User login
PIONEER-HF called “practice changing” for acute decompensated heart failure
CHICAGO – Initiation of angiotensin-neprilysin inhibition using sacubitril/valsartan during hospitalization for acute decompensated heart failure, instead of relying upon enalapril, resulted in a substantially greater reduction in N-terminal of the prohormone brain natriuretic peptide concentration and a markedly lower rate of rehospitalization with no safety downside in the PIONEER-HF trial, Eric J. Velazquez, MD, reported at the American Heart Association scientific sessions.

“We believe these results have clinical implications that support the in-hospital initiation of sacubitril/valsartan in stabilized patients with acute decompensated heart failure and reduced ejection fraction irrespective of prior ACE inhibitor or ARB [angiotensin II receptor blocker] use or prior diagnosis of heart failure,” said Dr. Velazquez, a professor of medicine and chief of the section of cardiovascular medicine at Yale University, New Haven, Conn., and physician in chief of the Heart and Vascular Center for the Yale-New Haven Health System.
Sacubitril/valsartan (Entresto) has a class I indication for treatment of symptomatic heart failure with reduced ejection fraction (HFrEF) in the AHA/American College of Cardiology guidelines. This strong recommendation is based largely upon the impressive results of the PARADIGM-HF trial, which in ambulatory outpatients demonstrated a lower risk of cardiovascular mortality or hospitalization for heart failure than enalapril (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
However, since patients with acute decompensated heart failure (ADHF) were excluded from PARADIGM-HF, the safety and effectiveness of starting such patients on the drug while hospitalized for acute decompensation was unknown.
PIONEER-HF was carried out to shed light on that issue and thereby address a major unmet need for better treatments for ADHF. Even though this condition accounts for more than 1 million hospitalizations annually in the United States, short-term rehospitalization and mortality rates in affected patients remain unacceptably high at 21% and 12%, respectively. And the standard-of-care treatment – decongestion with intravenous diuretics and hemodynamic support with inotropes and vasodilators – hasn’t changed in nearly half a century, Dr. Velazquez noted.
The trial included 881 patients hospitalized for acute decompensated HFrEF at 129 U.S. centers. The study population was diverse: 36% of participants were black and one-third of subjects had no diagnosis of heart failure prior to their hospitalization. After achieving hemodynamic stabilization, patients were randomized to receive sacubitril/valsartan or enalapril.
Key outcomes
The primary endpoint was change in N-terminal of the prohormone brain natriuretic peptide concentration from baseline to week 8. There was a 25% reduction in the enalapril group and a 45% reduction with sacubitril/valsartan. This translated to a highly significant 29% greater relative risk reduction with sacubitril/valsartan.
More eye opening was the between-group difference in the prespecified composite clinical endpoint comprising death, rehospitalization for heart failure, implantation of a left ventricular assist device, or listing for heart transplant during the 8-week study.
The rate was 16.8% in the enalapril group and 9.3% with sacubitril/valsartan. This worked out to a 46% relative risk reduction, with a number needed to treat of 13.
The composite result was driven by a 44% reduction in risk of heart failure rehospitalization in the sacubitril/valsartan group: 8.0% versus 13.8%. The sacubitril/valsartan group also had a numerically lower mortality rate: 2.3% versus 3.4%, although the number of fatalities was small and this 34% relative risk reduction didn’t achieve statistical significance.
Rates of the key safety outcomes – symptomatic hypotension, worsening renal function, hyperkalemia, and angioedema – didn’t differ between the two study arms. Of interest, however, all six cases of angioedema in the enalapril group occurred in black patients, while the only case in the sacubitril/valsartan group was in a white patient.
PIONEER-HF treatment strategy
Hemodynamic stabilization as a prelude to randomization to sacubitril/valsartan or enalapril required maintaining a systolic blood pressure of at least 100 mm Hg in the previous 6 hours, with no symptomatic hypotension, intensification of intravenous diuretics, or use of intravenous vasodilators during that time period, and no intravenous inotropes in the previous 24 hours.
Enalapril was titrated to a target dose of 10 mg twice daily. Sacubitril/valsartan was titrated to a target dose of 97/103 mg twice daily. Titration was carried out using an algorithm based upon systolic BP. If the SBP was at least 100 and less than 120 mm Hg at baseline, sacubitril/valsartan was initiated at 24/26 mg twice daily, enalapril at 2.5 mg b.i.d. If the SBP at randomization was 120 mm Hg or higher, the initial dosing was sacubitril/valsartan at 49/51 mm Hg b.i.d. or enalapril at 5 mg b.i.d. Up-titration occurred after 1 week, then biweekly through week 8.
PIONEER in perspective

Discussant Larry A. Allen, MD, a heart failure specialist at the University of Colorado at Denver, Aurora, predicted that this will be a practice-changing study.
“There has been a need for a study like PIONEER in heart failure,” he observed. While multiple randomized trials have advanced the treatment of ambulatory HFrEF patients, demonstrating benefit for initiation and intensification of treatment with ACE inhibitors, angiotensin II receptor blockers, beta-blockers, and mineralocorticoid receptor antagonists, the treatment of patients with ADHF has remained relatively static, marked by failed trials of once-promising novel agents including tolvaptan, nesiritide, and serelaxin.
“All the data is in ambulatory patients, but the action for the care of heart failure patients actually occurs largely in the hospital. Seventy percent of care provided in the U.S. to patients with heart failure occurs in the hospital setting. These patients are a captive audience at that time, and the transitions from inpatient to outpatient care are fragile,” Dr. Allen said.
He noted that the use of sacubitril/valsartan in routine practice as reflected in national registries has been “extremely low” – less than 15% among eligible patients – despite the drug having been approved more than 3 years ago. One major reason for the low uptake, in his view, is clinical inertia. That should melt away in what he termed “the post-PIONEER world.”
“I think one of the great things about this study is it keeps it simple. We now have a simpler algorithm for inpatient and subsequent outpatient management of heart failure with reduced ejection fraction. It’s easier for us to start with the treatment we want patients to be on, and it’s better for patients, too. Most importantly, this study reinforces the importance and safety of aggressive guideline-directed medical therapy starting from the beginning in most patients,” Dr. Allen said.
The study findings were published simultaneously in the New England Journal of Medicine (2018 Nov 11. doi: 10.1056/NEJMoa1812851).
PIONEER-HF was sponsored by Novartis. Dr. Velazquez reported receiving research grants from and serving as a consultant to that company and others. Dr. Allen reported having no financial conflicts.
CHICAGO – Initiation of angiotensin-neprilysin inhibition using sacubitril/valsartan during hospitalization for acute decompensated heart failure, instead of relying upon enalapril, resulted in a substantially greater reduction in N-terminal of the prohormone brain natriuretic peptide concentration and a markedly lower rate of rehospitalization with no safety downside in the PIONEER-HF trial, Eric J. Velazquez, MD, reported at the American Heart Association scientific sessions.
“We believe these results have clinical implications that support the in-hospital initiation of sacubitril/valsartan in stabilized patients with acute decompensated heart failure and reduced ejection fraction irrespective of prior ACE inhibitor or ARB [angiotensin II receptor blocker] use or prior diagnosis of heart failure,” said Dr. Velazquez, a professor of medicine and chief of the section of cardiovascular medicine at Yale University, New Haven, Conn., and physician in chief of the Heart and Vascular Center for the Yale-New Haven Health System.
Sacubitril/valsartan (Entresto) has a class I indication for treatment of symptomatic heart failure with reduced ejection fraction (HFrEF) in the AHA/American College of Cardiology guidelines. This strong recommendation is based largely upon the impressive results of the PARADIGM-HF trial, which in ambulatory outpatients demonstrated a lower risk of cardiovascular mortality or hospitalization for heart failure than enalapril (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
However, since patients with acute decompensated heart failure (ADHF) were excluded from PARADIGM-HF, the safety and effectiveness of starting such patients on the drug while hospitalized for acute decompensation was unknown.
PIONEER-HF was carried out to shed light on that issue and thereby address a major unmet need for better treatments for ADHF. Even though this condition accounts for more than 1 million hospitalizations annually in the United States, short-term rehospitalization and mortality rates in affected patients remain unacceptably high at 21% and 12%, respectively. And the standard-of-care treatment – decongestion with intravenous diuretics and hemodynamic support with inotropes and vasodilators – hasn’t changed in nearly half a century, Dr. Velazquez noted.
The trial included 881 patients hospitalized for acute decompensated HFrEF at 129 U.S. centers. The study population was diverse: 36% of participants were black and one-third of subjects had no diagnosis of heart failure prior to their hospitalization. After achieving hemodynamic stabilization, patients were randomized to receive sacubitril/valsartan or enalapril.
Key outcomes
The primary endpoint was change in N-terminal of the prohormone brain natriuretic peptide concentration from baseline to week 8. There was a 25% reduction in the enalapril group and a 45% reduction with sacubitril/valsartan. This translated to a highly significant 29% greater relative risk reduction with sacubitril/valsartan.
More eye opening was the between-group difference in the prespecified composite clinical endpoint comprising death, rehospitalization for heart failure, implantation of a left ventricular assist device, or listing for heart transplant during the 8-week study.
The rate was 16.8% in the enalapril group and 9.3% with sacubitril/valsartan. This worked out to a 46% relative risk reduction, with a number needed to treat of 13.
The composite result was driven by a 44% reduction in risk of heart failure rehospitalization in the sacubitril/valsartan group: 8.0% versus 13.8%. The sacubitril/valsartan group also had a numerically lower mortality rate: 2.3% versus 3.4%, although the number of fatalities was small and this 34% relative risk reduction didn’t achieve statistical significance.
Rates of the key safety outcomes – symptomatic hypotension, worsening renal function, hyperkalemia, and angioedema – didn’t differ between the two study arms. Of interest, however, all six cases of angioedema in the enalapril group occurred in black patients, while the only case in the sacubitril/valsartan group was in a white patient.
PIONEER-HF treatment strategy
Hemodynamic stabilization as a prelude to randomization to sacubitril/valsartan or enalapril required maintaining a systolic blood pressure of at least 100 mm Hg in the previous 6 hours, with no symptomatic hypotension, intensification of intravenous diuretics, or use of intravenous vasodilators during that time period, and no intravenous inotropes in the previous 24 hours.
Enalapril was titrated to a target dose of 10 mg twice daily. Sacubitril/valsartan was titrated to a target dose of 97/103 mg twice daily. Titration was carried out using an algorithm based upon systolic BP. If the SBP was at least 100 and less than 120 mm Hg at baseline, sacubitril/valsartan was initiated at 24/26 mg twice daily, enalapril at 2.5 mg b.i.d. If the SBP at randomization was 120 mm Hg or higher, the initial dosing was sacubitril/valsartan at 49/51 mm Hg b.i.d. or enalapril at 5 mg b.i.d. Up-titration occurred after 1 week, then biweekly through week 8.
PIONEER in perspective
Discussant Larry A. Allen, MD, a heart failure specialist at the University of Colorado at Denver, Aurora, predicted that this will be a practice-changing study.
“There has been a need for a study like PIONEER in heart failure,” he observed. While multiple randomized trials have advanced the treatment of ambulatory HFrEF patients, demonstrating benefit for initiation and intensification of treatment with ACE inhibitors, angiotensin II receptor blockers, beta-blockers, and mineralocorticoid receptor antagonists, the treatment of patients with ADHF has remained relatively static, marked by failed trials of once-promising novel agents including tolvaptan, nesiritide, and serelaxin.
“All the data is in ambulatory patients, but the action for the care of heart failure patients actually occurs largely in the hospital. Seventy percent of care provided in the U.S. to patients with heart failure occurs in the hospital setting. These patients are a captive audience at that time, and the transitions from inpatient to outpatient care are fragile,” Dr. Allen said.
He noted that the use of sacubitril/valsartan in routine practice as reflected in national registries has been “extremely low” – less than 15% among eligible patients – despite the drug having been approved more than 3 years ago. One major reason for the low uptake, in his view, is clinical inertia. That should melt away in what he termed “the post-PIONEER world.”
“I think one of the great things about this study is it keeps it simple. We now have a simpler algorithm for inpatient and subsequent outpatient management of heart failure with reduced ejection fraction. It’s easier for us to start with the treatment we want patients to be on, and it’s better for patients, too. Most importantly, this study reinforces the importance and safety of aggressive guideline-directed medical therapy starting from the beginning in most patients,” Dr. Allen said.
The study findings were published simultaneously in the New England Journal of Medicine (2018 Nov 11. doi: 10.1056/NEJMoa1812851).
PIONEER-HF was sponsored by Novartis. Dr. Velazquez reported receiving research grants from and serving as a consultant to that company and others. Dr. Allen reported having no financial conflicts.
CHICAGO – Initiation of angiotensin-neprilysin inhibition using sacubitril/valsartan during hospitalization for acute decompensated heart failure, instead of relying upon enalapril, resulted in a substantially greater reduction in N-terminal of the prohormone brain natriuretic peptide concentration and a markedly lower rate of rehospitalization with no safety downside in the PIONEER-HF trial, Eric J. Velazquez, MD, reported at the American Heart Association scientific sessions.
“We believe these results have clinical implications that support the in-hospital initiation of sacubitril/valsartan in stabilized patients with acute decompensated heart failure and reduced ejection fraction irrespective of prior ACE inhibitor or ARB [angiotensin II receptor blocker] use or prior diagnosis of heart failure,” said Dr. Velazquez, a professor of medicine and chief of the section of cardiovascular medicine at Yale University, New Haven, Conn., and physician in chief of the Heart and Vascular Center for the Yale-New Haven Health System.
Sacubitril/valsartan (Entresto) has a class I indication for treatment of symptomatic heart failure with reduced ejection fraction (HFrEF) in the AHA/American College of Cardiology guidelines. This strong recommendation is based largely upon the impressive results of the PARADIGM-HF trial, which in ambulatory outpatients demonstrated a lower risk of cardiovascular mortality or hospitalization for heart failure than enalapril (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
However, since patients with acute decompensated heart failure (ADHF) were excluded from PARADIGM-HF, the safety and effectiveness of starting such patients on the drug while hospitalized for acute decompensation was unknown.
PIONEER-HF was carried out to shed light on that issue and thereby address a major unmet need for better treatments for ADHF. Even though this condition accounts for more than 1 million hospitalizations annually in the United States, short-term rehospitalization and mortality rates in affected patients remain unacceptably high at 21% and 12%, respectively. And the standard-of-care treatment – decongestion with intravenous diuretics and hemodynamic support with inotropes and vasodilators – hasn’t changed in nearly half a century, Dr. Velazquez noted.
