User login
Daily sunscreen use will prevent more melanoma deaths than early detection
The dramatic advances in targeted therapies for late-stage melanoma capture the headlines, but a recent Australian study quietly concluded that according to Laura Korb Ferris, MD, PhD, a dermatologist and director of clinical trials in the department of dermatology at the University of Pittsburgh.

“I think it’s really important that we recognize the importance of preventing skin cancer, and not just early detection, not just treatment of late disease,” Dr. Ferris said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
She highlighted the Australian cost-effectiveness analysis, which used Markov modeling of data from two published population-based, randomized controlled trials carried out in Queensland, Australia.
The cost-effectiveness study compared the estimated long-term impact of three different approaches to control of melanoma: a primary prevention strategy, which basically consisted of promoting daily sunscreen use and other forms of sun protection; early detection through annual whole-body skin examinations by physicians starting at age 50; and no intervention. The analysis provided estimates of the number of cases of melanoma, deaths caused by melanoma, nonmelanoma skin cancers, and quality of life outcomes over the course of 30 years starting in 50-year-old men and women.
Primary prevention through sun protection was the clear winner, as shown by the results:
- A 44% reduction in the incidence of melanoma, compared with early detection via annual physician skin examinations.
- A 39% reduction in projected melanoma deaths compared with early detection, which in turn achieved only a 2% reduction when compared with no intervention.
- 27% fewer keratinocyte cancers excised than with annual skin examinations.
- A 21.7% reduction in societal costs, compared with an early-detection program.
Daily sunscreen use for primary prevention was also associated with a modest 0.1% increase in quality-adjusted life-years. “Prevention is low cost, low risk, and effective,” Dr. Ferris observed.
The investigators noted that, while residents of the Australian state of Queensland are mainly fair-skinned and confront high UV radiation levels throughout the year, somewhat limiting the generalizability of the study findings, the relationships between the costs of interventional strategies and their outcomes should be proportional in other countries.
True enough, but a strategy of annual skin examinations starting at age 50 years as modeled in the Australian study is not the most productive way to conduct a melanoma early-detection program, Dr. Ferris said. She noted that data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program show that the median age at diagnosis of melanoma in the United States is 65 years, while the median age at death caused by the malignancy is 71 years. That information is helpful in formulating strategies to improve early detection through more focused, higher-yield screening.

Case in point: European investigators have estimated that, by screening everyone age 50 years and older, 475 people need to be screened and an average of 19.6 lesions must be biopsied in order to detect one melanoma. But by reserving screening for those age 50 years and up who have any one of three risk factors – a personal history of melanoma, atypical nevi, or at least 40 common nevi – those numbers drop dramatically: 98 people need to be screened and 13.5 lesions biopsied to detect one melanoma. And by further narrowing the screened population to those age 65 years or older with any of the three risk factors, 63 seniors would need to be screened and 9.2 lesions excised to find one melanoma.
Total-body skin examinations are time-consuming for dermatologists. In a recent U.S. study, investigators determined that the additional face-to-face time required per skin cancer detected by doing a total-body skin exam in adults who present to a dermatologist for another reason is 4.5 hours. And that’s just the time involved in detecting any type of skin cancer.
“To get that number for melanoma, multiply by 15 to 20,” Dr. Ferris said.
The investigators also determined that, for each decade of advancing age and increment in lighter skin phototype, the number-needed-to-examine in order to identify one skin cancer of any type decreased.
“By focusing on patients who are older and have fair skin types we can get that time down to about 1 hour,” commented Dr. Ferris, who penned an editorial perspective on the study.
While many dermatologists recommend that people with a high common nevus count undergo frequent screening for melanoma because they are at particularly high risk for invasive disease, a couple of recent studies challenge that notion, she pointed out. One was a retrospective study of 326 consecutive new melanoma patients which found that patients with a higher nevus count had thinner melanomas and a greater likelihood of in situ melanoma. Patients who presented with invasive melanoma had a mean total nevus count of 31.5 lesions, while those with in situ melanoma averaged 57.2 nevi. Each additional nevus was associated with a 4% reduction in the likelihood of invasive melanoma, independent of age and sex.
The other study included 566 newly diagnosed melanoma patients in two U.S. centers. Among the 56% of patients who were younger than 60 years, those who had more than 50 total nevi were 68% less likely to have a thick melanoma in a logistic regression analysis that controlled for demographic factors, as well as anatomic location of the melanoma, histologic subtype, and skin cancer screening frequency. In contrast, younger patients with more than 5 atypical nevi were 2.43-fold more likely to have thicker melanomas than were those with no such lesions. The lesson, according to the investigators, is that total nevus count isn’t a reliable determinant of a patient’s risk status or the need for skin examinations.
Dr. Ferris reported no financial conflicts of interest regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
The dramatic advances in targeted therapies for late-stage melanoma capture the headlines, but a recent Australian study quietly concluded that according to Laura Korb Ferris, MD, PhD, a dermatologist and director of clinical trials in the department of dermatology at the University of Pittsburgh.
“I think it’s really important that we recognize the importance of preventing skin cancer, and not just early detection, not just treatment of late disease,” Dr. Ferris said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
She highlighted the Australian cost-effectiveness analysis, which used Markov modeling of data from two published population-based, randomized controlled trials carried out in Queensland, Australia.
The cost-effectiveness study compared the estimated long-term impact of three different approaches to control of melanoma: a primary prevention strategy, which basically consisted of promoting daily sunscreen use and other forms of sun protection; early detection through annual whole-body skin examinations by physicians starting at age 50; and no intervention. The analysis provided estimates of the number of cases of melanoma, deaths caused by melanoma, nonmelanoma skin cancers, and quality of life outcomes over the course of 30 years starting in 50-year-old men and women.
Primary prevention through sun protection was the clear winner, as shown by the results:
- A 44% reduction in the incidence of melanoma, compared with early detection via annual physician skin examinations.
- A 39% reduction in projected melanoma deaths compared with early detection, which in turn achieved only a 2% reduction when compared with no intervention.
- 27% fewer keratinocyte cancers excised than with annual skin examinations.
- A 21.7% reduction in societal costs, compared with an early-detection program.
Daily sunscreen use for primary prevention was also associated with a modest 0.1% increase in quality-adjusted life-years. “Prevention is low cost, low risk, and effective,” Dr. Ferris observed.
The investigators noted that, while residents of the Australian state of Queensland are mainly fair-skinned and confront high UV radiation levels throughout the year, somewhat limiting the generalizability of the study findings, the relationships between the costs of interventional strategies and their outcomes should be proportional in other countries.
True enough, but a strategy of annual skin examinations starting at age 50 years as modeled in the Australian study is not the most productive way to conduct a melanoma early-detection program, Dr. Ferris said. She noted that data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program show that the median age at diagnosis of melanoma in the United States is 65 years, while the median age at death caused by the malignancy is 71 years. That information is helpful in formulating strategies to improve early detection through more focused, higher-yield screening.
Case in point: European investigators have estimated that, by screening everyone age 50 years and older, 475 people need to be screened and an average of 19.6 lesions must be biopsied in order to detect one melanoma. But by reserving screening for those age 50 years and up who have any one of three risk factors – a personal history of melanoma, atypical nevi, or at least 40 common nevi – those numbers drop dramatically: 98 people need to be screened and 13.5 lesions biopsied to detect one melanoma. And by further narrowing the screened population to those age 65 years or older with any of the three risk factors, 63 seniors would need to be screened and 9.2 lesions excised to find one melanoma.
Total-body skin examinations are time-consuming for dermatologists. In a recent U.S. study, investigators determined that the additional face-to-face time required per skin cancer detected by doing a total-body skin exam in adults who present to a dermatologist for another reason is 4.5 hours. And that’s just the time involved in detecting any type of skin cancer.
“To get that number for melanoma, multiply by 15 to 20,” Dr. Ferris said.
The investigators also determined that, for each decade of advancing age and increment in lighter skin phototype, the number-needed-to-examine in order to identify one skin cancer of any type decreased.
“By focusing on patients who are older and have fair skin types we can get that time down to about 1 hour,” commented Dr. Ferris, who penned an editorial perspective on the study.
While many dermatologists recommend that people with a high common nevus count undergo frequent screening for melanoma because they are at particularly high risk for invasive disease, a couple of recent studies challenge that notion, she pointed out. One was a retrospective study of 326 consecutive new melanoma patients which found that patients with a higher nevus count had thinner melanomas and a greater likelihood of in situ melanoma. Patients who presented with invasive melanoma had a mean total nevus count of 31.5 lesions, while those with in situ melanoma averaged 57.2 nevi. Each additional nevus was associated with a 4% reduction in the likelihood of invasive melanoma, independent of age and sex.
The other study included 566 newly diagnosed melanoma patients in two U.S. centers. Among the 56% of patients who were younger than 60 years, those who had more than 50 total nevi were 68% less likely to have a thick melanoma in a logistic regression analysis that controlled for demographic factors, as well as anatomic location of the melanoma, histologic subtype, and skin cancer screening frequency. In contrast, younger patients with more than 5 atypical nevi were 2.43-fold more likely to have thicker melanomas than were those with no such lesions. The lesson, according to the investigators, is that total nevus count isn’t a reliable determinant of a patient’s risk status or the need for skin examinations.
Dr. Ferris reported no financial conflicts of interest regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
The dramatic advances in targeted therapies for late-stage melanoma capture the headlines, but a recent Australian study quietly concluded that according to Laura Korb Ferris, MD, PhD, a dermatologist and director of clinical trials in the department of dermatology at the University of Pittsburgh.
“I think it’s really important that we recognize the importance of preventing skin cancer, and not just early detection, not just treatment of late disease,” Dr. Ferris said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
She highlighted the Australian cost-effectiveness analysis, which used Markov modeling of data from two published population-based, randomized controlled trials carried out in Queensland, Australia.
The cost-effectiveness study compared the estimated long-term impact of three different approaches to control of melanoma: a primary prevention strategy, which basically consisted of promoting daily sunscreen use and other forms of sun protection; early detection through annual whole-body skin examinations by physicians starting at age 50; and no intervention. The analysis provided estimates of the number of cases of melanoma, deaths caused by melanoma, nonmelanoma skin cancers, and quality of life outcomes over the course of 30 years starting in 50-year-old men and women.
Primary prevention through sun protection was the clear winner, as shown by the results:
- A 44% reduction in the incidence of melanoma, compared with early detection via annual physician skin examinations.
- A 39% reduction in projected melanoma deaths compared with early detection, which in turn achieved only a 2% reduction when compared with no intervention.
- 27% fewer keratinocyte cancers excised than with annual skin examinations.
- A 21.7% reduction in societal costs, compared with an early-detection program.
Daily sunscreen use for primary prevention was also associated with a modest 0.1% increase in quality-adjusted life-years. “Prevention is low cost, low risk, and effective,” Dr. Ferris observed.
The investigators noted that, while residents of the Australian state of Queensland are mainly fair-skinned and confront high UV radiation levels throughout the year, somewhat limiting the generalizability of the study findings, the relationships between the costs of interventional strategies and their outcomes should be proportional in other countries.
True enough, but a strategy of annual skin examinations starting at age 50 years as modeled in the Australian study is not the most productive way to conduct a melanoma early-detection program, Dr. Ferris said. She noted that data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program show that the median age at diagnosis of melanoma in the United States is 65 years, while the median age at death caused by the malignancy is 71 years. That information is helpful in formulating strategies to improve early detection through more focused, higher-yield screening.
Case in point: European investigators have estimated that, by screening everyone age 50 years and older, 475 people need to be screened and an average of 19.6 lesions must be biopsied in order to detect one melanoma. But by reserving screening for those age 50 years and up who have any one of three risk factors – a personal history of melanoma, atypical nevi, or at least 40 common nevi – those numbers drop dramatically: 98 people need to be screened and 13.5 lesions biopsied to detect one melanoma. And by further narrowing the screened population to those age 65 years or older with any of the three risk factors, 63 seniors would need to be screened and 9.2 lesions excised to find one melanoma.
Total-body skin examinations are time-consuming for dermatologists. In a recent U.S. study, investigators determined that the additional face-to-face time required per skin cancer detected by doing a total-body skin exam in adults who present to a dermatologist for another reason is 4.5 hours. And that’s just the time involved in detecting any type of skin cancer.
“To get that number for melanoma, multiply by 15 to 20,” Dr. Ferris said.
The investigators also determined that, for each decade of advancing age and increment in lighter skin phototype, the number-needed-to-examine in order to identify one skin cancer of any type decreased.
“By focusing on patients who are older and have fair skin types we can get that time down to about 1 hour,” commented Dr. Ferris, who penned an editorial perspective on the study.
While many dermatologists recommend that people with a high common nevus count undergo frequent screening for melanoma because they are at particularly high risk for invasive disease, a couple of recent studies challenge that notion, she pointed out. One was a retrospective study of 326 consecutive new melanoma patients which found that patients with a higher nevus count had thinner melanomas and a greater likelihood of in situ melanoma. Patients who presented with invasive melanoma had a mean total nevus count of 31.5 lesions, while those with in situ melanoma averaged 57.2 nevi. Each additional nevus was associated with a 4% reduction in the likelihood of invasive melanoma, independent of age and sex.
The other study included 566 newly diagnosed melanoma patients in two U.S. centers. Among the 56% of patients who were younger than 60 years, those who had more than 50 total nevi were 68% less likely to have a thick melanoma in a logistic regression analysis that controlled for demographic factors, as well as anatomic location of the melanoma, histologic subtype, and skin cancer screening frequency. In contrast, younger patients with more than 5 atypical nevi were 2.43-fold more likely to have thicker melanomas than were those with no such lesions. The lesson, according to the investigators, is that total nevus count isn’t a reliable determinant of a patient’s risk status or the need for skin examinations.
Dr. Ferris reported no financial conflicts of interest regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
FROM THE CUTANEOUS MALIGNANCIES FORUM
International expert group agrees on redefining psoriasis severity
It’s high time to say farewell to the traditional categorization of psoriasis severity into mild, moderate, or severe disease, according to the International Psoriasis Council.
The mild/moderate/severe categorization is vague and defined differently by different organizations and in different countries. It often underestimates disease severity because it ignores psoriasis involvement in particularly tough-to-treat special areas, including the scalp, palms, soles, face, nails, and genitalia, Bruce E. Strober, MD, PhD, asserted at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year. He chaired an IPC project in which prominent psoriasis experts in 32 countries employed a Delphi consensus approach aimed at achieving agreement on a more practical recategorization of psoriasis severity for use in both daily clinical practice and enrolling appropriate participants in clinical trials. What emerged was a simplified dichotomous categorization system.
“What we came up with is a very sensible approach to defining whether patients should get either topical or systemic therapy. In fact, there are only two groups of patients in psoriasis: those who should get topicals alone, and those who should get systemic therapy. It’s topicals or systemics,” explained Dr. Strober, a dermatologist at Yale University, New Haven, Conn., who also works in private practice in Cromwell, Conn.
Under the IPC classification, psoriasis patients are candidates for systemic therapy if they meet at least one of three criteria: body surface area of involvement greater than 10%, disease involving the previously mentioned special areas, or failure of topical therapy.
“This approach is about practically treating patients who are in need,” Dr. Strober said. “If patients meet just one of these three criteria they can move on to our current toolbox of systemic therapies, be they older systemic treatments, apremilast, phototherapy, or 1 of the 11 biologics currently approved for the treatment of psoriasis. The key point is that for patients with moderate to severe psoriasis – or should I say, systemic therapy–appropriate psoriasis – treatment should be based on individual patient characteristics. We don’t work on a stepwise approach. If a patient walks in with more than 10% body surface area involved, don’t make them fail topicals; you can go right to systemics.”
