User login
For MD-IQ use only
Tiny hitchhikers like to ride in the trunk
Junk (germs) in the trunk
It’s been a long drive, and you’ve got a long way to go. You pull into a rest stop to use the bathroom and get some food. Quick, which order do you do those things in?
If you’re not a crazy person, you’d use the bathroom and then get your food. Who would bring food into a dirty bathroom? That’s kind of gross. Most people would take care of business, grab food, then get back in the car, eating along the way. Unfortunately, if you’re searching for a sanitary eating environment, your car may not actually be much better than that bathroom, according to new research from Aston University in Birmingham, England.
Let’s start off with the good news. The steering wheels of the five used cars that were swabbed for bacteria were pretty clean. Definitely cleaner than either of the toilet seats analyzed, likely thanks to increased usage of sanitizer, courtesy of the current pandemic. It’s easy to wipe down the steering wheel. Things break down, though, once we look elsewhere. The interiors of the five cars all contained just as much, if not more, bacteria than the toilet seats, with fecal matter commonly appearing on the driver’s seat.
The car interiors were less than sanitary, but they paled in comparison with the real winner here: the trunk. In each of the five cars, bacteria levels there far exceeded those in the toilets, and included everyone’s favorites – Escherichia coli and Staphylococcus aureus.
So, snacking on a bag of chips as you drive along is probably okay, but the food that popped out of its bag and spent the last 5 minutes rolling around the back? Perhaps less okay. You may want to wash it. Or burn it. Or torch the entire car for good measure like we’re about to do. Next time we’ll buy a car without poop in it.
Shut the lid when you flush
Maybe you’ve never thought about this, but it’s actually extremely important to shut the toilet lid when you flush. Just think of all those germs flying around from the force of the flush. Is your toothbrush anywhere near the toilet? Ew. Those pesky little bacteria and viruses are everywhere, and we know we can’t really escape them, but we should really do our best once we’re made aware of where to find them.

It seems like a no-brainer these days since we’ve all been really focused on cleanliness during the pandemic, but according to a poll in the United Kingdom, 55% of the 2,000 participants said they don’t put the lid down while flushing.
The OnePoll survey commissioned by Harpic, a company that makes toilet-cleaning products, also advised that toilet water isn’t even completely clean after flushed several times and can still be contaminated with many germs. Company researchers took specialized pictures of flushing toilets and they looked like tiny little Fourth of July fireworks shows, minus the sparklers. The pictures proved that droplets can go all over the place, including on bathroom users.
“There has never been a more important time to take extra care around our homes, although the risks associated with germ spread in unhygienic bathrooms are high, the solution to keeping them clean is simple,” a Harpic researcher said. Since other studies have shown that coronavirus can be found in feces, it’s become increasingly important to keep ourselves and others safe. Fireworks are pretty, but not when they come out of your toilet.
The latest in MRI fashion
Do you see that photo just below? Looks like something you could buy at the Lego store, right? Well, it’s not. Nor is it the proverbial thinking cap come to life.
(Did someone just say “come to life”? That reminds us of our favorite scene from Frosty the Snowman.)
Anywaaay, about the photo. That funny-looking chapeau is what we in the science business call a metamaterial.
Nope, metamaterials have nothing to do with Facebook parent company Meta. We checked. According to a statement from Boston University, they are engineered structures “created from small unit cells that might be unspectacular alone, but when grouped together in a precise way, get new superpowers not found in nature.”
Superpowers, eh? Who doesn’t want superpowers? Even if they come with a funny hat.
The unit cells, known as resonators, are just plastic tubes wrapped in copper wiring, but when they are grouped in an array and precisely arranged into a helmet, they can channel the magnetic field of the MRI machine during a scan. In theory, that would create “crisper images that can be captured at twice the normal speed,” Xin Zhang, PhD, and her team at BU’s Photonics Center explained in the university statement.
In the future, the metamaterial device could “be used in conjunction with cheaper low-field MRI machines to make the technology more widely available, particularly in the developing world,” they suggested. Or, like so many other superpowers, it could fall into the wrong hands. Like those of Lex Luthor. Or Mark Zuckerberg. Or Frosty the Snowman.
The highway of the mind
How fast can you think on your feet? Well, according to a recently published study, it could be a legitimate measure of intelligence. Here’s the science.

Researchers from the University of Würzburg in Germany and Indiana University have suggested that a person’s intelligence score measures the ability, based on certain neuronal networks and their communication structures, to switch between resting state and different task states.
The investigators set up a study to observe almost 800 people while they completed seven tasks. By monitoring brain activity with functional magnetic resonance imaging, the teams found that subjects who had higher intelligence scores required “less adjustment when switching between different cognitive states,” they said in a separate statement.
It comes down to the network architecture of their brains.
Kirsten Hilger, PhD, head of the German group, described it in terms of highways. The resting state of the brain is normal traffic. It’s always moving. Holiday traffic is the task. The ability to handle the increased flow of commuters is a function of the highway infrastructure. The better the infrastructure, the higher the intelligence.
So the next time you’re stuck in traffic, think how efficient your brain would be with such a task. The quicker, the better.
Junk (germs) in the trunk
It’s been a long drive, and you’ve got a long way to go. You pull into a rest stop to use the bathroom and get some food. Quick, which order do you do those things in?
If you’re not a crazy person, you’d use the bathroom and then get your food. Who would bring food into a dirty bathroom? That’s kind of gross. Most people would take care of business, grab food, then get back in the car, eating along the way. Unfortunately, if you’re searching for a sanitary eating environment, your car may not actually be much better than that bathroom, according to new research from Aston University in Birmingham, England.
Let’s start off with the good news. The steering wheels of the five used cars that were swabbed for bacteria were pretty clean. Definitely cleaner than either of the toilet seats analyzed, likely thanks to increased usage of sanitizer, courtesy of the current pandemic. It’s easy to wipe down the steering wheel. Things break down, though, once we look elsewhere. The interiors of the five cars all contained just as much, if not more, bacteria than the toilet seats, with fecal matter commonly appearing on the driver’s seat.
The car interiors were less than sanitary, but they paled in comparison with the real winner here: the trunk. In each of the five cars, bacteria levels there far exceeded those in the toilets, and included everyone’s favorites – Escherichia coli and Staphylococcus aureus.
So, snacking on a bag of chips as you drive along is probably okay, but the food that popped out of its bag and spent the last 5 minutes rolling around the back? Perhaps less okay. You may want to wash it. Or burn it. Or torch the entire car for good measure like we’re about to do. Next time we’ll buy a car without poop in it.
Shut the lid when you flush
Maybe you’ve never thought about this, but it’s actually extremely important to shut the toilet lid when you flush. Just think of all those germs flying around from the force of the flush. Is your toothbrush anywhere near the toilet? Ew. Those pesky little bacteria and viruses are everywhere, and we know we can’t really escape them, but we should really do our best once we’re made aware of where to find them.
It seems like a no-brainer these days since we’ve all been really focused on cleanliness during the pandemic, but according to a poll in the United Kingdom, 55% of the 2,000 participants said they don’t put the lid down while flushing.
The OnePoll survey commissioned by Harpic, a company that makes toilet-cleaning products, also advised that toilet water isn’t even completely clean after flushed several times and can still be contaminated with many germs. Company researchers took specialized pictures of flushing toilets and they looked like tiny little Fourth of July fireworks shows, minus the sparklers. The pictures proved that droplets can go all over the place, including on bathroom users.
“There has never been a more important time to take extra care around our homes, although the risks associated with germ spread in unhygienic bathrooms are high, the solution to keeping them clean is simple,” a Harpic researcher said. Since other studies have shown that coronavirus can be found in feces, it’s become increasingly important to keep ourselves and others safe. Fireworks are pretty, but not when they come out of your toilet.
The latest in MRI fashion
Do you see that photo just below? Looks like something you could buy at the Lego store, right? Well, it’s not. Nor is it the proverbial thinking cap come to life.
(Did someone just say “come to life”? That reminds us of our favorite scene from Frosty the Snowman.)
Anywaaay, about the photo. That funny-looking chapeau is what we in the science business call a metamaterial.
Nope, metamaterials have nothing to do with Facebook parent company Meta. We checked. According to a statement from Boston University, they are engineered structures “created from small unit cells that might be unspectacular alone, but when grouped together in a precise way, get new superpowers not found in nature.”
Superpowers, eh? Who doesn’t want superpowers? Even if they come with a funny hat.
The unit cells, known as resonators, are just plastic tubes wrapped in copper wiring, but when they are grouped in an array and precisely arranged into a helmet, they can channel the magnetic field of the MRI machine during a scan. In theory, that would create “crisper images that can be captured at twice the normal speed,” Xin Zhang, PhD, and her team at BU’s Photonics Center explained in the university statement.
In the future, the metamaterial device could “be used in conjunction with cheaper low-field MRI machines to make the technology more widely available, particularly in the developing world,” they suggested. Or, like so many other superpowers, it could fall into the wrong hands. Like those of Lex Luthor. Or Mark Zuckerberg. Or Frosty the Snowman.
The highway of the mind
How fast can you think on your feet? Well, according to a recently published study, it could be a legitimate measure of intelligence. Here’s the science.
Researchers from the University of Würzburg in Germany and Indiana University have suggested that a person’s intelligence score measures the ability, based on certain neuronal networks and their communication structures, to switch between resting state and different task states.
The investigators set up a study to observe almost 800 people while they completed seven tasks. By monitoring brain activity with functional magnetic resonance imaging, the teams found that subjects who had higher intelligence scores required “less adjustment when switching between different cognitive states,” they said in a separate statement.
It comes down to the network architecture of their brains.
Kirsten Hilger, PhD, head of the German group, described it in terms of highways. The resting state of the brain is normal traffic. It’s always moving. Holiday traffic is the task. The ability to handle the increased flow of commuters is a function of the highway infrastructure. The better the infrastructure, the higher the intelligence.
So the next time you’re stuck in traffic, think how efficient your brain would be with such a task. The quicker, the better.
Junk (germs) in the trunk
It’s been a long drive, and you’ve got a long way to go. You pull into a rest stop to use the bathroom and get some food. Quick, which order do you do those things in?
If you’re not a crazy person, you’d use the bathroom and then get your food. Who would bring food into a dirty bathroom? That’s kind of gross. Most people would take care of business, grab food, then get back in the car, eating along the way. Unfortunately, if you’re searching for a sanitary eating environment, your car may not actually be much better than that bathroom, according to new research from Aston University in Birmingham, England.
Let’s start off with the good news. The steering wheels of the five used cars that were swabbed for bacteria were pretty clean. Definitely cleaner than either of the toilet seats analyzed, likely thanks to increased usage of sanitizer, courtesy of the current pandemic. It’s easy to wipe down the steering wheel. Things break down, though, once we look elsewhere. The interiors of the five cars all contained just as much, if not more, bacteria than the toilet seats, with fecal matter commonly appearing on the driver’s seat.
The car interiors were less than sanitary, but they paled in comparison with the real winner here: the trunk. In each of the five cars, bacteria levels there far exceeded those in the toilets, and included everyone’s favorites – Escherichia coli and Staphylococcus aureus.
So, snacking on a bag of chips as you drive along is probably okay, but the food that popped out of its bag and spent the last 5 minutes rolling around the back? Perhaps less okay. You may want to wash it. Or burn it. Or torch the entire car for good measure like we’re about to do. Next time we’ll buy a car without poop in it.
Shut the lid when you flush
Maybe you’ve never thought about this, but it’s actually extremely important to shut the toilet lid when you flush. Just think of all those germs flying around from the force of the flush. Is your toothbrush anywhere near the toilet? Ew. Those pesky little bacteria and viruses are everywhere, and we know we can’t really escape them, but we should really do our best once we’re made aware of where to find them.
It seems like a no-brainer these days since we’ve all been really focused on cleanliness during the pandemic, but according to a poll in the United Kingdom, 55% of the 2,000 participants said they don’t put the lid down while flushing.
The OnePoll survey commissioned by Harpic, a company that makes toilet-cleaning products, also advised that toilet water isn’t even completely clean after flushed several times and can still be contaminated with many germs. Company researchers took specialized pictures of flushing toilets and they looked like tiny little Fourth of July fireworks shows, minus the sparklers. The pictures proved that droplets can go all over the place, including on bathroom users.
“There has never been a more important time to take extra care around our homes, although the risks associated with germ spread in unhygienic bathrooms are high, the solution to keeping them clean is simple,” a Harpic researcher said. Since other studies have shown that coronavirus can be found in feces, it’s become increasingly important to keep ourselves and others safe. Fireworks are pretty, but not when they come out of your toilet.
The latest in MRI fashion
Do you see that photo just below? Looks like something you could buy at the Lego store, right? Well, it’s not. Nor is it the proverbial thinking cap come to life.
(Did someone just say “come to life”? That reminds us of our favorite scene from Frosty the Snowman.)
Anywaaay, about the photo. That funny-looking chapeau is what we in the science business call a metamaterial.
Nope, metamaterials have nothing to do with Facebook parent company Meta. We checked. According to a statement from Boston University, they are engineered structures “created from small unit cells that might be unspectacular alone, but when grouped together in a precise way, get new superpowers not found in nature.”
Superpowers, eh? Who doesn’t want superpowers? Even if they come with a funny hat.
The unit cells, known as resonators, are just plastic tubes wrapped in copper wiring, but when they are grouped in an array and precisely arranged into a helmet, they can channel the magnetic field of the MRI machine during a scan. In theory, that would create “crisper images that can be captured at twice the normal speed,” Xin Zhang, PhD, and her team at BU’s Photonics Center explained in the university statement.
In the future, the metamaterial device could “be used in conjunction with cheaper low-field MRI machines to make the technology more widely available, particularly in the developing world,” they suggested. Or, like so many other superpowers, it could fall into the wrong hands. Like those of Lex Luthor. Or Mark Zuckerberg. Or Frosty the Snowman.
The highway of the mind
How fast can you think on your feet? Well, according to a recently published study, it could be a legitimate measure of intelligence. Here’s the science.
Researchers from the University of Würzburg in Germany and Indiana University have suggested that a person’s intelligence score measures the ability, based on certain neuronal networks and their communication structures, to switch between resting state and different task states.
The investigators set up a study to observe almost 800 people while they completed seven tasks. By monitoring brain activity with functional magnetic resonance imaging, the teams found that subjects who had higher intelligence scores required “less adjustment when switching between different cognitive states,” they said in a separate statement.
It comes down to the network architecture of their brains.
Kirsten Hilger, PhD, head of the German group, described it in terms of highways. The resting state of the brain is normal traffic. It’s always moving. Holiday traffic is the task. The ability to handle the increased flow of commuters is a function of the highway infrastructure. The better the infrastructure, the higher the intelligence.
So the next time you’re stuck in traffic, think how efficient your brain would be with such a task. The quicker, the better.
Repeat Laparoscopic Cholecystectomy for Duplicated Gallbladder After 16-Year Interval
Gallbladder duplication is a congenital abnormality of the hepatobiliary system and often is not considered in the evaluation of a patient with right upper quadrant pain. Accuracy of the most commonly used imaging study to assess for biliary disease, abdominal ultrasound, is highly dependent on the skills of the ultrasonographer, and given its relative rarity, this condition is often not considered prior to planned cholecystectomy.1 Small case reviews found that < 50% of gallbladder duplications are diagnosed preoperatively despite use of ultrasound or computed tomography (CT) scan.2-4 Failure to recognize duplicate gallbladder anatomy in symptomatic patients may result in incomplete surgical management, an increase in perioperative complications, and years of morbidity due to unresolved symptoms. Once a patient has had a cholecystectomy, symptoms are presumed to be due to a nonbiliary etiology and an extensive, often repetitive, workup is pursued before “repeat cholecystectomy” is considered.5
Case Presentation
A 63-year-old man was referred to gastroenterology for recurrent episodic right upper quadrant pain. He reported intermittent both right and left upper abdominal pain that was variable in quality. At times it was associated with an empty stomach prior to meals; at other times, onset was 30 to 60 minutes after meals. The patient also reported significant flatulence and bloating and intermittent loose stools. Sixteen years before, he underwent a laparoscopic cholecystectomy. He reported that the pain he experienced before the cholecystectomy never resolved after surgery but occurred less frequently. For the next 16 years, the patient did not seek evaluation of his ongoing but infrequent symptoms until his pain became a daily occurrence. The patient’s surgical history included a remote open vagotomy and antrectomy for peptic ulcer disease, laparoscopic appendectomy, and a laparoscopic cholecystectomy for reported biliary colic.
The gastroenterology evaluation included a colonoscopy and esophagogastroduodenoscopy (EGD); both were benign and without findings specific to identify the etiology for the patient’s pain. The patient was given a course of rifaximin 1200 mg daily for 7 days for possible bacterial overgrowth and placed on a proton pump inhibitor twice daily. Neither of these interventions helped resolve the patient’s symptoms. Further workup was pursued by gastroenterology to include a right upper quadrant ultrasound that showed a structure most consistent with a small gallbladder containing a small polyp vs stone. Magnetic resonance cholangiopancreatography (MRCP) also was performed and showed the presence of a small gallbladder with a small 2-mm filling defect and an otherwise benign biliary tree. MRCP images and EGD documented a Billroth 1 reconstruction at the time of his remote antrectomy and vagotomy (Figure 1).

The patient was referred to general surgery for consideration of a repeat cholecystectomy. He confirmed the history of intermittent upper abdominal pain for the past 16 years, which was similar to the symptoms he had experienced before his original laparoscopic cholecystectomy. On examination, the patient had a body mass index of 38, had a large upper midline incision from his prior antrectomy and vagotomy procedure, and several scars presumed to be port incision scars to the right lateral abdominal wall. Hospital records were obtained from the patient’s prior workup for biliary colic and cholecystectomy 16 years before. The preoperative abdominal ultrasound examination showed a mildly distended gallbladder but was notably described as “quite limited due to patient’s body habitus and liver is not well seen.” No additional imaging was documented in his presurgical evaluation notes and imaging records.
The operative report described a gallbladder that was densely adherent to adjacent fat and omental tissue with significant adhesions secondary to the prior vagotomy and antrectomy procedure. The cystic duct and artery were dissected free at the level of their junction with the gallbladder infundibulum. The cystic artery was divided with a harmonic scalpel. Following this the gallbladder body was dissected free from the liver bed in top-down fashion. A 0 Vicryl Endoloop suture was placed over the gallbladder and secured just past the origin of the cystic duct on the gallbladder infundibulum and the cystic duct divided above this suture. No surgical clips were used, which corresponded with the lack of surgical clips seen in imaging in his recent gastroenterology workup. No documentation of an intraoperative cholangiogram existed or was considered in the operative report.
The pathology report from this first cholecystectomy procedure noted the removed specimen to be an unopened 6-cm gallbladder containing 2 small yellow stones that otherwise were benign. At the time of this patient’s re-presentation to general surgery, there was suspicion that the patient’s prior surgical procedure had not been a cholecystectomy but rather a subtotal cholecystectomy. However, after appropriate workup and review of prior records, the patient had, indeed, previously undergone cholecystectomy and represented a rare case of gallbladder duplication resulting in abdominal pain for 16 years after his index operation.
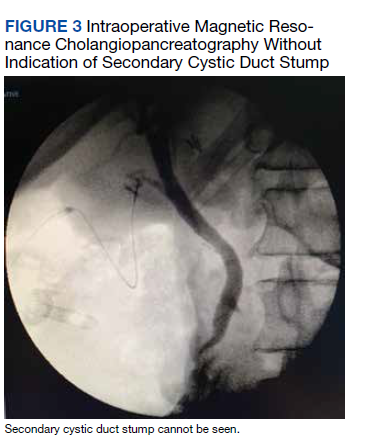
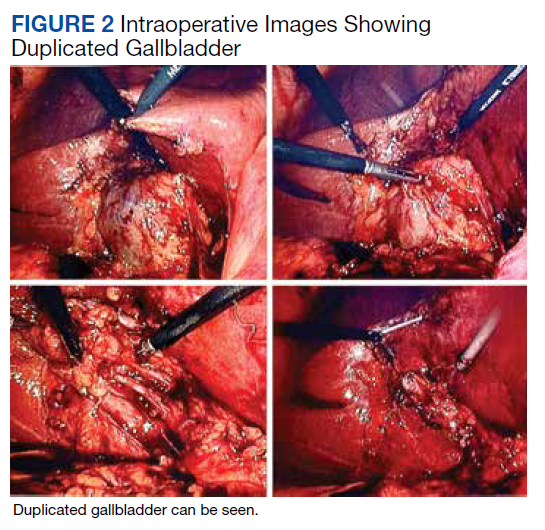
The patient was consented for repeat cholecystectomy and underwent a laparoscopic lysis of adhesions, cholecystectomy, and intraoperative cholangiogram. Significant scarring was found at the liver undersurface that would have been exposed during the original laparoscopic resection of the gallbladder from its liver bed. Deeper to this, a small saccular structure was identified as the duplicate gallbladder (Figure 2). Though the visualized gallbladder was small with a deep intrahepatic lie, the critical view of safety was achieved and was without additional variation. An intraoperative cholangiogram was performed to determine whether residual ductal stumps or other additional evidence of the previously removed gallbladder could be identified. The cholangiogram showed clear visualization of the cystic duct, common bile duct, right and left hepatic ducts, and contrast into the duodenum without abnormal variants. There was no visualized accessory or secondary cystic duct stump seen on the cholangiogram (Figure 3). Pathology of the repeat cholecystectomy specimen confirmed a 3-cm gallbladder with a distinct duct leading out of the gallbladder and the presence of several gallstones. The patient had an uneventful recovery after the repeat laparoscopic cholecystectomy with complete resolution of his upper abdominal pain.
