User login
Tool May Help Predict Persistent Postconcussion Symptoms
A clinical risk score may help identify which children and adolescents with recent head injury are at risk for persistent postconcussion symptoms, according to an investigation published March 8 in JAMA.
Approximately one-third of pediatric patients with concussion have ongoing somatic, cognitive, psychological, or behavioral symptoms at 28 days. At present, neurologists have no tools to help predict which patients will be affected in this way. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Roger Zemek, MD, a scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Canada, and his associates.

This prospective cohort study involved patients between ages 5 and 17 (median age, 12) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms. The investigators assessed 47 possible predictive variables for their usefulness in predicting persistent postconcussion symptoms in this cohort. The variables were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient and parent responses to weekly follow-up surveys during the month after the injury.
The investigators devised a clinical risk score using the following nine predictors that they found to be most accurate: age, gender, presence or absence of prior concussion, migraine history, presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to stratify the risk of persistent postconcussion symptoms: 0–3 points indicated low risk, 4–8 points indicated intermediate risk, and 9 or more points indicated high risk. Treating physicians also were asked to predict the likelihood of persistent postconcussion symptoms.
In the validation cohort, 291 of 883 participants (33%) met the criteria for persistent postconcussion symptoms. For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting persistent postconcussion symptoms. The clinical risk score has modest accuracy, however, at distinguishing between who will and who will not have persistent symptoms. This tool could be refined further, perhaps, by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, said Dr. Zemek and his associates.
—Mary Ann Moon
Suggested Reading
Zemek R, Barrowman N, Freedman SB, et al. Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA. 2016;315(10):1014-1025.
A clinical risk score may help identify which children and adolescents with recent head injury are at risk for persistent postconcussion symptoms, according to an investigation published March 8 in JAMA.
Approximately one-third of pediatric patients with concussion have ongoing somatic, cognitive, psychological, or behavioral symptoms at 28 days. At present, neurologists have no tools to help predict which patients will be affected in this way. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Roger Zemek, MD, a scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Canada, and his associates.
This prospective cohort study involved patients between ages 5 and 17 (median age, 12) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms. The investigators assessed 47 possible predictive variables for their usefulness in predicting persistent postconcussion symptoms in this cohort. The variables were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient and parent responses to weekly follow-up surveys during the month after the injury.
The investigators devised a clinical risk score using the following nine predictors that they found to be most accurate: age, gender, presence or absence of prior concussion, migraine history, presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to stratify the risk of persistent postconcussion symptoms: 0–3 points indicated low risk, 4–8 points indicated intermediate risk, and 9 or more points indicated high risk. Treating physicians also were asked to predict the likelihood of persistent postconcussion symptoms.
In the validation cohort, 291 of 883 participants (33%) met the criteria for persistent postconcussion symptoms. For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting persistent postconcussion symptoms. The clinical risk score has modest accuracy, however, at distinguishing between who will and who will not have persistent symptoms. This tool could be refined further, perhaps, by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, said Dr. Zemek and his associates.
—Mary Ann Moon
A clinical risk score may help identify which children and adolescents with recent head injury are at risk for persistent postconcussion symptoms, according to an investigation published March 8 in JAMA.
Approximately one-third of pediatric patients with concussion have ongoing somatic, cognitive, psychological, or behavioral symptoms at 28 days. At present, neurologists have no tools to help predict which patients will be affected in this way. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Roger Zemek, MD, a scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Canada, and his associates.
This prospective cohort study involved patients between ages 5 and 17 (median age, 12) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms. The investigators assessed 47 possible predictive variables for their usefulness in predicting persistent postconcussion symptoms in this cohort. The variables were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient and parent responses to weekly follow-up surveys during the month after the injury.
The investigators devised a clinical risk score using the following nine predictors that they found to be most accurate: age, gender, presence or absence of prior concussion, migraine history, presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to stratify the risk of persistent postconcussion symptoms: 0–3 points indicated low risk, 4–8 points indicated intermediate risk, and 9 or more points indicated high risk. Treating physicians also were asked to predict the likelihood of persistent postconcussion symptoms.
In the validation cohort, 291 of 883 participants (33%) met the criteria for persistent postconcussion symptoms. For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting persistent postconcussion symptoms. The clinical risk score has modest accuracy, however, at distinguishing between who will and who will not have persistent symptoms. This tool could be refined further, perhaps, by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, said Dr. Zemek and his associates.
—Mary Ann Moon
Suggested Reading
Zemek R, Barrowman N, Freedman SB, et al. Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA. 2016;315(10):1014-1025.
Suggested Reading
Zemek R, Barrowman N, Freedman SB, et al. Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA. 2016;315(10):1014-1025.

Increase in Blood Pressure May Improve Survival in TBI
SAN DIEGO—In the setting of traumatic brain injury (TBI), increases in systolic blood pressure after the blood pressure nadir are independently associated with improved survival in patients with hypotension. In addition, even substantial blood pressure increases do not seem to harm patients with normal blood pressure. These findings come from a subanalysis of the ongoing Excellence in Prehospital Injury Care (EPIC) TBI study.
“Little is known about the patterns of blood pressure in TBI in the field,” said Daniel W. Spaite, MD, Professor and Virginia Piper Endowed Chair of Emergency Medicine at the University of Arizona in Tucson, at the Annual Meeting of the National Association of EMS Physicians (NAEMSP). “For instance, nobody knows whether it’s better to have your blood pressure increasing, stable, or decreasing in the field with regard to outcome, especially mortality. Typical studies that do have EMS data linked only have a single blood pressure measurement documented, so there’s no knowledge of trends in EMS blood pressure in TBI.”

Dr. Spaite and his colleagues evaluated the association between mortality and increases in prehospital systolic blood pressure after the lowest recorded measurement in patients with major TBI who are part of the EPIC study, the statewide implementation of TBI guidelines from the Brain Trauma Foundation and the NAEMSP. Data sources include the Arizona State Trauma Registry, which has comprehensive hospital outcome data. “The cases are then linked, and the EMS patient care reports are carefully abstracted by the EPIC data team,” Dr. Spaite explained. “This included major TBI (which is, clinically, both moderate and severe) and all patients whose lowest systolic blood pressure was between 40 and 300 mmHg.”
The researchers used logistic regression to examine the association between the increase in EMS systolic blood pressure after the lowest EMS blood pressure recorded and its association with adjusted probability of death. They then separated the study population into four cohorts, based on each patient’s prehospital systolic blood pressure (ie, 40–89 mmHg, 90–139 mmHg, 140–159 mmHg, and 160–300 mmHg). In each cohort, they identified the independent association between the magnitude of increase in systolic blood pressure and the adjusted probability of death.
Dr. Spaite reported findings from 14,567 patients with TBI. More than two-thirds (68%) of participants were male, and their mean age was 45. The researchers observed that in the hypotensive cohort, mortality dropped significantly if the systolic blood pressure increased after the lowest recorded systolic blood pressure. “Improvements were dramatic with increases of 40–80 mmHg,” he said. In the normotensive group, increases in systolic blood pressure were associated with slight reductions in mortality. Large increases in systolic blood pressure, such as in the range of 70–90 mmHg, did not appear to be detrimental.In the mildly hypertensive group, large systolic increases were associated with higher mortality. “Interestingly, even if your lowest [systolic blood pressure] is between 140 and 159 mmHg, until you get above an increase of 40 mmHg above that, you don’t start seeing increases in mortality,” said Dr. Spaite. In the severely hypertensive group, mortality was higher with any subsequent increase in systolic blood pressure, “which doesn’t surprise any of us,” he said. “It’s dramatically higher if the increase is large.”
Dr. Spaite emphasized that the current analysis is based on observational data, “so this does not prove that treating hypotension improves outcome. … That direct question is part of the EPIC study itself and awaits the final analysis, hopefully in mid-2017. This is the first large report of blood pressure trends in the prehospital management of TBI.”
He concluded that the current findings in the hypotensive and normotensive cohorts “support guideline recommendations for restoring and optimizing cerebral perfusion in EMS TBI management. What is fascinating about the literature is that the focus in TBI has always been on hypotension, but there’s very little information about what’s the best or the optimal blood pressure.”
—Doug Brunk
SAN DIEGO—In the setting of traumatic brain injury (TBI), increases in systolic blood pressure after the blood pressure nadir are independently associated with improved survival in patients with hypotension. In addition, even substantial blood pressure increases do not seem to harm patients with normal blood pressure. These findings come from a subanalysis of the ongoing Excellence in Prehospital Injury Care (EPIC) TBI study.
“Little is known about the patterns of blood pressure in TBI in the field,” said Daniel W. Spaite, MD, Professor and Virginia Piper Endowed Chair of Emergency Medicine at the University of Arizona in Tucson, at the Annual Meeting of the National Association of EMS Physicians (NAEMSP). “For instance, nobody knows whether it’s better to have your blood pressure increasing, stable, or decreasing in the field with regard to outcome, especially mortality. Typical studies that do have EMS data linked only have a single blood pressure measurement documented, so there’s no knowledge of trends in EMS blood pressure in TBI.”
Dr. Spaite and his colleagues evaluated the association between mortality and increases in prehospital systolic blood pressure after the lowest recorded measurement in patients with major TBI who are part of the EPIC study, the statewide implementation of TBI guidelines from the Brain Trauma Foundation and the NAEMSP. Data sources include the Arizona State Trauma Registry, which has comprehensive hospital outcome data. “The cases are then linked, and the EMS patient care reports are carefully abstracted by the EPIC data team,” Dr. Spaite explained. “This included major TBI (which is, clinically, both moderate and severe) and all patients whose lowest systolic blood pressure was between 40 and 300 mmHg.”
The researchers used logistic regression to examine the association between the increase in EMS systolic blood pressure after the lowest EMS blood pressure recorded and its association with adjusted probability of death. They then separated the study population into four cohorts, based on each patient’s prehospital systolic blood pressure (ie, 40–89 mmHg, 90–139 mmHg, 140–159 mmHg, and 160–300 mmHg). In each cohort, they identified the independent association between the magnitude of increase in systolic blood pressure and the adjusted probability of death.
Dr. Spaite reported findings from 14,567 patients with TBI. More than two-thirds (68%) of participants were male, and their mean age was 45. The researchers observed that in the hypotensive cohort, mortality dropped significantly if the systolic blood pressure increased after the lowest recorded systolic blood pressure. “Improvements were dramatic with increases of 40–80 mmHg,” he said. In the normotensive group, increases in systolic blood pressure were associated with slight reductions in mortality. Large increases in systolic blood pressure, such as in the range of 70–90 mmHg, did not appear to be detrimental.In the mildly hypertensive group, large systolic increases were associated with higher mortality. “Interestingly, even if your lowest [systolic blood pressure] is between 140 and 159 mmHg, until you get above an increase of 40 mmHg above that, you don’t start seeing increases in mortality,” said Dr. Spaite. In the severely hypertensive group, mortality was higher with any subsequent increase in systolic blood pressure, “which doesn’t surprise any of us,” he said. “It’s dramatically higher if the increase is large.”
Dr. Spaite emphasized that the current analysis is based on observational data, “so this does not prove that treating hypotension improves outcome. … That direct question is part of the EPIC study itself and awaits the final analysis, hopefully in mid-2017. This is the first large report of blood pressure trends in the prehospital management of TBI.”
He concluded that the current findings in the hypotensive and normotensive cohorts “support guideline recommendations for restoring and optimizing cerebral perfusion in EMS TBI management. What is fascinating about the literature is that the focus in TBI has always been on hypotension, but there’s very little information about what’s the best or the optimal blood pressure.”
—Doug Brunk
SAN DIEGO—In the setting of traumatic brain injury (TBI), increases in systolic blood pressure after the blood pressure nadir are independently associated with improved survival in patients with hypotension. In addition, even substantial blood pressure increases do not seem to harm patients with normal blood pressure. These findings come from a subanalysis of the ongoing Excellence in Prehospital Injury Care (EPIC) TBI study.
“Little is known about the patterns of blood pressure in TBI in the field,” said Daniel W. Spaite, MD, Professor and Virginia Piper Endowed Chair of Emergency Medicine at the University of Arizona in Tucson, at the Annual Meeting of the National Association of EMS Physicians (NAEMSP). “For instance, nobody knows whether it’s better to have your blood pressure increasing, stable, or decreasing in the field with regard to outcome, especially mortality. Typical studies that do have EMS data linked only have a single blood pressure measurement documented, so there’s no knowledge of trends in EMS blood pressure in TBI.”
Dr. Spaite and his colleagues evaluated the association between mortality and increases in prehospital systolic blood pressure after the lowest recorded measurement in patients with major TBI who are part of the EPIC study, the statewide implementation of TBI guidelines from the Brain Trauma Foundation and the NAEMSP. Data sources include the Arizona State Trauma Registry, which has comprehensive hospital outcome data. “The cases are then linked, and the EMS patient care reports are carefully abstracted by the EPIC data team,” Dr. Spaite explained. “This included major TBI (which is, clinically, both moderate and severe) and all patients whose lowest systolic blood pressure was between 40 and 300 mmHg.”
