Our case presentation of PBD on the right upper arm in a female patient with a light skin tone is not classic, as PBD lesions usually manifest as well-demarcated scaly plaques on sun-protected sites in men with darker skin tones who are in the sixth to seventh decades of life.1
Dermoscopy of PBD in patients with lighter skin tones can present diagnostic challenges because characteristic clustered glomerular vessels may be faint or absent, particularly in small lesions such as this one. In such cases, PBD may instead demonstrate structureless brown pigmentation and irregular globules, patterns that overlap with pigmented actinic keratosis (PAK) and melanoma.3
Our case underscores the importance of maintaining a broad differential when evaluating small pigmented macules and reinforces biopsy as the diagnostic gold standard for PBD when dermoscopic findings are nonspecific.
- Mota AN, Piñeiro-Maceira J, Alves Mde F, et al. Pigmented Bowen’s disease. An Bras Dermatol. 2014;89:825-827. doi:10.1590 /abd1806-4841.20142725
- Lee JW, Hur J, Yeo KY, et al. A case of pigmented Bowen’s disease. Ann Dermatol. 2009;21:197-199. doi:10.5021/ad.2009.21.2.197
- Markowitz O. A Practical Guide to Dermoscopy. Philadelphia, PA: Wolters Kluwer; 2017.
- Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. doi:10.1111/jdv.12848
- Mota AN, Piñeiro-Maceira J, Alves Mde F, et al. Pigmented Bowen’s disease. An Bras Dermatol. 2014;89:825-827. doi:10.1590 /abd1806-4841.20142725
- Lee JW, Hur J, Yeo KY, et al. A case of pigmented Bowen’s disease. Ann Dermatol. 2009;21:197-199. doi:10.5021/ad.2009.21.2.197
