Cosmetic procedures carry inherent risks of adverse events. Transient and permanent alopecia are rare complications of these procedures. Although they have not been fully elucidated, several pathologic mechanisms for hair loss following cosmetic procedures have been proposed, including extravascular compression (a phenomenon that has been well documented in bedridden patients) as well as intravascular occlusion leading to inflammation and necrosis, which has been associated with hyaluronic acid (HA) fillers.¹ Cases of alopecia also have been reported following mesotherapy and calcium hydroxyapatite, deoxycholic acid, and botulinum toxin injections.² We report a case of alopecia resulting from poly-L-lactic acid (PLLA) injection in a 35-year-old woman with the intent to raise awareness of this rare adverse event.
Case Report
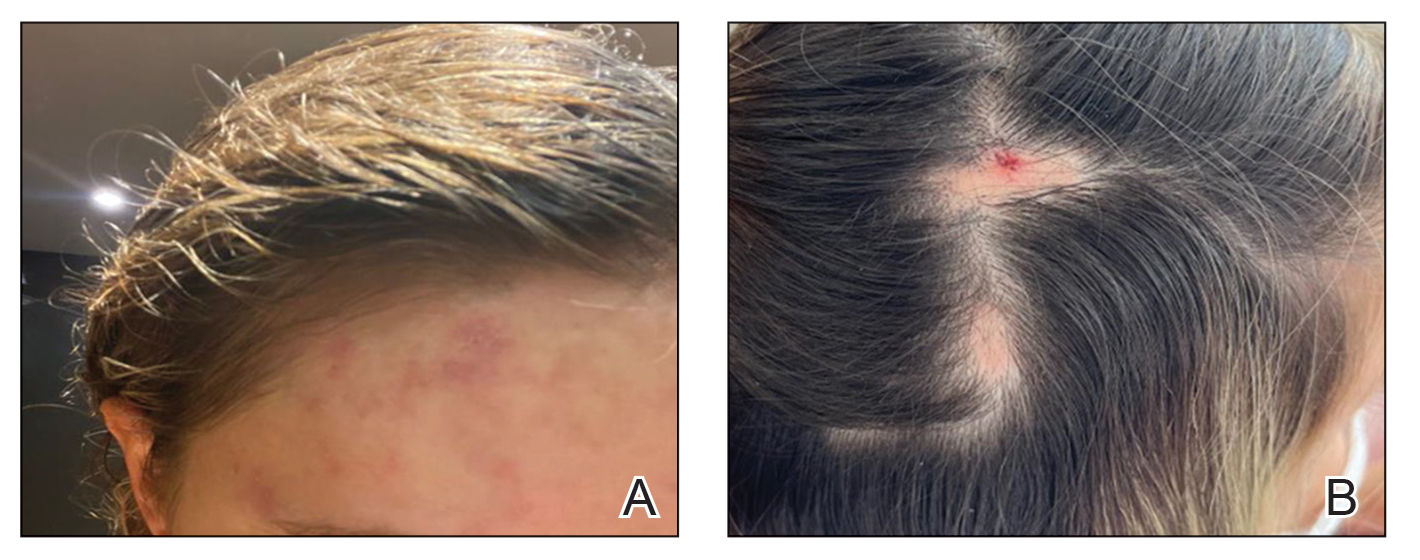
A healthy 35-year-old woman received aesthetic PLLA injections on the face and frontal hairline performed by an outside dermatologist using the vector technique. During the procedure, the patient experienced intense itchiness at the right temporal artery vascular territory and reported a substantial headache the next day. She also presented with erythema and edema of the frontal and right parietal scalp with a well-delimited livedoid vascular area along the temporal artery territory on the right side of the head 1 day after the procedure (Figure 1). These signs were reported to the outside dermatologist who performed the procedure, but they were not assumed to be adverse events at that time.
FIGURE 1. A, The patient presented with an ischemic event delimiting vascular territory in the frontal and temporal regions on the right hemiface 1 day following injection with poly-L-lactic acid. B, A single patch of alopecia (upper) started 27 days after the cosmetic procedure, and an additional patch of alopecia (lower) was noted on day 41.
The condition persisted for 4 days followed by the development of an irregular 3×2-cm patch of alopecia on the right parietal scalp. A 3-day course of self-administered oral prednisolone 0.2 mg/kg/d was prescribed.
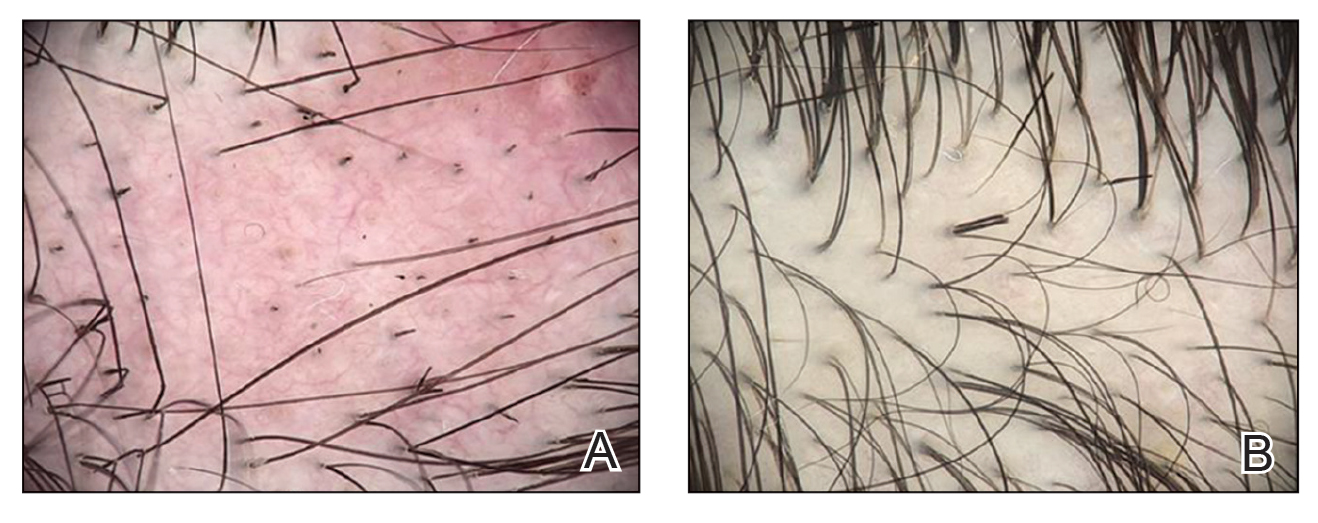
Twenty-seven days after the procedure, the patient presented to our trichology clinic for evaluation of a single patch of nonscarring alopecia on the right parietal scalp. Trichoscopy showed multiple yellow and black dots, broken hairs, pigment deposits, and an erythematous background mainly composed of linear telangiectatic vessels (Figure 2). Histopathologic analysis revealed a lymphocytic inflammatory infiltrate surrounding the follicular units that was compatible with an alopecia areata–like pattern as well as PLLA deposits in the subcutaneous tissue forming foreign body granulomas (Figure 3). The diagnosis of PLLA-induced alopecia was made based on the detection of PLLA at the biopsy site within the patchy alopecia.
FIGURE 2. A, Trichoscopy performed 27 days after the initial procedure showed multiple yellow and black dots and broken hairs in addition to an irregular vascular proliferation composed of ectatic vessels, erythema of the fundus, and pigment deposits. B, Partial hair regrowth was noted after 6 weeks of intralesional triamcinolone administered at the alopecic patch. Trichoscopy showed broken hairs as a possible sign of late inflammatory activity 3.5 months after poly-L-lactic acid injection.
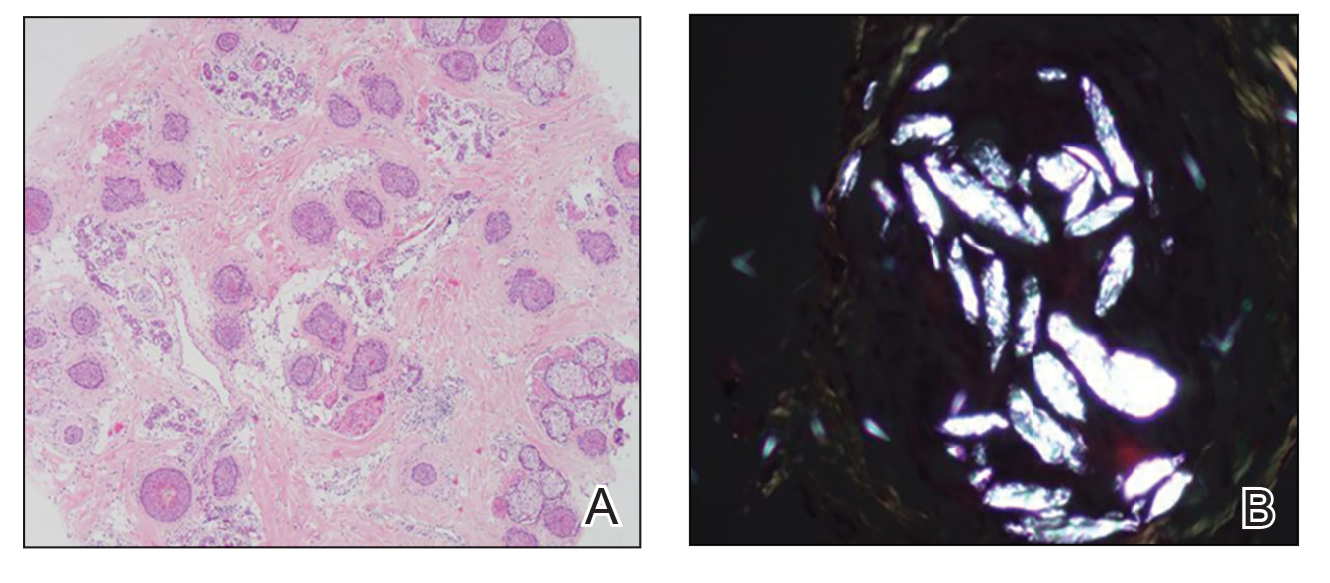
FIGURE 3. A, Histology showed a lymphocytic inflammatory infiltrate around the follicular units with increased catagen/telogen counts and miniaturization (H&E, original magnification ×200). B, Birefringence showed poly-L-lactic acid deposits in deeper sections of the subcutaneous tissue forming foreign body granulomas, confirming the diagnosis of alopecia induced by poly-L-lactic acid injection (original magnification ×400).
Intralesional triamcinolone acetonide 5 mg/mL was administered at 1-cm intervals in the subdermal space (0.1 mL/puncture site). After 14 days, the patient developed an additional patch of alopecia in the same vascular territory as the right temporal artery, positioned just beneath the initial patch, with similar trichoscopy findings. The patches were treated with intralesional triamcinolone acetonide for 3 additional sessions, administered every 4 weeks. Long-term monitoring of the patient revealed regrowth with comparable hair count to the unaffected contralateral scalp, indicative of a nonscarring alopecia.
Comment
Poly-L-lactic acid is a biostimulator synthesized from the α-hydroxy acid family in 1954 that has been safely used in suture materials, resorbable plates, and orthopedic screws.4 Alopecia has been reported as a systemic allergic reaction to biodegradable screws following an orthopedic procedure.5 Prior reports of embolization and retinal ischemia with PLLA have raised concerns regarding its occlusive potential.6-9
Approved by the US Food and Drug Administration in 2004 for soft tissue restoration in HIV-related lipoatrophy, PLLA was expanded to cosmetic applications in 2009. As previously reported with HA fillers, we hypothesize that extravascular compression resulting from the placement of the filler material (due to the volume injected in the scalp area) contributes to the development of alopecia plus PLLA embolism–induced ischemic alopecia in the affected areas.10 In our case, the diagnosis of PLLA-induced alopecia was confirmed based on the finding of the filler material in the subcutaneous tissue on histopathology, probably due to embolization. Moreover, trichoscopic findings were all similar to those described after HA embolization.11 The features found in our patient due to the PLLA local reaction were similar to those seen in other conditions such as alopecia areata, pressure alopecia, and chemotherapy-induced alopecia; therefore, histopathology confirmation is mandatory in cases of hair loss associated with PLLA.
The emergence of a secondary patch of alopecia prompts consideration of an intrinsic late inflammatory propensity of PLLA. Immune cells recognize PLLA as a foreign body, and subclinical inflammatory foreign body reactions can cause PLLA-induced collagen synthesis.12 This phenomenon underscores the need for further investigation into the immunologic implications of PLLA in alopecia pathogenesis.
The angiogenic properties of the anagen phase require an adequate blood supply for effective hair growth; therefore, the lack of blood and nutrient supply to the hair bulb triggers miniaturization, a possible explanation for the hair thinning found in the alopecic patch.13
Conclusion
Alopecia as an adverse effect of cosmetic procedures can be distressing for patients, even when reversible. A detailed understanding of scalp anatomy is critical for satisfactory outcomes with aesthetic procedures. Physicians must pay attention to the amount and area of material injected in order to avoid possible mechanisms of ischemia—embolization and/or extravascular compression—especially in highly vascularized areas.
We present a rare report of alopecia as an adverse event of PLLA injection. Dermatologists must be aware of this rare condition, and trichoscopy combined with histopathologic analysis are encouraged for early recognition and proper management.
References
Issa NT, Kaiser M, Martinez-Velasco A, et al. Alopecia after cosmetic injection procedures: a review. Dermatol Surg. 2022;48:855-861.
Alopecia with foreign body granulomas induced by Radiesse injection: a case report. J Cosmet Laser Ther. 2018;20:462-464.
Munia C, Parada M, de Alvarenga Morais MH. Changes in facial morphology using poly-L-lactic acid application according to vector technique: a case series. J Clin Aesthet Dermatol. 2022;15:38-42.
Attenello NH, Maas CS. Injectable fillers: review of material and properties. Facial Plast Surg. 2015;31:29-34.
Mastrokalos DS, Paessler HH. Allergic reaction to biodegradable interference poly-L-lactic acid screws after anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft. Arthroscopy. 2008;24:732-733.
Wu CW, Wu HJ. Retinal artery occlusion following cosmetic injection of poly-L-lactic acid. Taiwan J Ophthalmol. 2021;11:317-320.
Yuan JT, Chang TW, Yu SS, et al. Mental artery occlusion from poly-L-lactic acid injection at the lateral chin. Dermatol Surg. 2017;43:1402-1405.
Ragam A, Agemy SA, Dave SB, et al. Ipsilateral ophthalmic and cerebral infarctions after cosmetic polylactic acid injection into the forehead. J Neuroophthalmol. 2017;37:77-80.
Witmanowski H, Błochowiak K. Another face of dermal fillers. Postepy Dermatol Alergol. 2020;37:651-659.
Yang Q, Qiu L, Yi C, et al. Reversible alopecia with localized scalp necrosis after accidental embolization of the parietal artery with hyaluronic acid. Aesthetic Plast Surg. 2017;41:695-699.
Asz-Sigall D, Iñigo-Gomez K, Ortega-Springall MF, et al. Alopecia secondary to hyaluronic acid embolization: trichoscopic findings. Skin Appendage Disord. 2019;5:396-400.
Oh S, Lee JH, Kim HM, et al. Poly-L-lactic acid fillers improved dermal collagen synthesis by modulating M2 macrophage polarization in aged animal skin. Cells. 2023;12:1320. doi:10.3390/cells12091320
Natarelli N, Gahoonia N, Sivamani RK. Integrative and mechanistic approach to the hair growth cycle and hair loss. J Clin Med. 2023;12:893.2. Liu RF, Kuo TT, Chao YY, et al.
Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Michalany, Bagatin, and Nascimento are from the Federal University of São Paulo, Brazil. Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Bagatin, and Nascimento are from the Department of Dermatology, and Dr. Michalany is from the Department of Dermatopathology. Drs. Cortez de Almeida and Melo are from Department of Dermatology, Rio de Janeiro State University, Brazil.
Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Michalany, Cortez de Almeida, Melo, and Nascimento have no relevant financial disclosures to report. Dr. Bagatin is a speaker for L’Oréal and has received a research grant from Pierre Fabre Dermo-Cosmetique.
Correspondence: Gabriel Lazzeri Cortez, MD, Department of Dermatology, Federal University of São Paulo, Rua Botucatu, 740, Vila Clementino, São Paulo, 04023-062, Brazil (gabriel.cortez@unifesp.br).
Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Michalany, Bagatin, and Nascimento are from the Federal University of São Paulo, Brazil. Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Bagatin, and Nascimento are from the Department of Dermatology, and Dr. Michalany is from the Department of Dermatopathology. Drs. Cortez de Almeida and Melo are from Department of Dermatology, Rio de Janeiro State University, Brazil.
Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Michalany, Cortez de Almeida, Melo, and Nascimento have no relevant financial disclosures to report. Dr. Bagatin is a speaker for L’Oréal and has received a research grant from Pierre Fabre Dermo-Cosmetique.
Correspondence: Gabriel Lazzeri Cortez, MD, Department of Dermatology, Federal University of São Paulo, Rua Botucatu, 740, Vila Clementino, São Paulo, 04023-062, Brazil (gabriel.cortez@unifesp.br).
Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Michalany, Bagatin, and Nascimento are from the Federal University of São Paulo, Brazil. Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Bagatin, and Nascimento are from the Department of Dermatology, and Dr. Michalany is from the Department of Dermatopathology. Drs. Cortez de Almeida and Melo are from Department of Dermatology, Rio de Janeiro State University, Brazil.
Drs. Cortez, Hassun, Linhares, Pinheiro, Florenço, Michalany, Cortez de Almeida, Melo, and Nascimento have no relevant financial disclosures to report. Dr. Bagatin is a speaker for L’Oréal and has received a research grant from Pierre Fabre Dermo-Cosmetique.
