User login
Clinical trial enrollment linked to lower death rate in lung cancer patients
ALEXANDRIA, VA. – Patients with metastatic non–small cell lung cancer (NSCLC) who enrolled in clinical trials had a near 50% lower risk of death versus patients who received treatment outside a clinical trial, according to results of a single-center, retrospective medical record review.
Median survival was almost doubled for those patients with NSCLC enrolled in therapeutic drug trials, according to lead author Christina Merkhofer, MD, a hematology-oncology fellow at the University of Washington and Fred Hutchinson Cancer Center, both in Seattle.
The findings suggest that clinical trials, beyond supporting drug development, provide a direct benefit to NSCLC patients through provision of promising agents, enhanced supportive care, or both, according to Dr. Merkhofer and coauthors, who will present their findings in a poster at the Quality Care Symposium, sponsored by the American Society of Clinical Oncology.
The retrospective study included a total of 371 patients diagnosed with metastatic NSCLC between 2001 and 2015, of whom 118 (32%) enrolled in at least one clinical trial, Dr. Merkhofer reported at a press briefing ahead of the symposium.
Median survival was 838 days for the clinical trial enrollees versus 454 days for nonenrollees, according to the investigators. The risk of death was 47% lower (hazard ratio, 0.53; 95% confidence interval, 0.13-0.92; P = .002) for enrollees relative to nonenrollees after adjustment for variables including sex, performance status, smoking history, histology, presence of brain metastases, and EGFR/ALK status.
Based on this study by Dr. Merkhofer and colleagues, participating in therapeutic drug trials appears to improve survival in patients with advanced lung cancer, ASCO expert Merry-Jennifer Markham, MD, said in a statement.
Oncologists have a “duty” to enroll patients in clinical trials as appropriate, said Dr. Markham, chair of the Quality Care Symposium’s news planning team.
“We must work to better understand factors associated with enrollment so that the prospective benefits can be made accessible to all who are eligible,” she said.
The research is part of a larger investigation looking at “areas of uncertainty” in clinical trial participation, such as whether specific trial design characteristics are linked to survival benefit, according to Dr. Merkhofer.
“The study can support research evaluating health care policies or research that looks at incentives for patient participation in trials, such as financing transportation or lodging, [and] can help with research that addresses some of these important barriers to trial participation,” Dr. Merkhofer said in an ASCO press release.
Dr. Merkhofer had no disclosures related to the study. Her coauthors reported disclosures related to numerous pharmaceutical companies.
SOURCE: Merkhofer C et al. QCS2019, Abstract 137.
ALEXANDRIA, VA. – Patients with metastatic non–small cell lung cancer (NSCLC) who enrolled in clinical trials had a near 50% lower risk of death versus patients who received treatment outside a clinical trial, according to results of a single-center, retrospective medical record review.
Median survival was almost doubled for those patients with NSCLC enrolled in therapeutic drug trials, according to lead author Christina Merkhofer, MD, a hematology-oncology fellow at the University of Washington and Fred Hutchinson Cancer Center, both in Seattle.
The findings suggest that clinical trials, beyond supporting drug development, provide a direct benefit to NSCLC patients through provision of promising agents, enhanced supportive care, or both, according to Dr. Merkhofer and coauthors, who will present their findings in a poster at the Quality Care Symposium, sponsored by the American Society of Clinical Oncology.
The retrospective study included a total of 371 patients diagnosed with metastatic NSCLC between 2001 and 2015, of whom 118 (32%) enrolled in at least one clinical trial, Dr. Merkhofer reported at a press briefing ahead of the symposium.
Median survival was 838 days for the clinical trial enrollees versus 454 days for nonenrollees, according to the investigators. The risk of death was 47% lower (hazard ratio, 0.53; 95% confidence interval, 0.13-0.92; P = .002) for enrollees relative to nonenrollees after adjustment for variables including sex, performance status, smoking history, histology, presence of brain metastases, and EGFR/ALK status.
Based on this study by Dr. Merkhofer and colleagues, participating in therapeutic drug trials appears to improve survival in patients with advanced lung cancer, ASCO expert Merry-Jennifer Markham, MD, said in a statement.
Oncologists have a “duty” to enroll patients in clinical trials as appropriate, said Dr. Markham, chair of the Quality Care Symposium’s news planning team.
“We must work to better understand factors associated with enrollment so that the prospective benefits can be made accessible to all who are eligible,” she said.
The research is part of a larger investigation looking at “areas of uncertainty” in clinical trial participation, such as whether specific trial design characteristics are linked to survival benefit, according to Dr. Merkhofer.
“The study can support research evaluating health care policies or research that looks at incentives for patient participation in trials, such as financing transportation or lodging, [and] can help with research that addresses some of these important barriers to trial participation,” Dr. Merkhofer said in an ASCO press release.
Dr. Merkhofer had no disclosures related to the study. Her coauthors reported disclosures related to numerous pharmaceutical companies.
SOURCE: Merkhofer C et al. QCS2019, Abstract 137.
ALEXANDRIA, VA. – Patients with metastatic non–small cell lung cancer (NSCLC) who enrolled in clinical trials had a near 50% lower risk of death versus patients who received treatment outside a clinical trial, according to results of a single-center, retrospective medical record review.
Median survival was almost doubled for those patients with NSCLC enrolled in therapeutic drug trials, according to lead author Christina Merkhofer, MD, a hematology-oncology fellow at the University of Washington and Fred Hutchinson Cancer Center, both in Seattle.
The findings suggest that clinical trials, beyond supporting drug development, provide a direct benefit to NSCLC patients through provision of promising agents, enhanced supportive care, or both, according to Dr. Merkhofer and coauthors, who will present their findings in a poster at the Quality Care Symposium, sponsored by the American Society of Clinical Oncology.
The retrospective study included a total of 371 patients diagnosed with metastatic NSCLC between 2001 and 2015, of whom 118 (32%) enrolled in at least one clinical trial, Dr. Merkhofer reported at a press briefing ahead of the symposium.
Median survival was 838 days for the clinical trial enrollees versus 454 days for nonenrollees, according to the investigators. The risk of death was 47% lower (hazard ratio, 0.53; 95% confidence interval, 0.13-0.92; P = .002) for enrollees relative to nonenrollees after adjustment for variables including sex, performance status, smoking history, histology, presence of brain metastases, and EGFR/ALK status.
Based on this study by Dr. Merkhofer and colleagues, participating in therapeutic drug trials appears to improve survival in patients with advanced lung cancer, ASCO expert Merry-Jennifer Markham, MD, said in a statement.
Oncologists have a “duty” to enroll patients in clinical trials as appropriate, said Dr. Markham, chair of the Quality Care Symposium’s news planning team.
“We must work to better understand factors associated with enrollment so that the prospective benefits can be made accessible to all who are eligible,” she said.
The research is part of a larger investigation looking at “areas of uncertainty” in clinical trial participation, such as whether specific trial design characteristics are linked to survival benefit, according to Dr. Merkhofer.
“The study can support research evaluating health care policies or research that looks at incentives for patient participation in trials, such as financing transportation or lodging, [and] can help with research that addresses some of these important barriers to trial participation,” Dr. Merkhofer said in an ASCO press release.
Dr. Merkhofer had no disclosures related to the study. Her coauthors reported disclosures related to numerous pharmaceutical companies.
SOURCE: Merkhofer C et al. QCS2019, Abstract 137.
REPORTING FROM QCS 2019
Out-of-pocket cost of oral TKIs linked to poor lung cancer survival
ALEXANDRIA, VA. – Higher out-of-pocket costs for oral tyrosine kinase inhibitors (TKIs) were linked to inferior survival in patients with advanced, biomarker-positive lung cancers in an analysis of state-level registry data, an investigator reported at a press conference ahead of the Quality Care Symposium, sponsored by the American Society of Clinical Oncology.
Higher out-of-pocket cost burden was also linked to lower numbers of TKI prescriptions and shorter duration of TKI therapy in the study, which included patients diagnosed with EGFR- and ALK-positive non–small cell lung cancer (NSCLC) between 2010 and 2016.
The findings would suggest a need for a review of coverage for these effective medications, according to Bernardo H. L. Goulart, MD, a thoracic oncologist and health services researcher at the University of Washington and Fred Hutchinson Cancer Research Center, both in Seattle.
“Making sure that the cost to the patients is affordable could mitigate this financial toxicity, and hopefully help patients stay on therapy and derive the survival benefit that these medications are supposed to offer,” Dr. Goulart said in an interview.
The study included data on 106 patients with EGFR- and ALK-positive stage IV NSCLC in the Washington Surveillance, Epidemiology, and End Results registry who had at least one oral TKI prescription. Investigators linked that registry data with commercial and Medicare claims, then divided this patient cohort into quartiles based on out-of-pocket costs.
In the top quartile, the median monthly out-of-pocket cost for TKI treatment was $2,888, compared with just $1,431 in the other three quartiles – essentially half the cost, Dr. Goulart said.
Median survival in the patients in the top out-of-pocket cost quartile was just 9 months, compared with 22 months in the lower three quartiles, he added.
“That difference is remarkable,” Dr. Goulart said, adding that the survival in the top-cost quartile reflects a survival that might be expected with conventional, nontargeted chemotherapy, while survival in the remaining patients mirrored what might be expected based on clinical trials of TKIs in this setting.
Patients in the high-cost quartile were 2.31 times as likely to die as patients in the lower quartiles, according to results of a multivariable analysis that adjusted for patient, disease-specific, and financial characteristics including qualification for low-income subsidies.
The mean medication possession ratio, a measure of medication adherence, was lower in the high-cost quartile (1.06 vs. 1.20 for the lower three quartiles; P = .02), and median duration of therapy was likewise lower in the high-cost quartile (4 vs. 8 months; P less than .01), according to data reported in the study abstract.
While multiple previous studies have linked out-of-pocket costs to decreased adherence and duration of therapy, the present study is one of the few to evaluate the link between cost of oral cancer medications and survival, according to Dr. Goulart.
In one other recent study showing a relationship between financial toxicity and survival, researchers at Fred Hutch showing that Washington cancer patients who filed for bankruptcy were more likely to die, compared with cancer patients not filing for bankruptcy, even after adjustment for a variety of patient characteristics.
The present study results raise a “serious concern” that some patients are unable to afford their medications, which is having a detrimental effect on survival, Dr. Goulart said. Alternatively, the out-of-pocket costs may not have an effect on survival; rather, they may be a “marker of very poor insurance coverage” that reflects higher costs for multiple other aspects of their care.
“The out-of-pocket cost for these drugs can be pretty astronomical, and we have at least a plausible hypothesis that they are taking a toll on patient’s survival,” he added.
If the findings of this study are confirmed in more and larger studies, there could be important implications for health policy and oncology practice, according to Dr. Goulart.
“The biggest action would be to involve patient advocates and physician groups such as ASCO, and advocate for changes in policy for coverage and out-of-pocket costs for these oral TKIs, at least for the patients that have the mutations,” he explained.
Another action, according to Dr. Goulart, would be to try to equip oncology clinics everywhere with patient financial-assistance programs to link patients to entities that can help them afford the cost of TKIs.
“Patients who attend small, remote cancer clinics might not have access to a financial specialist who can help them navigate these costs,” he said.
Funding for the study came from the National Institutes of Health. Dr. Goulart reported disclosures related to Flatiron Health (travel, accommodations, and expenses).
SOURCE: Goulart BHL et al. SCS 2019, Abstract 3.
ALEXANDRIA, VA. – Higher out-of-pocket costs for oral tyrosine kinase inhibitors (TKIs) were linked to inferior survival in patients with advanced, biomarker-positive lung cancers in an analysis of state-level registry data, an investigator reported at a press conference ahead of the Quality Care Symposium, sponsored by the American Society of Clinical Oncology.
Higher out-of-pocket cost burden was also linked to lower numbers of TKI prescriptions and shorter duration of TKI therapy in the study, which included patients diagnosed with EGFR- and ALK-positive non–small cell lung cancer (NSCLC) between 2010 and 2016.
The findings would suggest a need for a review of coverage for these effective medications, according to Bernardo H. L. Goulart, MD, a thoracic oncologist and health services researcher at the University of Washington and Fred Hutchinson Cancer Research Center, both in Seattle.
“Making sure that the cost to the patients is affordable could mitigate this financial toxicity, and hopefully help patients stay on therapy and derive the survival benefit that these medications are supposed to offer,” Dr. Goulart said in an interview.
The study included data on 106 patients with EGFR- and ALK-positive stage IV NSCLC in the Washington Surveillance, Epidemiology, and End Results registry who had at least one oral TKI prescription. Investigators linked that registry data with commercial and Medicare claims, then divided this patient cohort into quartiles based on out-of-pocket costs.
In the top quartile, the median monthly out-of-pocket cost for TKI treatment was $2,888, compared with just $1,431 in the other three quartiles – essentially half the cost, Dr. Goulart said.
Median survival in the patients in the top out-of-pocket cost quartile was just 9 months, compared with 22 months in the lower three quartiles, he added.
“That difference is remarkable,” Dr. Goulart said, adding that the survival in the top-cost quartile reflects a survival that might be expected with conventional, nontargeted chemotherapy, while survival in the remaining patients mirrored what might be expected based on clinical trials of TKIs in this setting.
Patients in the high-cost quartile were 2.31 times as likely to die as patients in the lower quartiles, according to results of a multivariable analysis that adjusted for patient, disease-specific, and financial characteristics including qualification for low-income subsidies.
The mean medication possession ratio, a measure of medication adherence, was lower in the high-cost quartile (1.06 vs. 1.20 for the lower three quartiles; P = .02), and median duration of therapy was likewise lower in the high-cost quartile (4 vs. 8 months; P less than .01), according to data reported in the study abstract.
While multiple previous studies have linked out-of-pocket costs to decreased adherence and duration of therapy, the present study is one of the few to evaluate the link between cost of oral cancer medications and survival, according to Dr. Goulart.
In one other recent study showing a relationship between financial toxicity and survival, researchers at Fred Hutch showing that Washington cancer patients who filed for bankruptcy were more likely to die, compared with cancer patients not filing for bankruptcy, even after adjustment for a variety of patient characteristics.
The present study results raise a “serious concern” that some patients are unable to afford their medications, which is having a detrimental effect on survival, Dr. Goulart said. Alternatively, the out-of-pocket costs may not have an effect on survival; rather, they may be a “marker of very poor insurance coverage” that reflects higher costs for multiple other aspects of their care.
“The out-of-pocket cost for these drugs can be pretty astronomical, and we have at least a plausible hypothesis that they are taking a toll on patient’s survival,” he added.
If the findings of this study are confirmed in more and larger studies, there could be important implications for health policy and oncology practice, according to Dr. Goulart.
“The biggest action would be to involve patient advocates and physician groups such as ASCO, and advocate for changes in policy for coverage and out-of-pocket costs for these oral TKIs, at least for the patients that have the mutations,” he explained.
Another action, according to Dr. Goulart, would be to try to equip oncology clinics everywhere with patient financial-assistance programs to link patients to entities that can help them afford the cost of TKIs.
“Patients who attend small, remote cancer clinics might not have access to a financial specialist who can help them navigate these costs,” he said.
Funding for the study came from the National Institutes of Health. Dr. Goulart reported disclosures related to Flatiron Health (travel, accommodations, and expenses).
SOURCE: Goulart BHL et al. SCS 2019, Abstract 3.
ALEXANDRIA, VA. – Higher out-of-pocket costs for oral tyrosine kinase inhibitors (TKIs) were linked to inferior survival in patients with advanced, biomarker-positive lung cancers in an analysis of state-level registry data, an investigator reported at a press conference ahead of the Quality Care Symposium, sponsored by the American Society of Clinical Oncology.
Higher out-of-pocket cost burden was also linked to lower numbers of TKI prescriptions and shorter duration of TKI therapy in the study, which included patients diagnosed with EGFR- and ALK-positive non–small cell lung cancer (NSCLC) between 2010 and 2016.
The findings would suggest a need for a review of coverage for these effective medications, according to Bernardo H. L. Goulart, MD, a thoracic oncologist and health services researcher at the University of Washington and Fred Hutchinson Cancer Research Center, both in Seattle.
“Making sure that the cost to the patients is affordable could mitigate this financial toxicity, and hopefully help patients stay on therapy and derive the survival benefit that these medications are supposed to offer,” Dr. Goulart said in an interview.
The study included data on 106 patients with EGFR- and ALK-positive stage IV NSCLC in the Washington Surveillance, Epidemiology, and End Results registry who had at least one oral TKI prescription. Investigators linked that registry data with commercial and Medicare claims, then divided this patient cohort into quartiles based on out-of-pocket costs.
In the top quartile, the median monthly out-of-pocket cost for TKI treatment was $2,888, compared with just $1,431 in the other three quartiles – essentially half the cost, Dr. Goulart said.
Median survival in the patients in the top out-of-pocket cost quartile was just 9 months, compared with 22 months in the lower three quartiles, he added.
“That difference is remarkable,” Dr. Goulart said, adding that the survival in the top-cost quartile reflects a survival that might be expected with conventional, nontargeted chemotherapy, while survival in the remaining patients mirrored what might be expected based on clinical trials of TKIs in this setting.
Patients in the high-cost quartile were 2.31 times as likely to die as patients in the lower quartiles, according to results of a multivariable analysis that adjusted for patient, disease-specific, and financial characteristics including qualification for low-income subsidies.
The mean medication possession ratio, a measure of medication adherence, was lower in the high-cost quartile (1.06 vs. 1.20 for the lower three quartiles; P = .02), and median duration of therapy was likewise lower in the high-cost quartile (4 vs. 8 months; P less than .01), according to data reported in the study abstract.
While multiple previous studies have linked out-of-pocket costs to decreased adherence and duration of therapy, the present study is one of the few to evaluate the link between cost of oral cancer medications and survival, according to Dr. Goulart.
In one other recent study showing a relationship between financial toxicity and survival, researchers at Fred Hutch showing that Washington cancer patients who filed for bankruptcy were more likely to die, compared with cancer patients not filing for bankruptcy, even after adjustment for a variety of patient characteristics.
The present study results raise a “serious concern” that some patients are unable to afford their medications, which is having a detrimental effect on survival, Dr. Goulart said. Alternatively, the out-of-pocket costs may not have an effect on survival; rather, they may be a “marker of very poor insurance coverage” that reflects higher costs for multiple other aspects of their care.
“The out-of-pocket cost for these drugs can be pretty astronomical, and we have at least a plausible hypothesis that they are taking a toll on patient’s survival,” he added.
If the findings of this study are confirmed in more and larger studies, there could be important implications for health policy and oncology practice, according to Dr. Goulart.
“The biggest action would be to involve patient advocates and physician groups such as ASCO, and advocate for changes in policy for coverage and out-of-pocket costs for these oral TKIs, at least for the patients that have the mutations,” he explained.
