User login
Study reveals potential drivers of CLL

Photo courtesy of Dana-
Farber Cancer Institute
Researchers say they have identified dozens of genetic abnormalities that may drive chronic lymphocytic leukemia (CLL), including some that were never before linked to human cancer.
The team began to trace how some of these abnormalities affect the course of the disease and its susceptibility to treatment.
And they started tracking the evolutionary path of CLL as its genome spawns new groups and subgroups of tumor cells in a single patient.
“Sequencing the DNA of CLL has taught us a great deal about the genetic basis of the disease,” said Catherine Wu, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“Previous studies, however, were limited by the relatively small number of tumor tissue samples analyzed and by the fact that those samples were taken at different stages of the treatment process from patients treated with different drug agents.”
“In our new study, we wanted to determine if analyzing tissue samples from a large, similarly treated group of patients provides the statistical power necessary to study the disease in all its genetic diversity, to draw connections between certain mutations and the aggressiveness of the disease, and to chart the emergence of new mutations and their role in helping the disease advance. Our results demonstrate the range of insights to be gained by this approach.”
Dr Wu and her colleagues reported these results in Nature.
The researchers collected tumor and normal tissue samples from 538 patients with CLL and performed whole-exome sequencing on each sample.
In this way, the team identified 44 putative CLL driver genes, including 18 CLL mutated drivers that were previously identified and 26 additional putative CLL genes. About 34% of the CLL samples harbored a mutation in at least 1 of these 26 genes.
Nearly 9% of the patients had mutations in CLL genes in the MAPK-ERK pathway. The researchers therefore believe that further exploration of MAPK-ERK pathway inhibitors may be warranted.
The team found that mutations differed between IGHV-mutated and unmutated CLL. IGHV-unmutated CLL tended to have a higher proportion of most driving mutations, while only 3 driver genes were enriched in IGHV-mutated CLL—del(13q), MYD88, and CHD2.
The researchers also discovered that certain mutations were common in patients who had already undergone treatment.
Previous treatment was associated with enrichment in TP53 and BIRC3 mutations del(17p) and del(11q), as well as in mutated DDX3X and MAP2K1. The team therefore believes these mutations may help CLL rebound after initial therapy.
Another key finding was that therapy tended to produce shorter remissions in patients with mutations in TP53 or SF3B1.
“We found that genomic evolution after therapy is the rule rather than the exception,” Dr Wu noted. “Certain mutations were present in a greater number of leukemia cells within a sample after relapse, showing that these mutations, presumably, allow the tumor to persevere.” ![]()
Photo courtesy of Dana-
Farber Cancer Institute
Researchers say they have identified dozens of genetic abnormalities that may drive chronic lymphocytic leukemia (CLL), including some that were never before linked to human cancer.
The team began to trace how some of these abnormalities affect the course of the disease and its susceptibility to treatment.
And they started tracking the evolutionary path of CLL as its genome spawns new groups and subgroups of tumor cells in a single patient.
“Sequencing the DNA of CLL has taught us a great deal about the genetic basis of the disease,” said Catherine Wu, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“Previous studies, however, were limited by the relatively small number of tumor tissue samples analyzed and by the fact that those samples were taken at different stages of the treatment process from patients treated with different drug agents.”
“In our new study, we wanted to determine if analyzing tissue samples from a large, similarly treated group of patients provides the statistical power necessary to study the disease in all its genetic diversity, to draw connections between certain mutations and the aggressiveness of the disease, and to chart the emergence of new mutations and their role in helping the disease advance. Our results demonstrate the range of insights to be gained by this approach.”
Dr Wu and her colleagues reported these results in Nature.
The researchers collected tumor and normal tissue samples from 538 patients with CLL and performed whole-exome sequencing on each sample.
In this way, the team identified 44 putative CLL driver genes, including 18 CLL mutated drivers that were previously identified and 26 additional putative CLL genes. About 34% of the CLL samples harbored a mutation in at least 1 of these 26 genes.
Nearly 9% of the patients had mutations in CLL genes in the MAPK-ERK pathway. The researchers therefore believe that further exploration of MAPK-ERK pathway inhibitors may be warranted.
The team found that mutations differed between IGHV-mutated and unmutated CLL. IGHV-unmutated CLL tended to have a higher proportion of most driving mutations, while only 3 driver genes were enriched in IGHV-mutated CLL—del(13q), MYD88, and CHD2.
The researchers also discovered that certain mutations were common in patients who had already undergone treatment.
Previous treatment was associated with enrichment in TP53 and BIRC3 mutations del(17p) and del(11q), as well as in mutated DDX3X and MAP2K1. The team therefore believes these mutations may help CLL rebound after initial therapy.
Another key finding was that therapy tended to produce shorter remissions in patients with mutations in TP53 or SF3B1.
“We found that genomic evolution after therapy is the rule rather than the exception,” Dr Wu noted. “Certain mutations were present in a greater number of leukemia cells within a sample after relapse, showing that these mutations, presumably, allow the tumor to persevere.” ![]()
Photo courtesy of Dana-
Farber Cancer Institute
Researchers say they have identified dozens of genetic abnormalities that may drive chronic lymphocytic leukemia (CLL), including some that were never before linked to human cancer.
The team began to trace how some of these abnormalities affect the course of the disease and its susceptibility to treatment.
And they started tracking the evolutionary path of CLL as its genome spawns new groups and subgroups of tumor cells in a single patient.
“Sequencing the DNA of CLL has taught us a great deal about the genetic basis of the disease,” said Catherine Wu, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“Previous studies, however, were limited by the relatively small number of tumor tissue samples analyzed and by the fact that those samples were taken at different stages of the treatment process from patients treated with different drug agents.”
“In our new study, we wanted to determine if analyzing tissue samples from a large, similarly treated group of patients provides the statistical power necessary to study the disease in all its genetic diversity, to draw connections between certain mutations and the aggressiveness of the disease, and to chart the emergence of new mutations and their role in helping the disease advance. Our results demonstrate the range of insights to be gained by this approach.”
Dr Wu and her colleagues reported these results in Nature.
The researchers collected tumor and normal tissue samples from 538 patients with CLL and performed whole-exome sequencing on each sample.
In this way, the team identified 44 putative CLL driver genes, including 18 CLL mutated drivers that were previously identified and 26 additional putative CLL genes. About 34% of the CLL samples harbored a mutation in at least 1 of these 26 genes.
Nearly 9% of the patients had mutations in CLL genes in the MAPK-ERK pathway. The researchers therefore believe that further exploration of MAPK-ERK pathway inhibitors may be warranted.
The team found that mutations differed between IGHV-mutated and unmutated CLL. IGHV-unmutated CLL tended to have a higher proportion of most driving mutations, while only 3 driver genes were enriched in IGHV-mutated CLL—del(13q), MYD88, and CHD2.
The researchers also discovered that certain mutations were common in patients who had already undergone treatment.
Previous treatment was associated with enrichment in TP53 and BIRC3 mutations del(17p) and del(11q), as well as in mutated DDX3X and MAP2K1. The team therefore believes these mutations may help CLL rebound after initial therapy.
Another key finding was that therapy tended to produce shorter remissions in patients with mutations in TP53 or SF3B1.
“We found that genomic evolution after therapy is the rule rather than the exception,” Dr Wu noted. “Certain mutations were present in a greater number of leukemia cells within a sample after relapse, showing that these mutations, presumably, allow the tumor to persevere.” ![]()
NCCN creates tool to aid treatment decisions

patient and her father
Photo by Rhoda Baer
The National Comprehensive Cancer Network (NCCN) has developed a new tool to accompany its clinical practice guidelines.
The tool—known as NCCN Evidence Blocks™—is designed to provide additional information about guideline recommendations and help inform treatment decisions.
NCCN has already added Evidence Blocks to its guidelines for chronic myelogenous leukemia and multiple myeloma.
The organization hopes to have Evidence Blocks for all of its guidelines by early 2017.
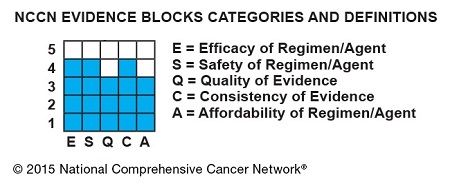
The Evidence Blocks provide a visual representation of 5 key value measures pertaining to guideline recommendations:
- Efficacy of treatment regimens
- Safety of regimens
- Quality and quantity of evidence supporting regimens
- Consistency of evidence supporting regimens
- Affordability of regimens. (This represents an estimate of overall total cost of a therapy, including but not limited to acquisition, administration, inpatient vs outpatient care, supportive care, infusions, toxicity monitoring, antiemetics and growth factors, and hospitalization.)
The Evidence Blocks are graphics of actual blocks that consist of 25 small squares. So each block has 5 rows and 5 columns.
Each of the 5 value measures—efficacy, safety, etc.—has a dedicated column within an Evidence Block, and each row of the Evidence Block represents a rating on a scale of 1 to 5. A score of 1 is unfavorable and a score of 5 is most favorable.
The rating of each value measure is shown by filling in the squares of the dedicated column—such as efficacy—up to the row that represents its assigned score—such as 4.
For example:
NCCN hopes this visual rating system will help patients and their physicians identify the optimal treatment based on clinical and economic considerations that are of the most value to the patient.
“Some patients will want an emerging therapy even with limited data,” said Robert W. Carlson, MD, chief executive officer of NCCN.
“Others will be most concerned about the expected side effects of the treatment indicated in the safety column. Still others may be very sensitive to cost. By considering the attributes of the range of possible therapies, the healthcare provider and the patient can discuss the benefits and drawbacks of each option and come to a decision most acceptable to the individual.”
By the end of 2015, NCCN expects to publish NCCN Evidence Blocks for systemic therapies (not surgery or radiation therapy) in the NCCN guidelines for breast, colon, non-small cell lung, and rectal cancers.
NCCN Evidence Blocks for systemic therapies are expected to be contained within the complete library of NCCN guidelines by the end of 2016.
In the near term, NCCN will continue to publish 2 sets of guidelines: those including NCCN Evidence Blocks and those without. The Evidence Blocks are not currently published in the NCCN Guidelines for Patients® and are intended for use in the US only.
For more information about NCCN Evidence Blocks, visit NCCN.org/EvidenceBlocks. ![]()
patient and her father
Photo by Rhoda Baer
The National Comprehensive Cancer Network (NCCN) has developed a new tool to accompany its clinical practice guidelines.
The tool—known as NCCN Evidence Blocks™—is designed to provide additional information about guideline recommendations and help inform treatment decisions.
NCCN has already added Evidence Blocks to its guidelines for chronic myelogenous leukemia and multiple myeloma.
The organization hopes to have Evidence Blocks for all of its guidelines by early 2017.
The Evidence Blocks provide a visual representation of 5 key value measures pertaining to guideline recommendations:
- Efficacy of treatment regimens
- Safety of regimens
- Quality and quantity of evidence supporting regimens
- Consistency of evidence supporting regimens
- Affordability of regimens. (This represents an estimate of overall total cost of a therapy, including but not limited to acquisition, administration, inpatient vs outpatient care, supportive care, infusions, toxicity monitoring, antiemetics and growth factors, and hospitalization.)
The Evidence Blocks are graphics of actual blocks that consist of 25 small squares. So each block has 5 rows and 5 columns.
Each of the 5 value measures—efficacy, safety, etc.—has a dedicated column within an Evidence Block, and each row of the Evidence Block represents a rating on a scale of 1 to 5. A score of 1 is unfavorable and a score of 5 is most favorable.
The rating of each value measure is shown by filling in the squares of the dedicated column—such as efficacy—up to the row that represents its assigned score—such as 4.
For example:
NCCN hopes this visual rating system will help patients and their physicians identify the optimal treatment based on clinical and economic considerations that are of the most value to the patient.
