User login
Birds, butterflies and bullfrogs: When patients ‘see things’
HISTORY: A sudden vision
Ms. K, 73, was in reasonably good health when one day she suddenly noticed red, green, and yellow birds and butterflies covering her wall.
Ms. K, who lives alone, was frightened at first, but she did not immediately alert anyone because she thought she “was just seeing things, and they’ll go away.”
Instead, she saw more visions over the next 3 months. She once “watched” as two doctors and a nun carried a middle-aged burn victim into her apartment. She remembers seeing the doctors put a “patch” over the woman’s body. To Ms. K, this experience seemed so shockingly real that she called 911, reporting, “That woman should have been in the hospital!”
She reports that a pack of butterflies once “followed” her to the market. She vividly recalls how they crawled about her shoes and legs as she entered the store. When asked if anyone noticed her insect-covered extremities, she replied matter-of-factly, “Maybe it’s not for them to see, maybe it’s just for me,” as if her hallucinations were a divine gift.
Ms. K’s hallucinations usually occur at home, where she spends most of her time. She says that the images are fleeting, lasting from a few seconds to several minutes, and that the creatures fly silently around her room.
Ms. K’s daughter grew concerned that the hallucinations were increasingly diminishing her mother’s ability to care for herself. She brought Ms. K into our emergency department, from which the patient was admitted.
On admission, Ms. K said she had lost 20 lbs within 6 months, and that “concentrating on those things in the house” was impairing her sleep. She denied recent illness, trauma, loss of conscious ness, changes in medications, seizures, drug or alcohol use, suicidal or homicidal ideation, or specific stress in her life. She added that she often cooks for herself—only to lose her appetite after seeing bugs and other creatures crawl into her food.
Her medical history includes hypertension, type 2 diabetes mellitus, peripheral vascular disease, urinary incontinence, gastroesophageal reflux, glaucoma in her left eye, and bilateral cataracts. She denies any psychiatric history and adds that she had never experienced hallucinations until about 3 months before hospitalization. She also denies any history of auditory, tactile, or olfactory hallucinations.
Would you suspect a primary psychotic illness? What clinical tests might help us understand Ms. K’s progressively debilitating visual hallucinations?
The authors’ observations
Ms. K’s case places us at the crossroads of psychiatric disturbances and medical conditions that can present as or precipitate apparent psychiatric symptoms. Delirium, dementia, psychosis, endocrinopathies, encephalitis, electrolyte disturbances, drug abuse/withdrawal, and occipital or temporal lobe seizures are all possible differential diagnoses (Table 1).
A cognitive function screening and a battery of laboratory tests, imaging scans, and neurologic and vision exams are needed to uncover the cause of her hallucinations.
EVALUATION: Looking for clues
Ms. K’s left pupil was fixed at 6 mm and did not respond to light, while the right pupil was regular and reactive to light at 3 mm. Using a Snellen eye chart, her visual acuity was poor: 20/100 to 20/200 in her right eye and less than 20/200 in the left eye. She scored a 29 out of 30 on the Folstein Mini-Mental State Examination (MMSE), indicating her cognition was intact. The remainder of the neurologic exam was unremarkable.
At admission, Ms. K’s medications included metoprolol, 100 mg qd, for hypertension; lansoprazole, 30 mg qd, for gastroesophageal reflux; tolterodine, 2 mg bid, and oxybutynin, 10 mg qd, for urinary incontinence; repaglinide, 2 mg bid, for type 2 diabetes; and three ophthalmic agents: brimonidine, prednisolone, and dorzolamide/timolol. The patient had been maintained on these medications for more than 2 years with no recent changes in dosing.
Results of Ms. K’s lab studies were normal, including a basic metabolic panel, CBC, liver function tests, urinalysis, B12, thyroid panel, rapid plasma reagin test, and urine drug screen.
A head CT without contrast revealed chronic small-vessel ischemic white matter disease and a chronic infarct of the left cerebellar hemisphere. No acute intracranial hemorrhages, masses, or other abnormalities were noted. No seizures were seen on EEG.
Table 1
Common causes of visual hallucinations
| Schizophrenia |
| Delirium |
| Dementias |
| Substance-induced psychosis |
| Electrolyte disturbances |
| Occipital and temporal lobe epilepsy |
| Charles Bonnet syndrome |
What do the laboratory and imaging tests reveal about Ms. K’s hallucinations? Is her diagnosis delirium? Alzheimer’s or other type of dementia? Schizophrenia?
The authors’ observations
Visual hallucinations—often of deceased parents or siblings, unknown intruders, and animals—can occur in up to 25% of patients with Alzheimer’s-type dementia.1 Also, patients with Lewy body dementia often present with well-formed visual hallucinations, which are thought to result from temporal lobe involvement by the characteristic Lewy bodies.
To diagnose dementia, DSM-IV requires the presence of multiple cognitive deficits manifested by memory impairment and one or more of the following:
- aphasia
- apraxia
- agnosia
- disturbance of executive functioning.2
Ms. K exhibited none of these characteristics, and she retained full executive function—she could balance her checkbook, buy groceries, and cook for herself. Also, her MMSE score was high.
Ms. K showed no consciousness fluctuations or attention deficits, two features commonly seen in delirium. She was alert and oriented throughout the interview, and her flow of thought, speech, language, and attention were appropriate. Therefore, delirium can be reasonably excluded.
The hallucinations probably do not signal onset of schizophrenia because of Ms. K’s age at presentation, lack of family history of psychotic disorder, and paucity of negative symptoms. Auditory hallucinations are much more common in psychosis, and isolated visual hallucinations rarely occur in schizophrenia.
Finally, Ms. K’s electrophysiologic, laboratory, and imaging studies revealed isolated systolic hypertension, low visual acuity, and a mild gait disturbance. Severe left lens opacification accounted for the patient’s discordant pupillary light reflex. None of these findings explained her visual hallucinations, however.
Is a non-psychiatric disorder causing Ms. K’s hallucinations? What type of medication might alleviate her symptoms?
The authors’ observations
Given Ms. K’s strong cognitive function and poor visual acuity, we concluded that her hallucinations may fit the criteria for Charles Bonnet syndrome (CBS), a poorly understood medical phenomenon.
CBS is characterized by complex visual hallucinations in visually impaired elderly patients without cognitive deficits (Table 2).3,4 Swiss philosopher Charles Bonnet first described the disorder in 1760 to explain the vivid visual hallucinations of his 89-year-old grandfather, who had severe cataracts but no cognitive deficits.3 Bonnet’s grandfather claimed to have visions of men, women, birds, buildings, and tapestries.3
CBS is increasingly recognized and reported, but the medical community has never formed a universally accepted definition for this phenomenon. Persons with CBS react positively or negatively to their hallucinations, and the images may stimulate anxiety, anger, or mild paranoia. Research has focused on prevalence, risk indicators, and treatment.
Table 2
Charles Bonnet syndrome: fast facts
|
Teunisse et al determined that visual hallucinations plague up to 14% of sight-impaired persons.4,5 The hallucinations vary widely: people, animals, flowers, vehicles, buildings, and sometimes complete scenes.4,5 Significant risk factors for CBS include advanced age and low visual acuity.4,5 Loneliness, introversion, and shyness are additional risk indicators in older, visually handicapped persons.6 Therefore, social isolation may be a predisposing factor.
Drug treatment of visual hallucinations in CBS currently includes antipsychotics, such as quetiapine (25 to 100 mg/d) and risperidone (0.25 to 1.0 mg/d).7 However, mixed results have been reported after use of antipsychotics in CBS; one patient’s visual hallucinations were exacerbated after risperidone was initiated.8 Case reports have also described the use of valproate, carbamazepine, and ondansetron in CBS.9-11
Empathy and patient education are the cornerstones of CBS treatment.3 Patients need to be reassured that their visions are benign. For many, simply increasing the amount of ambient light in the home can reduce hallucinations.
TREATMENT A frog in the toilet
Ms. K was started on quetiapine, 25 mg bid, to try to promote restorative sleep and resolve her hallucinations. Up to 18% of persons treated with quetiapine report somnolence as an adverse effect, vs. 3 to 8% of those treated with risperidone.12
During her hospital stay, Ms. K experienced no visual hallucinations during the day but reported seeing a grayish-brown bullfrog in the toilet at night. This hallucination did not frighten her; she would simply close the bathroom door and wait until the bullfrog “disappeared.”
Her sleep improved, as did her appetite. She participated in daily group sessions and socialized with other patients.
After 12 days, Ms. K was discharged. To decrease her social isolation, we encouraged her to participate in a day program for seniors. We also continued her on quetiapine, 25 mg bid.
Five months later, her primary care physician reports that Ms. K remains symptom free while maintaining her quetiapine dosage.
Related resources
- Royal National Institute of the Blind: Fact sheet for Charles Bonnet syndrome. Available at: http://www.rnib.org.uk/info/cbsfin.htm
- Verstraten PFJ. The Charles Bonnet syndrome: Development of a protocol for clinical practice in a multidisciplinary approach from assessment to intervention. Available at: http://www.rehab-syn.enter.iris.se/kc-syn/cb.htm
- Adamczyk DT. Optometric educators. Am I seeing things? Optometry Today June 18, 1999:37-9. Available at: http://www.optometry.co.uk/articles/19990618/Adamczyk.pdf
Drug brand names
- Brimonidine Ophthalmic • Alphagan
- Carbamazepine • Tegretol
- Dorzolamide/Timolol • Cosopt
- Lansoprazole • Prevacid
- Metoprolol • Toprol XL
- Ondansetron • Zofran
- Oxybutynin • Ditropan XL
- Quetiapine • Seroquel
- Repaglinide • Prandin
- Risperidone • Risperdal
- Tolterodine • Detrol
- Valproate • Depakote
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with competing manufacturers.
1. Geldmacher DS, Whitehouse PJ. Current concepts: evaluation of dementia. JAMA 1996;335:330-6.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, rev). Washington, DC: American Psychiatric Press, 2000.
3. Fernandez A, Lichtshein G, Vieweg WV. The Charles Bonnet syndrome: a review. J Nerv Ment Dis 1997;185:195-200.
4. Teunisse RJ, Cruysberg , JR, Hoefnagels WH, et al. Risk indicators for the Charles Bonnet syndrome. J Nerv Ment Dis 1998;186:190-2.
5. Teunisse RJ, Cruysberg J, Verbeek A, Zitman FG. The Charles Bonnet syndrome: a large prospective study in the Netherlands. A study of the prevalence of the Charles Bonnet syndrome and associated factors in 500 patients attending the University Department of Ophthalmology at Nijme. Br J Psychiatry 1995;166(2):254-7.
6. Teunisse RJ, Cruysberg JR, Hoefnagels WH, et al. Social and psychological characteristics of elderly visually handicapped patients with the Charles Bonnet Syndrome. Compr Psychiatry 1999;40(4):315-19.
7. Rovner BW. The Charles Bonnet syndrome: Visual hallucinations caused by visual impairment. Geriatrics 2002;57:45-6.
8. Kornreich C, Dan B, Verbanck P, Pelc I. Treating Charles Bonnet syndrome: understanding inconsistency. J Clin Psychopharmacol 2000;20(3):396.-
9. Hori H, Terao T, Shiraishi Y, Nakamura J. Treatment of Charles Bonnet syndrome with valproate. Int Clin Psychopharmacol 2000;15:117-19.
10. Batra A, Bartels M, Wormstall H. Therapeutic options in Charles Bonnet syndrome. Acta Psychiatr Scand 1997;96:129-33.
11. Nevins M. Charles Bonnet syndrome. J Am Geriatr Soc 1997;45:894.-
12. Brown C, Markowitz J, Moore T, Parker N. Atypical antipsychotics, part II: adverse effects, drug interactions, and efficacy. Ann Pharmacother 1999;33:210-17.
HISTORY: A sudden vision
Ms. K, 73, was in reasonably good health when one day she suddenly noticed red, green, and yellow birds and butterflies covering her wall.
Ms. K, who lives alone, was frightened at first, but she did not immediately alert anyone because she thought she “was just seeing things, and they’ll go away.”
Instead, she saw more visions over the next 3 months. She once “watched” as two doctors and a nun carried a middle-aged burn victim into her apartment. She remembers seeing the doctors put a “patch” over the woman’s body. To Ms. K, this experience seemed so shockingly real that she called 911, reporting, “That woman should have been in the hospital!”
She reports that a pack of butterflies once “followed” her to the market. She vividly recalls how they crawled about her shoes and legs as she entered the store. When asked if anyone noticed her insect-covered extremities, she replied matter-of-factly, “Maybe it’s not for them to see, maybe it’s just for me,” as if her hallucinations were a divine gift.
Ms. K’s hallucinations usually occur at home, where she spends most of her time. She says that the images are fleeting, lasting from a few seconds to several minutes, and that the creatures fly silently around her room.
Ms. K’s daughter grew concerned that the hallucinations were increasingly diminishing her mother’s ability to care for herself. She brought Ms. K into our emergency department, from which the patient was admitted.
On admission, Ms. K said she had lost 20 lbs within 6 months, and that “concentrating on those things in the house” was impairing her sleep. She denied recent illness, trauma, loss of conscious ness, changes in medications, seizures, drug or alcohol use, suicidal or homicidal ideation, or specific stress in her life. She added that she often cooks for herself—only to lose her appetite after seeing bugs and other creatures crawl into her food.
Her medical history includes hypertension, type 2 diabetes mellitus, peripheral vascular disease, urinary incontinence, gastroesophageal reflux, glaucoma in her left eye, and bilateral cataracts. She denies any psychiatric history and adds that she had never experienced hallucinations until about 3 months before hospitalization. She also denies any history of auditory, tactile, or olfactory hallucinations.
Would you suspect a primary psychotic illness? What clinical tests might help us understand Ms. K’s progressively debilitating visual hallucinations?
The authors’ observations
Ms. K’s case places us at the crossroads of psychiatric disturbances and medical conditions that can present as or precipitate apparent psychiatric symptoms. Delirium, dementia, psychosis, endocrinopathies, encephalitis, electrolyte disturbances, drug abuse/withdrawal, and occipital or temporal lobe seizures are all possible differential diagnoses (Table 1).
A cognitive function screening and a battery of laboratory tests, imaging scans, and neurologic and vision exams are needed to uncover the cause of her hallucinations.
EVALUATION: Looking for clues
Ms. K’s left pupil was fixed at 6 mm and did not respond to light, while the right pupil was regular and reactive to light at 3 mm. Using a Snellen eye chart, her visual acuity was poor: 20/100 to 20/200 in her right eye and less than 20/200 in the left eye. She scored a 29 out of 30 on the Folstein Mini-Mental State Examination (MMSE), indicating her cognition was intact. The remainder of the neurologic exam was unremarkable.
At admission, Ms. K’s medications included metoprolol, 100 mg qd, for hypertension; lansoprazole, 30 mg qd, for gastroesophageal reflux; tolterodine, 2 mg bid, and oxybutynin, 10 mg qd, for urinary incontinence; repaglinide, 2 mg bid, for type 2 diabetes; and three ophthalmic agents: brimonidine, prednisolone, and dorzolamide/timolol. The patient had been maintained on these medications for more than 2 years with no recent changes in dosing.
Results of Ms. K’s lab studies were normal, including a basic metabolic panel, CBC, liver function tests, urinalysis, B12, thyroid panel, rapid plasma reagin test, and urine drug screen.
A head CT without contrast revealed chronic small-vessel ischemic white matter disease and a chronic infarct of the left cerebellar hemisphere. No acute intracranial hemorrhages, masses, or other abnormalities were noted. No seizures were seen on EEG.
Table 1
Common causes of visual hallucinations
| Schizophrenia |
| Delirium |
| Dementias |
| Substance-induced psychosis |
| Electrolyte disturbances |
| Occipital and temporal lobe epilepsy |
| Charles Bonnet syndrome |
What do the laboratory and imaging tests reveal about Ms. K’s hallucinations? Is her diagnosis delirium? Alzheimer’s or other type of dementia? Schizophrenia?
The authors’ observations
Visual hallucinations—often of deceased parents or siblings, unknown intruders, and animals—can occur in up to 25% of patients with Alzheimer’s-type dementia.1 Also, patients with Lewy body dementia often present with well-formed visual hallucinations, which are thought to result from temporal lobe involvement by the characteristic Lewy bodies.
To diagnose dementia, DSM-IV requires the presence of multiple cognitive deficits manifested by memory impairment and one or more of the following:
- aphasia
- apraxia
- agnosia
- disturbance of executive functioning.2
Ms. K exhibited none of these characteristics, and she retained full executive function—she could balance her checkbook, buy groceries, and cook for herself. Also, her MMSE score was high.
Ms. K showed no consciousness fluctuations or attention deficits, two features commonly seen in delirium. She was alert and oriented throughout the interview, and her flow of thought, speech, language, and attention were appropriate. Therefore, delirium can be reasonably excluded.
The hallucinations probably do not signal onset of schizophrenia because of Ms. K’s age at presentation, lack of family history of psychotic disorder, and paucity of negative symptoms. Auditory hallucinations are much more common in psychosis, and isolated visual hallucinations rarely occur in schizophrenia.
Finally, Ms. K’s electrophysiologic, laboratory, and imaging studies revealed isolated systolic hypertension, low visual acuity, and a mild gait disturbance. Severe left lens opacification accounted for the patient’s discordant pupillary light reflex. None of these findings explained her visual hallucinations, however.
Is a non-psychiatric disorder causing Ms. K’s hallucinations? What type of medication might alleviate her symptoms?
The authors’ observations
Given Ms. K’s strong cognitive function and poor visual acuity, we concluded that her hallucinations may fit the criteria for Charles Bonnet syndrome (CBS), a poorly understood medical phenomenon.
CBS is characterized by complex visual hallucinations in visually impaired elderly patients without cognitive deficits (Table 2).3,4 Swiss philosopher Charles Bonnet first described the disorder in 1760 to explain the vivid visual hallucinations of his 89-year-old grandfather, who had severe cataracts but no cognitive deficits.3 Bonnet’s grandfather claimed to have visions of men, women, birds, buildings, and tapestries.3
CBS is increasingly recognized and reported, but the medical community has never formed a universally accepted definition for this phenomenon. Persons with CBS react positively or negatively to their hallucinations, and the images may stimulate anxiety, anger, or mild paranoia. Research has focused on prevalence, risk indicators, and treatment.
Table 2
Charles Bonnet syndrome: fast facts
|
Teunisse et al determined that visual hallucinations plague up to 14% of sight-impaired persons.4,5 The hallucinations vary widely: people, animals, flowers, vehicles, buildings, and sometimes complete scenes.4,5 Significant risk factors for CBS include advanced age and low visual acuity.4,5 Loneliness, introversion, and shyness are additional risk indicators in older, visually handicapped persons.6 Therefore, social isolation may be a predisposing factor.
Drug treatment of visual hallucinations in CBS currently includes antipsychotics, such as quetiapine (25 to 100 mg/d) and risperidone (0.25 to 1.0 mg/d).7 However, mixed results have been reported after use of antipsychotics in CBS; one patient’s visual hallucinations were exacerbated after risperidone was initiated.8 Case reports have also described the use of valproate, carbamazepine, and ondansetron in CBS.9-11
Empathy and patient education are the cornerstones of CBS treatment.3 Patients need to be reassured that their visions are benign. For many, simply increasing the amount of ambient light in the home can reduce hallucinations.
TREATMENT A frog in the toilet
Ms. K was started on quetiapine, 25 mg bid, to try to promote restorative sleep and resolve her hallucinations. Up to 18% of persons treated with quetiapine report somnolence as an adverse effect, vs. 3 to 8% of those treated with risperidone.12
During her hospital stay, Ms. K experienced no visual hallucinations during the day but reported seeing a grayish-brown bullfrog in the toilet at night. This hallucination did not frighten her; she would simply close the bathroom door and wait until the bullfrog “disappeared.”
Her sleep improved, as did her appetite. She participated in daily group sessions and socialized with other patients.
After 12 days, Ms. K was discharged. To decrease her social isolation, we encouraged her to participate in a day program for seniors. We also continued her on quetiapine, 25 mg bid.
Five months later, her primary care physician reports that Ms. K remains symptom free while maintaining her quetiapine dosage.
Related resources
- Royal National Institute of the Blind: Fact sheet for Charles Bonnet syndrome. Available at: http://www.rnib.org.uk/info/cbsfin.htm
- Verstraten PFJ. The Charles Bonnet syndrome: Development of a protocol for clinical practice in a multidisciplinary approach from assessment to intervention. Available at: http://www.rehab-syn.enter.iris.se/kc-syn/cb.htm
- Adamczyk DT. Optometric educators. Am I seeing things? Optometry Today June 18, 1999:37-9. Available at: http://www.optometry.co.uk/articles/19990618/Adamczyk.pdf
Drug brand names
- Brimonidine Ophthalmic • Alphagan
- Carbamazepine • Tegretol
- Dorzolamide/Timolol • Cosopt
- Lansoprazole • Prevacid
- Metoprolol • Toprol XL
- Ondansetron • Zofran
- Oxybutynin • Ditropan XL
- Quetiapine • Seroquel
- Repaglinide • Prandin
- Risperidone • Risperdal
- Tolterodine • Detrol
- Valproate • Depakote
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with competing manufacturers.
HISTORY: A sudden vision
Ms. K, 73, was in reasonably good health when one day she suddenly noticed red, green, and yellow birds and butterflies covering her wall.
Ms. K, who lives alone, was frightened at first, but she did not immediately alert anyone because she thought she “was just seeing things, and they’ll go away.”
Instead, she saw more visions over the next 3 months. She once “watched” as two doctors and a nun carried a middle-aged burn victim into her apartment. She remembers seeing the doctors put a “patch” over the woman’s body. To Ms. K, this experience seemed so shockingly real that she called 911, reporting, “That woman should have been in the hospital!”
She reports that a pack of butterflies once “followed” her to the market. She vividly recalls how they crawled about her shoes and legs as she entered the store. When asked if anyone noticed her insect-covered extremities, she replied matter-of-factly, “Maybe it’s not for them to see, maybe it’s just for me,” as if her hallucinations were a divine gift.
Ms. K’s hallucinations usually occur at home, where she spends most of her time. She says that the images are fleeting, lasting from a few seconds to several minutes, and that the creatures fly silently around her room.
Ms. K’s daughter grew concerned that the hallucinations were increasingly diminishing her mother’s ability to care for herself. She brought Ms. K into our emergency department, from which the patient was admitted.
On admission, Ms. K said she had lost 20 lbs within 6 months, and that “concentrating on those things in the house” was impairing her sleep. She denied recent illness, trauma, loss of conscious ness, changes in medications, seizures, drug or alcohol use, suicidal or homicidal ideation, or specific stress in her life. She added that she often cooks for herself—only to lose her appetite after seeing bugs and other creatures crawl into her food.
Her medical history includes hypertension, type 2 diabetes mellitus, peripheral vascular disease, urinary incontinence, gastroesophageal reflux, glaucoma in her left eye, and bilateral cataracts. She denies any psychiatric history and adds that she had never experienced hallucinations until about 3 months before hospitalization. She also denies any history of auditory, tactile, or olfactory hallucinations.
Would you suspect a primary psychotic illness? What clinical tests might help us understand Ms. K’s progressively debilitating visual hallucinations?
The authors’ observations
Ms. K’s case places us at the crossroads of psychiatric disturbances and medical conditions that can present as or precipitate apparent psychiatric symptoms. Delirium, dementia, psychosis, endocrinopathies, encephalitis, electrolyte disturbances, drug abuse/withdrawal, and occipital or temporal lobe seizures are all possible differential diagnoses (Table 1).
A cognitive function screening and a battery of laboratory tests, imaging scans, and neurologic and vision exams are needed to uncover the cause of her hallucinations.
EVALUATION: Looking for clues
Ms. K’s left pupil was fixed at 6 mm and did not respond to light, while the right pupil was regular and reactive to light at 3 mm. Using a Snellen eye chart, her visual acuity was poor: 20/100 to 20/200 in her right eye and less than 20/200 in the left eye. She scored a 29 out of 30 on the Folstein Mini-Mental State Examination (MMSE), indicating her cognition was intact. The remainder of the neurologic exam was unremarkable.
At admission, Ms. K’s medications included metoprolol, 100 mg qd, for hypertension; lansoprazole, 30 mg qd, for gastroesophageal reflux; tolterodine, 2 mg bid, and oxybutynin, 10 mg qd, for urinary incontinence; repaglinide, 2 mg bid, for type 2 diabetes; and three ophthalmic agents: brimonidine, prednisolone, and dorzolamide/timolol. The patient had been maintained on these medications for more than 2 years with no recent changes in dosing.
Results of Ms. K’s lab studies were normal, including a basic metabolic panel, CBC, liver function tests, urinalysis, B12, thyroid panel, rapid plasma reagin test, and urine drug screen.
A head CT without contrast revealed chronic small-vessel ischemic white matter disease and a chronic infarct of the left cerebellar hemisphere. No acute intracranial hemorrhages, masses, or other abnormalities were noted. No seizures were seen on EEG.
Table 1
Common causes of visual hallucinations
| Schizophrenia |
| Delirium |
| Dementias |
| Substance-induced psychosis |
| Electrolyte disturbances |
| Occipital and temporal lobe epilepsy |
| Charles Bonnet syndrome |
What do the laboratory and imaging tests reveal about Ms. K’s hallucinations? Is her diagnosis delirium? Alzheimer’s or other type of dementia? Schizophrenia?
The authors’ observations
Visual hallucinations—often of deceased parents or siblings, unknown intruders, and animals—can occur in up to 25% of patients with Alzheimer’s-type dementia.1 Also, patients with Lewy body dementia often present with well-formed visual hallucinations, which are thought to result from temporal lobe involvement by the characteristic Lewy bodies.
To diagnose dementia, DSM-IV requires the presence of multiple cognitive deficits manifested by memory impairment and one or more of the following:
- aphasia
- apraxia
- agnosia
- disturbance of executive functioning.2
Ms. K exhibited none of these characteristics, and she retained full executive function—she could balance her checkbook, buy groceries, and cook for herself. Also, her MMSE score was high.
Ms. K showed no consciousness fluctuations or attention deficits, two features commonly seen in delirium. She was alert and oriented throughout the interview, and her flow of thought, speech, language, and attention were appropriate. Therefore, delirium can be reasonably excluded.
The hallucinations probably do not signal onset of schizophrenia because of Ms. K’s age at presentation, lack of family history of psychotic disorder, and paucity of negative symptoms. Auditory hallucinations are much more common in psychosis, and isolated visual hallucinations rarely occur in schizophrenia.
Finally, Ms. K’s electrophysiologic, laboratory, and imaging studies revealed isolated systolic hypertension, low visual acuity, and a mild gait disturbance. Severe left lens opacification accounted for the patient’s discordant pupillary light reflex. None of these findings explained her visual hallucinations, however.
Is a non-psychiatric disorder causing Ms. K’s hallucinations? What type of medication might alleviate her symptoms?
The authors’ observations
Given Ms. K’s strong cognitive function and poor visual acuity, we concluded that her hallucinations may fit the criteria for Charles Bonnet syndrome (CBS), a poorly understood medical phenomenon.
CBS is characterized by complex visual hallucinations in visually impaired elderly patients without cognitive deficits (Table 2).3,4 Swiss philosopher Charles Bonnet first described the disorder in 1760 to explain the vivid visual hallucinations of his 89-year-old grandfather, who had severe cataracts but no cognitive deficits.3 Bonnet’s grandfather claimed to have visions of men, women, birds, buildings, and tapestries.3
CBS is increasingly recognized and reported, but the medical community has never formed a universally accepted definition for this phenomenon. Persons with CBS react positively or negatively to their hallucinations, and the images may stimulate anxiety, anger, or mild paranoia. Research has focused on prevalence, risk indicators, and treatment.
Table 2
Charles Bonnet syndrome: fast facts
|
Teunisse et al determined that visual hallucinations plague up to 14% of sight-impaired persons.4,5 The hallucinations vary widely: people, animals, flowers, vehicles, buildings, and sometimes complete scenes.4,5 Significant risk factors for CBS include advanced age and low visual acuity.4,5 Loneliness, introversion, and shyness are additional risk indicators in older, visually handicapped persons.6 Therefore, social isolation may be a predisposing factor.
Drug treatment of visual hallucinations in CBS currently includes antipsychotics, such as quetiapine (25 to 100 mg/d) and risperidone (0.25 to 1.0 mg/d).7 However, mixed results have been reported after use of antipsychotics in CBS; one patient’s visual hallucinations were exacerbated after risperidone was initiated.8 Case reports have also described the use of valproate, carbamazepine, and ondansetron in CBS.9-11
Empathy and patient education are the cornerstones of CBS treatment.3 Patients need to be reassured that their visions are benign. For many, simply increasing the amount of ambient light in the home can reduce hallucinations.
TREATMENT A frog in the toilet
Ms. K was started on quetiapine, 25 mg bid, to try to promote restorative sleep and resolve her hallucinations. Up to 18% of persons treated with quetiapine report somnolence as an adverse effect, vs. 3 to 8% of those treated with risperidone.12
During her hospital stay, Ms. K experienced no visual hallucinations during the day but reported seeing a grayish-brown bullfrog in the toilet at night. This hallucination did not frighten her; she would simply close the bathroom door and wait until the bullfrog “disappeared.”
Her sleep improved, as did her appetite. She participated in daily group sessions and socialized with other patients.
After 12 days, Ms. K was discharged. To decrease her social isolation, we encouraged her to participate in a day program for seniors. We also continued her on quetiapine, 25 mg bid.
Five months later, her primary care physician reports that Ms. K remains symptom free while maintaining her quetiapine dosage.
Related resources
- Royal National Institute of the Blind: Fact sheet for Charles Bonnet syndrome. Available at: http://www.rnib.org.uk/info/cbsfin.htm
- Verstraten PFJ. The Charles Bonnet syndrome: Development of a protocol for clinical practice in a multidisciplinary approach from assessment to intervention. Available at: http://www.rehab-syn.enter.iris.se/kc-syn/cb.htm
- Adamczyk DT. Optometric educators. Am I seeing things? Optometry Today June 18, 1999:37-9. Available at: http://www.optometry.co.uk/articles/19990618/Adamczyk.pdf
Drug brand names
- Brimonidine Ophthalmic • Alphagan
- Carbamazepine • Tegretol
- Dorzolamide/Timolol • Cosopt
- Lansoprazole • Prevacid
- Metoprolol • Toprol XL
- Ondansetron • Zofran
- Oxybutynin • Ditropan XL
- Quetiapine • Seroquel
- Repaglinide • Prandin
- Risperidone • Risperdal
- Tolterodine • Detrol
- Valproate • Depakote
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with competing manufacturers.
1. Geldmacher DS, Whitehouse PJ. Current concepts: evaluation of dementia. JAMA 1996;335:330-6.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, rev). Washington, DC: American Psychiatric Press, 2000.
3. Fernandez A, Lichtshein G, Vieweg WV. The Charles Bonnet syndrome: a review. J Nerv Ment Dis 1997;185:195-200.
4. Teunisse RJ, Cruysberg , JR, Hoefnagels WH, et al. Risk indicators for the Charles Bonnet syndrome. J Nerv Ment Dis 1998;186:190-2.
5. Teunisse RJ, Cruysberg J, Verbeek A, Zitman FG. The Charles Bonnet syndrome: a large prospective study in the Netherlands. A study of the prevalence of the Charles Bonnet syndrome and associated factors in 500 patients attending the University Department of Ophthalmology at Nijme. Br J Psychiatry 1995;166(2):254-7.
6. Teunisse RJ, Cruysberg JR, Hoefnagels WH, et al. Social and psychological characteristics of elderly visually handicapped patients with the Charles Bonnet Syndrome. Compr Psychiatry 1999;40(4):315-19.
7. Rovner BW. The Charles Bonnet syndrome: Visual hallucinations caused by visual impairment. Geriatrics 2002;57:45-6.
8. Kornreich C, Dan B, Verbanck P, Pelc I. Treating Charles Bonnet syndrome: understanding inconsistency. J Clin Psychopharmacol 2000;20(3):396.-
9. Hori H, Terao T, Shiraishi Y, Nakamura J. Treatment of Charles Bonnet syndrome with valproate. Int Clin Psychopharmacol 2000;15:117-19.
10. Batra A, Bartels M, Wormstall H. Therapeutic options in Charles Bonnet syndrome. Acta Psychiatr Scand 1997;96:129-33.
11. Nevins M. Charles Bonnet syndrome. J Am Geriatr Soc 1997;45:894.-
12. Brown C, Markowitz J, Moore T, Parker N. Atypical antipsychotics, part II: adverse effects, drug interactions, and efficacy. Ann Pharmacother 1999;33:210-17.
1. Geldmacher DS, Whitehouse PJ. Current concepts: evaluation of dementia. JAMA 1996;335:330-6.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, rev). Washington, DC: American Psychiatric Press, 2000.
3. Fernandez A, Lichtshein G, Vieweg WV. The Charles Bonnet syndrome: a review. J Nerv Ment Dis 1997;185:195-200.
4. Teunisse RJ, Cruysberg , JR, Hoefnagels WH, et al. Risk indicators for the Charles Bonnet syndrome. J Nerv Ment Dis 1998;186:190-2.
5. Teunisse RJ, Cruysberg J, Verbeek A, Zitman FG. The Charles Bonnet syndrome: a large prospective study in the Netherlands. A study of the prevalence of the Charles Bonnet syndrome and associated factors in 500 patients attending the University Department of Ophthalmology at Nijme. Br J Psychiatry 1995;166(2):254-7.
6. Teunisse RJ, Cruysberg JR, Hoefnagels WH, et al. Social and psychological characteristics of elderly visually handicapped patients with the Charles Bonnet Syndrome. Compr Psychiatry 1999;40(4):315-19.
7. Rovner BW. The Charles Bonnet syndrome: Visual hallucinations caused by visual impairment. Geriatrics 2002;57:45-6.
8. Kornreich C, Dan B, Verbanck P, Pelc I. Treating Charles Bonnet syndrome: understanding inconsistency. J Clin Psychopharmacol 2000;20(3):396.-
9. Hori H, Terao T, Shiraishi Y, Nakamura J. Treatment of Charles Bonnet syndrome with valproate. Int Clin Psychopharmacol 2000;15:117-19.
10. Batra A, Bartels M, Wormstall H. Therapeutic options in Charles Bonnet syndrome. Acta Psychiatr Scand 1997;96:129-33.
11. Nevins M. Charles Bonnet syndrome. J Am Geriatr Soc 1997;45:894.-
12. Brown C, Markowitz J, Moore T, Parker N. Atypical antipsychotics, part II: adverse effects, drug interactions, and efficacy. Ann Pharmacother 1999;33:210-17.
Preparing patients for life after bariatric surgery
With obesity on the rise, more people are seeking alternatives to failed diets, grueling exercise regimens, and prescription weight-loss agents with troublesome side effects.
Bariatric surgery offers hope to morbidly obese persons (defined as having a body mass index [BMI] 40 kg/m2) and to those with a BMI >34 kg/m2 who suffer hypertension, diabetes, and other comorbidities. The procedure produces significant short-term gains (diminished binge eating, weight loss, alleviation of depressed mood) and long-term benefits (improved self-image; increased HDL; lower apoprotein beta-containing lipoproteins; and lower LDL, blood pressure, and fasting blood glucose).
Too often, however, patients see bariatric surgery as a quick fix. Although hunger and stomach capacity are reduced, some patients do eat compulsively,1 and many regain weight after surgery. Patients also may not realize that they must make extensive lifestyle changes and adjust psychologically to life as a normal-weight person.
Suicide is a major cause of postoperative death, either because of poor psychosocial adjustment or the emergence of an occult personality disorder. Continued alcohol consumption and noncompliance with prescribed vitamin or mineral regimens can also be fatal.
Gauging patient readiness
A preoperative psychiatric evaluation can uncover mental disorders and other risk factors for postoperative noncompliance. Evaluate the following issues:
- What caused or contributed to the patient’s obesity? Bariatric surgery candidates have a high prevalence of psychopathology, including major depression, binge eating, and personality disorders.2,3 Untreated depression, bulimia, suicidality, and substance abuse are contraindications to bariatric surgery. Pre-existing major depression and binge-eating disorder are not, however.
- How does the patient perceive his or her body? Patients who have unrealistic perceptions about their bodies, such as those with eating disorders or psychoses, are poor surgical candidates. Such patients are unlikely to be satisfied with their postoperative body size.
- Why has the patient chosen to undergo bariatric surgery at this time? Ask whether he or she views it as a major procedure, and determine his or her level of conviction about receiving the surgery.
- Can the patient expect support from family and friends? Undue pressure from family members, such as a significant other’s dissatisfaction with the patient’s pre-operative body size, may lead to postoperative psychosocial maladjustment. A collateral history may be useful.
- Is the patient aware that postoperative behavioral changes will be needed? People will treat the patient differently and may even comment frequently about his or her new body size. Moreover, instead of eating as a coping mechanism, patients will need to find other ways to deal with unpleasant emotions.
- Does the patient understand the postoperative requirements? Reiterate that the patient must participate in group psychotherapy and follow postoperative instructions. The patient’s history of dieting, exercise, and weight-loss prescriptions may offer clues to prospective post-op compliance. Patients who have not complied with less invasive measures are not likely to be compliant after bariatric surgery.
Finally, to prevent miscommunication between patient and provider, ask the surgeon what he or she has told the patient about the procedure. A Minnesota Multiphasic Personality Inventory test can help confirm psychiatric diagnoses and determine whether the patient is being candid.
1. Saunders R. Compulsive eating and gastric bypass surgery: what does hunger have to do with it? Obes Surg 2001;11(6):757-61.
2. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am 2001;81(5):1001-24.
3. Glinski J, et al. The psychology of gastric bypass surgery. Obes Surg 2001;11:581-8.
Dr. Menaster practices psychiatry in San Francisco, CA
With obesity on the rise, more people are seeking alternatives to failed diets, grueling exercise regimens, and prescription weight-loss agents with troublesome side effects.
Bariatric surgery offers hope to morbidly obese persons (defined as having a body mass index [BMI] 40 kg/m2) and to those with a BMI >34 kg/m2 who suffer hypertension, diabetes, and other comorbidities. The procedure produces significant short-term gains (diminished binge eating, weight loss, alleviation of depressed mood) and long-term benefits (improved self-image; increased HDL; lower apoprotein beta-containing lipoproteins; and lower LDL, blood pressure, and fasting blood glucose).
Too often, however, patients see bariatric surgery as a quick fix. Although hunger and stomach capacity are reduced, some patients do eat compulsively,1 and many regain weight after surgery. Patients also may not realize that they must make extensive lifestyle changes and adjust psychologically to life as a normal-weight person.
Suicide is a major cause of postoperative death, either because of poor psychosocial adjustment or the emergence of an occult personality disorder. Continued alcohol consumption and noncompliance with prescribed vitamin or mineral regimens can also be fatal.
Gauging patient readiness
A preoperative psychiatric evaluation can uncover mental disorders and other risk factors for postoperative noncompliance. Evaluate the following issues:
- What caused or contributed to the patient’s obesity? Bariatric surgery candidates have a high prevalence of psychopathology, including major depression, binge eating, and personality disorders.2,3 Untreated depression, bulimia, suicidality, and substance abuse are contraindications to bariatric surgery. Pre-existing major depression and binge-eating disorder are not, however.
- How does the patient perceive his or her body? Patients who have unrealistic perceptions about their bodies, such as those with eating disorders or psychoses, are poor surgical candidates. Such patients are unlikely to be satisfied with their postoperative body size.
- Why has the patient chosen to undergo bariatric surgery at this time? Ask whether he or she views it as a major procedure, and determine his or her level of conviction about receiving the surgery.
- Can the patient expect support from family and friends? Undue pressure from family members, such as a significant other’s dissatisfaction with the patient’s pre-operative body size, may lead to postoperative psychosocial maladjustment. A collateral history may be useful.
- Is the patient aware that postoperative behavioral changes will be needed? People will treat the patient differently and may even comment frequently about his or her new body size. Moreover, instead of eating as a coping mechanism, patients will need to find other ways to deal with unpleasant emotions.
- Does the patient understand the postoperative requirements? Reiterate that the patient must participate in group psychotherapy and follow postoperative instructions. The patient’s history of dieting, exercise, and weight-loss prescriptions may offer clues to prospective post-op compliance. Patients who have not complied with less invasive measures are not likely to be compliant after bariatric surgery.
Finally, to prevent miscommunication between patient and provider, ask the surgeon what he or she has told the patient about the procedure. A Minnesota Multiphasic Personality Inventory test can help confirm psychiatric diagnoses and determine whether the patient is being candid.
With obesity on the rise, more people are seeking alternatives to failed diets, grueling exercise regimens, and prescription weight-loss agents with troublesome side effects.
Bariatric surgery offers hope to morbidly obese persons (defined as having a body mass index [BMI] 40 kg/m2) and to those with a BMI >34 kg/m2 who suffer hypertension, diabetes, and other comorbidities. The procedure produces significant short-term gains (diminished binge eating, weight loss, alleviation of depressed mood) and long-term benefits (improved self-image; increased HDL; lower apoprotein beta-containing lipoproteins; and lower LDL, blood pressure, and fasting blood glucose).
Too often, however, patients see bariatric surgery as a quick fix. Although hunger and stomach capacity are reduced, some patients do eat compulsively,1 and many regain weight after surgery. Patients also may not realize that they must make extensive lifestyle changes and adjust psychologically to life as a normal-weight person.
Suicide is a major cause of postoperative death, either because of poor psychosocial adjustment or the emergence of an occult personality disorder. Continued alcohol consumption and noncompliance with prescribed vitamin or mineral regimens can also be fatal.
Gauging patient readiness
A preoperative psychiatric evaluation can uncover mental disorders and other risk factors for postoperative noncompliance. Evaluate the following issues:
- What caused or contributed to the patient’s obesity? Bariatric surgery candidates have a high prevalence of psychopathology, including major depression, binge eating, and personality disorders.2,3 Untreated depression, bulimia, suicidality, and substance abuse are contraindications to bariatric surgery. Pre-existing major depression and binge-eating disorder are not, however.
- How does the patient perceive his or her body? Patients who have unrealistic perceptions about their bodies, such as those with eating disorders or psychoses, are poor surgical candidates. Such patients are unlikely to be satisfied with their postoperative body size.
- Why has the patient chosen to undergo bariatric surgery at this time? Ask whether he or she views it as a major procedure, and determine his or her level of conviction about receiving the surgery.
- Can the patient expect support from family and friends? Undue pressure from family members, such as a significant other’s dissatisfaction with the patient’s pre-operative body size, may lead to postoperative psychosocial maladjustment. A collateral history may be useful.
- Is the patient aware that postoperative behavioral changes will be needed? People will treat the patient differently and may even comment frequently about his or her new body size. Moreover, instead of eating as a coping mechanism, patients will need to find other ways to deal with unpleasant emotions.
- Does the patient understand the postoperative requirements? Reiterate that the patient must participate in group psychotherapy and follow postoperative instructions. The patient’s history of dieting, exercise, and weight-loss prescriptions may offer clues to prospective post-op compliance. Patients who have not complied with less invasive measures are not likely to be compliant after bariatric surgery.
Finally, to prevent miscommunication between patient and provider, ask the surgeon what he or she has told the patient about the procedure. A Minnesota Multiphasic Personality Inventory test can help confirm psychiatric diagnoses and determine whether the patient is being candid.
1. Saunders R. Compulsive eating and gastric bypass surgery: what does hunger have to do with it? Obes Surg 2001;11(6):757-61.
2. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am 2001;81(5):1001-24.
3. Glinski J, et al. The psychology of gastric bypass surgery. Obes Surg 2001;11:581-8.
Dr. Menaster practices psychiatry in San Francisco, CA
1. Saunders R. Compulsive eating and gastric bypass surgery: what does hunger have to do with it? Obes Surg 2001;11(6):757-61.
2. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am 2001;81(5):1001-24.
3. Glinski J, et al. The psychology of gastric bypass surgery. Obes Surg 2001;11:581-8.
Dr. Menaster practices psychiatry in San Francisco, CA
Psychiatric symptoms in Parkinson’s disease: A team approach to successful management
Depression, anxiety, and psychosis are common complications of Parkinson’s disease (PD) and of the medications used in antiparkinsonian treatment. These psychiatric problems impair patients’ functioning throughout the course of the chronic degenerative disease.
Because medication side effects often call for adjustments and trade-offs in PD treatment, a team effort by the psychiatrist, neurologist, patient, and caregiver is the most effective approach to decision-making. From our experience in such collaborations, here’s what you need to know about PD to be a most-valuable player on that treatment team.
Presentation of PD
The classic triad of PD features consists of a pill-rolling tremor, rigidity, and bradykinesia or slowness of movement. Other common features include postural instability, flexed posture, and other motor-freezing phenomena.
Freezing phenomena occur in the later stages of PD, as the response to dopaminergic therapy becomes erratic and unpredictable. Freezing can range from hesitation—such as when the patient tries to turn or is in a doorway—to transient episodes of total inability to move. These episodes are extremely distressing for both patients and caregivers.
Patients rarely present with the full complement of symptoms, but the presence of tremor at rest and/or bradykinesia is essential for the diagnosis. While motor signs dominate the presentation, cognitive symptoms such as shortened attention span, visuospatial impairment, personality changes, and dementia are also frequently present.
Average age of diagnosis is 60, and more men are affected than women (male-to-female ratio is 3:2). Many causative factors—including genetics and environmental toxins—have been implicated, but the disorder’s etiology remains unknown.
Drug treatment side effects
PD results from the loss of neurons in the substantia nigra that produce the neurotransmitter dopamine. Pharmacologic treatment emphasizes dopamine replacement, dopamine receptor stimulation, or prevention of enzymatic breakdown of dopamine in the synaptic cleft. As treatment of PD is symptomatic and not curative, medications are instituted only when the disease begins to cause functional impairment.
Treatment begins with dopamine agonists (Table). As dopamine agonist monotherapy becomes less effective, levodopa therapy is initiated. Blocking the enzymatic breakdown of dopamine with catechol-O-methyltransferase inhibitors is the next therapeutic strategy.
Within 5 years of starting levodopa therapy 75% of patients experience unsatisfactory motor response, from unpredictable fluctuations to wearing-off phenomena (in which a dose of levodopa does not last as long as it once did). Treatment of advanced PD is complicated by the emergence of psychiatric symptoms, such as hallucinations and psychosis, as dopamine levels are increased in an attempt to smooth the motor response.
The significantly distressing level of disability associated with the prominent side effects of pharmacologic treatment has led to interest in surgical interventions. These range from pallidotomy to implantation of basal ganglia stimulators to transplantation of fetal striatal neurons. The possibility of neuroprotection has also been extensively investigated, with mixed results.
Psychiatric complications of PD
Depression. Clearly, the stress of anticipating and coping with a relentless degenerative disease helps to trigger depression and anxiety in patients with PD. Depression is the most common psychiatric syndrome, with prevalence in PD as high as 42%.1 Patients with a history of depression are at particular risk.2 Those with recent deterioration or advancing severity of PD, akinesia, history of falls, or cognitive impairment are also at increased risk for depression.
Table
MEDICATIONS COMMONLY USED IN MANAGING PARKINSON’S DISEASE
| Medication class | Example | Indication for use |
|---|---|---|
| MAO-B inhibitor | Selegiline | ? Neuroprotection |
| Anticholinergic agents | Trihexyphenidyl, benztropine, biperiden, hyoscyamine, diphenhydramine | Tremor |
| Dopamine agonist | Pramipexole, pergolide, ropinirole | ? Neuroprotection Treatment of movement disorder |
| Dopamine replacement | Carbidopa-levodopa | Treatment of movement disorder |
| Catechol-O-methyltransferase inhibitor | Entacapone, tolcapone | Smooth motor fluctuations |
Depression correlates well with the patient’s perception of his or her degree of PD-related disability. Depression symptoms seem to peak early in the illness following diagnosis and in advanced disease.3
Patients may present with symptoms meeting diagnostic criteria ranging from dysthymic disorder to minor depression to major depressive disorder.1,4 Although they will frequently endorse suicidal ideation, patients with PD have a low rate of suicide. Diagnosing depression, however, may be difficult because its symptoms overlap with those of the underlying neurologic disease:
- Diminished affect and psychomotor slowing may be secondary to the motor features of parkinsonism.
- Diminished concentration may be secondary to cognitive decline rather than depression.
Patients also frequently have a chief complaint of diminished energy or fatigue that should trigger further investigation into other depressive symptoms.4,5
In addition to the obvious additional suffering it causes, depression in PD predicts impaired social, physical, and role functioning.6 Depression in the PD patient also results in higher distress for caregivers.7 In one study, depression was identified as a risk factor for development of psychosis in PD patients.8
Anxiety is a frequent problem for PD patients, with a prevalence of 33 to 40%.9,10 Anxiety in PD typically presents with symptoms of panic disorder, generalized anxiety disorder, or social phobia.11 It is comorbid with depression in up to 92% of cases and—like depression—frequently predates the onset of motor symptoms.12
Anxiety symptoms have been correlated, although not consistently, with the on-off motor phenomenon often found in advanced PD.13 They can also be an adverse effect of many of the antiparkinsonian medications, including anticholinergics, dopamine agonists, catechol-O-methyltransferase inhibitors, and selegiline. Both anxiety and depression have been associated with an increased risk for falls.14
Psychotic symptoms. Up to 25% of PD patients experience delusions or hallucinations.15 Risk factors include dementia, sleep disturbance, and—most commonly—the use of dopaminergic agents. Up to one-fifth of patients using dopaminergic drugs experience psychotic symptoms.16
Psychotic symptoms can occur with or without the clouded sensorium characteristic of delirium. Psychotic symptoms with an associated confusional state can be associated with use of anticholinergic agents and drugs such as selegiline and amantadine.17 Catechol-O-methyltransferase inhibitors cause more sustained dopaminergic activity of levodopa, which can result in psychotic symptoms. Therefore, the use of all known classes of antiparkinsonian medications has been associated with drug-induced psychosis.
In advanced PD, paranoid delusions, delusions of spousal infidelity, and visual hallucinations are common, whereas negative symptoms and thought disturbances are not.18 Psychosis may be a more important contributor to caregiver distress than the motor symptoms of PD and may be more likely than any other factor to lead to nursing home placement of the PD patient (Box 1).15
Psychiatric interventions
Goals for psychiatric treatment of depression, anxiety, and psychosis associated with PD seem relatively straightforward:
- improvement or remission of psychiatric symptoms
- restoration of optimal patient functioning.
Ideally, these goals would be achieved without causing sedation, orthostatic hypotension, or exacerbating motor symptoms. The older age of patients and the progressive nature of this neurodegenerative disorder predispose patients to cognitive side effects. Unfortunately, despite the high prevalence of psychiatric disturbances in PD, evidence with which to evaluate treatment efficacy and safety and to guide treatment selection is extremely limited.
For depression associated with PD, extensive clinical experience supports the efficacy of tricyclic antidepressants. Even so, selective serotonin reuptake inhibitors (SSRIs) are the preferred treatment, although only open-label trials and case reports support their efficacy.5,12 Compared with tricyclics, SSRIs exhibit a relative lack of problems with sedation, orthostatic hypotension, and memory-impairing anticholinergic side effects. While case reports have cited worsening of motor symptoms with SSRIs, a recent prospective study found no significant worsening of PD symptoms during treatment with citalopram, fluoxetine, fluvoxamine, or sertraline.19 Co-administration of an SSRI with selegiline is not absolutely contraindicated, but the combination does carry a very small risk of development of serotonin syndrome.1,5
Mr. J had a 6-year history of PD with pronounced bradykinesia and gait disturbance treated with amantadine and carbidopa-levodopa. His rigidity began to worsen, so the dosage of carbidopa-levodopa was increased. His wife then reported that he had increased confusion and balance problems. On evaluation, he was found to have a urinary tract infection. Following antibiotic treatment, mental status and gait returned to usual baseline.
One year later, Mr. J began having trouble getting out of bed, with unpredictable motor freezing episodes. Pramipexole was added to his regimen, and he began having prominent visual hallucinations. Low-dose trifluoperazine was added, and hallucinations improved. The patient became increasingly depressed, and sertraline was started.
Over the next year, his function progressively worsened, with increased motor freezing and unpredictable dyskinesias. Hallucinations complicated attempts to change his medications. Amantadine was stopped without improvement. He was referred for surgical evaluation, but because of his cognitive status and depression was deemed not to be a candidate.
He began to fall repeatedly and developed orthostatic hypotension. His clinical course continued to be complicated by hallucinations and delusions that his wife was being unfaithful. Ongoing psychosis and severe gait instability led to his admission to a nursing home.
Data are even more scant on the safe use of other antidepressants in PD. Electroconvulsive therapy has been proven helpful in refractory cases and sometimes results in transient motor symptom improvement.1,5,12 While clinical experience suggests that psychotherapy frequently helps, no extensive controlled studies exist. One small study suggests the efficacy of structured cognitive psychotherapy.20
Anxiety. No studies have examined the treatment of anxiety in PD patients. Given the extremely high comorbidity of anxiety with depression, antidepressants should probably be considered as a first-line pharmacotherapy. Benzodiazepines should be used cautiously, as they increase the risk of falls, sedation, and confusion in older patients. One small controlled study found that buspirone was well tolerated in PD patients at low dosages (10 to 40 mg/d), but anxiety did not improve. At high dosages (100 mg/d), anxiety worsened.21
Psychosis. Data on use of antipsychotic agents in PD are also limited, but some evidence supports their use in treating PD-related psychotic symptoms. While conventional antipsychotics can help control psychosis, the potential is high for worsening of parkinsonian symptoms due to D2 receptor blockade.
Among the atypical antipsychotics, clozapine has been most extensively studied in PD and has been shown in open and double-blind trials to be effective and well tolerated at low dosages (6.25 to 50 mg/d). A limited number of open studies of some of the newer atypicals have been performed. While extreme caution must be used in comparing data from these studies due to highly variable dosing and other study design issues, clozapine and quetiapine appear to be the agents best tolerated by PD patients.12,18,22 Initial antipsychotic dosing should be low and escalation cautious—regardless of the agent chosen—because of the dose-related potential for worsening of parkinsonian symptoms, sedation, and orthostatic hypotension.
A team approach to treatment
Because psychiatric and PD symptoms and treatments are closely interrelated, the psychiatrist, neurologist, patient, and caregiver must collaborate for the best therapeutic result. A simplistic approach to treatment can result in a catastrophic downward spiral in patient functioning.
Often, compromises must be made between optimal control of parkinsonian and psychiatric symptoms to achieve the best overall patient function. Patients and caregivers must be counseled about possible psychiatric symptoms associated with PD and antiparkinsonian therapy, as well as the potential for adverse effects from psychiatric medications. With this knowledge, patients and caregivers can help assess the severity of symptoms and set treatment priorities, depending on how symptoms may be affecting the patient’s level of functioning. For example, if an effective antiparkinsonian regimen has triggered infrequent, nondistressing hallucinations with preserved insight, intervention may not be required beyond patient and caregiver education (Box 2).
Patient workup. When intervention is required for psychiatric symptoms, it should begin with careful neurologic evaluation. Triggering factors such as infections (commonly urinary tract infections and pneumonia), metabolic disorders (hyperglycemia, hypothyroidism), subdural hematomas (if the patient is falling), and drug interactions should be ruled out or appropriately addressed.
Next, try to sequentially eliminate antiparkinsonian medications until the psychosis resolves or motor function worsens.23 Because of considerable overlap between PD symptoms and depression (psychomotor retardation, fatigue, and anergia), optimizing PD therapy sometimes can result in substantial psychiatric improvement. Some evidence also suggests that the dopamine agonist pramipexole may be effective in treating both PD and depression.5
When psychiatric medications are necessary for depression, anxiety, or psychosis, carefully review target symptoms, treatment expectations, and possible adverse effects with the patient and caregiver. Keep in mind the progressive nature of PD and, in addition to frequent monitoring, educate and encourage caregivers to immediately report any suspected adverse effects.
Any motor function deterioration should trigger a re-evaluation of psychotropic medications before you presume that the patient’s PD is progressing. Because antiparkinsonian drug regimens change over time, review the patient’s medications at each appointment, and alert patients and caregivers to potential psychiatric complications of any new medication.
Caregiver treatment In addition to treating the patient, it is important to monitor the impact of psychiatric symptoms and PD on the patient’s caregiver. Frequently assess whether the caregiver and patient have adequate social supports, and address any emerging needs. Useful interventions include caregiver counseling, referrals to support groups, and respite care.24
Mrs. K had a 4-year history of rapidly progressing PD treated with entacapone, carbidopa-levodopa, and a deep brain stimulator. Increasing periods of motor freezing, which were often accompanied by panic attacks, led her to become increasingly depressed and demanding of her caregiver husband. Eventually, she was admitted to an inpatient psychiatry unit because of suicidal ideation.
After a neurologic evaluation, the dosing times of her carbidopa-levodopa and entacapone were changed, but she continued to have panic attacks and remained depressed. Alprazolam promptly reduced her panic symptoms, and paroxetine was initiated for depression. A discussion with the patient and her husband revealed that they had some longstanding issues in their marriage that were exacerbated by Mrs K’s increasing dependency. The couple was referred for marital therapy, and Mrs. K agreed to begin attending a senior center.
Following discharge, the panic remained controlled and depression improved. Entacapone was replaced with tolcapone to see if motor freezing would decrease. Mrs. K’s movements improved, but her husband reported she had awakened on several nights with visual hallucinations. The hallucinations were infrequent, unaccompanied by agitation, and not distressing to the patient. Following a discussion of therapeutic options with Mrs. K and her husband, antipsychotic therapy was not instituted. The patient continues to live at home and attends the senior center regularly.
Related resources
- Parkinson’s Disease Foundation: http://www.pdf.org
- American Parkinson Disease Association: http://apdaparkinson.com
- National Parkinson Foundation: http://www.parkinson.org
- Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease 2001: treatment guidelines. Neurology 2001;56:5(suppl):S1-S88.
Drug brand names
- Alprazolam • Xanax
- Amantadine • Symmetrel
- Benztropine • Cogentin
- Biperiden • Akineton
- Buspirone • Buspar
- Carbidopa-levodopa • Sinemet
- Citalopram • Celexa
- Clozapine • Clozaril
- Entacapone • Comtan
- Fluvoxamine • Luvox
- Hyoscyamine • Levsin
- Paroxetine • Paxil
- Pergolide • Permax
- Pramipexole • Mirapex
- Ropinirole • Requip
- Selegeline • Eldepryl
- Sertraline • Zoloft
- Tolcapone • Tasmar
- Trihexyphenidyl • Artane
- Trifluoperazine • Stelazine
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Slaughter JR, Slaughter KA, Nichols D, et al. Prevalence, clinical manifestations, etiology, and treatment of depression in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 2001;13:187-96.
2. Starksein SE, Preziosi TJ, Bolduc PL, Robinson RG. Depression in Parkinson’s disease. J Nerv Ment Dis 1990;178:27-31.
3. Schrag A, Jahanshahi M, Quinn P. What contributes to depression in Parkinson’s disease? Psychological Medicine 2001;31:65-73.
4. Poewe W, Luginger E. Depression in Parkinson’s disease: impediments to recognition and treatment options. Neurology 2001;52(7):S002-S006.
5. Okun MS, Watts RL. Depression associated with Parkinson’s disease: clinical features and treatment. Neurology 2002;58:1(suppl):S63-S70.
6. Cole SA, Woodard JL, Juncos JL. Depression and disability in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1996;8(1):20-5.
7. Aarsland D, Larsen JP, et al. Mental symptoms in Parkinson’s disease are important contributors to caregiver distress. Int J Geriatr Psychiatry 1999;14(10):866-74.
8. Giladi N, Treves TA, Paleacu D, et al. Risk factors for dementia, depression and psychosis in long-standing Parkinson’s disease. J Neural Transm 2000;107(1):59-71.
