User login
Treatment of posttraumatic stress disorder
Traumatic events are extremely common, with as many as 60% of children experiencing some trauma by age 18 years. About 15% of these children will develop posttraumatic stress disorder (PTSD).
Case summary
Jane is a 13-year-old girl who presented because of steadily escalating angry outbursts with her mother, irritable mood, and anxiety since her father went to jail 2 years previously. Prior to the father’s departure from the family, he drank heavily and had been physically violent to Jane’s mother through most of Jane’s life.

Since these events, Jane has been extremely angry and irritable, often fighting extensively with her younger sister. She has severe difficulty separating from her mother, often following her around or demanding to know everything that her mother is doing. Jane herself reports that she feels worried, irritable, and sad much of the time. She is especially angry when thinking about anything related to her father. Jane won’t talk about her father to anyone, except occasionally her mother and one friend. She has difficulty falling asleep and has nightmares. She never thinks about the future, and instead just lives day to day. Images from the past come vividly into her mind. She has highly negative, hopeless views of the world, and doesn’t trust people, so she is unwilling to consider any therapy. Jane’s mother also is highly irritable and snaps at Jane over small things while in the office.
Discussion
The DSM-5 diagnostic criteria for PTSD require that an individual has been exposed to a severe stressor that threatens death, serious injury, or sexual violence through direct experience, witnessing the event happening to others, or learning that the event happened to a close family member or friend. Not all people who experience such events will develop PTSD, however. Additional symptoms are grouped into four areas (rather than three as in the DSM-IV), and a diagnosis requires one or two symptoms in each area:
• Intrusive symptoms including intrusive distressing memories, recurrent dreams with content related to the event, dissociative reactions such as flashbacks, intense distress at exposure to triggers that remind individuals of the event, or marked physiologic reactions to triggers.
• Avoidance of stimuli associated with the event, either memories or thoughts or external reminders.
• Negative cognitions manifesting as changes in thoughts and mood beginning or worsening after the event. These are an inability to remember the event, persistent negative beliefs about oneself or the world, distorted thoughts about the cause or results of the event, persistent negative emotional states such as anger or guilt, decreased participation in activities, feelings of estrangement from others, or an inability to experience positive emotions.
• Changes in arousal and reactivity as shown by irritable behavior, reckless behavior, hypervigilance, an exaggerated startle response, concentration problems, or sleep disturbance.
There are several screening instruments for the presence of a history of traumatic events as well as for symptoms of PTSD. The Child PTSD Symptom Scale (CPSS) is one example of a simple, readily available screening tool. More extensive assessment is an important part of treatment by mental health clinicians.
Treatment
Psychotherapy interventions are the core of treatment for PTSD in young people. Interventions based on cognitive-behavioral therapy (CBT) are the most extensively researched, with trauma-focused CBT (TF-CBT) being the specific intervention with the most research (13 randomized controlled trials showing efficacy) for children and adolescents. There are several other approaches that have evidence of efficacy through randomized controlled trials, and have been specifically studied for different ages, cultural groups, and focus of intervention (group, family, classroom). Child-parent psychotherapy focuses on traumatized 3-to 5-year-olds and works with both parent and child. Eye movement desensitization and preprocessing therapy (EMDR), extensively studied for adults, has some randomized controlled trials in children. The National Child Traumatic Stress Network (NCTSN) has a website listing evidence-based interventions with descriptions of the extent of the evidence for these and other interventions, including the population for which the intervention was designed and information on training and dissemination.
A recent meta-analysis by Morina et al. identified 39 randomized controlled trials with psychological interventions targeting PTSD in children and youth and found a large (0.83) overall effect size vs. wait list control, and a moderate (0.41) effect size vs. an active control such as supportive therapy. There were enough randomized controlled trials to analyze the TF-CBT–based interventions as a group, and these had even larger effect sizes: 1.44 vs. wait list and 0.66 vs. active control. The non-CBT approaches did not have enough studies to be evaluated separately (Clin Psychol Rev. 2016 Jul;47:41-54).
It is important to know which available therapists are trained in specific interventions such as TF-CBT and review the evidence behind other interventions that therapists are using. Advocacy for the training of local therapists, particularly therapists who are affiliated with your practice, can increase these resources.
The evidence for pharmacologic treatment for PTSD in children and adolescents, in contrast to adults, is very thin. In adults, SSRIs have shown a significant benefit, but there have been three randomized controlled trials examining this question in young people with no significant difference shown for the SSRI. One of these compared TF-CBT alone to TF-CBT plus sertraline, with no added benefit for sertraline. A second compared sertraline to placebo and showed no difference, and the third was an extremely brief trial of 1 week of fluoxetine for children with burns, with no effect. There are open label studies of citalopram that have shown some benefit.
Prazosin is an alpha-1 antagonist that decreases the effect of peripheral norepinephrine, which has been shown to decrease reactivity in adults through two randomized controlled trials, but there are case reports in adolescents only. Guanfacine, an alpha-2 agonist that acts centrally to decrease norepinephrine release, has one open label study of the extended-release form in adolescents showing benefit, but there are two negative randomized controlled trials in adults. Other agents such as second-generation antipsychotics and mood stabilizers (specifically carbamazepine and valproic acid) have open label studies in children only and have the potential for significant side effects.
Psychotherapy is clearly the treatment of choice for children and adolescents with PTSD; the difficulty is that avoidance and difficulty trusting people are core symptoms of PTSD, and can lead patients to be extremely reluctant to try therapy. As a pediatrician, you likely already have a trusting relationship with your patient and parent(s), which can provide an opening for discussion.
Psychoeducation about trauma and the specific trauma a child has experienced is a core component and often the first step of PTSD treatment. The NCTSN website provides a goldmine of information about specific types of trauma (found under the tab labeled trauma types), including common symptoms at different developmental stages and specific resources. By providing information to families in a sensitive way, clinicians can help people understand that they are not alone, that their struggles are common reactions to the type of trauma they have experienced, and that people can recover with therapy so that the trauma does not have to go on negatively affecting their lives.
Finally, noting a parent’s possible trauma, and encouraging that parent to get his or her own treatment in order to help the child, can be a crucial first step.
General references
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
Traumatic events are extremely common, with as many as 60% of children experiencing some trauma by age 18 years. About 15% of these children will develop posttraumatic stress disorder (PTSD).
Case summary
Jane is a 13-year-old girl who presented because of steadily escalating angry outbursts with her mother, irritable mood, and anxiety since her father went to jail 2 years previously. Prior to the father’s departure from the family, he drank heavily and had been physically violent to Jane’s mother through most of Jane’s life.
Since these events, Jane has been extremely angry and irritable, often fighting extensively with her younger sister. She has severe difficulty separating from her mother, often following her around or demanding to know everything that her mother is doing. Jane herself reports that she feels worried, irritable, and sad much of the time. She is especially angry when thinking about anything related to her father. Jane won’t talk about her father to anyone, except occasionally her mother and one friend. She has difficulty falling asleep and has nightmares. She never thinks about the future, and instead just lives day to day. Images from the past come vividly into her mind. She has highly negative, hopeless views of the world, and doesn’t trust people, so she is unwilling to consider any therapy. Jane’s mother also is highly irritable and snaps at Jane over small things while in the office.
Discussion
The DSM-5 diagnostic criteria for PTSD require that an individual has been exposed to a severe stressor that threatens death, serious injury, or sexual violence through direct experience, witnessing the event happening to others, or learning that the event happened to a close family member or friend. Not all people who experience such events will develop PTSD, however. Additional symptoms are grouped into four areas (rather than three as in the DSM-IV), and a diagnosis requires one or two symptoms in each area:
• Intrusive symptoms including intrusive distressing memories, recurrent dreams with content related to the event, dissociative reactions such as flashbacks, intense distress at exposure to triggers that remind individuals of the event, or marked physiologic reactions to triggers.
• Avoidance of stimuli associated with the event, either memories or thoughts or external reminders.