“Some patients will want an emerging therapy even with limited data,” said Robert W. Carlson, MD, chief executive officer of NCCN.
“Others will be most concerned about the expected side effects of the treatment indicated in the safety column. Still others may be very sensitive to cost. By considering the attributes of the range of possible therapies, the healthcare provider and the patient can discuss the benefits and drawbacks of each option and come to a decision most acceptable to the individual.”
By the end of 2015, NCCN expects to publish NCCN Evidence Blocks for systemic therapies (not surgery or radiation therapy) in the NCCN guidelines for breast, colon, non-small cell lung, and rectal cancers.
NCCN Evidence Blocks for systemic therapies are expected to be contained within the complete library of NCCN guidelines by the end of 2016.
In the near term, NCCN will continue to publish 2 sets of guidelines: those including NCCN Evidence Blocks and those without. The Evidence Blocks are not currently published in the NCCN Guidelines for Patients® and are intended for use in the US only.
For more information about NCCN Evidence Blocks, visit NCCN.org/EvidenceBlocks. ![]()
patient and her father
Photo by Rhoda Baer
The National Comprehensive Cancer Network (NCCN) has developed a new tool to accompany its clinical practice guidelines.
The tool—known as NCCN Evidence Blocks™—is designed to provide additional information about guideline recommendations and help inform treatment decisions.
NCCN has already added Evidence Blocks to its guidelines for chronic myelogenous leukemia and multiple myeloma.
The organization hopes to have Evidence Blocks for all of its guidelines by early 2017.
The Evidence Blocks provide a visual representation of 5 key value measures pertaining to guideline recommendations:
- Efficacy of treatment regimens
- Safety of regimens
- Quality and quantity of evidence supporting regimens
- Consistency of evidence supporting regimens
- Affordability of regimens. (This represents an estimate of overall total cost of a therapy, including but not limited to acquisition, administration, inpatient vs outpatient care, supportive care, infusions, toxicity monitoring, antiemetics and growth factors, and hospitalization.)
The Evidence Blocks are graphics of actual blocks that consist of 25 small squares. So each block has 5 rows and 5 columns.
Each of the 5 value measures—efficacy, safety, etc.—has a dedicated column within an Evidence Block, and each row of the Evidence Block represents a rating on a scale of 1 to 5. A score of 1 is unfavorable and a score of 5 is most favorable.
The rating of each value measure is shown by filling in the squares of the dedicated column—such as efficacy—up to the row that represents its assigned score—such as 4.
For example:
NCCN hopes this visual rating system will help patients and their physicians identify the optimal treatment based on clinical and economic considerations that are of the most value to the patient.
“Some patients will want an emerging therapy even with limited data,” said Robert W. Carlson, MD, chief executive officer of NCCN.
“Others will be most concerned about the expected side effects of the treatment indicated in the safety column. Still others may be very sensitive to cost. By considering the attributes of the range of possible therapies, the healthcare provider and the patient can discuss the benefits and drawbacks of each option and come to a decision most acceptable to the individual.”
By the end of 2015, NCCN expects to publish NCCN Evidence Blocks for systemic therapies (not surgery or radiation therapy) in the NCCN guidelines for breast, colon, non-small cell lung, and rectal cancers.
NCCN Evidence Blocks for systemic therapies are expected to be contained within the complete library of NCCN guidelines by the end of 2016.
In the near term, NCCN will continue to publish 2 sets of guidelines: those including NCCN Evidence Blocks and those without. The Evidence Blocks are not currently published in the NCCN Guidelines for Patients® and are intended for use in the US only.
For more information about NCCN Evidence Blocks, visit NCCN.org/EvidenceBlocks. ![]()
In ALL, early treatment decisions have “irrevocable” implications
SAN FRANCISCO – “The best opportunity to improve acute lymphoblastic leukemia (ALL) outcomes is to make the best evidence-based choices early at the time of diagnosis or early at the time of relapse. This is a disease where early choices are irrevocable, and if you make the wrong choices, patients suffer,” Dr. Joseph C. Alvarnas asserted at the National Comprehensive Cancer Network 10th Annual Congress: Hematologic Malignancies.
Hematologists must also stay up on novel agents being added to the ALL treatment armamentarium, he stressed. “The state of the art is one that evolves over the course of months, not over the course of years. So maintaining current [knowledge] in this is essential. And many of these patients benefit from being referred quickly to an expert institution,” he said.

Cytogenetics and genomics help risk-adapt therapy
“Cytogenetic, molecular, and genomic data are essential to making great early choices,” maintained Dr. Alvarnas, who is an associate clinical professor in the department of hematology & hematopoietic cell transplantation, and director of Value Based Analytics, at the City of Hope Comprehensive Cancer Center in Duarte, California.
Patients with Philadelphia chromosome (Ph)-positive ALL should receive tyrosine kinase inhibitors (TKIs) concomitantly with age-adapted induction and consolidation therapy, he recommended. In those with a poor response, a mutational analysis is key to guiding next steps.
“While in the young pediatric population – we are talking ages 5-10 years – there is a trend away from offering transplant to patients with Ph-positive disease because some of them are actually cured through the combination of induction pediatric regimens followed by TKI-based therapy, for adults, the standard of care until demonstrated otherwise is prompt referral for transplant,” he said.
Indeed, long-term survival is nearly doubled for Ph-positive patients if they have a transplant in a first complete remission versus later (54% vs 29%) (Blood. 2008;112;903-9).
Patients with the high-risk MLL rearrangement are likely to fare poorly and should also be considered for early transplant in first complete remission, according to Dr. Alvarnas.
A novel genetic subtype of ALL identified by looking at networks of genes – Ph-like ALL – has a poor prognosis, especially when affected patients are young adults as compared with children or adolescents (N Engl J Med. 2014;371:1005-15). Analyses have identified the presence of a cluster of genetic abnormalities involving ABL, JAK2, and RAS, among others.
“If you think strategically about how we might be able to better treat these patients … targeted agents like ruxolitinib (Jakafi), dasatinib (Sprycel), and crizotinib (Xalkori) may all play a role,” he said. “Now this is not ready for prime time yet – I’m not ready to advocate that you begin treating patients with targeted therapies. I think in fact this patient population should be referred to an academic cancer center for treatment on protocol. But as we look at what’s likely to change over the next year to 5 years, genomic alterations may make these patients better candidates for treatment with TKIs.”
Demographics can guide treatment choices as well
Patient demographics, especially age, should also be used to risk-adapt ALL therapy, according to Dr. Alvarnas. The adolescent and young adult (AYA) subset of patients – aged 15-39 – tend to be fitter and can therefore benefit from pediatric or pediatric-inspired regimens.
“These regimens don’t use novel therapeutics, for the most part; they increase the dose density or dose intensity of existing agents, particularly L-asparaginase. And a lot of adult doctors used to treating older patients don’t like L-asparaginase because of the significant morbidities, particularly pancreatitis, that can arise with this agent,” he said. “But when you get a younger, fitter group of patients, you can use very intensive doses of L-asparaginase not only with impunity, but with greater cure rates.”
AYA patients have superior event-free and overall survival when treated with a pediatric or pediatric-inspired regimen than when treated with an adult regimen (Blood. 2008;112:1646-54).
“So think of it this way: patients 15-39 years of age are receiving inferior therapy if they are receiving adult regimens,” Dr. Alvarnas said. “Now the caveat there is they have to be … physiologically fit, and there may be specific contraindications to these pediatric regimens. But this should be an opt out, not an opt in. The pediatric-inspired regimens are, I would say, the standard care for this population.”
At the other end of the age spectrum, patients 65 years and older with ALL have poorer outcomes, which may be due to both biology of disease and physiology. “We need to be very mindful and think carefully of how best to treat these patients in a patient-centric fashion,” he said.
He recommended consideration of comorbidities and use of a comprehensive geriatric assessment when contemplating care options for this age group. “We want to make sure that the therapy used matches the patient before us,” he added, pointing to an algorithm that is helpful in this setting (Blood. 2013;122:1366-75).
“Where it’s possible, I would encourage the use of clinical trials, particularly geared to the older age population. And that said, in the older, fitter patient with a good initial response to therapy, do not discount the appropriateness of allogeneic stem cell transplant,” Dr. Alvarnas advised.
At the same time, hematologists should have a frank discussion with these older patients about the goals of care and advanced directives, and should involve supportive care early.
“NCCN has an absolutely beautiful document on the care of older oncology patients as well as a beautiful set of guidelines regarding supportive care,” he added. “Please look at those. I think are an invaluable resource.”
Immunotherapy shows promise in the salvage setting
“At the time of salvage, immunotherapy-based approaches are very powerful, so don’t overtreat the patient with modalities that aren’t going to work,” Dr. Alvarnas recommended.
“Immunotherapeutic approaches are going to play an increasingly important role in patients with ALL, and we see these novel therapeutics completely upending what we knew about this disease even a year or two ago,” he said. A variety of monoclonal antibodies against CD20, CD19, CD22, and CD52 have shown promise when tested in various patient populations (Blood. 2015;125:4010-6).
This concept has been taken a step further with blinatumomab (Blincyto), an antibody having two antigen recognition sites that brings CD19-positive tumor cells in contact with T lymphocytes. It is the first such agent to be approved by the FDA for an ALL indication (currently for refractory or relapsed Ph-negative B-cell ALL). “It has nonoverlapping activity with cytotoxic chemotherapy, which makes it an ideal agent,” Dr. Alvarnas noted.
The main risk with blinatumomab is a cytokine release syndrome, which is most common in patients with a high disease burden and requires drug discontinuation and treatment with high-dose dexamethasone. Neurotoxicity is also noteworthy as it can be fatal.
Responses to blinatumomab tend to be dramatic and deep, but brief, according to Dr. Alvarnas. “Even though it’s profoundly powerful, it’s not a curative agent. It really provides a bridge towards cure, with that cure coming through the use of allogeneic stem cell transplant,” he elaborated. “So if someone relapses and you begin blinatumomab, get them referred very quickly to a transplant center.”
Another promising immunotherapy is inotuzumab ozagamicin, an antibody-drug conjugate that targets CD22-expressing cells. It has been associated with a complete response rate of 19%, although veno-occlusive toxicity has been problematic (Cancer. 2013;119:2728-36). “This agent has not yet received FDA approval, but it’s one that we are awaiting expectantly,” he said.
Finally, phase 1 trials from various academic centers have shown that chimeric antigen receptor (CAR) T-cell therapy achieves complete response rates of 67%-90% in patients with high-risk refractory disease, according to Dr. Alvarnas, who disclosed that he had no relevant financial relationships.
“This has lead to culmination in phase 2 trials, and I really do see this as an important component in the management of patients with relapsed and refractory ALL,” he concluded. “It’s not something that is available at every center. Right now it’s restricted largely to academic centers capable of producing these therapeutics in their own GLP [Good Laboratory Practice] facility.”
SAN FRANCISCO – “The best opportunity to improve acute lymphoblastic leukemia (ALL) outcomes is to make the best evidence-based choices early at the time of diagnosis or early at the time of relapse. This is a disease where early choices are irrevocable, and if you make the wrong choices, patients suffer,” Dr. Joseph C. Alvarnas asserted at the National Comprehensive Cancer Network 10th Annual Congress: Hematologic Malignancies.
Hematologists must also stay up on novel agents being added to the ALL treatment armamentarium, he stressed. “The state of the art is one that evolves over the course of months, not over the course of years. So maintaining current [knowledge] in this is essential. And many of these patients benefit from being referred quickly to an expert institution,” he said.
