User login
Solitary Nodular Lesion on the Scalp
The Diagnosis: Pilomatricoma
Pilomatricoma, first described by Malherbe and Chenantais1 in 1880, is a benign appendageal tumor derived from hair follicle matrix cells. It classically manifests as a solitary, asymptomatic, firm dermal nodule with a normal overlying epidermis. Less common morphologic variants include perforating, lymphagiectatic, keratoacanthomalike, pigmented, and anetodermalike surface changes.2 Inflammation and erosion through the skin surface are observed in the rare perforating variant, as seen in our patient. The average size is 1 cm, and it rarely exceeds 3 cm in diameter.3 The tumors predominantly occur on the head, neck, and upper extremities, with only 9.5% on the scalp.2 It may occur at any age, though it has a bimodal distribution with peaks in childhood and in adults older than 60 years. A slight preponderance in females has been observed with a female to male ratio of 1.5 to 1.2 Although our patient is black, most reported cases have occurred in individuals of European descent. Because cases of pilomatricoma are not systematically reported, it is uncertain if this finding represents a publication bias or if race is an actual risk factor. Multiple pilomatricomas and familial cases have been described in association with myotonic dystrophy, Turner syndrome, Gardner syndrome, Rubinstein-Taybi syndrome, polyfactorial coagulopathy, trisomy 9, xeroderma pigmentosum, and basal cell nevus syndrome.2,4
It has been shown that the proliferating cells of pilomatricomas stain with antibodies directed against Lef1 (lymphoid enhancer binding factor 1), a marker from hair matrix cells, providing biochemical evidence for the morphologic appearance of these neoplasms.5 Pilomatricomas have been associated with B-cell/chronic lymphocytic leukemia lymphoma 2 gene, BCL2, expression, a proto-oncogene that suppresses apoptosis in benign and malignant neoplasms, which may contribute to the pathogenesis of these tumors.6 Pilomatricomas also have been associated with β-catenin mutation, expression of Bmp2 (bone morphogenetic protein 2), and human hair keratin basic 1.7-9
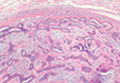
Definitive diagnosis is obtained through biopsy, looking for characteristic histopathologic findings. The lesion usually is found in the lower dermis and subcutaneous fat. However, in the perforating variant, the lesion is more superficial, located in the papillary and mid dermis, as seen in our patient.10
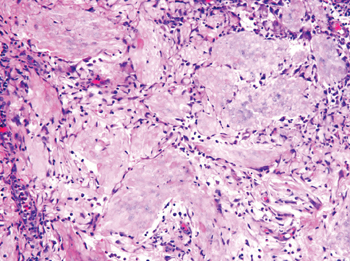
Pilomatricomas are sharply demarcated, often surrounded by a connective-tissue capsule. Histopathologic analysis reveals islands of epithelial cells comprised of 3 subtypes: basophilic cells with scant cytoplasm, shadow cells with a central pallor (Figure), and transitional cells between the former 2 cellular types.11 The number of basophilic and transitional cells is inversely related to the number of shadow cells. In older lesions, the shadow cells predominate, while the basophilic cells are few in number or absent. Calcium deposits are seen in 80% of lesions with von Kossa staining.12
Transformation into malignancy, known as pilomatrical carcinoma, is rare. These malignant neoplasms are characterized by aggressive biologic behavior such as recurrence, diffuse spread, or metastasis, or by cytologic abnormalities such as poor cellular organization, squamous differentiation, and conspicuous mitotic activity.13 The recent growth of the long-standing lesion in our patient might be interpreted as a sign of malignant transformation. However, this observation may be related to the intense inflammatory reaction supported by the histopathology.
Pilomatricomas are not associated with mortality. Pilomatrical carcinomas are uncommon but are locally invasive and can cause visceral metastases and death. Spontaneous regression has never been observed and medical treatment is ineffective. The treatment of choice is incision and curettage or surgical excision.14 Although recurrence has only been reported in 2.6% of cases from a large case series (N=228), patients should be monitored after surgical excision.12
1. Malherbe A, Chenantais J. Note sur l'epithelioma calcifie des glandes sebacees. Prog Med. 1880;8:826-828.
2. Julian CG, Bowers PW. A clinical review of 209 pilomatricomas. J Am Acad Dermatol. 1998;39(2, pt 1):191-195.
3. Lozzi GP, Soyer HP, Fruehauf J, et al. Giant pilomatricoma. Am J Dermatopathol. 2007;29:286-289.
4. Hubbard VG, Whittaker SJ. Multiple familial pilomatricomas: an unusual case. J Cutan Pathol. 2004;31:281-283.
5. Kizawa K, Toyoda M, Ito M, et al. Aberrantly differentiated cells in benign pilomatrixoma reflect the normal hair follicle: immunohistochemical analysis of Ca-binding S100A2, S100A3 and S100A6 proteins. Br J Dermatol. 2005;152:314-320.
6. Farrier S, Morgan M. bcl-2 expression in pilomatricoma. Am J Dermatopathol. 1997;19:254-257.
7. Park SW, Suh KS, Wang HY, et al. Beta-catenin expression in the transitional cell zone of pilomatricoma. Br J Dermatol. 2001;145:624-629.
8. Kurokawa I, Kusumoto K, Bessho K, et al. Immunohistochemical expression of bone morphogenetic protein-2 in pilomatricoma. Br J Dermatol. 2000;143:754-758.
9. Cribier B, Asch PH, Regnier C, et al. Expression of human hair keratin basic 1 in pilomatrixoma: a study of 128 cases. Br J Dermatol. 1999;140:600-604.
10. Bayle P, Bazex J, Lamant L, et al. Multiple perforating and non perforating pilomatricomas in a patient with Churg-Strauss syndrome and Rubinstein-Taybi syndrome. J Eur Acad Dermatol Venereol. 2004;18:607-610.
11. Elder D, Elenitsas R, Ragsdale BD. Pilomatricoma. In: Elder D, Elenitsas R, Jaworsky C, et al, eds. Histopathology of the Skin. 8th ed. Philadelphia, PA: Lippincott-Raven; 1997:757-759.