Correspondence: Gabriel Lazzeri Cortez, MD, Department of Dermatology, Federal University of São Paulo, Rua Botucatu, 740, Vila Clementino, São Paulo, 04023-062, Brazil (gabriel.cortez@unifesp.br).
Cosmetic procedures carry inherent risks of adverse events. Transient and permanent alopecia are rare complications of these procedures. Although they have not been fully elucidated, several pathologic mechanisms for hair loss following cosmetic procedures have been proposed, including extravascular compression (a phenomenon that has been well documented in bedridden patients) as well as intravascular occlusion leading to inflammation and necrosis, which has been associated with hyaluronic acid (HA) fillers.¹ Cases of alopecia also have been reported following mesotherapy and calcium hydroxyapatite, deoxycholic acid, and botulinum toxin injections.² We report a case of alopecia resulting from poly-L-lactic acid (PLLA) injection in a 35-year-old woman with the intent to raise awareness of this rare adverse event.
Case Report
A healthy 35-year-old woman received aesthetic PLLA injections on the face and frontal hairline performed by an outside dermatologist using the vector technique. During the procedure, the patient experienced intense itchiness at the right temporal artery vascular territory and reported a substantial headache the next day. She also presented with erythema and edema of the frontal and right parietal scalp with a well-delimited livedoid vascular area along the temporal artery territory on the right side of the head 1 day after the procedure (Figure 1). These signs were reported to the outside dermatologist who performed the procedure, but they were not assumed to be adverse events at that time.
FIGURE 1. A, The patient presented with an ischemic event delimiting vascular territory in the frontal and temporal regions on the right hemiface 1 day following injection with poly-L-lactic acid. B, A single patch of alopecia (upper) started 27 days after the cosmetic procedure, and an additional patch of alopecia (lower) was noted on day 41.
The condition persisted for 4 days followed by the development of an irregular 3×2-cm patch of alopecia on the right parietal scalp. A 3-day course of self-administered oral prednisolone 0.2 mg/kg/d was prescribed.
Twenty-seven days after the procedure, the patient presented to our trichology clinic for evaluation of a single patch of nonscarring alopecia on the right parietal scalp. Trichoscopy showed multiple yellow and black dots, broken hairs, pigment deposits, and an erythematous background mainly composed of linear telangiectatic vessels (Figure 2). Histopathologic analysis revealed a lymphocytic inflammatory infiltrate surrounding the follicular units that was compatible with an alopecia areata–like pattern as well as PLLA deposits in the subcutaneous tissue forming foreign body granulomas (Figure 3). The diagnosis of PLLA-induced alopecia was made based on the detection of PLLA at the biopsy site within the patchy alopecia.
FIGURE 2. A, Trichoscopy performed 27 days after the initial procedure showed multiple yellow and black dots and broken hairs in addition to an irregular vascular proliferation composed of ectatic vessels, erythema of the fundus, and pigment deposits. B, Partial hair regrowth was noted after 6 weeks of intralesional triamcinolone administered at the alopecic patch. Trichoscopy showed broken hairs as a possible sign of late inflammatory activity 3.5 months after poly-L-lactic acid injection.
FIGURE 3. A, Histology showed a lymphocytic inflammatory infiltrate around the follicular units with increased catagen/telogen counts and miniaturization (H&E, original magnification ×200). B, Birefringence showed poly-L-lactic acid deposits in deeper sections of the subcutaneous tissue forming foreign body granulomas, confirming the diagnosis of alopecia induced by poly-L-lactic acid injection (original magnification ×400).
Intralesional triamcinolone acetonide 5 mg/mL was administered at 1-cm intervals in the subdermal space (0.1 mL/puncture site). After 14 days, the patient developed an additional patch of alopecia in the same vascular territory as the right temporal artery, positioned just beneath the initial patch, with similar trichoscopy findings. The patches were treated with intralesional triamcinolone acetonide for 3 additional sessions, administered every 4 weeks. Long-term monitoring of the patient revealed regrowth with comparable hair count to the unaffected contralateral scalp, indicative of a nonscarring alopecia.
Comment
Poly-L-lactic acid is a biostimulator synthesized from the α-hydroxy acid family in 1954 that has been safely used in suture materials, resorbable plates, and orthopedic screws.4 Alopecia has been reported as a systemic allergic reaction to biodegradable screws following an orthopedic procedure.5 Prior reports of embolization and retinal ischemia with PLLA have raised concerns regarding its occlusive potential.6-9
Approved by the US Food and Drug Administration in 2004 for soft tissue restoration in HIV-related lipoatrophy, PLLA was expanded to cosmetic applications in 2009. As previously reported with HA fillers, we hypothesize that extravascular compression resulting from the placement of the filler material (due to the volume injected in the scalp area) contributes to the development of alopecia plus PLLA embolism–induced ischemic alopecia in the affected areas.10 In our case, the diagnosis of PLLA-induced alopecia was confirmed based on the finding of the filler material in the subcutaneous tissue on histopathology, probably due to embolization. Moreover, trichoscopic findings were all similar to those described after HA embolization.11 The features found in our patient due to the PLLA local reaction were similar to those seen in other conditions such as alopecia areata, pressure alopecia, and chemotherapy-induced alopecia; therefore, histopathology confirmation is mandatory in cases of hair loss associated with PLLA.
The emergence of a secondary patch of alopecia prompts consideration of an intrinsic late inflammatory propensity of PLLA. Immune cells recognize PLLA as a foreign body, and subclinical inflammatory foreign body reactions can cause PLLA-induced collagen synthesis.12 This phenomenon underscores the need for further investigation into the immunologic implications of PLLA in alopecia pathogenesis.
The angiogenic properties of the anagen phase require an adequate blood supply for effective hair growth; therefore, the lack of blood and nutrient supply to the hair bulb triggers miniaturization, a possible explanation for the hair thinning found in the alopecic patch.13
Conclusion
Alopecia as an adverse effect of cosmetic procedures can be distressing for patients, even when reversible. A detailed understanding of scalp anatomy is critical for satisfactory outcomes with aesthetic procedures. Physicians must pay attention to the amount and area of material injected in order to avoid possible mechanisms of ischemia—embolization and/or extravascular compression—especially in highly vascularized areas.
We present a rare report of alopecia as an adverse event of PLLA injection. Dermatologists must be aware of this rare condition, and trichoscopy combined with histopathologic analysis are encouraged for early recognition and proper management.
Cosmetic procedures carry inherent risks of adverse events. Transient and permanent alopecia are rare complications of these procedures. Although they have not been fully elucidated, several pathologic mechanisms for hair loss following cosmetic procedures have been proposed, including extravascular compression (a phenomenon that has been well documented in bedridden patients) as well as intravascular occlusion leading to inflammation and necrosis, which has been associated with hyaluronic acid (HA) fillers.¹ Cases of alopecia also have been reported following mesotherapy and calcium hydroxyapatite, deoxycholic acid, and botulinum toxin injections.² We report a case of alopecia resulting from poly-L-lactic acid (PLLA) injection in a 35-year-old woman with the intent to raise awareness of this rare adverse event.
Case Report
A healthy 35-year-old woman received aesthetic PLLA injections on the face and frontal hairline performed by an outside dermatologist using the vector technique. During the procedure, the patient experienced intense itchiness at the right temporal artery vascular territory and reported a substantial headache the next day. She also presented with erythema and edema of the frontal and right parietal scalp with a well-delimited livedoid vascular area along the temporal artery territory on the right side of the head 1 day after the procedure (Figure 1). These signs were reported to the outside dermatologist who performed the procedure, but they were not assumed to be adverse events at that time.
FIGURE 1. A, The patient presented with an ischemic event delimiting vascular territory in the frontal and temporal regions on the right hemiface 1 day following injection with poly-L-lactic acid. B, A single patch of alopecia (upper) started 27 days after the cosmetic procedure, and an additional patch of alopecia (lower) was noted on day 41.
The condition persisted for 4 days followed by the development of an irregular 3×2-cm patch of alopecia on the right parietal scalp. A 3-day course of self-administered oral prednisolone 0.2 mg/kg/d was prescribed.
Twenty-seven days after the procedure, the patient presented to our trichology clinic for evaluation of a single patch of nonscarring alopecia on the right parietal scalp. Trichoscopy showed multiple yellow and black dots, broken hairs, pigment deposits, and an erythematous background mainly composed of linear telangiectatic vessels (Figure 2). Histopathologic analysis revealed a lymphocytic inflammatory infiltrate surrounding the follicular units that was compatible with an alopecia areata–like pattern as well as PLLA deposits in the subcutaneous tissue forming foreign body granulomas (Figure 3). The diagnosis of PLLA-induced alopecia was made based on the detection of PLLA at the biopsy site within the patchy alopecia.
FIGURE 2. A, Trichoscopy performed 27 days after the initial procedure showed multiple yellow and black dots and broken hairs in addition to an irregular vascular proliferation composed of ectatic vessels, erythema of the fundus, and pigment deposits. B, Partial hair regrowth was noted after 6 weeks of intralesional triamcinolone administered at the alopecic patch. Trichoscopy showed broken hairs as a possible sign of late inflammatory activity 3.5 months after poly-L-lactic acid injection.
FIGURE 3. A, Histology showed a lymphocytic inflammatory infiltrate around the follicular units with increased catagen/telogen counts and miniaturization (H&E, original magnification ×200). B, Birefringence showed poly-L-lactic acid deposits in deeper sections of the subcutaneous tissue forming foreign body granulomas, confirming the diagnosis of alopecia induced by poly-L-lactic acid injection (original magnification ×400).
Intralesional triamcinolone acetonide 5 mg/mL was administered at 1-cm intervals in the subdermal space (0.1 mL/puncture site). After 14 days, the patient developed an additional patch of alopecia in the same vascular territory as the right temporal artery, positioned just beneath the initial patch, with similar trichoscopy findings. The patches were treated with intralesional triamcinolone acetonide for 3 additional sessions, administered every 4 weeks. Long-term monitoring of the patient revealed regrowth with comparable hair count to the unaffected contralateral scalp, indicative of a nonscarring alopecia.
Comment
Poly-L-lactic acid is a biostimulator synthesized from the α-hydroxy acid family in 1954 that has been safely used in suture materials, resorbable plates, and orthopedic screws.4 Alopecia has been reported as a systemic allergic reaction to biodegradable screws following an orthopedic procedure.5 Prior reports of embolization and retinal ischemia with PLLA have raised concerns regarding its occlusive potential.6-9
Approved by the US Food and Drug Administration in 2004 for soft tissue restoration in HIV-related lipoatrophy, PLLA was expanded to cosmetic applications in 2009. As previously reported with HA fillers, we hypothesize that extravascular compression resulting from the placement of the filler material (due to the volume injected in the scalp area) contributes to the development of alopecia plus PLLA embolism–induced ischemic alopecia in the affected areas.10 In our case, the diagnosis of PLLA-induced alopecia was confirmed based on the finding of the filler material in the subcutaneous tissue on histopathology, probably due to embolization. Moreover, trichoscopic findings were all similar to those described after HA embolization.11 The features found in our patient due to the PLLA local reaction were similar to those seen in other conditions such as alopecia areata, pressure alopecia, and chemotherapy-induced alopecia; therefore, histopathology confirmation is mandatory in cases of hair loss associated with PLLA.
The emergence of a secondary patch of alopecia prompts consideration of an intrinsic late inflammatory propensity of PLLA. Immune cells recognize PLLA as a foreign body, and subclinical inflammatory foreign body reactions can cause PLLA-induced collagen synthesis.12 This phenomenon underscores the need for further investigation into the immunologic implications of PLLA in alopecia pathogenesis.
The angiogenic properties of the anagen phase require an adequate blood supply for effective hair growth; therefore, the lack of blood and nutrient supply to the hair bulb triggers miniaturization, a possible explanation for the hair thinning found in the alopecic patch.13
Conclusion
Alopecia as an adverse effect of cosmetic procedures can be distressing for patients, even when reversible. A detailed understanding of scalp anatomy is critical for satisfactory outcomes with aesthetic procedures. Physicians must pay attention to the amount and area of material injected in order to avoid possible mechanisms of ischemia—embolization and/or extravascular compression—especially in highly vascularized areas.
We present a rare report of alopecia as an adverse event of PLLA injection. Dermatologists must be aware of this rare condition, and trichoscopy combined with histopathologic analysis are encouraged for early recognition and proper management.
References
Issa NT, Kaiser M, Martinez-Velasco A, et al. Alopecia after cosmetic injection procedures: a review. Dermatol Surg. 2022;48:855-861.
Alopecia with foreign body granulomas induced by Radiesse injection: a case report. J Cosmet Laser Ther. 2018;20:462-464.
Munia C, Parada M, de Alvarenga Morais MH. Changes in facial morphology using poly-L-lactic acid application according to vector technique: a case series. J Clin Aesthet Dermatol. 2022;15:38-42.
Attenello NH, Maas CS. Injectable fillers: review of material and properties. Facial Plast Surg. 2015;31:29-34.
Mastrokalos DS, Paessler HH. Allergic reaction to biodegradable interference poly-L-lactic acid screws after anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft. Arthroscopy. 2008;24:732-733.
Wu CW, Wu HJ. Retinal artery occlusion following cosmetic injection of poly-L-lactic acid. Taiwan J Ophthalmol. 2021;11:317-320.
Yuan JT, Chang TW, Yu SS, et al. Mental artery occlusion from poly-L-lactic acid injection at the lateral chin. Dermatol Surg. 2017;43:1402-1405.
Ragam A, Agemy SA, Dave SB, et al. Ipsilateral ophthalmic and cerebral infarctions after cosmetic polylactic acid injection into the forehead. J Neuroophthalmol. 2017;37:77-80.
Witmanowski H, Błochowiak K. Another face of dermal fillers. Postepy Dermatol Alergol. 2020;37:651-659.
Yang Q, Qiu L, Yi C, et al. Reversible alopecia with localized scalp necrosis after accidental embolization of the parietal artery with hyaluronic acid. Aesthetic Plast Surg. 2017;41:695-699.
Asz-Sigall D, Iñigo-Gomez K, Ortega-Springall MF, et al. Alopecia secondary to hyaluronic acid embolization: trichoscopic findings. Skin Appendage Disord. 2019;5:396-400.
Oh S, Lee JH, Kim HM, et al. Poly-L-lactic acid fillers improved dermal collagen synthesis by modulating M2 macrophage polarization in aged animal skin. Cells. 2023;12:1320. doi:10.3390/cells12091320
Natarelli N, Gahoonia N, Sivamani RK. Integrative and mechanistic approach to the hair growth cycle and hair loss. J Clin Med. 2023;12:893.2. Liu RF, Kuo TT, Chao YY, et al.
References
Issa NT, Kaiser M, Martinez-Velasco A, et al. Alopecia after cosmetic injection procedures: a review. Dermatol Surg. 2022;48:855-861.
Alopecia with foreign body granulomas induced by Radiesse injection: a case report. J Cosmet Laser Ther. 2018;20:462-464.
Munia C, Parada M, de Alvarenga Morais MH. Changes in facial morphology using poly-L-lactic acid application according to vector technique: a case series. J Clin Aesthet Dermatol. 2022;15:38-42.
Attenello NH, Maas CS. Injectable fillers: review of material and properties. Facial Plast Surg. 2015;31:29-34.
Mastrokalos DS, Paessler HH. Allergic reaction to biodegradable interference poly-L-lactic acid screws after anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft. Arthroscopy. 2008;24:732-733.
Wu CW, Wu HJ. Retinal artery occlusion following cosmetic injection of poly-L-lactic acid. Taiwan J Ophthalmol. 2021;11:317-320.
Yuan JT, Chang TW, Yu SS, et al. Mental artery occlusion from poly-L-lactic acid injection at the lateral chin. Dermatol Surg. 2017;43:1402-1405.
Ragam A, Agemy SA, Dave SB, et al. Ipsilateral ophthalmic and cerebral infarctions after cosmetic polylactic acid injection into the forehead. J Neuroophthalmol. 2017;37:77-80.
Witmanowski H, Błochowiak K. Another face of dermal fillers. Postepy Dermatol Alergol. 2020;37:651-659.
Yang Q, Qiu L, Yi C, et al. Reversible alopecia with localized scalp necrosis after accidental embolization of the parietal artery with hyaluronic acid. Aesthetic Plast Surg. 2017;41:695-699.
Asz-Sigall D, Iñigo-Gomez K, Ortega-Springall MF, et al. Alopecia secondary to hyaluronic acid embolization: trichoscopic findings. Skin Appendage Disord. 2019;5:396-400.
Oh S, Lee JH, Kim HM, et al. Poly-L-lactic acid fillers improved dermal collagen synthesis by modulating M2 macrophage polarization in aged animal skin. Cells. 2023;12:1320. doi:10.3390/cells12091320
Natarelli N, Gahoonia N, Sivamani RK. Integrative and mechanistic approach to the hair growth cycle and hair loss. J Clin Med. 2023;12:893.2. Liu RF, Kuo TT, Chao YY, et al.
Alopecia is a potential adverse event of poly-L-lactic acid (PLLA) injection, and prior reports of embolization and retinal ischemia with PLLA use raise the concern of its occlusive potential.
The combination of extravascular compression due to the presence of the filler material in the subcutaneous tissue as well as intravascular PLLA embolism may contribute to tissue ischemia–induced alopecia in the affected areas.
