User login
Serum vitamin D levels, atopy not significantly linked
SCOTTSDALE, ARIZ. – Serum vitamin D level was not significantly associated with atopic dermatitis or disease severity in a single-center study of more than 600 children and adolescents.
However, “we did observe a strong correlation between average serum vitamin D levels and skin type, as well as body mass index,” said Kavita Darji, a medical student at Saint Louis (Mo.) University, who presented the findings in a poster at the annual meeting of the Society for Investigative Dermatology. Those findings challenge the logic of following universal definitions of vitamin D deficiency, especially given the phenotypic heterogeneity of patients in the United States, she added in an interview.
Serum vitamin D testing is one of most common laboratory assays in this country, but clinicians still debate the risks and benefits of supplementing children and adolescents who test below the Endocrine Society’s threshold for sufficiency (30.0 ng/mL).
To identify factors affecting vitamin D levels, Ms. Darji and her associates reviewed electronic medical charts for patients under age 22 years at Saint Louis University medical centers between 2009 and 2014. The cohort of 655 patients was primarily white (64%) or black (29%), and was nearly equally balanced by gender; their average age was 10 years. The researchers analyzed only the first vitamin D serum measurement for each patient, and defined deficiency as a level under 20 ng/mL, insufficiency as a level between 20 and 29.9 ng/mL, and sufficiency as a level of at least 30 ng/mL.
Serum vitamin D levels were slightly lower among atopic patients, compared with those without atopy, but the difference did not reach statistical significance (about 25 ng/mL vs. about 38 ng/mL; P greater than .05). “We also did not find an association between AD severity and vitamin D level,” Ms. Darji reported. Instead, race and body mass index were the most significant predictors of vitamin D deficiency, probably because these factors directly affect cutaneous photo-induced vitamin D synthesis and the sequestration of fat-soluble vitamins in adipose tissue, she said.
Using the standard definitions, more than 50% of black patients were vitamin D deficient, while less than 30% had sufficient vitamin D levels. In contrast, about 25% of white patients were vitamin D deficient, while nearly 40% had sufficient vitamin D levels (P less than .0001 for proportions of deficiency by race). Furthermore, only about 10% of obese children (those who exceeded the 99th percentile of BMI for age) had sufficient vitamin D levels, compared with more than 40% of underweight children and about 30% of normal-weight children (P less than .00001).
Since vitamin D deficiency was more common among black and obese patients, “maybe they could benefit from a different cut-off value than the standard 30 ng per mL that we used,” Ms. Darji said. “The question is, do they really require these supplements? It may be beneficial to look at the unique characteristics of each patient before supplementing, because the risks of supplementation are considerable in terms of bone health and cardiovascular disease.”
Vitamin D levels did not vary significantly by gender or by month or season measured, Ms. Darji noted. She reported no funding sources and had no disclosures.
SCOTTSDALE, ARIZ. – Serum vitamin D level was not significantly associated with atopic dermatitis or disease severity in a single-center study of more than 600 children and adolescents.
However, “we did observe a strong correlation between average serum vitamin D levels and skin type, as well as body mass index,” said Kavita Darji, a medical student at Saint Louis (Mo.) University, who presented the findings in a poster at the annual meeting of the Society for Investigative Dermatology. Those findings challenge the logic of following universal definitions of vitamin D deficiency, especially given the phenotypic heterogeneity of patients in the United States, she added in an interview.
Serum vitamin D testing is one of most common laboratory assays in this country, but clinicians still debate the risks and benefits of supplementing children and adolescents who test below the Endocrine Society’s threshold for sufficiency (30.0 ng/mL).
To identify factors affecting vitamin D levels, Ms. Darji and her associates reviewed electronic medical charts for patients under age 22 years at Saint Louis University medical centers between 2009 and 2014. The cohort of 655 patients was primarily white (64%) or black (29%), and was nearly equally balanced by gender; their average age was 10 years. The researchers analyzed only the first vitamin D serum measurement for each patient, and defined deficiency as a level under 20 ng/mL, insufficiency as a level between 20 and 29.9 ng/mL, and sufficiency as a level of at least 30 ng/mL.
Serum vitamin D levels were slightly lower among atopic patients, compared with those without atopy, but the difference did not reach statistical significance (about 25 ng/mL vs. about 38 ng/mL; P greater than .05). “We also did not find an association between AD severity and vitamin D level,” Ms. Darji reported. Instead, race and body mass index were the most significant predictors of vitamin D deficiency, probably because these factors directly affect cutaneous photo-induced vitamin D synthesis and the sequestration of fat-soluble vitamins in adipose tissue, she said.
Using the standard definitions, more than 50% of black patients were vitamin D deficient, while less than 30% had sufficient vitamin D levels. In contrast, about 25% of white patients were vitamin D deficient, while nearly 40% had sufficient vitamin D levels (P less than .0001 for proportions of deficiency by race). Furthermore, only about 10% of obese children (those who exceeded the 99th percentile of BMI for age) had sufficient vitamin D levels, compared with more than 40% of underweight children and about 30% of normal-weight children (P less than .00001).
Since vitamin D deficiency was more common among black and obese patients, “maybe they could benefit from a different cut-off value than the standard 30 ng per mL that we used,” Ms. Darji said. “The question is, do they really require these supplements? It may be beneficial to look at the unique characteristics of each patient before supplementing, because the risks of supplementation are considerable in terms of bone health and cardiovascular disease.”
Vitamin D levels did not vary significantly by gender or by month or season measured, Ms. Darji noted. She reported no funding sources and had no disclosures.
SCOTTSDALE, ARIZ. – Serum vitamin D level was not significantly associated with atopic dermatitis or disease severity in a single-center study of more than 600 children and adolescents.
However, “we did observe a strong correlation between average serum vitamin D levels and skin type, as well as body mass index,” said Kavita Darji, a medical student at Saint Louis (Mo.) University, who presented the findings in a poster at the annual meeting of the Society for Investigative Dermatology. Those findings challenge the logic of following universal definitions of vitamin D deficiency, especially given the phenotypic heterogeneity of patients in the United States, she added in an interview.
Serum vitamin D testing is one of most common laboratory assays in this country, but clinicians still debate the risks and benefits of supplementing children and adolescents who test below the Endocrine Society’s threshold for sufficiency (30.0 ng/mL).
To identify factors affecting vitamin D levels, Ms. Darji and her associates reviewed electronic medical charts for patients under age 22 years at Saint Louis University medical centers between 2009 and 2014. The cohort of 655 patients was primarily white (64%) or black (29%), and was nearly equally balanced by gender; their average age was 10 years. The researchers analyzed only the first vitamin D serum measurement for each patient, and defined deficiency as a level under 20 ng/mL, insufficiency as a level between 20 and 29.9 ng/mL, and sufficiency as a level of at least 30 ng/mL.
Serum vitamin D levels were slightly lower among atopic patients, compared with those without atopy, but the difference did not reach statistical significance (about 25 ng/mL vs. about 38 ng/mL; P greater than .05). “We also did not find an association between AD severity and vitamin D level,” Ms. Darji reported. Instead, race and body mass index were the most significant predictors of vitamin D deficiency, probably because these factors directly affect cutaneous photo-induced vitamin D synthesis and the sequestration of fat-soluble vitamins in adipose tissue, she said.
Using the standard definitions, more than 50% of black patients were vitamin D deficient, while less than 30% had sufficient vitamin D levels. In contrast, about 25% of white patients were vitamin D deficient, while nearly 40% had sufficient vitamin D levels (P less than .0001 for proportions of deficiency by race). Furthermore, only about 10% of obese children (those who exceeded the 99th percentile of BMI for age) had sufficient vitamin D levels, compared with more than 40% of underweight children and about 30% of normal-weight children (P less than .00001).
Since vitamin D deficiency was more common among black and obese patients, “maybe they could benefit from a different cut-off value than the standard 30 ng per mL that we used,” Ms. Darji said. “The question is, do they really require these supplements? It may be beneficial to look at the unique characteristics of each patient before supplementing, because the risks of supplementation are considerable in terms of bone health and cardiovascular disease.”
Vitamin D levels did not vary significantly by gender or by month or season measured, Ms. Darji noted. She reported no funding sources and had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: Serum vitamin D was not a significant marker for pediatric atopic dermatitis or disease severity.
Major finding: The average serum vitamin D level was lower among patients with atopic dermatitis than healthy children, but the difference did not reach statistical significance.
Data source: A single-center retrospective review of electronic medical records from 655 patients aged 21 years and younger (average age, 10 years).
Disclosures: Ms. Darji reported no funding sources and had no disclosures.