- Markowitz O. A Practical Guide to Dermoscopy. Philadelphia, PA: Wolters Kluwer; 2017.
- Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. doi:10.1111/jdv.12848
Light-Brown Macule on the Upper Arm
Light-Brown Macule on the Upper Arm
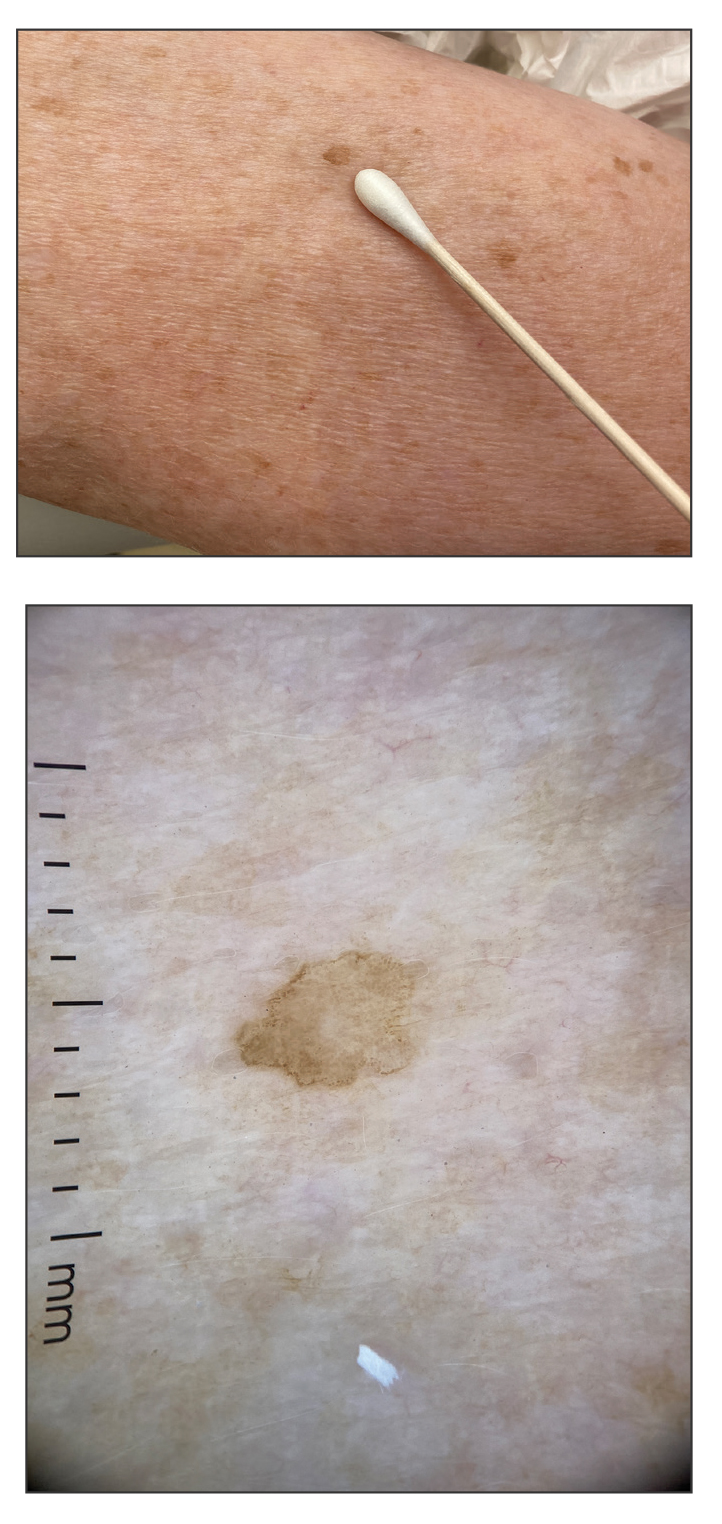
An otherwise healthy 61-year-old woman with a light skin tone presented to the dermatology clinic for evaluation of a pigmented lesion on the right anterior distal upper arm of approximately 6 months’ duration. The patient reported no personal history of nonmelanoma skin cancer, atypical nevi, or melanoma but noted she had a family history of melanoma. Physical examination revealed an asymptomatic light-brown macule on the right anterior distal upper arm measuring about 3 mm with notable border irregularity and delineation. Dermoscopy findings showed a darker brown area at the lateral edge adjacent to the larger, amorphous, lighter-brown area with irregular brown globules present throughout the lesion. A biopsy of the lesion was performed.

Dark-Brown Macule on the Periumbilical Skin
Dark-Brown Macule on the Periumbilical Skin
THE DIAGNOSIS: Seborrheic Keratosis
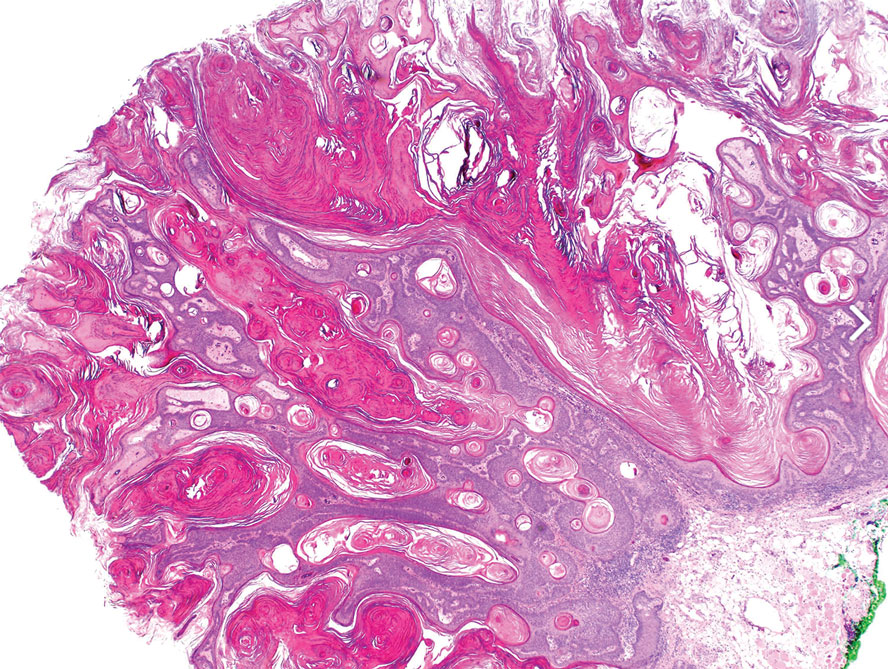
Histopathology revealed epidermal hyperplasia and hyperkeratosis with no notation of atypical melanocytic activity (Figure). There were no Kamino bodies, junctional nesting, or cytologic atypia. Based on these features as well as the clinical and dermoscopic findings, a diagnosis of an inflamed seborrheic keratosis (SK) was made. No further treatment was required following the shave biopsy, and the patient was reassured regarding the benign nature of the lesion.
