User login
Endoscopy Falls Short for Eosinophilic Esophagitis
Endoscopic findings alone are not sufficient to diagnose eosinophilic esophagitis and instead, biopsies are needed, reported Ms. Hannah P. Kim and her colleagues in the September issue of Clinical Gastroenterology and Hepatology.
Indeed, while findings like rings, strictures, and linear furrows ought to raise suspicion, a meta-analysis of more than 4,600 patients confirms that "low sensitivity and variable predictive values make them inadequate both for the diagnosis of EoE [eosinophilic esophagitis] and for the decision of whether or not to obtain biopsies."
Ms. Kim of the Center for Esophageal Diseases and Swallowing at the University of North Carolina, Chapel Hill, and her colleagues analyzed data from 80 articles and 20 abstracts that included a total of 4,678 patients with EoE and 2,742 patients without, who served as controls.
The studies were culled from PubMed, EMBASE, and gastroenterology meetings. All studies included in the analysis had more than 10 patients with EoE and provided information on the associated endoscopic findings. The mean age of participants ranged from 6 years to 55 years in the different studies.
In an analysis, the authors found that the overall pooled prevalence of esophageal rings in the sample was 44%. For strictures, the prevalence was 21%, and for linear furrows, 48% (Clin. Gastroenterol. Hepatol. 2012 [doi:10.1016/j.cgh.2012.04.019]).
Narrow-caliber esophagus findings had a pooled prevalence of only 9% of the total sample, while the presence of white plaques or exudates was 27%. Visible pallor or decreased vasculature on endoscopy was seen in 41% of patients, and erosive esophagitis in 17%.
"The endoscopic examination was normal in 17% of cases," added the authors.
They also found a difference in prevalence according to age of patients. For example, rings and strictures were more prevalent in adults (57% and 25%, respectively) than in children (11% and 8%; P less than .05 for each).
"On the other hand, white plaques and pallor or decreased vasculature were more prevalent in children (36% and 58%) than in adults (19% and 18%; P less than .05 for each)."
Finally, Ms. Kim and her associates assessed the overall sensitivity, specificity, pooled positive predictive value (PPV), and pooled negative predictive value (NPV) for each of the assessed endoscopic characteristics.
For rings, the overall sensitivity was 48%, the specificity was 91%, the PPV was 64%, and NPV was 84%. Strictures had an overall sensitivity of 15%, specificity of 95%, PPV of 51%, and NPV of 76%.
"The operating characteristics were slightly higher for linear furrows, with a sensitivity of 40%, specificity 95%, PPV 73%, and NPV 83%," wrote the authors.
And for the endoscopic finding of pallor and/or decreased vasculature, sensitivity was 43%, specificity 90%, PPV 65%, and NPV 79%.
"In contrast to the low sensitivity of individual endoscopic findings, when examining the presence of at least one endoscopic finding, an abnormal endoscopy had a sensitivity of 87%, specificity of 47%, PPV of 42%, and NPV of 89%," the authors added.
"Although endoscopic features of EoE such as esophageal rings, linear furrows, and white plaques or exudates are often considered to be typical features of EoE, these are not always identified by endoscopists," wrote the researchers.
And while most patients with EoE have abnormal findings on upper endoscopy examinations, "the sensitivity values of individual endoscopic findings were modest, and although the specificity values were higher, the predictive values were inadequate for diagnostic purposes."
"Esophageal biopsies should be obtained from all patients who present with symptoms of EoE, regardless of the endoscopic appearance of the esophagus."
The authors stated that the study was supported by grants from the National Institutes of Health and the Doris Duke Charitable Foundation. They stated that they had no individual disclosures.
Endoscopic findings alone are not sufficient to diagnose eosinophilic esophagitis and instead, biopsies are needed, reported Ms. Hannah P. Kim and her colleagues in the September issue of Clinical Gastroenterology and Hepatology.
Indeed, while findings like rings, strictures, and linear furrows ought to raise suspicion, a meta-analysis of more than 4,600 patients confirms that "low sensitivity and variable predictive values make them inadequate both for the diagnosis of EoE [eosinophilic esophagitis] and for the decision of whether or not to obtain biopsies."
Ms. Kim of the Center for Esophageal Diseases and Swallowing at the University of North Carolina, Chapel Hill, and her colleagues analyzed data from 80 articles and 20 abstracts that included a total of 4,678 patients with EoE and 2,742 patients without, who served as controls.
The studies were culled from PubMed, EMBASE, and gastroenterology meetings. All studies included in the analysis had more than 10 patients with EoE and provided information on the associated endoscopic findings. The mean age of participants ranged from 6 years to 55 years in the different studies.
In an analysis, the authors found that the overall pooled prevalence of esophageal rings in the sample was 44%. For strictures, the prevalence was 21%, and for linear furrows, 48% (Clin. Gastroenterol. Hepatol. 2012 [doi:10.1016/j.cgh.2012.04.019]).
Narrow-caliber esophagus findings had a pooled prevalence of only 9% of the total sample, while the presence of white plaques or exudates was 27%. Visible pallor or decreased vasculature on endoscopy was seen in 41% of patients, and erosive esophagitis in 17%.
"The endoscopic examination was normal in 17% of cases," added the authors.
They also found a difference in prevalence according to age of patients. For example, rings and strictures were more prevalent in adults (57% and 25%, respectively) than in children (11% and 8%; P less than .05 for each).
"On the other hand, white plaques and pallor or decreased vasculature were more prevalent in children (36% and 58%) than in adults (19% and 18%; P less than .05 for each)."
Finally, Ms. Kim and her associates assessed the overall sensitivity, specificity, pooled positive predictive value (PPV), and pooled negative predictive value (NPV) for each of the assessed endoscopic characteristics.
For rings, the overall sensitivity was 48%, the specificity was 91%, the PPV was 64%, and NPV was 84%. Strictures had an overall sensitivity of 15%, specificity of 95%, PPV of 51%, and NPV of 76%.
"The operating characteristics were slightly higher for linear furrows, with a sensitivity of 40%, specificity 95%, PPV 73%, and NPV 83%," wrote the authors.
And for the endoscopic finding of pallor and/or decreased vasculature, sensitivity was 43%, specificity 90%, PPV 65%, and NPV 79%.
"In contrast to the low sensitivity of individual endoscopic findings, when examining the presence of at least one endoscopic finding, an abnormal endoscopy had a sensitivity of 87%, specificity of 47%, PPV of 42%, and NPV of 89%," the authors added.
"Although endoscopic features of EoE such as esophageal rings, linear furrows, and white plaques or exudates are often considered to be typical features of EoE, these are not always identified by endoscopists," wrote the researchers.
And while most patients with EoE have abnormal findings on upper endoscopy examinations, "the sensitivity values of individual endoscopic findings were modest, and although the specificity values were higher, the predictive values were inadequate for diagnostic purposes."
"Esophageal biopsies should be obtained from all patients who present with symptoms of EoE, regardless of the endoscopic appearance of the esophagus."
The authors stated that the study was supported by grants from the National Institutes of Health and the Doris Duke Charitable Foundation. They stated that they had no individual disclosures.
Endoscopic findings alone are not sufficient to diagnose eosinophilic esophagitis and instead, biopsies are needed, reported Ms. Hannah P. Kim and her colleagues in the September issue of Clinical Gastroenterology and Hepatology.
Indeed, while findings like rings, strictures, and linear furrows ought to raise suspicion, a meta-analysis of more than 4,600 patients confirms that "low sensitivity and variable predictive values make them inadequate both for the diagnosis of EoE [eosinophilic esophagitis] and for the decision of whether or not to obtain biopsies."
Ms. Kim of the Center for Esophageal Diseases and Swallowing at the University of North Carolina, Chapel Hill, and her colleagues analyzed data from 80 articles and 20 abstracts that included a total of 4,678 patients with EoE and 2,742 patients without, who served as controls.
The studies were culled from PubMed, EMBASE, and gastroenterology meetings. All studies included in the analysis had more than 10 patients with EoE and provided information on the associated endoscopic findings. The mean age of participants ranged from 6 years to 55 years in the different studies.
In an analysis, the authors found that the overall pooled prevalence of esophageal rings in the sample was 44%. For strictures, the prevalence was 21%, and for linear furrows, 48% (Clin. Gastroenterol. Hepatol. 2012 [doi:10.1016/j.cgh.2012.04.019]).
Narrow-caliber esophagus findings had a pooled prevalence of only 9% of the total sample, while the presence of white plaques or exudates was 27%. Visible pallor or decreased vasculature on endoscopy was seen in 41% of patients, and erosive esophagitis in 17%.
"The endoscopic examination was normal in 17% of cases," added the authors.
They also found a difference in prevalence according to age of patients. For example, rings and strictures were more prevalent in adults (57% and 25%, respectively) than in children (11% and 8%; P less than .05 for each).
"On the other hand, white plaques and pallor or decreased vasculature were more prevalent in children (36% and 58%) than in adults (19% and 18%; P less than .05 for each)."
Finally, Ms. Kim and her associates assessed the overall sensitivity, specificity, pooled positive predictive value (PPV), and pooled negative predictive value (NPV) for each of the assessed endoscopic characteristics.
For rings, the overall sensitivity was 48%, the specificity was 91%, the PPV was 64%, and NPV was 84%. Strictures had an overall sensitivity of 15%, specificity of 95%, PPV of 51%, and NPV of 76%.
"The operating characteristics were slightly higher for linear furrows, with a sensitivity of 40%, specificity 95%, PPV 73%, and NPV 83%," wrote the authors.
And for the endoscopic finding of pallor and/or decreased vasculature, sensitivity was 43%, specificity 90%, PPV 65%, and NPV 79%.
"In contrast to the low sensitivity of individual endoscopic findings, when examining the presence of at least one endoscopic finding, an abnormal endoscopy had a sensitivity of 87%, specificity of 47%, PPV of 42%, and NPV of 89%," the authors added.
"Although endoscopic features of EoE such as esophageal rings, linear furrows, and white plaques or exudates are often considered to be typical features of EoE, these are not always identified by endoscopists," wrote the researchers.
And while most patients with EoE have abnormal findings on upper endoscopy examinations, "the sensitivity values of individual endoscopic findings were modest, and although the specificity values were higher, the predictive values were inadequate for diagnostic purposes."
"Esophageal biopsies should be obtained from all patients who present with symptoms of EoE, regardless of the endoscopic appearance of the esophagus."
The authors stated that the study was supported by grants from the National Institutes of Health and the Doris Duke Charitable Foundation. They stated that they had no individual disclosures.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Major Finding: On endoscopy, rings and strictures were more prevalent in adults (57% and 25%, respectively) than in children (11% and 8%; P less than .05 for each).
Data Source: A systematic review and meta-analysis of studies including more than 4,600 EoE patients and 2,700 controls.
Disclosures: The authors stated that the study was supported by grants from the National Institutes of Health and the Doris Duke Charitable Foundation. They stated that they had no individual disclosures.
Robotic Device for Gastric Neoplasia Found Safe in Five Patients
A novel robotic system designed to perform endoscopic submucosal dissection of early gastric neoplasia was safe and effective in a five-patient trial, reported Soo Jay Phee, Ph.D., and colleagues in Clinical Gastroenterology and Hepatology.
Indeed, the first human study of the robotic device showed that it achieved clear margins, no cases of major bleeding or perforation, and discharge within hours for several of the patients.
Dr. Phee of the School of Mechanical and Aerospace Engineering at Nanyang Technological University in Singapore and first author Dr. D. Nageshwar Reddy of the Asian Institute of Gastroenterology in Somajiguda, India, enrolled five patients from two centers in India and one in Hong Kong.
Only patients with gastric neoplasia limited to the mucosa, confirmed by biopsy and histopathology, were included.
All patients underwent endoscopic submucosal dissection with the assistance of a novel device called the Master and Slave Transluminal Endoscopic Robot (MASTER). The MASTER device has been described previously (Gastrointest. Endoscopy 2010;72:593-9).
According to the authors, the device is controlled by two operators, "one responsible for the steering of the endoscope while the other would be performing the submucosal dissection with the two robotic arms."
The investigators added, "The open edge of the mucosa with the tumor was grasped by one of the robotic arms to retract the mucosa and enhance exposure of the submucosa, while submucosal dissection was completed with the other L hook arm" (Clin. Gastroenterol. Hepatol. 2012 October [doi:10.1016/j.cgh.2012.05.019]).
All procedures were performed under general anesthesia and with ventilation by naso- or orotracheal intubation. All operators trained on porcine models prior to the study.
In the case of the first patient, a 41-year-old man with a 2-cm adenocarcinoma in the body of the stomach, "the submucosal dissection with the robotic system was successfully done in 19 minutes," reported the authors.
There was no bleeding for perforation, and histopathology of the specimen after retrieval showed intramucosal well-differentiated adenocarcinoma with clear resection margins. The patient was discharged after 12 hours.
The second case, a 60-year-old man, was found to have a 1.5-cm mucosal adenocarcinoma in the gastric antrum. "The submucosal dissection was completed in only 5 minutes," wrote the authors, with no complications, and clear margins on histopathology. The patient was discharged in 6 hours.
Similarly, the third patient (a 39-year-old man) had a 2-cm sessile lesion in the gastric antrum. Submucosal dissection with the MASTER was completed in 3 minutes, with no complications, clear margins, and discharge from the hospital 4 hours later.
