User login
Psoriasis, PsA increase temporomandibular disorder risk
Psoriasis may play a role in temporomandibular joint disorders, according to an observational study that compared psoriasis patients to individuals without the disorder.
The Italian study, conducted from January 2014 to December 2014, included 112 patients with psoriasis and a 112-person control group. Of the patients with psoriasis, 25 (22%) had psoriatic arthritis (PsA). Patients were examined for temporomandibular disorder (TMD) signs and symptoms based on the standardized Research Diagnostic Criteria for Temporomandibular Disorders. TMD was assessed through a questionnaire and a clinical examination.
Overall, patients with psoriasis experienced TMD symptoms significantly more frequently than did members of the control group, with 69% of the psoriasis group reporting one or more symptoms, compared with 24% of the controls. Most often, the patients with psoriasis reported suffering from tenderness or stiffness in the neck and shoulders, muscle pain on chewing, and the sensation of a stuck or locked jaw. The control group’s major complaint was tenderness or stiffness in the neck and shoulders.
Temporomandibular joint sounds and opening derangement, which are signs of TMD, also were more common in the patients with psoriasis than in the control group.
TMD symptoms and signs were even more common in the subset of patients with PsA, with 80% of these patients reporting symptoms. Additionally, a statistically significant increase in opening derangement, bruxism, and temporomandibular joint sounds occurred in patients with PsA, compared with psoriasis patents without arthritis and controls.
Temporomandibular joint sounds and opening derangement “were found to be more frequent and severe in patients with psoriasis and PsA than in the healthy subjects, this result being highly significant,” wrote Dr. Vito Crincoli and colleagues at the University of Bari (Italy). “Therefore, in addition to dermatological and rheumatological implications, psoriasis seems to play a role in TMJ disorders, causing an increase in orofacial pain and an altered chewing function.”
Read the full study in the International Journal of Medical Sciences (2015;12:341-8 [doi:10.7150/ijms.11288]).
Psoriasis may play a role in temporomandibular joint disorders, according to an observational study that compared psoriasis patients to individuals without the disorder.
The Italian study, conducted from January 2014 to December 2014, included 112 patients with psoriasis and a 112-person control group. Of the patients with psoriasis, 25 (22%) had psoriatic arthritis (PsA). Patients were examined for temporomandibular disorder (TMD) signs and symptoms based on the standardized Research Diagnostic Criteria for Temporomandibular Disorders. TMD was assessed through a questionnaire and a clinical examination.
Overall, patients with psoriasis experienced TMD symptoms significantly more frequently than did members of the control group, with 69% of the psoriasis group reporting one or more symptoms, compared with 24% of the controls. Most often, the patients with psoriasis reported suffering from tenderness or stiffness in the neck and shoulders, muscle pain on chewing, and the sensation of a stuck or locked jaw. The control group’s major complaint was tenderness or stiffness in the neck and shoulders.
Temporomandibular joint sounds and opening derangement, which are signs of TMD, also were more common in the patients with psoriasis than in the control group.
TMD symptoms and signs were even more common in the subset of patients with PsA, with 80% of these patients reporting symptoms. Additionally, a statistically significant increase in opening derangement, bruxism, and temporomandibular joint sounds occurred in patients with PsA, compared with psoriasis patents without arthritis and controls.
Temporomandibular joint sounds and opening derangement “were found to be more frequent and severe in patients with psoriasis and PsA than in the healthy subjects, this result being highly significant,” wrote Dr. Vito Crincoli and colleagues at the University of Bari (Italy). “Therefore, in addition to dermatological and rheumatological implications, psoriasis seems to play a role in TMJ disorders, causing an increase in orofacial pain and an altered chewing function.”
Read the full study in the International Journal of Medical Sciences (2015;12:341-8 [doi:10.7150/ijms.11288]).
Psoriasis may play a role in temporomandibular joint disorders, according to an observational study that compared psoriasis patients to individuals without the disorder.
The Italian study, conducted from January 2014 to December 2014, included 112 patients with psoriasis and a 112-person control group. Of the patients with psoriasis, 25 (22%) had psoriatic arthritis (PsA). Patients were examined for temporomandibular disorder (TMD) signs and symptoms based on the standardized Research Diagnostic Criteria for Temporomandibular Disorders. TMD was assessed through a questionnaire and a clinical examination.
Overall, patients with psoriasis experienced TMD symptoms significantly more frequently than did members of the control group, with 69% of the psoriasis group reporting one or more symptoms, compared with 24% of the controls. Most often, the patients with psoriasis reported suffering from tenderness or stiffness in the neck and shoulders, muscle pain on chewing, and the sensation of a stuck or locked jaw. The control group’s major complaint was tenderness or stiffness in the neck and shoulders.
Temporomandibular joint sounds and opening derangement, which are signs of TMD, also were more common in the patients with psoriasis than in the control group.
TMD symptoms and signs were even more common in the subset of patients with PsA, with 80% of these patients reporting symptoms. Additionally, a statistically significant increase in opening derangement, bruxism, and temporomandibular joint sounds occurred in patients with PsA, compared with psoriasis patents without arthritis and controls.
Temporomandibular joint sounds and opening derangement “were found to be more frequent and severe in patients with psoriasis and PsA than in the healthy subjects, this result being highly significant,” wrote Dr. Vito Crincoli and colleagues at the University of Bari (Italy). “Therefore, in addition to dermatological and rheumatological implications, psoriasis seems to play a role in TMJ disorders, causing an increase in orofacial pain and an altered chewing function.”
Read the full study in the International Journal of Medical Sciences (2015;12:341-8 [doi:10.7150/ijms.11288]).
FROM INTERNATIONAL JOURNAL OF MEDICAL SCIENCES
Chromosome deletion linked to PsA risk
A deletion between the ADAMTS9 and MAGI1 genes was associated with psoriatic arthritis and is unrelated to purely cutaneous psoriasis, according to Dr. Antonio Juliá of Vall d’Hebron Research Institute, Barcelona, and his associates.
Of 165 common copy number variants found in both the psoriatic arthritis (PsA) group and control group, only the ADAMTS9-MAGI1 deletion showed a significant association, with an odds ratio of 1.94. A deletion between the HLA-C and HLA-B genes was initially significant, but the association disappeared after correcting for alleles located at those genes already associated with PsA.
The ADAMTS9-MAGI1 deletion occurred significantly less often in patients with cutaneous psoriasis (PsC) than in PsA patients, and there was no significant difference in deletion frequency between the control group and the PsC group.
“It is possible, however, that once the specific biological mechanisms influenced by this genetic variation are identified, more targeted analysis will reveal association to other PsA phenotypes,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-207190)
A deletion between the ADAMTS9 and MAGI1 genes was associated with psoriatic arthritis and is unrelated to purely cutaneous psoriasis, according to Dr. Antonio Juliá of Vall d’Hebron Research Institute, Barcelona, and his associates.
