User login
For MD-IQ use only
First drug therapy approved for childhood GVHD
Specifically, the indication is for pediatric patients with cGVHD who have already been treated with one or more lines of systemic therapy. The manufacturers have also launched a new oral suspension formulation, in addition to capsules and tablets, which were already available.
Ibrutinib is already approved for use in adults with cGVHD.
The drug is also approved for use in several blood cancers, including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenström’s macroglobulinemia. All these approvals are for adult patients.
This is the first pediatric indication for the product and is “incredibly meaningful,” said Gauri Sunkersett, DO, associate medical director at AbbVie, which markets the drug together with Jansen. “As a pediatric oncologist, when my patients describe the physical pain they experience from simply hugging their parents, due to their cGVHD, the importance of researching alternative treatment options in this patient population is further validated.”
These children have already been through a lot, having been diagnosed with a leukemia or lymphoma and then undergoing chemotherapy and/or radiotherapy for a stem cell transplant. Just over half (52%-65%) of children who receive allogeneic transplants go on to develop cGVHD, in which the donor bone marrow or stem cells attack the recipient.
“Imagine going through a transplant and then being told you have a moderate to severe chronic disease that can sometimes also be life-threatening,” commented Paul A. Carpenter, MD, attending physician at Seattle Children’s Hospital. “If these children were between 1 and 12 and didn’t respond to steroid treatment, we didn’t have any rigorously studied treatment options – until now.”
The new indication was approved by the U.S. Food and Drug Administration on the basis of results from the iMAGINE trial, for which Dr. Carpenter was a principal investigator.
The phase 1/2 iMAGINE trial was an open-label, multicenter, single-arm trial conducted with 47 patients (mean age, 13 years; range, 1-19 years) with relapsed/refractory cGVHD who had received at least one prior systemic therapy. Ibrutinib was given at a dose of 420 mg orally once daily to patients aged 12 and older and at a dose of 240 mg/m2 orally once daily to patients who were younger than 12 years.
The overall response rate through week 25 was 60% (confidence interval, 95%, 44%-74%). The median duration of response was 5.3 months (95% CI, 2.8-8.8).
The safety profile was consistent with the established profile for ibrutinib. Observed adverse events in pediatric patients were consistent with those observed in adult patients with moderate to severe cGVHD, the companies noted.
The FDA noted that the most common (≥ 20%) adverse reactions, including laboratory abnormalities, were anemia, musculoskeletal pain, pyrexia, diarrhea, pneumonia, abdominal pain, stomatitis, thrombocytopenia, and headache.
Full prescribing information for ibrutinib is available here.
A version of this article first appeared on Medscape.com.
Specifically, the indication is for pediatric patients with cGVHD who have already been treated with one or more lines of systemic therapy. The manufacturers have also launched a new oral suspension formulation, in addition to capsules and tablets, which were already available.
Ibrutinib is already approved for use in adults with cGVHD.
The drug is also approved for use in several blood cancers, including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenström’s macroglobulinemia. All these approvals are for adult patients.
This is the first pediatric indication for the product and is “incredibly meaningful,” said Gauri Sunkersett, DO, associate medical director at AbbVie, which markets the drug together with Jansen. “As a pediatric oncologist, when my patients describe the physical pain they experience from simply hugging their parents, due to their cGVHD, the importance of researching alternative treatment options in this patient population is further validated.”
These children have already been through a lot, having been diagnosed with a leukemia or lymphoma and then undergoing chemotherapy and/or radiotherapy for a stem cell transplant. Just over half (52%-65%) of children who receive allogeneic transplants go on to develop cGVHD, in which the donor bone marrow or stem cells attack the recipient.
“Imagine going through a transplant and then being told you have a moderate to severe chronic disease that can sometimes also be life-threatening,” commented Paul A. Carpenter, MD, attending physician at Seattle Children’s Hospital. “If these children were between 1 and 12 and didn’t respond to steroid treatment, we didn’t have any rigorously studied treatment options – until now.”
The new indication was approved by the U.S. Food and Drug Administration on the basis of results from the iMAGINE trial, for which Dr. Carpenter was a principal investigator.
The phase 1/2 iMAGINE trial was an open-label, multicenter, single-arm trial conducted with 47 patients (mean age, 13 years; range, 1-19 years) with relapsed/refractory cGVHD who had received at least one prior systemic therapy. Ibrutinib was given at a dose of 420 mg orally once daily to patients aged 12 and older and at a dose of 240 mg/m2 orally once daily to patients who were younger than 12 years.
The overall response rate through week 25 was 60% (confidence interval, 95%, 44%-74%). The median duration of response was 5.3 months (95% CI, 2.8-8.8).
The safety profile was consistent with the established profile for ibrutinib. Observed adverse events in pediatric patients were consistent with those observed in adult patients with moderate to severe cGVHD, the companies noted.
The FDA noted that the most common (≥ 20%) adverse reactions, including laboratory abnormalities, were anemia, musculoskeletal pain, pyrexia, diarrhea, pneumonia, abdominal pain, stomatitis, thrombocytopenia, and headache.
Full prescribing information for ibrutinib is available here.
A version of this article first appeared on Medscape.com.
Specifically, the indication is for pediatric patients with cGVHD who have already been treated with one or more lines of systemic therapy. The manufacturers have also launched a new oral suspension formulation, in addition to capsules and tablets, which were already available.
Ibrutinib is already approved for use in adults with cGVHD.
The drug is also approved for use in several blood cancers, including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenström’s macroglobulinemia. All these approvals are for adult patients.
This is the first pediatric indication for the product and is “incredibly meaningful,” said Gauri Sunkersett, DO, associate medical director at AbbVie, which markets the drug together with Jansen. “As a pediatric oncologist, when my patients describe the physical pain they experience from simply hugging their parents, due to their cGVHD, the importance of researching alternative treatment options in this patient population is further validated.”
These children have already been through a lot, having been diagnosed with a leukemia or lymphoma and then undergoing chemotherapy and/or radiotherapy for a stem cell transplant. Just over half (52%-65%) of children who receive allogeneic transplants go on to develop cGVHD, in which the donor bone marrow or stem cells attack the recipient.
“Imagine going through a transplant and then being told you have a moderate to severe chronic disease that can sometimes also be life-threatening,” commented Paul A. Carpenter, MD, attending physician at Seattle Children’s Hospital. “If these children were between 1 and 12 and didn’t respond to steroid treatment, we didn’t have any rigorously studied treatment options – until now.”
The new indication was approved by the U.S. Food and Drug Administration on the basis of results from the iMAGINE trial, for which Dr. Carpenter was a principal investigator.
The phase 1/2 iMAGINE trial was an open-label, multicenter, single-arm trial conducted with 47 patients (mean age, 13 years; range, 1-19 years) with relapsed/refractory cGVHD who had received at least one prior systemic therapy. Ibrutinib was given at a dose of 420 mg orally once daily to patients aged 12 and older and at a dose of 240 mg/m2 orally once daily to patients who were younger than 12 years.
The overall response rate through week 25 was 60% (confidence interval, 95%, 44%-74%). The median duration of response was 5.3 months (95% CI, 2.8-8.8).
The safety profile was consistent with the established profile for ibrutinib. Observed adverse events in pediatric patients were consistent with those observed in adult patients with moderate to severe cGVHD, the companies noted.
The FDA noted that the most common (≥ 20%) adverse reactions, including laboratory abnormalities, were anemia, musculoskeletal pain, pyrexia, diarrhea, pneumonia, abdominal pain, stomatitis, thrombocytopenia, and headache.
Full prescribing information for ibrutinib is available here.
A version of this article first appeared on Medscape.com.
COMMENT & CONTROVERSY
How common is IUD perforation, expulsion, and malposition?
ROBERT L. BARBIERI, MD (APRIL 2022)
The seriousness of IUD embedment
I appreciated Dr. Barbieri’s comprehensive review of clinical problems regarding the intrauterine device (IUD). It is interesting that, in spite of your mention of IUD embedment in the myometrium, other publications regarding this phenomenon are seemingly absent (except for ours).1 Whether or not there is associated pain (and sometimes there is not), in our experience its removal can result in IUD fracture. As you stated, it is true that 3D transvaginal sonography perfectly enables this visualization, yet it is surprising that others have not experienced what we have. Nonetheless, it is encouraging to see that IUD embedment is seriously mentioned.
- Fernandez CM, Levine EM, Cabiya M, et al. Intrauterine device embedment resulting in its fracture: a case series. Arch Obstet Gynecol. 2021;2:1-4.
Elliot Levine, MD
Chicago, Illinois
Dr. Barbieri responds
I thank Dr. Levine for highlighting the important issue of IUD fracture and providing a reference to a case series of IUD fractures. Although such fracture is not common, when it does occur it may require a hysteroscopic procedure to remove all pieces of the IUD. In the cited case series, fracture was more commonly observed with the copper IUD than with the LNG-IUD. With regard to IUD malposition, 4 publications reviewed in my recent editorial describe the problem of an IUD arm embedded in the myometrium.1-4
References
- Benacerraf BR, Shipp TD, Bromley B. Three-dimensional ultrasound detection of abnormally located intrauterine contraceptive devices which are a source of pelvic pain and abnormal bleeding. Ultrasound Obstet Gynecol. 2009;34:110-115.
- Braaten KP, Benson CB, Maurer R, et al. Malpositioned intrauterine contraceptive devices: risk factors, outcomes and future pregnancies. Obstet Gynecol. 2011;118:1014-1020.
- Gerkowicz SA, Fiorentino DG, Kovacs AP, et al. Uterine structural abnormality and intrauterine device malposition: analysis of ultrasonographic and demographic variables of 517 patients. Am J Obstet Gynecol. 2019;220:183.e1-e8.
- Connolly CT, Fox NS. Incidence and risk factors for a malpositioned intrauterine device detected on three-dimensional ultrasound within eight weeks of placement. J Ultrasound Med. September 27, 2021.
Will NAAT replace microscopy for the identification of organisms causing vaginitis?
ROBERT L. BARBIERI, MD (MARCH 2022)
Follow-up questions on NAAT testing
The sensitivity of NAAT testing, as outlined in Dr. Barbieri’s editorial, is undoubtedly better than the clinical methods most clinicians are using. I appreciate the frustration we providers often experience in drawing conclusions for patients based on the Amsel criteria for bacterial vaginitis (BV). I am surprised by the low sensitivity of microscopy for yeast vaginitis. My follow-up questions are:
- Have the NAATs referenced been validated in clinical trials and proven to improve patient outcomes?
- Will the proposal to begin empiric therapy for both yeast vaginitis and BV in combination while waiting for NAAT results lead to an increase of resistant strains?
- What is the cost of NAAT for vaginitis, and is this cost effective in routine practice?
- Can NAATs be utilized to detect resistant strains of yeast or Gardnerella sp?
Alan Paul Gehrich, MD (COL, MC ret.)
Bethesda, Maryland
Dr. Barbieri responds
I thank Dr. Gehrich for raising the important issue of what is the optimal endpoint to assess the clinical utility of NAAT testing for vaginitis. Most studies of the use of NAAT to diagnose the cause of vaginitis focus on comparing NAAT results to standard clinical practice (microscopy and pH), and to a “gold standard.” In most studies the gold standards are Nugent scoring with Amsel criteria to resolve intermediate Nugent scores for bacterial vaginosis, culture for Candida, and culture for Trichomonas vaginalis. It is clear from multiple studies that NAAT provides superior sensitivity and specificity compared with standard clinical practice.1-3 As noted in the editorial, in a study of 466 patients with symptoms of vaginitis, standard office approaches to the diagnosis of vaginitis resulted in the failure to identify the correct infection in a large number of cases.4 For the diagnosis of BV, clinicians missed 42% of the cases identified by NAAT. For the diagnosis of Candida, clinicians missed 46% of the cases identified by NAAT. For the diagnosis of T vaginalis, clinicians missed 72% of the cases identified by NAAT. This resulted in clinicians not appropriately treating many infections detected by NAAT.
NAAT does provide information about the presence of Candida glabrata and Candida krusei, organisms which may be resistant to fluconazole. I agree with Dr. Gehrich that the optimal use of NAAT testing in practice is poorly studied with regard to treatment between sample collection and NAAT results. Cost of testing is a complex issue. Standard microscopy is relatively inexpensive, but performs poorly in clinical practice, resulting in misdiagnosis. NAAT testing is expensive but correctly identifies causes of vaginitis.
References
- Schwebke JR, Gaydos CA, Hyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56:e00252-18.
- Broache M, Cammarata CL, Stonebraker E, et al. Performance of vaginal panel assay compared with clinical diagnosis of vaginitis. Obstet Gynecol. 2021;138:853-859.
- Schwebke JR, Taylor SN, Ackerman N, et al. Clinical validation of the Aptima bacterial vaginosis and Aptima Candida/Trichomonas vaginalis assays: results from a prospective multi-center study. J Clin Microbiol. 2020;58:e01643-19. 4
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
How common is IUD perforation, expulsion, and malposition?
ROBERT L. BARBIERI, MD (APRIL 2022)
The seriousness of IUD embedment
I appreciated Dr. Barbieri’s comprehensive review of clinical problems regarding the intrauterine device (IUD). It is interesting that, in spite of your mention of IUD embedment in the myometrium, other publications regarding this phenomenon are seemingly absent (except for ours).1 Whether or not there is associated pain (and sometimes there is not), in our experience its removal can result in IUD fracture. As you stated, it is true that 3D transvaginal sonography perfectly enables this visualization, yet it is surprising that others have not experienced what we have. Nonetheless, it is encouraging to see that IUD embedment is seriously mentioned.
- Fernandez CM, Levine EM, Cabiya M, et al. Intrauterine device embedment resulting in its fracture: a case series. Arch Obstet Gynecol. 2021;2:1-4.
Elliot Levine, MD
Chicago, Illinois
Dr. Barbieri responds
I thank Dr. Levine for highlighting the important issue of IUD fracture and providing a reference to a case series of IUD fractures. Although such fracture is not common, when it does occur it may require a hysteroscopic procedure to remove all pieces of the IUD. In the cited case series, fracture was more commonly observed with the copper IUD than with the LNG-IUD. With regard to IUD malposition, 4 publications reviewed in my recent editorial describe the problem of an IUD arm embedded in the myometrium.1-4
References
- Benacerraf BR, Shipp TD, Bromley B. Three-dimensional ultrasound detection of abnormally located intrauterine contraceptive devices which are a source of pelvic pain and abnormal bleeding. Ultrasound Obstet Gynecol. 2009;34:110-115.
- Braaten KP, Benson CB, Maurer R, et al. Malpositioned intrauterine contraceptive devices: risk factors, outcomes and future pregnancies. Obstet Gynecol. 2011;118:1014-1020.
- Gerkowicz SA, Fiorentino DG, Kovacs AP, et al. Uterine structural abnormality and intrauterine device malposition: analysis of ultrasonographic and demographic variables of 517 patients. Am J Obstet Gynecol. 2019;220:183.e1-e8.
- Connolly CT, Fox NS. Incidence and risk factors for a malpositioned intrauterine device detected on three-dimensional ultrasound within eight weeks of placement. J Ultrasound Med. September 27, 2021.
Will NAAT replace microscopy for the identification of organisms causing vaginitis?
ROBERT L. BARBIERI, MD (MARCH 2022)
Follow-up questions on NAAT testing
The sensitivity of NAAT testing, as outlined in Dr. Barbieri’s editorial, is undoubtedly better than the clinical methods most clinicians are using. I appreciate the frustration we providers often experience in drawing conclusions for patients based on the Amsel criteria for bacterial vaginitis (BV). I am surprised by the low sensitivity of microscopy for yeast vaginitis. My follow-up questions are:
- Have the NAATs referenced been validated in clinical trials and proven to improve patient outcomes?
- Will the proposal to begin empiric therapy for both yeast vaginitis and BV in combination while waiting for NAAT results lead to an increase of resistant strains?
- What is the cost of NAAT for vaginitis, and is this cost effective in routine practice?
- Can NAATs be utilized to detect resistant strains of yeast or Gardnerella sp?
Alan Paul Gehrich, MD (COL, MC ret.)
Bethesda, Maryland
Dr. Barbieri responds
I thank Dr. Gehrich for raising the important issue of what is the optimal endpoint to assess the clinical utility of NAAT testing for vaginitis. Most studies of the use of NAAT to diagnose the cause of vaginitis focus on comparing NAAT results to standard clinical practice (microscopy and pH), and to a “gold standard.” In most studies the gold standards are Nugent scoring with Amsel criteria to resolve intermediate Nugent scores for bacterial vaginosis, culture for Candida, and culture for Trichomonas vaginalis. It is clear from multiple studies that NAAT provides superior sensitivity and specificity compared with standard clinical practice.1-3 As noted in the editorial, in a study of 466 patients with symptoms of vaginitis, standard office approaches to the diagnosis of vaginitis resulted in the failure to identify the correct infection in a large number of cases.4 For the diagnosis of BV, clinicians missed 42% of the cases identified by NAAT. For the diagnosis of Candida, clinicians missed 46% of the cases identified by NAAT. For the diagnosis of T vaginalis, clinicians missed 72% of the cases identified by NAAT. This resulted in clinicians not appropriately treating many infections detected by NAAT.
NAAT does provide information about the presence of Candida glabrata and Candida krusei, organisms which may be resistant to fluconazole. I agree with Dr. Gehrich that the optimal use of NAAT testing in practice is poorly studied with regard to treatment between sample collection and NAAT results. Cost of testing is a complex issue. Standard microscopy is relatively inexpensive, but performs poorly in clinical practice, resulting in misdiagnosis. NAAT testing is expensive but correctly identifies causes of vaginitis.
References
- Schwebke JR, Gaydos CA, Hyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56:e00252-18.
- Broache M, Cammarata CL, Stonebraker E, et al. Performance of vaginal panel assay compared with clinical diagnosis of vaginitis. Obstet Gynecol. 2021;138:853-859.
- Schwebke JR, Taylor SN, Ackerman N, et al. Clinical validation of the Aptima bacterial vaginosis and Aptima Candida/Trichomonas vaginalis assays: results from a prospective multi-center study. J Clin Microbiol. 2020;58:e01643-19. 4
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
How common is IUD perforation, expulsion, and malposition?
ROBERT L. BARBIERI, MD (APRIL 2022)
The seriousness of IUD embedment
I appreciated Dr. Barbieri’s comprehensive review of clinical problems regarding the intrauterine device (IUD). It is interesting that, in spite of your mention of IUD embedment in the myometrium, other publications regarding this phenomenon are seemingly absent (except for ours).1 Whether or not there is associated pain (and sometimes there is not), in our experience its removal can result in IUD fracture. As you stated, it is true that 3D transvaginal sonography perfectly enables this visualization, yet it is surprising that others have not experienced what we have. Nonetheless, it is encouraging to see that IUD embedment is seriously mentioned.
- Fernandez CM, Levine EM, Cabiya M, et al. Intrauterine device embedment resulting in its fracture: a case series. Arch Obstet Gynecol. 2021;2:1-4.