Another action, according to Dr. Goulart, would be to try to equip oncology clinics everywhere with patient financial-assistance programs to link patients to entities that can help them afford the cost of TKIs.
“Patients who attend small, remote cancer clinics might not have access to a financial specialist who can help them navigate these costs,” he said.
Funding for the study came from the National Institutes of Health. Dr. Goulart reported disclosures related to Flatiron Health (travel, accommodations, and expenses).
SOURCE: Goulart BHL et al. SCS 2019, Abstract 3.
REPORTING FROM QCS 2019
Lung Cancer – Regional Snapshot Kansas City VA
Open Clinical Trials for Patients With Lung Cancers (FULL)
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors or cosponsors nearly 1,000 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of August 1, 201 8 ; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Lung-MAP (multiple trials)
Lung-MAP (SWOG S1400) is a multidrug, multi-substudy, biomarker-driven squamous cell lung cancer clinical trial that uses state-of-the-art genomic profiling to match patients to substudies testing investigational treatments that may target the genomic alterations, or mutations, found to be driving the growth of their cancer.
ID: NCT02154490, NCT02595944, NCT02766335, NCT02785913, NCT02785939, NCT02926638, NCT02965378, NCT03373760, NCT03377556
Sponsor: Southwest Oncology Group
Locations: VA Connecticut Healthcare System-West Haven Campus; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Ann Arbor VAMC, Michigan; Kansas City VAMC, Missouri; VA New Jersey Health Care System, East Orange; Michael E. DeBakey VAMC Houston, Texas
ALCHEMIST: Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials (multiple trials)
A group of randomized clinical trials for patients with early-stage non-small cell lung cancer whose tumors have been completely removed by surgery.
ID: NCT02193282, NCT02194738, NCT02201992, NCT02595944
Sponsor: National Cancer Institute
Locations: Little Rock VAMC, Arkansas; VA Connecticut Healthcare System West Haven Campus; Atlanta VAMC, Decatur, Georgia; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Minneapolis VAMC, Minnesota; Saint Louis VAMC, Missouri; Veterans Affairs New York Harbor Healthcare System-Brooklyn Campus; Dayton VAMC, Ohio; William S. Middleton VAMC, Madison, Wisconsin
Veterans Affairs Lung Cancer Or Stereotactic Radiotherapy (VALOR)
The standard of care for stage I non-small cell lung cancer has historically been surgical resection in patients who are medically fit to tolerate an operation. Recent data now suggests that stereotactic radiotherapy may be a suitable alternative. This includes the results from a pooled analysis of two incomplete phase III studies that reported a 15% overall survival advantage with stereotactic radiotherapy at 3 years. While these data are promising, the median follow-up period was short, the results underpowered, and the findings were in contradiction to multiple retrospective studies that demonstrate the outcomes with surgery are likely equal or superior. Therefore, the herein trial aims to evaluate these two treatments in a prospective randomized fashion with a goal to compare the overall survival beyond 5 years. It has been designed to enroll patients who have a long life-expectancy, and are fit enough to tolerate an anatomic pulmonary resection with intraoperative lymph node sampling.
ID: NCT02984761
Sponsor: VA Office of Research and Development
Locations: Edward Hines Jr. VA Hospital, Hines, Illinois; Richard L. Roudebush VA Medical Center, Indianapolis, Indiana; Minneapolis VA Health Care System, Minnesota; Durham VAMC, North Carolina; Michael E. DeBakey VAMC, Houston, Texas; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Naloxegol in Treating Patients With Stage IIIB-IV Non-Small Cell Lung Cancer
This randomized pilot clinical trial studies the side effects and best dose of naloxegol and to see how well it works in treating patients with stage IIIB-IV non-small cell lung cancer. Naloxegol may relieve some of the side effects of opioid pain medication and fight off future growth in the cancer.
ID: NCT03087708
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Minneapolis VAMC, Minnesota; Kansas City VAMC, Missouri; VA Western New York Health Care System-Buffalo; Salisbury VAMC, North Carolina
Palliative Care Interventions for Outpatients Newly Diagnosed With Lung Cancer: Phase II (PCI2)
The focus of the study is to test a nurse-led telephone-based palliative care intervention on improving the delivery of care for patients with newly diagnosed lung cancer. The study is a three site randomized control trial to determine the efficacy of the intervention on improving patients’ quality of life, symptom burden, and satisfaction of care. Additionally, the study will test an innovative care delivery model to improve patients’ access to palliative care. The investigators will also determine the effect of the intervention on patient activation to discuss treatment preferences with their clinician and on clinician knowledge of patients’ goals of care.
ID: NCT03007953
Sponsor: VA Office of Research and Development
Locations: Birmingham VAMC, Alabama; VA Portland Health Care System, Oregon; VA Puget Sound Health Care System Seattle Division, Washington
Radiation Therapy Regimens in Treating Patients With Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide
Radiation therapy uses high-energy x-rays to kill tumor cells. Drugs used in chemotherapy, such as etoposide, carboplatin and cisplatin, work in different ways to stop the growth of tumor cells, either by killing the cells or by stopping them from dividing. It is not yet known which radiation therapy regimen is more effective when given together with chemotherapy in treating patients with limited-stage small cell lung cancer. This randomized phase III trial is comparing different chest radiation therapy regimens to see how well they work in treating patients with limited-stage small cell lung cancer.
ID: NCT00632853
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Baltimore VAMC, Maryland; Kansas City VAMC, Missouri; VA Western New York Health Care System, Buffalo, New York; Dayton VAMC, Ohio; Zablocki VAMC, Milwaukee, Wisconsin
Comparison of Different Types of Surgery in Treating Patients With Stage IA Non-Small Cell Lung Cancer
Wedge resection or segmentectomy may be less invasive types of surgery than lobectomy for non-small cell lung cancer and may have fewer side effects and improve recovery. It is not yet known whether wedge resection or segmentectomy are more effective than lobectomy in treating stage IA non-small cell lung cancer.
ID: NCT00499330
Sponsor: Alliance for Clinical Trials in Oncology
Locations: VA Loma Linda Healthcare System, California; VA Long Beach Medical Center, California; Richard L. Roudebush VAMC, Indianapolis, Indiana; Portland VAMC, Oregon
Lung Cancer Screening Decisions (VA-LCSDecTool)
Veterans have a high risk of developing lung in comparison to general populations due to their older age and smoking history. Recent evidence indicates that lung cancer screening with low dose CT scan reduces lung cancer mortality among older heavy smokers. However, the rates of false positive findings are high, requiring further testing and evaluation. Preliminary studies report that while some Veterans are enthusiastic about screening, others are highly reluctant. Patient preferences should be considered as part of an informed decision making process for this emerging paradigm of lung cancer control. Effective methods for preference assessment among Veterans have not yet been developed, evaluated, and integrated into clinical practice. The specific aims of this study are to 1) elicit patient and provider stakeholder input to inform the development of a lung cancer screening decision tool, 2) develop a web based Lung Cancer Screening Decision Tool (LCSDecTool) that incorporates patient and provider input, and 3) evaluate the impact of the LCSDecTool compared to usual care on the decision process, clinical outcomes, and quality of life.
ID
Sponsor: VA Office of Research and Development
Locations: VA Connecticut Healthcare System West Haven Campus; Corporal Michael J. Crescenz VAMC Philadelphia, Pennsylvania
Molecular Predictors of Cancer in Patients at High Risk of Lung Cancer
Using samples of blood, urine, sputum, and lung tissue from patients at high risk of cancer for laboratory studies may help doctors learn more about changes that may occur in DNA and identify biomarkers related to cancer.
ID: NCT00898313
Sponsor: Vanderbilt-Ingram Cancer Center
Location: VAMC Nashville, Tennessee
Improving Supportive Care for Patients With Thoracic Malignancies
The purpose of this study is to use a proactive approach to improve symptom management of patients with thoracic malignancies. In this pilot study, the investigators propose to evaluate the feasibility of using outbound, proactive telephone symptom assessment strategies and measure the efficacy of this approach on patient satisfaction with their care, patient activation, quality of life and use of healthcare resources.
ID: NCT03216109
Sponsor: Palo Alto Veterans Institute for Research
Location: VA Palo Alto Health Care System, California
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors or cosponsors nearly 1,000 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of August 1, 201 8 ; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Lung-MAP (multiple trials)
Lung-MAP (SWOG S1400) is a multidrug, multi-substudy, biomarker-driven squamous cell lung cancer clinical trial that uses state-of-the-art genomic profiling to match patients to substudies testing investigational treatments that may target the genomic alterations, or mutations, found to be driving the growth of their cancer.
ID: NCT02154490, NCT02595944, NCT02766335, NCT02785913, NCT02785939, NCT02926638, NCT02965378, NCT03373760, NCT03377556
Sponsor: Southwest Oncology Group
Locations: VA Connecticut Healthcare System-West Haven Campus; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Ann Arbor VAMC, Michigan; Kansas City VAMC, Missouri; VA New Jersey Health Care System, East Orange; Michael E. DeBakey VAMC Houston, Texas
ALCHEMIST: Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials (multiple trials)
A group of randomized clinical trials for patients with early-stage non-small cell lung cancer whose tumors have been completely removed by surgery.
ID: NCT02193282, NCT02194738, NCT02201992, NCT02595944
Sponsor: National Cancer Institute
Locations: Little Rock VAMC, Arkansas; VA Connecticut Healthcare System West Haven Campus; Atlanta VAMC, Decatur, Georgia; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Minneapolis VAMC, Minnesota; Saint Louis VAMC, Missouri; Veterans Affairs New York Harbor Healthcare System-Brooklyn Campus; Dayton VAMC, Ohio; William S. Middleton VAMC, Madison, Wisconsin
Veterans Affairs Lung Cancer Or Stereotactic Radiotherapy (VALOR)
The standard of care for stage I non-small cell lung cancer has historically been surgical resection in patients who are medically fit to tolerate an operation. Recent data now suggests that stereotactic radiotherapy may be a suitable alternative. This includes the results from a pooled analysis of two incomplete phase III studies that reported a 15% overall survival advantage with stereotactic radiotherapy at 3 years. While these data are promising, the median follow-up period was short, the results underpowered, and the findings were in contradiction to multiple retrospective studies that demonstrate the outcomes with surgery are likely equal or superior. Therefore, the herein trial aims to evaluate these two treatments in a prospective randomized fashion with a goal to compare the overall survival beyond 5 years. It has been designed to enroll patients who have a long life-expectancy, and are fit enough to tolerate an anatomic pulmonary resection with intraoperative lymph node sampling.
ID: NCT02984761
Sponsor: VA Office of Research and Development
Locations: Edward Hines Jr. VA Hospital, Hines, Illinois; Richard L. Roudebush VA Medical Center, Indianapolis, Indiana; Minneapolis VA Health Care System, Minnesota; Durham VAMC, North Carolina; Michael E. DeBakey VAMC, Houston, Texas; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Naloxegol in Treating Patients With Stage IIIB-IV Non-Small Cell Lung Cancer
This randomized pilot clinical trial studies the side effects and best dose of naloxegol and to see how well it works in treating patients with stage IIIB-IV non-small cell lung cancer. Naloxegol may relieve some of the side effects of opioid pain medication and fight off future growth in the cancer.
ID: NCT03087708
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Minneapolis VAMC, Minnesota; Kansas City VAMC, Missouri; VA Western New York Health Care System-Buffalo; Salisbury VAMC, North Carolina
Palliative Care Interventions for Outpatients Newly Diagnosed With Lung Cancer: Phase II (PCI2)
The focus of the study is to test a nurse-led telephone-based palliative care intervention on improving the delivery of care for patients with newly diagnosed lung cancer. The study is a three site randomized control trial to determine the efficacy of the intervention on improving patients’ quality of life, symptom burden, and satisfaction of care. Additionally, the study will test an innovative care delivery model to improve patients’ access to palliative care. The investigators will also determine the effect of the intervention on patient activation to discuss treatment preferences with their clinician and on clinician knowledge of patients’ goals of care.
ID: NCT03007953
Sponsor: VA Office of Research and Development
Locations: Birmingham VAMC, Alabama; VA Portland Health Care System, Oregon; VA Puget Sound Health Care System Seattle Division, Washington
Radiation Therapy Regimens in Treating Patients With Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide
Radiation therapy uses high-energy x-rays to kill tumor cells. Drugs used in chemotherapy, such as etoposide, carboplatin and cisplatin, work in different ways to stop the growth of tumor cells, either by killing the cells or by stopping them from dividing. It is not yet known which radiation therapy regimen is more effective when given together with chemotherapy in treating patients with limited-stage small cell lung cancer. This randomized phase III trial is comparing different chest radiation therapy regimens to see how well they work in treating patients with limited-stage small cell lung cancer.
ID: NCT00632853
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Baltimore VAMC, Maryland; Kansas City VAMC, Missouri; VA Western New York Health Care System, Buffalo, New York; Dayton VAMC, Ohio; Zablocki VAMC, Milwaukee, Wisconsin
Comparison of Different Types of Surgery in Treating Patients With Stage IA Non-Small Cell Lung Cancer
Wedge resection or segmentectomy may be less invasive types of surgery than lobectomy for non-small cell lung cancer and may have fewer side effects and improve recovery. It is not yet known whether wedge resection or segmentectomy are more effective than lobectomy in treating stage IA non-small cell lung cancer.
ID: NCT00499330
Sponsor: Alliance for Clinical Trials in Oncology
Locations: VA Loma Linda Healthcare System, California; VA Long Beach Medical Center, California; Richard L. Roudebush VAMC, Indianapolis, Indiana; Portland VAMC, Oregon
Lung Cancer Screening Decisions (VA-LCSDecTool)
Veterans have a high risk of developing lung in comparison to general populations due to their older age and smoking history. Recent evidence indicates that lung cancer screening with low dose CT scan reduces lung cancer mortality among older heavy smokers. However, the rates of false positive findings are high, requiring further testing and evaluation. Preliminary studies report that while some Veterans are enthusiastic about screening, others are highly reluctant. Patient preferences should be considered as part of an informed decision making process for this emerging paradigm of lung cancer control. Effective methods for preference assessment among Veterans have not yet been developed, evaluated, and integrated into clinical practice. The specific aims of this study are to 1) elicit patient and provider stakeholder input to inform the development of a lung cancer screening decision tool, 2) develop a web based Lung Cancer Screening Decision Tool (LCSDecTool) that incorporates patient and provider input, and 3) evaluate the impact of the LCSDecTool compared to usual care on the decision process, clinical outcomes, and quality of life.
ID
Sponsor: VA Office of Research and Development
Locations: VA Connecticut Healthcare System West Haven Campus; Corporal Michael J. Crescenz VAMC Philadelphia, Pennsylvania
Molecular Predictors of Cancer in Patients at High Risk of Lung Cancer
Using samples of blood, urine, sputum, and lung tissue from patients at high risk of cancer for laboratory studies may help doctors learn more about changes that may occur in DNA and identify biomarkers related to cancer.
ID: NCT00898313
Sponsor: Vanderbilt-Ingram Cancer Center
Location: VAMC Nashville, Tennessee
Improving Supportive Care for Patients With Thoracic Malignancies
The purpose of this study is to use a proactive approach to improve symptom management of patients with thoracic malignancies. In this pilot study, the investigators propose to evaluate the feasibility of using outbound, proactive telephone symptom assessment strategies and measure the efficacy of this approach on patient satisfaction with their care, patient activation, quality of life and use of healthcare resources.
ID: NCT03216109
Sponsor: Palo Alto Veterans Institute for Research
Location: VA Palo Alto Health Care System, California
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors or cosponsors nearly 1,000 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of August 1, 201 8 ; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Lung-MAP (multiple trials)
Lung-MAP (SWOG S1400) is a multidrug, multi-substudy, biomarker-driven squamous cell lung cancer clinical trial that uses state-of-the-art genomic profiling to match patients to substudies testing investigational treatments that may target the genomic alterations, or mutations, found to be driving the growth of their cancer.
ID: NCT02154490, NCT02595944, NCT02766335, NCT02785913, NCT02785939, NCT02926638, NCT02965378, NCT03373760, NCT03377556
Sponsor: Southwest Oncology Group
Locations: VA Connecticut Healthcare System-West Haven Campus; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Ann Arbor VAMC, Michigan; Kansas City VAMC, Missouri; VA New Jersey Health Care System, East Orange; Michael E. DeBakey VAMC Houston, Texas
ALCHEMIST: Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials (multiple trials)
A group of randomized clinical trials for patients with early-stage non-small cell lung cancer whose tumors have been completely removed by surgery.
ID: NCT02193282, NCT02194738, NCT02201992, NCT02595944
Sponsor: National Cancer Institute
Locations: Little Rock VAMC, Arkansas; VA Connecticut Healthcare System West Haven Campus; Atlanta VAMC, Decatur, Georgia; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Minneapolis VAMC, Minnesota; Saint Louis VAMC, Missouri; Veterans Affairs New York Harbor Healthcare System-Brooklyn Campus; Dayton VAMC, Ohio; William S. Middleton VAMC, Madison, Wisconsin
Veterans Affairs Lung Cancer Or Stereotactic Radiotherapy (VALOR)
The standard of care for stage I non-small cell lung cancer has historically been surgical resection in patients who are medically fit to tolerate an operation. Recent data now suggests that stereotactic radiotherapy may be a suitable alternative. This includes the results from a pooled analysis of two incomplete phase III studies that reported a 15% overall survival advantage with stereotactic radiotherapy at 3 years. While these data are promising, the median follow-up period was short, the results underpowered, and the findings were in contradiction to multiple retrospective studies that demonstrate the outcomes with surgery are likely equal or superior. Therefore, the herein trial aims to evaluate these two treatments in a prospective randomized fashion with a goal to compare the overall survival beyond 5 years. It has been designed to enroll patients who have a long life-expectancy, and are fit enough to tolerate an anatomic pulmonary resection with intraoperative lymph node sampling.
ID: NCT02984761
Sponsor: VA Office of Research and Development
Locations: Edward Hines Jr. VA Hospital, Hines, Illinois; Richard L. Roudebush VA Medical Center, Indianapolis, Indiana; Minneapolis VA Health Care System, Minnesota; Durham VAMC, North Carolina; Michael E. DeBakey VAMC, Houston, Texas; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Naloxegol in Treating Patients With Stage IIIB-IV Non-Small Cell Lung Cancer
This randomized pilot clinical trial studies the side effects and best dose of naloxegol and to see how well it works in treating patients with stage IIIB-IV non-small cell lung cancer. Naloxegol may relieve some of the side effects of opioid pain medication and fight off future growth in the cancer.