UTIs not caused by E. coli more likely in certain children
Certain children are more highly predisposed to contracting a urinary tract infection caused by a pathogen other than Escherichia coli, which is typically the most common cause of UTIs, a study showed.
“It may be clinically important to predict which children have UTIs caused by organisms other than E. coli because these organisms differ in their patterns of antimicrobial susceptibility,” wrote the study authors led by Nader Shaikh, MD, of the University of Pittsburgh. “Furthermore, some guidelines have suggested that screening for vesicoureteral reflux (VUR) with a voiding cystourethrogram (VCUG) should, at least in part, be based on whether an organism other than E. coli is recovered,” they wrote.

Dr. Shaikh and his coinvestigators examined the medical records of children in the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) trial and the Careful Urinary Tract Infection Evaluation (CUTIE), both of which were prospective multicenter studies. Children included in both studies were 2-71 months of age; RIVUR subjects had VUR grades 1-4 and presented with either a first or second febrile or symptomatic UTI, while CUTIE subjects presented with either their first or second UTI but not VUR (Ped Inf Dis J. 2016. doi:10.1097/INF.0000000000001301).
In total, 769 children from 19 centers were included from both studies, of which 703 (91%) were female and 596 (78%) were white. Nine percent of all the children had UTIs that were not caused by E. coli. Circumcised males had the highest odds ratio associated with non–E. coli UTIs, with an OR of 5.5 (95% CI, 1.18-17.1; P = .003). significantly higher than the 1.6 odds ratio for uncircumcised males (95% CI, 0.6-4.6; P = .35).
Hispanic children also had a higher risk (OR = 2.3; 95% CI, 1.1-4.6; P = .02) than either non-Hispanic children or females, which were reference cohorts. Other groups found to be at higher-than-normal risk for non–E. coli UTIs were children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02) and children with VUR grade 3 or 4 (OR = 2.2; 95% CI, 1.2-4.1; P = .01).
While more than 90% of children’s UTIs were caused by E. coli, the most common pathogens causing UTIs, causative organisms in the other 70 children were Proteus species (21 children, 30%), Klebsiella species (16, 23%), Enterococcus species (14, 20%), Enterobacter species (8, 11%), and “other species” (11, 16%).
“Children with UTIs caused by organisms other than E. coli were twice as likely to have high-grade VUR (grade 3 and 4), which is consistent with prior studies,” Dr. Shaikh and his coauthors noted, adding, “the association between Hispanic ethnicity and non-E. coli pathogens is novel and may be due to differences in genes involved with susceptibility to UTIs.”
There were no disclosures or sources of funding provided.
In this study of almost 800 children in the Pittsburgh area, the investigators sought to identify children at risk for urinary tract infections that more likely would have a bacterial organism not susceptible to standard first-line empiric antibiotic treatment.
They found that circumcised males, children with grade 3-4 vesicoureteral reflux, Hispanic children, and children without fever were more likely to have a UTI caused by organisms other than Escherichia coli and, therefore, less likely to respond to standard first-line antibiotic therapy. These investigators are the preeminent authorities in UTI management for children, so their findings should be viewed in that light.

|
Dr. Michael E. Pichichero |
The advance from the study is not a major one because all children with a suspected UTI should have a suitable culture specimen obtained before starting antibiotics, and the treatment choice continued or changed based on culture results. So really, the findings apply only to a decision about initial empiric treatment while awaiting culture results.
As a guide, if a clinician were to consider the diagnosis of UTI based on history, examination, and urinalysis, and the child was a circumcised male, a child with known grade 3 or 4 vesicoureteral reflux, Hispanic, or without fever, then the empiric antibiotic selected should be broader spectrum while awaiting urine culture results.
Michael E. Pichichero, MD, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
In this study of almost 800 children in the Pittsburgh area, the investigators sought to identify children at risk for urinary tract infections that more likely would have a bacterial organism not susceptible to standard first-line empiric antibiotic treatment.
They found that circumcised males, children with grade 3-4 vesicoureteral reflux, Hispanic children, and children without fever were more likely to have a UTI caused by organisms other than Escherichia coli and, therefore, less likely to respond to standard first-line antibiotic therapy. These investigators are the preeminent authorities in UTI management for children, so their findings should be viewed in that light.
|
|
Dr. Michael E. Pichichero |
The advance from the study is not a major one because all children with a suspected UTI should have a suitable culture specimen obtained before starting antibiotics, and the treatment choice continued or changed based on culture results. So really, the findings apply only to a decision about initial empiric treatment while awaiting culture results.
As a guide, if a clinician were to consider the diagnosis of UTI based on history, examination, and urinalysis, and the child was a circumcised male, a child with known grade 3 or 4 vesicoureteral reflux, Hispanic, or without fever, then the empiric antibiotic selected should be broader spectrum while awaiting urine culture results.
Michael E. Pichichero, MD, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
In this study of almost 800 children in the Pittsburgh area, the investigators sought to identify children at risk for urinary tract infections that more likely would have a bacterial organism not susceptible to standard first-line empiric antibiotic treatment.
They found that circumcised males, children with grade 3-4 vesicoureteral reflux, Hispanic children, and children without fever were more likely to have a UTI caused by organisms other than Escherichia coli and, therefore, less likely to respond to standard first-line antibiotic therapy. These investigators are the preeminent authorities in UTI management for children, so their findings should be viewed in that light.
|
|
Dr. Michael E. Pichichero |
The advance from the study is not a major one because all children with a suspected UTI should have a suitable culture specimen obtained before starting antibiotics, and the treatment choice continued or changed based on culture results. So really, the findings apply only to a decision about initial empiric treatment while awaiting culture results.
As a guide, if a clinician were to consider the diagnosis of UTI based on history, examination, and urinalysis, and the child was a circumcised male, a child with known grade 3 or 4 vesicoureteral reflux, Hispanic, or without fever, then the empiric antibiotic selected should be broader spectrum while awaiting urine culture results.
Michael E. Pichichero, MD, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
Certain children are more highly predisposed to contracting a urinary tract infection caused by a pathogen other than Escherichia coli, which is typically the most common cause of UTIs, a study showed.
“It may be clinically important to predict which children have UTIs caused by organisms other than E. coli because these organisms differ in their patterns of antimicrobial susceptibility,” wrote the study authors led by Nader Shaikh, MD, of the University of Pittsburgh. “Furthermore, some guidelines have suggested that screening for vesicoureteral reflux (VUR) with a voiding cystourethrogram (VCUG) should, at least in part, be based on whether an organism other than E. coli is recovered,” they wrote.
Dr. Shaikh and his coinvestigators examined the medical records of children in the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) trial and the Careful Urinary Tract Infection Evaluation (CUTIE), both of which were prospective multicenter studies. Children included in both studies were 2-71 months of age; RIVUR subjects had VUR grades 1-4 and presented with either a first or second febrile or symptomatic UTI, while CUTIE subjects presented with either their first or second UTI but not VUR (Ped Inf Dis J. 2016. doi:10.1097/INF.0000000000001301).
In total, 769 children from 19 centers were included from both studies, of which 703 (91%) were female and 596 (78%) were white. Nine percent of all the children had UTIs that were not caused by E. coli. Circumcised males had the highest odds ratio associated with non–E. coli UTIs, with an OR of 5.5 (95% CI, 1.18-17.1; P = .003). significantly higher than the 1.6 odds ratio for uncircumcised males (95% CI, 0.6-4.6; P = .35).
Hispanic children also had a higher risk (OR = 2.3; 95% CI, 1.1-4.6; P = .02) than either non-Hispanic children or females, which were reference cohorts. Other groups found to be at higher-than-normal risk for non–E. coli UTIs were children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02) and children with VUR grade 3 or 4 (OR = 2.2; 95% CI, 1.2-4.1; P = .01).
While more than 90% of children’s UTIs were caused by E. coli, the most common pathogens causing UTIs, causative organisms in the other 70 children were Proteus species (21 children, 30%), Klebsiella species (16, 23%), Enterococcus species (14, 20%), Enterobacter species (8, 11%), and “other species” (11, 16%).
“Children with UTIs caused by organisms other than E. coli were twice as likely to have high-grade VUR (grade 3 and 4), which is consistent with prior studies,” Dr. Shaikh and his coauthors noted, adding, “the association between Hispanic ethnicity and non-E. coli pathogens is novel and may be due to differences in genes involved with susceptibility to UTIs.”
There were no disclosures or sources of funding provided.
Certain children are more highly predisposed to contracting a urinary tract infection caused by a pathogen other than Escherichia coli, which is typically the most common cause of UTIs, a study showed.