Cytogenetics and genomics help risk-adapt therapy
“Cytogenetic, molecular, and genomic data are essential to making great early choices,” maintained Dr. Alvarnas, who is an associate clinical professor in the department of hematology & hematopoietic cell transplantation, and director of Value Based Analytics, at the City of Hope Comprehensive Cancer Center in Duarte, California.
Patients with Philadelphia chromosome (Ph)-positive ALL should receive tyrosine kinase inhibitors (TKIs) concomitantly with age-adapted induction and consolidation therapy, he recommended. In those with a poor response, a mutational analysis is key to guiding next steps.
“While in the young pediatric population – we are talking ages 5-10 years – there is a trend away from offering transplant to patients with Ph-positive disease because some of them are actually cured through the combination of induction pediatric regimens followed by TKI-based therapy, for adults, the standard of care until demonstrated otherwise is prompt referral for transplant,” he said.
Indeed, long-term survival is nearly doubled for Ph-positive patients if they have a transplant in a first complete remission versus later (54% vs 29%) (Blood. 2008;112;903-9).
Patients with the high-risk MLL rearrangement are likely to fare poorly and should also be considered for early transplant in first complete remission, according to Dr. Alvarnas.
A novel genetic subtype of ALL identified by looking at networks of genes – Ph-like ALL – has a poor prognosis, especially when affected patients are young adults as compared with children or adolescents (N Engl J Med. 2014;371:1005-15). Analyses have identified the presence of a cluster of genetic abnormalities involving ABL, JAK2, and RAS, among others.
“If you think strategically about how we might be able to better treat these patients … targeted agents like ruxolitinib (Jakafi), dasatinib (Sprycel), and crizotinib (Xalkori) may all play a role,” he said. “Now this is not ready for prime time yet – I’m not ready to advocate that you begin treating patients with targeted therapies. I think in fact this patient population should be referred to an academic cancer center for treatment on protocol. But as we look at what’s likely to change over the next year to 5 years, genomic alterations may make these patients better candidates for treatment with TKIs.”
Demographics can guide treatment choices as well
Patient demographics, especially age, should also be used to risk-adapt ALL therapy, according to Dr. Alvarnas. The adolescent and young adult (AYA) subset of patients – aged 15-39 – tend to be fitter and can therefore benefit from pediatric or pediatric-inspired regimens.
“These regimens don’t use novel therapeutics, for the most part; they increase the dose density or dose intensity of existing agents, particularly L-asparaginase. And a lot of adult doctors used to treating older patients don’t like L-asparaginase because of the significant morbidities, particularly pancreatitis, that can arise with this agent,” he said. “But when you get a younger, fitter group of patients, you can use very intensive doses of L-asparaginase not only with impunity, but with greater cure rates.”
AYA patients have superior event-free and overall survival when treated with a pediatric or pediatric-inspired regimen than when treated with an adult regimen (Blood. 2008;112:1646-54).
“So think of it this way: patients 15-39 years of age are receiving inferior therapy if they are receiving adult regimens,” Dr. Alvarnas said. “Now the caveat there is they have to be … physiologically fit, and there may be specific contraindications to these pediatric regimens. But this should be an opt out, not an opt in. The pediatric-inspired regimens are, I would say, the standard care for this population.”
At the other end of the age spectrum, patients 65 years and older with ALL have poorer outcomes, which may be due to both biology of disease and physiology. “We need to be very mindful and think carefully of how best to treat these patients in a patient-centric fashion,” he said.
He recommended consideration of comorbidities and use of a comprehensive geriatric assessment when contemplating care options for this age group. “We want to make sure that the therapy used matches the patient before us,” he added, pointing to an algorithm that is helpful in this setting (Blood. 2013;122:1366-75).
“Where it’s possible, I would encourage the use of clinical trials, particularly geared to the older age population. And that said, in the older, fitter patient with a good initial response to therapy, do not discount the appropriateness of allogeneic stem cell transplant,” Dr. Alvarnas advised.
At the same time, hematologists should have a frank discussion with these older patients about the goals of care and advanced directives, and should involve supportive care early.
“NCCN has an absolutely beautiful document on the care of older oncology patients as well as a beautiful set of guidelines regarding supportive care,” he added. “Please look at those. I think are an invaluable resource.”
Immunotherapy shows promise in the salvage setting
“At the time of salvage, immunotherapy-based approaches are very powerful, so don’t overtreat the patient with modalities that aren’t going to work,” Dr. Alvarnas recommended.
“Immunotherapeutic approaches are going to play an increasingly important role in patients with ALL, and we see these novel therapeutics completely upending what we knew about this disease even a year or two ago,” he said. A variety of monoclonal antibodies against CD20, CD19, CD22, and CD52 have shown promise when tested in various patient populations (Blood. 2015;125:4010-6).
This concept has been taken a step further with blinatumomab (Blincyto), an antibody having two antigen recognition sites that brings CD19-positive tumor cells in contact with T lymphocytes. It is the first such agent to be approved by the FDA for an ALL indication (currently for refractory or relapsed Ph-negative B-cell ALL). “It has nonoverlapping activity with cytotoxic chemotherapy, which makes it an ideal agent,” Dr. Alvarnas noted.
The main risk with blinatumomab is a cytokine release syndrome, which is most common in patients with a high disease burden and requires drug discontinuation and treatment with high-dose dexamethasone. Neurotoxicity is also noteworthy as it can be fatal.
Responses to blinatumomab tend to be dramatic and deep, but brief, according to Dr. Alvarnas. “Even though it’s profoundly powerful, it’s not a curative agent. It really provides a bridge towards cure, with that cure coming through the use of allogeneic stem cell transplant,” he elaborated. “So if someone relapses and you begin blinatumomab, get them referred very quickly to a transplant center.”
Another promising immunotherapy is inotuzumab ozagamicin, an antibody-drug conjugate that targets CD22-expressing cells. It has been associated with a complete response rate of 19%, although veno-occlusive toxicity has been problematic (Cancer. 2013;119:2728-36). “This agent has not yet received FDA approval, but it’s one that we are awaiting expectantly,” he said.
Finally, phase 1 trials from various academic centers have shown that chimeric antigen receptor (CAR) T-cell therapy achieves complete response rates of 67%-90% in patients with high-risk refractory disease, according to Dr. Alvarnas, who disclosed that he had no relevant financial relationships.
“This has lead to culmination in phase 2 trials, and I really do see this as an important component in the management of patients with relapsed and refractory ALL,” he concluded. “It’s not something that is available at every center. Right now it’s restricted largely to academic centers capable of producing these therapeutics in their own GLP [Good Laboratory Practice] facility.”
SAN FRANCISCO – “The best opportunity to improve acute lymphoblastic leukemia (ALL) outcomes is to make the best evidence-based choices early at the time of diagnosis or early at the time of relapse. This is a disease where early choices are irrevocable, and if you make the wrong choices, patients suffer,” Dr. Joseph C. Alvarnas asserted at the National Comprehensive Cancer Network 10th Annual Congress: Hematologic Malignancies.
Hematologists must also stay up on novel agents being added to the ALL treatment armamentarium, he stressed. “The state of the art is one that evolves over the course of months, not over the course of years. So maintaining current [knowledge] in this is essential. And many of these patients benefit from being referred quickly to an expert institution,” he said.
Cytogenetics and genomics help risk-adapt therapy
“Cytogenetic, molecular, and genomic data are essential to making great early choices,” maintained Dr. Alvarnas, who is an associate clinical professor in the department of hematology & hematopoietic cell transplantation, and director of Value Based Analytics, at the City of Hope Comprehensive Cancer Center in Duarte, California.
Patients with Philadelphia chromosome (Ph)-positive ALL should receive tyrosine kinase inhibitors (TKIs) concomitantly with age-adapted induction and consolidation therapy, he recommended. In those with a poor response, a mutational analysis is key to guiding next steps.
“While in the young pediatric population – we are talking ages 5-10 years – there is a trend away from offering transplant to patients with Ph-positive disease because some of them are actually cured through the combination of induction pediatric regimens followed by TKI-based therapy, for adults, the standard of care until demonstrated otherwise is prompt referral for transplant,” he said.
Indeed, long-term survival is nearly doubled for Ph-positive patients if they have a transplant in a first complete remission versus later (54% vs 29%) (Blood. 2008;112;903-9).
Patients with the high-risk MLL rearrangement are likely to fare poorly and should also be considered for early transplant in first complete remission, according to Dr. Alvarnas.
A novel genetic subtype of ALL identified by looking at networks of genes – Ph-like ALL – has a poor prognosis, especially when affected patients are young adults as compared with children or adolescents (N Engl J Med. 2014;371:1005-15). Analyses have identified the presence of a cluster of genetic abnormalities involving ABL, JAK2, and RAS, among others.
“If you think strategically about how we might be able to better treat these patients … targeted agents like ruxolitinib (Jakafi), dasatinib (Sprycel), and crizotinib (Xalkori) may all play a role,” he said. “Now this is not ready for prime time yet – I’m not ready to advocate that you begin treating patients with targeted therapies. I think in fact this patient population should be referred to an academic cancer center for treatment on protocol. But as we look at what’s likely to change over the next year to 5 years, genomic alterations may make these patients better candidates for treatment with TKIs.”
Demographics can guide treatment choices as well
Patient demographics, especially age, should also be used to risk-adapt ALL therapy, according to Dr. Alvarnas. The adolescent and young adult (AYA) subset of patients – aged 15-39 – tend to be fitter and can therefore benefit from pediatric or pediatric-inspired regimens.
“These regimens don’t use novel therapeutics, for the most part; they increase the dose density or dose intensity of existing agents, particularly L-asparaginase. And a lot of adult doctors used to treating older patients don’t like L-asparaginase because of the significant morbidities, particularly pancreatitis, that can arise with this agent,” he said. “But when you get a younger, fitter group of patients, you can use very intensive doses of L-asparaginase not only with impunity, but with greater cure rates.”
AYA patients have superior event-free and overall survival when treated with a pediatric or pediatric-inspired regimen than when treated with an adult regimen (Blood. 2008;112:1646-54).
“So think of it this way: patients 15-39 years of age are receiving inferior therapy if they are receiving adult regimens,” Dr. Alvarnas said. “Now the caveat there is they have to be … physiologically fit, and there may be specific contraindications to these pediatric regimens. But this should be an opt out, not an opt in. The pediatric-inspired regimens are, I would say, the standard care for this population.”
At the other end of the age spectrum, patients 65 years and older with ALL have poorer outcomes, which may be due to both biology of disease and physiology. “We need to be very mindful and think carefully of how best to treat these patients in a patient-centric fashion,” he said.
He recommended consideration of comorbidities and use of a comprehensive geriatric assessment when contemplating care options for this age group. “We want to make sure that the therapy used matches the patient before us,” he added, pointing to an algorithm that is helpful in this setting (Blood. 2013;122:1366-75).
“Where it’s possible, I would encourage the use of clinical trials, particularly geared to the older age population. And that said, in the older, fitter patient with a good initial response to therapy, do not discount the appropriateness of allogeneic stem cell transplant,” Dr. Alvarnas advised.
At the same time, hematologists should have a frank discussion with these older patients about the goals of care and advanced directives, and should involve supportive care early.
“NCCN has an absolutely beautiful document on the care of older oncology patients as well as a beautiful set of guidelines regarding supportive care,” he added. “Please look at those. I think are an invaluable resource.”
Immunotherapy shows promise in the salvage setting
“At the time of salvage, immunotherapy-based approaches are very powerful, so don’t overtreat the patient with modalities that aren’t going to work,” Dr. Alvarnas recommended.
“Immunotherapeutic approaches are going to play an increasingly important role in patients with ALL, and we see these novel therapeutics completely upending what we knew about this disease even a year or two ago,” he said. A variety of monoclonal antibodies against CD20, CD19, CD22, and CD52 have shown promise when tested in various patient populations (Blood. 2015;125:4010-6).
