User login
Compulsively checking social media linked with altered brain patterns in teens
Teens who compulsively checked social media networks showed different development patterns in parts of the brain that involve reward and punishment than did those who didn’t check their platforms as often, new research suggests.
Results were published online in JAMA Pediatrics.
Researchers, led by Maria T. Maza, of the department of psychology and neuroscience at University of North Carolina at Chapel Hill, included 169 6th- and 7th-grade students recruited from three public middle schools in rural North Carolina in a 3-year longitudinal cohort.
Participants reported how frequently they checked Facebook, Instagram, and Snapchat. Answers were grouped into eight score groups depending on their per-day check times: less than 1; 1; 2-3; 4-5; 6-10; 11-15; 16-20; or more than 20 times. Those groups were then broken into three categories: low (nonhabitual); moderate; and high (habitual).
Imaging shows reactions
Researchers used functional magnetic resonance imaging (fMRI) to see how different areas of the brain react when participants looked at a series of indicators, such as happy and angry faces, which mimic social media rewards, punishments, or neutral feedback.
The research team focused on adolescents, for whom social media participation and neural sensitivity to social feedback from peers are high.
They found that participants who frequently checked social media showed distinct brain patterns when anticipating social feedback compared with those who had moderate or low use, “suggesting that habitual social media checking early in adolescence is associated with divergent brain development over time.”
The affected regions of the brain included the networks that respond to motivation and cognitive control.
However, the study was not able to determine whether the differences are a good or bad thing.
“While for some individuals with habitual checking behaviors, an initial hyposensitivity to potential social rewards and punishments followed by hypersensitivity may contribute to checking behaviors on social media becoming compulsive and problematic, for others, this change in sensitivity may reflect an adaptive behavior that allows them to better navigate their increasingly digital environment,” the authors wrote.
Chicken-and-egg questions
David Rettew, MD, a child and adolescent psychiatrist at the Oregon Health & Science University in Portland, who was not part of this research, said in an interview that it’s not clear from this study which came first – different brain development in the teens prior to this study that caused compulsive checking, or checking behaviors that caused different brain development. The authors acknowledge this is a limitation of the study.
“Hopefully, someday researchers will look at some of these brain activation patterns before kids have been exposed to social media to help us sort some of these questions out,” Dr. Rettew said.
“It wasn’t as though the groups looked the same at baseline and then diverged as they used more and more social media,” Dr. Rettew said. “It looked like there were some baseline differences that could be traced back maybe years before the study even started.”
People hear “divergent brain development” associated with social media and naturally get alarmed, he acknowledged.
“I get that, but the study isn’t really equipped to tell us what should be happening in the brain and what changes may have implications for other parts of an adolescent’s life,” Dr. Rettew said, “In the end, what we have is an association between heavy social media use and certain brain activation patterns which is cool to see and measure.”
He agrees with the authors, however, that overuse of social media is concerning and studying its effects is important.
Seventy-eight percent of early adolescents check every hour
According to the paper, 78% of 13- to 17-year-olds report checking their devices at least every hour and 46% check “almost constantly.”
“Regardless of which brain regions light up when looking at various emoji responses to their Instagram post, I think it is valid already to have some concerns about youth who can’t stay off their phone for more than 10 minutes,” Dr. Rettew said. “Technology is here to stay, but how we can learn to use it rather than have it use us is probably the more pressing question at this point.”
One coauthor reports grants from the National Institute on Drug Abuse (NIDA) during the conduct of the study and grants from NIDA and the National Science Foundation outside the submitted work; a coauthor reports grants from the Winston Family Foundation; and a coauthor reports a grant from NIDA and funds from the Winston Family Foundation – both during the conduct of the study. No other disclosures were reported. Dr. Rettew is author of the book, “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.”
Teens who compulsively checked social media networks showed different development patterns in parts of the brain that involve reward and punishment than did those who didn’t check their platforms as often, new research suggests.
Results were published online in JAMA Pediatrics.
Researchers, led by Maria T. Maza, of the department of psychology and neuroscience at University of North Carolina at Chapel Hill, included 169 6th- and 7th-grade students recruited from three public middle schools in rural North Carolina in a 3-year longitudinal cohort.
Participants reported how frequently they checked Facebook, Instagram, and Snapchat. Answers were grouped into eight score groups depending on their per-day check times: less than 1; 1; 2-3; 4-5; 6-10; 11-15; 16-20; or more than 20 times. Those groups were then broken into three categories: low (nonhabitual); moderate; and high (habitual).
Imaging shows reactions
Researchers used functional magnetic resonance imaging (fMRI) to see how different areas of the brain react when participants looked at a series of indicators, such as happy and angry faces, which mimic social media rewards, punishments, or neutral feedback.
The research team focused on adolescents, for whom social media participation and neural sensitivity to social feedback from peers are high.
They found that participants who frequently checked social media showed distinct brain patterns when anticipating social feedback compared with those who had moderate or low use, “suggesting that habitual social media checking early in adolescence is associated with divergent brain development over time.”
The affected regions of the brain included the networks that respond to motivation and cognitive control.
However, the study was not able to determine whether the differences are a good or bad thing.
“While for some individuals with habitual checking behaviors, an initial hyposensitivity to potential social rewards and punishments followed by hypersensitivity may contribute to checking behaviors on social media becoming compulsive and problematic, for others, this change in sensitivity may reflect an adaptive behavior that allows them to better navigate their increasingly digital environment,” the authors wrote.
Chicken-and-egg questions
David Rettew, MD, a child and adolescent psychiatrist at the Oregon Health & Science University in Portland, who was not part of this research, said in an interview that it’s not clear from this study which came first – different brain development in the teens prior to this study that caused compulsive checking, or checking behaviors that caused different brain development. The authors acknowledge this is a limitation of the study.
“Hopefully, someday researchers will look at some of these brain activation patterns before kids have been exposed to social media to help us sort some of these questions out,” Dr. Rettew said.
“It wasn’t as though the groups looked the same at baseline and then diverged as they used more and more social media,” Dr. Rettew said. “It looked like there were some baseline differences that could be traced back maybe years before the study even started.”
People hear “divergent brain development” associated with social media and naturally get alarmed, he acknowledged.
“I get that, but the study isn’t really equipped to tell us what should be happening in the brain and what changes may have implications for other parts of an adolescent’s life,” Dr. Rettew said, “In the end, what we have is an association between heavy social media use and certain brain activation patterns which is cool to see and measure.”
He agrees with the authors, however, that overuse of social media is concerning and studying its effects is important.
Seventy-eight percent of early adolescents check every hour
According to the paper, 78% of 13- to 17-year-olds report checking their devices at least every hour and 46% check “almost constantly.”
“Regardless of which brain regions light up when looking at various emoji responses to their Instagram post, I think it is valid already to have some concerns about youth who can’t stay off their phone for more than 10 minutes,” Dr. Rettew said. “Technology is here to stay, but how we can learn to use it rather than have it use us is probably the more pressing question at this point.”
One coauthor reports grants from the National Institute on Drug Abuse (NIDA) during the conduct of the study and grants from NIDA and the National Science Foundation outside the submitted work; a coauthor reports grants from the Winston Family Foundation; and a coauthor reports a grant from NIDA and funds from the Winston Family Foundation – both during the conduct of the study. No other disclosures were reported. Dr. Rettew is author of the book, “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.”
Teens who compulsively checked social media networks showed different development patterns in parts of the brain that involve reward and punishment than did those who didn’t check their platforms as often, new research suggests.
Results were published online in JAMA Pediatrics.
Researchers, led by Maria T. Maza, of the department of psychology and neuroscience at University of North Carolina at Chapel Hill, included 169 6th- and 7th-grade students recruited from three public middle schools in rural North Carolina in a 3-year longitudinal cohort.
Participants reported how frequently they checked Facebook, Instagram, and Snapchat. Answers were grouped into eight score groups depending on their per-day check times: less than 1; 1; 2-3; 4-5; 6-10; 11-15; 16-20; or more than 20 times. Those groups were then broken into three categories: low (nonhabitual); moderate; and high (habitual).
Imaging shows reactions
Researchers used functional magnetic resonance imaging (fMRI) to see how different areas of the brain react when participants looked at a series of indicators, such as happy and angry faces, which mimic social media rewards, punishments, or neutral feedback.
The research team focused on adolescents, for whom social media participation and neural sensitivity to social feedback from peers are high.
They found that participants who frequently checked social media showed distinct brain patterns when anticipating social feedback compared with those who had moderate or low use, “suggesting that habitual social media checking early in adolescence is associated with divergent brain development over time.”
The affected regions of the brain included the networks that respond to motivation and cognitive control.
However, the study was not able to determine whether the differences are a good or bad thing.
“While for some individuals with habitual checking behaviors, an initial hyposensitivity to potential social rewards and punishments followed by hypersensitivity may contribute to checking behaviors on social media becoming compulsive and problematic, for others, this change in sensitivity may reflect an adaptive behavior that allows them to better navigate their increasingly digital environment,” the authors wrote.
Chicken-and-egg questions
David Rettew, MD, a child and adolescent psychiatrist at the Oregon Health & Science University in Portland, who was not part of this research, said in an interview that it’s not clear from this study which came first – different brain development in the teens prior to this study that caused compulsive checking, or checking behaviors that caused different brain development. The authors acknowledge this is a limitation of the study.
“Hopefully, someday researchers will look at some of these brain activation patterns before kids have been exposed to social media to help us sort some of these questions out,” Dr. Rettew said.
“It wasn’t as though the groups looked the same at baseline and then diverged as they used more and more social media,” Dr. Rettew said. “It looked like there were some baseline differences that could be traced back maybe years before the study even started.”
People hear “divergent brain development” associated with social media and naturally get alarmed, he acknowledged.
“I get that, but the study isn’t really equipped to tell us what should be happening in the brain and what changes may have implications for other parts of an adolescent’s life,” Dr. Rettew said, “In the end, what we have is an association between heavy social media use and certain brain activation patterns which is cool to see and measure.”
He agrees with the authors, however, that overuse of social media is concerning and studying its effects is important.
Seventy-eight percent of early adolescents check every hour
According to the paper, 78% of 13- to 17-year-olds report checking their devices at least every hour and 46% check “almost constantly.”
“Regardless of which brain regions light up when looking at various emoji responses to their Instagram post, I think it is valid already to have some concerns about youth who can’t stay off their phone for more than 10 minutes,” Dr. Rettew said. “Technology is here to stay, but how we can learn to use it rather than have it use us is probably the more pressing question at this point.”
One coauthor reports grants from the National Institute on Drug Abuse (NIDA) during the conduct of the study and grants from NIDA and the National Science Foundation outside the submitted work; a coauthor reports grants from the Winston Family Foundation; and a coauthor reports a grant from NIDA and funds from the Winston Family Foundation – both during the conduct of the study. No other disclosures were reported. Dr. Rettew is author of the book, “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.”
FROM JAMA PEDIATRICS
FDA considers regulating CBD products
The products can have drug-like effects on the body and contain CBD (cannabidiol) and THC (tetrahydrocannabinol). Both CBD and THC can be derived from hemp, which was legalized by Congress in 2018.
“Given what we know about the safety of CBD so far, it raises concerns for FDA about whether these existing regulatory pathways for food and dietary supplements are appropriate for this substance,” FDA Principal Deputy Commissioner Janet Woodcock, MD, told The Wall Street Journal.
A 2021 FDA report valued the CBD market at $4.6 billion and projected it to quadruple by 2026. The only FDA-approved CBD product is an oil called Epidiolex, which can be prescribed for the seizure-associated disease epilepsy. Research on CBD to treat other diseases is ongoing.
Food, beverage, and beauty products containing CBD are sold in stores and online in many forms, including oils, vaporized liquids, and oil-based capsules, but “research supporting the drug’s benefits is still limited,” the Mayo Clinic said.
Recently, investigations have found that many CBD products also contain THC, which can be derived from legal hemp in a form that is referred to as Delta 8 and produces a psychoactive high. The CDC warned in 2022 that people “mistook” THC products for CBD products, which are often sold at the same stores, and experienced “adverse events.”
The Centers for Disease Control and Prevention and FDA warn that much is unknown about CBD and delta-8 products. The CDC says known CBD risks include liver damage; interference with other drugs you are taking, which may lead to injury or serious side effects; drowsiness or sleepiness; diarrhea or changes in appetite; changes in mood, such as crankiness; potential negative effects on fetuses during pregnancy or on babies during breastfeeding; or unintentional poisoning of children when mistaking THC products for CBD products or due to containing other ingredients such as THC or pesticides.
“I don’t think that we can have the perfect be the enemy of the good when we’re looking at such a vast market that is so available and utilized,” Norman Birenbaum, a senior FDA adviser who is working on the regulatory issue, told the Journal. “You’ve got a widely unregulated market.”
A version of this article first appeared on WebMD.com.
The products can have drug-like effects on the body and contain CBD (cannabidiol) and THC (tetrahydrocannabinol). Both CBD and THC can be derived from hemp, which was legalized by Congress in 2018.
“Given what we know about the safety of CBD so far, it raises concerns for FDA about whether these existing regulatory pathways for food and dietary supplements are appropriate for this substance,” FDA Principal Deputy Commissioner Janet Woodcock, MD, told The Wall Street Journal.
A 2021 FDA report valued the CBD market at $4.6 billion and projected it to quadruple by 2026. The only FDA-approved CBD product is an oil called Epidiolex, which can be prescribed for the seizure-associated disease epilepsy. Research on CBD to treat other diseases is ongoing.
Food, beverage, and beauty products containing CBD are sold in stores and online in many forms, including oils, vaporized liquids, and oil-based capsules, but “research supporting the drug’s benefits is still limited,” the Mayo Clinic said.
Recently, investigations have found that many CBD products also contain THC, which can be derived from legal hemp in a form that is referred to as Delta 8 and produces a psychoactive high. The CDC warned in 2022 that people “mistook” THC products for CBD products, which are often sold at the same stores, and experienced “adverse events.”
The Centers for Disease Control and Prevention and FDA warn that much is unknown about CBD and delta-8 products. The CDC says known CBD risks include liver damage; interference with other drugs you are taking, which may lead to injury or serious side effects; drowsiness or sleepiness; diarrhea or changes in appetite; changes in mood, such as crankiness; potential negative effects on fetuses during pregnancy or on babies during breastfeeding; or unintentional poisoning of children when mistaking THC products for CBD products or due to containing other ingredients such as THC or pesticides.
“I don’t think that we can have the perfect be the enemy of the good when we’re looking at such a vast market that is so available and utilized,” Norman Birenbaum, a senior FDA adviser who is working on the regulatory issue, told the Journal. “You’ve got a widely unregulated market.”
A version of this article first appeared on WebMD.com.
The products can have drug-like effects on the body and contain CBD (cannabidiol) and THC (tetrahydrocannabinol). Both CBD and THC can be derived from hemp, which was legalized by Congress in 2018.
“Given what we know about the safety of CBD so far, it raises concerns for FDA about whether these existing regulatory pathways for food and dietary supplements are appropriate for this substance,” FDA Principal Deputy Commissioner Janet Woodcock, MD, told The Wall Street Journal.
A 2021 FDA report valued the CBD market at $4.6 billion and projected it to quadruple by 2026. The only FDA-approved CBD product is an oil called Epidiolex, which can be prescribed for the seizure-associated disease epilepsy. Research on CBD to treat other diseases is ongoing.
Food, beverage, and beauty products containing CBD are sold in stores and online in many forms, including oils, vaporized liquids, and oil-based capsules, but “research supporting the drug’s benefits is still limited,” the Mayo Clinic said.
Recently, investigations have found that many CBD products also contain THC, which can be derived from legal hemp in a form that is referred to as Delta 8 and produces a psychoactive high. The CDC warned in 2022 that people “mistook” THC products for CBD products, which are often sold at the same stores, and experienced “adverse events.”
The Centers for Disease Control and Prevention and FDA warn that much is unknown about CBD and delta-8 products. The CDC says known CBD risks include liver damage; interference with other drugs you are taking, which may lead to injury or serious side effects; drowsiness or sleepiness; diarrhea or changes in appetite; changes in mood, such as crankiness; potential negative effects on fetuses during pregnancy or on babies during breastfeeding; or unintentional poisoning of children when mistaking THC products for CBD products or due to containing other ingredients such as THC or pesticides.
“I don’t think that we can have the perfect be the enemy of the good when we’re looking at such a vast market that is so available and utilized,” Norman Birenbaum, a senior FDA adviser who is working on the regulatory issue, told the Journal. “You’ve got a widely unregulated market.”
A version of this article first appeared on WebMD.com.
Strong link between muscle strength, mobility, and brain health
A new study shows a strong correlation between muscle strength, mobility, and brain volume, including in the hippocampus that underlies memory function, in adults with Alzheimer’s disease (AD).
Investigators found statistically significant relationships between better handgrip strength and mobility and hippocampal and lobar brain volumes in 38 cognitively impaired adults with biomarker evidence of AD.
study investigator Cyrus Raji, MD, PhD, Mallinckrodt Institute of Radiology, Washington University, St. Louis, told this news organization.
The study was published online in the Journal of Alzheimer’s Disease.
Brain-body connection
The researchers measured handgrip strength in patients’ dominant and nondominant hands using a hand dynamometer and calculated handgrip asymmetry. Mobility was measured via the 2-minute walk test. Together, the test results were used to categorize patients as “frail” or “not frail.”
They measured regional brain volumes using Neuroreader (Brainreader), a U.S. Food and Drug Administration–approved software application that measures brain volumes on MRI scans.
The investigators found higher nondominant handgrip strength was significantly associated with larger volumes in the hippocampal volume (P = .02). In addition, higher dominant handgrip strength correlated with higher frontal lobe volume (P = .02).
Results also showed higher scores on the 2-minute walk test were associated with larger hippocampal (P = .04), frontal (P = .01), temporal (P = .03), parietal (P = .009), and occipital lobe (P = .005) volumes. Frailty was associated with reduced frontal, temporal, and parietal lobe volumes.
“In this study we combined objective evaluations of frailty with measurable determinants of brain structure on MRI to demonstrate a link between frailty and brain health in patients with both biomarker evidence of AD and cognitive impairment,” study investigator Somayeh Meysami, MD, with Pacific Brain Health Center, Pacific Neuroscience Institute Foundation (PNI), Santa Monica, Calif., told this news organization.
The researchers noted that it’s possible that interventions specifically focused on improving ambulatory mobility and handgrip strength could be beneficial in improving dementia trajectories.
‘Use it or lose it’
The chief limitation of the study is the cross-sectional design that precludes drawing firm conclusions about the causal relationships between handgrip strength and changes in brain structure.
In addition, the study used a relatively small convenience sample of outpatients from a specialty memory clinic.
The researchers say future longitudinal analyses with a larger sample size will be important to better understand the possible directions of causality between handgrip strength and progression of atrophy in AD.
However, despite these limitations, the findings emphasize the importance of “body-brain connections,” added David A. Merrill, MD, PhD, director of the Pacific Brain Health Center at PNI.
“Training our muscles helps sustain our brains and vice versa. It’s ‘use it or lose it’ for both body and mind. Exercise remains among the best strategies for maintaining a healthy body and mind with aging,” Dr. Merrill said in an interview.
“While it’s long been appreciated that aerobic training helps the brain, these findings add to the importance of strength training in supporting successful aging,” he added.
This work was supported by Providence St. Joseph Health, Seattle; Saint John’s Health Center Foundation; Pacific Neuroscience Institute Foundation; and the National Institutes of Health. Dr. Raji is a consultant for Brainreader, Apollo Health, Pacific Neuroscience Foundation, and Neurevolution. Dr. Merrill and Dr. Meysami reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new study shows a strong correlation between muscle strength, mobility, and brain volume, including in the hippocampus that underlies memory function, in adults with Alzheimer’s disease (AD).
Investigators found statistically significant relationships between better handgrip strength and mobility and hippocampal and lobar brain volumes in 38 cognitively impaired adults with biomarker evidence of AD.
study investigator Cyrus Raji, MD, PhD, Mallinckrodt Institute of Radiology, Washington University, St. Louis, told this news organization.
The study was published online in the Journal of Alzheimer’s Disease.
Brain-body connection
The researchers measured handgrip strength in patients’ dominant and nondominant hands using a hand dynamometer and calculated handgrip asymmetry. Mobility was measured via the 2-minute walk test. Together, the test results were used to categorize patients as “frail” or “not frail.”
They measured regional brain volumes using Neuroreader (Brainreader), a U.S. Food and Drug Administration–approved software application that measures brain volumes on MRI scans.
