User login
The Official Newspaper of the American Association for Thoracic Surgery
Surgery vs. waiting for flail leaflets
In patients with asymptomatic or minimally symptomatic mitral valve regurgitation as a result of flail mitral leaflets, early surgery yields better survival, lower risk of heart failure, and equivalent rates of atrial fibrillation, compared with watchful waiting, according to a report published online on August 13 in JAMA.
Overall long-term mortality is approximately 40% lower and HF risk approximately 60% lower for early surgery vs. watchful waiting. These benefits persist for up to 20 years and are seen across every important subgroup of patients, said Dr. Rakesh M. Suri of the Mayo Clinic, Rochester, Minn., and his associates.
These are the findings of a series of analyses of data from an international registry of consecutive patients diagnosed in routine clinical practice – the largest study in the world of the comparative effectiveness of early surgery vs. watchful waiting in patients without traditional indications for immediate surgery. The study results "emanate from institutions that together provide a very high rate of mitral valve repair (more than 90%) with low operative mortality, emphasizing that such results might also be achieved in routine practice at many advanced repair centers," the investigators noted.
Despite the safety and efficacy of current surgical correction of flail mitral leaflets, clinicians disagree as to the best approach for patients who have no or minimal HF symptoms, a left ventricular ejection fraction of 60% or more, and a left ventricular end-systolic diameter of 40 mm or more. Those who support watchful waiting consider the consequences of uncorrected mitral regurgitation to be benign, especially when weighed against the potential morbidity and mortality of early surgical intervention. North American guidelines favor early surgery while European guidelines favor watchful waiting.
The Mitral Regurgitation International Database (MIDA) – a registry of patients at two tertiary care centers in France, two in Italy, one in Belgium, and one in the United States – provided an ideal study population to compare the two approaches. For their study, Dr. Suri and his associates examined data for 1,021 of these patients who had been diagnosed in 1980-2004 and followed for up to 25 years (mean follow-up, 10.3 years).
This study included only patients who had no ischemic mitral regurgitation and no significant concomitant aortic valve disease, congenital heart disease, mitral stenosis, or previous valve surgery.
A total of 446 of these patients underwent early surgery (within 30 days of diagnosis) and 575 had watchful waiting at the discretion of their treating physicians. Importantly, 339 (59%) of the watchful-waiting group eventually were advised by their cardiologists to undergo valve repair, at a median of 1.65 years after diagnosis.
Overall, there were 319 deaths during follow-up.
The primary end points of this study were all-cause mortality at 5, 10, and 20 years.
In the initial, unadjusted analysis, survival was 95%, 86%, and 63%, respectively, with early surgery. In contrast, survival was significantly lower with watchful waiting, at 84% at 5 years, 69% at 10 years, and 41% at 20 years, the researchers said (JAMA 2013; 310:609-16).
The large survival benefit with early surgery was confirmed in a multivariable analysis that adjusted for patient age, sex, comorbidities, and the presence of subtle symptoms.
To account for differences between the two study groups in the propensity to undergo surgery, the investigators performed an analysis of the data in a set of 648 patients who were matched for age, comorbidities, and other factors. This analysis also showed a similar and distinct survival advantage with early surgery. Several subgroup analyses also confirmed the results.
Secondary end points were the incidence of heart failure and the onset of new atrial fibrillation during follow-up.
A total of 167 patients had at least one episode of HF. The rates were 7% with early surgery and 23% with watchful waiting at 10 years, and 10% vs. 35% at 20 years, showing a clear advantage for early surgery.
This strong advantage persisted in further analyses of the propensity-matched patients and in all other subgroups examined, at all time points examined.
New-onset AF developed in 227 patients overall. The rate was slightly higher in the early-surgery group during the immediate postoperative period but decreased thereafter and was equivalent between the two study groups at 5, 10, and 20 years.
"Long-term, the results are coherent by all methods used (direct comparison, adjusted comparison, propensity score matching, inverse probability weighing) that early surgical correction of mitral valve regurgitation was associated with a significant survival benefit (total mortality decrement of approximately 40%) and diminished HF risk (reduction of approximately 60%)," Dr. Suri and his associates wrote.
Dr. Suri reported ties to Edwards Lifesciences, Sorin Group, St. Jude Medical, and Abbott.
In patients with asymptomatic or minimally symptomatic mitral valve regurgitation as a result of flail mitral leaflets, early surgery yields better survival, lower risk of heart failure, and equivalent rates of atrial fibrillation, compared with watchful waiting, according to a report published online on August 13 in JAMA.
Overall long-term mortality is approximately 40% lower and HF risk approximately 60% lower for early surgery vs. watchful waiting. These benefits persist for up to 20 years and are seen across every important subgroup of patients, said Dr. Rakesh M. Suri of the Mayo Clinic, Rochester, Minn., and his associates.
These are the findings of a series of analyses of data from an international registry of consecutive patients diagnosed in routine clinical practice – the largest study in the world of the comparative effectiveness of early surgery vs. watchful waiting in patients without traditional indications for immediate surgery. The study results "emanate from institutions that together provide a very high rate of mitral valve repair (more than 90%) with low operative mortality, emphasizing that such results might also be achieved in routine practice at many advanced repair centers," the investigators noted.
Despite the safety and efficacy of current surgical correction of flail mitral leaflets, clinicians disagree as to the best approach for patients who have no or minimal HF symptoms, a left ventricular ejection fraction of 60% or more, and a left ventricular end-systolic diameter of 40 mm or more. Those who support watchful waiting consider the consequences of uncorrected mitral regurgitation to be benign, especially when weighed against the potential morbidity and mortality of early surgical intervention. North American guidelines favor early surgery while European guidelines favor watchful waiting.
The Mitral Regurgitation International Database (MIDA) – a registry of patients at two tertiary care centers in France, two in Italy, one in Belgium, and one in the United States – provided an ideal study population to compare the two approaches. For their study, Dr. Suri and his associates examined data for 1,021 of these patients who had been diagnosed in 1980-2004 and followed for up to 25 years (mean follow-up, 10.3 years).
This study included only patients who had no ischemic mitral regurgitation and no significant concomitant aortic valve disease, congenital heart disease, mitral stenosis, or previous valve surgery.
A total of 446 of these patients underwent early surgery (within 30 days of diagnosis) and 575 had watchful waiting at the discretion of their treating physicians. Importantly, 339 (59%) of the watchful-waiting group eventually were advised by their cardiologists to undergo valve repair, at a median of 1.65 years after diagnosis.
Overall, there were 319 deaths during follow-up.
The primary end points of this study were all-cause mortality at 5, 10, and 20 years.
In the initial, unadjusted analysis, survival was 95%, 86%, and 63%, respectively, with early surgery. In contrast, survival was significantly lower with watchful waiting, at 84% at 5 years, 69% at 10 years, and 41% at 20 years, the researchers said (JAMA 2013; 310:609-16).
The large survival benefit with early surgery was confirmed in a multivariable analysis that adjusted for patient age, sex, comorbidities, and the presence of subtle symptoms.
To account for differences between the two study groups in the propensity to undergo surgery, the investigators performed an analysis of the data in a set of 648 patients who were matched for age, comorbidities, and other factors. This analysis also showed a similar and distinct survival advantage with early surgery. Several subgroup analyses also confirmed the results.
Secondary end points were the incidence of heart failure and the onset of new atrial fibrillation during follow-up.
A total of 167 patients had at least one episode of HF. The rates were 7% with early surgery and 23% with watchful waiting at 10 years, and 10% vs. 35% at 20 years, showing a clear advantage for early surgery.
This strong advantage persisted in further analyses of the propensity-matched patients and in all other subgroups examined, at all time points examined.
New-onset AF developed in 227 patients overall. The rate was slightly higher in the early-surgery group during the immediate postoperative period but decreased thereafter and was equivalent between the two study groups at 5, 10, and 20 years.
"Long-term, the results are coherent by all methods used (direct comparison, adjusted comparison, propensity score matching, inverse probability weighing) that early surgical correction of mitral valve regurgitation was associated with a significant survival benefit (total mortality decrement of approximately 40%) and diminished HF risk (reduction of approximately 60%)," Dr. Suri and his associates wrote.
Dr. Suri reported ties to Edwards Lifesciences, Sorin Group, St. Jude Medical, and Abbott.
In patients with asymptomatic or minimally symptomatic mitral valve regurgitation as a result of flail mitral leaflets, early surgery yields better survival, lower risk of heart failure, and equivalent rates of atrial fibrillation, compared with watchful waiting, according to a report published online on August 13 in JAMA.
Overall long-term mortality is approximately 40% lower and HF risk approximately 60% lower for early surgery vs. watchful waiting. These benefits persist for up to 20 years and are seen across every important subgroup of patients, said Dr. Rakesh M. Suri of the Mayo Clinic, Rochester, Minn., and his associates.
These are the findings of a series of analyses of data from an international registry of consecutive patients diagnosed in routine clinical practice – the largest study in the world of the comparative effectiveness of early surgery vs. watchful waiting in patients without traditional indications for immediate surgery. The study results "emanate from institutions that together provide a very high rate of mitral valve repair (more than 90%) with low operative mortality, emphasizing that such results might also be achieved in routine practice at many advanced repair centers," the investigators noted.
Despite the safety and efficacy of current surgical correction of flail mitral leaflets, clinicians disagree as to the best approach for patients who have no or minimal HF symptoms, a left ventricular ejection fraction of 60% or more, and a left ventricular end-systolic diameter of 40 mm or more. Those who support watchful waiting consider the consequences of uncorrected mitral regurgitation to be benign, especially when weighed against the potential morbidity and mortality of early surgical intervention. North American guidelines favor early surgery while European guidelines favor watchful waiting.
The Mitral Regurgitation International Database (MIDA) – a registry of patients at two tertiary care centers in France, two in Italy, one in Belgium, and one in the United States – provided an ideal study population to compare the two approaches. For their study, Dr. Suri and his associates examined data for 1,021 of these patients who had been diagnosed in 1980-2004 and followed for up to 25 years (mean follow-up, 10.3 years).
This study included only patients who had no ischemic mitral regurgitation and no significant concomitant aortic valve disease, congenital heart disease, mitral stenosis, or previous valve surgery.
A total of 446 of these patients underwent early surgery (within 30 days of diagnosis) and 575 had watchful waiting at the discretion of their treating physicians. Importantly, 339 (59%) of the watchful-waiting group eventually were advised by their cardiologists to undergo valve repair, at a median of 1.65 years after diagnosis.
Overall, there were 319 deaths during follow-up.
The primary end points of this study were all-cause mortality at 5, 10, and 20 years.
In the initial, unadjusted analysis, survival was 95%, 86%, and 63%, respectively, with early surgery. In contrast, survival was significantly lower with watchful waiting, at 84% at 5 years, 69% at 10 years, and 41% at 20 years, the researchers said (JAMA 2013; 310:609-16).
The large survival benefit with early surgery was confirmed in a multivariable analysis that adjusted for patient age, sex, comorbidities, and the presence of subtle symptoms.
To account for differences between the two study groups in the propensity to undergo surgery, the investigators performed an analysis of the data in a set of 648 patients who were matched for age, comorbidities, and other factors. This analysis also showed a similar and distinct survival advantage with early surgery. Several subgroup analyses also confirmed the results.
Secondary end points were the incidence of heart failure and the onset of new atrial fibrillation during follow-up.
A total of 167 patients had at least one episode of HF. The rates were 7% with early surgery and 23% with watchful waiting at 10 years, and 10% vs. 35% at 20 years, showing a clear advantage for early surgery.
This strong advantage persisted in further analyses of the propensity-matched patients and in all other subgroups examined, at all time points examined.
New-onset AF developed in 227 patients overall. The rate was slightly higher in the early-surgery group during the immediate postoperative period but decreased thereafter and was equivalent between the two study groups at 5, 10, and 20 years.
"Long-term, the results are coherent by all methods used (direct comparison, adjusted comparison, propensity score matching, inverse probability weighing) that early surgical correction of mitral valve regurgitation was associated with a significant survival benefit (total mortality decrement of approximately 40%) and diminished HF risk (reduction of approximately 60%)," Dr. Suri and his associates wrote.
Dr. Suri reported ties to Edwards Lifesciences, Sorin Group, St. Jude Medical, and Abbott.
Major finding: Survival at 5, 10, and 20 years was 95%, 86%, and 63%, respectively, with early surgery, compared with 84%, 69%, and 41%, respectively, with watchful waiting.
Data source: Serial analyses of data on 1,021 patients with asymptomatic or minimally symptomatic mitral valve regurgitation caused by flail mitral leaflets who were advised to undergo early repair (446 subjects) or watchful waiting (575 subjects) and were followed for up to 25 years.
Disclosures: Dr. Suri reported ties to Edwards Lifesciences, Sorin Group, St. Jude Medical, and Abbott. His associates reported ties to Edwards Lifesciences, Valtech, and Abbott Vascular.
TSFRE announces a new Awards Program
Dear Colleague,
This is to officially announce the launch of the Thoracic Surgery Foundation for Research and Education (TSFRE) 2014 Awards Program. Please view the TSFRE Summer Newsletter with information about the 2014 Awards Program, including award descriptions, a timeline, links to download award applications, and a list of 2014 Research and Education Committee members (http://tinyurl.com/kfzdjz9).
Inside the issue you’ll find a special tribute to Dr. Carolyn E. Reed, a timely essay concerning the need to support cardiothoracic surgery research in today’s climate, and information about TSFRE’s mission and history of supporting cardiothoracic surgery research and education initiatives. You’ll also see the faces of many TSFRE supporters and friends.

I’d also like to mention that 2013 marks the 25th Anniversary of TSFRE. Since 1988, we have supported over $11 million toward cardiothoracic surgery research projects. We could not have accomplished this without the partnership of our society friends, the American Association for Thoracic Surgery (AATS), The Society of Thoracic Surgeons (STS), the Southern Thoracic Surgical Association (STSA), and the Western Thoracic Surgical Association (WTSA). And, we especially could not have achieved this without your support.
The quality and quantity of TSFRE-funded projects over the past 25 years have been phenomenal. Please join me today in making a contribution to the TSFRE 25th Anniversary Campaign by clicking on the link in the newsletter. Your donation will help ensure that TSFRE can continue funding important cardiothoracic surgery research and education for the next 25 years.
Thank you for your generosity as we head into our 25th year!
G. Alexander Patterson, M.D.
TSFRE President
Dear Colleague,
This is to officially announce the launch of the Thoracic Surgery Foundation for Research and Education (TSFRE) 2014 Awards Program. Please view the TSFRE Summer Newsletter with information about the 2014 Awards Program, including award descriptions, a timeline, links to download award applications, and a list of 2014 Research and Education Committee members (http://tinyurl.com/kfzdjz9).
Inside the issue you’ll find a special tribute to Dr. Carolyn E. Reed, a timely essay concerning the need to support cardiothoracic surgery research in today’s climate, and information about TSFRE’s mission and history of supporting cardiothoracic surgery research and education initiatives. You’ll also see the faces of many TSFRE supporters and friends.
