User login
In clinical practice, weight problems are very common. Among US women, about one-third are obese, with another one-quarter overweight. As we know, obesity is a risk factor for many medical problems, including diabetes, hypertension, elevated cholesterol, stroke, heart disease, many cancers, sleep apnea, and arthritis.1 Obesity is also a risk factor for a long list of serious obstetric problems, including gestational hypertension, preeclampsia, gestational diabetes, fetal malformations, macrosomia, stillbirth, prematurity, and an increased rate of cesarean delivery.
Clearly, collectively, we need to play more of an active role in our patients’ weight loss and subsequent weight-maintenance efforts. To help us achieve this goal, we should be familiar with our patients’ weight status and comorbidities and offer helpful nonpharmacologic weight-loss interventions. We also should be cognizant of current pharmacologic and surgical options, and, when appropriate, be prepared to counsel patients about their efficacy.
Routinely calculate BMI and assess comorbidities
The body mass index (BMI) of every patient should be calculated and recorded in her medical record.
Be familiar with her BMI. For white, Hispanic, and black women, overweight is defined as a BMI between 25 and 29 kg/m2, and obesity is defined by a BMI of 30 kg/m2 or more.2 For Asian women, overweight begins at a BMI of 23 kg/m2, and obesity begins at a BMI of 25 kg/m2.
If she’s overweight, determine her comorbidities. For your patients with a BMI of 25 kg/m2 or more, assess them for medical comorbidities such as hypertension, dyslipidemia, diabetes, heart disease, and sleep apnea, as the presence of any of these conditions markedly increases the risk of adverse health outcomes. To determine if metabolic syndrome is a concern, measure blood pressure; waist circumference; and fasting triglyceride, fasting glucose, and serum high-density lipoprotein (HDL)-cholesterol levels. To detect prediabetes or diabetes mellitus, consider the hemoglobin A1c (HbA1c) test. The American College of Obstetricians and Gynecologists recommends that clinicians test for diabetes in all women aged 45 and older every 3 years.3
Start with the basics—diet and exercise
It is very difficult for women, and men, who are overweight or obese to successfully lose weight and maintain a normal BMI over time. Many overweight or obese women have attempted to lose weight on many occasions by implementing changes in lifestyle, including diet and exercise, but have had only temporary success.
If your patient is motivated to begin a first or repeat attempt at weight loss, there are several helpful interventions you could recommend, including:
- consult with a nutritionist
- use smartphone apps to help
- support the diet plan (to track caloric intake, daily exercise, etc.)
- increase daily exercise to 1 hour
- join a group weight-loss program or support group
- eat breakfast every day
- avoid food binges on weekends and at night
- practice stress-reduction techniques.
If the combination of basic approaches do not result in her achieving sufficient weight loss, pharmacologic therapy can be considered.
Pharmacologic options
Pharmacologic therapy can be offered to all women with4:
- BMI of 30 kg/m2 or more
- BMI of 27 kg/m2 or more with comorbidities, such as hypertension, diabetes, dyslipidemia, or heart disease.
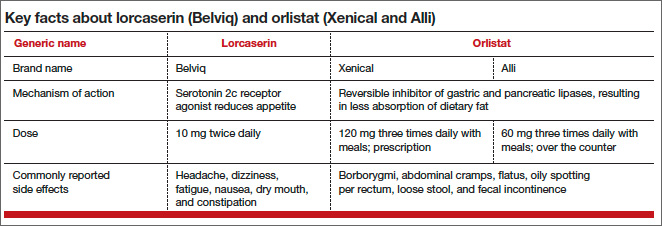
Pharmacologic options for long-term therapy include lorcaserin, orlistat, and phentermine-topiramate. Because of a risk of fetal malformations, women of childbearing age should have a monthly pregnancy test while taking phentermine-topiramate. Here, I focus on lorcaserin and orlistat, two agents that do not require monthly laboratory testing (TABLE). It is important to note that no weight-loss medicine should be prescribed to pregnant women.
