User login
Preclinical findings highlight value of Lynch syndrome for cancer vaccine development
ATLANTA – Lynch syndrome serves as an excellent platform for the development of immunoprevention cancer vaccines, and findings from a preclinical Lynch syndrome mouse model support ongoing research, according to Steven M. Lipkin, MD, PhD.
A novel vaccine, which included peptides encoding four intestinal cancer frameshift peptide (FSP) neoantigens derived from coding microsatellite (cMS) mutations in the genes Nacad, Maz, Xirp1, and Senp6 elicited strong antigen-specific cellular immune responses in the model, Dr. Lipkin, the Gladys and Roland Harriman Professor of Medicine and vice chair for research in the Sanford and Joan Weill Department of Medicine, Weill Cornell Medical College, New York, reported at the annual meeting of the American Association for Cancer Research.
CD4-specific T cell responses were detected for Maz, Nacad, and Senp6, and CD8-positive T cells were detected for Xirp1 and Nacad, he noted, explaining that the findings come in the wake of a recently completed clinical phase 1/2a trial that successfully demonstrated safety and immunogenicity of an FSP neoantigen-based vaccine in microsatellite unstable (MSI) colorectal cancer patients.
The current effort to further develop a cancer preventive vaccine against MSI cancers in Lynch syndrome using a preclinical mouse model involved a systematic database search to identify cMS sequences in the murine genome. Intestinal tumors obtained from Lynch syndrome mice were evaluated for mutations affecting these candidate cMS, and of 13 with a mutation frequency of 15% or higher, the 4 FSP neoantigens ultimately included in the vaccine elicited strong antigen-specific cellular immune responses.
Vaccination with peptides encoding these four intestinal cancer FSP neoantigens promoted antineoantigen immunity, reduced intestinal tumorigenicity, and prolonged overall survival, Dr. Lipkin said.
Further, based on preclinical data suggesting that naproxen in this setting might provide better risk-reducing effects, compared with aspirin (which has previously been shown to reduce colorectal cancer risk in Lynch syndrome patients), its addition to the vaccine did, indeed, improve response, he noted, explaining that naproxen worked as “sort of a super-aspirin,” that improved overall survival, compared with vaccine alone or nonsteroidal anti-inflammatory agents alone.
In a video interview, Dr. Lipkin describes his research and its potential implications for the immunoprevention of Lynch syndrome and other cancers.
Vaccination with as few as four mutations that occur across Lynch syndrome tumors induced complete cures in some mice and delays in disease onset in others, he said.
“[This is] a very simple approach, very effective,” he added, noting that the T cells are now being studied to better understand the biology of the effects. “The idea of immunoprevention ... is actually very exciting and ... can be expanded beyond this.”
Lynch syndrome is a “great place to start,” because of the high rate of mutations, which are the most immunogenic types of mutations, he said.
“If we can get this basic paradigm to work, I think we can expand it to other types of mutations – for example, KRAS or BRAF, which are seen frequently in lung cancers, colon cancers, stomach cancers, pancreatic cancers, and others,” he said, noting that a proposal for a phase 1 clinical trial has been submitted.
ATLANTA – Lynch syndrome serves as an excellent platform for the development of immunoprevention cancer vaccines, and findings from a preclinical Lynch syndrome mouse model support ongoing research, according to Steven M. Lipkin, MD, PhD.
A novel vaccine, which included peptides encoding four intestinal cancer frameshift peptide (FSP) neoantigens derived from coding microsatellite (cMS) mutations in the genes Nacad, Maz, Xirp1, and Senp6 elicited strong antigen-specific cellular immune responses in the model, Dr. Lipkin, the Gladys and Roland Harriman Professor of Medicine and vice chair for research in the Sanford and Joan Weill Department of Medicine, Weill Cornell Medical College, New York, reported at the annual meeting of the American Association for Cancer Research.
CD4-specific T cell responses were detected for Maz, Nacad, and Senp6, and CD8-positive T cells were detected for Xirp1 and Nacad, he noted, explaining that the findings come in the wake of a recently completed clinical phase 1/2a trial that successfully demonstrated safety and immunogenicity of an FSP neoantigen-based vaccine in microsatellite unstable (MSI) colorectal cancer patients.
The current effort to further develop a cancer preventive vaccine against MSI cancers in Lynch syndrome using a preclinical mouse model involved a systematic database search to identify cMS sequences in the murine genome. Intestinal tumors obtained from Lynch syndrome mice were evaluated for mutations affecting these candidate cMS, and of 13 with a mutation frequency of 15% or higher, the 4 FSP neoantigens ultimately included in the vaccine elicited strong antigen-specific cellular immune responses.
Vaccination with peptides encoding these four intestinal cancer FSP neoantigens promoted antineoantigen immunity, reduced intestinal tumorigenicity, and prolonged overall survival, Dr. Lipkin said.
Further, based on preclinical data suggesting that naproxen in this setting might provide better risk-reducing effects, compared with aspirin (which has previously been shown to reduce colorectal cancer risk in Lynch syndrome patients), its addition to the vaccine did, indeed, improve response, he noted, explaining that naproxen worked as “sort of a super-aspirin,” that improved overall survival, compared with vaccine alone or nonsteroidal anti-inflammatory agents alone.
In a video interview, Dr. Lipkin describes his research and its potential implications for the immunoprevention of Lynch syndrome and other cancers.
Vaccination with as few as four mutations that occur across Lynch syndrome tumors induced complete cures in some mice and delays in disease onset in others, he said.
“[This is] a very simple approach, very effective,” he added, noting that the T cells are now being studied to better understand the biology of the effects. “The idea of immunoprevention ... is actually very exciting and ... can be expanded beyond this.”
Lynch syndrome is a “great place to start,” because of the high rate of mutations, which are the most immunogenic types of mutations, he said.
“If we can get this basic paradigm to work, I think we can expand it to other types of mutations – for example, KRAS or BRAF, which are seen frequently in lung cancers, colon cancers, stomach cancers, pancreatic cancers, and others,” he said, noting that a proposal for a phase 1 clinical trial has been submitted.
ATLANTA – Lynch syndrome serves as an excellent platform for the development of immunoprevention cancer vaccines, and findings from a preclinical Lynch syndrome mouse model support ongoing research, according to Steven M. Lipkin, MD, PhD.
A novel vaccine, which included peptides encoding four intestinal cancer frameshift peptide (FSP) neoantigens derived from coding microsatellite (cMS) mutations in the genes Nacad, Maz, Xirp1, and Senp6 elicited strong antigen-specific cellular immune responses in the model, Dr. Lipkin, the Gladys and Roland Harriman Professor of Medicine and vice chair for research in the Sanford and Joan Weill Department of Medicine, Weill Cornell Medical College, New York, reported at the annual meeting of the American Association for Cancer Research.
CD4-specific T cell responses were detected for Maz, Nacad, and Senp6, and CD8-positive T cells were detected for Xirp1 and Nacad, he noted, explaining that the findings come in the wake of a recently completed clinical phase 1/2a trial that successfully demonstrated safety and immunogenicity of an FSP neoantigen-based vaccine in microsatellite unstable (MSI) colorectal cancer patients.
The current effort to further develop a cancer preventive vaccine against MSI cancers in Lynch syndrome using a preclinical mouse model involved a systematic database search to identify cMS sequences in the murine genome. Intestinal tumors obtained from Lynch syndrome mice were evaluated for mutations affecting these candidate cMS, and of 13 with a mutation frequency of 15% or higher, the 4 FSP neoantigens ultimately included in the vaccine elicited strong antigen-specific cellular immune responses.
Vaccination with peptides encoding these four intestinal cancer FSP neoantigens promoted antineoantigen immunity, reduced intestinal tumorigenicity, and prolonged overall survival, Dr. Lipkin said.
Further, based on preclinical data suggesting that naproxen in this setting might provide better risk-reducing effects, compared with aspirin (which has previously been shown to reduce colorectal cancer risk in Lynch syndrome patients), its addition to the vaccine did, indeed, improve response, he noted, explaining that naproxen worked as “sort of a super-aspirin,” that improved overall survival, compared with vaccine alone or nonsteroidal anti-inflammatory agents alone.
In a video interview, Dr. Lipkin describes his research and its potential implications for the immunoprevention of Lynch syndrome and other cancers.
Vaccination with as few as four mutations that occur across Lynch syndrome tumors induced complete cures in some mice and delays in disease onset in others, he said.
“[This is] a very simple approach, very effective,” he added, noting that the T cells are now being studied to better understand the biology of the effects. “The idea of immunoprevention ... is actually very exciting and ... can be expanded beyond this.”
Lynch syndrome is a “great place to start,” because of the high rate of mutations, which are the most immunogenic types of mutations, he said.
“If we can get this basic paradigm to work, I think we can expand it to other types of mutations – for example, KRAS or BRAF, which are seen frequently in lung cancers, colon cancers, stomach cancers, pancreatic cancers, and others,” he said, noting that a proposal for a phase 1 clinical trial has been submitted.