I’d also like to mention that 2013 marks the 25th Anniversary of TSFRE. Since 1988, we have supported over $11 million toward cardiothoracic surgery research projects. We could not have accomplished this without the partnership of our society friends, the American Association for Thoracic Surgery (AATS), The Society of Thoracic Surgeons (STS), the Southern Thoracic Surgical Association (STSA), and the Western Thoracic Surgical Association (WTSA). And, we especially could not have achieved this without your support.
The quality and quantity of TSFRE-funded projects over the past 25 years have been phenomenal. Please join me today in making a contribution to the TSFRE 25th Anniversary Campaign by clicking on the link in the newsletter. Your donation will help ensure that TSFRE can continue funding important cardiothoracic surgery research and education for the next 25 years.
Thank you for your generosity as we head into our 25th year!
G. Alexander Patterson, M.D.
TSFRE President
Dear Colleague,
This is to officially announce the launch of the Thoracic Surgery Foundation for Research and Education (TSFRE) 2014 Awards Program. Please view the TSFRE Summer Newsletter with information about the 2014 Awards Program, including award descriptions, a timeline, links to download award applications, and a list of 2014 Research and Education Committee members (http://tinyurl.com/kfzdjz9).
Inside the issue you’ll find a special tribute to Dr. Carolyn E. Reed, a timely essay concerning the need to support cardiothoracic surgery research in today’s climate, and information about TSFRE’s mission and history of supporting cardiothoracic surgery research and education initiatives. You’ll also see the faces of many TSFRE supporters and friends.
I’d also like to mention that 2013 marks the 25th Anniversary of TSFRE. Since 1988, we have supported over $11 million toward cardiothoracic surgery research projects. We could not have accomplished this without the partnership of our society friends, the American Association for Thoracic Surgery (AATS), The Society of Thoracic Surgeons (STS), the Southern Thoracic Surgical Association (STSA), and the Western Thoracic Surgical Association (WTSA). And, we especially could not have achieved this without your support.
The quality and quantity of TSFRE-funded projects over the past 25 years have been phenomenal. Please join me today in making a contribution to the TSFRE 25th Anniversary Campaign by clicking on the link in the newsletter. Your donation will help ensure that TSFRE can continue funding important cardiothoracic surgery research and education for the next 25 years.
Thank you for your generosity as we head into our 25th year!
G. Alexander Patterson, M.D.
TSFRE President

The new trainee curriculum arrives
Much anticipated by many, exciting to the tech-savvy among us, and unbeknownst to others, yet equally relevant to all: The new curriculum is here. Whether you are a trainee, an educator, or a thoracic surgeon interested in the future of our specialty, the unveiling of the new curriculum is of key significance.
In 1992, at the Joint Conference on Graduate Education in Thoracic Surgery, significant emphasis was placed upon curricular change for thoracic surgical education. In response, the Thoracic Surgery Directors Association (TSDA) initiated the comprehensive thoracic surgery curriculum project in order to develop a consensus as to the content that ought to be learned during thoracic surgical training. Published in 1994, and available online, the TSDA Curriculum was intended to serve as a study guide to individual trainees and a useful resource for Program Directors. While of enormous utility over the last 2 decades, the curriculum is getting a makeover.

Being released this July is a brand-new curriculum, with updated topics and an excitingly novel platform, as a collaborative project from several organizations committed to thoracic surgical education. The Joint Council on Thoracic Surgery Education (JCTSE) has been working closely with the TSDA, with significant input from the American Board of Thoracic Surgery (ABTS), the Society of Thoracic Surgeons (STS), and the Residency Review Committee (RRC) for Thoracic Surgery. Dr. Ara Vaporciyan, Program Director at the University of Texas MD Anderson Cancer Center and 2013 Secretary/Treasurer of the TSDA, has been a key player in the development of the new curriculum.
When asked about the impetus for developing a new curriculum, Dr. Vaporciyan acknowledges that the old curriculum was an enormous advantage when first introduced, but that, now, it is somewhat outdated, and, further, new technology allows us to deliver the content better and more efficiently. Further, Dr. Vaporciyan highlights the valuable aspect of the new curriculum that links its content to expectations of the ABTS for board certification and the requirements of the Accreditation Council for Graduate Medical Education (ACGME) Milestones project.
Similar to the old curriculum, the basic architecture of the new curriculum contains 88-90 separate topics. However, within the new curriculum, the topics have been selected to cover each element of the published learning objectives provided by the ABTS.
Specific topics were identified by appointed section editors (Cardiac: Drs. James Fann and Craig Baker, Thoracic: DRs. Stephen Yang and Ara Vaporciyan, Congenital: Drs. Ram Subramanyan and Winfield Wells). Approximately 20 topic editors from all over the country have helped populate the new curriculum with content, and have additionally provided some input toward the division of topics.
For many, the most exciting feature of the new curriculum relates to the way that the educational materials will be delivered. Using WebBrain software (TheBrain, Los Angeles) for content management, all topics are organized like a mind map. For example, on the main tree, one can click on Thoracic Surgery, then neoplasm of the lung, which then explodes into three related topics: medical knowledge, patient care, and technical skills, which each branch out further. As explained by Dr. Vaporciyan, "the learning objectives of the ABTS provide the structure of the tree – its trunk and main branches – while the content components, provided by the topic editors, serve as the leaves on the ends of the branches."
So what exactly makes up those leaves at the end of the branches? The multi-media material is 100% pre-existing, coming from six different textbooks, up-to-date literature, online presentations created by the TSDA, and societal guidelines. In addition to the WebBrain content management system, the new curriculum utilizes a Moodle-based (Moodle Pty. Ltd., Perth, Australia) platform for organizing specific lessons plans and weekly curricular goals. Moodle (modular object-oriented dynamic learning environment) is an e-learning software platform, also known as a virtual learning environment.
With features such as assignment submission, quiz completion, discussion forums, file download capabilities, and opportunities for instructors to track individual trainee use, the potential opportunities for future growth are enormous. Within the new TSDA curriculum, trainees will receive a weekly email (as they have with the previous version of the curriculum). This email will direct them to a Moodle course for that week, such as "cardiac disease 1," which will provide to direct links within the WebBrain to all of the topics expected to be covered that week, ultimately providing access to the relevant multi-media materials. Once one has accessed the WebBrain, he or she can surf anywhere within the content tree.
The curriculum will be released in two phases. Phase I entails releasing the content which has been populated onto the WebBrain, utilizing Moodle as the access point. Phase II, which is expected to occur over the coming year, will include a more robust Moodle site. These courses will be fleshed out to each include a multiple-choice quiz with feedback, a wiki page, opportunities for commentary, and a means of gathering feedback from end-users regarding the curriculum. Access to these courses will be free of charge to thoracic surgical residents in the United States and Canada, as well as to program coordinators and faculty. Graduating residents will have access for 1 additional year in order to use the curriculum as a tool to prepare for Boards.
Dr. Edward Verrier, JCTSE Surgical Director of Education, explains that "the curriculum revision is a number of years in conception, preparation, organization, and now implementation. It is the combined effort of a number of dedicated educators and societies with some financial support from industry."
Referencing Salman Kahn in The One World Schoolhouse: Education Reimagined, Dr. Verrier continues: "We believe that this educational tool, using both a learning management and content management electronic based platform, has the potential to ‘flip the classroom.’ With work hour restrictions for residents, a constantly increasing body of knowledge, and the challenges of teaching in the operating room, we believe the new Thoracic Surgery Curriculum has the potential to transform our current approach to surgical education."
So what does this mean for trainees? As stated by Dr. Vaporciyan, "the biggest benefit to the trainees is that, with this content and related quizzes, individuals will have the ability to assess their own needs, have immediate access to relevant content that is free of charge, and, importantly, it is the ABTS intent to ultimately derive the examination material from this new electronic curriculum." Yes, it’s true. The board has agreed that the new curriculum will serve as a template of the content for both the written and oral examinations, making this curriculum the ideal study source for trainees. Dr. John Calhoon, chair of the ABTS, reports that "it is our goal to make sure that we draw questions in the future from the content that is called for in our outline and encompassed by the efforts of this new curriculum’s editors." (And did I mention that it’s free and immediately accessible on the Internet?)
And what about for the educators out there – what does this mean for you? Vaporciyan highlights three key advantages for the teachers: 1) the curriculum is completely malleable, so you can take whatever topic you want your learners to focus upon, and you can add to it or separate topics in any way, such as rotation preparation or linear knowledge acquisition; 2) through learner management aspects of Moodle, you can track all of your learners’ progress; 3) the curriculum is linked to Milestones, which should dramatically assist with meeting this requirement of the ACGME.
As mentioned by Dr. Vaporciyan, the Milestones Project is an important recent endeavor of the ACGME, mandating that all specialty groups develop outcome-based goals for resident performance within the six domains of clinical competence. The milestones will be used by the ACGME to demonstrate accountability of effectiveness of education within ACGME-accredited programs, and, looking ahead, resident performance on milestones will become a source of normative data for the RRC to use in assessing residency programs and facilitating improvements. Linking the new curriculum to milestones will render it a great tool to program directors in ACGME-accredited programs. As explained by Dr. Calhoon, "the RRC is working with the Milestones effort to align the individual curricular modules so that residency training programs will find further synergy and utility in adapting or frankly using the curriculum ‘right off the shelf.’"
When asked about the new curriculum, President of the TSDA Dr. David Fullerton shares with us that "along with the other organizations within our specialty, the TSDA is committed to the education of our residents. The TSDA feels that the consolidation of our specialty’s curricular efforts in this way is a significant advance in thoracic surgical education." Further, Dr. Fullerton acknowledges that the new curriculum "will afford our residents immediate electronic access to important educational materials and will be flexible enough for adaption in individual programs." With gratitude on behalf of the TSDA, Dr. Fullerton congratulates all of the individuals who have contributed to making the Thoracic Surgery Curriculum a reality.
Clearly, this new curriculum has much to offer, for both the teacher and the student. It will be of significant interest to track use and observe associated relationships with subsequent board examination success.
In anticipation of an Aug. 1 launch, notifications regarding accessing the site were provided to residents and program directors via email throughout the month of July. More information on the new curriculum, as well as an introductory video, is found at www.tsda.org/education/thoracic-surgery-curricula.
And we will continue to follow and discuss the new curriculum in these pages of the Residents’ Corner.
Much anticipated by many, exciting to the tech-savvy among us, and unbeknownst to others, yet equally relevant to all: The new curriculum is here. Whether you are a trainee, an educator, or a thoracic surgeon interested in the future of our specialty, the unveiling of the new curriculum is of key significance.
In 1992, at the Joint Conference on Graduate Education in Thoracic Surgery, significant emphasis was placed upon curricular change for thoracic surgical education. In response, the Thoracic Surgery Directors Association (TSDA) initiated the comprehensive thoracic surgery curriculum project in order to develop a consensus as to the content that ought to be learned during thoracic surgical training. Published in 1994, and available online, the TSDA Curriculum was intended to serve as a study guide to individual trainees and a useful resource for Program Directors. While of enormous utility over the last 2 decades, the curriculum is getting a makeover.
Being released this July is a brand-new curriculum, with updated topics and an excitingly novel platform, as a collaborative project from several organizations committed to thoracic surgical education. The Joint Council on Thoracic Surgery Education (JCTSE) has been working closely with the TSDA, with significant input from the American Board of Thoracic Surgery (ABTS), the Society of Thoracic Surgeons (STS), and the Residency Review Committee (RRC) for Thoracic Surgery. Dr. Ara Vaporciyan, Program Director at the University of Texas MD Anderson Cancer Center and 2013 Secretary/Treasurer of the TSDA, has been a key player in the development of the new curriculum.
When asked about the impetus for developing a new curriculum, Dr. Vaporciyan acknowledges that the old curriculum was an enormous advantage when first introduced, but that, now, it is somewhat outdated, and, further, new technology allows us to deliver the content better and more efficiently. Further, Dr. Vaporciyan highlights the valuable aspect of the new curriculum that links its content to expectations of the ABTS for board certification and the requirements of the Accreditation Council for Graduate Medical Education (ACGME) Milestones project.
Similar to the old curriculum, the basic architecture of the new curriculum contains 88-90 separate topics. However, within the new curriculum, the topics have been selected to cover each element of the published learning objectives provided by the ABTS.
Specific topics were identified by appointed section editors (Cardiac: Drs. James Fann and Craig Baker, Thoracic: DRs. Stephen Yang and Ara Vaporciyan, Congenital: Drs. Ram Subramanyan and Winfield Wells). Approximately 20 topic editors from all over the country have helped populate the new curriculum with content, and have additionally provided some input toward the division of topics.
For many, the most exciting feature of the new curriculum relates to the way that the educational materials will be delivered. Using WebBrain software (TheBrain, Los Angeles) for content management, all topics are organized like a mind map. For example, on the main tree, one can click on Thoracic Surgery, then neoplasm of the lung, which then explodes into three related topics: medical knowledge, patient care, and technical skills, which each branch out further. As explained by Dr. Vaporciyan, "the learning objectives of the ABTS provide the structure of the tree – its trunk and main branches – while the content components, provided by the topic editors, serve as the leaves on the ends of the branches."
So what exactly makes up those leaves at the end of the branches? The multi-media material is 100% pre-existing, coming from six different textbooks, up-to-date literature, online presentations created by the TSDA, and societal guidelines. In addition to the WebBrain content management system, the new curriculum utilizes a Moodle-based (Moodle Pty. Ltd., Perth, Australia) platform for organizing specific lessons plans and weekly curricular goals. Moodle (modular object-oriented dynamic learning environment) is an e-learning software platform, also known as a virtual learning environment.
With features such as assignment submission, quiz completion, discussion forums, file download capabilities, and opportunities for instructors to track individual trainee use, the potential opportunities for future growth are enormous. Within the new TSDA curriculum, trainees will receive a weekly email (as they have with the previous version of the curriculum). This email will direct them to a Moodle course for that week, such as "cardiac disease 1," which will provide to direct links within the WebBrain to all of the topics expected to be covered that week, ultimately providing access to the relevant multi-media materials. Once one has accessed the WebBrain, he or she can surf anywhere within the content tree.
The curriculum will be released in two phases. Phase I entails releasing the content which has been populated onto the WebBrain, utilizing Moodle as the access point. Phase II, which is expected to occur over the coming year, will include a more robust Moodle site. These courses will be fleshed out to each include a multiple-choice quiz with feedback, a wiki page, opportunities for commentary, and a means of gathering feedback from end-users regarding the curriculum. Access to these courses will be free of charge to thoracic surgical residents in the United States and Canada, as well as to program coordinators and faculty. Graduating residents will have access for 1 additional year in order to use the curriculum as a tool to prepare for Boards.
Dr. Edward Verrier, JCTSE Surgical Director of Education, explains that "the curriculum revision is a number of years in conception, preparation, organization, and now implementation. It is the combined effort of a number of dedicated educators and societies with some financial support from industry."
