User login
No Change in Duration of Mechanical Ventilation with Acetazolamide for COPD Patients with Metabolic Alkalosis
Clinical question: Does acetazolamide decrease the duration of mechanical ventilation for patients with chronic obstructive pulmonary disease and metabolic alkalosis?
Bottom line: Although acetazolamide effectively decreased the levels of serum bicarbonate and the number of days with metabolic alkalosis in critically ill patients with chronic obstructive pulmonary disease (COPD) on mechanical ventilation, it did not produce a statistically significant difference in the duration of mechanical ventilation. However, this lack of statistical significance may have been due to an underpowered study. (LOE = 1b-)
Reference: Faisy C, Meziani F, Planquette B, et al, for the DIABOLO Investigators. Effect of acetazolamide vs placebo on duration of invasive mechanical ventilation among patients with chronic obstructive pulmonary disease. JAMA 2016;315(5):480-488.
Study design: Randomized controlled trial (double-blinded)
Funding source: Industry + govt
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis:
Acetazolamide is used as a respiratory stimulant for patients with COPD and metabolic alkalosis because of its ability to reduce serum bicarbonate, which may lead to a rise in minute ventilation. However, its clinical benefit has not been demonstrated previously in controlled trials.
Using concealed allocation, these investigators randomized patients with COPD who required invasive mechanical ventilation to receive either acetazolamide 500 mg intravenously twice daily (1000 mg if loop diuretics were also prescribed) or matching placebo up to 28 days. Only those patients found to have pure or mixed metabolic alkalosis received the treatment. The intention-to-treat population consisted of 380 patients and baseline characteristics were similar in both groups. The use of acetazolamide led to decreased levels of serum bicarbonate and fewer days with metabolic alkalosis but did not improve respiratory parameters such as respiratory rate, tidal volume, or minute ventilation.
For the primary outcome of duration of mechanical ventilation, the magnitude of the difference between the 2 groups was large, suggesting a clinically important effect, but the difference did not reach statistical significance (between-group difference -16 hours with acetazolamide; 95% CI -36.5 to 4.0 hours). The lack of statistical significance may be due to an underpowered study because of fewer-than-expected patients who received the treatment (more than 20% of patients in each group did not receive the assigned treatment because of lack of metabolic alkalosis or temporary contraindications) and a shorter-than-anticipated duration of mechanical ventilation in the placebo group.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does acetazolamide decrease the duration of mechanical ventilation for patients with chronic obstructive pulmonary disease and metabolic alkalosis?
Bottom line: Although acetazolamide effectively decreased the levels of serum bicarbonate and the number of days with metabolic alkalosis in critically ill patients with chronic obstructive pulmonary disease (COPD) on mechanical ventilation, it did not produce a statistically significant difference in the duration of mechanical ventilation. However, this lack of statistical significance may have been due to an underpowered study. (LOE = 1b-)
Reference: Faisy C, Meziani F, Planquette B, et al, for the DIABOLO Investigators. Effect of acetazolamide vs placebo on duration of invasive mechanical ventilation among patients with chronic obstructive pulmonary disease. JAMA 2016;315(5):480-488.
Study design: Randomized controlled trial (double-blinded)
Funding source: Industry + govt
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis:
Acetazolamide is used as a respiratory stimulant for patients with COPD and metabolic alkalosis because of its ability to reduce serum bicarbonate, which may lead to a rise in minute ventilation. However, its clinical benefit has not been demonstrated previously in controlled trials.
Using concealed allocation, these investigators randomized patients with COPD who required invasive mechanical ventilation to receive either acetazolamide 500 mg intravenously twice daily (1000 mg if loop diuretics were also prescribed) or matching placebo up to 28 days. Only those patients found to have pure or mixed metabolic alkalosis received the treatment. The intention-to-treat population consisted of 380 patients and baseline characteristics were similar in both groups. The use of acetazolamide led to decreased levels of serum bicarbonate and fewer days with metabolic alkalosis but did not improve respiratory parameters such as respiratory rate, tidal volume, or minute ventilation.
For the primary outcome of duration of mechanical ventilation, the magnitude of the difference between the 2 groups was large, suggesting a clinically important effect, but the difference did not reach statistical significance (between-group difference -16 hours with acetazolamide; 95% CI -36.5 to 4.0 hours). The lack of statistical significance may be due to an underpowered study because of fewer-than-expected patients who received the treatment (more than 20% of patients in each group did not receive the assigned treatment because of lack of metabolic alkalosis or temporary contraindications) and a shorter-than-anticipated duration of mechanical ventilation in the placebo group.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does acetazolamide decrease the duration of mechanical ventilation for patients with chronic obstructive pulmonary disease and metabolic alkalosis?
Bottom line: Although acetazolamide effectively decreased the levels of serum bicarbonate and the number of days with metabolic alkalosis in critically ill patients with chronic obstructive pulmonary disease (COPD) on mechanical ventilation, it did not produce a statistically significant difference in the duration of mechanical ventilation. However, this lack of statistical significance may have been due to an underpowered study. (LOE = 1b-)
Reference: Faisy C, Meziani F, Planquette B, et al, for the DIABOLO Investigators. Effect of acetazolamide vs placebo on duration of invasive mechanical ventilation among patients with chronic obstructive pulmonary disease. JAMA 2016;315(5):480-488.
Study design: Randomized controlled trial (double-blinded)
Funding source: Industry + govt
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis:
Acetazolamide is used as a respiratory stimulant for patients with COPD and metabolic alkalosis because of its ability to reduce serum bicarbonate, which may lead to a rise in minute ventilation. However, its clinical benefit has not been demonstrated previously in controlled trials.
Using concealed allocation, these investigators randomized patients with COPD who required invasive mechanical ventilation to receive either acetazolamide 500 mg intravenously twice daily (1000 mg if loop diuretics were also prescribed) or matching placebo up to 28 days. Only those patients found to have pure or mixed metabolic alkalosis received the treatment. The intention-to-treat population consisted of 380 patients and baseline characteristics were similar in both groups. The use of acetazolamide led to decreased levels of serum bicarbonate and fewer days with metabolic alkalosis but did not improve respiratory parameters such as respiratory rate, tidal volume, or minute ventilation.
For the primary outcome of duration of mechanical ventilation, the magnitude of the difference between the 2 groups was large, suggesting a clinically important effect, but the difference did not reach statistical significance (between-group difference -16 hours with acetazolamide; 95% CI -36.5 to 4.0 hours). The lack of statistical significance may be due to an underpowered study because of fewer-than-expected patients who received the treatment (more than 20% of patients in each group did not receive the assigned treatment because of lack of metabolic alkalosis or temporary contraindications) and a shorter-than-anticipated duration of mechanical ventilation in the placebo group.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Tamsulosin Effective as Expulsion Therapy for Distal Ureteric Stones
Clinical question: Is tamsulosin effective in the management of distal ureteric stones?
Bottom line: Tamsulosin promotes stone passage of ureteric stones that are 5 mm to 10 mm. You would need to treat 5 patients with tamsulosin to cause the expulsion of one such stone. Stones smaller than 5 mm have a high rate of spontaneous passage without any intervention. (LOE = 1b-)
Reference: Furyk JS, Chu K, Banks C et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 2016;67(1):86-95.
Study design: Randomized controlled trial (double-blinded)
Funding source: Foundation
Allocation: Concealed
Setting: Outpatient (primary care)
Synopsis: These authors recruited adult patients who presented to the emergency department with symptoms and imaging consistent with distal ureteric stones. Patients with fever, hypotension, stones larger than 10 mm, or kidney disease were excluded. Using concealed allocation, the investigators randomized the patients to receive either tamsulosin 0.4 mg daily or matching placebo for 28 days or until stone passage. The 2 groups had similar baseline characteristics and analysis was by intention to treat.