The longest procedure was done in a 51-year-old woman with a 3-cm early gastric cancer; this procedure took 50 minutes. She had no major bleeding or perforation, had clear margins on histopathology, and had a 3-day hospital stay.
Finally, a 50-year-old man with a 2.5-cm sessile polypoid in the inferior wall of the prepyloric canal underwent a 16-minute dissection. "Severe bleeding was encountered during the procedure and required exchange of the MASTER-mounted endoscope for a waterjet endoscope to stop the bleeding with coagulation grapser," wrote the authors.
"The pathology showed hyperplastic polyp with clear margins. He was discharged from hospital on day 3 after the procedure."
At 30 days’ follow-up, no complications were reported by any of the patients, and the follow-up endoscopy showed "complete healing" of the resection site. At 6 months, the three patients with data available were "doing well," according to the authors.
The study was supported by a MedTech Seeding Fund from the National University of Singapore. The authors reported having no other relevant financial disclosures.
A novel robotic system designed to perform endoscopic submucosal dissection of early gastric neoplasia was safe and effective in a five-patient trial, reported Soo Jay Phee, Ph.D., and colleagues in Clinical Gastroenterology and Hepatology.
Indeed, the first human study of the robotic device showed that it achieved clear margins, no cases of major bleeding or perforation, and discharge within hours for several of the patients.
Dr. Phee of the School of Mechanical and Aerospace Engineering at Nanyang Technological University in Singapore and first author Dr. D. Nageshwar Reddy of the Asian Institute of Gastroenterology in Somajiguda, India, enrolled five patients from two centers in India and one in Hong Kong.
Only patients with gastric neoplasia limited to the mucosa, confirmed by biopsy and histopathology, were included.
All patients underwent endoscopic submucosal dissection with the assistance of a novel device called the Master and Slave Transluminal Endoscopic Robot (MASTER). The MASTER device has been described previously (Gastrointest. Endoscopy 2010;72:593-9).
According to the authors, the device is controlled by two operators, "one responsible for the steering of the endoscope while the other would be performing the submucosal dissection with the two robotic arms."
The investigators added, "The open edge of the mucosa with the tumor was grasped by one of the robotic arms to retract the mucosa and enhance exposure of the submucosa, while submucosal dissection was completed with the other L hook arm" (Clin. Gastroenterol. Hepatol. 2012 October [doi:10.1016/j.cgh.2012.05.019]).
All procedures were performed under general anesthesia and with ventilation by naso- or orotracheal intubation. All operators trained on porcine models prior to the study.
In the case of the first patient, a 41-year-old man with a 2-cm adenocarcinoma in the body of the stomach, "the submucosal dissection with the robotic system was successfully done in 19 minutes," reported the authors.
There was no bleeding for perforation, and histopathology of the specimen after retrieval showed intramucosal well-differentiated adenocarcinoma with clear resection margins. The patient was discharged after 12 hours.
The second case, a 60-year-old man, was found to have a 1.5-cm mucosal adenocarcinoma in the gastric antrum. "The submucosal dissection was completed in only 5 minutes," wrote the authors, with no complications, and clear margins on histopathology. The patient was discharged in 6 hours.
Similarly, the third patient (a 39-year-old man) had a 2-cm sessile lesion in the gastric antrum. Submucosal dissection with the MASTER was completed in 3 minutes, with no complications, clear margins, and discharge from the hospital 4 hours later.
The longest procedure was done in a 51-year-old woman with a 3-cm early gastric cancer; this procedure took 50 minutes. She had no major bleeding or perforation, had clear margins on histopathology, and had a 3-day hospital stay.
Finally, a 50-year-old man with a 2.5-cm sessile polypoid in the inferior wall of the prepyloric canal underwent a 16-minute dissection. "Severe bleeding was encountered during the procedure and required exchange of the MASTER-mounted endoscope for a waterjet endoscope to stop the bleeding with coagulation grapser," wrote the authors.
"The pathology showed hyperplastic polyp with clear margins. He was discharged from hospital on day 3 after the procedure."
At 30 days’ follow-up, no complications were reported by any of the patients, and the follow-up endoscopy showed "complete healing" of the resection site. At 6 months, the three patients with data available were "doing well," according to the authors.
The study was supported by a MedTech Seeding Fund from the National University of Singapore. The authors reported having no other relevant financial disclosures.
A novel robotic system designed to perform endoscopic submucosal dissection of early gastric neoplasia was safe and effective in a five-patient trial, reported Soo Jay Phee, Ph.D., and colleagues in Clinical Gastroenterology and Hepatology.
Indeed, the first human study of the robotic device showed that it achieved clear margins, no cases of major bleeding or perforation, and discharge within hours for several of the patients.
Dr. Phee of the School of Mechanical and Aerospace Engineering at Nanyang Technological University in Singapore and first author Dr. D. Nageshwar Reddy of the Asian Institute of Gastroenterology in Somajiguda, India, enrolled five patients from two centers in India and one in Hong Kong.
Only patients with gastric neoplasia limited to the mucosa, confirmed by biopsy and histopathology, were included.
All patients underwent endoscopic submucosal dissection with the assistance of a novel device called the Master and Slave Transluminal Endoscopic Robot (MASTER). The MASTER device has been described previously (Gastrointest. Endoscopy 2010;72:593-9).
According to the authors, the device is controlled by two operators, "one responsible for the steering of the endoscope while the other would be performing the submucosal dissection with the two robotic arms."
The investigators added, "The open edge of the mucosa with the tumor was grasped by one of the robotic arms to retract the mucosa and enhance exposure of the submucosa, while submucosal dissection was completed with the other L hook arm" (Clin. Gastroenterol. Hepatol. 2012 October [doi:10.1016/j.cgh.2012.05.019]).
All procedures were performed under general anesthesia and with ventilation by naso- or orotracheal intubation. All operators trained on porcine models prior to the study.
In the case of the first patient, a 41-year-old man with a 2-cm adenocarcinoma in the body of the stomach, "the submucosal dissection with the robotic system was successfully done in 19 minutes," reported the authors.
There was no bleeding for perforation, and histopathology of the specimen after retrieval showed intramucosal well-differentiated adenocarcinoma with clear resection margins. The patient was discharged after 12 hours.
The second case, a 60-year-old man, was found to have a 1.5-cm mucosal adenocarcinoma in the gastric antrum. "The submucosal dissection was completed in only 5 minutes," wrote the authors, with no complications, and clear margins on histopathology. The patient was discharged in 6 hours.
Similarly, the third patient (a 39-year-old man) had a 2-cm sessile lesion in the gastric antrum. Submucosal dissection with the MASTER was completed in 3 minutes, with no complications, clear margins, and discharge from the hospital 4 hours later.
The longest procedure was done in a 51-year-old woman with a 3-cm early gastric cancer; this procedure took 50 minutes. She had no major bleeding or perforation, had clear margins on histopathology, and had a 3-day hospital stay.
Finally, a 50-year-old man with a 2.5-cm sessile polypoid in the inferior wall of the prepyloric canal underwent a 16-minute dissection. "Severe bleeding was encountered during the procedure and required exchange of the MASTER-mounted endoscope for a waterjet endoscope to stop the bleeding with coagulation grapser," wrote the authors.
"The pathology showed hyperplastic polyp with clear margins. He was discharged from hospital on day 3 after the procedure."
At 30 days’ follow-up, no complications were reported by any of the patients, and the follow-up endoscopy showed "complete healing" of the resection site. At 6 months, the three patients with data available were "doing well," according to the authors.
The study was supported by a MedTech Seeding Fund from the National University of Singapore. The authors reported having no other relevant financial disclosures.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Major Finding: Five patients who underwent endoscopic submucosal dissection of early-stage gastric neoplasia with the use of a novel robotic system had good 30-day outcomes and clear resection margins.
Data Source: The findings came from five case studies in India and Hong Kong.
Disclosures: The study was supported by a MedTech Seeding Fund from the National University of Singapore. The authors reported having no other relevant financial disclosures.
Upper GI Cancer Risk Elevated in AIDS
AIDS patients have a greater risk of esophageal and stomach malignancies, compared with the general population, reported E. Christina Persson, Ph.D., and her colleagues in Gastroenterology.
The researchers, led by Dr. Persson of the division of cancer epidemiology and genetics at the National Cancer Institute, analyzed data from nearly 2 million person-years recorded in the HIV/AIDS Cancer Match Study. The HACM study links state and metropolitan HIV/AIDS registries to the corresponding cancer registries.
The investigators limited their search to primary invasive carcinomas or non-Hodgkin’s lymphomas (NHLs) of the esophagus and stomach that were diagnosed between 1980 and 2007 (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.07.013]).
"Individuals diagnosed with first malignancies other than esophageal and stomach cancers were censored at date of diagnosis, and any subsequent malignancy was excluded," they said.
Additionally, the first 3 months after AIDS diagnosis were excluded from analysis, since NHL is AIDS-defining, and also because intensive medical evaluation in this period could artificially inflate cancer diagnoses.
AIDS patients were followed up until earliest cancer diagnosis, death, date of last registry coverage, or 10 years after AIDS diagnosis, whichever came first.
The researchers then ascertained the standardized incidence ratio (SIR) for the 596,955 AIDS patients (predominantly male) included in the study. This was calculated by dividing the observed counts in AIDS patients by expected counts, which were in turn estimated by applying general population incidence rates to the AIDS population in strata defined by age, race, sex, calendar year, and cancer registry.
During 1,920,274 person-years, the SIR for esophageal carcinoma was 1.69 in AIDS patients, compared with the general population (95% confidence interval, 1.37-2.07).
When the data were broken down by specific type of esophageal cancer, the SIR was higher for esophageal adenocarcinoma at 1.91 (95% CI, 1.31-2.70), and lower for squamous cell carcinoma of the esophagus at 1.47 (95% CI, 1.10-1.92).
The authors added that the elevated risk applied to all sites, "although the elevated risk of carcinoma of the middle esophagus was of borderline statistical significance."
The results were similar for carcinomas of the stomach. Compared with the general population, AIDS patients had a SIR of 1.44 for all carcinomas (95% CI, 1.17-1.76).
"All types of adenocarcinoma were elevated, including diffuse adenocarcinoma (SIR, 1.65; 95% CI, 1.08-2.41) and intestinal adenocarcinoma (SIR, 1.96; 95% CI, 0.94-3.61)," wrote Dr. Persson.
Moreover, the risk was elevated for both cardia and noncardia sites, "though only the SIR for noncardia stomach carcinoma was significant (SIR, 1.53; 95% CI, 1.12-2.05)."
The risks of non-Hodgkin’s lymphomas of the esophagus and stomach were dramatically elevated in the AIDS population, which was "not surprising," according to the authors: For the esophagus, the SIR was 261 (95% CI, 190-349) and for the stomach, it was 35.5 (95% CI, 31.9-39.5).
The authors also examined the risk of carcinoma adjusted for demographics, calendar year, and AIDS status. They found that CD4 count was not associated with the risk of either esophageal or stomach cancer.
Nor was there any decrease in the incidence rate over the calendar period of the study, even after the introduction of highly active antiretroviral therapy (HAART) in 1996.
According to the authors, this confirms that while "extended immunosuppression plays a role in the development of these cancers, ... HAART use after the development of AIDS may not be effective in halting this process."
The research was funded by the National Cancer Institute, the National Institutes of Health, and the Department of Health and Human Services. The authors declared no potential conflicts of interest.
Over the 30 years of the HIV pandemic, the risk of cancer has been found to be significantly elevated in HIV-infected persons. These include the three “AIDS-defining” cancers (Kaposi Sarcoma [KS], non-Hodgkin lymphoma [NHL], and cervical cancer) and a variety of “non AIDS-defining” cancers. Gastroenterologists have been most likely to encounter either visceral KS or hepatocellular carcinoma.
Dr. Persson and her colleagues used large population-based HIV and cancer registries to describe an increased risk of two additional malignancies, esophageal cancer (both squamous cell and adenocarcinoma) and stomach cancer in persons with AIDS, in addition to mucosa-associated lymphomas (NHL). NHL decreased in the era of effective antiretroviral therapy, but esophageal and gastric cancers remained elevated, and none was correlated with CD4 count.
HIV-associated cancers are often attributed to an infectious etiology, which presumably in the setting of impaired immunity and increased inflammation leads to a greater risk of cancer. Both Epstein-Barr virus and Helicobacter pylori have been associated with gastric cancer and NHL, and the role they play in HIV-associated gastrointestinal malignancies needs to be further defined. Additionally, the high prevalence of tobacco and alcohol use in HIV patients may contribute to the risk of gastrointestinal malignancies.
Gastroenterologists clearly now need to be familiar with several malignancies in persons with HIV, including KS, NHL, and gastric and esophageal carcinoma. It remains unknown whether strategies such as earlier initiation of antiretroviral therapy, eradication of H. pylori, and reducing alcohol and tobacco use are effective in reducing the burden of cancer in HIV-infected persons.
COREY CASPER, M.D., M.P.H., is an associate member of the divisions of public health science and clinical research in the department of vaccine and infectious disease at the Fred Hutchinson Cancer Research Center, Seattle, and an associate professor of medicine, epidemiology, and global health at the University of Washington, Seattle. He also is medical director of infection control, Seattle Cancer Care Alliance.