Referencing Salman Kahn in The One World Schoolhouse: Education Reimagined, Dr. Verrier continues: "We believe that this educational tool, using both a learning management and content management electronic based platform, has the potential to ‘flip the classroom.’ With work hour restrictions for residents, a constantly increasing body of knowledge, and the challenges of teaching in the operating room, we believe the new Thoracic Surgery Curriculum has the potential to transform our current approach to surgical education."
So what does this mean for trainees? As stated by Dr. Vaporciyan, "the biggest benefit to the trainees is that, with this content and related quizzes, individuals will have the ability to assess their own needs, have immediate access to relevant content that is free of charge, and, importantly, it is the ABTS intent to ultimately derive the examination material from this new electronic curriculum." Yes, it’s true. The board has agreed that the new curriculum will serve as a template of the content for both the written and oral examinations, making this curriculum the ideal study source for trainees. Dr. John Calhoon, chair of the ABTS, reports that "it is our goal to make sure that we draw questions in the future from the content that is called for in our outline and encompassed by the efforts of this new curriculum’s editors." (And did I mention that it’s free and immediately accessible on the Internet?)
And what about for the educators out there – what does this mean for you? Vaporciyan highlights three key advantages for the teachers: 1) the curriculum is completely malleable, so you can take whatever topic you want your learners to focus upon, and you can add to it or separate topics in any way, such as rotation preparation or linear knowledge acquisition; 2) through learner management aspects of Moodle, you can track all of your learners’ progress; 3) the curriculum is linked to Milestones, which should dramatically assist with meeting this requirement of the ACGME.
As mentioned by Dr. Vaporciyan, the Milestones Project is an important recent endeavor of the ACGME, mandating that all specialty groups develop outcome-based goals for resident performance within the six domains of clinical competence. The milestones will be used by the ACGME to demonstrate accountability of effectiveness of education within ACGME-accredited programs, and, looking ahead, resident performance on milestones will become a source of normative data for the RRC to use in assessing residency programs and facilitating improvements. Linking the new curriculum to milestones will render it a great tool to program directors in ACGME-accredited programs. As explained by Dr. Calhoon, "the RRC is working with the Milestones effort to align the individual curricular modules so that residency training programs will find further synergy and utility in adapting or frankly using the curriculum ‘right off the shelf.’"
When asked about the new curriculum, President of the TSDA Dr. David Fullerton shares with us that "along with the other organizations within our specialty, the TSDA is committed to the education of our residents. The TSDA feels that the consolidation of our specialty’s curricular efforts in this way is a significant advance in thoracic surgical education." Further, Dr. Fullerton acknowledges that the new curriculum "will afford our residents immediate electronic access to important educational materials and will be flexible enough for adaption in individual programs." With gratitude on behalf of the TSDA, Dr. Fullerton congratulates all of the individuals who have contributed to making the Thoracic Surgery Curriculum a reality.
Clearly, this new curriculum has much to offer, for both the teacher and the student. It will be of significant interest to track use and observe associated relationships with subsequent board examination success.
In anticipation of an Aug. 1 launch, notifications regarding accessing the site were provided to residents and program directors via email throughout the month of July. More information on the new curriculum, as well as an introductory video, is found at www.tsda.org/education/thoracic-surgery-curricula.
And we will continue to follow and discuss the new curriculum in these pages of the Residents’ Corner.
Much anticipated by many, exciting to the tech-savvy among us, and unbeknownst to others, yet equally relevant to all: The new curriculum is here. Whether you are a trainee, an educator, or a thoracic surgeon interested in the future of our specialty, the unveiling of the new curriculum is of key significance.
In 1992, at the Joint Conference on Graduate Education in Thoracic Surgery, significant emphasis was placed upon curricular change for thoracic surgical education. In response, the Thoracic Surgery Directors Association (TSDA) initiated the comprehensive thoracic surgery curriculum project in order to develop a consensus as to the content that ought to be learned during thoracic surgical training. Published in 1994, and available online, the TSDA Curriculum was intended to serve as a study guide to individual trainees and a useful resource for Program Directors. While of enormous utility over the last 2 decades, the curriculum is getting a makeover.
Being released this July is a brand-new curriculum, with updated topics and an excitingly novel platform, as a collaborative project from several organizations committed to thoracic surgical education. The Joint Council on Thoracic Surgery Education (JCTSE) has been working closely with the TSDA, with significant input from the American Board of Thoracic Surgery (ABTS), the Society of Thoracic Surgeons (STS), and the Residency Review Committee (RRC) for Thoracic Surgery. Dr. Ara Vaporciyan, Program Director at the University of Texas MD Anderson Cancer Center and 2013 Secretary/Treasurer of the TSDA, has been a key player in the development of the new curriculum.
When asked about the impetus for developing a new curriculum, Dr. Vaporciyan acknowledges that the old curriculum was an enormous advantage when first introduced, but that, now, it is somewhat outdated, and, further, new technology allows us to deliver the content better and more efficiently. Further, Dr. Vaporciyan highlights the valuable aspect of the new curriculum that links its content to expectations of the ABTS for board certification and the requirements of the Accreditation Council for Graduate Medical Education (ACGME) Milestones project.
Similar to the old curriculum, the basic architecture of the new curriculum contains 88-90 separate topics. However, within the new curriculum, the topics have been selected to cover each element of the published learning objectives provided by the ABTS.
Specific topics were identified by appointed section editors (Cardiac: Drs. James Fann and Craig Baker, Thoracic: DRs. Stephen Yang and Ara Vaporciyan, Congenital: Drs. Ram Subramanyan and Winfield Wells). Approximately 20 topic editors from all over the country have helped populate the new curriculum with content, and have additionally provided some input toward the division of topics.
For many, the most exciting feature of the new curriculum relates to the way that the educational materials will be delivered. Using WebBrain software (TheBrain, Los Angeles) for content management, all topics are organized like a mind map. For example, on the main tree, one can click on Thoracic Surgery, then neoplasm of the lung, which then explodes into three related topics: medical knowledge, patient care, and technical skills, which each branch out further. As explained by Dr. Vaporciyan, "the learning objectives of the ABTS provide the structure of the tree – its trunk and main branches – while the content components, provided by the topic editors, serve as the leaves on the ends of the branches."
So what exactly makes up those leaves at the end of the branches? The multi-media material is 100% pre-existing, coming from six different textbooks, up-to-date literature, online presentations created by the TSDA, and societal guidelines. In addition to the WebBrain content management system, the new curriculum utilizes a Moodle-based (Moodle Pty. Ltd., Perth, Australia) platform for organizing specific lessons plans and weekly curricular goals. Moodle (modular object-oriented dynamic learning environment) is an e-learning software platform, also known as a virtual learning environment.
With features such as assignment submission, quiz completion, discussion forums, file download capabilities, and opportunities for instructors to track individual trainee use, the potential opportunities for future growth are enormous. Within the new TSDA curriculum, trainees will receive a weekly email (as they have with the previous version of the curriculum). This email will direct them to a Moodle course for that week, such as "cardiac disease 1," which will provide to direct links within the WebBrain to all of the topics expected to be covered that week, ultimately providing access to the relevant multi-media materials. Once one has accessed the WebBrain, he or she can surf anywhere within the content tree.
The curriculum will be released in two phases. Phase I entails releasing the content which has been populated onto the WebBrain, utilizing Moodle as the access point. Phase II, which is expected to occur over the coming year, will include a more robust Moodle site. These courses will be fleshed out to each include a multiple-choice quiz with feedback, a wiki page, opportunities for commentary, and a means of gathering feedback from end-users regarding the curriculum. Access to these courses will be free of charge to thoracic surgical residents in the United States and Canada, as well as to program coordinators and faculty. Graduating residents will have access for 1 additional year in order to use the curriculum as a tool to prepare for Boards.
Dr. Edward Verrier, JCTSE Surgical Director of Education, explains that "the curriculum revision is a number of years in conception, preparation, organization, and now implementation. It is the combined effort of a number of dedicated educators and societies with some financial support from industry."
Referencing Salman Kahn in The One World Schoolhouse: Education Reimagined, Dr. Verrier continues: "We believe that this educational tool, using both a learning management and content management electronic based platform, has the potential to ‘flip the classroom.’ With work hour restrictions for residents, a constantly increasing body of knowledge, and the challenges of teaching in the operating room, we believe the new Thoracic Surgery Curriculum has the potential to transform our current approach to surgical education."
So what does this mean for trainees? As stated by Dr. Vaporciyan, "the biggest benefit to the trainees is that, with this content and related quizzes, individuals will have the ability to assess their own needs, have immediate access to relevant content that is free of charge, and, importantly, it is the ABTS intent to ultimately derive the examination material from this new electronic curriculum." Yes, it’s true. The board has agreed that the new curriculum will serve as a template of the content for both the written and oral examinations, making this curriculum the ideal study source for trainees. Dr. John Calhoon, chair of the ABTS, reports that "it is our goal to make sure that we draw questions in the future from the content that is called for in our outline and encompassed by the efforts of this new curriculum’s editors." (And did I mention that it’s free and immediately accessible on the Internet?)
And what about for the educators out there – what does this mean for you? Vaporciyan highlights three key advantages for the teachers: 1) the curriculum is completely malleable, so you can take whatever topic you want your learners to focus upon, and you can add to it or separate topics in any way, such as rotation preparation or linear knowledge acquisition; 2) through learner management aspects of Moodle, you can track all of your learners’ progress; 3) the curriculum is linked to Milestones, which should dramatically assist with meeting this requirement of the ACGME.
As mentioned by Dr. Vaporciyan, the Milestones Project is an important recent endeavor of the ACGME, mandating that all specialty groups develop outcome-based goals for resident performance within the six domains of clinical competence. The milestones will be used by the ACGME to demonstrate accountability of effectiveness of education within ACGME-accredited programs, and, looking ahead, resident performance on milestones will become a source of normative data for the RRC to use in assessing residency programs and facilitating improvements. Linking the new curriculum to milestones will render it a great tool to program directors in ACGME-accredited programs. As explained by Dr. Calhoon, "the RRC is working with the Milestones effort to align the individual curricular modules so that residency training programs will find further synergy and utility in adapting or frankly using the curriculum ‘right off the shelf.’"
When asked about the new curriculum, President of the TSDA Dr. David Fullerton shares with us that "along with the other organizations within our specialty, the TSDA is committed to the education of our residents. The TSDA feels that the consolidation of our specialty’s curricular efforts in this way is a significant advance in thoracic surgical education." Further, Dr. Fullerton acknowledges that the new curriculum "will afford our residents immediate electronic access to important educational materials and will be flexible enough for adaption in individual programs." With gratitude on behalf of the TSDA, Dr. Fullerton congratulates all of the individuals who have contributed to making the Thoracic Surgery Curriculum a reality.
Clearly, this new curriculum has much to offer, for both the teacher and the student. It will be of significant interest to track use and observe associated relationships with subsequent board examination success.
In anticipation of an Aug. 1 launch, notifications regarding accessing the site were provided to residents and program directors via email throughout the month of July. More information on the new curriculum, as well as an introductory video, is found at www.tsda.org/education/thoracic-surgery-curricula.
And we will continue to follow and discuss the new curriculum in these pages of the Residents’ Corner.

Similar cancer-free survival seen with EET, esophagectomy
ORLANDO – Mid- and long-term esophageal cancer–free survival rates are similar in patients with early esophageal adenocarcinoma who undergo endoscopic eradication therapy and those who undergo surgical resection, according to findings from a large population-based study.
Of 1,087 patients with early esophageal adenocarcinoma (EAC) who were included in the Surveillance, Epidemiology and End Results (SEER) database, 283 underwent endoscopic eradication therapy (EET), and 804 underwent surgical resection. No significant differences were seen between the groups with respect to 2-year esophageal cancer–free survival (93.5% and 89.6% in the EET and surgery groups, respectively) or 5-year survival (69.3% and 75.8%, respectively), Dr. Sachin Wani reported during a late-breaking abstract session at the annual Digestive Disease Week.
However, the EET group had higher mortality than the surgery group due to non-EAC causes (12.8% vs. 5.7% at 2 years, and 34.8% vs. 12.9% at 5 years), he said. Cardiovascular disease was the most common cause of non-EAC mortality.
Variables significantly associated with mortality were older age (hazard ratio, 1.02), stage T1a disease (compared with T0 disease; HR, 2.71), year of diagnosis (HR, 0.93), and radiation therapy (HR, 5.29), said Dr. Wani of the University of Colorado, Aurora.
Treatment arm was not a predictor of overall survival.
A time-trend analysis showed a significant increase in the proportion of patients with T0 disease undergoing endoscopic eradication therapy. A similar significant increase was noted in patients with stage T1a disease, as well, he said.
Notably, patients undergoing EET were significantly older than those undergoing surgery (70 vs. 63 years), and more likely to be diagnosed with T0 disease (32.5% vs. 23.1% of patients) with well-differentiated histology (33% vs. 24%). They also were less likely to be men, and less likely to receive radiation therapy.
"However, the overall follow-up in the endoscopy arm was shorter than for their surgical counterparts," Dr. Wani noted.
Regional variations were observed in the proportions of patients undergoing EET and surgery, he said.
The differences between the groups, along with the significant differences in non–EAC-related mortality between the treatment groups, highlight selection bias with respect to the therapies offered to patients with EAC, he said.
Patients included in this analysis were adults who had EAC between 1998 and 2009. EAC was defined as carcinoma in situ (T0 disease), or invasive tumor confined to the mucosa, lamina propria, and muscularis mucosae (T1a disease).
The vast majority of patients in the endoscopy arm underwent endoscopic mucosal resection alone; the vast majority in the surgery arm underwent esophagectomy plus partial or total gastrectomy, Dr. Wani said.
Though limited by the use of population-based data that lacked details on recurrences, pathology, staging modalities, and complications and morbidity, this study analyzed one of the largest cohorts of patients with EAC undergoing endoscopic therapy.
The findings are important, because EETs for EAC have gained wide acceptance, and have been endorsed by society guidelines despite a paucity of long-term data examining the differences in outcomes between EET and the gold standard of surgical resection, he said.
Indeed, esophagectomy has traditionally been considered the treatment of choice for EAC, but it is also associated with high morbidity and mortality, even in expert centers, he noted.
"The implications of our study? It really provides a greater degree of confidence in what we do on a daily basis and this whole concept of endoscopic eradication therapy for patients with early esophageal cancer. However we need long-term data – i.e., 5-year data, at least – with newer ablative therapies, such as radiofrequency ablation in combination with endoscopy mucosal resection," he said. Future studies should focus on identifying patient and provider determinants of optimal outcomes, he added.
Dr. Wani reported having no disclosures.
ORLANDO – Mid- and long-term esophageal cancer–free survival rates are similar in patients with early esophageal adenocarcinoma who undergo endoscopic eradication therapy and those who undergo surgical resection, according to findings from a large population-based study.
