User login
For MD-IQ use only
What’s lost, what’s saved
DDW is now history. While rejoicing that DDW happened (as opposed to when it couldn’t in 2020), the virtual format precluded all those hallway conversations, meetings with mentors and small group (after hour) discussions. This year, AGA saved substantial monies in travel costs. Of note, at Michigan Medicine, we track the miles patients did not have to travel because of our conversion to virtual care (currently about 30% of all ambulatory visits). To date, our “virtual first” protocol has saved over 24 million patient travel-miles since February 2020 (average of 62 miles per patient visit).

The pandemic forced rapid adoption of virtual care and alternative care delivery models. As patients adapted to telehealth, businesses saw opportunities. Health systems have begun to downsize their brick-and-mortar footprints for both clinical and office space. Hospital at Home models are developing as viable alternatives to inpatient care using a hybrid system of on-site nurses and remote physician supervision.
Digital health start-ups are developing rapidly, and equity funding for digital health companies has reached an all-time high of $26.5 billion in 2020. Multiple companies went public through traditional initial public offerings or special purpose acquisition companies. Sameer Berry, MD, recently collected an inventory of major GI digital health companies counted at least 16 with more appearing each month. These companies focus on management of a single condition (for example IBS or Celiac) or full-service virtual GI care that includes “at-risk” financial contracts

I am delighted to announce that Megan Adams, MD, JD, MSc, has been chosen to be the fourth editor in chief of GI & Hepatology News. She and her team will transition into editorial control during Fall 2021. I have known Megan since meeting her at an AGA young faculty function almost 10 years ago. She is extremely talented and knowledgeable about gastroenterology from a variety of viewpoints. She has recruited a strong and dedicated editorial board.
I have enjoyed the last 5 years leading the current board as we have brought breaking news to the GI community. I wish to publicly thank our editorial board and the Frontline staff who monthly publish AGA’s official newspaper.
John I. Allen, MD, MBA, AGAF
Editor in Chief
DDW is now history. While rejoicing that DDW happened (as opposed to when it couldn’t in 2020), the virtual format precluded all those hallway conversations, meetings with mentors and small group (after hour) discussions. This year, AGA saved substantial monies in travel costs. Of note, at Michigan Medicine, we track the miles patients did not have to travel because of our conversion to virtual care (currently about 30% of all ambulatory visits). To date, our “virtual first” protocol has saved over 24 million patient travel-miles since February 2020 (average of 62 miles per patient visit).
The pandemic forced rapid adoption of virtual care and alternative care delivery models. As patients adapted to telehealth, businesses saw opportunities. Health systems have begun to downsize their brick-and-mortar footprints for both clinical and office space. Hospital at Home models are developing as viable alternatives to inpatient care using a hybrid system of on-site nurses and remote physician supervision.
Digital health start-ups are developing rapidly, and equity funding for digital health companies has reached an all-time high of $26.5 billion in 2020. Multiple companies went public through traditional initial public offerings or special purpose acquisition companies. Sameer Berry, MD, recently collected an inventory of major GI digital health companies counted at least 16 with more appearing each month. These companies focus on management of a single condition (for example IBS or Celiac) or full-service virtual GI care that includes “at-risk” financial contracts
I am delighted to announce that Megan Adams, MD, JD, MSc, has been chosen to be the fourth editor in chief of GI & Hepatology News. She and her team will transition into editorial control during Fall 2021. I have known Megan since meeting her at an AGA young faculty function almost 10 years ago. She is extremely talented and knowledgeable about gastroenterology from a variety of viewpoints. She has recruited a strong and dedicated editorial board.
I have enjoyed the last 5 years leading the current board as we have brought breaking news to the GI community. I wish to publicly thank our editorial board and the Frontline staff who monthly publish AGA’s official newspaper.
John I. Allen, MD, MBA, AGAF
Editor in Chief
DDW is now history. While rejoicing that DDW happened (as opposed to when it couldn’t in 2020), the virtual format precluded all those hallway conversations, meetings with mentors and small group (after hour) discussions. This year, AGA saved substantial monies in travel costs. Of note, at Michigan Medicine, we track the miles patients did not have to travel because of our conversion to virtual care (currently about 30% of all ambulatory visits). To date, our “virtual first” protocol has saved over 24 million patient travel-miles since February 2020 (average of 62 miles per patient visit).
The pandemic forced rapid adoption of virtual care and alternative care delivery models. As patients adapted to telehealth, businesses saw opportunities. Health systems have begun to downsize their brick-and-mortar footprints for both clinical and office space. Hospital at Home models are developing as viable alternatives to inpatient care using a hybrid system of on-site nurses and remote physician supervision.
Digital health start-ups are developing rapidly, and equity funding for digital health companies has reached an all-time high of $26.5 billion in 2020. Multiple companies went public through traditional initial public offerings or special purpose acquisition companies. Sameer Berry, MD, recently collected an inventory of major GI digital health companies counted at least 16 with more appearing each month. These companies focus on management of a single condition (for example IBS or Celiac) or full-service virtual GI care that includes “at-risk” financial contracts
I am delighted to announce that Megan Adams, MD, JD, MSc, has been chosen to be the fourth editor in chief of GI & Hepatology News. She and her team will transition into editorial control during Fall 2021. I have known Megan since meeting her at an AGA young faculty function almost 10 years ago. She is extremely talented and knowledgeable about gastroenterology from a variety of viewpoints. She has recruited a strong and dedicated editorial board.
I have enjoyed the last 5 years leading the current board as we have brought breaking news to the GI community. I wish to publicly thank our editorial board and the Frontline staff who monthly publish AGA’s official newspaper.
John I. Allen, MD, MBA, AGAF
Editor in Chief

Question 2
Q2. Correct answer: D. Glucose hydrogen breath test.
Rationale
The etiology of small intestinal bacterial overgrowth (SIBO) is complex but may include an issue with altered antibacterial defense mechanisms, such as achlorhydria from atrophic gastritis. SIBO can be diagnosed by a glucose hydrogen breath test, and therefore, it is the best next step in the management of this patient's symptoms given the history of atrophic gastritis. Chromogranin A testing and video capsule endoscopy are used in the diagnostic evaluation of suspected carcinoid syndrome and inflammatory bowel disease, respectively, and may be indicated in the subsequent evaluation of this patient's symptoms. In addition, both of these diagnoses are unlikely to cause intermittent diarrhea. Eluxadoline is an agent that combines a mu-opioid receptor agonist and a delta-opioid receptor antagonist and is indicated for the treatment of irritable bowel syndrome - diarrhea predominant (IBS-D). The diagnosis of IBS requires the presence of abdominal pain and is unlikely in an elderly patient with new onset of symptoms; therefore, this is not the diagnosis in this patient's case.
Reference
Jan Bures et al. World J Gastroenterol. 2010 Jun 28;16(24):2978-90.
Q2. Correct answer: D. Glucose hydrogen breath test.
Rationale
The etiology of small intestinal bacterial overgrowth (SIBO) is complex but may include an issue with altered antibacterial defense mechanisms, such as achlorhydria from atrophic gastritis. SIBO can be diagnosed by a glucose hydrogen breath test, and therefore, it is the best next step in the management of this patient's symptoms given the history of atrophic gastritis. Chromogranin A testing and video capsule endoscopy are used in the diagnostic evaluation of suspected carcinoid syndrome and inflammatory bowel disease, respectively, and may be indicated in the subsequent evaluation of this patient's symptoms. In addition, both of these diagnoses are unlikely to cause intermittent diarrhea. Eluxadoline is an agent that combines a mu-opioid receptor agonist and a delta-opioid receptor antagonist and is indicated for the treatment of irritable bowel syndrome - diarrhea predominant (IBS-D). The diagnosis of IBS requires the presence of abdominal pain and is unlikely in an elderly patient with new onset of symptoms; therefore, this is not the diagnosis in this patient's case.
Reference
Jan Bures et al. World J Gastroenterol. 2010 Jun 28;16(24):2978-90.
Q2. Correct answer: D. Glucose hydrogen breath test.
Rationale
The etiology of small intestinal bacterial overgrowth (SIBO) is complex but may include an issue with altered antibacterial defense mechanisms, such as achlorhydria from atrophic gastritis. SIBO can be diagnosed by a glucose hydrogen breath test, and therefore, it is the best next step in the management of this patient's symptoms given the history of atrophic gastritis. Chromogranin A testing and video capsule endoscopy are used in the diagnostic evaluation of suspected carcinoid syndrome and inflammatory bowel disease, respectively, and may be indicated in the subsequent evaluation of this patient's symptoms. In addition, both of these diagnoses are unlikely to cause intermittent diarrhea. Eluxadoline is an agent that combines a mu-opioid receptor agonist and a delta-opioid receptor antagonist and is indicated for the treatment of irritable bowel syndrome - diarrhea predominant (IBS-D). The diagnosis of IBS requires the presence of abdominal pain and is unlikely in an elderly patient with new onset of symptoms; therefore, this is not the diagnosis in this patient's case.
Reference
Jan Bures et al. World J Gastroenterol. 2010 Jun 28;16(24):2978-90.
A 66-year-old woman with a history of atrophic gastritis presents for evaluation of intermittent diarrhea. She denies abdominal pain, weight loss, GI bleeding or a family history of colorectal neoplasia or IBD. Physical exam is normal. Labs including thyroid function testing, celiac screen and CRP are normal. A colonoscopy with random colon biopsies is normal.
Question 1
Q1. Correct answer: B. Expulsion of water-filled balloon in 3 minutes.
Rationale
The balloon expulsion test is highly suggestive of dyssynergia. A balloon expulsion time of greater than 2 minutes is abnormal. An absent RAIR can be seen in Hirschsprung's disease or megarectum. Defecation index equals maximum rectal pressure during attempted defecation divided by minimum anal residual pressure during attempted defecation. A normal defecation index is greater than 1.5. Decreased anal sphincter pressure during simulated defecation is normal and therefore not consistent with dyssynergic defecation.
References
Wald A et al. Am J Gastroenterol. 2014 Aug;109(8):1141-57.
Bharucha AE et al. Gastroenterology. 2013 Jan;144(1):218-38.
Q1. Correct answer: B. Expulsion of water-filled balloon in 3 minutes.
Rationale
The balloon expulsion test is highly suggestive of dyssynergia. A balloon expulsion time of greater than 2 minutes is abnormal. An absent RAIR can be seen in Hirschsprung's disease or megarectum. Defecation index equals maximum rectal pressure during attempted defecation divided by minimum anal residual pressure during attempted defecation. A normal defecation index is greater than 1.5. Decreased anal sphincter pressure during simulated defecation is normal and therefore not consistent with dyssynergic defecation.
References
Wald A et al. Am J Gastroenterol. 2014 Aug;109(8):1141-57.
Bharucha AE et al. Gastroenterology. 2013 Jan;144(1):218-38.
Q1. Correct answer: B. Expulsion of water-filled balloon in 3 minutes.
Rationale
The balloon expulsion test is highly suggestive of dyssynergia. A balloon expulsion time of greater than 2 minutes is abnormal. An absent RAIR can be seen in Hirschsprung's disease or megarectum. Defecation index equals maximum rectal pressure during attempted defecation divided by minimum anal residual pressure during attempted defecation. A normal defecation index is greater than 1.5. Decreased anal sphincter pressure during simulated defecation is normal and therefore not consistent with dyssynergic defecation.
References
Wald A et al. Am J Gastroenterol. 2014 Aug;109(8):1141-57.
Bharucha AE et al. Gastroenterology. 2013 Jan;144(1):218-38.
A 37-year-old woman with no significant past medical history presents for further evaluation of chronic constipation with straining. She denies significant abdominal pain, gastrointestinal bleeding, or weight loss. There is no family history of colorectal neoplasia or inflammatory bowel disease. She has not responded to many laxatives and undergoes anorectal manometry with balloon expulsion testing.
Hospitalist movers and shakers – May 2021
Rebecca Jaffe, MD, has been elevated to the permanent role of director of the division of hospital medicine at Thomas Jefferson University Hospital in Philadelphia. Dr. Jaffe has been the interim director since July 2020.

In the position, Dr. Jaffe will be responsible for leading an academic hospital medicine division that includes 36 faculty and 10 advanced-practice providers. She said her focus will be on developing physicians, advanced providers, and the inpatient practice model used while “educating the next generation of creative and compassionate clinicians.”
Dr. Jaffe is associate professor of medicine at Jefferson’s Sidney Kimmel Medical College and the hospital’s director of clinical learning environment improvement.
Christopher Freer, DO, recently was named the new senior vice president for emergency hospital medicine for RWJBarnabas Health (West Orange, N.J.). In a concurrent move, Maninder “Dolly” Abraham, MD, was named RWJBH’s chief of hospital medicine. The selections were made as RWJBH has become a direct employer for Envision Physician Services, a former hospital partner.
Dr. Freer has spent the past 5 years with RWJBH, where he has served as emergency services system director since 2015. He previously worked in leadership roles at Saint Barnabas Medical Center.
Dr. Abraham was previously medical director of Saint Barnabas’ hospitalist program, as well as a regional medical director with Envision during her 17 years of experience.
Sheetal Patel, MD, has been named the new regional medical director for Eagle Telemedicine (Cincinnati, Ohio), a physician-led company that provides telehospitalist services to hospitals around the country.
Dr. Patel will work closely with hospital administrators and medical directors to provide high-level telemedicine services, as well as devising processes and guidelines to guarantee streamlined care across Eagle’s facilities.
Dr. Patel has spent 4 years as a telehospitalist for Eagle, where she has been in charge of guiding on-site and remote staff members and providing training to new telehospitalists.
Timothy Crone, MD, MBA, has been elevated to the role of president of Cleveland Clinic Mercy Hospital (Canton, Ohio). The move comes as Cleveland Clinic recently added Mercy Medical Center as a full member of its health system.

Dr. Crone has served as chief medical officer at Cleveland Clinic Hillcrest Hospital in Cleveland since 2019. Previously, he was a medical director in enterprise business intelligence and analytics in medical operations at Cleveland Clinic’s main campus. He also was vice chairman of hospital medicine and has served as a staff hospitalist since 2010.