REPORTING FROM AACR 2019
Direct-to-consumer telemedicine visits may lead to pediatric antibiotic overprescribing
(ARIs), according to a study of antibiotic prescriptions for ARIs across 3 clinical settings.
“These differences in antibiotic prescribing for children contrast with previous studies of DTC telemedicine quality among adult patients in which quality differences have been smaller or nonexistent,” wrote Kristin N. Ray, MD, of Children’s Hospital of Pittsburgh, and her coauthors. The study was published in Pediatrics.
To determine quality of care during pediatric DTC telemedicine visits, the researchers embarked on a retrospective cohort study using 2015–2016 claims data from a large national commercial health plan. They identified visits for ARIs and matched them across 3 settings: DTC telemedicine, urgent care, and PCP offices. The matched sample included 4,604 DTC telemedicine visits, 38,408 urgent care visits, and 485,201 PCP visits.
Their analysis showed that children were more likely to be prescribed antibiotics at DTC telemedicine visits than in other settings (52% versus 42% for urgent care and 31% for PCP, P less than .001). In addition, they were less likely to receive guideline-concordant antibiotic management (59% versus 67% and 78%, P less than .001). This was primarily attributed to “antibiotic prescribing for visits with viral ARI diagnoses that do not warrant antibiotics,” antibiotics were appropriately not prescribed in only 54% of those DTC telemedicine visits, compared with 66% for urgent care and 80% for PCP (P less than .001).
The authors shared the limitations of their study, including a lack of sociodemographic or clinical data stemming from a reliance on insurance claims. They also noted that their analysis was limited to a specific health plan and its contracted DTC telemedicine vendor, recognizing that “antibiotic prescribing among other DTC telemedicine companies, models, and populations may differ.”
The study was funded by the National Institutes of Health and supported in part by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and gifts from Melvin Hall. The authors reported no conflicts of interest.
SOURCE: Ray KN et al. Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2018-2491.
These findings from this study illustrate the issues with direct-to-consumer (DTC) telemedicine, especially when treating children, according to Jeffrey S. Gerber, MD, medical director of the antimicrobial stewardship program at Children’s Hospital of Philadelphia.
The best way to get a 5-star rating after a DTC telemedicine visit is to prescribe an antibiotic, Dr. Gerber wrote, so it shouldn’t be surprising that doctors are handing them out at a higher rate than after an urgent care or a primary care visit. It should also be noted that this study covers a very specific privately insured population and that DTC telemedicine remains a “small piece of the pie,” for now, in terms of patient care.
But, he added, the most problematic element of this study may be that none of the 3 most common pediatric acute respiratory tract infection (ARTI) diagnoses should be followed with an immediate prescription, especially after a virtual visit.
“It could be argued that essentially no ARTI encounters should lead to antibiotic prescriptions solely on the basis of a DTC telemedicine visit,” he wrote, recognizing that – though there may be value for telemedicine in a screening capacity – the DTC version seems to be a “low quality encounter” at best and “a vehicle for antibiotic overuse” at worst.
These comments are adapted from an accompanying editorial (Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2019-0631 ). Dr. Gerber reported receiving personal fees from Medtronic outside the submitted work.
These findings from this study illustrate the issues with direct-to-consumer (DTC) telemedicine, especially when treating children, according to Jeffrey S. Gerber, MD, medical director of the antimicrobial stewardship program at Children’s Hospital of Philadelphia.
The best way to get a 5-star rating after a DTC telemedicine visit is to prescribe an antibiotic, Dr. Gerber wrote, so it shouldn’t be surprising that doctors are handing them out at a higher rate than after an urgent care or a primary care visit. It should also be noted that this study covers a very specific privately insured population and that DTC telemedicine remains a “small piece of the pie,” for now, in terms of patient care.
But, he added, the most problematic element of this study may be that none of the 3 most common pediatric acute respiratory tract infection (ARTI) diagnoses should be followed with an immediate prescription, especially after a virtual visit.
“It could be argued that essentially no ARTI encounters should lead to antibiotic prescriptions solely on the basis of a DTC telemedicine visit,” he wrote, recognizing that – though there may be value for telemedicine in a screening capacity – the DTC version seems to be a “low quality encounter” at best and “a vehicle for antibiotic overuse” at worst.
These comments are adapted from an accompanying editorial (Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2019-0631 ). Dr. Gerber reported receiving personal fees from Medtronic outside the submitted work.
These findings from this study illustrate the issues with direct-to-consumer (DTC) telemedicine, especially when treating children, according to Jeffrey S. Gerber, MD, medical director of the antimicrobial stewardship program at Children’s Hospital of Philadelphia.
The best way to get a 5-star rating after a DTC telemedicine visit is to prescribe an antibiotic, Dr. Gerber wrote, so it shouldn’t be surprising that doctors are handing them out at a higher rate than after an urgent care or a primary care visit. It should also be noted that this study covers a very specific privately insured population and that DTC telemedicine remains a “small piece of the pie,” for now, in terms of patient care.
But, he added, the most problematic element of this study may be that none of the 3 most common pediatric acute respiratory tract infection (ARTI) diagnoses should be followed with an immediate prescription, especially after a virtual visit.
“It could be argued that essentially no ARTI encounters should lead to antibiotic prescriptions solely on the basis of a DTC telemedicine visit,” he wrote, recognizing that – though there may be value for telemedicine in a screening capacity – the DTC version seems to be a “low quality encounter” at best and “a vehicle for antibiotic overuse” at worst.
These comments are adapted from an accompanying editorial (Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2019-0631 ). Dr. Gerber reported receiving personal fees from Medtronic outside the submitted work.
(ARIs), according to a study of antibiotic prescriptions for ARIs across 3 clinical settings.
“These differences in antibiotic prescribing for children contrast with previous studies of DTC telemedicine quality among adult patients in which quality differences have been smaller or nonexistent,” wrote Kristin N. Ray, MD, of Children’s Hospital of Pittsburgh, and her coauthors. The study was published in Pediatrics.
To determine quality of care during pediatric DTC telemedicine visits, the researchers embarked on a retrospective cohort study using 2015–2016 claims data from a large national commercial health plan. They identified visits for ARIs and matched them across 3 settings: DTC telemedicine, urgent care, and PCP offices. The matched sample included 4,604 DTC telemedicine visits, 38,408 urgent care visits, and 485,201 PCP visits.
Their analysis showed that children were more likely to be prescribed antibiotics at DTC telemedicine visits than in other settings (52% versus 42% for urgent care and 31% for PCP, P less than .001). In addition, they were less likely to receive guideline-concordant antibiotic management (59% versus 67% and 78%, P less than .001). This was primarily attributed to “antibiotic prescribing for visits with viral ARI diagnoses that do not warrant antibiotics,” antibiotics were appropriately not prescribed in only 54% of those DTC telemedicine visits, compared with 66% for urgent care and 80% for PCP (P less than .001).
The authors shared the limitations of their study, including a lack of sociodemographic or clinical data stemming from a reliance on insurance claims. They also noted that their analysis was limited to a specific health plan and its contracted DTC telemedicine vendor, recognizing that “antibiotic prescribing among other DTC telemedicine companies, models, and populations may differ.”
The study was funded by the National Institutes of Health and supported in part by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and gifts from Melvin Hall. The authors reported no conflicts of interest.
SOURCE: Ray KN et al. Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2018-2491.
(ARIs), according to a study of antibiotic prescriptions for ARIs across 3 clinical settings.
“These differences in antibiotic prescribing for children contrast with previous studies of DTC telemedicine quality among adult patients in which quality differences have been smaller or nonexistent,” wrote Kristin N. Ray, MD, of Children’s Hospital of Pittsburgh, and her coauthors. The study was published in Pediatrics.
To determine quality of care during pediatric DTC telemedicine visits, the researchers embarked on a retrospective cohort study using 2015–2016 claims data from a large national commercial health plan. They identified visits for ARIs and matched them across 3 settings: DTC telemedicine, urgent care, and PCP offices. The matched sample included 4,604 DTC telemedicine visits, 38,408 urgent care visits, and 485,201 PCP visits.
Their analysis showed that children were more likely to be prescribed antibiotics at DTC telemedicine visits than in other settings (52% versus 42% for urgent care and 31% for PCP, P less than .001). In addition, they were less likely to receive guideline-concordant antibiotic management (59% versus 67% and 78%, P less than .001). This was primarily attributed to “antibiotic prescribing for visits with viral ARI diagnoses that do not warrant antibiotics,” antibiotics were appropriately not prescribed in only 54% of those DTC telemedicine visits, compared with 66% for urgent care and 80% for PCP (P less than .001).
The authors shared the limitations of their study, including a lack of sociodemographic or clinical data stemming from a reliance on insurance claims. They also noted that their analysis was limited to a specific health plan and its contracted DTC telemedicine vendor, recognizing that “antibiotic prescribing among other DTC telemedicine companies, models, and populations may differ.”
The study was funded by the National Institutes of Health and supported in part by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and gifts from Melvin Hall. The authors reported no conflicts of interest.