Of 1,087 patients with early esophageal adenocarcinoma (EAC) who were included in the Surveillance, Epidemiology and End Results (SEER) database, 283 underwent endoscopic eradication therapy (EET), and 804 underwent surgical resection. No significant differences were seen between the groups with respect to 2-year esophageal cancer–free survival (93.5% and 89.6% in the EET and surgery groups, respectively) or 5-year survival (69.3% and 75.8%, respectively), Dr. Sachin Wani reported during a late-breaking abstract session at the annual Digestive Disease Week.
However, the EET group had higher mortality than the surgery group due to non-EAC causes (12.8% vs. 5.7% at 2 years, and 34.8% vs. 12.9% at 5 years), he said. Cardiovascular disease was the most common cause of non-EAC mortality.
Variables significantly associated with mortality were older age (hazard ratio, 1.02), stage T1a disease (compared with T0 disease; HR, 2.71), year of diagnosis (HR, 0.93), and radiation therapy (HR, 5.29), said Dr. Wani of the University of Colorado, Aurora.
Treatment arm was not a predictor of overall survival.
A time-trend analysis showed a significant increase in the proportion of patients with T0 disease undergoing endoscopic eradication therapy. A similar significant increase was noted in patients with stage T1a disease, as well, he said.
Notably, patients undergoing EET were significantly older than those undergoing surgery (70 vs. 63 years), and more likely to be diagnosed with T0 disease (32.5% vs. 23.1% of patients) with well-differentiated histology (33% vs. 24%). They also were less likely to be men, and less likely to receive radiation therapy.
"However, the overall follow-up in the endoscopy arm was shorter than for their surgical counterparts," Dr. Wani noted.
Regional variations were observed in the proportions of patients undergoing EET and surgery, he said.
The differences between the groups, along with the significant differences in non–EAC-related mortality between the treatment groups, highlight selection bias with respect to the therapies offered to patients with EAC, he said.
Patients included in this analysis were adults who had EAC between 1998 and 2009. EAC was defined as carcinoma in situ (T0 disease), or invasive tumor confined to the mucosa, lamina propria, and muscularis mucosae (T1a disease).
The vast majority of patients in the endoscopy arm underwent endoscopic mucosal resection alone; the vast majority in the surgery arm underwent esophagectomy plus partial or total gastrectomy, Dr. Wani said.
Though limited by the use of population-based data that lacked details on recurrences, pathology, staging modalities, and complications and morbidity, this study analyzed one of the largest cohorts of patients with EAC undergoing endoscopic therapy.
The findings are important, because EETs for EAC have gained wide acceptance, and have been endorsed by society guidelines despite a paucity of long-term data examining the differences in outcomes between EET and the gold standard of surgical resection, he said.
Indeed, esophagectomy has traditionally been considered the treatment of choice for EAC, but it is also associated with high morbidity and mortality, even in expert centers, he noted.
"The implications of our study? It really provides a greater degree of confidence in what we do on a daily basis and this whole concept of endoscopic eradication therapy for patients with early esophageal cancer. However we need long-term data – i.e., 5-year data, at least – with newer ablative therapies, such as radiofrequency ablation in combination with endoscopy mucosal resection," he said. Future studies should focus on identifying patient and provider determinants of optimal outcomes, he added.
Dr. Wani reported having no disclosures.
ORLANDO – Mid- and long-term esophageal cancer–free survival rates are similar in patients with early esophageal adenocarcinoma who undergo endoscopic eradication therapy and those who undergo surgical resection, according to findings from a large population-based study.
Of 1,087 patients with early esophageal adenocarcinoma (EAC) who were included in the Surveillance, Epidemiology and End Results (SEER) database, 283 underwent endoscopic eradication therapy (EET), and 804 underwent surgical resection. No significant differences were seen between the groups with respect to 2-year esophageal cancer–free survival (93.5% and 89.6% in the EET and surgery groups, respectively) or 5-year survival (69.3% and 75.8%, respectively), Dr. Sachin Wani reported during a late-breaking abstract session at the annual Digestive Disease Week.
However, the EET group had higher mortality than the surgery group due to non-EAC causes (12.8% vs. 5.7% at 2 years, and 34.8% vs. 12.9% at 5 years), he said. Cardiovascular disease was the most common cause of non-EAC mortality.
Variables significantly associated with mortality were older age (hazard ratio, 1.02), stage T1a disease (compared with T0 disease; HR, 2.71), year of diagnosis (HR, 0.93), and radiation therapy (HR, 5.29), said Dr. Wani of the University of Colorado, Aurora.
Treatment arm was not a predictor of overall survival.
A time-trend analysis showed a significant increase in the proportion of patients with T0 disease undergoing endoscopic eradication therapy. A similar significant increase was noted in patients with stage T1a disease, as well, he said.
Notably, patients undergoing EET were significantly older than those undergoing surgery (70 vs. 63 years), and more likely to be diagnosed with T0 disease (32.5% vs. 23.1% of patients) with well-differentiated histology (33% vs. 24%). They also were less likely to be men, and less likely to receive radiation therapy.
"However, the overall follow-up in the endoscopy arm was shorter than for their surgical counterparts," Dr. Wani noted.
Regional variations were observed in the proportions of patients undergoing EET and surgery, he said.
The differences between the groups, along with the significant differences in non–EAC-related mortality between the treatment groups, highlight selection bias with respect to the therapies offered to patients with EAC, he said.
Patients included in this analysis were adults who had EAC between 1998 and 2009. EAC was defined as carcinoma in situ (T0 disease), or invasive tumor confined to the mucosa, lamina propria, and muscularis mucosae (T1a disease).
The vast majority of patients in the endoscopy arm underwent endoscopic mucosal resection alone; the vast majority in the surgery arm underwent esophagectomy plus partial or total gastrectomy, Dr. Wani said.
Though limited by the use of population-based data that lacked details on recurrences, pathology, staging modalities, and complications and morbidity, this study analyzed one of the largest cohorts of patients with EAC undergoing endoscopic therapy.
The findings are important, because EETs for EAC have gained wide acceptance, and have been endorsed by society guidelines despite a paucity of long-term data examining the differences in outcomes between EET and the gold standard of surgical resection, he said.
Indeed, esophagectomy has traditionally been considered the treatment of choice for EAC, but it is also associated with high morbidity and mortality, even in expert centers, he noted.
"The implications of our study? It really provides a greater degree of confidence in what we do on a daily basis and this whole concept of endoscopic eradication therapy for patients with early esophageal cancer. However we need long-term data – i.e., 5-year data, at least – with newer ablative therapies, such as radiofrequency ablation in combination with endoscopy mucosal resection," he said. Future studies should focus on identifying patient and provider determinants of optimal outcomes, he added.
Dr. Wani reported having no disclosures.
Aortic valve-sparing surgery shows durability
MINNEAPOLIS – Despite the complexity of aortic valve–sparing techniques, early outcomes and 1-year survival were similar to those achieved with valve replacing during root replacement surgery in patients with Marfan syndrome in a prospective registry study.
Major adverse valve-related events (MAVREs) at 1 year were also comparable, although there was an increase, of course, in aortic valve regurgitation with valve sparing (7% vs. 0%), Dr. Joseph S. Coselli said at the annual meeting of the American Association for Thoracic Surgery.
"Follow-up is needed for this particular incident because we don’t know exactly what’s going to happen to these 2-plus aortic regurgitations," he said. "It’s quite possible they may remain stable over a long period of time and don’t represent a failure of the concept."

In an initial report from the international registry, valve-sparing techniques were the most common, and provided comparable 30-day outcomes in 151 patients (J. Thorac. Cardiovasc. Surg. 2009;137:1124-32).
The current analysis involved 316 patients, aged 4-70 years, who underwent aortic valve–sparing (AVS) (N = 239) or aortic valve–replacing (AVR) (N = 63 mechanical and 14 tissue) root replacement surgery at 19 centers between March 2005 and November 2010. The type of operation was determined by clinical factors, and by surgeon and patient preference. AVR surgery was considered the only option in 17% of patients. At 1 year, clinical follow-up was complete in 98% and imaging follow-up in 93%.
"Interestingly, when we started out this particular collection of patients, over 30% were receiving aortic valve replacement, but toward the end of this observational study, late 2010, virtually almost all patients were receiving aortic valve sparing," said Dr. Coselli, chief of adult cardiac surgery at Baylor College of Medicine, Texas Heart Institute, Houston.
AVS patients were younger (33 vs. 39 years); had smaller sinuses of Valsalva (49 vs. 53 mm); and had less acute dissection (3% vs. 9%), chronic dissection (3% vs. 12%), and previous cardiovascular surgery (5% vs. 14%).
Aortic-sparing techniques required significantly longer cardiopulmonary bypass time (195 vs. 152 minutes) and aortic clamp time (156 vs. 115 minutes), but cut ICU time from 46 hours with AVR surgery to 26 hours, ventilator support time from 12 to 8 hours, and hospital length of stay from 7 to 6 days, Dr. Coselli reported.
At 30 days, MAVREs were reported in 6 patients in the AVR group and 15 in the AVS group (P = .4), with no differences in nonstructural dysfunction (1 vs. 7), embolism (1 vs. 3), or bleeding (2 vs. 3 events).
Two AVS patients required early reoperation: One required same-day reintervention because of coronary artery kinking after a Florida sleeve procedure, and the second needed reintervention because of a coronary pseudoaneurysm 6 days after a David-V procedure, he said. Two early deaths occurred, one in each group, but neither was valve related.
One-year survival rates were 98% after AVS surgery and 97% after AVR surgery (4 vs. 2 deaths; P = .06).
At 1 year, MAVREs occurred in 8 AVR and 35 AVS patients (P = .5). There was no significant difference between AVR and AVS in freedom from valve-related death (1 vs. 2), embolism (2 vs. 4 events), reintervention (0 vs. 1), endocarditis (1 vs. 0), valve thrombosis (0 both), or valve-related morbidity (7 vs. 28), Dr. Coselli said.
The AVS group had significantly more nonstructural dysfunction/structural valve deterioration (23 events vs. 1 event; P = .04), but significantly less bleeding (3 vs. 5 events; P = .01).
In a Cox regression analysis at 1 year, the type of surgery was not associated with overall survival, MAVREs, or any other valve-related outcome, he said.
Dr. Coselli reported research support from St. Jude Medical; an educational grant, consultancy, and royalties from Vascutek Terumo; and research support, speaking for, and steering committee membership with Medtronic. Two coauthors reported consultant/advisory board participation with Medtronic or Edwards Lifesciences.
MINNEAPOLIS – Despite the complexity of aortic valve–sparing techniques, early outcomes and 1-year survival were similar to those achieved with valve replacing during root replacement surgery in patients with Marfan syndrome in a prospective registry study.
Major adverse valve-related events (MAVREs) at 1 year were also comparable, although there was an increase, of course, in aortic valve regurgitation with valve sparing (7% vs. 0%), Dr. Joseph S. Coselli said at the annual meeting of the American Association for Thoracic Surgery.
"Follow-up is needed for this particular incident because we don’t know exactly what’s going to happen to these 2-plus aortic regurgitations," he said. "It’s quite possible they may remain stable over a long period of time and don’t represent a failure of the concept."
In an initial report from the international registry, valve-sparing techniques were the most common, and provided comparable 30-day outcomes in 151 patients (J. Thorac. Cardiovasc. Surg. 2009;137:1124-32).
The current analysis involved 316 patients, aged 4-70 years, who underwent aortic valve–sparing (AVS) (N = 239) or aortic valve–replacing (AVR) (N = 63 mechanical and 14 tissue) root replacement surgery at 19 centers between March 2005 and November 2010. The type of operation was determined by clinical factors, and by surgeon and patient preference. AVR surgery was considered the only option in 17% of patients. At 1 year, clinical follow-up was complete in 98% and imaging follow-up in 93%.
"Interestingly, when we started out this particular collection of patients, over 30% were receiving aortic valve replacement, but toward the end of this observational study, late 2010, virtually almost all patients were receiving aortic valve sparing," said Dr. Coselli, chief of adult cardiac surgery at Baylor College of Medicine, Texas Heart Institute, Houston.
AVS patients were younger (33 vs. 39 years); had smaller sinuses of Valsalva (49 vs. 53 mm); and had less acute dissection (3% vs. 9%), chronic dissection (3% vs. 12%), and previous cardiovascular surgery (5% vs. 14%).
Aortic-sparing techniques required significantly longer cardiopulmonary bypass time (195 vs. 152 minutes) and aortic clamp time (156 vs. 115 minutes), but cut ICU time from 46 hours with AVR surgery to 26 hours, ventilator support time from 12 to 8 hours, and hospital length of stay from 7 to 6 days, Dr. Coselli reported.
At 30 days, MAVREs were reported in 6 patients in the AVR group and 15 in the AVS group (P = .4), with no differences in nonstructural dysfunction (1 vs. 7), embolism (1 vs. 3), or bleeding (2 vs. 3 events).
Two AVS patients required early reoperation: One required same-day reintervention because of coronary artery kinking after a Florida sleeve procedure, and the second needed reintervention because of a coronary pseudoaneurysm 6 days after a David-V procedure, he said. Two early deaths occurred, one in each group, but neither was valve related.
One-year survival rates were 98% after AVS surgery and 97% after AVR surgery (4 vs. 2 deaths; P = .06).
At 1 year, MAVREs occurred in 8 AVR and 35 AVS patients (P = .5). There was no significant difference between AVR and AVS in freedom from valve-related death (1 vs. 2), embolism (2 vs. 4 events), reintervention (0 vs. 1), endocarditis (1 vs. 0), valve thrombosis (0 both), or valve-related morbidity (7 vs. 28), Dr. Coselli said.
The AVS group had significantly more nonstructural dysfunction/structural valve deterioration (23 events vs. 1 event; P = .04), but significantly less bleeding (3 vs. 5 events; P = .01).
In a Cox regression analysis at 1 year, the type of surgery was not associated with overall survival, MAVREs, or any other valve-related outcome, he said.
Dr. Coselli reported research support from St. Jude Medical; an educational grant, consultancy, and royalties from Vascutek Terumo; and research support, speaking for, and steering committee membership with Medtronic. Two coauthors reported consultant/advisory board participation with Medtronic or Edwards Lifesciences.
MINNEAPOLIS – Despite the complexity of aortic valve–sparing techniques, early outcomes and 1-year survival were similar to those achieved with valve replacing during root replacement surgery in patients with Marfan syndrome in a prospective registry study.
Major adverse valve-related events (MAVREs) at 1 year were also comparable, although there was an increase, of course, in aortic valve regurgitation with valve sparing (7% vs. 0%), Dr. Joseph S. Coselli said at the annual meeting of the American Association for Thoracic Surgery.
"Follow-up is needed for this particular incident because we don’t know exactly what’s going to happen to these 2-plus aortic regurgitations," he said. "It’s quite possible they may remain stable over a long period of time and don’t represent a failure of the concept."