Elliot Levine, MD
Chicago, Illinois
Dr. Barbieri responds
I thank Dr. Levine for highlighting the important issue of IUD fracture and providing a reference to a case series of IUD fractures. Although such fracture is not common, when it does occur it may require a hysteroscopic procedure to remove all pieces of the IUD. In the cited case series, fracture was more commonly observed with the copper IUD than with the LNG-IUD. With regard to IUD malposition, 4 publications reviewed in my recent editorial describe the problem of an IUD arm embedded in the myometrium.1-4
References
- Benacerraf BR, Shipp TD, Bromley B. Three-dimensional ultrasound detection of abnormally located intrauterine contraceptive devices which are a source of pelvic pain and abnormal bleeding. Ultrasound Obstet Gynecol. 2009;34:110-115.
- Braaten KP, Benson CB, Maurer R, et al. Malpositioned intrauterine contraceptive devices: risk factors, outcomes and future pregnancies. Obstet Gynecol. 2011;118:1014-1020.
- Gerkowicz SA, Fiorentino DG, Kovacs AP, et al. Uterine structural abnormality and intrauterine device malposition: analysis of ultrasonographic and demographic variables of 517 patients. Am J Obstet Gynecol. 2019;220:183.e1-e8.
- Connolly CT, Fox NS. Incidence and risk factors for a malpositioned intrauterine device detected on three-dimensional ultrasound within eight weeks of placement. J Ultrasound Med. September 27, 2021.
Will NAAT replace microscopy for the identification of organisms causing vaginitis?
ROBERT L. BARBIERI, MD (MARCH 2022)
Follow-up questions on NAAT testing
The sensitivity of NAAT testing, as outlined in Dr. Barbieri’s editorial, is undoubtedly better than the clinical methods most clinicians are using. I appreciate the frustration we providers often experience in drawing conclusions for patients based on the Amsel criteria for bacterial vaginitis (BV). I am surprised by the low sensitivity of microscopy for yeast vaginitis. My follow-up questions are:
- Have the NAATs referenced been validated in clinical trials and proven to improve patient outcomes?
- Will the proposal to begin empiric therapy for both yeast vaginitis and BV in combination while waiting for NAAT results lead to an increase of resistant strains?
- What is the cost of NAAT for vaginitis, and is this cost effective in routine practice?
- Can NAATs be utilized to detect resistant strains of yeast or Gardnerella sp?
Alan Paul Gehrich, MD (COL, MC ret.)
Bethesda, Maryland
Dr. Barbieri responds
I thank Dr. Gehrich for raising the important issue of what is the optimal endpoint to assess the clinical utility of NAAT testing for vaginitis. Most studies of the use of NAAT to diagnose the cause of vaginitis focus on comparing NAAT results to standard clinical practice (microscopy and pH), and to a “gold standard.” In most studies the gold standards are Nugent scoring with Amsel criteria to resolve intermediate Nugent scores for bacterial vaginosis, culture for Candida, and culture for Trichomonas vaginalis. It is clear from multiple studies that NAAT provides superior sensitivity and specificity compared with standard clinical practice.1-3 As noted in the editorial, in a study of 466 patients with symptoms of vaginitis, standard office approaches to the diagnosis of vaginitis resulted in the failure to identify the correct infection in a large number of cases.4 For the diagnosis of BV, clinicians missed 42% of the cases identified by NAAT. For the diagnosis of Candida, clinicians missed 46% of the cases identified by NAAT. For the diagnosis of T vaginalis, clinicians missed 72% of the cases identified by NAAT. This resulted in clinicians not appropriately treating many infections detected by NAAT.
NAAT does provide information about the presence of Candida glabrata and Candida krusei, organisms which may be resistant to fluconazole. I agree with Dr. Gehrich that the optimal use of NAAT testing in practice is poorly studied with regard to treatment between sample collection and NAAT results. Cost of testing is a complex issue. Standard microscopy is relatively inexpensive, but performs poorly in clinical practice, resulting in misdiagnosis. NAAT testing is expensive but correctly identifies causes of vaginitis.
References
- Schwebke JR, Gaydos CA, Hyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56:e00252-18.
- Broache M, Cammarata CL, Stonebraker E, et al. Performance of vaginal panel assay compared with clinical diagnosis of vaginitis. Obstet Gynecol. 2021;138:853-859.
- Schwebke JR, Taylor SN, Ackerman N, et al. Clinical validation of the Aptima bacterial vaginosis and Aptima Candida/Trichomonas vaginalis assays: results from a prospective multi-center study. J Clin Microbiol. 2020;58:e01643-19. 4
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
Preparing for back to school amid monkeypox outbreak and ever-changing COVID landscape
Unlike last school year, there are now vaccines available for all over the age of 6 months, and home rapid antigen tests are more readily available. Additionally, many have now been exposed either by infection or vaccination to the virus.
The CDC has removed the recommendations for maintaining cohorts in the K-12 population. This changing landscape along with differing levels of personal risk make it challenging to counsel families about what to expect in terms of COVID this year.

The best defense that we currently have against COVID is the vaccine. Although it seems that many are susceptible to the virus despite the vaccine, those who have been vaccinated are less susceptible to serious disease, including young children.
As older children may be heading to college, it is important
to encourage them to isolate when they have symptoms, even when they test negative for COVID as we would all like to avoid being sick in general.
Additionally, they should pay attention to the COVID risk level in their area and wear masks, particularly when indoors, as the levels increase. College students should have a plan for where they can isolate when not feeling well. If anyone does test positive for COVID, they should follow the most recent quarantine guidelines, including wearing a well fitted mask when they do begin returning to activities.
Monkeypox
We now have a new health concern for this school year.
Monkeypox has come onto the scene with information changing as rapidly as information previously did for COVID. With this virus, we must particularly counsel those heading away to college to be careful to limit their exposure to this disease.
Dormitories and other congregate settings are high-risk locations for the spread of monkeypox. Particularly, students headed to stay in dormitories should be counseled about avoiding:
- sexual activity with those with lesions consistent with monkeypox;
- sharing eating and drinking utensils; and
- sleeping in the same bed as or sharing bedding or towels with anyone with a diagnosis of or lesions consistent with monkeypox.
Additionally, as with prevention of all infections, it is important to frequently wash hands or use alcohol-based sanitizer before eating, and avoid touching the face after using the restroom.
Guidance for those eligible for vaccines against monkeypox seems to be quickly changing as well.
At the time of this article, CDC guidance recommends the vaccine against monkeypox for:
- those considered to be at high risk for it, including those identified by public health officials as a contact of someone with monkeypox;
- those who are aware that a sexual partner had a diagnosis of monkeypox within the past 2 weeks;
- those with multiple sex partners in the past 2 weeks in an area with known monkeypox; and
- those whose jobs may expose them to monkeypox.
Currently, the CDC recommends the vaccine JYNNEOS, a two-dose vaccine that reaches maximum protection after fourteen days. Ultimately, guidance is likely to continue to quickly change for both COVID-19 and Monkeypox throughout the fall. It is possible that new vaccinations will become available, and families and physicians alike will have many questions.
Primary care offices should ensure that someone is keeping up to date with the latest guidance to share with the office so that physicians may share accurate information with their patients.
Families should be counseled that we anticipate information about monkeypox, particularly related to vaccinations, to continue to change, as it has during all stages of the COVID pandemic.
As always, patients should be reminded to continue regular routine vaccinations, including the annual influenza vaccine.
Dr. Wheat is a family physician at Erie Family Health Center and program director of Northwestern University’s McGaw Family Medicine residency program, both in Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
Unlike last school year, there are now vaccines available for all over the age of 6 months, and home rapid antigen tests are more readily available. Additionally, many have now been exposed either by infection or vaccination to the virus.
The CDC has removed the recommendations for maintaining cohorts in the K-12 population. This changing landscape along with differing levels of personal risk make it challenging to counsel families about what to expect in terms of COVID this year.
The best defense that we currently have against COVID is the vaccine. Although it seems that many are susceptible to the virus despite the vaccine, those who have been vaccinated are less susceptible to serious disease, including young children.
As older children may be heading to college, it is important
to encourage them to isolate when they have symptoms, even when they test negative for COVID as we would all like to avoid being sick in general.
Additionally, they should pay attention to the COVID risk level in their area and wear masks, particularly when indoors, as the levels increase. College students should have a plan for where they can isolate when not feeling well. If anyone does test positive for COVID, they should follow the most recent quarantine guidelines, including wearing a well fitted mask when they do begin returning to activities.
Monkeypox
We now have a new health concern for this school year.
Monkeypox has come onto the scene with information changing as rapidly as information previously did for COVID. With this virus, we must particularly counsel those heading away to college to be careful to limit their exposure to this disease.
Dormitories and other congregate settings are high-risk locations for the spread of monkeypox. Particularly, students headed to stay in dormitories should be counseled about avoiding:
- sexual activity with those with lesions consistent with monkeypox;
- sharing eating and drinking utensils; and
- sleeping in the same bed as or sharing bedding or towels with anyone with a diagnosis of or lesions consistent with monkeypox.
Additionally, as with prevention of all infections, it is important to frequently wash hands or use alcohol-based sanitizer before eating, and avoid touching the face after using the restroom.
Guidance for those eligible for vaccines against monkeypox seems to be quickly changing as well.
At the time of this article, CDC guidance recommends the vaccine against monkeypox for:
- those considered to be at high risk for it, including those identified by public health officials as a contact of someone with monkeypox;
- those who are aware that a sexual partner had a diagnosis of monkeypox within the past 2 weeks;
- those with multiple sex partners in the past 2 weeks in an area with known monkeypox; and
- those whose jobs may expose them to monkeypox.
Currently, the CDC recommends the vaccine JYNNEOS, a two-dose vaccine that reaches maximum protection after fourteen days. Ultimately, guidance is likely to continue to quickly change for both COVID-19 and Monkeypox throughout the fall. It is possible that new vaccinations will become available, and families and physicians alike will have many questions.
Primary care offices should ensure that someone is keeping up to date with the latest guidance to share with the office so that physicians may share accurate information with their patients.
Families should be counseled that we anticipate information about monkeypox, particularly related to vaccinations, to continue to change, as it has during all stages of the COVID pandemic.
As always, patients should be reminded to continue regular routine vaccinations, including the annual influenza vaccine.
Dr. Wheat is a family physician at Erie Family Health Center and program director of Northwestern University’s McGaw Family Medicine residency program, both in Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
Unlike last school year, there are now vaccines available for all over the age of 6 months, and home rapid antigen tests are more readily available. Additionally, many have now been exposed either by infection or vaccination to the virus.
The CDC has removed the recommendations for maintaining cohorts in the K-12 population. This changing landscape along with differing levels of personal risk make it challenging to counsel families about what to expect in terms of COVID this year.
The best defense that we currently have against COVID is the vaccine. Although it seems that many are susceptible to the virus despite the vaccine, those who have been vaccinated are less susceptible to serious disease, including young children.
As older children may be heading to college, it is important
to encourage them to isolate when they have symptoms, even when they test negative for COVID as we would all like to avoid being sick in general.
Additionally, they should pay attention to the COVID risk level in their area and wear masks, particularly when indoors, as the levels increase. College students should have a plan for where they can isolate when not feeling well. If anyone does test positive for COVID, they should follow the most recent quarantine guidelines, including wearing a well fitted mask when they do begin returning to activities.
Monkeypox
We now have a new health concern for this school year.
Monkeypox has come onto the scene with information changing as rapidly as information previously did for COVID. With this virus, we must particularly counsel those heading away to college to be careful to limit their exposure to this disease.
Dormitories and other congregate settings are high-risk locations for the spread of monkeypox. Particularly, students headed to stay in dormitories should be counseled about avoiding:
- sexual activity with those with lesions consistent with monkeypox;
- sharing eating and drinking utensils; and
- sleeping in the same bed as or sharing bedding or towels with anyone with a diagnosis of or lesions consistent with monkeypox.
Additionally, as with prevention of all infections, it is important to frequently wash hands or use alcohol-based sanitizer before eating, and avoid touching the face after using the restroom.
Guidance for those eligible for vaccines against monkeypox seems to be quickly changing as well.
At the time of this article, CDC guidance recommends the vaccine against monkeypox for:
- those considered to be at high risk for it, including those identified by public health officials as a contact of someone with monkeypox;
- those who are aware that a sexual partner had a diagnosis of monkeypox within the past 2 weeks;
- those with multiple sex partners in the past 2 weeks in an area with known monkeypox; and
- those whose jobs may expose them to monkeypox.
Currently, the CDC recommends the vaccine JYNNEOS, a two-dose vaccine that reaches maximum protection after fourteen days. Ultimately, guidance is likely to continue to quickly change for both COVID-19 and Monkeypox throughout the fall. It is possible that new vaccinations will become available, and families and physicians alike will have many questions.
Primary care offices should ensure that someone is keeping up to date with the latest guidance to share with the office so that physicians may share accurate information with their patients.
Families should be counseled that we anticipate information about monkeypox, particularly related to vaccinations, to continue to change, as it has during all stages of the COVID pandemic.
As always, patients should be reminded to continue regular routine vaccinations, including the annual influenza vaccine.
Dr. Wheat is a family physician at Erie Family Health Center and program director of Northwestern University’s McGaw Family Medicine residency program, both in Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
Postprandial Right Upper Quadrant Abdominal Pain
A 53-year-old male patient presented to the emergency department following a primary care office visit with sudden onset right upper quadrant abdominal pain that persisted for 3 weeks, worsening over the last 2 days. The abdominal pain worsened after eating or drinking and mildly improved with omeprazole. Associated symptoms included intermittent fever, night sweats, fatigue, and bloating since onset without vomiting or diarrhea. He reported a “complicated” cholecystectomy at an outside facility 6 months prior and that his “gallbladder was adhered to his duodenum,” though outside records were not available. Additional medical history included diverticulosis with prior flares of diverticulitis but no recent flares or treatments. His home medications included acetaminophen, naproxen, intranasal fluticasone, omeprazole, gabapentin, baclofen, trazodone, and antihistamines. He reported no tobacco or illicit drug use and stated he consumed a 6 pack of beer every 6 weeks.
Initial vital signs in the emergency department demonstrated an afebrile oral temperature with unremarkable blood pressure and pulse. He was alert and oriented and did not appear in significant acute distress. Physical examination of the abdomen demonstrated a nondistended abdomen, normal active bowel sounds in all 4 quadrants, and mild right upper and lower quadrant tenderness to soft and deep palpation with release.
Significant laboratory values included elevated C-reactive protein of 44.1 mg/L and mild leukocytosis of 11.1 K/µL (reference range, 4.00-10.60 K/µL). The basic metabolic panel, liver-associated enzymes, and lipase levels were within normal limits.
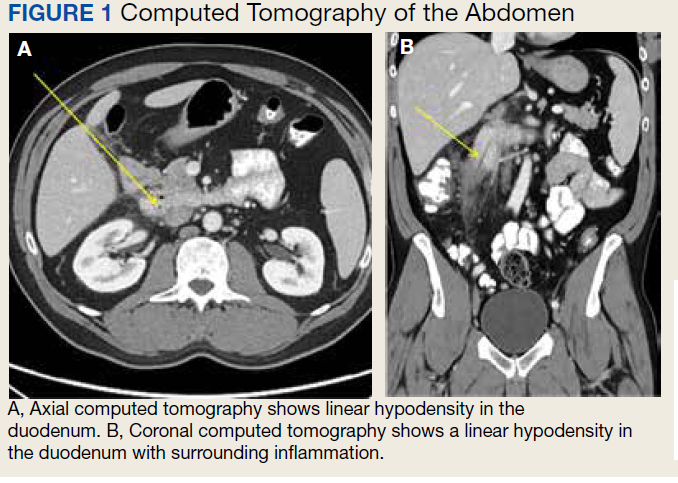
The initial imaging study was a computed tomography (CT) of the abdomen and pelvis with oral and IV contrast. The radiology report depicted a thin, needle-like hypodense foreign body approximately 8 cm in length in the proximal duodenum, slightly protruding extraluminally, and at least a moderate amount of surrounding inflammation without abscess or free air (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
Our Diagnosis
Based on the clinical history of postprandial abdominal pain with prior cholecystectomy and leukocytosis, the initial differential diagnosis included peptic ulcer disease, gastroesophageal reflux, or delayed sequela of the cholecystectomy 6 months prior. Although suspicion remained for possible delayed postoperative complications from the cholecystectomy, ultrasound and hepatobiliary iminodiacetic acid (HIDA) scan were not pursued based on CT imaging findings. The needle-like hypodensity in the duodenum with surrounding inflammation visualized on CT was concerning for an unidentified penetrating foreign body with a possible retroperitoneal microperforation.
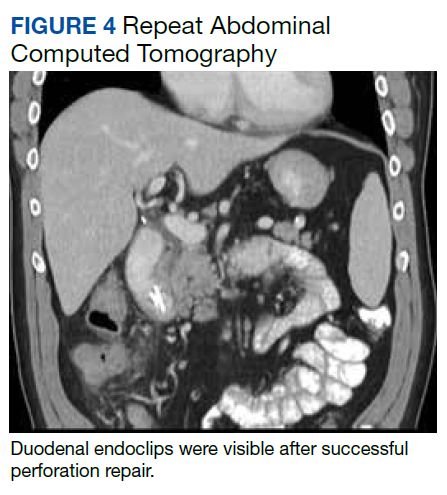
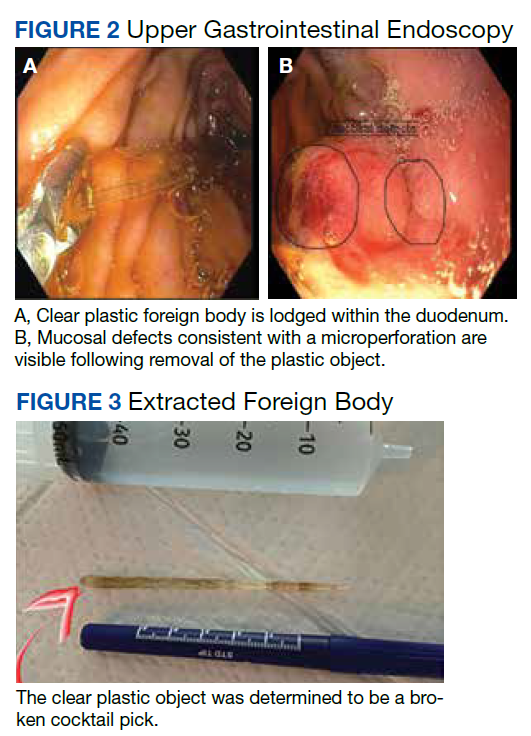
After these imaging findings were relayed from Radiology to the Gastroenterology Service, the patient underwent an upper gastrointestinal (GI) endoscopy to further evaluate the duodenum. Inspection revealed mild gastritis and a linear, clear piece of plastic with both ends firmly lodged within the mucosa from the distal duodenal bulb to the second portion of the duodenum; a significant mucosal defect of the bowel wall was visualized after careful extraction of the foreign body (Figure 2). The patient was diagnosed with a small duodenal perforation, which was sealed endoscopically with 2 endoclips. The extracted piece of plastic was examined and determined to be a broken cocktail pick (Figure 3). During discussion with the patient postprocedure, he stated that he ingested several olive martinis (which were served with cocktail picks) approximately 3 weeks prior to presentation and did not recall ingesting the cocktail pick. A repeat abdominal CT following the endoscopy demonstrated no leak or free air from the site of the repaired duodenal perforation (Figure 4). The patient avoided surgery and was permitted to resume a liquid diet prior to discharge.
