User login
Abs from transplanted AML patients enhance GvL effect in vitro

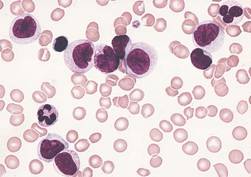
NEW YORK—Investigators have found that B cells may play a role in stimulating graft-versus-leukemia (GvL) responses in patients with acute myeloid leukemia (AML) who have undergone allogeneic hematopoietic stem cell transplant (HSCT).
The team created B cell lines from these patients, isolated AML-specific antibodies, and found that these antibodies can induce the death of AML cells through oncosis.
Oncosis is a non-apoptotic type of cell death that involves swelling and coagulation of the cytoplasm.
Mette Hazenberg, MD, PhD, from the Academic Medical Center in Amsterdam, The Netherlands, reported these findings at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference as poster B052.
The investigators cloned B cells from 3 high-risk AML patients who had a strong GvL response after HSCT.
The team transduced memory B cells from the patients’ peripheral blood using BCL-6 and BCL-xL. They then screened the B cells for those that produced antibodies that bound specifically to surface antigens on AML cell lines and blasts.
Six of the 15 AML antibodies retrieved from the patients bound specifically to snRNp200. In normal cells, snRNp200 is in the nucleus, but, in AML, it is exposed on the cell membrane.
The investigators then confirmed this by ELISA.
They found 7 of the 15 AML antibodies directly lysed AML blasts without the addition of effector cells or complement. Time-lapse images showed that cell death by the AML antibodies occurred rapidly, within minutes after incubation.
“The leukemia blasts popped like balloons,” Dr Hazenberg said.
The investigators confirmed that the antibodies induced cell death by oncosis and that oncosis occurred independently of temperature. The antibodies were cytotoxic at 4°C and 37°C.
Cytotoxicity of the antibodies could be blocked by the membrane stabilizer cytochalasin D but not by apoptosis inhibitors.
The team concluded that a potent GvL response could be mediated by these antibodies against tumor-associated antigens on AML cells.
Dr Hazenberg’s hope is that, at some point, these antibodies can be combined with chemotherapy—as is rituximab—so patients won’t need to undergo transplant. ![]()
NEW YORK—Investigators have found that B cells may play a role in stimulating graft-versus-leukemia (GvL) responses in patients with acute myeloid leukemia (AML) who have undergone allogeneic hematopoietic stem cell transplant (HSCT).
The team created B cell lines from these patients, isolated AML-specific antibodies, and found that these antibodies can induce the death of AML cells through oncosis.
Oncosis is a non-apoptotic type of cell death that involves swelling and coagulation of the cytoplasm.
Mette Hazenberg, MD, PhD, from the Academic Medical Center in Amsterdam, The Netherlands, reported these findings at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference as poster B052.
The investigators cloned B cells from 3 high-risk AML patients who had a strong GvL response after HSCT.
The team transduced memory B cells from the patients’ peripheral blood using BCL-6 and BCL-xL. They then screened the B cells for those that produced antibodies that bound specifically to surface antigens on AML cell lines and blasts.
Six of the 15 AML antibodies retrieved from the patients bound specifically to snRNp200. In normal cells, snRNp200 is in the nucleus, but, in AML, it is exposed on the cell membrane.
The investigators then confirmed this by ELISA.
They found 7 of the 15 AML antibodies directly lysed AML blasts without the addition of effector cells or complement. Time-lapse images showed that cell death by the AML antibodies occurred rapidly, within minutes after incubation.
“The leukemia blasts popped like balloons,” Dr Hazenberg said.
The investigators confirmed that the antibodies induced cell death by oncosis and that oncosis occurred independently of temperature. The antibodies were cytotoxic at 4°C and 37°C.
Cytotoxicity of the antibodies could be blocked by the membrane stabilizer cytochalasin D but not by apoptosis inhibitors.
The team concluded that a potent GvL response could be mediated by these antibodies against tumor-associated antigens on AML cells.
Dr Hazenberg’s hope is that, at some point, these antibodies can be combined with chemotherapy—as is rituximab—so patients won’t need to undergo transplant. ![]()
NEW YORK—Investigators have found that B cells may play a role in stimulating graft-versus-leukemia (GvL) responses in patients with acute myeloid leukemia (AML) who have undergone allogeneic hematopoietic stem cell transplant (HSCT).
The team created B cell lines from these patients, isolated AML-specific antibodies, and found that these antibodies can induce the death of AML cells through oncosis.
Oncosis is a non-apoptotic type of cell death that involves swelling and coagulation of the cytoplasm.
Mette Hazenberg, MD, PhD, from the Academic Medical Center in Amsterdam, The Netherlands, reported these findings at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference as poster B052.
The investigators cloned B cells from 3 high-risk AML patients who had a strong GvL response after HSCT.
The team transduced memory B cells from the patients’ peripheral blood using BCL-6 and BCL-xL. They then screened the B cells for those that produced antibodies that bound specifically to surface antigens on AML cell lines and blasts.
Six of the 15 AML antibodies retrieved from the patients bound specifically to snRNp200. In normal cells, snRNp200 is in the nucleus, but, in AML, it is exposed on the cell membrane.
The investigators then confirmed this by ELISA.
They found 7 of the 15 AML antibodies directly lysed AML blasts without the addition of effector cells or complement. Time-lapse images showed that cell death by the AML antibodies occurred rapidly, within minutes after incubation.
“The leukemia blasts popped like balloons,” Dr Hazenberg said.
The investigators confirmed that the antibodies induced cell death by oncosis and that oncosis occurred independently of temperature. The antibodies were cytotoxic at 4°C and 37°C.
Cytotoxicity of the antibodies could be blocked by the membrane stabilizer cytochalasin D but not by apoptosis inhibitors.
The team concluded that a potent GvL response could be mediated by these antibodies against tumor-associated antigens on AML cells.
Dr Hazenberg’s hope is that, at some point, these antibodies can be combined with chemotherapy—as is rituximab—so patients won’t need to undergo transplant. ![]()
Hospital readmission following transplantation: identifying risk factors and designing preventive measures
Background About 1 in 7 of all hospitalized patients is readmitted within 30 days of discharge. The cost of readmissions is significant, with Medicare readmissions alone costing the health care system an estimated $28 billion a year.
Objective To identify the rates of and causes for readmission within 100 days of patients receiving a hematopoietic stem cell transplant.
Methods We performed a retrospective review of 235 consecutive transplant recipients (autologous, n = 144; allogeneic, n = 91) to determine rates and causes for readmission within 100 days of patients receiving a transplant. Medical records and hospital readmissions were reviewed for each patient.
Results 36 allogeneic patients accounted for 56 readmissions. 23 autologous patients accounted for 26 readmissions. Autologous transplant recipients were most commonly readmitted for the development of a fever (n = 15 patients) or cardiopulmonary issues (n = 4). The most prevalent reasons for readmission in the allogeneic recipients included a fever (n = 21) or the development or exacerbation of graft-versus-host disease (n = 5). The readmission length of stay was 6 days (median range, 1-91 days) for allogeneic patients and 4 days (median range, 1-22 days) for autologous patients. There was no difference in survival between the readmitted and the non-readmitted cohorts (P = .55 for allogeneic patients; P = .24 for autologous patients). Although allogeneic graft recipients demonstrated a higher readmission rate (39.6%) compared with autologous recipients (16%), none of the variables examined, including age, gender, performance status, diagnosis, remission status at the time of transplant, comorbidities, type of preparative chemotherapy regimen or donor type, identified patients at increased risk for readmission.
Limitations Variations in clinical care, physician practices, and patient characteristics need to be considered when examining readmission rates. Most of the allogeneic patient population included unrelated donor recipients (65%) who received nonmyeloablative conditioning regimens (81% of allogeneic recipients). These features may not be characteristic of other centers.
Conclusions In these high-risk patients, readmissions following a transplant are common. Enhanced predischarge education by nurses and pharmacists, along with ongoing outpatient education and rigorous outpatient follow-up through phone calls or social media may decrease readmission rates.
Click on the PDF icon at the top of this introduction to read the full article.
Background About 1 in 7 of all hospitalized patients is readmitted within 30 days of discharge. The cost of readmissions is significant, with Medicare readmissions alone costing the health care system an estimated $28 billion a year.
Objective To identify the rates of and causes for readmission within 100 days of patients receiving a hematopoietic stem cell transplant.
Methods We performed a retrospective review of 235 consecutive transplant recipients (autologous, n = 144; allogeneic, n = 91) to determine rates and causes for readmission within 100 days of patients receiving a transplant. Medical records and hospital readmissions were reviewed for each patient.
Results 36 allogeneic patients accounted for 56 readmissions. 23 autologous patients accounted for 26 readmissions. Autologous transplant recipients were most commonly readmitted for the development of a fever (n = 15 patients) or cardiopulmonary issues (n = 4). The most prevalent reasons for readmission in the allogeneic recipients included a fever (n = 21) or the development or exacerbation of graft-versus-host disease (n = 5). The readmission length of stay was 6 days (median range, 1-91 days) for allogeneic patients and 4 days (median range, 1-22 days) for autologous patients. There was no difference in survival between the readmitted and the non-readmitted cohorts (P = .55 for allogeneic patients; P = .24 for autologous patients). Although allogeneic graft recipients demonstrated a higher readmission rate (39.6%) compared with autologous recipients (16%), none of the variables examined, including age, gender, performance status, diagnosis, remission status at the time of transplant, comorbidities, type of preparative chemotherapy regimen or donor type, identified patients at increased risk for readmission.
