User login
For MD-IQ use only
Cancer-related thyroidectomy linked to increased diabetes risk
People with thyroid cancer treated with thyroidectomy have as much as a 40% increased risk of developing type 2 diabetes, regardless of their age, with the elevated risk observed with low as well as high doses of postoperative levothyroxine, new research shows.
“This is the first population-based study to demonstrate an elevated risk of type 2 diabetes in postthyroidectomy patients with thyroid cancer, compared with that in matched controls,” wrote the authors of the research, published recently in the Journal of Clinical Endocrinology & Metabolism.
“Notably, there was a U-shaped relationship between postoperative levothyroxine dosage, a surrogate marker of TSH suppression, and the risk of type 2 diabetes,” said Hye Jin Yoo, MD, of the division of endocrinology and metabolism, Korea University College of Medicine, Seoul, and colleagues.
While other studies have linked thyroidectomy for thyroid cancer with an elevated risk for other metabolic conditions, including coronary heart disease and ischemic stroke, the relatively high diabetes risk is unexpected, said Tyler Drake, MD, an endocrinologist with the Minneapolis VA Health Care System.
“A 40% increased risk of diabetes is a big surprise,” he said in an interview.
“Diabetes is very common, with about one in 10 U.S. adults having type 2 diabetes, but a 40% increased risk in thyroid cancer patients is higher than I see in my clinical practice. [However], it is important to note that the [highest] risk was predominantly among the groups on the lowest and highest doses of levothyroxine,” said Dr. Drake, assistant professor of medicine at the University of Minnesota, Minneapolis.
U-shaped relationship between levothyroxine dose and diabetes risk
The findings are from a study of 36,377 patients with thyroid cancer in the National Health Insurance Service (NHIS) database in Korea who had undergone a thyroidectomy between 2004 and 2013.
The patients were matched 1:1 with controls who had nonthyroid cancers. Their mean age was 46.6 years, about 30% were male, and their mean body mass index was 23.8 kg/m2.
Over a mean follow-up of 6.6 years, the patients with thyroid cancer had a significantly higher risk of developing type 2 diabetes, at a rate of 47.5% (10,812) compared with 36.9% (9414; HR, 1.43; P < .001) in the control group, after adjustment for factors such as age, sex, BMI, smoking, drinking, systolic blood pressure, and fasting glucose.
The risk of type 2 diabetes among those with thyroid cancer was higher among the 83.2% of patients who underwent a total thyroidectomy compared with the 16.8% who had a unilateral lobectomy (HR, 1.06; P < .001).
In addition, those with thyroid cancer who received the lowest as well as highest dosages of levothyroxine had significantly higher risks of type 2 diabetes compared with controls (HR, 1.50 and 1.39, respectively; both P < .001).
A closer look at quartiles of levothyroxine dosing showed the first (lowest) quartile (defined as a mean levothyroxine dosage of < 101 mcg/day) was associated with an increased risk of type 2 diabetes compared with the second quartile group (101-127 mcg/day; HR, 1.45), as was the fourth quartile (≥ 150 mcg/day; HR, 1.37), while a decreased risk of type 2 diabetes was observed in the third quartile group (128-149 mcg/day versus the second quartile group; HR, 0.91).
“This result suggests a U-shaped relationship between the mean levothyroxine dosage and risk of type 2 diabetes in postthyroidectomy patients with thyroid cancer,” the authors said.
However, “consistent with previous studies, the present study showed that the highest risk of type 2 diabetes was observed in patients with thyroid cancer who were treated with the lowest mean dosage of levothyroxine,” they noted.
“This result suggests that inadequate supplementation of thyroid hormones may worsen glucose metabolism and should therefore be avoided.”
Potential mechanisms
Abnormal thyroid function, including hypo- and hyperthyroidism, following thyroidectomy and subsequent treatment with levothyroxine, is known to have potentially detrimental effects on glucose regulation among patients with thyroid cancer.
The potential mechanisms linking hypothyroidism with diabetes specifically include the possibility that insulin becomes unable to promote the utilization of glucose by muscles and adipose tissue. However, thyroid hormone replacement has been associated with a normalization of insulin sensitivity, the authors noted.
Meanwhile, glucose intolerance is common among patients with hyperthyroidism, largely due to an increase in hepatic glucose production, and likewise, the normalization of thyroid levels among those treated with methimazole has been linked to normalization of glucose and lipid metabolism alterations.
Dr. Drake noted that an important study limitation is that patients were analyzed based on their levothyroxine dose and not their TSH values, which the authors explain was due to the unavailability of the TSH values.
“By looking at levothyroxine doses, and not TSH values, it is possible some patients were being improperly treated with either too much or too little levothyroxine,” Dr. Drake noted.
Control group should have had hypothyroidism
The findings nevertheless shed light on the risk of diabetes following thyroidectomy for thyroid cancer, Anupam Kotwal, MD, commented on the study.
“This study is significant because it addresses an important topic exploring the link between thyroid dysfunction and metabolic disease, in this case ... hypothyroidism, due to surgery for thyroid cancer and type 2 diabetes,” Dr. Kotwal, assistant professor of medicine in the division of diabetes, endocrinology & metabolism at the University of Nebraska Medical Center, Omaha, said in an interview.
In terms of other limitations, Dr. Kotwal noted that the controls did not have hypothyroidism; therefore, “from this study, it is impossible to confirm whether hypothyroidism from any cause would be associated with higher incidence of diabetes or if it is specific to thyroid surgery for thyroid cancer.
“It would have been useful to have a control group of autoimmune primary hypothyroidism to evaluate the rate of diabetes during a similar follow-up duration,” Dr. Kotwal said.
“Hence, cohort studies with more granular data such as degree of TSH suppression and having a control group of hypothyroid patients due to autoimmune thyroid disease are needed to better understand this risk.”
Dr. Kotwal and Dr. Drake have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People with thyroid cancer treated with thyroidectomy have as much as a 40% increased risk of developing type 2 diabetes, regardless of their age, with the elevated risk observed with low as well as high doses of postoperative levothyroxine, new research shows.
“This is the first population-based study to demonstrate an elevated risk of type 2 diabetes in postthyroidectomy patients with thyroid cancer, compared with that in matched controls,” wrote the authors of the research, published recently in the Journal of Clinical Endocrinology & Metabolism.
“Notably, there was a U-shaped relationship between postoperative levothyroxine dosage, a surrogate marker of TSH suppression, and the risk of type 2 diabetes,” said Hye Jin Yoo, MD, of the division of endocrinology and metabolism, Korea University College of Medicine, Seoul, and colleagues.
While other studies have linked thyroidectomy for thyroid cancer with an elevated risk for other metabolic conditions, including coronary heart disease and ischemic stroke, the relatively high diabetes risk is unexpected, said Tyler Drake, MD, an endocrinologist with the Minneapolis VA Health Care System.
“A 40% increased risk of diabetes is a big surprise,” he said in an interview.
“Diabetes is very common, with about one in 10 U.S. adults having type 2 diabetes, but a 40% increased risk in thyroid cancer patients is higher than I see in my clinical practice. [However], it is important to note that the [highest] risk was predominantly among the groups on the lowest and highest doses of levothyroxine,” said Dr. Drake, assistant professor of medicine at the University of Minnesota, Minneapolis.
U-shaped relationship between levothyroxine dose and diabetes risk
The findings are from a study of 36,377 patients with thyroid cancer in the National Health Insurance Service (NHIS) database in Korea who had undergone a thyroidectomy between 2004 and 2013.
The patients were matched 1:1 with controls who had nonthyroid cancers. Their mean age was 46.6 years, about 30% were male, and their mean body mass index was 23.8 kg/m2.
Over a mean follow-up of 6.6 years, the patients with thyroid cancer had a significantly higher risk of developing type 2 diabetes, at a rate of 47.5% (10,812) compared with 36.9% (9414; HR, 1.43; P < .001) in the control group, after adjustment for factors such as age, sex, BMI, smoking, drinking, systolic blood pressure, and fasting glucose.
The risk of type 2 diabetes among those with thyroid cancer was higher among the 83.2% of patients who underwent a total thyroidectomy compared with the 16.8% who had a unilateral lobectomy (HR, 1.06; P < .001).
In addition, those with thyroid cancer who received the lowest as well as highest dosages of levothyroxine had significantly higher risks of type 2 diabetes compared with controls (HR, 1.50 and 1.39, respectively; both P < .001).
A closer look at quartiles of levothyroxine dosing showed the first (lowest) quartile (defined as a mean levothyroxine dosage of < 101 mcg/day) was associated with an increased risk of type 2 diabetes compared with the second quartile group (101-127 mcg/day; HR, 1.45), as was the fourth quartile (≥ 150 mcg/day; HR, 1.37), while a decreased risk of type 2 diabetes was observed in the third quartile group (128-149 mcg/day versus the second quartile group; HR, 0.91).
“This result suggests a U-shaped relationship between the mean levothyroxine dosage and risk of type 2 diabetes in postthyroidectomy patients with thyroid cancer,” the authors said.
However, “consistent with previous studies, the present study showed that the highest risk of type 2 diabetes was observed in patients with thyroid cancer who were treated with the lowest mean dosage of levothyroxine,” they noted.
“This result suggests that inadequate supplementation of thyroid hormones may worsen glucose metabolism and should therefore be avoided.”
Potential mechanisms
Abnormal thyroid function, including hypo- and hyperthyroidism, following thyroidectomy and subsequent treatment with levothyroxine, is known to have potentially detrimental effects on glucose regulation among patients with thyroid cancer.
The potential mechanisms linking hypothyroidism with diabetes specifically include the possibility that insulin becomes unable to promote the utilization of glucose by muscles and adipose tissue. However, thyroid hormone replacement has been associated with a normalization of insulin sensitivity, the authors noted.
Meanwhile, glucose intolerance is common among patients with hyperthyroidism, largely due to an increase in hepatic glucose production, and likewise, the normalization of thyroid levels among those treated with methimazole has been linked to normalization of glucose and lipid metabolism alterations.
Dr. Drake noted that an important study limitation is that patients were analyzed based on their levothyroxine dose and not their TSH values, which the authors explain was due to the unavailability of the TSH values.
“By looking at levothyroxine doses, and not TSH values, it is possible some patients were being improperly treated with either too much or too little levothyroxine,” Dr. Drake noted.
Control group should have had hypothyroidism
The findings nevertheless shed light on the risk of diabetes following thyroidectomy for thyroid cancer, Anupam Kotwal, MD, commented on the study.
“This study is significant because it addresses an important topic exploring the link between thyroid dysfunction and metabolic disease, in this case ... hypothyroidism, due to surgery for thyroid cancer and type 2 diabetes,” Dr. Kotwal, assistant professor of medicine in the division of diabetes, endocrinology & metabolism at the University of Nebraska Medical Center, Omaha, said in an interview.
In terms of other limitations, Dr. Kotwal noted that the controls did not have hypothyroidism; therefore, “from this study, it is impossible to confirm whether hypothyroidism from any cause would be associated with higher incidence of diabetes or if it is specific to thyroid surgery for thyroid cancer.
“It would have been useful to have a control group of autoimmune primary hypothyroidism to evaluate the rate of diabetes during a similar follow-up duration,” Dr. Kotwal said.
“Hence, cohort studies with more granular data such as degree of TSH suppression and having a control group of hypothyroid patients due to autoimmune thyroid disease are needed to better understand this risk.”
Dr. Kotwal and Dr. Drake have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People with thyroid cancer treated with thyroidectomy have as much as a 40% increased risk of developing type 2 diabetes, regardless of their age, with the elevated risk observed with low as well as high doses of postoperative levothyroxine, new research shows.
“This is the first population-based study to demonstrate an elevated risk of type 2 diabetes in postthyroidectomy patients with thyroid cancer, compared with that in matched controls,” wrote the authors of the research, published recently in the Journal of Clinical Endocrinology & Metabolism.
“Notably, there was a U-shaped relationship between postoperative levothyroxine dosage, a surrogate marker of TSH suppression, and the risk of type 2 diabetes,” said Hye Jin Yoo, MD, of the division of endocrinology and metabolism, Korea University College of Medicine, Seoul, and colleagues.
While other studies have linked thyroidectomy for thyroid cancer with an elevated risk for other metabolic conditions, including coronary heart disease and ischemic stroke, the relatively high diabetes risk is unexpected, said Tyler Drake, MD, an endocrinologist with the Minneapolis VA Health Care System.
“A 40% increased risk of diabetes is a big surprise,” he said in an interview.
“Diabetes is very common, with about one in 10 U.S. adults having type 2 diabetes, but a 40% increased risk in thyroid cancer patients is higher than I see in my clinical practice. [However], it is important to note that the [highest] risk was predominantly among the groups on the lowest and highest doses of levothyroxine,” said Dr. Drake, assistant professor of medicine at the University of Minnesota, Minneapolis.
U-shaped relationship between levothyroxine dose and diabetes risk
The findings are from a study of 36,377 patients with thyroid cancer in the National Health Insurance Service (NHIS) database in Korea who had undergone a thyroidectomy between 2004 and 2013.
The patients were matched 1:1 with controls who had nonthyroid cancers. Their mean age was 46.6 years, about 30% were male, and their mean body mass index was 23.8 kg/m2.
Over a mean follow-up of 6.6 years, the patients with thyroid cancer had a significantly higher risk of developing type 2 diabetes, at a rate of 47.5% (10,812) compared with 36.9% (9414; HR, 1.43; P < .001) in the control group, after adjustment for factors such as age, sex, BMI, smoking, drinking, systolic blood pressure, and fasting glucose.
The risk of type 2 diabetes among those with thyroid cancer was higher among the 83.2% of patients who underwent a total thyroidectomy compared with the 16.8% who had a unilateral lobectomy (HR, 1.06; P < .001).
In addition, those with thyroid cancer who received the lowest as well as highest dosages of levothyroxine had significantly higher risks of type 2 diabetes compared with controls (HR, 1.50 and 1.39, respectively; both P < .001).
A closer look at quartiles of levothyroxine dosing showed the first (lowest) quartile (defined as a mean levothyroxine dosage of < 101 mcg/day) was associated with an increased risk of type 2 diabetes compared with the second quartile group (101-127 mcg/day; HR, 1.45), as was the fourth quartile (≥ 150 mcg/day; HR, 1.37), while a decreased risk of type 2 diabetes was observed in the third quartile group (128-149 mcg/day versus the second quartile group; HR, 0.91).
“This result suggests a U-shaped relationship between the mean levothyroxine dosage and risk of type 2 diabetes in postthyroidectomy patients with thyroid cancer,” the authors said.
However, “consistent with previous studies, the present study showed that the highest risk of type 2 diabetes was observed in patients with thyroid cancer who were treated with the lowest mean dosage of levothyroxine,” they noted.
“This result suggests that inadequate supplementation of thyroid hormones may worsen glucose metabolism and should therefore be avoided.”
Potential mechanisms
Abnormal thyroid function, including hypo- and hyperthyroidism, following thyroidectomy and subsequent treatment with levothyroxine, is known to have potentially detrimental effects on glucose regulation among patients with thyroid cancer.
The potential mechanisms linking hypothyroidism with diabetes specifically include the possibility that insulin becomes unable to promote the utilization of glucose by muscles and adipose tissue. However, thyroid hormone replacement has been associated with a normalization of insulin sensitivity, the authors noted.
Meanwhile, glucose intolerance is common among patients with hyperthyroidism, largely due to an increase in hepatic glucose production, and likewise, the normalization of thyroid levels among those treated with methimazole has been linked to normalization of glucose and lipid metabolism alterations.
Dr. Drake noted that an important study limitation is that patients were analyzed based on their levothyroxine dose and not their TSH values, which the authors explain was due to the unavailability of the TSH values.
“By looking at levothyroxine doses, and not TSH values, it is possible some patients were being improperly treated with either too much or too little levothyroxine,” Dr. Drake noted.
Control group should have had hypothyroidism
The findings nevertheless shed light on the risk of diabetes following thyroidectomy for thyroid cancer, Anupam Kotwal, MD, commented on the study.
“This study is significant because it addresses an important topic exploring the link between thyroid dysfunction and metabolic disease, in this case ... hypothyroidism, due to surgery for thyroid cancer and type 2 diabetes,” Dr. Kotwal, assistant professor of medicine in the division of diabetes, endocrinology & metabolism at the University of Nebraska Medical Center, Omaha, said in an interview.
In terms of other limitations, Dr. Kotwal noted that the controls did not have hypothyroidism; therefore, “from this study, it is impossible to confirm whether hypothyroidism from any cause would be associated with higher incidence of diabetes or if it is specific to thyroid surgery for thyroid cancer.
“It would have been useful to have a control group of autoimmune primary hypothyroidism to evaluate the rate of diabetes during a similar follow-up duration,” Dr. Kotwal said.
“Hence, cohort studies with more granular data such as degree of TSH suppression and having a control group of hypothyroid patients due to autoimmune thyroid disease are needed to better understand this risk.”
Dr. Kotwal and Dr. Drake have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The road less traveled in gastroenterology and hepatology: Becoming a medical educator
How did you realize medical education was the pathway for you?
Near the end of medical school, I recall my friends and I casting predictions about what each person would be doing in twenty years. The projections offered up about my ultimate landing place were unanimous: a clinical researcher leading a gastroenterology division. I was excited when they said this to me. It made sense, as I had already done over 3 years of clinical research on inflammatory bowel disease at the time. But as I began leading various clinical research projects during my internal medicine residency, I realized that they were not generating a strong sense of fulfillment or passion for me. I greatly enjoyed the process of research and writing, but there still was something missing; I could no longer see the role of a funded clinical researcher sustaining me for the length of my medical and academic career.

Thus, at the end of my 2nd year of residency, I began to self-reflect more on the various aspects of my medical journey to elucidate my path forward. This process was jump-started by a humbling recognition from that year’s graduating class of medical students for my contributions to their education over the past 3 years. I had served as a teaching assistant for their pathophysiology course and then subsequently worked alongside many of them on their medicine rotations. I realized that helping foster their growth as physicians in a longitudinal way was unquestionably the most rewarding experience that I had had to date. With further reflection, I recognized that, amid the chaos of a busy call day, I most looked forward to the moments when I could teach the interns and students about the nuances of the patients being admitted. It never felt like an obligation but rather always left me feeling revitalized. So, by the beginning of my 3rd year of residency, I knew that I wanted to pursue a career within medical education.
Once you decided to become a medical educator, what were your next steps?
As I began to vocalize this change in career trajectory, I did not always encounter enthusiastic support. Because the medical educator pathway is more typical amongst the general medicine community, some faculty members advised me to avoid solely focusing on medical education as a specialist because academic success would be difficult to attain. But I had just recognized this could be my vocation within medicine, so I could not turn back now. Thus, I began to seek the mentorship of educators at my institution, and many of them wisely advised me to consider pursuing additional training in medical education to accrue the skill sets needed to lay the groundwork for a lifelong career. So, I participated in a 1-year medical education fellowship in conjunction with my chief residency year. This training was profoundly formative; I learned about the various theories on adult learning, as well as how to create curricula, how to teach effectively in a clinical environment, and how to deliver meaningful feedback to learners. But perhaps most importantly, I learned how to generate tangible evidence of productivity within medical education to allow for advancement in academia. This included rigorously studying the impact of educational interventions. It became clear to me by the end of this year that the pathways of medical education and researcher were not incongruent but could actually be quite complementary. In light of this, I designed and implemented a mandatory inpatient hepatology curriculum for internal medicine residents, for which I studied its immediate and long-term effects throughout my gastroenterology and hepatology fellowships as well as during my time as an attending. Currently, I am also investigating medical students’ exposure to liver disease through a multicenter assessment. Projects such as these would not have been feasible without dedicated mentorship, but as alluded to above, in contrast to the traditional clinical research paradigm, my mentors have often been from outside the fields of gastroenterology and hepatology.
What advice would you offer a junior faculty member interested in a career in medical education within gastroenterology and hepatology?
1. Just before I completed fellowship, I asked Holly Humphrey, MD, the former dean of the Pritzker School of Medicine at the University of Chicago, this same question. Her answer was simple and is worth sharing: “In the beginning, just focus on becoming the best clinician possible. The rest will fall into place with time.” So, I did exactly this. I continually tried to push the limits of my knowledge, always questioning standard clinical practices to understand the evidence behind (or not behind) them. This knowledge then naturally became the content of my teaching for trainees in the clinical environment so that eventually patient care and teaching were seamlessly integrated into the same day-to-day workflow. The more I taught trainees, the more my commitment to education was recognized by my institution.
2. Meet with leadership of your medical school, internal medicine residency program, and gastroenterology and hepatology fellowships early in the course of your career to assert your desire to contribute to their respective educational missions.
3. Create a teaching philosophy that clearly communicates “your fundamental beliefs about teaching and learning, why you hold those values and beliefs, and how you translate these claims into practice.”1 This document will act as a guiding force in your career by highlighting the themes and principles that you have already incorporated and will continue to incorporate into your teaching practices and educational activities. For example, it can provide clarity when you are in doubt of how to address a difficult learning environment or whether to accept a certain position.
4. Because of No. 1 and No. 2, you will start to be offered opportunities to formally become involved in curricula within undergraduate (UME) and graduate medical education (GME). It will likely begin with requests to lecture or precept small group sessions. Use these smaller opportunities not only to refine your teaching skills but to explore whether your career aspirations better align with UME or GME. With hard work and perseverance, the opportunities can progress to invitations to become a course director, join a curriculum committee, or become an associate program director for a residency or fellowship program (which at this point is why you want to know if you prefer working in UME, GME, or both).
5. Seek feedback often from your learners. It is the only way you will continue to improve your teaching skills and the learning environment you create. Furthermore, formal evaluations can be used in the promotion process.
6. Collaborate with and seek mentorship from fellow medical educators both at your own institution and at others. As previously mentioned, these relationships do not need to be (and are often not) with other gastroenterologists or hepatologists.
7. Seek out national opportunities related to medical education. Most of the gastroenterology and hepatology societies have one or more committees focused on medical training. The AGA Academy of Educators is a fantastic community of education-focused individuals within our specialty that provides opportunities for networking, funding, and career development. Furthermore, other general societies (for example, the Association of American Medical Colleges, American College of Physicians) may be interested in including subspecialty members in their educational committees and activities.
Dr. Mikolajczyk is an assistant professor of medicine and an associate program director for the Internal Medicine Residency Program at the University of Illinois Chicago. He is the lead faculty adviser for the Liver Fellow Network. He has no conflicts of interest to disclose.
How did you realize medical education was the pathway for you?
Near the end of medical school, I recall my friends and I casting predictions about what each person would be doing in twenty years. The projections offered up about my ultimate landing place were unanimous: a clinical researcher leading a gastroenterology division. I was excited when they said this to me. It made sense, as I had already done over 3 years of clinical research on inflammatory bowel disease at the time. But as I began leading various clinical research projects during my internal medicine residency, I realized that they were not generating a strong sense of fulfillment or passion for me. I greatly enjoyed the process of research and writing, but there still was something missing; I could no longer see the role of a funded clinical researcher sustaining me for the length of my medical and academic career.
Thus, at the end of my 2nd year of residency, I began to self-reflect more on the various aspects of my medical journey to elucidate my path forward. This process was jump-started by a humbling recognition from that year’s graduating class of medical students for my contributions to their education over the past 3 years. I had served as a teaching assistant for their pathophysiology course and then subsequently worked alongside many of them on their medicine rotations. I realized that helping foster their growth as physicians in a longitudinal way was unquestionably the most rewarding experience that I had had to date. With further reflection, I recognized that, amid the chaos of a busy call day, I most looked forward to the moments when I could teach the interns and students about the nuances of the patients being admitted. It never felt like an obligation but rather always left me feeling revitalized. So, by the beginning of my 3rd year of residency, I knew that I wanted to pursue a career within medical education.