Poly-L-lactic acid also may cause a local inflammatory reaction that is alopecia areata–like, which would explain its similar trichoscopy findings.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
What is the world’s most dangerous tree? According to Guinness World Records1 (and one unlucky contestant on the wilderness survival reality show Naked and Afraid,2 who got its sap in his eyes and needed to be evacuated for treatment), the manchineel tree (Hippomane mancinella) has earned this designation.1-3 Manchineel trees are part of the strand vegetation of islands in the West Indies and along the Caribbean coasts of South and Central America, where their copious root systems help reduce coastal erosion. In the United States, this poisonous tree grows along the southern edge of Florida’s Everglades National Park; the Florida Keys; and the US Virgin Islands, especially Virgin Islands National Park. Although the manchineel tree appears on several endangered species lists,4-6 there are places within its distribution where it is locally abundant and thus poses a risk to residents and visitors.
The first European description of manchineel toxicity was by Peter Martyr d’Anghiera, a court historian and geographer of Christopher Columbus’s patroness, Isabella I, Queen of Castile and Léon. In the early 1500s, Peter Martyr wrote that on Columbus’s second New World voyage in 1493, the crew encountered a mysterious tree that burned the skin and eyes of anyone who had contact with it.7 Columbus called the tree’s fruit manzanilla de la muerte (“little apple of death”) after several sailors became severely ill from eating the fruit.8,9 Manchineel lore is rife with tales of agonizing death after eating the applelike fruit, and several contemporaneous accounts describe indigenous Caribbean islanders using manchineel’s toxic sap as an arrow poison.10
Eating manchineel fruit is known to cause abdominal pain, burning sensations in the oropharynx, and esophageal spasms.11 Several case reports mention that consuming the fruit can create an exaggerated parasympathomimetic syndrome due to suspected anticholinesteraselike compounds.3,11,12 Ophthalmologic injuries include severe conjunctivitis—sometimes extensive enough to cause superficial punctate epithelial keratitis.5 Dermatologic injuries have been described, but reports on its histopathologic features are limited. We present a case of manchineel dermatitis in a patient who subsequently underwent a skin biopsy.
Case Report
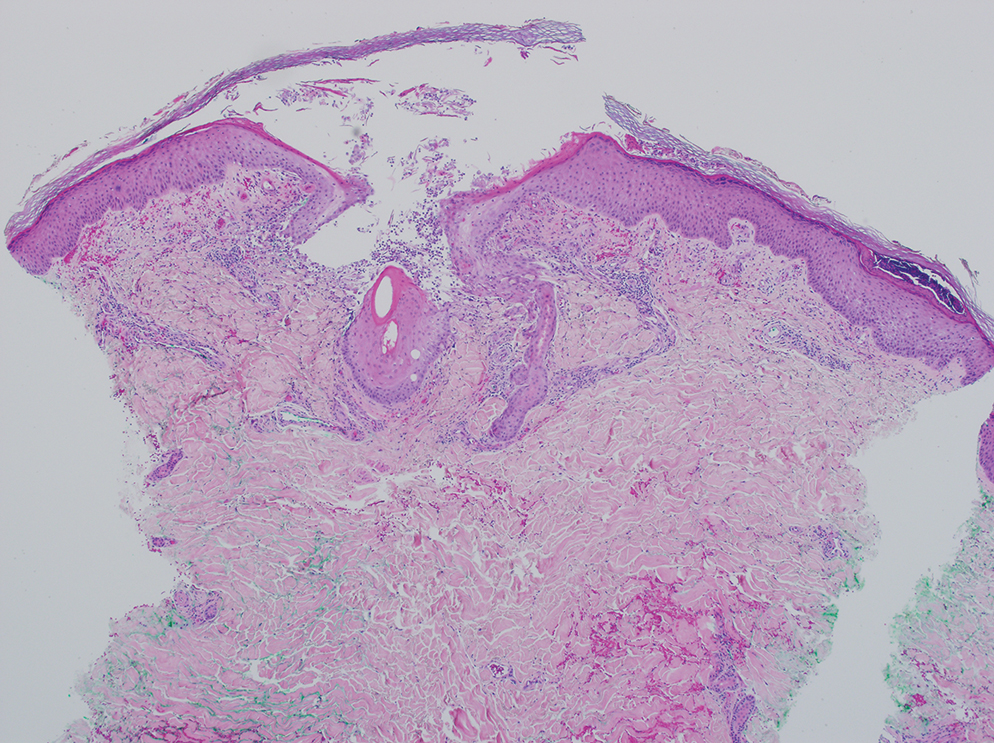
A 64-year-old physician (S.A.N.) came across a stand of manchineel trees while camping in the Virgin Islands National Park on St. John in the US Virgin Islands (Figure 1). The patient—who was knowledgeable about tropical ecology and was familiar with the tree—was curious about its purported cutaneous toxicity and applied the viscous white sap of a broken branchlet (Figure 2) to a patch of skin measuring 4 cm in diameter on the medial left calf. He took serial photographs of the site on days 2, 4 (Figure 3), 6, and 10 (Figure 4), showing the onset of erythema and the subsequent development of follicular pustules. On day 6, a 4-mm punch biopsy specimen was taken of the most prominent pustule. Histopathology showed a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which was consistent with irritant contact dermatitis (Figure 5). On day 8, the region became indurated and tender to pressure; however, there was no warmth, edema, purulent drainage, lymphangitic streaks, or other signs of infection. The region was never itchy; it was uncomfortable only with firm direct pressure. The patient applied hot compresses to the site for 10 minutes 1 to 2 times daily for roughly 2 weeks, and the affected area healed fully (without any additional intervention) in approximately 6 weeks.
FIGURE 1. Manchineel leaves with their characteristic shiny green upper surface and subtly serrated margins. Leaves have distinctive yellow-green mid ribs that are roughly as long as the petiole (stalk). An unripe manchineel fruit also is present.
FIGURE 2. Thick milky white sap drips copiously when a manchineel leaf, twig, or branch is disrupted. The sap is caustic to the skin and mucosae, thereby causing a severe irritant contact dermatitis. Minute pores (lenticels) used in gaseous exchange are scattered along woody twigs, branches, and stems.
FIGURE 3. An ill-defined red patch studded with follicular papules and pustules was visible 4 days after manchineel sap was applied to the leg.
FIGURE 4. An ill-defined red plaque with coalesced pustules and a near-confluent grayish hue to the epidermis was visible 10 days after manchineel sap was applied to the leg.
FIGURE 5. A punch biopsy from the left medial calf showed spongiosis and a subcorneal split; epidermal and follicular necrosis; a superficial mixed lymphocytic-neutrophilic infiltrate; and hemorrhage, consistent with an irritant contact dermatitis (H&E, original magnification ×4).
Comment
Manchineel is a member of the Euphorbiaceae (also known as the euphorb or spurge) family, a mainly tropical or subtropical plant family that includes many useful as well as many toxic species. Examples of useful plants include cassava (Manihot esculenta) and the rubber tree (Hevea brasiliensis). Many euphorbs have well-described toxicities, and many (eg, castor bean, Ricinus communis) are useful in some circumstances and toxic in others.6,12-14 Many euphorbs are known to cause skin reactions, usually due to toxins in the milky sap that directly irritate the skin or to latex compounds that can induce IgE-mediated contact dermatitis.9,14
Manchineel contains a complex mix of toxins, though no specific one has been identified as the main cause of the associated irritant contact dermatitis. Manchineel sap (and sap of many other euphorbs) contains phorbol esters that may cause direct pH-induced cytotoxicity leading to keratinocyte necrosis. Diterpenes may augment this cytotoxic effect via induction of proinflammatory cytokines.12 Pitts et al5 pointed to a mixture of oxygenated diterpene esters as the primary cause of toxicity and suggested that their water solubility explained occurrences of keratoconjunctivitis after contact with rainwater or dew from the manchineel tree.
All parts of the manchineel tree—fruit, leaves, wood, and sap—are poisonous. In a retrospective series of 97 cases of manchineel fruit ingestion, the most common symptoms were oropharyngeal pain (68% [66/97]), abdominal pain (42% [41/97]), and diarrhea (37% [36/97]). The same series identified 1 (1%) case of bradycardia and hypotension.3 Contact with the wood, exposure to sawdust, and inhalation of smoke from burning the wood can irritate the skin, conjunctivae, or nasopharynx. Rainwater or dew dripping from the leaves onto the skin can cause dermatitis and ophthalmitis, even without direct contact with the tree.4,5
Management—There is no specific treatment for manchineel dermatitis. Because it is an irritant reaction and not a type IV hypersensitivity reaction, topical corticosteroids have minimal benefit. A regimen consisting of a thorough cleansing, wet compresses, and observation, as most symptoms resolve spontaneously within a few days, has been recommended.4 Our patient used hot compresses, which he believes helped heal the site, although his symptoms lasted for several weeks.
Given that there is no specific treatment for manchineel dermatitis, the wisest approach is strict avoidance. On many Caribbean islands, visitors are warned about the manchineel tree, advised to avoid direct contact, and reminded to avoid standing beneath it during a rainstorm (Figure 6).
FIGURE 6. Sign from Virgin Islands National Park on St John, US Virgin Islands, warning visitors about manchineel trees and their hazards.
Conclusion
This article begins with a question: “What is the world’s most dangerous tree?” Many sources from the indexed medical literature as well as the popular press and social media state that it is the manchineel. Although all parts of the manchineel tree are highly toxic, human exposures are uncommon, and deaths are more apocryphal than actual.
Boucaud-Maitre D, Cachet X, Bouzidi C, et al. Severity of manchineel fruit (Hippomane mancinella) poisoning: a retrospective case series of 97 patients from French Poison Control Centers. Toxicon. 2019;161:28-32. doi:10.1016/j.toxicon.2019.02.014
Blue LM, Sailing C, Denapoles C, et al. Manchineel dermatitis in North American students in the Caribbean. J Travel Medicine. 2011;18:422-424. doi:10.1111/j.1708-8305.2011.00568.x
Lauter WM, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella, L. I. historical review. J Pharm Sci. 1952;41:199-201. https://doi.org/10.1002/jps.3030410412
Martyr P. De Orbe Novo: the Eight Decades of Peter Martyr d’Anghera. Vol 1. FA MacNutt (translator). GP Putnam’s Sons; 1912. Accessed October 14, 2024. https://gutenberg.org/cache/epub/12425/pg12425.txt
Fernandez de Ybarra AM. A forgotten medical worthy, Dr. Diego Alvarex Chanca, of Seville, Spain, and his letter describing the second voyage of Christopher Columbus to America. Med Library Hist J. 1906;4:246-263.
Muscat MK. Manchineel apple of death. EJIFCC. 2019;30:346-348.
Handler JS. Aspects of Amerindian ethnography in 17th century Barbados. Caribbean Studies. 1970;9:50-72.
Howard RA. Three experiences with the manchineel (Hippomane spp., Euphorbiaceae). Biotropica. 1981;13:224-227. https://doi.org/10.2307/2388129
Lauter WM, Foote PA. Investigation of the toxic principles of Hippomane mancinella L. II. Preliminary isolation of a toxic principle of the fruit. J Am Pharm Assoc. 1955;44:361-363. doi:10.1002/jps.3030440616
Carroll MN Jr, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella L. III. Toxic actions of extracts of Hippomane mancinella L. J Am Pharm Assoc. 1957;46:93-97. doi:10.1002/jps.3030460206
Drs. Munoz and Whitecar are from the Department of Dermatology, Walter Reed National Military Medical Center, Bethesda, Maryland. Dr. Norton is from the Department of Dermatology, Uniformed Services University, Bethesda.
The authors have no relevant financial disclosures to report.
Correspondence: Scott A. Norton, MD, MPH, MSc, Dermatologic Surgery Center of Washington, 5530 Wisconsin Avenue #820, Chevy Chase,MD 20815 (scottanorton@gmail.com).
Drs. Munoz and Whitecar are from the Department of Dermatology, Walter Reed National Military Medical Center, Bethesda, Maryland. Dr. Norton is from the Department of Dermatology, Uniformed Services University, Bethesda.
The authors have no relevant financial disclosures to report.
Correspondence: Scott A. Norton, MD, MPH, MSc, Dermatologic Surgery Center of Washington, 5530 Wisconsin Avenue #820, Chevy Chase,MD 20815 (scottanorton@gmail.com).
Drs. Munoz and Whitecar are from the Department of Dermatology, Walter Reed National Military Medical Center, Bethesda, Maryland. Dr. Norton is from the Department of Dermatology, Uniformed Services University, Bethesda.
The authors have no relevant financial disclosures to report.
Correspondence: Scott A. Norton, MD, MPH, MSc, Dermatologic Surgery Center of Washington, 5530 Wisconsin Avenue #820, Chevy Chase,MD 20815 (scottanorton@gmail.com).
What is the world’s most dangerous tree? According to Guinness World Records1 (and one unlucky contestant on the wilderness survival reality show Naked and Afraid,2 who got its sap in his eyes and needed to be evacuated for treatment), the manchineel tree (Hippomane mancinella) has earned this designation.1-3 Manchineel trees are part of the strand vegetation of islands in the West Indies and along the Caribbean coasts of South and Central America, where their copious root systems help reduce coastal erosion. In the United States, this poisonous tree grows along the southern edge of Florida’s Everglades National Park; the Florida Keys; and the US Virgin Islands, especially Virgin Islands National Park. Although the manchineel tree appears on several endangered species lists,4-6 there are places within its distribution where it is locally abundant and thus poses a risk to residents and visitors.
The first European description of manchineel toxicity was by Peter Martyr d’Anghiera, a court historian and geographer of Christopher Columbus’s patroness, Isabella I, Queen of Castile and Léon. In the early 1500s, Peter Martyr wrote that on Columbus’s second New World voyage in 1493, the crew encountered a mysterious tree that burned the skin and eyes of anyone who had contact with it.7 Columbus called the tree’s fruit manzanilla de la muerte (“little apple of death”) after several sailors became severely ill from eating the fruit.8,9 Manchineel lore is rife with tales of agonizing death after eating the applelike fruit, and several contemporaneous accounts describe indigenous Caribbean islanders using manchineel’s toxic sap as an arrow poison.10
Eating manchineel fruit is known to cause abdominal pain, burning sensations in the oropharynx, and esophageal spasms.11 Several case reports mention that consuming the fruit can create an exaggerated parasympathomimetic syndrome due to suspected anticholinesteraselike compounds.3,11,12 Ophthalmologic injuries include severe conjunctivitis—sometimes extensive enough to cause superficial punctate epithelial keratitis.5 Dermatologic injuries have been described, but reports on its histopathologic features are limited. We present a case of manchineel dermatitis in a patient who subsequently underwent a skin biopsy.
Case Report
A 64-year-old physician (S.A.N.) came across a stand of manchineel trees while camping in the Virgin Islands National Park on St. John in the US Virgin Islands (Figure 1). The patient—who was knowledgeable about tropical ecology and was familiar with the tree—was curious about its purported cutaneous toxicity and applied the viscous white sap of a broken branchlet (Figure 2) to a patch of skin measuring 4 cm in diameter on the medial left calf. He took serial photographs of the site on days 2, 4 (Figure 3), 6, and 10 (Figure 4), showing the onset of erythema and the subsequent development of follicular pustules. On day 6, a 4-mm punch biopsy specimen was taken of the most prominent pustule. Histopathology showed a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which was consistent with irritant contact dermatitis (Figure 5). On day 8, the region became indurated and tender to pressure; however, there was no warmth, edema, purulent drainage, lymphangitic streaks, or other signs of infection. The region was never itchy; it was uncomfortable only with firm direct pressure. The patient applied hot compresses to the site for 10 minutes 1 to 2 times daily for roughly 2 weeks, and the affected area healed fully (without any additional intervention) in approximately 6 weeks.
FIGURE 1. Manchineel leaves with their characteristic shiny green upper surface and subtly serrated margins. Leaves have distinctive yellow-green mid ribs that are roughly as long as the petiole (stalk). An unripe manchineel fruit also is present.
FIGURE 2. Thick milky white sap drips copiously when a manchineel leaf, twig, or branch is disrupted. The sap is caustic to the skin and mucosae, thereby causing a severe irritant contact dermatitis. Minute pores (lenticels) used in gaseous exchange are scattered along woody twigs, branches, and stems.
FIGURE 3. An ill-defined red patch studded with follicular papules and pustules was visible 4 days after manchineel sap was applied to the leg.
FIGURE 4. An ill-defined red plaque with coalesced pustules and a near-confluent grayish hue to the epidermis was visible 10 days after manchineel sap was applied to the leg.
FIGURE 5. A punch biopsy from the left medial calf showed spongiosis and a subcorneal split; epidermal and follicular necrosis; a superficial mixed lymphocytic-neutrophilic infiltrate; and hemorrhage, consistent with an irritant contact dermatitis (H&E, original magnification ×4).
Comment
Manchineel is a member of the Euphorbiaceae (also known as the euphorb or spurge) family, a mainly tropical or subtropical plant family that includes many useful as well as many toxic species. Examples of useful plants include cassava (Manihot esculenta) and the rubber tree (Hevea brasiliensis). Many euphorbs have well-described toxicities, and many (eg, castor bean, Ricinus communis) are useful in some circumstances and toxic in others.6,12-14 Many euphorbs are known to cause skin reactions, usually due to toxins in the milky sap that directly irritate the skin or to latex compounds that can induce IgE-mediated contact dermatitis.9,14
Manchineel contains a complex mix of toxins, though no specific one has been identified as the main cause of the associated irritant contact dermatitis. Manchineel sap (and sap of many other euphorbs) contains phorbol esters that may cause direct pH-induced cytotoxicity leading to keratinocyte necrosis. Diterpenes may augment this cytotoxic effect via induction of proinflammatory cytokines.12 Pitts et al5 pointed to a mixture of oxygenated diterpene esters as the primary cause of toxicity and suggested that their water solubility explained occurrences of keratoconjunctivitis after contact with rainwater or dew from the manchineel tree.