The researchers used logistic regression to examine the association between the increase in EMS systolic blood pressure after the lowest EMS blood pressure recorded and its association with adjusted probability of death. They then separated the study population into four cohorts, based on each patient’s prehospital systolic blood pressure (ie, 40–89 mmHg, 90–139 mmHg, 140–159 mmHg, and 160–300 mmHg). In each cohort, they identified the independent association between the magnitude of increase in systolic blood pressure and the adjusted probability of death.
Dr. Spaite reported findings from 14,567 patients with TBI. More than two-thirds (68%) of participants were male, and their mean age was 45. The researchers observed that in the hypotensive cohort, mortality dropped significantly if the systolic blood pressure increased after the lowest recorded systolic blood pressure. “Improvements were dramatic with increases of 40–80 mmHg,” he said. In the normotensive group, increases in systolic blood pressure were associated with slight reductions in mortality. Large increases in systolic blood pressure, such as in the range of 70–90 mmHg, did not appear to be detrimental.In the mildly hypertensive group, large systolic increases were associated with higher mortality. “Interestingly, even if your lowest [systolic blood pressure] is between 140 and 159 mmHg, until you get above an increase of 40 mmHg above that, you don’t start seeing increases in mortality,” said Dr. Spaite. In the severely hypertensive group, mortality was higher with any subsequent increase in systolic blood pressure, “which doesn’t surprise any of us,” he said. “It’s dramatically higher if the increase is large.”
Dr. Spaite emphasized that the current analysis is based on observational data, “so this does not prove that treating hypotension improves outcome. … That direct question is part of the EPIC study itself and awaits the final analysis, hopefully in mid-2017. This is the first large report of blood pressure trends in the prehospital management of TBI.”
He concluded that the current findings in the hypotensive and normotensive cohorts “support guideline recommendations for restoring and optimizing cerebral perfusion in EMS TBI management. What is fascinating about the literature is that the focus in TBI has always been on hypotension, but there’s very little information about what’s the best or the optimal blood pressure.”
—Doug Brunk

BRAIN Initiative Could Advance the Field of Neuromodulation
LAS VEGAS—Through various programs, the BRAIN Initiative seeks to fund research in 2016 that could advance the field of neuromodulation, according to a lecture given at the 19th Annual Meeting of the North American Neuromodulation Society. These investigations could affect the treatment of epilepsy, headache, Parkinson’s disease, or other neurologic disorders.
The BRAIN Initiative has two main objectives, said Stephanie Fertig, MBA, Director of Small Business Programs at the National Institute of Neurological Disorders and Stroke. The first is to foster the development of new technologies for mapping connections in the brain and discovering patterns of neural activity. The second goal is to use these new technologies, as well as existing technologies, to further neurologists’ understanding of how the neural circuit affects the function of the healthy or diseased brain. The initiative, which President Obama introduced in 2013, is a collaboration between federal agencies, including the National Science Foundation and NIH, private foundations, universities, and industry. Information on the BRAIN Initiative can be found online at www.braininitiative.nih.gov.
Researchers Invited to Apply for Funding
Several of the BRAIN Initiative’s programs are intended to promote the identification, development, and optimization of new technologies and approaches for large-scale recording and modulation in the nervous system. The goal is to foster research that will add to scientific understanding of the dynamic signaling in the nervous system, said Ms. Fertig. One program seeks applications to study new and untested ideas for recording and modulating technology, including ideas in the initial stages of conceptualization. Other programs aim to further proof-of-concept testing for such technology, as well as to enable the optimization of the technology with feedback from the user community.
Another of the initiative’s programs is intended to fund nonclinical and clinical studies that will help advance invasive recording or stimulating devices that could, in turn, treat CNS disorders and improve understanding of the human brain. Researchers will receive support for the implementation of clinical prototype devices, nonclinical safety and efficacy testing, design verification and validation activities, and pursuit of regulatory approval for a small clinical study. The program will consider clinical studies of acute or short-term procedures that entail nonsignificant risk (as determined by an Institutional Review Board), as well as those that entail a significant risk and require an Investigational Device Exemption (IDE) from the FDA. The BRAIN Initiative provides two options for researchers interested in funding for invasive devices, said Ms. Fertig. “One is if you need to do some nonclinical work before you get your IDE and then move into the clinic. That’s the phase translational to clinical research track. Then there’s the direct-to-clinical research program,” which is appropriate for investigators who do not need to perform nonclinical work and are ready for a clinical study.
Public–Private Partnership Program
The BRAIN Initiative also created a Public–Private Partnership Program to facilitate collaboration between clinical investigators and manufacturers of invasive recording or stimulating devices. This program is intended to promote clinical research and foster partnerships between clinical researchers and the developers of “next-generation implantable stimulating–recording devices,” said Ms. Fertig. Data about the safety and utility of such devices can be costly to obtain, but the Public–Private Partnership Program will enable researchers to use existing manufacturers’ safety data. To date, six device manufacturers (ie, Medtronic, Boston Scientific, Blackrock, NeuroPace, NeuroNexus, and Second Sight) have signed a memorandum of understanding with NIH to provide support and information on materials (eg, devices and software). The information will guide investigators who want to pursue specific agreements with manufacturers for the submission of research proposals to NIH. Furthermore, NIH has created templates of collaborative research agreements and confidential disclosure agreements to quicken the legal and administrative process for establishing partnerships between manufacturers and academic research institutions.
Funding Supports Device-Related Research
The BRAIN Initiative already has funded various studies that could lead to new invasive treatments for various neurologic disorders. Leigh R. Hochberg, MD, PhD, Director of the Neurotechnology Trials Unit at Massachusetts General Hospital in Boston, and associates received NIH support for the development of the BrainGate device. Dr. Hochberg created BrainGate, a brain implant system, to allow patients with quadriplegia to control external devices such as prosthetic arms by thought alone. Dr. Hochberg’s BRAIN project is to develop BrainGate into a fully implanted medical treatment system without external components. The goal is to enable patients to use the device independently on an ongoing basis.
In addition, Gregory A. Worrell, MD, PhD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and colleagues received funding to study wireless devices that measure brain activity, predict seizure onset, and deliver therapeutic stimulation to mitigate seizures. Dr. Worrell’s group initially plans to conduct a preclinical study to test one such device in dogs with epilepsy. If the device is successful, the group will perform a pilot clinical trial in patients with epilepsy.
Finally, Nicholas D. Schiff, MD, Jerold B. Katz Professor of Neurology and Neuroscience at Weill Cornell Medical College in New York, and colleagues received support for their efforts to develop device therapy for cognitive impairment associated with traumatic brain injury. They are focusing on a device that delivers deep brain stimulation to the thalamus, which they hypothesize may restore the disrupted circuit function that underlies the cognitive disability.
—Erik Greb
Suggested Reading
Brinkmann BH, Patterson EE, Vite C, et al. Forecasting seizures using intracranial EEG measures and SVM in naturally occurring canine epilepsy. PLoS One. 2015;10(8):e0133900.
Gummadavelli A, Motelow JE, Smith N, et al. Thalamic stimulation to improve level of consciousness after seizures: evaluation of electrophysiology and behavior. Epilepsia. 2015;56(1):114-124.
Hochberg LR, Bacher D, Jarosiewicz B, et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature. 2012;485(7398):372-375.
LAS VEGAS—Through various programs, the BRAIN Initiative seeks to fund research in 2016 that could advance the field of neuromodulation, according to a lecture given at the 19th Annual Meeting of the North American Neuromodulation Society. These investigations could affect the treatment of epilepsy, headache, Parkinson’s disease, or other neurologic disorders.
The BRAIN Initiative has two main objectives, said Stephanie Fertig, MBA, Director of Small Business Programs at the National Institute of Neurological Disorders and Stroke. The first is to foster the development of new technologies for mapping connections in the brain and discovering patterns of neural activity. The second goal is to use these new technologies, as well as existing technologies, to further neurologists’ understanding of how the neural circuit affects the function of the healthy or diseased brain. The initiative, which President Obama introduced in 2013, is a collaboration between federal agencies, including the National Science Foundation and NIH, private foundations, universities, and industry. Information on the BRAIN Initiative can be found online at www.braininitiative.nih.gov.
Researchers Invited to Apply for Funding
Several of the BRAIN Initiative’s programs are intended to promote the identification, development, and optimization of new technologies and approaches for large-scale recording and modulation in the nervous system. The goal is to foster research that will add to scientific understanding of the dynamic signaling in the nervous system, said Ms. Fertig. One program seeks applications to study new and untested ideas for recording and modulating technology, including ideas in the initial stages of conceptualization. Other programs aim to further proof-of-concept testing for such technology, as well as to enable the optimization of the technology with feedback from the user community.
Another of the initiative’s programs is intended to fund nonclinical and clinical studies that will help advance invasive recording or stimulating devices that could, in turn, treat CNS disorders and improve understanding of the human brain. Researchers will receive support for the implementation of clinical prototype devices, nonclinical safety and efficacy testing, design verification and validation activities, and pursuit of regulatory approval for a small clinical study. The program will consider clinical studies of acute or short-term procedures that entail nonsignificant risk (as determined by an Institutional Review Board), as well as those that entail a significant risk and require an Investigational Device Exemption (IDE) from the FDA. The BRAIN Initiative provides two options for researchers interested in funding for invasive devices, said Ms. Fertig. “One is if you need to do some nonclinical work before you get your IDE and then move into the clinic. That’s the phase translational to clinical research track. Then there’s the direct-to-clinical research program,” which is appropriate for investigators who do not need to perform nonclinical work and are ready for a clinical study.
Public–Private Partnership Program
The BRAIN Initiative also created a Public–Private Partnership Program to facilitate collaboration between clinical investigators and manufacturers of invasive recording or stimulating devices. This program is intended to promote clinical research and foster partnerships between clinical researchers and the developers of “next-generation implantable stimulating–recording devices,” said Ms. Fertig. Data about the safety and utility of such devices can be costly to obtain, but the Public–Private Partnership Program will enable researchers to use existing manufacturers’ safety data. To date, six device manufacturers (ie, Medtronic, Boston Scientific, Blackrock, NeuroPace, NeuroNexus, and Second Sight) have signed a memorandum of understanding with NIH to provide support and information on materials (eg, devices and software). The information will guide investigators who want to pursue specific agreements with manufacturers for the submission of research proposals to NIH. Furthermore, NIH has created templates of collaborative research agreements and confidential disclosure agreements to quicken the legal and administrative process for establishing partnerships between manufacturers and academic research institutions.
Funding Supports Device-Related Research
The BRAIN Initiative already has funded various studies that could lead to new invasive treatments for various neurologic disorders. Leigh R. Hochberg, MD, PhD, Director of the Neurotechnology Trials Unit at Massachusetts General Hospital in Boston, and associates received NIH support for the development of the BrainGate device. Dr. Hochberg created BrainGate, a brain implant system, to allow patients with quadriplegia to control external devices such as prosthetic arms by thought alone. Dr. Hochberg’s BRAIN project is to develop BrainGate into a fully implanted medical treatment system without external components. The goal is to enable patients to use the device independently on an ongoing basis.
In addition, Gregory A. Worrell, MD, PhD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and colleagues received funding to study wireless devices that measure brain activity, predict seizure onset, and deliver therapeutic stimulation to mitigate seizures. Dr. Worrell’s group initially plans to conduct a preclinical study to test one such device in dogs with epilepsy. If the device is successful, the group will perform a pilot clinical trial in patients with epilepsy.
Finally, Nicholas D. Schiff, MD, Jerold B. Katz Professor of Neurology and Neuroscience at Weill Cornell Medical College in New York, and colleagues received support for their efforts to develop device therapy for cognitive impairment associated with traumatic brain injury. They are focusing on a device that delivers deep brain stimulation to the thalamus, which they hypothesize may restore the disrupted circuit function that underlies the cognitive disability.
—Erik Greb
LAS VEGAS—Through various programs, the BRAIN Initiative seeks to fund research in 2016 that could advance the field of neuromodulation, according to a lecture given at the 19th Annual Meeting of the North American Neuromodulation Society. These investigations could affect the treatment of epilepsy, headache, Parkinson’s disease, or other neurologic disorders.
The BRAIN Initiative has two main objectives, said Stephanie Fertig, MBA, Director of Small Business Programs at the National Institute of Neurological Disorders and Stroke. The first is to foster the development of new technologies for mapping connections in the brain and discovering patterns of neural activity. The second goal is to use these new technologies, as well as existing technologies, to further neurologists’ understanding of how the neural circuit affects the function of the healthy or diseased brain. The initiative, which President Obama introduced in 2013, is a collaboration between federal agencies, including the National Science Foundation and NIH, private foundations, universities, and industry. Information on the BRAIN Initiative can be found online at www.braininitiative.nih.gov.
Researchers Invited to Apply for Funding
Several of the BRAIN Initiative’s programs are intended to promote the identification, development, and optimization of new technologies and approaches for large-scale recording and modulation in the nervous system. The goal is to foster research that will add to scientific understanding of the dynamic signaling in the nervous system, said Ms. Fertig. One program seeks applications to study new and untested ideas for recording and modulating technology, including ideas in the initial stages of conceptualization. Other programs aim to further proof-of-concept testing for such technology, as well as to enable the optimization of the technology with feedback from the user community.