• Negative cognitions manifesting as changes in thoughts and mood beginning or worsening after the event. These are an inability to remember the event, persistent negative beliefs about oneself or the world, distorted thoughts about the cause or results of the event, persistent negative emotional states such as anger or guilt, decreased participation in activities, feelings of estrangement from others, or an inability to experience positive emotions.
• Changes in arousal and reactivity as shown by irritable behavior, reckless behavior, hypervigilance, an exaggerated startle response, concentration problems, or sleep disturbance.
There are several screening instruments for the presence of a history of traumatic events as well as for symptoms of PTSD. The Child PTSD Symptom Scale (CPSS) is one example of a simple, readily available screening tool. More extensive assessment is an important part of treatment by mental health clinicians.
Treatment
Psychotherapy interventions are the core of treatment for PTSD in young people. Interventions based on cognitive-behavioral therapy (CBT) are the most extensively researched, with trauma-focused CBT (TF-CBT) being the specific intervention with the most research (13 randomized controlled trials showing efficacy) for children and adolescents. There are several other approaches that have evidence of efficacy through randomized controlled trials, and have been specifically studied for different ages, cultural groups, and focus of intervention (group, family, classroom). Child-parent psychotherapy focuses on traumatized 3-to 5-year-olds and works with both parent and child. Eye movement desensitization and preprocessing therapy (EMDR), extensively studied for adults, has some randomized controlled trials in children. The National Child Traumatic Stress Network (NCTSN) has a website listing evidence-based interventions with descriptions of the extent of the evidence for these and other interventions, including the population for which the intervention was designed and information on training and dissemination.
A recent meta-analysis by Morina et al. identified 39 randomized controlled trials with psychological interventions targeting PTSD in children and youth and found a large (0.83) overall effect size vs. wait list control, and a moderate (0.41) effect size vs. an active control such as supportive therapy. There were enough randomized controlled trials to analyze the TF-CBT–based interventions as a group, and these had even larger effect sizes: 1.44 vs. wait list and 0.66 vs. active control. The non-CBT approaches did not have enough studies to be evaluated separately (Clin Psychol Rev. 2016 Jul;47:41-54).
It is important to know which available therapists are trained in specific interventions such as TF-CBT and review the evidence behind other interventions that therapists are using. Advocacy for the training of local therapists, particularly therapists who are affiliated with your practice, can increase these resources.
The evidence for pharmacologic treatment for PTSD in children and adolescents, in contrast to adults, is very thin. In adults, SSRIs have shown a significant benefit, but there have been three randomized controlled trials examining this question in young people with no significant difference shown for the SSRI. One of these compared TF-CBT alone to TF-CBT plus sertraline, with no added benefit for sertraline. A second compared sertraline to placebo and showed no difference, and the third was an extremely brief trial of 1 week of fluoxetine for children with burns, with no effect. There are open label studies of citalopram that have shown some benefit.
Prazosin is an alpha-1 antagonist that decreases the effect of peripheral norepinephrine, which has been shown to decrease reactivity in adults through two randomized controlled trials, but there are case reports in adolescents only. Guanfacine, an alpha-2 agonist that acts centrally to decrease norepinephrine release, has one open label study of the extended-release form in adolescents showing benefit, but there are two negative randomized controlled trials in adults. Other agents such as second-generation antipsychotics and mood stabilizers (specifically carbamazepine and valproic acid) have open label studies in children only and have the potential for significant side effects.
Psychotherapy is clearly the treatment of choice for children and adolescents with PTSD; the difficulty is that avoidance and difficulty trusting people are core symptoms of PTSD, and can lead patients to be extremely reluctant to try therapy. As a pediatrician, you likely already have a trusting relationship with your patient and parent(s), which can provide an opening for discussion.
Psychoeducation about trauma and the specific trauma a child has experienced is a core component and often the first step of PTSD treatment. The NCTSN website provides a goldmine of information about specific types of trauma (found under the tab labeled trauma types), including common symptoms at different developmental stages and specific resources. By providing information to families in a sensitive way, clinicians can help people understand that they are not alone, that their struggles are common reactions to the type of trauma they have experienced, and that people can recover with therapy so that the trauma does not have to go on negatively affecting their lives.
Finally, noting a parent’s possible trauma, and encouraging that parent to get his or her own treatment in order to help the child, can be a crucial first step.
General references
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
Traumatic events are extremely common, with as many as 60% of children experiencing some trauma by age 18 years. About 15% of these children will develop posttraumatic stress disorder (PTSD).
Case summary
Jane is a 13-year-old girl who presented because of steadily escalating angry outbursts with her mother, irritable mood, and anxiety since her father went to jail 2 years previously. Prior to the father’s departure from the family, he drank heavily and had been physically violent to Jane’s mother through most of Jane’s life.
Since these events, Jane has been extremely angry and irritable, often fighting extensively with her younger sister. She has severe difficulty separating from her mother, often following her around or demanding to know everything that her mother is doing. Jane herself reports that she feels worried, irritable, and sad much of the time. She is especially angry when thinking about anything related to her father. Jane won’t talk about her father to anyone, except occasionally her mother and one friend. She has difficulty falling asleep and has nightmares. She never thinks about the future, and instead just lives day to day. Images from the past come vividly into her mind. She has highly negative, hopeless views of the world, and doesn’t trust people, so she is unwilling to consider any therapy. Jane’s mother also is highly irritable and snaps at Jane over small things while in the office.
Discussion
The DSM-5 diagnostic criteria for PTSD require that an individual has been exposed to a severe stressor that threatens death, serious injury, or sexual violence through direct experience, witnessing the event happening to others, or learning that the event happened to a close family member or friend. Not all people who experience such events will develop PTSD, however. Additional symptoms are grouped into four areas (rather than three as in the DSM-IV), and a diagnosis requires one or two symptoms in each area:
• Intrusive symptoms including intrusive distressing memories, recurrent dreams with content related to the event, dissociative reactions such as flashbacks, intense distress at exposure to triggers that remind individuals of the event, or marked physiologic reactions to triggers.
• Avoidance of stimuli associated with the event, either memories or thoughts or external reminders.
• Negative cognitions manifesting as changes in thoughts and mood beginning or worsening after the event. These are an inability to remember the event, persistent negative beliefs about oneself or the world, distorted thoughts about the cause or results of the event, persistent negative emotional states such as anger or guilt, decreased participation in activities, feelings of estrangement from others, or an inability to experience positive emotions.
• Changes in arousal and reactivity as shown by irritable behavior, reckless behavior, hypervigilance, an exaggerated startle response, concentration problems, or sleep disturbance.
There are several screening instruments for the presence of a history of traumatic events as well as for symptoms of PTSD. The Child PTSD Symptom Scale (CPSS) is one example of a simple, readily available screening tool. More extensive assessment is an important part of treatment by mental health clinicians.
Treatment
Psychotherapy interventions are the core of treatment for PTSD in young people. Interventions based on cognitive-behavioral therapy (CBT) are the most extensively researched, with trauma-focused CBT (TF-CBT) being the specific intervention with the most research (13 randomized controlled trials showing efficacy) for children and adolescents. There are several other approaches that have evidence of efficacy through randomized controlled trials, and have been specifically studied for different ages, cultural groups, and focus of intervention (group, family, classroom). Child-parent psychotherapy focuses on traumatized 3-to 5-year-olds and works with both parent and child. Eye movement desensitization and preprocessing therapy (EMDR), extensively studied for adults, has some randomized controlled trials in children. The National Child Traumatic Stress Network (NCTSN) has a website listing evidence-based interventions with descriptions of the extent of the evidence for these and other interventions, including the population for which the intervention was designed and information on training and dissemination.
A recent meta-analysis by Morina et al. identified 39 randomized controlled trials with psychological interventions targeting PTSD in children and youth and found a large (0.83) overall effect size vs. wait list control, and a moderate (0.41) effect size vs. an active control such as supportive therapy. There were enough randomized controlled trials to analyze the TF-CBT–based interventions as a group, and these had even larger effect sizes: 1.44 vs. wait list and 0.66 vs. active control. The non-CBT approaches did not have enough studies to be evaluated separately (Clin Psychol Rev. 2016 Jul;47:41-54).