12. Forbis R Jr, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606-618.
13. Wood MG, Parhizgar B, Beerman H. Malignant pilomatricoma. Arch Dermatol. 1984;120:770-773.
14. Thomas RW, Perkins JA, Ruegemer JL, et al. Surgical excision of pilomatrixoma of the head and neck: a retrospective review of 26 cases. Ear Nose Throat J. 1999;78:541, 544-546, 548.
The Diagnosis: Pilomatricoma
Pilomatricoma, first described by Malherbe and Chenantais1 in 1880, is a benign appendageal tumor derived from hair follicle matrix cells. It classically manifests as a solitary, asymptomatic, firm dermal nodule with a normal overlying epidermis. Less common morphologic variants include perforating, lymphagiectatic, keratoacanthomalike, pigmented, and anetodermalike surface changes.2 Inflammation and erosion through the skin surface are observed in the rare perforating variant, as seen in our patient. The average size is 1 cm, and it rarely exceeds 3 cm in diameter.3 The tumors predominantly occur on the head, neck, and upper extremities, with only 9.5% on the scalp.2 It may occur at any age, though it has a bimodal distribution with peaks in childhood and in adults older than 60 years. A slight preponderance in females has been observed with a female to male ratio of 1.5 to 1.2 Although our patient is black, most reported cases have occurred in individuals of European descent. Because cases of pilomatricoma are not systematically reported, it is uncertain if this finding represents a publication bias or if race is an actual risk factor. Multiple pilomatricomas and familial cases have been described in association with myotonic dystrophy, Turner syndrome, Gardner syndrome, Rubinstein-Taybi syndrome, polyfactorial coagulopathy, trisomy 9, xeroderma pigmentosum, and basal cell nevus syndrome.2,4
It has been shown that the proliferating cells of pilomatricomas stain with antibodies directed against Lef1 (lymphoid enhancer binding factor 1), a marker from hair matrix cells, providing biochemical evidence for the morphologic appearance of these neoplasms.5 Pilomatricomas have been associated with B-cell/chronic lymphocytic leukemia lymphoma 2 gene, BCL2, expression, a proto-oncogene that suppresses apoptosis in benign and malignant neoplasms, which may contribute to the pathogenesis of these tumors.6 Pilomatricomas also have been associated with β-catenin mutation, expression of Bmp2 (bone morphogenetic protein 2), and human hair keratin basic 1.7-9
Definitive diagnosis is obtained through biopsy, looking for characteristic histopathologic findings. The lesion usually is found in the lower dermis and subcutaneous fat. However, in the perforating variant, the lesion is more superficial, located in the papillary and mid dermis, as seen in our patient.10
Pilomatricomas are sharply demarcated, often surrounded by a connective-tissue capsule. Histopathologic analysis reveals islands of epithelial cells comprised of 3 subtypes: basophilic cells with scant cytoplasm, shadow cells with a central pallor (Figure), and transitional cells between the former 2 cellular types.11 The number of basophilic and transitional cells is inversely related to the number of shadow cells. In older lesions, the shadow cells predominate, while the basophilic cells are few in number or absent. Calcium deposits are seen in 80% of lesions with von Kossa staining.12
Transformation into malignancy, known as pilomatrical carcinoma, is rare. These malignant neoplasms are characterized by aggressive biologic behavior such as recurrence, diffuse spread, or metastasis, or by cytologic abnormalities such as poor cellular organization, squamous differentiation, and conspicuous mitotic activity.13 The recent growth of the long-standing lesion in our patient might be interpreted as a sign of malignant transformation. However, this observation may be related to the intense inflammatory reaction supported by the histopathology.
Pilomatricomas are not associated with mortality. Pilomatrical carcinomas are uncommon but are locally invasive and can cause visceral metastases and death. Spontaneous regression has never been observed and medical treatment is ineffective. The treatment of choice is incision and curettage or surgical excision.14 Although recurrence has only been reported in 2.6% of cases from a large case series (N=228), patients should be monitored after surgical excision.12
The Diagnosis: Pilomatricoma
Pilomatricoma, first described by Malherbe and Chenantais1 in 1880, is a benign appendageal tumor derived from hair follicle matrix cells. It classically manifests as a solitary, asymptomatic, firm dermal nodule with a normal overlying epidermis. Less common morphologic variants include perforating, lymphagiectatic, keratoacanthomalike, pigmented, and anetodermalike surface changes.2 Inflammation and erosion through the skin surface are observed in the rare perforating variant, as seen in our patient. The average size is 1 cm, and it rarely exceeds 3 cm in diameter.3 The tumors predominantly occur on the head, neck, and upper extremities, with only 9.5% on the scalp.2 It may occur at any age, though it has a bimodal distribution with peaks in childhood and in adults older than 60 years. A slight preponderance in females has been observed with a female to male ratio of 1.5 to 1.2 Although our patient is black, most reported cases have occurred in individuals of European descent. Because cases of pilomatricoma are not systematically reported, it is uncertain if this finding represents a publication bias or if race is an actual risk factor. Multiple pilomatricomas and familial cases have been described in association with myotonic dystrophy, Turner syndrome, Gardner syndrome, Rubinstein-Taybi syndrome, polyfactorial coagulopathy, trisomy 9, xeroderma pigmentosum, and basal cell nevus syndrome.2,4
It has been shown that the proliferating cells of pilomatricomas stain with antibodies directed against Lef1 (lymphoid enhancer binding factor 1), a marker from hair matrix cells, providing biochemical evidence for the morphologic appearance of these neoplasms.5 Pilomatricomas have been associated with B-cell/chronic lymphocytic leukemia lymphoma 2 gene, BCL2, expression, a proto-oncogene that suppresses apoptosis in benign and malignant neoplasms, which may contribute to the pathogenesis of these tumors.6 Pilomatricomas also have been associated with β-catenin mutation, expression of Bmp2 (bone morphogenetic protein 2), and human hair keratin basic 1.7-9
Definitive diagnosis is obtained through biopsy, looking for characteristic histopathologic findings. The lesion usually is found in the lower dermis and subcutaneous fat. However, in the perforating variant, the lesion is more superficial, located in the papillary and mid dermis, as seen in our patient.10
Pilomatricomas are sharply demarcated, often surrounded by a connective-tissue capsule. Histopathologic analysis reveals islands of epithelial cells comprised of 3 subtypes: basophilic cells with scant cytoplasm, shadow cells with a central pallor (Figure), and transitional cells between the former 2 cellular types.11 The number of basophilic and transitional cells is inversely related to the number of shadow cells. In older lesions, the shadow cells predominate, while the basophilic cells are few in number or absent. Calcium deposits are seen in 80% of lesions with von Kossa staining.12
Transformation into malignancy, known as pilomatrical carcinoma, is rare. These malignant neoplasms are characterized by aggressive biologic behavior such as recurrence, diffuse spread, or metastasis, or by cytologic abnormalities such as poor cellular organization, squamous differentiation, and conspicuous mitotic activity.13 The recent growth of the long-standing lesion in our patient might be interpreted as a sign of malignant transformation. However, this observation may be related to the intense inflammatory reaction supported by the histopathology.