Discussion
Foreign body ingestion in adults is most commonly unintentional with fish bones being the most common culprit.1 In unintentional instances of foreign body ingestion, many patients are not aware of the event, with dentures posing a significant well-known risk factor due to lack of palatal sensory feedback.2 Most ingested foreign bodies pass uninhibited through the GI tract without complications. However, less than 1% of ingested foreign bodies cause potentially life-threatening GI perforations.3
The risk of GI perforation due to foreign body ingestion is greatest with elongated, sharp objects, such as needles, bones, toothpicks, and cocktail picks. These objects tend to lodge at areas of narrowing or angulation, such as the appendix, ileocecal region, or as in this case, the duodenum.3 Passage of a foreign body through the duodenum is more likely to be inhibited if the object is longer than 6 cm and with a diameter > 2.5 cm.4 Signs of duodenal perforation are often subtle compared with jejunal or ileal perforations. Patients are commonly afebrile with normal white blood cell counts and are more likely to have chronic symptoms for > 3 days before the appropriate diagnosis of foreign body ingestion is made.1 Duodenal perforations may be more stable clinically compared with distal GI perforations in part due to the retroperitoneal location with relatively fewer bacteria present intraluminally. GI perforations may not occur acutely during passage of the foreign body but can present weeks, months, or even years later.5 Delayed onset of symptoms may happen when the foreign body becomes lodged and only partially perforates the bowel wall, resulting in a chronic inflammatory process. Other possible complications include fistulization and abscess formation from migrating linear sharp objects through the bowel wall, which is most observed with toothpicks and cocktail picks, specifically.5
Foreign bodies identified on plain radiographs commonly include radiopaque objects, such as glass, metallic objects, most animal bones and some fish bones, and some medications. However, radiolucent objects, such as toothpicks and cocktail picks, wood, plastic, most fish bones, and most medicines, often will not appear on radiographs. The diagnosis of ingested foreign body can therefore easily be delayed or overlooked on plain radiographs due to ingestion of radiolucent objects or lack of adequate patient history. A high index of suspicion is needed in such instances. The modality of choice for identifying GI perforation due to ingested foreign objects is CT.5 All of these commonly missed materials on radiographs will be visible on CT with variable densities. As an added benefit, CT also may reveal ingested objects not visualized on radiographs and show ancillary signs of perforation, such as extraluminal free air, localized inflammation, and fluid collections or abscess surrounding a segment of thickened bowel.5
Most ingested foreign bodies will pass through the GI system and can be managed with careful observation alone. However, upper endoscopy is emergently indicated in 3 scenarios of foreign body ingestion: (1) complete occlusion of the esophagus with salivary pooling due to risk of aspiration; (2) ingestion of batteries due to toxic substances; and (3) ingestion of sharp or pointed foreign bodies due to risk of perforation.4 Overall, endoscopic intervention is required in 20% of cases and surgical intervention remains rare at 1%.4 In the case of this patient, an emergent upper endoscopy was needed due to suspected duodenal perforation.
Treatment of duodenal perforations due to foreign bodies may involve conservative, surgical, or endoscopic management. Contained, small perforations in a stable patient may be treated conservatively with IV fluids, antibiotics, and proton pump inhibitors as they self-seal with omentum if the foreign body has passed.6 Retained duodenal foreign bodies pose a risk of persistent perforation or fistulization and must be removed. Anterior duodenal perforations pose a risk of peritonitis, whereas posterior duodenal perforations, although retroperitoneal and sparing the peritoneal cavity, may result in localized abscess formation necessitating foreign body removal. Endoscopic clipping is a modernized, less invasive way to close GI perforations. Through-the-scope clips (TTSCs) can close luminal defects < 2 cm in size.7 Defects > 1 cm may be repaired with combined TTSCs and endoloop or omental patching. Over-the-scope clips can close full thickness defects up to 2 to 3 cm with the advantage of being able to close leaks and fistulas involving inflamed or indurated tissue.7
Conclusions
Intestinal perforations related to foreign body ingestion are a rare complication occurring in < 1% of patients. Although most ingested foreign objects will pass through the GI tract, elongated or sharp objects pose a risk for perforation. In many cases, a history of foreign body ingestion is not obtained, and a high index of suspicion is required. Duodenal perforations due to foreign body ingestion should be included in the differential among the more common diagnoses of peptic ulcers, pancreatitis, and gallbladder disease in the setting of postprandial right upper quadrant abdominal pain. CT is the best modality for identifying foreign bodies, including objects that may be missed on plain radiographs.
1. Goh BK, Chow PK, Quah HM, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg. 2006;(30)372-377. doi:10.1007/s00268-005-0490-2
2. Bunker PG. The role of dentistry in problems of foreign body in the air and food passage. J Am Dent Assoc. 1962;(64):782-787. doi:10.14219/jada.archive.1962.0160
3. Hunter TB, Taljanovic MS. Foreign bodies. Radiographics. 2003;23(3):731-757. doi:10.1148/rg.233025137
4. Ambe P, Weber SA, Schauer M, Knoefel WT. Swallowed foreign bodies in adults. Dtsch Arztebl Int. 2012;109(50):869-875. doi:10.3238/arztebl.2012.0869
5. Kuzmich S, Burke CJ, Harvey CJ, et al. Perforation of gastrointestinal tract by poorly conspicuous ingested foreign bodies: radiological diagnosis. Br J Radiol. 2015;88(1050):20150086. doi:10.1259/bjr.20150086
6. Hill AG. Management of perforated duodenal ulcer. In: Holzheimer RG, Mannick JA, eds. Surgical Treatment: Evidence-Based and Problem-Oriented. Zuckschwerdt; 2001.
7. Rogalski P, Daniluk J, Baniukiewicz A, Wroblewski E, Dabrowski A. Endoscopic management of gastrointestinal perforations, leaks and fistulas. World J Gastroenterol. 2015;21(37):10542-10552. doi:10.3748/wjg.v21.i37.10542
A 53-year-old male patient presented to the emergency department following a primary care office visit with sudden onset right upper quadrant abdominal pain that persisted for 3 weeks, worsening over the last 2 days. The abdominal pain worsened after eating or drinking and mildly improved with omeprazole. Associated symptoms included intermittent fever, night sweats, fatigue, and bloating since onset without vomiting or diarrhea. He reported a “complicated” cholecystectomy at an outside facility 6 months prior and that his “gallbladder was adhered to his duodenum,” though outside records were not available. Additional medical history included diverticulosis with prior flares of diverticulitis but no recent flares or treatments. His home medications included acetaminophen, naproxen, intranasal fluticasone, omeprazole, gabapentin, baclofen, trazodone, and antihistamines. He reported no tobacco or illicit drug use and stated he consumed a 6 pack of beer every 6 weeks.
Initial vital signs in the emergency department demonstrated an afebrile oral temperature with unremarkable blood pressure and pulse. He was alert and oriented and did not appear in significant acute distress. Physical examination of the abdomen demonstrated a nondistended abdomen, normal active bowel sounds in all 4 quadrants, and mild right upper and lower quadrant tenderness to soft and deep palpation with release.
Significant laboratory values included elevated C-reactive protein of 44.1 mg/L and mild leukocytosis of 11.1 K/µL (reference range, 4.00-10.60 K/µL). The basic metabolic panel, liver-associated enzymes, and lipase levels were within normal limits.
The initial imaging study was a computed tomography (CT) of the abdomen and pelvis with oral and IV contrast. The radiology report depicted a thin, needle-like hypodense foreign body approximately 8 cm in length in the proximal duodenum, slightly protruding extraluminally, and at least a moderate amount of surrounding inflammation without abscess or free air (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
Our Diagnosis
Based on the clinical history of postprandial abdominal pain with prior cholecystectomy and leukocytosis, the initial differential diagnosis included peptic ulcer disease, gastroesophageal reflux, or delayed sequela of the cholecystectomy 6 months prior. Although suspicion remained for possible delayed postoperative complications from the cholecystectomy, ultrasound and hepatobiliary iminodiacetic acid (HIDA) scan were not pursued based on CT imaging findings. The needle-like hypodensity in the duodenum with surrounding inflammation visualized on CT was concerning for an unidentified penetrating foreign body with a possible retroperitoneal microperforation.
After these imaging findings were relayed from Radiology to the Gastroenterology Service, the patient underwent an upper gastrointestinal (GI) endoscopy to further evaluate the duodenum. Inspection revealed mild gastritis and a linear, clear piece of plastic with both ends firmly lodged within the mucosa from the distal duodenal bulb to the second portion of the duodenum; a significant mucosal defect of the bowel wall was visualized after careful extraction of the foreign body (Figure 2). The patient was diagnosed with a small duodenal perforation, which was sealed endoscopically with 2 endoclips. The extracted piece of plastic was examined and determined to be a broken cocktail pick (Figure 3). During discussion with the patient postprocedure, he stated that he ingested several olive martinis (which were served with cocktail picks) approximately 3 weeks prior to presentation and did not recall ingesting the cocktail pick. A repeat abdominal CT following the endoscopy demonstrated no leak or free air from the site of the repaired duodenal perforation (Figure 4). The patient avoided surgery and was permitted to resume a liquid diet prior to discharge.
Discussion
Foreign body ingestion in adults is most commonly unintentional with fish bones being the most common culprit.1 In unintentional instances of foreign body ingestion, many patients are not aware of the event, with dentures posing a significant well-known risk factor due to lack of palatal sensory feedback.2 Most ingested foreign bodies pass uninhibited through the GI tract without complications. However, less than 1% of ingested foreign bodies cause potentially life-threatening GI perforations.3
The risk of GI perforation due to foreign body ingestion is greatest with elongated, sharp objects, such as needles, bones, toothpicks, and cocktail picks. These objects tend to lodge at areas of narrowing or angulation, such as the appendix, ileocecal region, or as in this case, the duodenum.3 Passage of a foreign body through the duodenum is more likely to be inhibited if the object is longer than 6 cm and with a diameter > 2.5 cm.4 Signs of duodenal perforation are often subtle compared with jejunal or ileal perforations. Patients are commonly afebrile with normal white blood cell counts and are more likely to have chronic symptoms for > 3 days before the appropriate diagnosis of foreign body ingestion is made.1 Duodenal perforations may be more stable clinically compared with distal GI perforations in part due to the retroperitoneal location with relatively fewer bacteria present intraluminally. GI perforations may not occur acutely during passage of the foreign body but can present weeks, months, or even years later.5 Delayed onset of symptoms may happen when the foreign body becomes lodged and only partially perforates the bowel wall, resulting in a chronic inflammatory process. Other possible complications include fistulization and abscess formation from migrating linear sharp objects through the bowel wall, which is most observed with toothpicks and cocktail picks, specifically.5
Foreign bodies identified on plain radiographs commonly include radiopaque objects, such as glass, metallic objects, most animal bones and some fish bones, and some medications. However, radiolucent objects, such as toothpicks and cocktail picks, wood, plastic, most fish bones, and most medicines, often will not appear on radiographs. The diagnosis of ingested foreign body can therefore easily be delayed or overlooked on plain radiographs due to ingestion of radiolucent objects or lack of adequate patient history. A high index of suspicion is needed in such instances. The modality of choice for identifying GI perforation due to ingested foreign objects is CT.5 All of these commonly missed materials on radiographs will be visible on CT with variable densities. As an added benefit, CT also may reveal ingested objects not visualized on radiographs and show ancillary signs of perforation, such as extraluminal free air, localized inflammation, and fluid collections or abscess surrounding a segment of thickened bowel.5
Most ingested foreign bodies will pass through the GI system and can be managed with careful observation alone. However, upper endoscopy is emergently indicated in 3 scenarios of foreign body ingestion: (1) complete occlusion of the esophagus with salivary pooling due to risk of aspiration; (2) ingestion of batteries due to toxic substances; and (3) ingestion of sharp or pointed foreign bodies due to risk of perforation.4 Overall, endoscopic intervention is required in 20% of cases and surgical intervention remains rare at 1%.4 In the case of this patient, an emergent upper endoscopy was needed due to suspected duodenal perforation.
Treatment of duodenal perforations due to foreign bodies may involve conservative, surgical, or endoscopic management. Contained, small perforations in a stable patient may be treated conservatively with IV fluids, antibiotics, and proton pump inhibitors as they self-seal with omentum if the foreign body has passed.6 Retained duodenal foreign bodies pose a risk of persistent perforation or fistulization and must be removed. Anterior duodenal perforations pose a risk of peritonitis, whereas posterior duodenal perforations, although retroperitoneal and sparing the peritoneal cavity, may result in localized abscess formation necessitating foreign body removal. Endoscopic clipping is a modernized, less invasive way to close GI perforations. Through-the-scope clips (TTSCs) can close luminal defects < 2 cm in size.7 Defects > 1 cm may be repaired with combined TTSCs and endoloop or omental patching. Over-the-scope clips can close full thickness defects up to 2 to 3 cm with the advantage of being able to close leaks and fistulas involving inflamed or indurated tissue.7
Conclusions
Intestinal perforations related to foreign body ingestion are a rare complication occurring in < 1% of patients. Although most ingested foreign objects will pass through the GI tract, elongated or sharp objects pose a risk for perforation. In many cases, a history of foreign body ingestion is not obtained, and a high index of suspicion is required. Duodenal perforations due to foreign body ingestion should be included in the differential among the more common diagnoses of peptic ulcers, pancreatitis, and gallbladder disease in the setting of postprandial right upper quadrant abdominal pain. CT is the best modality for identifying foreign bodies, including objects that may be missed on plain radiographs.
A 53-year-old male patient presented to the emergency department following a primary care office visit with sudden onset right upper quadrant abdominal pain that persisted for 3 weeks, worsening over the last 2 days. The abdominal pain worsened after eating or drinking and mildly improved with omeprazole. Associated symptoms included intermittent fever, night sweats, fatigue, and bloating since onset without vomiting or diarrhea. He reported a “complicated” cholecystectomy at an outside facility 6 months prior and that his “gallbladder was adhered to his duodenum,” though outside records were not available. Additional medical history included diverticulosis with prior flares of diverticulitis but no recent flares or treatments. His home medications included acetaminophen, naproxen, intranasal fluticasone, omeprazole, gabapentin, baclofen, trazodone, and antihistamines. He reported no tobacco or illicit drug use and stated he consumed a 6 pack of beer every 6 weeks.
Initial vital signs in the emergency department demonstrated an afebrile oral temperature with unremarkable blood pressure and pulse. He was alert and oriented and did not appear in significant acute distress. Physical examination of the abdomen demonstrated a nondistended abdomen, normal active bowel sounds in all 4 quadrants, and mild right upper and lower quadrant tenderness to soft and deep palpation with release.
Significant laboratory values included elevated C-reactive protein of 44.1 mg/L and mild leukocytosis of 11.1 K/µL (reference range, 4.00-10.60 K/µL). The basic metabolic panel, liver-associated enzymes, and lipase levels were within normal limits.
The initial imaging study was a computed tomography (CT) of the abdomen and pelvis with oral and IV contrast. The radiology report depicted a thin, needle-like hypodense foreign body approximately 8 cm in length in the proximal duodenum, slightly protruding extraluminally, and at least a moderate amount of surrounding inflammation without abscess or free air (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
Our Diagnosis
Based on the clinical history of postprandial abdominal pain with prior cholecystectomy and leukocytosis, the initial differential diagnosis included peptic ulcer disease, gastroesophageal reflux, or delayed sequela of the cholecystectomy 6 months prior. Although suspicion remained for possible delayed postoperative complications from the cholecystectomy, ultrasound and hepatobiliary iminodiacetic acid (HIDA) scan were not pursued based on CT imaging findings. The needle-like hypodensity in the duodenum with surrounding inflammation visualized on CT was concerning for an unidentified penetrating foreign body with a possible retroperitoneal microperforation.
After these imaging findings were relayed from Radiology to the Gastroenterology Service, the patient underwent an upper gastrointestinal (GI) endoscopy to further evaluate the duodenum. Inspection revealed mild gastritis and a linear, clear piece of plastic with both ends firmly lodged within the mucosa from the distal duodenal bulb to the second portion of the duodenum; a significant mucosal defect of the bowel wall was visualized after careful extraction of the foreign body (Figure 2). The patient was diagnosed with a small duodenal perforation, which was sealed endoscopically with 2 endoclips. The extracted piece of plastic was examined and determined to be a broken cocktail pick (Figure 3). During discussion with the patient postprocedure, he stated that he ingested several olive martinis (which were served with cocktail picks) approximately 3 weeks prior to presentation and did not recall ingesting the cocktail pick. A repeat abdominal CT following the endoscopy demonstrated no leak or free air from the site of the repaired duodenal perforation (Figure 4). The patient avoided surgery and was permitted to resume a liquid diet prior to discharge.
Discussion
Foreign body ingestion in adults is most commonly unintentional with fish bones being the most common culprit.1 In unintentional instances of foreign body ingestion, many patients are not aware of the event, with dentures posing a significant well-known risk factor due to lack of palatal sensory feedback.2 Most ingested foreign bodies pass uninhibited through the GI tract without complications. However, less than 1% of ingested foreign bodies cause potentially life-threatening GI perforations.3
The risk of GI perforation due to foreign body ingestion is greatest with elongated, sharp objects, such as needles, bones, toothpicks, and cocktail picks. These objects tend to lodge at areas of narrowing or angulation, such as the appendix, ileocecal region, or as in this case, the duodenum.3 Passage of a foreign body through the duodenum is more likely to be inhibited if the object is longer than 6 cm and with a diameter > 2.5 cm.4 Signs of duodenal perforation are often subtle compared with jejunal or ileal perforations. Patients are commonly afebrile with normal white blood cell counts and are more likely to have chronic symptoms for > 3 days before the appropriate diagnosis of foreign body ingestion is made.1 Duodenal perforations may be more stable clinically compared with distal GI perforations in part due to the retroperitoneal location with relatively fewer bacteria present intraluminally. GI perforations may not occur acutely during passage of the foreign body but can present weeks, months, or even years later.5 Delayed onset of symptoms may happen when the foreign body becomes lodged and only partially perforates the bowel wall, resulting in a chronic inflammatory process. Other possible complications include fistulization and abscess formation from migrating linear sharp objects through the bowel wall, which is most observed with toothpicks and cocktail picks, specifically.5
Foreign bodies identified on plain radiographs commonly include radiopaque objects, such as glass, metallic objects, most animal bones and some fish bones, and some medications. However, radiolucent objects, such as toothpicks and cocktail picks, wood, plastic, most fish bones, and most medicines, often will not appear on radiographs. The diagnosis of ingested foreign body can therefore easily be delayed or overlooked on plain radiographs due to ingestion of radiolucent objects or lack of adequate patient history. A high index of suspicion is needed in such instances. The modality of choice for identifying GI perforation due to ingested foreign objects is CT.5 All of these commonly missed materials on radiographs will be visible on CT with variable densities. As an added benefit, CT also may reveal ingested objects not visualized on radiographs and show ancillary signs of perforation, such as extraluminal free air, localized inflammation, and fluid collections or abscess surrounding a segment of thickened bowel.5
Most ingested foreign bodies will pass through the GI system and can be managed with careful observation alone. However, upper endoscopy is emergently indicated in 3 scenarios of foreign body ingestion: (1) complete occlusion of the esophagus with salivary pooling due to risk of aspiration; (2) ingestion of batteries due to toxic substances; and (3) ingestion of sharp or pointed foreign bodies due to risk of perforation.4 Overall, endoscopic intervention is required in 20% of cases and surgical intervention remains rare at 1%.4 In the case of this patient, an emergent upper endoscopy was needed due to suspected duodenal perforation.