All parts of the manchineel tree—fruit, leaves, wood, and sap—are poisonous. In a retrospective series of 97 cases of manchineel fruit ingestion, the most common symptoms were oropharyngeal pain (68% [66/97]), abdominal pain (42% [41/97]), and diarrhea (37% [36/97]). The same series identified 1 (1%) case of bradycardia and hypotension.3 Contact with the wood, exposure to sawdust, and inhalation of smoke from burning the wood can irritate the skin, conjunctivae, or nasopharynx. Rainwater or dew dripping from the leaves onto the skin can cause dermatitis and ophthalmitis, even without direct contact with the tree.4,5
Management—There is no specific treatment for manchineel dermatitis. Because it is an irritant reaction and not a type IV hypersensitivity reaction, topical corticosteroids have minimal benefit. A regimen consisting of a thorough cleansing, wet compresses, and observation, as most symptoms resolve spontaneously within a few days, has been recommended.4 Our patient used hot compresses, which he believes helped heal the site, although his symptoms lasted for several weeks.
Given that there is no specific treatment for manchineel dermatitis, the wisest approach is strict avoidance. On many Caribbean islands, visitors are warned about the manchineel tree, advised to avoid direct contact, and reminded to avoid standing beneath it during a rainstorm (Figure 6).
FIGURE 6. Sign from Virgin Islands National Park on St John, US Virgin Islands, warning visitors about manchineel trees and their hazards.
Conclusion
This article begins with a question: “What is the world’s most dangerous tree?” Many sources from the indexed medical literature as well as the popular press and social media state that it is the manchineel. Although all parts of the manchineel tree are highly toxic, human exposures are uncommon, and deaths are more apocryphal than actual.
What is the world’s most dangerous tree? According to Guinness World Records1 (and one unlucky contestant on the wilderness survival reality show Naked and Afraid,2 who got its sap in his eyes and needed to be evacuated for treatment), the manchineel tree (Hippomane mancinella) has earned this designation.1-3 Manchineel trees are part of the strand vegetation of islands in the West Indies and along the Caribbean coasts of South and Central America, where their copious root systems help reduce coastal erosion. In the United States, this poisonous tree grows along the southern edge of Florida’s Everglades National Park; the Florida Keys; and the US Virgin Islands, especially Virgin Islands National Park. Although the manchineel tree appears on several endangered species lists,4-6 there are places within its distribution where it is locally abundant and thus poses a risk to residents and visitors.
The first European description of manchineel toxicity was by Peter Martyr d’Anghiera, a court historian and geographer of Christopher Columbus’s patroness, Isabella I, Queen of Castile and Léon. In the early 1500s, Peter Martyr wrote that on Columbus’s second New World voyage in 1493, the crew encountered a mysterious tree that burned the skin and eyes of anyone who had contact with it.7 Columbus called the tree’s fruit manzanilla de la muerte (“little apple of death”) after several sailors became severely ill from eating the fruit.8,9 Manchineel lore is rife with tales of agonizing death after eating the applelike fruit, and several contemporaneous accounts describe indigenous Caribbean islanders using manchineel’s toxic sap as an arrow poison.10
Eating manchineel fruit is known to cause abdominal pain, burning sensations in the oropharynx, and esophageal spasms.11 Several case reports mention that consuming the fruit can create an exaggerated parasympathomimetic syndrome due to suspected anticholinesteraselike compounds.3,11,12 Ophthalmologic injuries include severe conjunctivitis—sometimes extensive enough to cause superficial punctate epithelial keratitis.5 Dermatologic injuries have been described, but reports on its histopathologic features are limited. We present a case of manchineel dermatitis in a patient who subsequently underwent a skin biopsy.
Case Report
A 64-year-old physician (S.A.N.) came across a stand of manchineel trees while camping in the Virgin Islands National Park on St. John in the US Virgin Islands (Figure 1). The patient—who was knowledgeable about tropical ecology and was familiar with the tree—was curious about its purported cutaneous toxicity and applied the viscous white sap of a broken branchlet (Figure 2) to a patch of skin measuring 4 cm in diameter on the medial left calf. He took serial photographs of the site on days 2, 4 (Figure 3), 6, and 10 (Figure 4), showing the onset of erythema and the subsequent development of follicular pustules. On day 6, a 4-mm punch biopsy specimen was taken of the most prominent pustule. Histopathology showed a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which was consistent with irritant contact dermatitis (Figure 5). On day 8, the region became indurated and tender to pressure; however, there was no warmth, edema, purulent drainage, lymphangitic streaks, or other signs of infection. The region was never itchy; it was uncomfortable only with firm direct pressure. The patient applied hot compresses to the site for 10 minutes 1 to 2 times daily for roughly 2 weeks, and the affected area healed fully (without any additional intervention) in approximately 6 weeks.
FIGURE 1. Manchineel leaves with their characteristic shiny green upper surface and subtly serrated margins. Leaves have distinctive yellow-green mid ribs that are roughly as long as the petiole (stalk). An unripe manchineel fruit also is present.
FIGURE 2. Thick milky white sap drips copiously when a manchineel leaf, twig, or branch is disrupted. The sap is caustic to the skin and mucosae, thereby causing a severe irritant contact dermatitis. Minute pores (lenticels) used in gaseous exchange are scattered along woody twigs, branches, and stems.
FIGURE 3. An ill-defined red patch studded with follicular papules and pustules was visible 4 days after manchineel sap was applied to the leg.
FIGURE 4. An ill-defined red plaque with coalesced pustules and a near-confluent grayish hue to the epidermis was visible 10 days after manchineel sap was applied to the leg.
FIGURE 5. A punch biopsy from the left medial calf showed spongiosis and a subcorneal split; epidermal and follicular necrosis; a superficial mixed lymphocytic-neutrophilic infiltrate; and hemorrhage, consistent with an irritant contact dermatitis (H&E, original magnification ×4).
Comment
Manchineel is a member of the Euphorbiaceae (also known as the euphorb or spurge) family, a mainly tropical or subtropical plant family that includes many useful as well as many toxic species. Examples of useful plants include cassava (Manihot esculenta) and the rubber tree (Hevea brasiliensis). Many euphorbs have well-described toxicities, and many (eg, castor bean, Ricinus communis) are useful in some circumstances and toxic in others.6,12-14 Many euphorbs are known to cause skin reactions, usually due to toxins in the milky sap that directly irritate the skin or to latex compounds that can induce IgE-mediated contact dermatitis.9,14
Manchineel contains a complex mix of toxins, though no specific one has been identified as the main cause of the associated irritant contact dermatitis. Manchineel sap (and sap of many other euphorbs) contains phorbol esters that may cause direct pH-induced cytotoxicity leading to keratinocyte necrosis. Diterpenes may augment this cytotoxic effect via induction of proinflammatory cytokines.12 Pitts et al5 pointed to a mixture of oxygenated diterpene esters as the primary cause of toxicity and suggested that their water solubility explained occurrences of keratoconjunctivitis after contact with rainwater or dew from the manchineel tree.
All parts of the manchineel tree—fruit, leaves, wood, and sap—are poisonous. In a retrospective series of 97 cases of manchineel fruit ingestion, the most common symptoms were oropharyngeal pain (68% [66/97]), abdominal pain (42% [41/97]), and diarrhea (37% [36/97]). The same series identified 1 (1%) case of bradycardia and hypotension.3 Contact with the wood, exposure to sawdust, and inhalation of smoke from burning the wood can irritate the skin, conjunctivae, or nasopharynx. Rainwater or dew dripping from the leaves onto the skin can cause dermatitis and ophthalmitis, even without direct contact with the tree.4,5
Management—There is no specific treatment for manchineel dermatitis. Because it is an irritant reaction and not a type IV hypersensitivity reaction, topical corticosteroids have minimal benefit. A regimen consisting of a thorough cleansing, wet compresses, and observation, as most symptoms resolve spontaneously within a few days, has been recommended.4 Our patient used hot compresses, which he believes helped heal the site, although his symptoms lasted for several weeks.
Given that there is no specific treatment for manchineel dermatitis, the wisest approach is strict avoidance. On many Caribbean islands, visitors are warned about the manchineel tree, advised to avoid direct contact, and reminded to avoid standing beneath it during a rainstorm (Figure 6).
FIGURE 6. Sign from Virgin Islands National Park on St John, US Virgin Islands, warning visitors about manchineel trees and their hazards.
Conclusion
This article begins with a question: “What is the world’s most dangerous tree?” Many sources from the indexed medical literature as well as the popular press and social media state that it is the manchineel. Although all parts of the manchineel tree are highly toxic, human exposures are uncommon, and deaths are more apocryphal than actual.
Boucaud-Maitre D, Cachet X, Bouzidi C, et al. Severity of manchineel fruit (Hippomane mancinella) poisoning: a retrospective case series of 97 patients from French Poison Control Centers. Toxicon. 2019;161:28-32. doi:10.1016/j.toxicon.2019.02.014
Blue LM, Sailing C, Denapoles C, et al. Manchineel dermatitis in North American students in the Caribbean. J Travel Medicine. 2011;18:422-424. doi:10.1111/j.1708-8305.2011.00568.x
Lauter WM, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella, L. I. historical review. J Pharm Sci. 1952;41:199-201. https://doi.org/10.1002/jps.3030410412
Martyr P. De Orbe Novo: the Eight Decades of Peter Martyr d’Anghera. Vol 1. FA MacNutt (translator). GP Putnam’s Sons; 1912. Accessed October 14, 2024. https://gutenberg.org/cache/epub/12425/pg12425.txt
Fernandez de Ybarra AM. A forgotten medical worthy, Dr. Diego Alvarex Chanca, of Seville, Spain, and his letter describing the second voyage of Christopher Columbus to America. Med Library Hist J. 1906;4:246-263.
Muscat MK. Manchineel apple of death. EJIFCC. 2019;30:346-348.
Handler JS. Aspects of Amerindian ethnography in 17th century Barbados. Caribbean Studies. 1970;9:50-72.
Howard RA. Three experiences with the manchineel (Hippomane spp., Euphorbiaceae). Biotropica. 1981;13:224-227. https://doi.org/10.2307/2388129
Lauter WM, Foote PA. Investigation of the toxic principles of Hippomane mancinella L. II. Preliminary isolation of a toxic principle of the fruit. J Am Pharm Assoc. 1955;44:361-363. doi:10.1002/jps.3030440616
Carroll MN Jr, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella L. III. Toxic actions of extracts of Hippomane mancinella L. J Am Pharm Assoc. 1957;46:93-97. doi:10.1002/jps.3030460206
Boucaud-Maitre D, Cachet X, Bouzidi C, et al. Severity of manchineel fruit (Hippomane mancinella) poisoning: a retrospective case series of 97 patients from French Poison Control Centers. Toxicon. 2019;161:28-32. doi:10.1016/j.toxicon.2019.02.014
Blue LM, Sailing C, Denapoles C, et al. Manchineel dermatitis in North American students in the Caribbean. J Travel Medicine. 2011;18:422-424. doi:10.1111/j.1708-8305.2011.00568.x
Lauter WM, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella, L. I. historical review. J Pharm Sci. 1952;41:199-201. https://doi.org/10.1002/jps.3030410412
Martyr P. De Orbe Novo: the Eight Decades of Peter Martyr d’Anghera. Vol 1. FA MacNutt (translator). GP Putnam’s Sons; 1912. Accessed October 14, 2024. https://gutenberg.org/cache/epub/12425/pg12425.txt
Fernandez de Ybarra AM. A forgotten medical worthy, Dr. Diego Alvarex Chanca, of Seville, Spain, and his letter describing the second voyage of Christopher Columbus to America. Med Library Hist J. 1906;4:246-263.
Muscat MK. Manchineel apple of death. EJIFCC. 2019;30:346-348.
Handler JS. Aspects of Amerindian ethnography in 17th century Barbados. Caribbean Studies. 1970;9:50-72.
Howard RA. Three experiences with the manchineel (Hippomane spp., Euphorbiaceae). Biotropica. 1981;13:224-227. https://doi.org/10.2307/2388129
Lauter WM, Foote PA. Investigation of the toxic principles of Hippomane mancinella L. II. Preliminary isolation of a toxic principle of the fruit. J Am Pharm Assoc. 1955;44:361-363. doi:10.1002/jps.3030440616
Carroll MN Jr, Fox LE, Ariail WT. Investigation of the toxic principles of Hippomane mancinella L. III. Toxic actions of extracts of Hippomane mancinella L. J Am Pharm Assoc. 1957;46:93-97. doi:10.1002/jps.3030460206
Sap from the manchineel tree—found on the coasts of Caribbean islands, the Atlantic coastline of Central and northern South America, and parts of southernmost Florida—can cause severe dermatologic and ophthalmologic injuries. Eating its fruit can lead to oropharyngeal pain and diarrhea.
Histopathology of manchineel dermatitis reveals a subcorneal acantholytic blister and epidermal spongiosis overlying a mixed perivascular infiltrate and follicular necrosis, which is consistent with irritant contact dermatitis.
There is no specific treatment for manchineel dermatitis. Case reports advocate a thorough cleansing, application of wet compresses, and observation.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
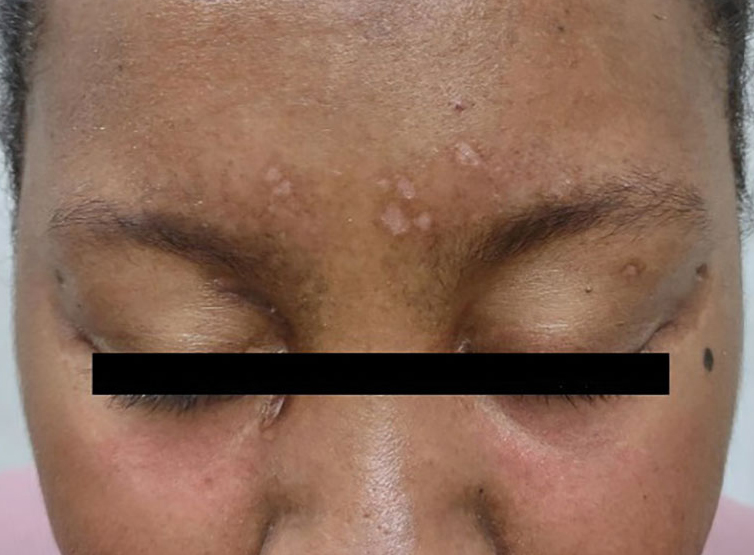
A previously healthy 31-year-old female active-duty Navy sailor working as a calibration technician developed a painful, erythematous, pruritic, indurated plaque on her left breast. The sailor was not lactating and had no known family history of malignancy. Initially, she was treated by her primary care practitioner for presumed mastitis with oral cephalexin and then with oral clindamycin with no symptom improvement. About 2 weeks after the completion of both antibiotic courses, she developed angioedema and periorbital edema (Figure 1), requiring highdose corticosteroids and antihistamines with a corticosteroid course of prednisone 40 mg daily tapered to 10 mg daily over 12 days and diphenhydramine 25 mg to use up to 4 times daily. Workup for both was acquired and hereditary angioedema was unremarkable. Two months later, the patient developed patches of alopecia, oral ulcerations, and hypopigmented plaques with a peripheral hyperpigmented rim on the central face and bilateral conchal bowls (Figure 2). She also developed hypopigmented papules with peripheral hyperpigmentation on the bilateral dorsal hands overlying the metacarpal and proximal interphalangeal joints, which eventually ulcerated (Figure 3). Laboratory evaluation, including tests for creatine kinase, aldolase, transaminases, lactate dehydrogenase, and autoantibodies (antiJo-1, anti-Mi-2, anti-MDA-5, anti-TIF-1, anti-NXP-2, and anti-SAEP), were unremarkable. A punch biopsy from a papule on the right dorsal hand showed superficial perivascular lymphohistiocytic inflammation with a subtle focal increase in dermal mucin, highlighted by the colloidal iron stain. Further evaluation of the left breast plaque revealed ER/PR+ HER2- stage IIIB inflammatory breast cancer.
FIGURE 1 Angioedema With Notable Periorbital Edema
FIGURE 2 Alopecia Patches, Hypopigmented Plaques, and Peripheral Hyperpigmented Rim on Central Face
FIGURE 3 Ulcerative Papules Overlying the Metacarpal and Proximal Interphalangeal Joints
DISCUSSION
Based on the clinical presentation and diagnosis of inflammatory breast cancer, the patient was diagnosed with paraneoplastic clinically amyopathic dermatomyositis (CADM). She was treated for her breast cancer with an initial chemotherapy regimen consisting of dose-dense cyclophosphamide and doxorubicin followed by paclitaxel. The patient underwent a mastectomy, axillary lymph node dissection, and 25 sessions of radiation therapy, and is currently continuing therapy with anastrozole 1 mg daily and ovarian suppression with leuprorelin 11.25 mg every 3 months. For the severe angioedema and dermatomyositis-like cutaneous findings, the patient was continued on high-dose corticosteroids at prednisone 60 mg daily with a prolonged taper to prednisone 10 mg daily. After about 10 months, she transitioned from prednisone 10 mg daily to hydrocortisone 30 mg daily and is currently tapering her hydrocortisone dosing. She was additionally started on monthly intravenous immunoglobulin, hydroxychloroquine 300 mg daily, and amlodipine 5 mg daily. The ulcerated papules on her hands were treated with topical clobetasol 0.05% ointment applied daily, topical tacrolimus 0.1% ointment applied daily, and multiple intralesional triamcinolone 5 mg/mL injections. With this regimen, the patient experienced significant improvement in her cutaneous symptoms.