ID: NCT03087708
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Minneapolis VAMC, Minnesota; Kansas City VAMC, Missouri; VA Western New York Health Care System-Buffalo; Salisbury VAMC, North Carolina
Palliative Care Interventions for Outpatients Newly Diagnosed With Lung Cancer: Phase II (PCI2)
The focus of the study is to test a nurse-led telephone-based palliative care intervention on improving the delivery of care for patients with newly diagnosed lung cancer. The study is a three site randomized control trial to determine the efficacy of the intervention on improving patients’ quality of life, symptom burden, and satisfaction of care. Additionally, the study will test an innovative care delivery model to improve patients’ access to palliative care. The investigators will also determine the effect of the intervention on patient activation to discuss treatment preferences with their clinician and on clinician knowledge of patients’ goals of care.
ID: NCT03007953
Sponsor: VA Office of Research and Development
Locations: Birmingham VAMC, Alabama; VA Portland Health Care System, Oregon; VA Puget Sound Health Care System Seattle Division, Washington
Radiation Therapy Regimens in Treating Patients With Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide
Radiation therapy uses high-energy x-rays to kill tumor cells. Drugs used in chemotherapy, such as etoposide, carboplatin and cisplatin, work in different ways to stop the growth of tumor cells, either by killing the cells or by stopping them from dividing. It is not yet known which radiation therapy regimen is more effective when given together with chemotherapy in treating patients with limited-stage small cell lung cancer. This randomized phase III trial is comparing different chest radiation therapy regimens to see how well they work in treating patients with limited-stage small cell lung cancer.
ID: NCT00632853
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Baltimore VAMC, Maryland; Kansas City VAMC, Missouri; VA Western New York Health Care System, Buffalo, New York; Dayton VAMC, Ohio; Zablocki VAMC, Milwaukee, Wisconsin
Comparison of Different Types of Surgery in Treating Patients With Stage IA Non-Small Cell Lung Cancer
Wedge resection or segmentectomy may be less invasive types of surgery than lobectomy for non-small cell lung cancer and may have fewer side effects and improve recovery. It is not yet known whether wedge resection or segmentectomy are more effective than lobectomy in treating stage IA non-small cell lung cancer.
ID: NCT00499330
Sponsor: Alliance for Clinical Trials in Oncology
Locations: VA Loma Linda Healthcare System, California; VA Long Beach Medical Center, California; Richard L. Roudebush VAMC, Indianapolis, Indiana; Portland VAMC, Oregon
Lung Cancer Screening Decisions (VA-LCSDecTool)
Veterans have a high risk of developing lung in comparison to general populations due to their older age and smoking history. Recent evidence indicates that lung cancer screening with low dose CT scan reduces lung cancer mortality among older heavy smokers. However, the rates of false positive findings are high, requiring further testing and evaluation. Preliminary studies report that while some Veterans are enthusiastic about screening, others are highly reluctant. Patient preferences should be considered as part of an informed decision making process for this emerging paradigm of lung cancer control. Effective methods for preference assessment among Veterans have not yet been developed, evaluated, and integrated into clinical practice. The specific aims of this study are to 1) elicit patient and provider stakeholder input to inform the development of a lung cancer screening decision tool, 2) develop a web based Lung Cancer Screening Decision Tool (LCSDecTool) that incorporates patient and provider input, and 3) evaluate the impact of the LCSDecTool compared to usual care on the decision process, clinical outcomes, and quality of life.
ID
Sponsor: VA Office of Research and Development
Locations: VA Connecticut Healthcare System West Haven Campus; Corporal Michael J. Crescenz VAMC Philadelphia, Pennsylvania
Molecular Predictors of Cancer in Patients at High Risk of Lung Cancer
Using samples of blood, urine, sputum, and lung tissue from patients at high risk of cancer for laboratory studies may help doctors learn more about changes that may occur in DNA and identify biomarkers related to cancer.
ID: NCT00898313
Sponsor: Vanderbilt-Ingram Cancer Center
Location: VAMC Nashville, Tennessee
Improving Supportive Care for Patients With Thoracic Malignancies
The purpose of this study is to use a proactive approach to improve symptom management of patients with thoracic malignancies. In this pilot study, the investigators propose to evaluate the feasibility of using outbound, proactive telephone symptom assessment strategies and measure the efficacy of this approach on patient satisfaction with their care, patient activation, quality of life and use of healthcare resources.
ID: NCT03216109
Sponsor: Palo Alto Veterans Institute for Research
Location: VA Palo Alto Health Care System, California
HIV drug may enhance efficacy of chemoradiation in locally advanced lung cancer
Administering an HIV drug concurrently with chemoradiotherapy resulted in promising local control and overall survival in patients with unresectable, locally advanced non–small cell lung cancer, researchers reported.
There was no overt exacerbation of the toxic effects of chemoradiotherapy with the addition of nelfinavir, a protease inhibitor, in the prospective, open-label, phase 1/2 study, the researchers wrote.
Nelfinavir plus chemoradiotherapy yielded a median progression-free survival of 11.7 months and median survival of 41.1 months, while the cumulative local failure incidence was 39% according to their report.
Those outcomes compare favorably with historical data, the investigators wrote in JAMA Oncology.
In benchmark results of the RTOG 0617 study of chemoradiotherapy in locally advanced non–small cell lung cancer, median overall survival was 28.7 months receiving radiotherapy at a standard dose of 60 Gy, and 20.3 months for those receiving high-dose (74 Gy) radiotherapy.
However, a randomized, phase 3 trial is needed to confirm these latest results with a protease inhibitor added to chemotherapy, according to Ramesh Rengan, MD, PhD, of the University of Washington, Seattle, and coinvestigators.
“As nelfinavir is a U.S. Food and Drug Administration–approved oral drug, this treatment approach is feasible and is potentially a readily exportable platform for daily clinical use,” Dr. Rengan and coauthors wrote.
In vitro and in vivo studies have shown that nelfinavir inhibited PI3K and Akt signaling, sensitized tumor cells to ionizing radiation, and improved tumor perfusion in animal models. “We hypothesize that it is these properties that drive the clinical results observed in this study,” Dr. Rengan and coauthors wrote.
They reported on a total of 35 patients with stage IIIA/IIIB non–small cell lung cancer who received nelfinavir at either 625 mg or 1,250 mg twice daily, starting 7-14 days before starting radiotherapy to 66.6 Gy at 1.8 Gy per fraction, and throughout the full course of radiotherapy.
There were no dose-limiting toxic effects observed in the study, and toxic effects were “acceptable,” with no grade 4 nonhematologic toxic effects seen, according to investigators. Leukopenia was the primary grade 3-4 hematologic toxic effect, observed in 2 of 5 patients receiving the lower nelfinavir dose and 18 of 30 at the higher dose.
Beyond non–small cell lung cancer, the efficacy and safety nelfinavir given concurrently with radiotherapy has been looked at in other disease settings. Data from those trials suggest that this protease inhibitor could “augment tumor response” not only in non–small cell lung cancer, but in locally advanced pancreatic cancer and glioblastoma, all of which are relatively radioresistant, according to Dr. Rengan and colleagues.
Study support came from grants from the National Institutes of Health and Abramson Cancer Center, and an American Society for Radiation Oncology training award to Dr. Rengan. Study authors reported disclosures related to Pfizer, 511 Pharma, Progenics Pharmaceuticals, Siemens, Actinium, AstraZeneca, Merck, Bristol-Myers Squibb, and others.
SOURCE: Rengan R et al. JAMA Oncol. 2019 Aug 22. doi: 10.1001/jamaoncol.2019.2095.
Administering an HIV drug concurrently with chemoradiotherapy resulted in promising local control and overall survival in patients with unresectable, locally advanced non–small cell lung cancer, researchers reported.
There was no overt exacerbation of the toxic effects of chemoradiotherapy with the addition of nelfinavir, a protease inhibitor, in the prospective, open-label, phase 1/2 study, the researchers wrote.
Nelfinavir plus chemoradiotherapy yielded a median progression-free survival of 11.7 months and median survival of 41.1 months, while the cumulative local failure incidence was 39% according to their report.
Those outcomes compare favorably with historical data, the investigators wrote in JAMA Oncology.
In benchmark results of the RTOG 0617 study of chemoradiotherapy in locally advanced non–small cell lung cancer, median overall survival was 28.7 months receiving radiotherapy at a standard dose of 60 Gy, and 20.3 months for those receiving high-dose (74 Gy) radiotherapy.
However, a randomized, phase 3 trial is needed to confirm these latest results with a protease inhibitor added to chemotherapy, according to Ramesh Rengan, MD, PhD, of the University of Washington, Seattle, and coinvestigators.
“As nelfinavir is a U.S. Food and Drug Administration–approved oral drug, this treatment approach is feasible and is potentially a readily exportable platform for daily clinical use,” Dr. Rengan and coauthors wrote.
In vitro and in vivo studies have shown that nelfinavir inhibited PI3K and Akt signaling, sensitized tumor cells to ionizing radiation, and improved tumor perfusion in animal models. “We hypothesize that it is these properties that drive the clinical results observed in this study,” Dr. Rengan and coauthors wrote.
They reported on a total of 35 patients with stage IIIA/IIIB non–small cell lung cancer who received nelfinavir at either 625 mg or 1,250 mg twice daily, starting 7-14 days before starting radiotherapy to 66.6 Gy at 1.8 Gy per fraction, and throughout the full course of radiotherapy.
There were no dose-limiting toxic effects observed in the study, and toxic effects were “acceptable,” with no grade 4 nonhematologic toxic effects seen, according to investigators. Leukopenia was the primary grade 3-4 hematologic toxic effect, observed in 2 of 5 patients receiving the lower nelfinavir dose and 18 of 30 at the higher dose.
Beyond non–small cell lung cancer, the efficacy and safety nelfinavir given concurrently with radiotherapy has been looked at in other disease settings. Data from those trials suggest that this protease inhibitor could “augment tumor response” not only in non–small cell lung cancer, but in locally advanced pancreatic cancer and glioblastoma, all of which are relatively radioresistant, according to Dr. Rengan and colleagues.
Study support came from grants from the National Institutes of Health and Abramson Cancer Center, and an American Society for Radiation Oncology training award to Dr. Rengan. Study authors reported disclosures related to Pfizer, 511 Pharma, Progenics Pharmaceuticals, Siemens, Actinium, AstraZeneca, Merck, Bristol-Myers Squibb, and others.
SOURCE: Rengan R et al. JAMA Oncol. 2019 Aug 22. doi: 10.1001/jamaoncol.2019.2095.
Administering an HIV drug concurrently with chemoradiotherapy resulted in promising local control and overall survival in patients with unresectable, locally advanced non–small cell lung cancer, researchers reported.
There was no overt exacerbation of the toxic effects of chemoradiotherapy with the addition of nelfinavir, a protease inhibitor, in the prospective, open-label, phase 1/2 study, the researchers wrote.
Nelfinavir plus chemoradiotherapy yielded a median progression-free survival of 11.7 months and median survival of 41.1 months, while the cumulative local failure incidence was 39% according to their report.
Those outcomes compare favorably with historical data, the investigators wrote in JAMA Oncology.
In benchmark results of the RTOG 0617 study of chemoradiotherapy in locally advanced non–small cell lung cancer, median overall survival was 28.7 months receiving radiotherapy at a standard dose of 60 Gy, and 20.3 months for those receiving high-dose (74 Gy) radiotherapy.
However, a randomized, phase 3 trial is needed to confirm these latest results with a protease inhibitor added to chemotherapy, according to Ramesh Rengan, MD, PhD, of the University of Washington, Seattle, and coinvestigators.
“As nelfinavir is a U.S. Food and Drug Administration–approved oral drug, this treatment approach is feasible and is potentially a readily exportable platform for daily clinical use,” Dr. Rengan and coauthors wrote.
In vitro and in vivo studies have shown that nelfinavir inhibited PI3K and Akt signaling, sensitized tumor cells to ionizing radiation, and improved tumor perfusion in animal models. “We hypothesize that it is these properties that drive the clinical results observed in this study,” Dr. Rengan and coauthors wrote.
They reported on a total of 35 patients with stage IIIA/IIIB non–small cell lung cancer who received nelfinavir at either 625 mg or 1,250 mg twice daily, starting 7-14 days before starting radiotherapy to 66.6 Gy at 1.8 Gy per fraction, and throughout the full course of radiotherapy.
There were no dose-limiting toxic effects observed in the study, and toxic effects were “acceptable,” with no grade 4 nonhematologic toxic effects seen, according to investigators. Leukopenia was the primary grade 3-4 hematologic toxic effect, observed in 2 of 5 patients receiving the lower nelfinavir dose and 18 of 30 at the higher dose.
Beyond non–small cell lung cancer, the efficacy and safety nelfinavir given concurrently with radiotherapy has been looked at in other disease settings. Data from those trials suggest that this protease inhibitor could “augment tumor response” not only in non–small cell lung cancer, but in locally advanced pancreatic cancer and glioblastoma, all of which are relatively radioresistant, according to Dr. Rengan and colleagues.
Study support came from grants from the National Institutes of Health and Abramson Cancer Center, and an American Society for Radiation Oncology training award to Dr. Rengan. Study authors reported disclosures related to Pfizer, 511 Pharma, Progenics Pharmaceuticals, Siemens, Actinium, AstraZeneca, Merck, Bristol-Myers Squibb, and others.
SOURCE: Rengan R et al. JAMA Oncol. 2019 Aug 22. doi: 10.1001/jamaoncol.2019.2095.
FROM JAMA ONCOLOGY
Molecular profiling a must in advanced NSCLC
All patients with locally advanced or metastatic non–small cell lung cancer (NSCLC) should undergo molecular testing for targetable mutations and for tumor expression of the programmed death–ligand 1 (PD-L1) protein, authors of a review of systemic therapies for NSCLC recommend.
Their opinion is based on evidence showing that 5-year overall survival rate for patients whose tumors have high levels of PD-L1 expression now exceeds 25%, and that patients with ALK-positive tumors have 5-year overall survival rates over 40%. In contrast, 5-year survival rates for patients with metastatic NSCLC prior to the 21st century were less than 5%, according to Kathryn C. Arbour, MD, and Gregory J. Riely, MD, PhD, from Memorial Sloan Kettering Cancer Center in New York.
“Improved understanding of the biology and molecular subtypes of non–small cell lung cancer have led to more biomarker-directed therapies for patients with metastatic disease. These biomarker-directed therapies and newer empirical treatment regimens have improved overall survival for patients with metastatic non–small cell lung cancer,” they wrote in JAMA.
The authors reviewed published studies of clinical trials of medical therapies for NSCLC, including articles on randomized trials, nonrandomized trials leading to practice changes or regulatory approval of new therapies for patients with locally advanced or metastatic NSCLC, and clinical practice guidelines.
Their review showed that approximately 30% of patients with NSCLC have molecular alterations predictive of response to treatment, such as mutations in EGFR, the gene encoding for epidermal growth factor receptor; rearrangements in the ALK (anaplastic lymphoma kinase) and ROS1 genes; and mutations in BRAF V600E.
Patients with somatic activating mutations in EGFR, which occur in approximately 20% of those with advanced NSCLC, have better progression-free survival when treated with an EGFR-target tyrosine kinase inhibitor such as gefitinib (Iressa), erlotinib (Tarceva), or afatinib (Gilotrif), compared with cytotoxic chemotherapy.
Similarly, they noted, patients with ALK rearrangements leading to overexpression of the ALK protein had better overall response rates and progression-free survival when treated with the ALK inhibitor crizotinib (Xalkori), compared with patients with ALK rearrangements treated with pemetrexed and a platinum agent.
For some patients without targetable mutations, immune checkpoint inhibitors either alone or in combination with chemotherapy have resulted in improvements in overall survival.
“These advances are substantial, but long-term durable responses remain uncommon for most patients. These insights into treating metastatic disease have informed the design of trials for new treatment strategies among patients with early-stage disease. The goal of NSCLC research is to understand and address mechanisms of resistant and refractory disease in patients with advanced disease and, ultimately, to increase cure rates,” the reviewers wrote.
The review was supported in part by a grant from the National Cancer Institute to Memorial Sloan Kettering. Dr. Arbour reported serving as a consultant to AstraZeneca and nonfinancial research support from Novartis and Takeda. Dr. Riely reported grants and nonfinancial support from Pfizer, Roche/Genentech/Chugai, Novartis, Merck, and Takeda; a patent pending for an alternate dosing of erlotinib for which he has no right to royalties; and payments from the National Comprehensive Cancer Network to participate in a committee overseeing solicitation and selection of grants to be awarded by AstraZeneca.
SOURCE: Arbour KC and Riely GJ. JAMA. 2019;322(8):764-74.
All patients with locally advanced or metastatic non–small cell lung cancer (NSCLC) should undergo molecular testing for targetable mutations and for tumor expression of the programmed death–ligand 1 (PD-L1) protein, authors of a review of systemic therapies for NSCLC recommend.
Their opinion is based on evidence showing that 5-year overall survival rate for patients whose tumors have high levels of PD-L1 expression now exceeds 25%, and that patients with ALK-positive tumors have 5-year overall survival rates over 40%. In contrast, 5-year survival rates for patients with metastatic NSCLC prior to the 21st century were less than 5%, according to Kathryn C. Arbour, MD, and Gregory J. Riely, MD, PhD, from Memorial Sloan Kettering Cancer Center in New York.
“Improved understanding of the biology and molecular subtypes of non–small cell lung cancer have led to more biomarker-directed therapies for patients with metastatic disease. These biomarker-directed therapies and newer empirical treatment regimens have improved overall survival for patients with metastatic non–small cell lung cancer,” they wrote in JAMA.
The authors reviewed published studies of clinical trials of medical therapies for NSCLC, including articles on randomized trials, nonrandomized trials leading to practice changes or regulatory approval of new therapies for patients with locally advanced or metastatic NSCLC, and clinical practice guidelines.
Their review showed that approximately 30% of patients with NSCLC have molecular alterations predictive of response to treatment, such as mutations in EGFR, the gene encoding for epidermal growth factor receptor; rearrangements in the ALK (anaplastic lymphoma kinase) and ROS1 genes; and mutations in BRAF V600E.
Patients with somatic activating mutations in EGFR, which occur in approximately 20% of those with advanced NSCLC, have better progression-free survival when treated with an EGFR-target tyrosine kinase inhibitor such as gefitinib (Iressa), erlotinib (Tarceva), or afatinib (Gilotrif), compared with cytotoxic chemotherapy.
Similarly, they noted, patients with ALK rearrangements leading to overexpression of the ALK protein had better overall response rates and progression-free survival when treated with the ALK inhibitor crizotinib (Xalkori), compared with patients with ALK rearrangements treated with pemetrexed and a platinum agent.
For some patients without targetable mutations, immune checkpoint inhibitors either alone or in combination with chemotherapy have resulted in improvements in overall survival.
“These advances are substantial, but long-term durable responses remain uncommon for most patients. These insights into treating metastatic disease have informed the design of trials for new treatment strategies among patients with early-stage disease. The goal of NSCLC research is to understand and address mechanisms of resistant and refractory disease in patients with advanced disease and, ultimately, to increase cure rates,” the reviewers wrote.