Lorcaserin
Lorcaserin is a selective serotonin 2c receptor agonist. Lorcaserin reduces appetite and food intake. Other serotonergic medications previously used for weight loss, such as fenfluramine, stimulated the serotonin 2b receptor, which may have contributed to an increased risk of cardiac valve disease. Because lorcaserin is a selective serotonin 2c receptor agonist, it is less likely to cause cardiac valve disease.
Lorcaserin is taken as a 10-mg tablet twice daily.5 In one large trial, approximately 50% of patients who took the drug for 12 months lost at least 5% of their body mass.6 For those patients taking lorcaserin who do not lose 5% or more of their body mass by 12 weeks of therapy, it is recommended that the medication be discontinued because successful weight loss may not occur with continued therapy. These women could be offered treatment with orlistat.
The most common side effects of lorcaserin are headache, dizziness, fatigue, nausea, dry mouth, and constipation. The drug is contraindicated in those with renal failure or in patients who are taking other serotonergic medications, such as selective serotonin reuptake inhibitors, bupropion, tricyclic antidepressants, or monoamine oxidase inhibitors.
Orlistat
Orlistat is a reversible inhibitor of gastric and pancreatic lipases, thereby inhibiting fat absorption. This leads to weight loss but also causes an increase in fecal fat excretion, which may cause side effects such as borborygmi, abdominal cramps, flatus, oily spotting per rectum, loose stool, and fecal incontinence. Orlistat is taken 3 times daily with meals. Only 1% of the orlistat dose is absorbed into the circulation, minimizing the drug’s effect on other organs and reducing the probability of a medication interaction.
Orlistat may reduce the absorption of vitamins A, D, E, and K. Patients taking the drug should take a daily vitamin pill at bedtime to maximize absorption of the vitamins. According to a 2004 study in which orlistat was combined with behavioral intervention over 12 months, the average weight loss was approximately 10% of patients’ baseline weight.7 (The control group in this study received a placebo tablet plus behavioral intervention and experienced a 5% weight loss.) When orlistat treatment continues as long as 36 months, the reduced weight is typically maintained. Orlistat treatment also has been shown to reduce blood pressure in hypertensive patients and improve their lipid profiles.8,9
You should be aware that some health plans place weight-loss medications on a restricted formulary list that requires preapproval. From my experience, if you prescribe a weight-loss drug you may occasionally be asked to complete a case synopsis on a structured form that is sent to the health insurer or pharmacy management team for review and
preapproval.
Bariatric surgery
Consider bariatric surgery for women with:
- BMI of 40 kg/m2 or more
- BMI of 35 kg/m2 or more with comorbidities and no success with diet, exercise, and weight-loss medications.
Many bariatric surgery programs require that candidates undergo a 6-month interval of diet, exercise, lifestyle change, and psychological assessment prior to scheduling surgery. Bariatric surgery is the medical intervention most likely to result in major weight loss.10
Related article: Consider bariatric surgery first for severely obese women Robert L. Barbieri, MD (April 2008)
Call for input
As obstetricians and gynecologists, our duty is to continually strive to improve the health of all women. Overweight and obesity are highly prevalent major health problems—for society as a whole as well as for many of the individual patients we treat in our practices. Can we, and should we, provide more options to our patients who are trying to lose weight by offering to prescribe lorcaserin or orlistat?
This is a question for all of us. I would like to know your viewpoint on this issue.
Weigh in on the discussion!
Email your letter to Dr. Barbieri at rbarbieri@frontlinemedcom.com
or contact us by:
email: obg@frontlinemedcom.com
fax: 973-206-9251
letter: OBG Management
7 Century Drive, Suite 302
Parsippany, NJ 07054
INSTANT POLL
• Do you think primary care providers routinely present the treatment options of diet/exercise, weight-loss medicines, and bariatric surgery to obese patients?
• Should ObGyns offer to prescribe lorcaserin or orlistat to their obese patients?
