User login
For MD-IQ use only
Yes, Russian docs should be shut out of medical associations, says ethicist
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at the NYU Grossman School of Medicine.
There are many difficult moral issues that are being fueled by the terrible war that Russia is waging against Ukraine. I think there is no way to justify anything that the Russians are doing. Ukraine did not do anything to violate Russian integrity, Russian territorial integrity, or anything by way of being aggressive toward Russia.
Russia decided at some point it wanted the Ukraine back. Putin has a dream, as the long-standing leader of Russia, to restore the Soviet empire, and Ukraine is top of the list of the places that he wants back for a variety of reasons.
We’re not here to debate the merits and demerits of this terrible act of war.
The European Society of Cardiology made a decision very recently to drop, as members, both Russia and Belarus, Russia’s ally in this aggressive war against Ukraine. They basically found it intolerable to have business as usual with these subsidiary cardiology societies as part of the ongoing activities of the European group.
The sole goal of this overarching European group is to reduce the health burden of cardiovascular disease. It doesn’t have political goals. It doesn’t have much to say about anything other than, “Let’s get evidence-based medicine used to try and prevent heart disease or treat heart disease.” So there’s noble intent.
Many of its members asked, “What are we doing in politics? Why are we punishing Russian and Belarussian cardiologists, acting as if somehow they are responsible for what the Russian army is doing or for what Putin has decided to do? Why are we acting against them? They are just trying to fight heart disease. That’s a legitimate goal for any doctor, public health official, or scientist.” They didn’t see, as members, why this exclusion had taken place.
I believe the exclusion is appropriate and some of the membership, obviously, in the European Society of Cardiology, agrees. It’s not because they’re holding doctors or scientists directly accountable for Putin’s war crimes, ethnic cleansing assault, or bombing and shelling of hospitals, maternity hospitals, and civilians.
They understand that these scientists and doctors have little to do with such things, but we are in a new form of warfare, and that warfare is basically economic and sociologic: turning Russia, as an inexcusably aggressive state, into a pariah.
The reason to break the ties is that that is the way to bring pressure upon Putin and his kleptocratic, oligarchic advisers to stop the attack, to try and bring down their economy, to say, “Business is not going to go on as usual. You will be excluded from normal scientific and medical commerce. We’re not going to be holding conferences or exchanging ideas,” and in my view, extending it to say, “We’re not taking your papers, we’re not publishing anything you do. We’re not even having you speak at our meetings until this war, this aggressive invasion, and these war crimes come to a halt.”
There is actually a basis for this action. It isn’t in the organization’s own bylaws, which as I said, are very simple — reduce cardiovascular disease burden — but they are a member of a broader group, the Biomedical Alliance in Europe, which does have a very explicit code of ethics.
I’m going to read you a little bit from that code. It says healthcare organizations should uphold and promote equality, diversity and inclusion, accountability, transparency, and equality. They also say that all members, including the European Society of Cardiology, should be committed both to the Declaration of Helsinki, a fundamental medical ethics document, and the Declaration of Geneva. These rules refer to the highest respect of human beings, responsible resource allocation, and preservation of the environment, among other things.
What the organization is doing is consistent with the code of ethics that the broader organization of all the medical societies of Europe say that these individual groups should be doing. You can’t collaborate with war criminals. You can’t act as if business as usual is going on. That’s not inclusive. That’s not respect for diversity.
I think the Ukrainian medical societies of cardiology and other specialties would find it grimly ironic to say that keeping Russian and Belarus members makes sense, given what’s going on in their country and what is happening to them. They’re under attack. They’re being killed. Their healthcare institutions are being indiscriminately shelled and bombed.
It’s very hard — and I understand that — to say we’re going to punish scientists. We’re going to, perhaps, even cause public health problems in Russia because we’re not going to collaborate right now with doctors and scientists in cardiology or any other medical specialty. I think it’s what has to be done.
We’re in a new era of trying to combat what is basically organized, international ethnic terrorism, complete with war crimes. We fight financially. We fight by isolating. We fight by excluding. It’s painful. It’s difficult. It’s somewhat unfair to individuals.
Only through that kind of pain are we going to get the kind of pressure that will achieve justice. I think that is a goal that we have to commend the European Society of Cardiology for honoring.
Dr. Caplan is director of the division of medical ethics at New York University. He is the author or editor of 35 books and 750 peer-reviewed articles as well as a frequent commentator in the media on bioethical issues. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (an unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at the NYU Grossman School of Medicine.
There are many difficult moral issues that are being fueled by the terrible war that Russia is waging against Ukraine. I think there is no way to justify anything that the Russians are doing. Ukraine did not do anything to violate Russian integrity, Russian territorial integrity, or anything by way of being aggressive toward Russia.
Russia decided at some point it wanted the Ukraine back. Putin has a dream, as the long-standing leader of Russia, to restore the Soviet empire, and Ukraine is top of the list of the places that he wants back for a variety of reasons.
We’re not here to debate the merits and demerits of this terrible act of war.
The European Society of Cardiology made a decision very recently to drop, as members, both Russia and Belarus, Russia’s ally in this aggressive war against Ukraine. They basically found it intolerable to have business as usual with these subsidiary cardiology societies as part of the ongoing activities of the European group.
The sole goal of this overarching European group is to reduce the health burden of cardiovascular disease. It doesn’t have political goals. It doesn’t have much to say about anything other than, “Let’s get evidence-based medicine used to try and prevent heart disease or treat heart disease.” So there’s noble intent.
Many of its members asked, “What are we doing in politics? Why are we punishing Russian and Belarussian cardiologists, acting as if somehow they are responsible for what the Russian army is doing or for what Putin has decided to do? Why are we acting against them? They are just trying to fight heart disease. That’s a legitimate goal for any doctor, public health official, or scientist.” They didn’t see, as members, why this exclusion had taken place.
I believe the exclusion is appropriate and some of the membership, obviously, in the European Society of Cardiology, agrees. It’s not because they’re holding doctors or scientists directly accountable for Putin’s war crimes, ethnic cleansing assault, or bombing and shelling of hospitals, maternity hospitals, and civilians.
They understand that these scientists and doctors have little to do with such things, but we are in a new form of warfare, and that warfare is basically economic and sociologic: turning Russia, as an inexcusably aggressive state, into a pariah.
The reason to break the ties is that that is the way to bring pressure upon Putin and his kleptocratic, oligarchic advisers to stop the attack, to try and bring down their economy, to say, “Business is not going to go on as usual. You will be excluded from normal scientific and medical commerce. We’re not going to be holding conferences or exchanging ideas,” and in my view, extending it to say, “We’re not taking your papers, we’re not publishing anything you do. We’re not even having you speak at our meetings until this war, this aggressive invasion, and these war crimes come to a halt.”
There is actually a basis for this action. It isn’t in the organization’s own bylaws, which as I said, are very simple — reduce cardiovascular disease burden — but they are a member of a broader group, the Biomedical Alliance in Europe, which does have a very explicit code of ethics.
I’m going to read you a little bit from that code. It says healthcare organizations should uphold and promote equality, diversity and inclusion, accountability, transparency, and equality. They also say that all members, including the European Society of Cardiology, should be committed both to the Declaration of Helsinki, a fundamental medical ethics document, and the Declaration of Geneva. These rules refer to the highest respect of human beings, responsible resource allocation, and preservation of the environment, among other things.
What the organization is doing is consistent with the code of ethics that the broader organization of all the medical societies of Europe say that these individual groups should be doing. You can’t collaborate with war criminals. You can’t act as if business as usual is going on. That’s not inclusive. That’s not respect for diversity.
I think the Ukrainian medical societies of cardiology and other specialties would find it grimly ironic to say that keeping Russian and Belarus members makes sense, given what’s going on in their country and what is happening to them. They’re under attack. They’re being killed. Their healthcare institutions are being indiscriminately shelled and bombed.
It’s very hard — and I understand that — to say we’re going to punish scientists. We’re going to, perhaps, even cause public health problems in Russia because we’re not going to collaborate right now with doctors and scientists in cardiology or any other medical specialty. I think it’s what has to be done.
We’re in a new era of trying to combat what is basically organized, international ethnic terrorism, complete with war crimes. We fight financially. We fight by isolating. We fight by excluding. It’s painful. It’s difficult. It’s somewhat unfair to individuals.
Only through that kind of pain are we going to get the kind of pressure that will achieve justice. I think that is a goal that we have to commend the European Society of Cardiology for honoring.
Dr. Caplan is director of the division of medical ethics at New York University. He is the author or editor of 35 books and 750 peer-reviewed articles as well as a frequent commentator in the media on bioethical issues. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (an unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at the NYU Grossman School of Medicine.
There are many difficult moral issues that are being fueled by the terrible war that Russia is waging against Ukraine. I think there is no way to justify anything that the Russians are doing. Ukraine did not do anything to violate Russian integrity, Russian territorial integrity, or anything by way of being aggressive toward Russia.
Russia decided at some point it wanted the Ukraine back. Putin has a dream, as the long-standing leader of Russia, to restore the Soviet empire, and Ukraine is top of the list of the places that he wants back for a variety of reasons.
We’re not here to debate the merits and demerits of this terrible act of war.
The European Society of Cardiology made a decision very recently to drop, as members, both Russia and Belarus, Russia’s ally in this aggressive war against Ukraine. They basically found it intolerable to have business as usual with these subsidiary cardiology societies as part of the ongoing activities of the European group.
The sole goal of this overarching European group is to reduce the health burden of cardiovascular disease. It doesn’t have political goals. It doesn’t have much to say about anything other than, “Let’s get evidence-based medicine used to try and prevent heart disease or treat heart disease.” So there’s noble intent.
Many of its members asked, “What are we doing in politics? Why are we punishing Russian and Belarussian cardiologists, acting as if somehow they are responsible for what the Russian army is doing or for what Putin has decided to do? Why are we acting against them? They are just trying to fight heart disease. That’s a legitimate goal for any doctor, public health official, or scientist.” They didn’t see, as members, why this exclusion had taken place.
I believe the exclusion is appropriate and some of the membership, obviously, in the European Society of Cardiology, agrees. It’s not because they’re holding doctors or scientists directly accountable for Putin’s war crimes, ethnic cleansing assault, or bombing and shelling of hospitals, maternity hospitals, and civilians.
They understand that these scientists and doctors have little to do with such things, but we are in a new form of warfare, and that warfare is basically economic and sociologic: turning Russia, as an inexcusably aggressive state, into a pariah.
The reason to break the ties is that that is the way to bring pressure upon Putin and his kleptocratic, oligarchic advisers to stop the attack, to try and bring down their economy, to say, “Business is not going to go on as usual. You will be excluded from normal scientific and medical commerce. We’re not going to be holding conferences or exchanging ideas,” and in my view, extending it to say, “We’re not taking your papers, we’re not publishing anything you do. We’re not even having you speak at our meetings until this war, this aggressive invasion, and these war crimes come to a halt.”
There is actually a basis for this action. It isn’t in the organization’s own bylaws, which as I said, are very simple — reduce cardiovascular disease burden — but they are a member of a broader group, the Biomedical Alliance in Europe, which does have a very explicit code of ethics.
I’m going to read you a little bit from that code. It says healthcare organizations should uphold and promote equality, diversity and inclusion, accountability, transparency, and equality. They also say that all members, including the European Society of Cardiology, should be committed both to the Declaration of Helsinki, a fundamental medical ethics document, and the Declaration of Geneva. These rules refer to the highest respect of human beings, responsible resource allocation, and preservation of the environment, among other things.
What the organization is doing is consistent with the code of ethics that the broader organization of all the medical societies of Europe say that these individual groups should be doing. You can’t collaborate with war criminals. You can’t act as if business as usual is going on. That’s not inclusive. That’s not respect for diversity.
I think the Ukrainian medical societies of cardiology and other specialties would find it grimly ironic to say that keeping Russian and Belarus members makes sense, given what’s going on in their country and what is happening to them. They’re under attack. They’re being killed. Their healthcare institutions are being indiscriminately shelled and bombed.
It’s very hard — and I understand that — to say we’re going to punish scientists. We’re going to, perhaps, even cause public health problems in Russia because we’re not going to collaborate right now with doctors and scientists in cardiology or any other medical specialty. I think it’s what has to be done.
We’re in a new era of trying to combat what is basically organized, international ethnic terrorism, complete with war crimes. We fight financially. We fight by isolating. We fight by excluding. It’s painful. It’s difficult. It’s somewhat unfair to individuals.
Only through that kind of pain are we going to get the kind of pressure that will achieve justice. I think that is a goal that we have to commend the European Society of Cardiology for honoring.
Dr. Caplan is director of the division of medical ethics at New York University. He is the author or editor of 35 books and 750 peer-reviewed articles as well as a frequent commentator in the media on bioethical issues. He has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (an unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
Lancet Commission reexamines the current approach to death
“The story of dying in the 21st century is a story of paradox.” This is the opening line of a report recently published in the Lancet, in which the Lancet Commission experts tackle what is, for many, a very sensitive topic: the end of life. The recommendations they present aim at “bringing death back into life.”
What makes the story a paradox is that, in end-of-life situations, many people are overtreated, and on the other hand, many people are undertreated.
In short, when all is said and done, “people die bad deaths.” A natural event, a natural part of life, has turned into something that people fear or, in some cases, refuse to even acknowledge or talk about.
This was the motivating factor for the Lancet Commission, a group of experts from various disciplines, to come together to try to better understand this complex concept. , as well as a balance between life and death.
This sensitive topic was explored by Marina Sozzi, PhD. She is the director of the Association for the Support and Assistance of People With Chronic and Oncological Diseases, a nonprofit organization that for more than 30 years has been dedicated to “providing palliative care and supporting individuals with oncological or other chronic and degenerative diseases.”
Call for rebalancing
To give people an idea of a better system in which life and death are in balance, the Lancet Commission experts described a realistic utopia, which they summarized in the following five principles:
- The social determinants of death, dying, and grieving are confronted.
- Dying is understood to be a relational and spiritual process rather than simply a physiological event.
- Networks of care provide support for people who are dying, those caring for them, and those grieving.
- Conversations and stories about everyday death, dying, and grief become common.
- Death is recognized as having value.
Achieving this utopia will not be easy, especially considering the current systems that are in place. “There have been tremendous medical advances over the last hundred years, particularly in increasing life expectancy and curing diseases that were once considered death sentences,” Dr. Sozzi explained. “Indeed, over the course of that time period, medical science acquired an enormous degree of social power, and matters of death – which in previous centuries had been within the purview of religions and houses of worship – were handed over to be handled by doctors and nurses.”
The COVID-19 pandemic has made the medical field’s role in matters of death more prominent: every day, people saw footage of dying people in hospital beds being cared for by health care professionals in masks and gowns. These patients were otherwise alone, their only contact with loved ones being over the phone or online. They died the ultimate medicalized deaths, stripped of almost all opportunities to get emotional support from family and friends.
New perspective needed
The Lancet Commission experts were certain about one point: The need to move away from the reductionist approach to death in order to integrate a more holistic approach, one that takes into account all of the dimensions of death without limiting itself only to the medical aspects.
“Medicine has its own take on the death phenomenon and on disease, which is a reductionist take,” said Dr. Sozzi, noting that, thanks to processes that make it possible to reduce phenomena to the measurable, medicine has managed to make tremendous progress. The same approach has been applied to the view of death, which has by and large become a biologic event.
“The problem is that, in reality, death is a much more complex phenomenon: cultural, social, involving families and society,” she explained. “Not all of these aspects are taken into consideration by medicine, and therefore, our culture has diminished its view of the death phenomenon.” Dr. Sozzi pointed out that, if looked upon more closely, the very question: “What did the person die of?” presupposes, in a certain sense, that it might have been possible to prevent that death – if only medicine had the right technology. So, death comes to be seen as something that could have been avoided.
Power of palliative care
Changing the approach to death requires a profound culture shift and, therefore, a lot of time. The good news is that, although there is still a long way to go, a few steps have been taken in this direction. “Talking about death, and even organizing courses aimed at health care professionals, is definitely easier these days than it was even just 10 years ago,” said Dr. Sozzi, citing, as an example, a project she developed for training nursing home operators in palliative care.
It is in palliative care where the greatest progress has been made in end-of-life matters. “The culture of palliative care allows us to think about death in very different terms and to recognize that moment when we should stop looking at curative care and direct our efforts at ‘comfort care.’ And this care of the dying has to be holistic,” Dr. Sozzi explained. She adds that we are increasingly talking about simultaneous palliative care – care that is not limited to the final days of a person’s life but that rather starts early on, when active treatments are still in place.
Dr. Sozzi mentioned Italy’s Law 38, which took effect in 2010. It regulates access to palliative care and pain management, expanding the right to receive these treatments to patients “in any health care setting, at any stage of life, and for any chronic or progressive condition which has no treatment or has a treatment that is not sufficient to stabilize it.”
A culture shift is also needed in this area; there has already been a movement away from general practitioners to health care professionals who can and must direct a patient to palliative care.
“We need to provide these doctors with more training and make them more aware of what a difference this kind of care can make throughout a patient’s life, not only during the final stages,” said Dr. Sozzi. Concerning training, she mentioned that Italy had recently introduced a specialization in palliative care for medical school graduates. This is another small step and one that adds a sense of dignity to this new approach to life and to death.
The experts’ recommendations
In attempting to find a balance between life and death, we must not look at the period prior to the 1900s as some kind of golden age. Dr. Sozzi explained that back then there was almost none of the medical technology now available to treat people at the end of life. “Palliative care has also set forth original technical aspects for eliminating pain. Without having eliminated a patient’s pain, I can hardly begin a discussion with them about spiritual aspects,” she said, emphasizing the importance of always contextualizing approaches to death.
The Lancet Commission experts assessed the approach to death in many different contexts. They recommended that, to best handle end-of-life matters in all their complexity, one should keep in mind the importance of relationships and networks across society.
They recommended that health care and social care professionals improve their skills and their capacity for taking care of dying patients and their families. When the patient has a life-limiting illness, a caring and compassionate approach should be taken when providing clear information about all interventions involved in palliative care, as well as when having conversations about death.
Governments and policy makers are advised to implement actions to allow all citizens to have the same access to necessary palliative care. In addition, all strategies and reports on social care and well-being more broadly should always include consideration of death, dying, and grieving. It’s an uphill climb, but one that must be made if we’re to build a new culture aimed at bringing death back into life. “As we continue stepping toward this new culture, let us each put a stone in place,” Dr. Sozzi concluded.
A version of this article first appeared on Medscape.com.
“The story of dying in the 21st century is a story of paradox.” This is the opening line of a report recently published in the Lancet, in which the Lancet Commission experts tackle what is, for many, a very sensitive topic: the end of life. The recommendations they present aim at “bringing death back into life.”
What makes the story a paradox is that, in end-of-life situations, many people are overtreated, and on the other hand, many people are undertreated.
In short, when all is said and done, “people die bad deaths.” A natural event, a natural part of life, has turned into something that people fear or, in some cases, refuse to even acknowledge or talk about.
This was the motivating factor for the Lancet Commission, a group of experts from various disciplines, to come together to try to better understand this complex concept. , as well as a balance between life and death.
This sensitive topic was explored by Marina Sozzi, PhD. She is the director of the Association for the Support and Assistance of People With Chronic and Oncological Diseases, a nonprofit organization that for more than 30 years has been dedicated to “providing palliative care and supporting individuals with oncological or other chronic and degenerative diseases.”
Call for rebalancing
To give people an idea of a better system in which life and death are in balance, the Lancet Commission experts described a realistic utopia, which they summarized in the following five principles:
- The social determinants of death, dying, and grieving are confronted.
- Dying is understood to be a relational and spiritual process rather than simply a physiological event.
- Networks of care provide support for people who are dying, those caring for them, and those grieving.
- Conversations and stories about everyday death, dying, and grief become common.
- Death is recognized as having value.
Achieving this utopia will not be easy, especially considering the current systems that are in place. “There have been tremendous medical advances over the last hundred years, particularly in increasing life expectancy and curing diseases that were once considered death sentences,” Dr. Sozzi explained. “Indeed, over the course of that time period, medical science acquired an enormous degree of social power, and matters of death – which in previous centuries had been within the purview of religions and houses of worship – were handed over to be handled by doctors and nurses.”
The COVID-19 pandemic has made the medical field’s role in matters of death more prominent: every day, people saw footage of dying people in hospital beds being cared for by health care professionals in masks and gowns. These patients were otherwise alone, their only contact with loved ones being over the phone or online. They died the ultimate medicalized deaths, stripped of almost all opportunities to get emotional support from family and friends.
New perspective needed
The Lancet Commission experts were certain about one point: The need to move away from the reductionist approach to death in order to integrate a more holistic approach, one that takes into account all of the dimensions of death without limiting itself only to the medical aspects.
“Medicine has its own take on the death phenomenon and on disease, which is a reductionist take,” said Dr. Sozzi, noting that, thanks to processes that make it possible to reduce phenomena to the measurable, medicine has managed to make tremendous progress. The same approach has been applied to the view of death, which has by and large become a biologic event.
“The problem is that, in reality, death is a much more complex phenomenon: cultural, social, involving families and society,” she explained. “Not all of these aspects are taken into consideration by medicine, and therefore, our culture has diminished its view of the death phenomenon.” Dr. Sozzi pointed out that, if looked upon more closely, the very question: “What did the person die of?” presupposes, in a certain sense, that it might have been possible to prevent that death – if only medicine had the right technology. So, death comes to be seen as something that could have been avoided.
Power of palliative care
Changing the approach to death requires a profound culture shift and, therefore, a lot of time. The good news is that, although there is still a long way to go, a few steps have been taken in this direction. “Talking about death, and even organizing courses aimed at health care professionals, is definitely easier these days than it was even just 10 years ago,” said Dr. Sozzi, citing, as an example, a project she developed for training nursing home operators in palliative care.
It is in palliative care where the greatest progress has been made in end-of-life matters. “The culture of palliative care allows us to think about death in very different terms and to recognize that moment when we should stop looking at curative care and direct our efforts at ‘comfort care.’ And this care of the dying has to be holistic,” Dr. Sozzi explained. She adds that we are increasingly talking about simultaneous palliative care – care that is not limited to the final days of a person’s life but that rather starts early on, when active treatments are still in place.
Dr. Sozzi mentioned Italy’s Law 38, which took effect in 2010. It regulates access to palliative care and pain management, expanding the right to receive these treatments to patients “in any health care setting, at any stage of life, and for any chronic or progressive condition which has no treatment or has a treatment that is not sufficient to stabilize it.”
A culture shift is also needed in this area; there has already been a movement away from general practitioners to health care professionals who can and must direct a patient to palliative care.
“We need to provide these doctors with more training and make them more aware of what a difference this kind of care can make throughout a patient’s life, not only during the final stages,” said Dr. Sozzi. Concerning training, she mentioned that Italy had recently introduced a specialization in palliative care for medical school graduates. This is another small step and one that adds a sense of dignity to this new approach to life and to death.
The experts’ recommendations
In attempting to find a balance between life and death, we must not look at the period prior to the 1900s as some kind of golden age. Dr. Sozzi explained that back then there was almost none of the medical technology now available to treat people at the end of life. “Palliative care has also set forth original technical aspects for eliminating pain. Without having eliminated a patient’s pain, I can hardly begin a discussion with them about spiritual aspects,” she said, emphasizing the importance of always contextualizing approaches to death.