This concept has been taken a step further with blinatumomab (Blincyto), an antibody having two antigen recognition sites that brings CD19-positive tumor cells in contact with T lymphocytes. It is the first such agent to be approved by the FDA for an ALL indication (currently for refractory or relapsed Ph-negative B-cell ALL). “It has nonoverlapping activity with cytotoxic chemotherapy, which makes it an ideal agent,” Dr. Alvarnas noted.
The main risk with blinatumomab is a cytokine release syndrome, which is most common in patients with a high disease burden and requires drug discontinuation and treatment with high-dose dexamethasone. Neurotoxicity is also noteworthy as it can be fatal.
Responses to blinatumomab tend to be dramatic and deep, but brief, according to Dr. Alvarnas. “Even though it’s profoundly powerful, it’s not a curative agent. It really provides a bridge towards cure, with that cure coming through the use of allogeneic stem cell transplant,” he elaborated. “So if someone relapses and you begin blinatumomab, get them referred very quickly to a transplant center.”
Another promising immunotherapy is inotuzumab ozagamicin, an antibody-drug conjugate that targets CD22-expressing cells. It has been associated with a complete response rate of 19%, although veno-occlusive toxicity has been problematic (Cancer. 2013;119:2728-36). “This agent has not yet received FDA approval, but it’s one that we are awaiting expectantly,” he said.
Finally, phase 1 trials from various academic centers have shown that chimeric antigen receptor (CAR) T-cell therapy achieves complete response rates of 67%-90% in patients with high-risk refractory disease, according to Dr. Alvarnas, who disclosed that he had no relevant financial relationships.
“This has lead to culmination in phase 2 trials, and I really do see this as an important component in the management of patients with relapsed and refractory ALL,” he concluded. “It’s not something that is available at every center. Right now it’s restricted largely to academic centers capable of producing these therapeutics in their own GLP [Good Laboratory Practice] facility.”
EXPERT ANALYSIS AT NCCN ANNUAL CONGRESS: HEMATOLOGIC MALIGNANCIES

COMP recommends orphan designations for KTE-C19

The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) has adopted positive opinions recommending orphan designation for KTE-C19 to treat acute lymphoblastic leukemia, chronic lymphocytic leukemia/small lymphocytic lymphoma, and follicular lymphoma.
KTE-C19 is an investigational chimeric antigen receptor (CAR) T-cell therapy designed to target CD19, a protein expressed on the surface of B cells.
The CAR T-cell therapy already has orphan designation for the treatment of diffuse large B-cell lymphoma in the US and the European Union (EU).
KTE-C19 also has COMP positive opinions for orphan designation in the EU for primary mediastinal B-cell lymphoma and mantle cell lymphoma.
About orphan designation
The COMP adopts an opinion on the granting of orphan designation, and that opinion is submitted to the European Commission for endorsement.
In the EU, orphan designation is granted to therapies intended to treat a life-threatening or chronically debilitating condition that affects no more than 5 in 10,000 persons and where no satisfactory treatment is available.
Companies that obtain orphan designation for a drug benefit from a number of incentives, including protocol assistance, a type of scientific advice specific for designated orphan medicines, and 10 years of market exclusivity once the medicine is approved. Fee reductions are also available, depending on the status of the sponsor and the type of service required.
KTE-C19 research
Last year, researchers reported results with KTE-C19 in the Journal of Clinical Oncology. The study included 15 patients with advanced B-cell malignancies.
The patients received a conditioning regimen of cyclophosphamide and fludarabine, followed 1 day later by a single infusion of the CAR T-cell therapy. The researchers noted that the conditioning regimen is known to be active against B-cell malignancies and could have made a direct contribution to patient responses.
Thirteen patients were evaluable for response. Eight patients achieved a complete response (CR), and 4 had a partial response (PR).
Of the 7 patients with chemotherapy-refractory diffuse large B-cell lymphoma, 4 achieved a CR, 2 achieved a PR, and 1 had stable disease. Of the 4 patients with chronic lymphocytic leukemia, 3 had a CR, and 1 had a PR. Among the 2 patients with indolent lymphomas, 1 achieved a CR, and 1 had a PR.
KTE-C19 was associated with fever, low blood pressure, focal neurological deficits, and delirium. Toxicities largely occurred in the first 2 weeks after infusion.
All but 2 patients experienced grade 3/4 adverse events. Four patients had grade 3/4 hypotension.
All patients had elevations in serum interferon gamma and/or interleukin 6 around the time of peak toxicity, but most did not develop elevations in serum tumor necrosis factor.
Neurologic toxicities included confusion and obtundation, which have been reported in previous studies. However, 3 patients developed unexpected neurologic abnormalities.
KTE-C19 is currently under investigation in a phase 1/2 trial (ZUMA-1) of patients with refractory, aggressive non-Hodgkin lymphomas. Kite Pharma, Inc., the company developing KTE-C19, plans to present top-line phase 1 data at the 2015 ASH Annual Meeting. ![]()
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) has adopted positive opinions recommending orphan designation for KTE-C19 to treat acute lymphoblastic leukemia, chronic lymphocytic leukemia/small lymphocytic lymphoma, and follicular lymphoma.
KTE-C19 is an investigational chimeric antigen receptor (CAR) T-cell therapy designed to target CD19, a protein expressed on the surface of B cells.
The CAR T-cell therapy already has orphan designation for the treatment of diffuse large B-cell lymphoma in the US and the European Union (EU).
KTE-C19 also has COMP positive opinions for orphan designation in the EU for primary mediastinal B-cell lymphoma and mantle cell lymphoma.
About orphan designation
The COMP adopts an opinion on the granting of orphan designation, and that opinion is submitted to the European Commission for endorsement.
In the EU, orphan designation is granted to therapies intended to treat a life-threatening or chronically debilitating condition that affects no more than 5 in 10,000 persons and where no satisfactory treatment is available.
Companies that obtain orphan designation for a drug benefit from a number of incentives, including protocol assistance, a type of scientific advice specific for designated orphan medicines, and 10 years of market exclusivity once the medicine is approved. Fee reductions are also available, depending on the status of the sponsor and the type of service required.
KTE-C19 research
Last year, researchers reported results with KTE-C19 in the Journal of Clinical Oncology. The study included 15 patients with advanced B-cell malignancies.
The patients received a conditioning regimen of cyclophosphamide and fludarabine, followed 1 day later by a single infusion of the CAR T-cell therapy. The researchers noted that the conditioning regimen is known to be active against B-cell malignancies and could have made a direct contribution to patient responses.
Thirteen patients were evaluable for response. Eight patients achieved a complete response (CR), and 4 had a partial response (PR).
Of the 7 patients with chemotherapy-refractory diffuse large B-cell lymphoma, 4 achieved a CR, 2 achieved a PR, and 1 had stable disease. Of the 4 patients with chronic lymphocytic leukemia, 3 had a CR, and 1 had a PR. Among the 2 patients with indolent lymphomas, 1 achieved a CR, and 1 had a PR.
KTE-C19 was associated with fever, low blood pressure, focal neurological deficits, and delirium. Toxicities largely occurred in the first 2 weeks after infusion.
All but 2 patients experienced grade 3/4 adverse events. Four patients had grade 3/4 hypotension.
All patients had elevations in serum interferon gamma and/or interleukin 6 around the time of peak toxicity, but most did not develop elevations in serum tumor necrosis factor.
Neurologic toxicities included confusion and obtundation, which have been reported in previous studies. However, 3 patients developed unexpected neurologic abnormalities.
KTE-C19 is currently under investigation in a phase 1/2 trial (ZUMA-1) of patients with refractory, aggressive non-Hodgkin lymphomas. Kite Pharma, Inc., the company developing KTE-C19, plans to present top-line phase 1 data at the 2015 ASH Annual Meeting. ![]()
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) has adopted positive opinions recommending orphan designation for KTE-C19 to treat acute lymphoblastic leukemia, chronic lymphocytic leukemia/small lymphocytic lymphoma, and follicular lymphoma.
KTE-C19 is an investigational chimeric antigen receptor (CAR) T-cell therapy designed to target CD19, a protein expressed on the surface of B cells.
The CAR T-cell therapy already has orphan designation for the treatment of diffuse large B-cell lymphoma in the US and the European Union (EU).
KTE-C19 also has COMP positive opinions for orphan designation in the EU for primary mediastinal B-cell lymphoma and mantle cell lymphoma.
About orphan designation
The COMP adopts an opinion on the granting of orphan designation, and that opinion is submitted to the European Commission for endorsement.
In the EU, orphan designation is granted to therapies intended to treat a life-threatening or chronically debilitating condition that affects no more than 5 in 10,000 persons and where no satisfactory treatment is available.
Companies that obtain orphan designation for a drug benefit from a number of incentives, including protocol assistance, a type of scientific advice specific for designated orphan medicines, and 10 years of market exclusivity once the medicine is approved. Fee reductions are also available, depending on the status of the sponsor and the type of service required.
KTE-C19 research
Last year, researchers reported results with KTE-C19 in the Journal of Clinical Oncology. The study included 15 patients with advanced B-cell malignancies.
The patients received a conditioning regimen of cyclophosphamide and fludarabine, followed 1 day later by a single infusion of the CAR T-cell therapy. The researchers noted that the conditioning regimen is known to be active against B-cell malignancies and could have made a direct contribution to patient responses.
Thirteen patients were evaluable for response. Eight patients achieved a complete response (CR), and 4 had a partial response (PR).
Of the 7 patients with chemotherapy-refractory diffuse large B-cell lymphoma, 4 achieved a CR, 2 achieved a PR, and 1 had stable disease. Of the 4 patients with chronic lymphocytic leukemia, 3 had a CR, and 1 had a PR. Among the 2 patients with indolent lymphomas, 1 achieved a CR, and 1 had a PR.
KTE-C19 was associated with fever, low blood pressure, focal neurological deficits, and delirium. Toxicities largely occurred in the first 2 weeks after infusion.
All but 2 patients experienced grade 3/4 adverse events. Four patients had grade 3/4 hypotension.
All patients had elevations in serum interferon gamma and/or interleukin 6 around the time of peak toxicity, but most did not develop elevations in serum tumor necrosis factor.
Neurologic toxicities included confusion and obtundation, which have been reported in previous studies. However, 3 patients developed unexpected neurologic abnormalities.
KTE-C19 is currently under investigation in a phase 1/2 trial (ZUMA-1) of patients with refractory, aggressive non-Hodgkin lymphomas. Kite Pharma, Inc., the company developing KTE-C19, plans to present top-line phase 1 data at the 2015 ASH Annual Meeting. ![]()
CML outcomes in the age of TKIs
CHICAGO – Major molecular response rates at 12 months were better among chronic myeloid leukemia patients treated with dasatinib/nilotinib vs. imatinib for first-line therapy, and among patients enrolled vs. not enrolled in clinical trials, in a retrospective review of patients treated with first-line tyrosine kinase inhibitors between 2002 and 2014.
The overall rates of major molecular response (MMR) at 12 and 24 months in the 51 patients in the study were 23.5% (12 patients) and 44.9% (22 patients), which was comparable to historical data, Dr. Isabelle Phuong Le reported in a poster at the American Society of Hematology Meeting on Hematologic Malignancies.
The MMR rate among those treated with dasatinib/nilotinib first line was 53%, compared with 10% for those treated with imatinib, said Dr. Le of the University of Texas Health Science Center, San Antonio.
Further the MMR rates at 12 and 24 months among those enrolled vs. not enrolled in clinical trials were 83% vs 15% and 100% vs. 45%, respectively, she noted.