Pilomatricomas are not associated with mortality. Pilomatrical carcinomas are uncommon but are locally invasive and can cause visceral metastases and death. Spontaneous regression has never been observed and medical treatment is ineffective. The treatment of choice is incision and curettage or surgical excision.14 Although recurrence has only been reported in 2.6% of cases from a large case series (N=228), patients should be monitored after surgical excision.12
1. Malherbe A, Chenantais J. Note sur l'epithelioma calcifie des glandes sebacees. Prog Med. 1880;8:826-828.
2. Julian CG, Bowers PW. A clinical review of 209 pilomatricomas. J Am Acad Dermatol. 1998;39(2, pt 1):191-195.
3. Lozzi GP, Soyer HP, Fruehauf J, et al. Giant pilomatricoma. Am J Dermatopathol. 2007;29:286-289.
4. Hubbard VG, Whittaker SJ. Multiple familial pilomatricomas: an unusual case. J Cutan Pathol. 2004;31:281-283.
5. Kizawa K, Toyoda M, Ito M, et al. Aberrantly differentiated cells in benign pilomatrixoma reflect the normal hair follicle: immunohistochemical analysis of Ca-binding S100A2, S100A3 and S100A6 proteins. Br J Dermatol. 2005;152:314-320.
6. Farrier S, Morgan M. bcl-2 expression in pilomatricoma. Am J Dermatopathol. 1997;19:254-257.
7. Park SW, Suh KS, Wang HY, et al. Beta-catenin expression in the transitional cell zone of pilomatricoma. Br J Dermatol. 2001;145:624-629.
8. Kurokawa I, Kusumoto K, Bessho K, et al. Immunohistochemical expression of bone morphogenetic protein-2 in pilomatricoma. Br J Dermatol. 2000;143:754-758.
9. Cribier B, Asch PH, Regnier C, et al. Expression of human hair keratin basic 1 in pilomatrixoma: a study of 128 cases. Br J Dermatol. 1999;140:600-604.
10. Bayle P, Bazex J, Lamant L, et al. Multiple perforating and non perforating pilomatricomas in a patient with Churg-Strauss syndrome and Rubinstein-Taybi syndrome. J Eur Acad Dermatol Venereol. 2004;18:607-610.
11. Elder D, Elenitsas R, Ragsdale BD. Pilomatricoma. In: Elder D, Elenitsas R, Jaworsky C, et al, eds. Histopathology of the Skin. 8th ed. Philadelphia, PA: Lippincott-Raven; 1997:757-759.
12. Forbis R Jr, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606-618.
13. Wood MG, Parhizgar B, Beerman H. Malignant pilomatricoma. Arch Dermatol. 1984;120:770-773.
14. Thomas RW, Perkins JA, Ruegemer JL, et al. Surgical excision of pilomatrixoma of the head and neck: a retrospective review of 26 cases. Ear Nose Throat J. 1999;78:541, 544-546, 548.
1. Malherbe A, Chenantais J. Note sur l'epithelioma calcifie des glandes sebacees. Prog Med. 1880;8:826-828.
2. Julian CG, Bowers PW. A clinical review of 209 pilomatricomas. J Am Acad Dermatol. 1998;39(2, pt 1):191-195.
3. Lozzi GP, Soyer HP, Fruehauf J, et al. Giant pilomatricoma. Am J Dermatopathol. 2007;29:286-289.
4. Hubbard VG, Whittaker SJ. Multiple familial pilomatricomas: an unusual case. J Cutan Pathol. 2004;31:281-283.
5. Kizawa K, Toyoda M, Ito M, et al. Aberrantly differentiated cells in benign pilomatrixoma reflect the normal hair follicle: immunohistochemical analysis of Ca-binding S100A2, S100A3 and S100A6 proteins. Br J Dermatol. 2005;152:314-320.
6. Farrier S, Morgan M. bcl-2 expression in pilomatricoma. Am J Dermatopathol. 1997;19:254-257.
7. Park SW, Suh KS, Wang HY, et al. Beta-catenin expression in the transitional cell zone of pilomatricoma. Br J Dermatol. 2001;145:624-629.
8. Kurokawa I, Kusumoto K, Bessho K, et al. Immunohistochemical expression of bone morphogenetic protein-2 in pilomatricoma. Br J Dermatol. 2000;143:754-758.
9. Cribier B, Asch PH, Regnier C, et al. Expression of human hair keratin basic 1 in pilomatrixoma: a study of 128 cases. Br J Dermatol. 1999;140:600-604.
10. Bayle P, Bazex J, Lamant L, et al. Multiple perforating and non perforating pilomatricomas in a patient with Churg-Strauss syndrome and Rubinstein-Taybi syndrome. J Eur Acad Dermatol Venereol. 2004;18:607-610.