In addition to his role as president, Dr. Crone plans to work in patient care at Mercy Hospital.
Just prior to the start of 2021, Wake Forest Baptist Health (Winston-Salem, N.C.) established a “Hospitalist at Home” program with the goal of reducing the length of time patients spend in the hospital.
Hospitalist at Home was created as the COVID-19 pandemic threatened hospital capacity. Wakehealth’s innovative approach involves developing an at-home plan with each patient before they leave the facility. Patients include those with COVID-19 who are stable but require supplemental oxygen or have diseases that need intravenous medication administration.
At home, a Wakehealth paramedic visits the patient while a hospitalist communicates and reviews the patient’s care plan via smartphone, tablet, or computer. The visits continue until the patient’s hospital-related care is complete.
The Multicare Health System (Tacoma, Wash.) has bulked up its hospitalist program by partnering with nationwide, physician-led health care provider Sound Physicians. The goal is to provide health care management at a regional level instead of individually per hospital.
Sound Physicians, which already contracts to provide hospitalist services at two Multicare facilities in Washington, transitioned its services to three other facilities as of April 5, 2021.
Conemaugh Meyersdale Medical Center (Meyersdale, Pa.) has started a hospitalist program at its facility in Somerset County. The program will be led by nurse practitioners Zeke Feyock and Sarah Piscatello.
Rebecca Jaffe, MD, has been elevated to the permanent role of director of the division of hospital medicine at Thomas Jefferson University Hospital in Philadelphia. Dr. Jaffe has been the interim director since July 2020.
In the position, Dr. Jaffe will be responsible for leading an academic hospital medicine division that includes 36 faculty and 10 advanced-practice providers. She said her focus will be on developing physicians, advanced providers, and the inpatient practice model used while “educating the next generation of creative and compassionate clinicians.”
Dr. Jaffe is associate professor of medicine at Jefferson’s Sidney Kimmel Medical College and the hospital’s director of clinical learning environment improvement.
Christopher Freer, DO, recently was named the new senior vice president for emergency hospital medicine for RWJBarnabas Health (West Orange, N.J.). In a concurrent move, Maninder “Dolly” Abraham, MD, was named RWJBH’s chief of hospital medicine. The selections were made as RWJBH has become a direct employer for Envision Physician Services, a former hospital partner.
Dr. Freer has spent the past 5 years with RWJBH, where he has served as emergency services system director since 2015. He previously worked in leadership roles at Saint Barnabas Medical Center.
Dr. Abraham was previously medical director of Saint Barnabas’ hospitalist program, as well as a regional medical director with Envision during her 17 years of experience.
Sheetal Patel, MD, has been named the new regional medical director for Eagle Telemedicine (Cincinnati, Ohio), a physician-led company that provides telehospitalist services to hospitals around the country.
Dr. Patel will work closely with hospital administrators and medical directors to provide high-level telemedicine services, as well as devising processes and guidelines to guarantee streamlined care across Eagle’s facilities.
Dr. Patel has spent 4 years as a telehospitalist for Eagle, where she has been in charge of guiding on-site and remote staff members and providing training to new telehospitalists.
Timothy Crone, MD, MBA, has been elevated to the role of president of Cleveland Clinic Mercy Hospital (Canton, Ohio). The move comes as Cleveland Clinic recently added Mercy Medical Center as a full member of its health system.
Dr. Crone has served as chief medical officer at Cleveland Clinic Hillcrest Hospital in Cleveland since 2019. Previously, he was a medical director in enterprise business intelligence and analytics in medical operations at Cleveland Clinic’s main campus. He also was vice chairman of hospital medicine and has served as a staff hospitalist since 2010.
In addition to his role as president, Dr. Crone plans to work in patient care at Mercy Hospital.
Just prior to the start of 2021, Wake Forest Baptist Health (Winston-Salem, N.C.) established a “Hospitalist at Home” program with the goal of reducing the length of time patients spend in the hospital.
Hospitalist at Home was created as the COVID-19 pandemic threatened hospital capacity. Wakehealth’s innovative approach involves developing an at-home plan with each patient before they leave the facility. Patients include those with COVID-19 who are stable but require supplemental oxygen or have diseases that need intravenous medication administration.
At home, a Wakehealth paramedic visits the patient while a hospitalist communicates and reviews the patient’s care plan via smartphone, tablet, or computer. The visits continue until the patient’s hospital-related care is complete.
The Multicare Health System (Tacoma, Wash.) has bulked up its hospitalist program by partnering with nationwide, physician-led health care provider Sound Physicians. The goal is to provide health care management at a regional level instead of individually per hospital.
Sound Physicians, which already contracts to provide hospitalist services at two Multicare facilities in Washington, transitioned its services to three other facilities as of April 5, 2021.
Conemaugh Meyersdale Medical Center (Meyersdale, Pa.) has started a hospitalist program at its facility in Somerset County. The program will be led by nurse practitioners Zeke Feyock and Sarah Piscatello.
Rebecca Jaffe, MD, has been elevated to the permanent role of director of the division of hospital medicine at Thomas Jefferson University Hospital in Philadelphia. Dr. Jaffe has been the interim director since July 2020.
In the position, Dr. Jaffe will be responsible for leading an academic hospital medicine division that includes 36 faculty and 10 advanced-practice providers. She said her focus will be on developing physicians, advanced providers, and the inpatient practice model used while “educating the next generation of creative and compassionate clinicians.”
Dr. Jaffe is associate professor of medicine at Jefferson’s Sidney Kimmel Medical College and the hospital’s director of clinical learning environment improvement.
Christopher Freer, DO, recently was named the new senior vice president for emergency hospital medicine for RWJBarnabas Health (West Orange, N.J.). In a concurrent move, Maninder “Dolly” Abraham, MD, was named RWJBH’s chief of hospital medicine. The selections were made as RWJBH has become a direct employer for Envision Physician Services, a former hospital partner.
Dr. Freer has spent the past 5 years with RWJBH, where he has served as emergency services system director since 2015. He previously worked in leadership roles at Saint Barnabas Medical Center.
Dr. Abraham was previously medical director of Saint Barnabas’ hospitalist program, as well as a regional medical director with Envision during her 17 years of experience.
Sheetal Patel, MD, has been named the new regional medical director for Eagle Telemedicine (Cincinnati, Ohio), a physician-led company that provides telehospitalist services to hospitals around the country.
Dr. Patel will work closely with hospital administrators and medical directors to provide high-level telemedicine services, as well as devising processes and guidelines to guarantee streamlined care across Eagle’s facilities.
Dr. Patel has spent 4 years as a telehospitalist for Eagle, where she has been in charge of guiding on-site and remote staff members and providing training to new telehospitalists.
Timothy Crone, MD, MBA, has been elevated to the role of president of Cleveland Clinic Mercy Hospital (Canton, Ohio). The move comes as Cleveland Clinic recently added Mercy Medical Center as a full member of its health system.
Dr. Crone has served as chief medical officer at Cleveland Clinic Hillcrest Hospital in Cleveland since 2019. Previously, he was a medical director in enterprise business intelligence and analytics in medical operations at Cleveland Clinic’s main campus. He also was vice chairman of hospital medicine and has served as a staff hospitalist since 2010.
In addition to his role as president, Dr. Crone plans to work in patient care at Mercy Hospital.
Just prior to the start of 2021, Wake Forest Baptist Health (Winston-Salem, N.C.) established a “Hospitalist at Home” program with the goal of reducing the length of time patients spend in the hospital.
Hospitalist at Home was created as the COVID-19 pandemic threatened hospital capacity. Wakehealth’s innovative approach involves developing an at-home plan with each patient before they leave the facility. Patients include those with COVID-19 who are stable but require supplemental oxygen or have diseases that need intravenous medication administration.
At home, a Wakehealth paramedic visits the patient while a hospitalist communicates and reviews the patient’s care plan via smartphone, tablet, or computer. The visits continue until the patient’s hospital-related care is complete.
The Multicare Health System (Tacoma, Wash.) has bulked up its hospitalist program by partnering with nationwide, physician-led health care provider Sound Physicians. The goal is to provide health care management at a regional level instead of individually per hospital.
Sound Physicians, which already contracts to provide hospitalist services at two Multicare facilities in Washington, transitioned its services to three other facilities as of April 5, 2021.
Conemaugh Meyersdale Medical Center (Meyersdale, Pa.) has started a hospitalist program at its facility in Somerset County. The program will be led by nurse practitioners Zeke Feyock and Sarah Piscatello.
Benefit from cooling temps for cardiac arrest does not differ in randomized trial
The first randomized controlled trial to compare specific temperatures for therapeutic hypothermia in comatose survivors of out-of-hospital cardiac arrest showed no differences in major outcomes, according to a single-center, double-blind study.

In the CAPITAL-CHILL trial, cooling temperatures of 31° C and 34° C were compared to explore the hypothesis that a lower temperature would improve major outcomes, explained Michel Le May, MD.
No differences for the primary composite outcome of all-cause mortality or poor neurologic outcome at 180 days were observed, he reported at the annual scientific sessions of the American College of Cardiology.
The study was completed over a period of almost 7 years in patients presumed to have had an out-of-hospital cardiac arrest and who were unconscious when they reached a center affiliated with the Ottawa Heart Institute, where Dr. Le May directs the regional STEMI (ST-elevation myocardial infarction) program. The initial rhythm at the time of the cardiac arrest was not an entry criterion.
Of 389 patients enrolled, the intention-to-treat analysis included 184 randomized to a cooling temperature of 31° C group and 183 to a temperature of 34° C. The assigned target temperature, reached with an endovascular device, was known only by the managing nurses.
31° C and 34° C are equivalent
There was a small numerical disadvantage for the lower temperature assignment, but none reached statistical significance. This was true of the primary outcome (48.4% vs. 45.4% for the higher temperature) and its components of mortality (43.5% vs. 41.0%) and poor neurologic outcome (4.9% vs. 4.4%). Poor neurologic outcome was defined as a Disability Rating Scale score of greater than 5.
Deaths were most common in the early part of the 180-day follow-up in both arms. On a Kaplan-Meier survival graph, Dr. Le May showed curves that he characterized as “almost superimposable.”
There were no significant differences for any subgroup stratifications, such as age 75 years or older versus younger, males versus females, presence versus absence or an initial shockable rhythm, percutaneous coronary intervention (PCI) within 24 hours versus later, and STEMI versus non-STEMI. In these analyses, the higher temperature was associated with a potential trend for benefit among females and those with a shockable rhythm.
There was no signal for a difference in neurologic outcomes on the Disability Rating Scale or the Modified Rankin Scale. On the latter, for example, 46% of those in the 31° C group and 44% of these in the 34° C group had a score of four or greater at the end of follow-up.
The baseline characteristics of the two groups were similar. About 80% were male; the average age was roughly 62 years. More than 80% of the cardiac arrests were witnessed with CPR being administered by bystanders in nearly 70%. Nearly 40% had a STEMI.
Interventions were similar. Almost all patients underwent coronary angiography, of which nearly 60% received a percutaneous coronary intervention. More than 50% received a stent. The time from arrest to randomization was slightly longer in the 31° C group (228 vs. 204 minutes). The time to balloon inflation from arrival at the cardiac center was also slightly longer (73 vs. 60 minutes).
There was a trend for an increased rate of seizures in the 31° C group (12.5% vs. 7.1%; P = .08), but other secondary outcomes, including pneumonia (67.8% vs. 63.4%), renal replacement therapy (9.2% vs. 9.3%), and stroke (4.4% vs. 1.6%), were similar in the 31° C and 34° C groups, respectively.
Bleeding, whether measured by transfusion (19.6% vs. 22.4%) or TIMI major bleed (23.4% vs. 19.7%) were similar in the 31° C and 34° C groups, respectively. Thrombosis, whether measured by stent thrombosis (1.2% vs. 2.2%) or deep venous thrombosis (11.4% vs. 10.9%) were similar in these two groups, respectively.
The length of stay in the cardiac intensive care unit was significantly greater in the 31° C group (10 vs. 7 days; P = .004). Some of this increased length of stay can be attributed to the longer rewarming process required for the greater cooling, according to Dr. Le May, but he acknowledged that it is not clear this provides a full explanation.
More trials like CAPITAL-CHILL needed
The validity of these findings is supported by several strengths of the methodology, according to Jeanne E. Poole, MD, director of the arrhythmia service and electrophysiology laboratory, University of Washington, Seattle. This includes the reliance of an endovascular device, which can accelerate the time to the target temperature and assure the precision with which it is reached and maintained.
Dr. Poole did note that many of the primary and secondary measures, including the rates of stroke, seizures, and major bleeds, even though not significantly different, favored the higher temperature. The slightly longer door-to-balloon times might have been a factor. For the higher rate of pneumonia in the 31° C group, she questioned whether the longer period of ventilation linked to a longer period of rewarming might have been a factor.
However, Dr. Poole praised the CAPITAL-CHILL trial for drawing attention to a group of patients for whom survival rates remain “dismally low.” She indicated that these types of high-level trials are needed to look for strategies to improve outcomes.
Dr. Le May and Dr. Poole report no potential conflicts of interest.
The first randomized controlled trial to compare specific temperatures for therapeutic hypothermia in comatose survivors of out-of-hospital cardiac arrest showed no differences in major outcomes, according to a single-center, double-blind study.
In the CAPITAL-CHILL trial, cooling temperatures of 31° C and 34° C were compared to explore the hypothesis that a lower temperature would improve major outcomes, explained Michel Le May, MD.
No differences for the primary composite outcome of all-cause mortality or poor neurologic outcome at 180 days were observed, he reported at the annual scientific sessions of the American College of Cardiology.
The study was completed over a period of almost 7 years in patients presumed to have had an out-of-hospital cardiac arrest and who were unconscious when they reached a center affiliated with the Ottawa Heart Institute, where Dr. Le May directs the regional STEMI (ST-elevation myocardial infarction) program. The initial rhythm at the time of the cardiac arrest was not an entry criterion.
Of 389 patients enrolled, the intention-to-treat analysis included 184 randomized to a cooling temperature of 31° C group and 183 to a temperature of 34° C. The assigned target temperature, reached with an endovascular device, was known only by the managing nurses.
