User login
Electroacupuncture promising for depression-related insomnia
In a study of more than 200 adults with depression and comorbid insomnia, change from baseline to week 8 on the Pittsburgh Sleep Quality Index (PSQI) was 3 points greater in the group receiving EA versus a group receiving sham acupuncture (SA) plus standard care, and 5 points greater vs a control group receiving standard care only. The improvements were sustained during a 24-week postintervention follow-up.
The EA group also showed significant improvement in depression, insomnia, self-rated anxiety, and total sleep time – all of which were not found in the SA or control groups.
“Based on the results of our trial, we recommend patients with depression and insomnia seek the treatment of EA as an alternative and complementary therapy for better results,” study investigator Shifen Xu, PhD, Shanghai (China) Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, told this news organization.
The findings were published online in JAMA Network Open.
Bidirectional relationship
“Sleep disturbance is the prominent symptom in patients with depression,” the investigators noted.
Depression and sleep issues have a bidirectional relationship, in that “poor sleep quality contributes to the development of depression, and having depression makes a person more likely to develop sleep issues,” they wrote.
Patients with co-occurring depression and sleep disorders are more difficult to treat and have a greater risk for relapse and recurrence of depression, they added.
Acupuncture may be an “effective drug-free approach to help treat mental illness and sleep disorders,” the researchers noted. A previous study suggested acupuncture may improve sleep efficacy and prolong total sleep in patients with primary insomnia.
“EA is the combination of traditional Chinese acupuncture with electric-impulse stimulation, and it can enhance the therapeutic effect of the acupoints throughout the needle retention time,” Dr. Xu said.
A previous pilot study of EA for depression-related insomnia showed significant improvements in sleep quality after EA treatment, but the sample size was small.
The current researchers, therefore, undertook the present study – with a larger sample size and comparison with SA and standard care. They divided 270 adults (mean age, 50.3 years; 71.9% women) at three tertiary hospitals in Shanghai into three groups, each consisting of 90 participants.
The EA plus standard care group and the SA plus standard care group received 30-minute treatments three times per week for 8 weeks. The control group received standard care only.
All participants had DSM-5–diagnosed depression; baseline PSQI scores greater than 7, with higher scores indicating worse sleep quality and a greater number or sleep disorders; and Hamilton Depression Rating Scales (HDRS-17) scores of 20-35, with higher scores indicating higher depression levels.
Patients with secondary depressive disorders caused by other conditions, medication, or psychotic disorders were excluded, as were patients with a history of alcohol abuse or drug dependence or those who had received acupuncture within the previous year.
Of the patients who completed the 8-week intervention, 83 were in the EA group, 81 in the SA group, and 83 in the control group. Almost all participants (91.5%) completed all outcome measurements by the end of the 24-week follow-up period (also known as week 32).
Calm mind, balanced mood
At the 8-week posttreatment assessment, which was the primary endpoint, the EA group had a mean reduction from baseline of 6.2 points (95% confidence interval, −6.9 to −5.6) in PSQI score.
There was a significant difference in PSQI score between the EA versus the SA group (−3.6 points; 95% CI, −4.4 to −2.8; P < .001) and vs the control group (−5.1 points; 95% CI, −6.0 to −4.2; P < .001).
The efficacy of EA in treating insomnia was sustained during the postintervention follow-up period when the EA group had a significantly greater reduction in PSQI score, compared with the SA group (−4.7; 95% CI, −5.4 to −3.9; P < .001) and the control group (−5.0; 95% CI, −5.8 to −4.1; P < .001).
Patients receiving EA also experienced significant (all P values < .001) improvement from baseline on secondary outcomes, including:
- Scores on the HDRS (−10.7; 95% CI, −11.8 to −9.7)
- Scores on the Insomnia Severity Index, (−7.6; 95% CI,−8.5 to −6.7)
- Scores on the Self-rated Anxiety Scale (−2.9; 95% CI, −4.1 to −1.7)
- Total sleep time, as recorded by sleep actigraphy (29.1 minutes; 95% CI, 21.5-36.7)
In addition, the EA group showed significant improvement in depression scores compared with the SA and control groups at both 8 and 32 weeks (all P values < .001).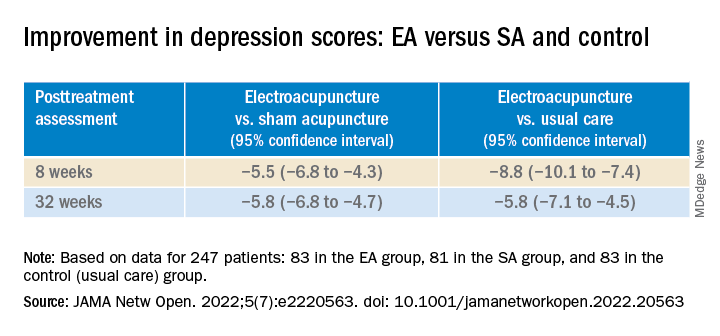
Participants in the EA group also had a 4.2% (95% CI, 2.6% - 5.8%) higher sleep efficiency score at week 8, compared with those in the SA group (P < .001).
In addition, they had lower scores on the Insomnia Severity Index and the Self-rated Anxiety Scale, and longer total sleep time, compared with the control group at week 8.
None of the participants reported any serious adverse events.
“Our findings constitute subjective and objective evidence of the efficacy and safety of EA with standard care in treating comorbid depression and insomnia compared with SA with standard care or standard care alone,” the investigators wrote.
“The acupoints we used in this trial mainly act on calming mind, relieving negative mood, and balancing the yin-yang,” Dr. Xu added.
Viable adjunctive treatment
Commenting on the study, Albert Yeung, MD, ScD, associate director of the Mass General Depression and Clinical Research Program and associate professor of psychiatry, Harvard Medical School, Boston, said that, with the evidence from this study, “acupuncture and/or electroacupuncture could be a viable adjunctive treatment for depressed patients who suffer from insomnia.”

Dr. Yeung, who was not involved with the study, is the coauthor of an accompanying editorial.
“More well-designed studies are warranted to provide evidence for integrating holistic treatment in medicine,” he said.
The study was funded by grants from the National Natural Science Foundation of China, and Shanghai Municipal Health. The investigators and Dr. Yeung reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a study of more than 200 adults with depression and comorbid insomnia, change from baseline to week 8 on the Pittsburgh Sleep Quality Index (PSQI) was 3 points greater in the group receiving EA versus a group receiving sham acupuncture (SA) plus standard care, and 5 points greater vs a control group receiving standard care only. The improvements were sustained during a 24-week postintervention follow-up.
The EA group also showed significant improvement in depression, insomnia, self-rated anxiety, and total sleep time – all of which were not found in the SA or control groups.
“Based on the results of our trial, we recommend patients with depression and insomnia seek the treatment of EA as an alternative and complementary therapy for better results,” study investigator Shifen Xu, PhD, Shanghai (China) Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, told this news organization.
The findings were published online in JAMA Network Open.
Bidirectional relationship
“Sleep disturbance is the prominent symptom in patients with depression,” the investigators noted.
Depression and sleep issues have a bidirectional relationship, in that “poor sleep quality contributes to the development of depression, and having depression makes a person more likely to develop sleep issues,” they wrote.
Patients with co-occurring depression and sleep disorders are more difficult to treat and have a greater risk for relapse and recurrence of depression, they added.
Acupuncture may be an “effective drug-free approach to help treat mental illness and sleep disorders,” the researchers noted. A previous study suggested acupuncture may improve sleep efficacy and prolong total sleep in patients with primary insomnia.
“EA is the combination of traditional Chinese acupuncture with electric-impulse stimulation, and it can enhance the therapeutic effect of the acupoints throughout the needle retention time,” Dr. Xu said.
A previous pilot study of EA for depression-related insomnia showed significant improvements in sleep quality after EA treatment, but the sample size was small.
The current researchers, therefore, undertook the present study – with a larger sample size and comparison with SA and standard care. They divided 270 adults (mean age, 50.3 years; 71.9% women) at three tertiary hospitals in Shanghai into three groups, each consisting of 90 participants.
The EA plus standard care group and the SA plus standard care group received 30-minute treatments three times per week for 8 weeks. The control group received standard care only.
All participants had DSM-5–diagnosed depression; baseline PSQI scores greater than 7, with higher scores indicating worse sleep quality and a greater number or sleep disorders; and Hamilton Depression Rating Scales (HDRS-17) scores of 20-35, with higher scores indicating higher depression levels.
Patients with secondary depressive disorders caused by other conditions, medication, or psychotic disorders were excluded, as were patients with a history of alcohol abuse or drug dependence or those who had received acupuncture within the previous year.
Of the patients who completed the 8-week intervention, 83 were in the EA group, 81 in the SA group, and 83 in the control group. Almost all participants (91.5%) completed all outcome measurements by the end of the 24-week follow-up period (also known as week 32).
Calm mind, balanced mood
At the 8-week posttreatment assessment, which was the primary endpoint, the EA group had a mean reduction from baseline of 6.2 points (95% confidence interval, −6.9 to −5.6) in PSQI score.
There was a significant difference in PSQI score between the EA versus the SA group (−3.6 points; 95% CI, −4.4 to −2.8; P < .001) and vs the control group (−5.1 points; 95% CI, −6.0 to −4.2; P < .001).
The efficacy of EA in treating insomnia was sustained during the postintervention follow-up period when the EA group had a significantly greater reduction in PSQI score, compared with the SA group (−4.7; 95% CI, −5.4 to −3.9; P < .001) and the control group (−5.0; 95% CI, −5.8 to −4.1; P < .001).
Patients receiving EA also experienced significant (all P values < .001) improvement from baseline on secondary outcomes, including:
- Scores on the HDRS (−10.7; 95% CI, −11.8 to −9.7)
- Scores on the Insomnia Severity Index, (−7.6; 95% CI,−8.5 to −6.7)
- Scores on the Self-rated Anxiety Scale (−2.9; 95% CI, −4.1 to −1.7)
- Total sleep time, as recorded by sleep actigraphy (29.1 minutes; 95% CI, 21.5-36.7)
In addition, the EA group showed significant improvement in depression scores compared with the SA and control groups at both 8 and 32 weeks (all P values < .001).
Participants in the EA group also had a 4.2% (95% CI, 2.6% - 5.8%) higher sleep efficiency score at week 8, compared with those in the SA group (P < .001).
In addition, they had lower scores on the Insomnia Severity Index and the Self-rated Anxiety Scale, and longer total sleep time, compared with the control group at week 8.
None of the participants reported any serious adverse events.
“Our findings constitute subjective and objective evidence of the efficacy and safety of EA with standard care in treating comorbid depression and insomnia compared with SA with standard care or standard care alone,” the investigators wrote.
“The acupoints we used in this trial mainly act on calming mind, relieving negative mood, and balancing the yin-yang,” Dr. Xu added.
Viable adjunctive treatment
Commenting on the study, Albert Yeung, MD, ScD, associate director of the Mass General Depression and Clinical Research Program and associate professor of psychiatry, Harvard Medical School, Boston, said that, with the evidence from this study, “acupuncture and/or electroacupuncture could be a viable adjunctive treatment for depressed patients who suffer from insomnia.”
Dr. Yeung, who was not involved with the study, is the coauthor of an accompanying editorial.
“More well-designed studies are warranted to provide evidence for integrating holistic treatment in medicine,” he said.
The study was funded by grants from the National Natural Science Foundation of China, and Shanghai Municipal Health. The investigators and Dr. Yeung reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a study of more than 200 adults with depression and comorbid insomnia, change from baseline to week 8 on the Pittsburgh Sleep Quality Index (PSQI) was 3 points greater in the group receiving EA versus a group receiving sham acupuncture (SA) plus standard care, and 5 points greater vs a control group receiving standard care only. The improvements were sustained during a 24-week postintervention follow-up.
The EA group also showed significant improvement in depression, insomnia, self-rated anxiety, and total sleep time – all of which were not found in the SA or control groups.
“Based on the results of our trial, we recommend patients with depression and insomnia seek the treatment of EA as an alternative and complementary therapy for better results,” study investigator Shifen Xu, PhD, Shanghai (China) Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, told this news organization.
The findings were published online in JAMA Network Open.
Bidirectional relationship
“Sleep disturbance is the prominent symptom in patients with depression,” the investigators noted.
Depression and sleep issues have a bidirectional relationship, in that “poor sleep quality contributes to the development of depression, and having depression makes a person more likely to develop sleep issues,” they wrote.
Patients with co-occurring depression and sleep disorders are more difficult to treat and have a greater risk for relapse and recurrence of depression, they added.
Acupuncture may be an “effective drug-free approach to help treat mental illness and sleep disorders,” the researchers noted. A previous study suggested acupuncture may improve sleep efficacy and prolong total sleep in patients with primary insomnia.
“EA is the combination of traditional Chinese acupuncture with electric-impulse stimulation, and it can enhance the therapeutic effect of the acupoints throughout the needle retention time,” Dr. Xu said.
A previous pilot study of EA for depression-related insomnia showed significant improvements in sleep quality after EA treatment, but the sample size was small.
The current researchers, therefore, undertook the present study – with a larger sample size and comparison with SA and standard care. They divided 270 adults (mean age, 50.3 years; 71.9% women) at three tertiary hospitals in Shanghai into three groups, each consisting of 90 participants.
The EA plus standard care group and the SA plus standard care group received 30-minute treatments three times per week for 8 weeks. The control group received standard care only.
All participants had DSM-5–diagnosed depression; baseline PSQI scores greater than 7, with higher scores indicating worse sleep quality and a greater number or sleep disorders; and Hamilton Depression Rating Scales (HDRS-17) scores of 20-35, with higher scores indicating higher depression levels.
Patients with secondary depressive disorders caused by other conditions, medication, or psychotic disorders were excluded, as were patients with a history of alcohol abuse or drug dependence or those who had received acupuncture within the previous year.
Of the patients who completed the 8-week intervention, 83 were in the EA group, 81 in the SA group, and 83 in the control group. Almost all participants (91.5%) completed all outcome measurements by the end of the 24-week follow-up period (also known as week 32).
Calm mind, balanced mood
At the 8-week posttreatment assessment, which was the primary endpoint, the EA group had a mean reduction from baseline of 6.2 points (95% confidence interval, −6.9 to −5.6) in PSQI score.
There was a significant difference in PSQI score between the EA versus the SA group (−3.6 points; 95% CI, −4.4 to −2.8; P < .001) and vs the control group (−5.1 points; 95% CI, −6.0 to −4.2; P < .001).
The efficacy of EA in treating insomnia was sustained during the postintervention follow-up period when the EA group had a significantly greater reduction in PSQI score, compared with the SA group (−4.7; 95% CI, −5.4 to −3.9; P < .001) and the control group (−5.0; 95% CI, −5.8 to −4.1; P < .001).
Patients receiving EA also experienced significant (all P values < .001) improvement from baseline on secondary outcomes, including:
- Scores on the HDRS (−10.7; 95% CI, −11.8 to −9.7)
- Scores on the Insomnia Severity Index, (−7.6; 95% CI,−8.5 to −6.7)
- Scores on the Self-rated Anxiety Scale (−2.9; 95% CI, −4.1 to −1.7)
- Total sleep time, as recorded by sleep actigraphy (29.1 minutes; 95% CI, 21.5-36.7)
In addition, the EA group showed significant improvement in depression scores compared with the SA and control groups at both 8 and 32 weeks (all P values < .001).
Participants in the EA group also had a 4.2% (95% CI, 2.6% - 5.8%) higher sleep efficiency score at week 8, compared with those in the SA group (P < .001).
In addition, they had lower scores on the Insomnia Severity Index and the Self-rated Anxiety Scale, and longer total sleep time, compared with the control group at week 8.
None of the participants reported any serious adverse events.
“Our findings constitute subjective and objective evidence of the efficacy and safety of EA with standard care in treating comorbid depression and insomnia compared with SA with standard care or standard care alone,” the investigators wrote.
“The acupoints we used in this trial mainly act on calming mind, relieving negative mood, and balancing the yin-yang,” Dr. Xu added.
Viable adjunctive treatment
Commenting on the study, Albert Yeung, MD, ScD, associate director of the Mass General Depression and Clinical Research Program and associate professor of psychiatry, Harvard Medical School, Boston, said that, with the evidence from this study, “acupuncture and/or electroacupuncture could be a viable adjunctive treatment for depressed patients who suffer from insomnia.”
Dr. Yeung, who was not involved with the study, is the coauthor of an accompanying editorial.
“More well-designed studies are warranted to provide evidence for integrating holistic treatment in medicine,” he said.
The study was funded by grants from the National Natural Science Foundation of China, and Shanghai Municipal Health. The investigators and Dr. Yeung reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Best meds for insomnia identified?
In a comprehensive comparative-effectiveness analysis, lemborexant and eszopiclone showed the best efficacy, acceptability, and tolerability for acute and long-term insomnia treatment.
However, eszopiclone may cause substantial side effects – and safety data on lemborexant were inconclusive, the researchers note.
Not surprisingly, short-acting, intermediate-acting, and long-acting benzodiazepines were effective in the acute treatment of insomnia, but they have unfavorable tolerability and safety profiles, and there are no long-term data on these issues.
