User login
No evidence to indicate significantly higher risk for cancer with JAKi vs bDMARD in RA
Key clinical point: Risk for first primary cancer was not significantly different among patients with rheumatoid arthritis (RA) receiving Janus kinase inhibitors (JAKi) vs biologic disease-modifying antirheumatic drugs (bDMARD). However, excess risk cannot be ruled out among those receiving JAKi.
Major finding: Patients with RA treated with JAKi had a numerically higher but not statistically significantly higher risk for first primary cancer (hazard ratio 1.41; 95% CI 0.76-2.37) compared with those treated with bDMARD.
Study details: Findings are from an observational cohort study including patients with RA without prior cancer diagnosis who initiated JAKi (n = 875) or bDMARD (n = 4247).
Disclosures: This study received financial support from the Danish Rheumatism Association and Danish Cancer Society. Several authors declared being employees of, receiving research grants and honoraria from, participating in advisory boards of, or serving on steering committees for various sources.
Source: Westermann R et al. Cancer risk in patients with rheumatoid arthritis treated with Janus kinase inhibitors: A nationwide Danish register-based cohort study. Rheumatology (Oxford). 2023 (Apr 13). Doi: 10.1093/rheumatology/kead163
Key clinical point: Risk for first primary cancer was not significantly different among patients with rheumatoid arthritis (RA) receiving Janus kinase inhibitors (JAKi) vs biologic disease-modifying antirheumatic drugs (bDMARD). However, excess risk cannot be ruled out among those receiving JAKi.
Major finding: Patients with RA treated with JAKi had a numerically higher but not statistically significantly higher risk for first primary cancer (hazard ratio 1.41; 95% CI 0.76-2.37) compared with those treated with bDMARD.
Study details: Findings are from an observational cohort study including patients with RA without prior cancer diagnosis who initiated JAKi (n = 875) or bDMARD (n = 4247).
Disclosures: This study received financial support from the Danish Rheumatism Association and Danish Cancer Society. Several authors declared being employees of, receiving research grants and honoraria from, participating in advisory boards of, or serving on steering committees for various sources.
Source: Westermann R et al. Cancer risk in patients with rheumatoid arthritis treated with Janus kinase inhibitors: A nationwide Danish register-based cohort study. Rheumatology (Oxford). 2023 (Apr 13). Doi: 10.1093/rheumatology/kead163
Key clinical point: Risk for first primary cancer was not significantly different among patients with rheumatoid arthritis (RA) receiving Janus kinase inhibitors (JAKi) vs biologic disease-modifying antirheumatic drugs (bDMARD). However, excess risk cannot be ruled out among those receiving JAKi.
Major finding: Patients with RA treated with JAKi had a numerically higher but not statistically significantly higher risk for first primary cancer (hazard ratio 1.41; 95% CI 0.76-2.37) compared with those treated with bDMARD.
Study details: Findings are from an observational cohort study including patients with RA without prior cancer diagnosis who initiated JAKi (n = 875) or bDMARD (n = 4247).
Disclosures: This study received financial support from the Danish Rheumatism Association and Danish Cancer Society. Several authors declared being employees of, receiving research grants and honoraria from, participating in advisory boards of, or serving on steering committees for various sources.
Source: Westermann R et al. Cancer risk in patients with rheumatoid arthritis treated with Janus kinase inhibitors: A nationwide Danish register-based cohort study. Rheumatology (Oxford). 2023 (Apr 13). Doi: 10.1093/rheumatology/kead163
HPV infection, HPV immunization, and RA prevalence: What is the link?
Key clinical point: Human papillomavirus (HPV) infection was associated with an increased prevalence of rheumatoid arthritis (RA), whereas HPV immunization lowered RA prevalence in adults aged 18-59 years.
Major finding: A significant association was observed between HPV infection and increased prevalence of RA (adjusted odds ratio [aOR] 1.074; 95% CI 1.071-1.076), whereas HPV immunization was associated with a significantly reduced RA prevalence (aOR 0.477; 95% CI 0.472-0.481).
Study details: Findings are from a population-based cohort study including adults age 18-59 years with complete data on HPV infection and history of RA (n = 15,677) and those with complete data on HPV vaccination and history of RA (n = 8944).
Disclosures: This study was supported by the Nanjing Medical University Science, China, and Technology Development Fund and other sources. The authors declared no conflicts of interest.
Source: Yang G et al. Association between human papillomavirus infection or immunization and risk for rheumatoid arthritis. Front Immunol. 2023;14:1130217 (Apr 14). Doi: 10.3389/fimmu.2023.1130217
Key clinical point: Human papillomavirus (HPV) infection was associated with an increased prevalence of rheumatoid arthritis (RA), whereas HPV immunization lowered RA prevalence in adults aged 18-59 years.
Major finding: A significant association was observed between HPV infection and increased prevalence of RA (adjusted odds ratio [aOR] 1.074; 95% CI 1.071-1.076), whereas HPV immunization was associated with a significantly reduced RA prevalence (aOR 0.477; 95% CI 0.472-0.481).
Study details: Findings are from a population-based cohort study including adults age 18-59 years with complete data on HPV infection and history of RA (n = 15,677) and those with complete data on HPV vaccination and history of RA (n = 8944).
Disclosures: This study was supported by the Nanjing Medical University Science, China, and Technology Development Fund and other sources. The authors declared no conflicts of interest.
Source: Yang G et al. Association between human papillomavirus infection or immunization and risk for rheumatoid arthritis. Front Immunol. 2023;14:1130217 (Apr 14). Doi: 10.3389/fimmu.2023.1130217
Key clinical point: Human papillomavirus (HPV) infection was associated with an increased prevalence of rheumatoid arthritis (RA), whereas HPV immunization lowered RA prevalence in adults aged 18-59 years.
Major finding: A significant association was observed between HPV infection and increased prevalence of RA (adjusted odds ratio [aOR] 1.074; 95% CI 1.071-1.076), whereas HPV immunization was associated with a significantly reduced RA prevalence (aOR 0.477; 95% CI 0.472-0.481).