Treatment of duodenal perforations due to foreign bodies may involve conservative, surgical, or endoscopic management. Contained, small perforations in a stable patient may be treated conservatively with IV fluids, antibiotics, and proton pump inhibitors as they self-seal with omentum if the foreign body has passed.6 Retained duodenal foreign bodies pose a risk of persistent perforation or fistulization and must be removed. Anterior duodenal perforations pose a risk of peritonitis, whereas posterior duodenal perforations, although retroperitoneal and sparing the peritoneal cavity, may result in localized abscess formation necessitating foreign body removal. Endoscopic clipping is a modernized, less invasive way to close GI perforations. Through-the-scope clips (TTSCs) can close luminal defects < 2 cm in size.7 Defects > 1 cm may be repaired with combined TTSCs and endoloop or omental patching. Over-the-scope clips can close full thickness defects up to 2 to 3 cm with the advantage of being able to close leaks and fistulas involving inflamed or indurated tissue.7
Conclusions
Intestinal perforations related to foreign body ingestion are a rare complication occurring in < 1% of patients. Although most ingested foreign objects will pass through the GI tract, elongated or sharp objects pose a risk for perforation. In many cases, a history of foreign body ingestion is not obtained, and a high index of suspicion is required. Duodenal perforations due to foreign body ingestion should be included in the differential among the more common diagnoses of peptic ulcers, pancreatitis, and gallbladder disease in the setting of postprandial right upper quadrant abdominal pain. CT is the best modality for identifying foreign bodies, including objects that may be missed on plain radiographs.
1. Goh BK, Chow PK, Quah HM, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg. 2006;(30)372-377. doi:10.1007/s00268-005-0490-2
2. Bunker PG. The role of dentistry in problems of foreign body in the air and food passage. J Am Dent Assoc. 1962;(64):782-787. doi:10.14219/jada.archive.1962.0160
3. Hunter TB, Taljanovic MS. Foreign bodies. Radiographics. 2003;23(3):731-757. doi:10.1148/rg.233025137
4. Ambe P, Weber SA, Schauer M, Knoefel WT. Swallowed foreign bodies in adults. Dtsch Arztebl Int. 2012;109(50):869-875. doi:10.3238/arztebl.2012.0869
5. Kuzmich S, Burke CJ, Harvey CJ, et al. Perforation of gastrointestinal tract by poorly conspicuous ingested foreign bodies: radiological diagnosis. Br J Radiol. 2015;88(1050):20150086. doi:10.1259/bjr.20150086
6. Hill AG. Management of perforated duodenal ulcer. In: Holzheimer RG, Mannick JA, eds. Surgical Treatment: Evidence-Based and Problem-Oriented. Zuckschwerdt; 2001.
7. Rogalski P, Daniluk J, Baniukiewicz A, Wroblewski E, Dabrowski A. Endoscopic management of gastrointestinal perforations, leaks and fistulas. World J Gastroenterol. 2015;21(37):10542-10552. doi:10.3748/wjg.v21.i37.10542
1. Goh BK, Chow PK, Quah HM, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg. 2006;(30)372-377. doi:10.1007/s00268-005-0490-2
2. Bunker PG. The role of dentistry in problems of foreign body in the air and food passage. J Am Dent Assoc. 1962;(64):782-787. doi:10.14219/jada.archive.1962.0160
3. Hunter TB, Taljanovic MS. Foreign bodies. Radiographics. 2003;23(3):731-757. doi:10.1148/rg.233025137
4. Ambe P, Weber SA, Schauer M, Knoefel WT. Swallowed foreign bodies in adults. Dtsch Arztebl Int. 2012;109(50):869-875. doi:10.3238/arztebl.2012.0869
5. Kuzmich S, Burke CJ, Harvey CJ, et al. Perforation of gastrointestinal tract by poorly conspicuous ingested foreign bodies: radiological diagnosis. Br J Radiol. 2015;88(1050):20150086. doi:10.1259/bjr.20150086
6. Hill AG. Management of perforated duodenal ulcer. In: Holzheimer RG, Mannick JA, eds. Surgical Treatment: Evidence-Based and Problem-Oriented. Zuckschwerdt; 2001.
7. Rogalski P, Daniluk J, Baniukiewicz A, Wroblewski E, Dabrowski A. Endoscopic management of gastrointestinal perforations, leaks and fistulas. World J Gastroenterol. 2015;21(37):10542-10552. doi:10.3748/wjg.v21.i37.10542
No fish can escape this net ... of COVID testing
Something about this COVID testing smells fishy
The Chinese have been challenging America’s political and economic hegemony (yes, we did have to look that one up – you’re rude to ask) for some time, but now they’ve gone too far. Are we going to just sit here and let China do something more ridiculous than us in response to COVID? No way!

Here’s the deal: The government of the Chinese coastal city of Xiamen has decided that it’s not just the workers on returning fishing boats who have the potential to introduce COVID to the rest of the population. The fish also present a problem. So when the authorities say that everyone needs to be tested before they can enter the city, they mean everyone.
An employee of the municipal ocean development bureau told local media that “all people in Xiamen City need nucleic acid testing, and the fish catches must be tested as well,” according to the Guardian, which also said that “TV news reports showed officials swabbing the mouths of fish and the underside of crabs.”
In the words of George Takei: “Oh my.”
Hold on there a second, George Takei, because we here in the good old US of A have still got Los Angeles, where COVID testing also has taken a nonhuman turn. The LA County public health department recently announced that pets are now eligible for a free SARS-CoV-2 test through veterinarians and other animal care facilities.
“Our goal is to test many different species of animals including wildlife (deer, bats, raccoons), pets (dogs, cats, hamsters, pocket pets), marine mammals (seals), and more,” Veterinary Public Health announced.
Hegemony restored.
Not even God could save them from worms
The Dark Ages may not have been as dark and violent as many people think, but there’s no denying that life in medieval Europe kind of sucked. The only real alternative to serfdom was a job with the Catholic Church. Medieval friars, for example, lived in stone buildings, had access to fresh fruits and vegetables, and even had latrines and running water. Luxuries compared with the life of the average peasant.

So why then, despite having access to more modern sanitation and amenities, did the friars have so many gut parasites? That’s the question raised by a group of researchers from the University of Cambridge, who conducted a study of 19 medieval friars buried at a local friary (Oh, doesn’t your town have one of those?) and 25 local people buried at a nonreligious cemetery during a similar time period. Of those 19 friars, 11 were infected with worms and parasites, compared with just 8 of 25 townspeople.
This doesn’t make a lot of sense. The friars had a good life by old-time standards: They had basic sanitation down and a solid diet. These things should lead to a healthier population. The problem, the researchers found, is two pronged and a vicious cycle. First off, the friars had plenty of fresh food, but they used human feces to fertilize their produce. There’s a reason modern practice for human waste fertilization is to let the waste compost for 6 months: The waiting period allows the parasites a chance to kindly die off, which prevents reinfection.
Secondly, the friars’ diet of fresh fruits and vegetables mixed together into a salad, while appealing to our modern-day sensibilities, was not a great choice. By comparison, laypeople tended to eat a boiled mishmash of whatever they could find, and while that’s kind of gross, the key here is that their food was cooked. And heat kills parasites. The uncooked salads did no such thing, so the monks ate infected food, expelled infected poop, and grew more infected food with their infected poop.
Once the worms arrived, they never left, making them the worst kind of house guest. Read the room, worms, take your dinner and move on. You don’t have to go home, but you can’t stay here.
What’s a shared genotype between friends?
Do you find it hard to tell the difference between Katy Perry and Zooey Deschanel? They look alike, but they’re not related. Or are they? According to new research, people who look and act very similar but are not related may share DNA.

“Our study provides a rare insight into human likeness by showing that people with extreme look-alike faces share common genotypes, whereas they are discordant at the epigenome and microbiome levels,” senior author Manel Esteller of the Josep Carreras Leukemia Research Institute in Barcelona said in a written statement. “Genomics clusters them together, and the rest sets them apart.”
The Internet has been a great source in being able to find look-alikes. The research team found photos of doppelgangers photographed by François Brunelle, a Canadian artist. Using facial recognition algorithms, the investigators were able to measure likeness between the each pair of look-alikes. The participants also completed a questionnaire about lifestyle and provided a saliva sample.
The results showed that the look-alikes had similar genotypes but different DNA methylation and microbiome landscapes. The look-alikes also seemed to have similarities in weight, height, and behaviors such as smoking, proving that doppelgangers not only look alike but also share common interests.
Next time someone tells you that you look like their best friend Steve, you won’t have to wonder much what Steve is like.
The secret to a good relationship? It’s a secret
Strong relationships are built on honesty and trust, right? Being open with your partner and/or friends is usually a good practice for keeping the relationship healthy, but the latest evidence suggests that maybe you shouldn’t share everything.

According to the first known study on the emotional, behavioral, and relational aspect of consumer behavior, not disclosing certain purchases to your partner can actually be a good thing for the relationship. How? Well, it all has to do with guilt.
In a series of studies, the researchers asked couples about their secret consumptions. The most commonly hidden thing by far was a product (65%).
“We found that 90% of people have recently kept everyday consumer behaviors a secret from a close other – like a friend or spouse – even though they also report that they don’t think their partner would care if they knew about it,” Kelley Gullo Wight, one of the study’s two lead authors, said in a written statement.
Keeping a hidden stash of chocolate produces guilt, which the researchers found to be the key factor, making the perpetrator want to do more in the relationship to ease that sense of betrayal or dishonesty. They called it a “greater relationship investment,” meaning the person is more likely to do a little extra for their partner, like shell out more money for the next anniversary gift or yield to watching their partner’s favorite program.
So don’t feel too bad about that secret Amazon purchase. As long as the other person doesn’t see the box, nobody has to know. Your relationship can only improve.
Something about this COVID testing smells fishy
The Chinese have been challenging America’s political and economic hegemony (yes, we did have to look that one up – you’re rude to ask) for some time, but now they’ve gone too far. Are we going to just sit here and let China do something more ridiculous than us in response to COVID? No way!
Here’s the deal: The government of the Chinese coastal city of Xiamen has decided that it’s not just the workers on returning fishing boats who have the potential to introduce COVID to the rest of the population. The fish also present a problem. So when the authorities say that everyone needs to be tested before they can enter the city, they mean everyone.
An employee of the municipal ocean development bureau told local media that “all people in Xiamen City need nucleic acid testing, and the fish catches must be tested as well,” according to the Guardian, which also said that “TV news reports showed officials swabbing the mouths of fish and the underside of crabs.”
In the words of George Takei: “Oh my.”
Hold on there a second, George Takei, because we here in the good old US of A have still got Los Angeles, where COVID testing also has taken a nonhuman turn. The LA County public health department recently announced that pets are now eligible for a free SARS-CoV-2 test through veterinarians and other animal care facilities.
“Our goal is to test many different species of animals including wildlife (deer, bats, raccoons), pets (dogs, cats, hamsters, pocket pets), marine mammals (seals), and more,” Veterinary Public Health announced.
Hegemony restored.
Not even God could save them from worms
The Dark Ages may not have been as dark and violent as many people think, but there’s no denying that life in medieval Europe kind of sucked. The only real alternative to serfdom was a job with the Catholic Church. Medieval friars, for example, lived in stone buildings, had access to fresh fruits and vegetables, and even had latrines and running water. Luxuries compared with the life of the average peasant.
So why then, despite having access to more modern sanitation and amenities, did the friars have so many gut parasites? That’s the question raised by a group of researchers from the University of Cambridge, who conducted a study of 19 medieval friars buried at a local friary (Oh, doesn’t your town have one of those?) and 25 local people buried at a nonreligious cemetery during a similar time period. Of those 19 friars, 11 were infected with worms and parasites, compared with just 8 of 25 townspeople.
This doesn’t make a lot of sense. The friars had a good life by old-time standards: They had basic sanitation down and a solid diet. These things should lead to a healthier population. The problem, the researchers found, is two pronged and a vicious cycle. First off, the friars had plenty of fresh food, but they used human feces to fertilize their produce. There’s a reason modern practice for human waste fertilization is to let the waste compost for 6 months: The waiting period allows the parasites a chance to kindly die off, which prevents reinfection.
Secondly, the friars’ diet of fresh fruits and vegetables mixed together into a salad, while appealing to our modern-day sensibilities, was not a great choice. By comparison, laypeople tended to eat a boiled mishmash of whatever they could find, and while that’s kind of gross, the key here is that their food was cooked. And heat kills parasites. The uncooked salads did no such thing, so the monks ate infected food, expelled infected poop, and grew more infected food with their infected poop.
Once the worms arrived, they never left, making them the worst kind of house guest. Read the room, worms, take your dinner and move on. You don’t have to go home, but you can’t stay here.
What’s a shared genotype between friends?
Do you find it hard to tell the difference between Katy Perry and Zooey Deschanel? They look alike, but they’re not related. Or are they? According to new research, people who look and act very similar but are not related may share DNA.
“Our study provides a rare insight into human likeness by showing that people with extreme look-alike faces share common genotypes, whereas they are discordant at the epigenome and microbiome levels,” senior author Manel Esteller of the Josep Carreras Leukemia Research Institute in Barcelona said in a written statement. “Genomics clusters them together, and the rest sets them apart.”
The Internet has been a great source in being able to find look-alikes. The research team found photos of doppelgangers photographed by François Brunelle, a Canadian artist. Using facial recognition algorithms, the investigators were able to measure likeness between the each pair of look-alikes. The participants also completed a questionnaire about lifestyle and provided a saliva sample.
The results showed that the look-alikes had similar genotypes but different DNA methylation and microbiome landscapes. The look-alikes also seemed to have similarities in weight, height, and behaviors such as smoking, proving that doppelgangers not only look alike but also share common interests.
Next time someone tells you that you look like their best friend Steve, you won’t have to wonder much what Steve is like.
The secret to a good relationship? It’s a secret
Strong relationships are built on honesty and trust, right? Being open with your partner and/or friends is usually a good practice for keeping the relationship healthy, but the latest evidence suggests that maybe you shouldn’t share everything.
According to the first known study on the emotional, behavioral, and relational aspect of consumer behavior, not disclosing certain purchases to your partner can actually be a good thing for the relationship. How? Well, it all has to do with guilt.
In a series of studies, the researchers asked couples about their secret consumptions. The most commonly hidden thing by far was a product (65%).
“We found that 90% of people have recently kept everyday consumer behaviors a secret from a close other – like a friend or spouse – even though they also report that they don’t think their partner would care if they knew about it,” Kelley Gullo Wight, one of the study’s two lead authors, said in a written statement.
Keeping a hidden stash of chocolate produces guilt, which the researchers found to be the key factor, making the perpetrator want to do more in the relationship to ease that sense of betrayal or dishonesty. They called it a “greater relationship investment,” meaning the person is more likely to do a little extra for their partner, like shell out more money for the next anniversary gift or yield to watching their partner’s favorite program.
So don’t feel too bad about that secret Amazon purchase. As long as the other person doesn’t see the box, nobody has to know. Your relationship can only improve.
Something about this COVID testing smells fishy
The Chinese have been challenging America’s political and economic hegemony (yes, we did have to look that one up – you’re rude to ask) for some time, but now they’ve gone too far. Are we going to just sit here and let China do something more ridiculous than us in response to COVID? No way!
Here’s the deal: The government of the Chinese coastal city of Xiamen has decided that it’s not just the workers on returning fishing boats who have the potential to introduce COVID to the rest of the population. The fish also present a problem. So when the authorities say that everyone needs to be tested before they can enter the city, they mean everyone.
An employee of the municipal ocean development bureau told local media that “all people in Xiamen City need nucleic acid testing, and the fish catches must be tested as well,” according to the Guardian, which also said that “TV news reports showed officials swabbing the mouths of fish and the underside of crabs.”
In the words of George Takei: “Oh my.”
Hold on there a second, George Takei, because we here in the good old US of A have still got Los Angeles, where COVID testing also has taken a nonhuman turn. The LA County public health department recently announced that pets are now eligible for a free SARS-CoV-2 test through veterinarians and other animal care facilities.
“Our goal is to test many different species of animals including wildlife (deer, bats, raccoons), pets (dogs, cats, hamsters, pocket pets), marine mammals (seals), and more,” Veterinary Public Health announced.
Hegemony restored.
Not even God could save them from worms
The Dark Ages may not have been as dark and violent as many people think, but there’s no denying that life in medieval Europe kind of sucked. The only real alternative to serfdom was a job with the Catholic Church. Medieval friars, for example, lived in stone buildings, had access to fresh fruits and vegetables, and even had latrines and running water. Luxuries compared with the life of the average peasant.
So why then, despite having access to more modern sanitation and amenities, did the friars have so many gut parasites? That’s the question raised by a group of researchers from the University of Cambridge, who conducted a study of 19 medieval friars buried at a local friary (Oh, doesn’t your town have one of those?) and 25 local people buried at a nonreligious cemetery during a similar time period. Of those 19 friars, 11 were infected with worms and parasites, compared with just 8 of 25 townspeople.
This doesn’t make a lot of sense. The friars had a good life by old-time standards: They had basic sanitation down and a solid diet. These things should lead to a healthier population. The problem, the researchers found, is two pronged and a vicious cycle. First off, the friars had plenty of fresh food, but they used human feces to fertilize their produce. There’s a reason modern practice for human waste fertilization is to let the waste compost for 6 months: The waiting period allows the parasites a chance to kindly die off, which prevents reinfection.