Seborrheic keratoses are benign epidermal growths that can manifest on any area of the skin except the palms and soles. They present clinically as tan, yellow, gray, brown, or black with a smooth, waxy, or verrucous surface. They range from 1 mm to several centimeters in diameter. Although SKs traditionally manifest more frequently in individuals with lighter skin tones, pigmented variants, such as dermatosis papulosa nigra, have been reported to occur more commonly and at younger ages in patients with skin of color.1
Dermoscopy of SK in patients with skin of color can present diagnostic challenges, as these lesions may display atypical pigmented patterns that overlap with melanocytic lesions, including Spitz nevi, particularly when starburstlike or globular structures are present.2 What sets inflamed SKs apart from other SKs is the lack of a heavily keratinized surface on both clinical and dermoscopic evaluation. Common histopathologic diagnostic criteria for Spitz nevi include Kamino bodies, uniform nuclear enlargement, and spindled or epithelioid nevus cells, which were not noted in our patient.3 Therefore, in presentations such as this, histopathology remains the gold standard for diagnosis.
The differential diagnosis in this case included benign nevus, dysplastic nevus, melanoma, and Spitz nevus. Benign nevi typically demonstrate uniform pigmentation and symmetric dermoscopic patterns. Dysplastic nevi may show architectural disorder and cytologic atypia but lack invasive features.3 Melanoma often exhibits asymmetry, atypical network patterns, and irregular pigmentation.4 Spitz nevi characteristically demonstrate large epithelioid or spindle cells with Kamino bodies on histopathology, which were absent in our patient.
- Greco MJ, Bhutta BS. Seborrheic keratosis. StatPearls [Internet]. StatPearls Publishing; 2025. Updated May 6, 2024. Accessed December 19, 2025. https://www.ncbi.nlm.nih.gov/books/NBK545285/
- Emanuel P, Cheng, H. Spitz naevus pathology. Accessed November 25, 2025. https://dermnetnz.org/topics/spitz-naevus-pathology.
- Wensley KE, Zito PM. Atypical mole. StatPearls [Internet]. StatPearls Publishing; 2025. Updated July 3, 2023. Accessed December 19, 2025. https://www.ncbi.nlm.nih.gov/books/NBK560606/
- Valenzuela FI, Hohnadel M. Dermatoscopic characteristics of melanoma versus benign lesions and nonmelanoma cancers. StatPearls [Internet]. StatPearls Publishing; 2025. Updated August 10, 2024. Accessed December 19, 2025. https://www.ncbi.nlm .nih.gov/books/NBK606113/
THE DIAGNOSIS: Seborrheic Keratosis
Histopathology revealed epidermal hyperplasia and hyperkeratosis with no notation of atypical melanocytic activity (Figure). There were no Kamino bodies, junctional nesting, or cytologic atypia. Based on these features as well as the clinical and dermoscopic findings, a diagnosis of an inflamed seborrheic keratosis (SK) was made. No further treatment was required following the shave biopsy, and the patient was reassured regarding the benign nature of the lesion.
Seborrheic keratoses are benign epidermal growths that can manifest on any area of the skin except the palms and soles. They present clinically as tan, yellow, gray, brown, or black with a smooth, waxy, or verrucous surface. They range from 1 mm to several centimeters in diameter. Although SKs traditionally manifest more frequently in individuals with lighter skin tones, pigmented variants, such as dermatosis papulosa nigra, have been reported to occur more commonly and at younger ages in patients with skin of color.1
Dermoscopy of SK in patients with skin of color can present diagnostic challenges, as these lesions may display atypical pigmented patterns that overlap with melanocytic lesions, including Spitz nevi, particularly when starburstlike or globular structures are present.2 What sets inflamed SKs apart from other SKs is the lack of a heavily keratinized surface on both clinical and dermoscopic evaluation. Common histopathologic diagnostic criteria for Spitz nevi include Kamino bodies, uniform nuclear enlargement, and spindled or epithelioid nevus cells, which were not noted in our patient.3 Therefore, in presentations such as this, histopathology remains the gold standard for diagnosis.
The differential diagnosis in this case included benign nevus, dysplastic nevus, melanoma, and Spitz nevus. Benign nevi typically demonstrate uniform pigmentation and symmetric dermoscopic patterns. Dysplastic nevi may show architectural disorder and cytologic atypia but lack invasive features.3 Melanoma often exhibits asymmetry, atypical network patterns, and irregular pigmentation.4 Spitz nevi characteristically demonstrate large epithelioid or spindle cells with Kamino bodies on histopathology, which were absent in our patient.