Patients in the analysis were adults with a mean age of 44.6 years who had chronic phase chronic myeloid leukemia (CML). Almost half (49%) were Hispanic, and 56.9% were women. Two-thirds (66.7%) received imatinib first line, and 33.3% received dasatinib/nilotinib first line. More than a third (37.2%) were younger than age 40 years, 15% had a language barrier, and 11.7% were enrolled in clinical trials.
No differences in the MMR rates at 12 and 24 months were seen between Hispanics and non-Hispanics, those with and without language barrier, or men and women, nor were any differences seen between those with more than three lines of therapy and those with three or fewer lines of therapy, or between patients older vs. younger than 40 years, although there was a trend toward improved response rates in older patients, she noted.
“Our patients have similar MMR rates at 12 months and 24 months compared to historical data,” Dr. Le wrote, noting that the findings regarding improved MMR rates with dasatinib/nilotinib were expected.
The findings regarding improved MMR rates among those enrolled in clinical trials could be due to “selective patients as clinical trial patients, more controlled and monitored treatment, frequent follow-ups, and better education regarding disease and treatment,” she said, concluding that “ we can improve treatment response rates in our patients with better disease education.”
Dr. Le reported having no disclosures.
CHICAGO – Major molecular response rates at 12 months were better among chronic myeloid leukemia patients treated with dasatinib/nilotinib vs. imatinib for first-line therapy, and among patients enrolled vs. not enrolled in clinical trials, in a retrospective review of patients treated with first-line tyrosine kinase inhibitors between 2002 and 2014.
The overall rates of major molecular response (MMR) at 12 and 24 months in the 51 patients in the study were 23.5% (12 patients) and 44.9% (22 patients), which was comparable to historical data, Dr. Isabelle Phuong Le reported in a poster at the American Society of Hematology Meeting on Hematologic Malignancies.
The MMR rate among those treated with dasatinib/nilotinib first line was 53%, compared with 10% for those treated with imatinib, said Dr. Le of the University of Texas Health Science Center, San Antonio.
Further the MMR rates at 12 and 24 months among those enrolled vs. not enrolled in clinical trials were 83% vs 15% and 100% vs. 45%, respectively, she noted.
Patients in the analysis were adults with a mean age of 44.6 years who had chronic phase chronic myeloid leukemia (CML). Almost half (49%) were Hispanic, and 56.9% were women. Two-thirds (66.7%) received imatinib first line, and 33.3% received dasatinib/nilotinib first line. More than a third (37.2%) were younger than age 40 years, 15% had a language barrier, and 11.7% were enrolled in clinical trials.
No differences in the MMR rates at 12 and 24 months were seen between Hispanics and non-Hispanics, those with and without language barrier, or men and women, nor were any differences seen between those with more than three lines of therapy and those with three or fewer lines of therapy, or between patients older vs. younger than 40 years, although there was a trend toward improved response rates in older patients, she noted.
“Our patients have similar MMR rates at 12 months and 24 months compared to historical data,” Dr. Le wrote, noting that the findings regarding improved MMR rates with dasatinib/nilotinib were expected.
The findings regarding improved MMR rates among those enrolled in clinical trials could be due to “selective patients as clinical trial patients, more controlled and monitored treatment, frequent follow-ups, and better education regarding disease and treatment,” she said, concluding that “ we can improve treatment response rates in our patients with better disease education.”
Dr. Le reported having no disclosures.
CHICAGO – Major molecular response rates at 12 months were better among chronic myeloid leukemia patients treated with dasatinib/nilotinib vs. imatinib for first-line therapy, and among patients enrolled vs. not enrolled in clinical trials, in a retrospective review of patients treated with first-line tyrosine kinase inhibitors between 2002 and 2014.
The overall rates of major molecular response (MMR) at 12 and 24 months in the 51 patients in the study were 23.5% (12 patients) and 44.9% (22 patients), which was comparable to historical data, Dr. Isabelle Phuong Le reported in a poster at the American Society of Hematology Meeting on Hematologic Malignancies.
The MMR rate among those treated with dasatinib/nilotinib first line was 53%, compared with 10% for those treated with imatinib, said Dr. Le of the University of Texas Health Science Center, San Antonio.
Further the MMR rates at 12 and 24 months among those enrolled vs. not enrolled in clinical trials were 83% vs 15% and 100% vs. 45%, respectively, she noted.
Patients in the analysis were adults with a mean age of 44.6 years who had chronic phase chronic myeloid leukemia (CML). Almost half (49%) were Hispanic, and 56.9% were women. Two-thirds (66.7%) received imatinib first line, and 33.3% received dasatinib/nilotinib first line. More than a third (37.2%) were younger than age 40 years, 15% had a language barrier, and 11.7% were enrolled in clinical trials.
No differences in the MMR rates at 12 and 24 months were seen between Hispanics and non-Hispanics, those with and without language barrier, or men and women, nor were any differences seen between those with more than three lines of therapy and those with three or fewer lines of therapy, or between patients older vs. younger than 40 years, although there was a trend toward improved response rates in older patients, she noted.
“Our patients have similar MMR rates at 12 months and 24 months compared to historical data,” Dr. Le wrote, noting that the findings regarding improved MMR rates with dasatinib/nilotinib were expected.
The findings regarding improved MMR rates among those enrolled in clinical trials could be due to “selective patients as clinical trial patients, more controlled and monitored treatment, frequent follow-ups, and better education regarding disease and treatment,” she said, concluding that “ we can improve treatment response rates in our patients with better disease education.”
Dr. Le reported having no disclosures.
AT MHM 2015
Key clinical point: Major molecular response rates at 12 months were better among CML patients treated with dasatinib/nilotinib vs. imatinib for first-line therapy, and among patients enrolled vs. not enrolled in clinical trials.
Major finding: The major molecular response rates at 12 and 24 months were 23.5% and 44.9%, which is comparable to historical data.
Data source: A retrospective review of 51 cases.
Disclosures: Dr. Le reported having no disclosures.
Computerized cognitive training benefits childhood cancer survivors

Conklin and Jason Ashford
Photo courtesy of St. Jude
Children’s Research Hospital
and Peter Barta
Cognitive training presented as a video game can help improve cognitive skills in childhood cancer survivors (CCSs), new research suggests.
CCSs who completed 20 to 30 training sessions with this game experienced significant improvements in working memory, attention, and the speed at which their brains process information.
However, these improvements did not translate to improved math or reading performance.
Heather Conklin, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and her colleagues conducted this research and described the results in the Journal of Clinical Oncology.
Study design
This study included 68 CCSs who had received cranial irradiation, intrathecal chemotherapy, or both for the treatment of acute lymphoblastic leukemia or brain tumors.
Participants were 8 to 16 years old, had completed treatment, and had been disease-free for at least a year. Prior to joining the study, all scored below expectations on measures of working memory.
The computerized intervention the CCSs used is called Cogmed (http://www.cogmed.com). It’s a working memory intervention that has previously demonstrated efficacy for individuals with developmental and acquired attention disorders as well as for healthy adults.
For this study, half the CCSs were randomized to begin using Cogmed immediately. The remaining survivors, who served as the control group, were given the opportunity to use Cogmed about 6 months later.
The CCSs assigned to Cogmed first were asked to complete 25 training sessions at home, along with weekly, telephone-based coaching. The training sessions lasted 30 to 45 minutes and included verbal and visual-spatial exercises that were presented as games and are designed to improve working memory.
CCSs who began training immediately underwent functional brain MRI before and soon after completing the intervention. The imaging tracked brain activity as the survivors completed a working memory exercise.
Results
CCSs who completed the intervention (n=30) showed greater improvements than controls on measures of working memory (P=0.002), attention (P=0.01), and processing speed (P=0.02).
The researchers said the benefits to working memory and attention were comparable to gains reported in previous studies of stimulant medications. And the gains from cognitive training moved the CCSs’ performance into the normal range.
Caregivers also reported significant improvement in the attention and executive functioning of CCSs who completed the training. (Executive functioning includes skills like planning and focus needed to juggle multiple tasks and get things done.)
“These results suggest that computerized cognitive training may help fill a void in management of cognitive late effects that impact quality of life for childhood cancer survivors, such as the likelihood they will complete school and live independently,” Dr Conklin said.
In addition, post-intervention brain imaging showed decreased activation of left lateral prefrontal and bilateral medial frontal areas.
“That suggests the intervention exercised and strengthened the well-established working memory network,” Dr Conklin said. “The implication is that the brain may operate more efficiently and have less need for compensatory strategies. Such training-induced neuroplasticity suggests the benefits might be sustained going forward.”
The researchers are now studying the possible benefits of starting brain training during treatment or combining it with other interventions. The team is also tracking whether the cognitive benefits are sustained and might eventually translate to the improved academic performance reported for other populations. ![]()
Conklin and Jason Ashford
Photo courtesy of St. Jude
Children’s Research Hospital
and Peter Barta
Cognitive training presented as a video game can help improve cognitive skills in childhood cancer survivors (CCSs), new research suggests.
CCSs who completed 20 to 30 training sessions with this game experienced significant improvements in working memory, attention, and the speed at which their brains process information.
However, these improvements did not translate to improved math or reading performance.
Heather Conklin, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and her colleagues conducted this research and described the results in the Journal of Clinical Oncology.
Study design
This study included 68 CCSs who had received cranial irradiation, intrathecal chemotherapy, or both for the treatment of acute lymphoblastic leukemia or brain tumors.
Participants were 8 to 16 years old, had completed treatment, and had been disease-free for at least a year. Prior to joining the study, all scored below expectations on measures of working memory.
The computerized intervention the CCSs used is called Cogmed (http://www.cogmed.com). It’s a working memory intervention that has previously demonstrated efficacy for individuals with developmental and acquired attention disorders as well as for healthy adults.
For this study, half the CCSs were randomized to begin using Cogmed immediately. The remaining survivors, who served as the control group, were given the opportunity to use Cogmed about 6 months later.
The CCSs assigned to Cogmed first were asked to complete 25 training sessions at home, along with weekly, telephone-based coaching. The training sessions lasted 30 to 45 minutes and included verbal and visual-spatial exercises that were presented as games and are designed to improve working memory.
CCSs who began training immediately underwent functional brain MRI before and soon after completing the intervention. The imaging tracked brain activity as the survivors completed a working memory exercise.
Results
CCSs who completed the intervention (n=30) showed greater improvements than controls on measures of working memory (P=0.002), attention (P=0.01), and processing speed (P=0.02).
The researchers said the benefits to working memory and attention were comparable to gains reported in previous studies of stimulant medications. And the gains from cognitive training moved the CCSs’ performance into the normal range.
Caregivers also reported significant improvement in the attention and executive functioning of CCSs who completed the training. (Executive functioning includes skills like planning and focus needed to juggle multiple tasks and get things done.)
“These results suggest that computerized cognitive training may help fill a void in management of cognitive late effects that impact quality of life for childhood cancer survivors, such as the likelihood they will complete school and live independently,” Dr Conklin said.
In addition, post-intervention brain imaging showed decreased activation of left lateral prefrontal and bilateral medial frontal areas.
“That suggests the intervention exercised and strengthened the well-established working memory network,” Dr Conklin said. “The implication is that the brain may operate more efficiently and have less need for compensatory strategies. Such training-induced neuroplasticity suggests the benefits might be sustained going forward.”
The researchers are now studying the possible benefits of starting brain training during treatment or combining it with other interventions. The team is also tracking whether the cognitive benefits are sustained and might eventually translate to the improved academic performance reported for other populations. ![]()
Conklin and Jason Ashford
Photo courtesy of St. Jude
Children’s Research Hospital
and Peter Barta
Cognitive training presented as a video game can help improve cognitive skills in childhood cancer survivors (CCSs), new research suggests.
CCSs who completed 20 to 30 training sessions with this game experienced significant improvements in working memory, attention, and the speed at which their brains process information.
However, these improvements did not translate to improved math or reading performance.