The trial included 881 patients hospitalized for acute decompensated HFrEF at 129 U.S. centers. The study population was diverse: 36% of participants were black and one-third of subjects had no diagnosis of heart failure prior to their hospitalization. After achieving hemodynamic stabilization, patients were randomized to receive sacubitril/valsartan or enalapril.
Key outcomes
The primary endpoint was change in N-terminal of the prohormone brain natriuretic peptide concentration from baseline to week 8. There was a 25% reduction in the enalapril group and a 45% reduction with sacubitril/valsartan. This translated to a highly significant 29% greater relative risk reduction with sacubitril/valsartan.
More eye opening was the between-group difference in the prespecified composite clinical endpoint comprising death, rehospitalization for heart failure, implantation of a left ventricular assist device, or listing for heart transplant during the 8-week study.
The rate was 16.8% in the enalapril group and 9.3% with sacubitril/valsartan. This worked out to a 46% relative risk reduction, with a number needed to treat of 13.
The composite result was driven by a 44% reduction in risk of heart failure rehospitalization in the sacubitril/valsartan group: 8.0% versus 13.8%. The sacubitril/valsartan group also had a numerically lower mortality rate: 2.3% versus 3.4%, although the number of fatalities was small and this 34% relative risk reduction didn’t achieve statistical significance.
Rates of the key safety outcomes – symptomatic hypotension, worsening renal function, hyperkalemia, and angioedema – didn’t differ between the two study arms. Of interest, however, all six cases of angioedema in the enalapril group occurred in black patients, while the only case in the sacubitril/valsartan group was in a white patient.
PIONEER-HF treatment strategy
Hemodynamic stabilization as a prelude to randomization to sacubitril/valsartan or enalapril required maintaining a systolic blood pressure of at least 100 mm Hg in the previous 6 hours, with no symptomatic hypotension, intensification of intravenous diuretics, or use of intravenous vasodilators during that time period, and no intravenous inotropes in the previous 24 hours.
Enalapril was titrated to a target dose of 10 mg twice daily. Sacubitril/valsartan was titrated to a target dose of 97/103 mg twice daily. Titration was carried out using an algorithm based upon systolic BP. If the SBP was at least 100 and less than 120 mm Hg at baseline, sacubitril/valsartan was initiated at 24/26 mg twice daily, enalapril at 2.5 mg b.i.d. If the SBP at randomization was 120 mm Hg or higher, the initial dosing was sacubitril/valsartan at 49/51 mm Hg b.i.d. or enalapril at 5 mg b.i.d. Up-titration occurred after 1 week, then biweekly through week 8.
PIONEER in perspective
Discussant Larry A. Allen, MD, a heart failure specialist at the University of Colorado at Denver, Aurora, predicted that this will be a practice-changing study.
“There has been a need for a study like PIONEER in heart failure,” he observed. While multiple randomized trials have advanced the treatment of ambulatory HFrEF patients, demonstrating benefit for initiation and intensification of treatment with ACE inhibitors, angiotensin II receptor blockers, beta-blockers, and mineralocorticoid receptor antagonists, the treatment of patients with ADHF has remained relatively static, marked by failed trials of once-promising novel agents including tolvaptan, nesiritide, and serelaxin.
“All the data is in ambulatory patients, but the action for the care of heart failure patients actually occurs largely in the hospital. Seventy percent of care provided in the U.S. to patients with heart failure occurs in the hospital setting. These patients are a captive audience at that time, and the transitions from inpatient to outpatient care are fragile,” Dr. Allen said.
He noted that the use of sacubitril/valsartan in routine practice as reflected in national registries has been “extremely low” – less than 15% among eligible patients – despite the drug having been approved more than 3 years ago. One major reason for the low uptake, in his view, is clinical inertia. That should melt away in what he termed “the post-PIONEER world.”
“I think one of the great things about this study is it keeps it simple. We now have a simpler algorithm for inpatient and subsequent outpatient management of heart failure with reduced ejection fraction. It’s easier for us to start with the treatment we want patients to be on, and it’s better for patients, too. Most importantly, this study reinforces the importance and safety of aggressive guideline-directed medical therapy starting from the beginning in most patients,” Dr. Allen said.
The study findings were published simultaneously in the New England Journal of Medicine (2018 Nov 11. doi: 10.1056/NEJMoa1812851).
PIONEER-HF was sponsored by Novartis. Dr. Velazquez reported receiving research grants from and serving as a consultant to that company and others. Dr. Allen reported having no financial conflicts.
REPORTING FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The rate of rehospitalization for heart failure during the next 2 months after initiation of sacubitril/valsartan during hospitalization for acute decompensated heart failure was 44% lower than with enalapril.
Study details: A randomized, multicenter trial involving 881 patients hospitalized for acute decompensated heart failure.
Disclosures: The PIONEER-HF trial was sponsored by Novartis. The presenter reported receiving research grants from and serving as a consultant to that company and others.
PIONEER-HF secures place for sacubitril/valsartan in this heart failure doc’s practice
CHICAGO – Dr. Larry A. Allen will now have an easier time of treating hospitalized patients with acute decompensated heart failure because of the results of the PIONEER-HF trial.
That study examined whether in-hospital initiation of sacubitril/valsartan compared to enalapril is safe and effective in ADHF, a treatment that hasn’t been studied well or taken up in clinical practice.
, showed comparable safety, and reduced composite endpoint of death, rehospitalization for heart failure, implantation of a left-ventricular implant device, and need for a transplant by 46%.
Dr. Allen, of the University of Colorado, Denver, was the designated discussant for the PIONEER-HF presentation at the American Heart Association scientific sessions. In an interview, he explained how these results will change his practice as a heart failure specialist. “It simplifies things: I don’t have to start on an old therapy in the hospital, get the patients back in clinic, and switch the over to this newer therapy. I can just start from the beginning with the therapy that I think will be most effective.”
To find out why, watch the complete interview.
CHICAGO – Dr. Larry A. Allen will now have an easier time of treating hospitalized patients with acute decompensated heart failure because of the results of the PIONEER-HF trial.
That study examined whether in-hospital initiation of sacubitril/valsartan compared to enalapril is safe and effective in ADHF, a treatment that hasn’t been studied well or taken up in clinical practice.
, showed comparable safety, and reduced composite endpoint of death, rehospitalization for heart failure, implantation of a left-ventricular implant device, and need for a transplant by 46%.
Dr. Allen, of the University of Colorado, Denver, was the designated discussant for the PIONEER-HF presentation at the American Heart Association scientific sessions. In an interview, he explained how these results will change his practice as a heart failure specialist. “It simplifies things: I don’t have to start on an old therapy in the hospital, get the patients back in clinic, and switch the over to this newer therapy. I can just start from the beginning with the therapy that I think will be most effective.”
To find out why, watch the complete interview.
CHICAGO – Dr. Larry A. Allen will now have an easier time of treating hospitalized patients with acute decompensated heart failure because of the results of the PIONEER-HF trial.
That study examined whether in-hospital initiation of sacubitril/valsartan compared to enalapril is safe and effective in ADHF, a treatment that hasn’t been studied well or taken up in clinical practice.
, showed comparable safety, and reduced composite endpoint of death, rehospitalization for heart failure, implantation of a left-ventricular implant device, and need for a transplant by 46%.
Dr. Allen, of the University of Colorado, Denver, was the designated discussant for the PIONEER-HF presentation at the American Heart Association scientific sessions. In an interview, he explained how these results will change his practice as a heart failure specialist. “It simplifies things: I don’t have to start on an old therapy in the hospital, get the patients back in clinic, and switch the over to this newer therapy. I can just start from the beginning with the therapy that I think will be most effective.”
To find out why, watch the complete interview.
REPORTING FROM AHA 2018
Vitamin D, fish oil circling the drain for primary prevention
CHICAGO – In what will surely come as a major disappointment to many millions of nutritional supplement enthusiasts, the daily use of vitamin D3 and/or omega-3 fatty acid capsules for a median of 5.3 years did not result in a lower incidence of invasive cancers or cardiovascular events than placebo in nearly 26,000 average-risk Americans who participated in the VITAL trial, JoAnn E. Manson, MD, reported at the American Heart Association scientific sessions.
VITAL (the Vitamin D and Omega-3 Trial) featured a 2x2 factorial design in which 25,871 subjects, including 5,016 black participants, were randomized in double-blind fashion to either vitamin D3, also known as cholecalciferol, at 2,000 IU/day and/or 1 g/day of omega-3 fatty acid, or placebo. The men had to be at least 50 years old, the women 55, and none had a baseline history of cardiovascular disease or invasive cancer. Their mean age was 67. Study pill adherence exceeded 83% over the course of 5.3 years.

This major study, funded by the National Institutes of Health, was designed to answer the question of whether two relatively inexpensive supplements with plausible mechanisms of potential benefit could be harnessed as effective agents for primary prevention of the two leading causes of death in the United States.
The simple answer turned out to be no. Invasive cancer of any type occurred in 793 patients in the vitamin D group and 824 placebo-treated controls, for a nonsignificant hazard ratio of 0.96. Major cardiovascular events – a composite of MI, stroke, or cardiovascular mortality – occurred in 396 and 409 patients, respectively, for a hazard ratio of 0.97.
Similarly, invasive cancer was diagnosed in 820 subjects in the omega-3 fatty acid group and 797 controls, while major cardiovascular events occurred in 386 patients taking fish oil and 419 on placebo. Again, the between-group differences were nonsignificant, noted Dr. Manson, chief of the division of preventive medicine and Brigham and Women’s Hospital and professor of medicine and women’s health at Harvard Medical School, Boston.
Buried within this vast data set were a few intriguing bright spots. For example, the prespecified secondary endpoint of total MIs was significantly reduced by 28% in patients using omega-3 fatty acid compared with placebo. In nonprespecified exploratory analyses, the risk of PCI was decreased by 22% in the omega-3 fatty acid group and total coronary heart disease events - a composite of MI, revascularization, or death due to coronary heart disease – was reduced by 17%. In black subjects, the use of omega-3 fatty acids reduced the risk of MIs by 77%.
Dietary fish consumption interacted with the effects of omega-3 supplementation. Subjects in the omega-3 group who ate less than the median 1.5 servings of fish per week had a statistically significant 19% relative risk reduction in major cardiovascular events and 40% fewer MIs than with placebo. In contrast, subjects who ate 1.5 or more fish servings derived no benefit from omega-3 supplements.
The most noteworthy finding in the vitamin D group was that, after excluding the first 2 years of follow-up, they had a 25% reduction in cancer mortality compared with controls.
However, Dr. Manson cautioned that these subgroup analyses should be interpreted with caution.
Discussant Jane Armitage, MD, went further, emphasizing that the primary study endpoints of invasive cancer and major cardiovascular events were negative for both vitamin D and fish oil.

“To drill down into the secondary endpoints is of some concern because I think there is often the risk of getting spurious results,” said Dr. Armitage, professor of clinical trials and epidemiology at the University of Oxford (England).
“I think the primary result that universal supplementation with vitamin D in a primary prevention population has not been shown to be beneficial is a robust result, and these other results need to be seen as hypothesis-generating,” according to Dr. Armitage.
She added that she thinks the VITAL trial is practice-changing.
“I think the general recommendation to take vitamin D is not supported by this paper,” she said.
The same holds true for omega-3 fatty acid supplementation based on the VITAL results, Dr. Armitage continued. She noted that the VITAL findings are consistent with a recent meta-analysis of 10 large trials of omega-3 which found no benefit in nearly 78,000 high-cardiovascular-risk subjects (JAMA Cardiol. 2018 Mar 1;3[3]:225-234).
VITAL vs. REDUCE-IT
The negative results in VITAL stood in sharp contrast to the findings of the REDUCE-IT trial, presented at the same late-breaker session by Deepak Bhatt, MD, of Harvard Medical School. In REDUCE-IT, icosapent ethyl, another fish-derived product, reduced major cardiovascular events by 25% in a study of more than 8,000 high-cardiovascular-risk patients with elevated triglycerides.
Why the difference in outcomes? Among the proposed explanations were that participants in VITAL got 1 g/day of omega-3 while those in REDUCE-IT got a much higher dose of 4 g/day of iscosapent ethyl, the REDUCE-IT population was at much higher cardiovascular risk, and icosapent ethyl has a mechanism of action that’s distinct from that of conventional fish oil products.
Dr. Manson said numerous ancillary studies from VITAL are underway and will begin appearing soon. These will look at the impact of vitamin D and fish oil supplementation on cognitive function, hypertension, atrial fibrillation, autoimmune disorders, bone health, depression, kidney disease, and other issues.
Simultaneously with her presentation at the AHA scientific sessions, the VITAL results were published online (N Engl J Med. 2018 Nov 10; doi: 10.1056/NEJMoa1809944 and 10.1056/NEJMoa1811403).
The study was sponsored by the National Institutes of Health. The presenter reported having no financial conflicts.
bjancin@mdedge.com
SOURCE: Manson JE. AHA Abstr. #19539
CHICAGO – In what will surely come as a major disappointment to many millions of nutritional supplement enthusiasts, the daily use of vitamin D3 and/or omega-3 fatty acid capsules for a median of 5.3 years did not result in a lower incidence of invasive cancers or cardiovascular events than placebo in nearly 26,000 average-risk Americans who participated in the VITAL trial, JoAnn E. Manson, MD, reported at the American Heart Association scientific sessions.
VITAL (the Vitamin D and Omega-3 Trial) featured a 2x2 factorial design in which 25,871 subjects, including 5,016 black participants, were randomized in double-blind fashion to either vitamin D3, also known as cholecalciferol, at 2,000 IU/day and/or 1 g/day of omega-3 fatty acid, or placebo. The men had to be at least 50 years old, the women 55, and none had a baseline history of cardiovascular disease or invasive cancer. Their mean age was 67. Study pill adherence exceeded 83% over the course of 5.3 years.
This major study, funded by the National Institutes of Health, was designed to answer the question of whether two relatively inexpensive supplements with plausible mechanisms of potential benefit could be harnessed as effective agents for primary prevention of the two leading causes of death in the United States.
The simple answer turned out to be no. Invasive cancer of any type occurred in 793 patients in the vitamin D group and 824 placebo-treated controls, for a nonsignificant hazard ratio of 0.96. Major cardiovascular events – a composite of MI, stroke, or cardiovascular mortality – occurred in 396 and 409 patients, respectively, for a hazard ratio of 0.97.
Similarly, invasive cancer was diagnosed in 820 subjects in the omega-3 fatty acid group and 797 controls, while major cardiovascular events occurred in 386 patients taking fish oil and 419 on placebo. Again, the between-group differences were nonsignificant, noted Dr. Manson, chief of the division of preventive medicine and Brigham and Women’s Hospital and professor of medicine and women’s health at Harvard Medical School, Boston.