“It may be clinically important to predict which children have UTIs caused by organisms other than E. coli because these organisms differ in their patterns of antimicrobial susceptibility,” wrote the study authors led by Nader Shaikh, MD, of the University of Pittsburgh. “Furthermore, some guidelines have suggested that screening for vesicoureteral reflux (VUR) with a voiding cystourethrogram (VCUG) should, at least in part, be based on whether an organism other than E. coli is recovered,” they wrote.
Dr. Shaikh and his coinvestigators examined the medical records of children in the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) trial and the Careful Urinary Tract Infection Evaluation (CUTIE), both of which were prospective multicenter studies. Children included in both studies were 2-71 months of age; RIVUR subjects had VUR grades 1-4 and presented with either a first or second febrile or symptomatic UTI, while CUTIE subjects presented with either their first or second UTI but not VUR (Ped Inf Dis J. 2016. doi:10.1097/INF.0000000000001301).
In total, 769 children from 19 centers were included from both studies, of which 703 (91%) were female and 596 (78%) were white. Nine percent of all the children had UTIs that were not caused by E. coli. Circumcised males had the highest odds ratio associated with non–E. coli UTIs, with an OR of 5.5 (95% CI, 1.18-17.1; P = .003). significantly higher than the 1.6 odds ratio for uncircumcised males (95% CI, 0.6-4.6; P = .35).
Hispanic children also had a higher risk (OR = 2.3; 95% CI, 1.1-4.6; P = .02) than either non-Hispanic children or females, which were reference cohorts. Other groups found to be at higher-than-normal risk for non–E. coli UTIs were children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02) and children with VUR grade 3 or 4 (OR = 2.2; 95% CI, 1.2-4.1; P = .01).
While more than 90% of children’s UTIs were caused by E. coli, the most common pathogens causing UTIs, causative organisms in the other 70 children were Proteus species (21 children, 30%), Klebsiella species (16, 23%), Enterococcus species (14, 20%), Enterobacter species (8, 11%), and “other species” (11, 16%).
“Children with UTIs caused by organisms other than E. coli were twice as likely to have high-grade VUR (grade 3 and 4), which is consistent with prior studies,” Dr. Shaikh and his coauthors noted, adding, “the association between Hispanic ethnicity and non-E. coli pathogens is novel and may be due to differences in genes involved with susceptibility to UTIs.”
There were no disclosures or sources of funding provided.
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
Key clinical point: Non–Escherichia coli urinary tract infections are more likely to occur in children who are uncircumcised, are Hispanic, have no fever, or have grade 3-4 vesicoureteral reflux.
Major finding: Circumcised males had an odds ratio of 5.5 (95% CI, 1.8-17.1; P = .003) of infection by pathogens other than E. coli; the odds ratio for Hispanic children (OR = 2.3; 95% CI, 1.1-4.6; P = .02), children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02), and children with grade 3-4 VUR (OR = 2.2; 95% CI, 1.2-4.1; P = .01) also were relatively high.
Data source: A review of data from two prospective multicenter studies involving 769 children with a UTI aged 2-71 months .
Disclosures: Funding sources and individual disclosures were not provided.

Psychiatric disorders often impair antiretroviral adherence in perinatally HIV-infected teens
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.

The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
AT AIDS 2016
Key clinical point: Look for and treat psychiatric disorders in perinatally HIV-infected adolescents as a means of optimizing their antiretroviral medication adherence.
Major finding: A majority of perinatally HIV-infected adolescents meet the criteria for at least one psychiatric diagnosis, and they are at significantly increased risk for poor medication adherence and viremia during the next 2-3 years.
Data source: The longitudinal CASAH study involving prospective follow-up of several hundred perinatally HIV-infected and perinatally exposed but uninfected subjects through adolescence and young adulthood.
Disclosures: The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.

Boxed for delivery
When our second daughter was born, she came home from the hospital in a box. All the babies born at Duke University Medical Center in 1973 were sent home in a cardboard box that had served as their bassinets during their stay in the newborn nursery. As I recall, the boxes were decorated with storks and musical notes; had spaces for the babies’ names, measurements, and birth dates; and had open slots that functioned as carrying handles.
Of course, 1973 predated crash-tested car seats, and so we put little Emily and her box in what we referred to as the “wayback” of our Ford Pinto wagon, a car that subsequently earned a reputation for turning into a fireball when involved in a rear-end collision. However, I believe I did take the extra precaution of “securing” the box in place with a bungee cord.

But Emily survived, and I filed away the memory of her cardboard bassinet until a few weeks ago when I read a story in the New York Times, “Why Finland’s Newborns Sleep in Cardboard Cribs” (Eli Rosenberg, July 6, 2016). It turns out the Finnish government gives out 40,000 cardboard boxes to pregnant women who agree to have a medical exam during the first trimester of their pregnancy. The gift boxes come along with 50 items of baby ware appropriate for Finland’s frigid climate, including a warm coat and a balaclava.
The baby box program began in the late 1930s as a way to encourage mothers to visit physicians. The current Finnish infant mortality is one of the lowest in the world and less than half of ours in the United States. There are some who have been tempted to attribute this dramatic decline to the baby box program. But it is hard to tease out one factor in a country that offers a 10-month paid parental leave and guarantees that a stay-at-home parent may return to his or her job at any time before the child’s third birthday.
Even without a broad social service support system, the cardboard box crib can save lives. For families who can’t afford a crib, the box offers a safer alternative to a couch with soft cushions and face-trapping gaps between its cushions, or to a bed shared with a sleep-deprived or inebriated parent, or to an antique crib with neck-pinching slats and layers of lead-laced paint.
Given this high costs of raising a child, the option of a no-cost cardboard box crib should appeal to most young families. But you know as well as I do that parents to be (and grandparents to be) are primed to buy and are focused on creating nurseries that match the images they see in the glossy magazines targeted at their vulnerable demographic.
It will require a major public relations campaign to counteract the image that bedding one’s precious newborn in a cardboard box conjures up. But maybe there is a role for us. If pediatricians began promoting the advantages of cardboard cribs, they might just catch on. On second thought, maybe we should focus our energies on promoting more child-friendly parental leave policies.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
When our second daughter was born, she came home from the hospital in a box. All the babies born at Duke University Medical Center in 1973 were sent home in a cardboard box that had served as their bassinets during their stay in the newborn nursery. As I recall, the boxes were decorated with storks and musical notes; had spaces for the babies’ names, measurements, and birth dates; and had open slots that functioned as carrying handles.
Of course, 1973 predated crash-tested car seats, and so we put little Emily and her box in what we referred to as the “wayback” of our Ford Pinto wagon, a car that subsequently earned a reputation for turning into a fireball when involved in a rear-end collision. However, I believe I did take the extra precaution of “securing” the box in place with a bungee cord.
But Emily survived, and I filed away the memory of her cardboard bassinet until a few weeks ago when I read a story in the New York Times, “Why Finland’s Newborns Sleep in Cardboard Cribs” (Eli Rosenberg, July 6, 2016). It turns out the Finnish government gives out 40,000 cardboard boxes to pregnant women who agree to have a medical exam during the first trimester of their pregnancy. The gift boxes come along with 50 items of baby ware appropriate for Finland’s frigid climate, including a warm coat and a balaclava.
The baby box program began in the late 1930s as a way to encourage mothers to visit physicians. The current Finnish infant mortality is one of the lowest in the world and less than half of ours in the United States. There are some who have been tempted to attribute this dramatic decline to the baby box program. But it is hard to tease out one factor in a country that offers a 10-month paid parental leave and guarantees that a stay-at-home parent may return to his or her job at any time before the child’s third birthday.
Even without a broad social service support system, the cardboard box crib can save lives. For families who can’t afford a crib, the box offers a safer alternative to a couch with soft cushions and face-trapping gaps between its cushions, or to a bed shared with a sleep-deprived or inebriated parent, or to an antique crib with neck-pinching slats and layers of lead-laced paint.
Given this high costs of raising a child, the option of a no-cost cardboard box crib should appeal to most young families. But you know as well as I do that parents to be (and grandparents to be) are primed to buy and are focused on creating nurseries that match the images they see in the glossy magazines targeted at their vulnerable demographic.
It will require a major public relations campaign to counteract the image that bedding one’s precious newborn in a cardboard box conjures up. But maybe there is a role for us. If pediatricians began promoting the advantages of cardboard cribs, they might just catch on. On second thought, maybe we should focus our energies on promoting more child-friendly parental leave policies.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
When our second daughter was born, she came home from the hospital in a box. All the babies born at Duke University Medical Center in 1973 were sent home in a cardboard box that had served as their bassinets during their stay in the newborn nursery. As I recall, the boxes were decorated with storks and musical notes; had spaces for the babies’ names, measurements, and birth dates; and had open slots that functioned as carrying handles.