Heather Conklin, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and her colleagues conducted this research and described the results in the Journal of Clinical Oncology.
Study design
This study included 68 CCSs who had received cranial irradiation, intrathecal chemotherapy, or both for the treatment of acute lymphoblastic leukemia or brain tumors.
Participants were 8 to 16 years old, had completed treatment, and had been disease-free for at least a year. Prior to joining the study, all scored below expectations on measures of working memory.
The computerized intervention the CCSs used is called Cogmed (http://www.cogmed.com). It’s a working memory intervention that has previously demonstrated efficacy for individuals with developmental and acquired attention disorders as well as for healthy adults.
For this study, half the CCSs were randomized to begin using Cogmed immediately. The remaining survivors, who served as the control group, were given the opportunity to use Cogmed about 6 months later.
The CCSs assigned to Cogmed first were asked to complete 25 training sessions at home, along with weekly, telephone-based coaching. The training sessions lasted 30 to 45 minutes and included verbal and visual-spatial exercises that were presented as games and are designed to improve working memory.
CCSs who began training immediately underwent functional brain MRI before and soon after completing the intervention. The imaging tracked brain activity as the survivors completed a working memory exercise.
Results
CCSs who completed the intervention (n=30) showed greater improvements than controls on measures of working memory (P=0.002), attention (P=0.01), and processing speed (P=0.02).
The researchers said the benefits to working memory and attention were comparable to gains reported in previous studies of stimulant medications. And the gains from cognitive training moved the CCSs’ performance into the normal range.
Caregivers also reported significant improvement in the attention and executive functioning of CCSs who completed the training. (Executive functioning includes skills like planning and focus needed to juggle multiple tasks and get things done.)
“These results suggest that computerized cognitive training may help fill a void in management of cognitive late effects that impact quality of life for childhood cancer survivors, such as the likelihood they will complete school and live independently,” Dr Conklin said.
In addition, post-intervention brain imaging showed decreased activation of left lateral prefrontal and bilateral medial frontal areas.
“That suggests the intervention exercised and strengthened the well-established working memory network,” Dr Conklin said. “The implication is that the brain may operate more efficiently and have less need for compensatory strategies. Such training-induced neuroplasticity suggests the benefits might be sustained going forward.”
The researchers are now studying the possible benefits of starting brain training during treatment or combining it with other interventions. The team is also tracking whether the cognitive benefits are sustained and might eventually translate to the improved academic performance reported for other populations. ![]()
Targeting a protein to improve AML treatment
Photo courtesy of VCU
Massey Cancer Center
Preclinical experiments have shown that blocking production of the protein CHD4 may help increase the effectiveness of first-line treatments for acute myeloid leukemia (AML).
Researchers found that depleting AML cells of CHD4 makes them more susceptible to standard chemotherapeutic agents by reducing the cells’ ability to repair DNA damage.
Depleting CHD4 also decreased AML cells’ ability to form colonies in vitro and tumors in vivo.
On the other hand, CHD4 depletion did not have detrimental effects on healthy bone marrow cells. The cells were no more sensitive to chemotherapy, and their growth was not affected.
Researchers reported these results in Blood.
“We are very encouraged by these findings,” said study author Gordon Ginder, MD, of Virginia Commonwealth University in Richmond.
“Targeting the CHD4 protein could allow us to reduce chemotherapy doses, which could potentially mean more effective first- and second-line treatments with fewer serious side effects.”
CHD4 is involved in silencing tumor suppressor genes in cancer cells. Recently, it has been shown to play a role in repairing DNA damage.
With their experiments, Dr Ginder and his colleagues found that CHD4 depletion severely restricted the ability of AML cells to develop colonies in soft agar models and establish tumors in mouse models.
In addition, blocking the production of CHD4 rendered AML cells more sensitive to daunorubicin and cytarabine, both in vitro and in vivo.
“This study builds on our team’s efforts to understand the molecular processes through which epigenetic regulators impact gene expression,” Dr Ginder said.
“Future studies will attempt to uncover the detailed mechanism through which CHD4 decreases the ability of AML cells to initiate leukemia and will look for potential ways to target this important protein. The fact that it functions as an enzyme suggests it may be druggable.” ![]()
Photo courtesy of VCU
Massey Cancer Center
Preclinical experiments have shown that blocking production of the protein CHD4 may help increase the effectiveness of first-line treatments for acute myeloid leukemia (AML).
Researchers found that depleting AML cells of CHD4 makes them more susceptible to standard chemotherapeutic agents by reducing the cells’ ability to repair DNA damage.
Depleting CHD4 also decreased AML cells’ ability to form colonies in vitro and tumors in vivo.
On the other hand, CHD4 depletion did not have detrimental effects on healthy bone marrow cells. The cells were no more sensitive to chemotherapy, and their growth was not affected.
Researchers reported these results in Blood.
“We are very encouraged by these findings,” said study author Gordon Ginder, MD, of Virginia Commonwealth University in Richmond.
“Targeting the CHD4 protein could allow us to reduce chemotherapy doses, which could potentially mean more effective first- and second-line treatments with fewer serious side effects.”
CHD4 is involved in silencing tumor suppressor genes in cancer cells. Recently, it has been shown to play a role in repairing DNA damage.
With their experiments, Dr Ginder and his colleagues found that CHD4 depletion severely restricted the ability of AML cells to develop colonies in soft agar models and establish tumors in mouse models.
In addition, blocking the production of CHD4 rendered AML cells more sensitive to daunorubicin and cytarabine, both in vitro and in vivo.
“This study builds on our team’s efforts to understand the molecular processes through which epigenetic regulators impact gene expression,” Dr Ginder said.
“Future studies will attempt to uncover the detailed mechanism through which CHD4 decreases the ability of AML cells to initiate leukemia and will look for potential ways to target this important protein. The fact that it functions as an enzyme suggests it may be druggable.” ![]()
Photo courtesy of VCU
Massey Cancer Center
Preclinical experiments have shown that blocking production of the protein CHD4 may help increase the effectiveness of first-line treatments for acute myeloid leukemia (AML).
Researchers found that depleting AML cells of CHD4 makes them more susceptible to standard chemotherapeutic agents by reducing the cells’ ability to repair DNA damage.
Depleting CHD4 also decreased AML cells’ ability to form colonies in vitro and tumors in vivo.
On the other hand, CHD4 depletion did not have detrimental effects on healthy bone marrow cells. The cells were no more sensitive to chemotherapy, and their growth was not affected.
Researchers reported these results in Blood.
“We are very encouraged by these findings,” said study author Gordon Ginder, MD, of Virginia Commonwealth University in Richmond.
“Targeting the CHD4 protein could allow us to reduce chemotherapy doses, which could potentially mean more effective first- and second-line treatments with fewer serious side effects.”
CHD4 is involved in silencing tumor suppressor genes in cancer cells. Recently, it has been shown to play a role in repairing DNA damage.
With their experiments, Dr Ginder and his colleagues found that CHD4 depletion severely restricted the ability of AML cells to develop colonies in soft agar models and establish tumors in mouse models.
In addition, blocking the production of CHD4 rendered AML cells more sensitive to daunorubicin and cytarabine, both in vitro and in vivo.
“This study builds on our team’s efforts to understand the molecular processes through which epigenetic regulators impact gene expression,” Dr Ginder said.
“Future studies will attempt to uncover the detailed mechanism through which CHD4 decreases the ability of AML cells to initiate leukemia and will look for potential ways to target this important protein. The fact that it functions as an enzyme suggests it may be druggable.” ![]()
CML: Select TKI based on comorbidities, monitor toxicity and adherence
CHICAGO – Chronic myeloid leukemia is highly treatable, and a “functional cure” appears to be within reach, according to Dr. Michael J. Mauro.
In fact, an “embarrassment of riches” exists when it comes to initial therapy for CML: In the United States there are five approved tyrosine kinase inhibitors (TKIs), and three are approved for front-line therapy, Dr. Mauro of Memorial Sloan Kettering Cancer Center, New York, said at the American Society of Hematology Meeting on Hematologic Malignancies.

Success, however, is contingent on managing reversible early toxicity, adherence to therapy, achieving landmarks of response, and remaining vigilant for late effects of therapy, he said.
Given the multitude of treatment options and the breadth of available data, Dr. Mauro said he counsels newly diagnosed patients that various treatment options are valid, and that “there may not be a right or wrong answer” for initial therapy. He also counsels patients that tolerability is manageable – and finding the right fit is an important process, and that response milestones are crucial and should be optimized.
It is important, he said, to discuss late toxicity concerns, to review comorbid conditions to help predict potential problems and identify risk, to consider the ramifications of potential toxicity, and to consider adherence.
“We need to portray therapy as really being medium- to long-term,” he said, noting that the urgency to think about treatment-free remission should be tempered by the reality that years of treatment are required first.
Risks and benefits of treatment should be discussed, and the acceptable balance determined in conjunction with the patient, he said, explaining that toxicities vary for the different TKIs.
Imatinib, for example, can be associated with edema/fluid retention, myalgias, hypophosphatemia, and gastrointestinal effects. Dasatinib can be associated with pleural/pericardial effusion, pulmonary arterial hypertension, and bleeding risk. Other toxicities associated with certain TKIs include pancreatic enzyme elevation, rash, and vascular adverse events.
Whether newly diagnosed patients should be directed away from certain agents remains unclear, as available data are open to interpretation, and the mechanism of action for some crucial late effects is unknown. Vascular disease should, however, be considered when making the decision, he said.
Given the available data on late toxicity with various therapies, a cardiovascular evaluation is advisable when initiating TKI therapy, he added.
Consider partnering with primary care, cardiology, or cardio-oncology specialists, and manage risk factors and findings of the evaluation as appropriate, irrespective of the CML, he said. Monitor for progression of cardiovascular risks or adverse events carefully, he added.
His approach for following recently diagnosed CML patients involves:
• A cardiovascular evaluation, at least including age- and comorbidity-appropriate studies, and an up-to-date cardiovascular risk profile. If nilotinib is used, he screens for peripheral, cerebral, and cardiovascular disease – an approach increasingly supported by data. If dasatinib is used, echocardiography is warranted to look for changes that suggest pulmonary hypertension. “And of course we should monitor blood pressure, lipid, and glycemic control,” he added.
• Initial studies, including bone marrow and quantitative polymerase chain reaction – international scale (qPCR IS).
• Lab studies every 1-2 weeks for at least 6 weeks, with titration thereafter as indicated, including for change in therapy.
• A 3-month assessment using qPCR IS. This is very important for following patient response, he said, noting that if the response surpasses compete cytogenetic remission and blood count is acceptable and stable, a repeat bone marrow study may be unnecessary.
• Sequential molecular analyses at least every 3 months.
• Repeat cardiovascular evaluation if/when indicated.
The 3-month response is an opportunity to critically appraise therapy choice and response trajectory; a therapy change is possible based on this assessment, he said. Responses at 6 and 12 months are also important, and changes in therapy for missed milestones at these time points are warranted as deeper remissions are sought.
At 18 months, the focus is on major molecular response, he added, noting that as patients get into deeper molecular remissions, plateaus and fluctuations are common; the nuances of determining who is well enough to consider for treatment-free remission remain to be sorted out in clinical trials.
In general, it appears that 3 years of therapy with about 2 years of optimal minimal residual disease is required prior to consideration for treatment-free remission, he said.
Dr. Mauro has consulted for and/or received research funding from Ariad, Bristol-Myers Squibb, Novartis, and Oregon Health & Science University.
CHICAGO – Chronic myeloid leukemia is highly treatable, and a “functional cure” appears to be within reach, according to Dr. Michael J. Mauro.