9. Shulman LM, Taback RL, Bean J, Weiner WJ. Comorbidity of the nonmotor symptoms of PD. Mov Disord 2001;16(3):507-10.
10. Walsh K, Bennett G. Parkinson’s disease and anxiety. Postgrad Med J 2001;77(904):89-93.
11. Richard IH, Schiffe RB, Kurler R. Anxiety and Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1996;8(4):383-92.
12. Menza MA. Psychiatric aspects of Parkinson’s disease. Psychiatric Ann 2002;32:99-104.
13. Richard IH, Justus AW, Kurlan R. Relationship between mood and motor fluctuations in PD. J Neuropsychiatry Clin Neurosci 2001;13(1):35-41.
14. Ashburn A, Stack E, Pickering CM, Ward CD. A community-dwelling sample of people with Parkinson’s disease: characteristics of fallers and non-fallers. Age Ageing 2001;30(1):47-52.
15. Wolters EC, Berendse HW. Management of psychosis in Parkinson’s disease. Curr Opin Neurol 2001;14(4):499-504.
16. Juncos JL. Management of psychotic aspects of Parkinson’s disease. J Clin Psychiatry 1999;60:8(suppl):42-53.
17. Wolters EC. Dopaminomimetic psychosis in Parkinson’s disease patients. Neurology 1999;52:7(suppl):S010-S013.
18. Friedman JH, Factor SA. Atypical antipsychotics in the treatment of drug-induced Parkinson’s disease. Mov Disord 2000;15(2):201-11.
19. Dell’Agnello G, Ceravolo R, et al. SSRIs do not worsen Parkinson’s disease: evidence from an open-label, prospective study. Clin Neuropharmacol 2001;24(4):221-27.
20. Dreisig H, Beckmann J, Wermuth L, et al. Psychological effects of structured cognitive psychotherapy in young patients with Parkinson’s disease (abstr). Nordic J Psychiatry 1999;53(3):217-21.
21. Ludwig CL, Weinberger DR, Bruno G, et al. Buspirone, Parkinson’s disease and the locus ceruleus. Clin Neuropharmacol 1986;9(4):373-8.
22. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs 2002;16(1):23-45.
23. Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease 2001: treatment guidelines. Neurology 2001;56:5(suppl):S1-S88.
24. Ellgring JH. Depression, psychosis, dementia: impact on the family. Neurology 1999;52:7(suppl 3):S17-S20.
Depression, anxiety, and psychosis are common complications of Parkinson’s disease (PD) and of the medications used in antiparkinsonian treatment. These psychiatric problems impair patients’ functioning throughout the course of the chronic degenerative disease.
Because medication side effects often call for adjustments and trade-offs in PD treatment, a team effort by the psychiatrist, neurologist, patient, and caregiver is the most effective approach to decision-making. From our experience in such collaborations, here’s what you need to know about PD to be a most-valuable player on that treatment team.
Presentation of PD
The classic triad of PD features consists of a pill-rolling tremor, rigidity, and bradykinesia or slowness of movement. Other common features include postural instability, flexed posture, and other motor-freezing phenomena.
Freezing phenomena occur in the later stages of PD, as the response to dopaminergic therapy becomes erratic and unpredictable. Freezing can range from hesitation—such as when the patient tries to turn or is in a doorway—to transient episodes of total inability to move. These episodes are extremely distressing for both patients and caregivers.
Patients rarely present with the full complement of symptoms, but the presence of tremor at rest and/or bradykinesia is essential for the diagnosis. While motor signs dominate the presentation, cognitive symptoms such as shortened attention span, visuospatial impairment, personality changes, and dementia are also frequently present.
Average age of diagnosis is 60, and more men are affected than women (male-to-female ratio is 3:2). Many causative factors—including genetics and environmental toxins—have been implicated, but the disorder’s etiology remains unknown.
Drug treatment side effects
PD results from the loss of neurons in the substantia nigra that produce the neurotransmitter dopamine. Pharmacologic treatment emphasizes dopamine replacement, dopamine receptor stimulation, or prevention of enzymatic breakdown of dopamine in the synaptic cleft. As treatment of PD is symptomatic and not curative, medications are instituted only when the disease begins to cause functional impairment.
Treatment begins with dopamine agonists (Table). As dopamine agonist monotherapy becomes less effective, levodopa therapy is initiated. Blocking the enzymatic breakdown of dopamine with catechol-O-methyltransferase inhibitors is the next therapeutic strategy.
Within 5 years of starting levodopa therapy 75% of patients experience unsatisfactory motor response, from unpredictable fluctuations to wearing-off phenomena (in which a dose of levodopa does not last as long as it once did). Treatment of advanced PD is complicated by the emergence of psychiatric symptoms, such as hallucinations and psychosis, as dopamine levels are increased in an attempt to smooth the motor response.
The significantly distressing level of disability associated with the prominent side effects of pharmacologic treatment has led to interest in surgical interventions. These range from pallidotomy to implantation of basal ganglia stimulators to transplantation of fetal striatal neurons. The possibility of neuroprotection has also been extensively investigated, with mixed results.
Psychiatric complications of PD
Depression. Clearly, the stress of anticipating and coping with a relentless degenerative disease helps to trigger depression and anxiety in patients with PD. Depression is the most common psychiatric syndrome, with prevalence in PD as high as 42%.1 Patients with a history of depression are at particular risk.2 Those with recent deterioration or advancing severity of PD, akinesia, history of falls, or cognitive impairment are also at increased risk for depression.
Table
MEDICATIONS COMMONLY USED IN MANAGING PARKINSON’S DISEASE
| Medication class | Example | Indication for use |
|---|---|---|
| MAO-B inhibitor | Selegiline | ? Neuroprotection |
| Anticholinergic agents | Trihexyphenidyl, benztropine, biperiden, hyoscyamine, diphenhydramine | Tremor |
| Dopamine agonist | Pramipexole, pergolide, ropinirole | ? Neuroprotection Treatment of movement disorder |
| Dopamine replacement | Carbidopa-levodopa | Treatment of movement disorder |
| Catechol-O-methyltransferase inhibitor | Entacapone, tolcapone | Smooth motor fluctuations |
Depression correlates well with the patient’s perception of his or her degree of PD-related disability. Depression symptoms seem to peak early in the illness following diagnosis and in advanced disease.3
Patients may present with symptoms meeting diagnostic criteria ranging from dysthymic disorder to minor depression to major depressive disorder.1,4 Although they will frequently endorse suicidal ideation, patients with PD have a low rate of suicide. Diagnosing depression, however, may be difficult because its symptoms overlap with those of the underlying neurologic disease:
- Diminished affect and psychomotor slowing may be secondary to the motor features of parkinsonism.
- Diminished concentration may be secondary to cognitive decline rather than depression.
Patients also frequently have a chief complaint of diminished energy or fatigue that should trigger further investigation into other depressive symptoms.4,5
In addition to the obvious additional suffering it causes, depression in PD predicts impaired social, physical, and role functioning.6 Depression in the PD patient also results in higher distress for caregivers.7 In one study, depression was identified as a risk factor for development of psychosis in PD patients.8
Anxiety is a frequent problem for PD patients, with a prevalence of 33 to 40%.9,10 Anxiety in PD typically presents with symptoms of panic disorder, generalized anxiety disorder, or social phobia.11 It is comorbid with depression in up to 92% of cases and—like depression—frequently predates the onset of motor symptoms.12
Anxiety symptoms have been correlated, although not consistently, with the on-off motor phenomenon often found in advanced PD.13 They can also be an adverse effect of many of the antiparkinsonian medications, including anticholinergics, dopamine agonists, catechol-O-methyltransferase inhibitors, and selegiline. Both anxiety and depression have been associated with an increased risk for falls.14
Psychotic symptoms. Up to 25% of PD patients experience delusions or hallucinations.15 Risk factors include dementia, sleep disturbance, and—most commonly—the use of dopaminergic agents. Up to one-fifth of patients using dopaminergic drugs experience psychotic symptoms.16
Psychotic symptoms can occur with or without the clouded sensorium characteristic of delirium. Psychotic symptoms with an associated confusional state can be associated with use of anticholinergic agents and drugs such as selegiline and amantadine.17 Catechol-O-methyltransferase inhibitors cause more sustained dopaminergic activity of levodopa, which can result in psychotic symptoms. Therefore, the use of all known classes of antiparkinsonian medications has been associated with drug-induced psychosis.
In advanced PD, paranoid delusions, delusions of spousal infidelity, and visual hallucinations are common, whereas negative symptoms and thought disturbances are not.18 Psychosis may be a more important contributor to caregiver distress than the motor symptoms of PD and may be more likely than any other factor to lead to nursing home placement of the PD patient (Box 1).15
Psychiatric interventions
Goals for psychiatric treatment of depression, anxiety, and psychosis associated with PD seem relatively straightforward:
- improvement or remission of psychiatric symptoms
- restoration of optimal patient functioning.
Ideally, these goals would be achieved without causing sedation, orthostatic hypotension, or exacerbating motor symptoms. The older age of patients and the progressive nature of this neurodegenerative disorder predispose patients to cognitive side effects. Unfortunately, despite the high prevalence of psychiatric disturbances in PD, evidence with which to evaluate treatment efficacy and safety and to guide treatment selection is extremely limited.
For depression associated with PD, extensive clinical experience supports the efficacy of tricyclic antidepressants. Even so, selective serotonin reuptake inhibitors (SSRIs) are the preferred treatment, although only open-label trials and case reports support their efficacy.5,12 Compared with tricyclics, SSRIs exhibit a relative lack of problems with sedation, orthostatic hypotension, and memory-impairing anticholinergic side effects. While case reports have cited worsening of motor symptoms with SSRIs, a recent prospective study found no significant worsening of PD symptoms during treatment with citalopram, fluoxetine, fluvoxamine, or sertraline.19 Co-administration of an SSRI with selegiline is not absolutely contraindicated, but the combination does carry a very small risk of development of serotonin syndrome.1,5
Mr. J had a 6-year history of PD with pronounced bradykinesia and gait disturbance treated with amantadine and carbidopa-levodopa. His rigidity began to worsen, so the dosage of carbidopa-levodopa was increased. His wife then reported that he had increased confusion and balance problems. On evaluation, he was found to have a urinary tract infection. Following antibiotic treatment, mental status and gait returned to usual baseline.
One year later, Mr. J began having trouble getting out of bed, with unpredictable motor freezing episodes. Pramipexole was added to his regimen, and he began having prominent visual hallucinations. Low-dose trifluoperazine was added, and hallucinations improved. The patient became increasingly depressed, and sertraline was started.
Over the next year, his function progressively worsened, with increased motor freezing and unpredictable dyskinesias. Hallucinations complicated attempts to change his medications. Amantadine was stopped without improvement. He was referred for surgical evaluation, but because of his cognitive status and depression was deemed not to be a candidate.
He began to fall repeatedly and developed orthostatic hypotension. His clinical course continued to be complicated by hallucinations and delusions that his wife was being unfaithful. Ongoing psychosis and severe gait instability led to his admission to a nursing home.
Data are even more scant on the safe use of other antidepressants in PD. Electroconvulsive therapy has been proven helpful in refractory cases and sometimes results in transient motor symptom improvement.1,5,12 While clinical experience suggests that psychotherapy frequently helps, no extensive controlled studies exist. One small study suggests the efficacy of structured cognitive psychotherapy.20
Anxiety. No studies have examined the treatment of anxiety in PD patients. Given the extremely high comorbidity of anxiety with depression, antidepressants should probably be considered as a first-line pharmacotherapy. Benzodiazepines should be used cautiously, as they increase the risk of falls, sedation, and confusion in older patients. One small controlled study found that buspirone was well tolerated in PD patients at low dosages (10 to 40 mg/d), but anxiety did not improve. At high dosages (100 mg/d), anxiety worsened.21
Psychosis. Data on use of antipsychotic agents in PD are also limited, but some evidence supports their use in treating PD-related psychotic symptoms. While conventional antipsychotics can help control psychosis, the potential is high for worsening of parkinsonian symptoms due to D2 receptor blockade.
Among the atypical antipsychotics, clozapine has been most extensively studied in PD and has been shown in open and double-blind trials to be effective and well tolerated at low dosages (6.25 to 50 mg/d). A limited number of open studies of some of the newer atypicals have been performed. While extreme caution must be used in comparing data from these studies due to highly variable dosing and other study design issues, clozapine and quetiapine appear to be the agents best tolerated by PD patients.12,18,22 Initial antipsychotic dosing should be low and escalation cautious—regardless of the agent chosen—because of the dose-related potential for worsening of parkinsonian symptoms, sedation, and orthostatic hypotension.
A team approach to treatment
Because psychiatric and PD symptoms and treatments are closely interrelated, the psychiatrist, neurologist, patient, and caregiver must collaborate for the best therapeutic result. A simplistic approach to treatment can result in a catastrophic downward spiral in patient functioning.
Often, compromises must be made between optimal control of parkinsonian and psychiatric symptoms to achieve the best overall patient function. Patients and caregivers must be counseled about possible psychiatric symptoms associated with PD and antiparkinsonian therapy, as well as the potential for adverse effects from psychiatric medications. With this knowledge, patients and caregivers can help assess the severity of symptoms and set treatment priorities, depending on how symptoms may be affecting the patient’s level of functioning. For example, if an effective antiparkinsonian regimen has triggered infrequent, nondistressing hallucinations with preserved insight, intervention may not be required beyond patient and caregiver education (Box 2).
Patient workup. When intervention is required for psychiatric symptoms, it should begin with careful neurologic evaluation. Triggering factors such as infections (commonly urinary tract infections and pneumonia), metabolic disorders (hyperglycemia, hypothyroidism), subdural hematomas (if the patient is falling), and drug interactions should be ruled out or appropriately addressed.
Next, try to sequentially eliminate antiparkinsonian medications until the psychosis resolves or motor function worsens.23 Because of considerable overlap between PD symptoms and depression (psychomotor retardation, fatigue, and anergia), optimizing PD therapy sometimes can result in substantial psychiatric improvement. Some evidence also suggests that the dopamine agonist pramipexole may be effective in treating both PD and depression.5
When psychiatric medications are necessary for depression, anxiety, or psychosis, carefully review target symptoms, treatment expectations, and possible adverse effects with the patient and caregiver. Keep in mind the progressive nature of PD and, in addition to frequent monitoring, educate and encourage caregivers to immediately report any suspected adverse effects.
Any motor function deterioration should trigger a re-evaluation of psychotropic medications before you presume that the patient’s PD is progressing. Because antiparkinsonian drug regimens change over time, review the patient’s medications at each appointment, and alert patients and caregivers to potential psychiatric complications of any new medication.
Caregiver treatment In addition to treating the patient, it is important to monitor the impact of psychiatric symptoms and PD on the patient’s caregiver. Frequently assess whether the caregiver and patient have adequate social supports, and address any emerging needs. Useful interventions include caregiver counseling, referrals to support groups, and respite care.24
Mrs. K had a 4-year history of rapidly progressing PD treated with entacapone, carbidopa-levodopa, and a deep brain stimulator. Increasing periods of motor freezing, which were often accompanied by panic attacks, led her to become increasingly depressed and demanding of her caregiver husband. Eventually, she was admitted to an inpatient psychiatry unit because of suicidal ideation.
After a neurologic evaluation, the dosing times of her carbidopa-levodopa and entacapone were changed, but she continued to have panic attacks and remained depressed. Alprazolam promptly reduced her panic symptoms, and paroxetine was initiated for depression. A discussion with the patient and her husband revealed that they had some longstanding issues in their marriage that were exacerbated by Mrs K’s increasing dependency. The couple was referred for marital therapy, and Mrs. K agreed to begin attending a senior center.
Following discharge, the panic remained controlled and depression improved. Entacapone was replaced with tolcapone to see if motor freezing would decrease. Mrs. K’s movements improved, but her husband reported she had awakened on several nights with visual hallucinations. The hallucinations were infrequent, unaccompanied by agitation, and not distressing to the patient. Following a discussion of therapeutic options with Mrs. K and her husband, antipsychotic therapy was not instituted. The patient continues to live at home and attends the senior center regularly.
Related resources
- Parkinson’s Disease Foundation: http://www.pdf.org
- American Parkinson Disease Association: http://apdaparkinson.com
- National Parkinson Foundation: http://www.parkinson.org
- Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease 2001: treatment guidelines. Neurology 2001;56:5(suppl):S1-S88.
Drug brand names
- Alprazolam • Xanax
- Amantadine • Symmetrel
- Benztropine • Cogentin
- Biperiden • Akineton
- Buspirone • Buspar
- Carbidopa-levodopa • Sinemet
- Citalopram • Celexa
- Clozapine • Clozaril
- Entacapone • Comtan
- Fluvoxamine • Luvox
- Hyoscyamine • Levsin
- Paroxetine • Paxil
- Pergolide • Permax
- Pramipexole • Mirapex
- Ropinirole • Requip
- Selegeline • Eldepryl
- Sertraline • Zoloft
- Tolcapone • Tasmar
- Trihexyphenidyl • Artane
- Trifluoperazine • Stelazine
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Depression, anxiety, and psychosis are common complications of Parkinson’s disease (PD) and of the medications used in antiparkinsonian treatment. These psychiatric problems impair patients’ functioning throughout the course of the chronic degenerative disease.
Because medication side effects often call for adjustments and trade-offs in PD treatment, a team effort by the psychiatrist, neurologist, patient, and caregiver is the most effective approach to decision-making. From our experience in such collaborations, here’s what you need to know about PD to be a most-valuable player on that treatment team.
Presentation of PD
The classic triad of PD features consists of a pill-rolling tremor, rigidity, and bradykinesia or slowness of movement. Other common features include postural instability, flexed posture, and other motor-freezing phenomena.
Freezing phenomena occur in the later stages of PD, as the response to dopaminergic therapy becomes erratic and unpredictable. Freezing can range from hesitation—such as when the patient tries to turn or is in a doorway—to transient episodes of total inability to move. These episodes are extremely distressing for both patients and caregivers.
Patients rarely present with the full complement of symptoms, but the presence of tremor at rest and/or bradykinesia is essential for the diagnosis. While motor signs dominate the presentation, cognitive symptoms such as shortened attention span, visuospatial impairment, personality changes, and dementia are also frequently present.
Average age of diagnosis is 60, and more men are affected than women (male-to-female ratio is 3:2). Many causative factors—including genetics and environmental toxins—have been implicated, but the disorder’s etiology remains unknown.
Drug treatment side effects
PD results from the loss of neurons in the substantia nigra that produce the neurotransmitter dopamine. Pharmacologic treatment emphasizes dopamine replacement, dopamine receptor stimulation, or prevention of enzymatic breakdown of dopamine in the synaptic cleft. As treatment of PD is symptomatic and not curative, medications are instituted only when the disease begins to cause functional impairment.
Treatment begins with dopamine agonists (Table). As dopamine agonist monotherapy becomes less effective, levodopa therapy is initiated. Blocking the enzymatic breakdown of dopamine with catechol-O-methyltransferase inhibitors is the next therapeutic strategy.
Within 5 years of starting levodopa therapy 75% of patients experience unsatisfactory motor response, from unpredictable fluctuations to wearing-off phenomena (in which a dose of levodopa does not last as long as it once did). Treatment of advanced PD is complicated by the emergence of psychiatric symptoms, such as hallucinations and psychosis, as dopamine levels are increased in an attempt to smooth the motor response.
The significantly distressing level of disability associated with the prominent side effects of pharmacologic treatment has led to interest in surgical interventions. These range from pallidotomy to implantation of basal ganglia stimulators to transplantation of fetal striatal neurons. The possibility of neuroprotection has also been extensively investigated, with mixed results.
Psychiatric complications of PD
Depression. Clearly, the stress of anticipating and coping with a relentless degenerative disease helps to trigger depression and anxiety in patients with PD. Depression is the most common psychiatric syndrome, with prevalence in PD as high as 42%.1 Patients with a history of depression are at particular risk.2 Those with recent deterioration or advancing severity of PD, akinesia, history of falls, or cognitive impairment are also at increased risk for depression.
Table
MEDICATIONS COMMONLY USED IN MANAGING PARKINSON’S DISEASE
| Medication class | Example | Indication for use |
|---|---|---|
| MAO-B inhibitor | Selegiline | ? Neuroprotection |
| Anticholinergic agents | Trihexyphenidyl, benztropine, biperiden, hyoscyamine, diphenhydramine | Tremor |
| Dopamine agonist | Pramipexole, pergolide, ropinirole | ? Neuroprotection Treatment of movement disorder |
| Dopamine replacement | Carbidopa-levodopa | Treatment of movement disorder |
| Catechol-O-methyltransferase inhibitor | Entacapone, tolcapone | Smooth motor fluctuations |
Depression correlates well with the patient’s perception of his or her degree of PD-related disability. Depression symptoms seem to peak early in the illness following diagnosis and in advanced disease.3
Patients may present with symptoms meeting diagnostic criteria ranging from dysthymic disorder to minor depression to major depressive disorder.1,4 Although they will frequently endorse suicidal ideation, patients with PD have a low rate of suicide. Diagnosing depression, however, may be difficult because its symptoms overlap with those of the underlying neurologic disease:
- Diminished affect and psychomotor slowing may be secondary to the motor features of parkinsonism.
- Diminished concentration may be secondary to cognitive decline rather than depression.
Patients also frequently have a chief complaint of diminished energy or fatigue that should trigger further investigation into other depressive symptoms.4,5
In addition to the obvious additional suffering it causes, depression in PD predicts impaired social, physical, and role functioning.6 Depression in the PD patient also results in higher distress for caregivers.7 In one study, depression was identified as a risk factor for development of psychosis in PD patients.8
Anxiety is a frequent problem for PD patients, with a prevalence of 33 to 40%.9,10 Anxiety in PD typically presents with symptoms of panic disorder, generalized anxiety disorder, or social phobia.11 It is comorbid with depression in up to 92% of cases and—like depression—frequently predates the onset of motor symptoms.12
Anxiety symptoms have been correlated, although not consistently, with the on-off motor phenomenon often found in advanced PD.13 They can also be an adverse effect of many of the antiparkinsonian medications, including anticholinergics, dopamine agonists, catechol-O-methyltransferase inhibitors, and selegiline. Both anxiety and depression have been associated with an increased risk for falls.14
Psychotic symptoms. Up to 25% of PD patients experience delusions or hallucinations.15 Risk factors include dementia, sleep disturbance, and—most commonly—the use of dopaminergic agents. Up to one-fifth of patients using dopaminergic drugs experience psychotic symptoms.16
Psychotic symptoms can occur with or without the clouded sensorium characteristic of delirium. Psychotic symptoms with an associated confusional state can be associated with use of anticholinergic agents and drugs such as selegiline and amantadine.17 Catechol-O-methyltransferase inhibitors cause more sustained dopaminergic activity of levodopa, which can result in psychotic symptoms. Therefore, the use of all known classes of antiparkinsonian medications has been associated with drug-induced psychosis.
In advanced PD, paranoid delusions, delusions of spousal infidelity, and visual hallucinations are common, whereas negative symptoms and thought disturbances are not.18 Psychosis may be a more important contributor to caregiver distress than the motor symptoms of PD and may be more likely than any other factor to lead to nursing home placement of the PD patient (Box 1).15
Psychiatric interventions
Goals for psychiatric treatment of depression, anxiety, and psychosis associated with PD seem relatively straightforward:
- improvement or remission of psychiatric symptoms
- restoration of optimal patient functioning.
Ideally, these goals would be achieved without causing sedation, orthostatic hypotension, or exacerbating motor symptoms. The older age of patients and the progressive nature of this neurodegenerative disorder predispose patients to cognitive side effects. Unfortunately, despite the high prevalence of psychiatric disturbances in PD, evidence with which to evaluate treatment efficacy and safety and to guide treatment selection is extremely limited.
For depression associated with PD, extensive clinical experience supports the efficacy of tricyclic antidepressants. Even so, selective serotonin reuptake inhibitors (SSRIs) are the preferred treatment, although only open-label trials and case reports support their efficacy.5,12 Compared with tricyclics, SSRIs exhibit a relative lack of problems with sedation, orthostatic hypotension, and memory-impairing anticholinergic side effects. While case reports have cited worsening of motor symptoms with SSRIs, a recent prospective study found no significant worsening of PD symptoms during treatment with citalopram, fluoxetine, fluvoxamine, or sertraline.19 Co-administration of an SSRI with selegiline is not absolutely contraindicated, but the combination does carry a very small risk of development of serotonin syndrome.1,5
Mr. J had a 6-year history of PD with pronounced bradykinesia and gait disturbance treated with amantadine and carbidopa-levodopa. His rigidity began to worsen, so the dosage of carbidopa-levodopa was increased. His wife then reported that he had increased confusion and balance problems. On evaluation, he was found to have a urinary tract infection. Following antibiotic treatment, mental status and gait returned to usual baseline.
One year later, Mr. J began having trouble getting out of bed, with unpredictable motor freezing episodes. Pramipexole was added to his regimen, and he began having prominent visual hallucinations. Low-dose trifluoperazine was added, and hallucinations improved. The patient became increasingly depressed, and sertraline was started.
Over the next year, his function progressively worsened, with increased motor freezing and unpredictable dyskinesias. Hallucinations complicated attempts to change his medications. Amantadine was stopped without improvement. He was referred for surgical evaluation, but because of his cognitive status and depression was deemed not to be a candidate.
He began to fall repeatedly and developed orthostatic hypotension. His clinical course continued to be complicated by hallucinations and delusions that his wife was being unfaithful. Ongoing psychosis and severe gait instability led to his admission to a nursing home.
Data are even more scant on the safe use of other antidepressants in PD. Electroconvulsive therapy has been proven helpful in refractory cases and sometimes results in transient motor symptom improvement.1,5,12 While clinical experience suggests that psychotherapy frequently helps, no extensive controlled studies exist. One small study suggests the efficacy of structured cognitive psychotherapy.20
Anxiety. No studies have examined the treatment of anxiety in PD patients. Given the extremely high comorbidity of anxiety with depression, antidepressants should probably be considered as a first-line pharmacotherapy. Benzodiazepines should be used cautiously, as they increase the risk of falls, sedation, and confusion in older patients. One small controlled study found that buspirone was well tolerated in PD patients at low dosages (10 to 40 mg/d), but anxiety did not improve. At high dosages (100 mg/d), anxiety worsened.21
Psychosis. Data on use of antipsychotic agents in PD are also limited, but some evidence supports their use in treating PD-related psychotic symptoms. While conventional antipsychotics can help control psychosis, the potential is high for worsening of parkinsonian symptoms due to D2 receptor blockade.
Among the atypical antipsychotics, clozapine has been most extensively studied in PD and has been shown in open and double-blind trials to be effective and well tolerated at low dosages (6.25 to 50 mg/d). A limited number of open studies of some of the newer atypicals have been performed. While extreme caution must be used in comparing data from these studies due to highly variable dosing and other study design issues, clozapine and quetiapine appear to be the agents best tolerated by PD patients.12,18,22 Initial antipsychotic dosing should be low and escalation cautious—regardless of the agent chosen—because of the dose-related potential for worsening of parkinsonian symptoms, sedation, and orthostatic hypotension.
A team approach to treatment
Because psychiatric and PD symptoms and treatments are closely interrelated, the psychiatrist, neurologist, patient, and caregiver must collaborate for the best therapeutic result. A simplistic approach to treatment can result in a catastrophic downward spiral in patient functioning.
Often, compromises must be made between optimal control of parkinsonian and psychiatric symptoms to achieve the best overall patient function. Patients and caregivers must be counseled about possible psychiatric symptoms associated with PD and antiparkinsonian therapy, as well as the potential for adverse effects from psychiatric medications. With this knowledge, patients and caregivers can help assess the severity of symptoms and set treatment priorities, depending on how symptoms may be affecting the patient’s level of functioning. For example, if an effective antiparkinsonian regimen has triggered infrequent, nondistressing hallucinations with preserved insight, intervention may not be required beyond patient and caregiver education (Box 2).
Patient workup. When intervention is required for psychiatric symptoms, it should begin with careful neurologic evaluation. Triggering factors such as infections (commonly urinary tract infections and pneumonia), metabolic disorders (hyperglycemia, hypothyroidism), subdural hematomas (if the patient is falling), and drug interactions should be ruled out or appropriately addressed.
Next, try to sequentially eliminate antiparkinsonian medications until the psychosis resolves or motor function worsens.23 Because of considerable overlap between PD symptoms and depression (psychomotor retardation, fatigue, and anergia), optimizing PD therapy sometimes can result in substantial psychiatric improvement. Some evidence also suggests that the dopamine agonist pramipexole may be effective in treating both PD and depression.5
When psychiatric medications are necessary for depression, anxiety, or psychosis, carefully review target symptoms, treatment expectations, and possible adverse effects with the patient and caregiver. Keep in mind the progressive nature of PD and, in addition to frequent monitoring, educate and encourage caregivers to immediately report any suspected adverse effects.
Any motor function deterioration should trigger a re-evaluation of psychotropic medications before you presume that the patient’s PD is progressing. Because antiparkinsonian drug regimens change over time, review the patient’s medications at each appointment, and alert patients and caregivers to potential psychiatric complications of any new medication.
Caregiver treatment In addition to treating the patient, it is important to monitor the impact of psychiatric symptoms and PD on the patient’s caregiver. Frequently assess whether the caregiver and patient have adequate social supports, and address any emerging needs. Useful interventions include caregiver counseling, referrals to support groups, and respite care.24
Mrs. K had a 4-year history of rapidly progressing PD treated with entacapone, carbidopa-levodopa, and a deep brain stimulator. Increasing periods of motor freezing, which were often accompanied by panic attacks, led her to become increasingly depressed and demanding of her caregiver husband. Eventually, she was admitted to an inpatient psychiatry unit because of suicidal ideation.
After a neurologic evaluation, the dosing times of her carbidopa-levodopa and entacapone were changed, but she continued to have panic attacks and remained depressed. Alprazolam promptly reduced her panic symptoms, and paroxetine was initiated for depression. A discussion with the patient and her husband revealed that they had some longstanding issues in their marriage that were exacerbated by Mrs K’s increasing dependency. The couple was referred for marital therapy, and Mrs. K agreed to begin attending a senior center.
Following discharge, the panic remained controlled and depression improved. Entacapone was replaced with tolcapone to see if motor freezing would decrease. Mrs. K’s movements improved, but her husband reported she had awakened on several nights with visual hallucinations. The hallucinations were infrequent, unaccompanied by agitation, and not distressing to the patient. Following a discussion of therapeutic options with Mrs. K and her husband, antipsychotic therapy was not instituted. The patient continues to live at home and attends the senior center regularly.
Related resources
- Parkinson’s Disease Foundation: http://www.pdf.org
- American Parkinson Disease Association: http://apdaparkinson.com
- National Parkinson Foundation: http://www.parkinson.org
- Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease 2001: treatment guidelines. Neurology 2001;56:5(suppl):S1-S88.
Drug brand names
- Alprazolam • Xanax
- Amantadine • Symmetrel
- Benztropine • Cogentin
- Biperiden • Akineton
- Buspirone • Buspar
- Carbidopa-levodopa • Sinemet
- Citalopram • Celexa
- Clozapine • Clozaril
- Entacapone • Comtan
- Fluvoxamine • Luvox
- Hyoscyamine • Levsin
- Paroxetine • Paxil
- Pergolide • Permax
- Pramipexole • Mirapex
- Ropinirole • Requip
- Selegeline • Eldepryl
- Sertraline • Zoloft
- Tolcapone • Tasmar
- Trihexyphenidyl • Artane
- Trifluoperazine • Stelazine
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Slaughter JR, Slaughter KA, Nichols D, et al. Prevalence, clinical manifestations, etiology, and treatment of depression in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 2001;13:187-96.
2. Starksein SE, Preziosi TJ, Bolduc PL, Robinson RG. Depression in Parkinson’s disease. J Nerv Ment Dis 1990;178:27-31.
3. Schrag A, Jahanshahi M, Quinn P. What contributes to depression in Parkinson’s disease? Psychological Medicine 2001;31:65-73.
4. Poewe W, Luginger E. Depression in Parkinson’s disease: impediments to recognition and treatment options. Neurology 2001;52(7):S002-S006.
5. Okun MS, Watts RL. Depression associated with Parkinson’s disease: clinical features and treatment. Neurology 2002;58:1(suppl):S63-S70.
6. Cole SA, Woodard JL, Juncos JL. Depression and disability in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1996;8(1):20-5.
7. Aarsland D, Larsen JP, et al. Mental symptoms in Parkinson’s disease are important contributors to caregiver distress. Int J Geriatr Psychiatry 1999;14(10):866-74.
8. Giladi N, Treves TA, Paleacu D, et al. Risk factors for dementia, depression and psychosis in long-standing Parkinson’s disease. J Neural Transm 2000;107(1):59-71.
9. Shulman LM, Taback RL, Bean J, Weiner WJ. Comorbidity of the nonmotor symptoms of PD. Mov Disord 2001;16(3):507-10.
10. Walsh K, Bennett G. Parkinson’s disease and anxiety. Postgrad Med J 2001;77(904):89-93.
11. Richard IH, Schiffe RB, Kurler R. Anxiety and Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1996;8(4):383-92.
12. Menza MA. Psychiatric aspects of Parkinson’s disease. Psychiatric Ann 2002;32:99-104.
13. Richard IH, Justus AW, Kurlan R. Relationship between mood and motor fluctuations in PD. J Neuropsychiatry Clin Neurosci 2001;13(1):35-41.
14. Ashburn A, Stack E, Pickering CM, Ward CD. A community-dwelling sample of people with Parkinson’s disease: characteristics of fallers and non-fallers. Age Ageing 2001;30(1):47-52.
15. Wolters EC, Berendse HW. Management of psychosis in Parkinson’s disease. Curr Opin Neurol 2001;14(4):499-504.
16. Juncos JL. Management of psychotic aspects of Parkinson’s disease. J Clin Psychiatry 1999;60:8(suppl):42-53.
17. Wolters EC. Dopaminomimetic psychosis in Parkinson’s disease patients. Neurology 1999;52:7(suppl):S010-S013.
18. Friedman JH, Factor SA. Atypical antipsychotics in the treatment of drug-induced Parkinson’s disease. Mov Disord 2000;15(2):201-11.
19. Dell’Agnello G, Ceravolo R, et al. SSRIs do not worsen Parkinson’s disease: evidence from an open-label, prospective study. Clin Neuropharmacol 2001;24(4):221-27.
20. Dreisig H, Beckmann J, Wermuth L, et al. Psychological effects of structured cognitive psychotherapy in young patients with Parkinson’s disease (abstr). Nordic J Psychiatry 1999;53(3):217-21.
21. Ludwig CL, Weinberger DR, Bruno G, et al. Buspirone, Parkinson’s disease and the locus ceruleus. Clin Neuropharmacol 1986;9(4):373-8.
22. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs 2002;16(1):23-45.
23. Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease 2001: treatment guidelines. Neurology 2001;56:5(suppl):S1-S88.
24. Ellgring JH. Depression, psychosis, dementia: impact on the family. Neurology 1999;52:7(suppl 3):S17-S20.
1. Slaughter JR, Slaughter KA, Nichols D, et al. Prevalence, clinical manifestations, etiology, and treatment of depression in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 2001;13:187-96.
2. Starksein SE, Preziosi TJ, Bolduc PL, Robinson RG. Depression in Parkinson’s disease. J Nerv Ment Dis 1990;178:27-31.
3. Schrag A, Jahanshahi M, Quinn P. What contributes to depression in Parkinson’s disease? Psychological Medicine 2001;31:65-73.
4. Poewe W, Luginger E. Depression in Parkinson’s disease: impediments to recognition and treatment options. Neurology 2001;52(7):S002-S006.
5. Okun MS, Watts RL. Depression associated with Parkinson’s disease: clinical features and treatment. Neurology 2002;58:1(suppl):S63-S70.
6. Cole SA, Woodard JL, Juncos JL. Depression and disability in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1996;8(1):20-5.
7. Aarsland D, Larsen JP, et al. Mental symptoms in Parkinson’s disease are important contributors to caregiver distress. Int J Geriatr Psychiatry 1999;14(10):866-74.
8. Giladi N, Treves TA, Paleacu D, et al. Risk factors for dementia, depression and psychosis in long-standing Parkinson’s disease. J Neural Transm 2000;107(1):59-71.
9. Shulman LM, Taback RL, Bean J, Weiner WJ. Comorbidity of the nonmotor symptoms of PD. Mov Disord 2001;16(3):507-10.
10. Walsh K, Bennett G. Parkinson’s disease and anxiety. Postgrad Med J 2001;77(904):89-93.
11. Richard IH, Schiffe RB, Kurler R. Anxiety and Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1996;8(4):383-92.
12. Menza MA. Psychiatric aspects of Parkinson’s disease. Psychiatric Ann 2002;32:99-104.
13. Richard IH, Justus AW, Kurlan R. Relationship between mood and motor fluctuations in PD. J Neuropsychiatry Clin Neurosci 2001;13(1):35-41.
14. Ashburn A, Stack E, Pickering CM, Ward CD. A community-dwelling sample of people with Parkinson’s disease: characteristics of fallers and non-fallers. Age Ageing 2001;30(1):47-52.
15. Wolters EC, Berendse HW. Management of psychosis in Parkinson’s disease. Curr Opin Neurol 2001;14(4):499-504.
16. Juncos JL. Management of psychotic aspects of Parkinson’s disease. J Clin Psychiatry 1999;60:8(suppl):42-53.
17. Wolters EC. Dopaminomimetic psychosis in Parkinson’s disease patients. Neurology 1999;52:7(suppl):S010-S013.
18. Friedman JH, Factor SA. Atypical antipsychotics in the treatment of drug-induced Parkinson’s disease. Mov Disord 2000;15(2):201-11.
19. Dell’Agnello G, Ceravolo R, et al. SSRIs do not worsen Parkinson’s disease: evidence from an open-label, prospective study. Clin Neuropharmacol 2001;24(4):221-27.
20. Dreisig H, Beckmann J, Wermuth L, et al. Psychological effects of structured cognitive psychotherapy in young patients with Parkinson’s disease (abstr). Nordic J Psychiatry 1999;53(3):217-21.
21. Ludwig CL, Weinberger DR, Bruno G, et al. Buspirone, Parkinson’s disease and the locus ceruleus. Clin Neuropharmacol 1986;9(4):373-8.
22. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs 2002;16(1):23-45.
23. Olanow CW, Watts RL, Koller WC. An algorithm (decision tree) for the management of Parkinson’s disease 2001: treatment guidelines. Neurology 2001;56:5(suppl):S1-S88.
24. Ellgring JH. Depression, psychosis, dementia: impact on the family. Neurology 1999;52:7(suppl 3):S17-S20.
Irritable bowel syndrome: Psychotherapy can improve GI symptoms and emotional health
A growing body of evidence suggests that psychiatrists have much to offer patients with severe irritable bowel syndrome (IBS). Behavioral and psychotherapeutic approaches are showing promise in relieving both GI and mood disturbances.
Treating patients with IBS with medications designed to influence only gut function can be frustrating. Those with refractory symptoms may be extremely sensitive to drug side effects, and they often report that medical management worsens or does not improve their symptoms. They experiment with alternative medicines and wander from physician to physician in a disappointing search for a “cure.”
Let’s look at evidence on the efficacy of individual and group behavioral therapies, hypnotherapy, biofeedback, and combination medical and behavioral treatment.
Psychotherapeutic approaches
IBS is a common gastrointestinal disorder that is characterized by abdominal discomfort and changes in bowel habits (Boxes 1 and 2). Patients with severe IBS symptoms often bring significant psychological impairment and psychosocial trauma to clinical encounters.1,2 They respond poorly to standard medical management, and evidence supporting the efficacy of medical treatments for IBS remains weak.3,4
Irritable bowel syndrome (IBS) is the most common disorder seen in gastrointestinal practice, representing more than 40% of all visits to gastroenterologists. Complaints of IBS also account for approximately 23% of office visits to primary care physicians.1
Key symptoms of this functional disorder are a pattern of lower abdominal discomfort and bloating accompanied by variable degrees of altered stool pattern—constipation, diarrhea, or intermittent constipation and diarrhea. IBS is most common in young patients, with onset rarely diagnosed after age 45. Its incidence is equal in men and women, but women are more likely to seek medical care for IBS symptoms.
The cause of IBS is unclear. Recent research suggests that changes in serotonin metabolism cause a pattern of visceral hypersensitivity and an altered sensation of pain. IBS is not a psychiatric disorder, but it can be worsened by comorbid psychopathology, particularly mood and anxiety disorders. Although patients tend to have either diarrhea-predominant or constipation-predominant IBS, the pathophysiology of both patterns seems similar.
In 1983, the first controlled trial of psychodynamic psychotherapy for IBS showed dramatic reductions in symptoms.5 A subsequent series of high-quality articles in the early 1990s also showed that interpersonal psychotherapy (with greater interaction between therapist and patient) could significantly decrease IBS symptoms.
Persistent improvement. In one randomized controlled trial,6 102 patients with IBS received either standard medical treatment or 10 hours of dynamically oriented individual psychotherapy in combination with standard medical treatment. After 3 months, patients who received psychotherapy showed significantly greater improvement in somatic symptoms and emotional well-being, compared with those who received medical treatment only.
Interestingly, this difference persisted 1 year after the study ended. GI symptoms and the emotional well-being of patients who received combination therapy continued to improve, whereas the physical and emotional status of those who received only standard medical treatment deteriorated.
In a second study,7 101 patients with severe IBS symptoms continued to receive medical treatment but were randomly divided into two groups:
- Study subjects received 8 hours of dynamically oriented psychotherapy.
- Control patients met with a psychiatrist who engaged in “supportive listening” but delivered no psychotherapy. This strategy was adopted to control for the effect of the psychiatrist’s presence.
Assessments included patients’ self-reports of symptoms, ratings of GI symptoms by the treating gastroenterologists, and measures of depression, anxiety, and health care utilization. Patients who received psychotherapy reported significant improvements in bowel symptoms (e.g., diarrhea, constipation, bloating, and abdominal pain). Likewise, the gastroenterologist who rated patients’ GI symptoms felt that those who received psychotherapy improved significantly across the entire spectrum of GI symptoms. The improvements were maintained at 1-year follow-up.
By comparison, the control patients reported worsening symptoms, as did subjects who dropped out. Patients who received psychotherapy also made significantly fewer outpatient visits to gastroenterologists, compared with controls (p<0.001).
Cognitive-behavioral therapy
Cognitive-behavioral therapy (CBT) is emerging as a major psychotherapeutic tool for treating mood disorders, anxiety disorders, and somatic syndromes associated with psychosocial distress. CBT also is showing promise for patients with moderate to severe IBS and those with IBS and concomitant anxiety or mood disorders. Studies consistently show that CBT is superior to standard medical management or the use of support groups or other behavioral treatments alone.
Reduced symptoms. In an early trial of CBT, 17 patients with IBS experienced significantly less abdominal pain and diarrhea after participating in a program of progressive relaxation, education about bowel functioning, use of thermal biofeedback, and stress coping techniques based on CBT. Overall, 64% of the patients improved.8
The same investigators then assigned 90 patients to 12 sessions of CBT, given over 8 weeks with or without meditation and biofeedback. Patients with axis I psychiatric diagnoses tended to respond poorly to CBT. The authors concluded that a careful pretreatment psychological workup is important to identify patients with IBS who would benefit most from CBT.9
As a follow-up, these investigators randomly assigned 20 patients to intensive individualized CBT (10 sessions over 8 weeks) or 8 weeks of daily GI symptom monitoring. Patients who received CBT had significantly fewer GI symptoms than did the symptom-monitoring group (p = 0.005). With CBT, 80% improved clinically, compared with only 10% in the control group. Improvements in the CBT group persisted at 3 months’ follow-up. Improved GI symptoms also were correlated with increased positive thoughts and reduced negative automatic thoughts (i.e., negative self-image).10
In the preceding 12 months, the patient has experienced at least 12 weeks or more (need not be consecutive) of abdominal discomfort or pain that has:
Two out of three features
- relieved with defecation, and/or
- onset associated with a change in frequency or stool, and/or
- onset associated with a change in form (appearance) of stool
Symptoms that cumulatively support the diagnosis
- Abnormal stool frequency (for research purposes, “abnormal” may be defined as >3 bowel movements per day and <3 bowel movements per week);
- abnormal stool form (lumpy/hard or loose/watery stool)
- abnormal stool passage (straining, urgency, or feeling of incomplete evacuation)
- passage of mucus
- bloating or abdominal distension.
* In the absence of structural or metabolic abnormalities to explain the symptoms
Source: Drossman DA, Corazziari E, Talley NJ, et al. Rome II: The functional gastrointestinal disorders (2nd ed). McLean, VA: Degnon Associates, 2000.
Group therapy. In a study of group rather than individualized CBT, 45 patients with severe IBS symptoms were randomly assigned to either a group CBT module (n = 25) or a waiting list control group (n = 20). Patients received eight 2-hour group CBT sessions over 3 months, then were followed an average of 2.25 years. Their abdominal pain, number of successful coping behavioral strategies, and avoidance of negative situations improved significantly—compared with the waiting list controls—and persisted during follow-up. The authors concluded that group CBT is effective for alleviating IBS symptoms and improving patients’ coping strategies.11
CBT vs. support groups. In a study comparing the effectiveness of CBT and an IBS self-help support group, 34 patients were randomly assigned to:
- individualized CBT (study group)
- a self-help support group
- or a symptom-monitoring waiting list (control group).
Each group was followed for 8 weeks. GI symptoms were reduced significantly in patients who received individualized CBT, compared with the support group or controls. Anxiety and depression in the CBT group also remained significantly improved 3 months later, compared with both other groups.12
Group psychotherapy
Group psychotherapy for IBS treatment can be more cost-effective than individual therapy, but its success depends on whether patients accept a group format. Data on the use of group psychotherapeutic approaches are largely favorable.
As described previously, one study demonstrated that group CBT reduced abdominal pain and diarrhea and improved symptoms overall.11 In another study, 20 patients with refractory IBS underwent 6 weeks of group behavioral and didactic psychotherapy. GI symptoms, dysphoria, and psychological distress improved significantly in all patients, and their interpersonal sensitivity and hostility were reduced. These improvements persisted 6 months later.12
A recent review suggests that cognitive-behavioral group psychotherapy may be highly effective in patients with IBS. These authors concluded that CBT can improve patients’ mood and other emotional symptoms, reduce their pain, and improve well-being and coping ability.14
Hypnotherapy
Researchers in Manchester, UK, have shown excellent results with hypnotherapy for patients with severe refractory IBS. Although their data seem to have established the ability of hypnotherapy to improve the GI and non-GI symptoms of IBS, corroborating evidence is needed from other centers. In this regard, some preliminary evidence is emerging.
Manchester group. In the first trial by the Manchester group, 30 patients received seven half-hour sessions of hypnotherapy (study group) or supportive psychotherapy and placebo (control group). Patients who received hypnotherapy also were given a tape for home autohypnosis after the third session.
Patients who received hypnotherapy improved dramatically in all GI symptoms— including abdominal pain, bloating, and bowel habits—and in their sense of well-being. This effect persisted 3 months later. The control patients’ abdominal pain, bloating, and well-being improved somewhat, but their bowel habits did not improve.15
The same investigators then studied 30 patients with IBS to assess the effect of hypnotherapy on rectal physiology. Fifteen patients received hypnotherapy, and 15 received relaxation exercises. Rectal sensitivity was measured using anorectal manometry at the start and finish of the intervention.
For patients with diarrhea-predominant IBS, rectal sensitivity was significantly reduced during hypnosis and after the full course of hypnotherapy, compared with controls (p<0.05). In patients with constipation-predominant IBS, a trend towards normalized rectal sensitivity did not reach statistical significance. The investigators concluded that symptomatic improvement of IBS after hypnotherapy may be related to changes in visceral sensitivity of the colon.16
These investigators later studied changes in distal colonic motility in 18 patients undergoing hypnotherapy for IBS. As the patients’ hypnotically induced anger or excitement increased, colonic motility decreased significantly (p<0.01) The investigators concluded that hypnosis may be a useful tool to investigate the effects of emotion on physiologic function.17
Using more contemporary outcome measures and diagnostic criteria, these investigators later showed that hypnotherapy significantly improved:
- IBS symptoms (abdominal pain and bloating, bowel habit, nausea, flatulence, urinary symptoms, lethargy, backache, and dyspareunia)
- quality of life (psychological and physical well-being, mood, locus of control, and work attitude).
Patients treated with hypnosis also took less time away from work (p = 0.02) and visited their physicians less often (p = 0.056), compared with controls.18
Other hypnosis studies. In the United States, another group randomly assigned 12 patients to gut-directed hypnotherapy or symptom monitoring. Subjects were matched by concurrent psychiatric diagnosis, susceptibility to hypnosis, and demographic features.
In findings similar to those of the Manchester group, primary IBS symptoms (abdominal pain, constipation, and flatulence) of patients who received hypnotherapy improved more than those of controls (p = 0.016). Anxiety, as measured by the Spielberger State-Trait Anxiety Inventory (STAXI), also decreased significantly. Treatment-induced gains were well-maintained 2 months later. No significant correlation was found between initial sensitivity to hypnosis and subsequent response to hypnotherapy. A positive relationship was seen between the presence of psychiatric diagnoses and overall levels of improvement.
This study suggests that hypnotherapy can be useful for treating IBS and can be easily adapted to different clinical settings and treatment populations.19 A similar study using gut-directed hypnotherapy found significant improvement in 27 IBS patients treated with short-term hypnosis, and symptom improvement persisted after treatment.20
Biofeedback
The role of biofeedback in IBS treatment remains ill-defined. To be considered as a treatment option, biofeedback must meet or exceed the benefits being achieved with psychotherapy, hypnotherapy, and other behavioral approaches.
In gastroenterology, biofeedback has been used mainly to treat constipation and specifically for outlet constipation due to pelvic floor dysfunction. Anorectal probes to measure rectal pressure in the resting state and during defecation can reveal a pattern of pelvic floor dysfunction. Studies have demonstrated up to 67% improvement in constipation symptoms using biofeedback. Use of anorectal biofeedback in adults with IBS also appears promising, but more controlled trials are needed.21
Anorectal biofeedback has also been used effectively to treat fecal incontinence in children and adults, achieving success rates of 70% or better. In IBS, however, the benefit of biofeedback is less clear. Studies of multicomponent treatment—combining biofeedback with CBT techniques—suggest improvement rates in the 50 to 60% range. However, these findings need to be compared with other treatments for IBS.
Combination treatment
Medical treatment of IBS is progressing. Antidepressant therapy, particularly using tricyclics, has shown moderate benefit.22 Newer medications such as alosetron and tegaserod, which modulate serotonin metabolism in the gut, have been developed. Alosetron and tegaserod have shown significantly greater efficacy compared with placebo for treatment of women with the diarrhea-predominant and constipation-predominant types of IBS, respectively.
Alosetron was voluntarily withdrawn from clinical use in 2000 because of reports of serious GI events associated with its use, including ischemic colitis in a small number of patients (about 3 women in 1,000). Because of the drug’s efficacy in IBS, however, the FDA recently approved its rerelease with a restricted indication—it is to be used only in women with severe diarrhea-predominant IBS who have not responded to conventional IBS treatment. The drug’s manufacturer also is implementing a risk management plan designed to reduce the potential for serious GI side effects.
Table
PSYCHOTHERAPY AS TREATMENT FOR IRRITABLE BOWEL SYNDROME
| Psychotherapeutic approach | Summary of research results |
|---|---|
| Psychodynamic therapy | Shown to be effective in reducing pain and dysphoric mood5 |
| Interpersonal psychotherapy | Effective in reducing pain, bloating, and health care utilization and improving emotional well-being7 |
| Cognitive-behavioral therapy | Improves coping skills and decreases helplessness and somatization14 |
| Group psychotherapy | Seems to be as efficacious as cognitive-behavioral therapy, with the added efficiency of a group model13 |
| Hypnotherapy | Highly effective for a spectrum of IBS symptoms15 |
| Biofeedback | Not useful for IBS per se, but helpful for pelvic floor dysfunction21 |
| Combination therapy | Emerging as a particularly useful strategy, combining medical and behavioral approaches23 |
Tegaserod, a serotonin-4 receptor (5HT4) agonist, was approved by the FDA in July. It is indicated for short-term treatment of women with IBS whose primary bowel symptom is constipation.
Combination therapy—medical management plus psychotherapy—may represent the future of IBS treatment (Table). This approach was examined recently in a randomized study of 24 IBS patients who received standard medical treatment alone or in combination with behavioral therapy. The behavioral component included patient education, helping patients shape a plausible model for their illness, progressive muscle relaxation, cognitive coping strategies, problem-solving education, and assertiveness and social skills training. All patients were treated in 10 individual therapy sessions of approximately 1 hour each by one of two psychotherapists across 10 weeks.
Compared with medical treatment alone, patients treated with combination therapy showed significantly improved GI symptoms (p < 0.001) and psychological symptoms (p = 0.01) in terms of both patient report and objective psychological measures. Outcomes are enhanced for patients with severe IBS, the investigators concluded, when behavioral therapy is added to thoughtful medical management.23
Related resource
- International Foundation for Functional Gastrointestinal Disorders. www.iffgd.org
Drug brand names
- Alosetron • Lotronex
- Tegaserod • Zelnorm
Disclosure
The author reports that he serves as a consultant to Novartis Pharmaceuticals Corp. He reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sandler R. Epidemiology of irritable bowel syndrome in the United States. Gastroenterology 1990;99:409-15.
2. Leserman J, Drossman DA, Li Z, et al. Sexual and physical abuse history in gastroenterology practice: how types of abuse impact health status. Psychosom Med 1996;58:4-15.
3. Klein KB. Controlled treatment trials in the irritable bowel syndrome: a critique. Gastroenterology 1988;95:232-41.
4. Jailwala J, Imperiale TF, Kroenke K. Pharmacologic treatment of the irritable bowel syndrome: a systematic review of randomized, controlled trials. Ann Intern Med 2000;133:136-47.
5. Svedlund J, Sjodin I, Ottosson JO, et al. Controlled study of psychotherapy in irritable bowel syndrome. Lancet 1983;ii:589-92.
6. Guthrie EA, Creed FH, Dawson D, et al. A controlled trial of psychological treatment for the irritable bowel syndrome. Gastroenterology 1991;100:450-7.
7. Guthrie EA, Creed FH, Dawson D, et al. A randomized controlled trial of psychotherapy in patients with refractory irritable bowel syndrome. Br J Psychiatry 1993;163:315-21.
8. Blanchard EB, Schwartz SP. Adaptation of a multi-component treatment program for irritable bowel syndrome to a small group format. Biofeedback Self-Regulation 1987;12:63-9.
9. Blanchard EB, Scharff L, Payne A, et al. Prediction of outcome from cognitive-behavioral treatment of irritable bowel syndrome. Behav Res Ther 1992;30:647-50.
10. Greene B, Blanchard EB. Cognitive therapy for irritable bowel syndrome. J Consult Clin Psychol 1994;62(3):576-82.
11. Van Dulmen AM, Fennis JFM, Bleijenberg G. Cognitive-behavioral group therapy for irritable bowel syndrome: effects and long-term follow-up. Psychosom Med 1996;58:508-14.
12. Payne A, Blanchard EB. A controlled comparison of cognitive therapy and self-help support groups in the treatment of irritable bowel syndrome. J Consult Clin Psychol 1995;63(5):779-86.
13. Wise TN, Cooper JN, Ahmed S. The efficacy of group therapy for patients with irritable bowel syndrome. Psychosomatics 1982;23:465-9.
14. Toner BB, Segal ZV, Emmott S, et al. Cognitive-behavioral group therapy for patients with irritable bowel syndrome. Int J Group Psychotherapy 1998;48(2):215-43.
15. Whorwell PJ, Prior A, Faragher EB. Controlled trial of hypnotherapy in the treatment of severe refractory irritable-bowel syndrome. Lancet 1984;2(8414):1232-43.
16. Prior A, Colgan SM, Whorwell PJ. Changes in rectal sensitivity after hypnotherapy in patients with irritable bowel syndrome. Gut 1990;31:896-8.
17. Whorwell PJ, Houghton LA, Taylor EE, et al. Physiological effects of emotion: assessment via hypnosis. Lancet 1992;340:69-72.
18. Houghton LA, Heyman DJ, Whorwell PJ. Symptomatology, quality of life and economic features of irritable bowel syndrome: the effect of hypnotherapy. Aliment Pharmacol Ther 1996;10(1):91-5.
19. Galovski TE, Blanchard EB. The treatment of irritable bowel syndrome with hypnotherapy. Appl Psychophysiol Biofeedback 1998;23(4):219-32.
20. Vidakovic-Vukic M. Hypnotherapy in the treatment of irritable bowel syndrome: methods and results in Amsterdam. Scandinavian University Press 1999;34(suppl 230):49-51.
21. Bassotti G, Whitehead WE. Biofeedback as a treatment approach to gastrointestinal tract disorders. Am J Gastroenterol 1994;89(2):158-64.
22. Jackson JL, O’Malley PG, et al. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72.
23. Heymann-Mönnikes I, Arnold R, Florin I, et al. The combination of medical treatment plus multicomponent behavioral therapy is superior to medical treatment alone in the therapy of irritable bowel syndrome. Am J Gastroenterol 2000;95:981-94.
A growing body of evidence suggests that psychiatrists have much to offer patients with severe irritable bowel syndrome (IBS). Behavioral and psychotherapeutic approaches are showing promise in relieving both GI and mood disturbances.
Treating patients with IBS with medications designed to influence only gut function can be frustrating. Those with refractory symptoms may be extremely sensitive to drug side effects, and they often report that medical management worsens or does not improve their symptoms. They experiment with alternative medicines and wander from physician to physician in a disappointing search for a “cure.”
Let’s look at evidence on the efficacy of individual and group behavioral therapies, hypnotherapy, biofeedback, and combination medical and behavioral treatment.
Psychotherapeutic approaches
IBS is a common gastrointestinal disorder that is characterized by abdominal discomfort and changes in bowel habits (Boxes 1 and 2). Patients with severe IBS symptoms often bring significant psychological impairment and psychosocial trauma to clinical encounters.1,2 They respond poorly to standard medical management, and evidence supporting the efficacy of medical treatments for IBS remains weak.3,4
Irritable bowel syndrome (IBS) is the most common disorder seen in gastrointestinal practice, representing more than 40% of all visits to gastroenterologists. Complaints of IBS also account for approximately 23% of office visits to primary care physicians.1
Key symptoms of this functional disorder are a pattern of lower abdominal discomfort and bloating accompanied by variable degrees of altered stool pattern—constipation, diarrhea, or intermittent constipation and diarrhea. IBS is most common in young patients, with onset rarely diagnosed after age 45. Its incidence is equal in men and women, but women are more likely to seek medical care for IBS symptoms.
The cause of IBS is unclear. Recent research suggests that changes in serotonin metabolism cause a pattern of visceral hypersensitivity and an altered sensation of pain. IBS is not a psychiatric disorder, but it can be worsened by comorbid psychopathology, particularly mood and anxiety disorders. Although patients tend to have either diarrhea-predominant or constipation-predominant IBS, the pathophysiology of both patterns seems similar.
In 1983, the first controlled trial of psychodynamic psychotherapy for IBS showed dramatic reductions in symptoms.5 A subsequent series of high-quality articles in the early 1990s also showed that interpersonal psychotherapy (with greater interaction between therapist and patient) could significantly decrease IBS symptoms.
Persistent improvement. In one randomized controlled trial,6 102 patients with IBS received either standard medical treatment or 10 hours of dynamically oriented individual psychotherapy in combination with standard medical treatment. After 3 months, patients who received psychotherapy showed significantly greater improvement in somatic symptoms and emotional well-being, compared with those who received medical treatment only.
Interestingly, this difference persisted 1 year after the study ended. GI symptoms and the emotional well-being of patients who received combination therapy continued to improve, whereas the physical and emotional status of those who received only standard medical treatment deteriorated.