Of 165 common copy number variants found in both the psoriatic arthritis (PsA) group and control group, only the ADAMTS9-MAGI1 deletion showed a significant association, with an odds ratio of 1.94. A deletion between the HLA-C and HLA-B genes was initially significant, but the association disappeared after correcting for alleles located at those genes already associated with PsA.
The ADAMTS9-MAGI1 deletion occurred significantly less often in patients with cutaneous psoriasis (PsC) than in PsA patients, and there was no significant difference in deletion frequency between the control group and the PsC group.
“It is possible, however, that once the specific biological mechanisms influenced by this genetic variation are identified, more targeted analysis will reveal association to other PsA phenotypes,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-207190)
A deletion between the ADAMTS9 and MAGI1 genes was associated with psoriatic arthritis and is unrelated to purely cutaneous psoriasis, according to Dr. Antonio Juliá of Vall d’Hebron Research Institute, Barcelona, and his associates.
Of 165 common copy number variants found in both the psoriatic arthritis (PsA) group and control group, only the ADAMTS9-MAGI1 deletion showed a significant association, with an odds ratio of 1.94. A deletion between the HLA-C and HLA-B genes was initially significant, but the association disappeared after correcting for alleles located at those genes already associated with PsA.
The ADAMTS9-MAGI1 deletion occurred significantly less often in patients with cutaneous psoriasis (PsC) than in PsA patients, and there was no significant difference in deletion frequency between the control group and the PsC group.
“It is possible, however, that once the specific biological mechanisms influenced by this genetic variation are identified, more targeted analysis will reveal association to other PsA phenotypes,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-207190)
BSR: Multiple benefits seen with intensive psoriatic arthritis therapy
MANCHESTER, U.K. – Multiple joint and skin benefits can be achieved by intensively treating patients with psoriatic arthritis until they achieve a set of minimal disease activity criteria, an expert said at the British Society for Rheumatology annual conference.
While data are mounting on the value of treating to target (otherwise known as tight control) in psoriatic arthritis (PsA), these data lag significantly behind that for inducing and maintaining remission in rheumatoid arthritis (RA), noted Dr. Philip Helliwell of the University of Leeds (England).
“There is half as much evidence in PsA as there is in rheumatoid arthritis,” he observed. “But we’ve also got a heterogeneous disease and what we are going to have to do moving forward is to find out how to treat different phenotypic expressions of psoriatic disease, and we’re beginning to work towards that now,” he said during a Special Interest Group on Spondyloarthropathies.
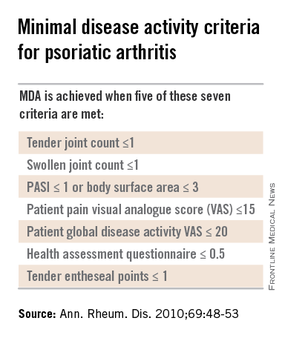
Dr. Helliwell is the principal investigator of the Tight Control of Psoriatic Arthritis (TICOPA) study, which he highlighted as an example of how targeting treatment to achieve minimal disease activity (MDA) criteria (Ann. Rheum. Dis. 2010;69:48-53) could be beneficial versus standard care.
A total of 206 patients with newly-diagnosed PsA were enrolled into the study and were randomized to receive either ‘tight control’ – meaning an intensive management strategy – or to standard care for 48 weeks.
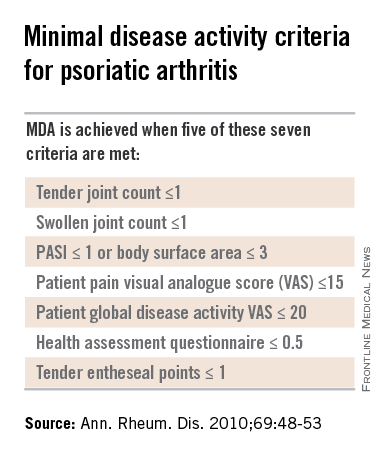
Intensive treatment involved starting with methotrexate at a dose of 15 mg/kg per week and rapidly escalating to 25 mg/kg per week at 6 weeks if needed. If patients did not achieve five out of a set of seven MDA criteria for PsA, then methotrexate was continued and sulfasalazine was added and dose escalated after 4-8 weeks.
If MDA was still not achieved and criteria for biologics were not met according to NICE guidance, then alternatives were swapping out sulfasalazine for cyclosporine or leflunomide, again increasing the doses. Patients who did get put onto a biologic could switch to another anti-TNF if they did not respond after 12 weeks.
The primary endpoint data from the trial have been reported previously and showed that a higher proportion of patients in the intensive management group achieved ACR20 at 48 weeks, compared with those in the standard care group (62% vs. 45%, respectively; P = .02). A higher percentage of intensively managed patients also achieved ACR50 (51% vs. 25%; P = .0004) and ACR70 (38% vs. 17%, P = .002).
Skin symptoms, measured via the Psoriasis Area and Severity Index (PASI) showed significant improvement favoring intensive therapy over standard care. PASI20 was achieved by 72% of intensively managed patients versus 52% of those who received standard care. PASI75 was achieved by 59% versus 33%, respectively, and PASI90 by 40% versus 20%, respectively.
The full results of the study will be published soon in The Lancet and will include details of a variety of secondary outcomes and the cost-effectiveness of the intensive management strategy versus the standard care approach.
One of the key secondary outcomes of the trial was to look at the effects of the two treatment strategies on other PsA symptoms, such as enthesitis, dactylitis, and nail symptoms. No differences between the groups were observed, however, with similar decreases seen in the tight control and standard care groups.
There were no statistically significant differences in radiologic outcomes, which included baseline and end-of-treatment changes in the total modified Sharp van der Heijde (SVdH) score, the erosion score, and joint-space narrowing (JSN) score.
While this might seem somewhat disappointing, “there wasn’t a lot of radiologic progression going on anyway,” Dr. Helliwell pointed out. Overall, there was a difference of about 5% in the percentage of patients with at least one joint erosion at baseline and after 48 weeks of treatment.
The majority of radiographic change that did occur was JSN of the hands, Dr. Helliwell said, adding that patients with JSN tended to be slightly older than those without, although this observation did not reach statistical significance.
“We’ve since looked for associations with ACPA [anticitrullinated protein antibodies] – about 7% of our patients were ACPA positive – but there is no relationship,” he added. There was also no significant association between levels of C-reactive protein levels and erosive disease.
There was a trend suggesting that patients with erosions may be more likely to have polyarticular disease than oligoarticular disease, so a next step would be to look at radiologic progression in these two groups of patients in more detail.
More adverse events were seen in the tight control arm, compared with the standard care arm, including more serious adverse events, but not all of these were related to study treatment and many adverse events were those to be expected with methotrexate treatment, Dr. Helliwell observed.