Of course, 1973 predated crash-tested car seats, and so we put little Emily and her box in what we referred to as the “wayback” of our Ford Pinto wagon, a car that subsequently earned a reputation for turning into a fireball when involved in a rear-end collision. However, I believe I did take the extra precaution of “securing” the box in place with a bungee cord.
But Emily survived, and I filed away the memory of her cardboard bassinet until a few weeks ago when I read a story in the New York Times, “Why Finland’s Newborns Sleep in Cardboard Cribs” (Eli Rosenberg, July 6, 2016). It turns out the Finnish government gives out 40,000 cardboard boxes to pregnant women who agree to have a medical exam during the first trimester of their pregnancy. The gift boxes come along with 50 items of baby ware appropriate for Finland’s frigid climate, including a warm coat and a balaclava.
The baby box program began in the late 1930s as a way to encourage mothers to visit physicians. The current Finnish infant mortality is one of the lowest in the world and less than half of ours in the United States. There are some who have been tempted to attribute this dramatic decline to the baby box program. But it is hard to tease out one factor in a country that offers a 10-month paid parental leave and guarantees that a stay-at-home parent may return to his or her job at any time before the child’s third birthday.
Even without a broad social service support system, the cardboard box crib can save lives. For families who can’t afford a crib, the box offers a safer alternative to a couch with soft cushions and face-trapping gaps between its cushions, or to a bed shared with a sleep-deprived or inebriated parent, or to an antique crib with neck-pinching slats and layers of lead-laced paint.
Given this high costs of raising a child, the option of a no-cost cardboard box crib should appeal to most young families. But you know as well as I do that parents to be (and grandparents to be) are primed to buy and are focused on creating nurseries that match the images they see in the glossy magazines targeted at their vulnerable demographic.
It will require a major public relations campaign to counteract the image that bedding one’s precious newborn in a cardboard box conjures up. But maybe there is a role for us. If pediatricians began promoting the advantages of cardboard cribs, they might just catch on. On second thought, maybe we should focus our energies on promoting more child-friendly parental leave policies.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

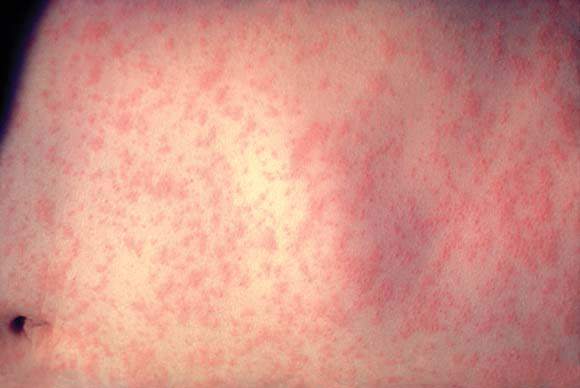
Approximately 9 million U.S. children, teens are vulnerable to measles infection
Of the almost 9 million children and adolescents aged 17 years and younger estimated to be measles susceptible in the United States, those 3 years and younger show the highest levels of risk for infection, according to the results of a study published in the American Journal of Epidemiology.
Robert A. Bednarczyk, MD, and his colleagues at Emory University, Atlanta, developed a model based on age-specific measles vaccination data from the National Immunization Survey–Teen collected between 2008 and 2013 (18 cumulative birth cohorts) to estimate the number of U.S. children (birth–age 12 years ) and adolescents (aged 13-17 years) susceptible to measles infection (Am J Epidemiol. 2016 Jul 15;184[2]:148-56).
The model was developed using the survey data in conjunction with assumptions designed to account for several potentially confounding variables. These included the effectiveness of the vaccine used, whether infants were protected by maternally derived, vaccine-induced antibodies, and any loss of immunity attributable to treatment for cancer during childhood. The model also allowed for an examination of susceptibility by different age groupings, as well as by state. Additionally, the study authors were able to estimate the impact of decreased measles-containing vaccine effectiveness on susceptibility to infection in adolescents.
Results from the model indicated that 12.5% of the over 69 million of U.S. children and adolescents in the 18 birth cohorts are susceptible to measles infection. Those with the highest percentage of susceptibility were children 3 years of age and younger (24.7%), compared with 9.0% of children and adolescents aged 4-17 years. Geographic differences in susceptibility also were apparent. In addition to the District of Columbia, 10 states had adolescent susceptibility levels of at least 6%, and 14 states each had over 20,000 susceptible adolescents.
Using the model to simulate a 1% decrease in vaccine effectiveness for both the first (93%-92%) and second (97%-96%) measles-containing vaccine doses, the study authors reported the addition of almost 1 million children and adolescents (13.4%) to the measles-susceptible category. This finding indicates that very small changes in vaccine effectiveness can have a substantial impact on susceptibility through a slow accumulation of additional susceptible children and adolescents each year, culminating in a steady decline in the proportion of children and adolescents immune to measles.
Regarding their overall findings, Dr. Bednarczyk and his colleagues stated, “the overall level of immunity to measles is generally at or higher than the operational threshold of 92%. This is compatible with the experience to date that, despite substantial numbers of importations, endemic measles transmission has not been reestablished.”
As for broader implications, the investigators said that “These estimates underscore the need to help public health professionals plan for future immunization programs and potential measles outbreaks, and to maintain appropriate levels of immunity in the population to prevent widespread transmission of this highly infectious disease.”
Of the almost 9 million children and adolescents aged 17 years and younger estimated to be measles susceptible in the United States, those 3 years and younger show the highest levels of risk for infection, according to the results of a study published in the American Journal of Epidemiology.
Robert A. Bednarczyk, MD, and his colleagues at Emory University, Atlanta, developed a model based on age-specific measles vaccination data from the National Immunization Survey–Teen collected between 2008 and 2013 (18 cumulative birth cohorts) to estimate the number of U.S. children (birth–age 12 years ) and adolescents (aged 13-17 years) susceptible to measles infection (Am J Epidemiol. 2016 Jul 15;184[2]:148-56).
The model was developed using the survey data in conjunction with assumptions designed to account for several potentially confounding variables. These included the effectiveness of the vaccine used, whether infants were protected by maternally derived, vaccine-induced antibodies, and any loss of immunity attributable to treatment for cancer during childhood. The model also allowed for an examination of susceptibility by different age groupings, as well as by state. Additionally, the study authors were able to estimate the impact of decreased measles-containing vaccine effectiveness on susceptibility to infection in adolescents.
Results from the model indicated that 12.5% of the over 69 million of U.S. children and adolescents in the 18 birth cohorts are susceptible to measles infection. Those with the highest percentage of susceptibility were children 3 years of age and younger (24.7%), compared with 9.0% of children and adolescents aged 4-17 years. Geographic differences in susceptibility also were apparent. In addition to the District of Columbia, 10 states had adolescent susceptibility levels of at least 6%, and 14 states each had over 20,000 susceptible adolescents.
Using the model to simulate a 1% decrease in vaccine effectiveness for both the first (93%-92%) and second (97%-96%) measles-containing vaccine doses, the study authors reported the addition of almost 1 million children and adolescents (13.4%) to the measles-susceptible category. This finding indicates that very small changes in vaccine effectiveness can have a substantial impact on susceptibility through a slow accumulation of additional susceptible children and adolescents each year, culminating in a steady decline in the proportion of children and adolescents immune to measles.
Regarding their overall findings, Dr. Bednarczyk and his colleagues stated, “the overall level of immunity to measles is generally at or higher than the operational threshold of 92%. This is compatible with the experience to date that, despite substantial numbers of importations, endemic measles transmission has not been reestablished.”
As for broader implications, the investigators said that “These estimates underscore the need to help public health professionals plan for future immunization programs and potential measles outbreaks, and to maintain appropriate levels of immunity in the population to prevent widespread transmission of this highly infectious disease.”
Of the almost 9 million children and adolescents aged 17 years and younger estimated to be measles susceptible in the United States, those 3 years and younger show the highest levels of risk for infection, according to the results of a study published in the American Journal of Epidemiology.
Robert A. Bednarczyk, MD, and his colleagues at Emory University, Atlanta, developed a model based on age-specific measles vaccination data from the National Immunization Survey–Teen collected between 2008 and 2013 (18 cumulative birth cohorts) to estimate the number of U.S. children (birth–age 12 years ) and adolescents (aged 13-17 years) susceptible to measles infection (Am J Epidemiol. 2016 Jul 15;184[2]:148-56).
The model was developed using the survey data in conjunction with assumptions designed to account for several potentially confounding variables. These included the effectiveness of the vaccine used, whether infants were protected by maternally derived, vaccine-induced antibodies, and any loss of immunity attributable to treatment for cancer during childhood. The model also allowed for an examination of susceptibility by different age groupings, as well as by state. Additionally, the study authors were able to estimate the impact of decreased measles-containing vaccine effectiveness on susceptibility to infection in adolescents.