The review was supported in part by a grant from the National Cancer Institute to Memorial Sloan Kettering. Dr. Arbour reported serving as a consultant to AstraZeneca and nonfinancial research support from Novartis and Takeda. Dr. Riely reported grants and nonfinancial support from Pfizer, Roche/Genentech/Chugai, Novartis, Merck, and Takeda; a patent pending for an alternate dosing of erlotinib for which he has no right to royalties; and payments from the National Comprehensive Cancer Network to participate in a committee overseeing solicitation and selection of grants to be awarded by AstraZeneca.
SOURCE: Arbour KC and Riely GJ. JAMA. 2019;322(8):764-74.
All patients with locally advanced or metastatic non–small cell lung cancer (NSCLC) should undergo molecular testing for targetable mutations and for tumor expression of the programmed death–ligand 1 (PD-L1) protein, authors of a review of systemic therapies for NSCLC recommend.
Their opinion is based on evidence showing that 5-year overall survival rate for patients whose tumors have high levels of PD-L1 expression now exceeds 25%, and that patients with ALK-positive tumors have 5-year overall survival rates over 40%. In contrast, 5-year survival rates for patients with metastatic NSCLC prior to the 21st century were less than 5%, according to Kathryn C. Arbour, MD, and Gregory J. Riely, MD, PhD, from Memorial Sloan Kettering Cancer Center in New York.
“Improved understanding of the biology and molecular subtypes of non–small cell lung cancer have led to more biomarker-directed therapies for patients with metastatic disease. These biomarker-directed therapies and newer empirical treatment regimens have improved overall survival for patients with metastatic non–small cell lung cancer,” they wrote in JAMA.
The authors reviewed published studies of clinical trials of medical therapies for NSCLC, including articles on randomized trials, nonrandomized trials leading to practice changes or regulatory approval of new therapies for patients with locally advanced or metastatic NSCLC, and clinical practice guidelines.
Their review showed that approximately 30% of patients with NSCLC have molecular alterations predictive of response to treatment, such as mutations in EGFR, the gene encoding for epidermal growth factor receptor; rearrangements in the ALK (anaplastic lymphoma kinase) and ROS1 genes; and mutations in BRAF V600E.
Patients with somatic activating mutations in EGFR, which occur in approximately 20% of those with advanced NSCLC, have better progression-free survival when treated with an EGFR-target tyrosine kinase inhibitor such as gefitinib (Iressa), erlotinib (Tarceva), or afatinib (Gilotrif), compared with cytotoxic chemotherapy.
Similarly, they noted, patients with ALK rearrangements leading to overexpression of the ALK protein had better overall response rates and progression-free survival when treated with the ALK inhibitor crizotinib (Xalkori), compared with patients with ALK rearrangements treated with pemetrexed and a platinum agent.
For some patients without targetable mutations, immune checkpoint inhibitors either alone or in combination with chemotherapy have resulted in improvements in overall survival.
“These advances are substantial, but long-term durable responses remain uncommon for most patients. These insights into treating metastatic disease have informed the design of trials for new treatment strategies among patients with early-stage disease. The goal of NSCLC research is to understand and address mechanisms of resistant and refractory disease in patients with advanced disease and, ultimately, to increase cure rates,” the reviewers wrote.
The review was supported in part by a grant from the National Cancer Institute to Memorial Sloan Kettering. Dr. Arbour reported serving as a consultant to AstraZeneca and nonfinancial research support from Novartis and Takeda. Dr. Riely reported grants and nonfinancial support from Pfizer, Roche/Genentech/Chugai, Novartis, Merck, and Takeda; a patent pending for an alternate dosing of erlotinib for which he has no right to royalties; and payments from the National Comprehensive Cancer Network to participate in a committee overseeing solicitation and selection of grants to be awarded by AstraZeneca.
SOURCE: Arbour KC and Riely GJ. JAMA. 2019;322(8):764-74.
FROM JAMA
Nivolumab yields long-term survival benefit in advanced NSCLC
The use of nivolumab is associated with a long-term survival benefit, compared with docetaxel in patients with previously treated advanced non–small cell lung cancer (NSCLC), according to a pooled analysis of four trials.
The survival outcomes comparing the two therapies demonstrates an extended survival advantage for nivolumab up to and past a duration of 4 years.
“We aimed to evaluate the long-term benefit of nivolumab and the effect of response and disease control on subsequent survival,” wrote Scott J. Antonia, MD, PhD, formally of the H. Lee Moffitt Cancer Center in Tampa and now at Duke Cancer Center, Durham, N.C., and colleagues. The findings were published in the Lancet Oncology.
The researchers combined data from four clinical studies (CheckMate 003, 017, 057, and 063) that assessed survival outcomes in patients receiving second-line or later nivolumab therapy. Across the four trials, a total of 664 patients were administered nivolumab.
The CheckMate 057 and 017 phase 3, randomized clinical trials compared docetaxel versus nivolumab in patients with previously treated nonsquamous and squamous NSCLC, respectively.
With respect to safety analyses, Dr. Antonia and colleagues included patients who were administered a minimum of one dose of nivolumab.
Across the four trials, the 4-year overall survival with nivolumab was 14% (11%-17%), including 11% (7%-16%) for patients with under 1% programmed death–ligand 1 expression, and 19% (15%-24%) for patients with a minimum of 1% programmed death–ligand 1 expression.
In CheckMate 057 and 017, the 4-year overall survival with nivolumab was 14% (11%-18%) versus 5% (3%-7%) in patients who received docetaxel.
With respect to safety, analysis of the long-term data did not reveal any novel safety signals.
The researchers acknowledged that a key limitation of the study was the exclusion of patients who were maintained in stable disease or in response at the point of data lock.
As a result, the findings likely minimize the survival advantage seen post–disease progression for nivolumab, compared with docetaxel.
“Additional analyses assessing the effect of various factors on long-term survival with immunotherapy versus chemotherapy are planned,” they wrote.
The study was funded by Bristol-Myers Squibb. The authors reported financial affiliations with AstraZeneca, Boehringer Ingelheim, Cellular Biomedicine Group, FLX Bio, Genentech, Novartis, Regeneron, and several others.
SOURCE: Antonia SJ et al. Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045(19)30407-3.
Recent advances in the treatment of metastatic non–small cell lung cancer are largely attributable to the arrival of checkpoint inhibitor therapy. As the body of evidence continues to grow, the long-term survival advantages seen with these agents are becoming increasingly apparent.
The findings of a combined analysis of four trials evaluating second-line nivolumab in patients with non–small cell lung cancer were recently reported. In comparison with historical data, which estimated 5-year overall survival rates to be less than 5%, the 4-year overall survival of 14% found by Dr. Antonia and colleagues is significant. The results suggest a plateau in overall survival of approximately 15% for patients in this setting.
With respect to safety, recent findings confirm that patients maintained on checkpoint inhibitor therapy should be closely monitored for the complete duration of exposure. In contrast to chemotherapy, there has been no evidence suggesting cumulative toxicity is related to immunotherapy treatment.
One question that remains from the current study is the ideal duration of checkpoint inhibitor therapy for patients who achieve an objective response. In addition, whether therapy should be maintained until adverse events or disease progression are seen also remains unclear. Various trials are presently ongoing in an attempt to help answer these remaining questions.
Pierre-Jean Souquet, MD, is affiliated with the University Hospital of Lyon (France). Sébastien Couraud, MD, PhD, is affiliated with the Université de Lyon (France). The authors reported financial affiliations with AstraZeneca, Bristol-Myers Squibb, Dohme, Merck, and Roche. These comments are adapted from their editorial (Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045(19)30508-X ).
Recent advances in the treatment of metastatic non–small cell lung cancer are largely attributable to the arrival of checkpoint inhibitor therapy. As the body of evidence continues to grow, the long-term survival advantages seen with these agents are becoming increasingly apparent.
The findings of a combined analysis of four trials evaluating second-line nivolumab in patients with non–small cell lung cancer were recently reported. In comparison with historical data, which estimated 5-year overall survival rates to be less than 5%, the 4-year overall survival of 14% found by Dr. Antonia and colleagues is significant. The results suggest a plateau in overall survival of approximately 15% for patients in this setting.
With respect to safety, recent findings confirm that patients maintained on checkpoint inhibitor therapy should be closely monitored for the complete duration of exposure. In contrast to chemotherapy, there has been no evidence suggesting cumulative toxicity is related to immunotherapy treatment.
One question that remains from the current study is the ideal duration of checkpoint inhibitor therapy for patients who achieve an objective response. In addition, whether therapy should be maintained until adverse events or disease progression are seen also remains unclear. Various trials are presently ongoing in an attempt to help answer these remaining questions.
Pierre-Jean Souquet, MD, is affiliated with the University Hospital of Lyon (France). Sébastien Couraud, MD, PhD, is affiliated with the Université de Lyon (France). The authors reported financial affiliations with AstraZeneca, Bristol-Myers Squibb, Dohme, Merck, and Roche. These comments are adapted from their editorial (Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045(19)30508-X ).
Recent advances in the treatment of metastatic non–small cell lung cancer are largely attributable to the arrival of checkpoint inhibitor therapy. As the body of evidence continues to grow, the long-term survival advantages seen with these agents are becoming increasingly apparent.
The findings of a combined analysis of four trials evaluating second-line nivolumab in patients with non–small cell lung cancer were recently reported. In comparison with historical data, which estimated 5-year overall survival rates to be less than 5%, the 4-year overall survival of 14% found by Dr. Antonia and colleagues is significant. The results suggest a plateau in overall survival of approximately 15% for patients in this setting.
With respect to safety, recent findings confirm that patients maintained on checkpoint inhibitor therapy should be closely monitored for the complete duration of exposure. In contrast to chemotherapy, there has been no evidence suggesting cumulative toxicity is related to immunotherapy treatment.
One question that remains from the current study is the ideal duration of checkpoint inhibitor therapy for patients who achieve an objective response. In addition, whether therapy should be maintained until adverse events or disease progression are seen also remains unclear. Various trials are presently ongoing in an attempt to help answer these remaining questions.
Pierre-Jean Souquet, MD, is affiliated with the University Hospital of Lyon (France). Sébastien Couraud, MD, PhD, is affiliated with the Université de Lyon (France). The authors reported financial affiliations with AstraZeneca, Bristol-Myers Squibb, Dohme, Merck, and Roche. These comments are adapted from their editorial (Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045(19)30508-X ).
The use of nivolumab is associated with a long-term survival benefit, compared with docetaxel in patients with previously treated advanced non–small cell lung cancer (NSCLC), according to a pooled analysis of four trials.
The survival outcomes comparing the two therapies demonstrates an extended survival advantage for nivolumab up to and past a duration of 4 years.
“We aimed to evaluate the long-term benefit of nivolumab and the effect of response and disease control on subsequent survival,” wrote Scott J. Antonia, MD, PhD, formally of the H. Lee Moffitt Cancer Center in Tampa and now at Duke Cancer Center, Durham, N.C., and colleagues. The findings were published in the Lancet Oncology.
The researchers combined data from four clinical studies (CheckMate 003, 017, 057, and 063) that assessed survival outcomes in patients receiving second-line or later nivolumab therapy. Across the four trials, a total of 664 patients were administered nivolumab.
The CheckMate 057 and 017 phase 3, randomized clinical trials compared docetaxel versus nivolumab in patients with previously treated nonsquamous and squamous NSCLC, respectively.
With respect to safety analyses, Dr. Antonia and colleagues included patients who were administered a minimum of one dose of nivolumab.
Across the four trials, the 4-year overall survival with nivolumab was 14% (11%-17%), including 11% (7%-16%) for patients with under 1% programmed death–ligand 1 expression, and 19% (15%-24%) for patients with a minimum of 1% programmed death–ligand 1 expression.
In CheckMate 057 and 017, the 4-year overall survival with nivolumab was 14% (11%-18%) versus 5% (3%-7%) in patients who received docetaxel.
With respect to safety, analysis of the long-term data did not reveal any novel safety signals.
The researchers acknowledged that a key limitation of the study was the exclusion of patients who were maintained in stable disease or in response at the point of data lock.
As a result, the findings likely minimize the survival advantage seen post–disease progression for nivolumab, compared with docetaxel.
“Additional analyses assessing the effect of various factors on long-term survival with immunotherapy versus chemotherapy are planned,” they wrote.
The study was funded by Bristol-Myers Squibb. The authors reported financial affiliations with AstraZeneca, Boehringer Ingelheim, Cellular Biomedicine Group, FLX Bio, Genentech, Novartis, Regeneron, and several others.
SOURCE: Antonia SJ et al. Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045(19)30407-3.
The use of nivolumab is associated with a long-term survival benefit, compared with docetaxel in patients with previously treated advanced non–small cell lung cancer (NSCLC), according to a pooled analysis of four trials.
The survival outcomes comparing the two therapies demonstrates an extended survival advantage for nivolumab up to and past a duration of 4 years.
“We aimed to evaluate the long-term benefit of nivolumab and the effect of response and disease control on subsequent survival,” wrote Scott J. Antonia, MD, PhD, formally of the H. Lee Moffitt Cancer Center in Tampa and now at Duke Cancer Center, Durham, N.C., and colleagues. The findings were published in the Lancet Oncology.
The researchers combined data from four clinical studies (CheckMate 003, 017, 057, and 063) that assessed survival outcomes in patients receiving second-line or later nivolumab therapy. Across the four trials, a total of 664 patients were administered nivolumab.
The CheckMate 057 and 017 phase 3, randomized clinical trials compared docetaxel versus nivolumab in patients with previously treated nonsquamous and squamous NSCLC, respectively.
With respect to safety analyses, Dr. Antonia and colleagues included patients who were administered a minimum of one dose of nivolumab.
Across the four trials, the 4-year overall survival with nivolumab was 14% (11%-17%), including 11% (7%-16%) for patients with under 1% programmed death–ligand 1 expression, and 19% (15%-24%) for patients with a minimum of 1% programmed death–ligand 1 expression.
In CheckMate 057 and 017, the 4-year overall survival with nivolumab was 14% (11%-18%) versus 5% (3%-7%) in patients who received docetaxel.
With respect to safety, analysis of the long-term data did not reveal any novel safety signals.
The researchers acknowledged that a key limitation of the study was the exclusion of patients who were maintained in stable disease or in response at the point of data lock.
As a result, the findings likely minimize the survival advantage seen post–disease progression for nivolumab, compared with docetaxel.
“Additional analyses assessing the effect of various factors on long-term survival with immunotherapy versus chemotherapy are planned,” they wrote.
The study was funded by Bristol-Myers Squibb. The authors reported financial affiliations with AstraZeneca, Boehringer Ingelheim, Cellular Biomedicine Group, FLX Bio, Genentech, Novartis, Regeneron, and several others.
SOURCE: Antonia SJ et al. Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045(19)30407-3.
FROM THE LANCET ONCOLOGY
Local treatment boosts survival for some with oligometastatic lung cancer
Adding local treatment to systemic therapy may extend survival among certain patients with oligometastatic non–small cell lung cancer (NSCLC), according to a retrospective look at more than 34,000 patients.
Surgical resection provided the greatest survival benefit, followed by external beam radiotherapy or thermal ablation (EBRT/TA), reported lead author Johannes Uhlig, MD, of University Medical Center Göttingen (Germany) and colleagues.
NSCLC patients with five or fewer metastatic sites (oligometastatic disease) are thought to achieve better outcomes than patients with more widely disseminated disease, the investigators noted in JAMA Network Open, but the benefit of local therapy for this population is unclear.
“A recent randomized, prospective study of 74 patients with oligometastatic NSCLC identified superior progression-free survival with local control after hypofractionated radiotherapy or surgical resection and radiotherapy compared with systemic therapy alone, suggesting an important application of local treatment options for patients with metastatic disease,” the investigators wrote.
To build on these findings, the investigators retrospectively evaluated 34,887 patients with stage IV NSCLC who had up to one distant metastatic lesion in the liver, lung, brain, or bone, as documented in the National Cancer Database. Treatment groups were divided into patients who received systemic therapy alone, surgical resection plus systemic therapy, or EBRT/TA plus systemic therapy. Multivariable Cox proportional hazards models were used to compare overall survival among the three groups.
Including a median follow-up of 39.4 months, data analysis showed that patients who underwent surgery and systemic therapy fared the best. Adding surgery reduced mortality risk by 38% and 41%, compared with EBRT/TA plus systemic therapy and systemic therapy alone, respectively (P less than .001 for both). Compared with systemic therapy alone, adding EBRT/TA reduced mortality risk by 5% (P = .002).
The impact of EBRT/TA varied among subgroups. For those with squamous cell carcinoma who had limited nodal disease, adding EBRT/TA resulted in a clear benefit, reducing mortality risk by 32% (P less than .001). Compared with systemic therapy alone, this benefit translated to higher survival rates for up to 3 years. Conversely, adding EBRT/TA increased risk of death by 39% among patients with extended local and distant adenocarcinoma (P less than .001). In this subgroup, survival rates over the next 3 years were higher among patients treated with systemic therapy alone.
“The present study supports a combined approach of local therapy in addition to systemic treatment for select patients with oligometastatic NSCLC,” the investigators concluded.
The study was funded by the U.S. Department of Defense. The investigators disclosed additional relationships with Bayer, AstraZeneca, Bristol-Myers Squibb, and others.
SOURCE: Uhlig et al. JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702.
Adding local treatment to systemic therapy may extend survival among certain patients with oligometastatic non–small cell lung cancer (NSCLC), according to a retrospective look at more than 34,000 patients.
Surgical resection provided the greatest survival benefit, followed by external beam radiotherapy or thermal ablation (EBRT/TA), reported lead author Johannes Uhlig, MD, of University Medical Center Göttingen (Germany) and colleagues.
NSCLC patients with five or fewer metastatic sites (oligometastatic disease) are thought to achieve better outcomes than patients with more widely disseminated disease, the investigators noted in JAMA Network Open, but the benefit of local therapy for this population is unclear.
“A recent randomized, prospective study of 74 patients with oligometastatic NSCLC identified superior progression-free survival with local control after hypofractionated radiotherapy or surgical resection and radiotherapy compared with systemic therapy alone, suggesting an important application of local treatment options for patients with metastatic disease,” the investigators wrote.
To build on these findings, the investigators retrospectively evaluated 34,887 patients with stage IV NSCLC who had up to one distant metastatic lesion in the liver, lung, brain, or bone, as documented in the National Cancer Database. Treatment groups were divided into patients who received systemic therapy alone, surgical resection plus systemic therapy, or EBRT/TA plus systemic therapy. Multivariable Cox proportional hazards models were used to compare overall survival among the three groups.