Once you decided to become a medical educator, what were your next steps?
As I began to vocalize this change in career trajectory, I did not always encounter enthusiastic support. Because the medical educator pathway is more typical amongst the general medicine community, some faculty members advised me to avoid solely focusing on medical education as a specialist because academic success would be difficult to attain. But I had just recognized this could be my vocation within medicine, so I could not turn back now. Thus, I began to seek the mentorship of educators at my institution, and many of them wisely advised me to consider pursuing additional training in medical education to accrue the skill sets needed to lay the groundwork for a lifelong career. So, I participated in a 1-year medical education fellowship in conjunction with my chief residency year. This training was profoundly formative; I learned about the various theories on adult learning, as well as how to create curricula, how to teach effectively in a clinical environment, and how to deliver meaningful feedback to learners. But perhaps most importantly, I learned how to generate tangible evidence of productivity within medical education to allow for advancement in academia. This included rigorously studying the impact of educational interventions. It became clear to me by the end of this year that the pathways of medical education and researcher were not incongruent but could actually be quite complementary. In light of this, I designed and implemented a mandatory inpatient hepatology curriculum for internal medicine residents, for which I studied its immediate and long-term effects throughout my gastroenterology and hepatology fellowships as well as during my time as an attending. Currently, I am also investigating medical students’ exposure to liver disease through a multicenter assessment. Projects such as these would not have been feasible without dedicated mentorship, but as alluded to above, in contrast to the traditional clinical research paradigm, my mentors have often been from outside the fields of gastroenterology and hepatology.
What advice would you offer a junior faculty member interested in a career in medical education within gastroenterology and hepatology?
1. Just before I completed fellowship, I asked Holly Humphrey, MD, the former dean of the Pritzker School of Medicine at the University of Chicago, this same question. Her answer was simple and is worth sharing: “In the beginning, just focus on becoming the best clinician possible. The rest will fall into place with time.” So, I did exactly this. I continually tried to push the limits of my knowledge, always questioning standard clinical practices to understand the evidence behind (or not behind) them. This knowledge then naturally became the content of my teaching for trainees in the clinical environment so that eventually patient care and teaching were seamlessly integrated into the same day-to-day workflow. The more I taught trainees, the more my commitment to education was recognized by my institution.
2. Meet with leadership of your medical school, internal medicine residency program, and gastroenterology and hepatology fellowships early in the course of your career to assert your desire to contribute to their respective educational missions.
3. Create a teaching philosophy that clearly communicates “your fundamental beliefs about teaching and learning, why you hold those values and beliefs, and how you translate these claims into practice.”1 This document will act as a guiding force in your career by highlighting the themes and principles that you have already incorporated and will continue to incorporate into your teaching practices and educational activities. For example, it can provide clarity when you are in doubt of how to address a difficult learning environment or whether to accept a certain position.
4. Because of No. 1 and No. 2, you will start to be offered opportunities to formally become involved in curricula within undergraduate (UME) and graduate medical education (GME). It will likely begin with requests to lecture or precept small group sessions. Use these smaller opportunities not only to refine your teaching skills but to explore whether your career aspirations better align with UME or GME. With hard work and perseverance, the opportunities can progress to invitations to become a course director, join a curriculum committee, or become an associate program director for a residency or fellowship program (which at this point is why you want to know if you prefer working in UME, GME, or both).
5. Seek feedback often from your learners. It is the only way you will continue to improve your teaching skills and the learning environment you create. Furthermore, formal evaluations can be used in the promotion process.
6. Collaborate with and seek mentorship from fellow medical educators both at your own institution and at others. As previously mentioned, these relationships do not need to be (and are often not) with other gastroenterologists or hepatologists.
7. Seek out national opportunities related to medical education. Most of the gastroenterology and hepatology societies have one or more committees focused on medical training. The AGA Academy of Educators is a fantastic community of education-focused individuals within our specialty that provides opportunities for networking, funding, and career development. Furthermore, other general societies (for example, the Association of American Medical Colleges, American College of Physicians) may be interested in including subspecialty members in their educational committees and activities.
Dr. Mikolajczyk is an assistant professor of medicine and an associate program director for the Internal Medicine Residency Program at the University of Illinois Chicago. He is the lead faculty adviser for the Liver Fellow Network. He has no conflicts of interest to disclose.
How did you realize medical education was the pathway for you?
Near the end of medical school, I recall my friends and I casting predictions about what each person would be doing in twenty years. The projections offered up about my ultimate landing place were unanimous: a clinical researcher leading a gastroenterology division. I was excited when they said this to me. It made sense, as I had already done over 3 years of clinical research on inflammatory bowel disease at the time. But as I began leading various clinical research projects during my internal medicine residency, I realized that they were not generating a strong sense of fulfillment or passion for me. I greatly enjoyed the process of research and writing, but there still was something missing; I could no longer see the role of a funded clinical researcher sustaining me for the length of my medical and academic career.
Thus, at the end of my 2nd year of residency, I began to self-reflect more on the various aspects of my medical journey to elucidate my path forward. This process was jump-started by a humbling recognition from that year’s graduating class of medical students for my contributions to their education over the past 3 years. I had served as a teaching assistant for their pathophysiology course and then subsequently worked alongside many of them on their medicine rotations. I realized that helping foster their growth as physicians in a longitudinal way was unquestionably the most rewarding experience that I had had to date. With further reflection, I recognized that, amid the chaos of a busy call day, I most looked forward to the moments when I could teach the interns and students about the nuances of the patients being admitted. It never felt like an obligation but rather always left me feeling revitalized. So, by the beginning of my 3rd year of residency, I knew that I wanted to pursue a career within medical education.
Once you decided to become a medical educator, what were your next steps?
As I began to vocalize this change in career trajectory, I did not always encounter enthusiastic support. Because the medical educator pathway is more typical amongst the general medicine community, some faculty members advised me to avoid solely focusing on medical education as a specialist because academic success would be difficult to attain. But I had just recognized this could be my vocation within medicine, so I could not turn back now. Thus, I began to seek the mentorship of educators at my institution, and many of them wisely advised me to consider pursuing additional training in medical education to accrue the skill sets needed to lay the groundwork for a lifelong career. So, I participated in a 1-year medical education fellowship in conjunction with my chief residency year. This training was profoundly formative; I learned about the various theories on adult learning, as well as how to create curricula, how to teach effectively in a clinical environment, and how to deliver meaningful feedback to learners. But perhaps most importantly, I learned how to generate tangible evidence of productivity within medical education to allow for advancement in academia. This included rigorously studying the impact of educational interventions. It became clear to me by the end of this year that the pathways of medical education and researcher were not incongruent but could actually be quite complementary. In light of this, I designed and implemented a mandatory inpatient hepatology curriculum for internal medicine residents, for which I studied its immediate and long-term effects throughout my gastroenterology and hepatology fellowships as well as during my time as an attending. Currently, I am also investigating medical students’ exposure to liver disease through a multicenter assessment. Projects such as these would not have been feasible without dedicated mentorship, but as alluded to above, in contrast to the traditional clinical research paradigm, my mentors have often been from outside the fields of gastroenterology and hepatology.
What advice would you offer a junior faculty member interested in a career in medical education within gastroenterology and hepatology?
1. Just before I completed fellowship, I asked Holly Humphrey, MD, the former dean of the Pritzker School of Medicine at the University of Chicago, this same question. Her answer was simple and is worth sharing: “In the beginning, just focus on becoming the best clinician possible. The rest will fall into place with time.” So, I did exactly this. I continually tried to push the limits of my knowledge, always questioning standard clinical practices to understand the evidence behind (or not behind) them. This knowledge then naturally became the content of my teaching for trainees in the clinical environment so that eventually patient care and teaching were seamlessly integrated into the same day-to-day workflow. The more I taught trainees, the more my commitment to education was recognized by my institution.
2. Meet with leadership of your medical school, internal medicine residency program, and gastroenterology and hepatology fellowships early in the course of your career to assert your desire to contribute to their respective educational missions.
3. Create a teaching philosophy that clearly communicates “your fundamental beliefs about teaching and learning, why you hold those values and beliefs, and how you translate these claims into practice.”1 This document will act as a guiding force in your career by highlighting the themes and principles that you have already incorporated and will continue to incorporate into your teaching practices and educational activities. For example, it can provide clarity when you are in doubt of how to address a difficult learning environment or whether to accept a certain position.
4. Because of No. 1 and No. 2, you will start to be offered opportunities to formally become involved in curricula within undergraduate (UME) and graduate medical education (GME). It will likely begin with requests to lecture or precept small group sessions. Use these smaller opportunities not only to refine your teaching skills but to explore whether your career aspirations better align with UME or GME. With hard work and perseverance, the opportunities can progress to invitations to become a course director, join a curriculum committee, or become an associate program director for a residency or fellowship program (which at this point is why you want to know if you prefer working in UME, GME, or both).
5. Seek feedback often from your learners. It is the only way you will continue to improve your teaching skills and the learning environment you create. Furthermore, formal evaluations can be used in the promotion process.
6. Collaborate with and seek mentorship from fellow medical educators both at your own institution and at others. As previously mentioned, these relationships do not need to be (and are often not) with other gastroenterologists or hepatologists.
7. Seek out national opportunities related to medical education. Most of the gastroenterology and hepatology societies have one or more committees focused on medical training. The AGA Academy of Educators is a fantastic community of education-focused individuals within our specialty that provides opportunities for networking, funding, and career development. Furthermore, other general societies (for example, the Association of American Medical Colleges, American College of Physicians) may be interested in including subspecialty members in their educational committees and activities.
Dr. Mikolajczyk is an assistant professor of medicine and an associate program director for the Internal Medicine Residency Program at the University of Illinois Chicago. He is the lead faculty adviser for the Liver Fellow Network. He has no conflicts of interest to disclose.
Specialists think it’s up to the PCP to recommend flu vaccines. But many patients don’t see a PCP every year
A new survey from the National Foundation for Infectious Diseases shows that, despite the recommendation that patients who have chronic illnesses receive annual flu vaccines, only 45% of these patients do get them. People with chronic diseases are at increased risk for serious flu-related complications, including hospitalization and death.

The survey looked at physicians’ practices toward flu vaccination and communication between health care providers (HCP) and their adult patients with chronic health conditions.
Overall, less than a third of HCPs (31%) said they recommend annual flu vaccination to all of their patients with chronic health conditions. There were some surprising differences between subspecialists. For example, 72% of patients with a heart problem who saw a cardiologist said that physician recommended the flu vaccine. The recommendation rate dropped to 32% of lung patients seeing a pulmonary physician and only 10% of people with diabetes who saw an endocrinologist.
There is quite a large gap between what physicians and patients say about their interactions. Fully 77% of HCPs who recommend annual flu vaccination say they tell patients when they are at higher risk of complications from influenza. Yet only 48% of patients say they have been given such information.
Although it is critically important information for patients to learn, their risk of influenza is often missing from the discussion. For example, patients with heart disease are six times more likely to have a heart attack within 7 days of flu infection. People with diabetes are six times more likely to be hospitalized from flu and three times more likely to die. Similarly, those with asthma or chronic obstructive pulmonary disorder are at a much higher risk of complications.
One problem is that Yet only 65% of patients with one of these chronic illnesses report seeing their primary care physician at least annually.
Much of the disparity between the patient’s perception of what they were told and the physician’s is “how the ‘recommendation’ is actually made,” William Schaffner, MD, NFID’s medical director and professor of medicine at Vanderbilt University, Nashville, Tenn., told this news organization. Dr. Schaffner offered the following example: At the end of the visit, the doctor might say: “It’s that time of the year again – you want to think about getting your flu shot.”
“The doctor thinks they’ve recommended that, but the doctor really has opened the door for you to think about it and leave [yourself] unvaccinated.”
Dr. Schaffner’s alternative? Tell the patient: “‘You’ll get your flu vaccine on the way out. Tom or Sally will give it to you.’ That’s a very different kind of recommendation. And it’s a much greater assurance of providing the vaccine.”
Another major problem, Dr. Schaffner said, is that many specialists “don’t think of vaccination as something that’s included with their routine care” even though they do direct much of the patient’s care. He said that physicians should be more “directive” in their care and that immunizations should be better integrated into routine practice.
Jody Lanard, MD, a retired risk communication consultant who spent many years working with the World Health Organization on disease outbreak communications, said in an interview that this disconnect between physician and patient reports “was really jarring. And it’s actionable!”
She offered several practical suggestions. For one, she said, “the messaging to the specialists has to be very, very empathic. We know you’re already overburdened. And here we’re asking you to do something that you think of as somebody else’s job.” But if your patient gets flu, then your job as the cardiologist or endocrinologist will become more complicated and time-consuming. So getting the patients vaccinated will be a good investment and will make your job easier.
Because of the disparity in patient and physician reports, Dr. Lanard suggested implementing a “feedback mechanism where they [the health care providers] give out the prescription, and then the office calls [the patient] to see if they’ve gotten the shot or not. Because that way it will help correct the mismatch between them thinking that they told the patient and the patient not hearing it.”
Asked about why there might be a big gap between what physicians report they said and what patients heard, Dr. Lanard explained that “physicians often communicate in [a manner] sort of like a checklist. And the patients are focused on one or two things that are high in their minds. And the physician was mentioning some things that are on a separate topic that are not on a patient’s list and it goes right past them.”
Dr. Lanard recommended brief storytelling instead of checklists. For example: “I’ve been treating your diabetes for 10 years. During this last flu season, several of my diabetic patients had a really hard time when they caught the flu. So now I’m trying harder to remember to remind you to get your flu shots.”
She urged HCPs to “make it more personal ... but it can still be scripted in advance as part of something that [you’re] remembering to do during the check.” She added that their professional associations may be able to send them suggested language they can adapt.
Finally, Dr. Lanard cautioned about vaccine myths. “The word myth is so insulting. It’s basically a word that sends the signal that you’re an idiot.”
She advised specialists to avoid the word “myth,” which will make the person defensive. Instead, say something like, “A lot of people, even some of my own family members, think the flu vaccine gives you the flu. ... But it doesn’t. And then you go into the reality.”
Dr. Lanard suggested that specialists implement the follow-up calls and close the feedback loop, saying: “If they did the survey a few years later, I bet that gap would narrow.”
Dr. Schaffner and Dr. Lanard disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new survey from the National Foundation for Infectious Diseases shows that, despite the recommendation that patients who have chronic illnesses receive annual flu vaccines, only 45% of these patients do get them. People with chronic diseases are at increased risk for serious flu-related complications, including hospitalization and death.
The survey looked at physicians’ practices toward flu vaccination and communication between health care providers (HCP) and their adult patients with chronic health conditions.
Overall, less than a third of HCPs (31%) said they recommend annual flu vaccination to all of their patients with chronic health conditions. There were some surprising differences between subspecialists. For example, 72% of patients with a heart problem who saw a cardiologist said that physician recommended the flu vaccine. The recommendation rate dropped to 32% of lung patients seeing a pulmonary physician and only 10% of people with diabetes who saw an endocrinologist.
There is quite a large gap between what physicians and patients say about their interactions. Fully 77% of HCPs who recommend annual flu vaccination say they tell patients when they are at higher risk of complications from influenza. Yet only 48% of patients say they have been given such information.
Although it is critically important information for patients to learn, their risk of influenza is often missing from the discussion. For example, patients with heart disease are six times more likely to have a heart attack within 7 days of flu infection. People with diabetes are six times more likely to be hospitalized from flu and three times more likely to die. Similarly, those with asthma or chronic obstructive pulmonary disorder are at a much higher risk of complications.
One problem is that Yet only 65% of patients with one of these chronic illnesses report seeing their primary care physician at least annually.
Much of the disparity between the patient’s perception of what they were told and the physician’s is “how the ‘recommendation’ is actually made,” William Schaffner, MD, NFID’s medical director and professor of medicine at Vanderbilt University, Nashville, Tenn., told this news organization. Dr. Schaffner offered the following example: At the end of the visit, the doctor might say: “It’s that time of the year again – you want to think about getting your flu shot.”
“The doctor thinks they’ve recommended that, but the doctor really has opened the door for you to think about it and leave [yourself] unvaccinated.”
Dr. Schaffner’s alternative? Tell the patient: “‘You’ll get your flu vaccine on the way out. Tom or Sally will give it to you.’ That’s a very different kind of recommendation. And it’s a much greater assurance of providing the vaccine.”
Another major problem, Dr. Schaffner said, is that many specialists “don’t think of vaccination as something that’s included with their routine care” even though they do direct much of the patient’s care. He said that physicians should be more “directive” in their care and that immunizations should be better integrated into routine practice.
Jody Lanard, MD, a retired risk communication consultant who spent many years working with the World Health Organization on disease outbreak communications, said in an interview that this disconnect between physician and patient reports “was really jarring. And it’s actionable!”
She offered several practical suggestions. For one, she said, “the messaging to the specialists has to be very, very empathic. We know you’re already overburdened. And here we’re asking you to do something that you think of as somebody else’s job.” But if your patient gets flu, then your job as the cardiologist or endocrinologist will become more complicated and time-consuming. So getting the patients vaccinated will be a good investment and will make your job easier.
Because of the disparity in patient and physician reports, Dr. Lanard suggested implementing a “feedback mechanism where they [the health care providers] give out the prescription, and then the office calls [the patient] to see if they’ve gotten the shot or not. Because that way it will help correct the mismatch between them thinking that they told the patient and the patient not hearing it.”
Asked about why there might be a big gap between what physicians report they said and what patients heard, Dr. Lanard explained that “physicians often communicate in [a manner] sort of like a checklist. And the patients are focused on one or two things that are high in their minds. And the physician was mentioning some things that are on a separate topic that are not on a patient’s list and it goes right past them.”
Dr. Lanard recommended brief storytelling instead of checklists. For example: “I’ve been treating your diabetes for 10 years. During this last flu season, several of my diabetic patients had a really hard time when they caught the flu. So now I’m trying harder to remember to remind you to get your flu shots.”
She urged HCPs to “make it more personal ... but it can still be scripted in advance as part of something that [you’re] remembering to do during the check.” She added that their professional associations may be able to send them suggested language they can adapt.
Finally, Dr. Lanard cautioned about vaccine myths. “The word myth is so insulting. It’s basically a word that sends the signal that you’re an idiot.”
She advised specialists to avoid the word “myth,” which will make the person defensive. Instead, say something like, “A lot of people, even some of my own family members, think the flu vaccine gives you the flu. ... But it doesn’t. And then you go into the reality.”
Dr. Lanard suggested that specialists implement the follow-up calls and close the feedback loop, saying: “If they did the survey a few years later, I bet that gap would narrow.”
Dr. Schaffner and Dr. Lanard disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new survey from the National Foundation for Infectious Diseases shows that, despite the recommendation that patients who have chronic illnesses receive annual flu vaccines, only 45% of these patients do get them. People with chronic diseases are at increased risk for serious flu-related complications, including hospitalization and death.
The survey looked at physicians’ practices toward flu vaccination and communication between health care providers (HCP) and their adult patients with chronic health conditions.
Overall, less than a third of HCPs (31%) said they recommend annual flu vaccination to all of their patients with chronic health conditions. There were some surprising differences between subspecialists. For example, 72% of patients with a heart problem who saw a cardiologist said that physician recommended the flu vaccine. The recommendation rate dropped to 32% of lung patients seeing a pulmonary physician and only 10% of people with diabetes who saw an endocrinologist.
There is quite a large gap between what physicians and patients say about their interactions. Fully 77% of HCPs who recommend annual flu vaccination say they tell patients when they are at higher risk of complications from influenza. Yet only 48% of patients say they have been given such information.
Although it is critically important information for patients to learn, their risk of influenza is often missing from the discussion. For example, patients with heart disease are six times more likely to have a heart attack within 7 days of flu infection. People with diabetes are six times more likely to be hospitalized from flu and three times more likely to die. Similarly, those with asthma or chronic obstructive pulmonary disorder are at a much higher risk of complications.
One problem is that Yet only 65% of patients with one of these chronic illnesses report seeing their primary care physician at least annually.
Much of the disparity between the patient’s perception of what they were told and the physician’s is “how the ‘recommendation’ is actually made,” William Schaffner, MD, NFID’s medical director and professor of medicine at Vanderbilt University, Nashville, Tenn., told this news organization. Dr. Schaffner offered the following example: At the end of the visit, the doctor might say: “It’s that time of the year again – you want to think about getting your flu shot.”
“The doctor thinks they’ve recommended that, but the doctor really has opened the door for you to think about it and leave [yourself] unvaccinated.”
Dr. Schaffner’s alternative? Tell the patient: “‘You’ll get your flu vaccine on the way out. Tom or Sally will give it to you.’ That’s a very different kind of recommendation. And it’s a much greater assurance of providing the vaccine.”
Another major problem, Dr. Schaffner said, is that many specialists “don’t think of vaccination as something that’s included with their routine care” even though they do direct much of the patient’s care. He said that physicians should be more “directive” in their care and that immunizations should be better integrated into routine practice.
Jody Lanard, MD, a retired risk communication consultant who spent many years working with the World Health Organization on disease outbreak communications, said in an interview that this disconnect between physician and patient reports “was really jarring. And it’s actionable!”
She offered several practical suggestions. For one, she said, “the messaging to the specialists has to be very, very empathic. We know you’re already overburdened. And here we’re asking you to do something that you think of as somebody else’s job.” But if your patient gets flu, then your job as the cardiologist or endocrinologist will become more complicated and time-consuming. So getting the patients vaccinated will be a good investment and will make your job easier.
Because of the disparity in patient and physician reports, Dr. Lanard suggested implementing a “feedback mechanism where they [the health care providers] give out the prescription, and then the office calls [the patient] to see if they’ve gotten the shot or not. Because that way it will help correct the mismatch between them thinking that they told the patient and the patient not hearing it.”
Asked about why there might be a big gap between what physicians report they said and what patients heard, Dr. Lanard explained that “physicians often communicate in [a manner] sort of like a checklist. And the patients are focused on one or two things that are high in their minds. And the physician was mentioning some things that are on a separate topic that are not on a patient’s list and it goes right past them.”
Dr. Lanard recommended brief storytelling instead of checklists. For example: “I’ve been treating your diabetes for 10 years. During this last flu season, several of my diabetic patients had a really hard time when they caught the flu. So now I’m trying harder to remember to remind you to get your flu shots.”
She urged HCPs to “make it more personal ... but it can still be scripted in advance as part of something that [you’re] remembering to do during the check.” She added that their professional associations may be able to send them suggested language they can adapt.
Finally, Dr. Lanard cautioned about vaccine myths. “The word myth is so insulting. It’s basically a word that sends the signal that you’re an idiot.”
She advised specialists to avoid the word “myth,” which will make the person defensive. Instead, say something like, “A lot of people, even some of my own family members, think the flu vaccine gives you the flu. ... But it doesn’t. And then you go into the reality.”
Dr. Lanard suggested that specialists implement the follow-up calls and close the feedback loop, saying: “If they did the survey a few years later, I bet that gap would narrow.”
Dr. Schaffner and Dr. Lanard disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Care via video teleconferencing can be as effective as in-person for some conditions

This was a finding of a new study published in Annals of Internal Medicine involving a review of literature on video teleconferencing (VTC) visits, which was authored by Jordan Albritton, PhD, MPH and his colleagues.
The authors found generally comparable patient outcomes as well as no differences in health care use, patient satisfaction, and quality of life when visits conducted using VTC were compared with usual care.
While VTC may work best for monitoring patients with chronic conditions, it can also be effective for acute care, said Dr. Albritton, who is a research public health analyst at RTI International in Research Triangle Park, N.C., in an interview.