Tell us—at rbarbieri@frontlinemedcom.com. Please include your name and city and state.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among U.S. adults, 1999–2008. JAMA. 2010;303:235–241.
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9414):157–163.
- American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 483. Primary and preventive care: periodic assessments. Obstet Gynecol. 2011;117(4):1008–1015.
- Lau DC; Obesity Canada Clinical Practice Guidelines Steering Committee and Expert Panel. Synopsis of the 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children. CMAJ. 2007;176(8):1103–1106.
- Chan EW, He Y, Chui CS, Wong AY, Lau WC, Wong IC. Efficacy and safety of lorcaserin in obese adults: a meta-analysis of 1-year randomized controlled trials (RCTs) and narrative review on short-term RCTs. Obes Rev. 2013;14(5):383–392.
- Fidler MC, Sanchez M, Raether B, et al; BLOSSOM Clinical Trial Group. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011;96(10):3067–3077.
- Torgerson JS, Hauptman J, Boldrin MN, Sjostrom L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155–161.
- Siebenhofer A, Jeitler K, Horvath K, Berghold A, Siering U, Semlitsch T. Long-term effects of weight-reducing drugs in hypertensive patients. Cochrane Database Syst Rev. 2013;3:CD007654.
- Tonstad S, Pometta D, Erkelens DW, et al. The effect of the gastrointestinal lipase inhibitor, orlistat, on serum lipids and lipoproteins in patients with primary hyperlipidemia. Eur J Clin Pharmacol. 1994;46(5):405–410.
- Barbieri RL. Consider bariatric surgery first for severely obese women. OBG Manag. 2008;20(4):9, 14, 16.
In clinical practice, weight problems are very common. Among US women, about one-third are obese, with another one-quarter overweight. As we know, obesity is a risk factor for many medical problems, including diabetes, hypertension, elevated cholesterol, stroke, heart disease, many cancers, sleep apnea, and arthritis.1 Obesity is also a risk factor for a long list of serious obstetric problems, including gestational hypertension, preeclampsia, gestational diabetes, fetal malformations, macrosomia, stillbirth, prematurity, and an increased rate of cesarean delivery.
Clearly, collectively, we need to play more of an active role in our patients’ weight loss and subsequent weight-maintenance efforts. To help us achieve this goal, we should be familiar with our patients’ weight status and comorbidities and offer helpful nonpharmacologic weight-loss interventions. We also should be cognizant of current pharmacologic and surgical options, and, when appropriate, be prepared to counsel patients about their efficacy.
Routinely calculate BMI and assess comorbidities
The body mass index (BMI) of every patient should be calculated and recorded in her medical record.
Be familiar with her BMI. For white, Hispanic, and black women, overweight is defined as a BMI between 25 and 29 kg/m2, and obesity is defined by a BMI of 30 kg/m2 or more.2 For Asian women, overweight begins at a BMI of 23 kg/m2, and obesity begins at a BMI of 25 kg/m2.
If she’s overweight, determine her comorbidities. For your patients with a BMI of 25 kg/m2 or more, assess them for medical comorbidities such as hypertension, dyslipidemia, diabetes, heart disease, and sleep apnea, as the presence of any of these conditions markedly increases the risk of adverse health outcomes. To determine if metabolic syndrome is a concern, measure blood pressure; waist circumference; and fasting triglyceride, fasting glucose, and serum high-density lipoprotein (HDL)-cholesterol levels. To detect prediabetes or diabetes mellitus, consider the hemoglobin A1c (HbA1c) test. The American College of Obstetricians and Gynecologists recommends that clinicians test for diabetes in all women aged 45 and older every 3 years.3
Start with the basics—diet and exercise
It is very difficult for women, and men, who are overweight or obese to successfully lose weight and maintain a normal BMI over time. Many overweight or obese women have attempted to lose weight on many occasions by implementing changes in lifestyle, including diet and exercise, but have had only temporary success.