For many insomnia medications, there is a “striking” and “appalling” lack of long-term data, study investigator Andrea Cipriani, MD, PhD, professor of psychiatry, University of Oxford, United Kingdom, noted during a press briefing.
“This is a call for regulators to raise the bar and ask for long-term data when companies submit an application for licensing insomnia drugs,” Dr. Cipriani said.
The findings were published online in The Lancet.
Prevalent, debilitating
Insomnia is highly prevalent, affecting up to 1 in 5 adults, and can have a profound impact on health, well-being, and productivity.
Sleep hygiene and cognitive-behavioral therapy for insomnia (CBT-I) are recommended first-line treatments, but they are often unavailable, which often leads patients and clinicians to turn to medications.
However, “insomnia drugs are not all created equal. Even within the same drug class there are differences,” Dr. Cipriani said.
In a large-scale systematic review and network meta-analysis, the researchers analyzed data from 154 double-blind, randomized controlled trials of medications (licensed or not) used for acute and long-term treatment of insomnia in 44,089 adults (mean age, 51.7 years; 63% women).
Results showed, for the acute treatment of insomnia, benzodiazepines, doxylamine, eszopiclone, lemborexant, seltorexant, zolpidem, and zopiclone were more effective than placebo (standardized mean difference range, 0.36-0.83; high-to-moderate certainty of evidence).
In addition, benzodiazepines, eszopiclone, zolpidem, and zopiclone were more effective than melatonin, ramelteon, and zaleplon (SMD, 0.27-0.71; moderate-to-very low certainty of evidence).
“Our results show that the melatonergic drugs melatonin and ramelteon are not really effective. The data do not support the regular use of these drugs,” co-investigator Phil Cowen, PhD, professor of psychopharmacology, University of Oxford, said at the briefing.
Best available evidence
What little long-term data is available suggest eszopiclone and lemborexant are more effective than placebo. Plus, eszopiclone is more effective than ramelteon and zolpidem but with “very low” certainty of evidence, the researchers report.
“There was insufficient evidence to support the prescription of benzodiazepines and zolpidem in long-term treatment,” they write.
Another problem was lack of data on other important outcomes, they add.
“We wanted to look at hangover effects, daytime sleepiness, [and] rebound effect, but often there was no data reported in trials. We need to collect data about these outcomes because they matter to clinicians and patients,” Dr. Cipriani said.
Summing up, the researchers note the current findings represent the “best available evidence base to guide the choice about pharmacological treatment for insomnia disorder in adults and will assist in shared decisionmaking between patients, carers, and their clinicians, as well as policy makers.”
They caution, however, that all statements comparing the merits of one drug with another “should be tempered by the potential limitations of the current analysis, the quality of the available evidence, the characteristics of the patient populations, and the uncertainties that might result from choice of dose or treatment setting.”
In addition, it is important to also consider nonpharmacologic treatments for insomnia disorder, as they are supported by “high-quality evidence and recommended as first-line treatment by guidelines,” the investigator write.
Shared decisionmaking
In an accompanying editorial, Myrto Samara, MD, University of Thessaly, Larissa, Greece, agrees with the researchers that discussion with patients is key.
“For insomnia treatment, patient-physician shared decisionmaking is crucial to decide when a pharmacological intervention is deemed necessary and which drug [is] to be given by considering the trade-offs for efficacy and side effects,” Dr. Samara writes.
The study was funded by the UK National Institute for Health Research (NIHR) Oxford Health Biomedical Research Center. Dr. Cipriani has received research and consultancy fees from the Italian Network for Pediatric Trials, CARIPLO Foundation, and Angelini Pharma, and is the chief and principal investigator of two trials of seltorexant in depression that are sponsored by Janssen. Dr. Samara has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a comprehensive comparative-effectiveness analysis, lemborexant and eszopiclone showed the best efficacy, acceptability, and tolerability for acute and long-term insomnia treatment.
However, eszopiclone may cause substantial side effects – and safety data on lemborexant were inconclusive, the researchers note.
Not surprisingly, short-acting, intermediate-acting, and long-acting benzodiazepines were effective in the acute treatment of insomnia, but they have unfavorable tolerability and safety profiles, and there are no long-term data on these issues.
For many insomnia medications, there is a “striking” and “appalling” lack of long-term data, study investigator Andrea Cipriani, MD, PhD, professor of psychiatry, University of Oxford, United Kingdom, noted during a press briefing.
“This is a call for regulators to raise the bar and ask for long-term data when companies submit an application for licensing insomnia drugs,” Dr. Cipriani said.
The findings were published online in The Lancet.
Prevalent, debilitating
Insomnia is highly prevalent, affecting up to 1 in 5 adults, and can have a profound impact on health, well-being, and productivity.
Sleep hygiene and cognitive-behavioral therapy for insomnia (CBT-I) are recommended first-line treatments, but they are often unavailable, which often leads patients and clinicians to turn to medications.
However, “insomnia drugs are not all created equal. Even within the same drug class there are differences,” Dr. Cipriani said.
In a large-scale systematic review and network meta-analysis, the researchers analyzed data from 154 double-blind, randomized controlled trials of medications (licensed or not) used for acute and long-term treatment of insomnia in 44,089 adults (mean age, 51.7 years; 63% women).
Results showed, for the acute treatment of insomnia, benzodiazepines, doxylamine, eszopiclone, lemborexant, seltorexant, zolpidem, and zopiclone were more effective than placebo (standardized mean difference range, 0.36-0.83; high-to-moderate certainty of evidence).
In addition, benzodiazepines, eszopiclone, zolpidem, and zopiclone were more effective than melatonin, ramelteon, and zaleplon (SMD, 0.27-0.71; moderate-to-very low certainty of evidence).
“Our results show that the melatonergic drugs melatonin and ramelteon are not really effective. The data do not support the regular use of these drugs,” co-investigator Phil Cowen, PhD, professor of psychopharmacology, University of Oxford, said at the briefing.
Best available evidence
What little long-term data is available suggest eszopiclone and lemborexant are more effective than placebo. Plus, eszopiclone is more effective than ramelteon and zolpidem but with “very low” certainty of evidence, the researchers report.
“There was insufficient evidence to support the prescription of benzodiazepines and zolpidem in long-term treatment,” they write.
Another problem was lack of data on other important outcomes, they add.
“We wanted to look at hangover effects, daytime sleepiness, [and] rebound effect, but often there was no data reported in trials. We need to collect data about these outcomes because they matter to clinicians and patients,” Dr. Cipriani said.
Summing up, the researchers note the current findings represent the “best available evidence base to guide the choice about pharmacological treatment for insomnia disorder in adults and will assist in shared decisionmaking between patients, carers, and their clinicians, as well as policy makers.”
They caution, however, that all statements comparing the merits of one drug with another “should be tempered by the potential limitations of the current analysis, the quality of the available evidence, the characteristics of the patient populations, and the uncertainties that might result from choice of dose or treatment setting.”
In addition, it is important to also consider nonpharmacologic treatments for insomnia disorder, as they are supported by “high-quality evidence and recommended as first-line treatment by guidelines,” the investigator write.
Shared decisionmaking
In an accompanying editorial, Myrto Samara, MD, University of Thessaly, Larissa, Greece, agrees with the researchers that discussion with patients is key.
“For insomnia treatment, patient-physician shared decisionmaking is crucial to decide when a pharmacological intervention is deemed necessary and which drug [is] to be given by considering the trade-offs for efficacy and side effects,” Dr. Samara writes.
The study was funded by the UK National Institute for Health Research (NIHR) Oxford Health Biomedical Research Center. Dr. Cipriani has received research and consultancy fees from the Italian Network for Pediatric Trials, CARIPLO Foundation, and Angelini Pharma, and is the chief and principal investigator of two trials of seltorexant in depression that are sponsored by Janssen. Dr. Samara has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a comprehensive comparative-effectiveness analysis, lemborexant and eszopiclone showed the best efficacy, acceptability, and tolerability for acute and long-term insomnia treatment.
However, eszopiclone may cause substantial side effects – and safety data on lemborexant were inconclusive, the researchers note.
Not surprisingly, short-acting, intermediate-acting, and long-acting benzodiazepines were effective in the acute treatment of insomnia, but they have unfavorable tolerability and safety profiles, and there are no long-term data on these issues.
For many insomnia medications, there is a “striking” and “appalling” lack of long-term data, study investigator Andrea Cipriani, MD, PhD, professor of psychiatry, University of Oxford, United Kingdom, noted during a press briefing.
“This is a call for regulators to raise the bar and ask for long-term data when companies submit an application for licensing insomnia drugs,” Dr. Cipriani said.
The findings were published online in The Lancet.
Prevalent, debilitating
Insomnia is highly prevalent, affecting up to 1 in 5 adults, and can have a profound impact on health, well-being, and productivity.
Sleep hygiene and cognitive-behavioral therapy for insomnia (CBT-I) are recommended first-line treatments, but they are often unavailable, which often leads patients and clinicians to turn to medications.
However, “insomnia drugs are not all created equal. Even within the same drug class there are differences,” Dr. Cipriani said.
In a large-scale systematic review and network meta-analysis, the researchers analyzed data from 154 double-blind, randomized controlled trials of medications (licensed or not) used for acute and long-term treatment of insomnia in 44,089 adults (mean age, 51.7 years; 63% women).
Results showed, for the acute treatment of insomnia, benzodiazepines, doxylamine, eszopiclone, lemborexant, seltorexant, zolpidem, and zopiclone were more effective than placebo (standardized mean difference range, 0.36-0.83; high-to-moderate certainty of evidence).
In addition, benzodiazepines, eszopiclone, zolpidem, and zopiclone were more effective than melatonin, ramelteon, and zaleplon (SMD, 0.27-0.71; moderate-to-very low certainty of evidence).
“Our results show that the melatonergic drugs melatonin and ramelteon are not really effective. The data do not support the regular use of these drugs,” co-investigator Phil Cowen, PhD, professor of psychopharmacology, University of Oxford, said at the briefing.
Best available evidence
What little long-term data is available suggest eszopiclone and lemborexant are more effective than placebo. Plus, eszopiclone is more effective than ramelteon and zolpidem but with “very low” certainty of evidence, the researchers report.
“There was insufficient evidence to support the prescription of benzodiazepines and zolpidem in long-term treatment,” they write.
Another problem was lack of data on other important outcomes, they add.
“We wanted to look at hangover effects, daytime sleepiness, [and] rebound effect, but often there was no data reported in trials. We need to collect data about these outcomes because they matter to clinicians and patients,” Dr. Cipriani said.
Summing up, the researchers note the current findings represent the “best available evidence base to guide the choice about pharmacological treatment for insomnia disorder in adults and will assist in shared decisionmaking between patients, carers, and their clinicians, as well as policy makers.”
They caution, however, that all statements comparing the merits of one drug with another “should be tempered by the potential limitations of the current analysis, the quality of the available evidence, the characteristics of the patient populations, and the uncertainties that might result from choice of dose or treatment setting.”
In addition, it is important to also consider nonpharmacologic treatments for insomnia disorder, as they are supported by “high-quality evidence and recommended as first-line treatment by guidelines,” the investigator write.
Shared decisionmaking
In an accompanying editorial, Myrto Samara, MD, University of Thessaly, Larissa, Greece, agrees with the researchers that discussion with patients is key.
“For insomnia treatment, patient-physician shared decisionmaking is crucial to decide when a pharmacological intervention is deemed necessary and which drug [is] to be given by considering the trade-offs for efficacy and side effects,” Dr. Samara writes.
The study was funded by the UK National Institute for Health Research (NIHR) Oxford Health Biomedical Research Center. Dr. Cipriani has received research and consultancy fees from the Italian Network for Pediatric Trials, CARIPLO Foundation, and Angelini Pharma, and is the chief and principal investigator of two trials of seltorexant in depression that are sponsored by Janssen. Dr. Samara has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LANCET
Do behavioral interventions improve nighttime sleep in children < 1 year old?
Most interventions resulted in at least modest improvements in sleep
A randomized controlled trial (RCT) of 279 newborn infants and their mothers evaluated developmentally appropriate sleep interventions.1 Mothers were given guidance on bedtime sleep routines, including starting the routine 30 to 45 minutes before bedtime, choosing age-appropriate calming bedtime activities, not using feeding as the last step before bedtime, and offering the child choices with their routine. Mothers were also given guidance on sleep location and behaviors, including recommendations on the best bedtime (between 7 and 8
These interventions were compared to a control group that received instructions on crib safety, sudden infant death syndrome prevention, and other sleep safety recommendations. Infant nocturnal sleep duration was determined by maternal report using the Brief Infant Sleep Questionnaire (BISQ). After 40 weeks, infants in the intervention group demonstrated longer sleep duration than did those in the control group (624.6 ± 67.6 minutes vs 602.9 ± 76.1 minutes; P = .01).1
An RCT of 82 infants (ages 2-4 months) and their mothers evaluated the effect of behavioral sleep interventions on maternal and infant sleep.2 Parents were offered either a 90-minute class and take-home booklet about behavioral sleep interventions or a 30-minute training on general infant safety with an accompanying pamphlet.
The behavioral interventions booklet included instructions on differentiating day and night routines for baby, avoiding digital devices and television in the evenings, playing more active games in the morning, dimming lights and reducing house noises in the afternoon, and having a consistent nighttime routine with consistent bedtime and sleep space. Participants completed an infant sleep diary prior to the intervention and repeated the sleep diary 8 weeks after the intervention. The infants whose mothers received the education on behavioral sleep interventions demonstrated an increase in nighttime sleep duration when compared to the control group (7.4 to 8.8 hours vs 7.3 to 7.5 hours; ANCOVA P < .001).
An RCT of 235 families with infants ages 6 to 8 months evaluated the effect of 45 minutes of nurse-provided education regarding normal infant sleep, effects of inadequate sleep, setting limits around infant sleep, importance of daytime routines, and negative sleep associations combined with a booklet and weekly phone follow-ups.3 This intervention was compared to routine infant education. At age 6 weeks, infants were monitored for 48 hours with actigraphy and the mothers completed a sleep diary to correlate activities. There was no difference in average nightly waking (2 nightly wakes; risk difference = –0.2%; 95% CI, –1.32 to 0.91).
An RCT of 268 families with infants (ages 2-3 weeks) evaluated the effect of 45 minutes of nurse-provided education on behavioral sleep interventions including the cyclical nature of infant sleep, environmental factors that influence sleep, and parent-independent sleep cues (eg, leaving a settling infant alone for 5 minutes before responding) combined with written information.4 This was compared to infants receiving standard care without parental sleep intervention education. Participants recorded sleep diaries for 7 days when their infant reached age 6 weeks and again at age 12 weeks. At both 6 weeks and 12 weeks, there was a significant increase in infant nocturnal sleep time in the intervention group vs the control group (mean difference [MD] at 6 weeks = 0.5 hours; 95% CI, 0.32 to 0.69 vs MD at 12 weeks = 0.64 hours; 95% CI, 0.19 to 0.89).
A nonrandomized controlled trial with 84 mothers and infants (ages 0-6 months) evaluated the effectiveness of a multifaceted intervention involving brief focused negotiation by pediatricians, motivational counseling by a health educator, and group parenting workshops, compared to mother–infant pairs receiving standard care.5 Parents completed the BISQ at 0 and 6 months to assess nocturnal sleep duration. At 6 months, the intervention group had a significantly higher increase in infant nocturnal sleep duration compared to the control group (mean increase = 1.9 vs 1.3 hours; P = .05).
In a prospective cohort study involving 79 infants (ages 3-24 months) with parent- or pediatrician-reported day and night sleep problems, parents were given education on the promotion of nighttime sleep by gradually reducing contact with the infant over several nights and only leaving the room after the infant fell asleep or allowing the child to self-soothe for 1-3 minutes.6 The intervention was performed over 3 weeks, with in-person follow-up performed on Day 15 and phone follow-up on Days 8 and 21. Infants in this study demonstrated an increase in the average hours of total night sleep from 10.2 to 10.5 hours (P < .001).
Editor’s takeaway
Providing behavioral recommendations to parents about infant sleep routines improves sleep duration. This increased sleep duration, and the supporting evidence, is modest, but the low cost and risk of these interventions make them worthwhile.