Buried within this vast data set were a few intriguing bright spots. For example, the prespecified secondary endpoint of total MIs was significantly reduced by 28% in patients using omega-3 fatty acid compared with placebo. In nonprespecified exploratory analyses, the risk of PCI was decreased by 22% in the omega-3 fatty acid group and total coronary heart disease events - a composite of MI, revascularization, or death due to coronary heart disease – was reduced by 17%. In black subjects, the use of omega-3 fatty acids reduced the risk of MIs by 77%.
Dietary fish consumption interacted with the effects of omega-3 supplementation. Subjects in the omega-3 group who ate less than the median 1.5 servings of fish per week had a statistically significant 19% relative risk reduction in major cardiovascular events and 40% fewer MIs than with placebo. In contrast, subjects who ate 1.5 or more fish servings derived no benefit from omega-3 supplements.
The most noteworthy finding in the vitamin D group was that, after excluding the first 2 years of follow-up, they had a 25% reduction in cancer mortality compared with controls.
However, Dr. Manson cautioned that these subgroup analyses should be interpreted with caution.
Discussant Jane Armitage, MD, went further, emphasizing that the primary study endpoints of invasive cancer and major cardiovascular events were negative for both vitamin D and fish oil.
“To drill down into the secondary endpoints is of some concern because I think there is often the risk of getting spurious results,” said Dr. Armitage, professor of clinical trials and epidemiology at the University of Oxford (England).
“I think the primary result that universal supplementation with vitamin D in a primary prevention population has not been shown to be beneficial is a robust result, and these other results need to be seen as hypothesis-generating,” according to Dr. Armitage.
She added that she thinks the VITAL trial is practice-changing.
“I think the general recommendation to take vitamin D is not supported by this paper,” she said.
The same holds true for omega-3 fatty acid supplementation based on the VITAL results, Dr. Armitage continued. She noted that the VITAL findings are consistent with a recent meta-analysis of 10 large trials of omega-3 which found no benefit in nearly 78,000 high-cardiovascular-risk subjects (JAMA Cardiol. 2018 Mar 1;3[3]:225-234).
VITAL vs. REDUCE-IT
The negative results in VITAL stood in sharp contrast to the findings of the REDUCE-IT trial, presented at the same late-breaker session by Deepak Bhatt, MD, of Harvard Medical School. In REDUCE-IT, icosapent ethyl, another fish-derived product, reduced major cardiovascular events by 25% in a study of more than 8,000 high-cardiovascular-risk patients with elevated triglycerides.
Why the difference in outcomes? Among the proposed explanations were that participants in VITAL got 1 g/day of omega-3 while those in REDUCE-IT got a much higher dose of 4 g/day of iscosapent ethyl, the REDUCE-IT population was at much higher cardiovascular risk, and icosapent ethyl has a mechanism of action that’s distinct from that of conventional fish oil products.
Dr. Manson said numerous ancillary studies from VITAL are underway and will begin appearing soon. These will look at the impact of vitamin D and fish oil supplementation on cognitive function, hypertension, atrial fibrillation, autoimmune disorders, bone health, depression, kidney disease, and other issues.
Simultaneously with her presentation at the AHA scientific sessions, the VITAL results were published online (N Engl J Med. 2018 Nov 10; doi: 10.1056/NEJMoa1809944 and 10.1056/NEJMoa1811403).
The study was sponsored by the National Institutes of Health. The presenter reported having no financial conflicts.
bjancin@mdedge.com
SOURCE: Manson JE. AHA Abstr. #19539
CHICAGO – In what will surely come as a major disappointment to many millions of nutritional supplement enthusiasts, the daily use of vitamin D3 and/or omega-3 fatty acid capsules for a median of 5.3 years did not result in a lower incidence of invasive cancers or cardiovascular events than placebo in nearly 26,000 average-risk Americans who participated in the VITAL trial, JoAnn E. Manson, MD, reported at the American Heart Association scientific sessions.
VITAL (the Vitamin D and Omega-3 Trial) featured a 2x2 factorial design in which 25,871 subjects, including 5,016 black participants, were randomized in double-blind fashion to either vitamin D3, also known as cholecalciferol, at 2,000 IU/day and/or 1 g/day of omega-3 fatty acid, or placebo. The men had to be at least 50 years old, the women 55, and none had a baseline history of cardiovascular disease or invasive cancer. Their mean age was 67. Study pill adherence exceeded 83% over the course of 5.3 years.
This major study, funded by the National Institutes of Health, was designed to answer the question of whether two relatively inexpensive supplements with plausible mechanisms of potential benefit could be harnessed as effective agents for primary prevention of the two leading causes of death in the United States.
The simple answer turned out to be no. Invasive cancer of any type occurred in 793 patients in the vitamin D group and 824 placebo-treated controls, for a nonsignificant hazard ratio of 0.96. Major cardiovascular events – a composite of MI, stroke, or cardiovascular mortality – occurred in 396 and 409 patients, respectively, for a hazard ratio of 0.97.
Similarly, invasive cancer was diagnosed in 820 subjects in the omega-3 fatty acid group and 797 controls, while major cardiovascular events occurred in 386 patients taking fish oil and 419 on placebo. Again, the between-group differences were nonsignificant, noted Dr. Manson, chief of the division of preventive medicine and Brigham and Women’s Hospital and professor of medicine and women’s health at Harvard Medical School, Boston.
Buried within this vast data set were a few intriguing bright spots. For example, the prespecified secondary endpoint of total MIs was significantly reduced by 28% in patients using omega-3 fatty acid compared with placebo. In nonprespecified exploratory analyses, the risk of PCI was decreased by 22% in the omega-3 fatty acid group and total coronary heart disease events - a composite of MI, revascularization, or death due to coronary heart disease – was reduced by 17%. In black subjects, the use of omega-3 fatty acids reduced the risk of MIs by 77%.
Dietary fish consumption interacted with the effects of omega-3 supplementation. Subjects in the omega-3 group who ate less than the median 1.5 servings of fish per week had a statistically significant 19% relative risk reduction in major cardiovascular events and 40% fewer MIs than with placebo. In contrast, subjects who ate 1.5 or more fish servings derived no benefit from omega-3 supplements.
The most noteworthy finding in the vitamin D group was that, after excluding the first 2 years of follow-up, they had a 25% reduction in cancer mortality compared with controls.
However, Dr. Manson cautioned that these subgroup analyses should be interpreted with caution.
Discussant Jane Armitage, MD, went further, emphasizing that the primary study endpoints of invasive cancer and major cardiovascular events were negative for both vitamin D and fish oil.
“To drill down into the secondary endpoints is of some concern because I think there is often the risk of getting spurious results,” said Dr. Armitage, professor of clinical trials and epidemiology at the University of Oxford (England).
“I think the primary result that universal supplementation with vitamin D in a primary prevention population has not been shown to be beneficial is a robust result, and these other results need to be seen as hypothesis-generating,” according to Dr. Armitage.
She added that she thinks the VITAL trial is practice-changing.
“I think the general recommendation to take vitamin D is not supported by this paper,” she said.
The same holds true for omega-3 fatty acid supplementation based on the VITAL results, Dr. Armitage continued. She noted that the VITAL findings are consistent with a recent meta-analysis of 10 large trials of omega-3 which found no benefit in nearly 78,000 high-cardiovascular-risk subjects (JAMA Cardiol. 2018 Mar 1;3[3]:225-234).
VITAL vs. REDUCE-IT
The negative results in VITAL stood in sharp contrast to the findings of the REDUCE-IT trial, presented at the same late-breaker session by Deepak Bhatt, MD, of Harvard Medical School. In REDUCE-IT, icosapent ethyl, another fish-derived product, reduced major cardiovascular events by 25% in a study of more than 8,000 high-cardiovascular-risk patients with elevated triglycerides.
Why the difference in outcomes? Among the proposed explanations were that participants in VITAL got 1 g/day of omega-3 while those in REDUCE-IT got a much higher dose of 4 g/day of iscosapent ethyl, the REDUCE-IT population was at much higher cardiovascular risk, and icosapent ethyl has a mechanism of action that’s distinct from that of conventional fish oil products.
Dr. Manson said numerous ancillary studies from VITAL are underway and will begin appearing soon. These will look at the impact of vitamin D and fish oil supplementation on cognitive function, hypertension, atrial fibrillation, autoimmune disorders, bone health, depression, kidney disease, and other issues.
Simultaneously with her presentation at the AHA scientific sessions, the VITAL results were published online (N Engl J Med. 2018 Nov 10; doi: 10.1056/NEJMoa1809944 and 10.1056/NEJMoa1811403).
The study was sponsored by the National Institutes of Health. The presenter reported having no financial conflicts.
bjancin@mdedge.com
SOURCE: Manson JE. AHA Abstr. #19539
REPORTING FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The primary cancer and cardiovascular outcomes were unaffected by either supplement in the VITAL study.
Study details: VITAL was a randomized, double-blind trial in which nearly 26,000 middle-age or older Americans at average cardiovascular risk were assigned to vitamin D3, omega-3 fatty acid, and placebo in a 2x2 factorial design and followed prospectively for a median of 5.3 years.
Disclosures: The study was sponsored by the National Institutes of Health. The presenter reported having no financial conflicts.
Source: Manson JE. AHA 2018 Abst. #19539.
Ask depressed patients about hypersomnia to screen for mixicity
BARCELONA – Hypersomnia is a novel, previously unappreciated factor useful in tipping the balance in favor of an underlying bipolar predisposition in patients with an acute major depressive episode, Andrea Murru, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.

“This may help us in clinical practice. It’s an effective, costless, and highly objective clinical measure. It’s one question, and it takes a second. It’s simply asking the patient: ‘Are you sleeping more hours at night than usual?’ It’s a very simple clinical question that could really change the focus of treatment for a patient,” said Dr. Murru, a clinical psychiatrist in the bipolar disorders program of the University of Barcelona.
He presented a post hoc analysis of 2,514 acutely depressed individuals who participated in the BRIDGE-II-MIX (Bipolar Disorders: Improving Diagnosis, Guidance and Education) study, an international, multicenter, cross-sectional, observational study aimed at better characterizing clinically valid mixed features of depression indicative of concurrent manic symptoms.
“This is one of a whole series of hypothesis-generating studies from BRIDGE-II-MIX that are trying to deal with the struggle of understanding whether all the elements that favor mixicity and an underpinning bipolar diathesis are fairly represented in the diagnostic criteria in DSM-5. And what we are basically finding is the DSM-5 criteria are leaving out important symptoms that really do play a role,” the psychiatrist said in an interview.
One of those missing factors, he continued, is hypersomnia. It was present in 16.8% of the study population, and he and his coinvestigators compared them in terms of clinical variables, current and past psychiatric symptoms, and sociodemographics with the 83.2% of patients with insomnia. That is, patients who got fewer hours of sleep than normal and felt fatigued during the next day were compared with those who felt a reduced need to sleep.
The two groups differed in important ways. Hypersomnia showed a powerful correlation with a physician diagnosis of major depressive episode with atypical features, being present in 32.2% of such patients, while a mere 1.8% had insomnia. Moreover, among patients diagnosed with bipolar disorder I or II, 20.6% reported hypersomnia, a significantly higher proportion than the 16% who had insomnia.
The finding that only 5% of BRIDGE-II-MIX participants with hypersomnia met DSM-5 criteria for a mixed-state specifier, a rate not significantly different from the 8.3% figure in those with insomnia, underscores the drawbacks of the DSM-5 criteria, according to Dr. Murru. He noted that, in contrast to the DSM-5 criteria, 32.9% of the hypersomniac patients with a major depressive episode met Research Diagnostic Criteria (RDC) for a mixed-state specifier, a rate significantly higher than the 27.6% figure in patients with insomnia.
Specifically, the individual RDC mixed-state specifiers that stood out as significantly more frequent among depressed patients with hypersomnia than insomnia were racing thoughts, by a margin of 15.1% to 10.6%; impulsivity, 16.8% versus 13.2%; distractibility, 29.6% versus 23.4%; hypersexuality, which was present in 4% of patients with hypersomnia but only 2.3% with insomnia; irritable mood, 33.1% versus 24.8%; and a history of insufficient response to previous antidepressant therapy, 34.3%, compared with 27.1% in insomniacs.
When Dr. Murru and his coinvestigators performed a stepwise linear regression analysis to identify significant predictors of hypersomnia in patients with a major depressive episode, they found that the sleep abnormality keeps some interesting company. Patients with current bulimia were 4.21-fold more likely to have hypersomnia than those without the eating disorder. Current social phobia was associated with a 1.77-fold increased risk of hypersomnia; mood lability on prior antidepressant therapy carried a 1.37-fold risk, as did current mood lability; prior attempted suicide was associated with a 1.31-fold increased risk; being overweight or obese was associated with a 1.42-fold risk; currently being on a mood stabilizer carried a 1.33-fold increased risk of hypersomnia; and currently being on an atypical antipsychotic agent had a 1.36-fold greater risk.
Dr. Murru concluded that the take-home message of this study – “Of course, conceding it’s highly exploratory nature intrinsic to a post hoc analysis,” he noted – is that hypersomnia should be included among the symptoms that trigger the “with mixed features” specifier in patients with a major depressive episode.
The BRIDGE-II-MIX study was sponsored by Sanofi-Aventis. Dr. Murru reported having no financial conflicts of interest regarding the study.
BARCELONA – Hypersomnia is a novel, previously unappreciated factor useful in tipping the balance in favor of an underlying bipolar predisposition in patients with an acute major depressive episode, Andrea Murru, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
“This may help us in clinical practice. It’s an effective, costless, and highly objective clinical measure. It’s one question, and it takes a second. It’s simply asking the patient: ‘Are you sleeping more hours at night than usual?’ It’s a very simple clinical question that could really change the focus of treatment for a patient,” said Dr. Murru, a clinical psychiatrist in the bipolar disorders program of the University of Barcelona.
He presented a post hoc analysis of 2,514 acutely depressed individuals who participated in the BRIDGE-II-MIX (Bipolar Disorders: Improving Diagnosis, Guidance and Education) study, an international, multicenter, cross-sectional, observational study aimed at better characterizing clinically valid mixed features of depression indicative of concurrent manic symptoms.
“This is one of a whole series of hypothesis-generating studies from BRIDGE-II-MIX that are trying to deal with the struggle of understanding whether all the elements that favor mixicity and an underpinning bipolar diathesis are fairly represented in the diagnostic criteria in DSM-5. And what we are basically finding is the DSM-5 criteria are leaving out important symptoms that really do play a role,” the psychiatrist said in an interview.