Including a median follow-up of 39.4 months, data analysis showed that patients who underwent surgery and systemic therapy fared the best. Adding surgery reduced mortality risk by 38% and 41%, compared with EBRT/TA plus systemic therapy and systemic therapy alone, respectively (P less than .001 for both). Compared with systemic therapy alone, adding EBRT/TA reduced mortality risk by 5% (P = .002).
The impact of EBRT/TA varied among subgroups. For those with squamous cell carcinoma who had limited nodal disease, adding EBRT/TA resulted in a clear benefit, reducing mortality risk by 32% (P less than .001). Compared with systemic therapy alone, this benefit translated to higher survival rates for up to 3 years. Conversely, adding EBRT/TA increased risk of death by 39% among patients with extended local and distant adenocarcinoma (P less than .001). In this subgroup, survival rates over the next 3 years were higher among patients treated with systemic therapy alone.
“The present study supports a combined approach of local therapy in addition to systemic treatment for select patients with oligometastatic NSCLC,” the investigators concluded.
The study was funded by the U.S. Department of Defense. The investigators disclosed additional relationships with Bayer, AstraZeneca, Bristol-Myers Squibb, and others.
SOURCE: Uhlig et al. JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702.
Adding local treatment to systemic therapy may extend survival among certain patients with oligometastatic non–small cell lung cancer (NSCLC), according to a retrospective look at more than 34,000 patients.
Surgical resection provided the greatest survival benefit, followed by external beam radiotherapy or thermal ablation (EBRT/TA), reported lead author Johannes Uhlig, MD, of University Medical Center Göttingen (Germany) and colleagues.
NSCLC patients with five or fewer metastatic sites (oligometastatic disease) are thought to achieve better outcomes than patients with more widely disseminated disease, the investigators noted in JAMA Network Open, but the benefit of local therapy for this population is unclear.
“A recent randomized, prospective study of 74 patients with oligometastatic NSCLC identified superior progression-free survival with local control after hypofractionated radiotherapy or surgical resection and radiotherapy compared with systemic therapy alone, suggesting an important application of local treatment options for patients with metastatic disease,” the investigators wrote.
To build on these findings, the investigators retrospectively evaluated 34,887 patients with stage IV NSCLC who had up to one distant metastatic lesion in the liver, lung, brain, or bone, as documented in the National Cancer Database. Treatment groups were divided into patients who received systemic therapy alone, surgical resection plus systemic therapy, or EBRT/TA plus systemic therapy. Multivariable Cox proportional hazards models were used to compare overall survival among the three groups.
Including a median follow-up of 39.4 months, data analysis showed that patients who underwent surgery and systemic therapy fared the best. Adding surgery reduced mortality risk by 38% and 41%, compared with EBRT/TA plus systemic therapy and systemic therapy alone, respectively (P less than .001 for both). Compared with systemic therapy alone, adding EBRT/TA reduced mortality risk by 5% (P = .002).
The impact of EBRT/TA varied among subgroups. For those with squamous cell carcinoma who had limited nodal disease, adding EBRT/TA resulted in a clear benefit, reducing mortality risk by 32% (P less than .001). Compared with systemic therapy alone, this benefit translated to higher survival rates for up to 3 years. Conversely, adding EBRT/TA increased risk of death by 39% among patients with extended local and distant adenocarcinoma (P less than .001). In this subgroup, survival rates over the next 3 years were higher among patients treated with systemic therapy alone.
“The present study supports a combined approach of local therapy in addition to systemic treatment for select patients with oligometastatic NSCLC,” the investigators concluded.
The study was funded by the U.S. Department of Defense. The investigators disclosed additional relationships with Bayer, AstraZeneca, Bristol-Myers Squibb, and others.
SOURCE: Uhlig et al. JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702.
FROM JAMA NETWORK OPEN
Key clinical point: Adding local treatment to systemic therapy may extend survival among certain patients with oligometastatic non–small cell lung cancer (NSCLC).
Major finding: Patients treated with a combination of surgical resection and systemic therapy had better overall survival than patients treated with systemic therapy alone (hazard ratio, 0.59).
Study details: A retrospective analysis of 34,887 patients with stage IV NSCLC.
Disclosures: The study was funded by the U.S. Department of Defense. The investigators disclosed additional relationships with Bayer, AstraZeneca, Bristol-Myers Squibb, and others.
Source: Uhlig J et al. JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702.
Adding chemo beats standard gefitinib for EGFR-mutated lung cancer
For patients with EGFR-mutated, advanced non–small cell lung cancer (NSCLC), adding pemetrexed and carboplatin to standard gefitinib therapy markedly extends progression free survival, but at the cost of twice as many serious toxicities, in a recent phase 3 trial.
Two previous phase 2 trials (J Clin Oncol. 2016 Sep 20;34[27]:3258-66 and Ann Oncol. 2015 Feb 10;26[5]:888-94) suggested that adding chemotherapy could improve outcomes over gefitinib alone, but this is the first study to clearly demonstrate better overall survival, reported lead author Vanita Noronha, MD, of Tata Memorial Hospital in Mumbai, India, and colleagues. They noted that this is the second regimen to demonstrate better overall survival than standard gefitinib for EGFR-mutated lung cancer, with dacomitinib being the first, as shown by the ARCHER 1050 trial.
The present study involved 350 patients with advanced, EGFR-mutated NSCLC who had an Eastern Cooperative Oncology (ECOG) performance status of 0-2 and were candidates for first-line palliative therapy. Approximately one-fifth of patients (21%) had a performance status of 2, and almost as many (18%) had brain metastases. After stratification for performance status and mutation type, patients were randomized in a 1:1 ratio to receive either gefitinib monotherapy (250 mg once daily) or gefitinib plus a chemotherapy combination of pemetrexed (500 mg/m2) and carboplatin (area under the curve of 5 with Calvert formula) on day 1 of four 21-day cycles. Subsequently, nonprogressing patients in the chemotherapy group received maintenance therapy with pemetrexed at the same dose and frequency. Treatment was continued until progression, toxicity, or withdrawal of consent. The primary endpoint was progression-free survival (PFS). Secondary outcomes included overall survival (OS), response rate, quality of life, and toxicity.
After a median follow-up of 17 months, the investigators found that adding chemotherapy to gefitinib resulted in a clear benefit, with estimated median PFS increasing from 8 months to 16 months (P less than .001). Estimated median overall survival also increased, with a figure not reached in the chemotherapy/gefitinib group, compared with 17 months among those who received gefitinib alone. Response rates echoed these findings, with more patients in the chemotherapy/gefitinib group achieving complete (2.9% vs. 0.6%) and partial remission (72.4% vs. 61.9%).
“[T]he PFS attained in our study is noteworthy, considering that 21% of our study patients had a [performance status] of 2, whereas the FLAURA study, [which demonstrated a PFS of 18.9 months with osimertinib], only included patients with a [performance status] of 1 or lower,” the investigators wrote. Their report is in Journal of Clinical Oncology.
Still, introducing chemotherapy was not without negative consequences. Compared with the gefitinib monotherapy group, patients who also received chemotherapy more often had grade 3 or higher adverse events (75% vs. 49.4%), and twice as many had clinically significant, serious toxicities (50.6% vs. 25.3%). The additional toxicities were predominantly due to myelosuppression and nephrotoxicity.
Despite these drawbacks, the investigators concluded that combination therapy was superior to gefitinib alone. “The combination of gefitinib, pemetrexed, and carboplatin represents a new standard first-line therapy for EGFR-mutant NSCLC,” the investigators concluded.
The study was funded by Tata Memorial Center Research Administration Council, Fresenius Kabi India, Lung Cancer Consortium India, and others. The investigators reported relationships with Roche, Biocon, Amgen, and others.
SOURCE: Noronha et al. Journal of Clinical Oncology. 2019 Aug 14. doi: 10.1200/JCO.19.01154.
For patients with EGFR-mutated, advanced non–small cell lung cancer (NSCLC), adding pemetrexed and carboplatin to standard gefitinib therapy markedly extends progression free survival, but at the cost of twice as many serious toxicities, in a recent phase 3 trial.
Two previous phase 2 trials (J Clin Oncol. 2016 Sep 20;34[27]:3258-66 and Ann Oncol. 2015 Feb 10;26[5]:888-94) suggested that adding chemotherapy could improve outcomes over gefitinib alone, but this is the first study to clearly demonstrate better overall survival, reported lead author Vanita Noronha, MD, of Tata Memorial Hospital in Mumbai, India, and colleagues. They noted that this is the second regimen to demonstrate better overall survival than standard gefitinib for EGFR-mutated lung cancer, with dacomitinib being the first, as shown by the ARCHER 1050 trial.
The present study involved 350 patients with advanced, EGFR-mutated NSCLC who had an Eastern Cooperative Oncology (ECOG) performance status of 0-2 and were candidates for first-line palliative therapy. Approximately one-fifth of patients (21%) had a performance status of 2, and almost as many (18%) had brain metastases. After stratification for performance status and mutation type, patients were randomized in a 1:1 ratio to receive either gefitinib monotherapy (250 mg once daily) or gefitinib plus a chemotherapy combination of pemetrexed (500 mg/m2) and carboplatin (area under the curve of 5 with Calvert formula) on day 1 of four 21-day cycles. Subsequently, nonprogressing patients in the chemotherapy group received maintenance therapy with pemetrexed at the same dose and frequency. Treatment was continued until progression, toxicity, or withdrawal of consent. The primary endpoint was progression-free survival (PFS). Secondary outcomes included overall survival (OS), response rate, quality of life, and toxicity.
After a median follow-up of 17 months, the investigators found that adding chemotherapy to gefitinib resulted in a clear benefit, with estimated median PFS increasing from 8 months to 16 months (P less than .001). Estimated median overall survival also increased, with a figure not reached in the chemotherapy/gefitinib group, compared with 17 months among those who received gefitinib alone. Response rates echoed these findings, with more patients in the chemotherapy/gefitinib group achieving complete (2.9% vs. 0.6%) and partial remission (72.4% vs. 61.9%).
“[T]he PFS attained in our study is noteworthy, considering that 21% of our study patients had a [performance status] of 2, whereas the FLAURA study, [which demonstrated a PFS of 18.9 months with osimertinib], only included patients with a [performance status] of 1 or lower,” the investigators wrote. Their report is in Journal of Clinical Oncology.
Still, introducing chemotherapy was not without negative consequences. Compared with the gefitinib monotherapy group, patients who also received chemotherapy more often had grade 3 or higher adverse events (75% vs. 49.4%), and twice as many had clinically significant, serious toxicities (50.6% vs. 25.3%). The additional toxicities were predominantly due to myelosuppression and nephrotoxicity.
Despite these drawbacks, the investigators concluded that combination therapy was superior to gefitinib alone. “The combination of gefitinib, pemetrexed, and carboplatin represents a new standard first-line therapy for EGFR-mutant NSCLC,” the investigators concluded.
The study was funded by Tata Memorial Center Research Administration Council, Fresenius Kabi India, Lung Cancer Consortium India, and others. The investigators reported relationships with Roche, Biocon, Amgen, and others.
SOURCE: Noronha et al. Journal of Clinical Oncology. 2019 Aug 14. doi: 10.1200/JCO.19.01154.
For patients with EGFR-mutated, advanced non–small cell lung cancer (NSCLC), adding pemetrexed and carboplatin to standard gefitinib therapy markedly extends progression free survival, but at the cost of twice as many serious toxicities, in a recent phase 3 trial.
Two previous phase 2 trials (J Clin Oncol. 2016 Sep 20;34[27]:3258-66 and Ann Oncol. 2015 Feb 10;26[5]:888-94) suggested that adding chemotherapy could improve outcomes over gefitinib alone, but this is the first study to clearly demonstrate better overall survival, reported lead author Vanita Noronha, MD, of Tata Memorial Hospital in Mumbai, India, and colleagues. They noted that this is the second regimen to demonstrate better overall survival than standard gefitinib for EGFR-mutated lung cancer, with dacomitinib being the first, as shown by the ARCHER 1050 trial.
The present study involved 350 patients with advanced, EGFR-mutated NSCLC who had an Eastern Cooperative Oncology (ECOG) performance status of 0-2 and were candidates for first-line palliative therapy. Approximately one-fifth of patients (21%) had a performance status of 2, and almost as many (18%) had brain metastases. After stratification for performance status and mutation type, patients were randomized in a 1:1 ratio to receive either gefitinib monotherapy (250 mg once daily) or gefitinib plus a chemotherapy combination of pemetrexed (500 mg/m2) and carboplatin (area under the curve of 5 with Calvert formula) on day 1 of four 21-day cycles. Subsequently, nonprogressing patients in the chemotherapy group received maintenance therapy with pemetrexed at the same dose and frequency. Treatment was continued until progression, toxicity, or withdrawal of consent. The primary endpoint was progression-free survival (PFS). Secondary outcomes included overall survival (OS), response rate, quality of life, and toxicity.
After a median follow-up of 17 months, the investigators found that adding chemotherapy to gefitinib resulted in a clear benefit, with estimated median PFS increasing from 8 months to 16 months (P less than .001). Estimated median overall survival also increased, with a figure not reached in the chemotherapy/gefitinib group, compared with 17 months among those who received gefitinib alone. Response rates echoed these findings, with more patients in the chemotherapy/gefitinib group achieving complete (2.9% vs. 0.6%) and partial remission (72.4% vs. 61.9%).
“[T]he PFS attained in our study is noteworthy, considering that 21% of our study patients had a [performance status] of 2, whereas the FLAURA study, [which demonstrated a PFS of 18.9 months with osimertinib], only included patients with a [performance status] of 1 or lower,” the investigators wrote. Their report is in Journal of Clinical Oncology.
Still, introducing chemotherapy was not without negative consequences. Compared with the gefitinib monotherapy group, patients who also received chemotherapy more often had grade 3 or higher adverse events (75% vs. 49.4%), and twice as many had clinically significant, serious toxicities (50.6% vs. 25.3%). The additional toxicities were predominantly due to myelosuppression and nephrotoxicity.
Despite these drawbacks, the investigators concluded that combination therapy was superior to gefitinib alone. “The combination of gefitinib, pemetrexed, and carboplatin represents a new standard first-line therapy for EGFR-mutant NSCLC,” the investigators concluded.
The study was funded by Tata Memorial Center Research Administration Council, Fresenius Kabi India, Lung Cancer Consortium India, and others. The investigators reported relationships with Roche, Biocon, Amgen, and others.
SOURCE: Noronha et al. Journal of Clinical Oncology. 2019 Aug 14. doi: 10.1200/JCO.19.01154.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Timely Diagnosis of Lung Cancer in a Dedicated VA Referral Unit with Endobronchial Ultrasound Capability (FULL)
Lung cancer is the leading cause of cancer death in the US, with 154 050 deaths in 2018.1 There have been many attempts to reduce mortality of the disease through early diagnosis with use of computed tomography (CT). The National Lung Cancer Screening trial showed that screening high-risk populations with low-dose CT (LDCT) can reduce mortality.2 However, implementing LDCT screening in the clinical setting has proven challenging, as illustrated by the VA Lung Cancer Screening Demonstration Project (LCSDP).3 A lung cancer diagnosis typically comprises several steps that require different medical specialties; this can lead to delays. In the LCSDP, the mean time to diagnosis was 137 days.3 There are no federal standards for timeliness of lung cancer diagnosis.
The nonprofit RAND Corporation is the only American research organization that has published guidelines specifying acceptable intervals for the diagnosis and treatment of lung cancer. In Quality of Care for Oncologic Conditions and HIV, RAND Corporation researchers propose management quality indicators: lung cancer diagnosis within 2 months of an abnormal radiologic study and treatment within 6 weeks of diagnosis.4 The Swedish Lung Cancer Study5 and the Canadian Strategy for Cancer Control6 both recommended a standard of about 30 days—half the time recommended by the RAND Corporation.
Bukhari and colleagues at the Dayton US Department of Veterans Affairs (VA) Medical Center (VAMC) conducted a quality improvement study that examined lung cancer diagnosis and management.7 They found the time (SD) from abnormal chest imaging to diagnosis was 35.5 (31.6) days. Of those veterans who received a lung cancer diagnosis, 89.2% had the diagnosis made within the 60 days recommended by the RAND Corporation. Although these results surpass those of the LCSDP, they can be exceeded.
Beyond the potential emotional distress of awaiting the final diagnosis of a lung lesion, a delay in diagnosis and treatment may adversely affect outcomes. LDCT screening has been shown to reduce mortality, which implies a link between survival and time to intervention. There is no published evidence that time to diagnosis in advanced stage lung cancer affects outcome. The National Cancer Database (NCDB) contains informtion on about 70% of the cancers diagnosed each year in the US.8 An analysis of 4984 patients with stage IA squamous cell lung cancer undergoing lobectomy from NCDB showed that earlier surgery was associated with an absolute decrease in 5-year mortality of 5% to 8%. 9 Hence, at least in early-stage disease, reduced time from initial suspect imaging to definitive treatment may improve survival.
A system that coordinates the requisite diagnostic steps and avoids delays should provide a significant improvement in patient care. The results of such an approach that utilized nurse navigators has been previously published. 10 Here, we present the results of a dedicated VA referral clinic with priority access to pulmonary consultation and procedures in place that are designed to expedite the diagnosis of potential lung cancer.
Methods
The John L. McClellan Memorial Veterans Hospital (JLMMVH) in Little Rock, Arkansas institutional review board approved this study, which was performed in accordance with the Declaration of Helsinki. Requirement for informed consent was waived, and patient confidentiality was maintained throughout.
We have developed a plan of care specifically to facilitate diagnosis and treatment of the large number of veterans referred to the JLMMVH Diagnostic Clinic for abnormal results of chest imaging. The clinic has priority access to same-day imaging and subspecialty consultation services. In the clinic, medical students and residents perform evaluations and a registered nurse (RN) manager coordinates care.
A Diagnostic Clinic consult for abnormal thoracic imaging immediately triggers an e-consult to an interventional pulmonologist (Figure). The RN manager and pulmonologist perform a joint review of records/imaging prior to scheduling, and the pulmonologist triages the patient. Triage options include follow-up imaging, bronchoscopy with endobronchial ultrasound (EBUS), endoscopic ultrasound (EUS), and CT-guided biopsy.