The investigators analyzed 20 randomized controlled trials of at least 50 patients and acceptable risk of bias in which VTC was used either for main or adjunct care delivery. Published from 2013 to 2019, these studies looked at care for diabetes and pain management, as well as some respiratory, neurologic, and cardiovascular conditions. Studies comparing VTC with usual care that did not involve any added in-person care were more likely to favor the VTC group, the investigators found.
“We excluded conditions such as substance use disorders, maternal care, and weight management for which there was sufficient prior evidence of the benefit of VTC,” Dr. Albritton said in an interview. “But I don’t think our results would have been substantially different if we had included these other diseases. We found general evidence in the literature that VTC is effective for a broader range of conditions.”
In some cases, such as if changes in a patient’s condition triggered an automatic virtual visit, the author said he thinks VTC may lead to even greater effectiveness.
“The doctor and patient could figure out on the spot what’s going on and perhaps change the medication,” Dr. Albritton explained.
In general agreement is Julia L. Frydman, MD, assistant professor in the Brookdale Department of Geriatric and Palliative Medicine at Icahn School of Medicine at Mount Sinai in New York, who was not involved in the RTI research.

“Telemedicine has promise across many medical subspecialties, and what we need now are more studies to understand the perspectives of patients, caregivers, and clinicians as well as the impact of telemedicine on health outcomes and healthcare utilization.”
In acknowledgment of their utility, video visits are on the rise in the United States. A 2020 survey found that 22% of patients and 80% of physicians reported having participated in a video visit, three times the rate of the previous year. The authors noted that policy changes enacted to support telehealth strategies during the pandemic are expected to remain in place, and although patients are returning to in-person care, the virtual visit market will likely continue growing.
Increased telemedicine use by older adults
“We’ve seen an exciting expansion of telemedicine use among older adults, and we need to focus on continuing to meet their needs,” Dr. Frydman said.
In a recent study of televisits during the pandemic, Dr. Frydman’s group found a fivefold greater uptake of remote consultations by seniors – from 5% to 25%. Although in-person visits were far more common among older adults.
A specific advantage of video-based over audio-only telehealth, noted Dr. Albritton, is that physicians can directly observe patients in their home environment. Sharing that view is Deepa Iyengar, MBBS/MD,MPH, professor of family medicine at McGovern Medical School at The University of Texas Health Science Center at Houston, where, she said, “the pandemic has put VTC use into overdrive.”

According to Dr. Iyengar, who was not involved in the RTI research, the video component definitely represents value-added over phone calls. “You can pick up visual cues on video that you might not see if the patient came in and you can see what the home environment is like – whether there are a lot of loose rugs on the floor or broken or missing light bulbs,” she said in an interview.
‘VTC is here to stay’
In other parts of the country, doctors are finding virtual care useful – and more common. “VTC is here to stay, for sure – the horse is out of the barn,” said Cheryl L. Wilkes, MD, an internist at Northwestern Medicine and assistant professor of medicine at Northwestern University in Chicago. “The RTI study shows no harm from VTC and also shows it may even improve clinical outcomes.”
Video visits can also save patients high parking fees at clinics and spare the sick or elderly from having to hire caregivers to bring them into the office or from having to walk blocks in dangerous weather conditions, she added. “And I can do a virtual visit on the fly or at night when a relative or caregiver is home from work to be there with the patient.”
In addition to being beneficial for following up with patients with chronic diseases such as hypertension or diabetes, VTC may be able to replace some visits that have traditionally required hands-on care, said Dr. Wilkes.
She said she knows a cardiologist who has refined a process whereby a patient – say, one who may have edema – is asked to perform a maneuver via VTC and then display the result to the doctor: The doctor says, “put your leg up and press on it hard for 10 seconds and then show me what it looks like,” according to Dr. Wilkes.
The key now is to identify the best persons across specialties from neurology to rheumatology to videotape ways they’ve created to help their patients participate virtually in consults traditionally done at the office, Dr. Wilkes noted.
But some conditions will always require palpation and the use of a stethoscope, according Dr. Iyengar.
“If someone has an ulcer, I have to be able to feel it,” she said.
And while some maternity care can be given virtually – for instance, if a mother-to be develops a bad cold – hands-on obstetrical care to check the position and health of the baby obviously has to be done in person. “So VTC is definitely going to be a welcome addition but not a replacement,” Dr. Iyengar said.
Gaps in research on VTC visits
Many questions remain regarding the overall usefulness of VTC visits for certain patient groups, according to the authors.
They highlighted, for example, the dearth of data on subgroups or on underserved and vulnerable populations, with no head-to-head studies identified in their review. In addition, they found no studies examining VTC versus usual care for patients with concurrent conditions or on its effect on health equity and disparities.
“It’s now our job to understand the ongoing barriers to telemedicine access, including the digital divide and the usability of telemedicine platforms, and design interventions that overcome them,” Dr. Frydman said. “At the same time, we need to make sure we’re understanding and respecting the preferences of older adults in terms of how they access health care.”
This study was supported by the Patient-Centered Outcomes Research Institute (PCORI). Dr. Albritton is employed by RTI International, the contractor responsible for conducting the research and developing the manuscript. Several coauthors disclosed support from or contracts with PCORI. One coauthor’s spouse holds stock in private health companies. Dr. Frydman, Dr. Iyengar, and Dr. Wilkes disclosed no competing interests relevant to their comments.
This was a finding of a new study published in Annals of Internal Medicine involving a review of literature on video teleconferencing (VTC) visits, which was authored by Jordan Albritton, PhD, MPH and his colleagues.
The authors found generally comparable patient outcomes as well as no differences in health care use, patient satisfaction, and quality of life when visits conducted using VTC were compared with usual care.
While VTC may work best for monitoring patients with chronic conditions, it can also be effective for acute care, said Dr. Albritton, who is a research public health analyst at RTI International in Research Triangle Park, N.C., in an interview.
The investigators analyzed 20 randomized controlled trials of at least 50 patients and acceptable risk of bias in which VTC was used either for main or adjunct care delivery. Published from 2013 to 2019, these studies looked at care for diabetes and pain management, as well as some respiratory, neurologic, and cardiovascular conditions. Studies comparing VTC with usual care that did not involve any added in-person care were more likely to favor the VTC group, the investigators found.
“We excluded conditions such as substance use disorders, maternal care, and weight management for which there was sufficient prior evidence of the benefit of VTC,” Dr. Albritton said in an interview. “But I don’t think our results would have been substantially different if we had included these other diseases. We found general evidence in the literature that VTC is effective for a broader range of conditions.”
In some cases, such as if changes in a patient’s condition triggered an automatic virtual visit, the author said he thinks VTC may lead to even greater effectiveness.
“The doctor and patient could figure out on the spot what’s going on and perhaps change the medication,” Dr. Albritton explained.
In general agreement is Julia L. Frydman, MD, assistant professor in the Brookdale Department of Geriatric and Palliative Medicine at Icahn School of Medicine at Mount Sinai in New York, who was not involved in the RTI research.
“Telemedicine has promise across many medical subspecialties, and what we need now are more studies to understand the perspectives of patients, caregivers, and clinicians as well as the impact of telemedicine on health outcomes and healthcare utilization.”
In acknowledgment of their utility, video visits are on the rise in the United States. A 2020 survey found that 22% of patients and 80% of physicians reported having participated in a video visit, three times the rate of the previous year. The authors noted that policy changes enacted to support telehealth strategies during the pandemic are expected to remain in place, and although patients are returning to in-person care, the virtual visit market will likely continue growing.
Increased telemedicine use by older adults
“We’ve seen an exciting expansion of telemedicine use among older adults, and we need to focus on continuing to meet their needs,” Dr. Frydman said.
In a recent study of televisits during the pandemic, Dr. Frydman’s group found a fivefold greater uptake of remote consultations by seniors – from 5% to 25%. Although in-person visits were far more common among older adults.
A specific advantage of video-based over audio-only telehealth, noted Dr. Albritton, is that physicians can directly observe patients in their home environment. Sharing that view is Deepa Iyengar, MBBS/MD,MPH, professor of family medicine at McGovern Medical School at The University of Texas Health Science Center at Houston, where, she said, “the pandemic has put VTC use into overdrive.”
According to Dr. Iyengar, who was not involved in the RTI research, the video component definitely represents value-added over phone calls. “You can pick up visual cues on video that you might not see if the patient came in and you can see what the home environment is like – whether there are a lot of loose rugs on the floor or broken or missing light bulbs,” she said in an interview.
‘VTC is here to stay’
In other parts of the country, doctors are finding virtual care useful – and more common. “VTC is here to stay, for sure – the horse is out of the barn,” said Cheryl L. Wilkes, MD, an internist at Northwestern Medicine and assistant professor of medicine at Northwestern University in Chicago. “The RTI study shows no harm from VTC and also shows it may even improve clinical outcomes.”
Video visits can also save patients high parking fees at clinics and spare the sick or elderly from having to hire caregivers to bring them into the office or from having to walk blocks in dangerous weather conditions, she added. “And I can do a virtual visit on the fly or at night when a relative or caregiver is home from work to be there with the patient.”
In addition to being beneficial for following up with patients with chronic diseases such as hypertension or diabetes, VTC may be able to replace some visits that have traditionally required hands-on care, said Dr. Wilkes.
She said she knows a cardiologist who has refined a process whereby a patient – say, one who may have edema – is asked to perform a maneuver via VTC and then display the result to the doctor: The doctor says, “put your leg up and press on it hard for 10 seconds and then show me what it looks like,” according to Dr. Wilkes.
The key now is to identify the best persons across specialties from neurology to rheumatology to videotape ways they’ve created to help their patients participate virtually in consults traditionally done at the office, Dr. Wilkes noted.
But some conditions will always require palpation and the use of a stethoscope, according Dr. Iyengar.
“If someone has an ulcer, I have to be able to feel it,” she said.
And while some maternity care can be given virtually – for instance, if a mother-to be develops a bad cold – hands-on obstetrical care to check the position and health of the baby obviously has to be done in person. “So VTC is definitely going to be a welcome addition but not a replacement,” Dr. Iyengar said.
Gaps in research on VTC visits
Many questions remain regarding the overall usefulness of VTC visits for certain patient groups, according to the authors.
They highlighted, for example, the dearth of data on subgroups or on underserved and vulnerable populations, with no head-to-head studies identified in their review. In addition, they found no studies examining VTC versus usual care for patients with concurrent conditions or on its effect on health equity and disparities.
“It’s now our job to understand the ongoing barriers to telemedicine access, including the digital divide and the usability of telemedicine platforms, and design interventions that overcome them,” Dr. Frydman said. “At the same time, we need to make sure we’re understanding and respecting the preferences of older adults in terms of how they access health care.”
This study was supported by the Patient-Centered Outcomes Research Institute (PCORI). Dr. Albritton is employed by RTI International, the contractor responsible for conducting the research and developing the manuscript. Several coauthors disclosed support from or contracts with PCORI. One coauthor’s spouse holds stock in private health companies. Dr. Frydman, Dr. Iyengar, and Dr. Wilkes disclosed no competing interests relevant to their comments.
This was a finding of a new study published in Annals of Internal Medicine involving a review of literature on video teleconferencing (VTC) visits, which was authored by Jordan Albritton, PhD, MPH and his colleagues.
The authors found generally comparable patient outcomes as well as no differences in health care use, patient satisfaction, and quality of life when visits conducted using VTC were compared with usual care.
While VTC may work best for monitoring patients with chronic conditions, it can also be effective for acute care, said Dr. Albritton, who is a research public health analyst at RTI International in Research Triangle Park, N.C., in an interview.
The investigators analyzed 20 randomized controlled trials of at least 50 patients and acceptable risk of bias in which VTC was used either for main or adjunct care delivery. Published from 2013 to 2019, these studies looked at care for diabetes and pain management, as well as some respiratory, neurologic, and cardiovascular conditions. Studies comparing VTC with usual care that did not involve any added in-person care were more likely to favor the VTC group, the investigators found.
“We excluded conditions such as substance use disorders, maternal care, and weight management for which there was sufficient prior evidence of the benefit of VTC,” Dr. Albritton said in an interview. “But I don’t think our results would have been substantially different if we had included these other diseases. We found general evidence in the literature that VTC is effective for a broader range of conditions.”
In some cases, such as if changes in a patient’s condition triggered an automatic virtual visit, the author said he thinks VTC may lead to even greater effectiveness.
“The doctor and patient could figure out on the spot what’s going on and perhaps change the medication,” Dr. Albritton explained.
In general agreement is Julia L. Frydman, MD, assistant professor in the Brookdale Department of Geriatric and Palliative Medicine at Icahn School of Medicine at Mount Sinai in New York, who was not involved in the RTI research.
“Telemedicine has promise across many medical subspecialties, and what we need now are more studies to understand the perspectives of patients, caregivers, and clinicians as well as the impact of telemedicine on health outcomes and healthcare utilization.”
In acknowledgment of their utility, video visits are on the rise in the United States. A 2020 survey found that 22% of patients and 80% of physicians reported having participated in a video visit, three times the rate of the previous year. The authors noted that policy changes enacted to support telehealth strategies during the pandemic are expected to remain in place, and although patients are returning to in-person care, the virtual visit market will likely continue growing.
Increased telemedicine use by older adults
“We’ve seen an exciting expansion of telemedicine use among older adults, and we need to focus on continuing to meet their needs,” Dr. Frydman said.
In a recent study of televisits during the pandemic, Dr. Frydman’s group found a fivefold greater uptake of remote consultations by seniors – from 5% to 25%. Although in-person visits were far more common among older adults.
A specific advantage of video-based over audio-only telehealth, noted Dr. Albritton, is that physicians can directly observe patients in their home environment. Sharing that view is Deepa Iyengar, MBBS/MD,MPH, professor of family medicine at McGovern Medical School at The University of Texas Health Science Center at Houston, where, she said, “the pandemic has put VTC use into overdrive.”
According to Dr. Iyengar, who was not involved in the RTI research, the video component definitely represents value-added over phone calls. “You can pick up visual cues on video that you might not see if the patient came in and you can see what the home environment is like – whether there are a lot of loose rugs on the floor or broken or missing light bulbs,” she said in an interview.
‘VTC is here to stay’
In other parts of the country, doctors are finding virtual care useful – and more common. “VTC is here to stay, for sure – the horse is out of the barn,” said Cheryl L. Wilkes, MD, an internist at Northwestern Medicine and assistant professor of medicine at Northwestern University in Chicago. “The RTI study shows no harm from VTC and also shows it may even improve clinical outcomes.”
Video visits can also save patients high parking fees at clinics and spare the sick or elderly from having to hire caregivers to bring them into the office or from having to walk blocks in dangerous weather conditions, she added. “And I can do a virtual visit on the fly or at night when a relative or caregiver is home from work to be there with the patient.”
In addition to being beneficial for following up with patients with chronic diseases such as hypertension or diabetes, VTC may be able to replace some visits that have traditionally required hands-on care, said Dr. Wilkes.
She said she knows a cardiologist who has refined a process whereby a patient – say, one who may have edema – is asked to perform a maneuver via VTC and then display the result to the doctor: The doctor says, “put your leg up and press on it hard for 10 seconds and then show me what it looks like,” according to Dr. Wilkes.
The key now is to identify the best persons across specialties from neurology to rheumatology to videotape ways they’ve created to help their patients participate virtually in consults traditionally done at the office, Dr. Wilkes noted.
But some conditions will always require palpation and the use of a stethoscope, according Dr. Iyengar.
“If someone has an ulcer, I have to be able to feel it,” she said.
And while some maternity care can be given virtually – for instance, if a mother-to be develops a bad cold – hands-on obstetrical care to check the position and health of the baby obviously has to be done in person. “So VTC is definitely going to be a welcome addition but not a replacement,” Dr. Iyengar said.
Gaps in research on VTC visits
Many questions remain regarding the overall usefulness of VTC visits for certain patient groups, according to the authors.
They highlighted, for example, the dearth of data on subgroups or on underserved and vulnerable populations, with no head-to-head studies identified in their review. In addition, they found no studies examining VTC versus usual care for patients with concurrent conditions or on its effect on health equity and disparities.
“It’s now our job to understand the ongoing barriers to telemedicine access, including the digital divide and the usability of telemedicine platforms, and design interventions that overcome them,” Dr. Frydman said. “At the same time, we need to make sure we’re understanding and respecting the preferences of older adults in terms of how they access health care.”
This study was supported by the Patient-Centered Outcomes Research Institute (PCORI). Dr. Albritton is employed by RTI International, the contractor responsible for conducting the research and developing the manuscript. Several coauthors disclosed support from or contracts with PCORI. One coauthor’s spouse holds stock in private health companies. Dr. Frydman, Dr. Iyengar, and Dr. Wilkes disclosed no competing interests relevant to their comments.
FROM ANNALS OF INTERNAL MEDICINE
The future of training: AGA EndoscopyNow Fellows Forum recap
Introduction
The virtual space has created new opportunities for gastroenterology fellows, but direct conversations about education and career development on the national level have been limited. On Oct. 16, 2021, the American Gastroenterological Association and EndoscopyNow hosted an online Fellows Forum titled “Navigating New Frontiers of Training in Gastroenterology.” Close to 100 fellows attended and had the chance to listen to discussions from a national panel of faculty with expertise in medical education, ask candid questions, and share experiences in breakout rooms specific to their year of training. Reading materials were also provided, which are cited throughout this article. What follows is a rundown of the discussion and points of particular interest for fellows.
What do fellows value?
Dr. Laura Raffals kicked off the event by asking fellows to create word clouds related to their challenges (“Balance” was the most common answer) and joys (“Family”). These answers underscore that, when faced with pressures to be 100% at work and home, it is human connection, particularly family, that sustains us. Fellows, however, worried that spending time with family conflicted with spending time on GI training and that they would be perceived as “that person who always leaves early.”1
Attendees discussed that “there are only 168 hours in a week,” (time is a zero-sum game), and it is important to be self-aware and honest about one’s personal values and commit the commensurate time and energy to those values. Consider personal development exercises.2 Faculty have a crucial role in coaching fellows on time management based on personal values.3
Has COVID-19 reduced fellows’ endoscopic skills?
One brave attendee asked: Is this generation of fellows “weaker” because of limited scoping during the pandemic? Faculty discussed that, even prepandemic, it was “not all about quantity; the quality of exposure matters just as much.” From their perspective, prepared, goal-directed, and helpful fellows would maximize learning during endoscopy blocks (see below). Lawrence Schiller, MD, providing the long view, reassured fellows that with a proactive attitude it all evens out in the end.
Fellows reflected that, although social isolation and burnout were rampant, some individuals stepped up to do extra work, supported colleagues with personal or family health issues, and scoped COVID-positive patients if others could not. In future years, the pandemic will be seen as a case study for those in leadership positions. The decisions that health systems, administrators, and providers made will be remembered, as well as how algorithms for “practice as usual” changed.4
What fellows can do to maximize endoscopic learning (attendings’ perspective):
- Know the patient before the case. Prior endoscopy reports, patient comorbidities, and medical history including details like anticoagulation use or issues with anesthesia.
- Help the work flow (and reduce the attending’s stress level). Consent patients and complete preprocedure paperwork if possible.
- Come into the scope block with a plan. Example: “I want to get to the cecum. The attending can withdraw, and I will take out polyps we find.”
- Ask about decision-making. Example: “Why did you choose to place a clip over that polypectomy site?” or “Why did you choose that instrument and not the other?”
- Give feedback on problematic behavior. Attendings that treat fellows like burdens and undermine fellow scope time should be reported. Fellows may be concerned about being perceived as a “troublemaker,” but discussing these situations with program directors is a civic duty.
How can we improve diversity?
We cannot wait for, and must instead proactively recruit, diverse trainees, as well as create inclusive environments. Mentorship is key. However, recent work showing imbalances in gender of mentor-mentees and extra pressure on women mentors raises concerns about sustainability.5,6 The panel suggested that interested fellows could engage students earlier in the pipeline, participate in community awareness and exposure programs, and dedicate education time to health equity.7 Fellows raised concerns about barriers for international medical graduates, which would require institutional and federal policy changes would to implement change.
How can fellows develop better practice patterns?
Sri Komanduri, MD, focused on complex endoscopic cases.8 Having live video, using polls, and listening to other attendings comment on cases was illuminating and sometimes humbling. The panel discussed that simulation labs could strongly enhance endoscopic skill training, but if unavailable, companies are often willing to sponsor events for teaching purposes.9 If training on specific topics is not offered at an institution, regional weekend courses are also an option.
Raman Muthusamy, MD, MS, discussed his philosophy towards endoscopic complications: be prepared and follow your instinct if something feels off. He and Dr. Ikuo Hirano emphasized the importance of following up with patients after a complication. The panel also suggested that fellows can build quality improvement experience by contributing to GI morbidity and mortality conferences or start them if not already offered.
Where is the future headed?
Amrita Sethi, MD, outlined the trend towards virtual platforms and getting the global GI community involved in education efforts. She pointed out the need for a gold standard on assessing competency in endoscopy. From a practice perspective, implementation of telemedicine in GI merits further study, as so far this technology has been attractive to providers and patients alike. Todd Baron, MD, stressed that newer technologies, including artificial intelligence, will not replace the endoscopist but may reduce the need for screening procedures and instead increase demand for specific diagnostic and therapeutic procedures. He used the examples of therapeutic applications of endoscopic ultrasound and the development of single-use duodenoscopes.
Concerns about transitioning from training to independent practice
During the third-year breakout session, fellows discussed anxieties about starting practice and living up to expectations: “What if it’s my first week and there’s something I can’t do?” Faculty recommended getting to know colleagues at a new institution, being confident in your training, and staying engaged with your own complications.10 Fellows described the surprising amount of time and energy they dedicated to the job search and got counseling from Dr. Schiller, who recommended defining what “success” and “satisfaction” look like (again, defining one’s values). He recommended that, for fellows looking at private practice positions, one should ask: How much autonomy do I want? How much business risk am I willing to accept? Fellows need more formal education on practice management and the “business side” of gastroenterology.11
Conclusions
The 2021 AGA EndoscopyNow forum was unique in its discussion of issues impacting GI fellows. The forum revealed that worries about personal well-being, training quality, and future career prospects have affected fellows everywhere: you are not alone. Presentations and lively conversation between seasoned faculty who reflected on career development, education, and medical management demonstrate the importance of seeking advice from colleagues and mentorship. Based on this event, future sessions with conversations between faculty and fellows to assess needs and set priorities for directions in training would be welcome.
Dr. Liu is a gastroenterology fellow, Northwestern University, Chicago. The author has no conflicts of interest to disclose.
References
1. Katzka DA and Proctor DD. Gastroenterology. 2009;136(4):1147-8.
2. Sull D and Houlder D. Do Your Commitments Match Your Convictions? Harv Bus Rev. 2005 Jan 1. https://hbr.org/2005/01/do-your-commitments-match-your-convictions.
3. Keswani RN et al. Gastroenterology. 2020;159(1):26-9.
4. Sethi A et al. Clin Gastroenterol Hepatol. 2020;18(8):1673-81.
5. Rabinowitz LG et al. Gastrointest Endosc. 2021;93(5):1047-56.e5.
6. Rabinowitz LG et al. Gastrointest Endosc. 2020;91(1):155-61.
7. Lee-Allen J, Shah BJ. Gastroenterology. 2021;160(6):1924-8.
8. Richter JM et al. Am J Gastroenterol. 2016;111(3):348-52.
9. Muthusamy VR and Komanduri S. Clin Gastroenterol Hepatol. 2019 Mar;17(4):580-3.
10. Liu H and Boyatzis RE. Front Psychol. 2021. doi: 10.3389/fpsyg.2021.685829.
11. Amann ST et al. “Words” to practice by: A guide to understand the business vernacular of a healthy practice. https://webfiles.gi.org/links/pm/TheHealthOfMyPracticeToolboxPMCommitteeToolbox.pdf.