Discussion
The first reported human case of gallbladder duplication was noted in a sacrificial victim of Emperor Augustus in 31 BCE. Sherren reported the first documented case of double accessory gallbladder in a living human in 1911.1,6 Though the exact incidence of gallbladder duplication is not fully known due to primary documentation from case reports, incidence is approximately 1 in 4000 to 5000 people. It was first formally classified by Boyden in 1926.7 Further anatomic classification based on morphology and embryogenesis was delineated by Harlaftis and colleagues in 1977, establishing type 1 and 2 structures of a duplicated gallbladder.8 Type 1 duplicated gallbladder anatomy shares a single cystic duct, whereas in type 2 each gallbladder has its own cystic duct. Later reports and studies identified triple gallbladders as well as trabecular variants with the most common classification used currently being the modified Harlaftis classification.9,10
The case presented here most likely represents either a Y-shaped type 1 primordial gallbladder or a type 2 accessory gallbladder based on historical data and intraoperative cholangiogram findings at the time of repeat cholecystectomy. Gallbladder duplication is clinically indistinguishable from regular gallbladder pathology preoperatively and can only be identified on imaging or intraoperatively.11 Prior case reports and studies have found that it is frequently missed on preoperative abdominal ultrasonography and CT in up to 50% of cases.12-14
The differential diagnosis of gallbladder duplication seen on preoperative imaging includes a gallbladder diverticulum, choledochal cyst, focal adenonomyomatosis, Phrygian cap, or folded gallbladder.1,2 Historically, the most definitive test for gallbladder duplication has been either intraoperative cholangiography, which can also clarify biliary anatomy, or endoscopic retrograde cholangiopancreatography with cholangiography.1,3 The debate over routine use of intraoperative cholangiography has been ongoing for the past several decades.15 Though intraoperative cholangiogram remains one of the most definitive tests for gallbladder duplication, given the overall low incidence of this variant, recommendation for routine intraoperative cholangiography solely to rule out gallbladder duplication cannot be definitively recommended based on our review of the literature. Currently, preoperative MRCP is the study of choice when there is concern from historical facts or from other imaging of gallbladder duplication as it is noninvasive and has a high degree of detail, particularly with 3D reconstructions.14,16 At the time of surgery, the most critical step to avoid inadvertent ductal injury is clear visualization of ductal anatomy and obtaining the critical view of safety.17 Though this will also assist in identifying some cases of gallbladder duplication, given the great variation of duplication, it will not prevent missing some variants. In our case, extensive local scarring from the patient’s prior antrectomy and vagotomy along with lack of the use of intraoperative cholangiography likely contributed to missing his duplication at the time of his index cholecystectomy.
Undiagnosed gallbladder duplication can lead to additional morbidity related to common entities associated with gallbladder pathology, such as biliary colic, cholecystitis, cholangitis, and pancreatitis. Additionally, case reports in the literature have documented more rare associations, such as empyema, carcinoma, cholecystoenteric fistula, and torsion, all associated with a duplicated gallbladder.18-21 Once identified pre- or intraoperatively, it is generally recommended that all gallbladders be removed in symptomatic patients and that intraoperative cholangiography be done to assure complete resection of the duplicated gallbladders and to avoid injury to the biliary trees.22-25
Conclusions
Gallbladder duplication and other congenital biliary anatomic variations should be considered before a biliary operation and included in the differential diagnosis when evaluating patients who have clinical symptoms consistent with biliary pathology. In addition, intraoperative cholangiogram should be performed during cholecystectomy if the inferior liver edge cannot be visualized well, as in the case of this patient where a prior foregut operation resulted in extensive adhesive disease. Intraoperative cholangiogram also should be considered in patients whose preoperative imaging does not visualize the right upper quadrant well due to patient habitus. Doing so may identify gallbladder duplication and allow for complete cholecystectomy as well as proper identification and management of cystic duct variants. Awareness and consideration of duplicated biliary variants can help prevent intraoperative complications related to biliary anomalies and avoid the morbidity related to recurrent biliary disease and the need for repeat operative procedures.
Acknowledgments
We extend our thanks to Veterans Affairs Puget Sound Healthcare System and the Departments of Surgery and Radiology for their support of this case report, and Lorrie Langdale, MD, and Roger Tatum, MD, for their mentorship of this project
1. Vezakis A, Pantiora E, Giannoulopoulos D, et al. A duplicated gallbladder in a patient presenting with acute cholangitis. A case study and a literature review. Ann Hepatol. 2019;18(1):240-245. doi:10.5604/01.3001.0012.7932
2. Barut Í, Tarhan ÖR, Dog^ru U, Bülbül M. Gallbladder duplication: diagnosed and treated by laparoscopy. Eur J Gen Med. 2006;3(3):142-145. doi:10.29333/ejgm/82396 3. Cozacov Y, Subhas G, Jacobs M, Parikh J. Total laparoscopic removal of accessory gallbladder: a case report and review of literature. World J Gastrointest Surg. 2015;7(12):398-402. doi:10.4240/wjgs.v7.i12.398
4. Musleh MG, Burnett H, Rajashanker B, Ammori BJ. Laparoscopic double cholecystectomy for duplicated gallbladder: a case report. Int J Surg Case Rep. 2017;41:502-504. Published 2017 Nov 27. doi:10.1016/j.ijscr.2017.11.046
5. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a duplicated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011;21(3):e156-e158. doi:10.1097/SLE.0b013e31821d47ce
6. Sherren J. A double gall-bladder removed by operation. Ann Surg. 1911;54(2):204-205. doi:10.1097/00000658-191108000-00009
7. Boyden EA. The accessory gall-bladder—an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anat. 1926; 38(2):177-231. doi:10.1002/aja.1000380202
8. Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surg Gynecol Obstet. 1977;145(6):928-934.
9. Kim RD, Zendejas I, Velopulos C, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009;39(6):536-539. doi:10.1007/s00595-008-3878-4
10. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010;45(2):443-446. doi:10.1016/j.jpedsurg.2009.12.015
11. Apolo Romero EX, Gálvez Salazar PF, Estrada Chandi JA, et al. Gallbladder duplication and cholecystitis. J Surg Case Rep. 2018;2018(7):rjy158. Published 2018 Jul 3. doi:10.1093/jscr/rjy158
12. Gorecki PJ, Andrei VE, Musacchio T, Schein M. Double gallbladder originating from left hepatic duct: a case report and review of literature. JSLS. 1998;2(4):337-339.
13. Cueto García J, Weber A, Serrano Berry F, Tanur Tatz B. Double gallbladder treated successfully by laparoscopy. J Laparoendosc Surg. 1993;3(2):153-155. doi:10.1089/lps.1993.3.153
14. Fazio V, Damiano G, Palumbo VD, et al. An unexpected surprise at the end of a “quiet” cholecystectomy. A case report and review of the literature. Ann Ital Chir. 2012;83(3):265-267.
15. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644. doi:10.1001/jama.289.13.1639
16. Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: a case report and review of the literature. Surg Radiol Anat. 2015;37(5):425-429. doi:10.1007/s00276-015-1456-1
17. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
18. Raymond SW, Thrift CB. Carcinoma of a duplicated gall bladder. Ill Med J. 1956;110(5):239-240.
19. Cunningham JJ. Empyema of a duplicated gallbladder: echographic findings. J Clin Ultrasound. 1980;8(6):511-512. doi:10.1002/jcu.1870080612
20. Recht W. Torsion of a double gallbladder; a report of a case and a review of the literature. Br J Surg. 1952;39(156):342-344. doi:10.1002/bjs.18003915616
21. Ritchie AW, Crucioli V. Double gallbladder with cholecystocolic fistula: a case report. Br J Surg. 1980;67(2):145-146. doi:10.1002/bjs.1800670226
22. Shapiro T, Rennie W. Duplicate gallbladder cholecystitis after open cholecystectomy. Ann Emerg Med. 1999;33(5):584-587. doi:10.1016/s0196-0644(99)70348-3
23. Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC. Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg. 2006;93(7):844-853. doi:10.1002/bjs.5333
24. Davidoff AM, Pappas TN, Murray EA, et al. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992;215(3):196-202. doi:10.1097/00000658-199203000-00002
25. Flowers JL, Zucker KA, Graham SM, Scovill WA, Imbembo AL, Bailey RW. Laparoscopic cholangiography. Results and indications. Ann Surg. 1992;215(3):209-216. doi:10.1097/00000658-199203000-00004
Gallbladder duplication is a congenital abnormality of the hepatobiliary system and often is not considered in the evaluation of a patient with right upper quadrant pain. Accuracy of the most commonly used imaging study to assess for biliary disease, abdominal ultrasound, is highly dependent on the skills of the ultrasonographer, and given its relative rarity, this condition is often not considered prior to planned cholecystectomy.1 Small case reviews found that < 50% of gallbladder duplications are diagnosed preoperatively despite use of ultrasound or computed tomography (CT) scan.2-4 Failure to recognize duplicate gallbladder anatomy in symptomatic patients may result in incomplete surgical management, an increase in perioperative complications, and years of morbidity due to unresolved symptoms. Once a patient has had a cholecystectomy, symptoms are presumed to be due to a nonbiliary etiology and an extensive, often repetitive, workup is pursued before “repeat cholecystectomy” is considered.5
Case Presentation
A 63-year-old man was referred to gastroenterology for recurrent episodic right upper quadrant pain. He reported intermittent both right and left upper abdominal pain that was variable in quality. At times it was associated with an empty stomach prior to meals; at other times, onset was 30 to 60 minutes after meals. The patient also reported significant flatulence and bloating and intermittent loose stools. Sixteen years before, he underwent a laparoscopic cholecystectomy. He reported that the pain he experienced before the cholecystectomy never resolved after surgery but occurred less frequently. For the next 16 years, the patient did not seek evaluation of his ongoing but infrequent symptoms until his pain became a daily occurrence. The patient’s surgical history included a remote open vagotomy and antrectomy for peptic ulcer disease, laparoscopic appendectomy, and a laparoscopic cholecystectomy for reported biliary colic.
The gastroenterology evaluation included a colonoscopy and esophagogastroduodenoscopy (EGD); both were benign and without findings specific to identify the etiology for the patient’s pain. The patient was given a course of rifaximin 1200 mg daily for 7 days for possible bacterial overgrowth and placed on a proton pump inhibitor twice daily. Neither of these interventions helped resolve the patient’s symptoms. Further workup was pursued by gastroenterology to include a right upper quadrant ultrasound that showed a structure most consistent with a small gallbladder containing a small polyp vs stone. Magnetic resonance cholangiopancreatography (MRCP) also was performed and showed the presence of a small gallbladder with a small 2-mm filling defect and an otherwise benign biliary tree. MRCP images and EGD documented a Billroth 1 reconstruction at the time of his remote antrectomy and vagotomy (Figure 1).
The patient was referred to general surgery for consideration of a repeat cholecystectomy. He confirmed the history of intermittent upper abdominal pain for the past 16 years, which was similar to the symptoms he had experienced before his original laparoscopic cholecystectomy. On examination, the patient had a body mass index of 38, had a large upper midline incision from his prior antrectomy and vagotomy procedure, and several scars presumed to be port incision scars to the right lateral abdominal wall. Hospital records were obtained from the patient’s prior workup for biliary colic and cholecystectomy 16 years before. The preoperative abdominal ultrasound examination showed a mildly distended gallbladder but was notably described as “quite limited due to patient’s body habitus and liver is not well seen.” No additional imaging was documented in his presurgical evaluation notes and imaging records.
The operative report described a gallbladder that was densely adherent to adjacent fat and omental tissue with significant adhesions secondary to the prior vagotomy and antrectomy procedure. The cystic duct and artery were dissected free at the level of their junction with the gallbladder infundibulum. The cystic artery was divided with a harmonic scalpel. Following this the gallbladder body was dissected free from the liver bed in top-down fashion. A 0 Vicryl Endoloop suture was placed over the gallbladder and secured just past the origin of the cystic duct on the gallbladder infundibulum and the cystic duct divided above this suture. No surgical clips were used, which corresponded with the lack of surgical clips seen in imaging in his recent gastroenterology workup. No documentation of an intraoperative cholangiogram existed or was considered in the operative report.
The pathology report from this first cholecystectomy procedure noted the removed specimen to be an unopened 6-cm gallbladder containing 2 small yellow stones that otherwise were benign. At the time of this patient’s re-presentation to general surgery, there was suspicion that the patient’s prior surgical procedure had not been a cholecystectomy but rather a subtotal cholecystectomy. However, after appropriate workup and review of prior records, the patient had, indeed, previously undergone cholecystectomy and represented a rare case of gallbladder duplication resulting in abdominal pain for 16 years after his index operation.
The patient was consented for repeat cholecystectomy and underwent a laparoscopic lysis of adhesions, cholecystectomy, and intraoperative cholangiogram. Significant scarring was found at the liver undersurface that would have been exposed during the original laparoscopic resection of the gallbladder from its liver bed. Deeper to this, a small saccular structure was identified as the duplicate gallbladder (Figure 2). Though the visualized gallbladder was small with a deep intrahepatic lie, the critical view of safety was achieved and was without additional variation. An intraoperative cholangiogram was performed to determine whether residual ductal stumps or other additional evidence of the previously removed gallbladder could be identified. The cholangiogram showed clear visualization of the cystic duct, common bile duct, right and left hepatic ducts, and contrast into the duodenum without abnormal variants. There was no visualized accessory or secondary cystic duct stump seen on the cholangiogram (Figure 3). Pathology of the repeat cholecystectomy specimen confirmed a 3-cm gallbladder with a distinct duct leading out of the gallbladder and the presence of several gallstones. The patient had an uneventful recovery after the repeat laparoscopic cholecystectomy with complete resolution of his upper abdominal pain.
Discussion
The first reported human case of gallbladder duplication was noted in a sacrificial victim of Emperor Augustus in 31 BCE. Sherren reported the first documented case of double accessory gallbladder in a living human in 1911.1,6 Though the exact incidence of gallbladder duplication is not fully known due to primary documentation from case reports, incidence is approximately 1 in 4000 to 5000 people. It was first formally classified by Boyden in 1926.7 Further anatomic classification based on morphology and embryogenesis was delineated by Harlaftis and colleagues in 1977, establishing type 1 and 2 structures of a duplicated gallbladder.8 Type 1 duplicated gallbladder anatomy shares a single cystic duct, whereas in type 2 each gallbladder has its own cystic duct. Later reports and studies identified triple gallbladders as well as trabecular variants with the most common classification used currently being the modified Harlaftis classification.9,10
The case presented here most likely represents either a Y-shaped type 1 primordial gallbladder or a type 2 accessory gallbladder based on historical data and intraoperative cholangiogram findings at the time of repeat cholecystectomy. Gallbladder duplication is clinically indistinguishable from regular gallbladder pathology preoperatively and can only be identified on imaging or intraoperatively.11 Prior case reports and studies have found that it is frequently missed on preoperative abdominal ultrasonography and CT in up to 50% of cases.12-14
The differential diagnosis of gallbladder duplication seen on preoperative imaging includes a gallbladder diverticulum, choledochal cyst, focal adenonomyomatosis, Phrygian cap, or folded gallbladder.1,2 Historically, the most definitive test for gallbladder duplication has been either intraoperative cholangiography, which can also clarify biliary anatomy, or endoscopic retrograde cholangiopancreatography with cholangiography.1,3 The debate over routine use of intraoperative cholangiography has been ongoing for the past several decades.15 Though intraoperative cholangiogram remains one of the most definitive tests for gallbladder duplication, given the overall low incidence of this variant, recommendation for routine intraoperative cholangiography solely to rule out gallbladder duplication cannot be definitively recommended based on our review of the literature. Currently, preoperative MRCP is the study of choice when there is concern from historical facts or from other imaging of gallbladder duplication as it is noninvasive and has a high degree of detail, particularly with 3D reconstructions.14,16 At the time of surgery, the most critical step to avoid inadvertent ductal injury is clear visualization of ductal anatomy and obtaining the critical view of safety.17 Though this will also assist in identifying some cases of gallbladder duplication, given the great variation of duplication, it will not prevent missing some variants. In our case, extensive local scarring from the patient’s prior antrectomy and vagotomy along with lack of the use of intraoperative cholangiography likely contributed to missing his duplication at the time of his index cholecystectomy.
Undiagnosed gallbladder duplication can lead to additional morbidity related to common entities associated with gallbladder pathology, such as biliary colic, cholecystitis, cholangitis, and pancreatitis. Additionally, case reports in the literature have documented more rare associations, such as empyema, carcinoma, cholecystoenteric fistula, and torsion, all associated with a duplicated gallbladder.18-21 Once identified pre- or intraoperatively, it is generally recommended that all gallbladders be removed in symptomatic patients and that intraoperative cholangiography be done to assure complete resection of the duplicated gallbladders and to avoid injury to the biliary trees.22-25
Conclusions
Gallbladder duplication and other congenital biliary anatomic variations should be considered before a biliary operation and included in the differential diagnosis when evaluating patients who have clinical symptoms consistent with biliary pathology. In addition, intraoperative cholangiogram should be performed during cholecystectomy if the inferior liver edge cannot be visualized well, as in the case of this patient where a prior foregut operation resulted in extensive adhesive disease. Intraoperative cholangiogram also should be considered in patients whose preoperative imaging does not visualize the right upper quadrant well due to patient habitus. Doing so may identify gallbladder duplication and allow for complete cholecystectomy as well as proper identification and management of cystic duct variants. Awareness and consideration of duplicated biliary variants can help prevent intraoperative complications related to biliary anomalies and avoid the morbidity related to recurrent biliary disease and the need for repeat operative procedures.
Acknowledgments
We extend our thanks to Veterans Affairs Puget Sound Healthcare System and the Departments of Surgery and Radiology for their support of this case report, and Lorrie Langdale, MD, and Roger Tatum, MD, for their mentorship of this project
Gallbladder duplication is a congenital abnormality of the hepatobiliary system and often is not considered in the evaluation of a patient with right upper quadrant pain. Accuracy of the most commonly used imaging study to assess for biliary disease, abdominal ultrasound, is highly dependent on the skills of the ultrasonographer, and given its relative rarity, this condition is often not considered prior to planned cholecystectomy.1 Small case reviews found that < 50% of gallbladder duplications are diagnosed preoperatively despite use of ultrasound or computed tomography (CT) scan.2-4 Failure to recognize duplicate gallbladder anatomy in symptomatic patients may result in incomplete surgical management, an increase in perioperative complications, and years of morbidity due to unresolved symptoms. Once a patient has had a cholecystectomy, symptoms are presumed to be due to a nonbiliary etiology and an extensive, often repetitive, workup is pursued before “repeat cholecystectomy” is considered.5
Case Presentation
A 63-year-old man was referred to gastroenterology for recurrent episodic right upper quadrant pain. He reported intermittent both right and left upper abdominal pain that was variable in quality. At times it was associated with an empty stomach prior to meals; at other times, onset was 30 to 60 minutes after meals. The patient also reported significant flatulence and bloating and intermittent loose stools. Sixteen years before, he underwent a laparoscopic cholecystectomy. He reported that the pain he experienced before the cholecystectomy never resolved after surgery but occurred less frequently. For the next 16 years, the patient did not seek evaluation of his ongoing but infrequent symptoms until his pain became a daily occurrence. The patient’s surgical history included a remote open vagotomy and antrectomy for peptic ulcer disease, laparoscopic appendectomy, and a laparoscopic cholecystectomy for reported biliary colic.
The gastroenterology evaluation included a colonoscopy and esophagogastroduodenoscopy (EGD); both were benign and without findings specific to identify the etiology for the patient’s pain. The patient was given a course of rifaximin 1200 mg daily for 7 days for possible bacterial overgrowth and placed on a proton pump inhibitor twice daily. Neither of these interventions helped resolve the patient’s symptoms. Further workup was pursued by gastroenterology to include a right upper quadrant ultrasound that showed a structure most consistent with a small gallbladder containing a small polyp vs stone. Magnetic resonance cholangiopancreatography (MRCP) also was performed and showed the presence of a small gallbladder with a small 2-mm filling defect and an otherwise benign biliary tree. MRCP images and EGD documented a Billroth 1 reconstruction at the time of his remote antrectomy and vagotomy (Figure 1).
The patient was referred to general surgery for consideration of a repeat cholecystectomy. He confirmed the history of intermittent upper abdominal pain for the past 16 years, which was similar to the symptoms he had experienced before his original laparoscopic cholecystectomy. On examination, the patient had a body mass index of 38, had a large upper midline incision from his prior antrectomy and vagotomy procedure, and several scars presumed to be port incision scars to the right lateral abdominal wall. Hospital records were obtained from the patient’s prior workup for biliary colic and cholecystectomy 16 years before. The preoperative abdominal ultrasound examination showed a mildly distended gallbladder but was notably described as “quite limited due to patient’s body habitus and liver is not well seen.” No additional imaging was documented in his presurgical evaluation notes and imaging records.