The Lancet Commission experts assessed the approach to death in many different contexts. They recommended that, to best handle end-of-life matters in all their complexity, one should keep in mind the importance of relationships and networks across society.
They recommended that health care and social care professionals improve their skills and their capacity for taking care of dying patients and their families. When the patient has a life-limiting illness, a caring and compassionate approach should be taken when providing clear information about all interventions involved in palliative care, as well as when having conversations about death.
Governments and policy makers are advised to implement actions to allow all citizens to have the same access to necessary palliative care. In addition, all strategies and reports on social care and well-being more broadly should always include consideration of death, dying, and grieving. It’s an uphill climb, but one that must be made if we’re to build a new culture aimed at bringing death back into life. “As we continue stepping toward this new culture, let us each put a stone in place,” Dr. Sozzi concluded.
A version of this article first appeared on Medscape.com.
“The story of dying in the 21st century is a story of paradox.” This is the opening line of a report recently published in the Lancet, in which the Lancet Commission experts tackle what is, for many, a very sensitive topic: the end of life. The recommendations they present aim at “bringing death back into life.”
What makes the story a paradox is that, in end-of-life situations, many people are overtreated, and on the other hand, many people are undertreated.
In short, when all is said and done, “people die bad deaths.” A natural event, a natural part of life, has turned into something that people fear or, in some cases, refuse to even acknowledge or talk about.
This was the motivating factor for the Lancet Commission, a group of experts from various disciplines, to come together to try to better understand this complex concept. , as well as a balance between life and death.
This sensitive topic was explored by Marina Sozzi, PhD. She is the director of the Association for the Support and Assistance of People With Chronic and Oncological Diseases, a nonprofit organization that for more than 30 years has been dedicated to “providing palliative care and supporting individuals with oncological or other chronic and degenerative diseases.”
Call for rebalancing
To give people an idea of a better system in which life and death are in balance, the Lancet Commission experts described a realistic utopia, which they summarized in the following five principles:
- The social determinants of death, dying, and grieving are confronted.
- Dying is understood to be a relational and spiritual process rather than simply a physiological event.
- Networks of care provide support for people who are dying, those caring for them, and those grieving.
- Conversations and stories about everyday death, dying, and grief become common.
- Death is recognized as having value.
Achieving this utopia will not be easy, especially considering the current systems that are in place. “There have been tremendous medical advances over the last hundred years, particularly in increasing life expectancy and curing diseases that were once considered death sentences,” Dr. Sozzi explained. “Indeed, over the course of that time period, medical science acquired an enormous degree of social power, and matters of death – which in previous centuries had been within the purview of religions and houses of worship – were handed over to be handled by doctors and nurses.”
The COVID-19 pandemic has made the medical field’s role in matters of death more prominent: every day, people saw footage of dying people in hospital beds being cared for by health care professionals in masks and gowns. These patients were otherwise alone, their only contact with loved ones being over the phone or online. They died the ultimate medicalized deaths, stripped of almost all opportunities to get emotional support from family and friends.
New perspective needed
The Lancet Commission experts were certain about one point: The need to move away from the reductionist approach to death in order to integrate a more holistic approach, one that takes into account all of the dimensions of death without limiting itself only to the medical aspects.
“Medicine has its own take on the death phenomenon and on disease, which is a reductionist take,” said Dr. Sozzi, noting that, thanks to processes that make it possible to reduce phenomena to the measurable, medicine has managed to make tremendous progress. The same approach has been applied to the view of death, which has by and large become a biologic event.
“The problem is that, in reality, death is a much more complex phenomenon: cultural, social, involving families and society,” she explained. “Not all of these aspects are taken into consideration by medicine, and therefore, our culture has diminished its view of the death phenomenon.” Dr. Sozzi pointed out that, if looked upon more closely, the very question: “What did the person die of?” presupposes, in a certain sense, that it might have been possible to prevent that death – if only medicine had the right technology. So, death comes to be seen as something that could have been avoided.
Power of palliative care
Changing the approach to death requires a profound culture shift and, therefore, a lot of time. The good news is that, although there is still a long way to go, a few steps have been taken in this direction. “Talking about death, and even organizing courses aimed at health care professionals, is definitely easier these days than it was even just 10 years ago,” said Dr. Sozzi, citing, as an example, a project she developed for training nursing home operators in palliative care.
It is in palliative care where the greatest progress has been made in end-of-life matters. “The culture of palliative care allows us to think about death in very different terms and to recognize that moment when we should stop looking at curative care and direct our efforts at ‘comfort care.’ And this care of the dying has to be holistic,” Dr. Sozzi explained. She adds that we are increasingly talking about simultaneous palliative care – care that is not limited to the final days of a person’s life but that rather starts early on, when active treatments are still in place.
Dr. Sozzi mentioned Italy’s Law 38, which took effect in 2010. It regulates access to palliative care and pain management, expanding the right to receive these treatments to patients “in any health care setting, at any stage of life, and for any chronic or progressive condition which has no treatment or has a treatment that is not sufficient to stabilize it.”
A culture shift is also needed in this area; there has already been a movement away from general practitioners to health care professionals who can and must direct a patient to palliative care.
“We need to provide these doctors with more training and make them more aware of what a difference this kind of care can make throughout a patient’s life, not only during the final stages,” said Dr. Sozzi. Concerning training, she mentioned that Italy had recently introduced a specialization in palliative care for medical school graduates. This is another small step and one that adds a sense of dignity to this new approach to life and to death.
The experts’ recommendations
In attempting to find a balance between life and death, we must not look at the period prior to the 1900s as some kind of golden age. Dr. Sozzi explained that back then there was almost none of the medical technology now available to treat people at the end of life. “Palliative care has also set forth original technical aspects for eliminating pain. Without having eliminated a patient’s pain, I can hardly begin a discussion with them about spiritual aspects,” she said, emphasizing the importance of always contextualizing approaches to death.
The Lancet Commission experts assessed the approach to death in many different contexts. They recommended that, to best handle end-of-life matters in all their complexity, one should keep in mind the importance of relationships and networks across society.
They recommended that health care and social care professionals improve their skills and their capacity for taking care of dying patients and their families. When the patient has a life-limiting illness, a caring and compassionate approach should be taken when providing clear information about all interventions involved in palliative care, as well as when having conversations about death.
Governments and policy makers are advised to implement actions to allow all citizens to have the same access to necessary palliative care. In addition, all strategies and reports on social care and well-being more broadly should always include consideration of death, dying, and grieving. It’s an uphill climb, but one that must be made if we’re to build a new culture aimed at bringing death back into life. “As we continue stepping toward this new culture, let us each put a stone in place,” Dr. Sozzi concluded.
A version of this article first appeared on Medscape.com.
FROM THE LANCET
First-year fellows guide to gastroenterology
After the excitement and the well-deserved celebrations of matching in a gastroenterology fellowship program, a whole new set of unanswered questions and worries can start forming in a first-year fellow’s mind. “I made it, but now what? How do I learn a whole new career skill like endoscopy? Is my GI knowledge solid and wide enough to manage patients and answer the medical team consult? How will I keep up with my reading and learning with a busy fellowship schedule? How do I balance growth in clinical knowledge, endoscopy, and research? Can I integrate ‘life’ alongside a busy fellowship?” All of these questions and more can be overwhelming to answer in the beginning. The following guide is designed to help you through this transition and navigate the various aspects of first-year fellowship.
First-year goals
It is important to keep in mind that you have 3 full years to become a well-rounded, highly skilled, and knowledgeable gastroenterologist and endoscopist. So, set realistic goals and expectations for your first year, but be mindful that this year also lays the solid foundations of who you will become as a clinician, educator, or researcher.

One of the main goals of fellowship is to learn and implement evidence-based medicine in the diagnosis and management of GI conditions, as well as to learn endoscopic skills and ethics, all while keeping the patient (as a whole person) at the center of what you do. According to a recently published article by Bollipo and colleagues,1 the overall growth as a gastroenterologist not only depends on acquisition of knowledge but also involves cultivating teamwork, communication, situational awareness, compassion, leadership, and situational awareness. Beyond your medical education, your professional growth is also dependent on intentionally working towards acquiring the following skills:
1. Manage your time efficiently and prioritize your daily tasks
2. Become a consultant: effectively communicate with others, teach, lead, and delegate as appropriate
3. Work as a team with colleagues, faculty, and endoscopy staff
4. Develop critical thinking, give and receive constructive feedback, and understand your skills, limitations, and growth potential
5. Identify mentors and potential niche area
6. Start building your professional network and your reputation
7. Get involved in national GI societies
Consults
Mindset
Shifting gear from residency to fellowship involves a shifting of your clinical mindset too, going from being part of a primary care team responsible for all aspects of a patient’s medical care, to that of a consulting team focused on a patient’s GI condition. It is important to find the right balance of refraining from micromanaging non-GI comorbidities while being fully aware of their impact on your diagnostic and therapeutic approach to the GI condition.

Let’s face it, you will not always get “exciting and interesting GI cases” consults, and on a busy day some consultations might feel unnecessary and frustrating to you. Remember that what seems obvious to you, based on your focused GI knowledge, might not be so simple to the primary team. In addition, every consult is an opportunity to improve your approach to patient care, as well as an opportunity to learn and teach others, from medical students to residents. So, always be professional and respectful when you pick up the phone, and build positive collaborative bridges between you and the medical or surgical consulting teams. Be the GI fellow others are not reluctant to call for help, and better, be the one who communicates GI pearls along the way, inspires others to join the field of gastroenterology, and positively represent the GI division.
Triage
When you answer your consult page, ask the primary team what specific question they have for you and/or what is the main GI complaint or test abnormality the patient has. This will help you assess the urgency and the complexity of the consult, and hence allow you to prioritize each consult (which one you need to see first and give the attending a heads-up), assign (or not) a rotating medical resident or student to the consult, tailor your preliminary recommendations to the primary team, and anticipate the need for a procedure. When you anticipate a procedure, assess its (semi-)urgency to get the process ready for same day or a bedside procedure by getting information on the patient’s vitals, basic labs, significant acute comorbidities, and supportive therapies in place. In other words, by judiciously obtaining key information from the primary team, you can efficiently triage the consults and keep your day organized and manageable (for the most part). Learn to divide and conquer the tasks of the day: split inpatient endoscopy and consults with your cofellows, assign appropriate consults and follow-ups to residents or students rotating on the GI service, and properly communicate with the primary team a plan of care (even a preliminary one) to avoid recurrent pages and interruptions. Some days the number or urgency of the consults and the required multitasking can be overwhelming: stop, breathe, and ask for help from your co-fellows and your attending. Remember, this is a fellowship, not a solo-ship and your program is here to support your work and growth.
Communication
Timely and efficient communication, between you and the different stakeholders, is crucial to provide optimal patient care and minimize the risk of “things falling through the cracks”. Convey to the primary team your recommendations and plan of care clearly, and use direct verbal communication (not just a note in the chart) when managing complex or urgent situations. Obtain information regarding current patient level of care (i.e., ICU), isolation precautions, and cardiac devices (i.e., left ventricular assist device). Keep the dialogue open with your attending about acutely ill patients and potentially urgent procedures. Inform the endoscopy suite early that you are adding a procedure on the same day, and communicate anticipated needs (such as intubation, fluoroscopy room, pediatric scope, stent). Using a “closed-loop” communication structure can ensure that your recommendations are received and implemented appropriately.2
Time management and structure

Having a structured routine to your day, in what seems to be a chaotic process of juggling different duties and being in different locations at once, will ensure that you efficiently complete your tasks in a timely manner. Find what works best for you, taking into account the challenges and resources available to you, such as the number of fellows and other trainees on the GI consult service, the average number of consults per day and their acuity, the availability of inpatient protocols for specific clinical situations (GI bleed, acute severe ulcerative colitis, etc.), and the time and style preferences of the rounding attending. We suggest the following schedule on a consult day: Round early in the morning and leave a note in the chart and/or communicate with the team key information, then review with the rotating trainees the patients they are following and personally reassess some patients as needed. Inform the endoscopy suite of the same day procedures and let your attending know of any issues that require immediate attention. Take your team and head to radiology and review the imaging studies on your patients. Learn and teach key points in diagnosis and therapeutic approach as you move through your day from the inpatient floors to the hallways. Divide consults during the day with your team and agree on a time to touch base. Review your patient list at the end of the day and assess which patients the GI service no longer need to follow and communicate that clearly to the primary team along with the appropriate outpatient GI care follow-up. Let the endoscopy suite know of any procedures you are adding for the next day along with their degree of urgency to allow the charge nurse to prioritize cases. When you leave the hospital, be intentional with your free time: Read about the GI conditions you have encountered, enjoy some fun relaxing time, and rest!
Call
Know your call environment and your emergency cart
Familiarize yourself with the locations where you could potentially perform an emergent case (i.e., the ICU, ED, operating room) and the relevant points of contact (such as the charge nurse, the anesthesia team, the on-call tech team) for overnight or weekend cases. Whether or not you have an endoscopy support team on call, learn to set up the emergency cart, find and check your equipment, and troubleshoot technical issues by soliciting an “in-service” from senior fellows or the endoscopy technical support staff. Before heading to an urgent case, double check that you have your “bleeder” or “food impaction” tools. For food impaction, consider obtaining rat tooth forceps, snares, Roth nets, and an overtube. For bleeding cases, obtain a therapeutic upper endoscope, hemostatic clips, clear caps, injection needles, epinephrine, HemosprayTM, banding kits, and the appropriate electrocautery/thermal set up.
What is an emergency?
Consults that require your immediate attention include food impactions, acute biliary conditions leading to septic shock, and hemodynamically unstable GI bleeds, especially variceal bleeds. Remember that patients who are hemodynamically unstable require adequate resuscitation before proceeding with any endoscopic intervention. Assess the need for intubation, the timing of the procedure, and the most optimal location to perform the procedure, depending on the time and acuity of the patients’ presentation, how they respond to resuscitation measures, and the resources and preferences of your institution.
The overnight ‘nonemergent’ call
Non-emergent consults can be addressed the next day, after reviewing the clinical information provided by the consulting team and the patient’s EMR to ensure no urgent measures are needed. Overnight call may include patient phone calls, from inquiries about colon prep (so familiarize yourself with the different prep instructions and how to troubleshoot prep difficulties) to GI symptoms that you will need to triage to either the ED or to an outpatient follow-up. Document all phone encounters in the EMR and route your note to the appropriate clinician and nurse or administrative assistant for follow-up.
The five E’s of endoscopy
Endoscopy training is a large component of a GI fellowship and can create achievement anxiety in many first-year fellows seeking the cecum! But there is more to endoscopy than technical skills: It is as important to adequately evaluate clinical situations, understand the indications and potential limitations and complications of the procedure, and assess how it will impact the management of the patient. And no, you don’t have to be a video gamer to be a good endoscopist; and yes, you will be able to regularly complete a colonoscopy before the end of your first year!
Evaluation
In order to improve your endoscopic skills, it is important to honestly assess your areas of proficiency and improvement and to welcome real-time constructive feedback from your teaching attending about your endoscopic skills range. Consider meeting regularly with your attending to discuss your short-term and long-term endoscopic goals and how to enhance your skills. This practice demonstrates responsibility, credibility, and accountability amongst your peers as well as a genuine commitment to your growth as an endoscopist.
Efficiency
In addition to focusing on the quality of your endoscopy, learn to be efficient in the pre- and postprocedure time flow. This entails any step from properly explaining the procedure to patients before they come to the endoscopy suite, making sure the needed endoscopy equipment and tools are available in your room, completing your personal setup (i.e., gowning up, setting up your bed/monitor height, testing your endoscope) even before time out, to discharging the patient and communicating key findings and plan of care to the primary team. Depending on the acuity of the procedure and patient’s comorbidities, certain procedures may need to be performed or completed by a more efficient and experienced senior fellow or attending; don’t let this situation trigger passive frustration in you, but rather use it as an active and engaging opportunity to learn.
Expectations
You (and all the other neighborhood kids) didn’t learn to ride a bike without falling, struggling, needing help, and practicing over and over again, and it goes the same when learning to scope as a first-year fellow. Keep this in mind to lessen frustration, set realistic expectations, and be patient with yourself and celebrate all the small victories. Set tangible goals with your attending prior to procedural days/rotations so they can help you hone in and perfect the desired endoscopy skills.
Ergonomics
In a recent study, endoscopy-related injury (ERI) was reported to occur in up to 75% of gastroenterologists.3 While your primary focus might be reaching the cecum, it is as crucial for you to learn how to prevent ERI to ensure your long term health and continued success in procedures.
Excellence over quantity
Your main focus as a trainee is to learn how to provide effective, efficient, and safe care to patients, including in endoscopy. The quality of the endoscopy you perform is much more important than the total number of procedures you do. Thus, it is key to take each procedure as a complete learning opportunity to perform a thorough evaluation, improve your technical skills, interpret the findings, and develop a therapeutic plan.
Work-life balance and burnout
Fellowship is a marathon and not a sprint, so you need to slow down after a busy workday and care for yourself and enjoy time with loved ones. The cognitive, physical, mental, and emotional demands for first-year fellows are arguably the highest during GI training and can lead to burnout. Signs of burnout include emotional exhaustion, loss of empathy, fatigue, depersonalization and detachment, and feelings of personal inadequacy.4 Antiburnout measures include respecting basic healthy life hygiene (eat and sleep well, regular physical activity), having a hobby, practicing meditation, avoiding taking work home, and having a healthy social network.5 Remember that your cofellows whom you share common experiences with are not only your colleagues but can also be your friends and your social support. If you are a parent juggling work and family, remember to ask for help from your peers if you need it and have an open discussion with your attending to find practical solutions to your schedule.
Professional growth in the field of gastroenterology
Becoming a successful gastroenterologist and endoscopist involves going above the “I” and into the inclusive “we.” Building collegial and professional relationships early on with different stakeholders will set you up for success during and beyond your fellowship.
Building relationships
Developing genuine collegial and collaborative relationships with cofellows and faculty will positively impact your wellness during fellowship but also build the foundation of your professional network necessary to your career growth. Be inclusive of your cofellows in your research projects and publications, and support and amplify their work as much as you amplify your own. Your cofellows or attendings are likely to be the ones to help you find the right job, invite you to speak at grand rounds, or sit on a GI committee and promote your postfellowship professional growth.
Mentorship, being an educator and role model
It is important to identify and seek out mentors, within or outside your fellowship program or institution, who can not only guide you in your career choices but also open doors for you and sponsor you to advance your career. On the other hand, you too can be a role model, mentor, and sponsor to medical residents and students interested in the field of GI. Teach others in didactic settings or on the consult service, include trainees in quality improvement projects and publications, and lead by example.
Research
Most academic GI programs have a baseline requirement of research. Choose and devise a project you can realistically complete despite your busy first-year schedule: expand on a residency research project, focus on a specific simple question triggered by a clinical situation you encountered, proceed with a retrospective chart review or quality improvement project, and include other fellows and trainees to divide tasks. Alternatively, devise a specific timeline with a research mentor to complete a larger research project during your three years of fellowship.
Involvement in GI societies/committees
Become a member of one (or all) of the national GI societies that align with your interests. Membership gives you access not only to peer-reviewed scientific articles and guidelines but also to fellow-focused programs, committees’ opportunities, early career research grants, and mentorship.6-10
Summary
The first year of a GI fellowship lays the foundation for your next 3 years: Be mindful of how you can optimize the opportunities at hand to learn, teach, build a solid reputation, and grow your professional network. But also remember you have 3 full years to accomplish all your goals, so be patient, pace yourself, and include others in your journey. Judiciously use the many resources within your program and GI societies to help you achieve your goals, reach out to others to overcome difficulties and barriers, and dedicate time to care for your personal health and growth. This is what a true comprehensive and healthy fellowship is all about!
Dr. Advani is with the division of gastroenterology and hepatology, Stony Brook (N.Y.) University Hospital. Dr. Saeed is with the division of gastroenterology and hepatology, University of Kentucky, Lexington. Dr. Charabaty is with the division of gastroenterology, Johns Hopkins University, Baltimore, and Johns Hopkins–Sibley Memorial Hospital, Washington. Dr. Advani and Dr. Saeed have no conflicts to disclose. Dr. Charabaty disclosed ties to AbbVie, Janssen, Takeda, Pfizer, and Bristol-Myers Squibb and is founder of @MondayNightIBD, and cofounder of Scrubs & Heels.
References
1. Bollipo S. Gastroenterology. 2020 Nov;159(5):1648-52.
2. Adams MA et al. Gastroenterology. 2014 Jan 1;146(1):5-9.
3. Pawa S et al. Am J Gastroenterol. 2021 Mar 1;116(3):530-8.
4. DeCross AJ. Gastroenterology. 2020 Jan 1;158(1):32-5.
5. Burke C et al. Am J Gastroenterol. 2017 Oct 1;112:S593-4.
6. Fellows Resources under Fellows & Early Career. American Gastroenterological Association. https://gastro.org/fellows-and-early-career/training-resources/fellows-resources/.
7. Trainee Courses and Events. American College of Gastroenterology. https://gi.org/trainees/trainee-courses-and-events/.
8. Trainee Resources. American Association for the Study of Liver Diseases. https://www.aasld.org/membership/hepatology-associates/trainee-resources.
9. First Year Fellows Courses under Education. American Society of Gastrointestinal Endoscopy. https://www.asge.org/home/education/advanced-education-training/first-year-fellow-(fyf)-courses.
10. Annual GI Fellow Summer Course Presentations. New York Society for Gastrointestinal Endoscopy. https://www.nysge.org/annual%20gi%20fellows%20summer%20course.
After the excitement and the well-deserved celebrations of matching in a gastroenterology fellowship program, a whole new set of unanswered questions and worries can start forming in a first-year fellow’s mind. “I made it, but now what? How do I learn a whole new career skill like endoscopy? Is my GI knowledge solid and wide enough to manage patients and answer the medical team consult? How will I keep up with my reading and learning with a busy fellowship schedule? How do I balance growth in clinical knowledge, endoscopy, and research? Can I integrate ‘life’ alongside a busy fellowship?” All of these questions and more can be overwhelming to answer in the beginning. The following guide is designed to help you through this transition and navigate the various aspects of first-year fellowship.
First-year goals
It is important to keep in mind that you have 3 full years to become a well-rounded, highly skilled, and knowledgeable gastroenterologist and endoscopist. So, set realistic goals and expectations for your first year, but be mindful that this year also lays the solid foundations of who you will become as a clinician, educator, or researcher.
One of the main goals of fellowship is to learn and implement evidence-based medicine in the diagnosis and management of GI conditions, as well as to learn endoscopic skills and ethics, all while keeping the patient (as a whole person) at the center of what you do. According to a recently published article by Bollipo and colleagues,1 the overall growth as a gastroenterologist not only depends on acquisition of knowledge but also involves cultivating teamwork, communication, situational awareness, compassion, leadership, and situational awareness. Beyond your medical education, your professional growth is also dependent on intentionally working towards acquiring the following skills:
1. Manage your time efficiently and prioritize your daily tasks
2. Become a consultant: effectively communicate with others, teach, lead, and delegate as appropriate
3. Work as a team with colleagues, faculty, and endoscopy staff
4. Develop critical thinking, give and receive constructive feedback, and understand your skills, limitations, and growth potential
5. Identify mentors and potential niche area
6. Start building your professional network and your reputation
7. Get involved in national GI societies
Consults
Mindset
Shifting gear from residency to fellowship involves a shifting of your clinical mindset too, going from being part of a primary care team responsible for all aspects of a patient’s medical care, to that of a consulting team focused on a patient’s GI condition. It is important to find the right balance of refraining from micromanaging non-GI comorbidities while being fully aware of their impact on your diagnostic and therapeutic approach to the GI condition.