Over the 30 years of the HIV pandemic, the risk of cancer has been found to be significantly elevated in HIV-infected persons. These include the three “AIDS-defining” cancers (Kaposi Sarcoma [KS], non-Hodgkin lymphoma [NHL], and cervical cancer) and a variety of “non AIDS-defining” cancers. Gastroenterologists have been most likely to encounter either visceral KS or hepatocellular carcinoma.
Dr. Persson and her colleagues used large population-based HIV and cancer registries to describe an increased risk of two additional malignancies, esophageal cancer (both squamous cell and adenocarcinoma) and stomach cancer in persons with AIDS, in addition to mucosa-associated lymphomas (NHL). NHL decreased in the era of effective antiretroviral therapy, but esophageal and gastric cancers remained elevated, and none was correlated with CD4 count.
HIV-associated cancers are often attributed to an infectious etiology, which presumably in the setting of impaired immunity and increased inflammation leads to a greater risk of cancer. Both Epstein-Barr virus and Helicobacter pylori have been associated with gastric cancer and NHL, and the role they play in HIV-associated gastrointestinal malignancies needs to be further defined. Additionally, the high prevalence of tobacco and alcohol use in HIV patients may contribute to the risk of gastrointestinal malignancies.
Gastroenterologists clearly now need to be familiar with several malignancies in persons with HIV, including KS, NHL, and gastric and esophageal carcinoma. It remains unknown whether strategies such as earlier initiation of antiretroviral therapy, eradication of H. pylori, and reducing alcohol and tobacco use are effective in reducing the burden of cancer in HIV-infected persons.
COREY CASPER, M.D., M.P.H., is an associate member of the divisions of public health science and clinical research in the department of vaccine and infectious disease at the Fred Hutchinson Cancer Research Center, Seattle, and an associate professor of medicine, epidemiology, and global health at the University of Washington, Seattle. He also is medical director of infection control, Seattle Cancer Care Alliance.
Over the 30 years of the HIV pandemic, the risk of cancer has been found to be significantly elevated in HIV-infected persons. These include the three “AIDS-defining” cancers (Kaposi Sarcoma [KS], non-Hodgkin lymphoma [NHL], and cervical cancer) and a variety of “non AIDS-defining” cancers. Gastroenterologists have been most likely to encounter either visceral KS or hepatocellular carcinoma.
Dr. Persson and her colleagues used large population-based HIV and cancer registries to describe an increased risk of two additional malignancies, esophageal cancer (both squamous cell and adenocarcinoma) and stomach cancer in persons with AIDS, in addition to mucosa-associated lymphomas (NHL). NHL decreased in the era of effective antiretroviral therapy, but esophageal and gastric cancers remained elevated, and none was correlated with CD4 count.
HIV-associated cancers are often attributed to an infectious etiology, which presumably in the setting of impaired immunity and increased inflammation leads to a greater risk of cancer. Both Epstein-Barr virus and Helicobacter pylori have been associated with gastric cancer and NHL, and the role they play in HIV-associated gastrointestinal malignancies needs to be further defined. Additionally, the high prevalence of tobacco and alcohol use in HIV patients may contribute to the risk of gastrointestinal malignancies.
Gastroenterologists clearly now need to be familiar with several malignancies in persons with HIV, including KS, NHL, and gastric and esophageal carcinoma. It remains unknown whether strategies such as earlier initiation of antiretroviral therapy, eradication of H. pylori, and reducing alcohol and tobacco use are effective in reducing the burden of cancer in HIV-infected persons.
COREY CASPER, M.D., M.P.H., is an associate member of the divisions of public health science and clinical research in the department of vaccine and infectious disease at the Fred Hutchinson Cancer Research Center, Seattle, and an associate professor of medicine, epidemiology, and global health at the University of Washington, Seattle. He also is medical director of infection control, Seattle Cancer Care Alliance.
AIDS patients have a greater risk of esophageal and stomach malignancies, compared with the general population, reported E. Christina Persson, Ph.D., and her colleagues in Gastroenterology.
The researchers, led by Dr. Persson of the division of cancer epidemiology and genetics at the National Cancer Institute, analyzed data from nearly 2 million person-years recorded in the HIV/AIDS Cancer Match Study. The HACM study links state and metropolitan HIV/AIDS registries to the corresponding cancer registries.
The investigators limited their search to primary invasive carcinomas or non-Hodgkin’s lymphomas (NHLs) of the esophagus and stomach that were diagnosed between 1980 and 2007 (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.07.013]).
"Individuals diagnosed with first malignancies other than esophageal and stomach cancers were censored at date of diagnosis, and any subsequent malignancy was excluded," they said.
Additionally, the first 3 months after AIDS diagnosis were excluded from analysis, since NHL is AIDS-defining, and also because intensive medical evaluation in this period could artificially inflate cancer diagnoses.
AIDS patients were followed up until earliest cancer diagnosis, death, date of last registry coverage, or 10 years after AIDS diagnosis, whichever came first.
The researchers then ascertained the standardized incidence ratio (SIR) for the 596,955 AIDS patients (predominantly male) included in the study. This was calculated by dividing the observed counts in AIDS patients by expected counts, which were in turn estimated by applying general population incidence rates to the AIDS population in strata defined by age, race, sex, calendar year, and cancer registry.
During 1,920,274 person-years, the SIR for esophageal carcinoma was 1.69 in AIDS patients, compared with the general population (95% confidence interval, 1.37-2.07).
When the data were broken down by specific type of esophageal cancer, the SIR was higher for esophageal adenocarcinoma at 1.91 (95% CI, 1.31-2.70), and lower for squamous cell carcinoma of the esophagus at 1.47 (95% CI, 1.10-1.92).
The authors added that the elevated risk applied to all sites, "although the elevated risk of carcinoma of the middle esophagus was of borderline statistical significance."
The results were similar for carcinomas of the stomach. Compared with the general population, AIDS patients had a SIR of 1.44 for all carcinomas (95% CI, 1.17-1.76).
"All types of adenocarcinoma were elevated, including diffuse adenocarcinoma (SIR, 1.65; 95% CI, 1.08-2.41) and intestinal adenocarcinoma (SIR, 1.96; 95% CI, 0.94-3.61)," wrote Dr. Persson.
Moreover, the risk was elevated for both cardia and noncardia sites, "though only the SIR for noncardia stomach carcinoma was significant (SIR, 1.53; 95% CI, 1.12-2.05)."
The risks of non-Hodgkin’s lymphomas of the esophagus and stomach were dramatically elevated in the AIDS population, which was "not surprising," according to the authors: For the esophagus, the SIR was 261 (95% CI, 190-349) and for the stomach, it was 35.5 (95% CI, 31.9-39.5).
The authors also examined the risk of carcinoma adjusted for demographics, calendar year, and AIDS status. They found that CD4 count was not associated with the risk of either esophageal or stomach cancer.
Nor was there any decrease in the incidence rate over the calendar period of the study, even after the introduction of highly active antiretroviral therapy (HAART) in 1996.
According to the authors, this confirms that while "extended immunosuppression plays a role in the development of these cancers, ... HAART use after the development of AIDS may not be effective in halting this process."
The research was funded by the National Cancer Institute, the National Institutes of Health, and the Department of Health and Human Services. The authors declared no potential conflicts of interest.
AIDS patients have a greater risk of esophageal and stomach malignancies, compared with the general population, reported E. Christina Persson, Ph.D., and her colleagues in Gastroenterology.
The researchers, led by Dr. Persson of the division of cancer epidemiology and genetics at the National Cancer Institute, analyzed data from nearly 2 million person-years recorded in the HIV/AIDS Cancer Match Study. The HACM study links state and metropolitan HIV/AIDS registries to the corresponding cancer registries.
The investigators limited their search to primary invasive carcinomas or non-Hodgkin’s lymphomas (NHLs) of the esophagus and stomach that were diagnosed between 1980 and 2007 (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.07.013]).
"Individuals diagnosed with first malignancies other than esophageal and stomach cancers were censored at date of diagnosis, and any subsequent malignancy was excluded," they said.
Additionally, the first 3 months after AIDS diagnosis were excluded from analysis, since NHL is AIDS-defining, and also because intensive medical evaluation in this period could artificially inflate cancer diagnoses.
AIDS patients were followed up until earliest cancer diagnosis, death, date of last registry coverage, or 10 years after AIDS diagnosis, whichever came first.
The researchers then ascertained the standardized incidence ratio (SIR) for the 596,955 AIDS patients (predominantly male) included in the study. This was calculated by dividing the observed counts in AIDS patients by expected counts, which were in turn estimated by applying general population incidence rates to the AIDS population in strata defined by age, race, sex, calendar year, and cancer registry.
During 1,920,274 person-years, the SIR for esophageal carcinoma was 1.69 in AIDS patients, compared with the general population (95% confidence interval, 1.37-2.07).
When the data were broken down by specific type of esophageal cancer, the SIR was higher for esophageal adenocarcinoma at 1.91 (95% CI, 1.31-2.70), and lower for squamous cell carcinoma of the esophagus at 1.47 (95% CI, 1.10-1.92).
The authors added that the elevated risk applied to all sites, "although the elevated risk of carcinoma of the middle esophagus was of borderline statistical significance."
The results were similar for carcinomas of the stomach. Compared with the general population, AIDS patients had a SIR of 1.44 for all carcinomas (95% CI, 1.17-1.76).
"All types of adenocarcinoma were elevated, including diffuse adenocarcinoma (SIR, 1.65; 95% CI, 1.08-2.41) and intestinal adenocarcinoma (SIR, 1.96; 95% CI, 0.94-3.61)," wrote Dr. Persson.
Moreover, the risk was elevated for both cardia and noncardia sites, "though only the SIR for noncardia stomach carcinoma was significant (SIR, 1.53; 95% CI, 1.12-2.05)."
The risks of non-Hodgkin’s lymphomas of the esophagus and stomach were dramatically elevated in the AIDS population, which was "not surprising," according to the authors: For the esophagus, the SIR was 261 (95% CI, 190-349) and for the stomach, it was 35.5 (95% CI, 31.9-39.5).
The authors also examined the risk of carcinoma adjusted for demographics, calendar year, and AIDS status. They found that CD4 count was not associated with the risk of either esophageal or stomach cancer.
Nor was there any decrease in the incidence rate over the calendar period of the study, even after the introduction of highly active antiretroviral therapy (HAART) in 1996.
According to the authors, this confirms that while "extended immunosuppression plays a role in the development of these cancers, ... HAART use after the development of AIDS may not be effective in halting this process."
The research was funded by the National Cancer Institute, the National Institutes of Health, and the Department of Health and Human Services. The authors declared no potential conflicts of interest.
FROM GASTROENTEROLOGY
Major Finding: The risk of developing cancer of the esophagus and stomach is increased by 69% and 44%, respectively, in people with AIDS, compared with the general population.
Data Source: This study was a review of nearly 2 million person-years of data from the HIV/AIDS Cancer Match Study.
Disclosures: The research was funded by the National Cancer Institute, the National Institutes of Health, and the Department of Health and Human Services. The authors declared no potential conflicts of interest.
Reversal of Lap-Band to Sleeve Gastrectomy Feasible
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Weight loss was more pronounced among patients who underwent reversal of Lap-Band to sleeve gastrectomy because of band slippage, erosion, or infection than because of dissatisfaction with weight loss (mean total BMI loss, –15.8 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
Data Source: The study consisted of 34 patients who underwent reversal of Lap-Band to sleeve gastrectomy at two centers from January 2004 to October 2011.
Disclosures: Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
Esophageal Cancer Survival Benefit Linked to Lymphadenectomy
SAN DIEGO – Removing 12-20 lymph nodes for node-negative patients and 8-25 lymph nodes for node-positive patients confers a survival advantage in esophageal cancer, according to a data analysis of more than 2,100 patients.
"The maximum survival advantage was seen when a minimum of 15 lymph nodes were removed in node-negative patients and 20 in the node-positive patients," Dr. Kenneth L. Meredith said.

The Surveillance Epidemiology and End Results (SEER) analysis also revealed that the benefit of adjuvant radiation therapy on survival in esophageal cancer is limited to those with node-positive disease, suggesting that the management of esophageal cancer remains a work in progress, Dr. Meredith said at the annual Digestive Disease Week.
"Currently the treatment for these patients includes esophagectomy with or without neoadjuvant therapy," Dr. Meredith said. "There are many approaches to esophagectomy, and there are a multitude of recommendations for nodal clearance of these patients. If you look at single and multi-institutional database reviews, their recommendation for nodal harvest is anywhere from 6 to 40. We decided to perform a more recent analysis of the SEER database."
Dr. Meredith, chief of esophagogastric oncology and director of esophageal research at Moffitt Cancer Center, Tampa, Fla., and his associates queried the database for patients who underwent esophagectomy for cancer between 2004 and 2008. They identified 2,109 patients and categorized them by nodal harvest: greater than or less than 5, 8, 10, 12, 15, 20, 25, and 30.
Of the 2,109 patients, 467 were treated with adjuvant radiation and 1,642 were not. Patients treated with neoadjuvant radiation were excluded from the analysis, as were those who had histologic subtypes of cancer that were not adenocarcinoma or squamous cell carcinoma.
Dr. Meredith reported that use of adjuvant radiation was associated with decreased survival in patients with stage I disease (hazard ratio, 2.73; P less than .0001), no benefit in stage II (P = .075), increased survival in stage III (HR, 0.71; P = .005), and no benefit in stage IV (P = .913).