The operative report described a gallbladder that was densely adherent to adjacent fat and omental tissue with significant adhesions secondary to the prior vagotomy and antrectomy procedure. The cystic duct and artery were dissected free at the level of their junction with the gallbladder infundibulum. The cystic artery was divided with a harmonic scalpel. Following this the gallbladder body was dissected free from the liver bed in top-down fashion. A 0 Vicryl Endoloop suture was placed over the gallbladder and secured just past the origin of the cystic duct on the gallbladder infundibulum and the cystic duct divided above this suture. No surgical clips were used, which corresponded with the lack of surgical clips seen in imaging in his recent gastroenterology workup. No documentation of an intraoperative cholangiogram existed or was considered in the operative report.
The pathology report from this first cholecystectomy procedure noted the removed specimen to be an unopened 6-cm gallbladder containing 2 small yellow stones that otherwise were benign. At the time of this patient’s re-presentation to general surgery, there was suspicion that the patient’s prior surgical procedure had not been a cholecystectomy but rather a subtotal cholecystectomy. However, after appropriate workup and review of prior records, the patient had, indeed, previously undergone cholecystectomy and represented a rare case of gallbladder duplication resulting in abdominal pain for 16 years after his index operation.
The patient was consented for repeat cholecystectomy and underwent a laparoscopic lysis of adhesions, cholecystectomy, and intraoperative cholangiogram. Significant scarring was found at the liver undersurface that would have been exposed during the original laparoscopic resection of the gallbladder from its liver bed. Deeper to this, a small saccular structure was identified as the duplicate gallbladder (Figure 2). Though the visualized gallbladder was small with a deep intrahepatic lie, the critical view of safety was achieved and was without additional variation. An intraoperative cholangiogram was performed to determine whether residual ductal stumps or other additional evidence of the previously removed gallbladder could be identified. The cholangiogram showed clear visualization of the cystic duct, common bile duct, right and left hepatic ducts, and contrast into the duodenum without abnormal variants. There was no visualized accessory or secondary cystic duct stump seen on the cholangiogram (Figure 3). Pathology of the repeat cholecystectomy specimen confirmed a 3-cm gallbladder with a distinct duct leading out of the gallbladder and the presence of several gallstones. The patient had an uneventful recovery after the repeat laparoscopic cholecystectomy with complete resolution of his upper abdominal pain.
Discussion
The first reported human case of gallbladder duplication was noted in a sacrificial victim of Emperor Augustus in 31 BCE. Sherren reported the first documented case of double accessory gallbladder in a living human in 1911.1,6 Though the exact incidence of gallbladder duplication is not fully known due to primary documentation from case reports, incidence is approximately 1 in 4000 to 5000 people. It was first formally classified by Boyden in 1926.7 Further anatomic classification based on morphology and embryogenesis was delineated by Harlaftis and colleagues in 1977, establishing type 1 and 2 structures of a duplicated gallbladder.8 Type 1 duplicated gallbladder anatomy shares a single cystic duct, whereas in type 2 each gallbladder has its own cystic duct. Later reports and studies identified triple gallbladders as well as trabecular variants with the most common classification used currently being the modified Harlaftis classification.9,10
The case presented here most likely represents either a Y-shaped type 1 primordial gallbladder or a type 2 accessory gallbladder based on historical data and intraoperative cholangiogram findings at the time of repeat cholecystectomy. Gallbladder duplication is clinically indistinguishable from regular gallbladder pathology preoperatively and can only be identified on imaging or intraoperatively.11 Prior case reports and studies have found that it is frequently missed on preoperative abdominal ultrasonography and CT in up to 50% of cases.12-14
The differential diagnosis of gallbladder duplication seen on preoperative imaging includes a gallbladder diverticulum, choledochal cyst, focal adenonomyomatosis, Phrygian cap, or folded gallbladder.1,2 Historically, the most definitive test for gallbladder duplication has been either intraoperative cholangiography, which can also clarify biliary anatomy, or endoscopic retrograde cholangiopancreatography with cholangiography.1,3 The debate over routine use of intraoperative cholangiography has been ongoing for the past several decades.15 Though intraoperative cholangiogram remains one of the most definitive tests for gallbladder duplication, given the overall low incidence of this variant, recommendation for routine intraoperative cholangiography solely to rule out gallbladder duplication cannot be definitively recommended based on our review of the literature. Currently, preoperative MRCP is the study of choice when there is concern from historical facts or from other imaging of gallbladder duplication as it is noninvasive and has a high degree of detail, particularly with 3D reconstructions.14,16 At the time of surgery, the most critical step to avoid inadvertent ductal injury is clear visualization of ductal anatomy and obtaining the critical view of safety.17 Though this will also assist in identifying some cases of gallbladder duplication, given the great variation of duplication, it will not prevent missing some variants. In our case, extensive local scarring from the patient’s prior antrectomy and vagotomy along with lack of the use of intraoperative cholangiography likely contributed to missing his duplication at the time of his index cholecystectomy.
Undiagnosed gallbladder duplication can lead to additional morbidity related to common entities associated with gallbladder pathology, such as biliary colic, cholecystitis, cholangitis, and pancreatitis. Additionally, case reports in the literature have documented more rare associations, such as empyema, carcinoma, cholecystoenteric fistula, and torsion, all associated with a duplicated gallbladder.18-21 Once identified pre- or intraoperatively, it is generally recommended that all gallbladders be removed in symptomatic patients and that intraoperative cholangiography be done to assure complete resection of the duplicated gallbladders and to avoid injury to the biliary trees.22-25
Conclusions
Gallbladder duplication and other congenital biliary anatomic variations should be considered before a biliary operation and included in the differential diagnosis when evaluating patients who have clinical symptoms consistent with biliary pathology. In addition, intraoperative cholangiogram should be performed during cholecystectomy if the inferior liver edge cannot be visualized well, as in the case of this patient where a prior foregut operation resulted in extensive adhesive disease. Intraoperative cholangiogram also should be considered in patients whose preoperative imaging does not visualize the right upper quadrant well due to patient habitus. Doing so may identify gallbladder duplication and allow for complete cholecystectomy as well as proper identification and management of cystic duct variants. Awareness and consideration of duplicated biliary variants can help prevent intraoperative complications related to biliary anomalies and avoid the morbidity related to recurrent biliary disease and the need for repeat operative procedures.
Acknowledgments
We extend our thanks to Veterans Affairs Puget Sound Healthcare System and the Departments of Surgery and Radiology for their support of this case report, and Lorrie Langdale, MD, and Roger Tatum, MD, for their mentorship of this project
1. Vezakis A, Pantiora E, Giannoulopoulos D, et al. A duplicated gallbladder in a patient presenting with acute cholangitis. A case study and a literature review. Ann Hepatol. 2019;18(1):240-245. doi:10.5604/01.3001.0012.7932
2. Barut Í, Tarhan ÖR, Dog^ru U, Bülbül M. Gallbladder duplication: diagnosed and treated by laparoscopy. Eur J Gen Med. 2006;3(3):142-145. doi:10.29333/ejgm/82396 3. Cozacov Y, Subhas G, Jacobs M, Parikh J. Total laparoscopic removal of accessory gallbladder: a case report and review of literature. World J Gastrointest Surg. 2015;7(12):398-402. doi:10.4240/wjgs.v7.i12.398
4. Musleh MG, Burnett H, Rajashanker B, Ammori BJ. Laparoscopic double cholecystectomy for duplicated gallbladder: a case report. Int J Surg Case Rep. 2017;41:502-504. Published 2017 Nov 27. doi:10.1016/j.ijscr.2017.11.046
5. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a duplicated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011;21(3):e156-e158. doi:10.1097/SLE.0b013e31821d47ce
6. Sherren J. A double gall-bladder removed by operation. Ann Surg. 1911;54(2):204-205. doi:10.1097/00000658-191108000-00009
7. Boyden EA. The accessory gall-bladder—an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anat. 1926; 38(2):177-231. doi:10.1002/aja.1000380202
8. Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surg Gynecol Obstet. 1977;145(6):928-934.
9. Kim RD, Zendejas I, Velopulos C, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009;39(6):536-539. doi:10.1007/s00595-008-3878-4
10. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010;45(2):443-446. doi:10.1016/j.jpedsurg.2009.12.015
11. Apolo Romero EX, Gálvez Salazar PF, Estrada Chandi JA, et al. Gallbladder duplication and cholecystitis. J Surg Case Rep. 2018;2018(7):rjy158. Published 2018 Jul 3. doi:10.1093/jscr/rjy158
12. Gorecki PJ, Andrei VE, Musacchio T, Schein M. Double gallbladder originating from left hepatic duct: a case report and review of literature. JSLS. 1998;2(4):337-339.
13. Cueto García J, Weber A, Serrano Berry F, Tanur Tatz B. Double gallbladder treated successfully by laparoscopy. J Laparoendosc Surg. 1993;3(2):153-155. doi:10.1089/lps.1993.3.153
14. Fazio V, Damiano G, Palumbo VD, et al. An unexpected surprise at the end of a “quiet” cholecystectomy. A case report and review of the literature. Ann Ital Chir. 2012;83(3):265-267.
15. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644. doi:10.1001/jama.289.13.1639
16. Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: a case report and review of the literature. Surg Radiol Anat. 2015;37(5):425-429. doi:10.1007/s00276-015-1456-1
17. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
18. Raymond SW, Thrift CB. Carcinoma of a duplicated gall bladder. Ill Med J. 1956;110(5):239-240.
19. Cunningham JJ. Empyema of a duplicated gallbladder: echographic findings. J Clin Ultrasound. 1980;8(6):511-512. doi:10.1002/jcu.1870080612
20. Recht W. Torsion of a double gallbladder; a report of a case and a review of the literature. Br J Surg. 1952;39(156):342-344. doi:10.1002/bjs.18003915616
21. Ritchie AW, Crucioli V. Double gallbladder with cholecystocolic fistula: a case report. Br J Surg. 1980;67(2):145-146. doi:10.1002/bjs.1800670226
22. Shapiro T, Rennie W. Duplicate gallbladder cholecystitis after open cholecystectomy. Ann Emerg Med. 1999;33(5):584-587. doi:10.1016/s0196-0644(99)70348-3
23. Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC. Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg. 2006;93(7):844-853. doi:10.1002/bjs.5333
24. Davidoff AM, Pappas TN, Murray EA, et al. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992;215(3):196-202. doi:10.1097/00000658-199203000-00002
25. Flowers JL, Zucker KA, Graham SM, Scovill WA, Imbembo AL, Bailey RW. Laparoscopic cholangiography. Results and indications. Ann Surg. 1992;215(3):209-216. doi:10.1097/00000658-199203000-00004
1. Vezakis A, Pantiora E, Giannoulopoulos D, et al. A duplicated gallbladder in a patient presenting with acute cholangitis. A case study and a literature review. Ann Hepatol. 2019;18(1):240-245. doi:10.5604/01.3001.0012.7932
2. Barut Í, Tarhan ÖR, Dog^ru U, Bülbül M. Gallbladder duplication: diagnosed and treated by laparoscopy. Eur J Gen Med. 2006;3(3):142-145. doi:10.29333/ejgm/82396 3. Cozacov Y, Subhas G, Jacobs M, Parikh J. Total laparoscopic removal of accessory gallbladder: a case report and review of literature. World J Gastrointest Surg. 2015;7(12):398-402. doi:10.4240/wjgs.v7.i12.398
4. Musleh MG, Burnett H, Rajashanker B, Ammori BJ. Laparoscopic double cholecystectomy for duplicated gallbladder: a case report. Int J Surg Case Rep. 2017;41:502-504. Published 2017 Nov 27. doi:10.1016/j.ijscr.2017.11.046
5. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a duplicated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011;21(3):e156-e158. doi:10.1097/SLE.0b013e31821d47ce
6. Sherren J. A double gall-bladder removed by operation. Ann Surg. 1911;54(2):204-205. doi:10.1097/00000658-191108000-00009
7. Boyden EA. The accessory gall-bladder—an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anat. 1926; 38(2):177-231. doi:10.1002/aja.1000380202
8. Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surg Gynecol Obstet. 1977;145(6):928-934.
9. Kim RD, Zendejas I, Velopulos C, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009;39(6):536-539. doi:10.1007/s00595-008-3878-4
10. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010;45(2):443-446. doi:10.1016/j.jpedsurg.2009.12.015
11. Apolo Romero EX, Gálvez Salazar PF, Estrada Chandi JA, et al. Gallbladder duplication and cholecystitis. J Surg Case Rep. 2018;2018(7):rjy158. Published 2018 Jul 3. doi:10.1093/jscr/rjy158
12. Gorecki PJ, Andrei VE, Musacchio T, Schein M. Double gallbladder originating from left hepatic duct: a case report and review of literature. JSLS. 1998;2(4):337-339.
13. Cueto García J, Weber A, Serrano Berry F, Tanur Tatz B. Double gallbladder treated successfully by laparoscopy. J Laparoendosc Surg. 1993;3(2):153-155. doi:10.1089/lps.1993.3.153
14. Fazio V, Damiano G, Palumbo VD, et al. An unexpected surprise at the end of a “quiet” cholecystectomy. A case report and review of the literature. Ann Ital Chir. 2012;83(3):265-267.
15. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644. doi:10.1001/jama.289.13.1639
16. Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: a case report and review of the literature. Surg Radiol Anat. 2015;37(5):425-429. doi:10.1007/s00276-015-1456-1
17. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
18. Raymond SW, Thrift CB. Carcinoma of a duplicated gall bladder. Ill Med J. 1956;110(5):239-240.
19. Cunningham JJ. Empyema of a duplicated gallbladder: echographic findings. J Clin Ultrasound. 1980;8(6):511-512. doi:10.1002/jcu.1870080612
20. Recht W. Torsion of a double gallbladder; a report of a case and a review of the literature. Br J Surg. 1952;39(156):342-344. doi:10.1002/bjs.18003915616
21. Ritchie AW, Crucioli V. Double gallbladder with cholecystocolic fistula: a case report. Br J Surg. 1980;67(2):145-146. doi:10.1002/bjs.1800670226
22. Shapiro T, Rennie W. Duplicate gallbladder cholecystitis after open cholecystectomy. Ann Emerg Med. 1999;33(5):584-587. doi:10.1016/s0196-0644(99)70348-3
23. Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC. Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg. 2006;93(7):844-853. doi:10.1002/bjs.5333
24. Davidoff AM, Pappas TN, Murray EA, et al. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992;215(3):196-202. doi:10.1097/00000658-199203000-00002
25. Flowers JL, Zucker KA, Graham SM, Scovill WA, Imbembo AL, Bailey RW. Laparoscopic cholangiography. Results and indications. Ann Surg. 1992;215(3):209-216. doi:10.1097/00000658-199203000-00004
FDA hints at deadlines to meet accelerated approval requirements
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
FROM JAMA ONCOLOGY
Too much marijuana can make you unpleasantly, dangerously sick
At the center of the emerging science on the unintended consequences of daily long-term use of marijuana lies a paradox.
For years, medical marijuana has been used to ease nausea from cancer chemotherapy and GI conditions. Now, with greater legalization comes growing awareness that chronic use of marijuana – also known as cannabis – can trigger a condition where, ironically, a person has hard-to-control vomiting and nausea.
Some people with the disorder, known as “cannabinoid hyperemesis syndrome,” also report crippling belly pain.
Linda can relate. The 33-year-old Oregon resident, who asked to remain anonymous to protect her privacy, refers to a medieval spiky metal ball on a chain when describing the pain.
“Picture a mace inside your stomach, pushing up inside your chest and, at the same time, exploding out,” she said.
To seek relief, she gets down on her knees, adopts a child’s yoga pose, and runs hot water in the bathroom for hours on end, a trick many with the disorder says has provided relief. She also occasionally goes outside and tries walking it off.
“I would just wander around my neighborhood, a lot of times at like 4 or 5 in the morning,” she said. “The fresh air helps a little bit. I just keep walking down the street, take about 10 steps, stop, vomit – walk a little bit more, stop, vomit.”
Her first experience with the disorder began in the middle of one night in 2017 while she was at a conference in Las Vegas.
“We went out to eat the night before, and I woke up about 4 in the morning with just the most intense pain I’ve ever had,” she said. “I found myself in a really hot shower in between throwing up everything and trying to say get some water down. I was sharing an Airbnb with my colleagues, so it was less than ideal.”
Many people with cannabinoid hyperemesis syndrome find relief from hot baths or showers. Researchers believe that hot water helps because temperature sensors in the skin send signals to the brain that can help ease the symptoms, at least for a while.
The problem is that people with this syndrome “can’t live in the water,” said emergency doctor and medical cannabis expert Leigh Vinocur, MD.
Fast-forward 6 months to another event in Boulder, Colo. Again, Linda woke up and could not stop vomiting.
“I was not feeling any better. Showering wasn’t helping. I ended up in the hospital,” she said.
She received opioids for her pain. But neither she nor the ED staff were quite sure what was happening. Her discharge paperwork read “cannabis allergy.”
Cannabinoid hyperemesis syndrome “shatters that image of cannabis only being a good thing. It’s a bold statement, but, you know, once you start to think about it, it’s like a little too much of anything isn’t good,” Linda said.
Experts suggest greater awareness is needed to identify this syndrome earlier, by both cannabinoid users and doctors. The bouts of vomiting, in particular, can get so severe that people can end up hospitalized with dehydration, electrolyte disorders, and weight loss.
The severe electrolyte imbalances “can really be life-threatening,” said David Johnson, MD, a professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk.
“By the time they come into emergency care, they’re in bad shape,” Dr. Vinocur agreed. “Many try to ignore it, but they continue to vomit.”
Genetic risk factors?
One mystery is why some regular marijuana users get this syndrome while others do not.
“I can say that not everybody gets this, thank goodness,” said Ethan Russo, MD. “But there has to be a reason that certain people are susceptible and others are not.”
Interestingly, a new study from Dr. Russo and colleagues suggests that genes play a role. They identified five genetic changes that could make a chronic marijuana user more likely to have cannabinoid hyperemesis syndrome in a study published July 5, 2021, in the journal Cannabis and Cannabinoid Research.
They compared 28 people with the disorder with 12 other high-frequency marijuana users without these symptoms.
The results are not final but could help guide future research, Dr. Russo said.
“What we’ve discovered – and it was far more than we expected – is that there’s a lot more to this than a hypersensitivity to cannabis,” said Dr. Russo, a neurologist and founder/CEO of CReDO Science, a firm that promotes cannabis research and develops commercial products.
Also, he said, those affected by cannabinoid hyperemesis syndrome could be at higher risk for other conditions, such as addiction to alcohol or other substances, dementia, diabetes, and heart disease.
“Most people with [cannabinoid hyperemesis syndrome] are going to be younger,” he said. “What we’ve demonstrated is there is a risk for more serious problems for decades to come. So someone who has these symptoms really deserves a look at this genetic screening.”
Battling disbelief
Getting back to the paradox, many users don’t believe marijuana can trigger serious vomiting and nausea because of its reputation for doing the opposite.
“Folks that have this are just uniquely resistant to the concept that cannabis is actually the problem and not the solution,” Dr. Russo said.
“It’s kind of counterintuitive because people think: ‘Oh, cannabis helps with nausea,’ so they use more of it,” said Dr. Vinocur, who is also a spokesperson for the American College of Emergency Physicians and runs a medical cannabis practice.
Most kinds of marijuana act in this way – doing opposite things at different doses. Once a certain threshold is passed, people with cannabinoid hyperemesis syndrome are “just uniquely susceptible and really can’t tolerate any significant amount of THC,” Dr. Russo said, referring to tetrahydrocannabinol, the substance that gets marijuana users high.
Once diagnosed, quitting is the most effective strategy. But it can be tough to persuade someone to stop using marijuana.
“You do have to try and convince them ... to try abstinence and to watch and see what happens,” Dr. Vinocur said.
People should “realize the root cause of this is its cannabinoid ingestion, and the treatment is really best directed at absolute avoidance,” Dr. Johnson said.
Unfortunately, evidence also shows that once a person stops using marijuana and gets relief, going back to marijuana or other forms of cannabinoids can cause the syndrome to start all over again.
“We’ve had people that quit for a month, a year, 2 years and upon resumption, almost invariably, they’re back into bouts of the hyperemesis along with all the other [symptoms],” Dr. Russo said.
Marijuana and cannabinoids can cause digestive problems, Dr. Johnson said, which may cause more problems.
What recent research reveals
Cannabinoid hyperemesis syndrome is a relatively young disorder – first described in 2004 – and early reports and case studies are giving way now to studies looking into potential treatments.
So far, the strongest evidence suggests a role for an over-the-counter cream called capsaicin to help manage symptoms, but more studies are needed.
Similar to hot showers, this ingredient from chili peppers can warm the skin and trigger the temperature-sensitive skin sensors to lessen the symptoms, Dr. Johnson said.
An October 2021 study in Spain looked at 54 ED visits among 29 people with cannabinoid hyperemesis syndrome. For the 75% treated with capsaicin, vomiting stopped after an average of 18 minutes.
Lead author Guillermo Burillo-Putze, MD, PhD, said he is most surprised by the growing number of new cases of the disorder.
“This should be of concern given the increase in cannabis use due to its legalization and permissiveness,” said Dr. Burillo-Putze, an emergency doctor at Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain.
Cannabinoid hyperemesis syndrome appears not to discriminate across racial and ethic groups. Although most studies to date include White participants, a July 2021 study of 29 people, 90% of whom were Black, found repeat visits to the ED were common.
The study found that 16 people returned 42 times to the ED and accounted for 10 hospital admissions, for example.
Cannabis conspiracy theories
“Unfortunately, this condition has become the subject of great speculation hinging on conspiracy theories as its true cause,” Dr. Russo noted in a September 2021 letter to the editor in the American Journal of Emergency Medicine.