11. Elder D, Elenitsas R, Ragsdale BD. Pilomatricoma. In: Elder D, Elenitsas R, Jaworsky C, et al, eds. Histopathology of the Skin. 8th ed. Philadelphia, PA: Lippincott-Raven; 1997:757-759.
12. Forbis R Jr, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606-618.
13. Wood MG, Parhizgar B, Beerman H. Malignant pilomatricoma. Arch Dermatol. 1984;120:770-773.
14. Thomas RW, Perkins JA, Ruegemer JL, et al. Surgical excision of pilomatrixoma of the head and neck: a retrospective review of 26 cases. Ear Nose Throat J. 1999;78:541, 544-546, 548.

An otherwise healthy 40-year-old man presented for examination of a solitary nodular lesion on the frontal aspect of the scalp of 1 year’s duration. The lesion had rapidly increased in size in the 2 weeks prior to presentation. He presented to the emergency department after he noted pain and drainage from the lesion. Biopsy of the lesion revealed islands of pale eosinophilic shadow cells with an intense dermal infiltrate consisting of lymphocytes, histiocytes, plasma cells, and neutrophils.

Double-Positive CD4+CD8+ Sézary Syndrome: An Unusual Phenotype With an Aggressive Clinical Course
Aggressive secondary squamous carcinoma appeared during BRAF inhibitor targeted therapy
A woman undergoing BRAF inhibitor targeted therapy for advanced melanoma has presented with invasive spindle cell squamous carcinoma masquerading as a secondary cutaneous squamous cell carcinoma, highlighting the importance of histologic evaluation of these lesions.
"Secondary cutaneous squamous cell carcinomas (cSCCs) are adverse effects of BRAF inhibitor targeted therapy for advanced melanoma," wrote Dr. Daniel N. Cohen and his associates online Feb. 26 in JAMA Dermatology.
The most commonly seen histologic type of secondary cutaneous squamous cell carcinomas is keratoacanthoma-like cSCC (cSCC-KA), which is thought to have a low risk of metastasis or recurrence, said lead author Dr. Cohen of the Vanderbilt University Medical Center, Nashville, Tenn.
In this case report, however, a woman in her 50s with BRAF-mutant metastatic melanoma developed more than 100 new cutaneous squamous proliferations across her face, trunk, and extremities within 4 weeks of starting treatment with the BRAF inhibitor dabrafenib as part of a clinical trial, with some lesions appearing to be a more aggressive type upon analysis.
The lesions began as acrochordons on her face and extremities, as well as new nevi on her torso and axilla. She also developed fever, chills, and fatigue and had enlarging, tender, and bleeding lesions on her trunk and extremities.
Seven large, tender, and indurated lesions were removed using a deep scoop shave biopsy, revealing a biphasic malignant growth pattern (JAMA Dermatology 2014 Feb 26 [doi:10.1001/jamadermatol.2013.7784]).
"The superficial portion demonstrated conventional cSCC-KA features of hyperkeratosis, epidermal acanthosis, and central core of glassy eosinophilic keratin with pseudopapillomatosis and a base with focal invasive lobules of cytologically atypical keratinocytes, consistent with previously reported cSCC-KA" the study authors reported.
However, they added, "in stark contrast to prior reports, the deep aspects of 6 of 7 lesions showed invasive spindled and epithelioid cells with monomorphic elongated nuclei with condensed chromatin and mitoses consistent with spindle cell squamous carcinoma, an aggressive subtype of squamous cell carcinoma."
The cells were strongly immunoreactive for cytokeratin CK5/6 and CK903, and both the squamous and spindle components were vimentin reactive and showed increased proliferation index. In contrast to the usual pattern of a spindle cell melanoma, the spindle tumor cells were also MART-1 and S100 negative.
The authors said this was the first known report of invasive spindle cell squamous carcinoma that mimicked keratoacanthoma-like secondary SCC appearing during BRAF inhibitor therapy and suggested that the discovery has implications for management of secondary squamous cell carcinoma.
"Because the clinical appearance of cSCC-KA and the spindle cell squamous carcinomas in our patient are indistinguishable, histologic evaluation of the entire lesion (via saucerization biopsy or incisional biopsy) is vital to prevent inadequate treatment of a deeply invasive process with a probable higher malignant potential," Dr. Cohen and his associates wrote.
The patient stopped BRAF inhibitor therapy and had no recurrence or new development of cutaneous secondary SCCs. A single later recurrence of melanoma was resected but she remains disease free.
One author declared a consultancy with Bristol-Myers Squibb and Genentech, as well as grant support from Genentech. There were no other financial disclosures reported.
A woman undergoing BRAF inhibitor targeted therapy for advanced melanoma has presented with invasive spindle cell squamous carcinoma masquerading as a secondary cutaneous squamous cell carcinoma, highlighting the importance of histologic evaluation of these lesions.
"Secondary cutaneous squamous cell carcinomas (cSCCs) are adverse effects of BRAF inhibitor targeted therapy for advanced melanoma," wrote Dr. Daniel N. Cohen and his associates online Feb. 26 in JAMA Dermatology.
The most commonly seen histologic type of secondary cutaneous squamous cell carcinomas is keratoacanthoma-like cSCC (cSCC-KA), which is thought to have a low risk of metastasis or recurrence, said lead author Dr. Cohen of the Vanderbilt University Medical Center, Nashville, Tenn.
In this case report, however, a woman in her 50s with BRAF-mutant metastatic melanoma developed more than 100 new cutaneous squamous proliferations across her face, trunk, and extremities within 4 weeks of starting treatment with the BRAF inhibitor dabrafenib as part of a clinical trial, with some lesions appearing to be a more aggressive type upon analysis.
The lesions began as acrochordons on her face and extremities, as well as new nevi on her torso and axilla. She also developed fever, chills, and fatigue and had enlarging, tender, and bleeding lesions on her trunk and extremities.
Seven large, tender, and indurated lesions were removed using a deep scoop shave biopsy, revealing a biphasic malignant growth pattern (JAMA Dermatology 2014 Feb 26 [doi:10.1001/jamadermatol.2013.7784]).