The median number of lymph nodes retracted from all patients was nine, "which is a little low by most standards," said Dr. Meredith.
Multivariate analysis revealed that among node-positive patients, the median survival with and without adjuvant radiation was 23 months and 20 months, respectively, and the 3-year survival rates were 34% and 26.7%, respectively (P = .023). Among node-negative patients, the 3-year survival with and without adjuvant radiation was 48.8% and 68.8%, respectively.
"The only lymph node cutoff we found was significant for all patients was that if you had more than five lymph nodes resected," Dr. Meredith said. "As you [removed more], lymph node harvesting did not translate into a survival benefit. However, when you subclassified whether they were node negative or node positive, a cutoff of 12 and 15, respectively, did translate into a survival benefit. In node-positive patients, those who had more than 8, 10, 12, 15, and 20 lymph nodes did translate into a survival benefit." He added that with regard to extended lymphadenectomy, or more than 20 lymph nodes resected in either cohort, no additional survival benefit was seen.
Dr. Meredith acknowledged certain limitations of the study, including its retrospective design and the fact that SEER lacks information on the nutritional status and performance status of patients. "There is also no information on margin status, chemotherapy, radiation dose, field design, and treatment technique," he said.
Dr. Meredith said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Removing 12-20 lymph nodes for node-negative patients and 8-25 lymph nodes for node-positive patients confers a survival advantage in esophageal cancer, according to a data analysis of more than 2,100 patients.
"The maximum survival advantage was seen when a minimum of 15 lymph nodes were removed in node-negative patients and 20 in the node-positive patients," Dr. Kenneth L. Meredith said.
The Surveillance Epidemiology and End Results (SEER) analysis also revealed that the benefit of adjuvant radiation therapy on survival in esophageal cancer is limited to those with node-positive disease, suggesting that the management of esophageal cancer remains a work in progress, Dr. Meredith said at the annual Digestive Disease Week.
"Currently the treatment for these patients includes esophagectomy with or without neoadjuvant therapy," Dr. Meredith said. "There are many approaches to esophagectomy, and there are a multitude of recommendations for nodal clearance of these patients. If you look at single and multi-institutional database reviews, their recommendation for nodal harvest is anywhere from 6 to 40. We decided to perform a more recent analysis of the SEER database."
Dr. Meredith, chief of esophagogastric oncology and director of esophageal research at Moffitt Cancer Center, Tampa, Fla., and his associates queried the database for patients who underwent esophagectomy for cancer between 2004 and 2008. They identified 2,109 patients and categorized them by nodal harvest: greater than or less than 5, 8, 10, 12, 15, 20, 25, and 30.
Of the 2,109 patients, 467 were treated with adjuvant radiation and 1,642 were not. Patients treated with neoadjuvant radiation were excluded from the analysis, as were those who had histologic subtypes of cancer that were not adenocarcinoma or squamous cell carcinoma.
Dr. Meredith reported that use of adjuvant radiation was associated with decreased survival in patients with stage I disease (hazard ratio, 2.73; P less than .0001), no benefit in stage II (P = .075), increased survival in stage III (HR, 0.71; P = .005), and no benefit in stage IV (P = .913).
The median number of lymph nodes retracted from all patients was nine, "which is a little low by most standards," said Dr. Meredith.
Multivariate analysis revealed that among node-positive patients, the median survival with and without adjuvant radiation was 23 months and 20 months, respectively, and the 3-year survival rates were 34% and 26.7%, respectively (P = .023). Among node-negative patients, the 3-year survival with and without adjuvant radiation was 48.8% and 68.8%, respectively.
"The only lymph node cutoff we found was significant for all patients was that if you had more than five lymph nodes resected," Dr. Meredith said. "As you [removed more], lymph node harvesting did not translate into a survival benefit. However, when you subclassified whether they were node negative or node positive, a cutoff of 12 and 15, respectively, did translate into a survival benefit. In node-positive patients, those who had more than 8, 10, 12, 15, and 20 lymph nodes did translate into a survival benefit." He added that with regard to extended lymphadenectomy, or more than 20 lymph nodes resected in either cohort, no additional survival benefit was seen.
Dr. Meredith acknowledged certain limitations of the study, including its retrospective design and the fact that SEER lacks information on the nutritional status and performance status of patients. "There is also no information on margin status, chemotherapy, radiation dose, field design, and treatment technique," he said.
Dr. Meredith said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Removing 12-20 lymph nodes for node-negative patients and 8-25 lymph nodes for node-positive patients confers a survival advantage in esophageal cancer, according to a data analysis of more than 2,100 patients.
"The maximum survival advantage was seen when a minimum of 15 lymph nodes were removed in node-negative patients and 20 in the node-positive patients," Dr. Kenneth L. Meredith said.
The Surveillance Epidemiology and End Results (SEER) analysis also revealed that the benefit of adjuvant radiation therapy on survival in esophageal cancer is limited to those with node-positive disease, suggesting that the management of esophageal cancer remains a work in progress, Dr. Meredith said at the annual Digestive Disease Week.
"Currently the treatment for these patients includes esophagectomy with or without neoadjuvant therapy," Dr. Meredith said. "There are many approaches to esophagectomy, and there are a multitude of recommendations for nodal clearance of these patients. If you look at single and multi-institutional database reviews, their recommendation for nodal harvest is anywhere from 6 to 40. We decided to perform a more recent analysis of the SEER database."
Dr. Meredith, chief of esophagogastric oncology and director of esophageal research at Moffitt Cancer Center, Tampa, Fla., and his associates queried the database for patients who underwent esophagectomy for cancer between 2004 and 2008. They identified 2,109 patients and categorized them by nodal harvest: greater than or less than 5, 8, 10, 12, 15, 20, 25, and 30.
Of the 2,109 patients, 467 were treated with adjuvant radiation and 1,642 were not. Patients treated with neoadjuvant radiation were excluded from the analysis, as were those who had histologic subtypes of cancer that were not adenocarcinoma or squamous cell carcinoma.
Dr. Meredith reported that use of adjuvant radiation was associated with decreased survival in patients with stage I disease (hazard ratio, 2.73; P less than .0001), no benefit in stage II (P = .075), increased survival in stage III (HR, 0.71; P = .005), and no benefit in stage IV (P = .913).
The median number of lymph nodes retracted from all patients was nine, "which is a little low by most standards," said Dr. Meredith.
Multivariate analysis revealed that among node-positive patients, the median survival with and without adjuvant radiation was 23 months and 20 months, respectively, and the 3-year survival rates were 34% and 26.7%, respectively (P = .023). Among node-negative patients, the 3-year survival with and without adjuvant radiation was 48.8% and 68.8%, respectively.
"The only lymph node cutoff we found was significant for all patients was that if you had more than five lymph nodes resected," Dr. Meredith said. "As you [removed more], lymph node harvesting did not translate into a survival benefit. However, when you subclassified whether they were node negative or node positive, a cutoff of 12 and 15, respectively, did translate into a survival benefit. In node-positive patients, those who had more than 8, 10, 12, 15, and 20 lymph nodes did translate into a survival benefit." He added that with regard to extended lymphadenectomy, or more than 20 lymph nodes resected in either cohort, no additional survival benefit was seen.
Dr. Meredith acknowledged certain limitations of the study, including its retrospective design and the fact that SEER lacks information on the nutritional status and performance status of patients. "There is also no information on margin status, chemotherapy, radiation dose, field design, and treatment technique," he said.
Dr. Meredith said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL DIGESTIVE DISEASE WEEK
BOLD Analysis Backs Safety of Sleeve Gastrectomy
SAN DIEGO – Laparoscopic sleeve gastrectomy is positioned between gastric banding and the laparoscopic gastric bypass for both safety and efficacy, results from the largest comparative study of its kind demonstrated.
The finding comes at a time when the Centers for Medicare and Medicaid Services is reviewing evidence to consider including sleeve gastrectomy as a covered benefit. Currently, gastric bypass, vertical banded gastroplasty, duodenal switch, and gastric banding are the only CMS-sanctioned bariatric procedures.

The study, which involved nearly 300,000 patients, "shows that across the board, regardless of the procedure, bariatric surgery is safe and effective," Dr. John M. Morton said in an interview at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "The emerging new procedure, the sleeve gastrectomy, is shown to be right between the bypass and the band. As a result, we have seen more interest from payers to cover it. In fact there are about 100 million lives that are covered. Our only outlier is CMS in deciding to cover. We hope that these data will help influence CMS in granting coverage for the sleeve gastrectomy."
Dr. Morton, associate professor of surgery and director of bariatric surgery at Stanford Hospitals and Clinics at Stanford (Calif.) University, and his associates examined BOLD (Bariatric Outcomes Longitudinal Database) to identify patients who had undergone laparoscopic Roux-en-Y gastric bypass (LRNYGB), gastric banding (LAGB), and sleeve gastrectomy (LSG) from June 2007 to December 2010. BOLD, the largest bariatric-specific database, is maintained by the ASMBS Bariatric Surgery Center of Excellence program, and includes more than 1,200 surgeons at 540 hospitals. Dr. Morton described the data as a "clinically rich" variable set that includes age, gender, race, insurance status, body mass index, excess body weight, and comorbidities.
"There is a definite need for more data around comparison of different procedures," Dr. Morton said at the meeting. "Our study hypothesis is very straightforward: Do demographics and outcomes for bariatric surgery vary by procedure?"
The primary outcomes were 30-day mortality, serious complications, and readmissions. The definitions of serious complications included death, anastomotic leakage, cardiac arrest, deep venous thrombosis, evisceration, heart failure and/or pulmonary edema, liver failure, and bleeding requiring transfusion.
Dr. Morton reported outcomes from 117,365 patients in the LAGB group, 138,222 in the LRNYGB group, and 16,139 in the LSG group. Patients in each group were generally the same age (a mean of 45, 46, and 45 years, respectively), mostly female (78%, 79%, and 74%), and mostly white (72%, 73%, and 72%). "The one area where there was a sizable difference was around self-pay," Dr. Morton said. About 21% of patients in the LSG group paid out-of-pocket, compared with 6% of those in the LAGB group and 2% of those in the LRNYGB group.
The proportion of preoperative comorbidities was similar among the three groups, with two exceptions. The prevalence of diabetes was highest in the LRNYGB group (37%, compared with 30% in the LSG group and 28% in the LAGB group; P less than .0001). A similar association was seen in the proportion of patients with five or more preoperative comorbidities (62%, 55%, and 52%, respectively; P less than .0001).
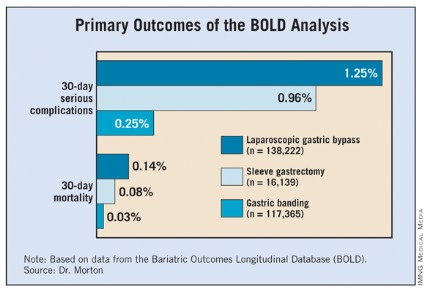
The mean length of stay was 0.7 days for the LAGB group, 1.9 days for the LSG group, and 2.3 days for the LRNYGB group. The percent change in BMI at 12 months was 7.6%, 13.4%, and 16.4%, respectively; the rate of 30-day serious complications was 0.25%, 0.96%, and 1.25%; and the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%. All differences between the groups were significant (P less than .0001).
"If you look at the remainder of the safety outcomes – everything from 30-day readmission to 30-day reoperation – it’s pretty much the same order, with the band group having the lowest [percentage], and the bypass having the highest, and the sleeve being right in between," Dr. Morton said. "When we looked at age greater than 65 in isolation, we found that the order of safety remains, with the banding having the least amount of mortality and the sleeve being right between the band procedure and the bypass."
Logistic regression analysis revealed several significant factors that predicted serious adverse events at 30 days: male gender (odds ratio, 1.67), having nonprivate insurance (OR, 1.15), stepwise progression with increasing age (for example, an OR of 1.27 for those aged 26-35 years and an OR of 4.42 for those above age 65), and stepwise progression with increasing BMI (for example, an OR of 1.37 for those with a BMI of 46-55 kg/m2 and an OR of 3.03 for those with a BMI greater than 65).
The invited discussant, Dr. Matthew M. Hutter, of Massachusetts General Hospital, Boston, described the size of the overall study cohort as remarkable. "What I find most interesting about this study is that it shows that sleeve gastrectomy – a brand-new, very complex procedure – can be introduced safely and effectively when performed under the standards of a bariatric accreditation program," Dr. Hutter said. "Other surgical procedures such as laparoscopic cholecystectomy or laparoscopic colectomy had very high morbidity and conversion rates when they were first implemented. However, this new complex procedure has been safe and effective from the get-go, and that is really quite impressive. The other remarkable finding is how consistent this is with all of the other major [bariatric surgery] data collection programs."
Dr. Morton acknowledged certain limitations of the study, including the fact that 1-year follow-up was available in only 60% of patients, while 30-day follow-up was available in 98% of the cohort. "Potentially, patients could have been admitted to other hospitals," he added. "These are research-consented patients, so about 70% consented. Some of this is surgeon-directed reporting."
Dr. Morton said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is positioned between gastric banding and the laparoscopic gastric bypass for both safety and efficacy, results from the largest comparative study of its kind demonstrated.
The finding comes at a time when the Centers for Medicare and Medicaid Services is reviewing evidence to consider including sleeve gastrectomy as a covered benefit. Currently, gastric bypass, vertical banded gastroplasty, duodenal switch, and gastric banding are the only CMS-sanctioned bariatric procedures.