European dermatologists often use the Psoriasis Area and Severity Index (PASI) score to characterize disease severity and monitor response to therapy. In contrast, American dermatologists generally find PASI too complex and time-consuming for use in clinical practice, relying instead on the amount of body surface area involved with psoriasis. Neither of these measures incorporates disease involvement in special areas, which when present ought to automatically place a patient in the systemic therapy–appropriate category, according to Dr. Strober.
“I find this [IPC recategorization] a very practical approach. I hope you write this down and use this in your own practice,” Dr. Strober said.
The full IPC report was published in the Journal of the American Academy of Dermatology.
The IPC psoriasis severity reclassification project was unfunded. Dr. Strober reported receiving institutional research funding from and serving as a paid consultant to more than two dozen pharmaceutical companies.
MedscapeLive and this news organization are owned by the same parent company.
It’s high time to say farewell to the traditional categorization of psoriasis severity into mild, moderate, or severe disease, according to the International Psoriasis Council.
The mild/moderate/severe categorization is vague and defined differently by different organizations and in different countries. It often underestimates disease severity because it ignores psoriasis involvement in particularly tough-to-treat special areas, including the scalp, palms, soles, face, nails, and genitalia, Bruce E. Strober, MD, PhD, asserted at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year. He chaired an IPC project in which prominent psoriasis experts in 32 countries employed a Delphi consensus approach aimed at achieving agreement on a more practical recategorization of psoriasis severity for use in both daily clinical practice and enrolling appropriate participants in clinical trials. What emerged was a simplified dichotomous categorization system.
“What we came up with is a very sensible approach to defining whether patients should get either topical or systemic therapy. In fact, there are only two groups of patients in psoriasis: those who should get topicals alone, and those who should get systemic therapy. It’s topicals or systemics,” explained Dr. Strober, a dermatologist at Yale University, New Haven, Conn., who also works in private practice in Cromwell, Conn.
Under the IPC classification, psoriasis patients are candidates for systemic therapy if they meet at least one of three criteria: body surface area of involvement greater than 10%, disease involving the previously mentioned special areas, or failure of topical therapy.
“This approach is about practically treating patients who are in need,” Dr. Strober said. “If patients meet just one of these three criteria they can move on to our current toolbox of systemic therapies, be they older systemic treatments, apremilast, phototherapy, or 1 of the 11 biologics currently approved for the treatment of psoriasis. The key point is that for patients with moderate to severe psoriasis – or should I say, systemic therapy–appropriate psoriasis – treatment should be based on individual patient characteristics. We don’t work on a stepwise approach. If a patient walks in with more than 10% body surface area involved, don’t make them fail topicals; you can go right to systemics.”
European dermatologists often use the Psoriasis Area and Severity Index (PASI) score to characterize disease severity and monitor response to therapy. In contrast, American dermatologists generally find PASI too complex and time-consuming for use in clinical practice, relying instead on the amount of body surface area involved with psoriasis. Neither of these measures incorporates disease involvement in special areas, which when present ought to automatically place a patient in the systemic therapy–appropriate category, according to Dr. Strober.
“I find this [IPC recategorization] a very practical approach. I hope you write this down and use this in your own practice,” Dr. Strober said.
The full IPC report was published in the Journal of the American Academy of Dermatology.
The IPC psoriasis severity reclassification project was unfunded. Dr. Strober reported receiving institutional research funding from and serving as a paid consultant to more than two dozen pharmaceutical companies.
MedscapeLive and this news organization are owned by the same parent company.
It’s high time to say farewell to the traditional categorization of psoriasis severity into mild, moderate, or severe disease, according to the International Psoriasis Council.
The mild/moderate/severe categorization is vague and defined differently by different organizations and in different countries. It often underestimates disease severity because it ignores psoriasis involvement in particularly tough-to-treat special areas, including the scalp, palms, soles, face, nails, and genitalia, Bruce E. Strober, MD, PhD, asserted at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year. He chaired an IPC project in which prominent psoriasis experts in 32 countries employed a Delphi consensus approach aimed at achieving agreement on a more practical recategorization of psoriasis severity for use in both daily clinical practice and enrolling appropriate participants in clinical trials. What emerged was a simplified dichotomous categorization system.
“What we came up with is a very sensible approach to defining whether patients should get either topical or systemic therapy. In fact, there are only two groups of patients in psoriasis: those who should get topicals alone, and those who should get systemic therapy. It’s topicals or systemics,” explained Dr. Strober, a dermatologist at Yale University, New Haven, Conn., who also works in private practice in Cromwell, Conn.
Under the IPC classification, psoriasis patients are candidates for systemic therapy if they meet at least one of three criteria: body surface area of involvement greater than 10%, disease involving the previously mentioned special areas, or failure of topical therapy.
“This approach is about practically treating patients who are in need,” Dr. Strober said. “If patients meet just one of these three criteria they can move on to our current toolbox of systemic therapies, be they older systemic treatments, apremilast, phototherapy, or 1 of the 11 biologics currently approved for the treatment of psoriasis. The key point is that for patients with moderate to severe psoriasis – or should I say, systemic therapy–appropriate psoriasis – treatment should be based on individual patient characteristics. We don’t work on a stepwise approach. If a patient walks in with more than 10% body surface area involved, don’t make them fail topicals; you can go right to systemics.”
European dermatologists often use the Psoriasis Area and Severity Index (PASI) score to characterize disease severity and monitor response to therapy. In contrast, American dermatologists generally find PASI too complex and time-consuming for use in clinical practice, relying instead on the amount of body surface area involved with psoriasis. Neither of these measures incorporates disease involvement in special areas, which when present ought to automatically place a patient in the systemic therapy–appropriate category, according to Dr. Strober.
“I find this [IPC recategorization] a very practical approach. I hope you write this down and use this in your own practice,” Dr. Strober said.
The full IPC report was published in the Journal of the American Academy of Dermatology.
The IPC psoriasis severity reclassification project was unfunded. Dr. Strober reported receiving institutional research funding from and serving as a paid consultant to more than two dozen pharmaceutical companies.
MedscapeLive and this news organization are owned by the same parent company.
FROM MEDSCAPELIVE LAS VEGAS DERMATOLOGY SEMINAR
The case for anti–IL-17 agents as first-line biologics in psoriatic arthritis
LAS VEGAS – at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year.

The 2018 joint American College of Rheumatology/National Psoriasis Association guidelines recommend the anti–tumor necrosis factor agents as first-line biologic therapy for PsA, with the anti–IL-17 biologics held in reserve as second-tier therapy for when the anti-TNFs don’t work. That’s largely because the guidance was developed before the compelling evidence for the anti–IL-17 agents as the biologics of choice was appreciated, according to Dr. Gordon, professor and chair of the department of dermatology at the Medical College of Wisconsin, Milwaukee.
“Many people go by these guidelines,” the dermatologist noted. “I think it’s really critical to look at the data and not just the guidelines because the guidelines don’t give full credit to the anti–IL-17 agents,” he added.
“Emerging psoriatic arthritis data may likely put this class of medications into the forefront of treatment for patients who have both psoriasis and psoriatic arthritis because you generally get higher responses for the skin disease than with anti-TNF therapy, and with similar responses in psoriatic arthritis.”
Two IL-17 inhibitors are approved for both PsA and psoriasis: secukinumab (Cosentyx) and ixekizumab (Taltz). In addition, brodalumab (Siliq), approved for psoriasis, is expected to receive an expanded indication for PsA based upon its strong showing in the AMVISION-1 and -2 trials. Data from those trials, as well as the FUTURE 2 trial for secukinumab and SPIRIT-P1 for ixekizumab, consistently document at least 20% improvement in the ACR criteria for PsA severity – that is, an ACR 20 response – in 50%-60% of patients on one of the three IL-17 inhibitors, as well as ACR 50 response rates of around 30%. Those outcomes are quite consistent with the impact of the anti-TNF biologics on joint disease. But the TNF inhibitors can’t touch the anti–IL-17 biologics when it comes to improvement in Psoriasis Area and Severity Index (PASI) scores: The anti–IL-17 agents have week-52 PASI 75 response rates in the range of 80%, PASI 90 response rates of 70%-75%, and PASI 100 response rates of 40%-55%, with the highest-end results being seen with brodalumab, he continued.
A point worth remembering when prescribing secukinumab is that the approved dose for PsA is 150 mg every 4 weeks, which is just half of the typical dose in psoriasis.
“I spend a lot of time convincing my rheumatology colleagues that if you’re treating both psoriasis and psoriatic arthritis, use the psoriasis dose. There’s some evidence that the higher dose provides some benefit in terms of prevention of permanent joint damage by x-ray,” Dr. Gordon said.
Evidence that TNF inhibitors inhibit permanent joint damage in patients with PsA has been considered a major advantage, establishing this medication class as first-line biologic therapy. But anti–IL-17 therapies appear to have a similar beneficial effect. That was demonstrated in the SPIRIT-P1 trial, where Sharp scores – a radiographic measure of progression of joint damage – were similar at 24 weeks in PsA patients randomized to ixekizumab as compared to adalimumab, with both biologics being superior to placebo. An Assessment of SpondyloArthritis International Society 20% improvement (ASAS 20) response or an ACR 50 response doesn’t capture what’s going on with regard to axial disease. That’s assessed through ASAS 20 and ASAS 40 responses – that is, at least 20% or 40% improvement, compared with baseline, in Assessment in Ankylosing Spondylitis scores. And in the MEASURE 1 and 2 trials, secukinumab achieved robust improvement in axial disease as reflected in favorable ASAS 20 and ASAS 40 responses through 52 weeks in patients with active ankylosing spondylitis.
“The anti–IL-17 agents do actually work in ankylosing spondylitis, which might be a surrogate for the treatment effect in axial psoriatic arthritis,” Dr. Gordon commented.
The phase 3b MAXIMISE trial presented at the 2019 EULAR meeting looked specifically at the impact of secukinumab in patients with psoriatic arthritis with axial involvement. An ASAS 20 response at week 12 was seen in 67% and 65% of patients randomized to secukinumab at 150 or 300 mg, respectively, if they were on concomitant methotrexate, and 64% and 61% if they were not, compared with ASAS 20 rates of 34% and 31% in placebo-treated controls.
“This is the only study of an anti–IL-17 agent that’s been done for axial disease to date in psoriatic arthritis. It’s very, very encouraging,” the dermatologist commented.
Durability of response and safety
“In terms of safety, the anti–IL-17s have been a truly remarkable success story. There are very low rates of things to be concerned about,” Dr. Gordon said.
Oral candidiasis occurs in 2%-4% of treated patients, but he noted, “It’s almost always very mild disease” that’s easily treatable with nystatin or, in the worst case, with some fluconazole.
Inflammatory bowel disease (IBD) as a side effect of anti–IL-17 therapy has been a controversial issue. Dr. Gordon’s interpretation of the evidence is that there probably is a very slight increase in the risk of developing ulcerative colitis, but not Crohn’s disease.
“This rate is extraordinarily low, so while it’s something that I consider, and if a patient has a personal history of IBD I will sometimes hesitate to use an anti–IL-17 agent, in patients who don’t have a personal history I’ll go ahead,” he explained.
There is a signal of a slight increase in risk of depression in patients on brodalumab, which isn’t the case for secukinumab or ixekizumab.
Importantly, large long-term extension studies with years of follow-up show that the initially low adverse event rates associated with the IL-17 inhibitors don’t increase over time; rather, they remain steady over years of use.
Long-term maintenance of response with these biologics is impressive. “It’s not perfect, but it’s still a tremendous advantage for patients, especially if you can get them through that initial period,” Dr. Gordon said.
For example, in the long-term extension of the UNCOVER-1 trial, psoriasis patients who had clear or almost clear skin at week 12 on ixekizumab and continued to take the medication open label for 5 years had PASI 75, 90, and 100 response rates of 94%, 82%, and 47%, respectively, at week 264.
What about IL-12/23 and IL-23 inhibitors in PsA?
In a separate presentation at the MedscapeLive seminar, Bruce E. Strober, MD, PhD, said that, although ustekinumab (Stelara) is approved for both psoriasis and PsA, the IL-12/-23 inhibitor’s efficacy in PsA is inconsistent and lower than other approved biologics. In contrast, the IL-23 inhibitor guselkumab (Tremfya), which also has the dual indications, is a strong performer in both. In the DISCOVER-2 trial, conducted in treatment-naive patients with PsA, guselkumab at the approved dose of 100 mg every 8 weeks achieved ACR 20, 50, and 70 rates of 64%, 31%, and 19%, respectively. It was also significantly better than placebo for resolution of enthesitis.

An important caveat: While radiographic inhibition of progression of joint disease occurred with guselkumab dosed at 100 mg every 4 weeks in DISCOVER-2, that’s not the approved dose. At 100 mg every 8 weeks – the FDA-approved dosing for both psoriatic arthritis and psoriasis – radiographic inhibition wasn’t better than with placebo, noted Dr. Strober, a dermatologist at Yale University, New Haven, Conn.
Dr. Gordon and Dr. Strober are clinical trialists who reported receiving research support and/or honoraria from more than a dozen pharmaceutical companies, including virtually all of those with biologics for dermatology.
MedscapeLive and this news organization are owned by the same parent company.
LAS VEGAS – at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year.
The 2018 joint American College of Rheumatology/National Psoriasis Association guidelines recommend the anti–tumor necrosis factor agents as first-line biologic therapy for PsA, with the anti–IL-17 biologics held in reserve as second-tier therapy for when the anti-TNFs don’t work. That’s largely because the guidance was developed before the compelling evidence for the anti–IL-17 agents as the biologics of choice was appreciated, according to Dr. Gordon, professor and chair of the department of dermatology at the Medical College of Wisconsin, Milwaukee.
“Many people go by these guidelines,” the dermatologist noted. “I think it’s really critical to look at the data and not just the guidelines because the guidelines don’t give full credit to the anti–IL-17 agents,” he added.
“Emerging psoriatic arthritis data may likely put this class of medications into the forefront of treatment for patients who have both psoriasis and psoriatic arthritis because you generally get higher responses for the skin disease than with anti-TNF therapy, and with similar responses in psoriatic arthritis.”
Two IL-17 inhibitors are approved for both PsA and psoriasis: secukinumab (Cosentyx) and ixekizumab (Taltz). In addition, brodalumab (Siliq), approved for psoriasis, is expected to receive an expanded indication for PsA based upon its strong showing in the AMVISION-1 and -2 trials. Data from those trials, as well as the FUTURE 2 trial for secukinumab and SPIRIT-P1 for ixekizumab, consistently document at least 20% improvement in the ACR criteria for PsA severity – that is, an ACR 20 response – in 50%-60% of patients on one of the three IL-17 inhibitors, as well as ACR 50 response rates of around 30%. Those outcomes are quite consistent with the impact of the anti-TNF biologics on joint disease. But the TNF inhibitors can’t touch the anti–IL-17 biologics when it comes to improvement in Psoriasis Area and Severity Index (PASI) scores: The anti–IL-17 agents have week-52 PASI 75 response rates in the range of 80%, PASI 90 response rates of 70%-75%, and PASI 100 response rates of 40%-55%, with the highest-end results being seen with brodalumab, he continued.
A point worth remembering when prescribing secukinumab is that the approved dose for PsA is 150 mg every 4 weeks, which is just half of the typical dose in psoriasis.