It is important to know which available therapists are trained in specific interventions such as TF-CBT and review the evidence behind other interventions that therapists are using. Advocacy for the training of local therapists, particularly therapists who are affiliated with your practice, can increase these resources.
The evidence for pharmacologic treatment for PTSD in children and adolescents, in contrast to adults, is very thin. In adults, SSRIs have shown a significant benefit, but there have been three randomized controlled trials examining this question in young people with no significant difference shown for the SSRI. One of these compared TF-CBT alone to TF-CBT plus sertraline, with no added benefit for sertraline. A second compared sertraline to placebo and showed no difference, and the third was an extremely brief trial of 1 week of fluoxetine for children with burns, with no effect. There are open label studies of citalopram that have shown some benefit.
Prazosin is an alpha-1 antagonist that decreases the effect of peripheral norepinephrine, which has been shown to decrease reactivity in adults through two randomized controlled trials, but there are case reports in adolescents only. Guanfacine, an alpha-2 agonist that acts centrally to decrease norepinephrine release, has one open label study of the extended-release form in adolescents showing benefit, but there are two negative randomized controlled trials in adults. Other agents such as second-generation antipsychotics and mood stabilizers (specifically carbamazepine and valproic acid) have open label studies in children only and have the potential for significant side effects.
Psychotherapy is clearly the treatment of choice for children and adolescents with PTSD; the difficulty is that avoidance and difficulty trusting people are core symptoms of PTSD, and can lead patients to be extremely reluctant to try therapy. As a pediatrician, you likely already have a trusting relationship with your patient and parent(s), which can provide an opening for discussion.
Psychoeducation about trauma and the specific trauma a child has experienced is a core component and often the first step of PTSD treatment. The NCTSN website provides a goldmine of information about specific types of trauma (found under the tab labeled trauma types), including common symptoms at different developmental stages and specific resources. By providing information to families in a sensitive way, clinicians can help people understand that they are not alone, that their struggles are common reactions to the type of trauma they have experienced, and that people can recover with therapy so that the trauma does not have to go on negatively affecting their lives.
Finally, noting a parent’s possible trauma, and encouraging that parent to get his or her own treatment in order to help the child, can be a crucial first step.
General references
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.

A prescription for health literacy
As physicians, we have a responsibility to stay abreast of the medical literature to provide state of the art pediatric care. We have at our disposal reliable resources to stay current, from professional organizations that provide us with updated practice guidelines, to scientific publications with cutting-edge medical research and clinical databases that offer support for medical decision making.
The greater public, however, does not have the luxury of a guide to navigate the health information ocean. In addition to traditional news outlets, such as television and the printed press, the advent of the Internet and social media have placed unprecedented amounts of medical information at everyone’s fingertips.1 But not all health information is created equal, and even “Dr. Google” has admitted its symptoms search engine has not been very helpful.2

Many websites, despite authoritarian-sounding domain names, are not impartial providers of medical information. The power of the media to shape public perception is perhaps nowhere more poignantly felt than in the pediatric community, where the now thoroughly debunked study by Dr. Andrew Wakefield that linked the MMR vaccine to autism continues to have lingering effects on vaccination rates.3,4
I recently completed an internship in medical journalism with ABC News in New York City to better understand how the news media provides health and medical information to millions of Americans. Lay medical journalists have the complicated task of reviewing new research, weighing its newsworthiness, and distilling complex concepts down to easy-to-digest sound bites. Working with medical correspondents and the editorial team, I reviewed new scientific studies, dissected their impact, and pondered their potential for a catchy headline. I also wrote content for medical segments and participated in educational Twitter chats. What made the headlines wasn’t always what I thought should make the headlines, and translating the results of a randomized, controlled trial into a 60-second script for television felt near impossible. Dipping my toes into medical journalism gave me a new appreciation of my role as a physician educator – avoiding health information overload and promoting meaningful health literacy for my patients.

The 24/7 medical news cycle is here to stay. Our patients will continue to use various media platforms for medical information whether we like it or not. It is our responsibility as pediatricians to help families get the most relevant and current medical information. By directing them to trustworthy sources, such as the American Academy of Pediatrics at healthychildren.org or the National Library of Medicine at www.nlm.nih.gov/medlineplus, we can strengthen our therapeutic alliance while promoting health literacy.
References
1. Interact J Med Res. 2015 Jun 22;4(2):e12.
3. “A Discredited Vaccine Study’s Continuing Impact on Public Health,” by Clyde Haberman, Feb. 1, 2015.
4. Ann Pharmacother. 2011 Oct;45(10):1302-4.
Dr. Talbot is a third-year resident at Monroe Carell Jr. Children’s Hospital at Vanderbilt in Nashville, Tenn. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
As physicians, we have a responsibility to stay abreast of the medical literature to provide state of the art pediatric care. We have at our disposal reliable resources to stay current, from professional organizations that provide us with updated practice guidelines, to scientific publications with cutting-edge medical research and clinical databases that offer support for medical decision making.
The greater public, however, does not have the luxury of a guide to navigate the health information ocean. In addition to traditional news outlets, such as television and the printed press, the advent of the Internet and social media have placed unprecedented amounts of medical information at everyone’s fingertips.1 But not all health information is created equal, and even “Dr. Google” has admitted its symptoms search engine has not been very helpful.2
Many websites, despite authoritarian-sounding domain names, are not impartial providers of medical information. The power of the media to shape public perception is perhaps nowhere more poignantly felt than in the pediatric community, where the now thoroughly debunked study by Dr. Andrew Wakefield that linked the MMR vaccine to autism continues to have lingering effects on vaccination rates.3,4
I recently completed an internship in medical journalism with ABC News in New York City to better understand how the news media provides health and medical information to millions of Americans. Lay medical journalists have the complicated task of reviewing new research, weighing its newsworthiness, and distilling complex concepts down to easy-to-digest sound bites. Working with medical correspondents and the editorial team, I reviewed new scientific studies, dissected their impact, and pondered their potential for a catchy headline. I also wrote content for medical segments and participated in educational Twitter chats. What made the headlines wasn’t always what I thought should make the headlines, and translating the results of a randomized, controlled trial into a 60-second script for television felt near impossible. Dipping my toes into medical journalism gave me a new appreciation of my role as a physician educator – avoiding health information overload and promoting meaningful health literacy for my patients.
The 24/7 medical news cycle is here to stay. Our patients will continue to use various media platforms for medical information whether we like it or not. It is our responsibility as pediatricians to help families get the most relevant and current medical information. By directing them to trustworthy sources, such as the American Academy of Pediatrics at healthychildren.org or the National Library of Medicine at www.nlm.nih.gov/medlineplus, we can strengthen our therapeutic alliance while promoting health literacy.
References
1. Interact J Med Res. 2015 Jun 22;4(2):e12.
3. “A Discredited Vaccine Study’s Continuing Impact on Public Health,” by Clyde Haberman, Feb. 1, 2015.
4. Ann Pharmacother. 2011 Oct;45(10):1302-4.
Dr. Talbot is a third-year resident at Monroe Carell Jr. Children’s Hospital at Vanderbilt in Nashville, Tenn. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
As physicians, we have a responsibility to stay abreast of the medical literature to provide state of the art pediatric care. We have at our disposal reliable resources to stay current, from professional organizations that provide us with updated practice guidelines, to scientific publications with cutting-edge medical research and clinical databases that offer support for medical decision making.