Let’s face it, you will not always get “exciting and interesting GI cases” consults, and on a busy day some consultations might feel unnecessary and frustrating to you. Remember that what seems obvious to you, based on your focused GI knowledge, might not be so simple to the primary team. In addition, every consult is an opportunity to improve your approach to patient care, as well as an opportunity to learn and teach others, from medical students to residents. So, always be professional and respectful when you pick up the phone, and build positive collaborative bridges between you and the medical or surgical consulting teams. Be the GI fellow others are not reluctant to call for help, and better, be the one who communicates GI pearls along the way, inspires others to join the field of gastroenterology, and positively represent the GI division.
Triage
When you answer your consult page, ask the primary team what specific question they have for you and/or what is the main GI complaint or test abnormality the patient has. This will help you assess the urgency and the complexity of the consult, and hence allow you to prioritize each consult (which one you need to see first and give the attending a heads-up), assign (or not) a rotating medical resident or student to the consult, tailor your preliminary recommendations to the primary team, and anticipate the need for a procedure. When you anticipate a procedure, assess its (semi-)urgency to get the process ready for same day or a bedside procedure by getting information on the patient’s vitals, basic labs, significant acute comorbidities, and supportive therapies in place. In other words, by judiciously obtaining key information from the primary team, you can efficiently triage the consults and keep your day organized and manageable (for the most part). Learn to divide and conquer the tasks of the day: split inpatient endoscopy and consults with your cofellows, assign appropriate consults and follow-ups to residents or students rotating on the GI service, and properly communicate with the primary team a plan of care (even a preliminary one) to avoid recurrent pages and interruptions. Some days the number or urgency of the consults and the required multitasking can be overwhelming: stop, breathe, and ask for help from your co-fellows and your attending. Remember, this is a fellowship, not a solo-ship and your program is here to support your work and growth.
Communication
Timely and efficient communication, between you and the different stakeholders, is crucial to provide optimal patient care and minimize the risk of “things falling through the cracks”. Convey to the primary team your recommendations and plan of care clearly, and use direct verbal communication (not just a note in the chart) when managing complex or urgent situations. Obtain information regarding current patient level of care (i.e., ICU), isolation precautions, and cardiac devices (i.e., left ventricular assist device). Keep the dialogue open with your attending about acutely ill patients and potentially urgent procedures. Inform the endoscopy suite early that you are adding a procedure on the same day, and communicate anticipated needs (such as intubation, fluoroscopy room, pediatric scope, stent). Using a “closed-loop” communication structure can ensure that your recommendations are received and implemented appropriately.2
Time management and structure
Having a structured routine to your day, in what seems to be a chaotic process of juggling different duties and being in different locations at once, will ensure that you efficiently complete your tasks in a timely manner. Find what works best for you, taking into account the challenges and resources available to you, such as the number of fellows and other trainees on the GI consult service, the average number of consults per day and their acuity, the availability of inpatient protocols for specific clinical situations (GI bleed, acute severe ulcerative colitis, etc.), and the time and style preferences of the rounding attending. We suggest the following schedule on a consult day: Round early in the morning and leave a note in the chart and/or communicate with the team key information, then review with the rotating trainees the patients they are following and personally reassess some patients as needed. Inform the endoscopy suite of the same day procedures and let your attending know of any issues that require immediate attention. Take your team and head to radiology and review the imaging studies on your patients. Learn and teach key points in diagnosis and therapeutic approach as you move through your day from the inpatient floors to the hallways. Divide consults during the day with your team and agree on a time to touch base. Review your patient list at the end of the day and assess which patients the GI service no longer need to follow and communicate that clearly to the primary team along with the appropriate outpatient GI care follow-up. Let the endoscopy suite know of any procedures you are adding for the next day along with their degree of urgency to allow the charge nurse to prioritize cases. When you leave the hospital, be intentional with your free time: Read about the GI conditions you have encountered, enjoy some fun relaxing time, and rest!
Call
Know your call environment and your emergency cart
Familiarize yourself with the locations where you could potentially perform an emergent case (i.e., the ICU, ED, operating room) and the relevant points of contact (such as the charge nurse, the anesthesia team, the on-call tech team) for overnight or weekend cases. Whether or not you have an endoscopy support team on call, learn to set up the emergency cart, find and check your equipment, and troubleshoot technical issues by soliciting an “in-service” from senior fellows or the endoscopy technical support staff. Before heading to an urgent case, double check that you have your “bleeder” or “food impaction” tools. For food impaction, consider obtaining rat tooth forceps, snares, Roth nets, and an overtube. For bleeding cases, obtain a therapeutic upper endoscope, hemostatic clips, clear caps, injection needles, epinephrine, HemosprayTM, banding kits, and the appropriate electrocautery/thermal set up.
What is an emergency?
Consults that require your immediate attention include food impactions, acute biliary conditions leading to septic shock, and hemodynamically unstable GI bleeds, especially variceal bleeds. Remember that patients who are hemodynamically unstable require adequate resuscitation before proceeding with any endoscopic intervention. Assess the need for intubation, the timing of the procedure, and the most optimal location to perform the procedure, depending on the time and acuity of the patients’ presentation, how they respond to resuscitation measures, and the resources and preferences of your institution.
The overnight ‘nonemergent’ call
Non-emergent consults can be addressed the next day, after reviewing the clinical information provided by the consulting team and the patient’s EMR to ensure no urgent measures are needed. Overnight call may include patient phone calls, from inquiries about colon prep (so familiarize yourself with the different prep instructions and how to troubleshoot prep difficulties) to GI symptoms that you will need to triage to either the ED or to an outpatient follow-up. Document all phone encounters in the EMR and route your note to the appropriate clinician and nurse or administrative assistant for follow-up.
The five E’s of endoscopy
Endoscopy training is a large component of a GI fellowship and can create achievement anxiety in many first-year fellows seeking the cecum! But there is more to endoscopy than technical skills: It is as important to adequately evaluate clinical situations, understand the indications and potential limitations and complications of the procedure, and assess how it will impact the management of the patient. And no, you don’t have to be a video gamer to be a good endoscopist; and yes, you will be able to regularly complete a colonoscopy before the end of your first year!
Evaluation
In order to improve your endoscopic skills, it is important to honestly assess your areas of proficiency and improvement and to welcome real-time constructive feedback from your teaching attending about your endoscopic skills range. Consider meeting regularly with your attending to discuss your short-term and long-term endoscopic goals and how to enhance your skills. This practice demonstrates responsibility, credibility, and accountability amongst your peers as well as a genuine commitment to your growth as an endoscopist.
Efficiency
In addition to focusing on the quality of your endoscopy, learn to be efficient in the pre- and postprocedure time flow. This entails any step from properly explaining the procedure to patients before they come to the endoscopy suite, making sure the needed endoscopy equipment and tools are available in your room, completing your personal setup (i.e., gowning up, setting up your bed/monitor height, testing your endoscope) even before time out, to discharging the patient and communicating key findings and plan of care to the primary team. Depending on the acuity of the procedure and patient’s comorbidities, certain procedures may need to be performed or completed by a more efficient and experienced senior fellow or attending; don’t let this situation trigger passive frustration in you, but rather use it as an active and engaging opportunity to learn.
Expectations
You (and all the other neighborhood kids) didn’t learn to ride a bike without falling, struggling, needing help, and practicing over and over again, and it goes the same when learning to scope as a first-year fellow. Keep this in mind to lessen frustration, set realistic expectations, and be patient with yourself and celebrate all the small victories. Set tangible goals with your attending prior to procedural days/rotations so they can help you hone in and perfect the desired endoscopy skills.
Ergonomics
In a recent study, endoscopy-related injury (ERI) was reported to occur in up to 75% of gastroenterologists.3 While your primary focus might be reaching the cecum, it is as crucial for you to learn how to prevent ERI to ensure your long term health and continued success in procedures.
Excellence over quantity
Your main focus as a trainee is to learn how to provide effective, efficient, and safe care to patients, including in endoscopy. The quality of the endoscopy you perform is much more important than the total number of procedures you do. Thus, it is key to take each procedure as a complete learning opportunity to perform a thorough evaluation, improve your technical skills, interpret the findings, and develop a therapeutic plan.
Work-life balance and burnout
Fellowship is a marathon and not a sprint, so you need to slow down after a busy workday and care for yourself and enjoy time with loved ones. The cognitive, physical, mental, and emotional demands for first-year fellows are arguably the highest during GI training and can lead to burnout. Signs of burnout include emotional exhaustion, loss of empathy, fatigue, depersonalization and detachment, and feelings of personal inadequacy.4 Antiburnout measures include respecting basic healthy life hygiene (eat and sleep well, regular physical activity), having a hobby, practicing meditation, avoiding taking work home, and having a healthy social network.5 Remember that your cofellows whom you share common experiences with are not only your colleagues but can also be your friends and your social support. If you are a parent juggling work and family, remember to ask for help from your peers if you need it and have an open discussion with your attending to find practical solutions to your schedule.
Professional growth in the field of gastroenterology
Becoming a successful gastroenterologist and endoscopist involves going above the “I” and into the inclusive “we.” Building collegial and professional relationships early on with different stakeholders will set you up for success during and beyond your fellowship.
Building relationships
Developing genuine collegial and collaborative relationships with cofellows and faculty will positively impact your wellness during fellowship but also build the foundation of your professional network necessary to your career growth. Be inclusive of your cofellows in your research projects and publications, and support and amplify their work as much as you amplify your own. Your cofellows or attendings are likely to be the ones to help you find the right job, invite you to speak at grand rounds, or sit on a GI committee and promote your postfellowship professional growth.
Mentorship, being an educator and role model
It is important to identify and seek out mentors, within or outside your fellowship program or institution, who can not only guide you in your career choices but also open doors for you and sponsor you to advance your career. On the other hand, you too can be a role model, mentor, and sponsor to medical residents and students interested in the field of GI. Teach others in didactic settings or on the consult service, include trainees in quality improvement projects and publications, and lead by example.
Research
Most academic GI programs have a baseline requirement of research. Choose and devise a project you can realistically complete despite your busy first-year schedule: expand on a residency research project, focus on a specific simple question triggered by a clinical situation you encountered, proceed with a retrospective chart review or quality improvement project, and include other fellows and trainees to divide tasks. Alternatively, devise a specific timeline with a research mentor to complete a larger research project during your three years of fellowship.
Involvement in GI societies/committees
Become a member of one (or all) of the national GI societies that align with your interests. Membership gives you access not only to peer-reviewed scientific articles and guidelines but also to fellow-focused programs, committees’ opportunities, early career research grants, and mentorship.6-10
Summary
The first year of a GI fellowship lays the foundation for your next 3 years: Be mindful of how you can optimize the opportunities at hand to learn, teach, build a solid reputation, and grow your professional network. But also remember you have 3 full years to accomplish all your goals, so be patient, pace yourself, and include others in your journey. Judiciously use the many resources within your program and GI societies to help you achieve your goals, reach out to others to overcome difficulties and barriers, and dedicate time to care for your personal health and growth. This is what a true comprehensive and healthy fellowship is all about!
Dr. Advani is with the division of gastroenterology and hepatology, Stony Brook (N.Y.) University Hospital. Dr. Saeed is with the division of gastroenterology and hepatology, University of Kentucky, Lexington. Dr. Charabaty is with the division of gastroenterology, Johns Hopkins University, Baltimore, and Johns Hopkins–Sibley Memorial Hospital, Washington. Dr. Advani and Dr. Saeed have no conflicts to disclose. Dr. Charabaty disclosed ties to AbbVie, Janssen, Takeda, Pfizer, and Bristol-Myers Squibb and is founder of @MondayNightIBD, and cofounder of Scrubs & Heels.
References
1. Bollipo S. Gastroenterology. 2020 Nov;159(5):1648-52.
2. Adams MA et al. Gastroenterology. 2014 Jan 1;146(1):5-9.
3. Pawa S et al. Am J Gastroenterol. 2021 Mar 1;116(3):530-8.
4. DeCross AJ. Gastroenterology. 2020 Jan 1;158(1):32-5.
5. Burke C et al. Am J Gastroenterol. 2017 Oct 1;112:S593-4.
6. Fellows Resources under Fellows & Early Career. American Gastroenterological Association. https://gastro.org/fellows-and-early-career/training-resources/fellows-resources/.
7. Trainee Courses and Events. American College of Gastroenterology. https://gi.org/trainees/trainee-courses-and-events/.
8. Trainee Resources. American Association for the Study of Liver Diseases. https://www.aasld.org/membership/hepatology-associates/trainee-resources.
9. First Year Fellows Courses under Education. American Society of Gastrointestinal Endoscopy. https://www.asge.org/home/education/advanced-education-training/first-year-fellow-(fyf)-courses.
10. Annual GI Fellow Summer Course Presentations. New York Society for Gastrointestinal Endoscopy. https://www.nysge.org/annual%20gi%20fellows%20summer%20course.
After the excitement and the well-deserved celebrations of matching in a gastroenterology fellowship program, a whole new set of unanswered questions and worries can start forming in a first-year fellow’s mind. “I made it, but now what? How do I learn a whole new career skill like endoscopy? Is my GI knowledge solid and wide enough to manage patients and answer the medical team consult? How will I keep up with my reading and learning with a busy fellowship schedule? How do I balance growth in clinical knowledge, endoscopy, and research? Can I integrate ‘life’ alongside a busy fellowship?” All of these questions and more can be overwhelming to answer in the beginning. The following guide is designed to help you through this transition and navigate the various aspects of first-year fellowship.
First-year goals
It is important to keep in mind that you have 3 full years to become a well-rounded, highly skilled, and knowledgeable gastroenterologist and endoscopist. So, set realistic goals and expectations for your first year, but be mindful that this year also lays the solid foundations of who you will become as a clinician, educator, or researcher.
One of the main goals of fellowship is to learn and implement evidence-based medicine in the diagnosis and management of GI conditions, as well as to learn endoscopic skills and ethics, all while keeping the patient (as a whole person) at the center of what you do. According to a recently published article by Bollipo and colleagues,1 the overall growth as a gastroenterologist not only depends on acquisition of knowledge but also involves cultivating teamwork, communication, situational awareness, compassion, leadership, and situational awareness. Beyond your medical education, your professional growth is also dependent on intentionally working towards acquiring the following skills:
1. Manage your time efficiently and prioritize your daily tasks
2. Become a consultant: effectively communicate with others, teach, lead, and delegate as appropriate
3. Work as a team with colleagues, faculty, and endoscopy staff
4. Develop critical thinking, give and receive constructive feedback, and understand your skills, limitations, and growth potential
5. Identify mentors and potential niche area
6. Start building your professional network and your reputation
7. Get involved in national GI societies
Consults
Mindset
Shifting gear from residency to fellowship involves a shifting of your clinical mindset too, going from being part of a primary care team responsible for all aspects of a patient’s medical care, to that of a consulting team focused on a patient’s GI condition. It is important to find the right balance of refraining from micromanaging non-GI comorbidities while being fully aware of their impact on your diagnostic and therapeutic approach to the GI condition.
Let’s face it, you will not always get “exciting and interesting GI cases” consults, and on a busy day some consultations might feel unnecessary and frustrating to you. Remember that what seems obvious to you, based on your focused GI knowledge, might not be so simple to the primary team. In addition, every consult is an opportunity to improve your approach to patient care, as well as an opportunity to learn and teach others, from medical students to residents. So, always be professional and respectful when you pick up the phone, and build positive collaborative bridges between you and the medical or surgical consulting teams. Be the GI fellow others are not reluctant to call for help, and better, be the one who communicates GI pearls along the way, inspires others to join the field of gastroenterology, and positively represent the GI division.
Triage
When you answer your consult page, ask the primary team what specific question they have for you and/or what is the main GI complaint or test abnormality the patient has. This will help you assess the urgency and the complexity of the consult, and hence allow you to prioritize each consult (which one you need to see first and give the attending a heads-up), assign (or not) a rotating medical resident or student to the consult, tailor your preliminary recommendations to the primary team, and anticipate the need for a procedure. When you anticipate a procedure, assess its (semi-)urgency to get the process ready for same day or a bedside procedure by getting information on the patient’s vitals, basic labs, significant acute comorbidities, and supportive therapies in place. In other words, by judiciously obtaining key information from the primary team, you can efficiently triage the consults and keep your day organized and manageable (for the most part). Learn to divide and conquer the tasks of the day: split inpatient endoscopy and consults with your cofellows, assign appropriate consults and follow-ups to residents or students rotating on the GI service, and properly communicate with the primary team a plan of care (even a preliminary one) to avoid recurrent pages and interruptions. Some days the number or urgency of the consults and the required multitasking can be overwhelming: stop, breathe, and ask for help from your co-fellows and your attending. Remember, this is a fellowship, not a solo-ship and your program is here to support your work and growth.
Communication
Timely and efficient communication, between you and the different stakeholders, is crucial to provide optimal patient care and minimize the risk of “things falling through the cracks”. Convey to the primary team your recommendations and plan of care clearly, and use direct verbal communication (not just a note in the chart) when managing complex or urgent situations. Obtain information regarding current patient level of care (i.e., ICU), isolation precautions, and cardiac devices (i.e., left ventricular assist device). Keep the dialogue open with your attending about acutely ill patients and potentially urgent procedures. Inform the endoscopy suite early that you are adding a procedure on the same day, and communicate anticipated needs (such as intubation, fluoroscopy room, pediatric scope, stent). Using a “closed-loop” communication structure can ensure that your recommendations are received and implemented appropriately.2
Time management and structure
Having a structured routine to your day, in what seems to be a chaotic process of juggling different duties and being in different locations at once, will ensure that you efficiently complete your tasks in a timely manner. Find what works best for you, taking into account the challenges and resources available to you, such as the number of fellows and other trainees on the GI consult service, the average number of consults per day and their acuity, the availability of inpatient protocols for specific clinical situations (GI bleed, acute severe ulcerative colitis, etc.), and the time and style preferences of the rounding attending. We suggest the following schedule on a consult day: Round early in the morning and leave a note in the chart and/or communicate with the team key information, then review with the rotating trainees the patients they are following and personally reassess some patients as needed. Inform the endoscopy suite of the same day procedures and let your attending know of any issues that require immediate attention. Take your team and head to radiology and review the imaging studies on your patients. Learn and teach key points in diagnosis and therapeutic approach as you move through your day from the inpatient floors to the hallways. Divide consults during the day with your team and agree on a time to touch base. Review your patient list at the end of the day and assess which patients the GI service no longer need to follow and communicate that clearly to the primary team along with the appropriate outpatient GI care follow-up. Let the endoscopy suite know of any procedures you are adding for the next day along with their degree of urgency to allow the charge nurse to prioritize cases. When you leave the hospital, be intentional with your free time: Read about the GI conditions you have encountered, enjoy some fun relaxing time, and rest!
Call
Know your call environment and your emergency cart
Familiarize yourself with the locations where you could potentially perform an emergent case (i.e., the ICU, ED, operating room) and the relevant points of contact (such as the charge nurse, the anesthesia team, the on-call tech team) for overnight or weekend cases. Whether or not you have an endoscopy support team on call, learn to set up the emergency cart, find and check your equipment, and troubleshoot technical issues by soliciting an “in-service” from senior fellows or the endoscopy technical support staff. Before heading to an urgent case, double check that you have your “bleeder” or “food impaction” tools. For food impaction, consider obtaining rat tooth forceps, snares, Roth nets, and an overtube. For bleeding cases, obtain a therapeutic upper endoscope, hemostatic clips, clear caps, injection needles, epinephrine, HemosprayTM, banding kits, and the appropriate electrocautery/thermal set up.
What is an emergency?
Consults that require your immediate attention include food impactions, acute biliary conditions leading to septic shock, and hemodynamically unstable GI bleeds, especially variceal bleeds. Remember that patients who are hemodynamically unstable require adequate resuscitation before proceeding with any endoscopic intervention. Assess the need for intubation, the timing of the procedure, and the most optimal location to perform the procedure, depending on the time and acuity of the patients’ presentation, how they respond to resuscitation measures, and the resources and preferences of your institution.
The overnight ‘nonemergent’ call
Non-emergent consults can be addressed the next day, after reviewing the clinical information provided by the consulting team and the patient’s EMR to ensure no urgent measures are needed. Overnight call may include patient phone calls, from inquiries about colon prep (so familiarize yourself with the different prep instructions and how to troubleshoot prep difficulties) to GI symptoms that you will need to triage to either the ED or to an outpatient follow-up. Document all phone encounters in the EMR and route your note to the appropriate clinician and nurse or administrative assistant for follow-up.
The five E’s of endoscopy
Endoscopy training is a large component of a GI fellowship and can create achievement anxiety in many first-year fellows seeking the cecum! But there is more to endoscopy than technical skills: It is as important to adequately evaluate clinical situations, understand the indications and potential limitations and complications of the procedure, and assess how it will impact the management of the patient. And no, you don’t have to be a video gamer to be a good endoscopist; and yes, you will be able to regularly complete a colonoscopy before the end of your first year!
Evaluation
In order to improve your endoscopic skills, it is important to honestly assess your areas of proficiency and improvement and to welcome real-time constructive feedback from your teaching attending about your endoscopic skills range. Consider meeting regularly with your attending to discuss your short-term and long-term endoscopic goals and how to enhance your skills. This practice demonstrates responsibility, credibility, and accountability amongst your peers as well as a genuine commitment to your growth as an endoscopist.
Efficiency
In addition to focusing on the quality of your endoscopy, learn to be efficient in the pre- and postprocedure time flow. This entails any step from properly explaining the procedure to patients before they come to the endoscopy suite, making sure the needed endoscopy equipment and tools are available in your room, completing your personal setup (i.e., gowning up, setting up your bed/monitor height, testing your endoscope) even before time out, to discharging the patient and communicating key findings and plan of care to the primary team. Depending on the acuity of the procedure and patient’s comorbidities, certain procedures may need to be performed or completed by a more efficient and experienced senior fellow or attending; don’t let this situation trigger passive frustration in you, but rather use it as an active and engaging opportunity to learn.
Expectations
You (and all the other neighborhood kids) didn’t learn to ride a bike without falling, struggling, needing help, and practicing over and over again, and it goes the same when learning to scope as a first-year fellow. Keep this in mind to lessen frustration, set realistic expectations, and be patient with yourself and celebrate all the small victories. Set tangible goals with your attending prior to procedural days/rotations so they can help you hone in and perfect the desired endoscopy skills.
Ergonomics
In a recent study, endoscopy-related injury (ERI) was reported to occur in up to 75% of gastroenterologists.3 While your primary focus might be reaching the cecum, it is as crucial for you to learn how to prevent ERI to ensure your long term health and continued success in procedures.
Excellence over quantity
Your main focus as a trainee is to learn how to provide effective, efficient, and safe care to patients, including in endoscopy. The quality of the endoscopy you perform is much more important than the total number of procedures you do. Thus, it is key to take each procedure as a complete learning opportunity to perform a thorough evaluation, improve your technical skills, interpret the findings, and develop a therapeutic plan.