Study details: Findings are from a population-based cohort study including adults age 18-59 years with complete data on HPV infection and history of RA (n = 15,677) and those with complete data on HPV vaccination and history of RA (n = 8944).
Disclosures: This study was supported by the Nanjing Medical University Science, China, and Technology Development Fund and other sources. The authors declared no conflicts of interest.
Source: Yang G et al. Association between human papillomavirus infection or immunization and risk for rheumatoid arthritis. Front Immunol. 2023;14:1130217 (Apr 14). Doi: 10.3389/fimmu.2023.1130217
Factors guiding sustained remission after withdrawal of combination therapy in RA
Key clinical point: Patients with rheumatoid arthritis (RA) with better overall disease activity and longer etanercept treatment duration are more likely to remain in remission after transition from methotrexate+etanercept combination therapy to methotrexate or etanercept monotherapy.
Major finding: At week 48, the likelihood of patients remaining in Simple Disease Activity Index-based remission or maintaining low disease activity was 1.12 times higher with long-term etanercept monotherapy (P = .044) but was 0.93 times lower with each 1-point increase in Patient Global Assessment of Disease Activity (P = .012) and C-reactive protein (P = .033).
Study details: Findings are from the phase 3, SEAM-RA trial including 253 patients with RA who achieved remission with 24 weeks of methotrexate+etanercept combination therapy and were randomly assigned to continue combination therapy or transition to methotrexate+placebo or etanercept+placebo.
Disclosures: A wholly owned subsidiary of Amgen Inc., Immunex, funded this study. Three authors declared being employees and stockholders of Amgen Inc., and four authors declared ties with various sources, including Amgen.
Source: Curtis JR R et al. Factors associated with maintenance of remission following change from combination therapy to monotherapy in patients with rheumatoid arthritis. J Rheumatol. 2023 (Apr 15). Doi: 10.3899/jrheum.2022-1008.
Key clinical point: Patients with rheumatoid arthritis (RA) with better overall disease activity and longer etanercept treatment duration are more likely to remain in remission after transition from methotrexate+etanercept combination therapy to methotrexate or etanercept monotherapy.
Major finding: At week 48, the likelihood of patients remaining in Simple Disease Activity Index-based remission or maintaining low disease activity was 1.12 times higher with long-term etanercept monotherapy (P = .044) but was 0.93 times lower with each 1-point increase in Patient Global Assessment of Disease Activity (P = .012) and C-reactive protein (P = .033).
Study details: Findings are from the phase 3, SEAM-RA trial including 253 patients with RA who achieved remission with 24 weeks of methotrexate+etanercept combination therapy and were randomly assigned to continue combination therapy or transition to methotrexate+placebo or etanercept+placebo.
Disclosures: A wholly owned subsidiary of Amgen Inc., Immunex, funded this study. Three authors declared being employees and stockholders of Amgen Inc., and four authors declared ties with various sources, including Amgen.
Source: Curtis JR R et al. Factors associated with maintenance of remission following change from combination therapy to monotherapy in patients with rheumatoid arthritis. J Rheumatol. 2023 (Apr 15). Doi: 10.3899/jrheum.2022-1008.
Key clinical point: Patients with rheumatoid arthritis (RA) with better overall disease activity and longer etanercept treatment duration are more likely to remain in remission after transition from methotrexate+etanercept combination therapy to methotrexate or etanercept monotherapy.
Major finding: At week 48, the likelihood of patients remaining in Simple Disease Activity Index-based remission or maintaining low disease activity was 1.12 times higher with long-term etanercept monotherapy (P = .044) but was 0.93 times lower with each 1-point increase in Patient Global Assessment of Disease Activity (P = .012) and C-reactive protein (P = .033).
Study details: Findings are from the phase 3, SEAM-RA trial including 253 patients with RA who achieved remission with 24 weeks of methotrexate+etanercept combination therapy and were randomly assigned to continue combination therapy or transition to methotrexate+placebo or etanercept+placebo.
Disclosures: A wholly owned subsidiary of Amgen Inc., Immunex, funded this study. Three authors declared being employees and stockholders of Amgen Inc., and four authors declared ties with various sources, including Amgen.
Source: Curtis JR R et al. Factors associated with maintenance of remission following change from combination therapy to monotherapy in patients with rheumatoid arthritis. J Rheumatol. 2023 (Apr 15). Doi: 10.3899/jrheum.2022-1008.
Tofacitinib withdrawal not a universal option for all patients with RA in remission
Key clinical point: Blanket withdrawal of tofacitinib may not be suitable for all patients with rheumatoid arthritis (RA) who have achieved clinical remission as more than half relapsed after tofacitinib discontinuation. However, the majority regained remission after tofacitinib resumption.
Major finding: At week 104, the tofacitinib vs methotrexate discontinuation group had a numerically lower Clinical Disease Activity Index-based sustained remission rate (29.2% vs 50.0%) and higher relapse rate (58.3% vs 35.0%). However, 71.4% vs 28.6% of patients regained remission on tofacitinib vs methotrexate resumption.
Study details: This prospective randomized controlled trial included 113 patients with RA and an inadequate response to methotrexate with or without biologic disease-modifying antirheumatic drugs who received 52 weeks of tofacitinib plus methotrexate treatment and thereafter, were randomly assigned to discontinue tofacitinib or methotrexate if experiencing clinical remission.
Disclosures: This study was supported by the Japan Society for the Promotion of Science, KAKENHI. Several authors declared receiving consulting fees, speaking fees, research grants, or honoraria from various sources.
Source: Kubo S et al. Sustained remission following the discontinuation of tofacitinib in patients with rheumatoid arthritis (XANADU study): An open-label randomised study. RMD Open. 2023;9(2):e003029 (Apr 25). Doi: 10.1136/rmdopen-2023-003029
Key clinical point: Blanket withdrawal of tofacitinib may not be suitable for all patients with rheumatoid arthritis (RA) who have achieved clinical remission as more than half relapsed after tofacitinib discontinuation. However, the majority regained remission after tofacitinib resumption.