But is the intensive approach cost-effective when compared to standard care? Data suggest that it is. Although the incremental cost-effectiveness ratio (ICER) initially exceeded the £20,000–£30,000 (about $31,000-$47,000) threshold used by the U.K. National Institute for Health and Care Excellence to judge if a new treatment is cost effective, allowing for certain factors enabled the ICER to be brought down to about £28,000 ($44,000), making it a cost-effective strategy.
PsA consists of five classical subtypes. The most common of these subtypes is polyarthritis (60% of patients), followed by oligoarthritis (30%). The remaining 10% of patients comprise those with arthritis mutilans, distal interphalangeal predominant disease, or spinal predominant disease. The clinical features of dactylitis and enthesitis are prevalent in about 40% and 50% of patients, respectively, and can occur in any subgroup.
Considering such heterogeneity in its presentation, the challenge now will be to determine if all clinical subgroups of PsA could benefit from treating to an MDA target with intensive management, or if one or other subgroups benefit more than another.
The TICOPA study was funded by Arthritis Research UK with support from Pfizer. Dr. Helliwell has received consulting fees from Pfizer.
Results of this study were published in the Lancet Sept. 30, 2015.
This article was updated October 6, 2015.
MANCHESTER, U.K. – Multiple joint and skin benefits can be achieved by intensively treating patients with psoriatic arthritis until they achieve a set of minimal disease activity criteria, an expert said at the British Society for Rheumatology annual conference.
While data are mounting on the value of treating to target (otherwise known as tight control) in psoriatic arthritis (PsA), these data lag significantly behind that for inducing and maintaining remission in rheumatoid arthritis (RA), noted Dr. Philip Helliwell of the University of Leeds (England).
“There is half as much evidence in PsA as there is in rheumatoid arthritis,” he observed. “But we’ve also got a heterogeneous disease and what we are going to have to do moving forward is to find out how to treat different phenotypic expressions of psoriatic disease, and we’re beginning to work towards that now,” he said during a Special Interest Group on Spondyloarthropathies.
Dr. Helliwell is the principal investigator of the Tight Control of Psoriatic Arthritis (TICOPA) study, which he highlighted as an example of how targeting treatment to achieve minimal disease activity (MDA) criteria (Ann. Rheum. Dis. 2010;69:48-53) could be beneficial versus standard care.
A total of 206 patients with newly-diagnosed PsA were enrolled into the study and were randomized to receive either ‘tight control’ – meaning an intensive management strategy – or to standard care for 48 weeks.
Intensive treatment involved starting with methotrexate at a dose of 15 mg/kg per week and rapidly escalating to 25 mg/kg per week at 6 weeks if needed. If patients did not achieve five out of a set of seven MDA criteria for PsA, then methotrexate was continued and sulfasalazine was added and dose escalated after 4-8 weeks.
If MDA was still not achieved and criteria for biologics were not met according to NICE guidance, then alternatives were swapping out sulfasalazine for cyclosporine or leflunomide, again increasing the doses. Patients who did get put onto a biologic could switch to another anti-TNF if they did not respond after 12 weeks.
The primary endpoint data from the trial have been reported previously and showed that a higher proportion of patients in the intensive management group achieved ACR20 at 48 weeks, compared with those in the standard care group (62% vs. 45%, respectively; P = .02). A higher percentage of intensively managed patients also achieved ACR50 (51% vs. 25%; P = .0004) and ACR70 (38% vs. 17%, P = .002).
Skin symptoms, measured via the Psoriasis Area and Severity Index (PASI) showed significant improvement favoring intensive therapy over standard care. PASI20 was achieved by 72% of intensively managed patients versus 52% of those who received standard care. PASI75 was achieved by 59% versus 33%, respectively, and PASI90 by 40% versus 20%, respectively.
The full results of the study will be published soon in The Lancet and will include details of a variety of secondary outcomes and the cost-effectiveness of the intensive management strategy versus the standard care approach.
One of the key secondary outcomes of the trial was to look at the effects of the two treatment strategies on other PsA symptoms, such as enthesitis, dactylitis, and nail symptoms. No differences between the groups were observed, however, with similar decreases seen in the tight control and standard care groups.
There were no statistically significant differences in radiologic outcomes, which included baseline and end-of-treatment changes in the total modified Sharp van der Heijde (SVdH) score, the erosion score, and joint-space narrowing (JSN) score.
While this might seem somewhat disappointing, “there wasn’t a lot of radiologic progression going on anyway,” Dr. Helliwell pointed out. Overall, there was a difference of about 5% in the percentage of patients with at least one joint erosion at baseline and after 48 weeks of treatment.
The majority of radiographic change that did occur was JSN of the hands, Dr. Helliwell said, adding that patients with JSN tended to be slightly older than those without, although this observation did not reach statistical significance.
“We’ve since looked for associations with ACPA [anticitrullinated protein antibodies] – about 7% of our patients were ACPA positive – but there is no relationship,” he added. There was also no significant association between levels of C-reactive protein levels and erosive disease.
There was a trend suggesting that patients with erosions may be more likely to have polyarticular disease than oligoarticular disease, so a next step would be to look at radiologic progression in these two groups of patients in more detail.
More adverse events were seen in the tight control arm, compared with the standard care arm, including more serious adverse events, but not all of these were related to study treatment and many adverse events were those to be expected with methotrexate treatment, Dr. Helliwell observed.
But is the intensive approach cost-effective when compared to standard care? Data suggest that it is. Although the incremental cost-effectiveness ratio (ICER) initially exceeded the £20,000–£30,000 (about $31,000-$47,000) threshold used by the U.K. National Institute for Health and Care Excellence to judge if a new treatment is cost effective, allowing for certain factors enabled the ICER to be brought down to about £28,000 ($44,000), making it a cost-effective strategy.
PsA consists of five classical subtypes. The most common of these subtypes is polyarthritis (60% of patients), followed by oligoarthritis (30%). The remaining 10% of patients comprise those with arthritis mutilans, distal interphalangeal predominant disease, or spinal predominant disease. The clinical features of dactylitis and enthesitis are prevalent in about 40% and 50% of patients, respectively, and can occur in any subgroup.
Considering such heterogeneity in its presentation, the challenge now will be to determine if all clinical subgroups of PsA could benefit from treating to an MDA target with intensive management, or if one or other subgroups benefit more than another.
The TICOPA study was funded by Arthritis Research UK with support from Pfizer. Dr. Helliwell has received consulting fees from Pfizer.
Results of this study were published in the Lancet Sept. 30, 2015.
This article was updated October 6, 2015.
MANCHESTER, U.K. – Multiple joint and skin benefits can be achieved by intensively treating patients with psoriatic arthritis until they achieve a set of minimal disease activity criteria, an expert said at the British Society for Rheumatology annual conference.