SOURCE: Ray KN et al. Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2018-2491.
FROM PEDIATRICS
Key clinical point: For children diagnosed with acute respiratory infections, antibiotic prescribing was higher and guideline-concordant antibiotic management was lower at direct-to-consumer (DTC) telemedicine visits.
Major finding: Children at DTC telemedicine visits were prescribed antibiotics for respiratory infections 52% of the time, compared with 42% at urgent care visits and 31% at primary care provider visits.
Study details: A retrospective cohort study of DTC telemedicine, urgent care, and primary care provider visits for acute respiratory infections and subsequent antibiotic prescriptions.
Disclosures: The study was funded by the National Institutes of Health and supported in part by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and gifts from Melvin Hall. The authors reported no conflicts of interest.
Source: Ray KN et al. Pediatrics. 2019 Apr 8. doi: 10.1542/peds.2018-2491.
Oscillatory ventilation reduced reintubation risk for preterm infants
Nasal high-frequency oscillatory ventilation, in a randomized trial of 206 preterm infants with respiratory failure.
Previous studies have supported the use of NHFOV as more effective for reducing CO2 and for lowering the risk of reintubation compared with NCPAP. But no randomized, controlled trials had compared the outcomes for preterm infants in particular, wrote Long Chen, MD, PhD, of Children’s Hospital of Chongqing Medical University, Chongqing, China, and colleagues.
Their study, published in Chest, was conducted at a single tertiary NICU in China between May 2017 and May 2018, and randomized infants with a gestational age less than 37 weeks to NHFOV (103 infants) or NCPAP (103 infants). Infants with major congenital abnormalities were excluded. The infants included 127 (61.7%) diagnosed with respiratory distress syndrome (RDS), 53 (25.7%) diagnosed with acute RDS (ARDS), and 26 (12.6%) diagnosed with both RDS and ARDS.
Overall, the reintubation rate within 6 hours was significantly lower among infants treated with NHFOV compared with those treated with NCPAP (15.5% vs. 34%, P = .002), and in the subset of infants with ARDS (23.5% vs. 52.6%, P = .032). Among infants with a gestational age of 32 weeks or less, reintuibation rates were also significantly lower among those treated with NHFOV (26.1% vs. 55.6%, P = .004).
In addition, PCO2 levels, 6 hours after extubation, were significantly lower among infants on NHFOV, compared with those on NCPAP (49.6 vs. 56.9 P = .00). The hospital stay, a secondary outcome, was significantly shorter among the infants treated with NHFOV, than those treated with NCPAP (22 days, vs. 27.6 days, P =.011).
Although the researchers observed some nasal trauma in NHFOV-treated patients, and intestinal dilation in both groups similar to side effects seen in previous studies, no feeding intolerance or skin lesions were associated with NHFOV. The study findings were consistent with those from previous studies, and suggested that the causes of respiratory failure might account for the differences between the treatment groups, they noted.
“RDS is primarily restrictive in the acute phase, and the high frequency oscillation over CPAP does not therefore bring any benefit. However, ARDS is both restrictive and obstructive in the acute phase due to the nature of ARDS,” and NHFOV is “able to improve oxygenation,” they added.
The study findings were limited by several factors including the use of data from a single center and the small number of infants younger than 28 weeks’ gestation, the researchers noted. However, they added, two international, multicenter, randomized controlled trials are in the works.
The study was supported by Social Livelihood Program of 38 Chongqing Science and Technology Commission, China. The researchers had no financial conflicts to disclose.
SOURCE: Long C et al. Chest. 2019; 155(4): 740-8.
Nasal high-frequency oscillatory ventilation, in a randomized trial of 206 preterm infants with respiratory failure.
Previous studies have supported the use of NHFOV as more effective for reducing CO2 and for lowering the risk of reintubation compared with NCPAP. But no randomized, controlled trials had compared the outcomes for preterm infants in particular, wrote Long Chen, MD, PhD, of Children’s Hospital of Chongqing Medical University, Chongqing, China, and colleagues.
Their study, published in Chest, was conducted at a single tertiary NICU in China between May 2017 and May 2018, and randomized infants with a gestational age less than 37 weeks to NHFOV (103 infants) or NCPAP (103 infants). Infants with major congenital abnormalities were excluded. The infants included 127 (61.7%) diagnosed with respiratory distress syndrome (RDS), 53 (25.7%) diagnosed with acute RDS (ARDS), and 26 (12.6%) diagnosed with both RDS and ARDS.
Overall, the reintubation rate within 6 hours was significantly lower among infants treated with NHFOV compared with those treated with NCPAP (15.5% vs. 34%, P = .002), and in the subset of infants with ARDS (23.5% vs. 52.6%, P = .032). Among infants with a gestational age of 32 weeks or less, reintuibation rates were also significantly lower among those treated with NHFOV (26.1% vs. 55.6%, P = .004).
In addition, PCO2 levels, 6 hours after extubation, were significantly lower among infants on NHFOV, compared with those on NCPAP (49.6 vs. 56.9 P = .00). The hospital stay, a secondary outcome, was significantly shorter among the infants treated with NHFOV, than those treated with NCPAP (22 days, vs. 27.6 days, P =.011).
Although the researchers observed some nasal trauma in NHFOV-treated patients, and intestinal dilation in both groups similar to side effects seen in previous studies, no feeding intolerance or skin lesions were associated with NHFOV. The study findings were consistent with those from previous studies, and suggested that the causes of respiratory failure might account for the differences between the treatment groups, they noted.
“RDS is primarily restrictive in the acute phase, and the high frequency oscillation over CPAP does not therefore bring any benefit. However, ARDS is both restrictive and obstructive in the acute phase due to the nature of ARDS,” and NHFOV is “able to improve oxygenation,” they added.
The study findings were limited by several factors including the use of data from a single center and the small number of infants younger than 28 weeks’ gestation, the researchers noted. However, they added, two international, multicenter, randomized controlled trials are in the works.
The study was supported by Social Livelihood Program of 38 Chongqing Science and Technology Commission, China. The researchers had no financial conflicts to disclose.
SOURCE: Long C et al. Chest. 2019; 155(4): 740-8.
Nasal high-frequency oscillatory ventilation, in a randomized trial of 206 preterm infants with respiratory failure.
Previous studies have supported the use of NHFOV as more effective for reducing CO2 and for lowering the risk of reintubation compared with NCPAP. But no randomized, controlled trials had compared the outcomes for preterm infants in particular, wrote Long Chen, MD, PhD, of Children’s Hospital of Chongqing Medical University, Chongqing, China, and colleagues.
Their study, published in Chest, was conducted at a single tertiary NICU in China between May 2017 and May 2018, and randomized infants with a gestational age less than 37 weeks to NHFOV (103 infants) or NCPAP (103 infants). Infants with major congenital abnormalities were excluded. The infants included 127 (61.7%) diagnosed with respiratory distress syndrome (RDS), 53 (25.7%) diagnosed with acute RDS (ARDS), and 26 (12.6%) diagnosed with both RDS and ARDS.
Overall, the reintubation rate within 6 hours was significantly lower among infants treated with NHFOV compared with those treated with NCPAP (15.5% vs. 34%, P = .002), and in the subset of infants with ARDS (23.5% vs. 52.6%, P = .032). Among infants with a gestational age of 32 weeks or less, reintuibation rates were also significantly lower among those treated with NHFOV (26.1% vs. 55.6%, P = .004).
In addition, PCO2 levels, 6 hours after extubation, were significantly lower among infants on NHFOV, compared with those on NCPAP (49.6 vs. 56.9 P = .00). The hospital stay, a secondary outcome, was significantly shorter among the infants treated with NHFOV, than those treated with NCPAP (22 days, vs. 27.6 days, P =.011).
Although the researchers observed some nasal trauma in NHFOV-treated patients, and intestinal dilation in both groups similar to side effects seen in previous studies, no feeding intolerance or skin lesions were associated with NHFOV. The study findings were consistent with those from previous studies, and suggested that the causes of respiratory failure might account for the differences between the treatment groups, they noted.
“RDS is primarily restrictive in the acute phase, and the high frequency oscillation over CPAP does not therefore bring any benefit. However, ARDS is both restrictive and obstructive in the acute phase due to the nature of ARDS,” and NHFOV is “able to improve oxygenation,” they added.
The study findings were limited by several factors including the use of data from a single center and the small number of infants younger than 28 weeks’ gestation, the researchers noted. However, they added, two international, multicenter, randomized controlled trials are in the works.
The study was supported by Social Livelihood Program of 38 Chongqing Science and Technology Commission, China. The researchers had no financial conflicts to disclose.
SOURCE: Long C et al. Chest. 2019; 155(4): 740-8.
FROM CHEST
Flu activity falling but still elevated
Measures of influenza activity fell again as the flu season continues to make its later-than-usual departure this year, according to the Centers for Disease Control and Prevention.