31° C and 34° C are equivalent
There was a small numerical disadvantage for the lower temperature assignment, but none reached statistical significance. This was true of the primary outcome (48.4% vs. 45.4% for the higher temperature) and its components of mortality (43.5% vs. 41.0%) and poor neurologic outcome (4.9% vs. 4.4%). Poor neurologic outcome was defined as a Disability Rating Scale score of greater than 5.
Deaths were most common in the early part of the 180-day follow-up in both arms. On a Kaplan-Meier survival graph, Dr. Le May showed curves that he characterized as “almost superimposable.”
There were no significant differences for any subgroup stratifications, such as age 75 years or older versus younger, males versus females, presence versus absence or an initial shockable rhythm, percutaneous coronary intervention (PCI) within 24 hours versus later, and STEMI versus non-STEMI. In these analyses, the higher temperature was associated with a potential trend for benefit among females and those with a shockable rhythm.
There was no signal for a difference in neurologic outcomes on the Disability Rating Scale or the Modified Rankin Scale. On the latter, for example, 46% of those in the 31° C group and 44% of these in the 34° C group had a score of four or greater at the end of follow-up.
The baseline characteristics of the two groups were similar. About 80% were male; the average age was roughly 62 years. More than 80% of the cardiac arrests were witnessed with CPR being administered by bystanders in nearly 70%. Nearly 40% had a STEMI.
Interventions were similar. Almost all patients underwent coronary angiography, of which nearly 60% received a percutaneous coronary intervention. More than 50% received a stent. The time from arrest to randomization was slightly longer in the 31° C group (228 vs. 204 minutes). The time to balloon inflation from arrival at the cardiac center was also slightly longer (73 vs. 60 minutes).
There was a trend for an increased rate of seizures in the 31° C group (12.5% vs. 7.1%; P = .08), but other secondary outcomes, including pneumonia (67.8% vs. 63.4%), renal replacement therapy (9.2% vs. 9.3%), and stroke (4.4% vs. 1.6%), were similar in the 31° C and 34° C groups, respectively.
Bleeding, whether measured by transfusion (19.6% vs. 22.4%) or TIMI major bleed (23.4% vs. 19.7%) were similar in the 31° C and 34° C groups, respectively. Thrombosis, whether measured by stent thrombosis (1.2% vs. 2.2%) or deep venous thrombosis (11.4% vs. 10.9%) were similar in these two groups, respectively.
The length of stay in the cardiac intensive care unit was significantly greater in the 31° C group (10 vs. 7 days; P = .004). Some of this increased length of stay can be attributed to the longer rewarming process required for the greater cooling, according to Dr. Le May, but he acknowledged that it is not clear this provides a full explanation.
More trials like CAPITAL-CHILL needed
The validity of these findings is supported by several strengths of the methodology, according to Jeanne E. Poole, MD, director of the arrhythmia service and electrophysiology laboratory, University of Washington, Seattle. This includes the reliance of an endovascular device, which can accelerate the time to the target temperature and assure the precision with which it is reached and maintained.
Dr. Poole did note that many of the primary and secondary measures, including the rates of stroke, seizures, and major bleeds, even though not significantly different, favored the higher temperature. The slightly longer door-to-balloon times might have been a factor. For the higher rate of pneumonia in the 31° C group, she questioned whether the longer period of ventilation linked to a longer period of rewarming might have been a factor.
However, Dr. Poole praised the CAPITAL-CHILL trial for drawing attention to a group of patients for whom survival rates remain “dismally low.” She indicated that these types of high-level trials are needed to look for strategies to improve outcomes.
Dr. Le May and Dr. Poole report no potential conflicts of interest.
The first randomized controlled trial to compare specific temperatures for therapeutic hypothermia in comatose survivors of out-of-hospital cardiac arrest showed no differences in major outcomes, according to a single-center, double-blind study.
In the CAPITAL-CHILL trial, cooling temperatures of 31° C and 34° C were compared to explore the hypothesis that a lower temperature would improve major outcomes, explained Michel Le May, MD.
No differences for the primary composite outcome of all-cause mortality or poor neurologic outcome at 180 days were observed, he reported at the annual scientific sessions of the American College of Cardiology.
The study was completed over a period of almost 7 years in patients presumed to have had an out-of-hospital cardiac arrest and who were unconscious when they reached a center affiliated with the Ottawa Heart Institute, where Dr. Le May directs the regional STEMI (ST-elevation myocardial infarction) program. The initial rhythm at the time of the cardiac arrest was not an entry criterion.
Of 389 patients enrolled, the intention-to-treat analysis included 184 randomized to a cooling temperature of 31° C group and 183 to a temperature of 34° C. The assigned target temperature, reached with an endovascular device, was known only by the managing nurses.
31° C and 34° C are equivalent
There was a small numerical disadvantage for the lower temperature assignment, but none reached statistical significance. This was true of the primary outcome (48.4% vs. 45.4% for the higher temperature) and its components of mortality (43.5% vs. 41.0%) and poor neurologic outcome (4.9% vs. 4.4%). Poor neurologic outcome was defined as a Disability Rating Scale score of greater than 5.
Deaths were most common in the early part of the 180-day follow-up in both arms. On a Kaplan-Meier survival graph, Dr. Le May showed curves that he characterized as “almost superimposable.”
There were no significant differences for any subgroup stratifications, such as age 75 years or older versus younger, males versus females, presence versus absence or an initial shockable rhythm, percutaneous coronary intervention (PCI) within 24 hours versus later, and STEMI versus non-STEMI. In these analyses, the higher temperature was associated with a potential trend for benefit among females and those with a shockable rhythm.
There was no signal for a difference in neurologic outcomes on the Disability Rating Scale or the Modified Rankin Scale. On the latter, for example, 46% of those in the 31° C group and 44% of these in the 34° C group had a score of four or greater at the end of follow-up.
The baseline characteristics of the two groups were similar. About 80% were male; the average age was roughly 62 years. More than 80% of the cardiac arrests were witnessed with CPR being administered by bystanders in nearly 70%. Nearly 40% had a STEMI.
Interventions were similar. Almost all patients underwent coronary angiography, of which nearly 60% received a percutaneous coronary intervention. More than 50% received a stent. The time from arrest to randomization was slightly longer in the 31° C group (228 vs. 204 minutes). The time to balloon inflation from arrival at the cardiac center was also slightly longer (73 vs. 60 minutes).
There was a trend for an increased rate of seizures in the 31° C group (12.5% vs. 7.1%; P = .08), but other secondary outcomes, including pneumonia (67.8% vs. 63.4%), renal replacement therapy (9.2% vs. 9.3%), and stroke (4.4% vs. 1.6%), were similar in the 31° C and 34° C groups, respectively.
Bleeding, whether measured by transfusion (19.6% vs. 22.4%) or TIMI major bleed (23.4% vs. 19.7%) were similar in the 31° C and 34° C groups, respectively. Thrombosis, whether measured by stent thrombosis (1.2% vs. 2.2%) or deep venous thrombosis (11.4% vs. 10.9%) were similar in these two groups, respectively.
The length of stay in the cardiac intensive care unit was significantly greater in the 31° C group (10 vs. 7 days; P = .004). Some of this increased length of stay can be attributed to the longer rewarming process required for the greater cooling, according to Dr. Le May, but he acknowledged that it is not clear this provides a full explanation.
More trials like CAPITAL-CHILL needed
The validity of these findings is supported by several strengths of the methodology, according to Jeanne E. Poole, MD, director of the arrhythmia service and electrophysiology laboratory, University of Washington, Seattle. This includes the reliance of an endovascular device, which can accelerate the time to the target temperature and assure the precision with which it is reached and maintained.
Dr. Poole did note that many of the primary and secondary measures, including the rates of stroke, seizures, and major bleeds, even though not significantly different, favored the higher temperature. The slightly longer door-to-balloon times might have been a factor. For the higher rate of pneumonia in the 31° C group, she questioned whether the longer period of ventilation linked to a longer period of rewarming might have been a factor.
However, Dr. Poole praised the CAPITAL-CHILL trial for drawing attention to a group of patients for whom survival rates remain “dismally low.” She indicated that these types of high-level trials are needed to look for strategies to improve outcomes.
Dr. Le May and Dr. Poole report no potential conflicts of interest.
FROM ACC 2021
The end of happy hour? No safe level of alcohol for the brain
There is no safe amount of alcohol consumption for the brain; even moderate drinking adversely affects brain structure and function, according a British study of more 25,000 adults.

“This is one of the largest studies of alcohol and brain health to date,” Anya Topiwala, DPhil, University of Oxford (England), told this news organization.
“There have been previous claims the relationship between alcohol and brain health are J-shaped (ie., small amounts are protective), but we formally tested this and did not find it to be the case. In fact, we found that any level of alcohol was associated with poorer brain health, compared to no alcohol,” Dr. Topiwala added.
The study, which has not yet been peer reviewed, was published online May 12 in MedRxiv.
Global impact on the brain
Participants provided detailed information on their alcohol intake. The cohort included 691 never-drinkers, 617 former drinkers, and 24,069 current drinkers.
Median alcohol intake was 13.5 units (102 g) weekly. Almost half of the sample (48.2%) were drinking above current UK low-risk guidelines (14 units, 112 g weekly), but few were heavy drinkers (>50 units, 400 g weekly).
After adjusting for all known potential confounders and multiple comparisons, a higher volume of alcohol consumed per week was associated with lower gray matter in “almost all areas of the brain,” Dr. Topiwala said in an interview.
Alcohol consumption accounted for up to 0.8% of gray matter volume variance. “The size of the effect is small, albeit greater than any other modifiable risk factor. These brain changes have been previously linked to aging, poorer performance on memory changes, and dementia,” Dr. Topiwala said.
Widespread negative associations were also found between drinking alcohol and all the measures of white matter integrity that were assessed. There was a significant positive association between alcohol consumption and resting-state functional connectivity.
Higher blood pressure and body mass index “steepened” the negative associations between alcohol and brain health, and binge drinking had additive negative effects on brain structure beyond the absolute volume consumed.
There was no evidence that the risk for alcohol-related brain harm differs according to the type of alcohol consumed (wine, beer, or spirits).
A key limitation of the study is that the study population from the UK Biobank represents a sample that is healthier, better educated, and less deprived and is characterized by less ethnic diversity than the general population. “As with any observational study, we cannot infer causality from association,” the authors note.
What remains unclear, they say, is the duration of drinking needed to cause an effect on the brain. It may be that vulnerability is increased during periods of life in which dynamic brain changes occur, such as adolescence and older age.
They also note that some studies of alcohol-dependent individuals have suggested that at least some brain damage is reversible upon abstinence. Whether that is true for moderate drinkers is unknown.
On the basis of their findings, there is “no safe dose of alcohol for the brain,” Dr. Topiwala and colleagues conclude. They suggest that current low-risk drinking guidelines be revisited to take account of brain effects.
Experts weigh in
Several experts weighed in on the study in a statement from the nonprofit UK Science Media Center.
Paul Matthews, MD, head of the department of brain sciences, Imperial College London, noted that this “carefully performed preliminary report extends our earlier UK Dementia Research Institute study of a smaller group from same UK Biobank population also showing that even moderate drinking is associated with greater atrophy of the brain, as well as injury to the heart and liver.”
Dr. Matthews said the investigators’ conclusion that there is no safe threshold below which alcohol consumption has no toxic effects “echoes our own. We join with them in suggesting that current public health guidelines concerning alcohol consumption may need to be revisited.”
Rebecca Dewey, PhD, research fellow in neuroimaging, University of Nottingham (England), cautioned that “the degree to which very small changes in brain volume are harmful” is unknown.
“While there was no threshold under which alcohol consumption did not cause changes in the brain, there may a degree of brain volume difference that is irrelevant to brain health. We don’t know what these people’s brains looked like before they drank alcohol, so the brain may have learned to cope/compensate,” Dewey said.
Sadie Boniface, PhD, head of research at the Institute of Alcohol Studies and visiting researcher at King’s College London, said, “While we can’t yet say for sure whether there is ‘no safe level’ of alcohol regarding brain health at the moment, it has been known for decades that heavy drinking is bad for brain health.
“We also shouldn’t forget alcohol affects all parts of the body and there are multiple health risks. For example, it is already known there is ‘no safe level’ of alcohol consumption for the seven types of cancer caused by alcohol, as identified by the UK chief medical officers,” Dr. Boniface said.
The study was supported in part by the Wellcome Trust, Li Ka Shing Center for Health Information and Discovery, the National Institutes of Health, and the UK Medical Research Council. Dr. Topiwala, Dr. Boniface, Dr. Dewey, and Dr. Matthews have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There is no safe amount of alcohol consumption for the brain; even moderate drinking adversely affects brain structure and function, according a British study of more 25,000 adults.
“This is one of the largest studies of alcohol and brain health to date,” Anya Topiwala, DPhil, University of Oxford (England), told this news organization.
“There have been previous claims the relationship between alcohol and brain health are J-shaped (ie., small amounts are protective), but we formally tested this and did not find it to be the case. In fact, we found that any level of alcohol was associated with poorer brain health, compared to no alcohol,” Dr. Topiwala added.
The study, which has not yet been peer reviewed, was published online May 12 in MedRxiv.
Global impact on the brain
Participants provided detailed information on their alcohol intake. The cohort included 691 never-drinkers, 617 former drinkers, and 24,069 current drinkers.
Median alcohol intake was 13.5 units (102 g) weekly. Almost half of the sample (48.2%) were drinking above current UK low-risk guidelines (14 units, 112 g weekly), but few were heavy drinkers (>50 units, 400 g weekly).
After adjusting for all known potential confounders and multiple comparisons, a higher volume of alcohol consumed per week was associated with lower gray matter in “almost all areas of the brain,” Dr. Topiwala said in an interview.
Alcohol consumption accounted for up to 0.8% of gray matter volume variance. “The size of the effect is small, albeit greater than any other modifiable risk factor. These brain changes have been previously linked to aging, poorer performance on memory changes, and dementia,” Dr. Topiwala said.