In an initial report from the international registry, valve-sparing techniques were the most common, and provided comparable 30-day outcomes in 151 patients (J. Thorac. Cardiovasc. Surg. 2009;137:1124-32).
The current analysis involved 316 patients, aged 4-70 years, who underwent aortic valve–sparing (AVS) (N = 239) or aortic valve–replacing (AVR) (N = 63 mechanical and 14 tissue) root replacement surgery at 19 centers between March 2005 and November 2010. The type of operation was determined by clinical factors, and by surgeon and patient preference. AVR surgery was considered the only option in 17% of patients. At 1 year, clinical follow-up was complete in 98% and imaging follow-up in 93%.
"Interestingly, when we started out this particular collection of patients, over 30% were receiving aortic valve replacement, but toward the end of this observational study, late 2010, virtually almost all patients were receiving aortic valve sparing," said Dr. Coselli, chief of adult cardiac surgery at Baylor College of Medicine, Texas Heart Institute, Houston.
AVS patients were younger (33 vs. 39 years); had smaller sinuses of Valsalva (49 vs. 53 mm); and had less acute dissection (3% vs. 9%), chronic dissection (3% vs. 12%), and previous cardiovascular surgery (5% vs. 14%).
Aortic-sparing techniques required significantly longer cardiopulmonary bypass time (195 vs. 152 minutes) and aortic clamp time (156 vs. 115 minutes), but cut ICU time from 46 hours with AVR surgery to 26 hours, ventilator support time from 12 to 8 hours, and hospital length of stay from 7 to 6 days, Dr. Coselli reported.
At 30 days, MAVREs were reported in 6 patients in the AVR group and 15 in the AVS group (P = .4), with no differences in nonstructural dysfunction (1 vs. 7), embolism (1 vs. 3), or bleeding (2 vs. 3 events).
Two AVS patients required early reoperation: One required same-day reintervention because of coronary artery kinking after a Florida sleeve procedure, and the second needed reintervention because of a coronary pseudoaneurysm 6 days after a David-V procedure, he said. Two early deaths occurred, one in each group, but neither was valve related.
One-year survival rates were 98% after AVS surgery and 97% after AVR surgery (4 vs. 2 deaths; P = .06).
At 1 year, MAVREs occurred in 8 AVR and 35 AVS patients (P = .5). There was no significant difference between AVR and AVS in freedom from valve-related death (1 vs. 2), embolism (2 vs. 4 events), reintervention (0 vs. 1), endocarditis (1 vs. 0), valve thrombosis (0 both), or valve-related morbidity (7 vs. 28), Dr. Coselli said.
The AVS group had significantly more nonstructural dysfunction/structural valve deterioration (23 events vs. 1 event; P = .04), but significantly less bleeding (3 vs. 5 events; P = .01).
In a Cox regression analysis at 1 year, the type of surgery was not associated with overall survival, MAVREs, or any other valve-related outcome, he said.
Dr. Coselli reported research support from St. Jude Medical; an educational grant, consultancy, and royalties from Vascutek Terumo; and research support, speaking for, and steering committee membership with Medtronic. Two coauthors reported consultant/advisory board participation with Medtronic or Edwards Lifesciences.
AT THE AATS ANNUAL MEETING
BRUISE CONTROL: Warfarin bests heparin bridging
DENVER – Uninterrupted warfarin therapy during pacemaker or implantable cardioverter-defibrillator surgery in patients at high thromboembolic risk proved superior to the guideline-recommended practice of discontinuing warfarin and bridging with heparin, according to a large, multicenter, randomized clinical trial.
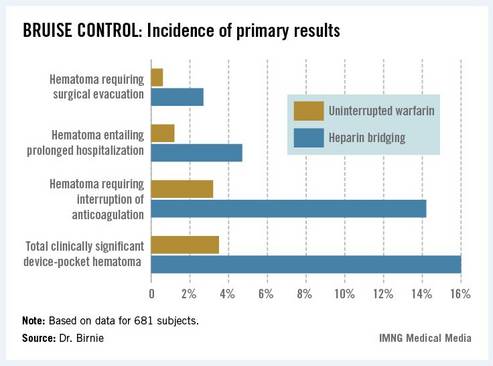
The primary outcome in the 17-center, 681-patient BRUISE CONTROL (Bridge or Continue Coumadin for Device Surgery Randomized Controlled Trial) was the incidence of clinically significant device-pocket hematoma. The rate was 16% in patients randomized to heparin bridging, compared with 3.5% with uninterrupted warfarin, Dr. David H. Birnie reported at the annual meeting of the Heart Rhythm Society.
These results are clearly practice changing. Heparin bridging has been the standard of care. It is recommended in this common clinical scenario in all of the major guidelines, but that’s bound to change as a result of BRUISE CONTROL, predicted Dr. Birnie of the University of Ottawa Heart Institute.
"This trial was a home run. It was unequivocally positive," he commented. "For sure, our clinical practice changed as soon as we saw those results."
Device-pocket hematoma is a "very nasty" complication of cardiac device surgery, Dr. Birnie noted. It is quite painful, can cause device infection, and is difficult to treat. Clinically significant device-pocket hematoma was defined in this trial as a hematoma resulting in prolonged hospitalization for an additional day or more, or interruption of oral anticoagulation for at least 24 hours, and/or requiring additional surgery. All three components of the primary endpoint were significantly less frequent in the uninterrupted warfarin group (see chart).
Performing device surgery in patients on uninterrupted warfarin with a median international normalized ratio (INR) of 2.3 was not associated with any increase in major perioperative bleeding or other surgical or thromboembolic complications. And patient satisfaction surveys indicated subjects greatly preferred having their procedure without stopping their warfarin.
BRUISE CONTROL was planned as a definitive 1,000-patient clinical trial. However, the Data and Safety Monitoring Board halted the study after an interim analysis involving the first 681 subjects.
Of note, this was a study restricted to patients at high stroke risk – greater than 5% annually – as defined by the presence of atrial fibrillation and a CHADS2 score of 3 or more or the presence of a mechanical heart valve.
Dr. Birnie said that although it seems counterintuitive to have less bleeding when cardiac device surgery is performed on a fully anticoagulated patient, as occurred in BRUISE CONTROL, he and his coinvestigators have an explanatory hypothesis: "When bleeding occurs in a fully anticoagulated patient, the operator can readily see it and address it. On the contrary, with bridging you get hemostasis at the time of surgery, but you may have missed a tiny little thing, and then 24 hours later when you start up your heparin bridging again, that’s when the bleeding occurs. It’s a physiologically plausible explanation," he said.
In a multivariate analysis, neither the use of pressure dressings, nor the use of sandbags, nor injection of antibleeding agents into the device pocket before closure had any significant impact on the incidence of clinically significant hematomas. Only three factors did: uninterrupted warfarin therapy, which reduced the risk by 84%; aspirin therapy, which doubled the risk; and the presence of diabetes mellitus, which was inexplicably associated with a 52% reduction in hematoma risk.
Each year roughly 1.6 million people worldwide undergo pacemaker or implantable cardioverter-defibrillator (ICD) implantation. Up to one-third of them are on long-term oral anticoagulation, most commonly with warfarin.
Dr. Birnie stressed that the BRUISE CONTROL findings have no relevance to patients on one of the new oral anticoagulants.
"The whole risk/benefit ratio of the new agents is completely different from warfarin. Their onset and offset of action is hours as opposed to the 5 days for warfarin," he noted.
With that point in mind, he and his coinvestigators have just started the BRUISE CONTROL-2 trial, which is examining whether it’s better to stop the new agents around the time of device surgery or continue the medication uninterrupted.
Simultaneous with Dr. Birnie’s presentation of the BRUISE CONTROL data in Denver, the study results were published online (N. Engl. J. Med. 2013 May 9 [doi: 10.1056/NEJMoa1302946]).
BRUISE CONTROL was funded by the Canadian Institutes of Health Research and the Ministry of Health and Long-Term Care of Ontario. Dr. Birnie reported having no conflicts of interest.
DENVER – Uninterrupted warfarin therapy during pacemaker or implantable cardioverter-defibrillator surgery in patients at high thromboembolic risk proved superior to the guideline-recommended practice of discontinuing warfarin and bridging with heparin, according to a large, multicenter, randomized clinical trial.
The primary outcome in the 17-center, 681-patient BRUISE CONTROL (Bridge or Continue Coumadin for Device Surgery Randomized Controlled Trial) was the incidence of clinically significant device-pocket hematoma. The rate was 16% in patients randomized to heparin bridging, compared with 3.5% with uninterrupted warfarin, Dr. David H. Birnie reported at the annual meeting of the Heart Rhythm Society.
These results are clearly practice changing. Heparin bridging has been the standard of care. It is recommended in this common clinical scenario in all of the major guidelines, but that’s bound to change as a result of BRUISE CONTROL, predicted Dr. Birnie of the University of Ottawa Heart Institute.
"This trial was a home run. It was unequivocally positive," he commented. "For sure, our clinical practice changed as soon as we saw those results."
Device-pocket hematoma is a "very nasty" complication of cardiac device surgery, Dr. Birnie noted. It is quite painful, can cause device infection, and is difficult to treat. Clinically significant device-pocket hematoma was defined in this trial as a hematoma resulting in prolonged hospitalization for an additional day or more, or interruption of oral anticoagulation for at least 24 hours, and/or requiring additional surgery. All three components of the primary endpoint were significantly less frequent in the uninterrupted warfarin group (see chart).
Performing device surgery in patients on uninterrupted warfarin with a median international normalized ratio (INR) of 2.3 was not associated with any increase in major perioperative bleeding or other surgical or thromboembolic complications. And patient satisfaction surveys indicated subjects greatly preferred having their procedure without stopping their warfarin.
BRUISE CONTROL was planned as a definitive 1,000-patient clinical trial. However, the Data and Safety Monitoring Board halted the study after an interim analysis involving the first 681 subjects.
Of note, this was a study restricted to patients at high stroke risk – greater than 5% annually – as defined by the presence of atrial fibrillation and a CHADS2 score of 3 or more or the presence of a mechanical heart valve.
Dr. Birnie said that although it seems counterintuitive to have less bleeding when cardiac device surgery is performed on a fully anticoagulated patient, as occurred in BRUISE CONTROL, he and his coinvestigators have an explanatory hypothesis: "When bleeding occurs in a fully anticoagulated patient, the operator can readily see it and address it. On the contrary, with bridging you get hemostasis at the time of surgery, but you may have missed a tiny little thing, and then 24 hours later when you start up your heparin bridging again, that’s when the bleeding occurs. It’s a physiologically plausible explanation," he said.
In a multivariate analysis, neither the use of pressure dressings, nor the use of sandbags, nor injection of antibleeding agents into the device pocket before closure had any significant impact on the incidence of clinically significant hematomas. Only three factors did: uninterrupted warfarin therapy, which reduced the risk by 84%; aspirin therapy, which doubled the risk; and the presence of diabetes mellitus, which was inexplicably associated with a 52% reduction in hematoma risk.
Each year roughly 1.6 million people worldwide undergo pacemaker or implantable cardioverter-defibrillator (ICD) implantation. Up to one-third of them are on long-term oral anticoagulation, most commonly with warfarin.
Dr. Birnie stressed that the BRUISE CONTROL findings have no relevance to patients on one of the new oral anticoagulants.
"The whole risk/benefit ratio of the new agents is completely different from warfarin. Their onset and offset of action is hours as opposed to the 5 days for warfarin," he noted.
With that point in mind, he and his coinvestigators have just started the BRUISE CONTROL-2 trial, which is examining whether it’s better to stop the new agents around the time of device surgery or continue the medication uninterrupted.
Simultaneous with Dr. Birnie’s presentation of the BRUISE CONTROL data in Denver, the study results were published online (N. Engl. J. Med. 2013 May 9 [doi: 10.1056/NEJMoa1302946]).
BRUISE CONTROL was funded by the Canadian Institutes of Health Research and the Ministry of Health and Long-Term Care of Ontario. Dr. Birnie reported having no conflicts of interest.
DENVER – Uninterrupted warfarin therapy during pacemaker or implantable cardioverter-defibrillator surgery in patients at high thromboembolic risk proved superior to the guideline-recommended practice of discontinuing warfarin and bridging with heparin, according to a large, multicenter, randomized clinical trial.
The primary outcome in the 17-center, 681-patient BRUISE CONTROL (Bridge or Continue Coumadin for Device Surgery Randomized Controlled Trial) was the incidence of clinically significant device-pocket hematoma. The rate was 16% in patients randomized to heparin bridging, compared with 3.5% with uninterrupted warfarin, Dr. David H. Birnie reported at the annual meeting of the Heart Rhythm Society.
These results are clearly practice changing. Heparin bridging has been the standard of care. It is recommended in this common clinical scenario in all of the major guidelines, but that’s bound to change as a result of BRUISE CONTROL, predicted Dr. Birnie of the University of Ottawa Heart Institute.
"This trial was a home run. It was unequivocally positive," he commented. "For sure, our clinical practice changed as soon as we saw those results."
Device-pocket hematoma is a "very nasty" complication of cardiac device surgery, Dr. Birnie noted. It is quite painful, can cause device infection, and is difficult to treat. Clinically significant device-pocket hematoma was defined in this trial as a hematoma resulting in prolonged hospitalization for an additional day or more, or interruption of oral anticoagulation for at least 24 hours, and/or requiring additional surgery. All three components of the primary endpoint were significantly less frequent in the uninterrupted warfarin group (see chart).
Performing device surgery in patients on uninterrupted warfarin with a median international normalized ratio (INR) of 2.3 was not associated with any increase in major perioperative bleeding or other surgical or thromboembolic complications. And patient satisfaction surveys indicated subjects greatly preferred having their procedure without stopping their warfarin.
BRUISE CONTROL was planned as a definitive 1,000-patient clinical trial. However, the Data and Safety Monitoring Board halted the study after an interim analysis involving the first 681 subjects.
Of note, this was a study restricted to patients at high stroke risk – greater than 5% annually – as defined by the presence of atrial fibrillation and a CHADS2 score of 3 or more or the presence of a mechanical heart valve.
Dr. Birnie said that although it seems counterintuitive to have less bleeding when cardiac device surgery is performed on a fully anticoagulated patient, as occurred in BRUISE CONTROL, he and his coinvestigators have an explanatory hypothesis: "When bleeding occurs in a fully anticoagulated patient, the operator can readily see it and address it. On the contrary, with bridging you get hemostasis at the time of surgery, but you may have missed a tiny little thing, and then 24 hours later when you start up your heparin bridging again, that’s when the bleeding occurs. It’s a physiologically plausible explanation," he said.
In a multivariate analysis, neither the use of pressure dressings, nor the use of sandbags, nor injection of antibleeding agents into the device pocket before closure had any significant impact on the incidence of clinically significant hematomas. Only three factors did: uninterrupted warfarin therapy, which reduced the risk by 84%; aspirin therapy, which doubled the risk; and the presence of diabetes mellitus, which was inexplicably associated with a 52% reduction in hematoma risk.