Major finding: At week 104, the tofacitinib vs methotrexate discontinuation group had a numerically lower Clinical Disease Activity Index-based sustained remission rate (29.2% vs 50.0%) and higher relapse rate (58.3% vs 35.0%). However, 71.4% vs 28.6% of patients regained remission on tofacitinib vs methotrexate resumption.
Study details: This prospective randomized controlled trial included 113 patients with RA and an inadequate response to methotrexate with or without biologic disease-modifying antirheumatic drugs who received 52 weeks of tofacitinib plus methotrexate treatment and thereafter, were randomly assigned to discontinue tofacitinib or methotrexate if experiencing clinical remission.
Disclosures: This study was supported by the Japan Society for the Promotion of Science, KAKENHI. Several authors declared receiving consulting fees, speaking fees, research grants, or honoraria from various sources.
Source: Kubo S et al. Sustained remission following the discontinuation of tofacitinib in patients with rheumatoid arthritis (XANADU study): An open-label randomised study. RMD Open. 2023;9(2):e003029 (Apr 25). Doi: 10.1136/rmdopen-2023-003029
Key clinical point: Blanket withdrawal of tofacitinib may not be suitable for all patients with rheumatoid arthritis (RA) who have achieved clinical remission as more than half relapsed after tofacitinib discontinuation. However, the majority regained remission after tofacitinib resumption.
Major finding: At week 104, the tofacitinib vs methotrexate discontinuation group had a numerically lower Clinical Disease Activity Index-based sustained remission rate (29.2% vs 50.0%) and higher relapse rate (58.3% vs 35.0%). However, 71.4% vs 28.6% of patients regained remission on tofacitinib vs methotrexate resumption.
Study details: This prospective randomized controlled trial included 113 patients with RA and an inadequate response to methotrexate with or without biologic disease-modifying antirheumatic drugs who received 52 weeks of tofacitinib plus methotrexate treatment and thereafter, were randomly assigned to discontinue tofacitinib or methotrexate if experiencing clinical remission.
Disclosures: This study was supported by the Japan Society for the Promotion of Science, KAKENHI. Several authors declared receiving consulting fees, speaking fees, research grants, or honoraria from various sources.
Source: Kubo S et al. Sustained remission following the discontinuation of tofacitinib in patients with rheumatoid arthritis (XANADU study): An open-label randomised study. RMD Open. 2023;9(2):e003029 (Apr 25). Doi: 10.1136/rmdopen-2023-003029
Joint damage repair: A rare phenomenon in early RA
Key clinical point: Repair of joint space narrowing occurred but was rare in patients with early rheumatoid arthritis (RA) who underwent 8 years of treatment to a target disease activity score (DAS) ≤ 2.4. Therefore, suppression of damage progression should be the focus of clinical care.
Major finding: Only 5.3% of patients showed repair of joint space narrowing and bone erosions after 8 years of treatment to a target of DAS ≤ 2.4. No significant association was observed between achieving repair and suppression of disease activity, duration of previous remission, or other predictors of repair.
Study details: Findings are from a subanalysis of BeSt study including 508 patients with severe early RA who were treated to a target of DAS ≤ 2.4 and followed for 8 years.
Disclosures: The BeSt study was supported by grants from the Dutch College of Health Insurances, Schering-Plough B.V., and Janssen B.V. The authors did not declare any conflicts of interest.
Source: van der Pol JA et al. Repair of joint damage in patients with rheumatoid arthritis does not relate to previous suppression of inflammation: A subanalysis after 8 years treat-to-target in the BeSt-trial. RMD Open. 2023;9(2):e002995 (Apr 25). Doi: 10.1136/rmdopen-2023-002995
Key clinical point: Repair of joint space narrowing occurred but was rare in patients with early rheumatoid arthritis (RA) who underwent 8 years of treatment to a target disease activity score (DAS) ≤ 2.4. Therefore, suppression of damage progression should be the focus of clinical care.
Major finding: Only 5.3% of patients showed repair of joint space narrowing and bone erosions after 8 years of treatment to a target of DAS ≤ 2.4. No significant association was observed between achieving repair and suppression of disease activity, duration of previous remission, or other predictors of repair.
Study details: Findings are from a subanalysis of BeSt study including 508 patients with severe early RA who were treated to a target of DAS ≤ 2.4 and followed for 8 years.
Disclosures: The BeSt study was supported by grants from the Dutch College of Health Insurances, Schering-Plough B.V., and Janssen B.V. The authors did not declare any conflicts of interest.
Source: van der Pol JA et al. Repair of joint damage in patients with rheumatoid arthritis does not relate to previous suppression of inflammation: A subanalysis after 8 years treat-to-target in the BeSt-trial. RMD Open. 2023;9(2):e002995 (Apr 25). Doi: 10.1136/rmdopen-2023-002995
Key clinical point: Repair of joint space narrowing occurred but was rare in patients with early rheumatoid arthritis (RA) who underwent 8 years of treatment to a target disease activity score (DAS) ≤ 2.4. Therefore, suppression of damage progression should be the focus of clinical care.
Major finding: Only 5.3% of patients showed repair of joint space narrowing and bone erosions after 8 years of treatment to a target of DAS ≤ 2.4. No significant association was observed between achieving repair and suppression of disease activity, duration of previous remission, or other predictors of repair.
Study details: Findings are from a subanalysis of BeSt study including 508 patients with severe early RA who were treated to a target of DAS ≤ 2.4 and followed for 8 years.
Disclosures: The BeSt study was supported by grants from the Dutch College of Health Insurances, Schering-Plough B.V., and Janssen B.V. The authors did not declare any conflicts of interest.