One of those missing factors, he continued, is hypersomnia. It was present in 16.8% of the study population, and he and his coinvestigators compared them in terms of clinical variables, current and past psychiatric symptoms, and sociodemographics with the 83.2% of patients with insomnia. That is, patients who got fewer hours of sleep than normal and felt fatigued during the next day were compared with those who felt a reduced need to sleep.
The two groups differed in important ways. Hypersomnia showed a powerful correlation with a physician diagnosis of major depressive episode with atypical features, being present in 32.2% of such patients, while a mere 1.8% had insomnia. Moreover, among patients diagnosed with bipolar disorder I or II, 20.6% reported hypersomnia, a significantly higher proportion than the 16% who had insomnia.
The finding that only 5% of BRIDGE-II-MIX participants with hypersomnia met DSM-5 criteria for a mixed-state specifier, a rate not significantly different from the 8.3% figure in those with insomnia, underscores the drawbacks of the DSM-5 criteria, according to Dr. Murru. He noted that, in contrast to the DSM-5 criteria, 32.9% of the hypersomniac patients with a major depressive episode met Research Diagnostic Criteria (RDC) for a mixed-state specifier, a rate significantly higher than the 27.6% figure in patients with insomnia.
Specifically, the individual RDC mixed-state specifiers that stood out as significantly more frequent among depressed patients with hypersomnia than insomnia were racing thoughts, by a margin of 15.1% to 10.6%; impulsivity, 16.8% versus 13.2%; distractibility, 29.6% versus 23.4%; hypersexuality, which was present in 4% of patients with hypersomnia but only 2.3% with insomnia; irritable mood, 33.1% versus 24.8%; and a history of insufficient response to previous antidepressant therapy, 34.3%, compared with 27.1% in insomniacs.
When Dr. Murru and his coinvestigators performed a stepwise linear regression analysis to identify significant predictors of hypersomnia in patients with a major depressive episode, they found that the sleep abnormality keeps some interesting company. Patients with current bulimia were 4.21-fold more likely to have hypersomnia than those without the eating disorder. Current social phobia was associated with a 1.77-fold increased risk of hypersomnia; mood lability on prior antidepressant therapy carried a 1.37-fold risk, as did current mood lability; prior attempted suicide was associated with a 1.31-fold increased risk; being overweight or obese was associated with a 1.42-fold risk; currently being on a mood stabilizer carried a 1.33-fold increased risk of hypersomnia; and currently being on an atypical antipsychotic agent had a 1.36-fold greater risk.
Dr. Murru concluded that the take-home message of this study – “Of course, conceding it’s highly exploratory nature intrinsic to a post hoc analysis,” he noted – is that hypersomnia should be included among the symptoms that trigger the “with mixed features” specifier in patients with a major depressive episode.
The BRIDGE-II-MIX study was sponsored by Sanofi-Aventis. Dr. Murru reported having no financial conflicts of interest regarding the study.
BARCELONA – Hypersomnia is a novel, previously unappreciated factor useful in tipping the balance in favor of an underlying bipolar predisposition in patients with an acute major depressive episode, Andrea Murru, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
“This may help us in clinical practice. It’s an effective, costless, and highly objective clinical measure. It’s one question, and it takes a second. It’s simply asking the patient: ‘Are you sleeping more hours at night than usual?’ It’s a very simple clinical question that could really change the focus of treatment for a patient,” said Dr. Murru, a clinical psychiatrist in the bipolar disorders program of the University of Barcelona.
He presented a post hoc analysis of 2,514 acutely depressed individuals who participated in the BRIDGE-II-MIX (Bipolar Disorders: Improving Diagnosis, Guidance and Education) study, an international, multicenter, cross-sectional, observational study aimed at better characterizing clinically valid mixed features of depression indicative of concurrent manic symptoms.
“This is one of a whole series of hypothesis-generating studies from BRIDGE-II-MIX that are trying to deal with the struggle of understanding whether all the elements that favor mixicity and an underpinning bipolar diathesis are fairly represented in the diagnostic criteria in DSM-5. And what we are basically finding is the DSM-5 criteria are leaving out important symptoms that really do play a role,” the psychiatrist said in an interview.
One of those missing factors, he continued, is hypersomnia. It was present in 16.8% of the study population, and he and his coinvestigators compared them in terms of clinical variables, current and past psychiatric symptoms, and sociodemographics with the 83.2% of patients with insomnia. That is, patients who got fewer hours of sleep than normal and felt fatigued during the next day were compared with those who felt a reduced need to sleep.
The two groups differed in important ways. Hypersomnia showed a powerful correlation with a physician diagnosis of major depressive episode with atypical features, being present in 32.2% of such patients, while a mere 1.8% had insomnia. Moreover, among patients diagnosed with bipolar disorder I or II, 20.6% reported hypersomnia, a significantly higher proportion than the 16% who had insomnia.
The finding that only 5% of BRIDGE-II-MIX participants with hypersomnia met DSM-5 criteria for a mixed-state specifier, a rate not significantly different from the 8.3% figure in those with insomnia, underscores the drawbacks of the DSM-5 criteria, according to Dr. Murru. He noted that, in contrast to the DSM-5 criteria, 32.9% of the hypersomniac patients with a major depressive episode met Research Diagnostic Criteria (RDC) for a mixed-state specifier, a rate significantly higher than the 27.6% figure in patients with insomnia.
Specifically, the individual RDC mixed-state specifiers that stood out as significantly more frequent among depressed patients with hypersomnia than insomnia were racing thoughts, by a margin of 15.1% to 10.6%; impulsivity, 16.8% versus 13.2%; distractibility, 29.6% versus 23.4%; hypersexuality, which was present in 4% of patients with hypersomnia but only 2.3% with insomnia; irritable mood, 33.1% versus 24.8%; and a history of insufficient response to previous antidepressant therapy, 34.3%, compared with 27.1% in insomniacs.
When Dr. Murru and his coinvestigators performed a stepwise linear regression analysis to identify significant predictors of hypersomnia in patients with a major depressive episode, they found that the sleep abnormality keeps some interesting company. Patients with current bulimia were 4.21-fold more likely to have hypersomnia than those without the eating disorder. Current social phobia was associated with a 1.77-fold increased risk of hypersomnia; mood lability on prior antidepressant therapy carried a 1.37-fold risk, as did current mood lability; prior attempted suicide was associated with a 1.31-fold increased risk; being overweight or obese was associated with a 1.42-fold risk; currently being on a mood stabilizer carried a 1.33-fold increased risk of hypersomnia; and currently being on an atypical antipsychotic agent had a 1.36-fold greater risk.
Dr. Murru concluded that the take-home message of this study – “Of course, conceding it’s highly exploratory nature intrinsic to a post hoc analysis,” he noted – is that hypersomnia should be included among the symptoms that trigger the “with mixed features” specifier in patients with a major depressive episode.
The BRIDGE-II-MIX study was sponsored by Sanofi-Aventis. Dr. Murru reported having no financial conflicts of interest regarding the study.
REPORTING FROM THE ECNP CONGRESS
Key clinical point: Ask patients with a major depressive episode about hypersomnia.
Major finding: Hypersomnia in patients with an acute major depressive episode clusters with numerous elements of a bipolar diathesis.
Study details: This was a post hoc analysis of 2,514 acutely depressed individuals who participated in an international, multicenter, cross-sectional, observational study.
Disclosures: The BRIDGE-II-MIX study was sponsored by Sanofi-Aventis. The presenter reported having no financial conflicts of interest regarding the study.
Novel theory explains SSRIs’ variable efficacy
BARCELONA – New evidence from the landmark 12-year-old STAR*D clinical trial provides fresh support for a novel Italian hypothesis that the efficacy of selective serotonin reuptake inhibitors in major depressive disorder results from their capacity to amplify the influence of living conditions upon mood.

“This hypothesis claims that SSRIs do not affect mood by themselves, but by increasing brain plasticity to render an individual more susceptible to the influence of living conditions. So in a positive environment, treatment leads to a beneficial outcome, and in a stressful environment it may lead to a worse prognosis,” Aurelia Viglione explained at the annual congress of the European College of Neuropsychopharmacology.
This originally was demonstrated by her senior coinvestigators in mouse studies, which showed increased brain plasticity and responsiveness of mood to living conditions in the presence of the serotonin boost provided by SSRIs. Now this animal research has been confirmed in a more clinically relevant fashion via a secondary analysis of the venerable National Institute of Mental Health–funded STAR*D (Sequenced Treatment Alternatives to Relieve Depression) data set, which Ms. Viglione presented at the ECNP congress.
This hypothesis, which she and her colleagues have dubbed the “undirected susceptibility to change” hypothesis of the mechanism of action of SSRIs, attempts to account for the drugs’ highly variable efficacy. As prescribing physicians and their often-frustrated patients with major depression are all too aware, the SSRIs – the most widely prescribed treatment for the disorder – induce remission in only 30%-40% of patients, while an additional 30%-40% fail to experience even a significant response. And despite much research effort, to date there is no reliable way to match the best antidepressant to a given individual in accord with the current priority to develop a personalized medicine approach.
The undirected susceptibility to change hypothesis provides a plausible explanation for these mixed clinical outcomes. The hypothesis posits that high serotonin levels lead to increased brain plasticity and consequent openness to change in mood, which can be for the better or worse – depending upon the quality of the surrounding environment.
Ms. Viglione, a PhD student in neuroscience at the University of Pisa (Italy), presented a study of a 591-patient subset of patients with major depression in STAR*D who received citalopram at 20 mg/day for 4 weeks, at which point the 40% of participants who weren’t showing a sufficiently favorable response trend had their citalopram increased to 40 mg/day. Patients’ living conditions were categorized as favorable or adverse based upon an amalgam of sociodemographic characteristics, including employment status, education, marital status, income, insurance status, ethnicity, drug abuse, and history of traumatic events. Treatment response was measured using the 16-item Quick Inventory of Depressive Symptomatology (QIDS-SR16) score.
. Patients were more likely to achieve remission as defined by a QIDS-SR16 score of 5 or less at week 6 if they had a college education, a job, higher income, and/or private health insurance than if those proxies for favorable living conditions were not present.
The impact of sociodemographic factors on change in mood was much larger in patients on citalopram at 40 mg/day than 20 mg/day. For example, having a college education rather than a high school education was independently associated with up to a 37-fold greater remission rate among patients on the higher dose of the SSRI, depending upon their sociodemographic status, compared with a 2-fold greater likelihood of remission in patients on citalopram at 20 mg/day.
“The correlation is very high. It’s a very huge effect,” Ms. Viglione commented.
On the other hand, the 40-mg dose also was associated with an increased likelihood of worsening in patients living in an unfavorable environment. For example, 35% of patients in the 40-mg group with only a high school degree showed worsening depression, compared with 21% on citalopram at 20 mg/day. And 40% of low-income patients on citalopram at 40 mg/day showed worsening depression, compared with 35% of low-income patients on 20 mg. These figures probably underestimate the true downside of higher-dose treatment in patients living in an adverse environment, because STAR*D guidelines called for treatment discontinuation in the setting of worsening depression, she noted.
The correlation between higher-dose SSRI therapy, sociodemographic environment, and change in depressive symptoms was not uniform across all symptom categories. Ms. Viglione and her colleagues grouped the elements of the QIDS-SR16 rating scale into three domains: core emotional symptoms, sleep/insomnia symptoms, and weight/appetite. They found that the impact of higher-dose therapy in combination with favorable living conditions was greatest on sleep/insomnia symptoms.
The next step for the Italian investigators will be to determine in a prospective study whether the undirected susceptibility to change hypothesis can predict which patients will benefit from SSRI therapy.
Ms. Viglione reported having no financial conflicts regarding her study, which was funded by the Italian Ministry of Health.
BARCELONA – New evidence from the landmark 12-year-old STAR*D clinical trial provides fresh support for a novel Italian hypothesis that the efficacy of selective serotonin reuptake inhibitors in major depressive disorder results from their capacity to amplify the influence of living conditions upon mood.
“This hypothesis claims that SSRIs do not affect mood by themselves, but by increasing brain plasticity to render an individual more susceptible to the influence of living conditions. So in a positive environment, treatment leads to a beneficial outcome, and in a stressful environment it may lead to a worse prognosis,” Aurelia Viglione explained at the annual congress of the European College of Neuropsychopharmacology.
This originally was demonstrated by her senior coinvestigators in mouse studies, which showed increased brain plasticity and responsiveness of mood to living conditions in the presence of the serotonin boost provided by SSRIs. Now this animal research has been confirmed in a more clinically relevant fashion via a secondary analysis of the venerable National Institute of Mental Health–funded STAR*D (Sequenced Treatment Alternatives to Relieve Depression) data set, which Ms. Viglione presented at the ECNP congress.
This hypothesis, which she and her colleagues have dubbed the “undirected susceptibility to change” hypothesis of the mechanism of action of SSRIs, attempts to account for the drugs’ highly variable efficacy. As prescribing physicians and their often-frustrated patients with major depression are all too aware, the SSRIs – the most widely prescribed treatment for the disorder – induce remission in only 30%-40% of patients, while an additional 30%-40% fail to experience even a significant response. And despite much research effort, to date there is no reliable way to match the best antidepressant to a given individual in accord with the current priority to develop a personalized medicine approach.
The undirected susceptibility to change hypothesis provides a plausible explanation for these mixed clinical outcomes. The hypothesis posits that high serotonin levels lead to increased brain plasticity and consequent openness to change in mood, which can be for the better or worse – depending upon the quality of the surrounding environment.
Ms. Viglione, a PhD student in neuroscience at the University of Pisa (Italy), presented a study of a 591-patient subset of patients with major depression in STAR*D who received citalopram at 20 mg/day for 4 weeks, at which point the 40% of participants who weren’t showing a sufficiently favorable response trend had their citalopram increased to 40 mg/day. Patients’ living conditions were categorized as favorable or adverse based upon an amalgam of sociodemographic characteristics, including employment status, education, marital status, income, insurance status, ethnicity, drug abuse, and history of traumatic events. Treatment response was measured using the 16-item Quick Inventory of Depressive Symptomatology (QIDS-SR16) score.
. Patients were more likely to achieve remission as defined by a QIDS-SR16 score of 5 or less at week 6 if they had a college education, a job, higher income, and/or private health insurance than if those proxies for favorable living conditions were not present.
The impact of sociodemographic factors on change in mood was much larger in patients on citalopram at 40 mg/day than 20 mg/day. For example, having a college education rather than a high school education was independently associated with up to a 37-fold greater remission rate among patients on the higher dose of the SSRI, depending upon their sociodemographic status, compared with a 2-fold greater likelihood of remission in patients on citalopram at 20 mg/day.
“The correlation is very high. It’s a very huge effect,” Ms. Viglione commented.