CADM is a rare autoimmune inflammatory disease featuring classic dermatomyositis-like cutaneous findings such as a heliotrope rash and Gottron papules. Ulcerative Gottron papules are less common than the typical erythematous papules and are associated more strongly with amyopathic disease.1 Paraneoplastic myositis poses a diagnostic challenge because it presents like an idiopathic dermatomyositis and often has a heterogeneous clinical presentation with additional manifestations, including periorbital edema, myalgias, dysphagia, and shortness of breath. If clinically suspected, laboratory tests (eg, creatine kinase, aldolase, transaminases, and lactate dehydrogenase) can assist in diagnosing paraneoplastic myositis. Additionally, serologic testing for autoantibodies such as anti-CADM-140, anti-Jo-1, anti-Mi-2, antiMDA-5, anti-TIF-1, anti-NXP-2, and antiSAE can assist the diagnosis and predict disease phenotype.1,2
Malignancy can precede, occur during, or develop after the diagnosis of CADM.3 Malignancies most often associated with CADM include ovarian, breast, and lung cancers.4 Despite the strong correlation with malignancy, there are currently no screening guidelines for malignancy upon inflammatory myositis diagnosis. Therefore, it is important to consider the entirety of a patient’s clinical presentation in establishing further evaluation in the initial diagnostic workup.
There are numerous systemic complications associated with inflammatory myositis and imaging modalities can help to rule out some of these conditions. CADM is strongly associated with the development of interstitial lung disease, so chest radiography and pulmonary function testing are often checked.1 Though cardiac and esophageal involvement are more commonly associated with classic dermatomyositis, it may be useful to obtain an electrocardiogram to rule out conduction abnormalities from myocardial involvement, along with esophageal manometry to evaluate for esophageal dysmotility.1,5
In the management of paraneoplastic CADM, the underlying malignancy should be treated first.6 If symptoms persist after the cancer is in remission, then CADM is treated with immunosuppressive medications such as methotrexate, mycophenolate mofetil, or azathioprine. Physical therapy can also provide further symptom relief for those suffering from proximal weakness.
CONCLUSIONS
Presumed mastitis, angioedema, and eczematous lesions for this patient were dermatologic manifestations of an underlying inflammatory breast cancer. This case highlights the importance of early recognition, the diagnosis of CADM and awareness of its association with underlying malignancy, especially within the primary care setting where most skin concerns are addressed. Early clinical suspicion and a swift diagnostic workup can further optimize multidisciplinary management, which is often required to treat malignancies.
References
Cao H, Xia Q, Pan M, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. 2016;43(9):1735-1742. doi:10.3899/jrheum.160024
Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. 2017;52(1):1-19. doi:10.1007/s12016-015-8510-y
Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208-215. doi:10.1007/s11926-011-0169-7
Udkoff J, Cohen PR. Amyopathic dermatomyositis: a concise review of clinical manifestations and associated malignancies. Am J Clin Dermatol. 2016;17(5): 509-518. doi:10.1007/s40257-016-0199-z
Fathi M, Lundberg IE, Tornling G. Pulmonary complications of polymyositis and dermatomyositis. Semin Respir Crit Care Med. 2007;28(4):451-458. doi:10.1055/s-2007-985666
Hendren E, Vinik O, Faragalla H, Haq R. Breast cancer and dermatomyositis: a case study and literature review. Curr Oncol. 2017;24(5):e429-e433. doi:10.3747/co.24.3696
Author and Disclosure Information
LT Logan Oliver, MD, USNa; CAPT Rachel Lee, MD, FACP, USNa; MAJ Michael Loncharich, MD, USAb; CPT Shena Kravitz, MD, USAb; MAJ Rebecca Wetzel, DO, USAb; CPT Jon Heald, DO, USAb
Correspondence: Logan Oliver (logan.oliver92@gmail.com)
Author affiliations aNaval Medical Center San Diego, California bWalter Reed National Military Medical Center, Bethesda, Maryland
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article
Fed Pract. 2024;41(10) Published online October 16. doi:10.12788/fp0517
LT Logan Oliver, MD, USNa; CAPT Rachel Lee, MD, FACP, USNa; MAJ Michael Loncharich, MD, USAb; CPT Shena Kravitz, MD, USAb; MAJ Rebecca Wetzel, DO, USAb; CPT Jon Heald, DO, USAb
Correspondence: Logan Oliver (logan.oliver92@gmail.com)
Author affiliations aNaval Medical Center San Diego, California bWalter Reed National Military Medical Center, Bethesda, Maryland
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article
Fed Pract. 2024;41(10) Published online October 16. doi:10.12788/fp0517
Author and Disclosure Information
LT Logan Oliver, MD, USNa; CAPT Rachel Lee, MD, FACP, USNa; MAJ Michael Loncharich, MD, USAb; CPT Shena Kravitz, MD, USAb; MAJ Rebecca Wetzel, DO, USAb; CPT Jon Heald, DO, USAb
Correspondence: Logan Oliver (logan.oliver92@gmail.com)
Author affiliations aNaval Medical Center San Diego, California bWalter Reed National Military Medical Center, Bethesda, Maryland
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article
Fed Pract. 2024;41(10) Published online October 16. doi:10.12788/fp0517
A previously healthy 31-year-old female active-duty Navy sailor working as a calibration technician developed a painful, erythematous, pruritic, indurated plaque on her left breast. The sailor was not lactating and had no known family history of malignancy. Initially, she was treated by her primary care practitioner for presumed mastitis with oral cephalexin and then with oral clindamycin with no symptom improvement. About 2 weeks after the completion of both antibiotic courses, she developed angioedema and periorbital edema (Figure 1), requiring highdose corticosteroids and antihistamines with a corticosteroid course of prednisone 40 mg daily tapered to 10 mg daily over 12 days and diphenhydramine 25 mg to use up to 4 times daily. Workup for both was acquired and hereditary angioedema was unremarkable. Two months later, the patient developed patches of alopecia, oral ulcerations, and hypopigmented plaques with a peripheral hyperpigmented rim on the central face and bilateral conchal bowls (Figure 2). She also developed hypopigmented papules with peripheral hyperpigmentation on the bilateral dorsal hands overlying the metacarpal and proximal interphalangeal joints, which eventually ulcerated (Figure 3). Laboratory evaluation, including tests for creatine kinase, aldolase, transaminases, lactate dehydrogenase, and autoantibodies (antiJo-1, anti-Mi-2, anti-MDA-5, anti-TIF-1, anti-NXP-2, and anti-SAEP), were unremarkable. A punch biopsy from a papule on the right dorsal hand showed superficial perivascular lymphohistiocytic inflammation with a subtle focal increase in dermal mucin, highlighted by the colloidal iron stain. Further evaluation of the left breast plaque revealed ER/PR+ HER2- stage IIIB inflammatory breast cancer.
FIGURE 1 Angioedema With Notable Periorbital Edema
FIGURE 2 Alopecia Patches, Hypopigmented Plaques, and Peripheral Hyperpigmented Rim on Central Face
FIGURE 3 Ulcerative Papules Overlying the Metacarpal and Proximal Interphalangeal Joints
DISCUSSION
Based on the clinical presentation and diagnosis of inflammatory breast cancer, the patient was diagnosed with paraneoplastic clinically amyopathic dermatomyositis (CADM). She was treated for her breast cancer with an initial chemotherapy regimen consisting of dose-dense cyclophosphamide and doxorubicin followed by paclitaxel. The patient underwent a mastectomy, axillary lymph node dissection, and 25 sessions of radiation therapy, and is currently continuing therapy with anastrozole 1 mg daily and ovarian suppression with leuprorelin 11.25 mg every 3 months. For the severe angioedema and dermatomyositis-like cutaneous findings, the patient was continued on high-dose corticosteroids at prednisone 60 mg daily with a prolonged taper to prednisone 10 mg daily. After about 10 months, she transitioned from prednisone 10 mg daily to hydrocortisone 30 mg daily and is currently tapering her hydrocortisone dosing. She was additionally started on monthly intravenous immunoglobulin, hydroxychloroquine 300 mg daily, and amlodipine 5 mg daily. The ulcerated papules on her hands were treated with topical clobetasol 0.05% ointment applied daily, topical tacrolimus 0.1% ointment applied daily, and multiple intralesional triamcinolone 5 mg/mL injections. With this regimen, the patient experienced significant improvement in her cutaneous symptoms.
CADM is a rare autoimmune inflammatory disease featuring classic dermatomyositis-like cutaneous findings such as a heliotrope rash and Gottron papules. Ulcerative Gottron papules are less common than the typical erythematous papules and are associated more strongly with amyopathic disease.1 Paraneoplastic myositis poses a diagnostic challenge because it presents like an idiopathic dermatomyositis and often has a heterogeneous clinical presentation with additional manifestations, including periorbital edema, myalgias, dysphagia, and shortness of breath. If clinically suspected, laboratory tests (eg, creatine kinase, aldolase, transaminases, and lactate dehydrogenase) can assist in diagnosing paraneoplastic myositis. Additionally, serologic testing for autoantibodies such as anti-CADM-140, anti-Jo-1, anti-Mi-2, antiMDA-5, anti-TIF-1, anti-NXP-2, and antiSAE can assist the diagnosis and predict disease phenotype.1,2
Malignancy can precede, occur during, or develop after the diagnosis of CADM.3 Malignancies most often associated with CADM include ovarian, breast, and lung cancers.4 Despite the strong correlation with malignancy, there are currently no screening guidelines for malignancy upon inflammatory myositis diagnosis. Therefore, it is important to consider the entirety of a patient’s clinical presentation in establishing further evaluation in the initial diagnostic workup.
There are numerous systemic complications associated with inflammatory myositis and imaging modalities can help to rule out some of these conditions. CADM is strongly associated with the development of interstitial lung disease, so chest radiography and pulmonary function testing are often checked.1 Though cardiac and esophageal involvement are more commonly associated with classic dermatomyositis, it may be useful to obtain an electrocardiogram to rule out conduction abnormalities from myocardial involvement, along with esophageal manometry to evaluate for esophageal dysmotility.1,5
In the management of paraneoplastic CADM, the underlying malignancy should be treated first.6 If symptoms persist after the cancer is in remission, then CADM is treated with immunosuppressive medications such as methotrexate, mycophenolate mofetil, or azathioprine. Physical therapy can also provide further symptom relief for those suffering from proximal weakness.
CONCLUSIONS
Presumed mastitis, angioedema, and eczematous lesions for this patient were dermatologic manifestations of an underlying inflammatory breast cancer. This case highlights the importance of early recognition, the diagnosis of CADM and awareness of its association with underlying malignancy, especially within the primary care setting where most skin concerns are addressed. Early clinical suspicion and a swift diagnostic workup can further optimize multidisciplinary management, which is often required to treat malignancies.
A previously healthy 31-year-old female active-duty Navy sailor working as a calibration technician developed a painful, erythematous, pruritic, indurated plaque on her left breast. The sailor was not lactating and had no known family history of malignancy. Initially, she was treated by her primary care practitioner for presumed mastitis with oral cephalexin and then with oral clindamycin with no symptom improvement. About 2 weeks after the completion of both antibiotic courses, she developed angioedema and periorbital edema (Figure 1), requiring highdose corticosteroids and antihistamines with a corticosteroid course of prednisone 40 mg daily tapered to 10 mg daily over 12 days and diphenhydramine 25 mg to use up to 4 times daily. Workup for both was acquired and hereditary angioedema was unremarkable. Two months later, the patient developed patches of alopecia, oral ulcerations, and hypopigmented plaques with a peripheral hyperpigmented rim on the central face and bilateral conchal bowls (Figure 2). She also developed hypopigmented papules with peripheral hyperpigmentation on the bilateral dorsal hands overlying the metacarpal and proximal interphalangeal joints, which eventually ulcerated (Figure 3). Laboratory evaluation, including tests for creatine kinase, aldolase, transaminases, lactate dehydrogenase, and autoantibodies (antiJo-1, anti-Mi-2, anti-MDA-5, anti-TIF-1, anti-NXP-2, and anti-SAEP), were unremarkable. A punch biopsy from a papule on the right dorsal hand showed superficial perivascular lymphohistiocytic inflammation with a subtle focal increase in dermal mucin, highlighted by the colloidal iron stain. Further evaluation of the left breast plaque revealed ER/PR+ HER2- stage IIIB inflammatory breast cancer.
FIGURE 1 Angioedema With Notable Periorbital Edema
FIGURE 2 Alopecia Patches, Hypopigmented Plaques, and Peripheral Hyperpigmented Rim on Central Face
FIGURE 3 Ulcerative Papules Overlying the Metacarpal and Proximal Interphalangeal Joints
DISCUSSION
Based on the clinical presentation and diagnosis of inflammatory breast cancer, the patient was diagnosed with paraneoplastic clinically amyopathic dermatomyositis (CADM). She was treated for her breast cancer with an initial chemotherapy regimen consisting of dose-dense cyclophosphamide and doxorubicin followed by paclitaxel. The patient underwent a mastectomy, axillary lymph node dissection, and 25 sessions of radiation therapy, and is currently continuing therapy with anastrozole 1 mg daily and ovarian suppression with leuprorelin 11.25 mg every 3 months. For the severe angioedema and dermatomyositis-like cutaneous findings, the patient was continued on high-dose corticosteroids at prednisone 60 mg daily with a prolonged taper to prednisone 10 mg daily. After about 10 months, she transitioned from prednisone 10 mg daily to hydrocortisone 30 mg daily and is currently tapering her hydrocortisone dosing. She was additionally started on monthly intravenous immunoglobulin, hydroxychloroquine 300 mg daily, and amlodipine 5 mg daily. The ulcerated papules on her hands were treated with topical clobetasol 0.05% ointment applied daily, topical tacrolimus 0.1% ointment applied daily, and multiple intralesional triamcinolone 5 mg/mL injections. With this regimen, the patient experienced significant improvement in her cutaneous symptoms.
CADM is a rare autoimmune inflammatory disease featuring classic dermatomyositis-like cutaneous findings such as a heliotrope rash and Gottron papules. Ulcerative Gottron papules are less common than the typical erythematous papules and are associated more strongly with amyopathic disease.1 Paraneoplastic myositis poses a diagnostic challenge because it presents like an idiopathic dermatomyositis and often has a heterogeneous clinical presentation with additional manifestations, including periorbital edema, myalgias, dysphagia, and shortness of breath. If clinically suspected, laboratory tests (eg, creatine kinase, aldolase, transaminases, and lactate dehydrogenase) can assist in diagnosing paraneoplastic myositis. Additionally, serologic testing for autoantibodies such as anti-CADM-140, anti-Jo-1, anti-Mi-2, antiMDA-5, anti-TIF-1, anti-NXP-2, and antiSAE can assist the diagnosis and predict disease phenotype.1,2
Malignancy can precede, occur during, or develop after the diagnosis of CADM.3 Malignancies most often associated with CADM include ovarian, breast, and lung cancers.4 Despite the strong correlation with malignancy, there are currently no screening guidelines for malignancy upon inflammatory myositis diagnosis. Therefore, it is important to consider the entirety of a patient’s clinical presentation in establishing further evaluation in the initial diagnostic workup.
There are numerous systemic complications associated with inflammatory myositis and imaging modalities can help to rule out some of these conditions. CADM is strongly associated with the development of interstitial lung disease, so chest radiography and pulmonary function testing are often checked.1 Though cardiac and esophageal involvement are more commonly associated with classic dermatomyositis, it may be useful to obtain an electrocardiogram to rule out conduction abnormalities from myocardial involvement, along with esophageal manometry to evaluate for esophageal dysmotility.1,5
In the management of paraneoplastic CADM, the underlying malignancy should be treated first.6 If symptoms persist after the cancer is in remission, then CADM is treated with immunosuppressive medications such as methotrexate, mycophenolate mofetil, or azathioprine. Physical therapy can also provide further symptom relief for those suffering from proximal weakness.
CONCLUSIONS
Presumed mastitis, angioedema, and eczematous lesions for this patient were dermatologic manifestations of an underlying inflammatory breast cancer. This case highlights the importance of early recognition, the diagnosis of CADM and awareness of its association with underlying malignancy, especially within the primary care setting where most skin concerns are addressed. Early clinical suspicion and a swift diagnostic workup can further optimize multidisciplinary management, which is often required to treat malignancies.