Source: van der Pol JA et al. Repair of joint damage in patients with rheumatoid arthritis does not relate to previous suppression of inflammation: A subanalysis after 8 years treat-to-target in the BeSt-trial. RMD Open. 2023;9(2):e002995 (Apr 25). Doi: 10.1136/rmdopen-2023-002995
Strong link between polycyclic aromatic hydrocarbons and raised rheumatoid arthritis risk
Key clinical point: Exposure to environmental polycyclic aromatic hydrocarbons (PAH) was significantly associated with an increased prevalence of rheumatoid arthritis (RA) in the US population, and PAH mediated the majority of the effects of smoking in RA.
Major finding: Risk of developing RA was significantly higher in participants in the highest vs lowest quartile of 1-hydroxynaphthalene level (adjusted odds ratio [aOR] 1.8; P = .020) and PAH body burden scores (aOR 2.2; P = .028). PAH body burden accounted for ~90% of the total effect of smoking on RA.
Study details: Findings are from a cross-sectional study including adult participants with (n = 1418) or without (n = 20,569) RA who underwent assessments for PAH, phthalate and plasticizer metabolite, and volatile organic compound body burden.
Disclosures: This study did not declare any specific funding source. The lead author declared receiving personal fees from Cleveland HeartLab, unrelated to this study, and holding a patent.
Source: Beidelschies M et al. Polycyclic aromatic hydrocarbons and risk of rheumatoid arthritis: A cross-sectional analysis of the National Health and Nutrition Examination Survey, 2007–2016. BMJ Open. 2023;13(5):e071514 (May 9). Doi: 10.1136/bmjopen-2022-071514
Key clinical point: Exposure to environmental polycyclic aromatic hydrocarbons (PAH) was significantly associated with an increased prevalence of rheumatoid arthritis (RA) in the US population, and PAH mediated the majority of the effects of smoking in RA.
Major finding: Risk of developing RA was significantly higher in participants in the highest vs lowest quartile of 1-hydroxynaphthalene level (adjusted odds ratio [aOR] 1.8; P = .020) and PAH body burden scores (aOR 2.2; P = .028). PAH body burden accounted for ~90% of the total effect of smoking on RA.
Study details: Findings are from a cross-sectional study including adult participants with (n = 1418) or without (n = 20,569) RA who underwent assessments for PAH, phthalate and plasticizer metabolite, and volatile organic compound body burden.
Disclosures: This study did not declare any specific funding source. The lead author declared receiving personal fees from Cleveland HeartLab, unrelated to this study, and holding a patent.
Source: Beidelschies M et al. Polycyclic aromatic hydrocarbons and risk of rheumatoid arthritis: A cross-sectional analysis of the National Health and Nutrition Examination Survey, 2007–2016. BMJ Open. 2023;13(5):e071514 (May 9). Doi: 10.1136/bmjopen-2022-071514
Key clinical point: Exposure to environmental polycyclic aromatic hydrocarbons (PAH) was significantly associated with an increased prevalence of rheumatoid arthritis (RA) in the US population, and PAH mediated the majority of the effects of smoking in RA.
Major finding: Risk of developing RA was significantly higher in participants in the highest vs lowest quartile of 1-hydroxynaphthalene level (adjusted odds ratio [aOR] 1.8; P = .020) and PAH body burden scores (aOR 2.2; P = .028). PAH body burden accounted for ~90% of the total effect of smoking on RA.
Study details: Findings are from a cross-sectional study including adult participants with (n = 1418) or without (n = 20,569) RA who underwent assessments for PAH, phthalate and plasticizer metabolite, and volatile organic compound body burden.
Disclosures: This study did not declare any specific funding source. The lead author declared receiving personal fees from Cleveland HeartLab, unrelated to this study, and holding a patent.
Source: Beidelschies M et al. Polycyclic aromatic hydrocarbons and risk of rheumatoid arthritis: A cross-sectional analysis of the National Health and Nutrition Examination Survey, 2007–2016. BMJ Open. 2023;13(5):e071514 (May 9). Doi: 10.1136/bmjopen-2022-071514
Skin changes and pain
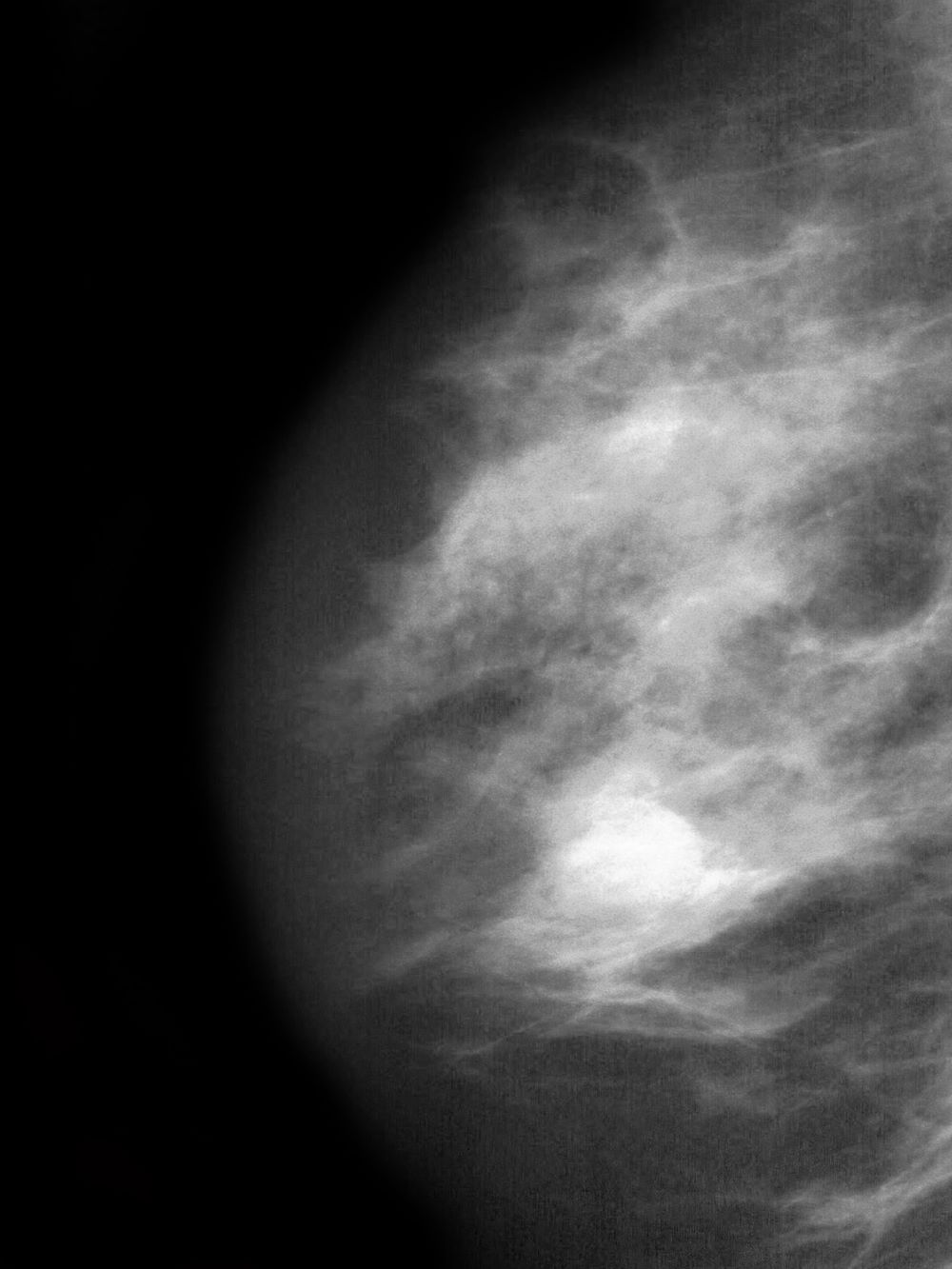
The history and findings in this case are suggestive of inflammatory breast cancer.
Breast cancer is the leading life-threatening cancer diagnosed and the second-leading cause of cancer-related deaths in women worldwide. In the United States, estimates suggest that 287,850 new cases of invasive breast cancer were diagnosed in 2022 and 43,250 women died of the disease. Globally, approximately 2.3 million new diagnoses and 685,000 breast cancer–related deaths were reported in 2020.