The study, which involved nearly 300,000 patients, "shows that across the board, regardless of the procedure, bariatric surgery is safe and effective," Dr. John M. Morton said in an interview at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "The emerging new procedure, the sleeve gastrectomy, is shown to be right between the bypass and the band. As a result, we have seen more interest from payers to cover it. In fact there are about 100 million lives that are covered. Our only outlier is CMS in deciding to cover. We hope that these data will help influence CMS in granting coverage for the sleeve gastrectomy."
Dr. Morton, associate professor of surgery and director of bariatric surgery at Stanford Hospitals and Clinics at Stanford (Calif.) University, and his associates examined BOLD (Bariatric Outcomes Longitudinal Database) to identify patients who had undergone laparoscopic Roux-en-Y gastric bypass (LRNYGB), gastric banding (LAGB), and sleeve gastrectomy (LSG) from June 2007 to December 2010. BOLD, the largest bariatric-specific database, is maintained by the ASMBS Bariatric Surgery Center of Excellence program, and includes more than 1,200 surgeons at 540 hospitals. Dr. Morton described the data as a "clinically rich" variable set that includes age, gender, race, insurance status, body mass index, excess body weight, and comorbidities.
"There is a definite need for more data around comparison of different procedures," Dr. Morton said at the meeting. "Our study hypothesis is very straightforward: Do demographics and outcomes for bariatric surgery vary by procedure?"
The primary outcomes were 30-day mortality, serious complications, and readmissions. The definitions of serious complications included death, anastomotic leakage, cardiac arrest, deep venous thrombosis, evisceration, heart failure and/or pulmonary edema, liver failure, and bleeding requiring transfusion.
Dr. Morton reported outcomes from 117,365 patients in the LAGB group, 138,222 in the LRNYGB group, and 16,139 in the LSG group. Patients in each group were generally the same age (a mean of 45, 46, and 45 years, respectively), mostly female (78%, 79%, and 74%), and mostly white (72%, 73%, and 72%). "The one area where there was a sizable difference was around self-pay," Dr. Morton said. About 21% of patients in the LSG group paid out-of-pocket, compared with 6% of those in the LAGB group and 2% of those in the LRNYGB group.
The proportion of preoperative comorbidities was similar among the three groups, with two exceptions. The prevalence of diabetes was highest in the LRNYGB group (37%, compared with 30% in the LSG group and 28% in the LAGB group; P less than .0001). A similar association was seen in the proportion of patients with five or more preoperative comorbidities (62%, 55%, and 52%, respectively; P less than .0001).
The mean length of stay was 0.7 days for the LAGB group, 1.9 days for the LSG group, and 2.3 days for the LRNYGB group. The percent change in BMI at 12 months was 7.6%, 13.4%, and 16.4%, respectively; the rate of 30-day serious complications was 0.25%, 0.96%, and 1.25%; and the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%. All differences between the groups were significant (P less than .0001).
"If you look at the remainder of the safety outcomes – everything from 30-day readmission to 30-day reoperation – it’s pretty much the same order, with the band group having the lowest [percentage], and the bypass having the highest, and the sleeve being right in between," Dr. Morton said. "When we looked at age greater than 65 in isolation, we found that the order of safety remains, with the banding having the least amount of mortality and the sleeve being right between the band procedure and the bypass."
Logistic regression analysis revealed several significant factors that predicted serious adverse events at 30 days: male gender (odds ratio, 1.67), having nonprivate insurance (OR, 1.15), stepwise progression with increasing age (for example, an OR of 1.27 for those aged 26-35 years and an OR of 4.42 for those above age 65), and stepwise progression with increasing BMI (for example, an OR of 1.37 for those with a BMI of 46-55 kg/m2 and an OR of 3.03 for those with a BMI greater than 65).
The invited discussant, Dr. Matthew M. Hutter, of Massachusetts General Hospital, Boston, described the size of the overall study cohort as remarkable. "What I find most interesting about this study is that it shows that sleeve gastrectomy – a brand-new, very complex procedure – can be introduced safely and effectively when performed under the standards of a bariatric accreditation program," Dr. Hutter said. "Other surgical procedures such as laparoscopic cholecystectomy or laparoscopic colectomy had very high morbidity and conversion rates when they were first implemented. However, this new complex procedure has been safe and effective from the get-go, and that is really quite impressive. The other remarkable finding is how consistent this is with all of the other major [bariatric surgery] data collection programs."
Dr. Morton acknowledged certain limitations of the study, including the fact that 1-year follow-up was available in only 60% of patients, while 30-day follow-up was available in 98% of the cohort. "Potentially, patients could have been admitted to other hospitals," he added. "These are research-consented patients, so about 70% consented. Some of this is surgeon-directed reporting."
Dr. Morton said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is positioned between gastric banding and the laparoscopic gastric bypass for both safety and efficacy, results from the largest comparative study of its kind demonstrated.
The finding comes at a time when the Centers for Medicare and Medicaid Services is reviewing evidence to consider including sleeve gastrectomy as a covered benefit. Currently, gastric bypass, vertical banded gastroplasty, duodenal switch, and gastric banding are the only CMS-sanctioned bariatric procedures.
The study, which involved nearly 300,000 patients, "shows that across the board, regardless of the procedure, bariatric surgery is safe and effective," Dr. John M. Morton said in an interview at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "The emerging new procedure, the sleeve gastrectomy, is shown to be right between the bypass and the band. As a result, we have seen more interest from payers to cover it. In fact there are about 100 million lives that are covered. Our only outlier is CMS in deciding to cover. We hope that these data will help influence CMS in granting coverage for the sleeve gastrectomy."
Dr. Morton, associate professor of surgery and director of bariatric surgery at Stanford Hospitals and Clinics at Stanford (Calif.) University, and his associates examined BOLD (Bariatric Outcomes Longitudinal Database) to identify patients who had undergone laparoscopic Roux-en-Y gastric bypass (LRNYGB), gastric banding (LAGB), and sleeve gastrectomy (LSG) from June 2007 to December 2010. BOLD, the largest bariatric-specific database, is maintained by the ASMBS Bariatric Surgery Center of Excellence program, and includes more than 1,200 surgeons at 540 hospitals. Dr. Morton described the data as a "clinically rich" variable set that includes age, gender, race, insurance status, body mass index, excess body weight, and comorbidities.
"There is a definite need for more data around comparison of different procedures," Dr. Morton said at the meeting. "Our study hypothesis is very straightforward: Do demographics and outcomes for bariatric surgery vary by procedure?"
The primary outcomes were 30-day mortality, serious complications, and readmissions. The definitions of serious complications included death, anastomotic leakage, cardiac arrest, deep venous thrombosis, evisceration, heart failure and/or pulmonary edema, liver failure, and bleeding requiring transfusion.
Dr. Morton reported outcomes from 117,365 patients in the LAGB group, 138,222 in the LRNYGB group, and 16,139 in the LSG group. Patients in each group were generally the same age (a mean of 45, 46, and 45 years, respectively), mostly female (78%, 79%, and 74%), and mostly white (72%, 73%, and 72%). "The one area where there was a sizable difference was around self-pay," Dr. Morton said. About 21% of patients in the LSG group paid out-of-pocket, compared with 6% of those in the LAGB group and 2% of those in the LRNYGB group.
The proportion of preoperative comorbidities was similar among the three groups, with two exceptions. The prevalence of diabetes was highest in the LRNYGB group (37%, compared with 30% in the LSG group and 28% in the LAGB group; P less than .0001). A similar association was seen in the proportion of patients with five or more preoperative comorbidities (62%, 55%, and 52%, respectively; P less than .0001).
The mean length of stay was 0.7 days for the LAGB group, 1.9 days for the LSG group, and 2.3 days for the LRNYGB group. The percent change in BMI at 12 months was 7.6%, 13.4%, and 16.4%, respectively; the rate of 30-day serious complications was 0.25%, 0.96%, and 1.25%; and the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%. All differences between the groups were significant (P less than .0001).
"If you look at the remainder of the safety outcomes – everything from 30-day readmission to 30-day reoperation – it’s pretty much the same order, with the band group having the lowest [percentage], and the bypass having the highest, and the sleeve being right in between," Dr. Morton said. "When we looked at age greater than 65 in isolation, we found that the order of safety remains, with the banding having the least amount of mortality and the sleeve being right between the band procedure and the bypass."
Logistic regression analysis revealed several significant factors that predicted serious adverse events at 30 days: male gender (odds ratio, 1.67), having nonprivate insurance (OR, 1.15), stepwise progression with increasing age (for example, an OR of 1.27 for those aged 26-35 years and an OR of 4.42 for those above age 65), and stepwise progression with increasing BMI (for example, an OR of 1.37 for those with a BMI of 46-55 kg/m2 and an OR of 3.03 for those with a BMI greater than 65).
The invited discussant, Dr. Matthew M. Hutter, of Massachusetts General Hospital, Boston, described the size of the overall study cohort as remarkable. "What I find most interesting about this study is that it shows that sleeve gastrectomy – a brand-new, very complex procedure – can be introduced safely and effectively when performed under the standards of a bariatric accreditation program," Dr. Hutter said. "Other surgical procedures such as laparoscopic cholecystectomy or laparoscopic colectomy had very high morbidity and conversion rates when they were first implemented. However, this new complex procedure has been safe and effective from the get-go, and that is really quite impressive. The other remarkable finding is how consistent this is with all of the other major [bariatric surgery] data collection programs."
Dr. Morton acknowledged certain limitations of the study, including the fact that 1-year follow-up was available in only 60% of patients, while 30-day follow-up was available in 98% of the cohort. "Potentially, patients could have been admitted to other hospitals," he added. "These are research-consented patients, so about 70% consented. Some of this is surgeon-directed reporting."
Dr. Morton said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: The rate of 30-day serious complications was 0.25% among those who underwent laparoscopic gastric banding, 0.96% among those who underwent laparoscopic sleeve gastrectomy, and 1.25% among those who underwent laparoscopic Roux-en-Y gastric bypass, while the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%, respectively.
Data Source: The data analysis was based on 271,726 patients from the Bariatric Outcomes Longitudinal Database who underwent bariatric surgery from June 2007 to December 2010.
Disclosures: Dr. Morton said that he had no relevant financial conflicts to disclose.
FDA Warns of QT Prolongation with Ondansetron Dose
Preliminary data indicate that a single 32-mg intravenous dose of ondansetron should be avoided because it may increase the risk of QT prolongation, along with the potentially fatal arrhythmia torsades de pointes, the Food and Drug Administration has announced.
GlaxoSmithKline, which manufactures ondansetron (Zofran), is removing the 32-mg single IV dose from the antinausea and vomiting drug’s label, according to an FDA statement.
The updated label will say that ondansetron, a 5-HT3 receptor antagonist, can continue to be used to treat adults and children with chemotherapy-induced nausea and vomiting at the dose of 0.15 mg/kg administered every 4 hours for three doses. "However, no single intravenous dose of ondansetron should exceed 16 mg due to the risk of QT prolongation," the FDA said.
The new data do not affect recommendations for oral doses of ondansetron (including the single 24-mg oral dose) used for chemotherapy-induced nausea and vomiting, the FDA noted. Recommendations on lower IV doses that are used to prevent postoperative nausea and vomiting (the other approved indication for ondansetron) also are unaffected.
Preliminary results of a study conducted by GlaxoSmithKline showed that QT prolongation "occurs in a dose-dependent manner," the FDA said. At the highest dose tested (the single 32-mg IV dose), the maximum mean difference in QTcF from placebo after baseline-correction was 20 msec. At the lower single dose tested (8 mg), the maximum mean difference in QTcF from placebo after baseline correction was 6 msec.
The FDA, which required GlaxoSmithKline to conduct the study, "will evaluate the final study results when available, and will work with GSK to explore an alternative single dose regimen that is both safe and effective for the prevention of chemotherapy-induced nausea and vomiting in adults," the FDA said.
It pointed out that ECG changes, including QT interval prolongation and torsades de pointes, have been reported in patients treated with ondansetron. In September 2011, the agency announced that it was reviewing the potential for QT prolongation with ondansetron.
Patients who have congenital long QT syndrome, heart failure, or bradyarrhythmias, or who are taking other medications that prolong the QT interval "may be at particular risk for QT prolongation" with ondansetron, the FDA warned.
The statement is available at www.fda.gov/Drugs/DrugSafety/ucm310190.htm. Serious adverse events associated with ondansetron should be reported to the FDA at 800-332-1088 or www.fda.gov/medwatch.
Preliminary data indicate that a single 32-mg intravenous dose of ondansetron should be avoided because it may increase the risk of QT prolongation, along with the potentially fatal arrhythmia torsades de pointes, the Food and Drug Administration has announced.
GlaxoSmithKline, which manufactures ondansetron (Zofran), is removing the 32-mg single IV dose from the antinausea and vomiting drug’s label, according to an FDA statement.
The updated label will say that ondansetron, a 5-HT3 receptor antagonist, can continue to be used to treat adults and children with chemotherapy-induced nausea and vomiting at the dose of 0.15 mg/kg administered every 4 hours for three doses. "However, no single intravenous dose of ondansetron should exceed 16 mg due to the risk of QT prolongation," the FDA said.