Each year roughly 1.6 million people worldwide undergo pacemaker or implantable cardioverter-defibrillator (ICD) implantation. Up to one-third of them are on long-term oral anticoagulation, most commonly with warfarin.
Dr. Birnie stressed that the BRUISE CONTROL findings have no relevance to patients on one of the new oral anticoagulants.
"The whole risk/benefit ratio of the new agents is completely different from warfarin. Their onset and offset of action is hours as opposed to the 5 days for warfarin," he noted.
With that point in mind, he and his coinvestigators have just started the BRUISE CONTROL-2 trial, which is examining whether it’s better to stop the new agents around the time of device surgery or continue the medication uninterrupted.
Simultaneous with Dr. Birnie’s presentation of the BRUISE CONTROL data in Denver, the study results were published online (N. Engl. J. Med. 2013 May 9 [doi: 10.1056/NEJMoa1302946]).
BRUISE CONTROL was funded by the Canadian Institutes of Health Research and the Ministry of Health and Long-Term Care of Ontario. Dr. Birnie reported having no conflicts of interest.
Major finding: The incidence of clinically significant device-pocket hematoma in patients at high thromboembolic risk who underwent pacemaker or implantable cardioverter-defibrillator surgery was 3.5% if they remained on full-dose warfarin, compared with 16% with the guideline-recommended, standard-of-care practice of interrupting warfarin in favor of heparin bridging.
Data source: BRUISE CONTROL was a 681-patient, 17-center randomized clinical trial.
Disclosures: BRUISE CONTROL was funded by the Canadian Institutes of Health Research and the Ministry of Health and Long-Term Care of Ontario. Dr. Birnie reported having no conflicts of interest.
Study: Reablate, don't medicate, after failed AF ablation
DENVER – After a failed first ablation procedure for paroxysmal atrial fibrillation, redo ablation proved more effective than did antiarrhythmic drug therapy in a randomized trial, Dr. Jonathan Steinberg reported at the annual meeting of the Heart Rhythm Society.
The success rate of a first ablation procedure in patients with symptomatic paroxysmal AF is typically about 60%. The question of what to do for the 40% who are nonresponders has been unclear, with no prior randomized clinical trial evidence available to guide decisions, noted Dr. Steinberg of Columbia University, New York.
The study comprised 154 patients with recurrent symptomatic paroxysmal AF 3 months after an initial ablation procedure involving only pulmonary vein isolation. All participants received an implantable loop recorder to track atrial arrhythmic events.
They were then randomized to redo ablation limited to reisolation of the pulmonary vein, which was successfully accomplished in all instances, or to guideline-based antiarrhythmic drug therapy. The choice of drug was left to individual investigator discretion. The three options were propafenone at 450-900 mg/day, sotalol at 160-320 mg/day, or flecainide at 200-400 mg/day. Propafenone was selected in the majority of cases, at an average dose of 579 mg/day.
The average AF burden as measured by implantable loop recorder at randomization was 15%. The primary study endpoint was AF burden at 36 months of follow-up, which was 5.6% in the redo-ablation group compared with 18.8% in the antiarrhythmic drug group.
Secondary endpoints uniformly favored redo ablation as well (see graphic).
Data from the implantable loop recorders was evaluated every 3 months during 3 years of follow-up. As early as 3 months into the study, the group given antiarrhythmic drugs had an AF burden of 3.3%, significantly higher than the 1.9% rate seen in the redo-ablation group.
Thereafter, the drug therapy group experienced a gradual increase in AF burden throughout the first 12-15 months, followed by a much more substantial increase during the remainder of the study.
"The redo-ablation group had a different pattern" of AF burden, Dr. Steinberg observed. "It was low throughout the first 12-15 months, with just a slight increase, and it then rose only gradually over time until the 36-month end of the study."
Freedom from any atrial tachy-arrhythmia at 1 year was 30% in the antiarrhythmic drug therapy group and 75% in the redo-ablation group. By 3 years, 12% of those in the drug therapy group were free of atrial tachyarrhythmias as were 58% in the redo-ablation group.
Complications in the redo-ablation group consisted of two cases of cardiac tamponade. In contrast, 49 patients, or 64%, in the antiarrhythmic drug therapy group discontinued medication because of intolerance or ineffectiveness.
Session cochair Dr. Gordon Tomaselli of Johns Hopkins University, Baltimore, said that in light of the potential proarrhythmic effects of virtually all antiarrhythmic drugs, it would have been useful to include a no-antiarrhythmic drug control group in the study.
Dr. Steinberg reported having no conflicts of interest.
DENVER – After a failed first ablation procedure for paroxysmal atrial fibrillation, redo ablation proved more effective than did antiarrhythmic drug therapy in a randomized trial, Dr. Jonathan Steinberg reported at the annual meeting of the Heart Rhythm Society.
The success rate of a first ablation procedure in patients with symptomatic paroxysmal AF is typically about 60%. The question of what to do for the 40% who are nonresponders has been unclear, with no prior randomized clinical trial evidence available to guide decisions, noted Dr. Steinberg of Columbia University, New York.
The study comprised 154 patients with recurrent symptomatic paroxysmal AF 3 months after an initial ablation procedure involving only pulmonary vein isolation. All participants received an implantable loop recorder to track atrial arrhythmic events.
They were then randomized to redo ablation limited to reisolation of the pulmonary vein, which was successfully accomplished in all instances, or to guideline-based antiarrhythmic drug therapy. The choice of drug was left to individual investigator discretion. The three options were propafenone at 450-900 mg/day, sotalol at 160-320 mg/day, or flecainide at 200-400 mg/day. Propafenone was selected in the majority of cases, at an average dose of 579 mg/day.
The average AF burden as measured by implantable loop recorder at randomization was 15%. The primary study endpoint was AF burden at 36 months of follow-up, which was 5.6% in the redo-ablation group compared with 18.8% in the antiarrhythmic drug group.
Secondary endpoints uniformly favored redo ablation as well (see graphic).
Data from the implantable loop recorders was evaluated every 3 months during 3 years of follow-up. As early as 3 months into the study, the group given antiarrhythmic drugs had an AF burden of 3.3%, significantly higher than the 1.9% rate seen in the redo-ablation group.
Thereafter, the drug therapy group experienced a gradual increase in AF burden throughout the first 12-15 months, followed by a much more substantial increase during the remainder of the study.
"The redo-ablation group had a different pattern" of AF burden, Dr. Steinberg observed. "It was low throughout the first 12-15 months, with just a slight increase, and it then rose only gradually over time until the 36-month end of the study."
Freedom from any atrial tachy-arrhythmia at 1 year was 30% in the antiarrhythmic drug therapy group and 75% in the redo-ablation group. By 3 years, 12% of those in the drug therapy group were free of atrial tachyarrhythmias as were 58% in the redo-ablation group.
Complications in the redo-ablation group consisted of two cases of cardiac tamponade. In contrast, 49 patients, or 64%, in the antiarrhythmic drug therapy group discontinued medication because of intolerance or ineffectiveness.
Session cochair Dr. Gordon Tomaselli of Johns Hopkins University, Baltimore, said that in light of the potential proarrhythmic effects of virtually all antiarrhythmic drugs, it would have been useful to include a no-antiarrhythmic drug control group in the study.
Dr. Steinberg reported having no conflicts of interest.
DENVER – After a failed first ablation procedure for paroxysmal atrial fibrillation, redo ablation proved more effective than did antiarrhythmic drug therapy in a randomized trial, Dr. Jonathan Steinberg reported at the annual meeting of the Heart Rhythm Society.
The success rate of a first ablation procedure in patients with symptomatic paroxysmal AF is typically about 60%. The question of what to do for the 40% who are nonresponders has been unclear, with no prior randomized clinical trial evidence available to guide decisions, noted Dr. Steinberg of Columbia University, New York.
The study comprised 154 patients with recurrent symptomatic paroxysmal AF 3 months after an initial ablation procedure involving only pulmonary vein isolation. All participants received an implantable loop recorder to track atrial arrhythmic events.
They were then randomized to redo ablation limited to reisolation of the pulmonary vein, which was successfully accomplished in all instances, or to guideline-based antiarrhythmic drug therapy. The choice of drug was left to individual investigator discretion. The three options were propafenone at 450-900 mg/day, sotalol at 160-320 mg/day, or flecainide at 200-400 mg/day. Propafenone was selected in the majority of cases, at an average dose of 579 mg/day.
The average AF burden as measured by implantable loop recorder at randomization was 15%. The primary study endpoint was AF burden at 36 months of follow-up, which was 5.6% in the redo-ablation group compared with 18.8% in the antiarrhythmic drug group.
Secondary endpoints uniformly favored redo ablation as well (see graphic).
Data from the implantable loop recorders was evaluated every 3 months during 3 years of follow-up. As early as 3 months into the study, the group given antiarrhythmic drugs had an AF burden of 3.3%, significantly higher than the 1.9% rate seen in the redo-ablation group.
Thereafter, the drug therapy group experienced a gradual increase in AF burden throughout the first 12-15 months, followed by a much more substantial increase during the remainder of the study.
"The redo-ablation group had a different pattern" of AF burden, Dr. Steinberg observed. "It was low throughout the first 12-15 months, with just a slight increase, and it then rose only gradually over time until the 36-month end of the study."
Freedom from any atrial tachy-arrhythmia at 1 year was 30% in the antiarrhythmic drug therapy group and 75% in the redo-ablation group. By 3 years, 12% of those in the drug therapy group were free of atrial tachyarrhythmias as were 58% in the redo-ablation group.
Complications in the redo-ablation group consisted of two cases of cardiac tamponade. In contrast, 49 patients, or 64%, in the antiarrhythmic drug therapy group discontinued medication because of intolerance or ineffectiveness.
Session cochair Dr. Gordon Tomaselli of Johns Hopkins University, Baltimore, said that in light of the potential proarrhythmic effects of virtually all antiarrhythmic drugs, it would have been useful to include a no-antiarrhythmic drug control group in the study.
Dr. Steinberg reported having no conflicts of interest.
Major Finding: At 3 years after a first ablation procedure had failed for symptomatic paroxysmal atrial fibrillation, 12% of those randomized to drug therapy and 58% of those in the redo-ablation group were free of atrial tachyarrhythmias.
Data Source: A randomized, prospective, multicenter clinical trial involving 154 patients whose atrial arrhythmia status was monitored via implantable loop recorder.
Disclosures: The presenter reported having no conflicts of interest.
Barrett's recurs in about one-third within 2 years after RFA
About one-third of patients with Barrett’s esophagus can expect recurrence of intestinal metaplasia by 2 years after obtaining complete remission with radiofrequency ablation.
The finding highlights the importance of frequent endoscopic surveillance in these patients, even after remission is achieved, wrote Dr. Milli Gupta and colleagues in the July issue of Gastroenterology.
In the study, Dr. Gupta, of the Mayo Clinic, Rochester, Minn., and her associates looked at 448 patients with Barrett’s treated with radiofrequency ablation (RFA) at three different tertiary referral centers (doi: .1053/j.gastro.2013.03.008).
The data were collected from patients treated and followed up in these centers from January 2003 to November 2011 as part of the Barrett’s Esophagus Translational Research Network consortium.
The patients’ mean age was 64 years, 85% were men, and the mean length of Barrett’s esophagus that was treated was 4.1 cm, the authors reported.
Looking at the indication for RFA, 11% had intramucosal esophageal adenocarcinoma, 60% had high-grade dysplasia, 15% had low-grade dysplasia, and 14% had nondysplastic BE.
Slightly more than half (55%) of patients also underwent endoscopic mucosal resection before RFA, and 1% had received cryotherapy.
After RFA, the authors found that by 1 year, roughly 26% of patients achieved complete remission of intestinal metaplasia (CRIM), defined as two negative endoscopies and histology clear of intestinal metaplasia.
That figure climbed to 56% by 2 years, and to 71% by 3 years, with 29% of patients receiving one RFA treatment session, 35% receiving two sessions, and the remaining percentage of patients undergoing 3-10 sessions before remission.
Adverse events occurred in 6.5% of patients, with stricture formation being the most common, followed by bleeding, mucosal tears, and hospitalizations for dysrhythmias.
However, using a Kaplan-Meier survival curve, they found that after CRIM was attained, 20% of patients would have recurrence of intestinal metaplasia by 1 year. Similarly, by 2 years after attainment of CRIM, the rate of recurrence was 33%.
"By 3 years, recurrences continued to occur, but precise estimates were difficult to establish because of the small number of at-risk subjects (n = 11), which made estimates of recurrence less precise," Dr. Gupta and her colleagues wrote.
According to the authors, the most common type of recurrence was intestinal metaplasia without dysplasia, which was seen in 78% of patients who recurred after CRIM.
The remaining patients who recurred (22%) developed dysplastic Barrett’s esophagus, with 11% showing high-grade dysplasia, 8% showing low-grade dysplasia, and 3% developing cancer.
There were no discernable endoscopic or patient factors associated with time to recurrence on univariate and multivariate analyses, the authors added.
"Despite the ability of RFA to achieve CRIM, recurrence of intestinal metaplasia and dysplasia appears to occur in a substantial proportion of subjects," wrote Dr. Gupta.
She pointed out that current recommendations call for intense surveillance at 3- to 6-month intervals, and if no recurrence is found, "surveillance generally is decreased to 6- to 12-month intervals."
However, "until predictive biomarkers are identified and available for clinical practice, endoscopic surveillance directed at the gastroesophageal junction and original BE [Barrett’s esophagus] segment should be continued."
Dr. Gupta had no conflicts of interest. Several of her coauthors disclosed financial relationships with drug makers, including the makers of therapies for Barrett’s esophagus. The study was funded by a grant from the National Institutes of Health. The Barrett’s Esophagus Translational Research Network consortium is funded by the National Cancer Institute.
About one-third of patients with Barrett’s esophagus can expect recurrence of intestinal metaplasia by 2 years after obtaining complete remission with radiofrequency ablation.
The finding highlights the importance of frequent endoscopic surveillance in these patients, even after remission is achieved, wrote Dr. Milli Gupta and colleagues in the July issue of Gastroenterology.
In the study, Dr. Gupta, of the Mayo Clinic, Rochester, Minn., and her associates looked at 448 patients with Barrett’s treated with radiofrequency ablation (RFA) at three different tertiary referral centers (doi: .1053/j.gastro.2013.03.008).
The data were collected from patients treated and followed up in these centers from January 2003 to November 2011 as part of the Barrett’s Esophagus Translational Research Network consortium.
The patients’ mean age was 64 years, 85% were men, and the mean length of Barrett’s esophagus that was treated was 4.1 cm, the authors reported.
Looking at the indication for RFA, 11% had intramucosal esophageal adenocarcinoma, 60% had high-grade dysplasia, 15% had low-grade dysplasia, and 14% had nondysplastic BE.
Slightly more than half (55%) of patients also underwent endoscopic mucosal resection before RFA, and 1% had received cryotherapy.