"The superficial portion demonstrated conventional cSCC-KA features of hyperkeratosis, epidermal acanthosis, and central core of glassy eosinophilic keratin with pseudopapillomatosis and a base with focal invasive lobules of cytologically atypical keratinocytes, consistent with previously reported cSCC-KA" the study authors reported.
However, they added, "in stark contrast to prior reports, the deep aspects of 6 of 7 lesions showed invasive spindled and epithelioid cells with monomorphic elongated nuclei with condensed chromatin and mitoses consistent with spindle cell squamous carcinoma, an aggressive subtype of squamous cell carcinoma."
The cells were strongly immunoreactive for cytokeratin CK5/6 and CK903, and both the squamous and spindle components were vimentin reactive and showed increased proliferation index. In contrast to the usual pattern of a spindle cell melanoma, the spindle tumor cells were also MART-1 and S100 negative.
The authors said this was the first known report of invasive spindle cell squamous carcinoma that mimicked keratoacanthoma-like secondary SCC appearing during BRAF inhibitor therapy and suggested that the discovery has implications for management of secondary squamous cell carcinoma.
"Because the clinical appearance of cSCC-KA and the spindle cell squamous carcinomas in our patient are indistinguishable, histologic evaluation of the entire lesion (via saucerization biopsy or incisional biopsy) is vital to prevent inadequate treatment of a deeply invasive process with a probable higher malignant potential," Dr. Cohen and his associates wrote.
The patient stopped BRAF inhibitor therapy and had no recurrence or new development of cutaneous secondary SCCs. A single later recurrence of melanoma was resected but she remains disease free.
One author declared a consultancy with Bristol-Myers Squibb and Genentech, as well as grant support from Genentech. There were no other financial disclosures reported.
A woman undergoing BRAF inhibitor targeted therapy for advanced melanoma has presented with invasive spindle cell squamous carcinoma masquerading as a secondary cutaneous squamous cell carcinoma, highlighting the importance of histologic evaluation of these lesions.
"Secondary cutaneous squamous cell carcinomas (cSCCs) are adverse effects of BRAF inhibitor targeted therapy for advanced melanoma," wrote Dr. Daniel N. Cohen and his associates online Feb. 26 in JAMA Dermatology.
The most commonly seen histologic type of secondary cutaneous squamous cell carcinomas is keratoacanthoma-like cSCC (cSCC-KA), which is thought to have a low risk of metastasis or recurrence, said lead author Dr. Cohen of the Vanderbilt University Medical Center, Nashville, Tenn.
In this case report, however, a woman in her 50s with BRAF-mutant metastatic melanoma developed more than 100 new cutaneous squamous proliferations across her face, trunk, and extremities within 4 weeks of starting treatment with the BRAF inhibitor dabrafenib as part of a clinical trial, with some lesions appearing to be a more aggressive type upon analysis.
The lesions began as acrochordons on her face and extremities, as well as new nevi on her torso and axilla. She also developed fever, chills, and fatigue and had enlarging, tender, and bleeding lesions on her trunk and extremities.
Seven large, tender, and indurated lesions were removed using a deep scoop shave biopsy, revealing a biphasic malignant growth pattern (JAMA Dermatology 2014 Feb 26 [doi:10.1001/jamadermatol.2013.7784]).
"The superficial portion demonstrated conventional cSCC-KA features of hyperkeratosis, epidermal acanthosis, and central core of glassy eosinophilic keratin with pseudopapillomatosis and a base with focal invasive lobules of cytologically atypical keratinocytes, consistent with previously reported cSCC-KA" the study authors reported.
However, they added, "in stark contrast to prior reports, the deep aspects of 6 of 7 lesions showed invasive spindled and epithelioid cells with monomorphic elongated nuclei with condensed chromatin and mitoses consistent with spindle cell squamous carcinoma, an aggressive subtype of squamous cell carcinoma."
The cells were strongly immunoreactive for cytokeratin CK5/6 and CK903, and both the squamous and spindle components were vimentin reactive and showed increased proliferation index. In contrast to the usual pattern of a spindle cell melanoma, the spindle tumor cells were also MART-1 and S100 negative.
The authors said this was the first known report of invasive spindle cell squamous carcinoma that mimicked keratoacanthoma-like secondary SCC appearing during BRAF inhibitor therapy and suggested that the discovery has implications for management of secondary squamous cell carcinoma.
"Because the clinical appearance of cSCC-KA and the spindle cell squamous carcinomas in our patient are indistinguishable, histologic evaluation of the entire lesion (via saucerization biopsy or incisional biopsy) is vital to prevent inadequate treatment of a deeply invasive process with a probable higher malignant potential," Dr. Cohen and his associates wrote.
The patient stopped BRAF inhibitor therapy and had no recurrence or new development of cutaneous secondary SCCs. A single later recurrence of melanoma was resected but she remains disease free.
One author declared a consultancy with Bristol-Myers Squibb and Genentech, as well as grant support from Genentech. There were no other financial disclosures reported.
FROM JAMA DERMATOLOGY
Major finding: A woman undergoing BRAF inhibitor targeted therapy for advanced melanoma has presented with invasive spindle cell squamous carcinoma masquerading as a secondary cutaneous squamous cell carcinoma.
Data source: Case report.
Disclosures: One author declared a consultancy with Bristol-Myers Squibb and Genentech, as well as grant support from Genentech. There were no other financial disclosures reported.
Chondroid Syringoma
Immunosuppressive therapy ups risk for skin cancers
HOLLYWOOD, FLA. – Current and previous use of thiopurines, biologics, and combination therapies are all independent risk factors for skin cancer, according to expert analysis given at a conference on inflammatory bowel diseases.
Although population-based cohort studies have shown that the baseline risk for nonmelanoma skin cancer in IBD has risen more than a third since the preimmunomodulator era, regardless of the mode of treatment, "Cutaneous side effects of immunomodulators and biologics are a rising concern in clinical practice," said Dr. Jean-Frederic Colombel of the Icahn School of Medicine at Mount Sinai in New York. "Patients with Crohn’s disease in particular have shown a twofold increased risk for nonmelanoma skin cancer, outside of any kind of immunomodulator or biologic therapy."