In fact, an “embarrassment of riches” exists when it comes to initial therapy for CML: In the United States there are five approved tyrosine kinase inhibitors (TKIs), and three are approved for front-line therapy, Dr. Mauro of Memorial Sloan Kettering Cancer Center, New York, said at the American Society of Hematology Meeting on Hematologic Malignancies.
Success, however, is contingent on managing reversible early toxicity, adherence to therapy, achieving landmarks of response, and remaining vigilant for late effects of therapy, he said.
Given the multitude of treatment options and the breadth of available data, Dr. Mauro said he counsels newly diagnosed patients that various treatment options are valid, and that “there may not be a right or wrong answer” for initial therapy. He also counsels patients that tolerability is manageable – and finding the right fit is an important process, and that response milestones are crucial and should be optimized.
It is important, he said, to discuss late toxicity concerns, to review comorbid conditions to help predict potential problems and identify risk, to consider the ramifications of potential toxicity, and to consider adherence.
“We need to portray therapy as really being medium- to long-term,” he said, noting that the urgency to think about treatment-free remission should be tempered by the reality that years of treatment are required first.
Risks and benefits of treatment should be discussed, and the acceptable balance determined in conjunction with the patient, he said, explaining that toxicities vary for the different TKIs.
Imatinib, for example, can be associated with edema/fluid retention, myalgias, hypophosphatemia, and gastrointestinal effects. Dasatinib can be associated with pleural/pericardial effusion, pulmonary arterial hypertension, and bleeding risk. Other toxicities associated with certain TKIs include pancreatic enzyme elevation, rash, and vascular adverse events.
Whether newly diagnosed patients should be directed away from certain agents remains unclear, as available data are open to interpretation, and the mechanism of action for some crucial late effects is unknown. Vascular disease should, however, be considered when making the decision, he said.
Given the available data on late toxicity with various therapies, a cardiovascular evaluation is advisable when initiating TKI therapy, he added.
Consider partnering with primary care, cardiology, or cardio-oncology specialists, and manage risk factors and findings of the evaluation as appropriate, irrespective of the CML, he said. Monitor for progression of cardiovascular risks or adverse events carefully, he added.
His approach for following recently diagnosed CML patients involves:
• A cardiovascular evaluation, at least including age- and comorbidity-appropriate studies, and an up-to-date cardiovascular risk profile. If nilotinib is used, he screens for peripheral, cerebral, and cardiovascular disease – an approach increasingly supported by data. If dasatinib is used, echocardiography is warranted to look for changes that suggest pulmonary hypertension. “And of course we should monitor blood pressure, lipid, and glycemic control,” he added.
• Initial studies, including bone marrow and quantitative polymerase chain reaction – international scale (qPCR IS).
• Lab studies every 1-2 weeks for at least 6 weeks, with titration thereafter as indicated, including for change in therapy.
• A 3-month assessment using qPCR IS. This is very important for following patient response, he said, noting that if the response surpasses compete cytogenetic remission and blood count is acceptable and stable, a repeat bone marrow study may be unnecessary.
• Sequential molecular analyses at least every 3 months.
• Repeat cardiovascular evaluation if/when indicated.
The 3-month response is an opportunity to critically appraise therapy choice and response trajectory; a therapy change is possible based on this assessment, he said. Responses at 6 and 12 months are also important, and changes in therapy for missed milestones at these time points are warranted as deeper remissions are sought.
At 18 months, the focus is on major molecular response, he added, noting that as patients get into deeper molecular remissions, plateaus and fluctuations are common; the nuances of determining who is well enough to consider for treatment-free remission remain to be sorted out in clinical trials.
In general, it appears that 3 years of therapy with about 2 years of optimal minimal residual disease is required prior to consideration for treatment-free remission, he said.
Dr. Mauro has consulted for and/or received research funding from Ariad, Bristol-Myers Squibb, Novartis, and Oregon Health & Science University.
CHICAGO – Chronic myeloid leukemia is highly treatable, and a “functional cure” appears to be within reach, according to Dr. Michael J. Mauro.
In fact, an “embarrassment of riches” exists when it comes to initial therapy for CML: In the United States there are five approved tyrosine kinase inhibitors (TKIs), and three are approved for front-line therapy, Dr. Mauro of Memorial Sloan Kettering Cancer Center, New York, said at the American Society of Hematology Meeting on Hematologic Malignancies.
Success, however, is contingent on managing reversible early toxicity, adherence to therapy, achieving landmarks of response, and remaining vigilant for late effects of therapy, he said.
Given the multitude of treatment options and the breadth of available data, Dr. Mauro said he counsels newly diagnosed patients that various treatment options are valid, and that “there may not be a right or wrong answer” for initial therapy. He also counsels patients that tolerability is manageable – and finding the right fit is an important process, and that response milestones are crucial and should be optimized.
It is important, he said, to discuss late toxicity concerns, to review comorbid conditions to help predict potential problems and identify risk, to consider the ramifications of potential toxicity, and to consider adherence.
“We need to portray therapy as really being medium- to long-term,” he said, noting that the urgency to think about treatment-free remission should be tempered by the reality that years of treatment are required first.
Risks and benefits of treatment should be discussed, and the acceptable balance determined in conjunction with the patient, he said, explaining that toxicities vary for the different TKIs.
Imatinib, for example, can be associated with edema/fluid retention, myalgias, hypophosphatemia, and gastrointestinal effects. Dasatinib can be associated with pleural/pericardial effusion, pulmonary arterial hypertension, and bleeding risk. Other toxicities associated with certain TKIs include pancreatic enzyme elevation, rash, and vascular adverse events.
Whether newly diagnosed patients should be directed away from certain agents remains unclear, as available data are open to interpretation, and the mechanism of action for some crucial late effects is unknown. Vascular disease should, however, be considered when making the decision, he said.
Given the available data on late toxicity with various therapies, a cardiovascular evaluation is advisable when initiating TKI therapy, he added.
Consider partnering with primary care, cardiology, or cardio-oncology specialists, and manage risk factors and findings of the evaluation as appropriate, irrespective of the CML, he said. Monitor for progression of cardiovascular risks or adverse events carefully, he added.
His approach for following recently diagnosed CML patients involves:
• A cardiovascular evaluation, at least including age- and comorbidity-appropriate studies, and an up-to-date cardiovascular risk profile. If nilotinib is used, he screens for peripheral, cerebral, and cardiovascular disease – an approach increasingly supported by data. If dasatinib is used, echocardiography is warranted to look for changes that suggest pulmonary hypertension. “And of course we should monitor blood pressure, lipid, and glycemic control,” he added.
• Initial studies, including bone marrow and quantitative polymerase chain reaction – international scale (qPCR IS).
• Lab studies every 1-2 weeks for at least 6 weeks, with titration thereafter as indicated, including for change in therapy.
• A 3-month assessment using qPCR IS. This is very important for following patient response, he said, noting that if the response surpasses compete cytogenetic remission and blood count is acceptable and stable, a repeat bone marrow study may be unnecessary.
• Sequential molecular analyses at least every 3 months.
• Repeat cardiovascular evaluation if/when indicated.
The 3-month response is an opportunity to critically appraise therapy choice and response trajectory; a therapy change is possible based on this assessment, he said. Responses at 6 and 12 months are also important, and changes in therapy for missed milestones at these time points are warranted as deeper remissions are sought.
At 18 months, the focus is on major molecular response, he added, noting that as patients get into deeper molecular remissions, plateaus and fluctuations are common; the nuances of determining who is well enough to consider for treatment-free remission remain to be sorted out in clinical trials.
In general, it appears that 3 years of therapy with about 2 years of optimal minimal residual disease is required prior to consideration for treatment-free remission, he said.
Dr. Mauro has consulted for and/or received research funding from Ariad, Bristol-Myers Squibb, Novartis, and Oregon Health & Science University.
EXPERT ANALYSIS FROM MHM 2015

Five epigenetic biomarkers define three CLL subgroups
Researchers have devised a simple and reproducible method of tracking the cellular origin of chronic lymphocytic leukemia (CLL) by applying five epigenetic biomarkers. By using this strategy, CLL patients can be categorized into three epigenetic subgroups with differential clinicobiologic features and outcomes – naive B-cell-like, intermediate, and memory B-cell-like CLL, according to a paper published in Leukemia.
Being able to identify CLL patients early on who are destined to progress would greatly help their clinical management, said Dr. Ana C. Queirós of the University of Barcelona and colleagues (Leukemia. 2015;29:598-605.
“We believe that the most relevant information obtained by the five epigenetic biomarkers is to classify CLL patients based on the putative cell of origin of the disease rather than being a mere additional prognostic biomarker,” the investigators wrote. “The recent advance in the genetics and cellular biology of CLL, including the present epigenetic classification, could result in the use of targeted therapies for specific subgroups of patients.”
In previous research, the authors identified the presence of three subgroups of CLL with different clinicobiologic features, and in this study they hypothesized that DNA methylation patterns associated with normal B cells could be used to classify CLL into three novel subgroups.
To test their hypothesis and to develop a clinically useful strategy, they identified five epigenetic biomarkers and established new quantitative DNA methylation assays, applying them to two independent series of CLL patients of different geographical origin.
The first epigenetic classification was determined in an initial cohort of 211 CLL patients and then validated in a series of 97 additional CLL patients.
To test the stability of these markers over time and after treatment, two or three sequential samples were analyzed from 27 CLL patients with a median difference between samples of 59 months (range, 5-114). In addition, specimens from 13 patients, from before and after treatment, also were analyzed.
In the initial 211 patients, the three subgroups had different levels of immunoglobulin heavy-chain locus (IGHV) mutation (P <.001) and VH gene usage (P <.03). There also were different clinical features and outcomes in regard to their time to first treatment and overall survival (P <.001), Dr. Queirós and associates reported.
After a Cox multivariate analysis, the final model showed that the epigenetic signature related to the cellular origin of CLL was the most important variable in predicting time to first treatment. Other important variables in the model were Binet stage, CD38 expression, LDH levels, and SF3B1 mutations.
The study was funded by the Spanish Ministry of Economy and Competitiveness (MINECO) through the Instituto de Salud Carlos III (ISCIII) and the Red Temática de Investigación del Cáncer (RTICC) of the ISCIII and project SAF2009-08663, the UK Medical Research Council, and the European Union’s Seventh Framework Programme through the Blueprint Consortium. The authors declared no conflicts of interest.
Researchers have devised a simple and reproducible method of tracking the cellular origin of chronic lymphocytic leukemia (CLL) by applying five epigenetic biomarkers. By using this strategy, CLL patients can be categorized into three epigenetic subgroups with differential clinicobiologic features and outcomes – naive B-cell-like, intermediate, and memory B-cell-like CLL, according to a paper published in Leukemia.
Being able to identify CLL patients early on who are destined to progress would greatly help their clinical management, said Dr. Ana C. Queirós of the University of Barcelona and colleagues (Leukemia. 2015;29:598-605.
“We believe that the most relevant information obtained by the five epigenetic biomarkers is to classify CLL patients based on the putative cell of origin of the disease rather than being a mere additional prognostic biomarker,” the investigators wrote. “The recent advance in the genetics and cellular biology of CLL, including the present epigenetic classification, could result in the use of targeted therapies for specific subgroups of patients.”
In previous research, the authors identified the presence of three subgroups of CLL with different clinicobiologic features, and in this study they hypothesized that DNA methylation patterns associated with normal B cells could be used to classify CLL into three novel subgroups.
To test their hypothesis and to develop a clinically useful strategy, they identified five epigenetic biomarkers and established new quantitative DNA methylation assays, applying them to two independent series of CLL patients of different geographical origin.
The first epigenetic classification was determined in an initial cohort of 211 CLL patients and then validated in a series of 97 additional CLL patients.
To test the stability of these markers over time and after treatment, two or three sequential samples were analyzed from 27 CLL patients with a median difference between samples of 59 months (range, 5-114). In addition, specimens from 13 patients, from before and after treatment, also were analyzed.