Widespread negative associations were also found between drinking alcohol and all the measures of white matter integrity that were assessed. There was a significant positive association between alcohol consumption and resting-state functional connectivity.
Higher blood pressure and body mass index “steepened” the negative associations between alcohol and brain health, and binge drinking had additive negative effects on brain structure beyond the absolute volume consumed.
There was no evidence that the risk for alcohol-related brain harm differs according to the type of alcohol consumed (wine, beer, or spirits).
A key limitation of the study is that the study population from the UK Biobank represents a sample that is healthier, better educated, and less deprived and is characterized by less ethnic diversity than the general population. “As with any observational study, we cannot infer causality from association,” the authors note.
What remains unclear, they say, is the duration of drinking needed to cause an effect on the brain. It may be that vulnerability is increased during periods of life in which dynamic brain changes occur, such as adolescence and older age.
They also note that some studies of alcohol-dependent individuals have suggested that at least some brain damage is reversible upon abstinence. Whether that is true for moderate drinkers is unknown.
On the basis of their findings, there is “no safe dose of alcohol for the brain,” Dr. Topiwala and colleagues conclude. They suggest that current low-risk drinking guidelines be revisited to take account of brain effects.
Experts weigh in
Several experts weighed in on the study in a statement from the nonprofit UK Science Media Center.
Paul Matthews, MD, head of the department of brain sciences, Imperial College London, noted that this “carefully performed preliminary report extends our earlier UK Dementia Research Institute study of a smaller group from same UK Biobank population also showing that even moderate drinking is associated with greater atrophy of the brain, as well as injury to the heart and liver.”
Dr. Matthews said the investigators’ conclusion that there is no safe threshold below which alcohol consumption has no toxic effects “echoes our own. We join with them in suggesting that current public health guidelines concerning alcohol consumption may need to be revisited.”
Rebecca Dewey, PhD, research fellow in neuroimaging, University of Nottingham (England), cautioned that “the degree to which very small changes in brain volume are harmful” is unknown.
“While there was no threshold under which alcohol consumption did not cause changes in the brain, there may a degree of brain volume difference that is irrelevant to brain health. We don’t know what these people’s brains looked like before they drank alcohol, so the brain may have learned to cope/compensate,” Dewey said.
Sadie Boniface, PhD, head of research at the Institute of Alcohol Studies and visiting researcher at King’s College London, said, “While we can’t yet say for sure whether there is ‘no safe level’ of alcohol regarding brain health at the moment, it has been known for decades that heavy drinking is bad for brain health.
“We also shouldn’t forget alcohol affects all parts of the body and there are multiple health risks. For example, it is already known there is ‘no safe level’ of alcohol consumption for the seven types of cancer caused by alcohol, as identified by the UK chief medical officers,” Dr. Boniface said.
The study was supported in part by the Wellcome Trust, Li Ka Shing Center for Health Information and Discovery, the National Institutes of Health, and the UK Medical Research Council. Dr. Topiwala, Dr. Boniface, Dr. Dewey, and Dr. Matthews have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There is no safe amount of alcohol consumption for the brain; even moderate drinking adversely affects brain structure and function, according a British study of more 25,000 adults.
“This is one of the largest studies of alcohol and brain health to date,” Anya Topiwala, DPhil, University of Oxford (England), told this news organization.
“There have been previous claims the relationship between alcohol and brain health are J-shaped (ie., small amounts are protective), but we formally tested this and did not find it to be the case. In fact, we found that any level of alcohol was associated with poorer brain health, compared to no alcohol,” Dr. Topiwala added.
The study, which has not yet been peer reviewed, was published online May 12 in MedRxiv.
Global impact on the brain
Participants provided detailed information on their alcohol intake. The cohort included 691 never-drinkers, 617 former drinkers, and 24,069 current drinkers.
Median alcohol intake was 13.5 units (102 g) weekly. Almost half of the sample (48.2%) were drinking above current UK low-risk guidelines (14 units, 112 g weekly), but few were heavy drinkers (>50 units, 400 g weekly).
After adjusting for all known potential confounders and multiple comparisons, a higher volume of alcohol consumed per week was associated with lower gray matter in “almost all areas of the brain,” Dr. Topiwala said in an interview.
Alcohol consumption accounted for up to 0.8% of gray matter volume variance. “The size of the effect is small, albeit greater than any other modifiable risk factor. These brain changes have been previously linked to aging, poorer performance on memory changes, and dementia,” Dr. Topiwala said.
Widespread negative associations were also found between drinking alcohol and all the measures of white matter integrity that were assessed. There was a significant positive association between alcohol consumption and resting-state functional connectivity.
Higher blood pressure and body mass index “steepened” the negative associations between alcohol and brain health, and binge drinking had additive negative effects on brain structure beyond the absolute volume consumed.
There was no evidence that the risk for alcohol-related brain harm differs according to the type of alcohol consumed (wine, beer, or spirits).
A key limitation of the study is that the study population from the UK Biobank represents a sample that is healthier, better educated, and less deprived and is characterized by less ethnic diversity than the general population. “As with any observational study, we cannot infer causality from association,” the authors note.
What remains unclear, they say, is the duration of drinking needed to cause an effect on the brain. It may be that vulnerability is increased during periods of life in which dynamic brain changes occur, such as adolescence and older age.
They also note that some studies of alcohol-dependent individuals have suggested that at least some brain damage is reversible upon abstinence. Whether that is true for moderate drinkers is unknown.
On the basis of their findings, there is “no safe dose of alcohol for the brain,” Dr. Topiwala and colleagues conclude. They suggest that current low-risk drinking guidelines be revisited to take account of brain effects.
Experts weigh in
Several experts weighed in on the study in a statement from the nonprofit UK Science Media Center.
Paul Matthews, MD, head of the department of brain sciences, Imperial College London, noted that this “carefully performed preliminary report extends our earlier UK Dementia Research Institute study of a smaller group from same UK Biobank population also showing that even moderate drinking is associated with greater atrophy of the brain, as well as injury to the heart and liver.”
Dr. Matthews said the investigators’ conclusion that there is no safe threshold below which alcohol consumption has no toxic effects “echoes our own. We join with them in suggesting that current public health guidelines concerning alcohol consumption may need to be revisited.”
Rebecca Dewey, PhD, research fellow in neuroimaging, University of Nottingham (England), cautioned that “the degree to which very small changes in brain volume are harmful” is unknown.
“While there was no threshold under which alcohol consumption did not cause changes in the brain, there may a degree of brain volume difference that is irrelevant to brain health. We don’t know what these people’s brains looked like before they drank alcohol, so the brain may have learned to cope/compensate,” Dewey said.
Sadie Boniface, PhD, head of research at the Institute of Alcohol Studies and visiting researcher at King’s College London, said, “While we can’t yet say for sure whether there is ‘no safe level’ of alcohol regarding brain health at the moment, it has been known for decades that heavy drinking is bad for brain health.
“We also shouldn’t forget alcohol affects all parts of the body and there are multiple health risks. For example, it is already known there is ‘no safe level’ of alcohol consumption for the seven types of cancer caused by alcohol, as identified by the UK chief medical officers,” Dr. Boniface said.
The study was supported in part by the Wellcome Trust, Li Ka Shing Center for Health Information and Discovery, the National Institutes of Health, and the UK Medical Research Council. Dr. Topiwala, Dr. Boniface, Dr. Dewey, and Dr. Matthews have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AHA reassures myocarditis rare after COVID vaccination, benefits overwhelm risks
The benefits of COVID-19 vaccination “enormously outweigh” the rare possible risk for heart-related complications, including myocarditis, the American Heart Association/American Stroke Association (ASA) says in new statement.
The message follows a Centers for Disease Control and Prevention report that the agency is monitoring the Vaccine Adverse Events Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) for cases of myocarditis that have been associated with the mRNA vaccines against SARS-CoV-2 from Pfizer and Moderna.
The “relatively few” reported cases myocarditis in adolescents or young adults have involved males more often than females, more often followed the second dose rather than the first, and were usually seen in the 4 days after vaccination, the CDC’s COVID-19 Vaccine Safety Technical Work Group (VaST) found.
“Most cases appear to be mild, and follow-up of cases is ongoing,” the CDC says. “Within CDC safety monitoring systems, rates of myocarditis reports in the window following COVID-19 vaccination have not differed from expected baseline rates.”
In their statement, the AHA/ASA “strongly urge” all adults and children 12 years and older to receive a COVID-19 vaccine as soon as possible.
“The evidence continues to indicate that the COVID-19 vaccines are nearly 100% effective at preventing death and hospitalization due to COVID-19 infection,” the groups say.
Although the investigation of cases of myocarditis related to COVID-19 vaccination is ongoing, the AHA/ASA notes that myocarditis is typically the result of an actual viral infection, “and it is yet to be determined if these cases have any correlation to receiving a COVID-19 vaccine.”
“We’ve lost hundreds of children, and there have been thousands who have been hospitalized, thousands who developed an inflammatory syndrome, and one of the pieces of that can be myocarditis,” Richard Besser, MD, president and CEO of the Robert Wood Johnson Foundation (RWJF), said today on ABC’s Good Morning America.
Still, “from my perspective, the risk of COVID is so much greater than any theoretical risk from the vaccine,” said Dr. Besser, former acting director of the CDC.
The symptoms that can occur after COVID-19 vaccination include tiredness, headache, muscle pain, chills, fever, and nausea, reminds the AHA/ASA statement. Such symptoms would “typically appear within 24-48 hours and usually pass within 36-48 hours after receiving the vaccine.”
All health care providers should be aware of the “very rare” adverse events that could be related to a COVID-19 vaccine, including myocarditis, blood clots, low platelets, and symptoms of severe inflammation, it says.
“Health care professionals should strongly consider inquiring about the timing of any recent COVID vaccination among patients presenting with these conditions, as needed, in order to provide appropriate treatment quickly,” the statement advises.
A version of this article first appeared on Medscape.com.
The benefits of COVID-19 vaccination “enormously outweigh” the rare possible risk for heart-related complications, including myocarditis, the American Heart Association/American Stroke Association (ASA) says in new statement.
The message follows a Centers for Disease Control and Prevention report that the agency is monitoring the Vaccine Adverse Events Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) for cases of myocarditis that have been associated with the mRNA vaccines against SARS-CoV-2 from Pfizer and Moderna.
The “relatively few” reported cases myocarditis in adolescents or young adults have involved males more often than females, more often followed the second dose rather than the first, and were usually seen in the 4 days after vaccination, the CDC’s COVID-19 Vaccine Safety Technical Work Group (VaST) found.
“Most cases appear to be mild, and follow-up of cases is ongoing,” the CDC says. “Within CDC safety monitoring systems, rates of myocarditis reports in the window following COVID-19 vaccination have not differed from expected baseline rates.”
In their statement, the AHA/ASA “strongly urge” all adults and children 12 years and older to receive a COVID-19 vaccine as soon as possible.
“The evidence continues to indicate that the COVID-19 vaccines are nearly 100% effective at preventing death and hospitalization due to COVID-19 infection,” the groups say.
Although the investigation of cases of myocarditis related to COVID-19 vaccination is ongoing, the AHA/ASA notes that myocarditis is typically the result of an actual viral infection, “and it is yet to be determined if these cases have any correlation to receiving a COVID-19 vaccine.”
“We’ve lost hundreds of children, and there have been thousands who have been hospitalized, thousands who developed an inflammatory syndrome, and one of the pieces of that can be myocarditis,” Richard Besser, MD, president and CEO of the Robert Wood Johnson Foundation (RWJF), said today on ABC’s Good Morning America.
Still, “from my perspective, the risk of COVID is so much greater than any theoretical risk from the vaccine,” said Dr. Besser, former acting director of the CDC.
The symptoms that can occur after COVID-19 vaccination include tiredness, headache, muscle pain, chills, fever, and nausea, reminds the AHA/ASA statement. Such symptoms would “typically appear within 24-48 hours and usually pass within 36-48 hours after receiving the vaccine.”
All health care providers should be aware of the “very rare” adverse events that could be related to a COVID-19 vaccine, including myocarditis, blood clots, low platelets, and symptoms of severe inflammation, it says.
“Health care professionals should strongly consider inquiring about the timing of any recent COVID vaccination among patients presenting with these conditions, as needed, in order to provide appropriate treatment quickly,” the statement advises.
A version of this article first appeared on Medscape.com.
The benefits of COVID-19 vaccination “enormously outweigh” the rare possible risk for heart-related complications, including myocarditis, the American Heart Association/American Stroke Association (ASA) says in new statement.
The message follows a Centers for Disease Control and Prevention report that the agency is monitoring the Vaccine Adverse Events Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) for cases of myocarditis that have been associated with the mRNA vaccines against SARS-CoV-2 from Pfizer and Moderna.
The “relatively few” reported cases myocarditis in adolescents or young adults have involved males more often than females, more often followed the second dose rather than the first, and were usually seen in the 4 days after vaccination, the CDC’s COVID-19 Vaccine Safety Technical Work Group (VaST) found.
“Most cases appear to be mild, and follow-up of cases is ongoing,” the CDC says. “Within CDC safety monitoring systems, rates of myocarditis reports in the window following COVID-19 vaccination have not differed from expected baseline rates.”
In their statement, the AHA/ASA “strongly urge” all adults and children 12 years and older to receive a COVID-19 vaccine as soon as possible.
“The evidence continues to indicate that the COVID-19 vaccines are nearly 100% effective at preventing death and hospitalization due to COVID-19 infection,” the groups say.
Although the investigation of cases of myocarditis related to COVID-19 vaccination is ongoing, the AHA/ASA notes that myocarditis is typically the result of an actual viral infection, “and it is yet to be determined if these cases have any correlation to receiving a COVID-19 vaccine.”
“We’ve lost hundreds of children, and there have been thousands who have been hospitalized, thousands who developed an inflammatory syndrome, and one of the pieces of that can be myocarditis,” Richard Besser, MD, president and CEO of the Robert Wood Johnson Foundation (RWJF), said today on ABC’s Good Morning America.
Still, “from my perspective, the risk of COVID is so much greater than any theoretical risk from the vaccine,” said Dr. Besser, former acting director of the CDC.