Limitations Variations in clinical care, physician practices, and patient characteristics need to be considered when examining readmission rates. Most of the allogeneic patient population included unrelated donor recipients (65%) who received nonmyeloablative conditioning regimens (81% of allogeneic recipients). These features may not be characteristic of other centers.
Conclusions In these high-risk patients, readmissions following a transplant are common. Enhanced predischarge education by nurses and pharmacists, along with ongoing outpatient education and rigorous outpatient follow-up through phone calls or social media may decrease readmission rates.
Click on the PDF icon at the top of this introduction to read the full article.
Background About 1 in 7 of all hospitalized patients is readmitted within 30 days of discharge. The cost of readmissions is significant, with Medicare readmissions alone costing the health care system an estimated $28 billion a year.
Objective To identify the rates of and causes for readmission within 100 days of patients receiving a hematopoietic stem cell transplant.
Methods We performed a retrospective review of 235 consecutive transplant recipients (autologous, n = 144; allogeneic, n = 91) to determine rates and causes for readmission within 100 days of patients receiving a transplant. Medical records and hospital readmissions were reviewed for each patient.
Results 36 allogeneic patients accounted for 56 readmissions. 23 autologous patients accounted for 26 readmissions. Autologous transplant recipients were most commonly readmitted for the development of a fever (n = 15 patients) or cardiopulmonary issues (n = 4). The most prevalent reasons for readmission in the allogeneic recipients included a fever (n = 21) or the development or exacerbation of graft-versus-host disease (n = 5). The readmission length of stay was 6 days (median range, 1-91 days) for allogeneic patients and 4 days (median range, 1-22 days) for autologous patients. There was no difference in survival between the readmitted and the non-readmitted cohorts (P = .55 for allogeneic patients; P = .24 for autologous patients). Although allogeneic graft recipients demonstrated a higher readmission rate (39.6%) compared with autologous recipients (16%), none of the variables examined, including age, gender, performance status, diagnosis, remission status at the time of transplant, comorbidities, type of preparative chemotherapy regimen or donor type, identified patients at increased risk for readmission.
Limitations Variations in clinical care, physician practices, and patient characteristics need to be considered when examining readmission rates. Most of the allogeneic patient population included unrelated donor recipients (65%) who received nonmyeloablative conditioning regimens (81% of allogeneic recipients). These features may not be characteristic of other centers.
Conclusions In these high-risk patients, readmissions following a transplant are common. Enhanced predischarge education by nurses and pharmacists, along with ongoing outpatient education and rigorous outpatient follow-up through phone calls or social media may decrease readmission rates.
Click on the PDF icon at the top of this introduction to read the full article.
Monitoring microbiome may help reduce infection in AML

Photo by Rhoda Baer
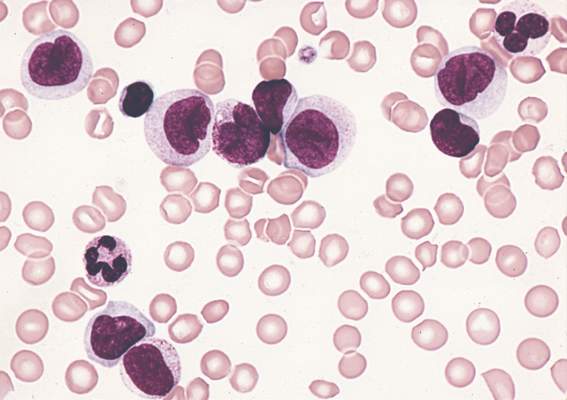
SAN DIEGO—Monitoring the microbiome during chemotherapy might help reduce infections in leukemia patients, according to research presented at ICAAC/ICC 2015.
The researchers studied buccal and fecal samples from patients with acute myeloid leukemia (AML) who were undergoing induction chemotherapy.
This revealed that decreased microbial diversity was associated with an increased risk of infection.
Jessica Galloway-Peña, PhD, of The University of Texas MD Anderson Cancer Center in Houston, and her colleagues described this work in a poster presentation at the meeting (poster B-993).
The team analyzed samples from 34 AML patients. All of the patients received prophylactic antimicrobials, and 91% received systemic antibiotics. The patients received an average of 5.4 different antibiotics for an average duration of 6.5 days.
The researchers collected buccal and fecal specimens from the patients every 96 hours over the course of induction chemotherapy. This yielded 276 buccal and 202 fecal samples—an average of 8 oral and 6 stool samples per patient.
The team used 16S rRNA V4 region sequencing to assign bacterial taxa and calculate α- and β-diversities. They had a total of 16,082,550 high-quality reads.
Analyzing these data, the researchers found that decreased microbial diversity, both at baseline and throughout induction, was associated with an increased risk of infection.
“We found the baseline microbial diversities from stool samples were significantly lower in patients that developed infections during chemotherapy compared to those that did not [P=0.006],” Dr Galloway-Peña said.
She and her colleagues also found that, overall, there was a significant decrease in oral (P=0.006) and intestinal (P<0.001) microbial diversity over the course of chemotherapy, although not all patients experienced decreases. There was a linear correlation between oral and stool microbiome changes (P=0.004).
In addition, over the course of induction, there was a significant increase (P=0.02) in the rates of bacterial domination (>30% of the microbiome dominated by 1 organism) by common causes of bacteremia, such as Streptococcus, Bacteriodes, Rothia, and Staphylococcus.
However, if patients were able to maintain a healthy microbiome overall or if they experienced an increase in microbial diversity over the induction course, they remained infection-free in the 90 days after induction.
Dr Galloway-Peña and her colleagues also assessed the role common antibiotics play in microbial diversity. And they found that carbapenems significantly decreased diversity.
There was a significant difference in oral and stool diversity when patients received carbapenems for at least 72 hours and when they did not (P=0.03). But there was no significant difference for piperacillin-tazobactam (P=1.0) or cefepime (P=0.48).
“This study shows that, in the future, doctors could use microbiome sampling in order to predict the chance of infectious complications during chemotherapy and that monitoring of a patient’s microbiome during induction chemotherapy could also predict their risk for microbial-related illness during subsequent treatments,” Dr Galloway-Peña said.
In addition, monitoring the microbiome could potentially mitigate the overuse of antimicrobials by allowing physicians to stratify patients according to their risk of developing an infection. ![]()
Photo by Rhoda Baer
SAN DIEGO—Monitoring the microbiome during chemotherapy might help reduce infections in leukemia patients, according to research presented at ICAAC/ICC 2015.
The researchers studied buccal and fecal samples from patients with acute myeloid leukemia (AML) who were undergoing induction chemotherapy.
This revealed that decreased microbial diversity was associated with an increased risk of infection.
Jessica Galloway-Peña, PhD, of The University of Texas MD Anderson Cancer Center in Houston, and her colleagues described this work in a poster presentation at the meeting (poster B-993).
The team analyzed samples from 34 AML patients. All of the patients received prophylactic antimicrobials, and 91% received systemic antibiotics. The patients received an average of 5.4 different antibiotics for an average duration of 6.5 days.
The researchers collected buccal and fecal specimens from the patients every 96 hours over the course of induction chemotherapy. This yielded 276 buccal and 202 fecal samples—an average of 8 oral and 6 stool samples per patient.
The team used 16S rRNA V4 region sequencing to assign bacterial taxa and calculate α- and β-diversities. They had a total of 16,082,550 high-quality reads.
Analyzing these data, the researchers found that decreased microbial diversity, both at baseline and throughout induction, was associated with an increased risk of infection.
“We found the baseline microbial diversities from stool samples were significantly lower in patients that developed infections during chemotherapy compared to those that did not [P=0.006],” Dr Galloway-Peña said.
She and her colleagues also found that, overall, there was a significant decrease in oral (P=0.006) and intestinal (P<0.001) microbial diversity over the course of chemotherapy, although not all patients experienced decreases. There was a linear correlation between oral and stool microbiome changes (P=0.004).
In addition, over the course of induction, there was a significant increase (P=0.02) in the rates of bacterial domination (>30% of the microbiome dominated by 1 organism) by common causes of bacteremia, such as Streptococcus, Bacteriodes, Rothia, and Staphylococcus.
However, if patients were able to maintain a healthy microbiome overall or if they experienced an increase in microbial diversity over the induction course, they remained infection-free in the 90 days after induction.
Dr Galloway-Peña and her colleagues also assessed the role common antibiotics play in microbial diversity. And they found that carbapenems significantly decreased diversity.
There was a significant difference in oral and stool diversity when patients received carbapenems for at least 72 hours and when they did not (P=0.03). But there was no significant difference for piperacillin-tazobactam (P=1.0) or cefepime (P=0.48).
“This study shows that, in the future, doctors could use microbiome sampling in order to predict the chance of infectious complications during chemotherapy and that monitoring of a patient’s microbiome during induction chemotherapy could also predict their risk for microbial-related illness during subsequent treatments,” Dr Galloway-Peña said.
In addition, monitoring the microbiome could potentially mitigate the overuse of antimicrobials by allowing physicians to stratify patients according to their risk of developing an infection. ![]()
Photo by Rhoda Baer
SAN DIEGO—Monitoring the microbiome during chemotherapy might help reduce infections in leukemia patients, according to research presented at ICAAC/ICC 2015.
The researchers studied buccal and fecal samples from patients with acute myeloid leukemia (AML) who were undergoing induction chemotherapy.
This revealed that decreased microbial diversity was associated with an increased risk of infection.
Jessica Galloway-Peña, PhD, of The University of Texas MD Anderson Cancer Center in Houston, and her colleagues described this work in a poster presentation at the meeting (poster B-993).