Another of the initiative’s programs is intended to fund nonclinical and clinical studies that will help advance invasive recording or stimulating devices that could, in turn, treat CNS disorders and improve understanding of the human brain. Researchers will receive support for the implementation of clinical prototype devices, nonclinical safety and efficacy testing, design verification and validation activities, and pursuit of regulatory approval for a small clinical study. The program will consider clinical studies of acute or short-term procedures that entail nonsignificant risk (as determined by an Institutional Review Board), as well as those that entail a significant risk and require an Investigational Device Exemption (IDE) from the FDA. The BRAIN Initiative provides two options for researchers interested in funding for invasive devices, said Ms. Fertig. “One is if you need to do some nonclinical work before you get your IDE and then move into the clinic. That’s the phase translational to clinical research track. Then there’s the direct-to-clinical research program,” which is appropriate for investigators who do not need to perform nonclinical work and are ready for a clinical study.
Public–Private Partnership Program
The BRAIN Initiative also created a Public–Private Partnership Program to facilitate collaboration between clinical investigators and manufacturers of invasive recording or stimulating devices. This program is intended to promote clinical research and foster partnerships between clinical researchers and the developers of “next-generation implantable stimulating–recording devices,” said Ms. Fertig. Data about the safety and utility of such devices can be costly to obtain, but the Public–Private Partnership Program will enable researchers to use existing manufacturers’ safety data. To date, six device manufacturers (ie, Medtronic, Boston Scientific, Blackrock, NeuroPace, NeuroNexus, and Second Sight) have signed a memorandum of understanding with NIH to provide support and information on materials (eg, devices and software). The information will guide investigators who want to pursue specific agreements with manufacturers for the submission of research proposals to NIH. Furthermore, NIH has created templates of collaborative research agreements and confidential disclosure agreements to quicken the legal and administrative process for establishing partnerships between manufacturers and academic research institutions.
Funding Supports Device-Related Research
The BRAIN Initiative already has funded various studies that could lead to new invasive treatments for various neurologic disorders. Leigh R. Hochberg, MD, PhD, Director of the Neurotechnology Trials Unit at Massachusetts General Hospital in Boston, and associates received NIH support for the development of the BrainGate device. Dr. Hochberg created BrainGate, a brain implant system, to allow patients with quadriplegia to control external devices such as prosthetic arms by thought alone. Dr. Hochberg’s BRAIN project is to develop BrainGate into a fully implanted medical treatment system without external components. The goal is to enable patients to use the device independently on an ongoing basis.
In addition, Gregory A. Worrell, MD, PhD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and colleagues received funding to study wireless devices that measure brain activity, predict seizure onset, and deliver therapeutic stimulation to mitigate seizures. Dr. Worrell’s group initially plans to conduct a preclinical study to test one such device in dogs with epilepsy. If the device is successful, the group will perform a pilot clinical trial in patients with epilepsy.
Finally, Nicholas D. Schiff, MD, Jerold B. Katz Professor of Neurology and Neuroscience at Weill Cornell Medical College in New York, and colleagues received support for their efforts to develop device therapy for cognitive impairment associated with traumatic brain injury. They are focusing on a device that delivers deep brain stimulation to the thalamus, which they hypothesize may restore the disrupted circuit function that underlies the cognitive disability.
—Erik Greb
Suggested Reading
Brinkmann BH, Patterson EE, Vite C, et al. Forecasting seizures using intracranial EEG measures and SVM in naturally occurring canine epilepsy. PLoS One. 2015;10(8):e0133900.
Gummadavelli A, Motelow JE, Smith N, et al. Thalamic stimulation to improve level of consciousness after seizures: evaluation of electrophysiology and behavior. Epilepsia. 2015;56(1):114-124.
Hochberg LR, Bacher D, Jarosiewicz B, et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature. 2012;485(7398):372-375.
Suggested Reading
Brinkmann BH, Patterson EE, Vite C, et al. Forecasting seizures using intracranial EEG measures and SVM in naturally occurring canine epilepsy. PLoS One. 2015;10(8):e0133900.
Gummadavelli A, Motelow JE, Smith N, et al. Thalamic stimulation to improve level of consciousness after seizures: evaluation of electrophysiology and behavior. Epilepsia. 2015;56(1):114-124.
Hochberg LR, Bacher D, Jarosiewicz B, et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature. 2012;485(7398):372-375.
Bert Vargas, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Bert B. Vargas, MD

Limiting Full-Contact Practice Reduces Football Concussions
WASHINGTON, DC—Limiting the amount of full-contact tackling that occurs in high school football practice reduces the rate of sports-related concussions among the athletes, according to a prospective study.
“Something as simple as saying they can’t tackle all the time, limiting the amount of minutes each month, reduced the incidence,” said Timothy A. McGuine, PhD, Senior Scientist at the University of Wisconsin, Madison, at the American Academy of Pediatrics Annual Meeting.
“The majority of sports-related concussions sustained in high school football practice occurred during full-contact activities,” he said. “The rate of sports-related concussions sustained in high school football practice was more than twice as high in the two seasons prior to a rule change limiting the amount and duration of full-contact activities.”
Testing a Tackle-Limiting Rule
In their study, Dr. McGuine and his associates tested the effects of a tackle-limiting rule implemented in 2014 in a state interscholastic athletic association for all players in grades 9 through 12. The rule prohibited full-contact play during the first practice week, and full contact was defined as “drills or game situations that occur at game speed when full tackles are made at a competitive pace and players are taken to the ground.” The players engaged in full-contact play for as long as 75 minutes total during the second week of practice and for a maximum of 60 min/week for all subsequent weeks in the practice season. The rule did not apply to games.
For data on the two years before the rule change, 2,081 athletes with a mean age of 16 reported their concussion history in the 2012 season, which included 36 schools, and the 2013 season, which included 18 schools. In 2014, licensed athletic trainers recorded the incidence and severity of each sports-related concussion for the 945 players at 26 schools. During all three seasons, almost half the concussions (46%) occurred during tackling. Although the overall rate of concussions dropped from 1.57 per 1,000 athletic exposures in the combined 2012 and 2013 seasons to 1.28 per 1,000 athletic exposures in the 2014 season, the difference was not significant. During the 2012 and 2013 seasons combined, 206 players (9%) sustained 211 concussions, compared with 67 players (7%) with 70 concussions in 2014.
The difference in concussions occurring during practice, however, did differ significantly before and after the rule change. The rate of concussions during practice in 2014 was 0.33 concussions per 1,000 athletic exposures, compared with 0.76 concussions per 1,000 exposures in the 2012 and 2013 seasons. Twelve of 15 concussions in 2014 practices occurred during full-contact practices, a rate of 0.57 per 1,000 exposures, and 82 of 86 concussions in the 2012 and 2013 seasons occurred during full contact practices, a rate of 0.87 per 1,000 exposures.
The investigators observed no difference in concussion rate during the games following the rule change. The 2014 rate of concussions during games was 5.74 per 1,000 exposures, compared with 5.81 per 1,000 exposures in the combined 2012 and 2013 seasons. The severity of concussions sustained before and after the rule change also did not differ, and athletes’ years of football-playing experience had no effect on the concussion incidence in 2014.
To Tackle or Not to Tackle?
Despite the relationship between full-contact play and concussions, Dr. McGuine said that he would not support banning tackling from football.
“I think the benefits of the sport far outweigh the risks,” Dr. McGuine said. “Concussions particularly have transcended a sports issue and become a public health issue and have become political, and I’m very much against legislators, policy makers, [and] associations making blanket rules without the evidence to back those,” he said. “There are lingering long-term effects from all orthopedic injuries, but we’re focusing on concussions.”
Equipment modification is unlikely to make much difference in concussion rates either, said Dr. McGuine, whose previous study on football helmets found that the brand and model did not influence concussion risk. “Concussions are multifactorial,” he said. “We can’t just limit the amount of force transmitted to the brain and say we’re going to stop these injuries from occurring.”
One important strategy for reducing concussions is increasing parents’ and athletes’ awareness about multiple injuries and about ways to reduce the risk, Dr. McGuine said.
“Concussions are like any other injury [such as] ankle sprains, knee injuries and surgeries, [and] shoulder dislocations,” he said. “If you have one, you’re more susceptible to having another one, as opposed to somebody who never had that injury, so the problems are repeat injuries and lingering injuries.” Any of these injuries can have a lasting effect on a young athlete’s quality of life, Dr. McGuine added.
Another way to decrease the incidence of concussions is to enforce rules against leading, or lowering, athletes’ heads during tackling.
“A big issue now is penalizing players for leading with their head and face, but I think we need to be consistent there, too,” Dr. McGuine said. “We can’t penalize defensive players for lowering their helmet if we’re not going to penalize running backs and wide receivers.”
—Tara Haelle
WASHINGTON, DC—Limiting the amount of full-contact tackling that occurs in high school football practice reduces the rate of sports-related concussions among the athletes, according to a prospective study.
“Something as simple as saying they can’t tackle all the time, limiting the amount of minutes each month, reduced the incidence,” said Timothy A. McGuine, PhD, Senior Scientist at the University of Wisconsin, Madison, at the American Academy of Pediatrics Annual Meeting.
“The majority of sports-related concussions sustained in high school football practice occurred during full-contact activities,” he said. “The rate of sports-related concussions sustained in high school football practice was more than twice as high in the two seasons prior to a rule change limiting the amount and duration of full-contact activities.”
Testing a Tackle-Limiting Rule
In their study, Dr. McGuine and his associates tested the effects of a tackle-limiting rule implemented in 2014 in a state interscholastic athletic association for all players in grades 9 through 12. The rule prohibited full-contact play during the first practice week, and full contact was defined as “drills or game situations that occur at game speed when full tackles are made at a competitive pace and players are taken to the ground.” The players engaged in full-contact play for as long as 75 minutes total during the second week of practice and for a maximum of 60 min/week for all subsequent weeks in the practice season. The rule did not apply to games.
For data on the two years before the rule change, 2,081 athletes with a mean age of 16 reported their concussion history in the 2012 season, which included 36 schools, and the 2013 season, which included 18 schools. In 2014, licensed athletic trainers recorded the incidence and severity of each sports-related concussion for the 945 players at 26 schools. During all three seasons, almost half the concussions (46%) occurred during tackling. Although the overall rate of concussions dropped from 1.57 per 1,000 athletic exposures in the combined 2012 and 2013 seasons to 1.28 per 1,000 athletic exposures in the 2014 season, the difference was not significant. During the 2012 and 2013 seasons combined, 206 players (9%) sustained 211 concussions, compared with 67 players (7%) with 70 concussions in 2014.
The difference in concussions occurring during practice, however, did differ significantly before and after the rule change. The rate of concussions during practice in 2014 was 0.33 concussions per 1,000 athletic exposures, compared with 0.76 concussions per 1,000 exposures in the 2012 and 2013 seasons. Twelve of 15 concussions in 2014 practices occurred during full-contact practices, a rate of 0.57 per 1,000 exposures, and 82 of 86 concussions in the 2012 and 2013 seasons occurred during full contact practices, a rate of 0.87 per 1,000 exposures.
The investigators observed no difference in concussion rate during the games following the rule change. The 2014 rate of concussions during games was 5.74 per 1,000 exposures, compared with 5.81 per 1,000 exposures in the combined 2012 and 2013 seasons. The severity of concussions sustained before and after the rule change also did not differ, and athletes’ years of football-playing experience had no effect on the concussion incidence in 2014.
To Tackle or Not to Tackle?
Despite the relationship between full-contact play and concussions, Dr. McGuine said that he would not support banning tackling from football.
“I think the benefits of the sport far outweigh the risks,” Dr. McGuine said. “Concussions particularly have transcended a sports issue and become a public health issue and have become political, and I’m very much against legislators, policy makers, [and] associations making blanket rules without the evidence to back those,” he said. “There are lingering long-term effects from all orthopedic injuries, but we’re focusing on concussions.”
Equipment modification is unlikely to make much difference in concussion rates either, said Dr. McGuine, whose previous study on football helmets found that the brand and model did not influence concussion risk. “Concussions are multifactorial,” he said. “We can’t just limit the amount of force transmitted to the brain and say we’re going to stop these injuries from occurring.”
One important strategy for reducing concussions is increasing parents’ and athletes’ awareness about multiple injuries and about ways to reduce the risk, Dr. McGuine said.
“Concussions are like any other injury [such as] ankle sprains, knee injuries and surgeries, [and] shoulder dislocations,” he said. “If you have one, you’re more susceptible to having another one, as opposed to somebody who never had that injury, so the problems are repeat injuries and lingering injuries.” Any of these injuries can have a lasting effect on a young athlete’s quality of life, Dr. McGuine added.
Another way to decrease the incidence of concussions is to enforce rules against leading, or lowering, athletes’ heads during tackling.
“A big issue now is penalizing players for leading with their head and face, but I think we need to be consistent there, too,” Dr. McGuine said. “We can’t penalize defensive players for lowering their helmet if we’re not going to penalize running backs and wide receivers.”
—Tara Haelle
WASHINGTON, DC—Limiting the amount of full-contact tackling that occurs in high school football practice reduces the rate of sports-related concussions among the athletes, according to a prospective study.