Work-life balance and burnout
Fellowship is a marathon and not a sprint, so you need to slow down after a busy workday and care for yourself and enjoy time with loved ones. The cognitive, physical, mental, and emotional demands for first-year fellows are arguably the highest during GI training and can lead to burnout. Signs of burnout include emotional exhaustion, loss of empathy, fatigue, depersonalization and detachment, and feelings of personal inadequacy.4 Antiburnout measures include respecting basic healthy life hygiene (eat and sleep well, regular physical activity), having a hobby, practicing meditation, avoiding taking work home, and having a healthy social network.5 Remember that your cofellows whom you share common experiences with are not only your colleagues but can also be your friends and your social support. If you are a parent juggling work and family, remember to ask for help from your peers if you need it and have an open discussion with your attending to find practical solutions to your schedule.
Professional growth in the field of gastroenterology
Becoming a successful gastroenterologist and endoscopist involves going above the “I” and into the inclusive “we.” Building collegial and professional relationships early on with different stakeholders will set you up for success during and beyond your fellowship.
Building relationships
Developing genuine collegial and collaborative relationships with cofellows and faculty will positively impact your wellness during fellowship but also build the foundation of your professional network necessary to your career growth. Be inclusive of your cofellows in your research projects and publications, and support and amplify their work as much as you amplify your own. Your cofellows or attendings are likely to be the ones to help you find the right job, invite you to speak at grand rounds, or sit on a GI committee and promote your postfellowship professional growth.
Mentorship, being an educator and role model
It is important to identify and seek out mentors, within or outside your fellowship program or institution, who can not only guide you in your career choices but also open doors for you and sponsor you to advance your career. On the other hand, you too can be a role model, mentor, and sponsor to medical residents and students interested in the field of GI. Teach others in didactic settings or on the consult service, include trainees in quality improvement projects and publications, and lead by example.
Research
Most academic GI programs have a baseline requirement of research. Choose and devise a project you can realistically complete despite your busy first-year schedule: expand on a residency research project, focus on a specific simple question triggered by a clinical situation you encountered, proceed with a retrospective chart review or quality improvement project, and include other fellows and trainees to divide tasks. Alternatively, devise a specific timeline with a research mentor to complete a larger research project during your three years of fellowship.
Involvement in GI societies/committees
Become a member of one (or all) of the national GI societies that align with your interests. Membership gives you access not only to peer-reviewed scientific articles and guidelines but also to fellow-focused programs, committees’ opportunities, early career research grants, and mentorship.6-10
Summary
The first year of a GI fellowship lays the foundation for your next 3 years: Be mindful of how you can optimize the opportunities at hand to learn, teach, build a solid reputation, and grow your professional network. But also remember you have 3 full years to accomplish all your goals, so be patient, pace yourself, and include others in your journey. Judiciously use the many resources within your program and GI societies to help you achieve your goals, reach out to others to overcome difficulties and barriers, and dedicate time to care for your personal health and growth. This is what a true comprehensive and healthy fellowship is all about!
Dr. Advani is with the division of gastroenterology and hepatology, Stony Brook (N.Y.) University Hospital. Dr. Saeed is with the division of gastroenterology and hepatology, University of Kentucky, Lexington. Dr. Charabaty is with the division of gastroenterology, Johns Hopkins University, Baltimore, and Johns Hopkins–Sibley Memorial Hospital, Washington. Dr. Advani and Dr. Saeed have no conflicts to disclose. Dr. Charabaty disclosed ties to AbbVie, Janssen, Takeda, Pfizer, and Bristol-Myers Squibb and is founder of @MondayNightIBD, and cofounder of Scrubs & Heels.
References
1. Bollipo S. Gastroenterology. 2020 Nov;159(5):1648-52.
2. Adams MA et al. Gastroenterology. 2014 Jan 1;146(1):5-9.
3. Pawa S et al. Am J Gastroenterol. 2021 Mar 1;116(3):530-8.
4. DeCross AJ. Gastroenterology. 2020 Jan 1;158(1):32-5.
5. Burke C et al. Am J Gastroenterol. 2017 Oct 1;112:S593-4.
6. Fellows Resources under Fellows & Early Career. American Gastroenterological Association. https://gastro.org/fellows-and-early-career/training-resources/fellows-resources/.
7. Trainee Courses and Events. American College of Gastroenterology. https://gi.org/trainees/trainee-courses-and-events/.
8. Trainee Resources. American Association for the Study of Liver Diseases. https://www.aasld.org/membership/hepatology-associates/trainee-resources.
9. First Year Fellows Courses under Education. American Society of Gastrointestinal Endoscopy. https://www.asge.org/home/education/advanced-education-training/first-year-fellow-(fyf)-courses.
10. Annual GI Fellow Summer Course Presentations. New York Society for Gastrointestinal Endoscopy. https://www.nysge.org/annual%20gi%20fellows%20summer%20course.
The central role of informed consent in novel procedures
Mrs. Jones is a 44-year-old woman who has struggled with her weight. She has a body mass index (BMI) of 35 kg/m2 and hypertension requiring daily medication. She has tried various diets over the years and has never been able to exercise consistently. She desperately wants to lose weight to improve her confidence and to avoid developing diabetes and dialysis that her parents required. She has considered weight loss surgery but is afraid after her best friend died following uterine fibroid surgery. She saw a billboard that advertised a new weight loss procedure without surgery. She looked up the procedure, found Dr. Indo on the university medical center’s website, and booked an appointment. Dr. Indo talked about performing an incisionless procedure done with an endoscope through her mouth. It would make her stomach into a tube to reduce the amount of food she could eat as well as prevent some absorption of food in her intestines. When Mrs. Jones asked how many of these the doctor had performed, Dr. Indo remarked she personally had done “several” in the past few years including training. Dr. Indo reassured Mrs. Jones that the procedure has been performed hundreds of times around the country and has been shown to be safe. Dr. Indo also explained that studies were still ongoing, including possibly at the university medical center, but that she had never personally seen any serious complications or death, and only one patient she knew of converted to a traditional bariatric surgery.

Obesity is a large international public health problem, with the World Health Organization estimating that there are 600 million obese adults worldwide.1 Bariatric surgery has been an effective way to improve complications related to obesity and quality of life. Endoscopic approaches to bariatric surgery have appeared since at least the late 1980s and, similarly to their traditional surgical counterparts, work in two main categories: restrictive or malabsorptive.1 Restrictive endoscopic bariatric therapies (EBTs) include intragastric balloons (IGB) that are filled with saline or gas to decrease intragastric luminal size, endoscopic sleeve gastroplasty that makes full-thickness plications of the gastric wall to tubularize the stomach like a sleeve gastrectomy, and AspireAssist where patients use a percutaneous gastrostomy to remove part of an ingested meal.1 Malabsorptive procedures include bypass sleeves that use a stentlike device to bypass absorption of food in the duodenum and proximal jejunum, the incisionless magnetic anastomosis system (IMAS) that creates a gastrojejunal bypass for diverting absorption, and duodenal mucosal resurfacing (DMR) that ablates the duodenal mucosa.1,2
The benefits of EBTs over traditional bariatric surgery are that they have a lower risk profile, there is limited anatomic alternation, and they are potentially reversible.1 Although no formal guidelines exist in the United States for the use of EBTs, the American Society for Gastrointestinal Endoscopy (ASGE) preliminary recommendations describe EBTs as applicable for patients who have failed lifestyle interventions and have BMIs between 30 and 45.1 While some of these techniques were first described in the 1980s, many individual companies and devices still do not have Food and Drug Administration approval and some have even had approval withdrawn. While traditional bariatric surgery may have complication rates up to 17%, EBTs are not without complications.1 Endoscopic barriers can migrate and occlude, cause pancreatitis, cause liver abscesses from biliary occlusion, and more severely cause GI bleeding and perforations.1 Many EBTs are also temporary treatments with IGBs and barrier bypasses placed only for 6-12 months.1 While there have been some studies looking at individual outcomes of the various EBTs, large prospective research trials looking at safety and efficacy, especially when comparing EBT to traditional bariatric surgery or in combination, are lacking.
Continued innovation in medicine and technology is critical to improving patient care. New innovations in medicine have allowed us to treat more disease, save lives, reduce complications, and better care for patients. But what exactly is innovation and when does it become research? The landmark Belmont Report in 1979 distinguishes research from innovative therapy, calling research “an activity designed to test a hypothesis, permit conclusions to be drawn, and thereby to develop or contribute to generalizable knowledge.”3 Patients in research thus bear the risks while others stand to benefit. The report affirms then that routine medical practice involves interventions designed specifically to benefit the individual patient. The European Association for Endoscopic Surgery defines innovations as any “significant modification of a standard technique, a new application of or new indication for an established technique, or an alternative combination of an established technique with another therapeutic modality.”4 As such, innovations should eventually be formally studied with institutional review board (IRB) approval and protocols to establish safety and efficacy. Another complicating factor is that there is no FDA approval for surgical and procedural techniques as there is for medications and certain devices. Therefore, no robust regulatory mechanisms exist to ensure patient safety and benefit. Further complicating matters is that innovative procedures often start as modifications of techniques and are often done regularly to fit specific situations – for example, an additional stitch in a different location or in a different orientation to what is done in the standard fashion. However, true innovations should be distinguished from these modifications. Perhaps then another way to think about the two is to splinter them into three types of activity: research, routine accepted practice, and innovative medicine.5
Given this potential for blurred lines about novel approaches to medical conditions, how do we communicate this to patients? This is where the role of informed consent becomes essential. Informed consent is key to respecting patients’ autonomy – a central tenet of medical ethics. For patients to make autonomous choices they need basic facts to make informed decisions.6 These facts must be unbiased and free from conflicts, and they must not only be truthful but also be comprehensive and free from omission. It is in this informed consent process that we must explain that a technique or procedure is new, outline the risks and benefits, and share our actual experiences with said procedure especially if it is limited.7 We must also be aware of how certain biases and conflicts can affect our decisions to adapt and recommend innovative therapies. We may have incentives to offer innovative therapies to be on the “cutting edge” and attract patients. We may have explicit financial gain if working directly with device manufacturers or reimbursed by our institutions per procedure. Conflicts of interest are not only financial, but they can also be the prospects of promotion or career advancement.3 Institutions as well are incentivized to advertise the “latest” to bolster their prestige and reputations. Ultimately, we should act to the highest levels of professionalism, and ethics, by ignoring benefit to ourselves as physicians and always focusing on the benefits for our patients.7
What about when patients ask for specific innovative procedures as Mrs. Jones did above? What is our responsibility then? In situations where patients specifically push for a new procedure, it remains our duty to inform patients about the novelty of the procedure and the limited study of its safety and efficacy. When speaking about the “experience” with a novel procedure, it is tempting to speak globally and broadly. For example, Dr. Indo spoke about the procedure being done hundreds of times across the country and being safe in this context. It is our duty to be transparent, disclose our own experiences, and consider our own skills when recommending a novel procedure.7 It should be noted that patients are a vulnerable population and many times at the mercy of our recommendations. We’ve often heard patients say “Whatever you say doc; You’re the doctor;” or “I’ll do what you think is best” when presented with treatment options. This is an incredible amount of power, and we must protect this trust patients place in us by clearly acknowledging the uncertainties of new procedures and placing their benefit over our own potential gain.
Dr. Williams is a general surgery resident at the University of Chicago and a fellow at the MacLean Center for clinical medical ethics. Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, vice chairman for ethics, professional development, and wellness, and chief of endocrine surgery, department of surgery, and the associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago. The authors have no conflicts to disclose.
References
1. Goyal H et al. Ther Adv Gastrointest Endosc. 2021;14. doi: 10.1177/2631774520984627.
2. Machytka E et al. Gastrointestinal Endosc. 2017;86(5):904-12. doi: 10.1016/j.gie.2017.07.009.
3. Eastwood GL. J Gastroenterol Hepatol (Australia). 2015;30(S1):8-11. doi: 10.1111/jgh.12755.
4. Neugebauer EAM et al. Surg Endosc. 2010;24(7):1594-1615. doi: 10.1007/s00464-009-0818-3.
5. Eaton, ML and Kennedy, DL. Innovation in Medical Technology: Ethical Issues and Challenges. Baltimore: Johns Hopkins University Press, 2007.
6. Angelos P. Ann Thorac Surg. 2019;108(6):1611-2. doi: 10.1016/j.athoracsur.2019.08.010.
7. Angelos P. Virtual Mentor. 2011;13(1):6-9. doi: 10.1001/virtualmentor.2011.13.1.ccas1-1101.
Mrs. Jones is a 44-year-old woman who has struggled with her weight. She has a body mass index (BMI) of 35 kg/m2 and hypertension requiring daily medication. She has tried various diets over the years and has never been able to exercise consistently. She desperately wants to lose weight to improve her confidence and to avoid developing diabetes and dialysis that her parents required. She has considered weight loss surgery but is afraid after her best friend died following uterine fibroid surgery. She saw a billboard that advertised a new weight loss procedure without surgery. She looked up the procedure, found Dr. Indo on the university medical center’s website, and booked an appointment. Dr. Indo talked about performing an incisionless procedure done with an endoscope through her mouth. It would make her stomach into a tube to reduce the amount of food she could eat as well as prevent some absorption of food in her intestines. When Mrs. Jones asked how many of these the doctor had performed, Dr. Indo remarked she personally had done “several” in the past few years including training. Dr. Indo reassured Mrs. Jones that the procedure has been performed hundreds of times around the country and has been shown to be safe. Dr. Indo also explained that studies were still ongoing, including possibly at the university medical center, but that she had never personally seen any serious complications or death, and only one patient she knew of converted to a traditional bariatric surgery.
Obesity is a large international public health problem, with the World Health Organization estimating that there are 600 million obese adults worldwide.1 Bariatric surgery has been an effective way to improve complications related to obesity and quality of life. Endoscopic approaches to bariatric surgery have appeared since at least the late 1980s and, similarly to their traditional surgical counterparts, work in two main categories: restrictive or malabsorptive.1 Restrictive endoscopic bariatric therapies (EBTs) include intragastric balloons (IGB) that are filled with saline or gas to decrease intragastric luminal size, endoscopic sleeve gastroplasty that makes full-thickness plications of the gastric wall to tubularize the stomach like a sleeve gastrectomy, and AspireAssist where patients use a percutaneous gastrostomy to remove part of an ingested meal.1 Malabsorptive procedures include bypass sleeves that use a stentlike device to bypass absorption of food in the duodenum and proximal jejunum, the incisionless magnetic anastomosis system (IMAS) that creates a gastrojejunal bypass for diverting absorption, and duodenal mucosal resurfacing (DMR) that ablates the duodenal mucosa.1,2
The benefits of EBTs over traditional bariatric surgery are that they have a lower risk profile, there is limited anatomic alternation, and they are potentially reversible.1 Although no formal guidelines exist in the United States for the use of EBTs, the American Society for Gastrointestinal Endoscopy (ASGE) preliminary recommendations describe EBTs as applicable for patients who have failed lifestyle interventions and have BMIs between 30 and 45.1 While some of these techniques were first described in the 1980s, many individual companies and devices still do not have Food and Drug Administration approval and some have even had approval withdrawn. While traditional bariatric surgery may have complication rates up to 17%, EBTs are not without complications.1 Endoscopic barriers can migrate and occlude, cause pancreatitis, cause liver abscesses from biliary occlusion, and more severely cause GI bleeding and perforations.1 Many EBTs are also temporary treatments with IGBs and barrier bypasses placed only for 6-12 months.1 While there have been some studies looking at individual outcomes of the various EBTs, large prospective research trials looking at safety and efficacy, especially when comparing EBT to traditional bariatric surgery or in combination, are lacking.
Continued innovation in medicine and technology is critical to improving patient care. New innovations in medicine have allowed us to treat more disease, save lives, reduce complications, and better care for patients. But what exactly is innovation and when does it become research? The landmark Belmont Report in 1979 distinguishes research from innovative therapy, calling research “an activity designed to test a hypothesis, permit conclusions to be drawn, and thereby to develop or contribute to generalizable knowledge.”3 Patients in research thus bear the risks while others stand to benefit. The report affirms then that routine medical practice involves interventions designed specifically to benefit the individual patient. The European Association for Endoscopic Surgery defines innovations as any “significant modification of a standard technique, a new application of or new indication for an established technique, or an alternative combination of an established technique with another therapeutic modality.”4 As such, innovations should eventually be formally studied with institutional review board (IRB) approval and protocols to establish safety and efficacy. Another complicating factor is that there is no FDA approval for surgical and procedural techniques as there is for medications and certain devices. Therefore, no robust regulatory mechanisms exist to ensure patient safety and benefit. Further complicating matters is that innovative procedures often start as modifications of techniques and are often done regularly to fit specific situations – for example, an additional stitch in a different location or in a different orientation to what is done in the standard fashion. However, true innovations should be distinguished from these modifications. Perhaps then another way to think about the two is to splinter them into three types of activity: research, routine accepted practice, and innovative medicine.5
Given this potential for blurred lines about novel approaches to medical conditions, how do we communicate this to patients? This is where the role of informed consent becomes essential. Informed consent is key to respecting patients’ autonomy – a central tenet of medical ethics. For patients to make autonomous choices they need basic facts to make informed decisions.6 These facts must be unbiased and free from conflicts, and they must not only be truthful but also be comprehensive and free from omission. It is in this informed consent process that we must explain that a technique or procedure is new, outline the risks and benefits, and share our actual experiences with said procedure especially if it is limited.7 We must also be aware of how certain biases and conflicts can affect our decisions to adapt and recommend innovative therapies. We may have incentives to offer innovative therapies to be on the “cutting edge” and attract patients. We may have explicit financial gain if working directly with device manufacturers or reimbursed by our institutions per procedure. Conflicts of interest are not only financial, but they can also be the prospects of promotion or career advancement.3 Institutions as well are incentivized to advertise the “latest” to bolster their prestige and reputations. Ultimately, we should act to the highest levels of professionalism, and ethics, by ignoring benefit to ourselves as physicians and always focusing on the benefits for our patients.7
What about when patients ask for specific innovative procedures as Mrs. Jones did above? What is our responsibility then? In situations where patients specifically push for a new procedure, it remains our duty to inform patients about the novelty of the procedure and the limited study of its safety and efficacy. When speaking about the “experience” with a novel procedure, it is tempting to speak globally and broadly. For example, Dr. Indo spoke about the procedure being done hundreds of times across the country and being safe in this context. It is our duty to be transparent, disclose our own experiences, and consider our own skills when recommending a novel procedure.7 It should be noted that patients are a vulnerable population and many times at the mercy of our recommendations. We’ve often heard patients say “Whatever you say doc; You’re the doctor;” or “I’ll do what you think is best” when presented with treatment options. This is an incredible amount of power, and we must protect this trust patients place in us by clearly acknowledging the uncertainties of new procedures and placing their benefit over our own potential gain.
Dr. Williams is a general surgery resident at the University of Chicago and a fellow at the MacLean Center for clinical medical ethics. Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, vice chairman for ethics, professional development, and wellness, and chief of endocrine surgery, department of surgery, and the associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago. The authors have no conflicts to disclose.
References
1. Goyal H et al. Ther Adv Gastrointest Endosc. 2021;14. doi: 10.1177/2631774520984627.
2. Machytka E et al. Gastrointestinal Endosc. 2017;86(5):904-12. doi: 10.1016/j.gie.2017.07.009.
3. Eastwood GL. J Gastroenterol Hepatol (Australia). 2015;30(S1):8-11. doi: 10.1111/jgh.12755.
4. Neugebauer EAM et al. Surg Endosc. 2010;24(7):1594-1615. doi: 10.1007/s00464-009-0818-3.
5. Eaton, ML and Kennedy, DL. Innovation in Medical Technology: Ethical Issues and Challenges. Baltimore: Johns Hopkins University Press, 2007.
6. Angelos P. Ann Thorac Surg. 2019;108(6):1611-2. doi: 10.1016/j.athoracsur.2019.08.010.
7. Angelos P. Virtual Mentor. 2011;13(1):6-9. doi: 10.1001/virtualmentor.2011.13.1.ccas1-1101.
Mrs. Jones is a 44-year-old woman who has struggled with her weight. She has a body mass index (BMI) of 35 kg/m2 and hypertension requiring daily medication. She has tried various diets over the years and has never been able to exercise consistently. She desperately wants to lose weight to improve her confidence and to avoid developing diabetes and dialysis that her parents required. She has considered weight loss surgery but is afraid after her best friend died following uterine fibroid surgery. She saw a billboard that advertised a new weight loss procedure without surgery. She looked up the procedure, found Dr. Indo on the university medical center’s website, and booked an appointment. Dr. Indo talked about performing an incisionless procedure done with an endoscope through her mouth. It would make her stomach into a tube to reduce the amount of food she could eat as well as prevent some absorption of food in her intestines. When Mrs. Jones asked how many of these the doctor had performed, Dr. Indo remarked she personally had done “several” in the past few years including training. Dr. Indo reassured Mrs. Jones that the procedure has been performed hundreds of times around the country and has been shown to be safe. Dr. Indo also explained that studies were still ongoing, including possibly at the university medical center, but that she had never personally seen any serious complications or death, and only one patient she knew of converted to a traditional bariatric surgery.
Obesity is a large international public health problem, with the World Health Organization estimating that there are 600 million obese adults worldwide.1 Bariatric surgery has been an effective way to improve complications related to obesity and quality of life. Endoscopic approaches to bariatric surgery have appeared since at least the late 1980s and, similarly to their traditional surgical counterparts, work in two main categories: restrictive or malabsorptive.1 Restrictive endoscopic bariatric therapies (EBTs) include intragastric balloons (IGB) that are filled with saline or gas to decrease intragastric luminal size, endoscopic sleeve gastroplasty that makes full-thickness plications of the gastric wall to tubularize the stomach like a sleeve gastrectomy, and AspireAssist where patients use a percutaneous gastrostomy to remove part of an ingested meal.1 Malabsorptive procedures include bypass sleeves that use a stentlike device to bypass absorption of food in the duodenum and proximal jejunum, the incisionless magnetic anastomosis system (IMAS) that creates a gastrojejunal bypass for diverting absorption, and duodenal mucosal resurfacing (DMR) that ablates the duodenal mucosa.1,2
The benefits of EBTs over traditional bariatric surgery are that they have a lower risk profile, there is limited anatomic alternation, and they are potentially reversible.1 Although no formal guidelines exist in the United States for the use of EBTs, the American Society for Gastrointestinal Endoscopy (ASGE) preliminary recommendations describe EBTs as applicable for patients who have failed lifestyle interventions and have BMIs between 30 and 45.1 While some of these techniques were first described in the 1980s, many individual companies and devices still do not have Food and Drug Administration approval and some have even had approval withdrawn. While traditional bariatric surgery may have complication rates up to 17%, EBTs are not without complications.1 Endoscopic barriers can migrate and occlude, cause pancreatitis, cause liver abscesses from biliary occlusion, and more severely cause GI bleeding and perforations.1 Many EBTs are also temporary treatments with IGBs and barrier bypasses placed only for 6-12 months.1 While there have been some studies looking at individual outcomes of the various EBTs, large prospective research trials looking at safety and efficacy, especially when comparing EBT to traditional bariatric surgery or in combination, are lacking.