Some “myth busting” is in order, he said.
For example, cannabinoid hyperemesis syndrome does not happen because of exposure to products from a tree called neem or from pesticides applied to marijuana plants during cultivation, Dr. Russo said. It can also occur with high-dose synthetic cannabinoids.
The state of recreational and medical marijuana
Recreational marijuana is legal in 18 states, Washington, D.C., and Guam as of January 2022, according to a report in U.S. News. More states permit medical marijuana use – 37 in total, plus Washington, D.C., according to Britannica ProCon.
One of the states where only medicinal use is legal is Maryland, which is where Dr. Vinocur practices.
“We are seeing increasing numbers of cases” of cannabinoid hyperemesis syndrome, she said.
In addition to chronic use or higher doses, it’s likely that the higher potency levels of THC in the legal marijuana industry trigger the syndrome in some people as well.
Linda estimates she ended up in emergency rooms at least a half-dozen times in the last 5 years. In April 2021, she had a “pretty serious event.” She blames it on traveling a lot for work, not eating right, and not getting enough sleep. She broke her 2-year abstinence with alcohol.
“I basically didn’t listen to my body and paid a pretty significant price for it,” she said.
Linda did not stop altogether but said she “drastically changed the types and form of the cannabis I was using.”
“I can tell you on the record that I would be a hundred percent dead without this plant,” she said.
“The prospect of living without it was more detrimental to me than all of those things I just described to you, because addiction runs in my family and I had opiate problems myself that I overcame with cannabis.”
A version of this article first appeared on Medscape.com.
At the center of the emerging science on the unintended consequences of daily long-term use of marijuana lies a paradox.
For years, medical marijuana has been used to ease nausea from cancer chemotherapy and GI conditions. Now, with greater legalization comes growing awareness that chronic use of marijuana – also known as cannabis – can trigger a condition where, ironically, a person has hard-to-control vomiting and nausea.
Some people with the disorder, known as “cannabinoid hyperemesis syndrome,” also report crippling belly pain.
Linda can relate. The 33-year-old Oregon resident, who asked to remain anonymous to protect her privacy, refers to a medieval spiky metal ball on a chain when describing the pain.
“Picture a mace inside your stomach, pushing up inside your chest and, at the same time, exploding out,” she said.
To seek relief, she gets down on her knees, adopts a child’s yoga pose, and runs hot water in the bathroom for hours on end, a trick many with the disorder says has provided relief. She also occasionally goes outside and tries walking it off.
“I would just wander around my neighborhood, a lot of times at like 4 or 5 in the morning,” she said. “The fresh air helps a little bit. I just keep walking down the street, take about 10 steps, stop, vomit – walk a little bit more, stop, vomit.”
Her first experience with the disorder began in the middle of one night in 2017 while she was at a conference in Las Vegas.
“We went out to eat the night before, and I woke up about 4 in the morning with just the most intense pain I’ve ever had,” she said. “I found myself in a really hot shower in between throwing up everything and trying to say get some water down. I was sharing an Airbnb with my colleagues, so it was less than ideal.”
Many people with cannabinoid hyperemesis syndrome find relief from hot baths or showers. Researchers believe that hot water helps because temperature sensors in the skin send signals to the brain that can help ease the symptoms, at least for a while.
The problem is that people with this syndrome “can’t live in the water,” said emergency doctor and medical cannabis expert Leigh Vinocur, MD.
Fast-forward 6 months to another event in Boulder, Colo. Again, Linda woke up and could not stop vomiting.
“I was not feeling any better. Showering wasn’t helping. I ended up in the hospital,” she said.
She received opioids for her pain. But neither she nor the ED staff were quite sure what was happening. Her discharge paperwork read “cannabis allergy.”
Cannabinoid hyperemesis syndrome “shatters that image of cannabis only being a good thing. It’s a bold statement, but, you know, once you start to think about it, it’s like a little too much of anything isn’t good,” Linda said.
Experts suggest greater awareness is needed to identify this syndrome earlier, by both cannabinoid users and doctors. The bouts of vomiting, in particular, can get so severe that people can end up hospitalized with dehydration, electrolyte disorders, and weight loss.
The severe electrolyte imbalances “can really be life-threatening,” said David Johnson, MD, a professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk.
“By the time they come into emergency care, they’re in bad shape,” Dr. Vinocur agreed. “Many try to ignore it, but they continue to vomit.”
Genetic risk factors?
One mystery is why some regular marijuana users get this syndrome while others do not.
“I can say that not everybody gets this, thank goodness,” said Ethan Russo, MD. “But there has to be a reason that certain people are susceptible and others are not.”
Interestingly, a new study from Dr. Russo and colleagues suggests that genes play a role. They identified five genetic changes that could make a chronic marijuana user more likely to have cannabinoid hyperemesis syndrome in a study published July 5, 2021, in the journal Cannabis and Cannabinoid Research.
They compared 28 people with the disorder with 12 other high-frequency marijuana users without these symptoms.
The results are not final but could help guide future research, Dr. Russo said.
“What we’ve discovered – and it was far more than we expected – is that there’s a lot more to this than a hypersensitivity to cannabis,” said Dr. Russo, a neurologist and founder/CEO of CReDO Science, a firm that promotes cannabis research and develops commercial products.
Also, he said, those affected by cannabinoid hyperemesis syndrome could be at higher risk for other conditions, such as addiction to alcohol or other substances, dementia, diabetes, and heart disease.
“Most people with [cannabinoid hyperemesis syndrome] are going to be younger,” he said. “What we’ve demonstrated is there is a risk for more serious problems for decades to come. So someone who has these symptoms really deserves a look at this genetic screening.”
Battling disbelief
Getting back to the paradox, many users don’t believe marijuana can trigger serious vomiting and nausea because of its reputation for doing the opposite.
“Folks that have this are just uniquely resistant to the concept that cannabis is actually the problem and not the solution,” Dr. Russo said.
“It’s kind of counterintuitive because people think: ‘Oh, cannabis helps with nausea,’ so they use more of it,” said Dr. Vinocur, who is also a spokesperson for the American College of Emergency Physicians and runs a medical cannabis practice.
Most kinds of marijuana act in this way – doing opposite things at different doses. Once a certain threshold is passed, people with cannabinoid hyperemesis syndrome are “just uniquely susceptible and really can’t tolerate any significant amount of THC,” Dr. Russo said, referring to tetrahydrocannabinol, the substance that gets marijuana users high.
Once diagnosed, quitting is the most effective strategy. But it can be tough to persuade someone to stop using marijuana.
“You do have to try and convince them ... to try abstinence and to watch and see what happens,” Dr. Vinocur said.
People should “realize the root cause of this is its cannabinoid ingestion, and the treatment is really best directed at absolute avoidance,” Dr. Johnson said.
Unfortunately, evidence also shows that once a person stops using marijuana and gets relief, going back to marijuana or other forms of cannabinoids can cause the syndrome to start all over again.
“We’ve had people that quit for a month, a year, 2 years and upon resumption, almost invariably, they’re back into bouts of the hyperemesis along with all the other [symptoms],” Dr. Russo said.
Marijuana and cannabinoids can cause digestive problems, Dr. Johnson said, which may cause more problems.
What recent research reveals
Cannabinoid hyperemesis syndrome is a relatively young disorder – first described in 2004 – and early reports and case studies are giving way now to studies looking into potential treatments.
So far, the strongest evidence suggests a role for an over-the-counter cream called capsaicin to help manage symptoms, but more studies are needed.
Similar to hot showers, this ingredient from chili peppers can warm the skin and trigger the temperature-sensitive skin sensors to lessen the symptoms, Dr. Johnson said.
An October 2021 study in Spain looked at 54 ED visits among 29 people with cannabinoid hyperemesis syndrome. For the 75% treated with capsaicin, vomiting stopped after an average of 18 minutes.
Lead author Guillermo Burillo-Putze, MD, PhD, said he is most surprised by the growing number of new cases of the disorder.
“This should be of concern given the increase in cannabis use due to its legalization and permissiveness,” said Dr. Burillo-Putze, an emergency doctor at Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain.
Cannabinoid hyperemesis syndrome appears not to discriminate across racial and ethic groups. Although most studies to date include White participants, a July 2021 study of 29 people, 90% of whom were Black, found repeat visits to the ED were common.
The study found that 16 people returned 42 times to the ED and accounted for 10 hospital admissions, for example.
Cannabis conspiracy theories
“Unfortunately, this condition has become the subject of great speculation hinging on conspiracy theories as its true cause,” Dr. Russo noted in a September 2021 letter to the editor in the American Journal of Emergency Medicine.
Some “myth busting” is in order, he said.
For example, cannabinoid hyperemesis syndrome does not happen because of exposure to products from a tree called neem or from pesticides applied to marijuana plants during cultivation, Dr. Russo said. It can also occur with high-dose synthetic cannabinoids.
The state of recreational and medical marijuana
Recreational marijuana is legal in 18 states, Washington, D.C., and Guam as of January 2022, according to a report in U.S. News. More states permit medical marijuana use – 37 in total, plus Washington, D.C., according to Britannica ProCon.
One of the states where only medicinal use is legal is Maryland, which is where Dr. Vinocur practices.
“We are seeing increasing numbers of cases” of cannabinoid hyperemesis syndrome, she said.
In addition to chronic use or higher doses, it’s likely that the higher potency levels of THC in the legal marijuana industry trigger the syndrome in some people as well.
Linda estimates she ended up in emergency rooms at least a half-dozen times in the last 5 years. In April 2021, she had a “pretty serious event.” She blames it on traveling a lot for work, not eating right, and not getting enough sleep. She broke her 2-year abstinence with alcohol.
“I basically didn’t listen to my body and paid a pretty significant price for it,” she said.
Linda did not stop altogether but said she “drastically changed the types and form of the cannabis I was using.”
“I can tell you on the record that I would be a hundred percent dead without this plant,” she said.
“The prospect of living without it was more detrimental to me than all of those things I just described to you, because addiction runs in my family and I had opiate problems myself that I overcame with cannabis.”
A version of this article first appeared on Medscape.com.
At the center of the emerging science on the unintended consequences of daily long-term use of marijuana lies a paradox.
For years, medical marijuana has been used to ease nausea from cancer chemotherapy and GI conditions. Now, with greater legalization comes growing awareness that chronic use of marijuana – also known as cannabis – can trigger a condition where, ironically, a person has hard-to-control vomiting and nausea.
Some people with the disorder, known as “cannabinoid hyperemesis syndrome,” also report crippling belly pain.
Linda can relate. The 33-year-old Oregon resident, who asked to remain anonymous to protect her privacy, refers to a medieval spiky metal ball on a chain when describing the pain.
“Picture a mace inside your stomach, pushing up inside your chest and, at the same time, exploding out,” she said.
To seek relief, she gets down on her knees, adopts a child’s yoga pose, and runs hot water in the bathroom for hours on end, a trick many with the disorder says has provided relief. She also occasionally goes outside and tries walking it off.
“I would just wander around my neighborhood, a lot of times at like 4 or 5 in the morning,” she said. “The fresh air helps a little bit. I just keep walking down the street, take about 10 steps, stop, vomit – walk a little bit more, stop, vomit.”
Her first experience with the disorder began in the middle of one night in 2017 while she was at a conference in Las Vegas.
“We went out to eat the night before, and I woke up about 4 in the morning with just the most intense pain I’ve ever had,” she said. “I found myself in a really hot shower in between throwing up everything and trying to say get some water down. I was sharing an Airbnb with my colleagues, so it was less than ideal.”
Many people with cannabinoid hyperemesis syndrome find relief from hot baths or showers. Researchers believe that hot water helps because temperature sensors in the skin send signals to the brain that can help ease the symptoms, at least for a while.
The problem is that people with this syndrome “can’t live in the water,” said emergency doctor and medical cannabis expert Leigh Vinocur, MD.
Fast-forward 6 months to another event in Boulder, Colo. Again, Linda woke up and could not stop vomiting.
“I was not feeling any better. Showering wasn’t helping. I ended up in the hospital,” she said.
She received opioids for her pain. But neither she nor the ED staff were quite sure what was happening. Her discharge paperwork read “cannabis allergy.”
Cannabinoid hyperemesis syndrome “shatters that image of cannabis only being a good thing. It’s a bold statement, but, you know, once you start to think about it, it’s like a little too much of anything isn’t good,” Linda said.
Experts suggest greater awareness is needed to identify this syndrome earlier, by both cannabinoid users and doctors. The bouts of vomiting, in particular, can get so severe that people can end up hospitalized with dehydration, electrolyte disorders, and weight loss.
The severe electrolyte imbalances “can really be life-threatening,” said David Johnson, MD, a professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk.
“By the time they come into emergency care, they’re in bad shape,” Dr. Vinocur agreed. “Many try to ignore it, but they continue to vomit.”
Genetic risk factors?
One mystery is why some regular marijuana users get this syndrome while others do not.
“I can say that not everybody gets this, thank goodness,” said Ethan Russo, MD. “But there has to be a reason that certain people are susceptible and others are not.”
Interestingly, a new study from Dr. Russo and colleagues suggests that genes play a role. They identified five genetic changes that could make a chronic marijuana user more likely to have cannabinoid hyperemesis syndrome in a study published July 5, 2021, in the journal Cannabis and Cannabinoid Research.
They compared 28 people with the disorder with 12 other high-frequency marijuana users without these symptoms.
The results are not final but could help guide future research, Dr. Russo said.
“What we’ve discovered – and it was far more than we expected – is that there’s a lot more to this than a hypersensitivity to cannabis,” said Dr. Russo, a neurologist and founder/CEO of CReDO Science, a firm that promotes cannabis research and develops commercial products.
Also, he said, those affected by cannabinoid hyperemesis syndrome could be at higher risk for other conditions, such as addiction to alcohol or other substances, dementia, diabetes, and heart disease.
“Most people with [cannabinoid hyperemesis syndrome] are going to be younger,” he said. “What we’ve demonstrated is there is a risk for more serious problems for decades to come. So someone who has these symptoms really deserves a look at this genetic screening.”
Battling disbelief
Getting back to the paradox, many users don’t believe marijuana can trigger serious vomiting and nausea because of its reputation for doing the opposite.
“Folks that have this are just uniquely resistant to the concept that cannabis is actually the problem and not the solution,” Dr. Russo said.
“It’s kind of counterintuitive because people think: ‘Oh, cannabis helps with nausea,’ so they use more of it,” said Dr. Vinocur, who is also a spokesperson for the American College of Emergency Physicians and runs a medical cannabis practice.
Most kinds of marijuana act in this way – doing opposite things at different doses. Once a certain threshold is passed, people with cannabinoid hyperemesis syndrome are “just uniquely susceptible and really can’t tolerate any significant amount of THC,” Dr. Russo said, referring to tetrahydrocannabinol, the substance that gets marijuana users high.
Once diagnosed, quitting is the most effective strategy. But it can be tough to persuade someone to stop using marijuana.
“You do have to try and convince them ... to try abstinence and to watch and see what happens,” Dr. Vinocur said.
People should “realize the root cause of this is its cannabinoid ingestion, and the treatment is really best directed at absolute avoidance,” Dr. Johnson said.
Unfortunately, evidence also shows that once a person stops using marijuana and gets relief, going back to marijuana or other forms of cannabinoids can cause the syndrome to start all over again.
“We’ve had people that quit for a month, a year, 2 years and upon resumption, almost invariably, they’re back into bouts of the hyperemesis along with all the other [symptoms],” Dr. Russo said.
Marijuana and cannabinoids can cause digestive problems, Dr. Johnson said, which may cause more problems.
What recent research reveals
Cannabinoid hyperemesis syndrome is a relatively young disorder – first described in 2004 – and early reports and case studies are giving way now to studies looking into potential treatments.
So far, the strongest evidence suggests a role for an over-the-counter cream called capsaicin to help manage symptoms, but more studies are needed.
Similar to hot showers, this ingredient from chili peppers can warm the skin and trigger the temperature-sensitive skin sensors to lessen the symptoms, Dr. Johnson said.
An October 2021 study in Spain looked at 54 ED visits among 29 people with cannabinoid hyperemesis syndrome. For the 75% treated with capsaicin, vomiting stopped after an average of 18 minutes.
Lead author Guillermo Burillo-Putze, MD, PhD, said he is most surprised by the growing number of new cases of the disorder.
“This should be of concern given the increase in cannabis use due to its legalization and permissiveness,” said Dr. Burillo-Putze, an emergency doctor at Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain.
Cannabinoid hyperemesis syndrome appears not to discriminate across racial and ethic groups. Although most studies to date include White participants, a July 2021 study of 29 people, 90% of whom were Black, found repeat visits to the ED were common.
The study found that 16 people returned 42 times to the ED and accounted for 10 hospital admissions, for example.
Cannabis conspiracy theories
“Unfortunately, this condition has become the subject of great speculation hinging on conspiracy theories as its true cause,” Dr. Russo noted in a September 2021 letter to the editor in the American Journal of Emergency Medicine.
Some “myth busting” is in order, he said.
For example, cannabinoid hyperemesis syndrome does not happen because of exposure to products from a tree called neem or from pesticides applied to marijuana plants during cultivation, Dr. Russo said. It can also occur with high-dose synthetic cannabinoids.
The state of recreational and medical marijuana
Recreational marijuana is legal in 18 states, Washington, D.C., and Guam as of January 2022, according to a report in U.S. News. More states permit medical marijuana use – 37 in total, plus Washington, D.C., according to Britannica ProCon.
One of the states where only medicinal use is legal is Maryland, which is where Dr. Vinocur practices.
“We are seeing increasing numbers of cases” of cannabinoid hyperemesis syndrome, she said.
In addition to chronic use or higher doses, it’s likely that the higher potency levels of THC in the legal marijuana industry trigger the syndrome in some people as well.
Linda estimates she ended up in emergency rooms at least a half-dozen times in the last 5 years. In April 2021, she had a “pretty serious event.” She blames it on traveling a lot for work, not eating right, and not getting enough sleep. She broke her 2-year abstinence with alcohol.
“I basically didn’t listen to my body and paid a pretty significant price for it,” she said.
Linda did not stop altogether but said she “drastically changed the types and form of the cannabis I was using.”
“I can tell you on the record that I would be a hundred percent dead without this plant,” she said.
“The prospect of living without it was more detrimental to me than all of those things I just described to you, because addiction runs in my family and I had opiate problems myself that I overcame with cannabis.”
A version of this article first appeared on Medscape.com.
A third person living with HIV has been cured by transplant
In a first, If she remains off treatment without any hint of HIV, she would be only the third person in the world – after the Berlin Patient and the London Patient – to be cured through a transplant.
“Her own virus could not infect her cells,” said Yvonne Bryson, MD, chief of pediatric infectious diseases at the University of California, Los Angeles, who presented the study at the Conference on Retroviruses and Opportunistic Infections, which both presenters and the audience attended remotely.
The middle-aged New York woman of mixed race, who has asked that her specific race and age not be shared to protect her privacy, was diagnosed with HIV in 2013 when she was still in the very early stages of infection. She started treatment immediately and quickly achieved an undetectable viral load. An undetectable viral load not only prevents someone from transmitting HIV to others but also reduces or eliminates HIV replication, which means fewer variants and less time for the virus to infiltrate cells where it can hide.
But in 2017, she was diagnosed with leukemia. As a last resort to cure her of the cancer, she received a combination of adult stem cells from a relative’s blood that closely matched her own and umbilical cord blood obtained from a cord blood bank. That particular sample of cord blood was selected for its genetic mutation against the CCR5 receptor on immune cells, CD4 T cells. That mutation makes the immune system resistant to HIV.
The two previous HIV cures, of Berlin Patient Timothy Ray Brown and London Patient Adam Castillejo, also used stem cell transplantation with a CCR5 mutation, but theirs were bone marrow transplants. Bone marrow transplants are more arduous than cord blood transplants, which are commonly used in pediatric cancer treatment.
In this case, the physicians treating her used both.
“This allows the adult cells to accelerate and grow up until the cord blood takes over,” said Dr. Bryson. During her presentation, Dr. Bryson pointed to two types of data: First, she presented data showing the level of HIV in the patient’s blood. Soon after HIV diagnosis and treatment, her viral load dropped to undetectable levels. She had a spike of virus when she received the transplant, but then it went back to undetectable and has stayed that way ever since.
Meanwhile, following the transplant, her immune system started rebuilding itself using the new, HIV-resistant cells provided in the transplant. As her care team watched, no graft-versus-host (GVH) disease, a common side effect of stem cell transplants, emerged. In fact, the transplant went so well that she was discharged early from the hospital.
One hundred days after the transplant, the immune system contained within the cord blood had taken over. Her CD4 immune cells returned to normal levels a little more than a year after the transplant. By 27 months, she decided to stop all HIV treatment to see if the transplant had worked.
This was the real test. But as Dr. Bryson and colleagues continued to watch her HIV viral load and her CD4 counts and search for infectious virus, they didn’t find any. She tested negative for HIV by antibody test. Dr. Bryson grew 75 million of her cells in a lab to look for any HIV. None. Aside from one blip in detectable HIV DNA at 14 weeks, researchers never found HIV in the patient again.
“Her cells are resistant to HIV now – both her own strains and laboratory strains,” Dr. Bryson told this news organization. “It’s been 14 months since then. She has no rebound and no detectable virus.”
The presentation drew as raucous as praise gets in a virtual environment. The comments began pouring in.