In the initial 211 patients, the three subgroups had different levels of immunoglobulin heavy-chain locus (IGHV) mutation (P <.001) and VH gene usage (P <.03). There also were different clinical features and outcomes in regard to their time to first treatment and overall survival (P <.001), Dr. Queirós and associates reported.
After a Cox multivariate analysis, the final model showed that the epigenetic signature related to the cellular origin of CLL was the most important variable in predicting time to first treatment. Other important variables in the model were Binet stage, CD38 expression, LDH levels, and SF3B1 mutations.
The study was funded by the Spanish Ministry of Economy and Competitiveness (MINECO) through the Instituto de Salud Carlos III (ISCIII) and the Red Temática de Investigación del Cáncer (RTICC) of the ISCIII and project SAF2009-08663, the UK Medical Research Council, and the European Union’s Seventh Framework Programme through the Blueprint Consortium. The authors declared no conflicts of interest.
Researchers have devised a simple and reproducible method of tracking the cellular origin of chronic lymphocytic leukemia (CLL) by applying five epigenetic biomarkers. By using this strategy, CLL patients can be categorized into three epigenetic subgroups with differential clinicobiologic features and outcomes – naive B-cell-like, intermediate, and memory B-cell-like CLL, according to a paper published in Leukemia.
Being able to identify CLL patients early on who are destined to progress would greatly help their clinical management, said Dr. Ana C. Queirós of the University of Barcelona and colleagues (Leukemia. 2015;29:598-605.
“We believe that the most relevant information obtained by the five epigenetic biomarkers is to classify CLL patients based on the putative cell of origin of the disease rather than being a mere additional prognostic biomarker,” the investigators wrote. “The recent advance in the genetics and cellular biology of CLL, including the present epigenetic classification, could result in the use of targeted therapies for specific subgroups of patients.”
In previous research, the authors identified the presence of three subgroups of CLL with different clinicobiologic features, and in this study they hypothesized that DNA methylation patterns associated with normal B cells could be used to classify CLL into three novel subgroups.
To test their hypothesis and to develop a clinically useful strategy, they identified five epigenetic biomarkers and established new quantitative DNA methylation assays, applying them to two independent series of CLL patients of different geographical origin.
The first epigenetic classification was determined in an initial cohort of 211 CLL patients and then validated in a series of 97 additional CLL patients.
To test the stability of these markers over time and after treatment, two or three sequential samples were analyzed from 27 CLL patients with a median difference between samples of 59 months (range, 5-114). In addition, specimens from 13 patients, from before and after treatment, also were analyzed.
In the initial 211 patients, the three subgroups had different levels of immunoglobulin heavy-chain locus (IGHV) mutation (P <.001) and VH gene usage (P <.03). There also were different clinical features and outcomes in regard to their time to first treatment and overall survival (P <.001), Dr. Queirós and associates reported.
After a Cox multivariate analysis, the final model showed that the epigenetic signature related to the cellular origin of CLL was the most important variable in predicting time to first treatment. Other important variables in the model were Binet stage, CD38 expression, LDH levels, and SF3B1 mutations.
The study was funded by the Spanish Ministry of Economy and Competitiveness (MINECO) through the Instituto de Salud Carlos III (ISCIII) and the Red Temática de Investigación del Cáncer (RTICC) of the ISCIII and project SAF2009-08663, the UK Medical Research Council, and the European Union’s Seventh Framework Programme through the Blueprint Consortium. The authors declared no conflicts of interest.
FROM LEUKEMIA
Key clinical point: A new strategy allows CLL patients to be categorized into three epigenetic subgroups with differential clinicobiologic features and outcomes.
Major finding: Epigenetic classification was the strongest predictor of time to treatment (P <.001), along with Binet stage (P <.001); these findings were corroborated in a validation series (n = 97).
Data source: A prediction model formulated using five epigenetic biomarkers that was able to classify CLL patients accurately into the three subgroups.
Disclosures: The study was funded by the Spanish Ministry of Economy and Competitiveness (MINECO) through the Instituto de Salud Carlos III (ISCIII) and the Red Temática de Investigación del Cáncer (RTICC) of the ISCIII and project SAF2009-08663, the UK Medical Research Council, and the European Union’s Seventh Framework Programme through the Blueprint Consortium. The authors declared no conflicts of interest.
Cancer survivors have poor diets, study suggests

New research suggests that cancer survivors in the US may need dietary interventions to improve their health.
The study showed that, overall, cancer survivors did not adhere to federal dietary guidelines as well as a matched control population.
Cancer survivors tended to consume more empty calories and less fiber than controls.
Fang Fang Zhang, MD, PhD, of Tufts University in Boston, Massachusetts, and his colleagues reported these findings in Cancer.
The team evaluated the diets of 1533 adult cancer survivors who participated in the National Health and Nutrition Examination Survey from 1999 to 2010. The investigators also assessed the diets of 3075 individuals who had no history of cancer and were matched to the cancer survivors by age, sex, and race/ethnicity.
The goal was to determine how subjects’ diets aligned with advice from the 2010 Dietary Guidelines for Americans, which was jointly issued by the Department of Agriculture and the Department of Health and Human Services.
Cancer survivors had poor adherence to the guidelines, with a total Healthy Eating Index score of 47.2 out of 100, compared with a score of 48.3 in the adults without a history of cancer (P=0.03).
Cancer survivors had a significantly lower mean score for empty calories compared to the noncancer group—13.6 and 14.4, respectively (P=0.001). This suggested the cancer group had a higher consumption of calories from solid fats, alcohol, and added sugars.
Cancer survivors also had significantly lower dietary intake of fiber than the noncancer group—15.0 and 15.9 g per day, respectively (P=0.02).
Compared to recommended values, cancer survivors had low dietary intakes of vitamin D (31% of the recommended intake), vitamin E (47%), potassium (55%), and calcium (73%) but high intakes of saturated fat (112%) and sodium (133%).
The investigators noted that diet quality in cancer survivors increased linearly with age. The older the age, the better the diet quality.
Survivors with lower education (high school or less) had significantly worse diet quality than those with higher education. And survivors who were current smokers had significantly worse diet quality than non-smokers or former smokers.
For the 4 major cancer types in the US (breast, prostate, lung, and colorectal), breast cancer survivors had the best diet quality, and lung cancer survivors had the worst diet quality.
The investigators said that knowing how well cancer survivors adhere to federal dietary guidelines can help inform evidence-based priorities for improving their nutritional intake.
“Dietary changes that include more fiber, fruit, and vegetables in the diet and less fat, sodium, and added sugar would be important for cancer survivors,” Dr Zhang said.
“Oncology care providers can play critical roles in reinforcing the importance of a healthful diet and can refer patients to registered dietitians who are experts in oncology care or to other reputable sources in order to improve survivors’ overall health.” ![]()
New research suggests that cancer survivors in the US may need dietary interventions to improve their health.
The study showed that, overall, cancer survivors did not adhere to federal dietary guidelines as well as a matched control population.
Cancer survivors tended to consume more empty calories and less fiber than controls.
Fang Fang Zhang, MD, PhD, of Tufts University in Boston, Massachusetts, and his colleagues reported these findings in Cancer.
The team evaluated the diets of 1533 adult cancer survivors who participated in the National Health and Nutrition Examination Survey from 1999 to 2010. The investigators also assessed the diets of 3075 individuals who had no history of cancer and were matched to the cancer survivors by age, sex, and race/ethnicity.
The goal was to determine how subjects’ diets aligned with advice from the 2010 Dietary Guidelines for Americans, which was jointly issued by the Department of Agriculture and the Department of Health and Human Services.
Cancer survivors had poor adherence to the guidelines, with a total Healthy Eating Index score of 47.2 out of 100, compared with a score of 48.3 in the adults without a history of cancer (P=0.03).
Cancer survivors had a significantly lower mean score for empty calories compared to the noncancer group—13.6 and 14.4, respectively (P=0.001). This suggested the cancer group had a higher consumption of calories from solid fats, alcohol, and added sugars.
Cancer survivors also had significantly lower dietary intake of fiber than the noncancer group—15.0 and 15.9 g per day, respectively (P=0.02).
Compared to recommended values, cancer survivors had low dietary intakes of vitamin D (31% of the recommended intake), vitamin E (47%), potassium (55%), and calcium (73%) but high intakes of saturated fat (112%) and sodium (133%).
The investigators noted that diet quality in cancer survivors increased linearly with age. The older the age, the better the diet quality.
Survivors with lower education (high school or less) had significantly worse diet quality than those with higher education. And survivors who were current smokers had significantly worse diet quality than non-smokers or former smokers.
For the 4 major cancer types in the US (breast, prostate, lung, and colorectal), breast cancer survivors had the best diet quality, and lung cancer survivors had the worst diet quality.
The investigators said that knowing how well cancer survivors adhere to federal dietary guidelines can help inform evidence-based priorities for improving their nutritional intake.
“Dietary changes that include more fiber, fruit, and vegetables in the diet and less fat, sodium, and added sugar would be important for cancer survivors,” Dr Zhang said.
“Oncology care providers can play critical roles in reinforcing the importance of a healthful diet and can refer patients to registered dietitians who are experts in oncology care or to other reputable sources in order to improve survivors’ overall health.” ![]()
New research suggests that cancer survivors in the US may need dietary interventions to improve their health.
The study showed that, overall, cancer survivors did not adhere to federal dietary guidelines as well as a matched control population.
Cancer survivors tended to consume more empty calories and less fiber than controls.
Fang Fang Zhang, MD, PhD, of Tufts University in Boston, Massachusetts, and his colleagues reported these findings in Cancer.
The team evaluated the diets of 1533 adult cancer survivors who participated in the National Health and Nutrition Examination Survey from 1999 to 2010. The investigators also assessed the diets of 3075 individuals who had no history of cancer and were matched to the cancer survivors by age, sex, and race/ethnicity.
The goal was to determine how subjects’ diets aligned with advice from the 2010 Dietary Guidelines for Americans, which was jointly issued by the Department of Agriculture and the Department of Health and Human Services.
Cancer survivors had poor adherence to the guidelines, with a total Healthy Eating Index score of 47.2 out of 100, compared with a score of 48.3 in the adults without a history of cancer (P=0.03).
Cancer survivors had a significantly lower mean score for empty calories compared to the noncancer group—13.6 and 14.4, respectively (P=0.001). This suggested the cancer group had a higher consumption of calories from solid fats, alcohol, and added sugars.
Cancer survivors also had significantly lower dietary intake of fiber than the noncancer group—15.0 and 15.9 g per day, respectively (P=0.02).
Compared to recommended values, cancer survivors had low dietary intakes of vitamin D (31% of the recommended intake), vitamin E (47%), potassium (55%), and calcium (73%) but high intakes of saturated fat (112%) and sodium (133%).
The investigators noted that diet quality in cancer survivors increased linearly with age. The older the age, the better the diet quality.
Survivors with lower education (high school or less) had significantly worse diet quality than those with higher education. And survivors who were current smokers had significantly worse diet quality than non-smokers or former smokers.
For the 4 major cancer types in the US (breast, prostate, lung, and colorectal), breast cancer survivors had the best diet quality, and lung cancer survivors had the worst diet quality.
The investigators said that knowing how well cancer survivors adhere to federal dietary guidelines can help inform evidence-based priorities for improving their nutritional intake.
“Dietary changes that include more fiber, fruit, and vegetables in the diet and less fat, sodium, and added sugar would be important for cancer survivors,” Dr Zhang said.
“Oncology care providers can play critical roles in reinforcing the importance of a healthful diet and can refer patients to registered dietitians who are experts in oncology care or to other reputable sources in order to improve survivors’ overall health.” ![]()