The primary outcome was stone expulsion as confirmed by computed tomography (CT) and time to stone expulsion was defined by self-reported passage of stone or 48-hour pain-free period. Compliance to the study medications was poor in both groups, and almost one-fifth of the patients did not have follow-up imaging. Of the approximately 80% of patients in each group who underwent follow-up CT, there was no difference in the percentage of patients with passed stones (87% in the tamsulosin group vs 82% in the placebo group; P = .22). In the subset of patients with larger stones (5 mm -10 mm), the tamsulosin group had a significantly higher rate of stone passage than the placebo group (83% vs 61%; P = .03). There were no significant differences detected in time to stone passage, pain, analgesia requirements, need for urological intervention, or adverse events.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Is tamsulosin effective in the management of distal ureteric stones?
Bottom line: Tamsulosin promotes stone passage of ureteric stones that are 5 mm to 10 mm. You would need to treat 5 patients with tamsulosin to cause the expulsion of one such stone. Stones smaller than 5 mm have a high rate of spontaneous passage without any intervention. (LOE = 1b-)
Reference: Furyk JS, Chu K, Banks C et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 2016;67(1):86-95.
Study design: Randomized controlled trial (double-blinded)
Funding source: Foundation
Allocation: Concealed
Setting: Outpatient (primary care)
Synopsis: These authors recruited adult patients who presented to the emergency department with symptoms and imaging consistent with distal ureteric stones. Patients with fever, hypotension, stones larger than 10 mm, or kidney disease were excluded. Using concealed allocation, the investigators randomized the patients to receive either tamsulosin 0.4 mg daily or matching placebo for 28 days or until stone passage. The 2 groups had similar baseline characteristics and analysis was by intention to treat.
The primary outcome was stone expulsion as confirmed by computed tomography (CT) and time to stone expulsion was defined by self-reported passage of stone or 48-hour pain-free period. Compliance to the study medications was poor in both groups, and almost one-fifth of the patients did not have follow-up imaging. Of the approximately 80% of patients in each group who underwent follow-up CT, there was no difference in the percentage of patients with passed stones (87% in the tamsulosin group vs 82% in the placebo group; P = .22). In the subset of patients with larger stones (5 mm -10 mm), the tamsulosin group had a significantly higher rate of stone passage than the placebo group (83% vs 61%; P = .03). There were no significant differences detected in time to stone passage, pain, analgesia requirements, need for urological intervention, or adverse events.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Is tamsulosin effective in the management of distal ureteric stones?
Bottom line: Tamsulosin promotes stone passage of ureteric stones that are 5 mm to 10 mm. You would need to treat 5 patients with tamsulosin to cause the expulsion of one such stone. Stones smaller than 5 mm have a high rate of spontaneous passage without any intervention. (LOE = 1b-)
Reference: Furyk JS, Chu K, Banks C et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 2016;67(1):86-95.
Study design: Randomized controlled trial (double-blinded)
Funding source: Foundation
Allocation: Concealed
Setting: Outpatient (primary care)
Synopsis: These authors recruited adult patients who presented to the emergency department with symptoms and imaging consistent with distal ureteric stones. Patients with fever, hypotension, stones larger than 10 mm, or kidney disease were excluded. Using concealed allocation, the investigators randomized the patients to receive either tamsulosin 0.4 mg daily or matching placebo for 28 days or until stone passage. The 2 groups had similar baseline characteristics and analysis was by intention to treat.
The primary outcome was stone expulsion as confirmed by computed tomography (CT) and time to stone expulsion was defined by self-reported passage of stone or 48-hour pain-free period. Compliance to the study medications was poor in both groups, and almost one-fifth of the patients did not have follow-up imaging. Of the approximately 80% of patients in each group who underwent follow-up CT, there was no difference in the percentage of patients with passed stones (87% in the tamsulosin group vs 82% in the placebo group; P = .22). In the subset of patients with larger stones (5 mm -10 mm), the tamsulosin group had a significantly higher rate of stone passage than the placebo group (83% vs 61%; P = .03). There were no significant differences detected in time to stone passage, pain, analgesia requirements, need for urological intervention, or adverse events.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
SHM Offering Webinars on Reducing Readmissions, Optimizing Glycemic Control
This April, the Society of Hospital Medicine (SHM) will offer two free live webinars on how two of its signature mentored implementation programs are changing the way hospitals manage two key issues: readmissions and glycemic control.
Project BOOST is an evidence-based approach to reduce preventable admissions, decrease average length of stay, and improve patient satisfaction. It includes one year of individualized mentoring from a physician leader with expertise in clinical quality, on-site mentoring and training from leaders in the field, access to an online tool kit with clinical resources, and more. Find out how to get involved with Project BOOST and take the first steps toward reducing readmissions with our complimentary webinar in April.
Learn more at www.hospitalmedicine.org/BOOST.
Another signature program, SHM’s Glycemic Control Mentored Implementation Program, has supported the development and implementation of glycemic control in more than 100 hospitals nationwide. Added benefits include data collection and analysis tools, monthly coaching calls with mentors, SHM-facilitated calls and live webinars, and access to an online web-based glycemic control collaborative to share best practices.
Join more than 100 hospitals working with SHM to improve glycemic control at an upcoming free live webinar. More information is available at www.hospitalmedicine.org/gc.
A comprehensive suite of mentored implementation programs offered through SHM’s Center for Hospital Innovation and Improvement is designed to provide institutions with coaching by national physician experts to map current processes, identify root causes of deficiencies, and tailor interventions to the unique needs of the institution for sustainable results.
For more information, visit www.hospitalmedicine.org and click on Quality & Innovation.
This April, the Society of Hospital Medicine (SHM) will offer two free live webinars on how two of its signature mentored implementation programs are changing the way hospitals manage two key issues: readmissions and glycemic control.
Project BOOST is an evidence-based approach to reduce preventable admissions, decrease average length of stay, and improve patient satisfaction. It includes one year of individualized mentoring from a physician leader with expertise in clinical quality, on-site mentoring and training from leaders in the field, access to an online tool kit with clinical resources, and more. Find out how to get involved with Project BOOST and take the first steps toward reducing readmissions with our complimentary webinar in April.
Learn more at www.hospitalmedicine.org/BOOST.
Another signature program, SHM’s Glycemic Control Mentored Implementation Program, has supported the development and implementation of glycemic control in more than 100 hospitals nationwide. Added benefits include data collection and analysis tools, monthly coaching calls with mentors, SHM-facilitated calls and live webinars, and access to an online web-based glycemic control collaborative to share best practices.
Join more than 100 hospitals working with SHM to improve glycemic control at an upcoming free live webinar. More information is available at www.hospitalmedicine.org/gc.
A comprehensive suite of mentored implementation programs offered through SHM’s Center for Hospital Innovation and Improvement is designed to provide institutions with coaching by national physician experts to map current processes, identify root causes of deficiencies, and tailor interventions to the unique needs of the institution for sustainable results.
For more information, visit www.hospitalmedicine.org and click on Quality & Innovation.
This April, the Society of Hospital Medicine (SHM) will offer two free live webinars on how two of its signature mentored implementation programs are changing the way hospitals manage two key issues: readmissions and glycemic control.
Project BOOST is an evidence-based approach to reduce preventable admissions, decrease average length of stay, and improve patient satisfaction. It includes one year of individualized mentoring from a physician leader with expertise in clinical quality, on-site mentoring and training from leaders in the field, access to an online tool kit with clinical resources, and more. Find out how to get involved with Project BOOST and take the first steps toward reducing readmissions with our complimentary webinar in April.