1. Paul IM, Savage JS, Anzman-Frasca S, et al. INSIGHT responsive parenting intervention and infant sleep. Pediatrics. 2016;138:e20160762. doi:10.1542/peds.2016-0762
2. Rouzafzoon M, Farnam F, Khakbazan Z. The effects of infant behavioural sleep interventions on maternal sleep and mood, and infant sleep: a randomised controlled trial. J Sleep Res. 2021;30:e13344. doi: 10.1111/jsr.13344
3. Hall WA, Hutton E, Brant RF, et al. A randomized controlled trial of an intervention for infants’ behavioral sleep problems. BMC Pediatr. 2015;15:181. doi:10.1186/s12887-015-0492-7
4. Symon BG, Marley JE, Martin AJ, et al. Effect of a consultation teaching behaviour modification on sleep performance in infants: a randomised controlled trial. Med J Aust. 2005;182:215-218. doi: 10.5694/j.1326-5377.2005.tb06669.x
5. Taveras EM, Blackburn K, Gillman MW, et al. First steps for mommy and me: a pilot intervention to improve nutrition and physical activity behaviors of postpartum mothers and their infants. Matern Child Health J. 2011;15:1217-1227. doi: 10.1007/s10995-010-0696-2
6. Skuladottir A, Thome M, Ramel A. Improving day and night sleep problems in infants by changing day time sleep rhythm: a single group before and after study. Int J Nurs Stud. 2005;42:843-850. doi: 10.1016/j.ijnurstu.2004.12.004
Most interventions resulted in at least modest improvements in sleep
A randomized controlled trial (RCT) of 279 newborn infants and their mothers evaluated developmentally appropriate sleep interventions.1 Mothers were given guidance on bedtime sleep routines, including starting the routine 30 to 45 minutes before bedtime, choosing age-appropriate calming bedtime activities, not using feeding as the last step before bedtime, and offering the child choices with their routine. Mothers were also given guidance on sleep location and behaviors, including recommendations on the best bedtime (between 7 and 8
These interventions were compared to a control group that received instructions on crib safety, sudden infant death syndrome prevention, and other sleep safety recommendations. Infant nocturnal sleep duration was determined by maternal report using the Brief Infant Sleep Questionnaire (BISQ). After 40 weeks, infants in the intervention group demonstrated longer sleep duration than did those in the control group (624.6 ± 67.6 minutes vs 602.9 ± 76.1 minutes; P = .01).1
An RCT of 82 infants (ages 2-4 months) and their mothers evaluated the effect of behavioral sleep interventions on maternal and infant sleep.2 Parents were offered either a 90-minute class and take-home booklet about behavioral sleep interventions or a 30-minute training on general infant safety with an accompanying pamphlet.
The behavioral interventions booklet included instructions on differentiating day and night routines for baby, avoiding digital devices and television in the evenings, playing more active games in the morning, dimming lights and reducing house noises in the afternoon, and having a consistent nighttime routine with consistent bedtime and sleep space. Participants completed an infant sleep diary prior to the intervention and repeated the sleep diary 8 weeks after the intervention. The infants whose mothers received the education on behavioral sleep interventions demonstrated an increase in nighttime sleep duration when compared to the control group (7.4 to 8.8 hours vs 7.3 to 7.5 hours; ANCOVA P < .001).
An RCT of 235 families with infants ages 6 to 8 months evaluated the effect of 45 minutes of nurse-provided education regarding normal infant sleep, effects of inadequate sleep, setting limits around infant sleep, importance of daytime routines, and negative sleep associations combined with a booklet and weekly phone follow-ups.3 This intervention was compared to routine infant education. At age 6 weeks, infants were monitored for 48 hours with actigraphy and the mothers completed a sleep diary to correlate activities. There was no difference in average nightly waking (2 nightly wakes; risk difference = –0.2%; 95% CI, –1.32 to 0.91).
An RCT of 268 families with infants (ages 2-3 weeks) evaluated the effect of 45 minutes of nurse-provided education on behavioral sleep interventions including the cyclical nature of infant sleep, environmental factors that influence sleep, and parent-independent sleep cues (eg, leaving a settling infant alone for 5 minutes before responding) combined with written information.4 This was compared to infants receiving standard care without parental sleep intervention education. Participants recorded sleep diaries for 7 days when their infant reached age 6 weeks and again at age 12 weeks. At both 6 weeks and 12 weeks, there was a significant increase in infant nocturnal sleep time in the intervention group vs the control group (mean difference [MD] at 6 weeks = 0.5 hours; 95% CI, 0.32 to 0.69 vs MD at 12 weeks = 0.64 hours; 95% CI, 0.19 to 0.89).
A nonrandomized controlled trial with 84 mothers and infants (ages 0-6 months) evaluated the effectiveness of a multifaceted intervention involving brief focused negotiation by pediatricians, motivational counseling by a health educator, and group parenting workshops, compared to mother–infant pairs receiving standard care.5 Parents completed the BISQ at 0 and 6 months to assess nocturnal sleep duration. At 6 months, the intervention group had a significantly higher increase in infant nocturnal sleep duration compared to the control group (mean increase = 1.9 vs 1.3 hours; P = .05).
In a prospective cohort study involving 79 infants (ages 3-24 months) with parent- or pediatrician-reported day and night sleep problems, parents were given education on the promotion of nighttime sleep by gradually reducing contact with the infant over several nights and only leaving the room after the infant fell asleep or allowing the child to self-soothe for 1-3 minutes.6 The intervention was performed over 3 weeks, with in-person follow-up performed on Day 15 and phone follow-up on Days 8 and 21. Infants in this study demonstrated an increase in the average hours of total night sleep from 10.2 to 10.5 hours (P < .001).
Editor’s takeaway
Providing behavioral recommendations to parents about infant sleep routines improves sleep duration. This increased sleep duration, and the supporting evidence, is modest, but the low cost and risk of these interventions make them worthwhile.
Most interventions resulted in at least modest improvements in sleep
A randomized controlled trial (RCT) of 279 newborn infants and their mothers evaluated developmentally appropriate sleep interventions.1 Mothers were given guidance on bedtime sleep routines, including starting the routine 30 to 45 minutes before bedtime, choosing age-appropriate calming bedtime activities, not using feeding as the last step before bedtime, and offering the child choices with their routine. Mothers were also given guidance on sleep location and behaviors, including recommendations on the best bedtime (between 7 and 8
These interventions were compared to a control group that received instructions on crib safety, sudden infant death syndrome prevention, and other sleep safety recommendations. Infant nocturnal sleep duration was determined by maternal report using the Brief Infant Sleep Questionnaire (BISQ). After 40 weeks, infants in the intervention group demonstrated longer sleep duration than did those in the control group (624.6 ± 67.6 minutes vs 602.9 ± 76.1 minutes; P = .01).1
An RCT of 82 infants (ages 2-4 months) and their mothers evaluated the effect of behavioral sleep interventions on maternal and infant sleep.2 Parents were offered either a 90-minute class and take-home booklet about behavioral sleep interventions or a 30-minute training on general infant safety with an accompanying pamphlet.
The behavioral interventions booklet included instructions on differentiating day and night routines for baby, avoiding digital devices and television in the evenings, playing more active games in the morning, dimming lights and reducing house noises in the afternoon, and having a consistent nighttime routine with consistent bedtime and sleep space. Participants completed an infant sleep diary prior to the intervention and repeated the sleep diary 8 weeks after the intervention. The infants whose mothers received the education on behavioral sleep interventions demonstrated an increase in nighttime sleep duration when compared to the control group (7.4 to 8.8 hours vs 7.3 to 7.5 hours; ANCOVA P < .001).
An RCT of 235 families with infants ages 6 to 8 months evaluated the effect of 45 minutes of nurse-provided education regarding normal infant sleep, effects of inadequate sleep, setting limits around infant sleep, importance of daytime routines, and negative sleep associations combined with a booklet and weekly phone follow-ups.3 This intervention was compared to routine infant education. At age 6 weeks, infants were monitored for 48 hours with actigraphy and the mothers completed a sleep diary to correlate activities. There was no difference in average nightly waking (2 nightly wakes; risk difference = –0.2%; 95% CI, –1.32 to 0.91).
An RCT of 268 families with infants (ages 2-3 weeks) evaluated the effect of 45 minutes of nurse-provided education on behavioral sleep interventions including the cyclical nature of infant sleep, environmental factors that influence sleep, and parent-independent sleep cues (eg, leaving a settling infant alone for 5 minutes before responding) combined with written information.4 This was compared to infants receiving standard care without parental sleep intervention education. Participants recorded sleep diaries for 7 days when their infant reached age 6 weeks and again at age 12 weeks. At both 6 weeks and 12 weeks, there was a significant increase in infant nocturnal sleep time in the intervention group vs the control group (mean difference [MD] at 6 weeks = 0.5 hours; 95% CI, 0.32 to 0.69 vs MD at 12 weeks = 0.64 hours; 95% CI, 0.19 to 0.89).
A nonrandomized controlled trial with 84 mothers and infants (ages 0-6 months) evaluated the effectiveness of a multifaceted intervention involving brief focused negotiation by pediatricians, motivational counseling by a health educator, and group parenting workshops, compared to mother–infant pairs receiving standard care.5 Parents completed the BISQ at 0 and 6 months to assess nocturnal sleep duration. At 6 months, the intervention group had a significantly higher increase in infant nocturnal sleep duration compared to the control group (mean increase = 1.9 vs 1.3 hours; P = .05).
In a prospective cohort study involving 79 infants (ages 3-24 months) with parent- or pediatrician-reported day and night sleep problems, parents were given education on the promotion of nighttime sleep by gradually reducing contact with the infant over several nights and only leaving the room after the infant fell asleep or allowing the child to self-soothe for 1-3 minutes.6 The intervention was performed over 3 weeks, with in-person follow-up performed on Day 15 and phone follow-up on Days 8 and 21. Infants in this study demonstrated an increase in the average hours of total night sleep from 10.2 to 10.5 hours (P < .001).
Editor’s takeaway
Providing behavioral recommendations to parents about infant sleep routines improves sleep duration. This increased sleep duration, and the supporting evidence, is modest, but the low cost and risk of these interventions make them worthwhile.
1. Paul IM, Savage JS, Anzman-Frasca S, et al. INSIGHT responsive parenting intervention and infant sleep. Pediatrics. 2016;138:e20160762. doi:10.1542/peds.2016-0762
2. Rouzafzoon M, Farnam F, Khakbazan Z. The effects of infant behavioural sleep interventions on maternal sleep and mood, and infant sleep: a randomised controlled trial. J Sleep Res. 2021;30:e13344. doi: 10.1111/jsr.13344
3. Hall WA, Hutton E, Brant RF, et al. A randomized controlled trial of an intervention for infants’ behavioral sleep problems. BMC Pediatr. 2015;15:181. doi:10.1186/s12887-015-0492-7
4. Symon BG, Marley JE, Martin AJ, et al. Effect of a consultation teaching behaviour modification on sleep performance in infants: a randomised controlled trial. Med J Aust. 2005;182:215-218. doi: 10.5694/j.1326-5377.2005.tb06669.x
5. Taveras EM, Blackburn K, Gillman MW, et al. First steps for mommy and me: a pilot intervention to improve nutrition and physical activity behaviors of postpartum mothers and their infants. Matern Child Health J. 2011;15:1217-1227. doi: 10.1007/s10995-010-0696-2
6. Skuladottir A, Thome M, Ramel A. Improving day and night sleep problems in infants by changing day time sleep rhythm: a single group before and after study. Int J Nurs Stud. 2005;42:843-850. doi: 10.1016/j.ijnurstu.2004.12.004
1. Paul IM, Savage JS, Anzman-Frasca S, et al. INSIGHT responsive parenting intervention and infant sleep. Pediatrics. 2016;138:e20160762. doi:10.1542/peds.2016-0762
2. Rouzafzoon M, Farnam F, Khakbazan Z. The effects of infant behavioural sleep interventions on maternal sleep and mood, and infant sleep: a randomised controlled trial. J Sleep Res. 2021;30:e13344. doi: 10.1111/jsr.13344
3. Hall WA, Hutton E, Brant RF, et al. A randomized controlled trial of an intervention for infants’ behavioral sleep problems. BMC Pediatr. 2015;15:181. doi:10.1186/s12887-015-0492-7
4. Symon BG, Marley JE, Martin AJ, et al. Effect of a consultation teaching behaviour modification on sleep performance in infants: a randomised controlled trial. Med J Aust. 2005;182:215-218. doi: 10.5694/j.1326-5377.2005.tb06669.x
5. Taveras EM, Blackburn K, Gillman MW, et al. First steps for mommy and me: a pilot intervention to improve nutrition and physical activity behaviors of postpartum mothers and their infants. Matern Child Health J. 2011;15:1217-1227. doi: 10.1007/s10995-010-0696-2
6. Skuladottir A, Thome M, Ramel A. Improving day and night sleep problems in infants by changing day time sleep rhythm: a single group before and after study. Int J Nurs Stud. 2005;42:843-850. doi: 10.1016/j.ijnurstu.2004.12.004
EVIDENCE-BASED ANSWER:
YES. Infants respond to behavioral interventions, although objective data are limited. Behavioral interventions include establishing regular daytime and sleep routines for the infant, reducing environmental noises or distractions, and allowing for self-soothing at bedtime (strength of recommendation: B, based on multiple randomized and nonrandomized studies).
Nocturnal sleep key to successful kindergarten adjustment
Children who regularly slept 10-plus hours per night, particularly just before starting kindergarten, transitioned more successfully to kindergarten than those with less regular sleeping patterns, an observational study found. The effect held across the kindergarten year regardless of socioeconomic and health covariates, according to a new study by Douglas M. Teti, PhD, a developmental scientist and a professor of pediatrics at Penn State University, University Park, and colleagues.
“These effects were ubiquitous, extending to socioemotional learning engagement and academic domains,” they wrote online in Pediatrics

Furthermore, it was the regularity of sufficient nocturnal sleep that appeared to be more important for school adjustment than overall amounts of sleep accumulated across the day or the proportion of 24-hour periods in which children got 10 or more hours of sleep.
The American Academy of Sleep Medicine has recommended that 3- to 5-year-olds get 10-13 hours of sleep per day, including naps.
The findings by Dr. Teti’s group suggest that family-based interventions to establish consistent patterns of sufficient nighttime sleep should begin 5 or 6 months before the start of kindergarten.
“The importance of sleep as a predictor of school functioning in children is well-established, but relatively less is known about how sleep impacts children as they make their first transition into formal schooling,” Dr. Teti told this news organization. “School readiness and adjustment can be impacted by many factors, including socioeconomic status, child health, and missed days of school, but few studies have isolated the role of sleep in the transition to kindergarten net of these other influences, and few studies have examined the role that sleep plays on children’s school functioning throughout the full kindergarten year.”
The study
During 2016-2019, the researcher recruited 230 families from three Pennsylvania school districts, of which 221 completed the study. At several time points, the study examined three different measures of child sleep duration in 7-day bursts: at pre-kindergarten (July to August), early kindergarten (late September), mid-kindergarten (late November), and late kindergarten (mid-to-late April), using wrist actigraphy. These measures included:
- mean amounts of child sleep per 24-hour period across the full week
- proportion of 24-hour periods per week that children slept 10 or more hours
- proportion of nighttime sleep periods per week that children slept 10 or more hours
Outcomes at the designated school year time points were provided by 64 teachers blinded to the pupils’ sleep histories and by assessments administered by project staff.
Among the sleep measures examined, regularity of nighttime sleep involving 10 or more hours of sleep over the nocturnal period, especially at the pre-kindergarten stage, consistently predicted more favorable outcomes in socioemotional, learning engagement, and academic domains. These findings were controlled for income-to-poverty threshold ratios, child health status, and number of missed school days.
The study results generally align with those of previous studies, showing the importance of sleep for children’s school functioning, Dr. Teti told this news organization. “But they differed significantly in terms of finding that it was the regularity of 10-plus hours concentrated during the nighttime sleep period that was most important for predicting school adjustment, in particular, regular or sufficient sleep that occurred prior to the start of kindergarten.”
Calling the study “thought provoking,” Michael B. Grosso, MD, chair of pediatrics at Huntington (N.Y.) Hospital, said it confirms a robust correlation between total sleep duration and outcomes important to successful adjustment to kindergarten. “And we find out that uninterrupted sleep time of 10 hours or more seems to matter as well.”
In his view, the biggest limitation to the analysis is the one inherent to any observational study, “which is that association cannot prove causality. The authors did attempt to control for other health factors, but that can be hard to do,” he said. “The point is that if a child faces any of several health challenges, from sleep apnea to uncontrolled asthma, to ADHD or an autistic spectrum disorder, those issues will cause disrupted, abnormal sleep and also interfere with the outcomes the study addresses. In other words, it’s hard to know if sleep is affecting kindergarten adjustment or whether some X factor is affecting sleep and also affecting kindergarten performance.”
Getting children into bed earlier in long bright evenings of spring and summer before onset of kindergarten may not be easy, Dr. Teti acknowledged. “Arranging children’s sleep schedule as they approach kindergarten so that most, if not all, of their sleep takes place during the night – and as a corollary, reducing the frequency of naps during the day – should help children shift into sleeping nighttime primarily if not exclusively,” he said.
If necessary, he added, parents can work with sleep professionals to gradually concentrate children’s sleep during the night. They should normalize earlier bedtimes by reducing access to electronic screens before bedtime and removing televisions from their bedrooms. “A consistent bedtime routine should be a central feature of parental attempts to shape better, more regular sleep in their children.”
Dr. Grosso added that pediatricians need to talk about the importance of consistent routines and especially adequate sleep when counseling parents during pre-school health supervision visits. “And as the authors mention, it’s hard to ensure good sleep hygiene for children if parents aren’t also getting a good night sleep. It all goes together.”
This study was supported by the National Institutes of Health. The authors had no competing interests to declare. Dr. Grosso disclosed no relevant conflicts of interest.