References
Cao H, Xia Q, Pan M, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. 2016;43(9):1735-1742. doi:10.3899/jrheum.160024
Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. 2017;52(1):1-19. doi:10.1007/s12016-015-8510-y
Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208-215. doi:10.1007/s11926-011-0169-7
Udkoff J, Cohen PR. Amyopathic dermatomyositis: a concise review of clinical manifestations and associated malignancies. Am J Clin Dermatol. 2016;17(5): 509-518. doi:10.1007/s40257-016-0199-z
Fathi M, Lundberg IE, Tornling G. Pulmonary complications of polymyositis and dermatomyositis. Semin Respir Crit Care Med. 2007;28(4):451-458. doi:10.1055/s-2007-985666
Hendren E, Vinik O, Faragalla H, Haq R. Breast cancer and dermatomyositis: a case study and literature review. Curr Oncol. 2017;24(5):e429-e433. doi:10.3747/co.24.3696
References
Cao H, Xia Q, Pan M, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. 2016;43(9):1735-1742. doi:10.3899/jrheum.160024
Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. 2017;52(1):1-19. doi:10.1007/s12016-015-8510-y
Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208-215. doi:10.1007/s11926-011-0169-7
Udkoff J, Cohen PR. Amyopathic dermatomyositis: a concise review of clinical manifestations and associated malignancies. Am J Clin Dermatol. 2016;17(5): 509-518. doi:10.1007/s40257-016-0199-z
Fathi M, Lundberg IE, Tornling G. Pulmonary complications of polymyositis and dermatomyositis. Semin Respir Crit Care Med. 2007;28(4):451-458. doi:10.1055/s-2007-985666
Hendren E, Vinik O, Faragalla H, Haq R. Breast cancer and dermatomyositis: a case study and literature review. Curr Oncol. 2017;24(5):e429-e433. doi:10.3747/co.24.3696
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Fed Pract. 2024;41(10). Published online October 15. doi:10.12788/fp.0516
Author and Disclosure Information
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
Splenic abscesses are a rare occurrence that represent a marginal proportion of intra-abdominal infections. One study found splenic abscesses in only 0.14% to 0.70% of autopsies and none of the 540 abdominal abscesses they examined originated in the spleen.1 Patients with splenic abscesses tend to present with nonspecific symptoms such as fevers, chills, and abdominal pain.2 Imaging modalities such as abdominal ultrasound and computed tomography (CT) are vital to the workup and diagnosis identification.2 Splenic abscesses are generally associated with another underlying process, as seen in patients who are affected by endocarditis, trauma, metastatic infection, splenic infarction, or neoplasia.2
Pleural effusions, or the buildup of fluid within the pleural space, is a common condition typically secondary to another disease.3 Clinical identification of the primary condition may be challenging.3 In the absence of a clear etiology, such as obvious signs of congestive heart failure, further differentiation relies upon pleural fluid analysis, beginning with the distinction between exudate (inflammatory) and transudate (noninflammatory). 3,4 This distinction can be made using Light’s criteria, which relies on protein and lactate dehydrogenase (LDH) ratios between the pleural fluid and serum (Table 1).5 Though rare, half of splenic abscesses are associated with pleural effusion.6 As an inflammatory condition, splenic abscesses have been classically described as a cause of exudative pleural effusions.5,6
A myelodysplastic syndrome is a group of diseases that arise from malignant hematopoietic stem cells, leading to the proliferation of the malignant cells and faulty production of other bone marrow products.7 These disorders can range from single to multilineage dysplasia. Cells are often left in an immature blast form, unable to function appropriately, and vulnerable to destruction. Patients with myeloproliferative disorders frequently suffer from leukopenia and infections attributable to known quantitative and qualitative defects of neutrophils.8
CASE PRESENTATION
A male aged 80 years presented to the Central Texas Veterans Affairs Hospital (CTVAH) with shortness of breath, weight loss, and fever. On admission, his medical history was notable for atrial fibrillation, myelodysplastic syndrome, hypertension, hyperlipidemia, stable ascending aortic aneurysm, and Vitamin B12 deficiency. A chest CT showed a large left pleural effusion (Figure 1). Additionally, the radiology report noted a nonspecific 4- to 5-cm lobulated subdiaphragmatic mass within the anterior dome of the spleen with surrounding soft tissue swelling and splenomegaly (Figure 2).
A, coronal view; B, sagittal view. Opacification of the left pleural cavity was nearly total and pockets of air in collapsed left lung can be seen.
A, coronal view; B, sagittal view. Opacification of the left pleural cavity was nearly total and pockets of air in collapsed left lung can be seen.
Initial thoracentesis was performed with 1500 mL of straw-colored fluid negative for bacteria, fungi, malignancy, and acid-fast organisms (Tables 2 and 3). The pleural effusion persisted, requiring a second thoracentesis 2 days later that was positive for Escherichia coli (E coli). Given the exudative nature and positive culture, a chest tube was placed, and the pleural effusion was therefore felt to be an empyema, arousing suspicion that the splenic mass seen on CT was an abscess. The site was accessed by interventional radiology, purulent fluid aspirated, and a drain was placed. Cultures grew E coli sensitive to ceftriaxone. Despite receiving intravenous ceftriaxone 2 g daily, the pleural effusion became further complicated due to chest tube obstruction and persistent drainage.
The patient was discharged to Baylor Scott & White Medical Center in Temple, Texas where he underwent decortication with cardiothoracic surgery with several pleural adhesions noted. Following surgery the patient was readmitted to CTVAH and continued ceftriaxone therapy following the infectious disease specialist's recommendation. He was discharged with plans to return to CTVAH for continued care. The patient was readmitted and transitioned to oral levofloxacin 500 mg daily and received physical and occupational therapy. He showed dramatic improvement on this regimen, with a 3-week follow-up CT that indicated only a small left pleural effusion and a 28 mm × 11 mm × 10 mm lesion in the anterior superior spleen. The patient had not returned for further evaluation by thoracic surgery; however, he has continued to see CTVAH primary care without reported recurrence of symptoms.
DISCUSSION
Splenic abscesses are a rare condition typically characterized by hematogenous spread of bacteria from another source, most commonly the endocardium.2 Other differential diagnoses include bacteremia or spread from an intra-abdominal site.2 Staphylococcus aureus and E coli are the most common bacteria seen in splenic abscesses. 2 Treatment includes antibiotics, percutaneous drainage, and, as a last resort, splenectomy.2
Our patient was found to have grown E coli, but no source indicative of spread was identified. He had negative blood cultures, negative findings for intra-abdominal pathologies on CT scans, and a negative echocardiogram for endocarditis. A bronchoscopy showed no evidence of a source from the lungs, and specimens taken from the pleural adhesions were negative for malignancy and bacteria.
This patient had risk factors for the illness, namely his history of being immunocompromised secondary to myelodysplastic syndrome.7 Accordingly, the patient showed persistent leukopenia with neutropenia and lymphocytopenia, which would not be expected for most patients with such an extensive infection. 8 While being immunocompromised undoubtedly contributed to the severity of the patient’s presentation and slow recovery, it does not explain the etiology or origin of his infection. This patient differs from current literature in that his splenic abscess was truly idiopathic rather than resulting from an alternative source.
Complications of splenic abscesses include pleural effusions, as seen with this patient, as well as pneumonia, pneumothorax, hemorrhage, subphrenic abscess, and intraabdominal perforation, among others.2 We determined conclusively that the patient’s pleural effusion was secondary to the splenic abscess, and excluded other bacterial foci strongly suggests that the spleen was the origin of the illness.
CONCLUSIONS
This case suggests splenic abscesses should be considered when evaluating pleural effusion. It further demonstrates that the spleen may be the central source of infection in the absence of iatrogenic inoculation or bacteremia. We hope our findings may lead to earlier identification in similar scenarios and improved patient outcomes in a multidisciplinary approach.
References
Lee WS, Choi ST, Kim KK. Splenic abscess: a single institution study and review of the literature. Yonsei Med J. 2011;52(2):288-292. doi:10.3349/ymj.2011.52.2.288
Lotfollahzadeh S, Mathew G, Zemaitis MR. Splenic Abscess. In: StatPearls. StatPearls Publishing; June 3, 2023.
Jany B, Welte T. Pleural effusion in adults-etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2019;116(21):377- 386. doi:10.3238/arztebl.2019.0377
Light RW. Pleural effusions. Med Clin North Am. 2011;95(6):1055-1070. doi:10.1016/j.mcna.2011.08.005
Feller-Kopman D, Light R. Pleural Disease. N Engl J Med. 2018;378(18):1754. doi:10.1056/NEJMc1803858
Ferreiro L, Casal A, Toubes ME, et al. Pleural effusion due to nonmalignant gastrointestinal disease. ERJ Open Res. 2023;9(3):00290-2022. doi:10.1183/23120541.00290-2022
Madison Demmera; Mitchell Clarka; Tayler Acton DOb,c; Nikhil Seth MDa,d
Author affiliations: aTexas A&M School of Medicine, Bryan bCentral Texas Veterans Affairs Hospital, Temple cBaylor College of Medicine, Houston, Texas dBaylor Scott and White Health, Temple, Texas
Author disclosures: The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Correspondence: Madison Demmer (mpdemmer@tamu.edu)
Fed Pract. 2024;41(9)e509. Published online September 23. doi:10.12788/fp.0509
Madison Demmera; Mitchell Clarka; Tayler Acton DOb,c; Nikhil Seth MDa,d
Author affiliations: aTexas A&M School of Medicine, Bryan bCentral Texas Veterans Affairs Hospital, Temple cBaylor College of Medicine, Houston, Texas dBaylor Scott and White Health, Temple, Texas
Author disclosures: The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Correspondence: Madison Demmer (mpdemmer@tamu.edu)
Fed Pract. 2024;41(9)e509. Published online September 23. doi:10.12788/fp.0509
Author and Disclosure Information
Madison Demmera; Mitchell Clarka; Tayler Acton DOb,c; Nikhil Seth MDa,d
Author affiliations: aTexas A&M School of Medicine, Bryan bCentral Texas Veterans Affairs Hospital, Temple cBaylor College of Medicine, Houston, Texas dBaylor Scott and White Health, Temple, Texas
Author disclosures: The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Correspondence: Madison Demmer (mpdemmer@tamu.edu)
Fed Pract. 2024;41(9)e509. Published online September 23. doi:10.12788/fp.0509
Splenic abscesses are a rare occurrence that represent a marginal proportion of intra-abdominal infections. One study found splenic abscesses in only 0.14% to 0.70% of autopsies and none of the 540 abdominal abscesses they examined originated in the spleen.1 Patients with splenic abscesses tend to present with nonspecific symptoms such as fevers, chills, and abdominal pain.2 Imaging modalities such as abdominal ultrasound and computed tomography (CT) are vital to the workup and diagnosis identification.2 Splenic abscesses are generally associated with another underlying process, as seen in patients who are affected by endocarditis, trauma, metastatic infection, splenic infarction, or neoplasia.2
Pleural effusions, or the buildup of fluid within the pleural space, is a common condition typically secondary to another disease.3 Clinical identification of the primary condition may be challenging.3 In the absence of a clear etiology, such as obvious signs of congestive heart failure, further differentiation relies upon pleural fluid analysis, beginning with the distinction between exudate (inflammatory) and transudate (noninflammatory). 3,4 This distinction can be made using Light’s criteria, which relies on protein and lactate dehydrogenase (LDH) ratios between the pleural fluid and serum (Table 1).5 Though rare, half of splenic abscesses are associated with pleural effusion.6 As an inflammatory condition, splenic abscesses have been classically described as a cause of exudative pleural effusions.5,6
A myelodysplastic syndrome is a group of diseases that arise from malignant hematopoietic stem cells, leading to the proliferation of the malignant cells and faulty production of other bone marrow products.7 These disorders can range from single to multilineage dysplasia. Cells are often left in an immature blast form, unable to function appropriately, and vulnerable to destruction. Patients with myeloproliferative disorders frequently suffer from leukopenia and infections attributable to known quantitative and qualitative defects of neutrophils.8
CASE PRESENTATION
A male aged 80 years presented to the Central Texas Veterans Affairs Hospital (CTVAH) with shortness of breath, weight loss, and fever. On admission, his medical history was notable for atrial fibrillation, myelodysplastic syndrome, hypertension, hyperlipidemia, stable ascending aortic aneurysm, and Vitamin B12 deficiency. A chest CT showed a large left pleural effusion (Figure 1). Additionally, the radiology report noted a nonspecific 4- to 5-cm lobulated subdiaphragmatic mass within the anterior dome of the spleen with surrounding soft tissue swelling and splenomegaly (Figure 2).
A, coronal view; B, sagittal view. Opacification of the left pleural cavity was nearly total and pockets of air in collapsed left lung can be seen.
A, coronal view; B, sagittal view. Opacification of the left pleural cavity was nearly total and pockets of air in collapsed left lung can be seen.
Initial thoracentesis was performed with 1500 mL of straw-colored fluid negative for bacteria, fungi, malignancy, and acid-fast organisms (Tables 2 and 3). The pleural effusion persisted, requiring a second thoracentesis 2 days later that was positive for Escherichia coli (E coli). Given the exudative nature and positive culture, a chest tube was placed, and the pleural effusion was therefore felt to be an empyema, arousing suspicion that the splenic mass seen on CT was an abscess. The site was accessed by interventional radiology, purulent fluid aspirated, and a drain was placed. Cultures grew E coli sensitive to ceftriaxone. Despite receiving intravenous ceftriaxone 2 g daily, the pleural effusion became further complicated due to chest tube obstruction and persistent drainage.
The patient was discharged to Baylor Scott & White Medical Center in Temple, Texas where he underwent decortication with cardiothoracic surgery with several pleural adhesions noted. Following surgery the patient was readmitted to CTVAH and continued ceftriaxone therapy following the infectious disease specialist's recommendation. He was discharged with plans to return to CTVAH for continued care. The patient was readmitted and transitioned to oral levofloxacin 500 mg daily and received physical and occupational therapy. He showed dramatic improvement on this regimen, with a 3-week follow-up CT that indicated only a small left pleural effusion and a 28 mm × 11 mm × 10 mm lesion in the anterior superior spleen. The patient had not returned for further evaluation by thoracic surgery; however, he has continued to see CTVAH primary care without reported recurrence of symptoms.
DISCUSSION
Splenic abscesses are a rare condition typically characterized by hematogenous spread of bacteria from another source, most commonly the endocardium.2 Other differential diagnoses include bacteremia or spread from an intra-abdominal site.2 Staphylococcus aureus and E coli are the most common bacteria seen in splenic abscesses. 2 Treatment includes antibiotics, percutaneous drainage, and, as a last resort, splenectomy.2
Our patient was found to have grown E coli, but no source indicative of spread was identified. He had negative blood cultures, negative findings for intra-abdominal pathologies on CT scans, and a negative echocardiogram for endocarditis. A bronchoscopy showed no evidence of a source from the lungs, and specimens taken from the pleural adhesions were negative for malignancy and bacteria.
This patient had risk factors for the illness, namely his history of being immunocompromised secondary to myelodysplastic syndrome.7 Accordingly, the patient showed persistent leukopenia with neutropenia and lymphocytopenia, which would not be expected for most patients with such an extensive infection. 8 While being immunocompromised undoubtedly contributed to the severity of the patient’s presentation and slow recovery, it does not explain the etiology or origin of his infection. This patient differs from current literature in that his splenic abscess was truly idiopathic rather than resulting from an alternative source.
Complications of splenic abscesses include pleural effusions, as seen with this patient, as well as pneumonia, pneumothorax, hemorrhage, subphrenic abscess, and intraabdominal perforation, among others.2 We determined conclusively that the patient’s pleural effusion was secondary to the splenic abscess, and excluded other bacterial foci strongly suggests that the spleen was the origin of the illness.
CONCLUSIONS
This case suggests splenic abscesses should be considered when evaluating pleural effusion. It further demonstrates that the spleen may be the central source of infection in the absence of iatrogenic inoculation or bacteremia. We hope our findings may lead to earlier identification in similar scenarios and improved patient outcomes in a multidisciplinary approach.
Splenic abscesses are a rare occurrence that represent a marginal proportion of intra-abdominal infections. One study found splenic abscesses in only 0.14% to 0.70% of autopsies and none of the 540 abdominal abscesses they examined originated in the spleen.1 Patients with splenic abscesses tend to present with nonspecific symptoms such as fevers, chills, and abdominal pain.2 Imaging modalities such as abdominal ultrasound and computed tomography (CT) are vital to the workup and diagnosis identification.2 Splenic abscesses are generally associated with another underlying process, as seen in patients who are affected by endocarditis, trauma, metastatic infection, splenic infarction, or neoplasia.2
Pleural effusions, or the buildup of fluid within the pleural space, is a common condition typically secondary to another disease.3 Clinical identification of the primary condition may be challenging.3 In the absence of a clear etiology, such as obvious signs of congestive heart failure, further differentiation relies upon pleural fluid analysis, beginning with the distinction between exudate (inflammatory) and transudate (noninflammatory). 3,4 This distinction can be made using Light’s criteria, which relies on protein and lactate dehydrogenase (LDH) ratios between the pleural fluid and serum (Table 1).5 Though rare, half of splenic abscesses are associated with pleural effusion.6 As an inflammatory condition, splenic abscesses have been classically described as a cause of exudative pleural effusions.5,6
A myelodysplastic syndrome is a group of diseases that arise from malignant hematopoietic stem cells, leading to the proliferation of the malignant cells and faulty production of other bone marrow products.7 These disorders can range from single to multilineage dysplasia. Cells are often left in an immature blast form, unable to function appropriately, and vulnerable to destruction. Patients with myeloproliferative disorders frequently suffer from leukopenia and infections attributable to known quantitative and qualitative defects of neutrophils.8
CASE PRESENTATION
A male aged 80 years presented to the Central Texas Veterans Affairs Hospital (CTVAH) with shortness of breath, weight loss, and fever. On admission, his medical history was notable for atrial fibrillation, myelodysplastic syndrome, hypertension, hyperlipidemia, stable ascending aortic aneurysm, and Vitamin B12 deficiency. A chest CT showed a large left pleural effusion (Figure 1). Additionally, the radiology report noted a nonspecific 4- to 5-cm lobulated subdiaphragmatic mass within the anterior dome of the spleen with surrounding soft tissue swelling and splenomegaly (Figure 2).
A, coronal view; B, sagittal view. Opacification of the left pleural cavity was nearly total and pockets of air in collapsed left lung can be seen.
A, coronal view; B, sagittal view. Opacification of the left pleural cavity was nearly total and pockets of air in collapsed left lung can be seen.
Initial thoracentesis was performed with 1500 mL of straw-colored fluid negative for bacteria, fungi, malignancy, and acid-fast organisms (Tables 2 and 3). The pleural effusion persisted, requiring a second thoracentesis 2 days later that was positive for Escherichia coli (E coli). Given the exudative nature and positive culture, a chest tube was placed, and the pleural effusion was therefore felt to be an empyema, arousing suspicion that the splenic mass seen on CT was an abscess. The site was accessed by interventional radiology, purulent fluid aspirated, and a drain was placed. Cultures grew E coli sensitive to ceftriaxone. Despite receiving intravenous ceftriaxone 2 g daily, the pleural effusion became further complicated due to chest tube obstruction and persistent drainage.