“Something as simple as saying they can’t tackle all the time, limiting the amount of minutes each month, reduced the incidence,” said Timothy A. McGuine, PhD, Senior Scientist at the University of Wisconsin, Madison, at the American Academy of Pediatrics Annual Meeting.
“The majority of sports-related concussions sustained in high school football practice occurred during full-contact activities,” he said. “The rate of sports-related concussions sustained in high school football practice was more than twice as high in the two seasons prior to a rule change limiting the amount and duration of full-contact activities.”
Testing a Tackle-Limiting Rule
In their study, Dr. McGuine and his associates tested the effects of a tackle-limiting rule implemented in 2014 in a state interscholastic athletic association for all players in grades 9 through 12. The rule prohibited full-contact play during the first practice week, and full contact was defined as “drills or game situations that occur at game speed when full tackles are made at a competitive pace and players are taken to the ground.” The players engaged in full-contact play for as long as 75 minutes total during the second week of practice and for a maximum of 60 min/week for all subsequent weeks in the practice season. The rule did not apply to games.
For data on the two years before the rule change, 2,081 athletes with a mean age of 16 reported their concussion history in the 2012 season, which included 36 schools, and the 2013 season, which included 18 schools. In 2014, licensed athletic trainers recorded the incidence and severity of each sports-related concussion for the 945 players at 26 schools. During all three seasons, almost half the concussions (46%) occurred during tackling. Although the overall rate of concussions dropped from 1.57 per 1,000 athletic exposures in the combined 2012 and 2013 seasons to 1.28 per 1,000 athletic exposures in the 2014 season, the difference was not significant. During the 2012 and 2013 seasons combined, 206 players (9%) sustained 211 concussions, compared with 67 players (7%) with 70 concussions in 2014.
The difference in concussions occurring during practice, however, did differ significantly before and after the rule change. The rate of concussions during practice in 2014 was 0.33 concussions per 1,000 athletic exposures, compared with 0.76 concussions per 1,000 exposures in the 2012 and 2013 seasons. Twelve of 15 concussions in 2014 practices occurred during full-contact practices, a rate of 0.57 per 1,000 exposures, and 82 of 86 concussions in the 2012 and 2013 seasons occurred during full contact practices, a rate of 0.87 per 1,000 exposures.
The investigators observed no difference in concussion rate during the games following the rule change. The 2014 rate of concussions during games was 5.74 per 1,000 exposures, compared with 5.81 per 1,000 exposures in the combined 2012 and 2013 seasons. The severity of concussions sustained before and after the rule change also did not differ, and athletes’ years of football-playing experience had no effect on the concussion incidence in 2014.
To Tackle or Not to Tackle?
Despite the relationship between full-contact play and concussions, Dr. McGuine said that he would not support banning tackling from football.
“I think the benefits of the sport far outweigh the risks,” Dr. McGuine said. “Concussions particularly have transcended a sports issue and become a public health issue and have become political, and I’m very much against legislators, policy makers, [and] associations making blanket rules without the evidence to back those,” he said. “There are lingering long-term effects from all orthopedic injuries, but we’re focusing on concussions.”
Equipment modification is unlikely to make much difference in concussion rates either, said Dr. McGuine, whose previous study on football helmets found that the brand and model did not influence concussion risk. “Concussions are multifactorial,” he said. “We can’t just limit the amount of force transmitted to the brain and say we’re going to stop these injuries from occurring.”
One important strategy for reducing concussions is increasing parents’ and athletes’ awareness about multiple injuries and about ways to reduce the risk, Dr. McGuine said.
“Concussions are like any other injury [such as] ankle sprains, knee injuries and surgeries, [and] shoulder dislocations,” he said. “If you have one, you’re more susceptible to having another one, as opposed to somebody who never had that injury, so the problems are repeat injuries and lingering injuries.” Any of these injuries can have a lasting effect on a young athlete’s quality of life, Dr. McGuine added.
Another way to decrease the incidence of concussions is to enforce rules against leading, or lowering, athletes’ heads during tackling.
“A big issue now is penalizing players for leading with their head and face, but I think we need to be consistent there, too,” Dr. McGuine said. “We can’t penalize defensive players for lowering their helmet if we’re not going to penalize running backs and wide receivers.”
—Tara Haelle
Idiopathic Intracranial Hypertension in Pregnancy
A 27-year-old white woman presented to the clinic with headaches and decreased vision through her reading glasses while performing near tasks. Her medical history was significant for herpes simplex, hyperlipidemia, and migraine headaches with aura. Her migraines began following an earlier motor vehicle accident, and her most recent magnetic resonance imaging (MRI) showed no abnormalities. Her current medications included prophylactic acyclovir for herpes and acetaminophen and caffeine tablets as needed for headache. She reported no other trauma or surgery and no known allergies. The patient’s best-corrected Snellen visual acuities in both eyes were 20/20 (distance) and 20/30 (near).
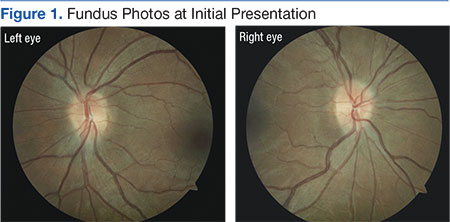
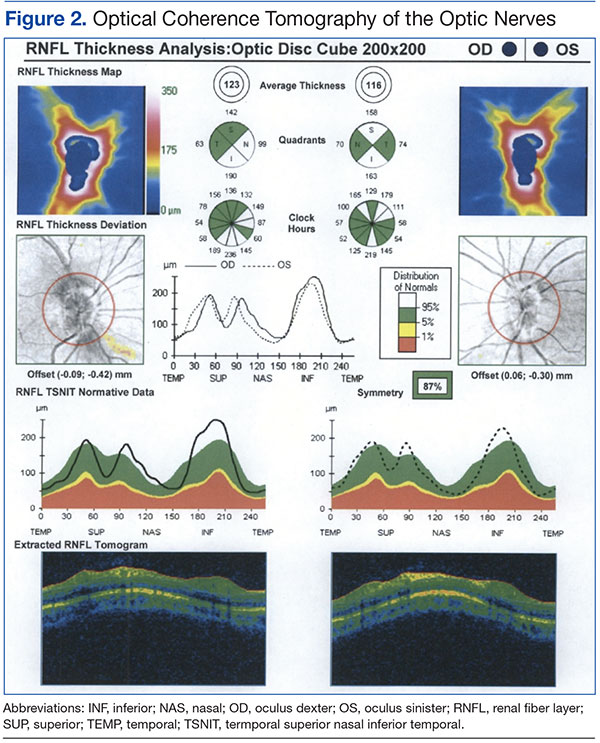
Preliminary testing, including pupils, extraocular motilities, confrontation fields, and color vision, were all within normal limits. Her slit-lamp examination was unremarkable. A dilated fundus examination revealed crowded, elevated discs without vessel obscuration, hemorrhage, hyperemia, or drusen (Figure 1). The fundus examination was otherwise unremarkable. Optical coherence tomography of the optic nerves showed increased nerve fiber layer thickness in both eyes (Figure 2). Her blood pressure (BP) at this visit was 106/77 mm/Hg.
The diagnosis based on these findings was bilateral optic nerve elevation with long-standing migraine headaches. The plan was for the patient to return to the clinic for repeat visual field testing and B-scan ultrasonography to rule out buried optic nerve head drusen.
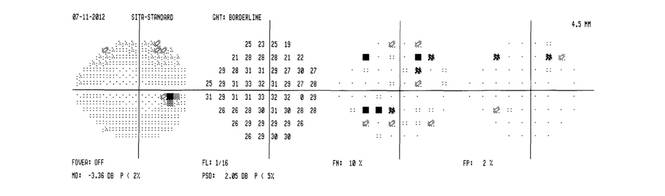
Two months later, the patient presented to the clinic 19 weeks pregnant and reported that her headaches had increased in frequency, but she had no diplopia. All preliminary testing, including visual acuities, pupil reaction, color vision, and slit-lamp examination remained normal. Fundus examination showed the patient’s nerves were unchanged in appearance from the initial presentation. Visual fields revealed an enlarged blind spot in the right eye and paracentral defects in the left eye. The B-scan testing was negative for optic nerve drusen. Due to the increased frequency of headaches, pregnancy, and suspicious optic nerves, an urgent consult was placed to neurology.
At the neurology appointment 1 month later, the patient was diagnosed with migraine headache syndrome and idiopathic intracranial hypertension (IIH). The neurologist believed her headaches might have been resulting from analgesic rebound. He suggested that the patient discontinue or decrease use of oral butalbital, acetaminophen and caffeine tablets, and other forms of caffeine. It was decided that divalproxen sodium and verapamil were not feasible due to pregnancy. The neurologist started her on oral acetazolamide 500 mg twice daily.
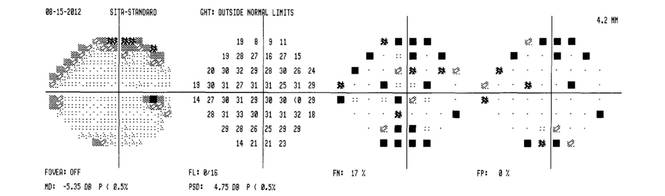
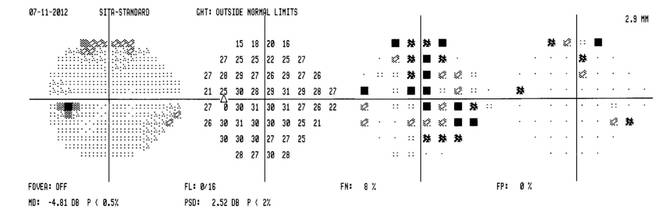
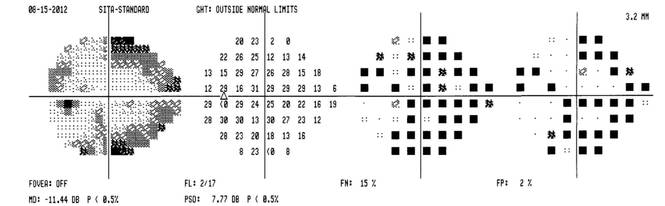
The patient returned to her obstetrician 1 month later for a routine follow-up; the headaches had worsened and were now accompanied by nausea and vomiting twice daily on average. Her medications still included acetaminophen and caffeine tablets, although it had been recommended she discontinue them, prochlorperazine, and acetazolamide. Due to the worsening of her symptoms and visual fields (eFigure 1), the obstetrician recommended that the patient deliver by cesarean section at 38 to 39 weeks.
(eFigure 1.Visual Fields at Follow-up 1 and 2)
Right eye
Left Eye
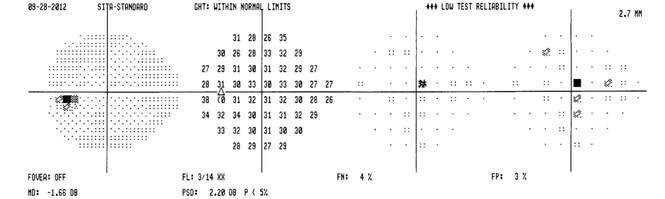
Following an uncomplicated cesarean delivery at 38 weeks, the patient returned to the clinic for visual field testing. Humphrey visual fields were full in the right eye and showed some scattered central depressions in the left. Both eyes were significantly improved from previous fields (eFigure 2) . The patient had discontinued acetazolamide and reported minor tension headaches she believed were due to lack of sleep but stated that she was no longer having migraines. There was no papilledema noted on fundus examination, and Snellen distance visual acuity measured 20/20 in both eyes. An MRI had been performed after delivery and was negative for intracranial hemorrhage, mass, or hydrocephalus).
(eFigure 2. Visual Fields Postpartum)
Right eye
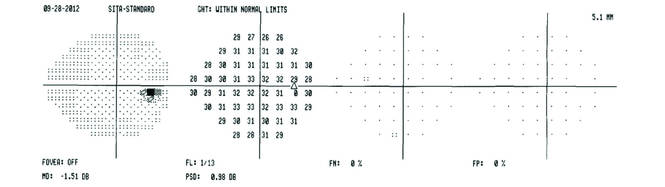
Left eye
Three months later, the patient returned for her yearly comprehensive examination. At that visit, she reported a decrease in frequency of the migraine headaches. Optical coherence tomography was performed and showed a significant decrease in optic nerve head swelling.
Related: Diabetes on the Rise Among Other Pregnancy Problems
Clinical Picture
Idiopathic intracranial hypertension presents clinically with signs and symptoms of increased intracranial pressure (ICP). Headache is the most common symptom, usually presenting as daily and pulsatile.1 Nausea may be associated with the headache, although vomiting is rare, and the headache may awaken the patient. The headache may remain after resolution of elevated ICP (Table).2
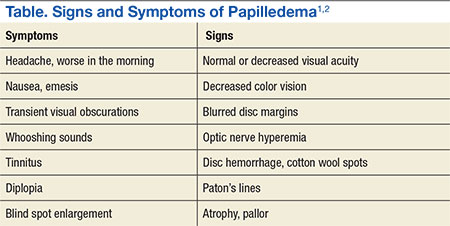
Papilledema is the most common sign of IIH.1,2 Visual loss associated with papilledema is generally mild at first but progressive. Transient blur lasts usually 30 seconds and may be monocular or binocular.1 The cause is thought to be related to transient ischemia of the optic nerve.1 Vision loss is typically reversible with resolution of optic nerve swelling, but 25% of patients may develop optic atrophy, which results in permanent vision loss.2 Common patterns of visual abnormalities include enlargement of the physiologic blind spot, inferonasal and arcuate defects, and eventually severe peripheral constriction.1,2 It is imperative that all patients with IIH have visual field testing performed.