Children who regularly slept 10-plus hours per night, particularly just before starting kindergarten, transitioned more successfully to kindergarten than those with less regular sleeping patterns, an observational study found. The effect held across the kindergarten year regardless of socioeconomic and health covariates, according to a new study by Douglas M. Teti, PhD, a developmental scientist and a professor of pediatrics at Penn State University, University Park, and colleagues.
“These effects were ubiquitous, extending to socioemotional learning engagement and academic domains,” they wrote online in Pediatrics
Furthermore, it was the regularity of sufficient nocturnal sleep that appeared to be more important for school adjustment than overall amounts of sleep accumulated across the day or the proportion of 24-hour periods in which children got 10 or more hours of sleep.
The American Academy of Sleep Medicine has recommended that 3- to 5-year-olds get 10-13 hours of sleep per day, including naps.
The findings by Dr. Teti’s group suggest that family-based interventions to establish consistent patterns of sufficient nighttime sleep should begin 5 or 6 months before the start of kindergarten.
“The importance of sleep as a predictor of school functioning in children is well-established, but relatively less is known about how sleep impacts children as they make their first transition into formal schooling,” Dr. Teti told this news organization. “School readiness and adjustment can be impacted by many factors, including socioeconomic status, child health, and missed days of school, but few studies have isolated the role of sleep in the transition to kindergarten net of these other influences, and few studies have examined the role that sleep plays on children’s school functioning throughout the full kindergarten year.”
The study
During 2016-2019, the researcher recruited 230 families from three Pennsylvania school districts, of which 221 completed the study. At several time points, the study examined three different measures of child sleep duration in 7-day bursts: at pre-kindergarten (July to August), early kindergarten (late September), mid-kindergarten (late November), and late kindergarten (mid-to-late April), using wrist actigraphy. These measures included:
- mean amounts of child sleep per 24-hour period across the full week
- proportion of 24-hour periods per week that children slept 10 or more hours
- proportion of nighttime sleep periods per week that children slept 10 or more hours
Outcomes at the designated school year time points were provided by 64 teachers blinded to the pupils’ sleep histories and by assessments administered by project staff.
Among the sleep measures examined, regularity of nighttime sleep involving 10 or more hours of sleep over the nocturnal period, especially at the pre-kindergarten stage, consistently predicted more favorable outcomes in socioemotional, learning engagement, and academic domains. These findings were controlled for income-to-poverty threshold ratios, child health status, and number of missed school days.
The study results generally align with those of previous studies, showing the importance of sleep for children’s school functioning, Dr. Teti told this news organization. “But they differed significantly in terms of finding that it was the regularity of 10-plus hours concentrated during the nighttime sleep period that was most important for predicting school adjustment, in particular, regular or sufficient sleep that occurred prior to the start of kindergarten.”
Calling the study “thought provoking,” Michael B. Grosso, MD, chair of pediatrics at Huntington (N.Y.) Hospital, said it confirms a robust correlation between total sleep duration and outcomes important to successful adjustment to kindergarten. “And we find out that uninterrupted sleep time of 10 hours or more seems to matter as well.”
In his view, the biggest limitation to the analysis is the one inherent to any observational study, “which is that association cannot prove causality. The authors did attempt to control for other health factors, but that can be hard to do,” he said. “The point is that if a child faces any of several health challenges, from sleep apnea to uncontrolled asthma, to ADHD or an autistic spectrum disorder, those issues will cause disrupted, abnormal sleep and also interfere with the outcomes the study addresses. In other words, it’s hard to know if sleep is affecting kindergarten adjustment or whether some X factor is affecting sleep and also affecting kindergarten performance.”
Getting children into bed earlier in long bright evenings of spring and summer before onset of kindergarten may not be easy, Dr. Teti acknowledged. “Arranging children’s sleep schedule as they approach kindergarten so that most, if not all, of their sleep takes place during the night – and as a corollary, reducing the frequency of naps during the day – should help children shift into sleeping nighttime primarily if not exclusively,” he said.
If necessary, he added, parents can work with sleep professionals to gradually concentrate children’s sleep during the night. They should normalize earlier bedtimes by reducing access to electronic screens before bedtime and removing televisions from their bedrooms. “A consistent bedtime routine should be a central feature of parental attempts to shape better, more regular sleep in their children.”
Dr. Grosso added that pediatricians need to talk about the importance of consistent routines and especially adequate sleep when counseling parents during pre-school health supervision visits. “And as the authors mention, it’s hard to ensure good sleep hygiene for children if parents aren’t also getting a good night sleep. It all goes together.”
This study was supported by the National Institutes of Health. The authors had no competing interests to declare. Dr. Grosso disclosed no relevant conflicts of interest.
Children who regularly slept 10-plus hours per night, particularly just before starting kindergarten, transitioned more successfully to kindergarten than those with less regular sleeping patterns, an observational study found. The effect held across the kindergarten year regardless of socioeconomic and health covariates, according to a new study by Douglas M. Teti, PhD, a developmental scientist and a professor of pediatrics at Penn State University, University Park, and colleagues.
“These effects were ubiquitous, extending to socioemotional learning engagement and academic domains,” they wrote online in Pediatrics
Furthermore, it was the regularity of sufficient nocturnal sleep that appeared to be more important for school adjustment than overall amounts of sleep accumulated across the day or the proportion of 24-hour periods in which children got 10 or more hours of sleep.
The American Academy of Sleep Medicine has recommended that 3- to 5-year-olds get 10-13 hours of sleep per day, including naps.
The findings by Dr. Teti’s group suggest that family-based interventions to establish consistent patterns of sufficient nighttime sleep should begin 5 or 6 months before the start of kindergarten.
“The importance of sleep as a predictor of school functioning in children is well-established, but relatively less is known about how sleep impacts children as they make their first transition into formal schooling,” Dr. Teti told this news organization. “School readiness and adjustment can be impacted by many factors, including socioeconomic status, child health, and missed days of school, but few studies have isolated the role of sleep in the transition to kindergarten net of these other influences, and few studies have examined the role that sleep plays on children’s school functioning throughout the full kindergarten year.”
The study
During 2016-2019, the researcher recruited 230 families from three Pennsylvania school districts, of which 221 completed the study. At several time points, the study examined three different measures of child sleep duration in 7-day bursts: at pre-kindergarten (July to August), early kindergarten (late September), mid-kindergarten (late November), and late kindergarten (mid-to-late April), using wrist actigraphy. These measures included:
- mean amounts of child sleep per 24-hour period across the full week
- proportion of 24-hour periods per week that children slept 10 or more hours
- proportion of nighttime sleep periods per week that children slept 10 or more hours
Outcomes at the designated school year time points were provided by 64 teachers blinded to the pupils’ sleep histories and by assessments administered by project staff.
Among the sleep measures examined, regularity of nighttime sleep involving 10 or more hours of sleep over the nocturnal period, especially at the pre-kindergarten stage, consistently predicted more favorable outcomes in socioemotional, learning engagement, and academic domains. These findings were controlled for income-to-poverty threshold ratios, child health status, and number of missed school days.
The study results generally align with those of previous studies, showing the importance of sleep for children’s school functioning, Dr. Teti told this news organization. “But they differed significantly in terms of finding that it was the regularity of 10-plus hours concentrated during the nighttime sleep period that was most important for predicting school adjustment, in particular, regular or sufficient sleep that occurred prior to the start of kindergarten.”
Calling the study “thought provoking,” Michael B. Grosso, MD, chair of pediatrics at Huntington (N.Y.) Hospital, said it confirms a robust correlation between total sleep duration and outcomes important to successful adjustment to kindergarten. “And we find out that uninterrupted sleep time of 10 hours or more seems to matter as well.”
In his view, the biggest limitation to the analysis is the one inherent to any observational study, “which is that association cannot prove causality. The authors did attempt to control for other health factors, but that can be hard to do,” he said. “The point is that if a child faces any of several health challenges, from sleep apnea to uncontrolled asthma, to ADHD or an autistic spectrum disorder, those issues will cause disrupted, abnormal sleep and also interfere with the outcomes the study addresses. In other words, it’s hard to know if sleep is affecting kindergarten adjustment or whether some X factor is affecting sleep and also affecting kindergarten performance.”
Getting children into bed earlier in long bright evenings of spring and summer before onset of kindergarten may not be easy, Dr. Teti acknowledged. “Arranging children’s sleep schedule as they approach kindergarten so that most, if not all, of their sleep takes place during the night – and as a corollary, reducing the frequency of naps during the day – should help children shift into sleeping nighttime primarily if not exclusively,” he said.
If necessary, he added, parents can work with sleep professionals to gradually concentrate children’s sleep during the night. They should normalize earlier bedtimes by reducing access to electronic screens before bedtime and removing televisions from their bedrooms. “A consistent bedtime routine should be a central feature of parental attempts to shape better, more regular sleep in their children.”
Dr. Grosso added that pediatricians need to talk about the importance of consistent routines and especially adequate sleep when counseling parents during pre-school health supervision visits. “And as the authors mention, it’s hard to ensure good sleep hygiene for children if parents aren’t also getting a good night sleep. It all goes together.”
This study was supported by the National Institutes of Health. The authors had no competing interests to declare. Dr. Grosso disclosed no relevant conflicts of interest.
FROM PEDIATRICS
New AHA checklist: Only one in five adults has optimal heart health
About 80% of American adults have low to moderate cardiovascular (CV) health based on the American Heart Association checklist for optimal heart health, which now includes healthy sleep as an essential component for heart health.
With the addition of sleep, “Life’s Essential 8” replaces the AHA’s “Life’s Simple 7” checklist.
“The new metric of sleep duration reflects the latest research findings: Sleep impacts overall health, and people who have healthier sleep patterns manage health factors such as weight, blood pressure, or risk for type 2 diabetes more effectively,” AHA President Donald M. Lloyd-Jones, MD, said in a news release.

“In addition, advances in ways to measure sleep, such as with wearable devices, now offer people the ability to reliably and routinely monitor their sleep habits at home,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University in Chicago.
The AHA Presidential Advisory – Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct on Cardiovascular Health – was published online in the journal Circulation.
A companion paper published simultaneously in Circulation reports the first study using Life’s Essential 8.
Overall, the results show that CV health of the U.S. population is “suboptimal, and we see important differences across age and sociodemographic groups,” Dr. Lloyd-Jones said.
Refining Life’s Simple 7
The AHA first defined the seven metrics for optimal CV health in 2010. After 12 years and more than 2,400 scientific papers on the topic, new discoveries in CV health and ways to measure it provided an opportunity to revisit each health component in more detail and provide updates as needed, the AHA explains.
“We felt it was the right time to conduct a comprehensive review of the latest research to refine the existing metrics and consider any new metrics that add value to assessing cardiovascular health for all people,” Dr. Lloyd-Jones said.
Four of the original metrics have been redefined for consistency with newer clinical guidelines or compatibility with new measurement tools, and the scoring system can now also be applied to anyone ages 2 and older. Here is a snapshot of Life’s Essential 8 metrics, including updates.
1. Diet (updated)
The tool includes a new guide to assess diet quality for adults and children at the individual and population level. At the population level, dietary assessment is based on daily intake of elements in the Dietary Approaches to Stop Hypertension (DASH) eating pattern. For individuals, the Mediterranean Eating Pattern for Americans (MEPA) is used to assess and monitor cardiovascular health.
2. Physical activity (no changes)
Physical activity continues to be measured by the total number of minutes of moderate or vigorous physical activity per week, as defined by the U.S. Physical Activity Guidelines for Americans (2nd edition). The optimal level is 150 minutes (2.5 hours) of moderate physical activity or more per week or 75 minutes per week of vigorous-intensity physical activity for adults; 420 minutes (7 hours) or more per week for children ages 6 and older; and age-specific modifications for younger children.
3. Nicotine exposure (updated)
Use of inhaled nicotine-delivery systems, which includes e-cigarettes or vaping devices, has been added since the previous metric monitored only traditional, combustible cigarettes. This reflects use by adults and youth and their implications on long-term health. Second-hand smoke exposure for children and adults has also been added.
4. Sleep duration (new)
Sleep duration is associated with CV health. Measured by average hours of sleep per night, the ideal level is 7-9 hours daily for adults. Ideal daily sleep ranges for children are 10-16 hours per 24 hours for ages 5 and younger; 9-12 hours for ages 6-12 years; and 8-10 hours for ages 13-18 years.
5. Body mass index (no changes)
The AHA acknowledges that body mass index (BMI) is an imperfect metric. Yet, because it’s easily calculated and widely available, BMI continues as a “reasonable” gauge to assess weight categories that may lead to health problems. BMI of 18.5-24.9 is associated with the highest levels of CV health. The AHA notes that BMI ranges and the subsequent health risks associated with them may differ among people from diverse racial or ethnic backgrounds or ancestry. This aligns with the World Health Organization recommendations to adjust BMI ranges for people of Asian or Pacific Islander ancestry because recent evidence indicates their risk of conditions such as CVD or type 2 diabetes is higher at a lower BMI.
6. Blood lipids (updated)
The metric for blood lipids (cholesterol and triglycerides) is updated to use non-HDL cholesterol as the preferred number to monitor, rather than total cholesterol. This shift is made because non-HDL cholesterol can be measured without fasting beforehand (thereby increasing its availability at any time of day and implementation at more appointments) and reliably calculated among all people.
7. Blood glucose (updated)
This metric is expanded to include the option of hemoglobin A1c readings or blood glucose levels for people with or without type 1 or 2 diabetes or prediabetes.
8. Blood pressure (no changes)
Blood pressure criteria remain unchanged from 2017 guidance that established levels less than 120/80 mm Hg as optimal, and defined hypertension as 130-139 mm Hg systolic pressure or 80-89 mm Hg diastolic pressure.
‘Concerning’ new data
Results of the first study using Life’s Essential 8 show that the overall CV health of the U.S. population is “well below ideal,” with 80% of adults scoring at a low or moderate level, the researchers report.
Data for the analysis came from 2013-2018 U.S. National Health and Nutrition Examination surveys (NHANES) of more than 13,500 adults aged 20-79 years and nearly 9,900 children aged 2-19 years. Among the key findings:
- The average CV health score based on Life’s Essential 8 was 64.7 for adults and 65.5 for children – in the moderate range on the 0-100 scale.
- Only 0.45% of adults had a perfect score of 100; 20% had high CV health (score of 80 or higher), 63% moderate (score of 50-79), and 18% had low CV health (score of less than 50).
- Adult women had higher average CV health scores (67) compared with men (62.5).
- In general, adults scored lowest in the areas of diet, physical activity, and BMI.
- CV health scores were generally lower at older ages.
- Non-Hispanic Asian Americans had a higher average CV health score than other racial/ethnic groups. Non-Hispanic Whites had the second highest average CV health score, followed, in order, by Hispanic (other than Mexican), Mexican, and non-Hispanic Blacks.
- Children’s diet scores were low, at an average of 40.6.
- Adult sociodemographic groups varied notably in CV health scores for diet, nicotine exposure, blood glucose, and blood pressure.
“These data represent the first look at the cardiovascular health of the U.S. population using the AHA’s new Life’s Essential 8 scoring algorithm,” Dr. Lloyd-Jones said.
“Life’s Essential 8 is a major step forward in our ability to identify when cardiovascular health can be preserved and when it is suboptimal. It should energize efforts to improve cardiovascular health for all people and at every life stage,” Dr. Lloyd-Jones added.
“Analyses like this can help policymakers, communities, clinicians, and the public to understand the opportunities to intervene to improve and maintain optimal cardiovascular health across the life course,” he said.
This research had no commercial funding. The authors have no reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About 80% of American adults have low to moderate cardiovascular (CV) health based on the American Heart Association checklist for optimal heart health, which now includes healthy sleep as an essential component for heart health.
With the addition of sleep, “Life’s Essential 8” replaces the AHA’s “Life’s Simple 7” checklist.
“The new metric of sleep duration reflects the latest research findings: Sleep impacts overall health, and people who have healthier sleep patterns manage health factors such as weight, blood pressure, or risk for type 2 diabetes more effectively,” AHA President Donald M. Lloyd-Jones, MD, said in a news release.
“In addition, advances in ways to measure sleep, such as with wearable devices, now offer people the ability to reliably and routinely monitor their sleep habits at home,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University in Chicago.
The AHA Presidential Advisory – Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct on Cardiovascular Health – was published online in the journal Circulation.
A companion paper published simultaneously in Circulation reports the first study using Life’s Essential 8.
Overall, the results show that CV health of the U.S. population is “suboptimal, and we see important differences across age and sociodemographic groups,” Dr. Lloyd-Jones said.
Refining Life’s Simple 7
The AHA first defined the seven metrics for optimal CV health in 2010. After 12 years and more than 2,400 scientific papers on the topic, new discoveries in CV health and ways to measure it provided an opportunity to revisit each health component in more detail and provide updates as needed, the AHA explains.
“We felt it was the right time to conduct a comprehensive review of the latest research to refine the existing metrics and consider any new metrics that add value to assessing cardiovascular health for all people,” Dr. Lloyd-Jones said.