Results from the model indicated that 12.5% of the over 69 million of U.S. children and adolescents in the 18 birth cohorts are susceptible to measles infection. Those with the highest percentage of susceptibility were children 3 years of age and younger (24.7%), compared with 9.0% of children and adolescents aged 4-17 years. Geographic differences in susceptibility also were apparent. In addition to the District of Columbia, 10 states had adolescent susceptibility levels of at least 6%, and 14 states each had over 20,000 susceptible adolescents.
Using the model to simulate a 1% decrease in vaccine effectiveness for both the first (93%-92%) and second (97%-96%) measles-containing vaccine doses, the study authors reported the addition of almost 1 million children and adolescents (13.4%) to the measles-susceptible category. This finding indicates that very small changes in vaccine effectiveness can have a substantial impact on susceptibility through a slow accumulation of additional susceptible children and adolescents each year, culminating in a steady decline in the proportion of children and adolescents immune to measles.
Regarding their overall findings, Dr. Bednarczyk and his colleagues stated, “the overall level of immunity to measles is generally at or higher than the operational threshold of 92%. This is compatible with the experience to date that, despite substantial numbers of importations, endemic measles transmission has not been reestablished.”
As for broader implications, the investigators said that “These estimates underscore the need to help public health professionals plan for future immunization programs and potential measles outbreaks, and to maintain appropriate levels of immunity in the population to prevent widespread transmission of this highly infectious disease.”
Key clinical point: U.S. children younger than 3 years of age have a high estimated susceptibility to measles infection.
Major finding: An estimated 12.5% of U.S. children and adolescents 17 years and younger are susceptible to measles infection, with differences in susceptibility levels detected for specific age ranges and states. Small decreases in vaccine effectiveness can have a large impact on susceptibility levels.
Data sources: National Immunization Survey–Teen collected between 2008 and 2013.
Disclosures: The study was conducted without grant support. All authors reported no conflicts of interest.
Links found between NAFLD, type 2 diabetes, and NASH in children
Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this co-morbidity is also associated with a greater risk of nonalcoholic steatohepatitis, according to a cross-sectional study published online Aug. 1 in JAMA Pediatrics.
The study used data from 675 children with biopsy-confirmed nonalcoholic fatty liver disease (NAFLD) who were enrolled in the NASH Clinical Research Network. The mean age of the children was 12.6 years, and they had a mean BMI of 32.5. Most of the children in the study were boys and Hispanic.
Overall, 23.4% of study participants had prediabetes and 6.5% met the clinical criteria for type 2 diabetes. However, girls with NAFLD had a 60% greater risk of prediabetes and a fivefold greater risk of type 2 diabetes than boys, even after controlling for BMI and waist circumference (JAMA Pediatr. 2016 Aug 1. doi: 10.1001/jamapediatrics.2016.1971), reported Dr. Kimberly P. Newton and her coauthors.
The researchers also noted a significant association between nonalcoholic steatohepatitis (NASH) and glucose metabolism. Individuals with type 2 diabetes were three times more likely to also have NASH, while those with prediabetes had a 90% higher incidence of NASH, compared with individuals with normal glucose metabolism. They also found that those with NASH had significantly higher mean fasting glucose and insulin concentrations than children without NASH.
Dr. Newton, of the University of California, San Diego, and her coauthors wrote that while abnormal glucose metabolism is known to be common in adults with NAFLD, and that type diabetes is a risk factor for progression to NASH and liver-related mortality, the association in children with NAFLD is less well understood.
“Among our cohort, the prevalence of children with type 2 diabetes was much higher than would be expected based on contributions from obesity alone,” they wrote. “Although systemic insulin resistance is believed be important in the pathogenesis of both pediatric NAFLD and type 2 diabetes, to our knowledge, there are no longitudinal studies that evaluate the cause-effect relationship between these two associated conditions.”
The authors drew particular attention to the threefold higher odds of NASH in children with NAFLD and type 2 diabetes, pointing out that while the prognostic implications of NASH in childhood are not fully known, the NASH phenotype is associated with a “substantially” greater risk of cirrhosis. This risk is likely to be compounded by the presence of type 2 diabetes.
“Our study advances the literature by showing that as early as childhood, prediabetes and type 2 diabetes emerge as clear risk factors for NASH with potential downstream implications for future morbidity and mortality.”
Commenting on the greater incidence of prediabetes and type 2 diabetes among girls with NAFLD, the authors said this had been observed in other studies and that sex differences represented a major unmet research need.
The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this co-morbidity is also associated with a greater risk of nonalcoholic steatohepatitis, according to a cross-sectional study published online Aug. 1 in JAMA Pediatrics.
The study used data from 675 children with biopsy-confirmed nonalcoholic fatty liver disease (NAFLD) who were enrolled in the NASH Clinical Research Network. The mean age of the children was 12.6 years, and they had a mean BMI of 32.5. Most of the children in the study were boys and Hispanic.
Overall, 23.4% of study participants had prediabetes and 6.5% met the clinical criteria for type 2 diabetes. However, girls with NAFLD had a 60% greater risk of prediabetes and a fivefold greater risk of type 2 diabetes than boys, even after controlling for BMI and waist circumference (JAMA Pediatr. 2016 Aug 1. doi: 10.1001/jamapediatrics.2016.1971), reported Dr. Kimberly P. Newton and her coauthors.
The researchers also noted a significant association between nonalcoholic steatohepatitis (NASH) and glucose metabolism. Individuals with type 2 diabetes were three times more likely to also have NASH, while those with prediabetes had a 90% higher incidence of NASH, compared with individuals with normal glucose metabolism. They also found that those with NASH had significantly higher mean fasting glucose and insulin concentrations than children without NASH.
Dr. Newton, of the University of California, San Diego, and her coauthors wrote that while abnormal glucose metabolism is known to be common in adults with NAFLD, and that type diabetes is a risk factor for progression to NASH and liver-related mortality, the association in children with NAFLD is less well understood.
“Among our cohort, the prevalence of children with type 2 diabetes was much higher than would be expected based on contributions from obesity alone,” they wrote. “Although systemic insulin resistance is believed be important in the pathogenesis of both pediatric NAFLD and type 2 diabetes, to our knowledge, there are no longitudinal studies that evaluate the cause-effect relationship between these two associated conditions.”
The authors drew particular attention to the threefold higher odds of NASH in children with NAFLD and type 2 diabetes, pointing out that while the prognostic implications of NASH in childhood are not fully known, the NASH phenotype is associated with a “substantially” greater risk of cirrhosis. This risk is likely to be compounded by the presence of type 2 diabetes.
“Our study advances the literature by showing that as early as childhood, prediabetes and type 2 diabetes emerge as clear risk factors for NASH with potential downstream implications for future morbidity and mortality.”
Commenting on the greater incidence of prediabetes and type 2 diabetes among girls with NAFLD, the authors said this had been observed in other studies and that sex differences represented a major unmet research need.
The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this co-morbidity is also associated with a greater risk of nonalcoholic steatohepatitis, according to a cross-sectional study published online Aug. 1 in JAMA Pediatrics.
The study used data from 675 children with biopsy-confirmed nonalcoholic fatty liver disease (NAFLD) who were enrolled in the NASH Clinical Research Network. The mean age of the children was 12.6 years, and they had a mean BMI of 32.5. Most of the children in the study were boys and Hispanic.
Overall, 23.4% of study participants had prediabetes and 6.5% met the clinical criteria for type 2 diabetes. However, girls with NAFLD had a 60% greater risk of prediabetes and a fivefold greater risk of type 2 diabetes than boys, even after controlling for BMI and waist circumference (JAMA Pediatr. 2016 Aug 1. doi: 10.1001/jamapediatrics.2016.1971), reported Dr. Kimberly P. Newton and her coauthors.
The researchers also noted a significant association between nonalcoholic steatohepatitis (NASH) and glucose metabolism. Individuals with type 2 diabetes were three times more likely to also have NASH, while those with prediabetes had a 90% higher incidence of NASH, compared with individuals with normal glucose metabolism. They also found that those with NASH had significantly higher mean fasting glucose and insulin concentrations than children without NASH.
Dr. Newton, of the University of California, San Diego, and her coauthors wrote that while abnormal glucose metabolism is known to be common in adults with NAFLD, and that type diabetes is a risk factor for progression to NASH and liver-related mortality, the association in children with NAFLD is less well understood.
“Among our cohort, the prevalence of children with type 2 diabetes was much higher than would be expected based on contributions from obesity alone,” they wrote. “Although systemic insulin resistance is believed be important in the pathogenesis of both pediatric NAFLD and type 2 diabetes, to our knowledge, there are no longitudinal studies that evaluate the cause-effect relationship between these two associated conditions.”