THE DIAGNOSIS: Seborrheic Keratosis
Histopathology revealed epidermal hyperplasia and hyperkeratosis with no notation of atypical melanocytic activity (Figure). There were no Kamino bodies, junctional nesting, or cytologic atypia. Based on these features as well as the clinical and dermoscopic findings, a diagnosis of an inflamed seborrheic keratosis (SK) was made. No further treatment was required following the shave biopsy, and the patient was reassured regarding the benign nature of the lesion.
Seborrheic keratoses are benign epidermal growths that can manifest on any area of the skin except the palms and soles. They present clinically as tan, yellow, gray, brown, or black with a smooth, waxy, or verrucous surface. They range from 1 mm to several centimeters in diameter. Although SKs traditionally manifest more frequently in individuals with lighter skin tones, pigmented variants, such as dermatosis papulosa nigra, have been reported to occur more commonly and at younger ages in patients with skin of color.1
Dermoscopy of SK in patients with skin of color can present diagnostic challenges, as these lesions may display atypical pigmented patterns that overlap with melanocytic lesions, including Spitz nevi, particularly when starburstlike or globular structures are present.2 What sets inflamed SKs apart from other SKs is the lack of a heavily keratinized surface on both clinical and dermoscopic evaluation. Common histopathologic diagnostic criteria for Spitz nevi include Kamino bodies, uniform nuclear enlargement, and spindled or epithelioid nevus cells, which were not noted in our patient.3 Therefore, in presentations such as this, histopathology remains the gold standard for diagnosis.
The differential diagnosis in this case included benign nevus, dysplastic nevus, melanoma, and Spitz nevus. Benign nevi typically demonstrate uniform pigmentation and symmetric dermoscopic patterns. Dysplastic nevi may show architectural disorder and cytologic atypia but lack invasive features.3 Melanoma often exhibits asymmetry, atypical network patterns, and irregular pigmentation.4 Spitz nevi characteristically demonstrate large epithelioid or spindle cells with Kamino bodies on histopathology, which were absent in our patient.
- Greco MJ, Bhutta BS. Seborrheic keratosis. StatPearls [Internet]. StatPearls Publishing; 2025. Updated May 6, 2024. Accessed December 19, 2025. https://www.ncbi.nlm.nih.gov/books/NBK545285/
- Emanuel P, Cheng, H. Spitz naevus pathology. Accessed November 25, 2025. https://dermnetnz.org/topics/spitz-naevus-pathology.
- Wensley KE, Zito PM. Atypical mole. StatPearls [Internet]. StatPearls Publishing; 2025. Updated July 3, 2023. Accessed December 19, 2025. https://www.ncbi.nlm.nih.gov/books/NBK560606/
- Valenzuela FI, Hohnadel M. Dermatoscopic characteristics of melanoma versus benign lesions and nonmelanoma cancers. StatPearls [Internet]. StatPearls Publishing; 2025. Updated August 10, 2024. Accessed December 19, 2025. https://www.ncbi.nlm .nih.gov/books/NBK606113/
- Greco MJ, Bhutta BS. Seborrheic keratosis. StatPearls [Internet]. StatPearls Publishing; 2025. Updated May 6, 2024. Accessed December 19, 2025. https://www.ncbi.nlm.nih.gov/books/NBK545285/
- Emanuel P, Cheng, H. Spitz naevus pathology. Accessed November 25, 2025. https://dermnetnz.org/topics/spitz-naevus-pathology.
- Wensley KE, Zito PM. Atypical mole. StatPearls [Internet]. StatPearls Publishing; 2025. Updated July 3, 2023. Accessed December 19, 2025. https://www.ncbi.nlm.nih.gov/books/NBK560606/
- Valenzuela FI, Hohnadel M. Dermatoscopic characteristics of melanoma versus benign lesions and nonmelanoma cancers. StatPearls [Internet]. StatPearls Publishing; 2025. Updated August 10, 2024. Accessed December 19, 2025. https://www.ncbi.nlm .nih.gov/books/NBK606113/
Dark-Brown Macule on the Periumbilical Skin
Dark-Brown Macule on the Periumbilical Skin
A 33-year-old man with moderately to deeply pigmented skin presented to the dermatology department with a dark-brown macule in the periumbilical area of more than 1 year’s duration. The patient was otherwise healthy and reported no personal or family history of atypical nevi, nonmelanoma skin cancer, or melanoma. Dermoscopy of the lesion showed a dark brown macule less than 2 mm in diameter with a starburst like pattern and a blue-hued border. A shave biopsy of the lesion was performed.