Four of the original metrics have been redefined for consistency with newer clinical guidelines or compatibility with new measurement tools, and the scoring system can now also be applied to anyone ages 2 and older. Here is a snapshot of Life’s Essential 8 metrics, including updates.
1. Diet (updated)
The tool includes a new guide to assess diet quality for adults and children at the individual and population level. At the population level, dietary assessment is based on daily intake of elements in the Dietary Approaches to Stop Hypertension (DASH) eating pattern. For individuals, the Mediterranean Eating Pattern for Americans (MEPA) is used to assess and monitor cardiovascular health.
2. Physical activity (no changes)
Physical activity continues to be measured by the total number of minutes of moderate or vigorous physical activity per week, as defined by the U.S. Physical Activity Guidelines for Americans (2nd edition). The optimal level is 150 minutes (2.5 hours) of moderate physical activity or more per week or 75 minutes per week of vigorous-intensity physical activity for adults; 420 minutes (7 hours) or more per week for children ages 6 and older; and age-specific modifications for younger children.
3. Nicotine exposure (updated)
Use of inhaled nicotine-delivery systems, which includes e-cigarettes or vaping devices, has been added since the previous metric monitored only traditional, combustible cigarettes. This reflects use by adults and youth and their implications on long-term health. Second-hand smoke exposure for children and adults has also been added.
4. Sleep duration (new)
Sleep duration is associated with CV health. Measured by average hours of sleep per night, the ideal level is 7-9 hours daily for adults. Ideal daily sleep ranges for children are 10-16 hours per 24 hours for ages 5 and younger; 9-12 hours for ages 6-12 years; and 8-10 hours for ages 13-18 years.
5. Body mass index (no changes)
The AHA acknowledges that body mass index (BMI) is an imperfect metric. Yet, because it’s easily calculated and widely available, BMI continues as a “reasonable” gauge to assess weight categories that may lead to health problems. BMI of 18.5-24.9 is associated with the highest levels of CV health. The AHA notes that BMI ranges and the subsequent health risks associated with them may differ among people from diverse racial or ethnic backgrounds or ancestry. This aligns with the World Health Organization recommendations to adjust BMI ranges for people of Asian or Pacific Islander ancestry because recent evidence indicates their risk of conditions such as CVD or type 2 diabetes is higher at a lower BMI.
6. Blood lipids (updated)
The metric for blood lipids (cholesterol and triglycerides) is updated to use non-HDL cholesterol as the preferred number to monitor, rather than total cholesterol. This shift is made because non-HDL cholesterol can be measured without fasting beforehand (thereby increasing its availability at any time of day and implementation at more appointments) and reliably calculated among all people.
7. Blood glucose (updated)
This metric is expanded to include the option of hemoglobin A1c readings or blood glucose levels for people with or without type 1 or 2 diabetes or prediabetes.
8. Blood pressure (no changes)
Blood pressure criteria remain unchanged from 2017 guidance that established levels less than 120/80 mm Hg as optimal, and defined hypertension as 130-139 mm Hg systolic pressure or 80-89 mm Hg diastolic pressure.
‘Concerning’ new data
Results of the first study using Life’s Essential 8 show that the overall CV health of the U.S. population is “well below ideal,” with 80% of adults scoring at a low or moderate level, the researchers report.
Data for the analysis came from 2013-2018 U.S. National Health and Nutrition Examination surveys (NHANES) of more than 13,500 adults aged 20-79 years and nearly 9,900 children aged 2-19 years. Among the key findings:
- The average CV health score based on Life’s Essential 8 was 64.7 for adults and 65.5 for children – in the moderate range on the 0-100 scale.
- Only 0.45% of adults had a perfect score of 100; 20% had high CV health (score of 80 or higher), 63% moderate (score of 50-79), and 18% had low CV health (score of less than 50).
- Adult women had higher average CV health scores (67) compared with men (62.5).
- In general, adults scored lowest in the areas of diet, physical activity, and BMI.
- CV health scores were generally lower at older ages.
- Non-Hispanic Asian Americans had a higher average CV health score than other racial/ethnic groups. Non-Hispanic Whites had the second highest average CV health score, followed, in order, by Hispanic (other than Mexican), Mexican, and non-Hispanic Blacks.
- Children’s diet scores were low, at an average of 40.6.
- Adult sociodemographic groups varied notably in CV health scores for diet, nicotine exposure, blood glucose, and blood pressure.
“These data represent the first look at the cardiovascular health of the U.S. population using the AHA’s new Life’s Essential 8 scoring algorithm,” Dr. Lloyd-Jones said.
“Life’s Essential 8 is a major step forward in our ability to identify when cardiovascular health can be preserved and when it is suboptimal. It should energize efforts to improve cardiovascular health for all people and at every life stage,” Dr. Lloyd-Jones added.
“Analyses like this can help policymakers, communities, clinicians, and the public to understand the opportunities to intervene to improve and maintain optimal cardiovascular health across the life course,” he said.
This research had no commercial funding. The authors have no reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About 80% of American adults have low to moderate cardiovascular (CV) health based on the American Heart Association checklist for optimal heart health, which now includes healthy sleep as an essential component for heart health.
With the addition of sleep, “Life’s Essential 8” replaces the AHA’s “Life’s Simple 7” checklist.
“The new metric of sleep duration reflects the latest research findings: Sleep impacts overall health, and people who have healthier sleep patterns manage health factors such as weight, blood pressure, or risk for type 2 diabetes more effectively,” AHA President Donald M. Lloyd-Jones, MD, said in a news release.
“In addition, advances in ways to measure sleep, such as with wearable devices, now offer people the ability to reliably and routinely monitor their sleep habits at home,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University in Chicago.
The AHA Presidential Advisory – Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct on Cardiovascular Health – was published online in the journal Circulation.
A companion paper published simultaneously in Circulation reports the first study using Life’s Essential 8.
Overall, the results show that CV health of the U.S. population is “suboptimal, and we see important differences across age and sociodemographic groups,” Dr. Lloyd-Jones said.
Refining Life’s Simple 7
The AHA first defined the seven metrics for optimal CV health in 2010. After 12 years and more than 2,400 scientific papers on the topic, new discoveries in CV health and ways to measure it provided an opportunity to revisit each health component in more detail and provide updates as needed, the AHA explains.
“We felt it was the right time to conduct a comprehensive review of the latest research to refine the existing metrics and consider any new metrics that add value to assessing cardiovascular health for all people,” Dr. Lloyd-Jones said.
Four of the original metrics have been redefined for consistency with newer clinical guidelines or compatibility with new measurement tools, and the scoring system can now also be applied to anyone ages 2 and older. Here is a snapshot of Life’s Essential 8 metrics, including updates.
1. Diet (updated)
The tool includes a new guide to assess diet quality for adults and children at the individual and population level. At the population level, dietary assessment is based on daily intake of elements in the Dietary Approaches to Stop Hypertension (DASH) eating pattern. For individuals, the Mediterranean Eating Pattern for Americans (MEPA) is used to assess and monitor cardiovascular health.
2. Physical activity (no changes)
Physical activity continues to be measured by the total number of minutes of moderate or vigorous physical activity per week, as defined by the U.S. Physical Activity Guidelines for Americans (2nd edition). The optimal level is 150 minutes (2.5 hours) of moderate physical activity or more per week or 75 minutes per week of vigorous-intensity physical activity for adults; 420 minutes (7 hours) or more per week for children ages 6 and older; and age-specific modifications for younger children.
3. Nicotine exposure (updated)
Use of inhaled nicotine-delivery systems, which includes e-cigarettes or vaping devices, has been added since the previous metric monitored only traditional, combustible cigarettes. This reflects use by adults and youth and their implications on long-term health. Second-hand smoke exposure for children and adults has also been added.
4. Sleep duration (new)
Sleep duration is associated with CV health. Measured by average hours of sleep per night, the ideal level is 7-9 hours daily for adults. Ideal daily sleep ranges for children are 10-16 hours per 24 hours for ages 5 and younger; 9-12 hours for ages 6-12 years; and 8-10 hours for ages 13-18 years.
5. Body mass index (no changes)
The AHA acknowledges that body mass index (BMI) is an imperfect metric. Yet, because it’s easily calculated and widely available, BMI continues as a “reasonable” gauge to assess weight categories that may lead to health problems. BMI of 18.5-24.9 is associated with the highest levels of CV health. The AHA notes that BMI ranges and the subsequent health risks associated with them may differ among people from diverse racial or ethnic backgrounds or ancestry. This aligns with the World Health Organization recommendations to adjust BMI ranges for people of Asian or Pacific Islander ancestry because recent evidence indicates their risk of conditions such as CVD or type 2 diabetes is higher at a lower BMI.
6. Blood lipids (updated)
The metric for blood lipids (cholesterol and triglycerides) is updated to use non-HDL cholesterol as the preferred number to monitor, rather than total cholesterol. This shift is made because non-HDL cholesterol can be measured without fasting beforehand (thereby increasing its availability at any time of day and implementation at more appointments) and reliably calculated among all people.
7. Blood glucose (updated)
This metric is expanded to include the option of hemoglobin A1c readings or blood glucose levels for people with or without type 1 or 2 diabetes or prediabetes.
8. Blood pressure (no changes)
Blood pressure criteria remain unchanged from 2017 guidance that established levels less than 120/80 mm Hg as optimal, and defined hypertension as 130-139 mm Hg systolic pressure or 80-89 mm Hg diastolic pressure.
‘Concerning’ new data
Results of the first study using Life’s Essential 8 show that the overall CV health of the U.S. population is “well below ideal,” with 80% of adults scoring at a low or moderate level, the researchers report.
Data for the analysis came from 2013-2018 U.S. National Health and Nutrition Examination surveys (NHANES) of more than 13,500 adults aged 20-79 years and nearly 9,900 children aged 2-19 years. Among the key findings:
- The average CV health score based on Life’s Essential 8 was 64.7 for adults and 65.5 for children – in the moderate range on the 0-100 scale.
- Only 0.45% of adults had a perfect score of 100; 20% had high CV health (score of 80 or higher), 63% moderate (score of 50-79), and 18% had low CV health (score of less than 50).
- Adult women had higher average CV health scores (67) compared with men (62.5).
- In general, adults scored lowest in the areas of diet, physical activity, and BMI.
- CV health scores were generally lower at older ages.
- Non-Hispanic Asian Americans had a higher average CV health score than other racial/ethnic groups. Non-Hispanic Whites had the second highest average CV health score, followed, in order, by Hispanic (other than Mexican), Mexican, and non-Hispanic Blacks.
- Children’s diet scores were low, at an average of 40.6.
- Adult sociodemographic groups varied notably in CV health scores for diet, nicotine exposure, blood glucose, and blood pressure.
“These data represent the first look at the cardiovascular health of the U.S. population using the AHA’s new Life’s Essential 8 scoring algorithm,” Dr. Lloyd-Jones said.
“Life’s Essential 8 is a major step forward in our ability to identify when cardiovascular health can be preserved and when it is suboptimal. It should energize efforts to improve cardiovascular health for all people and at every life stage,” Dr. Lloyd-Jones added.
“Analyses like this can help policymakers, communities, clinicians, and the public to understand the opportunities to intervene to improve and maintain optimal cardiovascular health across the life course,” he said.
This research had no commercial funding. The authors have no reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Lifestyle medicine eases anxiety symptoms
Despite the availability of effective treatment strategies, including pharmacotherapy, psychotherapy, and combination therapy, the prevalence of anxiety continues to increase, especially in low-income and conflict-ridden countries, Vincent Wing-Hei Wong, a PhD student at The Chinese University of Hong Kong, and colleagues wrote.
Previous studies have shown that lifestyle factors including diet, sleep, and sedentary behavior are involved in the development of anxiety symptoms, but the impact of lifestyle medicine (LM) as a treatment for anxiety has not been well studied, they wrote.
In a meta-analysis published in the Journal of Affective Disorders, the researchers identified 53 randomized, controlled trials with a total of 18,894 participants. Anxiety symptoms were measured using self-report questionnaires including the Hospital Anxiety and Depression Scale, the Depression Anxiety and Stress Scale, and the General Anxiety Disorder–7. Random-effects models were used to assess the effect of the intervention at immediate post treatment, short-term follow-up (1-3 months post treatment), medium follow-up (4-6 months), and long-term follow-up (7 months or more).
The studies included various combinations of LM intervention involving exercise, stress management, and sleep management. The interventions ranged from 1 month to 4 years, with an average duration of 6.3 months.
Overall, patients randomized to multicomponent LM interventions showed significantly improved symptoms compared to controls immediately after treatment and at short-term follow-up (P < .001 for both).
However, no significant differences were noted between the multicomponent LM intervention and control groups at medium-term follow-up, the researchers said. Only one study included data on long-term effects, so these effects were not evaluated in a meta-analysis, and more research is needed.
In a subgroup analysis, the effect was greatest for individuals with moderate anxiety symptoms at baseline (P < .05). “Our results could perhaps be explained by the occurrence of floor effect; those with higher baseline anxiety symptoms have greater room for improvement relative to those with fewer symptoms,” the researchers wrote.
The study findings were limited by several factors including the risk of overall bias and publication bias for the selected studies, as well as the limited degree of improvement because most patients had minimal anxiety symptoms at baseline, the researchers noted. Other limitations included the small number of studies for subgroup comparisons and the use of self-reports.
However, the results were strengthened by the use of broad search terms to capture multiple lifestyle determinants, and the diverse study populations and backgrounds from individuals in 19 countries.
The results support findings from previous studies, and support the value of multicomponent LM interventions for patients with anxiety in the short-term and immediately after treatment, the researchers emphasized.
“The LM approach, which leverages a range of universal lifestyle measures to manage anxiety and other common mental disorders such as depression, may be a viable solution to address the huge mental health burden through empowering individuals to practice self-management,” they concluded.
However, the researchers acknowledged the need for more randomized, controlled trials targeting patients with higher baseline anxiety levels or anxiety disorders, and using technology to improve treatment adherence.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Despite the availability of effective treatment strategies, including pharmacotherapy, psychotherapy, and combination therapy, the prevalence of anxiety continues to increase, especially in low-income and conflict-ridden countries, Vincent Wing-Hei Wong, a PhD student at The Chinese University of Hong Kong, and colleagues wrote.
Previous studies have shown that lifestyle factors including diet, sleep, and sedentary behavior are involved in the development of anxiety symptoms, but the impact of lifestyle medicine (LM) as a treatment for anxiety has not been well studied, they wrote.
In a meta-analysis published in the Journal of Affective Disorders, the researchers identified 53 randomized, controlled trials with a total of 18,894 participants. Anxiety symptoms were measured using self-report questionnaires including the Hospital Anxiety and Depression Scale, the Depression Anxiety and Stress Scale, and the General Anxiety Disorder–7. Random-effects models were used to assess the effect of the intervention at immediate post treatment, short-term follow-up (1-3 months post treatment), medium follow-up (4-6 months), and long-term follow-up (7 months or more).
The studies included various combinations of LM intervention involving exercise, stress management, and sleep management. The interventions ranged from 1 month to 4 years, with an average duration of 6.3 months.
Overall, patients randomized to multicomponent LM interventions showed significantly improved symptoms compared to controls immediately after treatment and at short-term follow-up (P < .001 for both).
However, no significant differences were noted between the multicomponent LM intervention and control groups at medium-term follow-up, the researchers said. Only one study included data on long-term effects, so these effects were not evaluated in a meta-analysis, and more research is needed.
In a subgroup analysis, the effect was greatest for individuals with moderate anxiety symptoms at baseline (P < .05). “Our results could perhaps be explained by the occurrence of floor effect; those with higher baseline anxiety symptoms have greater room for improvement relative to those with fewer symptoms,” the researchers wrote.
The study findings were limited by several factors including the risk of overall bias and publication bias for the selected studies, as well as the limited degree of improvement because most patients had minimal anxiety symptoms at baseline, the researchers noted. Other limitations included the small number of studies for subgroup comparisons and the use of self-reports.
However, the results were strengthened by the use of broad search terms to capture multiple lifestyle determinants, and the diverse study populations and backgrounds from individuals in 19 countries.
The results support findings from previous studies, and support the value of multicomponent LM interventions for patients with anxiety in the short-term and immediately after treatment, the researchers emphasized.
“The LM approach, which leverages a range of universal lifestyle measures to manage anxiety and other common mental disorders such as depression, may be a viable solution to address the huge mental health burden through empowering individuals to practice self-management,” they concluded.
However, the researchers acknowledged the need for more randomized, controlled trials targeting patients with higher baseline anxiety levels or anxiety disorders, and using technology to improve treatment adherence.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Despite the availability of effective treatment strategies, including pharmacotherapy, psychotherapy, and combination therapy, the prevalence of anxiety continues to increase, especially in low-income and conflict-ridden countries, Vincent Wing-Hei Wong, a PhD student at The Chinese University of Hong Kong, and colleagues wrote.
Previous studies have shown that lifestyle factors including diet, sleep, and sedentary behavior are involved in the development of anxiety symptoms, but the impact of lifestyle medicine (LM) as a treatment for anxiety has not been well studied, they wrote.