About one-third of patients with IIH experience diplopia. This binocular, horizontal diplopia is caused by a sixth nerve palsy in 10% to 20% of patients.1 Cranial nerves II, VI, and VII make a 90-degree bend and seem to be prone to damage at the site of the bend.1
Pulse-synchronous tinnitus is common in IIH as well.2,3 This generally occurs unilaterally and may be eliminated by jugular compression or the head turning to the ipsilateral side.1,3 The sound is caused by the transmission of an increase in the vascular pulse due to high pressure on the cerebrospinal fluid (CSF).1,3
Idiopathic intracranial hypertension most typically presents in obese women of childbearing age.1-3 An increasing degree of obesity is generally associated with an increased risk of vision loss.1,2 Men seem to have worse acuity and visual fields at presentation than do women.2 Men are less likely to report headaches than are women and, therefore, have double the likelihood of severe vision loss.2 Hence, closer monitoring and more aggressive intervention is recommended for men due to their lesser tendency for headaches.2 Black patients also demonstrate more aggressive disease and, therefore, require closer monitoring and early aggressive intervention.1,2
Papilledema is the most common sign of IIH and may be caused by several processes. In this case, most were ruled out given the patient’s normal visual acuities, pupillary reaction, color vision testing, BP measurement, and B-scan imaging. The patient’s systemic history was negative for thyroid-related disease, diabetes, hypertension, autoimmune disease, or infection. She had no family history of vision loss or hereditary ocular conditions. The most recent MRI was negative for any long-standing space-occupying lesion or hydrocephalus.
Pathophysiology
Several mechanisms leading to increased ICP have been proposed. These include increased brain water content, excess CSF production, reduced CSF absorption, and increased cerebral venous pressure.2,3 There is also a suspicion of the role of sex hormones in IIH due to its high predilection for females.2
The role of vitamin A metabolism has also been studied in IIH.1 Retinol levels are elevated in the CSF of patients with IIH. Patients may ingest an abnormally large amount of vitamin A, metabolize it abnormally, or be sensitive to its effects.2,4 The function of adipose tissue as an actively secreting endocrine tissue may play a role in IIH due to its release of adipose tissue-derived retinol binding protein.2 Other adipose-produced cytokines include leptin, which has been implicated in IIH due to its elevated levels found in the CSF of patients with IIH.2
Stenosis of the cerebral sinuses is another proposed mechanism of IIH.1-3 Cerebrospinal fluid exits the cranium into the venous sinuses via the arachnoid villi.2 An obstruction in these sinuses may impair CSF outflow and result in intracranial hypertension. Microthrombosis caused by hypercoaguable disorders may result in increased cerebral venous pressure and impaired CSF absorption as well.2,4
Some medications have been found in association with IIH. These include tetracycline, cyclosporine, lithium, nalidixic acid, nitrofurantoin, oral contraceptives, levonorgestrel, danaxol, and tamoxifen.1-4 Tetracycline seems to have the strongest association with IIH and should be discontinued in those patients where the association is very likely to be the causative factor.2 The link to oral contraceptives may occur simply due to their association with young women most at risk for IIH.1-3
Related:Young Man With Headache, Confusion, and Hearing Loss
Management
The goals of treatment with IIH are to preserve vision and relieve symptoms, particularly headache. The general recommendation is that pregnant women with IIH should be managed and treated the same as any other patient with IIH. However, imaging and some drug contraindications exist between these 2 groups.
The diagnostic test for IIH is a lumbar puncture, which is also the most effective treatment.1-3,5 Lumbar puncture should be performed in the relaxed lateral decubitus position without sedation.1-3 The opening pressure should be measured and is the most clinically significant diagnostic tool for diagnosis of IIH. Opening pressures of > 250 mm H2O are diagnostic of IIH.1-3,5
Weight loss is an essential part of treatment in obese patients with IIH.1-3 A low-calorie, low-salt diet with mild fluid restriction seems to reverse the symptoms of IIH. A 5% to 10% reduction in body weight may reduce symptoms and signs of IIH.2
Carbonic anhydrase inhibitors (CAIs), such as acetalzolamide, have a multifactorial role in IIH.4 They are usually prescribed in 1 to 2 grams over several doses and function by decreasing CSF production.1 Carbonic anhydrase inhibitors also are known to change the taste of foods and may, therefore, aid in weight loss.1,2 Patients prescribed CAIs commonly experience a tingling in their fingers, toes, and perioral region, an indication that the medication is working.1,2 A rare but serious adverse effect (AE) is aplastic anemia, which generally occurs in the first 6 months of treatment in elderly patients.1 The use of CAIs in pregnancy is controversial, and although rare complications are reported, it is considered a class C drug.5
In patients with rapidly progressive vision loss but with minimal headache, optic nerve sheath fenestration (ONSF) is the surgical treatment of choice.2,3,6 In this procedure, a window or series of slits are created behind the globe in the optic nerve sheath.1 About 50% of patients achieve adequate headache control with ONSF, especially for frontal headaches.1,2
For patients with vision loss, papilledema, and headache that do not respond to medical therapy, a CSF diversion procedure is the preferred treatment. Cerebrospinal fluid diversion with ventriculoperitoneal or lumboperitoneal shunts may prevent progressive loss of vision.1,4,6 However, variable response rates and shunt failure requiring subsequent revisions are common and may occur in as many as half of patients undergoing these procedures.1
Increased intracranial venous pressure due to stenosis of the venous sinuses has been thought to be a possible cause of IIH. Stenting of the transverse venous sinus stenosis has been shown to reduce cerebral venous pressure, reduce ICP, and improve symptoms in patients with IIH.1-3 It is unclear whether elevations in ICP cause transverse sinus stenosis or whether transverse sinus stenosis causes increased ICP.2 Regardless, stents have a high rate of complications, including subdural hemorrhage, venous sinus perforation, in-stent thrombosis, and recurrent stenosis proximal to the stent.2
Steroids have been used to treat IIH in the past, although their mechanism of action remains unclear.2 There may be recurrence of papilledema if they are tapered too quickly. Due to their association with long-term AEs, including weight gain, they should be avoided.2
Management in Pregnancy
Several studies agree that vision loss occurs in the same frequency in pregnant and nonpregnant patients with IIH.4,7 Idiopathic intracranial hypertension can occur in any trimester in pregnancy. It has been found that patients have the same spontaneous abortion rate and visual outcomes as the general population.6-8 It has also been concluded that treatment should be the same in both patient populations with slight variability in the use of acetazolamide.4,6,7
The use of dilating drops during pregnancy is controversial. Although there have been no teratogenic effects reported with use of topical anesthetics and dilating drops, all drugs should be avoided during the first trimester.7-10 Guidelines have been established by the American Congress of Obstetricians and Gynecologists for X-ray examination and exposure during pregnancy. It has been determined that exposure from a single diagnostic X-ray procedure does not result in harmful fetal effects.11 Magnetic resonance imaging is not associated with any known adverse fetal effects and is a better imaging option during pregnancy, because it is not associated with the use of ionizing radiation.11
The use of CAIs in the first trimester is controversial.4,7 Some believe it should be avoided because it is a Pregnancy Category C drug. However, a single case of sacrococcygeal teratoma has been reported in humans; therefore, some believe this is not a strong basis for withholding the medication in patients with the potential risk for severe vision loss.4,7 In this case, a consult to the patient’s obstetrician was made, and the use of acetazolamide had no effect on the health of the baby.
In pregnant women with IIH with progressive vision loss, failed treatment, or nonadherence, surgery may be necessary. Optic nerve sheath fenestration is preferred due to lower morbidity and mortality compared with shunting procedures.1,2,4,6 The growing fetus may be affected by the peritoneal end of the shunt.4
Related: 49-Year-Old Woman With a Broken Heart
Conclusions
Vision loss associated with IIH can be severe and permanent if left untreated. The best treatments and often the most effective involve weight loss and lumbar puncture. Acetazolamide has been a proven effective treatment in some patients, but some debate exists over the safety of its use during pregnancy. This patient did not have any AEs from its use; however, it did not prove valuable in her treatment. Studies often disagree on the use of acetazolamide in pregnancy; however, all agree that proper patient counseling on potential AEs and management by an obstetrician are important. With proper management, pregnant women with IIH have had outcomes similar to those of the general population.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010;28(3):593-617.
2. Bruce BB, Biousee V, Newman NJ. Update on idiopathic intracranial hypertension. Am J Ophthalmol. 2011;152(2):163-169.
3. Fields JD, Javendani PP, Falardeau J, et al. Dural venous sinus angioplasty and stenting for the treatment of idiopathic intracranial hypertension. J Neurointerv Surg. 2013;5(1):62-68.
4. Evans RW, Lee AG. Idiopathic intracranial hypertension in pregnancy. Headache. 2010;50(9):1513-1515.
5. Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002;59(10):1492-1495.
6. Martínez-Varea A, Diago-Almela VJ, Abad-Carrascosa A, Perales-Marín A. Progressive visual loss in a pregnant woman with idiopathic intracranial hypertension. Eur J Obstet Gynecol Reprod Biol. 2012;163(1):117-122.
7. Falardeau J, Lobb B, Golden S, Maxfield SD, Tanne E. The use of acetazolamide during pregnancy in intracranial hypertension patients. J Neuroophthalmol. 2013;33(1):9-12.
8. Dinn RB, Harris A, Marcus PS. Ocular changes in pregnancy. Obstet Gynecol Surg. 2003;58(2):137-144.
9. Shultz KL, Birnbaum AD, Goldstein DA. Ocular disease in pregnancy. Curr Opin Ophthalmol. 2005;16(5):308-314.
10. Chung CY, Kwok AKH, Chung KL. Use of ophthalmic medications during pregnancy. Hong Kong Med J. 2004;10(3):191-195.
11. American Congress of Obstetricians and Gynecologists. Committee Opinion. Guidelines for diagnostic imaging during pregnancy. American Congress of Obstetricians and Gynecologists Website. http://www.acog.org/-/media/Committee-Opinions/Committee-on-Obstetric-Practice/co299.pdf. Published 2004. Accessed October 9, 2015.
A 27-year-old white woman presented to the clinic with headaches and decreased vision through her reading glasses while performing near tasks. Her medical history was significant for herpes simplex, hyperlipidemia, and migraine headaches with aura. Her migraines began following an earlier motor vehicle accident, and her most recent magnetic resonance imaging (MRI) showed no abnormalities. Her current medications included prophylactic acyclovir for herpes and acetaminophen and caffeine tablets as needed for headache. She reported no other trauma or surgery and no known allergies. The patient’s best-corrected Snellen visual acuities in both eyes were 20/20 (distance) and 20/30 (near).
Preliminary testing, including pupils, extraocular motilities, confrontation fields, and color vision, were all within normal limits. Her slit-lamp examination was unremarkable. A dilated fundus examination revealed crowded, elevated discs without vessel obscuration, hemorrhage, hyperemia, or drusen (Figure 1). The fundus examination was otherwise unremarkable. Optical coherence tomography of the optic nerves showed increased nerve fiber layer thickness in both eyes (Figure 2). Her blood pressure (BP) at this visit was 106/77 mm/Hg.
The diagnosis based on these findings was bilateral optic nerve elevation with long-standing migraine headaches. The plan was for the patient to return to the clinic for repeat visual field testing and B-scan ultrasonography to rule out buried optic nerve head drusen.
Two months later, the patient presented to the clinic 19 weeks pregnant and reported that her headaches had increased in frequency, but she had no diplopia. All preliminary testing, including visual acuities, pupil reaction, color vision, and slit-lamp examination remained normal. Fundus examination showed the patient’s nerves were unchanged in appearance from the initial presentation. Visual fields revealed an enlarged blind spot in the right eye and paracentral defects in the left eye. The B-scan testing was negative for optic nerve drusen. Due to the increased frequency of headaches, pregnancy, and suspicious optic nerves, an urgent consult was placed to neurology.
At the neurology appointment 1 month later, the patient was diagnosed with migraine headache syndrome and idiopathic intracranial hypertension (IIH). The neurologist believed her headaches might have been resulting from analgesic rebound. He suggested that the patient discontinue or decrease use of oral butalbital, acetaminophen and caffeine tablets, and other forms of caffeine. It was decided that divalproxen sodium and verapamil were not feasible due to pregnancy. The neurologist started her on oral acetazolamide 500 mg twice daily.
The patient returned to her obstetrician 1 month later for a routine follow-up; the headaches had worsened and were now accompanied by nausea and vomiting twice daily on average. Her medications still included acetaminophen and caffeine tablets, although it had been recommended she discontinue them, prochlorperazine, and acetazolamide. Due to the worsening of her symptoms and visual fields (eFigure 1), the obstetrician recommended that the patient deliver by cesarean section at 38 to 39 weeks.