If your patient is motivated to begin a first or repeat attempt at weight loss, there are several helpful interventions you could recommend, including:
- consult with a nutritionist
- use smartphone apps to help
- support the diet plan (to track caloric intake, daily exercise, etc.)
- increase daily exercise to 1 hour
- join a group weight-loss program or support group
- eat breakfast every day
- avoid food binges on weekends and at night
- practice stress-reduction techniques.
If the combination of basic approaches do not result in her achieving sufficient weight loss, pharmacologic therapy can be considered.
Pharmacologic options
Pharmacologic therapy can be offered to all women with4:
- BMI of 30 kg/m2 or more
- BMI of 27 kg/m2 or more with comorbidities, such as hypertension, diabetes, dyslipidemia, or heart disease.
Pharmacologic options for long-term therapy include lorcaserin, orlistat, and phentermine-topiramate. Because of a risk of fetal malformations, women of childbearing age should have a monthly pregnancy test while taking phentermine-topiramate. Here, I focus on lorcaserin and orlistat, two agents that do not require monthly laboratory testing (TABLE). It is important to note that no weight-loss medicine should be prescribed to pregnant women.
Lorcaserin
Lorcaserin is a selective serotonin 2c receptor agonist. Lorcaserin reduces appetite and food intake. Other serotonergic medications previously used for weight loss, such as fenfluramine, stimulated the serotonin 2b receptor, which may have contributed to an increased risk of cardiac valve disease. Because lorcaserin is a selective serotonin 2c receptor agonist, it is less likely to cause cardiac valve disease.
Lorcaserin is taken as a 10-mg tablet twice daily.5 In one large trial, approximately 50% of patients who took the drug for 12 months lost at least 5% of their body mass.6 For those patients taking lorcaserin who do not lose 5% or more of their body mass by 12 weeks of therapy, it is recommended that the medication be discontinued because successful weight loss may not occur with continued therapy. These women could be offered treatment with orlistat.
The most common side effects of lorcaserin are headache, dizziness, fatigue, nausea, dry mouth, and constipation. The drug is contraindicated in those with renal failure or in patients who are taking other serotonergic medications, such as selective serotonin reuptake inhibitors, bupropion, tricyclic antidepressants, or monoamine oxidase inhibitors.
Orlistat
Orlistat is a reversible inhibitor of gastric and pancreatic lipases, thereby inhibiting fat absorption. This leads to weight loss but also causes an increase in fecal fat excretion, which may cause side effects such as borborygmi, abdominal cramps, flatus, oily spotting per rectum, loose stool, and fecal incontinence. Orlistat is taken 3 times daily with meals. Only 1% of the orlistat dose is absorbed into the circulation, minimizing the drug’s effect on other organs and reducing the probability of a medication interaction.
Orlistat may reduce the absorption of vitamins A, D, E, and K. Patients taking the drug should take a daily vitamin pill at bedtime to maximize absorption of the vitamins. According to a 2004 study in which orlistat was combined with behavioral intervention over 12 months, the average weight loss was approximately 10% of patients’ baseline weight.7 (The control group in this study received a placebo tablet plus behavioral intervention and experienced a 5% weight loss.) When orlistat treatment continues as long as 36 months, the reduced weight is typically maintained. Orlistat treatment also has been shown to reduce blood pressure in hypertensive patients and improve their lipid profiles.8,9
You should be aware that some health plans place weight-loss medications on a restricted formulary list that requires preapproval. From my experience, if you prescribe a weight-loss drug you may occasionally be asked to complete a case synopsis on a structured form that is sent to the health insurer or pharmacy management team for review and
preapproval.
Bariatric surgery
Consider bariatric surgery for women with:
- BMI of 40 kg/m2 or more
- BMI of 35 kg/m2 or more with comorbidities and no success with diet, exercise, and weight-loss medications.