“I spend a lot of time convincing my rheumatology colleagues that if you’re treating both psoriasis and psoriatic arthritis, use the psoriasis dose. There’s some evidence that the higher dose provides some benefit in terms of prevention of permanent joint damage by x-ray,” Dr. Gordon said.
Evidence that TNF inhibitors inhibit permanent joint damage in patients with PsA has been considered a major advantage, establishing this medication class as first-line biologic therapy. But anti–IL-17 therapies appear to have a similar beneficial effect. That was demonstrated in the SPIRIT-P1 trial, where Sharp scores – a radiographic measure of progression of joint damage – were similar at 24 weeks in PsA patients randomized to ixekizumab as compared to adalimumab, with both biologics being superior to placebo. An Assessment of SpondyloArthritis International Society 20% improvement (ASAS 20) response or an ACR 50 response doesn’t capture what’s going on with regard to axial disease. That’s assessed through ASAS 20 and ASAS 40 responses – that is, at least 20% or 40% improvement, compared with baseline, in Assessment in Ankylosing Spondylitis scores. And in the MEASURE 1 and 2 trials, secukinumab achieved robust improvement in axial disease as reflected in favorable ASAS 20 and ASAS 40 responses through 52 weeks in patients with active ankylosing spondylitis.
“The anti–IL-17 agents do actually work in ankylosing spondylitis, which might be a surrogate for the treatment effect in axial psoriatic arthritis,” Dr. Gordon commented.
The phase 3b MAXIMISE trial presented at the 2019 EULAR meeting looked specifically at the impact of secukinumab in patients with psoriatic arthritis with axial involvement. An ASAS 20 response at week 12 was seen in 67% and 65% of patients randomized to secukinumab at 150 or 300 mg, respectively, if they were on concomitant methotrexate, and 64% and 61% if they were not, compared with ASAS 20 rates of 34% and 31% in placebo-treated controls.
“This is the only study of an anti–IL-17 agent that’s been done for axial disease to date in psoriatic arthritis. It’s very, very encouraging,” the dermatologist commented.
Durability of response and safety
“In terms of safety, the anti–IL-17s have been a truly remarkable success story. There are very low rates of things to be concerned about,” Dr. Gordon said.
Oral candidiasis occurs in 2%-4% of treated patients, but he noted, “It’s almost always very mild disease” that’s easily treatable with nystatin or, in the worst case, with some fluconazole.
Inflammatory bowel disease (IBD) as a side effect of anti–IL-17 therapy has been a controversial issue. Dr. Gordon’s interpretation of the evidence is that there probably is a very slight increase in the risk of developing ulcerative colitis, but not Crohn’s disease.
“This rate is extraordinarily low, so while it’s something that I consider, and if a patient has a personal history of IBD I will sometimes hesitate to use an anti–IL-17 agent, in patients who don’t have a personal history I’ll go ahead,” he explained.
There is a signal of a slight increase in risk of depression in patients on brodalumab, which isn’t the case for secukinumab or ixekizumab.
Importantly, large long-term extension studies with years of follow-up show that the initially low adverse event rates associated with the IL-17 inhibitors don’t increase over time; rather, they remain steady over years of use.
Long-term maintenance of response with these biologics is impressive. “It’s not perfect, but it’s still a tremendous advantage for patients, especially if you can get them through that initial period,” Dr. Gordon said.
For example, in the long-term extension of the UNCOVER-1 trial, psoriasis patients who had clear or almost clear skin at week 12 on ixekizumab and continued to take the medication open label for 5 years had PASI 75, 90, and 100 response rates of 94%, 82%, and 47%, respectively, at week 264.
What about IL-12/23 and IL-23 inhibitors in PsA?
In a separate presentation at the MedscapeLive seminar, Bruce E. Strober, MD, PhD, said that, although ustekinumab (Stelara) is approved for both psoriasis and PsA, the IL-12/-23 inhibitor’s efficacy in PsA is inconsistent and lower than other approved biologics. In contrast, the IL-23 inhibitor guselkumab (Tremfya), which also has the dual indications, is a strong performer in both. In the DISCOVER-2 trial, conducted in treatment-naive patients with PsA, guselkumab at the approved dose of 100 mg every 8 weeks achieved ACR 20, 50, and 70 rates of 64%, 31%, and 19%, respectively. It was also significantly better than placebo for resolution of enthesitis.
An important caveat: While radiographic inhibition of progression of joint disease occurred with guselkumab dosed at 100 mg every 4 weeks in DISCOVER-2, that’s not the approved dose. At 100 mg every 8 weeks – the FDA-approved dosing for both psoriatic arthritis and psoriasis – radiographic inhibition wasn’t better than with placebo, noted Dr. Strober, a dermatologist at Yale University, New Haven, Conn.
Dr. Gordon and Dr. Strober are clinical trialists who reported receiving research support and/or honoraria from more than a dozen pharmaceutical companies, including virtually all of those with biologics for dermatology.
MedscapeLive and this news organization are owned by the same parent company.
LAS VEGAS – at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year.
The 2018 joint American College of Rheumatology/National Psoriasis Association guidelines recommend the anti–tumor necrosis factor agents as first-line biologic therapy for PsA, with the anti–IL-17 biologics held in reserve as second-tier therapy for when the anti-TNFs don’t work. That’s largely because the guidance was developed before the compelling evidence for the anti–IL-17 agents as the biologics of choice was appreciated, according to Dr. Gordon, professor and chair of the department of dermatology at the Medical College of Wisconsin, Milwaukee.
“Many people go by these guidelines,” the dermatologist noted. “I think it’s really critical to look at the data and not just the guidelines because the guidelines don’t give full credit to the anti–IL-17 agents,” he added.
“Emerging psoriatic arthritis data may likely put this class of medications into the forefront of treatment for patients who have both psoriasis and psoriatic arthritis because you generally get higher responses for the skin disease than with anti-TNF therapy, and with similar responses in psoriatic arthritis.”
Two IL-17 inhibitors are approved for both PsA and psoriasis: secukinumab (Cosentyx) and ixekizumab (Taltz). In addition, brodalumab (Siliq), approved for psoriasis, is expected to receive an expanded indication for PsA based upon its strong showing in the AMVISION-1 and -2 trials. Data from those trials, as well as the FUTURE 2 trial for secukinumab and SPIRIT-P1 for ixekizumab, consistently document at least 20% improvement in the ACR criteria for PsA severity – that is, an ACR 20 response – in 50%-60% of patients on one of the three IL-17 inhibitors, as well as ACR 50 response rates of around 30%. Those outcomes are quite consistent with the impact of the anti-TNF biologics on joint disease. But the TNF inhibitors can’t touch the anti–IL-17 biologics when it comes to improvement in Psoriasis Area and Severity Index (PASI) scores: The anti–IL-17 agents have week-52 PASI 75 response rates in the range of 80%, PASI 90 response rates of 70%-75%, and PASI 100 response rates of 40%-55%, with the highest-end results being seen with brodalumab, he continued.
A point worth remembering when prescribing secukinumab is that the approved dose for PsA is 150 mg every 4 weeks, which is just half of the typical dose in psoriasis.
“I spend a lot of time convincing my rheumatology colleagues that if you’re treating both psoriasis and psoriatic arthritis, use the psoriasis dose. There’s some evidence that the higher dose provides some benefit in terms of prevention of permanent joint damage by x-ray,” Dr. Gordon said.
Evidence that TNF inhibitors inhibit permanent joint damage in patients with PsA has been considered a major advantage, establishing this medication class as first-line biologic therapy. But anti–IL-17 therapies appear to have a similar beneficial effect. That was demonstrated in the SPIRIT-P1 trial, where Sharp scores – a radiographic measure of progression of joint damage – were similar at 24 weeks in PsA patients randomized to ixekizumab as compared to adalimumab, with both biologics being superior to placebo. An Assessment of SpondyloArthritis International Society 20% improvement (ASAS 20) response or an ACR 50 response doesn’t capture what’s going on with regard to axial disease. That’s assessed through ASAS 20 and ASAS 40 responses – that is, at least 20% or 40% improvement, compared with baseline, in Assessment in Ankylosing Spondylitis scores. And in the MEASURE 1 and 2 trials, secukinumab achieved robust improvement in axial disease as reflected in favorable ASAS 20 and ASAS 40 responses through 52 weeks in patients with active ankylosing spondylitis.
“The anti–IL-17 agents do actually work in ankylosing spondylitis, which might be a surrogate for the treatment effect in axial psoriatic arthritis,” Dr. Gordon commented.
The phase 3b MAXIMISE trial presented at the 2019 EULAR meeting looked specifically at the impact of secukinumab in patients with psoriatic arthritis with axial involvement. An ASAS 20 response at week 12 was seen in 67% and 65% of patients randomized to secukinumab at 150 or 300 mg, respectively, if they were on concomitant methotrexate, and 64% and 61% if they were not, compared with ASAS 20 rates of 34% and 31% in placebo-treated controls.
“This is the only study of an anti–IL-17 agent that’s been done for axial disease to date in psoriatic arthritis. It’s very, very encouraging,” the dermatologist commented.
Durability of response and safety
“In terms of safety, the anti–IL-17s have been a truly remarkable success story. There are very low rates of things to be concerned about,” Dr. Gordon said.
Oral candidiasis occurs in 2%-4% of treated patients, but he noted, “It’s almost always very mild disease” that’s easily treatable with nystatin or, in the worst case, with some fluconazole.
Inflammatory bowel disease (IBD) as a side effect of anti–IL-17 therapy has been a controversial issue. Dr. Gordon’s interpretation of the evidence is that there probably is a very slight increase in the risk of developing ulcerative colitis, but not Crohn’s disease.
“This rate is extraordinarily low, so while it’s something that I consider, and if a patient has a personal history of IBD I will sometimes hesitate to use an anti–IL-17 agent, in patients who don’t have a personal history I’ll go ahead,” he explained.
There is a signal of a slight increase in risk of depression in patients on brodalumab, which isn’t the case for secukinumab or ixekizumab.
Importantly, large long-term extension studies with years of follow-up show that the initially low adverse event rates associated with the IL-17 inhibitors don’t increase over time; rather, they remain steady over years of use.
Long-term maintenance of response with these biologics is impressive. “It’s not perfect, but it’s still a tremendous advantage for patients, especially if you can get them through that initial period,” Dr. Gordon said.
For example, in the long-term extension of the UNCOVER-1 trial, psoriasis patients who had clear or almost clear skin at week 12 on ixekizumab and continued to take the medication open label for 5 years had PASI 75, 90, and 100 response rates of 94%, 82%, and 47%, respectively, at week 264.
What about IL-12/23 and IL-23 inhibitors in PsA?
In a separate presentation at the MedscapeLive seminar, Bruce E. Strober, MD, PhD, said that, although ustekinumab (Stelara) is approved for both psoriasis and PsA, the IL-12/-23 inhibitor’s efficacy in PsA is inconsistent and lower than other approved biologics. In contrast, the IL-23 inhibitor guselkumab (Tremfya), which also has the dual indications, is a strong performer in both. In the DISCOVER-2 trial, conducted in treatment-naive patients with PsA, guselkumab at the approved dose of 100 mg every 8 weeks achieved ACR 20, 50, and 70 rates of 64%, 31%, and 19%, respectively. It was also significantly better than placebo for resolution of enthesitis.
An important caveat: While radiographic inhibition of progression of joint disease occurred with guselkumab dosed at 100 mg every 4 weeks in DISCOVER-2, that’s not the approved dose. At 100 mg every 8 weeks – the FDA-approved dosing for both psoriatic arthritis and psoriasis – radiographic inhibition wasn’t better than with placebo, noted Dr. Strober, a dermatologist at Yale University, New Haven, Conn.
Dr. Gordon and Dr. Strober are clinical trialists who reported receiving research support and/or honoraria from more than a dozen pharmaceutical companies, including virtually all of those with biologics for dermatology.
MedscapeLive and this news organization are owned by the same parent company.
FROM MEDSCAPELIVE LAS VEGAS DERMATOLOGY SEMINAR
Expanded indications likely for apremilast
Big changes are coming in the use of oral apremilast, currently approved for moderate to severe psoriasis and plaque psoriasis in adults, Bruce E. Strober, MD, PhD, predicted at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year.
“We’ll have , meaning we can use this drug in patients in whom we typically think about using only topical therapies. Keep on the lookout: I think the mild to moderate indication may be coming next year, and that’s going to really shake up the whole landscape of psoriasis therapy,” said Dr. Strober, a dermatologist at Yale University in New Haven, Conn., and Central Connecticut Dermatology in Cromwell, Conn.
Mild or moderate psoriasis
Apremilast manufacturer Amgen has announced positive topline results from the phase 3 ADVANCE trial, a multicenter, placebo-controlled, double-blind, study of 595 patients with mild or moderate psoriasis as defined by an involved body surface area of 2%-15% and a Psoriasis Area and Severity Index score of 2-15. Participants were randomized to the approved dose of apremilast (Otezla) – 30 mg twice daily – or placebo for 16 weeks, followed by 16 weeks of open-label apremilast for all. The full study findings haven’t yet been published or presented at a medical conference, but Amgen announced that the results were positive for all primary and secondary endpoints, and the company plans to file a request with the Food and Drug Administration for an expanded indication for the oral agent.
Pediatric studies
A recently published phase 2, open-label, 1-year study of apremilast in 42 children and adolescents with moderate to severe plaque psoriasis demonstrated that weight-based dosing is the best approach in the pediatric population. The study, which serves as the template for coming phase 3 trials, showed that dosing apremilast at 20 mg twice daily in youths weighing not more than 35 kg and 30 mg twice daily in those who weighed more provided pharmacokinetic exposure similar to that achieved with apremilast at the standard adult dose of 30 mg twice daily. Most participants liked the taste of the tablet.
“My prediction is apremilast will have efficacy in children and teenagers comparable to what it has in adults, with a similar safety and adverse event profile,” Dr. Strober said.
Apremilast works by blocking phosphodiesterase type 4, thereby reducing cyclic AMP metabolism, with a resultant increase in cyclic AMP levels. Cyclic AMP is a regulator of inflammation. Boosting its level has the effect of decreasing tumor necrosis factor and other proinflammatory cytokines while increasing anti-inflammatory mediators, such as interleukin-10.
Dr. Strober characterized apremilast’s efficacy as “modest” by contemporary standards in adults with moderate to severe psoriasis, with week 16 PASI 75 rates of about 30% in randomized trials, compared with 5% in placebo-treated controls. He considers it a good option in patients with moderate disease who are needle phobic and in those averse to the inconvenience of laboratory monitoring. The drug is useful in treating psoriasis in especially challenging locations. Apremilast is specifically approved for scalp psoriasis, and Dr. Strober has anecdotally found it helpful in patients with palmoplantar psoriasis or genital psoriasis.
“Apremilast has tolerability issues: first and foremost diarrhea, nausea, and headache. Probably 15%-20% of patients have nausea or diarrhea ranging from mild to severe, and 1 in 20 have headache. You have to warn patients,” he said.
Roughly 1% of patients experience depressed mood. “I’ve seen it in a few patients. I definitely believe it’s real, so query patients about mood changes while taking apremilast,” the dermatologist advised.
One in 5 patients loses 5% of body weight during the first 6 months on apremilast, but there’s no additional weight loss thereafter. It’s wrong to characterize the oral agent as a weight-loss drug, though, since 80% of patients don’t lose weight, Dr. Strober noted.