The greater public, however, does not have the luxury of a guide to navigate the health information ocean. In addition to traditional news outlets, such as television and the printed press, the advent of the Internet and social media have placed unprecedented amounts of medical information at everyone’s fingertips.1 But not all health information is created equal, and even “Dr. Google” has admitted its symptoms search engine has not been very helpful.2
Many websites, despite authoritarian-sounding domain names, are not impartial providers of medical information. The power of the media to shape public perception is perhaps nowhere more poignantly felt than in the pediatric community, where the now thoroughly debunked study by Dr. Andrew Wakefield that linked the MMR vaccine to autism continues to have lingering effects on vaccination rates.3,4
I recently completed an internship in medical journalism with ABC News in New York City to better understand how the news media provides health and medical information to millions of Americans. Lay medical journalists have the complicated task of reviewing new research, weighing its newsworthiness, and distilling complex concepts down to easy-to-digest sound bites. Working with medical correspondents and the editorial team, I reviewed new scientific studies, dissected their impact, and pondered their potential for a catchy headline. I also wrote content for medical segments and participated in educational Twitter chats. What made the headlines wasn’t always what I thought should make the headlines, and translating the results of a randomized, controlled trial into a 60-second script for television felt near impossible. Dipping my toes into medical journalism gave me a new appreciation of my role as a physician educator – avoiding health information overload and promoting meaningful health literacy for my patients.
The 24/7 medical news cycle is here to stay. Our patients will continue to use various media platforms for medical information whether we like it or not. It is our responsibility as pediatricians to help families get the most relevant and current medical information. By directing them to trustworthy sources, such as the American Academy of Pediatrics at healthychildren.org or the National Library of Medicine at www.nlm.nih.gov/medlineplus, we can strengthen our therapeutic alliance while promoting health literacy.
References
1. Interact J Med Res. 2015 Jun 22;4(2):e12.
3. “A Discredited Vaccine Study’s Continuing Impact on Public Health,” by Clyde Haberman, Feb. 1, 2015.
4. Ann Pharmacother. 2011 Oct;45(10):1302-4.
Dr. Talbot is a third-year resident at Monroe Carell Jr. Children’s Hospital at Vanderbilt in Nashville, Tenn. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.

Study Links Severe Childhood Eczema to Sedentary Behaviors
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Study links severe childhood eczema to sedentary behaviors
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: A large national study linked severe atopic dermatitis to sedentary behaviors and screen time.
Major finding: Compared with children without eczema, those with severe disease were about 60% less likely to exercise at least once a week (OR, 0.39).
Data source: An analysis of data for 131,783 children from the National Survey of Children’s Health.
Disclosures: The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
Consider home phototherapy for some pediatric patients
MINNEAPOLIS, MINN. – For a select subset of pediatric dermatology patients, home phototherapy may represent a safe, effective, and even affordable alternative to office visits. Some families whose children are in treatment for vitiligo, psoriasis, and atopic dermatitis may find that the expense and learning curve of administering treatment at home are worthwhile, but dermatologists must select those families carefully.
Leslie Castelo-Soccio, MD, PhD, professor of pediatric dermatology at the Children’s Hospital of Philadelphia, gave an overview of medical phototherapy for childhood skin diseases at the annual meeting of the Society for Pediatric Dermatology.
For vitiligo, narrow-band UVB’s (NBUVB) effectiveness is maximized if treatment is begun relatively early, and if results are going to happen, they’ll show up fairly quickly. “If there’s no response after six months, stop the therapy,” Dr. Castelo-Soccio said.
Although the literature shows NBUVB to be effective in treating atopic dermatitis, Dr. Castelo-Soccio noted that most pediatric atopic dermatitis studies have been small and retrospective and conducted in a population with severe disease.
Regarding psoriasis in children, the literature shows “higher numbers of patients with near-complete or complete response,” she said.
The experience of NBUVB for pediatric dermatologic conditions at the Children’s Hospital of Philadelphia supports the idea that “the best responses are seen after at least 40 treatments,” and that 6 months is enough time to see whether a patient will respond. The best responders at her institution are children with facial vitiligo. “Of course, you get a better response with compliance,” she noted.
The experience of her patients falls in line with the data about side effects, in which the most common adverse events are reactivation of HSV and burning.
Families ask about cancer risk, but “there are no published data on the risk of skin cancer in long-term phototherapy in children,” she said. At this point, the best pediatric dermatologists can do is to extrapolate risk from data on phototherapy for neonatal jaundice, but even those data are inconclusive, she said.
Dr. Castelo-Soccio noted that it’s pretty common for families to request home treatment: “When you start talking to patients about phototherapy, the thing I always get questions about is, ‘Why can’t I do it at home?’ ” She prefers to initiate treatment in the clinic and then assess suitability for home therapy after a relationship has been established.
The ideal patient, said Dr. Castelo-Soccio, is one whose family has been diligent about coming to appointments and who otherwise demonstrates excellent compliance.
At first blush, the cost of acquiring a home device – often in the $2,000 range – might seem prohibitive for many families. The upfront cost may be worth it for some, since office visits involve copayments and lost time from school and work for multiple treatments weekly over a period of months. A big commute to the doctor’s office for treatment may further tip the scales toward home treatment. “I wouldn’t hesitate to offer this option to the right family,” she said.
Dr. Castelo-Soccio said she’s had some limited success getting insurance reimbursement for home phototherapy, especially if success has already been seen with office-based treatment.
NBUVB therapy has limitations, though. Some that have particular relevance for the pediatric population involve the challenges of safe delivery, including using appropriate eye wear and ensuring lack of movement. Each of these problems can be even more of a challenge at home, reinforcing the need to select appropriate patients for home phototherapy, she added.
Dr. Castelo-Soccio said she provides information about all of the various phototherapy devices to her patients and their parents, letting them make the choice. “All of the companies are really good about helping with paperwork” to apply for insurance reimbursement, she said. Options range from the bulkiest and most expensive – a full phototherapy box – to three-panel arrays, single panels, hand-foot devices, and even hand-held devices. The latter can be had for less than $1,000 and may be best suited for targeting smaller areas.
Features to look for in home phototherapy devices include a dosimeter accuracy sensor, which adjusts the treatment time to deliver the same dose, even if dust or aging lamps reduce output. User-friendly timers also are helpful for families, said Dr. Castelo-Soccio. A safety lock-out will allow only a certain number of treatments before the unit must be reset by the physician and is a reassuring feature. Each activation counts as a treatment, however, so families and physicians must be aware that if a hand-held unit is used to treat multiple small lesions in different body areas, a single treatment session will involve many device activations, each of which will be registered as a treatment.
Dr. Castelo-Soccio had no relevant financial disclosures.
On Twitter @karioakes
MINNEAPOLIS, MINN. – For a select subset of pediatric dermatology patients, home phototherapy may represent a safe, effective, and even affordable alternative to office visits. Some families whose children are in treatment for vitiligo, psoriasis, and atopic dermatitis may find that the expense and learning curve of administering treatment at home are worthwhile, but dermatologists must select those families carefully.
Leslie Castelo-Soccio, MD, PhD, professor of pediatric dermatology at the Children’s Hospital of Philadelphia, gave an overview of medical phototherapy for childhood skin diseases at the annual meeting of the Society for Pediatric Dermatology.
For vitiligo, narrow-band UVB’s (NBUVB) effectiveness is maximized if treatment is begun relatively early, and if results are going to happen, they’ll show up fairly quickly. “If there’s no response after six months, stop the therapy,” Dr. Castelo-Soccio said.
Although the literature shows NBUVB to be effective in treating atopic dermatitis, Dr. Castelo-Soccio noted that most pediatric atopic dermatitis studies have been small and retrospective and conducted in a population with severe disease.
Regarding psoriasis in children, the literature shows “higher numbers of patients with near-complete or complete response,” she said.
The experience of NBUVB for pediatric dermatologic conditions at the Children’s Hospital of Philadelphia supports the idea that “the best responses are seen after at least 40 treatments,” and that 6 months is enough time to see whether a patient will respond. The best responders at her institution are children with facial vitiligo. “Of course, you get a better response with compliance,” she noted.
The experience of her patients falls in line with the data about side effects, in which the most common adverse events are reactivation of HSV and burning.