(eFigure 1.Visual Fields at Follow-up 1 and 2)
Right eye
Left Eye
Following an uncomplicated cesarean delivery at 38 weeks, the patient returned to the clinic for visual field testing. Humphrey visual fields were full in the right eye and showed some scattered central depressions in the left. Both eyes were significantly improved from previous fields (eFigure 2) . The patient had discontinued acetazolamide and reported minor tension headaches she believed were due to lack of sleep but stated that she was no longer having migraines. There was no papilledema noted on fundus examination, and Snellen distance visual acuity measured 20/20 in both eyes. An MRI had been performed after delivery and was negative for intracranial hemorrhage, mass, or hydrocephalus).
(eFigure 2. Visual Fields Postpartum)
Right eye
Left eye
Three months later, the patient returned for her yearly comprehensive examination. At that visit, she reported a decrease in frequency of the migraine headaches. Optical coherence tomography was performed and showed a significant decrease in optic nerve head swelling.
Related: Diabetes on the Rise Among Other Pregnancy Problems
Clinical Picture
Idiopathic intracranial hypertension presents clinically with signs and symptoms of increased intracranial pressure (ICP). Headache is the most common symptom, usually presenting as daily and pulsatile.1 Nausea may be associated with the headache, although vomiting is rare, and the headache may awaken the patient. The headache may remain after resolution of elevated ICP (Table).2
Papilledema is the most common sign of IIH.1,2 Visual loss associated with papilledema is generally mild at first but progressive. Transient blur lasts usually 30 seconds and may be monocular or binocular.1 The cause is thought to be related to transient ischemia of the optic nerve.1 Vision loss is typically reversible with resolution of optic nerve swelling, but 25% of patients may develop optic atrophy, which results in permanent vision loss.2 Common patterns of visual abnormalities include enlargement of the physiologic blind spot, inferonasal and arcuate defects, and eventually severe peripheral constriction.1,2 It is imperative that all patients with IIH have visual field testing performed.
About one-third of patients with IIH experience diplopia. This binocular, horizontal diplopia is caused by a sixth nerve palsy in 10% to 20% of patients.1 Cranial nerves II, VI, and VII make a 90-degree bend and seem to be prone to damage at the site of the bend.1
Pulse-synchronous tinnitus is common in IIH as well.2,3 This generally occurs unilaterally and may be eliminated by jugular compression or the head turning to the ipsilateral side.1,3 The sound is caused by the transmission of an increase in the vascular pulse due to high pressure on the cerebrospinal fluid (CSF).1,3
Idiopathic intracranial hypertension most typically presents in obese women of childbearing age.1-3 An increasing degree of obesity is generally associated with an increased risk of vision loss.1,2 Men seem to have worse acuity and visual fields at presentation than do women.2 Men are less likely to report headaches than are women and, therefore, have double the likelihood of severe vision loss.2 Hence, closer monitoring and more aggressive intervention is recommended for men due to their lesser tendency for headaches.2 Black patients also demonstrate more aggressive disease and, therefore, require closer monitoring and early aggressive intervention.1,2
Papilledema is the most common sign of IIH and may be caused by several processes. In this case, most were ruled out given the patient’s normal visual acuities, pupillary reaction, color vision testing, BP measurement, and B-scan imaging. The patient’s systemic history was negative for thyroid-related disease, diabetes, hypertension, autoimmune disease, or infection. She had no family history of vision loss or hereditary ocular conditions. The most recent MRI was negative for any long-standing space-occupying lesion or hydrocephalus.
Pathophysiology
Several mechanisms leading to increased ICP have been proposed. These include increased brain water content, excess CSF production, reduced CSF absorption, and increased cerebral venous pressure.2,3 There is also a suspicion of the role of sex hormones in IIH due to its high predilection for females.2
The role of vitamin A metabolism has also been studied in IIH.1 Retinol levels are elevated in the CSF of patients with IIH. Patients may ingest an abnormally large amount of vitamin A, metabolize it abnormally, or be sensitive to its effects.2,4 The function of adipose tissue as an actively secreting endocrine tissue may play a role in IIH due to its release of adipose tissue-derived retinol binding protein.2 Other adipose-produced cytokines include leptin, which has been implicated in IIH due to its elevated levels found in the CSF of patients with IIH.2
Stenosis of the cerebral sinuses is another proposed mechanism of IIH.1-3 Cerebrospinal fluid exits the cranium into the venous sinuses via the arachnoid villi.2 An obstruction in these sinuses may impair CSF outflow and result in intracranial hypertension. Microthrombosis caused by hypercoaguable disorders may result in increased cerebral venous pressure and impaired CSF absorption as well.2,4
Some medications have been found in association with IIH. These include tetracycline, cyclosporine, lithium, nalidixic acid, nitrofurantoin, oral contraceptives, levonorgestrel, danaxol, and tamoxifen.1-4 Tetracycline seems to have the strongest association with IIH and should be discontinued in those patients where the association is very likely to be the causative factor.2 The link to oral contraceptives may occur simply due to their association with young women most at risk for IIH.1-3
Related:Young Man With Headache, Confusion, and Hearing Loss
Management
The goals of treatment with IIH are to preserve vision and relieve symptoms, particularly headache. The general recommendation is that pregnant women with IIH should be managed and treated the same as any other patient with IIH. However, imaging and some drug contraindications exist between these 2 groups.
The diagnostic test for IIH is a lumbar puncture, which is also the most effective treatment.1-3,5 Lumbar puncture should be performed in the relaxed lateral decubitus position without sedation.1-3 The opening pressure should be measured and is the most clinically significant diagnostic tool for diagnosis of IIH. Opening pressures of > 250 mm H2O are diagnostic of IIH.1-3,5
Weight loss is an essential part of treatment in obese patients with IIH.1-3 A low-calorie, low-salt diet with mild fluid restriction seems to reverse the symptoms of IIH. A 5% to 10% reduction in body weight may reduce symptoms and signs of IIH.2
Carbonic anhydrase inhibitors (CAIs), such as acetalzolamide, have a multifactorial role in IIH.4 They are usually prescribed in 1 to 2 grams over several doses and function by decreasing CSF production.1 Carbonic anhydrase inhibitors also are known to change the taste of foods and may, therefore, aid in weight loss.1,2 Patients prescribed CAIs commonly experience a tingling in their fingers, toes, and perioral region, an indication that the medication is working.1,2 A rare but serious adverse effect (AE) is aplastic anemia, which generally occurs in the first 6 months of treatment in elderly patients.1 The use of CAIs in pregnancy is controversial, and although rare complications are reported, it is considered a class C drug.5
In patients with rapidly progressive vision loss but with minimal headache, optic nerve sheath fenestration (ONSF) is the surgical treatment of choice.2,3,6 In this procedure, a window or series of slits are created behind the globe in the optic nerve sheath.1 About 50% of patients achieve adequate headache control with ONSF, especially for frontal headaches.1,2
For patients with vision loss, papilledema, and headache that do not respond to medical therapy, a CSF diversion procedure is the preferred treatment. Cerebrospinal fluid diversion with ventriculoperitoneal or lumboperitoneal shunts may prevent progressive loss of vision.1,4,6 However, variable response rates and shunt failure requiring subsequent revisions are common and may occur in as many as half of patients undergoing these procedures.1
Increased intracranial venous pressure due to stenosis of the venous sinuses has been thought to be a possible cause of IIH. Stenting of the transverse venous sinus stenosis has been shown to reduce cerebral venous pressure, reduce ICP, and improve symptoms in patients with IIH.1-3 It is unclear whether elevations in ICP cause transverse sinus stenosis or whether transverse sinus stenosis causes increased ICP.2 Regardless, stents have a high rate of complications, including subdural hemorrhage, venous sinus perforation, in-stent thrombosis, and recurrent stenosis proximal to the stent.2
Steroids have been used to treat IIH in the past, although their mechanism of action remains unclear.2 There may be recurrence of papilledema if they are tapered too quickly. Due to their association with long-term AEs, including weight gain, they should be avoided.2
Management in Pregnancy
Several studies agree that vision loss occurs in the same frequency in pregnant and nonpregnant patients with IIH.4,7 Idiopathic intracranial hypertension can occur in any trimester in pregnancy. It has been found that patients have the same spontaneous abortion rate and visual outcomes as the general population.6-8 It has also been concluded that treatment should be the same in both patient populations with slight variability in the use of acetazolamide.4,6,7
The use of dilating drops during pregnancy is controversial. Although there have been no teratogenic effects reported with use of topical anesthetics and dilating drops, all drugs should be avoided during the first trimester.7-10 Guidelines have been established by the American Congress of Obstetricians and Gynecologists for X-ray examination and exposure during pregnancy. It has been determined that exposure from a single diagnostic X-ray procedure does not result in harmful fetal effects.11 Magnetic resonance imaging is not associated with any known adverse fetal effects and is a better imaging option during pregnancy, because it is not associated with the use of ionizing radiation.11
The use of CAIs in the first trimester is controversial.4,7 Some believe it should be avoided because it is a Pregnancy Category C drug. However, a single case of sacrococcygeal teratoma has been reported in humans; therefore, some believe this is not a strong basis for withholding the medication in patients with the potential risk for severe vision loss.4,7 In this case, a consult to the patient’s obstetrician was made, and the use of acetazolamide had no effect on the health of the baby.
In pregnant women with IIH with progressive vision loss, failed treatment, or nonadherence, surgery may be necessary. Optic nerve sheath fenestration is preferred due to lower morbidity and mortality compared with shunting procedures.1,2,4,6 The growing fetus may be affected by the peritoneal end of the shunt.4
Related: 49-Year-Old Woman With a Broken Heart
Conclusions
Vision loss associated with IIH can be severe and permanent if left untreated. The best treatments and often the most effective involve weight loss and lumbar puncture. Acetazolamide has been a proven effective treatment in some patients, but some debate exists over the safety of its use during pregnancy. This patient did not have any AEs from its use; however, it did not prove valuable in her treatment. Studies often disagree on the use of acetazolamide in pregnancy; however, all agree that proper patient counseling on potential AEs and management by an obstetrician are important. With proper management, pregnant women with IIH have had outcomes similar to those of the general population.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
A 27-year-old white woman presented to the clinic with headaches and decreased vision through her reading glasses while performing near tasks. Her medical history was significant for herpes simplex, hyperlipidemia, and migraine headaches with aura. Her migraines began following an earlier motor vehicle accident, and her most recent magnetic resonance imaging (MRI) showed no abnormalities. Her current medications included prophylactic acyclovir for herpes and acetaminophen and caffeine tablets as needed for headache. She reported no other trauma or surgery and no known allergies. The patient’s best-corrected Snellen visual acuities in both eyes were 20/20 (distance) and 20/30 (near).
Preliminary testing, including pupils, extraocular motilities, confrontation fields, and color vision, were all within normal limits. Her slit-lamp examination was unremarkable. A dilated fundus examination revealed crowded, elevated discs without vessel obscuration, hemorrhage, hyperemia, or drusen (Figure 1). The fundus examination was otherwise unremarkable. Optical coherence tomography of the optic nerves showed increased nerve fiber layer thickness in both eyes (Figure 2). Her blood pressure (BP) at this visit was 106/77 mm/Hg.
The diagnosis based on these findings was bilateral optic nerve elevation with long-standing migraine headaches. The plan was for the patient to return to the clinic for repeat visual field testing and B-scan ultrasonography to rule out buried optic nerve head drusen.
Two months later, the patient presented to the clinic 19 weeks pregnant and reported that her headaches had increased in frequency, but she had no diplopia. All preliminary testing, including visual acuities, pupil reaction, color vision, and slit-lamp examination remained normal. Fundus examination showed the patient’s nerves were unchanged in appearance from the initial presentation. Visual fields revealed an enlarged blind spot in the right eye and paracentral defects in the left eye. The B-scan testing was negative for optic nerve drusen. Due to the increased frequency of headaches, pregnancy, and suspicious optic nerves, an urgent consult was placed to neurology.
At the neurology appointment 1 month later, the patient was diagnosed with migraine headache syndrome and idiopathic intracranial hypertension (IIH). The neurologist believed her headaches might have been resulting from analgesic rebound. He suggested that the patient discontinue or decrease use of oral butalbital, acetaminophen and caffeine tablets, and other forms of caffeine. It was decided that divalproxen sodium and verapamil were not feasible due to pregnancy. The neurologist started her on oral acetazolamide 500 mg twice daily.
The patient returned to her obstetrician 1 month later for a routine follow-up; the headaches had worsened and were now accompanied by nausea and vomiting twice daily on average. Her medications still included acetaminophen and caffeine tablets, although it had been recommended she discontinue them, prochlorperazine, and acetazolamide. Due to the worsening of her symptoms and visual fields (eFigure 1), the obstetrician recommended that the patient deliver by cesarean section at 38 to 39 weeks.
(eFigure 1.Visual Fields at Follow-up 1 and 2)
Right eye
Left Eye
Following an uncomplicated cesarean delivery at 38 weeks, the patient returned to the clinic for visual field testing. Humphrey visual fields were full in the right eye and showed some scattered central depressions in the left. Both eyes were significantly improved from previous fields (eFigure 2) . The patient had discontinued acetazolamide and reported minor tension headaches she believed were due to lack of sleep but stated that she was no longer having migraines. There was no papilledema noted on fundus examination, and Snellen distance visual acuity measured 20/20 in both eyes. An MRI had been performed after delivery and was negative for intracranial hemorrhage, mass, or hydrocephalus).