The team analyzed samples from 34 AML patients. All of the patients received prophylactic antimicrobials, and 91% received systemic antibiotics. The patients received an average of 5.4 different antibiotics for an average duration of 6.5 days.
The researchers collected buccal and fecal specimens from the patients every 96 hours over the course of induction chemotherapy. This yielded 276 buccal and 202 fecal samples—an average of 8 oral and 6 stool samples per patient.
The team used 16S rRNA V4 region sequencing to assign bacterial taxa and calculate α- and β-diversities. They had a total of 16,082,550 high-quality reads.
Analyzing these data, the researchers found that decreased microbial diversity, both at baseline and throughout induction, was associated with an increased risk of infection.
“We found the baseline microbial diversities from stool samples were significantly lower in patients that developed infections during chemotherapy compared to those that did not [P=0.006],” Dr Galloway-Peña said.
She and her colleagues also found that, overall, there was a significant decrease in oral (P=0.006) and intestinal (P<0.001) microbial diversity over the course of chemotherapy, although not all patients experienced decreases. There was a linear correlation between oral and stool microbiome changes (P=0.004).
In addition, over the course of induction, there was a significant increase (P=0.02) in the rates of bacterial domination (>30% of the microbiome dominated by 1 organism) by common causes of bacteremia, such as Streptococcus, Bacteriodes, Rothia, and Staphylococcus.
However, if patients were able to maintain a healthy microbiome overall or if they experienced an increase in microbial diversity over the induction course, they remained infection-free in the 90 days after induction.
Dr Galloway-Peña and her colleagues also assessed the role common antibiotics play in microbial diversity. And they found that carbapenems significantly decreased diversity.
There was a significant difference in oral and stool diversity when patients received carbapenems for at least 72 hours and when they did not (P=0.03). But there was no significant difference for piperacillin-tazobactam (P=1.0) or cefepime (P=0.48).
“This study shows that, in the future, doctors could use microbiome sampling in order to predict the chance of infectious complications during chemotherapy and that monitoring of a patient’s microbiome during induction chemotherapy could also predict their risk for microbial-related illness during subsequent treatments,” Dr Galloway-Peña said.
In addition, monitoring the microbiome could potentially mitigate the overuse of antimicrobials by allowing physicians to stratify patients according to their risk of developing an infection. ![]()
Insights from the 5-year follow-up of CTL019 in CLL

Photo courtesy of the
University of Pennsylvania
NEW YORK—The 5-year follow-up of the phase 1 trial of CTL019 in relapsed or refractory chronic lymphoblastic leukemia (CLL) is allowing investigators to define more clearly who will respond to chimeric antigen receptor (CAR) T cells directed against CD19.
One thing investigators have determined is that persistence of the CARs is essential for long-term responses.
In the first 2 patients who achieved a complete remission (CR), CAR T cells persisted for more than 4 years. In addition, no patient in CR has relapsed to date.
Of the 14 patients enrolled in the trial, 4 (28%) achieved a CR, 4 (28%) achieved a partial response, and 6 (43%) had no response, for an overall response rate of 57%.
These results were recently published in Science Translational Medicine.
Carl June, MD, of the University of Pennsylvania in Philadelphia, shared some insights into the research with attendees at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
Dr June explained that CTL019 is a CD19-directed single chain variable fragment with a 4-1BB signaling module that transduces T cells with a lentiviral vector. The technology was developed at the University of Pennsylvania and subsequently licensed to Novartis.
In the phase 1 trial of CTL019 in CLL, patients who achieved complete remission have very high levels of CARs—100% of the circulating T cells—but the non-responders don’t. The CARs engrafted in non-responders but did not proliferate.
“So the biomarker correlate of success is persistence and proliferation, in CLL at least,” Dr June said.
The investigators performed IGH next-generation sequencing and found no detectable CLL clones in the complete responders, including 1 patient at 3.5 years and another at 4 years post-infusion.
“There was no clinically evident disease in these patients,” Dr June said, “and so the responses are durable.”
The team also believes that at least a subset of the cells remains functional because the patients still had B-cell aplasia.
The investigators have not observed a CD19 loss in any CLL patient who responded.
“Patients who have gone into remission stay in remission,” Dr June added.
Kinetics of delayed CR
Dr June discussed in detail Patient 10, whose response was somewhat different from the other complete responders. Patient 10 achieved a CR, but the response was delayed. It took 51 days after infusion, compared to about 10 days in the other complete responders.
Patient 10 was initially scored as a failure at the 28-day evaluation. Eventually, he had marked improvement, and, by a year, he was in CR.
He required hospitalization for tumor lysis syndrome and treatment with tocilizumab for cytokine release syndrome.
Patient 10 had a single cell that investigators surmise could have been responsible for the tumor elimination.
“In fact, on day 28, when he still had tumor, his CARs were polyclonal,” Dr June said. “So we stained and isolated his CARs by sorting, and, at time of tumor elimination, he had descendants of 1 CAR.”
Nevertheless, Patient 10’s response is durable. He is now 81 years old and remains engrafted with CAR19 cells.
Investigators hypothesize that the kinetics and CAR proliferation were so different in Patient 10 because Tet2 was disrupted by the integration of the CAR into the intronic region.
“What we don’t know is whether Tet2 was a passenger or a driver here,” Dr June observed. “Did it actually aid the function of the CAR cells or was it just a marker?”
He noted that Tet2 has been shown in acute myeloid leukemia to increase stem cell renewal, “and it may well have done that in this patient.” ![]()
Photo courtesy of the
University of Pennsylvania
NEW YORK—The 5-year follow-up of the phase 1 trial of CTL019 in relapsed or refractory chronic lymphoblastic leukemia (CLL) is allowing investigators to define more clearly who will respond to chimeric antigen receptor (CAR) T cells directed against CD19.
One thing investigators have determined is that persistence of the CARs is essential for long-term responses.
In the first 2 patients who achieved a complete remission (CR), CAR T cells persisted for more than 4 years. In addition, no patient in CR has relapsed to date.
Of the 14 patients enrolled in the trial, 4 (28%) achieved a CR, 4 (28%) achieved a partial response, and 6 (43%) had no response, for an overall response rate of 57%.
These results were recently published in Science Translational Medicine.
Carl June, MD, of the University of Pennsylvania in Philadelphia, shared some insights into the research with attendees at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
Dr June explained that CTL019 is a CD19-directed single chain variable fragment with a 4-1BB signaling module that transduces T cells with a lentiviral vector. The technology was developed at the University of Pennsylvania and subsequently licensed to Novartis.
In the phase 1 trial of CTL019 in CLL, patients who achieved complete remission have very high levels of CARs—100% of the circulating T cells—but the non-responders don’t. The CARs engrafted in non-responders but did not proliferate.
“So the biomarker correlate of success is persistence and proliferation, in CLL at least,” Dr June said.
The investigators performed IGH next-generation sequencing and found no detectable CLL clones in the complete responders, including 1 patient at 3.5 years and another at 4 years post-infusion.
“There was no clinically evident disease in these patients,” Dr June said, “and so the responses are durable.”
The team also believes that at least a subset of the cells remains functional because the patients still had B-cell aplasia.
The investigators have not observed a CD19 loss in any CLL patient who responded.
“Patients who have gone into remission stay in remission,” Dr June added.
Kinetics of delayed CR
Dr June discussed in detail Patient 10, whose response was somewhat different from the other complete responders. Patient 10 achieved a CR, but the response was delayed. It took 51 days after infusion, compared to about 10 days in the other complete responders.
Patient 10 was initially scored as a failure at the 28-day evaluation. Eventually, he had marked improvement, and, by a year, he was in CR.
He required hospitalization for tumor lysis syndrome and treatment with tocilizumab for cytokine release syndrome.
Patient 10 had a single cell that investigators surmise could have been responsible for the tumor elimination.
“In fact, on day 28, when he still had tumor, his CARs were polyclonal,” Dr June said. “So we stained and isolated his CARs by sorting, and, at time of tumor elimination, he had descendants of 1 CAR.”
Nevertheless, Patient 10’s response is durable. He is now 81 years old and remains engrafted with CAR19 cells.
Investigators hypothesize that the kinetics and CAR proliferation were so different in Patient 10 because Tet2 was disrupted by the integration of the CAR into the intronic region.
“What we don’t know is whether Tet2 was a passenger or a driver here,” Dr June observed. “Did it actually aid the function of the CAR cells or was it just a marker?”
He noted that Tet2 has been shown in acute myeloid leukemia to increase stem cell renewal, “and it may well have done that in this patient.” ![]()
Photo courtesy of the
University of Pennsylvania
NEW YORK—The 5-year follow-up of the phase 1 trial of CTL019 in relapsed or refractory chronic lymphoblastic leukemia (CLL) is allowing investigators to define more clearly who will respond to chimeric antigen receptor (CAR) T cells directed against CD19.
One thing investigators have determined is that persistence of the CARs is essential for long-term responses.
In the first 2 patients who achieved a complete remission (CR), CAR T cells persisted for more than 4 years. In addition, no patient in CR has relapsed to date.
Of the 14 patients enrolled in the trial, 4 (28%) achieved a CR, 4 (28%) achieved a partial response, and 6 (43%) had no response, for an overall response rate of 57%.
These results were recently published in Science Translational Medicine.
Carl June, MD, of the University of Pennsylvania in Philadelphia, shared some insights into the research with attendees at the inaugural CRI-CIMT-EATI-AACR International Cancer Immunotherapy Conference.
Dr June explained that CTL019 is a CD19-directed single chain variable fragment with a 4-1BB signaling module that transduces T cells with a lentiviral vector. The technology was developed at the University of Pennsylvania and subsequently licensed to Novartis.