After RFA, the authors found that by 1 year, roughly 26% of patients achieved complete remission of intestinal metaplasia (CRIM), defined as two negative endoscopies and histology clear of intestinal metaplasia.
That figure climbed to 56% by 2 years, and to 71% by 3 years, with 29% of patients receiving one RFA treatment session, 35% receiving two sessions, and the remaining percentage of patients undergoing 3-10 sessions before remission.
Adverse events occurred in 6.5% of patients, with stricture formation being the most common, followed by bleeding, mucosal tears, and hospitalizations for dysrhythmias.
However, using a Kaplan-Meier survival curve, they found that after CRIM was attained, 20% of patients would have recurrence of intestinal metaplasia by 1 year. Similarly, by 2 years after attainment of CRIM, the rate of recurrence was 33%.
"By 3 years, recurrences continued to occur, but precise estimates were difficult to establish because of the small number of at-risk subjects (n = 11), which made estimates of recurrence less precise," Dr. Gupta and her colleagues wrote.
According to the authors, the most common type of recurrence was intestinal metaplasia without dysplasia, which was seen in 78% of patients who recurred after CRIM.
The remaining patients who recurred (22%) developed dysplastic Barrett’s esophagus, with 11% showing high-grade dysplasia, 8% showing low-grade dysplasia, and 3% developing cancer.
There were no discernable endoscopic or patient factors associated with time to recurrence on univariate and multivariate analyses, the authors added.
"Despite the ability of RFA to achieve CRIM, recurrence of intestinal metaplasia and dysplasia appears to occur in a substantial proportion of subjects," wrote Dr. Gupta.
She pointed out that current recommendations call for intense surveillance at 3- to 6-month intervals, and if no recurrence is found, "surveillance generally is decreased to 6- to 12-month intervals."
However, "until predictive biomarkers are identified and available for clinical practice, endoscopic surveillance directed at the gastroesophageal junction and original BE [Barrett’s esophagus] segment should be continued."
Dr. Gupta had no conflicts of interest. Several of her coauthors disclosed financial relationships with drug makers, including the makers of therapies for Barrett’s esophagus. The study was funded by a grant from the National Institutes of Health. The Barrett’s Esophagus Translational Research Network consortium is funded by the National Cancer Institute.
About one-third of patients with Barrett’s esophagus can expect recurrence of intestinal metaplasia by 2 years after obtaining complete remission with radiofrequency ablation.
The finding highlights the importance of frequent endoscopic surveillance in these patients, even after remission is achieved, wrote Dr. Milli Gupta and colleagues in the July issue of Gastroenterology.
In the study, Dr. Gupta, of the Mayo Clinic, Rochester, Minn., and her associates looked at 448 patients with Barrett’s treated with radiofrequency ablation (RFA) at three different tertiary referral centers (doi: .1053/j.gastro.2013.03.008).
The data were collected from patients treated and followed up in these centers from January 2003 to November 2011 as part of the Barrett’s Esophagus Translational Research Network consortium.
The patients’ mean age was 64 years, 85% were men, and the mean length of Barrett’s esophagus that was treated was 4.1 cm, the authors reported.
Looking at the indication for RFA, 11% had intramucosal esophageal adenocarcinoma, 60% had high-grade dysplasia, 15% had low-grade dysplasia, and 14% had nondysplastic BE.
Slightly more than half (55%) of patients also underwent endoscopic mucosal resection before RFA, and 1% had received cryotherapy.
After RFA, the authors found that by 1 year, roughly 26% of patients achieved complete remission of intestinal metaplasia (CRIM), defined as two negative endoscopies and histology clear of intestinal metaplasia.
That figure climbed to 56% by 2 years, and to 71% by 3 years, with 29% of patients receiving one RFA treatment session, 35% receiving two sessions, and the remaining percentage of patients undergoing 3-10 sessions before remission.
Adverse events occurred in 6.5% of patients, with stricture formation being the most common, followed by bleeding, mucosal tears, and hospitalizations for dysrhythmias.
However, using a Kaplan-Meier survival curve, they found that after CRIM was attained, 20% of patients would have recurrence of intestinal metaplasia by 1 year. Similarly, by 2 years after attainment of CRIM, the rate of recurrence was 33%.
"By 3 years, recurrences continued to occur, but precise estimates were difficult to establish because of the small number of at-risk subjects (n = 11), which made estimates of recurrence less precise," Dr. Gupta and her colleagues wrote.
According to the authors, the most common type of recurrence was intestinal metaplasia without dysplasia, which was seen in 78% of patients who recurred after CRIM.
The remaining patients who recurred (22%) developed dysplastic Barrett’s esophagus, with 11% showing high-grade dysplasia, 8% showing low-grade dysplasia, and 3% developing cancer.
There were no discernable endoscopic or patient factors associated with time to recurrence on univariate and multivariate analyses, the authors added.
"Despite the ability of RFA to achieve CRIM, recurrence of intestinal metaplasia and dysplasia appears to occur in a substantial proportion of subjects," wrote Dr. Gupta.
She pointed out that current recommendations call for intense surveillance at 3- to 6-month intervals, and if no recurrence is found, "surveillance generally is decreased to 6- to 12-month intervals."
However, "until predictive biomarkers are identified and available for clinical practice, endoscopic surveillance directed at the gastroesophageal junction and original BE [Barrett’s esophagus] segment should be continued."
Dr. Gupta had no conflicts of interest. Several of her coauthors disclosed financial relationships with drug makers, including the makers of therapies for Barrett’s esophagus. The study was funded by a grant from the National Institutes of Health. The Barrett’s Esophagus Translational Research Network consortium is funded by the National Cancer Institute.
Major finding: At 2 years after attainment of complete remission of intestinal metaplasia in Barrett’s esophagus treated with radiofrequency ablation, 33% of patients experienced a recurrence of dysplasia.
Data source: A total of 448 patients from the Barrett’s Esophagus Translational Research Network consortium.
Disclosures: Dr. Gupta had no conflicts of interest. Several of her coauthors disclosed financial relationships with drug makers, including the makers of therapies for Barrett’s esophagus. The study was funded by a grant from the National Institutes of Health. The Barrett’s Esophagus Translational Research Network consortium is funded by the National Cancer Institute.
Risks for poorer outcomes of ASO for TGA
Neoaortic root dilation and neoaortic valve regurgitation are common complications in infants with transposition of the great arteries who undergo an arterial switch operation for repair, and the risk of developing these changes in the neoaorta increases over time, according to the results of a retrospective database study of patients at Children’s Hospital of Wisconsin.
In addition, when dilation occurs, the dimensions may progressively enlarge over time, making it important to maintain lifelong surveillance of this population.
Although perioperative mortality and long-term survival (assessed up to 30 years) has improved in more recent eras for use of an arterial switch operation (ASO) for transposition of the great arteries (TGA), these long-term studies have also shown important late complications that may contribute to late morbidity and the need for reoperation, according to Dr. Jennifer G. Co-Vu and her colleagues at the Medical College of Wisconsin, Milwaukee.
They performed their study to determine the prevalence of neoaortic root dilation and neoaortic valve regurgitation in patients treated at their institution and to determine risk factors involved in the development of these late complications.
Out of 247 patients with TGA treated with an ASO at the hospital, there were 124 patients who had at least one available postoperative transthoracic echocardiogram at least 1 year after the ASO. Median age of these patients was 0.2 months at the time of their ASO and 7.2 years at their last follow-up; 71% were boys (Ann. Thorac. Surg. 2013;95:1654-9).
Retrospective measurements of the neoaortic annulus and root were performed on all available transthoracic echocardiograms and the severity of neoaortic valve regurgitation was determined by assessing the width of the color Doppler jet of regurgitation measured at the level of the valve in the parasternal long-axis view. A jet width of 1-4 mm was defined as trivial to mild; 4-6 mm was defined as moderate; and greater than 6 mm indicated severe regurgitation, according to the researchers. Significant regurgitation was defined as moderate or severe. Significant neoaortic annulus dilation was defined as a z score of 2.5 or greater.
They evaluated potential risk factors for the development of neoaortic root dilation, annulus dilation, and neoaortic valve regurgitation.
Significant neoaortic root dilation developed in 88 of 124 (66%) of the patients during follow-up, with the probability of being free from a root diameter z score of 2.5 or greater of 84%, 67%, 47%, and 32% at 1, 5, 10, and 15 years, respectively. Significant risk factors predicting neoaortic root dilation using multivariate analysis were a history of double outlet right ventricle (DORV), previous pulmonary artery (PA) banding, and length of follow-up. A history of ventricular septal defect (VSD), coarctation, left ventricular outflow tract obstruction, and age at ASO were not significant risk factors.
Significant annulus dilation occurred in 54% of patients, with significant risk factors including a history of VSD, history of DORV, and the presence of a dilated neoaortic root. History of PA banding and length of follow-up were not significant. Moderate or severe neoaortic valve regurgitation occurred in 17 of 124 (14%) of the patients, with a probability of being free of these levels of regurgitation of 96%, 92%, 89%, and 75% at 1, 5, 10, and 15 years, respectively. The significant risk factors for regurgitation were history of DORV, VSD, left ventricular outflow tract obstruction, and length of follow-up. No patient in the series required reintervention on the neoaorta.
The authors had no disclosures.
Most people living with congenital heart disease are now adults. Unfortunately the majority of these adults, for unclear reasons, are not receiving expert care by congenital heart specialists. Perhaps some of these adults have a misperception that they are cured. Dr. Co-Vu and coauthors at the Medical College of Wisconsin confirm that the highly successful arterial switch operation is not a "cure."
| Dr. Williams |
Their important, carefully executed echo study demonstrates important progressive increases in measured diameters of the neoaortic annulus and neoaortic root over the first 15 years of life. The
authors point out that the dilation has not as yet led to a need for reintervention, and the late prevalence of neoaortic regurgitation is not high, although it too is slowly increasing over time. Their message is a clarion call for lifelong clinical surveillance following an arterial switch operation – a message that should be applied to all patients with congenital heart disease.
Dr. William G. Williams is executive director of the Congenital Heart Surgeons’ Society Data Center, Toronto, and emeritus professor of surgery, University of Toronto, and an associate medical editor for Thoracic Surgery News.
Most people living with congenital heart disease are now adults. Unfortunately the majority of these adults, for unclear reasons, are not receiving expert care by congenital heart specialists. Perhaps some of these adults have a misperception that they are cured. Dr. Co-Vu and coauthors at the Medical College of Wisconsin confirm that the highly successful arterial switch operation is not a "cure."
| Dr. Williams |
Their important, carefully executed echo study demonstrates important progressive increases in measured diameters of the neoaortic annulus and neoaortic root over the first 15 years of life. The
authors point out that the dilation has not as yet led to a need for reintervention, and the late prevalence of neoaortic regurgitation is not high, although it too is slowly increasing over time. Their message is a clarion call for lifelong clinical surveillance following an arterial switch operation – a message that should be applied to all patients with congenital heart disease.
Dr. William G. Williams is executive director of the Congenital Heart Surgeons’ Society Data Center, Toronto, and emeritus professor of surgery, University of Toronto, and an associate medical editor for Thoracic Surgery News.
Most people living with congenital heart disease are now adults. Unfortunately the majority of these adults, for unclear reasons, are not receiving expert care by congenital heart specialists. Perhaps some of these adults have a misperception that they are cured. Dr. Co-Vu and coauthors at the Medical College of Wisconsin confirm that the highly successful arterial switch operation is not a "cure."
| Dr. Williams |
Their important, carefully executed echo study demonstrates important progressive increases in measured diameters of the neoaortic annulus and neoaortic root over the first 15 years of life. The
authors point out that the dilation has not as yet led to a need for reintervention, and the late prevalence of neoaortic regurgitation is not high, although it too is slowly increasing over time. Their message is a clarion call for lifelong clinical surveillance following an arterial switch operation – a message that should be applied to all patients with congenital heart disease.
Dr. William G. Williams is executive director of the Congenital Heart Surgeons’ Society Data Center, Toronto, and emeritus professor of surgery, University of Toronto, and an associate medical editor for Thoracic Surgery News.
Neoaortic root dilation and neoaortic valve regurgitation are common complications in infants with transposition of the great arteries who undergo an arterial switch operation for repair, and the risk of developing these changes in the neoaorta increases over time, according to the results of a retrospective database study of patients at Children’s Hospital of Wisconsin.
In addition, when dilation occurs, the dimensions may progressively enlarge over time, making it important to maintain lifelong surveillance of this population.
Although perioperative mortality and long-term survival (assessed up to 30 years) has improved in more recent eras for use of an arterial switch operation (ASO) for transposition of the great arteries (TGA), these long-term studies have also shown important late complications that may contribute to late morbidity and the need for reoperation, according to Dr. Jennifer G. Co-Vu and her colleagues at the Medical College of Wisconsin, Milwaukee.
They performed their study to determine the prevalence of neoaortic root dilation and neoaortic valve regurgitation in patients treated at their institution and to determine risk factors involved in the development of these late complications.
Out of 247 patients with TGA treated with an ASO at the hospital, there were 124 patients who had at least one available postoperative transthoracic echocardiogram at least 1 year after the ASO. Median age of these patients was 0.2 months at the time of their ASO and 7.2 years at their last follow-up; 71% were boys (Ann. Thorac. Surg. 2013;95:1654-9).
Retrospective measurements of the neoaortic annulus and root were performed on all available transthoracic echocardiograms and the severity of neoaortic valve regurgitation was determined by assessing the width of the color Doppler jet of regurgitation measured at the level of the valve in the parasternal long-axis view. A jet width of 1-4 mm was defined as trivial to mild; 4-6 mm was defined as moderate; and greater than 6 mm indicated severe regurgitation, according to the researchers. Significant regurgitation was defined as moderate or severe. Significant neoaortic annulus dilation was defined as a z score of 2.5 or greater.
They evaluated potential risk factors for the development of neoaortic root dilation, annulus dilation, and neoaortic valve regurgitation.
Significant neoaortic root dilation developed in 88 of 124 (66%) of the patients during follow-up, with the probability of being free from a root diameter z score of 2.5 or greater of 84%, 67%, 47%, and 32% at 1, 5, 10, and 15 years, respectively. Significant risk factors predicting neoaortic root dilation using multivariate analysis were a history of double outlet right ventricle (DORV), previous pulmonary artery (PA) banding, and length of follow-up. A history of ventricular septal defect (VSD), coarctation, left ventricular outflow tract obstruction, and age at ASO were not significant risk factors.
Significant annulus dilation occurred in 54% of patients, with significant risk factors including a history of VSD, history of DORV, and the presence of a dilated neoaortic root. History of PA banding and length of follow-up were not significant. Moderate or severe neoaortic valve regurgitation occurred in 17 of 124 (14%) of the patients, with a probability of being free of these levels of regurgitation of 96%, 92%, 89%, and 75% at 1, 5, 10, and 15 years, respectively. The significant risk factors for regurgitation were history of DORV, VSD, left ventricular outflow tract obstruction, and length of follow-up. No patient in the series required reintervention on the neoaorta.