Learn more at www.hospitalmedicine.org/BOOST.
Another signature program, SHM’s Glycemic Control Mentored Implementation Program, has supported the development and implementation of glycemic control in more than 100 hospitals nationwide. Added benefits include data collection and analysis tools, monthly coaching calls with mentors, SHM-facilitated calls and live webinars, and access to an online web-based glycemic control collaborative to share best practices.
Join more than 100 hospitals working with SHM to improve glycemic control at an upcoming free live webinar. More information is available at www.hospitalmedicine.org/gc.
A comprehensive suite of mentored implementation programs offered through SHM’s Center for Hospital Innovation and Improvement is designed to provide institutions with coaching by national physician experts to map current processes, identify root causes of deficiencies, and tailor interventions to the unique needs of the institution for sustainable results.
For more information, visit www.hospitalmedicine.org and click on Quality & Innovation.
Study Shows Non-diabetics can Benefit from Taking the Diabetes Drug Pioglitaztione
NEW YORK (Reuters Health) - The diabetes drug pioglitazone, given to non-diabetics with a recent history of stroke or transient ischemic attack (TIA), prevented subsequent strokes and reduced their odds of developing type 2 diabetes, a long-term multicenter study has concluded.
But the drug also increased the risk of fracture, weight gain, and edema.
After nearly five years of follow-up, the rate of stroke or heart attack was 11.8% with placebo and 9.0% with the drug (p=0.007). The target dose was 45 mg daily.
"That 25% relative reduction is a huge effect for a stroke trial," coauthor Dr. Wayne Clark, director of the Oregon Stroke Center at Oregon Health and Science University, told Reuters Health by phone. "That's on the same realm as aspirin and a big effect for stroke.
"We're always expecting negative results these days," because so many stroke drugs have failed in previous tests, he said. "This was a positive surprise."
Dr. Clark said he was particularly taken aback by the rate that diabetes developed in pioglitazone recipients. It manifested in 3.8% of drug recipients versus 7.7% of placebo
recipients (p<0.001).
"I didn't expect that at all," he said. "That has much wider implications and might take confirmatory studies."
The 3,876 volunteers studied at 179 sites worldwide were not diabetic but they had developed insulin resistance at the time of enrollment.
Drug therapy did not reduce mortality.The results of the study, known as IRIS, were presented February 17 at the American Heart Association and the American
Stroke Association's International Stroke Conference in Los Angeles, and online in the New England Journal of Medicine.
"The findings suggest that the administration of pioglitazone in 100 patients similar to those in our trial for about five years could prevent three patients from having a
stroke or myocardial infarction," the researchers wrote in the Journal. "However, during the same period, the treatment would be expected to result in bone fractures requiring surgery or hospitalization in two patients.
"It seems reasonable to consider individual treatment preference and risk of drug-related adverse events in addition to potential benefits when making patient-specific decisions regarding therapy," they concluded.
Serious fractures occurred in 5.1% of drug recipients versus 3.2% among placebo patients (p=0.003). A weight gain of more than 4.5 kg was seen in 52.2% of pioglitazone recipientscompared with 33.7% for placebo, and rates of edema were 35.6% with the drug versus 24.9% with placebo (both p<0.001).
The drug has been plagued by suspicions that it might increase the risk of heart failure and bladder cancer. In this study, 74 pioglitazone recipients developed heart failure versus 71 in the placebo group (p=0.80). A dozen drug recipients were diagnosed with bladder cancer compared with eight cases in the placebo group (p=0.37).
Dr. Clark said, "All of the stuff we're doing for risk-factor reduction -- blood pressure reduction, stop smoking and giving aspirin -- they're all on the same level of relative improvement, and all of those are widely used. Aspirin has a list of side effects that will fill up three pages."
At the start of the study, all of the volunteers were insulin resistant, at least 40 years old, and had experienced an ischemic stroke or TIA in the previous six months. Diabetics were excluded as were patients with heart failure, active liver disease, and an increased risk of bladder cancer.
By the end of the study, 60% of the pioglitazone patients were still taking their medicine compared with 67% of placebo recipients. The most common reason for discontinuing was edema or weight gain.
The National Institute of Neurological Disorders and Stroke funded this study. Eleven coauthors reported disclosures.
NEW YORK (Reuters Health) - The diabetes drug pioglitazone, given to non-diabetics with a recent history of stroke or transient ischemic attack (TIA), prevented subsequent strokes and reduced their odds of developing type 2 diabetes, a long-term multicenter study has concluded.
But the drug also increased the risk of fracture, weight gain, and edema.
After nearly five years of follow-up, the rate of stroke or heart attack was 11.8% with placebo and 9.0% with the drug (p=0.007). The target dose was 45 mg daily.
"That 25% relative reduction is a huge effect for a stroke trial," coauthor Dr. Wayne Clark, director of the Oregon Stroke Center at Oregon Health and Science University, told Reuters Health by phone. "That's on the same realm as aspirin and a big effect for stroke.
"We're always expecting negative results these days," because so many stroke drugs have failed in previous tests, he said. "This was a positive surprise."
Dr. Clark said he was particularly taken aback by the rate that diabetes developed in pioglitazone recipients. It manifested in 3.8% of drug recipients versus 7.7% of placebo
recipients (p<0.001).
"I didn't expect that at all," he said. "That has much wider implications and might take confirmatory studies."
The 3,876 volunteers studied at 179 sites worldwide were not diabetic but they had developed insulin resistance at the time of enrollment.
Drug therapy did not reduce mortality.The results of the study, known as IRIS, were presented February 17 at the American Heart Association and the American
Stroke Association's International Stroke Conference in Los Angeles, and online in the New England Journal of Medicine.
"The findings suggest that the administration of pioglitazone in 100 patients similar to those in our trial for about five years could prevent three patients from having a
stroke or myocardial infarction," the researchers wrote in the Journal. "However, during the same period, the treatment would be expected to result in bone fractures requiring surgery or hospitalization in two patients.
"It seems reasonable to consider individual treatment preference and risk of drug-related adverse events in addition to potential benefits when making patient-specific decisions regarding therapy," they concluded.
Serious fractures occurred in 5.1% of drug recipients versus 3.2% among placebo patients (p=0.003). A weight gain of more than 4.5 kg was seen in 52.2% of pioglitazone recipientscompared with 33.7% for placebo, and rates of edema were 35.6% with the drug versus 24.9% with placebo (both p<0.001).
The drug has been plagued by suspicions that it might increase the risk of heart failure and bladder cancer. In this study, 74 pioglitazone recipients developed heart failure versus 71 in the placebo group (p=0.80). A dozen drug recipients were diagnosed with bladder cancer compared with eight cases in the placebo group (p=0.37).
Dr. Clark said, "All of the stuff we're doing for risk-factor reduction -- blood pressure reduction, stop smoking and giving aspirin -- they're all on the same level of relative improvement, and all of those are widely used. Aspirin has a list of side effects that will fill up three pages."
At the start of the study, all of the volunteers were insulin resistant, at least 40 years old, and had experienced an ischemic stroke or TIA in the previous six months. Diabetics were excluded as were patients with heart failure, active liver disease, and an increased risk of bladder cancer.
By the end of the study, 60% of the pioglitazone patients were still taking their medicine compared with 67% of placebo recipients. The most common reason for discontinuing was edema or weight gain.
The National Institute of Neurological Disorders and Stroke funded this study. Eleven coauthors reported disclosures.