While data are mounting on the value of treating to target (otherwise known as tight control) in psoriatic arthritis (PsA), these data lag significantly behind that for inducing and maintaining remission in rheumatoid arthritis (RA), noted Dr. Philip Helliwell of the University of Leeds (England).
“There is half as much evidence in PsA as there is in rheumatoid arthritis,” he observed. “But we’ve also got a heterogeneous disease and what we are going to have to do moving forward is to find out how to treat different phenotypic expressions of psoriatic disease, and we’re beginning to work towards that now,” he said during a Special Interest Group on Spondyloarthropathies.
Dr. Helliwell is the principal investigator of the Tight Control of Psoriatic Arthritis (TICOPA) study, which he highlighted as an example of how targeting treatment to achieve minimal disease activity (MDA) criteria (Ann. Rheum. Dis. 2010;69:48-53) could be beneficial versus standard care.
A total of 206 patients with newly-diagnosed PsA were enrolled into the study and were randomized to receive either ‘tight control’ – meaning an intensive management strategy – or to standard care for 48 weeks.
Intensive treatment involved starting with methotrexate at a dose of 15 mg/kg per week and rapidly escalating to 25 mg/kg per week at 6 weeks if needed. If patients did not achieve five out of a set of seven MDA criteria for PsA, then methotrexate was continued and sulfasalazine was added and dose escalated after 4-8 weeks.
If MDA was still not achieved and criteria for biologics were not met according to NICE guidance, then alternatives were swapping out sulfasalazine for cyclosporine or leflunomide, again increasing the doses. Patients who did get put onto a biologic could switch to another anti-TNF if they did not respond after 12 weeks.
The primary endpoint data from the trial have been reported previously and showed that a higher proportion of patients in the intensive management group achieved ACR20 at 48 weeks, compared with those in the standard care group (62% vs. 45%, respectively; P = .02). A higher percentage of intensively managed patients also achieved ACR50 (51% vs. 25%; P = .0004) and ACR70 (38% vs. 17%, P = .002).
Skin symptoms, measured via the Psoriasis Area and Severity Index (PASI) showed significant improvement favoring intensive therapy over standard care. PASI20 was achieved by 72% of intensively managed patients versus 52% of those who received standard care. PASI75 was achieved by 59% versus 33%, respectively, and PASI90 by 40% versus 20%, respectively.
The full results of the study will be published soon in The Lancet and will include details of a variety of secondary outcomes and the cost-effectiveness of the intensive management strategy versus the standard care approach.
One of the key secondary outcomes of the trial was to look at the effects of the two treatment strategies on other PsA symptoms, such as enthesitis, dactylitis, and nail symptoms. No differences between the groups were observed, however, with similar decreases seen in the tight control and standard care groups.
There were no statistically significant differences in radiologic outcomes, which included baseline and end-of-treatment changes in the total modified Sharp van der Heijde (SVdH) score, the erosion score, and joint-space narrowing (JSN) score.
While this might seem somewhat disappointing, “there wasn’t a lot of radiologic progression going on anyway,” Dr. Helliwell pointed out. Overall, there was a difference of about 5% in the percentage of patients with at least one joint erosion at baseline and after 48 weeks of treatment.
The majority of radiographic change that did occur was JSN of the hands, Dr. Helliwell said, adding that patients with JSN tended to be slightly older than those without, although this observation did not reach statistical significance.
“We’ve since looked for associations with ACPA [anticitrullinated protein antibodies] – about 7% of our patients were ACPA positive – but there is no relationship,” he added. There was also no significant association between levels of C-reactive protein levels and erosive disease.
There was a trend suggesting that patients with erosions may be more likely to have polyarticular disease than oligoarticular disease, so a next step would be to look at radiologic progression in these two groups of patients in more detail.
More adverse events were seen in the tight control arm, compared with the standard care arm, including more serious adverse events, but not all of these were related to study treatment and many adverse events were those to be expected with methotrexate treatment, Dr. Helliwell observed.
But is the intensive approach cost-effective when compared to standard care? Data suggest that it is. Although the incremental cost-effectiveness ratio (ICER) initially exceeded the £20,000–£30,000 (about $31,000-$47,000) threshold used by the U.K. National Institute for Health and Care Excellence to judge if a new treatment is cost effective, allowing for certain factors enabled the ICER to be brought down to about £28,000 ($44,000), making it a cost-effective strategy.
PsA consists of five classical subtypes. The most common of these subtypes is polyarthritis (60% of patients), followed by oligoarthritis (30%). The remaining 10% of patients comprise those with arthritis mutilans, distal interphalangeal predominant disease, or spinal predominant disease. The clinical features of dactylitis and enthesitis are prevalent in about 40% and 50% of patients, respectively, and can occur in any subgroup.
Considering such heterogeneity in its presentation, the challenge now will be to determine if all clinical subgroups of PsA could benefit from treating to an MDA target with intensive management, or if one or other subgroups benefit more than another.
The TICOPA study was funded by Arthritis Research UK with support from Pfizer. Dr. Helliwell has received consulting fees from Pfizer.
Results of this study were published in the Lancet Sept. 30, 2015.
This article was updated October 6, 2015.
EXPERT ANALYSIS AT RHEUMATOLOGY 2015
New psoriatic arthritis risk locus unrelated to psoriasis found
The PTPN22 gene was significantly associated with susceptibility to psoriatic arthritis but was not related to psoriasis risk, according to Dr. John Bowes and his associates.
In a total sample of 3,139 psoriatic arthritis (PsA) cases and 11,078 controls, the investigators tested 13 single-nucleotide polymorphisms and found 2 to be significantly associated with PsA, rs4795067 and rs2476601. The single-nucleotide polymorphism rs4795067, which maps to the NOS2 gene, was already known as a risk locus, but rs2476601, which maps to PTPN22, was not. The odds ratio for PTPN22 was 1.32, slightly more than the OR for the previously known NOS2 locus at 1.22.
“The identification of PsA-specific loci is vital in terms of understanding the different pathways involved, which may require different treatments, and for future screening strategies to identify subjects at risk of developing PsA in patients with psoriasis,” the investigators wrote.
Read the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-207187).
The PTPN22 gene was significantly associated with susceptibility to psoriatic arthritis but was not related to psoriasis risk, according to Dr. John Bowes and his associates.
In a total sample of 3,139 psoriatic arthritis (PsA) cases and 11,078 controls, the investigators tested 13 single-nucleotide polymorphisms and found 2 to be significantly associated with PsA, rs4795067 and rs2476601. The single-nucleotide polymorphism rs4795067, which maps to the NOS2 gene, was already known as a risk locus, but rs2476601, which maps to PTPN22, was not. The odds ratio for PTPN22 was 1.32, slightly more than the OR for the previously known NOS2 locus at 1.22.
“The identification of PsA-specific loci is vital in terms of understanding the different pathways involved, which may require different treatments, and for future screening strategies to identify subjects at risk of developing PsA in patients with psoriasis,” the investigators wrote.