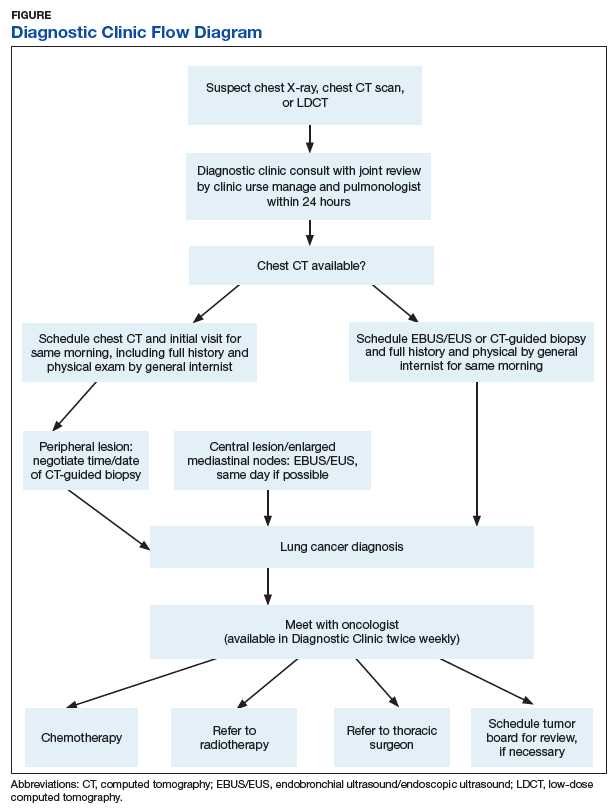
The RN manager then schedules a clinic visit that includes a medical evaluation by clinic staff and any indicated procedures on the same day. The interventional pulmonologist performs EBUS, EUS with the convex curvilinear bronchoscope, or both combined as indicated for diagnosis and staging. All procedures are performed in the JLMMVH bronchoscopy suite with standard conscious sedation using midazolam and fentanyl. Any other relevant procedures, such as pleural tap, also are performed at time of procedure. The pulmonologist and an attending pathologist interpret biopsies obtained in the bronchoscopy suite.
We performed a retrospective chart review of patients diagnosed with primary lung cancer through referral to the JLMMVH Diagnostic Clinic. The primary outcome was time from initial suspect chest imaging to cancer diagnosis. The study population consisted of patients referred for abnormal thoracic imaging between January 1, 2013 and December 31, 2016 and subsequently diagnosed with a primary lung cancer.
Subjects were excluded if (1) the patient was referred from outside our care network and a delay of > 10 days occurred between initial lesion imaging and referral; (2) the patient did not show up for appointments or chose to delay evaluation following referral; (3) biopsy demonstrated a nonlung primary cancer; and (4) serious intercurrent illness interrupted the diagnostic plan. In some cases, the radiologist or consulting pulmonologist had judged the lung lesion too small for immediate biopsy and recommended repeat imaging at a later date.
Patients were included in the study if the follow- up imaging led to a lung cancer diagnosis. However, because the interval between the initial imaging and the follow-up imaging in these patients did not represent a systems delay problem, the date of the scheduled follow-up abnormal imaging, which resulted in initiation of a potential cancer evaluation, served as the index suspect imaging date for this study.
Patient electronic medical records were reviewed and the following data were abstracted: date of the abnormal imaging that led to referral and time from abnormal chest X-ray to chest CT scan if applicable; date of referral and date of clinic visit; date of biopsy; date of lung cancer diagnosis; method of obtaining diagnostic specimen; lung cancer type and stage; type and date of treatment initiation or decision for supportive care only; and decision to seek further evaluation or care outside of our system.
All patients diagnosed with lung cancer during the study period were reviewed for inclusion, hence no required sample-size estimate was calculated. All outcomes were assessed as calendar days. The primary outcome was the time from the index suspect chest imaging study to the date of diagnosis of lung cancer. Prior to the initiation of our study, we chose this more stringent 30-day recommendation of the Canadian6 and Swedish5 studies as the comparator for our primary outcome, although data with respect to the 60-day Rand Corporation guidelines also are reported.4
Statistical Methods
The mean time to lung cancer diagnosis in our cohort was compared with this 30-day standard using a 2-sided Mann–Whitney U test. Normality of data distribution was determined using the Kolmogorov–Smirnov test. For statistical significance testing a P value of .05 was used. Statistical calculations were performed using R statistical software version 3.2.4. Secondary outcomes consisted of time from diagnosis to treatment; proportion of subjects diagnosed within 60 days; time from initial clinic visit to biopsy; and time from biopsy to diagnosis.
Results
Overall, 222 patients were diagnosed with a malignant lung lesion, of which 63 were excluded from analysis: 22 cancelled or did not appear for appointments, declined further evaluation, or completed evaluation outside of our network; 13 had the diagnosis made prior to Diagnostic Clinic visit; 13 proved to have a nonlung primary tumor presenting in the lung or mediastinal nodes; 12 were delayed > 10 days in referral from an outside network; and 3 had an intervening serious acute medical problem forcing delay in the diagnostic process.
Of the 159 included subjects, 154 (96.9%) were male, and the mean (SD) age was 67.6 (8.1) years. For 76 subjects, the abnormal chest X-ray and subsequent chest CT scan were performed the same day or the lung lesion had initially been noted on a CT scan. For 54 subjects, there was a delay of ≥ 1 week in obtaining a chest CT scan. The mean (SD) time from placement of the Diagnostic Clinic consultation by the primary care provider (PCP) or other provider and the initial Diagnostic Clinic visit was 6.3 (4.4) days. The mean (SD) time from suspect imaging to diagnosis (primary outcome) was 22.6(16.6) days.
The distribution of this outcome was nonnormal (Kolmogorov-Smirnov test P < .01). When compared with the standard of 30 days, the primary outcome of 22.6 days was significantly shorter (2-sided Mann–Whitney U test P < .01). Three-quarters (76.1%) of subjects were diagnosed within 30 days and 95.0% of subjects were diagnosed within 60 days of the initial imaging. For the 8 subjects diagnosed after 60 days, contributing factors included PCP delay in Diagnostic Clinic consultation, initial negative biopsy, delay in performance of chest CT scan prior to consultation, and outsourcing of positron emission tomography (PET) scans.
Overall, 57 (35.8%) of the subjects underwent biopsy on the day of their Diagnostic Clinic visit: 14 underwent CT-guided biopsy and 43 underwent EBUS/EUS. Within 2 days of the initial visit 106 subjects (66.7%) had undergone biopsy. The mean (SD) time from initial Diagnostic Clinic visit to biopsy was 6.3 (9.5) days. The mean (SD) interval was 1.8 (3.0) days for EBUS/ EUS and 11.3 (11.7) days for CT-guided biopsy. The mean (SD) interval from biopsy to diagnosis was 3.2 (6.2) days with 64 cases (40.3%) diagnosed the day of biopsy.
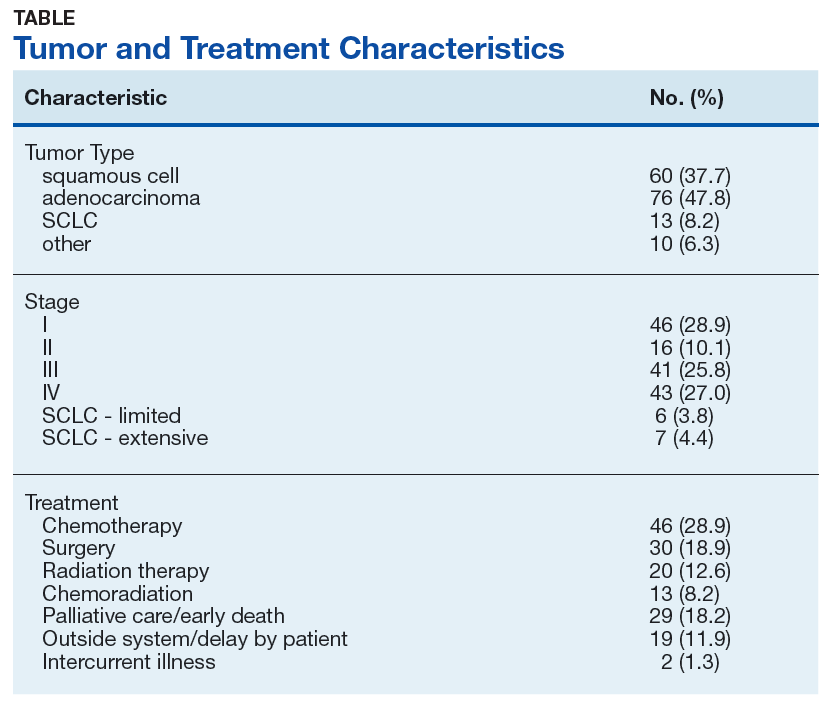
Excluding subjects whose treatment was delayed by patient choice or intercurrent illness, and those who left the VA system to seek treatment elsewhere (n = 21), 24 opted for palliative care, 5 died before treatment could be initiated, and 109 underwent treatment for their tumors (Table). The mean times (SD) from diagnosis to treatment were: chemotherapy alone 34.7 (25.3) days; chemoradiation 37.0 (22.8) days; surgery 44.3 (24.4) days; radiation therapy alone 47.9 (26.0) days. With respect to the RAND Corporation recommended diagnosis to treatment time, 60.9% of chemotherapy alone, 61.5% of chemoradiation, 66.7% of surgery, and 45.0% of radiation therapy alone treatments were initiated within the 6-week window.
Discussion
This retrospective case study demonstrates the effectiveness of a dedicated diagnostic clinic with priority EBUS/EUS access in diagnosing lung cancer within the VA system. Although there is no universally accepted quality standard for comparison, the RAND Corporation recommendation of 60 days from abnormal imaging to diagnosis and the Dayton VAMC published mean of 35.5 days are guideposts; however, the results from the Dayton VAMC may have been affected negatively by some subjects undergoing serial imaging for asymptomatic nodules. We chose a more stringent standard of 30 days as recommended by Swedish and Canadian task forces.
When diagnosing lung cancer, the overriding purpose of the Diagnostic Clinic is to minimize system delays. The method is to have as simple a task as possible for the PCP or other provider who identifies a lung nodule or mass and submits a single consultation request to the Diagnostic Clinic. Once this consultation is placed, the clinic RN manager oversees all further steps required for diagnosis and referral for treatment. The key factor in achieving a mean diagnosis time of 22.6 days is the cooperation between the RN manager and the interventional pulmonologist. When a consultation is received, the RN manager and pulmonologist review the data together and schedule the initial clinic visit; the goal is same-day biopsy, which is achieved in more than one-third of cases. Not all patients with a chest image suspected for lung cancer had it ordered by their PCP. For this reason, a Diagnostic Clinic consultation is available to all health care providers in our system. Many patients reach the clinic after the discovery of a suspect chest X-ray during an emergency department visit, a regularly scheduled subspecialty appointment, or during a preoperative evaluation.
The mean time from initial visit to biopsy was 1.8 days for EBUS/EUS compared with an interval of 11.3 days for CT-guided biopsy. This difference reflects the pulmonologist’s involvement in initial scheduling of Diagnostic Clinic patients. The ability of the pulmonologist to provide an accurate assessment of sample adequacy and a preliminary diagnosis at bedside, with concurrent confirmation by a staff pathologist, permitted the Diagnostic Clinic to inform 40.3% of patients of the finding of malignancy on the day of biopsy. A published comparison of the onsite review of biopsy material showed our pulmonologist and staff pathologists to be equally accurate in their interpretations.11
Sources of Delays
While this study documents the shortest intervals from suspect imaging to diagnosis reported to date, it also identifies sources of system delay in diagnosing lung cancer that JLMMVH could further optimize. The first is the time from initial abnormal chest X-ray imaging to performance of the chest CT scan. On occasion, the index lung lesion is identified unexpectedly on an outpatient or emergency department chest CT scan. With greater use of LDCT lung cancer screening, the initial detection of suspect lesions by CT scanning will increase in the future. However, the PCP most often investigates a patient complaint with a standard chest X-ray that reveals a suspect nodule or mass. When ordered by the PCP as an outpatient test, scheduling of the follow-up chest CT scan is not given priority. More than a third of subjects experienced a delay ≥ 1 week in obtaining a chest CT scan ordered by the PCP; for 29 subjects the delay was ≥ 3weeks. At JLMMVH, the Diagnostic Clinic is given priority in scheduling CT scans. Hence, for suspect lung lesions, the chest CT scan, if not already obtained, is generally performed on the morning of the clinic visit. Educating the PCP to refer the patient immediately to the Diagnostic Clinic rather than waiting to obtain an outpatient chest CT scan may remove this source of unnecessary delay.
Scheduling a CT-guided fine needle aspiration of a lung lesion is another source of system delay. When the chest CT scan is available at the time of the Diagnostic Clinic referral, the clinic visit is scheduled for the earliest day a required CT-guided biopsy can be performed. However, the mean time of 11.3 days from initial Diagnostic Clinic visit to CT-guided biopsy is indicative of the backlog faced by the interventional radiologists.
Although infrequent, PET scans that are required before biopsy can lead to substantial delays. PET scans are performed at our university affiliate, and the joint VA-university lung tumor board sometimes generates requests for such scans prior to tissue diagnosis, yet another source of delay.
The time from referral receipt to the Diagnostic Clinic visit averaged 6.3 days. This delay usually was determined by the availability of the CT-guided biopsy or the dedicated interventional pulmonologist. Although other interventional pulmonologists at JLMMVH may perform the requisite diagnostic procedures, they are not always available for immediate review of imaging studies of referred patients nor can their schedules flexibly accommodate the number of patients seen in our clinic for evaluation.
Lung Cancer Diagnosis
Prompt diagnosis in the setting of a worrisome chest X-ray may help decrease patient anxiety, but does the clinic improve lung cancer treatment outcomes? Such improvement has been demonstrated only in stage IA squamous cell lung cancer.9 Of our study population, 37.7% had squamous cell carcinoma, and 85.5% had non-small cell lung cancer. Of those with non-small cell lung cancer, 28.9% had a clinical stage I tumor. Stage I squamous cell carcinoma, the type of tumor most likely to benefit from early diagnosis and treatment, was diagnosed in 11.3% of patients. With the increased application of LDCT screening, the proportion of veterans identified with early stage lung cancer may rise. The Providence VAMC in Rhode Island reported its results from instituting LDCT screening.12 Prior to screening, 28% of patients diagnosed with lung cancer had a stage I tumor. Following the introduction of LDCT screening, 49% diagnosed by LDCT screening had a stage I tumor. Nearly a third of their patients diagnosed with lung cancer through LDCT screening had squamous cell tumor histology. Thus, we can anticipate an increasing number of veterans with early stage lung cancer who would benefit from timely diagnosis.
The JLMMVH is a referral center for the entire state of Arkansas. Quite a few of its referred patients come from a long distance, which may require overnight housing and other related travel expenses. Apart from any potential outcome benefit, the efficiencies of the system described herein include the minimization of extra trips, an inconvenience and cost to both patient and JLMMVH.
Although the primary task of the clinic is diagnosis, we also seek to facilitate timely treatment. Our lack of an on-site PET scanner and radiation therapy, resources present on-site at the Dayton VAMC, contribute to longer therapy wait times. The shortest mean wait time at JLMMVH is for chemotherapy alone (34.7 days), in part because the JLMMVH oncologists, performing initial consultations 2 to 3 times weekly in the Diagnostic Clinic, are more readily available than are our thoracic surgeons or radiation therapists. Yet overall, JLMMVH patients often face delay from the time of lung cancer diagnosis to initiation of treatment.
The Connecticut Veterans Affairs Healthcare System has published the results of changes in lung cancer management associated with a nurse navigator system.10 Prior to creating the position of cancer care coordinator, filled by an advanced practice RNs, the mean time from clinical suspicion of lung cancer to treatment was 117 days. After 4 years of such care navigation, this waiting time had decreased to 52.4 days. Associated with this dramatic improvement in overall waiting time were decreases in the turnaround time required for performance of CT and PET scans. With respect to this big picture view of lung cancer care, our Diagnostic Clinic serves as a model for the initial step of diagnosis. Coordination and streamlining of the various steps from diagnosis to definitive therapy shall require a more system-wide effort involving all the key players in cancer care.
Conclusion
We have developed a care pathway based in a dedicated diagnostic clinic and have been able to document the shortest interval from abnormality to diagnosis of lung cancer reported in the literature to date. Efficient functioning of this clinic is dependent upon the close cooperation between a full-time RN clinic manager and an interventional pulmonologist experienced in lung cancer management and able to interpret cytologic samples at the time of biopsy. Shortening the delay between diagnosis and definitive therapy remains a challenge and may benefit from the oncology nurse navigator model previously described within the VA system. 10
1. American Cancer Society. Cancer Facts & Figures. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf. Accessed July 13, 2019.
2. National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Eng J Med. 2011;365(5):395-409.
3. Kinsinger LS, Anderson C, Kim J, et al. Implementation of lung cancer screening in the Veterans Health Administration. JAMA Intern Med. 2017;177(3):399-406.
4. Asch SM, Kerr EA, Hamilton EG, Reifel JL, McGlynn EA, eds. Quality of Care for Oncologic Conditions and HIV: A Review of the Literature and Quality Indicators. Santa Monica, CA: RAND Corporation; 2000.
5. Hillerdal G. [Recommendations from the Swedish Lung Cancer Study Group: Shorter waiting times are demanded for quality in diagnostic work-ups for lung care.] Swedish Med J 1999; 96: 4691.
6. Simunovic M, Gagliardi A, McCready D, Coates A, Levine M, DePetrillo D. A snapshot of waiting times for cancer surgery provided by surgeons affiliated with regional cancer centres in Ontario. CMAJ. 2001;165(4):421-425. [Canadian Strategy for Cancer Control]
7. Bukhari A, Kumar G, Rajsheker R, Markert R. Timeliness of lung cancer diagnosis and treatment. Fed Pract. 2017;34(suppl 1):24S-29S.
8. Bilimoria KY, Ko CY, Tomlinson JS, et al. Wait times for cancer surgery in the United States: trends and predictors of delays. Ann Surg. 2011;253(4):779-785.
9. Yang CJ, Wang H, Kumar A, et al. Impact of timing of lobectomy on survival for clinical stage IA lung squamous cell carcinoma. Chest. 2017;152(6):1239-1250.
10. Hunnibell LS, Rose MG, Connery DM, et al. Using nurse navigation to improve timeliness of lung cancer care at a veterans hospital. Clin J Oncol Nurs. 2012;16(1):29-36.
11. Meena N, Jeffus S, Massoll N, et al. Rapid onsite evaluation: a comparison of cytopathologist and pulmonologist performance. Cancer Cytopatho. 2016;124(4):279-84.
12. Okereke IC, Bates MF, Jankowich MD, et al. Effects of implementation of lung cancer screening at one Veterans Affairs Medical Center. Chest 2016;150(5):1023-1029.
Lung cancer is the leading cause of cancer death in the US, with 154 050 deaths in 2018.1 There have been many attempts to reduce mortality of the disease through early diagnosis with use of computed tomography (CT). The National Lung Cancer Screening trial showed that screening high-risk populations with low-dose CT (LDCT) can reduce mortality.2 However, implementing LDCT screening in the clinical setting has proven challenging, as illustrated by the VA Lung Cancer Screening Demonstration Project (LCSDP).3 A lung cancer diagnosis typically comprises several steps that require different medical specialties; this can lead to delays. In the LCSDP, the mean time to diagnosis was 137 days.3 There are no federal standards for timeliness of lung cancer diagnosis.