In a second study,7 101 patients with severe IBS symptoms continued to receive medical treatment but were randomly divided into two groups:
- Study subjects received 8 hours of dynamically oriented psychotherapy.
- Control patients met with a psychiatrist who engaged in “supportive listening” but delivered no psychotherapy. This strategy was adopted to control for the effect of the psychiatrist’s presence.
Assessments included patients’ self-reports of symptoms, ratings of GI symptoms by the treating gastroenterologists, and measures of depression, anxiety, and health care utilization. Patients who received psychotherapy reported significant improvements in bowel symptoms (e.g., diarrhea, constipation, bloating, and abdominal pain). Likewise, the gastroenterologist who rated patients’ GI symptoms felt that those who received psychotherapy improved significantly across the entire spectrum of GI symptoms. The improvements were maintained at 1-year follow-up.
By comparison, the control patients reported worsening symptoms, as did subjects who dropped out. Patients who received psychotherapy also made significantly fewer outpatient visits to gastroenterologists, compared with controls (p<0.001).
Cognitive-behavioral therapy
Cognitive-behavioral therapy (CBT) is emerging as a major psychotherapeutic tool for treating mood disorders, anxiety disorders, and somatic syndromes associated with psychosocial distress. CBT also is showing promise for patients with moderate to severe IBS and those with IBS and concomitant anxiety or mood disorders. Studies consistently show that CBT is superior to standard medical management or the use of support groups or other behavioral treatments alone.
Reduced symptoms. In an early trial of CBT, 17 patients with IBS experienced significantly less abdominal pain and diarrhea after participating in a program of progressive relaxation, education about bowel functioning, use of thermal biofeedback, and stress coping techniques based on CBT. Overall, 64% of the patients improved.8
The same investigators then assigned 90 patients to 12 sessions of CBT, given over 8 weeks with or without meditation and biofeedback. Patients with axis I psychiatric diagnoses tended to respond poorly to CBT. The authors concluded that a careful pretreatment psychological workup is important to identify patients with IBS who would benefit most from CBT.9
As a follow-up, these investigators randomly assigned 20 patients to intensive individualized CBT (10 sessions over 8 weeks) or 8 weeks of daily GI symptom monitoring. Patients who received CBT had significantly fewer GI symptoms than did the symptom-monitoring group (p = 0.005). With CBT, 80% improved clinically, compared with only 10% in the control group. Improvements in the CBT group persisted at 3 months’ follow-up. Improved GI symptoms also were correlated with increased positive thoughts and reduced negative automatic thoughts (i.e., negative self-image).10
In the preceding 12 months, the patient has experienced at least 12 weeks or more (need not be consecutive) of abdominal discomfort or pain that has:
Two out of three features
- relieved with defecation, and/or
- onset associated with a change in frequency or stool, and/or
- onset associated with a change in form (appearance) of stool
Symptoms that cumulatively support the diagnosis
- Abnormal stool frequency (for research purposes, “abnormal” may be defined as >3 bowel movements per day and <3 bowel movements per week);
- abnormal stool form (lumpy/hard or loose/watery stool)
- abnormal stool passage (straining, urgency, or feeling of incomplete evacuation)
- passage of mucus
- bloating or abdominal distension.
* In the absence of structural or metabolic abnormalities to explain the symptoms
Source: Drossman DA, Corazziari E, Talley NJ, et al. Rome II: The functional gastrointestinal disorders (2nd ed). McLean, VA: Degnon Associates, 2000.
Group therapy. In a study of group rather than individualized CBT, 45 patients with severe IBS symptoms were randomly assigned to either a group CBT module (n = 25) or a waiting list control group (n = 20). Patients received eight 2-hour group CBT sessions over 3 months, then were followed an average of 2.25 years. Their abdominal pain, number of successful coping behavioral strategies, and avoidance of negative situations improved significantly—compared with the waiting list controls—and persisted during follow-up. The authors concluded that group CBT is effective for alleviating IBS symptoms and improving patients’ coping strategies.11
CBT vs. support groups. In a study comparing the effectiveness of CBT and an IBS self-help support group, 34 patients were randomly assigned to:
- individualized CBT (study group)
- a self-help support group
- or a symptom-monitoring waiting list (control group).
Each group was followed for 8 weeks. GI symptoms were reduced significantly in patients who received individualized CBT, compared with the support group or controls. Anxiety and depression in the CBT group also remained significantly improved 3 months later, compared with both other groups.12
Group psychotherapy
Group psychotherapy for IBS treatment can be more cost-effective than individual therapy, but its success depends on whether patients accept a group format. Data on the use of group psychotherapeutic approaches are largely favorable.
As described previously, one study demonstrated that group CBT reduced abdominal pain and diarrhea and improved symptoms overall.11 In another study, 20 patients with refractory IBS underwent 6 weeks of group behavioral and didactic psychotherapy. GI symptoms, dysphoria, and psychological distress improved significantly in all patients, and their interpersonal sensitivity and hostility were reduced. These improvements persisted 6 months later.12
A recent review suggests that cognitive-behavioral group psychotherapy may be highly effective in patients with IBS. These authors concluded that CBT can improve patients’ mood and other emotional symptoms, reduce their pain, and improve well-being and coping ability.14
Hypnotherapy
Researchers in Manchester, UK, have shown excellent results with hypnotherapy for patients with severe refractory IBS. Although their data seem to have established the ability of hypnotherapy to improve the GI and non-GI symptoms of IBS, corroborating evidence is needed from other centers. In this regard, some preliminary evidence is emerging.
Manchester group. In the first trial by the Manchester group, 30 patients received seven half-hour sessions of hypnotherapy (study group) or supportive psychotherapy and placebo (control group). Patients who received hypnotherapy also were given a tape for home autohypnosis after the third session.
Patients who received hypnotherapy improved dramatically in all GI symptoms— including abdominal pain, bloating, and bowel habits—and in their sense of well-being. This effect persisted 3 months later. The control patients’ abdominal pain, bloating, and well-being improved somewhat, but their bowel habits did not improve.15
The same investigators then studied 30 patients with IBS to assess the effect of hypnotherapy on rectal physiology. Fifteen patients received hypnotherapy, and 15 received relaxation exercises. Rectal sensitivity was measured using anorectal manometry at the start and finish of the intervention.
For patients with diarrhea-predominant IBS, rectal sensitivity was significantly reduced during hypnosis and after the full course of hypnotherapy, compared with controls (p<0.05). In patients with constipation-predominant IBS, a trend towards normalized rectal sensitivity did not reach statistical significance. The investigators concluded that symptomatic improvement of IBS after hypnotherapy may be related to changes in visceral sensitivity of the colon.16
These investigators later studied changes in distal colonic motility in 18 patients undergoing hypnotherapy for IBS. As the patients’ hypnotically induced anger or excitement increased, colonic motility decreased significantly (p<0.01) The investigators concluded that hypnosis may be a useful tool to investigate the effects of emotion on physiologic function.17
Using more contemporary outcome measures and diagnostic criteria, these investigators later showed that hypnotherapy significantly improved:
- IBS symptoms (abdominal pain and bloating, bowel habit, nausea, flatulence, urinary symptoms, lethargy, backache, and dyspareunia)
- quality of life (psychological and physical well-being, mood, locus of control, and work attitude).
Patients treated with hypnosis also took less time away from work (p = 0.02) and visited their physicians less often (p = 0.056), compared with controls.18
Other hypnosis studies. In the United States, another group randomly assigned 12 patients to gut-directed hypnotherapy or symptom monitoring. Subjects were matched by concurrent psychiatric diagnosis, susceptibility to hypnosis, and demographic features.
In findings similar to those of the Manchester group, primary IBS symptoms (abdominal pain, constipation, and flatulence) of patients who received hypnotherapy improved more than those of controls (p = 0.016). Anxiety, as measured by the Spielberger State-Trait Anxiety Inventory (STAXI), also decreased significantly. Treatment-induced gains were well-maintained 2 months later. No significant correlation was found between initial sensitivity to hypnosis and subsequent response to hypnotherapy. A positive relationship was seen between the presence of psychiatric diagnoses and overall levels of improvement.
This study suggests that hypnotherapy can be useful for treating IBS and can be easily adapted to different clinical settings and treatment populations.19 A similar study using gut-directed hypnotherapy found significant improvement in 27 IBS patients treated with short-term hypnosis, and symptom improvement persisted after treatment.20
Biofeedback
The role of biofeedback in IBS treatment remains ill-defined. To be considered as a treatment option, biofeedback must meet or exceed the benefits being achieved with psychotherapy, hypnotherapy, and other behavioral approaches.
In gastroenterology, biofeedback has been used mainly to treat constipation and specifically for outlet constipation due to pelvic floor dysfunction. Anorectal probes to measure rectal pressure in the resting state and during defecation can reveal a pattern of pelvic floor dysfunction. Studies have demonstrated up to 67% improvement in constipation symptoms using biofeedback. Use of anorectal biofeedback in adults with IBS also appears promising, but more controlled trials are needed.21
Anorectal biofeedback has also been used effectively to treat fecal incontinence in children and adults, achieving success rates of 70% or better. In IBS, however, the benefit of biofeedback is less clear. Studies of multicomponent treatment—combining biofeedback with CBT techniques—suggest improvement rates in the 50 to 60% range. However, these findings need to be compared with other treatments for IBS.
Combination treatment
Medical treatment of IBS is progressing. Antidepressant therapy, particularly using tricyclics, has shown moderate benefit.22 Newer medications such as alosetron and tegaserod, which modulate serotonin metabolism in the gut, have been developed. Alosetron and tegaserod have shown significantly greater efficacy compared with placebo for treatment of women with the diarrhea-predominant and constipation-predominant types of IBS, respectively.
Alosetron was voluntarily withdrawn from clinical use in 2000 because of reports of serious GI events associated with its use, including ischemic colitis in a small number of patients (about 3 women in 1,000). Because of the drug’s efficacy in IBS, however, the FDA recently approved its rerelease with a restricted indication—it is to be used only in women with severe diarrhea-predominant IBS who have not responded to conventional IBS treatment. The drug’s manufacturer also is implementing a risk management plan designed to reduce the potential for serious GI side effects.
Table
PSYCHOTHERAPY AS TREATMENT FOR IRRITABLE BOWEL SYNDROME
| Psychotherapeutic approach | Summary of research results |
|---|---|
| Psychodynamic therapy | Shown to be effective in reducing pain and dysphoric mood5 |
| Interpersonal psychotherapy | Effective in reducing pain, bloating, and health care utilization and improving emotional well-being7 |
| Cognitive-behavioral therapy | Improves coping skills and decreases helplessness and somatization14 |
| Group psychotherapy | Seems to be as efficacious as cognitive-behavioral therapy, with the added efficiency of a group model13 |
| Hypnotherapy | Highly effective for a spectrum of IBS symptoms15 |
| Biofeedback | Not useful for IBS per se, but helpful for pelvic floor dysfunction21 |
| Combination therapy | Emerging as a particularly useful strategy, combining medical and behavioral approaches23 |
Tegaserod, a serotonin-4 receptor (5HT4) agonist, was approved by the FDA in July. It is indicated for short-term treatment of women with IBS whose primary bowel symptom is constipation.
Combination therapy—medical management plus psychotherapy—may represent the future of IBS treatment (Table). This approach was examined recently in a randomized study of 24 IBS patients who received standard medical treatment alone or in combination with behavioral therapy. The behavioral component included patient education, helping patients shape a plausible model for their illness, progressive muscle relaxation, cognitive coping strategies, problem-solving education, and assertiveness and social skills training. All patients were treated in 10 individual therapy sessions of approximately 1 hour each by one of two psychotherapists across 10 weeks.
Compared with medical treatment alone, patients treated with combination therapy showed significantly improved GI symptoms (p < 0.001) and psychological symptoms (p = 0.01) in terms of both patient report and objective psychological measures. Outcomes are enhanced for patients with severe IBS, the investigators concluded, when behavioral therapy is added to thoughtful medical management.23
Related resource
- International Foundation for Functional Gastrointestinal Disorders. www.iffgd.org
Drug brand names
- Alosetron • Lotronex
- Tegaserod • Zelnorm
Disclosure
The author reports that he serves as a consultant to Novartis Pharmaceuticals Corp. He reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
A growing body of evidence suggests that psychiatrists have much to offer patients with severe irritable bowel syndrome (IBS). Behavioral and psychotherapeutic approaches are showing promise in relieving both GI and mood disturbances.
Treating patients with IBS with medications designed to influence only gut function can be frustrating. Those with refractory symptoms may be extremely sensitive to drug side effects, and they often report that medical management worsens or does not improve their symptoms. They experiment with alternative medicines and wander from physician to physician in a disappointing search for a “cure.”
Let’s look at evidence on the efficacy of individual and group behavioral therapies, hypnotherapy, biofeedback, and combination medical and behavioral treatment.
Psychotherapeutic approaches
IBS is a common gastrointestinal disorder that is characterized by abdominal discomfort and changes in bowel habits (Boxes 1 and 2). Patients with severe IBS symptoms often bring significant psychological impairment and psychosocial trauma to clinical encounters.1,2 They respond poorly to standard medical management, and evidence supporting the efficacy of medical treatments for IBS remains weak.3,4
Irritable bowel syndrome (IBS) is the most common disorder seen in gastrointestinal practice, representing more than 40% of all visits to gastroenterologists. Complaints of IBS also account for approximately 23% of office visits to primary care physicians.1
Key symptoms of this functional disorder are a pattern of lower abdominal discomfort and bloating accompanied by variable degrees of altered stool pattern—constipation, diarrhea, or intermittent constipation and diarrhea. IBS is most common in young patients, with onset rarely diagnosed after age 45. Its incidence is equal in men and women, but women are more likely to seek medical care for IBS symptoms.
The cause of IBS is unclear. Recent research suggests that changes in serotonin metabolism cause a pattern of visceral hypersensitivity and an altered sensation of pain. IBS is not a psychiatric disorder, but it can be worsened by comorbid psychopathology, particularly mood and anxiety disorders. Although patients tend to have either diarrhea-predominant or constipation-predominant IBS, the pathophysiology of both patterns seems similar.
In 1983, the first controlled trial of psychodynamic psychotherapy for IBS showed dramatic reductions in symptoms.5 A subsequent series of high-quality articles in the early 1990s also showed that interpersonal psychotherapy (with greater interaction between therapist and patient) could significantly decrease IBS symptoms.
Persistent improvement. In one randomized controlled trial,6 102 patients with IBS received either standard medical treatment or 10 hours of dynamically oriented individual psychotherapy in combination with standard medical treatment. After 3 months, patients who received psychotherapy showed significantly greater improvement in somatic symptoms and emotional well-being, compared with those who received medical treatment only.
Interestingly, this difference persisted 1 year after the study ended. GI symptoms and the emotional well-being of patients who received combination therapy continued to improve, whereas the physical and emotional status of those who received only standard medical treatment deteriorated.
In a second study,7 101 patients with severe IBS symptoms continued to receive medical treatment but were randomly divided into two groups:
- Study subjects received 8 hours of dynamically oriented psychotherapy.
- Control patients met with a psychiatrist who engaged in “supportive listening” but delivered no psychotherapy. This strategy was adopted to control for the effect of the psychiatrist’s presence.
Assessments included patients’ self-reports of symptoms, ratings of GI symptoms by the treating gastroenterologists, and measures of depression, anxiety, and health care utilization. Patients who received psychotherapy reported significant improvements in bowel symptoms (e.g., diarrhea, constipation, bloating, and abdominal pain). Likewise, the gastroenterologist who rated patients’ GI symptoms felt that those who received psychotherapy improved significantly across the entire spectrum of GI symptoms. The improvements were maintained at 1-year follow-up.
By comparison, the control patients reported worsening symptoms, as did subjects who dropped out. Patients who received psychotherapy also made significantly fewer outpatient visits to gastroenterologists, compared with controls (p<0.001).
Cognitive-behavioral therapy
Cognitive-behavioral therapy (CBT) is emerging as a major psychotherapeutic tool for treating mood disorders, anxiety disorders, and somatic syndromes associated with psychosocial distress. CBT also is showing promise for patients with moderate to severe IBS and those with IBS and concomitant anxiety or mood disorders. Studies consistently show that CBT is superior to standard medical management or the use of support groups or other behavioral treatments alone.
Reduced symptoms. In an early trial of CBT, 17 patients with IBS experienced significantly less abdominal pain and diarrhea after participating in a program of progressive relaxation, education about bowel functioning, use of thermal biofeedback, and stress coping techniques based on CBT. Overall, 64% of the patients improved.8
The same investigators then assigned 90 patients to 12 sessions of CBT, given over 8 weeks with or without meditation and biofeedback. Patients with axis I psychiatric diagnoses tended to respond poorly to CBT. The authors concluded that a careful pretreatment psychological workup is important to identify patients with IBS who would benefit most from CBT.9
As a follow-up, these investigators randomly assigned 20 patients to intensive individualized CBT (10 sessions over 8 weeks) or 8 weeks of daily GI symptom monitoring. Patients who received CBT had significantly fewer GI symptoms than did the symptom-monitoring group (p = 0.005). With CBT, 80% improved clinically, compared with only 10% in the control group. Improvements in the CBT group persisted at 3 months’ follow-up. Improved GI symptoms also were correlated with increased positive thoughts and reduced negative automatic thoughts (i.e., negative self-image).10
In the preceding 12 months, the patient has experienced at least 12 weeks or more (need not be consecutive) of abdominal discomfort or pain that has:
Two out of three features
- relieved with defecation, and/or
- onset associated with a change in frequency or stool, and/or
- onset associated with a change in form (appearance) of stool
Symptoms that cumulatively support the diagnosis
- Abnormal stool frequency (for research purposes, “abnormal” may be defined as >3 bowel movements per day and <3 bowel movements per week);
- abnormal stool form (lumpy/hard or loose/watery stool)
- abnormal stool passage (straining, urgency, or feeling of incomplete evacuation)
- passage of mucus
- bloating or abdominal distension.
* In the absence of structural or metabolic abnormalities to explain the symptoms
Source: Drossman DA, Corazziari E, Talley NJ, et al. Rome II: The functional gastrointestinal disorders (2nd ed). McLean, VA: Degnon Associates, 2000.
Group therapy. In a study of group rather than individualized CBT, 45 patients with severe IBS symptoms were randomly assigned to either a group CBT module (n = 25) or a waiting list control group (n = 20). Patients received eight 2-hour group CBT sessions over 3 months, then were followed an average of 2.25 years. Their abdominal pain, number of successful coping behavioral strategies, and avoidance of negative situations improved significantly—compared with the waiting list controls—and persisted during follow-up. The authors concluded that group CBT is effective for alleviating IBS symptoms and improving patients’ coping strategies.11
CBT vs. support groups. In a study comparing the effectiveness of CBT and an IBS self-help support group, 34 patients were randomly assigned to:
- individualized CBT (study group)
- a self-help support group
- or a symptom-monitoring waiting list (control group).
Each group was followed for 8 weeks. GI symptoms were reduced significantly in patients who received individualized CBT, compared with the support group or controls. Anxiety and depression in the CBT group also remained significantly improved 3 months later, compared with both other groups.12
Group psychotherapy
Group psychotherapy for IBS treatment can be more cost-effective than individual therapy, but its success depends on whether patients accept a group format. Data on the use of group psychotherapeutic approaches are largely favorable.
As described previously, one study demonstrated that group CBT reduced abdominal pain and diarrhea and improved symptoms overall.11 In another study, 20 patients with refractory IBS underwent 6 weeks of group behavioral and didactic psychotherapy. GI symptoms, dysphoria, and psychological distress improved significantly in all patients, and their interpersonal sensitivity and hostility were reduced. These improvements persisted 6 months later.12
A recent review suggests that cognitive-behavioral group psychotherapy may be highly effective in patients with IBS. These authors concluded that CBT can improve patients’ mood and other emotional symptoms, reduce their pain, and improve well-being and coping ability.14
Hypnotherapy
Researchers in Manchester, UK, have shown excellent results with hypnotherapy for patients with severe refractory IBS. Although their data seem to have established the ability of hypnotherapy to improve the GI and non-GI symptoms of IBS, corroborating evidence is needed from other centers. In this regard, some preliminary evidence is emerging.
Manchester group. In the first trial by the Manchester group, 30 patients received seven half-hour sessions of hypnotherapy (study group) or supportive psychotherapy and placebo (control group). Patients who received hypnotherapy also were given a tape for home autohypnosis after the third session.
Patients who received hypnotherapy improved dramatically in all GI symptoms— including abdominal pain, bloating, and bowel habits—and in their sense of well-being. This effect persisted 3 months later. The control patients’ abdominal pain, bloating, and well-being improved somewhat, but their bowel habits did not improve.15
The same investigators then studied 30 patients with IBS to assess the effect of hypnotherapy on rectal physiology. Fifteen patients received hypnotherapy, and 15 received relaxation exercises. Rectal sensitivity was measured using anorectal manometry at the start and finish of the intervention.
For patients with diarrhea-predominant IBS, rectal sensitivity was significantly reduced during hypnosis and after the full course of hypnotherapy, compared with controls (p<0.05). In patients with constipation-predominant IBS, a trend towards normalized rectal sensitivity did not reach statistical significance. The investigators concluded that symptomatic improvement of IBS after hypnotherapy may be related to changes in visceral sensitivity of the colon.16
These investigators later studied changes in distal colonic motility in 18 patients undergoing hypnotherapy for IBS. As the patients’ hypnotically induced anger or excitement increased, colonic motility decreased significantly (p<0.01) The investigators concluded that hypnosis may be a useful tool to investigate the effects of emotion on physiologic function.17
Using more contemporary outcome measures and diagnostic criteria, these investigators later showed that hypnotherapy significantly improved:
- IBS symptoms (abdominal pain and bloating, bowel habit, nausea, flatulence, urinary symptoms, lethargy, backache, and dyspareunia)
- quality of life (psychological and physical well-being, mood, locus of control, and work attitude).
Patients treated with hypnosis also took less time away from work (p = 0.02) and visited their physicians less often (p = 0.056), compared with controls.18
Other hypnosis studies. In the United States, another group randomly assigned 12 patients to gut-directed hypnotherapy or symptom monitoring. Subjects were matched by concurrent psychiatric diagnosis, susceptibility to hypnosis, and demographic features.
In findings similar to those of the Manchester group, primary IBS symptoms (abdominal pain, constipation, and flatulence) of patients who received hypnotherapy improved more than those of controls (p = 0.016). Anxiety, as measured by the Spielberger State-Trait Anxiety Inventory (STAXI), also decreased significantly. Treatment-induced gains were well-maintained 2 months later. No significant correlation was found between initial sensitivity to hypnosis and subsequent response to hypnotherapy. A positive relationship was seen between the presence of psychiatric diagnoses and overall levels of improvement.
This study suggests that hypnotherapy can be useful for treating IBS and can be easily adapted to different clinical settings and treatment populations.19 A similar study using gut-directed hypnotherapy found significant improvement in 27 IBS patients treated with short-term hypnosis, and symptom improvement persisted after treatment.20
Biofeedback
The role of biofeedback in IBS treatment remains ill-defined. To be considered as a treatment option, biofeedback must meet or exceed the benefits being achieved with psychotherapy, hypnotherapy, and other behavioral approaches.
In gastroenterology, biofeedback has been used mainly to treat constipation and specifically for outlet constipation due to pelvic floor dysfunction. Anorectal probes to measure rectal pressure in the resting state and during defecation can reveal a pattern of pelvic floor dysfunction. Studies have demonstrated up to 67% improvement in constipation symptoms using biofeedback. Use of anorectal biofeedback in adults with IBS also appears promising, but more controlled trials are needed.21
Anorectal biofeedback has also been used effectively to treat fecal incontinence in children and adults, achieving success rates of 70% or better. In IBS, however, the benefit of biofeedback is less clear. Studies of multicomponent treatment—combining biofeedback with CBT techniques—suggest improvement rates in the 50 to 60% range. However, these findings need to be compared with other treatments for IBS.
Combination treatment
Medical treatment of IBS is progressing. Antidepressant therapy, particularly using tricyclics, has shown moderate benefit.22 Newer medications such as alosetron and tegaserod, which modulate serotonin metabolism in the gut, have been developed. Alosetron and tegaserod have shown significantly greater efficacy compared with placebo for treatment of women with the diarrhea-predominant and constipation-predominant types of IBS, respectively.
Alosetron was voluntarily withdrawn from clinical use in 2000 because of reports of serious GI events associated with its use, including ischemic colitis in a small number of patients (about 3 women in 1,000). Because of the drug’s efficacy in IBS, however, the FDA recently approved its rerelease with a restricted indication—it is to be used only in women with severe diarrhea-predominant IBS who have not responded to conventional IBS treatment. The drug’s manufacturer also is implementing a risk management plan designed to reduce the potential for serious GI side effects.
Table
PSYCHOTHERAPY AS TREATMENT FOR IRRITABLE BOWEL SYNDROME
| Psychotherapeutic approach | Summary of research results |
|---|---|
| Psychodynamic therapy | Shown to be effective in reducing pain and dysphoric mood5 |
| Interpersonal psychotherapy | Effective in reducing pain, bloating, and health care utilization and improving emotional well-being7 |
| Cognitive-behavioral therapy | Improves coping skills and decreases helplessness and somatization14 |
| Group psychotherapy | Seems to be as efficacious as cognitive-behavioral therapy, with the added efficiency of a group model13 |
| Hypnotherapy | Highly effective for a spectrum of IBS symptoms15 |
| Biofeedback | Not useful for IBS per se, but helpful for pelvic floor dysfunction21 |
| Combination therapy | Emerging as a particularly useful strategy, combining medical and behavioral approaches23 |
Tegaserod, a serotonin-4 receptor (5HT4) agonist, was approved by the FDA in July. It is indicated for short-term treatment of women with IBS whose primary bowel symptom is constipation.
Combination therapy—medical management plus psychotherapy—may represent the future of IBS treatment (Table). This approach was examined recently in a randomized study of 24 IBS patients who received standard medical treatment alone or in combination with behavioral therapy. The behavioral component included patient education, helping patients shape a plausible model for their illness, progressive muscle relaxation, cognitive coping strategies, problem-solving education, and assertiveness and social skills training. All patients were treated in 10 individual therapy sessions of approximately 1 hour each by one of two psychotherapists across 10 weeks.
Compared with medical treatment alone, patients treated with combination therapy showed significantly improved GI symptoms (p < 0.001) and psychological symptoms (p = 0.01) in terms of both patient report and objective psychological measures. Outcomes are enhanced for patients with severe IBS, the investigators concluded, when behavioral therapy is added to thoughtful medical management.23
Related resource
- International Foundation for Functional Gastrointestinal Disorders. www.iffgd.org
Drug brand names
- Alosetron • Lotronex
- Tegaserod • Zelnorm
Disclosure
The author reports that he serves as a consultant to Novartis Pharmaceuticals Corp. He reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sandler R. Epidemiology of irritable bowel syndrome in the United States. Gastroenterology 1990;99:409-15.
2. Leserman J, Drossman DA, Li Z, et al. Sexual and physical abuse history in gastroenterology practice: how types of abuse impact health status. Psychosom Med 1996;58:4-15.
3. Klein KB. Controlled treatment trials in the irritable bowel syndrome: a critique. Gastroenterology 1988;95:232-41.
4. Jailwala J, Imperiale TF, Kroenke K. Pharmacologic treatment of the irritable bowel syndrome: a systematic review of randomized, controlled trials. Ann Intern Med 2000;133:136-47.
5. Svedlund J, Sjodin I, Ottosson JO, et al. Controlled study of psychotherapy in irritable bowel syndrome. Lancet 1983;ii:589-92.
6. Guthrie EA, Creed FH, Dawson D, et al. A controlled trial of psychological treatment for the irritable bowel syndrome. Gastroenterology 1991;100:450-7.
7. Guthrie EA, Creed FH, Dawson D, et al. A randomized controlled trial of psychotherapy in patients with refractory irritable bowel syndrome. Br J Psychiatry 1993;163:315-21.
8. Blanchard EB, Schwartz SP. Adaptation of a multi-component treatment program for irritable bowel syndrome to a small group format. Biofeedback Self-Regulation 1987;12:63-9.
9. Blanchard EB, Scharff L, Payne A, et al. Prediction of outcome from cognitive-behavioral treatment of irritable bowel syndrome. Behav Res Ther 1992;30:647-50.
10. Greene B, Blanchard EB. Cognitive therapy for irritable bowel syndrome. J Consult Clin Psychol 1994;62(3):576-82.
11. Van Dulmen AM, Fennis JFM, Bleijenberg G. Cognitive-behavioral group therapy for irritable bowel syndrome: effects and long-term follow-up. Psychosom Med 1996;58:508-14.
12. Payne A, Blanchard EB. A controlled comparison of cognitive therapy and self-help support groups in the treatment of irritable bowel syndrome. J Consult Clin Psychol 1995;63(5):779-86.
13. Wise TN, Cooper JN, Ahmed S. The efficacy of group therapy for patients with irritable bowel syndrome. Psychosomatics 1982;23:465-9.
14. Toner BB, Segal ZV, Emmott S, et al. Cognitive-behavioral group therapy for patients with irritable bowel syndrome. Int J Group Psychotherapy 1998;48(2):215-43.
15. Whorwell PJ, Prior A, Faragher EB. Controlled trial of hypnotherapy in the treatment of severe refractory irritable-bowel syndrome. Lancet 1984;2(8414):1232-43.
16. Prior A, Colgan SM, Whorwell PJ. Changes in rectal sensitivity after hypnotherapy in patients with irritable bowel syndrome. Gut 1990;31:896-8.
17. Whorwell PJ, Houghton LA, Taylor EE, et al. Physiological effects of emotion: assessment via hypnosis. Lancet 1992;340:69-72.
18. Houghton LA, Heyman DJ, Whorwell PJ. Symptomatology, quality of life and economic features of irritable bowel syndrome: the effect of hypnotherapy. Aliment Pharmacol Ther 1996;10(1):91-5.
19. Galovski TE, Blanchard EB. The treatment of irritable bowel syndrome with hypnotherapy. Appl Psychophysiol Biofeedback 1998;23(4):219-32.
20. Vidakovic-Vukic M. Hypnotherapy in the treatment of irritable bowel syndrome: methods and results in Amsterdam. Scandinavian University Press 1999;34(suppl 230):49-51.
21. Bassotti G, Whitehead WE. Biofeedback as a treatment approach to gastrointestinal tract disorders. Am J Gastroenterol 1994;89(2):158-64.
22. Jackson JL, O’Malley PG, et al. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72.
23. Heymann-Mönnikes I, Arnold R, Florin I, et al. The combination of medical treatment plus multicomponent behavioral therapy is superior to medical treatment alone in the therapy of irritable bowel syndrome. Am J Gastroenterol 2000;95:981-94.
1. Sandler R. Epidemiology of irritable bowel syndrome in the United States. Gastroenterology 1990;99:409-15.
2. Leserman J, Drossman DA, Li Z, et al. Sexual and physical abuse history in gastroenterology practice: how types of abuse impact health status. Psychosom Med 1996;58:4-15.
3. Klein KB. Controlled treatment trials in the irritable bowel syndrome: a critique. Gastroenterology 1988;95:232-41.
4. Jailwala J, Imperiale TF, Kroenke K. Pharmacologic treatment of the irritable bowel syndrome: a systematic review of randomized, controlled trials. Ann Intern Med 2000;133:136-47.
5. Svedlund J, Sjodin I, Ottosson JO, et al. Controlled study of psychotherapy in irritable bowel syndrome. Lancet 1983;ii:589-92.
6. Guthrie EA, Creed FH, Dawson D, et al. A controlled trial of psychological treatment for the irritable bowel syndrome. Gastroenterology 1991;100:450-7.
7. Guthrie EA, Creed FH, Dawson D, et al. A randomized controlled trial of psychotherapy in patients with refractory irritable bowel syndrome. Br J Psychiatry 1993;163:315-21.
8. Blanchard EB, Schwartz SP. Adaptation of a multi-component treatment program for irritable bowel syndrome to a small group format. Biofeedback Self-Regulation 1987;12:63-9.
9. Blanchard EB, Scharff L, Payne A, et al. Prediction of outcome from cognitive-behavioral treatment of irritable bowel syndrome. Behav Res Ther 1992;30:647-50.
10. Greene B, Blanchard EB. Cognitive therapy for irritable bowel syndrome. J Consult Clin Psychol 1994;62(3):576-82.
11. Van Dulmen AM, Fennis JFM, Bleijenberg G. Cognitive-behavioral group therapy for irritable bowel syndrome: effects and long-term follow-up. Psychosom Med 1996;58:508-14.
12. Payne A, Blanchard EB. A controlled comparison of cognitive therapy and self-help support groups in the treatment of irritable bowel syndrome. J Consult Clin Psychol 1995;63(5):779-86.
13. Wise TN, Cooper JN, Ahmed S. The efficacy of group therapy for patients with irritable bowel syndrome. Psychosomatics 1982;23:465-9.
14. Toner BB, Segal ZV, Emmott S, et al. Cognitive-behavioral group therapy for patients with irritable bowel syndrome. Int J Group Psychotherapy 1998;48(2):215-43.
15. Whorwell PJ, Prior A, Faragher EB. Controlled trial of hypnotherapy in the treatment of severe refractory irritable-bowel syndrome. Lancet 1984;2(8414):1232-43.
16. Prior A, Colgan SM, Whorwell PJ. Changes in rectal sensitivity after hypnotherapy in patients with irritable bowel syndrome. Gut 1990;31:896-8.
17. Whorwell PJ, Houghton LA, Taylor EE, et al. Physiological effects of emotion: assessment via hypnosis. Lancet 1992;340:69-72.
18. Houghton LA, Heyman DJ, Whorwell PJ. Symptomatology, quality of life and economic features of irritable bowel syndrome: the effect of hypnotherapy. Aliment Pharmacol Ther 1996;10(1):91-5.
19. Galovski TE, Blanchard EB. The treatment of irritable bowel syndrome with hypnotherapy. Appl Psychophysiol Biofeedback 1998;23(4):219-32.
20. Vidakovic-Vukic M. Hypnotherapy in the treatment of irritable bowel syndrome: methods and results in Amsterdam. Scandinavian University Press 1999;34(suppl 230):49-51.
21. Bassotti G, Whitehead WE. Biofeedback as a treatment approach to gastrointestinal tract disorders. Am J Gastroenterol 1994;89(2):158-64.
22. Jackson JL, O’Malley PG, et al. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72.
23. Heymann-Mönnikes I, Arnold R, Florin I, et al. The combination of medical treatment plus multicomponent behavioral therapy is superior to medical treatment alone in the therapy of irritable bowel syndrome. Am J Gastroenterol 2000;95:981-94.
Hypertension: Pitfalls to prescribing for patients with high blood pressure
Roughly 50 million adult Americans have hypertension.1 Chances are some of them are—or soon will be—under your care.
Hypertension is common among patients with psychiatric disorders, particularly in those with chronic mental conditions.2 Medication-associated weight gain and other reactions to psychotropics, drug-drug interactions, lack of exercise, adverse dietary habits, and pre-existing medical conditions all predispose psychiatric patients to hypertension.
Yet hypertension often goes undetected in psychiatric patients. Hypertension many times is asymptomatic—about 50% of all people with the disorder don’t even know they have it.3 Some symptoms of uncontrolled hypertension—fatigue, headache, palpitations, and dizziness—are also associated with many psychiatric disorders. As a result, psychiatrists may attempt to manage the symptoms but miss the hypertension.
Psychiatrists need to be alert for hypertension, either as a possible contributing factor to a mental disorder or as a potential side effect of a psychiatric disorder or treatment. The following diagnostic and treatment strategies will help you detect and manage this common condition.
Causes of hypertension in mental illness
The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure defines elevated blood pressure as 140 mm Hg systolic and/or 90 mm Hg diastolic. The diagnosis of hypertension should be based on the average of two or more blood pressure readings at each of two or more visits after initial screening.
All patients with elevated blood pressure have an underlying physiologic abnormality that is causing their hypertension. The disorder falls within the following two categories:
- essential hypertension, emanating from an unknown cause
- secondary hypertension, resulting from an underlying, discoverable, often treatable cause.
Researchers have speculated that certain psychiatric disorders might cause, or be risk factors for, hypertension. Anxiety or panic disorders have been associated with acute (and perhaps chronic) blood pressure elevations.2 Some research suggests that patients with alexithymia are at risk for developing hypertension.4
Other studies suggest that hypertensive patients with certain psychological disorders (e.g., depression) or social factors (e.g., substance abuse) are less likely than nonaffected patients to self-report the presence of hypertension and less likely to receive medical attention for it.5
Psychiatric drugs also may affect blood pressure by one of two mechanisms:
- Pharmacodynamic—direct effects at the site of action (e.g., receptors) via physiologic mechanisms (Table 1). For example, amphetamines act directly on the sympathetic nervous system to elevate blood pressure.
- Pharmacokinetic—indirect effects on blood pressure via drug/drug interactions that alter the absorption, distribution, metabolism, or clearance of antihypertensive medications. Thiazide diuretics, angiotensin-converting enzyme (ACE) inhibitors, and salt intake restrictions can raise lithium levels. The calcium-channel blockers verapamil and diltiazem can unpredictably increase or decrease lithium levels, but the combination generally is safe. Verapamil also raises tricyclic antidepressant levels. Monoamine oxidase inhibitors (MAOIs) used in tandem with the antihypertensive reserpine can cause hypomania. Beta-blocker levels are increased when used in concert with selective serotonin reuptake inhibitors. Use of carbamazepine with calcium-channel blockers can elevate carbamazapine levels and diminish the effectiveness of the calcium-channel blocker.
Table 1
POSSIBLE PHARMACODYNAMIC EFFECTS OFPSYCHIATRIC MEDICATIONS ON BLOOD PRESSURE
| Psychiatric medication | Effect on blood pressure |
|---|---|
| Amphetamines | ▲ |
| Benzodiazepines | Withdrawal may cause ▲ |
| Tricyclic antidepressants | ▲ or ▼ (postural hypotension or supine hypertension) |
| Methylphenidate | ▲ |
| Monoamine oxidase inhibitors | ▲ may precipitate an acute hypertensive crisis, especially with foods with high tyramine content (e.g., red wines, aged cheeses) |
| Lithium | ▼ via direct effect on renal concentrating ability |
| Venlafaxine | ▲ dose-related, <1% incidence |
| Antipsychotics (both typical and atypical) | ▼ |
Symptoms, complications of high blood pressure
Symptoms that may be associated with high blood pressure include headaches, dizziness, lightheadedness, fatigue, palpitations, and chest discomfort. Patients may also experience symptoms secondary to end-organ damage (e.g., shortness of breath from congestive heart failure).
Most people, however, experience no symptoms when their blood pressure is elevated. This is one reason most people with hypertension do not adequately control their blood pressure.
Aside from the long-term end-organ damage caused by persistently elevated blood pressure, hypertension also has been found to cause psychiatric disorders, though not directly. For example, post-MI depression is well-recognized. Hypertension may also cause multi-infarct dementia with resultant depression, paranoia, or other psychotic features.
The psychological burden of having chronic and usually incurable (though controllable) hypertension may worsen depression or anxiety disorders. Patients with a chronic psychiatric illness generally have a higher incidence of chronic medical problems.
Likewise, patients with chronic medical disorders have a higher incidence of psychiatric complaints.6
Patient evaluation
When evaluating the patient with elevated blood pressure, it is important to:
- detect and confirm hypertension
- detect target-organ disease (e.g., renal damage or congestive heart failure)
- identify other cardiovascular risk factors (e.g., diabetes mellitus, hyperlipidemia, obesity)
- identify secondary causes of hypertension, such as endocrine abnormalities (e.g., hyperaldosteronism, thyroid disorders), kidney disease, obstructive sleep apnea, and response to medications.
Table 2
ANTIHYPERTENSIVE MEDICATIONS AND SIDE EFFECTS
| Antihypertensive class | Agent(s) | Possible associated psychiatric symptoms |
|---|---|---|
| Beta-adrenergic blocking agents | Propranolol, atenolol, metoprolol, others | Fatigue, depression, psychosis, delirium, anxiety, sexual dysfunction, nightmares, hallucinations* |
| Angiotensin-converting enzyme (ACE) inhibitors | Captopril, enalapril, lisinopril, ramipril, others | Mania, anxiety, hallucinations |
| Angiotensin II receptor blockers (ARBs or AIIAs) | Losartan, valsartan, others | Probably same as ACE inhibitors |
| Diuretics | Hydrochlorothiazide, furosemide | Sexual dysfunction, depression |
| Calcium-channel blockers | Nifedipine, verapamil, diltiazem | Dizziness, headache, flushing, tachycardia, depression |
| Alpha-adrenergic blockers | Prazosin, terazosin, doxazosin | Syncope, dizziness and vertigo, palpitations, drowsiness, weakness, confusion |
| Central alpha-adrenergic agonists | Clonidine, methyldopa | Drowsiness, sedation, fatigue, depression, impotence, delirium, psychosis, nightmares, amnesia |
| Direct vasodilators | Hydralazine, minoxidil | Tachycardia, headache, dizziness |
| Peripheral adrenergic neuron antagonists | Reserpine, guanadrel | Drowsiness, depression, nightmares, tardive dyskinesia |
| *May occur with ophthalmic preparations | ||
A thorough history and physical examination should be performed to assess these four areas. Routine laboratory testing for the hypertensive patient should include a urinalysis, a complete blood count, an assessment of blood chemistries (potassium, sodium, creatinine, fasting glucose, fasting lipid profile), and a 12-lead electrocardiogram.
Treating hypertension
Many medications are used to treat hypertension. Most classes of antihypertensive agents have been shown to be about equally effective in lowering blood pressure.

All other factors being equal, the sixth report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC-VI) recommends initial treatment with a diuretic or beta-blocker. These classes of drugs have been shown to significantly reduce overall hypertension-related mortality.
Most patients with hypertension—particularly the elderly, patients with diabetes mellitus, and those with renal disease—will need two or more agents to control their blood pressure. Avoid prescribing agents that may worsen an existing condition (e.g., beta-blockers may worsen bronchospasm in patients with asthma). Use agents that may help improve comorbid conditions (e.g., beta-blockers have been shown to reduce mortality in patients with previous MI).
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC), which has issued six previous reports on hypertension control, is expected to issue updated recommendations within the next year. Angiotensin-converting enzyme inhibitors, calcium-channel blockers, and angiotensin II receptor antagonists may then be recommended as initial treatment options, along with the previously preferred classes of diuretics and beta-blockers.
A wealth of data has been obtained from multiple randomized, controlled studies since JNC released its most recent report in 1997. Turner et al used genetic analysis to identify individuals with essential hypertension who had a common genetic mutation that resulted in a renal absorption defect. Study participants with this mutation responded much better to diuretic therapy (which specifically targeted the underlying defect) than did those without the defect.8
In the future, determination of genetic polymorphism before prescribing medications may reduce side effects and increase efficacy in treating a variety of disorders, including hypertension.
Potential side effects, some of which mimic or are commonly found in psychiatric disorders, must be considered when choosing an antihypertensive agent. Table 2 lists nine classes of antihypertensives and some associated side effects. Also consider the agent’s cost, convenience of administration, direct-to-consumer advertising, and the patient’s age or race. For example, beta-blockers tend to be less effective in black or elderly patients than in other demographic groups.
Nonpharmacologic hypertension management emphasizes weight reduction, moderation of alcohol intake, regular aerobic exercise, dietary restriction of sodium, and smoking cessation. Most studies of these behavioral interventions have demonstrated a short-term benefit in decreasing blood pressure, but long-term adherence to them is disappointing. Relaxation therapies and biofeedback have been advocated for hypertension, but proof of their efficacy is lacking.7
As more is learned about genetic and other causes of hypertension, more-effective treatments for hypertension could become available (Box).
Treating high-risk groups
Special considerations apply to two patient groups with a high prevalence of hypertension—those age 65 and older and those with diabetes.
Older patients. Treatment benefits are more pronounced in patients age 65 or older because of their greater absolute risk for cardiovascular events. Also, systolic blood pressures increase with aging as the arterial tree becomes progressively less distensible.
Older patients often will require more than one drug to control their blood pressure. The initial dosages should be low and gradually titrated upward as needed. To minimize side effects, use smaller doses of multiple agents that are well tolerated instead of high-dose monotherapy.
A diuretic is often recommended as initial treatment for older patients, though a long-acting dihydropyridine calcium-channel blocker is a reasonable alternative. An ACE inhibitor is recommended for older patients with diabetes, systolic congestive heart failure, or previous MI. An alpha blocker should not be used as initial therapy for hypertension in the elderly because of relative lack of efficacy in preventing cardiovascular events.
Patients with diabetes. Aggressive blood pressure control is especially important in the patient with diabetes, which is the leading cause of end-stage renal disease. Most patients with diabetes also have hypertension—which accelerates their renal disease as well as cardiovascular disease. Blood pressure control goals significantly below 140/90 mm Hg are recommended (120 to 135 mm Hg systolic, 80 to 85 mm Hg diastolic) if diabetes is present.
ACE inhibitors or angiotensin receptor blockers are preferred for initial treatment of hypertension in diabetes, especially if proteinuria is present. Some authorities feel the level of blood pressure control in diabetes is more important than the agent(s) chosen to achieve that control. Most patients with hypertension and diabetes are not controlled on a single antihypertensive drug, and a diuretic is often added.
Psychological aspects of hypertension management
The diagnosis of hypertension and a resulting perception of loss of health or longevity may trigger a grief reaction in some patients.
Several psychological aspects to hypertension treatment make it difficult to achieve long-term control. Patients may become discouraged as dosages are increased and more medications are added. Asymptomatic patients may have no incentive to control their blood pressure. Many report, “I don’t feel any better” when their blood pressure comes down.
Because the goal of hypertension therapy is control rather than cure, the patient must commit to long-term treatment. Lifestyle changes such as dietary sodium restriction, smoking cessation, and weight loss may be difficult to achieve, especially for patients already dealing with a psychiatric disorder.
Also, the cost of treatment—the price of medications and initial and follow-up laboratory studies, plus the expense of follow-up office visits (possibly requiring time off work)—may be high.
Psychiatrists can help by offering moral support and encouraging patients to manage their medical problems, risk factors, and overall health. Psychiatrists can also educate patients on the importance of blood pressure control in preventing cardiovascular morbidity and mortality.
Brief cognitive-behaviorial therapy can identify the individual’s state of change (precontemplation, contemplation, preparation, action, or maintenance). Process techniques (such as consciousness-raising, commitment, or self-reevaluation) appropriate to the stage of change may then be employed.
For example, a patient in the precontemplation stage may resist returning to his or her primary care doctor to begin treatment for high blood pressure, employing such reasoning as, “I can’t afford those expensive office visits, and the medications would cost too much anyway.”
The psychiatrist might then apply consciousness-raising to motivate the patient: “How serious do you think it is to have high blood pressure that isn’t controlled? Are you aware that many people with high blood pressure are treated by means other than medications, or that many blood pressure medications are inexpensive?”
Providing relaxation techniques or a 12-week course of buproprion also can enhance the efficacy of smoking cessation efforts.
Related resources
- Drugs for hypertension. The Medical Letter 2001;43(1099):17-22.
- Some drugs that cause psychiatric symptoms. The Medical Letter 1998;40(1020):21-4.
- Hypertension—Journal of the American Heart Association. http://hyper.ahajournals.org/
- National Heart, Lung, and Blood institute’s Cardiovascular information site. http://www.nhlbi.nih.gov/health/public/heart/index.htm#hbp
Drug brand names
- Bupropion • Wellbutrin
- Guanadrel • Hylorel
- Lisinopril • Prinivil, Zestril
- Losartan • Hyzaar
- Ramipril • Altace
- Reserpine • Diutensen-R
- Valsartan • Diovan
- Venlafaxine • Effexor
- (Numerous other drugs mentioned in this article are available generically)
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kaplan NK. Hypertension in the population at large. In: NK Kaplan, ed. Clinical hypertension (7th ed). Baltimore: Williams & Wilkins, 1998.
2. Yates WR, et al. Cardiovascular risk factors and psychiatric illness. Medical Update for Psychiatrists 1998;3(6):196-201.
3. Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
4. Todarello O, Taylor GJ, Parker JD, Fanelli M. Alexithymia in essential hypertensive and psychiatric outpatients: a compartative study. J Psychosom Res 1995;39(8):987-94.
5. Horwitz S, Prados-Torres A, et al. The influence of psychological and social factors on accuracy of self reported blood pressure. J Clin Epidemiol 1997;50(4):411-18.
6. Adamis D, Ball C. Physical morbidity in elderly psychiatric inpatients: prevalence and possible relations between the major mental disorders and physical illness. Int J Geriatr Psychiatry 2000;15:248-53.
7. Dubbert PM. Behavioral (life-style) modification in the prevention and treatment of hypertension. Clin Psychol Rev 1995;15(3):187-216.
8. Turner ST, et al. C825T polymorphism of the G protein beta(3)-subunit and antihypertensive response to a thiazide diuretic. Hypertension 2001;37(2 Part 2):739-43.
Roughly 50 million adult Americans have hypertension.1 Chances are some of them are—or soon will be—under your care.
Hypertension is common among patients with psychiatric disorders, particularly in those with chronic mental conditions.2 Medication-associated weight gain and other reactions to psychotropics, drug-drug interactions, lack of exercise, adverse dietary habits, and pre-existing medical conditions all predispose psychiatric patients to hypertension.
Yet hypertension often goes undetected in psychiatric patients. Hypertension many times is asymptomatic—about 50% of all people with the disorder don’t even know they have it.3 Some symptoms of uncontrolled hypertension—fatigue, headache, palpitations, and dizziness—are also associated with many psychiatric disorders. As a result, psychiatrists may attempt to manage the symptoms but miss the hypertension.
Psychiatrists need to be alert for hypertension, either as a possible contributing factor to a mental disorder or as a potential side effect of a psychiatric disorder or treatment. The following diagnostic and treatment strategies will help you detect and manage this common condition.
Causes of hypertension in mental illness
The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure defines elevated blood pressure as 140 mm Hg systolic and/or 90 mm Hg diastolic. The diagnosis of hypertension should be based on the average of two or more blood pressure readings at each of two or more visits after initial screening.
All patients with elevated blood pressure have an underlying physiologic abnormality that is causing their hypertension. The disorder falls within the following two categories:
- essential hypertension, emanating from an unknown cause
- secondary hypertension, resulting from an underlying, discoverable, often treatable cause.
Researchers have speculated that certain psychiatric disorders might cause, or be risk factors for, hypertension. Anxiety or panic disorders have been associated with acute (and perhaps chronic) blood pressure elevations.2 Some research suggests that patients with alexithymia are at risk for developing hypertension.4
Other studies suggest that hypertensive patients with certain psychological disorders (e.g., depression) or social factors (e.g., substance abuse) are less likely than nonaffected patients to self-report the presence of hypertension and less likely to receive medical attention for it.5
Psychiatric drugs also may affect blood pressure by one of two mechanisms:
- Pharmacodynamic—direct effects at the site of action (e.g., receptors) via physiologic mechanisms (Table 1). For example, amphetamines act directly on the sympathetic nervous system to elevate blood pressure.
- Pharmacokinetic—indirect effects on blood pressure via drug/drug interactions that alter the absorption, distribution, metabolism, or clearance of antihypertensive medications. Thiazide diuretics, angiotensin-converting enzyme (ACE) inhibitors, and salt intake restrictions can raise lithium levels. The calcium-channel blockers verapamil and diltiazem can unpredictably increase or decrease lithium levels, but the combination generally is safe. Verapamil also raises tricyclic antidepressant levels. Monoamine oxidase inhibitors (MAOIs) used in tandem with the antihypertensive reserpine can cause hypomania. Beta-blocker levels are increased when used in concert with selective serotonin reuptake inhibitors. Use of carbamazepine with calcium-channel blockers can elevate carbamazapine levels and diminish the effectiveness of the calcium-channel blocker.
Table 1
POSSIBLE PHARMACODYNAMIC EFFECTS OFPSYCHIATRIC MEDICATIONS ON BLOOD PRESSURE
| Psychiatric medication | Effect on blood pressure |
|---|---|
| Amphetamines | ▲ |
| Benzodiazepines | Withdrawal may cause ▲ |
| Tricyclic antidepressants | ▲ or ▼ (postural hypotension or supine hypertension) |
| Methylphenidate | ▲ |
| Monoamine oxidase inhibitors | ▲ may precipitate an acute hypertensive crisis, especially with foods with high tyramine content (e.g., red wines, aged cheeses) |
| Lithium | ▼ via direct effect on renal concentrating ability |
| Venlafaxine | ▲ dose-related, <1% incidence |
| Antipsychotics (both typical and atypical) | ▼ |
Symptoms, complications of high blood pressure
Symptoms that may be associated with high blood pressure include headaches, dizziness, lightheadedness, fatigue, palpitations, and chest discomfort. Patients may also experience symptoms secondary to end-organ damage (e.g., shortness of breath from congestive heart failure).
Most people, however, experience no symptoms when their blood pressure is elevated. This is one reason most people with hypertension do not adequately control their blood pressure.
Aside from the long-term end-organ damage caused by persistently elevated blood pressure, hypertension also has been found to cause psychiatric disorders, though not directly. For example, post-MI depression is well-recognized. Hypertension may also cause multi-infarct dementia with resultant depression, paranoia, or other psychotic features.
The psychological burden of having chronic and usually incurable (though controllable) hypertension may worsen depression or anxiety disorders. Patients with a chronic psychiatric illness generally have a higher incidence of chronic medical problems.
Likewise, patients with chronic medical disorders have a higher incidence of psychiatric complaints.6
Patient evaluation
When evaluating the patient with elevated blood pressure, it is important to:
- detect and confirm hypertension
- detect target-organ disease (e.g., renal damage or congestive heart failure)
- identify other cardiovascular risk factors (e.g., diabetes mellitus, hyperlipidemia, obesity)
- identify secondary causes of hypertension, such as endocrine abnormalities (e.g., hyperaldosteronism, thyroid disorders), kidney disease, obstructive sleep apnea, and response to medications.
Table 2
ANTIHYPERTENSIVE MEDICATIONS AND SIDE EFFECTS
| Antihypertensive class | Agent(s) | Possible associated psychiatric symptoms |
|---|---|---|
| Beta-adrenergic blocking agents | Propranolol, atenolol, metoprolol, others | Fatigue, depression, psychosis, delirium, anxiety, sexual dysfunction, nightmares, hallucinations* |
| Angiotensin-converting enzyme (ACE) inhibitors | Captopril, enalapril, lisinopril, ramipril, others | Mania, anxiety, hallucinations |
| Angiotensin II receptor blockers (ARBs or AIIAs) | Losartan, valsartan, others | Probably same as ACE inhibitors |
| Diuretics | Hydrochlorothiazide, furosemide | Sexual dysfunction, depression |
| Calcium-channel blockers | Nifedipine, verapamil, diltiazem | Dizziness, headache, flushing, tachycardia, depression |
| Alpha-adrenergic blockers | Prazosin, terazosin, doxazosin | Syncope, dizziness and vertigo, palpitations, drowsiness, weakness, confusion |
| Central alpha-adrenergic agonists | Clonidine, methyldopa | Drowsiness, sedation, fatigue, depression, impotence, delirium, psychosis, nightmares, amnesia |
| Direct vasodilators | Hydralazine, minoxidil | Tachycardia, headache, dizziness |
| Peripheral adrenergic neuron antagonists | Reserpine, guanadrel | Drowsiness, depression, nightmares, tardive dyskinesia |
| *May occur with ophthalmic preparations | ||
A thorough history and physical examination should be performed to assess these four areas. Routine laboratory testing for the hypertensive patient should include a urinalysis, a complete blood count, an assessment of blood chemistries (potassium, sodium, creatinine, fasting glucose, fasting lipid profile), and a 12-lead electrocardiogram.
Treating hypertension
Many medications are used to treat hypertension. Most classes of antihypertensive agents have been shown to be about equally effective in lowering blood pressure.
All other factors being equal, the sixth report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC-VI) recommends initial treatment with a diuretic or beta-blocker. These classes of drugs have been shown to significantly reduce overall hypertension-related mortality.
Most patients with hypertension—particularly the elderly, patients with diabetes mellitus, and those with renal disease—will need two or more agents to control their blood pressure. Avoid prescribing agents that may worsen an existing condition (e.g., beta-blockers may worsen bronchospasm in patients with asthma). Use agents that may help improve comorbid conditions (e.g., beta-blockers have been shown to reduce mortality in patients with previous MI).
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC), which has issued six previous reports on hypertension control, is expected to issue updated recommendations within the next year. Angiotensin-converting enzyme inhibitors, calcium-channel blockers, and angiotensin II receptor antagonists may then be recommended as initial treatment options, along with the previously preferred classes of diuretics and beta-blockers.
A wealth of data has been obtained from multiple randomized, controlled studies since JNC released its most recent report in 1997. Turner et al used genetic analysis to identify individuals with essential hypertension who had a common genetic mutation that resulted in a renal absorption defect. Study participants with this mutation responded much better to diuretic therapy (which specifically targeted the underlying defect) than did those without the defect.8
In the future, determination of genetic polymorphism before prescribing medications may reduce side effects and increase efficacy in treating a variety of disorders, including hypertension.
Potential side effects, some of which mimic or are commonly found in psychiatric disorders, must be considered when choosing an antihypertensive agent. Table 2 lists nine classes of antihypertensives and some associated side effects. Also consider the agent’s cost, convenience of administration, direct-to-consumer advertising, and the patient’s age or race. For example, beta-blockers tend to be less effective in black or elderly patients than in other demographic groups.
Nonpharmacologic hypertension management emphasizes weight reduction, moderation of alcohol intake, regular aerobic exercise, dietary restriction of sodium, and smoking cessation. Most studies of these behavioral interventions have demonstrated a short-term benefit in decreasing blood pressure, but long-term adherence to them is disappointing. Relaxation therapies and biofeedback have been advocated for hypertension, but proof of their efficacy is lacking.7
As more is learned about genetic and other causes of hypertension, more-effective treatments for hypertension could become available (Box).
Treating high-risk groups
Special considerations apply to two patient groups with a high prevalence of hypertension—those age 65 and older and those with diabetes.
Older patients. Treatment benefits are more pronounced in patients age 65 or older because of their greater absolute risk for cardiovascular events. Also, systolic blood pressures increase with aging as the arterial tree becomes progressively less distensible.
Older patients often will require more than one drug to control their blood pressure. The initial dosages should be low and gradually titrated upward as needed. To minimize side effects, use smaller doses of multiple agents that are well tolerated instead of high-dose monotherapy.
A diuretic is often recommended as initial treatment for older patients, though a long-acting dihydropyridine calcium-channel blocker is a reasonable alternative. An ACE inhibitor is recommended for older patients with diabetes, systolic congestive heart failure, or previous MI. An alpha blocker should not be used as initial therapy for hypertension in the elderly because of relative lack of efficacy in preventing cardiovascular events.
Patients with diabetes. Aggressive blood pressure control is especially important in the patient with diabetes, which is the leading cause of end-stage renal disease. Most patients with diabetes also have hypertension—which accelerates their renal disease as well as cardiovascular disease. Blood pressure control goals significantly below 140/90 mm Hg are recommended (120 to 135 mm Hg systolic, 80 to 85 mm Hg diastolic) if diabetes is present.
ACE inhibitors or angiotensin receptor blockers are preferred for initial treatment of hypertension in diabetes, especially if proteinuria is present. Some authorities feel the level of blood pressure control in diabetes is more important than the agent(s) chosen to achieve that control. Most patients with hypertension and diabetes are not controlled on a single antihypertensive drug, and a diuretic is often added.
Psychological aspects of hypertension management
The diagnosis of hypertension and a resulting perception of loss of health or longevity may trigger a grief reaction in some patients.
Several psychological aspects to hypertension treatment make it difficult to achieve long-term control. Patients may become discouraged as dosages are increased and more medications are added. Asymptomatic patients may have no incentive to control their blood pressure. Many report, “I don’t feel any better” when their blood pressure comes down.