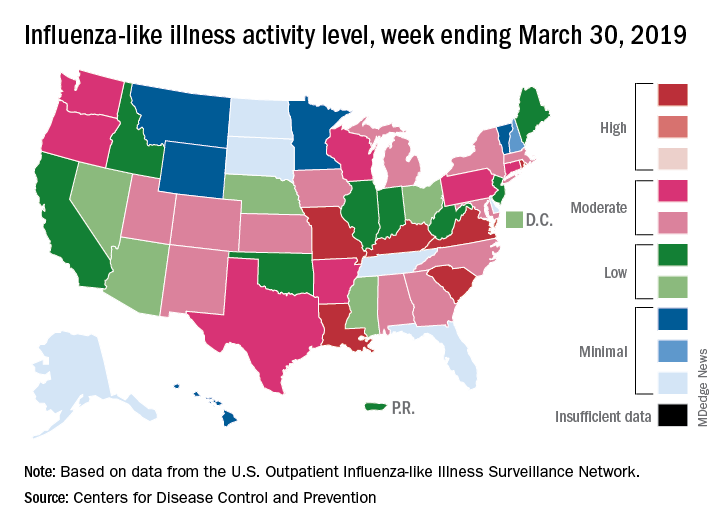
On the geographic front, the map of influenza-like illness (ILI) activity for the week ending March 30 shows that only 6 states are at level 10 on the CDC’s 1-10 scale, compared with 11 for the previous week, and that those same 6 states make up the entire membership of the high range of levels 8-10, which is down from 20 states a week ago, data from the CDC’s Outpatient ILI Surveillance Network show.
The proportion of outpatient visits for ILI, now at 3.2%, dropped for the sixth consecutive week after reaching its season high of 5.1% back in mid-February. The outpatient rate has now been at or above the national baseline of 2.2% for 19 weeks this season, the CDC’s influenza division said April 5, noting that the average for the past five seasons is 16 weeks.
Six flu-related pediatric deaths were reported in the week ending March 30, and the total is now 82 for the 2018-2019 season. Five of the six occurred during previous weeks of this season, and one occurred in the 2017-2018 season, the CDC said.
Measures of influenza activity fell again as the flu season continues to make its later-than-usual departure this year, according to the Centers for Disease Control and Prevention.
On the geographic front, the map of influenza-like illness (ILI) activity for the week ending March 30 shows that only 6 states are at level 10 on the CDC’s 1-10 scale, compared with 11 for the previous week, and that those same 6 states make up the entire membership of the high range of levels 8-10, which is down from 20 states a week ago, data from the CDC’s Outpatient ILI Surveillance Network show.
The proportion of outpatient visits for ILI, now at 3.2%, dropped for the sixth consecutive week after reaching its season high of 5.1% back in mid-February. The outpatient rate has now been at or above the national baseline of 2.2% for 19 weeks this season, the CDC’s influenza division said April 5, noting that the average for the past five seasons is 16 weeks.
Six flu-related pediatric deaths were reported in the week ending March 30, and the total is now 82 for the 2018-2019 season. Five of the six occurred during previous weeks of this season, and one occurred in the 2017-2018 season, the CDC said.
Measures of influenza activity fell again as the flu season continues to make its later-than-usual departure this year, according to the Centers for Disease Control and Prevention.
On the geographic front, the map of influenza-like illness (ILI) activity for the week ending March 30 shows that only 6 states are at level 10 on the CDC’s 1-10 scale, compared with 11 for the previous week, and that those same 6 states make up the entire membership of the high range of levels 8-10, which is down from 20 states a week ago, data from the CDC’s Outpatient ILI Surveillance Network show.
The proportion of outpatient visits for ILI, now at 3.2%, dropped for the sixth consecutive week after reaching its season high of 5.1% back in mid-February. The outpatient rate has now been at or above the national baseline of 2.2% for 19 weeks this season, the CDC’s influenza division said April 5, noting that the average for the past five seasons is 16 weeks.
Six flu-related pediatric deaths were reported in the week ending March 30, and the total is now 82 for the 2018-2019 season. Five of the six occurred during previous weeks of this season, and one occurred in the 2017-2018 season, the CDC said.
Abatacept appears safe for RA patients with COPD
Concerns about abatacept (Orencia)-related lung disease in patients with rheumatoid arthritis appear to be unfounded, a large U.S. database review has determined.

Safety signals seen in a small subset of patients in the 2006 ASSURE study likely arose from chance, Samy Suissa, PhD, and his colleagues wrote in Seminars in Arthritis & Rheumatism. Patients in that study with preexisting chronic obstructive pulmonary disease (COPD) were 84% more likely to develop an exacerbation or other lung disorder than were those taking a placebo comparator.
The new database study contradicted that finding.
“Our study suggests that these numerical differences in ASSURE are expected results of random variation and thus compatible with chance,” Dr. Suissa of Jewish General Hospital and McGill University, both in Montreal, and his coauthors wrote. “Moreover, our findings are consistent with two studies of the safety of abatacept in the context of interstitial lung disease, albeit a different respiratory disease than COPD.”
The year-long ASSURE trial reported on the safety of abatacept in 959 patients versus 482 assigned to placebo. The safety signal arose in a subgroup of 54 patients with COPD, 37 of whom were assigned to abatacept and 17 to placebo. Among these were four serious respiratory adverse events (COPD exacerbation, worsening of COPD, bronchitis, and pneumonia) in four patients taking abatacept and none in the placebo arm.
“It is useful to note that this difference of 11% versus 0% rate is compatible with chance [exact P = .31], while the exact 95% confidence interval for the odds ratio is wide and includes unity ... The trial also reported more mild-moderate respiratory events with abatacept than with placebo [43.2% vs. 23.5%], including cough, rhonchi, COPD exacerbation, COPD, dyspnea, and nasal congestion. This difference resulted in an odds ration of 1.84,” with a wide confidence interval that included unity (0.48-8.63).
Nevertheless, these findings led to the addition of a warning in the prescribing insert: “Adult COPD patients treated with Orencia developed adverse events more frequently than those treated with placebo, including COPD exacerbations, cough, rhonchi, and dyspnea. Use of Orencia in patients with RA and COPD should be undertaken with caution and such patients should be monitored for worsening of their respiratory status.”
Dr. Suissa’s team used the U.S. MarketScan prescribing database to asses the risk of respiratory adverse events associated with abatacept, compared with other biologic disease-modifying antirheumatic drugs (DMARDs) in a real-world setting.
The cohort comprised 1,807 patients with rheumatoid arthritis and COPD who started a new prescription for abatacept, matched in time to 3,547 who initiated another biologic DMARD. The primary endpoint was the combined risk of hospitalization for COPD exacerbation, bronchitis, and hospitalized pneumonia or influenza.
The most common comparator biologic DMARDs were etanercept, adalimumab, rituximab, and infliximab.
For patients with COPD and comparator patients, the incidence rates for COPD exacerbation were 1.2 per 100 person-years with abatacept and 2.1 per 100 person-years with a different biologic DMARD; for bronchitis, the respective rates were 4.2 and 5.3; for hospitalized pneumonia or influenza, 3.6 and 2.6; and for outpatient pneumonia or flu, 14.7 and 14.4. For the combined endpoint, the incidence rate was 8.7 per 100 person-years with abatacept and 9.9 per 100 person-years with other biologic DMARDs.
The adjusted hazard ratio of the combined endpoint with abatacept versus that with other biologic DMARDs was a nonsignificant risk of 0.87. The hazard ratio with abatacept was 0.60 for hospitalized COPD; 0.80 for bronchitis; 1.39 for hospitalized pneumonia and flu; and 1.05 for outpatient pneumonia and flu. None of these associations was statistically significant.
“One exception was the risk of hospitalization for pneumonia or influenza, which was higher with abatacept among patients with more severe COPD,” at 6.99, than it was with other biologic DMARDs, the authors noted.
Dr. Suissa disclosed relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, and Novartis.
SOURCE: Suissa S et al. Semin Arthritis Rheum. 2019 Mar 16. doi: 10.1016j.semarthrit.2019.03.007.
Concerns about abatacept (Orencia)-related lung disease in patients with rheumatoid arthritis appear to be unfounded, a large U.S. database review has determined.
Safety signals seen in a small subset of patients in the 2006 ASSURE study likely arose from chance, Samy Suissa, PhD, and his colleagues wrote in Seminars in Arthritis & Rheumatism. Patients in that study with preexisting chronic obstructive pulmonary disease (COPD) were 84% more likely to develop an exacerbation or other lung disorder than were those taking a placebo comparator.
The new database study contradicted that finding.
“Our study suggests that these numerical differences in ASSURE are expected results of random variation and thus compatible with chance,” Dr. Suissa of Jewish General Hospital and McGill University, both in Montreal, and his coauthors wrote. “Moreover, our findings are consistent with two studies of the safety of abatacept in the context of interstitial lung disease, albeit a different respiratory disease than COPD.”