Many bariatric surgery programs require that candidates undergo a 6-month interval of diet, exercise, lifestyle change, and psychological assessment prior to scheduling surgery. Bariatric surgery is the medical intervention most likely to result in major weight loss.10
Related article: Consider bariatric surgery first for severely obese women Robert L. Barbieri, MD (April 2008)
Call for input
As obstetricians and gynecologists, our duty is to continually strive to improve the health of all women. Overweight and obesity are highly prevalent major health problems—for society as a whole as well as for many of the individual patients we treat in our practices. Can we, and should we, provide more options to our patients who are trying to lose weight by offering to prescribe lorcaserin or orlistat?
This is a question for all of us. I would like to know your viewpoint on this issue.
Weigh in on the discussion!
Email your letter to Dr. Barbieri at rbarbieri@frontlinemedcom.com
or contact us by:
email: obg@frontlinemedcom.com
fax: 973-206-9251
letter: OBG Management
7 Century Drive, Suite 302
Parsippany, NJ 07054
INSTANT POLL
• Do you think primary care providers routinely present the treatment options of diet/exercise, weight-loss medicines, and bariatric surgery to obese patients?
• Should ObGyns offer to prescribe lorcaserin or orlistat to their obese patients?
Tell us—at rbarbieri@frontlinemedcom.com. Please include your name and city and state.
In clinical practice, weight problems are very common. Among US women, about one-third are obese, with another one-quarter overweight. As we know, obesity is a risk factor for many medical problems, including diabetes, hypertension, elevated cholesterol, stroke, heart disease, many cancers, sleep apnea, and arthritis.1 Obesity is also a risk factor for a long list of serious obstetric problems, including gestational hypertension, preeclampsia, gestational diabetes, fetal malformations, macrosomia, stillbirth, prematurity, and an increased rate of cesarean delivery.
Clearly, collectively, we need to play more of an active role in our patients’ weight loss and subsequent weight-maintenance efforts. To help us achieve this goal, we should be familiar with our patients’ weight status and comorbidities and offer helpful nonpharmacologic weight-loss interventions. We also should be cognizant of current pharmacologic and surgical options, and, when appropriate, be prepared to counsel patients about their efficacy.
Routinely calculate BMI and assess comorbidities
The body mass index (BMI) of every patient should be calculated and recorded in her medical record.
Be familiar with her BMI. For white, Hispanic, and black women, overweight is defined as a BMI between 25 and 29 kg/m2, and obesity is defined by a BMI of 30 kg/m2 or more.2 For Asian women, overweight begins at a BMI of 23 kg/m2, and obesity begins at a BMI of 25 kg/m2.
If she’s overweight, determine her comorbidities. For your patients with a BMI of 25 kg/m2 or more, assess them for medical comorbidities such as hypertension, dyslipidemia, diabetes, heart disease, and sleep apnea, as the presence of any of these conditions markedly increases the risk of adverse health outcomes. To determine if metabolic syndrome is a concern, measure blood pressure; waist circumference; and fasting triglyceride, fasting glucose, and serum high-density lipoprotein (HDL)-cholesterol levels. To detect prediabetes or diabetes mellitus, consider the hemoglobin A1c (HbA1c) test. The American College of Obstetricians and Gynecologists recommends that clinicians test for diabetes in all women aged 45 and older every 3 years.3
Start with the basics—diet and exercise
It is very difficult for women, and men, who are overweight or obese to successfully lose weight and maintain a normal BMI over time. Many overweight or obese women have attempted to lose weight on many occasions by implementing changes in lifestyle, including diet and exercise, but have had only temporary success.
If your patient is motivated to begin a first or repeat attempt at weight loss, there are several helpful interventions you could recommend, including:
- consult with a nutritionist
- use smartphone apps to help
- support the diet plan (to track caloric intake, daily exercise, etc.)
- increase daily exercise to 1 hour
- join a group weight-loss program or support group
- eat breakfast every day
- avoid food binges on weekends and at night
- practice stress-reduction techniques.