Families ask about cancer risk, but “there are no published data on the risk of skin cancer in long-term phototherapy in children,” she said. At this point, the best pediatric dermatologists can do is to extrapolate risk from data on phototherapy for neonatal jaundice, but even those data are inconclusive, she said.
Dr. Castelo-Soccio noted that it’s pretty common for families to request home treatment: “When you start talking to patients about phototherapy, the thing I always get questions about is, ‘Why can’t I do it at home?’ ” She prefers to initiate treatment in the clinic and then assess suitability for home therapy after a relationship has been established.
The ideal patient, said Dr. Castelo-Soccio, is one whose family has been diligent about coming to appointments and who otherwise demonstrates excellent compliance.
At first blush, the cost of acquiring a home device – often in the $2,000 range – might seem prohibitive for many families. The upfront cost may be worth it for some, since office visits involve copayments and lost time from school and work for multiple treatments weekly over a period of months. A big commute to the doctor’s office for treatment may further tip the scales toward home treatment. “I wouldn’t hesitate to offer this option to the right family,” she said.
Dr. Castelo-Soccio said she’s had some limited success getting insurance reimbursement for home phototherapy, especially if success has already been seen with office-based treatment.
NBUVB therapy has limitations, though. Some that have particular relevance for the pediatric population involve the challenges of safe delivery, including using appropriate eye wear and ensuring lack of movement. Each of these problems can be even more of a challenge at home, reinforcing the need to select appropriate patients for home phototherapy, she added.
Dr. Castelo-Soccio said she provides information about all of the various phototherapy devices to her patients and their parents, letting them make the choice. “All of the companies are really good about helping with paperwork” to apply for insurance reimbursement, she said. Options range from the bulkiest and most expensive – a full phototherapy box – to three-panel arrays, single panels, hand-foot devices, and even hand-held devices. The latter can be had for less than $1,000 and may be best suited for targeting smaller areas.
Features to look for in home phototherapy devices include a dosimeter accuracy sensor, which adjusts the treatment time to deliver the same dose, even if dust or aging lamps reduce output. User-friendly timers also are helpful for families, said Dr. Castelo-Soccio. A safety lock-out will allow only a certain number of treatments before the unit must be reset by the physician and is a reassuring feature. Each activation counts as a treatment, however, so families and physicians must be aware that if a hand-held unit is used to treat multiple small lesions in different body areas, a single treatment session will involve many device activations, each of which will be registered as a treatment.
Dr. Castelo-Soccio had no relevant financial disclosures.
On Twitter @karioakes
MINNEAPOLIS, MINN. – For a select subset of pediatric dermatology patients, home phototherapy may represent a safe, effective, and even affordable alternative to office visits. Some families whose children are in treatment for vitiligo, psoriasis, and atopic dermatitis may find that the expense and learning curve of administering treatment at home are worthwhile, but dermatologists must select those families carefully.
Leslie Castelo-Soccio, MD, PhD, professor of pediatric dermatology at the Children’s Hospital of Philadelphia, gave an overview of medical phototherapy for childhood skin diseases at the annual meeting of the Society for Pediatric Dermatology.
For vitiligo, narrow-band UVB’s (NBUVB) effectiveness is maximized if treatment is begun relatively early, and if results are going to happen, they’ll show up fairly quickly. “If there’s no response after six months, stop the therapy,” Dr. Castelo-Soccio said.
Although the literature shows NBUVB to be effective in treating atopic dermatitis, Dr. Castelo-Soccio noted that most pediatric atopic dermatitis studies have been small and retrospective and conducted in a population with severe disease.
Regarding psoriasis in children, the literature shows “higher numbers of patients with near-complete or complete response,” she said.
The experience of NBUVB for pediatric dermatologic conditions at the Children’s Hospital of Philadelphia supports the idea that “the best responses are seen after at least 40 treatments,” and that 6 months is enough time to see whether a patient will respond. The best responders at her institution are children with facial vitiligo. “Of course, you get a better response with compliance,” she noted.
The experience of her patients falls in line with the data about side effects, in which the most common adverse events are reactivation of HSV and burning.
Families ask about cancer risk, but “there are no published data on the risk of skin cancer in long-term phototherapy in children,” she said. At this point, the best pediatric dermatologists can do is to extrapolate risk from data on phototherapy for neonatal jaundice, but even those data are inconclusive, she said.
Dr. Castelo-Soccio noted that it’s pretty common for families to request home treatment: “When you start talking to patients about phototherapy, the thing I always get questions about is, ‘Why can’t I do it at home?’ ” She prefers to initiate treatment in the clinic and then assess suitability for home therapy after a relationship has been established.
The ideal patient, said Dr. Castelo-Soccio, is one whose family has been diligent about coming to appointments and who otherwise demonstrates excellent compliance.
At first blush, the cost of acquiring a home device – often in the $2,000 range – might seem prohibitive for many families. The upfront cost may be worth it for some, since office visits involve copayments and lost time from school and work for multiple treatments weekly over a period of months. A big commute to the doctor’s office for treatment may further tip the scales toward home treatment. “I wouldn’t hesitate to offer this option to the right family,” she said.
Dr. Castelo-Soccio said she’s had some limited success getting insurance reimbursement for home phototherapy, especially if success has already been seen with office-based treatment.
NBUVB therapy has limitations, though. Some that have particular relevance for the pediatric population involve the challenges of safe delivery, including using appropriate eye wear and ensuring lack of movement. Each of these problems can be even more of a challenge at home, reinforcing the need to select appropriate patients for home phototherapy, she added.
Dr. Castelo-Soccio said she provides information about all of the various phototherapy devices to her patients and their parents, letting them make the choice. “All of the companies are really good about helping with paperwork” to apply for insurance reimbursement, she said. Options range from the bulkiest and most expensive – a full phototherapy box – to three-panel arrays, single panels, hand-foot devices, and even hand-held devices. The latter can be had for less than $1,000 and may be best suited for targeting smaller areas.
Features to look for in home phototherapy devices include a dosimeter accuracy sensor, which adjusts the treatment time to deliver the same dose, even if dust or aging lamps reduce output. User-friendly timers also are helpful for families, said Dr. Castelo-Soccio. A safety lock-out will allow only a certain number of treatments before the unit must be reset by the physician and is a reassuring feature. Each activation counts as a treatment, however, so families and physicians must be aware that if a hand-held unit is used to treat multiple small lesions in different body areas, a single treatment session will involve many device activations, each of which will be registered as a treatment.
Dr. Castelo-Soccio had no relevant financial disclosures.
On Twitter @karioakes
EXPERT ANALYSIS FROM THE SPD ANNUAL MEETING
Syndecan-1 may predict kidney injury after ped heart surgery
Acute kidney injury is a common complication after pediatric cardiac surgery, but measuring for a specific genetic protein immediately after cardiac surgery may improve cardiac surgeons’ ability to predict patients at higher risk of AKI, according to researchers from Brazil. The study results are in the July issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152-178-86).
“Plasma syndecan-1 levels measured early in the postoperative period were independently associated with severe acute kidney injury,” wrote Candice Torres de Melo Bezerra Cavalcante, MD, of Heart Hospital of Messejana and Federal University of Ceará.
Their prospective cohort study involved 289 pediatric patients who had cardiac surgery at their institution between September 2013 and December 2014.
Dr. Cavalcante and colleagues acknowledged that the traditional biomarker for renal function, serum creatinine, only increases appreciably after the glomerular filtration rate declines 50%, impairing physicians’ ability to detect AKI early enough to treat it. “This delay can explain, in part the, negative results in AKI therapeutic clinical trials,” they wrote.
They evaluated two different endothelial biomarkers in addition to syndecan-1 with regard to their capacity for predicting severe AKI: plasma ICAM-1, a marker of endothelial cell activation; and E-selectin, an endothelial cell adhesion molecule. Syndecan-1 works as a biomarker of injury to the glycocalyx protein that surrounds endothelial cell membranes that acts as a permeability barrier and prevents the cells from adhering to blood. They found that median syndecan-1 levels soon after surgery were higher in patients with severe AKI, 103.6 vs. 42.3 ng/mL.