On the other hand, the 40-mg dose also was associated with an increased likelihood of worsening in patients living in an unfavorable environment. For example, 35% of patients in the 40-mg group with only a high school degree showed worsening depression, compared with 21% on citalopram at 20 mg/day. And 40% of low-income patients on citalopram at 40 mg/day showed worsening depression, compared with 35% of low-income patients on 20 mg. These figures probably underestimate the true downside of higher-dose treatment in patients living in an adverse environment, because STAR*D guidelines called for treatment discontinuation in the setting of worsening depression, she noted.
The correlation between higher-dose SSRI therapy, sociodemographic environment, and change in depressive symptoms was not uniform across all symptom categories. Ms. Viglione and her colleagues grouped the elements of the QIDS-SR16 rating scale into three domains: core emotional symptoms, sleep/insomnia symptoms, and weight/appetite. They found that the impact of higher-dose therapy in combination with favorable living conditions was greatest on sleep/insomnia symptoms.
The next step for the Italian investigators will be to determine in a prospective study whether the undirected susceptibility to change hypothesis can predict which patients will benefit from SSRI therapy.
Ms. Viglione reported having no financial conflicts regarding her study, which was funded by the Italian Ministry of Health.
BARCELONA – New evidence from the landmark 12-year-old STAR*D clinical trial provides fresh support for a novel Italian hypothesis that the efficacy of selective serotonin reuptake inhibitors in major depressive disorder results from their capacity to amplify the influence of living conditions upon mood.
“This hypothesis claims that SSRIs do not affect mood by themselves, but by increasing brain plasticity to render an individual more susceptible to the influence of living conditions. So in a positive environment, treatment leads to a beneficial outcome, and in a stressful environment it may lead to a worse prognosis,” Aurelia Viglione explained at the annual congress of the European College of Neuropsychopharmacology.
This originally was demonstrated by her senior coinvestigators in mouse studies, which showed increased brain plasticity and responsiveness of mood to living conditions in the presence of the serotonin boost provided by SSRIs. Now this animal research has been confirmed in a more clinically relevant fashion via a secondary analysis of the venerable National Institute of Mental Health–funded STAR*D (Sequenced Treatment Alternatives to Relieve Depression) data set, which Ms. Viglione presented at the ECNP congress.
This hypothesis, which she and her colleagues have dubbed the “undirected susceptibility to change” hypothesis of the mechanism of action of SSRIs, attempts to account for the drugs’ highly variable efficacy. As prescribing physicians and their often-frustrated patients with major depression are all too aware, the SSRIs – the most widely prescribed treatment for the disorder – induce remission in only 30%-40% of patients, while an additional 30%-40% fail to experience even a significant response. And despite much research effort, to date there is no reliable way to match the best antidepressant to a given individual in accord with the current priority to develop a personalized medicine approach.
The undirected susceptibility to change hypothesis provides a plausible explanation for these mixed clinical outcomes. The hypothesis posits that high serotonin levels lead to increased brain plasticity and consequent openness to change in mood, which can be for the better or worse – depending upon the quality of the surrounding environment.
Ms. Viglione, a PhD student in neuroscience at the University of Pisa (Italy), presented a study of a 591-patient subset of patients with major depression in STAR*D who received citalopram at 20 mg/day for 4 weeks, at which point the 40% of participants who weren’t showing a sufficiently favorable response trend had their citalopram increased to 40 mg/day. Patients’ living conditions were categorized as favorable or adverse based upon an amalgam of sociodemographic characteristics, including employment status, education, marital status, income, insurance status, ethnicity, drug abuse, and history of traumatic events. Treatment response was measured using the 16-item Quick Inventory of Depressive Symptomatology (QIDS-SR16) score.
. Patients were more likely to achieve remission as defined by a QIDS-SR16 score of 5 or less at week 6 if they had a college education, a job, higher income, and/or private health insurance than if those proxies for favorable living conditions were not present.
The impact of sociodemographic factors on change in mood was much larger in patients on citalopram at 40 mg/day than 20 mg/day. For example, having a college education rather than a high school education was independently associated with up to a 37-fold greater remission rate among patients on the higher dose of the SSRI, depending upon their sociodemographic status, compared with a 2-fold greater likelihood of remission in patients on citalopram at 20 mg/day.
“The correlation is very high. It’s a very huge effect,” Ms. Viglione commented.
On the other hand, the 40-mg dose also was associated with an increased likelihood of worsening in patients living in an unfavorable environment. For example, 35% of patients in the 40-mg group with only a high school degree showed worsening depression, compared with 21% on citalopram at 20 mg/day. And 40% of low-income patients on citalopram at 40 mg/day showed worsening depression, compared with 35% of low-income patients on 20 mg. These figures probably underestimate the true downside of higher-dose treatment in patients living in an adverse environment, because STAR*D guidelines called for treatment discontinuation in the setting of worsening depression, she noted.
The correlation between higher-dose SSRI therapy, sociodemographic environment, and change in depressive symptoms was not uniform across all symptom categories. Ms. Viglione and her colleagues grouped the elements of the QIDS-SR16 rating scale into three domains: core emotional symptoms, sleep/insomnia symptoms, and weight/appetite. They found that the impact of higher-dose therapy in combination with favorable living conditions was greatest on sleep/insomnia symptoms.
The next step for the Italian investigators will be to determine in a prospective study whether the undirected susceptibility to change hypothesis can predict which patients will benefit from SSRI therapy.
Ms. Viglione reported having no financial conflicts regarding her study, which was funded by the Italian Ministry of Health.
REPORTING FROM THE ECNP CONGRESS
Key clinical point: There’s a new hypothesis to explain the mixed results of selective serotonin reuptake inhibitors for major depression.
Major finding: Improvement in symptoms of major depression was strongly correlated with SSRI dose and patients’ living conditions.
Study details: This secondary analysis of the STAR*D data set included 591 patients who received citalopram for major depression.
Disclosures: The presenter reported having no financial conflicts regarding the study, funded by the Italian Ministry of Health.
Mood stabilizers protect bipolar patients from suicide
BARCELONA – Lithium and valproic acid are the treatments of choice for patients with bipolar disorder at increased risk for suicide, according to the findings of a large Finnish national study.
“We found that – surprise, surprise – lithium and valproic acid had the lowest risk of anyone committing suicide on them. And funnily enough, some antidepressants seemed to be correlated with a higher risk of committing suicide,” Markku Lähteenvuo, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
However, he suspects that the correlation between antidepressant therapy and suicide in bipolar patients probably was caused by confounding by indication.
“I wouldn’t have as a take-home message that SSRI [selective serotonin reuptake inhibitor] antidepressants are bad for you; it’s probably rather that these are really bad cases, treatment gets initiated when someone gets worse, and the antidepressants just aren’t quick enough to really give an effect. It takes 3-4 weeks for an SSRI to really kick in, whereas mood stabilizers like lithium and valproic acid usually kick in almost immediately, within a couple of days to a week,” explained Dr. Lähteenvuo, a forensic psychiatrist at Niuvanniemi Hospital and the University of Eastern Finland, in Kuopio.
He presented a study of all suicides among the 18,018 Finnish patients hospitalized for bipolar disorder nationwide during 1996-2012. Using prospective national databases to follow patients for a mean of 7.2 years, he and his coinvestigators were able to determine what medications they were on when they committed suicide and the likelihood they were actually taking their prescribed medications at the time.
In a multivariate proportional hazards analysis adjusted for concomitant psychotropic medications, duration of bipolar illness, intervals of drug exposure and nonexposure, age, sex, and number of hospitalizations for suicidality within the prior 2 years, bipolar patients on lithium had a 67% lower risk of suicide than did those not on the drug. Those on valproic acid were 39% less likely to commit suicide than those not on that mood stabilizer. And bipolar patients on lithium were 42% less likely to die from suicide than those on valproic acid.
At the other extreme, patients on antidepressants were in aggregate 28% more likely to commit suicide than those who were not. This risk varied considerably according to the specific antidepressant: for example, escitalopram and mirtazapine were associated with 71% and 57% greater risks of suicide, respectively, than in patients not on those antidepressants, while patients on paroxetine, venlafaxine, or sertraline were not at increased risk.
Also, the use of sedatives was associated with a 52% greater likelihood of suicide, and benzodiazepines were linked to a 21% increase in risk. Again, as with antidepressants, these associations with increased risk of completed suicide could be attributable in part or in whole to confounding by indication, the psychiatrist noted. He and his colleagues are conducting further analyses examining that possibility.
Pending the outcome of that closer look, however, Dr. Lähteenvuo believes the study’s message to clinicians is clear: “The use of lithium is getting less and less common all the time because of side effects. That’s also true for valproic acid. Many bipolar patients are now prescribed only antidepressants, even though all the guidelines advise against it due to the risk of hypomania. We think that this is a bad trend and that lithium and valproic acid should be prescribed more. Also, as a safety precaution, anyone with bipolar disorder on antidepressants or benzodiazepines or sedatives should be followed especially closely for suicidal signals, because they could carry a really highly increased risk – up to 50% – due to the medication as well.”
He reported having no financial conflicts regarding the study, funded by the Finnish government.
Dr. Lähteenvuo also was first author of a recent study showing that among the various drugs prescribed for treatment of bipolar disorder, lithium was the clear winner for prevention of rehospitalization in the same national Finnish population of more than 18,000 bipolar patients (JAMA Psychiatry. 2018;75[4]:347-55). One expert named this among the top four studies of the year in the field of mood disorders.
BARCELONA – Lithium and valproic acid are the treatments of choice for patients with bipolar disorder at increased risk for suicide, according to the findings of a large Finnish national study.
“We found that – surprise, surprise – lithium and valproic acid had the lowest risk of anyone committing suicide on them. And funnily enough, some antidepressants seemed to be correlated with a higher risk of committing suicide,” Markku Lähteenvuo, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
However, he suspects that the correlation between antidepressant therapy and suicide in bipolar patients probably was caused by confounding by indication.
“I wouldn’t have as a take-home message that SSRI [selective serotonin reuptake inhibitor] antidepressants are bad for you; it’s probably rather that these are really bad cases, treatment gets initiated when someone gets worse, and the antidepressants just aren’t quick enough to really give an effect. It takes 3-4 weeks for an SSRI to really kick in, whereas mood stabilizers like lithium and valproic acid usually kick in almost immediately, within a couple of days to a week,” explained Dr. Lähteenvuo, a forensic psychiatrist at Niuvanniemi Hospital and the University of Eastern Finland, in Kuopio.
He presented a study of all suicides among the 18,018 Finnish patients hospitalized for bipolar disorder nationwide during 1996-2012. Using prospective national databases to follow patients for a mean of 7.2 years, he and his coinvestigators were able to determine what medications they were on when they committed suicide and the likelihood they were actually taking their prescribed medications at the time.
In a multivariate proportional hazards analysis adjusted for concomitant psychotropic medications, duration of bipolar illness, intervals of drug exposure and nonexposure, age, sex, and number of hospitalizations for suicidality within the prior 2 years, bipolar patients on lithium had a 67% lower risk of suicide than did those not on the drug. Those on valproic acid were 39% less likely to commit suicide than those not on that mood stabilizer. And bipolar patients on lithium were 42% less likely to die from suicide than those on valproic acid.
At the other extreme, patients on antidepressants were in aggregate 28% more likely to commit suicide than those who were not. This risk varied considerably according to the specific antidepressant: for example, escitalopram and mirtazapine were associated with 71% and 57% greater risks of suicide, respectively, than in patients not on those antidepressants, while patients on paroxetine, venlafaxine, or sertraline were not at increased risk.
Also, the use of sedatives was associated with a 52% greater likelihood of suicide, and benzodiazepines were linked to a 21% increase in risk. Again, as with antidepressants, these associations with increased risk of completed suicide could be attributable in part or in whole to confounding by indication, the psychiatrist noted. He and his colleagues are conducting further analyses examining that possibility.
Pending the outcome of that closer look, however, Dr. Lähteenvuo believes the study’s message to clinicians is clear: “The use of lithium is getting less and less common all the time because of side effects. That’s also true for valproic acid. Many bipolar patients are now prescribed only antidepressants, even though all the guidelines advise against it due to the risk of hypomania. We think that this is a bad trend and that lithium and valproic acid should be prescribed more. Also, as a safety precaution, anyone with bipolar disorder on antidepressants or benzodiazepines or sedatives should be followed especially closely for suicidal signals, because they could carry a really highly increased risk – up to 50% – due to the medication as well.”
He reported having no financial conflicts regarding the study, funded by the Finnish government.
Dr. Lähteenvuo also was first author of a recent study showing that among the various drugs prescribed for treatment of bipolar disorder, lithium was the clear winner for prevention of rehospitalization in the same national Finnish population of more than 18,000 bipolar patients (JAMA Psychiatry. 2018;75[4]:347-55). One expert named this among the top four studies of the year in the field of mood disorders.
BARCELONA – Lithium and valproic acid are the treatments of choice for patients with bipolar disorder at increased risk for suicide, according to the findings of a large Finnish national study.
“We found that – surprise, surprise – lithium and valproic acid had the lowest risk of anyone committing suicide on them. And funnily enough, some antidepressants seemed to be correlated with a higher risk of committing suicide,” Markku Lähteenvuo, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
However, he suspects that the correlation between antidepressant therapy and suicide in bipolar patients probably was caused by confounding by indication.
“I wouldn’t have as a take-home message that SSRI [selective serotonin reuptake inhibitor] antidepressants are bad for you; it’s probably rather that these are really bad cases, treatment gets initiated when someone gets worse, and the antidepressants just aren’t quick enough to really give an effect. It takes 3-4 weeks for an SSRI to really kick in, whereas mood stabilizers like lithium and valproic acid usually kick in almost immediately, within a couple of days to a week,” explained Dr. Lähteenvuo, a forensic psychiatrist at Niuvanniemi Hospital and the University of Eastern Finland, in Kuopio.
He presented a study of all suicides among the 18,018 Finnish patients hospitalized for bipolar disorder nationwide during 1996-2012. Using prospective national databases to follow patients for a mean of 7.2 years, he and his coinvestigators were able to determine what medications they were on when they committed suicide and the likelihood they were actually taking their prescribed medications at the time.
In a multivariate proportional hazards analysis adjusted for concomitant psychotropic medications, duration of bipolar illness, intervals of drug exposure and nonexposure, age, sex, and number of hospitalizations for suicidality within the prior 2 years, bipolar patients on lithium had a 67% lower risk of suicide than did those not on the drug. Those on valproic acid were 39% less likely to commit suicide than those not on that mood stabilizer. And bipolar patients on lithium were 42% less likely to die from suicide than those on valproic acid.