Thiopurine use has been associated with a twofold increased risk of nonmelanoma skin cancer that persists even after withdrawal from the medication, although there is not an increased risk for melanoma, according to Dr. Colombel.
In a comparative analysis of studies published primarily since 2011, he noted an epidemiologic study with an A level of evidence for nearly 10,000 IBD patients undergoing thiopurine treatment that had an increased risk for NMSC with an odds ratio of approximately 2.2 (95% CI, 1.24-3.81).
"What is very important to note is that the risk of nonmelanoma skin cancer persists even after the antimetabolite has been stopped," said Dr. Colombel, referring to data from the CESAME study that indicated, regardless of age, past and current thiopurine use was associated with higher incidence rates of NMSC.
To date, other immunomodulators have not been associated with NMSC, said Dr. Colombel. "What we are observing is quite specific to azathioprine."
Thiopurines are not considered a risk factor for melanoma, said Dr. Colombel. He cited a study of records from a health care claims database for the period between 1997 and 2009. In the study, 209 melanoma cases were matched with 823 controls. Exposure to thiopurines was associated with an OR of 1.1 for melanoma. In that same study, patients exposed to biologics were found to have an increased risk of melanoma, although the risk was higher in patients with Crohn’s disease than those with ulcerative colitis (OR, 1.94 vs. 1.73).
Biologics may also increase the risk of NMSC, although currently the data are "controversial" said Dr. Colombel. "The results are more difficult to interpret."
The risk for NMSC in IBD patients exposed to biologics was evaluated in three studies published between 2010 and 2013. One study indicated no significant increased risk for either past or current biologic use (OR 1.14, 95% CI 0.95-1.36).
Another study indicated a twofold increased risk for patients who’d withdrawn from biologic therapy (OR 2.07, 95% CI 1.28-3.33) and who had persistent use (OR 2.18, 95% CI, 1.07-4.46).
A third study showed a 2.3 increased NMSC risk (95% CI, 1.44-3.47).
In a meta-analysis published in 2013, the pooled relative risk for melanoma in IBD patients exposed to biologics was not shown to be significant (RR, 1.10).
Combination therapy has been found to increase the risk of NMSC nearly fourfold, said Dr. Colombel.
Even though more data are needed, Dr. Colombel said that all patients who are scheduled to start immunosuppression should be informed of the potential for dermatologic complications. "Personally, I am now sending all my patients to a dermatologist for a baseline evaluation," he said.
The conference was sponsored by the Crohn’s & Colitis Foundation of America. Dr. Colombel reported many disclosures, including Abbott Laboratories, Bristol-Myers Squibb, Genentech, Inc., Pfizer Inc. and sanofi-aventis, among others.
HOLLYWOOD, FLA. – Current and previous use of thiopurines, biologics, and combination therapies are all independent risk factors for skin cancer, according to expert analysis given at a conference on inflammatory bowel diseases.
Although population-based cohort studies have shown that the baseline risk for nonmelanoma skin cancer in IBD has risen more than a third since the preimmunomodulator era, regardless of the mode of treatment, "Cutaneous side effects of immunomodulators and biologics are a rising concern in clinical practice," said Dr. Jean-Frederic Colombel of the Icahn School of Medicine at Mount Sinai in New York. "Patients with Crohn’s disease in particular have shown a twofold increased risk for nonmelanoma skin cancer, outside of any kind of immunomodulator or biologic therapy."
Thiopurine use has been associated with a twofold increased risk of nonmelanoma skin cancer that persists even after withdrawal from the medication, although there is not an increased risk for melanoma, according to Dr. Colombel.
In a comparative analysis of studies published primarily since 2011, he noted an epidemiologic study with an A level of evidence for nearly 10,000 IBD patients undergoing thiopurine treatment that had an increased risk for NMSC with an odds ratio of approximately 2.2 (95% CI, 1.24-3.81).
"What is very important to note is that the risk of nonmelanoma skin cancer persists even after the antimetabolite has been stopped," said Dr. Colombel, referring to data from the CESAME study that indicated, regardless of age, past and current thiopurine use was associated with higher incidence rates of NMSC.
To date, other immunomodulators have not been associated with NMSC, said Dr. Colombel. "What we are observing is quite specific to azathioprine."
Thiopurines are not considered a risk factor for melanoma, said Dr. Colombel. He cited a study of records from a health care claims database for the period between 1997 and 2009. In the study, 209 melanoma cases were matched with 823 controls. Exposure to thiopurines was associated with an OR of 1.1 for melanoma. In that same study, patients exposed to biologics were found to have an increased risk of melanoma, although the risk was higher in patients with Crohn’s disease than those with ulcerative colitis (OR, 1.94 vs. 1.73).
Biologics may also increase the risk of NMSC, although currently the data are "controversial" said Dr. Colombel. "The results are more difficult to interpret."
The risk for NMSC in IBD patients exposed to biologics was evaluated in three studies published between 2010 and 2013. One study indicated no significant increased risk for either past or current biologic use (OR 1.14, 95% CI 0.95-1.36).
Another study indicated a twofold increased risk for patients who’d withdrawn from biologic therapy (OR 2.07, 95% CI 1.28-3.33) and who had persistent use (OR 2.18, 95% CI, 1.07-4.46).
A third study showed a 2.3 increased NMSC risk (95% CI, 1.44-3.47).
In a meta-analysis published in 2013, the pooled relative risk for melanoma in IBD patients exposed to biologics was not shown to be significant (RR, 1.10).
Combination therapy has been found to increase the risk of NMSC nearly fourfold, said Dr. Colombel.
Even though more data are needed, Dr. Colombel said that all patients who are scheduled to start immunosuppression should be informed of the potential for dermatologic complications. "Personally, I am now sending all my patients to a dermatologist for a baseline evaluation," he said.