The year-long ASSURE trial reported on the safety of abatacept in 959 patients versus 482 assigned to placebo. The safety signal arose in a subgroup of 54 patients with COPD, 37 of whom were assigned to abatacept and 17 to placebo. Among these were four serious respiratory adverse events (COPD exacerbation, worsening of COPD, bronchitis, and pneumonia) in four patients taking abatacept and none in the placebo arm.
“It is useful to note that this difference of 11% versus 0% rate is compatible with chance [exact P = .31], while the exact 95% confidence interval for the odds ratio is wide and includes unity ... The trial also reported more mild-moderate respiratory events with abatacept than with placebo [43.2% vs. 23.5%], including cough, rhonchi, COPD exacerbation, COPD, dyspnea, and nasal congestion. This difference resulted in an odds ration of 1.84,” with a wide confidence interval that included unity (0.48-8.63).
Nevertheless, these findings led to the addition of a warning in the prescribing insert: “Adult COPD patients treated with Orencia developed adverse events more frequently than those treated with placebo, including COPD exacerbations, cough, rhonchi, and dyspnea. Use of Orencia in patients with RA and COPD should be undertaken with caution and such patients should be monitored for worsening of their respiratory status.”
Dr. Suissa’s team used the U.S. MarketScan prescribing database to asses the risk of respiratory adverse events associated with abatacept, compared with other biologic disease-modifying antirheumatic drugs (DMARDs) in a real-world setting.
The cohort comprised 1,807 patients with rheumatoid arthritis and COPD who started a new prescription for abatacept, matched in time to 3,547 who initiated another biologic DMARD. The primary endpoint was the combined risk of hospitalization for COPD exacerbation, bronchitis, and hospitalized pneumonia or influenza.
The most common comparator biologic DMARDs were etanercept, adalimumab, rituximab, and infliximab.
For patients with COPD and comparator patients, the incidence rates for COPD exacerbation were 1.2 per 100 person-years with abatacept and 2.1 per 100 person-years with a different biologic DMARD; for bronchitis, the respective rates were 4.2 and 5.3; for hospitalized pneumonia or influenza, 3.6 and 2.6; and for outpatient pneumonia or flu, 14.7 and 14.4. For the combined endpoint, the incidence rate was 8.7 per 100 person-years with abatacept and 9.9 per 100 person-years with other biologic DMARDs.
The adjusted hazard ratio of the combined endpoint with abatacept versus that with other biologic DMARDs was a nonsignificant risk of 0.87. The hazard ratio with abatacept was 0.60 for hospitalized COPD; 0.80 for bronchitis; 1.39 for hospitalized pneumonia and flu; and 1.05 for outpatient pneumonia and flu. None of these associations was statistically significant.
“One exception was the risk of hospitalization for pneumonia or influenza, which was higher with abatacept among patients with more severe COPD,” at 6.99, than it was with other biologic DMARDs, the authors noted.
Dr. Suissa disclosed relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, and Novartis.
SOURCE: Suissa S et al. Semin Arthritis Rheum. 2019 Mar 16. doi: 10.1016j.semarthrit.2019.03.007.
Concerns about abatacept (Orencia)-related lung disease in patients with rheumatoid arthritis appear to be unfounded, a large U.S. database review has determined.
Safety signals seen in a small subset of patients in the 2006 ASSURE study likely arose from chance, Samy Suissa, PhD, and his colleagues wrote in Seminars in Arthritis & Rheumatism. Patients in that study with preexisting chronic obstructive pulmonary disease (COPD) were 84% more likely to develop an exacerbation or other lung disorder than were those taking a placebo comparator.
The new database study contradicted that finding.
“Our study suggests that these numerical differences in ASSURE are expected results of random variation and thus compatible with chance,” Dr. Suissa of Jewish General Hospital and McGill University, both in Montreal, and his coauthors wrote. “Moreover, our findings are consistent with two studies of the safety of abatacept in the context of interstitial lung disease, albeit a different respiratory disease than COPD.”
The year-long ASSURE trial reported on the safety of abatacept in 959 patients versus 482 assigned to placebo. The safety signal arose in a subgroup of 54 patients with COPD, 37 of whom were assigned to abatacept and 17 to placebo. Among these were four serious respiratory adverse events (COPD exacerbation, worsening of COPD, bronchitis, and pneumonia) in four patients taking abatacept and none in the placebo arm.
“It is useful to note that this difference of 11% versus 0% rate is compatible with chance [exact P = .31], while the exact 95% confidence interval for the odds ratio is wide and includes unity ... The trial also reported more mild-moderate respiratory events with abatacept than with placebo [43.2% vs. 23.5%], including cough, rhonchi, COPD exacerbation, COPD, dyspnea, and nasal congestion. This difference resulted in an odds ration of 1.84,” with a wide confidence interval that included unity (0.48-8.63).
Nevertheless, these findings led to the addition of a warning in the prescribing insert: “Adult COPD patients treated with Orencia developed adverse events more frequently than those treated with placebo, including COPD exacerbations, cough, rhonchi, and dyspnea. Use of Orencia in patients with RA and COPD should be undertaken with caution and such patients should be monitored for worsening of their respiratory status.”
Dr. Suissa’s team used the U.S. MarketScan prescribing database to asses the risk of respiratory adverse events associated with abatacept, compared with other biologic disease-modifying antirheumatic drugs (DMARDs) in a real-world setting.
The cohort comprised 1,807 patients with rheumatoid arthritis and COPD who started a new prescription for abatacept, matched in time to 3,547 who initiated another biologic DMARD. The primary endpoint was the combined risk of hospitalization for COPD exacerbation, bronchitis, and hospitalized pneumonia or influenza.
The most common comparator biologic DMARDs were etanercept, adalimumab, rituximab, and infliximab.
For patients with COPD and comparator patients, the incidence rates for COPD exacerbation were 1.2 per 100 person-years with abatacept and 2.1 per 100 person-years with a different biologic DMARD; for bronchitis, the respective rates were 4.2 and 5.3; for hospitalized pneumonia or influenza, 3.6 and 2.6; and for outpatient pneumonia or flu, 14.7 and 14.4. For the combined endpoint, the incidence rate was 8.7 per 100 person-years with abatacept and 9.9 per 100 person-years with other biologic DMARDs.
The adjusted hazard ratio of the combined endpoint with abatacept versus that with other biologic DMARDs was a nonsignificant risk of 0.87. The hazard ratio with abatacept was 0.60 for hospitalized COPD; 0.80 for bronchitis; 1.39 for hospitalized pneumonia and flu; and 1.05 for outpatient pneumonia and flu. None of these associations was statistically significant.
“One exception was the risk of hospitalization for pneumonia or influenza, which was higher with abatacept among patients with more severe COPD,” at 6.99, than it was with other biologic DMARDs, the authors noted.
Dr. Suissa disclosed relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, and Novartis.
SOURCE: Suissa S et al. Semin Arthritis Rheum. 2019 Mar 16. doi: 10.1016j.semarthrit.2019.03.007.
FROM SEMINARS IN ARTHRITIS & RHEUMATISM
NIH to undertake first in-human trial of universal influenza vaccine
The National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health, is launching the first in-human trial of a universal influenza vaccine candidate.

The experimental vaccine, H1ssF_3928, is derived from the stem of an H1N1 virus and has a surface made from hemagglutinin and ferritin. By including only the stem of the virus, which changes less than the head, the vaccine should require fewer updates. A similar vaccine made from the same materials was shown to be safe and well tolerated in humans.
The clinical trial (NCT03814720) will be conducted at the NIH Clinical Center in Bethesda, Md., and will gradually enroll at least 53 healthy adults aged 18-70 years. The first 5 participants will receive one 20-mcg intramuscular injection of the vaccine; the other 48 participants will receive two 60-mcg vaccinations 16 weeks apart. Patients will return for 9-11 follow-ups over a 12- to 15-month period, and will provide blood samples for analysis of anti-influenza antibodies.
“Seasonal influenza is a perpetual public health challenge, and we continually face the possibility of an influenza pandemic resulting from the emergence and spread of novel influenza viruses. This phase 1 clinical trial is a step forward in our efforts to develop a durable and broadly protective universal influenza vaccine,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said in the press release.
Find the full press release on the NIH website.
The National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health, is launching the first in-human trial of a universal influenza vaccine candidate.
The experimental vaccine, H1ssF_3928, is derived from the stem of an H1N1 virus and has a surface made from hemagglutinin and ferritin. By including only the stem of the virus, which changes less than the head, the vaccine should require fewer updates. A similar vaccine made from the same materials was shown to be safe and well tolerated in humans.
The clinical trial (NCT03814720) will be conducted at the NIH Clinical Center in Bethesda, Md., and will gradually enroll at least 53 healthy adults aged 18-70 years. The first 5 participants will receive one 20-mcg intramuscular injection of the vaccine; the other 48 participants will receive two 60-mcg vaccinations 16 weeks apart. Patients will return for 9-11 follow-ups over a 12- to 15-month period, and will provide blood samples for analysis of anti-influenza antibodies.