Introduction
The virtual space has created new opportunities for gastroenterology fellows, but direct conversations about education and career development on the national level have been limited. On Oct. 16, 2021, the American Gastroenterological Association and EndoscopyNow hosted an online Fellows Forum titled “Navigating New Frontiers of Training in Gastroenterology.” Close to 100 fellows attended and had the chance to listen to discussions from a national panel of faculty with expertise in medical education, ask candid questions, and share experiences in breakout rooms specific to their year of training. Reading materials were also provided, which are cited throughout this article. What follows is a rundown of the discussion and points of particular interest for fellows.
What do fellows value?
Dr. Laura Raffals kicked off the event by asking fellows to create word clouds related to their challenges (“Balance” was the most common answer) and joys (“Family”). These answers underscore that, when faced with pressures to be 100% at work and home, it is human connection, particularly family, that sustains us. Fellows, however, worried that spending time with family conflicted with spending time on GI training and that they would be perceived as “that person who always leaves early.”1
Attendees discussed that “there are only 168 hours in a week,” (time is a zero-sum game), and it is important to be self-aware and honest about one’s personal values and commit the commensurate time and energy to those values. Consider personal development exercises.2 Faculty have a crucial role in coaching fellows on time management based on personal values.3
Has COVID-19 reduced fellows’ endoscopic skills?
One brave attendee asked: Is this generation of fellows “weaker” because of limited scoping during the pandemic? Faculty discussed that, even prepandemic, it was “not all about quantity; the quality of exposure matters just as much.” From their perspective, prepared, goal-directed, and helpful fellows would maximize learning during endoscopy blocks (see below). Lawrence Schiller, MD, providing the long view, reassured fellows that with a proactive attitude it all evens out in the end.
Fellows reflected that, although social isolation and burnout were rampant, some individuals stepped up to do extra work, supported colleagues with personal or family health issues, and scoped COVID-positive patients if others could not. In future years, the pandemic will be seen as a case study for those in leadership positions. The decisions that health systems, administrators, and providers made will be remembered, as well as how algorithms for “practice as usual” changed.4
What fellows can do to maximize endoscopic learning (attendings’ perspective):
- Know the patient before the case. Prior endoscopy reports, patient comorbidities, and medical history including details like anticoagulation use or issues with anesthesia.
- Help the work flow (and reduce the attending’s stress level). Consent patients and complete preprocedure paperwork if possible.
- Come into the scope block with a plan. Example: “I want to get to the cecum. The attending can withdraw, and I will take out polyps we find.”
- Ask about decision-making. Example: “Why did you choose to place a clip over that polypectomy site?” or “Why did you choose that instrument and not the other?”
- Give feedback on problematic behavior. Attendings that treat fellows like burdens and undermine fellow scope time should be reported. Fellows may be concerned about being perceived as a “troublemaker,” but discussing these situations with program directors is a civic duty.
How can we improve diversity?
We cannot wait for, and must instead proactively recruit, diverse trainees, as well as create inclusive environments. Mentorship is key. However, recent work showing imbalances in gender of mentor-mentees and extra pressure on women mentors raises concerns about sustainability.5,6 The panel suggested that interested fellows could engage students earlier in the pipeline, participate in community awareness and exposure programs, and dedicate education time to health equity.7 Fellows raised concerns about barriers for international medical graduates, which would require institutional and federal policy changes would to implement change.
How can fellows develop better practice patterns?
Sri Komanduri, MD, focused on complex endoscopic cases.8 Having live video, using polls, and listening to other attendings comment on cases was illuminating and sometimes humbling. The panel discussed that simulation labs could strongly enhance endoscopic skill training, but if unavailable, companies are often willing to sponsor events for teaching purposes.9 If training on specific topics is not offered at an institution, regional weekend courses are also an option.
Raman Muthusamy, MD, MS, discussed his philosophy towards endoscopic complications: be prepared and follow your instinct if something feels off. He and Dr. Ikuo Hirano emphasized the importance of following up with patients after a complication. The panel also suggested that fellows can build quality improvement experience by contributing to GI morbidity and mortality conferences or start them if not already offered.
Where is the future headed?
Amrita Sethi, MD, outlined the trend towards virtual platforms and getting the global GI community involved in education efforts. She pointed out the need for a gold standard on assessing competency in endoscopy. From a practice perspective, implementation of telemedicine in GI merits further study, as so far this technology has been attractive to providers and patients alike. Todd Baron, MD, stressed that newer technologies, including artificial intelligence, will not replace the endoscopist but may reduce the need for screening procedures and instead increase demand for specific diagnostic and therapeutic procedures. He used the examples of therapeutic applications of endoscopic ultrasound and the development of single-use duodenoscopes.
Concerns about transitioning from training to independent practice
During the third-year breakout session, fellows discussed anxieties about starting practice and living up to expectations: “What if it’s my first week and there’s something I can’t do?” Faculty recommended getting to know colleagues at a new institution, being confident in your training, and staying engaged with your own complications.10 Fellows described the surprising amount of time and energy they dedicated to the job search and got counseling from Dr. Schiller, who recommended defining what “success” and “satisfaction” look like (again, defining one’s values). He recommended that, for fellows looking at private practice positions, one should ask: How much autonomy do I want? How much business risk am I willing to accept? Fellows need more formal education on practice management and the “business side” of gastroenterology.11
Conclusions
The 2021 AGA EndoscopyNow forum was unique in its discussion of issues impacting GI fellows. The forum revealed that worries about personal well-being, training quality, and future career prospects have affected fellows everywhere: you are not alone. Presentations and lively conversation between seasoned faculty who reflected on career development, education, and medical management demonstrate the importance of seeking advice from colleagues and mentorship. Based on this event, future sessions with conversations between faculty and fellows to assess needs and set priorities for directions in training would be welcome.
Dr. Liu is a gastroenterology fellow, Northwestern University, Chicago. The author has no conflicts of interest to disclose.
References
1. Katzka DA and Proctor DD. Gastroenterology. 2009;136(4):1147-8.
2. Sull D and Houlder D. Do Your Commitments Match Your Convictions? Harv Bus Rev. 2005 Jan 1. https://hbr.org/2005/01/do-your-commitments-match-your-convictions.
3. Keswani RN et al. Gastroenterology. 2020;159(1):26-9.
4. Sethi A et al. Clin Gastroenterol Hepatol. 2020;18(8):1673-81.
5. Rabinowitz LG et al. Gastrointest Endosc. 2021;93(5):1047-56.e5.
6. Rabinowitz LG et al. Gastrointest Endosc. 2020;91(1):155-61.
7. Lee-Allen J, Shah BJ. Gastroenterology. 2021;160(6):1924-8.
8. Richter JM et al. Am J Gastroenterol. 2016;111(3):348-52.
9. Muthusamy VR and Komanduri S. Clin Gastroenterol Hepatol. 2019 Mar;17(4):580-3.
10. Liu H and Boyatzis RE. Front Psychol. 2021. doi: 10.3389/fpsyg.2021.685829.
11. Amann ST et al. “Words” to practice by: A guide to understand the business vernacular of a healthy practice. https://webfiles.gi.org/links/pm/TheHealthOfMyPracticeToolboxPMCommitteeToolbox.pdf.
Introduction
The virtual space has created new opportunities for gastroenterology fellows, but direct conversations about education and career development on the national level have been limited. On Oct. 16, 2021, the American Gastroenterological Association and EndoscopyNow hosted an online Fellows Forum titled “Navigating New Frontiers of Training in Gastroenterology.” Close to 100 fellows attended and had the chance to listen to discussions from a national panel of faculty with expertise in medical education, ask candid questions, and share experiences in breakout rooms specific to their year of training. Reading materials were also provided, which are cited throughout this article. What follows is a rundown of the discussion and points of particular interest for fellows.
What do fellows value?
Dr. Laura Raffals kicked off the event by asking fellows to create word clouds related to their challenges (“Balance” was the most common answer) and joys (“Family”). These answers underscore that, when faced with pressures to be 100% at work and home, it is human connection, particularly family, that sustains us. Fellows, however, worried that spending time with family conflicted with spending time on GI training and that they would be perceived as “that person who always leaves early.”1
Attendees discussed that “there are only 168 hours in a week,” (time is a zero-sum game), and it is important to be self-aware and honest about one’s personal values and commit the commensurate time and energy to those values. Consider personal development exercises.2 Faculty have a crucial role in coaching fellows on time management based on personal values.3
Has COVID-19 reduced fellows’ endoscopic skills?
One brave attendee asked: Is this generation of fellows “weaker” because of limited scoping during the pandemic? Faculty discussed that, even prepandemic, it was “not all about quantity; the quality of exposure matters just as much.” From their perspective, prepared, goal-directed, and helpful fellows would maximize learning during endoscopy blocks (see below). Lawrence Schiller, MD, providing the long view, reassured fellows that with a proactive attitude it all evens out in the end.
Fellows reflected that, although social isolation and burnout were rampant, some individuals stepped up to do extra work, supported colleagues with personal or family health issues, and scoped COVID-positive patients if others could not. In future years, the pandemic will be seen as a case study for those in leadership positions. The decisions that health systems, administrators, and providers made will be remembered, as well as how algorithms for “practice as usual” changed.4
What fellows can do to maximize endoscopic learning (attendings’ perspective):
- Know the patient before the case. Prior endoscopy reports, patient comorbidities, and medical history including details like anticoagulation use or issues with anesthesia.
- Help the work flow (and reduce the attending’s stress level). Consent patients and complete preprocedure paperwork if possible.
- Come into the scope block with a plan. Example: “I want to get to the cecum. The attending can withdraw, and I will take out polyps we find.”
- Ask about decision-making. Example: “Why did you choose to place a clip over that polypectomy site?” or “Why did you choose that instrument and not the other?”
- Give feedback on problematic behavior. Attendings that treat fellows like burdens and undermine fellow scope time should be reported. Fellows may be concerned about being perceived as a “troublemaker,” but discussing these situations with program directors is a civic duty.
How can we improve diversity?
We cannot wait for, and must instead proactively recruit, diverse trainees, as well as create inclusive environments. Mentorship is key. However, recent work showing imbalances in gender of mentor-mentees and extra pressure on women mentors raises concerns about sustainability.5,6 The panel suggested that interested fellows could engage students earlier in the pipeline, participate in community awareness and exposure programs, and dedicate education time to health equity.7 Fellows raised concerns about barriers for international medical graduates, which would require institutional and federal policy changes would to implement change.
How can fellows develop better practice patterns?
Sri Komanduri, MD, focused on complex endoscopic cases.8 Having live video, using polls, and listening to other attendings comment on cases was illuminating and sometimes humbling. The panel discussed that simulation labs could strongly enhance endoscopic skill training, but if unavailable, companies are often willing to sponsor events for teaching purposes.9 If training on specific topics is not offered at an institution, regional weekend courses are also an option.
Raman Muthusamy, MD, MS, discussed his philosophy towards endoscopic complications: be prepared and follow your instinct if something feels off. He and Dr. Ikuo Hirano emphasized the importance of following up with patients after a complication. The panel also suggested that fellows can build quality improvement experience by contributing to GI morbidity and mortality conferences or start them if not already offered.
Where is the future headed?
Amrita Sethi, MD, outlined the trend towards virtual platforms and getting the global GI community involved in education efforts. She pointed out the need for a gold standard on assessing competency in endoscopy. From a practice perspective, implementation of telemedicine in GI merits further study, as so far this technology has been attractive to providers and patients alike. Todd Baron, MD, stressed that newer technologies, including artificial intelligence, will not replace the endoscopist but may reduce the need for screening procedures and instead increase demand for specific diagnostic and therapeutic procedures. He used the examples of therapeutic applications of endoscopic ultrasound and the development of single-use duodenoscopes.
Concerns about transitioning from training to independent practice
During the third-year breakout session, fellows discussed anxieties about starting practice and living up to expectations: “What if it’s my first week and there’s something I can’t do?” Faculty recommended getting to know colleagues at a new institution, being confident in your training, and staying engaged with your own complications.10 Fellows described the surprising amount of time and energy they dedicated to the job search and got counseling from Dr. Schiller, who recommended defining what “success” and “satisfaction” look like (again, defining one’s values). He recommended that, for fellows looking at private practice positions, one should ask: How much autonomy do I want? How much business risk am I willing to accept? Fellows need more formal education on practice management and the “business side” of gastroenterology.11
Conclusions
The 2021 AGA EndoscopyNow forum was unique in its discussion of issues impacting GI fellows. The forum revealed that worries about personal well-being, training quality, and future career prospects have affected fellows everywhere: you are not alone. Presentations and lively conversation between seasoned faculty who reflected on career development, education, and medical management demonstrate the importance of seeking advice from colleagues and mentorship. Based on this event, future sessions with conversations between faculty and fellows to assess needs and set priorities for directions in training would be welcome.
Dr. Liu is a gastroenterology fellow, Northwestern University, Chicago. The author has no conflicts of interest to disclose.
References
1. Katzka DA and Proctor DD. Gastroenterology. 2009;136(4):1147-8.
2. Sull D and Houlder D. Do Your Commitments Match Your Convictions? Harv Bus Rev. 2005 Jan 1. https://hbr.org/2005/01/do-your-commitments-match-your-convictions.
3. Keswani RN et al. Gastroenterology. 2020;159(1):26-9.
4. Sethi A et al. Clin Gastroenterol Hepatol. 2020;18(8):1673-81.
5. Rabinowitz LG et al. Gastrointest Endosc. 2021;93(5):1047-56.e5.
6. Rabinowitz LG et al. Gastrointest Endosc. 2020;91(1):155-61.
7. Lee-Allen J, Shah BJ. Gastroenterology. 2021;160(6):1924-8.
8. Richter JM et al. Am J Gastroenterol. 2016;111(3):348-52.
9. Muthusamy VR and Komanduri S. Clin Gastroenterol Hepatol. 2019 Mar;17(4):580-3.
10. Liu H and Boyatzis RE. Front Psychol. 2021. doi: 10.3389/fpsyg.2021.685829.
11. Amann ST et al. “Words” to practice by: A guide to understand the business vernacular of a healthy practice. https://webfiles.gi.org/links/pm/TheHealthOfMyPracticeToolboxPMCommitteeToolbox.pdf.
Nephrogenic Systemic Fibrosis in the Setting of Transient Renal Insufficiency
Nephrogenic systemic fibrosis (NSF) is a rare debilitating disorder characterized by dermal plaques, joint contractures, and fibrosis of the skin with possible involvement of muscles and internal organs.1-3 Originally identified in 1997 as nephrogenic fibrosing dermopathy to describe its characteristic cutaneous thickening and hardening, the name was changed to NSF to more accurately reflect the noncutaneous manifestations present in other organ tissues.2,4,5 Nephrogenic systemic fibrosis occurs in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents (GBCAs) used in magnetic resonance angiography and magnetic resonance imaging. There is no predilection for age, sex, or ethnicity.
Nephrogenic systemic fibrosis may develop over a period of days to several weeks. However, there have been cases of NSF developing 10 years after gadolinium exposure.2 In most cases, patients have a history of severe chronic renal disease requiring hemodialysis. There have been a few reported cases of NSF occurring in patients with resolved acute kidney injury or resolved acute on chronic renal disease.1,6-10 We present a case of NSF occurring in a patient with resolved transient renal insufficiency and no history of chronic renal disease.
Case Report
A 68-year-old woman presented with new dark, painless, pink plaques on the right thigh and calf. The patient stated the condition started and got worse after she was hospitalized 12 years prior for lower extremity cellulitis, sepsis, and acute renal failure. The patient developed complications during that hospital stay and underwent a renal biopsy and renal artery embolization requiring use of a GBCA. After the procedure, she noticed skin hardening in the extremities and decreased mobility in both legs while she was still in the hospital. It was thought that the lower leg changes were due to cellulitis. Therefore, when the renal issues resolved, she was discharged. Her skin and joint changes remained stable until 6 years later when she noticed new pink plaques appearing. Her medical history was positive for breast cancer, which was surgically and medically treated 16 years prior to presentation.
On presentation, physical examination revealed dark pink, hyperpigmented plaques on the right leg and a firm hypopigmented broad linear plaque on the right forearm. Palpation of the legs revealed thickened sclerotic plaques from the thighs down to the ankles (Figure 1). The plaques were not tender to palpation. She did have a decreased range of motion with eversion and inversion of the feet and ankles.
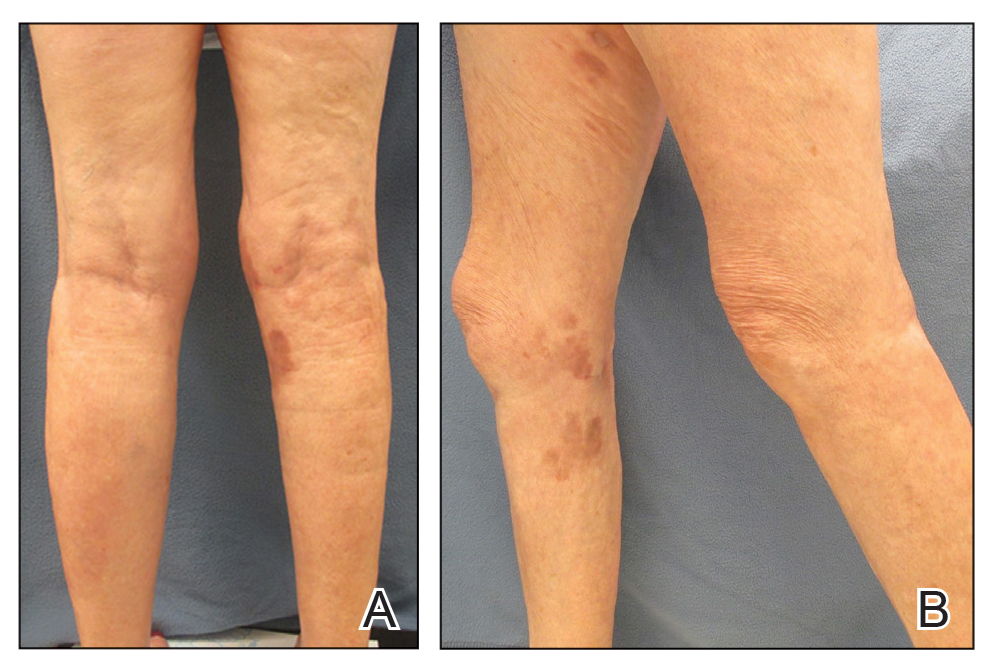
Biopsies from the right medial leg and right volar forearm showed increased bland dermal spindle cellularity associated with numerous round to ovoid osteoid aggregates encircling elastic fibers and surrounded by osteoblasts (Figure 2). CD34 immunohistochemistry showed general retention of staining within the dermal fibroblast population, and elastin stain showed general retention of elastic fiber bundles and thickening.
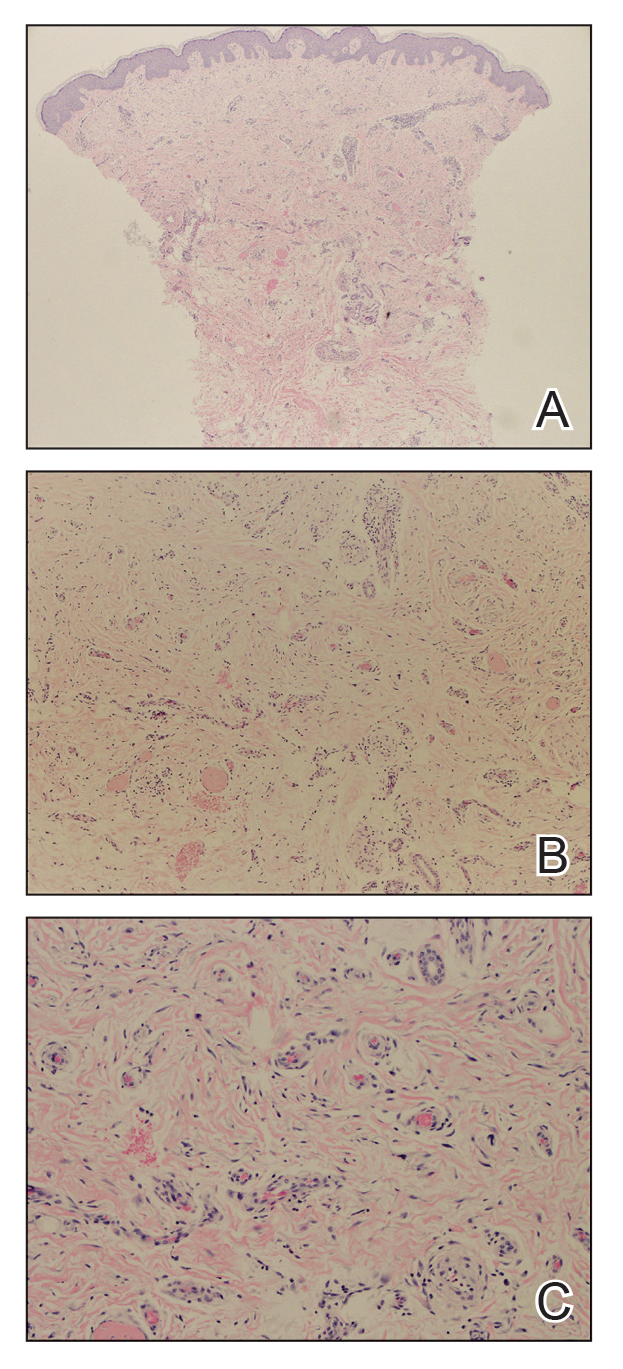
Laboratory workup included a complete blood cell count, comprehensive metabolic panel, thyroid-stimulating hormone level, and serum protein electrophoresis; results were all within reference range. The patient also had a urine element profile from an outside provider 1 month after presenting to our office that showed an elevated urine gadolinium level of 4.146 μg/g (reference range, 0–0.019 μg/g). The patient’s skin lesions have remained stable, and she is now working with physical therapy to help with her range of motion.