Because the goal of hypertension therapy is control rather than cure, the patient must commit to long-term treatment. Lifestyle changes such as dietary sodium restriction, smoking cessation, and weight loss may be difficult to achieve, especially for patients already dealing with a psychiatric disorder.
Also, the cost of treatment—the price of medications and initial and follow-up laboratory studies, plus the expense of follow-up office visits (possibly requiring time off work)—may be high.
Psychiatrists can help by offering moral support and encouraging patients to manage their medical problems, risk factors, and overall health. Psychiatrists can also educate patients on the importance of blood pressure control in preventing cardiovascular morbidity and mortality.
Brief cognitive-behaviorial therapy can identify the individual’s state of change (precontemplation, contemplation, preparation, action, or maintenance). Process techniques (such as consciousness-raising, commitment, or self-reevaluation) appropriate to the stage of change may then be employed.
For example, a patient in the precontemplation stage may resist returning to his or her primary care doctor to begin treatment for high blood pressure, employing such reasoning as, “I can’t afford those expensive office visits, and the medications would cost too much anyway.”
The psychiatrist might then apply consciousness-raising to motivate the patient: “How serious do you think it is to have high blood pressure that isn’t controlled? Are you aware that many people with high blood pressure are treated by means other than medications, or that many blood pressure medications are inexpensive?”
Providing relaxation techniques or a 12-week course of buproprion also can enhance the efficacy of smoking cessation efforts.
Related resources
- Drugs for hypertension. The Medical Letter 2001;43(1099):17-22.
- Some drugs that cause psychiatric symptoms. The Medical Letter 1998;40(1020):21-4.
- Hypertension—Journal of the American Heart Association. http://hyper.ahajournals.org/
- National Heart, Lung, and Blood institute’s Cardiovascular information site. http://www.nhlbi.nih.gov/health/public/heart/index.htm#hbp
Drug brand names
- Bupropion • Wellbutrin
- Guanadrel • Hylorel
- Lisinopril • Prinivil, Zestril
- Losartan • Hyzaar
- Ramipril • Altace
- Reserpine • Diutensen-R
- Valsartan • Diovan
- Venlafaxine • Effexor
- (Numerous other drugs mentioned in this article are available generically)
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Roughly 50 million adult Americans have hypertension.1 Chances are some of them are—or soon will be—under your care.
Hypertension is common among patients with psychiatric disorders, particularly in those with chronic mental conditions.2 Medication-associated weight gain and other reactions to psychotropics, drug-drug interactions, lack of exercise, adverse dietary habits, and pre-existing medical conditions all predispose psychiatric patients to hypertension.
Yet hypertension often goes undetected in psychiatric patients. Hypertension many times is asymptomatic—about 50% of all people with the disorder don’t even know they have it.3 Some symptoms of uncontrolled hypertension—fatigue, headache, palpitations, and dizziness—are also associated with many psychiatric disorders. As a result, psychiatrists may attempt to manage the symptoms but miss the hypertension.
Psychiatrists need to be alert for hypertension, either as a possible contributing factor to a mental disorder or as a potential side effect of a psychiatric disorder or treatment. The following diagnostic and treatment strategies will help you detect and manage this common condition.
Causes of hypertension in mental illness
The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure defines elevated blood pressure as 140 mm Hg systolic and/or 90 mm Hg diastolic. The diagnosis of hypertension should be based on the average of two or more blood pressure readings at each of two or more visits after initial screening.
All patients with elevated blood pressure have an underlying physiologic abnormality that is causing their hypertension. The disorder falls within the following two categories:
- essential hypertension, emanating from an unknown cause
- secondary hypertension, resulting from an underlying, discoverable, often treatable cause.
Researchers have speculated that certain psychiatric disorders might cause, or be risk factors for, hypertension. Anxiety or panic disorders have been associated with acute (and perhaps chronic) blood pressure elevations.2 Some research suggests that patients with alexithymia are at risk for developing hypertension.4
Other studies suggest that hypertensive patients with certain psychological disorders (e.g., depression) or social factors (e.g., substance abuse) are less likely than nonaffected patients to self-report the presence of hypertension and less likely to receive medical attention for it.5
Psychiatric drugs also may affect blood pressure by one of two mechanisms:
- Pharmacodynamic—direct effects at the site of action (e.g., receptors) via physiologic mechanisms (Table 1). For example, amphetamines act directly on the sympathetic nervous system to elevate blood pressure.
- Pharmacokinetic—indirect effects on blood pressure via drug/drug interactions that alter the absorption, distribution, metabolism, or clearance of antihypertensive medications. Thiazide diuretics, angiotensin-converting enzyme (ACE) inhibitors, and salt intake restrictions can raise lithium levels. The calcium-channel blockers verapamil and diltiazem can unpredictably increase or decrease lithium levels, but the combination generally is safe. Verapamil also raises tricyclic antidepressant levels. Monoamine oxidase inhibitors (MAOIs) used in tandem with the antihypertensive reserpine can cause hypomania. Beta-blocker levels are increased when used in concert with selective serotonin reuptake inhibitors. Use of carbamazepine with calcium-channel blockers can elevate carbamazapine levels and diminish the effectiveness of the calcium-channel blocker.
Table 1
POSSIBLE PHARMACODYNAMIC EFFECTS OFPSYCHIATRIC MEDICATIONS ON BLOOD PRESSURE
| Psychiatric medication | Effect on blood pressure |
|---|---|
| Amphetamines | ▲ |
| Benzodiazepines | Withdrawal may cause ▲ |
| Tricyclic antidepressants | ▲ or ▼ (postural hypotension or supine hypertension) |
| Methylphenidate | ▲ |
| Monoamine oxidase inhibitors | ▲ may precipitate an acute hypertensive crisis, especially with foods with high tyramine content (e.g., red wines, aged cheeses) |
| Lithium | ▼ via direct effect on renal concentrating ability |
| Venlafaxine | ▲ dose-related, <1% incidence |
| Antipsychotics (both typical and atypical) | ▼ |
Symptoms, complications of high blood pressure
Symptoms that may be associated with high blood pressure include headaches, dizziness, lightheadedness, fatigue, palpitations, and chest discomfort. Patients may also experience symptoms secondary to end-organ damage (e.g., shortness of breath from congestive heart failure).
Most people, however, experience no symptoms when their blood pressure is elevated. This is one reason most people with hypertension do not adequately control their blood pressure.
Aside from the long-term end-organ damage caused by persistently elevated blood pressure, hypertension also has been found to cause psychiatric disorders, though not directly. For example, post-MI depression is well-recognized. Hypertension may also cause multi-infarct dementia with resultant depression, paranoia, or other psychotic features.
The psychological burden of having chronic and usually incurable (though controllable) hypertension may worsen depression or anxiety disorders. Patients with a chronic psychiatric illness generally have a higher incidence of chronic medical problems.
Likewise, patients with chronic medical disorders have a higher incidence of psychiatric complaints.6
Patient evaluation
When evaluating the patient with elevated blood pressure, it is important to:
- detect and confirm hypertension
- detect target-organ disease (e.g., renal damage or congestive heart failure)
- identify other cardiovascular risk factors (e.g., diabetes mellitus, hyperlipidemia, obesity)
- identify secondary causes of hypertension, such as endocrine abnormalities (e.g., hyperaldosteronism, thyroid disorders), kidney disease, obstructive sleep apnea, and response to medications.
Table 2
ANTIHYPERTENSIVE MEDICATIONS AND SIDE EFFECTS
| Antihypertensive class | Agent(s) | Possible associated psychiatric symptoms |
|---|---|---|
| Beta-adrenergic blocking agents | Propranolol, atenolol, metoprolol, others | Fatigue, depression, psychosis, delirium, anxiety, sexual dysfunction, nightmares, hallucinations* |
| Angiotensin-converting enzyme (ACE) inhibitors | Captopril, enalapril, lisinopril, ramipril, others | Mania, anxiety, hallucinations |
| Angiotensin II receptor blockers (ARBs or AIIAs) | Losartan, valsartan, others | Probably same as ACE inhibitors |
| Diuretics | Hydrochlorothiazide, furosemide | Sexual dysfunction, depression |
| Calcium-channel blockers | Nifedipine, verapamil, diltiazem | Dizziness, headache, flushing, tachycardia, depression |
| Alpha-adrenergic blockers | Prazosin, terazosin, doxazosin | Syncope, dizziness and vertigo, palpitations, drowsiness, weakness, confusion |
| Central alpha-adrenergic agonists | Clonidine, methyldopa | Drowsiness, sedation, fatigue, depression, impotence, delirium, psychosis, nightmares, amnesia |
| Direct vasodilators | Hydralazine, minoxidil | Tachycardia, headache, dizziness |
| Peripheral adrenergic neuron antagonists | Reserpine, guanadrel | Drowsiness, depression, nightmares, tardive dyskinesia |
| *May occur with ophthalmic preparations | ||
A thorough history and physical examination should be performed to assess these four areas. Routine laboratory testing for the hypertensive patient should include a urinalysis, a complete blood count, an assessment of blood chemistries (potassium, sodium, creatinine, fasting glucose, fasting lipid profile), and a 12-lead electrocardiogram.
Treating hypertension
Many medications are used to treat hypertension. Most classes of antihypertensive agents have been shown to be about equally effective in lowering blood pressure.
All other factors being equal, the sixth report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC-VI) recommends initial treatment with a diuretic or beta-blocker. These classes of drugs have been shown to significantly reduce overall hypertension-related mortality.
Most patients with hypertension—particularly the elderly, patients with diabetes mellitus, and those with renal disease—will need two or more agents to control their blood pressure. Avoid prescribing agents that may worsen an existing condition (e.g., beta-blockers may worsen bronchospasm in patients with asthma). Use agents that may help improve comorbid conditions (e.g., beta-blockers have been shown to reduce mortality in patients with previous MI).
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC), which has issued six previous reports on hypertension control, is expected to issue updated recommendations within the next year. Angiotensin-converting enzyme inhibitors, calcium-channel blockers, and angiotensin II receptor antagonists may then be recommended as initial treatment options, along with the previously preferred classes of diuretics and beta-blockers.
A wealth of data has been obtained from multiple randomized, controlled studies since JNC released its most recent report in 1997. Turner et al used genetic analysis to identify individuals with essential hypertension who had a common genetic mutation that resulted in a renal absorption defect. Study participants with this mutation responded much better to diuretic therapy (which specifically targeted the underlying defect) than did those without the defect.8
In the future, determination of genetic polymorphism before prescribing medications may reduce side effects and increase efficacy in treating a variety of disorders, including hypertension.
Potential side effects, some of which mimic or are commonly found in psychiatric disorders, must be considered when choosing an antihypertensive agent. Table 2 lists nine classes of antihypertensives and some associated side effects. Also consider the agent’s cost, convenience of administration, direct-to-consumer advertising, and the patient’s age or race. For example, beta-blockers tend to be less effective in black or elderly patients than in other demographic groups.
Nonpharmacologic hypertension management emphasizes weight reduction, moderation of alcohol intake, regular aerobic exercise, dietary restriction of sodium, and smoking cessation. Most studies of these behavioral interventions have demonstrated a short-term benefit in decreasing blood pressure, but long-term adherence to them is disappointing. Relaxation therapies and biofeedback have been advocated for hypertension, but proof of their efficacy is lacking.7
As more is learned about genetic and other causes of hypertension, more-effective treatments for hypertension could become available (Box).
Treating high-risk groups
Special considerations apply to two patient groups with a high prevalence of hypertension—those age 65 and older and those with diabetes.
Older patients. Treatment benefits are more pronounced in patients age 65 or older because of their greater absolute risk for cardiovascular events. Also, systolic blood pressures increase with aging as the arterial tree becomes progressively less distensible.
Older patients often will require more than one drug to control their blood pressure. The initial dosages should be low and gradually titrated upward as needed. To minimize side effects, use smaller doses of multiple agents that are well tolerated instead of high-dose monotherapy.
A diuretic is often recommended as initial treatment for older patients, though a long-acting dihydropyridine calcium-channel blocker is a reasonable alternative. An ACE inhibitor is recommended for older patients with diabetes, systolic congestive heart failure, or previous MI. An alpha blocker should not be used as initial therapy for hypertension in the elderly because of relative lack of efficacy in preventing cardiovascular events.
Patients with diabetes. Aggressive blood pressure control is especially important in the patient with diabetes, which is the leading cause of end-stage renal disease. Most patients with diabetes also have hypertension—which accelerates their renal disease as well as cardiovascular disease. Blood pressure control goals significantly below 140/90 mm Hg are recommended (120 to 135 mm Hg systolic, 80 to 85 mm Hg diastolic) if diabetes is present.
ACE inhibitors or angiotensin receptor blockers are preferred for initial treatment of hypertension in diabetes, especially if proteinuria is present. Some authorities feel the level of blood pressure control in diabetes is more important than the agent(s) chosen to achieve that control. Most patients with hypertension and diabetes are not controlled on a single antihypertensive drug, and a diuretic is often added.
Psychological aspects of hypertension management
The diagnosis of hypertension and a resulting perception of loss of health or longevity may trigger a grief reaction in some patients.
Several psychological aspects to hypertension treatment make it difficult to achieve long-term control. Patients may become discouraged as dosages are increased and more medications are added. Asymptomatic patients may have no incentive to control their blood pressure. Many report, “I don’t feel any better” when their blood pressure comes down.
Because the goal of hypertension therapy is control rather than cure, the patient must commit to long-term treatment. Lifestyle changes such as dietary sodium restriction, smoking cessation, and weight loss may be difficult to achieve, especially for patients already dealing with a psychiatric disorder.
Also, the cost of treatment—the price of medications and initial and follow-up laboratory studies, plus the expense of follow-up office visits (possibly requiring time off work)—may be high.
Psychiatrists can help by offering moral support and encouraging patients to manage their medical problems, risk factors, and overall health. Psychiatrists can also educate patients on the importance of blood pressure control in preventing cardiovascular morbidity and mortality.
Brief cognitive-behaviorial therapy can identify the individual’s state of change (precontemplation, contemplation, preparation, action, or maintenance). Process techniques (such as consciousness-raising, commitment, or self-reevaluation) appropriate to the stage of change may then be employed.
For example, a patient in the precontemplation stage may resist returning to his or her primary care doctor to begin treatment for high blood pressure, employing such reasoning as, “I can’t afford those expensive office visits, and the medications would cost too much anyway.”
The psychiatrist might then apply consciousness-raising to motivate the patient: “How serious do you think it is to have high blood pressure that isn’t controlled? Are you aware that many people with high blood pressure are treated by means other than medications, or that many blood pressure medications are inexpensive?”
Providing relaxation techniques or a 12-week course of buproprion also can enhance the efficacy of smoking cessation efforts.
Related resources
- Drugs for hypertension. The Medical Letter 2001;43(1099):17-22.
- Some drugs that cause psychiatric symptoms. The Medical Letter 1998;40(1020):21-4.
- Hypertension—Journal of the American Heart Association. http://hyper.ahajournals.org/
- National Heart, Lung, and Blood institute’s Cardiovascular information site. http://www.nhlbi.nih.gov/health/public/heart/index.htm#hbp
Drug brand names
- Bupropion • Wellbutrin
- Guanadrel • Hylorel
- Lisinopril • Prinivil, Zestril
- Losartan • Hyzaar
- Ramipril • Altace
- Reserpine • Diutensen-R
- Valsartan • Diovan
- Venlafaxine • Effexor
- (Numerous other drugs mentioned in this article are available generically)
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kaplan NK. Hypertension in the population at large. In: NK Kaplan, ed. Clinical hypertension (7th ed). Baltimore: Williams & Wilkins, 1998.
2. Yates WR, et al. Cardiovascular risk factors and psychiatric illness. Medical Update for Psychiatrists 1998;3(6):196-201.
3. Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
4. Todarello O, Taylor GJ, Parker JD, Fanelli M. Alexithymia in essential hypertensive and psychiatric outpatients: a compartative study. J Psychosom Res 1995;39(8):987-94.
5. Horwitz S, Prados-Torres A, et al. The influence of psychological and social factors on accuracy of self reported blood pressure. J Clin Epidemiol 1997;50(4):411-18.
6. Adamis D, Ball C. Physical morbidity in elderly psychiatric inpatients: prevalence and possible relations between the major mental disorders and physical illness. Int J Geriatr Psychiatry 2000;15:248-53.
7. Dubbert PM. Behavioral (life-style) modification in the prevention and treatment of hypertension. Clin Psychol Rev 1995;15(3):187-216.
8. Turner ST, et al. C825T polymorphism of the G protein beta(3)-subunit and antihypertensive response to a thiazide diuretic. Hypertension 2001;37(2 Part 2):739-43.
1. Kaplan NK. Hypertension in the population at large. In: NK Kaplan, ed. Clinical hypertension (7th ed). Baltimore: Williams & Wilkins, 1998.
2. Yates WR, et al. Cardiovascular risk factors and psychiatric illness. Medical Update for Psychiatrists 1998;3(6):196-201.
3. Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
4. Todarello O, Taylor GJ, Parker JD, Fanelli M. Alexithymia in essential hypertensive and psychiatric outpatients: a compartative study. J Psychosom Res 1995;39(8):987-94.
5. Horwitz S, Prados-Torres A, et al. The influence of psychological and social factors on accuracy of self reported blood pressure. J Clin Epidemiol 1997;50(4):411-18.
6. Adamis D, Ball C. Physical morbidity in elderly psychiatric inpatients: prevalence and possible relations between the major mental disorders and physical illness. Int J Geriatr Psychiatry 2000;15:248-53.
7. Dubbert PM. Behavioral (life-style) modification in the prevention and treatment of hypertension. Clin Psychol Rev 1995;15(3):187-216.
8. Turner ST, et al. C825T polymorphism of the G protein beta(3)-subunit and antihypertensive response to a thiazide diuretic. Hypertension 2001;37(2 Part 2):739-43.
Weight control and antipsychotics: How to tip the scales away from diabetes and heart disease
Weight gain is a potential problem for all patients who require treatment with antipsychotics. Those with schizophrenia face double jeopardy. Both the disorder and the use of virtually any available antipsychotic drug may be associated with weight gain, new-onset glucose intolerance, and type 2 diabetes mellitus.
Because of the cardiovascular risks and other morbidity associated with weight gain and glucose dysregulation,1 the psychiatrist must remain vigilant and manage these complications aggressively. In this article, we offer insights into the prevention and management of metabolic complications associated with the use of antipsychotic agents in patients with schizophrenia.
Weight gain and antipsychotics
Weight change was recognized as a feature of schizophrenia even before antipsychotic drugs were introduced in the 1950s.2 Schizophrenia—independent of drug treatment—also is a risk factor for the development of type 2 diabetes. In persons with schizophrenia, serum glucose levels increase more slowly, decline more gradually, and represent higher-than-normal reference values.3
Figure 1 WEIGHT GAIN ASSOCIATED WITH ANTIPSYCHOTIC DRUG ADMINISTRATION
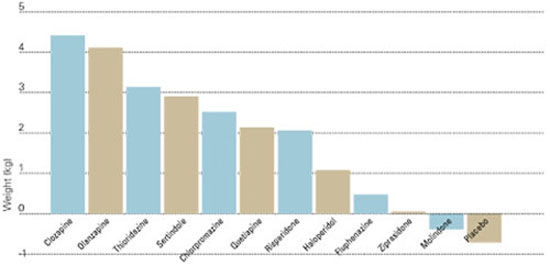
Values represent estimates of drug-induced weight gain after 10 weeks of drug administration.
Source: Allison et al. Am J Psychiatry 1999;156:1686-96; Brecher et al. Int J Psychiatry Clin Pract 2000;4:287-92.In 1999, Allison et al assessed the effects of conventional and atypical antipsychotics on body weight. Using 81 published articles, they estimated and compared weight changes associated with 10 antipsychotic agents and a placebo when given at standard dosages for 10 weeks.4 Comparative data on quetiapine, which were insufficient in 1999, have since been added (Figure 1).5
Patients who received a placebo lost 0.74 kg across 10 weeks. Weight changes with the conventional agents ranged from a reduction of 0.39 kg with molindone to an increase of 3.19 kg with thioridazine. Weight gains also were seen with all of the newer atypical agents, including clozapine (+4.45 kg), olanzapine (+4.15 kg), risperidone (+2.10 kg), and ziprasidone (+0.04 kg).
Fontaine et al have estimated that weight gain in patients with schizophrenia has its greatest impact on mortality in two scenarios:
- when patients are overweight before they start antipsychotic medication
- with greater degrees of weight gain across 10 years (Figure 2).
Whatever a patient’s starting weight, substantial weight gain with antipsychotic therapy increases the risk of impaired glucose tolerance and hypertension (Figure 3).6
Schizophrenia and diabetes
The prevalence of type 2 diabetes in patients with schizophrenia increased from 4.2% in 1956 to 17.2% in 1968, related in part to the introduction of phenothiazines.7 A recent study of data collected by the Schizophrenia Patient Outcomes Research Team (PORT)2 found higher rates of diabetes in persons with schizophrenia (lifetime prevalence, 14.9%) than in the general population (approximately 7.3%).1 Most patients in the PORT study were taking older antipsychotics, the use of which has occasionally been associated with carbohydrate dysregulation.
Figure 2 INCREASED MORTALITY ASSOCIATED WITH WEIGHT GAIN
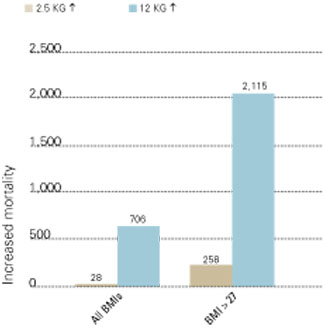
Number of deaths associated with weight gains of 2.5 and 12 kg over 10 years, as related to all body mass index measurements (BMIs) and BMIs >27 (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.The prevalence of new-onset diabetes with use of specific antipsychotics is unknown. Most information is contained in case reports, and proper epidemiologic studies await publication.
The most detailed report—a pooled study of published cases related to clozapine use—comes from the FDA’s Center for Drug Evaluation and Research.8 In this study, the authors identified 384 reports of diabetes that developed (in 242 patients) or was exacerbated (in 54 patients) in association with clozapine. Patient mean age was 40, and diabetes occurred more commonly in women than in men.
Diabetes developed most commonly within 6 months of starting treatment with clozapine, and one patient developed diabetes after a single 500-mg dose. Metabolic acidosis or ketosis occurred in 80 cases, and 25 subjects died during hyperglycemic episodes. Stopping clozapine or reducing the dosage improved glycemic control in 46 patients.8
Figure 3 INCREASED MORBIDITY ASSOCIATED WITH WEIGHT GAIN
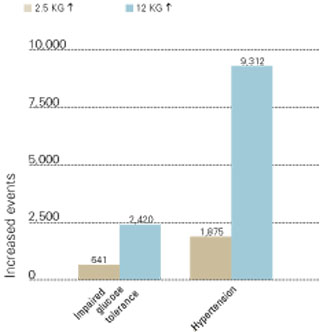
New cases of impaired glucose tolerance and hypertension that developed with weight gains of 2.5 and 12 kg over 10 years (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.During antipsychotic therapy, it is important to measure patients’ fasting plasma glucose at least annually—and more often for high-risk patients (Table 1). The American Diabetes Association defines diabetes as a fasting serum or plasma glucose 126 mg/dl or a 2-hour postprandial serum or plasma glucose 200 mg/dl. In all patients, these tests should be repeated to confirm the diagnosis. Oral glucose tolerance testing is less convenient than fasting plasma glucose testing but more sensitive in identifying changes in carbohydrate metabolism.
As with weight gain, it is easier to prevent diabetes than to treat it. The psychiatrist can best help the patient with emerging carbohydrate dysregulation by collaborating with an internist, family physician, or endocrinologist.
Table 1
FACTORS RELATED TO HIGH RISK OF DEVELOPING TYPE 2 DIABETES
|
| Source: American Diabetes Association |
Weight gain with diabetes drugs Weight gain is associated not only with the use of antipsychotics but also with four classes of oral agents used to treat type 2 diabetes: sulfonylureas, meglitinides, phenylalanine derivatives, and thiazolidinediones. One class—biguanides—contributes to weight reduction, and one—alpha-glucosidase inhibitors—has a variable effect on body weight. These drugs also vary in their effects on serum lipids, including total cholesterol, LDL and HDL cholesterol, and triglycerides (Table 2).9
Many patients with type 2 diabetes require more than one agent to control plasma glucose. With time, insulin deficiency becomes more marked, and insulin therapy is frequently added to the regimen. Hypertension and hyperlipidemia are also very common in patients with type 2 diabetes and require medication to reduce the risk of cardiovascular events.10 As a result, the diabetic patient requiring antipsychotic drugs will likely need polypharmacy, and many of the drugs that might be used may lead to weight gain.
Assessing, managing weight gain
During each visit for the patient with schizophrenia, it is important to routinely weigh those receiving antipsychotics and ask about polydipsia and polyuria, which are early signs of incipient diabetes. A patient who is gaining significant weight (7% of baseline) while taking an antipsychotic and has risk factors for cardiovascular events (e.g., smoking, hypertension, hypertriglyceridemia) is a candidate for a change in antipsychotics.
Try to weigh patients at approximately the same time of day at each visit to compensate for possible diurnal weight changes related to polydipsia-hyponatremia syndrome.11 Patients with this syndrome can gain 5 to 10 lbs (or more) per day and excrete the retained fluid at night. It occurs in 5 to 10% of chronically psychotic patients requiring institutional care and in 1 to 2% of outpatients. Patients with schizophrenia complicated by this syndrome may manifest polydipsia and polyuria secondary to psychosis rather than emerging diabetes. Thus, the clinician must be alert to both diabetes and the polydipsia-hyponatremia syndrome in this setting.
Weight-control approaches
Patients who are taking sedating antipsychotics (e.g., clozapine, olanzapine, or low-potency phenothiazines) may gain up to 30 lbs per year if they become physically inactive and do not reduce their food consumption. Thus, it is important to work with such patients to decrease their caloric intake.
A weight-loss program that produces a loss of 0.5 to 1% of body weight per week is considered safe and acceptable.12 Mild to moderate obesity may be managed by reducing food intake by 500 calories and exercising 30 minutes each day.
CBT Cognitive-behavioral therapy (CBT) may help stem weight gain associated with antipsychotic use. Umbricht et al provided CBT to six patients with chronic psychosis who were receiving clozapine or olanzapine. Therapists in group and individual sessions focused on the causes of weight gain, lowcalorie nutrition, weight-loss guidelines, exercise programs, and relaxation strategies. Across 8 weeks, patients’ mean BMI decreased from 29.6 to 25.1 kg/m2
Table 2
METABOLIC EFFECTS OF ORAL ANTIHYPERGLYCEMIC DRUGS
| Class | Body weight | Total cholesterol | LDL | HDL | Triglycerides |
|---|---|---|---|---|---|
| Sulfonylureas Glipizide Glyburide Glimepiride | ▲ | ◄► | ◄► | ◄► | ◄► |
| Meglitinides Repaglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Phenylalanine derivatives Nateglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Biguanides Metformin | ▼ | ▼ | ▼ | ▲ | ▼ |
| Thiazolidinediones Pioglitazone Rosiglitazone | ▲ | ▲ | ▲ | ▲ | ▼ |
| Alpha-glucosidase inhibitors Acarbose Miglitol | ◄► | ◄► | ◄► | ◄► | ◄► |
| ▲ Increase ▼ Decrease ◄► Neutral effect/no change | |||||
Weight management program The Weight Watchers weight management program has shown mild success when offered to men and women with schizophrenia or schizoaffective disorder. Twenty-one patients who had gained an average of 32 lbs while taking olanzapine were enrolled in a Weight Watchers program at a psychiatric center.14 Mean starting BMI was 32 kg/m2 among the 11 patients who completed the 10-week program. Those 11 lost an average of 5 lbs.
All seven men lost weight. Three of the four women gained weight, and one woman lost 13 lbs. Study subjects remained clinically stable during the 10-week study. Two of the three women who did not lose weight had disabling psychiatric symptoms. Participation rates were similar to those of typical Weight Watchers clientele, suggesting that patients requiring antipsychotics might benefit from treatments used for other obese patients.
Patient education Educating patients about nutrition and exercise may help them control their rate of weight gain during antipsychotic therapy.
Littrell et al provided such an educational program for 1 hour per week for 4 months to six men and six women taking olanzapine for schizophrenia or schizoaffective disorder.15 Patients in the behavioral group gained 0.5 kg, compared with a control group that gained 2.9 kg. Mean increase in BMI was less for the behavioral group (0.3 kg/m2) than for the control patients (0.9 kg/m2). Men in both groups gained more weight than did women.
Pharmacologic approaches
Antiobesity medications are generally reserved for patients with a BMI 30 kg/m2 (threshold for obesity) or for those with a BMI 27 kg/m2 (threshold for overweight is 25 kg/m2) who have additional risk factors for cardiovascular disease, stroke, or diabetes.16
For patients with schizophrenia, who typically have a BMI 27 kg/m2, the presence of these risk factors alone may be enough to warrant consideration of an antiobesity agent. Adding any new drug to a patient’s regimen, however, increases the risk of an adverse interaction.
Antiobesity drugs work by a variety of mechanisms, including decreasing appetite, decreasing fat absorption, and increasing energy expenditure. Drugs may reduce caloric intake by decreasing appetite (anorectic drugs) or increasing satiety (appetite suppressants). Centrally-acting sympathomimetics or serotonergic drugs may suppress appetite.
In studies up to 2 years, the appetite suppressant sibutramine, with mixed serotonergic and noradrenergic reuptake inhibition properties, has been shown to cause more weight loss than a placebo in populations without schizophrenia.17 According to one case report, sibutramine use was associated with new-onset psychosis.18
Common side effects of sibutramine include headache, dry mouth, anorexia, constipation, and insomnia. Regular monitoring of blood pressure is required. Do not prescribe this drug for patients with cardiovascular disease, and avoid co-prescribing with MAO inhibitors and serotonergics.

Orlistat reduces fat absorption from the GI tract.19 Common side effects are largely confined to the GI tract and include oily spotting, flatulence, fecal urgency, fatty/oily stool, and oily evacuation.
Combination therapies
Researchers are studying whether adding adjunctive agents to antipsychotics reduces weight gain.
Clozapine plus quetiapine A group of 65 patients who experienced a mean body weight increase of 6.5 kg while taking clozapine for 6 months were then given clozapine plus quetiapine at chlorpromazine-equivalent dosing during the next 10 months. The patients lost a mean of 4.2 kg, and their glycemic control improved. Elevated glycosylated hemoglobin (HbA1c) became normal in those subjects (20% of participants) who had developed type 2 diabetes while taking clozapine alone. The authors theorized that the weight loss diminished insulin resistance, leading to better control of serum glucose levels.20
Olanzapine plus amantadine A group of 12 outpatients with axis I or II diagnoses had responded well clinically to olanzapine but had gained an average 7.3 kg over 1 to 11 months. In an open-label study, they continued their dosages of olanzapine and also were given amantadine, 100 to 300 mg/d. Amantadine was chosen for this trial because of its possible release of dopamine.
No dietary changes were made, but subjects gained no additional weight after amantadine was added. Over the next 3 to 6 months, they lost a mean 3.5 kg, which was 50% of the weight gain associated with olanzapine administration.21
Clozapine plus topiramate In clinical trials, the anticonvulsant topiramate has been associated with significant weight loss for up to 12 months in patients with seizure disorders.22 This agent, which also has mood-stabilizing effects, may be useful both for mood stabilization and weight loss in tandem with antipsychotic therapy.
In a case study,23 a 29-year-old man with schizophrenia who failed several trials of antipsychotic drugs experienced significant improvement with clozapine, 800 mg/d. Over 2 years, however, he developed myoclonic jerks and gained 45.5 kg (a 49% increase over baseline). When topiramate was added, starting with 25 mg/d and increasing to 125 mg/d, his mood improved and the myoclonic jerks stopped. During 5 months of combination therapy, the patient lost 21 kg without changing his eating habits.
Olanzapine and nizatidine Agents that block histamine (H 2) receptors in the digestive tract may be associated with weight loss when given at high doses, although the mechanism by which they contribute to weight loss is unclear. In a double-blind, placebo-controlled study,24 the H 2 blocker nizatidine was given to patients with schizophrenia who were taking olanzapine, 5 to 20 mg/d. In a 16-week trial, 132 patients were randomized to receive adjunctive treatment with low-dose nizatidine (150 mg bid), high-dose nizatidine (300 mg bid), or a placebo.
After 16 weeks, nizatidine demonstrated a dose-response effect when combined with olanzapine. Average weight gain was:
- 5.51 kg with a placebo
- 4.41 kg with low-dose nizatidine
- 2.76 kg with high-dose nizatidine (p =0.02 compared with a placebo).
In the high-dose nizatidine group, only 6% of patients gained more than 10 kg, and weight gain leveled off by week eight. Adverse events and clinical improvements were similar in the three groups.
Related resources
- Weight gain: A growing problem in schizophrenia management. J Clin Psychiatry 2001;62(suppl 7).
- Weight gain associated with the use of psychotropic medications. J Clin Psychiatry 1999;60(suppl 2).
- Effects of atypical antipsychotics on body weight and glucose regulation. J Clin Psychiatry 2001;62(suppl 23).
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
Drug brand names
- Amantadine • Symmetrel
- Clozapine • Clozaril
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Orlistat • Xenical
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sibutramine • Meridia
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
1. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-1200.
2. Dixon L, Weiden P, Delahanty J, et al. Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 2000;26:903-12.
3. Braceland FJ, Meduna LJ, Vaichulis JA. Delayed action of insulin in schizophrenia. Am J Psychiatry 1945;102:108-10.
4. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
5. Brecher M, Rak IW, Westhead EK. The long-term effect of quetiapine (“Seroquel’) monotherapy on weight in patients with schizophrenia. Int J Psychiatry Clin Pract 2000;4:287-92.
6. Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshiminarayanan M. Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 2001;101:277-88.
7. Theonnard-Neumann E. Phenothiazines and diabetes in hospitalized women. Am J Psychiatry 1968;124:978-82.
8. Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. Am J Med 2001;111:716-23.
9. Pendergrass ML. Pathophysiology and management of type 2 diabetes. In: Giles TD, Sowers JR, Weber MA (eds). Diabetes & cardiovascular disease: a practical primer. New Orleans: Institute of Professional Education, 2000;15-40.
10. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults. Findings from the Third National Health and Nutrition Examination Survey. JAMA 2002;287:356-9.
11. Vieweg WVR, Leadbetter RA. The polydipsia-hyponatremia syndrome. Epidemiology, clinical features, and treatment. CNS Drugs 1997;7:121-38.
12. Thomas PR. Weighing the options: criteria for evaluating weight management programs. Washington, DC: National Academy Press, 1995.
13. Umbricht D, Flury H, Bridler R. Cognitive behavioral therapy for weight gain. Am J Psychiatry 2001;158:971.-
14. Ball M, Coons V, Buchanan R. A program for treating olanzapine-related weight gain. Psychiatric Services 2001;52:967-9.
15. Littrell KH, Petty RG, Hilligoss NM, Peabody CD, Johnson CG. Educational interventions for the management of antipsychotic-related weight gain. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31, 2001.
16. Greenberg I, Chan S, Blackburn GL. Nonpharmacologic and pharmacologic management of weight gain. J Clin Psychiatry 1999;60(suppl 21):31-6.
17. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized controlled trial. JAMA 2001;286:1331-9.
18. Taflinski T, Chojnacka J. Sibutramine-associated psychotic episode. Am J Psychiatry 2001;157:2057-8.
19. Glazer G. Long-term pharmacotherapy of obesity 2000. Arch Intern Med 2001;161:1814-24.
20. Reinstein M, Sirotovskaya L, Jones L. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18:99-104.
21. Floris M, Lejeune J, Deberdt W. Effect of amantadine on weight gain during olanzapine treatment. Eur Neuropsychopharmacol 2001;11:181-2.
22. Norton J, Potter D, Edwards K. Sustained weight loss associated with topiramate [abstract]. Epilepsia 1997;38(suppl 3):60.-
23. Dursun SM, Devarajan S. Clozapine weight gain, plus topiramate weight loss. Can J Psychiatry 2000;45:198.-
24. Breier A, Tanaka Y, Roychowdhury S, Clark WS. Nizatidine for the prevention of olanzapine-associated weight gain in schizophrenia and related disorders. A randomized controlled double blind study. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31 2001.
Weight gain is a potential problem for all patients who require treatment with antipsychotics. Those with schizophrenia face double jeopardy. Both the disorder and the use of virtually any available antipsychotic drug may be associated with weight gain, new-onset glucose intolerance, and type 2 diabetes mellitus.
Because of the cardiovascular risks and other morbidity associated with weight gain and glucose dysregulation,1 the psychiatrist must remain vigilant and manage these complications aggressively. In this article, we offer insights into the prevention and management of metabolic complications associated with the use of antipsychotic agents in patients with schizophrenia.
Weight gain and antipsychotics
Weight change was recognized as a feature of schizophrenia even before antipsychotic drugs were introduced in the 1950s.2 Schizophrenia—independent of drug treatment—also is a risk factor for the development of type 2 diabetes. In persons with schizophrenia, serum glucose levels increase more slowly, decline more gradually, and represent higher-than-normal reference values.3
Figure 1 WEIGHT GAIN ASSOCIATED WITH ANTIPSYCHOTIC DRUG ADMINISTRATION
Values represent estimates of drug-induced weight gain after 10 weeks of drug administration.
Source: Allison et al. Am J Psychiatry 1999;156:1686-96; Brecher et al. Int J Psychiatry Clin Pract 2000;4:287-92.In 1999, Allison et al assessed the effects of conventional and atypical antipsychotics on body weight. Using 81 published articles, they estimated and compared weight changes associated with 10 antipsychotic agents and a placebo when given at standard dosages for 10 weeks.4 Comparative data on quetiapine, which were insufficient in 1999, have since been added (Figure 1).5
Patients who received a placebo lost 0.74 kg across 10 weeks. Weight changes with the conventional agents ranged from a reduction of 0.39 kg with molindone to an increase of 3.19 kg with thioridazine. Weight gains also were seen with all of the newer atypical agents, including clozapine (+4.45 kg), olanzapine (+4.15 kg), risperidone (+2.10 kg), and ziprasidone (+0.04 kg).
Fontaine et al have estimated that weight gain in patients with schizophrenia has its greatest impact on mortality in two scenarios:
- when patients are overweight before they start antipsychotic medication
- with greater degrees of weight gain across 10 years (Figure 2).
Whatever a patient’s starting weight, substantial weight gain with antipsychotic therapy increases the risk of impaired glucose tolerance and hypertension (Figure 3).6
Schizophrenia and diabetes
The prevalence of type 2 diabetes in patients with schizophrenia increased from 4.2% in 1956 to 17.2% in 1968, related in part to the introduction of phenothiazines.7 A recent study of data collected by the Schizophrenia Patient Outcomes Research Team (PORT)2 found higher rates of diabetes in persons with schizophrenia (lifetime prevalence, 14.9%) than in the general population (approximately 7.3%).1 Most patients in the PORT study were taking older antipsychotics, the use of which has occasionally been associated with carbohydrate dysregulation.
Figure 2 INCREASED MORTALITY ASSOCIATED WITH WEIGHT GAIN
Number of deaths associated with weight gains of 2.5 and 12 kg over 10 years, as related to all body mass index measurements (BMIs) and BMIs >27 (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.The prevalence of new-onset diabetes with use of specific antipsychotics is unknown. Most information is contained in case reports, and proper epidemiologic studies await publication.
The most detailed report—a pooled study of published cases related to clozapine use—comes from the FDA’s Center for Drug Evaluation and Research.8 In this study, the authors identified 384 reports of diabetes that developed (in 242 patients) or was exacerbated (in 54 patients) in association with clozapine. Patient mean age was 40, and diabetes occurred more commonly in women than in men.
Diabetes developed most commonly within 6 months of starting treatment with clozapine, and one patient developed diabetes after a single 500-mg dose. Metabolic acidosis or ketosis occurred in 80 cases, and 25 subjects died during hyperglycemic episodes. Stopping clozapine or reducing the dosage improved glycemic control in 46 patients.8
Figure 3 INCREASED MORBIDITY ASSOCIATED WITH WEIGHT GAIN
New cases of impaired glucose tolerance and hypertension that developed with weight gains of 2.5 and 12 kg over 10 years (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.During antipsychotic therapy, it is important to measure patients’ fasting plasma glucose at least annually—and more often for high-risk patients (Table 1). The American Diabetes Association defines diabetes as a fasting serum or plasma glucose 126 mg/dl or a 2-hour postprandial serum or plasma glucose 200 mg/dl. In all patients, these tests should be repeated to confirm the diagnosis. Oral glucose tolerance testing is less convenient than fasting plasma glucose testing but more sensitive in identifying changes in carbohydrate metabolism.
As with weight gain, it is easier to prevent diabetes than to treat it. The psychiatrist can best help the patient with emerging carbohydrate dysregulation by collaborating with an internist, family physician, or endocrinologist.
Table 1
FACTORS RELATED TO HIGH RISK OF DEVELOPING TYPE 2 DIABETES
|
| Source: American Diabetes Association |
Weight gain with diabetes drugs Weight gain is associated not only with the use of antipsychotics but also with four classes of oral agents used to treat type 2 diabetes: sulfonylureas, meglitinides, phenylalanine derivatives, and thiazolidinediones. One class—biguanides—contributes to weight reduction, and one—alpha-glucosidase inhibitors—has a variable effect on body weight. These drugs also vary in their effects on serum lipids, including total cholesterol, LDL and HDL cholesterol, and triglycerides (Table 2).9
Many patients with type 2 diabetes require more than one agent to control plasma glucose. With time, insulin deficiency becomes more marked, and insulin therapy is frequently added to the regimen. Hypertension and hyperlipidemia are also very common in patients with type 2 diabetes and require medication to reduce the risk of cardiovascular events.10 As a result, the diabetic patient requiring antipsychotic drugs will likely need polypharmacy, and many of the drugs that might be used may lead to weight gain.
Assessing, managing weight gain
During each visit for the patient with schizophrenia, it is important to routinely weigh those receiving antipsychotics and ask about polydipsia and polyuria, which are early signs of incipient diabetes. A patient who is gaining significant weight (7% of baseline) while taking an antipsychotic and has risk factors for cardiovascular events (e.g., smoking, hypertension, hypertriglyceridemia) is a candidate for a change in antipsychotics.
Try to weigh patients at approximately the same time of day at each visit to compensate for possible diurnal weight changes related to polydipsia-hyponatremia syndrome.11 Patients with this syndrome can gain 5 to 10 lbs (or more) per day and excrete the retained fluid at night. It occurs in 5 to 10% of chronically psychotic patients requiring institutional care and in 1 to 2% of outpatients. Patients with schizophrenia complicated by this syndrome may manifest polydipsia and polyuria secondary to psychosis rather than emerging diabetes. Thus, the clinician must be alert to both diabetes and the polydipsia-hyponatremia syndrome in this setting.
Weight-control approaches
Patients who are taking sedating antipsychotics (e.g., clozapine, olanzapine, or low-potency phenothiazines) may gain up to 30 lbs per year if they become physically inactive and do not reduce their food consumption. Thus, it is important to work with such patients to decrease their caloric intake.
A weight-loss program that produces a loss of 0.5 to 1% of body weight per week is considered safe and acceptable.12 Mild to moderate obesity may be managed by reducing food intake by 500 calories and exercising 30 minutes each day.
CBT Cognitive-behavioral therapy (CBT) may help stem weight gain associated with antipsychotic use. Umbricht et al provided CBT to six patients with chronic psychosis who were receiving clozapine or olanzapine. Therapists in group and individual sessions focused on the causes of weight gain, lowcalorie nutrition, weight-loss guidelines, exercise programs, and relaxation strategies. Across 8 weeks, patients’ mean BMI decreased from 29.6 to 25.1 kg/m2
Table 2
METABOLIC EFFECTS OF ORAL ANTIHYPERGLYCEMIC DRUGS
| Class | Body weight | Total cholesterol | LDL | HDL | Triglycerides |
|---|---|---|---|---|---|
| Sulfonylureas Glipizide Glyburide Glimepiride | ▲ | ◄► | ◄► | ◄► | ◄► |
| Meglitinides Repaglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Phenylalanine derivatives Nateglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Biguanides Metformin | ▼ | ▼ | ▼ | ▲ | ▼ |
| Thiazolidinediones Pioglitazone Rosiglitazone | ▲ | ▲ | ▲ | ▲ | ▼ |
| Alpha-glucosidase inhibitors Acarbose Miglitol | ◄► | ◄► | ◄► | ◄► | ◄► |
| ▲ Increase ▼ Decrease ◄► Neutral effect/no change | |||||
Weight management program The Weight Watchers weight management program has shown mild success when offered to men and women with schizophrenia or schizoaffective disorder. Twenty-one patients who had gained an average of 32 lbs while taking olanzapine were enrolled in a Weight Watchers program at a psychiatric center.14 Mean starting BMI was 32 kg/m2 among the 11 patients who completed the 10-week program. Those 11 lost an average of 5 lbs.
All seven men lost weight. Three of the four women gained weight, and one woman lost 13 lbs. Study subjects remained clinically stable during the 10-week study. Two of the three women who did not lose weight had disabling psychiatric symptoms. Participation rates were similar to those of typical Weight Watchers clientele, suggesting that patients requiring antipsychotics might benefit from treatments used for other obese patients.
Patient education Educating patients about nutrition and exercise may help them control their rate of weight gain during antipsychotic therapy.
Littrell et al provided such an educational program for 1 hour per week for 4 months to six men and six women taking olanzapine for schizophrenia or schizoaffective disorder.15 Patients in the behavioral group gained 0.5 kg, compared with a control group that gained 2.9 kg. Mean increase in BMI was less for the behavioral group (0.3 kg/m2) than for the control patients (0.9 kg/m2). Men in both groups gained more weight than did women.
Pharmacologic approaches
Antiobesity medications are generally reserved for patients with a BMI 30 kg/m2 (threshold for obesity) or for those with a BMI 27 kg/m2 (threshold for overweight is 25 kg/m2) who have additional risk factors for cardiovascular disease, stroke, or diabetes.16
For patients with schizophrenia, who typically have a BMI 27 kg/m2, the presence of these risk factors alone may be enough to warrant consideration of an antiobesity agent. Adding any new drug to a patient’s regimen, however, increases the risk of an adverse interaction.
Antiobesity drugs work by a variety of mechanisms, including decreasing appetite, decreasing fat absorption, and increasing energy expenditure. Drugs may reduce caloric intake by decreasing appetite (anorectic drugs) or increasing satiety (appetite suppressants). Centrally-acting sympathomimetics or serotonergic drugs may suppress appetite.
In studies up to 2 years, the appetite suppressant sibutramine, with mixed serotonergic and noradrenergic reuptake inhibition properties, has been shown to cause more weight loss than a placebo in populations without schizophrenia.17 According to one case report, sibutramine use was associated with new-onset psychosis.18
Common side effects of sibutramine include headache, dry mouth, anorexia, constipation, and insomnia. Regular monitoring of blood pressure is required. Do not prescribe this drug for patients with cardiovascular disease, and avoid co-prescribing with MAO inhibitors and serotonergics.
Orlistat reduces fat absorption from the GI tract.19 Common side effects are largely confined to the GI tract and include oily spotting, flatulence, fecal urgency, fatty/oily stool, and oily evacuation.
Combination therapies
Researchers are studying whether adding adjunctive agents to antipsychotics reduces weight gain.
Clozapine plus quetiapine A group of 65 patients who experienced a mean body weight increase of 6.5 kg while taking clozapine for 6 months were then given clozapine plus quetiapine at chlorpromazine-equivalent dosing during the next 10 months. The patients lost a mean of 4.2 kg, and their glycemic control improved. Elevated glycosylated hemoglobin (HbA1c) became normal in those subjects (20% of participants) who had developed type 2 diabetes while taking clozapine alone. The authors theorized that the weight loss diminished insulin resistance, leading to better control of serum glucose levels.20
Olanzapine plus amantadine A group of 12 outpatients with axis I or II diagnoses had responded well clinically to olanzapine but had gained an average 7.3 kg over 1 to 11 months. In an open-label study, they continued their dosages of olanzapine and also were given amantadine, 100 to 300 mg/d. Amantadine was chosen for this trial because of its possible release of dopamine.
No dietary changes were made, but subjects gained no additional weight after amantadine was added. Over the next 3 to 6 months, they lost a mean 3.5 kg, which was 50% of the weight gain associated with olanzapine administration.21
Clozapine plus topiramate In clinical trials, the anticonvulsant topiramate has been associated with significant weight loss for up to 12 months in patients with seizure disorders.22 This agent, which also has mood-stabilizing effects, may be useful both for mood stabilization and weight loss in tandem with antipsychotic therapy.
In a case study,23 a 29-year-old man with schizophrenia who failed several trials of antipsychotic drugs experienced significant improvement with clozapine, 800 mg/d. Over 2 years, however, he developed myoclonic jerks and gained 45.5 kg (a 49% increase over baseline). When topiramate was added, starting with 25 mg/d and increasing to 125 mg/d, his mood improved and the myoclonic jerks stopped. During 5 months of combination therapy, the patient lost 21 kg without changing his eating habits.
Olanzapine and nizatidine Agents that block histamine (H 2) receptors in the digestive tract may be associated with weight loss when given at high doses, although the mechanism by which they contribute to weight loss is unclear. In a double-blind, placebo-controlled study,24 the H 2 blocker nizatidine was given to patients with schizophrenia who were taking olanzapine, 5 to 20 mg/d. In a 16-week trial, 132 patients were randomized to receive adjunctive treatment with low-dose nizatidine (150 mg bid), high-dose nizatidine (300 mg bid), or a placebo.
After 16 weeks, nizatidine demonstrated a dose-response effect when combined with olanzapine. Average weight gain was:
- 5.51 kg with a placebo
- 4.41 kg with low-dose nizatidine
- 2.76 kg with high-dose nizatidine (p =0.02 compared with a placebo).
In the high-dose nizatidine group, only 6% of patients gained more than 10 kg, and weight gain leveled off by week eight. Adverse events and clinical improvements were similar in the three groups.
Related resources
- Weight gain: A growing problem in schizophrenia management. J Clin Psychiatry 2001;62(suppl 7).
- Weight gain associated with the use of psychotropic medications. J Clin Psychiatry 1999;60(suppl 2).
- Effects of atypical antipsychotics on body weight and glucose regulation. J Clin Psychiatry 2001;62(suppl 23).
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
Drug brand names
- Amantadine • Symmetrel
- Clozapine • Clozaril
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Orlistat • Xenical
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sibutramine • Meridia
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
Weight gain is a potential problem for all patients who require treatment with antipsychotics. Those with schizophrenia face double jeopardy. Both the disorder and the use of virtually any available antipsychotic drug may be associated with weight gain, new-onset glucose intolerance, and type 2 diabetes mellitus.
Because of the cardiovascular risks and other morbidity associated with weight gain and glucose dysregulation,1 the psychiatrist must remain vigilant and manage these complications aggressively. In this article, we offer insights into the prevention and management of metabolic complications associated with the use of antipsychotic agents in patients with schizophrenia.
Weight gain and antipsychotics
Weight change was recognized as a feature of schizophrenia even before antipsychotic drugs were introduced in the 1950s.2 Schizophrenia—independent of drug treatment—also is a risk factor for the development of type 2 diabetes. In persons with schizophrenia, serum glucose levels increase more slowly, decline more gradually, and represent higher-than-normal reference values.3
Figure 1 WEIGHT GAIN ASSOCIATED WITH ANTIPSYCHOTIC DRUG ADMINISTRATION
Values represent estimates of drug-induced weight gain after 10 weeks of drug administration.
Source: Allison et al. Am J Psychiatry 1999;156:1686-96; Brecher et al. Int J Psychiatry Clin Pract 2000;4:287-92.In 1999, Allison et al assessed the effects of conventional and atypical antipsychotics on body weight. Using 81 published articles, they estimated and compared weight changes associated with 10 antipsychotic agents and a placebo when given at standard dosages for 10 weeks.4 Comparative data on quetiapine, which were insufficient in 1999, have since been added (Figure 1).5
Patients who received a placebo lost 0.74 kg across 10 weeks. Weight changes with the conventional agents ranged from a reduction of 0.39 kg with molindone to an increase of 3.19 kg with thioridazine. Weight gains also were seen with all of the newer atypical agents, including clozapine (+4.45 kg), olanzapine (+4.15 kg), risperidone (+2.10 kg), and ziprasidone (+0.04 kg).
Fontaine et al have estimated that weight gain in patients with schizophrenia has its greatest impact on mortality in two scenarios:
- when patients are overweight before they start antipsychotic medication
- with greater degrees of weight gain across 10 years (Figure 2).
Whatever a patient’s starting weight, substantial weight gain with antipsychotic therapy increases the risk of impaired glucose tolerance and hypertension (Figure 3).6
Schizophrenia and diabetes
The prevalence of type 2 diabetes in patients with schizophrenia increased from 4.2% in 1956 to 17.2% in 1968, related in part to the introduction of phenothiazines.7 A recent study of data collected by the Schizophrenia Patient Outcomes Research Team (PORT)2 found higher rates of diabetes in persons with schizophrenia (lifetime prevalence, 14.9%) than in the general population (approximately 7.3%).1 Most patients in the PORT study were taking older antipsychotics, the use of which has occasionally been associated with carbohydrate dysregulation.
Figure 2 INCREASED MORTALITY ASSOCIATED WITH WEIGHT GAIN
Number of deaths associated with weight gains of 2.5 and 12 kg over 10 years, as related to all body mass index measurements (BMIs) and BMIs >27 (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.The prevalence of new-onset diabetes with use of specific antipsychotics is unknown. Most information is contained in case reports, and proper epidemiologic studies await publication.
The most detailed report—a pooled study of published cases related to clozapine use—comes from the FDA’s Center for Drug Evaluation and Research.8 In this study, the authors identified 384 reports of diabetes that developed (in 242 patients) or was exacerbated (in 54 patients) in association with clozapine. Patient mean age was 40, and diabetes occurred more commonly in women than in men.
Diabetes developed most commonly within 6 months of starting treatment with clozapine, and one patient developed diabetes after a single 500-mg dose. Metabolic acidosis or ketosis occurred in 80 cases, and 25 subjects died during hyperglycemic episodes. Stopping clozapine or reducing the dosage improved glycemic control in 46 patients.8
Figure 3 INCREASED MORBIDITY ASSOCIATED WITH WEIGHT GAIN
New cases of impaired glucose tolerance and hypertension that developed with weight gains of 2.5 and 12 kg over 10 years (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.During antipsychotic therapy, it is important to measure patients’ fasting plasma glucose at least annually—and more often for high-risk patients (Table 1). The American Diabetes Association defines diabetes as a fasting serum or plasma glucose 126 mg/dl or a 2-hour postprandial serum or plasma glucose 200 mg/dl. In all patients, these tests should be repeated to confirm the diagnosis. Oral glucose tolerance testing is less convenient than fasting plasma glucose testing but more sensitive in identifying changes in carbohydrate metabolism.
As with weight gain, it is easier to prevent diabetes than to treat it. The psychiatrist can best help the patient with emerging carbohydrate dysregulation by collaborating with an internist, family physician, or endocrinologist.
Table 1
FACTORS RELATED TO HIGH RISK OF DEVELOPING TYPE 2 DIABETES
|
| Source: American Diabetes Association |
Weight gain with diabetes drugs Weight gain is associated not only with the use of antipsychotics but also with four classes of oral agents used to treat type 2 diabetes: sulfonylureas, meglitinides, phenylalanine derivatives, and thiazolidinediones. One class—biguanides—contributes to weight reduction, and one—alpha-glucosidase inhibitors—has a variable effect on body weight. These drugs also vary in their effects on serum lipids, including total cholesterol, LDL and HDL cholesterol, and triglycerides (Table 2).9
Many patients with type 2 diabetes require more than one agent to control plasma glucose. With time, insulin deficiency becomes more marked, and insulin therapy is frequently added to the regimen. Hypertension and hyperlipidemia are also very common in patients with type 2 diabetes and require medication to reduce the risk of cardiovascular events.10 As a result, the diabetic patient requiring antipsychotic drugs will likely need polypharmacy, and many of the drugs that might be used may lead to weight gain.
Assessing, managing weight gain
During each visit for the patient with schizophrenia, it is important to routinely weigh those receiving antipsychotics and ask about polydipsia and polyuria, which are early signs of incipient diabetes. A patient who is gaining significant weight (7% of baseline) while taking an antipsychotic and has risk factors for cardiovascular events (e.g., smoking, hypertension, hypertriglyceridemia) is a candidate for a change in antipsychotics.
Try to weigh patients at approximately the same time of day at each visit to compensate for possible diurnal weight changes related to polydipsia-hyponatremia syndrome.11 Patients with this syndrome can gain 5 to 10 lbs (or more) per day and excrete the retained fluid at night. It occurs in 5 to 10% of chronically psychotic patients requiring institutional care and in 1 to 2% of outpatients. Patients with schizophrenia complicated by this syndrome may manifest polydipsia and polyuria secondary to psychosis rather than emerging diabetes. Thus, the clinician must be alert to both diabetes and the polydipsia-hyponatremia syndrome in this setting.
Weight-control approaches
Patients who are taking sedating antipsychotics (e.g., clozapine, olanzapine, or low-potency phenothiazines) may gain up to 30 lbs per year if they become physically inactive and do not reduce their food consumption. Thus, it is important to work with such patients to decrease their caloric intake.
A weight-loss program that produces a loss of 0.5 to 1% of body weight per week is considered safe and acceptable.12 Mild to moderate obesity may be managed by reducing food intake by 500 calories and exercising 30 minutes each day.
CBT Cognitive-behavioral therapy (CBT) may help stem weight gain associated with antipsychotic use. Umbricht et al provided CBT to six patients with chronic psychosis who were receiving clozapine or olanzapine. Therapists in group and individual sessions focused on the causes of weight gain, lowcalorie nutrition, weight-loss guidelines, exercise programs, and relaxation strategies. Across 8 weeks, patients’ mean BMI decreased from 29.6 to 25.1 kg/m2
Table 2
METABOLIC EFFECTS OF ORAL ANTIHYPERGLYCEMIC DRUGS
| Class | Body weight | Total cholesterol | LDL | HDL | Triglycerides |
|---|---|---|---|---|---|
| Sulfonylureas Glipizide Glyburide Glimepiride | ▲ | ◄► | ◄► | ◄► | ◄► |
| Meglitinides Repaglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Phenylalanine derivatives Nateglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Biguanides Metformin | ▼ | ▼ | ▼ | ▲ | ▼ |
| Thiazolidinediones Pioglitazone Rosiglitazone | ▲ | ▲ | ▲ | ▲ | ▼ |
| Alpha-glucosidase inhibitors Acarbose Miglitol | ◄► | ◄► | ◄► | ◄► | ◄► |
| ▲ Increase ▼ Decrease ◄► Neutral effect/no change | |||||
Weight management program The Weight Watchers weight management program has shown mild success when offered to men and women with schizophrenia or schizoaffective disorder. Twenty-one patients who had gained an average of 32 lbs while taking olanzapine were enrolled in a Weight Watchers program at a psychiatric center.14 Mean starting BMI was 32 kg/m2 among the 11 patients who completed the 10-week program. Those 11 lost an average of 5 lbs.
All seven men lost weight. Three of the four women gained weight, and one woman lost 13 lbs. Study subjects remained clinically stable during the 10-week study. Two of the three women who did not lose weight had disabling psychiatric symptoms. Participation rates were similar to those of typical Weight Watchers clientele, suggesting that patients requiring antipsychotics might benefit from treatments used for other obese patients.
Patient education Educating patients about nutrition and exercise may help them control their rate of weight gain during antipsychotic therapy.