Read the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-207187).
The PTPN22 gene was significantly associated with susceptibility to psoriatic arthritis but was not related to psoriasis risk, according to Dr. John Bowes and his associates.
In a total sample of 3,139 psoriatic arthritis (PsA) cases and 11,078 controls, the investigators tested 13 single-nucleotide polymorphisms and found 2 to be significantly associated with PsA, rs4795067 and rs2476601. The single-nucleotide polymorphism rs4795067, which maps to the NOS2 gene, was already known as a risk locus, but rs2476601, which maps to PTPN22, was not. The odds ratio for PTPN22 was 1.32, slightly more than the OR for the previously known NOS2 locus at 1.22.
“The identification of PsA-specific loci is vital in terms of understanding the different pathways involved, which may require different treatments, and for future screening strategies to identify subjects at risk of developing PsA in patients with psoriasis,” the investigators wrote.
Read the full study in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-207187).
New teaching tool could help doctors screen for PsA
A new teaching tool based on the acronym mnemonic PSA may help doctors to screen for psoriatic arthritis in patients with psoriasis or a strong family history of it.
The tool tells physicians to ask patients whether they are experiencing core features of psoriatic arthritis (PsA). Such features are tied to the acronym PSA. P stands for pain in the joints, S stands for stiffness more than 30 minutes after a period of inactivity and for sausage digits, and A represents axial spine involvement or back pain associated with stiffness that improves with activity. If patients with psoriasis and/or a strong family history of psoriasis say they are experiencing at least two of those features, then they “would have a higher than average chance of a PsA diagnosis,” according to Jeffrey M. Cohen and his colleagues.
Benefits of the tool include its ease of use and short administration time; it also covers “the core domains” of the disease, just like many of the current PsA screening tools.
The tool is limited, however, because it is unlikely to be as specific as the longer PsA screening instruments and it calls for questioning patients about features of PsA that are also features of other pathologies. Additionally, the tool is more specific to diagnosing seronegative peripheral and axial spondyloarthritides than inflammatory arthritis. It also is useful for distinguishing between noninflammatory arthritis and inflammatory arthritis.
“We feel this teaching tool, while not specific for PsA, will help the nonrheumatologist begin to differentiate inflammatory from noninflammatory musculoskeletal pain and therefore prompt an appropriate referral for work-up,” the researchers wrote.
Read the full paper in the Journal of the American Academy of Dermatology (doi:10.1016/j.jaad.2014.12.008).
A new teaching tool based on the acronym mnemonic PSA may help doctors to screen for psoriatic arthritis in patients with psoriasis or a strong family history of it.
The tool tells physicians to ask patients whether they are experiencing core features of psoriatic arthritis (PsA). Such features are tied to the acronym PSA. P stands for pain in the joints, S stands for stiffness more than 30 minutes after a period of inactivity and for sausage digits, and A represents axial spine involvement or back pain associated with stiffness that improves with activity. If patients with psoriasis and/or a strong family history of psoriasis say they are experiencing at least two of those features, then they “would have a higher than average chance of a PsA diagnosis,” according to Jeffrey M. Cohen and his colleagues.
Benefits of the tool include its ease of use and short administration time; it also covers “the core domains” of the disease, just like many of the current PsA screening tools.
The tool is limited, however, because it is unlikely to be as specific as the longer PsA screening instruments and it calls for questioning patients about features of PsA that are also features of other pathologies. Additionally, the tool is more specific to diagnosing seronegative peripheral and axial spondyloarthritides than inflammatory arthritis. It also is useful for distinguishing between noninflammatory arthritis and inflammatory arthritis.
“We feel this teaching tool, while not specific for PsA, will help the nonrheumatologist begin to differentiate inflammatory from noninflammatory musculoskeletal pain and therefore prompt an appropriate referral for work-up,” the researchers wrote.
Read the full paper in the Journal of the American Academy of Dermatology (doi:10.1016/j.jaad.2014.12.008).
A new teaching tool based on the acronym mnemonic PSA may help doctors to screen for psoriatic arthritis in patients with psoriasis or a strong family history of it.
The tool tells physicians to ask patients whether they are experiencing core features of psoriatic arthritis (PsA). Such features are tied to the acronym PSA. P stands for pain in the joints, S stands for stiffness more than 30 minutes after a period of inactivity and for sausage digits, and A represents axial spine involvement or back pain associated with stiffness that improves with activity. If patients with psoriasis and/or a strong family history of psoriasis say they are experiencing at least two of those features, then they “would have a higher than average chance of a PsA diagnosis,” according to Jeffrey M. Cohen and his colleagues.
Benefits of the tool include its ease of use and short administration time; it also covers “the core domains” of the disease, just like many of the current PsA screening tools.
The tool is limited, however, because it is unlikely to be as specific as the longer PsA screening instruments and it calls for questioning patients about features of PsA that are also features of other pathologies. Additionally, the tool is more specific to diagnosing seronegative peripheral and axial spondyloarthritides than inflammatory arthritis. It also is useful for distinguishing between noninflammatory arthritis and inflammatory arthritis.
“We feel this teaching tool, while not specific for PsA, will help the nonrheumatologist begin to differentiate inflammatory from noninflammatory musculoskeletal pain and therefore prompt an appropriate referral for work-up,” the researchers wrote.
Read the full paper in the Journal of the American Academy of Dermatology (doi:10.1016/j.jaad.2014.12.008).
Systemic psoriasis treatment may resolve subclinical enthesitis
Psoriasis patients with ultrasonographic enthesitis who undergo systemic treatments can experience significant reductions in morphologic abnormalities in as little as 6 months, according to the findings of a two-center prospective study published in Joint Bone Spine.
“Here, we showed that subclinical enthesitis of both [psoriasis] and PsA [psoriatic arthritis] population improve under systemic treatment,” wrote lead author Dr. Emilie Acquacalda of the University Hospital of Nice (France) and her associates. “Both patients under methotrexate and biologics had a reduction of the enthesitis at US [ultrasonographic] examination.”
The investigators enrolled 34 patients – 22 with psoriasis and 12 with symptomatic PsA – for whom US assessments were taken at baseline. Abnormalities, specifically hypoechogenicity and thickness, were noted in 86.4% (19) of psoriasis patients and 97.1% (33) of the total population. Enthesitis was found in 95 of the 340 entheses examined at baseline, 57 of which were in psoriasis patients (Joint Bone Spine 2015 April 13 [doi:10.1016/j.jbspin.2015.01.016]).
Psoriasis patients were given systemic treatment consisting of methotrexate and/or biologic therapies, which were infliximab, adalimumab, etanercept, and ustekinumab. At 6 months, 23 patients were assessed (11 refused ultrasonography), 13 of whom had psoriasis and 10 of whom had PsA. Of these subjects, 12 received methotrexate alone and 11 received it with a biologic.