(eFigure 2. Visual Fields Postpartum)
Right eye
Left eye
Three months later, the patient returned for her yearly comprehensive examination. At that visit, she reported a decrease in frequency of the migraine headaches. Optical coherence tomography was performed and showed a significant decrease in optic nerve head swelling.
Related: Diabetes on the Rise Among Other Pregnancy Problems
Clinical Picture
Idiopathic intracranial hypertension presents clinically with signs and symptoms of increased intracranial pressure (ICP). Headache is the most common symptom, usually presenting as daily and pulsatile.1 Nausea may be associated with the headache, although vomiting is rare, and the headache may awaken the patient. The headache may remain after resolution of elevated ICP (Table).2
Papilledema is the most common sign of IIH.1,2 Visual loss associated with papilledema is generally mild at first but progressive. Transient blur lasts usually 30 seconds and may be monocular or binocular.1 The cause is thought to be related to transient ischemia of the optic nerve.1 Vision loss is typically reversible with resolution of optic nerve swelling, but 25% of patients may develop optic atrophy, which results in permanent vision loss.2 Common patterns of visual abnormalities include enlargement of the physiologic blind spot, inferonasal and arcuate defects, and eventually severe peripheral constriction.1,2 It is imperative that all patients with IIH have visual field testing performed.
About one-third of patients with IIH experience diplopia. This binocular, horizontal diplopia is caused by a sixth nerve palsy in 10% to 20% of patients.1 Cranial nerves II, VI, and VII make a 90-degree bend and seem to be prone to damage at the site of the bend.1
Pulse-synchronous tinnitus is common in IIH as well.2,3 This generally occurs unilaterally and may be eliminated by jugular compression or the head turning to the ipsilateral side.1,3 The sound is caused by the transmission of an increase in the vascular pulse due to high pressure on the cerebrospinal fluid (CSF).1,3
Idiopathic intracranial hypertension most typically presents in obese women of childbearing age.1-3 An increasing degree of obesity is generally associated with an increased risk of vision loss.1,2 Men seem to have worse acuity and visual fields at presentation than do women.2 Men are less likely to report headaches than are women and, therefore, have double the likelihood of severe vision loss.2 Hence, closer monitoring and more aggressive intervention is recommended for men due to their lesser tendency for headaches.2 Black patients also demonstrate more aggressive disease and, therefore, require closer monitoring and early aggressive intervention.1,2
Papilledema is the most common sign of IIH and may be caused by several processes. In this case, most were ruled out given the patient’s normal visual acuities, pupillary reaction, color vision testing, BP measurement, and B-scan imaging. The patient’s systemic history was negative for thyroid-related disease, diabetes, hypertension, autoimmune disease, or infection. She had no family history of vision loss or hereditary ocular conditions. The most recent MRI was negative for any long-standing space-occupying lesion or hydrocephalus.
Pathophysiology
Several mechanisms leading to increased ICP have been proposed. These include increased brain water content, excess CSF production, reduced CSF absorption, and increased cerebral venous pressure.2,3 There is also a suspicion of the role of sex hormones in IIH due to its high predilection for females.2
The role of vitamin A metabolism has also been studied in IIH.1 Retinol levels are elevated in the CSF of patients with IIH. Patients may ingest an abnormally large amount of vitamin A, metabolize it abnormally, or be sensitive to its effects.2,4 The function of adipose tissue as an actively secreting endocrine tissue may play a role in IIH due to its release of adipose tissue-derived retinol binding protein.2 Other adipose-produced cytokines include leptin, which has been implicated in IIH due to its elevated levels found in the CSF of patients with IIH.2
Stenosis of the cerebral sinuses is another proposed mechanism of IIH.1-3 Cerebrospinal fluid exits the cranium into the venous sinuses via the arachnoid villi.2 An obstruction in these sinuses may impair CSF outflow and result in intracranial hypertension. Microthrombosis caused by hypercoaguable disorders may result in increased cerebral venous pressure and impaired CSF absorption as well.2,4
Some medications have been found in association with IIH. These include tetracycline, cyclosporine, lithium, nalidixic acid, nitrofurantoin, oral contraceptives, levonorgestrel, danaxol, and tamoxifen.1-4 Tetracycline seems to have the strongest association with IIH and should be discontinued in those patients where the association is very likely to be the causative factor.2 The link to oral contraceptives may occur simply due to their association with young women most at risk for IIH.1-3
Related:Young Man With Headache, Confusion, and Hearing Loss
Management
The goals of treatment with IIH are to preserve vision and relieve symptoms, particularly headache. The general recommendation is that pregnant women with IIH should be managed and treated the same as any other patient with IIH. However, imaging and some drug contraindications exist between these 2 groups.
The diagnostic test for IIH is a lumbar puncture, which is also the most effective treatment.1-3,5 Lumbar puncture should be performed in the relaxed lateral decubitus position without sedation.1-3 The opening pressure should be measured and is the most clinically significant diagnostic tool for diagnosis of IIH. Opening pressures of > 250 mm H2O are diagnostic of IIH.1-3,5
Weight loss is an essential part of treatment in obese patients with IIH.1-3 A low-calorie, low-salt diet with mild fluid restriction seems to reverse the symptoms of IIH. A 5% to 10% reduction in body weight may reduce symptoms and signs of IIH.2
Carbonic anhydrase inhibitors (CAIs), such as acetalzolamide, have a multifactorial role in IIH.4 They are usually prescribed in 1 to 2 grams over several doses and function by decreasing CSF production.1 Carbonic anhydrase inhibitors also are known to change the taste of foods and may, therefore, aid in weight loss.1,2 Patients prescribed CAIs commonly experience a tingling in their fingers, toes, and perioral region, an indication that the medication is working.1,2 A rare but serious adverse effect (AE) is aplastic anemia, which generally occurs in the first 6 months of treatment in elderly patients.1 The use of CAIs in pregnancy is controversial, and although rare complications are reported, it is considered a class C drug.5
In patients with rapidly progressive vision loss but with minimal headache, optic nerve sheath fenestration (ONSF) is the surgical treatment of choice.2,3,6 In this procedure, a window or series of slits are created behind the globe in the optic nerve sheath.1 About 50% of patients achieve adequate headache control with ONSF, especially for frontal headaches.1,2
For patients with vision loss, papilledema, and headache that do not respond to medical therapy, a CSF diversion procedure is the preferred treatment. Cerebrospinal fluid diversion with ventriculoperitoneal or lumboperitoneal shunts may prevent progressive loss of vision.1,4,6 However, variable response rates and shunt failure requiring subsequent revisions are common and may occur in as many as half of patients undergoing these procedures.1
Increased intracranial venous pressure due to stenosis of the venous sinuses has been thought to be a possible cause of IIH. Stenting of the transverse venous sinus stenosis has been shown to reduce cerebral venous pressure, reduce ICP, and improve symptoms in patients with IIH.1-3 It is unclear whether elevations in ICP cause transverse sinus stenosis or whether transverse sinus stenosis causes increased ICP.2 Regardless, stents have a high rate of complications, including subdural hemorrhage, venous sinus perforation, in-stent thrombosis, and recurrent stenosis proximal to the stent.2
Steroids have been used to treat IIH in the past, although their mechanism of action remains unclear.2 There may be recurrence of papilledema if they are tapered too quickly. Due to their association with long-term AEs, including weight gain, they should be avoided.2
Management in Pregnancy
Several studies agree that vision loss occurs in the same frequency in pregnant and nonpregnant patients with IIH.4,7 Idiopathic intracranial hypertension can occur in any trimester in pregnancy. It has been found that patients have the same spontaneous abortion rate and visual outcomes as the general population.6-8 It has also been concluded that treatment should be the same in both patient populations with slight variability in the use of acetazolamide.4,6,7
The use of dilating drops during pregnancy is controversial. Although there have been no teratogenic effects reported with use of topical anesthetics and dilating drops, all drugs should be avoided during the first trimester.7-10 Guidelines have been established by the American Congress of Obstetricians and Gynecologists for X-ray examination and exposure during pregnancy. It has been determined that exposure from a single diagnostic X-ray procedure does not result in harmful fetal effects.11 Magnetic resonance imaging is not associated with any known adverse fetal effects and is a better imaging option during pregnancy, because it is not associated with the use of ionizing radiation.11
The use of CAIs in the first trimester is controversial.4,7 Some believe it should be avoided because it is a Pregnancy Category C drug. However, a single case of sacrococcygeal teratoma has been reported in humans; therefore, some believe this is not a strong basis for withholding the medication in patients with the potential risk for severe vision loss.4,7 In this case, a consult to the patient’s obstetrician was made, and the use of acetazolamide had no effect on the health of the baby.
In pregnant women with IIH with progressive vision loss, failed treatment, or nonadherence, surgery may be necessary. Optic nerve sheath fenestration is preferred due to lower morbidity and mortality compared with shunting procedures.1,2,4,6 The growing fetus may be affected by the peritoneal end of the shunt.4
Related: 49-Year-Old Woman With a Broken Heart
Conclusions
Vision loss associated with IIH can be severe and permanent if left untreated. The best treatments and often the most effective involve weight loss and lumbar puncture. Acetazolamide has been a proven effective treatment in some patients, but some debate exists over the safety of its use during pregnancy. This patient did not have any AEs from its use; however, it did not prove valuable in her treatment. Studies often disagree on the use of acetazolamide in pregnancy; however, all agree that proper patient counseling on potential AEs and management by an obstetrician are important. With proper management, pregnant women with IIH have had outcomes similar to those of the general population.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010;28(3):593-617.
2. Bruce BB, Biousee V, Newman NJ. Update on idiopathic intracranial hypertension. Am J Ophthalmol. 2011;152(2):163-169.
3. Fields JD, Javendani PP, Falardeau J, et al. Dural venous sinus angioplasty and stenting for the treatment of idiopathic intracranial hypertension. J Neurointerv Surg. 2013;5(1):62-68.
4. Evans RW, Lee AG. Idiopathic intracranial hypertension in pregnancy. Headache. 2010;50(9):1513-1515.
5. Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002;59(10):1492-1495.
6. Martínez-Varea A, Diago-Almela VJ, Abad-Carrascosa A, Perales-Marín A. Progressive visual loss in a pregnant woman with idiopathic intracranial hypertension. Eur J Obstet Gynecol Reprod Biol. 2012;163(1):117-122.
7. Falardeau J, Lobb B, Golden S, Maxfield SD, Tanne E. The use of acetazolamide during pregnancy in intracranial hypertension patients. J Neuroophthalmol. 2013;33(1):9-12.
8. Dinn RB, Harris A, Marcus PS. Ocular changes in pregnancy. Obstet Gynecol Surg. 2003;58(2):137-144.
9. Shultz KL, Birnbaum AD, Goldstein DA. Ocular disease in pregnancy. Curr Opin Ophthalmol. 2005;16(5):308-314.
10. Chung CY, Kwok AKH, Chung KL. Use of ophthalmic medications during pregnancy. Hong Kong Med J. 2004;10(3):191-195.
11. American Congress of Obstetricians and Gynecologists. Committee Opinion. Guidelines for diagnostic imaging during pregnancy. American Congress of Obstetricians and Gynecologists Website. http://www.acog.org/-/media/Committee-Opinions/Committee-on-Obstetric-Practice/co299.pdf. Published 2004. Accessed October 9, 2015.
1. Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010;28(3):593-617.
2. Bruce BB, Biousee V, Newman NJ. Update on idiopathic intracranial hypertension. Am J Ophthalmol. 2011;152(2):163-169.
3. Fields JD, Javendani PP, Falardeau J, et al. Dural venous sinus angioplasty and stenting for the treatment of idiopathic intracranial hypertension. J Neurointerv Surg. 2013;5(1):62-68.
4. Evans RW, Lee AG. Idiopathic intracranial hypertension in pregnancy. Headache. 2010;50(9):1513-1515.
5. Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002;59(10):1492-1495.
6. Martínez-Varea A, Diago-Almela VJ, Abad-Carrascosa A, Perales-Marín A. Progressive visual loss in a pregnant woman with idiopathic intracranial hypertension. Eur J Obstet Gynecol Reprod Biol. 2012;163(1):117-122.
7. Falardeau J, Lobb B, Golden S, Maxfield SD, Tanne E. The use of acetazolamide during pregnancy in intracranial hypertension patients. J Neuroophthalmol. 2013;33(1):9-12.
8. Dinn RB, Harris A, Marcus PS. Ocular changes in pregnancy. Obstet Gynecol Surg. 2003;58(2):137-144.
9. Shultz KL, Birnbaum AD, Goldstein DA. Ocular disease in pregnancy. Curr Opin Ophthalmol. 2005;16(5):308-314.
10. Chung CY, Kwok AKH, Chung KL. Use of ophthalmic medications during pregnancy. Hong Kong Med J. 2004;10(3):191-195.
11. American Congress of Obstetricians and Gynecologists. Committee Opinion. Guidelines for diagnostic imaging during pregnancy. American Congress of Obstetricians and Gynecologists Website. http://www.acog.org/-/media/Committee-Opinions/Committee-on-Obstetric-Practice/co299.pdf. Published 2004. Accessed October 9, 2015.