Littrell et al provided such an educational program for 1 hour per week for 4 months to six men and six women taking olanzapine for schizophrenia or schizoaffective disorder.15 Patients in the behavioral group gained 0.5 kg, compared with a control group that gained 2.9 kg. Mean increase in BMI was less for the behavioral group (0.3 kg/m2) than for the control patients (0.9 kg/m2). Men in both groups gained more weight than did women.
Pharmacologic approaches
Antiobesity medications are generally reserved for patients with a BMI 30 kg/m2 (threshold for obesity) or for those with a BMI 27 kg/m2 (threshold for overweight is 25 kg/m2) who have additional risk factors for cardiovascular disease, stroke, or diabetes.16
For patients with schizophrenia, who typically have a BMI 27 kg/m2, the presence of these risk factors alone may be enough to warrant consideration of an antiobesity agent. Adding any new drug to a patient’s regimen, however, increases the risk of an adverse interaction.
Antiobesity drugs work by a variety of mechanisms, including decreasing appetite, decreasing fat absorption, and increasing energy expenditure. Drugs may reduce caloric intake by decreasing appetite (anorectic drugs) or increasing satiety (appetite suppressants). Centrally-acting sympathomimetics or serotonergic drugs may suppress appetite.
In studies up to 2 years, the appetite suppressant sibutramine, with mixed serotonergic and noradrenergic reuptake inhibition properties, has been shown to cause more weight loss than a placebo in populations without schizophrenia.17 According to one case report, sibutramine use was associated with new-onset psychosis.18
Common side effects of sibutramine include headache, dry mouth, anorexia, constipation, and insomnia. Regular monitoring of blood pressure is required. Do not prescribe this drug for patients with cardiovascular disease, and avoid co-prescribing with MAO inhibitors and serotonergics.
Orlistat reduces fat absorption from the GI tract.19 Common side effects are largely confined to the GI tract and include oily spotting, flatulence, fecal urgency, fatty/oily stool, and oily evacuation.
Combination therapies
Researchers are studying whether adding adjunctive agents to antipsychotics reduces weight gain.
Clozapine plus quetiapine A group of 65 patients who experienced a mean body weight increase of 6.5 kg while taking clozapine for 6 months were then given clozapine plus quetiapine at chlorpromazine-equivalent dosing during the next 10 months. The patients lost a mean of 4.2 kg, and their glycemic control improved. Elevated glycosylated hemoglobin (HbA1c) became normal in those subjects (20% of participants) who had developed type 2 diabetes while taking clozapine alone. The authors theorized that the weight loss diminished insulin resistance, leading to better control of serum glucose levels.20
Olanzapine plus amantadine A group of 12 outpatients with axis I or II diagnoses had responded well clinically to olanzapine but had gained an average 7.3 kg over 1 to 11 months. In an open-label study, they continued their dosages of olanzapine and also were given amantadine, 100 to 300 mg/d. Amantadine was chosen for this trial because of its possible release of dopamine.
No dietary changes were made, but subjects gained no additional weight after amantadine was added. Over the next 3 to 6 months, they lost a mean 3.5 kg, which was 50% of the weight gain associated with olanzapine administration.21
Clozapine plus topiramate In clinical trials, the anticonvulsant topiramate has been associated with significant weight loss for up to 12 months in patients with seizure disorders.22 This agent, which also has mood-stabilizing effects, may be useful both for mood stabilization and weight loss in tandem with antipsychotic therapy.
In a case study,23 a 29-year-old man with schizophrenia who failed several trials of antipsychotic drugs experienced significant improvement with clozapine, 800 mg/d. Over 2 years, however, he developed myoclonic jerks and gained 45.5 kg (a 49% increase over baseline). When topiramate was added, starting with 25 mg/d and increasing to 125 mg/d, his mood improved and the myoclonic jerks stopped. During 5 months of combination therapy, the patient lost 21 kg without changing his eating habits.
Olanzapine and nizatidine Agents that block histamine (H 2) receptors in the digestive tract may be associated with weight loss when given at high doses, although the mechanism by which they contribute to weight loss is unclear. In a double-blind, placebo-controlled study,24 the H 2 blocker nizatidine was given to patients with schizophrenia who were taking olanzapine, 5 to 20 mg/d. In a 16-week trial, 132 patients were randomized to receive adjunctive treatment with low-dose nizatidine (150 mg bid), high-dose nizatidine (300 mg bid), or a placebo.
After 16 weeks, nizatidine demonstrated a dose-response effect when combined with olanzapine. Average weight gain was:
- 5.51 kg with a placebo
- 4.41 kg with low-dose nizatidine
- 2.76 kg with high-dose nizatidine (p =0.02 compared with a placebo).
In the high-dose nizatidine group, only 6% of patients gained more than 10 kg, and weight gain leveled off by week eight. Adverse events and clinical improvements were similar in the three groups.
Related resources
- Weight gain: A growing problem in schizophrenia management. J Clin Psychiatry 2001;62(suppl 7).
- Weight gain associated with the use of psychotropic medications. J Clin Psychiatry 1999;60(suppl 2).
- Effects of atypical antipsychotics on body weight and glucose regulation. J Clin Psychiatry 2001;62(suppl 23).
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
Drug brand names
- Amantadine • Symmetrel
- Clozapine • Clozaril
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Orlistat • Xenical
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sibutramine • Meridia
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
1. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-1200.
2. Dixon L, Weiden P, Delahanty J, et al. Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 2000;26:903-12.
3. Braceland FJ, Meduna LJ, Vaichulis JA. Delayed action of insulin in schizophrenia. Am J Psychiatry 1945;102:108-10.
4. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
5. Brecher M, Rak IW, Westhead EK. The long-term effect of quetiapine (“Seroquel’) monotherapy on weight in patients with schizophrenia. Int J Psychiatry Clin Pract 2000;4:287-92.
6. Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshiminarayanan M. Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 2001;101:277-88.
7. Theonnard-Neumann E. Phenothiazines and diabetes in hospitalized women. Am J Psychiatry 1968;124:978-82.
8. Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. Am J Med 2001;111:716-23.
9. Pendergrass ML. Pathophysiology and management of type 2 diabetes. In: Giles TD, Sowers JR, Weber MA (eds). Diabetes & cardiovascular disease: a practical primer. New Orleans: Institute of Professional Education, 2000;15-40.
10. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults. Findings from the Third National Health and Nutrition Examination Survey. JAMA 2002;287:356-9.
11. Vieweg WVR, Leadbetter RA. The polydipsia-hyponatremia syndrome. Epidemiology, clinical features, and treatment. CNS Drugs 1997;7:121-38.
12. Thomas PR. Weighing the options: criteria for evaluating weight management programs. Washington, DC: National Academy Press, 1995.
13. Umbricht D, Flury H, Bridler R. Cognitive behavioral therapy for weight gain. Am J Psychiatry 2001;158:971.-
14. Ball M, Coons V, Buchanan R. A program for treating olanzapine-related weight gain. Psychiatric Services 2001;52:967-9.
15. Littrell KH, Petty RG, Hilligoss NM, Peabody CD, Johnson CG. Educational interventions for the management of antipsychotic-related weight gain. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31, 2001.
16. Greenberg I, Chan S, Blackburn GL. Nonpharmacologic and pharmacologic management of weight gain. J Clin Psychiatry 1999;60(suppl 21):31-6.
17. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized controlled trial. JAMA 2001;286:1331-9.
18. Taflinski T, Chojnacka J. Sibutramine-associated psychotic episode. Am J Psychiatry 2001;157:2057-8.
19. Glazer G. Long-term pharmacotherapy of obesity 2000. Arch Intern Med 2001;161:1814-24.
20. Reinstein M, Sirotovskaya L, Jones L. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18:99-104.
21. Floris M, Lejeune J, Deberdt W. Effect of amantadine on weight gain during olanzapine treatment. Eur Neuropsychopharmacol 2001;11:181-2.
22. Norton J, Potter D, Edwards K. Sustained weight loss associated with topiramate [abstract]. Epilepsia 1997;38(suppl 3):60.-
23. Dursun SM, Devarajan S. Clozapine weight gain, plus topiramate weight loss. Can J Psychiatry 2000;45:198.-
24. Breier A, Tanaka Y, Roychowdhury S, Clark WS. Nizatidine for the prevention of olanzapine-associated weight gain in schizophrenia and related disorders. A randomized controlled double blind study. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31 2001.
1. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-1200.
2. Dixon L, Weiden P, Delahanty J, et al. Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 2000;26:903-12.
3. Braceland FJ, Meduna LJ, Vaichulis JA. Delayed action of insulin in schizophrenia. Am J Psychiatry 1945;102:108-10.
4. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
5. Brecher M, Rak IW, Westhead EK. The long-term effect of quetiapine (“Seroquel’) monotherapy on weight in patients with schizophrenia. Int J Psychiatry Clin Pract 2000;4:287-92.
6. Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshiminarayanan M. Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 2001;101:277-88.
7. Theonnard-Neumann E. Phenothiazines and diabetes in hospitalized women. Am J Psychiatry 1968;124:978-82.
8. Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. Am J Med 2001;111:716-23.
9. Pendergrass ML. Pathophysiology and management of type 2 diabetes. In: Giles TD, Sowers JR, Weber MA (eds). Diabetes & cardiovascular disease: a practical primer. New Orleans: Institute of Professional Education, 2000;15-40.
10. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults. Findings from the Third National Health and Nutrition Examination Survey. JAMA 2002;287:356-9.
11. Vieweg WVR, Leadbetter RA. The polydipsia-hyponatremia syndrome. Epidemiology, clinical features, and treatment. CNS Drugs 1997;7:121-38.
12. Thomas PR. Weighing the options: criteria for evaluating weight management programs. Washington, DC: National Academy Press, 1995.
13. Umbricht D, Flury H, Bridler R. Cognitive behavioral therapy for weight gain. Am J Psychiatry 2001;158:971.-
14. Ball M, Coons V, Buchanan R. A program for treating olanzapine-related weight gain. Psychiatric Services 2001;52:967-9.
15. Littrell KH, Petty RG, Hilligoss NM, Peabody CD, Johnson CG. Educational interventions for the management of antipsychotic-related weight gain. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31, 2001.
16. Greenberg I, Chan S, Blackburn GL. Nonpharmacologic and pharmacologic management of weight gain. J Clin Psychiatry 1999;60(suppl 21):31-6.
17. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized controlled trial. JAMA 2001;286:1331-9.
18. Taflinski T, Chojnacka J. Sibutramine-associated psychotic episode. Am J Psychiatry 2001;157:2057-8.
19. Glazer G. Long-term pharmacotherapy of obesity 2000. Arch Intern Med 2001;161:1814-24.
20. Reinstein M, Sirotovskaya L, Jones L. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18:99-104.
21. Floris M, Lejeune J, Deberdt W. Effect of amantadine on weight gain during olanzapine treatment. Eur Neuropsychopharmacol 2001;11:181-2.
22. Norton J, Potter D, Edwards K. Sustained weight loss associated with topiramate [abstract]. Epilepsia 1997;38(suppl 3):60.-
23. Dursun SM, Devarajan S. Clozapine weight gain, plus topiramate weight loss. Can J Psychiatry 2000;45:198.-
24. Breier A, Tanaka Y, Roychowdhury S, Clark WS. Nizatidine for the prevention of olanzapine-associated weight gain in schizophrenia and related disorders. A randomized controlled double blind study. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31 2001.
Weight control and antipsychotics: How to tip the scales away from diabetes and heart disease
Weight gain is a potential problem for all patients who require treatment with antipsychotics. Those with schizophrenia face double jeopardy. Both the disorder and the use of virtually any available antipsychotic drug may be associated with weight gain, new-onset glucose intolerance, and type 2 diabetes mellitus.
Because of the cardiovascular risks and other morbidity associated with weight gain and glucose dysregulation,1 the psychiatrist must remain vigilant and manage these complications aggressively. In this article, we offer insights into the prevention and management of metabolic complications associated with the use of antipsychotic agents in patients with schizophrenia.
Weight gain and antipsychotics
Weight change was recognized as a feature of schizophrenia even before antipsychotic drugs were introduced in the 1950s.2 Schizophrenia—independent of drug treatment—also is a risk factor for the development of type 2 diabetes. In persons with schizophrenia, serum glucose levels increase more slowly, decline more gradually, and represent higher-than-normal reference values.3
Figure 1 WEIGHT GAIN ASSOCIATED WITH ANTIPSYCHOTIC DRUG ADMINISTRATION
Values represent estimates of drug-induced weight gain after 10 weeks of drug administration.
Source: Allison et al. Am J Psychiatry 1999;156:1686-96; Brecher et al. Int J Psychiatry Clin Pract 2000;4:287-92.In 1999, Allison et al assessed the effects of conventional and atypical antipsychotics on body weight. Using 81 published articles, they estimated and compared weight changes associated with 10 antipsychotic agents and a placebo when given at standard dosages for 10 weeks.4 Comparative data on quetiapine, which were insufficient in 1999, have since been added (Figure 1).5
Patients who received a placebo lost 0.74 kg across 10 weeks. Weight changes with the conventional agents ranged from a reduction of 0.39 kg with molindone to an increase of 3.19 kg with thioridazine. Weight gains also were seen with all of the newer atypical agents, including clozapine (+4.45 kg), olanzapine (+4.15 kg), risperidone (+2.10 kg), and ziprasidone (+0.04 kg).
Fontaine et al have estimated that weight gain in patients with schizophrenia has its greatest impact on mortality in two scenarios:
- when patients are overweight before they start antipsychotic medication
- with greater degrees of weight gain across 10 years (Figure 2).
Whatever a patient’s starting weight, substantial weight gain with antipsychotic therapy increases the risk of impaired glucose tolerance and hypertension (Figure 3).6
Schizophrenia and diabetes
The prevalence of type 2 diabetes in patients with schizophrenia increased from 4.2% in 1956 to 17.2% in 1968, related in part to the introduction of phenothiazines.7 A recent study of data collected by the Schizophrenia Patient Outcomes Research Team (PORT)2 found higher rates of diabetes in persons with schizophrenia (lifetime prevalence, 14.9%) than in the general population (approximately 7.3%).1 Most patients in the PORT study were taking older antipsychotics, the use of which has occasionally been associated with carbohydrate dysregulation.
Figure 2 INCREASED MORTALITY ASSOCIATED WITH WEIGHT GAIN
Number of deaths associated with weight gains of 2.5 and 12 kg over 10 years, as related to all body mass index measurements (BMIs) and BMIs >27 (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.The prevalence of new-onset diabetes with use of specific antipsychotics is unknown. Most information is contained in case reports, and proper epidemiologic studies await publication.
The most detailed report—a pooled study of published cases related to clozapine use—comes from the FDA’s Center for Drug Evaluation and Research.8 In this study, the authors identified 384 reports of diabetes that developed (in 242 patients) or was exacerbated (in 54 patients) in association with clozapine. Patient mean age was 40, and diabetes occurred more commonly in women than in men.
Diabetes developed most commonly within 6 months of starting treatment with clozapine, and one patient developed diabetes after a single 500-mg dose. Metabolic acidosis or ketosis occurred in 80 cases, and 25 subjects died during hyperglycemic episodes. Stopping clozapine or reducing the dosage improved glycemic control in 46 patients.8
Figure 3 INCREASED MORBIDITY ASSOCIATED WITH WEIGHT GAIN
New cases of impaired glucose tolerance and hypertension that developed with weight gains of 2.5 and 12 kg over 10 years (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.During antipsychotic therapy, it is important to measure patients’ fasting plasma glucose at least annually—and more often for high-risk patients (Table 1). The American Diabetes Association defines diabetes as a fasting serum or plasma glucose 126 mg/dl or a 2-hour postprandial serum or plasma glucose 200 mg/dl. In all patients, these tests should be repeated to confirm the diagnosis. Oral glucose tolerance testing is less convenient than fasting plasma glucose testing but more sensitive in identifying changes in carbohydrate metabolism.
As with weight gain, it is easier to prevent diabetes than to treat it. The psychiatrist can best help the patient with emerging carbohydrate dysregulation by collaborating with an internist, family physician, or endocrinologist.
Table 1
FACTORS RELATED TO HIGH RISK OF DEVELOPING TYPE 2 DIABETES
|
| Source: American Diabetes Association |
Weight gain with diabetes drugs Weight gain is associated not only with the use of antipsychotics but also with four classes of oral agents used to treat type 2 diabetes: sulfonylureas, meglitinides, phenylalanine derivatives, and thiazolidinediones. One class—biguanides—contributes to weight reduction, and one—alpha-glucosidase inhibitors—has a variable effect on body weight. These drugs also vary in their effects on serum lipids, including total cholesterol, LDL and HDL cholesterol, and triglycerides (Table 2).9
Many patients with type 2 diabetes require more than one agent to control plasma glucose. With time, insulin deficiency becomes more marked, and insulin therapy is frequently added to the regimen. Hypertension and hyperlipidemia are also very common in patients with type 2 diabetes and require medication to reduce the risk of cardiovascular events.10 As a result, the diabetic patient requiring antipsychotic drugs will likely need polypharmacy, and many of the drugs that might be used may lead to weight gain.
Assessing, managing weight gain
During each visit for the patient with schizophrenia, it is important to routinely weigh those receiving antipsychotics and ask about polydipsia and polyuria, which are early signs of incipient diabetes. A patient who is gaining significant weight (7% of baseline) while taking an antipsychotic and has risk factors for cardiovascular events (e.g., smoking, hypertension, hypertriglyceridemia) is a candidate for a change in antipsychotics.
Try to weigh patients at approximately the same time of day at each visit to compensate for possible diurnal weight changes related to polydipsia-hyponatremia syndrome.11 Patients with this syndrome can gain 5 to 10 lbs (or more) per day and excrete the retained fluid at night. It occurs in 5 to 10% of chronically psychotic patients requiring institutional care and in 1 to 2% of outpatients. Patients with schizophrenia complicated by this syndrome may manifest polydipsia and polyuria secondary to psychosis rather than emerging diabetes. Thus, the clinician must be alert to both diabetes and the polydipsia-hyponatremia syndrome in this setting.
Weight-control approaches
Patients who are taking sedating antipsychotics (e.g., clozapine, olanzapine, or low-potency phenothiazines) may gain up to 30 lbs per year if they become physically inactive and do not reduce their food consumption. Thus, it is important to work with such patients to decrease their caloric intake.
A weight-loss program that produces a loss of 0.5 to 1% of body weight per week is considered safe and acceptable.12 Mild to moderate obesity may be managed by reducing food intake by 500 calories and exercising 30 minutes each day.
CBT Cognitive-behavioral therapy (CBT) may help stem weight gain associated with antipsychotic use. Umbricht et al provided CBT to six patients with chronic psychosis who were receiving clozapine or olanzapine. Therapists in group and individual sessions focused on the causes of weight gain, lowcalorie nutrition, weight-loss guidelines, exercise programs, and relaxation strategies. Across 8 weeks, patients’ mean BMI decreased from 29.6 to 25.1 kg/m2
Table 2
METABOLIC EFFECTS OF ORAL ANTIHYPERGLYCEMIC DRUGS
| Class | Body weight | Total cholesterol | LDL | HDL | Triglycerides |
|---|---|---|---|---|---|
| Sulfonylureas Glipizide Glyburide Glimepiride | ▲ | ◄► | ◄► | ◄► | ◄► |
| Meglitinides Repaglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Phenylalanine derivatives Nateglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Biguanides Metformin | ▼ | ▼ | ▼ | ▲ | ▼ |
| Thiazolidinediones Pioglitazone Rosiglitazone | ▲ | ▲ | ▲ | ▲ | ▼ |
| Alpha-glucosidase inhibitors Acarbose Miglitol | ◄► | ◄► | ◄► | ◄► | ◄► |
| ▲ Increase ▼ Decrease ◄► Neutral effect/no change | |||||
Weight management program The Weight Watchers weight management program has shown mild success when offered to men and women with schizophrenia or schizoaffective disorder. Twenty-one patients who had gained an average of 32 lbs while taking olanzapine were enrolled in a Weight Watchers program at a psychiatric center.14 Mean starting BMI was 32 kg/m2 among the 11 patients who completed the 10-week program. Those 11 lost an average of 5 lbs.
All seven men lost weight. Three of the four women gained weight, and one woman lost 13 lbs. Study subjects remained clinically stable during the 10-week study. Two of the three women who did not lose weight had disabling psychiatric symptoms. Participation rates were similar to those of typical Weight Watchers clientele, suggesting that patients requiring antipsychotics might benefit from treatments used for other obese patients.
Patient education Educating patients about nutrition and exercise may help them control their rate of weight gain during antipsychotic therapy.
Littrell et al provided such an educational program for 1 hour per week for 4 months to six men and six women taking olanzapine for schizophrenia or schizoaffective disorder.15 Patients in the behavioral group gained 0.5 kg, compared with a control group that gained 2.9 kg. Mean increase in BMI was less for the behavioral group (0.3 kg/m2) than for the control patients (0.9 kg/m2). Men in both groups gained more weight than did women.
Pharmacologic approaches
Antiobesity medications are generally reserved for patients with a BMI 30 kg/m2 (threshold for obesity) or for those with a BMI 27 kg/m2 (threshold for overweight is 25 kg/m2) who have additional risk factors for cardiovascular disease, stroke, or diabetes.16
For patients with schizophrenia, who typically have a BMI 27 kg/m2, the presence of these risk factors alone may be enough to warrant consideration of an antiobesity agent. Adding any new drug to a patient’s regimen, however, increases the risk of an adverse interaction.
Antiobesity drugs work by a variety of mechanisms, including decreasing appetite, decreasing fat absorption, and increasing energy expenditure. Drugs may reduce caloric intake by decreasing appetite (anorectic drugs) or increasing satiety (appetite suppressants). Centrally-acting sympathomimetics or serotonergic drugs may suppress appetite.
In studies up to 2 years, the appetite suppressant sibutramine, with mixed serotonergic and noradrenergic reuptake inhibition properties, has been shown to cause more weight loss than a placebo in populations without schizophrenia.17 According to one case report, sibutramine use was associated with new-onset psychosis.18
Common side effects of sibutramine include headache, dry mouth, anorexia, constipation, and insomnia. Regular monitoring of blood pressure is required. Do not prescribe this drug for patients with cardiovascular disease, and avoid co-prescribing with MAO inhibitors and serotonergics.
Orlistat reduces fat absorption from the GI tract.19 Common side effects are largely confined to the GI tract and include oily spotting, flatulence, fecal urgency, fatty/oily stool, and oily evacuation.
Combination therapies
Researchers are studying whether adding adjunctive agents to antipsychotics reduces weight gain.
Clozapine plus quetiapine A group of 65 patients who experienced a mean body weight increase of 6.5 kg while taking clozapine for 6 months were then given clozapine plus quetiapine at chlorpromazine-equivalent dosing during the next 10 months. The patients lost a mean of 4.2 kg, and their glycemic control improved. Elevated glycosylated hemoglobin (HbA1c) became normal in those subjects (20% of participants) who had developed type 2 diabetes while taking clozapine alone. The authors theorized that the weight loss diminished insulin resistance, leading to better control of serum glucose levels.20
Olanzapine plus amantadine A group of 12 outpatients with axis I or II diagnoses had responded well clinically to olanzapine but had gained an average 7.3 kg over 1 to 11 months. In an open-label study, they continued their dosages of olanzapine and also were given amantadine, 100 to 300 mg/d. Amantadine was chosen for this trial because of its possible release of dopamine.
No dietary changes were made, but subjects gained no additional weight after amantadine was added. Over the next 3 to 6 months, they lost a mean 3.5 kg, which was 50% of the weight gain associated with olanzapine administration.21
Clozapine plus topiramate In clinical trials, the anticonvulsant topiramate has been associated with significant weight loss for up to 12 months in patients with seizure disorders.22 This agent, which also has mood-stabilizing effects, may be useful both for mood stabilization and weight loss in tandem with antipsychotic therapy.
In a case study,23 a 29-year-old man with schizophrenia who failed several trials of antipsychotic drugs experienced significant improvement with clozapine, 800 mg/d. Over 2 years, however, he developed myoclonic jerks and gained 45.5 kg (a 49% increase over baseline). When topiramate was added, starting with 25 mg/d and increasing to 125 mg/d, his mood improved and the myoclonic jerks stopped. During 5 months of combination therapy, the patient lost 21 kg without changing his eating habits.
Olanzapine and nizatidine Agents that block histamine (H 2) receptors in the digestive tract may be associated with weight loss when given at high doses, although the mechanism by which they contribute to weight loss is unclear. In a double-blind, placebo-controlled study,24 the H 2 blocker nizatidine was given to patients with schizophrenia who were taking olanzapine, 5 to 20 mg/d. In a 16-week trial, 132 patients were randomized to receive adjunctive treatment with low-dose nizatidine (150 mg bid), high-dose nizatidine (300 mg bid), or a placebo.
After 16 weeks, nizatidine demonstrated a dose-response effect when combined with olanzapine. Average weight gain was:
- 5.51 kg with a placebo
- 4.41 kg with low-dose nizatidine
- 2.76 kg with high-dose nizatidine (p =0.02 compared with a placebo).
In the high-dose nizatidine group, only 6% of patients gained more than 10 kg, and weight gain leveled off by week eight. Adverse events and clinical improvements were similar in the three groups.
Related resources
- Weight gain: A growing problem in schizophrenia management. J Clin Psychiatry 2001;62(suppl 7).
- Weight gain associated with the use of psychotropic medications. J Clin Psychiatry 1999;60(suppl 2).
- Effects of atypical antipsychotics on body weight and glucose regulation. J Clin Psychiatry 2001;62(suppl 23).
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
Drug brand names
- Amantadine • Symmetrel
- Clozapine • Clozaril
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Orlistat • Xenical
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sibutramine • Meridia
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
1. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-1200.
2. Dixon L, Weiden P, Delahanty J, et al. Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 2000;26:903-12.
3. Braceland FJ, Meduna LJ, Vaichulis JA. Delayed action of insulin in schizophrenia. Am J Psychiatry 1945;102:108-10.
4. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
5. Brecher M, Rak IW, Westhead EK. The long-term effect of quetiapine (“Seroquel’) monotherapy on weight in patients with schizophrenia. Int J Psychiatry Clin Pract 2000;4:287-92.
6. Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshiminarayanan M. Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 2001;101:277-88.
7. Theonnard-Neumann E. Phenothiazines and diabetes in hospitalized women. Am J Psychiatry 1968;124:978-82.
8. Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. Am J Med 2001;111:716-23.
9. Pendergrass ML. Pathophysiology and management of type 2 diabetes. In: Giles TD, Sowers JR, Weber MA (eds). Diabetes & cardiovascular disease: a practical primer. New Orleans: Institute of Professional Education, 2000;15-40.
10. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults. Findings from the Third National Health and Nutrition Examination Survey. JAMA 2002;287:356-9.
11. Vieweg WVR, Leadbetter RA. The polydipsia-hyponatremia syndrome. Epidemiology, clinical features, and treatment. CNS Drugs 1997;7:121-38.
12. Thomas PR. Weighing the options: criteria for evaluating weight management programs. Washington, DC: National Academy Press, 1995.
13. Umbricht D, Flury H, Bridler R. Cognitive behavioral therapy for weight gain. Am J Psychiatry 2001;158:971.-
14. Ball M, Coons V, Buchanan R. A program for treating olanzapine-related weight gain. Psychiatric Services 2001;52:967-9.
15. Littrell KH, Petty RG, Hilligoss NM, Peabody CD, Johnson CG. Educational interventions for the management of antipsychotic-related weight gain. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31, 2001.
16. Greenberg I, Chan S, Blackburn GL. Nonpharmacologic and pharmacologic management of weight gain. J Clin Psychiatry 1999;60(suppl 21):31-6.
17. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized controlled trial. JAMA 2001;286:1331-9.
18. Taflinski T, Chojnacka J. Sibutramine-associated psychotic episode. Am J Psychiatry 2001;157:2057-8.
19. Glazer G. Long-term pharmacotherapy of obesity 2000. Arch Intern Med 2001;161:1814-24.
20. Reinstein M, Sirotovskaya L, Jones L. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18:99-104.
21. Floris M, Lejeune J, Deberdt W. Effect of amantadine on weight gain during olanzapine treatment. Eur Neuropsychopharmacol 2001;11:181-2.
22. Norton J, Potter D, Edwards K. Sustained weight loss associated with topiramate [abstract]. Epilepsia 1997;38(suppl 3):60.-
23. Dursun SM, Devarajan S. Clozapine weight gain, plus topiramate weight loss. Can J Psychiatry 2000;45:198.-
24. Breier A, Tanaka Y, Roychowdhury S, Clark WS. Nizatidine for the prevention of olanzapine-associated weight gain in schizophrenia and related disorders. A randomized controlled double blind study. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31 2001.
Weight gain is a potential problem for all patients who require treatment with antipsychotics. Those with schizophrenia face double jeopardy. Both the disorder and the use of virtually any available antipsychotic drug may be associated with weight gain, new-onset glucose intolerance, and type 2 diabetes mellitus.
Because of the cardiovascular risks and other morbidity associated with weight gain and glucose dysregulation,1 the psychiatrist must remain vigilant and manage these complications aggressively. In this article, we offer insights into the prevention and management of metabolic complications associated with the use of antipsychotic agents in patients with schizophrenia.
Weight gain and antipsychotics
Weight change was recognized as a feature of schizophrenia even before antipsychotic drugs were introduced in the 1950s.2 Schizophrenia—independent of drug treatment—also is a risk factor for the development of type 2 diabetes. In persons with schizophrenia, serum glucose levels increase more slowly, decline more gradually, and represent higher-than-normal reference values.3
Figure 1 WEIGHT GAIN ASSOCIATED WITH ANTIPSYCHOTIC DRUG ADMINISTRATION
Values represent estimates of drug-induced weight gain after 10 weeks of drug administration.
Source: Allison et al. Am J Psychiatry 1999;156:1686-96; Brecher et al. Int J Psychiatry Clin Pract 2000;4:287-92.In 1999, Allison et al assessed the effects of conventional and atypical antipsychotics on body weight. Using 81 published articles, they estimated and compared weight changes associated with 10 antipsychotic agents and a placebo when given at standard dosages for 10 weeks.4 Comparative data on quetiapine, which were insufficient in 1999, have since been added (Figure 1).5
Patients who received a placebo lost 0.74 kg across 10 weeks. Weight changes with the conventional agents ranged from a reduction of 0.39 kg with molindone to an increase of 3.19 kg with thioridazine. Weight gains also were seen with all of the newer atypical agents, including clozapine (+4.45 kg), olanzapine (+4.15 kg), risperidone (+2.10 kg), and ziprasidone (+0.04 kg).
Fontaine et al have estimated that weight gain in patients with schizophrenia has its greatest impact on mortality in two scenarios:
- when patients are overweight before they start antipsychotic medication
- with greater degrees of weight gain across 10 years (Figure 2).
Whatever a patient’s starting weight, substantial weight gain with antipsychotic therapy increases the risk of impaired glucose tolerance and hypertension (Figure 3).6
Schizophrenia and diabetes
The prevalence of type 2 diabetes in patients with schizophrenia increased from 4.2% in 1956 to 17.2% in 1968, related in part to the introduction of phenothiazines.7 A recent study of data collected by the Schizophrenia Patient Outcomes Research Team (PORT)2 found higher rates of diabetes in persons with schizophrenia (lifetime prevalence, 14.9%) than in the general population (approximately 7.3%).1 Most patients in the PORT study were taking older antipsychotics, the use of which has occasionally been associated with carbohydrate dysregulation.
Figure 2 INCREASED MORTALITY ASSOCIATED WITH WEIGHT GAIN
Number of deaths associated with weight gains of 2.5 and 12 kg over 10 years, as related to all body mass index measurements (BMIs) and BMIs >27 (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.The prevalence of new-onset diabetes with use of specific antipsychotics is unknown. Most information is contained in case reports, and proper epidemiologic studies await publication.
The most detailed report—a pooled study of published cases related to clozapine use—comes from the FDA’s Center for Drug Evaluation and Research.8 In this study, the authors identified 384 reports of diabetes that developed (in 242 patients) or was exacerbated (in 54 patients) in association with clozapine. Patient mean age was 40, and diabetes occurred more commonly in women than in men.
Diabetes developed most commonly within 6 months of starting treatment with clozapine, and one patient developed diabetes after a single 500-mg dose. Metabolic acidosis or ketosis occurred in 80 cases, and 25 subjects died during hyperglycemic episodes. Stopping clozapine or reducing the dosage improved glycemic control in 46 patients.8
Figure 3 INCREASED MORBIDITY ASSOCIATED WITH WEIGHT GAIN
New cases of impaired glucose tolerance and hypertension that developed with weight gains of 2.5 and 12 kg over 10 years (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.During antipsychotic therapy, it is important to measure patients’ fasting plasma glucose at least annually—and more often for high-risk patients (Table 1). The American Diabetes Association defines diabetes as a fasting serum or plasma glucose 126 mg/dl or a 2-hour postprandial serum or plasma glucose 200 mg/dl. In all patients, these tests should be repeated to confirm the diagnosis. Oral glucose tolerance testing is less convenient than fasting plasma glucose testing but more sensitive in identifying changes in carbohydrate metabolism.
As with weight gain, it is easier to prevent diabetes than to treat it. The psychiatrist can best help the patient with emerging carbohydrate dysregulation by collaborating with an internist, family physician, or endocrinologist.
Table 1
FACTORS RELATED TO HIGH RISK OF DEVELOPING TYPE 2 DIABETES
|
| Source: American Diabetes Association |
Weight gain with diabetes drugs Weight gain is associated not only with the use of antipsychotics but also with four classes of oral agents used to treat type 2 diabetes: sulfonylureas, meglitinides, phenylalanine derivatives, and thiazolidinediones. One class—biguanides—contributes to weight reduction, and one—alpha-glucosidase inhibitors—has a variable effect on body weight. These drugs also vary in their effects on serum lipids, including total cholesterol, LDL and HDL cholesterol, and triglycerides (Table 2).9
Many patients with type 2 diabetes require more than one agent to control plasma glucose. With time, insulin deficiency becomes more marked, and insulin therapy is frequently added to the regimen. Hypertension and hyperlipidemia are also very common in patients with type 2 diabetes and require medication to reduce the risk of cardiovascular events.10 As a result, the diabetic patient requiring antipsychotic drugs will likely need polypharmacy, and many of the drugs that might be used may lead to weight gain.
Assessing, managing weight gain
During each visit for the patient with schizophrenia, it is important to routinely weigh those receiving antipsychotics and ask about polydipsia and polyuria, which are early signs of incipient diabetes. A patient who is gaining significant weight (7% of baseline) while taking an antipsychotic and has risk factors for cardiovascular events (e.g., smoking, hypertension, hypertriglyceridemia) is a candidate for a change in antipsychotics.
Try to weigh patients at approximately the same time of day at each visit to compensate for possible diurnal weight changes related to polydipsia-hyponatremia syndrome.11 Patients with this syndrome can gain 5 to 10 lbs (or more) per day and excrete the retained fluid at night. It occurs in 5 to 10% of chronically psychotic patients requiring institutional care and in 1 to 2% of outpatients. Patients with schizophrenia complicated by this syndrome may manifest polydipsia and polyuria secondary to psychosis rather than emerging diabetes. Thus, the clinician must be alert to both diabetes and the polydipsia-hyponatremia syndrome in this setting.
Weight-control approaches
Patients who are taking sedating antipsychotics (e.g., clozapine, olanzapine, or low-potency phenothiazines) may gain up to 30 lbs per year if they become physically inactive and do not reduce their food consumption. Thus, it is important to work with such patients to decrease their caloric intake.
A weight-loss program that produces a loss of 0.5 to 1% of body weight per week is considered safe and acceptable.12 Mild to moderate obesity may be managed by reducing food intake by 500 calories and exercising 30 minutes each day.
CBT Cognitive-behavioral therapy (CBT) may help stem weight gain associated with antipsychotic use. Umbricht et al provided CBT to six patients with chronic psychosis who were receiving clozapine or olanzapine. Therapists in group and individual sessions focused on the causes of weight gain, lowcalorie nutrition, weight-loss guidelines, exercise programs, and relaxation strategies. Across 8 weeks, patients’ mean BMI decreased from 29.6 to 25.1 kg/m2
Table 2
METABOLIC EFFECTS OF ORAL ANTIHYPERGLYCEMIC DRUGS
| Class | Body weight | Total cholesterol | LDL | HDL | Triglycerides |
|---|---|---|---|---|---|
| Sulfonylureas Glipizide Glyburide Glimepiride | ▲ | ◄► | ◄► | ◄► | ◄► |
| Meglitinides Repaglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Phenylalanine derivatives Nateglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Biguanides Metformin | ▼ | ▼ | ▼ | ▲ | ▼ |
| Thiazolidinediones Pioglitazone Rosiglitazone | ▲ | ▲ | ▲ | ▲ | ▼ |
| Alpha-glucosidase inhibitors Acarbose Miglitol | ◄► | ◄► | ◄► | ◄► | ◄► |
| ▲ Increase ▼ Decrease ◄► Neutral effect/no change | |||||
Weight management program The Weight Watchers weight management program has shown mild success when offered to men and women with schizophrenia or schizoaffective disorder. Twenty-one patients who had gained an average of 32 lbs while taking olanzapine were enrolled in a Weight Watchers program at a psychiatric center.14 Mean starting BMI was 32 kg/m2 among the 11 patients who completed the 10-week program. Those 11 lost an average of 5 lbs.
All seven men lost weight. Three of the four women gained weight, and one woman lost 13 lbs. Study subjects remained clinically stable during the 10-week study. Two of the three women who did not lose weight had disabling psychiatric symptoms. Participation rates were similar to those of typical Weight Watchers clientele, suggesting that patients requiring antipsychotics might benefit from treatments used for other obese patients.
Patient education Educating patients about nutrition and exercise may help them control their rate of weight gain during antipsychotic therapy.
Littrell et al provided such an educational program for 1 hour per week for 4 months to six men and six women taking olanzapine for schizophrenia or schizoaffective disorder.15 Patients in the behavioral group gained 0.5 kg, compared with a control group that gained 2.9 kg. Mean increase in BMI was less for the behavioral group (0.3 kg/m2) than for the control patients (0.9 kg/m2). Men in both groups gained more weight than did women.
Pharmacologic approaches
Antiobesity medications are generally reserved for patients with a BMI 30 kg/m2 (threshold for obesity) or for those with a BMI 27 kg/m2 (threshold for overweight is 25 kg/m2) who have additional risk factors for cardiovascular disease, stroke, or diabetes.16
For patients with schizophrenia, who typically have a BMI 27 kg/m2, the presence of these risk factors alone may be enough to warrant consideration of an antiobesity agent. Adding any new drug to a patient’s regimen, however, increases the risk of an adverse interaction.
Antiobesity drugs work by a variety of mechanisms, including decreasing appetite, decreasing fat absorption, and increasing energy expenditure. Drugs may reduce caloric intake by decreasing appetite (anorectic drugs) or increasing satiety (appetite suppressants). Centrally-acting sympathomimetics or serotonergic drugs may suppress appetite.
In studies up to 2 years, the appetite suppressant sibutramine, with mixed serotonergic and noradrenergic reuptake inhibition properties, has been shown to cause more weight loss than a placebo in populations without schizophrenia.17 According to one case report, sibutramine use was associated with new-onset psychosis.18
Common side effects of sibutramine include headache, dry mouth, anorexia, constipation, and insomnia. Regular monitoring of blood pressure is required. Do not prescribe this drug for patients with cardiovascular disease, and avoid co-prescribing with MAO inhibitors and serotonergics.
Orlistat reduces fat absorption from the GI tract.19 Common side effects are largely confined to the GI tract and include oily spotting, flatulence, fecal urgency, fatty/oily stool, and oily evacuation.
Combination therapies
Researchers are studying whether adding adjunctive agents to antipsychotics reduces weight gain.
Clozapine plus quetiapine A group of 65 patients who experienced a mean body weight increase of 6.5 kg while taking clozapine for 6 months were then given clozapine plus quetiapine at chlorpromazine-equivalent dosing during the next 10 months. The patients lost a mean of 4.2 kg, and their glycemic control improved. Elevated glycosylated hemoglobin (HbA1c) became normal in those subjects (20% of participants) who had developed type 2 diabetes while taking clozapine alone. The authors theorized that the weight loss diminished insulin resistance, leading to better control of serum glucose levels.20
Olanzapine plus amantadine A group of 12 outpatients with axis I or II diagnoses had responded well clinically to olanzapine but had gained an average 7.3 kg over 1 to 11 months. In an open-label study, they continued their dosages of olanzapine and also were given amantadine, 100 to 300 mg/d. Amantadine was chosen for this trial because of its possible release of dopamine.
No dietary changes were made, but subjects gained no additional weight after amantadine was added. Over the next 3 to 6 months, they lost a mean 3.5 kg, which was 50% of the weight gain associated with olanzapine administration.21
Clozapine plus topiramate In clinical trials, the anticonvulsant topiramate has been associated with significant weight loss for up to 12 months in patients with seizure disorders.22 This agent, which also has mood-stabilizing effects, may be useful both for mood stabilization and weight loss in tandem with antipsychotic therapy.
In a case study,23 a 29-year-old man with schizophrenia who failed several trials of antipsychotic drugs experienced significant improvement with clozapine, 800 mg/d. Over 2 years, however, he developed myoclonic jerks and gained 45.5 kg (a 49% increase over baseline). When topiramate was added, starting with 25 mg/d and increasing to 125 mg/d, his mood improved and the myoclonic jerks stopped. During 5 months of combination therapy, the patient lost 21 kg without changing his eating habits.
Olanzapine and nizatidine Agents that block histamine (H 2) receptors in the digestive tract may be associated with weight loss when given at high doses, although the mechanism by which they contribute to weight loss is unclear. In a double-blind, placebo-controlled study,24 the H 2 blocker nizatidine was given to patients with schizophrenia who were taking olanzapine, 5 to 20 mg/d. In a 16-week trial, 132 patients were randomized to receive adjunctive treatment with low-dose nizatidine (150 mg bid), high-dose nizatidine (300 mg bid), or a placebo.
After 16 weeks, nizatidine demonstrated a dose-response effect when combined with olanzapine. Average weight gain was:
- 5.51 kg with a placebo
- 4.41 kg with low-dose nizatidine
- 2.76 kg with high-dose nizatidine (p =0.02 compared with a placebo).
In the high-dose nizatidine group, only 6% of patients gained more than 10 kg, and weight gain leveled off by week eight. Adverse events and clinical improvements were similar in the three groups.
Related resources
- Weight gain: A growing problem in schizophrenia management. J Clin Psychiatry 2001;62(suppl 7).
- Weight gain associated with the use of psychotropic medications. J Clin Psychiatry 1999;60(suppl 2).
- Effects of atypical antipsychotics on body weight and glucose regulation. J Clin Psychiatry 2001;62(suppl 23).
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
Drug brand names
- Amantadine • Symmetrel
- Clozapine • Clozaril
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Orlistat • Xenical
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sibutramine • Meridia
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
Weight gain is a potential problem for all patients who require treatment with antipsychotics. Those with schizophrenia face double jeopardy. Both the disorder and the use of virtually any available antipsychotic drug may be associated with weight gain, new-onset glucose intolerance, and type 2 diabetes mellitus.
Because of the cardiovascular risks and other morbidity associated with weight gain and glucose dysregulation,1 the psychiatrist must remain vigilant and manage these complications aggressively. In this article, we offer insights into the prevention and management of metabolic complications associated with the use of antipsychotic agents in patients with schizophrenia.
Weight gain and antipsychotics
Weight change was recognized as a feature of schizophrenia even before antipsychotic drugs were introduced in the 1950s.2 Schizophrenia—independent of drug treatment—also is a risk factor for the development of type 2 diabetes. In persons with schizophrenia, serum glucose levels increase more slowly, decline more gradually, and represent higher-than-normal reference values.3
Figure 1 WEIGHT GAIN ASSOCIATED WITH ANTIPSYCHOTIC DRUG ADMINISTRATION
Values represent estimates of drug-induced weight gain after 10 weeks of drug administration.
Source: Allison et al. Am J Psychiatry 1999;156:1686-96; Brecher et al. Int J Psychiatry Clin Pract 2000;4:287-92.In 1999, Allison et al assessed the effects of conventional and atypical antipsychotics on body weight. Using 81 published articles, they estimated and compared weight changes associated with 10 antipsychotic agents and a placebo when given at standard dosages for 10 weeks.4 Comparative data on quetiapine, which were insufficient in 1999, have since been added (Figure 1).5
Patients who received a placebo lost 0.74 kg across 10 weeks. Weight changes with the conventional agents ranged from a reduction of 0.39 kg with molindone to an increase of 3.19 kg with thioridazine. Weight gains also were seen with all of the newer atypical agents, including clozapine (+4.45 kg), olanzapine (+4.15 kg), risperidone (+2.10 kg), and ziprasidone (+0.04 kg).
Fontaine et al have estimated that weight gain in patients with schizophrenia has its greatest impact on mortality in two scenarios:
- when patients are overweight before they start antipsychotic medication
- with greater degrees of weight gain across 10 years (Figure 2).
Whatever a patient’s starting weight, substantial weight gain with antipsychotic therapy increases the risk of impaired glucose tolerance and hypertension (Figure 3).6
Schizophrenia and diabetes
The prevalence of type 2 diabetes in patients with schizophrenia increased from 4.2% in 1956 to 17.2% in 1968, related in part to the introduction of phenothiazines.7 A recent study of data collected by the Schizophrenia Patient Outcomes Research Team (PORT)2 found higher rates of diabetes in persons with schizophrenia (lifetime prevalence, 14.9%) than in the general population (approximately 7.3%).1 Most patients in the PORT study were taking older antipsychotics, the use of which has occasionally been associated with carbohydrate dysregulation.
Figure 2 INCREASED MORTALITY ASSOCIATED WITH WEIGHT GAIN
Number of deaths associated with weight gains of 2.5 and 12 kg over 10 years, as related to all body mass index measurements (BMIs) and BMIs >27 (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.The prevalence of new-onset diabetes with use of specific antipsychotics is unknown. Most information is contained in case reports, and proper epidemiologic studies await publication.
The most detailed report—a pooled study of published cases related to clozapine use—comes from the FDA’s Center for Drug Evaluation and Research.8 In this study, the authors identified 384 reports of diabetes that developed (in 242 patients) or was exacerbated (in 54 patients) in association with clozapine. Patient mean age was 40, and diabetes occurred more commonly in women than in men.
Diabetes developed most commonly within 6 months of starting treatment with clozapine, and one patient developed diabetes after a single 500-mg dose. Metabolic acidosis or ketosis occurred in 80 cases, and 25 subjects died during hyperglycemic episodes. Stopping clozapine or reducing the dosage improved glycemic control in 46 patients.8
Figure 3 INCREASED MORBIDITY ASSOCIATED WITH WEIGHT GAIN
New cases of impaired glucose tolerance and hypertension that developed with weight gains of 2.5 and 12 kg over 10 years (per 100,000 persons in U.S. population).
Source: Fontaine et al. Psychiatry Res 2001;101:277-88.During antipsychotic therapy, it is important to measure patients’ fasting plasma glucose at least annually—and more often for high-risk patients (Table 1). The American Diabetes Association defines diabetes as a fasting serum or plasma glucose 126 mg/dl or a 2-hour postprandial serum or plasma glucose 200 mg/dl. In all patients, these tests should be repeated to confirm the diagnosis. Oral glucose tolerance testing is less convenient than fasting plasma glucose testing but more sensitive in identifying changes in carbohydrate metabolism.
As with weight gain, it is easier to prevent diabetes than to treat it. The psychiatrist can best help the patient with emerging carbohydrate dysregulation by collaborating with an internist, family physician, or endocrinologist.
Table 1
FACTORS RELATED TO HIGH RISK OF DEVELOPING TYPE 2 DIABETES
|
| Source: American Diabetes Association |
Weight gain with diabetes drugs Weight gain is associated not only with the use of antipsychotics but also with four classes of oral agents used to treat type 2 diabetes: sulfonylureas, meglitinides, phenylalanine derivatives, and thiazolidinediones. One class—biguanides—contributes to weight reduction, and one—alpha-glucosidase inhibitors—has a variable effect on body weight. These drugs also vary in their effects on serum lipids, including total cholesterol, LDL and HDL cholesterol, and triglycerides (Table 2).9
Many patients with type 2 diabetes require more than one agent to control plasma glucose. With time, insulin deficiency becomes more marked, and insulin therapy is frequently added to the regimen. Hypertension and hyperlipidemia are also very common in patients with type 2 diabetes and require medication to reduce the risk of cardiovascular events.10 As a result, the diabetic patient requiring antipsychotic drugs will likely need polypharmacy, and many of the drugs that might be used may lead to weight gain.
Assessing, managing weight gain
During each visit for the patient with schizophrenia, it is important to routinely weigh those receiving antipsychotics and ask about polydipsia and polyuria, which are early signs of incipient diabetes. A patient who is gaining significant weight (7% of baseline) while taking an antipsychotic and has risk factors for cardiovascular events (e.g., smoking, hypertension, hypertriglyceridemia) is a candidate for a change in antipsychotics.
Try to weigh patients at approximately the same time of day at each visit to compensate for possible diurnal weight changes related to polydipsia-hyponatremia syndrome.11 Patients with this syndrome can gain 5 to 10 lbs (or more) per day and excrete the retained fluid at night. It occurs in 5 to 10% of chronically psychotic patients requiring institutional care and in 1 to 2% of outpatients. Patients with schizophrenia complicated by this syndrome may manifest polydipsia and polyuria secondary to psychosis rather than emerging diabetes. Thus, the clinician must be alert to both diabetes and the polydipsia-hyponatremia syndrome in this setting.
Weight-control approaches
Patients who are taking sedating antipsychotics (e.g., clozapine, olanzapine, or low-potency phenothiazines) may gain up to 30 lbs per year if they become physically inactive and do not reduce their food consumption. Thus, it is important to work with such patients to decrease their caloric intake.
A weight-loss program that produces a loss of 0.5 to 1% of body weight per week is considered safe and acceptable.12 Mild to moderate obesity may be managed by reducing food intake by 500 calories and exercising 30 minutes each day.
CBT Cognitive-behavioral therapy (CBT) may help stem weight gain associated with antipsychotic use. Umbricht et al provided CBT to six patients with chronic psychosis who were receiving clozapine or olanzapine. Therapists in group and individual sessions focused on the causes of weight gain, lowcalorie nutrition, weight-loss guidelines, exercise programs, and relaxation strategies. Across 8 weeks, patients’ mean BMI decreased from 29.6 to 25.1 kg/m2
Table 2
METABOLIC EFFECTS OF ORAL ANTIHYPERGLYCEMIC DRUGS
| Class | Body weight | Total cholesterol | LDL | HDL | Triglycerides |
|---|---|---|---|---|---|
| Sulfonylureas Glipizide Glyburide Glimepiride | ▲ | ◄► | ◄► | ◄► | ◄► |
| Meglitinides Repaglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Phenylalanine derivatives Nateglinide | ▲ | ◄► | ◄► | ◄► | ◄► |
| Biguanides Metformin | ▼ | ▼ | ▼ | ▲ | ▼ |
| Thiazolidinediones Pioglitazone Rosiglitazone | ▲ | ▲ | ▲ | ▲ | ▼ |
| Alpha-glucosidase inhibitors Acarbose Miglitol | ◄► | ◄► | ◄► | ◄► | ◄► |
| ▲ Increase ▼ Decrease ◄► Neutral effect/no change | |||||
Weight management program The Weight Watchers weight management program has shown mild success when offered to men and women with schizophrenia or schizoaffective disorder. Twenty-one patients who had gained an average of 32 lbs while taking olanzapine were enrolled in a Weight Watchers program at a psychiatric center.14 Mean starting BMI was 32 kg/m2 among the 11 patients who completed the 10-week program. Those 11 lost an average of 5 lbs.
All seven men lost weight. Three of the four women gained weight, and one woman lost 13 lbs. Study subjects remained clinically stable during the 10-week study. Two of the three women who did not lose weight had disabling psychiatric symptoms. Participation rates were similar to those of typical Weight Watchers clientele, suggesting that patients requiring antipsychotics might benefit from treatments used for other obese patients.
Patient education Educating patients about nutrition and exercise may help them control their rate of weight gain during antipsychotic therapy.
Littrell et al provided such an educational program for 1 hour per week for 4 months to six men and six women taking olanzapine for schizophrenia or schizoaffective disorder.15 Patients in the behavioral group gained 0.5 kg, compared with a control group that gained 2.9 kg. Mean increase in BMI was less for the behavioral group (0.3 kg/m2) than for the control patients (0.9 kg/m2). Men in both groups gained more weight than did women.
Pharmacologic approaches
Antiobesity medications are generally reserved for patients with a BMI 30 kg/m2 (threshold for obesity) or for those with a BMI 27 kg/m2 (threshold for overweight is 25 kg/m2) who have additional risk factors for cardiovascular disease, stroke, or diabetes.16
For patients with schizophrenia, who typically have a BMI 27 kg/m2, the presence of these risk factors alone may be enough to warrant consideration of an antiobesity agent. Adding any new drug to a patient’s regimen, however, increases the risk of an adverse interaction.
Antiobesity drugs work by a variety of mechanisms, including decreasing appetite, decreasing fat absorption, and increasing energy expenditure. Drugs may reduce caloric intake by decreasing appetite (anorectic drugs) or increasing satiety (appetite suppressants). Centrally-acting sympathomimetics or serotonergic drugs may suppress appetite.
In studies up to 2 years, the appetite suppressant sibutramine, with mixed serotonergic and noradrenergic reuptake inhibition properties, has been shown to cause more weight loss than a placebo in populations without schizophrenia.17 According to one case report, sibutramine use was associated with new-onset psychosis.18
Common side effects of sibutramine include headache, dry mouth, anorexia, constipation, and insomnia. Regular monitoring of blood pressure is required. Do not prescribe this drug for patients with cardiovascular disease, and avoid co-prescribing with MAO inhibitors and serotonergics.
Orlistat reduces fat absorption from the GI tract.19 Common side effects are largely confined to the GI tract and include oily spotting, flatulence, fecal urgency, fatty/oily stool, and oily evacuation.
Combination therapies
Researchers are studying whether adding adjunctive agents to antipsychotics reduces weight gain.
Clozapine plus quetiapine A group of 65 patients who experienced a mean body weight increase of 6.5 kg while taking clozapine for 6 months were then given clozapine plus quetiapine at chlorpromazine-equivalent dosing during the next 10 months. The patients lost a mean of 4.2 kg, and their glycemic control improved. Elevated glycosylated hemoglobin (HbA1c) became normal in those subjects (20% of participants) who had developed type 2 diabetes while taking clozapine alone. The authors theorized that the weight loss diminished insulin resistance, leading to better control of serum glucose levels.20
Olanzapine plus amantadine A group of 12 outpatients with axis I or II diagnoses had responded well clinically to olanzapine but had gained an average 7.3 kg over 1 to 11 months. In an open-label study, they continued their dosages of olanzapine and also were given amantadine, 100 to 300 mg/d. Amantadine was chosen for this trial because of its possible release of dopamine.
No dietary changes were made, but subjects gained no additional weight after amantadine was added. Over the next 3 to 6 months, they lost a mean 3.5 kg, which was 50% of the weight gain associated with olanzapine administration.21
Clozapine plus topiramate In clinical trials, the anticonvulsant topiramate has been associated with significant weight loss for up to 12 months in patients with seizure disorders.22 This agent, which also has mood-stabilizing effects, may be useful both for mood stabilization and weight loss in tandem with antipsychotic therapy.
In a case study,23 a 29-year-old man with schizophrenia who failed several trials of antipsychotic drugs experienced significant improvement with clozapine, 800 mg/d. Over 2 years, however, he developed myoclonic jerks and gained 45.5 kg (a 49% increase over baseline). When topiramate was added, starting with 25 mg/d and increasing to 125 mg/d, his mood improved and the myoclonic jerks stopped. During 5 months of combination therapy, the patient lost 21 kg without changing his eating habits.
Olanzapine and nizatidine Agents that block histamine (H 2) receptors in the digestive tract may be associated with weight loss when given at high doses, although the mechanism by which they contribute to weight loss is unclear. In a double-blind, placebo-controlled study,24 the H 2 blocker nizatidine was given to patients with schizophrenia who were taking olanzapine, 5 to 20 mg/d. In a 16-week trial, 132 patients were randomized to receive adjunctive treatment with low-dose nizatidine (150 mg bid), high-dose nizatidine (300 mg bid), or a placebo.
After 16 weeks, nizatidine demonstrated a dose-response effect when combined with olanzapine. Average weight gain was:
- 5.51 kg with a placebo
- 4.41 kg with low-dose nizatidine
- 2.76 kg with high-dose nizatidine (p =0.02 compared with a placebo).
In the high-dose nizatidine group, only 6% of patients gained more than 10 kg, and weight gain leveled off by week eight. Adverse events and clinical improvements were similar in the three groups.
Related resources
- Weight gain: A growing problem in schizophrenia management. J Clin Psychiatry 2001;62(suppl 7).
- Weight gain associated with the use of psychotropic medications. J Clin Psychiatry 1999;60(suppl 2).
- Effects of atypical antipsychotics on body weight and glucose regulation. J Clin Psychiatry 2001;62(suppl 23).
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
Drug brand names
- Amantadine • Symmetrel
- Clozapine • Clozaril
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Orlistat • Xenical
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sibutramine • Meridia
- Topiramate • Topamax
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
1. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-1200.
2. Dixon L, Weiden P, Delahanty J, et al. Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 2000;26:903-12.
3. Braceland FJ, Meduna LJ, Vaichulis JA. Delayed action of insulin in schizophrenia. Am J Psychiatry 1945;102:108-10.
4. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
5. Brecher M, Rak IW, Westhead EK. The long-term effect of quetiapine (“Seroquel’) monotherapy on weight in patients with schizophrenia. Int J Psychiatry Clin Pract 2000;4:287-92.
6. Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshiminarayanan M. Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 2001;101:277-88.
7. Theonnard-Neumann E. Phenothiazines and diabetes in hospitalized women. Am J Psychiatry 1968;124:978-82.
8. Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. Am J Med 2001;111:716-23.
9. Pendergrass ML. Pathophysiology and management of type 2 diabetes. In: Giles TD, Sowers JR, Weber MA (eds). Diabetes & cardiovascular disease: a practical primer. New Orleans: Institute of Professional Education, 2000;15-40.
10. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults. Findings from the Third National Health and Nutrition Examination Survey. JAMA 2002;287:356-9.
11. Vieweg WVR, Leadbetter RA. The polydipsia-hyponatremia syndrome. Epidemiology, clinical features, and treatment. CNS Drugs 1997;7:121-38.
12. Thomas PR. Weighing the options: criteria for evaluating weight management programs. Washington, DC: National Academy Press, 1995.
13. Umbricht D, Flury H, Bridler R. Cognitive behavioral therapy for weight gain. Am J Psychiatry 2001;158:971.-
14. Ball M, Coons V, Buchanan R. A program for treating olanzapine-related weight gain. Psychiatric Services 2001;52:967-9.
15. Littrell KH, Petty RG, Hilligoss NM, Peabody CD, Johnson CG. Educational interventions for the management of antipsychotic-related weight gain. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31, 2001.
16. Greenberg I, Chan S, Blackburn GL. Nonpharmacologic and pharmacologic management of weight gain. J Clin Psychiatry 1999;60(suppl 21):31-6.
17. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized controlled trial. JAMA 2001;286:1331-9.
18. Taflinski T, Chojnacka J. Sibutramine-associated psychotic episode. Am J Psychiatry 2001;157:2057-8.
19. Glazer G. Long-term pharmacotherapy of obesity 2000. Arch Intern Med 2001;161:1814-24.
20. Reinstein M, Sirotovskaya L, Jones L. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18:99-104.
21. Floris M, Lejeune J, Deberdt W. Effect of amantadine on weight gain during olanzapine treatment. Eur Neuropsychopharmacol 2001;11:181-2.