The new data do not affect recommendations for oral doses of ondansetron (including the single 24-mg oral dose) used for chemotherapy-induced nausea and vomiting, the FDA noted. Recommendations on lower IV doses that are used to prevent postoperative nausea and vomiting (the other approved indication for ondansetron) also are unaffected.
Preliminary results of a study conducted by GlaxoSmithKline showed that QT prolongation "occurs in a dose-dependent manner," the FDA said. At the highest dose tested (the single 32-mg IV dose), the maximum mean difference in QTcF from placebo after baseline-correction was 20 msec. At the lower single dose tested (8 mg), the maximum mean difference in QTcF from placebo after baseline correction was 6 msec.
The FDA, which required GlaxoSmithKline to conduct the study, "will evaluate the final study results when available, and will work with GSK to explore an alternative single dose regimen that is both safe and effective for the prevention of chemotherapy-induced nausea and vomiting in adults," the FDA said.
It pointed out that ECG changes, including QT interval prolongation and torsades de pointes, have been reported in patients treated with ondansetron. In September 2011, the agency announced that it was reviewing the potential for QT prolongation with ondansetron.
Patients who have congenital long QT syndrome, heart failure, or bradyarrhythmias, or who are taking other medications that prolong the QT interval "may be at particular risk for QT prolongation" with ondansetron, the FDA warned.
The statement is available at www.fda.gov/Drugs/DrugSafety/ucm310190.htm. Serious adverse events associated with ondansetron should be reported to the FDA at 800-332-1088 or www.fda.gov/medwatch.
Preliminary data indicate that a single 32-mg intravenous dose of ondansetron should be avoided because it may increase the risk of QT prolongation, along with the potentially fatal arrhythmia torsades de pointes, the Food and Drug Administration has announced.
GlaxoSmithKline, which manufactures ondansetron (Zofran), is removing the 32-mg single IV dose from the antinausea and vomiting drug’s label, according to an FDA statement.
The updated label will say that ondansetron, a 5-HT3 receptor antagonist, can continue to be used to treat adults and children with chemotherapy-induced nausea and vomiting at the dose of 0.15 mg/kg administered every 4 hours for three doses. "However, no single intravenous dose of ondansetron should exceed 16 mg due to the risk of QT prolongation," the FDA said.
The new data do not affect recommendations for oral doses of ondansetron (including the single 24-mg oral dose) used for chemotherapy-induced nausea and vomiting, the FDA noted. Recommendations on lower IV doses that are used to prevent postoperative nausea and vomiting (the other approved indication for ondansetron) also are unaffected.
Preliminary results of a study conducted by GlaxoSmithKline showed that QT prolongation "occurs in a dose-dependent manner," the FDA said. At the highest dose tested (the single 32-mg IV dose), the maximum mean difference in QTcF from placebo after baseline-correction was 20 msec. At the lower single dose tested (8 mg), the maximum mean difference in QTcF from placebo after baseline correction was 6 msec.
The FDA, which required GlaxoSmithKline to conduct the study, "will evaluate the final study results when available, and will work with GSK to explore an alternative single dose regimen that is both safe and effective for the prevention of chemotherapy-induced nausea and vomiting in adults," the FDA said.
It pointed out that ECG changes, including QT interval prolongation and torsades de pointes, have been reported in patients treated with ondansetron. In September 2011, the agency announced that it was reviewing the potential for QT prolongation with ondansetron.
Patients who have congenital long QT syndrome, heart failure, or bradyarrhythmias, or who are taking other medications that prolong the QT interval "may be at particular risk for QT prolongation" with ondansetron, the FDA warned.
The statement is available at www.fda.gov/Drugs/DrugSafety/ucm310190.htm. Serious adverse events associated with ondansetron should be reported to the FDA at 800-332-1088 or www.fda.gov/medwatch.
Aerosolized Fluticasone for EoE Improved Histology but Not Dysphagia
Aerosolized fluticasone decreases esophageal eosinophilia in adults with eosinophilic esophagitis but does not relieve the symptomatic dysphagia caused by the allergic inflammatory disease, Dr. Jeffrey A. Alexander and his colleagues reported in the July issue of Clinical Gastroenterology and Hepatology.
In a double-blind, placebo-controlled trial conducted by Dr. Alexander of the Mayo Clinic, Rochester, Minn., and his coauthors, 42 adults with eosinophilic esophagitis (EoE) were randomly assigned to receive 880 mcg of aerosolized fluticasone twice daily (21) or to use a placebo inhaler twice daily (21) for 6 weeks.
The study’s primary end point was complete symptom response, and secondary end points were partial symptom response, partial and complete histologic response, and eosinophil-derived neurotoxin response to treatment using Fisher’s exact test (Clin. Gastroenterol. Hepatol. 2012 July [doi:10.1016/j.cgh.2012.03.018]).
The study subjects were recruited from the Esophageal Clinic at Mayo Clinic Rochester during 2005-2009 for management of newly diagnosed EoE. Subjects had symptomatic dysphagia, had a peak eosinophil count of at least 20 eosinophils per high-power field on esophageal biopsy, and demonstrated at least 90% compliance with the study requirement that they keep symptom logs for review by phone interview after weeks 2 and 4, and at study completion.
For symptom assessment, a complete response was defined as an answer of "no" to the question: "In the past 2 weeks, have you had trouble swallowing, not associated with other cold symptoms?" on the Mayo Dysphagia Questionnaire–2 week, while an answer of "yes" along with a two-level or one-level decrease in frequency was considered a partial response. An answer of "yes" and a one-level decrease in one variable (either frequency or severity), plus an increase in the other variable, was classified as no response, the authors wrote.
A structured phone interview to assess side effects was conducted at weeks 2 and 4, and again at study completion, along with a physical exam, endoscopy, and 24-hour urine cortisol.
Six patients in the placebo group and two in the treatment group dropped out for reasons unrelated to the treatment. Of the 15 subjects who received 6 weeks of fluticasone, 11 had a complete histologic response, defined as a greater than 90% decrease in mean eosinophil count, compared with none of the 15 placebo subjects based on intention-to-treat analysis. By per-protocol analysis, "the histologic response was observed in 68% of subjects that received fluticasone [13/19], compared to none of those that received placebo," the authors wrote.
Analysis of symptom data in the treatment group showed that a complete dysphagia response occurred in 42.9% by intent-to-treat and 47.4% per protocol, neither of which was better than the respective placebo responses of 28.6% and 40.0%, according to the authors. Similarly, "the per-protocol analysis for a complete or partial response rate for fluticasone was 63.2%, versus a 46.7% response rate for placebo," representing a nonsignificant difference, they said.
The authors hypothesized that the factors contributing to the discrepancy between symptomatic and histologic responses include a possible underappreciation at endoscopy of esophageal stricture and small-caliber esophagus, and the possibility that esophageal narrowing may require dilation to relieve symptomatic dysphagia despite a histologic response.
In addition, "changes in esophageal compliance related to fibrosis may be important," they wrote, as a decrease in esophageal distensibility and compliance has been shown in EoE, which could well be a cause of dysphagia. Candida infections, which developed in 31.6% of the treatment group and none of the placebo group, could potentially lead to persistent dysphagia despite a histologic response, they said. Most likely, however, the discrepancy "reflects a waxing and waning of dysphagia in this disease," they concluded.
The study findings are limited by the relatively small sample size and the unexpectedly high dropout rate in the placebo group, which "left us somewhat underpowered for our primary end point," the authors wrote. Also, gastroesophageal reflux disease was not categorically excluded in all of the patients prior to enrollment. "While we would have liked to adjust for baseline differences in erosive esophagitis and PPI [protein pump inhibitor] use between treatment and placebo groups, this is beyond the limits of a dataset this size," they said.
The treatment was safe and well tolerated, but further study is needed to evaluate the optimal dose of therapy, length of therapy, and long-term safety of topical fluticasone, as well as other steroid medications. "Furthermore," the authors wrote, "delivery systems need to be developed that are easier to use and provide more direct drug delivery to the esophagus."
Dr. Alexander disclosed a financial relationship with Meritage Pharmacia.
Aerosolized fluticasone decreases esophageal eosinophilia in adults with eosinophilic esophagitis but does not relieve the symptomatic dysphagia caused by the allergic inflammatory disease, Dr. Jeffrey A. Alexander and his colleagues reported in the July issue of Clinical Gastroenterology and Hepatology.
In a double-blind, placebo-controlled trial conducted by Dr. Alexander of the Mayo Clinic, Rochester, Minn., and his coauthors, 42 adults with eosinophilic esophagitis (EoE) were randomly assigned to receive 880 mcg of aerosolized fluticasone twice daily (21) or to use a placebo inhaler twice daily (21) for 6 weeks.
The study’s primary end point was complete symptom response, and secondary end points were partial symptom response, partial and complete histologic response, and eosinophil-derived neurotoxin response to treatment using Fisher’s exact test (Clin. Gastroenterol. Hepatol. 2012 July [doi:10.1016/j.cgh.2012.03.018]).
The study subjects were recruited from the Esophageal Clinic at Mayo Clinic Rochester during 2005-2009 for management of newly diagnosed EoE. Subjects had symptomatic dysphagia, had a peak eosinophil count of at least 20 eosinophils per high-power field on esophageal biopsy, and demonstrated at least 90% compliance with the study requirement that they keep symptom logs for review by phone interview after weeks 2 and 4, and at study completion.
For symptom assessment, a complete response was defined as an answer of "no" to the question: "In the past 2 weeks, have you had trouble swallowing, not associated with other cold symptoms?" on the Mayo Dysphagia Questionnaire–2 week, while an answer of "yes" along with a two-level or one-level decrease in frequency was considered a partial response. An answer of "yes" and a one-level decrease in one variable (either frequency or severity), plus an increase in the other variable, was classified as no response, the authors wrote.
A structured phone interview to assess side effects was conducted at weeks 2 and 4, and again at study completion, along with a physical exam, endoscopy, and 24-hour urine cortisol.
Six patients in the placebo group and two in the treatment group dropped out for reasons unrelated to the treatment. Of the 15 subjects who received 6 weeks of fluticasone, 11 had a complete histologic response, defined as a greater than 90% decrease in mean eosinophil count, compared with none of the 15 placebo subjects based on intention-to-treat analysis. By per-protocol analysis, "the histologic response was observed in 68% of subjects that received fluticasone [13/19], compared to none of those that received placebo," the authors wrote.
Analysis of symptom data in the treatment group showed that a complete dysphagia response occurred in 42.9% by intent-to-treat and 47.4% per protocol, neither of which was better than the respective placebo responses of 28.6% and 40.0%, according to the authors. Similarly, "the per-protocol analysis for a complete or partial response rate for fluticasone was 63.2%, versus a 46.7% response rate for placebo," representing a nonsignificant difference, they said.
The authors hypothesized that the factors contributing to the discrepancy between symptomatic and histologic responses include a possible underappreciation at endoscopy of esophageal stricture and small-caliber esophagus, and the possibility that esophageal narrowing may require dilation to relieve symptomatic dysphagia despite a histologic response.
In addition, "changes in esophageal compliance related to fibrosis may be important," they wrote, as a decrease in esophageal distensibility and compliance has been shown in EoE, which could well be a cause of dysphagia. Candida infections, which developed in 31.6% of the treatment group and none of the placebo group, could potentially lead to persistent dysphagia despite a histologic response, they said. Most likely, however, the discrepancy "reflects a waxing and waning of dysphagia in this disease," they concluded.
The study findings are limited by the relatively small sample size and the unexpectedly high dropout rate in the placebo group, which "left us somewhat underpowered for our primary end point," the authors wrote. Also, gastroesophageal reflux disease was not categorically excluded in all of the patients prior to enrollment. "While we would have liked to adjust for baseline differences in erosive esophagitis and PPI [protein pump inhibitor] use between treatment and placebo groups, this is beyond the limits of a dataset this size," they said.
The treatment was safe and well tolerated, but further study is needed to evaluate the optimal dose of therapy, length of therapy, and long-term safety of topical fluticasone, as well as other steroid medications. "Furthermore," the authors wrote, "delivery systems need to be developed that are easier to use and provide more direct drug delivery to the esophagus."
Dr. Alexander disclosed a financial relationship with Meritage Pharmacia.
Aerosolized fluticasone decreases esophageal eosinophilia in adults with eosinophilic esophagitis but does not relieve the symptomatic dysphagia caused by the allergic inflammatory disease, Dr. Jeffrey A. Alexander and his colleagues reported in the July issue of Clinical Gastroenterology and Hepatology.
In a double-blind, placebo-controlled trial conducted by Dr. Alexander of the Mayo Clinic, Rochester, Minn., and his coauthors, 42 adults with eosinophilic esophagitis (EoE) were randomly assigned to receive 880 mcg of aerosolized fluticasone twice daily (21) or to use a placebo inhaler twice daily (21) for 6 weeks.
The study’s primary end point was complete symptom response, and secondary end points were partial symptom response, partial and complete histologic response, and eosinophil-derived neurotoxin response to treatment using Fisher’s exact test (Clin. Gastroenterol. Hepatol. 2012 July [doi:10.1016/j.cgh.2012.03.018]).
The study subjects were recruited from the Esophageal Clinic at Mayo Clinic Rochester during 2005-2009 for management of newly diagnosed EoE. Subjects had symptomatic dysphagia, had a peak eosinophil count of at least 20 eosinophils per high-power field on esophageal biopsy, and demonstrated at least 90% compliance with the study requirement that they keep symptom logs for review by phone interview after weeks 2 and 4, and at study completion.