Comment
Gadolinium Causing Fibrosis—The incidence of NSF varies according to the severity of renal impairment, dosage level of GBCA used, and the history of GBCA use. In patients with normal renal function, gadolinium is excreted within 90 minutes. In patients with severe renal disease, the half-life can increase to up to 34.3 hours.11 Reduced renal clearance and increased half-life of gadolinium lead to prolonged excretion, causing the GBCA to become unstable and dissociate into its constituents, leading to tissue deposition of Gd3+ cations. This dissociation is thought to be due to differences in the stability of the various chelation complexes among the different formulations of GBCAs.12 The mechanism by which the dissociated gadolinium causes the fibrosis in the skin or other organs of the body is still unknown. Furthermore, even patients with normal renal function who undergo repeated administration of GBCA have been found to have higher levels of Gd3+ in their tissues, even in the absence of symptoms.13
Diagnosing NSF—In 2011, Girardi et al14 created a clinical and histopathological scoring system to help diagnose NSF. Clinical findings can be broken down into major criteria and minor criteria. Major criteria consist of patterned plaques, joint contractures, cobblestoning, marked induration, or peau d’orange change. Minor criteria consist of puckering, linear banding, superficial plaques or patches, dermal papules, and scleral plaques. Histopathologic findings include increased dermal cellularity (score +1), CD34+ cells with tram tracking (score +1), thickened or thin collagen bundles (score +1), preserved elastic fibers (score −1), septal involvement (score +1), and osseous metaplasia (score +3)(eTable).14
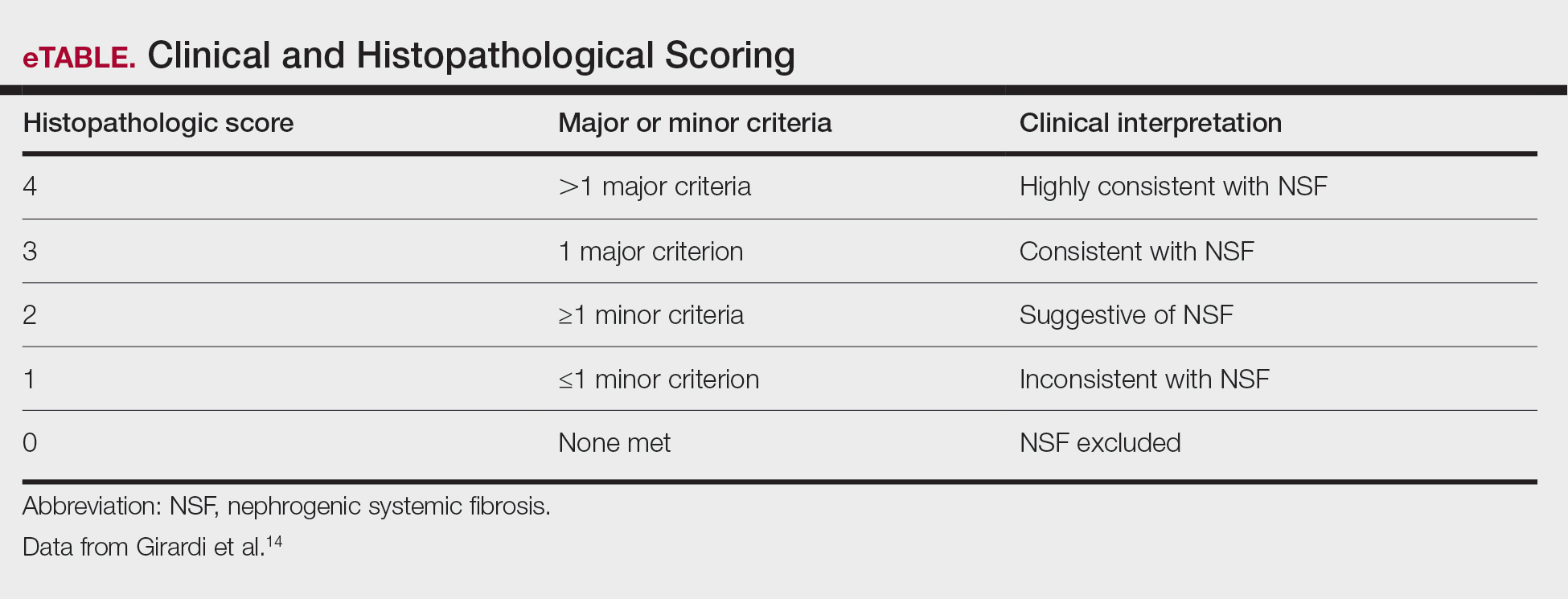
Differential Diagnosis—The differential diagnosis of NSF includes scleromyxedema, scleroderma, eosinophilic fasciitis, eosinophilia-myalgia syndrome, lipodermatosclerosis, morphea, and chronic graft-vs-host disease. Histopathologic examination of scleromyxedema can look identical to NSF. Therefore, a review of the patient’s medical history, prior hospitalizations, and prior gadolinium exposure is important. Appropriate laboratory workups should be ordered to rule out the other differential diagnoses.
NSF and Kidney Injury—A PubMed search of articles indexed for MEDLINE using the terms NSF with kidney injury revealed 7 cases of NSF occurring in patients who either had resolved acute kidney injury or resolved acute on chronic kidney disease.1,6-10 Of those cases, 3 reported NSF occurring in patients with completely resolved acute kidney injury.6,7,10 One of those cases involved a 65-year-old man who developed acute renal failure due to acute tubular necrosis.7 He had no history of renal disease prior to hospitalization. His skin lesions continued to improve as his renal function normalized back to baseline after discharge.7 The second case involved a 42-year-old man who had repeated exposure to GBCAs during a brief period of acute kidney injury.6 Nephrogenic systemic fibrosis developed after his renal function normalized. The authors did not mention if there was clinical improvement.6 The third case involved a 22-year-old man who developed acute renal failure after ingestion of hair dye. He did not have a history of chronic renal disease, and as he recovered from the acute kidney injury, almost all of the skin lesions cleared after 1 year.10
Our patient did not have a history of chronic renal disease when she presented to the hospital for sepsis and acute tubular necrosis. Unlike 2 of the prior cases, she did not notice improvement of the skin lesions as the renal function returned to baseline. She continued to experience changes in the skin, even up to 5 years after, and then stabilized. Throughout that time, her renal function was normal. Interestingly, despite having a normal creatinine level, the patient had an elevated gadolinium level on the urine gadolinium test, which typically is not a standard test for NSF. However, the elevated value does shed light on the persistence of gadolinium in the patient despite her exposure having been more than 10 years earlier.
Treatment of NSF—There is no gold standard treatment of NSF, and reversing the fibrosis has proven to be difficult. Avoidance of GBCAs in acute kidney injury or chronic severe renal disease, as recommended by the US Food and Drug Administration, is key to preventing this debilitating disease.15 Restoration of renal function is essential for excreting the gadolinium and improvement in NSF.12 Physical and occupational therapy can improve joint mobility. Therapies such as extracorporeal photopheresis, sodium thiosulfate, pentoxifylline, glucocorticoids, plasmapheresis, intravenous immunoglobulin, cyclophosphamide, imatinib mesylate, intralesional interferon alfa, topical calcipotriene, corticosteroids, and UVA1 light therapy have been used with varying results.12 It has been suggested that renal transplantation can stop the progression of NSF. However, in the cases we reviewed, renal transplantation would not have benefited those patients because their renal function normalized.6,7,10 Additionally, even though our patient’s renal function normalized after discharge from the hospital, she continued to see more skin lesions developing, likely due to the accumulated gadolinium that was already in her tissue. The possibility of chelation therapy to remove the gadolinium has been proposed. In 1 case study involving deferoxamine injected intramuscularly in a patient with NSF, the urine excretion of gadolinium increased almost 2-fold, but there was no change in the serum concentration level of gadolinium or improvement in the patient’s clinical symptoms.16 We anticipate that our patient’s symptoms will slowly improve, as her body is still excreting the gadolinium. Our patient also was added to the International NSF Registry that was created by Dr. Shawn E. Cowper at the Yale School of Medicine (New Haven, Connecticut).
Conclusion
We report a rare case of NSF occurring in a patient with resolved acute kidney injury and no history of chronic renal disease. Our patient initially did not improve after her renal function normalized, as she continued to develop lesions 10 years after the exposure. Her elevated urine gadolinium excretion level also sheds light on the persistence of gadolinium in her body despite her normal renal function 10 years after her exposure. Although her clinical symptoms have stabilized, our case reiterates the complex pathology of this entity and challenge regarding treatment options. Physicians should be aware that NSF can still occur in healthy patients with no chronic renal disease who have had an episode of acute renal insufficiency along with exposure to a GBCA.
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383-393.
- Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21:1104-1108.
- Larson KN, Gagnon AL, Darling MD, et al. Nephrogenic systemic fibrosis manifesting a decade after exposure to gadolinium. JAMA Dermatol. 2015;151:1117-1120.
- Mendoza FA, Artlett CM, Sandorfi N, et al. Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum. 2006;35:238-249.
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903-906.
- Lu CF, Hsiao CH, Tjiu JW. Nephrogenic systemic fibrosis developed after recovery from acute renal failure: gadolinium as a possible aetiological factor. J Eur Acad Dermatol Venereol. 2009;23:339-340.
- Cassis TB, Jackson JM, Sonnier GB, et al. Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol. 2006;45:56-59.
- Swartz RD, Crofford LJ, Phan SH, et al. Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med. 2003;114:563-572.
- Mackay-Wiggan JM, Cohen DJ, Hardy MA, et al. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol. 2003;48:55-60.
- Reddy IS, Somani VK, Swarnalata G, et al. Nephrogenic systemic fibrosis following hair-dye ingestion induced acute renal failure. Indian J Dermatol Venereol Leprol. 2006;76:400-403.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006;17:2359-2362.
- Cheong BYC, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Inst J. 2010;37:508-515.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29:365-376.
- Girardi M, Kay J, Elston DM, et al. Nephrogenic systemic fibrosis: clinicopathological definition and workup recommendations. J Am Acad Dermatol. 2011;65:1095-1106.
- US Food and Drug Administration. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. Updated February 6, 2018. Accessed November 22, 2021. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm
- Leung N, Pittelkow MR, Lee CU, et al. Chelation of gadolinium with deferoxamine in a patient with nephrogenic systemic fibrosis. NDT Plus. 2009;2:309-311.
Nephrogenic systemic fibrosis (NSF) is a rare debilitating disorder characterized by dermal plaques, joint contractures, and fibrosis of the skin with possible involvement of muscles and internal organs.1-3 Originally identified in 1997 as nephrogenic fibrosing dermopathy to describe its characteristic cutaneous thickening and hardening, the name was changed to NSF to more accurately reflect the noncutaneous manifestations present in other organ tissues.2,4,5 Nephrogenic systemic fibrosis occurs in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents (GBCAs) used in magnetic resonance angiography and magnetic resonance imaging. There is no predilection for age, sex, or ethnicity.
Nephrogenic systemic fibrosis may develop over a period of days to several weeks. However, there have been cases of NSF developing 10 years after gadolinium exposure.2 In most cases, patients have a history of severe chronic renal disease requiring hemodialysis. There have been a few reported cases of NSF occurring in patients with resolved acute kidney injury or resolved acute on chronic renal disease.1,6-10 We present a case of NSF occurring in a patient with resolved transient renal insufficiency and no history of chronic renal disease.
Case Report
A 68-year-old woman presented with new dark, painless, pink plaques on the right thigh and calf. The patient stated the condition started and got worse after she was hospitalized 12 years prior for lower extremity cellulitis, sepsis, and acute renal failure. The patient developed complications during that hospital stay and underwent a renal biopsy and renal artery embolization requiring use of a GBCA. After the procedure, she noticed skin hardening in the extremities and decreased mobility in both legs while she was still in the hospital. It was thought that the lower leg changes were due to cellulitis. Therefore, when the renal issues resolved, she was discharged. Her skin and joint changes remained stable until 6 years later when she noticed new pink plaques appearing. Her medical history was positive for breast cancer, which was surgically and medically treated 16 years prior to presentation.
On presentation, physical examination revealed dark pink, hyperpigmented plaques on the right leg and a firm hypopigmented broad linear plaque on the right forearm. Palpation of the legs revealed thickened sclerotic plaques from the thighs down to the ankles (Figure 1). The plaques were not tender to palpation. She did have a decreased range of motion with eversion and inversion of the feet and ankles.
Biopsies from the right medial leg and right volar forearm showed increased bland dermal spindle cellularity associated with numerous round to ovoid osteoid aggregates encircling elastic fibers and surrounded by osteoblasts (Figure 2). CD34 immunohistochemistry showed general retention of staining within the dermal fibroblast population, and elastin stain showed general retention of elastic fiber bundles and thickening.
Laboratory workup included a complete blood cell count, comprehensive metabolic panel, thyroid-stimulating hormone level, and serum protein electrophoresis; results were all within reference range. The patient also had a urine element profile from an outside provider 1 month after presenting to our office that showed an elevated urine gadolinium level of 4.146 μg/g (reference range, 0–0.019 μg/g). The patient’s skin lesions have remained stable, and she is now working with physical therapy to help with her range of motion.
Comment
Gadolinium Causing Fibrosis—The incidence of NSF varies according to the severity of renal impairment, dosage level of GBCA used, and the history of GBCA use. In patients with normal renal function, gadolinium is excreted within 90 minutes. In patients with severe renal disease, the half-life can increase to up to 34.3 hours.11 Reduced renal clearance and increased half-life of gadolinium lead to prolonged excretion, causing the GBCA to become unstable and dissociate into its constituents, leading to tissue deposition of Gd3+ cations. This dissociation is thought to be due to differences in the stability of the various chelation complexes among the different formulations of GBCAs.12 The mechanism by which the dissociated gadolinium causes the fibrosis in the skin or other organs of the body is still unknown. Furthermore, even patients with normal renal function who undergo repeated administration of GBCA have been found to have higher levels of Gd3+ in their tissues, even in the absence of symptoms.13
Diagnosing NSF—In 2011, Girardi et al14 created a clinical and histopathological scoring system to help diagnose NSF. Clinical findings can be broken down into major criteria and minor criteria. Major criteria consist of patterned plaques, joint contractures, cobblestoning, marked induration, or peau d’orange change. Minor criteria consist of puckering, linear banding, superficial plaques or patches, dermal papules, and scleral plaques. Histopathologic findings include increased dermal cellularity (score +1), CD34+ cells with tram tracking (score +1), thickened or thin collagen bundles (score +1), preserved elastic fibers (score −1), septal involvement (score +1), and osseous metaplasia (score +3)(eTable).14
Differential Diagnosis—The differential diagnosis of NSF includes scleromyxedema, scleroderma, eosinophilic fasciitis, eosinophilia-myalgia syndrome, lipodermatosclerosis, morphea, and chronic graft-vs-host disease. Histopathologic examination of scleromyxedema can look identical to NSF. Therefore, a review of the patient’s medical history, prior hospitalizations, and prior gadolinium exposure is important. Appropriate laboratory workups should be ordered to rule out the other differential diagnoses.
NSF and Kidney Injury—A PubMed search of articles indexed for MEDLINE using the terms NSF with kidney injury revealed 7 cases of NSF occurring in patients who either had resolved acute kidney injury or resolved acute on chronic kidney disease.1,6-10 Of those cases, 3 reported NSF occurring in patients with completely resolved acute kidney injury.6,7,10 One of those cases involved a 65-year-old man who developed acute renal failure due to acute tubular necrosis.7 He had no history of renal disease prior to hospitalization. His skin lesions continued to improve as his renal function normalized back to baseline after discharge.7 The second case involved a 42-year-old man who had repeated exposure to GBCAs during a brief period of acute kidney injury.6 Nephrogenic systemic fibrosis developed after his renal function normalized. The authors did not mention if there was clinical improvement.6 The third case involved a 22-year-old man who developed acute renal failure after ingestion of hair dye. He did not have a history of chronic renal disease, and as he recovered from the acute kidney injury, almost all of the skin lesions cleared after 1 year.10
Our patient did not have a history of chronic renal disease when she presented to the hospital for sepsis and acute tubular necrosis. Unlike 2 of the prior cases, she did not notice improvement of the skin lesions as the renal function returned to baseline. She continued to experience changes in the skin, even up to 5 years after, and then stabilized. Throughout that time, her renal function was normal. Interestingly, despite having a normal creatinine level, the patient had an elevated gadolinium level on the urine gadolinium test, which typically is not a standard test for NSF. However, the elevated value does shed light on the persistence of gadolinium in the patient despite her exposure having been more than 10 years earlier.
Treatment of NSF—There is no gold standard treatment of NSF, and reversing the fibrosis has proven to be difficult. Avoidance of GBCAs in acute kidney injury or chronic severe renal disease, as recommended by the US Food and Drug Administration, is key to preventing this debilitating disease.15 Restoration of renal function is essential for excreting the gadolinium and improvement in NSF.12 Physical and occupational therapy can improve joint mobility. Therapies such as extracorporeal photopheresis, sodium thiosulfate, pentoxifylline, glucocorticoids, plasmapheresis, intravenous immunoglobulin, cyclophosphamide, imatinib mesylate, intralesional interferon alfa, topical calcipotriene, corticosteroids, and UVA1 light therapy have been used with varying results.12 It has been suggested that renal transplantation can stop the progression of NSF. However, in the cases we reviewed, renal transplantation would not have benefited those patients because their renal function normalized.6,7,10 Additionally, even though our patient’s renal function normalized after discharge from the hospital, she continued to see more skin lesions developing, likely due to the accumulated gadolinium that was already in her tissue. The possibility of chelation therapy to remove the gadolinium has been proposed. In 1 case study involving deferoxamine injected intramuscularly in a patient with NSF, the urine excretion of gadolinium increased almost 2-fold, but there was no change in the serum concentration level of gadolinium or improvement in the patient’s clinical symptoms.16 We anticipate that our patient’s symptoms will slowly improve, as her body is still excreting the gadolinium. Our patient also was added to the International NSF Registry that was created by Dr. Shawn E. Cowper at the Yale School of Medicine (New Haven, Connecticut).
Conclusion
We report a rare case of NSF occurring in a patient with resolved acute kidney injury and no history of chronic renal disease. Our patient initially did not improve after her renal function normalized, as she continued to develop lesions 10 years after the exposure. Her elevated urine gadolinium excretion level also sheds light on the persistence of gadolinium in her body despite her normal renal function 10 years after her exposure. Although her clinical symptoms have stabilized, our case reiterates the complex pathology of this entity and challenge regarding treatment options. Physicians should be aware that NSF can still occur in healthy patients with no chronic renal disease who have had an episode of acute renal insufficiency along with exposure to a GBCA.
Nephrogenic systemic fibrosis (NSF) is a rare debilitating disorder characterized by dermal plaques, joint contractures, and fibrosis of the skin with possible involvement of muscles and internal organs.1-3 Originally identified in 1997 as nephrogenic fibrosing dermopathy to describe its characteristic cutaneous thickening and hardening, the name was changed to NSF to more accurately reflect the noncutaneous manifestations present in other organ tissues.2,4,5 Nephrogenic systemic fibrosis occurs in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents (GBCAs) used in magnetic resonance angiography and magnetic resonance imaging. There is no predilection for age, sex, or ethnicity.
Nephrogenic systemic fibrosis may develop over a period of days to several weeks. However, there have been cases of NSF developing 10 years after gadolinium exposure.2 In most cases, patients have a history of severe chronic renal disease requiring hemodialysis. There have been a few reported cases of NSF occurring in patients with resolved acute kidney injury or resolved acute on chronic renal disease.1,6-10 We present a case of NSF occurring in a patient with resolved transient renal insufficiency and no history of chronic renal disease.
Case Report
A 68-year-old woman presented with new dark, painless, pink plaques on the right thigh and calf. The patient stated the condition started and got worse after she was hospitalized 12 years prior for lower extremity cellulitis, sepsis, and acute renal failure. The patient developed complications during that hospital stay and underwent a renal biopsy and renal artery embolization requiring use of a GBCA. After the procedure, she noticed skin hardening in the extremities and decreased mobility in both legs while she was still in the hospital. It was thought that the lower leg changes were due to cellulitis. Therefore, when the renal issues resolved, she was discharged. Her skin and joint changes remained stable until 6 years later when she noticed new pink plaques appearing. Her medical history was positive for breast cancer, which was surgically and medically treated 16 years prior to presentation.
On presentation, physical examination revealed dark pink, hyperpigmented plaques on the right leg and a firm hypopigmented broad linear plaque on the right forearm. Palpation of the legs revealed thickened sclerotic plaques from the thighs down to the ankles (Figure 1). The plaques were not tender to palpation. She did have a decreased range of motion with eversion and inversion of the feet and ankles.
Biopsies from the right medial leg and right volar forearm showed increased bland dermal spindle cellularity associated with numerous round to ovoid osteoid aggregates encircling elastic fibers and surrounded by osteoblasts (Figure 2). CD34 immunohistochemistry showed general retention of staining within the dermal fibroblast population, and elastin stain showed general retention of elastic fiber bundles and thickening.
Laboratory workup included a complete blood cell count, comprehensive metabolic panel, thyroid-stimulating hormone level, and serum protein electrophoresis; results were all within reference range. The patient also had a urine element profile from an outside provider 1 month after presenting to our office that showed an elevated urine gadolinium level of 4.146 μg/g (reference range, 0–0.019 μg/g). The patient’s skin lesions have remained stable, and she is now working with physical therapy to help with her range of motion.
Comment
Gadolinium Causing Fibrosis—The incidence of NSF varies according to the severity of renal impairment, dosage level of GBCA used, and the history of GBCA use. In patients with normal renal function, gadolinium is excreted within 90 minutes. In patients with severe renal disease, the half-life can increase to up to 34.3 hours.11 Reduced renal clearance and increased half-life of gadolinium lead to prolonged excretion, causing the GBCA to become unstable and dissociate into its constituents, leading to tissue deposition of Gd3+ cations. This dissociation is thought to be due to differences in the stability of the various chelation complexes among the different formulations of GBCAs.12 The mechanism by which the dissociated gadolinium causes the fibrosis in the skin or other organs of the body is still unknown. Furthermore, even patients with normal renal function who undergo repeated administration of GBCA have been found to have higher levels of Gd3+ in their tissues, even in the absence of symptoms.13
Diagnosing NSF—In 2011, Girardi et al14 created a clinical and histopathological scoring system to help diagnose NSF. Clinical findings can be broken down into major criteria and minor criteria. Major criteria consist of patterned plaques, joint contractures, cobblestoning, marked induration, or peau d’orange change. Minor criteria consist of puckering, linear banding, superficial plaques or patches, dermal papules, and scleral plaques. Histopathologic findings include increased dermal cellularity (score +1), CD34+ cells with tram tracking (score +1), thickened or thin collagen bundles (score +1), preserved elastic fibers (score −1), septal involvement (score +1), and osseous metaplasia (score +3)(eTable).14
Differential Diagnosis—The differential diagnosis of NSF includes scleromyxedema, scleroderma, eosinophilic fasciitis, eosinophilia-myalgia syndrome, lipodermatosclerosis, morphea, and chronic graft-vs-host disease. Histopathologic examination of scleromyxedema can look identical to NSF. Therefore, a review of the patient’s medical history, prior hospitalizations, and prior gadolinium exposure is important. Appropriate laboratory workups should be ordered to rule out the other differential diagnoses.
NSF and Kidney Injury—A PubMed search of articles indexed for MEDLINE using the terms NSF with kidney injury revealed 7 cases of NSF occurring in patients who either had resolved acute kidney injury or resolved acute on chronic kidney disease.1,6-10 Of those cases, 3 reported NSF occurring in patients with completely resolved acute kidney injury.6,7,10 One of those cases involved a 65-year-old man who developed acute renal failure due to acute tubular necrosis.7 He had no history of renal disease prior to hospitalization. His skin lesions continued to improve as his renal function normalized back to baseline after discharge.7 The second case involved a 42-year-old man who had repeated exposure to GBCAs during a brief period of acute kidney injury.6 Nephrogenic systemic fibrosis developed after his renal function normalized. The authors did not mention if there was clinical improvement.6 The third case involved a 22-year-old man who developed acute renal failure after ingestion of hair dye. He did not have a history of chronic renal disease, and as he recovered from the acute kidney injury, almost all of the skin lesions cleared after 1 year.10
Our patient did not have a history of chronic renal disease when she presented to the hospital for sepsis and acute tubular necrosis. Unlike 2 of the prior cases, she did not notice improvement of the skin lesions as the renal function returned to baseline. She continued to experience changes in the skin, even up to 5 years after, and then stabilized. Throughout that time, her renal function was normal. Interestingly, despite having a normal creatinine level, the patient had an elevated gadolinium level on the urine gadolinium test, which typically is not a standard test for NSF. However, the elevated value does shed light on the persistence of gadolinium in the patient despite her exposure having been more than 10 years earlier.