22. Norton J, Potter D, Edwards K. Sustained weight loss associated with topiramate [abstract]. Epilepsia 1997;38(suppl 3):60.-
23. Dursun SM, Devarajan S. Clozapine weight gain, plus topiramate weight loss. Can J Psychiatry 2000;45:198.-
24. Breier A, Tanaka Y, Roychowdhury S, Clark WS. Nizatidine for the prevention of olanzapine-associated weight gain in schizophrenia and related disorders. A randomized controlled double blind study. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31 2001.
1. Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA 2001;286:1195-1200.
2. Dixon L, Weiden P, Delahanty J, et al. Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 2000;26:903-12.
3. Braceland FJ, Meduna LJ, Vaichulis JA. Delayed action of insulin in schizophrenia. Am J Psychiatry 1945;102:108-10.
4. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: a comprehensive research synthesis. Am J Psychiatry 1999;156:1686-96.
5. Brecher M, Rak IW, Westhead EK. The long-term effect of quetiapine (“Seroquel’) monotherapy on weight in patients with schizophrenia. Int J Psychiatry Clin Pract 2000;4:287-92.
6. Fontaine KR, Heo M, Harrigan EP, Shear CL, Lakshiminarayanan M. Estimating the consequences of anti-psychotic induced weight gain on health and mortality rate. Psychiatry Res 2001;101:277-88.
7. Theonnard-Neumann E. Phenothiazines and diabetes in hospitalized women. Am J Psychiatry 1968;124:978-82.
8. Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. Am J Med 2001;111:716-23.
9. Pendergrass ML. Pathophysiology and management of type 2 diabetes. In: Giles TD, Sowers JR, Weber MA (eds). Diabetes & cardiovascular disease: a practical primer. New Orleans: Institute of Professional Education, 2000;15-40.
10. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults. Findings from the Third National Health and Nutrition Examination Survey. JAMA 2002;287:356-9.
11. Vieweg WVR, Leadbetter RA. The polydipsia-hyponatremia syndrome. Epidemiology, clinical features, and treatment. CNS Drugs 1997;7:121-38.
12. Thomas PR. Weighing the options: criteria for evaluating weight management programs. Washington, DC: National Academy Press, 1995.
13. Umbricht D, Flury H, Bridler R. Cognitive behavioral therapy for weight gain. Am J Psychiatry 2001;158:971.-
14. Ball M, Coons V, Buchanan R. A program for treating olanzapine-related weight gain. Psychiatric Services 2001;52:967-9.
15. Littrell KH, Petty RG, Hilligoss NM, Peabody CD, Johnson CG. Educational interventions for the management of antipsychotic-related weight gain. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31, 2001.
16. Greenberg I, Chan S, Blackburn GL. Nonpharmacologic and pharmacologic management of weight gain. J Clin Psychiatry 1999;60(suppl 21):31-6.
17. Wirth A, Krause J. Long-term weight loss with sibutramine: a randomized controlled trial. JAMA 2001;286:1331-9.
18. Taflinski T, Chojnacka J. Sibutramine-associated psychotic episode. Am J Psychiatry 2001;157:2057-8.
19. Glazer G. Long-term pharmacotherapy of obesity 2000. Arch Intern Med 2001;161:1814-24.
20. Reinstein M, Sirotovskaya L, Jones L. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18:99-104.
21. Floris M, Lejeune J, Deberdt W. Effect of amantadine on weight gain during olanzapine treatment. Eur Neuropsychopharmacol 2001;11:181-2.
22. Norton J, Potter D, Edwards K. Sustained weight loss associated with topiramate [abstract]. Epilepsia 1997;38(suppl 3):60.-
23. Dursun SM, Devarajan S. Clozapine weight gain, plus topiramate weight loss. Can J Psychiatry 2000;45:198.-
24. Breier A, Tanaka Y, Roychowdhury S, Clark WS. Nizatidine for the prevention of olanzapine-associated weight gain in schizophrenia and related disorders. A randomized controlled double blind study. 41st annual meeting of the New Clinical Drug Evaluation Unit, Phoenix, AZ, May 28-31 2001.
Eating baby powder controls her urge to purge
History: An inpatient discovery
Ms. A, 20, presented to the emergency room with an exacerbation of asthma due to noncompliance with medications. A review of her systems and a physical exam revealed significant bilateral shortness of breath, wheezes, and rhonchi.
A single mother who lives with her two daughters, ages 5 and 2, Ms. A is 28 weeks pregnant with her third child. After receiving albuterol nebulizers for her asthma, she was admitted to the obstetrics and gynecology floor for monitoring of maternal and fetal status. There, a nursing staff member observed her eating baby powder.
The psychiatric team evaluated Ms. A and learned that, during her first pregnancy at age 15, she grew uncomfortable with her increased weight and started purging. Standing at 5 feet, 6 inches, Ms. A weighed as much as 220 during the pregnancy; her weight fell to 170 pounds after delivery. When she presented to us she lamented, “All of my friends are still thin.”
The stress of being a single teenage mother and going to school, combined with disgust over her physical appearance, provoked her purging. She did not think purging would help her lose weight but would prevent her from gaining more even as she ate as much as she wanted.
For 11 months after the birth of her first child, she purged three to four times daily. She could eat as many as five “value meals” within 2 to 3 hours at fast-food restaurants. Eating relaxed her and made her feel comfortable, but the frequency of purging escalated to five to six times daily and the vomiting was physically exhausting, painful, and caused esophageal damage.
At age 17, Ms. A became pregnant with her second child. In the first 2 to 3 months, she continued to eat large quantities of food but purged less often (two to three times daily).
One day in the third month of this pregnancy, Ms. A watched as her mother used medicated powder on her own child, and the powder's scent stimulated within Ms. A an urge to taste it. Before long Ms. A was eating the powder regularly and had stopped purging. She recalled purging only three times during the remaining 6 months of the pregnancy. The craving for powder replaced both her desire to vomit and the need to binge on food. She returned to regular binging and purging (once or twice weekly) after her second child was born, however.
In your view, which should be addressed first, the bulimia or the obsession with baby powder? Or should both be addressed in tandem?
Commentary
This case displays a form of adult pica for baby powder, which has only been described in the literature for pediatric pica.1,2 She displays no cognitive deficits or psychological disorders (e.g., mental retardation, schizophrenia) that are commonly associated with pica.3-6 Pregnancy, which is also common in pica, did exist in this patient and may provide some physiologic or psychological insight into the patient’s disorder.7 The patient’s bulimia nervosa, however, gives an unusual twist to this case.
In the 18th century, pica was classified together with bulimia simply as an erroneous or aberrant appetite (Box 1).8 Pica has been known to occur with—and can be a symptom of—bulimia and anorexia, but it is rarely cited.8,10 As in other eating disorders, affected individuals are ashamed of their weight, body shape, and body image.13
The term pica has evolved over centuries to describe the compulsive ingestion of non-nutritive substances or unusual food cravings. Its etymology stems from the Latin word for magpie (genus Pica), a bird said to pick up, carry away, and presumably eat a myriad of objects.
The word was first used in 1563 by Thomas Gale, who noted this consumption of unusual foodstuffs in pregnant women and children.8 In contemporary literature, the word “craving” is often used instead of pica to minimize social judgment toward practices that deviate from “normal.”
An estimated 20% of pregnant women are believed to have a history of pica, but the documented prevalence of these cravings may be underestimated because women often are embarrassed to disclose the behavior.9
Pica has been speculated to be a form of aggression, a result of compulsive neuroses, or a manifestation of oral fixation because of its association with thumb sucking.1 In the end, pica is a poorly understood disorder.
Scientists question the etiology of pica. Early psychiatric hypotheses focused on societal expectations of women’s outward beauty. A higher prevalence of pica has been recognized in mentally retarded persons and patients with schizophrenia.3-6
Pica is most frequently observed in children, pregnant women, and patients from a low socioeconomic background.10,11 More comprehensive studies have explored geophagia (a craving to eat chalk, clay, or dirt) in Africa and the southern United States.12
Comorbid bulimia and pica disorders tend to work together to accomplish a similar task: weight loss/control. Eating non-nutritive substances occupies space in the stomach, creating a sense of satiety without taking in calories. Therefore, this behavior acts as a substitute for binging in the patient with bulimia.14
One study identified eight themes associated with pica during pregnancy: keeping practices secret, singularity of the experience, extravagant means for obtaining the craved substance, fears for the effects on the fetus, yielding or not yielding to the cravings, use of the substances as medication, pica and lack of food intake, and sensory experiences other than taste.2 All eight of these themes were present in Ms. A.
Evaluation: Needing more and more
By her third pregnancy, Ms. A’s obsession with powder started to take hold. She found it easier to conceal the purging from her partner, so she began purging more often (twice daily) to offset her cravings for the baby powder. Purging was a last resort for the patient and her only means of off-setting her desire for the powder, which relieved her urge to vomit. She ate baby powder throughout the day, even awaking two to three times at night to ingest a few spoonfuls.
Until she presented to us, Ms. A had followed a daily ritual. At 10:30 a.m., when the local drug store opens, she superficially tested the consistency of a certain brand of powder available on the shelves. She then purchased one case (six 14-ounce containers) of powder, went home and sampled each container, and rated them in quality from 1 to 6, with 1 being the bottle of powder she ate that day. The next morning, regardless of how many cases of powder were piled in her closet, she went to the drug store and repeated the process.
Ms. A felt comfortable eating the talc-based powder in her apartment and her mother’s house. She kept some baby powder in her desk at work, but she regularly took an hour-long lunch break to drive back to her apartment and satisfy her craving. She also carried powder in the car, tasting it while driving.
When asked how the powder made her feel, Ms. A replied: “Powder is like nothing else. It makes me feel content and at ease.” Whenever she was irritated, or if the children were frustrating her, she would take a spoonful of powder.
In the beginning, she consumed approximately one 14-ounce bottle per month. When she presented 28 weeks pregnant with her third child, she could not imagine life without baby powder. A spoonful satisfied her for only 5 to 10 minutes before she would desire more. No other substance quelled the cravings. She had tried edible substitutes such as confectioners sugar, cornstarch, and ice chips, but nothing offered the satisfaction she got from powder.
When she is unable to ingest powder, she develops a headache, begins to sweat, gets extremely anxious and irritable, cries profusely, and becomes depressed. If she is abstinent more than 2 days she is unable to sleep and becomes preoccupied with the powder. If powder is not available, she binges and induces vomiting to stifle her craving.
In the hospital she craved powder 2 days after it was removed from her access. She became extremely anxious and distressed. She then ordered as much food as possible so she could purge and forget about the powder.
How would you explain the patient’s psychopathological attraction to baby powder?
Commentary
Patients with pica typically express satisfaction from consuming non-nutrient substances (Box 2). Ms. A’s motive for eating the powder stemmed from what she perceived as its soothing properties.
Other reported cases have alluded to the sensation generated by the texture of soil or chalk in the mouth. Some of these patients also described the importance of the soil’s taste—i.e., particle size—as being second to its texture.12 The desire to experience a certain texture, color, odor, and taste are important components in pica cravings.10
| Object | Specific disorder |
|---|---|
| Burnt matches | Cautopyreiophagia |
| Earth (chalk, clay, dirt) | Geophagia |
| Feces | Coprophagia |
| Hair | Tricophagia |
| Ice | Pagophagia |
| Laundry starch, cornstarch | Amylophagia |
| Lead paint chips | Plumbophagia |
| Raw potatoes | Geomelophagia |
| Stones | Lithophagia |
Other known objects of pica—Ashes, baking soda, balloons, carrots, celery, chewing gum, cigarette butts, cloth, coal, coca leaf, coffee grounds/beans, cotton balls, concrete, crayons, croutons, detergent, grass, hard candy, insects, lavatory fresheners, latex gloves, licorice, lint, metal, milk, newsprint, oats, oyster shells, paper, parsley, plant leaves, pencil erasers, plastic, popcorn, powder puffs, salt, soap, string, thread, toilet tissue, tomato seeds, twigs, vinegar, wood.
Pica appears to meet the individual’s need for mental relaxation and sensory pleasure15 in much the same way that alcohol or drug abusers satisfy their intense desire for euphoria and relaxation. Scientists theorize that alcohol and drug abuse may be exacerbated by or result from a neurochemical imbalance. A similar hypothesis may explain this “variant” in pica patients.
Pregnant women often develop taste aversions for items that are potentially harmful to the developing fetus, such as alcohol and coffee. Expectant mothers may develop utter disgust and provocation of nausea toward items they enjoyed while not gravid. Aversions to foods and other items during pregnancy might be the consequence of homeostatic factors that have evolved as general feto-protective mechanisms.16,17 The metabolic changes that accompany the gravid state might alter olfactory and taste sensitivity.17
If a pregnancy-related change in chemical balance can cause taste aversion, certainly a similar situation could evolve into pica. In laboratory rats, intraventricular injection of exogenous neuropeptide Y, a hormone with documented CNS activity, caused taste aversions and elicited geophagia.18
Ms. A’s ingestion of baby powder itself did not harm the fetus. Stephen Emery, MD, director of perinatal ultrasound at the Cleveland Clinic, notes that talc is inert and the powder’s perfumes probably are benign. He adds, however, that because the powder often has replaced real food, Ms. A placed her unborn child at risk via malnourishment.
Further evaluation: A ‘pleasant’ appearance
Ms. A’s medical history revealed chronic asthma since childhood and gastroesophageal reflux disease. According to her social history, she is dating the father of her expectant child. She has been smoking one pack of cigarettes per day for 2 years but says she does not drink alcohol and has never abused illicit drugs.
Her lab values were as follows (with normal ranges in parentheses): blood urea, 4 mg/dl (9-23); serum iron, 69 mg/dl (42-135); calcium 8.7 mg/dl (8.5-10.5); magnesium, 1.6 mg/dl (1.8-2.4); phosphate, 2.4 mg/dl (2.7-4.6); hemoglobin, 10.0 g/dl (12.0-14.0); hematocrit, 31.1% (37.0-47.0); mean corpuscular volume, 86.4 fl (81-99).
Ms. A appeared well-nourished, appropriately dressed, and well-groomed during our examination. She was alert, oriented and cooperative, and held a pleasant conversation with good eye contact. Her mood was depressed and anxious, and her affect was congruent. Speech was normal in rate, tone, and volume. Her thoughts were well organized and goal-directed. She denied suicidal ideation but had thoughts of harming her fetus. She denied any perceptual disturbances. No intellectual impairment was evident, and her insight and judgment were preserved.
What is the psychiatric diagnosis for this patient? Also, in your view, how likely is she to harm her fetus or her two children? How would you assess and manage that risk?
Commentary
The physiologic cause of pica may be metabolic disturbances in iron, zinc, calcium, potassium, lead, and magnesium.10,19-22 Ice pica typically is associated with iron deficiency and low hemoglobin levels,14,20,23,24 although other forms of pica have been linked to iron deficiency.12,25 Some studies show iron deficiency in nearly half of patients who display ice pica;20,26 correcting the iron deficiency relieves the cravings for the desired substances.7,14 Scientists are split as to whether pica results in the deficiency of certain minerals or whether mineral deficiencies cause pica. Mineral deficiencies may alter appetite-regulating brain enzymes that can lead to these cravings.7,10,11,23
Ms. A’s laboratory values demonstrated decreased hemoglobin, hematocrit, and magnesium levels. Magnesium replacement did not change her eating behavior. Her mild anemia may simply have been an effect of pregnancy.
Treatment: Confronting comorbid depression
Ms. A’s diagnosis was pica, bulimia nervosa-purging type, with comorbid depressive disorder NOS.
She was placed on the selective serotonin reuptake inhibitor sertraline, 12.5 mg/d. The dosage was increased gradually to 50 mg qd. Supportive psychotherapy was provided during the patient’s hospital course.
After her discharge, cognitive therapy was initiated. Ms. A was asked to keep a journal utilizing the “triple column technique,” through which she described a situation in one column, explained the symptoms or unwanted behaviors and emotions evoked by that situation in the second, and wrote down her thoughts in the third.
Ms. A was monitored for signs and symptoms of postpartum depression. After this careful assessment, in which two psychiatrists and the ob/gyn team participated, we concluded that the patient’s transient thoughts of harming her fetus had fully resolved.
Ms. A was educated about nutrition and healthy exercise, as well as birth control options. We also asked to see her as an outpatient.
In the ensuing months, Ms. A reported moderate depressive symptoms but described a significant decrease in her craving for, and consumption of, powder. She continued follow-up treatment with her physician at the women’s care center. Ms. A decided to stop taking sertraline after 2 months because she felt it was not helping her depression and was causing fatigue.
When we followed up after 6 months, Ms. A reported that she and her baby were doing well. She told us that her powder cravings had decreased markedly.
Related resources
- Alliance for Eating Disorders Awareness. www.eatingdisorderinfo.org
- Stein DJ, Bouwer C, van Heerden B. Pica and the obsessive spectrum disorders. S Afr Med J 1996; 86(12 suppl):1586-8, 1591-2.
Drug brand names
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
1. Robischon P. Pica practice and other hand-mouth behavior and children’s development level. Nurs Res 1971;20(1):4-16.
2. Cooksey NR. Pica and olfactory craving of pregnancy: How deep are the secrets? Birth 1995;22(3):129-37.
3. Danford DE, Smith JC, Huber AM. Pica and mineral status in the mentally retarded. Am J Clin Nutr 1982;35(5):958-67.
4. Jawed SH, Krishnan VH, et al. Worsening of pica as a symptom of Depressive illness in a person with severe mental handicap. Br J Psychiatry 1993;162:835-7.
5. Sturmey P. Pica and developmental disability. J Am Board Fam Pract 2001;14(1):80-1.
6. Tracy JI, de Leon J, Qureshi G, et al. Repetitive behaviors in schizophrenia: a single disturbance or discrete symptoms? Schizophr Res 1996;20(1-2):221-9.
7. Federman DG, Kirsner RS, Federman GS. Pica: Are you hungry for the facts? Conn Med 1997;61(4):207-9.
8. Parry-Jones B, Parry-Jones WL. Pica: symptom or eating disorder? A historical perspective. Br J Psychiatry. 1992;160:341-54.
9. Goldstein M. Adult pica: A clinical nexus of physiology and psychodynamics. Psychosom 1998;39:465-9.
10. Danford DE. Pica and nutrition. Annu Rev Nutr 1982;2:303-22.
11. Jackson WC, Martin JP. Amylophagia presenting as gestational diabetes. Arch Fam Med 2000;9(7):649-52.
12. Geissler PW, Prince RJ, Levene M, et al. Perceptions of soil-eating and anemia among pregnant women on the Kenyan coast. Soc Sci Med 1999;48(8):1069-79.
13. Parry-Jones B. Historical terminology of eating disorders. Psychol Med 1991;21:21-8.
14. Rose EA, Porcerelli JH, Neale AV. Pica: common but commonly missed. J Am Board Fam Pract 2000;13(5):353-8.
15. Castiglia PT. Pica. J Pediatr Health Care 1993;7(4):174-5.
16. Fairburn CG, Stein A, Jones R. Eating habits and eating disorders during pregnancy. Psychosom Med 1992;54(6):665-72.
17. Hook EB. Dietary cravings and aversions during pregnancy. Am J Clin Nutr 1978;31(8):1355-62.
18. Madden LJ, Seeley RJ, Woods SC. Intraventricular neuropeptide Y decreases need induced sodium appetite and increases pica in rats. Behav Neurosci 1999;113:826-32.
19. Appel RG, Bleyer AJ. Pica associated with renal and electrolyte disorders. Int J Artif Organs 1999;22(11):726-9.
20. Crosby WH. Pica. JAMA 1976;235(25):2765.-
21. Lofts RH, Schroeder SR, Maier RH. Effects of serum zinc supplementation on pica behavior of persons with mental retardation. Am J Ment Retard 1990;95(1):103-9.
22. Siklar Z, Gulten T, Dallor Y, Gunay S. Pica and intoxication in childhood. Clin Pediatr (Phila) 2000;39(10):624-5.
23. Rainville AJ. Pica practices of pregnant women are associated with lower maternal hemoglobin level at delivery. J Am Diet Assoc 1998;98(3):293-6.
24. Rothenberg SJ, Manalo M, Jiang J, et al. Maternal blood lead level during pregnancy in South Central Los Angeles. Arch Environ Health 1999;54(3):151-7.
25. Marinella MA. “Tomatophagia” and iron-deficiency anemia. N Engl J Med 1999;341(1):60-1.
26. Crosby WH. Pica: A compulsion caused by iron deficiency. Br J Haematol 1976;34(2):341-2.
History: An inpatient discovery
Ms. A, 20, presented to the emergency room with an exacerbation of asthma due to noncompliance with medications. A review of her systems and a physical exam revealed significant bilateral shortness of breath, wheezes, and rhonchi.
A single mother who lives with her two daughters, ages 5 and 2, Ms. A is 28 weeks pregnant with her third child. After receiving albuterol nebulizers for her asthma, she was admitted to the obstetrics and gynecology floor for monitoring of maternal and fetal status. There, a nursing staff member observed her eating baby powder.
The psychiatric team evaluated Ms. A and learned that, during her first pregnancy at age 15, she grew uncomfortable with her increased weight and started purging. Standing at 5 feet, 6 inches, Ms. A weighed as much as 220 during the pregnancy; her weight fell to 170 pounds after delivery. When she presented to us she lamented, “All of my friends are still thin.”
The stress of being a single teenage mother and going to school, combined with disgust over her physical appearance, provoked her purging. She did not think purging would help her lose weight but would prevent her from gaining more even as she ate as much as she wanted.
For 11 months after the birth of her first child, she purged three to four times daily. She could eat as many as five “value meals” within 2 to 3 hours at fast-food restaurants. Eating relaxed her and made her feel comfortable, but the frequency of purging escalated to five to six times daily and the vomiting was physically exhausting, painful, and caused esophageal damage.
At age 17, Ms. A became pregnant with her second child. In the first 2 to 3 months, she continued to eat large quantities of food but purged less often (two to three times daily).
One day in the third month of this pregnancy, Ms. A watched as her mother used medicated powder on her own child, and the powder's scent stimulated within Ms. A an urge to taste it. Before long Ms. A was eating the powder regularly and had stopped purging. She recalled purging only three times during the remaining 6 months of the pregnancy. The craving for powder replaced both her desire to vomit and the need to binge on food. She returned to regular binging and purging (once or twice weekly) after her second child was born, however.
In your view, which should be addressed first, the bulimia or the obsession with baby powder? Or should both be addressed in tandem?
Commentary
This case displays a form of adult pica for baby powder, which has only been described in the literature for pediatric pica.1,2 She displays no cognitive deficits or psychological disorders (e.g., mental retardation, schizophrenia) that are commonly associated with pica.3-6 Pregnancy, which is also common in pica, did exist in this patient and may provide some physiologic or psychological insight into the patient’s disorder.7 The patient’s bulimia nervosa, however, gives an unusual twist to this case.
In the 18th century, pica was classified together with bulimia simply as an erroneous or aberrant appetite (Box 1).8 Pica has been known to occur with—and can be a symptom of—bulimia and anorexia, but it is rarely cited.8,10 As in other eating disorders, affected individuals are ashamed of their weight, body shape, and body image.13
The term pica has evolved over centuries to describe the compulsive ingestion of non-nutritive substances or unusual food cravings. Its etymology stems from the Latin word for magpie (genus Pica), a bird said to pick up, carry away, and presumably eat a myriad of objects.
The word was first used in 1563 by Thomas Gale, who noted this consumption of unusual foodstuffs in pregnant women and children.8 In contemporary literature, the word “craving” is often used instead of pica to minimize social judgment toward practices that deviate from “normal.”
An estimated 20% of pregnant women are believed to have a history of pica, but the documented prevalence of these cravings may be underestimated because women often are embarrassed to disclose the behavior.9
Pica has been speculated to be a form of aggression, a result of compulsive neuroses, or a manifestation of oral fixation because of its association with thumb sucking.1 In the end, pica is a poorly understood disorder.
Scientists question the etiology of pica. Early psychiatric hypotheses focused on societal expectations of women’s outward beauty. A higher prevalence of pica has been recognized in mentally retarded persons and patients with schizophrenia.3-6
Pica is most frequently observed in children, pregnant women, and patients from a low socioeconomic background.10,11 More comprehensive studies have explored geophagia (a craving to eat chalk, clay, or dirt) in Africa and the southern United States.12
Comorbid bulimia and pica disorders tend to work together to accomplish a similar task: weight loss/control. Eating non-nutritive substances occupies space in the stomach, creating a sense of satiety without taking in calories. Therefore, this behavior acts as a substitute for binging in the patient with bulimia.14
One study identified eight themes associated with pica during pregnancy: keeping practices secret, singularity of the experience, extravagant means for obtaining the craved substance, fears for the effects on the fetus, yielding or not yielding to the cravings, use of the substances as medication, pica and lack of food intake, and sensory experiences other than taste.2 All eight of these themes were present in Ms. A.
Evaluation: Needing more and more
By her third pregnancy, Ms. A’s obsession with powder started to take hold. She found it easier to conceal the purging from her partner, so she began purging more often (twice daily) to offset her cravings for the baby powder. Purging was a last resort for the patient and her only means of off-setting her desire for the powder, which relieved her urge to vomit. She ate baby powder throughout the day, even awaking two to three times at night to ingest a few spoonfuls.
Until she presented to us, Ms. A had followed a daily ritual. At 10:30 a.m., when the local drug store opens, she superficially tested the consistency of a certain brand of powder available on the shelves. She then purchased one case (six 14-ounce containers) of powder, went home and sampled each container, and rated them in quality from 1 to 6, with 1 being the bottle of powder she ate that day. The next morning, regardless of how many cases of powder were piled in her closet, she went to the drug store and repeated the process.
Ms. A felt comfortable eating the talc-based powder in her apartment and her mother’s house. She kept some baby powder in her desk at work, but she regularly took an hour-long lunch break to drive back to her apartment and satisfy her craving. She also carried powder in the car, tasting it while driving.
When asked how the powder made her feel, Ms. A replied: “Powder is like nothing else. It makes me feel content and at ease.” Whenever she was irritated, or if the children were frustrating her, she would take a spoonful of powder.
In the beginning, she consumed approximately one 14-ounce bottle per month. When she presented 28 weeks pregnant with her third child, she could not imagine life without baby powder. A spoonful satisfied her for only 5 to 10 minutes before she would desire more. No other substance quelled the cravings. She had tried edible substitutes such as confectioners sugar, cornstarch, and ice chips, but nothing offered the satisfaction she got from powder.
When she is unable to ingest powder, she develops a headache, begins to sweat, gets extremely anxious and irritable, cries profusely, and becomes depressed. If she is abstinent more than 2 days she is unable to sleep and becomes preoccupied with the powder. If powder is not available, she binges and induces vomiting to stifle her craving.
In the hospital she craved powder 2 days after it was removed from her access. She became extremely anxious and distressed. She then ordered as much food as possible so she could purge and forget about the powder.
How would you explain the patient’s psychopathological attraction to baby powder?
Commentary
Patients with pica typically express satisfaction from consuming non-nutrient substances (Box 2). Ms. A’s motive for eating the powder stemmed from what she perceived as its soothing properties.
Other reported cases have alluded to the sensation generated by the texture of soil or chalk in the mouth. Some of these patients also described the importance of the soil’s taste—i.e., particle size—as being second to its texture.12 The desire to experience a certain texture, color, odor, and taste are important components in pica cravings.10
| Object | Specific disorder |
|---|---|
| Burnt matches | Cautopyreiophagia |
| Earth (chalk, clay, dirt) | Geophagia |
| Feces | Coprophagia |
| Hair | Tricophagia |
| Ice | Pagophagia |
| Laundry starch, cornstarch | Amylophagia |
| Lead paint chips | Plumbophagia |
| Raw potatoes | Geomelophagia |
| Stones | Lithophagia |
Other known objects of pica—Ashes, baking soda, balloons, carrots, celery, chewing gum, cigarette butts, cloth, coal, coca leaf, coffee grounds/beans, cotton balls, concrete, crayons, croutons, detergent, grass, hard candy, insects, lavatory fresheners, latex gloves, licorice, lint, metal, milk, newsprint, oats, oyster shells, paper, parsley, plant leaves, pencil erasers, plastic, popcorn, powder puffs, salt, soap, string, thread, toilet tissue, tomato seeds, twigs, vinegar, wood.
Pica appears to meet the individual’s need for mental relaxation and sensory pleasure15 in much the same way that alcohol or drug abusers satisfy their intense desire for euphoria and relaxation. Scientists theorize that alcohol and drug abuse may be exacerbated by or result from a neurochemical imbalance. A similar hypothesis may explain this “variant” in pica patients.
Pregnant women often develop taste aversions for items that are potentially harmful to the developing fetus, such as alcohol and coffee. Expectant mothers may develop utter disgust and provocation of nausea toward items they enjoyed while not gravid. Aversions to foods and other items during pregnancy might be the consequence of homeostatic factors that have evolved as general feto-protective mechanisms.16,17 The metabolic changes that accompany the gravid state might alter olfactory and taste sensitivity.17
If a pregnancy-related change in chemical balance can cause taste aversion, certainly a similar situation could evolve into pica. In laboratory rats, intraventricular injection of exogenous neuropeptide Y, a hormone with documented CNS activity, caused taste aversions and elicited geophagia.18
Ms. A’s ingestion of baby powder itself did not harm the fetus. Stephen Emery, MD, director of perinatal ultrasound at the Cleveland Clinic, notes that talc is inert and the powder’s perfumes probably are benign. He adds, however, that because the powder often has replaced real food, Ms. A placed her unborn child at risk via malnourishment.
Further evaluation: A ‘pleasant’ appearance
Ms. A’s medical history revealed chronic asthma since childhood and gastroesophageal reflux disease. According to her social history, she is dating the father of her expectant child. She has been smoking one pack of cigarettes per day for 2 years but says she does not drink alcohol and has never abused illicit drugs.
Her lab values were as follows (with normal ranges in parentheses): blood urea, 4 mg/dl (9-23); serum iron, 69 mg/dl (42-135); calcium 8.7 mg/dl (8.5-10.5); magnesium, 1.6 mg/dl (1.8-2.4); phosphate, 2.4 mg/dl (2.7-4.6); hemoglobin, 10.0 g/dl (12.0-14.0); hematocrit, 31.1% (37.0-47.0); mean corpuscular volume, 86.4 fl (81-99).
Ms. A appeared well-nourished, appropriately dressed, and well-groomed during our examination. She was alert, oriented and cooperative, and held a pleasant conversation with good eye contact. Her mood was depressed and anxious, and her affect was congruent. Speech was normal in rate, tone, and volume. Her thoughts were well organized and goal-directed. She denied suicidal ideation but had thoughts of harming her fetus. She denied any perceptual disturbances. No intellectual impairment was evident, and her insight and judgment were preserved.
What is the psychiatric diagnosis for this patient? Also, in your view, how likely is she to harm her fetus or her two children? How would you assess and manage that risk?
Commentary
The physiologic cause of pica may be metabolic disturbances in iron, zinc, calcium, potassium, lead, and magnesium.10,19-22 Ice pica typically is associated with iron deficiency and low hemoglobin levels,14,20,23,24 although other forms of pica have been linked to iron deficiency.12,25 Some studies show iron deficiency in nearly half of patients who display ice pica;20,26 correcting the iron deficiency relieves the cravings for the desired substances.7,14 Scientists are split as to whether pica results in the deficiency of certain minerals or whether mineral deficiencies cause pica. Mineral deficiencies may alter appetite-regulating brain enzymes that can lead to these cravings.7,10,11,23
Ms. A’s laboratory values demonstrated decreased hemoglobin, hematocrit, and magnesium levels. Magnesium replacement did not change her eating behavior. Her mild anemia may simply have been an effect of pregnancy.
Treatment: Confronting comorbid depression
Ms. A’s diagnosis was pica, bulimia nervosa-purging type, with comorbid depressive disorder NOS.
She was placed on the selective serotonin reuptake inhibitor sertraline, 12.5 mg/d. The dosage was increased gradually to 50 mg qd. Supportive psychotherapy was provided during the patient’s hospital course.
After her discharge, cognitive therapy was initiated. Ms. A was asked to keep a journal utilizing the “triple column technique,” through which she described a situation in one column, explained the symptoms or unwanted behaviors and emotions evoked by that situation in the second, and wrote down her thoughts in the third.
Ms. A was monitored for signs and symptoms of postpartum depression. After this careful assessment, in which two psychiatrists and the ob/gyn team participated, we concluded that the patient’s transient thoughts of harming her fetus had fully resolved.
Ms. A was educated about nutrition and healthy exercise, as well as birth control options. We also asked to see her as an outpatient.
In the ensuing months, Ms. A reported moderate depressive symptoms but described a significant decrease in her craving for, and consumption of, powder. She continued follow-up treatment with her physician at the women’s care center. Ms. A decided to stop taking sertraline after 2 months because she felt it was not helping her depression and was causing fatigue.
When we followed up after 6 months, Ms. A reported that she and her baby were doing well. She told us that her powder cravings had decreased markedly.
Related resources
- Alliance for Eating Disorders Awareness. www.eatingdisorderinfo.org
- Stein DJ, Bouwer C, van Heerden B. Pica and the obsessive spectrum disorders. S Afr Med J 1996; 86(12 suppl):1586-8, 1591-2.
Drug brand names
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
History: An inpatient discovery
Ms. A, 20, presented to the emergency room with an exacerbation of asthma due to noncompliance with medications. A review of her systems and a physical exam revealed significant bilateral shortness of breath, wheezes, and rhonchi.
A single mother who lives with her two daughters, ages 5 and 2, Ms. A is 28 weeks pregnant with her third child. After receiving albuterol nebulizers for her asthma, she was admitted to the obstetrics and gynecology floor for monitoring of maternal and fetal status. There, a nursing staff member observed her eating baby powder.
The psychiatric team evaluated Ms. A and learned that, during her first pregnancy at age 15, she grew uncomfortable with her increased weight and started purging. Standing at 5 feet, 6 inches, Ms. A weighed as much as 220 during the pregnancy; her weight fell to 170 pounds after delivery. When she presented to us she lamented, “All of my friends are still thin.”
The stress of being a single teenage mother and going to school, combined with disgust over her physical appearance, provoked her purging. She did not think purging would help her lose weight but would prevent her from gaining more even as she ate as much as she wanted.
For 11 months after the birth of her first child, she purged three to four times daily. She could eat as many as five “value meals” within 2 to 3 hours at fast-food restaurants. Eating relaxed her and made her feel comfortable, but the frequency of purging escalated to five to six times daily and the vomiting was physically exhausting, painful, and caused esophageal damage.
At age 17, Ms. A became pregnant with her second child. In the first 2 to 3 months, she continued to eat large quantities of food but purged less often (two to three times daily).
One day in the third month of this pregnancy, Ms. A watched as her mother used medicated powder on her own child, and the powder's scent stimulated within Ms. A an urge to taste it. Before long Ms. A was eating the powder regularly and had stopped purging. She recalled purging only three times during the remaining 6 months of the pregnancy. The craving for powder replaced both her desire to vomit and the need to binge on food. She returned to regular binging and purging (once or twice weekly) after her second child was born, however.
In your view, which should be addressed first, the bulimia or the obsession with baby powder? Or should both be addressed in tandem?
Commentary
This case displays a form of adult pica for baby powder, which has only been described in the literature for pediatric pica.1,2 She displays no cognitive deficits or psychological disorders (e.g., mental retardation, schizophrenia) that are commonly associated with pica.3-6 Pregnancy, which is also common in pica, did exist in this patient and may provide some physiologic or psychological insight into the patient’s disorder.7 The patient’s bulimia nervosa, however, gives an unusual twist to this case.
In the 18th century, pica was classified together with bulimia simply as an erroneous or aberrant appetite (Box 1).8 Pica has been known to occur with—and can be a symptom of—bulimia and anorexia, but it is rarely cited.8,10 As in other eating disorders, affected individuals are ashamed of their weight, body shape, and body image.13
The term pica has evolved over centuries to describe the compulsive ingestion of non-nutritive substances or unusual food cravings. Its etymology stems from the Latin word for magpie (genus Pica), a bird said to pick up, carry away, and presumably eat a myriad of objects.
The word was first used in 1563 by Thomas Gale, who noted this consumption of unusual foodstuffs in pregnant women and children.8 In contemporary literature, the word “craving” is often used instead of pica to minimize social judgment toward practices that deviate from “normal.”
An estimated 20% of pregnant women are believed to have a history of pica, but the documented prevalence of these cravings may be underestimated because women often are embarrassed to disclose the behavior.9
Pica has been speculated to be a form of aggression, a result of compulsive neuroses, or a manifestation of oral fixation because of its association with thumb sucking.1 In the end, pica is a poorly understood disorder.
Scientists question the etiology of pica. Early psychiatric hypotheses focused on societal expectations of women’s outward beauty. A higher prevalence of pica has been recognized in mentally retarded persons and patients with schizophrenia.3-6
Pica is most frequently observed in children, pregnant women, and patients from a low socioeconomic background.10,11 More comprehensive studies have explored geophagia (a craving to eat chalk, clay, or dirt) in Africa and the southern United States.12
Comorbid bulimia and pica disorders tend to work together to accomplish a similar task: weight loss/control. Eating non-nutritive substances occupies space in the stomach, creating a sense of satiety without taking in calories. Therefore, this behavior acts as a substitute for binging in the patient with bulimia.14
One study identified eight themes associated with pica during pregnancy: keeping practices secret, singularity of the experience, extravagant means for obtaining the craved substance, fears for the effects on the fetus, yielding or not yielding to the cravings, use of the substances as medication, pica and lack of food intake, and sensory experiences other than taste.2 All eight of these themes were present in Ms. A.
Evaluation: Needing more and more
By her third pregnancy, Ms. A’s obsession with powder started to take hold. She found it easier to conceal the purging from her partner, so she began purging more often (twice daily) to offset her cravings for the baby powder. Purging was a last resort for the patient and her only means of off-setting her desire for the powder, which relieved her urge to vomit. She ate baby powder throughout the day, even awaking two to three times at night to ingest a few spoonfuls.
Until she presented to us, Ms. A had followed a daily ritual. At 10:30 a.m., when the local drug store opens, she superficially tested the consistency of a certain brand of powder available on the shelves. She then purchased one case (six 14-ounce containers) of powder, went home and sampled each container, and rated them in quality from 1 to 6, with 1 being the bottle of powder she ate that day. The next morning, regardless of how many cases of powder were piled in her closet, she went to the drug store and repeated the process.
Ms. A felt comfortable eating the talc-based powder in her apartment and her mother’s house. She kept some baby powder in her desk at work, but she regularly took an hour-long lunch break to drive back to her apartment and satisfy her craving. She also carried powder in the car, tasting it while driving.
When asked how the powder made her feel, Ms. A replied: “Powder is like nothing else. It makes me feel content and at ease.” Whenever she was irritated, or if the children were frustrating her, she would take a spoonful of powder.
In the beginning, she consumed approximately one 14-ounce bottle per month. When she presented 28 weeks pregnant with her third child, she could not imagine life without baby powder. A spoonful satisfied her for only 5 to 10 minutes before she would desire more. No other substance quelled the cravings. She had tried edible substitutes such as confectioners sugar, cornstarch, and ice chips, but nothing offered the satisfaction she got from powder.
When she is unable to ingest powder, she develops a headache, begins to sweat, gets extremely anxious and irritable, cries profusely, and becomes depressed. If she is abstinent more than 2 days she is unable to sleep and becomes preoccupied with the powder. If powder is not available, she binges and induces vomiting to stifle her craving.
In the hospital she craved powder 2 days after it was removed from her access. She became extremely anxious and distressed. She then ordered as much food as possible so she could purge and forget about the powder.
How would you explain the patient’s psychopathological attraction to baby powder?
Commentary
Patients with pica typically express satisfaction from consuming non-nutrient substances (Box 2). Ms. A’s motive for eating the powder stemmed from what she perceived as its soothing properties.
Other reported cases have alluded to the sensation generated by the texture of soil or chalk in the mouth. Some of these patients also described the importance of the soil’s taste—i.e., particle size—as being second to its texture.12 The desire to experience a certain texture, color, odor, and taste are important components in pica cravings.10
| Object | Specific disorder |
|---|---|
| Burnt matches | Cautopyreiophagia |
| Earth (chalk, clay, dirt) | Geophagia |
| Feces | Coprophagia |
| Hair | Tricophagia |
| Ice | Pagophagia |
| Laundry starch, cornstarch | Amylophagia |
| Lead paint chips | Plumbophagia |
| Raw potatoes | Geomelophagia |
| Stones | Lithophagia |
Other known objects of pica—Ashes, baking soda, balloons, carrots, celery, chewing gum, cigarette butts, cloth, coal, coca leaf, coffee grounds/beans, cotton balls, concrete, crayons, croutons, detergent, grass, hard candy, insects, lavatory fresheners, latex gloves, licorice, lint, metal, milk, newsprint, oats, oyster shells, paper, parsley, plant leaves, pencil erasers, plastic, popcorn, powder puffs, salt, soap, string, thread, toilet tissue, tomato seeds, twigs, vinegar, wood.
Pica appears to meet the individual’s need for mental relaxation and sensory pleasure15 in much the same way that alcohol or drug abusers satisfy their intense desire for euphoria and relaxation. Scientists theorize that alcohol and drug abuse may be exacerbated by or result from a neurochemical imbalance. A similar hypothesis may explain this “variant” in pica patients.
Pregnant women often develop taste aversions for items that are potentially harmful to the developing fetus, such as alcohol and coffee. Expectant mothers may develop utter disgust and provocation of nausea toward items they enjoyed while not gravid. Aversions to foods and other items during pregnancy might be the consequence of homeostatic factors that have evolved as general feto-protective mechanisms.16,17 The metabolic changes that accompany the gravid state might alter olfactory and taste sensitivity.17
If a pregnancy-related change in chemical balance can cause taste aversion, certainly a similar situation could evolve into pica. In laboratory rats, intraventricular injection of exogenous neuropeptide Y, a hormone with documented CNS activity, caused taste aversions and elicited geophagia.18
Ms. A’s ingestion of baby powder itself did not harm the fetus. Stephen Emery, MD, director of perinatal ultrasound at the Cleveland Clinic, notes that talc is inert and the powder’s perfumes probably are benign. He adds, however, that because the powder often has replaced real food, Ms. A placed her unborn child at risk via malnourishment.
Further evaluation: A ‘pleasant’ appearance
Ms. A’s medical history revealed chronic asthma since childhood and gastroesophageal reflux disease. According to her social history, she is dating the father of her expectant child. She has been smoking one pack of cigarettes per day for 2 years but says she does not drink alcohol and has never abused illicit drugs.
Her lab values were as follows (with normal ranges in parentheses): blood urea, 4 mg/dl (9-23); serum iron, 69 mg/dl (42-135); calcium 8.7 mg/dl (8.5-10.5); magnesium, 1.6 mg/dl (1.8-2.4); phosphate, 2.4 mg/dl (2.7-4.6); hemoglobin, 10.0 g/dl (12.0-14.0); hematocrit, 31.1% (37.0-47.0); mean corpuscular volume, 86.4 fl (81-99).
Ms. A appeared well-nourished, appropriately dressed, and well-groomed during our examination. She was alert, oriented and cooperative, and held a pleasant conversation with good eye contact. Her mood was depressed and anxious, and her affect was congruent. Speech was normal in rate, tone, and volume. Her thoughts were well organized and goal-directed. She denied suicidal ideation but had thoughts of harming her fetus. She denied any perceptual disturbances. No intellectual impairment was evident, and her insight and judgment were preserved.
What is the psychiatric diagnosis for this patient? Also, in your view, how likely is she to harm her fetus or her two children? How would you assess and manage that risk?
Commentary
The physiologic cause of pica may be metabolic disturbances in iron, zinc, calcium, potassium, lead, and magnesium.10,19-22 Ice pica typically is associated with iron deficiency and low hemoglobin levels,14,20,23,24 although other forms of pica have been linked to iron deficiency.12,25 Some studies show iron deficiency in nearly half of patients who display ice pica;20,26 correcting the iron deficiency relieves the cravings for the desired substances.7,14 Scientists are split as to whether pica results in the deficiency of certain minerals or whether mineral deficiencies cause pica. Mineral deficiencies may alter appetite-regulating brain enzymes that can lead to these cravings.7,10,11,23
Ms. A’s laboratory values demonstrated decreased hemoglobin, hematocrit, and magnesium levels. Magnesium replacement did not change her eating behavior. Her mild anemia may simply have been an effect of pregnancy.
Treatment: Confronting comorbid depression
Ms. A’s diagnosis was pica, bulimia nervosa-purging type, with comorbid depressive disorder NOS.
She was placed on the selective serotonin reuptake inhibitor sertraline, 12.5 mg/d. The dosage was increased gradually to 50 mg qd. Supportive psychotherapy was provided during the patient’s hospital course.
After her discharge, cognitive therapy was initiated. Ms. A was asked to keep a journal utilizing the “triple column technique,” through which she described a situation in one column, explained the symptoms or unwanted behaviors and emotions evoked by that situation in the second, and wrote down her thoughts in the third.
Ms. A was monitored for signs and symptoms of postpartum depression. After this careful assessment, in which two psychiatrists and the ob/gyn team participated, we concluded that the patient’s transient thoughts of harming her fetus had fully resolved.
Ms. A was educated about nutrition and healthy exercise, as well as birth control options. We also asked to see her as an outpatient.
In the ensuing months, Ms. A reported moderate depressive symptoms but described a significant decrease in her craving for, and consumption of, powder. She continued follow-up treatment with her physician at the women’s care center. Ms. A decided to stop taking sertraline after 2 months because she felt it was not helping her depression and was causing fatigue.
When we followed up after 6 months, Ms. A reported that she and her baby were doing well. She told us that her powder cravings had decreased markedly.
Related resources
- Alliance for Eating Disorders Awareness. www.eatingdisorderinfo.org
- Stein DJ, Bouwer C, van Heerden B. Pica and the obsessive spectrum disorders. S Afr Med J 1996; 86(12 suppl):1586-8, 1591-2.
Drug brand names
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article.
1. Robischon P. Pica practice and other hand-mouth behavior and children’s development level. Nurs Res 1971;20(1):4-16.
2. Cooksey NR. Pica and olfactory craving of pregnancy: How deep are the secrets? Birth 1995;22(3):129-37.
3. Danford DE, Smith JC, Huber AM. Pica and mineral status in the mentally retarded. Am J Clin Nutr 1982;35(5):958-67.
4. Jawed SH, Krishnan VH, et al. Worsening of pica as a symptom of Depressive illness in a person with severe mental handicap. Br J Psychiatry 1993;162:835-7.
5. Sturmey P. Pica and developmental disability. J Am Board Fam Pract 2001;14(1):80-1.
6. Tracy JI, de Leon J, Qureshi G, et al. Repetitive behaviors in schizophrenia: a single disturbance or discrete symptoms? Schizophr Res 1996;20(1-2):221-9.
7. Federman DG, Kirsner RS, Federman GS. Pica: Are you hungry for the facts? Conn Med 1997;61(4):207-9.
8. Parry-Jones B, Parry-Jones WL. Pica: symptom or eating disorder? A historical perspective. Br J Psychiatry. 1992;160:341-54.
9. Goldstein M. Adult pica: A clinical nexus of physiology and psychodynamics. Psychosom 1998;39:465-9.
10. Danford DE. Pica and nutrition. Annu Rev Nutr 1982;2:303-22.
11. Jackson WC, Martin JP. Amylophagia presenting as gestational diabetes. Arch Fam Med 2000;9(7):649-52.
12. Geissler PW, Prince RJ, Levene M, et al. Perceptions of soil-eating and anemia among pregnant women on the Kenyan coast. Soc Sci Med 1999;48(8):1069-79.
13. Parry-Jones B. Historical terminology of eating disorders. Psychol Med 1991;21:21-8.
14. Rose EA, Porcerelli JH, Neale AV. Pica: common but commonly missed. J Am Board Fam Pract 2000;13(5):353-8.
15. Castiglia PT. Pica. J Pediatr Health Care 1993;7(4):174-5.
16. Fairburn CG, Stein A, Jones R. Eating habits and eating disorders during pregnancy. Psychosom Med 1992;54(6):665-72.
17. Hook EB. Dietary cravings and aversions during pregnancy. Am J Clin Nutr 1978;31(8):1355-62.
18. Madden LJ, Seeley RJ, Woods SC. Intraventricular neuropeptide Y decreases need induced sodium appetite and increases pica in rats. Behav Neurosci 1999;113:826-32.
19. Appel RG, Bleyer AJ. Pica associated with renal and electrolyte disorders. Int J Artif Organs 1999;22(11):726-9.
20. Crosby WH. Pica. JAMA 1976;235(25):2765.-
21. Lofts RH, Schroeder SR, Maier RH. Effects of serum zinc supplementation on pica behavior of persons with mental retardation. Am J Ment Retard 1990;95(1):103-9.
22. Siklar Z, Gulten T, Dallor Y, Gunay S. Pica and intoxication in childhood. Clin Pediatr (Phila) 2000;39(10):624-5.
23. Rainville AJ. Pica practices of pregnant women are associated with lower maternal hemoglobin level at delivery. J Am Diet Assoc 1998;98(3):293-6.
24. Rothenberg SJ, Manalo M, Jiang J, et al. Maternal blood lead level during pregnancy in South Central Los Angeles. Arch Environ Health 1999;54(3):151-7.
25. Marinella MA. “Tomatophagia” and iron-deficiency anemia. N Engl J Med 1999;341(1):60-1.
26. Crosby WH. Pica: A compulsion caused by iron deficiency. Br J Haematol 1976;34(2):341-2.
1. Robischon P. Pica practice and other hand-mouth behavior and children’s development level. Nurs Res 1971;20(1):4-16.
2. Cooksey NR. Pica and olfactory craving of pregnancy: How deep are the secrets? Birth 1995;22(3):129-37.
3. Danford DE, Smith JC, Huber AM. Pica and mineral status in the mentally retarded. Am J Clin Nutr 1982;35(5):958-67.
4. Jawed SH, Krishnan VH, et al. Worsening of pica as a symptom of Depressive illness in a person with severe mental handicap. Br J Psychiatry 1993;162:835-7.
5. Sturmey P. Pica and developmental disability. J Am Board Fam Pract 2001;14(1):80-1.
6. Tracy JI, de Leon J, Qureshi G, et al. Repetitive behaviors in schizophrenia: a single disturbance or discrete symptoms? Schizophr Res 1996;20(1-2):221-9.
7. Federman DG, Kirsner RS, Federman GS. Pica: Are you hungry for the facts? Conn Med 1997;61(4):207-9.
8. Parry-Jones B, Parry-Jones WL. Pica: symptom or eating disorder? A historical perspective. Br J Psychiatry. 1992;160:341-54.
9. Goldstein M. Adult pica: A clinical nexus of physiology and psychodynamics. Psychosom 1998;39:465-9.
10. Danford DE. Pica and nutrition. Annu Rev Nutr 1982;2:303-22.
11. Jackson WC, Martin JP. Amylophagia presenting as gestational diabetes. Arch Fam Med 2000;9(7):649-52.
12. Geissler PW, Prince RJ, Levene M, et al. Perceptions of soil-eating and anemia among pregnant women on the Kenyan coast. Soc Sci Med 1999;48(8):1069-79.
13. Parry-Jones B. Historical terminology of eating disorders. Psychol Med 1991;21:21-8.
14. Rose EA, Porcerelli JH, Neale AV. Pica: common but commonly missed. J Am Board Fam Pract 2000;13(5):353-8.
15. Castiglia PT. Pica. J Pediatr Health Care 1993;7(4):174-5.
16. Fairburn CG, Stein A, Jones R. Eating habits and eating disorders during pregnancy. Psychosom Med 1992;54(6):665-72.
17. Hook EB. Dietary cravings and aversions during pregnancy. Am J Clin Nutr 1978;31(8):1355-62.
18. Madden LJ, Seeley RJ, Woods SC. Intraventricular neuropeptide Y decreases need induced sodium appetite and increases pica in rats. Behav Neurosci 1999;113:826-32.
19. Appel RG, Bleyer AJ. Pica associated with renal and electrolyte disorders. Int J Artif Organs 1999;22(11):726-9.
20. Crosby WH. Pica. JAMA 1976;235(25):2765.-
21. Lofts RH, Schroeder SR, Maier RH. Effects of serum zinc supplementation on pica behavior of persons with mental retardation. Am J Ment Retard 1990;95(1):103-9.
22. Siklar Z, Gulten T, Dallor Y, Gunay S. Pica and intoxication in childhood. Clin Pediatr (Phila) 2000;39(10):624-5.
23. Rainville AJ. Pica practices of pregnant women are associated with lower maternal hemoglobin level at delivery. J Am Diet Assoc 1998;98(3):293-6.
24. Rothenberg SJ, Manalo M, Jiang J, et al. Maternal blood lead level during pregnancy in South Central Los Angeles. Arch Environ Health 1999;54(3):151-7.
25. Marinella MA. “Tomatophagia” and iron-deficiency anemia. N Engl J Med 1999;341(1):60-1.
26. Crosby WH. Pica: A compulsion caused by iron deficiency. Br J Haematol 1976;34(2):341-2.
Strategies to prevent fatal arrhythmias in patients taking antipsychotics
Before approving the antipsychotic agent ziprasidone last year, the Food and Drug Administration required specific safety data on whether the drug might cause the life-threatening arrhythmia known as torsade de pointes.
The FDA’s action, which delayed the drug’s approval for 3 years, underscores growing concern about the risk of cardiovascular effects with the use of antipsychotic and other agents known to prolong the cardiac QT interval. This concern has led to withdrawal of some drugs before reaching the market (e.g., the atypical neuroleptic sertindole), the addition of “black box” warnings in the labeling of some antipsychotics, and withdrawal from the market of antihistamines terfenadine and astemizole and the GI stimulant cisapride.
Torsade de pointes is a polymorphic ventricular tachycardia (VT), a rare arrhythmia that can cause sudden death. Because torsade can occur with the use of some antipsychotics, the psychiatrist needs to consider cardiovascular safety when selecting among available agents. To help with these decisions, here is information about the documented and potential electrocardiographic features of commonly prescribed antipsychotic drugs, as well as background on QT interval prolongation and torsade de pointes.
Torsade de pointes
Named for a ballet movement, torsade de pointes describes bursts of “twisting of the points,” a variation of the morphology of the QRS vector about the isoelectric axis from positive to net negative and back again. As seen on an ECG (Figure 1), the first beat of torsade de pointes is a normal ventricular complex preceded by a P wave. This is followed by a premature ventricular contraction (PVC) with a short coupling interval. After a compensatory pause, a second normal beat is followed by a second PVC, which is the first beat of a polymorphic VT. We know tachycardia is present because the ventricular beats appear close together. We know the arrhythmia is ventricular in origin because the ventricular complexes are wide. Finally, we note the ventricular complexes vary in configuration—that is, the shape (morphology) varies from beat to beat.
Figure 1 Typical ECG features of torsade de pointes
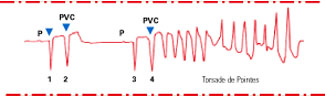
Sinus beat with normal ventricular complex (1) followed by premature ventricular contraction (PVC) (2) with short coupling interval. After a long pause (long refractory period), another sinus beat (3) is followed by another PVC (4) with a short coupling interval. The second PVC (4) is the first beat of polymorphic ventricular tachycardiaIn torsade, the stimulus for the VT moves within the ventricle, changing its shape from beat to beat. This multifocal VT differs from the more common unifocal VT, in which all the QRS complexes appear the same.
Drug-induced torsade de pointes
Although the term torsade de pointes was first described in 1966,1 the drug-induced form of this arrhythmia has been recognized for nearly a century.
Quinidine Around 1920, cardiologists first used quinidine to help restore normal sinus rhythm in patients with atrial fibrillation, most commonly due to rheumatic heart disease.2
In 1964, Selzer and Wray3 studied the use of quinidine to convert atrial fibrillation to normal sinus rhythm in more than 200 patients seen during 4 years in a cardiopulmonary clinic. In a subgroup of eight patients, these researchers documented 10 reactions (including five documented episodes of ventricular fibrillation/ventricular flutter) among 36 syncopal episodes that developed within 1 to 6.5 hours of quinidine administration. Symptoms were nonspecific and included nausea, faintness, and feeling ill. It is now recognized that torsade de pointes was the principal rhythm disturbance in those eight patients. Syncope usually occurs early in treatment and may be found in 5% to 10% of patients taking quinidine.
TCAs and antipsychotics Tricyclic antidepressants (TCAs) and antipsychotics that have quinidine-like properties (e.g., thioridazine) also may be associated with QT interval prolongation and torsade de pointes.4-9 In high doses (particularly in overdose), TCAs may induce widening of the QRS complex. Fowler et al reported episodes of VT in five patients taking thioridazine—one of whom died.10
Mehtonen et al reported sudden unexpected deaths associated with antipsychotic or antidepressant drugs among 31 women and 18 men in a survey of autopsies performed from 1985 to 1988 in Finland. The authors documented therapeutic use of phenothiazines in all but 3 of the 49 cases. Thioridazine was involved in more than half the deaths. In 15 of the deaths, thioridazine was the only antipsychotic drug taken. Drugs other than thioridazine were documented in only 5 of the 49 sudden cardiac deaths.11
Figure 2 Normal ECG in sinus rhythm
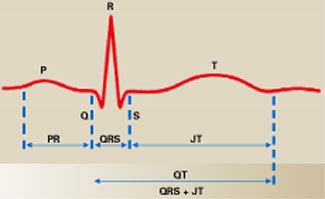
In this typical lead II of a surface ECG, the P wave (atrial depolarization) leads to right and left atrial contraction and the QRS complex (ventricular depolarization) leads to left and right ventricular contraction. The ST segment represents isoelectric ventricular repolarization, and the T wave represents directional repolarization. The QT interval includes both ventricular depolarization (QRS complex) and ventricular repolarization (JT interval, or ST segment plus T wave).
QT interval as a marker for torsade
The incidence of torsade is unknown, but it is an uncommon cardiac abnormality. In the United States, torsade probably accounts for less than 5% of the 300,000 sudden cardiac deaths that occur each year. Because torsade de pointes is rare, regulatory agencies and clinicians use the QT interval as a surrogate ECG marker for risk of torsade de pointes. Heart rate can affect the QT interval, so various formulae are used to correct the QT interval for heart rate (QTc).
What is the QT interval? In a normal ECG (Figure 2), the P wave derives from right and left atrial electrical depolarization. The pacemaker of the heart is located in the sino-atrial node (SAN) in the superior portion of the right atrium. From the SAN, electrical signals travel down three intra-atrial pathways, activating the right atrium, then travel to the atrioventricular node (AVN). Bachmann’s bundle—a fourth atrial pathway—passes from the SAN to depolarize the left atrium. From the AVN, the electrical signal travels through the left and right bundle branches to activate their respective ventricles.
Electrical depolarization of the left and right ventricles produces the QRS complex. Most of the electrical forces making up this complex arise in the left ventricle, which is much larger than the right ventricle.
The electrical circuitry of the heart activates the left and right atria in such a fashion that these chambers eject blood into their respective ventricles just before these chambers contract. Optimal ventricular filling maximizes ventricular ejection of blood (Starling’s law). Ventricular repolarization (JT interval—electrical recovery) follows ventricular depolarization. On the surface ECG, the JT interval consists of an isoelectric event—the ST segment running from the end of the QRS complex to the beginning of the T wave—and the T wave itself (directional electrical recovery).
The QT interval, then, consists of both ventricular depolarization (QRS complex) and ventricular repolarization (JT interval). Ventricular repolarization makes up by far the greater portion of the QT interval.
Correcting the QT interval (QTc) In 1920, Bazett noted that as the heart rate slowed, the QT interval lengthened.12 From personal and reported observations, he derived an equation called the Bazett formula that corrects (or normalizes) the QT interval to a heart rate of 60 beats/min (QTc). In the Bazett formula, the QTc interval is the measured QT interval divided by the square root of the RR interval (time between sequential QRS complexes—the determinant of heart rate) measured in seconds (QTc = QT/RR).