The conference was sponsored by the Crohn’s & Colitis Foundation of America. Dr. Colombel reported many disclosures, including Abbott Laboratories, Bristol-Myers Squibb, Genentech, Inc., Pfizer Inc. and sanofi-aventis, among others.
HOLLYWOOD, FLA. – Current and previous use of thiopurines, biologics, and combination therapies are all independent risk factors for skin cancer, according to expert analysis given at a conference on inflammatory bowel diseases.
Although population-based cohort studies have shown that the baseline risk for nonmelanoma skin cancer in IBD has risen more than a third since the preimmunomodulator era, regardless of the mode of treatment, "Cutaneous side effects of immunomodulators and biologics are a rising concern in clinical practice," said Dr. Jean-Frederic Colombel of the Icahn School of Medicine at Mount Sinai in New York. "Patients with Crohn’s disease in particular have shown a twofold increased risk for nonmelanoma skin cancer, outside of any kind of immunomodulator or biologic therapy."
Thiopurine use has been associated with a twofold increased risk of nonmelanoma skin cancer that persists even after withdrawal from the medication, although there is not an increased risk for melanoma, according to Dr. Colombel.
In a comparative analysis of studies published primarily since 2011, he noted an epidemiologic study with an A level of evidence for nearly 10,000 IBD patients undergoing thiopurine treatment that had an increased risk for NMSC with an odds ratio of approximately 2.2 (95% CI, 1.24-3.81).
"What is very important to note is that the risk of nonmelanoma skin cancer persists even after the antimetabolite has been stopped," said Dr. Colombel, referring to data from the CESAME study that indicated, regardless of age, past and current thiopurine use was associated with higher incidence rates of NMSC.
To date, other immunomodulators have not been associated with NMSC, said Dr. Colombel. "What we are observing is quite specific to azathioprine."
Thiopurines are not considered a risk factor for melanoma, said Dr. Colombel. He cited a study of records from a health care claims database for the period between 1997 and 2009. In the study, 209 melanoma cases were matched with 823 controls. Exposure to thiopurines was associated with an OR of 1.1 for melanoma. In that same study, patients exposed to biologics were found to have an increased risk of melanoma, although the risk was higher in patients with Crohn’s disease than those with ulcerative colitis (OR, 1.94 vs. 1.73).
Biologics may also increase the risk of NMSC, although currently the data are "controversial" said Dr. Colombel. "The results are more difficult to interpret."
The risk for NMSC in IBD patients exposed to biologics was evaluated in three studies published between 2010 and 2013. One study indicated no significant increased risk for either past or current biologic use (OR 1.14, 95% CI 0.95-1.36).
Another study indicated a twofold increased risk for patients who’d withdrawn from biologic therapy (OR 2.07, 95% CI 1.28-3.33) and who had persistent use (OR 2.18, 95% CI, 1.07-4.46).
A third study showed a 2.3 increased NMSC risk (95% CI, 1.44-3.47).
In a meta-analysis published in 2013, the pooled relative risk for melanoma in IBD patients exposed to biologics was not shown to be significant (RR, 1.10).
Combination therapy has been found to increase the risk of NMSC nearly fourfold, said Dr. Colombel.
Even though more data are needed, Dr. Colombel said that all patients who are scheduled to start immunosuppression should be informed of the potential for dermatologic complications. "Personally, I am now sending all my patients to a dermatologist for a baseline evaluation," he said.
The conference was sponsored by the Crohn’s & Colitis Foundation of America. Dr. Colombel reported many disclosures, including Abbott Laboratories, Bristol-Myers Squibb, Genentech, Inc., Pfizer Inc. and sanofi-aventis, among others.
EXPERT ANALYSIS FROM 2013 ADVANCES IN IBD

Multiple Familial Trichodiscomas

Growing Ears, Noses, and Skin: The New Frontier in Dermatology and Dermatologic Surgery?

In an article published online in Maclean’s magazine on October 15, 2013, the concept of developing artificial body parts is discussed. The technology now exists for scientists to grow tissue organs, such as ears, noses, and fingers. Several groups of investigators, including Anthony Atala, MD (Wake Forest Institute for Regenerative Medicine, Winston-Salem, North Carolina) and Alexander Seifalian, PhD (University College London, England), are busy making ears by creating a biodegradable scaffold onto which cells—either stem cells from the patient or cells that have been harvested from the patient’s original organ—are layered and permitted to multiply. The cell-layered scaffold is then placed in a bioreactor for a couple of weeks. Once ready, the new ear is transplanted onto the patient; subsequently, the scaffold melts away.
Dr. Atala’s laboratory also is busy growing fingers. Meanwhile, Dr. Seifalian grew a nose (inside the patient’s own arm) in only 3 months after the patient lost his nose to skin cancer. He made a mold based on the patient’s original nose, created a scaffold composed of nanocomposite material, added the patient’s stem cells to the scaffold, and put the nose in a bioreactor to mature. Meanwhile, he placed a tissue expander in the patient’s arm and subsequently inserted the nose into the arm so that it could become vascularized and covered by skin. The nose was transplanted to the patient’s face; additional surgery is planned to open the nostrils, followed by seeding them with stem cells to return his sense of smell.
Marc Jeschke, MD, PhD (Ross Tilley Burn Centre, Sunnybrook Health Sciences Centre, Toronto, Ontario) is developing a bioprinter to create skin. The bioprinter dispenses different types of cells (grown from the patient’s own cells) into a hydrogel matrix in 3 dimensions. Currently, Dr. Jeschke is working with mice; however, in a few years, he anticipates treating human patients. Other investigators, such as Michael C. McAlpine (Princeton University, New Jersey), recently used a commercial 3-dimensional printer to make an ear; the “inks” included calf cells and a silver nanoparticle paste that formed a coiled antenna inside the cartilage that was capable of receiving electromagnetic signals and transmitting them to the brain.
What’s the issue?