Treatment of NSF—There is no gold standard treatment of NSF, and reversing the fibrosis has proven to be difficult. Avoidance of GBCAs in acute kidney injury or chronic severe renal disease, as recommended by the US Food and Drug Administration, is key to preventing this debilitating disease.15 Restoration of renal function is essential for excreting the gadolinium and improvement in NSF.12 Physical and occupational therapy can improve joint mobility. Therapies such as extracorporeal photopheresis, sodium thiosulfate, pentoxifylline, glucocorticoids, plasmapheresis, intravenous immunoglobulin, cyclophosphamide, imatinib mesylate, intralesional interferon alfa, topical calcipotriene, corticosteroids, and UVA1 light therapy have been used with varying results.12 It has been suggested that renal transplantation can stop the progression of NSF. However, in the cases we reviewed, renal transplantation would not have benefited those patients because their renal function normalized.6,7,10 Additionally, even though our patient’s renal function normalized after discharge from the hospital, she continued to see more skin lesions developing, likely due to the accumulated gadolinium that was already in her tissue. The possibility of chelation therapy to remove the gadolinium has been proposed. In 1 case study involving deferoxamine injected intramuscularly in a patient with NSF, the urine excretion of gadolinium increased almost 2-fold, but there was no change in the serum concentration level of gadolinium or improvement in the patient’s clinical symptoms.16 We anticipate that our patient’s symptoms will slowly improve, as her body is still excreting the gadolinium. Our patient also was added to the International NSF Registry that was created by Dr. Shawn E. Cowper at the Yale School of Medicine (New Haven, Connecticut).
Conclusion
We report a rare case of NSF occurring in a patient with resolved acute kidney injury and no history of chronic renal disease. Our patient initially did not improve after her renal function normalized, as she continued to develop lesions 10 years after the exposure. Her elevated urine gadolinium excretion level also sheds light on the persistence of gadolinium in her body despite her normal renal function 10 years after her exposure. Although her clinical symptoms have stabilized, our case reiterates the complex pathology of this entity and challenge regarding treatment options. Physicians should be aware that NSF can still occur in healthy patients with no chronic renal disease who have had an episode of acute renal insufficiency along with exposure to a GBCA.
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383-393.
- Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21:1104-1108.
- Larson KN, Gagnon AL, Darling MD, et al. Nephrogenic systemic fibrosis manifesting a decade after exposure to gadolinium. JAMA Dermatol. 2015;151:1117-1120.
- Mendoza FA, Artlett CM, Sandorfi N, et al. Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum. 2006;35:238-249.
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903-906.
- Lu CF, Hsiao CH, Tjiu JW. Nephrogenic systemic fibrosis developed after recovery from acute renal failure: gadolinium as a possible aetiological factor. J Eur Acad Dermatol Venereol. 2009;23:339-340.
- Cassis TB, Jackson JM, Sonnier GB, et al. Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol. 2006;45:56-59.
- Swartz RD, Crofford LJ, Phan SH, et al. Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med. 2003;114:563-572.
- Mackay-Wiggan JM, Cohen DJ, Hardy MA, et al. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol. 2003;48:55-60.
- Reddy IS, Somani VK, Swarnalata G, et al. Nephrogenic systemic fibrosis following hair-dye ingestion induced acute renal failure. Indian J Dermatol Venereol Leprol. 2006;76:400-403.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006;17:2359-2362.
- Cheong BYC, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Inst J. 2010;37:508-515.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29:365-376.
- Girardi M, Kay J, Elston DM, et al. Nephrogenic systemic fibrosis: clinicopathological definition and workup recommendations. J Am Acad Dermatol. 2011;65:1095-1106.
- US Food and Drug Administration. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. Updated February 6, 2018. Accessed November 22, 2021. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm
- Leung N, Pittelkow MR, Lee CU, et al. Chelation of gadolinium with deferoxamine in a patient with nephrogenic systemic fibrosis. NDT Plus. 2009;2:309-311.
- Cowper SE, Su LD, Bhawan J, et al. Nephrogenic fibrosing dermopathy. Am J Dermatopathol. 2001;23:383-393.
- Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21:1104-1108.
- Larson KN, Gagnon AL, Darling MD, et al. Nephrogenic systemic fibrosis manifesting a decade after exposure to gadolinium. JAMA Dermatol. 2015;151:1117-1120.
- Mendoza FA, Artlett CM, Sandorfi N, et al. Description of 12 cases of nephrogenic fibrosing dermopathy and review of the literature. Semin Arthritis Rheum. 2006;35:238-249.
- Ting WW, Stone MS, Madison KC, et al. Nephrogenic fibrosing dermopathy with systemic involvement. Arch Dermatol. 2003;139:903-906.
- Lu CF, Hsiao CH, Tjiu JW. Nephrogenic systemic fibrosis developed after recovery from acute renal failure: gadolinium as a possible aetiological factor. J Eur Acad Dermatol Venereol. 2009;23:339-340.
- Cassis TB, Jackson JM, Sonnier GB, et al. Nephrogenic fibrosing dermopathy in a patient with acute renal failure never requiring dialysis. Int J Dermatol. 2006;45:56-59.
- Swartz RD, Crofford LJ, Phan SH, et al. Nephrogenic fibrosing dermopathy: a novel cutaneous fibrosing disorder in patients with renal failure. Am J Med. 2003;114:563-572.
- Mackay-Wiggan JM, Cohen DJ, Hardy MA, et al. Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). J Am Acad Dermatol. 2003;48:55-60.
- Reddy IS, Somani VK, Swarnalata G, et al. Nephrogenic systemic fibrosis following hair-dye ingestion induced acute renal failure. Indian J Dermatol Venereol Leprol. 2006;76:400-403.
- Marckmann P, Skov L, Rossen K, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol. 2006;17:2359-2362.
- Cheong BYC, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Inst J. 2010;37:508-515.
- Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed mechanisms. BioMetals. 2016;29:365-376.
- Girardi M, Kay J, Elston DM, et al. Nephrogenic systemic fibrosis: clinicopathological definition and workup recommendations. J Am Acad Dermatol. 2011;65:1095-1106.
- US Food and Drug Administration. FDA Drug Safety Communication: new warnings for using gadolinium-based contrast agents in patients with kidney dysfunction. Updated February 6, 2018. Accessed November 22, 2021. http://www.fda.gov/Drugs/DrugSafety/ucm223966.htm
- Leung N, Pittelkow MR, Lee CU, et al. Chelation of gadolinium with deferoxamine in a patient with nephrogenic systemic fibrosis. NDT Plus. 2009;2:309-311.
Practice Points
- Nephrogenic systemic fibrosis may occur in patients with a history of renal insufficiency and exposure to gadolinium-based contrast agents.
- Nephrogenic systemic fibrosis may develop over a period of days to several years after exposure.
- Symptoms of this rare disease can progress and get worse even after renal function normalizes.
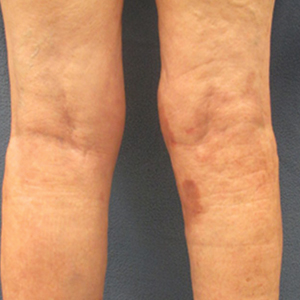
Sleep disorders and cancer: It’s complicated
Sleep apnea and other types of sleep disorders appear to elevate the risk for some types of cancer, specifically prostate cancer, more so than others. But the overall risk can be highly variable, and some sleep problems were found to be associated with a lower risk for cancer and cancer-related death, an analysis of a large observational cohort study of cardiovascular patients found.
Results of the analysis were published online in the journal Cancer Epidemiology. Investigators analyzed the presence of sleep apnea and insomnia and cancer risk in more than 8,500 patients in the Cardiovascular Health Study (CHS). “The fact that we observed certain sleep problems, like apneas, to be associated with elevated risk of some cancers but not others reflects the fact that cancer is a heterogeneous disease,” senior author Amanda Phipps, PhD, said in an interview. Dr. Phipps is an associate professor of epidemiology at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
Variable cancer links
The researchers assessed sleep problems in two groups in the CHS: an incident cancer group of 3,930 patients and a cancer mortality group of 4,580 patients. Within those respective groups, the investigators identified 885 first-incident cancers and 804 cancer deaths with a median follow-up of 12 and 14 years. The average age of the study population was 73 years, and 57% were women.
Sleep apnea symptoms (SAS) were associated with a lower risk for incident cancers – a 16% lower baseline risk and a 24% lower time-dependent risk. The study showed no association between cancer incidence and daytime sleepiness and apneas.
However, there was a significantly elevated risk relationship between sleep problems and prostate cancer. A time-dependent analysis of apnea showed more than double the risk (hazard ratio, 2.34), and baseline snoring carried a 69% greater risk. There was also a dose-response relationship for baseline cumulative SAS, compared with not having symptoms: an HR of 1.30 for one symptom, and 2.22 for two or more symptoms.
Risks for lymphatic or hematopoietic cancers were also associated with baseline daytime sleepiness (HR, 1.81), but not with insomnia (HR, 0.54).
With regard to cancer mortality, the study found no relationship between sleep problems and cancer death. In fact, it found an overall inverse relationship with snoring (time-dependent HR, 0.73; cumulative average HR, 0.67) and baseline apnea (HR, 0.69). Likewise, patients reporting SAS had lower risks than those having no SAS: an HR of 0.90 for one symptom and 0.75 for multiple symptoms. No relationships were found between any insomnia symptom and cancer death.
“We know the pathways that lead to prostate cancer can be very different than the pathways that lead to colorectal cancer,” Dr. Phipps said. “What we don’t yet understand is why these associations differ or what mechanisms are responsible for these cancer site-specific associations.”
Need for sleep assessment
The findings don’t change much for how clinicians should evaluate cancer risks in patients with sleep problems, Dr. Phipps said. “Other studies have clearly demonstrated the implications that sleep apnea has for a variety of other important health conditions – such as cardiovascular disease – so there are already plenty of good reasons for clinicians to ask their patients about their sleep and to connect patients with resources for the diagnosis and treatment of sleep apnea,” she added. “This study provides another possible reason.”
These findings provide context for future studies of the relationship between sleep problems and cancer. “But, given that sleep is something we all do and given that sleep problems are so pervasive, it’s important that we keep trying to better understand this relationship,” Dr. Phipps said.
“My hope is that future cancer studies will build in more detailed, longitudinal information on sleep patterns to help us fill current gaps in knowledge.”
Dr. Phipps has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sleep apnea and other types of sleep disorders appear to elevate the risk for some types of cancer, specifically prostate cancer, more so than others. But the overall risk can be highly variable, and some sleep problems were found to be associated with a lower risk for cancer and cancer-related death, an analysis of a large observational cohort study of cardiovascular patients found.
Results of the analysis were published online in the journal Cancer Epidemiology. Investigators analyzed the presence of sleep apnea and insomnia and cancer risk in more than 8,500 patients in the Cardiovascular Health Study (CHS). “The fact that we observed certain sleep problems, like apneas, to be associated with elevated risk of some cancers but not others reflects the fact that cancer is a heterogeneous disease,” senior author Amanda Phipps, PhD, said in an interview. Dr. Phipps is an associate professor of epidemiology at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
Variable cancer links
The researchers assessed sleep problems in two groups in the CHS: an incident cancer group of 3,930 patients and a cancer mortality group of 4,580 patients. Within those respective groups, the investigators identified 885 first-incident cancers and 804 cancer deaths with a median follow-up of 12 and 14 years. The average age of the study population was 73 years, and 57% were women.
Sleep apnea symptoms (SAS) were associated with a lower risk for incident cancers – a 16% lower baseline risk and a 24% lower time-dependent risk. The study showed no association between cancer incidence and daytime sleepiness and apneas.
However, there was a significantly elevated risk relationship between sleep problems and prostate cancer. A time-dependent analysis of apnea showed more than double the risk (hazard ratio, 2.34), and baseline snoring carried a 69% greater risk. There was also a dose-response relationship for baseline cumulative SAS, compared with not having symptoms: an HR of 1.30 for one symptom, and 2.22 for two or more symptoms.
Risks for lymphatic or hematopoietic cancers were also associated with baseline daytime sleepiness (HR, 1.81), but not with insomnia (HR, 0.54).
With regard to cancer mortality, the study found no relationship between sleep problems and cancer death. In fact, it found an overall inverse relationship with snoring (time-dependent HR, 0.73; cumulative average HR, 0.67) and baseline apnea (HR, 0.69). Likewise, patients reporting SAS had lower risks than those having no SAS: an HR of 0.90 for one symptom and 0.75 for multiple symptoms. No relationships were found between any insomnia symptom and cancer death.
“We know the pathways that lead to prostate cancer can be very different than the pathways that lead to colorectal cancer,” Dr. Phipps said. “What we don’t yet understand is why these associations differ or what mechanisms are responsible for these cancer site-specific associations.”
Need for sleep assessment
The findings don’t change much for how clinicians should evaluate cancer risks in patients with sleep problems, Dr. Phipps said. “Other studies have clearly demonstrated the implications that sleep apnea has for a variety of other important health conditions – such as cardiovascular disease – so there are already plenty of good reasons for clinicians to ask their patients about their sleep and to connect patients with resources for the diagnosis and treatment of sleep apnea,” she added. “This study provides another possible reason.”
These findings provide context for future studies of the relationship between sleep problems and cancer. “But, given that sleep is something we all do and given that sleep problems are so pervasive, it’s important that we keep trying to better understand this relationship,” Dr. Phipps said.
“My hope is that future cancer studies will build in more detailed, longitudinal information on sleep patterns to help us fill current gaps in knowledge.”
Dr. Phipps has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sleep apnea and other types of sleep disorders appear to elevate the risk for some types of cancer, specifically prostate cancer, more so than others. But the overall risk can be highly variable, and some sleep problems were found to be associated with a lower risk for cancer and cancer-related death, an analysis of a large observational cohort study of cardiovascular patients found.
Results of the analysis were published online in the journal Cancer Epidemiology. Investigators analyzed the presence of sleep apnea and insomnia and cancer risk in more than 8,500 patients in the Cardiovascular Health Study (CHS). “The fact that we observed certain sleep problems, like apneas, to be associated with elevated risk of some cancers but not others reflects the fact that cancer is a heterogeneous disease,” senior author Amanda Phipps, PhD, said in an interview. Dr. Phipps is an associate professor of epidemiology at the University of Washington and the Fred Hutchinson Cancer Research Center, both in Seattle.
Variable cancer links
The researchers assessed sleep problems in two groups in the CHS: an incident cancer group of 3,930 patients and a cancer mortality group of 4,580 patients. Within those respective groups, the investigators identified 885 first-incident cancers and 804 cancer deaths with a median follow-up of 12 and 14 years. The average age of the study population was 73 years, and 57% were women.
Sleep apnea symptoms (SAS) were associated with a lower risk for incident cancers – a 16% lower baseline risk and a 24% lower time-dependent risk. The study showed no association between cancer incidence and daytime sleepiness and apneas.
However, there was a significantly elevated risk relationship between sleep problems and prostate cancer. A time-dependent analysis of apnea showed more than double the risk (hazard ratio, 2.34), and baseline snoring carried a 69% greater risk. There was also a dose-response relationship for baseline cumulative SAS, compared with not having symptoms: an HR of 1.30 for one symptom, and 2.22 for two or more symptoms.
Risks for lymphatic or hematopoietic cancers were also associated with baseline daytime sleepiness (HR, 1.81), but not with insomnia (HR, 0.54).
With regard to cancer mortality, the study found no relationship between sleep problems and cancer death. In fact, it found an overall inverse relationship with snoring (time-dependent HR, 0.73; cumulative average HR, 0.67) and baseline apnea (HR, 0.69). Likewise, patients reporting SAS had lower risks than those having no SAS: an HR of 0.90 for one symptom and 0.75 for multiple symptoms. No relationships were found between any insomnia symptom and cancer death.
“We know the pathways that lead to prostate cancer can be very different than the pathways that lead to colorectal cancer,” Dr. Phipps said. “What we don’t yet understand is why these associations differ or what mechanisms are responsible for these cancer site-specific associations.”
Need for sleep assessment
The findings don’t change much for how clinicians should evaluate cancer risks in patients with sleep problems, Dr. Phipps said. “Other studies have clearly demonstrated the implications that sleep apnea has for a variety of other important health conditions – such as cardiovascular disease – so there are already plenty of good reasons for clinicians to ask their patients about their sleep and to connect patients with resources for the diagnosis and treatment of sleep apnea,” she added. “This study provides another possible reason.”
These findings provide context for future studies of the relationship between sleep problems and cancer. “But, given that sleep is something we all do and given that sleep problems are so pervasive, it’s important that we keep trying to better understand this relationship,” Dr. Phipps said.
“My hope is that future cancer studies will build in more detailed, longitudinal information on sleep patterns to help us fill current gaps in knowledge.”
Dr. Phipps has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CANCER EPIDEMIOLOGY
ASH meeting: Diversity, inclusion, immunotherapy, and COVID-19
In 2021, the American Society of Hematology will be hosting its annual meeting in a hybrid format. Content will be presented both live and in person at the Georgia World Congress Center in Atlanta and also online for those who can’t or don’t want to be there in person.
Inevitably during the ongoing pandemic, the meeting will contain key sessions on COVID-19 in hematology, including a plenary presentation outlining a biologic mechanism for the increased coagulopathy with SARS-CoV-2 infections.
In addition, there will be a scientific symposium on COVID-19 vaccination in immunocompromised patients and a special moderated session summarizing nine abstracts on the science of thrombosis in COVID-19, outcomes in patients with hematologic disease, and vaccine responses.
And speaking of COVID, lest anyone forget, annual meeting attendees will be required to be fully vaccinated and masked. Free COVID-19 testing will be available at stations situated throughout the convention center.
Diversifying care
chair of the ASH committee on communications and chief of the division of hematology at the Sylvester Comprehensive Cancer Center at the University of Miami.
For example, investigators at Massachusetts General Hospital in Boston will present new data on code-status transitions among patients with poor-prognosis high-risk acute myeloid leukemia (AML) who are approaching the end of life. Their findings suggest that physician-patient discussions about the goals of care may occur too late in the course of illness for many patients (abstract 109).
“While there have been many advances in the treatment of acute myeloid leukemia, and in fact there has been significant progress even among high-risk patients, addressing end-of-life issues is an often neglected area,” commented briefing participant Martin A. Tallman, MD, from Memorial Sloan Kettering Cancer Center, New York, who is also the current ASH president.
On a more upbeat note, Dr. Tallman also pointed to the results of the phase 3, randomized AGILE trial as an example of progress in AML, especially for patients with newly diagnosed high-risk disease who have mutations in IDH1. This trial investigated a new approach to treatment, with a combination of the combination of the IDH1 inhibitor ivosidenib (Tibsovo) and azacitidine, and compared it with azacitidine alone. The investigators assessed impact on event-free survival, overall survival, and clinical responses (abstract 697).
Dr. Tallman also highlighted abstracts touching on racial, social, and socioeconomic contributors to health care disparities among children with acute lymphoblastic leukemia (ALL; abstract 211) and on clinical trial enrollment characteristics and outcomes for Black and Hispanic adolescents and young adults with ALL (abstract 337).
Immunotherapy advances
Some of the most eagerly awaited abstracts will be highlighting advances in immunotherapy for hematologic malignancies, and these were previewed by Cynthia E. Dunbar, MD, ASH secretary and chief of the Translational Stem Cell Biology Branch within the Intramural Research Program of the National Heart, Lung, and Blood Institute in Bethesda, Md.
These abstracts include the primary analysis of the ZUMA-7 trial, a randomized, phase 3 study comparing the chimeric antigen receptor T-cell (CAR T) construct axicabtagene ciloleucel (axi-cel; Yescarta) with standard of care in patients with relapsed or refractory large B-cell lymphomas (LBCLs; abstract 2) and the interim analysis of the randomized, phase 3 Transform Study comparing the CAR T construct lisocabtagene maralecleucl (liso-cel; Breyanzi) with salvage chemotherapy in patients with relapsed/refractory LBCL (abstract 91).
“Over 500 patients were enrolled in the two studies, and both abstracts report significantly longer survival without relapse in the CAR T arm – for instance, fourfold higher in ZUMA-7, compared to standard of care,” Dr. Dunbar said at the briefing.
“These abstracts provide really critical information to patients, their treating physicians, and the payers who are trying to decide whether use of these expensive, complex, and potentially toxic CAR T-cell therapies are justified, compared to standard therapy,” she said.
Dr. Dunbar also highlighted an abstract on the addition of the anti-CD38 monoclonal antibody isatuximab (Sarclisa) to lenalidomide, bortezomib, and dexamethasone as induction therapy for patients with newly diagnosed multiple myeloma who are eligible for stem cell transplantation (abstract 463).
“The authors report that patients on the isatuximab arm had significantly fewer tumor cells following treatment,” Dr. Dunbar said. “We have come a long way beyond treating myeloma with a single drug, with remissions now measured in many years instead of 1 or 2 following initiation of treatment, and this abstract is another demonstration that novel combinations of multiple agents are really making a difference in this very debilitating disease.”
She also cited an abstract (abstract 127) on monotherapy with the novel bispecific T-cell–engaging monoclonal antibody mosunetuzumab for treatment of patients with follicular lymphoma that has relapsed or is refractory to at least two prior lines of therapy.
Old disorders, new insights
Other abstracts highlighted at the premeeting press briefing included a study that found a high prevalence of monoclonal gammopathy in persons at risk for multiple myeloma (abstract 152) and another with the surprising finding that clonal hematopoiesis, a risk factor myeloid malignancies, may be protective against Alzheimer’s disease (abstract 5).
In addition, a long-term follow-up study of patients with transfusion-dependent beta-thalassemia treated with gene therapy showed that some patients have become transfusion independent and iron homeostasis was restored (abstract 573).
Presentations from CDC and FDA
Dr. Sekeres highlighted other events of interest scheduled for ASH 2021, including a Grassroots Network Lunch featuring a discussion with Rochelle Walensky, MD, MPH, director of the Centers for Disease Control and Prevention in Atlanta, and a joint symposium between ASH and the Food and Drug Administration on newly approved drugs in hematology.
Dr. Sekeres has disclosed consulting/advising for Novartis, Takea/Millennium, and Bristol-Myers Squibb. Dr. Dunbar reported no relevant conflicts of interest. Dr. Tallman disclosed consulting/advising with and research funding from multiple entities.
A version of this article first appeared on Medscape.com.
In 2021, the American Society of Hematology will be hosting its annual meeting in a hybrid format. Content will be presented both live and in person at the Georgia World Congress Center in Atlanta and also online for those who can’t or don’t want to be there in person.
Inevitably during the ongoing pandemic, the meeting will contain key sessions on COVID-19 in hematology, including a plenary presentation outlining a biologic mechanism for the increased coagulopathy with SARS-CoV-2 infections.
In addition, there will be a scientific symposium on COVID-19 vaccination in immunocompromised patients and a special moderated session summarizing nine abstracts on the science of thrombosis in COVID-19, outcomes in patients with hematologic disease, and vaccine responses.
And speaking of COVID, lest anyone forget, annual meeting attendees will be required to be fully vaccinated and masked. Free COVID-19 testing will be available at stations situated throughout the convention center.
Diversifying care
chair of the ASH committee on communications and chief of the division of hematology at the Sylvester Comprehensive Cancer Center at the University of Miami.
For example, investigators at Massachusetts General Hospital in Boston will present new data on code-status transitions among patients with poor-prognosis high-risk acute myeloid leukemia (AML) who are approaching the end of life. Their findings suggest that physician-patient discussions about the goals of care may occur too late in the course of illness for many patients (abstract 109).
“While there have been many advances in the treatment of acute myeloid leukemia, and in fact there has been significant progress even among high-risk patients, addressing end-of-life issues is an often neglected area,” commented briefing participant Martin A. Tallman, MD, from Memorial Sloan Kettering Cancer Center, New York, who is also the current ASH president.
On a more upbeat note, Dr. Tallman also pointed to the results of the phase 3, randomized AGILE trial as an example of progress in AML, especially for patients with newly diagnosed high-risk disease who have mutations in IDH1. This trial investigated a new approach to treatment, with a combination of the combination of the IDH1 inhibitor ivosidenib (Tibsovo) and azacitidine, and compared it with azacitidine alone. The investigators assessed impact on event-free survival, overall survival, and clinical responses (abstract 697).
Dr. Tallman also highlighted abstracts touching on racial, social, and socioeconomic contributors to health care disparities among children with acute lymphoblastic leukemia (ALL; abstract 211) and on clinical trial enrollment characteristics and outcomes for Black and Hispanic adolescents and young adults with ALL (abstract 337).