“Seasonal influenza is a perpetual public health challenge, and we continually face the possibility of an influenza pandemic resulting from the emergence and spread of novel influenza viruses. This phase 1 clinical trial is a step forward in our efforts to develop a durable and broadly protective universal influenza vaccine,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said in the press release.
Find the full press release on the NIH website.
The National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health, is launching the first in-human trial of a universal influenza vaccine candidate.
The experimental vaccine, H1ssF_3928, is derived from the stem of an H1N1 virus and has a surface made from hemagglutinin and ferritin. By including only the stem of the virus, which changes less than the head, the vaccine should require fewer updates. A similar vaccine made from the same materials was shown to be safe and well tolerated in humans.
The clinical trial (NCT03814720) will be conducted at the NIH Clinical Center in Bethesda, Md., and will gradually enroll at least 53 healthy adults aged 18-70 years. The first 5 participants will receive one 20-mcg intramuscular injection of the vaccine; the other 48 participants will receive two 60-mcg vaccinations 16 weeks apart. Patients will return for 9-11 follow-ups over a 12- to 15-month period, and will provide blood samples for analysis of anti-influenza antibodies.
“Seasonal influenza is a perpetual public health challenge, and we continually face the possibility of an influenza pandemic resulting from the emergence and spread of novel influenza viruses. This phase 1 clinical trial is a step forward in our efforts to develop a durable and broadly protective universal influenza vaccine,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said in the press release.
Find the full press release on the NIH website.
FDA concerned about e-cigs/seizures in youth
the agency announced April 3.

Between 2010 and early 2019, the FDA and poison control centers received 35 reports of seizures that mentioned the use of e-cigarettes. Most reports involved youth or young adults, and the reports have increased slightly since June 2018, the announcement says.
“We want to be clear that we don’t yet know if there’s a direct relationship between the use of e-cigarettes and a risk of seizure,” said FDA Commissioner Scott Gottlieb, MD, and Principal Deputy Commissioner Amy Abernethy, MD, PhD, in a statement. “We believe these 35 cases warrant scientific investigation into whether there is in fact a connection.”
In addition, the FDA is trying to determine whether any e-cigarette product-specific factors may be associated with the risk of seizures.
Seizures have been reported after a few puffs or up to 1 day after e-cigarette use and among first-time and experienced users. A few patients had a prior history of seizures or also used other substances, such as marijuana or amphetamines.
“While 35 cases may not seem like much compared to the total number of people using e-cigarettes, we are nonetheless concerned by these reported cases. We also recognized that not all of the cases may be reported,” Dr. Gottlieb and Dr. Abernethy said.
Although seizures are known side effects of nicotine toxicity and have been reported in the context of intentional or accidental swallowing of e-cigarette liquid, the voluntary reports of seizures occurring with vaping could represent a new safety issue, the FDA said.
The agency encouraged people to report cases via an online safety reporting portal. It also provided redacted case reports that involve vaping and seizures.
the agency announced April 3.
Between 2010 and early 2019, the FDA and poison control centers received 35 reports of seizures that mentioned the use of e-cigarettes. Most reports involved youth or young adults, and the reports have increased slightly since June 2018, the announcement says.
“We want to be clear that we don’t yet know if there’s a direct relationship between the use of e-cigarettes and a risk of seizure,” said FDA Commissioner Scott Gottlieb, MD, and Principal Deputy Commissioner Amy Abernethy, MD, PhD, in a statement. “We believe these 35 cases warrant scientific investigation into whether there is in fact a connection.”
In addition, the FDA is trying to determine whether any e-cigarette product-specific factors may be associated with the risk of seizures.
Seizures have been reported after a few puffs or up to 1 day after e-cigarette use and among first-time and experienced users. A few patients had a prior history of seizures or also used other substances, such as marijuana or amphetamines.
“While 35 cases may not seem like much compared to the total number of people using e-cigarettes, we are nonetheless concerned by these reported cases. We also recognized that not all of the cases may be reported,” Dr. Gottlieb and Dr. Abernethy said.
Although seizures are known side effects of nicotine toxicity and have been reported in the context of intentional or accidental swallowing of e-cigarette liquid, the voluntary reports of seizures occurring with vaping could represent a new safety issue, the FDA said.
The agency encouraged people to report cases via an online safety reporting portal. It also provided redacted case reports that involve vaping and seizures.
the agency announced April 3.
Between 2010 and early 2019, the FDA and poison control centers received 35 reports of seizures that mentioned the use of e-cigarettes. Most reports involved youth or young adults, and the reports have increased slightly since June 2018, the announcement says.
“We want to be clear that we don’t yet know if there’s a direct relationship between the use of e-cigarettes and a risk of seizure,” said FDA Commissioner Scott Gottlieb, MD, and Principal Deputy Commissioner Amy Abernethy, MD, PhD, in a statement. “We believe these 35 cases warrant scientific investigation into whether there is in fact a connection.”
In addition, the FDA is trying to determine whether any e-cigarette product-specific factors may be associated with the risk of seizures.
Seizures have been reported after a few puffs or up to 1 day after e-cigarette use and among first-time and experienced users. A few patients had a prior history of seizures or also used other substances, such as marijuana or amphetamines.
“While 35 cases may not seem like much compared to the total number of people using e-cigarettes, we are nonetheless concerned by these reported cases. We also recognized that not all of the cases may be reported,” Dr. Gottlieb and Dr. Abernethy said.
Although seizures are known side effects of nicotine toxicity and have been reported in the context of intentional or accidental swallowing of e-cigarette liquid, the voluntary reports of seizures occurring with vaping could represent a new safety issue, the FDA said.
The agency encouraged people to report cases via an online safety reporting portal. It also provided redacted case reports that involve vaping and seizures.
Noninfected children of HIV-positive mothers have high rates of obesity
NEW ORLEANS – than are those with no such exposure, according to research that provides a compelling link between inflammatory activity in utero and subsequent risk of metabolic disorders.
Most supportive of that link was a near-linear inverse relationship between CD4 counts during the time of pregnancy and risk of both obesity and reactive respiratory disease more than a decade later, according to research presented by Lindsay Fourman, MD, an instructor in medicine at Massachusetts General Hospital, Boston, during the annual meeting of the Endocrine Society.
In this video interview, Dr. Fourman discusses the effort to understand the long-term health consequences of being exposed to HIV and antiretroviral therapies while in utero, a group known by the acronym HIV-exposed uninfected (HEU). With effective therapies now routinely preventing mother-to-child transmission, this population of children is growing quickly.
For this study, 50 HEU individuals were identified from a patient database. They were matched in a 3:1 ratio to a control group for a variety of demographic and socioeconomic variables. At a median age of 18 years, the HEU population was found to have a “strikingly” higher rate of obesity, compared with controls (42% vs. 25%, respectively; P = .04). The rate of reactive airway disease was similarly increased in the HEU group (40% vs. 24%; P = .04).
These data are important for considering health risks in an HEU population, but Dr. Fourman explained that it provides support for looking at metabolic risks from other in utero exposures linked to upregulated inflammation, such as gestational diabetes or obesity.
Dr Fourman and her colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Fourman L et al. ENDO 2019, Session P10 (SAT-256).
NEW ORLEANS – than are those with no such exposure, according to research that provides a compelling link between inflammatory activity in utero and subsequent risk of metabolic disorders.
Most supportive of that link was a near-linear inverse relationship between CD4 counts during the time of pregnancy and risk of both obesity and reactive respiratory disease more than a decade later, according to research presented by Lindsay Fourman, MD, an instructor in medicine at Massachusetts General Hospital, Boston, during the annual meeting of the Endocrine Society.
In this video interview, Dr. Fourman discusses the effort to understand the long-term health consequences of being exposed to HIV and antiretroviral therapies while in utero, a group known by the acronym HIV-exposed uninfected (HEU). With effective therapies now routinely preventing mother-to-child transmission, this population of children is growing quickly.
For this study, 50 HEU individuals were identified from a patient database. They were matched in a 3:1 ratio to a control group for a variety of demographic and socioeconomic variables. At a median age of 18 years, the HEU population was found to have a “strikingly” higher rate of obesity, compared with controls (42% vs. 25%, respectively; P = .04). The rate of reactive airway disease was similarly increased in the HEU group (40% vs. 24%; P = .04).
These data are important for considering health risks in an HEU population, but Dr. Fourman explained that it provides support for looking at metabolic risks from other in utero exposures linked to upregulated inflammation, such as gestational diabetes or obesity.
Dr Fourman and her colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Fourman L et al. ENDO 2019, Session P10 (SAT-256).
NEW ORLEANS – than are those with no such exposure, according to research that provides a compelling link between inflammatory activity in utero and subsequent risk of metabolic disorders.
Most supportive of that link was a near-linear inverse relationship between CD4 counts during the time of pregnancy and risk of both obesity and reactive respiratory disease more than a decade later, according to research presented by Lindsay Fourman, MD, an instructor in medicine at Massachusetts General Hospital, Boston, during the annual meeting of the Endocrine Society.