Secondly, the friars’ diet of fresh fruits and vegetables mixed together into a salad, while appealing to our modern-day sensibilities, was not a great choice. By comparison, laypeople tended to eat a boiled mishmash of whatever they could find, and while that’s kind of gross, the key here is that their food was cooked. And heat kills parasites. The uncooked salads did no such thing, so the monks ate infected food, expelled infected poop, and grew more infected food with their infected poop.
Once the worms arrived, they never left, making them the worst kind of house guest. Read the room, worms, take your dinner and move on. You don’t have to go home, but you can’t stay here.
What’s a shared genotype between friends?
Do you find it hard to tell the difference between Katy Perry and Zooey Deschanel? They look alike, but they’re not related. Or are they? According to new research, people who look and act very similar but are not related may share DNA.
“Our study provides a rare insight into human likeness by showing that people with extreme look-alike faces share common genotypes, whereas they are discordant at the epigenome and microbiome levels,” senior author Manel Esteller of the Josep Carreras Leukemia Research Institute in Barcelona said in a written statement. “Genomics clusters them together, and the rest sets them apart.”
The Internet has been a great source in being able to find look-alikes. The research team found photos of doppelgangers photographed by François Brunelle, a Canadian artist. Using facial recognition algorithms, the investigators were able to measure likeness between the each pair of look-alikes. The participants also completed a questionnaire about lifestyle and provided a saliva sample.
The results showed that the look-alikes had similar genotypes but different DNA methylation and microbiome landscapes. The look-alikes also seemed to have similarities in weight, height, and behaviors such as smoking, proving that doppelgangers not only look alike but also share common interests.
Next time someone tells you that you look like their best friend Steve, you won’t have to wonder much what Steve is like.
The secret to a good relationship? It’s a secret
Strong relationships are built on honesty and trust, right? Being open with your partner and/or friends is usually a good practice for keeping the relationship healthy, but the latest evidence suggests that maybe you shouldn’t share everything.
According to the first known study on the emotional, behavioral, and relational aspect of consumer behavior, not disclosing certain purchases to your partner can actually be a good thing for the relationship. How? Well, it all has to do with guilt.
In a series of studies, the researchers asked couples about their secret consumptions. The most commonly hidden thing by far was a product (65%).
“We found that 90% of people have recently kept everyday consumer behaviors a secret from a close other – like a friend or spouse – even though they also report that they don’t think their partner would care if they knew about it,” Kelley Gullo Wight, one of the study’s two lead authors, said in a written statement.
Keeping a hidden stash of chocolate produces guilt, which the researchers found to be the key factor, making the perpetrator want to do more in the relationship to ease that sense of betrayal or dishonesty. They called it a “greater relationship investment,” meaning the person is more likely to do a little extra for their partner, like shell out more money for the next anniversary gift or yield to watching their partner’s favorite program.
So don’t feel too bad about that secret Amazon purchase. As long as the other person doesn’t see the box, nobody has to know. Your relationship can only improve.
One hour of walking per week may boost longevity for octogenarians
Adults aged 85 years and older who logged an hour or more of walking each week had a 40% reduced risk of all-cause mortality compared with less active peers, according to data from more than 7,000 individuals.
“Aging is accompanied by reduced physical activity and increased sedentary behavior, and reduced physical activity is associated with decreased life expectancy,” Moo-Nyun Jin, MD, of Inje University Sanggye Paik Hospital, Seoul, South Korea, said in an interview.
Reduced physical activity was especially likely in the elderly during the COVID-19 pandemic, he added.
“Promoting walking may be a simple way to help older adults avoid inactivity and encourage an active lifestyle for all-cause and cardiovascular mortality risk reduction,” Dr. Jin said.
Although walking is generally an easy form of exercise for the older adult population, the specific benefit of walking on reducing mortality has not been well studied, according to Dr. Jin and colleagues.
For adults of any age, current guidelines recommend at least 150 minutes per week of moderate activity or 75 minutes per week of vigorous activity, but the amount of physical activity tends to decline with age, and activity recommendations are more difficult to meet, the authors wrote in a press release accompanying their study.
In the study, to be presented at the European Society of Cardiology Congress on Aug. 28 (Abstract 85643), the researchers reviewed data from 7,047 adults aged 85 years and older who participated in the Korean National Health Screening Program. The average age of the study population was 87 years, and 68% were women. Participants completed questionnaires about the amount of time spent in leisure time activities each week, including walking at a slow pace, moderate activity (such as cycling or brisk walking), and vigorous activity (such as running).
Those who walked at a slow pace for at least 1 hour per week had a 40% reduced risk of all-cause mortality and a 39% reduced risk of cardiovascular mortality, compared with inactive participants.
The proportions of participants who reported walking, moderate activity, and vigorous intensity physical activity were 42.5%, 14.7%, and 11.0%, respectively. Roughly one-third (33%) of those who reported slow walking each week also reported moderate or vigorous physical activity.
However, walking for 1 hour per week significantly reduced the risk for all-cause mortality and cardiovascular mortality among individuals who reported walking only, without other moderate or vigorous physical activity (hazard ratio, 0.50 and 0.46, respectively).
“Walking was linked with a lower likelihood of dying in older adults, regardless of whether or not they did any moderate to vigorous intensity physical activity,” Dr. Jin told this news organization. “Our study indicates that walking even just 1 hour every week is advantageous to those aged 85 years and older compared to being inactive.”
The hour of walking need not be in long bouts, 10 minutes each day will do, Dr. Jin added.
The participants were divided into five groups based on reported amount of weekly walking. More than half (57.5%) reported no slow walking, 8.5% walked less than 1 hour per week, 12.0% walked 1-2 hours, 8.7% walked 2-3 hours, and 13.3% walked more than 3 hours.
Although the study was limited by the reliance on self-reports, the results were strengthened by the large sample size and support the value of easy walking for adults aged 85 years and older compared to being inactive.
“Walking may present an opportunity for promoting physical activity among the elderly population, offering a simple way to avoid inactivity and increase physical activity,” said Dr. Jin. However, more research is needed to evaluate the association between mortality and walking by objective measurement of walking levels, using a device such as a smart watch, he noted.
Results are preliminary
“This is an observational study, not an experiment, so it means causality cannot be presumed,” said Maria Fiatarone Singh, MD, a geriatrician with a focus on exercise physiology at the University of Sydney, in an interview. “In other words, it is possible that diseases resulting in mortality prevented people from walking rather than the other way around,” she noted. The only published experimental study on exercise and mortality in older adults was conducted by Dr. Fiatarone Singh and colleagues in Norway. In that study, published in the British Medical Journal in 2020, high-intensity training programs were associated with reduced all-cause mortality compared with inactive controls and individuals who engaged in moderate intensity exercise.
The current study “would have needed to control for many factors related to mortality, such as cardiovascular disease, hypertension, diabetes, malnutrition, and dementia to see what residual benefit might be related to walking,” Dr. Fiatarone Singh said.
“Although walking seems easy and safe, in fact people who are frail, sarcopenic, osteoporotic, or have fallen are recommended to do resistance and balance training rather than walking, and add walking later when they are able to do it safely,” she emphasized.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Fiatarone Singh had no financial conflicts to disclose.
Adults aged 85 years and older who logged an hour or more of walking each week had a 40% reduced risk of all-cause mortality compared with less active peers, according to data from more than 7,000 individuals.
“Aging is accompanied by reduced physical activity and increased sedentary behavior, and reduced physical activity is associated with decreased life expectancy,” Moo-Nyun Jin, MD, of Inje University Sanggye Paik Hospital, Seoul, South Korea, said in an interview.
Reduced physical activity was especially likely in the elderly during the COVID-19 pandemic, he added.
“Promoting walking may be a simple way to help older adults avoid inactivity and encourage an active lifestyle for all-cause and cardiovascular mortality risk reduction,” Dr. Jin said.
Although walking is generally an easy form of exercise for the older adult population, the specific benefit of walking on reducing mortality has not been well studied, according to Dr. Jin and colleagues.
For adults of any age, current guidelines recommend at least 150 minutes per week of moderate activity or 75 minutes per week of vigorous activity, but the amount of physical activity tends to decline with age, and activity recommendations are more difficult to meet, the authors wrote in a press release accompanying their study.
In the study, to be presented at the European Society of Cardiology Congress on Aug. 28 (Abstract 85643), the researchers reviewed data from 7,047 adults aged 85 years and older who participated in the Korean National Health Screening Program. The average age of the study population was 87 years, and 68% were women. Participants completed questionnaires about the amount of time spent in leisure time activities each week, including walking at a slow pace, moderate activity (such as cycling or brisk walking), and vigorous activity (such as running).
Those who walked at a slow pace for at least 1 hour per week had a 40% reduced risk of all-cause mortality and a 39% reduced risk of cardiovascular mortality, compared with inactive participants.
The proportions of participants who reported walking, moderate activity, and vigorous intensity physical activity were 42.5%, 14.7%, and 11.0%, respectively. Roughly one-third (33%) of those who reported slow walking each week also reported moderate or vigorous physical activity.
However, walking for 1 hour per week significantly reduced the risk for all-cause mortality and cardiovascular mortality among individuals who reported walking only, without other moderate or vigorous physical activity (hazard ratio, 0.50 and 0.46, respectively).
“Walking was linked with a lower likelihood of dying in older adults, regardless of whether or not they did any moderate to vigorous intensity physical activity,” Dr. Jin told this news organization. “Our study indicates that walking even just 1 hour every week is advantageous to those aged 85 years and older compared to being inactive.”
The hour of walking need not be in long bouts, 10 minutes each day will do, Dr. Jin added.
The participants were divided into five groups based on reported amount of weekly walking. More than half (57.5%) reported no slow walking, 8.5% walked less than 1 hour per week, 12.0% walked 1-2 hours, 8.7% walked 2-3 hours, and 13.3% walked more than 3 hours.
Although the study was limited by the reliance on self-reports, the results were strengthened by the large sample size and support the value of easy walking for adults aged 85 years and older compared to being inactive.
“Walking may present an opportunity for promoting physical activity among the elderly population, offering a simple way to avoid inactivity and increase physical activity,” said Dr. Jin. However, more research is needed to evaluate the association between mortality and walking by objective measurement of walking levels, using a device such as a smart watch, he noted.
Results are preliminary
“This is an observational study, not an experiment, so it means causality cannot be presumed,” said Maria Fiatarone Singh, MD, a geriatrician with a focus on exercise physiology at the University of Sydney, in an interview. “In other words, it is possible that diseases resulting in mortality prevented people from walking rather than the other way around,” she noted. The only published experimental study on exercise and mortality in older adults was conducted by Dr. Fiatarone Singh and colleagues in Norway. In that study, published in the British Medical Journal in 2020, high-intensity training programs were associated with reduced all-cause mortality compared with inactive controls and individuals who engaged in moderate intensity exercise.
The current study “would have needed to control for many factors related to mortality, such as cardiovascular disease, hypertension, diabetes, malnutrition, and dementia to see what residual benefit might be related to walking,” Dr. Fiatarone Singh said.
“Although walking seems easy and safe, in fact people who are frail, sarcopenic, osteoporotic, or have fallen are recommended to do resistance and balance training rather than walking, and add walking later when they are able to do it safely,” she emphasized.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Fiatarone Singh had no financial conflicts to disclose.
Adults aged 85 years and older who logged an hour or more of walking each week had a 40% reduced risk of all-cause mortality compared with less active peers, according to data from more than 7,000 individuals.
“Aging is accompanied by reduced physical activity and increased sedentary behavior, and reduced physical activity is associated with decreased life expectancy,” Moo-Nyun Jin, MD, of Inje University Sanggye Paik Hospital, Seoul, South Korea, said in an interview.
Reduced physical activity was especially likely in the elderly during the COVID-19 pandemic, he added.
“Promoting walking may be a simple way to help older adults avoid inactivity and encourage an active lifestyle for all-cause and cardiovascular mortality risk reduction,” Dr. Jin said.
Although walking is generally an easy form of exercise for the older adult population, the specific benefit of walking on reducing mortality has not been well studied, according to Dr. Jin and colleagues.
For adults of any age, current guidelines recommend at least 150 minutes per week of moderate activity or 75 minutes per week of vigorous activity, but the amount of physical activity tends to decline with age, and activity recommendations are more difficult to meet, the authors wrote in a press release accompanying their study.
In the study, to be presented at the European Society of Cardiology Congress on Aug. 28 (Abstract 85643), the researchers reviewed data from 7,047 adults aged 85 years and older who participated in the Korean National Health Screening Program. The average age of the study population was 87 years, and 68% were women. Participants completed questionnaires about the amount of time spent in leisure time activities each week, including walking at a slow pace, moderate activity (such as cycling or brisk walking), and vigorous activity (such as running).
Those who walked at a slow pace for at least 1 hour per week had a 40% reduced risk of all-cause mortality and a 39% reduced risk of cardiovascular mortality, compared with inactive participants.
The proportions of participants who reported walking, moderate activity, and vigorous intensity physical activity were 42.5%, 14.7%, and 11.0%, respectively. Roughly one-third (33%) of those who reported slow walking each week also reported moderate or vigorous physical activity.
However, walking for 1 hour per week significantly reduced the risk for all-cause mortality and cardiovascular mortality among individuals who reported walking only, without other moderate or vigorous physical activity (hazard ratio, 0.50 and 0.46, respectively).
“Walking was linked with a lower likelihood of dying in older adults, regardless of whether or not they did any moderate to vigorous intensity physical activity,” Dr. Jin told this news organization. “Our study indicates that walking even just 1 hour every week is advantageous to those aged 85 years and older compared to being inactive.”
The hour of walking need not be in long bouts, 10 minutes each day will do, Dr. Jin added.
The participants were divided into five groups based on reported amount of weekly walking. More than half (57.5%) reported no slow walking, 8.5% walked less than 1 hour per week, 12.0% walked 1-2 hours, 8.7% walked 2-3 hours, and 13.3% walked more than 3 hours.
Although the study was limited by the reliance on self-reports, the results were strengthened by the large sample size and support the value of easy walking for adults aged 85 years and older compared to being inactive.
“Walking may present an opportunity for promoting physical activity among the elderly population, offering a simple way to avoid inactivity and increase physical activity,” said Dr. Jin. However, more research is needed to evaluate the association between mortality and walking by objective measurement of walking levels, using a device such as a smart watch, he noted.
Results are preliminary
“This is an observational study, not an experiment, so it means causality cannot be presumed,” said Maria Fiatarone Singh, MD, a geriatrician with a focus on exercise physiology at the University of Sydney, in an interview. “In other words, it is possible that diseases resulting in mortality prevented people from walking rather than the other way around,” she noted. The only published experimental study on exercise and mortality in older adults was conducted by Dr. Fiatarone Singh and colleagues in Norway. In that study, published in the British Medical Journal in 2020, high-intensity training programs were associated with reduced all-cause mortality compared with inactive controls and individuals who engaged in moderate intensity exercise.
The current study “would have needed to control for many factors related to mortality, such as cardiovascular disease, hypertension, diabetes, malnutrition, and dementia to see what residual benefit might be related to walking,” Dr. Fiatarone Singh said.
“Although walking seems easy and safe, in fact people who are frail, sarcopenic, osteoporotic, or have fallen are recommended to do resistance and balance training rather than walking, and add walking later when they are able to do it safely,” she emphasized.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Fiatarone Singh had no financial conflicts to disclose.
FROM ESC CONGRESS 2022
Digital therapy may ‘rewire’ the brain to improve tinnitus
, new research suggests. In a randomized controlled trial, results at 12 weeks showed patients with tinnitus reported clinically meaningful reductions in ratings of annoyance, inability to ignore, unpleasantness, and loudness after using a digital polytherapeutic app prototype that focuses on relief, relaxation, and attention-focused retraining. In addition, their improvements were significantly greater than for the control group, which received a common white noise app.
Researchers called the results “promising” for a condition that has no cure and few successful treatments. “What this therapy does is essentially rewire the brain in a way that de-emphasizes the sound of the tinnitus to a background noise that has no meaning or relevance to the listener,” lead author Grant Searchfield, PhD, associate professor of audiology at the University of Auckland, New Zealand, said in a press release.
The findings were published online in Frontiers in Neurology.
Worldwide problem
A recent study showed more than 740 million adults worldwide (nearly 15% of the population) have experienced at least one symptom of tinnitus – and about 120 million are severely affected. Tinnitus is the perception of a ringing, buzzing, whistling, or hissing noise in one or both ears when no external source of the sound is present. Often caused by damage to the auditory system, tinnitus can also be a symptom of a wide range of medical conditions and has been identified as a side effect of COVID-19 vaccination. In its most severe form, which is associated with hearing loss, tinnitus can also affect a patient’s mental, emotional, and social health.
For the current study, participants with tinnitus were randomly assigned to a popular app that uses white noise (control group, n = 30) or to the UpSilent app (n = 31). The UpSilent group received a smartphone app, Bluetooth bone conduction headphones, a Bluetooth neck pillow speaker for sleep, and written counseling materials. Participants in the control group received a widely available app called “White Noise” and in-ear wired headphones.
‘Quicker and more effective’
Both groups reported reductions in ratings of annoyance, inability to ignore, unpleasantness, and loudness at 12 weeks. But significantly more of the UpSilent group reported clinically meaningful improvement compared with the control group (65% vs. 43%, respectively; P = .049).
“Earlier trials have found white noise, goal-based counseling, goal-oriented games, and other technology-based therapies are effective for some people some of the time,” Dr. Searchfield said. “This is quicker and more effective, taking 12 weeks rather than 12 months for more individuals to gain some control,” he added.
The investigators noted that the study was not designed to determine which of the app’s functions of passive listening, active listening, or counseling contributed to symptom improvement.
The next step will be to refine the prototype and proceed to larger local and international trials with a view toward approval by the U.S. Food and Drug Administration, they reported.
The researchers hope the app will be clinically available in about 6 months.
The study was funded by Return on Science, Auckland UniServices. Dr. Searchfield is a founder and scientific officer for TrueSilence, a spinout company of the University of Auckland, and has a financial interest in TrueSilence. His coauthor has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a randomized controlled trial, results at 12 weeks showed patients with tinnitus reported clinically meaningful reductions in ratings of annoyance, inability to ignore, unpleasantness, and loudness after using a digital polytherapeutic app prototype that focuses on relief, relaxation, and attention-focused retraining. In addition, their improvements were significantly greater than for the control group, which received a common white noise app.
Researchers called the results “promising” for a condition that has no cure and few successful treatments. “What this therapy does is essentially rewire the brain in a way that de-emphasizes the sound of the tinnitus to a background noise that has no meaning or relevance to the listener,” lead author Grant Searchfield, PhD, associate professor of audiology at the University of Auckland, New Zealand, said in a press release.
The findings were published online in Frontiers in Neurology.
Worldwide problem
A recent study showed more than 740 million adults worldwide (nearly 15% of the population) have experienced at least one symptom of tinnitus – and about 120 million are severely affected. Tinnitus is the perception of a ringing, buzzing, whistling, or hissing noise in one or both ears when no external source of the sound is present. Often caused by damage to the auditory system, tinnitus can also be a symptom of a wide range of medical conditions and has been identified as a side effect of COVID-19 vaccination. In its most severe form, which is associated with hearing loss, tinnitus can also affect a patient’s mental, emotional, and social health.