Immunotherapy advances
Some of the most eagerly awaited abstracts will be highlighting advances in immunotherapy for hematologic malignancies, and these were previewed by Cynthia E. Dunbar, MD, ASH secretary and chief of the Translational Stem Cell Biology Branch within the Intramural Research Program of the National Heart, Lung, and Blood Institute in Bethesda, Md.
These abstracts include the primary analysis of the ZUMA-7 trial, a randomized, phase 3 study comparing the chimeric antigen receptor T-cell (CAR T) construct axicabtagene ciloleucel (axi-cel; Yescarta) with standard of care in patients with relapsed or refractory large B-cell lymphomas (LBCLs; abstract 2) and the interim analysis of the randomized, phase 3 Transform Study comparing the CAR T construct lisocabtagene maralecleucl (liso-cel; Breyanzi) with salvage chemotherapy in patients with relapsed/refractory LBCL (abstract 91).
“Over 500 patients were enrolled in the two studies, and both abstracts report significantly longer survival without relapse in the CAR T arm – for instance, fourfold higher in ZUMA-7, compared to standard of care,” Dr. Dunbar said at the briefing.
“These abstracts provide really critical information to patients, their treating physicians, and the payers who are trying to decide whether use of these expensive, complex, and potentially toxic CAR T-cell therapies are justified, compared to standard therapy,” she said.
Dr. Dunbar also highlighted an abstract on the addition of the anti-CD38 monoclonal antibody isatuximab (Sarclisa) to lenalidomide, bortezomib, and dexamethasone as induction therapy for patients with newly diagnosed multiple myeloma who are eligible for stem cell transplantation (abstract 463).
“The authors report that patients on the isatuximab arm had significantly fewer tumor cells following treatment,” Dr. Dunbar said. “We have come a long way beyond treating myeloma with a single drug, with remissions now measured in many years instead of 1 or 2 following initiation of treatment, and this abstract is another demonstration that novel combinations of multiple agents are really making a difference in this very debilitating disease.”
She also cited an abstract (abstract 127) on monotherapy with the novel bispecific T-cell–engaging monoclonal antibody mosunetuzumab for treatment of patients with follicular lymphoma that has relapsed or is refractory to at least two prior lines of therapy.
Old disorders, new insights
Other abstracts highlighted at the premeeting press briefing included a study that found a high prevalence of monoclonal gammopathy in persons at risk for multiple myeloma (abstract 152) and another with the surprising finding that clonal hematopoiesis, a risk factor myeloid malignancies, may be protective against Alzheimer’s disease (abstract 5).
In addition, a long-term follow-up study of patients with transfusion-dependent beta-thalassemia treated with gene therapy showed that some patients have become transfusion independent and iron homeostasis was restored (abstract 573).
Presentations from CDC and FDA
Dr. Sekeres highlighted other events of interest scheduled for ASH 2021, including a Grassroots Network Lunch featuring a discussion with Rochelle Walensky, MD, MPH, director of the Centers for Disease Control and Prevention in Atlanta, and a joint symposium between ASH and the Food and Drug Administration on newly approved drugs in hematology.
Dr. Sekeres has disclosed consulting/advising for Novartis, Takea/Millennium, and Bristol-Myers Squibb. Dr. Dunbar reported no relevant conflicts of interest. Dr. Tallman disclosed consulting/advising with and research funding from multiple entities.
A version of this article first appeared on Medscape.com.
In 2021, the American Society of Hematology will be hosting its annual meeting in a hybrid format. Content will be presented both live and in person at the Georgia World Congress Center in Atlanta and also online for those who can’t or don’t want to be there in person.
Inevitably during the ongoing pandemic, the meeting will contain key sessions on COVID-19 in hematology, including a plenary presentation outlining a biologic mechanism for the increased coagulopathy with SARS-CoV-2 infections.
In addition, there will be a scientific symposium on COVID-19 vaccination in immunocompromised patients and a special moderated session summarizing nine abstracts on the science of thrombosis in COVID-19, outcomes in patients with hematologic disease, and vaccine responses.
And speaking of COVID, lest anyone forget, annual meeting attendees will be required to be fully vaccinated and masked. Free COVID-19 testing will be available at stations situated throughout the convention center.
Diversifying care
chair of the ASH committee on communications and chief of the division of hematology at the Sylvester Comprehensive Cancer Center at the University of Miami.
For example, investigators at Massachusetts General Hospital in Boston will present new data on code-status transitions among patients with poor-prognosis high-risk acute myeloid leukemia (AML) who are approaching the end of life. Their findings suggest that physician-patient discussions about the goals of care may occur too late in the course of illness for many patients (abstract 109).
“While there have been many advances in the treatment of acute myeloid leukemia, and in fact there has been significant progress even among high-risk patients, addressing end-of-life issues is an often neglected area,” commented briefing participant Martin A. Tallman, MD, from Memorial Sloan Kettering Cancer Center, New York, who is also the current ASH president.
On a more upbeat note, Dr. Tallman also pointed to the results of the phase 3, randomized AGILE trial as an example of progress in AML, especially for patients with newly diagnosed high-risk disease who have mutations in IDH1. This trial investigated a new approach to treatment, with a combination of the combination of the IDH1 inhibitor ivosidenib (Tibsovo) and azacitidine, and compared it with azacitidine alone. The investigators assessed impact on event-free survival, overall survival, and clinical responses (abstract 697).
Dr. Tallman also highlighted abstracts touching on racial, social, and socioeconomic contributors to health care disparities among children with acute lymphoblastic leukemia (ALL; abstract 211) and on clinical trial enrollment characteristics and outcomes for Black and Hispanic adolescents and young adults with ALL (abstract 337).
Immunotherapy advances
Some of the most eagerly awaited abstracts will be highlighting advances in immunotherapy for hematologic malignancies, and these were previewed by Cynthia E. Dunbar, MD, ASH secretary and chief of the Translational Stem Cell Biology Branch within the Intramural Research Program of the National Heart, Lung, and Blood Institute in Bethesda, Md.
These abstracts include the primary analysis of the ZUMA-7 trial, a randomized, phase 3 study comparing the chimeric antigen receptor T-cell (CAR T) construct axicabtagene ciloleucel (axi-cel; Yescarta) with standard of care in patients with relapsed or refractory large B-cell lymphomas (LBCLs; abstract 2) and the interim analysis of the randomized, phase 3 Transform Study comparing the CAR T construct lisocabtagene maralecleucl (liso-cel; Breyanzi) with salvage chemotherapy in patients with relapsed/refractory LBCL (abstract 91).
“Over 500 patients were enrolled in the two studies, and both abstracts report significantly longer survival without relapse in the CAR T arm – for instance, fourfold higher in ZUMA-7, compared to standard of care,” Dr. Dunbar said at the briefing.
“These abstracts provide really critical information to patients, their treating physicians, and the payers who are trying to decide whether use of these expensive, complex, and potentially toxic CAR T-cell therapies are justified, compared to standard therapy,” she said.
Dr. Dunbar also highlighted an abstract on the addition of the anti-CD38 monoclonal antibody isatuximab (Sarclisa) to lenalidomide, bortezomib, and dexamethasone as induction therapy for patients with newly diagnosed multiple myeloma who are eligible for stem cell transplantation (abstract 463).
“The authors report that patients on the isatuximab arm had significantly fewer tumor cells following treatment,” Dr. Dunbar said. “We have come a long way beyond treating myeloma with a single drug, with remissions now measured in many years instead of 1 or 2 following initiation of treatment, and this abstract is another demonstration that novel combinations of multiple agents are really making a difference in this very debilitating disease.”
She also cited an abstract (abstract 127) on monotherapy with the novel bispecific T-cell–engaging monoclonal antibody mosunetuzumab for treatment of patients with follicular lymphoma that has relapsed or is refractory to at least two prior lines of therapy.
Old disorders, new insights
Other abstracts highlighted at the premeeting press briefing included a study that found a high prevalence of monoclonal gammopathy in persons at risk for multiple myeloma (abstract 152) and another with the surprising finding that clonal hematopoiesis, a risk factor myeloid malignancies, may be protective against Alzheimer’s disease (abstract 5).
In addition, a long-term follow-up study of patients with transfusion-dependent beta-thalassemia treated with gene therapy showed that some patients have become transfusion independent and iron homeostasis was restored (abstract 573).
Presentations from CDC and FDA
Dr. Sekeres highlighted other events of interest scheduled for ASH 2021, including a Grassroots Network Lunch featuring a discussion with Rochelle Walensky, MD, MPH, director of the Centers for Disease Control and Prevention in Atlanta, and a joint symposium between ASH and the Food and Drug Administration on newly approved drugs in hematology.
Dr. Sekeres has disclosed consulting/advising for Novartis, Takea/Millennium, and Bristol-Myers Squibb. Dr. Dunbar reported no relevant conflicts of interest. Dr. Tallman disclosed consulting/advising with and research funding from multiple entities.
A version of this article first appeared on Medscape.com.
Residency programs readjust during COVID
Hospitalist-honed agility proves invaluable
It could be argued that hospital medicine in the United States was made vital by a major infectious disease epidemic – the HIV/AIDS crisis – said Emily Gottenborg, MD, a hospitalist and program director of hospitalist training at the University of Colorado at Denver, Aurora. Certainly, it was born out of the need for change, for physicians who could coordinate complex patient care plans and serve as the “quarterbacks” of the hospital. “As a result, we have always been very nimble and ready to embrace change,” said Dr. Gottenborg.

That hospitalist-honed agility and penchant for innovation has proven to be invaluable during the current COVID-19 pandemic as hospital medicine–focused residency programs have been forced to pivot quickly and modify their agendas. From managing the pandemic’s impact on residents’ day-to-day experiences, to carefully balancing educational needs and goals, program leaders have worked tirelessly to ensure that residents continue to receive excellent training.
The overarching theme across U.S.-based residency programs is that the educational changes and challenges during the COVID-19 pandemic have often been one and the same.
Service versus education
At the beginning of the pandemic, trainees at the University of Pittsburgh Medical Center were limited in seeing COVID patients in order to curb exposure. But now that COVID appears to be the new normal, “I think the question becomes: ‘How do we incorporate our trainees to take care of COVID patients since it seems it will be staying around for a while?’ ” said Rachna Rawal, MD, a hospitalist and clinical assistant professor of medicine at UPMC.
This dilemma highlights the conflict between service and education. Residents have been motivated and eager to help, which has been beneficial whenever there is a surge. “At the same time, you want to preserve their education, and it’s a very difficult balance at times,” said Dr. Rawal. It’s also challenging to figure out the safest way for residents to see patients, as well as how to include medical students, since interns and residents serve as important educational resources for them.
Keeping trainees involved with daily virtual conferences rather than in-person interactions raises the question of whether or not the engagement is equivalent. “It’s harder to keep them accountable when they’re not in person, but it’s also not worth the risk given the COVID numbers at times,” Dr. Rawal said. The goal has become to make sure residents stay safe while still feeling that they are getting a good education.
A balancing act
“I think early on, there was a lot of pride in what we were doing, that we were on the front line managing this thing that was emerging,” said Daniel Ricotta, MD, a hospitalist and associate program director of the internal medicine residency at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston. “And now I think people are starting to feel a little bit weary.”

It has been demanding trying to manage ongoing educational needs through this time. “At the end of the day, residents are still trainees and have to be trained and educated. They’re not just worker bees taking care of patients,” Dr. Ricotta said. Residents need a well-rounded clinical experience – “they can’t just take care of COVID patients and then be able to graduate as general internists,” he said – but that becomes onerous when the hospital is full of patients with COVID.
Along with balancing residents’ clinical immersion, Dr. Ricotta said there has been the challenge of doing “the content-based teaching from didactics that occur in the context of clinical work, but are somewhat separated when you need to limit the number of people in the rooms and try to keep as many people at home as possible when they’re not taking care of patients in order to limit their level of risk.” Adjusting and readjusting both of these aspects has had a major impact on residents’ day-to-day education.
“A big part of residency is community,” noted Dr. Ricotta, but the sense of community has been disrupted because some of the bonding experiences residents used to do outside the hospital to build that community have necessarily gone by the wayside. This particularly affects interns from around the country who are meeting each other for the first time. “We actually had a normal intern orientation this year, but last year, when everything was virtual, we were trying to find ways to bridge relationships in a way that was safe and socially distanced,” he said.
Improving quality
UC Denver is unique in that they have a 3-year program specifically for hospital medicine residents, said Dr. Gottenborg. Right away, “our residents rose to the challenge and wanted to be part of the workforce that helps care for this critical population of [COVID] patients.” The residents were able to run the ICUs and take care of COVID patients, but in exchange, they had to give up some of their elective rotation time.
One aspect of the UC Denver hospital medicine residency program is participation in projects that focus on how to improve the health care system. Over the past year, the residents worked on one project in particular that focused on restructuring the guidelines for consulting physical therapists. Since many patients end up needing a physical therapist for a variety of reasons, a full hospital puts increased strain on their workload, making their time more precious.
“[The project] forced us to think about the right criteria to consult them,” explained Dr. Gottenborg. “We cut down essentially all the inappropriate consults to PT, opening their time. That project was driven by how the residents were experiencing the pandemic in the hospital.”
Learning to adapt
“The training environment during this pandemic has been tumultuous for both our residents and medical students,” said Alan M. Hall, MD, associate professor of internal medicine and pediatrics and assistant dean of curriculum integration at the University of Kentucky, Lexington. Along with treating patients with COVID-19, he said trainees have also had to cope with anxiety about getting the virus themselves or inadvertently bringing it home to their families.

Like most medical schools, University of Kentucky students were shifted away from clinical rotations and into alternative and online education for a time. When they returned to in-person education, the students were initially restricted from seeing patients with confirmed or suspected COVID-19 in order to reduce their personal risk and to conserve personal protective equipment.
This especially impacted certain rotations, such as pediatrics. Because respiratory symptoms are common in this population, students were greatly limited in the number of new patients they could see. Now they are given the option to see patients with COVID-19 if they want to.
“Our residents have had to adapt to seemingly endless changes during this pandemic,” Dr. Hall said. For example, at the beginning of the surge, the internal medicine residents trained for a completely new clinical model, though this ultimately never needed to be implemented. Then they had to adjust to extremely high census numbers that continue to have an effect on almost all of their rotations.
Conversely, the pediatrics residents saw far fewer inpatients last winter than they typically would. This made it more difficult for them to feel comfortable when census numbers increased with common diagnoses like bronchiolitis. “However, those respiratory viruses that were hibernating last winter caused an unusual and challenging summer surge,” Dr. Hall said.
The biggest challenge though “is knowing that there is not a perfect solution for this global pandemic’s effect on medical education,” said Dr. Hall. “We can’t possibly perfectly balance the safety of our learners and their families with the dangers of COVID-19.”
Leadership discussions
As a residency program leader, Dr. Ricotta said there are conversations about multiple topics, including maintaining a safe learning environment; providing important aspects of residency training; whether to go back to full in-person teaching, keep doing virtual teaching, or implement a hybrid model; and how to help residents understand the balance between their personal and professional lives, especially in terms of safety.
“They have to their lives outside of the hospital, but we also are trying to instill ... what their responsibility is to society, to their patients, and to each other,” said Dr. Ricotta.
A more recent discussion has been about how to manage the COVID vaccine boosters. “We can’t have everyone getting vaccines at the same time because they might have symptoms afterward, and then be out sick – you’re missing half your workforce,” Dr. Ricotta said. But staggering residents’ booster shots created yet another dilemma around deciding who received the booster sooner rather than later.
The biggest consideration for Dr. Gottenborg’s leadership team was deciding whether to use their residents to help with the COVID surges or keep them in a traditional residency experience. While the residents wanted to be part of the pandemic response, there were many factors to consider. Ultimately, they came up with a balance between the amount of time residents should spend taking care of COVID patients while also assuring that they leave the program with all the skills and experiences they need.
Though Dr. Hall works more closely with medical students than residents, he sees the challenges and effects as being similar. Creating harmony between a safe learning environment and students’ educational goals has been the topic of endless discussions. This includes decisions as to whether or not students should be involved in person in certain activities such as large classroom didactics, written exams, seeing patients in clinical settings, and small group discussions.
Recruitment effects
When it comes to recruiting during a global pandemic, the experiences and predictions are mixed. Dr. Hall believes virtual interviews are making recruitment easier, but in turn, the fact that they are virtual also makes it harder for the applicant to get a good feel for the program and the people involved in it.
Dr. Ricotta reported that recruitment numbers have been fairly steady at Beth Israel Deaconess over the last few years. “In addition to the critical care physicians, hospital medicine was really the front line of this pandemic and so in some ways, we gained some recognition that we may not have had otherwise,” said Dr. Ricotta. He believes this has the benefit of attracting some residents, but at the same time, it could potentially scare others away from what they perceive as a demanding, grueling job. “I think it has been mixed. It’s dependent on the person.”
At UC Denver, Dr. Gottenborg said they are seeing a rapid rise in the number of applications and interest in their programs. Still, “I think this could go both ways,” she acknowledged. With the focus on hospital medicine in the media, medical students are more aware of the specialty and what it involves. “I think the sense of mission is really exemplified and everyone is talking about it,” she said. This is evident in the arrival this summer of the first new class of interns since the pandemic. “They’re incredibly passionate about the work,” said Dr. Gottenborg.
However, there is also the notable increase in physician burnout since the pandemic started. That this has been regularly featured in the media leaves Dr. Gottenborg to wonder if prospective residents will shy away from hospital medicine because they believe it is an area that leads to burnout. “I hope that’s not the case,” she said.
“I would actually argue [recruitment] is easier,” said Dr. Rawal. Like Dr. Hall, she sees virtual interviews as a big benefit to prospective trainees because they don’t have to spend a large amount of money on travel, food, and other expenses like they did before, a welcome relief for residents with significant debt. “I think that is one very big positive from the pandemic,” she said. Her trainees were advised to make a final list and consider going to see the top two or three in person, but “at this point, there’s really no expectation to go see all 15 places that you look into.”
Dr. Rawal also pointed out that recruitment is affected by whether or not trainees are expected to see COVID patients. “I know in some places they aren’t and in some places they are, so it just depends on where you are and what you’re looking for,” she said.
Shifts in education
It remains to be seen if all the educational changes will be permanent, though it appears that many will remain. Dr. Hall hopes that virtual visits to provide care to patients who have difficulty getting to physical clinics will continue to be a focus for hospital medicine trainees. “For medical students, I think this will allow us to better assess what content can best be delivered in person, synchronously online, or asynchronously through recorded content,” he said.
Dr. Ricotta predicts that virtual conferences will become more pervasive as academic hospitals continue to acquire more community hospitals, especially for grand rounds. “The virtual teaching that occurred in the residency program because it’s required by the [Accreditation Council for Graduate Medical Education] has, I think, informed how academic centers do ongoing faculty development, professional development, and obviously education for the residents,” Dr. Ricotta said. “I think virtual teaching is here to stay.” This includes telehealth training, which had not been a widespread part of residency education before now.
Trainees have been given tools to handle high patient censuses and learned a whole new set of communication skills, thanks to the pandemic, said Dr. Rawal. There has been a focus on learning how to advocate for the vaccine, along with education on situations like how to have conversations with patients who don’t believe they have COVID, even when their tests are positive. “Learning to handle these situations and still be a physician and provide appropriate care regardless of the patient’s views is very important. This is not something I learned in my training because it never came up,” she said.
Dr. Gottenborg has been impressed by the resident workforce’s response across all specialties throughout these difficult days. “They were universally ready to dive in and work long hours and care for these very sick patients and ultimately share their experiences so that we could do it better as these patients continue to flow through our systems,” she said. “It has been very invigorating.”
The pandemic has also put a spotlight on the importance of being flexible, as well as various problems with how health care systems operate, “which, for people in our field, gets us both excited and gives us a lot of work to do,” said Dr. Gottenborg. “Our residents see that and feel that and will hopefully continue to hold that torch in hospital medicine.”
In spite of everything, Dr. Rawal believes this is an exhilarating time to be a trainee. “They’re getting an opportunity that none of us got. Usually, when policies are made, we really don’t see the immediate impact.” But with recent mandates like masks and social distancing, “the rate of change that they get to see things happen is exciting. They’re going to be a very exciting group of physicians.”
Hospitalist-honed agility proves invaluable
Hospitalist-honed agility proves invaluable
It could be argued that hospital medicine in the United States was made vital by a major infectious disease epidemic – the HIV/AIDS crisis – said Emily Gottenborg, MD, a hospitalist and program director of hospitalist training at the University of Colorado at Denver, Aurora. Certainly, it was born out of the need for change, for physicians who could coordinate complex patient care plans and serve as the “quarterbacks” of the hospital. “As a result, we have always been very nimble and ready to embrace change,” said Dr. Gottenborg.
That hospitalist-honed agility and penchant for innovation has proven to be invaluable during the current COVID-19 pandemic as hospital medicine–focused residency programs have been forced to pivot quickly and modify their agendas. From managing the pandemic’s impact on residents’ day-to-day experiences, to carefully balancing educational needs and goals, program leaders have worked tirelessly to ensure that residents continue to receive excellent training.
The overarching theme across U.S.-based residency programs is that the educational changes and challenges during the COVID-19 pandemic have often been one and the same.
Service versus education
At the beginning of the pandemic, trainees at the University of Pittsburgh Medical Center were limited in seeing COVID patients in order to curb exposure. But now that COVID appears to be the new normal, “I think the question becomes: ‘How do we incorporate our trainees to take care of COVID patients since it seems it will be staying around for a while?’ ” said Rachna Rawal, MD, a hospitalist and clinical assistant professor of medicine at UPMC.
This dilemma highlights the conflict between service and education. Residents have been motivated and eager to help, which has been beneficial whenever there is a surge. “At the same time, you want to preserve their education, and it’s a very difficult balance at times,” said Dr. Rawal. It’s also challenging to figure out the safest way for residents to see patients, as well as how to include medical students, since interns and residents serve as important educational resources for them.
Keeping trainees involved with daily virtual conferences rather than in-person interactions raises the question of whether or not the engagement is equivalent. “It’s harder to keep them accountable when they’re not in person, but it’s also not worth the risk given the COVID numbers at times,” Dr. Rawal said. The goal has become to make sure residents stay safe while still feeling that they are getting a good education.
A balancing act
“I think early on, there was a lot of pride in what we were doing, that we were on the front line managing this thing that was emerging,” said Daniel Ricotta, MD, a hospitalist and associate program director of the internal medicine residency at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston. “And now I think people are starting to feel a little bit weary.”
It has been demanding trying to manage ongoing educational needs through this time. “At the end of the day, residents are still trainees and have to be trained and educated. They’re not just worker bees taking care of patients,” Dr. Ricotta said. Residents need a well-rounded clinical experience – “they can’t just take care of COVID patients and then be able to graduate as general internists,” he said – but that becomes onerous when the hospital is full of patients with COVID.
Along with balancing residents’ clinical immersion, Dr. Ricotta said there has been the challenge of doing “the content-based teaching from didactics that occur in the context of clinical work, but are somewhat separated when you need to limit the number of people in the rooms and try to keep as many people at home as possible when they’re not taking care of patients in order to limit their level of risk.” Adjusting and readjusting both of these aspects has had a major impact on residents’ day-to-day education.
“A big part of residency is community,” noted Dr. Ricotta, but the sense of community has been disrupted because some of the bonding experiences residents used to do outside the hospital to build that community have necessarily gone by the wayside. This particularly affects interns from around the country who are meeting each other for the first time. “We actually had a normal intern orientation this year, but last year, when everything was virtual, we were trying to find ways to bridge relationships in a way that was safe and socially distanced,” he said.