“Although syndecan-1 is not a renal-specific biomarker, there has been recent increasing evidence that endothelial injury has an important role in AKI pathophysiology,” the researchers noted.
Study results showed the higher the level of syndecan-1, the greater the adjusted odds ratio (OR) for severe AKI. Levels of less than 17 ng/mL were considered normal; 17.1-46.7 ng/mL carried an adjusted OR of 1.42; 47.4-93.1 ng/mL had an adjusted OR of 2.05; and levels 96.3 or greater had an OR of 8.87.
“Maintenance of endothelial glycocalyx integrity can be a therapeutic target to reduce AKI in this setting,” the researchers wrote.
The authors acknowledged that the study was done at a single center that had dialysis and death rates three and five times higher, respectively, than those of developed countries; and it measured syndecan-1 at only one time point almost immediately after the operation.
“Adding postoperative syndecan-1, even when using a clinical model that already incorporates variables from renal angina index, results in significant improvement in the capacity to predict severe AKI,” Dr. Cavalcante and colleagues concluded.
They had no financial relationships to disclose.
Results of AKI in heart surgery patients have been “sobering,” with up to 56% of these patients being diagnosed with AKI, but research such as that by Dr. Cavalcante and colleagues represents a new approach to improving outcomes by combining clinical risk factors with specific biomarkers to identify patients at risk, Petros V. Anagnostopoulos, MD, of American Family Children’s Hospital, University of Wisconsin, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152[1]:187-8).
Dr. Anagnostopoulos acknowledged problems with traditional markers for renal function. “An ideal biomarker should be sensitive, easy to measure, reproducible, and inexpensive,” he said. “Finally, when combined with clinical prediction models, it should potentiate the discrimination of these models.”
Syndecan-1 answers that call, he said. “It peaks early and is cheap, fast, and easy to measure with readily available methods, which makes it an ideal early biomarker of AKI,” Dr. Anagnostopoulos said. Even so, he pointed out potential shortcomings of syndecan-1: It is not renal specific and it does not increase before the operation.
But he applauded Dr. Cavalcante and colleagues for pursuing research to combine clinical risk factors with specific biomarkers. “It is very likely that this type of clinical research will become prevalent in the near future and will hopefully produce results that will allow better individual patient-specific risk stratification,” Dr. Anagnostopoulos said.
He had no financial relationships to disclose.
Results of AKI in heart surgery patients have been “sobering,” with up to 56% of these patients being diagnosed with AKI, but research such as that by Dr. Cavalcante and colleagues represents a new approach to improving outcomes by combining clinical risk factors with specific biomarkers to identify patients at risk, Petros V. Anagnostopoulos, MD, of American Family Children’s Hospital, University of Wisconsin, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152[1]:187-8).
Dr. Anagnostopoulos acknowledged problems with traditional markers for renal function. “An ideal biomarker should be sensitive, easy to measure, reproducible, and inexpensive,” he said. “Finally, when combined with clinical prediction models, it should potentiate the discrimination of these models.”
Syndecan-1 answers that call, he said. “It peaks early and is cheap, fast, and easy to measure with readily available methods, which makes it an ideal early biomarker of AKI,” Dr. Anagnostopoulos said. Even so, he pointed out potential shortcomings of syndecan-1: It is not renal specific and it does not increase before the operation.
But he applauded Dr. Cavalcante and colleagues for pursuing research to combine clinical risk factors with specific biomarkers. “It is very likely that this type of clinical research will become prevalent in the near future and will hopefully produce results that will allow better individual patient-specific risk stratification,” Dr. Anagnostopoulos said.
He had no financial relationships to disclose.
Results of AKI in heart surgery patients have been “sobering,” with up to 56% of these patients being diagnosed with AKI, but research such as that by Dr. Cavalcante and colleagues represents a new approach to improving outcomes by combining clinical risk factors with specific biomarkers to identify patients at risk, Petros V. Anagnostopoulos, MD, of American Family Children’s Hospital, University of Wisconsin, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152[1]:187-8).
Dr. Anagnostopoulos acknowledged problems with traditional markers for renal function. “An ideal biomarker should be sensitive, easy to measure, reproducible, and inexpensive,” he said. “Finally, when combined with clinical prediction models, it should potentiate the discrimination of these models.”
Syndecan-1 answers that call, he said. “It peaks early and is cheap, fast, and easy to measure with readily available methods, which makes it an ideal early biomarker of AKI,” Dr. Anagnostopoulos said. Even so, he pointed out potential shortcomings of syndecan-1: It is not renal specific and it does not increase before the operation.
But he applauded Dr. Cavalcante and colleagues for pursuing research to combine clinical risk factors with specific biomarkers. “It is very likely that this type of clinical research will become prevalent in the near future and will hopefully produce results that will allow better individual patient-specific risk stratification,” Dr. Anagnostopoulos said.
He had no financial relationships to disclose.
Acute kidney injury is a common complication after pediatric cardiac surgery, but measuring for a specific genetic protein immediately after cardiac surgery may improve cardiac surgeons’ ability to predict patients at higher risk of AKI, according to researchers from Brazil. The study results are in the July issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152-178-86).
“Plasma syndecan-1 levels measured early in the postoperative period were independently associated with severe acute kidney injury,” wrote Candice Torres de Melo Bezerra Cavalcante, MD, of Heart Hospital of Messejana and Federal University of Ceará.
Their prospective cohort study involved 289 pediatric patients who had cardiac surgery at their institution between September 2013 and December 2014.
Dr. Cavalcante and colleagues acknowledged that the traditional biomarker for renal function, serum creatinine, only increases appreciably after the glomerular filtration rate declines 50%, impairing physicians’ ability to detect AKI early enough to treat it. “This delay can explain, in part the, negative results in AKI therapeutic clinical trials,” they wrote.
They evaluated two different endothelial biomarkers in addition to syndecan-1 with regard to their capacity for predicting severe AKI: plasma ICAM-1, a marker of endothelial cell activation; and E-selectin, an endothelial cell adhesion molecule. Syndecan-1 works as a biomarker of injury to the glycocalyx protein that surrounds endothelial cell membranes that acts as a permeability barrier and prevents the cells from adhering to blood. They found that median syndecan-1 levels soon after surgery were higher in patients with severe AKI, 103.6 vs. 42.3 ng/mL.
“Although syndecan-1 is not a renal-specific biomarker, there has been recent increasing evidence that endothelial injury has an important role in AKI pathophysiology,” the researchers noted.
Study results showed the higher the level of syndecan-1, the greater the adjusted odds ratio (OR) for severe AKI. Levels of less than 17 ng/mL were considered normal; 17.1-46.7 ng/mL carried an adjusted OR of 1.42; 47.4-93.1 ng/mL had an adjusted OR of 2.05; and levels 96.3 or greater had an OR of 8.87.
“Maintenance of endothelial glycocalyx integrity can be a therapeutic target to reduce AKI in this setting,” the researchers wrote.
The authors acknowledged that the study was done at a single center that had dialysis and death rates three and five times higher, respectively, than those of developed countries; and it measured syndecan-1 at only one time point almost immediately after the operation.
“Adding postoperative syndecan-1, even when using a clinical model that already incorporates variables from renal angina index, results in significant improvement in the capacity to predict severe AKI,” Dr. Cavalcante and colleagues concluded.
They had no financial relationships to disclose.
Acute kidney injury is a common complication after pediatric cardiac surgery, but measuring for a specific genetic protein immediately after cardiac surgery may improve cardiac surgeons’ ability to predict patients at higher risk of AKI, according to researchers from Brazil. The study results are in the July issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152-178-86).
“Plasma syndecan-1 levels measured early in the postoperative period were independently associated with severe acute kidney injury,” wrote Candice Torres de Melo Bezerra Cavalcante, MD, of Heart Hospital of Messejana and Federal University of Ceará.