NEW YORK (Reuters Health) - The diabetes drug pioglitazone, given to non-diabetics with a recent history of stroke or transient ischemic attack (TIA), prevented subsequent strokes and reduced their odds of developing type 2 diabetes, a long-term multicenter study has concluded.
But the drug also increased the risk of fracture, weight gain, and edema.
After nearly five years of follow-up, the rate of stroke or heart attack was 11.8% with placebo and 9.0% with the drug (p=0.007). The target dose was 45 mg daily.
"That 25% relative reduction is a huge effect for a stroke trial," coauthor Dr. Wayne Clark, director of the Oregon Stroke Center at Oregon Health and Science University, told Reuters Health by phone. "That's on the same realm as aspirin and a big effect for stroke.
"We're always expecting negative results these days," because so many stroke drugs have failed in previous tests, he said. "This was a positive surprise."
Dr. Clark said he was particularly taken aback by the rate that diabetes developed in pioglitazone recipients. It manifested in 3.8% of drug recipients versus 7.7% of placebo
recipients (p<0.001).
"I didn't expect that at all," he said. "That has much wider implications and might take confirmatory studies."
The 3,876 volunteers studied at 179 sites worldwide were not diabetic but they had developed insulin resistance at the time of enrollment.
Drug therapy did not reduce mortality.The results of the study, known as IRIS, were presented February 17 at the American Heart Association and the American
Stroke Association's International Stroke Conference in Los Angeles, and online in the New England Journal of Medicine.
"The findings suggest that the administration of pioglitazone in 100 patients similar to those in our trial for about five years could prevent three patients from having a
stroke or myocardial infarction," the researchers wrote in the Journal. "However, during the same period, the treatment would be expected to result in bone fractures requiring surgery or hospitalization in two patients.
"It seems reasonable to consider individual treatment preference and risk of drug-related adverse events in addition to potential benefits when making patient-specific decisions regarding therapy," they concluded.
Serious fractures occurred in 5.1% of drug recipients versus 3.2% among placebo patients (p=0.003). A weight gain of more than 4.5 kg was seen in 52.2% of pioglitazone recipientscompared with 33.7% for placebo, and rates of edema were 35.6% with the drug versus 24.9% with placebo (both p<0.001).
The drug has been plagued by suspicions that it might increase the risk of heart failure and bladder cancer. In this study, 74 pioglitazone recipients developed heart failure versus 71 in the placebo group (p=0.80). A dozen drug recipients were diagnosed with bladder cancer compared with eight cases in the placebo group (p=0.37).
Dr. Clark said, "All of the stuff we're doing for risk-factor reduction -- blood pressure reduction, stop smoking and giving aspirin -- they're all on the same level of relative improvement, and all of those are widely used. Aspirin has a list of side effects that will fill up three pages."
At the start of the study, all of the volunteers were insulin resistant, at least 40 years old, and had experienced an ischemic stroke or TIA in the previous six months. Diabetics were excluded as were patients with heart failure, active liver disease, and an increased risk of bladder cancer.
By the end of the study, 60% of the pioglitazone patients were still taking their medicine compared with 67% of placebo recipients. The most common reason for discontinuing was edema or weight gain.
The National Institute of Neurological Disorders and Stroke funded this study. Eleven coauthors reported disclosures.
Key Elements of Critical Care
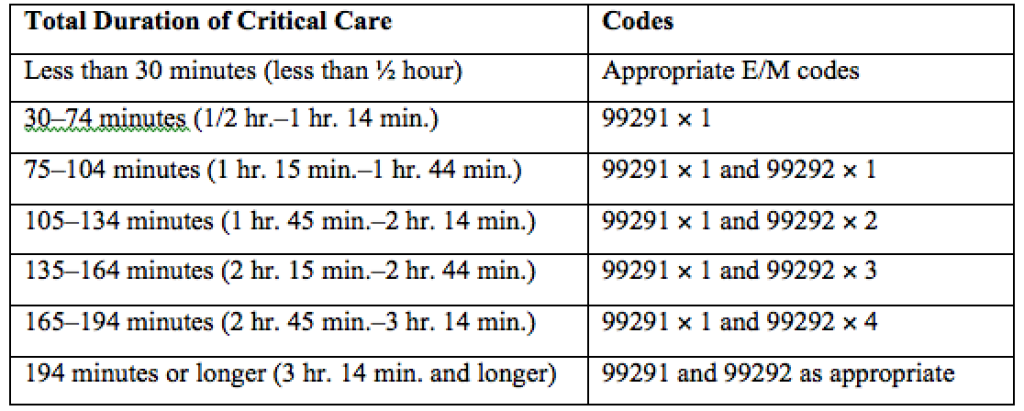
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.

Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1

Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
QI and Patient Safety: No Longer Just an Elective for Trainees
The demand for training in healthcare quality and patient safety, for both medical students and residents, has never been higher. The Quality and Safety Educators Academy (QSEA, sites.hospitalmedicine.org/qsea) responds to that demand by providing medical educators with the knowledge and tools to integrate quality improvement and safety concepts into their curricula.
Sponsored by the Society of Hospital Medicine (SHM) and the Alliance for Academic Internal Medicine (AAIM), QSEA 2016 is a two-and-a-half-day course designed as a faculty development program. This year, QSEA will be held at Tempe Mission Palms Hotel and Conference Center in Tempe, Ariz., from May 23 to 25.
Attendees will enjoy a hands-on, interactive learning environment with a 10-to-1 student-to-faculty ratio. Participants will develop a professional network and leave with a tool kit of educational resources and curricular tools for quality and safety education.
Think QSEA is for you? Make plans to attend now if you are:
- A program director or assistant program director interested in acquiring new curricular ideas to help meet the ACGME requirements, which require residency programs to integrate quality and safety in their curriculum
- A medical school leader or clerkship director developing quality and safety curricula for students
- A faculty member beginning a new role or expanding an existing role in quality and safety education
- A quality and safety leader who wishes to extend influence and effectiveness by learning strategies to teach and engage trainees
QSEA has sold out each of the past four years, so don’t delay. Register online at sites.hospitalmedicine.org/qsea/register.html or via phone at 800-843-3360. Questions? Email meetings@hospitalmedicine.org. TH
Brett Radler is SHM’s communications coordinator.
The demand for training in healthcare quality and patient safety, for both medical students and residents, has never been higher. The Quality and Safety Educators Academy (QSEA, sites.hospitalmedicine.org/qsea) responds to that demand by providing medical educators with the knowledge and tools to integrate quality improvement and safety concepts into their curricula.
Sponsored by the Society of Hospital Medicine (SHM) and the Alliance for Academic Internal Medicine (AAIM), QSEA 2016 is a two-and-a-half-day course designed as a faculty development program. This year, QSEA will be held at Tempe Mission Palms Hotel and Conference Center in Tempe, Ariz., from May 23 to 25.
Attendees will enjoy a hands-on, interactive learning environment with a 10-to-1 student-to-faculty ratio. Participants will develop a professional network and leave with a tool kit of educational resources and curricular tools for quality and safety education.
Think QSEA is for you? Make plans to attend now if you are:
- A program director or assistant program director interested in acquiring new curricular ideas to help meet the ACGME requirements, which require residency programs to integrate quality and safety in their curriculum
- A medical school leader or clerkship director developing quality and safety curricula for students
- A faculty member beginning a new role or expanding an existing role in quality and safety education
- A quality and safety leader who wishes to extend influence and effectiveness by learning strategies to teach and engage trainees
QSEA has sold out each of the past four years, so don’t delay. Register online at sites.hospitalmedicine.org/qsea/register.html or via phone at 800-843-3360. Questions? Email meetings@hospitalmedicine.org. TH
Brett Radler is SHM’s communications coordinator.