Inflammatory breast cancer is a rare and highly aggressive subtype of locally advanced breast cancer. In the United States, inflammatory breast cancer accounts for approximately 2%-4% of breast cancer cases. Although its incidence is rare, 7% of breast cancer caused mortality is attributed to inflammatory breast cancer. Cases of inflammatory breast cancer tend to be diagnosed at a younger age compared with noninflammatory breast cancer cases. Risk factors include African-American race and obesity.
The symptoms of inflammatory breast cancer can vary broadly, ranging from subtle skin erythema to diffuse breast involvement with skin dimpling and nipple inversion. Diagnostic criteria include erythema occupying at least one third of the breast, edema, peau d'orange, and/or warmth, with or without an underlying mass; rapid onset (< 3 months); and pathologic confirmation of invasive breast carcinoma. Histologic findings include florid tumor emboli that obstruct dermal lymphatics, which results in swelling and inflammation of the affected breast.
Inflammatory breast cancer has been associated with a poor prognosis. However, treatment advances are helping to improve outcomes. Currently, 5-year survival rates are reported to be 40%-70%, with a median survival of 2-4 years. According to 2023 guidelines from the National Comprehensive Cancer Network (NCCN), the first-line treatment of inflammatory breast cancer involves neoadjuvant chemotherapy, modified radical mastectomy, and adjuvant radiation to the chest wall and regional nodes. Endocrine treatment should also be given to patients who are ER-positive and/or PR-positive (sequential chemotherapy followed by endocrine therapy). For patients who are HER2-positive, up to 1 year of HER2-targeted therapy should be given. HER2-targeted therapies can be administered concurrently with radiation and with endocrine therapy if indicated.
Delayed reconstruction after mastectomy remains the clinical standard for inflammatory breast cancer. This is because the need to resect involved skin negates the benefit of skin-sparing mastectomy for immediate reconstruction. Moreover, high rates of local and distant recurrence warrant comprehensive regional node irradiation in a timely fashion, which may be more challenging or subject to delay after immediate reconstruction. Rarely, the extent of skin excision at the time of mastectomy prohibits primary or local closure. In such cases, reconstruction of the chest wall defect with autologous tissue is required, and concomitant immediate reconstruction may be undertaken.
Detailed guidance on the treatment of inflammatory breast cancer, in the first line and beyond, are available from the NCCN.
Avan J. Armaghani, MD, Assistant Member, Department of Breast Oncology, Moffitt Cancer Center, University of South Florida, Tampa, FL.
Avan J. Armaghani, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are suggestive of inflammatory breast cancer.
Breast cancer is the leading life-threatening cancer diagnosed and the second-leading cause of cancer-related deaths in women worldwide. In the United States, estimates suggest that 287,850 new cases of invasive breast cancer were diagnosed in 2022 and 43,250 women died of the disease. Globally, approximately 2.3 million new diagnoses and 685,000 breast cancer–related deaths were reported in 2020.
Inflammatory breast cancer is a rare and highly aggressive subtype of locally advanced breast cancer. In the United States, inflammatory breast cancer accounts for approximately 2%-4% of breast cancer cases. Although its incidence is rare, 7% of breast cancer caused mortality is attributed to inflammatory breast cancer. Cases of inflammatory breast cancer tend to be diagnosed at a younger age compared with noninflammatory breast cancer cases. Risk factors include African-American race and obesity.
The symptoms of inflammatory breast cancer can vary broadly, ranging from subtle skin erythema to diffuse breast involvement with skin dimpling and nipple inversion. Diagnostic criteria include erythema occupying at least one third of the breast, edema, peau d'orange, and/or warmth, with or without an underlying mass; rapid onset (< 3 months); and pathologic confirmation of invasive breast carcinoma. Histologic findings include florid tumor emboli that obstruct dermal lymphatics, which results in swelling and inflammation of the affected breast.