Topical PDE-4 inhibitor shows promise
Separately at the Las Vegas meeting, Linda Stein Gold, MD, provided highlights of a phase 2b randomized trial of a topical cream formulation of an extremely potent PDE-4 inhibitor, roflumilast, in patients with chronic plaque psoriasis. This molecule is a couple hundred times more effective at inhibiting the PDE-4 receptor than either oral apremilast or topical crisaborole (Eucrisa). And as a once-daily topical agent with very little systemic absorption, roflumilast cream sidesteps the tolerability issues that accompany apremilast.
“Roflumilast is currently available as an oral formulation for treatment of [chronic obstructive pulmonary disease], so it has a fairly well-established safety profile,” noted Dr. Stein Gold, director of dermatology clinical research at the Henry Ford Health System in Detroit.
The 12-week, multicenter, phase 2b study sponsored by Arcutis Biotherapeutics included 331 patients with chronic plaque psoriasis who were randomized to once-daily 0.3% roflumilast cream, 0.15% roflumilast cream, or vehicle. Three-quarters of participants had baseline moderate disease.
A week-8 Investigator’s Global Assessment (IGA) score of 0 or 1, meaning clear skin or almost clear, plus at least a 2-grade improvement from baseline occurred in 32% of the high-dose roflumilast group, 25% of those on the 0.15% formulation, and 10% of controls. On the secondary endpoint of improvement in tough-to-treat intertriginous psoriasis, at week 12 an intertriginous IGA score of 0 or 1 plus at least a 2-point improvement from baseline was seen in 86% of the 0.3% roflumilast cream group, 50% on low-dose therapy, and 29% of controls. Moreover, the clinical improvements in IGA and itch kicked in quickly, with significant separation from placebo by week 2, Dr. Stein Gold noted.
The phase 3 program is now recruiting participants.
Dr. Strober and Dr. Stein Gold reported receiving research funding from and serving as consultants to Amgen and numerous other pharmaceutical companies.
MedscapeLive and this news organization are owned by the same parent company.
Big changes are coming in the use of oral apremilast, currently approved for moderate to severe psoriasis and plaque psoriasis in adults, Bruce E. Strober, MD, PhD, predicted at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year.
“We’ll have , meaning we can use this drug in patients in whom we typically think about using only topical therapies. Keep on the lookout: I think the mild to moderate indication may be coming next year, and that’s going to really shake up the whole landscape of psoriasis therapy,” said Dr. Strober, a dermatologist at Yale University in New Haven, Conn., and Central Connecticut Dermatology in Cromwell, Conn.
Mild or moderate psoriasis
Apremilast manufacturer Amgen has announced positive topline results from the phase 3 ADVANCE trial, a multicenter, placebo-controlled, double-blind, study of 595 patients with mild or moderate psoriasis as defined by an involved body surface area of 2%-15% and a Psoriasis Area and Severity Index score of 2-15. Participants were randomized to the approved dose of apremilast (Otezla) – 30 mg twice daily – or placebo for 16 weeks, followed by 16 weeks of open-label apremilast for all. The full study findings haven’t yet been published or presented at a medical conference, but Amgen announced that the results were positive for all primary and secondary endpoints, and the company plans to file a request with the Food and Drug Administration for an expanded indication for the oral agent.
Pediatric studies
A recently published phase 2, open-label, 1-year study of apremilast in 42 children and adolescents with moderate to severe plaque psoriasis demonstrated that weight-based dosing is the best approach in the pediatric population. The study, which serves as the template for coming phase 3 trials, showed that dosing apremilast at 20 mg twice daily in youths weighing not more than 35 kg and 30 mg twice daily in those who weighed more provided pharmacokinetic exposure similar to that achieved with apremilast at the standard adult dose of 30 mg twice daily. Most participants liked the taste of the tablet.
“My prediction is apremilast will have efficacy in children and teenagers comparable to what it has in adults, with a similar safety and adverse event profile,” Dr. Strober said.
Apremilast works by blocking phosphodiesterase type 4, thereby reducing cyclic AMP metabolism, with a resultant increase in cyclic AMP levels. Cyclic AMP is a regulator of inflammation. Boosting its level has the effect of decreasing tumor necrosis factor and other proinflammatory cytokines while increasing anti-inflammatory mediators, such as interleukin-10.
Dr. Strober characterized apremilast’s efficacy as “modest” by contemporary standards in adults with moderate to severe psoriasis, with week 16 PASI 75 rates of about 30% in randomized trials, compared with 5% in placebo-treated controls. He considers it a good option in patients with moderate disease who are needle phobic and in those averse to the inconvenience of laboratory monitoring. The drug is useful in treating psoriasis in especially challenging locations. Apremilast is specifically approved for scalp psoriasis, and Dr. Strober has anecdotally found it helpful in patients with palmoplantar psoriasis or genital psoriasis.
“Apremilast has tolerability issues: first and foremost diarrhea, nausea, and headache. Probably 15%-20% of patients have nausea or diarrhea ranging from mild to severe, and 1 in 20 have headache. You have to warn patients,” he said.
Roughly 1% of patients experience depressed mood. “I’ve seen it in a few patients. I definitely believe it’s real, so query patients about mood changes while taking apremilast,” the dermatologist advised.
One in 5 patients loses 5% of body weight during the first 6 months on apremilast, but there’s no additional weight loss thereafter. It’s wrong to characterize the oral agent as a weight-loss drug, though, since 80% of patients don’t lose weight, Dr. Strober noted.
Topical PDE-4 inhibitor shows promise
Separately at the Las Vegas meeting, Linda Stein Gold, MD, provided highlights of a phase 2b randomized trial of a topical cream formulation of an extremely potent PDE-4 inhibitor, roflumilast, in patients with chronic plaque psoriasis. This molecule is a couple hundred times more effective at inhibiting the PDE-4 receptor than either oral apremilast or topical crisaborole (Eucrisa). And as a once-daily topical agent with very little systemic absorption, roflumilast cream sidesteps the tolerability issues that accompany apremilast.
“Roflumilast is currently available as an oral formulation for treatment of [chronic obstructive pulmonary disease], so it has a fairly well-established safety profile,” noted Dr. Stein Gold, director of dermatology clinical research at the Henry Ford Health System in Detroit.
The 12-week, multicenter, phase 2b study sponsored by Arcutis Biotherapeutics included 331 patients with chronic plaque psoriasis who were randomized to once-daily 0.3% roflumilast cream, 0.15% roflumilast cream, or vehicle. Three-quarters of participants had baseline moderate disease.
A week-8 Investigator’s Global Assessment (IGA) score of 0 or 1, meaning clear skin or almost clear, plus at least a 2-grade improvement from baseline occurred in 32% of the high-dose roflumilast group, 25% of those on the 0.15% formulation, and 10% of controls. On the secondary endpoint of improvement in tough-to-treat intertriginous psoriasis, at week 12 an intertriginous IGA score of 0 or 1 plus at least a 2-point improvement from baseline was seen in 86% of the 0.3% roflumilast cream group, 50% on low-dose therapy, and 29% of controls. Moreover, the clinical improvements in IGA and itch kicked in quickly, with significant separation from placebo by week 2, Dr. Stein Gold noted.
The phase 3 program is now recruiting participants.
Dr. Strober and Dr. Stein Gold reported receiving research funding from and serving as consultants to Amgen and numerous other pharmaceutical companies.
MedscapeLive and this news organization are owned by the same parent company.
Big changes are coming in the use of oral apremilast, currently approved for moderate to severe psoriasis and plaque psoriasis in adults, Bruce E. Strober, MD, PhD, predicted at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually this year.
“We’ll have , meaning we can use this drug in patients in whom we typically think about using only topical therapies. Keep on the lookout: I think the mild to moderate indication may be coming next year, and that’s going to really shake up the whole landscape of psoriasis therapy,” said Dr. Strober, a dermatologist at Yale University in New Haven, Conn., and Central Connecticut Dermatology in Cromwell, Conn.
Mild or moderate psoriasis
Apremilast manufacturer Amgen has announced positive topline results from the phase 3 ADVANCE trial, a multicenter, placebo-controlled, double-blind, study of 595 patients with mild or moderate psoriasis as defined by an involved body surface area of 2%-15% and a Psoriasis Area and Severity Index score of 2-15. Participants were randomized to the approved dose of apremilast (Otezla) – 30 mg twice daily – or placebo for 16 weeks, followed by 16 weeks of open-label apremilast for all. The full study findings haven’t yet been published or presented at a medical conference, but Amgen announced that the results were positive for all primary and secondary endpoints, and the company plans to file a request with the Food and Drug Administration for an expanded indication for the oral agent.
Pediatric studies
A recently published phase 2, open-label, 1-year study of apremilast in 42 children and adolescents with moderate to severe plaque psoriasis demonstrated that weight-based dosing is the best approach in the pediatric population. The study, which serves as the template for coming phase 3 trials, showed that dosing apremilast at 20 mg twice daily in youths weighing not more than 35 kg and 30 mg twice daily in those who weighed more provided pharmacokinetic exposure similar to that achieved with apremilast at the standard adult dose of 30 mg twice daily. Most participants liked the taste of the tablet.
“My prediction is apremilast will have efficacy in children and teenagers comparable to what it has in adults, with a similar safety and adverse event profile,” Dr. Strober said.
Apremilast works by blocking phosphodiesterase type 4, thereby reducing cyclic AMP metabolism, with a resultant increase in cyclic AMP levels. Cyclic AMP is a regulator of inflammation. Boosting its level has the effect of decreasing tumor necrosis factor and other proinflammatory cytokines while increasing anti-inflammatory mediators, such as interleukin-10.
Dr. Strober characterized apremilast’s efficacy as “modest” by contemporary standards in adults with moderate to severe psoriasis, with week 16 PASI 75 rates of about 30% in randomized trials, compared with 5% in placebo-treated controls. He considers it a good option in patients with moderate disease who are needle phobic and in those averse to the inconvenience of laboratory monitoring. The drug is useful in treating psoriasis in especially challenging locations. Apremilast is specifically approved for scalp psoriasis, and Dr. Strober has anecdotally found it helpful in patients with palmoplantar psoriasis or genital psoriasis.
“Apremilast has tolerability issues: first and foremost diarrhea, nausea, and headache. Probably 15%-20% of patients have nausea or diarrhea ranging from mild to severe, and 1 in 20 have headache. You have to warn patients,” he said.
Roughly 1% of patients experience depressed mood. “I’ve seen it in a few patients. I definitely believe it’s real, so query patients about mood changes while taking apremilast,” the dermatologist advised.
One in 5 patients loses 5% of body weight during the first 6 months on apremilast, but there’s no additional weight loss thereafter. It’s wrong to characterize the oral agent as a weight-loss drug, though, since 80% of patients don’t lose weight, Dr. Strober noted.
Topical PDE-4 inhibitor shows promise
Separately at the Las Vegas meeting, Linda Stein Gold, MD, provided highlights of a phase 2b randomized trial of a topical cream formulation of an extremely potent PDE-4 inhibitor, roflumilast, in patients with chronic plaque psoriasis. This molecule is a couple hundred times more effective at inhibiting the PDE-4 receptor than either oral apremilast or topical crisaborole (Eucrisa). And as a once-daily topical agent with very little systemic absorption, roflumilast cream sidesteps the tolerability issues that accompany apremilast.
“Roflumilast is currently available as an oral formulation for treatment of [chronic obstructive pulmonary disease], so it has a fairly well-established safety profile,” noted Dr. Stein Gold, director of dermatology clinical research at the Henry Ford Health System in Detroit.
The 12-week, multicenter, phase 2b study sponsored by Arcutis Biotherapeutics included 331 patients with chronic plaque psoriasis who were randomized to once-daily 0.3% roflumilast cream, 0.15% roflumilast cream, or vehicle. Three-quarters of participants had baseline moderate disease.
A week-8 Investigator’s Global Assessment (IGA) score of 0 or 1, meaning clear skin or almost clear, plus at least a 2-grade improvement from baseline occurred in 32% of the high-dose roflumilast group, 25% of those on the 0.15% formulation, and 10% of controls. On the secondary endpoint of improvement in tough-to-treat intertriginous psoriasis, at week 12 an intertriginous IGA score of 0 or 1 plus at least a 2-point improvement from baseline was seen in 86% of the 0.3% roflumilast cream group, 50% on low-dose therapy, and 29% of controls. Moreover, the clinical improvements in IGA and itch kicked in quickly, with significant separation from placebo by week 2, Dr. Stein Gold noted.
The phase 3 program is now recruiting participants.
Dr. Strober and Dr. Stein Gold reported receiving research funding from and serving as consultants to Amgen and numerous other pharmaceutical companies.
MedscapeLive and this news organization are owned by the same parent company.
FROM MEDSCAPELIVE LAS VEGAS DERMATOLOGY SEMINAR
Merino wool clothing improves atopic dermatitis, studies find
Conventional wisdom holds that Joseph F. Fowler, Jr., MD, said at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually.

“We’ve always though that wool is bad in atopics, right? Indeed, rough wool might be. But fine wool garments can actually improve atopic dermatitis, probably because wool is the most breathable fabric and has the best temperature regulation qualities of any fabric we can wear,” said Dr. Fowler, a dermatologist at the University of Louisville (Ky).
He was first author of a randomized, 12-week, crossover, assessor-blinded clinical trial which showed precisely that. And a second, similarly designed study, this one conducted in Australia, also concluded that fine merino wool assists in the management of AD.
The study by Dr. Fowler and coinvestigators included 50 children and adults with mild or moderate AD who either wore top-and-bottom base layer merino wool ensembles for 6 weeks and then switched to their regular nonwoolen clothing, or vice versa. The mean Eczema Area and Severity Index (EASI) score in those initially randomized to merino wool improved from a mean baseline of 4.5 to 1.7 at week 6, a significantly greater improvement than in the group wearing their regular clothing. Similarly, those who switched to merino wool after 6 weeks experienced a significant decrease in EASI scores from that point on to week 12, while those who switched from merino wool to their regular clothing did not.
Mean Dermatology Life Quality Index (DLQI) scores in patients who wore merino wool first improved from 6.9 at baseline to 3.4 at week 6. Those who wore their regular clothing first went from a mean baseline DLQI of 6.7 to 6.2 at week 6 – a nonsignificant change – but then improved to a week 12 mean DLQI of 3.7 while wearing wool. There was no improvement in DLQI scores while participants were wearing their regular clothing.
Static Investigator’s Global Assessment scores showed significantly greater improvement while patients wore merino wool garments than their regular clothing.
The Australian study included 39 patients with mild to moderate AD aged between 4 weeks and 3 years. This, too, was a 12-week, randomized, crossover, assessor-blinded clinical trial. Participating children wore merino wool for 6 weeks and cotton ensembles chosen by their parents for an equal time. The primary endpoint was change in the SCORing Atopic Dermatitis (SCORAD) index after each 6-week period. The mean 7.6-point greater SCORAD reduction at 6 weeks while wearing merino wool, compared with cotton, was “a pretty impressive reduction,” Dr. Fowler observed.
Reductions in the secondary endpoints of Atopic Dermatitis Severity Index and Infants’ Dermatitis Quality of Life Index while wearing merino wool followed suit. In contrast, switching from wool to cotton resulted in an increase in both scores. Also, use of topical corticosteroids was significantly reduced while patients wore merino wool.
Wool harvested from merino sheep is characterized by fine-diameter fibers. In Dr. Fowler’s study the mean fiber diameter was 17.5 mcm. This makes for a soft fabric with outstanding moisture absorbance capacity, a quality that’s beneficial in patients with AD, since their lesional skin loses the ability to regulate moisture, the dermatologist explained.
Both randomized trials were funded by Australian Wool Innovation and the Australian government.
MedscapeLive and this news organization are owned by the same parent company.