In the phase 1 trial of CTL019 in CLL, patients who achieved complete remission have very high levels of CARs—100% of the circulating T cells—but the non-responders don’t. The CARs engrafted in non-responders but did not proliferate.
“So the biomarker correlate of success is persistence and proliferation, in CLL at least,” Dr June said.
The investigators performed IGH next-generation sequencing and found no detectable CLL clones in the complete responders, including 1 patient at 3.5 years and another at 4 years post-infusion.
“There was no clinically evident disease in these patients,” Dr June said, “and so the responses are durable.”
The team also believes that at least a subset of the cells remains functional because the patients still had B-cell aplasia.
The investigators have not observed a CD19 loss in any CLL patient who responded.
“Patients who have gone into remission stay in remission,” Dr June added.
Kinetics of delayed CR
Dr June discussed in detail Patient 10, whose response was somewhat different from the other complete responders. Patient 10 achieved a CR, but the response was delayed. It took 51 days after infusion, compared to about 10 days in the other complete responders.
Patient 10 was initially scored as a failure at the 28-day evaluation. Eventually, he had marked improvement, and, by a year, he was in CR.
He required hospitalization for tumor lysis syndrome and treatment with tocilizumab for cytokine release syndrome.
Patient 10 had a single cell that investigators surmise could have been responsible for the tumor elimination.
“In fact, on day 28, when he still had tumor, his CARs were polyclonal,” Dr June said. “So we stained and isolated his CARs by sorting, and, at time of tumor elimination, he had descendants of 1 CAR.”
Nevertheless, Patient 10’s response is durable. He is now 81 years old and remains engrafted with CAR19 cells.
Investigators hypothesize that the kinetics and CAR proliferation were so different in Patient 10 because Tet2 was disrupted by the integration of the CAR into the intronic region.
“What we don’t know is whether Tet2 was a passenger or a driver here,” Dr June observed. “Did it actually aid the function of the CAR cells or was it just a marker?”
He noted that Tet2 has been shown in acute myeloid leukemia to increase stem cell renewal, “and it may well have done that in this patient.” ![]()
Cytarabine Combination: Long-term Effects
Low-dose cytarabine in combination with valproic acid and all-transretinoic acid (ATRA) is used in stabilizing treatment for patients with acute myeloid leukemia (AML) who aren’t candidates for intensive therapy. In vivo studies have shown that the triple-drug treatment has immunomodulatory effects. But researchers from University of Bergen, Norway, say little was known about both the acute and long-term effects of such treatment on the T-cell system.
Related: Signaling Pathways and Novel Inhibitors in Chronic Lymphocytic Leukemia
To find out, they conducted an in vitro study to examine the effects of cytarabine, valproic acid, and ATRA on activated T cells, testing cytarabine at concentrations reached during in vivo treatment with high doses, conventional doses, and low doses.
The researchers found that cytarabine—especially when combined with valproic acid and ATRA—can reduce T-cell viability and proliferation, alter the activation-induced expression of membrane molecules, and reduce the release of several cytokines. Cytarabine’s effects on T-cell activation were concentration dependent: Reduced viability was seen only at the higher concentrations. However, the researchers note that cytarabine had immunoregulatory effects even at lower levels. When cytarabine was combined with valproic acid and ATRA, the researchers observed no or minor effects on T-cell viability.
Related: Blast Phase Chronic Myelogenous Leukemia
Only cytarabine 44 μM had both antiproliferative and proapoptotic effects. The drug reduced AML cell viability only at 0.5 and 0.05 μM, not at the lowest concentration; but it inhibited AML cell proliferation even at 0.01 μM. By contrast, T-cell proliferation was inhibited only at concentrations ≥ 0.35 μM.
Based on the proliferation studies, the researchers conclude that primary AML cells are more susceptible to cytarabine than are normal T cells, which suggests, they add, a therapeutic window for cytarabine treatment that “makes it possible to achieve antileukemic effects in vivo before severe T-cell toxicity occurs.”
Related:HIV-Negative Patients at Risk for Pneumocystosis
The triple-drug combination’s direct effects on the T cells may be offset by other effects on immunocompetent cells; the researchers say the possible risk of immunosuppression should be further investigated.
Source
Ersvaer E, Brenner AK, Vetås K, Reikvam H, Bruserud Ø. BMC Pharmacol Toxicol. 2015;16:12.
doi: 10.1186/s40360-015-0012-2.
Low-dose cytarabine in combination with valproic acid and all-transretinoic acid (ATRA) is used in stabilizing treatment for patients with acute myeloid leukemia (AML) who aren’t candidates for intensive therapy. In vivo studies have shown that the triple-drug treatment has immunomodulatory effects. But researchers from University of Bergen, Norway, say little was known about both the acute and long-term effects of such treatment on the T-cell system.
Related: Signaling Pathways and Novel Inhibitors in Chronic Lymphocytic Leukemia
To find out, they conducted an in vitro study to examine the effects of cytarabine, valproic acid, and ATRA on activated T cells, testing cytarabine at concentrations reached during in vivo treatment with high doses, conventional doses, and low doses.
The researchers found that cytarabine—especially when combined with valproic acid and ATRA—can reduce T-cell viability and proliferation, alter the activation-induced expression of membrane molecules, and reduce the release of several cytokines. Cytarabine’s effects on T-cell activation were concentration dependent: Reduced viability was seen only at the higher concentrations. However, the researchers note that cytarabine had immunoregulatory effects even at lower levels. When cytarabine was combined with valproic acid and ATRA, the researchers observed no or minor effects on T-cell viability.
Related: Blast Phase Chronic Myelogenous Leukemia
Only cytarabine 44 μM had both antiproliferative and proapoptotic effects. The drug reduced AML cell viability only at 0.5 and 0.05 μM, not at the lowest concentration; but it inhibited AML cell proliferation even at 0.01 μM. By contrast, T-cell proliferation was inhibited only at concentrations ≥ 0.35 μM.
Based on the proliferation studies, the researchers conclude that primary AML cells are more susceptible to cytarabine than are normal T cells, which suggests, they add, a therapeutic window for cytarabine treatment that “makes it possible to achieve antileukemic effects in vivo before severe T-cell toxicity occurs.”
Related:HIV-Negative Patients at Risk for Pneumocystosis
The triple-drug combination’s direct effects on the T cells may be offset by other effects on immunocompetent cells; the researchers say the possible risk of immunosuppression should be further investigated.
Source
Ersvaer E, Brenner AK, Vetås K, Reikvam H, Bruserud Ø. BMC Pharmacol Toxicol. 2015;16:12.
doi: 10.1186/s40360-015-0012-2.
Low-dose cytarabine in combination with valproic acid and all-transretinoic acid (ATRA) is used in stabilizing treatment for patients with acute myeloid leukemia (AML) who aren’t candidates for intensive therapy. In vivo studies have shown that the triple-drug treatment has immunomodulatory effects. But researchers from University of Bergen, Norway, say little was known about both the acute and long-term effects of such treatment on the T-cell system.
Related: Signaling Pathways and Novel Inhibitors in Chronic Lymphocytic Leukemia
To find out, they conducted an in vitro study to examine the effects of cytarabine, valproic acid, and ATRA on activated T cells, testing cytarabine at concentrations reached during in vivo treatment with high doses, conventional doses, and low doses.
The researchers found that cytarabine—especially when combined with valproic acid and ATRA—can reduce T-cell viability and proliferation, alter the activation-induced expression of membrane molecules, and reduce the release of several cytokines. Cytarabine’s effects on T-cell activation were concentration dependent: Reduced viability was seen only at the higher concentrations. However, the researchers note that cytarabine had immunoregulatory effects even at lower levels. When cytarabine was combined with valproic acid and ATRA, the researchers observed no or minor effects on T-cell viability.
Related: Blast Phase Chronic Myelogenous Leukemia
Only cytarabine 44 μM had both antiproliferative and proapoptotic effects. The drug reduced AML cell viability only at 0.5 and 0.05 μM, not at the lowest concentration; but it inhibited AML cell proliferation even at 0.01 μM. By contrast, T-cell proliferation was inhibited only at concentrations ≥ 0.35 μM.
Based on the proliferation studies, the researchers conclude that primary AML cells are more susceptible to cytarabine than are normal T cells, which suggests, they add, a therapeutic window for cytarabine treatment that “makes it possible to achieve antileukemic effects in vivo before severe T-cell toxicity occurs.”
Related:HIV-Negative Patients at Risk for Pneumocystosis
The triple-drug combination’s direct effects on the T cells may be offset by other effects on immunocompetent cells; the researchers say the possible risk of immunosuppression should be further investigated.
Source
Ersvaer E, Brenner AK, Vetås K, Reikvam H, Bruserud Ø. BMC Pharmacol Toxicol. 2015;16:12.
doi: 10.1186/s40360-015-0012-2.
mAb gets priority review as maintenance in CLL

Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted priority review for an application for ofatumumab (Arzerra) as maintenance therapy in
patients with relapsed chronic lymphocytic leukemia (CLL).
The FDA grants priority review to investigational therapies that, if approved, may offer significant improvements in the treatment, prevention, or diagnosis of a serious condition.
The designation shortens the review period from 10 months to 6 months.
Ofatumumab is a human monoclonal antibody (mAb) designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
The mAb is already FDA-approved to treat patients with CLL that is refractory to fludarabine and alemtuzumab. Ofatumumab is also approved for use in combination with chlorambucil to treat previously untreated patients with CLL for whom fludarabine-based therapy is considered inappropriate.
The FDA said it aims to complete its review of the application for ofatumumab as maintenance therapy in relapsed CLL by January 21, 2016.