Inflammatory breast cancer has been associated with a poor prognosis. However, treatment advances are helping to improve outcomes. Currently, 5-year survival rates are reported to be 40%-70%, with a median survival of 2-4 years. According to 2023 guidelines from the National Comprehensive Cancer Network (NCCN), the first-line treatment of inflammatory breast cancer involves neoadjuvant chemotherapy, modified radical mastectomy, and adjuvant radiation to the chest wall and regional nodes. Endocrine treatment should also be given to patients who are ER-positive and/or PR-positive (sequential chemotherapy followed by endocrine therapy). For patients who are HER2-positive, up to 1 year of HER2-targeted therapy should be given. HER2-targeted therapies can be administered concurrently with radiation and with endocrine therapy if indicated.
Delayed reconstruction after mastectomy remains the clinical standard for inflammatory breast cancer. This is because the need to resect involved skin negates the benefit of skin-sparing mastectomy for immediate reconstruction. Moreover, high rates of local and distant recurrence warrant comprehensive regional node irradiation in a timely fashion, which may be more challenging or subject to delay after immediate reconstruction. Rarely, the extent of skin excision at the time of mastectomy prohibits primary or local closure. In such cases, reconstruction of the chest wall defect with autologous tissue is required, and concomitant immediate reconstruction may be undertaken.
Detailed guidance on the treatment of inflammatory breast cancer, in the first line and beyond, are available from the NCCN.
Avan J. Armaghani, MD, Assistant Member, Department of Breast Oncology, Moffitt Cancer Center, University of South Florida, Tampa, FL.
Avan J. Armaghani, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are suggestive of inflammatory breast cancer.
Breast cancer is the leading life-threatening cancer diagnosed and the second-leading cause of cancer-related deaths in women worldwide. In the United States, estimates suggest that 287,850 new cases of invasive breast cancer were diagnosed in 2022 and 43,250 women died of the disease. Globally, approximately 2.3 million new diagnoses and 685,000 breast cancer–related deaths were reported in 2020.
Inflammatory breast cancer is a rare and highly aggressive subtype of locally advanced breast cancer. In the United States, inflammatory breast cancer accounts for approximately 2%-4% of breast cancer cases. Although its incidence is rare, 7% of breast cancer caused mortality is attributed to inflammatory breast cancer. Cases of inflammatory breast cancer tend to be diagnosed at a younger age compared with noninflammatory breast cancer cases. Risk factors include African-American race and obesity.
The symptoms of inflammatory breast cancer can vary broadly, ranging from subtle skin erythema to diffuse breast involvement with skin dimpling and nipple inversion. Diagnostic criteria include erythema occupying at least one third of the breast, edema, peau d'orange, and/or warmth, with or without an underlying mass; rapid onset (< 3 months); and pathologic confirmation of invasive breast carcinoma. Histologic findings include florid tumor emboli that obstruct dermal lymphatics, which results in swelling and inflammation of the affected breast.
Inflammatory breast cancer has been associated with a poor prognosis. However, treatment advances are helping to improve outcomes. Currently, 5-year survival rates are reported to be 40%-70%, with a median survival of 2-4 years. According to 2023 guidelines from the National Comprehensive Cancer Network (NCCN), the first-line treatment of inflammatory breast cancer involves neoadjuvant chemotherapy, modified radical mastectomy, and adjuvant radiation to the chest wall and regional nodes. Endocrine treatment should also be given to patients who are ER-positive and/or PR-positive (sequential chemotherapy followed by endocrine therapy). For patients who are HER2-positive, up to 1 year of HER2-targeted therapy should be given. HER2-targeted therapies can be administered concurrently with radiation and with endocrine therapy if indicated.
Delayed reconstruction after mastectomy remains the clinical standard for inflammatory breast cancer. This is because the need to resect involved skin negates the benefit of skin-sparing mastectomy for immediate reconstruction. Moreover, high rates of local and distant recurrence warrant comprehensive regional node irradiation in a timely fashion, which may be more challenging or subject to delay after immediate reconstruction. Rarely, the extent of skin excision at the time of mastectomy prohibits primary or local closure. In such cases, reconstruction of the chest wall defect with autologous tissue is required, and concomitant immediate reconstruction may be undertaken.
Detailed guidance on the treatment of inflammatory breast cancer, in the first line and beyond, are available from the NCCN.
Avan J. Armaghani, MD, Assistant Member, Department of Breast Oncology, Moffitt Cancer Center, University of South Florida, Tampa, FL.