If the combination of basic approaches do not result in her achieving sufficient weight loss, pharmacologic therapy can be considered.
Pharmacologic options
Pharmacologic therapy can be offered to all women with4:
- BMI of 30 kg/m2 or more
- BMI of 27 kg/m2 or more with comorbidities, such as hypertension, diabetes, dyslipidemia, or heart disease.
Pharmacologic options for long-term therapy include lorcaserin, orlistat, and phentermine-topiramate. Because of a risk of fetal malformations, women of childbearing age should have a monthly pregnancy test while taking phentermine-topiramate. Here, I focus on lorcaserin and orlistat, two agents that do not require monthly laboratory testing (TABLE). It is important to note that no weight-loss medicine should be prescribed to pregnant women.
Lorcaserin
Lorcaserin is a selective serotonin 2c receptor agonist. Lorcaserin reduces appetite and food intake. Other serotonergic medications previously used for weight loss, such as fenfluramine, stimulated the serotonin 2b receptor, which may have contributed to an increased risk of cardiac valve disease. Because lorcaserin is a selective serotonin 2c receptor agonist, it is less likely to cause cardiac valve disease.
Lorcaserin is taken as a 10-mg tablet twice daily.5 In one large trial, approximately 50% of patients who took the drug for 12 months lost at least 5% of their body mass.6 For those patients taking lorcaserin who do not lose 5% or more of their body mass by 12 weeks of therapy, it is recommended that the medication be discontinued because successful weight loss may not occur with continued therapy. These women could be offered treatment with orlistat.
The most common side effects of lorcaserin are headache, dizziness, fatigue, nausea, dry mouth, and constipation. The drug is contraindicated in those with renal failure or in patients who are taking other serotonergic medications, such as selective serotonin reuptake inhibitors, bupropion, tricyclic antidepressants, or monoamine oxidase inhibitors.
Orlistat
Orlistat is a reversible inhibitor of gastric and pancreatic lipases, thereby inhibiting fat absorption. This leads to weight loss but also causes an increase in fecal fat excretion, which may cause side effects such as borborygmi, abdominal cramps, flatus, oily spotting per rectum, loose stool, and fecal incontinence. Orlistat is taken 3 times daily with meals. Only 1% of the orlistat dose is absorbed into the circulation, minimizing the drug’s effect on other organs and reducing the probability of a medication interaction.
Orlistat may reduce the absorption of vitamins A, D, E, and K. Patients taking the drug should take a daily vitamin pill at bedtime to maximize absorption of the vitamins. According to a 2004 study in which orlistat was combined with behavioral intervention over 12 months, the average weight loss was approximately 10% of patients’ baseline weight.7 (The control group in this study received a placebo tablet plus behavioral intervention and experienced a 5% weight loss.) When orlistat treatment continues as long as 36 months, the reduced weight is typically maintained. Orlistat treatment also has been shown to reduce blood pressure in hypertensive patients and improve their lipid profiles.8,9
You should be aware that some health plans place weight-loss medications on a restricted formulary list that requires preapproval. From my experience, if you prescribe a weight-loss drug you may occasionally be asked to complete a case synopsis on a structured form that is sent to the health insurer or pharmacy management team for review and
preapproval.
Bariatric surgery
Consider bariatric surgery for women with:
- BMI of 40 kg/m2 or more
- BMI of 35 kg/m2 or more with comorbidities and no success with diet, exercise, and weight-loss medications.
Many bariatric surgery programs require that candidates undergo a 6-month interval of diet, exercise, lifestyle change, and psychological assessment prior to scheduling surgery. Bariatric surgery is the medical intervention most likely to result in major weight loss.10
Related article: Consider bariatric surgery first for severely obese women Robert L. Barbieri, MD (April 2008)
Call for input
As obstetricians and gynecologists, our duty is to continually strive to improve the health of all women. Overweight and obesity are highly prevalent major health problems—for society as a whole as well as for many of the individual patients we treat in our practices. Can we, and should we, provide more options to our patients who are trying to lose weight by offering to prescribe lorcaserin or orlistat?