Conventional wisdom holds that Joseph F. Fowler, Jr., MD, said at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually.
“We’ve always though that wool is bad in atopics, right? Indeed, rough wool might be. But fine wool garments can actually improve atopic dermatitis, probably because wool is the most breathable fabric and has the best temperature regulation qualities of any fabric we can wear,” said Dr. Fowler, a dermatologist at the University of Louisville (Ky).
He was first author of a randomized, 12-week, crossover, assessor-blinded clinical trial which showed precisely that. And a second, similarly designed study, this one conducted in Australia, also concluded that fine merino wool assists in the management of AD.
The study by Dr. Fowler and coinvestigators included 50 children and adults with mild or moderate AD who either wore top-and-bottom base layer merino wool ensembles for 6 weeks and then switched to their regular nonwoolen clothing, or vice versa. The mean Eczema Area and Severity Index (EASI) score in those initially randomized to merino wool improved from a mean baseline of 4.5 to 1.7 at week 6, a significantly greater improvement than in the group wearing their regular clothing. Similarly, those who switched to merino wool after 6 weeks experienced a significant decrease in EASI scores from that point on to week 12, while those who switched from merino wool to their regular clothing did not.
Mean Dermatology Life Quality Index (DLQI) scores in patients who wore merino wool first improved from 6.9 at baseline to 3.4 at week 6. Those who wore their regular clothing first went from a mean baseline DLQI of 6.7 to 6.2 at week 6 – a nonsignificant change – but then improved to a week 12 mean DLQI of 3.7 while wearing wool. There was no improvement in DLQI scores while participants were wearing their regular clothing.
Static Investigator’s Global Assessment scores showed significantly greater improvement while patients wore merino wool garments than their regular clothing.
The Australian study included 39 patients with mild to moderate AD aged between 4 weeks and 3 years. This, too, was a 12-week, randomized, crossover, assessor-blinded clinical trial. Participating children wore merino wool for 6 weeks and cotton ensembles chosen by their parents for an equal time. The primary endpoint was change in the SCORing Atopic Dermatitis (SCORAD) index after each 6-week period. The mean 7.6-point greater SCORAD reduction at 6 weeks while wearing merino wool, compared with cotton, was “a pretty impressive reduction,” Dr. Fowler observed.
Reductions in the secondary endpoints of Atopic Dermatitis Severity Index and Infants’ Dermatitis Quality of Life Index while wearing merino wool followed suit. In contrast, switching from wool to cotton resulted in an increase in both scores. Also, use of topical corticosteroids was significantly reduced while patients wore merino wool.
Wool harvested from merino sheep is characterized by fine-diameter fibers. In Dr. Fowler’s study the mean fiber diameter was 17.5 mcm. This makes for a soft fabric with outstanding moisture absorbance capacity, a quality that’s beneficial in patients with AD, since their lesional skin loses the ability to regulate moisture, the dermatologist explained.
Both randomized trials were funded by Australian Wool Innovation and the Australian government.
MedscapeLive and this news organization are owned by the same parent company.
Conventional wisdom holds that Joseph F. Fowler, Jr., MD, said at MedscapeLive’s annual Las Vegas Dermatology Seminar, held virtually.
“We’ve always though that wool is bad in atopics, right? Indeed, rough wool might be. But fine wool garments can actually improve atopic dermatitis, probably because wool is the most breathable fabric and has the best temperature regulation qualities of any fabric we can wear,” said Dr. Fowler, a dermatologist at the University of Louisville (Ky).
He was first author of a randomized, 12-week, crossover, assessor-blinded clinical trial which showed precisely that. And a second, similarly designed study, this one conducted in Australia, also concluded that fine merino wool assists in the management of AD.
The study by Dr. Fowler and coinvestigators included 50 children and adults with mild or moderate AD who either wore top-and-bottom base layer merino wool ensembles for 6 weeks and then switched to their regular nonwoolen clothing, or vice versa. The mean Eczema Area and Severity Index (EASI) score in those initially randomized to merino wool improved from a mean baseline of 4.5 to 1.7 at week 6, a significantly greater improvement than in the group wearing their regular clothing. Similarly, those who switched to merino wool after 6 weeks experienced a significant decrease in EASI scores from that point on to week 12, while those who switched from merino wool to their regular clothing did not.
Mean Dermatology Life Quality Index (DLQI) scores in patients who wore merino wool first improved from 6.9 at baseline to 3.4 at week 6. Those who wore their regular clothing first went from a mean baseline DLQI of 6.7 to 6.2 at week 6 – a nonsignificant change – but then improved to a week 12 mean DLQI of 3.7 while wearing wool. There was no improvement in DLQI scores while participants were wearing their regular clothing.
Static Investigator’s Global Assessment scores showed significantly greater improvement while patients wore merino wool garments than their regular clothing.
The Australian study included 39 patients with mild to moderate AD aged between 4 weeks and 3 years. This, too, was a 12-week, randomized, crossover, assessor-blinded clinical trial. Participating children wore merino wool for 6 weeks and cotton ensembles chosen by their parents for an equal time. The primary endpoint was change in the SCORing Atopic Dermatitis (SCORAD) index after each 6-week period. The mean 7.6-point greater SCORAD reduction at 6 weeks while wearing merino wool, compared with cotton, was “a pretty impressive reduction,” Dr. Fowler observed.
Reductions in the secondary endpoints of Atopic Dermatitis Severity Index and Infants’ Dermatitis Quality of Life Index while wearing merino wool followed suit. In contrast, switching from wool to cotton resulted in an increase in both scores. Also, use of topical corticosteroids was significantly reduced while patients wore merino wool.
Wool harvested from merino sheep is characterized by fine-diameter fibers. In Dr. Fowler’s study the mean fiber diameter was 17.5 mcm. This makes for a soft fabric with outstanding moisture absorbance capacity, a quality that’s beneficial in patients with AD, since their lesional skin loses the ability to regulate moisture, the dermatologist explained.
Both randomized trials were funded by Australian Wool Innovation and the Australian government.
MedscapeLive and this news organization are owned by the same parent company.
FROM MEDSCAPELIVE LAS VEGAS DERMATOLOGY SEMINAR
Potential new option: 1-month DAPT post DES, then aspirin alone
One month of dual-antiplatelet therapy followed by aspirin monotherapy in patients who’ve received a drug-eluting stent proved noninferior to 6-12 months of DAPT for a composite 1-year endpoint of cardiovascular events or major bleeding in the large, randomized One-Month DAPT trial.

This is the first test of such a strategy. Other trials of short-course DAPT, such as the successful TWILIGHT trial, have dropped the aspirin and continued the P2Y12 inhibitor. But aspirin monotherapy after a single month of DAPT is an attractive alternative in patients undergoing PCI for noncomplex lesions, Myeong-Ki Hong, MD, PhD, said in presenting his results at the American Heart Association scientific sessions.
“In everyday clinical practice, people receiving P2Y12 receptor blockers usually complain of several episodes of minor bleeding. And the cost. Those are strong factors in patient noncompliance,” he said, adding, “I think aspirin monotherapy is more comfortable for the physician and the patient.”
The One-Month DAPT trial included 3,020 patients who underwent percutaneous coronary intervention with drug-eluting stents (DES) at 23 Korean centers. They were split roughly 60/40 between patients with stable angina and those with acute coronary syndrome involving unstable angina. Patients with complex coronary lesions or acute MI were not eligible for enrollment. Participants were randomized to receive either the polymer-free drug-coated BioFreedom stent, in which case they got 1 month of DAPT followed by 11 months of aspirin antiplatelet monotherapy, or they received 6 or 12 months of DAPT in conjunction with a thick-strut BioMatrix or an Ultimaster polymer-based DES. The reason for using different stents in the two study arms is that only the polymer-free stent completes drug release within 1 month; other contemporary DESs release their drug for 3-4 months, and it’s risky to discontinue one of the antiplatelet agents during drug elution, said Dr. Hong, professor of cardiology at Yonsei University in Seoul, South Korea.
Patients with stable angina fared best
The primary endpoint in this noninferiority trial was the 1-year composite of cardiac death, MI, target vessel revascularization, stroke, or major bleeding. The incidence was 5.9% in the 1-month DAPT group, statistically noninferior to the 6.5% figure in the 6- or 12-month DAPT group. The major bleeding rate at 1 year was 1.7% with 1 month of DAPT and 2.5% with 6-12 months of DAPT, a nonsignificant difference. Of note, the primary composite endpoint occurred in 5.1% of patients with stable angina who were randomized to 1 month of DAPT, compared with 7.6% with 6 or 12 months of DAPT, a statistically significant difference that translated into a 33% relative risk reduction. In contrast, in patients with unstable angina the primary endpoint occurred in 7.2% of those on 1 month of DAPT and 5.1% with 6 or 12 months of DAPT, a trend that didn’t reach significance.
Roughly 75% of patients in the long-DAPT arm were assigned to 12 months of DAPT. That’s because the trial began in 2015, before clinical practice guidelines declared 6 months of DAPT to be the recommendation in patients with stable coronary artery disease. The choice of 6 versus 12 months of DAPT in the trial was left up to the patient’s physician.
Discussant Roisin Colleran, MBBCh, said the study addresses “an unmet clinical need” for improved antiplatelet regimens following PCI with DES.
Trial’s shortcomings temper reaction
“After a period of short DAPT, aspirin monotherapy may be preferable to P2Y12 monotherapy because it’s cheaper, with fewer off-target side effects, less variation in treatment response, and fewer contraindications,” said Dr. Colleran, a cardiologist at Mater Private Hospital, Dublin.
That being said, she shared several reservations about the study. For one, none of the three stents used in the trial is approved by the Food and Drug Administration. The results may not be generalizable to non–East Asian populations. The use of 12 months of DAPT in stable angina patients is out of step with current U.S. and European practice guidelines, which recommend 6 months. And 17% of patients in the 1-month DAPT group were noncompliant with that strategy, meaning they continued on DAPT; had that reverse noncompliance rate been lower, the between-group difference in the primary endpoint might have become statistically significant.
Dr. Hong said he thinks the study findings are applicable elsewhere in the world. The 1-month DAPT followed by aspirin monotherapy strategy is attractive in elderly patients, those on oral anticoagulation for atrial fibrillation, individuals who need to undergo noncardiac surgery, and in the large group of stable patients with noncomplex coronary lesions.
“Let’s provide these patients with some options,” the cardiologist urged.
He is particularly keen on the combination of a polymer-free stent with a drug-elution period of less than 1 month.
“Is polymer perfect? I don’t think so. The polymer is a foreign body. It’s fantastic, but in 5 or 10 years the polymer may cause irritation and chronic inflammation and a new lesion,” Dr. Hong said.
Session moderator Wayne B. Batchelor, MD, commented on the battle for stent market share: “It almost appears that we’re getting to a ceiling point with coronary interventions whereby at a year we’re getting such low ischemic event rates – they’re often in the 5%-7% range – that all of these [head-to-head] studies are noninferiority studies, because it’s just the only way to do these comparisons nowadays. We can’t do 10-, 15-, or 20,000-patient trials. But these noninferiority margins are quite broad.”
“Are we stuck just saying: ‘All stents are equal,’ or are we going to be able to get to the point that we can show that a healing stent is superior?” asked Dr. Batchelor, director of interventional cardiology and interventional cardiology research at the Inova Medical Group in Falls Church, Va.
“I think it’s going to be very hard to beat the current technology,” observed panelist Alexandre Abizaid, MD, PhD, of the Dante Pazzanese Institute of Cardiology in São Paulo. “Even though the polymers are durable, they’re biocompatible, and they’re hard to beat. It’s not going to be easy to show superiority. Maybe in patient subsets.”
Dr. Hong reported having no financial conflicts of interest regarding the One-Month DAPT trial, funded by DIO, Cardinal Health Korea, and Terumo.
One month of dual-antiplatelet therapy followed by aspirin monotherapy in patients who’ve received a drug-eluting stent proved noninferior to 6-12 months of DAPT for a composite 1-year endpoint of cardiovascular events or major bleeding in the large, randomized One-Month DAPT trial.
This is the first test of such a strategy. Other trials of short-course DAPT, such as the successful TWILIGHT trial, have dropped the aspirin and continued the P2Y12 inhibitor. But aspirin monotherapy after a single month of DAPT is an attractive alternative in patients undergoing PCI for noncomplex lesions, Myeong-Ki Hong, MD, PhD, said in presenting his results at the American Heart Association scientific sessions.
“In everyday clinical practice, people receiving P2Y12 receptor blockers usually complain of several episodes of minor bleeding. And the cost. Those are strong factors in patient noncompliance,” he said, adding, “I think aspirin monotherapy is more comfortable for the physician and the patient.”
The One-Month DAPT trial included 3,020 patients who underwent percutaneous coronary intervention with drug-eluting stents (DES) at 23 Korean centers. They were split roughly 60/40 between patients with stable angina and those with acute coronary syndrome involving unstable angina. Patients with complex coronary lesions or acute MI were not eligible for enrollment. Participants were randomized to receive either the polymer-free drug-coated BioFreedom stent, in which case they got 1 month of DAPT followed by 11 months of aspirin antiplatelet monotherapy, or they received 6 or 12 months of DAPT in conjunction with a thick-strut BioMatrix or an Ultimaster polymer-based DES. The reason for using different stents in the two study arms is that only the polymer-free stent completes drug release within 1 month; other contemporary DESs release their drug for 3-4 months, and it’s risky to discontinue one of the antiplatelet agents during drug elution, said Dr. Hong, professor of cardiology at Yonsei University in Seoul, South Korea.
Patients with stable angina fared best
The primary endpoint in this noninferiority trial was the 1-year composite of cardiac death, MI, target vessel revascularization, stroke, or major bleeding. The incidence was 5.9% in the 1-month DAPT group, statistically noninferior to the 6.5% figure in the 6- or 12-month DAPT group. The major bleeding rate at 1 year was 1.7% with 1 month of DAPT and 2.5% with 6-12 months of DAPT, a nonsignificant difference. Of note, the primary composite endpoint occurred in 5.1% of patients with stable angina who were randomized to 1 month of DAPT, compared with 7.6% with 6 or 12 months of DAPT, a statistically significant difference that translated into a 33% relative risk reduction. In contrast, in patients with unstable angina the primary endpoint occurred in 7.2% of those on 1 month of DAPT and 5.1% with 6 or 12 months of DAPT, a trend that didn’t reach significance.
Roughly 75% of patients in the long-DAPT arm were assigned to 12 months of DAPT. That’s because the trial began in 2015, before clinical practice guidelines declared 6 months of DAPT to be the recommendation in patients with stable coronary artery disease. The choice of 6 versus 12 months of DAPT in the trial was left up to the patient’s physician.
Discussant Roisin Colleran, MBBCh, said the study addresses “an unmet clinical need” for improved antiplatelet regimens following PCI with DES.
Trial’s shortcomings temper reaction
“After a period of short DAPT, aspirin monotherapy may be preferable to P2Y12 monotherapy because it’s cheaper, with fewer off-target side effects, less variation in treatment response, and fewer contraindications,” said Dr. Colleran, a cardiologist at Mater Private Hospital, Dublin.
That being said, she shared several reservations about the study. For one, none of the three stents used in the trial is approved by the Food and Drug Administration. The results may not be generalizable to non–East Asian populations. The use of 12 months of DAPT in stable angina patients is out of step with current U.S. and European practice guidelines, which recommend 6 months. And 17% of patients in the 1-month DAPT group were noncompliant with that strategy, meaning they continued on DAPT; had that reverse noncompliance rate been lower, the between-group difference in the primary endpoint might have become statistically significant.