Morphologic abnormalities in the psoriasis population decreased significantly, from 30% (39 of 130) at baseline to 17.7% (23 of 130; P = .021). Psoriasis patients who took methotrexate had the most significant decreases, with methotrexate alone reducing the proportion of abnormalities from 28.8% (23 of 30) at baseline to 15% (12 of 80; P = .035), Dr. Acquacalda and her associates reported.
Treatment with biologics also showed promise, with abnormality rates dropping from 32% (16 of 80) to 22% (11 of 80), but the results were not statistically significant (P = .359). Overall, PsA patients saw enthesitis improvement from 33% (33 of 100) to 24% (24 of 100) over the 6-month study period, but the difference was not statistically significant (P = .164), they said.
The authors also noted that the relatively small number of subjects in their study prohibits them from making any definitive conclusions about the efficacy of systemic and biological treatments, but urged that “long-term follow-up studies of [psoriasis] patients with and without subclinical enthesitis are warranted to determine if they have a predictive value of future PsA, and to determine if rapid introduction of a systemic treatment could impact this evolution.”
The authors did not report any relevant conflicts of interest.
Psoriasis patients with ultrasonographic enthesitis who undergo systemic treatments can experience significant reductions in morphologic abnormalities in as little as 6 months, according to the findings of a two-center prospective study published in Joint Bone Spine.
“Here, we showed that subclinical enthesitis of both [psoriasis] and PsA [psoriatic arthritis] population improve under systemic treatment,” wrote lead author Dr. Emilie Acquacalda of the University Hospital of Nice (France) and her associates. “Both patients under methotrexate and biologics had a reduction of the enthesitis at US [ultrasonographic] examination.”
The investigators enrolled 34 patients – 22 with psoriasis and 12 with symptomatic PsA – for whom US assessments were taken at baseline. Abnormalities, specifically hypoechogenicity and thickness, were noted in 86.4% (19) of psoriasis patients and 97.1% (33) of the total population. Enthesitis was found in 95 of the 340 entheses examined at baseline, 57 of which were in psoriasis patients (Joint Bone Spine 2015 April 13 [doi:10.1016/j.jbspin.2015.01.016]).
Psoriasis patients were given systemic treatment consisting of methotrexate and/or biologic therapies, which were infliximab, adalimumab, etanercept, and ustekinumab. At 6 months, 23 patients were assessed (11 refused ultrasonography), 13 of whom had psoriasis and 10 of whom had PsA. Of these subjects, 12 received methotrexate alone and 11 received it with a biologic.
Morphologic abnormalities in the psoriasis population decreased significantly, from 30% (39 of 130) at baseline to 17.7% (23 of 130; P = .021). Psoriasis patients who took methotrexate had the most significant decreases, with methotrexate alone reducing the proportion of abnormalities from 28.8% (23 of 30) at baseline to 15% (12 of 80; P = .035), Dr. Acquacalda and her associates reported.
Treatment with biologics also showed promise, with abnormality rates dropping from 32% (16 of 80) to 22% (11 of 80), but the results were not statistically significant (P = .359). Overall, PsA patients saw enthesitis improvement from 33% (33 of 100) to 24% (24 of 100) over the 6-month study period, but the difference was not statistically significant (P = .164), they said.
The authors also noted that the relatively small number of subjects in their study prohibits them from making any definitive conclusions about the efficacy of systemic and biological treatments, but urged that “long-term follow-up studies of [psoriasis] patients with and without subclinical enthesitis are warranted to determine if they have a predictive value of future PsA, and to determine if rapid introduction of a systemic treatment could impact this evolution.”
The authors did not report any relevant conflicts of interest.
Psoriasis patients with ultrasonographic enthesitis who undergo systemic treatments can experience significant reductions in morphologic abnormalities in as little as 6 months, according to the findings of a two-center prospective study published in Joint Bone Spine.
“Here, we showed that subclinical enthesitis of both [psoriasis] and PsA [psoriatic arthritis] population improve under systemic treatment,” wrote lead author Dr. Emilie Acquacalda of the University Hospital of Nice (France) and her associates. “Both patients under methotrexate and biologics had a reduction of the enthesitis at US [ultrasonographic] examination.”
The investigators enrolled 34 patients – 22 with psoriasis and 12 with symptomatic PsA – for whom US assessments were taken at baseline. Abnormalities, specifically hypoechogenicity and thickness, were noted in 86.4% (19) of psoriasis patients and 97.1% (33) of the total population. Enthesitis was found in 95 of the 340 entheses examined at baseline, 57 of which were in psoriasis patients (Joint Bone Spine 2015 April 13 [doi:10.1016/j.jbspin.2015.01.016]).
Psoriasis patients were given systemic treatment consisting of methotrexate and/or biologic therapies, which were infliximab, adalimumab, etanercept, and ustekinumab. At 6 months, 23 patients were assessed (11 refused ultrasonography), 13 of whom had psoriasis and 10 of whom had PsA. Of these subjects, 12 received methotrexate alone and 11 received it with a biologic.
Morphologic abnormalities in the psoriasis population decreased significantly, from 30% (39 of 130) at baseline to 17.7% (23 of 130; P = .021). Psoriasis patients who took methotrexate had the most significant decreases, with methotrexate alone reducing the proportion of abnormalities from 28.8% (23 of 30) at baseline to 15% (12 of 80; P = .035), Dr. Acquacalda and her associates reported.
Treatment with biologics also showed promise, with abnormality rates dropping from 32% (16 of 80) to 22% (11 of 80), but the results were not statistically significant (P = .359). Overall, PsA patients saw enthesitis improvement from 33% (33 of 100) to 24% (24 of 100) over the 6-month study period, but the difference was not statistically significant (P = .164), they said.
The authors also noted that the relatively small number of subjects in their study prohibits them from making any definitive conclusions about the efficacy of systemic and biological treatments, but urged that “long-term follow-up studies of [psoriasis] patients with and without subclinical enthesitis are warranted to determine if they have a predictive value of future PsA, and to determine if rapid introduction of a systemic treatment could impact this evolution.”
The authors did not report any relevant conflicts of interest.
FROM JOINT BONE SPINE
Key clinical point: Systemic treatment of ultrasonographic enthesitis in psoriasis patients significantly mitigates morphologic abnormalities within 6 months.
Major finding: Psoriasis patients with ultrasonographic morphological abnormalities decreased from 30% to 17.7% (P = .021); treatment with methotrexate alone decreased the rate of enthesitis from 28.8% of entheses to 15% (P = .035).
Data source: Prospective study of 34 patients receiving treatment in two centers over the course of 6 months.
Disclosures: The authors did not report any relevant conflicts of interest.
New tool aims to improve monitoring of psoriatic arthritis
Austrian researchers have developed and validated a new five-question self-assessment survey for psoriatic arthritis patients to monitor their disease activity, according to a report published online in BMC Musculoskeletal Disorders.