The Bazett formula is most widely used to estimate the QTc interval, although at least 20 other formulae have been developed in response to the original’s perceived inadequacies.13-15 Bazett’s formula is used in most automated interpretations of the ECG.
Up to age 55, the normal QTc interval ranges from 350 to 430 msec for men and 350 to 450 msec for women, and it tends to increase with age. Most cases of torsade occur when the QT or QTc interval is greater than 500 msec.14 A QTc interval between 450 and 500 msec is cause for concern; a QTc interval that exceeds 500 msec is cause for alarm.
Factors that cause variations in QTc
Factors that can affect the QTc interval and increase the risk of torsade de pointes include electrolyte imbalances, medication use and overdose, cardiac disease, liver disease, endocrine disorders such as diabetes and hypothyroidism, and CNS injury (Table 1).
Table 1
Risk factors contributing to QTc interval prolongation
| Risk factor | Causes/implications |
|---|---|
| Sex (female) | QT intervals longer in women than in men QT interval longer during first half of menstrual cycle |
| Age (elderly) | Increased risk for CAD Multiple medications Pharmacokinetic/pharmacodynamic changes |
| Electrolyte imbalance Hypokalemia, hypomagnesemia Hypocalcemia | Diuretic use Excessive vomiting or diarrhea Postprandial hypokalemia |
| Congenital long QT syndrome | Associated with torsade and sudden death |
| Cardiac disease, with history of acute or chronic myocardial ischemia, CHF, cardiac arrhythmias, bradycardia | Increased risk of cardiac arrhythmias |
| Drugs known to prolong QTc interval | May potentiate QTc prolongation |
| Medication overdose with drugs that prolong the QTc interval | QTc prolongation generally dose-dependent |
| Concomitant medications, liver disease | Adverse events with cytochrome P-450 enzyme system inhibition, leading to increased drug levels that can increase QT interval |
| Endocrine/metabolic disorders Diabetes, obesity Hypothyroidism, pituitary insufficiency | Via electrolytes or cardiovascular disease |
| CNS injury Stroke, infection, trauma | Via autonomic nervous system dysfunction |
Circadian patterns The QTc interval varies throughout the 24-hour day, with nocturnal values about 20 msec greater than daytime measurements. These differences are driven by changes in autonomic (sympathetic and parasympathetic) tone.16,17 In 20 normal subjects, circadian variability was 76 ± 19 msec (range 35 to 108 msec) from day to night.17 This circadian variation may be accentuated in patients with cardiovascular disease.
Sex. At birth, QTc interval measurements do no vary by sex.18 At puberty, however, the male QTc interval shortens and remains shorter than its female counterpart by about 20 msec until age 50 to 55, coincident with a decline in male testosterone levels. This sex difference appears to be androgen driven. About 70% of torsade de pointes cases occur in women.18
Menstrual cycle QTc interval measurements are stable throughout the menstrual cycle if quinidine-like drugs are not given.
Variations were seen, however, when Rodriguez et al studied the effect of IV low-dose ibutilide (an antiarrhythmic agent known to prolong the QT interval) on the QTc intervals of 58 healthy subjects (38 men and 20 women, ages 21 to 40). During 1 month, men were studied once and women studied three times, coincident with the three phases of the menstrual cycle. The greatest increase in QTc intervals measurements occurred in women during the first half of their menstrual cycles.19
Age and cardiovascular disease Two congenital long QT syndromes may be associated with sudden death, mostly in children and young adults:
- The Jervell and Lange-Nielsen syndrome is marked by severe congenital deafness and autosomal recessive inheritance.
- The Romano-Ward syndrome has normal hearing and autosomal dominant inheritance.20
Congenital long QT syndrome (LQTS) occurs in about one in 5,000 births and accounts for about 3,000 to 4,000 deaths per year in the United States. Nine percent of pediatric LQTS subjects present with sudden cardiac death. More than 71% of patients will die before age 15 if not treated.
Elderly persons tend to have longer QTc intervals than do younger subjects, even when both groups are free of cardiovascular disease.21 Also, age-matched subjects with cardiovascular disease tend to have longer QTc intervals than do those free of cardiovascular disease.
Electrolytes Electrolyte disturbances, particularly hypokalemia and hypomagnesemia, may contribute to or even cause QT interval prolongation.22
Hypokalemia prolongs the cardiac action potential and may cause early afterdepolarization, leading to torsade.23 Low potassium levels reduce the net outward potassium current during phase 3 of the cardiac action potential. Hypomagnesemia may contribute to gross U wave alternans, lengthening the cardiac action potential and setting the stage for torsade.24 Various factors may contribute to electrolyte disturbances, including use of diuretics and excessive vomiting and diarrhea. Even postprandial states may induce hypokalemia.
Intensive exercise and agitation may be associated with hypokalemia.25 Serum potassium may be lower in severely agitated patients (3.59 mmol/L) than in mildly agitated patients (3.79 mmol/L). The mean QTc interval of psychiatric emergency patients may be prolonged (453±40 msec),5 with QTc intervals of psychiatric inpatients longer than those of psychiatric outpatients. Altered potassium states probably explain these observations. Mechanisms that link exercise and agitation with hypokalemia remain to be elucidated.
Metabolic factors Drugs may alter phase 3 potassium flow, thereby disrupting the synchrony of action of individual cardiac cells during repolarization. This change may induce early afterdepolarizations and torsade.23
Five percent to 10% of Americans of European descent have genetic profiles that make them poor metabolizers of drugs that are metabolized by the cytochrome P-450 isoenzyme 2D6. The Pfizer Inc. 054 study assessed the potential for metabolic inhibitors such as paroxetine to raise antipsychotic drug levels in these patients and induce QTc interval prolongation.26
In response to FDA concerns about QTc interval prolongation associated with the use of ziprasidone, Pfizer studied the potential for QTc interval prolongation when antipsychotics are given with and without metabolic inhibitors of cytochrome P-450 isoenzymes 2D6 (paroxetine), 3A4 (ketoconazole), and 1A2 (fluvoxamine). The study population of 183 subjects (mean age:men, 37.1 years, women 38.8 years) was three-quarters young men with schizophrenia, in good health otherwise and possessing normal ECGs—i.e., patients with a low risk of developing cardiac arrhythmias.
Figure 3 Antipsychotic drugs and QTc interval changes
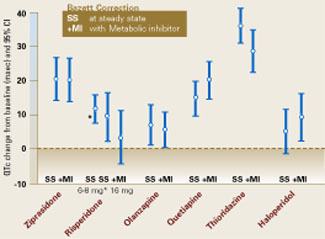
Six antipsychotic drugs and QTc interval changes from baseline when given with and without metabolic inhibitors. QTc interval changes (in msec) when given without a metabolic inhibitor were ziprasidone, 20.3; risperidone, 11.6; olanzapine, 6.8; quetiapine, 14.5; thioridazine, 35.6; and haloperidol 4.7.
Reprinted from: “FDA Psychopharmacological Drugs Advisory Committee. 19 July 2000. Briefing Documents for Zeldox Capsules (Ziprasidone HCL). Pfizer.” Available from Central Research Division, Pfizer, Inc., Eastern Point Road, Groton, CT 06340, (860) 441-4100.Over the course of about 1 week, daily doses were escalated to ziprasidone, 160 mg; risperidone, 8 mg and 16 mg; olanzapine, 20 mg; quetiapine, 750 mg; thioridazine, 300 mg; and haloperidol, 15 mg. Thioridazine (35.6 msec) and ziprasidone (20.3 msec) showed the greatest QTc interval increase following drug administration (Figure 3). Co-administration of a metabolic inhibitor did not further prolong the QTc interval for these two drugs.
Of the six drugs studied, only thioridazine and ziprasidone showed QTc interval increases 5% compared with baseline measurements.
Co-administration of a metabolic inhibitor caused the greatest increase in QTc intervals for quetiapine (from 14.5 to 19.7 msec). This value closely approached the steady-state ziprasidone measurement (20.3 msec). Because quetiapine is more likely than the other antipsychotic drugs studied to increase heart rate, it may be argued that the Bazett formula’s limitations in estimating the QTc interval at higher heart rates contributed to the quetiapine study findings.
Table 2
Relative risk of QTc interval prolongation with common antipsychotic agents
| Risk level | Agent |
|---|---|
| ECG required or strongly recommended before prescribing (most commonly associated with QTc interval prolongation and torsade de pointes) | Thioridazine Mesoridazine Droperidol Pimozide Haloperidol in large doses IV (commonly ≥ 100 mg/d) |
| Mild to moderate risk of QTc interval prolongation (~20 msec) when prescribed alone or with a metabolic inhibitor | Quetiapine Ziprasidone Chlorpromazine |
| Little or no risk of QTc interval prolongation (~20 msec) when prescribed alone or with a metabolic inhibitor | Haloperidol (oral) Olanzapine Risperidone Clozapine |
Recommendations
Taking a careful history is key to cardiovascular assessment before prescribing an antipsychotic. An ECG is indicated for patients with:
- Personal or family history of syncope or sudden death;
- Personal history of angina pectoris, myocardial infarction, congestive heart failure, cardiac arrhythmias, hypokalemia, hypomagnesemia, or significant cardiac risk factors.
The relative cardiovascular risks associated with antipsychotic agents are shown in Table 2.
An ECG also is required or strongly recommended before prescribing the antipsychotic drugs most commonly associated with QT prolongation and torsade de pointes—droperidol, haloperidol in large doses IV (commonly 100 mg/d), mesoridazine, pimozide, and thioridazine.
The FDA has strengthened the warning labels required for these agents, adding “black box” warnings about the risks of prolonged QTc intervals, torsade de pointes, and sudden death for droperidol, mesoridazine, and thioridazine. Thioridazine, for example, is indicated only for patients with schizophrenia who fail to show an acceptable response to other antipsychotic drugs. Its use is contraindicated in patients who take:
- fluvoxamine, propranolol, and pindolol;
- any drug that inhibits the cytochrome P-450 2D6 isoenzyme (e.g., fluoxetine, paroxetine);
- agents known to prolong the QTc interval.
Use of thioridazine also is contraindicated in patients known to have reduced levels of the cytochrome P450 2D6 isozyme, as well as in patients with congenital LQTS or a history of cardiac arrhythmias. Psychiatrists are advised to read the warnings and prescribing information in the labeling of all antipsychotics for potential cardiovascular side effects.
When the psychiatrist receives a report of suspected QTc interval prolongation on a patient’s ECG, the following steps are recommended:
- Obtain another ECG.
- Assess serum potassium, magnesium, calcium, and thyroid hormone levels.
In patients with confirmed QTc interval prolongation, any complaint of palpitations, presyncope, or syncope are grounds for urgent referral to a cardiologist.
Related resources
- European Society of Cardiology guidelines: www.escardio.org/scinfo/Guidelines/Haverkamp.pdf
- Sudden Arrhythmia Death Syndromes Foundation (SADSF): www.sads.org (800) 786-7723.
- Drugs that prolong the QT interval and/or induce torsade de pointes. Georgetown Center for Education and Research Therapeutics: www.torsades.org
1. Dessertenne F. Tachycardie ventriculaire a deux foyers opposes variables. Arch Mal Coeur Vaiss 1966;59(2):263-72.
2. Clark-Kennedy AE. Quinidine in the treatment of auricular fibrillation. Quart J Med 1922;16:204-35.
3. Selzer A, Wray W. Quinidine syncope. Paroxysmal ventricular fibrillation occurring during treatment of chronic atrial arrhythmias. Circulation 1964;30:17-26.
4. Reilly JG, Ayis SA, Ferrier IN, Jones SJ, Thomas SHL. QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients. Lancet 2000;355:1048-52.
5. Hatta K, Takahashi T, Nakamura H, Yamashiro H, Yonezawa Y. Prolonged QT interval in acute psychotic patients. Psychiatry Res 2000;94(3):279-85.
6. Welch R. Antipsychotic agents and QT changes. J Psychiatry Neurosci 2000;25(2):154-60.
7. Fayek M, Kingsbury SJ, Zada J, Simpson GM. Cardiac effects of antipsychotic medications. Psychiatr Serv 2001;52(5):607-9.
8. Kelly HG, Fay JE, Laverty SG. Thioridazine hydrochloride (Mellaril): its effect on the electrocardiogram and a report of two fatalities with electrocardiographic abnormalities. Can Med Assoc J 1963;89:546-54.
9. Donatini B, LeBlaye I, Krupp P. Transient cardiac pacing is insufficiently used to treat arrhythmia associated with thioridazine. Cardiology 1992;81(6):340-1.
10. Fowler NO, McCall D, et al. Electrocardiographic changes and cardiac arrhythmias in patients receiving psychotropic drugs. Am J Cardiol 1976;37:223-30.
11. Mehtonen OP, Aranko K, Malkonen L, Vapaatalo H. A survey of sudden death associated with the use of antipsychotic or antidepressant drugs: 49 cases in Finland. Acta Psychiatr Scand 1991;84:58-64.
12 Bazett HC. An analysis of the time-relations of electrocardiograms. Heart 1920;7:353-70.
13. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: techniques and limitations. Am J Cardiol 1993;72(suppl):17B-22B.
14. Bednar MM, et al. The QT Interval. Prog Cardiovas Dis 2001;43(5, pt 2):1-45.
15. Malik M. Problems of heart rate correction in assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol 2001;12(4):411-20.
16. Browne K, Prystowsky E, Heger JJ, Chilson DA, Zipes DP. Prolongation of the Q-T interval in man during sleep. Am J Cardiol 1983;52(1):55-9.
17. Morganroth J, Brozovich FV, McDonald JT, Jacobs RA. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67(8):774-6.
18. Woosley R, Sketch MH. Gender and drug-induced torsade de pointes. Bethesda, Md: American College of Cardiology, 1998; ACCEL 30, No. 2.
19. Rodriguez I, Kilborn MJ, Liu XK, Pezzullo JC, Woosley RL. Drug-induced QT prolongation in women during the menstrual cycle. JAMA 2001;285(10):1322-6.
20. Vincent GM. Long QT syndrome. Cardiology Clinics 1999;18:309-25.
21. Khan SP, Dahlvani S, Vieweg WVR, Bernardo NL, Lewis RE. Electrocardiographic QT interval in a geropsychiatric inpatient population: a preliminary study. Med Psychiatr 1998;1:71-4.
22. Compton SJ, Lux RL, Ramsey MR, et al. Genetically defined therapy of inherited long-QT syndrome. Correction of abnormal repolarization by potassium. Circulation 1996;94(5):1018-22.
23. Tan HL, Hou CJY, Lauer MR, Sung RJ. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122(9):701-14.
24. Jackman WM, Friday KJ, Anderson JL, et al. The long QT syndromes: a critical review, new clinical observations, and a unifying hypothesis. Prog Cardiovas Dis 1988;31(2):115-72.
25. Hatta K, Takahashi T, Nakamura H, et al. Hypokalemia and agitation in acute psychotic patients. Psychiatry Res 1999;86(1):85-8.
26. Food and Drug Administration Advisory Committee: Zeldox capsules (ziprasidone): summary of efficacy and safety and overall benefit risk relationship. Bethesda, Md: Food and Drug Administration, July 19, 2000.
Before approving the antipsychotic agent ziprasidone last year, the Food and Drug Administration required specific safety data on whether the drug might cause the life-threatening arrhythmia known as torsade de pointes.
The FDA’s action, which delayed the drug’s approval for 3 years, underscores growing concern about the risk of cardiovascular effects with the use of antipsychotic and other agents known to prolong the cardiac QT interval. This concern has led to withdrawal of some drugs before reaching the market (e.g., the atypical neuroleptic sertindole), the addition of “black box” warnings in the labeling of some antipsychotics, and withdrawal from the market of antihistamines terfenadine and astemizole and the GI stimulant cisapride.
Torsade de pointes is a polymorphic ventricular tachycardia (VT), a rare arrhythmia that can cause sudden death. Because torsade can occur with the use of some antipsychotics, the psychiatrist needs to consider cardiovascular safety when selecting among available agents. To help with these decisions, here is information about the documented and potential electrocardiographic features of commonly prescribed antipsychotic drugs, as well as background on QT interval prolongation and torsade de pointes.
Torsade de pointes
Named for a ballet movement, torsade de pointes describes bursts of “twisting of the points,” a variation of the morphology of the QRS vector about the isoelectric axis from positive to net negative and back again. As seen on an ECG (Figure 1), the first beat of torsade de pointes is a normal ventricular complex preceded by a P wave. This is followed by a premature ventricular contraction (PVC) with a short coupling interval. After a compensatory pause, a second normal beat is followed by a second PVC, which is the first beat of a polymorphic VT. We know tachycardia is present because the ventricular beats appear close together. We know the arrhythmia is ventricular in origin because the ventricular complexes are wide. Finally, we note the ventricular complexes vary in configuration—that is, the shape (morphology) varies from beat to beat.
Figure 1 Typical ECG features of torsade de pointes
Sinus beat with normal ventricular complex (1) followed by premature ventricular contraction (PVC) (2) with short coupling interval. After a long pause (long refractory period), another sinus beat (3) is followed by another PVC (4) with a short coupling interval. The second PVC (4) is the first beat of polymorphic ventricular tachycardiaIn torsade, the stimulus for the VT moves within the ventricle, changing its shape from beat to beat. This multifocal VT differs from the more common unifocal VT, in which all the QRS complexes appear the same.
Drug-induced torsade de pointes
Although the term torsade de pointes was first described in 1966,1 the drug-induced form of this arrhythmia has been recognized for nearly a century.
Quinidine Around 1920, cardiologists first used quinidine to help restore normal sinus rhythm in patients with atrial fibrillation, most commonly due to rheumatic heart disease.2
In 1964, Selzer and Wray3 studied the use of quinidine to convert atrial fibrillation to normal sinus rhythm in more than 200 patients seen during 4 years in a cardiopulmonary clinic. In a subgroup of eight patients, these researchers documented 10 reactions (including five documented episodes of ventricular fibrillation/ventricular flutter) among 36 syncopal episodes that developed within 1 to 6.5 hours of quinidine administration. Symptoms were nonspecific and included nausea, faintness, and feeling ill. It is now recognized that torsade de pointes was the principal rhythm disturbance in those eight patients. Syncope usually occurs early in treatment and may be found in 5% to 10% of patients taking quinidine.
TCAs and antipsychotics Tricyclic antidepressants (TCAs) and antipsychotics that have quinidine-like properties (e.g., thioridazine) also may be associated with QT interval prolongation and torsade de pointes.4-9 In high doses (particularly in overdose), TCAs may induce widening of the QRS complex. Fowler et al reported episodes of VT in five patients taking thioridazine—one of whom died.10
Mehtonen et al reported sudden unexpected deaths associated with antipsychotic or antidepressant drugs among 31 women and 18 men in a survey of autopsies performed from 1985 to 1988 in Finland. The authors documented therapeutic use of phenothiazines in all but 3 of the 49 cases. Thioridazine was involved in more than half the deaths. In 15 of the deaths, thioridazine was the only antipsychotic drug taken. Drugs other than thioridazine were documented in only 5 of the 49 sudden cardiac deaths.11
Figure 2 Normal ECG in sinus rhythm
In this typical lead II of a surface ECG, the P wave (atrial depolarization) leads to right and left atrial contraction and the QRS complex (ventricular depolarization) leads to left and right ventricular contraction. The ST segment represents isoelectric ventricular repolarization, and the T wave represents directional repolarization. The QT interval includes both ventricular depolarization (QRS complex) and ventricular repolarization (JT interval, or ST segment plus T wave).
QT interval as a marker for torsade
The incidence of torsade is unknown, but it is an uncommon cardiac abnormality. In the United States, torsade probably accounts for less than 5% of the 300,000 sudden cardiac deaths that occur each year. Because torsade de pointes is rare, regulatory agencies and clinicians use the QT interval as a surrogate ECG marker for risk of torsade de pointes. Heart rate can affect the QT interval, so various formulae are used to correct the QT interval for heart rate (QTc).
What is the QT interval? In a normal ECG (Figure 2), the P wave derives from right and left atrial electrical depolarization. The pacemaker of the heart is located in the sino-atrial node (SAN) in the superior portion of the right atrium. From the SAN, electrical signals travel down three intra-atrial pathways, activating the right atrium, then travel to the atrioventricular node (AVN). Bachmann’s bundle—a fourth atrial pathway—passes from the SAN to depolarize the left atrium. From the AVN, the electrical signal travels through the left and right bundle branches to activate their respective ventricles.
Electrical depolarization of the left and right ventricles produces the QRS complex. Most of the electrical forces making up this complex arise in the left ventricle, which is much larger than the right ventricle.
The electrical circuitry of the heart activates the left and right atria in such a fashion that these chambers eject blood into their respective ventricles just before these chambers contract. Optimal ventricular filling maximizes ventricular ejection of blood (Starling’s law). Ventricular repolarization (JT interval—electrical recovery) follows ventricular depolarization. On the surface ECG, the JT interval consists of an isoelectric event—the ST segment running from the end of the QRS complex to the beginning of the T wave—and the T wave itself (directional electrical recovery).
The QT interval, then, consists of both ventricular depolarization (QRS complex) and ventricular repolarization (JT interval). Ventricular repolarization makes up by far the greater portion of the QT interval.
Correcting the QT interval (QTc) In 1920, Bazett noted that as the heart rate slowed, the QT interval lengthened.12 From personal and reported observations, he derived an equation called the Bazett formula that corrects (or normalizes) the QT interval to a heart rate of 60 beats/min (QTc). In the Bazett formula, the QTc interval is the measured QT interval divided by the square root of the RR interval (time between sequential QRS complexes—the determinant of heart rate) measured in seconds (QTc = QT/RR).
The Bazett formula is most widely used to estimate the QTc interval, although at least 20 other formulae have been developed in response to the original’s perceived inadequacies.13-15 Bazett’s formula is used in most automated interpretations of the ECG.
Up to age 55, the normal QTc interval ranges from 350 to 430 msec for men and 350 to 450 msec for women, and it tends to increase with age. Most cases of torsade occur when the QT or QTc interval is greater than 500 msec.14 A QTc interval between 450 and 500 msec is cause for concern; a QTc interval that exceeds 500 msec is cause for alarm.
Factors that cause variations in QTc
Factors that can affect the QTc interval and increase the risk of torsade de pointes include electrolyte imbalances, medication use and overdose, cardiac disease, liver disease, endocrine disorders such as diabetes and hypothyroidism, and CNS injury (Table 1).
Table 1
Risk factors contributing to QTc interval prolongation
| Risk factor | Causes/implications |
|---|---|
| Sex (female) | QT intervals longer in women than in men QT interval longer during first half of menstrual cycle |
| Age (elderly) | Increased risk for CAD Multiple medications Pharmacokinetic/pharmacodynamic changes |
| Electrolyte imbalance Hypokalemia, hypomagnesemia Hypocalcemia | Diuretic use Excessive vomiting or diarrhea Postprandial hypokalemia |
| Congenital long QT syndrome | Associated with torsade and sudden death |
| Cardiac disease, with history of acute or chronic myocardial ischemia, CHF, cardiac arrhythmias, bradycardia | Increased risk of cardiac arrhythmias |
| Drugs known to prolong QTc interval | May potentiate QTc prolongation |
| Medication overdose with drugs that prolong the QTc interval | QTc prolongation generally dose-dependent |
| Concomitant medications, liver disease | Adverse events with cytochrome P-450 enzyme system inhibition, leading to increased drug levels that can increase QT interval |
| Endocrine/metabolic disorders Diabetes, obesity Hypothyroidism, pituitary insufficiency | Via electrolytes or cardiovascular disease |
| CNS injury Stroke, infection, trauma | Via autonomic nervous system dysfunction |
Circadian patterns The QTc interval varies throughout the 24-hour day, with nocturnal values about 20 msec greater than daytime measurements. These differences are driven by changes in autonomic (sympathetic and parasympathetic) tone.16,17 In 20 normal subjects, circadian variability was 76 ± 19 msec (range 35 to 108 msec) from day to night.17 This circadian variation may be accentuated in patients with cardiovascular disease.
Sex. At birth, QTc interval measurements do no vary by sex.18 At puberty, however, the male QTc interval shortens and remains shorter than its female counterpart by about 20 msec until age 50 to 55, coincident with a decline in male testosterone levels. This sex difference appears to be androgen driven. About 70% of torsade de pointes cases occur in women.18
Menstrual cycle QTc interval measurements are stable throughout the menstrual cycle if quinidine-like drugs are not given.
Variations were seen, however, when Rodriguez et al studied the effect of IV low-dose ibutilide (an antiarrhythmic agent known to prolong the QT interval) on the QTc intervals of 58 healthy subjects (38 men and 20 women, ages 21 to 40). During 1 month, men were studied once and women studied three times, coincident with the three phases of the menstrual cycle. The greatest increase in QTc intervals measurements occurred in women during the first half of their menstrual cycles.19
Age and cardiovascular disease Two congenital long QT syndromes may be associated with sudden death, mostly in children and young adults:
- The Jervell and Lange-Nielsen syndrome is marked by severe congenital deafness and autosomal recessive inheritance.
- The Romano-Ward syndrome has normal hearing and autosomal dominant inheritance.20
Congenital long QT syndrome (LQTS) occurs in about one in 5,000 births and accounts for about 3,000 to 4,000 deaths per year in the United States. Nine percent of pediatric LQTS subjects present with sudden cardiac death. More than 71% of patients will die before age 15 if not treated.
Elderly persons tend to have longer QTc intervals than do younger subjects, even when both groups are free of cardiovascular disease.21 Also, age-matched subjects with cardiovascular disease tend to have longer QTc intervals than do those free of cardiovascular disease.
Electrolytes Electrolyte disturbances, particularly hypokalemia and hypomagnesemia, may contribute to or even cause QT interval prolongation.22
Hypokalemia prolongs the cardiac action potential and may cause early afterdepolarization, leading to torsade.23 Low potassium levels reduce the net outward potassium current during phase 3 of the cardiac action potential. Hypomagnesemia may contribute to gross U wave alternans, lengthening the cardiac action potential and setting the stage for torsade.24 Various factors may contribute to electrolyte disturbances, including use of diuretics and excessive vomiting and diarrhea. Even postprandial states may induce hypokalemia.
Intensive exercise and agitation may be associated with hypokalemia.25 Serum potassium may be lower in severely agitated patients (3.59 mmol/L) than in mildly agitated patients (3.79 mmol/L). The mean QTc interval of psychiatric emergency patients may be prolonged (453±40 msec),5 with QTc intervals of psychiatric inpatients longer than those of psychiatric outpatients. Altered potassium states probably explain these observations. Mechanisms that link exercise and agitation with hypokalemia remain to be elucidated.
Metabolic factors Drugs may alter phase 3 potassium flow, thereby disrupting the synchrony of action of individual cardiac cells during repolarization. This change may induce early afterdepolarizations and torsade.23
Five percent to 10% of Americans of European descent have genetic profiles that make them poor metabolizers of drugs that are metabolized by the cytochrome P-450 isoenzyme 2D6. The Pfizer Inc. 054 study assessed the potential for metabolic inhibitors such as paroxetine to raise antipsychotic drug levels in these patients and induce QTc interval prolongation.26
In response to FDA concerns about QTc interval prolongation associated with the use of ziprasidone, Pfizer studied the potential for QTc interval prolongation when antipsychotics are given with and without metabolic inhibitors of cytochrome P-450 isoenzymes 2D6 (paroxetine), 3A4 (ketoconazole), and 1A2 (fluvoxamine). The study population of 183 subjects (mean age:men, 37.1 years, women 38.8 years) was three-quarters young men with schizophrenia, in good health otherwise and possessing normal ECGs—i.e., patients with a low risk of developing cardiac arrhythmias.
Figure 3 Antipsychotic drugs and QTc interval changes
Six antipsychotic drugs and QTc interval changes from baseline when given with and without metabolic inhibitors. QTc interval changes (in msec) when given without a metabolic inhibitor were ziprasidone, 20.3; risperidone, 11.6; olanzapine, 6.8; quetiapine, 14.5; thioridazine, 35.6; and haloperidol 4.7.
Reprinted from: “FDA Psychopharmacological Drugs Advisory Committee. 19 July 2000. Briefing Documents for Zeldox Capsules (Ziprasidone HCL). Pfizer.” Available from Central Research Division, Pfizer, Inc., Eastern Point Road, Groton, CT 06340, (860) 441-4100.Over the course of about 1 week, daily doses were escalated to ziprasidone, 160 mg; risperidone, 8 mg and 16 mg; olanzapine, 20 mg; quetiapine, 750 mg; thioridazine, 300 mg; and haloperidol, 15 mg. Thioridazine (35.6 msec) and ziprasidone (20.3 msec) showed the greatest QTc interval increase following drug administration (Figure 3). Co-administration of a metabolic inhibitor did not further prolong the QTc interval for these two drugs.
Of the six drugs studied, only thioridazine and ziprasidone showed QTc interval increases 5% compared with baseline measurements.
Co-administration of a metabolic inhibitor caused the greatest increase in QTc intervals for quetiapine (from 14.5 to 19.7 msec). This value closely approached the steady-state ziprasidone measurement (20.3 msec). Because quetiapine is more likely than the other antipsychotic drugs studied to increase heart rate, it may be argued that the Bazett formula’s limitations in estimating the QTc interval at higher heart rates contributed to the quetiapine study findings.
Table 2
Relative risk of QTc interval prolongation with common antipsychotic agents
| Risk level | Agent |
|---|---|
| ECG required or strongly recommended before prescribing (most commonly associated with QTc interval prolongation and torsade de pointes) | Thioridazine Mesoridazine Droperidol Pimozide Haloperidol in large doses IV (commonly ≥ 100 mg/d) |
| Mild to moderate risk of QTc interval prolongation (~20 msec) when prescribed alone or with a metabolic inhibitor | Quetiapine Ziprasidone Chlorpromazine |
| Little or no risk of QTc interval prolongation (~20 msec) when prescribed alone or with a metabolic inhibitor | Haloperidol (oral) Olanzapine Risperidone Clozapine |
Recommendations
Taking a careful history is key to cardiovascular assessment before prescribing an antipsychotic. An ECG is indicated for patients with:
- Personal or family history of syncope or sudden death;
- Personal history of angina pectoris, myocardial infarction, congestive heart failure, cardiac arrhythmias, hypokalemia, hypomagnesemia, or significant cardiac risk factors.
The relative cardiovascular risks associated with antipsychotic agents are shown in Table 2.
An ECG also is required or strongly recommended before prescribing the antipsychotic drugs most commonly associated with QT prolongation and torsade de pointes—droperidol, haloperidol in large doses IV (commonly 100 mg/d), mesoridazine, pimozide, and thioridazine.
The FDA has strengthened the warning labels required for these agents, adding “black box” warnings about the risks of prolonged QTc intervals, torsade de pointes, and sudden death for droperidol, mesoridazine, and thioridazine. Thioridazine, for example, is indicated only for patients with schizophrenia who fail to show an acceptable response to other antipsychotic drugs. Its use is contraindicated in patients who take:
- fluvoxamine, propranolol, and pindolol;
- any drug that inhibits the cytochrome P-450 2D6 isoenzyme (e.g., fluoxetine, paroxetine);
- agents known to prolong the QTc interval.
Use of thioridazine also is contraindicated in patients known to have reduced levels of the cytochrome P450 2D6 isozyme, as well as in patients with congenital LQTS or a history of cardiac arrhythmias. Psychiatrists are advised to read the warnings and prescribing information in the labeling of all antipsychotics for potential cardiovascular side effects.
When the psychiatrist receives a report of suspected QTc interval prolongation on a patient’s ECG, the following steps are recommended:
- Obtain another ECG.
- Assess serum potassium, magnesium, calcium, and thyroid hormone levels.
In patients with confirmed QTc interval prolongation, any complaint of palpitations, presyncope, or syncope are grounds for urgent referral to a cardiologist.
Related resources
- European Society of Cardiology guidelines: www.escardio.org/scinfo/Guidelines/Haverkamp.pdf
- Sudden Arrhythmia Death Syndromes Foundation (SADSF): www.sads.org (800) 786-7723.
- Drugs that prolong the QT interval and/or induce torsade de pointes. Georgetown Center for Education and Research Therapeutics: www.torsades.org
Before approving the antipsychotic agent ziprasidone last year, the Food and Drug Administration required specific safety data on whether the drug might cause the life-threatening arrhythmia known as torsade de pointes.
The FDA’s action, which delayed the drug’s approval for 3 years, underscores growing concern about the risk of cardiovascular effects with the use of antipsychotic and other agents known to prolong the cardiac QT interval. This concern has led to withdrawal of some drugs before reaching the market (e.g., the atypical neuroleptic sertindole), the addition of “black box” warnings in the labeling of some antipsychotics, and withdrawal from the market of antihistamines terfenadine and astemizole and the GI stimulant cisapride.
Torsade de pointes is a polymorphic ventricular tachycardia (VT), a rare arrhythmia that can cause sudden death. Because torsade can occur with the use of some antipsychotics, the psychiatrist needs to consider cardiovascular safety when selecting among available agents. To help with these decisions, here is information about the documented and potential electrocardiographic features of commonly prescribed antipsychotic drugs, as well as background on QT interval prolongation and torsade de pointes.
Torsade de pointes
Named for a ballet movement, torsade de pointes describes bursts of “twisting of the points,” a variation of the morphology of the QRS vector about the isoelectric axis from positive to net negative and back again. As seen on an ECG (Figure 1), the first beat of torsade de pointes is a normal ventricular complex preceded by a P wave. This is followed by a premature ventricular contraction (PVC) with a short coupling interval. After a compensatory pause, a second normal beat is followed by a second PVC, which is the first beat of a polymorphic VT. We know tachycardia is present because the ventricular beats appear close together. We know the arrhythmia is ventricular in origin because the ventricular complexes are wide. Finally, we note the ventricular complexes vary in configuration—that is, the shape (morphology) varies from beat to beat.
Figure 1 Typical ECG features of torsade de pointes
Sinus beat with normal ventricular complex (1) followed by premature ventricular contraction (PVC) (2) with short coupling interval. After a long pause (long refractory period), another sinus beat (3) is followed by another PVC (4) with a short coupling interval. The second PVC (4) is the first beat of polymorphic ventricular tachycardiaIn torsade, the stimulus for the VT moves within the ventricle, changing its shape from beat to beat. This multifocal VT differs from the more common unifocal VT, in which all the QRS complexes appear the same.
Drug-induced torsade de pointes
Although the term torsade de pointes was first described in 1966,1 the drug-induced form of this arrhythmia has been recognized for nearly a century.
Quinidine Around 1920, cardiologists first used quinidine to help restore normal sinus rhythm in patients with atrial fibrillation, most commonly due to rheumatic heart disease.2
In 1964, Selzer and Wray3 studied the use of quinidine to convert atrial fibrillation to normal sinus rhythm in more than 200 patients seen during 4 years in a cardiopulmonary clinic. In a subgroup of eight patients, these researchers documented 10 reactions (including five documented episodes of ventricular fibrillation/ventricular flutter) among 36 syncopal episodes that developed within 1 to 6.5 hours of quinidine administration. Symptoms were nonspecific and included nausea, faintness, and feeling ill. It is now recognized that torsade de pointes was the principal rhythm disturbance in those eight patients. Syncope usually occurs early in treatment and may be found in 5% to 10% of patients taking quinidine.
TCAs and antipsychotics Tricyclic antidepressants (TCAs) and antipsychotics that have quinidine-like properties (e.g., thioridazine) also may be associated with QT interval prolongation and torsade de pointes.4-9 In high doses (particularly in overdose), TCAs may induce widening of the QRS complex. Fowler et al reported episodes of VT in five patients taking thioridazine—one of whom died.10
Mehtonen et al reported sudden unexpected deaths associated with antipsychotic or antidepressant drugs among 31 women and 18 men in a survey of autopsies performed from 1985 to 1988 in Finland. The authors documented therapeutic use of phenothiazines in all but 3 of the 49 cases. Thioridazine was involved in more than half the deaths. In 15 of the deaths, thioridazine was the only antipsychotic drug taken. Drugs other than thioridazine were documented in only 5 of the 49 sudden cardiac deaths.11
Figure 2 Normal ECG in sinus rhythm
In this typical lead II of a surface ECG, the P wave (atrial depolarization) leads to right and left atrial contraction and the QRS complex (ventricular depolarization) leads to left and right ventricular contraction. The ST segment represents isoelectric ventricular repolarization, and the T wave represents directional repolarization. The QT interval includes both ventricular depolarization (QRS complex) and ventricular repolarization (JT interval, or ST segment plus T wave).
QT interval as a marker for torsade
The incidence of torsade is unknown, but it is an uncommon cardiac abnormality. In the United States, torsade probably accounts for less than 5% of the 300,000 sudden cardiac deaths that occur each year. Because torsade de pointes is rare, regulatory agencies and clinicians use the QT interval as a surrogate ECG marker for risk of torsade de pointes. Heart rate can affect the QT interval, so various formulae are used to correct the QT interval for heart rate (QTc).
What is the QT interval? In a normal ECG (Figure 2), the P wave derives from right and left atrial electrical depolarization. The pacemaker of the heart is located in the sino-atrial node (SAN) in the superior portion of the right atrium. From the SAN, electrical signals travel down three intra-atrial pathways, activating the right atrium, then travel to the atrioventricular node (AVN). Bachmann’s bundle—a fourth atrial pathway—passes from the SAN to depolarize the left atrium. From the AVN, the electrical signal travels through the left and right bundle branches to activate their respective ventricles.
Electrical depolarization of the left and right ventricles produces the QRS complex. Most of the electrical forces making up this complex arise in the left ventricle, which is much larger than the right ventricle.
The electrical circuitry of the heart activates the left and right atria in such a fashion that these chambers eject blood into their respective ventricles just before these chambers contract. Optimal ventricular filling maximizes ventricular ejection of blood (Starling’s law). Ventricular repolarization (JT interval—electrical recovery) follows ventricular depolarization. On the surface ECG, the JT interval consists of an isoelectric event—the ST segment running from the end of the QRS complex to the beginning of the T wave—and the T wave itself (directional electrical recovery).
The QT interval, then, consists of both ventricular depolarization (QRS complex) and ventricular repolarization (JT interval). Ventricular repolarization makes up by far the greater portion of the QT interval.
Correcting the QT interval (QTc) In 1920, Bazett noted that as the heart rate slowed, the QT interval lengthened.12 From personal and reported observations, he derived an equation called the Bazett formula that corrects (or normalizes) the QT interval to a heart rate of 60 beats/min (QTc). In the Bazett formula, the QTc interval is the measured QT interval divided by the square root of the RR interval (time between sequential QRS complexes—the determinant of heart rate) measured in seconds (QTc = QT/RR).
The Bazett formula is most widely used to estimate the QTc interval, although at least 20 other formulae have been developed in response to the original’s perceived inadequacies.13-15 Bazett’s formula is used in most automated interpretations of the ECG.
Up to age 55, the normal QTc interval ranges from 350 to 430 msec for men and 350 to 450 msec for women, and it tends to increase with age. Most cases of torsade occur when the QT or QTc interval is greater than 500 msec.14 A QTc interval between 450 and 500 msec is cause for concern; a QTc interval that exceeds 500 msec is cause for alarm.
Factors that cause variations in QTc
Factors that can affect the QTc interval and increase the risk of torsade de pointes include electrolyte imbalances, medication use and overdose, cardiac disease, liver disease, endocrine disorders such as diabetes and hypothyroidism, and CNS injury (Table 1).
Table 1
Risk factors contributing to QTc interval prolongation
| Risk factor | Causes/implications |
|---|---|
| Sex (female) | QT intervals longer in women than in men QT interval longer during first half of menstrual cycle |
| Age (elderly) | Increased risk for CAD Multiple medications Pharmacokinetic/pharmacodynamic changes |
| Electrolyte imbalance Hypokalemia, hypomagnesemia Hypocalcemia | Diuretic use Excessive vomiting or diarrhea Postprandial hypokalemia |
| Congenital long QT syndrome | Associated with torsade and sudden death |
| Cardiac disease, with history of acute or chronic myocardial ischemia, CHF, cardiac arrhythmias, bradycardia | Increased risk of cardiac arrhythmias |
| Drugs known to prolong QTc interval | May potentiate QTc prolongation |
| Medication overdose with drugs that prolong the QTc interval | QTc prolongation generally dose-dependent |
| Concomitant medications, liver disease | Adverse events with cytochrome P-450 enzyme system inhibition, leading to increased drug levels that can increase QT interval |
| Endocrine/metabolic disorders Diabetes, obesity Hypothyroidism, pituitary insufficiency | Via electrolytes or cardiovascular disease |
| CNS injury Stroke, infection, trauma | Via autonomic nervous system dysfunction |
Circadian patterns The QTc interval varies throughout the 24-hour day, with nocturnal values about 20 msec greater than daytime measurements. These differences are driven by changes in autonomic (sympathetic and parasympathetic) tone.16,17 In 20 normal subjects, circadian variability was 76 ± 19 msec (range 35 to 108 msec) from day to night.17 This circadian variation may be accentuated in patients with cardiovascular disease.
Sex. At birth, QTc interval measurements do no vary by sex.18 At puberty, however, the male QTc interval shortens and remains shorter than its female counterpart by about 20 msec until age 50 to 55, coincident with a decline in male testosterone levels. This sex difference appears to be androgen driven. About 70% of torsade de pointes cases occur in women.18
Menstrual cycle QTc interval measurements are stable throughout the menstrual cycle if quinidine-like drugs are not given.
Variations were seen, however, when Rodriguez et al studied the effect of IV low-dose ibutilide (an antiarrhythmic agent known to prolong the QT interval) on the QTc intervals of 58 healthy subjects (38 men and 20 women, ages 21 to 40). During 1 month, men were studied once and women studied three times, coincident with the three phases of the menstrual cycle. The greatest increase in QTc intervals measurements occurred in women during the first half of their menstrual cycles.19
Age and cardiovascular disease Two congenital long QT syndromes may be associated with sudden death, mostly in children and young adults:
- The Jervell and Lange-Nielsen syndrome is marked by severe congenital deafness and autosomal recessive inheritance.
- The Romano-Ward syndrome has normal hearing and autosomal dominant inheritance.20
Congenital long QT syndrome (LQTS) occurs in about one in 5,000 births and accounts for about 3,000 to 4,000 deaths per year in the United States. Nine percent of pediatric LQTS subjects present with sudden cardiac death. More than 71% of patients will die before age 15 if not treated.
Elderly persons tend to have longer QTc intervals than do younger subjects, even when both groups are free of cardiovascular disease.21 Also, age-matched subjects with cardiovascular disease tend to have longer QTc intervals than do those free of cardiovascular disease.
Electrolytes Electrolyte disturbances, particularly hypokalemia and hypomagnesemia, may contribute to or even cause QT interval prolongation.22
Hypokalemia prolongs the cardiac action potential and may cause early afterdepolarization, leading to torsade.23 Low potassium levels reduce the net outward potassium current during phase 3 of the cardiac action potential. Hypomagnesemia may contribute to gross U wave alternans, lengthening the cardiac action potential and setting the stage for torsade.24 Various factors may contribute to electrolyte disturbances, including use of diuretics and excessive vomiting and diarrhea. Even postprandial states may induce hypokalemia.
Intensive exercise and agitation may be associated with hypokalemia.25 Serum potassium may be lower in severely agitated patients (3.59 mmol/L) than in mildly agitated patients (3.79 mmol/L). The mean QTc interval of psychiatric emergency patients may be prolonged (453±40 msec),5 with QTc intervals of psychiatric inpatients longer than those of psychiatric outpatients. Altered potassium states probably explain these observations. Mechanisms that link exercise and agitation with hypokalemia remain to be elucidated.
Metabolic factors Drugs may alter phase 3 potassium flow, thereby disrupting the synchrony of action of individual cardiac cells during repolarization. This change may induce early afterdepolarizations and torsade.23
Five percent to 10% of Americans of European descent have genetic profiles that make them poor metabolizers of drugs that are metabolized by the cytochrome P-450 isoenzyme 2D6. The Pfizer Inc. 054 study assessed the potential for metabolic inhibitors such as paroxetine to raise antipsychotic drug levels in these patients and induce QTc interval prolongation.26
In response to FDA concerns about QTc interval prolongation associated with the use of ziprasidone, Pfizer studied the potential for QTc interval prolongation when antipsychotics are given with and without metabolic inhibitors of cytochrome P-450 isoenzymes 2D6 (paroxetine), 3A4 (ketoconazole), and 1A2 (fluvoxamine). The study population of 183 subjects (mean age:men, 37.1 years, women 38.8 years) was three-quarters young men with schizophrenia, in good health otherwise and possessing normal ECGs—i.e., patients with a low risk of developing cardiac arrhythmias.
Figure 3 Antipsychotic drugs and QTc interval changes
Six antipsychotic drugs and QTc interval changes from baseline when given with and without metabolic inhibitors. QTc interval changes (in msec) when given without a metabolic inhibitor were ziprasidone, 20.3; risperidone, 11.6; olanzapine, 6.8; quetiapine, 14.5; thioridazine, 35.6; and haloperidol 4.7.
Reprinted from: “FDA Psychopharmacological Drugs Advisory Committee. 19 July 2000. Briefing Documents for Zeldox Capsules (Ziprasidone HCL). Pfizer.” Available from Central Research Division, Pfizer, Inc., Eastern Point Road, Groton, CT 06340, (860) 441-4100.Over the course of about 1 week, daily doses were escalated to ziprasidone, 160 mg; risperidone, 8 mg and 16 mg; olanzapine, 20 mg; quetiapine, 750 mg; thioridazine, 300 mg; and haloperidol, 15 mg. Thioridazine (35.6 msec) and ziprasidone (20.3 msec) showed the greatest QTc interval increase following drug administration (Figure 3). Co-administration of a metabolic inhibitor did not further prolong the QTc interval for these two drugs.
Of the six drugs studied, only thioridazine and ziprasidone showed QTc interval increases 5% compared with baseline measurements.
Co-administration of a metabolic inhibitor caused the greatest increase in QTc intervals for quetiapine (from 14.5 to 19.7 msec). This value closely approached the steady-state ziprasidone measurement (20.3 msec). Because quetiapine is more likely than the other antipsychotic drugs studied to increase heart rate, it may be argued that the Bazett formula’s limitations in estimating the QTc interval at higher heart rates contributed to the quetiapine study findings.
Table 2
Relative risk of QTc interval prolongation with common antipsychotic agents
| Risk level | Agent |
|---|---|
| ECG required or strongly recommended before prescribing (most commonly associated with QTc interval prolongation and torsade de pointes) | Thioridazine Mesoridazine Droperidol Pimozide Haloperidol in large doses IV (commonly ≥ 100 mg/d) |
| Mild to moderate risk of QTc interval prolongation (~20 msec) when prescribed alone or with a metabolic inhibitor | Quetiapine Ziprasidone Chlorpromazine |
| Little or no risk of QTc interval prolongation (~20 msec) when prescribed alone or with a metabolic inhibitor | Haloperidol (oral) Olanzapine Risperidone Clozapine |
Recommendations
Taking a careful history is key to cardiovascular assessment before prescribing an antipsychotic. An ECG is indicated for patients with:
- Personal or family history of syncope or sudden death;
- Personal history of angina pectoris, myocardial infarction, congestive heart failure, cardiac arrhythmias, hypokalemia, hypomagnesemia, or significant cardiac risk factors.
The relative cardiovascular risks associated with antipsychotic agents are shown in Table 2.
An ECG also is required or strongly recommended before prescribing the antipsychotic drugs most commonly associated with QT prolongation and torsade de pointes—droperidol, haloperidol in large doses IV (commonly 100 mg/d), mesoridazine, pimozide, and thioridazine.
The FDA has strengthened the warning labels required for these agents, adding “black box” warnings about the risks of prolonged QTc intervals, torsade de pointes, and sudden death for droperidol, mesoridazine, and thioridazine. Thioridazine, for example, is indicated only for patients with schizophrenia who fail to show an acceptable response to other antipsychotic drugs. Its use is contraindicated in patients who take:
- fluvoxamine, propranolol, and pindolol;
- any drug that inhibits the cytochrome P-450 2D6 isoenzyme (e.g., fluoxetine, paroxetine);
- agents known to prolong the QTc interval.
Use of thioridazine also is contraindicated in patients known to have reduced levels of the cytochrome P450 2D6 isozyme, as well as in patients with congenital LQTS or a history of cardiac arrhythmias. Psychiatrists are advised to read the warnings and prescribing information in the labeling of all antipsychotics for potential cardiovascular side effects.
When the psychiatrist receives a report of suspected QTc interval prolongation on a patient’s ECG, the following steps are recommended:
- Obtain another ECG.
- Assess serum potassium, magnesium, calcium, and thyroid hormone levels.
In patients with confirmed QTc interval prolongation, any complaint of palpitations, presyncope, or syncope are grounds for urgent referral to a cardiologist.
Related resources
- European Society of Cardiology guidelines: www.escardio.org/scinfo/Guidelines/Haverkamp.pdf
- Sudden Arrhythmia Death Syndromes Foundation (SADSF): www.sads.org (800) 786-7723.
- Drugs that prolong the QT interval and/or induce torsade de pointes. Georgetown Center for Education and Research Therapeutics: www.torsades.org
1. Dessertenne F. Tachycardie ventriculaire a deux foyers opposes variables. Arch Mal Coeur Vaiss 1966;59(2):263-72.
2. Clark-Kennedy AE. Quinidine in the treatment of auricular fibrillation. Quart J Med 1922;16:204-35.
3. Selzer A, Wray W. Quinidine syncope. Paroxysmal ventricular fibrillation occurring during treatment of chronic atrial arrhythmias. Circulation 1964;30:17-26.
4. Reilly JG, Ayis SA, Ferrier IN, Jones SJ, Thomas SHL. QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients. Lancet 2000;355:1048-52.
5. Hatta K, Takahashi T, Nakamura H, Yamashiro H, Yonezawa Y. Prolonged QT interval in acute psychotic patients. Psychiatry Res 2000;94(3):279-85.
6. Welch R. Antipsychotic agents and QT changes. J Psychiatry Neurosci 2000;25(2):154-60.
7. Fayek M, Kingsbury SJ, Zada J, Simpson GM. Cardiac effects of antipsychotic medications. Psychiatr Serv 2001;52(5):607-9.
8. Kelly HG, Fay JE, Laverty SG. Thioridazine hydrochloride (Mellaril): its effect on the electrocardiogram and a report of two fatalities with electrocardiographic abnormalities. Can Med Assoc J 1963;89:546-54.
9. Donatini B, LeBlaye I, Krupp P. Transient cardiac pacing is insufficiently used to treat arrhythmia associated with thioridazine. Cardiology 1992;81(6):340-1.
10. Fowler NO, McCall D, et al. Electrocardiographic changes and cardiac arrhythmias in patients receiving psychotropic drugs. Am J Cardiol 1976;37:223-30.
11. Mehtonen OP, Aranko K, Malkonen L, Vapaatalo H. A survey of sudden death associated with the use of antipsychotic or antidepressant drugs: 49 cases in Finland. Acta Psychiatr Scand 1991;84:58-64.
12 Bazett HC. An analysis of the time-relations of electrocardiograms. Heart 1920;7:353-70.
13. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: techniques and limitations. Am J Cardiol 1993;72(suppl):17B-22B.
14. Bednar MM, et al. The QT Interval. Prog Cardiovas Dis 2001;43(5, pt 2):1-45.
15. Malik M. Problems of heart rate correction in assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol 2001;12(4):411-20.
16. Browne K, Prystowsky E, Heger JJ, Chilson DA, Zipes DP. Prolongation of the Q-T interval in man during sleep. Am J Cardiol 1983;52(1):55-9.
17. Morganroth J, Brozovich FV, McDonald JT, Jacobs RA. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67(8):774-6.
18. Woosley R, Sketch MH. Gender and drug-induced torsade de pointes. Bethesda, Md: American College of Cardiology, 1998; ACCEL 30, No. 2.
19. Rodriguez I, Kilborn MJ, Liu XK, Pezzullo JC, Woosley RL. Drug-induced QT prolongation in women during the menstrual cycle. JAMA 2001;285(10):1322-6.
20. Vincent GM. Long QT syndrome. Cardiology Clinics 1999;18:309-25.
21. Khan SP, Dahlvani S, Vieweg WVR, Bernardo NL, Lewis RE. Electrocardiographic QT interval in a geropsychiatric inpatient population: a preliminary study. Med Psychiatr 1998;1:71-4.
22. Compton SJ, Lux RL, Ramsey MR, et al. Genetically defined therapy of inherited long-QT syndrome. Correction of abnormal repolarization by potassium. Circulation 1996;94(5):1018-22.
23. Tan HL, Hou CJY, Lauer MR, Sung RJ. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122(9):701-14.
24. Jackman WM, Friday KJ, Anderson JL, et al. The long QT syndromes: a critical review, new clinical observations, and a unifying hypothesis. Prog Cardiovas Dis 1988;31(2):115-72.
25. Hatta K, Takahashi T, Nakamura H, et al. Hypokalemia and agitation in acute psychotic patients. Psychiatry Res 1999;86(1):85-8.
26. Food and Drug Administration Advisory Committee: Zeldox capsules (ziprasidone): summary of efficacy and safety and overall benefit risk relationship. Bethesda, Md: Food and Drug Administration, July 19, 2000.
1. Dessertenne F. Tachycardie ventriculaire a deux foyers opposes variables. Arch Mal Coeur Vaiss 1966;59(2):263-72.
2. Clark-Kennedy AE. Quinidine in the treatment of auricular fibrillation. Quart J Med 1922;16:204-35.
3. Selzer A, Wray W. Quinidine syncope. Paroxysmal ventricular fibrillation occurring during treatment of chronic atrial arrhythmias. Circulation 1964;30:17-26.
4. Reilly JG, Ayis SA, Ferrier IN, Jones SJ, Thomas SHL. QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients. Lancet 2000;355:1048-52.
5. Hatta K, Takahashi T, Nakamura H, Yamashiro H, Yonezawa Y. Prolonged QT interval in acute psychotic patients. Psychiatry Res 2000;94(3):279-85.
6. Welch R. Antipsychotic agents and QT changes. J Psychiatry Neurosci 2000;25(2):154-60.
7. Fayek M, Kingsbury SJ, Zada J, Simpson GM. Cardiac effects of antipsychotic medications. Psychiatr Serv 2001;52(5):607-9.
8. Kelly HG, Fay JE, Laverty SG. Thioridazine hydrochloride (Mellaril): its effect on the electrocardiogram and a report of two fatalities with electrocardiographic abnormalities. Can Med Assoc J 1963;89:546-54.
9. Donatini B, LeBlaye I, Krupp P. Transient cardiac pacing is insufficiently used to treat arrhythmia associated with thioridazine. Cardiology 1992;81(6):340-1.
10. Fowler NO, McCall D, et al. Electrocardiographic changes and cardiac arrhythmias in patients receiving psychotropic drugs. Am J Cardiol 1976;37:223-30.
11. Mehtonen OP, Aranko K, Malkonen L, Vapaatalo H. A survey of sudden death associated with the use of antipsychotic or antidepressant drugs: 49 cases in Finland. Acta Psychiatr Scand 1991;84:58-64.
12 Bazett HC. An analysis of the time-relations of electrocardiograms. Heart 1920;7:353-70.
13. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: techniques and limitations. Am J Cardiol 1993;72(suppl):17B-22B.
14. Bednar MM, et al. The QT Interval. Prog Cardiovas Dis 2001;43(5, pt 2):1-45.
15. Malik M. Problems of heart rate correction in assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol 2001;12(4):411-20.
16. Browne K, Prystowsky E, Heger JJ, Chilson DA, Zipes DP. Prolongation of the Q-T interval in man during sleep. Am J Cardiol 1983;52(1):55-9.
17. Morganroth J, Brozovich FV, McDonald JT, Jacobs RA. Variability of the QT measurement in healthy men, with implications for selection of an abnormal QT value to predict drug toxicity and proarrhythmia. Am J Cardiol 1991;67(8):774-6.
18. Woosley R, Sketch MH. Gender and drug-induced torsade de pointes. Bethesda, Md: American College of Cardiology, 1998; ACCEL 30, No. 2.
19. Rodriguez I, Kilborn MJ, Liu XK, Pezzullo JC, Woosley RL. Drug-induced QT prolongation in women during the menstrual cycle. JAMA 2001;285(10):1322-6.
20. Vincent GM. Long QT syndrome. Cardiology Clinics 1999;18:309-25.
21. Khan SP, Dahlvani S, Vieweg WVR, Bernardo NL, Lewis RE. Electrocardiographic QT interval in a geropsychiatric inpatient population: a preliminary study. Med Psychiatr 1998;1:71-4.
22. Compton SJ, Lux RL, Ramsey MR, et al. Genetically defined therapy of inherited long-QT syndrome. Correction of abnormal repolarization by potassium. Circulation 1996;94(5):1018-22.
23. Tan HL, Hou CJY, Lauer MR, Sung RJ. Electrophysiologic mechanisms of the long QT interval syndromes and torsade de pointes. Ann Intern Med 1995;122(9):701-14.
24. Jackman WM, Friday KJ, Anderson JL, et al. The long QT syndromes: a critical review, new clinical observations, and a unifying hypothesis. Prog Cardiovas Dis 1988;31(2):115-72.
25. Hatta K, Takahashi T, Nakamura H, et al. Hypokalemia and agitation in acute psychotic patients. Psychiatry Res 1999;86(1):85-8.
26. Food and Drug Administration Advisory Committee: Zeldox capsules (ziprasidone): summary of efficacy and safety and overall benefit risk relationship. Bethesda, Md: Food and Drug Administration, July 19, 2000.
Psychiatric illness or thyroid disease? Don’t be misled by false lab tests
Psychiatrists commonly order thyroid testing and are often the first to confront abnormal thyroid test results. As thyroid testing has become more sophisticated and sensitive (Box 1), the interpretation and management of abnormal or slightly abnormal results has become increasingly complex. What’s more, older individuals, hospitalized patients, and those with psychiatric illness often present with subtle laboratory abnormalities.
Hyperthyroidism and hypothyroidism are highly prevalent disorders, especially in women and the elderly. Thyroid dysfunction is the second most common endocrine disorder after diabetes among elders. In the three cases that follow, some of the problems and solutions in dealing with thyroid testing are presented.
Case 1: Depression and thyroid abnormalities
J.R., 67, has a history of hypertension. She was referred for evaluation of depressive symptoms. She reports 3 months of increasing fatigue, lethargy, and poor motivation. Her weight has increased by 10 pounds over this period. Her physical exam, ECG, and chest x-ray are normal. She is well groomed and slightly overweight. Her medications have not changed recently and include hydrochlorothiazide 25 mg/d and an aspirin a day.
J.R. reports no history of treatment for psychiatric illness, denies current use of alcohol, tobacco, or illicit drugs, exhibits no abnormal movements or psychomotor changes, and her speech is articulate. Her mood is depressed, and her affect is restricted. She is not suicidal or homicidal, and her exam reveals no psychotic features.
Challenge Patients with thyroid abnormalities often present with psychiatric complaints. Classically, hypothyroidism can present like a depressive episode with similar symptoms of fatigue, anhedonia, weight gain, and sleep disturbance. Patients with hypothyroidism, however, may have physical complaints as well, which should alert the clinician to an underlying thyroid disorder. Typical physical complaints include hair loss, weight gain, dry skin, cold intolerance, constipation, muscle cramps, and joint pains. Women may also complain of menstrual disturbances such as menorrhagia, and may have trouble with fertility.
An elevated or decreased TSH suggests thyroid dysfunction and should always be evaluated.
A low free T4 confirms the diagnosis of hypothyroidism. A low total T3 or free T3 is not always present but is associated with severe forms of hypothyroidism. The hallmark of hyperthyroidism is an elevated free T4 level or free T3 level or both. In a primary thyroid disorder, the TSH is below 0.1 U/L or undetectable.