In this video interview, Dr. Fourman discusses the effort to understand the long-term health consequences of being exposed to HIV and antiretroviral therapies while in utero, a group known by the acronym HIV-exposed uninfected (HEU). With effective therapies now routinely preventing mother-to-child transmission, this population of children is growing quickly.
For this study, 50 HEU individuals were identified from a patient database. They were matched in a 3:1 ratio to a control group for a variety of demographic and socioeconomic variables. At a median age of 18 years, the HEU population was found to have a “strikingly” higher rate of obesity, compared with controls (42% vs. 25%, respectively; P = .04). The rate of reactive airway disease was similarly increased in the HEU group (40% vs. 24%; P = .04).
These data are important for considering health risks in an HEU population, but Dr. Fourman explained that it provides support for looking at metabolic risks from other in utero exposures linked to upregulated inflammation, such as gestational diabetes or obesity.
Dr Fourman and her colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Fourman L et al. ENDO 2019, Session P10 (SAT-256).
REPORTING FROM ENDO 2019

In obesity-related asthma, a new hormonal target
NEW ORLEANS – A hormone that is oversecreted in obesity may provide a pathway from adipose to lung tissue in individuals with both obesity and asthma, according to new research presented at the annual meeting of the Endocrine Society.
“Obesity-related asthma is a really understudied and new phenomenon. It’s a unique complication of obesity,” said Furkan Burak, MD, in a video interview after an obesity-focused press conference.
“In addition to being a standalone disease, obesity mostly comes as a package. And that’s the problem,” said Dr. Burak, pointing to obesity-related asthma’s clustering with diseases such as diabetes and atherosclerosis.
Asthma affects 10% of the world population, and it’s becoming increasingly understood that said Dr. Burak, an endocrinology fellow at Brigham and Women’s Hospital, Boston.
“There are two types of asthma related to obesity,” he said. Classic allergic asthma can get worse with obesity; however, asthma can sometimes occur de novo in adults, particularly women, with obesity. “What is important is … that they are less responsive to classic treatments,” such as steroids and beta-agonists. “And the problem is not small: Of asthmatics, 40% are obese. It’s a therapeutic problem, and we are not able to treat them well.”
The fatty acid binding protein 4, aP2, a hormone that is released by adipose tissue, travels to distant organs and regulates metabolic responses. Levels of aP2 are known to be increased in obesity, particularly in individuals with asthma, said Dr. Burak.
Citing work done at Brigham and Women’s Hospital and at Boston’s Harvard Medical School, as well as elsewhere, Dr. Burak and his collaborators noted in the abstract accompanying the presentation that “increased serum aP2 levels strongly correlate with poor metabolic, inflammatory, and cardiovascular outcomes in multiple independent human studies.”
Dr. Burak said he and his colleagues are trying to sort out “how a fat-tissue–borne hormone could potentially cause a problem in the lung.”
A big clue came with the discovery that patients with asthma and obesity have elevated levels of aP2 within their airways when bronchoalveolar lavage is performed, suggesting that the hormone may be the pathological mediator linking obesity to asthma – “a direct link between the fat tissue and the lung,” he said.
Serum aP2 levels were available from the Nurse’s Health Study, so Dr. Burak and his colleagues looked at those levels in randomly selected study participants. “We found that aP2 levels were elevated 25.6% – significantly – in asthmatics, compared with nonasthmatics, but only in obese and overweight [participants, and] not in lean” participants, he said.
Dr. Burak and his colleagues compared 525 individuals with body mass indices of less than 25 kg/m2, of whom 15 had asthma, with 385 individuals with body mass indices of more than 25, of whom 15 of whom had asthma.
Collecting bronchoalveolar lavage fluid from individuals with asthma showed a mean increase of 23% in aP2 levels in patients with obesity compared with lean individuals.
These data taken together show both systemic and local elevations of aP2 in human obesity. “That could contribute to the airway hyperreactivity and to the asthma pathogenesis,” which would confirm findings from animal studies, said Dr. Burak.
Further investigation will focus on individuals who are haploinsufficient for aP2. The group already is known to have lower risk for dyslipidemia, diabetes, and cardiovascular disease, but Dr. Burak and his collaborators also will determine whether asthma incidence is also lower.
The eventual goal is to attack aP2 as a therapeutic target. “Can we inhibit and target aP2 therapeutically in the context of obesity to treat obesity-related asthma? We have a big hope for that.”
Dr. Burak and his colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Burak MF et al. ENDO 2019, Session OR01-1.
NEW ORLEANS – A hormone that is oversecreted in obesity may provide a pathway from adipose to lung tissue in individuals with both obesity and asthma, according to new research presented at the annual meeting of the Endocrine Society.
“Obesity-related asthma is a really understudied and new phenomenon. It’s a unique complication of obesity,” said Furkan Burak, MD, in a video interview after an obesity-focused press conference.
“In addition to being a standalone disease, obesity mostly comes as a package. And that’s the problem,” said Dr. Burak, pointing to obesity-related asthma’s clustering with diseases such as diabetes and atherosclerosis.
Asthma affects 10% of the world population, and it’s becoming increasingly understood that said Dr. Burak, an endocrinology fellow at Brigham and Women’s Hospital, Boston.
“There are two types of asthma related to obesity,” he said. Classic allergic asthma can get worse with obesity; however, asthma can sometimes occur de novo in adults, particularly women, with obesity. “What is important is … that they are less responsive to classic treatments,” such as steroids and beta-agonists. “And the problem is not small: Of asthmatics, 40% are obese. It’s a therapeutic problem, and we are not able to treat them well.”
The fatty acid binding protein 4, aP2, a hormone that is released by adipose tissue, travels to distant organs and regulates metabolic responses. Levels of aP2 are known to be increased in obesity, particularly in individuals with asthma, said Dr. Burak.
Citing work done at Brigham and Women’s Hospital and at Boston’s Harvard Medical School, as well as elsewhere, Dr. Burak and his collaborators noted in the abstract accompanying the presentation that “increased serum aP2 levels strongly correlate with poor metabolic, inflammatory, and cardiovascular outcomes in multiple independent human studies.”
Dr. Burak said he and his colleagues are trying to sort out “how a fat-tissue–borne hormone could potentially cause a problem in the lung.”
A big clue came with the discovery that patients with asthma and obesity have elevated levels of aP2 within their airways when bronchoalveolar lavage is performed, suggesting that the hormone may be the pathological mediator linking obesity to asthma – “a direct link between the fat tissue and the lung,” he said.
Serum aP2 levels were available from the Nurse’s Health Study, so Dr. Burak and his colleagues looked at those levels in randomly selected study participants. “We found that aP2 levels were elevated 25.6% – significantly – in asthmatics, compared with nonasthmatics, but only in obese and overweight [participants, and] not in lean” participants, he said.
Dr. Burak and his colleagues compared 525 individuals with body mass indices of less than 25 kg/m2, of whom 15 had asthma, with 385 individuals with body mass indices of more than 25, of whom 15 of whom had asthma.
Collecting bronchoalveolar lavage fluid from individuals with asthma showed a mean increase of 23% in aP2 levels in patients with obesity compared with lean individuals.
These data taken together show both systemic and local elevations of aP2 in human obesity. “That could contribute to the airway hyperreactivity and to the asthma pathogenesis,” which would confirm findings from animal studies, said Dr. Burak.
Further investigation will focus on individuals who are haploinsufficient for aP2. The group already is known to have lower risk for dyslipidemia, diabetes, and cardiovascular disease, but Dr. Burak and his collaborators also will determine whether asthma incidence is also lower.
The eventual goal is to attack aP2 as a therapeutic target. “Can we inhibit and target aP2 therapeutically in the context of obesity to treat obesity-related asthma? We have a big hope for that.”
Dr. Burak and his colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Burak MF et al. ENDO 2019, Session OR01-1.
NEW ORLEANS – A hormone that is oversecreted in obesity may provide a pathway from adipose to lung tissue in individuals with both obesity and asthma, according to new research presented at the annual meeting of the Endocrine Society.
“Obesity-related asthma is a really understudied and new phenomenon. It’s a unique complication of obesity,” said Furkan Burak, MD, in a video interview after an obesity-focused press conference.
“In addition to being a standalone disease, obesity mostly comes as a package. And that’s the problem,” said Dr. Burak, pointing to obesity-related asthma’s clustering with diseases such as diabetes and atherosclerosis.
Asthma affects 10% of the world population, and it’s becoming increasingly understood that said Dr. Burak, an endocrinology fellow at Brigham and Women’s Hospital, Boston.
“There are two types of asthma related to obesity,” he said. Classic allergic asthma can get worse with obesity; however, asthma can sometimes occur de novo in adults, particularly women, with obesity. “What is important is … that they are less responsive to classic treatments,” such as steroids and beta-agonists. “And the problem is not small: Of asthmatics, 40% are obese. It’s a therapeutic problem, and we are not able to treat them well.”