PROLONG trial
The application for ofatumumab as maintenance is based on interim results from the phase 3 PROLONG (OMB112517) trial, which were presented at ASH 2014.
In this trial, researchers compared ofatumumab maintenance to no further treatment in patients with a complete or partial response after second-
or third-line treatment for CLL.
Interim results suggested that ofatumumab significantly improves progression-free survival but not overall survival.
The median progression-free survival was about 29 months in patients who received ofatumumab and about 15 months for patients who did not receive
maintenance (P<0.0001).
There was no significant difference in the median overall survival, which was not reached in either treatment arm.
Ofatumumab development
Ofatumumab is approved in more than 50 countries worldwide as monotherapy for CLL patients who are refractory to fludarabine and alemtuzumab.
In the European Union, ofatumumab is approved for use in combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and who are not eligible for fludarabine-based therapy.
Ofatumumab is not approved anywhere in the world as maintenance therapy for relapsed CLL. The drug is being developed by Genmab and Novartis. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted priority review for an application for ofatumumab (Arzerra) as maintenance therapy in
patients with relapsed chronic lymphocytic leukemia (CLL).
The FDA grants priority review to investigational therapies that, if approved, may offer significant improvements in the treatment, prevention, or diagnosis of a serious condition.
The designation shortens the review period from 10 months to 6 months.
Ofatumumab is a human monoclonal antibody (mAb) designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
The mAb is already FDA-approved to treat patients with CLL that is refractory to fludarabine and alemtuzumab. Ofatumumab is also approved for use in combination with chlorambucil to treat previously untreated patients with CLL for whom fludarabine-based therapy is considered inappropriate.
The FDA said it aims to complete its review of the application for ofatumumab as maintenance therapy in relapsed CLL by January 21, 2016.
PROLONG trial
The application for ofatumumab as maintenance is based on interim results from the phase 3 PROLONG (OMB112517) trial, which were presented at ASH 2014.
In this trial, researchers compared ofatumumab maintenance to no further treatment in patients with a complete or partial response after second-
or third-line treatment for CLL.
Interim results suggested that ofatumumab significantly improves progression-free survival but not overall survival.
The median progression-free survival was about 29 months in patients who received ofatumumab and about 15 months for patients who did not receive
maintenance (P<0.0001).
There was no significant difference in the median overall survival, which was not reached in either treatment arm.
Ofatumumab development
Ofatumumab is approved in more than 50 countries worldwide as monotherapy for CLL patients who are refractory to fludarabine and alemtuzumab.
In the European Union, ofatumumab is approved for use in combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and who are not eligible for fludarabine-based therapy.
Ofatumumab is not approved anywhere in the world as maintenance therapy for relapsed CLL. The drug is being developed by Genmab and Novartis. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted priority review for an application for ofatumumab (Arzerra) as maintenance therapy in
patients with relapsed chronic lymphocytic leukemia (CLL).
The FDA grants priority review to investigational therapies that, if approved, may offer significant improvements in the treatment, prevention, or diagnosis of a serious condition.
The designation shortens the review period from 10 months to 6 months.
Ofatumumab is a human monoclonal antibody (mAb) designed to target CD20 on the surface of CLL cells and normal B lymphocytes.
The mAb is already FDA-approved to treat patients with CLL that is refractory to fludarabine and alemtuzumab. Ofatumumab is also approved for use in combination with chlorambucil to treat previously untreated patients with CLL for whom fludarabine-based therapy is considered inappropriate.
The FDA said it aims to complete its review of the application for ofatumumab as maintenance therapy in relapsed CLL by January 21, 2016.
PROLONG trial
The application for ofatumumab as maintenance is based on interim results from the phase 3 PROLONG (OMB112517) trial, which were presented at ASH 2014.
In this trial, researchers compared ofatumumab maintenance to no further treatment in patients with a complete or partial response after second-
or third-line treatment for CLL.
Interim results suggested that ofatumumab significantly improves progression-free survival but not overall survival.
The median progression-free survival was about 29 months in patients who received ofatumumab and about 15 months for patients who did not receive
maintenance (P<0.0001).
There was no significant difference in the median overall survival, which was not reached in either treatment arm.
Ofatumumab development
Ofatumumab is approved in more than 50 countries worldwide as monotherapy for CLL patients who are refractory to fludarabine and alemtuzumab.
In the European Union, ofatumumab is approved for use in combination with chlorambucil or bendamustine to treat CLL patients who have not received prior therapy and who are not eligible for fludarabine-based therapy.
Ofatumumab is not approved anywhere in the world as maintenance therapy for relapsed CLL. The drug is being developed by Genmab and Novartis. ![]()
CDK inhibitor active against lymphoma too

HOUSTON—Preclinical data suggest the second-generation cyclin-dependent kinase (CDK) inhibitor CYC065 is active against lymphomas as well as leukemias.
Previous research showed that CYC065 can fight acute myeloid leukemia (AML) in vitro and in vivo.
New research shows that CYC065 can decrease cell viability in a range of B-cell lymphoma cell lines, and the drug synergizes with both venetoclax and cytarabine.
Sheelagh Frame, PhD, and her colleagues presented these results at the SOHO 2015 Annual Meeting (poster 213). All of the investigators involved in the research are employees of Cyclacel Ltd., the company developing CYC065.
The investigators analyzed the anticancer activity of CYC065 in a range of cell lines and found that CYC065 induced apoptosis by inhibiting the expression of CDK9-dependent oncogenic transcripts, including Mcl-1, c-Myc, Hoxa9, and Meis1.
Results in AML
Experiments in the AML-MLL cell line MOLM-13 showed that short pulses of CYC065 (6 hours), rather than continuous treatment, were sufficient to achieve maximal cytotoxicity.
CYC065 induced apoptosis, in a dose-dependent manner, in other AML cell lines as well, including EOL-1 (MLL-PTD), MV4-11 (MLL-AF4, FLT3-ITD, and trisomy chr 8), HL60 (Myc amplified), and Kasumi-1.
The investigators noted that AML cell lines with MLL rearrangements were especially sensitive to CYC065, and the reliance of AML on Mcl-1 confers sensitivity to CYC065.
They also found evidence to suggest that Bak and Bcl-xL levels may be predictive of CYC065 response in AML. Cell lines that were less sensitive to treatment had high levels of Bcl-xL and negligible levels of Bak.
B-cell lymphomas
In B-cell lymphoma cell lines, the investigators observed a dose-dependent reduction in cell viability after CYC065 treatment (8-hour pulses).
CYC065 proved most effective in cell lines without genomic alterations associated with poor prognosis (HT and U-698-M) and in cell lines with Myc rearrangements (SU-DHL-8 and WILL-1).
The drug also decreased cell viability—but to a lesser degree—in cell lines with Bcl-2 rearrangements (SU-DHL-4 and U2932) and in double-hit lymphoma cell lines (MAVER-1, RI-1, SC-1, and SU-DHL-10).
The investigators therefore theorized that combining CYC065 with a Bcl-2 inhibitor might prove more effective in these cell lines.
CYC065 in combination
CYC065 synergized with the Bcl-2 inhibitor venetoclax in all B-cell lymphoma cell lines tested. The drugs were “strongly synergistic” in U2932 and RI-1 cell lines but simply “synergistic” in SU-CHL-4 and MAVER-1 cell lines.
CYC065 also synergized with cytarabine to fight AML. The combination proved synergistic at a range of doses in the HL60 and MV4-11 cell lines.
Considering these results together, the investigators concluded that CYC065 has shown potential for treating a range of leukemias and lymphomas with unmet clinical need, including MLL-rearranged leukemia and Myc-driven lymphoma.
And the drug might prove effective in combination with standard cytotoxic agents or agents targeting apoptotic regulators. ![]()
HOUSTON—Preclinical data suggest the second-generation cyclin-dependent kinase (CDK) inhibitor CYC065 is active against lymphomas as well as leukemias.
Previous research showed that CYC065 can fight acute myeloid leukemia (AML) in vitro and in vivo.
New research shows that CYC065 can decrease cell viability in a range of B-cell lymphoma cell lines, and the drug synergizes with both venetoclax and cytarabine.
Sheelagh Frame, PhD, and her colleagues presented these results at the SOHO 2015 Annual Meeting (poster 213). All of the investigators involved in the research are employees of Cyclacel Ltd., the company developing CYC065.
The investigators analyzed the anticancer activity of CYC065 in a range of cell lines and found that CYC065 induced apoptosis by inhibiting the expression of CDK9-dependent oncogenic transcripts, including Mcl-1, c-Myc, Hoxa9, and Meis1.
Results in AML
Experiments in the AML-MLL cell line MOLM-13 showed that short pulses of CYC065 (6 hours), rather than continuous treatment, were sufficient to achieve maximal cytotoxicity.
CYC065 induced apoptosis, in a dose-dependent manner, in other AML cell lines as well, including EOL-1 (MLL-PTD), MV4-11 (MLL-AF4, FLT3-ITD, and trisomy chr 8), HL60 (Myc amplified), and Kasumi-1.
The investigators noted that AML cell lines with MLL rearrangements were especially sensitive to CYC065, and the reliance of AML on Mcl-1 confers sensitivity to CYC065.
They also found evidence to suggest that Bak and Bcl-xL levels may be predictive of CYC065 response in AML. Cell lines that were less sensitive to treatment had high levels of Bcl-xL and negligible levels of Bak.
B-cell lymphomas
In B-cell lymphoma cell lines, the investigators observed a dose-dependent reduction in cell viability after CYC065 treatment (8-hour pulses).