The demand for training in healthcare quality and patient safety, for both medical students and residents, has never been higher. The Quality and Safety Educators Academy (QSEA, sites.hospitalmedicine.org/qsea) responds to that demand by providing medical educators with the knowledge and tools to integrate quality improvement and safety concepts into their curricula.
Sponsored by the Society of Hospital Medicine (SHM) and the Alliance for Academic Internal Medicine (AAIM), QSEA 2016 is a two-and-a-half-day course designed as a faculty development program. This year, QSEA will be held at Tempe Mission Palms Hotel and Conference Center in Tempe, Ariz., from May 23 to 25.
Attendees will enjoy a hands-on, interactive learning environment with a 10-to-1 student-to-faculty ratio. Participants will develop a professional network and leave with a tool kit of educational resources and curricular tools for quality and safety education.
Think QSEA is for you? Make plans to attend now if you are:
- A program director or assistant program director interested in acquiring new curricular ideas to help meet the ACGME requirements, which require residency programs to integrate quality and safety in their curriculum
- A medical school leader or clerkship director developing quality and safety curricula for students
- A faculty member beginning a new role or expanding an existing role in quality and safety education
- A quality and safety leader who wishes to extend influence and effectiveness by learning strategies to teach and engage trainees
QSEA has sold out each of the past four years, so don’t delay. Register online at sites.hospitalmedicine.org/qsea/register.html or via phone at 800-843-3360. Questions? Email meetings@hospitalmedicine.org. TH
Brett Radler is SHM’s communications coordinator.
Medicare Grants Billing Code for Hospitalists
PHILADELPHIA—The Society of Hospital Medicine (SHM) is pleased to announce the introduction of a dedicated billing code for hospitalists by the Centers for Medicare & Medicaid Services (CMS). This decision comes in response to concerted advocacy efforts from SHM for CMS to recognize the specialty. This is a monumental step for hospital medicine, which continues to be the fastest growing medical specialty in the United States with over 48,000 practitioners identifying as hospitalists, growing from approximately 1,000 in the mid-1990s.
“We see each day that hospitalists are driving positive change in healthcare, and this recognition by CMS affirms that hospital medicine is growing both in scope and impact,” notes Laurence Wellikson, MD, MHM, CEO of SHM. “The ability for hospital medicine practitioners to differentiate themselves from providers in other specialties will have a huge impact, particularly for upcoming value-based or pay-for-performance programs.”
Until now, hospitalists could only compare performance to that of practitioners in internal medicine or another related specialty. This new billing code will allow hospitalists to appropriately benchmark and focus improvement efforts with others in the hospital medicine specialty, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Despite varied training backgrounds, hospitalists have become focused within their own unique specialty, dedicated to providing care to hospitalized patients and working toward high-quality, patient-centered care in the hospital. They have developed institutional-based skills that differentiate them from practitioners in other specialties, such as internal and family medicine. Their specialized expertise includes improving both the efficiency and safety of care for hospitalized patients and the ability to manage and innovate in a hospital’s team-based environment.
This momentous decision coincides with the twenty-year anniversary of the coining of the term ‘hospitalist’ by Robert Wachter, MD, MHM, and Lee Goldman, MD in the New England Journal of Medicine. In recognition of this anniversary, SHM introduced a year-long celebration, the “Year of the Hospitalist,” to commemorate the specialty’s continued success and bright future.
“We have known who we are for years, and the special role that hospitalists play in the well-being of our patients, communities and health systems,” explains Brian Harte, MD, SFHM, president-elect of SHM. “The hospitalist provider code will provide Medicare and other players in the healthcare system an important new tool to better understand and acknowledge the critical role we play in the care of hospitalized patients nationwide.”
Lisa Zoks is SHM's Vice-President of Communications.
ABOUT SHM
Representing the fastest growing specialty in modern healthcare, SHM is the leading medical society for more than 48,000 hospitalists and their patients. SHM is dedicated to promoting the highest quality care for all hospitalized patients and overall excellence in the practice of hospital medicine through quality improvement, education, advocacy and research. Over the past decade, studies have shown that hospitalists can contribute to decreased patient lengths of stay, reductions in hospital costs and readmission rates, and increased patient satisfaction.
PHILADELPHIA—The Society of Hospital Medicine (SHM) is pleased to announce the introduction of a dedicated billing code for hospitalists by the Centers for Medicare & Medicaid Services (CMS). This decision comes in response to concerted advocacy efforts from SHM for CMS to recognize the specialty. This is a monumental step for hospital medicine, which continues to be the fastest growing medical specialty in the United States with over 48,000 practitioners identifying as hospitalists, growing from approximately 1,000 in the mid-1990s.
“We see each day that hospitalists are driving positive change in healthcare, and this recognition by CMS affirms that hospital medicine is growing both in scope and impact,” notes Laurence Wellikson, MD, MHM, CEO of SHM. “The ability for hospital medicine practitioners to differentiate themselves from providers in other specialties will have a huge impact, particularly for upcoming value-based or pay-for-performance programs.”
Until now, hospitalists could only compare performance to that of practitioners in internal medicine or another related specialty. This new billing code will allow hospitalists to appropriately benchmark and focus improvement efforts with others in the hospital medicine specialty, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Despite varied training backgrounds, hospitalists have become focused within their own unique specialty, dedicated to providing care to hospitalized patients and working toward high-quality, patient-centered care in the hospital. They have developed institutional-based skills that differentiate them from practitioners in other specialties, such as internal and family medicine. Their specialized expertise includes improving both the efficiency and safety of care for hospitalized patients and the ability to manage and innovate in a hospital’s team-based environment.
This momentous decision coincides with the twenty-year anniversary of the coining of the term ‘hospitalist’ by Robert Wachter, MD, MHM, and Lee Goldman, MD in the New England Journal of Medicine. In recognition of this anniversary, SHM introduced a year-long celebration, the “Year of the Hospitalist,” to commemorate the specialty’s continued success and bright future.
“We have known who we are for years, and the special role that hospitalists play in the well-being of our patients, communities and health systems,” explains Brian Harte, MD, SFHM, president-elect of SHM. “The hospitalist provider code will provide Medicare and other players in the healthcare system an important new tool to better understand and acknowledge the critical role we play in the care of hospitalized patients nationwide.”
Lisa Zoks is SHM's Vice-President of Communications.
ABOUT SHM
Representing the fastest growing specialty in modern healthcare, SHM is the leading medical society for more than 48,000 hospitalists and their patients. SHM is dedicated to promoting the highest quality care for all hospitalized patients and overall excellence in the practice of hospital medicine through quality improvement, education, advocacy and research. Over the past decade, studies have shown that hospitalists can contribute to decreased patient lengths of stay, reductions in hospital costs and readmission rates, and increased patient satisfaction.
PHILADELPHIA—The Society of Hospital Medicine (SHM) is pleased to announce the introduction of a dedicated billing code for hospitalists by the Centers for Medicare & Medicaid Services (CMS). This decision comes in response to concerted advocacy efforts from SHM for CMS to recognize the specialty. This is a monumental step for hospital medicine, which continues to be the fastest growing medical specialty in the United States with over 48,000 practitioners identifying as hospitalists, growing from approximately 1,000 in the mid-1990s.
“We see each day that hospitalists are driving positive change in healthcare, and this recognition by CMS affirms that hospital medicine is growing both in scope and impact,” notes Laurence Wellikson, MD, MHM, CEO of SHM. “The ability for hospital medicine practitioners to differentiate themselves from providers in other specialties will have a huge impact, particularly for upcoming value-based or pay-for-performance programs.”