Dr. Hong said he thinks the study findings are applicable elsewhere in the world. The 1-month DAPT followed by aspirin monotherapy strategy is attractive in elderly patients, those on oral anticoagulation for atrial fibrillation, individuals who need to undergo noncardiac surgery, and in the large group of stable patients with noncomplex coronary lesions.
“Let’s provide these patients with some options,” the cardiologist urged.
He is particularly keen on the combination of a polymer-free stent with a drug-elution period of less than 1 month.
“Is polymer perfect? I don’t think so. The polymer is a foreign body. It’s fantastic, but in 5 or 10 years the polymer may cause irritation and chronic inflammation and a new lesion,” Dr. Hong said.
Session moderator Wayne B. Batchelor, MD, commented on the battle for stent market share: “It almost appears that we’re getting to a ceiling point with coronary interventions whereby at a year we’re getting such low ischemic event rates – they’re often in the 5%-7% range – that all of these [head-to-head] studies are noninferiority studies, because it’s just the only way to do these comparisons nowadays. We can’t do 10-, 15-, or 20,000-patient trials. But these noninferiority margins are quite broad.”
“Are we stuck just saying: ‘All stents are equal,’ or are we going to be able to get to the point that we can show that a healing stent is superior?” asked Dr. Batchelor, director of interventional cardiology and interventional cardiology research at the Inova Medical Group in Falls Church, Va.
“I think it’s going to be very hard to beat the current technology,” observed panelist Alexandre Abizaid, MD, PhD, of the Dante Pazzanese Institute of Cardiology in São Paulo. “Even though the polymers are durable, they’re biocompatible, and they’re hard to beat. It’s not going to be easy to show superiority. Maybe in patient subsets.”
Dr. Hong reported having no financial conflicts of interest regarding the One-Month DAPT trial, funded by DIO, Cardinal Health Korea, and Terumo.
One month of dual-antiplatelet therapy followed by aspirin monotherapy in patients who’ve received a drug-eluting stent proved noninferior to 6-12 months of DAPT for a composite 1-year endpoint of cardiovascular events or major bleeding in the large, randomized One-Month DAPT trial.
This is the first test of such a strategy. Other trials of short-course DAPT, such as the successful TWILIGHT trial, have dropped the aspirin and continued the P2Y12 inhibitor. But aspirin monotherapy after a single month of DAPT is an attractive alternative in patients undergoing PCI for noncomplex lesions, Myeong-Ki Hong, MD, PhD, said in presenting his results at the American Heart Association scientific sessions.
“In everyday clinical practice, people receiving P2Y12 receptor blockers usually complain of several episodes of minor bleeding. And the cost. Those are strong factors in patient noncompliance,” he said, adding, “I think aspirin monotherapy is more comfortable for the physician and the patient.”
The One-Month DAPT trial included 3,020 patients who underwent percutaneous coronary intervention with drug-eluting stents (DES) at 23 Korean centers. They were split roughly 60/40 between patients with stable angina and those with acute coronary syndrome involving unstable angina. Patients with complex coronary lesions or acute MI were not eligible for enrollment. Participants were randomized to receive either the polymer-free drug-coated BioFreedom stent, in which case they got 1 month of DAPT followed by 11 months of aspirin antiplatelet monotherapy, or they received 6 or 12 months of DAPT in conjunction with a thick-strut BioMatrix or an Ultimaster polymer-based DES. The reason for using different stents in the two study arms is that only the polymer-free stent completes drug release within 1 month; other contemporary DESs release their drug for 3-4 months, and it’s risky to discontinue one of the antiplatelet agents during drug elution, said Dr. Hong, professor of cardiology at Yonsei University in Seoul, South Korea.
Patients with stable angina fared best
The primary endpoint in this noninferiority trial was the 1-year composite of cardiac death, MI, target vessel revascularization, stroke, or major bleeding. The incidence was 5.9% in the 1-month DAPT group, statistically noninferior to the 6.5% figure in the 6- or 12-month DAPT group. The major bleeding rate at 1 year was 1.7% with 1 month of DAPT and 2.5% with 6-12 months of DAPT, a nonsignificant difference. Of note, the primary composite endpoint occurred in 5.1% of patients with stable angina who were randomized to 1 month of DAPT, compared with 7.6% with 6 or 12 months of DAPT, a statistically significant difference that translated into a 33% relative risk reduction. In contrast, in patients with unstable angina the primary endpoint occurred in 7.2% of those on 1 month of DAPT and 5.1% with 6 or 12 months of DAPT, a trend that didn’t reach significance.
Roughly 75% of patients in the long-DAPT arm were assigned to 12 months of DAPT. That’s because the trial began in 2015, before clinical practice guidelines declared 6 months of DAPT to be the recommendation in patients with stable coronary artery disease. The choice of 6 versus 12 months of DAPT in the trial was left up to the patient’s physician.
Discussant Roisin Colleran, MBBCh, said the study addresses “an unmet clinical need” for improved antiplatelet regimens following PCI with DES.
Trial’s shortcomings temper reaction
“After a period of short DAPT, aspirin monotherapy may be preferable to P2Y12 monotherapy because it’s cheaper, with fewer off-target side effects, less variation in treatment response, and fewer contraindications,” said Dr. Colleran, a cardiologist at Mater Private Hospital, Dublin.
That being said, she shared several reservations about the study. For one, none of the three stents used in the trial is approved by the Food and Drug Administration. The results may not be generalizable to non–East Asian populations. The use of 12 months of DAPT in stable angina patients is out of step with current U.S. and European practice guidelines, which recommend 6 months. And 17% of patients in the 1-month DAPT group were noncompliant with that strategy, meaning they continued on DAPT; had that reverse noncompliance rate been lower, the between-group difference in the primary endpoint might have become statistically significant.
Dr. Hong said he thinks the study findings are applicable elsewhere in the world. The 1-month DAPT followed by aspirin monotherapy strategy is attractive in elderly patients, those on oral anticoagulation for atrial fibrillation, individuals who need to undergo noncardiac surgery, and in the large group of stable patients with noncomplex coronary lesions.
“Let’s provide these patients with some options,” the cardiologist urged.
He is particularly keen on the combination of a polymer-free stent with a drug-elution period of less than 1 month.
“Is polymer perfect? I don’t think so. The polymer is a foreign body. It’s fantastic, but in 5 or 10 years the polymer may cause irritation and chronic inflammation and a new lesion,” Dr. Hong said.
Session moderator Wayne B. Batchelor, MD, commented on the battle for stent market share: “It almost appears that we’re getting to a ceiling point with coronary interventions whereby at a year we’re getting such low ischemic event rates – they’re often in the 5%-7% range – that all of these [head-to-head] studies are noninferiority studies, because it’s just the only way to do these comparisons nowadays. We can’t do 10-, 15-, or 20,000-patient trials. But these noninferiority margins are quite broad.”
“Are we stuck just saying: ‘All stents are equal,’ or are we going to be able to get to the point that we can show that a healing stent is superior?” asked Dr. Batchelor, director of interventional cardiology and interventional cardiology research at the Inova Medical Group in Falls Church, Va.
“I think it’s going to be very hard to beat the current technology,” observed panelist Alexandre Abizaid, MD, PhD, of the Dante Pazzanese Institute of Cardiology in São Paulo. “Even though the polymers are durable, they’re biocompatible, and they’re hard to beat. It’s not going to be easy to show superiority. Maybe in patient subsets.”
Dr. Hong reported having no financial conflicts of interest regarding the One-Month DAPT trial, funded by DIO, Cardinal Health Korea, and Terumo.
FROM AHA 2020
Mitotic rate makes comeback as melanoma prognosticator
at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.

Dr. Kashani-Sabet, a dermatologist, director of the melanoma research program, and senior scientist at the California Pacific Medical Center Research Institute, San Francisco, was first author of a large recently published study that made a strong case for reincorporation of mitotic index into the American Joint Cancer Committee (AJCC) melanoma staging system.
Mitotic index was included in the 7th edition of the AJCC classification system, but was dropped from the current 8th edition in part because of concern it could potentially lead to overtreatment of patients with very thin melanomas of less than 0.5-mm thickness.
However, mitotic rate, like tumor thickness, is a continuous variable. And like tumor thickness, mitotic rate has a nonlinear relationship with survival. That’s why the AJCC staging system utilizes unequally spaced tumor thickness cut points of 1, 2, and 4 mm to define T1-T4 disease. But until the study led by Dr. Kashani-Sabet, optimal cut points for mitotic rate hadn’t been defined.
He and his coinvestigators at Melanoma Institute Australia collected a dataset comprising 5,050 patients with primary cutaneous melanoma in Australia and Northern California, all of whom either died of metastatic melanoma or remained distant metastasis–free for at least 8 years of follow-up. Median follow-up of the cohort was 9.5 years.
The investigators developed computer-generated cut points for mitotic rate and its impact on survival for each melanoma T category, then assessed their value in randomly split training and validation sets from their large cohort. For T1 melanoma, the optimal cut point proved to be 2 mitoses/mm2; more than two was independently associated with increased mortality risk. For T2 disease, the optimal cut point was 4, for T3 it was 6, and for T4 it was 7 mitoses/mm2.
A key study finding: In a multivariate regression analysis, tumor thickness was associated with survival, with an odds ratio of 1.58, ulceration had an odds ratio of 1.55, and mitotic rate by cut point had an odds ratio of 5.38. Each of these three characteristics was independently associated with survival (P < .00005). Dr. Kashani-Sabet said that, despite the more than threefold greater odds ratio for mitotic rate, compared with ulceration, in a Kaplan-Meier analysis, the survival impact of ulceration being present was “virtually identical” to an elevated mitotic rate in each T category.
He and his coinvestigators proposed a revised T-category system which incorporates this new insight. There is no change in tumor thickness to define T1-T4 melanoma: T1 is less than 1.0 mm, T2 is greater than 1-2.0 mm, T3 is greater than 2.01-4.0 mm, and T4 is greater than 4.0 mm. But now, within each T category the proposal is that the “a” designation indicates neither ulceration nor an elevated mitotic rate is present, while “b” means ulceration and/or an elevated mitotic rate using the optimal cut point for that T category is present. In their Australian/Northern California dataset, these new T categories showed a distinct separation in cumulative survival.
Dr. Kashani-Sabet and coworkers have submitted a proposal to validate their results using the AJCC database. Based upon a first look at the numbers, “We think it’s really very likely that these observations can be reproduced in this most important of datasets,” he predicted.

During a panel discussion, Sancy Leachman, MD, PhD, offered a recent example from her own practice where an elevated mitotic index as defined by Dr. Kashani-Sabet and coworkers served as a red flag.
“I had a patient with a 0.3-mm melanoma with three mitoses. I did a sentinel lymph node biopsy on the patient, and she was positive,” said Dr. Leachman, professor and chair of the department of dermatology at Oregon Health & Science University, Portland.
Dr. Kashani-Sabet commented that, while an elevated mitotic index is clearly not an absolute requirement for metastasis, when present it’s a prognostically important finding.
Moreover, as adjuvant therapies of proven value in node-positive disease increasingly come under study in node-negative melanoma, it will be critical to identify the high-risk node-negative subgroup for whom such therapies should be targeted.
“While T4 tumors and ulcerated melanomas are clearly high risk, they’re not going to capture every patient who has a very high risk of distant metastases and death. I think mitotic rate is another pathway to identify patients who very well might benefit and should be candidates for inclusion in those adjuvant therapy trials as we’re moving more into node-negative patients,” according to Dr. Kashani-Sabet.
He reported having no financial conflicts of interest regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
Dr. Kashani-Sabet, a dermatologist, director of the melanoma research program, and senior scientist at the California Pacific Medical Center Research Institute, San Francisco, was first author of a large recently published study that made a strong case for reincorporation of mitotic index into the American Joint Cancer Committee (AJCC) melanoma staging system.
Mitotic index was included in the 7th edition of the AJCC classification system, but was dropped from the current 8th edition in part because of concern it could potentially lead to overtreatment of patients with very thin melanomas of less than 0.5-mm thickness.
However, mitotic rate, like tumor thickness, is a continuous variable. And like tumor thickness, mitotic rate has a nonlinear relationship with survival. That’s why the AJCC staging system utilizes unequally spaced tumor thickness cut points of 1, 2, and 4 mm to define T1-T4 disease. But until the study led by Dr. Kashani-Sabet, optimal cut points for mitotic rate hadn’t been defined.
He and his coinvestigators at Melanoma Institute Australia collected a dataset comprising 5,050 patients with primary cutaneous melanoma in Australia and Northern California, all of whom either died of metastatic melanoma or remained distant metastasis–free for at least 8 years of follow-up. Median follow-up of the cohort was 9.5 years.
The investigators developed computer-generated cut points for mitotic rate and its impact on survival for each melanoma T category, then assessed their value in randomly split training and validation sets from their large cohort. For T1 melanoma, the optimal cut point proved to be 2 mitoses/mm2; more than two was independently associated with increased mortality risk. For T2 disease, the optimal cut point was 4, for T3 it was 6, and for T4 it was 7 mitoses/mm2.
A key study finding: In a multivariate regression analysis, tumor thickness was associated with survival, with an odds ratio of 1.58, ulceration had an odds ratio of 1.55, and mitotic rate by cut point had an odds ratio of 5.38. Each of these three characteristics was independently associated with survival (P < .00005). Dr. Kashani-Sabet said that, despite the more than threefold greater odds ratio for mitotic rate, compared with ulceration, in a Kaplan-Meier analysis, the survival impact of ulceration being present was “virtually identical” to an elevated mitotic rate in each T category.
He and his coinvestigators proposed a revised T-category system which incorporates this new insight. There is no change in tumor thickness to define T1-T4 melanoma: T1 is less than 1.0 mm, T2 is greater than 1-2.0 mm, T3 is greater than 2.01-4.0 mm, and T4 is greater than 4.0 mm. But now, within each T category the proposal is that the “a” designation indicates neither ulceration nor an elevated mitotic rate is present, while “b” means ulceration and/or an elevated mitotic rate using the optimal cut point for that T category is present. In their Australian/Northern California dataset, these new T categories showed a distinct separation in cumulative survival.
Dr. Kashani-Sabet and coworkers have submitted a proposal to validate their results using the AJCC database. Based upon a first look at the numbers, “We think it’s really very likely that these observations can be reproduced in this most important of datasets,” he predicted.
During a panel discussion, Sancy Leachman, MD, PhD, offered a recent example from her own practice where an elevated mitotic index as defined by Dr. Kashani-Sabet and coworkers served as a red flag.
“I had a patient with a 0.3-mm melanoma with three mitoses. I did a sentinel lymph node biopsy on the patient, and she was positive,” said Dr. Leachman, professor and chair of the department of dermatology at Oregon Health & Science University, Portland.
Dr. Kashani-Sabet commented that, while an elevated mitotic index is clearly not an absolute requirement for metastasis, when present it’s a prognostically important finding.
Moreover, as adjuvant therapies of proven value in node-positive disease increasingly come under study in node-negative melanoma, it will be critical to identify the high-risk node-negative subgroup for whom such therapies should be targeted.
“While T4 tumors and ulcerated melanomas are clearly high risk, they’re not going to capture every patient who has a very high risk of distant metastases and death. I think mitotic rate is another pathway to identify patients who very well might benefit and should be candidates for inclusion in those adjuvant therapy trials as we’re moving more into node-negative patients,” according to Dr. Kashani-Sabet.
He reported having no financial conflicts of interest regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medical Education.