The authors drew particular attention to the threefold higher odds of NASH in children with NAFLD and type 2 diabetes, pointing out that while the prognostic implications of NASH in childhood are not fully known, the NASH phenotype is associated with a “substantially” greater risk of cirrhosis. This risk is likely to be compounded by the presence of type 2 diabetes.
“Our study advances the literature by showing that as early as childhood, prediabetes and type 2 diabetes emerge as clear risk factors for NASH with potential downstream implications for future morbidity and mortality.”
Commenting on the greater incidence of prediabetes and type 2 diabetes among girls with NAFLD, the authors said this had been observed in other studies and that sex differences represented a major unmet research need.
The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
FROM JAMA PEDIATRICS
Key clinical point: Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this combination also is associated with a greater risk of nonalcoholic steatohepatitis.
Major finding: Among children with biopsy-diagnosed non-alcoholic fatty liver disease, 23.4% had prediabetes and 6.5% met the clinical criteria for type 2 diabetes.
Data source: Cross-sectional study of 675 children with biopsy-confirmed nonalcoholic fatty liver disease enrolled in the NASH Clinical Research Network.
Disclosures: The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
Gene therapy shows promise for severe hemophilia A

Image by Spencer Phillips
ORLANDO—An investigational gene therapy can safely reduce bleeding in patients with severe hemophilia A, a phase 1/2 study suggests.
The therapy is BMN 270, a recombinant adeno-associated virus (AAV) vector coding for human coagulation factor VIII (FVIII).
Six of the 7 patients treated with the highest dose of BMN 270 had FVIII levels above 50%, and the number of bleeding events fell substantially from baseline.
None of the patients developed inhibitors to FVIII, there were no serious adverse events, and none of the patients discontinued the therapy due to safety reasons.
John Pasi, PhD, of Barts and the London School of Medicine and Dentistry in London, UK, presented the results of this study in a late-breaking oral presentation at the World Federation of Hemophilia 2016 World Congress.* The research was funded by BioMarin Pharmaceutical Inc.
This phase 1/2 dose-escalation study was designed to evaluate the safety and efficacy of BMN 270 in up to 12 patients with severe hemophilia A.
The primary endpoints are to assess the safety of a single dose of BMN 270 and the change from baseline of FVIII expression level at 16 weeks after infusion.
Secondary endpoints include assessing the impact of BMN 270 on the frequency of FVIII replacement therapy, the number of bleeding episodes requiring treatment, and any potential immune responses. Patients will be monitored for safety and durability of effect for 5 years.
Thus far, 9 patients with severe hemophilia A have received a single dose of BMN 270—1 at 6×1012 vg/kg, 1 at 2×1013 vg/kg, and 7 at 6 x 1013 vg/kg.
As of the July 6 data cutoff, post-treatment follow-up ranges from 12 weeks to 28 weeks.
Safety
The most common adverse events were arthralgia (9 events in 6 subjects), contusion (6 events in 3 subjects), back pain (4 events in 3 subjects), and ALT elevation (6 events in 6 subjects).
No clinically relevant sustained rises in ALT levels or other markers of liver toxicity have been observed.
The maximum ALT levels were between 23 U/L and 82 U/L (less than 2 times the upper limit of normal, which is 43 U/L for the central laboratory in this study) approximately 12 weeks after gene delivery and generally declined over the next few weeks. ALT rises have not been associated with any decrease in FVIII levels.
A steroid regimen administered to all high-dose patients has been well-tolerated. Patients are successfully tapering off of steroids. Two patients have been off steroid therapy for up to 2.5 weeks, with no adverse impact on FVIII expression or ALT levels.
Efficacy
The patient treated at the lowest dose (6×1012 vg/kg) had no change from baseline in FVIII levels. The patient treated at the mid-dose (2×1013 vg/kg) had a stable FVIII activity level greater than 2 IU/dL for more than 28 weeks.
All 7 patients treated at the highest dose (6×1013 vg/kg) had FVIII activity levels greater than 10 IU/dL after week 10.
As of each patient’s most recent reading, 6 of the 7 patients in the high-dose group had FVIII levels above 50%, as a percentage calculated based on the numbers of IU/dL. The seventh patient had levels above 10%.
Four patients who have been followed the longest had a mean FVIII level of 146% at their 20-week visit. Two patients with FVIII levels above 200% had no unexpected events or need for medical intervention.
For the 7 patients treated at the high dose, the median annualized bleeding rate measured from the day of gene transfer to the data cutoff fell from 20 to 5.
After week 7 post-infusion, there were no bleeds in 6 of the 7 patients. There were 10 bleeds from weeks 0 through 2 post-infusion, 7 bleeds from weeks 3 through 8, and 2 bleeds from weeks 9 through 28. From weeks 2 through 28, all but 1 bleed occurred in a single subject who is the lowest responder.
All of the patients in the high-dose cohort have switched to receiving FVIII therapy on-demand. Six of them were previously receiving FVIII therapy as prophylaxis.
“These data provide strong proof-of-concept evidence that restoration of clotting function may be achieved by gene therapy,” Dr Pasi said. “For the first time, patients have reason to hope to avoid bleeding and the opportunity to live a normal life.” ![]()
Image by Spencer Phillips
ORLANDO—An investigational gene therapy can safely reduce bleeding in patients with severe hemophilia A, a phase 1/2 study suggests.
The therapy is BMN 270, a recombinant adeno-associated virus (AAV) vector coding for human coagulation factor VIII (FVIII).
Six of the 7 patients treated with the highest dose of BMN 270 had FVIII levels above 50%, and the number of bleeding events fell substantially from baseline.
None of the patients developed inhibitors to FVIII, there were no serious adverse events, and none of the patients discontinued the therapy due to safety reasons.
John Pasi, PhD, of Barts and the London School of Medicine and Dentistry in London, UK, presented the results of this study in a late-breaking oral presentation at the World Federation of Hemophilia 2016 World Congress.* The research was funded by BioMarin Pharmaceutical Inc.
This phase 1/2 dose-escalation study was designed to evaluate the safety and efficacy of BMN 270 in up to 12 patients with severe hemophilia A.
The primary endpoints are to assess the safety of a single dose of BMN 270 and the change from baseline of FVIII expression level at 16 weeks after infusion.
Secondary endpoints include assessing the impact of BMN 270 on the frequency of FVIII replacement therapy, the number of bleeding episodes requiring treatment, and any potential immune responses. Patients will be monitored for safety and durability of effect for 5 years.
Thus far, 9 patients with severe hemophilia A have received a single dose of BMN 270—1 at 6×1012 vg/kg, 1 at 2×1013 vg/kg, and 7 at 6 x 1013 vg/kg.
As of the July 6 data cutoff, post-treatment follow-up ranges from 12 weeks to 28 weeks.
Safety
The most common adverse events were arthralgia (9 events in 6 subjects), contusion (6 events in 3 subjects), back pain (4 events in 3 subjects), and ALT elevation (6 events in 6 subjects).
No clinically relevant sustained rises in ALT levels or other markers of liver toxicity have been observed.
The maximum ALT levels were between 23 U/L and 82 U/L (less than 2 times the upper limit of normal, which is 43 U/L for the central laboratory in this study) approximately 12 weeks after gene delivery and generally declined over the next few weeks. ALT rises have not been associated with any decrease in FVIII levels.
A steroid regimen administered to all high-dose patients has been well-tolerated. Patients are successfully tapering off of steroids. Two patients have been off steroid therapy for up to 2.5 weeks, with no adverse impact on FVIII expression or ALT levels.
Efficacy
The patient treated at the lowest dose (6×1012 vg/kg) had no change from baseline in FVIII levels. The patient treated at the mid-dose (2×1013 vg/kg) had a stable FVIII activity level greater than 2 IU/dL for more than 28 weeks.
All 7 patients treated at the highest dose (6×1013 vg/kg) had FVIII activity levels greater than 10 IU/dL after week 10.
As of each patient’s most recent reading, 6 of the 7 patients in the high-dose group had FVIII levels above 50%, as a percentage calculated based on the numbers of IU/dL. The seventh patient had levels above 10%.
Four patients who have been followed the longest had a mean FVIII level of 146% at their 20-week visit. Two patients with FVIII levels above 200% had no unexpected events or need for medical intervention.
For the 7 patients treated at the high dose, the median annualized bleeding rate measured from the day of gene transfer to the data cutoff fell from 20 to 5.
After week 7 post-infusion, there were no bleeds in 6 of the 7 patients. There were 10 bleeds from weeks 0 through 2 post-infusion, 7 bleeds from weeks 3 through 8, and 2 bleeds from weeks 9 through 28. From weeks 2 through 28, all but 1 bleed occurred in a single subject who is the lowest responder.