Continued innovation in medicine and technology is critical to improving patient care. New innovations in medicine have allowed us to treat more disease, save lives, reduce complications, and better care for patients. But what exactly is innovation and when does it become research? The landmark Belmont Report in 1979 distinguishes research from innovative therapy, calling research “an activity designed to test a hypothesis, permit conclusions to be drawn, and thereby to develop or contribute to generalizable knowledge.”3 Patients in research thus bear the risks while others stand to benefit. The report affirms then that routine medical practice involves interventions designed specifically to benefit the individual patient. The European Association for Endoscopic Surgery defines innovations as any “significant modification of a standard technique, a new application of or new indication for an established technique, or an alternative combination of an established technique with another therapeutic modality.”4 As such, innovations should eventually be formally studied with institutional review board (IRB) approval and protocols to establish safety and efficacy. Another complicating factor is that there is no FDA approval for surgical and procedural techniques as there is for medications and certain devices. Therefore, no robust regulatory mechanisms exist to ensure patient safety and benefit. Further complicating matters is that innovative procedures often start as modifications of techniques and are often done regularly to fit specific situations – for example, an additional stitch in a different location or in a different orientation to what is done in the standard fashion. However, true innovations should be distinguished from these modifications. Perhaps then another way to think about the two is to splinter them into three types of activity: research, routine accepted practice, and innovative medicine.5
Given this potential for blurred lines about novel approaches to medical conditions, how do we communicate this to patients? This is where the role of informed consent becomes essential. Informed consent is key to respecting patients’ autonomy – a central tenet of medical ethics. For patients to make autonomous choices they need basic facts to make informed decisions.6 These facts must be unbiased and free from conflicts, and they must not only be truthful but also be comprehensive and free from omission. It is in this informed consent process that we must explain that a technique or procedure is new, outline the risks and benefits, and share our actual experiences with said procedure especially if it is limited.7 We must also be aware of how certain biases and conflicts can affect our decisions to adapt and recommend innovative therapies. We may have incentives to offer innovative therapies to be on the “cutting edge” and attract patients. We may have explicit financial gain if working directly with device manufacturers or reimbursed by our institutions per procedure. Conflicts of interest are not only financial, but they can also be the prospects of promotion or career advancement.3 Institutions as well are incentivized to advertise the “latest” to bolster their prestige and reputations. Ultimately, we should act to the highest levels of professionalism, and ethics, by ignoring benefit to ourselves as physicians and always focusing on the benefits for our patients.7
What about when patients ask for specific innovative procedures as Mrs. Jones did above? What is our responsibility then? In situations where patients specifically push for a new procedure, it remains our duty to inform patients about the novelty of the procedure and the limited study of its safety and efficacy. When speaking about the “experience” with a novel procedure, it is tempting to speak globally and broadly. For example, Dr. Indo spoke about the procedure being done hundreds of times across the country and being safe in this context. It is our duty to be transparent, disclose our own experiences, and consider our own skills when recommending a novel procedure.7 It should be noted that patients are a vulnerable population and many times at the mercy of our recommendations. We’ve often heard patients say “Whatever you say doc; You’re the doctor;” or “I’ll do what you think is best” when presented with treatment options. This is an incredible amount of power, and we must protect this trust patients place in us by clearly acknowledging the uncertainties of new procedures and placing their benefit over our own potential gain.
Dr. Williams is a general surgery resident at the University of Chicago and a fellow at the MacLean Center for clinical medical ethics. Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, vice chairman for ethics, professional development, and wellness, and chief of endocrine surgery, department of surgery, and the associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago. The authors have no conflicts to disclose.
References
1. Goyal H et al. Ther Adv Gastrointest Endosc. 2021;14. doi: 10.1177/2631774520984627.
2. Machytka E et al. Gastrointestinal Endosc. 2017;86(5):904-12. doi: 10.1016/j.gie.2017.07.009.
3. Eastwood GL. J Gastroenterol Hepatol (Australia). 2015;30(S1):8-11. doi: 10.1111/jgh.12755.
4. Neugebauer EAM et al. Surg Endosc. 2010;24(7):1594-1615. doi: 10.1007/s00464-009-0818-3.
5. Eaton, ML and Kennedy, DL. Innovation in Medical Technology: Ethical Issues and Challenges. Baltimore: Johns Hopkins University Press, 2007.
6. Angelos P. Ann Thorac Surg. 2019;108(6):1611-2. doi: 10.1016/j.athoracsur.2019.08.010.
7. Angelos P. Virtual Mentor. 2011;13(1):6-9. doi: 10.1001/virtualmentor.2011.13.1.ccas1-1101.
Integrating psychogastroenterology into GI care
Psychogastroenterology, or gastrointestinal psychology, refers to psychosocial research and clinical practice related to GI conditions. This field is situated within a biopsychosocial model of illness and grounded in an understanding of the gut-brain axis. A key feature of GI psychology intervention is behavioral symptom management. Commonly referred to as “brain-gut psychotherapies,” the primary goal of these interventions is to reduce GI symptoms and their impact on those experiencing them. Additionally, GI-focused psychotherapies can help patients with GI disorders cope with their symptoms, diagnosis, or treatment.
GI psychology providers
GI-focused psychotherapies are typically provided by clinical health psychologists (PhDs or PsyDs) with specialized training in GI disorders, although sometimes they are provided by a clinical social worker or advanced-practice nursing provider. Psychologists that identify GI as their primary specialty area often refer to themselves as “GI psychologists.” Psychologists that treat patients with a variety of medical concerns, which may include GI disorders, typically refer to themselves with the broader term, “health psychologists.”
Interventions
A variety of psychological treatments have been applied to GI populations, including cognitive behavioral therapy (CBT), gut-directed hypnotherapy (GDH), psychodynamic interpersonal therapy, relaxation training, and mindfulness-based stress reduction. Psychological therapies have been shown to be useful in a variety of GI disorders, with a number needed to treat of four in IBS.1 Common ingredients of GI-focused psychotherapy interventions include psychoeducation regarding the gut-brain relationship and relaxation strategies to provide in-the-moment tools to deescalate the body’s stress response.
CBT and GDH are the most commonly used interventions across a range of GI conditions, with the bulk of empirical evidence in IBS.2-5 CBT is a theoretical orientation in which thoughts and behaviors are understood to be modifiable factors that impact emotions and physical sensations. When utilized in a GI setting (i.e., GI-CBT), treatment aims to address GI-specific outcomes such as reducing GI symptoms, optimizing health care utilization, and improving quality of life. These interventions target cognitive and behavioral factors common among GI patient populations, such as GI-specific anxiety, symptom hypervigilance, and rigid coping strategies. See Figure 1 for a GI-CBT model.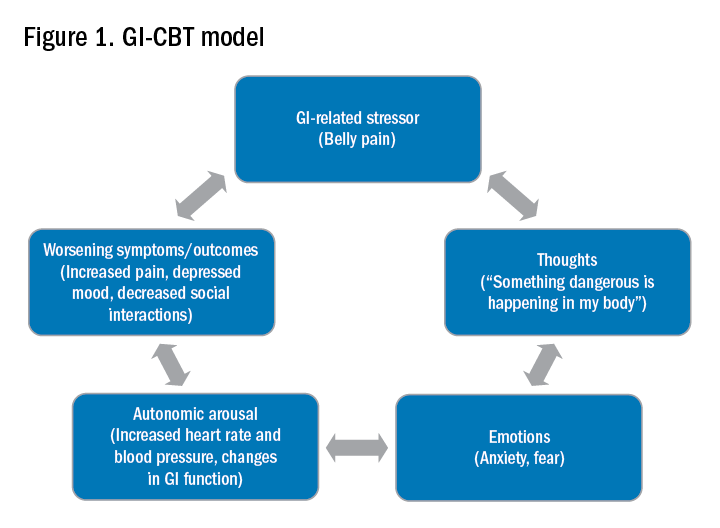
While research studies often implement manualized protocols, in clinical practice many GI psychologists use cognitive-behavioral interventions flexibly to tailor them to each patient’s presentation, while also integrating theory and practice from other types of therapies such as acceptance and commitment therapy (ACT; pronounced as one word). ACT, a “new wave” therapy derived from traditional CBT, emphasizes acceptance of distress (including GI symptoms), with a focus on engaging in values-based activities rather than symptom reduction.
Clinical hypnotherapy is utilized in a variety of medical specialties and has been studied in GI disorders for over 30 years. There are two evidence-based gut-directed hypnotherapy protocols, the Manchester6 and the North Carolina,7 that are widely used by GI psychologists. Though the exact mechanisms of hypnotherapy are unknown, it is thought to improve GI symptoms by modulating autonomic arousal and nerve sensitivity in the GI tract.
Evaluation
GI psychologists typically meet with patients for a 1-hour evaluation to determine appropriateness for psychogastroenterology intervention and develop a treatment plan. If GI-focused psychotherapy is indicated, patients are typically offered a course of treatment ranging from four to eight sessions. Depending on the nature of the patient’s concerns, longer courses of treatment may be offered, such as for with patients with active inflammatory bowel disease undergoing changes in medical treatment.
Appropriateness for psychogastroenterology treatment
Ideal patients are those who are psychologically stable and whose distress is primarily related to GI concerns, as opposed to family, work, or other situational stressors. While these other stressors can certainly impact GI symptoms, general mental health professionals are best suited to assist patients with these concerns. Patients experiencing more severe mental health concerns may be recommended to pursue a different treatment, such as mental health treatment for depression or anxiety or specialized treatments for trauma, eating disorders, or substance use. In both cases, once these general, non-GI, stressors or significant mental health concerns are more optimally managed, patients are likely to benefit from a GI-focused psychological treatment. Note, however, that because a GI psychologist’s particular practice can vary because of interest, experience, and institutional factors, it is best to connect directly with the GI psychologist you work with to clarify the types of referrals they are comfortable seeing and any specific characteristics of their practice.
Best practice recommendations for gastroenterologists
Developing a collaborative relationship with the GI psychologist, as well as any therapists to whom you regularly refer patients, is key to the success of integrated care. When talking to patients about the referral, refer to the GI psychologist as your colleague and a member of the treatment team. Maintain communication with the GI psychologist, and let the patient know that you are doing so.
When referring a patient, do so after you have completed your work-up and have optimized basic medical management for their condition but suspect that psychosocial factors may be negatively impacting their symptoms or ability to cope. Present the referral as an evaluation rather than implying a guarantee of treatment. This is particularly helpful in those cases where the patient is recommended to pursue a different treatment prior to GI-focused psychotherapy. Additionally, avoid telling patients that they are being referred for a specific intervention such as “a referral for CBT” or “a referral for hypnotherapy,” as the GI psychologist will recommend the most appropriate treatment for the patient upon evaluation. See Figure 2 for example scripts to use when referring.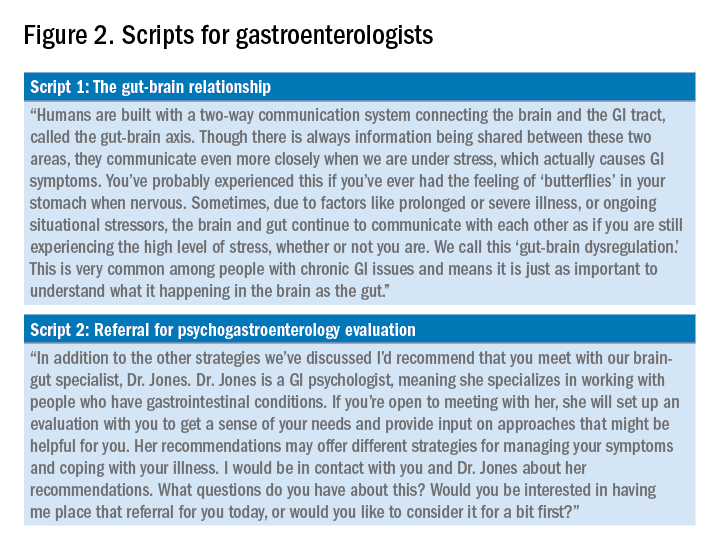
Expect to maintain communication with the GI psychologist after making the referral. GI psychologists typically send the referring provider a written summary following the initial evaluation and conclusion of treatment and, in some cases, provide updates throughout. Be prepared to answer questions or provide input as requested. Not only may the psychologist have questions about the medical diagnosis or treatment, but they may enlist your help for medical expert opinion during treatment to address misinformation, which can often fuel concerns like treatment nonadherence or anxiety.
Identifying a psychogastroenterology provider
In recent years there has been significant growth in the training and hiring of GI psychologists, and it is increasingly common for GI psychologists to be employed at academic medical centers. However, the majority of gastroenterologists do not have access to a fully integrated or co-located GI psychologist. In these cases, gastroenterologists should search for other health psychology options in their area, such as psychologists or clinical social workers with experience with patients with chronic medical conditions and CBT. One positive product of the COVID-19 pandemic is that telemedicine has become increasingly utilized, and in some cases GI psychologists are able to provide virtual therapy to patients across state lines. However, this should be confirmed with the therapy practice as there are numerous factors to consider regarding virtual practice.
Dr. Bedell is assistant professor in the department of psychiatry and behavioral neuroscience at the University of Chicago. She has no conflicts of interest to disclose.
Resources available
To locate a GI psychology provider in your area: Search the Rome Psychogastroenterology directory (https://romegipsych.org/).
To locate general mental health providers: Search the Psychology Today website using the therapist finder function, which allows patients or providers to search by insurance, location, and specialty area (www.psychologytoday.com/us). The patient can also request a list of in-network psychotherapy providers from their insurance company and may find it helpful to cross-check these providers for potential fit by searching them online.
References
1. Ford AC et al. Effect of antidepressants and psychological therapies in irritable bowel syndrome: An updated systematic review and meta-analysis. Am J Gastroenterol. 2019 Jan;114(1):21-39. doi: 10.1038/s41395-018-0222-5.
2. Laird KT et al. Short-term and long-term efficacy of psychological therapies for irritable bowel syndrome: A systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2016 Jul;14(7):937-47.e4. doi: 10.1016/j.cgh.2015.11.020.
3. Lackner JM et al. Improvement in gastrointestinal symptoms after cognitive behavior therapy for refractory irritable bowel syndrome. Gastroenterology. 2018 Jul;155(1):47-57. doi: 10.1053/j.gastro.2018.03.063.
4. Lövdahl J et al. Nurse-administered, gut-directed hypnotherapy in IBS: Efficacy and factors predicting a positive response. Am J Clin Hypn. 2015 Jul;58(1):100-14. doi: 10.1080/00029157.2015.1030492.
5. Smith GD. Effect of nurse-led gut-directed hypnotherapy upon health-related quality of life in patients with irritable bowel syndrome. J Clin Nurs. 2006 Jun;15(6):678-84. doi: 10.1111/j.1365-2702.2006.01356.x.
6. Gonsalkorale WM. Gut-directed hypnotherapy: the Manchester approach for treatment of irritable bowel syndrome. Int J Clin Exp Hypn. 2006 Jan;54(1):27-50. doi: 10.1080/00207140500323030.
7. Palsson OS. Standardized hypnosis treatment for irritable bowel syndrome: The North Carolina protocol. Int J Clin Exp Hypn. 2006 Jan;54(1):51-64. doi: 10.1080/00207140500322933.
Psychogastroenterology, or gastrointestinal psychology, refers to psychosocial research and clinical practice related to GI conditions. This field is situated within a biopsychosocial model of illness and grounded in an understanding of the gut-brain axis. A key feature of GI psychology intervention is behavioral symptom management. Commonly referred to as “brain-gut psychotherapies,” the primary goal of these interventions is to reduce GI symptoms and their impact on those experiencing them. Additionally, GI-focused psychotherapies can help patients with GI disorders cope with their symptoms, diagnosis, or treatment.
GI psychology providers
GI-focused psychotherapies are typically provided by clinical health psychologists (PhDs or PsyDs) with specialized training in GI disorders, although sometimes they are provided by a clinical social worker or advanced-practice nursing provider. Psychologists that identify GI as their primary specialty area often refer to themselves as “GI psychologists.” Psychologists that treat patients with a variety of medical concerns, which may include GI disorders, typically refer to themselves with the broader term, “health psychologists.”
Interventions
A variety of psychological treatments have been applied to GI populations, including cognitive behavioral therapy (CBT), gut-directed hypnotherapy (GDH), psychodynamic interpersonal therapy, relaxation training, and mindfulness-based stress reduction. Psychological therapies have been shown to be useful in a variety of GI disorders, with a number needed to treat of four in IBS.1 Common ingredients of GI-focused psychotherapy interventions include psychoeducation regarding the gut-brain relationship and relaxation strategies to provide in-the-moment tools to deescalate the body’s stress response.
CBT and GDH are the most commonly used interventions across a range of GI conditions, with the bulk of empirical evidence in IBS.2-5 CBT is a theoretical orientation in which thoughts and behaviors are understood to be modifiable factors that impact emotions and physical sensations. When utilized in a GI setting (i.e., GI-CBT), treatment aims to address GI-specific outcomes such as reducing GI symptoms, optimizing health care utilization, and improving quality of life. These interventions target cognitive and behavioral factors common among GI patient populations, such as GI-specific anxiety, symptom hypervigilance, and rigid coping strategies. See Figure 1 for a GI-CBT model.
While research studies often implement manualized protocols, in clinical practice many GI psychologists use cognitive-behavioral interventions flexibly to tailor them to each patient’s presentation, while also integrating theory and practice from other types of therapies such as acceptance and commitment therapy (ACT; pronounced as one word). ACT, a “new wave” therapy derived from traditional CBT, emphasizes acceptance of distress (including GI symptoms), with a focus on engaging in values-based activities rather than symptom reduction.
Clinical hypnotherapy is utilized in a variety of medical specialties and has been studied in GI disorders for over 30 years. There are two evidence-based gut-directed hypnotherapy protocols, the Manchester6 and the North Carolina,7 that are widely used by GI psychologists. Though the exact mechanisms of hypnotherapy are unknown, it is thought to improve GI symptoms by modulating autonomic arousal and nerve sensitivity in the GI tract.
Evaluation
GI psychologists typically meet with patients for a 1-hour evaluation to determine appropriateness for psychogastroenterology intervention and develop a treatment plan. If GI-focused psychotherapy is indicated, patients are typically offered a course of treatment ranging from four to eight sessions. Depending on the nature of the patient’s concerns, longer courses of treatment may be offered, such as for with patients with active inflammatory bowel disease undergoing changes in medical treatment.
Appropriateness for psychogastroenterology treatment
Ideal patients are those who are psychologically stable and whose distress is primarily related to GI concerns, as opposed to family, work, or other situational stressors. While these other stressors can certainly impact GI symptoms, general mental health professionals are best suited to assist patients with these concerns. Patients experiencing more severe mental health concerns may be recommended to pursue a different treatment, such as mental health treatment for depression or anxiety or specialized treatments for trauma, eating disorders, or substance use. In both cases, once these general, non-GI, stressors or significant mental health concerns are more optimally managed, patients are likely to benefit from a GI-focused psychological treatment. Note, however, that because a GI psychologist’s particular practice can vary because of interest, experience, and institutional factors, it is best to connect directly with the GI psychologist you work with to clarify the types of referrals they are comfortable seeing and any specific characteristics of their practice.
Best practice recommendations for gastroenterologists
Developing a collaborative relationship with the GI psychologist, as well as any therapists to whom you regularly refer patients, is key to the success of integrated care. When talking to patients about the referral, refer to the GI psychologist as your colleague and a member of the treatment team. Maintain communication with the GI psychologist, and let the patient know that you are doing so.
When referring a patient, do so after you have completed your work-up and have optimized basic medical management for their condition but suspect that psychosocial factors may be negatively impacting their symptoms or ability to cope. Present the referral as an evaluation rather than implying a guarantee of treatment. This is particularly helpful in those cases where the patient is recommended to pursue a different treatment prior to GI-focused psychotherapy. Additionally, avoid telling patients that they are being referred for a specific intervention such as “a referral for CBT” or “a referral for hypnotherapy,” as the GI psychologist will recommend the most appropriate treatment for the patient upon evaluation. See Figure 2 for example scripts to use when referring.
Expect to maintain communication with the GI psychologist after making the referral. GI psychologists typically send the referring provider a written summary following the initial evaluation and conclusion of treatment and, in some cases, provide updates throughout. Be prepared to answer questions or provide input as requested. Not only may the psychologist have questions about the medical diagnosis or treatment, but they may enlist your help for medical expert opinion during treatment to address misinformation, which can often fuel concerns like treatment nonadherence or anxiety.
Identifying a psychogastroenterology provider
In recent years there has been significant growth in the training and hiring of GI psychologists, and it is increasingly common for GI psychologists to be employed at academic medical centers. However, the majority of gastroenterologists do not have access to a fully integrated or co-located GI psychologist. In these cases, gastroenterologists should search for other health psychology options in their area, such as psychologists or clinical social workers with experience with patients with chronic medical conditions and CBT. One positive product of the COVID-19 pandemic is that telemedicine has become increasingly utilized, and in some cases GI psychologists are able to provide virtual therapy to patients across state lines. However, this should be confirmed with the therapy practice as there are numerous factors to consider regarding virtual practice.
Dr. Bedell is assistant professor in the department of psychiatry and behavioral neuroscience at the University of Chicago. She has no conflicts of interest to disclose.
Resources available
To locate a GI psychology provider in your area: Search the Rome Psychogastroenterology directory (https://romegipsych.org/).
To locate general mental health providers: Search the Psychology Today website using the therapist finder function, which allows patients or providers to search by insurance, location, and specialty area (www.psychologytoday.com/us). The patient can also request a list of in-network psychotherapy providers from their insurance company and may find it helpful to cross-check these providers for potential fit by searching them online.
References
1. Ford AC et al. Effect of antidepressants and psychological therapies in irritable bowel syndrome: An updated systematic review and meta-analysis. Am J Gastroenterol. 2019 Jan;114(1):21-39. doi: 10.1038/s41395-018-0222-5.
2. Laird KT et al. Short-term and long-term efficacy of psychological therapies for irritable bowel syndrome: A systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2016 Jul;14(7):937-47.e4. doi: 10.1016/j.cgh.2015.11.020.
3. Lackner JM et al. Improvement in gastrointestinal symptoms after cognitive behavior therapy for refractory irritable bowel syndrome. Gastroenterology. 2018 Jul;155(1):47-57. doi: 10.1053/j.gastro.2018.03.063.
4. Lövdahl J et al. Nurse-administered, gut-directed hypnotherapy in IBS: Efficacy and factors predicting a positive response. Am J Clin Hypn. 2015 Jul;58(1):100-14. doi: 10.1080/00029157.2015.1030492.
5. Smith GD. Effect of nurse-led gut-directed hypnotherapy upon health-related quality of life in patients with irritable bowel syndrome. J Clin Nurs. 2006 Jun;15(6):678-84. doi: 10.1111/j.1365-2702.2006.01356.x.
6. Gonsalkorale WM. Gut-directed hypnotherapy: the Manchester approach for treatment of irritable bowel syndrome. Int J Clin Exp Hypn. 2006 Jan;54(1):27-50. doi: 10.1080/00207140500323030.
7. Palsson OS. Standardized hypnosis treatment for irritable bowel syndrome: The North Carolina protocol. Int J Clin Exp Hypn. 2006 Jan;54(1):51-64. doi: 10.1080/00207140500322933.