The nonprofit RAND Corporation is the only American research organization that has published guidelines specifying acceptable intervals for the diagnosis and treatment of lung cancer. In Quality of Care for Oncologic Conditions and HIV, RAND Corporation researchers propose management quality indicators: lung cancer diagnosis within 2 months of an abnormal radiologic study and treatment within 6 weeks of diagnosis.4 The Swedish Lung Cancer Study5 and the Canadian Strategy for Cancer Control6 both recommended a standard of about 30 days—half the time recommended by the RAND Corporation.
Bukhari and colleagues at the Dayton US Department of Veterans Affairs (VA) Medical Center (VAMC) conducted a quality improvement study that examined lung cancer diagnosis and management.7 They found the time (SD) from abnormal chest imaging to diagnosis was 35.5 (31.6) days. Of those veterans who received a lung cancer diagnosis, 89.2% had the diagnosis made within the 60 days recommended by the RAND Corporation. Although these results surpass those of the LCSDP, they can be exceeded.
Beyond the potential emotional distress of awaiting the final diagnosis of a lung lesion, a delay in diagnosis and treatment may adversely affect outcomes. LDCT screening has been shown to reduce mortality, which implies a link between survival and time to intervention. There is no published evidence that time to diagnosis in advanced stage lung cancer affects outcome. The National Cancer Database (NCDB) contains informtion on about 70% of the cancers diagnosed each year in the US.8 An analysis of 4984 patients with stage IA squamous cell lung cancer undergoing lobectomy from NCDB showed that earlier surgery was associated with an absolute decrease in 5-year mortality of 5% to 8%. 9 Hence, at least in early-stage disease, reduced time from initial suspect imaging to definitive treatment may improve survival.
A system that coordinates the requisite diagnostic steps and avoids delays should provide a significant improvement in patient care. The results of such an approach that utilized nurse navigators has been previously published. 10 Here, we present the results of a dedicated VA referral clinic with priority access to pulmonary consultation and procedures in place that are designed to expedite the diagnosis of potential lung cancer.
Methods
The John L. McClellan Memorial Veterans Hospital (JLMMVH) in Little Rock, Arkansas institutional review board approved this study, which was performed in accordance with the Declaration of Helsinki. Requirement for informed consent was waived, and patient confidentiality was maintained throughout.
We have developed a plan of care specifically to facilitate diagnosis and treatment of the large number of veterans referred to the JLMMVH Diagnostic Clinic for abnormal results of chest imaging. The clinic has priority access to same-day imaging and subspecialty consultation services. In the clinic, medical students and residents perform evaluations and a registered nurse (RN) manager coordinates care.
A Diagnostic Clinic consult for abnormal thoracic imaging immediately triggers an e-consult to an interventional pulmonologist (Figure). The RN manager and pulmonologist perform a joint review of records/imaging prior to scheduling, and the pulmonologist triages the patient. Triage options include follow-up imaging, bronchoscopy with endobronchial ultrasound (EBUS), endoscopic ultrasound (EUS), and CT-guided biopsy.
The RN manager then schedules a clinic visit that includes a medical evaluation by clinic staff and any indicated procedures on the same day. The interventional pulmonologist performs EBUS, EUS with the convex curvilinear bronchoscope, or both combined as indicated for diagnosis and staging. All procedures are performed in the JLMMVH bronchoscopy suite with standard conscious sedation using midazolam and fentanyl. Any other relevant procedures, such as pleural tap, also are performed at time of procedure. The pulmonologist and an attending pathologist interpret biopsies obtained in the bronchoscopy suite.
We performed a retrospective chart review of patients diagnosed with primary lung cancer through referral to the JLMMVH Diagnostic Clinic. The primary outcome was time from initial suspect chest imaging to cancer diagnosis. The study population consisted of patients referred for abnormal thoracic imaging between January 1, 2013 and December 31, 2016 and subsequently diagnosed with a primary lung cancer.
Subjects were excluded if (1) the patient was referred from outside our care network and a delay of > 10 days occurred between initial lesion imaging and referral; (2) the patient did not show up for appointments or chose to delay evaluation following referral; (3) biopsy demonstrated a nonlung primary cancer; and (4) serious intercurrent illness interrupted the diagnostic plan. In some cases, the radiologist or consulting pulmonologist had judged the lung lesion too small for immediate biopsy and recommended repeat imaging at a later date.
Patients were included in the study if the follow- up imaging led to a lung cancer diagnosis. However, because the interval between the initial imaging and the follow-up imaging in these patients did not represent a systems delay problem, the date of the scheduled follow-up abnormal imaging, which resulted in initiation of a potential cancer evaluation, served as the index suspect imaging date for this study.
Patient electronic medical records were reviewed and the following data were abstracted: date of the abnormal imaging that led to referral and time from abnormal chest X-ray to chest CT scan if applicable; date of referral and date of clinic visit; date of biopsy; date of lung cancer diagnosis; method of obtaining diagnostic specimen; lung cancer type and stage; type and date of treatment initiation or decision for supportive care only; and decision to seek further evaluation or care outside of our system.
All patients diagnosed with lung cancer during the study period were reviewed for inclusion, hence no required sample-size estimate was calculated. All outcomes were assessed as calendar days. The primary outcome was the time from the index suspect chest imaging study to the date of diagnosis of lung cancer. Prior to the initiation of our study, we chose this more stringent 30-day recommendation of the Canadian6 and Swedish5 studies as the comparator for our primary outcome, although data with respect to the 60-day Rand Corporation guidelines also are reported.4
Statistical Methods
The mean time to lung cancer diagnosis in our cohort was compared with this 30-day standard using a 2-sided Mann–Whitney U test. Normality of data distribution was determined using the Kolmogorov–Smirnov test. For statistical significance testing a P value of .05 was used. Statistical calculations were performed using R statistical software version 3.2.4. Secondary outcomes consisted of time from diagnosis to treatment; proportion of subjects diagnosed within 60 days; time from initial clinic visit to biopsy; and time from biopsy to diagnosis.
Results
Overall, 222 patients were diagnosed with a malignant lung lesion, of which 63 were excluded from analysis: 22 cancelled or did not appear for appointments, declined further evaluation, or completed evaluation outside of our network; 13 had the diagnosis made prior to Diagnostic Clinic visit; 13 proved to have a nonlung primary tumor presenting in the lung or mediastinal nodes; 12 were delayed > 10 days in referral from an outside network; and 3 had an intervening serious acute medical problem forcing delay in the diagnostic process.
Of the 159 included subjects, 154 (96.9%) were male, and the mean (SD) age was 67.6 (8.1) years. For 76 subjects, the abnormal chest X-ray and subsequent chest CT scan were performed the same day or the lung lesion had initially been noted on a CT scan. For 54 subjects, there was a delay of ≥ 1 week in obtaining a chest CT scan. The mean (SD) time from placement of the Diagnostic Clinic consultation by the primary care provider (PCP) or other provider and the initial Diagnostic Clinic visit was 6.3 (4.4) days. The mean (SD) time from suspect imaging to diagnosis (primary outcome) was 22.6(16.6) days.
The distribution of this outcome was nonnormal (Kolmogorov-Smirnov test P < .01). When compared with the standard of 30 days, the primary outcome of 22.6 days was significantly shorter (2-sided Mann–Whitney U test P < .01). Three-quarters (76.1%) of subjects were diagnosed within 30 days and 95.0% of subjects were diagnosed within 60 days of the initial imaging. For the 8 subjects diagnosed after 60 days, contributing factors included PCP delay in Diagnostic Clinic consultation, initial negative biopsy, delay in performance of chest CT scan prior to consultation, and outsourcing of positron emission tomography (PET) scans.
Overall, 57 (35.8%) of the subjects underwent biopsy on the day of their Diagnostic Clinic visit: 14 underwent CT-guided biopsy and 43 underwent EBUS/EUS. Within 2 days of the initial visit 106 subjects (66.7%) had undergone biopsy. The mean (SD) time from initial Diagnostic Clinic visit to biopsy was 6.3 (9.5) days. The mean (SD) interval was 1.8 (3.0) days for EBUS/ EUS and 11.3 (11.7) days for CT-guided biopsy. The mean (SD) interval from biopsy to diagnosis was 3.2 (6.2) days with 64 cases (40.3%) diagnosed the day of biopsy.
Excluding subjects whose treatment was delayed by patient choice or intercurrent illness, and those who left the VA system to seek treatment elsewhere (n = 21), 24 opted for palliative care, 5 died before treatment could be initiated, and 109 underwent treatment for their tumors (Table). The mean times (SD) from diagnosis to treatment were: chemotherapy alone 34.7 (25.3) days; chemoradiation 37.0 (22.8) days; surgery 44.3 (24.4) days; radiation therapy alone 47.9 (26.0) days. With respect to the RAND Corporation recommended diagnosis to treatment time, 60.9% of chemotherapy alone, 61.5% of chemoradiation, 66.7% of surgery, and 45.0% of radiation therapy alone treatments were initiated within the 6-week window.
Discussion
This retrospective case study demonstrates the effectiveness of a dedicated diagnostic clinic with priority EBUS/EUS access in diagnosing lung cancer within the VA system. Although there is no universally accepted quality standard for comparison, the RAND Corporation recommendation of 60 days from abnormal imaging to diagnosis and the Dayton VAMC published mean of 35.5 days are guideposts; however, the results from the Dayton VAMC may have been affected negatively by some subjects undergoing serial imaging for asymptomatic nodules. We chose a more stringent standard of 30 days as recommended by Swedish and Canadian task forces.
When diagnosing lung cancer, the overriding purpose of the Diagnostic Clinic is to minimize system delays. The method is to have as simple a task as possible for the PCP or other provider who identifies a lung nodule or mass and submits a single consultation request to the Diagnostic Clinic. Once this consultation is placed, the clinic RN manager oversees all further steps required for diagnosis and referral for treatment. The key factor in achieving a mean diagnosis time of 22.6 days is the cooperation between the RN manager and the interventional pulmonologist. When a consultation is received, the RN manager and pulmonologist review the data together and schedule the initial clinic visit; the goal is same-day biopsy, which is achieved in more than one-third of cases. Not all patients with a chest image suspected for lung cancer had it ordered by their PCP. For this reason, a Diagnostic Clinic consultation is available to all health care providers in our system. Many patients reach the clinic after the discovery of a suspect chest X-ray during an emergency department visit, a regularly scheduled subspecialty appointment, or during a preoperative evaluation.
The mean time from initial visit to biopsy was 1.8 days for EBUS/EUS compared with an interval of 11.3 days for CT-guided biopsy. This difference reflects the pulmonologist’s involvement in initial scheduling of Diagnostic Clinic patients. The ability of the pulmonologist to provide an accurate assessment of sample adequacy and a preliminary diagnosis at bedside, with concurrent confirmation by a staff pathologist, permitted the Diagnostic Clinic to inform 40.3% of patients of the finding of malignancy on the day of biopsy. A published comparison of the onsite review of biopsy material showed our pulmonologist and staff pathologists to be equally accurate in their interpretations.11
Sources of Delays
While this study documents the shortest intervals from suspect imaging to diagnosis reported to date, it also identifies sources of system delay in diagnosing lung cancer that JLMMVH could further optimize. The first is the time from initial abnormal chest X-ray imaging to performance of the chest CT scan. On occasion, the index lung lesion is identified unexpectedly on an outpatient or emergency department chest CT scan. With greater use of LDCT lung cancer screening, the initial detection of suspect lesions by CT scanning will increase in the future. However, the PCP most often investigates a patient complaint with a standard chest X-ray that reveals a suspect nodule or mass. When ordered by the PCP as an outpatient test, scheduling of the follow-up chest CT scan is not given priority. More than a third of subjects experienced a delay ≥ 1 week in obtaining a chest CT scan ordered by the PCP; for 29 subjects the delay was ≥ 3weeks. At JLMMVH, the Diagnostic Clinic is given priority in scheduling CT scans. Hence, for suspect lung lesions, the chest CT scan, if not already obtained, is generally performed on the morning of the clinic visit. Educating the PCP to refer the patient immediately to the Diagnostic Clinic rather than waiting to obtain an outpatient chest CT scan may remove this source of unnecessary delay.
Scheduling a CT-guided fine needle aspiration of a lung lesion is another source of system delay. When the chest CT scan is available at the time of the Diagnostic Clinic referral, the clinic visit is scheduled for the earliest day a required CT-guided biopsy can be performed. However, the mean time of 11.3 days from initial Diagnostic Clinic visit to CT-guided biopsy is indicative of the backlog faced by the interventional radiologists.
Although infrequent, PET scans that are required before biopsy can lead to substantial delays. PET scans are performed at our university affiliate, and the joint VA-university lung tumor board sometimes generates requests for such scans prior to tissue diagnosis, yet another source of delay.
The time from referral receipt to the Diagnostic Clinic visit averaged 6.3 days. This delay usually was determined by the availability of the CT-guided biopsy or the dedicated interventional pulmonologist. Although other interventional pulmonologists at JLMMVH may perform the requisite diagnostic procedures, they are not always available for immediate review of imaging studies of referred patients nor can their schedules flexibly accommodate the number of patients seen in our clinic for evaluation.
Lung Cancer Diagnosis
Prompt diagnosis in the setting of a worrisome chest X-ray may help decrease patient anxiety, but does the clinic improve lung cancer treatment outcomes? Such improvement has been demonstrated only in stage IA squamous cell lung cancer.9 Of our study population, 37.7% had squamous cell carcinoma, and 85.5% had non-small cell lung cancer. Of those with non-small cell lung cancer, 28.9% had a clinical stage I tumor. Stage I squamous cell carcinoma, the type of tumor most likely to benefit from early diagnosis and treatment, was diagnosed in 11.3% of patients. With the increased application of LDCT screening, the proportion of veterans identified with early stage lung cancer may rise. The Providence VAMC in Rhode Island reported its results from instituting LDCT screening.12 Prior to screening, 28% of patients diagnosed with lung cancer had a stage I tumor. Following the introduction of LDCT screening, 49% diagnosed by LDCT screening had a stage I tumor. Nearly a third of their patients diagnosed with lung cancer through LDCT screening had squamous cell tumor histology. Thus, we can anticipate an increasing number of veterans with early stage lung cancer who would benefit from timely diagnosis.
The JLMMVH is a referral center for the entire state of Arkansas. Quite a few of its referred patients come from a long distance, which may require overnight housing and other related travel expenses. Apart from any potential outcome benefit, the efficiencies of the system described herein include the minimization of extra trips, an inconvenience and cost to both patient and JLMMVH.
Although the primary task of the clinic is diagnosis, we also seek to facilitate timely treatment. Our lack of an on-site PET scanner and radiation therapy, resources present on-site at the Dayton VAMC, contribute to longer therapy wait times. The shortest mean wait time at JLMMVH is for chemotherapy alone (34.7 days), in part because the JLMMVH oncologists, performing initial consultations 2 to 3 times weekly in the Diagnostic Clinic, are more readily available than are our thoracic surgeons or radiation therapists. Yet overall, JLMMVH patients often face delay from the time of lung cancer diagnosis to initiation of treatment.
The Connecticut Veterans Affairs Healthcare System has published the results of changes in lung cancer management associated with a nurse navigator system.10 Prior to creating the position of cancer care coordinator, filled by an advanced practice RNs, the mean time from clinical suspicion of lung cancer to treatment was 117 days. After 4 years of such care navigation, this waiting time had decreased to 52.4 days. Associated with this dramatic improvement in overall waiting time were decreases in the turnaround time required for performance of CT and PET scans. With respect to this big picture view of lung cancer care, our Diagnostic Clinic serves as a model for the initial step of diagnosis. Coordination and streamlining of the various steps from diagnosis to definitive therapy shall require a more system-wide effort involving all the key players in cancer care.
Conclusion
We have developed a care pathway based in a dedicated diagnostic clinic and have been able to document the shortest interval from abnormality to diagnosis of lung cancer reported in the literature to date. Efficient functioning of this clinic is dependent upon the close cooperation between a full-time RN clinic manager and an interventional pulmonologist experienced in lung cancer management and able to interpret cytologic samples at the time of biopsy. Shortening the delay between diagnosis and definitive therapy remains a challenge and may benefit from the oncology nurse navigator model previously described within the VA system. 10
Lung cancer is the leading cause of cancer death in the US, with 154 050 deaths in 2018.1 There have been many attempts to reduce mortality of the disease through early diagnosis with use of computed tomography (CT). The National Lung Cancer Screening trial showed that screening high-risk populations with low-dose CT (LDCT) can reduce mortality.2 However, implementing LDCT screening in the clinical setting has proven challenging, as illustrated by the VA Lung Cancer Screening Demonstration Project (LCSDP).3 A lung cancer diagnosis typically comprises several steps that require different medical specialties; this can lead to delays. In the LCSDP, the mean time to diagnosis was 137 days.3 There are no federal standards for timeliness of lung cancer diagnosis.
The nonprofit RAND Corporation is the only American research organization that has published guidelines specifying acceptable intervals for the diagnosis and treatment of lung cancer. In Quality of Care for Oncologic Conditions and HIV, RAND Corporation researchers propose management quality indicators: lung cancer diagnosis within 2 months of an abnormal radiologic study and treatment within 6 weeks of diagnosis.4 The Swedish Lung Cancer Study5 and the Canadian Strategy for Cancer Control6 both recommended a standard of about 30 days—half the time recommended by the RAND Corporation.
Bukhari and colleagues at the Dayton US Department of Veterans Affairs (VA) Medical Center (VAMC) conducted a quality improvement study that examined lung cancer diagnosis and management.7 They found the time (SD) from abnormal chest imaging to diagnosis was 35.5 (31.6) days. Of those veterans who received a lung cancer diagnosis, 89.2% had the diagnosis made within the 60 days recommended by the RAND Corporation. Although these results surpass those of the LCSDP, they can be exceeded.
Beyond the potential emotional distress of awaiting the final diagnosis of a lung lesion, a delay in diagnosis and treatment may adversely affect outcomes. LDCT screening has been shown to reduce mortality, which implies a link between survival and time to intervention. There is no published evidence that time to diagnosis in advanced stage lung cancer affects outcome. The National Cancer Database (NCDB) contains informtion on about 70% of the cancers diagnosed each year in the US.8 An analysis of 4984 patients with stage IA squamous cell lung cancer undergoing lobectomy from NCDB showed that earlier surgery was associated with an absolute decrease in 5-year mortality of 5% to 8%. 9 Hence, at least in early-stage disease, reduced time from initial suspect imaging to definitive treatment may improve survival.