Until now, hospitalists could only compare performance to that of practitioners in internal medicine or another related specialty. This new billing code will allow hospitalists to appropriately benchmark and focus improvement efforts with others in the hospital medicine specialty, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Despite varied training backgrounds, hospitalists have become focused within their own unique specialty, dedicated to providing care to hospitalized patients and working toward high-quality, patient-centered care in the hospital. They have developed institutional-based skills that differentiate them from practitioners in other specialties, such as internal and family medicine. Their specialized expertise includes improving both the efficiency and safety of care for hospitalized patients and the ability to manage and innovate in a hospital’s team-based environment.
This momentous decision coincides with the twenty-year anniversary of the coining of the term ‘hospitalist’ by Robert Wachter, MD, MHM, and Lee Goldman, MD in the New England Journal of Medicine. In recognition of this anniversary, SHM introduced a year-long celebration, the “Year of the Hospitalist,” to commemorate the specialty’s continued success and bright future.
“We have known who we are for years, and the special role that hospitalists play in the well-being of our patients, communities and health systems,” explains Brian Harte, MD, SFHM, president-elect of SHM. “The hospitalist provider code will provide Medicare and other players in the healthcare system an important new tool to better understand and acknowledge the critical role we play in the care of hospitalized patients nationwide.”
Lisa Zoks is SHM's Vice-President of Communications.
ABOUT SHM
Representing the fastest growing specialty in modern healthcare, SHM is the leading medical society for more than 48,000 hospitalists and their patients. SHM is dedicated to promoting the highest quality care for all hospitalized patients and overall excellence in the practice of hospital medicine through quality improvement, education, advocacy and research. Over the past decade, studies have shown that hospitalists can contribute to decreased patient lengths of stay, reductions in hospital costs and readmission rates, and increased patient satisfaction.
Sharing Notes for Better Doctor-Patient Communication
Excellent communication between physicians and patients is a crucial element of hospital quality, but it’s also an ongoing challenge for many institutions. One physician wondered whether letting patients read their physicians’ notes could help.
“I wanted to find new methods to improve patient understanding of their medical care plan,” says Craig Weinert, MD, MPH, medical director for adult inpatient services at the University of Minnesota Medical Center and author of “Giving Doctors’ Daily Progress Notes to Hospitalized Patients and Families to Improve Patient Experience” in the American Journal of Medical Quality. “It seemed logical to me that giving patients access to the same information that all the other members of the healthcare team were reading would improve communication. This is the overall hypothesis of the Open Notes movement.”
Another reason Dr. Weinert pursued the study: In his clinical job as an intensivist, he encounters frequent disagreements with patients’ families regarding prognosis and goals of care.
“No one has figured out how to increase the alignment of prognosis between the family and the medical team,” Dr. Weinert says. “I think having the families read the doctors’ notes, where the issues with poor-prognosis multi-organ failure are repeatedly spelled out, might help families more quickly grasp the futility of continuing care.”
During the study, hospitalized patients or family members on six wards of a university hospital received a printed copy of their medical team’s daily progress notes. Surveys afterward showed 74% to 86% of patients and family members responded favorably. Physicians were mostly satisfied, too.
“Most doctors, at the end of the study, thought that Open Notes went better than they had predicted,” Dr. Weinert says.
Complete transparency of medical records is the future of medicine, he says. It’s what patients want, “especially the younger generation.”
“Over the next 10 years,” he says, “I predict ... all [electronic medical record] vendors will have electronic portals that allow clinic and hospitalized patients access to almost everything in the EMR.”
Reference
1. Weinert C. Giving doctors’ daily progress notes to hospitalized patients and families to improve patient experience. Am J Med Qual. 2015. doi:10.1177/1062860615610424.
Excellent communication between physicians and patients is a crucial element of hospital quality, but it’s also an ongoing challenge for many institutions. One physician wondered whether letting patients read their physicians’ notes could help.
“I wanted to find new methods to improve patient understanding of their medical care plan,” says Craig Weinert, MD, MPH, medical director for adult inpatient services at the University of Minnesota Medical Center and author of “Giving Doctors’ Daily Progress Notes to Hospitalized Patients and Families to Improve Patient Experience” in the American Journal of Medical Quality. “It seemed logical to me that giving patients access to the same information that all the other members of the healthcare team were reading would improve communication. This is the overall hypothesis of the Open Notes movement.”
Another reason Dr. Weinert pursued the study: In his clinical job as an intensivist, he encounters frequent disagreements with patients’ families regarding prognosis and goals of care.
“No one has figured out how to increase the alignment of prognosis between the family and the medical team,” Dr. Weinert says. “I think having the families read the doctors’ notes, where the issues with poor-prognosis multi-organ failure are repeatedly spelled out, might help families more quickly grasp the futility of continuing care.”
During the study, hospitalized patients or family members on six wards of a university hospital received a printed copy of their medical team’s daily progress notes. Surveys afterward showed 74% to 86% of patients and family members responded favorably. Physicians were mostly satisfied, too.
“Most doctors, at the end of the study, thought that Open Notes went better than they had predicted,” Dr. Weinert says.
Complete transparency of medical records is the future of medicine, he says. It’s what patients want, “especially the younger generation.”
“Over the next 10 years,” he says, “I predict ... all [electronic medical record] vendors will have electronic portals that allow clinic and hospitalized patients access to almost everything in the EMR.”
Reference
1. Weinert C. Giving doctors’ daily progress notes to hospitalized patients and families to improve patient experience. Am J Med Qual. 2015. doi:10.1177/1062860615610424.
Excellent communication between physicians and patients is a crucial element of hospital quality, but it’s also an ongoing challenge for many institutions. One physician wondered whether letting patients read their physicians’ notes could help.
“I wanted to find new methods to improve patient understanding of their medical care plan,” says Craig Weinert, MD, MPH, medical director for adult inpatient services at the University of Minnesota Medical Center and author of “Giving Doctors’ Daily Progress Notes to Hospitalized Patients and Families to Improve Patient Experience” in the American Journal of Medical Quality. “It seemed logical to me that giving patients access to the same information that all the other members of the healthcare team were reading would improve communication. This is the overall hypothesis of the Open Notes movement.”
Another reason Dr. Weinert pursued the study: In his clinical job as an intensivist, he encounters frequent disagreements with patients’ families regarding prognosis and goals of care.
“No one has figured out how to increase the alignment of prognosis between the family and the medical team,” Dr. Weinert says. “I think having the families read the doctors’ notes, where the issues with poor-prognosis multi-organ failure are repeatedly spelled out, might help families more quickly grasp the futility of continuing care.”
During the study, hospitalized patients or family members on six wards of a university hospital received a printed copy of their medical team’s daily progress notes. Surveys afterward showed 74% to 86% of patients and family members responded favorably. Physicians were mostly satisfied, too.
“Most doctors, at the end of the study, thought that Open Notes went better than they had predicted,” Dr. Weinert says.
Complete transparency of medical records is the future of medicine, he says. It’s what patients want, “especially the younger generation.”
“Over the next 10 years,” he says, “I predict ... all [electronic medical record] vendors will have electronic portals that allow clinic and hospitalized patients access to almost everything in the EMR.”
Reference
1. Weinert C. Giving doctors’ daily progress notes to hospitalized patients and families to improve patient experience. Am J Med Qual. 2015. doi:10.1177/1062860615610424.
Elderly Patients Hospitalized For Cancer are More likely to Have Complications Afterward Compared to the Middle-Aged
(Reuters Health) - Elderly patients hospitalized for cancer surgery are more likely to have complications afterward compared to the middle-aged, particularly when they have several other health problems, a U.S. study suggests.