“Impressive results,” wrote Jim Hoxie, MD, professor emeritus at the University of Pennsylvania, Philadelphia.
“Exciting case,” wrote Allison Agwu, MD, a professor of pediatrics at Johns Hopkins University, Baltimore.
And Dennis Copertino, a research specialist at Weill Cornell Medicine, New York, wrote: “Thank you so much for translating this important cure strategy to people of color.”
Most donors with CCR5 mutations are White, Dr. Bryson said, suggesting that this approach, in a mixed-race woman, could expand the pool of people living with HIV and cancer who are good candidates for the approach.
But other observers had questions, ones that may require more research to answer. Some asked why this woman’s virus, after transplantation, wasn’t just immune to viruses with CCR5 but also another variant, called CXCR4, that one wouldn’t expect. Luis Montaner, DVM, director of the Immunopathogenesis Laboratory at the Wistar Institute in Philadelphia, wondered whether it was more than the blood that had cleared HIV. Did it get into the tissue, too? That question has not yet been answered.
For Carl Dieffenbach, PhD, director of the division of AIDS at the National Institute of Allergy and Infectious Diseases, the lack of GVH disease was a powerful and hopeful finding.
“There’s been this ongoing hypothesis that maybe graft-versus-host disease was needed at some level to help clear out every last single CD4+ T cell that may or may not have been harboring replication-competent virus,” Dr. Dieffenbach said in an interview. “But there was no GVH disease. That’s incredible. It’s a wonderful thing.”
Now the challenge is to move from a single case to making cure available to other people living with HIV.
The case also got cure researchers thinking.
Dr. Montaner called the case “an encouraging roadmap supporting anti-CCR5 strategies by CRISPR Cas9,” studies that are now underway.
Steven Deeks, MD, called the case “perhaps a model for how we might do this using a person’s own cells. Because we were never really going to be transplanting cells from another person as a scalable cure.”
For people living with HIV, particularly women of color, the results raise hopes and questions. Nina Martinez knows something about being a “first.” In 2019, she was the first American woman of color living with HIV to donate a kidney to another person living with the virus. To her, the excitement over the first woman of color being cured of HIV just shines a light on how very White and male HIV cure studies have been until now.
“For me, I’m not looking for a cure in which the successful step forward is me getting cancer,” she said in an interview. “I’m looking at, what’s going to be sustainable? I want to know what’s going to work for a group of people.”
Gina Marie Brown, a social worker living with HIV in New Orleans, is also thinking of groups of people.
“Every time we get a breakthrough, it’s like the sun is taken from behind the clouds a little more,” said Ms. Brown. “I think about people in the South, who bear a huge burden of HIV. I think about trans women. I think about Black women, and gay, bisexual, and same-gender-loving men. This could really impact HIV – in the same way that PrEP [pre-exposure prophylaxis] has, the same way that one pill once a day has.”
When Ms. Brown was diagnosed with HIV 22 years ago, she started to plan her funeral.
“That’s how much I thought HIV was a death sentence,” she told this news organization. “Oh my goodness! Glad you stuck around, Gina.”
The study was funded by the National Institutes of Health. Dr. Bryson, Dr. Dieffenbach, Dr. Deeks, and Dr. Montaner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a first, If she remains off treatment without any hint of HIV, she would be only the third person in the world – after the Berlin Patient and the London Patient – to be cured through a transplant.
“Her own virus could not infect her cells,” said Yvonne Bryson, MD, chief of pediatric infectious diseases at the University of California, Los Angeles, who presented the study at the Conference on Retroviruses and Opportunistic Infections, which both presenters and the audience attended remotely.
The middle-aged New York woman of mixed race, who has asked that her specific race and age not be shared to protect her privacy, was diagnosed with HIV in 2013 when she was still in the very early stages of infection. She started treatment immediately and quickly achieved an undetectable viral load. An undetectable viral load not only prevents someone from transmitting HIV to others but also reduces or eliminates HIV replication, which means fewer variants and less time for the virus to infiltrate cells where it can hide.
But in 2017, she was diagnosed with leukemia. As a last resort to cure her of the cancer, she received a combination of adult stem cells from a relative’s blood that closely matched her own and umbilical cord blood obtained from a cord blood bank. That particular sample of cord blood was selected for its genetic mutation against the CCR5 receptor on immune cells, CD4 T cells. That mutation makes the immune system resistant to HIV.
The two previous HIV cures, of Berlin Patient Timothy Ray Brown and London Patient Adam Castillejo, also used stem cell transplantation with a CCR5 mutation, but theirs were bone marrow transplants. Bone marrow transplants are more arduous than cord blood transplants, which are commonly used in pediatric cancer treatment.
In this case, the physicians treating her used both.
“This allows the adult cells to accelerate and grow up until the cord blood takes over,” said Dr. Bryson. During her presentation, Dr. Bryson pointed to two types of data: First, she presented data showing the level of HIV in the patient’s blood. Soon after HIV diagnosis and treatment, her viral load dropped to undetectable levels. She had a spike of virus when she received the transplant, but then it went back to undetectable and has stayed that way ever since.
Meanwhile, following the transplant, her immune system started rebuilding itself using the new, HIV-resistant cells provided in the transplant. As her care team watched, no graft-versus-host (GVH) disease, a common side effect of stem cell transplants, emerged. In fact, the transplant went so well that she was discharged early from the hospital.
One hundred days after the transplant, the immune system contained within the cord blood had taken over. Her CD4 immune cells returned to normal levels a little more than a year after the transplant. By 27 months, she decided to stop all HIV treatment to see if the transplant had worked.
This was the real test. But as Dr. Bryson and colleagues continued to watch her HIV viral load and her CD4 counts and search for infectious virus, they didn’t find any. She tested negative for HIV by antibody test. Dr. Bryson grew 75 million of her cells in a lab to look for any HIV. None. Aside from one blip in detectable HIV DNA at 14 weeks, researchers never found HIV in the patient again.
“Her cells are resistant to HIV now – both her own strains and laboratory strains,” Dr. Bryson told this news organization. “It’s been 14 months since then. She has no rebound and no detectable virus.”
The presentation drew as raucous as praise gets in a virtual environment. The comments began pouring in.
“Impressive results,” wrote Jim Hoxie, MD, professor emeritus at the University of Pennsylvania, Philadelphia.
“Exciting case,” wrote Allison Agwu, MD, a professor of pediatrics at Johns Hopkins University, Baltimore.
And Dennis Copertino, a research specialist at Weill Cornell Medicine, New York, wrote: “Thank you so much for translating this important cure strategy to people of color.”
Most donors with CCR5 mutations are White, Dr. Bryson said, suggesting that this approach, in a mixed-race woman, could expand the pool of people living with HIV and cancer who are good candidates for the approach.
But other observers had questions, ones that may require more research to answer. Some asked why this woman’s virus, after transplantation, wasn’t just immune to viruses with CCR5 but also another variant, called CXCR4, that one wouldn’t expect. Luis Montaner, DVM, director of the Immunopathogenesis Laboratory at the Wistar Institute in Philadelphia, wondered whether it was more than the blood that had cleared HIV. Did it get into the tissue, too? That question has not yet been answered.
For Carl Dieffenbach, PhD, director of the division of AIDS at the National Institute of Allergy and Infectious Diseases, the lack of GVH disease was a powerful and hopeful finding.
“There’s been this ongoing hypothesis that maybe graft-versus-host disease was needed at some level to help clear out every last single CD4+ T cell that may or may not have been harboring replication-competent virus,” Dr. Dieffenbach said in an interview. “But there was no GVH disease. That’s incredible. It’s a wonderful thing.”
Now the challenge is to move from a single case to making cure available to other people living with HIV.
The case also got cure researchers thinking.
Dr. Montaner called the case “an encouraging roadmap supporting anti-CCR5 strategies by CRISPR Cas9,” studies that are now underway.
Steven Deeks, MD, called the case “perhaps a model for how we might do this using a person’s own cells. Because we were never really going to be transplanting cells from another person as a scalable cure.”
For people living with HIV, particularly women of color, the results raise hopes and questions. Nina Martinez knows something about being a “first.” In 2019, she was the first American woman of color living with HIV to donate a kidney to another person living with the virus. To her, the excitement over the first woman of color being cured of HIV just shines a light on how very White and male HIV cure studies have been until now.
“For me, I’m not looking for a cure in which the successful step forward is me getting cancer,” she said in an interview. “I’m looking at, what’s going to be sustainable? I want to know what’s going to work for a group of people.”
Gina Marie Brown, a social worker living with HIV in New Orleans, is also thinking of groups of people.
“Every time we get a breakthrough, it’s like the sun is taken from behind the clouds a little more,” said Ms. Brown. “I think about people in the South, who bear a huge burden of HIV. I think about trans women. I think about Black women, and gay, bisexual, and same-gender-loving men. This could really impact HIV – in the same way that PrEP [pre-exposure prophylaxis] has, the same way that one pill once a day has.”
When Ms. Brown was diagnosed with HIV 22 years ago, she started to plan her funeral.
“That’s how much I thought HIV was a death sentence,” she told this news organization. “Oh my goodness! Glad you stuck around, Gina.”
The study was funded by the National Institutes of Health. Dr. Bryson, Dr. Dieffenbach, Dr. Deeks, and Dr. Montaner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a first, If she remains off treatment without any hint of HIV, she would be only the third person in the world – after the Berlin Patient and the London Patient – to be cured through a transplant.
“Her own virus could not infect her cells,” said Yvonne Bryson, MD, chief of pediatric infectious diseases at the University of California, Los Angeles, who presented the study at the Conference on Retroviruses and Opportunistic Infections, which both presenters and the audience attended remotely.
The middle-aged New York woman of mixed race, who has asked that her specific race and age not be shared to protect her privacy, was diagnosed with HIV in 2013 when she was still in the very early stages of infection. She started treatment immediately and quickly achieved an undetectable viral load. An undetectable viral load not only prevents someone from transmitting HIV to others but also reduces or eliminates HIV replication, which means fewer variants and less time for the virus to infiltrate cells where it can hide.
But in 2017, she was diagnosed with leukemia. As a last resort to cure her of the cancer, she received a combination of adult stem cells from a relative’s blood that closely matched her own and umbilical cord blood obtained from a cord blood bank. That particular sample of cord blood was selected for its genetic mutation against the CCR5 receptor on immune cells, CD4 T cells. That mutation makes the immune system resistant to HIV.
The two previous HIV cures, of Berlin Patient Timothy Ray Brown and London Patient Adam Castillejo, also used stem cell transplantation with a CCR5 mutation, but theirs were bone marrow transplants. Bone marrow transplants are more arduous than cord blood transplants, which are commonly used in pediatric cancer treatment.
In this case, the physicians treating her used both.
“This allows the adult cells to accelerate and grow up until the cord blood takes over,” said Dr. Bryson. During her presentation, Dr. Bryson pointed to two types of data: First, she presented data showing the level of HIV in the patient’s blood. Soon after HIV diagnosis and treatment, her viral load dropped to undetectable levels. She had a spike of virus when she received the transplant, but then it went back to undetectable and has stayed that way ever since.
Meanwhile, following the transplant, her immune system started rebuilding itself using the new, HIV-resistant cells provided in the transplant. As her care team watched, no graft-versus-host (GVH) disease, a common side effect of stem cell transplants, emerged. In fact, the transplant went so well that she was discharged early from the hospital.
One hundred days after the transplant, the immune system contained within the cord blood had taken over. Her CD4 immune cells returned to normal levels a little more than a year after the transplant. By 27 months, she decided to stop all HIV treatment to see if the transplant had worked.
This was the real test. But as Dr. Bryson and colleagues continued to watch her HIV viral load and her CD4 counts and search for infectious virus, they didn’t find any. She tested negative for HIV by antibody test. Dr. Bryson grew 75 million of her cells in a lab to look for any HIV. None. Aside from one blip in detectable HIV DNA at 14 weeks, researchers never found HIV in the patient again.
“Her cells are resistant to HIV now – both her own strains and laboratory strains,” Dr. Bryson told this news organization. “It’s been 14 months since then. She has no rebound and no detectable virus.”
The presentation drew as raucous as praise gets in a virtual environment. The comments began pouring in.
“Impressive results,” wrote Jim Hoxie, MD, professor emeritus at the University of Pennsylvania, Philadelphia.
“Exciting case,” wrote Allison Agwu, MD, a professor of pediatrics at Johns Hopkins University, Baltimore.
And Dennis Copertino, a research specialist at Weill Cornell Medicine, New York, wrote: “Thank you so much for translating this important cure strategy to people of color.”
Most donors with CCR5 mutations are White, Dr. Bryson said, suggesting that this approach, in a mixed-race woman, could expand the pool of people living with HIV and cancer who are good candidates for the approach.
But other observers had questions, ones that may require more research to answer. Some asked why this woman’s virus, after transplantation, wasn’t just immune to viruses with CCR5 but also another variant, called CXCR4, that one wouldn’t expect. Luis Montaner, DVM, director of the Immunopathogenesis Laboratory at the Wistar Institute in Philadelphia, wondered whether it was more than the blood that had cleared HIV. Did it get into the tissue, too? That question has not yet been answered.
For Carl Dieffenbach, PhD, director of the division of AIDS at the National Institute of Allergy and Infectious Diseases, the lack of GVH disease was a powerful and hopeful finding.
“There’s been this ongoing hypothesis that maybe graft-versus-host disease was needed at some level to help clear out every last single CD4+ T cell that may or may not have been harboring replication-competent virus,” Dr. Dieffenbach said in an interview. “But there was no GVH disease. That’s incredible. It’s a wonderful thing.”
Now the challenge is to move from a single case to making cure available to other people living with HIV.
The case also got cure researchers thinking.
Dr. Montaner called the case “an encouraging roadmap supporting anti-CCR5 strategies by CRISPR Cas9,” studies that are now underway.
Steven Deeks, MD, called the case “perhaps a model for how we might do this using a person’s own cells. Because we were never really going to be transplanting cells from another person as a scalable cure.”
For people living with HIV, particularly women of color, the results raise hopes and questions. Nina Martinez knows something about being a “first.” In 2019, she was the first American woman of color living with HIV to donate a kidney to another person living with the virus. To her, the excitement over the first woman of color being cured of HIV just shines a light on how very White and male HIV cure studies have been until now.
“For me, I’m not looking for a cure in which the successful step forward is me getting cancer,” she said in an interview. “I’m looking at, what’s going to be sustainable? I want to know what’s going to work for a group of people.”
Gina Marie Brown, a social worker living with HIV in New Orleans, is also thinking of groups of people.
“Every time we get a breakthrough, it’s like the sun is taken from behind the clouds a little more,” said Ms. Brown. “I think about people in the South, who bear a huge burden of HIV. I think about trans women. I think about Black women, and gay, bisexual, and same-gender-loving men. This could really impact HIV – in the same way that PrEP [pre-exposure prophylaxis] has, the same way that one pill once a day has.”
When Ms. Brown was diagnosed with HIV 22 years ago, she started to plan her funeral.
“That’s how much I thought HIV was a death sentence,” she told this news organization. “Oh my goodness! Glad you stuck around, Gina.”
The study was funded by the National Institutes of Health. Dr. Bryson, Dr. Dieffenbach, Dr. Deeks, and Dr. Montaner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CROI 2022
Blind optimism only works in fantasy football. Time to get realistic
In the age of COVID, what exactly does it mean to be optimistic? I get this question quite a bit from virtually everyone I meet in one form or another through my work with the George Washington Resiliency and Well-Being Center in Washington, D.C. Giving a lecture on resilience and staying positive can be a significant challenge. Especially when we wake up to the news that 1 of every 100 older Americans has died secondary to COVID. The mind doesn’t really know how to process this type of loss. It is hard to maintain any form of a positive attitude when you’re still struggling just to accept the magnitude of what humanity has experienced over the past 2 years.

In “Resilience: The Science of Mastering Life’s Greatest Challenges,” (Cambridge, England: Cambridge University Press, 2018), Steven M. Southwick, MD, and Dennis S. Charney, MD, identify 10 critical factors associated with very resilient individuals. The authors based their work on science, personal experience, and interviews of people who have literally been through hell and back. One of the critical factors they identified is optimism.
“Optimism ignites resilience, providing energy to power the other resilience factors. It facilitates an active and creative approach to coping with challenging situations.”
Dr. Southwick and Dr. Charney are a lot smarter than me and far more patient to weave all this data together into a coherent story about optimism. Sounds like a damn good factor to focus a lecture on in my book! Slight problem: In my experience, many health professionals are already expert optimists. They literally eat, sleep, and sincerely breathe this stuff. So if we are going to talk about optimism, then we need to discuss realistic optimism.
How does realistic optimism differ from, say, blind optimism? Dr. Southwick and Dr. Charney’s review of the literature points to three features worthy of highlighting.
Realistic vs. blind optimism: Take-home points
- In realistic optimism, we notice the negative but don’t stay engaged with it. Realistic optimists moved on from problems that were not solvable.
- Blind optimism can lead to underestimating risk, overestimating abilities, and inadequate preparation.
Growing up in northeast Ohio, I can absolutely embrace the concept of realistic optimism. It’s overcast in Cleveland 8 months out of the year. To hope for 3 sunny days in a row in April is genuinely a fools’ errand. So you learn over time, the sun will shine; you just have to at times wait 3-4 months for it to occur.
From a skill perspective, realistic optimism could be conceptualized as a great mix of radical acceptance, emotion regulation, and focused problem solving. This is all fine, but to be realistically optimistic, we must first stop wishing for a better tomorrow. You may say, I don’t wish for or see rainbows and unicorns, et cetera, et cetera. Okay, so you don’t verbalize your wishes, but on a small level, you may engage in wishful thinking. Here are a few wishful thoughts that I would daydream about, which were not realistically optimistic at various points:
- “Once we get enough COVID-19 tests, things will improve.”
- “All we need to do is get vaccines, and then the new normal is right there.”
- “Once everyone gets the booster, then we got this thing beat.”
At this point, you could argue that I was engaged in blind optimism. I consider the above statements blind for a couple of reasons. They weren’t balanced (both positive and negative), didn’t have a clear definition of the outcome, and were more focused on external events I couldn’t control. These statements were the equivalent of wishes, and I don’t have a magic lamp with a genie, so I need to let go of my wishful thinking first. Let me rephrase that: I need to forcefully toss it into the sea of COVID variants and start figuring out how I’m going to tread water for another 6-12 months. So with this in mind, here are my initial thoughts on ways to navigate the next year of the pandemic:
- A multilayered form of protection gives me the best chance to survive the next 6 months of the pandemic.
- It will take time, but I’ll process the loss associated with a workplace that will never be the same.
- Until we have positivity test rates lower than 2% across the globe, COVID will remain a substantial disruption to humanity.
- I can’t bring back missed graduation or the first day of school, but I can share ways that I’ve countered and survived loneliness in my life with my children.
Okay, this is the starting point – hopefully not pessimistic, or blindly optimistic, just realistic. Now I can address other important topics, such as planning to rebuild my disappointing fantasy football team. I was No. 1 in our GW department of psychiatry fantasy football league until my star running back Derrick Henry went down. My residents will become attendings and still give me grief about this for many years to follow, and that is a very good thing.
Everyone be well and safe.
Dr. Norris is associate dean of student affairs; associate professor, department of psychiatry, George Washington University; chief wellness officer, GW Hospital, GW Medical Faculty Associates, and the GW School of Medicine and Health Sciences (GWU Medical Enterprise), Washington. He has disclosed having no relevant financial relationships. A version of this article first appeared on Medscape.com.
In the age of COVID, what exactly does it mean to be optimistic? I get this question quite a bit from virtually everyone I meet in one form or another through my work with the George Washington Resiliency and Well-Being Center in Washington, D.C. Giving a lecture on resilience and staying positive can be a significant challenge. Especially when we wake up to the news that 1 of every 100 older Americans has died secondary to COVID. The mind doesn’t really know how to process this type of loss. It is hard to maintain any form of a positive attitude when you’re still struggling just to accept the magnitude of what humanity has experienced over the past 2 years.
In “Resilience: The Science of Mastering Life’s Greatest Challenges,” (Cambridge, England: Cambridge University Press, 2018), Steven M. Southwick, MD, and Dennis S. Charney, MD, identify 10 critical factors associated with very resilient individuals. The authors based their work on science, personal experience, and interviews of people who have literally been through hell and back. One of the critical factors they identified is optimism.
“Optimism ignites resilience, providing energy to power the other resilience factors. It facilitates an active and creative approach to coping with challenging situations.”
Dr. Southwick and Dr. Charney are a lot smarter than me and far more patient to weave all this data together into a coherent story about optimism. Sounds like a damn good factor to focus a lecture on in my book! Slight problem: In my experience, many health professionals are already expert optimists. They literally eat, sleep, and sincerely breathe this stuff. So if we are going to talk about optimism, then we need to discuss realistic optimism.
How does realistic optimism differ from, say, blind optimism? Dr. Southwick and Dr. Charney’s review of the literature points to three features worthy of highlighting.
Realistic vs. blind optimism: Take-home points
- In realistic optimism, we notice the negative but don’t stay engaged with it. Realistic optimists moved on from problems that were not solvable.
- Blind optimism can lead to underestimating risk, overestimating abilities, and inadequate preparation.
Growing up in northeast Ohio, I can absolutely embrace the concept of realistic optimism. It’s overcast in Cleveland 8 months out of the year. To hope for 3 sunny days in a row in April is genuinely a fools’ errand. So you learn over time, the sun will shine; you just have to at times wait 3-4 months for it to occur.