Avan J. Armaghani, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
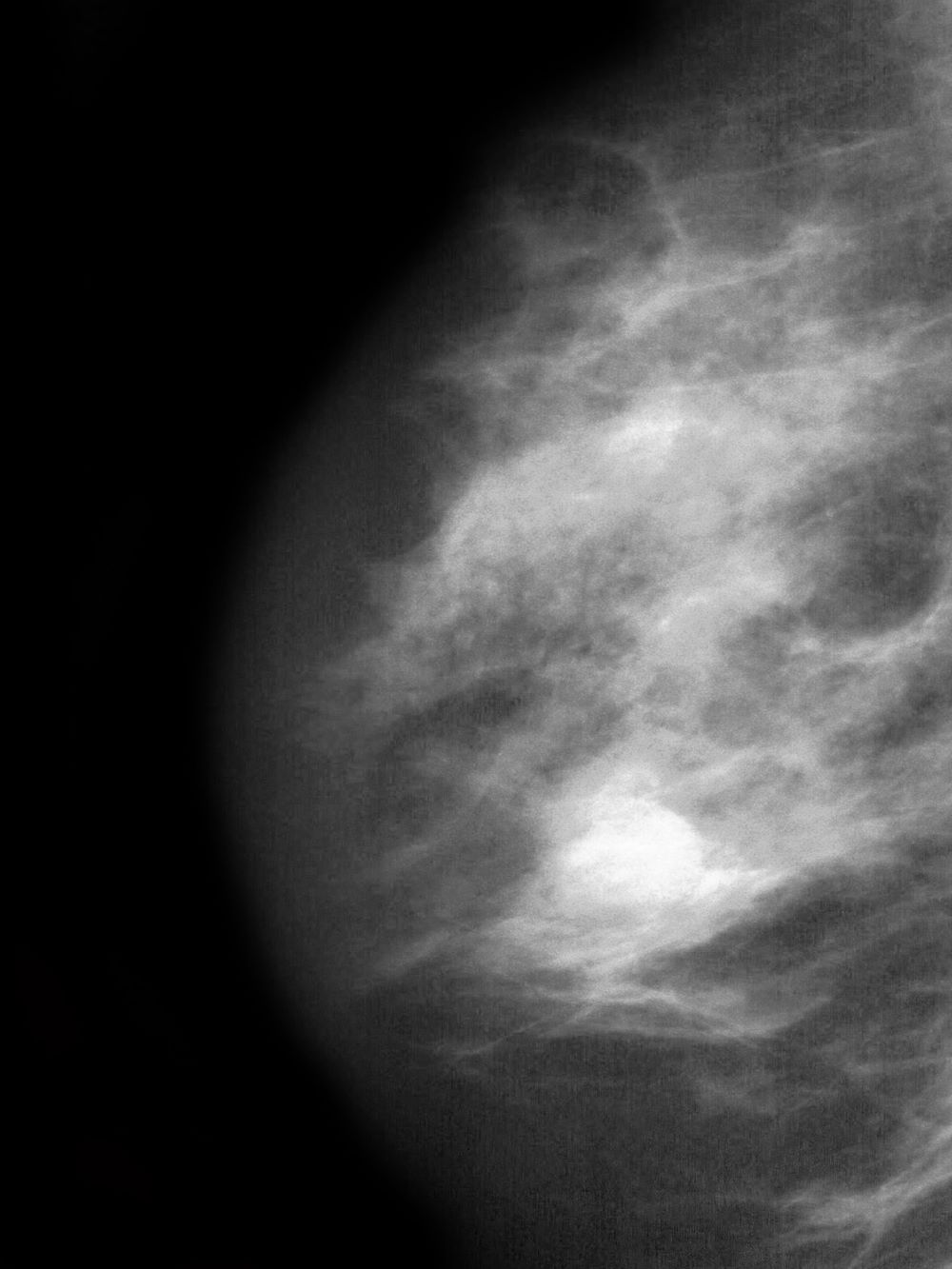
A 51-year-old nonsmoking Black woman presents with a lump in her left breast, as well as associated skin changes and pain of approximately 3 months' duration. The patient last underwent routine screening breast imaging 2 years earlier. The patient is 5 ft 7 in and weighs 200 lb (BMI 31.3). Previous medical history is unremarkable. There is a family history of breast cancer (maternal aunt) and lung cancer (maternal uncle). Physical examination reveals a palpable abnormality in the left breast with edema, skin thickening, and peau d'orange. More than one third of the breast is erythematous. A bilateral mammography reveals an irregular mass and calcifications in the upper outer quadrant of the left breast as well as numerous additional masses and focal asymmetries involving the upper outer and lower outer quadrant of the left breast that extend into the inner left breast. A 1.6-cm mass in the upper left breast is noted, with total abnormality spanning 12.7 cm. Left axillary lymphadenopathy is also observed. Skin punch biopsy of the affected breast reveals dermal lymphatic invasion by tumor cells and tumor emboli. Left axial fine-needle aspiration biopsy reveals malignant cells.
Single-strain probiotic lactobacilli: An up-and-coming adjuvant therapy for atopic dermatitis
Key clinical point: Adjuvant supplementation with single-strain probiotic lactobacilli significantly reduced the SCORing Atopic Dermatitis (SCORAD) index in young patients with atopic dermatitis (AD).
Major finding: The single-strain probiotic lactobacilli vs placebo group had a significant reduction in the SCORAD index (mean difference −4.50; P = .003).
Study details: Findings are from a meta-analysis of 14 studies involving 1124 patients aged 0-18 years with AD who received single-strain probiotic lactobacilli (n = 574) or placebo (n = 550).
Disclosures: This study was funded by the Slovenian Research Agency. The authors declared no conflicts of interest.
Source: Fijan S et al. Single-strain probiotic lactobacilli for the treatment of atopic dermatitis in children: A systematic review and meta-analysis. Pharmaceutics. 2023;15(4):1256 (Apr 17). Doi: 10.3390/pharmaceutics15041256
Key clinical point: Adjuvant supplementation with single-strain probiotic lactobacilli significantly reduced the SCORing Atopic Dermatitis (SCORAD) index in young patients with atopic dermatitis (AD).
Major finding: The single-strain probiotic lactobacilli vs placebo group had a significant reduction in the SCORAD index (mean difference −4.50; P = .003).
Study details: Findings are from a meta-analysis of 14 studies involving 1124 patients aged 0-18 years with AD who received single-strain probiotic lactobacilli (n = 574) or placebo (n = 550).
Disclosures: This study was funded by the Slovenian Research Agency. The authors declared no conflicts of interest.
Source: Fijan S et al. Single-strain probiotic lactobacilli for the treatment of atopic dermatitis in children: A systematic review and meta-analysis. Pharmaceutics. 2023;15(4):1256 (Apr 17). Doi: 10.3390/pharmaceutics15041256
Key clinical point: Adjuvant supplementation with single-strain probiotic lactobacilli significantly reduced the SCORing Atopic Dermatitis (SCORAD) index in young patients with atopic dermatitis (AD).
Major finding: The single-strain probiotic lactobacilli vs placebo group had a significant reduction in the SCORAD index (mean difference −4.50; P = .003).