For the current study, participants with tinnitus were randomly assigned to a popular app that uses white noise (control group, n = 30) or to the UpSilent app (n = 31). The UpSilent group received a smartphone app, Bluetooth bone conduction headphones, a Bluetooth neck pillow speaker for sleep, and written counseling materials. Participants in the control group received a widely available app called “White Noise” and in-ear wired headphones.
‘Quicker and more effective’
Both groups reported reductions in ratings of annoyance, inability to ignore, unpleasantness, and loudness at 12 weeks. But significantly more of the UpSilent group reported clinically meaningful improvement compared with the control group (65% vs. 43%, respectively; P = .049).
“Earlier trials have found white noise, goal-based counseling, goal-oriented games, and other technology-based therapies are effective for some people some of the time,” Dr. Searchfield said. “This is quicker and more effective, taking 12 weeks rather than 12 months for more individuals to gain some control,” he added.
The investigators noted that the study was not designed to determine which of the app’s functions of passive listening, active listening, or counseling contributed to symptom improvement.
The next step will be to refine the prototype and proceed to larger local and international trials with a view toward approval by the U.S. Food and Drug Administration, they reported.
The researchers hope the app will be clinically available in about 6 months.
The study was funded by Return on Science, Auckland UniServices. Dr. Searchfield is a founder and scientific officer for TrueSilence, a spinout company of the University of Auckland, and has a financial interest in TrueSilence. His coauthor has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a randomized controlled trial, results at 12 weeks showed patients with tinnitus reported clinically meaningful reductions in ratings of annoyance, inability to ignore, unpleasantness, and loudness after using a digital polytherapeutic app prototype that focuses on relief, relaxation, and attention-focused retraining. In addition, their improvements were significantly greater than for the control group, which received a common white noise app.
Researchers called the results “promising” for a condition that has no cure and few successful treatments. “What this therapy does is essentially rewire the brain in a way that de-emphasizes the sound of the tinnitus to a background noise that has no meaning or relevance to the listener,” lead author Grant Searchfield, PhD, associate professor of audiology at the University of Auckland, New Zealand, said in a press release.
The findings were published online in Frontiers in Neurology.
Worldwide problem
A recent study showed more than 740 million adults worldwide (nearly 15% of the population) have experienced at least one symptom of tinnitus – and about 120 million are severely affected. Tinnitus is the perception of a ringing, buzzing, whistling, or hissing noise in one or both ears when no external source of the sound is present. Often caused by damage to the auditory system, tinnitus can also be a symptom of a wide range of medical conditions and has been identified as a side effect of COVID-19 vaccination. In its most severe form, which is associated with hearing loss, tinnitus can also affect a patient’s mental, emotional, and social health.
For the current study, participants with tinnitus were randomly assigned to a popular app that uses white noise (control group, n = 30) or to the UpSilent app (n = 31). The UpSilent group received a smartphone app, Bluetooth bone conduction headphones, a Bluetooth neck pillow speaker for sleep, and written counseling materials. Participants in the control group received a widely available app called “White Noise” and in-ear wired headphones.
‘Quicker and more effective’
Both groups reported reductions in ratings of annoyance, inability to ignore, unpleasantness, and loudness at 12 weeks. But significantly more of the UpSilent group reported clinically meaningful improvement compared with the control group (65% vs. 43%, respectively; P = .049).
“Earlier trials have found white noise, goal-based counseling, goal-oriented games, and other technology-based therapies are effective for some people some of the time,” Dr. Searchfield said. “This is quicker and more effective, taking 12 weeks rather than 12 months for more individuals to gain some control,” he added.
The investigators noted that the study was not designed to determine which of the app’s functions of passive listening, active listening, or counseling contributed to symptom improvement.
The next step will be to refine the prototype and proceed to larger local and international trials with a view toward approval by the U.S. Food and Drug Administration, they reported.
The researchers hope the app will be clinically available in about 6 months.
The study was funded by Return on Science, Auckland UniServices. Dr. Searchfield is a founder and scientific officer for TrueSilence, a spinout company of the University of Auckland, and has a financial interest in TrueSilence. His coauthor has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM FRONTIERS IN NEUROLOGY
Multiple Eruptive Dermatofibromas Associated With Down Syndrome
To the Editor:
Dermatofibromas (also known as fibrous histiocytomas) are benign fibrous nodules that most often arise as solitary lesions on the lower extremities. Multiple eruptive dermatofibromas (MEDFs) are uncommon and have been defined as more than 15 in number1 or 5 to 8 dermatofibromas appearing within 4 months.2 They have been reported in association with a number of conditions of immune dysregulation such as systemic lupus erythematosus, Sjögren syndrome, HIV infection, and leukemia.3 Multiple eruptive dermatofibromas also have been described in patients with Down syndrome (DS).4-7 We report a case of MEDFs in a patient with DS and review the literature on the association between MEDFs and DS.
A 38-year-old woman with DS, hidradenitis suppurativa, and hypothyroidism presented with multiple cutaneous lesions developing over the last year. The lesions continued to increase in number but were otherwise asymptomatic. Physical examination revealed approximately 20 rubbery, pink-tan papules measuring less than 1 cm in diameter that were scattered along the trunk (Figure, A), arms, and legs (Figure, B).
 consistent with dermatofibromas on the upper back and left leg")
The patient had no known history of immunosuppression or rheumatologic disease and was otherwise healthy. Basic laboratory tests including a complete blood cell count and antinuclear antibody titer were within reference range. The lesions were clinically consistent with dermatofibromas, but due to their increasing number within a short period of time, a biopsy of a representative lesion was performed to confirm the diagnosis.
The exact incidence of MEDFs is unknown, but they are rare, with one review finding only 50 cases reported from 1960 to 2002.8 They are increasingly recognized as a sign of potential immune dysregulation. Approximately 56% to 70% of cases are seen in patients with an underlying disease state; 80% are immune mediated.8,9 Interestingly, DS has long been associated with notable immune dysfunction,10,11 with evidence suggesting that trisomy 21 may result in widespread changes in gene expression that can lead to interferon activation.12
A PubMed search of articles indexed for MEDLINE using the terms dermatofibroma and Down, dermatofibroma and Down syndrome, eruptive dermatofibroma and Down syndrome, and multiple dermatofibroma and Down syndrome revealed 6 cases of MEDFs in patients with DS that have been reported since 2005.4-7 An additional report by Honda et al13 described a patient with DS who developed 7 dermatofibromas, but no time frame of development was specified. We reviewed the characteristics of 8 patients with DS with MEDFs, which included our patient (Table). The average age at time of presentation was 39 years (median age, 40 years). Six patients (75%) were female and 2 (25%) were male. Dermatofibromas were reported to appear over the course of months to years. Comorbidities included psoriatic arthritis (treated with methotrexate),6 thyroid disorders (ie, Graves disease),6 hypercholesterolemia,6 hidradenitis suppurativa, long-standing mild lymphopenia (1.4×109/L [reference range, 1.5−4.0×109/L]),4 and acute megakaryoblastic leukemia13 treated 15 years before the appearance of dermatofibromas.

Many dermatologic conditions have been reported at increased rates in individuals with DS, including seborrheic dermatitis, alopecia areata, syringomas, elastosis perforans serpiginosa, cutis marmorata, xerosis, and palmoplantar hyperkeratosis.14,15 Although drawing conclusions about associations between MEDFs and DS is limited by our small sample size, we have reported this case and reviewed existing cases of MEDFs in DS to highlight a potential association that may be underrecognized or underreported. More evidence is needed to determine the strength of the association between MEDFs and DS, but dermatologists should be aware that MEDFs may be an additional skin finding associated with DS that is related to the syndrome’s immune dysregulation.
- Baraf CS, Shapiro L. Multiple histiocytomas: report of a case. Arch Dermatol. 1970;101:588-590.
- Ammirati CT, Mann C, Hornstra IK. Multiple eruptive dermatofibromas in three men with HIV infection. Dermatology. 1997;4:344-348.
- Zaccaria E, Rebora A, Rongioletti F. Multiple eruptive dermatofibromas and immunosuppression: report of two cases and review of the literature. Int J Dermatol. 2008;47:723-727.
- Lamb RC, Gangopadhyay M, MacDonald A. Multiple dermatofibromas in Down syndrome. Int J Dermatol. 2014;53:E274-E275.
- Monteagudo B, Álvarez-Fernández JC, Iglesias B, et al. Multiple eruptive dermatofibromas in a patient with Down’s syndrome [article in Spanish]. Actas Dermosifiliogr. 2005;96:199.
- Monteagudo B, Suárez-Amor O, Cabanillas M, et al. Down syndrome: another cause of immunosuppression associated with multiple eruptive dermatofibroma? [article in Spanish]. Dermatol Online J. 2009;15:15.
- Tanaka M, Hoashi T, Serizawa N, et al. Multiple unilaterally localized dermatofibromas in a patient with Down syndrome. J Dermatol. 2017;44:1074-1076.
- Niiyama S, Katsuoka K, Happle R, et al. Multiple eruptive dermatofibromas: a review of the literature. Acta Derm Venereol. 2002;82:241-244.
- Her Y, Ku SH, Kim KH. A case of multiple eruptive dermatofibromas in a healthy adult. Ann Dermatol. 2014;26:539-540.
- Bertotto A, Arcangeli C, Crupi S, et al. T cell response to anti-CD3 antibody in Down’s syndrome. Arch Dis Child. 1987;62:1148-1151.
- Kusters MA, Verstegen RH, Gemen EF, et al. Intrinsic defect of the immune system in children with Down syndrome: a review. Clin Exp Immunol. 2009;156:189-193.
- Sullivan KD, Evans D, Pandey A, et al. Trisomy 21 causes changes in the circulating proteome indicative of chronic inflammation. Sci Rep. 2017;7:14818.
- Honda M, Tomimura S, de Vega S, et al. Multiple dermatofibromas in a patient with Down syndrome. J Dermatol. 2016;43:346-348.
- Daneshpazhooh M, Nazemi TM, Bigdeloo L, et al. Mucocutaneous findings in 100 children with Down syndrome. Pediatr Dermatol. 2007;24:317-320.
- Madan V, Williams J, Lear JT. Dermatological manifestations of Down’s syndrome. Clin Exp Dermatol. 2006;31:623-629.
To the Editor:
Dermatofibromas (also known as fibrous histiocytomas) are benign fibrous nodules that most often arise as solitary lesions on the lower extremities. Multiple eruptive dermatofibromas (MEDFs) are uncommon and have been defined as more than 15 in number1 or 5 to 8 dermatofibromas appearing within 4 months.2 They have been reported in association with a number of conditions of immune dysregulation such as systemic lupus erythematosus, Sjögren syndrome, HIV infection, and leukemia.3 Multiple eruptive dermatofibromas also have been described in patients with Down syndrome (DS).4-7 We report a case of MEDFs in a patient with DS and review the literature on the association between MEDFs and DS.
A 38-year-old woman with DS, hidradenitis suppurativa, and hypothyroidism presented with multiple cutaneous lesions developing over the last year. The lesions continued to increase in number but were otherwise asymptomatic. Physical examination revealed approximately 20 rubbery, pink-tan papules measuring less than 1 cm in diameter that were scattered along the trunk (Figure, A), arms, and legs (Figure, B).
The patient had no known history of immunosuppression or rheumatologic disease and was otherwise healthy. Basic laboratory tests including a complete blood cell count and antinuclear antibody titer were within reference range. The lesions were clinically consistent with dermatofibromas, but due to their increasing number within a short period of time, a biopsy of a representative lesion was performed to confirm the diagnosis.
The exact incidence of MEDFs is unknown, but they are rare, with one review finding only 50 cases reported from 1960 to 2002.8 They are increasingly recognized as a sign of potential immune dysregulation. Approximately 56% to 70% of cases are seen in patients with an underlying disease state; 80% are immune mediated.8,9 Interestingly, DS has long been associated with notable immune dysfunction,10,11 with evidence suggesting that trisomy 21 may result in widespread changes in gene expression that can lead to interferon activation.12
A PubMed search of articles indexed for MEDLINE using the terms dermatofibroma and Down, dermatofibroma and Down syndrome, eruptive dermatofibroma and Down syndrome, and multiple dermatofibroma and Down syndrome revealed 6 cases of MEDFs in patients with DS that have been reported since 2005.4-7 An additional report by Honda et al13 described a patient with DS who developed 7 dermatofibromas, but no time frame of development was specified. We reviewed the characteristics of 8 patients with DS with MEDFs, which included our patient (Table). The average age at time of presentation was 39 years (median age, 40 years). Six patients (75%) were female and 2 (25%) were male. Dermatofibromas were reported to appear over the course of months to years. Comorbidities included psoriatic arthritis (treated with methotrexate),6 thyroid disorders (ie, Graves disease),6 hypercholesterolemia,6 hidradenitis suppurativa, long-standing mild lymphopenia (1.4×109/L [reference range, 1.5−4.0×109/L]),4 and acute megakaryoblastic leukemia13 treated 15 years before the appearance of dermatofibromas.
Many dermatologic conditions have been reported at increased rates in individuals with DS, including seborrheic dermatitis, alopecia areata, syringomas, elastosis perforans serpiginosa, cutis marmorata, xerosis, and palmoplantar hyperkeratosis.14,15 Although drawing conclusions about associations between MEDFs and DS is limited by our small sample size, we have reported this case and reviewed existing cases of MEDFs in DS to highlight a potential association that may be underrecognized or underreported. More evidence is needed to determine the strength of the association between MEDFs and DS, but dermatologists should be aware that MEDFs may be an additional skin finding associated with DS that is related to the syndrome’s immune dysregulation.
To the Editor:
Dermatofibromas (also known as fibrous histiocytomas) are benign fibrous nodules that most often arise as solitary lesions on the lower extremities. Multiple eruptive dermatofibromas (MEDFs) are uncommon and have been defined as more than 15 in number1 or 5 to 8 dermatofibromas appearing within 4 months.2 They have been reported in association with a number of conditions of immune dysregulation such as systemic lupus erythematosus, Sjögren syndrome, HIV infection, and leukemia.3 Multiple eruptive dermatofibromas also have been described in patients with Down syndrome (DS).4-7 We report a case of MEDFs in a patient with DS and review the literature on the association between MEDFs and DS.
A 38-year-old woman with DS, hidradenitis suppurativa, and hypothyroidism presented with multiple cutaneous lesions developing over the last year. The lesions continued to increase in number but were otherwise asymptomatic. Physical examination revealed approximately 20 rubbery, pink-tan papules measuring less than 1 cm in diameter that were scattered along the trunk (Figure, A), arms, and legs (Figure, B).
The patient had no known history of immunosuppression or rheumatologic disease and was otherwise healthy. Basic laboratory tests including a complete blood cell count and antinuclear antibody titer were within reference range. The lesions were clinically consistent with dermatofibromas, but due to their increasing number within a short period of time, a biopsy of a representative lesion was performed to confirm the diagnosis.
The exact incidence of MEDFs is unknown, but they are rare, with one review finding only 50 cases reported from 1960 to 2002.8 They are increasingly recognized as a sign of potential immune dysregulation. Approximately 56% to 70% of cases are seen in patients with an underlying disease state; 80% are immune mediated.8,9 Interestingly, DS has long been associated with notable immune dysfunction,10,11 with evidence suggesting that trisomy 21 may result in widespread changes in gene expression that can lead to interferon activation.12
A PubMed search of articles indexed for MEDLINE using the terms dermatofibroma and Down, dermatofibroma and Down syndrome, eruptive dermatofibroma and Down syndrome, and multiple dermatofibroma and Down syndrome revealed 6 cases of MEDFs in patients with DS that have been reported since 2005.4-7 An additional report by Honda et al13 described a patient with DS who developed 7 dermatofibromas, but no time frame of development was specified. We reviewed the characteristics of 8 patients with DS with MEDFs, which included our patient (Table). The average age at time of presentation was 39 years (median age, 40 years). Six patients (75%) were female and 2 (25%) were male. Dermatofibromas were reported to appear over the course of months to years. Comorbidities included psoriatic arthritis (treated with methotrexate),6 thyroid disorders (ie, Graves disease),6 hypercholesterolemia,6 hidradenitis suppurativa, long-standing mild lymphopenia (1.4×109/L [reference range, 1.5−4.0×109/L]),4 and acute megakaryoblastic leukemia13 treated 15 years before the appearance of dermatofibromas.
Many dermatologic conditions have been reported at increased rates in individuals with DS, including seborrheic dermatitis, alopecia areata, syringomas, elastosis perforans serpiginosa, cutis marmorata, xerosis, and palmoplantar hyperkeratosis.14,15 Although drawing conclusions about associations between MEDFs and DS is limited by our small sample size, we have reported this case and reviewed existing cases of MEDFs in DS to highlight a potential association that may be underrecognized or underreported. More evidence is needed to determine the strength of the association between MEDFs and DS, but dermatologists should be aware that MEDFs may be an additional skin finding associated with DS that is related to the syndrome’s immune dysregulation.
- Baraf CS, Shapiro L. Multiple histiocytomas: report of a case. Arch Dermatol. 1970;101:588-590.
- Ammirati CT, Mann C, Hornstra IK. Multiple eruptive dermatofibromas in three men with HIV infection. Dermatology. 1997;4:344-348.
- Zaccaria E, Rebora A, Rongioletti F. Multiple eruptive dermatofibromas and immunosuppression: report of two cases and review of the literature. Int J Dermatol. 2008;47:723-727.
- Lamb RC, Gangopadhyay M, MacDonald A. Multiple dermatofibromas in Down syndrome. Int J Dermatol. 2014;53:E274-E275.
- Monteagudo B, Álvarez-Fernández JC, Iglesias B, et al. Multiple eruptive dermatofibromas in a patient with Down’s syndrome [article in Spanish]. Actas Dermosifiliogr. 2005;96:199.
- Monteagudo B, Suárez-Amor O, Cabanillas M, et al. Down syndrome: another cause of immunosuppression associated with multiple eruptive dermatofibroma? [article in Spanish]. Dermatol Online J. 2009;15:15.
- Tanaka M, Hoashi T, Serizawa N, et al. Multiple unilaterally localized dermatofibromas in a patient with Down syndrome. J Dermatol. 2017;44:1074-1076.
- Niiyama S, Katsuoka K, Happle R, et al. Multiple eruptive dermatofibromas: a review of the literature. Acta Derm Venereol. 2002;82:241-244.
- Her Y, Ku SH, Kim KH. A case of multiple eruptive dermatofibromas in a healthy adult. Ann Dermatol. 2014;26:539-540.
- Bertotto A, Arcangeli C, Crupi S, et al. T cell response to anti-CD3 antibody in Down’s syndrome. Arch Dis Child. 1987;62:1148-1151.