Psychogastroenterology, or gastrointestinal psychology, refers to psychosocial research and clinical practice related to GI conditions. This field is situated within a biopsychosocial model of illness and grounded in an understanding of the gut-brain axis. A key feature of GI psychology intervention is behavioral symptom management. Commonly referred to as “brain-gut psychotherapies,” the primary goal of these interventions is to reduce GI symptoms and their impact on those experiencing them. Additionally, GI-focused psychotherapies can help patients with GI disorders cope with their symptoms, diagnosis, or treatment.
GI psychology providers
GI-focused psychotherapies are typically provided by clinical health psychologists (PhDs or PsyDs) with specialized training in GI disorders, although sometimes they are provided by a clinical social worker or advanced-practice nursing provider. Psychologists that identify GI as their primary specialty area often refer to themselves as “GI psychologists.” Psychologists that treat patients with a variety of medical concerns, which may include GI disorders, typically refer to themselves with the broader term, “health psychologists.”
Interventions
A variety of psychological treatments have been applied to GI populations, including cognitive behavioral therapy (CBT), gut-directed hypnotherapy (GDH), psychodynamic interpersonal therapy, relaxation training, and mindfulness-based stress reduction. Psychological therapies have been shown to be useful in a variety of GI disorders, with a number needed to treat of four in IBS.1 Common ingredients of GI-focused psychotherapy interventions include psychoeducation regarding the gut-brain relationship and relaxation strategies to provide in-the-moment tools to deescalate the body’s stress response.
CBT and GDH are the most commonly used interventions across a range of GI conditions, with the bulk of empirical evidence in IBS.2-5 CBT is a theoretical orientation in which thoughts and behaviors are understood to be modifiable factors that impact emotions and physical sensations. When utilized in a GI setting (i.e., GI-CBT), treatment aims to address GI-specific outcomes such as reducing GI symptoms, optimizing health care utilization, and improving quality of life. These interventions target cognitive and behavioral factors common among GI patient populations, such as GI-specific anxiety, symptom hypervigilance, and rigid coping strategies. See Figure 1 for a GI-CBT model.
While research studies often implement manualized protocols, in clinical practice many GI psychologists use cognitive-behavioral interventions flexibly to tailor them to each patient’s presentation, while also integrating theory and practice from other types of therapies such as acceptance and commitment therapy (ACT; pronounced as one word). ACT, a “new wave” therapy derived from traditional CBT, emphasizes acceptance of distress (including GI symptoms), with a focus on engaging in values-based activities rather than symptom reduction.
Clinical hypnotherapy is utilized in a variety of medical specialties and has been studied in GI disorders for over 30 years. There are two evidence-based gut-directed hypnotherapy protocols, the Manchester6 and the North Carolina,7 that are widely used by GI psychologists. Though the exact mechanisms of hypnotherapy are unknown, it is thought to improve GI symptoms by modulating autonomic arousal and nerve sensitivity in the GI tract.
Evaluation
GI psychologists typically meet with patients for a 1-hour evaluation to determine appropriateness for psychogastroenterology intervention and develop a treatment plan. If GI-focused psychotherapy is indicated, patients are typically offered a course of treatment ranging from four to eight sessions. Depending on the nature of the patient’s concerns, longer courses of treatment may be offered, such as for with patients with active inflammatory bowel disease undergoing changes in medical treatment.
Appropriateness for psychogastroenterology treatment
Ideal patients are those who are psychologically stable and whose distress is primarily related to GI concerns, as opposed to family, work, or other situational stressors. While these other stressors can certainly impact GI symptoms, general mental health professionals are best suited to assist patients with these concerns. Patients experiencing more severe mental health concerns may be recommended to pursue a different treatment, such as mental health treatment for depression or anxiety or specialized treatments for trauma, eating disorders, or substance use. In both cases, once these general, non-GI, stressors or significant mental health concerns are more optimally managed, patients are likely to benefit from a GI-focused psychological treatment. Note, however, that because a GI psychologist’s particular practice can vary because of interest, experience, and institutional factors, it is best to connect directly with the GI psychologist you work with to clarify the types of referrals they are comfortable seeing and any specific characteristics of their practice.
Best practice recommendations for gastroenterologists
Developing a collaborative relationship with the GI psychologist, as well as any therapists to whom you regularly refer patients, is key to the success of integrated care. When talking to patients about the referral, refer to the GI psychologist as your colleague and a member of the treatment team. Maintain communication with the GI psychologist, and let the patient know that you are doing so.
When referring a patient, do so after you have completed your work-up and have optimized basic medical management for their condition but suspect that psychosocial factors may be negatively impacting their symptoms or ability to cope. Present the referral as an evaluation rather than implying a guarantee of treatment. This is particularly helpful in those cases where the patient is recommended to pursue a different treatment prior to GI-focused psychotherapy. Additionally, avoid telling patients that they are being referred for a specific intervention such as “a referral for CBT” or “a referral for hypnotherapy,” as the GI psychologist will recommend the most appropriate treatment for the patient upon evaluation. See Figure 2 for example scripts to use when referring.
Expect to maintain communication with the GI psychologist after making the referral. GI psychologists typically send the referring provider a written summary following the initial evaluation and conclusion of treatment and, in some cases, provide updates throughout. Be prepared to answer questions or provide input as requested. Not only may the psychologist have questions about the medical diagnosis or treatment, but they may enlist your help for medical expert opinion during treatment to address misinformation, which can often fuel concerns like treatment nonadherence or anxiety.
Identifying a psychogastroenterology provider
In recent years there has been significant growth in the training and hiring of GI psychologists, and it is increasingly common for GI psychologists to be employed at academic medical centers. However, the majority of gastroenterologists do not have access to a fully integrated or co-located GI psychologist. In these cases, gastroenterologists should search for other health psychology options in their area, such as psychologists or clinical social workers with experience with patients with chronic medical conditions and CBT. One positive product of the COVID-19 pandemic is that telemedicine has become increasingly utilized, and in some cases GI psychologists are able to provide virtual therapy to patients across state lines. However, this should be confirmed with the therapy practice as there are numerous factors to consider regarding virtual practice.
Dr. Bedell is assistant professor in the department of psychiatry and behavioral neuroscience at the University of Chicago. She has no conflicts of interest to disclose.
Resources available
To locate a GI psychology provider in your area: Search the Rome Psychogastroenterology directory (https://romegipsych.org/).
To locate general mental health providers: Search the Psychology Today website using the therapist finder function, which allows patients or providers to search by insurance, location, and specialty area (www.psychologytoday.com/us). The patient can also request a list of in-network psychotherapy providers from their insurance company and may find it helpful to cross-check these providers for potential fit by searching them online.
References
1. Ford AC et al. Effect of antidepressants and psychological therapies in irritable bowel syndrome: An updated systematic review and meta-analysis. Am J Gastroenterol. 2019 Jan;114(1):21-39. doi: 10.1038/s41395-018-0222-5.
2. Laird KT et al. Short-term and long-term efficacy of psychological therapies for irritable bowel syndrome: A systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2016 Jul;14(7):937-47.e4. doi: 10.1016/j.cgh.2015.11.020.
3. Lackner JM et al. Improvement in gastrointestinal symptoms after cognitive behavior therapy for refractory irritable bowel syndrome. Gastroenterology. 2018 Jul;155(1):47-57. doi: 10.1053/j.gastro.2018.03.063.
4. Lövdahl J et al. Nurse-administered, gut-directed hypnotherapy in IBS: Efficacy and factors predicting a positive response. Am J Clin Hypn. 2015 Jul;58(1):100-14. doi: 10.1080/00029157.2015.1030492.
5. Smith GD. Effect of nurse-led gut-directed hypnotherapy upon health-related quality of life in patients with irritable bowel syndrome. J Clin Nurs. 2006 Jun;15(6):678-84. doi: 10.1111/j.1365-2702.2006.01356.x.
6. Gonsalkorale WM. Gut-directed hypnotherapy: the Manchester approach for treatment of irritable bowel syndrome. Int J Clin Exp Hypn. 2006 Jan;54(1):27-50. doi: 10.1080/00207140500323030.
7. Palsson OS. Standardized hypnosis treatment for irritable bowel syndrome: The North Carolina protocol. Int J Clin Exp Hypn. 2006 Jan;54(1):51-64. doi: 10.1080/00207140500322933.
Adverse skin effects of cancer immunotherapy reviewed
Immune checkpoint inhibitors (ICIs) have unquestionably revolutionized the care of patients with malignant melanoma, non-small cell lung cancer, and other types of cancer.
, according to members of a European Academy of Dermatology and Venereology (EADV) task force.
“The desirable, immune-mediated oncologic response is often achieved at the cost of immune-related adverse events (irAEs) that may potentially affect any organ system,” they write in a position statement on the management of ICI-derived dermatologic adverse events.
Recommendations from the EADV “Dermatology for Cancer Patients” task force have been published in the Journal of the European Academy of Dermatology and Venereology.
Task force members developed the recommendations based on clinical experience from published data and came up with specific recommendations for treating cutaneous toxicities associated with dermatologic immune-related adverse events (dirAEs) that occur in patients receiving immunotherapy with an ICI.
ICIs include the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy, Bristol Myers Squibb), and inhibitors of programmed death protein 1 (PD-1) and its ligand (PD-L1), including nivolumab (Opdivo, Bristol Myers Squibb), pembrolizumab (Keytruda, Merck), and other agents.
“The basic principle of management is that the interventions should be tailored to serve the equilibrium between patients’ relief from the symptoms and signs of skin toxicity and the preservation of an unimpeded oncologic treatment,” they write.
The recommendations are in line with those included in a 2021 update of the American Society of Clinical Oncology (ASCO) guidelines on the management of irAEs in patients treated with ICIs across the whole range of organ systems, said Milan J. Anadkat, MD, professor of dermatology and director of dermatology clinical trials at Washington University School of Medicine, St. Louis. Dr. Anadkat was a coauthor of the ASCO guideline update.
Although the European recommendations focus only on dermatologic side effects of ICIs in patients with cancer, “that doesn’t diminish their importance. They do a good job of summarizing how to approach and how to manage it depending on the severity of the toxicities and the various types of toxicities,” he told this news organization.
Having a paper focused exclusively on the dermatologic side effects of ICIs allows the inclusion of photographs that can help clinicians identify specific conditions that may require referral to a dermatologist, he said.
Both Dr. Anadkat and the authors of the European recommendations noted that dermatologic irAEs are more common with CTLA-4 inhibition than with PD-1/PD-L1 inhibition.
“It has to do with where the target is,” Dr. Anadkat said. “CTLA-4 inhibition works on a central aspect of the immune system, so it’s a much less specific site, whereas PD-1 affects an interaction at the site of the tumor cell itself, so it’s a little more specific.”
Pruritus
ICI-induced pruritus can occur without apparent skin changes, they write, noting that in a recent study of patients with dirAEs, about one-third had isolated pruritus.
The task force members cite a meta-analysis indicating a pruritus incidence of 13.2% for patients treated with nivolumab and 20.2% for patients treated with pembrolizumab but respective grade 3 pruritus rates of only 0.5% and 2.3%. The reported incidence of pruritus with ipilimumab was 47% in a different study.
Recommended treatments include topical moisturizers with or without medium-to-high potency corticosteroids for grade 1 reactions, non-sedating histamines and/or GABA agonists such as pregabalin, or gabapentin for grade 2 pruritus, and suspension of ICIs until pruritus improves in patients with grade 3 pruritus.
Maculopapular rash
Maculopapular or eczema-like rashes may occur in up to 68% of patients who receive a CTLA-4 inhibitor and up to 20% of those who receive a PD1/PD-L1 inhibitor, the authors note. Rashes commonly appear within 3-6 weeks of initiating therapy.
“The clinical presentation is nonspecific and consists of a rapid onset of multiple minimally scaly, erythematous macules and papules, congregating into plaques. Lesions are mostly located on trunk and extensor surfaces of the extremities and the face is generally spared,” they write.
Maculopapular rashes are typically accompanied by itching but could be asymptomatic, they noted.
Mild (grade 1) rashes may respond to moisturizers and topical potent or super-potent corticosteroids. Patients with grade 2 rash should also receive oral antihistamines. Systemic corticosteroids may be considered for patients with grade 3 rashes but only after other dirAEs that may require specific management, such as psoriasis, are ruled out.
Psoriasis-like rash
The most common form of psoriasis seen in patients treated with ICIs is psoriasis vulgaris with plaques, but other clinical variants are also seen, the authors note.
“Topical agents (corticosteroids, Vitamin D analogues) are prescribed in Grades 1/2 and supplementary” to systemic treatment for patients with grade 3 or recalcitrant lesions, they write. “If skin-directed therapies fail to provide symptomatic control,” systemic treatment and narrow band UVB phototherapy “should be considered,” they add.
Evidence regarding the use of systemic therapies to treat psoriasis-like rash associated with ICIs is sparse. Acitretin can be safely used in patients with cancer. Low-dose methotrexate is also safe to use except in patients with non-melanoma skin cancers. Cyclosporine, however, should be avoided because of the potential for tumor-promoting effects, they emphasized.
The recommendations also cover treatment of lichen planus-like and vitiligo-like rashes, as well as hair and nail changes, autoimmune bullous disorders, and oral mucosal dirAEs.
In addition, the recommendations cover severe cutaneous adverse reactions as well as serious, potentially life-threatening dirAEs, including Stevens-Johnson syndrome/TEN, acute generalized exanthematous pustulosis (AGEP), and drug reaction with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS).
“The dose of corticosteroids may be adapted to the severity of DRESS. The therapeutic benefit of systemic corticosteroids in the management of SJS/TEN remains controversial, and some authors favor treatment with cyclosporine. However, the use of corticosteroids in this context of ICI treatment appears reasonable and should be proposed. Short courses of steroids seem also effective in AGEP,” the task force members write.
The recommendations did not have outside funding. Of the 19 authors, 6 disclosed relationships with various pharmaceutical companies, including AbbVie, Leo Pharma, Boehringer Ingelheim, Bristol Myers Squibb, and/or Janssen. Dr. Anadkat disclosed previous relationships with Merck, Bristol Myers Squibb, and current relationships with others.
A version of this article first appeared on Medscape.com.
Immune checkpoint inhibitors (ICIs) have unquestionably revolutionized the care of patients with malignant melanoma, non-small cell lung cancer, and other types of cancer.
, according to members of a European Academy of Dermatology and Venereology (EADV) task force.
“The desirable, immune-mediated oncologic response is often achieved at the cost of immune-related adverse events (irAEs) that may potentially affect any organ system,” they write in a position statement on the management of ICI-derived dermatologic adverse events.
Recommendations from the EADV “Dermatology for Cancer Patients” task force have been published in the Journal of the European Academy of Dermatology and Venereology.
Task force members developed the recommendations based on clinical experience from published data and came up with specific recommendations for treating cutaneous toxicities associated with dermatologic immune-related adverse events (dirAEs) that occur in patients receiving immunotherapy with an ICI.
ICIs include the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy, Bristol Myers Squibb), and inhibitors of programmed death protein 1 (PD-1) and its ligand (PD-L1), including nivolumab (Opdivo, Bristol Myers Squibb), pembrolizumab (Keytruda, Merck), and other agents.
“The basic principle of management is that the interventions should be tailored to serve the equilibrium between patients’ relief from the symptoms and signs of skin toxicity and the preservation of an unimpeded oncologic treatment,” they write.
The recommendations are in line with those included in a 2021 update of the American Society of Clinical Oncology (ASCO) guidelines on the management of irAEs in patients treated with ICIs across the whole range of organ systems, said Milan J. Anadkat, MD, professor of dermatology and director of dermatology clinical trials at Washington University School of Medicine, St. Louis. Dr. Anadkat was a coauthor of the ASCO guideline update.
Although the European recommendations focus only on dermatologic side effects of ICIs in patients with cancer, “that doesn’t diminish their importance. They do a good job of summarizing how to approach and how to manage it depending on the severity of the toxicities and the various types of toxicities,” he told this news organization.
Having a paper focused exclusively on the dermatologic side effects of ICIs allows the inclusion of photographs that can help clinicians identify specific conditions that may require referral to a dermatologist, he said.
Both Dr. Anadkat and the authors of the European recommendations noted that dermatologic irAEs are more common with CTLA-4 inhibition than with PD-1/PD-L1 inhibition.
“It has to do with where the target is,” Dr. Anadkat said. “CTLA-4 inhibition works on a central aspect of the immune system, so it’s a much less specific site, whereas PD-1 affects an interaction at the site of the tumor cell itself, so it’s a little more specific.”
Pruritus
ICI-induced pruritus can occur without apparent skin changes, they write, noting that in a recent study of patients with dirAEs, about one-third had isolated pruritus.
The task force members cite a meta-analysis indicating a pruritus incidence of 13.2% for patients treated with nivolumab and 20.2% for patients treated with pembrolizumab but respective grade 3 pruritus rates of only 0.5% and 2.3%. The reported incidence of pruritus with ipilimumab was 47% in a different study.
Recommended treatments include topical moisturizers with or without medium-to-high potency corticosteroids for grade 1 reactions, non-sedating histamines and/or GABA agonists such as pregabalin, or gabapentin for grade 2 pruritus, and suspension of ICIs until pruritus improves in patients with grade 3 pruritus.
Maculopapular rash
Maculopapular or eczema-like rashes may occur in up to 68% of patients who receive a CTLA-4 inhibitor and up to 20% of those who receive a PD1/PD-L1 inhibitor, the authors note. Rashes commonly appear within 3-6 weeks of initiating therapy.
“The clinical presentation is nonspecific and consists of a rapid onset of multiple minimally scaly, erythematous macules and papules, congregating into plaques. Lesions are mostly located on trunk and extensor surfaces of the extremities and the face is generally spared,” they write.
Maculopapular rashes are typically accompanied by itching but could be asymptomatic, they noted.
Mild (grade 1) rashes may respond to moisturizers and topical potent or super-potent corticosteroids. Patients with grade 2 rash should also receive oral antihistamines. Systemic corticosteroids may be considered for patients with grade 3 rashes but only after other dirAEs that may require specific management, such as psoriasis, are ruled out.
Psoriasis-like rash
The most common form of psoriasis seen in patients treated with ICIs is psoriasis vulgaris with plaques, but other clinical variants are also seen, the authors note.
“Topical agents (corticosteroids, Vitamin D analogues) are prescribed in Grades 1/2 and supplementary” to systemic treatment for patients with grade 3 or recalcitrant lesions, they write. “If skin-directed therapies fail to provide symptomatic control,” systemic treatment and narrow band UVB phototherapy “should be considered,” they add.
Evidence regarding the use of systemic therapies to treat psoriasis-like rash associated with ICIs is sparse. Acitretin can be safely used in patients with cancer. Low-dose methotrexate is also safe to use except in patients with non-melanoma skin cancers. Cyclosporine, however, should be avoided because of the potential for tumor-promoting effects, they emphasized.
The recommendations also cover treatment of lichen planus-like and vitiligo-like rashes, as well as hair and nail changes, autoimmune bullous disorders, and oral mucosal dirAEs.
In addition, the recommendations cover severe cutaneous adverse reactions as well as serious, potentially life-threatening dirAEs, including Stevens-Johnson syndrome/TEN, acute generalized exanthematous pustulosis (AGEP), and drug reaction with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS).
“The dose of corticosteroids may be adapted to the severity of DRESS. The therapeutic benefit of systemic corticosteroids in the management of SJS/TEN remains controversial, and some authors favor treatment with cyclosporine. However, the use of corticosteroids in this context of ICI treatment appears reasonable and should be proposed. Short courses of steroids seem also effective in AGEP,” the task force members write.
The recommendations did not have outside funding. Of the 19 authors, 6 disclosed relationships with various pharmaceutical companies, including AbbVie, Leo Pharma, Boehringer Ingelheim, Bristol Myers Squibb, and/or Janssen. Dr. Anadkat disclosed previous relationships with Merck, Bristol Myers Squibb, and current relationships with others.
A version of this article first appeared on Medscape.com.
Immune checkpoint inhibitors (ICIs) have unquestionably revolutionized the care of patients with malignant melanoma, non-small cell lung cancer, and other types of cancer.
, according to members of a European Academy of Dermatology and Venereology (EADV) task force.
“The desirable, immune-mediated oncologic response is often achieved at the cost of immune-related adverse events (irAEs) that may potentially affect any organ system,” they write in a position statement on the management of ICI-derived dermatologic adverse events.
Recommendations from the EADV “Dermatology for Cancer Patients” task force have been published in the Journal of the European Academy of Dermatology and Venereology.
Task force members developed the recommendations based on clinical experience from published data and came up with specific recommendations for treating cutaneous toxicities associated with dermatologic immune-related adverse events (dirAEs) that occur in patients receiving immunotherapy with an ICI.
ICIs include the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy, Bristol Myers Squibb), and inhibitors of programmed death protein 1 (PD-1) and its ligand (PD-L1), including nivolumab (Opdivo, Bristol Myers Squibb), pembrolizumab (Keytruda, Merck), and other agents.
“The basic principle of management is that the interventions should be tailored to serve the equilibrium between patients’ relief from the symptoms and signs of skin toxicity and the preservation of an unimpeded oncologic treatment,” they write.
The recommendations are in line with those included in a 2021 update of the American Society of Clinical Oncology (ASCO) guidelines on the management of irAEs in patients treated with ICIs across the whole range of organ systems, said Milan J. Anadkat, MD, professor of dermatology and director of dermatology clinical trials at Washington University School of Medicine, St. Louis. Dr. Anadkat was a coauthor of the ASCO guideline update.
Although the European recommendations focus only on dermatologic side effects of ICIs in patients with cancer, “that doesn’t diminish their importance. They do a good job of summarizing how to approach and how to manage it depending on the severity of the toxicities and the various types of toxicities,” he told this news organization.
Having a paper focused exclusively on the dermatologic side effects of ICIs allows the inclusion of photographs that can help clinicians identify specific conditions that may require referral to a dermatologist, he said.
Both Dr. Anadkat and the authors of the European recommendations noted that dermatologic irAEs are more common with CTLA-4 inhibition than with PD-1/PD-L1 inhibition.
“It has to do with where the target is,” Dr. Anadkat said. “CTLA-4 inhibition works on a central aspect of the immune system, so it’s a much less specific site, whereas PD-1 affects an interaction at the site of the tumor cell itself, so it’s a little more specific.”
Pruritus
ICI-induced pruritus can occur without apparent skin changes, they write, noting that in a recent study of patients with dirAEs, about one-third had isolated pruritus.
The task force members cite a meta-analysis indicating a pruritus incidence of 13.2% for patients treated with nivolumab and 20.2% for patients treated with pembrolizumab but respective grade 3 pruritus rates of only 0.5% and 2.3%. The reported incidence of pruritus with ipilimumab was 47% in a different study.
Recommended treatments include topical moisturizers with or without medium-to-high potency corticosteroids for grade 1 reactions, non-sedating histamines and/or GABA agonists such as pregabalin, or gabapentin for grade 2 pruritus, and suspension of ICIs until pruritus improves in patients with grade 3 pruritus.
Maculopapular rash
Maculopapular or eczema-like rashes may occur in up to 68% of patients who receive a CTLA-4 inhibitor and up to 20% of those who receive a PD1/PD-L1 inhibitor, the authors note. Rashes commonly appear within 3-6 weeks of initiating therapy.
“The clinical presentation is nonspecific and consists of a rapid onset of multiple minimally scaly, erythematous macules and papules, congregating into plaques. Lesions are mostly located on trunk and extensor surfaces of the extremities and the face is generally spared,” they write.