The symptoms that can occur after COVID-19 vaccination include tiredness, headache, muscle pain, chills, fever, and nausea, reminds the AHA/ASA statement. Such symptoms would “typically appear within 24-48 hours and usually pass within 36-48 hours after receiving the vaccine.”
All health care providers should be aware of the “very rare” adverse events that could be related to a COVID-19 vaccine, including myocarditis, blood clots, low platelets, and symptoms of severe inflammation, it says.
“Health care professionals should strongly consider inquiring about the timing of any recent COVID vaccination among patients presenting with these conditions, as needed, in order to provide appropriate treatment quickly,” the statement advises.
A version of this article first appeared on Medscape.com.
Bullous Pemphigoid Triggered by Liraglutide
To the Editor:
Bullous pemphigoid (BP) is an autoimmune blistering disease that typically affects the elderly, with an incidence of approximately 7 new cases per million.1 The pathogenesis of BP involves autoantibodies to BP antigens 180 and 230 at the dermoepidermal junction. Bullous pemphigoid has been associated with the use of multiple medications; vaccines; and physical damage to the skin, including trauma, radiation, and surgery.2
Several classes of medications may cause BP; one study described an association of BP with loop diuretics,3 while others found higher incidences of BP in patients taking aldosterone antagonists and neuroleptics.4 We describe a case of drug-triggered BP to liraglutide, a glucagonlike peptide 1 (GLP-1) receptor agonist.
A 75-year-old man presented to dermatology for evaluation of a vesicular eruption on the head, neck, trunk, and arms of 6 months’ duration. The eruption developed 2 weeks after starting liraglutide 1.2 mg subcutaneously daily for diabetes mellitus. The patient had a medical history of type 2 diabetes mellitus, hypertension, stroke, and prostate cancer treated with prostatectomy, and he also was taking insulin. Liraglutide was discontinued shortly after the onset of the eruption.
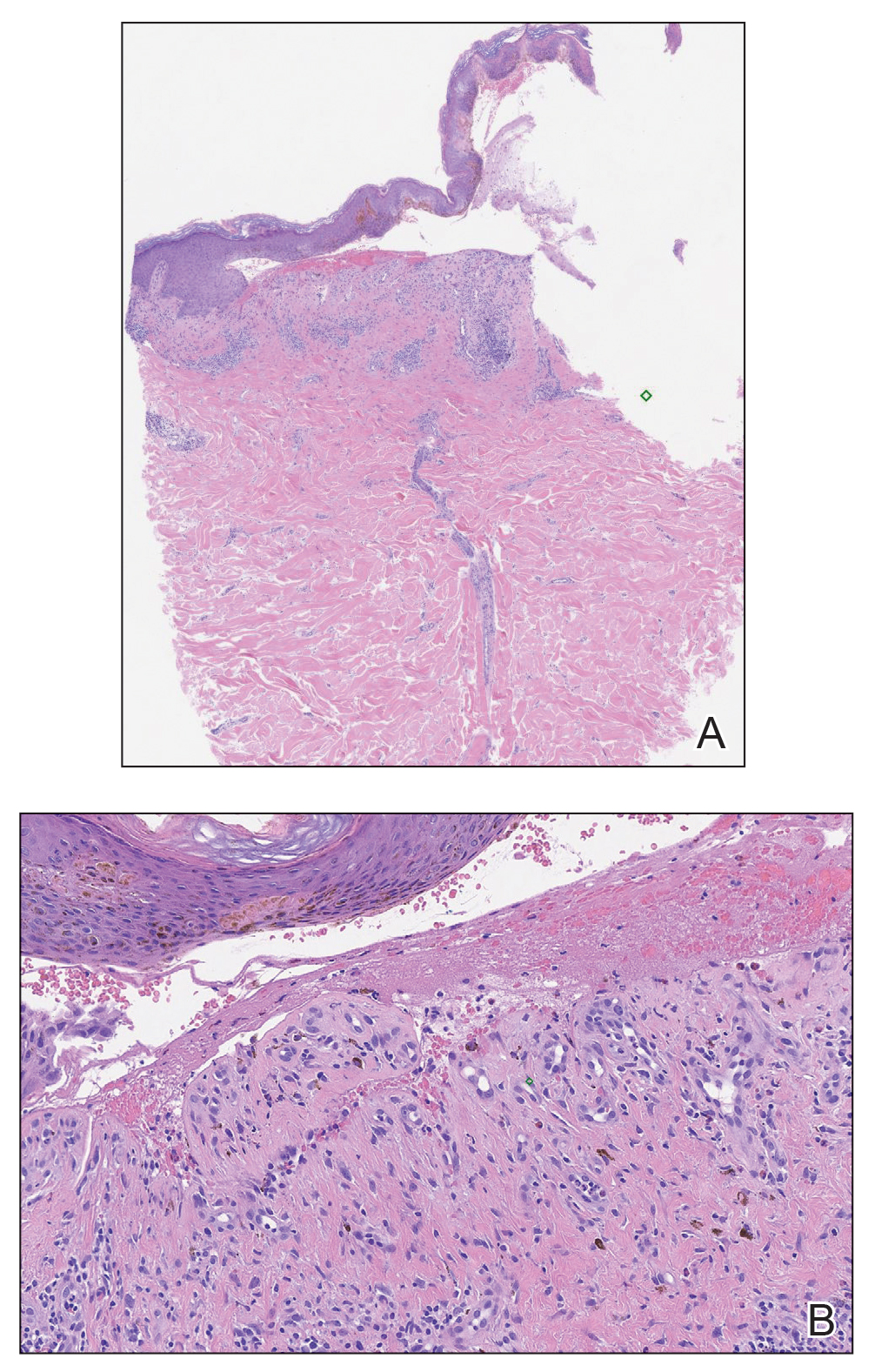
Physical examination revealed annular plaques on the head, neck, trunk, and arms with central hypopigmentation and hyperpigmented borders (Figure 1). Two tense bullae were evident on the left flank (Figure 2). Histopathology revealed a subepidermal blister, mixed perivascular infiltrate with numerous eosinophils, and pigment incontinence (Figure 3). Direct immunofluorescence showed linear deposition of IgG and C3 along the basement membrane zone that was localized to the roof of the blister on salt-split analysis. No microorganisms were identified on periodic acid–Schiff, Grocott-Gomori methenamine-silver, acid-fast bacilli, and Fite stains. The patient initially was treated with clobetasol ointment 0.05%, leading to marginal improvement. He declined treatment with prednisone or dapsone, and he was started on doxycycline. Seven months after stopping liraglutide and starting doxycycline, the patient had no blisters, but residual pigmentary changes remained.


Two types of BP have been described in response to medications: drug-induced BP and drug-triggered BP. Drug-induced BP presents as an acute, self-limited eruption that typically resolves after withdrawal of the offending agent. It tends to involve a younger population and may present with mucosal involvement and target lesions on the palms and soles. Direct immunofluorescence shows linear IgG and C3 deposition at the basement membrane zone. Patients tend to respond quickly to systemic corticosteroids and have low recurrence rates. Drug-triggered BP is a chronic form of BP that is caused by a medication and is not resolved with removal of the offending agent.5 Therefore, drug-triggered BP is more difficult to detect, especially in patients taking multiple medications.
Our patient represents a case of drug-triggered BP to liraglutide. Liraglutide is a GLP-1 receptor agonist that is US Food and Drug Administration approved for the treatment of type 2 diabetes mellitus. Glucagonlike peptide 1 is an incretin hormone that is secreted by the intestine during digestion. It binds to the GLP-1 receptor leading to an increase in glucose-dependent insulin secretion and a decrease in glucagon secretion.6 Glucagonlike peptide 1 agonists also affect the immune system; liraglutide has been shown to modestly improve psoriasis, reduce the number of dermal gamma delta T cells, and decrease IL-17 expression.7 Glucagonlike peptide 1 agonists also produce anti-inflammatory effects on multiple organs including the liver, brain, vasculature, kidney, and skin.8
Dipeptidyl peptidase 4 (DPP-4) inhibitors that function to inhibit the degradation of GLP-1 and other peptides also have been reported to cause BP. In several patients, the DPP-4 inhibitors vildagliptin and sitagliptin caused drug-induced BP that resolved with discontinuation of the medication.9 Dipeptidyl peptidase 4 is expressed in various organ systems including the skin, and inhibition of DPP-4 enhances eosinophil mobilization in the blood and recruitment to the skin in animal models.10
Although the pathogenesis of BP involves autoantibodies to BP antigens 180 and 230, these antibodies are not sufficient to cause disease, as antibasement antibodies have been detected in patients without clinically evident BP. These patients, however, may be more susceptible to developing medication-induced BP. Several hypotheses regarding the pathogenesis of medication-induced BP have been proposed, including immune dysregulation, molecular mimicry, and cross-reactivity to a prior sensitizing agent.5 Liraglutide and the DPP-4 inhibitors affect the immune system, supporting the hypothesis of immune dysregulation; however, the exact mechanism of how immune modulating medications such as GLP-1 agonists and DPP-4 inhibitors cause BP remains unclear.
The effects of liraglutide and the DPP-4 inhibitors on the immune system may play a role in the pathogenesis of drug-triggered BP and drug-induced BP, respectively. Additional studies of the immunomodulatory effects of GLP-1 agonists and DPP-4 inhibitors may help elucidate the pathogenesis of drug-triggered or drug-induced BP.
- Serwin AB, Musialkowska E, Piascik M. Incidence and mortality of bullous pemphigoid in north-east Poland (Podlaskie Province), 1999-2012: a retrospective bicentric cohort study. Int J Dermatol. 2014;53:E432-E437.
- Danescu S, Chiorean R, Macovei V, et al. Role of physical factors in the pathogenesis of bullous pemphigoid: case report series and a comprehensive review of the published work. J Dermatol. 2016;43:134-130.
- Lloyd-Lavery A, Chi CC, Wojnarowska F, et al. The associations between bullous pemphigoid and drug use: a UK case-control study. JAMA Dermatol. 2013;149:58-62.
- Bastuji-Garin S, Joly P, Picard-Dahan C, et al. Drugs associated with bullous pemphigoid. a case-control study. Arch Dermatol. 1996;132:272-276.
- Stavropoulos PG, Soura E, Antoniou C. Drug-induced pemphigoid: a review of the literature. J Eur Acad Dermatol Venereol. 2014;28:1133-1140.
- Triplitt C, Solis-Herrera C. GLP-1 receptor agonists: practical considerations for clinical practice. Diabetes Educ. 2015;41(suppl 1):32S-46S.
- Buysschaert M, Baeck M, Preumont V, et al. Improvement of psoriasis during glucagon-like peptide-1 analogue therapy in type 2 diabetes is associated with decreasing dermal gammadelta T-cell number: a prospective case-series study. Br J Dermatol. 2014;171:155-161.
- Lee YS, Jun HS. Anti-inflammatory effects of GLP-1-based therapies beyond glucose control. Mediators Inflamm. 2016;2016:3094642.
- Skandalis K, Spirova M, Gaitanis G, et al Drug-induced bullous pemphigoid in diabetes mellitus patients receiving dipeptidyl peptidase-IV inhibitors plus metformin. J Eur Acad Dermatol Venereol. 2012;26:249-253.
- Forssmann U, Stoetzer C, Stephan M, et al. Inhibition of CD26/dipeptidyl peptidase IV enhances CCL11/eotaxin-mediated recruitment of eosinophils in vivo. J Immunol. 2008;181:1120-1127.
To the Editor:
Bullous pemphigoid (BP) is an autoimmune blistering disease that typically affects the elderly, with an incidence of approximately 7 new cases per million.1 The pathogenesis of BP involves autoantibodies to BP antigens 180 and 230 at the dermoepidermal junction. Bullous pemphigoid has been associated with the use of multiple medications; vaccines; and physical damage to the skin, including trauma, radiation, and surgery.2
Several classes of medications may cause BP; one study described an association of BP with loop diuretics,3 while others found higher incidences of BP in patients taking aldosterone antagonists and neuroleptics.4 We describe a case of drug-triggered BP to liraglutide, a glucagonlike peptide 1 (GLP-1) receptor agonist.
A 75-year-old man presented to dermatology for evaluation of a vesicular eruption on the head, neck, trunk, and arms of 6 months’ duration. The eruption developed 2 weeks after starting liraglutide 1.2 mg subcutaneously daily for diabetes mellitus. The patient had a medical history of type 2 diabetes mellitus, hypertension, stroke, and prostate cancer treated with prostatectomy, and he also was taking insulin. Liraglutide was discontinued shortly after the onset of the eruption.
Physical examination revealed annular plaques on the head, neck, trunk, and arms with central hypopigmentation and hyperpigmented borders (Figure 1). Two tense bullae were evident on the left flank (Figure 2). Histopathology revealed a subepidermal blister, mixed perivascular infiltrate with numerous eosinophils, and pigment incontinence (Figure 3). Direct immunofluorescence showed linear deposition of IgG and C3 along the basement membrane zone that was localized to the roof of the blister on salt-split analysis. No microorganisms were identified on periodic acid–Schiff, Grocott-Gomori methenamine-silver, acid-fast bacilli, and Fite stains. The patient initially was treated with clobetasol ointment 0.05%, leading to marginal improvement. He declined treatment with prednisone or dapsone, and he was started on doxycycline. Seven months after stopping liraglutide and starting doxycycline, the patient had no blisters, but residual pigmentary changes remained.
Two types of BP have been described in response to medications: drug-induced BP and drug-triggered BP. Drug-induced BP presents as an acute, self-limited eruption that typically resolves after withdrawal of the offending agent. It tends to involve a younger population and may present with mucosal involvement and target lesions on the palms and soles. Direct immunofluorescence shows linear IgG and C3 deposition at the basement membrane zone. Patients tend to respond quickly to systemic corticosteroids and have low recurrence rates. Drug-triggered BP is a chronic form of BP that is caused by a medication and is not resolved with removal of the offending agent.5 Therefore, drug-triggered BP is more difficult to detect, especially in patients taking multiple medications.