CYC065 proved most effective in cell lines without genomic alterations associated with poor prognosis (HT and U-698-M) and in cell lines with Myc rearrangements (SU-DHL-8 and WILL-1).
The drug also decreased cell viability—but to a lesser degree—in cell lines with Bcl-2 rearrangements (SU-DHL-4 and U2932) and in double-hit lymphoma cell lines (MAVER-1, RI-1, SC-1, and SU-DHL-10).
The investigators therefore theorized that combining CYC065 with a Bcl-2 inhibitor might prove more effective in these cell lines.
CYC065 in combination
CYC065 synergized with the Bcl-2 inhibitor venetoclax in all B-cell lymphoma cell lines tested. The drugs were “strongly synergistic” in U2932 and RI-1 cell lines but simply “synergistic” in SU-CHL-4 and MAVER-1 cell lines.
CYC065 also synergized with cytarabine to fight AML. The combination proved synergistic at a range of doses in the HL60 and MV4-11 cell lines.
Considering these results together, the investigators concluded that CYC065 has shown potential for treating a range of leukemias and lymphomas with unmet clinical need, including MLL-rearranged leukemia and Myc-driven lymphoma.
And the drug might prove effective in combination with standard cytotoxic agents or agents targeting apoptotic regulators. ![]()
HOUSTON—Preclinical data suggest the second-generation cyclin-dependent kinase (CDK) inhibitor CYC065 is active against lymphomas as well as leukemias.
Previous research showed that CYC065 can fight acute myeloid leukemia (AML) in vitro and in vivo.
New research shows that CYC065 can decrease cell viability in a range of B-cell lymphoma cell lines, and the drug synergizes with both venetoclax and cytarabine.
Sheelagh Frame, PhD, and her colleagues presented these results at the SOHO 2015 Annual Meeting (poster 213). All of the investigators involved in the research are employees of Cyclacel Ltd., the company developing CYC065.
The investigators analyzed the anticancer activity of CYC065 in a range of cell lines and found that CYC065 induced apoptosis by inhibiting the expression of CDK9-dependent oncogenic transcripts, including Mcl-1, c-Myc, Hoxa9, and Meis1.
Results in AML
Experiments in the AML-MLL cell line MOLM-13 showed that short pulses of CYC065 (6 hours), rather than continuous treatment, were sufficient to achieve maximal cytotoxicity.
CYC065 induced apoptosis, in a dose-dependent manner, in other AML cell lines as well, including EOL-1 (MLL-PTD), MV4-11 (MLL-AF4, FLT3-ITD, and trisomy chr 8), HL60 (Myc amplified), and Kasumi-1.
The investigators noted that AML cell lines with MLL rearrangements were especially sensitive to CYC065, and the reliance of AML on Mcl-1 confers sensitivity to CYC065.
They also found evidence to suggest that Bak and Bcl-xL levels may be predictive of CYC065 response in AML. Cell lines that were less sensitive to treatment had high levels of Bcl-xL and negligible levels of Bak.
B-cell lymphomas
In B-cell lymphoma cell lines, the investigators observed a dose-dependent reduction in cell viability after CYC065 treatment (8-hour pulses).
CYC065 proved most effective in cell lines without genomic alterations associated with poor prognosis (HT and U-698-M) and in cell lines with Myc rearrangements (SU-DHL-8 and WILL-1).
The drug also decreased cell viability—but to a lesser degree—in cell lines with Bcl-2 rearrangements (SU-DHL-4 and U2932) and in double-hit lymphoma cell lines (MAVER-1, RI-1, SC-1, and SU-DHL-10).
The investigators therefore theorized that combining CYC065 with a Bcl-2 inhibitor might prove more effective in these cell lines.
CYC065 in combination
CYC065 synergized with the Bcl-2 inhibitor venetoclax in all B-cell lymphoma cell lines tested. The drugs were “strongly synergistic” in U2932 and RI-1 cell lines but simply “synergistic” in SU-CHL-4 and MAVER-1 cell lines.
CYC065 also synergized with cytarabine to fight AML. The combination proved synergistic at a range of doses in the HL60 and MV4-11 cell lines.
Considering these results together, the investigators concluded that CYC065 has shown potential for treating a range of leukemias and lymphomas with unmet clinical need, including MLL-rearranged leukemia and Myc-driven lymphoma.
And the drug might prove effective in combination with standard cytotoxic agents or agents targeting apoptotic regulators. ![]()
Advances in AML understanding could translate to improved therapy
An understanding of the various molecular differences between acute myeloid leukemia (AML) particles is guiding the search for new drug combinations targeting a variety of AML cellular processes, according to research published in the New England Journal of Medicine.
After a brief overview of disease classification and prognostic factors for AML, the authors, led by Dr. Hartmut Döhner of University Hospital Ulm in Germany, described a number of new treatment strategies. These approaches include directly addressing mutant proteins by targeting mutation-specific dependencies, developing inhibitors that could cut down on the occurrence of mutations in receptor tyrosine kinase genes, and developing new epigenetic therapies based on targeting specific mutant metabolic enzymes such as IDH1 and IDH2.
Other strategies, such as antibody therapy that focuses on the development of new monoclonal antibodies targeting CD33, and new formulations of older cytotoxic agents, also are being developed or are in clinical trial stages; however, many of these developments have not yet been translated into clinical practice, the researchers noted.
“New compounds hold promise to improve treatment outcomes; however, it is unlikely that any of these compounds, when used as single agents, will cure the disease. A major challenge will be to identify predictors for a response to specific agents, which will allow for the rational design of combinatorial therapies,” they wrote.
Dr. Döhner and a coauthor disclosed ties with several pharmaceutical companies.
Read the article here.
An understanding of the various molecular differences between acute myeloid leukemia (AML) particles is guiding the search for new drug combinations targeting a variety of AML cellular processes, according to research published in the New England Journal of Medicine.
After a brief overview of disease classification and prognostic factors for AML, the authors, led by Dr. Hartmut Döhner of University Hospital Ulm in Germany, described a number of new treatment strategies. These approaches include directly addressing mutant proteins by targeting mutation-specific dependencies, developing inhibitors that could cut down on the occurrence of mutations in receptor tyrosine kinase genes, and developing new epigenetic therapies based on targeting specific mutant metabolic enzymes such as IDH1 and IDH2.
Other strategies, such as antibody therapy that focuses on the development of new monoclonal antibodies targeting CD33, and new formulations of older cytotoxic agents, also are being developed or are in clinical trial stages; however, many of these developments have not yet been translated into clinical practice, the researchers noted.
“New compounds hold promise to improve treatment outcomes; however, it is unlikely that any of these compounds, when used as single agents, will cure the disease. A major challenge will be to identify predictors for a response to specific agents, which will allow for the rational design of combinatorial therapies,” they wrote.
Dr. Döhner and a coauthor disclosed ties with several pharmaceutical companies.
Read the article here.
An understanding of the various molecular differences between acute myeloid leukemia (AML) particles is guiding the search for new drug combinations targeting a variety of AML cellular processes, according to research published in the New England Journal of Medicine.
After a brief overview of disease classification and prognostic factors for AML, the authors, led by Dr. Hartmut Döhner of University Hospital Ulm in Germany, described a number of new treatment strategies. These approaches include directly addressing mutant proteins by targeting mutation-specific dependencies, developing inhibitors that could cut down on the occurrence of mutations in receptor tyrosine kinase genes, and developing new epigenetic therapies based on targeting specific mutant metabolic enzymes such as IDH1 and IDH2.
Other strategies, such as antibody therapy that focuses on the development of new monoclonal antibodies targeting CD33, and new formulations of older cytotoxic agents, also are being developed or are in clinical trial stages; however, many of these developments have not yet been translated into clinical practice, the researchers noted.
“New compounds hold promise to improve treatment outcomes; however, it is unlikely that any of these compounds, when used as single agents, will cure the disease. A major challenge will be to identify predictors for a response to specific agents, which will allow for the rational design of combinatorial therapies,” they wrote.
Dr. Döhner and a coauthor disclosed ties with several pharmaceutical companies.
Read the article here.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Improving Access to Care for Veterans Referred for Stem Cell Transplant Using Video-Based Telemedicine
Purpose: The primary purpose of this quality improvement project was to decrease the time from referral to evaluation for stem cell transplant patients to < 30 days.
Background: Stem cell transplant patients referred to the VA Tennessee Valley Healthcare System (VATVHS) from throughout the U.S. require complex coordination of care, including travel and lodging at government expense. Coordination of care for this patient population was becoming labor intensive and inefficient. The prospect of travelling far from home for an extended evaluation creates an undue amount of stress and expense for some veterans. As the number of referrals increased, we sought methods to improve both the cost and efficiency associated with the referral process.
Methods: We implemented the videobased telemedicine evaluation system at VATVHS in July 2014. Our method for implementation involved the creation of a pretransplant evaluation template geared toward video-based telemedicine. Criteria for inclusion depended on the home VA’s ability to schedule and conduct video-based telemedicine. The attending physician assigned to the referral made the final decision as to whether the referred veteran was appropriate for video-based telemedicine or required an inperson evaluation. The time to evaluation from referral was our primary goal for improvement. Travel and lodging savings and reduction of clinic days were secondary measures of improvement.
Data Analysis: From July 9, 2014, to April 8, 2015, we evaluated 51 patient referrals using video-based telemedicine.
Results: We were able to decrease patient evaluation times from > 30 days to 19.4 days, a 35% reduction in time from referral to evaluation. Additionally, we were able to reduce air travel costs by $50,000 and lodging costs by $31,000. We were also able to decrease clinic days at VATVHS by 02 (2 patient clinic visits per evaluation).