In a meta-analysis published in the Journal of Affective Disorders, the researchers identified 53 randomized, controlled trials with a total of 18,894 participants. Anxiety symptoms were measured using self-report questionnaires including the Hospital Anxiety and Depression Scale, the Depression Anxiety and Stress Scale, and the General Anxiety Disorder–7. Random-effects models were used to assess the effect of the intervention at immediate post treatment, short-term follow-up (1-3 months post treatment), medium follow-up (4-6 months), and long-term follow-up (7 months or more).
The studies included various combinations of LM intervention involving exercise, stress management, and sleep management. The interventions ranged from 1 month to 4 years, with an average duration of 6.3 months.
Overall, patients randomized to multicomponent LM interventions showed significantly improved symptoms compared to controls immediately after treatment and at short-term follow-up (P < .001 for both).
However, no significant differences were noted between the multicomponent LM intervention and control groups at medium-term follow-up, the researchers said. Only one study included data on long-term effects, so these effects were not evaluated in a meta-analysis, and more research is needed.
In a subgroup analysis, the effect was greatest for individuals with moderate anxiety symptoms at baseline (P < .05). “Our results could perhaps be explained by the occurrence of floor effect; those with higher baseline anxiety symptoms have greater room for improvement relative to those with fewer symptoms,” the researchers wrote.
The study findings were limited by several factors including the risk of overall bias and publication bias for the selected studies, as well as the limited degree of improvement because most patients had minimal anxiety symptoms at baseline, the researchers noted. Other limitations included the small number of studies for subgroup comparisons and the use of self-reports.
However, the results were strengthened by the use of broad search terms to capture multiple lifestyle determinants, and the diverse study populations and backgrounds from individuals in 19 countries.
The results support findings from previous studies, and support the value of multicomponent LM interventions for patients with anxiety in the short-term and immediately after treatment, the researchers emphasized.
“The LM approach, which leverages a range of universal lifestyle measures to manage anxiety and other common mental disorders such as depression, may be a viable solution to address the huge mental health burden through empowering individuals to practice self-management,” they concluded.
However, the researchers acknowledged the need for more randomized, controlled trials targeting patients with higher baseline anxiety levels or anxiety disorders, and using technology to improve treatment adherence.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF AFFECTIVE DISORDERS
Childhood melatonin poisonings skyrocket in the past 10 years
The number of children in the United States who unintentionally ingested melatonin supplements over the past 10 years has skyrocketed to the point where, as of 2021, melatonin ingestions by children accounted for almost 5% of all poisonings reported to poison control centers in the United States, data from the National Poison Data System (NPDS) indicate.
This compared with only 0.6% of melatonin ingestions reported to poison control centers in 2012, the authors added.
“Basically the number of pediatric melatonin ingestions increased 530% from 8,337 in 2012 to 52,563 in 2021 so it’s a 6.3-fold increase from the beginning of the study until the end,” Michael Toce, MD, one of the study authors and attending, pediatric emergency medicine/medical toxicology, Boston Children’s Hospital, said in an interview.
“And I think the biggest driver of this increase is simply that sales of melatonin have increased astronomically so there is just more melatonin at home and studies have shown there is a correlation between the amount of an individual medication in the home and the risk of pediatric exposure – so simply put: The more of a single substance in a home, the greater the chance that a child is going to get into it,” he underscored.
The study was published in the Morbidity and Mortality Weekly Report .
Melatonin ingestions
All cases of single substance melatonin ingestions involving children and adolescents between Jan. 1, 2012, and Dec. 31, 2021, were included in the analysis. During the 10-year study interval, 260,435 pediatric melatonin ingestions were reported to the NPDS. Over 94% of the reported ingestions were unintentional and 99% occurred in the home.
Over 88% of them were managed on-site; most involved young male children aged 5 years and under, and almost 83% of children who ingested melatonin supplements remained asymptomatic. On the other hand, 27,795 patients sought care at a health care facility and close to 15% of them were hospitalized. Among all melatonin ingestions, 1.6% resulted in more serious outcomes; more serious outcomes being defined as a moderate or major effects or death. Five children required mechanical ventilation in order to treat their symptoms and 2 patients died.
The largest number of patients who were hospitalized were adolescents who took melatonin intentionally but the largest increase in the rate of exposure was in young, unintentional patients, as Dr. Toce observed. Interestingly, the largest yearly increase in pediatric melatonin ingestions – almost 38% – coincided with the onset of the COVID-19 pandemic.
“This might be related to increased accessibility of melatonin during the pandemic, as children spent more time at home because of stay-at-home orders and school closures,” the authors speculate. Moreover, sleep disturbances were common during the pandemic, leading to a greater likelihood that parents were buying melatonin and thus exposing children to more melatonin at home.
Taken appropriately and at normal does, melatonin in itself is quite safe, as Dr. Toce stressed. However, “for any substance, the dose makes the poison, so taken in any significant quantity, anything is going to be dangerous.” Moreover, it’s important to appreciate that melatonin, at least in the United States, is regulated as a dietary supplement, not as a pharmaceutical.
“Thus, it doesn’t get the same rigorous testing that something like acetaminophen does by the FDA and that means two things,” Dr. Toce noted. First, if the product says that each gummy contains 3 mg of melatonin, no independent body is verifying whether or not that statement is true so there could be 3 mg of melatonin in each gummy or there could be 10 mg,.
Secondly, because there is no impartial oversight for dietary supplements, there may in fact be no melatonin at all in the product or something else may be added to it that might be harmful. “Just because something is sold over-the-counter does not necessarily mean that it’s safe,” Dr. Toce stressed. To keep children safe from pharmaceuticals and supplements, he recommended several generic poison prevention tips. This advice could be passed on to patients who are parents.
- Keep all pharmaceuticals and supplements preferably locked away so there is less risk of children and adolescents taking products either unintentionally or intentionally
- If parents have no place to lock their products up, put them out of reach, high-up so children cannot easily access them
- Keep the product in the original child-resistant packaging as opposed to taking the pills out of the packaging and putting it in a plastic bag bag. “Certainly we’ve seen that when medications are moved into a non–child-resistant container, ingestions go up,” Dr. Toce warned
- Don’t refer to any medicine or supplement a child might take as “candy.” “A lot of children have difficulty taking medications so some families will say: ‘It’s time for your candy,’ ” Dr. Toce explained. Then, if a child does discover the “candy” on a table where they have access to it, they will not recognize it as medication and they’re likely to pop it into their mouth, thinking it is candy.
Lastly, and most importantly, parents who are considering trying a melatonin supplement to help a child sleep better should first establish a stable sleep routine for their child. “They also need to limit caffeinated beverages before bed as well as screen time,” Dr. Toce added.
And they should talk with their primary care provider as to whether or not initiation of a melatonin supplement is appropriate for their child – “and not just jump right into giving them melatonin without first discussing whether it is appropriate to do so,” Dr. Toce stressed.
Remarkable rise
In a comment on his own experience with melatonin poisoning over recent years, toxicology expert Kevin Osterhoudt, MD, of the University of Pennsylvania, Philadelphia and the Children’s Hospital of Philadelphia, noted that it has been their experience that there has been a remarkable rise in poison center reports of children ingesting melatonin in the recent past. For example, the Poison Control Center at CHOP received nearly 4,000 calls involving melatonin ingestion by children 5 years old or younger in the 5 years between 2017 and 2021 with increasing numbers every year.
“The [current study] supports that our regional observation that this has been a national trend,” Dr. Osterhoudt said. Dr. Osterhoudt agreed with Dr. Toce that good sleep is healthy, and it is very important to develop good sleep habits and a regular bedtime routine in order to do so. “In some situations, melatonin may be useful as a short-term sleep aid and that’s a good discussion to have with your child’s health care provider.”
If parents do decide to give their child a melatonin supplement, they need to keep in mind that melatonin may alter how the body handles other drugs such as those used to treat epilepsy or blood clotting. They also need to know experts are still uncertain about how melatonin affects the body over the long term and whether it is safe for mothers to take during pregnancy.
Dr. Osterhoudt offered his own recommendations for safe melatonin use in the home:
- Discuss planned melatonin use with your health care provider.
- Buy only high-quality supplements by looking for the “USP Verified” mark.
- Insist that manufacturers sell products in child-resistant bottles.
- Periodically inspect the medications in your home and dispose of medications that are no longer being used.
- Program the phone number of your regional poison control center into your phone; poison center experts are available 24/7 to answer questions and concerns about ingestions of melatonin (in the United States the number is 1-800-222-1222).
The study authors and neither Dr. Toce nor Dr. Osterhoudt had any relevant conflicts of interest to declare.
The number of children in the United States who unintentionally ingested melatonin supplements over the past 10 years has skyrocketed to the point where, as of 2021, melatonin ingestions by children accounted for almost 5% of all poisonings reported to poison control centers in the United States, data from the National Poison Data System (NPDS) indicate.
This compared with only 0.6% of melatonin ingestions reported to poison control centers in 2012, the authors added.
“Basically the number of pediatric melatonin ingestions increased 530% from 8,337 in 2012 to 52,563 in 2021 so it’s a 6.3-fold increase from the beginning of the study until the end,” Michael Toce, MD, one of the study authors and attending, pediatric emergency medicine/medical toxicology, Boston Children’s Hospital, said in an interview.
“And I think the biggest driver of this increase is simply that sales of melatonin have increased astronomically so there is just more melatonin at home and studies have shown there is a correlation between the amount of an individual medication in the home and the risk of pediatric exposure – so simply put: The more of a single substance in a home, the greater the chance that a child is going to get into it,” he underscored.
The study was published in the Morbidity and Mortality Weekly Report .
Melatonin ingestions
All cases of single substance melatonin ingestions involving children and adolescents between Jan. 1, 2012, and Dec. 31, 2021, were included in the analysis. During the 10-year study interval, 260,435 pediatric melatonin ingestions were reported to the NPDS. Over 94% of the reported ingestions were unintentional and 99% occurred in the home.
Over 88% of them were managed on-site; most involved young male children aged 5 years and under, and almost 83% of children who ingested melatonin supplements remained asymptomatic. On the other hand, 27,795 patients sought care at a health care facility and close to 15% of them were hospitalized. Among all melatonin ingestions, 1.6% resulted in more serious outcomes; more serious outcomes being defined as a moderate or major effects or death. Five children required mechanical ventilation in order to treat their symptoms and 2 patients died.
The largest number of patients who were hospitalized were adolescents who took melatonin intentionally but the largest increase in the rate of exposure was in young, unintentional patients, as Dr. Toce observed. Interestingly, the largest yearly increase in pediatric melatonin ingestions – almost 38% – coincided with the onset of the COVID-19 pandemic.
“This might be related to increased accessibility of melatonin during the pandemic, as children spent more time at home because of stay-at-home orders and school closures,” the authors speculate. Moreover, sleep disturbances were common during the pandemic, leading to a greater likelihood that parents were buying melatonin and thus exposing children to more melatonin at home.
Taken appropriately and at normal does, melatonin in itself is quite safe, as Dr. Toce stressed. However, “for any substance, the dose makes the poison, so taken in any significant quantity, anything is going to be dangerous.” Moreover, it’s important to appreciate that melatonin, at least in the United States, is regulated as a dietary supplement, not as a pharmaceutical.
“Thus, it doesn’t get the same rigorous testing that something like acetaminophen does by the FDA and that means two things,” Dr. Toce noted. First, if the product says that each gummy contains 3 mg of melatonin, no independent body is verifying whether or not that statement is true so there could be 3 mg of melatonin in each gummy or there could be 10 mg,.
Secondly, because there is no impartial oversight for dietary supplements, there may in fact be no melatonin at all in the product or something else may be added to it that might be harmful. “Just because something is sold over-the-counter does not necessarily mean that it’s safe,” Dr. Toce stressed. To keep children safe from pharmaceuticals and supplements, he recommended several generic poison prevention tips. This advice could be passed on to patients who are parents.
- Keep all pharmaceuticals and supplements preferably locked away so there is less risk of children and adolescents taking products either unintentionally or intentionally
- If parents have no place to lock their products up, put them out of reach, high-up so children cannot easily access them
- Keep the product in the original child-resistant packaging as opposed to taking the pills out of the packaging and putting it in a plastic bag bag. “Certainly we’ve seen that when medications are moved into a non–child-resistant container, ingestions go up,” Dr. Toce warned
- Don’t refer to any medicine or supplement a child might take as “candy.” “A lot of children have difficulty taking medications so some families will say: ‘It’s time for your candy,’ ” Dr. Toce explained. Then, if a child does discover the “candy” on a table where they have access to it, they will not recognize it as medication and they’re likely to pop it into their mouth, thinking it is candy.
Lastly, and most importantly, parents who are considering trying a melatonin supplement to help a child sleep better should first establish a stable sleep routine for their child. “They also need to limit caffeinated beverages before bed as well as screen time,” Dr. Toce added.
And they should talk with their primary care provider as to whether or not initiation of a melatonin supplement is appropriate for their child – “and not just jump right into giving them melatonin without first discussing whether it is appropriate to do so,” Dr. Toce stressed.
Remarkable rise
In a comment on his own experience with melatonin poisoning over recent years, toxicology expert Kevin Osterhoudt, MD, of the University of Pennsylvania, Philadelphia and the Children’s Hospital of Philadelphia, noted that it has been their experience that there has been a remarkable rise in poison center reports of children ingesting melatonin in the recent past. For example, the Poison Control Center at CHOP received nearly 4,000 calls involving melatonin ingestion by children 5 years old or younger in the 5 years between 2017 and 2021 with increasing numbers every year.
“The [current study] supports that our regional observation that this has been a national trend,” Dr. Osterhoudt said. Dr. Osterhoudt agreed with Dr. Toce that good sleep is healthy, and it is very important to develop good sleep habits and a regular bedtime routine in order to do so. “In some situations, melatonin may be useful as a short-term sleep aid and that’s a good discussion to have with your child’s health care provider.”
If parents do decide to give their child a melatonin supplement, they need to keep in mind that melatonin may alter how the body handles other drugs such as those used to treat epilepsy or blood clotting. They also need to know experts are still uncertain about how melatonin affects the body over the long term and whether it is safe for mothers to take during pregnancy.
Dr. Osterhoudt offered his own recommendations for safe melatonin use in the home:
- Discuss planned melatonin use with your health care provider.
- Buy only high-quality supplements by looking for the “USP Verified” mark.
- Insist that manufacturers sell products in child-resistant bottles.
- Periodically inspect the medications in your home and dispose of medications that are no longer being used.
- Program the phone number of your regional poison control center into your phone; poison center experts are available 24/7 to answer questions and concerns about ingestions of melatonin (in the United States the number is 1-800-222-1222).
The study authors and neither Dr. Toce nor Dr. Osterhoudt had any relevant conflicts of interest to declare.
The number of children in the United States who unintentionally ingested melatonin supplements over the past 10 years has skyrocketed to the point where, as of 2021, melatonin ingestions by children accounted for almost 5% of all poisonings reported to poison control centers in the United States, data from the National Poison Data System (NPDS) indicate.
This compared with only 0.6% of melatonin ingestions reported to poison control centers in 2012, the authors added.
“Basically the number of pediatric melatonin ingestions increased 530% from 8,337 in 2012 to 52,563 in 2021 so it’s a 6.3-fold increase from the beginning of the study until the end,” Michael Toce, MD, one of the study authors and attending, pediatric emergency medicine/medical toxicology, Boston Children’s Hospital, said in an interview.
“And I think the biggest driver of this increase is simply that sales of melatonin have increased astronomically so there is just more melatonin at home and studies have shown there is a correlation between the amount of an individual medication in the home and the risk of pediatric exposure – so simply put: The more of a single substance in a home, the greater the chance that a child is going to get into it,” he underscored.
The study was published in the Morbidity and Mortality Weekly Report .
Melatonin ingestions
All cases of single substance melatonin ingestions involving children and adolescents between Jan. 1, 2012, and Dec. 31, 2021, were included in the analysis. During the 10-year study interval, 260,435 pediatric melatonin ingestions were reported to the NPDS. Over 94% of the reported ingestions were unintentional and 99% occurred in the home.
Over 88% of them were managed on-site; most involved young male children aged 5 years and under, and almost 83% of children who ingested melatonin supplements remained asymptomatic. On the other hand, 27,795 patients sought care at a health care facility and close to 15% of them were hospitalized. Among all melatonin ingestions, 1.6% resulted in more serious outcomes; more serious outcomes being defined as a moderate or major effects or death. Five children required mechanical ventilation in order to treat their symptoms and 2 patients died.
The largest number of patients who were hospitalized were adolescents who took melatonin intentionally but the largest increase in the rate of exposure was in young, unintentional patients, as Dr. Toce observed. Interestingly, the largest yearly increase in pediatric melatonin ingestions – almost 38% – coincided with the onset of the COVID-19 pandemic.
“This might be related to increased accessibility of melatonin during the pandemic, as children spent more time at home because of stay-at-home orders and school closures,” the authors speculate. Moreover, sleep disturbances were common during the pandemic, leading to a greater likelihood that parents were buying melatonin and thus exposing children to more melatonin at home.