Their prospective cohort study involved 289 pediatric patients who had cardiac surgery at their institution between September 2013 and December 2014.
Dr. Cavalcante and colleagues acknowledged that the traditional biomarker for renal function, serum creatinine, only increases appreciably after the glomerular filtration rate declines 50%, impairing physicians’ ability to detect AKI early enough to treat it. “This delay can explain, in part the, negative results in AKI therapeutic clinical trials,” they wrote.
They evaluated two different endothelial biomarkers in addition to syndecan-1 with regard to their capacity for predicting severe AKI: plasma ICAM-1, a marker of endothelial cell activation; and E-selectin, an endothelial cell adhesion molecule. Syndecan-1 works as a biomarker of injury to the glycocalyx protein that surrounds endothelial cell membranes that acts as a permeability barrier and prevents the cells from adhering to blood. They found that median syndecan-1 levels soon after surgery were higher in patients with severe AKI, 103.6 vs. 42.3 ng/mL.
“Although syndecan-1 is not a renal-specific biomarker, there has been recent increasing evidence that endothelial injury has an important role in AKI pathophysiology,” the researchers noted.
Study results showed the higher the level of syndecan-1, the greater the adjusted odds ratio (OR) for severe AKI. Levels of less than 17 ng/mL were considered normal; 17.1-46.7 ng/mL carried an adjusted OR of 1.42; 47.4-93.1 ng/mL had an adjusted OR of 2.05; and levels 96.3 or greater had an OR of 8.87.
“Maintenance of endothelial glycocalyx integrity can be a therapeutic target to reduce AKI in this setting,” the researchers wrote.
The authors acknowledged that the study was done at a single center that had dialysis and death rates three and five times higher, respectively, than those of developed countries; and it measured syndecan-1 at only one time point almost immediately after the operation.
“Adding postoperative syndecan-1, even when using a clinical model that already incorporates variables from renal angina index, results in significant improvement in the capacity to predict severe AKI,” Dr. Cavalcante and colleagues concluded.
They had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: The biomarker syndecan-1 may aid in determining acute kidney injury risk for children having cardiac surgery.
Major finding: Children with elevated levels of syndecan-1 had a two- to ninefold greater risk of acute kidney injury.
Data source: Single-institution, prospective cohort study of 289 pediatric patients who had cardiac surgery from September 2013 to December 2014.
Disclosures: Dr. Cavalcante and coauthors had no financial relationships to disclose.
9-valent, Quadrivalent HPV Vaccines Have Comparable Safety
The 9-valent human papillomavirus vaccine was well tolerated in 16-26 year olds and had a safety profile comparable to that of the quadrivalent vaccine, according to an analysis of seven phase III trials.
“The demonstrated efficacy and favorable safety profile of the 9vHPV vaccine support widespread vaccination programs,” reported Dr. Edson D. Moreira Jr. and his associates in Pediatrics.
Vaccines were given in a three-dose regimen: 15,776 male and female patients received at least one dose of the 9-valent vaccine and 7,391 control subjects received at least one dose of the quadrivalent vaccine.
Frequencies of vaccine-related systemic adverse events such as headache and pyrexia were “generally similar” between the two vaccine groups, the investigators reported.
Compared with the quadrivalent vaccine, the 9-valent vaccine was associated with significantly more frequent adverse events at the injection site, including pain (84% vs. 90%), swelling (29% vs. 40%), and erythema (34% vs. 26%). Most of these reactions in both groups were mild to moderate in intensity, however.
Discontinuations and vaccine-related serious adverse events in the 9-valent vaccine group were rare (0.1% and less than 0.1%, respectively).
Read the full study here (doi:10.1542/peds.2015-4387).
The 9-valent human papillomavirus vaccine was well tolerated in 16-26 year olds and had a safety profile comparable to that of the quadrivalent vaccine, according to an analysis of seven phase III trials.
“The demonstrated efficacy and favorable safety profile of the 9vHPV vaccine support widespread vaccination programs,” reported Dr. Edson D. Moreira Jr. and his associates in Pediatrics.
Vaccines were given in a three-dose regimen: 15,776 male and female patients received at least one dose of the 9-valent vaccine and 7,391 control subjects received at least one dose of the quadrivalent vaccine.
Frequencies of vaccine-related systemic adverse events such as headache and pyrexia were “generally similar” between the two vaccine groups, the investigators reported.
Compared with the quadrivalent vaccine, the 9-valent vaccine was associated with significantly more frequent adverse events at the injection site, including pain (84% vs. 90%), swelling (29% vs. 40%), and erythema (34% vs. 26%). Most of these reactions in both groups were mild to moderate in intensity, however.
Discontinuations and vaccine-related serious adverse events in the 9-valent vaccine group were rare (0.1% and less than 0.1%, respectively).
Read the full study here (doi:10.1542/peds.2015-4387).
The 9-valent human papillomavirus vaccine was well tolerated in 16-26 year olds and had a safety profile comparable to that of the quadrivalent vaccine, according to an analysis of seven phase III trials.
“The demonstrated efficacy and favorable safety profile of the 9vHPV vaccine support widespread vaccination programs,” reported Dr. Edson D. Moreira Jr. and his associates in Pediatrics.
Vaccines were given in a three-dose regimen: 15,776 male and female patients received at least one dose of the 9-valent vaccine and 7,391 control subjects received at least one dose of the quadrivalent vaccine.
Frequencies of vaccine-related systemic adverse events such as headache and pyrexia were “generally similar” between the two vaccine groups, the investigators reported.
Compared with the quadrivalent vaccine, the 9-valent vaccine was associated with significantly more frequent adverse events at the injection site, including pain (84% vs. 90%), swelling (29% vs. 40%), and erythema (34% vs. 26%). Most of these reactions in both groups were mild to moderate in intensity, however.
Discontinuations and vaccine-related serious adverse events in the 9-valent vaccine group were rare (0.1% and less than 0.1%, respectively).
Read the full study here (doi:10.1542/peds.2015-4387).
FROM PEDIATRICS
9-valent, quadrivalent HPV vaccines have comparable safety
The 9-valent human papillomavirus vaccine was well tolerated in 16-26 year olds and had a safety profile comparable to that of the quadrivalent vaccine, according to an analysis of seven phase III trials.
“The demonstrated efficacy and favorable safety profile of the 9vHPV vaccine support widespread vaccination programs,” reported Dr. Edson D. Moreira Jr. and his associates in Pediatrics.
Vaccines were given in a three-dose regimen: 15,776 male and female patients received at least one dose of the 9-valent vaccine and 7,391 control subjects received at least one dose of the quadrivalent vaccine.
Frequencies of vaccine-related systemic adverse events such as headache and pyrexia were “generally similar” between the two vaccine groups, the investigators reported.
Compared with the quadrivalent vaccine, the 9-valent vaccine was associated with significantly more frequent adverse events at the injection site, including pain (84% vs. 90%), swelling (29% vs. 40%), and erythema (34% vs. 26%). Most of these reactions in both groups were mild to moderate in intensity, however.
Discontinuations and vaccine-related serious adverse events in the 9-valent vaccine group were rare (0.1% and less than 0.1%, respectively).
Read the full study here (doi:10.1542/peds.2015-4387).
The 9-valent human papillomavirus vaccine was well tolerated in 16-26 year olds and had a safety profile comparable to that of the quadrivalent vaccine, according to an analysis of seven phase III trials.
“The demonstrated efficacy and favorable safety profile of the 9vHPV vaccine support widespread vaccination programs,” reported Dr. Edson D. Moreira Jr. and his associates in Pediatrics.
Vaccines were given in a three-dose regimen: 15,776 male and female patients received at least one dose of the 9-valent vaccine and 7,391 control subjects received at least one dose of the quadrivalent vaccine.
Frequencies of vaccine-related systemic adverse events such as headache and pyrexia were “generally similar” between the two vaccine groups, the investigators reported.