All of the patients in the high-dose cohort have switched to receiving FVIII therapy on-demand. Six of them were previously receiving FVIII therapy as prophylaxis.
“These data provide strong proof-of-concept evidence that restoration of clotting function may be achieved by gene therapy,” Dr Pasi said. “For the first time, patients have reason to hope to avoid bleeding and the opportunity to live a normal life.” ![]()
Image by Spencer Phillips
ORLANDO—An investigational gene therapy can safely reduce bleeding in patients with severe hemophilia A, a phase 1/2 study suggests.
The therapy is BMN 270, a recombinant adeno-associated virus (AAV) vector coding for human coagulation factor VIII (FVIII).
Six of the 7 patients treated with the highest dose of BMN 270 had FVIII levels above 50%, and the number of bleeding events fell substantially from baseline.
None of the patients developed inhibitors to FVIII, there were no serious adverse events, and none of the patients discontinued the therapy due to safety reasons.
John Pasi, PhD, of Barts and the London School of Medicine and Dentistry in London, UK, presented the results of this study in a late-breaking oral presentation at the World Federation of Hemophilia 2016 World Congress.* The research was funded by BioMarin Pharmaceutical Inc.
This phase 1/2 dose-escalation study was designed to evaluate the safety and efficacy of BMN 270 in up to 12 patients with severe hemophilia A.
The primary endpoints are to assess the safety of a single dose of BMN 270 and the change from baseline of FVIII expression level at 16 weeks after infusion.
Secondary endpoints include assessing the impact of BMN 270 on the frequency of FVIII replacement therapy, the number of bleeding episodes requiring treatment, and any potential immune responses. Patients will be monitored for safety and durability of effect for 5 years.
Thus far, 9 patients with severe hemophilia A have received a single dose of BMN 270—1 at 6×1012 vg/kg, 1 at 2×1013 vg/kg, and 7 at 6 x 1013 vg/kg.
As of the July 6 data cutoff, post-treatment follow-up ranges from 12 weeks to 28 weeks.
Safety
The most common adverse events were arthralgia (9 events in 6 subjects), contusion (6 events in 3 subjects), back pain (4 events in 3 subjects), and ALT elevation (6 events in 6 subjects).
No clinically relevant sustained rises in ALT levels or other markers of liver toxicity have been observed.
The maximum ALT levels were between 23 U/L and 82 U/L (less than 2 times the upper limit of normal, which is 43 U/L for the central laboratory in this study) approximately 12 weeks after gene delivery and generally declined over the next few weeks. ALT rises have not been associated with any decrease in FVIII levels.
A steroid regimen administered to all high-dose patients has been well-tolerated. Patients are successfully tapering off of steroids. Two patients have been off steroid therapy for up to 2.5 weeks, with no adverse impact on FVIII expression or ALT levels.
Efficacy
The patient treated at the lowest dose (6×1012 vg/kg) had no change from baseline in FVIII levels. The patient treated at the mid-dose (2×1013 vg/kg) had a stable FVIII activity level greater than 2 IU/dL for more than 28 weeks.
All 7 patients treated at the highest dose (6×1013 vg/kg) had FVIII activity levels greater than 10 IU/dL after week 10.
As of each patient’s most recent reading, 6 of the 7 patients in the high-dose group had FVIII levels above 50%, as a percentage calculated based on the numbers of IU/dL. The seventh patient had levels above 10%.
Four patients who have been followed the longest had a mean FVIII level of 146% at their 20-week visit. Two patients with FVIII levels above 200% had no unexpected events or need for medical intervention.
For the 7 patients treated at the high dose, the median annualized bleeding rate measured from the day of gene transfer to the data cutoff fell from 20 to 5.
After week 7 post-infusion, there were no bleeds in 6 of the 7 patients. There were 10 bleeds from weeks 0 through 2 post-infusion, 7 bleeds from weeks 3 through 8, and 2 bleeds from weeks 9 through 28. From weeks 2 through 28, all but 1 bleed occurred in a single subject who is the lowest responder.
All of the patients in the high-dose cohort have switched to receiving FVIII therapy on-demand. Six of them were previously receiving FVIII therapy as prophylaxis.
“These data provide strong proof-of-concept evidence that restoration of clotting function may be achieved by gene therapy,” Dr Pasi said. “For the first time, patients have reason to hope to avoid bleeding and the opportunity to live a normal life.” ![]()
PHM16: Promoting, Teaching Pediatric High Value Care
As we embark on Choosing Wisely, pediatric hospitalists gathered to attend this fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high value care are plenty and essentially universal to academic and community sites: we have had no formal teaching, there is cultural resistance and there is lack of transparency on costs and charges.
Perhaps the questions we should be asking ourselves, our trainees and our families are:
- Instead of “What’s the matter?” ask “What matters?”
- Instead of asking “Will that test change our management?” ask “Does that test benefit the patient? What are the harms of the test?”
Thinking about effects of tests downstream, the “testing cascade” can be a great mental exercise for the higher-level learner to understand the value, the unknowns we face in our daily decisions and simultaneously improving our understanding of best practices.
A toolkit was provided to help bring back resources and methods to teach high value care in morning report/ case conference settings, bedside teaching and family discussions.
One point is clear though—there is still a long way to go to move the pendulum to the side of value based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary values—family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
This serves as an exciting time to unite and better our understanding on why we do what we do and deliberately think about downstream effects. High value care curriculum for medical students, residents, fellows and even faculty is an area ripe for further educational and clinical research.
When asking for the Pediatric Value Meal, this is one where I will not Super size it!
Dr. Akshata Hopkins, MD FAAP, is an academic hospitalist at Johns Hopkins All Children's Hospital, St. Petersburg, Fla.
As we embark on Choosing Wisely, pediatric hospitalists gathered to attend this fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high value care are plenty and essentially universal to academic and community sites: we have had no formal teaching, there is cultural resistance and there is lack of transparency on costs and charges.
Perhaps the questions we should be asking ourselves, our trainees and our families are:
- Instead of “What’s the matter?” ask “What matters?”
- Instead of asking “Will that test change our management?” ask “Does that test benefit the patient? What are the harms of the test?”
Thinking about effects of tests downstream, the “testing cascade” can be a great mental exercise for the higher-level learner to understand the value, the unknowns we face in our daily decisions and simultaneously improving our understanding of best practices.
A toolkit was provided to help bring back resources and methods to teach high value care in morning report/ case conference settings, bedside teaching and family discussions.
One point is clear though—there is still a long way to go to move the pendulum to the side of value based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary values—family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
This serves as an exciting time to unite and better our understanding on why we do what we do and deliberately think about downstream effects. High value care curriculum for medical students, residents, fellows and even faculty is an area ripe for further educational and clinical research.
When asking for the Pediatric Value Meal, this is one where I will not Super size it!
Dr. Akshata Hopkins, MD FAAP, is an academic hospitalist at Johns Hopkins All Children's Hospital, St. Petersburg, Fla.
As we embark on Choosing Wisely, pediatric hospitalists gathered to attend this fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high value care are plenty and essentially universal to academic and community sites: we have had no formal teaching, there is cultural resistance and there is lack of transparency on costs and charges.
Perhaps the questions we should be asking ourselves, our trainees and our families are:
- Instead of “What’s the matter?” ask “What matters?”
- Instead of asking “Will that test change our management?” ask “Does that test benefit the patient? What are the harms of the test?”
Thinking about effects of tests downstream, the “testing cascade” can be a great mental exercise for the higher-level learner to understand the value, the unknowns we face in our daily decisions and simultaneously improving our understanding of best practices.
A toolkit was provided to help bring back resources and methods to teach high value care in morning report/ case conference settings, bedside teaching and family discussions.
One point is clear though—there is still a long way to go to move the pendulum to the side of value based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary values—family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
This serves as an exciting time to unite and better our understanding on why we do what we do and deliberately think about downstream effects. High value care curriculum for medical students, residents, fellows and even faculty is an area ripe for further educational and clinical research.
When asking for the Pediatric Value Meal, this is one where I will not Super size it!
Dr. Akshata Hopkins, MD FAAP, is an academic hospitalist at Johns Hopkins All Children's Hospital, St. Petersburg, Fla.
ED Visits Rise With Age in Children, Young Adults With Diabetes
The rate of diabetes-related emergency department visits was 464.5 per 100,000 U.S. population among Americans under age 30 in 2012, with young adults heading to the ED far more often than children, according to the Agency for Healthcare Research and Quality.