Taken appropriately and at normal does, melatonin in itself is quite safe, as Dr. Toce stressed. However, “for any substance, the dose makes the poison, so taken in any significant quantity, anything is going to be dangerous.” Moreover, it’s important to appreciate that melatonin, at least in the United States, is regulated as a dietary supplement, not as a pharmaceutical.
“Thus, it doesn’t get the same rigorous testing that something like acetaminophen does by the FDA and that means two things,” Dr. Toce noted. First, if the product says that each gummy contains 3 mg of melatonin, no independent body is verifying whether or not that statement is true so there could be 3 mg of melatonin in each gummy or there could be 10 mg,.
Secondly, because there is no impartial oversight for dietary supplements, there may in fact be no melatonin at all in the product or something else may be added to it that might be harmful. “Just because something is sold over-the-counter does not necessarily mean that it’s safe,” Dr. Toce stressed. To keep children safe from pharmaceuticals and supplements, he recommended several generic poison prevention tips. This advice could be passed on to patients who are parents.
- Keep all pharmaceuticals and supplements preferably locked away so there is less risk of children and adolescents taking products either unintentionally or intentionally
- If parents have no place to lock their products up, put them out of reach, high-up so children cannot easily access them
- Keep the product in the original child-resistant packaging as opposed to taking the pills out of the packaging and putting it in a plastic bag bag. “Certainly we’ve seen that when medications are moved into a non–child-resistant container, ingestions go up,” Dr. Toce warned
- Don’t refer to any medicine or supplement a child might take as “candy.” “A lot of children have difficulty taking medications so some families will say: ‘It’s time for your candy,’ ” Dr. Toce explained. Then, if a child does discover the “candy” on a table where they have access to it, they will not recognize it as medication and they’re likely to pop it into their mouth, thinking it is candy.
Lastly, and most importantly, parents who are considering trying a melatonin supplement to help a child sleep better should first establish a stable sleep routine for their child. “They also need to limit caffeinated beverages before bed as well as screen time,” Dr. Toce added.
And they should talk with their primary care provider as to whether or not initiation of a melatonin supplement is appropriate for their child – “and not just jump right into giving them melatonin without first discussing whether it is appropriate to do so,” Dr. Toce stressed.
Remarkable rise
In a comment on his own experience with melatonin poisoning over recent years, toxicology expert Kevin Osterhoudt, MD, of the University of Pennsylvania, Philadelphia and the Children’s Hospital of Philadelphia, noted that it has been their experience that there has been a remarkable rise in poison center reports of children ingesting melatonin in the recent past. For example, the Poison Control Center at CHOP received nearly 4,000 calls involving melatonin ingestion by children 5 years old or younger in the 5 years between 2017 and 2021 with increasing numbers every year.
“The [current study] supports that our regional observation that this has been a national trend,” Dr. Osterhoudt said. Dr. Osterhoudt agreed with Dr. Toce that good sleep is healthy, and it is very important to develop good sleep habits and a regular bedtime routine in order to do so. “In some situations, melatonin may be useful as a short-term sleep aid and that’s a good discussion to have with your child’s health care provider.”
If parents do decide to give their child a melatonin supplement, they need to keep in mind that melatonin may alter how the body handles other drugs such as those used to treat epilepsy or blood clotting. They also need to know experts are still uncertain about how melatonin affects the body over the long term and whether it is safe for mothers to take during pregnancy.
Dr. Osterhoudt offered his own recommendations for safe melatonin use in the home:
- Discuss planned melatonin use with your health care provider.
- Buy only high-quality supplements by looking for the “USP Verified” mark.
- Insist that manufacturers sell products in child-resistant bottles.
- Periodically inspect the medications in your home and dispose of medications that are no longer being used.
- Program the phone number of your regional poison control center into your phone; poison center experts are available 24/7 to answer questions and concerns about ingestions of melatonin (in the United States the number is 1-800-222-1222).
The study authors and neither Dr. Toce nor Dr. Osterhoudt had any relevant conflicts of interest to declare.
FROM THE MMWR
Study links sleep and objective, subjective cognition
CHARLOTTE, N.C. – , preliminary findings from a pilot study of objective and subjective cognitive measures have shown.
The pilot study underscored the important role of objective sleep measures to better understand discrepancies when patients’ own reports of everyday cognitive function don’t align with objective cognitive profiles, Amy Costa, MA, a graduate student in psychology at the University of Missouri-Columbia, said in reporting the results at the annual meeting of the Associated Professional Sleep Societies.

“Between our previously published paper and these new pilot results, we’re reporting evidence that suggests sleep is playing a role between the objective and subjective cognition relationship,” Ms. Costa said in an interview. “It is possible that these older adults who are sleeping poorly may be worse at understanding how well they’re doing cognitively. That’s really important for doctors. For example, if we can’t diagnose someone with mild cognitive impairment or Alzheimer’s disease or other types of dementia earlier, then we can’t intervene as quickly.”
Sleep efficiency, cognition, and patient complaints
These findings are in agreement with those Ms. Costa and colleagues recently published in the Journal of Clinical Sleep Medicine, she said.
The current pilot study included 35 older adults with an average age of 69 years who had insomnia complaints. They completed one night of home-based polysomnography – specifically with the Sleep Profiler PSG2TM – and a battery of cognitive tests. Their average sleep deficiency was 57%, “indicating potentially pretty severe insomnia,” Ms. Costa said.
“We found that sleep efficiency – that is the percentage of time spent sleeping while in bed – moderated the association between self reports and objective measures of cognitive distractibility,” Ms. Costa said in reporting the results. “In other words, our findings suggest that individuals with lower sleep efficiency who are performing the worst cognitively have the least amount of complaints. Basically, this can be thought of as that they are overestimating their cognitive performance.”
Sleep stage versus working memory and distractibility
The pilot study also focused on how the percentage of lighter-stage sleep, or N1 sleep, moderated the associations between working memory, as measured by Sternberg performance, and memory, distractibility, and blunders measured with the Cognitive Failures Questionnaire.
At the highest percentage of N1 sleep, worse working memory was associated with fewer complaints about memory, distractibility, and blunders, Ms. Costa said.
“The percentage of lighter-stage N1 sleep and sleep efficiency moderated the association between cognitive flexibility and distractibility,” Ms. Costa said. At the lowest percentage of N1 sleep, worse cognitive flexibility was associated with more distractibility, while at the highest percentage of N1 sleep worse cognitive flexibility showed a reverse effect; it was linked to less distractibility. The lowest percentage of sleep efficiency showed an association between worse cognitive flexibility and less distractibility, but the highest percentage of SE showed an association between worse cognitive flexibility and more distractibility.
“So in terms of evaluating their cognitive performance, the worse working memory was associated with more blunder complaints in individuals with the lowest percentage of N1,” she said. “So whenever individuals were spending less time in N1, they were able to better recognized their cognitive ability.”
She added, “Overall, more light and more fragmented sleep moderated the association between worse objective and less cognitive complaints, suggesting that these individuals might be overestimating their cognitive abilities.”
The findings indicate that evaluation of objective sleep should consider objectively measured N1 and sleep efficiency to better understand when subjective cognitive complaints and neurophysiological/objective cognitive profiles don’t align, she said.
Important indicators of cognitive deficits
“Specifically, for an older adult who comes into the clinic with complaints of waking up during the night, low sleep efficiency and more lighter-stage sleep might be really important indicators that they are probably not going to be the best at identifying their cognitive abilities or deficits,” she said.
Future directions for this research include collecting more data and looking at other sleep measures, such as using rapid-eye movement sleep, as potential moderators for the relationship between cognitive outcomes, evaluating sleep architecture more closely, and evaluating outcomes in a longitudinal study, Ms. Costa said.
The importance of objectively measured sleep
“Studies like this one using objectively measured sleep are important because much of the prior literature relied on self-reported sleep measures,” said Brendan P. Lucey, MD, associate professor of neurology and head of the sleep medicine section at Washington University School of Medicine in St. Louis. “This study suggests how objectively measured sleep may mediate discrepancies in objective/subjective cognitive dysfunction. Future studies need to work out if we need to add objective sleep measures when evaluating cognitive complaints in older adults.”

Dr. Lucey, who was not involved in the study, voiced one concern with the pilot study methodology the future research should address: the use of the Sleep Profiler PSG2TM to measure N1 sleep, which, as he noted, records a single-channel electroencephalogram over the forehead. “Scoring N1 sleep relies on attenuation of the alpha rhythm over the occipital region and the Sleep Profiler is not as accurate as in-lab polysomnography for this sleep stage,” he said.
The pilot study received funding from the American Academy of Sleep Medicine Foundation. Ms. Costa and her coauthors have no disclosures. Dr. Lucey disclosed relationships with Merck, Eli Lilly, Eisai, and Beacon Biosignals.
CHARLOTTE, N.C. – , preliminary findings from a pilot study of objective and subjective cognitive measures have shown.
The pilot study underscored the important role of objective sleep measures to better understand discrepancies when patients’ own reports of everyday cognitive function don’t align with objective cognitive profiles, Amy Costa, MA, a graduate student in psychology at the University of Missouri-Columbia, said in reporting the results at the annual meeting of the Associated Professional Sleep Societies.
“Between our previously published paper and these new pilot results, we’re reporting evidence that suggests sleep is playing a role between the objective and subjective cognition relationship,” Ms. Costa said in an interview. “It is possible that these older adults who are sleeping poorly may be worse at understanding how well they’re doing cognitively. That’s really important for doctors. For example, if we can’t diagnose someone with mild cognitive impairment or Alzheimer’s disease or other types of dementia earlier, then we can’t intervene as quickly.”
Sleep efficiency, cognition, and patient complaints
These findings are in agreement with those Ms. Costa and colleagues recently published in the Journal of Clinical Sleep Medicine, she said.
The current pilot study included 35 older adults with an average age of 69 years who had insomnia complaints. They completed one night of home-based polysomnography – specifically with the Sleep Profiler PSG2TM – and a battery of cognitive tests. Their average sleep deficiency was 57%, “indicating potentially pretty severe insomnia,” Ms. Costa said.
“We found that sleep efficiency – that is the percentage of time spent sleeping while in bed – moderated the association between self reports and objective measures of cognitive distractibility,” Ms. Costa said in reporting the results. “In other words, our findings suggest that individuals with lower sleep efficiency who are performing the worst cognitively have the least amount of complaints. Basically, this can be thought of as that they are overestimating their cognitive performance.”
Sleep stage versus working memory and distractibility
The pilot study also focused on how the percentage of lighter-stage sleep, or N1 sleep, moderated the associations between working memory, as measured by Sternberg performance, and memory, distractibility, and blunders measured with the Cognitive Failures Questionnaire.
At the highest percentage of N1 sleep, worse working memory was associated with fewer complaints about memory, distractibility, and blunders, Ms. Costa said.
“The percentage of lighter-stage N1 sleep and sleep efficiency moderated the association between cognitive flexibility and distractibility,” Ms. Costa said. At the lowest percentage of N1 sleep, worse cognitive flexibility was associated with more distractibility, while at the highest percentage of N1 sleep worse cognitive flexibility showed a reverse effect; it was linked to less distractibility. The lowest percentage of sleep efficiency showed an association between worse cognitive flexibility and less distractibility, but the highest percentage of SE showed an association between worse cognitive flexibility and more distractibility.
“So in terms of evaluating their cognitive performance, the worse working memory was associated with more blunder complaints in individuals with the lowest percentage of N1,” she said. “So whenever individuals were spending less time in N1, they were able to better recognized their cognitive ability.”
She added, “Overall, more light and more fragmented sleep moderated the association between worse objective and less cognitive complaints, suggesting that these individuals might be overestimating their cognitive abilities.”
The findings indicate that evaluation of objective sleep should consider objectively measured N1 and sleep efficiency to better understand when subjective cognitive complaints and neurophysiological/objective cognitive profiles don’t align, she said.
Important indicators of cognitive deficits
“Specifically, for an older adult who comes into the clinic with complaints of waking up during the night, low sleep efficiency and more lighter-stage sleep might be really important indicators that they are probably not going to be the best at identifying their cognitive abilities or deficits,” she said.
Future directions for this research include collecting more data and looking at other sleep measures, such as using rapid-eye movement sleep, as potential moderators for the relationship between cognitive outcomes, evaluating sleep architecture more closely, and evaluating outcomes in a longitudinal study, Ms. Costa said.
The importance of objectively measured sleep
“Studies like this one using objectively measured sleep are important because much of the prior literature relied on self-reported sleep measures,” said Brendan P. Lucey, MD, associate professor of neurology and head of the sleep medicine section at Washington University School of Medicine in St. Louis. “This study suggests how objectively measured sleep may mediate discrepancies in objective/subjective cognitive dysfunction. Future studies need to work out if we need to add objective sleep measures when evaluating cognitive complaints in older adults.”
Dr. Lucey, who was not involved in the study, voiced one concern with the pilot study methodology the future research should address: the use of the Sleep Profiler PSG2TM to measure N1 sleep, which, as he noted, records a single-channel electroencephalogram over the forehead. “Scoring N1 sleep relies on attenuation of the alpha rhythm over the occipital region and the Sleep Profiler is not as accurate as in-lab polysomnography for this sleep stage,” he said.
The pilot study received funding from the American Academy of Sleep Medicine Foundation. Ms. Costa and her coauthors have no disclosures. Dr. Lucey disclosed relationships with Merck, Eli Lilly, Eisai, and Beacon Biosignals.
CHARLOTTE, N.C. – , preliminary findings from a pilot study of objective and subjective cognitive measures have shown.
The pilot study underscored the important role of objective sleep measures to better understand discrepancies when patients’ own reports of everyday cognitive function don’t align with objective cognitive profiles, Amy Costa, MA, a graduate student in psychology at the University of Missouri-Columbia, said in reporting the results at the annual meeting of the Associated Professional Sleep Societies.
“Between our previously published paper and these new pilot results, we’re reporting evidence that suggests sleep is playing a role between the objective and subjective cognition relationship,” Ms. Costa said in an interview. “It is possible that these older adults who are sleeping poorly may be worse at understanding how well they’re doing cognitively. That’s really important for doctors. For example, if we can’t diagnose someone with mild cognitive impairment or Alzheimer’s disease or other types of dementia earlier, then we can’t intervene as quickly.”
Sleep efficiency, cognition, and patient complaints
These findings are in agreement with those Ms. Costa and colleagues recently published in the Journal of Clinical Sleep Medicine, she said.
The current pilot study included 35 older adults with an average age of 69 years who had insomnia complaints. They completed one night of home-based polysomnography – specifically with the Sleep Profiler PSG2TM – and a battery of cognitive tests. Their average sleep deficiency was 57%, “indicating potentially pretty severe insomnia,” Ms. Costa said.
“We found that sleep efficiency – that is the percentage of time spent sleeping while in bed – moderated the association between self reports and objective measures of cognitive distractibility,” Ms. Costa said in reporting the results. “In other words, our findings suggest that individuals with lower sleep efficiency who are performing the worst cognitively have the least amount of complaints. Basically, this can be thought of as that they are overestimating their cognitive performance.”
Sleep stage versus working memory and distractibility
The pilot study also focused on how the percentage of lighter-stage sleep, or N1 sleep, moderated the associations between working memory, as measured by Sternberg performance, and memory, distractibility, and blunders measured with the Cognitive Failures Questionnaire.
At the highest percentage of N1 sleep, worse working memory was associated with fewer complaints about memory, distractibility, and blunders, Ms. Costa said.
“The percentage of lighter-stage N1 sleep and sleep efficiency moderated the association between cognitive flexibility and distractibility,” Ms. Costa said. At the lowest percentage of N1 sleep, worse cognitive flexibility was associated with more distractibility, while at the highest percentage of N1 sleep worse cognitive flexibility showed a reverse effect; it was linked to less distractibility. The lowest percentage of sleep efficiency showed an association between worse cognitive flexibility and less distractibility, but the highest percentage of SE showed an association between worse cognitive flexibility and more distractibility.
“So in terms of evaluating their cognitive performance, the worse working memory was associated with more blunder complaints in individuals with the lowest percentage of N1,” she said. “So whenever individuals were spending less time in N1, they were able to better recognized their cognitive ability.”
She added, “Overall, more light and more fragmented sleep moderated the association between worse objective and less cognitive complaints, suggesting that these individuals might be overestimating their cognitive abilities.”
The findings indicate that evaluation of objective sleep should consider objectively measured N1 and sleep efficiency to better understand when subjective cognitive complaints and neurophysiological/objective cognitive profiles don’t align, she said.
Important indicators of cognitive deficits
“Specifically, for an older adult who comes into the clinic with complaints of waking up during the night, low sleep efficiency and more lighter-stage sleep might be really important indicators that they are probably not going to be the best at identifying their cognitive abilities or deficits,” she said.
Future directions for this research include collecting more data and looking at other sleep measures, such as using rapid-eye movement sleep, as potential moderators for the relationship between cognitive outcomes, evaluating sleep architecture more closely, and evaluating outcomes in a longitudinal study, Ms. Costa said.