The patient was discharged to Baylor Scott & White Medical Center in Temple, Texas where he underwent decortication with cardiothoracic surgery with several pleural adhesions noted. Following surgery the patient was readmitted to CTVAH and continued ceftriaxone therapy following the infectious disease specialist's recommendation. He was discharged with plans to return to CTVAH for continued care. The patient was readmitted and transitioned to oral levofloxacin 500 mg daily and received physical and occupational therapy. He showed dramatic improvement on this regimen, with a 3-week follow-up CT that indicated only a small left pleural effusion and a 28 mm × 11 mm × 10 mm lesion in the anterior superior spleen. The patient had not returned for further evaluation by thoracic surgery; however, he has continued to see CTVAH primary care without reported recurrence of symptoms.
DISCUSSION
Splenic abscesses are a rare condition typically characterized by hematogenous spread of bacteria from another source, most commonly the endocardium.2 Other differential diagnoses include bacteremia or spread from an intra-abdominal site.2 Staphylococcus aureus and E coli are the most common bacteria seen in splenic abscesses. 2 Treatment includes antibiotics, percutaneous drainage, and, as a last resort, splenectomy.2
Our patient was found to have grown E coli, but no source indicative of spread was identified. He had negative blood cultures, negative findings for intra-abdominal pathologies on CT scans, and a negative echocardiogram for endocarditis. A bronchoscopy showed no evidence of a source from the lungs, and specimens taken from the pleural adhesions were negative for malignancy and bacteria.
This patient had risk factors for the illness, namely his history of being immunocompromised secondary to myelodysplastic syndrome.7 Accordingly, the patient showed persistent leukopenia with neutropenia and lymphocytopenia, which would not be expected for most patients with such an extensive infection. 8 While being immunocompromised undoubtedly contributed to the severity of the patient’s presentation and slow recovery, it does not explain the etiology or origin of his infection. This patient differs from current literature in that his splenic abscess was truly idiopathic rather than resulting from an alternative source.
Complications of splenic abscesses include pleural effusions, as seen with this patient, as well as pneumonia, pneumothorax, hemorrhage, subphrenic abscess, and intraabdominal perforation, among others.2 We determined conclusively that the patient’s pleural effusion was secondary to the splenic abscess, and excluded other bacterial foci strongly suggests that the spleen was the origin of the illness.
CONCLUSIONS
This case suggests splenic abscesses should be considered when evaluating pleural effusion. It further demonstrates that the spleen may be the central source of infection in the absence of iatrogenic inoculation or bacteremia. We hope our findings may lead to earlier identification in similar scenarios and improved patient outcomes in a multidisciplinary approach.
References
Lee WS, Choi ST, Kim KK. Splenic abscess: a single institution study and review of the literature. Yonsei Med J. 2011;52(2):288-292. doi:10.3349/ymj.2011.52.2.288
Lotfollahzadeh S, Mathew G, Zemaitis MR. Splenic Abscess. In: StatPearls. StatPearls Publishing; June 3, 2023.
Jany B, Welte T. Pleural effusion in adults-etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2019;116(21):377- 386. doi:10.3238/arztebl.2019.0377
Light RW. Pleural effusions. Med Clin North Am. 2011;95(6):1055-1070. doi:10.1016/j.mcna.2011.08.005
Feller-Kopman D, Light R. Pleural Disease. N Engl J Med. 2018;378(18):1754. doi:10.1056/NEJMc1803858
Ferreiro L, Casal A, Toubes ME, et al. Pleural effusion due to nonmalignant gastrointestinal disease. ERJ Open Res. 2023;9(3):00290-2022. doi:10.1183/23120541.00290-2022
Toma A, Fenaux P, Dreyfus F, Cordonnier C. Infections in myelodysplastic syndromes. Haematologica. 2012;97(10):1459- 1470. doi:10.3324/haematol2012.063420
References
Lee WS, Choi ST, Kim KK. Splenic abscess: a single institution study and review of the literature. Yonsei Med J. 2011;52(2):288-292. doi:10.3349/ymj.2011.52.2.288
Lotfollahzadeh S, Mathew G, Zemaitis MR. Splenic Abscess. In: StatPearls. StatPearls Publishing; June 3, 2023.
Jany B, Welte T. Pleural effusion in adults-etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2019;116(21):377- 386. doi:10.3238/arztebl.2019.0377
Light RW. Pleural effusions. Med Clin North Am. 2011;95(6):1055-1070. doi:10.1016/j.mcna.2011.08.005
Feller-Kopman D, Light R. Pleural Disease. N Engl J Med. 2018;378(18):1754. doi:10.1056/NEJMc1803858
Ferreiro L, Casal A, Toubes ME, et al. Pleural effusion due to nonmalignant gastrointestinal disease. ERJ Open Res. 2023;9(3):00290-2022. doi:10.1183/23120541.00290-2022
Bevacizumab, an anti-vascular endothelial growth factor monoclonal antibody, is known to inhibit angiogenesis and prevent carcinogenesis. Recent evidence from the IMbrave050 trial indicates that combining bevacizumab with atezolizumab enhances recurrence-free survival (RFS) in high-risk HCC patients undergoing curative treatments. Bevacizumab is notorious for causing endothelial dysfunction that may provoke vasospasm, leading to central hypoperfusion, hypertension, and, albeit rarely, PRES. Similarly, immunotherapy, including atezolizumab, has been implicated in PRES, underscoring a potential risk when these therapies are administered concurrently.
Case Presentation
A 64-year-old woman with a history of hepatitis C and alcoholic cirrhosis was diagnosed with stage II (T2 N0 M0) HCC. Following partial hepatectomy, we proceeded with adjuvant systemic therapy with atezolizumab and bevacizumab (per the IMbrave050 trial). After her 2nd treatment, she developed altered mental status, seizures, and severe hypertension. Labs revealed acute kidney injury and elevated creatinine kinase levels suggesting rhabdomyolysis. Computed tomography head showed no acute findings, but magnetic resonance imaging of the brain identified increased flair attenuated inversion recovery (FLAIR) signal in the brain’s posterior regions, indicating PRES. Symptomatic management with anti-hypertensives and intravenous fluids led to the recovery of mental status to baseline. Further therapy with bevacizumab and atezolizumab was then held off.
Discussion
Therapeutic advances in HCC management through the IMbrave050 trial demonstrate the efficacy of bevacizumab and atezolizumab in reducing RFS, without highlighting the serious side effects like PRES. To our knowledge, this is the first case reported where PRES occurred with the simultaneous use of atezolizumab and bevacizumab. Since both drugs can individually cause PRES, there might be a heightened risk with the co-administration, signaling a critical need for vigilant monitoring and further research into this treatment modality’s long-term safety profile.
Bevacizumab, an anti-vascular endothelial growth factor monoclonal antibody, is known to inhibit angiogenesis and prevent carcinogenesis. Recent evidence from the IMbrave050 trial indicates that combining bevacizumab with atezolizumab enhances recurrence-free survival (RFS) in high-risk HCC patients undergoing curative treatments. Bevacizumab is notorious for causing endothelial dysfunction that may provoke vasospasm, leading to central hypoperfusion, hypertension, and, albeit rarely, PRES. Similarly, immunotherapy, including atezolizumab, has been implicated in PRES, underscoring a potential risk when these therapies are administered concurrently.
Case Presentation
A 64-year-old woman with a history of hepatitis C and alcoholic cirrhosis was diagnosed with stage II (T2 N0 M0) HCC. Following partial hepatectomy, we proceeded with adjuvant systemic therapy with atezolizumab and bevacizumab (per the IMbrave050 trial). After her 2nd treatment, she developed altered mental status, seizures, and severe hypertension. Labs revealed acute kidney injury and elevated creatinine kinase levels suggesting rhabdomyolysis. Computed tomography head showed no acute findings, but magnetic resonance imaging of the brain identified increased flair attenuated inversion recovery (FLAIR) signal in the brain’s posterior regions, indicating PRES. Symptomatic management with anti-hypertensives and intravenous fluids led to the recovery of mental status to baseline. Further therapy with bevacizumab and atezolizumab was then held off.
Discussion
Therapeutic advances in HCC management through the IMbrave050 trial demonstrate the efficacy of bevacizumab and atezolizumab in reducing RFS, without highlighting the serious side effects like PRES. To our knowledge, this is the first case reported where PRES occurred with the simultaneous use of atezolizumab and bevacizumab. Since both drugs can individually cause PRES, there might be a heightened risk with the co-administration, signaling a critical need for vigilant monitoring and further research into this treatment modality’s long-term safety profile.
Background
Bevacizumab, an anti-vascular endothelial growth factor monoclonal antibody, is known to inhibit angiogenesis and prevent carcinogenesis. Recent evidence from the IMbrave050 trial indicates that combining bevacizumab with atezolizumab enhances recurrence-free survival (RFS) in high-risk HCC patients undergoing curative treatments. Bevacizumab is notorious for causing endothelial dysfunction that may provoke vasospasm, leading to central hypoperfusion, hypertension, and, albeit rarely, PRES. Similarly, immunotherapy, including atezolizumab, has been implicated in PRES, underscoring a potential risk when these therapies are administered concurrently.
Case Presentation
A 64-year-old woman with a history of hepatitis C and alcoholic cirrhosis was diagnosed with stage II (T2 N0 M0) HCC. Following partial hepatectomy, we proceeded with adjuvant systemic therapy with atezolizumab and bevacizumab (per the IMbrave050 trial). After her 2nd treatment, she developed altered mental status, seizures, and severe hypertension. Labs revealed acute kidney injury and elevated creatinine kinase levels suggesting rhabdomyolysis. Computed tomography head showed no acute findings, but magnetic resonance imaging of the brain identified increased flair attenuated inversion recovery (FLAIR) signal in the brain’s posterior regions, indicating PRES. Symptomatic management with anti-hypertensives and intravenous fluids led to the recovery of mental status to baseline. Further therapy with bevacizumab and atezolizumab was then held off.
Discussion
Therapeutic advances in HCC management through the IMbrave050 trial demonstrate the efficacy of bevacizumab and atezolizumab in reducing RFS, without highlighting the serious side effects like PRES. To our knowledge, this is the first case reported where PRES occurred with the simultaneous use of atezolizumab and bevacizumab. Since both drugs can individually cause PRES, there might be a heightened risk with the co-administration, signaling a critical need for vigilant monitoring and further research into this treatment modality’s long-term safety profile.
Goblet cell adenocarcinoma (GCA), also known as goblet cell carcinoid, is a rare and distinct type of cancer originating from the appendix. It is characterized by cells that exhibit both mucinous and neuroendocrine differentiation, presenting a more aggressive nature compared to conventional carcinoids and a higher propensity for metastasis.
Case Presentation
A 60-year-old male presented with complaints of abdominal pain, nausea, vomiting, constipation, and weight loss worsening in the last month. He had a history of heavy alcohol intake, smoking, and family history of colon cancer in his grandfather. Initial workup with abdominal CT revealed findings suggestive of early bowel obstruction and possible malignancy. Subsequent EGD showed esophagitis, and colonoscopy identified a cecal mass. Biopsies confirmed malignant cells of enteric type with goblet cell features. Staging CT during hospitalization did not reveal distant metastasis initially. However, diagnostic laparoscopy later identified widespread peritoneal carcinomatosis, precluding surgical intervention. The case was discussed in tumor boards, leading to the initiation of palliative FOLFOX + Bevacizumab chemotherapy. After completing 7 cycles, restaging imaging showed stable disease. Subsequently, the patient experienced worsening obstructive symptoms with CT abdomen and pelvis demonstrating disease progression. Given his condition, decompressive gastrostomy was not feasible. The patient decided to transition to comfort measures only.
Discussion
Goblet cell adenocarcinoma is a rare appendiceal tumor with amphicrine differentiation, occurring at a rate of 0.01–0.05 per 100,000 individuals annually and comprising approximately 15% of all appendiceal neoplasms. These tumors often disseminate within the peritoneum, contributing to their aggressive behavior and challenging management.
Conclusions
Metastatic goblet cell adenocarcinoma presents significant treatment challenges and is associated with a poor prognosis. Tailored treatment strategies, vigilant monitoring, and ongoing research efforts are essential for optimizing patient outcomes and enhancing quality of life in this aggressive cancer
Goblet cell adenocarcinoma (GCA), also known as goblet cell carcinoid, is a rare and distinct type of cancer originating from the appendix. It is characterized by cells that exhibit both mucinous and neuroendocrine differentiation, presenting a more aggressive nature compared to conventional carcinoids and a higher propensity for metastasis.
Case Presentation
A 60-year-old male presented with complaints of abdominal pain, nausea, vomiting, constipation, and weight loss worsening in the last month. He had a history of heavy alcohol intake, smoking, and family history of colon cancer in his grandfather. Initial workup with abdominal CT revealed findings suggestive of early bowel obstruction and possible malignancy. Subsequent EGD showed esophagitis, and colonoscopy identified a cecal mass. Biopsies confirmed malignant cells of enteric type with goblet cell features. Staging CT during hospitalization did not reveal distant metastasis initially. However, diagnostic laparoscopy later identified widespread peritoneal carcinomatosis, precluding surgical intervention. The case was discussed in tumor boards, leading to the initiation of palliative FOLFOX + Bevacizumab chemotherapy. After completing 7 cycles, restaging imaging showed stable disease. Subsequently, the patient experienced worsening obstructive symptoms with CT abdomen and pelvis demonstrating disease progression. Given his condition, decompressive gastrostomy was not feasible. The patient decided to transition to comfort measures only.
Discussion
Goblet cell adenocarcinoma is a rare appendiceal tumor with amphicrine differentiation, occurring at a rate of 0.01–0.05 per 100,000 individuals annually and comprising approximately 15% of all appendiceal neoplasms. These tumors often disseminate within the peritoneum, contributing to their aggressive behavior and challenging management.
Conclusions
Metastatic goblet cell adenocarcinoma presents significant treatment challenges and is associated with a poor prognosis. Tailored treatment strategies, vigilant monitoring, and ongoing research efforts are essential for optimizing patient outcomes and enhancing quality of life in this aggressive cancer
Background
Goblet cell adenocarcinoma (GCA), also known as goblet cell carcinoid, is a rare and distinct type of cancer originating from the appendix. It is characterized by cells that exhibit both mucinous and neuroendocrine differentiation, presenting a more aggressive nature compared to conventional carcinoids and a higher propensity for metastasis.
Case Presentation
A 60-year-old male presented with complaints of abdominal pain, nausea, vomiting, constipation, and weight loss worsening in the last month. He had a history of heavy alcohol intake, smoking, and family history of colon cancer in his grandfather. Initial workup with abdominal CT revealed findings suggestive of early bowel obstruction and possible malignancy. Subsequent EGD showed esophagitis, and colonoscopy identified a cecal mass. Biopsies confirmed malignant cells of enteric type with goblet cell features. Staging CT during hospitalization did not reveal distant metastasis initially. However, diagnostic laparoscopy later identified widespread peritoneal carcinomatosis, precluding surgical intervention. The case was discussed in tumor boards, leading to the initiation of palliative FOLFOX + Bevacizumab chemotherapy. After completing 7 cycles, restaging imaging showed stable disease. Subsequently, the patient experienced worsening obstructive symptoms with CT abdomen and pelvis demonstrating disease progression. Given his condition, decompressive gastrostomy was not feasible. The patient decided to transition to comfort measures only.
Discussion
Goblet cell adenocarcinoma is a rare appendiceal tumor with amphicrine differentiation, occurring at a rate of 0.01–0.05 per 100,000 individuals annually and comprising approximately 15% of all appendiceal neoplasms. These tumors often disseminate within the peritoneum, contributing to their aggressive behavior and challenging management.
Conclusions
Metastatic goblet cell adenocarcinoma presents significant treatment challenges and is associated with a poor prognosis. Tailored treatment strategies, vigilant monitoring, and ongoing research efforts are essential for optimizing patient outcomes and enhancing quality of life in this aggressive cancer
Cholangiocarcinoma (CCA) is a rare and aggressive cancer of the biliary system, accounting for 15% of primary liver cancers. Most CCAs arise spontaneously, with risk factors including primary biliary cirrhosis, liver fluke infection, and biliary malformations. A newly described variant, Inhibin-positive Cholangioblastic (solid-tubulocystic) intrahepatic cholangiocarcinoma (iCCA), mimics neuroendocrine tumors (NET). This report presents a case of this new variant.
Case Presentation
A 53-year-old female with a history of alcohol use disorder and no family history of liver cancer presented with watery diarrhea for a month. Blood tests, including tumor markers, were normal. An ultrasound revealed a large mass in the right hepatic lobe. CT and MRI scans suggested a hemangioma. Due to the mass’s size and spontaneous bleeding risk, she underwent surgical resection. The mass was initially thought to be a hemangioma but was later identified as poorly differentiated intrahepatic CCA with a solid and tubulocystic structure. Pathology showed strong staining for Cytokeratin (CK) 7, CK-19, and Inhibin, and weak staining for synaptophysin, confirming a diagnosis of cholangioblastic iCCA. Genetic testing revealed no actionable variations. She was started on capecitabine for 8 cycles. Follow-up imaging showed no disease recurrence or metastasis.
Discussion
CCA often presents at advanced stages with symptoms like weight loss and jaundice. Diagnosis involves clinical assessment, lab work, and imaging, particularly MRI. Cholangioblastic Intrahepatic CCA (iCCA) is a newly described variant of cholangiocarcinoma. There have been 16 reported cases of the disease. Initially, it was thought to be a NET as it expressed Chromogranin, insulinoma-associated protein-1, and Synaptophysin. Almost half of the reported cases were diagnosed as NET initially. One tool clinicians can use to differentiate them is inhibin. Inhibin has been documented in all of the reported cases of Cholangioblastic iCCA. A novel inhibin-positive cholangioblastic iCCA variant with a Nipped-B-like protein and nucleus accumbens associated-1 (NIPBL-NACC1) fusion transcript has been reported recently, further helping differentiate the two. There is no standard of therapy for this variant. It’s managed similarly to CCAs, relying on surgical resection as the primary treatment. Limited data shows varied responses to neoadjuvant and adjuvant therapy.