Overall, almost one in 10 adults age 55 and older had at least one post-operative issue like delirium, dehydration, falls, fractures, pressure ulcers or unusual weight loss, the study of nearly 1 million cancer surgery patients found.
These setbacks were even more common when patients were at least 65 years old, had two or more other serious health problems in addition to malignancies, or had surgeries for tumors of the digestive system or nearby organs.
But the odds were worst for people over 75 - about 46 percent of them had at least one complication, compared with 22 percent of adults aged 55 to 64.
"With the population aging, it's becoming increasingly important to consider not only the survival benefits of cancer surgery but the impact on functionality, vitality and quality of life," said lead study author Dr. Hung-Jui Tan, a researcher in urologic oncology at the University of California, Los Angeles.
While the events studied here are specific to the initial hospitalization, they can carry potential long-term ramifications," Tan added by email.
To see how age influences the risk of post-operative complications, Tan and colleagues reviewed hospital admission records for a nationwide sample of 940,000 adults age 55 and older who had cancer surgery from 2009 to 2011.
Compared with patients who were under age 65, those who were 65 to 74 years old were 23 percent more likely to have complications, while the over-75 group had 66 percent higher odds, researchers report in the Journal of Clinical Oncology.
Complications were most likely when patients were having surgery for cancers of the bladder, ovary, colon, rectum, pancreas or stomach.
After suffering post-operative setbacks, patients were also more likely to have further complications during their hospital stay, to remain in the hospital longer and to have more costly care. They were also more likely to die in the hospital and less likely to be discharged to home.
One limitation of the study is its reliance on administrative claims data, which is designed for billing purposes and might not always reflect the nuances of patients' medical conditions, the authors note. In addition, it's possible that some complications may have resulted from conditions patients had before they arrived at the hospital for cancer surgery.
The study can't prove that advanced age directly causes post-operative problems. But the findings suggest doctors and patients should consider these potential risks when deciding the best course of treatment, Tan said.
Patients should also understand that not all complications are equally devastating to quality of life. Dehydration and weight loss, for example, are nutritional problems that might be treated with fluids, noted Dr. Siri Rostoft, a geriatric medicine researcher at Oslo University Hospital in Norway.
"Cancer is often a lethal disease if left untreated that causes conditions such as bleeding, obstruction of the intestines, and pain," Rostoft, who wasn't involved in the study, said by email. "Not treating patients may be worse for their quality of life than operating."
Still, the findings add to a growing body of data on post-operative complications that may help doctors and patients decide if the potential benefits of surgery outweigh the possible risks, Dr. Steven Cunningham, a researcher at Saint Agnes Hospital and Cancer Institute in Baltimore who wasn't involved in the study, said by email.
Complications in the study were more likely at non-teaching hospitals and facilities that did fewer cancer surgeries, a factor that patients should also consider when they have a choice about where to go for surgery, noted Dr. Kwok-Leung Cheung, a researcher at the University of Nottingham in the U.K. and member of the surgical task force for the International Society of Geriatric Oncology.
Knowing when not to operate also matters, Cheung, who wasn't involved in the study, added by email.
"The surgeon should seriously consider the intensity of surgery, which has been identified as one of the important factors with post operative problems," Cheung added. "The use of minimally invasive techniques including laparoscopic and robotic surgery should be considered wherever appropriate."
(Reuters Health) - Elderly patients hospitalized for cancer surgery are more likely to have complications afterward compared to the middle-aged, particularly when they have several other health problems, a U.S. study suggests.
Overall, almost one in 10 adults age 55 and older had at least one post-operative issue like delirium, dehydration, falls, fractures, pressure ulcers or unusual weight loss, the study of nearly 1 million cancer surgery patients found.
These setbacks were even more common when patients were at least 65 years old, had two or more other serious health problems in addition to malignancies, or had surgeries for tumors of the digestive system or nearby organs.
But the odds were worst for people over 75 - about 46 percent of them had at least one complication, compared with 22 percent of adults aged 55 to 64.
"With the population aging, it's becoming increasingly important to consider not only the survival benefits of cancer surgery but the impact on functionality, vitality and quality of life," said lead study author Dr. Hung-Jui Tan, a researcher in urologic oncology at the University of California, Los Angeles.
While the events studied here are specific to the initial hospitalization, they can carry potential long-term ramifications," Tan added by email.
To see how age influences the risk of post-operative complications, Tan and colleagues reviewed hospital admission records for a nationwide sample of 940,000 adults age 55 and older who had cancer surgery from 2009 to 2011.
Compared with patients who were under age 65, those who were 65 to 74 years old were 23 percent more likely to have complications, while the over-75 group had 66 percent higher odds, researchers report in the Journal of Clinical Oncology.
Complications were most likely when patients were having surgery for cancers of the bladder, ovary, colon, rectum, pancreas or stomach.
After suffering post-operative setbacks, patients were also more likely to have further complications during their hospital stay, to remain in the hospital longer and to have more costly care. They were also more likely to die in the hospital and less likely to be discharged to home.
One limitation of the study is its reliance on administrative claims data, which is designed for billing purposes and might not always reflect the nuances of patients' medical conditions, the authors note. In addition, it's possible that some complications may have resulted from conditions patients had before they arrived at the hospital for cancer surgery.
The study can't prove that advanced age directly causes post-operative problems. But the findings suggest doctors and patients should consider these potential risks when deciding the best course of treatment, Tan said.
Patients should also understand that not all complications are equally devastating to quality of life. Dehydration and weight loss, for example, are nutritional problems that might be treated with fluids, noted Dr. Siri Rostoft, a geriatric medicine researcher at Oslo University Hospital in Norway.
"Cancer is often a lethal disease if left untreated that causes conditions such as bleeding, obstruction of the intestines, and pain," Rostoft, who wasn't involved in the study, said by email. "Not treating patients may be worse for their quality of life than operating."
Still, the findings add to a growing body of data on post-operative complications that may help doctors and patients decide if the potential benefits of surgery outweigh the possible risks, Dr. Steven Cunningham, a researcher at Saint Agnes Hospital and Cancer Institute in Baltimore who wasn't involved in the study, said by email.
Complications in the study were more likely at non-teaching hospitals and facilities that did fewer cancer surgeries, a factor that patients should also consider when they have a choice about where to go for surgery, noted Dr. Kwok-Leung Cheung, a researcher at the University of Nottingham in the U.K. and member of the surgical task force for the International Society of Geriatric Oncology.
Knowing when not to operate also matters, Cheung, who wasn't involved in the study, added by email.
"The surgeon should seriously consider the intensity of surgery, which has been identified as one of the important factors with post operative problems," Cheung added. "The use of minimally invasive techniques including laparoscopic and robotic surgery should be considered wherever appropriate."
(Reuters Health) - Elderly patients hospitalized for cancer surgery are more likely to have complications afterward compared to the middle-aged, particularly when they have several other health problems, a U.S. study suggests.
Overall, almost one in 10 adults age 55 and older had at least one post-operative issue like delirium, dehydration, falls, fractures, pressure ulcers or unusual weight loss, the study of nearly 1 million cancer surgery patients found.
These setbacks were even more common when patients were at least 65 years old, had two or more other serious health problems in addition to malignancies, or had surgeries for tumors of the digestive system or nearby organs.
But the odds were worst for people over 75 - about 46 percent of them had at least one complication, compared with 22 percent of adults aged 55 to 64.
"With the population aging, it's becoming increasingly important to consider not only the survival benefits of cancer surgery but the impact on functionality, vitality and quality of life," said lead study author Dr. Hung-Jui Tan, a researcher in urologic oncology at the University of California, Los Angeles.
While the events studied here are specific to the initial hospitalization, they can carry potential long-term ramifications," Tan added by email.