Here is a description of these tests and what they mean:
- TSH (thyroid-stimulating hormone) is a pituitary hormone that acts on the thyroid gland to increase thyroid hormone secretion. Measurement of TSH is the most sensitive test to screen for hypothyroidism and hyperthyroidism as long as a second-generation assay is used (0.05 mIU/L). Thyroid testing should always begin just with the TSH test. Ordering a free T4 test at the same time is redundant and costly.
- T4 (thyroxine) is best and most accurately measured in its unbound free form. Of all the tests that measure thyroxine, free T4 most accurately reflects unbound thyroid hormone, which is physiologically active. Also, several variables (e.g. pregnancy, disease states, medications) alter total T4 levels by increasing or decreasing thyroid binding hormones. A free T4 test should always follow an abnormal TSH.
- T3 (triiodothyronine) is produced in the thyroid and in peripheral tissues via the enzymatic conversion of T4. Like T4, it is bound and unbound in the serum by thyroid binding globulin, and either form can be measured. T3 should be measured when the TSH is abnormal but the free T4 is within normal limits.
- T3 resin uptake is used to calculate indirectly free T4 and should only be ordered if a free T4 test is unavailable.
- Thyroid antibody tests can help uncover the underlying cause of thyroid dysfunction. These tests lack sensitivity and specificity and should not be used to rule out cancer. Thyroid peroxidase antibodies (antithyroglobulin) and antimicrosomal antibodies are associated with Hashimoto’s thyroiditis and Graves’ disease. Thyroid-stimulating immunoglobulin (TSI) or thyroid-stimulating hormone receptor antibodies are almost always unique to Graves’ disease.
- A radioactive iodine uptake thyroid scan (RAIU) is the best test to determine the cause of hyperthyroidism. Uptake is elevated in most common conditions causing hyperthyroidism, but the pattern of uptake differs. In the context of hyperthyroidism, absent uptake should raise a red flag for nonfunctioning nodules that can be either benign or malignant. A thyroid scan is unhelpful and should not be ordered in working up hypothyroidism.
- Thyroid ultrasound can characterize gland size and nodularity but cannot distinguish benign from malignant masses.
- Fine-needle aspiration biopsy (FNAB) is the best test to distinguish benign and malignant nodules.
What makes the diagnosis difficult and often missed is that some patients have hypothyroidism with minimal or no symptoms. This is especially true in elders because many of the signs and symptoms of hypothyroidism are attributed to “normal” aging. In one recent review of women older than 70 who were screened in an office-based setting, 2% were diagnosed with unsuspected overt hypothyroidism.1 Because classical exam and laboratory findings associated with hypothyroidism tend to present later in the disorder, many patients with thyroid dysfunction have “normal” exams.
Exam findings associated with a hypo-functioning thyroid may include an enlarged thyroid gland (goiter) or nonpalpable gland, non-pitting edema (myxedema), sinus bradycardia, decrease in body temperature, and delayed relaxation of the deep tendon reflexes. Secondary laboratory abnormalities associated with hypothyroidism include normacytic anemia and elevated lipoproteins. Without specific thyroid testing, a “normal” physical does not rule out thyroid dysfunction.
Hyperthyroidism can also manifest as a depression in elders, known as “apathetic hyperthyroidism.” Patients report decreased cognition, depression, and fatigue, and often experience unexplained weight loss, muscle weakness, or atrial fibrillation. Therefore, elderly patients presenting with depression may have a hyper- or hypo-functioning thyroid.
Case 1 concluded The treating psychiatrist diagnosed the patient with major depression. In addition to treatment with an antidepressant, the patient underwent laboratory testing, including a complete blood count, metabolic panel, and TSH (thyroid stimulating hormone). Test results were normal except for a TSH of 64 mU/L, consistent with hypothyroidism. The patient was referred to her primary care physician to begin thyroid hormone replacement.
Comment Although psychiatric symptoms may be caused by clinically important thyroid dysfunction, thyroid function testing may uncover abnormalities of questionable clinical significance. The prevalence of abnormal thyroid hormone levels in hospitalized psychiatric patients ranges from 3% to 32%.2 High thyroid levels (free T4 index and total T4) are associated with acutely psychotic patients such as those with schizophrenia, affective psychosis, and amphetamine abuses. Most studies show that these changes are transient and often normalize with correction of the psychiatric condition, usually within 10 days. Many researchers believe these findings are consistent with euthyroid sick syndrome (Box 2).3
Depressed patients and those with bipolar disorder often present with altered measures of the hypothalamic-pituitary-thyroid (HPT) axis. These abnormalities include mildly elevated or depressed T3, T4 and TSH levels and are not indicative of true thyroid dysfunction (Table 1). It has been debated whether these patients differ in prognosis from psychiatric patients without such abnormalities, although data in depressed patients suggest equivalent outcomes.4 Furthermore, there is no clear evidence that thyroid supplementation benefits depressed patients with mildly elevated TSH with normal T4 and T3 values.5
The prevalence of thyroid disorders in the general population depends largely on the age, sex, and iodine consumption of the population studied. Women in general face a greater risk of overt thyroid dysfunction than do men, and elders face a greater risk than do the young. High dietary iodine consumption is associated with autoimmune hypothyroidism, especially in the aged. Iodine deficiency facilitates the development of hyperthyroidism secondary to toxic nodular goiter.
Table 1
INTERPRETING TEST RESULTS
| Cause | TSH | Free T4 | Free T3 |
|---|---|---|---|
| Hypothyroidism | Increased | Decreased | Normal or decreased |
| Hypothyroidism | Decreased | Increased | Increased |
| Subclinical hypothyroidism | Increased | Normal | Normal |
| Subclinical hypothyroidism | Decreased | Normal | Normal |
| Euthyroid sick syndrome | Normal or decreased | Normal or decreased | Decreased |
| Hypothalamic pituitary disorder | Decreased | Decreased | Normal or decreased |
| Hypothalamic pituitary disorder | Increased | Increased | Normal or decreased |
A number of other risk factors should also clue the clinician to thyroid dysfunction (Table 2).
Case 2: Subclinical thyroid abnormalities
S.J., 34, has a history of panic disorder that has been well controlled with a selective serotonin reuptake inhibitor (SSRI). He is referred to a primary care physician for an annual physical exam. His blood pressure is elevated as it has been on several occasions over the past year. His physical exam is otherwise normal. Laboratory and ECG test results are normal, except for an elevated TSH at 12 mU/L. Follow-up free T4 and free T3 tests are within normal limits. S.J. agrees to eat less salt to address his hypertension.
Challenge An elevated or decreased TSH with a normal thyroxine level (Table 1) is referred to as a “subclinical” thyroid disorder, which is more common than overt thyroid disorders. Women and elders are at greatest risk for subclinical hypothyroidism. In patients older than 60, the rate can be as high as 17% in women and 15% in men.6 The rate largely depends on the number of patients receiving exogenous thyroid hormone—16% in populations including individuals receiving exogenous thyroid hormone and as low as 0.6-1.1% in populations without such patients.1 Chronic subclinical hypothyroidism or mild thyroid failure is the most common condition found in thyroid function screening.
Table 2
WHEN TO CONSIDER THYROID DYSFUNCTION
|
Although patients with subclinical abnormalities appear to be symptom-free, there are clinical implications for these patients. Subclinical hyperthyroidism in the elderly increases the risk for atrial fibrillation and osteoporosis. Postmenopausal women with chronically low TSH measures have lower bone density, especially in cortical bone (e.g., the forearm and hip). Subclinical hypothyroidism is associated with lipid abnormalities and progression to overt hypothyroidism. More recently it has become apparent that this “subclinical” syndrome is not as symptom-free as once assumed, with dry skin, cold intolerance, and easy fatigability more common than in euthyroid patients.7
Case 2 concluded Three months later, repeat testing reveals a negative thyroid antibody test, a TSH elevated to 9 mU/L, and a free T4 and fasting lipid profile within normal limits. S.J. and his physician discuss the pros and cons of thyroid replacement and decide to retest his thyroid function in 6 months with a repeat TSH.
Comment Should individuals with subclinical disorders be treated? How frequently should their thyroid function tests be monitored? The answers vary greatly among clinicians.
Some experts argue that treatment improves behavioral function and decreases lipid levels. Some clinicians take a “wait and see” approach because values can normalize in approximately 10% of patients.6,8 Others treat based on presence of symptoms and risk of progression to overt thyroid failure (Table 2). If treatment is elected, only partial supplementation is usually needed. Most clinicians will start with a dose of 25 ug/d of T4 with adjustment every 6 to 8 weeks until the TSH is normalized.
Unless subclinical hyperthyroidism is secondary to over-replacement with exogenous thyroid hormone, this condtion can be more difficult to treat than subclinical hypothyroidism. Antithyroid therapy should be discussed with patients who have symptoms suggestive of hyperthyroidism, osteoporosis, recurrent atrial fibrillation, or thyroid gland nodules. Consultation with an endocrinologist can help clarify the risks and benefits and determine the specific antithyroid treatment appropriate for each patient.
Case 3: Medications and thyroid abnormalities
R.K., 56, has a long history of bipolar disorder. Upon presenting to his psychiatrist for routine follow-up, he reports a lack of energy but denies other symptoms of mania or depression. He periodically leaves work early or takes a short nap in his office to combat the fatigue. He feels that this may simply be part of “getting old.” He denies any new medical problems and has seen his family physician in the last year. He states that he has been compliant with his medications, lithium and olanzapine. He appears slightly withdrawn and blunted but otherwise there are no abnormal features.
His lithium level, thyroid function, or kidney function had not been checked for 7 months. Subsequent testing reveals an elevated TSH (50 mU/L), a normal kidney profile, and a lithium level in the therapeutic range.
Challenge In psychiatric settings, lithium carbonate is the drug most commonly associated with decreased thyroid function. Lithium interferes with both thyroid hormone synthesis and secretion. One-half of those taking lithium chronically develop goiter, and 40% develop subclinical or overt hypothyroidism.9-11
Many patients treated with lithium test positive for antithyroid antibodies. It is unclear if this finding represents a chronic autoimmune thyroiditis or is secondary to lithium treatment itself. In any case, patients taking lithium face an increased risk of thyroid failure. Other risk factors for thyroid failure include female gender and duration of treatment. Lithium dosage does not seem to be related to risk.
Clinicians differ on the frequency of thyroid monitoring for patients taking lithium. For patients without a history of thyroid dysfunction, annual TSH testing is likely sufficient.
Other medications affecting thyroid hormone production include methimazole, propylthiouracil, and iodide-containing drugs and dyes. Methimazole and propylthiouracil are given to patients intentionally with overt hyperthyroidism and interfere with hormone synthesis. Patients receiving medications or dyes containing iodide may also be susceptible to hypothyroidism. These agents are partially deiodinated after they are given and therefore can cause transient or prolonged decreases in thyroid production.
In consultative work, psychiatrists often confront abnormal thyroid tests in critically ill patients. Euthyroid sick syndrome can be a challenge to distinguish from ill patients with true thyroid or pituitary dysfunction. This syndrome is common in hospitalized patients and has been documented in more than 50% of patients in some settings.14
Abnormal thyroid tests are observed in a variety of medical conditions including heart failure, myocardial infarction, renal failure, liver disease, infections, stress, trauma, starvation, and autoimmune disorders. There is considerable debate about the meaning of these test abnormalities, and to date no conclusive intervention to correct abnormalities has proven to be consistently effective in ill patients.
The complex results of testing contribute to the confusion. An isolated low T3 is the most common lab abnormality found in nonthyroidal illness, related to a decrease in T4 enzymatic conversion to T3. Many disease states decrease this enzyme’s (5’-deiodinase) activity. Unlike T3, TSH and T4 levels stay within normal limits in mild to moderately ill patients.
In patients who are moderately ill or who have been ill for a longer time, T4 levels fall with T3. In more severe and critically ill patients, the TSH level can decrease as well.
T4 can be elevated in sick patients without thyroid dysfunction. With this pattern, the TSH and T3 levels are normal or high. The clinical meaning of these abnormalities is unclear. Some studies suggest that the degree of thyroid hormone suppression correlates with disease severity and prognosis. Both decreased T3 and T4 levels have been shown to correlate with mortality in some disease states.15 Debate remains as to whether these findings represent a maladaptive process or a protective response to illness.
III patients with hyperthyroidism generally have an elevated serum free T4 and T3 with an undetectable TSH. Ill patients with true hypothyroidism will have a TSH greater than 20 to 30 mU/ml with suppressed T4 and T3 levels. Diagnosis is more difficult when TSH levels are mildly abnormal or when the clinician is trying to distinguish secondary hypothyroidism from the low T3, T4, and TSH pattern found in many critically ill patients. Secondary testing or clinical findings such as an enlarged gland, the presence of thyroid antibodies, or abnormalities in other pituitary hormones may point to an underlying thyroid or pituitary problem in ill patients.
Some oral cholecystographic agents and the antiarrhythmic medication amiodarone are excreted slowly and can be associated with more prolonged decreases in thyroid hormone production. Iodide and medications containing iodide may precipitate a longer enduring hypothyroidism in patients with chronic autoimmune thyroiditis and in those with hyperthyroidism who have received radioactive iodine therapy or have undergone partial thyroidectomy.
The cholesterol-lowering bile acid sequestrants colestipol and cholestyramine can also inhibit thyroid reabsorption from the intestine, potentially leading to hypothyroidism. Patients dependent on exogenous T4 or who have an underlying decreased thyroid function may develop hypothyroidism.
Table 3
WHICH MEDICATIONS CAN CAUSE THYROID DYSFUNCTION?
| Drugs that increase thyroid hormone secretion Iodide-containing medication Amiodarone Providone-iodine antiseptics X-ray contrast media containing iodine | Drugs that increase hepatic metabolism of T4 and T3 Phenobarbital Rifampin Phenytoin Carbamazepine |
| Drugs that decrease TBG,* causing a relative increase in unbound thyroid Androgens Anabolic steroids | Drugs that decrease T4 absorption Colestipol Cholestyramine Aluminum hydroxide Ferrous sulfate Sucralfate |
| Drugs that decrease thyroid hormone secretion Lithium carbonate Iodide Amiodarone | Drugs that increase TBG,* causing a relative decrease in unbound thyroid Estrogens Tamoxifen Heroin and methadone |
| *Thyroxine-binding globulin Table adapted from: Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333(25):1688-94. | |
Drugs that alter thyroid hormone metabolism can also be problematic. Although thyroid hormone is metabolized mostly by deiodination, it also undergoes glucuronidation and sulfation. Phenobarbital, rifampin, phenytoin, and carbamazepine all increase T4 and T3 metabolism by inducing these hepatic enzymes. In patients with no thyroid disease, phenytoin and carbamazepine can decrease circulating free T4 levels by 20% to 40%.12 Patients receiving T4 replacement may need their dosage increased or risk hypothyroidism if placed on one of these medications (Table 3).
Several medications alter total T4 and T3 levels by increasing or decreasing thyroid-binding proteins. Examples include estrogens, androgens, anabolic steroids, methadone, and heroin. Most thyroid hormone circulates as bound, but it is the unbound form that is active in peripheral tissues. Patients thus can experience changes in the binding proteins, while the proportion of unbound (“free”) hormone at the tissue level remains unaffected.
Because this unbound form remains relatively unchanged, the patient with normal thyroid function remains euthyroid despite alterations in total thyroid levels. When patients with hypothyroidism start one of these medications, their replacement hormone dosage may need to be adjusted.
Related resources
- American Association of Clinical Endocrinologists. www.aace.com
- Clinical practice guidelines for evaluation and treatment of hypothyroidism and hyperthyroidism. Position statement on subclinical hypothyroidism and pregnancy
- Thyroid Federation International. www.thyroid-fed.org
- Online videos regarding thyroid disease (patient-directed). Patient handouts on thyroid disease
- Jameson JL, Weetman AP. Disorders of the thyroid gland. In: Harrison’s Principles of Internal Medicine. 15th ed. New York: McGraw-Hill; 2001:2060-84
Drug brand names
- Amiodorone • Pacerone, Cordarone
- Colestipol • Colestid
- Methimazole • Tapazole
- Olanzapine • Zyprexa, Zyprexa Zydis
- Rifampin • Rifadin, Rimactane
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article.
1. Helfand M, Redfern CC. Screening for thyroid disease: an update. Ann Intern Med 1998;129(2):144-58.
2. Arem R, Cusi K. Thyroid function testing in psychiatric illness usefulness and limitations. Trends Endocrinol Metab 1997;8:282-87.
3. Nader S, Warner MD, Doyle S, Peabody CA. Euthyroid sick syndrome in psychiatric inpatients. Biol Psychiatry 1996;40(12):1288-93.
4. Fava M, Labbate LA, Abraham ME. Hypothyroidism and hyperthyroidism in major depression. J Clin Psychiatry 1995;56(5):186-92.
5. Jackson IM. The thyroid axis and depression. Thyroid 1998;8(10):951-56.
6. Samuels MH. Subclinical thyroid disease in the elderly. Thyroid 1998;8(9):803-13.
7. Staub JJ, Althaus BU, Engler H, Ryff AS, Trabucco P, Marquardt K, et al. Spectrum of subclinical and overt hypothyroidism: effect on thyrotropin, prolactin, and thyroid reserve, and metabolic impact on peripheral target tissues. Am J Med 1992;92(6):631-42.
8. Ayala AR, Wartofsky L. Minimally symptomatic (subclinical) hypothyroidism. Endocrinologist 1997;7:44-50.
9. Spaulding SW, Burrow GN, Bermudez F, Himmelhoch JM. The inhibitory effect of lithium on thyroid hormone release in both euthyroid and thyrotoxic patients. J Clin Endocrinol Metab 1972;35(6):905-11.
10. Perrild H, Hegedus L Baastrup PC, Kayser L, Kastberg S. Thyroid function and ultrasonically determined thyroid size in patients receiving long-term lithium treatment. Am J Psychiatry 1990;147(11):1518-21.
11. Bocchetta A, Bernardi F, Peditzi M. Thyroid abnormalities during lithium treatment. Acta Psychiatr Scand 1991;83(3):193-98.
12. Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333(25):1688-94.
13. Mandel SJ, Larsen PR, Seely EW, Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N Engl J Med 1990;323(2):91-6.
14. Chopra IJ. Clinical review 86: euthyroid sick syndrome: is it a misnomer? J Clin Endocrinol Metab 1997;82(2):329-34.
15. Camacho PM, Dwarkanathan AA. Sick euthyroid syndrome, what to do when thyroid function tests are abnormal in critically ill patients. Postgrad Med 1999;105(4):215-19.
16. Woeber KA. Update of management of hyperthyroidism and hypothyroidism. Arch Fam Med 2000;9(8):743-47.
Psychiatrists commonly order thyroid testing and are often the first to confront abnormal thyroid test results. As thyroid testing has become more sophisticated and sensitive (Box 1), the interpretation and management of abnormal or slightly abnormal results has become increasingly complex. What’s more, older individuals, hospitalized patients, and those with psychiatric illness often present with subtle laboratory abnormalities.
Hyperthyroidism and hypothyroidism are highly prevalent disorders, especially in women and the elderly. Thyroid dysfunction is the second most common endocrine disorder after diabetes among elders. In the three cases that follow, some of the problems and solutions in dealing with thyroid testing are presented.
Case 1: Depression and thyroid abnormalities
J.R., 67, has a history of hypertension. She was referred for evaluation of depressive symptoms. She reports 3 months of increasing fatigue, lethargy, and poor motivation. Her weight has increased by 10 pounds over this period. Her physical exam, ECG, and chest x-ray are normal. She is well groomed and slightly overweight. Her medications have not changed recently and include hydrochlorothiazide 25 mg/d and an aspirin a day.
J.R. reports no history of treatment for psychiatric illness, denies current use of alcohol, tobacco, or illicit drugs, exhibits no abnormal movements or psychomotor changes, and her speech is articulate. Her mood is depressed, and her affect is restricted. She is not suicidal or homicidal, and her exam reveals no psychotic features.
Challenge Patients with thyroid abnormalities often present with psychiatric complaints. Classically, hypothyroidism can present like a depressive episode with similar symptoms of fatigue, anhedonia, weight gain, and sleep disturbance. Patients with hypothyroidism, however, may have physical complaints as well, which should alert the clinician to an underlying thyroid disorder. Typical physical complaints include hair loss, weight gain, dry skin, cold intolerance, constipation, muscle cramps, and joint pains. Women may also complain of menstrual disturbances such as menorrhagia, and may have trouble with fertility.
An elevated or decreased TSH suggests thyroid dysfunction and should always be evaluated.
A low free T4 confirms the diagnosis of hypothyroidism. A low total T3 or free T3 is not always present but is associated with severe forms of hypothyroidism. The hallmark of hyperthyroidism is an elevated free T4 level or free T3 level or both. In a primary thyroid disorder, the TSH is below 0.1 U/L or undetectable.
Here is a description of these tests and what they mean:
- TSH (thyroid-stimulating hormone) is a pituitary hormone that acts on the thyroid gland to increase thyroid hormone secretion. Measurement of TSH is the most sensitive test to screen for hypothyroidism and hyperthyroidism as long as a second-generation assay is used (0.05 mIU/L). Thyroid testing should always begin just with the TSH test. Ordering a free T4 test at the same time is redundant and costly.
- T4 (thyroxine) is best and most accurately measured in its unbound free form. Of all the tests that measure thyroxine, free T4 most accurately reflects unbound thyroid hormone, which is physiologically active. Also, several variables (e.g. pregnancy, disease states, medications) alter total T4 levels by increasing or decreasing thyroid binding hormones. A free T4 test should always follow an abnormal TSH.
- T3 (triiodothyronine) is produced in the thyroid and in peripheral tissues via the enzymatic conversion of T4. Like T4, it is bound and unbound in the serum by thyroid binding globulin, and either form can be measured. T3 should be measured when the TSH is abnormal but the free T4 is within normal limits.
- T3 resin uptake is used to calculate indirectly free T4 and should only be ordered if a free T4 test is unavailable.
- Thyroid antibody tests can help uncover the underlying cause of thyroid dysfunction. These tests lack sensitivity and specificity and should not be used to rule out cancer. Thyroid peroxidase antibodies (antithyroglobulin) and antimicrosomal antibodies are associated with Hashimoto’s thyroiditis and Graves’ disease. Thyroid-stimulating immunoglobulin (TSI) or thyroid-stimulating hormone receptor antibodies are almost always unique to Graves’ disease.
- A radioactive iodine uptake thyroid scan (RAIU) is the best test to determine the cause of hyperthyroidism. Uptake is elevated in most common conditions causing hyperthyroidism, but the pattern of uptake differs. In the context of hyperthyroidism, absent uptake should raise a red flag for nonfunctioning nodules that can be either benign or malignant. A thyroid scan is unhelpful and should not be ordered in working up hypothyroidism.
- Thyroid ultrasound can characterize gland size and nodularity but cannot distinguish benign from malignant masses.
- Fine-needle aspiration biopsy (FNAB) is the best test to distinguish benign and malignant nodules.
What makes the diagnosis difficult and often missed is that some patients have hypothyroidism with minimal or no symptoms. This is especially true in elders because many of the signs and symptoms of hypothyroidism are attributed to “normal” aging. In one recent review of women older than 70 who were screened in an office-based setting, 2% were diagnosed with unsuspected overt hypothyroidism.1 Because classical exam and laboratory findings associated with hypothyroidism tend to present later in the disorder, many patients with thyroid dysfunction have “normal” exams.
Exam findings associated with a hypo-functioning thyroid may include an enlarged thyroid gland (goiter) or nonpalpable gland, non-pitting edema (myxedema), sinus bradycardia, decrease in body temperature, and delayed relaxation of the deep tendon reflexes. Secondary laboratory abnormalities associated with hypothyroidism include normacytic anemia and elevated lipoproteins. Without specific thyroid testing, a “normal” physical does not rule out thyroid dysfunction.
Hyperthyroidism can also manifest as a depression in elders, known as “apathetic hyperthyroidism.” Patients report decreased cognition, depression, and fatigue, and often experience unexplained weight loss, muscle weakness, or atrial fibrillation. Therefore, elderly patients presenting with depression may have a hyper- or hypo-functioning thyroid.
Case 1 concluded The treating psychiatrist diagnosed the patient with major depression. In addition to treatment with an antidepressant, the patient underwent laboratory testing, including a complete blood count, metabolic panel, and TSH (thyroid stimulating hormone). Test results were normal except for a TSH of 64 mU/L, consistent with hypothyroidism. The patient was referred to her primary care physician to begin thyroid hormone replacement.
Comment Although psychiatric symptoms may be caused by clinically important thyroid dysfunction, thyroid function testing may uncover abnormalities of questionable clinical significance. The prevalence of abnormal thyroid hormone levels in hospitalized psychiatric patients ranges from 3% to 32%.2 High thyroid levels (free T4 index and total T4) are associated with acutely psychotic patients such as those with schizophrenia, affective psychosis, and amphetamine abuses. Most studies show that these changes are transient and often normalize with correction of the psychiatric condition, usually within 10 days. Many researchers believe these findings are consistent with euthyroid sick syndrome (Box 2).3
Depressed patients and those with bipolar disorder often present with altered measures of the hypothalamic-pituitary-thyroid (HPT) axis. These abnormalities include mildly elevated or depressed T3, T4 and TSH levels and are not indicative of true thyroid dysfunction (Table 1). It has been debated whether these patients differ in prognosis from psychiatric patients without such abnormalities, although data in depressed patients suggest equivalent outcomes.4 Furthermore, there is no clear evidence that thyroid supplementation benefits depressed patients with mildly elevated TSH with normal T4 and T3 values.5
The prevalence of thyroid disorders in the general population depends largely on the age, sex, and iodine consumption of the population studied. Women in general face a greater risk of overt thyroid dysfunction than do men, and elders face a greater risk than do the young. High dietary iodine consumption is associated with autoimmune hypothyroidism, especially in the aged. Iodine deficiency facilitates the development of hyperthyroidism secondary to toxic nodular goiter.
Table 1
INTERPRETING TEST RESULTS
| Cause | TSH | Free T4 | Free T3 |
|---|---|---|---|
| Hypothyroidism | Increased | Decreased | Normal or decreased |
| Hypothyroidism | Decreased | Increased | Increased |
| Subclinical hypothyroidism | Increased | Normal | Normal |
| Subclinical hypothyroidism | Decreased | Normal | Normal |
| Euthyroid sick syndrome | Normal or decreased | Normal or decreased | Decreased |
| Hypothalamic pituitary disorder | Decreased | Decreased | Normal or decreased |
| Hypothalamic pituitary disorder | Increased | Increased | Normal or decreased |
A number of other risk factors should also clue the clinician to thyroid dysfunction (Table 2).
Case 2: Subclinical thyroid abnormalities
S.J., 34, has a history of panic disorder that has been well controlled with a selective serotonin reuptake inhibitor (SSRI). He is referred to a primary care physician for an annual physical exam. His blood pressure is elevated as it has been on several occasions over the past year. His physical exam is otherwise normal. Laboratory and ECG test results are normal, except for an elevated TSH at 12 mU/L. Follow-up free T4 and free T3 tests are within normal limits. S.J. agrees to eat less salt to address his hypertension.
Challenge An elevated or decreased TSH with a normal thyroxine level (Table 1) is referred to as a “subclinical” thyroid disorder, which is more common than overt thyroid disorders. Women and elders are at greatest risk for subclinical hypothyroidism. In patients older than 60, the rate can be as high as 17% in women and 15% in men.6 The rate largely depends on the number of patients receiving exogenous thyroid hormone—16% in populations including individuals receiving exogenous thyroid hormone and as low as 0.6-1.1% in populations without such patients.1 Chronic subclinical hypothyroidism or mild thyroid failure is the most common condition found in thyroid function screening.
Table 2
WHEN TO CONSIDER THYROID DYSFUNCTION
|
Although patients with subclinical abnormalities appear to be symptom-free, there are clinical implications for these patients. Subclinical hyperthyroidism in the elderly increases the risk for atrial fibrillation and osteoporosis. Postmenopausal women with chronically low TSH measures have lower bone density, especially in cortical bone (e.g., the forearm and hip). Subclinical hypothyroidism is associated with lipid abnormalities and progression to overt hypothyroidism. More recently it has become apparent that this “subclinical” syndrome is not as symptom-free as once assumed, with dry skin, cold intolerance, and easy fatigability more common than in euthyroid patients.7
Case 2 concluded Three months later, repeat testing reveals a negative thyroid antibody test, a TSH elevated to 9 mU/L, and a free T4 and fasting lipid profile within normal limits. S.J. and his physician discuss the pros and cons of thyroid replacement and decide to retest his thyroid function in 6 months with a repeat TSH.
Comment Should individuals with subclinical disorders be treated? How frequently should their thyroid function tests be monitored? The answers vary greatly among clinicians.
Some experts argue that treatment improves behavioral function and decreases lipid levels. Some clinicians take a “wait and see” approach because values can normalize in approximately 10% of patients.6,8 Others treat based on presence of symptoms and risk of progression to overt thyroid failure (Table 2). If treatment is elected, only partial supplementation is usually needed. Most clinicians will start with a dose of 25 ug/d of T4 with adjustment every 6 to 8 weeks until the TSH is normalized.
Unless subclinical hyperthyroidism is secondary to over-replacement with exogenous thyroid hormone, this condtion can be more difficult to treat than subclinical hypothyroidism. Antithyroid therapy should be discussed with patients who have symptoms suggestive of hyperthyroidism, osteoporosis, recurrent atrial fibrillation, or thyroid gland nodules. Consultation with an endocrinologist can help clarify the risks and benefits and determine the specific antithyroid treatment appropriate for each patient.
Case 3: Medications and thyroid abnormalities
R.K., 56, has a long history of bipolar disorder. Upon presenting to his psychiatrist for routine follow-up, he reports a lack of energy but denies other symptoms of mania or depression. He periodically leaves work early or takes a short nap in his office to combat the fatigue. He feels that this may simply be part of “getting old.” He denies any new medical problems and has seen his family physician in the last year. He states that he has been compliant with his medications, lithium and olanzapine. He appears slightly withdrawn and blunted but otherwise there are no abnormal features.
His lithium level, thyroid function, or kidney function had not been checked for 7 months. Subsequent testing reveals an elevated TSH (50 mU/L), a normal kidney profile, and a lithium level in the therapeutic range.
Challenge In psychiatric settings, lithium carbonate is the drug most commonly associated with decreased thyroid function. Lithium interferes with both thyroid hormone synthesis and secretion. One-half of those taking lithium chronically develop goiter, and 40% develop subclinical or overt hypothyroidism.9-11
Many patients treated with lithium test positive for antithyroid antibodies. It is unclear if this finding represents a chronic autoimmune thyroiditis or is secondary to lithium treatment itself. In any case, patients taking lithium face an increased risk of thyroid failure. Other risk factors for thyroid failure include female gender and duration of treatment. Lithium dosage does not seem to be related to risk.
Clinicians differ on the frequency of thyroid monitoring for patients taking lithium. For patients without a history of thyroid dysfunction, annual TSH testing is likely sufficient.
Other medications affecting thyroid hormone production include methimazole, propylthiouracil, and iodide-containing drugs and dyes. Methimazole and propylthiouracil are given to patients intentionally with overt hyperthyroidism and interfere with hormone synthesis. Patients receiving medications or dyes containing iodide may also be susceptible to hypothyroidism. These agents are partially deiodinated after they are given and therefore can cause transient or prolonged decreases in thyroid production.
In consultative work, psychiatrists often confront abnormal thyroid tests in critically ill patients. Euthyroid sick syndrome can be a challenge to distinguish from ill patients with true thyroid or pituitary dysfunction. This syndrome is common in hospitalized patients and has been documented in more than 50% of patients in some settings.14
Abnormal thyroid tests are observed in a variety of medical conditions including heart failure, myocardial infarction, renal failure, liver disease, infections, stress, trauma, starvation, and autoimmune disorders. There is considerable debate about the meaning of these test abnormalities, and to date no conclusive intervention to correct abnormalities has proven to be consistently effective in ill patients.
The complex results of testing contribute to the confusion. An isolated low T3 is the most common lab abnormality found in nonthyroidal illness, related to a decrease in T4 enzymatic conversion to T3. Many disease states decrease this enzyme’s (5’-deiodinase) activity. Unlike T3, TSH and T4 levels stay within normal limits in mild to moderately ill patients.
In patients who are moderately ill or who have been ill for a longer time, T4 levels fall with T3. In more severe and critically ill patients, the TSH level can decrease as well.
T4 can be elevated in sick patients without thyroid dysfunction. With this pattern, the TSH and T3 levels are normal or high. The clinical meaning of these abnormalities is unclear. Some studies suggest that the degree of thyroid hormone suppression correlates with disease severity and prognosis. Both decreased T3 and T4 levels have been shown to correlate with mortality in some disease states.15 Debate remains as to whether these findings represent a maladaptive process or a protective response to illness.
III patients with hyperthyroidism generally have an elevated serum free T4 and T3 with an undetectable TSH. Ill patients with true hypothyroidism will have a TSH greater than 20 to 30 mU/ml with suppressed T4 and T3 levels. Diagnosis is more difficult when TSH levels are mildly abnormal or when the clinician is trying to distinguish secondary hypothyroidism from the low T3, T4, and TSH pattern found in many critically ill patients. Secondary testing or clinical findings such as an enlarged gland, the presence of thyroid antibodies, or abnormalities in other pituitary hormones may point to an underlying thyroid or pituitary problem in ill patients.
Some oral cholecystographic agents and the antiarrhythmic medication amiodarone are excreted slowly and can be associated with more prolonged decreases in thyroid hormone production. Iodide and medications containing iodide may precipitate a longer enduring hypothyroidism in patients with chronic autoimmune thyroiditis and in those with hyperthyroidism who have received radioactive iodine therapy or have undergone partial thyroidectomy.
The cholesterol-lowering bile acid sequestrants colestipol and cholestyramine can also inhibit thyroid reabsorption from the intestine, potentially leading to hypothyroidism. Patients dependent on exogenous T4 or who have an underlying decreased thyroid function may develop hypothyroidism.
Table 3
WHICH MEDICATIONS CAN CAUSE THYROID DYSFUNCTION?
| Drugs that increase thyroid hormone secretion Iodide-containing medication Amiodarone Providone-iodine antiseptics X-ray contrast media containing iodine | Drugs that increase hepatic metabolism of T4 and T3 Phenobarbital Rifampin Phenytoin Carbamazepine |
| Drugs that decrease TBG,* causing a relative increase in unbound thyroid Androgens Anabolic steroids | Drugs that decrease T4 absorption Colestipol Cholestyramine Aluminum hydroxide Ferrous sulfate Sucralfate |
| Drugs that decrease thyroid hormone secretion Lithium carbonate Iodide Amiodarone | Drugs that increase TBG,* causing a relative decrease in unbound thyroid Estrogens Tamoxifen Heroin and methadone |
| *Thyroxine-binding globulin Table adapted from: Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333(25):1688-94. | |
Drugs that alter thyroid hormone metabolism can also be problematic. Although thyroid hormone is metabolized mostly by deiodination, it also undergoes glucuronidation and sulfation. Phenobarbital, rifampin, phenytoin, and carbamazepine all increase T4 and T3 metabolism by inducing these hepatic enzymes. In patients with no thyroid disease, phenytoin and carbamazepine can decrease circulating free T4 levels by 20% to 40%.12 Patients receiving T4 replacement may need their dosage increased or risk hypothyroidism if placed on one of these medications (Table 3).
Several medications alter total T4 and T3 levels by increasing or decreasing thyroid-binding proteins. Examples include estrogens, androgens, anabolic steroids, methadone, and heroin. Most thyroid hormone circulates as bound, but it is the unbound form that is active in peripheral tissues. Patients thus can experience changes in the binding proteins, while the proportion of unbound (“free”) hormone at the tissue level remains unaffected.
Because this unbound form remains relatively unchanged, the patient with normal thyroid function remains euthyroid despite alterations in total thyroid levels. When patients with hypothyroidism start one of these medications, their replacement hormone dosage may need to be adjusted.
Related resources
- American Association of Clinical Endocrinologists. www.aace.com
- Clinical practice guidelines for evaluation and treatment of hypothyroidism and hyperthyroidism. Position statement on subclinical hypothyroidism and pregnancy
- Thyroid Federation International. www.thyroid-fed.org
- Online videos regarding thyroid disease (patient-directed). Patient handouts on thyroid disease
- Jameson JL, Weetman AP. Disorders of the thyroid gland. In: Harrison’s Principles of Internal Medicine. 15th ed. New York: McGraw-Hill; 2001:2060-84
Drug brand names
- Amiodorone • Pacerone, Cordarone
- Colestipol • Colestid
- Methimazole • Tapazole
- Olanzapine • Zyprexa, Zyprexa Zydis
- Rifampin • Rifadin, Rimactane
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article.
Psychiatrists commonly order thyroid testing and are often the first to confront abnormal thyroid test results. As thyroid testing has become more sophisticated and sensitive (Box 1), the interpretation and management of abnormal or slightly abnormal results has become increasingly complex. What’s more, older individuals, hospitalized patients, and those with psychiatric illness often present with subtle laboratory abnormalities.
Hyperthyroidism and hypothyroidism are highly prevalent disorders, especially in women and the elderly. Thyroid dysfunction is the second most common endocrine disorder after diabetes among elders. In the three cases that follow, some of the problems and solutions in dealing with thyroid testing are presented.
Case 1: Depression and thyroid abnormalities
J.R., 67, has a history of hypertension. She was referred for evaluation of depressive symptoms. She reports 3 months of increasing fatigue, lethargy, and poor motivation. Her weight has increased by 10 pounds over this period. Her physical exam, ECG, and chest x-ray are normal. She is well groomed and slightly overweight. Her medications have not changed recently and include hydrochlorothiazide 25 mg/d and an aspirin a day.
J.R. reports no history of treatment for psychiatric illness, denies current use of alcohol, tobacco, or illicit drugs, exhibits no abnormal movements or psychomotor changes, and her speech is articulate. Her mood is depressed, and her affect is restricted. She is not suicidal or homicidal, and her exam reveals no psychotic features.
Challenge Patients with thyroid abnormalities often present with psychiatric complaints. Classically, hypothyroidism can present like a depressive episode with similar symptoms of fatigue, anhedonia, weight gain, and sleep disturbance. Patients with hypothyroidism, however, may have physical complaints as well, which should alert the clinician to an underlying thyroid disorder. Typical physical complaints include hair loss, weight gain, dry skin, cold intolerance, constipation, muscle cramps, and joint pains. Women may also complain of menstrual disturbances such as menorrhagia, and may have trouble with fertility.
An elevated or decreased TSH suggests thyroid dysfunction and should always be evaluated.
A low free T4 confirms the diagnosis of hypothyroidism. A low total T3 or free T3 is not always present but is associated with severe forms of hypothyroidism. The hallmark of hyperthyroidism is an elevated free T4 level or free T3 level or both. In a primary thyroid disorder, the TSH is below 0.1 U/L or undetectable.
Here is a description of these tests and what they mean:
- TSH (thyroid-stimulating hormone) is a pituitary hormone that acts on the thyroid gland to increase thyroid hormone secretion. Measurement of TSH is the most sensitive test to screen for hypothyroidism and hyperthyroidism as long as a second-generation assay is used (0.05 mIU/L). Thyroid testing should always begin just with the TSH test. Ordering a free T4 test at the same time is redundant and costly.
- T4 (thyroxine) is best and most accurately measured in its unbound free form. Of all the tests that measure thyroxine, free T4 most accurately reflects unbound thyroid hormone, which is physiologically active. Also, several variables (e.g. pregnancy, disease states, medications) alter total T4 levels by increasing or decreasing thyroid binding hormones. A free T4 test should always follow an abnormal TSH.
- T3 (triiodothyronine) is produced in the thyroid and in peripheral tissues via the enzymatic conversion of T4. Like T4, it is bound and unbound in the serum by thyroid binding globulin, and either form can be measured. T3 should be measured when the TSH is abnormal but the free T4 is within normal limits.
- T3 resin uptake is used to calculate indirectly free T4 and should only be ordered if a free T4 test is unavailable.
- Thyroid antibody tests can help uncover the underlying cause of thyroid dysfunction. These tests lack sensitivity and specificity and should not be used to rule out cancer. Thyroid peroxidase antibodies (antithyroglobulin) and antimicrosomal antibodies are associated with Hashimoto’s thyroiditis and Graves’ disease. Thyroid-stimulating immunoglobulin (TSI) or thyroid-stimulating hormone receptor antibodies are almost always unique to Graves’ disease.
- A radioactive iodine uptake thyroid scan (RAIU) is the best test to determine the cause of hyperthyroidism. Uptake is elevated in most common conditions causing hyperthyroidism, but the pattern of uptake differs. In the context of hyperthyroidism, absent uptake should raise a red flag for nonfunctioning nodules that can be either benign or malignant. A thyroid scan is unhelpful and should not be ordered in working up hypothyroidism.
- Thyroid ultrasound can characterize gland size and nodularity but cannot distinguish benign from malignant masses.
- Fine-needle aspiration biopsy (FNAB) is the best test to distinguish benign and malignant nodules.
What makes the diagnosis difficult and often missed is that some patients have hypothyroidism with minimal or no symptoms. This is especially true in elders because many of the signs and symptoms of hypothyroidism are attributed to “normal” aging. In one recent review of women older than 70 who were screened in an office-based setting, 2% were diagnosed with unsuspected overt hypothyroidism.1 Because classical exam and laboratory findings associated with hypothyroidism tend to present later in the disorder, many patients with thyroid dysfunction have “normal” exams.
Exam findings associated with a hypo-functioning thyroid may include an enlarged thyroid gland (goiter) or nonpalpable gland, non-pitting edema (myxedema), sinus bradycardia, decrease in body temperature, and delayed relaxation of the deep tendon reflexes. Secondary laboratory abnormalities associated with hypothyroidism include normacytic anemia and elevated lipoproteins. Without specific thyroid testing, a “normal” physical does not rule out thyroid dysfunction.
Hyperthyroidism can also manifest as a depression in elders, known as “apathetic hyperthyroidism.” Patients report decreased cognition, depression, and fatigue, and often experience unexplained weight loss, muscle weakness, or atrial fibrillation. Therefore, elderly patients presenting with depression may have a hyper- or hypo-functioning thyroid.
Case 1 concluded The treating psychiatrist diagnosed the patient with major depression. In addition to treatment with an antidepressant, the patient underwent laboratory testing, including a complete blood count, metabolic panel, and TSH (thyroid stimulating hormone). Test results were normal except for a TSH of 64 mU/L, consistent with hypothyroidism. The patient was referred to her primary care physician to begin thyroid hormone replacement.
Comment Although psychiatric symptoms may be caused by clinically important thyroid dysfunction, thyroid function testing may uncover abnormalities of questionable clinical significance. The prevalence of abnormal thyroid hormone levels in hospitalized psychiatric patients ranges from 3% to 32%.2 High thyroid levels (free T4 index and total T4) are associated with acutely psychotic patients such as those with schizophrenia, affective psychosis, and amphetamine abuses. Most studies show that these changes are transient and often normalize with correction of the psychiatric condition, usually within 10 days. Many researchers believe these findings are consistent with euthyroid sick syndrome (Box 2).3
Depressed patients and those with bipolar disorder often present with altered measures of the hypothalamic-pituitary-thyroid (HPT) axis. These abnormalities include mildly elevated or depressed T3, T4 and TSH levels and are not indicative of true thyroid dysfunction (Table 1). It has been debated whether these patients differ in prognosis from psychiatric patients without such abnormalities, although data in depressed patients suggest equivalent outcomes.4 Furthermore, there is no clear evidence that thyroid supplementation benefits depressed patients with mildly elevated TSH with normal T4 and T3 values.5
The prevalence of thyroid disorders in the general population depends largely on the age, sex, and iodine consumption of the population studied. Women in general face a greater risk of overt thyroid dysfunction than do men, and elders face a greater risk than do the young. High dietary iodine consumption is associated with autoimmune hypothyroidism, especially in the aged. Iodine deficiency facilitates the development of hyperthyroidism secondary to toxic nodular goiter.
Table 1
INTERPRETING TEST RESULTS
| Cause | TSH | Free T4 | Free T3 |
|---|---|---|---|
| Hypothyroidism | Increased | Decreased | Normal or decreased |
| Hypothyroidism | Decreased | Increased | Increased |
| Subclinical hypothyroidism | Increased | Normal | Normal |
| Subclinical hypothyroidism | Decreased | Normal | Normal |
| Euthyroid sick syndrome | Normal or decreased | Normal or decreased | Decreased |
| Hypothalamic pituitary disorder | Decreased | Decreased | Normal or decreased |
| Hypothalamic pituitary disorder | Increased | Increased | Normal or decreased |
A number of other risk factors should also clue the clinician to thyroid dysfunction (Table 2).
Case 2: Subclinical thyroid abnormalities
S.J., 34, has a history of panic disorder that has been well controlled with a selective serotonin reuptake inhibitor (SSRI). He is referred to a primary care physician for an annual physical exam. His blood pressure is elevated as it has been on several occasions over the past year. His physical exam is otherwise normal. Laboratory and ECG test results are normal, except for an elevated TSH at 12 mU/L. Follow-up free T4 and free T3 tests are within normal limits. S.J. agrees to eat less salt to address his hypertension.
Challenge An elevated or decreased TSH with a normal thyroxine level (Table 1) is referred to as a “subclinical” thyroid disorder, which is more common than overt thyroid disorders. Women and elders are at greatest risk for subclinical hypothyroidism. In patients older than 60, the rate can be as high as 17% in women and 15% in men.6 The rate largely depends on the number of patients receiving exogenous thyroid hormone—16% in populations including individuals receiving exogenous thyroid hormone and as low as 0.6-1.1% in populations without such patients.1 Chronic subclinical hypothyroidism or mild thyroid failure is the most common condition found in thyroid function screening.
Table 2
WHEN TO CONSIDER THYROID DYSFUNCTION
|
Although patients with subclinical abnormalities appear to be symptom-free, there are clinical implications for these patients. Subclinical hyperthyroidism in the elderly increases the risk for atrial fibrillation and osteoporosis. Postmenopausal women with chronically low TSH measures have lower bone density, especially in cortical bone (e.g., the forearm and hip). Subclinical hypothyroidism is associated with lipid abnormalities and progression to overt hypothyroidism. More recently it has become apparent that this “subclinical” syndrome is not as symptom-free as once assumed, with dry skin, cold intolerance, and easy fatigability more common than in euthyroid patients.7
Case 2 concluded Three months later, repeat testing reveals a negative thyroid antibody test, a TSH elevated to 9 mU/L, and a free T4 and fasting lipid profile within normal limits. S.J. and his physician discuss the pros and cons of thyroid replacement and decide to retest his thyroid function in 6 months with a repeat TSH.
Comment Should individuals with subclinical disorders be treated? How frequently should their thyroid function tests be monitored? The answers vary greatly among clinicians.
Some experts argue that treatment improves behavioral function and decreases lipid levels. Some clinicians take a “wait and see” approach because values can normalize in approximately 10% of patients.6,8 Others treat based on presence of symptoms and risk of progression to overt thyroid failure (Table 2). If treatment is elected, only partial supplementation is usually needed. Most clinicians will start with a dose of 25 ug/d of T4 with adjustment every 6 to 8 weeks until the TSH is normalized.
Unless subclinical hyperthyroidism is secondary to over-replacement with exogenous thyroid hormone, this condtion can be more difficult to treat than subclinical hypothyroidism. Antithyroid therapy should be discussed with patients who have symptoms suggestive of hyperthyroidism, osteoporosis, recurrent atrial fibrillation, or thyroid gland nodules. Consultation with an endocrinologist can help clarify the risks and benefits and determine the specific antithyroid treatment appropriate for each patient.
Case 3: Medications and thyroid abnormalities
R.K., 56, has a long history of bipolar disorder. Upon presenting to his psychiatrist for routine follow-up, he reports a lack of energy but denies other symptoms of mania or depression. He periodically leaves work early or takes a short nap in his office to combat the fatigue. He feels that this may simply be part of “getting old.” He denies any new medical problems and has seen his family physician in the last year. He states that he has been compliant with his medications, lithium and olanzapine. He appears slightly withdrawn and blunted but otherwise there are no abnormal features.
His lithium level, thyroid function, or kidney function had not been checked for 7 months. Subsequent testing reveals an elevated TSH (50 mU/L), a normal kidney profile, and a lithium level in the therapeutic range.
Challenge In psychiatric settings, lithium carbonate is the drug most commonly associated with decreased thyroid function. Lithium interferes with both thyroid hormone synthesis and secretion. One-half of those taking lithium chronically develop goiter, and 40% develop subclinical or overt hypothyroidism.9-11
Many patients treated with lithium test positive for antithyroid antibodies. It is unclear if this finding represents a chronic autoimmune thyroiditis or is secondary to lithium treatment itself. In any case, patients taking lithium face an increased risk of thyroid failure. Other risk factors for thyroid failure include female gender and duration of treatment. Lithium dosage does not seem to be related to risk.
Clinicians differ on the frequency of thyroid monitoring for patients taking lithium. For patients without a history of thyroid dysfunction, annual TSH testing is likely sufficient.
Other medications affecting thyroid hormone production include methimazole, propylthiouracil, and iodide-containing drugs and dyes. Methimazole and propylthiouracil are given to patients intentionally with overt hyperthyroidism and interfere with hormone synthesis. Patients receiving medications or dyes containing iodide may also be susceptible to hypothyroidism. These agents are partially deiodinated after they are given and therefore can cause transient or prolonged decreases in thyroid production.
In consultative work, psychiatrists often confront abnormal thyroid tests in critically ill patients. Euthyroid sick syndrome can be a challenge to distinguish from ill patients with true thyroid or pituitary dysfunction. This syndrome is common in hospitalized patients and has been documented in more than 50% of patients in some settings.14
Abnormal thyroid tests are observed in a variety of medical conditions including heart failure, myocardial infarction, renal failure, liver disease, infections, stress, trauma, starvation, and autoimmune disorders. There is considerable debate about the meaning of these test abnormalities, and to date no conclusive intervention to correct abnormalities has proven to be consistently effective in ill patients.
The complex results of testing contribute to the confusion. An isolated low T3 is the most common lab abnormality found in nonthyroidal illness, related to a decrease in T4 enzymatic conversion to T3. Many disease states decrease this enzyme’s (5’-deiodinase) activity. Unlike T3, TSH and T4 levels stay within normal limits in mild to moderately ill patients.
In patients who are moderately ill or who have been ill for a longer time, T4 levels fall with T3. In more severe and critically ill patients, the TSH level can decrease as well.
T4 can be elevated in sick patients without thyroid dysfunction. With this pattern, the TSH and T3 levels are normal or high. The clinical meaning of these abnormalities is unclear. Some studies suggest that the degree of thyroid hormone suppression correlates with disease severity and prognosis. Both decreased T3 and T4 levels have been shown to correlate with mortality in some disease states.15 Debate remains as to whether these findings represent a maladaptive process or a protective response to illness.
III patients with hyperthyroidism generally have an elevated serum free T4 and T3 with an undetectable TSH. Ill patients with true hypothyroidism will have a TSH greater than 20 to 30 mU/ml with suppressed T4 and T3 levels. Diagnosis is more difficult when TSH levels are mildly abnormal or when the clinician is trying to distinguish secondary hypothyroidism from the low T3, T4, and TSH pattern found in many critically ill patients. Secondary testing or clinical findings such as an enlarged gland, the presence of thyroid antibodies, or abnormalities in other pituitary hormones may point to an underlying thyroid or pituitary problem in ill patients.
Some oral cholecystographic agents and the antiarrhythmic medication amiodarone are excreted slowly and can be associated with more prolonged decreases in thyroid hormone production. Iodide and medications containing iodide may precipitate a longer enduring hypothyroidism in patients with chronic autoimmune thyroiditis and in those with hyperthyroidism who have received radioactive iodine therapy or have undergone partial thyroidectomy.
The cholesterol-lowering bile acid sequestrants colestipol and cholestyramine can also inhibit thyroid reabsorption from the intestine, potentially leading to hypothyroidism. Patients dependent on exogenous T4 or who have an underlying decreased thyroid function may develop hypothyroidism.
Table 3
WHICH MEDICATIONS CAN CAUSE THYROID DYSFUNCTION?
| Drugs that increase thyroid hormone secretion Iodide-containing medication Amiodarone Providone-iodine antiseptics X-ray contrast media containing iodine | Drugs that increase hepatic metabolism of T4 and T3 Phenobarbital Rifampin Phenytoin Carbamazepine |
| Drugs that decrease TBG,* causing a relative increase in unbound thyroid Androgens Anabolic steroids | Drugs that decrease T4 absorption Colestipol Cholestyramine Aluminum hydroxide Ferrous sulfate Sucralfate |
| Drugs that decrease thyroid hormone secretion Lithium carbonate Iodide Amiodarone | Drugs that increase TBG,* causing a relative decrease in unbound thyroid Estrogens Tamoxifen Heroin and methadone |
| *Thyroxine-binding globulin Table adapted from: Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333(25):1688-94. | |
Drugs that alter thyroid hormone metabolism can also be problematic. Although thyroid hormone is metabolized mostly by deiodination, it also undergoes glucuronidation and sulfation. Phenobarbital, rifampin, phenytoin, and carbamazepine all increase T4 and T3 metabolism by inducing these hepatic enzymes. In patients with no thyroid disease, phenytoin and carbamazepine can decrease circulating free T4 levels by 20% to 40%.12 Patients receiving T4 replacement may need their dosage increased or risk hypothyroidism if placed on one of these medications (Table 3).
Several medications alter total T4 and T3 levels by increasing or decreasing thyroid-binding proteins. Examples include estrogens, androgens, anabolic steroids, methadone, and heroin. Most thyroid hormone circulates as bound, but it is the unbound form that is active in peripheral tissues. Patients thus can experience changes in the binding proteins, while the proportion of unbound (“free”) hormone at the tissue level remains unaffected.
Because this unbound form remains relatively unchanged, the patient with normal thyroid function remains euthyroid despite alterations in total thyroid levels. When patients with hypothyroidism start one of these medications, their replacement hormone dosage may need to be adjusted.
Related resources
- American Association of Clinical Endocrinologists. www.aace.com
- Clinical practice guidelines for evaluation and treatment of hypothyroidism and hyperthyroidism. Position statement on subclinical hypothyroidism and pregnancy
- Thyroid Federation International. www.thyroid-fed.org
- Online videos regarding thyroid disease (patient-directed). Patient handouts on thyroid disease
- Jameson JL, Weetman AP. Disorders of the thyroid gland. In: Harrison’s Principles of Internal Medicine. 15th ed. New York: McGraw-Hill; 2001:2060-84
Drug brand names
- Amiodorone • Pacerone, Cordarone
- Colestipol • Colestid
- Methimazole • Tapazole
- Olanzapine • Zyprexa, Zyprexa Zydis
- Rifampin • Rifadin, Rimactane
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article.
1. Helfand M, Redfern CC. Screening for thyroid disease: an update. Ann Intern Med 1998;129(2):144-58.
2. Arem R, Cusi K. Thyroid function testing in psychiatric illness usefulness and limitations. Trends Endocrinol Metab 1997;8:282-87.
3. Nader S, Warner MD, Doyle S, Peabody CA. Euthyroid sick syndrome in psychiatric inpatients. Biol Psychiatry 1996;40(12):1288-93.
4. Fava M, Labbate LA, Abraham ME. Hypothyroidism and hyperthyroidism in major depression. J Clin Psychiatry 1995;56(5):186-92.
5. Jackson IM. The thyroid axis and depression. Thyroid 1998;8(10):951-56.
6. Samuels MH. Subclinical thyroid disease in the elderly. Thyroid 1998;8(9):803-13.
7. Staub JJ, Althaus BU, Engler H, Ryff AS, Trabucco P, Marquardt K, et al. Spectrum of subclinical and overt hypothyroidism: effect on thyrotropin, prolactin, and thyroid reserve, and metabolic impact on peripheral target tissues. Am J Med 1992;92(6):631-42.
8. Ayala AR, Wartofsky L. Minimally symptomatic (subclinical) hypothyroidism. Endocrinologist 1997;7:44-50.
9. Spaulding SW, Burrow GN, Bermudez F, Himmelhoch JM. The inhibitory effect of lithium on thyroid hormone release in both euthyroid and thyrotoxic patients. J Clin Endocrinol Metab 1972;35(6):905-11.
10. Perrild H, Hegedus L Baastrup PC, Kayser L, Kastberg S. Thyroid function and ultrasonically determined thyroid size in patients receiving long-term lithium treatment. Am J Psychiatry 1990;147(11):1518-21.
11. Bocchetta A, Bernardi F, Peditzi M. Thyroid abnormalities during lithium treatment. Acta Psychiatr Scand 1991;83(3):193-98.
12. Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333(25):1688-94.
13. Mandel SJ, Larsen PR, Seely EW, Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N Engl J Med 1990;323(2):91-6.
14. Chopra IJ. Clinical review 86: euthyroid sick syndrome: is it a misnomer? J Clin Endocrinol Metab 1997;82(2):329-34.
15. Camacho PM, Dwarkanathan AA. Sick euthyroid syndrome, what to do when thyroid function tests are abnormal in critically ill patients. Postgrad Med 1999;105(4):215-19.
16. Woeber KA. Update of management of hyperthyroidism and hypothyroidism. Arch Fam Med 2000;9(8):743-47.
1. Helfand M, Redfern CC. Screening for thyroid disease: an update. Ann Intern Med 1998;129(2):144-58.
2. Arem R, Cusi K. Thyroid function testing in psychiatric illness usefulness and limitations. Trends Endocrinol Metab 1997;8:282-87.
3. Nader S, Warner MD, Doyle S, Peabody CA. Euthyroid sick syndrome in psychiatric inpatients. Biol Psychiatry 1996;40(12):1288-93.
4. Fava M, Labbate LA, Abraham ME. Hypothyroidism and hyperthyroidism in major depression. J Clin Psychiatry 1995;56(5):186-92.
5. Jackson IM. The thyroid axis and depression. Thyroid 1998;8(10):951-56.
6. Samuels MH. Subclinical thyroid disease in the elderly. Thyroid 1998;8(9):803-13.
7. Staub JJ, Althaus BU, Engler H, Ryff AS, Trabucco P, Marquardt K, et al. Spectrum of subclinical and overt hypothyroidism: effect on thyrotropin, prolactin, and thyroid reserve, and metabolic impact on peripheral target tissues. Am J Med 1992;92(6):631-42.
8. Ayala AR, Wartofsky L. Minimally symptomatic (subclinical) hypothyroidism. Endocrinologist 1997;7:44-50.
9. Spaulding SW, Burrow GN, Bermudez F, Himmelhoch JM. The inhibitory effect of lithium on thyroid hormone release in both euthyroid and thyrotoxic patients. J Clin Endocrinol Metab 1972;35(6):905-11.
10. Perrild H, Hegedus L Baastrup PC, Kayser L, Kastberg S. Thyroid function and ultrasonically determined thyroid size in patients receiving long-term lithium treatment. Am J Psychiatry 1990;147(11):1518-21.
11. Bocchetta A, Bernardi F, Peditzi M. Thyroid abnormalities during lithium treatment. Acta Psychiatr Scand 1991;83(3):193-98.
12. Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333(25):1688-94.
13. Mandel SJ, Larsen PR, Seely EW, Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N Engl J Med 1990;323(2):91-6.
14. Chopra IJ. Clinical review 86: euthyroid sick syndrome: is it a misnomer? J Clin Endocrinol Metab 1997;82(2):329-34.
15. Camacho PM, Dwarkanathan AA. Sick euthyroid syndrome, what to do when thyroid function tests are abnormal in critically ill patients. Postgrad Med 1999;105(4):215-19.
16. Woeber KA. Update of management of hyperthyroidism and hypothyroidism. Arch Fam Med 2000;9(8):743-47.