The investigators found higher nondominant handgrip strength was significantly associated with larger volumes in the hippocampal volume (P = .02). In addition, higher dominant handgrip strength correlated with higher frontal lobe volume (P = .02).
Results also showed higher scores on the 2-minute walk test were associated with larger hippocampal (P = .04), frontal (P = .01), temporal (P = .03), parietal (P = .009), and occipital lobe (P = .005) volumes. Frailty was associated with reduced frontal, temporal, and parietal lobe volumes.
“In this study we combined objective evaluations of frailty with measurable determinants of brain structure on MRI to demonstrate a link between frailty and brain health in patients with both biomarker evidence of AD and cognitive impairment,” study investigator Somayeh Meysami, MD, with Pacific Brain Health Center, Pacific Neuroscience Institute Foundation (PNI), Santa Monica, Calif., told this news organization.
The researchers noted that it’s possible that interventions specifically focused on improving ambulatory mobility and handgrip strength could be beneficial in improving dementia trajectories.
‘Use it or lose it’
The chief limitation of the study is the cross-sectional design that precludes drawing firm conclusions about the causal relationships between handgrip strength and changes in brain structure.
In addition, the study used a relatively small convenience sample of outpatients from a specialty memory clinic.
The researchers say future longitudinal analyses with a larger sample size will be important to better understand the possible directions of causality between handgrip strength and progression of atrophy in AD.
However, despite these limitations, the findings emphasize the importance of “body-brain connections,” added David A. Merrill, MD, PhD, director of the Pacific Brain Health Center at PNI.
“Training our muscles helps sustain our brains and vice versa. It’s ‘use it or lose it’ for both body and mind. Exercise remains among the best strategies for maintaining a healthy body and mind with aging,” Dr. Merrill said in an interview.
“While it’s long been appreciated that aerobic training helps the brain, these findings add to the importance of strength training in supporting successful aging,” he added.
This work was supported by Providence St. Joseph Health, Seattle; Saint John’s Health Center Foundation; Pacific Neuroscience Institute Foundation; and the National Institutes of Health. Dr. Raji is a consultant for Brainreader, Apollo Health, Pacific Neuroscience Foundation, and Neurevolution. Dr. Merrill and Dr. Meysami reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
A new study shows a strong correlation between muscle strength, mobility, and brain volume, including in the hippocampus that underlies memory function, in adults with Alzheimer’s disease (AD).
Investigators found statistically significant relationships between better handgrip strength and mobility and hippocampal and lobar brain volumes in 38 cognitively impaired adults with biomarker evidence of AD.
study investigator Cyrus Raji, MD, PhD, Mallinckrodt Institute of Radiology, Washington University, St. Louis, told this news organization.
The study was published online in the Journal of Alzheimer’s Disease.
Brain-body connection
The researchers measured handgrip strength in patients’ dominant and nondominant hands using a hand dynamometer and calculated handgrip asymmetry. Mobility was measured via the 2-minute walk test. Together, the test results were used to categorize patients as “frail” or “not frail.”
They measured regional brain volumes using Neuroreader (Brainreader), a U.S. Food and Drug Administration–approved software application that measures brain volumes on MRI scans.
The investigators found higher nondominant handgrip strength was significantly associated with larger volumes in the hippocampal volume (P = .02). In addition, higher dominant handgrip strength correlated with higher frontal lobe volume (P = .02).
Results also showed higher scores on the 2-minute walk test were associated with larger hippocampal (P = .04), frontal (P = .01), temporal (P = .03), parietal (P = .009), and occipital lobe (P = .005) volumes. Frailty was associated with reduced frontal, temporal, and parietal lobe volumes.
“In this study we combined objective evaluations of frailty with measurable determinants of brain structure on MRI to demonstrate a link between frailty and brain health in patients with both biomarker evidence of AD and cognitive impairment,” study investigator Somayeh Meysami, MD, with Pacific Brain Health Center, Pacific Neuroscience Institute Foundation (PNI), Santa Monica, Calif., told this news organization.
The researchers noted that it’s possible that interventions specifically focused on improving ambulatory mobility and handgrip strength could be beneficial in improving dementia trajectories.
‘Use it or lose it’
The chief limitation of the study is the cross-sectional design that precludes drawing firm conclusions about the causal relationships between handgrip strength and changes in brain structure.
In addition, the study used a relatively small convenience sample of outpatients from a specialty memory clinic.
The researchers say future longitudinal analyses with a larger sample size will be important to better understand the possible directions of causality between handgrip strength and progression of atrophy in AD.
However, despite these limitations, the findings emphasize the importance of “body-brain connections,” added David A. Merrill, MD, PhD, director of the Pacific Brain Health Center at PNI.
“Training our muscles helps sustain our brains and vice versa. It’s ‘use it or lose it’ for both body and mind. Exercise remains among the best strategies for maintaining a healthy body and mind with aging,” Dr. Merrill said in an interview.
“While it’s long been appreciated that aerobic training helps the brain, these findings add to the importance of strength training in supporting successful aging,” he added.
This work was supported by Providence St. Joseph Health, Seattle; Saint John’s Health Center Foundation; Pacific Neuroscience Institute Foundation; and the National Institutes of Health. Dr. Raji is a consultant for Brainreader, Apollo Health, Pacific Neuroscience Foundation, and Neurevolution. Dr. Merrill and Dr. Meysami reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF ALZHEIMER’S DISEASE
Alzheimer’s Association to CMS: Ditch restraints on amyloid drugs
In a letter addressed to CMS administrator Chiquita Brooks-LaSure, MPP, the association has asked the agency to remove the requirements for “coverage with evidence development” in its national coverage determination for FDA-approved anti-amyloid monoclonal antibodies.
The CMS coverage restrictions for anti-amyloid drugs were finalized in April on the basis of data available at the time.
Since then, new data from the CLARITY AD trial “clearly demonstrate a meaningful clinical benefit” from the investigational anti-amyloid agent lecanemab (Eisai/Biogen), Robert Egge, chief public policy officer for the Alzheimer’s Association, told this news organization.
The CLARITY AD results were published in the New England Journal of Medicine. Lecanemab is currently under accelerated review at the FDA.
The Alzheimer’s Association’s letter to the CMS includes a joint statement signed by more than 200 AD researchers and experts. All agree that the lecanemab results represent “significant new evidence” that necessitates reconsidering the restrictions on anti-amyloid agents.
“CMS has said it would look at new evidence, and now that evidence is here. We believe CMS recognizes this evidence for lecanemab is stronger than that for many treatments Medicare routinely covers,” Mr. Egge said.
‘No time to waste’
“With the timing of accelerated approvals for both lecanemab and donanemab in the next few months, the Alzheimer’s Association wants to ensure, if approved, that patients can access these treatments,” Mr. Egge noted.
“Because revisions to National Coverage Determinations can be a lengthy process, CMS needs to act quickly to minimize delays. People living with Alzheimer’s disease don’t have time to waste,” he added.
The Alzheimer’s Association estimates that every day, more than 2,000 individuals aged 65 or older may transition from mild dementia due to AD to a more advanced stage of the disease in which they may no longer be eligible for lecanemab and the other anti-amyloid agents currently being tested.
“Each day matters when it comes to slowing the progression of this disease,” Joanne Pike, DrPH, president and incoming chief executive officer for the Alzheimer’s Association, noted in a news release.
“The current CMS policy to severely limit access to these treatments eliminates people’s options, is resulting in continued irreversible disease progression, and contributes to greater health inequities. That’s not acceptable,” Dr. Pike said.
A version of this article first appeared on Medscape.com.
In a letter addressed to CMS administrator Chiquita Brooks-LaSure, MPP, the association has asked the agency to remove the requirements for “coverage with evidence development” in its national coverage determination for FDA-approved anti-amyloid monoclonal antibodies.
The CMS coverage restrictions for anti-amyloid drugs were finalized in April on the basis of data available at the time.
Since then, new data from the CLARITY AD trial “clearly demonstrate a meaningful clinical benefit” from the investigational anti-amyloid agent lecanemab (Eisai/Biogen), Robert Egge, chief public policy officer for the Alzheimer’s Association, told this news organization.
The CLARITY AD results were published in the New England Journal of Medicine. Lecanemab is currently under accelerated review at the FDA.
The Alzheimer’s Association’s letter to the CMS includes a joint statement signed by more than 200 AD researchers and experts. All agree that the lecanemab results represent “significant new evidence” that necessitates reconsidering the restrictions on anti-amyloid agents.
“CMS has said it would look at new evidence, and now that evidence is here. We believe CMS recognizes this evidence for lecanemab is stronger than that for many treatments Medicare routinely covers,” Mr. Egge said.
‘No time to waste’
“With the timing of accelerated approvals for both lecanemab and donanemab in the next few months, the Alzheimer’s Association wants to ensure, if approved, that patients can access these treatments,” Mr. Egge noted.
“Because revisions to National Coverage Determinations can be a lengthy process, CMS needs to act quickly to minimize delays. People living with Alzheimer’s disease don’t have time to waste,” he added.
The Alzheimer’s Association estimates that every day, more than 2,000 individuals aged 65 or older may transition from mild dementia due to AD to a more advanced stage of the disease in which they may no longer be eligible for lecanemab and the other anti-amyloid agents currently being tested.
“Each day matters when it comes to slowing the progression of this disease,” Joanne Pike, DrPH, president and incoming chief executive officer for the Alzheimer’s Association, noted in a news release.
“The current CMS policy to severely limit access to these treatments eliminates people’s options, is resulting in continued irreversible disease progression, and contributes to greater health inequities. That’s not acceptable,” Dr. Pike said.
A version of this article first appeared on Medscape.com.
In a letter addressed to CMS administrator Chiquita Brooks-LaSure, MPP, the association has asked the agency to remove the requirements for “coverage with evidence development” in its national coverage determination for FDA-approved anti-amyloid monoclonal antibodies.
The CMS coverage restrictions for anti-amyloid drugs were finalized in April on the basis of data available at the time.
Since then, new data from the CLARITY AD trial “clearly demonstrate a meaningful clinical benefit” from the investigational anti-amyloid agent lecanemab (Eisai/Biogen), Robert Egge, chief public policy officer for the Alzheimer’s Association, told this news organization.
The CLARITY AD results were published in the New England Journal of Medicine. Lecanemab is currently under accelerated review at the FDA.
The Alzheimer’s Association’s letter to the CMS includes a joint statement signed by more than 200 AD researchers and experts. All agree that the lecanemab results represent “significant new evidence” that necessitates reconsidering the restrictions on anti-amyloid agents.
“CMS has said it would look at new evidence, and now that evidence is here. We believe CMS recognizes this evidence for lecanemab is stronger than that for many treatments Medicare routinely covers,” Mr. Egge said.
‘No time to waste’
“With the timing of accelerated approvals for both lecanemab and donanemab in the next few months, the Alzheimer’s Association wants to ensure, if approved, that patients can access these treatments,” Mr. Egge noted.
“Because revisions to National Coverage Determinations can be a lengthy process, CMS needs to act quickly to minimize delays. People living with Alzheimer’s disease don’t have time to waste,” he added.
The Alzheimer’s Association estimates that every day, more than 2,000 individuals aged 65 or older may transition from mild dementia due to AD to a more advanced stage of the disease in which they may no longer be eligible for lecanemab and the other anti-amyloid agents currently being tested.
“Each day matters when it comes to slowing the progression of this disease,” Joanne Pike, DrPH, president and incoming chief executive officer for the Alzheimer’s Association, noted in a news release.
“The current CMS policy to severely limit access to these treatments eliminates people’s options, is resulting in continued irreversible disease progression, and contributes to greater health inequities. That’s not acceptable,” Dr. Pike said.
A version of this article first appeared on Medscape.com.
Cluster headache tied to high risk of mental and neurologic disorders
, leading to significant disability and absenteeism, new research shows.
Results from a Swedish register-based study also showed that patients with cluster headache had a sixfold increased risk for central nervous system disorders and a twofold increased risk for musculoskeletal disorders.
Although cluster headaches are often more prevalent in men, researchers found that multimorbidity rates were significantly higher in women. In addition, rates of external injuries were significantly higher among individuals with cluster headache than among persons without cluster headache.
“The findings very clearly indicate that cluster headache patients suffer from other health issues as well and that they are at risk of having longer periods of times when they cannot work,” said lead investigator Caroline Ran, PhD, a research specialist in the department of neuroscience at the Karolinska Institutet, Stockholm.
“It’s really important for clinicians to look at cluster headache from a broader perspective and make sure that patients are followed up so that they don’t risk ending up in a situation where they have several comorbidities,” Dr. Ran added.
The findings were published online in Neurology.
‘Striking’ finding
Cluster headache is one of the most severe and debilitating types of headache. It causes intense pain behind the eyes, which has been described as being worse than pain associated with childbirth or kidney stones.
Attacks can occur multiple times in a single day and can last up to 3 hours. Cluster headache is rare, occurring in about 1 in 1,000 individuals, and is more common in men. Underdiagnosis is common – especially in women.
The study drew on two Swedish population-based registries and included 3,240 patients with cluster headache aged 16-64 years and 16,200 matched control persons. The analysis covered medical visits from 2001 to 2010.
Results showed that 91.9% of participants with cluster headache had some type of multimorbidity. By comparison, 77.6% of the control group had some type of multimorbidity (odds ratio, 3.26; P < .0001).
Prior studies have shown a higher incidence of mental health and behavioral disorders among patients with cluster headache. However, when the researchers removed those conditions along with external injuries from the dataset, patients with headache were still significantly more likely to have multiple co-occurring illnesses (86.7% vs. 68.8%; OR, 2.95; P < .0001).
The most common comorbid conditions in the overall cluster headache group were diseases of the nervous system (OR, 5.9; 95% CI, 5.46 -6.42); 51.8% of the cluster headache group reported these disorders, compared with just 15.4% of the control group.
Diseases of the eye, the respiratory, gastrointestinal, and musculoskeletal systems, and connective tissue were also significantly more common among patients with cluster headache.
“For each diagnosis that we investigated, we found a higher incidence in the cluster headache group, and we thought this was a very striking finding and worth discussing in the clinical setting that these patients are at risk of general ill health,” Dr. Ran said.
Risky behavior?
Another novel finding was the higher rate of external injuries among the cluster headache group, compared with the control group. The finding seems to back up the theory that patients with cluster headache are more likely to engage in risky behaviors, the researchers noted.
In the cluster headache group, external injuries were reported by 47.1% of men and 41% of women, versus 34.9% and 26.0%, respectively, in the control group.
“Now we can also show that cluster headache patients have more injuries and that is totally unrelated to the biological health of the individuals, so that could also indicate higher risk taking,” Dr. Ran said.
Overall multimorbidity rates and diagnoses in each medical category except external injury were higher among women with cluster headache than men with headaches. In addition, the mean number of days on sick leave and disability pension was higher among women with cluster headache than among men with cluster headache (83.71 days vs. 52.56 days).
Overall, the mean number of sickness absence and disability pension net days in 2010 was nearly twice as high in the cluster headache group as in the control group (63.15 days vs. 34.08 days).
Removing mental and behavioral health disorders from the mix did not lower those numbers.
“Our numbers indicate that the mental health issues that are related to cluster headache might not impact their work situation as much as the other comorbidities,” Dr. Ran said.
Struggle is real
Commenting on the findings, Heidi Schwarz, MD, professor of clinical neurology at the University of Rochester (N.Y.) Medical Center, called the study a “valuable contribution” to the field and to the treatment of cluster headache.
“It’s a good study that addresses factors that really need to be considered as you take care of these patients,” said Dr. Schwarz, who was not involved with the research.
“The most salient features of this is that cluster headache is quite disabling, and if you add a comorbidity to it, it’s even more disabling,” she said.
Dr. Schwarz noted that cluster headache is often misdiagnosed as migraine or is overlooked altogether, especially in women. These data underscore that, although cluster headache is more common in men, it affects women too and could lead to even greater disability.
“This has a direct impact on patient quality of life, and in the end, that really should be what we’re looking to enhance,” Dr. Schwarz said. “When a patient with cluster comes in and they tell you they’re really struggling, believe them because it’s quite real.”
The findings also fill a gap in the literature and offer the kind of data that could not be collected in the United States, she noted. Sweden provides paid sick time for all workers aged 16 and older and offers a disability pension to all workers whose ability to work is temporarily or permanently inhibited because of illness or injury.
“You will never get this kind of data in the United States because this kind of data comes from two datasets that are extremely inclusive and detailed in a society, Sweden, where they have a social support system,” Dr. Schwarz said.
The study was funded by the Swedish Research Council, the Swedish Brain Foundation, and Mellby Gård, Region Stockholm, Märta Lundkvist stiftelse and Karolinska Institutet research funds. Dr. Ran and Dr. Schwarz report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, leading to significant disability and absenteeism, new research shows.
Results from a Swedish register-based study also showed that patients with cluster headache had a sixfold increased risk for central nervous system disorders and a twofold increased risk for musculoskeletal disorders.
Although cluster headaches are often more prevalent in men, researchers found that multimorbidity rates were significantly higher in women. In addition, rates of external injuries were significantly higher among individuals with cluster headache than among persons without cluster headache.
“The findings very clearly indicate that cluster headache patients suffer from other health issues as well and that they are at risk of having longer periods of times when they cannot work,” said lead investigator Caroline Ran, PhD, a research specialist in the department of neuroscience at the Karolinska Institutet, Stockholm.
“It’s really important for clinicians to look at cluster headache from a broader perspective and make sure that patients are followed up so that they don’t risk ending up in a situation where they have several comorbidities,” Dr. Ran added.
The findings were published online in Neurology.
‘Striking’ finding
Cluster headache is one of the most severe and debilitating types of headache. It causes intense pain behind the eyes, which has been described as being worse than pain associated with childbirth or kidney stones.
Attacks can occur multiple times in a single day and can last up to 3 hours. Cluster headache is rare, occurring in about 1 in 1,000 individuals, and is more common in men. Underdiagnosis is common – especially in women.
The study drew on two Swedish population-based registries and included 3,240 patients with cluster headache aged 16-64 years and 16,200 matched control persons. The analysis covered medical visits from 2001 to 2010.
Results showed that 91.9% of participants with cluster headache had some type of multimorbidity. By comparison, 77.6% of the control group had some type of multimorbidity (odds ratio, 3.26; P < .0001).
Prior studies have shown a higher incidence of mental health and behavioral disorders among patients with cluster headache. However, when the researchers removed those conditions along with external injuries from the dataset, patients with headache were still significantly more likely to have multiple co-occurring illnesses (86.7% vs. 68.8%; OR, 2.95; P < .0001).
The most common comorbid conditions in the overall cluster headache group were diseases of the nervous system (OR, 5.9; 95% CI, 5.46 -6.42); 51.8% of the cluster headache group reported these disorders, compared with just 15.4% of the control group.
Diseases of the eye, the respiratory, gastrointestinal, and musculoskeletal systems, and connective tissue were also significantly more common among patients with cluster headache.
“For each diagnosis that we investigated, we found a higher incidence in the cluster headache group, and we thought this was a very striking finding and worth discussing in the clinical setting that these patients are at risk of general ill health,” Dr. Ran said.
Risky behavior?
Another novel finding was the higher rate of external injuries among the cluster headache group, compared with the control group. The finding seems to back up the theory that patients with cluster headache are more likely to engage in risky behaviors, the researchers noted.
In the cluster headache group, external injuries were reported by 47.1% of men and 41% of women, versus 34.9% and 26.0%, respectively, in the control group.
“Now we can also show that cluster headache patients have more injuries and that is totally unrelated to the biological health of the individuals, so that could also indicate higher risk taking,” Dr. Ran said.
Overall multimorbidity rates and diagnoses in each medical category except external injury were higher among women with cluster headache than men with headaches. In addition, the mean number of days on sick leave and disability pension was higher among women with cluster headache than among men with cluster headache (83.71 days vs. 52.56 days).
Overall, the mean number of sickness absence and disability pension net days in 2010 was nearly twice as high in the cluster headache group as in the control group (63.15 days vs. 34.08 days).
Removing mental and behavioral health disorders from the mix did not lower those numbers.
“Our numbers indicate that the mental health issues that are related to cluster headache might not impact their work situation as much as the other comorbidities,” Dr. Ran said.
Struggle is real
Commenting on the findings, Heidi Schwarz, MD, professor of clinical neurology at the University of Rochester (N.Y.) Medical Center, called the study a “valuable contribution” to the field and to the treatment of cluster headache.
“It’s a good study that addresses factors that really need to be considered as you take care of these patients,” said Dr. Schwarz, who was not involved with the research.