From a skill perspective, realistic optimism could be conceptualized as a great mix of radical acceptance, emotion regulation, and focused problem solving. This is all fine, but to be realistically optimistic, we must first stop wishing for a better tomorrow. You may say, I don’t wish for or see rainbows and unicorns, et cetera, et cetera. Okay, so you don’t verbalize your wishes, but on a small level, you may engage in wishful thinking. Here are a few wishful thoughts that I would daydream about, which were not realistically optimistic at various points:
- “Once we get enough COVID-19 tests, things will improve.”
- “All we need to do is get vaccines, and then the new normal is right there.”
- “Once everyone gets the booster, then we got this thing beat.”
At this point, you could argue that I was engaged in blind optimism. I consider the above statements blind for a couple of reasons. They weren’t balanced (both positive and negative), didn’t have a clear definition of the outcome, and were more focused on external events I couldn’t control. These statements were the equivalent of wishes, and I don’t have a magic lamp with a genie, so I need to let go of my wishful thinking first. Let me rephrase that: I need to forcefully toss it into the sea of COVID variants and start figuring out how I’m going to tread water for another 6-12 months. So with this in mind, here are my initial thoughts on ways to navigate the next year of the pandemic:
- A multilayered form of protection gives me the best chance to survive the next 6 months of the pandemic.
- It will take time, but I’ll process the loss associated with a workplace that will never be the same.
- Until we have positivity test rates lower than 2% across the globe, COVID will remain a substantial disruption to humanity.
- I can’t bring back missed graduation or the first day of school, but I can share ways that I’ve countered and survived loneliness in my life with my children.
Okay, this is the starting point – hopefully not pessimistic, or blindly optimistic, just realistic. Now I can address other important topics, such as planning to rebuild my disappointing fantasy football team. I was No. 1 in our GW department of psychiatry fantasy football league until my star running back Derrick Henry went down. My residents will become attendings and still give me grief about this for many years to follow, and that is a very good thing.
Everyone be well and safe.
Dr. Norris is associate dean of student affairs; associate professor, department of psychiatry, George Washington University; chief wellness officer, GW Hospital, GW Medical Faculty Associates, and the GW School of Medicine and Health Sciences (GWU Medical Enterprise), Washington. He has disclosed having no relevant financial relationships. A version of this article first appeared on Medscape.com.
In the age of COVID, what exactly does it mean to be optimistic? I get this question quite a bit from virtually everyone I meet in one form or another through my work with the George Washington Resiliency and Well-Being Center in Washington, D.C. Giving a lecture on resilience and staying positive can be a significant challenge. Especially when we wake up to the news that 1 of every 100 older Americans has died secondary to COVID. The mind doesn’t really know how to process this type of loss. It is hard to maintain any form of a positive attitude when you’re still struggling just to accept the magnitude of what humanity has experienced over the past 2 years.
In “Resilience: The Science of Mastering Life’s Greatest Challenges,” (Cambridge, England: Cambridge University Press, 2018), Steven M. Southwick, MD, and Dennis S. Charney, MD, identify 10 critical factors associated with very resilient individuals. The authors based their work on science, personal experience, and interviews of people who have literally been through hell and back. One of the critical factors they identified is optimism.
“Optimism ignites resilience, providing energy to power the other resilience factors. It facilitates an active and creative approach to coping with challenging situations.”
Dr. Southwick and Dr. Charney are a lot smarter than me and far more patient to weave all this data together into a coherent story about optimism. Sounds like a damn good factor to focus a lecture on in my book! Slight problem: In my experience, many health professionals are already expert optimists. They literally eat, sleep, and sincerely breathe this stuff. So if we are going to talk about optimism, then we need to discuss realistic optimism.
How does realistic optimism differ from, say, blind optimism? Dr. Southwick and Dr. Charney’s review of the literature points to three features worthy of highlighting.
Realistic vs. blind optimism: Take-home points
- In realistic optimism, we notice the negative but don’t stay engaged with it. Realistic optimists moved on from problems that were not solvable.
- Blind optimism can lead to underestimating risk, overestimating abilities, and inadequate preparation.
Growing up in northeast Ohio, I can absolutely embrace the concept of realistic optimism. It’s overcast in Cleveland 8 months out of the year. To hope for 3 sunny days in a row in April is genuinely a fools’ errand. So you learn over time, the sun will shine; you just have to at times wait 3-4 months for it to occur.
From a skill perspective, realistic optimism could be conceptualized as a great mix of radical acceptance, emotion regulation, and focused problem solving. This is all fine, but to be realistically optimistic, we must first stop wishing for a better tomorrow. You may say, I don’t wish for or see rainbows and unicorns, et cetera, et cetera. Okay, so you don’t verbalize your wishes, but on a small level, you may engage in wishful thinking. Here are a few wishful thoughts that I would daydream about, which were not realistically optimistic at various points:
- “Once we get enough COVID-19 tests, things will improve.”
- “All we need to do is get vaccines, and then the new normal is right there.”
- “Once everyone gets the booster, then we got this thing beat.”
At this point, you could argue that I was engaged in blind optimism. I consider the above statements blind for a couple of reasons. They weren’t balanced (both positive and negative), didn’t have a clear definition of the outcome, and were more focused on external events I couldn’t control. These statements were the equivalent of wishes, and I don’t have a magic lamp with a genie, so I need to let go of my wishful thinking first. Let me rephrase that: I need to forcefully toss it into the sea of COVID variants and start figuring out how I’m going to tread water for another 6-12 months. So with this in mind, here are my initial thoughts on ways to navigate the next year of the pandemic:
- A multilayered form of protection gives me the best chance to survive the next 6 months of the pandemic.
- It will take time, but I’ll process the loss associated with a workplace that will never be the same.
- Until we have positivity test rates lower than 2% across the globe, COVID will remain a substantial disruption to humanity.
- I can’t bring back missed graduation or the first day of school, but I can share ways that I’ve countered and survived loneliness in my life with my children.
Okay, this is the starting point – hopefully not pessimistic, or blindly optimistic, just realistic. Now I can address other important topics, such as planning to rebuild my disappointing fantasy football team. I was No. 1 in our GW department of psychiatry fantasy football league until my star running back Derrick Henry went down. My residents will become attendings and still give me grief about this for many years to follow, and that is a very good thing.
Everyone be well and safe.
Dr. Norris is associate dean of student affairs; associate professor, department of psychiatry, George Washington University; chief wellness officer, GW Hospital, GW Medical Faculty Associates, and the GW School of Medicine and Health Sciences (GWU Medical Enterprise), Washington. He has disclosed having no relevant financial relationships. A version of this article first appeared on Medscape.com.
Derms in survey say climate change is impacting their patients
in which the majority of participants said their patients are already being impacted.
Almost 80% of the 148 participants who responded to an electronic survey reported this belief.

The survey was designed and distributed to the membership of various dermatological organizations by Misha Rosenbach, MD, and coauthors. The results were published in the British Journal of Dermatology.
Asked also about specific types of climate-driven phenomena with a current – or future – impact on their patients, 80.1% reported that they believed that increased exposure to ultraviolet radiation (UVR) is impactful, or will be. Changes in temporal or geographic patterns of vector-borne illnesses were affirmed by 78.7%, and an increase in social displacement caused by extreme weather or other events was affirmed by 67.1% as having an impact on their patients currently or in the future.
Other phenomena affirmed by respondents as already having an impact or impacting patients in the future were an increased incidence of heat exposure or heat-related illness (58.2%); an increase in rates of inflammatory skin disease flares (43.2%); increased incidence of waterborne infections (42.5%); and increased rates of allergic contact dermatitis (29.5%).
The survey was sent to the membership of the American Society of Dermatologic Surgery, the Society for Pediatric Dermatology, the Society for Investigative Dermatology, and the American Academy of Dermatology’s Climate Change Expert Resource Group (ERG), among other organizations.
The study design and membership overlap made it impossible to calculate a response rate, the authors said, but they estimated it to be about 10%.
Almost all respondents were from the United States, and most (86.3%) practiced in an academic setting. The findings are similar to those of an online survey of members of the International Society of Dermatology (ISD), published in 2020, which found that 89% of 158 respondents believed climate change will impact the incidence of skin diseases in their area.
“Physicians, including dermatologists, are starting to understand the impact of the climate crisis on both their patients and themselves ... both through lived experiences and [issues raised] more in the scientific literature and in meetings,” Dr. Rosenbach, associate professor of dermatology at the University of Pennsylvania, Philadelphia, said in an interview.
A majority of participants in the U.S. survey agreed they have a responsibility to bring awareness of the health effects of climate change to patients (77.2%) and to policymakers (88.6%). (In the ISD survey, 88% said they believed that dermatologists should play an advocacy role in climate change-related issues).
Only a minority of respondents in the U.S. survey said that they would feel comfortable discussing climate change with their patients (37.2%). Almost one-third of the respondents said they would like to be better informed about climate change before doing so. And 81.8% said they would like to read more about the dermatological effects of climate change in scientific journals.
“There continues to be unfilled interest in education and advocacy regarding climate change, suggesting a ‘practice gap’ even among dermatologists,” Dr. Rosenbach and his colleagues wrote, noting opportunities for professional organizations and journals to provide more resources and “actionable items” regarding climate change.
Some dermatologists have been taking action, in the meantime, to reduce the carbon footprint of their practices and institutions. Reductions in facility energy consumption, and reductions in medical waste/optimization of recycling, were each reported by more than one-third of survey respondents.
And almost half indicated that their practice or institution had increased capacity for telemedicine or telecommuting in response to climate change. Only 8% said their practice or institution had divested from fossil fuel stocks and/or bonds.
“There are a lot of sustainability-in-medicine solutions that are actually cost-neutral or cost-saving for practices,” said Dr. Rosenbach, who is a founder and co-chair of the AAD’s ERG on Climate Change and Environmental Issues.
Research in dermatology is starting to quantify the environmental impact of some of these changes. In a research letter also published in the British Journal of Dermatology, researchers from Cardiff University and the department of dermatology at University Hospital of Wales, described how they determined that reusable surgical packs used for skin surgery are more sustainable than single-use packs because of their reduced cost and reduced greenhouse gas emissions.
Such single-site reports are “early feeders” into what will become a stream of larger studies quantifying the impact of measures taken in dermatology, Dr. Rosenbach said.
Across medicine, there is evidence that health care professionals are now seeing climate change as a threat to their patients. In a multinational survey published last year in The Lancet Planetary Health, 77% of 3,977 participants said that climate change will cause a moderate or great deal of harm for their patients.
Climate change will be discussed at the AAD’s annual meeting in late March in a session devoted to the topic, and as part of a broader session on controversies in dermatology.
Dr. Rosenbach and two of the five authors of the dermatology research letter are members of the AAD’s ERG on climate change, but in the publication they noted that they were not writing on behalf of the AAD. None of the authors reported any disclosures, and there was no funding source for the survey.
in which the majority of participants said their patients are already being impacted.
Almost 80% of the 148 participants who responded to an electronic survey reported this belief.
The survey was designed and distributed to the membership of various dermatological organizations by Misha Rosenbach, MD, and coauthors. The results were published in the British Journal of Dermatology.
Asked also about specific types of climate-driven phenomena with a current – or future – impact on their patients, 80.1% reported that they believed that increased exposure to ultraviolet radiation (UVR) is impactful, or will be. Changes in temporal or geographic patterns of vector-borne illnesses were affirmed by 78.7%, and an increase in social displacement caused by extreme weather or other events was affirmed by 67.1% as having an impact on their patients currently or in the future.
Other phenomena affirmed by respondents as already having an impact or impacting patients in the future were an increased incidence of heat exposure or heat-related illness (58.2%); an increase in rates of inflammatory skin disease flares (43.2%); increased incidence of waterborne infections (42.5%); and increased rates of allergic contact dermatitis (29.5%).
The survey was sent to the membership of the American Society of Dermatologic Surgery, the Society for Pediatric Dermatology, the Society for Investigative Dermatology, and the American Academy of Dermatology’s Climate Change Expert Resource Group (ERG), among other organizations.
The study design and membership overlap made it impossible to calculate a response rate, the authors said, but they estimated it to be about 10%.
Almost all respondents were from the United States, and most (86.3%) practiced in an academic setting. The findings are similar to those of an online survey of members of the International Society of Dermatology (ISD), published in 2020, which found that 89% of 158 respondents believed climate change will impact the incidence of skin diseases in their area.
“Physicians, including dermatologists, are starting to understand the impact of the climate crisis on both their patients and themselves ... both through lived experiences and [issues raised] more in the scientific literature and in meetings,” Dr. Rosenbach, associate professor of dermatology at the University of Pennsylvania, Philadelphia, said in an interview.
A majority of participants in the U.S. survey agreed they have a responsibility to bring awareness of the health effects of climate change to patients (77.2%) and to policymakers (88.6%). (In the ISD survey, 88% said they believed that dermatologists should play an advocacy role in climate change-related issues).
Only a minority of respondents in the U.S. survey said that they would feel comfortable discussing climate change with their patients (37.2%). Almost one-third of the respondents said they would like to be better informed about climate change before doing so. And 81.8% said they would like to read more about the dermatological effects of climate change in scientific journals.
“There continues to be unfilled interest in education and advocacy regarding climate change, suggesting a ‘practice gap’ even among dermatologists,” Dr. Rosenbach and his colleagues wrote, noting opportunities for professional organizations and journals to provide more resources and “actionable items” regarding climate change.
Some dermatologists have been taking action, in the meantime, to reduce the carbon footprint of their practices and institutions. Reductions in facility energy consumption, and reductions in medical waste/optimization of recycling, were each reported by more than one-third of survey respondents.
And almost half indicated that their practice or institution had increased capacity for telemedicine or telecommuting in response to climate change. Only 8% said their practice or institution had divested from fossil fuel stocks and/or bonds.
“There are a lot of sustainability-in-medicine solutions that are actually cost-neutral or cost-saving for practices,” said Dr. Rosenbach, who is a founder and co-chair of the AAD’s ERG on Climate Change and Environmental Issues.
Research in dermatology is starting to quantify the environmental impact of some of these changes. In a research letter also published in the British Journal of Dermatology, researchers from Cardiff University and the department of dermatology at University Hospital of Wales, described how they determined that reusable surgical packs used for skin surgery are more sustainable than single-use packs because of their reduced cost and reduced greenhouse gas emissions.
Such single-site reports are “early feeders” into what will become a stream of larger studies quantifying the impact of measures taken in dermatology, Dr. Rosenbach said.
Across medicine, there is evidence that health care professionals are now seeing climate change as a threat to their patients. In a multinational survey published last year in The Lancet Planetary Health, 77% of 3,977 participants said that climate change will cause a moderate or great deal of harm for their patients.
Climate change will be discussed at the AAD’s annual meeting in late March in a session devoted to the topic, and as part of a broader session on controversies in dermatology.
Dr. Rosenbach and two of the five authors of the dermatology research letter are members of the AAD’s ERG on climate change, but in the publication they noted that they were not writing on behalf of the AAD. None of the authors reported any disclosures, and there was no funding source for the survey.
in which the majority of participants said their patients are already being impacted.
Almost 80% of the 148 participants who responded to an electronic survey reported this belief.
The survey was designed and distributed to the membership of various dermatological organizations by Misha Rosenbach, MD, and coauthors. The results were published in the British Journal of Dermatology.
Asked also about specific types of climate-driven phenomena with a current – or future – impact on their patients, 80.1% reported that they believed that increased exposure to ultraviolet radiation (UVR) is impactful, or will be. Changes in temporal or geographic patterns of vector-borne illnesses were affirmed by 78.7%, and an increase in social displacement caused by extreme weather or other events was affirmed by 67.1% as having an impact on their patients currently or in the future.
Other phenomena affirmed by respondents as already having an impact or impacting patients in the future were an increased incidence of heat exposure or heat-related illness (58.2%); an increase in rates of inflammatory skin disease flares (43.2%); increased incidence of waterborne infections (42.5%); and increased rates of allergic contact dermatitis (29.5%).
The survey was sent to the membership of the American Society of Dermatologic Surgery, the Society for Pediatric Dermatology, the Society for Investigative Dermatology, and the American Academy of Dermatology’s Climate Change Expert Resource Group (ERG), among other organizations.
The study design and membership overlap made it impossible to calculate a response rate, the authors said, but they estimated it to be about 10%.
Almost all respondents were from the United States, and most (86.3%) practiced in an academic setting. The findings are similar to those of an online survey of members of the International Society of Dermatology (ISD), published in 2020, which found that 89% of 158 respondents believed climate change will impact the incidence of skin diseases in their area.
“Physicians, including dermatologists, are starting to understand the impact of the climate crisis on both their patients and themselves ... both through lived experiences and [issues raised] more in the scientific literature and in meetings,” Dr. Rosenbach, associate professor of dermatology at the University of Pennsylvania, Philadelphia, said in an interview.
A majority of participants in the U.S. survey agreed they have a responsibility to bring awareness of the health effects of climate change to patients (77.2%) and to policymakers (88.6%). (In the ISD survey, 88% said they believed that dermatologists should play an advocacy role in climate change-related issues).
Only a minority of respondents in the U.S. survey said that they would feel comfortable discussing climate change with their patients (37.2%). Almost one-third of the respondents said they would like to be better informed about climate change before doing so. And 81.8% said they would like to read more about the dermatological effects of climate change in scientific journals.
“There continues to be unfilled interest in education and advocacy regarding climate change, suggesting a ‘practice gap’ even among dermatologists,” Dr. Rosenbach and his colleagues wrote, noting opportunities for professional organizations and journals to provide more resources and “actionable items” regarding climate change.
Some dermatologists have been taking action, in the meantime, to reduce the carbon footprint of their practices and institutions. Reductions in facility energy consumption, and reductions in medical waste/optimization of recycling, were each reported by more than one-third of survey respondents.
And almost half indicated that their practice or institution had increased capacity for telemedicine or telecommuting in response to climate change. Only 8% said their practice or institution had divested from fossil fuel stocks and/or bonds.
“There are a lot of sustainability-in-medicine solutions that are actually cost-neutral or cost-saving for practices,” said Dr. Rosenbach, who is a founder and co-chair of the AAD’s ERG on Climate Change and Environmental Issues.
Research in dermatology is starting to quantify the environmental impact of some of these changes. In a research letter also published in the British Journal of Dermatology, researchers from Cardiff University and the department of dermatology at University Hospital of Wales, described how they determined that reusable surgical packs used for skin surgery are more sustainable than single-use packs because of their reduced cost and reduced greenhouse gas emissions.
Such single-site reports are “early feeders” into what will become a stream of larger studies quantifying the impact of measures taken in dermatology, Dr. Rosenbach said.
Across medicine, there is evidence that health care professionals are now seeing climate change as a threat to their patients. In a multinational survey published last year in The Lancet Planetary Health, 77% of 3,977 participants said that climate change will cause a moderate or great deal of harm for their patients.
Climate change will be discussed at the AAD’s annual meeting in late March in a session devoted to the topic, and as part of a broader session on controversies in dermatology.
Dr. Rosenbach and two of the five authors of the dermatology research letter are members of the AAD’s ERG on climate change, but in the publication they noted that they were not writing on behalf of the AAD. None of the authors reported any disclosures, and there was no funding source for the survey.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Clinical data affirm dupilumab for chronic nasal polyps
In a specialty clinic, dupilumab (Dupixent) injections significantly improved symptoms for patients with chronic rhinosinusitis with nasal polyps, based on provisional data from more than 100 adults.
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a significant burden among working-age adults. Symptom control remains a challenge for many of these patients, and the cost in lost productivity and health care consumption can be substantial, write Rik J.L. van der Lans, MD, of the University of Amsterdam, and colleagues.
Dupilumab, a biologic that targets components of the type 2 inflammatory pathway, represents a new option that has shown effectiveness in clinical trials for regulatory approval, they said.
A new observational study tests dupilumab in patients who met criteria for biological treatment proposed in a recent major systematic review. The findings were published in the journal Allergy.
In the study, the researchers identified 131 adults older than 18 years (mean age 51.7) with CRSwNP treated at a single tertiary care center. Participants received 300 mg of dupilumab subcutaneous injection every 2 weeks for at least 12 weeks.
The primary outcomes were scores on several measures, including the SinoNasal Outcome Test-22 (SNOT-22, scale of 0-110), the bilateral Nasal Polyp Score (NPS, scale of 0-8), and the Sniffin’ Sticks-12 identification test (SSIT-12, scale of 0-6 anosmia, 7-10 hyposmia, 11-12 normosmia).
The mean scores on all three outcomes improved significantly from baseline to both 24 weeks and 48 weeks. Scores on the SNOT-22 improved from 52.4 at baseline to 18.5 and 16.8 at weeks 24 and 48, respectively. NPS improved from 5.4 at baseline to 1.6 and 1.0, respectively. SSIT-12 scores improved from 3.6 at baseline to 7.3 and 8.3, respectively.
At baseline, 95.8% of the patients had uncontrolled chronic rhinosinusitis, but at 24 and 48 weeks, respectively, 24.3% and 6.2% were uncontrolled.
Approximately half of the patients experienced treatment-emergent adverse events, but these were “mild and decreased in occurrence and intensity throughout treatment,” the researchers say.
For patients with a strong response, the researchers also tested an extension of the interval between doses to 4 weeks and 6 weeks, in a provisional indication of continued established control at these timepoints.