The authors had no disclosures.
Neoaortic root dilation and neoaortic valve regurgitation are common complications in infants with transposition of the great arteries who undergo an arterial switch operation for repair, and the risk of developing these changes in the neoaorta increases over time, according to the results of a retrospective database study of patients at Children’s Hospital of Wisconsin.
In addition, when dilation occurs, the dimensions may progressively enlarge over time, making it important to maintain lifelong surveillance of this population.
Although perioperative mortality and long-term survival (assessed up to 30 years) has improved in more recent eras for use of an arterial switch operation (ASO) for transposition of the great arteries (TGA), these long-term studies have also shown important late complications that may contribute to late morbidity and the need for reoperation, according to Dr. Jennifer G. Co-Vu and her colleagues at the Medical College of Wisconsin, Milwaukee.
They performed their study to determine the prevalence of neoaortic root dilation and neoaortic valve regurgitation in patients treated at their institution and to determine risk factors involved in the development of these late complications.
Out of 247 patients with TGA treated with an ASO at the hospital, there were 124 patients who had at least one available postoperative transthoracic echocardiogram at least 1 year after the ASO. Median age of these patients was 0.2 months at the time of their ASO and 7.2 years at their last follow-up; 71% were boys (Ann. Thorac. Surg. 2013;95:1654-9).
Retrospective measurements of the neoaortic annulus and root were performed on all available transthoracic echocardiograms and the severity of neoaortic valve regurgitation was determined by assessing the width of the color Doppler jet of regurgitation measured at the level of the valve in the parasternal long-axis view. A jet width of 1-4 mm was defined as trivial to mild; 4-6 mm was defined as moderate; and greater than 6 mm indicated severe regurgitation, according to the researchers. Significant regurgitation was defined as moderate or severe. Significant neoaortic annulus dilation was defined as a z score of 2.5 or greater.
They evaluated potential risk factors for the development of neoaortic root dilation, annulus dilation, and neoaortic valve regurgitation.
Significant neoaortic root dilation developed in 88 of 124 (66%) of the patients during follow-up, with the probability of being free from a root diameter z score of 2.5 or greater of 84%, 67%, 47%, and 32% at 1, 5, 10, and 15 years, respectively. Significant risk factors predicting neoaortic root dilation using multivariate analysis were a history of double outlet right ventricle (DORV), previous pulmonary artery (PA) banding, and length of follow-up. A history of ventricular septal defect (VSD), coarctation, left ventricular outflow tract obstruction, and age at ASO were not significant risk factors.
Significant annulus dilation occurred in 54% of patients, with significant risk factors including a history of VSD, history of DORV, and the presence of a dilated neoaortic root. History of PA banding and length of follow-up were not significant. Moderate or severe neoaortic valve regurgitation occurred in 17 of 124 (14%) of the patients, with a probability of being free of these levels of regurgitation of 96%, 92%, 89%, and 75% at 1, 5, 10, and 15 years, respectively. The significant risk factors for regurgitation were history of DORV, VSD, left ventricular outflow tract obstruction, and length of follow-up. No patient in the series required reintervention on the neoaorta.
The authors had no disclosures.
Erythropoietin cuts heart surgery transfusions
MINNEAPOLIS – A single high dose of human recombinant erythropoietin given 2 days before heart surgery reduced blood transfusions by 65%, without substantially increasing mortality or morbidity in the prospective, randomized SHOT trial.
Patients who received 80,000 IU of erythropoietin (Eprex) in a single bolus plus iron supplementation until discharge needed 0.39 blood units/patient, compared with 1.12 units/patient for those receiving standard care involving thromboelastography and tranexamic acid (P less than .001; risk ratio, 0.338).

All-cause mortality at 45 days postoperative was 3.0% with erythropoietin and 3.33%
without it (P = .26), Dr. Luca Weltert said at the annual meeting of the American Association for Thoracic Surgery.
The investigators undertook the SHOT (Blood Sparing Strategies: Single Shot High Dose Erythropoietin Two Days Before Heart Surgery) trial because their original erythropoietin protocol proved too compli- cated for everyday use. The protocol was incorporated
into the 2012 Society of
Thoracic Surgeons and Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines, but consisted of five different doses of erythropoietin in 5 days, totaling 52,000 IU, he explained.
Invited discussant Dr. Victor Ferraris, of the Lexington (Ky.) Veterans Affairs Medical Center, questioned whether the high dose of erythropoietin increased thromboembolic events, in light of the black box warnings added to erythropoiesis-stimulating agents due to an increased risk for thromboembolic events in patients with malignancy and an increased risk of serious cardiovascular events in patients with chronic kidney disease when the hemoglobin level exceeds 12 g/dL.
Thromboembolic events were not significantly different between groups, and the trial did not include cancer patients, said Dr. Weltert of the European Hospital in Rome.
Major nonfatal adverse events at 45 days were reported in 4.33% of erythropoietin and 5.67% of control patients (P = .13). Specifically, there were no differences in neurologic complications (4 vs. 5 events, respectively), long-term wound infection (4 in both groups), deep vein thrombosis (2 vs. 5), onset of acute hypertension (1 vs. 2), and new-onset renal failure (2 vs. 1).
Attendees continued this line of questioning, asking how reliable the negative finding is and whether the investigators could have missed a population with a positive result. The efficacy endpoint was based on a minimal sample size of 400 patients, and the trial enrolled 600 consecutive "all comers," Dr. Weltert said, but he added that 3,000 - 4,000 patients would be needed for the safety endpoint, "so the samples are ridiculously small to really state strongly that there is no harm for a subgroup."
The two study arms were well matched, with 35% of all patients undergoing coronary artery bypass grafting, 31% valve surgery, roughly 20% repair of the ascending aorta, and other in about 14%. The mean logistic EuroScore was 9.94 in the erythropoietin group and 10.12 in the control group, and the mean ages were 72.9 and 70.4 years, respectively.
Mean hemoglobin levels on day 4 postoperative was significantly higher in the erythropoietin group than in controls (10.21 vs. 9.01 g/dL; P = .02), Dr. Weltert said.
There were no significant differences between the erythropoietin and control groups in intensive care unit stay (2.71 vs. 2.60 days, respectively), perioperative myocardial infarction (7 vs. 7), cardiac tamponade (3 vs. 5), or need for reintubation (13 vs. 15).
An attendee asked whether hemoglobin levels drifted between days 3 and 4 postoperatively, as this can confound the decision to transfuse after cardiac surgery, and whether the investigators looked at another potential confounder, hemoglobin trigger, since no less than five randomized controlled trials have shown that a hemoglobin level of 7-8 g/dL should be used as a transfusion trigger.
Dr. Weltert said the team picked day 4 to check hemoglobin levels for practical reasons because that’s the day when you see the biggest drift and that the erythropoietin group fared better. He went on to say, "The trigger is extremely important, and I think it will be the very next step in bloodless surgery."
The investigators did compare costs for the two strategies, with standard care ringing up at 336 euros (U.S.$434), vs. 297 euros (U.S.$383) for the erythropoietin protocol (P = .05).
The European Hospital sponsored the study. Dr. Weltert reported no relevant disclosures.
MINNEAPOLIS – A single high dose of human recombinant erythropoietin given 2 days before heart surgery reduced blood transfusions by 65%, without substantially increasing mortality or morbidity in the prospective, randomized SHOT trial.
Patients who received 80,000 IU of erythropoietin (Eprex) in a single bolus plus iron supplementation until discharge needed 0.39 blood units/patient, compared with 1.12 units/patient for those receiving standard care involving thromboelastography and tranexamic acid (P less than .001; risk ratio, 0.338).
All-cause mortality at 45 days postoperative was 3.0% with erythropoietin and 3.33%
without it (P = .26), Dr. Luca Weltert said at the annual meeting of the American Association for Thoracic Surgery.
The investigators undertook the SHOT (Blood Sparing Strategies: Single Shot High Dose Erythropoietin Two Days Before Heart Surgery) trial because their original erythropoietin protocol proved too compli- cated for everyday use. The protocol was incorporated
into the 2012 Society of
Thoracic Surgeons and Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines, but consisted of five different doses of erythropoietin in 5 days, totaling 52,000 IU, he explained.
Invited discussant Dr. Victor Ferraris, of the Lexington (Ky.) Veterans Affairs Medical Center, questioned whether the high dose of erythropoietin increased thromboembolic events, in light of the black box warnings added to erythropoiesis-stimulating agents due to an increased risk for thromboembolic events in patients with malignancy and an increased risk of serious cardiovascular events in patients with chronic kidney disease when the hemoglobin level exceeds 12 g/dL.
Thromboembolic events were not significantly different between groups, and the trial did not include cancer patients, said Dr. Weltert of the European Hospital in Rome.
Major nonfatal adverse events at 45 days were reported in 4.33% of erythropoietin and 5.67% of control patients (P = .13). Specifically, there were no differences in neurologic complications (4 vs. 5 events, respectively), long-term wound infection (4 in both groups), deep vein thrombosis (2 vs. 5), onset of acute hypertension (1 vs. 2), and new-onset renal failure (2 vs. 1).
Attendees continued this line of questioning, asking how reliable the negative finding is and whether the investigators could have missed a population with a positive result. The efficacy endpoint was based on a minimal sample size of 400 patients, and the trial enrolled 600 consecutive "all comers," Dr. Weltert said, but he added that 3,000 - 4,000 patients would be needed for the safety endpoint, "so the samples are ridiculously small to really state strongly that there is no harm for a subgroup."
The two study arms were well matched, with 35% of all patients undergoing coronary artery bypass grafting, 31% valve surgery, roughly 20% repair of the ascending aorta, and other in about 14%. The mean logistic EuroScore was 9.94 in the erythropoietin group and 10.12 in the control group, and the mean ages were 72.9 and 70.4 years, respectively.
Mean hemoglobin levels on day 4 postoperative was significantly higher in the erythropoietin group than in controls (10.21 vs. 9.01 g/dL; P = .02), Dr. Weltert said.
There were no significant differences between the erythropoietin and control groups in intensive care unit stay (2.71 vs. 2.60 days, respectively), perioperative myocardial infarction (7 vs. 7), cardiac tamponade (3 vs. 5), or need for reintubation (13 vs. 15).
An attendee asked whether hemoglobin levels drifted between days 3 and 4 postoperatively, as this can confound the decision to transfuse after cardiac surgery, and whether the investigators looked at another potential confounder, hemoglobin trigger, since no less than five randomized controlled trials have shown that a hemoglobin level of 7-8 g/dL should be used as a transfusion trigger.
Dr. Weltert said the team picked day 4 to check hemoglobin levels for practical reasons because that’s the day when you see the biggest drift and that the erythropoietin group fared better. He went on to say, "The trigger is extremely important, and I think it will be the very next step in bloodless surgery."
The investigators did compare costs for the two strategies, with standard care ringing up at 336 euros (U.S.$434), vs. 297 euros (U.S.$383) for the erythropoietin protocol (P = .05).
The European Hospital sponsored the study. Dr. Weltert reported no relevant disclosures.
MINNEAPOLIS – A single high dose of human recombinant erythropoietin given 2 days before heart surgery reduced blood transfusions by 65%, without substantially increasing mortality or morbidity in the prospective, randomized SHOT trial.
Patients who received 80,000 IU of erythropoietin (Eprex) in a single bolus plus iron supplementation until discharge needed 0.39 blood units/patient, compared with 1.12 units/patient for those receiving standard care involving thromboelastography and tranexamic acid (P less than .001; risk ratio, 0.338).
All-cause mortality at 45 days postoperative was 3.0% with erythropoietin and 3.33%
without it (P = .26), Dr. Luca Weltert said at the annual meeting of the American Association for Thoracic Surgery.
The investigators undertook the SHOT (Blood Sparing Strategies: Single Shot High Dose Erythropoietin Two Days Before Heart Surgery) trial because their original erythropoietin protocol proved too compli- cated for everyday use. The protocol was incorporated
into the 2012 Society of
Thoracic Surgeons and Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines, but consisted of five different doses of erythropoietin in 5 days, totaling 52,000 IU, he explained.
Invited discussant Dr. Victor Ferraris, of the Lexington (Ky.) Veterans Affairs Medical Center, questioned whether the high dose of erythropoietin increased thromboembolic events, in light of the black box warnings added to erythropoiesis-stimulating agents due to an increased risk for thromboembolic events in patients with malignancy and an increased risk of serious cardiovascular events in patients with chronic kidney disease when the hemoglobin level exceeds 12 g/dL.
Thromboembolic events were not significantly different between groups, and the trial did not include cancer patients, said Dr. Weltert of the European Hospital in Rome.
Major nonfatal adverse events at 45 days were reported in 4.33% of erythropoietin and 5.67% of control patients (P = .13). Specifically, there were no differences in neurologic complications (4 vs. 5 events, respectively), long-term wound infection (4 in both groups), deep vein thrombosis (2 vs. 5), onset of acute hypertension (1 vs. 2), and new-onset renal failure (2 vs. 1).
Attendees continued this line of questioning, asking how reliable the negative finding is and whether the investigators could have missed a population with a positive result. The efficacy endpoint was based on a minimal sample size of 400 patients, and the trial enrolled 600 consecutive "all comers," Dr. Weltert said, but he added that 3,000 - 4,000 patients would be needed for the safety endpoint, "so the samples are ridiculously small to really state strongly that there is no harm for a subgroup."
The two study arms were well matched, with 35% of all patients undergoing coronary artery bypass grafting, 31% valve surgery, roughly 20% repair of the ascending aorta, and other in about 14%. The mean logistic EuroScore was 9.94 in the erythropoietin group and 10.12 in the control group, and the mean ages were 72.9 and 70.4 years, respectively.
Mean hemoglobin levels on day 4 postoperative was significantly higher in the erythropoietin group than in controls (10.21 vs. 9.01 g/dL; P = .02), Dr. Weltert said.
There were no significant differences between the erythropoietin and control groups in intensive care unit stay (2.71 vs. 2.60 days, respectively), perioperative myocardial infarction (7 vs. 7), cardiac tamponade (3 vs. 5), or need for reintubation (13 vs. 15).
An attendee asked whether hemoglobin levels drifted between days 3 and 4 postoperatively, as this can confound the decision to transfuse after cardiac surgery, and whether the investigators looked at another potential confounder, hemoglobin trigger, since no less than five randomized controlled trials have shown that a hemoglobin level of 7-8 g/dL should be used as a transfusion trigger.
Dr. Weltert said the team picked day 4 to check hemoglobin levels for practical reasons because that’s the day when you see the biggest drift and that the erythropoietin group fared better. He went on to say, "The trigger is extremely important, and I think it will be the very next step in bloodless surgery."
The investigators did compare costs for the two strategies, with standard care ringing up at 336 euros (U.S.$434), vs. 297 euros (U.S.$383) for the erythropoietin protocol (P = .05).
The European Hospital sponsored the study. Dr. Weltert reported no relevant disclosures.
AT THE AATS ANNUAL MEETING