- Kusters MA, Verstegen RH, Gemen EF, et al. Intrinsic defect of the immune system in children with Down syndrome: a review. Clin Exp Immunol. 2009;156:189-193.
- Sullivan KD, Evans D, Pandey A, et al. Trisomy 21 causes changes in the circulating proteome indicative of chronic inflammation. Sci Rep. 2017;7:14818.
- Honda M, Tomimura S, de Vega S, et al. Multiple dermatofibromas in a patient with Down syndrome. J Dermatol. 2016;43:346-348.
- Daneshpazhooh M, Nazemi TM, Bigdeloo L, et al. Mucocutaneous findings in 100 children with Down syndrome. Pediatr Dermatol. 2007;24:317-320.
- Madan V, Williams J, Lear JT. Dermatological manifestations of Down’s syndrome. Clin Exp Dermatol. 2006;31:623-629.
- Baraf CS, Shapiro L. Multiple histiocytomas: report of a case. Arch Dermatol. 1970;101:588-590.
- Ammirati CT, Mann C, Hornstra IK. Multiple eruptive dermatofibromas in three men with HIV infection. Dermatology. 1997;4:344-348.
- Zaccaria E, Rebora A, Rongioletti F. Multiple eruptive dermatofibromas and immunosuppression: report of two cases and review of the literature. Int J Dermatol. 2008;47:723-727.
- Lamb RC, Gangopadhyay M, MacDonald A. Multiple dermatofibromas in Down syndrome. Int J Dermatol. 2014;53:E274-E275.
- Monteagudo B, Álvarez-Fernández JC, Iglesias B, et al. Multiple eruptive dermatofibromas in a patient with Down’s syndrome [article in Spanish]. Actas Dermosifiliogr. 2005;96:199.
- Monteagudo B, Suárez-Amor O, Cabanillas M, et al. Down syndrome: another cause of immunosuppression associated with multiple eruptive dermatofibroma? [article in Spanish]. Dermatol Online J. 2009;15:15.
- Tanaka M, Hoashi T, Serizawa N, et al. Multiple unilaterally localized dermatofibromas in a patient with Down syndrome. J Dermatol. 2017;44:1074-1076.
- Niiyama S, Katsuoka K, Happle R, et al. Multiple eruptive dermatofibromas: a review of the literature. Acta Derm Venereol. 2002;82:241-244.
- Her Y, Ku SH, Kim KH. A case of multiple eruptive dermatofibromas in a healthy adult. Ann Dermatol. 2014;26:539-540.
- Bertotto A, Arcangeli C, Crupi S, et al. T cell response to anti-CD3 antibody in Down’s syndrome. Arch Dis Child. 1987;62:1148-1151.
- Kusters MA, Verstegen RH, Gemen EF, et al. Intrinsic defect of the immune system in children with Down syndrome: a review. Clin Exp Immunol. 2009;156:189-193.
- Sullivan KD, Evans D, Pandey A, et al. Trisomy 21 causes changes in the circulating proteome indicative of chronic inflammation. Sci Rep. 2017;7:14818.
- Honda M, Tomimura S, de Vega S, et al. Multiple dermatofibromas in a patient with Down syndrome. J Dermatol. 2016;43:346-348.
- Daneshpazhooh M, Nazemi TM, Bigdeloo L, et al. Mucocutaneous findings in 100 children with Down syndrome. Pediatr Dermatol. 2007;24:317-320.
- Madan V, Williams J, Lear JT. Dermatological manifestations of Down’s syndrome. Clin Exp Dermatol. 2006;31:623-629.
Practice Points
- Although dermatofibromas are common and benign skin lesions, multiple eruptive dermatofibromas have been associated with a number of underlying conditions, particularly those associated with immune dysregulation.
- The immune dysregulation reported in Down syndrome may explain the appearance of multiple dermatofibromas.
 consistent with dermatofibromas")
Patients with cancer get valuable second opinion for free
Halfway through her first round of chemotherapy, with hair falling out, weight down, and her brain in a fog, Carolyn Hackett sat down for a Zoom meeting with a team of oncologists.
She didn’t even want a second opinion, but a friend had insisted that she get one, and she had agreed for the sake of their friendship.
But that Zoom meeting likely saved her life. The team of five specialists who had been reviewing her case for a week explained that she had been misdiagnosed. The original pathologist was mistaken. She didn’t have Hodgkin lymphoma; her cancer was really non-Hodgkin T-cell lymphoma. And the chemotherapy regimen she was in the middle of would do nothing to stop it.
The panel of doctors who populated Hackett’s computer screen during that December 2020 Zoom call were all volunteers with an organization called thesecondopinion, based in San Francisco.
The group, organized in 1969, currently offers free second opinions to at least three California patients with cancer each week. Patients meet for an average of 30-40 minutes – though there is really no limit – with a panel of doctors who have expertise in their specific case.
More than 70 cancer-related specialists, both current and retired, make up the roster of volunteers. A paid staffer rounds up a patient’s medical records, imaging and pathology slides. And a team of four to five doctors spends a week reviewing each case.
Then they meet directly with the patient and their doctor to answer questions and deliver their consensus.
Ms. Hackett was in disbelief after her meeting with thesecondopinion. Her diagnosis had gone from bad to worse, but the new information had changed her life. Without it, she would have surely continued chemotherapy and died.
On top of the new acccurate diagnosis, Ms. Hackett said it was a relief and reassurance when the team of volunteer doctors honored and included her oncologist. “I’m a nurse,” she said, and so she knows through experience that medicine comes with egos and frequent risk of lawsuits. But the team from thesecondopinion never criticized her doctor – after all, it wasn’t his mistake anyway – nor did they suggest legal action. Instead, they immediately included him as part of the team and sent him a letter detailing the panel concensus, she said, which made her feel safe.
Second opinions are big business
“And rightly so,” says Alan Venook, MD, a professor of medicine at UCSF with experience and expertise in gastrointestinal malignancies who was approached for comment but is not associated with thesecondopinion. Cancer is an increasingly a sub-specialized area, and every patient should get a second opinion, he said in an interview.
What is unique to an appointment with thesecondopinion, however, is the price tag – $0.
By comparison, a virtual second opinion at the Cleveland Clinic comes at a flat rate of $1,850, and at the Dana-Farber Cancer Institute, Boston, the cost is $2,400.
At UCSF, a second opinion from Dr. Venook and his colleagues will cost patients a couple thousand dollars out-of-pocket, he said. “Many patients don’t have the luxury of paying for a second opinion,” he said.
More than looking for misdiagnosis
Research shows that getting a second opinion can significantly change the course of a patient’s disease and treatment. A 2017 study by the Mayo Clinic found that at their institution, around 22% of second opinions changed the diagnosis, and 66% of patients received a refined or redefined diagnosis.
However, a misdiagnosis – such the case presented by Ms. Hackett – is a rare occurrence at thesecondopinion, said Howard Kleckner, MD, a medical oncologist and the organization’s medical director.
“We aren’t in the business to look for mistakes,” he said.
More often, thesecondopinion panels are about clarifying and helping patients understand the disease and options they have.”People with cancer need to make a peace with it and make peace with the treatment,” Dr. Kleckner said.
He estimates that 90% of the patients that come to the group already have the right diagnosis and treatment plan because, he says, there are “very good doctors in the state and in the Bay Area in particular.”
And even in the case of the remaining 10% of patients whose second opinion differs from their first, it’s largely a case of differences in the staging the disease or treatment options, Dr. Kleckner said.
“We aren’t coming up with brilliant suggestions. Often we are agreeing with what’s already been said,” said David Lakes, MD, a retired medical oncologist who has been volunteering with thesecondopinion for more than 30 years. “But we often see people understand for the first time.”
Both Dr. Kleckner and Dr. Lakes say that the organization attracts a certain kind of doctor, who tends to be an excellent communicator and really cares about helping the patients.
Many of these doctors are retired, but they want to keep doing the work, and they understand which pieces of information are most important for patients to know, Dr. Kleckner told this news organization. They are also willing to do this kind of work even when they won’t get paid, Dr. Kleckner said.
Part of that comes with gray hair and storied careers, Dr. Lakes added. “Retired people have experience and judgment and communication skills that a lot of younger doctors don’t have,” he commented. They often have more experience with some of the tough stuff, like exploring the goals of treatment, discontinuing treatment, and end-of-life care, and they also have more time to engage patients on their emotional health, he said.
Dr. Venook said that the services provided free-of-charge by these volunteers is “laudable,” and their thorough review of all the diagnostic information is “to their credit.” But he questions whether every second opinion provided by the organization is an expert one, since the doctors are no longer practicing. Oncology is a particularly fast-moving field, with many new developments and novel drugs launched in recent years.
“Second opinions are incredibly helpful but [have] to be [provided] by a knowledgeable expert who gets all the details and gives it serious thought,” Dr. Venook said.
Dr. Lakes says that he is constantly evaluating whether he is entitled to keep offering second opinions when he isn’t practicing; so far the answer remains a yes. Although he now has to spend more time researching treatment options like biologics, he still feels adept at engaging with patients and helping patients understand where they are in their illness and the potential benefits of fourth- or fifth-line treatments.
Another strength of thesecondopinion model lies in numbers. Most of the time second opinions are given by one doctor, Dr. Kleckner pointed out. In contrast, thesecondopinion provides the patient with access to a whole team of specialists.
“Sometimes people on the panels don’t completely agree,” Dr. Lakes said. So, before meeting with the patient on Zoom, the doctors review the case together for about half an hour and come up with a consensus. This way there’s no mixed messaging and as little anxiety for the patient as possible, he said.
The fact that patients have direct access to the panel of experts who review their cases is unique in itself, Dr. Kleckner said.
Many hospitals have tumor boards, but they are reserved for physicians, he pointed out. Patients get to hear the board’s opinion secondhand through their primary doctor or oncologist.
But at thesecondopinion, the patient gets to engage with the doctors directly. There is time to review up to four questions that the patient has submitted before the meeting and also time for any additional questions that may have arisen during the course of the meeting.
In oncology, and medicine in general, patients are often shuffled from one specialist to another, Dr. Lakes said. But often, there is no one who takes a steps back to see the whole picture.
That’s part of what thesecondopinion offers, he said. “We have the time, the experience, and no skin in the game. We can think about [the cases] in an intellectual way without feeling like we are in the hot seat or in charge.”
Thanks to her second opinion, Ms. Hackett was able to get connected with an oncologist in San Francisco who specializes in the type of cancer she actually had. She went on to receive nine rounds of a monoclonal antibody treatment formulated for her specific cancer. She is now in remission 6 months after finishing that therapy.
Scans in late July showed that she was cancer-free and doing really well. “I’m so grateful to them. I’m so impressed with thesecondopinion, I can’t believe it,” she said. “I’m alive because of them.”
A version of this article first appeared on Medscape.com.
Halfway through her first round of chemotherapy, with hair falling out, weight down, and her brain in a fog, Carolyn Hackett sat down for a Zoom meeting with a team of oncologists.
She didn’t even want a second opinion, but a friend had insisted that she get one, and she had agreed for the sake of their friendship.
But that Zoom meeting likely saved her life. The team of five specialists who had been reviewing her case for a week explained that she had been misdiagnosed. The original pathologist was mistaken. She didn’t have Hodgkin lymphoma; her cancer was really non-Hodgkin T-cell lymphoma. And the chemotherapy regimen she was in the middle of would do nothing to stop it.
The panel of doctors who populated Hackett’s computer screen during that December 2020 Zoom call were all volunteers with an organization called thesecondopinion, based in San Francisco.
The group, organized in 1969, currently offers free second opinions to at least three California patients with cancer each week. Patients meet for an average of 30-40 minutes – though there is really no limit – with a panel of doctors who have expertise in their specific case.
More than 70 cancer-related specialists, both current and retired, make up the roster of volunteers. A paid staffer rounds up a patient’s medical records, imaging and pathology slides. And a team of four to five doctors spends a week reviewing each case.
Then they meet directly with the patient and their doctor to answer questions and deliver their consensus.
Ms. Hackett was in disbelief after her meeting with thesecondopinion. Her diagnosis had gone from bad to worse, but the new information had changed her life. Without it, she would have surely continued chemotherapy and died.
On top of the new acccurate diagnosis, Ms. Hackett said it was a relief and reassurance when the team of volunteer doctors honored and included her oncologist. “I’m a nurse,” she said, and so she knows through experience that medicine comes with egos and frequent risk of lawsuits. But the team from thesecondopinion never criticized her doctor – after all, it wasn’t his mistake anyway – nor did they suggest legal action. Instead, they immediately included him as part of the team and sent him a letter detailing the panel concensus, she said, which made her feel safe.
Second opinions are big business
“And rightly so,” says Alan Venook, MD, a professor of medicine at UCSF with experience and expertise in gastrointestinal malignancies who was approached for comment but is not associated with thesecondopinion. Cancer is an increasingly a sub-specialized area, and every patient should get a second opinion, he said in an interview.
What is unique to an appointment with thesecondopinion, however, is the price tag – $0.
By comparison, a virtual second opinion at the Cleveland Clinic comes at a flat rate of $1,850, and at the Dana-Farber Cancer Institute, Boston, the cost is $2,400.
At UCSF, a second opinion from Dr. Venook and his colleagues will cost patients a couple thousand dollars out-of-pocket, he said. “Many patients don’t have the luxury of paying for a second opinion,” he said.
More than looking for misdiagnosis
Research shows that getting a second opinion can significantly change the course of a patient’s disease and treatment. A 2017 study by the Mayo Clinic found that at their institution, around 22% of second opinions changed the diagnosis, and 66% of patients received a refined or redefined diagnosis.
However, a misdiagnosis – such the case presented by Ms. Hackett – is a rare occurrence at thesecondopinion, said Howard Kleckner, MD, a medical oncologist and the organization’s medical director.
“We aren’t in the business to look for mistakes,” he said.
More often, thesecondopinion panels are about clarifying and helping patients understand the disease and options they have.”People with cancer need to make a peace with it and make peace with the treatment,” Dr. Kleckner said.
He estimates that 90% of the patients that come to the group already have the right diagnosis and treatment plan because, he says, there are “very good doctors in the state and in the Bay Area in particular.”
And even in the case of the remaining 10% of patients whose second opinion differs from their first, it’s largely a case of differences in the staging the disease or treatment options, Dr. Kleckner said.
“We aren’t coming up with brilliant suggestions. Often we are agreeing with what’s already been said,” said David Lakes, MD, a retired medical oncologist who has been volunteering with thesecondopinion for more than 30 years. “But we often see people understand for the first time.”
Both Dr. Kleckner and Dr. Lakes say that the organization attracts a certain kind of doctor, who tends to be an excellent communicator and really cares about helping the patients.
Many of these doctors are retired, but they want to keep doing the work, and they understand which pieces of information are most important for patients to know, Dr. Kleckner told this news organization. They are also willing to do this kind of work even when they won’t get paid, Dr. Kleckner said.
Part of that comes with gray hair and storied careers, Dr. Lakes added. “Retired people have experience and judgment and communication skills that a lot of younger doctors don’t have,” he commented. They often have more experience with some of the tough stuff, like exploring the goals of treatment, discontinuing treatment, and end-of-life care, and they also have more time to engage patients on their emotional health, he said.
Dr. Venook said that the services provided free-of-charge by these volunteers is “laudable,” and their thorough review of all the diagnostic information is “to their credit.” But he questions whether every second opinion provided by the organization is an expert one, since the doctors are no longer practicing. Oncology is a particularly fast-moving field, with many new developments and novel drugs launched in recent years.
“Second opinions are incredibly helpful but [have] to be [provided] by a knowledgeable expert who gets all the details and gives it serious thought,” Dr. Venook said.
Dr. Lakes says that he is constantly evaluating whether he is entitled to keep offering second opinions when he isn’t practicing; so far the answer remains a yes. Although he now has to spend more time researching treatment options like biologics, he still feels adept at engaging with patients and helping patients understand where they are in their illness and the potential benefits of fourth- or fifth-line treatments.
Another strength of thesecondopinion model lies in numbers. Most of the time second opinions are given by one doctor, Dr. Kleckner pointed out. In contrast, thesecondopinion provides the patient with access to a whole team of specialists.
“Sometimes people on the panels don’t completely agree,” Dr. Lakes said. So, before meeting with the patient on Zoom, the doctors review the case together for about half an hour and come up with a consensus. This way there’s no mixed messaging and as little anxiety for the patient as possible, he said.
The fact that patients have direct access to the panel of experts who review their cases is unique in itself, Dr. Kleckner said.
Many hospitals have tumor boards, but they are reserved for physicians, he pointed out. Patients get to hear the board’s opinion secondhand through their primary doctor or oncologist.
But at thesecondopinion, the patient gets to engage with the doctors directly. There is time to review up to four questions that the patient has submitted before the meeting and also time for any additional questions that may have arisen during the course of the meeting.
In oncology, and medicine in general, patients are often shuffled from one specialist to another, Dr. Lakes said. But often, there is no one who takes a steps back to see the whole picture.
That’s part of what thesecondopinion offers, he said. “We have the time, the experience, and no skin in the game. We can think about [the cases] in an intellectual way without feeling like we are in the hot seat or in charge.”
Thanks to her second opinion, Ms. Hackett was able to get connected with an oncologist in San Francisco who specializes in the type of cancer she actually had. She went on to receive nine rounds of a monoclonal antibody treatment formulated for her specific cancer. She is now in remission 6 months after finishing that therapy.
Scans in late July showed that she was cancer-free and doing really well. “I’m so grateful to them. I’m so impressed with thesecondopinion, I can’t believe it,” she said. “I’m alive because of them.”
A version of this article first appeared on Medscape.com.
Halfway through her first round of chemotherapy, with hair falling out, weight down, and her brain in a fog, Carolyn Hackett sat down for a Zoom meeting with a team of oncologists.
She didn’t even want a second opinion, but a friend had insisted that she get one, and she had agreed for the sake of their friendship.
But that Zoom meeting likely saved her life. The team of five specialists who had been reviewing her case for a week explained that she had been misdiagnosed. The original pathologist was mistaken. She didn’t have Hodgkin lymphoma; her cancer was really non-Hodgkin T-cell lymphoma. And the chemotherapy regimen she was in the middle of would do nothing to stop it.
The panel of doctors who populated Hackett’s computer screen during that December 2020 Zoom call were all volunteers with an organization called thesecondopinion, based in San Francisco.
The group, organized in 1969, currently offers free second opinions to at least three California patients with cancer each week. Patients meet for an average of 30-40 minutes – though there is really no limit – with a panel of doctors who have expertise in their specific case.
More than 70 cancer-related specialists, both current and retired, make up the roster of volunteers. A paid staffer rounds up a patient’s medical records, imaging and pathology slides. And a team of four to five doctors spends a week reviewing each case.
Then they meet directly with the patient and their doctor to answer questions and deliver their consensus.