At the other extreme, patients on antidepressants were in aggregate 28% more likely to commit suicide than those who were not. This risk varied considerably according to the specific antidepressant: for example, escitalopram and mirtazapine were associated with 71% and 57% greater risks of suicide, respectively, than in patients not on those antidepressants, while patients on paroxetine, venlafaxine, or sertraline were not at increased risk.
Also, the use of sedatives was associated with a 52% greater likelihood of suicide, and benzodiazepines were linked to a 21% increase in risk. Again, as with antidepressants, these associations with increased risk of completed suicide could be attributable in part or in whole to confounding by indication, the psychiatrist noted. He and his colleagues are conducting further analyses examining that possibility.
Pending the outcome of that closer look, however, Dr. Lähteenvuo believes the study’s message to clinicians is clear: “The use of lithium is getting less and less common all the time because of side effects. That’s also true for valproic acid. Many bipolar patients are now prescribed only antidepressants, even though all the guidelines advise against it due to the risk of hypomania. We think that this is a bad trend and that lithium and valproic acid should be prescribed more. Also, as a safety precaution, anyone with bipolar disorder on antidepressants or benzodiazepines or sedatives should be followed especially closely for suicidal signals, because they could carry a really highly increased risk – up to 50% – due to the medication as well.”
He reported having no financial conflicts regarding the study, funded by the Finnish government.
Dr. Lähteenvuo also was first author of a recent study showing that among the various drugs prescribed for treatment of bipolar disorder, lithium was the clear winner for prevention of rehospitalization in the same national Finnish population of more than 18,000 bipolar patients (JAMA Psychiatry. 2018;75[4]:347-55). One expert named this among the top four studies of the year in the field of mood disorders.
REPORTING FROM THE ECNP CONGRESS
Key clinical point: Lithium and valproic acid protect patients with bipolar disorder from suicide.
Major finding: The likelihood of suicide was reduced by two-thirds in bipolar patients on lithium, compared with that of patients not on the mood stabilizer.
Study details: This was a retrospective study of more than 18,000 Finnish patients hospitalized at some point for bipolar disorder and the medications they were on when a subset of them committed suicide.
Disclosures: The presenter reported having no financial conflicts regarding the study, funded by the Finnish government.
Study confirms advice to halt methotrexate when giving flu vaccine to RA patients
CHICAGO – Discontinuing methotrexate for 2 weeks in patients with RA starting the day they receive the seasonal influenza vaccine significantly improves the vaccine’s immunogenicity without aggravating disease activity, Kevin L. Winthrop, MD, reported at the annual meeting of the American College of Rheumatology.

“I think this is potentially clinically practice changing because now there are two studies showing the same thing,” said Dr. Winthrop, a professor of public health and preventive medicine at Oregon Health & Science University, Portland.
Based upon these prospective randomized studies, which he conducted together with investigators at Seoul National University in South Korea, initiating a 2-week halt of methotrexate on the day the influenza vaccine is given to patients with RA is now his routine practice, and he recommends other physicians do the same.
The first prospective, randomized trial included 199 RA patients on stable doses of methotrexate who were assigned to one of four groups in conjunction with seasonal influenza vaccination. One group continued their methotrexate as usual, the second stopped the drug for 1 month prior to vaccination and then restarted it at the time of vaccination, the third group halted methotrexate for 2 weeks before and 2 weeks after vaccination, and the fourth suspended methotrexate for 4 weeks starting on the day they got their flu shot. Everyone received trivalent influenza vaccine containing H1N1, H3N2, and B/Yamagata.
The lowest rate of satisfactory vaccine response as defined by at least a 300% titer increase 1 month after vaccination occurred in the group that continued their methotrexate as usual. The group that halted the drug for 2 weeks before and 2 weeks after influenza vaccination had a 51% satisfactory vaccine response against all three antigens, compared with a 31.5% rate in the methotrexate-as-usual group. RA flare rates ranged from 21% to 39% across the four study arms, differences that weren’t statistically significant (Ann Rheum Dis. 2017 Sep;76[9]:1559-65).
Next Dr. Winthrop and his colleagues conducted a confirmatory prospective, multicenter, randomized trial in which they sought to nail down the optimal duration and timing of methotrexate discontinuation. A total of 320 RA patients on stable doses of methotrexate were assigned to halt the drug for 2 weeks starting at the time they received a quadrivalent seasonal influenza vaccine containing H1N1, H3N2, B/Yamagata, and B/Victoria strains, or to continue their methotrexate throughout.
A satisfactory vaccine response was achieved in 75.5% of the group that discontinued the drug, significantly better than the 54.5% rate in the methotrexate continuers. The absolute difference in seroprotection was greater in patients who halted their methotrexate for 2 weeks after vaccination for all four antigens: an absolute 11% difference for H1N1, 16% for H3N2, 12% for B/Yamagata, and 15% for B/Victoria (Ann Rheum Dis. 2018 Jun;77[6]:898-904).
“It does seem to be a nice strategy. The percentage of people who flared their RA during their 2 weeks off methotrexate was very low, so there seems to be a good reason to do this,” according to Dr. Winthrop.
Some rheumatologists he has spoken with initially balked at the plausibility of the results.
“I had the same thought about these studies: It doesn’t make sense to me in terms of how methotrexate works, and why we would see this effect acutely by stopping methotrexate for just 2 weeks?” he said.
But then a coinvestigator drilled down deeper into the data and came up with the explanation: The benefit in terms of enhanced flu vaccine immunogenicity through temporary withholding of methotrexate was confined to the subgroup of RA patients with high baseline levels of B-cell activation factor (BAFF). In contrast, withholding methotrexate didn’t affect the vaccine response in patients with low or normal baseline BAFF (Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214025).
“I don’t know how to check anyone’s BAFF levels. I don’t think there’s a commercial test out there. But this does help explain why we saw this observation. So I think I would still hold everyone’s methotrexate for 2 weeks. That’s how I approach it. And they may get benefit from it, and they may not,” he said.
Dr. Winthrop reported having no financial conflicts regarding the study, which was funded by GC Pharma.
CHICAGO – Discontinuing methotrexate for 2 weeks in patients with RA starting the day they receive the seasonal influenza vaccine significantly improves the vaccine’s immunogenicity without aggravating disease activity, Kevin L. Winthrop, MD, reported at the annual meeting of the American College of Rheumatology.
“I think this is potentially clinically practice changing because now there are two studies showing the same thing,” said Dr. Winthrop, a professor of public health and preventive medicine at Oregon Health & Science University, Portland.
Based upon these prospective randomized studies, which he conducted together with investigators at Seoul National University in South Korea, initiating a 2-week halt of methotrexate on the day the influenza vaccine is given to patients with RA is now his routine practice, and he recommends other physicians do the same.
The first prospective, randomized trial included 199 RA patients on stable doses of methotrexate who were assigned to one of four groups in conjunction with seasonal influenza vaccination. One group continued their methotrexate as usual, the second stopped the drug for 1 month prior to vaccination and then restarted it at the time of vaccination, the third group halted methotrexate for 2 weeks before and 2 weeks after vaccination, and the fourth suspended methotrexate for 4 weeks starting on the day they got their flu shot. Everyone received trivalent influenza vaccine containing H1N1, H3N2, and B/Yamagata.
The lowest rate of satisfactory vaccine response as defined by at least a 300% titer increase 1 month after vaccination occurred in the group that continued their methotrexate as usual. The group that halted the drug for 2 weeks before and 2 weeks after influenza vaccination had a 51% satisfactory vaccine response against all three antigens, compared with a 31.5% rate in the methotrexate-as-usual group. RA flare rates ranged from 21% to 39% across the four study arms, differences that weren’t statistically significant (Ann Rheum Dis. 2017 Sep;76[9]:1559-65).
Next Dr. Winthrop and his colleagues conducted a confirmatory prospective, multicenter, randomized trial in which they sought to nail down the optimal duration and timing of methotrexate discontinuation. A total of 320 RA patients on stable doses of methotrexate were assigned to halt the drug for 2 weeks starting at the time they received a quadrivalent seasonal influenza vaccine containing H1N1, H3N2, B/Yamagata, and B/Victoria strains, or to continue their methotrexate throughout.
A satisfactory vaccine response was achieved in 75.5% of the group that discontinued the drug, significantly better than the 54.5% rate in the methotrexate continuers. The absolute difference in seroprotection was greater in patients who halted their methotrexate for 2 weeks after vaccination for all four antigens: an absolute 11% difference for H1N1, 16% for H3N2, 12% for B/Yamagata, and 15% for B/Victoria (Ann Rheum Dis. 2018 Jun;77[6]:898-904).
“It does seem to be a nice strategy. The percentage of people who flared their RA during their 2 weeks off methotrexate was very low, so there seems to be a good reason to do this,” according to Dr. Winthrop.
Some rheumatologists he has spoken with initially balked at the plausibility of the results.
“I had the same thought about these studies: It doesn’t make sense to me in terms of how methotrexate works, and why we would see this effect acutely by stopping methotrexate for just 2 weeks?” he said.
But then a coinvestigator drilled down deeper into the data and came up with the explanation: The benefit in terms of enhanced flu vaccine immunogenicity through temporary withholding of methotrexate was confined to the subgroup of RA patients with high baseline levels of B-cell activation factor (BAFF). In contrast, withholding methotrexate didn’t affect the vaccine response in patients with low or normal baseline BAFF (Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214025).
“I don’t know how to check anyone’s BAFF levels. I don’t think there’s a commercial test out there. But this does help explain why we saw this observation. So I think I would still hold everyone’s methotrexate for 2 weeks. That’s how I approach it. And they may get benefit from it, and they may not,” he said.
Dr. Winthrop reported having no financial conflicts regarding the study, which was funded by GC Pharma.
CHICAGO – Discontinuing methotrexate for 2 weeks in patients with RA starting the day they receive the seasonal influenza vaccine significantly improves the vaccine’s immunogenicity without aggravating disease activity, Kevin L. Winthrop, MD, reported at the annual meeting of the American College of Rheumatology.
“I think this is potentially clinically practice changing because now there are two studies showing the same thing,” said Dr. Winthrop, a professor of public health and preventive medicine at Oregon Health & Science University, Portland.
Based upon these prospective randomized studies, which he conducted together with investigators at Seoul National University in South Korea, initiating a 2-week halt of methotrexate on the day the influenza vaccine is given to patients with RA is now his routine practice, and he recommends other physicians do the same.
The first prospective, randomized trial included 199 RA patients on stable doses of methotrexate who were assigned to one of four groups in conjunction with seasonal influenza vaccination. One group continued their methotrexate as usual, the second stopped the drug for 1 month prior to vaccination and then restarted it at the time of vaccination, the third group halted methotrexate for 2 weeks before and 2 weeks after vaccination, and the fourth suspended methotrexate for 4 weeks starting on the day they got their flu shot. Everyone received trivalent influenza vaccine containing H1N1, H3N2, and B/Yamagata.
The lowest rate of satisfactory vaccine response as defined by at least a 300% titer increase 1 month after vaccination occurred in the group that continued their methotrexate as usual. The group that halted the drug for 2 weeks before and 2 weeks after influenza vaccination had a 51% satisfactory vaccine response against all three antigens, compared with a 31.5% rate in the methotrexate-as-usual group. RA flare rates ranged from 21% to 39% across the four study arms, differences that weren’t statistically significant (Ann Rheum Dis. 2017 Sep;76[9]:1559-65).
Next Dr. Winthrop and his colleagues conducted a confirmatory prospective, multicenter, randomized trial in which they sought to nail down the optimal duration and timing of methotrexate discontinuation. A total of 320 RA patients on stable doses of methotrexate were assigned to halt the drug for 2 weeks starting at the time they received a quadrivalent seasonal influenza vaccine containing H1N1, H3N2, B/Yamagata, and B/Victoria strains, or to continue their methotrexate throughout.
A satisfactory vaccine response was achieved in 75.5% of the group that discontinued the drug, significantly better than the 54.5% rate in the methotrexate continuers. The absolute difference in seroprotection was greater in patients who halted their methotrexate for 2 weeks after vaccination for all four antigens: an absolute 11% difference for H1N1, 16% for H3N2, 12% for B/Yamagata, and 15% for B/Victoria (Ann Rheum Dis. 2018 Jun;77[6]:898-904).
“It does seem to be a nice strategy. The percentage of people who flared their RA during their 2 weeks off methotrexate was very low, so there seems to be a good reason to do this,” according to Dr. Winthrop.
Some rheumatologists he has spoken with initially balked at the plausibility of the results.
“I had the same thought about these studies: It doesn’t make sense to me in terms of how methotrexate works, and why we would see this effect acutely by stopping methotrexate for just 2 weeks?” he said.
But then a coinvestigator drilled down deeper into the data and came up with the explanation: The benefit in terms of enhanced flu vaccine immunogenicity through temporary withholding of methotrexate was confined to the subgroup of RA patients with high baseline levels of B-cell activation factor (BAFF). In contrast, withholding methotrexate didn’t affect the vaccine response in patients with low or normal baseline BAFF (Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214025).
“I don’t know how to check anyone’s BAFF levels. I don’t think there’s a commercial test out there. But this does help explain why we saw this observation. So I think I would still hold everyone’s methotrexate for 2 weeks. That’s how I approach it. And they may get benefit from it, and they may not,” he said.
Dr. Winthrop reported having no financial conflicts regarding the study, which was funded by GC Pharma.
REPORTING FROM THE ACR ANNUAL MEETING
Dueling SLE classification criteria: And the winner is...
CHICAGO – Newer isn’t necessarily better – especially when it comes to the plethora of SLE classification criteria, according to Michelle A. Petri, MD, professor of medicine and director of the Hopkins Lupus Center at Johns Hopkins University, Baltimore.

“We have an embarrassment of criteria for lupus right now, and everyone wants to know if one is better than the others,” the rheumatologist said at the annual meeting of the American College of Rheumatology.
She and several coinvestigators who are members of the Systemic Lupus International Collaborating Clinics (SLICC) set out to learn the answer. They developed a new, modified, weighted version of the 2012 SLICC criteria and compared its sensitivity and specificity for SLE diagnosis by 690 physicians with three other major classification systems: the 1997 update to ACR-11 criteria, the nonweighted SLICC 2012 criteria, and the proposed EULAR/ACR criteria, which uses a differentially weighted approach in which the various possible disease manifestations are each assigned a different point score. In contrast, the revised ACR-11 and SLICC 2012 criteria count each SLE manifestation equally.