Cholangiocarcinoma (CCA) is a rare and aggressive cancer of the biliary system, accounting for 15% of primary liver cancers. Most CCAs arise spontaneously, with risk factors including primary biliary cirrhosis, liver fluke infection, and biliary malformations. A newly described variant, Inhibin-positive Cholangioblastic (solid-tubulocystic) intrahepatic cholangiocarcinoma (iCCA), mimics neuroendocrine tumors (NET). This report presents a case of this new variant.
Case Presentation
A 53-year-old female with a history of alcohol use disorder and no family history of liver cancer presented with watery diarrhea for a month. Blood tests, including tumor markers, were normal. An ultrasound revealed a large mass in the right hepatic lobe. CT and MRI scans suggested a hemangioma. Due to the mass’s size and spontaneous bleeding risk, she underwent surgical resection. The mass was initially thought to be a hemangioma but was later identified as poorly differentiated intrahepatic CCA with a solid and tubulocystic structure. Pathology showed strong staining for Cytokeratin (CK) 7, CK-19, and Inhibin, and weak staining for synaptophysin, confirming a diagnosis of cholangioblastic iCCA. Genetic testing revealed no actionable variations. She was started on capecitabine for 8 cycles. Follow-up imaging showed no disease recurrence or metastasis.
Discussion
CCA often presents at advanced stages with symptoms like weight loss and jaundice. Diagnosis involves clinical assessment, lab work, and imaging, particularly MRI. Cholangioblastic Intrahepatic CCA (iCCA) is a newly described variant of cholangiocarcinoma. There have been 16 reported cases of the disease. Initially, it was thought to be a NET as it expressed Chromogranin, insulinoma-associated protein-1, and Synaptophysin. Almost half of the reported cases were diagnosed as NET initially. One tool clinicians can use to differentiate them is inhibin. Inhibin has been documented in all of the reported cases of Cholangioblastic iCCA. A novel inhibin-positive cholangioblastic iCCA variant with a Nipped-B-like protein and nucleus accumbens associated-1 (NIPBL-NACC1) fusion transcript has been reported recently, further helping differentiate the two. There is no standard of therapy for this variant. It’s managed similarly to CCAs, relying on surgical resection as the primary treatment. Limited data shows varied responses to neoadjuvant and adjuvant therapy.
Background
Cholangiocarcinoma (CCA) is a rare and aggressive cancer of the biliary system, accounting for 15% of primary liver cancers. Most CCAs arise spontaneously, with risk factors including primary biliary cirrhosis, liver fluke infection, and biliary malformations. A newly described variant, Inhibin-positive Cholangioblastic (solid-tubulocystic) intrahepatic cholangiocarcinoma (iCCA), mimics neuroendocrine tumors (NET). This report presents a case of this new variant.
Case Presentation
A 53-year-old female with a history of alcohol use disorder and no family history of liver cancer presented with watery diarrhea for a month. Blood tests, including tumor markers, were normal. An ultrasound revealed a large mass in the right hepatic lobe. CT and MRI scans suggested a hemangioma. Due to the mass’s size and spontaneous bleeding risk, she underwent surgical resection. The mass was initially thought to be a hemangioma but was later identified as poorly differentiated intrahepatic CCA with a solid and tubulocystic structure. Pathology showed strong staining for Cytokeratin (CK) 7, CK-19, and Inhibin, and weak staining for synaptophysin, confirming a diagnosis of cholangioblastic iCCA. Genetic testing revealed no actionable variations. She was started on capecitabine for 8 cycles. Follow-up imaging showed no disease recurrence or metastasis.
Discussion
CCA often presents at advanced stages with symptoms like weight loss and jaundice. Diagnosis involves clinical assessment, lab work, and imaging, particularly MRI. Cholangioblastic Intrahepatic CCA (iCCA) is a newly described variant of cholangiocarcinoma. There have been 16 reported cases of the disease. Initially, it was thought to be a NET as it expressed Chromogranin, insulinoma-associated protein-1, and Synaptophysin. Almost half of the reported cases were diagnosed as NET initially. One tool clinicians can use to differentiate them is inhibin. Inhibin has been documented in all of the reported cases of Cholangioblastic iCCA. A novel inhibin-positive cholangioblastic iCCA variant with a Nipped-B-like protein and nucleus accumbens associated-1 (NIPBL-NACC1) fusion transcript has been reported recently, further helping differentiate the two. There is no standard of therapy for this variant. It’s managed similarly to CCAs, relying on surgical resection as the primary treatment. Limited data shows varied responses to neoadjuvant and adjuvant therapy.
Ampulla of Vater is an extremely rare site for neuroendocrine tumors (NET), accounting for less than 0.3% of gastrointestinal (GI) and 2% of ampullary malignancies. This case report highlights the circuitous diagnosis of this rare tumor in a patient with a history of primary biliary cholangitis presenting with epigastric pain and severe pruritis.
Case Presentation
A 58-year-old female with history of sarcoidosis and primary biliary cholangitis status post sphincterotomy eight months prior, presented with worsening epigastric pain, fatigue, and weight loss over 6 months. Physical exam showed right upper quadrant tenderness. Labs revealed elevated alanine and aspartate aminotransferases at 415 and 195 units/L, with bilirubin of 0.3 mg/dl. Computerized tomography (CT) revealed a 2.3x3.2x4.0 cm peripancreatic hypodensity associated with phlegmon, pancreatic ductal dilation and pneumobilia. Magnetic resonance imaging (MRI) demonstrated a pancreatic head mass. Positron emission tomogram (PET) was negative for distant metastases. After discussion of management options, patient opted for Whipple procedure. The surgical pathology was consistent with invasive ampullary ductal carcinoma of the small intestine, pancreaticobiliary type. However, staining for synaptophysin and chromogranin were positive, with Ki-67 < 55%. Tumor board review confirmed neuroendocrine tumor of the ampulla of Vater. NCCN guidelines recommended active surveillance due to locoregional disease without positive margins or lymph nodes, advising routine follow-up and imaging.
Discussion
Neuroendocrine tumors (NET) at the Ampulla of Vater are exceedingly rare. Often manifesting as obstructive jaundice, they pose diagnostic hurdles, especially in patients with anatomical variations like scarring from primary biliary cholangitis. In a case series of 20 ampullary tumors, only one was neuroendocrine, highlighting their rarity. Accurate diagnosis, achieved through surgical biopsy and immunohistochemical testing, is crucial for appropriate management. Following NCCN guidelines for gastrointestinal NETs, our patient avoided unnecessary systemic treatment meant for adenocarcinoma, preserving her quality of life. Reporting such cases is essential for advancing understanding and refining patient care.
Conclusions
This case had evolving diagnoses, altering both the prognosis and treatment standards. Comorbid primary biliary cholangitis and high-grade tumor complexity posed diagnostic challenges, which was finally confirmed by surgical biopsy. Reporting such cases is vital in aiding tumor management and patient outcomes.
Ampulla of Vater is an extremely rare site for neuroendocrine tumors (NET), accounting for less than 0.3% of gastrointestinal (GI) and 2% of ampullary malignancies. This case report highlights the circuitous diagnosis of this rare tumor in a patient with a history of primary biliary cholangitis presenting with epigastric pain and severe pruritis.
Case Presentation
A 58-year-old female with history of sarcoidosis and primary biliary cholangitis status post sphincterotomy eight months prior, presented with worsening epigastric pain, fatigue, and weight loss over 6 months. Physical exam showed right upper quadrant tenderness. Labs revealed elevated alanine and aspartate aminotransferases at 415 and 195 units/L, with bilirubin of 0.3 mg/dl. Computerized tomography (CT) revealed a 2.3x3.2x4.0 cm peripancreatic hypodensity associated with phlegmon, pancreatic ductal dilation and pneumobilia. Magnetic resonance imaging (MRI) demonstrated a pancreatic head mass. Positron emission tomogram (PET) was negative for distant metastases. After discussion of management options, patient opted for Whipple procedure. The surgical pathology was consistent with invasive ampullary ductal carcinoma of the small intestine, pancreaticobiliary type. However, staining for synaptophysin and chromogranin were positive, with Ki-67 < 55%. Tumor board review confirmed neuroendocrine tumor of the ampulla of Vater. NCCN guidelines recommended active surveillance due to locoregional disease without positive margins or lymph nodes, advising routine follow-up and imaging.
Discussion
Neuroendocrine tumors (NET) at the Ampulla of Vater are exceedingly rare. Often manifesting as obstructive jaundice, they pose diagnostic hurdles, especially in patients with anatomical variations like scarring from primary biliary cholangitis. In a case series of 20 ampullary tumors, only one was neuroendocrine, highlighting their rarity. Accurate diagnosis, achieved through surgical biopsy and immunohistochemical testing, is crucial for appropriate management. Following NCCN guidelines for gastrointestinal NETs, our patient avoided unnecessary systemic treatment meant for adenocarcinoma, preserving her quality of life. Reporting such cases is essential for advancing understanding and refining patient care.
Conclusions
This case had evolving diagnoses, altering both the prognosis and treatment standards. Comorbid primary biliary cholangitis and high-grade tumor complexity posed diagnostic challenges, which was finally confirmed by surgical biopsy. Reporting such cases is vital in aiding tumor management and patient outcomes.
Background
Ampulla of Vater is an extremely rare site for neuroendocrine tumors (NET), accounting for less than 0.3% of gastrointestinal (GI) and 2% of ampullary malignancies. This case report highlights the circuitous diagnosis of this rare tumor in a patient with a history of primary biliary cholangitis presenting with epigastric pain and severe pruritis.
Case Presentation
A 58-year-old female with history of sarcoidosis and primary biliary cholangitis status post sphincterotomy eight months prior, presented with worsening epigastric pain, fatigue, and weight loss over 6 months. Physical exam showed right upper quadrant tenderness. Labs revealed elevated alanine and aspartate aminotransferases at 415 and 195 units/L, with bilirubin of 0.3 mg/dl. Computerized tomography (CT) revealed a 2.3x3.2x4.0 cm peripancreatic hypodensity associated with phlegmon, pancreatic ductal dilation and pneumobilia. Magnetic resonance imaging (MRI) demonstrated a pancreatic head mass. Positron emission tomogram (PET) was negative for distant metastases. After discussion of management options, patient opted for Whipple procedure. The surgical pathology was consistent with invasive ampullary ductal carcinoma of the small intestine, pancreaticobiliary type. However, staining for synaptophysin and chromogranin were positive, with Ki-67 < 55%. Tumor board review confirmed neuroendocrine tumor of the ampulla of Vater. NCCN guidelines recommended active surveillance due to locoregional disease without positive margins or lymph nodes, advising routine follow-up and imaging.
Discussion
Neuroendocrine tumors (NET) at the Ampulla of Vater are exceedingly rare. Often manifesting as obstructive jaundice, they pose diagnostic hurdles, especially in patients with anatomical variations like scarring from primary biliary cholangitis. In a case series of 20 ampullary tumors, only one was neuroendocrine, highlighting their rarity. Accurate diagnosis, achieved through surgical biopsy and immunohistochemical testing, is crucial for appropriate management. Following NCCN guidelines for gastrointestinal NETs, our patient avoided unnecessary systemic treatment meant for adenocarcinoma, preserving her quality of life. Reporting such cases is essential for advancing understanding and refining patient care.
Conclusions
This case had evolving diagnoses, altering both the prognosis and treatment standards. Comorbid primary biliary cholangitis and high-grade tumor complexity posed diagnostic challenges, which was finally confirmed by surgical biopsy. Reporting such cases is vital in aiding tumor management and patient outcomes.
CML is usually classified in chronic phase (CP), accelerated phase (AP) and/or Blast phase (BP). Studies have described another provisional entity as Preleukemic phase of CML which precedes CP and is without leukocytosis and blood features of CP phase of CML. Here we will present a case of metastatic prostate cancer, where next-generation sequencing showed BCR-ABL1 but no overt leukocytosis and then later developed clinical CML after 11 months.
Case Presentation
Our patient was 87-yr-old male with history of metastatic prostate cancer, who presented with elevated PSA levels and new bony metastasis. He underwent next-generation-sequencing (foundation one liquid cdx) in April 2022. It did not show reportable alterations related to prostate cancer but BCR-ABL1 (p210) fusion was detected. It also showed ASXL1-S846fs5 and TET2-Q1548 that are also markers of clonal hematopoiesis. In March 2023 (11 months after the finding of BCR-ABL1), he developed asymptomatic leukocytosis, Workup showed BCR-ABL1(210) of 44% in peripheral blood and bone marrow showed 9% blasts. He was started on Imatinib after shared decision-making and considering the toxicity profile and comorbidities. He followed up regularly with improvement in leukocytosis.
Discussion
The diagnosis of CML is first suspected by typical findings in blood and/or bone marrow and then confirmed by presence of Philadelphia chromosome. Along with chronic and accelerated phases, there is another term described in few cases called “preleukemic or smoldering or aleukemic phase.” This is not a wellestablished term but mostly defined as normal leukocyte count with presence of BCR/ABL1 fusion gene/ ph chromosome. Preleukemic phase of CML is mostly underdiagnosed or misdiagnosed. Our case is unique in that BCR/ABL1 fusion was detected incidentally on next-generation sequencing and patient progressed to chronic phase of CML 11 months later. Upon literature review, few case reports and case series documenting aleukemic/preleukemic phase of CML but timing from the appearance of BCR/ABL1 mutation to actual development to leukocytosis is not well documented. Especially in the era of NGS testing, patients with incidental BCR-ABL1 should be evaluated further irrespective of normal WBC. Further studies need to be done to recognize this early and decrease the delay in treatment.
CML is usually classified in chronic phase (CP), accelerated phase (AP) and/or Blast phase (BP). Studies have described another provisional entity as Preleukemic phase of CML which precedes CP and is without leukocytosis and blood features of CP phase of CML. Here we will present a case of metastatic prostate cancer, where next-generation sequencing showed BCR-ABL1 but no overt leukocytosis and then later developed clinical CML after 11 months.
Case Presentation
Our patient was 87-yr-old male with history of metastatic prostate cancer, who presented with elevated PSA levels and new bony metastasis. He underwent next-generation-sequencing (foundation one liquid cdx) in April 2022. It did not show reportable alterations related to prostate cancer but BCR-ABL1 (p210) fusion was detected. It also showed ASXL1-S846fs5 and TET2-Q1548 that are also markers of clonal hematopoiesis. In March 2023 (11 months after the finding of BCR-ABL1), he developed asymptomatic leukocytosis, Workup showed BCR-ABL1(210) of 44% in peripheral blood and bone marrow showed 9% blasts. He was started on Imatinib after shared decision-making and considering the toxicity profile and comorbidities. He followed up regularly with improvement in leukocytosis.
Discussion
The diagnosis of CML is first suspected by typical findings in blood and/or bone marrow and then confirmed by presence of Philadelphia chromosome. Along with chronic and accelerated phases, there is another term described in few cases called “preleukemic or smoldering or aleukemic phase.” This is not a wellestablished term but mostly defined as normal leukocyte count with presence of BCR/ABL1 fusion gene/ ph chromosome. Preleukemic phase of CML is mostly underdiagnosed or misdiagnosed. Our case is unique in that BCR/ABL1 fusion was detected incidentally on next-generation sequencing and patient progressed to chronic phase of CML 11 months later. Upon literature review, few case reports and case series documenting aleukemic/preleukemic phase of CML but timing from the appearance of BCR/ABL1 mutation to actual development to leukocytosis is not well documented. Especially in the era of NGS testing, patients with incidental BCR-ABL1 should be evaluated further irrespective of normal WBC. Further studies need to be done to recognize this early and decrease the delay in treatment.
Background
CML is usually classified in chronic phase (CP), accelerated phase (AP) and/or Blast phase (BP). Studies have described another provisional entity as Preleukemic phase of CML which precedes CP and is without leukocytosis and blood features of CP phase of CML. Here we will present a case of metastatic prostate cancer, where next-generation sequencing showed BCR-ABL1 but no overt leukocytosis and then later developed clinical CML after 11 months.
Case Presentation
Our patient was 87-yr-old male with history of metastatic prostate cancer, who presented with elevated PSA levels and new bony metastasis. He underwent next-generation-sequencing (foundation one liquid cdx) in April 2022. It did not show reportable alterations related to prostate cancer but BCR-ABL1 (p210) fusion was detected. It also showed ASXL1-S846fs5 and TET2-Q1548 that are also markers of clonal hematopoiesis. In March 2023 (11 months after the finding of BCR-ABL1), he developed asymptomatic leukocytosis, Workup showed BCR-ABL1(210) of 44% in peripheral blood and bone marrow showed 9% blasts. He was started on Imatinib after shared decision-making and considering the toxicity profile and comorbidities. He followed up regularly with improvement in leukocytosis.
Discussion
The diagnosis of CML is first suspected by typical findings in blood and/or bone marrow and then confirmed by presence of Philadelphia chromosome. Along with chronic and accelerated phases, there is another term described in few cases called “preleukemic or smoldering or aleukemic phase.” This is not a wellestablished term but mostly defined as normal leukocyte count with presence of BCR/ABL1 fusion gene/ ph chromosome. Preleukemic phase of CML is mostly underdiagnosed or misdiagnosed. Our case is unique in that BCR/ABL1 fusion was detected incidentally on next-generation sequencing and patient progressed to chronic phase of CML 11 months later. Upon literature review, few case reports and case series documenting aleukemic/preleukemic phase of CML but timing from the appearance of BCR/ABL1 mutation to actual development to leukocytosis is not well documented. Especially in the era of NGS testing, patients with incidental BCR-ABL1 should be evaluated further irrespective of normal WBC. Further studies need to be done to recognize this early and decrease the delay in treatment.