Hypothermia Therapy in Traumatic Brain Injury
In patients with an intracranial pressure of more than 20 mm Hg after traumatic brain injury (TBI), therapeutic hypothermia plus standard care to reduce intracranial pressure did not result in outcomes better than those with standard care alone, according to a study of 387 patients with TBI. Researchers found:
• Stage 3 treatments were needed to control intracranial pressure in 54% of controls and 44% of the hypothermia group.
• Adjusted common odds ratio for the Extended Glasgow Outcome Scale (GOS-E) was 1.53, indicating a worse outcome in the hypothermia group vs controls.
• A favorable outcome occurred in 26% of the hypothermia group vs 37% in controls.
Citation: Andrews PJ, Sinclair HL, Rodriguez A, et al. Hypothermia for intracranial hypertension after traumatic brain injury. [Published online ahead of print October 7, 2015]. N Engl J Med. doi: 10.1056/NEJMoa1507581.
In patients with an intracranial pressure of more than 20 mm Hg after traumatic brain injury (TBI), therapeutic hypothermia plus standard care to reduce intracranial pressure did not result in outcomes better than those with standard care alone, according to a study of 387 patients with TBI. Researchers found:
• Stage 3 treatments were needed to control intracranial pressure in 54% of controls and 44% of the hypothermia group.
• Adjusted common odds ratio for the Extended Glasgow Outcome Scale (GOS-E) was 1.53, indicating a worse outcome in the hypothermia group vs controls.
• A favorable outcome occurred in 26% of the hypothermia group vs 37% in controls.
Citation: Andrews PJ, Sinclair HL, Rodriguez A, et al. Hypothermia for intracranial hypertension after traumatic brain injury. [Published online ahead of print October 7, 2015]. N Engl J Med. doi: 10.1056/NEJMoa1507581.
In patients with an intracranial pressure of more than 20 mm Hg after traumatic brain injury (TBI), therapeutic hypothermia plus standard care to reduce intracranial pressure did not result in outcomes better than those with standard care alone, according to a study of 387 patients with TBI. Researchers found:
• Stage 3 treatments were needed to control intracranial pressure in 54% of controls and 44% of the hypothermia group.
• Adjusted common odds ratio for the Extended Glasgow Outcome Scale (GOS-E) was 1.53, indicating a worse outcome in the hypothermia group vs controls.
• A favorable outcome occurred in 26% of the hypothermia group vs 37% in controls.
Citation: Andrews PJ, Sinclair HL, Rodriguez A, et al. Hypothermia for intracranial hypertension after traumatic brain injury. [Published online ahead of print October 7, 2015]. N Engl J Med. doi: 10.1056/NEJMoa1507581.
Helping Veterans Manage Pain
Patients with a history of traumatic brain injury (TBI) may be coping with lingering pain in safe and healthy ways, but there are still many areas where their health care practitioners can help, according to a pilot study of how veterans with TBI are managing their pain.
Researchers from VA Western New York Healthcare System in Buffalo, State University of New York in Buffalo, and the Syracuse VAMC in New York surveyed 24 outpatients with a history of mild-to-moderate TBI. Participants completed a series of self-reports, including the Pain Outcomes Questionnaire and Pain Symptom Survey pain scale.
Related: Veterans' Health and Opioid Safety—Contexts, Risks, and Outreach Implications
Most rated their health as average or better, although more than half reported having pain at least 3 days per week, and more than one-third reported having pain daily. About two-thirds reported headache and/or lower back pain; 54% had joint pain, and 42% had neck pain. The researchers note that the pain was not necessarily attributable to TBI, although factors such as the number and severity of injuries might have played a role.
Related: TBI Biomarker Development on the Horizon
The veterans were mostly using exercise, nonopioid analgesics, and rest to manage their pain. They also used, to a lesser degree, heat therapy, antidepressants, and opioids. Only regular use of antidepressants was associated with greater benefit.
The takeaway for practitioners, the researchers suggest, is multifaceted. First, they need to be prepared to manage pain of various etiologies in the context of other comorbid conditions. Second, the survey indicates that patients may be underusing some effective pain management tools: 10 of 14 possible strategies in the survey were endorsed by fewer than half the veterans.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Third, the researchers suggest that because some of the participants were concerned about exercise leading to reinjury, it might be helpful to provide additional education and support about the value of pacing (ie, moderate exercise and rest vs overexertion followed by extended bed rest). VA mental health providers, they add, could also address common anxieties about reinjury and offer nonpharmacologic interventions. Studies of veterans with pain and posttraumatic stress disorder, for instance, have shown that cognitive behavioral approaches such as progressive muscle relaxation, biofeedback, and diaphragmatic breathing, which were underused in the survey group, are effective and well received.
Source
King PR, Beehler GP, Wade MJ. Mil Med. 2015;180(8):863-868.
doi: 10.7205/MILMED-D-14-00472.
Patients with a history of traumatic brain injury (TBI) may be coping with lingering pain in safe and healthy ways, but there are still many areas where their health care practitioners can help, according to a pilot study of how veterans with TBI are managing their pain.
Researchers from VA Western New York Healthcare System in Buffalo, State University of New York in Buffalo, and the Syracuse VAMC in New York surveyed 24 outpatients with a history of mild-to-moderate TBI. Participants completed a series of self-reports, including the Pain Outcomes Questionnaire and Pain Symptom Survey pain scale.
Related: Veterans' Health and Opioid Safety—Contexts, Risks, and Outreach Implications
Most rated their health as average or better, although more than half reported having pain at least 3 days per week, and more than one-third reported having pain daily. About two-thirds reported headache and/or lower back pain; 54% had joint pain, and 42% had neck pain. The researchers note that the pain was not necessarily attributable to TBI, although factors such as the number and severity of injuries might have played a role.
Related: TBI Biomarker Development on the Horizon
The veterans were mostly using exercise, nonopioid analgesics, and rest to manage their pain. They also used, to a lesser degree, heat therapy, antidepressants, and opioids. Only regular use of antidepressants was associated with greater benefit.
The takeaway for practitioners, the researchers suggest, is multifaceted. First, they need to be prepared to manage pain of various etiologies in the context of other comorbid conditions. Second, the survey indicates that patients may be underusing some effective pain management tools: 10 of 14 possible strategies in the survey were endorsed by fewer than half the veterans.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Third, the researchers suggest that because some of the participants were concerned about exercise leading to reinjury, it might be helpful to provide additional education and support about the value of pacing (ie, moderate exercise and rest vs overexertion followed by extended bed rest). VA mental health providers, they add, could also address common anxieties about reinjury and offer nonpharmacologic interventions. Studies of veterans with pain and posttraumatic stress disorder, for instance, have shown that cognitive behavioral approaches such as progressive muscle relaxation, biofeedback, and diaphragmatic breathing, which were underused in the survey group, are effective and well received.
Source
King PR, Beehler GP, Wade MJ. Mil Med. 2015;180(8):863-868.
doi: 10.7205/MILMED-D-14-00472.
Patients with a history of traumatic brain injury (TBI) may be coping with lingering pain in safe and healthy ways, but there are still many areas where their health care practitioners can help, according to a pilot study of how veterans with TBI are managing their pain.
Researchers from VA Western New York Healthcare System in Buffalo, State University of New York in Buffalo, and the Syracuse VAMC in New York surveyed 24 outpatients with a history of mild-to-moderate TBI. Participants completed a series of self-reports, including the Pain Outcomes Questionnaire and Pain Symptom Survey pain scale.
Related: Veterans' Health and Opioid Safety—Contexts, Risks, and Outreach Implications
Most rated their health as average or better, although more than half reported having pain at least 3 days per week, and more than one-third reported having pain daily. About two-thirds reported headache and/or lower back pain; 54% had joint pain, and 42% had neck pain. The researchers note that the pain was not necessarily attributable to TBI, although factors such as the number and severity of injuries might have played a role.
Related: TBI Biomarker Development on the Horizon
The veterans were mostly using exercise, nonopioid analgesics, and rest to manage their pain. They also used, to a lesser degree, heat therapy, antidepressants, and opioids. Only regular use of antidepressants was associated with greater benefit.
The takeaway for practitioners, the researchers suggest, is multifaceted. First, they need to be prepared to manage pain of various etiologies in the context of other comorbid conditions. Second, the survey indicates that patients may be underusing some effective pain management tools: 10 of 14 possible strategies in the survey were endorsed by fewer than half the veterans.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Third, the researchers suggest that because some of the participants were concerned about exercise leading to reinjury, it might be helpful to provide additional education and support about the value of pacing (ie, moderate exercise and rest vs overexertion followed by extended bed rest). VA mental health providers, they add, could also address common anxieties about reinjury and offer nonpharmacologic interventions. Studies of veterans with pain and posttraumatic stress disorder, for instance, have shown that cognitive behavioral approaches such as progressive muscle relaxation, biofeedback, and diaphragmatic breathing, which were underused in the survey group, are effective and well received.
Source
King PR, Beehler GP, Wade MJ. Mil Med. 2015;180(8):863-868.
doi: 10.7205/MILMED-D-14-00472.
TBI Biomarker Development on the Horizon
A number of advanced efforts in traumatic brain injury (TBI) research are on the verge of reporting new data, according to a roundtable discussion that took place during the Military Health System Research Symposium on August 19. Among the most notable is in the area of biomarker development.
A 2,000-patient pivotal trial recently closed, and analysis should be completed by the end of the year. By March 2016, the research team expects to submit for FDA clearance a first-ever blood test for TBI. In addition, TBI research is currently being conducted in the areas of eye movement and balance.
Related: Brain Training for TBI Patients
A problem with assessing and treating the complexities of TBI up to this point is that although there are hundreds of measures of brain function, the evidence isn’t strong enough to provide a gold standard. “The whole area of drugs in neuroscience has been very difficult,” said Col. Dallas Hack, MD, senior medical advisor to the principal assistant for research and technology. “We have a couple of major efforts that are aimed at solving the problems of achieving results that can be measured according to the standards required to have them approved.”
Related: Stopping TBI-Related Brain Degeneration
To address the lack of a gold standard, the TBI Endpoints Development multiyear effort is making progress to give validity to the many existing measures of brain injury. Another effort is the VA/DoD Chronic Effects of Neurotrauma Consortium (CENC), a federally funded program that identifies gaps in research and provides support services for scientific, clinical, and translational research projects focused on the long-term effects of mild TBI in veterans and active-duty service members.
For information about the CENC, click here.
A number of advanced efforts in traumatic brain injury (TBI) research are on the verge of reporting new data, according to a roundtable discussion that took place during the Military Health System Research Symposium on August 19. Among the most notable is in the area of biomarker development.
A 2,000-patient pivotal trial recently closed, and analysis should be completed by the end of the year. By March 2016, the research team expects to submit for FDA clearance a first-ever blood test for TBI. In addition, TBI research is currently being conducted in the areas of eye movement and balance.
Related: Brain Training for TBI Patients
A problem with assessing and treating the complexities of TBI up to this point is that although there are hundreds of measures of brain function, the evidence isn’t strong enough to provide a gold standard. “The whole area of drugs in neuroscience has been very difficult,” said Col. Dallas Hack, MD, senior medical advisor to the principal assistant for research and technology. “We have a couple of major efforts that are aimed at solving the problems of achieving results that can be measured according to the standards required to have them approved.”
Related: Stopping TBI-Related Brain Degeneration
To address the lack of a gold standard, the TBI Endpoints Development multiyear effort is making progress to give validity to the many existing measures of brain injury. Another effort is the VA/DoD Chronic Effects of Neurotrauma Consortium (CENC), a federally funded program that identifies gaps in research and provides support services for scientific, clinical, and translational research projects focused on the long-term effects of mild TBI in veterans and active-duty service members.
For information about the CENC, click here.
A number of advanced efforts in traumatic brain injury (TBI) research are on the verge of reporting new data, according to a roundtable discussion that took place during the Military Health System Research Symposium on August 19. Among the most notable is in the area of biomarker development.
A 2,000-patient pivotal trial recently closed, and analysis should be completed by the end of the year. By March 2016, the research team expects to submit for FDA clearance a first-ever blood test for TBI. In addition, TBI research is currently being conducted in the areas of eye movement and balance.
Related: Brain Training for TBI Patients
A problem with assessing and treating the complexities of TBI up to this point is that although there are hundreds of measures of brain function, the evidence isn’t strong enough to provide a gold standard. “The whole area of drugs in neuroscience has been very difficult,” said Col. Dallas Hack, MD, senior medical advisor to the principal assistant for research and technology. “We have a couple of major efforts that are aimed at solving the problems of achieving results that can be measured according to the standards required to have them approved.”
Related: Stopping TBI-Related Brain Degeneration
To address the lack of a gold standard, the TBI Endpoints Development multiyear effort is making progress to give validity to the many existing measures of brain injury. Another effort is the VA/DoD Chronic Effects of Neurotrauma Consortium (CENC), a federally funded program that identifies gaps in research and provides support services for scientific, clinical, and translational research projects focused on the long-term effects of mild TBI in veterans and active-duty service members.
For information about the CENC, click here.