The importance of objectively measured sleep
“Studies like this one using objectively measured sleep are important because much of the prior literature relied on self-reported sleep measures,” said Brendan P. Lucey, MD, associate professor of neurology and head of the sleep medicine section at Washington University School of Medicine in St. Louis. “This study suggests how objectively measured sleep may mediate discrepancies in objective/subjective cognitive dysfunction. Future studies need to work out if we need to add objective sleep measures when evaluating cognitive complaints in older adults.”
Dr. Lucey, who was not involved in the study, voiced one concern with the pilot study methodology the future research should address: the use of the Sleep Profiler PSG2TM to measure N1 sleep, which, as he noted, records a single-channel electroencephalogram over the forehead. “Scoring N1 sleep relies on attenuation of the alpha rhythm over the occipital region and the Sleep Profiler is not as accurate as in-lab polysomnography for this sleep stage,” he said.
The pilot study received funding from the American Academy of Sleep Medicine Foundation. Ms. Costa and her coauthors have no disclosures. Dr. Lucey disclosed relationships with Merck, Eli Lilly, Eisai, and Beacon Biosignals.
AT SLEEP 2022
Children with autism experience more severe sleep apnea
Symptoms of obstructive sleep apnea (OSA) were significantly more common in children with autism spectrum disorder (ASD), compared with controls, based on data from 166 individuals up to age 18 years.
Autism spectrum disorder affects approximately 1 in 54 children in the United States, and recent studies have shown an increased risk of obstructive sleep apnea in this population, compared with the general pediatric population, wrote Pooja Santapuram, MD, of Vanderbilt University, Nashville, Tenn., and colleagues.
In a study published in the International Journal of Pediatric Ototrhinolaryngology , the researchers reviewed data from 166 children and adolescents up to 18 years of age with OSA who underwent adenotonsillectomy at a single center between 2019 and 2021. The primary objective was to assess OSA symptoms in children with and without ASD. The study population included 75 children with ASD and 91 controls. The average age of both the ASD group and control group was approximately 73 months.
OSA meets ASD
Obstructive sleep apnea is common in autism spectrum disorder. Children with OSA can present with a range of symptoms, including loud snoring, excessive daytime sleepiness, and changes in cognitive function. Some of these symptoms can overlap with and exacerbate symptoms of ASD, potentially delaying OSA diagnosis in children with both conditions. The primary objective of this study was to assess between-group difference in OSA symptomatology and age at OSA diagnosis in children with and without ASD. To do so, a retrospective chart review was conducted on the 166 pediatric patients.
Overall, significantly more OSA symptoms were reported in children with ASD, compared with controls (P < .001).
Lower autism severity was associated with an increased number of reported OSA symptoms (P = .006). There was not a significant between-group difference in age at OSA diagnosis (P = .999); however, lower autism severity was also associated with an increased age at diagnosis (P = .002). These findings suggest that OSA may present with a higher symptom burden in children with ASD, and children with lower ASD severity often experience delays in OSA diagnosis.
Interestingly, despite the known associations between obesity and OSA, children with an increased body mass index were not diagnosed with OSA at an earlier age in this sample population, the researchers indicated.
Because the current study revealed that children with less severe ASD are more likely to report an increased number of OSA symptoms and be diagnosed at a later age than children without ASD, clinicians should have a heightened sense for OSA evaluation in children with ASD, particularly in children with a lower severity of ASD and an increased BMI, the researchers concluded.
The research study was not externally funded, and the researchers reported that they had no conflicts of interest.
Symptoms of obstructive sleep apnea (OSA) were significantly more common in children with autism spectrum disorder (ASD), compared with controls, based on data from 166 individuals up to age 18 years.
Autism spectrum disorder affects approximately 1 in 54 children in the United States, and recent studies have shown an increased risk of obstructive sleep apnea in this population, compared with the general pediatric population, wrote Pooja Santapuram, MD, of Vanderbilt University, Nashville, Tenn., and colleagues.
In a study published in the International Journal of Pediatric Ototrhinolaryngology , the researchers reviewed data from 166 children and adolescents up to 18 years of age with OSA who underwent adenotonsillectomy at a single center between 2019 and 2021. The primary objective was to assess OSA symptoms in children with and without ASD. The study population included 75 children with ASD and 91 controls. The average age of both the ASD group and control group was approximately 73 months.
OSA meets ASD
Obstructive sleep apnea is common in autism spectrum disorder. Children with OSA can present with a range of symptoms, including loud snoring, excessive daytime sleepiness, and changes in cognitive function. Some of these symptoms can overlap with and exacerbate symptoms of ASD, potentially delaying OSA diagnosis in children with both conditions. The primary objective of this study was to assess between-group difference in OSA symptomatology and age at OSA diagnosis in children with and without ASD. To do so, a retrospective chart review was conducted on the 166 pediatric patients.
Overall, significantly more OSA symptoms were reported in children with ASD, compared with controls (P < .001).
Lower autism severity was associated with an increased number of reported OSA symptoms (P = .006). There was not a significant between-group difference in age at OSA diagnosis (P = .999); however, lower autism severity was also associated with an increased age at diagnosis (P = .002). These findings suggest that OSA may present with a higher symptom burden in children with ASD, and children with lower ASD severity often experience delays in OSA diagnosis.
Interestingly, despite the known associations between obesity and OSA, children with an increased body mass index were not diagnosed with OSA at an earlier age in this sample population, the researchers indicated.
Because the current study revealed that children with less severe ASD are more likely to report an increased number of OSA symptoms and be diagnosed at a later age than children without ASD, clinicians should have a heightened sense for OSA evaluation in children with ASD, particularly in children with a lower severity of ASD and an increased BMI, the researchers concluded.
The research study was not externally funded, and the researchers reported that they had no conflicts of interest.
Symptoms of obstructive sleep apnea (OSA) were significantly more common in children with autism spectrum disorder (ASD), compared with controls, based on data from 166 individuals up to age 18 years.
Autism spectrum disorder affects approximately 1 in 54 children in the United States, and recent studies have shown an increased risk of obstructive sleep apnea in this population, compared with the general pediatric population, wrote Pooja Santapuram, MD, of Vanderbilt University, Nashville, Tenn., and colleagues.
In a study published in the International Journal of Pediatric Ototrhinolaryngology , the researchers reviewed data from 166 children and adolescents up to 18 years of age with OSA who underwent adenotonsillectomy at a single center between 2019 and 2021. The primary objective was to assess OSA symptoms in children with and without ASD. The study population included 75 children with ASD and 91 controls. The average age of both the ASD group and control group was approximately 73 months.
OSA meets ASD
Obstructive sleep apnea is common in autism spectrum disorder. Children with OSA can present with a range of symptoms, including loud snoring, excessive daytime sleepiness, and changes in cognitive function. Some of these symptoms can overlap with and exacerbate symptoms of ASD, potentially delaying OSA diagnosis in children with both conditions. The primary objective of this study was to assess between-group difference in OSA symptomatology and age at OSA diagnosis in children with and without ASD. To do so, a retrospective chart review was conducted on the 166 pediatric patients.
Overall, significantly more OSA symptoms were reported in children with ASD, compared with controls (P < .001).
Lower autism severity was associated with an increased number of reported OSA symptoms (P = .006). There was not a significant between-group difference in age at OSA diagnosis (P = .999); however, lower autism severity was also associated with an increased age at diagnosis (P = .002). These findings suggest that OSA may present with a higher symptom burden in children with ASD, and children with lower ASD severity often experience delays in OSA diagnosis.
Interestingly, despite the known associations between obesity and OSA, children with an increased body mass index were not diagnosed with OSA at an earlier age in this sample population, the researchers indicated.
Because the current study revealed that children with less severe ASD are more likely to report an increased number of OSA symptoms and be diagnosed at a later age than children without ASD, clinicians should have a heightened sense for OSA evaluation in children with ASD, particularly in children with a lower severity of ASD and an increased BMI, the researchers concluded.
The research study was not externally funded, and the researchers reported that they had no conflicts of interest.
FROM THE INTERNATIONAL JOURNAL OF PEDIATRIC OTORHINOLARYNGOLOGY
Longer circadian rhythms linked to severe depression in teens
, according to results from a European study.
A range of psychiatric symptoms and conditions has been linked to sleep pathologies, wrote Liisa Kuula, PhD, of the University of Helsinki, Finland, and colleagues. Some research suggests that late circadian rhythms and irregular sleep patterns increase the risk for psychiatric conditions, but the association has not been well studied, especially in adolescents, although the onset of psychiatric problems often occurs at this age, they said.

In a study published in the Journal of Psychiatric Research (2022 Apr 4. doi: 10.1016/j.jpsychires.2022.03.056.), the investigators reviewed data from 342 adolescents who were part of SleepHelsinki! a large cohort study of delayed sleep phase disorder (DSPD) in adolescents. The mean age of the participants was 17.4 years, and 70% were female.
The participants completed the Mini International Neuropsychiatric Interview (MINI) and wore temperature loggers for 3 days to assess circadian rhythms. The primary outcome was the impact of circadian dynamics on different psychiatric problems. Delayed Sleep Phase (DSP) behavior was defined as going to sleep later than 1 a.m. at least three times a week.
Circadian length was determined through the temperature loggers worn for 3 days. Most participants also completed 1-week GeneActiv Original actigraphy measurements (wearing the actigraph for 1 week) and responded to the Morningness-Eveningness Questionnaire, which divided participants into three circadian preference groups: morning, intermediate, and evening. Sleep duration was calculated as total sleep time, sleep quality was estimated by sleep efficiency, and sleep timing was assessed by the midpoint of the sleep period.
Overall, the MINI interview results suggested that approximately one-third (36%) of the teens had at least one psychiatric problem, and 21% had comorbid conditions.
Severe depression was significantly associated with a longer circadian period (P = .002), while suicidality was significantly associated with a later midpoint and more irregular sleep (P = .007 for both).
Participants with agoraphobia slept longer than did those without, the researchers noted (P = .013). However, sleep duration was not significantly associated with other psychiatric conditions.
Manic episodes and psychotic disorders were associated with irregular sleep timing (P < .018 and P < .017, respectively).
When the researchers examined DSP and circadian preferences, they found that 21.5% of individuals with suicidality had characteristics of DSP, as did 21.5% of those with panic disorder.
Individuals with a preference for eveningness were significantly more likely to meet criteria for severe depression, panic disorder, generalized anxiety disorder, and obsessive-compulsive disorder than were those without a preference for eveningness, the researchers noted.
“Our findings are the first to encompass diverse circadian measures alongside an array of psychiatric symptoms in such a focused age range,” the researchers wrote in their discussion. The data reflect results from other studies and extend the likely role of circadian patterns in mental wellbeing, they said.
The study findings were limited by several factors including the lack of actual diagnoses from medical records and use of self-reported symptoms, the researchers noted. Other limitations included the lack of polysomnography data and small size of subgroups of the study sample.
However, the results were strengthened by the heterogenous study population and use of multiple measures to examine sleep and circadian rhythms, as well as consideration of personal circadian preferences, the researchers said.
“The importance of overall synchronization with environment is perhaps best highlighted by response to treatment: most psychopathologic symptoms benefit from sleep-targeted therapeutic approaches,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
, according to results from a European study.
A range of psychiatric symptoms and conditions has been linked to sleep pathologies, wrote Liisa Kuula, PhD, of the University of Helsinki, Finland, and colleagues. Some research suggests that late circadian rhythms and irregular sleep patterns increase the risk for psychiatric conditions, but the association has not been well studied, especially in adolescents, although the onset of psychiatric problems often occurs at this age, they said.
In a study published in the Journal of Psychiatric Research (2022 Apr 4. doi: 10.1016/j.jpsychires.2022.03.056.), the investigators reviewed data from 342 adolescents who were part of SleepHelsinki! a large cohort study of delayed sleep phase disorder (DSPD) in adolescents. The mean age of the participants was 17.4 years, and 70% were female.
The participants completed the Mini International Neuropsychiatric Interview (MINI) and wore temperature loggers for 3 days to assess circadian rhythms. The primary outcome was the impact of circadian dynamics on different psychiatric problems. Delayed Sleep Phase (DSP) behavior was defined as going to sleep later than 1 a.m. at least three times a week.
Circadian length was determined through the temperature loggers worn for 3 days. Most participants also completed 1-week GeneActiv Original actigraphy measurements (wearing the actigraph for 1 week) and responded to the Morningness-Eveningness Questionnaire, which divided participants into three circadian preference groups: morning, intermediate, and evening. Sleep duration was calculated as total sleep time, sleep quality was estimated by sleep efficiency, and sleep timing was assessed by the midpoint of the sleep period.
Overall, the MINI interview results suggested that approximately one-third (36%) of the teens had at least one psychiatric problem, and 21% had comorbid conditions.
Severe depression was significantly associated with a longer circadian period (P = .002), while suicidality was significantly associated with a later midpoint and more irregular sleep (P = .007 for both).
Participants with agoraphobia slept longer than did those without, the researchers noted (P = .013). However, sleep duration was not significantly associated with other psychiatric conditions.
Manic episodes and psychotic disorders were associated with irregular sleep timing (P < .018 and P < .017, respectively).
When the researchers examined DSP and circadian preferences, they found that 21.5% of individuals with suicidality had characteristics of DSP, as did 21.5% of those with panic disorder.
Individuals with a preference for eveningness were significantly more likely to meet criteria for severe depression, panic disorder, generalized anxiety disorder, and obsessive-compulsive disorder than were those without a preference for eveningness, the researchers noted.
“Our findings are the first to encompass diverse circadian measures alongside an array of psychiatric symptoms in such a focused age range,” the researchers wrote in their discussion. The data reflect results from other studies and extend the likely role of circadian patterns in mental wellbeing, they said.
The study findings were limited by several factors including the lack of actual diagnoses from medical records and use of self-reported symptoms, the researchers noted. Other limitations included the lack of polysomnography data and small size of subgroups of the study sample.
However, the results were strengthened by the heterogenous study population and use of multiple measures to examine sleep and circadian rhythms, as well as consideration of personal circadian preferences, the researchers said.
“The importance of overall synchronization with environment is perhaps best highlighted by response to treatment: most psychopathologic symptoms benefit from sleep-targeted therapeutic approaches,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
, according to results from a European study.
A range of psychiatric symptoms and conditions has been linked to sleep pathologies, wrote Liisa Kuula, PhD, of the University of Helsinki, Finland, and colleagues. Some research suggests that late circadian rhythms and irregular sleep patterns increase the risk for psychiatric conditions, but the association has not been well studied, especially in adolescents, although the onset of psychiatric problems often occurs at this age, they said.
In a study published in the Journal of Psychiatric Research (2022 Apr 4. doi: 10.1016/j.jpsychires.2022.03.056.), the investigators reviewed data from 342 adolescents who were part of SleepHelsinki! a large cohort study of delayed sleep phase disorder (DSPD) in adolescents. The mean age of the participants was 17.4 years, and 70% were female.
The participants completed the Mini International Neuropsychiatric Interview (MINI) and wore temperature loggers for 3 days to assess circadian rhythms. The primary outcome was the impact of circadian dynamics on different psychiatric problems. Delayed Sleep Phase (DSP) behavior was defined as going to sleep later than 1 a.m. at least three times a week.
Circadian length was determined through the temperature loggers worn for 3 days. Most participants also completed 1-week GeneActiv Original actigraphy measurements (wearing the actigraph for 1 week) and responded to the Morningness-Eveningness Questionnaire, which divided participants into three circadian preference groups: morning, intermediate, and evening. Sleep duration was calculated as total sleep time, sleep quality was estimated by sleep efficiency, and sleep timing was assessed by the midpoint of the sleep period.
Overall, the MINI interview results suggested that approximately one-third (36%) of the teens had at least one psychiatric problem, and 21% had comorbid conditions.
Severe depression was significantly associated with a longer circadian period (P = .002), while suicidality was significantly associated with a later midpoint and more irregular sleep (P = .007 for both).
Participants with agoraphobia slept longer than did those without, the researchers noted (P = .013). However, sleep duration was not significantly associated with other psychiatric conditions.
Manic episodes and psychotic disorders were associated with irregular sleep timing (P < .018 and P < .017, respectively).
When the researchers examined DSP and circadian preferences, they found that 21.5% of individuals with suicidality had characteristics of DSP, as did 21.5% of those with panic disorder.
Individuals with a preference for eveningness were significantly more likely to meet criteria for severe depression, panic disorder, generalized anxiety disorder, and obsessive-compulsive disorder than were those without a preference for eveningness, the researchers noted.
“Our findings are the first to encompass diverse circadian measures alongside an array of psychiatric symptoms in such a focused age range,” the researchers wrote in their discussion. The data reflect results from other studies and extend the likely role of circadian patterns in mental wellbeing, they said.
The study findings were limited by several factors including the lack of actual diagnoses from medical records and use of self-reported symptoms, the researchers noted. Other limitations included the lack of polysomnography data and small size of subgroups of the study sample.
However, the results were strengthened by the heterogenous study population and use of multiple measures to examine sleep and circadian rhythms, as well as consideration of personal circadian preferences, the researchers said.
“The importance of overall synchronization with environment is perhaps best highlighted by response to treatment: most psychopathologic symptoms benefit from sleep-targeted therapeutic approaches,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF PSYCHIATRIC RESEARCH