“The most salient features of this is that cluster headache is quite disabling, and if you add a comorbidity to it, it’s even more disabling,” she said.
Dr. Schwarz noted that cluster headache is often misdiagnosed as migraine or is overlooked altogether, especially in women. These data underscore that, although cluster headache is more common in men, it affects women too and could lead to even greater disability.
“This has a direct impact on patient quality of life, and in the end, that really should be what we’re looking to enhance,” Dr. Schwarz said. “When a patient with cluster comes in and they tell you they’re really struggling, believe them because it’s quite real.”
The findings also fill a gap in the literature and offer the kind of data that could not be collected in the United States, she noted. Sweden provides paid sick time for all workers aged 16 and older and offers a disability pension to all workers whose ability to work is temporarily or permanently inhibited because of illness or injury.
“You will never get this kind of data in the United States because this kind of data comes from two datasets that are extremely inclusive and detailed in a society, Sweden, where they have a social support system,” Dr. Schwarz said.
The study was funded by the Swedish Research Council, the Swedish Brain Foundation, and Mellby Gård, Region Stockholm, Märta Lundkvist stiftelse and Karolinska Institutet research funds. Dr. Ran and Dr. Schwarz report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, leading to significant disability and absenteeism, new research shows.
Results from a Swedish register-based study also showed that patients with cluster headache had a sixfold increased risk for central nervous system disorders and a twofold increased risk for musculoskeletal disorders.
Although cluster headaches are often more prevalent in men, researchers found that multimorbidity rates were significantly higher in women. In addition, rates of external injuries were significantly higher among individuals with cluster headache than among persons without cluster headache.
“The findings very clearly indicate that cluster headache patients suffer from other health issues as well and that they are at risk of having longer periods of times when they cannot work,” said lead investigator Caroline Ran, PhD, a research specialist in the department of neuroscience at the Karolinska Institutet, Stockholm.
“It’s really important for clinicians to look at cluster headache from a broader perspective and make sure that patients are followed up so that they don’t risk ending up in a situation where they have several comorbidities,” Dr. Ran added.
The findings were published online in Neurology.
‘Striking’ finding
Cluster headache is one of the most severe and debilitating types of headache. It causes intense pain behind the eyes, which has been described as being worse than pain associated with childbirth or kidney stones.
Attacks can occur multiple times in a single day and can last up to 3 hours. Cluster headache is rare, occurring in about 1 in 1,000 individuals, and is more common in men. Underdiagnosis is common – especially in women.
The study drew on two Swedish population-based registries and included 3,240 patients with cluster headache aged 16-64 years and 16,200 matched control persons. The analysis covered medical visits from 2001 to 2010.
Results showed that 91.9% of participants with cluster headache had some type of multimorbidity. By comparison, 77.6% of the control group had some type of multimorbidity (odds ratio, 3.26; P < .0001).
Prior studies have shown a higher incidence of mental health and behavioral disorders among patients with cluster headache. However, when the researchers removed those conditions along with external injuries from the dataset, patients with headache were still significantly more likely to have multiple co-occurring illnesses (86.7% vs. 68.8%; OR, 2.95; P < .0001).
The most common comorbid conditions in the overall cluster headache group were diseases of the nervous system (OR, 5.9; 95% CI, 5.46 -6.42); 51.8% of the cluster headache group reported these disorders, compared with just 15.4% of the control group.
Diseases of the eye, the respiratory, gastrointestinal, and musculoskeletal systems, and connective tissue were also significantly more common among patients with cluster headache.
“For each diagnosis that we investigated, we found a higher incidence in the cluster headache group, and we thought this was a very striking finding and worth discussing in the clinical setting that these patients are at risk of general ill health,” Dr. Ran said.
Risky behavior?
Another novel finding was the higher rate of external injuries among the cluster headache group, compared with the control group. The finding seems to back up the theory that patients with cluster headache are more likely to engage in risky behaviors, the researchers noted.
In the cluster headache group, external injuries were reported by 47.1% of men and 41% of women, versus 34.9% and 26.0%, respectively, in the control group.
“Now we can also show that cluster headache patients have more injuries and that is totally unrelated to the biological health of the individuals, so that could also indicate higher risk taking,” Dr. Ran said.
Overall multimorbidity rates and diagnoses in each medical category except external injury were higher among women with cluster headache than men with headaches. In addition, the mean number of days on sick leave and disability pension was higher among women with cluster headache than among men with cluster headache (83.71 days vs. 52.56 days).
Overall, the mean number of sickness absence and disability pension net days in 2010 was nearly twice as high in the cluster headache group as in the control group (63.15 days vs. 34.08 days).
Removing mental and behavioral health disorders from the mix did not lower those numbers.
“Our numbers indicate that the mental health issues that are related to cluster headache might not impact their work situation as much as the other comorbidities,” Dr. Ran said.
Struggle is real
Commenting on the findings, Heidi Schwarz, MD, professor of clinical neurology at the University of Rochester (N.Y.) Medical Center, called the study a “valuable contribution” to the field and to the treatment of cluster headache.
“It’s a good study that addresses factors that really need to be considered as you take care of these patients,” said Dr. Schwarz, who was not involved with the research.
“The most salient features of this is that cluster headache is quite disabling, and if you add a comorbidity to it, it’s even more disabling,” she said.
Dr. Schwarz noted that cluster headache is often misdiagnosed as migraine or is overlooked altogether, especially in women. These data underscore that, although cluster headache is more common in men, it affects women too and could lead to even greater disability.
“This has a direct impact on patient quality of life, and in the end, that really should be what we’re looking to enhance,” Dr. Schwarz said. “When a patient with cluster comes in and they tell you they’re really struggling, believe them because it’s quite real.”
The findings also fill a gap in the literature and offer the kind of data that could not be collected in the United States, she noted. Sweden provides paid sick time for all workers aged 16 and older and offers a disability pension to all workers whose ability to work is temporarily or permanently inhibited because of illness or injury.
“You will never get this kind of data in the United States because this kind of data comes from two datasets that are extremely inclusive and detailed in a society, Sweden, where they have a social support system,” Dr. Schwarz said.
The study was funded by the Swedish Research Council, the Swedish Brain Foundation, and Mellby Gård, Region Stockholm, Märta Lundkvist stiftelse and Karolinska Institutet research funds. Dr. Ran and Dr. Schwarz report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Annual U.S. Parkinson’s disease incidence 50% higher than earlier estimates
according to new research that investigators say highlights the growing strain on clinical services and the need for more research funding.
In an analysis of five databases and more than 15 million people, about 60,000-90,000 individuals older than 45 years are estimated to be diagnosed with Parkinson’s disease each year – which is far more than the previous estimate of around 40,000-60,000 new cases annually.
This is the latest study to update decades-old epidemiologic data on Parkinson’s disease incidence and prevalence. Previous incidence rates came from small, single-population studies that are now more than 25 years old.
“In the advocacy community, we’ve been earnest about the impact of people living with Parkinson’s disease, and what we really lacked was sufficient data to be able to demonstrate the urgency of our need,” said study coinvestigator James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, New York.
“We wanted to revise these numbers, highlight that they are larger than people anticipated, and use it as a call to action to change the approach we have toward Parkinson’s,” Dr. Beck said.
The findings were published online in NPJ Parkinson’s Disease.
Updating an outdated model
The study builds on the Parkinson’s Prevalence Project, a 2018 initiative that used a new model to calculate Parkinson’s disease prevalence. Before then, federal prevalence data was based on a 40-year-old study of just 26 Parkinson’s disease cases in one small county in rural Mississippi.
Dr. Beck and others used a more sophisticated model, using data from five separate cohort studies. They estimated the total number of patients living with Parkinson’s disease in the United States to be 930,000, which is far higher than the 650,000 the old model predicted.
Researchers then moved on to the current project, developing a new method to estimate Parkinson’s disease incidence.
The project included 2012 data on more than 15 million individuals in the United States and Canada. The investigators drew from three large insurance databases (Kaiser Permanente Northern California, Ontario Health Care, and Medicare) and two long-term epidemiologic studies (the Honolulu-Asia Aging Study and the Rochester Epidemiology Project).
On the basis of their analysis, the investigators proposed a working Parkinson’s disease incident rate estimate of 47-77 cases per 100,000 people aged 45 years or older. Limiting the analysis to those aged 65 or older raised the incidence to 108-212 per 100,000 people.
That translates to 60,000-95,000 new cases each year among adults aged 45 years or older. Using the Medicare administrative database alone for this same time period suggests an annual incidence of nearly 90,000 for individuals aged 65 or older.
“The numbers we’re proposing are conservative,” Dr. Beck said. “The true numbers are probably north of 90,000.”
Incidence rates increased with age and were higher in men. The researchers also identified clusters of counties with higher incidence rates in parts of the country called the “Parkinson’s belt.”
That geographic area mirrors the Rust Belt and includes parts of the Northeastern and Midwestern United States with a long history of industrial manufacturing that used heavy metals and industrial solvents, which are environmental factors linked to risk for Parkinson’s disease.
Cases were also higher in southern California, southeastern Texas, and Florida – agricultural regions with high pesticide use, which is also a risk factor for Parkinson’s disease. Central Pennsylvania also had higher incidence rates.
Why the increase?
The increase in cases could be the result of the more comprehensive estimation model used, the researchers noted. Or it could be improved detection, the aging population, a rise in sedentary lifestyles, increased exposure to environmental risk factors, or even the sharp decline in smoking in the United States, as some studies have shown that smokers have a lower Parkinson’s disease risk.
“The short answer is, we don’t know; and the long answer is, it’s all the above,” Dr. Beck said.
Although about 15% of Parkinson’s disease cases have a genetic basis, the cause is unknown in the majority of cases. In addition, diagnosis is difficult because there is no blood test or scan that detects the disease.
“Diagnosis requires a skilled clinician with real familiarity with Parkinson’s. And we have a real shortage of neurologists in this country to not only be able to diagnose but also to treat the condition,” Dr. Beck said.
That was one motivation for doing the study: to highlight what experts say is a pending clinical crisis for patients with Parkinson’s disease, he added.
The investigators also wanted to raise awareness about the scope of the disorder – not just about prevalence and incidence but also what those data mean for the health care industry, research aims, drug development and health care coverage, and policies.
In a 2020 study, the same researchers calculated a cost of $52 billion per year for medical and nonmedical costs related to Parkinson’s disease, which works out to about $26,000 per year per patient. That figure is expected to surpass $79 billion by 2030.
“This is an urgent condition for many people who live with the disease. And to the extent we can get our country to recognize that and really make the investment now, this is an area where a stitch in time saves nine,” Dr. Beck said.
“If we can invest some money now, we have a chance to really make a difference in the future,” he added.
‘Groundbreaking’ findings
Commenting on the findings, Jori Fleisher, MD, MSCE, associate professor of neurological sciences at Rush University Medical Center, Chicago, called the results “groundbreaking” and said that they validate what clinicians have been seeing in real-world practice.
“The findings reflect what a lot of us in practice have been appreciating anecdotally, which is that it seems that Parkinson’s is being diagnosed more frequently and that the incidence has been rising,” said Dr. Fleisher, who was not involved with the study.
She noted that the use of multiple datasets is one element of the methodology that makes the data so significant.
“There has been great work out of individual centers; but no matter how good your study methods are within that one population, you’re drawing conclusions based on that one population,” Dr. Fleisher said.
This research, together with the previous work by the group on prevalence data, could go a long way toward raising awareness about the scope of Parkinson’s disease in the United States – which could lead to earlier diagnosis, more research funding, and increased attention on the need for more clinicians who specialize in movement disorders, she added.
“This should increase research funding across the spectrum, including everything from the basic science to translational research, clinical research and implementation, and health services research,” Dr. Fleisher said.
The study was supported by the Parkinson’s Foundation, The Michael J. Fox Foundation for Parkinson’s Research, and the Institute for Clinical Evaluative Sciences. Dr. Beck and Dr. Fleisher reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to new research that investigators say highlights the growing strain on clinical services and the need for more research funding.
In an analysis of five databases and more than 15 million people, about 60,000-90,000 individuals older than 45 years are estimated to be diagnosed with Parkinson’s disease each year – which is far more than the previous estimate of around 40,000-60,000 new cases annually.
This is the latest study to update decades-old epidemiologic data on Parkinson’s disease incidence and prevalence. Previous incidence rates came from small, single-population studies that are now more than 25 years old.
“In the advocacy community, we’ve been earnest about the impact of people living with Parkinson’s disease, and what we really lacked was sufficient data to be able to demonstrate the urgency of our need,” said study coinvestigator James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, New York.
“We wanted to revise these numbers, highlight that they are larger than people anticipated, and use it as a call to action to change the approach we have toward Parkinson’s,” Dr. Beck said.
The findings were published online in NPJ Parkinson’s Disease.
Updating an outdated model
The study builds on the Parkinson’s Prevalence Project, a 2018 initiative that used a new model to calculate Parkinson’s disease prevalence. Before then, federal prevalence data was based on a 40-year-old study of just 26 Parkinson’s disease cases in one small county in rural Mississippi.
Dr. Beck and others used a more sophisticated model, using data from five separate cohort studies. They estimated the total number of patients living with Parkinson’s disease in the United States to be 930,000, which is far higher than the 650,000 the old model predicted.
Researchers then moved on to the current project, developing a new method to estimate Parkinson’s disease incidence.
The project included 2012 data on more than 15 million individuals in the United States and Canada. The investigators drew from three large insurance databases (Kaiser Permanente Northern California, Ontario Health Care, and Medicare) and two long-term epidemiologic studies (the Honolulu-Asia Aging Study and the Rochester Epidemiology Project).
On the basis of their analysis, the investigators proposed a working Parkinson’s disease incident rate estimate of 47-77 cases per 100,000 people aged 45 years or older. Limiting the analysis to those aged 65 or older raised the incidence to 108-212 per 100,000 people.
That translates to 60,000-95,000 new cases each year among adults aged 45 years or older. Using the Medicare administrative database alone for this same time period suggests an annual incidence of nearly 90,000 for individuals aged 65 or older.
“The numbers we’re proposing are conservative,” Dr. Beck said. “The true numbers are probably north of 90,000.”
Incidence rates increased with age and were higher in men. The researchers also identified clusters of counties with higher incidence rates in parts of the country called the “Parkinson’s belt.”
That geographic area mirrors the Rust Belt and includes parts of the Northeastern and Midwestern United States with a long history of industrial manufacturing that used heavy metals and industrial solvents, which are environmental factors linked to risk for Parkinson’s disease.
Cases were also higher in southern California, southeastern Texas, and Florida – agricultural regions with high pesticide use, which is also a risk factor for Parkinson’s disease. Central Pennsylvania also had higher incidence rates.
Why the increase?
The increase in cases could be the result of the more comprehensive estimation model used, the researchers noted. Or it could be improved detection, the aging population, a rise in sedentary lifestyles, increased exposure to environmental risk factors, or even the sharp decline in smoking in the United States, as some studies have shown that smokers have a lower Parkinson’s disease risk.
“The short answer is, we don’t know; and the long answer is, it’s all the above,” Dr. Beck said.
Although about 15% of Parkinson’s disease cases have a genetic basis, the cause is unknown in the majority of cases. In addition, diagnosis is difficult because there is no blood test or scan that detects the disease.
“Diagnosis requires a skilled clinician with real familiarity with Parkinson’s. And we have a real shortage of neurologists in this country to not only be able to diagnose but also to treat the condition,” Dr. Beck said.
That was one motivation for doing the study: to highlight what experts say is a pending clinical crisis for patients with Parkinson’s disease, he added.
The investigators also wanted to raise awareness about the scope of the disorder – not just about prevalence and incidence but also what those data mean for the health care industry, research aims, drug development and health care coverage, and policies.
In a 2020 study, the same researchers calculated a cost of $52 billion per year for medical and nonmedical costs related to Parkinson’s disease, which works out to about $26,000 per year per patient. That figure is expected to surpass $79 billion by 2030.
“This is an urgent condition for many people who live with the disease. And to the extent we can get our country to recognize that and really make the investment now, this is an area where a stitch in time saves nine,” Dr. Beck said.
“If we can invest some money now, we have a chance to really make a difference in the future,” he added.
‘Groundbreaking’ findings
Commenting on the findings, Jori Fleisher, MD, MSCE, associate professor of neurological sciences at Rush University Medical Center, Chicago, called the results “groundbreaking” and said that they validate what clinicians have been seeing in real-world practice.
“The findings reflect what a lot of us in practice have been appreciating anecdotally, which is that it seems that Parkinson’s is being diagnosed more frequently and that the incidence has been rising,” said Dr. Fleisher, who was not involved with the study.
She noted that the use of multiple datasets is one element of the methodology that makes the data so significant.
“There has been great work out of individual centers; but no matter how good your study methods are within that one population, you’re drawing conclusions based on that one population,” Dr. Fleisher said.
This research, together with the previous work by the group on prevalence data, could go a long way toward raising awareness about the scope of Parkinson’s disease in the United States – which could lead to earlier diagnosis, more research funding, and increased attention on the need for more clinicians who specialize in movement disorders, she added.
“This should increase research funding across the spectrum, including everything from the basic science to translational research, clinical research and implementation, and health services research,” Dr. Fleisher said.
The study was supported by the Parkinson’s Foundation, The Michael J. Fox Foundation for Parkinson’s Research, and the Institute for Clinical Evaluative Sciences. Dr. Beck and Dr. Fleisher reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to new research that investigators say highlights the growing strain on clinical services and the need for more research funding.
In an analysis of five databases and more than 15 million people, about 60,000-90,000 individuals older than 45 years are estimated to be diagnosed with Parkinson’s disease each year – which is far more than the previous estimate of around 40,000-60,000 new cases annually.
This is the latest study to update decades-old epidemiologic data on Parkinson’s disease incidence and prevalence. Previous incidence rates came from small, single-population studies that are now more than 25 years old.
“In the advocacy community, we’ve been earnest about the impact of people living with Parkinson’s disease, and what we really lacked was sufficient data to be able to demonstrate the urgency of our need,” said study coinvestigator James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, New York.
“We wanted to revise these numbers, highlight that they are larger than people anticipated, and use it as a call to action to change the approach we have toward Parkinson’s,” Dr. Beck said.
The findings were published online in NPJ Parkinson’s Disease.
Updating an outdated model
The study builds on the Parkinson’s Prevalence Project, a 2018 initiative that used a new model to calculate Parkinson’s disease prevalence. Before then, federal prevalence data was based on a 40-year-old study of just 26 Parkinson’s disease cases in one small county in rural Mississippi.
Dr. Beck and others used a more sophisticated model, using data from five separate cohort studies. They estimated the total number of patients living with Parkinson’s disease in the United States to be 930,000, which is far higher than the 650,000 the old model predicted.
Researchers then moved on to the current project, developing a new method to estimate Parkinson’s disease incidence.
The project included 2012 data on more than 15 million individuals in the United States and Canada. The investigators drew from three large insurance databases (Kaiser Permanente Northern California, Ontario Health Care, and Medicare) and two long-term epidemiologic studies (the Honolulu-Asia Aging Study and the Rochester Epidemiology Project).
On the basis of their analysis, the investigators proposed a working Parkinson’s disease incident rate estimate of 47-77 cases per 100,000 people aged 45 years or older. Limiting the analysis to those aged 65 or older raised the incidence to 108-212 per 100,000 people.
That translates to 60,000-95,000 new cases each year among adults aged 45 years or older. Using the Medicare administrative database alone for this same time period suggests an annual incidence of nearly 90,000 for individuals aged 65 or older.
“The numbers we’re proposing are conservative,” Dr. Beck said. “The true numbers are probably north of 90,000.”
Incidence rates increased with age and were higher in men. The researchers also identified clusters of counties with higher incidence rates in parts of the country called the “Parkinson’s belt.”
That geographic area mirrors the Rust Belt and includes parts of the Northeastern and Midwestern United States with a long history of industrial manufacturing that used heavy metals and industrial solvents, which are environmental factors linked to risk for Parkinson’s disease.
Cases were also higher in southern California, southeastern Texas, and Florida – agricultural regions with high pesticide use, which is also a risk factor for Parkinson’s disease. Central Pennsylvania also had higher incidence rates.
Why the increase?
The increase in cases could be the result of the more comprehensive estimation model used, the researchers noted. Or it could be improved detection, the aging population, a rise in sedentary lifestyles, increased exposure to environmental risk factors, or even the sharp decline in smoking in the United States, as some studies have shown that smokers have a lower Parkinson’s disease risk.
“The short answer is, we don’t know; and the long answer is, it’s all the above,” Dr. Beck said.