Implications: Video-based telemedicine is an efficient, costeffective, convenient method of conducting initial evaluations for stem cell transplant patients. Further implementation of video-based telemedicine could serve to improve efficiency of evaluations, reduce the financial burden associated with travel and lodging, and serve to increase patient satisfaction by reducing travel time.
Purpose: The primary purpose of this quality improvement project was to decrease the time from referral to evaluation for stem cell transplant patients to < 30 days.
Background: Stem cell transplant patients referred to the VA Tennessee Valley Healthcare System (VATVHS) from throughout the U.S. require complex coordination of care, including travel and lodging at government expense. Coordination of care for this patient population was becoming labor intensive and inefficient. The prospect of travelling far from home for an extended evaluation creates an undue amount of stress and expense for some veterans. As the number of referrals increased, we sought methods to improve both the cost and efficiency associated with the referral process.
Methods: We implemented the videobased telemedicine evaluation system at VATVHS in July 2014. Our method for implementation involved the creation of a pretransplant evaluation template geared toward video-based telemedicine. Criteria for inclusion depended on the home VA’s ability to schedule and conduct video-based telemedicine. The attending physician assigned to the referral made the final decision as to whether the referred veteran was appropriate for video-based telemedicine or required an inperson evaluation. The time to evaluation from referral was our primary goal for improvement. Travel and lodging savings and reduction of clinic days were secondary measures of improvement.
Data Analysis: From July 9, 2014, to April 8, 2015, we evaluated 51 patient referrals using video-based telemedicine.
Results: We were able to decrease patient evaluation times from > 30 days to 19.4 days, a 35% reduction in time from referral to evaluation. Additionally, we were able to reduce air travel costs by $50,000 and lodging costs by $31,000. We were also able to decrease clinic days at VATVHS by 02 (2 patient clinic visits per evaluation).
Implications: Video-based telemedicine is an efficient, costeffective, convenient method of conducting initial evaluations for stem cell transplant patients. Further implementation of video-based telemedicine could serve to improve efficiency of evaluations, reduce the financial burden associated with travel and lodging, and serve to increase patient satisfaction by reducing travel time.
Purpose: The primary purpose of this quality improvement project was to decrease the time from referral to evaluation for stem cell transplant patients to < 30 days.
Background: Stem cell transplant patients referred to the VA Tennessee Valley Healthcare System (VATVHS) from throughout the U.S. require complex coordination of care, including travel and lodging at government expense. Coordination of care for this patient population was becoming labor intensive and inefficient. The prospect of travelling far from home for an extended evaluation creates an undue amount of stress and expense for some veterans. As the number of referrals increased, we sought methods to improve both the cost and efficiency associated with the referral process.
Methods: We implemented the videobased telemedicine evaluation system at VATVHS in July 2014. Our method for implementation involved the creation of a pretransplant evaluation template geared toward video-based telemedicine. Criteria for inclusion depended on the home VA’s ability to schedule and conduct video-based telemedicine. The attending physician assigned to the referral made the final decision as to whether the referred veteran was appropriate for video-based telemedicine or required an inperson evaluation. The time to evaluation from referral was our primary goal for improvement. Travel and lodging savings and reduction of clinic days were secondary measures of improvement.
Data Analysis: From July 9, 2014, to April 8, 2015, we evaluated 51 patient referrals using video-based telemedicine.
Results: We were able to decrease patient evaluation times from > 30 days to 19.4 days, a 35% reduction in time from referral to evaluation. Additionally, we were able to reduce air travel costs by $50,000 and lodging costs by $31,000. We were also able to decrease clinic days at VATVHS by 02 (2 patient clinic visits per evaluation).
Implications: Video-based telemedicine is an efficient, costeffective, convenient method of conducting initial evaluations for stem cell transplant patients. Further implementation of video-based telemedicine could serve to improve efficiency of evaluations, reduce the financial burden associated with travel and lodging, and serve to increase patient satisfaction by reducing travel time.
HELIOS trial: Ibrutinib safely boosts survival in CLL/SLL
CHICAGO – Adding ibrutinib to bendamustine and rituximab improved outcomes without significantly reducing safety in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) in the randomized, placebo-controlled, phase III HELIOS trial.
Efficacy results from the double-blind HELIOS trial, as reported by Dr. Asher Alban Chanan-Khan at the 2015 meeting of the American Society of Clinical Oncology, showed that adding ibrutinib to bendamustine and rituximab (BR) significantly extended progression-free survival, compared with BR plus placebo, in patients with CLL/SLL; the risk of progression and death was reduced by 80%.
The current findings, reported by Dr. Chanan-Khan at the American Society of Hematology Meeting on Hematologic Malignancies, demonstrate that this improvement was achieved without sacrificing safety, and they characterize the management of adverse events.
In 578 patients with active chronic CLL/SLL following at least one prior line of systemic therapy who were randomized to receive 420 mg of ibrutinib plus BR or placebo plus BR for six cycles, exposure was 14.7 months and 12.8 months, respectively. Infection rates were similar in the two groups, but exposure-adjusted analysis showed an overall lower infection rate in the ibrutinib group, compared with the placebo group (10.3/100 vs. 11.2/100 patient months), and the rates of grade 3 or higher infections was similar in the groups, said Dr. Chanan-Khan of the Mayo Clinic, Jacksonville, Fla.
The rates of all-grade and grade 3/4 anemia were 22.3% and 3.5%, respectively, in the ibrutinib group, and 28.9% and 8.0%, respectively, in the BR group. The ibrutinib patients also required fewer transfusions – most often red blood cell transfusions (23% vs. 29% in the BR group).This may have been a reflection of restoration of the hematopoietic system in the ibrutinib group, said Dr. Chanan-Khan.
Grade 3/4 neutropenia was similar in the groups (53.7% and 50.5%), but fewer patients discontinued treatment due to treatment-related neutropenia with ibrutinib (1% vs. 2.8%), he noted.
Thrombocytopenia occurred slightly more often in the ibrutinib group (30.7% vs. 24%), but grade 3/4 events occurred in 15% of patients in each group.
Atrial fibrillation (AF) occurred in a small number of patients, but was observed more often with ibrutinib (7.3% vs. 2.8% overall, and 2.8% vs. 0.7% for grade 3/4 AF). Only seven patients required dose interruption – for a median duration of 7 days – to manage AF.
“No dose reductions were required,” said Dr. Chanan-Khan, adding that four patients, all with grade 3/4 AF and all in the ibrutinib group, discontinued therapy because of AF.
“We then analyzed our data to identify potential risk factors for predisposition to AF ... no one baseline risk factor could be identified as causative. However, most patients who developed AF had a known risk factor,” he said.
He added that among those with a prior history of AF, 28% on the ibrutinib arm, and only 9% on the placebo arm, developed AF.
Baseline cardiac comorbidities also were found to have no effect on progression-free survival in either arm.
“We therefore concluded that the risk of AF is low at around 5%, it does not impact progression-free survival, prior history of AF is not a contraindication in the absence of any great freak event, ibrutinib dose interruption or reduction is not warranted, and you should treat CLL patients first for CLL and manage AF second,” he said.
Another important factor that often impacts clinical decision making is the use of anticoagulants or antiplatelet agents and the bleeding risk with ibrutinib, he said, noting that more than 40% of patients in the ibrutinib arm were using such agents.
“We did not see any impact on the progression-free survival outcomes on either of the arms in patients who were on anticoagulant or antiplatelet therapy,” he said.
Bleeding occurred in 31% and 14.6% of patients in the ibrutinib and placebo groups, respectively, and most cases involved grade 1 bruises and contusions. Only four patients discontinued therapy because of bleeding.
The rates of grade 3/4 major bleeding and major hemorrhage events were low in both groups, at less than 4%, and two patients discontinued therapy because of major bleeding. Two patients in the ibrutinib arm died because of major bleeding, including one who had a large preexisting abdominal aortic aneurysm, and one who experienced a large postsurgical intestinal perforation.
“Overall, these data support the use of ibrutinib in patients on concurrent anticoagulant or antiplatelet therapy, with no significantly increased major risk of bleeding with ibrutinib vs. placebo, and most bleeding events being grade 1 in nature,” said Dr. Chanan-Khan.
The rate of treatment-related lymphocytosis – a known pharmacodynamic effect of ibrutinib – occurred in 7% and 5.9% of the ibrutinib and placebo group patients, and most cases resolved within 2 weeks.
Based on the results of the 2014 phase III RESONATE trial and others looking at ibrutinib as a single-agent treatment for CLL, the agent is considered a new standard of care in patients with previously treated CLL/SLL. HELIOS was the first study to investigate ibrutinib in combination with BR.
“Considering the significant improvement in progression-free survival and overall survival, ibrutinib has a strong overall risk-benefit profile,” Dr. Chanan-Khan concluded.
The HELIOS study was sponsored by Janssen Pharmaceuticals. Dr. Chanan-Khan reported having no disclosures.
CHICAGO – Adding ibrutinib to bendamustine and rituximab improved outcomes without significantly reducing safety in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) in the randomized, placebo-controlled, phase III HELIOS trial.
Efficacy results from the double-blind HELIOS trial, as reported by Dr. Asher Alban Chanan-Khan at the 2015 meeting of the American Society of Clinical Oncology, showed that adding ibrutinib to bendamustine and rituximab (BR) significantly extended progression-free survival, compared with BR plus placebo, in patients with CLL/SLL; the risk of progression and death was reduced by 80%.
The current findings, reported by Dr. Chanan-Khan at the American Society of Hematology Meeting on Hematologic Malignancies, demonstrate that this improvement was achieved without sacrificing safety, and they characterize the management of adverse events.