Compared with the quadrivalent vaccine, the 9-valent vaccine was associated with significantly more frequent adverse events at the injection site, including pain (84% vs. 90%), swelling (29% vs. 40%), and erythema (34% vs. 26%). Most of these reactions in both groups were mild to moderate in intensity, however.
Discontinuations and vaccine-related serious adverse events in the 9-valent vaccine group were rare (0.1% and less than 0.1%, respectively).
Read the full study here (doi:10.1542/peds.2015-4387).
The 9-valent human papillomavirus vaccine was well tolerated in 16-26 year olds and had a safety profile comparable to that of the quadrivalent vaccine, according to an analysis of seven phase III trials.
“The demonstrated efficacy and favorable safety profile of the 9vHPV vaccine support widespread vaccination programs,” reported Dr. Edson D. Moreira Jr. and his associates in Pediatrics.
Vaccines were given in a three-dose regimen: 15,776 male and female patients received at least one dose of the 9-valent vaccine and 7,391 control subjects received at least one dose of the quadrivalent vaccine.
Frequencies of vaccine-related systemic adverse events such as headache and pyrexia were “generally similar” between the two vaccine groups, the investigators reported.
Compared with the quadrivalent vaccine, the 9-valent vaccine was associated with significantly more frequent adverse events at the injection site, including pain (84% vs. 90%), swelling (29% vs. 40%), and erythema (34% vs. 26%). Most of these reactions in both groups were mild to moderate in intensity, however.
Discontinuations and vaccine-related serious adverse events in the 9-valent vaccine group were rare (0.1% and less than 0.1%, respectively).
Read the full study here (doi:10.1542/peds.2015-4387).
FROM PEDIATRICS
Teen birth rate continues to decline
The U.S teen birth rate has dropped for another consecutive year, adding to the long-term decline in teen pregnancy, according to a federal report on trends in child health and well being.

In 2014, the teen birth rate was 11 births per 1,000 girls’ aged 15-17 years, down from 12 per 1,000 in 2013. Racial and ethinic disparities in the teen birth rate have also dropped significantly since 1995 – with the difference between the highest and lowest rates dropping from 55 points in 1995 to 17 points in 2014. But substantial disparities persist.
The report also found that the percentages of 10th and 12th-graders in all racial and ethnic groups who binge-drink were the lowest in 2015 since the report started in 1980. The percentage of uninsured children also declined, falling from 7% in 2013 to 5% in 2014. However, there was no improvement in the rate of childhood obesity. During 2011-2014, 19% of children aged 6-17 years were obese.
The annual report is published by the Federal Interagency Forum on Child and Family Statistics, a working group of 23 federal agencies that collect, analyze and report data on conditions and trends related to child and family well-being. The report tracks 41 health and social indicators.
Read the full 2016 America’s Children Report here.
The U.S teen birth rate has dropped for another consecutive year, adding to the long-term decline in teen pregnancy, according to a federal report on trends in child health and well being.
In 2014, the teen birth rate was 11 births per 1,000 girls’ aged 15-17 years, down from 12 per 1,000 in 2013. Racial and ethinic disparities in the teen birth rate have also dropped significantly since 1995 – with the difference between the highest and lowest rates dropping from 55 points in 1995 to 17 points in 2014. But substantial disparities persist.
The report also found that the percentages of 10th and 12th-graders in all racial and ethnic groups who binge-drink were the lowest in 2015 since the report started in 1980. The percentage of uninsured children also declined, falling from 7% in 2013 to 5% in 2014. However, there was no improvement in the rate of childhood obesity. During 2011-2014, 19% of children aged 6-17 years were obese.
The annual report is published by the Federal Interagency Forum on Child and Family Statistics, a working group of 23 federal agencies that collect, analyze and report data on conditions and trends related to child and family well-being. The report tracks 41 health and social indicators.
Read the full 2016 America’s Children Report here.
The U.S teen birth rate has dropped for another consecutive year, adding to the long-term decline in teen pregnancy, according to a federal report on trends in child health and well being.
In 2014, the teen birth rate was 11 births per 1,000 girls’ aged 15-17 years, down from 12 per 1,000 in 2013. Racial and ethinic disparities in the teen birth rate have also dropped significantly since 1995 – with the difference between the highest and lowest rates dropping from 55 points in 1995 to 17 points in 2014. But substantial disparities persist.
The report also found that the percentages of 10th and 12th-graders in all racial and ethnic groups who binge-drink were the lowest in 2015 since the report started in 1980. The percentage of uninsured children also declined, falling from 7% in 2013 to 5% in 2014. However, there was no improvement in the rate of childhood obesity. During 2011-2014, 19% of children aged 6-17 years were obese.
The annual report is published by the Federal Interagency Forum on Child and Family Statistics, a working group of 23 federal agencies that collect, analyze and report data on conditions and trends related to child and family well-being. The report tracks 41 health and social indicators.
Read the full 2016 America’s Children Report here.

Number of U.S. Zika-related poor pregnancy outcomes rise to 16
One pregnancy loss with birth defects related to Zika virus was reported in the week ending July 7, 2016, along with two liveborn infants with Zika-related birth defects, according to the Centers for Disease Control and Prevention.
That brings the total number of Zika-related poor birth outcomes in the United States to seven pregnancy losses and nine liveborn infants with birth defects, the CDC reported July 14.
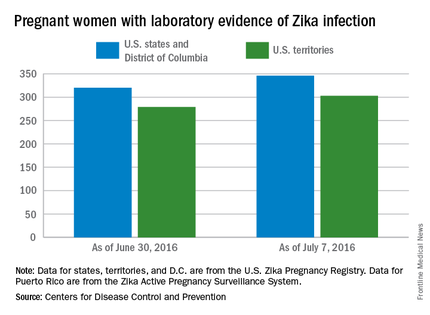
All three of the latest Zika-related poor outcomes occurred in the 50 states and the District of Columbia. Of the 16 total poor outcomes so far, 15 have occurred in the 50 states and D.C.; one pregnancy loss has been reported in the U.S. territories. State- or territorial-level data are not being reported to protect the privacy of affected women and children, the CDC said.
The CDC also reported that 346 pregnant women in the 50 states and D.C. and 303 women in U.S. territories have had laboratory evidence of Zika virus infection, for a total of 649 nationwide as of July 7.
The figures for states, territories, and the District of Columbia reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
One pregnancy loss with birth defects related to Zika virus was reported in the week ending July 7, 2016, along with two liveborn infants with Zika-related birth defects, according to the Centers for Disease Control and Prevention.
That brings the total number of Zika-related poor birth outcomes in the United States to seven pregnancy losses and nine liveborn infants with birth defects, the CDC reported July 14.
All three of the latest Zika-related poor outcomes occurred in the 50 states and the District of Columbia. Of the 16 total poor outcomes so far, 15 have occurred in the 50 states and D.C.; one pregnancy loss has been reported in the U.S. territories. State- or territorial-level data are not being reported to protect the privacy of affected women and children, the CDC said.
The CDC also reported that 346 pregnant women in the 50 states and D.C. and 303 women in U.S. territories have had laboratory evidence of Zika virus infection, for a total of 649 nationwide as of July 7.
The figures for states, territories, and the District of Columbia reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
One pregnancy loss with birth defects related to Zika virus was reported in the week ending July 7, 2016, along with two liveborn infants with Zika-related birth defects, according to the Centers for Disease Control and Prevention.
That brings the total number of Zika-related poor birth outcomes in the United States to seven pregnancy losses and nine liveborn infants with birth defects, the CDC reported July 14.
All three of the latest Zika-related poor outcomes occurred in the 50 states and the District of Columbia. Of the 16 total poor outcomes so far, 15 have occurred in the 50 states and D.C.; one pregnancy loss has been reported in the U.S. territories. State- or territorial-level data are not being reported to protect the privacy of affected women and children, the CDC said.
The CDC also reported that 346 pregnant women in the 50 states and D.C. and 303 women in U.S. territories have had laboratory evidence of Zika virus infection, for a total of 649 nationwide as of July 7.
The figures for states, territories, and the District of Columbia reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.