To see how age influences the risk of post-operative complications, Tan and colleagues reviewed hospital admission records for a nationwide sample of 940,000 adults age 55 and older who had cancer surgery from 2009 to 2011.
Compared with patients who were under age 65, those who were 65 to 74 years old were 23 percent more likely to have complications, while the over-75 group had 66 percent higher odds, researchers report in the Journal of Clinical Oncology.
Complications were most likely when patients were having surgery for cancers of the bladder, ovary, colon, rectum, pancreas or stomach.
After suffering post-operative setbacks, patients were also more likely to have further complications during their hospital stay, to remain in the hospital longer and to have more costly care. They were also more likely to die in the hospital and less likely to be discharged to home.
One limitation of the study is its reliance on administrative claims data, which is designed for billing purposes and might not always reflect the nuances of patients' medical conditions, the authors note. In addition, it's possible that some complications may have resulted from conditions patients had before they arrived at the hospital for cancer surgery.
The study can't prove that advanced age directly causes post-operative problems. But the findings suggest doctors and patients should consider these potential risks when deciding the best course of treatment, Tan said.
Patients should also understand that not all complications are equally devastating to quality of life. Dehydration and weight loss, for example, are nutritional problems that might be treated with fluids, noted Dr. Siri Rostoft, a geriatric medicine researcher at Oslo University Hospital in Norway.
"Cancer is often a lethal disease if left untreated that causes conditions such as bleeding, obstruction of the intestines, and pain," Rostoft, who wasn't involved in the study, said by email. "Not treating patients may be worse for their quality of life than operating."
Still, the findings add to a growing body of data on post-operative complications that may help doctors and patients decide if the potential benefits of surgery outweigh the possible risks, Dr. Steven Cunningham, a researcher at Saint Agnes Hospital and Cancer Institute in Baltimore who wasn't involved in the study, said by email.
Complications in the study were more likely at non-teaching hospitals and facilities that did fewer cancer surgeries, a factor that patients should also consider when they have a choice about where to go for surgery, noted Dr. Kwok-Leung Cheung, a researcher at the University of Nottingham in the U.K. and member of the surgical task force for the International Society of Geriatric Oncology.
Knowing when not to operate also matters, Cheung, who wasn't involved in the study, added by email.
"The surgeon should seriously consider the intensity of surgery, which has been identified as one of the important factors with post operative problems," Cheung added. "The use of minimally invasive techniques including laparoscopic and robotic surgery should be considered wherever appropriate."
Latest Study of Hospitalist Malpractice Claims Now Available
A study of closed malpractice claims involving more than 2,100 hospitalists shows that claims* arising from hospitalist care are more likely to have a higher injury severity than claims against other physician specialties. This latest analysis of allegations made by patients against hospitalists—and the factors that led to these claims—was produced by The Doctors Company, the nation’s largest physician-owned medical malpractice insurer.
The study also shows that the vast majority of claims against hospitalists were diagnosis related (36%), involved improper management of treatment (31%), or were the result of a medication-related error (11%).
The study is based on 464 claims against hospitalists that closed from 2007 to 2014. All claims were studied regardless of their ultimate outcome.
The research is unique compared with other studies of malpractice claims because it includes expert insights into the specific elements that led to the patient injury. Findings by expert physician reviewers were consistent with the patients’ allegations—that their problems arose from incorrect or delayed diagnoses. Reviewers noted that 35% of the cases resulted from an inadequate initial assessment, consequently decreasing the chance that the hospitalist would arrive at the correct diagnosis.
The study also includes 15 examples of malpractice cases, lists the conditions that were most commonly involved in incorrect or delayed diagnoses, and provides risk-mitigation strategies.
“We hope that the information presented in this study will prompt physicians to collaborate with hospital leadership to identify system weaknesses, thereby reducing the risk of harm to patients,” says study co-author David B. Troxel, MD, medical director of the The Doctors Company.
Copies of the full study will be available at The Doctors Company’s exhibit space at HM16 or at www.thedoctors.com/hospitaliststudy.
*A written notice, demand, lawsuit, arbitration proceeding, or screening panel in which a demand is made for money or a bill reduction and that alleges injury, disability, sickness, disease, or death of a patient arising from the physician’s rendering or failing to render professional services.
A study of closed malpractice claims involving more than 2,100 hospitalists shows that claims* arising from hospitalist care are more likely to have a higher injury severity than claims against other physician specialties. This latest analysis of allegations made by patients against hospitalists—and the factors that led to these claims—was produced by The Doctors Company, the nation’s largest physician-owned medical malpractice insurer.
The study also shows that the vast majority of claims against hospitalists were diagnosis related (36%), involved improper management of treatment (31%), or were the result of a medication-related error (11%).
The study is based on 464 claims against hospitalists that closed from 2007 to 2014. All claims were studied regardless of their ultimate outcome.
The research is unique compared with other studies of malpractice claims because it includes expert insights into the specific elements that led to the patient injury. Findings by expert physician reviewers were consistent with the patients’ allegations—that their problems arose from incorrect or delayed diagnoses. Reviewers noted that 35% of the cases resulted from an inadequate initial assessment, consequently decreasing the chance that the hospitalist would arrive at the correct diagnosis.
The study also includes 15 examples of malpractice cases, lists the conditions that were most commonly involved in incorrect or delayed diagnoses, and provides risk-mitigation strategies.
“We hope that the information presented in this study will prompt physicians to collaborate with hospital leadership to identify system weaknesses, thereby reducing the risk of harm to patients,” says study co-author David B. Troxel, MD, medical director of the The Doctors Company.
Copies of the full study will be available at The Doctors Company’s exhibit space at HM16 or at www.thedoctors.com/hospitaliststudy.
*A written notice, demand, lawsuit, arbitration proceeding, or screening panel in which a demand is made for money or a bill reduction and that alleges injury, disability, sickness, disease, or death of a patient arising from the physician’s rendering or failing to render professional services.
A study of closed malpractice claims involving more than 2,100 hospitalists shows that claims* arising from hospitalist care are more likely to have a higher injury severity than claims against other physician specialties. This latest analysis of allegations made by patients against hospitalists—and the factors that led to these claims—was produced by The Doctors Company, the nation’s largest physician-owned medical malpractice insurer.
The study also shows that the vast majority of claims against hospitalists were diagnosis related (36%), involved improper management of treatment (31%), or were the result of a medication-related error (11%).
The study is based on 464 claims against hospitalists that closed from 2007 to 2014. All claims were studied regardless of their ultimate outcome.
The research is unique compared with other studies of malpractice claims because it includes expert insights into the specific elements that led to the patient injury. Findings by expert physician reviewers were consistent with the patients’ allegations—that their problems arose from incorrect or delayed diagnoses. Reviewers noted that 35% of the cases resulted from an inadequate initial assessment, consequently decreasing the chance that the hospitalist would arrive at the correct diagnosis.
The study also includes 15 examples of malpractice cases, lists the conditions that were most commonly involved in incorrect or delayed diagnoses, and provides risk-mitigation strategies.
“We hope that the information presented in this study will prompt physicians to collaborate with hospital leadership to identify system weaknesses, thereby reducing the risk of harm to patients,” says study co-author David B. Troxel, MD, medical director of the The Doctors Company.
Copies of the full study will be available at The Doctors Company’s exhibit space at HM16 or at www.thedoctors.com/hospitaliststudy.
*A written notice, demand, lawsuit, arbitration proceeding, or screening panel in which a demand is made for money or a bill reduction and that alleges injury, disability, sickness, disease, or death of a patient arising from the physician’s rendering or failing to render professional services.