In 578 patients with active chronic CLL/SLL following at least one prior line of systemic therapy who were randomized to receive 420 mg of ibrutinib plus BR or placebo plus BR for six cycles, exposure was 14.7 months and 12.8 months, respectively. Infection rates were similar in the two groups, but exposure-adjusted analysis showed an overall lower infection rate in the ibrutinib group, compared with the placebo group (10.3/100 vs. 11.2/100 patient months), and the rates of grade 3 or higher infections was similar in the groups, said Dr. Chanan-Khan of the Mayo Clinic, Jacksonville, Fla.
The rates of all-grade and grade 3/4 anemia were 22.3% and 3.5%, respectively, in the ibrutinib group, and 28.9% and 8.0%, respectively, in the BR group. The ibrutinib patients also required fewer transfusions – most often red blood cell transfusions (23% vs. 29% in the BR group).This may have been a reflection of restoration of the hematopoietic system in the ibrutinib group, said Dr. Chanan-Khan.
Grade 3/4 neutropenia was similar in the groups (53.7% and 50.5%), but fewer patients discontinued treatment due to treatment-related neutropenia with ibrutinib (1% vs. 2.8%), he noted.
Thrombocytopenia occurred slightly more often in the ibrutinib group (30.7% vs. 24%), but grade 3/4 events occurred in 15% of patients in each group.
Atrial fibrillation (AF) occurred in a small number of patients, but was observed more often with ibrutinib (7.3% vs. 2.8% overall, and 2.8% vs. 0.7% for grade 3/4 AF). Only seven patients required dose interruption – for a median duration of 7 days – to manage AF.
“No dose reductions were required,” said Dr. Chanan-Khan, adding that four patients, all with grade 3/4 AF and all in the ibrutinib group, discontinued therapy because of AF.
“We then analyzed our data to identify potential risk factors for predisposition to AF ... no one baseline risk factor could be identified as causative. However, most patients who developed AF had a known risk factor,” he said.
He added that among those with a prior history of AF, 28% on the ibrutinib arm, and only 9% on the placebo arm, developed AF.
Baseline cardiac comorbidities also were found to have no effect on progression-free survival in either arm.
“We therefore concluded that the risk of AF is low at around 5%, it does not impact progression-free survival, prior history of AF is not a contraindication in the absence of any great freak event, ibrutinib dose interruption or reduction is not warranted, and you should treat CLL patients first for CLL and manage AF second,” he said.
Another important factor that often impacts clinical decision making is the use of anticoagulants or antiplatelet agents and the bleeding risk with ibrutinib, he said, noting that more than 40% of patients in the ibrutinib arm were using such agents.
“We did not see any impact on the progression-free survival outcomes on either of the arms in patients who were on anticoagulant or antiplatelet therapy,” he said.
Bleeding occurred in 31% and 14.6% of patients in the ibrutinib and placebo groups, respectively, and most cases involved grade 1 bruises and contusions. Only four patients discontinued therapy because of bleeding.
The rates of grade 3/4 major bleeding and major hemorrhage events were low in both groups, at less than 4%, and two patients discontinued therapy because of major bleeding. Two patients in the ibrutinib arm died because of major bleeding, including one who had a large preexisting abdominal aortic aneurysm, and one who experienced a large postsurgical intestinal perforation.
“Overall, these data support the use of ibrutinib in patients on concurrent anticoagulant or antiplatelet therapy, with no significantly increased major risk of bleeding with ibrutinib vs. placebo, and most bleeding events being grade 1 in nature,” said Dr. Chanan-Khan.
The rate of treatment-related lymphocytosis – a known pharmacodynamic effect of ibrutinib – occurred in 7% and 5.9% of the ibrutinib and placebo group patients, and most cases resolved within 2 weeks.
Based on the results of the 2014 phase III RESONATE trial and others looking at ibrutinib as a single-agent treatment for CLL, the agent is considered a new standard of care in patients with previously treated CLL/SLL. HELIOS was the first study to investigate ibrutinib in combination with BR.
“Considering the significant improvement in progression-free survival and overall survival, ibrutinib has a strong overall risk-benefit profile,” Dr. Chanan-Khan concluded.
The HELIOS study was sponsored by Janssen Pharmaceuticals. Dr. Chanan-Khan reported having no disclosures.
CHICAGO – Adding ibrutinib to bendamustine and rituximab improved outcomes without significantly reducing safety in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) in the randomized, placebo-controlled, phase III HELIOS trial.
Efficacy results from the double-blind HELIOS trial, as reported by Dr. Asher Alban Chanan-Khan at the 2015 meeting of the American Society of Clinical Oncology, showed that adding ibrutinib to bendamustine and rituximab (BR) significantly extended progression-free survival, compared with BR plus placebo, in patients with CLL/SLL; the risk of progression and death was reduced by 80%.
The current findings, reported by Dr. Chanan-Khan at the American Society of Hematology Meeting on Hematologic Malignancies, demonstrate that this improvement was achieved without sacrificing safety, and they characterize the management of adverse events.
In 578 patients with active chronic CLL/SLL following at least one prior line of systemic therapy who were randomized to receive 420 mg of ibrutinib plus BR or placebo plus BR for six cycles, exposure was 14.7 months and 12.8 months, respectively. Infection rates were similar in the two groups, but exposure-adjusted analysis showed an overall lower infection rate in the ibrutinib group, compared with the placebo group (10.3/100 vs. 11.2/100 patient months), and the rates of grade 3 or higher infections was similar in the groups, said Dr. Chanan-Khan of the Mayo Clinic, Jacksonville, Fla.
The rates of all-grade and grade 3/4 anemia were 22.3% and 3.5%, respectively, in the ibrutinib group, and 28.9% and 8.0%, respectively, in the BR group. The ibrutinib patients also required fewer transfusions – most often red blood cell transfusions (23% vs. 29% in the BR group).This may have been a reflection of restoration of the hematopoietic system in the ibrutinib group, said Dr. Chanan-Khan.
Grade 3/4 neutropenia was similar in the groups (53.7% and 50.5%), but fewer patients discontinued treatment due to treatment-related neutropenia with ibrutinib (1% vs. 2.8%), he noted.
Thrombocytopenia occurred slightly more often in the ibrutinib group (30.7% vs. 24%), but grade 3/4 events occurred in 15% of patients in each group.
Atrial fibrillation (AF) occurred in a small number of patients, but was observed more often with ibrutinib (7.3% vs. 2.8% overall, and 2.8% vs. 0.7% for grade 3/4 AF). Only seven patients required dose interruption – for a median duration of 7 days – to manage AF.
“No dose reductions were required,” said Dr. Chanan-Khan, adding that four patients, all with grade 3/4 AF and all in the ibrutinib group, discontinued therapy because of AF.
“We then analyzed our data to identify potential risk factors for predisposition to AF ... no one baseline risk factor could be identified as causative. However, most patients who developed AF had a known risk factor,” he said.
He added that among those with a prior history of AF, 28% on the ibrutinib arm, and only 9% on the placebo arm, developed AF.
Baseline cardiac comorbidities also were found to have no effect on progression-free survival in either arm.
“We therefore concluded that the risk of AF is low at around 5%, it does not impact progression-free survival, prior history of AF is not a contraindication in the absence of any great freak event, ibrutinib dose interruption or reduction is not warranted, and you should treat CLL patients first for CLL and manage AF second,” he said.
Another important factor that often impacts clinical decision making is the use of anticoagulants or antiplatelet agents and the bleeding risk with ibrutinib, he said, noting that more than 40% of patients in the ibrutinib arm were using such agents.
“We did not see any impact on the progression-free survival outcomes on either of the arms in patients who were on anticoagulant or antiplatelet therapy,” he said.
Bleeding occurred in 31% and 14.6% of patients in the ibrutinib and placebo groups, respectively, and most cases involved grade 1 bruises and contusions. Only four patients discontinued therapy because of bleeding.
The rates of grade 3/4 major bleeding and major hemorrhage events were low in both groups, at less than 4%, and two patients discontinued therapy because of major bleeding. Two patients in the ibrutinib arm died because of major bleeding, including one who had a large preexisting abdominal aortic aneurysm, and one who experienced a large postsurgical intestinal perforation.
“Overall, these data support the use of ibrutinib in patients on concurrent anticoagulant or antiplatelet therapy, with no significantly increased major risk of bleeding with ibrutinib vs. placebo, and most bleeding events being grade 1 in nature,” said Dr. Chanan-Khan.
The rate of treatment-related lymphocytosis – a known pharmacodynamic effect of ibrutinib – occurred in 7% and 5.9% of the ibrutinib and placebo group patients, and most cases resolved within 2 weeks.
Based on the results of the 2014 phase III RESONATE trial and others looking at ibrutinib as a single-agent treatment for CLL, the agent is considered a new standard of care in patients with previously treated CLL/SLL. HELIOS was the first study to investigate ibrutinib in combination with BR.
“Considering the significant improvement in progression-free survival and overall survival, ibrutinib has a strong overall risk-benefit profile,” Dr. Chanan-Khan concluded.
The HELIOS study was sponsored by Janssen Pharmaceuticals. Dr. Chanan-Khan reported having no disclosures.
AT MHM 2015
Key clinical point: Adding ibrutinib to bendamustine and rituximab improved outcomes without significantly reducing safety in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL).
Major finding: The overall infection rate was lower in the ibrutinib group than in the placebo group (10.3/100 vs. 11.2/100 patient months).
Data source: The phase III HELIOS study involving 578 patients.
Disclosures: Janssen Pharmaceuticals sponsored the study. Dr. Chanan-Khan reported having no disclosures.