The study findings were limited by several factors, including the potential for selection bias, and data from only the first patient cohort, the researchers noted. However, the results were strengthened by the real-life context, standardized indications, and long-term follow up for almost a year, they said.
More research is needed on nonacademic patient cohorts, but the current data confirm the effectiveness of dupilumab as an add-on for difficult-to-treat CRSwNP, they concluded. The findings also validate the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS2020) inclusion criteria for biologic treatment, they said.
The new study is important because of the need for verification of results from randomized controlled trials using real-world data, Dr. Van der Lans told this news organization.
“For example, differences in treatment efficacy might result from differing indication criteria, and the inclusion/exclusion criteria in the RCTs might have excluded patients one would encounter in daily practice,” he said. “With our prospective observational cohort, we are seeking to verify efficacy, monitor pharmacovigilance, and evaluate and advance the indication criteria and positioning of biologicals registered for CRSwNP, such as dupilumab.”
These cross-sectional results suggest dupilumab is more effective in preventing possibly harmful escape treatments, such as oral corticosteroids and/or surgery, than reported by the registration trials.
“Additionally, it appears possible to maintain established CRS-control during response-dependent, stepwise, interdose interval prolongation of up to 6 weeks, which is officially an off-label dosing interval,” he said. “This would greatly benefit patients’ treatment burden and direct costs,” he said. However, both findings require corroboration by anticipated longitudinal results in 2022, he noted.
The key message for clinicians in practice: “Biologicals like dupilumab are a potent and promising treatment for severe CRSwNP when conventional medical and surgical therapy fails,” he emphasized.
Looking ahead, important research objectives include head-on comparison studies of the diverse biological agents, establishing biomarkers to guide preferential therapy, and evaluating the economics of biologics compared with conventional therapy, Dr. Van der Lans added. Such research is vital not only for improving patient-centered care but to sustain the use of biologicals in a health-economic perspective.
One of the greatest criticisms of biologic therapy for CRSwNP is cost, particularly in a setting of ever-increasing health care costs. A recent review noted the average cost per year is greater than $30,000.
Real-life study verifies effectiveness
“As the authors pointed out, this is a real-life, prospective observational cohort with a decently large size, evaluating the therapeutic efficacy of add-on dupilumab,” said Seong H. Cho, MD, of the University of South Florida, Tampa, in an interview.
“Dupilumab is the first FDA-approved biologic to treat severe chronic rhinosinusitis with nasal polyps based on two phase 3 clinical trials,” said Dr. Cho, who was not involved with the study. “It has been more than 2 years since dupilumab was approved for severe CRSwNP by the FDA and EMA. This real-life, prospective, observational study with a decent size verified the efficacy of dupilumab as an add-on treatment when used with a proper indication such as EPOS2020 indication criteria.
“I am not surprised by the efficacy of dupilumab on severe CRSwNP, based on my clinical experience. My clinical observation is similar to the results of this study. This study verifies that dupilumab is highly efficacious in treating refractory and severe CRSwNP in a real-life setting by improving all subjective and objective clinical outcomes such as SNOT-22, NPS, and smell test score,” he said. The study also confirms that a stepwise, interdose interval prolongation from every 2-4 weeks for CRSwNP patients with good response should be a consideration for clinical practice, he added.
The cost-effectiveness of dupilumab is the main barrier to more consistent use, Dr. Cho said. “There is no evidence that dupilumab can change the course of the disease, and we don’t know how long patients need to be on this drug. Therefore, nasal polyps need to be refractory and severe enough to use dupilumab and other biologics,” he explained.
Consequently, proper indication criteria, such as the EPOS2020 indication criteria for biologics, should be established before initiating dupilumab, Dr. Cho noted.
“Generally, endoscopic sinus surgery would be preferred in sinus-surgery naive CRSwNP patients, unless surgery is contraindicated or refused by patients because of cost-effectiveness rather than the superior efficacy,” he said. “If surgery fails, then dupilumab can be considered. In addition, proper evaluation of nasal polyp severity would be important.”
“One should establish an objective NPS by endoscopic exam before initiation of dupilumab. This baseline score would be an important marker to assess the efficacy of dupilumab in the course of treatment.”
Monitoring of the NPS together with the patient’s symptom improvement would be essential to implementing a stepwise, interdose interval prolongation to reduce the cost, he emphasized.
“The most crucial additional research is establishing suitable biomarkers for the response of dupilumab and other biologics,” said Dr. Cho. “Overall, the performance of dupilumab seems to be good. But there are patients unresponsive to dupilumab, even more to other recently FDA-approved biologics for CRSwNP.”
Blood eosinophils and exhaled nitric oxide can be a good biomarker for type 2 asthma, Dr. Cho added. “Still, there is no evidence that these biomarkers are decent for CRSwNP, even though CRSwNP is mostly considered as type 2 disease. Therefore, it would be essential to find promising biomarkers for severe CRSwNP.”
Dr. Van der Lans disclosed serving as a consultant for GlaxoSmithKline, and several coauthors disclosed relationships with companies including Sanofi and Novartis. The patient registry from which the study population was drawn is cofunded by Sanofi and Novartis. Dr. Cho has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a specialty clinic, dupilumab (Dupixent) injections significantly improved symptoms for patients with chronic rhinosinusitis with nasal polyps, based on provisional data from more than 100 adults.
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a significant burden among working-age adults. Symptom control remains a challenge for many of these patients, and the cost in lost productivity and health care consumption can be substantial, write Rik J.L. van der Lans, MD, of the University of Amsterdam, and colleagues.
Dupilumab, a biologic that targets components of the type 2 inflammatory pathway, represents a new option that has shown effectiveness in clinical trials for regulatory approval, they said.
A new observational study tests dupilumab in patients who met criteria for biological treatment proposed in a recent major systematic review. The findings were published in the journal Allergy.
In the study, the researchers identified 131 adults older than 18 years (mean age 51.7) with CRSwNP treated at a single tertiary care center. Participants received 300 mg of dupilumab subcutaneous injection every 2 weeks for at least 12 weeks.
The primary outcomes were scores on several measures, including the SinoNasal Outcome Test-22 (SNOT-22, scale of 0-110), the bilateral Nasal Polyp Score (NPS, scale of 0-8), and the Sniffin’ Sticks-12 identification test (SSIT-12, scale of 0-6 anosmia, 7-10 hyposmia, 11-12 normosmia).
The mean scores on all three outcomes improved significantly from baseline to both 24 weeks and 48 weeks. Scores on the SNOT-22 improved from 52.4 at baseline to 18.5 and 16.8 at weeks 24 and 48, respectively. NPS improved from 5.4 at baseline to 1.6 and 1.0, respectively. SSIT-12 scores improved from 3.6 at baseline to 7.3 and 8.3, respectively.
At baseline, 95.8% of the patients had uncontrolled chronic rhinosinusitis, but at 24 and 48 weeks, respectively, 24.3% and 6.2% were uncontrolled.
Approximately half of the patients experienced treatment-emergent adverse events, but these were “mild and decreased in occurrence and intensity throughout treatment,” the researchers say.
For patients with a strong response, the researchers also tested an extension of the interval between doses to 4 weeks and 6 weeks, in a provisional indication of continued established control at these timepoints.
The study findings were limited by several factors, including the potential for selection bias, and data from only the first patient cohort, the researchers noted. However, the results were strengthened by the real-life context, standardized indications, and long-term follow up for almost a year, they said.
More research is needed on nonacademic patient cohorts, but the current data confirm the effectiveness of dupilumab as an add-on for difficult-to-treat CRSwNP, they concluded. The findings also validate the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS2020) inclusion criteria for biologic treatment, they said.
The new study is important because of the need for verification of results from randomized controlled trials using real-world data, Dr. Van der Lans told this news organization.
“For example, differences in treatment efficacy might result from differing indication criteria, and the inclusion/exclusion criteria in the RCTs might have excluded patients one would encounter in daily practice,” he said. “With our prospective observational cohort, we are seeking to verify efficacy, monitor pharmacovigilance, and evaluate and advance the indication criteria and positioning of biologicals registered for CRSwNP, such as dupilumab.”
These cross-sectional results suggest dupilumab is more effective in preventing possibly harmful escape treatments, such as oral corticosteroids and/or surgery, than reported by the registration trials.
“Additionally, it appears possible to maintain established CRS-control during response-dependent, stepwise, interdose interval prolongation of up to 6 weeks, which is officially an off-label dosing interval,” he said. “This would greatly benefit patients’ treatment burden and direct costs,” he said. However, both findings require corroboration by anticipated longitudinal results in 2022, he noted.
The key message for clinicians in practice: “Biologicals like dupilumab are a potent and promising treatment for severe CRSwNP when conventional medical and surgical therapy fails,” he emphasized.
Looking ahead, important research objectives include head-on comparison studies of the diverse biological agents, establishing biomarkers to guide preferential therapy, and evaluating the economics of biologics compared with conventional therapy, Dr. Van der Lans added. Such research is vital not only for improving patient-centered care but to sustain the use of biologicals in a health-economic perspective.
One of the greatest criticisms of biologic therapy for CRSwNP is cost, particularly in a setting of ever-increasing health care costs. A recent review noted the average cost per year is greater than $30,000.
Real-life study verifies effectiveness
“As the authors pointed out, this is a real-life, prospective observational cohort with a decently large size, evaluating the therapeutic efficacy of add-on dupilumab,” said Seong H. Cho, MD, of the University of South Florida, Tampa, in an interview.
“Dupilumab is the first FDA-approved biologic to treat severe chronic rhinosinusitis with nasal polyps based on two phase 3 clinical trials,” said Dr. Cho, who was not involved with the study. “It has been more than 2 years since dupilumab was approved for severe CRSwNP by the FDA and EMA. This real-life, prospective, observational study with a decent size verified the efficacy of dupilumab as an add-on treatment when used with a proper indication such as EPOS2020 indication criteria.
“I am not surprised by the efficacy of dupilumab on severe CRSwNP, based on my clinical experience. My clinical observation is similar to the results of this study. This study verifies that dupilumab is highly efficacious in treating refractory and severe CRSwNP in a real-life setting by improving all subjective and objective clinical outcomes such as SNOT-22, NPS, and smell test score,” he said. The study also confirms that a stepwise, interdose interval prolongation from every 2-4 weeks for CRSwNP patients with good response should be a consideration for clinical practice, he added.
The cost-effectiveness of dupilumab is the main barrier to more consistent use, Dr. Cho said. “There is no evidence that dupilumab can change the course of the disease, and we don’t know how long patients need to be on this drug. Therefore, nasal polyps need to be refractory and severe enough to use dupilumab and other biologics,” he explained.
Consequently, proper indication criteria, such as the EPOS2020 indication criteria for biologics, should be established before initiating dupilumab, Dr. Cho noted.
“Generally, endoscopic sinus surgery would be preferred in sinus-surgery naive CRSwNP patients, unless surgery is contraindicated or refused by patients because of cost-effectiveness rather than the superior efficacy,” he said. “If surgery fails, then dupilumab can be considered. In addition, proper evaluation of nasal polyp severity would be important.”
“One should establish an objective NPS by endoscopic exam before initiation of dupilumab. This baseline score would be an important marker to assess the efficacy of dupilumab in the course of treatment.”
Monitoring of the NPS together with the patient’s symptom improvement would be essential to implementing a stepwise, interdose interval prolongation to reduce the cost, he emphasized.
“The most crucial additional research is establishing suitable biomarkers for the response of dupilumab and other biologics,” said Dr. Cho. “Overall, the performance of dupilumab seems to be good. But there are patients unresponsive to dupilumab, even more to other recently FDA-approved biologics for CRSwNP.”
Blood eosinophils and exhaled nitric oxide can be a good biomarker for type 2 asthma, Dr. Cho added. “Still, there is no evidence that these biomarkers are decent for CRSwNP, even though CRSwNP is mostly considered as type 2 disease. Therefore, it would be essential to find promising biomarkers for severe CRSwNP.”
Dr. Van der Lans disclosed serving as a consultant for GlaxoSmithKline, and several coauthors disclosed relationships with companies including Sanofi and Novartis. The patient registry from which the study population was drawn is cofunded by Sanofi and Novartis. Dr. Cho has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a specialty clinic, dupilumab (Dupixent) injections significantly improved symptoms for patients with chronic rhinosinusitis with nasal polyps, based on provisional data from more than 100 adults.
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a significant burden among working-age adults. Symptom control remains a challenge for many of these patients, and the cost in lost productivity and health care consumption can be substantial, write Rik J.L. van der Lans, MD, of the University of Amsterdam, and colleagues.
Dupilumab, a biologic that targets components of the type 2 inflammatory pathway, represents a new option that has shown effectiveness in clinical trials for regulatory approval, they said.
A new observational study tests dupilumab in patients who met criteria for biological treatment proposed in a recent major systematic review. The findings were published in the journal Allergy.
In the study, the researchers identified 131 adults older than 18 years (mean age 51.7) with CRSwNP treated at a single tertiary care center. Participants received 300 mg of dupilumab subcutaneous injection every 2 weeks for at least 12 weeks.
The primary outcomes were scores on several measures, including the SinoNasal Outcome Test-22 (SNOT-22, scale of 0-110), the bilateral Nasal Polyp Score (NPS, scale of 0-8), and the Sniffin’ Sticks-12 identification test (SSIT-12, scale of 0-6 anosmia, 7-10 hyposmia, 11-12 normosmia).
The mean scores on all three outcomes improved significantly from baseline to both 24 weeks and 48 weeks. Scores on the SNOT-22 improved from 52.4 at baseline to 18.5 and 16.8 at weeks 24 and 48, respectively. NPS improved from 5.4 at baseline to 1.6 and 1.0, respectively. SSIT-12 scores improved from 3.6 at baseline to 7.3 and 8.3, respectively.
At baseline, 95.8% of the patients had uncontrolled chronic rhinosinusitis, but at 24 and 48 weeks, respectively, 24.3% and 6.2% were uncontrolled.
Approximately half of the patients experienced treatment-emergent adverse events, but these were “mild and decreased in occurrence and intensity throughout treatment,” the researchers say.
For patients with a strong response, the researchers also tested an extension of the interval between doses to 4 weeks and 6 weeks, in a provisional indication of continued established control at these timepoints.
The study findings were limited by several factors, including the potential for selection bias, and data from only the first patient cohort, the researchers noted. However, the results were strengthened by the real-life context, standardized indications, and long-term follow up for almost a year, they said.
More research is needed on nonacademic patient cohorts, but the current data confirm the effectiveness of dupilumab as an add-on for difficult-to-treat CRSwNP, they concluded. The findings also validate the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS2020) inclusion criteria for biologic treatment, they said.
The new study is important because of the need for verification of results from randomized controlled trials using real-world data, Dr. Van der Lans told this news organization.
“For example, differences in treatment efficacy might result from differing indication criteria, and the inclusion/exclusion criteria in the RCTs might have excluded patients one would encounter in daily practice,” he said. “With our prospective observational cohort, we are seeking to verify efficacy, monitor pharmacovigilance, and evaluate and advance the indication criteria and positioning of biologicals registered for CRSwNP, such as dupilumab.”
These cross-sectional results suggest dupilumab is more effective in preventing possibly harmful escape treatments, such as oral corticosteroids and/or surgery, than reported by the registration trials.
“Additionally, it appears possible to maintain established CRS-control during response-dependent, stepwise, interdose interval prolongation of up to 6 weeks, which is officially an off-label dosing interval,” he said. “This would greatly benefit patients’ treatment burden and direct costs,” he said. However, both findings require corroboration by anticipated longitudinal results in 2022, he noted.
The key message for clinicians in practice: “Biologicals like dupilumab are a potent and promising treatment for severe CRSwNP when conventional medical and surgical therapy fails,” he emphasized.
Looking ahead, important research objectives include head-on comparison studies of the diverse biological agents, establishing biomarkers to guide preferential therapy, and evaluating the economics of biologics compared with conventional therapy, Dr. Van der Lans added. Such research is vital not only for improving patient-centered care but to sustain the use of biologicals in a health-economic perspective.
One of the greatest criticisms of biologic therapy for CRSwNP is cost, particularly in a setting of ever-increasing health care costs. A recent review noted the average cost per year is greater than $30,000.
Real-life study verifies effectiveness
“As the authors pointed out, this is a real-life, prospective observational cohort with a decently large size, evaluating the therapeutic efficacy of add-on dupilumab,” said Seong H. Cho, MD, of the University of South Florida, Tampa, in an interview.
“Dupilumab is the first FDA-approved biologic to treat severe chronic rhinosinusitis with nasal polyps based on two phase 3 clinical trials,” said Dr. Cho, who was not involved with the study. “It has been more than 2 years since dupilumab was approved for severe CRSwNP by the FDA and EMA. This real-life, prospective, observational study with a decent size verified the efficacy of dupilumab as an add-on treatment when used with a proper indication such as EPOS2020 indication criteria.
“I am not surprised by the efficacy of dupilumab on severe CRSwNP, based on my clinical experience. My clinical observation is similar to the results of this study. This study verifies that dupilumab is highly efficacious in treating refractory and severe CRSwNP in a real-life setting by improving all subjective and objective clinical outcomes such as SNOT-22, NPS, and smell test score,” he said. The study also confirms that a stepwise, interdose interval prolongation from every 2-4 weeks for CRSwNP patients with good response should be a consideration for clinical practice, he added.
The cost-effectiveness of dupilumab is the main barrier to more consistent use, Dr. Cho said. “There is no evidence that dupilumab can change the course of the disease, and we don’t know how long patients need to be on this drug. Therefore, nasal polyps need to be refractory and severe enough to use dupilumab and other biologics,” he explained.
Consequently, proper indication criteria, such as the EPOS2020 indication criteria for biologics, should be established before initiating dupilumab, Dr. Cho noted.
“Generally, endoscopic sinus surgery would be preferred in sinus-surgery naive CRSwNP patients, unless surgery is contraindicated or refused by patients because of cost-effectiveness rather than the superior efficacy,” he said. “If surgery fails, then dupilumab can be considered. In addition, proper evaluation of nasal polyp severity would be important.”
“One should establish an objective NPS by endoscopic exam before initiation of dupilumab. This baseline score would be an important marker to assess the efficacy of dupilumab in the course of treatment.”
Monitoring of the NPS together with the patient’s symptom improvement would be essential to implementing a stepwise, interdose interval prolongation to reduce the cost, he emphasized.
“The most crucial additional research is establishing suitable biomarkers for the response of dupilumab and other biologics,” said Dr. Cho. “Overall, the performance of dupilumab seems to be good. But there are patients unresponsive to dupilumab, even more to other recently FDA-approved biologics for CRSwNP.”
Blood eosinophils and exhaled nitric oxide can be a good biomarker for type 2 asthma, Dr. Cho added. “Still, there is no evidence that these biomarkers are decent for CRSwNP, even though CRSwNP is mostly considered as type 2 disease. Therefore, it would be essential to find promising biomarkers for severe CRSwNP.”
Dr. Van der Lans disclosed serving as a consultant for GlaxoSmithKline, and several coauthors disclosed relationships with companies including Sanofi and Novartis. The patient registry from which the study population was drawn is cofunded by Sanofi and Novartis. Dr. Cho has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ALLERGY
Sepsis common cause of ICU admissions in patients with MS
Sepsis is an alarmingly common cause behind ICU admissions in patients with multiple sclerosis (MS), a retrospective, population-based cohort study indicates.
Furthermore, it contributes to a disproportionately high percentage of the short-term mortality risk among patients with MS admitted to the ICU, findings also show. Short-term mortality risk was defined in the study as a combination of in-hospital death or discharge to hospice.
“We found that the risk of short-term mortality in critically ill patients with MS is four times higher among those with sepsis ... so sepsis appears to be comparatively more lethal among patients with MS than in the general population,” Lavi Oud, MD, professor of medicine, Texas Tech University HSC at the Permian Basin, Odessa, said in an email.
“[Although] the specific mechanisms underlying the markedly higher risk of sepsis among patients with MS compared to the general population remain to be fully elucidated ... it’s thought that the risk may stem from the dysfunction of the immune system in these patients related to MS itself and to the potentially adverse effect of the immunomodulating therapy we use in these patients,” he added.
The study was published online Jan. 11 in the Journal of Critical Care.
Sepsis rates
The Texas Inpatient Public Use Data File was used to identify adults with a diagnosis of MS admitted to the hospital between 2010 and 2017. Among the 19,837 patients with MS admitted to the ICU during the study interval, almost one-third (31.5%) had sepsis, investigators report. “The rate of sepsis among ICU admissions increased with age, ranging from 20.8% among those aged 18-44 to 39.4% among those aged 65 years or older,” investigators note.
The most common site of infection among MS patients admitted to the ICU were urinary in nature (65.2%), followed by respiratory (36.1%). A smaller proportion of infections (7.6%) involved the skin and soft tissues, researchers note. A full one-quarter of patients developed septic shock in response to their infection while the length of stay among patients with sepsis (mean of 10.9 days) was substantially longer than it was for those without sepsis (mean of 5.6 days), they observe.
At a mean total hospital cost of $121,797 for each ICU patient with sepsis, the cost of caring for each patient was nearly twofold higher than the mean total cost of taking care of ICU patients without sepsis (mean total cost, $65,179). On adjusted analysis, sepsis was associated with a 42.7% (95% confidence interval, 38.9-46.5; P < .0001) longer length of hospital stay and a 26.2% (95% CI, 23.1-29.1; P < .0001) higher total hospital cost compared with patients without sepsis, the authors point out.