Young adults aged 18-29 years made diabetes-related ED visits at a rate of 905 per 100,000 in 2012, compared with 149 per 100,000 for children 17 and under. Narrowing down the age groups shows even greater differences: The rate was 47 per 100,000 for children aged 5 years and under, 95 for children aged 6-9, 193 for 10- to 13-year-olds, 316.5 for those aged 14-17, 607 for 18- to 21-year-olds, 889 for 22- to 25-year-olds, and 1,236 for those aged 26-29 years, the AHRQ reported.
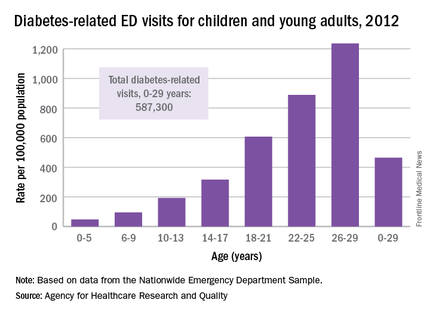
Patients aged 5 years and under were, however, the most likely to be admitted to the hospital in 2012: 29% of their diabetes-related ED visits resulted in admission, compared with 26% for those aged 26-29. Those aged 22-25 years were the least likely to be admitted, with 18% staying after their ED visit, and the overall admission rate for those aged 0-29 years was 23.5%, the report noted.
The ED visit rate for diabetes was higher for females than for males aged 0-29 years – 569 per 100,000 vs. 355 – but males were more likely to be admitted – 27% vs. 21% for females, according to data from the Nationwide Emergency Department Sample.
The rate of diabetes-related emergency department visits was 464.5 per 100,000 U.S. population among Americans under age 30 in 2012, with young adults heading to the ED far more often than children, according to the Agency for Healthcare Research and Quality.
Young adults aged 18-29 years made diabetes-related ED visits at a rate of 905 per 100,000 in 2012, compared with 149 per 100,000 for children 17 and under. Narrowing down the age groups shows even greater differences: The rate was 47 per 100,000 for children aged 5 years and under, 95 for children aged 6-9, 193 for 10- to 13-year-olds, 316.5 for those aged 14-17, 607 for 18- to 21-year-olds, 889 for 22- to 25-year-olds, and 1,236 for those aged 26-29 years, the AHRQ reported.
Patients aged 5 years and under were, however, the most likely to be admitted to the hospital in 2012: 29% of their diabetes-related ED visits resulted in admission, compared with 26% for those aged 26-29. Those aged 22-25 years were the least likely to be admitted, with 18% staying after their ED visit, and the overall admission rate for those aged 0-29 years was 23.5%, the report noted.
The ED visit rate for diabetes was higher for females than for males aged 0-29 years – 569 per 100,000 vs. 355 – but males were more likely to be admitted – 27% vs. 21% for females, according to data from the Nationwide Emergency Department Sample.
The rate of diabetes-related emergency department visits was 464.5 per 100,000 U.S. population among Americans under age 30 in 2012, with young adults heading to the ED far more often than children, according to the Agency for Healthcare Research and Quality.
Young adults aged 18-29 years made diabetes-related ED visits at a rate of 905 per 100,000 in 2012, compared with 149 per 100,000 for children 17 and under. Narrowing down the age groups shows even greater differences: The rate was 47 per 100,000 for children aged 5 years and under, 95 for children aged 6-9, 193 for 10- to 13-year-olds, 316.5 for those aged 14-17, 607 for 18- to 21-year-olds, 889 for 22- to 25-year-olds, and 1,236 for those aged 26-29 years, the AHRQ reported.
Patients aged 5 years and under were, however, the most likely to be admitted to the hospital in 2012: 29% of their diabetes-related ED visits resulted in admission, compared with 26% for those aged 26-29. Those aged 22-25 years were the least likely to be admitted, with 18% staying after their ED visit, and the overall admission rate for those aged 0-29 years was 23.5%, the report noted.
The ED visit rate for diabetes was higher for females than for males aged 0-29 years – 569 per 100,000 vs. 355 – but males were more likely to be admitted – 27% vs. 21% for females, according to data from the Nationwide Emergency Department Sample.
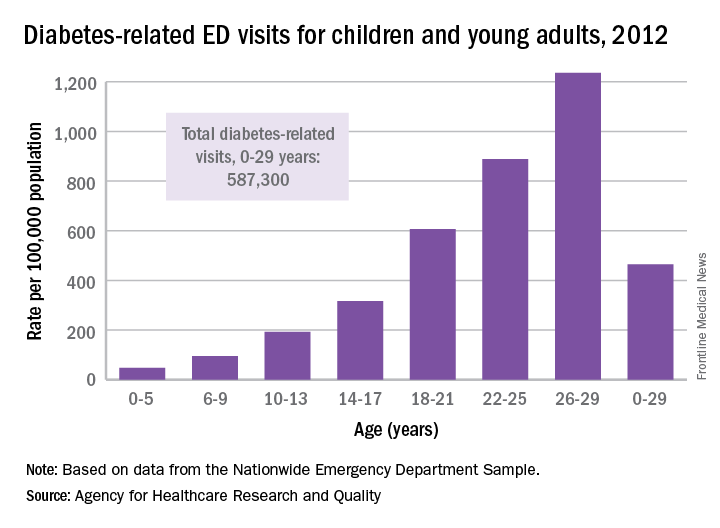
C6 EIA testing can guide Lyme disease treatment in children
The C6 Lyme enzyme immunoassay is an effective diagnostic tool for children who are being tested for Lyme disease, according to Susan C. Lipsett, MD, and her associates.
Of the 944 samples collected for the study, 114 were positive for Lyme disease. The sensitivity of C6 enzyme immunoassay (EIA) testing alone was 79.8% and the specificity was 94.2%, slightly less than the standard two-tiered testing approach, which had a sensitivity of 81.6% and a specificity of 98.8%. The specificity of C6 EIA testing was increased to 98.6% when a supplemental immunoblot was added to testing.
The specificity of C6 EIA testing alone was significantly lower than standard testing in the control group. When the supplemental immunoblot was added to testing, the specificity of C6 EIA testing did match the specificity of standard testing in children who did not have Lyme disease.
“Although supplemental immunoblots are still required to confirm a Lyme disease diagnosis, our study supports using the C6 EIA as a first-line diagnostic test in children undergoing evaluation for Lyme disease. In the appropriate clinical scenario, the C6 EIA could limit unnecessary procedures and allow for prompt initiation of appropriate therapy,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (doi:10.1093/cid/ciw427).
The C6 Lyme enzyme immunoassay is an effective diagnostic tool for children who are being tested for Lyme disease, according to Susan C. Lipsett, MD, and her associates.
Of the 944 samples collected for the study, 114 were positive for Lyme disease. The sensitivity of C6 enzyme immunoassay (EIA) testing alone was 79.8% and the specificity was 94.2%, slightly less than the standard two-tiered testing approach, which had a sensitivity of 81.6% and a specificity of 98.8%. The specificity of C6 EIA testing was increased to 98.6% when a supplemental immunoblot was added to testing.
The specificity of C6 EIA testing alone was significantly lower than standard testing in the control group. When the supplemental immunoblot was added to testing, the specificity of C6 EIA testing did match the specificity of standard testing in children who did not have Lyme disease.
“Although supplemental immunoblots are still required to confirm a Lyme disease diagnosis, our study supports using the C6 EIA as a first-line diagnostic test in children undergoing evaluation for Lyme disease. In the appropriate clinical scenario, the C6 EIA could limit unnecessary procedures and allow for prompt initiation of appropriate therapy,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (doi:10.1093/cid/ciw427).
The C6 Lyme enzyme immunoassay is an effective diagnostic tool for children who are being tested for Lyme disease, according to Susan C. Lipsett, MD, and her associates.
Of the 944 samples collected for the study, 114 were positive for Lyme disease. The sensitivity of C6 enzyme immunoassay (EIA) testing alone was 79.8% and the specificity was 94.2%, slightly less than the standard two-tiered testing approach, which had a sensitivity of 81.6% and a specificity of 98.8%. The specificity of C6 EIA testing was increased to 98.6% when a supplemental immunoblot was added to testing.
The specificity of C6 EIA testing alone was significantly lower than standard testing in the control group. When the supplemental immunoblot was added to testing, the specificity of C6 EIA testing did match the specificity of standard testing in children who did not have Lyme disease.
“Although supplemental immunoblots are still required to confirm a Lyme disease diagnosis, our study supports using the C6 EIA as a first-line diagnostic test in children undergoing evaluation for Lyme disease. In the appropriate clinical scenario, the C6 EIA could limit unnecessary procedures and allow for prompt initiation of appropriate therapy,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (doi:10.1093/cid/ciw427).
FROM CLINICAL INFECTIOUS DISEASES