The Stockerau Activity Score for Psoriatic Arthritis (SASPA) was developed by the team responsible for the Rheumatoid Arthritis Disease Activity Index (RADAI-5) and is similar to it. Using a variety of statistical tests, Dr. Burkhard F. Leeb of the Karl Landsteiner Institute for Clinical Rheumatology in Stockerau, Austria, and his colleagues demonstrated SASPA’s reliability, convergent validity, and sensitivity to change in 152 adult psoriatic arthritis outpatients. For example, they found a Cronbach’s alpha for SASPA of 0.875, indicating high internal consistency and reliability (BMC Musculoskelet. Disord. 2015;16:73).
There are several psoriatic arthritis assessment tools already that work for between-group comparisons but “may not be fully suitable for assessing individual patients,” the investigators wrote.
With SASPA, however, they noted that “inter-physician, but also intra-physician variations in assessing joints or global disease activity are eliminated, and other pitfalls of joint counts are avoided.”
The study was supported by the Karl Landsteiner Institute for Clinical Rheumatology. The authors said that they had no financial disclosures.
Austrian researchers have developed and validated a new five-question self-assessment survey for psoriatic arthritis patients to monitor their disease activity, according to a report published online in BMC Musculoskeletal Disorders.
The Stockerau Activity Score for Psoriatic Arthritis (SASPA) was developed by the team responsible for the Rheumatoid Arthritis Disease Activity Index (RADAI-5) and is similar to it. Using a variety of statistical tests, Dr. Burkhard F. Leeb of the Karl Landsteiner Institute for Clinical Rheumatology in Stockerau, Austria, and his colleagues demonstrated SASPA’s reliability, convergent validity, and sensitivity to change in 152 adult psoriatic arthritis outpatients. For example, they found a Cronbach’s alpha for SASPA of 0.875, indicating high internal consistency and reliability (BMC Musculoskelet. Disord. 2015;16:73).
There are several psoriatic arthritis assessment tools already that work for between-group comparisons but “may not be fully suitable for assessing individual patients,” the investigators wrote.
With SASPA, however, they noted that “inter-physician, but also intra-physician variations in assessing joints or global disease activity are eliminated, and other pitfalls of joint counts are avoided.”
The study was supported by the Karl Landsteiner Institute for Clinical Rheumatology. The authors said that they had no financial disclosures.
Austrian researchers have developed and validated a new five-question self-assessment survey for psoriatic arthritis patients to monitor their disease activity, according to a report published online in BMC Musculoskeletal Disorders.
The Stockerau Activity Score for Psoriatic Arthritis (SASPA) was developed by the team responsible for the Rheumatoid Arthritis Disease Activity Index (RADAI-5) and is similar to it. Using a variety of statistical tests, Dr. Burkhard F. Leeb of the Karl Landsteiner Institute for Clinical Rheumatology in Stockerau, Austria, and his colleagues demonstrated SASPA’s reliability, convergent validity, and sensitivity to change in 152 adult psoriatic arthritis outpatients. For example, they found a Cronbach’s alpha for SASPA of 0.875, indicating high internal consistency and reliability (BMC Musculoskelet. Disord. 2015;16:73).
There are several psoriatic arthritis assessment tools already that work for between-group comparisons but “may not be fully suitable for assessing individual patients,” the investigators wrote.
With SASPA, however, they noted that “inter-physician, but also intra-physician variations in assessing joints or global disease activity are eliminated, and other pitfalls of joint counts are avoided.”
The study was supported by the Karl Landsteiner Institute for Clinical Rheumatology. The authors said that they had no financial disclosures.
FROM BMC MUSCULOSKELETAL DISORDERS
Key clinical point: A brief, five-question assessment tool may be a good way to routinely monitor psoriatic arthritis patients.
Major finding: The Stockerau Activity Score for Psoriatic Arthritis (SASPA) had a Cronbach’s alpha of 0.875, indicating high internal consistency and reliability.
Data source: An observational study of 152 outpatients with psoriatic arthritis.
Disclosures: The study was supported by the Karl Landsteiner Institute for Clinical Rheumatology. The authors said they had no financial disclosures.
Older psoriasis patients experience more adverse events
Serious adverse events are more likely in patients older than 65 years undergoing psoriasis therapy, though whether these events are because of the treatment itself or other risk factors remains unclear, according to Dr. Carolina Medina and her associates.
In a review of data from 1,793 psoriasis patients enrolled in a national registry in Spain (10% of whom were older than 65 years), the overall risk of any adverse event was not significantly higher in the older group (drug group adjusted hazard ratio 1.09). However, the risk of serious adverse events was much greater (drug group adjusted HR, 3.2). Biologic exposure decreased the risk of adverse events in both younger and older patients, compared with those receiving classic therapy, even after adjustments for age (HR, 0.7, age adjusted), the researchers noted.
“These results are reassuring, although uncontrolled confounding could not be excluded as an explanation for these findings, and the power of the study to detect differences was low,” they concluded.
Find the full study in the Journal of the European Academy of Dermatology and Venereology (doi: 10.1111/jdv.12688).
Serious adverse events are more likely in patients older than 65 years undergoing psoriasis therapy, though whether these events are because of the treatment itself or other risk factors remains unclear, according to Dr. Carolina Medina and her associates.
In a review of data from 1,793 psoriasis patients enrolled in a national registry in Spain (10% of whom were older than 65 years), the overall risk of any adverse event was not significantly higher in the older group (drug group adjusted hazard ratio 1.09). However, the risk of serious adverse events was much greater (drug group adjusted HR, 3.2). Biologic exposure decreased the risk of adverse events in both younger and older patients, compared with those receiving classic therapy, even after adjustments for age (HR, 0.7, age adjusted), the researchers noted.
“These results are reassuring, although uncontrolled confounding could not be excluded as an explanation for these findings, and the power of the study to detect differences was low,” they concluded.
Find the full study in the Journal of the European Academy of Dermatology and Venereology (doi: 10.1111/jdv.12688).
Serious adverse events are more likely in patients older than 65 years undergoing psoriasis therapy, though whether these events are because of the treatment itself or other risk factors remains unclear, according to Dr. Carolina Medina and her associates.
In a review of data from 1,793 psoriasis patients enrolled in a national registry in Spain (10% of whom were older than 65 years), the overall risk of any adverse event was not significantly higher in the older group (drug group adjusted hazard ratio 1.09). However, the risk of serious adverse events was much greater (drug group adjusted HR, 3.2). Biologic exposure decreased the risk of adverse events in both younger and older patients, compared with those receiving classic therapy, even after adjustments for age (HR, 0.7, age adjusted), the researchers noted.
“These results are reassuring, although uncontrolled confounding could not be excluded as an explanation for these findings, and the power of the study to detect differences was low,” they concluded.