Dr. Kashani-Sabet, a dermatologist, director of the melanoma research program, and senior scientist at the California Pacific Medical Center Research Institute, San Francisco, was first author of a large recently published study that made a strong case for reincorporation of mitotic index into the American Joint Cancer Committee (AJCC) melanoma staging system.
Mitotic index was included in the 7th edition of the AJCC classification system, but was dropped from the current 8th edition in part because of concern it could potentially lead to overtreatment of patients with very thin melanomas of less than 0.5-mm thickness.
However, mitotic rate, like tumor thickness, is a continuous variable. And like tumor thickness, mitotic rate has a nonlinear relationship with survival. That’s why the AJCC staging system utilizes unequally spaced tumor thickness cut points of 1, 2, and 4 mm to define T1-T4 disease. But until the study led by Dr. Kashani-Sabet, optimal cut points for mitotic rate hadn’t been defined.
He and his coinvestigators at Melanoma Institute Australia collected a dataset comprising 5,050 patients with primary cutaneous melanoma in Australia and Northern California, all of whom either died of metastatic melanoma or remained distant metastasis–free for at least 8 years of follow-up. Median follow-up of the cohort was 9.5 years.
The investigators developed computer-generated cut points for mitotic rate and its impact on survival for each melanoma T category, then assessed their value in randomly split training and validation sets from their large cohort. For T1 melanoma, the optimal cut point proved to be 2 mitoses/mm2; more than two was independently associated with increased mortality risk. For T2 disease, the optimal cut point was 4, for T3 it was 6, and for T4 it was 7 mitoses/mm2.
A key study finding: In a multivariate regression analysis, tumor thickness was associated with survival, with an odds ratio of 1.58, ulceration had an odds ratio of 1.55, and mitotic rate by cut point had an odds ratio of 5.38. Each of these three characteristics was independently associated with survival (P < .00005). Dr. Kashani-Sabet said that, despite the more than threefold greater odds ratio for mitotic rate, compared with ulceration, in a Kaplan-Meier analysis, the survival impact of ulceration being present was “virtually identical” to an elevated mitotic rate in each T category.
He and his coinvestigators proposed a revised T-category system which incorporates this new insight. There is no change in tumor thickness to define T1-T4 melanoma: T1 is less than 1.0 mm, T2 is greater than 1-2.0 mm, T3 is greater than 2.01-4.0 mm, and T4 is greater than 4.0 mm. But now, within each T category the proposal is that the “a” designation indicates neither ulceration nor an elevated mitotic rate is present, while “b” means ulceration and/or an elevated mitotic rate using the optimal cut point for that T category is present. In their Australian/Northern California dataset, these new T categories showed a distinct separation in cumulative survival.
Dr. Kashani-Sabet and coworkers have submitted a proposal to validate their results using the AJCC database. Based upon a first look at the numbers, “We think it’s really very likely that these observations can be reproduced in this most important of datasets,” he predicted.
During a panel discussion, Sancy Leachman, MD, PhD, offered a recent example from her own practice where an elevated mitotic index as defined by Dr. Kashani-Sabet and coworkers served as a red flag.
“I had a patient with a 0.3-mm melanoma with three mitoses. I did a sentinel lymph node biopsy on the patient, and she was positive,” said Dr. Leachman, professor and chair of the department of dermatology at Oregon Health & Science University, Portland.
Dr. Kashani-Sabet commented that, while an elevated mitotic index is clearly not an absolute requirement for metastasis, when present it’s a prognostically important finding.
Moreover, as adjuvant therapies of proven value in node-positive disease increasingly come under study in node-negative melanoma, it will be critical to identify the high-risk node-negative subgroup for whom such therapies should be targeted.
“While T4 tumors and ulcerated melanomas are clearly high risk, they’re not going to capture every patient who has a very high risk of distant metastases and death. I think mitotic rate is another pathway to identify patients who very well might benefit and should be candidates for inclusion in those adjuvant therapy trials as we’re moving more into node-negative patients,” according to Dr. Kashani-Sabet.
He reported having no financial conflicts of interest regarding his presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
FROM THE CUTANEOUS MALIGNANCIES FORUM
Improvements in chronic hand eczema seen with oral gusacitinib in phase 2 study
in a phase 2b, randomized trial, Howard Sofen, MD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
The once-daily drug proved effective for this challenging condition, regardless of whether an individual’s chronic hand eczema was driven chiefly by irritant contact dermatitis, allergic contact dermatitis, or atopic dermatitis, added Dr. Sofen, medical director of Dermatology Research Associates, Los Angeles, and chief of the dermatology division at LA County/Olive View Medical Center.
Gusacitinib is a once-daily oral inhibitor of Janus kinase 1, 2, and 3, tyrosine kinase 2, and spleen tyrosine kinase (SYK). As such, it targets the Th1, Th2, Th17, and Th22 cytokine pathways, as well as SYK-mediated interleukin-17 signaling of keratinocyte proliferation and differentiation. Thus, its spectrum of activity makes it a candidate for the treatment of a variety of other inflammatory dermatologic diseases, although chronic hand eczema alone affects an estimated 7 million Americans, the dermatologist noted.
The phase 2b, double-blind, 16-week, multicenter, randomized trial included 97 patients who were randomized to oral gusacitinib as monotherapy at 40 or 80 mg once daily or placebo. All participants had chronic hand eczema of more than 6 months duration that was refractory to potent or superpotent topical and/or systemic steroids. Participants were split 60/40 between those with severe chronic hand eczema, defined by a baseline score on the 0-4 Physician’s Global Assessment scale, and moderate disease, with a PGA of 3.
The primary endpoint was the percent improvement in modified total lesion severity score (mTLSS) at week 16 from a mean baseline of 13.2. A clearcut dose response was evident: Gusacitinib at 80 mg/day achieved a 69.5% decrease, while 40 mg brought a 40% reduction, which wasn’t significantly better than the 33.5% decrease in placebo-treated controls.
The rapidity of response was noteworthy in these steroid-refractory patients. The 80-mg group showed significant separation from placebo by 2 weeks, with a mean 40.1% reduction in mTLSS versus 13.6% with placebo.
The secondary endpoint was achievement of a PGA score of 0 or 1 – that is, clear or almost clear – with a 2-grade improvement over placebo. This was achieved in 31.3% of patients assigned to the higher dose of gusacitinib at week 16, a success rate fivefold higher than the 6.3% rate in controls. The two groups separated on this endpoint at week 2, the first assessment. At week 8 there was an eightfold difference in response: 25% in patients on gusacitinib at 80 mg, 3.1% with placebo.
The other secondary endpoint was improvement in itch as measured by the mTLSS pruritus 0-3 subscore. As for the other outcomes, the improvement in itch was rapid. At week 2, patients on gusacitinib at 80 mg averaged a 43.1% reduction from their baseline pruritus score, compared with 4.6% with placebo. At week 16, the reductions were 65.7% and 29.8%, respectively.
Both doses of gusacitinib were well tolerated, according to Dr. Sofer. No thromboembolic events, major adverse cardiovascular events, or opportunistic infections occurred during the short 16-week study. The drug’s safety profile was consistent with what’s been seen in a collective gusacitinib clinical trial experience totaling more than 350 patients: mild to moderate nasopharyngitis, headache, asymptomatic elevations in creatine phosphokinase, and a slight increase in HDL cholesterol accompanied by a small reduction in LDL cholesterol.
Dr. Sofen reported receiving research funding from and serving as a consultant to Asana BioSciences, the study sponsor, as well as more than half a dozen other pharmaceutical companies.
in a phase 2b, randomized trial, Howard Sofen, MD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
The once-daily drug proved effective for this challenging condition, regardless of whether an individual’s chronic hand eczema was driven chiefly by irritant contact dermatitis, allergic contact dermatitis, or atopic dermatitis, added Dr. Sofen, medical director of Dermatology Research Associates, Los Angeles, and chief of the dermatology division at LA County/Olive View Medical Center.
Gusacitinib is a once-daily oral inhibitor of Janus kinase 1, 2, and 3, tyrosine kinase 2, and spleen tyrosine kinase (SYK). As such, it targets the Th1, Th2, Th17, and Th22 cytokine pathways, as well as SYK-mediated interleukin-17 signaling of keratinocyte proliferation and differentiation. Thus, its spectrum of activity makes it a candidate for the treatment of a variety of other inflammatory dermatologic diseases, although chronic hand eczema alone affects an estimated 7 million Americans, the dermatologist noted.
The phase 2b, double-blind, 16-week, multicenter, randomized trial included 97 patients who were randomized to oral gusacitinib as monotherapy at 40 or 80 mg once daily or placebo. All participants had chronic hand eczema of more than 6 months duration that was refractory to potent or superpotent topical and/or systemic steroids. Participants were split 60/40 between those with severe chronic hand eczema, defined by a baseline score on the 0-4 Physician’s Global Assessment scale, and moderate disease, with a PGA of 3.
The primary endpoint was the percent improvement in modified total lesion severity score (mTLSS) at week 16 from a mean baseline of 13.2. A clearcut dose response was evident: Gusacitinib at 80 mg/day achieved a 69.5% decrease, while 40 mg brought a 40% reduction, which wasn’t significantly better than the 33.5% decrease in placebo-treated controls.
The rapidity of response was noteworthy in these steroid-refractory patients. The 80-mg group showed significant separation from placebo by 2 weeks, with a mean 40.1% reduction in mTLSS versus 13.6% with placebo.
The secondary endpoint was achievement of a PGA score of 0 or 1 – that is, clear or almost clear – with a 2-grade improvement over placebo. This was achieved in 31.3% of patients assigned to the higher dose of gusacitinib at week 16, a success rate fivefold higher than the 6.3% rate in controls. The two groups separated on this endpoint at week 2, the first assessment. At week 8 there was an eightfold difference in response: 25% in patients on gusacitinib at 80 mg, 3.1% with placebo.
The other secondary endpoint was improvement in itch as measured by the mTLSS pruritus 0-3 subscore. As for the other outcomes, the improvement in itch was rapid. At week 2, patients on gusacitinib at 80 mg averaged a 43.1% reduction from their baseline pruritus score, compared with 4.6% with placebo. At week 16, the reductions were 65.7% and 29.8%, respectively.
Both doses of gusacitinib were well tolerated, according to Dr. Sofer. No thromboembolic events, major adverse cardiovascular events, or opportunistic infections occurred during the short 16-week study. The drug’s safety profile was consistent with what’s been seen in a collective gusacitinib clinical trial experience totaling more than 350 patients: mild to moderate nasopharyngitis, headache, asymptomatic elevations in creatine phosphokinase, and a slight increase in HDL cholesterol accompanied by a small reduction in LDL cholesterol.
Dr. Sofen reported receiving research funding from and serving as a consultant to Asana BioSciences, the study sponsor, as well as more than half a dozen other pharmaceutical companies.
in a phase 2b, randomized trial, Howard Sofen, MD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
The once-daily drug proved effective for this challenging condition, regardless of whether an individual’s chronic hand eczema was driven chiefly by irritant contact dermatitis, allergic contact dermatitis, or atopic dermatitis, added Dr. Sofen, medical director of Dermatology Research Associates, Los Angeles, and chief of the dermatology division at LA County/Olive View Medical Center.
Gusacitinib is a once-daily oral inhibitor of Janus kinase 1, 2, and 3, tyrosine kinase 2, and spleen tyrosine kinase (SYK). As such, it targets the Th1, Th2, Th17, and Th22 cytokine pathways, as well as SYK-mediated interleukin-17 signaling of keratinocyte proliferation and differentiation. Thus, its spectrum of activity makes it a candidate for the treatment of a variety of other inflammatory dermatologic diseases, although chronic hand eczema alone affects an estimated 7 million Americans, the dermatologist noted.
The phase 2b, double-blind, 16-week, multicenter, randomized trial included 97 patients who were randomized to oral gusacitinib as monotherapy at 40 or 80 mg once daily or placebo. All participants had chronic hand eczema of more than 6 months duration that was refractory to potent or superpotent topical and/or systemic steroids. Participants were split 60/40 between those with severe chronic hand eczema, defined by a baseline score on the 0-4 Physician’s Global Assessment scale, and moderate disease, with a PGA of 3.
The primary endpoint was the percent improvement in modified total lesion severity score (mTLSS) at week 16 from a mean baseline of 13.2. A clearcut dose response was evident: Gusacitinib at 80 mg/day achieved a 69.5% decrease, while 40 mg brought a 40% reduction, which wasn’t significantly better than the 33.5% decrease in placebo-treated controls.
The rapidity of response was noteworthy in these steroid-refractory patients. The 80-mg group showed significant separation from placebo by 2 weeks, with a mean 40.1% reduction in mTLSS versus 13.6% with placebo.
The secondary endpoint was achievement of a PGA score of 0 or 1 – that is, clear or almost clear – with a 2-grade improvement over placebo. This was achieved in 31.3% of patients assigned to the higher dose of gusacitinib at week 16, a success rate fivefold higher than the 6.3% rate in controls. The two groups separated on this endpoint at week 2, the first assessment. At week 8 there was an eightfold difference in response: 25% in patients on gusacitinib at 80 mg, 3.1% with placebo.
The other secondary endpoint was improvement in itch as measured by the mTLSS pruritus 0-3 subscore. As for the other outcomes, the improvement in itch was rapid. At week 2, patients on gusacitinib at 80 mg averaged a 43.1% reduction from their baseline pruritus score, compared with 4.6% with placebo. At week 16, the reductions were 65.7% and 29.8%, respectively.
Both doses of gusacitinib were well tolerated, according to Dr. Sofer. No thromboembolic events, major adverse cardiovascular events, or opportunistic infections occurred during the short 16-week study. The drug’s safety profile was consistent with what’s been seen in a collective gusacitinib clinical trial experience totaling more than 350 patients: mild to moderate nasopharyngitis, headache, asymptomatic elevations in creatine phosphokinase, and a slight increase in HDL cholesterol accompanied by a small reduction in LDL cholesterol.
Dr. Sofen reported receiving research funding from and serving as a consultant to Asana BioSciences, the study sponsor, as well as more than half a dozen other pharmaceutical companies.
FROM THE EADV CONGRESS
Tildrakizumab for psoriasis shows durable efficacy over 5 years
The full during more than 5,400 patient-years of prospective follow-up, Diamont Thaçi, MD, PhD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
For example, 89% of patients who had a PASI-75 response on the 100-mg dose of tildrakizumab (Ilumya) – the dose approved in the United States – at week 28 in the parent reSURFACE 1 and reSURFACE 2 trials maintained their PASI-75 response throughout the next 4½ years in the long-term extension study, as did 93% of those with a week 28 PASI-75 response on 200 mg, a dose approved elsewhere, said Dr. Thaçi, professor of dermatology and director of the Comprehensive Center for Inflammation Medicine at Lübeck (Germany) University.
The same held true for PASI-90, a response achieved by 71% of participants on 100 mg of tildrakizumab at week 28 and 66% at week 244, and by 73% of those on the 200-mg dose at week 28 and 70% at 5 years. A PASI-100 response was documented at week 28 in 29% of patients on the lower dose and 37% of those on 200 mg, with week 244 PASI-100 rates of 33% and 41%, respectively.
The long-term extension study enrolled 622 patients with moderate to severe chronic plaque psoriasis with at least a PASI-75 response to 100 mg or 200 mg of the humanized monoclonal antibody interleukin-23p19 inhibitor at week 28 in reSURFACE 1 or 2, or who were partial or nonresponders to etanercept in reSURFACE 2 and were then switched to tildrakizumab at 200 mg. Five hundred and forty-five of the 622 patients (88%) completed the full 5 years of the extension study.