The ability to grow tissue organs is going to revolutionize the surgical management of patients who need solid organ replacement; kidneys, lungs, pancreases, spleens, and tracheas have already been successfully grown. Indeed several investigators are making ears and noses. How long will it be before flaps and grafts to repair wound defects following extensive and deforming skin cancer surgery are replaced by ears and noses that are grown from the patient’s own tissue cells or stem cells? Although it seems like science fiction today, how soon will it be before a cutaneous 3-dimensional printer becomes a standard piece of equipment in the dermatologist and dermatologic surgeon’s office for use to create skin to cover postoperative sites that cannot be closed by directly bringing the wound edges together?
In an article published online in Maclean’s magazine on October 15, 2013, the concept of developing artificial body parts is discussed. The technology now exists for scientists to grow tissue organs, such as ears, noses, and fingers. Several groups of investigators, including Anthony Atala, MD (Wake Forest Institute for Regenerative Medicine, Winston-Salem, North Carolina) and Alexander Seifalian, PhD (University College London, England), are busy making ears by creating a biodegradable scaffold onto which cells—either stem cells from the patient or cells that have been harvested from the patient’s original organ—are layered and permitted to multiply. The cell-layered scaffold is then placed in a bioreactor for a couple of weeks. Once ready, the new ear is transplanted onto the patient; subsequently, the scaffold melts away.
Dr. Atala’s laboratory also is busy growing fingers. Meanwhile, Dr. Seifalian grew a nose (inside the patient’s own arm) in only 3 months after the patient lost his nose to skin cancer. He made a mold based on the patient’s original nose, created a scaffold composed of nanocomposite material, added the patient’s stem cells to the scaffold, and put the nose in a bioreactor to mature. Meanwhile, he placed a tissue expander in the patient’s arm and subsequently inserted the nose into the arm so that it could become vascularized and covered by skin. The nose was transplanted to the patient’s face; additional surgery is planned to open the nostrils, followed by seeding them with stem cells to return his sense of smell.
Marc Jeschke, MD, PhD (Ross Tilley Burn Centre, Sunnybrook Health Sciences Centre, Toronto, Ontario) is developing a bioprinter to create skin. The bioprinter dispenses different types of cells (grown from the patient’s own cells) into a hydrogel matrix in 3 dimensions. Currently, Dr. Jeschke is working with mice; however, in a few years, he anticipates treating human patients. Other investigators, such as Michael C. McAlpine (Princeton University, New Jersey), recently used a commercial 3-dimensional printer to make an ear; the “inks” included calf cells and a silver nanoparticle paste that formed a coiled antenna inside the cartilage that was capable of receiving electromagnetic signals and transmitting them to the brain.
What’s the issue?
The ability to grow tissue organs is going to revolutionize the surgical management of patients who need solid organ replacement; kidneys, lungs, pancreases, spleens, and tracheas have already been successfully grown. Indeed several investigators are making ears and noses. How long will it be before flaps and grafts to repair wound defects following extensive and deforming skin cancer surgery are replaced by ears and noses that are grown from the patient’s own tissue cells or stem cells? Although it seems like science fiction today, how soon will it be before a cutaneous 3-dimensional printer becomes a standard piece of equipment in the dermatologist and dermatologic surgeon’s office for use to create skin to cover postoperative sites that cannot be closed by directly bringing the wound edges together?
In an article published online in Maclean’s magazine on October 15, 2013, the concept of developing artificial body parts is discussed. The technology now exists for scientists to grow tissue organs, such as ears, noses, and fingers. Several groups of investigators, including Anthony Atala, MD (Wake Forest Institute for Regenerative Medicine, Winston-Salem, North Carolina) and Alexander Seifalian, PhD (University College London, England), are busy making ears by creating a biodegradable scaffold onto which cells—either stem cells from the patient or cells that have been harvested from the patient’s original organ—are layered and permitted to multiply. The cell-layered scaffold is then placed in a bioreactor for a couple of weeks. Once ready, the new ear is transplanted onto the patient; subsequently, the scaffold melts away.
Dr. Atala’s laboratory also is busy growing fingers. Meanwhile, Dr. Seifalian grew a nose (inside the patient’s own arm) in only 3 months after the patient lost his nose to skin cancer. He made a mold based on the patient’s original nose, created a scaffold composed of nanocomposite material, added the patient’s stem cells to the scaffold, and put the nose in a bioreactor to mature. Meanwhile, he placed a tissue expander in the patient’s arm and subsequently inserted the nose into the arm so that it could become vascularized and covered by skin. The nose was transplanted to the patient’s face; additional surgery is planned to open the nostrils, followed by seeding them with stem cells to return his sense of smell.
Marc Jeschke, MD, PhD (Ross Tilley Burn Centre, Sunnybrook Health Sciences Centre, Toronto, Ontario) is developing a bioprinter to create skin. The bioprinter dispenses different types of cells (grown from the patient’s own cells) into a hydrogel matrix in 3 dimensions. Currently, Dr. Jeschke is working with mice; however, in a few years, he anticipates treating human patients. Other investigators, such as Michael C. McAlpine (Princeton University, New Jersey), recently used a commercial 3-dimensional printer to make an ear; the “inks” included calf cells and a silver nanoparticle paste that formed a coiled antenna inside the cartilage that was capable of receiving electromagnetic signals and transmitting them to the brain.
What’s the issue?
The ability to grow tissue organs is going to revolutionize the surgical management of patients who need solid organ replacement; kidneys, lungs, pancreases, spleens, and tracheas have already been successfully grown. Indeed several investigators are making ears and noses. How long will it be before flaps and grafts to repair wound defects following extensive and deforming skin cancer surgery are replaced by ears and noses that are grown from the patient’s own tissue cells or stem cells? Although it seems like science fiction today, how soon will it be before a cutaneous 3-dimensional printer becomes a standard piece of equipment in the dermatologist and dermatologic surgeon’s office for use to create skin to cover postoperative sites that cannot be closed by directly bringing the wound edges together?

Endocrine Mucin-Producing Sweat Gland Carcinoma
Eccrine Porocarcinoma: A Report of 2 Cases and Review of the Literature
Test your knowledge on eccrine porocarcinoma with MD-IQ: the medical intelligence quiz. Click here to answer 5 questions.