Ms. Hackett was in disbelief after her meeting with thesecondopinion. Her diagnosis had gone from bad to worse, but the new information had changed her life. Without it, she would have surely continued chemotherapy and died.
On top of the new acccurate diagnosis, Ms. Hackett said it was a relief and reassurance when the team of volunteer doctors honored and included her oncologist. “I’m a nurse,” she said, and so she knows through experience that medicine comes with egos and frequent risk of lawsuits. But the team from thesecondopinion never criticized her doctor – after all, it wasn’t his mistake anyway – nor did they suggest legal action. Instead, they immediately included him as part of the team and sent him a letter detailing the panel concensus, she said, which made her feel safe.
Second opinions are big business
“And rightly so,” says Alan Venook, MD, a professor of medicine at UCSF with experience and expertise in gastrointestinal malignancies who was approached for comment but is not associated with thesecondopinion. Cancer is an increasingly a sub-specialized area, and every patient should get a second opinion, he said in an interview.
What is unique to an appointment with thesecondopinion, however, is the price tag – $0.
By comparison, a virtual second opinion at the Cleveland Clinic comes at a flat rate of $1,850, and at the Dana-Farber Cancer Institute, Boston, the cost is $2,400.
At UCSF, a second opinion from Dr. Venook and his colleagues will cost patients a couple thousand dollars out-of-pocket, he said. “Many patients don’t have the luxury of paying for a second opinion,” he said.
More than looking for misdiagnosis
Research shows that getting a second opinion can significantly change the course of a patient’s disease and treatment. A 2017 study by the Mayo Clinic found that at their institution, around 22% of second opinions changed the diagnosis, and 66% of patients received a refined or redefined diagnosis.
However, a misdiagnosis – such the case presented by Ms. Hackett – is a rare occurrence at thesecondopinion, said Howard Kleckner, MD, a medical oncologist and the organization’s medical director.
“We aren’t in the business to look for mistakes,” he said.
More often, thesecondopinion panels are about clarifying and helping patients understand the disease and options they have.”People with cancer need to make a peace with it and make peace with the treatment,” Dr. Kleckner said.
He estimates that 90% of the patients that come to the group already have the right diagnosis and treatment plan because, he says, there are “very good doctors in the state and in the Bay Area in particular.”
And even in the case of the remaining 10% of patients whose second opinion differs from their first, it’s largely a case of differences in the staging the disease or treatment options, Dr. Kleckner said.
“We aren’t coming up with brilliant suggestions. Often we are agreeing with what’s already been said,” said David Lakes, MD, a retired medical oncologist who has been volunteering with thesecondopinion for more than 30 years. “But we often see people understand for the first time.”
Both Dr. Kleckner and Dr. Lakes say that the organization attracts a certain kind of doctor, who tends to be an excellent communicator and really cares about helping the patients.
Many of these doctors are retired, but they want to keep doing the work, and they understand which pieces of information are most important for patients to know, Dr. Kleckner told this news organization. They are also willing to do this kind of work even when they won’t get paid, Dr. Kleckner said.
Part of that comes with gray hair and storied careers, Dr. Lakes added. “Retired people have experience and judgment and communication skills that a lot of younger doctors don’t have,” he commented. They often have more experience with some of the tough stuff, like exploring the goals of treatment, discontinuing treatment, and end-of-life care, and they also have more time to engage patients on their emotional health, he said.
Dr. Venook said that the services provided free-of-charge by these volunteers is “laudable,” and their thorough review of all the diagnostic information is “to their credit.” But he questions whether every second opinion provided by the organization is an expert one, since the doctors are no longer practicing. Oncology is a particularly fast-moving field, with many new developments and novel drugs launched in recent years.
“Second opinions are incredibly helpful but [have] to be [provided] by a knowledgeable expert who gets all the details and gives it serious thought,” Dr. Venook said.
Dr. Lakes says that he is constantly evaluating whether he is entitled to keep offering second opinions when he isn’t practicing; so far the answer remains a yes. Although he now has to spend more time researching treatment options like biologics, he still feels adept at engaging with patients and helping patients understand where they are in their illness and the potential benefits of fourth- or fifth-line treatments.
Another strength of thesecondopinion model lies in numbers. Most of the time second opinions are given by one doctor, Dr. Kleckner pointed out. In contrast, thesecondopinion provides the patient with access to a whole team of specialists.
“Sometimes people on the panels don’t completely agree,” Dr. Lakes said. So, before meeting with the patient on Zoom, the doctors review the case together for about half an hour and come up with a consensus. This way there’s no mixed messaging and as little anxiety for the patient as possible, he said.
The fact that patients have direct access to the panel of experts who review their cases is unique in itself, Dr. Kleckner said.
Many hospitals have tumor boards, but they are reserved for physicians, he pointed out. Patients get to hear the board’s opinion secondhand through their primary doctor or oncologist.
But at thesecondopinion, the patient gets to engage with the doctors directly. There is time to review up to four questions that the patient has submitted before the meeting and also time for any additional questions that may have arisen during the course of the meeting.
In oncology, and medicine in general, patients are often shuffled from one specialist to another, Dr. Lakes said. But often, there is no one who takes a steps back to see the whole picture.
That’s part of what thesecondopinion offers, he said. “We have the time, the experience, and no skin in the game. We can think about [the cases] in an intellectual way without feeling like we are in the hot seat or in charge.”
Thanks to her second opinion, Ms. Hackett was able to get connected with an oncologist in San Francisco who specializes in the type of cancer she actually had. She went on to receive nine rounds of a monoclonal antibody treatment formulated for her specific cancer. She is now in remission 6 months after finishing that therapy.
Scans in late July showed that she was cancer-free and doing really well. “I’m so grateful to them. I’m so impressed with thesecondopinion, I can’t believe it,” she said. “I’m alive because of them.”
A version of this article first appeared on Medscape.com.
‘I missed it’: Coping with medical error
Thursday night
It was 9 o’clock at night when my phone rang. I didn’t recognize the number but decided to answer it anyway. It was my doctor.

“Chase, I got your labs back and you have a critically low level. I spoke with someone at the hospital, I think I know what is happening, but I need you to go to the pharmacy right now and get a medicine.” She explained further and as I listened electric currents ran through my thighs until I could barely feel my legs.
“I’m so sorry, Chase. I missed it. It was low the last time we did your labs 9 months ago, and I missed it.”
In disbelief, I continued to listen as she instructed me about the next steps I was to take and prepared me for what was to come the next day.
“If you notice any changes overnight, go straight to the ED.”
My chest tingled and I could barely breathe. My mind struggled to comprehend what was happening. I looked at my husband sitting close by on the couch. He looked concerned. I tuned back in and heard her say: “Is your husband there? Can I talk to him?”
“Yes,” is all I could manage, and I handed him the phone. I sat while he listened and asked his questions. My breathing came back under my control, my legs felt wiry, and restlessness set in. “I have to get out of here,” I thought. “I have to go and pick up this medicine.”
Monday afternoon
I am sitting across from a PGY3 resident I have been treating since his intern year, as part of his treatment plan for managing a chronic mental illness that began in medical school. Earlier in the day, I received an urgent message from him requesting an emergency appointment.
Within a few minutes of sitting down, the story from his weekend call shift tumbled out of him. His speech became pressured, and his eyes welled with tears as he recounted in detail the steps he had taken to care for a very sick patient overnight.
“I missed it.” The dam broke and he sat sobbing in front of me, his body trembling.
I sat silently across from him. Willing him to breathe.
In time, his breathing came back under his control, and he slowly regained his composure. He continued: “I got the imaging, and I missed a bleed.”
Failure and shame
I can recall memorable moments from my training when I came to understand that what I initially perceived to be a mistake was instead part of the work. An example from our practice involves a patient whom I was comanaging with her primary care provider (PCP). She was not doing well following a critical work event. When I met with her after the event, she admitted having thoughts of suicide, refused a voluntary inpatient admission, and would not have met criteria for an involuntary admission. My hands were tied.
Together we created a plan to keep her safe, which included paging her PCP after hours if needed. I told her PCP before leaving that night that he might hear from her and that if she reached out, she would require hospitalization.
I arrived at work the following day, and her PCP shared with me that our patient had overdosed on medication, paged him, and was admitted to the unit.
He seemed forlorn.
I was both relieved by the news and confused by his reaction. I had hoped that she would choose a higher level of care than what we could provide her as an outpatient. I said: “This is good. She followed the plan.”
Her overdose was, of course, not part of the plan. She was struggling with several internal conflicts, including having mixed feelings about coming into the hospital; but, when the critical moment happened and she was faced with a decision to call for help or possibly die, she chose to call her PCP and have him paged as we had talked about.
I looked at her PCP. “You helped get her to where she needed to be.”
In the years of working side by side with medically trained colleagues, I have time and again needed to reframe for them that what they perceive to be a “failure” or a “crisis” is often a catalyst for change. The patient I comanaged with the PCP was a highly skilled caregiver and, as such, had been having a hard time asking for help. The hospitalization that her PCP facilitated allowed her to receive the care she needed and created an opportunity for family and friends to show up for her. Their support fed her, and she only made gains from that point on.
My training had taught me that respecting a patient’s autonomy was of the utmost importance. This instills confidence in patients as the authority in their lives. For a clinician to do this, a certain amount of helplessness must be tolerated. As I became better at identifying these moments of helplessness, feelings of failure and shame transformed.
Medical error
Sitting across from the PGY3 resident who I had met with weekly for the past 3 years, I thought about his error.
I thought about my phone call 4 nights earlier. My doctor was called at home by a lab technician, who never met their patients but was simply following protocol and alerted my doctor to the worsening number that she should have been aware of 9 months earlier.
Just like my doctor’s lapse of attention, my patient’s error was not a moment of helplessness to be tolerated. These were mistakes, and there was no way around it.
“People make mistakes.” I said simply.
We sat silently for a time.
I don’t remember who broke the silence. The conversation that followed was centered on our humanity and our capability for both compassion and fallibility. Afterward, I wondered who my doctor confided in and hoped she had a similar conversation.
Dr. Levesque is a clinical psychologist and clinical assistant professor of psychiatry at the Geisel School of Medicine at Dartmouth, Hanover, N.H., where she also serves on the Committee for a Respectful Learning Environment.
A version of this article first appeared on Medscape.com.
Thursday night
It was 9 o’clock at night when my phone rang. I didn’t recognize the number but decided to answer it anyway. It was my doctor.
“Chase, I got your labs back and you have a critically low level. I spoke with someone at the hospital, I think I know what is happening, but I need you to go to the pharmacy right now and get a medicine.” She explained further and as I listened electric currents ran through my thighs until I could barely feel my legs.
“I’m so sorry, Chase. I missed it. It was low the last time we did your labs 9 months ago, and I missed it.”
In disbelief, I continued to listen as she instructed me about the next steps I was to take and prepared me for what was to come the next day.
“If you notice any changes overnight, go straight to the ED.”
My chest tingled and I could barely breathe. My mind struggled to comprehend what was happening. I looked at my husband sitting close by on the couch. He looked concerned. I tuned back in and heard her say: “Is your husband there? Can I talk to him?”
“Yes,” is all I could manage, and I handed him the phone. I sat while he listened and asked his questions. My breathing came back under my control, my legs felt wiry, and restlessness set in. “I have to get out of here,” I thought. “I have to go and pick up this medicine.”
Monday afternoon
I am sitting across from a PGY3 resident I have been treating since his intern year, as part of his treatment plan for managing a chronic mental illness that began in medical school. Earlier in the day, I received an urgent message from him requesting an emergency appointment.
Within a few minutes of sitting down, the story from his weekend call shift tumbled out of him. His speech became pressured, and his eyes welled with tears as he recounted in detail the steps he had taken to care for a very sick patient overnight.
“I missed it.” The dam broke and he sat sobbing in front of me, his body trembling.
I sat silently across from him. Willing him to breathe.
In time, his breathing came back under his control, and he slowly regained his composure. He continued: “I got the imaging, and I missed a bleed.”
Failure and shame
I can recall memorable moments from my training when I came to understand that what I initially perceived to be a mistake was instead part of the work. An example from our practice involves a patient whom I was comanaging with her primary care provider (PCP). She was not doing well following a critical work event. When I met with her after the event, she admitted having thoughts of suicide, refused a voluntary inpatient admission, and would not have met criteria for an involuntary admission. My hands were tied.
Together we created a plan to keep her safe, which included paging her PCP after hours if needed. I told her PCP before leaving that night that he might hear from her and that if she reached out, she would require hospitalization.
I arrived at work the following day, and her PCP shared with me that our patient had overdosed on medication, paged him, and was admitted to the unit.
He seemed forlorn.
I was both relieved by the news and confused by his reaction. I had hoped that she would choose a higher level of care than what we could provide her as an outpatient. I said: “This is good. She followed the plan.”
Her overdose was, of course, not part of the plan. She was struggling with several internal conflicts, including having mixed feelings about coming into the hospital; but, when the critical moment happened and she was faced with a decision to call for help or possibly die, she chose to call her PCP and have him paged as we had talked about.
I looked at her PCP. “You helped get her to where she needed to be.”
In the years of working side by side with medically trained colleagues, I have time and again needed to reframe for them that what they perceive to be a “failure” or a “crisis” is often a catalyst for change. The patient I comanaged with the PCP was a highly skilled caregiver and, as such, had been having a hard time asking for help. The hospitalization that her PCP facilitated allowed her to receive the care she needed and created an opportunity for family and friends to show up for her. Their support fed her, and she only made gains from that point on.
My training had taught me that respecting a patient’s autonomy was of the utmost importance. This instills confidence in patients as the authority in their lives. For a clinician to do this, a certain amount of helplessness must be tolerated. As I became better at identifying these moments of helplessness, feelings of failure and shame transformed.
Medical error
Sitting across from the PGY3 resident who I had met with weekly for the past 3 years, I thought about his error.
I thought about my phone call 4 nights earlier. My doctor was called at home by a lab technician, who never met their patients but was simply following protocol and alerted my doctor to the worsening number that she should have been aware of 9 months earlier.
Just like my doctor’s lapse of attention, my patient’s error was not a moment of helplessness to be tolerated. These were mistakes, and there was no way around it.
“People make mistakes.” I said simply.
We sat silently for a time.
I don’t remember who broke the silence. The conversation that followed was centered on our humanity and our capability for both compassion and fallibility. Afterward, I wondered who my doctor confided in and hoped she had a similar conversation.
Dr. Levesque is a clinical psychologist and clinical assistant professor of psychiatry at the Geisel School of Medicine at Dartmouth, Hanover, N.H., where she also serves on the Committee for a Respectful Learning Environment.
A version of this article first appeared on Medscape.com.
Thursday night
It was 9 o’clock at night when my phone rang. I didn’t recognize the number but decided to answer it anyway. It was my doctor.
“Chase, I got your labs back and you have a critically low level. I spoke with someone at the hospital, I think I know what is happening, but I need you to go to the pharmacy right now and get a medicine.” She explained further and as I listened electric currents ran through my thighs until I could barely feel my legs.
“I’m so sorry, Chase. I missed it. It was low the last time we did your labs 9 months ago, and I missed it.”
In disbelief, I continued to listen as she instructed me about the next steps I was to take and prepared me for what was to come the next day.
“If you notice any changes overnight, go straight to the ED.”
My chest tingled and I could barely breathe. My mind struggled to comprehend what was happening. I looked at my husband sitting close by on the couch. He looked concerned. I tuned back in and heard her say: “Is your husband there? Can I talk to him?”
“Yes,” is all I could manage, and I handed him the phone. I sat while he listened and asked his questions. My breathing came back under my control, my legs felt wiry, and restlessness set in. “I have to get out of here,” I thought. “I have to go and pick up this medicine.”
Monday afternoon
I am sitting across from a PGY3 resident I have been treating since his intern year, as part of his treatment plan for managing a chronic mental illness that began in medical school. Earlier in the day, I received an urgent message from him requesting an emergency appointment.
Within a few minutes of sitting down, the story from his weekend call shift tumbled out of him. His speech became pressured, and his eyes welled with tears as he recounted in detail the steps he had taken to care for a very sick patient overnight.
“I missed it.” The dam broke and he sat sobbing in front of me, his body trembling.
I sat silently across from him. Willing him to breathe.
In time, his breathing came back under his control, and he slowly regained his composure. He continued: “I got the imaging, and I missed a bleed.”
Failure and shame
I can recall memorable moments from my training when I came to understand that what I initially perceived to be a mistake was instead part of the work. An example from our practice involves a patient whom I was comanaging with her primary care provider (PCP). She was not doing well following a critical work event. When I met with her after the event, she admitted having thoughts of suicide, refused a voluntary inpatient admission, and would not have met criteria for an involuntary admission. My hands were tied.
Together we created a plan to keep her safe, which included paging her PCP after hours if needed. I told her PCP before leaving that night that he might hear from her and that if she reached out, she would require hospitalization.
I arrived at work the following day, and her PCP shared with me that our patient had overdosed on medication, paged him, and was admitted to the unit.
He seemed forlorn.
I was both relieved by the news and confused by his reaction. I had hoped that she would choose a higher level of care than what we could provide her as an outpatient. I said: “This is good. She followed the plan.”
Her overdose was, of course, not part of the plan. She was struggling with several internal conflicts, including having mixed feelings about coming into the hospital; but, when the critical moment happened and she was faced with a decision to call for help or possibly die, she chose to call her PCP and have him paged as we had talked about.
I looked at her PCP. “You helped get her to where she needed to be.”
In the years of working side by side with medically trained colleagues, I have time and again needed to reframe for them that what they perceive to be a “failure” or a “crisis” is often a catalyst for change. The patient I comanaged with the PCP was a highly skilled caregiver and, as such, had been having a hard time asking for help. The hospitalization that her PCP facilitated allowed her to receive the care she needed and created an opportunity for family and friends to show up for her. Their support fed her, and she only made gains from that point on.
My training had taught me that respecting a patient’s autonomy was of the utmost importance. This instills confidence in patients as the authority in their lives. For a clinician to do this, a certain amount of helplessness must be tolerated. As I became better at identifying these moments of helplessness, feelings of failure and shame transformed.
Medical error
Sitting across from the PGY3 resident who I had met with weekly for the past 3 years, I thought about his error.
I thought about my phone call 4 nights earlier. My doctor was called at home by a lab technician, who never met their patients but was simply following protocol and alerted my doctor to the worsening number that she should have been aware of 9 months earlier.
Just like my doctor’s lapse of attention, my patient’s error was not a moment of helplessness to be tolerated. These were mistakes, and there was no way around it.
“People make mistakes.” I said simply.
We sat silently for a time.
I don’t remember who broke the silence. The conversation that followed was centered on our humanity and our capability for both compassion and fallibility. Afterward, I wondered who my doctor confided in and hoped she had a similar conversation.
Dr. Levesque is a clinical psychologist and clinical assistant professor of psychiatry at the Geisel School of Medicine at Dartmouth, Hanover, N.H., where she also serves on the Committee for a Respectful Learning Environment.
A version of this article first appeared on Medscape.com.