Maculopapular rashes are typically accompanied by itching but could be asymptomatic, they noted.
Mild (grade 1) rashes may respond to moisturizers and topical potent or super-potent corticosteroids. Patients with grade 2 rash should also receive oral antihistamines. Systemic corticosteroids may be considered for patients with grade 3 rashes but only after other dirAEs that may require specific management, such as psoriasis, are ruled out.
Psoriasis-like rash
The most common form of psoriasis seen in patients treated with ICIs is psoriasis vulgaris with plaques, but other clinical variants are also seen, the authors note.
“Topical agents (corticosteroids, Vitamin D analogues) are prescribed in Grades 1/2 and supplementary” to systemic treatment for patients with grade 3 or recalcitrant lesions, they write. “If skin-directed therapies fail to provide symptomatic control,” systemic treatment and narrow band UVB phototherapy “should be considered,” they add.
Evidence regarding the use of systemic therapies to treat psoriasis-like rash associated with ICIs is sparse. Acitretin can be safely used in patients with cancer. Low-dose methotrexate is also safe to use except in patients with non-melanoma skin cancers. Cyclosporine, however, should be avoided because of the potential for tumor-promoting effects, they emphasized.
The recommendations also cover treatment of lichen planus-like and vitiligo-like rashes, as well as hair and nail changes, autoimmune bullous disorders, and oral mucosal dirAEs.
In addition, the recommendations cover severe cutaneous adverse reactions as well as serious, potentially life-threatening dirAEs, including Stevens-Johnson syndrome/TEN, acute generalized exanthematous pustulosis (AGEP), and drug reaction with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS).
“The dose of corticosteroids may be adapted to the severity of DRESS. The therapeutic benefit of systemic corticosteroids in the management of SJS/TEN remains controversial, and some authors favor treatment with cyclosporine. However, the use of corticosteroids in this context of ICI treatment appears reasonable and should be proposed. Short courses of steroids seem also effective in AGEP,” the task force members write.
The recommendations did not have outside funding. Of the 19 authors, 6 disclosed relationships with various pharmaceutical companies, including AbbVie, Leo Pharma, Boehringer Ingelheim, Bristol Myers Squibb, and/or Janssen. Dr. Anadkat disclosed previous relationships with Merck, Bristol Myers Squibb, and current relationships with others.
A version of this article first appeared on Medscape.com.
Common eye disorder in children tied to mental illness
Misaligned eyes in children are associated with an increased prevalence of mental illness, results of a large study suggest.
“Psychiatrists who have a patient with depression or anxiety and notice that patient also has strabismus might think about the link between those two conditions and refer that patient,” study investigator Stacy L. Pineles, MD, professor, department of ophthalmology, University of California, Los Angeles, told this news organization.

The study was published online March 10 in JAMA Ophthalmology.
A common condition
Strabismus, a condition in which the eyes don’t line up or are “crossed,” is one of the most common eye diseases in children, with some estimates suggesting it affects more than 1.5 million American youth.
Patients with strabismus have problems making eye contact and are affected socially and functionally, said Dr. Pineles. They’re often met with a negative bias, as shown by children’s responses to pictures of faces with and without strabismus, she said.
There is a signal from previous research suggesting that strabismus is linked to a higher risk of mental illness. However, most of these studies were small and had relatively homogenous populations, said Dr. Pineles.
The new study includes over 12 million children (mean age, 8.0 years) from a private health insurance claims database that represents diverse races and ethnicities as well as geographic regions across the United States.
The sample included 352,636 children with strabismus and 11,652,553 children with no diagnosed eye disease who served as controls. Most participants were White (51.6%), came from a family with an annual household income of $40,000 or more (51.0%), had point-of-service insurance (68.7%), and had at least one comorbid condition (64.5%).
The study evaluated five mental illness diagnoses. These included anxiety disorder, depressive disorder, substance use or addictive disorder, bipolar disorder, and schizophrenia.
Overall, children with strabismus had a higher prevalence of all these illnesses, with the exception of substance use disorder.
After adjusting for age, sex, race and ethnicity, census region, education level of caregiver, family net worth, and presence of at least one comorbid condition, the odds ratios among those with versus without strabismus were: 2.01 (95% confidence interval, 1.99-2.04; P < .001) for anxiety disorder, 1.83 (95% CI, 1.76-1.90; P < .001) for schizophrenia, 1.64 (95% CI, 1.59-1.70; P < .001) for bipolar disorder, and 1.61 (95% CI, 1.59-1.63; P < .001) for depressive disorder.
Substance use disorder had a negative unadjusted association with strabismus, but after adjustment for confounders, the association was not significant (OR, 0.99; 95% CI, 0.97-1.02; P = .48).
Dr. Pineles noted that the study participants, who were all under age 19, may be too young to have substance use disorders.
The results for substance use disorders provided something of an “internal control” and reaffirmed results for the other four conditions, said Dr. Pineles.
“When you do research on such a large database, you’re very likely to find significant associations; the dataset is so large that even very small differences become statistically significant. It was interesting that not everything gave us a positive association.”
Researchers divided the strabismus group into those with esotropia, where the eyes turn inward (52.2%), exotropia, where they turn outward (46.3%), and hypertropia, where one eye wanders upward (12.5%). Investigators found that all three conditions were associated with increased risk of anxiety disorder, depressive disorder, bipolar disorders, and schizophrenia.
Investigators note that rates in the current study were lower than in previous studies, which showed that children with congenital esotropia were 2.6 times more likely to receive a mental health diagnosis, and children with intermittent exotropia were 2.7 times more likely to receive a mental health diagnosis.
“It is probable that our study found a lower risk than these studies, because our study was cross-sectional and claims based, whereas these studies observed the children to early adulthood and were based on medical records,” the investigators note.
It’s impossible to determine from this study how strabismus is connected to mental illness. However, Dr. Pineles believes depression and anxiety might be tied to strabismus via teasing, which affects self-esteem, although genetics could also play a role. For conditions such as schizophrenia, a shared genetic link with strabismus might be more likely, she added.
“Schizophrenia is a pretty severe diagnosis, so just being teased or having poor self-esteem is probably not enough” to develop schizophrenia.
Based on her clinical experience, Dr. Pineles said that realigning the eyes of patients with milder forms of depression or anxiety “definitely anecdotally helps these patients a lot.”
Dr. Pineles and colleagues have another paper in press that examines mental illnesses and other serious eye disorders in children and shows similar findings, she said.
Implications for insurance coverage?
In an accompanying editorial, experts, led by S. Grace Prakalapakorn, MD, department of ophthalmology and pediatrics, Duke University Medical Center, Durham, N.C., noted the exclusion of children covered under government insurance or without insurance is an important study limitation, largely because socioeconomic status is a risk factor for poor mental health.
The editorialists point to studies showing that surgical correction of ocular misalignments may be associated with reduced anxiety and depression. However, health insurance coverage for such surgical correction “may not be available owing to a misconception that these conditions are ‘cosmetic’.”
Evidence of the broader association of strabismus with physical and mental health “may play an important role in shifting policy to promote insurance coverage for timely strabismus care,” they write.
As many mental health disorders begin in childhood or adolescence, “it is paramount to identify, address, and, if possible, prevent mental health disorders at a young age, because failure to intervene in a timely fashion can have lifelong health consequences,” say Dr. Prakalapakorn and colleagues.
With mental health conditions and disorders increasing worldwide, compounded by the stressors of the COVID-19 pandemic, additional studies are needed to explore the causal relationships between ocular and psychiatric phenomena, their treatment, and outcomes, they add.
The study was supported by a grant from the National Eye Institute and an unrestricted grant from Research to Prevent Blindness. Dr. Pineles has reported no relevant conflicts of interest. Commentary author Manpreet K. Singh, MD, has reported receiving research support from Stanford’s Maternal Child Health Research Institute and Stanford’s Department of Psychiatry and Behavioral Sciences, the National Institute of Mental Health, the National Institute on Aging, the Patient-Centered Outcomes Research Institute, Johnson & Johnson, Allergan, and the Brain and Behavior Research Foundation; serving on the advisory board for Sunovion and Skyland Trail; serving as a consultant for Johnson & Johnson; previously serving as a consultant for X, the moonshot factory, Alphabet, and Limbix Health; receiving honoraria from the American Academy of Child and Adolescent Psychiatry; and receiving royalties from American Psychiatric Association Publishing and Thrive Global. Commentary author Nathan Congdon, MD, has reported receiving personal fees from Belkin Vision outside the submitted work.
A version of this article first appeared on Medscape.com.
Misaligned eyes in children are associated with an increased prevalence of mental illness, results of a large study suggest.
“Psychiatrists who have a patient with depression or anxiety and notice that patient also has strabismus might think about the link between those two conditions and refer that patient,” study investigator Stacy L. Pineles, MD, professor, department of ophthalmology, University of California, Los Angeles, told this news organization.
The study was published online March 10 in JAMA Ophthalmology.
A common condition
Strabismus, a condition in which the eyes don’t line up or are “crossed,” is one of the most common eye diseases in children, with some estimates suggesting it affects more than 1.5 million American youth.
Patients with strabismus have problems making eye contact and are affected socially and functionally, said Dr. Pineles. They’re often met with a negative bias, as shown by children’s responses to pictures of faces with and without strabismus, she said.
There is a signal from previous research suggesting that strabismus is linked to a higher risk of mental illness. However, most of these studies were small and had relatively homogenous populations, said Dr. Pineles.
The new study includes over 12 million children (mean age, 8.0 years) from a private health insurance claims database that represents diverse races and ethnicities as well as geographic regions across the United States.
The sample included 352,636 children with strabismus and 11,652,553 children with no diagnosed eye disease who served as controls. Most participants were White (51.6%), came from a family with an annual household income of $40,000 or more (51.0%), had point-of-service insurance (68.7%), and had at least one comorbid condition (64.5%).
The study evaluated five mental illness diagnoses. These included anxiety disorder, depressive disorder, substance use or addictive disorder, bipolar disorder, and schizophrenia.
Overall, children with strabismus had a higher prevalence of all these illnesses, with the exception of substance use disorder.
After adjusting for age, sex, race and ethnicity, census region, education level of caregiver, family net worth, and presence of at least one comorbid condition, the odds ratios among those with versus without strabismus were: 2.01 (95% confidence interval, 1.99-2.04; P < .001) for anxiety disorder, 1.83 (95% CI, 1.76-1.90; P < .001) for schizophrenia, 1.64 (95% CI, 1.59-1.70; P < .001) for bipolar disorder, and 1.61 (95% CI, 1.59-1.63; P < .001) for depressive disorder.
Substance use disorder had a negative unadjusted association with strabismus, but after adjustment for confounders, the association was not significant (OR, 0.99; 95% CI, 0.97-1.02; P = .48).
Dr. Pineles noted that the study participants, who were all under age 19, may be too young to have substance use disorders.
The results for substance use disorders provided something of an “internal control” and reaffirmed results for the other four conditions, said Dr. Pineles.
“When you do research on such a large database, you’re very likely to find significant associations; the dataset is so large that even very small differences become statistically significant. It was interesting that not everything gave us a positive association.”
Researchers divided the strabismus group into those with esotropia, where the eyes turn inward (52.2%), exotropia, where they turn outward (46.3%), and hypertropia, where one eye wanders upward (12.5%). Investigators found that all three conditions were associated with increased risk of anxiety disorder, depressive disorder, bipolar disorders, and schizophrenia.
Investigators note that rates in the current study were lower than in previous studies, which showed that children with congenital esotropia were 2.6 times more likely to receive a mental health diagnosis, and children with intermittent exotropia were 2.7 times more likely to receive a mental health diagnosis.
“It is probable that our study found a lower risk than these studies, because our study was cross-sectional and claims based, whereas these studies observed the children to early adulthood and were based on medical records,” the investigators note.
It’s impossible to determine from this study how strabismus is connected to mental illness. However, Dr. Pineles believes depression and anxiety might be tied to strabismus via teasing, which affects self-esteem, although genetics could also play a role. For conditions such as schizophrenia, a shared genetic link with strabismus might be more likely, she added.
“Schizophrenia is a pretty severe diagnosis, so just being teased or having poor self-esteem is probably not enough” to develop schizophrenia.
Based on her clinical experience, Dr. Pineles said that realigning the eyes of patients with milder forms of depression or anxiety “definitely anecdotally helps these patients a lot.”
Dr. Pineles and colleagues have another paper in press that examines mental illnesses and other serious eye disorders in children and shows similar findings, she said.
Implications for insurance coverage?
In an accompanying editorial, experts, led by S. Grace Prakalapakorn, MD, department of ophthalmology and pediatrics, Duke University Medical Center, Durham, N.C., noted the exclusion of children covered under government insurance or without insurance is an important study limitation, largely because socioeconomic status is a risk factor for poor mental health.
The editorialists point to studies showing that surgical correction of ocular misalignments may be associated with reduced anxiety and depression. However, health insurance coverage for such surgical correction “may not be available owing to a misconception that these conditions are ‘cosmetic’.”
Evidence of the broader association of strabismus with physical and mental health “may play an important role in shifting policy to promote insurance coverage for timely strabismus care,” they write.
As many mental health disorders begin in childhood or adolescence, “it is paramount to identify, address, and, if possible, prevent mental health disorders at a young age, because failure to intervene in a timely fashion can have lifelong health consequences,” say Dr. Prakalapakorn and colleagues.
With mental health conditions and disorders increasing worldwide, compounded by the stressors of the COVID-19 pandemic, additional studies are needed to explore the causal relationships between ocular and psychiatric phenomena, their treatment, and outcomes, they add.
The study was supported by a grant from the National Eye Institute and an unrestricted grant from Research to Prevent Blindness. Dr. Pineles has reported no relevant conflicts of interest. Commentary author Manpreet K. Singh, MD, has reported receiving research support from Stanford’s Maternal Child Health Research Institute and Stanford’s Department of Psychiatry and Behavioral Sciences, the National Institute of Mental Health, the National Institute on Aging, the Patient-Centered Outcomes Research Institute, Johnson & Johnson, Allergan, and the Brain and Behavior Research Foundation; serving on the advisory board for Sunovion and Skyland Trail; serving as a consultant for Johnson & Johnson; previously serving as a consultant for X, the moonshot factory, Alphabet, and Limbix Health; receiving honoraria from the American Academy of Child and Adolescent Psychiatry; and receiving royalties from American Psychiatric Association Publishing and Thrive Global. Commentary author Nathan Congdon, MD, has reported receiving personal fees from Belkin Vision outside the submitted work.
A version of this article first appeared on Medscape.com.
Misaligned eyes in children are associated with an increased prevalence of mental illness, results of a large study suggest.
“Psychiatrists who have a patient with depression or anxiety and notice that patient also has strabismus might think about the link between those two conditions and refer that patient,” study investigator Stacy L. Pineles, MD, professor, department of ophthalmology, University of California, Los Angeles, told this news organization.
The study was published online March 10 in JAMA Ophthalmology.
A common condition
Strabismus, a condition in which the eyes don’t line up or are “crossed,” is one of the most common eye diseases in children, with some estimates suggesting it affects more than 1.5 million American youth.
Patients with strabismus have problems making eye contact and are affected socially and functionally, said Dr. Pineles. They’re often met with a negative bias, as shown by children’s responses to pictures of faces with and without strabismus, she said.
There is a signal from previous research suggesting that strabismus is linked to a higher risk of mental illness. However, most of these studies were small and had relatively homogenous populations, said Dr. Pineles.
The new study includes over 12 million children (mean age, 8.0 years) from a private health insurance claims database that represents diverse races and ethnicities as well as geographic regions across the United States.
The sample included 352,636 children with strabismus and 11,652,553 children with no diagnosed eye disease who served as controls. Most participants were White (51.6%), came from a family with an annual household income of $40,000 or more (51.0%), had point-of-service insurance (68.7%), and had at least one comorbid condition (64.5%).
The study evaluated five mental illness diagnoses. These included anxiety disorder, depressive disorder, substance use or addictive disorder, bipolar disorder, and schizophrenia.
Overall, children with strabismus had a higher prevalence of all these illnesses, with the exception of substance use disorder.
After adjusting for age, sex, race and ethnicity, census region, education level of caregiver, family net worth, and presence of at least one comorbid condition, the odds ratios among those with versus without strabismus were: 2.01 (95% confidence interval, 1.99-2.04; P < .001) for anxiety disorder, 1.83 (95% CI, 1.76-1.90; P < .001) for schizophrenia, 1.64 (95% CI, 1.59-1.70; P < .001) for bipolar disorder, and 1.61 (95% CI, 1.59-1.63; P < .001) for depressive disorder.
Substance use disorder had a negative unadjusted association with strabismus, but after adjustment for confounders, the association was not significant (OR, 0.99; 95% CI, 0.97-1.02; P = .48).
Dr. Pineles noted that the study participants, who were all under age 19, may be too young to have substance use disorders.
The results for substance use disorders provided something of an “internal control” and reaffirmed results for the other four conditions, said Dr. Pineles.
“When you do research on such a large database, you’re very likely to find significant associations; the dataset is so large that even very small differences become statistically significant. It was interesting that not everything gave us a positive association.”
Researchers divided the strabismus group into those with esotropia, where the eyes turn inward (52.2%), exotropia, where they turn outward (46.3%), and hypertropia, where one eye wanders upward (12.5%). Investigators found that all three conditions were associated with increased risk of anxiety disorder, depressive disorder, bipolar disorders, and schizophrenia.
Investigators note that rates in the current study were lower than in previous studies, which showed that children with congenital esotropia were 2.6 times more likely to receive a mental health diagnosis, and children with intermittent exotropia were 2.7 times more likely to receive a mental health diagnosis.
“It is probable that our study found a lower risk than these studies, because our study was cross-sectional and claims based, whereas these studies observed the children to early adulthood and were based on medical records,” the investigators note.
It’s impossible to determine from this study how strabismus is connected to mental illness. However, Dr. Pineles believes depression and anxiety might be tied to strabismus via teasing, which affects self-esteem, although genetics could also play a role. For conditions such as schizophrenia, a shared genetic link with strabismus might be more likely, she added.
“Schizophrenia is a pretty severe diagnosis, so just being teased or having poor self-esteem is probably not enough” to develop schizophrenia.
Based on her clinical experience, Dr. Pineles said that realigning the eyes of patients with milder forms of depression or anxiety “definitely anecdotally helps these patients a lot.”
Dr. Pineles and colleagues have another paper in press that examines mental illnesses and other serious eye disorders in children and shows similar findings, she said.
Implications for insurance coverage?
In an accompanying editorial, experts, led by S. Grace Prakalapakorn, MD, department of ophthalmology and pediatrics, Duke University Medical Center, Durham, N.C., noted the exclusion of children covered under government insurance or without insurance is an important study limitation, largely because socioeconomic status is a risk factor for poor mental health.
The editorialists point to studies showing that surgical correction of ocular misalignments may be associated with reduced anxiety and depression. However, health insurance coverage for such surgical correction “may not be available owing to a misconception that these conditions are ‘cosmetic’.”
Evidence of the broader association of strabismus with physical and mental health “may play an important role in shifting policy to promote insurance coverage for timely strabismus care,” they write.
As many mental health disorders begin in childhood or adolescence, “it is paramount to identify, address, and, if possible, prevent mental health disorders at a young age, because failure to intervene in a timely fashion can have lifelong health consequences,” say Dr. Prakalapakorn and colleagues.
With mental health conditions and disorders increasing worldwide, compounded by the stressors of the COVID-19 pandemic, additional studies are needed to explore the causal relationships between ocular and psychiatric phenomena, their treatment, and outcomes, they add.
The study was supported by a grant from the National Eye Institute and an unrestricted grant from Research to Prevent Blindness. Dr. Pineles has reported no relevant conflicts of interest. Commentary author Manpreet K. Singh, MD, has reported receiving research support from Stanford’s Maternal Child Health Research Institute and Stanford’s Department of Psychiatry and Behavioral Sciences, the National Institute of Mental Health, the National Institute on Aging, the Patient-Centered Outcomes Research Institute, Johnson & Johnson, Allergan, and the Brain and Behavior Research Foundation; serving on the advisory board for Sunovion and Skyland Trail; serving as a consultant for Johnson & Johnson; previously serving as a consultant for X, the moonshot factory, Alphabet, and Limbix Health; receiving honoraria from the American Academy of Child and Adolescent Psychiatry; and receiving royalties from American Psychiatric Association Publishing and Thrive Global. Commentary author Nathan Congdon, MD, has reported receiving personal fees from Belkin Vision outside the submitted work.
A version of this article first appeared on Medscape.com.
U.S. primary care seen lagging in key markers
In delivery of primary care, including access and coordination, the U.S. trails well behind 10 other wealthy countries, according to a new report from the Commonwealth Fund.
The document, released March 15, concludes that the shortcomings in the U.S. system – from a lack of a relationship with a primary care physician to unequal access to after-hours care – “disproportionately affect Black and Latinx communities and rural areas, exacerbating disparities that have widened during the COVID-19 pandemic.”
“This report really shows that the U.S. is falling behind. We know that a strong primary care system yields better health outcomes. We have a lot to learn from other high-income countries,” coauthor Munira Z. Gunja, MPH, a senior researcher for the Commonwealth Fund’s International Program in Health Policy and Practice Innovations, told this news organization. “At baseline, we really need to make sure that everyone has health insurance in this country so they can actually use primary care services, and we need to increase the supply of those services.”
The report draws from the Commonwealth Fund’s 2019 and 2020 International Health Policy Surveys and the 2020 International Profiles of Health Care Systems. Among the main points:
- U.S. adults are the least likely to have a regular physician or place of care or a long-standing relationship with a primary care provider: 43% of American adults have a long-term relationship with a primary care doctor, compared with highs of 71% in Germany and the Netherlands.
- Access to home visits or after-hours care – excluding emergency department visits – is lowest in the United States (45%). In the Netherlands, Norway, New Zealand, and Germany, the rate is 90% to 96%.
- Half of primary care providers in the United States report adequate coordination with specialists and hospitals – around the average for the 11 countries studied.
‘Dismal mess’
Experts reacted to the report with a mix of concern and frustration – but not surprise.
“The results in this report are not surprising, and we have known them all for a number of years now,” Timothy Hoff, PhD, a health policy expert at Northeastern University, Boston, said. “Primary care doctors remain the backbone of our primary care system. But there are too few of them in the United States, and there likely will remain too few of them in the future. This opens the door to other and more diverse forms of innovation that will be required to help complement the work they do.”
Dr. Hoff, author of Searching for the Family Doctor: Primary Care on the Brink, added that comparing the United States to smaller countries like Norway or the United Kingdom is “somewhat problematic.”
“Our system has to take care of several hundred million people, trapped in a fragmented and market-based delivery system focused on specialty care, each of whom may have a different insurance plan,” he said. “Doing some of the things very small countries with government-funded insurance and a history of strong primary care delivery do in taking care of far fewer citizens is not realistic.”
Jeffrey Borkan, MD, PhD, chair and professor in the department of family medicine at the Alpert Medical School of Brown University, Providence, R.I., said the most shocking finding in the report is that despite spending far more on health care than any other country, “we cannot manage to provide one of the least expensive and most efficacious services: a relationship with a primary care doctor.”
Arthur Caplan, PhD, director of the Division of Medical Ethics at New York University Langone Medical Center, called primary care in this country “a dismal mess. It has been for many years. This is especially so in mental health. Access in many counties is nonexistent, and many primary care physicians are opting into boutique care.”