Although about 15% of Parkinson’s disease cases have a genetic basis, the cause is unknown in the majority of cases. In addition, diagnosis is difficult because there is no blood test or scan that detects the disease.
“Diagnosis requires a skilled clinician with real familiarity with Parkinson’s. And we have a real shortage of neurologists in this country to not only be able to diagnose but also to treat the condition,” Dr. Beck said.
That was one motivation for doing the study: to highlight what experts say is a pending clinical crisis for patients with Parkinson’s disease, he added.
The investigators also wanted to raise awareness about the scope of the disorder – not just about prevalence and incidence but also what those data mean for the health care industry, research aims, drug development and health care coverage, and policies.
In a 2020 study, the same researchers calculated a cost of $52 billion per year for medical and nonmedical costs related to Parkinson’s disease, which works out to about $26,000 per year per patient. That figure is expected to surpass $79 billion by 2030.
“This is an urgent condition for many people who live with the disease. And to the extent we can get our country to recognize that and really make the investment now, this is an area where a stitch in time saves nine,” Dr. Beck said.
“If we can invest some money now, we have a chance to really make a difference in the future,” he added.
‘Groundbreaking’ findings
Commenting on the findings, Jori Fleisher, MD, MSCE, associate professor of neurological sciences at Rush University Medical Center, Chicago, called the results “groundbreaking” and said that they validate what clinicians have been seeing in real-world practice.
“The findings reflect what a lot of us in practice have been appreciating anecdotally, which is that it seems that Parkinson’s is being diagnosed more frequently and that the incidence has been rising,” said Dr. Fleisher, who was not involved with the study.
She noted that the use of multiple datasets is one element of the methodology that makes the data so significant.
“There has been great work out of individual centers; but no matter how good your study methods are within that one population, you’re drawing conclusions based on that one population,” Dr. Fleisher said.
This research, together with the previous work by the group on prevalence data, could go a long way toward raising awareness about the scope of Parkinson’s disease in the United States – which could lead to earlier diagnosis, more research funding, and increased attention on the need for more clinicians who specialize in movement disorders, she added.
“This should increase research funding across the spectrum, including everything from the basic science to translational research, clinical research and implementation, and health services research,” Dr. Fleisher said.
The study was supported by the Parkinson’s Foundation, The Michael J. Fox Foundation for Parkinson’s Research, and the Institute for Clinical Evaluative Sciences. Dr. Beck and Dr. Fleisher reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NPJ PARKINSON’S DISEASE
Antipsychotic shows benefit for Alzheimer’s agitation
SAN FRANCISCO – In a widely anticipated report,
Members of a panel of dementia specialists here at the 15th Clinical Trials on Alzheimer’s Disease (CTAD) conference said that the results were encouraging. But they also noted that the available data make it difficult to understand the impact of the drug on the day-to-day life on patients.
“I’d like to be able to translate that into something else to understand the risk benefit calculus,” said neurologist and neuroscientist Alireza Atri, MD, PhD, of Banner Sun Health Research Institute in Phoenix. “How does it affect the patients themselves, their quality of life, and the family members and their burden?”
Currently, there’s no Food and Drug Administration–approved treatment for agitation in AD.
In 2015, the FDA approved brexpiprazole, an oral medication, as a treatment for schizophrenia and an adjunctive treatment for major depressive disorder (MDD). It is an expensive drug with an average retail price per GoodRx of $1,582 per month, and no generic is available.
Researchers released the results of a trio of phase 3 clinical trials at CTAD that examined various doses of brexpiprazole. The results of the first two trials had been released earlier in 2018.
Three trials
All trials were multicenter, 12-week, randomized, double-blind and placebo-controlled.
Study participants were aged 55-90 years, had probable AD diagnoses, and had agitation per various scales. The average age in the groups was 74 years, 56.0%-61.7% were women, and 94.3%-98.1% were White.
The first trial examined two fixed doses (1 mg/d, n = 137; and 2 mg/d, n = 140) or placebo (n = 136). “The study initially included a 0.5 mg/day arm,” the researchers reported, “which was removed in a protocol amendment, and patients randomized to that arm were not included in efficacy analyses.”
The second trial looked at a flexible dose (0.5-2 mg/d, n = 133) or placebo (n = 137).
In a CTAD presentation, Nanco Hefting of Lundbeck, a codeveloper of the drug, said that the researchers learned from the first two trials that 2 mg/d might be an appropriate dose, and the FDA recommended they also examine 3 mg/day. As a result, the third trial examined two fixed doses (2 mg/d, n = 75; 3 mg/d, n = 153; or placebo, n = 117).
In the third trial, both the placebo and drug groups improved per a measurement of agitation; those in the drug group improved somewhat more.
The mean change in baseline on the Cohen-Mansfield Agitation Inventory scale – the primary endpoint – was –5.32 for the 2-mg/d and 3-mg/d groups vs. placebo (P = .0026); the score in the placebo group fell by about 18 and by about 22 in the drug group.
The key secondary endpoint was an improvement from baseline to week 12 in the Clinical Global Impression–Severity (CGI-S) score related to agitation. Compared with the placebo group, this score was –0.27 in the drug group (P = .0078). Both scores hovered around –1.0.
Safety data show the percentage of treatment-emergent events ranged from 45.9% in the placebo group to 49.0%-56.8% for brexpiprazole in the three trials. The percentage of these events leading to discontinuation was 6.3% among those receiving the drug and 3.4% in the placebo group.
University of Exeter dementia researcher Clive Ballard, MD, MB ChB, one of the panelists who discussed the research after the CTAD presentation, praised the trials as “well-conducted” and said that he was pleased that subjects in institutions were included. “It’s not an easy environment to do trials in. They should be really commended for doing for doing that.”
But he echoed fellow panelist Dr. Atri by noting that more data are needed to understand how well the drug works. “I would like to see the effect sizes and a little bit more detail to understand the clinical meaningfulness of that level of benefit.”
What’s next? A spokeswoman for Otsuka, a codeveloper of brexpiprazole, said that it hopes to hear in 2023 about a supplemental new drug application that was filed in November 2022.
Otsuka and Lundbeck funded the research. Mr. Hefting is an employee of Lundbeck, and several other authors work for Lundbeck or Otsuka. The single non-employee author reports various disclosures. Disclosures for Dr. Atri and Dr. Ballard were not provided.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – In a widely anticipated report,
Members of a panel of dementia specialists here at the 15th Clinical Trials on Alzheimer’s Disease (CTAD) conference said that the results were encouraging. But they also noted that the available data make it difficult to understand the impact of the drug on the day-to-day life on patients.
“I’d like to be able to translate that into something else to understand the risk benefit calculus,” said neurologist and neuroscientist Alireza Atri, MD, PhD, of Banner Sun Health Research Institute in Phoenix. “How does it affect the patients themselves, their quality of life, and the family members and their burden?”
Currently, there’s no Food and Drug Administration–approved treatment for agitation in AD.
In 2015, the FDA approved brexpiprazole, an oral medication, as a treatment for schizophrenia and an adjunctive treatment for major depressive disorder (MDD). It is an expensive drug with an average retail price per GoodRx of $1,582 per month, and no generic is available.
Researchers released the results of a trio of phase 3 clinical trials at CTAD that examined various doses of brexpiprazole. The results of the first two trials had been released earlier in 2018.
Three trials
All trials were multicenter, 12-week, randomized, double-blind and placebo-controlled.
Study participants were aged 55-90 years, had probable AD diagnoses, and had agitation per various scales. The average age in the groups was 74 years, 56.0%-61.7% were women, and 94.3%-98.1% were White.
The first trial examined two fixed doses (1 mg/d, n = 137; and 2 mg/d, n = 140) or placebo (n = 136). “The study initially included a 0.5 mg/day arm,” the researchers reported, “which was removed in a protocol amendment, and patients randomized to that arm were not included in efficacy analyses.”
The second trial looked at a flexible dose (0.5-2 mg/d, n = 133) or placebo (n = 137).
In a CTAD presentation, Nanco Hefting of Lundbeck, a codeveloper of the drug, said that the researchers learned from the first two trials that 2 mg/d might be an appropriate dose, and the FDA recommended they also examine 3 mg/day. As a result, the third trial examined two fixed doses (2 mg/d, n = 75; 3 mg/d, n = 153; or placebo, n = 117).
In the third trial, both the placebo and drug groups improved per a measurement of agitation; those in the drug group improved somewhat more.
The mean change in baseline on the Cohen-Mansfield Agitation Inventory scale – the primary endpoint – was –5.32 for the 2-mg/d and 3-mg/d groups vs. placebo (P = .0026); the score in the placebo group fell by about 18 and by about 22 in the drug group.
The key secondary endpoint was an improvement from baseline to week 12 in the Clinical Global Impression–Severity (CGI-S) score related to agitation. Compared with the placebo group, this score was –0.27 in the drug group (P = .0078). Both scores hovered around –1.0.
Safety data show the percentage of treatment-emergent events ranged from 45.9% in the placebo group to 49.0%-56.8% for brexpiprazole in the three trials. The percentage of these events leading to discontinuation was 6.3% among those receiving the drug and 3.4% in the placebo group.
University of Exeter dementia researcher Clive Ballard, MD, MB ChB, one of the panelists who discussed the research after the CTAD presentation, praised the trials as “well-conducted” and said that he was pleased that subjects in institutions were included. “It’s not an easy environment to do trials in. They should be really commended for doing for doing that.”
But he echoed fellow panelist Dr. Atri by noting that more data are needed to understand how well the drug works. “I would like to see the effect sizes and a little bit more detail to understand the clinical meaningfulness of that level of benefit.”
What’s next? A spokeswoman for Otsuka, a codeveloper of brexpiprazole, said that it hopes to hear in 2023 about a supplemental new drug application that was filed in November 2022.
Otsuka and Lundbeck funded the research. Mr. Hefting is an employee of Lundbeck, and several other authors work for Lundbeck or Otsuka. The single non-employee author reports various disclosures. Disclosures for Dr. Atri and Dr. Ballard were not provided.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – In a widely anticipated report,
Members of a panel of dementia specialists here at the 15th Clinical Trials on Alzheimer’s Disease (CTAD) conference said that the results were encouraging. But they also noted that the available data make it difficult to understand the impact of the drug on the day-to-day life on patients.
“I’d like to be able to translate that into something else to understand the risk benefit calculus,” said neurologist and neuroscientist Alireza Atri, MD, PhD, of Banner Sun Health Research Institute in Phoenix. “How does it affect the patients themselves, their quality of life, and the family members and their burden?”
Currently, there’s no Food and Drug Administration–approved treatment for agitation in AD.
In 2015, the FDA approved brexpiprazole, an oral medication, as a treatment for schizophrenia and an adjunctive treatment for major depressive disorder (MDD). It is an expensive drug with an average retail price per GoodRx of $1,582 per month, and no generic is available.
Researchers released the results of a trio of phase 3 clinical trials at CTAD that examined various doses of brexpiprazole. The results of the first two trials had been released earlier in 2018.
Three trials
All trials were multicenter, 12-week, randomized, double-blind and placebo-controlled.
Study participants were aged 55-90 years, had probable AD diagnoses, and had agitation per various scales. The average age in the groups was 74 years, 56.0%-61.7% were women, and 94.3%-98.1% were White.
The first trial examined two fixed doses (1 mg/d, n = 137; and 2 mg/d, n = 140) or placebo (n = 136). “The study initially included a 0.5 mg/day arm,” the researchers reported, “which was removed in a protocol amendment, and patients randomized to that arm were not included in efficacy analyses.”
The second trial looked at a flexible dose (0.5-2 mg/d, n = 133) or placebo (n = 137).
In a CTAD presentation, Nanco Hefting of Lundbeck, a codeveloper of the drug, said that the researchers learned from the first two trials that 2 mg/d might be an appropriate dose, and the FDA recommended they also examine 3 mg/day. As a result, the third trial examined two fixed doses (2 mg/d, n = 75; 3 mg/d, n = 153; or placebo, n = 117).
In the third trial, both the placebo and drug groups improved per a measurement of agitation; those in the drug group improved somewhat more.
The mean change in baseline on the Cohen-Mansfield Agitation Inventory scale – the primary endpoint – was –5.32 for the 2-mg/d and 3-mg/d groups vs. placebo (P = .0026); the score in the placebo group fell by about 18 and by about 22 in the drug group.
The key secondary endpoint was an improvement from baseline to week 12 in the Clinical Global Impression–Severity (CGI-S) score related to agitation. Compared with the placebo group, this score was –0.27 in the drug group (P = .0078). Both scores hovered around –1.0.
Safety data show the percentage of treatment-emergent events ranged from 45.9% in the placebo group to 49.0%-56.8% for brexpiprazole in the three trials. The percentage of these events leading to discontinuation was 6.3% among those receiving the drug and 3.4% in the placebo group.
University of Exeter dementia researcher Clive Ballard, MD, MB ChB, one of the panelists who discussed the research after the CTAD presentation, praised the trials as “well-conducted” and said that he was pleased that subjects in institutions were included. “It’s not an easy environment to do trials in. They should be really commended for doing for doing that.”
But he echoed fellow panelist Dr. Atri by noting that more data are needed to understand how well the drug works. “I would like to see the effect sizes and a little bit more detail to understand the clinical meaningfulness of that level of benefit.”
What’s next? A spokeswoman for Otsuka, a codeveloper of brexpiprazole, said that it hopes to hear in 2023 about a supplemental new drug application that was filed in November 2022.
Otsuka and Lundbeck funded the research. Mr. Hefting is an employee of Lundbeck, and several other authors work for Lundbeck or Otsuka. The single non-employee author reports various disclosures. Disclosures for Dr. Atri and Dr. Ballard were not provided.
A version of this article first appeared on Medscape.com.
AT CTAD 2022
Patient With Severe Headache After IV Immunoglobulin
A 35-year-old woman with a history of hypothyroidism and idiopathic small fiber autonomic and sensory neuropathy presented to the emergency department (ED) 48 hours after IV immunoglobulin (IG) infusion with a severe headache, nausea, neck stiffness, photophobia, and episodes of intense positional eye pressure. The patient reported previous episodes of headaches post-IVIG infusion but not nearly as severe. On ED arrival, the patient was afebrile with vital signs within normal limits. Initial laboratory results were notable for levels within reference range parameters: 5.9 × 109/L white blood cell (WBC) count, 13.3 g/dL hemoglobin, 38.7% hematocrit, and 279 × 109/L platelet count; there were no abnormal urinalysis findings, and she was negative for human chorionic gonadotropin.
Due to the patient’s symptoms concerning for an acute intracranial process, a brain computed tomography (CT) without contrast was ordered. The CT demonstrated no intracranial abnormalities, but the patient’s symptoms continued to worsen. The patient was started on IV fluids and 1 g IV acetaminophen and underwent a lumbar puncture (LP). Her opening pressure was elevated at 29 cm H2O (reference range, 6-20 cm), and the fluid was notably clear. During the LP, 25 mL of cerebrospinal fluid (CSF) was collected for laboratory analysis to include a polymerase chain reaction (PCR) panel and cultures, and a closing pressure of 12 cm H2O was recorded at the end of the procedure with the patient reporting some relief of pressure. The patient was admitted to the medicine ward for further workup and observations.The patient’s meningitis/encephalitis PCR panel detected no pathogens in the CSF, but her WBC count was 84 × 109/L (reference range, 4-11) with 30 segmented neutrophils (reference range, 0-6) and red blood cell count of 24 (reference range, 0-1); her normal glucose at 60 mg/dL (reference range, 40-70) and protein of 33 mg/dL (reference range, 15-45) were within normal parameters. Brain magnetic resonance images with and without contrast was inconsistent with any acute intracranial pathology to include subarachnoid hemorrhage or central nervous system neoplasm (Figure 1). Bacterial and fungal cultures were negative.
- What is your diagnosis?
- How would you treat this patient?
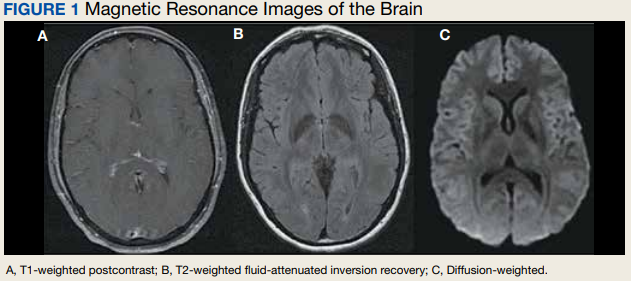
Discussion
Aseptic meningitis presents with a typical clinical picture of meningitis to include headache, stiffened neck, and photophobia. In the event of negative CSF bacterial and fungal cultures and negative viral PCR, a diagnosis of aseptic meningitis is considered.1 Though the differential for aseptic meningitis is broad, in the immunocompetent patient, the most common etiology of aseptic meningitis in the United States is by far viral, and specifically, enterovirus (50.9%). It is less commonly caused by herpes simplex virus (8.3%), varicella zoster virus, and finally, the mosquito-borne St. Louis encephalitis and West Nile viruses typically acquired in the summer or early fall months. Other infectious agents that can present with aseptic meningitis are spirochetes (Lyme disease and syphilis), tuberculous meningitis, fungal infections (cryptococcal meningitis), and other bacterial infections that have a negative culture.
The patient’s history, physical examination, vital signs, imaging, and lumbar puncture findings were most concerning for drug-induced aseptic meningitis (DIAM) secondary to her recent IVIG infusion. An algorithm can be used to work through the diagnostic approach (Figure 2).3,4 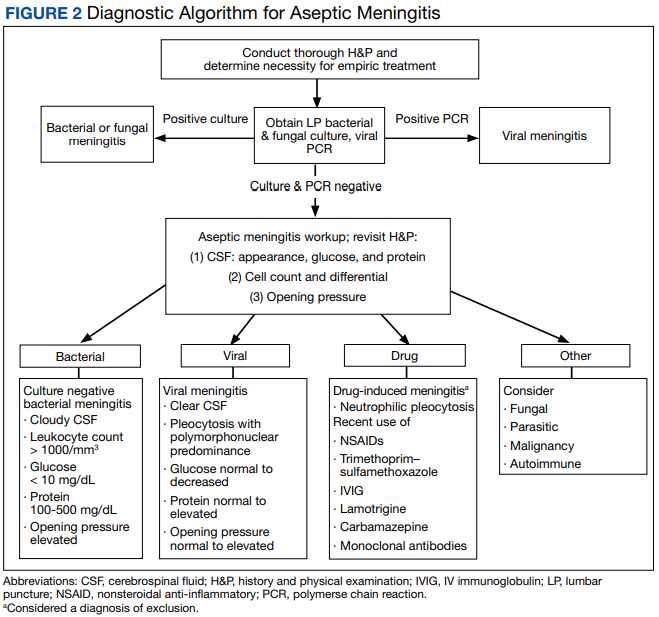
Immediate and delayed adverse reactions to IVIG are known risks for IVIG therapy. About 1% to 15% of patients who receive IVIG will experience mild immediate reactions to the infusion.6 These immediate reactions include fever (78.6%), acrocyanosis (71.4%), rash (64.3%), headache (57.1%), shortness of breath (42.8%), hypotension (35.7%), and chest pain (21.4%).
IVIG is an increasingly used biologic pharmacologic agent used for a variety of medical conditions. This can be attributed to its multifaceted properties and ability to fight infection when given as replacement therapy and provide immunomodulation in conjunction with its more well-known anti-inflammatory properties.8 The number of conditions that can potentially benefit from IVIG is so vast that the American Academy of Allergy, Asthma and Immunology had to divide the indication for IVIG therapy into definitely beneficial, probably beneficial, may provide benefit, and unlikely to provide benefit categories.8
Conclusions
We encourage heightened clinical suspicion of DIAM in patients who have recently undergone IVIG infusion and present with meningeal signs (stiff neck, headache, photophobia, and ear/eye pressure) without any evidence of infection on physical examination or laboratory results. With such, we hope to improve clinician suspicion, detection, as well as patient education and outcomes in cases of DIAM.
1. Kareva L, Mironska K, Stavric K, Hasani A. Adverse reactions to intravenous immunoglobulins—our experience. Open Access Maced J Med Sci. 2018;6(12):2359-2362. doi:10.3889/oamjms.2018.513
2. Mount HR, Boyle SD. Aseptic and bacterial meningitis: evaluation, treatment, and prevention. Am Fam Physician. 2017;96(5):314-322.
3. Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
4. Connolly KJ, Hammer SM. The acute aseptic meningitis syndrome. Infect Dis Clin North Am. 1990;4(4):599-622.
5. Jolles S, Sewell WA, Leighton C. Drug-induced aseptic meningitis: diagnosis and management. Drug Saf. 2000;22(3):215-226. doi:10.2165/00002018-200022030-00005
6. Yelehe-Okouma M, Czmil-Garon J, Pape E, Petitpain N, Gillet P. Drug-induced aseptic meningitis: a mini-review. Fundam Clin Pharmacol. 2018;32(3):252-260. doi:10.1111/fcp.12349
7. Kepa L, Oczko-Grzesik B, Stolarz W, Sobala-Szczygiel B. Drug-induced aseptic meningitis in suspected central nervous system infections. J Clin Neurosci. 2005;12(5):562-564. doi:10.1016/j.jocn.2004.08.024
8. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1-S46. doi:10.1016/j.jaci.2016.09.023
9. Kaarthigeyan K, Burli VV. Aseptic meningitis following intravenous immunoglobulin therapy of common variable immunodeficiency. J Pediatr Neurosci. 2011;6(2):160-161. doi:10.4103/1817-1745.92858
A 35-year-old woman with a history of hypothyroidism and idiopathic small fiber autonomic and sensory neuropathy presented to the emergency department (ED) 48 hours after IV immunoglobulin (IG) infusion with a severe headache, nausea, neck stiffness, photophobia, and episodes of intense positional eye pressure. The patient reported previous episodes of headaches post-IVIG infusion but not nearly as severe. On ED arrival, the patient was afebrile with vital signs within normal limits. Initial laboratory results were notable for levels within reference range parameters: 5.9 × 109/L white blood cell (WBC) count, 13.3 g/dL hemoglobin, 38.7% hematocrit, and 279 × 109/L platelet count; there were no abnormal urinalysis findings, and she was negative for human chorionic gonadotropin.
Due to the patient’s symptoms concerning for an acute intracranial process, a brain computed tomography (CT) without contrast was ordered. The CT demonstrated no intracranial abnormalities, but the patient’s symptoms continued to worsen. The patient was started on IV fluids and 1 g IV acetaminophen and underwent a lumbar puncture (LP). Her opening pressure was elevated at 29 cm H2O (reference range, 6-20 cm), and the fluid was notably clear. During the LP, 25 mL of cerebrospinal fluid (CSF) was collected for laboratory analysis to include a polymerase chain reaction (PCR) panel and cultures, and a closing pressure of 12 cm H2O was recorded at the end of the procedure with the patient reporting some relief of pressure. The patient was admitted to the medicine ward for further workup and observations.The patient’s meningitis/encephalitis PCR panel detected no pathogens in the CSF, but her WBC count was 84 × 109/L (reference range, 4-11) with 30 segmented neutrophils (reference range, 0-6) and red blood cell count of 24 (reference range, 0-1); her normal glucose at 60 mg/dL (reference range, 40-70) and protein of 33 mg/dL (reference range, 15-45) were within normal parameters. Brain magnetic resonance images with and without contrast was inconsistent with any acute intracranial pathology to include subarachnoid hemorrhage or central nervous system neoplasm (Figure 1). Bacterial and fungal cultures were negative.
- What is your diagnosis?
- How would you treat this patient?
Discussion
Aseptic meningitis presents with a typical clinical picture of meningitis to include headache, stiffened neck, and photophobia. In the event of negative CSF bacterial and fungal cultures and negative viral PCR, a diagnosis of aseptic meningitis is considered.1 Though the differential for aseptic meningitis is broad, in the immunocompetent patient, the most common etiology of aseptic meningitis in the United States is by far viral, and specifically, enterovirus (50.9%). It is less commonly caused by herpes simplex virus (8.3%), varicella zoster virus, and finally, the mosquito-borne St. Louis encephalitis and West Nile viruses typically acquired in the summer or early fall months. Other infectious agents that can present with aseptic meningitis are spirochetes (Lyme disease and syphilis), tuberculous meningitis, fungal infections (cryptococcal meningitis), and other bacterial infections that have a negative culture.
The patient’s history, physical examination, vital signs, imaging, and lumbar puncture findings were most concerning for drug-induced aseptic meningitis (DIAM) secondary to her recent IVIG infusion. An algorithm can be used to work through the diagnostic approach (Figure 2).3,4
Immediate and delayed adverse reactions to IVIG are known risks for IVIG therapy. About 1% to 15% of patients who receive IVIG will experience mild immediate reactions to the infusion.6 These immediate reactions include fever (78.6%), acrocyanosis (71.4%), rash (64.3%), headache (57.1%), shortness of breath (42.8%), hypotension (35.7%), and chest pain (21.4%).
IVIG is an increasingly used biologic pharmacologic agent used for a variety of medical conditions. This can be attributed to its multifaceted properties and ability to fight infection when given as replacement therapy and provide immunomodulation in conjunction with its more well-known anti-inflammatory properties.8 The number of conditions that can potentially benefit from IVIG is so vast that the American Academy of Allergy, Asthma and Immunology had to divide the indication for IVIG therapy into definitely beneficial, probably beneficial, may provide benefit, and unlikely to provide benefit categories.8
Conclusions
We encourage heightened clinical suspicion of DIAM in patients who have recently undergone IVIG infusion and present with meningeal signs (stiff neck, headache, photophobia, and ear/eye pressure) without any evidence of infection on physical examination or laboratory results. With such, we hope to improve clinician suspicion, detection, as well as patient education and outcomes in cases of DIAM.
A 35-year-old woman with a history of hypothyroidism and idiopathic small fiber autonomic and sensory neuropathy presented to the emergency department (ED) 48 hours after IV immunoglobulin (IG) infusion with a severe headache, nausea, neck stiffness, photophobia, and episodes of intense positional eye pressure. The patient reported previous episodes of headaches post-IVIG infusion but not nearly as severe. On ED arrival, the patient was afebrile with vital signs within normal limits. Initial laboratory results were notable for levels within reference range parameters: 5.9 × 109/L white blood cell (WBC) count, 13.3 g/dL hemoglobin, 38.7% hematocrit, and 279 × 109/L platelet count; there were no abnormal urinalysis findings, and she was negative for human chorionic gonadotropin.
Due to the patient’s symptoms concerning for an acute intracranial process, a brain computed tomography (CT) without contrast was ordered. The CT demonstrated no intracranial abnormalities, but the patient’s symptoms continued to worsen. The patient was started on IV fluids and 1 g IV acetaminophen and underwent a lumbar puncture (LP). Her opening pressure was elevated at 29 cm H2O (reference range, 6-20 cm), and the fluid was notably clear. During the LP, 25 mL of cerebrospinal fluid (CSF) was collected for laboratory analysis to include a polymerase chain reaction (PCR) panel and cultures, and a closing pressure of 12 cm H2O was recorded at the end of the procedure with the patient reporting some relief of pressure. The patient was admitted to the medicine ward for further workup and observations.The patient’s meningitis/encephalitis PCR panel detected no pathogens in the CSF, but her WBC count was 84 × 109/L (reference range, 4-11) with 30 segmented neutrophils (reference range, 0-6) and red blood cell count of 24 (reference range, 0-1); her normal glucose at 60 mg/dL (reference range, 40-70) and protein of 33 mg/dL (reference range, 15-45) were within normal parameters. Brain magnetic resonance images with and without contrast was inconsistent with any acute intracranial pathology to include subarachnoid hemorrhage or central nervous system neoplasm (Figure 1). Bacterial and fungal cultures were negative.
- What is your diagnosis?
- How would you treat this patient?
Discussion
Aseptic meningitis presents with a typical clinical picture of meningitis to include headache, stiffened neck, and photophobia. In the event of negative CSF bacterial and fungal cultures and negative viral PCR, a diagnosis of aseptic meningitis is considered.1 Though the differential for aseptic meningitis is broad, in the immunocompetent patient, the most common etiology of aseptic meningitis in the United States is by far viral, and specifically, enterovirus (50.9%). It is less commonly caused by herpes simplex virus (8.3%), varicella zoster virus, and finally, the mosquito-borne St. Louis encephalitis and West Nile viruses typically acquired in the summer or early fall months. Other infectious agents that can present with aseptic meningitis are spirochetes (Lyme disease and syphilis), tuberculous meningitis, fungal infections (cryptococcal meningitis), and other bacterial infections that have a negative culture.
The patient’s history, physical examination, vital signs, imaging, and lumbar puncture findings were most concerning for drug-induced aseptic meningitis (DIAM) secondary to her recent IVIG infusion. An algorithm can be used to work through the diagnostic approach (Figure 2).3,4
Immediate and delayed adverse reactions to IVIG are known risks for IVIG therapy. About 1% to 15% of patients who receive IVIG will experience mild immediate reactions to the infusion.6 These immediate reactions include fever (78.6%), acrocyanosis (71.4%), rash (64.3%), headache (57.1%), shortness of breath (42.8%), hypotension (35.7%), and chest pain (21.4%).
IVIG is an increasingly used biologic pharmacologic agent used for a variety of medical conditions. This can be attributed to its multifaceted properties and ability to fight infection when given as replacement therapy and provide immunomodulation in conjunction with its more well-known anti-inflammatory properties.8 The number of conditions that can potentially benefit from IVIG is so vast that the American Academy of Allergy, Asthma and Immunology had to divide the indication for IVIG therapy into definitely beneficial, probably beneficial, may provide benefit, and unlikely to provide benefit categories.8
Conclusions
We encourage heightened clinical suspicion of DIAM in patients who have recently undergone IVIG infusion and present with meningeal signs (stiff neck, headache, photophobia, and ear/eye pressure) without any evidence of infection on physical examination or laboratory results. With such, we hope to improve clinician suspicion, detection, as well as patient education and outcomes in cases of DIAM.
1. Kareva L, Mironska K, Stavric K, Hasani A. Adverse reactions to intravenous immunoglobulins—our experience. Open Access Maced J Med Sci. 2018;6(12):2359-2362. doi:10.3889/oamjms.2018.513
2. Mount HR, Boyle SD. Aseptic and bacterial meningitis: evaluation, treatment, and prevention. Am Fam Physician. 2017;96(5):314-322.
3. Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
4. Connolly KJ, Hammer SM. The acute aseptic meningitis syndrome. Infect Dis Clin North Am. 1990;4(4):599-622.
5. Jolles S, Sewell WA, Leighton C. Drug-induced aseptic meningitis: diagnosis and management. Drug Saf. 2000;22(3):215-226. doi:10.2165/00002018-200022030-00005
6. Yelehe-Okouma M, Czmil-Garon J, Pape E, Petitpain N, Gillet P. Drug-induced aseptic meningitis: a mini-review. Fundam Clin Pharmacol. 2018;32(3):252-260. doi:10.1111/fcp.12349
7. Kepa L, Oczko-Grzesik B, Stolarz W, Sobala-Szczygiel B. Drug-induced aseptic meningitis in suspected central nervous system infections. J Clin Neurosci. 2005;12(5):562-564. doi:10.1016/j.jocn.2004.08.024
8. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1-S46. doi:10.1016/j.jaci.2016.09.023
9. Kaarthigeyan K, Burli VV. Aseptic meningitis following intravenous immunoglobulin therapy of common variable immunodeficiency. J Pediatr Neurosci. 2011;6(2):160-161. doi:10.4103/1817-1745.92858
1. Kareva L, Mironska K, Stavric K, Hasani A. Adverse reactions to intravenous immunoglobulins—our experience. Open Access Maced J Med Sci. 2018;6(12):2359-2362. doi:10.3889/oamjms.2018.513
2. Mount HR, Boyle SD. Aseptic and bacterial meningitis: evaluation, treatment, and prevention. Am Fam Physician. 2017;96(5):314-322.
3. Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
4. Connolly KJ, Hammer SM. The acute aseptic meningitis syndrome. Infect Dis Clin North Am. 1990;4(4):599-622.
5. Jolles S, Sewell WA, Leighton C. Drug-induced aseptic meningitis: diagnosis and management. Drug Saf. 2000;22(3):215-226. doi:10.2165/00002018-200022030-00005
6. Yelehe-Okouma M, Czmil-Garon J, Pape E, Petitpain N, Gillet P. Drug-induced aseptic meningitis: a mini-review. Fundam Clin Pharmacol. 2018;32(3):252-260. doi:10.1111/fcp.12349
7. Kepa L, Oczko-Grzesik B, Stolarz W, Sobala-Szczygiel B. Drug-induced aseptic meningitis in suspected central nervous system infections. J Clin Neurosci. 2005;12(5):562-564. doi:10.1016/j.jocn.2004.08.024
8. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1-S46. doi:10.1016/j.jaci.2016.09.023
9. Kaarthigeyan K, Burli VV. Aseptic meningitis following intravenous immunoglobulin therapy of common variable immunodeficiency. J Pediatr Neurosci. 2011;6(2):160-161. doi:10.4103/1817-1745.92858
Noninvasive laser therapy tied to improved short-term memory
Investigators compared the effect of 1,064 nm of tPBM delivered over a 12-minute session to the right PFC vs. three other treatment arms: delivery of the same intervention to the left PFC, delivery of the intervention at a lower frequency, and a sham intervention.
All participants were shown a series of items prior to the intervention and asked to recall them after the intervention. Those who received tPBM 1,064 nm to the right PFC showed a superior performance of up to 25% in the memory tasks compared with the other groups.
Patients with attention-related conditions, such as attention deficit hyperactivity disorder, “could benefit from this type of treatment, which is safe, simple, and noninvasive, with no side effects,” coinvestigator Dongwei Li, a visiting PhD student at the Centre for Human Brain Health, University of Birmingham, England, said in a news release.
The findings were published online in Science Advances.
Differing wavelengths
The researchers note that “in the past decades,” noninvasive brain stimulation technology using transcranial application of direct or alternating electrical or magnetic fields “has been proven to be useful” in the improvement of working memory (WM).
When applied to the right PFC, tPBM has been shown to improve accuracy and speed of reaction time in WM tasks and improvements in “high-order cognitive functions,” such as sustained attention, emotion, and executive functions.
The investigators wanted to assess the impact of tPBM applied to different parts of the brain and at different wavelengths. They conducted four double-blind, sham-controlled experiments encompassing 90 neurotypical college students (mean age, 22 years). Each student participated in only one of the four experiments.
All completed two different tPBM sessions, separated by a week, in which sham and active tPBM were compared. Two different types of change-detection memory tasks were given: one requiring participants to remember the orientation of a series of items before and after the intervention and one other requiring them to remember the color of the items (experiments 1 and 2).
A series of follow-up experiments focused on comparing different wavelengths (1,064 nm vs. 852 nm) and different stimulation sites (right vs. left PFC; experiments 3 and 4).
EEG recordings were obtained during the intervention and the memory tasks.
Each experiment consisted of one active tPBM session and one sham tPBM session, with sessions consisting of 12 minutes of laser light (or sham) intervention. These sessions were conducted on the first and the seventh day; then, on the eighth day, participants were asked to report (or guess) which session was the active tPBM session.
Stimulating astrocytes
Results showed that, compared with sham tPBM, there was an improvement in WM capacity and scores by the 1,064 nm intervention in the orientation as well as the color task.
Participants who received the targeted treatment were able to remember between four and five test objects, whereas those with the treatment variations were only able to remember between three and four objects.
“These results support the hypothesis that 1,064 nm tPBM on the right PFC enhances WM capacity,” the investigators wrote.
They also found improvements in WM in participants receiving tPBM vs. sham regardless of whether their performance in the WM task was at a low or high level. This finding held true in both the orientation and the color tasks.
“Therefore, participants with good and poor WM capacity improved after 1,064 nm tPBM,” the researchers noted.
In addition, participants were unable to guess or report whether they had received sham or active tPBM.
EEG monitoring showed changes in brain activity that predicted the improvements in memory performance. In particular, 1,064 tPBM applied to the right PFC increased occipitoparietal contralateral delay activity (CDA), with CDA mediating the WM improvement.
This is “consistent with previous research that CDA is indicative of the number of maintained objects in visual working memory,” the investigators wrote.
Pearson correlation analyses showed that the differences in CDA set-size effects between active and sham session “correlated positively” with the behavioral differences between these sessions. For the orientation task, the r was 0.446 (P < .04); and for the color task, the r was .563 (P < .02).
No similar improvements were found with the 852 nm tPBM.
“We need further research to understand exactly why the tPBM is having this positive effect,” coinvestigator Ole Jensen, PhD, professor in translational neuroscience and codirector of the Centre for Human Brain Health, said in the release.
“It’s possible that the light is stimulating the astrocytes – the powerplants – in the nerve cells within the PFC, and this has a positive effect on the cells’ efficiency,” he noted.
Dr. Jensen added that his team “will also be investigating how long the effects might last. Clearly, if these experiments are to lead to a clinical intervention, we will need to see long-lasting benefits.”
Beneficial cognitive, emotional effects
Commenting for this news organization, Francisco Gonzalez-Lima, PhD, professor in the department of psychology, University of Texas at Austin, called the study “well done.”
Dr. Gonzalez-Lima was one of the first researchers to demonstrate that 1,064 nm transcranial infrared laser stimulation “produces beneficial cognitive and emotional effects in humans, including improving visual working memory,” he said.
The current study “reported an additional brain effect linked to the improved visual working memory that consists of an EEG-derived response, which is a new finding,” noted Dr. Gonzales-Lima, who was not involved with the new research.
He added that the same laser method “has been found by the Gonzalez-Lima lab to be effective at improving cognition in older adults and depressed and bipolar patients.”
The study was supported by the National Natural Science Foundation of China, the Ministry of Science and Technology of the People’s Republic of China, and the National Defence Basic Scientific Research Program of China. The investigators and Dr. Gonzalez-Lima report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators compared the effect of 1,064 nm of tPBM delivered over a 12-minute session to the right PFC vs. three other treatment arms: delivery of the same intervention to the left PFC, delivery of the intervention at a lower frequency, and a sham intervention.
All participants were shown a series of items prior to the intervention and asked to recall them after the intervention. Those who received tPBM 1,064 nm to the right PFC showed a superior performance of up to 25% in the memory tasks compared with the other groups.
Patients with attention-related conditions, such as attention deficit hyperactivity disorder, “could benefit from this type of treatment, which is safe, simple, and noninvasive, with no side effects,” coinvestigator Dongwei Li, a visiting PhD student at the Centre for Human Brain Health, University of Birmingham, England, said in a news release.
The findings were published online in Science Advances.
Differing wavelengths
The researchers note that “in the past decades,” noninvasive brain stimulation technology using transcranial application of direct or alternating electrical or magnetic fields “has been proven to be useful” in the improvement of working memory (WM).
When applied to the right PFC, tPBM has been shown to improve accuracy and speed of reaction time in WM tasks and improvements in “high-order cognitive functions,” such as sustained attention, emotion, and executive functions.
The investigators wanted to assess the impact of tPBM applied to different parts of the brain and at different wavelengths. They conducted four double-blind, sham-controlled experiments encompassing 90 neurotypical college students (mean age, 22 years). Each student participated in only one of the four experiments.
All completed two different tPBM sessions, separated by a week, in which sham and active tPBM were compared. Two different types of change-detection memory tasks were given: one requiring participants to remember the orientation of a series of items before and after the intervention and one other requiring them to remember the color of the items (experiments 1 and 2).
A series of follow-up experiments focused on comparing different wavelengths (1,064 nm vs. 852 nm) and different stimulation sites (right vs. left PFC; experiments 3 and 4).
EEG recordings were obtained during the intervention and the memory tasks.
Each experiment consisted of one active tPBM session and one sham tPBM session, with sessions consisting of 12 minutes of laser light (or sham) intervention. These sessions were conducted on the first and the seventh day; then, on the eighth day, participants were asked to report (or guess) which session was the active tPBM session.
Stimulating astrocytes
Results showed that, compared with sham tPBM, there was an improvement in WM capacity and scores by the 1,064 nm intervention in the orientation as well as the color task.
Participants who received the targeted treatment were able to remember between four and five test objects, whereas those with the treatment variations were only able to remember between three and four objects.
“These results support the hypothesis that 1,064 nm tPBM on the right PFC enhances WM capacity,” the investigators wrote.
They also found improvements in WM in participants receiving tPBM vs. sham regardless of whether their performance in the WM task was at a low or high level. This finding held true in both the orientation and the color tasks.
“Therefore, participants with good and poor WM capacity improved after 1,064 nm tPBM,” the researchers noted.
In addition, participants were unable to guess or report whether they had received sham or active tPBM.
EEG monitoring showed changes in brain activity that predicted the improvements in memory performance. In particular, 1,064 tPBM applied to the right PFC increased occipitoparietal contralateral delay activity (CDA), with CDA mediating the WM improvement.
This is “consistent with previous research that CDA is indicative of the number of maintained objects in visual working memory,” the investigators wrote.
Pearson correlation analyses showed that the differences in CDA set-size effects between active and sham session “correlated positively” with the behavioral differences between these sessions. For the orientation task, the r was 0.446 (P < .04); and for the color task, the r was .563 (P < .02).
No similar improvements were found with the 852 nm tPBM.
“We need further research to understand exactly why the tPBM is having this positive effect,” coinvestigator Ole Jensen, PhD, professor in translational neuroscience and codirector of the Centre for Human Brain Health, said in the release.
“It’s possible that the light is stimulating the astrocytes – the powerplants – in the nerve cells within the PFC, and this has a positive effect on the cells’ efficiency,” he noted.
Dr. Jensen added that his team “will also be investigating how long the effects might last. Clearly, if these experiments are to lead to a clinical intervention, we will need to see long-lasting benefits.”
Beneficial cognitive, emotional effects
Commenting for this news organization, Francisco Gonzalez-Lima, PhD, professor in the department of psychology, University of Texas at Austin, called the study “well done.”
Dr. Gonzalez-Lima was one of the first researchers to demonstrate that 1,064 nm transcranial infrared laser stimulation “produces beneficial cognitive and emotional effects in humans, including improving visual working memory,” he said.
The current study “reported an additional brain effect linked to the improved visual working memory that consists of an EEG-derived response, which is a new finding,” noted Dr. Gonzales-Lima, who was not involved with the new research.
He added that the same laser method “has been found by the Gonzalez-Lima lab to be effective at improving cognition in older adults and depressed and bipolar patients.”
The study was supported by the National Natural Science Foundation of China, the Ministry of Science and Technology of the People’s Republic of China, and the National Defence Basic Scientific Research Program of China. The investigators and Dr. Gonzalez-Lima report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators compared the effect of 1,064 nm of tPBM delivered over a 12-minute session to the right PFC vs. three other treatment arms: delivery of the same intervention to the left PFC, delivery of the intervention at a lower frequency, and a sham intervention.
All participants were shown a series of items prior to the intervention and asked to recall them after the intervention. Those who received tPBM 1,064 nm to the right PFC showed a superior performance of up to 25% in the memory tasks compared with the other groups.
Patients with attention-related conditions, such as attention deficit hyperactivity disorder, “could benefit from this type of treatment, which is safe, simple, and noninvasive, with no side effects,” coinvestigator Dongwei Li, a visiting PhD student at the Centre for Human Brain Health, University of Birmingham, England, said in a news release.
The findings were published online in Science Advances.
Differing wavelengths
The researchers note that “in the past decades,” noninvasive brain stimulation technology using transcranial application of direct or alternating electrical or magnetic fields “has been proven to be useful” in the improvement of working memory (WM).
When applied to the right PFC, tPBM has been shown to improve accuracy and speed of reaction time in WM tasks and improvements in “high-order cognitive functions,” such as sustained attention, emotion, and executive functions.
The investigators wanted to assess the impact of tPBM applied to different parts of the brain and at different wavelengths. They conducted four double-blind, sham-controlled experiments encompassing 90 neurotypical college students (mean age, 22 years). Each student participated in only one of the four experiments.
All completed two different tPBM sessions, separated by a week, in which sham and active tPBM were compared. Two different types of change-detection memory tasks were given: one requiring participants to remember the orientation of a series of items before and after the intervention and one other requiring them to remember the color of the items (experiments 1 and 2).
A series of follow-up experiments focused on comparing different wavelengths (1,064 nm vs. 852 nm) and different stimulation sites (right vs. left PFC; experiments 3 and 4).
EEG recordings were obtained during the intervention and the memory tasks.
Each experiment consisted of one active tPBM session and one sham tPBM session, with sessions consisting of 12 minutes of laser light (or sham) intervention. These sessions were conducted on the first and the seventh day; then, on the eighth day, participants were asked to report (or guess) which session was the active tPBM session.
Stimulating astrocytes
Results showed that, compared with sham tPBM, there was an improvement in WM capacity and scores by the 1,064 nm intervention in the orientation as well as the color task.
Participants who received the targeted treatment were able to remember between four and five test objects, whereas those with the treatment variations were only able to remember between three and four objects.
“These results support the hypothesis that 1,064 nm tPBM on the right PFC enhances WM capacity,” the investigators wrote.
They also found improvements in WM in participants receiving tPBM vs. sham regardless of whether their performance in the WM task was at a low or high level. This finding held true in both the orientation and the color tasks.
“Therefore, participants with good and poor WM capacity improved after 1,064 nm tPBM,” the researchers noted.
In addition, participants were unable to guess or report whether they had received sham or active tPBM.
EEG monitoring showed changes in brain activity that predicted the improvements in memory performance. In particular, 1,064 tPBM applied to the right PFC increased occipitoparietal contralateral delay activity (CDA), with CDA mediating the WM improvement.
This is “consistent with previous research that CDA is indicative of the number of maintained objects in visual working memory,” the investigators wrote.
Pearson correlation analyses showed that the differences in CDA set-size effects between active and sham session “correlated positively” with the behavioral differences between these sessions. For the orientation task, the r was 0.446 (P < .04); and for the color task, the r was .563 (P < .02).
No similar improvements were found with the 852 nm tPBM.
“We need further research to understand exactly why the tPBM is having this positive effect,” coinvestigator Ole Jensen, PhD, professor in translational neuroscience and codirector of the Centre for Human Brain Health, said in the release.
“It’s possible that the light is stimulating the astrocytes – the powerplants – in the nerve cells within the PFC, and this has a positive effect on the cells’ efficiency,” he noted.
Dr. Jensen added that his team “will also be investigating how long the effects might last. Clearly, if these experiments are to lead to a clinical intervention, we will need to see long-lasting benefits.”
Beneficial cognitive, emotional effects
Commenting for this news organization, Francisco Gonzalez-Lima, PhD, professor in the department of psychology, University of Texas at Austin, called the study “well done.”
Dr. Gonzalez-Lima was one of the first researchers to demonstrate that 1,064 nm transcranial infrared laser stimulation “produces beneficial cognitive and emotional effects in humans, including improving visual working memory,” he said.
The current study “reported an additional brain effect linked to the improved visual working memory that consists of an EEG-derived response, which is a new finding,” noted Dr. Gonzales-Lima, who was not involved with the new research.
He added that the same laser method “has been found by the Gonzalez-Lima lab to be effective at improving cognition in older adults and depressed and bipolar patients.”
The study was supported by the National Natural Science Foundation of China, the Ministry of Science and Technology of the People’s Republic of China, and the National Defence Basic Scientific Research Program of China. The investigators and Dr. Gonzalez-Lima report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SCIENCE ADVANCES
A Transdisciplinary Program for Care of Veterans With Neurocognitive Disorders
Dementia is a devastating condition resulting in major functional, emotional, and financial impact on patients, their caregivers, and families. Approximately 6.5 million Americans are living with Alzheimer disease (AD), the most common of many causes of dementia.1 The prevalence of AD could increase to 12.7 million Americans by 2050 as the population ages.1 Studies suggest that dementia, also known as major neurocognitive disorder, is common and underdiagnosed among US veterans, a population with a mean age of 65 years.2 During cognitive screening, memory impairment is present in approximately 20% of veterans aged ≥ 75 years who have not been diagnosed with a neurocognitive disorder.3 In addition, veterans might be particularly vulnerable to dementia at an earlier age than the general population because of vascular risk factors and traumatic brain injuries.4 These concerns highlight the need for effective dementia care programs at US Department of Veterans Affairs (VA) facilities.
The US health care system often does not adequately address the needs of patients with dementia and their caregivers.5 Dementia care requires specialized medical care among collaborating professionals and caregiver and psychosocial interventions and services. However, the US health care system is fragmented with different clinicians and services siloed into separate practices and most dementia care occurring in primary care settings.6 Primary care professionals (PCPs) often are uncomfortable diagnosing and managing dementia because of time constraints, lack of expertise and training, and inability to deal with the range of care needs.7 PCPs do not identify approximately 42% of their patients with dementia and, when recognized, do not adhere to dementia care guidelines and address caregiver needs.8-10 Research indicates that caregiver support improves dementia care by teaching behavioral management skills and caregiver coping strategies, allowing patients to stay at home and delay institutionalization.6,11,12 Clinicians underuse available resources and do not incorporate them in their patient care.10 These community services benefit patients and caregivers and significantly improve the overall quality of care.6
Memory clinics have emerged to address these deficiencies when managing dementia.13 The most effective memory clinics maximize the use of specialists with different expertise in dementia care, particularly integrated programs where disciplines function together rather than independently.1,5,14 Systematic reviews and meta-analyses have documented the effectiveness of collaborative care management programs.11,12,15 Integration of dementia care management is associated with earlier diagnosis and interventions, decreased functional and cognitive symptom severity, decreased or delayed institutionalization, improved quality of life for patients and caregivers, enhanced overall quality of care and cost-effectiveness, and better integration of community services.11,12,14-19 In these programs, designating a dementia care manager (DCM) as the patient’s advocate facilitates the integrated structure, increases the quality of care, helps caregivers, facilitates adherence to dementia practice guidelines, and prevents behavioral and psychological symptoms of dementia (BPSD).1,6,11,12,20,21
The best interprofessional model for dementia care might be the transdisciplinary model that includes a DCM. To meet the specific demands of dementia care, there must be a high level of interprofessional collaboration rather than multiple health care professionals (HCPs) delivering care in isolation—an approach that is time consuming and often difficult to implement.22 Whereas multidisciplinary care refers to delivery of parallel services and interdisciplinary care implies a joint formulation, transdisciplinary care aims to maximize integration of HCPs and their specific expertise and contributions through interactions and discussions that deliver focused input to the lead physician. The transdisciplinary model addresses needs that often are missed and can minimize disparities in the quality of dementia care.23 A DCM is an integral part of our program, facilitating understanding and implementation of the final care plan and providing long-term follow-up and care. We outline a conference-centered transdisciplinary dementia care model with a social worker as DCM (SW-DCM) at our VA medical center.
Program Description
In 2020, the VA Greater Los Angeles Healthcare System (VAGLAHS) in California established a multispecialty clinic dedicated to evaluation and treatment of veterans with memory and neurocognitive disorders and to provide support for their caregivers and families. With the agreement of leadership in mental health, neurology, and geriatrics services on the importance of collaboration for dementia care, the psychiatry and neurology services created a joint Memory and Neurobehavior Clinic, which completed its first 2 years of operation as a full-day program. In recent months, the clinic has scheduled 24 veterans per day, approximately 50% new evaluations and 50% follow-up patients, with wait times of < 2 months. There is a mean of 12 intake or lead physicians who could attend sessions in the morning, afternoon, or both. The general clinic flow consists of a 2-hour intake evaluation of new referrals by the lead physician followed by a clinic conference with transdisciplinary discussion. The DCM then follows up with the veteran/caregiver presenting a final care plan individualized to the veterans, caregivers, and families.
The Memory and Neurobehavior team includes behavioral neurologists, geriatric psychiatrists, neuropsychologists, geriatric fellows, advanced clinical nurses, and social workers who function as the DCM (Table 1). 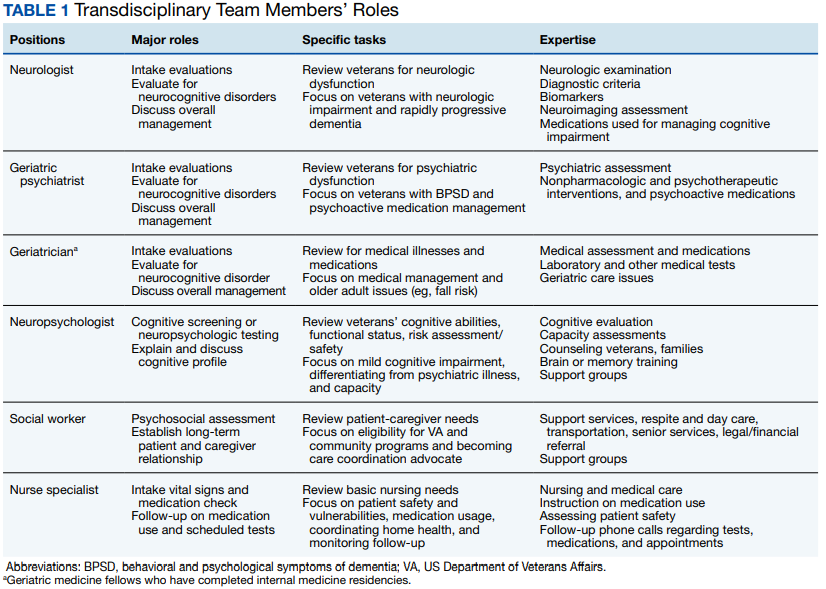
Procedures
Before the office visit, the coordinating geriatric psychiatrist triages veterans to neurology, psychiatry, or geriatric physicians based on the clinical presentation, history of neurologic signs or symptoms, BPSD or psychiatric history, functional decline, or comorbid medical illnesses. Although veterans often have overlapping concerns, the triage process aims to coordinate the intake evaluations with the most indicated and available specialist with the intention to notify the other specialists during the transdisciplinary conference.
Referrals to the program occur from many sources, notably from primary care (70.8%), mental health (16.7%), and specialty clinics (12.5%). The clinic also receives referrals from the affiliated Veterans Cognitive Assessment and Management Program, which provides dementia evaluation and support via telehealth screening. This VAGLAHS program services a diverse population of veterans: 87% male; 43% aged > 65 years (75% in our clinic); 51% non-Hispanic White; 19% non-Hispanic African American; 16% Hispanic; 4% Asian; and 1% Native American. This population receives care at regional VA medical centers and community-based outpatient clinics over a wide geographic service area.
The initial standardized assessments by intake or lead physicians includes mental status screening with the Montreal Cognitive Assessment (with certified clinicians), the Neurobehavioral Status Examination for a more detailed assessment of cognitive domains, the Columbia-Suicide Severity Rating Scale, the Patient Health Questionnaire for depression screening, and assessment for impairments in instrumental or basic activities of daily living. This initial evaluation aims to apply clinical guidelines and diagnostic criteria for the differential diagnosis of neurocognitive disorders, determine eligibility for cognitive-enhancing medications and techniques, assess for BPSD and the need for nonpharmacologic or pharmacologic interventions, determine functional status, and evaluate the need for supervision, safety concerns, and evidence of neglect or abuse.
As part of its mission, the clinic is charged with implementing the VA Dementia System of Care (DSOC). The stated goals of the DSOC are to provide individualized person-centered dementia care to help veterans experiencing dementia and their caregivers maintain a positive and optimal quality of life and create an environment where VA medical center staff understand the health care needs of veterans with dementia and their caregivers’ role. As part of this initiative, the clinic includes (1) coordination of care through a SW-DCM; (2) 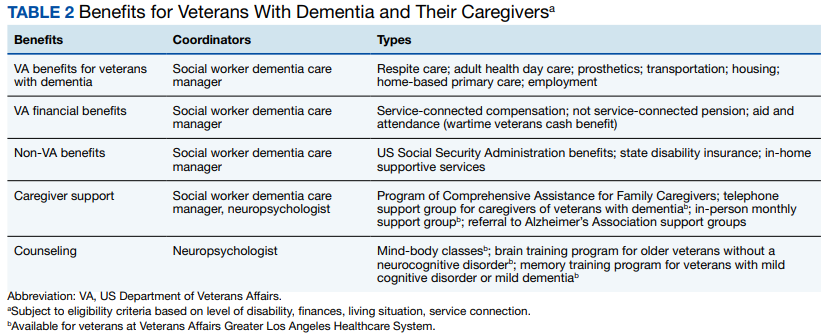
Transdisciplinary Conference
Clinic conferences are held after the veterans are seen. Staff gather to discuss the patient and review management. All team members are present, as well as the head of the clinical clerical staff who can facilitate appointments, make lobby and wait times more bearable for our patients and caregivers, and help manage emergencies. Although this is an in-person conference, the COVID-19 pandemic has allowed us to include staff who screen at remote sites via videoconferencing, similar to other VA programs.24 The Memory and Neurobehavior Clinic has two ≤ 90-minute conferences daily. The lead physicians and their senior attendings present the new intake evaluations (4-6 at each conference session) with a preliminary formulation and questions for discussion. The moderator solicits contributions from the different disciplines, going from one to the next and recording their responses for each veteran. Further specialists are available for consultation through the conference mechanism if necessary. The final assessment is reviewed, a diagnosis is established, and a tailored, individualized care plan for adjusting or optimizing the veteran’s care is presented to the lead physician who makes the final determination. At the close of the conference, the team’s discussion is recorded along with the lead physician’s original detailed intake evaluation. Currently, the records go into the Computerized Patient Record System, but we are making plans to transition to Cerner as it is implemented.
During the discussion, team members review several areas of consideration. If there is neuroimaging, neurologists review the images projected on a large computer screen. Team members also will assess for the need to obtain biomarker studies, such as blood, cerebrospinal fluid, or positron emission tomography. Psychiatrists could review management of BPSD and use of psychotropic agents, and neuropsychologists might consider the need for more precise cognitive testing and whether a capacity assessment is indicated. Social work might bring up the need for a durable power of attorney as well as applicable caregiver and community resources. Geriatric medicine and nursing could provide input into medical management and care and the ability of veterans and caregivers to follow the prescribed regimen. Further areas of discussion include driving safety and restrictions on driving (as required in California) and the presence of guns in the home. Finally, brief education is provided in short 10-to-15-minute lectures covering pertinent topics so staff remain up-to-date in this changing field.
Postconference Continuity
After the conference, the SW-DCM continues to provide support throughout the disease course, helping veterans and their caregivers understand and follow through on the team’s recommendations. The SW-DCM, who is experienced and trained in case management, forms an ongoing relationship with the veterans and their caregivers and remains an advocate for their care. The SW-DCM communicates the final plan by phone and, when necessary, requests the lead physician to call to clarify any poorly understood or technical aspects of the care plan. About 50% of our veterans—primarily those who do not have a neurocognitive disorder or have mild cognitive impairment—return to their PCPs with our care plan consultation; about 25% are already enrolled in geriatric and other programs with long-term follow-up. The assigned SW-DCM follows up with the remaining veterans and caregivers regularly by phone, facilitates communication with other team members, and endeavors to assure postvisit continuity of care and support during advancing stages of the disease. In addition, the SW-DCM can provide supportive counseling and psychotherapy for stressed caregivers, refer to support groups and cognitive rehabilitation programs, and help develop long-term goals and consideration for supervised living environments. The nurse specialist participates with follow-up calls regarding medications and scheduled tests and appointments, clearing up confusion about instructions, avoiding medication errors, and providing education in dementia care. Both social worker and nurse are present throughout the week, reachable by phone, and, in turn, able to contact the clinic physicians for veterans’ needs.
Discussion
Because of the heterogenous medical and psychosocial needs of veterans with dementia and their caregivers, a transdisciplinary team with a dedicated DCM might offer the most effective and efficient model for dementia care. We present a transdisciplinary program that incorporates dementia specialists in a single evaluation by maximizing their time through a conference-centered program. Our program involves neurologists, psychiatrists, geriatricians, psychologists, nurses, and social workers collaborating and communicating to enact effective dementia care. It further meets the goals of the VA-DSOC in implementing individualized patient and caregiver care.
This transdisciplinary model addresses a number of issues, starting with the differential diagnosis of underlying neurologic conditions. Within the transdisciplinary team, the neurologist can provide specific insights into any neurologic findings and illnesses, such as Alzheimer disease and other neurodegenerative dementias, vascular dementia syndromes, normal pressure hydrocephalus, Creutzfeldt-Jakob disease, neurosyphilis, and others. Most veterans with dementia experience BPSD at some point during of their illness. The psychiatrists on the transdisciplinary team can maximize management of BPSD with nonpharmacologic interventions and the fewest and least aversive psychoactive medications. Our program also addresses the need for more precise cognitive evaluation. Neuropsychologists are present and available for administrating neuropsychologic tests and interpreting cognitive performance and any earlier neuropsychologic testing. This model also cares for the caregivers and assesses their needs. The social worker—as well as other members of the team—can provide caregivers with strategies for coping with disruptive and other behaviors related to dementia, counsel them on how to manage the veteran’s functional decline, and aid in establishing a safe living space. Because the social worker serves as a DCM, these coping and adjustment questions occupy significant clinical attention between appointments. This transdisciplinary model places the patient’s illness in the context of their functional status, diagnoses, and medications. The team geriatrician and the nurse specialist are indispensable resources. The clinic conference provides a teaching venue for staff and trainees and a mechanism to discuss new developments in dementia care, such as the increasing need to assess individuals with mild cognitive impairment.25 This model depends on the DCM’s invaluable role in ensuring implementation of the dementia care plan and continuity of care.
Conclusions
We describe effective dementia care with a transdisciplinary team in a conference setting and with the participation of a dedicated DCM.5 To date, this program appears to be an efficient, sustainable application of the limited resources allocated to dementia care. Nevertheless, we are collecting data to compare with performance measures, track use, and assess the programs effects on continuity of care. We look forward to presenting metrics from our program that show improvement in the health care for veterans experiencing a devastating and increasingly common disorder.
1. 2022 Alzheimer’s disease facts and figures. Alzheimers Dement. 2022;18(4):700-789. doi:10.1002/alz.12638
2. National Center for Veterans Analysis and Statistics. Profile of veterans: 2016. Accessed October 12, 2022. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2016.pdf
3. Chodosh J, Sultzer DL, Lee ML, et al. Memory impairment among primary care veterans. Aging Ment Health. 2007;11(4):444-450. doi:10.1080/13607860601086272
4. Kennedy E, Panahi S, Stewart IJ, et al. Traumatic brain injury and early onset dementia in post 9-11 veterans. Brain Inj. 2022;36(5):620-627. doi:10.1080/02699052.2022.20338465. Heintz H, Monette P, Epstein-Lubow G, Smith L, Rowlett S, Forester BP. Emerging collaborative care models for dementia care in the primary care setting: a narrative review. Am J Geriatr Psychiatry. 2020;28(3):320-330. doi:10.1016/j.jagp.2019.07.015
6. Reuben DB, Evertson LC, Wenger NS, et al. The University of California at Los Angeles Alzheimer’s and Dementia Care program for comprehensive, coordinated, patient-centered care: preliminary data. J Am Geriatr Soc. 2013;61(12):2214-2218. doi:10.1111/jgs.12562
7. Apesoa-Varano EC, Barker JC, Hinton L. Curing and caring: the work of primary care physicians with dementia patients. Qual Health Res. 2011;21(11):1469-1483. doi:10.1177/1049732311412788
8. Creavin ST, Noel-Storr AH, Langdon RJ, et al. Clinical judgement by primary care physicians for the diagnosis of all-cause dementia or cognitive impairment in symptomatic people. Cochrane Database Syst Rev. 2022;6:CD012558. doi:10.1002/14651858.CD012558.pub2
9. Sivananthan SN, Puyat JH, McGrail KM. Variations in self-reported practice of physicians providing clinical care to individuals with dementia: a systematic review. J Am Geriatr Soc. 2013;61(8):1277-1285. doi:10.1111/jgs.12368
10. Rosen CS, Chow HC, Greenbaum MA, et al. How well are clinicians following dementia practice guidelines? Alzheimer Dis Assoc Disord. 2002;16(1):15-23. doi:10.1097/00002093-200201000-00003
11. Reilly S, Miranda-Castillo C, Malouf R, et al. Case management approaches to home support for people with dementia. Cochrane Database Syst Rev. 2015;1:CD008345. doi:10.1002/14651858.CD008345.pub2
12. Tam-Tham H, Cepoiu-Martin M, Ronksley PE, Maxwell CJ, Hemmelgarn BR. Dementia case management and risk of long-term care placement: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2013;28(9):889-902. doi:10.1002/gps.3906
13. Jolley D, Benbow SM, Grizzell M. Memory clinics. Postgrad Med J. 2006;82(965):199-206. doi:10.1136/pgmj.2005.040592
14. Muhlichen F, Michalowsky B, Radke A, et al. Tasks and activities of an effective collaborative dementia care management program in German primary care. J Alzheimers Dis. 2022;87(4):1615-1625. doi:10.3233/JAD-215656
15. Somme D, Trouve H, Drame M, Gagnon D, Couturier Y, Saint-Jean O. Analysis of case management programs for patients with dementia: a systematic review. Alzheimers Dement. 2012;8(5):426-436. doi:10.1016/j.jalz.2011.06.004
16. Ramakers IH, Verhey FR. Development of memory clinics in the Netherlands: 1998 to 2009. Aging Ment Health. 2011;15(1):34-39. doi:10.1080/13607863.2010.519321
17. LaMantia MA, Alder CA, Callahan CM, et al. The aging brain care medical home: preliminary data. J Am Geriatr Soc. 2015;63(6):1209-1213. doi:10.1111/jgs.13447
18. Rubinsztein JS, van Rensburg MJ, Al-Salihy Z, et al. A memory clinic v. traditional community mental health team service: comparison of costs and quality. BJPsych Bull. 2015;39(1):6-11. doi:10.1192/pb.bp.113.044263
19. Lee L, Hillier LM, Harvey D. Integrating community services into primary care: improving the quality of dementia care. Neurodegener Dis Manag. 2014;4(1):11-21. doi:10.2217/nmt.13.72
20. Bass DM, Judge KS, Snow AL, et al. Caregiver outcomes of partners in dementia care: effect of a care coordination program for veterans with dementia and their family members and friends. J Am Geriatr Soc. 2013;61(8):1377-1386. doi:10.1111/jgs.12362
21. Callahan CM, Boustani MA, Unverzagt FW, et al. Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial. JAMA. 2006;295(18):2148-2157. doi:10.1001/jama.295.18.2148
22. Leggett A, Connell C, Dubin L, et al. Dementia care across a tertiary care health system: what exists now and what needs to change. J Am Med Dir Assoc. 2019;20(10):1307-12 e1. doi:10.1016/j.jamda.2019.04.006
23. Brown AF, Vassar SD, Connor KI, Vickrey BG. Collaborative care management reduces disparities in dementia care quality for caregivers with less education. J Am Geriatr Soc. 2013;61(2):243-251. doi:10.1111/jgs.12079
24. Powers BB, Homer MC, Morone N, Edmonds N, Rossi MI. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
25. Galvin JE, Aisen P, Langbaum JB, et al. Early stages of Alzheimer’s Disease: evolving the care team for optimal patient management. Front Neurol. 2020;11:592302. doi:10.3389/fneur.2020.592302
Dementia is a devastating condition resulting in major functional, emotional, and financial impact on patients, their caregivers, and families. Approximately 6.5 million Americans are living with Alzheimer disease (AD), the most common of many causes of dementia.1 The prevalence of AD could increase to 12.7 million Americans by 2050 as the population ages.1 Studies suggest that dementia, also known as major neurocognitive disorder, is common and underdiagnosed among US veterans, a population with a mean age of 65 years.2 During cognitive screening, memory impairment is present in approximately 20% of veterans aged ≥ 75 years who have not been diagnosed with a neurocognitive disorder.3 In addition, veterans might be particularly vulnerable to dementia at an earlier age than the general population because of vascular risk factors and traumatic brain injuries.4 These concerns highlight the need for effective dementia care programs at US Department of Veterans Affairs (VA) facilities.
The US health care system often does not adequately address the needs of patients with dementia and their caregivers.5 Dementia care requires specialized medical care among collaborating professionals and caregiver and psychosocial interventions and services. However, the US health care system is fragmented with different clinicians and services siloed into separate practices and most dementia care occurring in primary care settings.6 Primary care professionals (PCPs) often are uncomfortable diagnosing and managing dementia because of time constraints, lack of expertise and training, and inability to deal with the range of care needs.7 PCPs do not identify approximately 42% of their patients with dementia and, when recognized, do not adhere to dementia care guidelines and address caregiver needs.8-10 Research indicates that caregiver support improves dementia care by teaching behavioral management skills and caregiver coping strategies, allowing patients to stay at home and delay institutionalization.6,11,12 Clinicians underuse available resources and do not incorporate them in their patient care.10 These community services benefit patients and caregivers and significantly improve the overall quality of care.6
Memory clinics have emerged to address these deficiencies when managing dementia.13 The most effective memory clinics maximize the use of specialists with different expertise in dementia care, particularly integrated programs where disciplines function together rather than independently.1,5,14 Systematic reviews and meta-analyses have documented the effectiveness of collaborative care management programs.11,12,15 Integration of dementia care management is associated with earlier diagnosis and interventions, decreased functional and cognitive symptom severity, decreased or delayed institutionalization, improved quality of life for patients and caregivers, enhanced overall quality of care and cost-effectiveness, and better integration of community services.11,12,14-19 In these programs, designating a dementia care manager (DCM) as the patient’s advocate facilitates the integrated structure, increases the quality of care, helps caregivers, facilitates adherence to dementia practice guidelines, and prevents behavioral and psychological symptoms of dementia (BPSD).1,6,11,12,20,21
The best interprofessional model for dementia care might be the transdisciplinary model that includes a DCM. To meet the specific demands of dementia care, there must be a high level of interprofessional collaboration rather than multiple health care professionals (HCPs) delivering care in isolation—an approach that is time consuming and often difficult to implement.22 Whereas multidisciplinary care refers to delivery of parallel services and interdisciplinary care implies a joint formulation, transdisciplinary care aims to maximize integration of HCPs and their specific expertise and contributions through interactions and discussions that deliver focused input to the lead physician. The transdisciplinary model addresses needs that often are missed and can minimize disparities in the quality of dementia care.23 A DCM is an integral part of our program, facilitating understanding and implementation of the final care plan and providing long-term follow-up and care. We outline a conference-centered transdisciplinary dementia care model with a social worker as DCM (SW-DCM) at our VA medical center.
Program Description
In 2020, the VA Greater Los Angeles Healthcare System (VAGLAHS) in California established a multispecialty clinic dedicated to evaluation and treatment of veterans with memory and neurocognitive disorders and to provide support for their caregivers and families. With the agreement of leadership in mental health, neurology, and geriatrics services on the importance of collaboration for dementia care, the psychiatry and neurology services created a joint Memory and Neurobehavior Clinic, which completed its first 2 years of operation as a full-day program. In recent months, the clinic has scheduled 24 veterans per day, approximately 50% new evaluations and 50% follow-up patients, with wait times of < 2 months. There is a mean of 12 intake or lead physicians who could attend sessions in the morning, afternoon, or both. The general clinic flow consists of a 2-hour intake evaluation of new referrals by the lead physician followed by a clinic conference with transdisciplinary discussion. The DCM then follows up with the veteran/caregiver presenting a final care plan individualized to the veterans, caregivers, and families.
The Memory and Neurobehavior team includes behavioral neurologists, geriatric psychiatrists, neuropsychologists, geriatric fellows, advanced clinical nurses, and social workers who function as the DCM (Table 1).
Procedures
Before the office visit, the coordinating geriatric psychiatrist triages veterans to neurology, psychiatry, or geriatric physicians based on the clinical presentation, history of neurologic signs or symptoms, BPSD or psychiatric history, functional decline, or comorbid medical illnesses. Although veterans often have overlapping concerns, the triage process aims to coordinate the intake evaluations with the most indicated and available specialist with the intention to notify the other specialists during the transdisciplinary conference.
Referrals to the program occur from many sources, notably from primary care (70.8%), mental health (16.7%), and specialty clinics (12.5%). The clinic also receives referrals from the affiliated Veterans Cognitive Assessment and Management Program, which provides dementia evaluation and support via telehealth screening. This VAGLAHS program services a diverse population of veterans: 87% male; 43% aged > 65 years (75% in our clinic); 51% non-Hispanic White; 19% non-Hispanic African American; 16% Hispanic; 4% Asian; and 1% Native American. This population receives care at regional VA medical centers and community-based outpatient clinics over a wide geographic service area.
The initial standardized assessments by intake or lead physicians includes mental status screening with the Montreal Cognitive Assessment (with certified clinicians), the Neurobehavioral Status Examination for a more detailed assessment of cognitive domains, the Columbia-Suicide Severity Rating Scale, the Patient Health Questionnaire for depression screening, and assessment for impairments in instrumental or basic activities of daily living. This initial evaluation aims to apply clinical guidelines and diagnostic criteria for the differential diagnosis of neurocognitive disorders, determine eligibility for cognitive-enhancing medications and techniques, assess for BPSD and the need for nonpharmacologic or pharmacologic interventions, determine functional status, and evaluate the need for supervision, safety concerns, and evidence of neglect or abuse.
As part of its mission, the clinic is charged with implementing the VA Dementia System of Care (DSOC). The stated goals of the DSOC are to provide individualized person-centered dementia care to help veterans experiencing dementia and their caregivers maintain a positive and optimal quality of life and create an environment where VA medical center staff understand the health care needs of veterans with dementia and their caregivers’ role. As part of this initiative, the clinic includes (1) coordination of care through a SW-DCM; (2)
Transdisciplinary Conference
Clinic conferences are held after the veterans are seen. Staff gather to discuss the patient and review management. All team members are present, as well as the head of the clinical clerical staff who can facilitate appointments, make lobby and wait times more bearable for our patients and caregivers, and help manage emergencies. Although this is an in-person conference, the COVID-19 pandemic has allowed us to include staff who screen at remote sites via videoconferencing, similar to other VA programs.24 The Memory and Neurobehavior Clinic has two ≤ 90-minute conferences daily. The lead physicians and their senior attendings present the new intake evaluations (4-6 at each conference session) with a preliminary formulation and questions for discussion. The moderator solicits contributions from the different disciplines, going from one to the next and recording their responses for each veteran. Further specialists are available for consultation through the conference mechanism if necessary. The final assessment is reviewed, a diagnosis is established, and a tailored, individualized care plan for adjusting or optimizing the veteran’s care is presented to the lead physician who makes the final determination. At the close of the conference, the team’s discussion is recorded along with the lead physician’s original detailed intake evaluation. Currently, the records go into the Computerized Patient Record System, but we are making plans to transition to Cerner as it is implemented.
During the discussion, team members review several areas of consideration. If there is neuroimaging, neurologists review the images projected on a large computer screen. Team members also will assess for the need to obtain biomarker studies, such as blood, cerebrospinal fluid, or positron emission tomography. Psychiatrists could review management of BPSD and use of psychotropic agents, and neuropsychologists might consider the need for more precise cognitive testing and whether a capacity assessment is indicated. Social work might bring up the need for a durable power of attorney as well as applicable caregiver and community resources. Geriatric medicine and nursing could provide input into medical management and care and the ability of veterans and caregivers to follow the prescribed regimen. Further areas of discussion include driving safety and restrictions on driving (as required in California) and the presence of guns in the home. Finally, brief education is provided in short 10-to-15-minute lectures covering pertinent topics so staff remain up-to-date in this changing field.
Postconference Continuity
After the conference, the SW-DCM continues to provide support throughout the disease course, helping veterans and their caregivers understand and follow through on the team’s recommendations. The SW-DCM, who is experienced and trained in case management, forms an ongoing relationship with the veterans and their caregivers and remains an advocate for their care. The SW-DCM communicates the final plan by phone and, when necessary, requests the lead physician to call to clarify any poorly understood or technical aspects of the care plan. About 50% of our veterans—primarily those who do not have a neurocognitive disorder or have mild cognitive impairment—return to their PCPs with our care plan consultation; about 25% are already enrolled in geriatric and other programs with long-term follow-up. The assigned SW-DCM follows up with the remaining veterans and caregivers regularly by phone, facilitates communication with other team members, and endeavors to assure postvisit continuity of care and support during advancing stages of the disease. In addition, the SW-DCM can provide supportive counseling and psychotherapy for stressed caregivers, refer to support groups and cognitive rehabilitation programs, and help develop long-term goals and consideration for supervised living environments. The nurse specialist participates with follow-up calls regarding medications and scheduled tests and appointments, clearing up confusion about instructions, avoiding medication errors, and providing education in dementia care. Both social worker and nurse are present throughout the week, reachable by phone, and, in turn, able to contact the clinic physicians for veterans’ needs.
Discussion
Because of the heterogenous medical and psychosocial needs of veterans with dementia and their caregivers, a transdisciplinary team with a dedicated DCM might offer the most effective and efficient model for dementia care. We present a transdisciplinary program that incorporates dementia specialists in a single evaluation by maximizing their time through a conference-centered program. Our program involves neurologists, psychiatrists, geriatricians, psychologists, nurses, and social workers collaborating and communicating to enact effective dementia care. It further meets the goals of the VA-DSOC in implementing individualized patient and caregiver care.
This transdisciplinary model addresses a number of issues, starting with the differential diagnosis of underlying neurologic conditions. Within the transdisciplinary team, the neurologist can provide specific insights into any neurologic findings and illnesses, such as Alzheimer disease and other neurodegenerative dementias, vascular dementia syndromes, normal pressure hydrocephalus, Creutzfeldt-Jakob disease, neurosyphilis, and others. Most veterans with dementia experience BPSD at some point during of their illness. The psychiatrists on the transdisciplinary team can maximize management of BPSD with nonpharmacologic interventions and the fewest and least aversive psychoactive medications. Our program also addresses the need for more precise cognitive evaluation. Neuropsychologists are present and available for administrating neuropsychologic tests and interpreting cognitive performance and any earlier neuropsychologic testing. This model also cares for the caregivers and assesses their needs. The social worker—as well as other members of the team—can provide caregivers with strategies for coping with disruptive and other behaviors related to dementia, counsel them on how to manage the veteran’s functional decline, and aid in establishing a safe living space. Because the social worker serves as a DCM, these coping and adjustment questions occupy significant clinical attention between appointments. This transdisciplinary model places the patient’s illness in the context of their functional status, diagnoses, and medications. The team geriatrician and the nurse specialist are indispensable resources. The clinic conference provides a teaching venue for staff and trainees and a mechanism to discuss new developments in dementia care, such as the increasing need to assess individuals with mild cognitive impairment.25 This model depends on the DCM’s invaluable role in ensuring implementation of the dementia care plan and continuity of care.
Conclusions
We describe effective dementia care with a transdisciplinary team in a conference setting and with the participation of a dedicated DCM.5 To date, this program appears to be an efficient, sustainable application of the limited resources allocated to dementia care. Nevertheless, we are collecting data to compare with performance measures, track use, and assess the programs effects on continuity of care. We look forward to presenting metrics from our program that show improvement in the health care for veterans experiencing a devastating and increasingly common disorder.
Dementia is a devastating condition resulting in major functional, emotional, and financial impact on patients, their caregivers, and families. Approximately 6.5 million Americans are living with Alzheimer disease (AD), the most common of many causes of dementia.1 The prevalence of AD could increase to 12.7 million Americans by 2050 as the population ages.1 Studies suggest that dementia, also known as major neurocognitive disorder, is common and underdiagnosed among US veterans, a population with a mean age of 65 years.2 During cognitive screening, memory impairment is present in approximately 20% of veterans aged ≥ 75 years who have not been diagnosed with a neurocognitive disorder.3 In addition, veterans might be particularly vulnerable to dementia at an earlier age than the general population because of vascular risk factors and traumatic brain injuries.4 These concerns highlight the need for effective dementia care programs at US Department of Veterans Affairs (VA) facilities.
The US health care system often does not adequately address the needs of patients with dementia and their caregivers.5 Dementia care requires specialized medical care among collaborating professionals and caregiver and psychosocial interventions and services. However, the US health care system is fragmented with different clinicians and services siloed into separate practices and most dementia care occurring in primary care settings.6 Primary care professionals (PCPs) often are uncomfortable diagnosing and managing dementia because of time constraints, lack of expertise and training, and inability to deal with the range of care needs.7 PCPs do not identify approximately 42% of their patients with dementia and, when recognized, do not adhere to dementia care guidelines and address caregiver needs.8-10 Research indicates that caregiver support improves dementia care by teaching behavioral management skills and caregiver coping strategies, allowing patients to stay at home and delay institutionalization.6,11,12 Clinicians underuse available resources and do not incorporate them in their patient care.10 These community services benefit patients and caregivers and significantly improve the overall quality of care.6
Memory clinics have emerged to address these deficiencies when managing dementia.13 The most effective memory clinics maximize the use of specialists with different expertise in dementia care, particularly integrated programs where disciplines function together rather than independently.1,5,14 Systematic reviews and meta-analyses have documented the effectiveness of collaborative care management programs.11,12,15 Integration of dementia care management is associated with earlier diagnosis and interventions, decreased functional and cognitive symptom severity, decreased or delayed institutionalization, improved quality of life for patients and caregivers, enhanced overall quality of care and cost-effectiveness, and better integration of community services.11,12,14-19 In these programs, designating a dementia care manager (DCM) as the patient’s advocate facilitates the integrated structure, increases the quality of care, helps caregivers, facilitates adherence to dementia practice guidelines, and prevents behavioral and psychological symptoms of dementia (BPSD).1,6,11,12,20,21
The best interprofessional model for dementia care might be the transdisciplinary model that includes a DCM. To meet the specific demands of dementia care, there must be a high level of interprofessional collaboration rather than multiple health care professionals (HCPs) delivering care in isolation—an approach that is time consuming and often difficult to implement.22 Whereas multidisciplinary care refers to delivery of parallel services and interdisciplinary care implies a joint formulation, transdisciplinary care aims to maximize integration of HCPs and their specific expertise and contributions through interactions and discussions that deliver focused input to the lead physician. The transdisciplinary model addresses needs that often are missed and can minimize disparities in the quality of dementia care.23 A DCM is an integral part of our program, facilitating understanding and implementation of the final care plan and providing long-term follow-up and care. We outline a conference-centered transdisciplinary dementia care model with a social worker as DCM (SW-DCM) at our VA medical center.
Program Description
In 2020, the VA Greater Los Angeles Healthcare System (VAGLAHS) in California established a multispecialty clinic dedicated to evaluation and treatment of veterans with memory and neurocognitive disorders and to provide support for their caregivers and families. With the agreement of leadership in mental health, neurology, and geriatrics services on the importance of collaboration for dementia care, the psychiatry and neurology services created a joint Memory and Neurobehavior Clinic, which completed its first 2 years of operation as a full-day program. In recent months, the clinic has scheduled 24 veterans per day, approximately 50% new evaluations and 50% follow-up patients, with wait times of < 2 months. There is a mean of 12 intake or lead physicians who could attend sessions in the morning, afternoon, or both. The general clinic flow consists of a 2-hour intake evaluation of new referrals by the lead physician followed by a clinic conference with transdisciplinary discussion. The DCM then follows up with the veteran/caregiver presenting a final care plan individualized to the veterans, caregivers, and families.
The Memory and Neurobehavior team includes behavioral neurologists, geriatric psychiatrists, neuropsychologists, geriatric fellows, advanced clinical nurses, and social workers who function as the DCM (Table 1).
Procedures
Before the office visit, the coordinating geriatric psychiatrist triages veterans to neurology, psychiatry, or geriatric physicians based on the clinical presentation, history of neurologic signs or symptoms, BPSD or psychiatric history, functional decline, or comorbid medical illnesses. Although veterans often have overlapping concerns, the triage process aims to coordinate the intake evaluations with the most indicated and available specialist with the intention to notify the other specialists during the transdisciplinary conference.
Referrals to the program occur from many sources, notably from primary care (70.8%), mental health (16.7%), and specialty clinics (12.5%). The clinic also receives referrals from the affiliated Veterans Cognitive Assessment and Management Program, which provides dementia evaluation and support via telehealth screening. This VAGLAHS program services a diverse population of veterans: 87% male; 43% aged > 65 years (75% in our clinic); 51% non-Hispanic White; 19% non-Hispanic African American; 16% Hispanic; 4% Asian; and 1% Native American. This population receives care at regional VA medical centers and community-based outpatient clinics over a wide geographic service area.
The initial standardized assessments by intake or lead physicians includes mental status screening with the Montreal Cognitive Assessment (with certified clinicians), the Neurobehavioral Status Examination for a more detailed assessment of cognitive domains, the Columbia-Suicide Severity Rating Scale, the Patient Health Questionnaire for depression screening, and assessment for impairments in instrumental or basic activities of daily living. This initial evaluation aims to apply clinical guidelines and diagnostic criteria for the differential diagnosis of neurocognitive disorders, determine eligibility for cognitive-enhancing medications and techniques, assess for BPSD and the need for nonpharmacologic or pharmacologic interventions, determine functional status, and evaluate the need for supervision, safety concerns, and evidence of neglect or abuse.
As part of its mission, the clinic is charged with implementing the VA Dementia System of Care (DSOC). The stated goals of the DSOC are to provide individualized person-centered dementia care to help veterans experiencing dementia and their caregivers maintain a positive and optimal quality of life and create an environment where VA medical center staff understand the health care needs of veterans with dementia and their caregivers’ role. As part of this initiative, the clinic includes (1) coordination of care through a SW-DCM; (2)
Transdisciplinary Conference
Clinic conferences are held after the veterans are seen. Staff gather to discuss the patient and review management. All team members are present, as well as the head of the clinical clerical staff who can facilitate appointments, make lobby and wait times more bearable for our patients and caregivers, and help manage emergencies. Although this is an in-person conference, the COVID-19 pandemic has allowed us to include staff who screen at remote sites via videoconferencing, similar to other VA programs.24 The Memory and Neurobehavior Clinic has two ≤ 90-minute conferences daily. The lead physicians and their senior attendings present the new intake evaluations (4-6 at each conference session) with a preliminary formulation and questions for discussion. The moderator solicits contributions from the different disciplines, going from one to the next and recording their responses for each veteran. Further specialists are available for consultation through the conference mechanism if necessary. The final assessment is reviewed, a diagnosis is established, and a tailored, individualized care plan for adjusting or optimizing the veteran’s care is presented to the lead physician who makes the final determination. At the close of the conference, the team’s discussion is recorded along with the lead physician’s original detailed intake evaluation. Currently, the records go into the Computerized Patient Record System, but we are making plans to transition to Cerner as it is implemented.
During the discussion, team members review several areas of consideration. If there is neuroimaging, neurologists review the images projected on a large computer screen. Team members also will assess for the need to obtain biomarker studies, such as blood, cerebrospinal fluid, or positron emission tomography. Psychiatrists could review management of BPSD and use of psychotropic agents, and neuropsychologists might consider the need for more precise cognitive testing and whether a capacity assessment is indicated. Social work might bring up the need for a durable power of attorney as well as applicable caregiver and community resources. Geriatric medicine and nursing could provide input into medical management and care and the ability of veterans and caregivers to follow the prescribed regimen. Further areas of discussion include driving safety and restrictions on driving (as required in California) and the presence of guns in the home. Finally, brief education is provided in short 10-to-15-minute lectures covering pertinent topics so staff remain up-to-date in this changing field.
Postconference Continuity
After the conference, the SW-DCM continues to provide support throughout the disease course, helping veterans and their caregivers understand and follow through on the team’s recommendations. The SW-DCM, who is experienced and trained in case management, forms an ongoing relationship with the veterans and their caregivers and remains an advocate for their care. The SW-DCM communicates the final plan by phone and, when necessary, requests the lead physician to call to clarify any poorly understood or technical aspects of the care plan. About 50% of our veterans—primarily those who do not have a neurocognitive disorder or have mild cognitive impairment—return to their PCPs with our care plan consultation; about 25% are already enrolled in geriatric and other programs with long-term follow-up. The assigned SW-DCM follows up with the remaining veterans and caregivers regularly by phone, facilitates communication with other team members, and endeavors to assure postvisit continuity of care and support during advancing stages of the disease. In addition, the SW-DCM can provide supportive counseling and psychotherapy for stressed caregivers, refer to support groups and cognitive rehabilitation programs, and help develop long-term goals and consideration for supervised living environments. The nurse specialist participates with follow-up calls regarding medications and scheduled tests and appointments, clearing up confusion about instructions, avoiding medication errors, and providing education in dementia care. Both social worker and nurse are present throughout the week, reachable by phone, and, in turn, able to contact the clinic physicians for veterans’ needs.
Discussion
Because of the heterogenous medical and psychosocial needs of veterans with dementia and their caregivers, a transdisciplinary team with a dedicated DCM might offer the most effective and efficient model for dementia care. We present a transdisciplinary program that incorporates dementia specialists in a single evaluation by maximizing their time through a conference-centered program. Our program involves neurologists, psychiatrists, geriatricians, psychologists, nurses, and social workers collaborating and communicating to enact effective dementia care. It further meets the goals of the VA-DSOC in implementing individualized patient and caregiver care.
This transdisciplinary model addresses a number of issues, starting with the differential diagnosis of underlying neurologic conditions. Within the transdisciplinary team, the neurologist can provide specific insights into any neurologic findings and illnesses, such as Alzheimer disease and other neurodegenerative dementias, vascular dementia syndromes, normal pressure hydrocephalus, Creutzfeldt-Jakob disease, neurosyphilis, and others. Most veterans with dementia experience BPSD at some point during of their illness. The psychiatrists on the transdisciplinary team can maximize management of BPSD with nonpharmacologic interventions and the fewest and least aversive psychoactive medications. Our program also addresses the need for more precise cognitive evaluation. Neuropsychologists are present and available for administrating neuropsychologic tests and interpreting cognitive performance and any earlier neuropsychologic testing. This model also cares for the caregivers and assesses their needs. The social worker—as well as other members of the team—can provide caregivers with strategies for coping with disruptive and other behaviors related to dementia, counsel them on how to manage the veteran’s functional decline, and aid in establishing a safe living space. Because the social worker serves as a DCM, these coping and adjustment questions occupy significant clinical attention between appointments. This transdisciplinary model places the patient’s illness in the context of their functional status, diagnoses, and medications. The team geriatrician and the nurse specialist are indispensable resources. The clinic conference provides a teaching venue for staff and trainees and a mechanism to discuss new developments in dementia care, such as the increasing need to assess individuals with mild cognitive impairment.25 This model depends on the DCM’s invaluable role in ensuring implementation of the dementia care plan and continuity of care.
Conclusions
We describe effective dementia care with a transdisciplinary team in a conference setting and with the participation of a dedicated DCM.5 To date, this program appears to be an efficient, sustainable application of the limited resources allocated to dementia care. Nevertheless, we are collecting data to compare with performance measures, track use, and assess the programs effects on continuity of care. We look forward to presenting metrics from our program that show improvement in the health care for veterans experiencing a devastating and increasingly common disorder.
1. 2022 Alzheimer’s disease facts and figures. Alzheimers Dement. 2022;18(4):700-789. doi:10.1002/alz.12638
2. National Center for Veterans Analysis and Statistics. Profile of veterans: 2016. Accessed October 12, 2022. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2016.pdf
3. Chodosh J, Sultzer DL, Lee ML, et al. Memory impairment among primary care veterans. Aging Ment Health. 2007;11(4):444-450. doi:10.1080/13607860601086272
4. Kennedy E, Panahi S, Stewart IJ, et al. Traumatic brain injury and early onset dementia in post 9-11 veterans. Brain Inj. 2022;36(5):620-627. doi:10.1080/02699052.2022.20338465. Heintz H, Monette P, Epstein-Lubow G, Smith L, Rowlett S, Forester BP. Emerging collaborative care models for dementia care in the primary care setting: a narrative review. Am J Geriatr Psychiatry. 2020;28(3):320-330. doi:10.1016/j.jagp.2019.07.015
6. Reuben DB, Evertson LC, Wenger NS, et al. The University of California at Los Angeles Alzheimer’s and Dementia Care program for comprehensive, coordinated, patient-centered care: preliminary data. J Am Geriatr Soc. 2013;61(12):2214-2218. doi:10.1111/jgs.12562
7. Apesoa-Varano EC, Barker JC, Hinton L. Curing and caring: the work of primary care physicians with dementia patients. Qual Health Res. 2011;21(11):1469-1483. doi:10.1177/1049732311412788
8. Creavin ST, Noel-Storr AH, Langdon RJ, et al. Clinical judgement by primary care physicians for the diagnosis of all-cause dementia or cognitive impairment in symptomatic people. Cochrane Database Syst Rev. 2022;6:CD012558. doi:10.1002/14651858.CD012558.pub2
9. Sivananthan SN, Puyat JH, McGrail KM. Variations in self-reported practice of physicians providing clinical care to individuals with dementia: a systematic review. J Am Geriatr Soc. 2013;61(8):1277-1285. doi:10.1111/jgs.12368
10. Rosen CS, Chow HC, Greenbaum MA, et al. How well are clinicians following dementia practice guidelines? Alzheimer Dis Assoc Disord. 2002;16(1):15-23. doi:10.1097/00002093-200201000-00003
11. Reilly S, Miranda-Castillo C, Malouf R, et al. Case management approaches to home support for people with dementia. Cochrane Database Syst Rev. 2015;1:CD008345. doi:10.1002/14651858.CD008345.pub2
12. Tam-Tham H, Cepoiu-Martin M, Ronksley PE, Maxwell CJ, Hemmelgarn BR. Dementia case management and risk of long-term care placement: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2013;28(9):889-902. doi:10.1002/gps.3906
13. Jolley D, Benbow SM, Grizzell M. Memory clinics. Postgrad Med J. 2006;82(965):199-206. doi:10.1136/pgmj.2005.040592
14. Muhlichen F, Michalowsky B, Radke A, et al. Tasks and activities of an effective collaborative dementia care management program in German primary care. J Alzheimers Dis. 2022;87(4):1615-1625. doi:10.3233/JAD-215656
15. Somme D, Trouve H, Drame M, Gagnon D, Couturier Y, Saint-Jean O. Analysis of case management programs for patients with dementia: a systematic review. Alzheimers Dement. 2012;8(5):426-436. doi:10.1016/j.jalz.2011.06.004
16. Ramakers IH, Verhey FR. Development of memory clinics in the Netherlands: 1998 to 2009. Aging Ment Health. 2011;15(1):34-39. doi:10.1080/13607863.2010.519321
17. LaMantia MA, Alder CA, Callahan CM, et al. The aging brain care medical home: preliminary data. J Am Geriatr Soc. 2015;63(6):1209-1213. doi:10.1111/jgs.13447
18. Rubinsztein JS, van Rensburg MJ, Al-Salihy Z, et al. A memory clinic v. traditional community mental health team service: comparison of costs and quality. BJPsych Bull. 2015;39(1):6-11. doi:10.1192/pb.bp.113.044263
19. Lee L, Hillier LM, Harvey D. Integrating community services into primary care: improving the quality of dementia care. Neurodegener Dis Manag. 2014;4(1):11-21. doi:10.2217/nmt.13.72
20. Bass DM, Judge KS, Snow AL, et al. Caregiver outcomes of partners in dementia care: effect of a care coordination program for veterans with dementia and their family members and friends. J Am Geriatr Soc. 2013;61(8):1377-1386. doi:10.1111/jgs.12362
21. Callahan CM, Boustani MA, Unverzagt FW, et al. Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial. JAMA. 2006;295(18):2148-2157. doi:10.1001/jama.295.18.2148
22. Leggett A, Connell C, Dubin L, et al. Dementia care across a tertiary care health system: what exists now and what needs to change. J Am Med Dir Assoc. 2019;20(10):1307-12 e1. doi:10.1016/j.jamda.2019.04.006
23. Brown AF, Vassar SD, Connor KI, Vickrey BG. Collaborative care management reduces disparities in dementia care quality for caregivers with less education. J Am Geriatr Soc. 2013;61(2):243-251. doi:10.1111/jgs.12079
24. Powers BB, Homer MC, Morone N, Edmonds N, Rossi MI. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
25. Galvin JE, Aisen P, Langbaum JB, et al. Early stages of Alzheimer’s Disease: evolving the care team for optimal patient management. Front Neurol. 2020;11:592302. doi:10.3389/fneur.2020.592302
1. 2022 Alzheimer’s disease facts and figures. Alzheimers Dement. 2022;18(4):700-789. doi:10.1002/alz.12638
2. National Center for Veterans Analysis and Statistics. Profile of veterans: 2016. Accessed October 12, 2022. https://www.va.gov/vetdata/docs/SpecialReports/Profile_of_Veterans_2016.pdf
3. Chodosh J, Sultzer DL, Lee ML, et al. Memory impairment among primary care veterans. Aging Ment Health. 2007;11(4):444-450. doi:10.1080/13607860601086272
4. Kennedy E, Panahi S, Stewart IJ, et al. Traumatic brain injury and early onset dementia in post 9-11 veterans. Brain Inj. 2022;36(5):620-627. doi:10.1080/02699052.2022.20338465. Heintz H, Monette P, Epstein-Lubow G, Smith L, Rowlett S, Forester BP. Emerging collaborative care models for dementia care in the primary care setting: a narrative review. Am J Geriatr Psychiatry. 2020;28(3):320-330. doi:10.1016/j.jagp.2019.07.015
6. Reuben DB, Evertson LC, Wenger NS, et al. The University of California at Los Angeles Alzheimer’s and Dementia Care program for comprehensive, coordinated, patient-centered care: preliminary data. J Am Geriatr Soc. 2013;61(12):2214-2218. doi:10.1111/jgs.12562
7. Apesoa-Varano EC, Barker JC, Hinton L. Curing and caring: the work of primary care physicians with dementia patients. Qual Health Res. 2011;21(11):1469-1483. doi:10.1177/1049732311412788
8. Creavin ST, Noel-Storr AH, Langdon RJ, et al. Clinical judgement by primary care physicians for the diagnosis of all-cause dementia or cognitive impairment in symptomatic people. Cochrane Database Syst Rev. 2022;6:CD012558. doi:10.1002/14651858.CD012558.pub2
9. Sivananthan SN, Puyat JH, McGrail KM. Variations in self-reported practice of physicians providing clinical care to individuals with dementia: a systematic review. J Am Geriatr Soc. 2013;61(8):1277-1285. doi:10.1111/jgs.12368
10. Rosen CS, Chow HC, Greenbaum MA, et al. How well are clinicians following dementia practice guidelines? Alzheimer Dis Assoc Disord. 2002;16(1):15-23. doi:10.1097/00002093-200201000-00003
11. Reilly S, Miranda-Castillo C, Malouf R, et al. Case management approaches to home support for people with dementia. Cochrane Database Syst Rev. 2015;1:CD008345. doi:10.1002/14651858.CD008345.pub2
12. Tam-Tham H, Cepoiu-Martin M, Ronksley PE, Maxwell CJ, Hemmelgarn BR. Dementia case management and risk of long-term care placement: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2013;28(9):889-902. doi:10.1002/gps.3906
13. Jolley D, Benbow SM, Grizzell M. Memory clinics. Postgrad Med J. 2006;82(965):199-206. doi:10.1136/pgmj.2005.040592
14. Muhlichen F, Michalowsky B, Radke A, et al. Tasks and activities of an effective collaborative dementia care management program in German primary care. J Alzheimers Dis. 2022;87(4):1615-1625. doi:10.3233/JAD-215656
15. Somme D, Trouve H, Drame M, Gagnon D, Couturier Y, Saint-Jean O. Analysis of case management programs for patients with dementia: a systematic review. Alzheimers Dement. 2012;8(5):426-436. doi:10.1016/j.jalz.2011.06.004
16. Ramakers IH, Verhey FR. Development of memory clinics in the Netherlands: 1998 to 2009. Aging Ment Health. 2011;15(1):34-39. doi:10.1080/13607863.2010.519321
17. LaMantia MA, Alder CA, Callahan CM, et al. The aging brain care medical home: preliminary data. J Am Geriatr Soc. 2015;63(6):1209-1213. doi:10.1111/jgs.13447
18. Rubinsztein JS, van Rensburg MJ, Al-Salihy Z, et al. A memory clinic v. traditional community mental health team service: comparison of costs and quality. BJPsych Bull. 2015;39(1):6-11. doi:10.1192/pb.bp.113.044263
19. Lee L, Hillier LM, Harvey D. Integrating community services into primary care: improving the quality of dementia care. Neurodegener Dis Manag. 2014;4(1):11-21. doi:10.2217/nmt.13.72
20. Bass DM, Judge KS, Snow AL, et al. Caregiver outcomes of partners in dementia care: effect of a care coordination program for veterans with dementia and their family members and friends. J Am Geriatr Soc. 2013;61(8):1377-1386. doi:10.1111/jgs.12362
21. Callahan CM, Boustani MA, Unverzagt FW, et al. Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial. JAMA. 2006;295(18):2148-2157. doi:10.1001/jama.295.18.2148
22. Leggett A, Connell C, Dubin L, et al. Dementia care across a tertiary care health system: what exists now and what needs to change. J Am Med Dir Assoc. 2019;20(10):1307-12 e1. doi:10.1016/j.jamda.2019.04.006
23. Brown AF, Vassar SD, Connor KI, Vickrey BG. Collaborative care management reduces disparities in dementia care quality for caregivers with less education. J Am Geriatr Soc. 2013;61(2):243-251. doi:10.1111/jgs.12079
24. Powers BB, Homer MC, Morone N, Edmonds N, Rossi MI. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
25. Galvin JE, Aisen P, Langbaum JB, et al. Early stages of Alzheimer’s Disease: evolving the care team for optimal patient management. Front Neurol. 2020;11:592302. doi:10.3389/fneur.2020.592302