Very few patients left the study because of loss of efficacy or adverse events. Indeed, the exposure-adjusted rate of drug-related serious adverse events was 0.8 cases per 100 patient-years at tildrakizumab 100 mg and 0.5 per 100 patient-years at 200 mg. Moreover, the rates of drug-related serious adverse events leading to treatment continuation were 0.3 and 0.2 per 100 patient-years at the 100-mg and 200-mg doses. Rates of treatment-emergent severe infection were 1.2 and 1.3 per 100 patient-years on the lower and higher doses. Major adverse cardiovascular events occurred at rates of 0.5 and 0.7 cases per 100 patient-years.
“I think the adverse events are generally similar to what has been seen with other biologics, but slightly less with tildrakizumab. Registries will provide a clearer picture. What’s interesting is that even if you double the dosage you don’t see an increase in side effects,” Dr. Thaçi said.
Asked what happens when a tildrakizumab responder stops taking the monoclonal antibody, he replied, “This is something very interesting we see with the IL-23 inhibitors: The disease comes back very slowly. It takes months, and sometimes years, for the patient to lose the PASI-75 or even the PASI-90 response. But we still consider that continuous treatment is probably the better way to go because we cannot be sure who will lose or regain response. At the moment we don’t have a biomarker to tell us what we should do in our daily practice.”
Dr. Thaçi reported serving as an adviser to and paid investigator for Almirall, the study sponsor, and approximately 20 other pharmaceutical companies.
The full during more than 5,400 patient-years of prospective follow-up, Diamont Thaçi, MD, PhD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
For example, 89% of patients who had a PASI-75 response on the 100-mg dose of tildrakizumab (Ilumya) – the dose approved in the United States – at week 28 in the parent reSURFACE 1 and reSURFACE 2 trials maintained their PASI-75 response throughout the next 4½ years in the long-term extension study, as did 93% of those with a week 28 PASI-75 response on 200 mg, a dose approved elsewhere, said Dr. Thaçi, professor of dermatology and director of the Comprehensive Center for Inflammation Medicine at Lübeck (Germany) University.
The same held true for PASI-90, a response achieved by 71% of participants on 100 mg of tildrakizumab at week 28 and 66% at week 244, and by 73% of those on the 200-mg dose at week 28 and 70% at 5 years. A PASI-100 response was documented at week 28 in 29% of patients on the lower dose and 37% of those on 200 mg, with week 244 PASI-100 rates of 33% and 41%, respectively.
The long-term extension study enrolled 622 patients with moderate to severe chronic plaque psoriasis with at least a PASI-75 response to 100 mg or 200 mg of the humanized monoclonal antibody interleukin-23p19 inhibitor at week 28 in reSURFACE 1 or 2, or who were partial or nonresponders to etanercept in reSURFACE 2 and were then switched to tildrakizumab at 200 mg. Five hundred and forty-five of the 622 patients (88%) completed the full 5 years of the extension study.
Very few patients left the study because of loss of efficacy or adverse events. Indeed, the exposure-adjusted rate of drug-related serious adverse events was 0.8 cases per 100 patient-years at tildrakizumab 100 mg and 0.5 per 100 patient-years at 200 mg. Moreover, the rates of drug-related serious adverse events leading to treatment continuation were 0.3 and 0.2 per 100 patient-years at the 100-mg and 200-mg doses. Rates of treatment-emergent severe infection were 1.2 and 1.3 per 100 patient-years on the lower and higher doses. Major adverse cardiovascular events occurred at rates of 0.5 and 0.7 cases per 100 patient-years.
“I think the adverse events are generally similar to what has been seen with other biologics, but slightly less with tildrakizumab. Registries will provide a clearer picture. What’s interesting is that even if you double the dosage you don’t see an increase in side effects,” Dr. Thaçi said.
Asked what happens when a tildrakizumab responder stops taking the monoclonal antibody, he replied, “This is something very interesting we see with the IL-23 inhibitors: The disease comes back very slowly. It takes months, and sometimes years, for the patient to lose the PASI-75 or even the PASI-90 response. But we still consider that continuous treatment is probably the better way to go because we cannot be sure who will lose or regain response. At the moment we don’t have a biomarker to tell us what we should do in our daily practice.”
Dr. Thaçi reported serving as an adviser to and paid investigator for Almirall, the study sponsor, and approximately 20 other pharmaceutical companies.
The full during more than 5,400 patient-years of prospective follow-up, Diamont Thaçi, MD, PhD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
For example, 89% of patients who had a PASI-75 response on the 100-mg dose of tildrakizumab (Ilumya) – the dose approved in the United States – at week 28 in the parent reSURFACE 1 and reSURFACE 2 trials maintained their PASI-75 response throughout the next 4½ years in the long-term extension study, as did 93% of those with a week 28 PASI-75 response on 200 mg, a dose approved elsewhere, said Dr. Thaçi, professor of dermatology and director of the Comprehensive Center for Inflammation Medicine at Lübeck (Germany) University.
The same held true for PASI-90, a response achieved by 71% of participants on 100 mg of tildrakizumab at week 28 and 66% at week 244, and by 73% of those on the 200-mg dose at week 28 and 70% at 5 years. A PASI-100 response was documented at week 28 in 29% of patients on the lower dose and 37% of those on 200 mg, with week 244 PASI-100 rates of 33% and 41%, respectively.
The long-term extension study enrolled 622 patients with moderate to severe chronic plaque psoriasis with at least a PASI-75 response to 100 mg or 200 mg of the humanized monoclonal antibody interleukin-23p19 inhibitor at week 28 in reSURFACE 1 or 2, or who were partial or nonresponders to etanercept in reSURFACE 2 and were then switched to tildrakizumab at 200 mg. Five hundred and forty-five of the 622 patients (88%) completed the full 5 years of the extension study.
Very few patients left the study because of loss of efficacy or adverse events. Indeed, the exposure-adjusted rate of drug-related serious adverse events was 0.8 cases per 100 patient-years at tildrakizumab 100 mg and 0.5 per 100 patient-years at 200 mg. Moreover, the rates of drug-related serious adverse events leading to treatment continuation were 0.3 and 0.2 per 100 patient-years at the 100-mg and 200-mg doses. Rates of treatment-emergent severe infection were 1.2 and 1.3 per 100 patient-years on the lower and higher doses. Major adverse cardiovascular events occurred at rates of 0.5 and 0.7 cases per 100 patient-years.
“I think the adverse events are generally similar to what has been seen with other biologics, but slightly less with tildrakizumab. Registries will provide a clearer picture. What’s interesting is that even if you double the dosage you don’t see an increase in side effects,” Dr. Thaçi said.
Asked what happens when a tildrakizumab responder stops taking the monoclonal antibody, he replied, “This is something very interesting we see with the IL-23 inhibitors: The disease comes back very slowly. It takes months, and sometimes years, for the patient to lose the PASI-75 or even the PASI-90 response. But we still consider that continuous treatment is probably the better way to go because we cannot be sure who will lose or regain response. At the moment we don’t have a biomarker to tell us what we should do in our daily practice.”
Dr. Thaçi reported serving as an adviser to and paid investigator for Almirall, the study sponsor, and approximately 20 other pharmaceutical companies.
FROM THE EADV CONGRESS
Inattention to heightened CV risk common theme in clozapine deaths teaser
Death while on clozapine for schizophrenia is often associated with substandard treatment of cardiometabolic risk factors, Sharon Taub, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
“Inadequate treatment for metabolic syndrome was found to be a mortality predictor while on clozapine therapy. Patients who died were less likely to receive appropriate treatment for hyperlipidemia and type 2 diabetes, despite having been diagnosed with those conditions,” she said in presenting the results of her retrospective cohort study.
“Better preventive care, with special attention to those conditions, might prevent morbidity and improve life expectancy in this population,” concluded Dr. Taub of Geha Mental Health Center in Petah Tikva, Israel, and Tel Aviv University.
She reported on all 1,817 patients on clozapine for schizophrenia included in a large Israeli health care electronic medical records database, of whom 112, or 6.2%, died during 2 years of follow-up. Mortality while on the atypical antipsychotic was associated with a higher prevalence of hyperlipidemia, type 2 diabetes, hypertension, known ischemic heart disease, and a history of acute MI, compared with survivors.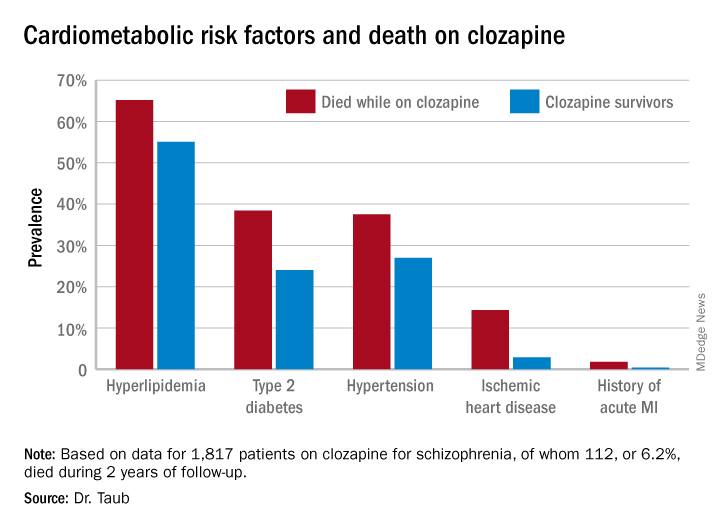
Similarly, only 16.3% of those known to have type 2 diabetes who died while on clozapine were on hypoglycemic agents, compared with 67.1% of diabetic survivors. The between-group difference in the use of antihypertensive drug therapy for patients diagnosed with hypertension – 28.6% in nonsurvivors on clozapine, 40.1% in survivors – did not achieve statistical significance.
In a multivariate analysis adjusted for age, sex, and socioeconomic status, schizophrenia patients with type 2 diabetes who weren’t on hypoglycemic medication were at 695% increased risk of mortality, compared with those who were. Similarly, hyperlipidemic patients on clozapine who weren’t on a statin had a 579% increase in mortality risk.
Patients who died while on clozapine had no increased risk of use of medical services while living in the community.
This evidence of a pattern of inadequate care with regard to management of cardiometabolic risk factors in patients on clozapine is disturbing for several reasons. For one, clozapine is known to be associated with increased risk of serious side effects, including development or worsening of metabolic syndrome. Also, clozapine is an important drug in psychiatric practice: “Clozapine is the only antipsychotic indicated for refractory schizophrenia. It is highly effective in treatment-resistant disease, present in 25%-30% of individuals with schizophrenia,” Dr. Taub noted. “Clozapine is underused, mostly because of severe side effects. Its administration is often postponed.”
She reported having no financial conflicts regarding her study, which was voted by conference attendees one of the top presentations at ECNP 2020.
Death while on clozapine for schizophrenia is often associated with substandard treatment of cardiometabolic risk factors, Sharon Taub, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
“Inadequate treatment for metabolic syndrome was found to be a mortality predictor while on clozapine therapy. Patients who died were less likely to receive appropriate treatment for hyperlipidemia and type 2 diabetes, despite having been diagnosed with those conditions,” she said in presenting the results of her retrospective cohort study.
“Better preventive care, with special attention to those conditions, might prevent morbidity and improve life expectancy in this population,” concluded Dr. Taub of Geha Mental Health Center in Petah Tikva, Israel, and Tel Aviv University.
She reported on all 1,817 patients on clozapine for schizophrenia included in a large Israeli health care electronic medical records database, of whom 112, or 6.2%, died during 2 years of follow-up. Mortality while on the atypical antipsychotic was associated with a higher prevalence of hyperlipidemia, type 2 diabetes, hypertension, known ischemic heart disease, and a history of acute MI, compared with survivors.
Similarly, only 16.3% of those known to have type 2 diabetes who died while on clozapine were on hypoglycemic agents, compared with 67.1% of diabetic survivors. The between-group difference in the use of antihypertensive drug therapy for patients diagnosed with hypertension – 28.6% in nonsurvivors on clozapine, 40.1% in survivors – did not achieve statistical significance.
In a multivariate analysis adjusted for age, sex, and socioeconomic status, schizophrenia patients with type 2 diabetes who weren’t on hypoglycemic medication were at 695% increased risk of mortality, compared with those who were. Similarly, hyperlipidemic patients on clozapine who weren’t on a statin had a 579% increase in mortality risk.
Patients who died while on clozapine had no increased risk of use of medical services while living in the community.
This evidence of a pattern of inadequate care with regard to management of cardiometabolic risk factors in patients on clozapine is disturbing for several reasons. For one, clozapine is known to be associated with increased risk of serious side effects, including development or worsening of metabolic syndrome. Also, clozapine is an important drug in psychiatric practice: “Clozapine is the only antipsychotic indicated for refractory schizophrenia. It is highly effective in treatment-resistant disease, present in 25%-30% of individuals with schizophrenia,” Dr. Taub noted. “Clozapine is underused, mostly because of severe side effects. Its administration is often postponed.”
She reported having no financial conflicts regarding her study, which was voted by conference attendees one of the top presentations at ECNP 2020.
Death while on clozapine for schizophrenia is often associated with substandard treatment of cardiometabolic risk factors, Sharon Taub, MD, reported at the virtual congress of the European College of Neuropsychopharmacology.
“Inadequate treatment for metabolic syndrome was found to be a mortality predictor while on clozapine therapy. Patients who died were less likely to receive appropriate treatment for hyperlipidemia and type 2 diabetes, despite having been diagnosed with those conditions,” she said in presenting the results of her retrospective cohort study.
“Better preventive care, with special attention to those conditions, might prevent morbidity and improve life expectancy in this population,” concluded Dr. Taub of Geha Mental Health Center in Petah Tikva, Israel, and Tel Aviv University.
She reported on all 1,817 patients on clozapine for schizophrenia included in a large Israeli health care electronic medical records database, of whom 112, or 6.2%, died during 2 years of follow-up. Mortality while on the atypical antipsychotic was associated with a higher prevalence of hyperlipidemia, type 2 diabetes, hypertension, known ischemic heart disease, and a history of acute MI, compared with survivors.
Similarly, only 16.3% of those known to have type 2 diabetes who died while on clozapine were on hypoglycemic agents, compared with 67.1% of diabetic survivors. The between-group difference in the use of antihypertensive drug therapy for patients diagnosed with hypertension – 28.6% in nonsurvivors on clozapine, 40.1% in survivors – did not achieve statistical significance.
In a multivariate analysis adjusted for age, sex, and socioeconomic status, schizophrenia patients with type 2 diabetes who weren’t on hypoglycemic medication were at 695% increased risk of mortality, compared with those who were. Similarly, hyperlipidemic patients on clozapine who weren’t on a statin had a 579% increase in mortality risk.
Patients who died while on clozapine had no increased risk of use of medical services while living in the community.
This evidence of a pattern of inadequate care with regard to management of cardiometabolic risk factors in patients on clozapine is disturbing for several reasons. For one, clozapine is known to be associated with increased risk of serious side effects, including development or worsening of metabolic syndrome. Also, clozapine is an important drug in psychiatric practice: “Clozapine is the only antipsychotic indicated for refractory schizophrenia. It is highly effective in treatment-resistant disease, present in 25%-30% of individuals with schizophrenia,” Dr. Taub noted. “Clozapine is underused, mostly because of severe side effects. Its administration is often postponed.”
She reported having no financial conflicts regarding her study, which was voted by conference attendees one of the top presentations at ECNP 2020.
FROM ECNP 2020