A system that coordinates the requisite diagnostic steps and avoids delays should provide a significant improvement in patient care. The results of such an approach that utilized nurse navigators has been previously published. 10 Here, we present the results of a dedicated VA referral clinic with priority access to pulmonary consultation and procedures in place that are designed to expedite the diagnosis of potential lung cancer.
Methods
The John L. McClellan Memorial Veterans Hospital (JLMMVH) in Little Rock, Arkansas institutional review board approved this study, which was performed in accordance with the Declaration of Helsinki. Requirement for informed consent was waived, and patient confidentiality was maintained throughout.
We have developed a plan of care specifically to facilitate diagnosis and treatment of the large number of veterans referred to the JLMMVH Diagnostic Clinic for abnormal results of chest imaging. The clinic has priority access to same-day imaging and subspecialty consultation services. In the clinic, medical students and residents perform evaluations and a registered nurse (RN) manager coordinates care.
A Diagnostic Clinic consult for abnormal thoracic imaging immediately triggers an e-consult to an interventional pulmonologist (Figure). The RN manager and pulmonologist perform a joint review of records/imaging prior to scheduling, and the pulmonologist triages the patient. Triage options include follow-up imaging, bronchoscopy with endobronchial ultrasound (EBUS), endoscopic ultrasound (EUS), and CT-guided biopsy.
The RN manager then schedules a clinic visit that includes a medical evaluation by clinic staff and any indicated procedures on the same day. The interventional pulmonologist performs EBUS, EUS with the convex curvilinear bronchoscope, or both combined as indicated for diagnosis and staging. All procedures are performed in the JLMMVH bronchoscopy suite with standard conscious sedation using midazolam and fentanyl. Any other relevant procedures, such as pleural tap, also are performed at time of procedure. The pulmonologist and an attending pathologist interpret biopsies obtained in the bronchoscopy suite.
We performed a retrospective chart review of patients diagnosed with primary lung cancer through referral to the JLMMVH Diagnostic Clinic. The primary outcome was time from initial suspect chest imaging to cancer diagnosis. The study population consisted of patients referred for abnormal thoracic imaging between January 1, 2013 and December 31, 2016 and subsequently diagnosed with a primary lung cancer.
Subjects were excluded if (1) the patient was referred from outside our care network and a delay of > 10 days occurred between initial lesion imaging and referral; (2) the patient did not show up for appointments or chose to delay evaluation following referral; (3) biopsy demonstrated a nonlung primary cancer; and (4) serious intercurrent illness interrupted the diagnostic plan. In some cases, the radiologist or consulting pulmonologist had judged the lung lesion too small for immediate biopsy and recommended repeat imaging at a later date.
Patients were included in the study if the follow- up imaging led to a lung cancer diagnosis. However, because the interval between the initial imaging and the follow-up imaging in these patients did not represent a systems delay problem, the date of the scheduled follow-up abnormal imaging, which resulted in initiation of a potential cancer evaluation, served as the index suspect imaging date for this study.
Patient electronic medical records were reviewed and the following data were abstracted: date of the abnormal imaging that led to referral and time from abnormal chest X-ray to chest CT scan if applicable; date of referral and date of clinic visit; date of biopsy; date of lung cancer diagnosis; method of obtaining diagnostic specimen; lung cancer type and stage; type and date of treatment initiation or decision for supportive care only; and decision to seek further evaluation or care outside of our system.
All patients diagnosed with lung cancer during the study period were reviewed for inclusion, hence no required sample-size estimate was calculated. All outcomes were assessed as calendar days. The primary outcome was the time from the index suspect chest imaging study to the date of diagnosis of lung cancer. Prior to the initiation of our study, we chose this more stringent 30-day recommendation of the Canadian6 and Swedish5 studies as the comparator for our primary outcome, although data with respect to the 60-day Rand Corporation guidelines also are reported.4
Statistical Methods
The mean time to lung cancer diagnosis in our cohort was compared with this 30-day standard using a 2-sided Mann–Whitney U test. Normality of data distribution was determined using the Kolmogorov–Smirnov test. For statistical significance testing a P value of .05 was used. Statistical calculations were performed using R statistical software version 3.2.4. Secondary outcomes consisted of time from diagnosis to treatment; proportion of subjects diagnosed within 60 days; time from initial clinic visit to biopsy; and time from biopsy to diagnosis.
Results
Overall, 222 patients were diagnosed with a malignant lung lesion, of which 63 were excluded from analysis: 22 cancelled or did not appear for appointments, declined further evaluation, or completed evaluation outside of our network; 13 had the diagnosis made prior to Diagnostic Clinic visit; 13 proved to have a nonlung primary tumor presenting in the lung or mediastinal nodes; 12 were delayed > 10 days in referral from an outside network; and 3 had an intervening serious acute medical problem forcing delay in the diagnostic process.
Of the 159 included subjects, 154 (96.9%) were male, and the mean (SD) age was 67.6 (8.1) years. For 76 subjects, the abnormal chest X-ray and subsequent chest CT scan were performed the same day or the lung lesion had initially been noted on a CT scan. For 54 subjects, there was a delay of ≥ 1 week in obtaining a chest CT scan. The mean (SD) time from placement of the Diagnostic Clinic consultation by the primary care provider (PCP) or other provider and the initial Diagnostic Clinic visit was 6.3 (4.4) days. The mean (SD) time from suspect imaging to diagnosis (primary outcome) was 22.6(16.6) days.
The distribution of this outcome was nonnormal (Kolmogorov-Smirnov test P < .01). When compared with the standard of 30 days, the primary outcome of 22.6 days was significantly shorter (2-sided Mann–Whitney U test P < .01). Three-quarters (76.1%) of subjects were diagnosed within 30 days and 95.0% of subjects were diagnosed within 60 days of the initial imaging. For the 8 subjects diagnosed after 60 days, contributing factors included PCP delay in Diagnostic Clinic consultation, initial negative biopsy, delay in performance of chest CT scan prior to consultation, and outsourcing of positron emission tomography (PET) scans.
Overall, 57 (35.8%) of the subjects underwent biopsy on the day of their Diagnostic Clinic visit: 14 underwent CT-guided biopsy and 43 underwent EBUS/EUS. Within 2 days of the initial visit 106 subjects (66.7%) had undergone biopsy. The mean (SD) time from initial Diagnostic Clinic visit to biopsy was 6.3 (9.5) days. The mean (SD) interval was 1.8 (3.0) days for EBUS/ EUS and 11.3 (11.7) days for CT-guided biopsy. The mean (SD) interval from biopsy to diagnosis was 3.2 (6.2) days with 64 cases (40.3%) diagnosed the day of biopsy.
Excluding subjects whose treatment was delayed by patient choice or intercurrent illness, and those who left the VA system to seek treatment elsewhere (n = 21), 24 opted for palliative care, 5 died before treatment could be initiated, and 109 underwent treatment for their tumors (Table). The mean times (SD) from diagnosis to treatment were: chemotherapy alone 34.7 (25.3) days; chemoradiation 37.0 (22.8) days; surgery 44.3 (24.4) days; radiation therapy alone 47.9 (26.0) days. With respect to the RAND Corporation recommended diagnosis to treatment time, 60.9% of chemotherapy alone, 61.5% of chemoradiation, 66.7% of surgery, and 45.0% of radiation therapy alone treatments were initiated within the 6-week window.
Discussion
This retrospective case study demonstrates the effectiveness of a dedicated diagnostic clinic with priority EBUS/EUS access in diagnosing lung cancer within the VA system. Although there is no universally accepted quality standard for comparison, the RAND Corporation recommendation of 60 days from abnormal imaging to diagnosis and the Dayton VAMC published mean of 35.5 days are guideposts; however, the results from the Dayton VAMC may have been affected negatively by some subjects undergoing serial imaging for asymptomatic nodules. We chose a more stringent standard of 30 days as recommended by Swedish and Canadian task forces.
When diagnosing lung cancer, the overriding purpose of the Diagnostic Clinic is to minimize system delays. The method is to have as simple a task as possible for the PCP or other provider who identifies a lung nodule or mass and submits a single consultation request to the Diagnostic Clinic. Once this consultation is placed, the clinic RN manager oversees all further steps required for diagnosis and referral for treatment. The key factor in achieving a mean diagnosis time of 22.6 days is the cooperation between the RN manager and the interventional pulmonologist. When a consultation is received, the RN manager and pulmonologist review the data together and schedule the initial clinic visit; the goal is same-day biopsy, which is achieved in more than one-third of cases. Not all patients with a chest image suspected for lung cancer had it ordered by their PCP. For this reason, a Diagnostic Clinic consultation is available to all health care providers in our system. Many patients reach the clinic after the discovery of a suspect chest X-ray during an emergency department visit, a regularly scheduled subspecialty appointment, or during a preoperative evaluation.
The mean time from initial visit to biopsy was 1.8 days for EBUS/EUS compared with an interval of 11.3 days for CT-guided biopsy. This difference reflects the pulmonologist’s involvement in initial scheduling of Diagnostic Clinic patients. The ability of the pulmonologist to provide an accurate assessment of sample adequacy and a preliminary diagnosis at bedside, with concurrent confirmation by a staff pathologist, permitted the Diagnostic Clinic to inform 40.3% of patients of the finding of malignancy on the day of biopsy. A published comparison of the onsite review of biopsy material showed our pulmonologist and staff pathologists to be equally accurate in their interpretations.11
Sources of Delays
While this study documents the shortest intervals from suspect imaging to diagnosis reported to date, it also identifies sources of system delay in diagnosing lung cancer that JLMMVH could further optimize. The first is the time from initial abnormal chest X-ray imaging to performance of the chest CT scan. On occasion, the index lung lesion is identified unexpectedly on an outpatient or emergency department chest CT scan. With greater use of LDCT lung cancer screening, the initial detection of suspect lesions by CT scanning will increase in the future. However, the PCP most often investigates a patient complaint with a standard chest X-ray that reveals a suspect nodule or mass. When ordered by the PCP as an outpatient test, scheduling of the follow-up chest CT scan is not given priority. More than a third of subjects experienced a delay ≥ 1 week in obtaining a chest CT scan ordered by the PCP; for 29 subjects the delay was ≥ 3weeks. At JLMMVH, the Diagnostic Clinic is given priority in scheduling CT scans. Hence, for suspect lung lesions, the chest CT scan, if not already obtained, is generally performed on the morning of the clinic visit. Educating the PCP to refer the patient immediately to the Diagnostic Clinic rather than waiting to obtain an outpatient chest CT scan may remove this source of unnecessary delay.
Scheduling a CT-guided fine needle aspiration of a lung lesion is another source of system delay. When the chest CT scan is available at the time of the Diagnostic Clinic referral, the clinic visit is scheduled for the earliest day a required CT-guided biopsy can be performed. However, the mean time of 11.3 days from initial Diagnostic Clinic visit to CT-guided biopsy is indicative of the backlog faced by the interventional radiologists.
Although infrequent, PET scans that are required before biopsy can lead to substantial delays. PET scans are performed at our university affiliate, and the joint VA-university lung tumor board sometimes generates requests for such scans prior to tissue diagnosis, yet another source of delay.
The time from referral receipt to the Diagnostic Clinic visit averaged 6.3 days. This delay usually was determined by the availability of the CT-guided biopsy or the dedicated interventional pulmonologist. Although other interventional pulmonologists at JLMMVH may perform the requisite diagnostic procedures, they are not always available for immediate review of imaging studies of referred patients nor can their schedules flexibly accommodate the number of patients seen in our clinic for evaluation.
Lung Cancer Diagnosis
Prompt diagnosis in the setting of a worrisome chest X-ray may help decrease patient anxiety, but does the clinic improve lung cancer treatment outcomes? Such improvement has been demonstrated only in stage IA squamous cell lung cancer.9 Of our study population, 37.7% had squamous cell carcinoma, and 85.5% had non-small cell lung cancer. Of those with non-small cell lung cancer, 28.9% had a clinical stage I tumor. Stage I squamous cell carcinoma, the type of tumor most likely to benefit from early diagnosis and treatment, was diagnosed in 11.3% of patients. With the increased application of LDCT screening, the proportion of veterans identified with early stage lung cancer may rise. The Providence VAMC in Rhode Island reported its results from instituting LDCT screening.12 Prior to screening, 28% of patients diagnosed with lung cancer had a stage I tumor. Following the introduction of LDCT screening, 49% diagnosed by LDCT screening had a stage I tumor. Nearly a third of their patients diagnosed with lung cancer through LDCT screening had squamous cell tumor histology. Thus, we can anticipate an increasing number of veterans with early stage lung cancer who would benefit from timely diagnosis.
The JLMMVH is a referral center for the entire state of Arkansas. Quite a few of its referred patients come from a long distance, which may require overnight housing and other related travel expenses. Apart from any potential outcome benefit, the efficiencies of the system described herein include the minimization of extra trips, an inconvenience and cost to both patient and JLMMVH.
Although the primary task of the clinic is diagnosis, we also seek to facilitate timely treatment. Our lack of an on-site PET scanner and radiation therapy, resources present on-site at the Dayton VAMC, contribute to longer therapy wait times. The shortest mean wait time at JLMMVH is for chemotherapy alone (34.7 days), in part because the JLMMVH oncologists, performing initial consultations 2 to 3 times weekly in the Diagnostic Clinic, are more readily available than are our thoracic surgeons or radiation therapists. Yet overall, JLMMVH patients often face delay from the time of lung cancer diagnosis to initiation of treatment.
The Connecticut Veterans Affairs Healthcare System has published the results of changes in lung cancer management associated with a nurse navigator system.10 Prior to creating the position of cancer care coordinator, filled by an advanced practice RNs, the mean time from clinical suspicion of lung cancer to treatment was 117 days. After 4 years of such care navigation, this waiting time had decreased to 52.4 days. Associated with this dramatic improvement in overall waiting time were decreases in the turnaround time required for performance of CT and PET scans. With respect to this big picture view of lung cancer care, our Diagnostic Clinic serves as a model for the initial step of diagnosis. Coordination and streamlining of the various steps from diagnosis to definitive therapy shall require a more system-wide effort involving all the key players in cancer care.
Conclusion
We have developed a care pathway based in a dedicated diagnostic clinic and have been able to document the shortest interval from abnormality to diagnosis of lung cancer reported in the literature to date. Efficient functioning of this clinic is dependent upon the close cooperation between a full-time RN clinic manager and an interventional pulmonologist experienced in lung cancer management and able to interpret cytologic samples at the time of biopsy. Shortening the delay between diagnosis and definitive therapy remains a challenge and may benefit from the oncology nurse navigator model previously described within the VA system. 10
1. American Cancer Society. Cancer Facts & Figures. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf. Accessed July 13, 2019.
2. National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Eng J Med. 2011;365(5):395-409.
3. Kinsinger LS, Anderson C, Kim J, et al. Implementation of lung cancer screening in the Veterans Health Administration. JAMA Intern Med. 2017;177(3):399-406.
4. Asch SM, Kerr EA, Hamilton EG, Reifel JL, McGlynn EA, eds. Quality of Care for Oncologic Conditions and HIV: A Review of the Literature and Quality Indicators. Santa Monica, CA: RAND Corporation; 2000.
5. Hillerdal G. [Recommendations from the Swedish Lung Cancer Study Group: Shorter waiting times are demanded for quality in diagnostic work-ups for lung care.] Swedish Med J 1999; 96: 4691.
6. Simunovic M, Gagliardi A, McCready D, Coates A, Levine M, DePetrillo D. A snapshot of waiting times for cancer surgery provided by surgeons affiliated with regional cancer centres in Ontario. CMAJ. 2001;165(4):421-425. [Canadian Strategy for Cancer Control]
7. Bukhari A, Kumar G, Rajsheker R, Markert R. Timeliness of lung cancer diagnosis and treatment. Fed Pract. 2017;34(suppl 1):24S-29S.
8. Bilimoria KY, Ko CY, Tomlinson JS, et al. Wait times for cancer surgery in the United States: trends and predictors of delays. Ann Surg. 2011;253(4):779-785.
9. Yang CJ, Wang H, Kumar A, et al. Impact of timing of lobectomy on survival for clinical stage IA lung squamous cell carcinoma. Chest. 2017;152(6):1239-1250.
10. Hunnibell LS, Rose MG, Connery DM, et al. Using nurse navigation to improve timeliness of lung cancer care at a veterans hospital. Clin J Oncol Nurs. 2012;16(1):29-36.
11. Meena N, Jeffus S, Massoll N, et al. Rapid onsite evaluation: a comparison of cytopathologist and pulmonologist performance. Cancer Cytopatho. 2016;124(4):279-84.
12. Okereke IC, Bates MF, Jankowich MD, et al. Effects of implementation of lung cancer screening at one Veterans Affairs Medical Center. Chest 2016;150(5):1023-1029.
1. American Cancer Society. Cancer Facts & Figures. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf. Accessed July 13, 2019.
2. National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Eng J Med. 2011;365(5):395-409.
3. Kinsinger LS, Anderson C, Kim J, et al. Implementation of lung cancer screening in the Veterans Health Administration. JAMA Intern Med. 2017;177(3):399-406.
4. Asch SM, Kerr EA, Hamilton EG, Reifel JL, McGlynn EA, eds. Quality of Care for Oncologic Conditions and HIV: A Review of the Literature and Quality Indicators. Santa Monica, CA: RAND Corporation; 2000.
5. Hillerdal G. [Recommendations from the Swedish Lung Cancer Study Group: Shorter waiting times are demanded for quality in diagnostic work-ups for lung care.] Swedish Med J 1999; 96: 4691.
6. Simunovic M, Gagliardi A, McCready D, Coates A, Levine M, DePetrillo D. A snapshot of waiting times for cancer surgery provided by surgeons affiliated with regional cancer centres in Ontario. CMAJ. 2001;165(4):421-425. [Canadian Strategy for Cancer Control]
7. Bukhari A, Kumar G, Rajsheker R, Markert R. Timeliness of lung cancer diagnosis and treatment. Fed Pract. 2017;34(suppl 1):24S-29S.
8. Bilimoria KY, Ko CY, Tomlinson JS, et al. Wait times for cancer surgery in the United States: trends and predictors of delays. Ann Surg. 2011;253(4):779-785.
9. Yang CJ, Wang H, Kumar A, et al. Impact of timing of lobectomy on survival for clinical stage IA lung squamous cell carcinoma. Chest. 2017;152(6):1239-1250.
10. Hunnibell LS, Rose MG, Connery DM, et al. Using nurse navigation to improve timeliness of lung cancer care at a veterans hospital. Clin J Oncol Nurs. 2012;16(1):29-36.
11. Meena N, Jeffus S, Massoll N, et al. Rapid onsite evaluation: a comparison of cytopathologist and pulmonologist performance. Cancer Cytopatho. 2016;124(4):279-84.
12. Okereke IC, Bates MF, Jankowich MD, et al. Effects of implementation of lung cancer screening at one Veterans Affairs Medical Center. Chest 2016;150(5):1023-1029.