Indeed, ICU admissions with sepsis accounted for 47.3% of all hospital days and for 46.1% of the aggregate hospital charges among all MS patients admitted to the ICU.
“The adjusted probability of short-term mortality was 13.4% (95% CI, 13.0-13.7) among ICU admissions with sepsis and 3.3% (95% CI, 3.2-3.4) among ICU admissions without sepsis,” the authors report.
This translated into a 44% higher risk of short-term mortality at an adjusted odds ratio of 1.44 (95% CI, 1.23-1.69; P < .0001) for those with sepsis, compared with those without, they add. Among all ICU admissions, sepsis was reported in over two-thirds of documented short-term mortality events. The risk of short-term mortality was also almost threefold higher among patients with sepsis who were age 65 years and older compared with patients aged 18-44.
As Dr. Oud noted, there is no specific test for sepsis, and it can initially present in an atypical manner, especially in older, frailer, chronically ill patients as well as in patients with immune dysfunction. “Thus, considering sepsis as a possible cause of new deterioration in a patient’s condition is essential, along with the timely start of sepsis-related care,” Dr. Oud observed.
A limitation of the study was that the dataset did not include information on the type of MS a patient had, the duration of their illness, the treatment received, the level of disease activity, or the level of disability.
The study had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sepsis is an alarmingly common cause behind ICU admissions in patients with multiple sclerosis (MS), a retrospective, population-based cohort study indicates.
Furthermore, it contributes to a disproportionately high percentage of the short-term mortality risk among patients with MS admitted to the ICU, findings also show. Short-term mortality risk was defined in the study as a combination of in-hospital death or discharge to hospice.
“We found that the risk of short-term mortality in critically ill patients with MS is four times higher among those with sepsis ... so sepsis appears to be comparatively more lethal among patients with MS than in the general population,” Lavi Oud, MD, professor of medicine, Texas Tech University HSC at the Permian Basin, Odessa, said in an email.
“[Although] the specific mechanisms underlying the markedly higher risk of sepsis among patients with MS compared to the general population remain to be fully elucidated ... it’s thought that the risk may stem from the dysfunction of the immune system in these patients related to MS itself and to the potentially adverse effect of the immunomodulating therapy we use in these patients,” he added.
The study was published online Jan. 11 in the Journal of Critical Care.
Sepsis rates
The Texas Inpatient Public Use Data File was used to identify adults with a diagnosis of MS admitted to the hospital between 2010 and 2017. Among the 19,837 patients with MS admitted to the ICU during the study interval, almost one-third (31.5%) had sepsis, investigators report. “The rate of sepsis among ICU admissions increased with age, ranging from 20.8% among those aged 18-44 to 39.4% among those aged 65 years or older,” investigators note.
The most common site of infection among MS patients admitted to the ICU were urinary in nature (65.2%), followed by respiratory (36.1%). A smaller proportion of infections (7.6%) involved the skin and soft tissues, researchers note. A full one-quarter of patients developed septic shock in response to their infection while the length of stay among patients with sepsis (mean of 10.9 days) was substantially longer than it was for those without sepsis (mean of 5.6 days), they observe.
At a mean total hospital cost of $121,797 for each ICU patient with sepsis, the cost of caring for each patient was nearly twofold higher than the mean total cost of taking care of ICU patients without sepsis (mean total cost, $65,179). On adjusted analysis, sepsis was associated with a 42.7% (95% confidence interval, 38.9-46.5; P < .0001) longer length of hospital stay and a 26.2% (95% CI, 23.1-29.1; P < .0001) higher total hospital cost compared with patients without sepsis, the authors point out.
Indeed, ICU admissions with sepsis accounted for 47.3% of all hospital days and for 46.1% of the aggregate hospital charges among all MS patients admitted to the ICU.
“The adjusted probability of short-term mortality was 13.4% (95% CI, 13.0-13.7) among ICU admissions with sepsis and 3.3% (95% CI, 3.2-3.4) among ICU admissions without sepsis,” the authors report.
This translated into a 44% higher risk of short-term mortality at an adjusted odds ratio of 1.44 (95% CI, 1.23-1.69; P < .0001) for those with sepsis, compared with those without, they add. Among all ICU admissions, sepsis was reported in over two-thirds of documented short-term mortality events. The risk of short-term mortality was also almost threefold higher among patients with sepsis who were age 65 years and older compared with patients aged 18-44.
As Dr. Oud noted, there is no specific test for sepsis, and it can initially present in an atypical manner, especially in older, frailer, chronically ill patients as well as in patients with immune dysfunction. “Thus, considering sepsis as a possible cause of new deterioration in a patient’s condition is essential, along with the timely start of sepsis-related care,” Dr. Oud observed.
A limitation of the study was that the dataset did not include information on the type of MS a patient had, the duration of their illness, the treatment received, the level of disease activity, or the level of disability.
The study had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sepsis is an alarmingly common cause behind ICU admissions in patients with multiple sclerosis (MS), a retrospective, population-based cohort study indicates.
Furthermore, it contributes to a disproportionately high percentage of the short-term mortality risk among patients with MS admitted to the ICU, findings also show. Short-term mortality risk was defined in the study as a combination of in-hospital death or discharge to hospice.
“We found that the risk of short-term mortality in critically ill patients with MS is four times higher among those with sepsis ... so sepsis appears to be comparatively more lethal among patients with MS than in the general population,” Lavi Oud, MD, professor of medicine, Texas Tech University HSC at the Permian Basin, Odessa, said in an email.
“[Although] the specific mechanisms underlying the markedly higher risk of sepsis among patients with MS compared to the general population remain to be fully elucidated ... it’s thought that the risk may stem from the dysfunction of the immune system in these patients related to MS itself and to the potentially adverse effect of the immunomodulating therapy we use in these patients,” he added.
The study was published online Jan. 11 in the Journal of Critical Care.
Sepsis rates
The Texas Inpatient Public Use Data File was used to identify adults with a diagnosis of MS admitted to the hospital between 2010 and 2017. Among the 19,837 patients with MS admitted to the ICU during the study interval, almost one-third (31.5%) had sepsis, investigators report. “The rate of sepsis among ICU admissions increased with age, ranging from 20.8% among those aged 18-44 to 39.4% among those aged 65 years or older,” investigators note.
The most common site of infection among MS patients admitted to the ICU were urinary in nature (65.2%), followed by respiratory (36.1%). A smaller proportion of infections (7.6%) involved the skin and soft tissues, researchers note. A full one-quarter of patients developed septic shock in response to their infection while the length of stay among patients with sepsis (mean of 10.9 days) was substantially longer than it was for those without sepsis (mean of 5.6 days), they observe.
At a mean total hospital cost of $121,797 for each ICU patient with sepsis, the cost of caring for each patient was nearly twofold higher than the mean total cost of taking care of ICU patients without sepsis (mean total cost, $65,179). On adjusted analysis, sepsis was associated with a 42.7% (95% confidence interval, 38.9-46.5; P < .0001) longer length of hospital stay and a 26.2% (95% CI, 23.1-29.1; P < .0001) higher total hospital cost compared with patients without sepsis, the authors point out.
Indeed, ICU admissions with sepsis accounted for 47.3% of all hospital days and for 46.1% of the aggregate hospital charges among all MS patients admitted to the ICU.
“The adjusted probability of short-term mortality was 13.4% (95% CI, 13.0-13.7) among ICU admissions with sepsis and 3.3% (95% CI, 3.2-3.4) among ICU admissions without sepsis,” the authors report.
This translated into a 44% higher risk of short-term mortality at an adjusted odds ratio of 1.44 (95% CI, 1.23-1.69; P < .0001) for those with sepsis, compared with those without, they add. Among all ICU admissions, sepsis was reported in over two-thirds of documented short-term mortality events. The risk of short-term mortality was also almost threefold higher among patients with sepsis who were age 65 years and older compared with patients aged 18-44.
As Dr. Oud noted, there is no specific test for sepsis, and it can initially present in an atypical manner, especially in older, frailer, chronically ill patients as well as in patients with immune dysfunction. “Thus, considering sepsis as a possible cause of new deterioration in a patient’s condition is essential, along with the timely start of sepsis-related care,” Dr. Oud observed.
A limitation of the study was that the dataset did not include information on the type of MS a patient had, the duration of their illness, the treatment received, the level of disease activity, or the level of disability.
The study had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CRITICAL CARE
Sarcoidosis Presenting as Telangiectatic Macules
To the Editor:
Sarcoidosis is a multisystem, noncaseating, granulomatous disorder thought to occur from a combination of immunologic, genetic, and environmental factors.1 Often referred to as the “great imitator,” the cutaneous manifestations of sarcoidosis encompass many morphologies, including papules, plaques, nodules, and scars.1 We report an unusual case of sarcoidosis presenting as telangiectatic macules on the lower extremities.
A woman in her early 30s presented with a burning, pruritic, erythematous, telangiectatic eruption on the lower extremities with concurrent ankle swelling of 4 weeks’ duration. The patient denied any fevers, chills, recent infections, or new medications. Evaluation by her primary care physician during the time of the eruption included unremarkable antinuclear antibodies, thyroid stimulating hormone level, complete blood cell count, comprehensive metabolic panel, urinalysis, chest radiography, and lower-extremity Doppler ultrasonography.
Physical examination at the current presentation revealed numerous scattered, faint, erythematous, blanchable macules on the lower extremities along with mild pitting edema (Figure 1). The patient’s current medications included cetirizine, which she had been taking for years, as well as an intrauterine device. A punch biopsy from the right lower leg revealed small, well-demarcated sarcoidal granulomatous inflammation surrounding vascular structures and skin appendages (Figure 2). No foreign bodies were observed with polarized light microscopy. Microscopic findings suggestive of an infection, including caseation necrosis and suppurative inflammation, also were absent. Angiotensin-converting enzyme levels were normal. Myeloperoxidase and proteinase 3 IgG antibody levels were evaluated due to potential vascular involvement but were negative. An infectious cause of the sarcoidal granulomas was unlikely given histopathologic findings and negative tuberculosis skin testing, which the patient underwent annually for her job, so a tissue culture was not performed. The patient was prescribed triamcinolone acetonide cream 0.1% for the itching and burning at the initial visit and was continued on this treatment after the diagnosis of sarcoidosis was made. At 2-month follow-up, the patient’s eruption had nearly resolved with topical therapy.

Cutaneous manifestation occurs in 20% to 35% of sarcoidosis cases and may develop in the presence or absence of systemic disease. Approximately 60% of individuals with cutaneous sarcoidosis are found to have systemic involvement; therefore, careful monitoring and diagnostic workup are important in the management of these patients.2 While most cases of cutaneous sarcoidosis are papular, it is important for clinicians to maintain a level of suspicion for sarcoidosis in any uncertain dermatologic presentation.1,2 Evidence of telangiectasias has been shown in rarer forms of sarcoidosis (eg, angiolupoid), but the lesions usually are confined to the face, ears, or neck.3 Granulomatous vasculitis has been reported in a small number of individuals with ulcerative sarcoidosis.4 In our case, no ulcerations were present, possibly indicating an early lesion or an entirely novel process. Lastly, although reticular dermal granulomas are found in drug-induced interstitial granulomatous dermatitis, these lesions often are dispersed interstitially amongst collagen bundles and are associated with necrobiosis of collagen and eosinophilic/neutrophilic infiltrates.5 The lack of these characteristic pathologic findings in our patient along with no known reported cases of cetirizine-induced granulomatous dermatitis led us to rule out reticular dermal granulomas as a diagnosis. We present our case as a reminder of the diversity of cutaneous sarcoidosis manifestations and the importance of early diagnosis of these lesions.
.")
- Haimovic A, Sanchez M, Judson MA, et al. Sarcoidosis: a comprehensive review and update for the dermatologist: part I. cutaneous disease. J Am Acad Dermatol. 2012;66:699.E1-E18.
- Yanardag H, Tetikkurt C, Bilir M, et al. Diagnosis of cutaneous sarcoidosis; clinical and the prognostic significance of skin lesions. Multidiscip Respir Med. 2013;8:26.
- Arias-Santiago S, Fernández-Pugnaire MA, Aneiros- Fernández J, et al. Recurrent telangiectasias on the cheek: angiolupoid sarcoidosis. Am J Med. 2010;123:E7-E8.
- Wei C-H, Huang Y-H, Shih Y-C, et al. Sarcoidosis with cutaneous granulomatous vasculitis. Australas J Dermatol. 2010;51:198-201.
- Peroni A, Colato C, Schena D, et al. Interstitial granulomatous dermatitis: a distinct entity with characteristic histological and clinical pattern. Br J Dermatol. 2012;166:775-783.
To the Editor:
Sarcoidosis is a multisystem, noncaseating, granulomatous disorder thought to occur from a combination of immunologic, genetic, and environmental factors.1 Often referred to as the “great imitator,” the cutaneous manifestations of sarcoidosis encompass many morphologies, including papules, plaques, nodules, and scars.1 We report an unusual case of sarcoidosis presenting as telangiectatic macules on the lower extremities.
A woman in her early 30s presented with a burning, pruritic, erythematous, telangiectatic eruption on the lower extremities with concurrent ankle swelling of 4 weeks’ duration. The patient denied any fevers, chills, recent infections, or new medications. Evaluation by her primary care physician during the time of the eruption included unremarkable antinuclear antibodies, thyroid stimulating hormone level, complete blood cell count, comprehensive metabolic panel, urinalysis, chest radiography, and lower-extremity Doppler ultrasonography.
Physical examination at the current presentation revealed numerous scattered, faint, erythematous, blanchable macules on the lower extremities along with mild pitting edema (Figure 1). The patient’s current medications included cetirizine, which she had been taking for years, as well as an intrauterine device. A punch biopsy from the right lower leg revealed small, well-demarcated sarcoidal granulomatous inflammation surrounding vascular structures and skin appendages (Figure 2). No foreign bodies were observed with polarized light microscopy. Microscopic findings suggestive of an infection, including caseation necrosis and suppurative inflammation, also were absent. Angiotensin-converting enzyme levels were normal. Myeloperoxidase and proteinase 3 IgG antibody levels were evaluated due to potential vascular involvement but were negative. An infectious cause of the sarcoidal granulomas was unlikely given histopathologic findings and negative tuberculosis skin testing, which the patient underwent annually for her job, so a tissue culture was not performed. The patient was prescribed triamcinolone acetonide cream 0.1% for the itching and burning at the initial visit and was continued on this treatment after the diagnosis of sarcoidosis was made. At 2-month follow-up, the patient’s eruption had nearly resolved with topical therapy.
Cutaneous manifestation occurs in 20% to 35% of sarcoidosis cases and may develop in the presence or absence of systemic disease. Approximately 60% of individuals with cutaneous sarcoidosis are found to have systemic involvement; therefore, careful monitoring and diagnostic workup are important in the management of these patients.2 While most cases of cutaneous sarcoidosis are papular, it is important for clinicians to maintain a level of suspicion for sarcoidosis in any uncertain dermatologic presentation.1,2 Evidence of telangiectasias has been shown in rarer forms of sarcoidosis (eg, angiolupoid), but the lesions usually are confined to the face, ears, or neck.3 Granulomatous vasculitis has been reported in a small number of individuals with ulcerative sarcoidosis.4 In our case, no ulcerations were present, possibly indicating an early lesion or an entirely novel process. Lastly, although reticular dermal granulomas are found in drug-induced interstitial granulomatous dermatitis, these lesions often are dispersed interstitially amongst collagen bundles and are associated with necrobiosis of collagen and eosinophilic/neutrophilic infiltrates.5 The lack of these characteristic pathologic findings in our patient along with no known reported cases of cetirizine-induced granulomatous dermatitis led us to rule out reticular dermal granulomas as a diagnosis. We present our case as a reminder of the diversity of cutaneous sarcoidosis manifestations and the importance of early diagnosis of these lesions.
To the Editor:
Sarcoidosis is a multisystem, noncaseating, granulomatous disorder thought to occur from a combination of immunologic, genetic, and environmental factors.1 Often referred to as the “great imitator,” the cutaneous manifestations of sarcoidosis encompass many morphologies, including papules, plaques, nodules, and scars.1 We report an unusual case of sarcoidosis presenting as telangiectatic macules on the lower extremities.
A woman in her early 30s presented with a burning, pruritic, erythematous, telangiectatic eruption on the lower extremities with concurrent ankle swelling of 4 weeks’ duration. The patient denied any fevers, chills, recent infections, or new medications. Evaluation by her primary care physician during the time of the eruption included unremarkable antinuclear antibodies, thyroid stimulating hormone level, complete blood cell count, comprehensive metabolic panel, urinalysis, chest radiography, and lower-extremity Doppler ultrasonography.
Physical examination at the current presentation revealed numerous scattered, faint, erythematous, blanchable macules on the lower extremities along with mild pitting edema (Figure 1). The patient’s current medications included cetirizine, which she had been taking for years, as well as an intrauterine device. A punch biopsy from the right lower leg revealed small, well-demarcated sarcoidal granulomatous inflammation surrounding vascular structures and skin appendages (Figure 2). No foreign bodies were observed with polarized light microscopy. Microscopic findings suggestive of an infection, including caseation necrosis and suppurative inflammation, also were absent. Angiotensin-converting enzyme levels were normal. Myeloperoxidase and proteinase 3 IgG antibody levels were evaluated due to potential vascular involvement but were negative. An infectious cause of the sarcoidal granulomas was unlikely given histopathologic findings and negative tuberculosis skin testing, which the patient underwent annually for her job, so a tissue culture was not performed. The patient was prescribed triamcinolone acetonide cream 0.1% for the itching and burning at the initial visit and was continued on this treatment after the diagnosis of sarcoidosis was made. At 2-month follow-up, the patient’s eruption had nearly resolved with topical therapy.
Cutaneous manifestation occurs in 20% to 35% of sarcoidosis cases and may develop in the presence or absence of systemic disease. Approximately 60% of individuals with cutaneous sarcoidosis are found to have systemic involvement; therefore, careful monitoring and diagnostic workup are important in the management of these patients.2 While most cases of cutaneous sarcoidosis are papular, it is important for clinicians to maintain a level of suspicion for sarcoidosis in any uncertain dermatologic presentation.1,2 Evidence of telangiectasias has been shown in rarer forms of sarcoidosis (eg, angiolupoid), but the lesions usually are confined to the face, ears, or neck.3 Granulomatous vasculitis has been reported in a small number of individuals with ulcerative sarcoidosis.4 In our case, no ulcerations were present, possibly indicating an early lesion or an entirely novel process. Lastly, although reticular dermal granulomas are found in drug-induced interstitial granulomatous dermatitis, these lesions often are dispersed interstitially amongst collagen bundles and are associated with necrobiosis of collagen and eosinophilic/neutrophilic infiltrates.5 The lack of these characteristic pathologic findings in our patient along with no known reported cases of cetirizine-induced granulomatous dermatitis led us to rule out reticular dermal granulomas as a diagnosis. We present our case as a reminder of the diversity of cutaneous sarcoidosis manifestations and the importance of early diagnosis of these lesions.
- Haimovic A, Sanchez M, Judson MA, et al. Sarcoidosis: a comprehensive review and update for the dermatologist: part I. cutaneous disease. J Am Acad Dermatol. 2012;66:699.E1-E18.
- Yanardag H, Tetikkurt C, Bilir M, et al. Diagnosis of cutaneous sarcoidosis; clinical and the prognostic significance of skin lesions. Multidiscip Respir Med. 2013;8:26.
- Arias-Santiago S, Fernández-Pugnaire MA, Aneiros- Fernández J, et al. Recurrent telangiectasias on the cheek: angiolupoid sarcoidosis. Am J Med. 2010;123:E7-E8.
- Wei C-H, Huang Y-H, Shih Y-C, et al. Sarcoidosis with cutaneous granulomatous vasculitis. Australas J Dermatol. 2010;51:198-201.
- Peroni A, Colato C, Schena D, et al. Interstitial granulomatous dermatitis: a distinct entity with characteristic histological and clinical pattern. Br J Dermatol. 2012;166:775-783.
- Haimovic A, Sanchez M, Judson MA, et al. Sarcoidosis: a comprehensive review and update for the dermatologist: part I. cutaneous disease. J Am Acad Dermatol. 2012;66:699.E1-E18.
- Yanardag H, Tetikkurt C, Bilir M, et al. Diagnosis of cutaneous sarcoidosis; clinical and the prognostic significance of skin lesions. Multidiscip Respir Med. 2013;8:26.
- Arias-Santiago S, Fernández-Pugnaire MA, Aneiros- Fernández J, et al. Recurrent telangiectasias on the cheek: angiolupoid sarcoidosis. Am J Med. 2010;123:E7-E8.
- Wei C-H, Huang Y-H, Shih Y-C, et al. Sarcoidosis with cutaneous granulomatous vasculitis. Australas J Dermatol. 2010;51:198-201.
- Peroni A, Colato C, Schena D, et al. Interstitial granulomatous dermatitis: a distinct entity with characteristic histological and clinical pattern. Br J Dermatol. 2012;166:775-783.
Practice Points
- Cutaneous manifestations of sarcoidosis can encompass numerous morphologies. A high degree of suspicion should be maintained for any uncertain dermatologic presentation.
- Although papular eruptions are the most common cutaneous findings in sarcoidosis, this case report illustrates a less common vascular-appearing presentation.
- A systemic workup is indicated in any presentation of sarcoidosis.