Find the full study in the Journal of the European Academy of Dermatology and Venereology (doi: 10.1111/jdv.12688).
Late-onset psoriasis genetics identified
Certain genetic loci are likely associated with late-onset psoriasis, based on data from a study of 543 cases and 4,373 healthy controls. Previous studies have shown 36 genetic loci linked to early-onset psoriasis (younger than 40 years), but the genetics of late-onset psoriasis (aged 40 years and older) have not been well studied, wrote Harry L. Hébert, a PhD candidate at the University of Manchester, England, and his colleagues.
In their genotyping analysis, the two loci HLA-C and IL12B, shown to be associated with early-onset psoriasis, also were significantly associated with late-onset disease, as were six other loci. In addition, IL1R1 on chromosome 2q13 was uniquely associated with late-onset psoriasis.
Find the full study online in the British Journal of Dermatology (2015;172:933-9 [doi:10.1111/bjd.13340]).
Certain genetic loci are likely associated with late-onset psoriasis, based on data from a study of 543 cases and 4,373 healthy controls. Previous studies have shown 36 genetic loci linked to early-onset psoriasis (younger than 40 years), but the genetics of late-onset psoriasis (aged 40 years and older) have not been well studied, wrote Harry L. Hébert, a PhD candidate at the University of Manchester, England, and his colleagues.
In their genotyping analysis, the two loci HLA-C and IL12B, shown to be associated with early-onset psoriasis, also were significantly associated with late-onset disease, as were six other loci. In addition, IL1R1 on chromosome 2q13 was uniquely associated with late-onset psoriasis.
Find the full study online in the British Journal of Dermatology (2015;172:933-9 [doi:10.1111/bjd.13340]).
Certain genetic loci are likely associated with late-onset psoriasis, based on data from a study of 543 cases and 4,373 healthy controls. Previous studies have shown 36 genetic loci linked to early-onset psoriasis (younger than 40 years), but the genetics of late-onset psoriasis (aged 40 years and older) have not been well studied, wrote Harry L. Hébert, a PhD candidate at the University of Manchester, England, and his colleagues.
In their genotyping analysis, the two loci HLA-C and IL12B, shown to be associated with early-onset psoriasis, also were significantly associated with late-onset disease, as were six other loci. In addition, IL1R1 on chromosome 2q13 was uniquely associated with late-onset psoriasis.
Find the full study online in the British Journal of Dermatology (2015;172:933-9 [doi:10.1111/bjd.13340]).
New psoriatic arthritis screening tool passes initial validation
The second version of the Toronto Psoriatic Arthritis screen performed well at identifying psoriatic arthritis in 336 psoriasis patients, 131 psoriatic arthritis patients, and 89 individuals in the general population, according to Dr. Brian Tom and his associates.
The sensitivities of the capped and uncapped version of the ToPAS 2 system were the same across all measured groups (92.0%) when the cutpoint was 7 for ToPAS2_cap and 8 for ToPAS2_uncap, although the sensitivity for ToPAS2_uncap was slightly lower when the cutpoint was 9 (84.0% vs. 87.2)%. Both were higher than the original ToPAS index (sensitivity 86.6%), which did not include a spinal domain. However, the specificity of the original ToPAS index across all measured groups was slightly higher (80.5%-95.5%) than with ToPAS2_cap and ToPAS2_uncap (73.8%-89.9% and 71.6%-91.0%).
Besides the addition of a spinal domain, the ToPAS 2 “incorporates further pictures of cutaneous psoriasis, joint inflammation, and dactylitis to improve its performance, as well as more carefully worded questions regarding spinal involvement,” the investigators wrote.
While the specificity is lower with ToPAS 2, this should not be a major issue, because “for the purposes of identifying patients whom dermatologists or primary care physicians should refer to a rheumatologist, the specificity is not as important, because patients with rheumatological disorders other than PsA would benefit from a rheumatologist’s consultation,” the investigators said.
Find the full study in Journal of Rheumatology (doi:10.3899/jrheum.140857).
The second version of the Toronto Psoriatic Arthritis screen performed well at identifying psoriatic arthritis in 336 psoriasis patients, 131 psoriatic arthritis patients, and 89 individuals in the general population, according to Dr. Brian Tom and his associates.
The sensitivities of the capped and uncapped version of the ToPAS 2 system were the same across all measured groups (92.0%) when the cutpoint was 7 for ToPAS2_cap and 8 for ToPAS2_uncap, although the sensitivity for ToPAS2_uncap was slightly lower when the cutpoint was 9 (84.0% vs. 87.2)%. Both were higher than the original ToPAS index (sensitivity 86.6%), which did not include a spinal domain. However, the specificity of the original ToPAS index across all measured groups was slightly higher (80.5%-95.5%) than with ToPAS2_cap and ToPAS2_uncap (73.8%-89.9% and 71.6%-91.0%).
Besides the addition of a spinal domain, the ToPAS 2 “incorporates further pictures of cutaneous psoriasis, joint inflammation, and dactylitis to improve its performance, as well as more carefully worded questions regarding spinal involvement,” the investigators wrote.
While the specificity is lower with ToPAS 2, this should not be a major issue, because “for the purposes of identifying patients whom dermatologists or primary care physicians should refer to a rheumatologist, the specificity is not as important, because patients with rheumatological disorders other than PsA would benefit from a rheumatologist’s consultation,” the investigators said.
Find the full study in Journal of Rheumatology (doi:10.3899/jrheum.140857).
The second version of the Toronto Psoriatic Arthritis screen performed well at identifying psoriatic arthritis in 336 psoriasis patients, 131 psoriatic arthritis patients, and 89 individuals in the general population, according to Dr. Brian Tom and his associates.
The sensitivities of the capped and uncapped version of the ToPAS 2 system were the same across all measured groups (92.0%) when the cutpoint was 7 for ToPAS2_cap and 8 for ToPAS2_uncap, although the sensitivity for ToPAS2_uncap was slightly lower when the cutpoint was 9 (84.0% vs. 87.2)%. Both were higher than the original ToPAS index (sensitivity 86.6%), which did not include a spinal domain. However, the specificity of the original ToPAS index across all measured groups was slightly higher (80.5%-95.5%) than with ToPAS2_cap and ToPAS2_uncap (73.8%-89.9% and 71.6%-91.0%).
Besides the addition of a spinal domain, the ToPAS 2 “incorporates further pictures of cutaneous psoriasis, joint inflammation, and dactylitis to improve its performance, as well as more carefully worded questions regarding spinal involvement,” the investigators wrote.
While the specificity is lower with ToPAS 2, this should not be a major issue, because “for the purposes of identifying patients whom dermatologists or primary care physicians should refer to a rheumatologist, the specificity is not as important, because patients with rheumatological disorders other than PsA would benefit from a rheumatologist’s consultation,” the investigators said.
Find the full study in Journal of Rheumatology (doi:10.3899/jrheum.140857).