Study details: Findings are from a meta-analysis of 14 studies involving 1124 patients aged 0-18 years with AD who received single-strain probiotic lactobacilli (n = 574) or placebo (n = 550).
Disclosures: This study was funded by the Slovenian Research Agency. The authors declared no conflicts of interest.
Source: Fijan S et al. Single-strain probiotic lactobacilli for the treatment of atopic dermatitis in children: A systematic review and meta-analysis. Pharmaceutics. 2023;15(4):1256 (Apr 17). Doi: 10.3390/pharmaceutics15041256
Low diversity in skin microbiome in infancy raises risk for atopic dermatitis in high-risk children
Key clinical point: A lower alpha diversity in infancy is associated with an increased risk for atopic dermatitis (AD) in children of parents with atopy.
Major finding: Overall, the skin microbiome at birth and 2 months of age was not associated with the subsequent development of AD (P = .2). However, a lower alpha diversity at 2 months of age was significantly associated with an increased risk for AD during the first 2 years in children with at least 1 parent (adjusted hazard ratio [aHR] 1.67; P = .03) or both parents (aHR 4.44; P = .04) with a history of atopy.
Study details: Findings are from a prospective analysis of 300 children born to term, of which 153 had a parental history of atopy.
Disclosures: This study was funded by The Leo Foundation and others. Some authors declared serving as speakers, advisors, or consultants for or receiving research grants or speaker or consulting honoraria from various organizations, including the study funders.
Source: Halling AS et al. Reduced skin microbiome diversity in infancy is associated with increased risk of atopic dermatitis in high-risk children. J Invest Dermatol. 2023 (Apr 19). Doi: 10.1016/j.jid.2023.03.1682
Key clinical point: A lower alpha diversity in infancy is associated with an increased risk for atopic dermatitis (AD) in children of parents with atopy.
Major finding: Overall, the skin microbiome at birth and 2 months of age was not associated with the subsequent development of AD (P = .2). However, a lower alpha diversity at 2 months of age was significantly associated with an increased risk for AD during the first 2 years in children with at least 1 parent (adjusted hazard ratio [aHR] 1.67; P = .03) or both parents (aHR 4.44; P = .04) with a history of atopy.
Study details: Findings are from a prospective analysis of 300 children born to term, of which 153 had a parental history of atopy.
Disclosures: This study was funded by The Leo Foundation and others. Some authors declared serving as speakers, advisors, or consultants for or receiving research grants or speaker or consulting honoraria from various organizations, including the study funders.
Source: Halling AS et al. Reduced skin microbiome diversity in infancy is associated with increased risk of atopic dermatitis in high-risk children. J Invest Dermatol. 2023 (Apr 19). Doi: 10.1016/j.jid.2023.03.1682
Key clinical point: A lower alpha diversity in infancy is associated with an increased risk for atopic dermatitis (AD) in children of parents with atopy.
Major finding: Overall, the skin microbiome at birth and 2 months of age was not associated with the subsequent development of AD (P = .2). However, a lower alpha diversity at 2 months of age was significantly associated with an increased risk for AD during the first 2 years in children with at least 1 parent (adjusted hazard ratio [aHR] 1.67; P = .03) or both parents (aHR 4.44; P = .04) with a history of atopy.
Study details: Findings are from a prospective analysis of 300 children born to term, of which 153 had a parental history of atopy.
Disclosures: This study was funded by The Leo Foundation and others. Some authors declared serving as speakers, advisors, or consultants for or receiving research grants or speaker or consulting honoraria from various organizations, including the study funders.
Source: Halling AS et al. Reduced skin microbiome diversity in infancy is associated with increased risk of atopic dermatitis in high-risk children. J Invest Dermatol. 2023 (Apr 19). Doi: 10.1016/j.jid.2023.03.1682
Meta-analysis shows unidirectional association between atopic dermatitis and rheumatoid arthritis
Key clinical point: Patients with atopic dermatitis (AD) have a 1.28-fold increased risk of developing rheumatoid arthritis (RA) but patients with RA do not have an increased risk of developing AD.
Major finding: Patients with AD had a significantly increased risk of developing RA (odds ratio [OR] 1.28; P < .001). However, the risk of developing AD in patients with RA was not significant (OR 1.10; P = .52).
Study details: The data come from a systematic review and meta-analysis of nine studies that investigated the association between AD and RA.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Williams RC et al. The uni-directional association of atopic dermatitis and rheumatoid arthritis: A systematic review and meta‑analysis. Arch Dermatol Res. 2023 (Apr 12). Doi: 10.1007/s00403-023-02619-0
Key clinical point: Patients with atopic dermatitis (AD) have a 1.28-fold increased risk of developing rheumatoid arthritis (RA) but patients with RA do not have an increased risk of developing AD.
Major finding: Patients with AD had a significantly increased risk of developing RA (odds ratio [OR] 1.28; P < .001). However, the risk of developing AD in patients with RA was not significant (OR 1.10; P = .52).
Study details: The data come from a systematic review and meta-analysis of nine studies that investigated the association between AD and RA.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Williams RC et al. The uni-directional association of atopic dermatitis and rheumatoid arthritis: A systematic review and meta‑analysis. Arch Dermatol Res. 2023 (Apr 12). Doi: 10.1007/s00403-023-02619-0
Key clinical point: Patients with atopic dermatitis (AD) have a 1.28-fold increased risk of developing rheumatoid arthritis (RA) but patients with RA do not have an increased risk of developing AD.
Major finding: Patients with AD had a significantly increased risk of developing RA (odds ratio [OR] 1.28; P < .001). However, the risk of developing AD in patients with RA was not significant (OR 1.10; P = .52).
Study details: The data come from a systematic review and meta-analysis of nine studies that investigated the association between AD and RA.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Williams RC et al. The uni-directional association of atopic dermatitis and rheumatoid arthritis: A systematic review and meta‑analysis. Arch Dermatol Res. 2023 (Apr 12). Doi: 10.1007/s00403-023-02619-0