For symptom assessment, a complete response was defined as an answer of "no" to the question: "In the past 2 weeks, have you had trouble swallowing, not associated with other cold symptoms?" on the Mayo Dysphagia Questionnaire–2 week, while an answer of "yes" along with a two-level or one-level decrease in frequency was considered a partial response. An answer of "yes" and a one-level decrease in one variable (either frequency or severity), plus an increase in the other variable, was classified as no response, the authors wrote.
A structured phone interview to assess side effects was conducted at weeks 2 and 4, and again at study completion, along with a physical exam, endoscopy, and 24-hour urine cortisol.
Six patients in the placebo group and two in the treatment group dropped out for reasons unrelated to the treatment. Of the 15 subjects who received 6 weeks of fluticasone, 11 had a complete histologic response, defined as a greater than 90% decrease in mean eosinophil count, compared with none of the 15 placebo subjects based on intention-to-treat analysis. By per-protocol analysis, "the histologic response was observed in 68% of subjects that received fluticasone [13/19], compared to none of those that received placebo," the authors wrote.
Analysis of symptom data in the treatment group showed that a complete dysphagia response occurred in 42.9% by intent-to-treat and 47.4% per protocol, neither of which was better than the respective placebo responses of 28.6% and 40.0%, according to the authors. Similarly, "the per-protocol analysis for a complete or partial response rate for fluticasone was 63.2%, versus a 46.7% response rate for placebo," representing a nonsignificant difference, they said.
The authors hypothesized that the factors contributing to the discrepancy between symptomatic and histologic responses include a possible underappreciation at endoscopy of esophageal stricture and small-caliber esophagus, and the possibility that esophageal narrowing may require dilation to relieve symptomatic dysphagia despite a histologic response.
In addition, "changes in esophageal compliance related to fibrosis may be important," they wrote, as a decrease in esophageal distensibility and compliance has been shown in EoE, which could well be a cause of dysphagia. Candida infections, which developed in 31.6% of the treatment group and none of the placebo group, could potentially lead to persistent dysphagia despite a histologic response, they said. Most likely, however, the discrepancy "reflects a waxing and waning of dysphagia in this disease," they concluded.
The study findings are limited by the relatively small sample size and the unexpectedly high dropout rate in the placebo group, which "left us somewhat underpowered for our primary end point," the authors wrote. Also, gastroesophageal reflux disease was not categorically excluded in all of the patients prior to enrollment. "While we would have liked to adjust for baseline differences in erosive esophagitis and PPI [protein pump inhibitor] use between treatment and placebo groups, this is beyond the limits of a dataset this size," they said.
The treatment was safe and well tolerated, but further study is needed to evaluate the optimal dose of therapy, length of therapy, and long-term safety of topical fluticasone, as well as other steroid medications. "Furthermore," the authors wrote, "delivery systems need to be developed that are easier to use and provide more direct drug delivery to the esophagus."
Dr. Alexander disclosed a financial relationship with Meritage Pharmacia.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
H. Pylori Infection, Colonic Neoplasms Linked
SAN DIEGO – Patients with Helicobacter pylori infection face a significantly increased risk for developing colonic neoplasms, according to what is believed to be the largest investigation of the association.
Several studies have suggested that H. pylori infection is a risk factor for colonic neoplasms, but all of them involved relatively small case populations, Dr. Amnon Sonnenberg explained at the annual Digestive Disease Week.
Dr. Sonnenberg, a gastroenterologist with the Portland (Ore.) VA Medical Center, investigated the relationship between H. pylori infection and the presence of colonic neoplasms in 156,269 patients who had undergone both a colonoscopy and an esophagogastroduodenoscopy. Surgical pathology samples from all the patients were stored in an electronic database at the Miraca Research Institute, a specialized gastrointestinal lab that serves private outpatient endoscopy centers throughout the United States. More than 1,500 gastroenterologists contributed to the database between January 2008 and December 2011.
Patients were an average age of 58 years, and 59% were female. Among the total, 16,759 (11%) had H. pylori gastritis on immunochemistry. The prevalence of H. pylori gastritis was 9% in patients without polyps, 11% in patients with hyperplastic polyps, 12% in patients with adenoma, 14% in patients with advanced adenoma, 15% in patients with villous adenoma or polyps with high-grade dysplasia, and 18% in patients with colonic adenocarcinoma.
There was a slight trend for the prevalence of H. pylori to rise with the increasing number, as well as the size, of adenomatous polyps. The prevalence of H. pylori was similar for all colon sites.
Significant associations also were noted between the development of colonic adenoma and the following other types of gastric histopathology: intestinal metaplasia, gastric adenoma, gastric cancer, and gastric lymphoma. Similar but even more significant associations were seen between advanced adenoma and these types of gastric histopathology.

Multivariate logistic regression confirmed that the development of H. pylori gastritis was associated with advanced age, male gender, hyperplastic polyps, adenoma, villous adenoma or high-grade dysplasia, and adenocarcinoma.
"H. pylori gastritis confers an increased risk for colonic neoplasm," concluded Dr. Sonnenberg, who is also professor of medicine in the division of gastroenterology and hepatology at Oregon Health and Science University.
"The risk applies to all types of colonic neoplasms and appears to increase with advancing stage of the neoplasm from hyperplastic and adenomatous polyps to tubulovillous adenoma, adenoma with high-grade dysplasia, and adenocarcinoma. Such risk is not limited to chronic active gastritis but is found in other types of gastric histopathology related to H. pylori, such as gastric intestinal metaplasia, gastric adenoma, gastric lymphoma, and gastric cancer," he said.
Long-term infection with H. pylori "may be related to elevated gastrin levels that may act as a growth factor," he speculated.
Dr. Sonnenberg disclosed having received a research grant from Takeda Pharmaceutical Company. No support was received for this study.
SAN DIEGO – Patients with Helicobacter pylori infection face a significantly increased risk for developing colonic neoplasms, according to what is believed to be the largest investigation of the association.
Several studies have suggested that H. pylori infection is a risk factor for colonic neoplasms, but all of them involved relatively small case populations, Dr. Amnon Sonnenberg explained at the annual Digestive Disease Week.
Dr. Sonnenberg, a gastroenterologist with the Portland (Ore.) VA Medical Center, investigated the relationship between H. pylori infection and the presence of colonic neoplasms in 156,269 patients who had undergone both a colonoscopy and an esophagogastroduodenoscopy. Surgical pathology samples from all the patients were stored in an electronic database at the Miraca Research Institute, a specialized gastrointestinal lab that serves private outpatient endoscopy centers throughout the United States. More than 1,500 gastroenterologists contributed to the database between January 2008 and December 2011.
Patients were an average age of 58 years, and 59% were female. Among the total, 16,759 (11%) had H. pylori gastritis on immunochemistry. The prevalence of H. pylori gastritis was 9% in patients without polyps, 11% in patients with hyperplastic polyps, 12% in patients with adenoma, 14% in patients with advanced adenoma, 15% in patients with villous adenoma or polyps with high-grade dysplasia, and 18% in patients with colonic adenocarcinoma.
There was a slight trend for the prevalence of H. pylori to rise with the increasing number, as well as the size, of adenomatous polyps. The prevalence of H. pylori was similar for all colon sites.
Significant associations also were noted between the development of colonic adenoma and the following other types of gastric histopathology: intestinal metaplasia, gastric adenoma, gastric cancer, and gastric lymphoma. Similar but even more significant associations were seen between advanced adenoma and these types of gastric histopathology.
Multivariate logistic regression confirmed that the development of H. pylori gastritis was associated with advanced age, male gender, hyperplastic polyps, adenoma, villous adenoma or high-grade dysplasia, and adenocarcinoma.
"H. pylori gastritis confers an increased risk for colonic neoplasm," concluded Dr. Sonnenberg, who is also professor of medicine in the division of gastroenterology and hepatology at Oregon Health and Science University.
"The risk applies to all types of colonic neoplasms and appears to increase with advancing stage of the neoplasm from hyperplastic and adenomatous polyps to tubulovillous adenoma, adenoma with high-grade dysplasia, and adenocarcinoma. Such risk is not limited to chronic active gastritis but is found in other types of gastric histopathology related to H. pylori, such as gastric intestinal metaplasia, gastric adenoma, gastric lymphoma, and gastric cancer," he said.
Long-term infection with H. pylori "may be related to elevated gastrin levels that may act as a growth factor," he speculated.
Dr. Sonnenberg disclosed having received a research grant from Takeda Pharmaceutical Company. No support was received for this study.
SAN DIEGO – Patients with Helicobacter pylori infection face a significantly increased risk for developing colonic neoplasms, according to what is believed to be the largest investigation of the association.
Several studies have suggested that H. pylori infection is a risk factor for colonic neoplasms, but all of them involved relatively small case populations, Dr. Amnon Sonnenberg explained at the annual Digestive Disease Week.
Dr. Sonnenberg, a gastroenterologist with the Portland (Ore.) VA Medical Center, investigated the relationship between H. pylori infection and the presence of colonic neoplasms in 156,269 patients who had undergone both a colonoscopy and an esophagogastroduodenoscopy. Surgical pathology samples from all the patients were stored in an electronic database at the Miraca Research Institute, a specialized gastrointestinal lab that serves private outpatient endoscopy centers throughout the United States. More than 1,500 gastroenterologists contributed to the database between January 2008 and December 2011.
Patients were an average age of 58 years, and 59% were female. Among the total, 16,759 (11%) had H. pylori gastritis on immunochemistry. The prevalence of H. pylori gastritis was 9% in patients without polyps, 11% in patients with hyperplastic polyps, 12% in patients with adenoma, 14% in patients with advanced adenoma, 15% in patients with villous adenoma or polyps with high-grade dysplasia, and 18% in patients with colonic adenocarcinoma.
There was a slight trend for the prevalence of H. pylori to rise with the increasing number, as well as the size, of adenomatous polyps. The prevalence of H. pylori was similar for all colon sites.
Significant associations also were noted between the development of colonic adenoma and the following other types of gastric histopathology: intestinal metaplasia, gastric adenoma, gastric cancer, and gastric lymphoma. Similar but even more significant associations were seen between advanced adenoma and these types of gastric histopathology.
Multivariate logistic regression confirmed that the development of H. pylori gastritis was associated with advanced age, male gender, hyperplastic polyps, adenoma, villous adenoma or high-grade dysplasia, and adenocarcinoma.
"H. pylori gastritis confers an increased risk for colonic neoplasm," concluded Dr. Sonnenberg, who is also professor of medicine in the division of gastroenterology and hepatology at Oregon Health and Science University.
"The risk applies to all types of colonic neoplasms and appears to increase with advancing stage of the neoplasm from hyperplastic and adenomatous polyps to tubulovillous adenoma, adenoma with high-grade dysplasia, and adenocarcinoma. Such risk is not limited to chronic active gastritis but is found in other types of gastric histopathology related to H. pylori, such as gastric intestinal metaplasia, gastric adenoma, gastric lymphoma, and gastric cancer," he said.
Long-term infection with H. pylori "may be related to elevated gastrin levels that may act as a growth factor," he speculated.
Dr. Sonnenberg disclosed having received a research grant from Takeda Pharmaceutical Company. No support was received for this study.
FROM THE ANNUAL DIGESTIVE DISEASE WEEK
Major Finding: The prevalence of H. pylori gastritis was 9% in patients without polyps, 11% in patients with hyperplastic polyps, 12% in patients with adenoma, 14% in patients with advanced adenoma, 15% in patients with villous adenoma or polyps with high-grade dysplasia, and 18% in patients with colonic adenocarcinoma.
Data Source: Findings are based on an analysis of pathology data from 156,269 patients who had undergone both a colonoscopy and an esophagogastroduodenoscopy.
Disclosures: Dr. Sonnenberg disclosed having received a research grant from Takeda Pharmaceutical Company. No support was received for this study.
Fundoplication Doesn't Diminish Efficacy of Ablation in Barrett's Patients
SAN DIEGO – Radiofrequency ablation was found to be safe and effective in treating Barrett’s esophagus patients, whether or not they had undergone a prior fundoplication, based on results from a multicenter registry study.
"Gastroesophageal reflux causes esophageal mucosal injury and inflammation that may impair healing and squamous re-epithelialization after treatment of Barrett’s esophagus [BE] with radiofrequency ablation [RFA]," Dr. Nicholas J. Shaheen said at the annual Digestive Disease Week.

"It is unclear if fundoplication surgery, as a mechanical barrier to all reflux, improves treatment outcomes of RFA for BE. Similarly, some have postulated that change in the conformation of the hiatus with surgery might make ablation problematic."
Dr. Shaheen, director of the Center for Esophageal Diseases and Swallowing at the University of North Carolina, Chapel Hill, and his associates conducted the largest study of its kind, he said. They evaluated records from the RFA Patient Registry to assess the relationship between prior fundoplication and both efficacy and safety outcomes in patients with BE who were treated with RFA.
The registry comprises 113 community-based and 35 academic-affiliated medical institutions in the United States. "About 75% of these institutions are private practices, so this is an interesting snapshot of RFA as it’s practiced outside of tertiary care centers," Dr. Shaheen said.