Long story short: “The two newly derived weighted classification rules did not perform better than the existing list-based rules in terms of overall agreement,” according to Dr. Petri.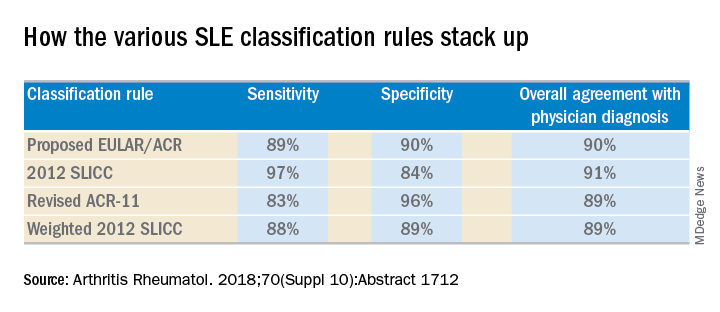
“We don’t think that weighting all the criteria, which is what the EULAR/ACR and weighted SLICC 2012 rules do, adds to the performance of the criteria set, and in fact it makes it much more difficult for clinicians to use when there’s a complicated weighting system, unless it’s web-based or there’s an app for it. And to be honest, clinicians are so busy that they’re probably not going to take time out in a clinic visit to go use the web or an app. Our criteria need to be user friendly,” she continued.
So which of the four classification systems is most user friendly? The EULAR/ACR criteria can be dismissed on that score because they are supposed to be used only for research, according to the rheumatologist.
“I think the SLICC 2012 criteria are very useful for clinicians because they have the highest sensitivity. And what a clinician wants is not to miss a diagnosis and to start treatment early,” Dr. Petri said.
To develop the weighted SLICC criteria, whose future at this point doesn’t look bright, she and her coinvestigators redeployed the same physician-rated patient scenarios used to develop the nonweighted 2012 SLICC classification criteria and assigned each of the potential manifestations of SLE a specific point score. For example, acute cutaneous manifestations received 16 points, serositis 9, oral ulcers 16, thrombocytopenia 15, and so forth. Under this system, a patient with a score of at least 56 points, or lupus nephritis, or least one clinical and one immunologic component of SLE was classified as having the disease.
Dr. Petri reported having no financial conflicts regarding her study, supported by the National Institutes of Health.
SOURCE: Petri MA et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1712.
CHICAGO – Newer isn’t necessarily better – especially when it comes to the plethora of SLE classification criteria, according to Michelle A. Petri, MD, professor of medicine and director of the Hopkins Lupus Center at Johns Hopkins University, Baltimore.
“We have an embarrassment of criteria for lupus right now, and everyone wants to know if one is better than the others,” the rheumatologist said at the annual meeting of the American College of Rheumatology.
She and several coinvestigators who are members of the Systemic Lupus International Collaborating Clinics (SLICC) set out to learn the answer. They developed a new, modified, weighted version of the 2012 SLICC criteria and compared its sensitivity and specificity for SLE diagnosis by 690 physicians with three other major classification systems: the 1997 update to ACR-11 criteria, the nonweighted SLICC 2012 criteria, and the proposed EULAR/ACR criteria, which uses a differentially weighted approach in which the various possible disease manifestations are each assigned a different point score. In contrast, the revised ACR-11 and SLICC 2012 criteria count each SLE manifestation equally.
Long story short: “The two newly derived weighted classification rules did not perform better than the existing list-based rules in terms of overall agreement,” according to Dr. Petri.
“We don’t think that weighting all the criteria, which is what the EULAR/ACR and weighted SLICC 2012 rules do, adds to the performance of the criteria set, and in fact it makes it much more difficult for clinicians to use when there’s a complicated weighting system, unless it’s web-based or there’s an app for it. And to be honest, clinicians are so busy that they’re probably not going to take time out in a clinic visit to go use the web or an app. Our criteria need to be user friendly,” she continued.
So which of the four classification systems is most user friendly? The EULAR/ACR criteria can be dismissed on that score because they are supposed to be used only for research, according to the rheumatologist.
“I think the SLICC 2012 criteria are very useful for clinicians because they have the highest sensitivity. And what a clinician wants is not to miss a diagnosis and to start treatment early,” Dr. Petri said.
To develop the weighted SLICC criteria, whose future at this point doesn’t look bright, she and her coinvestigators redeployed the same physician-rated patient scenarios used to develop the nonweighted 2012 SLICC classification criteria and assigned each of the potential manifestations of SLE a specific point score. For example, acute cutaneous manifestations received 16 points, serositis 9, oral ulcers 16, thrombocytopenia 15, and so forth. Under this system, a patient with a score of at least 56 points, or lupus nephritis, or least one clinical and one immunologic component of SLE was classified as having the disease.
Dr. Petri reported having no financial conflicts regarding her study, supported by the National Institutes of Health.
SOURCE: Petri MA et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1712.
CHICAGO – Newer isn’t necessarily better – especially when it comes to the plethora of SLE classification criteria, according to Michelle A. Petri, MD, professor of medicine and director of the Hopkins Lupus Center at Johns Hopkins University, Baltimore.
“We have an embarrassment of criteria for lupus right now, and everyone wants to know if one is better than the others,” the rheumatologist said at the annual meeting of the American College of Rheumatology.
She and several coinvestigators who are members of the Systemic Lupus International Collaborating Clinics (SLICC) set out to learn the answer. They developed a new, modified, weighted version of the 2012 SLICC criteria and compared its sensitivity and specificity for SLE diagnosis by 690 physicians with three other major classification systems: the 1997 update to ACR-11 criteria, the nonweighted SLICC 2012 criteria, and the proposed EULAR/ACR criteria, which uses a differentially weighted approach in which the various possible disease manifestations are each assigned a different point score. In contrast, the revised ACR-11 and SLICC 2012 criteria count each SLE manifestation equally.
Long story short: “The two newly derived weighted classification rules did not perform better than the existing list-based rules in terms of overall agreement,” according to Dr. Petri.
“We don’t think that weighting all the criteria, which is what the EULAR/ACR and weighted SLICC 2012 rules do, adds to the performance of the criteria set, and in fact it makes it much more difficult for clinicians to use when there’s a complicated weighting system, unless it’s web-based or there’s an app for it. And to be honest, clinicians are so busy that they’re probably not going to take time out in a clinic visit to go use the web or an app. Our criteria need to be user friendly,” she continued.
So which of the four classification systems is most user friendly? The EULAR/ACR criteria can be dismissed on that score because they are supposed to be used only for research, according to the rheumatologist.
“I think the SLICC 2012 criteria are very useful for clinicians because they have the highest sensitivity. And what a clinician wants is not to miss a diagnosis and to start treatment early,” Dr. Petri said.
To develop the weighted SLICC criteria, whose future at this point doesn’t look bright, she and her coinvestigators redeployed the same physician-rated patient scenarios used to develop the nonweighted 2012 SLICC classification criteria and assigned each of the potential manifestations of SLE a specific point score. For example, acute cutaneous manifestations received 16 points, serositis 9, oral ulcers 16, thrombocytopenia 15, and so forth. Under this system, a patient with a score of at least 56 points, or lupus nephritis, or least one clinical and one immunologic component of SLE was classified as having the disease.
Dr. Petri reported having no financial conflicts regarding her study, supported by the National Institutes of Health.
SOURCE: Petri MA et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1712.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: The 2012 SLICC SLE classification criteria are best suited for clinical practice.
Major finding:
Study details: This study compared the sensitivity, specificity, and overall agreement with physician diagnosis of four different sets of SLE classification criteria.
Disclosures: The study was supported by the National Institutes of Health. The presenter reported having no financial conflicts.
Source: Petri MA et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1712.
Ligelizumab outperformed omalizumab for refractory chronic spontaneous urticaria
.

“For sure, ligelizumab is the highlight of this year in urticariology,” Marcus Maurer, MD, declared at the annual congress of the European Academy of Dermatology and Venereology. An ongoing phase 3 trial will now compare more than 1,000 patients with CSU who will be randomized to ligelizumab, omalizumab, or placebo.
Like omalizumab (Xolair), which is approved in the United States and Europe for treatment of CSU, ligelizumab is a humanized anti-IgE monoclonal antibody. But the investigational agent binds to IgE with greater affinity than omalizumab, and this translated into greater therapeutic efficacy in the multicenter, double-blind, placebo-controlled clinical trial, explained Dr. Maurer, professor of dermatology and allergy at Charité University in Berlin.
Study participants, all refractory to histamine1 antihistamines and in many cases to leukotriene receptor antagonists as well, were randomized to omalizumab at 300 mg, placebo, or to ligelizumab at 24 mg, 72 mg, or 240 mg administered by subcutaneous injection every 4 weeks for 20 weeks. The study showed that the effective dose of ligelizumab lies somewhere between 72 and 240 mg; the 24-mg dose won’t be pursued in further studies.
“Three things are important in the comparison between ligelizumab and omalizumab: First, ligelizumab works faster – and omalizumab is a fast-working drug in urticaria. As early as week 4 after initiation of treatment, ligelizumab resulted in a significantly higher response rate,” he said.
Second, a complete response rate as defined by an Urticaria Activity Score over the past 7 days (UAS7) of 0 was achieved by more than 50% of patients on ligelizumab at 240 mg, a rate twice that seen in the omalizumab group. Indeed, more patients were symptom-free on ligelizumab at 72 mg or 240 mg than on omalizumab throughout the 20-week study.
And third, time to relapse after treatment discontinuation was markedly longer with ligelizumab.
“Once you stop the treatment, we expect patients to come back because we didn’t cure the disease, we blocked the signs and symptoms by blocking mast cell degranulation. Relapse after the last injection occurred at about 4 weeks with omalizumab versus 10 weeks for ligelizumab on average. That’s amazing,” Dr. Maurer said.
At week 20, the mean reductions from baseline in UAS7 scores were 13.6 points with placebo, 15.2 points with the lowest dose of ligelizumab, 18.2 points with omalizumab, 23.1 points with ligelizumab at 72 mg, and 22.5 points for ligelizumab at 240 mg.
The side effect profiles for both biologics were essentially the same as for placebo with the exception of a 5.9% rate of mild injection site reactions with ligelizumab at the 240-mg dose versus 2.3% with placebo.
Many clinicians have noticed a significant limitation of omalizumab: It is less effective in patients with more complex CSU having an autoimmune overlay, type 2b angioedema, and/or long disease duration.
“This does not seem to be the case with ligelizumab. Even for the difficult-to-treat subpopulations of CSU, ligelizumab appears to be a drug that can protect against mast cell degranulation. We see a reduction in angioedema activity; we see a reduction in wheal size and number; we see a reduction in the itch – so across all the symptoms in the difficult subpopulations, this is the better drug. Now we have to make it work in the phase 3 trials to bring it to clinical practice,” he said.
Dr. Maurer reported receiving research funding from and serving as an advisor to and paid speaker for Novartis, which markets omalizumab and is developing ligelizumab.
.
“For sure, ligelizumab is the highlight of this year in urticariology,” Marcus Maurer, MD, declared at the annual congress of the European Academy of Dermatology and Venereology. An ongoing phase 3 trial will now compare more than 1,000 patients with CSU who will be randomized to ligelizumab, omalizumab, or placebo.
Like omalizumab (Xolair), which is approved in the United States and Europe for treatment of CSU, ligelizumab is a humanized anti-IgE monoclonal antibody. But the investigational agent binds to IgE with greater affinity than omalizumab, and this translated into greater therapeutic efficacy in the multicenter, double-blind, placebo-controlled clinical trial, explained Dr. Maurer, professor of dermatology and allergy at Charité University in Berlin.
Study participants, all refractory to histamine1 antihistamines and in many cases to leukotriene receptor antagonists as well, were randomized to omalizumab at 300 mg, placebo, or to ligelizumab at 24 mg, 72 mg, or 240 mg administered by subcutaneous injection every 4 weeks for 20 weeks. The study showed that the effective dose of ligelizumab lies somewhere between 72 and 240 mg; the 24-mg dose won’t be pursued in further studies.
“Three things are important in the comparison between ligelizumab and omalizumab: First, ligelizumab works faster – and omalizumab is a fast-working drug in urticaria. As early as week 4 after initiation of treatment, ligelizumab resulted in a significantly higher response rate,” he said.
Second, a complete response rate as defined by an Urticaria Activity Score over the past 7 days (UAS7) of 0 was achieved by more than 50% of patients on ligelizumab at 240 mg, a rate twice that seen in the omalizumab group. Indeed, more patients were symptom-free on ligelizumab at 72 mg or 240 mg than on omalizumab throughout the 20-week study.
And third, time to relapse after treatment discontinuation was markedly longer with ligelizumab.
“Once you stop the treatment, we expect patients to come back because we didn’t cure the disease, we blocked the signs and symptoms by blocking mast cell degranulation. Relapse after the last injection occurred at about 4 weeks with omalizumab versus 10 weeks for ligelizumab on average. That’s amazing,” Dr. Maurer said.
At week 20, the mean reductions from baseline in UAS7 scores were 13.6 points with placebo, 15.2 points with the lowest dose of ligelizumab, 18.2 points with omalizumab, 23.1 points with ligelizumab at 72 mg, and 22.5 points for ligelizumab at 240 mg.
The side effect profiles for both biologics were essentially the same as for placebo with the exception of a 5.9% rate of mild injection site reactions with ligelizumab at the 240-mg dose versus 2.3% with placebo.
Many clinicians have noticed a significant limitation of omalizumab: It is less effective in patients with more complex CSU having an autoimmune overlay, type 2b angioedema, and/or long disease duration.
“This does not seem to be the case with ligelizumab. Even for the difficult-to-treat subpopulations of CSU, ligelizumab appears to be a drug that can protect against mast cell degranulation. We see a reduction in angioedema activity; we see a reduction in wheal size and number; we see a reduction in the itch – so across all the symptoms in the difficult subpopulations, this is the better drug. Now we have to make it work in the phase 3 trials to bring it to clinical practice,” he said.
Dr. Maurer reported receiving research funding from and serving as an advisor to and paid speaker for Novartis, which markets omalizumab and is developing ligelizumab.
.
“For sure, ligelizumab is the highlight of this year in urticariology,” Marcus Maurer, MD, declared at the annual congress of the European Academy of Dermatology and Venereology. An ongoing phase 3 trial will now compare more than 1,000 patients with CSU who will be randomized to ligelizumab, omalizumab, or placebo.
Like omalizumab (Xolair), which is approved in the United States and Europe for treatment of CSU, ligelizumab is a humanized anti-IgE monoclonal antibody. But the investigational agent binds to IgE with greater affinity than omalizumab, and this translated into greater therapeutic efficacy in the multicenter, double-blind, placebo-controlled clinical trial, explained Dr. Maurer, professor of dermatology and allergy at Charité University in Berlin.
Study participants, all refractory to histamine1 antihistamines and in many cases to leukotriene receptor antagonists as well, were randomized to omalizumab at 300 mg, placebo, or to ligelizumab at 24 mg, 72 mg, or 240 mg administered by subcutaneous injection every 4 weeks for 20 weeks. The study showed that the effective dose of ligelizumab lies somewhere between 72 and 240 mg; the 24-mg dose won’t be pursued in further studies.