Our patient represents a case of drug-triggered BP to liraglutide. Liraglutide is a GLP-1 receptor agonist that is US Food and Drug Administration approved for the treatment of type 2 diabetes mellitus. Glucagonlike peptide 1 is an incretin hormone that is secreted by the intestine during digestion. It binds to the GLP-1 receptor leading to an increase in glucose-dependent insulin secretion and a decrease in glucagon secretion.6 Glucagonlike peptide 1 agonists also affect the immune system; liraglutide has been shown to modestly improve psoriasis, reduce the number of dermal gamma delta T cells, and decrease IL-17 expression.7 Glucagonlike peptide 1 agonists also produce anti-inflammatory effects on multiple organs including the liver, brain, vasculature, kidney, and skin.8
Dipeptidyl peptidase 4 (DPP-4) inhibitors that function to inhibit the degradation of GLP-1 and other peptides also have been reported to cause BP. In several patients, the DPP-4 inhibitors vildagliptin and sitagliptin caused drug-induced BP that resolved with discontinuation of the medication.9 Dipeptidyl peptidase 4 is expressed in various organ systems including the skin, and inhibition of DPP-4 enhances eosinophil mobilization in the blood and recruitment to the skin in animal models.10
Although the pathogenesis of BP involves autoantibodies to BP antigens 180 and 230, these antibodies are not sufficient to cause disease, as antibasement antibodies have been detected in patients without clinically evident BP. These patients, however, may be more susceptible to developing medication-induced BP. Several hypotheses regarding the pathogenesis of medication-induced BP have been proposed, including immune dysregulation, molecular mimicry, and cross-reactivity to a prior sensitizing agent.5 Liraglutide and the DPP-4 inhibitors affect the immune system, supporting the hypothesis of immune dysregulation; however, the exact mechanism of how immune modulating medications such as GLP-1 agonists and DPP-4 inhibitors cause BP remains unclear.
The effects of liraglutide and the DPP-4 inhibitors on the immune system may play a role in the pathogenesis of drug-triggered BP and drug-induced BP, respectively. Additional studies of the immunomodulatory effects of GLP-1 agonists and DPP-4 inhibitors may help elucidate the pathogenesis of drug-triggered or drug-induced BP.
To the Editor:
Bullous pemphigoid (BP) is an autoimmune blistering disease that typically affects the elderly, with an incidence of approximately 7 new cases per million.1 The pathogenesis of BP involves autoantibodies to BP antigens 180 and 230 at the dermoepidermal junction. Bullous pemphigoid has been associated with the use of multiple medications; vaccines; and physical damage to the skin, including trauma, radiation, and surgery.2
Several classes of medications may cause BP; one study described an association of BP with loop diuretics,3 while others found higher incidences of BP in patients taking aldosterone antagonists and neuroleptics.4 We describe a case of drug-triggered BP to liraglutide, a glucagonlike peptide 1 (GLP-1) receptor agonist.
A 75-year-old man presented to dermatology for evaluation of a vesicular eruption on the head, neck, trunk, and arms of 6 months’ duration. The eruption developed 2 weeks after starting liraglutide 1.2 mg subcutaneously daily for diabetes mellitus. The patient had a medical history of type 2 diabetes mellitus, hypertension, stroke, and prostate cancer treated with prostatectomy, and he also was taking insulin. Liraglutide was discontinued shortly after the onset of the eruption.
Physical examination revealed annular plaques on the head, neck, trunk, and arms with central hypopigmentation and hyperpigmented borders (Figure 1). Two tense bullae were evident on the left flank (Figure 2). Histopathology revealed a subepidermal blister, mixed perivascular infiltrate with numerous eosinophils, and pigment incontinence (Figure 3). Direct immunofluorescence showed linear deposition of IgG and C3 along the basement membrane zone that was localized to the roof of the blister on salt-split analysis. No microorganisms were identified on periodic acid–Schiff, Grocott-Gomori methenamine-silver, acid-fast bacilli, and Fite stains. The patient initially was treated with clobetasol ointment 0.05%, leading to marginal improvement. He declined treatment with prednisone or dapsone, and he was started on doxycycline. Seven months after stopping liraglutide and starting doxycycline, the patient had no blisters, but residual pigmentary changes remained.
Two types of BP have been described in response to medications: drug-induced BP and drug-triggered BP. Drug-induced BP presents as an acute, self-limited eruption that typically resolves after withdrawal of the offending agent. It tends to involve a younger population and may present with mucosal involvement and target lesions on the palms and soles. Direct immunofluorescence shows linear IgG and C3 deposition at the basement membrane zone. Patients tend to respond quickly to systemic corticosteroids and have low recurrence rates. Drug-triggered BP is a chronic form of BP that is caused by a medication and is not resolved with removal of the offending agent.5 Therefore, drug-triggered BP is more difficult to detect, especially in patients taking multiple medications.
Our patient represents a case of drug-triggered BP to liraglutide. Liraglutide is a GLP-1 receptor agonist that is US Food and Drug Administration approved for the treatment of type 2 diabetes mellitus. Glucagonlike peptide 1 is an incretin hormone that is secreted by the intestine during digestion. It binds to the GLP-1 receptor leading to an increase in glucose-dependent insulin secretion and a decrease in glucagon secretion.6 Glucagonlike peptide 1 agonists also affect the immune system; liraglutide has been shown to modestly improve psoriasis, reduce the number of dermal gamma delta T cells, and decrease IL-17 expression.7 Glucagonlike peptide 1 agonists also produce anti-inflammatory effects on multiple organs including the liver, brain, vasculature, kidney, and skin.8
Dipeptidyl peptidase 4 (DPP-4) inhibitors that function to inhibit the degradation of GLP-1 and other peptides also have been reported to cause BP. In several patients, the DPP-4 inhibitors vildagliptin and sitagliptin caused drug-induced BP that resolved with discontinuation of the medication.9 Dipeptidyl peptidase 4 is expressed in various organ systems including the skin, and inhibition of DPP-4 enhances eosinophil mobilization in the blood and recruitment to the skin in animal models.10
Although the pathogenesis of BP involves autoantibodies to BP antigens 180 and 230, these antibodies are not sufficient to cause disease, as antibasement antibodies have been detected in patients without clinically evident BP. These patients, however, may be more susceptible to developing medication-induced BP. Several hypotheses regarding the pathogenesis of medication-induced BP have been proposed, including immune dysregulation, molecular mimicry, and cross-reactivity to a prior sensitizing agent.5 Liraglutide and the DPP-4 inhibitors affect the immune system, supporting the hypothesis of immune dysregulation; however, the exact mechanism of how immune modulating medications such as GLP-1 agonists and DPP-4 inhibitors cause BP remains unclear.
The effects of liraglutide and the DPP-4 inhibitors on the immune system may play a role in the pathogenesis of drug-triggered BP and drug-induced BP, respectively. Additional studies of the immunomodulatory effects of GLP-1 agonists and DPP-4 inhibitors may help elucidate the pathogenesis of drug-triggered or drug-induced BP.
- Serwin AB, Musialkowska E, Piascik M. Incidence and mortality of bullous pemphigoid in north-east Poland (Podlaskie Province), 1999-2012: a retrospective bicentric cohort study. Int J Dermatol. 2014;53:E432-E437.
- Danescu S, Chiorean R, Macovei V, et al. Role of physical factors in the pathogenesis of bullous pemphigoid: case report series and a comprehensive review of the published work. J Dermatol. 2016;43:134-130.
- Lloyd-Lavery A, Chi CC, Wojnarowska F, et al. The associations between bullous pemphigoid and drug use: a UK case-control study. JAMA Dermatol. 2013;149:58-62.
- Bastuji-Garin S, Joly P, Picard-Dahan C, et al. Drugs associated with bullous pemphigoid. a case-control study. Arch Dermatol. 1996;132:272-276.
- Stavropoulos PG, Soura E, Antoniou C. Drug-induced pemphigoid: a review of the literature. J Eur Acad Dermatol Venereol. 2014;28:1133-1140.
- Triplitt C, Solis-Herrera C. GLP-1 receptor agonists: practical considerations for clinical practice. Diabetes Educ. 2015;41(suppl 1):32S-46S.
- Buysschaert M, Baeck M, Preumont V, et al. Improvement of psoriasis during glucagon-like peptide-1 analogue therapy in type 2 diabetes is associated with decreasing dermal gammadelta T-cell number: a prospective case-series study. Br J Dermatol. 2014;171:155-161.
- Lee YS, Jun HS. Anti-inflammatory effects of GLP-1-based therapies beyond glucose control. Mediators Inflamm. 2016;2016:3094642.
- Skandalis K, Spirova M, Gaitanis G, et al Drug-induced bullous pemphigoid in diabetes mellitus patients receiving dipeptidyl peptidase-IV inhibitors plus metformin. J Eur Acad Dermatol Venereol. 2012;26:249-253.
- Forssmann U, Stoetzer C, Stephan M, et al. Inhibition of CD26/dipeptidyl peptidase IV enhances CCL11/eotaxin-mediated recruitment of eosinophils in vivo. J Immunol. 2008;181:1120-1127.
- Serwin AB, Musialkowska E, Piascik M. Incidence and mortality of bullous pemphigoid in north-east Poland (Podlaskie Province), 1999-2012: a retrospective bicentric cohort study. Int J Dermatol. 2014;53:E432-E437.
- Danescu S, Chiorean R, Macovei V, et al. Role of physical factors in the pathogenesis of bullous pemphigoid: case report series and a comprehensive review of the published work. J Dermatol. 2016;43:134-130.
- Lloyd-Lavery A, Chi CC, Wojnarowska F, et al. The associations between bullous pemphigoid and drug use: a UK case-control study. JAMA Dermatol. 2013;149:58-62.
- Bastuji-Garin S, Joly P, Picard-Dahan C, et al. Drugs associated with bullous pemphigoid. a case-control study. Arch Dermatol. 1996;132:272-276.
- Stavropoulos PG, Soura E, Antoniou C. Drug-induced pemphigoid: a review of the literature. J Eur Acad Dermatol Venereol. 2014;28:1133-1140.
- Triplitt C, Solis-Herrera C. GLP-1 receptor agonists: practical considerations for clinical practice. Diabetes Educ. 2015;41(suppl 1):32S-46S.
- Buysschaert M, Baeck M, Preumont V, et al. Improvement of psoriasis during glucagon-like peptide-1 analogue therapy in type 2 diabetes is associated with decreasing dermal gammadelta T-cell number: a prospective case-series study. Br J Dermatol. 2014;171:155-161.
- Lee YS, Jun HS. Anti-inflammatory effects of GLP-1-based therapies beyond glucose control. Mediators Inflamm. 2016;2016:3094642.
- Skandalis K, Spirova M, Gaitanis G, et al Drug-induced bullous pemphigoid in diabetes mellitus patients receiving dipeptidyl peptidase-IV inhibitors plus metformin. J Eur Acad Dermatol Venereol. 2012;26:249-253.
- Forssmann U, Stoetzer C, Stephan M, et al. Inhibition of CD26/dipeptidyl peptidase IV enhances CCL11/eotaxin-mediated recruitment of eosinophils in vivo. J Immunol. 2008;181:1120-1127.
Practice Points
- Liraglutide and dipeptidyl peptidase 4 inhibitors, medications used in the treatment of diabetes mellitus, may be linked to the development of bullous pemphigoid (BP).
- Further study of the mechanism of action of these medications may lead to improved understanding of the pathogenesis of BP.

Physicians’ trust in health care leadership drops in pandemic
according to a survey conducted by NORC at the University of Chicago on behalf of the American Board of Internal Medicine Foundation.
Survey results, released May 21, indicate that 30% of physicians say their trust in the U.S. health care system and health care leadership has decreased during the pandemic. Only 18% reported an increase in trust.
Physicians, however, have great trust in their fellow clinicians.
In the survey of 600 physicians, 94% said they trust doctors within their practice; 85% trusted doctors outside of their practice; and 89% trusted nurses. That trust increased during the pandemic, with 41% saying their trust in fellow physicians rose and 37% saying their trust in nurses did.
In a separate survey, NORC asked patients about their trust in various aspects of health care. Among 2,069 respondents, a wide majority reported that they trust doctors (84%) and nurses (85%), but only 64% trusted the health care system as a whole. One in three consumers (32%) said their trust in the health care system decreased during the pandemic, compared with 11% who said their trust increased.
The ABIM Foundation released the research findings on May 21 as part of Building Trust, a national campaign that aims to boost trust among patients, clinicians, system leaders, researchers, and others.
Richard J. Baron, MD, president and chief executive officer of the ABIM Foundation, said in an interview, “Clearly there’s lower trust in health care organization leaders and executives, and that’s troubling.
“Science by itself is not enough,” he said. “Becoming trustworthy has to be a core project of everybody in health care.”
Deterioration in physicians’ trust during the pandemic comes in part from failed promises of adequate personal protective equipment and some physicians’ loss of income as a result of the crisis, Dr. Baron said.
He added that the vaccine rollout was very uneven and that policies as to which elective procedures could be performed were handled differently in different parts of the country.
He also noted that, early on, transparency was lacking as to how many COVID patients hospitals were treating, which may have contributed to the decrease in trust in the system.
Fear of being known as ‘the COVID hospital’
Hospitals were afraid of being known as “the COVID hospital” and losing patients who were afraid to come there, Dr. Baron said.
He said the COVID-19 epidemic exacerbated problems regarding trust, but that trust has been declining for some time. The Building Trust campaign will focus on solutions in breaches of trust as physicians move increasingly toward being employees of huge systems, according to Dr. Baron.
However, trust works both ways, Dr. Baron notes. Physicians can be champions for their health care system or “throw the system under the bus,” he said.
For example, if a patient complains about the appointment system, clinicians who trust their institutions may say the system usually works and that they will try to make sure the patient has a better experience next time. Clinicians without trust may say they agree that the health care system doesn’t know what it is doing, and patients may further lose confidence when physicians validate their complaint, and patients may then go elsewhere.
78% of patients trust primary care doctor
When asked whether they trust their primary care physician, 78% of patients said yes. However, trust in doctors was higher among people who were older (90%), White (82%), or had high income (89%). Among people reporting lower trust, 25% said their physician spends too little time with them, and 14% said their doctor does not know or listen to them.