Improving quality
UC Denver is unique in that they have a 3-year program specifically for hospital medicine residents, said Dr. Gottenborg. Right away, “our residents rose to the challenge and wanted to be part of the workforce that helps care for this critical population of [COVID] patients.” The residents were able to run the ICUs and take care of COVID patients, but in exchange, they had to give up some of their elective rotation time.
One aspect of the UC Denver hospital medicine residency program is participation in projects that focus on how to improve the health care system. Over the past year, the residents worked on one project in particular that focused on restructuring the guidelines for consulting physical therapists. Since many patients end up needing a physical therapist for a variety of reasons, a full hospital puts increased strain on their workload, making their time more precious.
“[The project] forced us to think about the right criteria to consult them,” explained Dr. Gottenborg. “We cut down essentially all the inappropriate consults to PT, opening their time. That project was driven by how the residents were experiencing the pandemic in the hospital.”
Learning to adapt
“The training environment during this pandemic has been tumultuous for both our residents and medical students,” said Alan M. Hall, MD, associate professor of internal medicine and pediatrics and assistant dean of curriculum integration at the University of Kentucky, Lexington. Along with treating patients with COVID-19, he said trainees have also had to cope with anxiety about getting the virus themselves or inadvertently bringing it home to their families.
Like most medical schools, University of Kentucky students were shifted away from clinical rotations and into alternative and online education for a time. When they returned to in-person education, the students were initially restricted from seeing patients with confirmed or suspected COVID-19 in order to reduce their personal risk and to conserve personal protective equipment.
This especially impacted certain rotations, such as pediatrics. Because respiratory symptoms are common in this population, students were greatly limited in the number of new patients they could see. Now they are given the option to see patients with COVID-19 if they want to.
“Our residents have had to adapt to seemingly endless changes during this pandemic,” Dr. Hall said. For example, at the beginning of the surge, the internal medicine residents trained for a completely new clinical model, though this ultimately never needed to be implemented. Then they had to adjust to extremely high census numbers that continue to have an effect on almost all of their rotations.
Conversely, the pediatrics residents saw far fewer inpatients last winter than they typically would. This made it more difficult for them to feel comfortable when census numbers increased with common diagnoses like bronchiolitis. “However, those respiratory viruses that were hibernating last winter caused an unusual and challenging summer surge,” Dr. Hall said.
The biggest challenge though “is knowing that there is not a perfect solution for this global pandemic’s effect on medical education,” said Dr. Hall. “We can’t possibly perfectly balance the safety of our learners and their families with the dangers of COVID-19.”
Leadership discussions
As a residency program leader, Dr. Ricotta said there are conversations about multiple topics, including maintaining a safe learning environment; providing important aspects of residency training; whether to go back to full in-person teaching, keep doing virtual teaching, or implement a hybrid model; and how to help residents understand the balance between their personal and professional lives, especially in terms of safety.
“They have to their lives outside of the hospital, but we also are trying to instill ... what their responsibility is to society, to their patients, and to each other,” said Dr. Ricotta.
A more recent discussion has been about how to manage the COVID vaccine boosters. “We can’t have everyone getting vaccines at the same time because they might have symptoms afterward, and then be out sick – you’re missing half your workforce,” Dr. Ricotta said. But staggering residents’ booster shots created yet another dilemma around deciding who received the booster sooner rather than later.
The biggest consideration for Dr. Gottenborg’s leadership team was deciding whether to use their residents to help with the COVID surges or keep them in a traditional residency experience. While the residents wanted to be part of the pandemic response, there were many factors to consider. Ultimately, they came up with a balance between the amount of time residents should spend taking care of COVID patients while also assuring that they leave the program with all the skills and experiences they need.
Though Dr. Hall works more closely with medical students than residents, he sees the challenges and effects as being similar. Creating harmony between a safe learning environment and students’ educational goals has been the topic of endless discussions. This includes decisions as to whether or not students should be involved in person in certain activities such as large classroom didactics, written exams, seeing patients in clinical settings, and small group discussions.
Recruitment effects
When it comes to recruiting during a global pandemic, the experiences and predictions are mixed. Dr. Hall believes virtual interviews are making recruitment easier, but in turn, the fact that they are virtual also makes it harder for the applicant to get a good feel for the program and the people involved in it.
Dr. Ricotta reported that recruitment numbers have been fairly steady at Beth Israel Deaconess over the last few years. “In addition to the critical care physicians, hospital medicine was really the front line of this pandemic and so in some ways, we gained some recognition that we may not have had otherwise,” said Dr. Ricotta. He believes this has the benefit of attracting some residents, but at the same time, it could potentially scare others away from what they perceive as a demanding, grueling job. “I think it has been mixed. It’s dependent on the person.”
At UC Denver, Dr. Gottenborg said they are seeing a rapid rise in the number of applications and interest in their programs. Still, “I think this could go both ways,” she acknowledged. With the focus on hospital medicine in the media, medical students are more aware of the specialty and what it involves. “I think the sense of mission is really exemplified and everyone is talking about it,” she said. This is evident in the arrival this summer of the first new class of interns since the pandemic. “They’re incredibly passionate about the work,” said Dr. Gottenborg.
However, there is also the notable increase in physician burnout since the pandemic started. That this has been regularly featured in the media leaves Dr. Gottenborg to wonder if prospective residents will shy away from hospital medicine because they believe it is an area that leads to burnout. “I hope that’s not the case,” she said.
“I would actually argue [recruitment] is easier,” said Dr. Rawal. Like Dr. Hall, she sees virtual interviews as a big benefit to prospective trainees because they don’t have to spend a large amount of money on travel, food, and other expenses like they did before, a welcome relief for residents with significant debt. “I think that is one very big positive from the pandemic,” she said. Her trainees were advised to make a final list and consider going to see the top two or three in person, but “at this point, there’s really no expectation to go see all 15 places that you look into.”
Dr. Rawal also pointed out that recruitment is affected by whether or not trainees are expected to see COVID patients. “I know in some places they aren’t and in some places they are, so it just depends on where you are and what you’re looking for,” she said.
Shifts in education
It remains to be seen if all the educational changes will be permanent, though it appears that many will remain. Dr. Hall hopes that virtual visits to provide care to patients who have difficulty getting to physical clinics will continue to be a focus for hospital medicine trainees. “For medical students, I think this will allow us to better assess what content can best be delivered in person, synchronously online, or asynchronously through recorded content,” he said.
Dr. Ricotta predicts that virtual conferences will become more pervasive as academic hospitals continue to acquire more community hospitals, especially for grand rounds. “The virtual teaching that occurred in the residency program because it’s required by the [Accreditation Council for Graduate Medical Education] has, I think, informed how academic centers do ongoing faculty development, professional development, and obviously education for the residents,” Dr. Ricotta said. “I think virtual teaching is here to stay.” This includes telehealth training, which had not been a widespread part of residency education before now.
Trainees have been given tools to handle high patient censuses and learned a whole new set of communication skills, thanks to the pandemic, said Dr. Rawal. There has been a focus on learning how to advocate for the vaccine, along with education on situations like how to have conversations with patients who don’t believe they have COVID, even when their tests are positive. “Learning to handle these situations and still be a physician and provide appropriate care regardless of the patient’s views is very important. This is not something I learned in my training because it never came up,” she said.
Dr. Gottenborg has been impressed by the resident workforce’s response across all specialties throughout these difficult days. “They were universally ready to dive in and work long hours and care for these very sick patients and ultimately share their experiences so that we could do it better as these patients continue to flow through our systems,” she said. “It has been very invigorating.”
The pandemic has also put a spotlight on the importance of being flexible, as well as various problems with how health care systems operate, “which, for people in our field, gets us both excited and gives us a lot of work to do,” said Dr. Gottenborg. “Our residents see that and feel that and will hopefully continue to hold that torch in hospital medicine.”
In spite of everything, Dr. Rawal believes this is an exhilarating time to be a trainee. “They’re getting an opportunity that none of us got. Usually, when policies are made, we really don’t see the immediate impact.” But with recent mandates like masks and social distancing, “the rate of change that they get to see things happen is exciting. They’re going to be a very exciting group of physicians.”
It could be argued that hospital medicine in the United States was made vital by a major infectious disease epidemic – the HIV/AIDS crisis – said Emily Gottenborg, MD, a hospitalist and program director of hospitalist training at the University of Colorado at Denver, Aurora. Certainly, it was born out of the need for change, for physicians who could coordinate complex patient care plans and serve as the “quarterbacks” of the hospital. “As a result, we have always been very nimble and ready to embrace change,” said Dr. Gottenborg.
That hospitalist-honed agility and penchant for innovation has proven to be invaluable during the current COVID-19 pandemic as hospital medicine–focused residency programs have been forced to pivot quickly and modify their agendas. From managing the pandemic’s impact on residents’ day-to-day experiences, to carefully balancing educational needs and goals, program leaders have worked tirelessly to ensure that residents continue to receive excellent training.
The overarching theme across U.S.-based residency programs is that the educational changes and challenges during the COVID-19 pandemic have often been one and the same.
Service versus education
At the beginning of the pandemic, trainees at the University of Pittsburgh Medical Center were limited in seeing COVID patients in order to curb exposure. But now that COVID appears to be the new normal, “I think the question becomes: ‘How do we incorporate our trainees to take care of COVID patients since it seems it will be staying around for a while?’ ” said Rachna Rawal, MD, a hospitalist and clinical assistant professor of medicine at UPMC.
This dilemma highlights the conflict between service and education. Residents have been motivated and eager to help, which has been beneficial whenever there is a surge. “At the same time, you want to preserve their education, and it’s a very difficult balance at times,” said Dr. Rawal. It’s also challenging to figure out the safest way for residents to see patients, as well as how to include medical students, since interns and residents serve as important educational resources for them.
Keeping trainees involved with daily virtual conferences rather than in-person interactions raises the question of whether or not the engagement is equivalent. “It’s harder to keep them accountable when they’re not in person, but it’s also not worth the risk given the COVID numbers at times,” Dr. Rawal said. The goal has become to make sure residents stay safe while still feeling that they are getting a good education.
A balancing act
“I think early on, there was a lot of pride in what we were doing, that we were on the front line managing this thing that was emerging,” said Daniel Ricotta, MD, a hospitalist and associate program director of the internal medicine residency at Beth Israel Deaconess Medical Center and assistant professor of medicine at Harvard Medical School, both in Boston. “And now I think people are starting to feel a little bit weary.”
It has been demanding trying to manage ongoing educational needs through this time. “At the end of the day, residents are still trainees and have to be trained and educated. They’re not just worker bees taking care of patients,” Dr. Ricotta said. Residents need a well-rounded clinical experience – “they can’t just take care of COVID patients and then be able to graduate as general internists,” he said – but that becomes onerous when the hospital is full of patients with COVID.
Along with balancing residents’ clinical immersion, Dr. Ricotta said there has been the challenge of doing “the content-based teaching from didactics that occur in the context of clinical work, but are somewhat separated when you need to limit the number of people in the rooms and try to keep as many people at home as possible when they’re not taking care of patients in order to limit their level of risk.” Adjusting and readjusting both of these aspects has had a major impact on residents’ day-to-day education.
“A big part of residency is community,” noted Dr. Ricotta, but the sense of community has been disrupted because some of the bonding experiences residents used to do outside the hospital to build that community have necessarily gone by the wayside. This particularly affects interns from around the country who are meeting each other for the first time. “We actually had a normal intern orientation this year, but last year, when everything was virtual, we were trying to find ways to bridge relationships in a way that was safe and socially distanced,” he said.
Improving quality
UC Denver is unique in that they have a 3-year program specifically for hospital medicine residents, said Dr. Gottenborg. Right away, “our residents rose to the challenge and wanted to be part of the workforce that helps care for this critical population of [COVID] patients.” The residents were able to run the ICUs and take care of COVID patients, but in exchange, they had to give up some of their elective rotation time.
One aspect of the UC Denver hospital medicine residency program is participation in projects that focus on how to improve the health care system. Over the past year, the residents worked on one project in particular that focused on restructuring the guidelines for consulting physical therapists. Since many patients end up needing a physical therapist for a variety of reasons, a full hospital puts increased strain on their workload, making their time more precious.
“[The project] forced us to think about the right criteria to consult them,” explained Dr. Gottenborg. “We cut down essentially all the inappropriate consults to PT, opening their time. That project was driven by how the residents were experiencing the pandemic in the hospital.”
Learning to adapt
“The training environment during this pandemic has been tumultuous for both our residents and medical students,” said Alan M. Hall, MD, associate professor of internal medicine and pediatrics and assistant dean of curriculum integration at the University of Kentucky, Lexington. Along with treating patients with COVID-19, he said trainees have also had to cope with anxiety about getting the virus themselves or inadvertently bringing it home to their families.
Like most medical schools, University of Kentucky students were shifted away from clinical rotations and into alternative and online education for a time. When they returned to in-person education, the students were initially restricted from seeing patients with confirmed or suspected COVID-19 in order to reduce their personal risk and to conserve personal protective equipment.
This especially impacted certain rotations, such as pediatrics. Because respiratory symptoms are common in this population, students were greatly limited in the number of new patients they could see. Now they are given the option to see patients with COVID-19 if they want to.
“Our residents have had to adapt to seemingly endless changes during this pandemic,” Dr. Hall said. For example, at the beginning of the surge, the internal medicine residents trained for a completely new clinical model, though this ultimately never needed to be implemented. Then they had to adjust to extremely high census numbers that continue to have an effect on almost all of their rotations.
Conversely, the pediatrics residents saw far fewer inpatients last winter than they typically would. This made it more difficult for them to feel comfortable when census numbers increased with common diagnoses like bronchiolitis. “However, those respiratory viruses that were hibernating last winter caused an unusual and challenging summer surge,” Dr. Hall said.
The biggest challenge though “is knowing that there is not a perfect solution for this global pandemic’s effect on medical education,” said Dr. Hall. “We can’t possibly perfectly balance the safety of our learners and their families with the dangers of COVID-19.”
Leadership discussions
As a residency program leader, Dr. Ricotta said there are conversations about multiple topics, including maintaining a safe learning environment; providing important aspects of residency training; whether to go back to full in-person teaching, keep doing virtual teaching, or implement a hybrid model; and how to help residents understand the balance between their personal and professional lives, especially in terms of safety.
“They have to their lives outside of the hospital, but we also are trying to instill ... what their responsibility is to society, to their patients, and to each other,” said Dr. Ricotta.
A more recent discussion has been about how to manage the COVID vaccine boosters. “We can’t have everyone getting vaccines at the same time because they might have symptoms afterward, and then be out sick – you’re missing half your workforce,” Dr. Ricotta said. But staggering residents’ booster shots created yet another dilemma around deciding who received the booster sooner rather than later.
The biggest consideration for Dr. Gottenborg’s leadership team was deciding whether to use their residents to help with the COVID surges or keep them in a traditional residency experience. While the residents wanted to be part of the pandemic response, there were many factors to consider. Ultimately, they came up with a balance between the amount of time residents should spend taking care of COVID patients while also assuring that they leave the program with all the skills and experiences they need.
Though Dr. Hall works more closely with medical students than residents, he sees the challenges and effects as being similar. Creating harmony between a safe learning environment and students’ educational goals has been the topic of endless discussions. This includes decisions as to whether or not students should be involved in person in certain activities such as large classroom didactics, written exams, seeing patients in clinical settings, and small group discussions.
Recruitment effects
When it comes to recruiting during a global pandemic, the experiences and predictions are mixed. Dr. Hall believes virtual interviews are making recruitment easier, but in turn, the fact that they are virtual also makes it harder for the applicant to get a good feel for the program and the people involved in it.
Dr. Ricotta reported that recruitment numbers have been fairly steady at Beth Israel Deaconess over the last few years. “In addition to the critical care physicians, hospital medicine was really the front line of this pandemic and so in some ways, we gained some recognition that we may not have had otherwise,” said Dr. Ricotta. He believes this has the benefit of attracting some residents, but at the same time, it could potentially scare others away from what they perceive as a demanding, grueling job. “I think it has been mixed. It’s dependent on the person.”
At UC Denver, Dr. Gottenborg said they are seeing a rapid rise in the number of applications and interest in their programs. Still, “I think this could go both ways,” she acknowledged. With the focus on hospital medicine in the media, medical students are more aware of the specialty and what it involves. “I think the sense of mission is really exemplified and everyone is talking about it,” she said. This is evident in the arrival this summer of the first new class of interns since the pandemic. “They’re incredibly passionate about the work,” said Dr. Gottenborg.
However, there is also the notable increase in physician burnout since the pandemic started. That this has been regularly featured in the media leaves Dr. Gottenborg to wonder if prospective residents will shy away from hospital medicine because they believe it is an area that leads to burnout. “I hope that’s not the case,” she said.
“I would actually argue [recruitment] is easier,” said Dr. Rawal. Like Dr. Hall, she sees virtual interviews as a big benefit to prospective trainees because they don’t have to spend a large amount of money on travel, food, and other expenses like they did before, a welcome relief for residents with significant debt. “I think that is one very big positive from the pandemic,” she said. Her trainees were advised to make a final list and consider going to see the top two or three in person, but “at this point, there’s really no expectation to go see all 15 places that you look into.”
Dr. Rawal also pointed out that recruitment is affected by whether or not trainees are expected to see COVID patients. “I know in some places they aren’t and in some places they are, so it just depends on where you are and what you’re looking for,” she said.
Shifts in education
It remains to be seen if all the educational changes will be permanent, though it appears that many will remain. Dr. Hall hopes that virtual visits to provide care to patients who have difficulty getting to physical clinics will continue to be a focus for hospital medicine trainees. “For medical students, I think this will allow us to better assess what content can best be delivered in person, synchronously online, or asynchronously through recorded content,” he said.
Dr. Ricotta predicts that virtual conferences will become more pervasive as academic hospitals continue to acquire more community hospitals, especially for grand rounds. “The virtual teaching that occurred in the residency program because it’s required by the [Accreditation Council for Graduate Medical Education] has, I think, informed how academic centers do ongoing faculty development, professional development, and obviously education for the residents,” Dr. Ricotta said. “I think virtual teaching is here to stay.” This includes telehealth training, which had not been a widespread part of residency education before now.
Trainees have been given tools to handle high patient censuses and learned a whole new set of communication skills, thanks to the pandemic, said Dr. Rawal. There has been a focus on learning how to advocate for the vaccine, along with education on situations like how to have conversations with patients who don’t believe they have COVID, even when their tests are positive. “Learning to handle these situations and still be a physician and provide appropriate care regardless of the patient’s views is very important. This is not something I learned in my training because it never came up,” she said.
Dr. Gottenborg has been impressed by the resident workforce’s response across all specialties throughout these difficult days. “They were universally ready to dive in and work long hours and care for these very sick patients and ultimately share their experiences so that we could do it better as these patients continue to flow through our systems,” she said. “It has been very invigorating.”
The pandemic has also put a spotlight on the importance of being flexible, as well as various problems with how health care systems operate, “which, for people in our field, gets us both excited and gives us a lot of work to do,” said Dr. Gottenborg. “Our residents see that and feel that and will hopefully continue to hold that torch in hospital medicine.”
In spite of everything, Dr. Rawal believes this is an exhilarating time to be a trainee. “They’re getting an opportunity that none of us got. Usually, when policies are made, we really don’t see the immediate impact.” But with recent mandates like masks and social distancing, “the rate of change that they get to see things happen is exciting. They’re going to be a very exciting group of physicians.”
Misinterpretation is a science, not an art
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?

Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.

A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.

We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?
Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.
A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.
We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!
It isn’t autocorrect’s fault this time, we swear
We’ve come a long way with communication technology. Back in the day, when Gondor needed to call for aid, they had to pull off the greatest signal fire montage of all time. Now we can send each other texts back and forth in an instant. (“Hey Theoden, send army, need help pls” doesn’t quite have the same gravitas though.) The question is, how do our brains keep up with such rapidly advancing technology?
Er, they don’t. Not really. Instead, our brains create shortcuts called “good-enough language processing,” which is exactly what it sounds like.
Psychologists and psycholinguists have been studying misinterpretations such as good-enough language processing since the 1970s. Recently, however, psycholinguists from the Centre for Language and Brain at Higher School of Economics in Moscow have found that, when it comes to reading comprehension over text, older adults are using their knowledge of the world over how it’s grammatically formed in the sentence.
In the study, 349 people were asked to read and interpret four sentences, the third of which (translated from Russian) was: “Misha met the firefighter’s dentist, who had put out a fire in the warehouse.” When asked who put the fire out, 79% of older adults (aged 55 years and older), utilizing good-enough language processing, said the firefighter put out the fire. You probably glossed over that sentence and assumed the same thing. But this time, the dentist was the real hero.
That said, adolescents (aged 13-17) and young adults (aged 20-30) weren’t much better, and got that particular sentence wrong 63%-68% of the time. According to the researchers, good-enough language processing forms in adolescence and intensifies throughout adulthood.
Moral of the story? We should utilize signal fires more often. Less room for misinterpretation. When the beacons of Minas Tirith were lit, Rohan answered.
Singing … your … lungs … out
There’s nothing quite like a karaoke bar to unleash your inner rock star. Hey, why not just go for it, everyone is just as bad at singing as you. That’s part of the fun.
A 25-year-old man named Wang Zhe may have taken the karaoke concept a bit too far, however. While out with friends at a birthday party, Mr. Zhe let loose on a song with a particularly large number of high notes. He tried his best, gamely attacking the song until he felt a pain in his chest. He didn’t think much of it, although he did cut his performance short, but then he awoke the next morning unable to breathe properly.
After a trip to the hospital, he explained the sequence of events to the doctors, and an x-ray found that the culprit of the pain and difficulty breathing was a life-threatening condition in which air bubbles are created between the chest and lung. All the force Mr. Zhe had used trying to sing made air sacks in his lung burst, causing the air bubbles and his lung to be compressed to 15% of what it should be. Mr. Zhe needed surgery to remove the air bubbles, but fortunately turned out just fine.
So, if you’re ever at a karaoke bar, looking for a song to sing, maybe avoid the ones with super high notes and stick with something a little lower. We’re picturing something like Paul Robeson singing Ol’ Man River. That oughta do the trick.
And the word of the year is …
Flibbertigibbet. Bamboozle. Gobbledygook. If the LOTME staff had any say, those would be the words of the year every year, but sadly, we’re not in charge of such things. Instead, we’ll just have to defer to Oxford and Merriam-Webster, both of whom have recently chosen their words of the year. No word yet on whether or not they made their announcement at a red carpet gala dinner attended by all the most fashionable and powerful words out there, but we’re hoping that’s what happened.
We’ll start with Oxford, since they did choose first. We all know Oxford is the bad boy of the dictionary world, so they’ve chosen a casual colloquialism related to the big COVID-sized elephant in the room (or should it be elephant-sized COVID in the room?): Vax. According to them, while vax has been hanging around since the 1980s, it’s only been in the past year that it’s exploded in popularity in a wide range of contexts (we can’t imagine what those would be). According to Oxford, “as a short pithy word, it appeals, perhaps especially to media commentators, when more formal alternatives are much more long-winded.”
Speaking of long-winded, that brings us to Merriam-Webster, the sheltered nerd of the dictionary world. Clearly they’re too good for vax, so they’ve gone with vaccine as their 2021 word of the year. Vaccine, according to Merriam-Webster, carries two big stories: The impressive and herculean feat of bringing a COVID-19 vaccine so quickly to so many people, and the complex political and social upheaval between vaccine supporters and deniers.
Vaccine also serves as a great bookend for Merriam-Webster’s 2020 word of the year: Pandemic. In 2020, the pandemic started, and in 2021, thanks to the vaccine, the pandemic ends. That’s how it works, right? We have a vaccine, it’s all over now. What’s that? Omicron? No! Bad COVID! You do that outside, not on the carpet!