“Three things are important in the comparison between ligelizumab and omalizumab: First, ligelizumab works faster – and omalizumab is a fast-working drug in urticaria. As early as week 4 after initiation of treatment, ligelizumab resulted in a significantly higher response rate,” he said.
Second, a complete response rate as defined by an Urticaria Activity Score over the past 7 days (UAS7) of 0 was achieved by more than 50% of patients on ligelizumab at 240 mg, a rate twice that seen in the omalizumab group. Indeed, more patients were symptom-free on ligelizumab at 72 mg or 240 mg than on omalizumab throughout the 20-week study.
And third, time to relapse after treatment discontinuation was markedly longer with ligelizumab.
“Once you stop the treatment, we expect patients to come back because we didn’t cure the disease, we blocked the signs and symptoms by blocking mast cell degranulation. Relapse after the last injection occurred at about 4 weeks with omalizumab versus 10 weeks for ligelizumab on average. That’s amazing,” Dr. Maurer said.
At week 20, the mean reductions from baseline in UAS7 scores were 13.6 points with placebo, 15.2 points with the lowest dose of ligelizumab, 18.2 points with omalizumab, 23.1 points with ligelizumab at 72 mg, and 22.5 points for ligelizumab at 240 mg.
The side effect profiles for both biologics were essentially the same as for placebo with the exception of a 5.9% rate of mild injection site reactions with ligelizumab at the 240-mg dose versus 2.3% with placebo.
Many clinicians have noticed a significant limitation of omalizumab: It is less effective in patients with more complex CSU having an autoimmune overlay, type 2b angioedema, and/or long disease duration.
“This does not seem to be the case with ligelizumab. Even for the difficult-to-treat subpopulations of CSU, ligelizumab appears to be a drug that can protect against mast cell degranulation. We see a reduction in angioedema activity; we see a reduction in wheal size and number; we see a reduction in the itch – so across all the symptoms in the difficult subpopulations, this is the better drug. Now we have to make it work in the phase 3 trials to bring it to clinical practice,” he said.
Dr. Maurer reported receiving research funding from and serving as an advisor to and paid speaker for Novartis, which markets omalizumab and is developing ligelizumab.
REPORTING FROM THE EADV CONGRESS
Key clinical point: Ligelizumab shows considerable promise for chronic spontaneous urticaria.
Major finding: The complete response rate was two times higher with ligelizumab than it was with omalizumab.
Study details: This phase 2b randomized, double-blind, multicenter, active- and placebo-controlled, 20-week study included 382 patients with chronic spontaneous urticaria.
Disclosures: The presenter reported receiving research funding from and serving as an advisor to and paid speaker for Novartis, which is developing ligelizumab.
Secukinumab shows promise in hidradenitis suppurativa
PARIS – David Rosmarin, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.

“It was especially notable that secukinumab was effective in five of the six patients who had previously failed anti-TNF [tumor necrosis factor] therapy,” said Dr. Rosmarin, a dermatologist at Tufts University, Boston.
At present, the sole medication approved for treatment of hidradenitis suppurativa (HS) is the TNF inhibitor adalimumab (Humira). The rationale for investigating secukinumab (Cosentyx), a biologic that blocks the interleukin-17A receptor and is approved for treatment of psoriasis, psoriatic arthritis, and ankylosing spondylitis, lies in the observation that HS lesions exhibit an increased ratio of Th17- to T-regulatory cells, compared with normal skin. Lesional skin also features elevated IL-17 levels. These abnormalities can be reversed by anti-TNF therapy, he explained.
Dr. Rosmarin presented a 28-week, open-label study in which 18 patients with moderate to severe HS received an induction regimen consisting of 300 mg secukinumab given subcutaneously once weekly for 5 weeks and were then randomized to the same dose of the biologic given either every 2 or 4 weeks until week 24.
The primary endpoint was achievement of a Hidradenitis Suppurativa Clinical Response (HiSCR) at 24 weeks. This requires no increase in the number of draining fistulae or abscesses, compared with baseline, plus at least a 50% reduction in total inflammatory nodules. Secondary endpoints were the mean change from baseline in the Sartorius Scale as well as on the Dermatology Life Quality Index (DLQI).
Participants were an average of 33 years and had a disease duration of 12 years; 14 patients were Hurley Stage II, the rest Stage III. Their mean baseline DLQI was 12.
“Patients with hidradenitis suppurativa have a horrible quality of life,” Dr. Rosmarin commented. “When we compare it to patients who have atopic dermatitis, psoriasis, or chronic idiopathic urticaria, oftentimes patients with hidradenitis suppurativa suffer the worst and have the most quality of life impairment.”
Of the 18 patients, 14 – 7 of 9 in each group – achieved HiSCR. This included five of the six patients who were previous nonresponders to adalimumab or another anti-TNF biologic.
“The other thing we noticed was the rapidity of response, which is important to a lot of our patients. It took an average of 7 weeks to achieve HiSCR, and eight patients achieved HiSCR during the induction phase of treatment,” the dermatologist said.
Mean scores on the Sartorius Scale dropped by 28%. Similarly, scores on the DLQI improved by a mean of 3.6 points, or 26%. Nine patients experienced a reduction of 5 points or more on the DLQI. “This happened largely in the first 1-2 months of therapy,” Dr. Rosmarin continued.
Secukinumab was well tolerated. There were no treatment discontinuations because of adverse events. Four patients, all in the biweekly dosing arm, developed Candida infections, all easily cured using topical ketoconazole.
The next step will be to conduct a large, placebo-controlled, randomized trial to firmly establish the efficacy of secukinumab for HS. Also, the optimal dosing of the biologic for induction and long-term maintenance therapy have yet to be determined. Over the long term, it will be important to see whether marked improvement in HS is accompanied by a reduction in the elevated cardiovascular risk associated with this inflammatory disease, he added.
In 2019, a trial will get underway to compare two doses of secukinumab for patients with HS. Based on a search of clinical trials at ClinicalTrials.gov, a wide range of monoclonal antibody therapies are being investigated for the treatment of HS.
The results of this preliminary study of secukinumab emphasize the importance of the Th17 pathway in HS and open the door to alternative strategies targeting this pathway. Dr. Rosmarin noted that he and his coinvestigators have collected a case series of positive responses to guselkumab (Tremfya), which targets the IL-23 p19 subunit, which also lies along the Th17 pathway.
The secukinumab study was sponsored by Novartis. Dr. Rosmarin reported serving as a consultant to or on speakers’ bureaus for that company and more than half a dozen other pharmaceutical companies.
PARIS – David Rosmarin, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
“It was especially notable that secukinumab was effective in five of the six patients who had previously failed anti-TNF [tumor necrosis factor] therapy,” said Dr. Rosmarin, a dermatologist at Tufts University, Boston.
At present, the sole medication approved for treatment of hidradenitis suppurativa (HS) is the TNF inhibitor adalimumab (Humira). The rationale for investigating secukinumab (Cosentyx), a biologic that blocks the interleukin-17A receptor and is approved for treatment of psoriasis, psoriatic arthritis, and ankylosing spondylitis, lies in the observation that HS lesions exhibit an increased ratio of Th17- to T-regulatory cells, compared with normal skin. Lesional skin also features elevated IL-17 levels. These abnormalities can be reversed by anti-TNF therapy, he explained.
Dr. Rosmarin presented a 28-week, open-label study in which 18 patients with moderate to severe HS received an induction regimen consisting of 300 mg secukinumab given subcutaneously once weekly for 5 weeks and were then randomized to the same dose of the biologic given either every 2 or 4 weeks until week 24.
The primary endpoint was achievement of a Hidradenitis Suppurativa Clinical Response (HiSCR) at 24 weeks. This requires no increase in the number of draining fistulae or abscesses, compared with baseline, plus at least a 50% reduction in total inflammatory nodules. Secondary endpoints were the mean change from baseline in the Sartorius Scale as well as on the Dermatology Life Quality Index (DLQI).
Participants were an average of 33 years and had a disease duration of 12 years; 14 patients were Hurley Stage II, the rest Stage III. Their mean baseline DLQI was 12.
“Patients with hidradenitis suppurativa have a horrible quality of life,” Dr. Rosmarin commented. “When we compare it to patients who have atopic dermatitis, psoriasis, or chronic idiopathic urticaria, oftentimes patients with hidradenitis suppurativa suffer the worst and have the most quality of life impairment.”
Of the 18 patients, 14 – 7 of 9 in each group – achieved HiSCR. This included five of the six patients who were previous nonresponders to adalimumab or another anti-TNF biologic.
“The other thing we noticed was the rapidity of response, which is important to a lot of our patients. It took an average of 7 weeks to achieve HiSCR, and eight patients achieved HiSCR during the induction phase of treatment,” the dermatologist said.
Mean scores on the Sartorius Scale dropped by 28%. Similarly, scores on the DLQI improved by a mean of 3.6 points, or 26%. Nine patients experienced a reduction of 5 points or more on the DLQI. “This happened largely in the first 1-2 months of therapy,” Dr. Rosmarin continued.
Secukinumab was well tolerated. There were no treatment discontinuations because of adverse events. Four patients, all in the biweekly dosing arm, developed Candida infections, all easily cured using topical ketoconazole.
The next step will be to conduct a large, placebo-controlled, randomized trial to firmly establish the efficacy of secukinumab for HS. Also, the optimal dosing of the biologic for induction and long-term maintenance therapy have yet to be determined. Over the long term, it will be important to see whether marked improvement in HS is accompanied by a reduction in the elevated cardiovascular risk associated with this inflammatory disease, he added.
In 2019, a trial will get underway to compare two doses of secukinumab for patients with HS. Based on a search of clinical trials at ClinicalTrials.gov, a wide range of monoclonal antibody therapies are being investigated for the treatment of HS.
The results of this preliminary study of secukinumab emphasize the importance of the Th17 pathway in HS and open the door to alternative strategies targeting this pathway. Dr. Rosmarin noted that he and his coinvestigators have collected a case series of positive responses to guselkumab (Tremfya), which targets the IL-23 p19 subunit, which also lies along the Th17 pathway.
The secukinumab study was sponsored by Novartis. Dr. Rosmarin reported serving as a consultant to or on speakers’ bureaus for that company and more than half a dozen other pharmaceutical companies.
PARIS – David Rosmarin, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
“It was especially notable that secukinumab was effective in five of the six patients who had previously failed anti-TNF [tumor necrosis factor] therapy,” said Dr. Rosmarin, a dermatologist at Tufts University, Boston.
At present, the sole medication approved for treatment of hidradenitis suppurativa (HS) is the TNF inhibitor adalimumab (Humira). The rationale for investigating secukinumab (Cosentyx), a biologic that blocks the interleukin-17A receptor and is approved for treatment of psoriasis, psoriatic arthritis, and ankylosing spondylitis, lies in the observation that HS lesions exhibit an increased ratio of Th17- to T-regulatory cells, compared with normal skin. Lesional skin also features elevated IL-17 levels. These abnormalities can be reversed by anti-TNF therapy, he explained.
Dr. Rosmarin presented a 28-week, open-label study in which 18 patients with moderate to severe HS received an induction regimen consisting of 300 mg secukinumab given subcutaneously once weekly for 5 weeks and were then randomized to the same dose of the biologic given either every 2 or 4 weeks until week 24.
The primary endpoint was achievement of a Hidradenitis Suppurativa Clinical Response (HiSCR) at 24 weeks. This requires no increase in the number of draining fistulae or abscesses, compared with baseline, plus at least a 50% reduction in total inflammatory nodules. Secondary endpoints were the mean change from baseline in the Sartorius Scale as well as on the Dermatology Life Quality Index (DLQI).
Participants were an average of 33 years and had a disease duration of 12 years; 14 patients were Hurley Stage II, the rest Stage III. Their mean baseline DLQI was 12.
“Patients with hidradenitis suppurativa have a horrible quality of life,” Dr. Rosmarin commented. “When we compare it to patients who have atopic dermatitis, psoriasis, or chronic idiopathic urticaria, oftentimes patients with hidradenitis suppurativa suffer the worst and have the most quality of life impairment.”
Of the 18 patients, 14 – 7 of 9 in each group – achieved HiSCR. This included five of the six patients who were previous nonresponders to adalimumab or another anti-TNF biologic.
“The other thing we noticed was the rapidity of response, which is important to a lot of our patients. It took an average of 7 weeks to achieve HiSCR, and eight patients achieved HiSCR during the induction phase of treatment,” the dermatologist said.
Mean scores on the Sartorius Scale dropped by 28%. Similarly, scores on the DLQI improved by a mean of 3.6 points, or 26%. Nine patients experienced a reduction of 5 points or more on the DLQI. “This happened largely in the first 1-2 months of therapy,” Dr. Rosmarin continued.
Secukinumab was well tolerated. There were no treatment discontinuations because of adverse events. Four patients, all in the biweekly dosing arm, developed Candida infections, all easily cured using topical ketoconazole.
The next step will be to conduct a large, placebo-controlled, randomized trial to firmly establish the efficacy of secukinumab for HS. Also, the optimal dosing of the biologic for induction and long-term maintenance therapy have yet to be determined. Over the long term, it will be important to see whether marked improvement in HS is accompanied by a reduction in the elevated cardiovascular risk associated with this inflammatory disease, he added.
In 2019, a trial will get underway to compare two doses of secukinumab for patients with HS. Based on a search of clinical trials at ClinicalTrials.gov, a wide range of monoclonal antibody therapies are being investigated for the treatment of HS.
The results of this preliminary study of secukinumab emphasize the importance of the Th17 pathway in HS and open the door to alternative strategies targeting this pathway. Dr. Rosmarin noted that he and his coinvestigators have collected a case series of positive responses to guselkumab (Tremfya), which targets the IL-23 p19 subunit, which also lies along the Th17 pathway.
The secukinumab study was sponsored by Novartis. Dr. Rosmarin reported serving as a consultant to or on speakers’ bureaus for that company and more than half a dozen other pharmaceutical companies.
REPORTING FROM THE EADV CONGRESS
Key clinical point: Secukinumab shows considerable promise for treatment of hidradenitis suppurativa.
Major finding: Hidradenitis suppurativa improved markedly in response to secukinumab in 14 of 18 patients.
Study details: This prospective, open-label, 28-week study included 18 patients with hidradenitis suppurativa who were randomized to one of two secukinumab dosing regimens.
Disclosures: The study was sponsored by Novartis. The presenter reported serving as a consultant to or on speakers’ bureaus for that company and more than half a dozen other pharmaceutical companies.