This is a question for all of us. I would like to know your viewpoint on this issue.
Weigh in on the discussion!
Email your letter to Dr. Barbieri at rbarbieri@frontlinemedcom.com
or contact us by:
email: obg@frontlinemedcom.com
fax: 973-206-9251
letter: OBG Management
7 Century Drive, Suite 302
Parsippany, NJ 07054
INSTANT POLL
• Do you think primary care providers routinely present the treatment options of diet/exercise, weight-loss medicines, and bariatric surgery to obese patients?
• Should ObGyns offer to prescribe lorcaserin or orlistat to their obese patients?
Tell us—at rbarbieri@frontlinemedcom.com. Please include your name and city and state.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among U.S. adults, 1999–2008. JAMA. 2010;303:235–241.
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9414):157–163.
- American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 483. Primary and preventive care: periodic assessments. Obstet Gynecol. 2011;117(4):1008–1015.
- Lau DC; Obesity Canada Clinical Practice Guidelines Steering Committee and Expert Panel. Synopsis of the 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children. CMAJ. 2007;176(8):1103–1106.
- Chan EW, He Y, Chui CS, Wong AY, Lau WC, Wong IC. Efficacy and safety of lorcaserin in obese adults: a meta-analysis of 1-year randomized controlled trials (RCTs) and narrative review on short-term RCTs. Obes Rev. 2013;14(5):383–392.
- Fidler MC, Sanchez M, Raether B, et al; BLOSSOM Clinical Trial Group. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011;96(10):3067–3077.
- Torgerson JS, Hauptman J, Boldrin MN, Sjostrom L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155–161.
- Siebenhofer A, Jeitler K, Horvath K, Berghold A, Siering U, Semlitsch T. Long-term effects of weight-reducing drugs in hypertensive patients. Cochrane Database Syst Rev. 2013;3:CD007654.
- Tonstad S, Pometta D, Erkelens DW, et al. The effect of the gastrointestinal lipase inhibitor, orlistat, on serum lipids and lipoproteins in patients with primary hyperlipidemia. Eur J Clin Pharmacol. 1994;46(5):405–410.
- Barbieri RL. Consider bariatric surgery first for severely obese women. OBG Manag. 2008;20(4):9, 14, 16.
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among U.S. adults, 1999–2008. JAMA. 2010;303:235–241.
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9414):157–163.
- American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 483. Primary and preventive care: periodic assessments. Obstet Gynecol. 2011;117(4):1008–1015.
- Lau DC; Obesity Canada Clinical Practice Guidelines Steering Committee and Expert Panel. Synopsis of the 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children. CMAJ. 2007;176(8):1103–1106.
- Chan EW, He Y, Chui CS, Wong AY, Lau WC, Wong IC. Efficacy and safety of lorcaserin in obese adults: a meta-analysis of 1-year randomized controlled trials (RCTs) and narrative review on short-term RCTs. Obes Rev. 2013;14(5):383–392.
- Fidler MC, Sanchez M, Raether B, et al; BLOSSOM Clinical Trial Group. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011;96(10):3067–3077.
- Torgerson JS, Hauptman J, Boldrin MN, Sjostrom L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155–161.
- Siebenhofer A, Jeitler K, Horvath K, Berghold A, Siering U, Semlitsch T. Long-term effects of weight-reducing drugs in hypertensive patients. Cochrane Database Syst Rev. 2013;3:CD007654.
- Tonstad S, Pometta D, Erkelens DW, et al. The effect of the gastrointestinal lipase inhibitor, orlistat, on serum lipids and lipoproteins in patients with primary hyperlipidemia. Eur J Clin Pharmacol. 1994;46(5):405–410.
- Barbieri RL. Consider bariatric surgery first for severely obese women. OBG Manag. 2008;20(4):9, 14, 16.