R. Shawn Martin, CEO of the 133,000-member American Academy of Family Physicians, said, “None of this surprises me. I think these are trendlines; we have been following this for many, many years here at the Academy.”
Mr. Martin added that he was disappointed that the recent, large investments in sharing and digitizing information have not closed the gaps that hinder the efficient and widespread delivery of primary care.
The findings in the report weren’t all bad. More primary care providers in the United States (30%) screen their patients for social needs such as housing, food security, and transportation – the highest among all 11 nations studied.
Also, Commonwealth Fund said the proportion of patients who said they received information on meeting their social needs and screening for domestic violence or social isolation was low everywhere. However, the percentage in the United States, Canada, and Norway was the highest, at 9%. Sweden had the lowest rate for such screenings, at 1%.
The researchers noted that social determinants of health account for as much as 55% of health outcomes. “In some countries, like the United States, the higher rates of receiving such information may be a response to the higher rates of material hardship, along with a weaker safety net,” the report states.
Ms. Gunja and her colleagues suggested several options for changes in policies, including narrowing the wage gap between primary care providers and higher-paid specialists; subsidizing medical school tuition to give students incentives to enter primary care; investing in telehealth to make primary care more accessible; and rewarding and holding providers accountable for continuity of care.
“The U.S. had the largest wage gap and highest tuition fees among the countries we studied,” Ms. Gunja told this news organization..
Researchers noted that U.S. patients could benefit from the introduction of incentives such as those paid in New Zealand to primary health organizations, which receive additional funding per capita to promote health and coordinate care.
But Dr. Caplan was skeptical that those measures would do much to correct the problems.
“We have no will to fix this ongoing, scandalous situation,” he said. “Specialist care still pays inordinately large salaries. Nurses and physician extenders are underused. Academic prestige does little to reward primary care. Plus, patients are not pressing for better access. Sorry, but I see no solutions pending in the current climate. Obamacare barely survived.”
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In delivery of primary care, including access and coordination, the U.S. trails well behind 10 other wealthy countries, according to a new report from the Commonwealth Fund.
The document, released March 15, concludes that the shortcomings in the U.S. system – from a lack of a relationship with a primary care physician to unequal access to after-hours care – “disproportionately affect Black and Latinx communities and rural areas, exacerbating disparities that have widened during the COVID-19 pandemic.”
“This report really shows that the U.S. is falling behind. We know that a strong primary care system yields better health outcomes. We have a lot to learn from other high-income countries,” coauthor Munira Z. Gunja, MPH, a senior researcher for the Commonwealth Fund’s International Program in Health Policy and Practice Innovations, told this news organization. “At baseline, we really need to make sure that everyone has health insurance in this country so they can actually use primary care services, and we need to increase the supply of those services.”
The report draws from the Commonwealth Fund’s 2019 and 2020 International Health Policy Surveys and the 2020 International Profiles of Health Care Systems. Among the main points:
- U.S. adults are the least likely to have a regular physician or place of care or a long-standing relationship with a primary care provider: 43% of American adults have a long-term relationship with a primary care doctor, compared with highs of 71% in Germany and the Netherlands.
- Access to home visits or after-hours care – excluding emergency department visits – is lowest in the United States (45%). In the Netherlands, Norway, New Zealand, and Germany, the rate is 90% to 96%.
- Half of primary care providers in the United States report adequate coordination with specialists and hospitals – around the average for the 11 countries studied.
‘Dismal mess’
Experts reacted to the report with a mix of concern and frustration – but not surprise.
“The results in this report are not surprising, and we have known them all for a number of years now,” Timothy Hoff, PhD, a health policy expert at Northeastern University, Boston, said. “Primary care doctors remain the backbone of our primary care system. But there are too few of them in the United States, and there likely will remain too few of them in the future. This opens the door to other and more diverse forms of innovation that will be required to help complement the work they do.”
Dr. Hoff, author of Searching for the Family Doctor: Primary Care on the Brink, added that comparing the United States to smaller countries like Norway or the United Kingdom is “somewhat problematic.”
“Our system has to take care of several hundred million people, trapped in a fragmented and market-based delivery system focused on specialty care, each of whom may have a different insurance plan,” he said. “Doing some of the things very small countries with government-funded insurance and a history of strong primary care delivery do in taking care of far fewer citizens is not realistic.”
Jeffrey Borkan, MD, PhD, chair and professor in the department of family medicine at the Alpert Medical School of Brown University, Providence, R.I., said the most shocking finding in the report is that despite spending far more on health care than any other country, “we cannot manage to provide one of the least expensive and most efficacious services: a relationship with a primary care doctor.”
Arthur Caplan, PhD, director of the Division of Medical Ethics at New York University Langone Medical Center, called primary care in this country “a dismal mess. It has been for many years. This is especially so in mental health. Access in many counties is nonexistent, and many primary care physicians are opting into boutique care.”
R. Shawn Martin, CEO of the 133,000-member American Academy of Family Physicians, said, “None of this surprises me. I think these are trendlines; we have been following this for many, many years here at the Academy.”
Mr. Martin added that he was disappointed that the recent, large investments in sharing and digitizing information have not closed the gaps that hinder the efficient and widespread delivery of primary care.
The findings in the report weren’t all bad. More primary care providers in the United States (30%) screen their patients for social needs such as housing, food security, and transportation – the highest among all 11 nations studied.
Also, Commonwealth Fund said the proportion of patients who said they received information on meeting their social needs and screening for domestic violence or social isolation was low everywhere. However, the percentage in the United States, Canada, and Norway was the highest, at 9%. Sweden had the lowest rate for such screenings, at 1%.
The researchers noted that social determinants of health account for as much as 55% of health outcomes. “In some countries, like the United States, the higher rates of receiving such information may be a response to the higher rates of material hardship, along with a weaker safety net,” the report states.
Ms. Gunja and her colleagues suggested several options for changes in policies, including narrowing the wage gap between primary care providers and higher-paid specialists; subsidizing medical school tuition to give students incentives to enter primary care; investing in telehealth to make primary care more accessible; and rewarding and holding providers accountable for continuity of care.
“The U.S. had the largest wage gap and highest tuition fees among the countries we studied,” Ms. Gunja told this news organization..
Researchers noted that U.S. patients could benefit from the introduction of incentives such as those paid in New Zealand to primary health organizations, which receive additional funding per capita to promote health and coordinate care.
But Dr. Caplan was skeptical that those measures would do much to correct the problems.
“We have no will to fix this ongoing, scandalous situation,” he said. “Specialist care still pays inordinately large salaries. Nurses and physician extenders are underused. Academic prestige does little to reward primary care. Plus, patients are not pressing for better access. Sorry, but I see no solutions pending in the current climate. Obamacare barely survived.”
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In delivery of primary care, including access and coordination, the U.S. trails well behind 10 other wealthy countries, according to a new report from the Commonwealth Fund.
The document, released March 15, concludes that the shortcomings in the U.S. system – from a lack of a relationship with a primary care physician to unequal access to after-hours care – “disproportionately affect Black and Latinx communities and rural areas, exacerbating disparities that have widened during the COVID-19 pandemic.”
“This report really shows that the U.S. is falling behind. We know that a strong primary care system yields better health outcomes. We have a lot to learn from other high-income countries,” coauthor Munira Z. Gunja, MPH, a senior researcher for the Commonwealth Fund’s International Program in Health Policy and Practice Innovations, told this news organization. “At baseline, we really need to make sure that everyone has health insurance in this country so they can actually use primary care services, and we need to increase the supply of those services.”
The report draws from the Commonwealth Fund’s 2019 and 2020 International Health Policy Surveys and the 2020 International Profiles of Health Care Systems. Among the main points:
- U.S. adults are the least likely to have a regular physician or place of care or a long-standing relationship with a primary care provider: 43% of American adults have a long-term relationship with a primary care doctor, compared with highs of 71% in Germany and the Netherlands.
- Access to home visits or after-hours care – excluding emergency department visits – is lowest in the United States (45%). In the Netherlands, Norway, New Zealand, and Germany, the rate is 90% to 96%.
- Half of primary care providers in the United States report adequate coordination with specialists and hospitals – around the average for the 11 countries studied.
‘Dismal mess’
Experts reacted to the report with a mix of concern and frustration – but not surprise.
“The results in this report are not surprising, and we have known them all for a number of years now,” Timothy Hoff, PhD, a health policy expert at Northeastern University, Boston, said. “Primary care doctors remain the backbone of our primary care system. But there are too few of them in the United States, and there likely will remain too few of them in the future. This opens the door to other and more diverse forms of innovation that will be required to help complement the work they do.”
Dr. Hoff, author of Searching for the Family Doctor: Primary Care on the Brink, added that comparing the United States to smaller countries like Norway or the United Kingdom is “somewhat problematic.”
“Our system has to take care of several hundred million people, trapped in a fragmented and market-based delivery system focused on specialty care, each of whom may have a different insurance plan,” he said. “Doing some of the things very small countries with government-funded insurance and a history of strong primary care delivery do in taking care of far fewer citizens is not realistic.”
Jeffrey Borkan, MD, PhD, chair and professor in the department of family medicine at the Alpert Medical School of Brown University, Providence, R.I., said the most shocking finding in the report is that despite spending far more on health care than any other country, “we cannot manage to provide one of the least expensive and most efficacious services: a relationship with a primary care doctor.”
Arthur Caplan, PhD, director of the Division of Medical Ethics at New York University Langone Medical Center, called primary care in this country “a dismal mess. It has been for many years. This is especially so in mental health. Access in many counties is nonexistent, and many primary care physicians are opting into boutique care.”
R. Shawn Martin, CEO of the 133,000-member American Academy of Family Physicians, said, “None of this surprises me. I think these are trendlines; we have been following this for many, many years here at the Academy.”
Mr. Martin added that he was disappointed that the recent, large investments in sharing and digitizing information have not closed the gaps that hinder the efficient and widespread delivery of primary care.
The findings in the report weren’t all bad. More primary care providers in the United States (30%) screen their patients for social needs such as housing, food security, and transportation – the highest among all 11 nations studied.
Also, Commonwealth Fund said the proportion of patients who said they received information on meeting their social needs and screening for domestic violence or social isolation was low everywhere. However, the percentage in the United States, Canada, and Norway was the highest, at 9%. Sweden had the lowest rate for such screenings, at 1%.
The researchers noted that social determinants of health account for as much as 55% of health outcomes. “In some countries, like the United States, the higher rates of receiving such information may be a response to the higher rates of material hardship, along with a weaker safety net,” the report states.
Ms. Gunja and her colleagues suggested several options for changes in policies, including narrowing the wage gap between primary care providers and higher-paid specialists; subsidizing medical school tuition to give students incentives to enter primary care; investing in telehealth to make primary care more accessible; and rewarding and holding providers accountable for continuity of care.
“The U.S. had the largest wage gap and highest tuition fees among the countries we studied,” Ms. Gunja told this news organization..
Researchers noted that U.S. patients could benefit from the introduction of incentives such as those paid in New Zealand to primary health organizations, which receive additional funding per capita to promote health and coordinate care.
But Dr. Caplan was skeptical that those measures would do much to correct the problems.
“We have no will to fix this ongoing, scandalous situation,” he said. “Specialist care still pays inordinately large salaries. Nurses and physician extenders are underused. Academic prestige does little to reward primary care. Plus, patients are not pressing for better access. Sorry, but I see no solutions pending in the current climate. Obamacare barely survived.”
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Empagliflozin scores topline win in EMPA-KIDNEY trial
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.

In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.
In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.
In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Cancer patients vulnerable to COVID misinformation
For the past 2 years, oncology practitioners around the world have struggled with the same dilemma: how to maintain their patients’ cancer care without exposing them to COVID-19. Regardless of the country, language, or even which wave of the pandemic, the conversations have likely been very similar: weighing risks versuss benefits, and individualizing each patient’s pandemic cancer plan.
But one question most oncologists have probably overlooked in these discussions is about where their patients get their COVID information – or misinformation.
Surprisingly, this seemingly small detail could make a big difference in a patient’s prognosis.
A recent study found that building on an earlier finding of similar vulnerabilities among parents of children with cancer, compared with parents of healthy children.
“It doesn’t matter what you search for, there is an overwhelming level of information online,” the lead author on both studies, Jeanine Guidry, PhD, from Virginia Commonwealth University’s Massey Cancer Center in Richmond, said in an interview. “If misinformation is the first thing you encounter about a topic, you’re much more likely to believe it and it’s going to be very hard to convince you otherwise.”
Before the pandemic, Dr. Guidry, who is director of the Media+Health Lab at VCU, had already been studying vaccine misinformation on Pinterest and Instagram.
So when data coming out at the start of the pandemic suggested that an increase in pediatric cancer mortality might be partially because of COVID-19 misinformation, she jumped on it.
Dr. Guidry and associates designed a questionnaire involving COVID misinformation statements available online and found that parents of children with cancer were significantly more likely to endorse them, compared with parents of healthy children.
“Our advice to clinicians is you may have an issue here,” Dr. Guidry said in an interview. “You may want to check where they get their news, and if there’s any pieces of misinformation that could be harmful.”
Some beliefs, such as eating more garlic protects against COVID, are not particularly harmful, she acknowledged, but others – such as drinking bleach being protective – are quite harmful, and they often stem from the same misinformation sources.
Both of Dr. Guidry’s studies involved surveys of either adult patients with cancer or parents of children with cancer.
The adult patient survey was conducted June 1-15, 2020, and included 897 respondents, of whom 287 were patients in active treatment for cancer, 301 were survivors not currently in treatment, and 309 had no cancer history.
The parents’ survey, conducted in May 2020, included 735 parents of children aged 2-17 years, 315 of whom had children currently undergoing cancer treatment, and 420 of whom had children with no history of cancer.
Among the misinformation they were asked to agree or disagree with were statements such as “it is unsafe to receive mail from China,” “antibiotics can prevent and treat COVID-19,” and “COVID is less deadly than the ‘flu,’ ” among others.
The surveys revealed that the patients in current treatment for cancer and the parents of patients in current treatment were most likely to endorse COVID misinformation. Results from the parents’ survey showed that “believing misinformation was also more likely for fathers, younger parents, and parents with higher perceived stress from COVID-19,” the authors wrote. Among adult patients and controls, patients in active treatment were most likely to believe misinformation, with cancer survivors no longer in treatment being the least likely to believe it, compared with healthy controls who were in between.
Why the difference? The authors suggested that patients in active treatment “may seek out more information on the internet or via social media where they are more exposed to misinformation,” whereas survivors no longer undergoing treatment may be more “media savvy and have learned to be wary of questionable health information.”
In their articles, Dr. Guidry and associates advised oncologists to be aware of their patients’ potential to endorse COVID misinformation and to “proactively address this in routine visits as well as tailored written materials.” This is easier said than done, she commented, acknowledging that keeping up with the latest misinformation is a challenge.
The misinformation statements her group used in their surveys were popular early in the pandemic, but “some of them have shown fairly remarkable staying power and some have been replaced,” she said. She invited interested clinicians to contact her team for guidance on newer misinformation.
Ultimately, she believes most patients with cancer who endorse misinformation are simply afraid, and looking for help. “They’re already dealing with a level of stress from their illness and then they’re thrown into a pandemic,” Dr. Guidry said. “At some point you just want a solution. Hydroxychloroquine? Great! Horse dewormer? Fantastic! Just wanting to control the situation and not having something else to deal with.”
Both studies were funded by the National Cancer Institute at the National Institutes of Health. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For the past 2 years, oncology practitioners around the world have struggled with the same dilemma: how to maintain their patients’ cancer care without exposing them to COVID-19. Regardless of the country, language, or even which wave of the pandemic, the conversations have likely been very similar: weighing risks versuss benefits, and individualizing each patient’s pandemic cancer plan.
But one question most oncologists have probably overlooked in these discussions is about where their patients get their COVID information – or misinformation.
Surprisingly, this seemingly small detail could make a big difference in a patient’s prognosis.
A recent study found that building on an earlier finding of similar vulnerabilities among parents of children with cancer, compared with parents of healthy children.
“It doesn’t matter what you search for, there is an overwhelming level of information online,” the lead author on both studies, Jeanine Guidry, PhD, from Virginia Commonwealth University’s Massey Cancer Center in Richmond, said in an interview. “If misinformation is the first thing you encounter about a topic, you’re much more likely to believe it and it’s going to be very hard to convince you otherwise.”
Before the pandemic, Dr. Guidry, who is director of the Media+Health Lab at VCU, had already been studying vaccine misinformation on Pinterest and Instagram.
So when data coming out at the start of the pandemic suggested that an increase in pediatric cancer mortality might be partially because of COVID-19 misinformation, she jumped on it.
Dr. Guidry and associates designed a questionnaire involving COVID misinformation statements available online and found that parents of children with cancer were significantly more likely to endorse them, compared with parents of healthy children.
“Our advice to clinicians is you may have an issue here,” Dr. Guidry said in an interview. “You may want to check where they get their news, and if there’s any pieces of misinformation that could be harmful.”
Some beliefs, such as eating more garlic protects against COVID, are not particularly harmful, she acknowledged, but others – such as drinking bleach being protective – are quite harmful, and they often stem from the same misinformation sources.
Both of Dr. Guidry’s studies involved surveys of either adult patients with cancer or parents of children with cancer.
The adult patient survey was conducted June 1-15, 2020, and included 897 respondents, of whom 287 were patients in active treatment for cancer, 301 were survivors not currently in treatment, and 309 had no cancer history.
The parents’ survey, conducted in May 2020, included 735 parents of children aged 2-17 years, 315 of whom had children currently undergoing cancer treatment, and 420 of whom had children with no history of cancer.
Among the misinformation they were asked to agree or disagree with were statements such as “it is unsafe to receive mail from China,” “antibiotics can prevent and treat COVID-19,” and “COVID is less deadly than the ‘flu,’ ” among others.
The surveys revealed that the patients in current treatment for cancer and the parents of patients in current treatment were most likely to endorse COVID misinformation. Results from the parents’ survey showed that “believing misinformation was also more likely for fathers, younger parents, and parents with higher perceived stress from COVID-19,” the authors wrote. Among adult patients and controls, patients in active treatment were most likely to believe misinformation, with cancer survivors no longer in treatment being the least likely to believe it, compared with healthy controls who were in between.
Why the difference? The authors suggested that patients in active treatment “may seek out more information on the internet or via social media where they are more exposed to misinformation,” whereas survivors no longer undergoing treatment may be more “media savvy and have learned to be wary of questionable health information.”
In their articles, Dr. Guidry and associates advised oncologists to be aware of their patients’ potential to endorse COVID misinformation and to “proactively address this in routine visits as well as tailored written materials.” This is easier said than done, she commented, acknowledging that keeping up with the latest misinformation is a challenge.
The misinformation statements her group used in their surveys were popular early in the pandemic, but “some of them have shown fairly remarkable staying power and some have been replaced,” she said. She invited interested clinicians to contact her team for guidance on newer misinformation.
Ultimately, she believes most patients with cancer who endorse misinformation are simply afraid, and looking for help. “They’re already dealing with a level of stress from their illness and then they’re thrown into a pandemic,” Dr. Guidry said. “At some point you just want a solution. Hydroxychloroquine? Great! Horse dewormer? Fantastic! Just wanting to control the situation and not having something else to deal with.”
Both studies were funded by the National Cancer Institute at the National Institutes of Health. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For the past 2 years, oncology practitioners around the world have struggled with the same dilemma: how to maintain their patients’ cancer care without exposing them to COVID-19. Regardless of the country, language, or even which wave of the pandemic, the conversations have likely been very similar: weighing risks versuss benefits, and individualizing each patient’s pandemic cancer plan.
But one question most oncologists have probably overlooked in these discussions is about where their patients get their COVID information – or misinformation.
Surprisingly, this seemingly small detail could make a big difference in a patient’s prognosis.
A recent study found that building on an earlier finding of similar vulnerabilities among parents of children with cancer, compared with parents of healthy children.
“It doesn’t matter what you search for, there is an overwhelming level of information online,” the lead author on both studies, Jeanine Guidry, PhD, from Virginia Commonwealth University’s Massey Cancer Center in Richmond, said in an interview. “If misinformation is the first thing you encounter about a topic, you’re much more likely to believe it and it’s going to be very hard to convince you otherwise.”
Before the pandemic, Dr. Guidry, who is director of the Media+Health Lab at VCU, had already been studying vaccine misinformation on Pinterest and Instagram.
So when data coming out at the start of the pandemic suggested that an increase in pediatric cancer mortality might be partially because of COVID-19 misinformation, she jumped on it.
Dr. Guidry and associates designed a questionnaire involving COVID misinformation statements available online and found that parents of children with cancer were significantly more likely to endorse them, compared with parents of healthy children.
“Our advice to clinicians is you may have an issue here,” Dr. Guidry said in an interview. “You may want to check where they get their news, and if there’s any pieces of misinformation that could be harmful.”
Some beliefs, such as eating more garlic protects against COVID, are not particularly harmful, she acknowledged, but others – such as drinking bleach being protective – are quite harmful, and they often stem from the same misinformation sources.
Both of Dr. Guidry’s studies involved surveys of either adult patients with cancer or parents of children with cancer.
The adult patient survey was conducted June 1-15, 2020, and included 897 respondents, of whom 287 were patients in active treatment for cancer, 301 were survivors not currently in treatment, and 309 had no cancer history.
The parents’ survey, conducted in May 2020, included 735 parents of children aged 2-17 years, 315 of whom had children currently undergoing cancer treatment, and 420 of whom had children with no history of cancer.
Among the misinformation they were asked to agree or disagree with were statements such as “it is unsafe to receive mail from China,” “antibiotics can prevent and treat COVID-19,” and “COVID is less deadly than the ‘flu,’ ” among others.
The surveys revealed that the patients in current treatment for cancer and the parents of patients in current treatment were most likely to endorse COVID misinformation. Results from the parents’ survey showed that “believing misinformation was also more likely for fathers, younger parents, and parents with higher perceived stress from COVID-19,” the authors wrote. Among adult patients and controls, patients in active treatment were most likely to believe misinformation, with cancer survivors no longer in treatment being the least likely to believe it, compared with healthy controls who were in between.
Why the difference? The authors suggested that patients in active treatment “may seek out more information on the internet or via social media where they are more exposed to misinformation,” whereas survivors no longer undergoing treatment may be more “media savvy and have learned to be wary of questionable health information.”
In their articles, Dr. Guidry and associates advised oncologists to be aware of their patients’ potential to endorse COVID misinformation and to “proactively address this in routine visits as well as tailored written materials.” This is easier said than done, she commented, acknowledging that keeping up with the latest misinformation is a challenge.
The misinformation statements her group used in their surveys were popular early in the pandemic, but “some of them have shown fairly remarkable staying power and some have been replaced,” she said. She invited interested clinicians to contact her team for guidance on newer misinformation.
Ultimately, she believes most patients with cancer who endorse misinformation are simply afraid, and looking for help. “They’re already dealing with a level of stress from their illness and then they’re thrown into a pandemic,” Dr. Guidry said. “At some point you just want a solution. Hydroxychloroquine? Great! Horse dewormer? Fantastic! Just wanting to control the situation and not having something else to deal with.”
Both studies were funded by the National Cancer Institute at the National Institutes of Health. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PATIENT EDUCATION AND COUNSELING