The fatty acid binding protein 4, aP2, a hormone that is released by adipose tissue, travels to distant organs and regulates metabolic responses. Levels of aP2 are known to be increased in obesity, particularly in individuals with asthma, said Dr. Burak.
Citing work done at Brigham and Women’s Hospital and at Boston’s Harvard Medical School, as well as elsewhere, Dr. Burak and his collaborators noted in the abstract accompanying the presentation that “increased serum aP2 levels strongly correlate with poor metabolic, inflammatory, and cardiovascular outcomes in multiple independent human studies.”
Dr. Burak said he and his colleagues are trying to sort out “how a fat-tissue–borne hormone could potentially cause a problem in the lung.”
A big clue came with the discovery that patients with asthma and obesity have elevated levels of aP2 within their airways when bronchoalveolar lavage is performed, suggesting that the hormone may be the pathological mediator linking obesity to asthma – “a direct link between the fat tissue and the lung,” he said.
Serum aP2 levels were available from the Nurse’s Health Study, so Dr. Burak and his colleagues looked at those levels in randomly selected study participants. “We found that aP2 levels were elevated 25.6% – significantly – in asthmatics, compared with nonasthmatics, but only in obese and overweight [participants, and] not in lean” participants, he said.
Dr. Burak and his colleagues compared 525 individuals with body mass indices of less than 25 kg/m2, of whom 15 had asthma, with 385 individuals with body mass indices of more than 25, of whom 15 of whom had asthma.
Collecting bronchoalveolar lavage fluid from individuals with asthma showed a mean increase of 23% in aP2 levels in patients with obesity compared with lean individuals.
These data taken together show both systemic and local elevations of aP2 in human obesity. “That could contribute to the airway hyperreactivity and to the asthma pathogenesis,” which would confirm findings from animal studies, said Dr. Burak.
Further investigation will focus on individuals who are haploinsufficient for aP2. The group already is known to have lower risk for dyslipidemia, diabetes, and cardiovascular disease, but Dr. Burak and his collaborators also will determine whether asthma incidence is also lower.
The eventual goal is to attack aP2 as a therapeutic target. “Can we inhibit and target aP2 therapeutically in the context of obesity to treat obesity-related asthma? We have a big hope for that.”
Dr. Burak and his colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Burak MF et al. ENDO 2019, Session OR01-1.
REPORTING FROM ENDO 2019
Measles: Latest weekly count is the highest of the year
according to the Centers for Disease Control and Prevention.
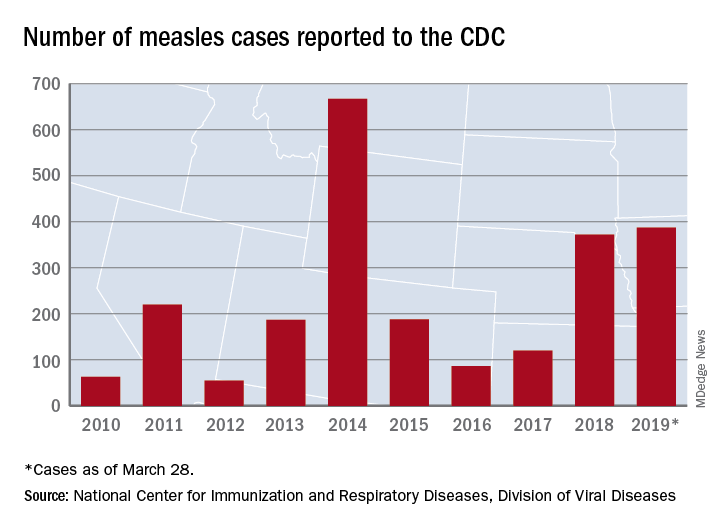
The 73 new cases of measles reported to the CDC during the week ending March 28 – more than any other single week so far in 2019 – brings the total number of cases for the year to 387, the CDC reported April 1. That surpasses the 372 reported in 2018 and is now the highest annual count since 667 cases were reported in 2014.
The ongoing outbreak in Rockland County, N.Y., which resulted in 6 new cases there last week and 52 for the year, prompted County Executive Ed Day to declare a state of emergency effective March 27 that bars unvaccinated individuals under age 18 years from public places for the next 30 days unless they receive an MMR vaccination.
“As this outbreak has continued our inspectors have begun to meet resistance from those they are trying to protect. They have been hung up on or told not to call again. They’ve been told ‘we’re not discussing this, do not come back,’ when visiting the homes of infected individuals as part of their investigations. This type of response is unacceptable and irresponsible. It endangers the health and well-being of others and displays a shocking lack of responsibility and concern for others in our community,” Mr. Day said in a written statement.
In addition to Rockland County, the CDC is currently tracking five other outbreaks: New York City, mainly Brooklyn (33 new cases last week); Washington state (74 cases for the year, but no new cases in the last week); New Jersey (10 total cases, with 8 related to an outbreak in Ocean and Monmouth Counties); and two in California (16 total cases, with 11 related to the outbreaks). One of the California outbreaks and the New Jersey outbreak are new, but the CDC is no longer reporting outbreaks in Texas and Illinois, so the total stays at six nationwide.
In related news from California, state Sen. Richard Pan (D), a pediatrician, and Assemblywoman Lorena Gonzalez (D) introduced a bill to monitor vaccine exemptions “by requiring the state health department to vet each medical exemption form written by physicians [and to] maintain a database of exemptions that would allow officials to monitor which doctors are granting the exemptions,” the Los Angeles Times reported.
according to the Centers for Disease Control and Prevention.
The 73 new cases of measles reported to the CDC during the week ending March 28 – more than any other single week so far in 2019 – brings the total number of cases for the year to 387, the CDC reported April 1. That surpasses the 372 reported in 2018 and is now the highest annual count since 667 cases were reported in 2014.
The ongoing outbreak in Rockland County, N.Y., which resulted in 6 new cases there last week and 52 for the year, prompted County Executive Ed Day to declare a state of emergency effective March 27 that bars unvaccinated individuals under age 18 years from public places for the next 30 days unless they receive an MMR vaccination.
“As this outbreak has continued our inspectors have begun to meet resistance from those they are trying to protect. They have been hung up on or told not to call again. They’ve been told ‘we’re not discussing this, do not come back,’ when visiting the homes of infected individuals as part of their investigations. This type of response is unacceptable and irresponsible. It endangers the health and well-being of others and displays a shocking lack of responsibility and concern for others in our community,” Mr. Day said in a written statement.
In addition to Rockland County, the CDC is currently tracking five other outbreaks: New York City, mainly Brooklyn (33 new cases last week); Washington state (74 cases for the year, but no new cases in the last week); New Jersey (10 total cases, with 8 related to an outbreak in Ocean and Monmouth Counties); and two in California (16 total cases, with 11 related to the outbreaks). One of the California outbreaks and the New Jersey outbreak are new, but the CDC is no longer reporting outbreaks in Texas and Illinois, so the total stays at six nationwide.
In related news from California, state Sen. Richard Pan (D), a pediatrician, and Assemblywoman Lorena Gonzalez (D) introduced a bill to monitor vaccine exemptions “by requiring the state health department to vet each medical exemption form written by physicians [and to] maintain a database of exemptions that would allow officials to monitor which doctors are granting the exemptions,” the Los Angeles Times reported.
according to the Centers for Disease Control and Prevention.
The 73 new cases of measles reported to the CDC during the week ending March 28 – more than any other single week so far in 2019 – brings the total number of cases for the year to 387, the CDC reported April 1. That surpasses the 372 reported in 2018 and is now the highest annual count since 667 cases were reported in 2014.
The ongoing outbreak in Rockland County, N.Y., which resulted in 6 new cases there last week and 52 for the year, prompted County Executive Ed Day to declare a state of emergency effective March 27 that bars unvaccinated individuals under age 18 years from public places for the next 30 days unless they receive an MMR vaccination.
“As this outbreak has continued our inspectors have begun to meet resistance from those they are trying to protect. They have been hung up on or told not to call again. They’ve been told ‘we’re not discussing this, do not come back,’ when visiting the homes of infected individuals as part of their investigations. This type of response is unacceptable and irresponsible. It endangers the health and well-being of others and displays a shocking lack of responsibility and concern for others in our community,” Mr. Day said in a written statement.
In addition to Rockland County, the CDC is currently tracking five other outbreaks: New York City, mainly Brooklyn (33 new cases last week); Washington state (74 cases for the year, but no new cases in the last week); New Jersey (10 total cases, with 8 related to an outbreak in Ocean and Monmouth Counties); and two in California (16 total cases, with 11 related to the outbreaks). One of the California outbreaks and the New Jersey outbreak are new, but the CDC is no longer reporting outbreaks in Texas and Illinois, so the total stays at six nationwide.
In related news from California, state Sen. Richard Pan (D), a pediatrician, and Assemblywoman Lorena Gonzalez (D) introduced a bill to monitor vaccine exemptions “by requiring the state health department to vet each medical exemption form written by physicians [and to] maintain a database of exemptions that would allow officials to monitor which doctors are granting the exemptions,” the Los Angeles Times reported.