The survey shows that government agencies have work to do to earn trust. Responses indicate that 43% of physicians said they have “complete trust” in government health care agencies, such as the U.S. Food and Drug Administration and the Centers for Disease Control and Prevention, which is substantially higher than other parts of the health care system. However, trust in agencies declined for 43% of physician respondents and increased for 21%.
Dhruv Khullar, MD, MPP, of the department of health policy and economics at Weill Cornell Medical College in New York, told this news organization the survey results match what he sees anecdotally in medicine – that physicians have been losing trust in the system but not in their colleagues.
He said the sample size of 600 is enough to be influential, though he said he would like to know the response rate, which was not calculated for this survey.
He added that, in large part, physicians’ lack of trust in their systems may come from generally being asked to see more patients and to meet more metrics during the same or shorter periods.
Physicians’ lack of trust in the system can have significant consequences, he said. It can lead to burnout, which has been linked with poorer quality of care and physician turnover, he noted.
COVID-19 led some physicians to wonder whether their system had their best interests at heart, insofar as access to adequate medicines and supplies as well as emotional support were inconsistent, Dr. Khullar said.
He said that to regain trust health care systems need to ask themselves questions in three areas. The first is whether their goals are focused on the best interest of the organization or the best interest of the patient.
“Next is competency,” Dr. Khullar said. “Maybe your motives are right, but are you able to deliver? Are you delivering a good product, whether clinical services or something else?”
The third area is transparency, he said. “Are you going to be honest and forthright in what we’re doing and where we’re going?”
Caroline Pearson, senior vice president of health care strategy for NORC, said the emailed survey was conducted between Dec. 29, 2020, and Feb. 5, 2021, with a health care survey partner that maintains a nationwide panel of physicians across specialties.
She said this report is fairly novel insofar as surveys are more typically conducted regarding patients’ trust of their doctors or of the health care system.
Ms. Pearson said because health care is delivered in teams, understanding the level of trust among the entities helps ensure that care will be delivered effectively and seamlessly with high quality.
“We want our patients to trust our doctors, but we really want doctors to trust each other and trust the hospitals and systems in which they’re working,” she said.
Dr. Baron, Ms. Pearson, and Dr. Khullar report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a survey conducted by NORC at the University of Chicago on behalf of the American Board of Internal Medicine Foundation.
Survey results, released May 21, indicate that 30% of physicians say their trust in the U.S. health care system and health care leadership has decreased during the pandemic. Only 18% reported an increase in trust.
Physicians, however, have great trust in their fellow clinicians.
In the survey of 600 physicians, 94% said they trust doctors within their practice; 85% trusted doctors outside of their practice; and 89% trusted nurses. That trust increased during the pandemic, with 41% saying their trust in fellow physicians rose and 37% saying their trust in nurses did.
In a separate survey, NORC asked patients about their trust in various aspects of health care. Among 2,069 respondents, a wide majority reported that they trust doctors (84%) and nurses (85%), but only 64% trusted the health care system as a whole. One in three consumers (32%) said their trust in the health care system decreased during the pandemic, compared with 11% who said their trust increased.
The ABIM Foundation released the research findings on May 21 as part of Building Trust, a national campaign that aims to boost trust among patients, clinicians, system leaders, researchers, and others.
Richard J. Baron, MD, president and chief executive officer of the ABIM Foundation, said in an interview, “Clearly there’s lower trust in health care organization leaders and executives, and that’s troubling.
“Science by itself is not enough,” he said. “Becoming trustworthy has to be a core project of everybody in health care.”
Deterioration in physicians’ trust during the pandemic comes in part from failed promises of adequate personal protective equipment and some physicians’ loss of income as a result of the crisis, Dr. Baron said.
He added that the vaccine rollout was very uneven and that policies as to which elective procedures could be performed were handled differently in different parts of the country.
He also noted that, early on, transparency was lacking as to how many COVID patients hospitals were treating, which may have contributed to the decrease in trust in the system.
Fear of being known as ‘the COVID hospital’
Hospitals were afraid of being known as “the COVID hospital” and losing patients who were afraid to come there, Dr. Baron said.
He said the COVID-19 epidemic exacerbated problems regarding trust, but that trust has been declining for some time. The Building Trust campaign will focus on solutions in breaches of trust as physicians move increasingly toward being employees of huge systems, according to Dr. Baron.
However, trust works both ways, Dr. Baron notes. Physicians can be champions for their health care system or “throw the system under the bus,” he said.
For example, if a patient complains about the appointment system, clinicians who trust their institutions may say the system usually works and that they will try to make sure the patient has a better experience next time. Clinicians without trust may say they agree that the health care system doesn’t know what it is doing, and patients may further lose confidence when physicians validate their complaint, and patients may then go elsewhere.
78% of patients trust primary care doctor
When asked whether they trust their primary care physician, 78% of patients said yes. However, trust in doctors was higher among people who were older (90%), White (82%), or had high income (89%). Among people reporting lower trust, 25% said their physician spends too little time with them, and 14% said their doctor does not know or listen to them.
The survey shows that government agencies have work to do to earn trust. Responses indicate that 43% of physicians said they have “complete trust” in government health care agencies, such as the U.S. Food and Drug Administration and the Centers for Disease Control and Prevention, which is substantially higher than other parts of the health care system. However, trust in agencies declined for 43% of physician respondents and increased for 21%.
Dhruv Khullar, MD, MPP, of the department of health policy and economics at Weill Cornell Medical College in New York, told this news organization the survey results match what he sees anecdotally in medicine – that physicians have been losing trust in the system but not in their colleagues.
He said the sample size of 600 is enough to be influential, though he said he would like to know the response rate, which was not calculated for this survey.
He added that, in large part, physicians’ lack of trust in their systems may come from generally being asked to see more patients and to meet more metrics during the same or shorter periods.
Physicians’ lack of trust in the system can have significant consequences, he said. It can lead to burnout, which has been linked with poorer quality of care and physician turnover, he noted.
COVID-19 led some physicians to wonder whether their system had their best interests at heart, insofar as access to adequate medicines and supplies as well as emotional support were inconsistent, Dr. Khullar said.
He said that to regain trust health care systems need to ask themselves questions in three areas. The first is whether their goals are focused on the best interest of the organization or the best interest of the patient.
“Next is competency,” Dr. Khullar said. “Maybe your motives are right, but are you able to deliver? Are you delivering a good product, whether clinical services or something else?”
The third area is transparency, he said. “Are you going to be honest and forthright in what we’re doing and where we’re going?”
Caroline Pearson, senior vice president of health care strategy for NORC, said the emailed survey was conducted between Dec. 29, 2020, and Feb. 5, 2021, with a health care survey partner that maintains a nationwide panel of physicians across specialties.
She said this report is fairly novel insofar as surveys are more typically conducted regarding patients’ trust of their doctors or of the health care system.
Ms. Pearson said because health care is delivered in teams, understanding the level of trust among the entities helps ensure that care will be delivered effectively and seamlessly with high quality.
“We want our patients to trust our doctors, but we really want doctors to trust each other and trust the hospitals and systems in which they’re working,” she said.
Dr. Baron, Ms. Pearson, and Dr. Khullar report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a survey conducted by NORC at the University of Chicago on behalf of the American Board of Internal Medicine Foundation.
Survey results, released May 21, indicate that 30% of physicians say their trust in the U.S. health care system and health care leadership has decreased during the pandemic. Only 18% reported an increase in trust.
Physicians, however, have great trust in their fellow clinicians.
In the survey of 600 physicians, 94% said they trust doctors within their practice; 85% trusted doctors outside of their practice; and 89% trusted nurses. That trust increased during the pandemic, with 41% saying their trust in fellow physicians rose and 37% saying their trust in nurses did.
In a separate survey, NORC asked patients about their trust in various aspects of health care. Among 2,069 respondents, a wide majority reported that they trust doctors (84%) and nurses (85%), but only 64% trusted the health care system as a whole. One in three consumers (32%) said their trust in the health care system decreased during the pandemic, compared with 11% who said their trust increased.
The ABIM Foundation released the research findings on May 21 as part of Building Trust, a national campaign that aims to boost trust among patients, clinicians, system leaders, researchers, and others.
Richard J. Baron, MD, president and chief executive officer of the ABIM Foundation, said in an interview, “Clearly there’s lower trust in health care organization leaders and executives, and that’s troubling.
“Science by itself is not enough,” he said. “Becoming trustworthy has to be a core project of everybody in health care.”
Deterioration in physicians’ trust during the pandemic comes in part from failed promises of adequate personal protective equipment and some physicians’ loss of income as a result of the crisis, Dr. Baron said.
He added that the vaccine rollout was very uneven and that policies as to which elective procedures could be performed were handled differently in different parts of the country.
He also noted that, early on, transparency was lacking as to how many COVID patients hospitals were treating, which may have contributed to the decrease in trust in the system.
Fear of being known as ‘the COVID hospital’
Hospitals were afraid of being known as “the COVID hospital” and losing patients who were afraid to come there, Dr. Baron said.
He said the COVID-19 epidemic exacerbated problems regarding trust, but that trust has been declining for some time. The Building Trust campaign will focus on solutions in breaches of trust as physicians move increasingly toward being employees of huge systems, according to Dr. Baron.
However, trust works both ways, Dr. Baron notes. Physicians can be champions for their health care system or “throw the system under the bus,” he said.
For example, if a patient complains about the appointment system, clinicians who trust their institutions may say the system usually works and that they will try to make sure the patient has a better experience next time. Clinicians without trust may say they agree that the health care system doesn’t know what it is doing, and patients may further lose confidence when physicians validate their complaint, and patients may then go elsewhere.
78% of patients trust primary care doctor
When asked whether they trust their primary care physician, 78% of patients said yes. However, trust in doctors was higher among people who were older (90%), White (82%), or had high income (89%). Among people reporting lower trust, 25% said their physician spends too little time with them, and 14% said their doctor does not know or listen to them.
The survey shows that government agencies have work to do to earn trust. Responses indicate that 43% of physicians said they have “complete trust” in government health care agencies, such as the U.S. Food and Drug Administration and the Centers for Disease Control and Prevention, which is substantially higher than other parts of the health care system. However, trust in agencies declined for 43% of physician respondents and increased for 21%.
Dhruv Khullar, MD, MPP, of the department of health policy and economics at Weill Cornell Medical College in New York, told this news organization the survey results match what he sees anecdotally in medicine – that physicians have been losing trust in the system but not in their colleagues.
He said the sample size of 600 is enough to be influential, though he said he would like to know the response rate, which was not calculated for this survey.
He added that, in large part, physicians’ lack of trust in their systems may come from generally being asked to see more patients and to meet more metrics during the same or shorter periods.
Physicians’ lack of trust in the system can have significant consequences, he said. It can lead to burnout, which has been linked with poorer quality of care and physician turnover, he noted.
COVID-19 led some physicians to wonder whether their system had their best interests at heart, insofar as access to adequate medicines and supplies as well as emotional support were inconsistent, Dr. Khullar said.
He said that to regain trust health care systems need to ask themselves questions in three areas. The first is whether their goals are focused on the best interest of the organization or the best interest of the patient.
“Next is competency,” Dr. Khullar said. “Maybe your motives are right, but are you able to deliver? Are you delivering a good product, whether clinical services or something else?”
The third area is transparency, he said. “Are you going to be honest and forthright in what we’re doing and where we’re going?”
Caroline Pearson, senior vice president of health care strategy for NORC, said the emailed survey was conducted between Dec. 29, 2020, and Feb. 5, 2021, with a health care survey partner that maintains a nationwide panel of physicians across specialties.
She said this report is fairly novel insofar as surveys are more typically conducted regarding patients’ trust of their doctors or of the health care system.
Ms. Pearson said because health care is delivered in teams, understanding the level of trust among the entities helps ensure that care will be delivered effectively and seamlessly with high quality.
“We want our patients to trust our doctors, but we really want doctors to trust each other and trust the hospitals and systems in which they’re working,” she said.
Dr. Baron, Ms. Pearson, and Dr. Khullar report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rituximab superior to mycophenolate mofetil in pemphigus vulgaris study
Mycophenolate mofetil, commonly used as a first-line corticosteroid-sparing agent for moderate to severe cases of the autoimmune blistering skin condition pemphigus vulgaris, has been found to be inferior to the biologic agent rituximab.

Mycophenolate mofetil is widely accepted as a first-in-line corticosteroid-sparing agent for pemphigus vulgaris, but few studies have compared the effectiveness of the two treatments for pemphigus vulgaris. The European Academy of Dermatology and Venereology recommends rituximab (Rituxan), a CD20 inhibitor, as first-line treatment for patients with new-onset cases of moderate to severe intensity or for patients who fail to achieve clinical remission with systemic corticosteroids with or without other immunosuppressive treatments.
In the current study, published online on May 19, 2021, in the New England Journal of Medicine, researchers led by Victoria P. Werth, MD, professor of dermatology at the University of Pennsylvania, Philadelphia, conducted a randomized, controlled trial of 135 patients (mean age, 48 years; 53% women) with moderate to severe pemphigus vulgaris with 67 receiving rituximab and 68 receiving mycophenolate mofetil (99% of patients in the rituximab group and 85% of patients in the mycophenolate mofetil group completed the trial).
Patients in the rituximab group received 1,000 mg of IV rituximab on days 1, 15, 168, and 182 of the study, plus twice-daily oral placebo. Intravenous methylprednisolone at 100 mg was administered before each rituximab infusion to reduce infusion-related reactions. Patients in the second group were given mycophenolate mofetil orally twice daily, starting at 1 g/day in divided doses and adjusted to 2 g/day in divided doses by week 2. They also received placebo infusions on days 1, 15, 168, and 182 of the study.
Patients in both groups received oral glucocorticoids throughout the course of the trial: an average of 3,545 mg for the rituximab treatment group and a cumulative dose of 5,140 mg for the group treated with mycophenolate mofetil, a statistically significant difference (P < .001). Outcomes based on 62 patients treated with rituximab and 63 on MMF, a modified intention-to-treat group.