All study patients had BE confirmed by endoscopy and histology, and had undergone treatment with RFA. Enrollment commenced in July 2007 and ended in July 2011. Data were gleaned from standard case report forms and included demographics; relevant medical history; histologic grade prior to treatment; endoscopic findings; dates and total number of RFA treatment sessions; and ablation outcomes and complications.
"The vast amount of data is prospective, but less than 15% is retrospective," Dr. Shaheen said. "This is a registry study, so we could not mandate treatment, but a treatment protocol was suggested." Twice-daily use of proton pump inhibitors (PPIs) was recommended to everyone in the study, including those post fundoplication.
The mean age of patients was 61 years, and the majority were white. The mean pretreatment length of BE was about 4 cm, and patients received an average of 2.5 treatments with RFA. "Importantly, in this registry, about half of the patients had nondysplastic disease," Dr. Shaheen said. "Also, roughly 20% in each group had low- and high-grade dysplasia."
Dr. Shaheen reported results from the safety cohort, which included 5,537 patients who received RFA, and results from the efficacy cohort, which included 2,466 patients with biopsies performed 12 months after enrollment. Safety outcomes included perforation, stricture that required dilation, bleeding that required hospitalization or transfusion, and hospitalization. Efficacy outcomes included complete eradication of intestinal metaplasia and dysplasia.
Among patients in the safety cohort, 301 had a prior fundoplication, whereas 5,236 had received medical therapy only. Patients in the fundoplication group had a somewhat lower mean age than those in the medical therapy group (59 vs. 62 years, P = .0002), and were slightly less likely to be African American (0.3% vs. 1.6%, P = .03) or Hispanic (0.7% vs. 2.6%, P = .03). In the fundoplication group, the length of BE was greater (5.0 cm vs. 4.1 cm, P less than .0001), and the prevalence of nondysplastic BE was higher (53% vs. 49%, P = .05).
In addition, fewer patients in the fundoplication group were taking twice-daily PPIs compared with those in the medical therapy group (82% vs. 95%, P less than .001). There were no significant between-group differences in the rates of bleeding, hospitalization, or stricture.
Among patients in the efficacy cohort, 136 had a prior fundoplication and 2,330 had received medical therapy only. The fundoplication patients were slightly younger than the medical therapy patients (59 vs. 62 years, P = .004), had a somewhat greater length of BE (5.0 cm vs. 4.3 cm, P = .009), and were less likely to be taking twice-daily PPIs (75% vs. 93%, P less than .001).
Rates of complete eradication of intestinal metaplasia were 71% in the fundoplication group vs. 73% in the medical therapy group, a nonsignificant difference, while the rate of complete eradication of dysplasia was identical in both groups at 87%.
Among patients who had nondysplastic BE, 75% in the fundoplication group achieved complete eradication of intestinal metaplasia, compared with 81% in the medical therapy group, a nonsignificant difference.
Regarding combined efficacy for dysplastic BE and intramucosal carcinoma, 67% of patients in the fundoplication group achieved complete eradication of intestinal metaplasia, compared with 66% in the medical therapy group, and both groups had a rate of 87% for complete eradication of dysplasia; none of these differences were significant.
Dr. Shaheen acknowledged certain limitations of the study, including the fact that the functional status of the fundoplications was not known. "All we know is that some patients had them," he said. "These are observational data and subject to selection bias. Also note that this is hardly a pure comparison, because the people who got fundoplication were also getting PPIs. However, one might expect that to bias the study in favor of fundoplication, to the degree that the addition of PPIs helps."
The study was funded by Covidien, which provided the RFA equipment used in the study, and by grants from the National Institutes of Health. Dr. Shaheen disclosed that he has consulting relationships with numerous pharmaceutical and medical device companies, but none with Covidien.
SAN DIEGO – Radiofrequency ablation was found to be safe and effective in treating Barrett’s esophagus patients, whether or not they had undergone a prior fundoplication, based on results from a multicenter registry study.
"Gastroesophageal reflux causes esophageal mucosal injury and inflammation that may impair healing and squamous re-epithelialization after treatment of Barrett’s esophagus [BE] with radiofrequency ablation [RFA]," Dr. Nicholas J. Shaheen said at the annual Digestive Disease Week.
"It is unclear if fundoplication surgery, as a mechanical barrier to all reflux, improves treatment outcomes of RFA for BE. Similarly, some have postulated that change in the conformation of the hiatus with surgery might make ablation problematic."
Dr. Shaheen, director of the Center for Esophageal Diseases and Swallowing at the University of North Carolina, Chapel Hill, and his associates conducted the largest study of its kind, he said. They evaluated records from the RFA Patient Registry to assess the relationship between prior fundoplication and both efficacy and safety outcomes in patients with BE who were treated with RFA.
The registry comprises 113 community-based and 35 academic-affiliated medical institutions in the United States. "About 75% of these institutions are private practices, so this is an interesting snapshot of RFA as it’s practiced outside of tertiary care centers," Dr. Shaheen said.
All study patients had BE confirmed by endoscopy and histology, and had undergone treatment with RFA. Enrollment commenced in July 2007 and ended in July 2011. Data were gleaned from standard case report forms and included demographics; relevant medical history; histologic grade prior to treatment; endoscopic findings; dates and total number of RFA treatment sessions; and ablation outcomes and complications.
"The vast amount of data is prospective, but less than 15% is retrospective," Dr. Shaheen said. "This is a registry study, so we could not mandate treatment, but a treatment protocol was suggested." Twice-daily use of proton pump inhibitors (PPIs) was recommended to everyone in the study, including those post fundoplication.
The mean age of patients was 61 years, and the majority were white. The mean pretreatment length of BE was about 4 cm, and patients received an average of 2.5 treatments with RFA. "Importantly, in this registry, about half of the patients had nondysplastic disease," Dr. Shaheen said. "Also, roughly 20% in each group had low- and high-grade dysplasia."
Dr. Shaheen reported results from the safety cohort, which included 5,537 patients who received RFA, and results from the efficacy cohort, which included 2,466 patients with biopsies performed 12 months after enrollment. Safety outcomes included perforation, stricture that required dilation, bleeding that required hospitalization or transfusion, and hospitalization. Efficacy outcomes included complete eradication of intestinal metaplasia and dysplasia.
Among patients in the safety cohort, 301 had a prior fundoplication, whereas 5,236 had received medical therapy only. Patients in the fundoplication group had a somewhat lower mean age than those in the medical therapy group (59 vs. 62 years, P = .0002), and were slightly less likely to be African American (0.3% vs. 1.6%, P = .03) or Hispanic (0.7% vs. 2.6%, P = .03). In the fundoplication group, the length of BE was greater (5.0 cm vs. 4.1 cm, P less than .0001), and the prevalence of nondysplastic BE was higher (53% vs. 49%, P = .05).
In addition, fewer patients in the fundoplication group were taking twice-daily PPIs compared with those in the medical therapy group (82% vs. 95%, P less than .001). There were no significant between-group differences in the rates of bleeding, hospitalization, or stricture.
Among patients in the efficacy cohort, 136 had a prior fundoplication and 2,330 had received medical therapy only. The fundoplication patients were slightly younger than the medical therapy patients (59 vs. 62 years, P = .004), had a somewhat greater length of BE (5.0 cm vs. 4.3 cm, P = .009), and were less likely to be taking twice-daily PPIs (75% vs. 93%, P less than .001).
Rates of complete eradication of intestinal metaplasia were 71% in the fundoplication group vs. 73% in the medical therapy group, a nonsignificant difference, while the rate of complete eradication of dysplasia was identical in both groups at 87%.
Among patients who had nondysplastic BE, 75% in the fundoplication group achieved complete eradication of intestinal metaplasia, compared with 81% in the medical therapy group, a nonsignificant difference.
Regarding combined efficacy for dysplastic BE and intramucosal carcinoma, 67% of patients in the fundoplication group achieved complete eradication of intestinal metaplasia, compared with 66% in the medical therapy group, and both groups had a rate of 87% for complete eradication of dysplasia; none of these differences were significant.
Dr. Shaheen acknowledged certain limitations of the study, including the fact that the functional status of the fundoplications was not known. "All we know is that some patients had them," he said. "These are observational data and subject to selection bias. Also note that this is hardly a pure comparison, because the people who got fundoplication were also getting PPIs. However, one might expect that to bias the study in favor of fundoplication, to the degree that the addition of PPIs helps."
The study was funded by Covidien, which provided the RFA equipment used in the study, and by grants from the National Institutes of Health. Dr. Shaheen disclosed that he has consulting relationships with numerous pharmaceutical and medical device companies, but none with Covidien.
SAN DIEGO – Radiofrequency ablation was found to be safe and effective in treating Barrett’s esophagus patients, whether or not they had undergone a prior fundoplication, based on results from a multicenter registry study.
"Gastroesophageal reflux causes esophageal mucosal injury and inflammation that may impair healing and squamous re-epithelialization after treatment of Barrett’s esophagus [BE] with radiofrequency ablation [RFA]," Dr. Nicholas J. Shaheen said at the annual Digestive Disease Week.
"It is unclear if fundoplication surgery, as a mechanical barrier to all reflux, improves treatment outcomes of RFA for BE. Similarly, some have postulated that change in the conformation of the hiatus with surgery might make ablation problematic."
Dr. Shaheen, director of the Center for Esophageal Diseases and Swallowing at the University of North Carolina, Chapel Hill, and his associates conducted the largest study of its kind, he said. They evaluated records from the RFA Patient Registry to assess the relationship between prior fundoplication and both efficacy and safety outcomes in patients with BE who were treated with RFA.
The registry comprises 113 community-based and 35 academic-affiliated medical institutions in the United States. "About 75% of these institutions are private practices, so this is an interesting snapshot of RFA as it’s practiced outside of tertiary care centers," Dr. Shaheen said.
All study patients had BE confirmed by endoscopy and histology, and had undergone treatment with RFA. Enrollment commenced in July 2007 and ended in July 2011. Data were gleaned from standard case report forms and included demographics; relevant medical history; histologic grade prior to treatment; endoscopic findings; dates and total number of RFA treatment sessions; and ablation outcomes and complications.
"The vast amount of data is prospective, but less than 15% is retrospective," Dr. Shaheen said. "This is a registry study, so we could not mandate treatment, but a treatment protocol was suggested." Twice-daily use of proton pump inhibitors (PPIs) was recommended to everyone in the study, including those post fundoplication.
The mean age of patients was 61 years, and the majority were white. The mean pretreatment length of BE was about 4 cm, and patients received an average of 2.5 treatments with RFA. "Importantly, in this registry, about half of the patients had nondysplastic disease," Dr. Shaheen said. "Also, roughly 20% in each group had low- and high-grade dysplasia."
Dr. Shaheen reported results from the safety cohort, which included 5,537 patients who received RFA, and results from the efficacy cohort, which included 2,466 patients with biopsies performed 12 months after enrollment. Safety outcomes included perforation, stricture that required dilation, bleeding that required hospitalization or transfusion, and hospitalization. Efficacy outcomes included complete eradication of intestinal metaplasia and dysplasia.
Among patients in the safety cohort, 301 had a prior fundoplication, whereas 5,236 had received medical therapy only. Patients in the fundoplication group had a somewhat lower mean age than those in the medical therapy group (59 vs. 62 years, P = .0002), and were slightly less likely to be African American (0.3% vs. 1.6%, P = .03) or Hispanic (0.7% vs. 2.6%, P = .03). In the fundoplication group, the length of BE was greater (5.0 cm vs. 4.1 cm, P less than .0001), and the prevalence of nondysplastic BE was higher (53% vs. 49%, P = .05).
In addition, fewer patients in the fundoplication group were taking twice-daily PPIs compared with those in the medical therapy group (82% vs. 95%, P less than .001). There were no significant between-group differences in the rates of bleeding, hospitalization, or stricture.
Among patients in the efficacy cohort, 136 had a prior fundoplication and 2,330 had received medical therapy only. The fundoplication patients were slightly younger than the medical therapy patients (59 vs. 62 years, P = .004), had a somewhat greater length of BE (5.0 cm vs. 4.3 cm, P = .009), and were less likely to be taking twice-daily PPIs (75% vs. 93%, P less than .001).
Rates of complete eradication of intestinal metaplasia were 71% in the fundoplication group vs. 73% in the medical therapy group, a nonsignificant difference, while the rate of complete eradication of dysplasia was identical in both groups at 87%.
Among patients who had nondysplastic BE, 75% in the fundoplication group achieved complete eradication of intestinal metaplasia, compared with 81% in the medical therapy group, a nonsignificant difference.
Regarding combined efficacy for dysplastic BE and intramucosal carcinoma, 67% of patients in the fundoplication group achieved complete eradication of intestinal metaplasia, compared with 66% in the medical therapy group, and both groups had a rate of 87% for complete eradication of dysplasia; none of these differences were significant.
Dr. Shaheen acknowledged certain limitations of the study, including the fact that the functional status of the fundoplications was not known. "All we know is that some patients had them," he said. "These are observational data and subject to selection bias. Also note that this is hardly a pure comparison, because the people who got fundoplication were also getting PPIs. However, one might expect that to bias the study in favor of fundoplication, to the degree that the addition of PPIs helps."
The study was funded by Covidien, which provided the RFA equipment used in the study, and by grants from the National Institutes of Health. Dr. Shaheen disclosed that he has consulting relationships with numerous pharmaceutical and medical device companies, but none with Covidien.
FROM THE ANNUAL DIGESTIVE DISEASE WEEK