By week 52, 25 patients (40%) who were treated with rituximab experienced complete sustained remission (the primary endpoint), compared with 6 patients (10%) in the mycophenolate mofetil group (95% confidence interval, 15-45, P < .001).
Only six patients in the rituximab group experienced a disease flare as compared with 44 patients in the mycophenolate mofetil group (adjusted rate ratio, 0.12; 95% CI, 0.05-0.29; P < .001). Serious adverse events occurred in 15 of 67 patients (22%) in the rituximab group and in 10 of 68 (15%) in the mycophenolate mofetil group with 3 patients in the rituximab group and 26 in the mycophenolate mofetil receiving rescue therapy.
Second to remission, the goal of treatment for pemphigus vulgaris is to reduce the use of glucocorticoids, Dr. Werth and colleagues wrote, adding: “The results of this trial showed that rituximab was superior to mycophenolate mofetil in producing sustained complete remission over 52 weeks among patients with moderate to severe pemphigus vulgaris. Rituximab had a greater glucocorticoid-sparing effect than mycophenolate mofetil, but more patients in this group had serious adverse events.”
Most adverse events in the rituximab group were limited to infusion-related reactions, but serious adverse events occurred in 15 patients (including pneumonia and upper respiratory tract infection, cellulitis and acute pyelonephritis, viral pneumonia, and skin infection). Ten patients in the mycophenolate mofetil group experienced serious adverse events (pneumonia and influenza, cellulitis and sepsis, herpes zoster, and pyelonephritis).
The current study had several limitations, primarily its small size. Plus, the authors noted a short follow-up period after glucocorticoids were stopped.
Mycophenolate mofetil, along with immunosuppressants, is approved in the United States as a treatment for organ rejection in patients who have received kidney, heart or liver transplants. But it is also used off label for pemphigus vulgaris and in rheumatology as a treatment for lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease (Crohn’s disease), inflammatory eye disease (uveitis) as well as kidney and skin disorders.
In the 2018 treatment guidelines for pemphigus by the European Dermatology Forum and the EADV, mycophenolate mofetil is recommended as a first-line corticosteroid sparing agent for pemphigus vulgaris.
Rituximab was approved in 2018 as the first biologic therapy for patients with pemphigus vulgaris and is currently recommended as a treatment for patients with pemphigus. But how well it works in comparison with the long-established mycophenolate mofetil hasn’t been extensively studied.
Other smaller studies show that mycophenolate mofetil has a treatment effect, but those studies were small. The Ritux 3 trial, published in The Lancet showed that rituximab plus glucocorticoids as opposed to glucocorticoids alone was beneficial in treating pemphigus.
“Rituximab has moved toward first-line therapy for moderate to severe pemphigus as recommended by an international panel of experts,” Dr. Werth said in an interview.
In her practice, Dr. Werth said that she has observed similar outcomes in clinical practice for patients prescribed oral mycophenolate mofetil. “Patients take a long time to get to remission and frequently end up staying on prednisone and long-term mycophenolate mofetil,” she said. She uses mycophenolate mofetil less often since rituximab has been shown to be effective for many patients, but mycophenolate mofetil “still has a place for patients who don’t want, or can’t tolerate, rituximab, or for cases in which rituximab doesn’t work.”
This study was supported by a grant from Hoffmann–La Roche. Dr. Werth disclosed having served as a consultant to Genentech on pemphigus, and that the University of Pennsylvania has received a grant/contract to perform a rituximab–mycophenolate mofetil trial for pemphigus vulgaris.
Mycophenolate mofetil, commonly used as a first-line corticosteroid-sparing agent for moderate to severe cases of the autoimmune blistering skin condition pemphigus vulgaris, has been found to be inferior to the biologic agent rituximab.
Mycophenolate mofetil is widely accepted as a first-in-line corticosteroid-sparing agent for pemphigus vulgaris, but few studies have compared the effectiveness of the two treatments for pemphigus vulgaris. The European Academy of Dermatology and Venereology recommends rituximab (Rituxan), a CD20 inhibitor, as first-line treatment for patients with new-onset cases of moderate to severe intensity or for patients who fail to achieve clinical remission with systemic corticosteroids with or without other immunosuppressive treatments.
In the current study, published online on May 19, 2021, in the New England Journal of Medicine, researchers led by Victoria P. Werth, MD, professor of dermatology at the University of Pennsylvania, Philadelphia, conducted a randomized, controlled trial of 135 patients (mean age, 48 years; 53% women) with moderate to severe pemphigus vulgaris with 67 receiving rituximab and 68 receiving mycophenolate mofetil (99% of patients in the rituximab group and 85% of patients in the mycophenolate mofetil group completed the trial).
Patients in the rituximab group received 1,000 mg of IV rituximab on days 1, 15, 168, and 182 of the study, plus twice-daily oral placebo. Intravenous methylprednisolone at 100 mg was administered before each rituximab infusion to reduce infusion-related reactions. Patients in the second group were given mycophenolate mofetil orally twice daily, starting at 1 g/day in divided doses and adjusted to 2 g/day in divided doses by week 2. They also received placebo infusions on days 1, 15, 168, and 182 of the study.
Patients in both groups received oral glucocorticoids throughout the course of the trial: an average of 3,545 mg for the rituximab treatment group and a cumulative dose of 5,140 mg for the group treated with mycophenolate mofetil, a statistically significant difference (P < .001). Outcomes based on 62 patients treated with rituximab and 63 on MMF, a modified intention-to-treat group.
By week 52, 25 patients (40%) who were treated with rituximab experienced complete sustained remission (the primary endpoint), compared with 6 patients (10%) in the mycophenolate mofetil group (95% confidence interval, 15-45, P < .001).
Only six patients in the rituximab group experienced a disease flare as compared with 44 patients in the mycophenolate mofetil group (adjusted rate ratio, 0.12; 95% CI, 0.05-0.29; P < .001). Serious adverse events occurred in 15 of 67 patients (22%) in the rituximab group and in 10 of 68 (15%) in the mycophenolate mofetil group with 3 patients in the rituximab group and 26 in the mycophenolate mofetil receiving rescue therapy.
Second to remission, the goal of treatment for pemphigus vulgaris is to reduce the use of glucocorticoids, Dr. Werth and colleagues wrote, adding: “The results of this trial showed that rituximab was superior to mycophenolate mofetil in producing sustained complete remission over 52 weeks among patients with moderate to severe pemphigus vulgaris. Rituximab had a greater glucocorticoid-sparing effect than mycophenolate mofetil, but more patients in this group had serious adverse events.”
Most adverse events in the rituximab group were limited to infusion-related reactions, but serious adverse events occurred in 15 patients (including pneumonia and upper respiratory tract infection, cellulitis and acute pyelonephritis, viral pneumonia, and skin infection). Ten patients in the mycophenolate mofetil group experienced serious adverse events (pneumonia and influenza, cellulitis and sepsis, herpes zoster, and pyelonephritis).
The current study had several limitations, primarily its small size. Plus, the authors noted a short follow-up period after glucocorticoids were stopped.
Mycophenolate mofetil, along with immunosuppressants, is approved in the United States as a treatment for organ rejection in patients who have received kidney, heart or liver transplants. But it is also used off label for pemphigus vulgaris and in rheumatology as a treatment for lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease (Crohn’s disease), inflammatory eye disease (uveitis) as well as kidney and skin disorders.
In the 2018 treatment guidelines for pemphigus by the European Dermatology Forum and the EADV, mycophenolate mofetil is recommended as a first-line corticosteroid sparing agent for pemphigus vulgaris.
Rituximab was approved in 2018 as the first biologic therapy for patients with pemphigus vulgaris and is currently recommended as a treatment for patients with pemphigus. But how well it works in comparison with the long-established mycophenolate mofetil hasn’t been extensively studied.
Other smaller studies show that mycophenolate mofetil has a treatment effect, but those studies were small. The Ritux 3 trial, published in The Lancet showed that rituximab plus glucocorticoids as opposed to glucocorticoids alone was beneficial in treating pemphigus.
“Rituximab has moved toward first-line therapy for moderate to severe pemphigus as recommended by an international panel of experts,” Dr. Werth said in an interview.
In her practice, Dr. Werth said that she has observed similar outcomes in clinical practice for patients prescribed oral mycophenolate mofetil. “Patients take a long time to get to remission and frequently end up staying on prednisone and long-term mycophenolate mofetil,” she said. She uses mycophenolate mofetil less often since rituximab has been shown to be effective for many patients, but mycophenolate mofetil “still has a place for patients who don’t want, or can’t tolerate, rituximab, or for cases in which rituximab doesn’t work.”
This study was supported by a grant from Hoffmann–La Roche. Dr. Werth disclosed having served as a consultant to Genentech on pemphigus, and that the University of Pennsylvania has received a grant/contract to perform a rituximab–mycophenolate mofetil trial for pemphigus vulgaris.
Mycophenolate mofetil, commonly used as a first-line corticosteroid-sparing agent for moderate to severe cases of the autoimmune blistering skin condition pemphigus vulgaris, has been found to be inferior to the biologic agent rituximab.
Mycophenolate mofetil is widely accepted as a first-in-line corticosteroid-sparing agent for pemphigus vulgaris, but few studies have compared the effectiveness of the two treatments for pemphigus vulgaris. The European Academy of Dermatology and Venereology recommends rituximab (Rituxan), a CD20 inhibitor, as first-line treatment for patients with new-onset cases of moderate to severe intensity or for patients who fail to achieve clinical remission with systemic corticosteroids with or without other immunosuppressive treatments.
In the current study, published online on May 19, 2021, in the New England Journal of Medicine, researchers led by Victoria P. Werth, MD, professor of dermatology at the University of Pennsylvania, Philadelphia, conducted a randomized, controlled trial of 135 patients (mean age, 48 years; 53% women) with moderate to severe pemphigus vulgaris with 67 receiving rituximab and 68 receiving mycophenolate mofetil (99% of patients in the rituximab group and 85% of patients in the mycophenolate mofetil group completed the trial).
Patients in the rituximab group received 1,000 mg of IV rituximab on days 1, 15, 168, and 182 of the study, plus twice-daily oral placebo. Intravenous methylprednisolone at 100 mg was administered before each rituximab infusion to reduce infusion-related reactions. Patients in the second group were given mycophenolate mofetil orally twice daily, starting at 1 g/day in divided doses and adjusted to 2 g/day in divided doses by week 2. They also received placebo infusions on days 1, 15, 168, and 182 of the study.
Patients in both groups received oral glucocorticoids throughout the course of the trial: an average of 3,545 mg for the rituximab treatment group and a cumulative dose of 5,140 mg for the group treated with mycophenolate mofetil, a statistically significant difference (P < .001). Outcomes based on 62 patients treated with rituximab and 63 on MMF, a modified intention-to-treat group.
By week 52, 25 patients (40%) who were treated with rituximab experienced complete sustained remission (the primary endpoint), compared with 6 patients (10%) in the mycophenolate mofetil group (95% confidence interval, 15-45, P < .001).
Only six patients in the rituximab group experienced a disease flare as compared with 44 patients in the mycophenolate mofetil group (adjusted rate ratio, 0.12; 95% CI, 0.05-0.29; P < .001). Serious adverse events occurred in 15 of 67 patients (22%) in the rituximab group and in 10 of 68 (15%) in the mycophenolate mofetil group with 3 patients in the rituximab group and 26 in the mycophenolate mofetil receiving rescue therapy.
Second to remission, the goal of treatment for pemphigus vulgaris is to reduce the use of glucocorticoids, Dr. Werth and colleagues wrote, adding: “The results of this trial showed that rituximab was superior to mycophenolate mofetil in producing sustained complete remission over 52 weeks among patients with moderate to severe pemphigus vulgaris. Rituximab had a greater glucocorticoid-sparing effect than mycophenolate mofetil, but more patients in this group had serious adverse events.”
Most adverse events in the rituximab group were limited to infusion-related reactions, but serious adverse events occurred in 15 patients (including pneumonia and upper respiratory tract infection, cellulitis and acute pyelonephritis, viral pneumonia, and skin infection). Ten patients in the mycophenolate mofetil group experienced serious adverse events (pneumonia and influenza, cellulitis and sepsis, herpes zoster, and pyelonephritis).
The current study had several limitations, primarily its small size. Plus, the authors noted a short follow-up period after glucocorticoids were stopped.
Mycophenolate mofetil, along with immunosuppressants, is approved in the United States as a treatment for organ rejection in patients who have received kidney, heart or liver transplants. But it is also used off label for pemphigus vulgaris and in rheumatology as a treatment for lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease (Crohn’s disease), inflammatory eye disease (uveitis) as well as kidney and skin disorders.
In the 2018 treatment guidelines for pemphigus by the European Dermatology Forum and the EADV, mycophenolate mofetil is recommended as a first-line corticosteroid sparing agent for pemphigus vulgaris.
Rituximab was approved in 2018 as the first biologic therapy for patients with pemphigus vulgaris and is currently recommended as a treatment for patients with pemphigus. But how well it works in comparison with the long-established mycophenolate mofetil hasn’t been extensively studied.
Other smaller studies show that mycophenolate mofetil has a treatment effect, but those studies were small. The Ritux 3 trial, published in The Lancet showed that rituximab plus glucocorticoids as opposed to glucocorticoids alone was beneficial in treating pemphigus.
“Rituximab has moved toward first-line therapy for moderate to severe pemphigus as recommended by an international panel of experts,” Dr. Werth said in an interview.
In her practice, Dr. Werth said that she has observed similar outcomes in clinical practice for patients prescribed oral mycophenolate mofetil. “Patients take a long time to get to remission and frequently end up staying on prednisone and long-term mycophenolate mofetil,” she said. She uses mycophenolate mofetil less often since rituximab has been shown to be effective for many patients, but mycophenolate mofetil “still has a place for patients who don’t want, or can’t tolerate, rituximab, or for cases in which rituximab doesn’t work.”
This study was supported by a grant from Hoffmann–La Roche. Dr. Werth disclosed having served as a consultant to Genentech on pemphigus, and that the University of Pennsylvania has received a grant/contract to perform a rituximab–mycophenolate mofetil trial for pemphigus vulgaris.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE