User login
For MD-IQ use only
FDA approves first-in-class drug for follicular lymphoma
This product is a first-in-class bispecific antibody that is designed to target CD20 on the surface of B cells and CD3 on the surface of T cells. This dual targeting activates and redirects a patient’s existing T cells to engage and eliminate target B cells by releasing cytotoxic proteins into the B cells, according to the manufacturer, Genentech.
Mosunetuzumab-axgb is administered as an intravenous infusion for a fixed duration, which allows for time off therapy, and can be infused in an outpatient setting, the company noted.
The drug was granted an accelerated approval on the basis of response rate data from the phase 2 GO29781 trial. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial, the company noted.
The GO29781 study was carried out in individuals with pretreated follicular lymphoma, including those who were at high risk for disease progression or whose disease was refractory to prior therapies.
A complete response was achieved in 60% of patients (54 of 90).
An objective response rate (a combination of complete and partial responses) was seen in 80% of patients who received the drug, with a majority maintaining responses for at least 18 months.
The median duration of response among those who responded was 22.8 months.
Safety data come from 218 patients with hematologic cancers who received mosunetuzumab-axgb at the recommended dose. The most common adverse event was cytokine release syndrome (39%), which can be severe and life-threatening. The median duration of cytokine release syndrome events was 3 days (range, 1-29 days). Other common adverse events (≥ 20%) included fatigue, rash, pyrexia, and headache.
“This approval is a significant milestone for people with relapsed or refractory follicular lymphoma, who have had limited treatment options until now,” said Elizabeth Budde, MD, PhD, from the City of Hope, Los Angeles, division of lymphoma, and clinical trial investigator.
Dr. Budde presented data on mosunetuzumab-axgb at the 2021 annual meeting of the American Society of Hematology, as reported by this news organization.
She noted that the 60% complete response rate seen with this new drug contrasts with the 14% that has been seen for historical controls.
“We have seen deep and durable responses in heavily pretreated, high-risk relapsed/refractory follicular lymphoma patients with fixed-duration treatment. We also observed a very favorable tolerability profile, with most cytokine release syndrome confined to cycle 1 and low grade, and treatment administration is without mandatory hospitalization,” she commented at the time.
A lymphoma specialist who was not involved in the study told this news organization at the time that he was favorably impressed by the findings.
“To me, the single-agent data looks really outstanding, with a response rate of 80%, a complete response rate of 60%, and a median duration of response of 23 months, and really very acceptable rates of cytokine release syndrome,” commented Brad S. Kahl, MD, from the Siteman Cancer Center and Washington University in St. Louis.
“I think as a single agent – if it does get approval – it will be a really valuable addition to the armamentarium in follicular lymphoma,” he added.
A version of this article first appeared on Medscape.com.
This product is a first-in-class bispecific antibody that is designed to target CD20 on the surface of B cells and CD3 on the surface of T cells. This dual targeting activates and redirects a patient’s existing T cells to engage and eliminate target B cells by releasing cytotoxic proteins into the B cells, according to the manufacturer, Genentech.
Mosunetuzumab-axgb is administered as an intravenous infusion for a fixed duration, which allows for time off therapy, and can be infused in an outpatient setting, the company noted.
The drug was granted an accelerated approval on the basis of response rate data from the phase 2 GO29781 trial. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial, the company noted.
The GO29781 study was carried out in individuals with pretreated follicular lymphoma, including those who were at high risk for disease progression or whose disease was refractory to prior therapies.
A complete response was achieved in 60% of patients (54 of 90).
An objective response rate (a combination of complete and partial responses) was seen in 80% of patients who received the drug, with a majority maintaining responses for at least 18 months.
The median duration of response among those who responded was 22.8 months.
Safety data come from 218 patients with hematologic cancers who received mosunetuzumab-axgb at the recommended dose. The most common adverse event was cytokine release syndrome (39%), which can be severe and life-threatening. The median duration of cytokine release syndrome events was 3 days (range, 1-29 days). Other common adverse events (≥ 20%) included fatigue, rash, pyrexia, and headache.
“This approval is a significant milestone for people with relapsed or refractory follicular lymphoma, who have had limited treatment options until now,” said Elizabeth Budde, MD, PhD, from the City of Hope, Los Angeles, division of lymphoma, and clinical trial investigator.
Dr. Budde presented data on mosunetuzumab-axgb at the 2021 annual meeting of the American Society of Hematology, as reported by this news organization.
She noted that the 60% complete response rate seen with this new drug contrasts with the 14% that has been seen for historical controls.
“We have seen deep and durable responses in heavily pretreated, high-risk relapsed/refractory follicular lymphoma patients with fixed-duration treatment. We also observed a very favorable tolerability profile, with most cytokine release syndrome confined to cycle 1 and low grade, and treatment administration is without mandatory hospitalization,” she commented at the time.
A lymphoma specialist who was not involved in the study told this news organization at the time that he was favorably impressed by the findings.
“To me, the single-agent data looks really outstanding, with a response rate of 80%, a complete response rate of 60%, and a median duration of response of 23 months, and really very acceptable rates of cytokine release syndrome,” commented Brad S. Kahl, MD, from the Siteman Cancer Center and Washington University in St. Louis.
“I think as a single agent – if it does get approval – it will be a really valuable addition to the armamentarium in follicular lymphoma,” he added.
A version of this article first appeared on Medscape.com.
This product is a first-in-class bispecific antibody that is designed to target CD20 on the surface of B cells and CD3 on the surface of T cells. This dual targeting activates and redirects a patient’s existing T cells to engage and eliminate target B cells by releasing cytotoxic proteins into the B cells, according to the manufacturer, Genentech.
Mosunetuzumab-axgb is administered as an intravenous infusion for a fixed duration, which allows for time off therapy, and can be infused in an outpatient setting, the company noted.
The drug was granted an accelerated approval on the basis of response rate data from the phase 2 GO29781 trial. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial, the company noted.
The GO29781 study was carried out in individuals with pretreated follicular lymphoma, including those who were at high risk for disease progression or whose disease was refractory to prior therapies.
A complete response was achieved in 60% of patients (54 of 90).
An objective response rate (a combination of complete and partial responses) was seen in 80% of patients who received the drug, with a majority maintaining responses for at least 18 months.
The median duration of response among those who responded was 22.8 months.
Safety data come from 218 patients with hematologic cancers who received mosunetuzumab-axgb at the recommended dose. The most common adverse event was cytokine release syndrome (39%), which can be severe and life-threatening. The median duration of cytokine release syndrome events was 3 days (range, 1-29 days). Other common adverse events (≥ 20%) included fatigue, rash, pyrexia, and headache.
“This approval is a significant milestone for people with relapsed or refractory follicular lymphoma, who have had limited treatment options until now,” said Elizabeth Budde, MD, PhD, from the City of Hope, Los Angeles, division of lymphoma, and clinical trial investigator.
Dr. Budde presented data on mosunetuzumab-axgb at the 2021 annual meeting of the American Society of Hematology, as reported by this news organization.
She noted that the 60% complete response rate seen with this new drug contrasts with the 14% that has been seen for historical controls.
“We have seen deep and durable responses in heavily pretreated, high-risk relapsed/refractory follicular lymphoma patients with fixed-duration treatment. We also observed a very favorable tolerability profile, with most cytokine release syndrome confined to cycle 1 and low grade, and treatment administration is without mandatory hospitalization,” she commented at the time.
A lymphoma specialist who was not involved in the study told this news organization at the time that he was favorably impressed by the findings.
“To me, the single-agent data looks really outstanding, with a response rate of 80%, a complete response rate of 60%, and a median duration of response of 23 months, and really very acceptable rates of cytokine release syndrome,” commented Brad S. Kahl, MD, from the Siteman Cancer Center and Washington University in St. Louis.
“I think as a single agent – if it does get approval – it will be a really valuable addition to the armamentarium in follicular lymphoma,” he added.
A version of this article first appeared on Medscape.com.
The trauma of sudden death
“It is one of life’s most self-evident truths that everything fades, that we fear the fading, and that we must live, nonetheless, in the face of the fear.” – Irvin D. Yalom, MD, Existential Psychotherapy, 1980
The email was titled simply, “A sorrowful note,” and I knew that someone had died. I held my breath and read as Dr. Jimmy Potash informed our entire department that Dr. Cait McFarland died in a car accident on December 7 while driving to work at West Cecil Health Center, Conowingo, Md., where she was director of psychiatry.

Sadness swelled as I remembered the outspoken resident who was interested in LGBTQ issues. Cait graduated from the Johns Hopkins residency program in 2020, she had recently married a social worker in the department, and the plan was for her to return to Hopkins full-time in July 2023 to be director of a clinic focused on mental health for people who are transgendered.
Sudden deaths are tragic and jarring and they call to the surface our losses from the past. These deaths don’t stand alone – I found myself thinking of my editor at Medscape, Dr. Bret Stetka, who died unexpectedly in August 2022, and then of Dr. Lidia Palcan Wenz, a psychiatrist I trained with, who died in a motor vehicle accident in 2004. Lidia’s husband also died in the accident, while their two young children in the back seat survived – this tragedy haunted me for some time. None of these people was close to me, but I am no stranger to the impact of unexpected death: My parents and brother all died from cardiac events, and any sudden death is a reminder of those losses.
Julia Riddle, MD, trained with Cait McFarland and was her close friend for years. “I don’t have a belief in ‘the afterlife’ but do like to think of the people that I have lost together in my memory – as if they are all suddenly in a new room together. And, with each loss, all the other occupants of that room come freshly to life again,” Dr. Riddle said.
Death is our shared destination in life, but sudden and unexpected deaths carry their own weight. There is no chance to tie up loose ends, to repair riffs, to say goodbye. Nothing is put in order, and the life that was to be lived goes on for some time as bills arrive, social and work events go unattended, vacations are canceled, and there is the awkward moment of running into someone who didn’t know your loved one has died.
Roger Lewin, MD, is a psychiatrist and writer in Towson, Md. He has both personal and professional experience with sudden death. “There is no way to prepare beforehand, so we have to get ready for what has already happened, and that is hard,” he said. “We invent a life for ourselves and others that extends into the future, and that gets interrupted.”
Most people become ill and die on a vaguely predictable schedule. There may be a chance to plan, to know and honor the wishes of the individual, and often there is the opportunity for loved ones to begin the grieving process gradually as death approaches. For those who are elderly, there may be a sense that this is the natural order of things – which may or may not temper the intensity of the grief for those who remain. If the person has suffered, the end may come with relief.
Still, I sometimes find myself surprised at the length and intensity of anguish that some people experience after losing a loved one who has lived a long and full life, who declined and suffered, but whose absence remains a gaping wound that takes years to form a scar.
Sudden death is not rare; accidents, homicide, and suicide are the top killers among young people, and cardiovascular deaths are number one among those who are older. Natural disasters and terrorist attacks can cause catastrophic numbers of sudden deaths and leave survivors to grieve not only the dead, but the loss of all that was familiar to them.
Psychiatry has been a bit lost as to how we approach grief. We often hear patients talk about anxiety surrounding death and illness, be it a fear of death or a longing for it. These fears can seem irrational – I am reminded of a patient who was afraid to eat romaine because of news reports that it was responsible for food poisoning in other states, but not Maryland, where the person lived. I found it odd that he worried about eating lettuce, but not about smoking two packs of cigarettes a day.
But our fears are like that – they move to what the media sensationalizes, or to what may be remote, because otherwise no one would get in a car or clear their walkway of snow. Life is most easily lived with a bit of denial: We shut out the reality that we can be here one moment, overscheduled and overwhelmed, with deadlines, mortgage payments, and summer vacation plans, oblivious to the fact that life may end at any moment. The early months of COVID-19 felt like a global game of Russian roulette, with each venture out a pull of the trigger and everyone’s defenses stripped bare.
While death belongs to us all, we relegate it to the disciplines of religion, philosophy, the arts, and psychology. Religion offers answers – whether a heaven, a hell, or continual reincarnation until the individual attains enlightenment, there is a destination. Perhaps it will be pleasant, perhaps not, and for some there is the hope that one gets to be the driver by having the right beliefs or doing good deeds, while others are comforted by the hope of being reunited with loved ones.
“The suddenness endures and the shock lasts – it’s like a meteor that creates a crater and we revisit it in different ways from different angles,” Dr. Lewin said. “It may leap on us unexpectedly, often many years later.”
Patients talk about death, and when their fears seem unrealistic we may long to reassure them, yet there is no reassurance and psychiatry grasps for how to help. Psychiatry has looked to draw lines for when normal grief crosses to abnormal. Is it an adjustment disorder, complicated grief, “prolonged” grief, pathology in need of medication and medicalization, or something one experiences individually, sometimes for a very long time even with treatment?
One justification for pathologizing “prolonged” reactions includes the fact that insurers will pay for treatment only if there is a diagnosis code, and shouldn’t people in distress be entitled to psychotherapy or medication? Yet there is something offensive about telling someone that they are mentally ill if they don’t grieve along a prescribed timeline, as much as there is about denying them the possible benefits of therapy or medication if they seek it, but are suffering in all the “right” ways. Psychiatry’s approach to death is inelegant at best.
In his poignant podcast series, All There Is, Anderson Cooper is tasked with sorting through his mother’s apartment after her death at age 95. In the course of packing up her belongings, he brings on other guests to talk about their emotional reactions to death. Mr. Cooper’s mother, Gloria Vanderbilt, died at an advanced age, but his father died after a brief cardiac illness when Mr. Cooper was a child, and his brother died by suicide when he was 21. He uses these experiences as a springboard to examine childhood losses, the aftermath of suicide, and the loneliness of grief.
“Loss and grief is this universal experience that we will all go through multiple times in our lives,” Mr. Cooper says, “And yet it leaves us feeling so alone and so separated from other people. At least it does me and has my entire life.”
When we talk about grief and loss, we talk about “getting over it,” or “moving on.” But loss doesn’t work that way – time usually eases the pain, leaving scars that are part of the road map for who we are on the journey that defines us.
Sudden death is hard, and the unexpected death of a young person is tragic. For Cait McFarland, there are the decades she won’t get to experience. For her family and friends, it may be excruciating, and for all the patients who have lost a psychiatrist, may time bring healing and peace.
The Dr. Caitlin McFarland Educational Fund for LGBTQI+ Mental Health is being established, and donations are being accepted at https://www.gofundme.com/f/in-memory-of-cait-mcfarland.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She has disclosed no relevant financial relationships.
“It is one of life’s most self-evident truths that everything fades, that we fear the fading, and that we must live, nonetheless, in the face of the fear.” – Irvin D. Yalom, MD, Existential Psychotherapy, 1980
The email was titled simply, “A sorrowful note,” and I knew that someone had died. I held my breath and read as Dr. Jimmy Potash informed our entire department that Dr. Cait McFarland died in a car accident on December 7 while driving to work at West Cecil Health Center, Conowingo, Md., where she was director of psychiatry.
Sadness swelled as I remembered the outspoken resident who was interested in LGBTQ issues. Cait graduated from the Johns Hopkins residency program in 2020, she had recently married a social worker in the department, and the plan was for her to return to Hopkins full-time in July 2023 to be director of a clinic focused on mental health for people who are transgendered.
Sudden deaths are tragic and jarring and they call to the surface our losses from the past. These deaths don’t stand alone – I found myself thinking of my editor at Medscape, Dr. Bret Stetka, who died unexpectedly in August 2022, and then of Dr. Lidia Palcan Wenz, a psychiatrist I trained with, who died in a motor vehicle accident in 2004. Lidia’s husband also died in the accident, while their two young children in the back seat survived – this tragedy haunted me for some time. None of these people was close to me, but I am no stranger to the impact of unexpected death: My parents and brother all died from cardiac events, and any sudden death is a reminder of those losses.
Julia Riddle, MD, trained with Cait McFarland and was her close friend for years. “I don’t have a belief in ‘the afterlife’ but do like to think of the people that I have lost together in my memory – as if they are all suddenly in a new room together. And, with each loss, all the other occupants of that room come freshly to life again,” Dr. Riddle said.
Death is our shared destination in life, but sudden and unexpected deaths carry their own weight. There is no chance to tie up loose ends, to repair riffs, to say goodbye. Nothing is put in order, and the life that was to be lived goes on for some time as bills arrive, social and work events go unattended, vacations are canceled, and there is the awkward moment of running into someone who didn’t know your loved one has died.
Roger Lewin, MD, is a psychiatrist and writer in Towson, Md. He has both personal and professional experience with sudden death. “There is no way to prepare beforehand, so we have to get ready for what has already happened, and that is hard,” he said. “We invent a life for ourselves and others that extends into the future, and that gets interrupted.”
Most people become ill and die on a vaguely predictable schedule. There may be a chance to plan, to know and honor the wishes of the individual, and often there is the opportunity for loved ones to begin the grieving process gradually as death approaches. For those who are elderly, there may be a sense that this is the natural order of things – which may or may not temper the intensity of the grief for those who remain. If the person has suffered, the end may come with relief.
Still, I sometimes find myself surprised at the length and intensity of anguish that some people experience after losing a loved one who has lived a long and full life, who declined and suffered, but whose absence remains a gaping wound that takes years to form a scar.
Sudden death is not rare; accidents, homicide, and suicide are the top killers among young people, and cardiovascular deaths are number one among those who are older. Natural disasters and terrorist attacks can cause catastrophic numbers of sudden deaths and leave survivors to grieve not only the dead, but the loss of all that was familiar to them.
Psychiatry has been a bit lost as to how we approach grief. We often hear patients talk about anxiety surrounding death and illness, be it a fear of death or a longing for it. These fears can seem irrational – I am reminded of a patient who was afraid to eat romaine because of news reports that it was responsible for food poisoning in other states, but not Maryland, where the person lived. I found it odd that he worried about eating lettuce, but not about smoking two packs of cigarettes a day.
But our fears are like that – they move to what the media sensationalizes, or to what may be remote, because otherwise no one would get in a car or clear their walkway of snow. Life is most easily lived with a bit of denial: We shut out the reality that we can be here one moment, overscheduled and overwhelmed, with deadlines, mortgage payments, and summer vacation plans, oblivious to the fact that life may end at any moment. The early months of COVID-19 felt like a global game of Russian roulette, with each venture out a pull of the trigger and everyone’s defenses stripped bare.
While death belongs to us all, we relegate it to the disciplines of religion, philosophy, the arts, and psychology. Religion offers answers – whether a heaven, a hell, or continual reincarnation until the individual attains enlightenment, there is a destination. Perhaps it will be pleasant, perhaps not, and for some there is the hope that one gets to be the driver by having the right beliefs or doing good deeds, while others are comforted by the hope of being reunited with loved ones.
“The suddenness endures and the shock lasts – it’s like a meteor that creates a crater and we revisit it in different ways from different angles,” Dr. Lewin said. “It may leap on us unexpectedly, often many years later.”
Patients talk about death, and when their fears seem unrealistic we may long to reassure them, yet there is no reassurance and psychiatry grasps for how to help. Psychiatry has looked to draw lines for when normal grief crosses to abnormal. Is it an adjustment disorder, complicated grief, “prolonged” grief, pathology in need of medication and medicalization, or something one experiences individually, sometimes for a very long time even with treatment?
One justification for pathologizing “prolonged” reactions includes the fact that insurers will pay for treatment only if there is a diagnosis code, and shouldn’t people in distress be entitled to psychotherapy or medication? Yet there is something offensive about telling someone that they are mentally ill if they don’t grieve along a prescribed timeline, as much as there is about denying them the possible benefits of therapy or medication if they seek it, but are suffering in all the “right” ways. Psychiatry’s approach to death is inelegant at best.
In his poignant podcast series, All There Is, Anderson Cooper is tasked with sorting through his mother’s apartment after her death at age 95. In the course of packing up her belongings, he brings on other guests to talk about their emotional reactions to death. Mr. Cooper’s mother, Gloria Vanderbilt, died at an advanced age, but his father died after a brief cardiac illness when Mr. Cooper was a child, and his brother died by suicide when he was 21. He uses these experiences as a springboard to examine childhood losses, the aftermath of suicide, and the loneliness of grief.
“Loss and grief is this universal experience that we will all go through multiple times in our lives,” Mr. Cooper says, “And yet it leaves us feeling so alone and so separated from other people. At least it does me and has my entire life.”
When we talk about grief and loss, we talk about “getting over it,” or “moving on.” But loss doesn’t work that way – time usually eases the pain, leaving scars that are part of the road map for who we are on the journey that defines us.
Sudden death is hard, and the unexpected death of a young person is tragic. For Cait McFarland, there are the decades she won’t get to experience. For her family and friends, it may be excruciating, and for all the patients who have lost a psychiatrist, may time bring healing and peace.
The Dr. Caitlin McFarland Educational Fund for LGBTQI+ Mental Health is being established, and donations are being accepted at https://www.gofundme.com/f/in-memory-of-cait-mcfarland.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She has disclosed no relevant financial relationships.
“It is one of life’s most self-evident truths that everything fades, that we fear the fading, and that we must live, nonetheless, in the face of the fear.” – Irvin D. Yalom, MD, Existential Psychotherapy, 1980
The email was titled simply, “A sorrowful note,” and I knew that someone had died. I held my breath and read as Dr. Jimmy Potash informed our entire department that Dr. Cait McFarland died in a car accident on December 7 while driving to work at West Cecil Health Center, Conowingo, Md., where she was director of psychiatry.
Sadness swelled as I remembered the outspoken resident who was interested in LGBTQ issues. Cait graduated from the Johns Hopkins residency program in 2020, she had recently married a social worker in the department, and the plan was for her to return to Hopkins full-time in July 2023 to be director of a clinic focused on mental health for people who are transgendered.
Sudden deaths are tragic and jarring and they call to the surface our losses from the past. These deaths don’t stand alone – I found myself thinking of my editor at Medscape, Dr. Bret Stetka, who died unexpectedly in August 2022, and then of Dr. Lidia Palcan Wenz, a psychiatrist I trained with, who died in a motor vehicle accident in 2004. Lidia’s husband also died in the accident, while their two young children in the back seat survived – this tragedy haunted me for some time. None of these people was close to me, but I am no stranger to the impact of unexpected death: My parents and brother all died from cardiac events, and any sudden death is a reminder of those losses.
Julia Riddle, MD, trained with Cait McFarland and was her close friend for years. “I don’t have a belief in ‘the afterlife’ but do like to think of the people that I have lost together in my memory – as if they are all suddenly in a new room together. And, with each loss, all the other occupants of that room come freshly to life again,” Dr. Riddle said.
Death is our shared destination in life, but sudden and unexpected deaths carry their own weight. There is no chance to tie up loose ends, to repair riffs, to say goodbye. Nothing is put in order, and the life that was to be lived goes on for some time as bills arrive, social and work events go unattended, vacations are canceled, and there is the awkward moment of running into someone who didn’t know your loved one has died.
Roger Lewin, MD, is a psychiatrist and writer in Towson, Md. He has both personal and professional experience with sudden death. “There is no way to prepare beforehand, so we have to get ready for what has already happened, and that is hard,” he said. “We invent a life for ourselves and others that extends into the future, and that gets interrupted.”
Most people become ill and die on a vaguely predictable schedule. There may be a chance to plan, to know and honor the wishes of the individual, and often there is the opportunity for loved ones to begin the grieving process gradually as death approaches. For those who are elderly, there may be a sense that this is the natural order of things – which may or may not temper the intensity of the grief for those who remain. If the person has suffered, the end may come with relief.
Still, I sometimes find myself surprised at the length and intensity of anguish that some people experience after losing a loved one who has lived a long and full life, who declined and suffered, but whose absence remains a gaping wound that takes years to form a scar.
Sudden death is not rare; accidents, homicide, and suicide are the top killers among young people, and cardiovascular deaths are number one among those who are older. Natural disasters and terrorist attacks can cause catastrophic numbers of sudden deaths and leave survivors to grieve not only the dead, but the loss of all that was familiar to them.
Psychiatry has been a bit lost as to how we approach grief. We often hear patients talk about anxiety surrounding death and illness, be it a fear of death or a longing for it. These fears can seem irrational – I am reminded of a patient who was afraid to eat romaine because of news reports that it was responsible for food poisoning in other states, but not Maryland, where the person lived. I found it odd that he worried about eating lettuce, but not about smoking two packs of cigarettes a day.
But our fears are like that – they move to what the media sensationalizes, or to what may be remote, because otherwise no one would get in a car or clear their walkway of snow. Life is most easily lived with a bit of denial: We shut out the reality that we can be here one moment, overscheduled and overwhelmed, with deadlines, mortgage payments, and summer vacation plans, oblivious to the fact that life may end at any moment. The early months of COVID-19 felt like a global game of Russian roulette, with each venture out a pull of the trigger and everyone’s defenses stripped bare.
While death belongs to us all, we relegate it to the disciplines of religion, philosophy, the arts, and psychology. Religion offers answers – whether a heaven, a hell, or continual reincarnation until the individual attains enlightenment, there is a destination. Perhaps it will be pleasant, perhaps not, and for some there is the hope that one gets to be the driver by having the right beliefs or doing good deeds, while others are comforted by the hope of being reunited with loved ones.
“The suddenness endures and the shock lasts – it’s like a meteor that creates a crater and we revisit it in different ways from different angles,” Dr. Lewin said. “It may leap on us unexpectedly, often many years later.”
Patients talk about death, and when their fears seem unrealistic we may long to reassure them, yet there is no reassurance and psychiatry grasps for how to help. Psychiatry has looked to draw lines for when normal grief crosses to abnormal. Is it an adjustment disorder, complicated grief, “prolonged” grief, pathology in need of medication and medicalization, or something one experiences individually, sometimes for a very long time even with treatment?
One justification for pathologizing “prolonged” reactions includes the fact that insurers will pay for treatment only if there is a diagnosis code, and shouldn’t people in distress be entitled to psychotherapy or medication? Yet there is something offensive about telling someone that they are mentally ill if they don’t grieve along a prescribed timeline, as much as there is about denying them the possible benefits of therapy or medication if they seek it, but are suffering in all the “right” ways. Psychiatry’s approach to death is inelegant at best.
In his poignant podcast series, All There Is, Anderson Cooper is tasked with sorting through his mother’s apartment after her death at age 95. In the course of packing up her belongings, he brings on other guests to talk about their emotional reactions to death. Mr. Cooper’s mother, Gloria Vanderbilt, died at an advanced age, but his father died after a brief cardiac illness when Mr. Cooper was a child, and his brother died by suicide when he was 21. He uses these experiences as a springboard to examine childhood losses, the aftermath of suicide, and the loneliness of grief.
“Loss and grief is this universal experience that we will all go through multiple times in our lives,” Mr. Cooper says, “And yet it leaves us feeling so alone and so separated from other people. At least it does me and has my entire life.”
When we talk about grief and loss, we talk about “getting over it,” or “moving on.” But loss doesn’t work that way – time usually eases the pain, leaving scars that are part of the road map for who we are on the journey that defines us.
Sudden death is hard, and the unexpected death of a young person is tragic. For Cait McFarland, there are the decades she won’t get to experience. For her family and friends, it may be excruciating, and for all the patients who have lost a psychiatrist, may time bring healing and peace.
The Dr. Caitlin McFarland Educational Fund for LGBTQI+ Mental Health is being established, and donations are being accepted at https://www.gofundme.com/f/in-memory-of-cait-mcfarland.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, Baltimore. She has disclosed no relevant financial relationships.
A doctor saves a drowning family in a dangerous river
Is There a Doctor in the House? is a new series telling these stories.
I live on the Maumee River in Ohio, about 50 yards from the water. I had an early quit time and came home to meet my wife for lunch. Afterward, I went up to my barn across the main road to tinker around. It was a nice day out, so my wife had opened some windows. Suddenly, she heard screaming from the river. It did not sound like fun.
She ran down to the river’s edge and saw a dad and three boys struggling in the water. She phoned me screaming: “They’re drowning! They’re drowning!” I jumped in my truck and drove up our driveway through the yard right down to the river.
My wife was on the phone with 911 at that point, and I could see them about 75-100 yards out. The dad had two of the boys clinging around his neck. They were going under the water and coming up and going under again. The other boy was just floating nearby, face down, motionless.
I threw my shoes and scrubs off and started to walk towards the water. My wife screamed at me, “You’re not going in there!” I said, “I’m not going to stand here and watch this. It’s not going to happen.”
I’m not a kid anymore, but I was a high school swimmer, and to this day I work out all the time. I felt like I had to try something. So, I went in the water despite my wife yelling and I swam towards them.
What happens when you get in that deep water is that you panic. You can’t hear anyone because of the rapids, and your instinct is to swim back towards where you went in, which is against the current. Unless you’re a very strong swimmer, you’re just wasting your time, swimming in place.
But these guys weren’t trying to go anywhere. Dad was just trying to stay up and keep the boys alive. He was in about 10 feet of water. What they didn’t see or just didn’t know: About 20 yards upstream from that deep water is a little island.
When I got to them, I yelled at the dad to move towards the island, “Go backwards! Go back!” I flipped the boy over who wasn’t moving. He was the oldest of the three, around 10 or 11 years old. When I turned him over, he was blue and wasn’t breathing. I put my fingers on his neck and didn’t feel a pulse.
So, I’m treading water, holding him. I put an arm behind his back and started doing chest compressions on him. I probably did a dozen to 15 compressions – nothing. I thought, I’ve got to get some air in this kid. So, I gave him two deep breaths and then started doing compressions again. I know ACLS and CPR training would say we don’t do that anymore. But I couldn’t just sit there and give up. Shortly after that, he coughed out a large amount of water and started breathing.
The dad and the other two boys had made it to the island. So, I started moving towards it with the boy. It was a few minutes before he regained consciousness. Of course, he was unaware of what had happened. He started to scream, because here’s this strange man holding him. But he was breathing. That’s all I cared about.
When we got to the island, I saw that my neighbor downstream had launched his canoe. He’s a retired gentleman who lives next to me, a very physically fit man. He started rolling as hard as he could towards us, against the stream. I kind of gave him a thumbs up, like, “we’re safe now. We’re standing.” We loaded the kids and the dad in the canoe and made it back against the stream to the parking lot where they went in.
All this took probably 10 or 15 minutes, and by then the paramedics were there. Life Flight had been dispatched up by my barn where there’s room to land. So, they drove up there in the ambulance. The boy I revived was flown to the hospital. The others went in the ambulance.
I know all the ED docs, so I talked to somebody later who, with permission from the family, said they were all doing fine. They were getting x-rays on the boy’s lungs. And then I heard the dad and two boys were released that night. The other boy I worked on was observed overnight and discharged the following morning.
Four or 5 days later, I heard from their pediatrician, who also had permission to share. He sent me a very nice note through Epic that he had seen the boys. Besides some mental trauma, they were all healthy and doing fine.
The family lives in the area and the kids go to school 5 miles from my house. So, the following weekend they came over. It was Father’s Day, which was kind of cool. They brought me some flowers and candy and a card the boys had drawn to thank me.
I learned that the dad had brought the boys to the fishing site. They were horsing around in knee deep water. One of the boys walked off a little way and didn’t realize there was a drop off. He went in, and of course the dad went after him, and the other two followed.
I said to the parents: “Look, things like this happen for a reason. People like your son are saved and go on in this world because they’ve got special things to do. I can’t wait to see what kind of man he becomes.”
Two or 3 months later, it was football season, and I got at a message from the dad saying their son was playing football on Saturday at the school. He wondered if I could drop by. So, I kind of snuck over and watched, but I didn’t go say hi. There’s trauma there, and I didn’t want them to have to relive that.
I’m very fortunate that I exercise every day and I know how to do CPR and swim. And thank God the boy was floating when I got to him, or I never would’ve found him. The Maumee River is known as the “muddy Maumee.” You can’t see anything under the water.
Depending on the time of year, the river can be almost dry or overflowing into the parking lot with the current rushing hard. If it had been like that, I wouldn’t have considered going in. And they wouldn’t they have been there in the first place. They’d have been a mile downstream.
I took a risk. I could have gone out there and had the dad and two other kids jump on top of me. Then we all would have been in trouble. But like I told my wife, I couldn’t stand there and watch it. I’m just not that person.
I think it was also about being a dad myself and having grandkids now. Doctor or no doctor, I felt like I was in reasonably good shape and I had to go in there to help. This dad was trying his butt off, but three little kids is too many. You can’t do that by yourself. They were not going to make it.
I go to the hospital and I save lives as part of my job, and I don’t even come home and talk about it. But this is a whole different thing. Being able to save someone’s life when put in this situation is very gratifying. It’s a tremendous feeling. There’s a reason that young man is here today, and I’ll be watching for great things from him.
A version of this article first appeared on Medscape.com.
Daniel Cassavar, MD, is a cardiologist with ProMedica in Perrysburg, Ohio.
Is There a Doctor in the House? is a new series telling these stories.
I live on the Maumee River in Ohio, about 50 yards from the water. I had an early quit time and came home to meet my wife for lunch. Afterward, I went up to my barn across the main road to tinker around. It was a nice day out, so my wife had opened some windows. Suddenly, she heard screaming from the river. It did not sound like fun.
She ran down to the river’s edge and saw a dad and three boys struggling in the water. She phoned me screaming: “They’re drowning! They’re drowning!” I jumped in my truck and drove up our driveway through the yard right down to the river.
My wife was on the phone with 911 at that point, and I could see them about 75-100 yards out. The dad had two of the boys clinging around his neck. They were going under the water and coming up and going under again. The other boy was just floating nearby, face down, motionless.
I threw my shoes and scrubs off and started to walk towards the water. My wife screamed at me, “You’re not going in there!” I said, “I’m not going to stand here and watch this. It’s not going to happen.”
I’m not a kid anymore, but I was a high school swimmer, and to this day I work out all the time. I felt like I had to try something. So, I went in the water despite my wife yelling and I swam towards them.
What happens when you get in that deep water is that you panic. You can’t hear anyone because of the rapids, and your instinct is to swim back towards where you went in, which is against the current. Unless you’re a very strong swimmer, you’re just wasting your time, swimming in place.
But these guys weren’t trying to go anywhere. Dad was just trying to stay up and keep the boys alive. He was in about 10 feet of water. What they didn’t see or just didn’t know: About 20 yards upstream from that deep water is a little island.
When I got to them, I yelled at the dad to move towards the island, “Go backwards! Go back!” I flipped the boy over who wasn’t moving. He was the oldest of the three, around 10 or 11 years old. When I turned him over, he was blue and wasn’t breathing. I put my fingers on his neck and didn’t feel a pulse.
So, I’m treading water, holding him. I put an arm behind his back and started doing chest compressions on him. I probably did a dozen to 15 compressions – nothing. I thought, I’ve got to get some air in this kid. So, I gave him two deep breaths and then started doing compressions again. I know ACLS and CPR training would say we don’t do that anymore. But I couldn’t just sit there and give up. Shortly after that, he coughed out a large amount of water and started breathing.
The dad and the other two boys had made it to the island. So, I started moving towards it with the boy. It was a few minutes before he regained consciousness. Of course, he was unaware of what had happened. He started to scream, because here’s this strange man holding him. But he was breathing. That’s all I cared about.
When we got to the island, I saw that my neighbor downstream had launched his canoe. He’s a retired gentleman who lives next to me, a very physically fit man. He started rolling as hard as he could towards us, against the stream. I kind of gave him a thumbs up, like, “we’re safe now. We’re standing.” We loaded the kids and the dad in the canoe and made it back against the stream to the parking lot where they went in.
All this took probably 10 or 15 minutes, and by then the paramedics were there. Life Flight had been dispatched up by my barn where there’s room to land. So, they drove up there in the ambulance. The boy I revived was flown to the hospital. The others went in the ambulance.
I know all the ED docs, so I talked to somebody later who, with permission from the family, said they were all doing fine. They were getting x-rays on the boy’s lungs. And then I heard the dad and two boys were released that night. The other boy I worked on was observed overnight and discharged the following morning.
Four or 5 days later, I heard from their pediatrician, who also had permission to share. He sent me a very nice note through Epic that he had seen the boys. Besides some mental trauma, they were all healthy and doing fine.
The family lives in the area and the kids go to school 5 miles from my house. So, the following weekend they came over. It was Father’s Day, which was kind of cool. They brought me some flowers and candy and a card the boys had drawn to thank me.
I learned that the dad had brought the boys to the fishing site. They were horsing around in knee deep water. One of the boys walked off a little way and didn’t realize there was a drop off. He went in, and of course the dad went after him, and the other two followed.
I said to the parents: “Look, things like this happen for a reason. People like your son are saved and go on in this world because they’ve got special things to do. I can’t wait to see what kind of man he becomes.”
Two or 3 months later, it was football season, and I got at a message from the dad saying their son was playing football on Saturday at the school. He wondered if I could drop by. So, I kind of snuck over and watched, but I didn’t go say hi. There’s trauma there, and I didn’t want them to have to relive that.
I’m very fortunate that I exercise every day and I know how to do CPR and swim. And thank God the boy was floating when I got to him, or I never would’ve found him. The Maumee River is known as the “muddy Maumee.” You can’t see anything under the water.
Depending on the time of year, the river can be almost dry or overflowing into the parking lot with the current rushing hard. If it had been like that, I wouldn’t have considered going in. And they wouldn’t they have been there in the first place. They’d have been a mile downstream.
I took a risk. I could have gone out there and had the dad and two other kids jump on top of me. Then we all would have been in trouble. But like I told my wife, I couldn’t stand there and watch it. I’m just not that person.
I think it was also about being a dad myself and having grandkids now. Doctor or no doctor, I felt like I was in reasonably good shape and I had to go in there to help. This dad was trying his butt off, but three little kids is too many. You can’t do that by yourself. They were not going to make it.
I go to the hospital and I save lives as part of my job, and I don’t even come home and talk about it. But this is a whole different thing. Being able to save someone’s life when put in this situation is very gratifying. It’s a tremendous feeling. There’s a reason that young man is here today, and I’ll be watching for great things from him.
A version of this article first appeared on Medscape.com.
Daniel Cassavar, MD, is a cardiologist with ProMedica in Perrysburg, Ohio.
Is There a Doctor in the House? is a new series telling these stories.
I live on the Maumee River in Ohio, about 50 yards from the water. I had an early quit time and came home to meet my wife for lunch. Afterward, I went up to my barn across the main road to tinker around. It was a nice day out, so my wife had opened some windows. Suddenly, she heard screaming from the river. It did not sound like fun.
She ran down to the river’s edge and saw a dad and three boys struggling in the water. She phoned me screaming: “They’re drowning! They’re drowning!” I jumped in my truck and drove up our driveway through the yard right down to the river.
My wife was on the phone with 911 at that point, and I could see them about 75-100 yards out. The dad had two of the boys clinging around his neck. They were going under the water and coming up and going under again. The other boy was just floating nearby, face down, motionless.
I threw my shoes and scrubs off and started to walk towards the water. My wife screamed at me, “You’re not going in there!” I said, “I’m not going to stand here and watch this. It’s not going to happen.”
I’m not a kid anymore, but I was a high school swimmer, and to this day I work out all the time. I felt like I had to try something. So, I went in the water despite my wife yelling and I swam towards them.
What happens when you get in that deep water is that you panic. You can’t hear anyone because of the rapids, and your instinct is to swim back towards where you went in, which is against the current. Unless you’re a very strong swimmer, you’re just wasting your time, swimming in place.
But these guys weren’t trying to go anywhere. Dad was just trying to stay up and keep the boys alive. He was in about 10 feet of water. What they didn’t see or just didn’t know: About 20 yards upstream from that deep water is a little island.
When I got to them, I yelled at the dad to move towards the island, “Go backwards! Go back!” I flipped the boy over who wasn’t moving. He was the oldest of the three, around 10 or 11 years old. When I turned him over, he was blue and wasn’t breathing. I put my fingers on his neck and didn’t feel a pulse.
So, I’m treading water, holding him. I put an arm behind his back and started doing chest compressions on him. I probably did a dozen to 15 compressions – nothing. I thought, I’ve got to get some air in this kid. So, I gave him two deep breaths and then started doing compressions again. I know ACLS and CPR training would say we don’t do that anymore. But I couldn’t just sit there and give up. Shortly after that, he coughed out a large amount of water and started breathing.
The dad and the other two boys had made it to the island. So, I started moving towards it with the boy. It was a few minutes before he regained consciousness. Of course, he was unaware of what had happened. He started to scream, because here’s this strange man holding him. But he was breathing. That’s all I cared about.
When we got to the island, I saw that my neighbor downstream had launched his canoe. He’s a retired gentleman who lives next to me, a very physically fit man. He started rolling as hard as he could towards us, against the stream. I kind of gave him a thumbs up, like, “we’re safe now. We’re standing.” We loaded the kids and the dad in the canoe and made it back against the stream to the parking lot where they went in.
All this took probably 10 or 15 minutes, and by then the paramedics were there. Life Flight had been dispatched up by my barn where there’s room to land. So, they drove up there in the ambulance. The boy I revived was flown to the hospital. The others went in the ambulance.
I know all the ED docs, so I talked to somebody later who, with permission from the family, said they were all doing fine. They were getting x-rays on the boy’s lungs. And then I heard the dad and two boys were released that night. The other boy I worked on was observed overnight and discharged the following morning.
Four or 5 days later, I heard from their pediatrician, who also had permission to share. He sent me a very nice note through Epic that he had seen the boys. Besides some mental trauma, they were all healthy and doing fine.
The family lives in the area and the kids go to school 5 miles from my house. So, the following weekend they came over. It was Father’s Day, which was kind of cool. They brought me some flowers and candy and a card the boys had drawn to thank me.
I learned that the dad had brought the boys to the fishing site. They were horsing around in knee deep water. One of the boys walked off a little way and didn’t realize there was a drop off. He went in, and of course the dad went after him, and the other two followed.
I said to the parents: “Look, things like this happen for a reason. People like your son are saved and go on in this world because they’ve got special things to do. I can’t wait to see what kind of man he becomes.”
Two or 3 months later, it was football season, and I got at a message from the dad saying their son was playing football on Saturday at the school. He wondered if I could drop by. So, I kind of snuck over and watched, but I didn’t go say hi. There’s trauma there, and I didn’t want them to have to relive that.
I’m very fortunate that I exercise every day and I know how to do CPR and swim. And thank God the boy was floating when I got to him, or I never would’ve found him. The Maumee River is known as the “muddy Maumee.” You can’t see anything under the water.
Depending on the time of year, the river can be almost dry or overflowing into the parking lot with the current rushing hard. If it had been like that, I wouldn’t have considered going in. And they wouldn’t they have been there in the first place. They’d have been a mile downstream.
I took a risk. I could have gone out there and had the dad and two other kids jump on top of me. Then we all would have been in trouble. But like I told my wife, I couldn’t stand there and watch it. I’m just not that person.
I think it was also about being a dad myself and having grandkids now. Doctor or no doctor, I felt like I was in reasonably good shape and I had to go in there to help. This dad was trying his butt off, but three little kids is too many. You can’t do that by yourself. They were not going to make it.
I go to the hospital and I save lives as part of my job, and I don’t even come home and talk about it. But this is a whole different thing. Being able to save someone’s life when put in this situation is very gratifying. It’s a tremendous feeling. There’s a reason that young man is here today, and I’ll be watching for great things from him.
A version of this article first appeared on Medscape.com.
Daniel Cassavar, MD, is a cardiologist with ProMedica in Perrysburg, Ohio.
All the National Health Service wants for Christmas is tea and biscuits
Three cups of tea, two biscuit packs, and a Christmas study from the BMJ
Warning: The following content may contain excessive Britishness. Continue at your own risk.
It’s no secret that the world economy is in an … interesting spot right now. Belt tightening is occurring around the world despite the holiday season, and hospitals across the pond in Great Britain are no exception.

It was a simple sign that prompted the study, published in the Christmas edition of the BMJ: “Please do not take excessive quantities of these refreshments.” And if we all know one thing, you do not get between Brits and their tea and biscuits. So the researchers behind the study drafted a survey and sent it around to nearly 2,000 British health care workers and asked what they considered to be excessive consumption of work-provided hot drinks and biscuits.
In the hot drinks department (tea and coffee, though we appreciate the two people who voiced a preference for free hot whiskey, if it was available) the survey participants decreed that 3.32 drinks was the maximum before consumption became excessive. That’s pretty close to the actual number of hot drinks respondents drank daily (3.04), so it’s pretty fair to say that British health care workers do a good job of self-limiting.
It’s much the same story with biscuits: Health care workers reported that consuming 2.25 packets of free biscuits would be excessive. Notably, doctors would take more than nondoctors (2.35 vs. 2.14 – typical doctor behavior), and those who had been in their role for less than 2 years would consume nearly 3 packets a day before calling it quits.
The study did not include an official cost analysis, but calculations conducted on a biscuit wrapper (that’s not a joke, by the way) estimated that the combined cost for providing every National Health Service employee with three free drinks and two free biscuit packages a day would be about 160 million pounds a year. Now, that’s a lot of money for tea and biscuits, but, they added, it’s a meager 0.1% of the NHS annual budget. They also noted that most employees consider free hot drinks a more valuable workplace perk than free support for mental health.
In conclusion, the authors wrote, “As a target for cost-saving initiatives, limiting free refreshment consumption is really scraping the biscuit barrel (although some limits on hot whiskey availability may be necessary), and implementing, or continuing, perks that improve staff morale seems justifiable. … Healthcare employers should allow biscuits and hot drinks to be freely available to staff, and they should leave these grateful recipients to judge for themselves what constitutes reasonable consumption.”
Now there’s a Christmas sentiment we can all get behind.
We come not to bury sugar, but to improve it
When we think about sugar, healthy isn’t the first thing that comes to mind. Research also shows that artificial sweeteners, as well as processed foods in general, are bad for your body and brain. People, however, love the stuff. That’s why one of the leading brands in processed foods, Kraft Heinz, partnered with the Wyss Institute for Biologically Inspired Engineering at Harvard to find a way to reduce consumers’ sugar consumption.

The question that Kraft Heinz presented to Wyss was this: How could it reduce the fructose in its products without losing the functionality of regular sugar.
The Wyss team’s approach seems pretty simple: Use a naturally occurring enzyme to convert sugar to fiber. The trick was to add the enzymes into the food so they could convert the sugar to fiber after being consumed. The enzymes also needed to be able to be added to existing food products without changing their existing recipes, Kraft Heinz insisted.
How does it work? The crafted enzyme is encapsulated to remain dormant in the food until exposed to an increased pH level, as is found in the GI tract between the stomach and the intestine. It reduces the amount of sugar absorbed in the bloodstream and creates a healthy prebiotic fiber, the institute explained.
This opens a whole new window for consumers. People with diabetes can enjoy their favorite cookies from time to time, while parents can feel less guilty about their children bathing their chicken nuggets in unholy amounts of ketchup.
New genes, or not new genes? That is the question
… and the police report that no capybaras were harmed in the incident. What a relief. Now Action News 8 brings you Carol Espinosa’s exclusive interview with legendary scientist and zombie, Charles Darwin.
Carol: Thanks, Daryl. Tell us, Prof. Darwin, what have you been up to lately?
Prof. Darwin: Please, Carol, call me Chuck. As always, I’ve got my hands full with the whole evolution thing. The big news right now is a study published in Cell Reports that offers evidence of the continuing evolution of humans. Can I eat your brain now?
Carol: No, Chuck, you may not. So people are still evolving? It sure seems like we’ve reverted to survival of the dumbest.
Chuck Darwin: Good one, Carol, but evolution hasn’t stopped. The investigators used a previously published dataset of functionally relevant new genes to create an ancestral tree comparing humans with other vertebrate species. By tracking the genes across evolution, they found 155 from regions of unique DNA that arose from scratch and not from duplication events in the existing genome. That’s a big deal.
Carol: Anything made from scratch is always better. Everyone knows that. What else can you tell us, Chuck?
Chuck Darwin: So these 155 genes didn’t exist when humans separated from chimpanzees nearly 7 million years ago. Turns out that 44 of them are associated with growth defects in cell cultures and three “have disease-associated DNA markers that point to connections with ailments such as muscular dystrophy, retinitis pigmentosa, and Alazami syndrome.” At least that’s what the investigators said in a written statement. I must say, Carol, that your brain is looking particularly delicious tonight.
Carol: Ironic. For years I’ve been hoping a man would appreciate me for my brain, and now I get this. Back to you, Daryl.
Three cups of tea, two biscuit packs, and a Christmas study from the BMJ
Warning: The following content may contain excessive Britishness. Continue at your own risk.
It’s no secret that the world economy is in an … interesting spot right now. Belt tightening is occurring around the world despite the holiday season, and hospitals across the pond in Great Britain are no exception.
It was a simple sign that prompted the study, published in the Christmas edition of the BMJ: “Please do not take excessive quantities of these refreshments.” And if we all know one thing, you do not get between Brits and their tea and biscuits. So the researchers behind the study drafted a survey and sent it around to nearly 2,000 British health care workers and asked what they considered to be excessive consumption of work-provided hot drinks and biscuits.
In the hot drinks department (tea and coffee, though we appreciate the two people who voiced a preference for free hot whiskey, if it was available) the survey participants decreed that 3.32 drinks was the maximum before consumption became excessive. That’s pretty close to the actual number of hot drinks respondents drank daily (3.04), so it’s pretty fair to say that British health care workers do a good job of self-limiting.
It’s much the same story with biscuits: Health care workers reported that consuming 2.25 packets of free biscuits would be excessive. Notably, doctors would take more than nondoctors (2.35 vs. 2.14 – typical doctor behavior), and those who had been in their role for less than 2 years would consume nearly 3 packets a day before calling it quits.
The study did not include an official cost analysis, but calculations conducted on a biscuit wrapper (that’s not a joke, by the way) estimated that the combined cost for providing every National Health Service employee with three free drinks and two free biscuit packages a day would be about 160 million pounds a year. Now, that’s a lot of money for tea and biscuits, but, they added, it’s a meager 0.1% of the NHS annual budget. They also noted that most employees consider free hot drinks a more valuable workplace perk than free support for mental health.
In conclusion, the authors wrote, “As a target for cost-saving initiatives, limiting free refreshment consumption is really scraping the biscuit barrel (although some limits on hot whiskey availability may be necessary), and implementing, or continuing, perks that improve staff morale seems justifiable. … Healthcare employers should allow biscuits and hot drinks to be freely available to staff, and they should leave these grateful recipients to judge for themselves what constitutes reasonable consumption.”
Now there’s a Christmas sentiment we can all get behind.
We come not to bury sugar, but to improve it
When we think about sugar, healthy isn’t the first thing that comes to mind. Research also shows that artificial sweeteners, as well as processed foods in general, are bad for your body and brain. People, however, love the stuff. That’s why one of the leading brands in processed foods, Kraft Heinz, partnered with the Wyss Institute for Biologically Inspired Engineering at Harvard to find a way to reduce consumers’ sugar consumption.
The question that Kraft Heinz presented to Wyss was this: How could it reduce the fructose in its products without losing the functionality of regular sugar.
The Wyss team’s approach seems pretty simple: Use a naturally occurring enzyme to convert sugar to fiber. The trick was to add the enzymes into the food so they could convert the sugar to fiber after being consumed. The enzymes also needed to be able to be added to existing food products without changing their existing recipes, Kraft Heinz insisted.
How does it work? The crafted enzyme is encapsulated to remain dormant in the food until exposed to an increased pH level, as is found in the GI tract between the stomach and the intestine. It reduces the amount of sugar absorbed in the bloodstream and creates a healthy prebiotic fiber, the institute explained.
This opens a whole new window for consumers. People with diabetes can enjoy their favorite cookies from time to time, while parents can feel less guilty about their children bathing their chicken nuggets in unholy amounts of ketchup.
New genes, or not new genes? That is the question
… and the police report that no capybaras were harmed in the incident. What a relief. Now Action News 8 brings you Carol Espinosa’s exclusive interview with legendary scientist and zombie, Charles Darwin.
Carol: Thanks, Daryl. Tell us, Prof. Darwin, what have you been up to lately?
Prof. Darwin: Please, Carol, call me Chuck. As always, I’ve got my hands full with the whole evolution thing. The big news right now is a study published in Cell Reports that offers evidence of the continuing evolution of humans. Can I eat your brain now?
Carol: No, Chuck, you may not. So people are still evolving? It sure seems like we’ve reverted to survival of the dumbest.
Chuck Darwin: Good one, Carol, but evolution hasn’t stopped. The investigators used a previously published dataset of functionally relevant new genes to create an ancestral tree comparing humans with other vertebrate species. By tracking the genes across evolution, they found 155 from regions of unique DNA that arose from scratch and not from duplication events in the existing genome. That’s a big deal.
Carol: Anything made from scratch is always better. Everyone knows that. What else can you tell us, Chuck?
Chuck Darwin: So these 155 genes didn’t exist when humans separated from chimpanzees nearly 7 million years ago. Turns out that 44 of them are associated with growth defects in cell cultures and three “have disease-associated DNA markers that point to connections with ailments such as muscular dystrophy, retinitis pigmentosa, and Alazami syndrome.” At least that’s what the investigators said in a written statement. I must say, Carol, that your brain is looking particularly delicious tonight.
Carol: Ironic. For years I’ve been hoping a man would appreciate me for my brain, and now I get this. Back to you, Daryl.
Three cups of tea, two biscuit packs, and a Christmas study from the BMJ
Warning: The following content may contain excessive Britishness. Continue at your own risk.
It’s no secret that the world economy is in an … interesting spot right now. Belt tightening is occurring around the world despite the holiday season, and hospitals across the pond in Great Britain are no exception.
It was a simple sign that prompted the study, published in the Christmas edition of the BMJ: “Please do not take excessive quantities of these refreshments.” And if we all know one thing, you do not get between Brits and their tea and biscuits. So the researchers behind the study drafted a survey and sent it around to nearly 2,000 British health care workers and asked what they considered to be excessive consumption of work-provided hot drinks and biscuits.
In the hot drinks department (tea and coffee, though we appreciate the two people who voiced a preference for free hot whiskey, if it was available) the survey participants decreed that 3.32 drinks was the maximum before consumption became excessive. That’s pretty close to the actual number of hot drinks respondents drank daily (3.04), so it’s pretty fair to say that British health care workers do a good job of self-limiting.
It’s much the same story with biscuits: Health care workers reported that consuming 2.25 packets of free biscuits would be excessive. Notably, doctors would take more than nondoctors (2.35 vs. 2.14 – typical doctor behavior), and those who had been in their role for less than 2 years would consume nearly 3 packets a day before calling it quits.
The study did not include an official cost analysis, but calculations conducted on a biscuit wrapper (that’s not a joke, by the way) estimated that the combined cost for providing every National Health Service employee with three free drinks and two free biscuit packages a day would be about 160 million pounds a year. Now, that’s a lot of money for tea and biscuits, but, they added, it’s a meager 0.1% of the NHS annual budget. They also noted that most employees consider free hot drinks a more valuable workplace perk than free support for mental health.
In conclusion, the authors wrote, “As a target for cost-saving initiatives, limiting free refreshment consumption is really scraping the biscuit barrel (although some limits on hot whiskey availability may be necessary), and implementing, or continuing, perks that improve staff morale seems justifiable. … Healthcare employers should allow biscuits and hot drinks to be freely available to staff, and they should leave these grateful recipients to judge for themselves what constitutes reasonable consumption.”
Now there’s a Christmas sentiment we can all get behind.
We come not to bury sugar, but to improve it
When we think about sugar, healthy isn’t the first thing that comes to mind. Research also shows that artificial sweeteners, as well as processed foods in general, are bad for your body and brain. People, however, love the stuff. That’s why one of the leading brands in processed foods, Kraft Heinz, partnered with the Wyss Institute for Biologically Inspired Engineering at Harvard to find a way to reduce consumers’ sugar consumption.
The question that Kraft Heinz presented to Wyss was this: How could it reduce the fructose in its products without losing the functionality of regular sugar.
The Wyss team’s approach seems pretty simple: Use a naturally occurring enzyme to convert sugar to fiber. The trick was to add the enzymes into the food so they could convert the sugar to fiber after being consumed. The enzymes also needed to be able to be added to existing food products without changing their existing recipes, Kraft Heinz insisted.
How does it work? The crafted enzyme is encapsulated to remain dormant in the food until exposed to an increased pH level, as is found in the GI tract between the stomach and the intestine. It reduces the amount of sugar absorbed in the bloodstream and creates a healthy prebiotic fiber, the institute explained.
This opens a whole new window for consumers. People with diabetes can enjoy their favorite cookies from time to time, while parents can feel less guilty about their children bathing their chicken nuggets in unholy amounts of ketchup.
New genes, or not new genes? That is the question
… and the police report that no capybaras were harmed in the incident. What a relief. Now Action News 8 brings you Carol Espinosa’s exclusive interview with legendary scientist and zombie, Charles Darwin.
Carol: Thanks, Daryl. Tell us, Prof. Darwin, what have you been up to lately?
Prof. Darwin: Please, Carol, call me Chuck. As always, I’ve got my hands full with the whole evolution thing. The big news right now is a study published in Cell Reports that offers evidence of the continuing evolution of humans. Can I eat your brain now?
Carol: No, Chuck, you may not. So people are still evolving? It sure seems like we’ve reverted to survival of the dumbest.
Chuck Darwin: Good one, Carol, but evolution hasn’t stopped. The investigators used a previously published dataset of functionally relevant new genes to create an ancestral tree comparing humans with other vertebrate species. By tracking the genes across evolution, they found 155 from regions of unique DNA that arose from scratch and not from duplication events in the existing genome. That’s a big deal.
Carol: Anything made from scratch is always better. Everyone knows that. What else can you tell us, Chuck?
Chuck Darwin: So these 155 genes didn’t exist when humans separated from chimpanzees nearly 7 million years ago. Turns out that 44 of them are associated with growth defects in cell cultures and three “have disease-associated DNA markers that point to connections with ailments such as muscular dystrophy, retinitis pigmentosa, and Alazami syndrome.” At least that’s what the investigators said in a written statement. I must say, Carol, that your brain is looking particularly delicious tonight.
Carol: Ironic. For years I’ve been hoping a man would appreciate me for my brain, and now I get this. Back to you, Daryl.
AGA News - February 2023
AGA members advocate for GI during Alliance of Specialty Medicine fly-in
In December, six AGA members joined more than 100 specialty doctors organized by the Alliance of Specialty Medicine, a coalition that represents specialty physicians, to meet with House and Senate offices and discuss pressing policy priorities.
Members spoke on behalf of GI and stressed the need for Congress to act immediately on the upcoming Medicare cuts, and discussed step therapy protocols, prior authorization reform, and the role of artificial intelligence in the specialty.
Our members represented GI well throughout the day’s meetings!
AGA PAC Board Member and Congressional Advocate Dr. Sadeea Abbasi spoke to House Leader Kevin McCarthy (R-CA) about challenges specialty doctors are facing and petitioned for Congress to mitigate the nearly 10 percent Medicare payment cuts before the end of the 117th Congress.
Additionally, AGA Government Affairs Committee Chair Dr. Rotonya Carr engaged with several members of Congress on issues impacting specialty care and discussed the future of AI in medicine with Rep. Mariannette Miller-Meeks (R-IA), who is an ophthalmologist.
Thank you to all our members who spoke on behalf of GI! We appreciate our AGA leaders who took time to participate!
- Sadeea Abbasi, MD, PhD
- Dawn B. Beaulieu, MD, AGAF
- Brent Burnette, MD
- Rotonya M. Carr, MD, FACP
- Peter S. Margolis, MD, AGAF
- Suzette Rivera MacMurray, MD
Learn how AGA is advocating for you. Visit gastro.org/advocacy.
AGA workshops champion women in GI
At AGA, we’re committed to supporting, empowering, and amplifying women in GI. As part of our ongoing efforts, we were thrilled to host nearly 250 women at four Women in GI regional workshops this fall. These workshops provided women across the country with opportunities to develop their personal and professional networks, participate in leadership development seminars, receive career mentoring, and engage in various wellness practices.
Following the conclusion of the regional workshops, we hosted the AGA Women’s Leadership Collaboration Conference at the AGA national office in Bethesda, Md.
I can’t stop talking about this weekend! What a profound experience! I continue to be inspired by this group of women, our mission, and the far-reaching impact of this collaboration. Each one of us was absolutely transformed this weekend. And the radius of that impact is immeasurable! – Dr. Bahar Adeli, TJUH–Albert Einstein Medical Center

During the two-day conference, 22 delegates discussed workplace experiences, reported on their region’s workshop, and participated in strategy development exercises to further gender equity in GI, which included identifying tactics and ideas for action.
This unique event brought together delegates from each regional workshop, including 2023 Dr. Maria Leo-Lieber scholarship winners Alyssa Parian and Alexandra Livanos, who attended the Northeast workshop. It was a great time of collaboration and connection with the AGA #WomenInGI community!
Thank you to everyone who participated and made the events a success. We look forward to uplifting all women in GI and identifying ways to support the community in the coming year.
AGA thanks Johnson & Johnson Health Care Systems, Inc. for their support of this program.
Help move innovation forward at the 2023 AGA Tech Summit
Innovative technologies for endoscopy, advanced imaging, and bariatric care are a few of the topics that will headline the 2023 AGA Tech Summit, March 9-10, 2023, at the Grand Hyatt San Francisco. Registration is now open. Visit techsummit.gastro.org to secure your spot.

The Tech Summit is where GI innovators, clinicians, medical device companies, venture capitalists and regulatory agencies meet to foster the development and adoption of GI technologies. It is the perfect venue for:
- All innovators, entrepreneurs and clinicians who want to build their professional networks in the GI space.
- Early-stage GI companies who want to showcase their technologies and find new ideas for further innovations that will improve patient care.
- GI fellows who want an exclusive and immersive behind-the-scenes look into the MedTech world.
Learn more by visiting techsummit.gastro.org.
AGA members advocate for GI during Alliance of Specialty Medicine fly-in
In December, six AGA members joined more than 100 specialty doctors organized by the Alliance of Specialty Medicine, a coalition that represents specialty physicians, to meet with House and Senate offices and discuss pressing policy priorities.
Members spoke on behalf of GI and stressed the need for Congress to act immediately on the upcoming Medicare cuts, and discussed step therapy protocols, prior authorization reform, and the role of artificial intelligence in the specialty.
Our members represented GI well throughout the day’s meetings!
AGA PAC Board Member and Congressional Advocate Dr. Sadeea Abbasi spoke to House Leader Kevin McCarthy (R-CA) about challenges specialty doctors are facing and petitioned for Congress to mitigate the nearly 10 percent Medicare payment cuts before the end of the 117th Congress.
Additionally, AGA Government Affairs Committee Chair Dr. Rotonya Carr engaged with several members of Congress on issues impacting specialty care and discussed the future of AI in medicine with Rep. Mariannette Miller-Meeks (R-IA), who is an ophthalmologist.
Thank you to all our members who spoke on behalf of GI! We appreciate our AGA leaders who took time to participate!
- Sadeea Abbasi, MD, PhD
- Dawn B. Beaulieu, MD, AGAF
- Brent Burnette, MD
- Rotonya M. Carr, MD, FACP
- Peter S. Margolis, MD, AGAF
- Suzette Rivera MacMurray, MD
Learn how AGA is advocating for you. Visit gastro.org/advocacy.
AGA workshops champion women in GI
At AGA, we’re committed to supporting, empowering, and amplifying women in GI. As part of our ongoing efforts, we were thrilled to host nearly 250 women at four Women in GI regional workshops this fall. These workshops provided women across the country with opportunities to develop their personal and professional networks, participate in leadership development seminars, receive career mentoring, and engage in various wellness practices.
Following the conclusion of the regional workshops, we hosted the AGA Women’s Leadership Collaboration Conference at the AGA national office in Bethesda, Md.
I can’t stop talking about this weekend! What a profound experience! I continue to be inspired by this group of women, our mission, and the far-reaching impact of this collaboration. Each one of us was absolutely transformed this weekend. And the radius of that impact is immeasurable! – Dr. Bahar Adeli, TJUH–Albert Einstein Medical Center
During the two-day conference, 22 delegates discussed workplace experiences, reported on their region’s workshop, and participated in strategy development exercises to further gender equity in GI, which included identifying tactics and ideas for action.
This unique event brought together delegates from each regional workshop, including 2023 Dr. Maria Leo-Lieber scholarship winners Alyssa Parian and Alexandra Livanos, who attended the Northeast workshop. It was a great time of collaboration and connection with the AGA #WomenInGI community!
Thank you to everyone who participated and made the events a success. We look forward to uplifting all women in GI and identifying ways to support the community in the coming year.
AGA thanks Johnson & Johnson Health Care Systems, Inc. for their support of this program.
Help move innovation forward at the 2023 AGA Tech Summit
Innovative technologies for endoscopy, advanced imaging, and bariatric care are a few of the topics that will headline the 2023 AGA Tech Summit, March 9-10, 2023, at the Grand Hyatt San Francisco. Registration is now open. Visit techsummit.gastro.org to secure your spot.
The Tech Summit is where GI innovators, clinicians, medical device companies, venture capitalists and regulatory agencies meet to foster the development and adoption of GI technologies. It is the perfect venue for:
- All innovators, entrepreneurs and clinicians who want to build their professional networks in the GI space.
- Early-stage GI companies who want to showcase their technologies and find new ideas for further innovations that will improve patient care.
- GI fellows who want an exclusive and immersive behind-the-scenes look into the MedTech world.
Learn more by visiting techsummit.gastro.org.
AGA members advocate for GI during Alliance of Specialty Medicine fly-in
In December, six AGA members joined more than 100 specialty doctors organized by the Alliance of Specialty Medicine, a coalition that represents specialty physicians, to meet with House and Senate offices and discuss pressing policy priorities.
Members spoke on behalf of GI and stressed the need for Congress to act immediately on the upcoming Medicare cuts, and discussed step therapy protocols, prior authorization reform, and the role of artificial intelligence in the specialty.
Our members represented GI well throughout the day’s meetings!
AGA PAC Board Member and Congressional Advocate Dr. Sadeea Abbasi spoke to House Leader Kevin McCarthy (R-CA) about challenges specialty doctors are facing and petitioned for Congress to mitigate the nearly 10 percent Medicare payment cuts before the end of the 117th Congress.
Additionally, AGA Government Affairs Committee Chair Dr. Rotonya Carr engaged with several members of Congress on issues impacting specialty care and discussed the future of AI in medicine with Rep. Mariannette Miller-Meeks (R-IA), who is an ophthalmologist.
Thank you to all our members who spoke on behalf of GI! We appreciate our AGA leaders who took time to participate!
- Sadeea Abbasi, MD, PhD
- Dawn B. Beaulieu, MD, AGAF
- Brent Burnette, MD
- Rotonya M. Carr, MD, FACP
- Peter S. Margolis, MD, AGAF
- Suzette Rivera MacMurray, MD
Learn how AGA is advocating for you. Visit gastro.org/advocacy.
AGA workshops champion women in GI
At AGA, we’re committed to supporting, empowering, and amplifying women in GI. As part of our ongoing efforts, we were thrilled to host nearly 250 women at four Women in GI regional workshops this fall. These workshops provided women across the country with opportunities to develop their personal and professional networks, participate in leadership development seminars, receive career mentoring, and engage in various wellness practices.
Following the conclusion of the regional workshops, we hosted the AGA Women’s Leadership Collaboration Conference at the AGA national office in Bethesda, Md.
I can’t stop talking about this weekend! What a profound experience! I continue to be inspired by this group of women, our mission, and the far-reaching impact of this collaboration. Each one of us was absolutely transformed this weekend. And the radius of that impact is immeasurable! – Dr. Bahar Adeli, TJUH–Albert Einstein Medical Center
During the two-day conference, 22 delegates discussed workplace experiences, reported on their region’s workshop, and participated in strategy development exercises to further gender equity in GI, which included identifying tactics and ideas for action.
This unique event brought together delegates from each regional workshop, including 2023 Dr. Maria Leo-Lieber scholarship winners Alyssa Parian and Alexandra Livanos, who attended the Northeast workshop. It was a great time of collaboration and connection with the AGA #WomenInGI community!
Thank you to everyone who participated and made the events a success. We look forward to uplifting all women in GI and identifying ways to support the community in the coming year.
AGA thanks Johnson & Johnson Health Care Systems, Inc. for their support of this program.
Help move innovation forward at the 2023 AGA Tech Summit
Innovative technologies for endoscopy, advanced imaging, and bariatric care are a few of the topics that will headline the 2023 AGA Tech Summit, March 9-10, 2023, at the Grand Hyatt San Francisco. Registration is now open. Visit techsummit.gastro.org to secure your spot.
The Tech Summit is where GI innovators, clinicians, medical device companies, venture capitalists and regulatory agencies meet to foster the development and adoption of GI technologies. It is the perfect venue for:
- All innovators, entrepreneurs and clinicians who want to build their professional networks in the GI space.
- Early-stage GI companies who want to showcase their technologies and find new ideas for further innovations that will improve patient care.
- GI fellows who want an exclusive and immersive behind-the-scenes look into the MedTech world.
Learn more by visiting techsummit.gastro.org.
Is there hope in the fight against aging?
For many years, it has been believed that the aging process is inevitable and that age-related diseases cannot be prevented or reversed. For example, the U.S. Food and Drug Administration does not recognize aging as an indication for drug approval because there are no markers to determine whether possible treatments have a significant impact on the hallmarks of aging.
The field of geroscience aims to find ways to change this by delaying the onset of age-related diseases or by extending the life span. Those mechanisms contribute to the vulnerability of older adults. The presentations focused on identifying biomarkers of aging and on the search for interventions to prevent and treat age-related diseases.
Perspectives from this meeting were published in a report.
An abridged glossary
- Senescent cells: These are old cells with irreversibly damaged DNA; they strongly resist apoptosis. Thus, they are not eliminated and continue to secrete pathogenic proinflammatory molecules.
- Senolytics: This is a class of compounds that promote the removal of senescent cells from the body.
- Autophagy: This is a process that promotes protein degradation, which is attenuated with aging and that impedes the aggregation of proteins harmful to cell function, particularly those of the central nervous system.
- Proteostasis: This is the dynamic regulation of protein homeostasis.
- Epigenetics: This is the field of biology that studies phenotype changes that are not caused by changes in DNA sequencing and that continue to affect cellular division.
- Metabolome: This refers to small molecules that make up the building blocks of all organismal features, from cell membranes to metabolic cycles to genes and proteins.
- Translational research: This involves applying primary research results to clinical research and vice versa.
Possible research topics
Senescence not only occurs with age but also drives aging. At the meeting, evidence was provided that senescent cells may exacerbate the clinical course of older adults in cases of infections (for example, COVID-19) as they lead to cytokine storms.
Experiments on old mice that have undergone genetic modification of senescent cells or the administration of “senolytic cocktails” composed of dasatinib plus quercetin protected the animals from the effects of viral infections. This finding corroborates the idea that factors involved in biological aging increase vulnerability and could be modified through treatment.
Alzheimer’s disease is an example of the effects of cellular senescence. Senescent cells develop a senescence-associated secretory phenotype that can be toxic to neighboring healthy cells and can allow senescence to propagate within tissues. This effect makes Alzheimer’s disease an essential focal point when studying the use of senolytics. In addition, agents that stimulate autophagy may be of interest for treating degenerative diseases.
Assessing therapeutic effects
It may be possible to assess the therapeutic effects of drug candidates using the following biomarkers.
- Growth hormone and type 1 insulin-like growth factor (IGF-1): Older adults are often prescribed growth hormone. However, recent data suggest that doing so is not advantageous to this patient population, because it antagonizes proteostasis and other cell maintenance mechanisms in older age. Experimental studies and studies conducted on centenarians suggest that low growth hormone and IGF-1 levels contribute to longevity and may be therapeutic biomarkers.
- Epigenetics: DNA methylation is a method that offers an “epigenetic clock” to compare biological age with chronologic age. Higher epigenetic age was associated with increased mortality risk, breast cancer, and nonalcoholic fatty liver disease. Therefore, it could also be a therapeutic biomarker.
- Metabolomics: Studying metabolomes facilitates the identification of the link between genetic polymorphisms and longevity, as most polymorphisms explain less than 0.5% of longevity variations.
- New translational strategy: It is common practice to treat each age-related disease individually. An alternative strategy would be to target the hallmarks of biological aging to prevent these diseases from developing. The rate of biological aging correlates with the speed of damage accumulation at the macromolecular, organelle, and cellular levels. It also affects the capacity of the body to repair this damage. The assessment of biomarkers would make possibile research into the effects of short- and long-term treatments that minimize damage and enhance resilience related to diseases common with aging.
New translational research
The report highlights two translational research models: the in-depth study of centenarians and the analysis of how immune aging makes older adults vulnerable to COVID-19. The impact of impaired immunity on aging became particularly evident during the pandemic. However, to home in on immunity as a therapeutic target and to better understand immune resilience, the specific nature of immune and biological deficits still need to be defined.
Metformin is among the therapeutic agents under investigation in cutting-edge clinical research. Its effect on aging will be studied in the Targeting Aging with Metformin (TAME) clinical trial. This trial is the first to study aging outcomes. The goal is to create a regulatory framework that future therapies can follow to achieve FDA approval.
There are three promising therapeutic platforms among the cutting-edge research studies. The first aims to produce adenosine triphosphate, levels of which decline dramatically with aging. The second aims to promote autophagy to remove cellular waste to treat neurodegenerative diseases. The third reprograms the epigenome to a younger state.
Research on mitochondrial dysfunction is relevant because it is highly involved in age-related diseases. Mitochondrial-derived peptides could potentially serve as biomarkers of mitochondrial function in aging studies and become promising therapeutic targets in age-related diseases. One of these peptides, humanin, has been demonstrated to exert protective effects on the heart, brain, and liver. Researchers observed that mitochondrial proteins are age-dependent and are suppressed by growth hormone and IGF-1. They also found that humanin levels are correlated with endothelial function. Data from animal studies have shown that sustained humanin levels are positively linked to longevity; these findings are mirrored in data from centenarians and their offspring, who have higher levels of humanin.
The formation of a Translational Geroscience Network composed of several scientists from various institutions should accelerate the application of this understanding. Despite the ongoing investigational and clinical studies, senolytics should not be regarded as extending life span or treating certain conditions, because their full safety profiles have not yet been elucidated.
Conclusion
Geroscience faces challenges in dealing with age-related problems. It is hoped that these challenges will be overcome through investigational and clinical studies on the mechanisms involved in aging. In-depth study of the interactions of underlying mechanisms of aging are needed to answer the following questions:
- Is there a hierarchical relationship among these mechanisms?
- Are there organ or cell-type differences in the interactions among these mechanisms?
- Is it possible to achieve a synergistic effect through combined interventions targeting several of the processes that drive aging?
It is complicated, but researchers are starting to see the light at the end of the tunnel.
This article was translated from the Medscape Portuguese edition and a version appeared on Medscape.com.
For many years, it has been believed that the aging process is inevitable and that age-related diseases cannot be prevented or reversed. For example, the U.S. Food and Drug Administration does not recognize aging as an indication for drug approval because there are no markers to determine whether possible treatments have a significant impact on the hallmarks of aging.
The field of geroscience aims to find ways to change this by delaying the onset of age-related diseases or by extending the life span. Those mechanisms contribute to the vulnerability of older adults. The presentations focused on identifying biomarkers of aging and on the search for interventions to prevent and treat age-related diseases.
Perspectives from this meeting were published in a report.
An abridged glossary
- Senescent cells: These are old cells with irreversibly damaged DNA; they strongly resist apoptosis. Thus, they are not eliminated and continue to secrete pathogenic proinflammatory molecules.
- Senolytics: This is a class of compounds that promote the removal of senescent cells from the body.
- Autophagy: This is a process that promotes protein degradation, which is attenuated with aging and that impedes the aggregation of proteins harmful to cell function, particularly those of the central nervous system.
- Proteostasis: This is the dynamic regulation of protein homeostasis.
- Epigenetics: This is the field of biology that studies phenotype changes that are not caused by changes in DNA sequencing and that continue to affect cellular division.
- Metabolome: This refers to small molecules that make up the building blocks of all organismal features, from cell membranes to metabolic cycles to genes and proteins.
- Translational research: This involves applying primary research results to clinical research and vice versa.
Possible research topics
Senescence not only occurs with age but also drives aging. At the meeting, evidence was provided that senescent cells may exacerbate the clinical course of older adults in cases of infections (for example, COVID-19) as they lead to cytokine storms.
Experiments on old mice that have undergone genetic modification of senescent cells or the administration of “senolytic cocktails” composed of dasatinib plus quercetin protected the animals from the effects of viral infections. This finding corroborates the idea that factors involved in biological aging increase vulnerability and could be modified through treatment.
Alzheimer’s disease is an example of the effects of cellular senescence. Senescent cells develop a senescence-associated secretory phenotype that can be toxic to neighboring healthy cells and can allow senescence to propagate within tissues. This effect makes Alzheimer’s disease an essential focal point when studying the use of senolytics. In addition, agents that stimulate autophagy may be of interest for treating degenerative diseases.
Assessing therapeutic effects
It may be possible to assess the therapeutic effects of drug candidates using the following biomarkers.
- Growth hormone and type 1 insulin-like growth factor (IGF-1): Older adults are often prescribed growth hormone. However, recent data suggest that doing so is not advantageous to this patient population, because it antagonizes proteostasis and other cell maintenance mechanisms in older age. Experimental studies and studies conducted on centenarians suggest that low growth hormone and IGF-1 levels contribute to longevity and may be therapeutic biomarkers.
- Epigenetics: DNA methylation is a method that offers an “epigenetic clock” to compare biological age with chronologic age. Higher epigenetic age was associated with increased mortality risk, breast cancer, and nonalcoholic fatty liver disease. Therefore, it could also be a therapeutic biomarker.
- Metabolomics: Studying metabolomes facilitates the identification of the link between genetic polymorphisms and longevity, as most polymorphisms explain less than 0.5% of longevity variations.
- New translational strategy: It is common practice to treat each age-related disease individually. An alternative strategy would be to target the hallmarks of biological aging to prevent these diseases from developing. The rate of biological aging correlates with the speed of damage accumulation at the macromolecular, organelle, and cellular levels. It also affects the capacity of the body to repair this damage. The assessment of biomarkers would make possibile research into the effects of short- and long-term treatments that minimize damage and enhance resilience related to diseases common with aging.
New translational research
The report highlights two translational research models: the in-depth study of centenarians and the analysis of how immune aging makes older adults vulnerable to COVID-19. The impact of impaired immunity on aging became particularly evident during the pandemic. However, to home in on immunity as a therapeutic target and to better understand immune resilience, the specific nature of immune and biological deficits still need to be defined.
Metformin is among the therapeutic agents under investigation in cutting-edge clinical research. Its effect on aging will be studied in the Targeting Aging with Metformin (TAME) clinical trial. This trial is the first to study aging outcomes. The goal is to create a regulatory framework that future therapies can follow to achieve FDA approval.
There are three promising therapeutic platforms among the cutting-edge research studies. The first aims to produce adenosine triphosphate, levels of which decline dramatically with aging. The second aims to promote autophagy to remove cellular waste to treat neurodegenerative diseases. The third reprograms the epigenome to a younger state.
Research on mitochondrial dysfunction is relevant because it is highly involved in age-related diseases. Mitochondrial-derived peptides could potentially serve as biomarkers of mitochondrial function in aging studies and become promising therapeutic targets in age-related diseases. One of these peptides, humanin, has been demonstrated to exert protective effects on the heart, brain, and liver. Researchers observed that mitochondrial proteins are age-dependent and are suppressed by growth hormone and IGF-1. They also found that humanin levels are correlated with endothelial function. Data from animal studies have shown that sustained humanin levels are positively linked to longevity; these findings are mirrored in data from centenarians and their offspring, who have higher levels of humanin.
The formation of a Translational Geroscience Network composed of several scientists from various institutions should accelerate the application of this understanding. Despite the ongoing investigational and clinical studies, senolytics should not be regarded as extending life span or treating certain conditions, because their full safety profiles have not yet been elucidated.
Conclusion
Geroscience faces challenges in dealing with age-related problems. It is hoped that these challenges will be overcome through investigational and clinical studies on the mechanisms involved in aging. In-depth study of the interactions of underlying mechanisms of aging are needed to answer the following questions:
- Is there a hierarchical relationship among these mechanisms?
- Are there organ or cell-type differences in the interactions among these mechanisms?
- Is it possible to achieve a synergistic effect through combined interventions targeting several of the processes that drive aging?
It is complicated, but researchers are starting to see the light at the end of the tunnel.
This article was translated from the Medscape Portuguese edition and a version appeared on Medscape.com.
For many years, it has been believed that the aging process is inevitable and that age-related diseases cannot be prevented or reversed. For example, the U.S. Food and Drug Administration does not recognize aging as an indication for drug approval because there are no markers to determine whether possible treatments have a significant impact on the hallmarks of aging.
The field of geroscience aims to find ways to change this by delaying the onset of age-related diseases or by extending the life span. Those mechanisms contribute to the vulnerability of older adults. The presentations focused on identifying biomarkers of aging and on the search for interventions to prevent and treat age-related diseases.
Perspectives from this meeting were published in a report.
An abridged glossary
- Senescent cells: These are old cells with irreversibly damaged DNA; they strongly resist apoptosis. Thus, they are not eliminated and continue to secrete pathogenic proinflammatory molecules.
- Senolytics: This is a class of compounds that promote the removal of senescent cells from the body.
- Autophagy: This is a process that promotes protein degradation, which is attenuated with aging and that impedes the aggregation of proteins harmful to cell function, particularly those of the central nervous system.
- Proteostasis: This is the dynamic regulation of protein homeostasis.
- Epigenetics: This is the field of biology that studies phenotype changes that are not caused by changes in DNA sequencing and that continue to affect cellular division.
- Metabolome: This refers to small molecules that make up the building blocks of all organismal features, from cell membranes to metabolic cycles to genes and proteins.
- Translational research: This involves applying primary research results to clinical research and vice versa.
Possible research topics
Senescence not only occurs with age but also drives aging. At the meeting, evidence was provided that senescent cells may exacerbate the clinical course of older adults in cases of infections (for example, COVID-19) as they lead to cytokine storms.
Experiments on old mice that have undergone genetic modification of senescent cells or the administration of “senolytic cocktails” composed of dasatinib plus quercetin protected the animals from the effects of viral infections. This finding corroborates the idea that factors involved in biological aging increase vulnerability and could be modified through treatment.
Alzheimer’s disease is an example of the effects of cellular senescence. Senescent cells develop a senescence-associated secretory phenotype that can be toxic to neighboring healthy cells and can allow senescence to propagate within tissues. This effect makes Alzheimer’s disease an essential focal point when studying the use of senolytics. In addition, agents that stimulate autophagy may be of interest for treating degenerative diseases.
Assessing therapeutic effects
It may be possible to assess the therapeutic effects of drug candidates using the following biomarkers.
- Growth hormone and type 1 insulin-like growth factor (IGF-1): Older adults are often prescribed growth hormone. However, recent data suggest that doing so is not advantageous to this patient population, because it antagonizes proteostasis and other cell maintenance mechanisms in older age. Experimental studies and studies conducted on centenarians suggest that low growth hormone and IGF-1 levels contribute to longevity and may be therapeutic biomarkers.
- Epigenetics: DNA methylation is a method that offers an “epigenetic clock” to compare biological age with chronologic age. Higher epigenetic age was associated with increased mortality risk, breast cancer, and nonalcoholic fatty liver disease. Therefore, it could also be a therapeutic biomarker.
- Metabolomics: Studying metabolomes facilitates the identification of the link between genetic polymorphisms and longevity, as most polymorphisms explain less than 0.5% of longevity variations.
- New translational strategy: It is common practice to treat each age-related disease individually. An alternative strategy would be to target the hallmarks of biological aging to prevent these diseases from developing. The rate of biological aging correlates with the speed of damage accumulation at the macromolecular, organelle, and cellular levels. It also affects the capacity of the body to repair this damage. The assessment of biomarkers would make possibile research into the effects of short- and long-term treatments that minimize damage and enhance resilience related to diseases common with aging.
New translational research
The report highlights two translational research models: the in-depth study of centenarians and the analysis of how immune aging makes older adults vulnerable to COVID-19. The impact of impaired immunity on aging became particularly evident during the pandemic. However, to home in on immunity as a therapeutic target and to better understand immune resilience, the specific nature of immune and biological deficits still need to be defined.
Metformin is among the therapeutic agents under investigation in cutting-edge clinical research. Its effect on aging will be studied in the Targeting Aging with Metformin (TAME) clinical trial. This trial is the first to study aging outcomes. The goal is to create a regulatory framework that future therapies can follow to achieve FDA approval.
There are three promising therapeutic platforms among the cutting-edge research studies. The first aims to produce adenosine triphosphate, levels of which decline dramatically with aging. The second aims to promote autophagy to remove cellular waste to treat neurodegenerative diseases. The third reprograms the epigenome to a younger state.
Research on mitochondrial dysfunction is relevant because it is highly involved in age-related diseases. Mitochondrial-derived peptides could potentially serve as biomarkers of mitochondrial function in aging studies and become promising therapeutic targets in age-related diseases. One of these peptides, humanin, has been demonstrated to exert protective effects on the heart, brain, and liver. Researchers observed that mitochondrial proteins are age-dependent and are suppressed by growth hormone and IGF-1. They also found that humanin levels are correlated with endothelial function. Data from animal studies have shown that sustained humanin levels are positively linked to longevity; these findings are mirrored in data from centenarians and their offspring, who have higher levels of humanin.
The formation of a Translational Geroscience Network composed of several scientists from various institutions should accelerate the application of this understanding. Despite the ongoing investigational and clinical studies, senolytics should not be regarded as extending life span or treating certain conditions, because their full safety profiles have not yet been elucidated.
Conclusion
Geroscience faces challenges in dealing with age-related problems. It is hoped that these challenges will be overcome through investigational and clinical studies on the mechanisms involved in aging. In-depth study of the interactions of underlying mechanisms of aging are needed to answer the following questions:
- Is there a hierarchical relationship among these mechanisms?
- Are there organ or cell-type differences in the interactions among these mechanisms?
- Is it possible to achieve a synergistic effect through combined interventions targeting several of the processes that drive aging?
It is complicated, but researchers are starting to see the light at the end of the tunnel.
This article was translated from the Medscape Portuguese edition and a version appeared on Medscape.com.
What length antibiotic course for prostatitis?
PARIS – To date, studies of antibiotic course length for treating urinary tract infections in men have been patchy and retrospective.
Through recent randomized trials, guidelines can now be based on more solid data.
In sum, to maximize clinical and microbiologic success, a nonfebrile urinary tract infection is treated for 7 days, and a febrile urinary tract infection is treated for a minimum of 14 days.
At the 116th conference of the French urology association, Matthieu Lafaurie, MD, of the Multidisciplinary Infectious Diseases Unit U21, Saint Louis Hospital, Paris, reviewed the literature on this subject.
Guidelines for men
The European Association of Urology made its position clear in a text updated in 2022. It stated: Therefore, treatment with antimicrobial drugs that penetrate the prostate tissue is needed in men presenting with symptoms of a urinary tract infection.” In its classification of prostatitis, the National Institutes of Health distinguishes between acute prostatitis (symptoms of a urinary tract infection; stage I) and chronic prostatitis (recurrent infection with the same microorganism; stage II).
Although the French-language Society of Infectious Diseases distinguishes between febrile and nonfebrile urinary tract infections in males, the academic body does not take into account whether the patient has a fever when determining which antibiotic should be given and how long the course should be: A minimum of 14 days’ treatment is recommended when opting for fluoroquinolones, trimethoprim-sulfamethoxazole (cotrimoxazole), or injectable beta-lactam antibiotics, and at least 21 days is recommended for other drugs or in cases in which there is an underlying urologic condition that has not been treated.
Yet the EAU recommends treating cystitis with antibiotics for at least 7 days, preferably with cotrimoxazole or fluoroquinolone, depending on the results of sensitivity testing. For acute prostatitis, the length of treatment with fluoroquinolones should be at least 14 days.
Nonfebrile infections
Participation of men in studies of the treatment of complicated cystitis is variable; at most only 10% of patients in such trials are men. There are few data specific to men with nonfebrile urinary tract infections, and most studies are retrospective and involve small cohorts. One of these is a community-based study that involved 422 men aged 18-104 years who presented with nonfebrile urinary tract infection (acute dysuria, frequency of urination and/or urgency of urination, temperature < 38° C, no general symptoms). Antibiotic treatment was prescribed in 60% of cases. In more than 55% of cases, the length of the course of treatment was 1–7 days. Treatment was with cotrimoxazole, quinolones, and nitrofurantoin.
Another observational retrospective study showed benefit with nitrofurantoin (50 mg/8 h in 94% of cases; 69 patients) and pivmecillinam (200 mg/8 h in 65% of cases; 200 mg/12 h in 30% of patients; 57 patients) in treating lower urinary tract infections in men. The median treatment duration was 7 days. The failure rate was 1.4% and 12%, respectively, for these treatments. Compared to the so-called gold-standard treatment, trimethoprim (10 days/800 mg/12 h; 45 patients), the recurrence rate was 11% and 26% for nitrofurantoin and pivmecillinam versus 7% for trimethoprim. The most significant relapse rate with pivmecillinam was when treatment was given for fewer than 7 days.
This is the only risk factor for further antibiotic treatment and/or recurrence. There was no significant difference between the three drugs with regard to other parameters (urinary tract infection symptoms, benign prostatic hypertrophy, prostate cancer, gram-positive bacteria, etc).
Another retrospective, European study of nitrofurantoin that was published in 2015 included 485 patients (100 mg twice daily in 71% of cases). Clinical cure was defined as an absence of signs or symptoms of a urinary tract infection for 14 days after stopping nitrofurantoin, without use of other antibiotics. The cure rate was 77%. Better efficacy was achieved for patients with gram-negative (vs. gram-positive) bacteria. The treatment duration did not differ significantly (clinical success was achieved when the treatment was taken for 8.6 ± 3.6 days; clinical failure occurred when the treatment was taken for 9.3 ± 6.9 days; P = .28).
Regarding pivmecillinam, a retrospective 2010-2016 study involved 21,864 adults and included 2,524 men who had been treated empirically with pivmecillinam (400 mg three times daily) for significant bacteriuria (Escherichia coli) and a lower urinary tract infection. The researchers concluded that for men, the success rate was identical whether the treatment lasted 5 or 7 days.
An American community-based (urologists, primary care physicians, general medicine services) retrospective cohort study involving 573 men with nonfebrile lower urinary tract infections was conducted from 2011 to 2015. The patients received antibiotic treatment with fluoroquinolones (69.7%), cotrimoxazole (21.2%), nitrofurantoin (5.3%), trimethoprim, beta-lactam antibiotics, or aminoglycosides. No clinical advantage was seen in treating men with urinary tract infections for longer than 7 days.
There are some data on the use of fosfomycin. In an observational retrospective study, 25 men of 52 male adults with leukocyturia and E. coli greater than 105, ESBL, were treated with fosfomycin trometamol 3 g on days 1, 3, 5. Clinical and microbiologic success was achieved for 94% and 78.5%, respectively. No distinction was made between the sexes.
These results were confirmed in a retrospective, observational study involving 18 men (of a total of 75 adults) with no fever or hyperleukocytosis who received the same fosfomycin trometamol regimen. The rate of clinical cure or sterile urine microscopy and culture was 69% at 13 days. The risk failure factor was, as expected, infection with Klebsiella pneumoniae, which was slightly susceptible to fosfomycin, unlike E. coli.
The most recent study in this field was published in 2021. It was also the first randomized, double-blind, placebo-controlled study. In all, 272 men older than 18 years were prescribed either ciprofloxacin or cotrimoxazole for 7-14 days to treat a nonfebrile urinary tract infection. To be eligible for the trial, patients were required to have disease of new onset with at least one of the following symptoms: dysuria, frequency of urination, urgency of urination, hematuria, costovertebral angle tenderness, or perineal, flank, or suprapubic pain. Urine microscopy and culture were not necessary; the approach was wholly symptomatic. Treatment was prescribed for 7 days. Patients were randomly allocated on day 8 to receive treatment for the following 7 days (molecule or placebo). The primary outcome was resolution of clinical symptoms of urinary tract infection by 14 days after completion of active antibiotic treatment. In an intention-to-treat or per-protocol analysis, the difference in efficacy between the two molecules was largely below the required 10%. The treatment duration noninferiority margin was 7 days, compared with 14 days.
“In 2022, with regard to the duration of treatment of nonfebrile urinary tract infections in men, the not completely irrefutable evidence does, however, stack up in favor of the possibility of a 7-day or even 5-day course,” pointed out Dr. Lafaurie. “Fluoroquinolones [such as] ofloxacin, levofloxacin, ciprofloxacin, as well as cotrimoxazole and other antibiotics, such as pivmecillinam, nitrofurantoin, or fosfomycin trometamol, can be used, despite the fact that they pass less easily into the prostate – a not-so-obvious benefit.”
Febrile infections
In terms of febrile urinary tract infections, a single-center, prospective, open-label study from 2003 involved 72 male inpatients who were randomly to receive treatment either for 2 weeks or 4 weeks. Treatment consisted of ciprofloxacin 500 mg twice daily. This study provided most of the evidence to justify the recommended 14-day antibiotic course.
Another noninferiority, randomized, placebo-controlled study published in 2017 compared 7- and 14-day treatment with ciprofloxacin 500 mg to placebo twice per week. In men, 7 days of antibiotic therapy was inferior to 14 days during a short-term follow-up but was not inferior during a longer follow-up.
A decisive study, which is currently in the submission phase, could silence debate. “In our noninferiority, multicenter, randomized, double-blind, placebo-controlled study, we have enrolled 240 men over the age of 18 years with a febrile infection documented by a fever of 38° C or more, clinical signs of infection, and leukocyturia at least above 10/mm3 and with symptoms lasting less than 3 months,” said Dr. Lafaurie, the trial coordinator.
The primary outcome for efficacy was microbiologic and clinical success after 6 weeks. Patients received either ofloxacin, ceftriaxone, or cefotaxime (two third-generation cephalosporins in the beta-lactam family).
“We clearly show that, for a 7-day course, the clinical success rate is 55.7%, and for a 14-day course, this goes up to 77.6%, with no difference in terms of adverse effects or selection of resistant bacteria. The predictive factors for success are a 14-day treatment and being under the age of 50 years,” said Dr. Lafaurie.
“Unlike nonfebrile urinary tract infections in men, a 7-day course is insufficient for patients with febrile urinary tract infections, and a minimum of 14 days is required to achieve clinical and microbiological success,” he concluded.
This article was translated from the Medscape French edition. A version appeared on Medscape.com.
PARIS – To date, studies of antibiotic course length for treating urinary tract infections in men have been patchy and retrospective.
Through recent randomized trials, guidelines can now be based on more solid data.
In sum, to maximize clinical and microbiologic success, a nonfebrile urinary tract infection is treated for 7 days, and a febrile urinary tract infection is treated for a minimum of 14 days.
At the 116th conference of the French urology association, Matthieu Lafaurie, MD, of the Multidisciplinary Infectious Diseases Unit U21, Saint Louis Hospital, Paris, reviewed the literature on this subject.
Guidelines for men
The European Association of Urology made its position clear in a text updated in 2022. It stated: Therefore, treatment with antimicrobial drugs that penetrate the prostate tissue is needed in men presenting with symptoms of a urinary tract infection.” In its classification of prostatitis, the National Institutes of Health distinguishes between acute prostatitis (symptoms of a urinary tract infection; stage I) and chronic prostatitis (recurrent infection with the same microorganism; stage II).
Although the French-language Society of Infectious Diseases distinguishes between febrile and nonfebrile urinary tract infections in males, the academic body does not take into account whether the patient has a fever when determining which antibiotic should be given and how long the course should be: A minimum of 14 days’ treatment is recommended when opting for fluoroquinolones, trimethoprim-sulfamethoxazole (cotrimoxazole), or injectable beta-lactam antibiotics, and at least 21 days is recommended for other drugs or in cases in which there is an underlying urologic condition that has not been treated.
Yet the EAU recommends treating cystitis with antibiotics for at least 7 days, preferably with cotrimoxazole or fluoroquinolone, depending on the results of sensitivity testing. For acute prostatitis, the length of treatment with fluoroquinolones should be at least 14 days.
Nonfebrile infections
Participation of men in studies of the treatment of complicated cystitis is variable; at most only 10% of patients in such trials are men. There are few data specific to men with nonfebrile urinary tract infections, and most studies are retrospective and involve small cohorts. One of these is a community-based study that involved 422 men aged 18-104 years who presented with nonfebrile urinary tract infection (acute dysuria, frequency of urination and/or urgency of urination, temperature < 38° C, no general symptoms). Antibiotic treatment was prescribed in 60% of cases. In more than 55% of cases, the length of the course of treatment was 1–7 days. Treatment was with cotrimoxazole, quinolones, and nitrofurantoin.
Another observational retrospective study showed benefit with nitrofurantoin (50 mg/8 h in 94% of cases; 69 patients) and pivmecillinam (200 mg/8 h in 65% of cases; 200 mg/12 h in 30% of patients; 57 patients) in treating lower urinary tract infections in men. The median treatment duration was 7 days. The failure rate was 1.4% and 12%, respectively, for these treatments. Compared to the so-called gold-standard treatment, trimethoprim (10 days/800 mg/12 h; 45 patients), the recurrence rate was 11% and 26% for nitrofurantoin and pivmecillinam versus 7% for trimethoprim. The most significant relapse rate with pivmecillinam was when treatment was given for fewer than 7 days.
This is the only risk factor for further antibiotic treatment and/or recurrence. There was no significant difference between the three drugs with regard to other parameters (urinary tract infection symptoms, benign prostatic hypertrophy, prostate cancer, gram-positive bacteria, etc).
Another retrospective, European study of nitrofurantoin that was published in 2015 included 485 patients (100 mg twice daily in 71% of cases). Clinical cure was defined as an absence of signs or symptoms of a urinary tract infection for 14 days after stopping nitrofurantoin, without use of other antibiotics. The cure rate was 77%. Better efficacy was achieved for patients with gram-negative (vs. gram-positive) bacteria. The treatment duration did not differ significantly (clinical success was achieved when the treatment was taken for 8.6 ± 3.6 days; clinical failure occurred when the treatment was taken for 9.3 ± 6.9 days; P = .28).
Regarding pivmecillinam, a retrospective 2010-2016 study involved 21,864 adults and included 2,524 men who had been treated empirically with pivmecillinam (400 mg three times daily) for significant bacteriuria (Escherichia coli) and a lower urinary tract infection. The researchers concluded that for men, the success rate was identical whether the treatment lasted 5 or 7 days.
An American community-based (urologists, primary care physicians, general medicine services) retrospective cohort study involving 573 men with nonfebrile lower urinary tract infections was conducted from 2011 to 2015. The patients received antibiotic treatment with fluoroquinolones (69.7%), cotrimoxazole (21.2%), nitrofurantoin (5.3%), trimethoprim, beta-lactam antibiotics, or aminoglycosides. No clinical advantage was seen in treating men with urinary tract infections for longer than 7 days.
There are some data on the use of fosfomycin. In an observational retrospective study, 25 men of 52 male adults with leukocyturia and E. coli greater than 105, ESBL, were treated with fosfomycin trometamol 3 g on days 1, 3, 5. Clinical and microbiologic success was achieved for 94% and 78.5%, respectively. No distinction was made between the sexes.
These results were confirmed in a retrospective, observational study involving 18 men (of a total of 75 adults) with no fever or hyperleukocytosis who received the same fosfomycin trometamol regimen. The rate of clinical cure or sterile urine microscopy and culture was 69% at 13 days. The risk failure factor was, as expected, infection with Klebsiella pneumoniae, which was slightly susceptible to fosfomycin, unlike E. coli.
The most recent study in this field was published in 2021. It was also the first randomized, double-blind, placebo-controlled study. In all, 272 men older than 18 years were prescribed either ciprofloxacin or cotrimoxazole for 7-14 days to treat a nonfebrile urinary tract infection. To be eligible for the trial, patients were required to have disease of new onset with at least one of the following symptoms: dysuria, frequency of urination, urgency of urination, hematuria, costovertebral angle tenderness, or perineal, flank, or suprapubic pain. Urine microscopy and culture were not necessary; the approach was wholly symptomatic. Treatment was prescribed for 7 days. Patients were randomly allocated on day 8 to receive treatment for the following 7 days (molecule or placebo). The primary outcome was resolution of clinical symptoms of urinary tract infection by 14 days after completion of active antibiotic treatment. In an intention-to-treat or per-protocol analysis, the difference in efficacy between the two molecules was largely below the required 10%. The treatment duration noninferiority margin was 7 days, compared with 14 days.
“In 2022, with regard to the duration of treatment of nonfebrile urinary tract infections in men, the not completely irrefutable evidence does, however, stack up in favor of the possibility of a 7-day or even 5-day course,” pointed out Dr. Lafaurie. “Fluoroquinolones [such as] ofloxacin, levofloxacin, ciprofloxacin, as well as cotrimoxazole and other antibiotics, such as pivmecillinam, nitrofurantoin, or fosfomycin trometamol, can be used, despite the fact that they pass less easily into the prostate – a not-so-obvious benefit.”
Febrile infections
In terms of febrile urinary tract infections, a single-center, prospective, open-label study from 2003 involved 72 male inpatients who were randomly to receive treatment either for 2 weeks or 4 weeks. Treatment consisted of ciprofloxacin 500 mg twice daily. This study provided most of the evidence to justify the recommended 14-day antibiotic course.
Another noninferiority, randomized, placebo-controlled study published in 2017 compared 7- and 14-day treatment with ciprofloxacin 500 mg to placebo twice per week. In men, 7 days of antibiotic therapy was inferior to 14 days during a short-term follow-up but was not inferior during a longer follow-up.
A decisive study, which is currently in the submission phase, could silence debate. “In our noninferiority, multicenter, randomized, double-blind, placebo-controlled study, we have enrolled 240 men over the age of 18 years with a febrile infection documented by a fever of 38° C or more, clinical signs of infection, and leukocyturia at least above 10/mm3 and with symptoms lasting less than 3 months,” said Dr. Lafaurie, the trial coordinator.
The primary outcome for efficacy was microbiologic and clinical success after 6 weeks. Patients received either ofloxacin, ceftriaxone, or cefotaxime (two third-generation cephalosporins in the beta-lactam family).
“We clearly show that, for a 7-day course, the clinical success rate is 55.7%, and for a 14-day course, this goes up to 77.6%, with no difference in terms of adverse effects or selection of resistant bacteria. The predictive factors for success are a 14-day treatment and being under the age of 50 years,” said Dr. Lafaurie.
“Unlike nonfebrile urinary tract infections in men, a 7-day course is insufficient for patients with febrile urinary tract infections, and a minimum of 14 days is required to achieve clinical and microbiological success,” he concluded.
This article was translated from the Medscape French edition. A version appeared on Medscape.com.
PARIS – To date, studies of antibiotic course length for treating urinary tract infections in men have been patchy and retrospective.
Through recent randomized trials, guidelines can now be based on more solid data.
In sum, to maximize clinical and microbiologic success, a nonfebrile urinary tract infection is treated for 7 days, and a febrile urinary tract infection is treated for a minimum of 14 days.
At the 116th conference of the French urology association, Matthieu Lafaurie, MD, of the Multidisciplinary Infectious Diseases Unit U21, Saint Louis Hospital, Paris, reviewed the literature on this subject.
Guidelines for men
The European Association of Urology made its position clear in a text updated in 2022. It stated: Therefore, treatment with antimicrobial drugs that penetrate the prostate tissue is needed in men presenting with symptoms of a urinary tract infection.” In its classification of prostatitis, the National Institutes of Health distinguishes between acute prostatitis (symptoms of a urinary tract infection; stage I) and chronic prostatitis (recurrent infection with the same microorganism; stage II).
Although the French-language Society of Infectious Diseases distinguishes between febrile and nonfebrile urinary tract infections in males, the academic body does not take into account whether the patient has a fever when determining which antibiotic should be given and how long the course should be: A minimum of 14 days’ treatment is recommended when opting for fluoroquinolones, trimethoprim-sulfamethoxazole (cotrimoxazole), or injectable beta-lactam antibiotics, and at least 21 days is recommended for other drugs or in cases in which there is an underlying urologic condition that has not been treated.
Yet the EAU recommends treating cystitis with antibiotics for at least 7 days, preferably with cotrimoxazole or fluoroquinolone, depending on the results of sensitivity testing. For acute prostatitis, the length of treatment with fluoroquinolones should be at least 14 days.
Nonfebrile infections
Participation of men in studies of the treatment of complicated cystitis is variable; at most only 10% of patients in such trials are men. There are few data specific to men with nonfebrile urinary tract infections, and most studies are retrospective and involve small cohorts. One of these is a community-based study that involved 422 men aged 18-104 years who presented with nonfebrile urinary tract infection (acute dysuria, frequency of urination and/or urgency of urination, temperature < 38° C, no general symptoms). Antibiotic treatment was prescribed in 60% of cases. In more than 55% of cases, the length of the course of treatment was 1–7 days. Treatment was with cotrimoxazole, quinolones, and nitrofurantoin.
Another observational retrospective study showed benefit with nitrofurantoin (50 mg/8 h in 94% of cases; 69 patients) and pivmecillinam (200 mg/8 h in 65% of cases; 200 mg/12 h in 30% of patients; 57 patients) in treating lower urinary tract infections in men. The median treatment duration was 7 days. The failure rate was 1.4% and 12%, respectively, for these treatments. Compared to the so-called gold-standard treatment, trimethoprim (10 days/800 mg/12 h; 45 patients), the recurrence rate was 11% and 26% for nitrofurantoin and pivmecillinam versus 7% for trimethoprim. The most significant relapse rate with pivmecillinam was when treatment was given for fewer than 7 days.
This is the only risk factor for further antibiotic treatment and/or recurrence. There was no significant difference between the three drugs with regard to other parameters (urinary tract infection symptoms, benign prostatic hypertrophy, prostate cancer, gram-positive bacteria, etc).
Another retrospective, European study of nitrofurantoin that was published in 2015 included 485 patients (100 mg twice daily in 71% of cases). Clinical cure was defined as an absence of signs or symptoms of a urinary tract infection for 14 days after stopping nitrofurantoin, without use of other antibiotics. The cure rate was 77%. Better efficacy was achieved for patients with gram-negative (vs. gram-positive) bacteria. The treatment duration did not differ significantly (clinical success was achieved when the treatment was taken for 8.6 ± 3.6 days; clinical failure occurred when the treatment was taken for 9.3 ± 6.9 days; P = .28).
Regarding pivmecillinam, a retrospective 2010-2016 study involved 21,864 adults and included 2,524 men who had been treated empirically with pivmecillinam (400 mg three times daily) for significant bacteriuria (Escherichia coli) and a lower urinary tract infection. The researchers concluded that for men, the success rate was identical whether the treatment lasted 5 or 7 days.
An American community-based (urologists, primary care physicians, general medicine services) retrospective cohort study involving 573 men with nonfebrile lower urinary tract infections was conducted from 2011 to 2015. The patients received antibiotic treatment with fluoroquinolones (69.7%), cotrimoxazole (21.2%), nitrofurantoin (5.3%), trimethoprim, beta-lactam antibiotics, or aminoglycosides. No clinical advantage was seen in treating men with urinary tract infections for longer than 7 days.
There are some data on the use of fosfomycin. In an observational retrospective study, 25 men of 52 male adults with leukocyturia and E. coli greater than 105, ESBL, were treated with fosfomycin trometamol 3 g on days 1, 3, 5. Clinical and microbiologic success was achieved for 94% and 78.5%, respectively. No distinction was made between the sexes.
These results were confirmed in a retrospective, observational study involving 18 men (of a total of 75 adults) with no fever or hyperleukocytosis who received the same fosfomycin trometamol regimen. The rate of clinical cure or sterile urine microscopy and culture was 69% at 13 days. The risk failure factor was, as expected, infection with Klebsiella pneumoniae, which was slightly susceptible to fosfomycin, unlike E. coli.
The most recent study in this field was published in 2021. It was also the first randomized, double-blind, placebo-controlled study. In all, 272 men older than 18 years were prescribed either ciprofloxacin or cotrimoxazole for 7-14 days to treat a nonfebrile urinary tract infection. To be eligible for the trial, patients were required to have disease of new onset with at least one of the following symptoms: dysuria, frequency of urination, urgency of urination, hematuria, costovertebral angle tenderness, or perineal, flank, or suprapubic pain. Urine microscopy and culture were not necessary; the approach was wholly symptomatic. Treatment was prescribed for 7 days. Patients were randomly allocated on day 8 to receive treatment for the following 7 days (molecule or placebo). The primary outcome was resolution of clinical symptoms of urinary tract infection by 14 days after completion of active antibiotic treatment. In an intention-to-treat or per-protocol analysis, the difference in efficacy between the two molecules was largely below the required 10%. The treatment duration noninferiority margin was 7 days, compared with 14 days.
“In 2022, with regard to the duration of treatment of nonfebrile urinary tract infections in men, the not completely irrefutable evidence does, however, stack up in favor of the possibility of a 7-day or even 5-day course,” pointed out Dr. Lafaurie. “Fluoroquinolones [such as] ofloxacin, levofloxacin, ciprofloxacin, as well as cotrimoxazole and other antibiotics, such as pivmecillinam, nitrofurantoin, or fosfomycin trometamol, can be used, despite the fact that they pass less easily into the prostate – a not-so-obvious benefit.”
Febrile infections
In terms of febrile urinary tract infections, a single-center, prospective, open-label study from 2003 involved 72 male inpatients who were randomly to receive treatment either for 2 weeks or 4 weeks. Treatment consisted of ciprofloxacin 500 mg twice daily. This study provided most of the evidence to justify the recommended 14-day antibiotic course.
Another noninferiority, randomized, placebo-controlled study published in 2017 compared 7- and 14-day treatment with ciprofloxacin 500 mg to placebo twice per week. In men, 7 days of antibiotic therapy was inferior to 14 days during a short-term follow-up but was not inferior during a longer follow-up.
A decisive study, which is currently in the submission phase, could silence debate. “In our noninferiority, multicenter, randomized, double-blind, placebo-controlled study, we have enrolled 240 men over the age of 18 years with a febrile infection documented by a fever of 38° C or more, clinical signs of infection, and leukocyturia at least above 10/mm3 and with symptoms lasting less than 3 months,” said Dr. Lafaurie, the trial coordinator.
The primary outcome for efficacy was microbiologic and clinical success after 6 weeks. Patients received either ofloxacin, ceftriaxone, or cefotaxime (two third-generation cephalosporins in the beta-lactam family).
“We clearly show that, for a 7-day course, the clinical success rate is 55.7%, and for a 14-day course, this goes up to 77.6%, with no difference in terms of adverse effects or selection of resistant bacteria. The predictive factors for success are a 14-day treatment and being under the age of 50 years,” said Dr. Lafaurie.
“Unlike nonfebrile urinary tract infections in men, a 7-day course is insufficient for patients with febrile urinary tract infections, and a minimum of 14 days is required to achieve clinical and microbiological success,” he concluded.
This article was translated from the Medscape French edition. A version appeared on Medscape.com.
New test that detects 14 cancers focuses on sugars, not DNA
The leader in this field is the Galleri test (from GRAIL) which is already in clinical use in some health care networks across the United States. That test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating tumor (or cell-free) DNA (cfDNA) in a blood sample.
The new test, under development by Swedish biotechnology company Elypta AB, has a different premise. It can detect 14 cancer types based on the analysis of glycosaminoglycans, which are a diverse group of polysaccharides that are altered by the presence of tumors. Using plasma and urine samples, the method had a 41.6%-62.3% sensitivity for detecting stage I cancer at 95% specificity.
In comparison, say the authors, other assays have reported 39%-73% sensitivity to stage I cancers, but these estimates are usually limited to 12 cancer types that are considered “high-signal,” and the assays perform poorly in cancers that emit little cfDNA, such as genitourinary and brain malignancies.
“The main advantage of glycosaminoglycans appears to be that they change in the blood and urine at the earliest stages of cancer,” said study author Francesco Gatto, PhD, founder and chief scientific officer at Elypta. “Consequently, this method showed an impressive detection rate in stage I compared to other emerging methods.”
The study was published online in Proceedings of the National Academy of Sciences.
Combine tests?
Dr. Gatto commented that he “could envision that one day we may be able to combine these methods.”
“The same blood specimen could be used to test both glycosaminoglycans and genomic biomarkers,” said Dr. Gatto. “This strategy could hopefully detect even more cancers than with either method alone, and the resulting performance may well be sufficient as a one-stop-shop screening program.”
So how does the new test from Elypta compare with the Galleri test?
“Galleri and similar methods mostly focused on information coming from molecules of DNA naturally floating in the blood,” explained Dr. Gatto. “It makes sense to conduct research there because cancers typically start with events in the DNA.”
He noted that the current study explored a new layer of information, molecules called glycosaminoglycans, that participate in the metabolism of cancer.
“This method detected many cancers that the previous methods missed, and a substantial proportion of these were at stage I,” said Dr. Gatto. “Cancer is a complex disease, so the most layers of information we can probe noninvasively, say with a blood test, the more likely we can catch more cancers at its earliest stage.”
Other platforms typically rely on sequencing and detecting cancer-derived fractions of cfDNA, but these methods have challenges that can interfere with their usage. For example, some cancer types do not shed sufficient cfDNA and it cannot be accurately measured.
“An advantage on focusing on glycosaminoglycans is that the method does not require next-generation sequencing or similarly complex assays because glycosaminoglycans are informative with less than 10 simultaneous measurements as opposed to Galleri that looks at over 1 million DNA methylation sites,” he said.
“This makes the assay behind the test much cheaper and robust – we estimated a 5-10 times lower cost difference,” Dr. Gatto said.
Prospective and comparative data needed
In a comment, Eric Klein, MD, emeritus chair of the Glickman Urological and Kidney Institute at the Cleveland Clinic explained that the “only accurate way to know how a test will perform in an intended-use population is to actually test it in that population. It’s not possible to extrapolate results directly from a case-control study.”
Cancers shed many different biologic markers into body fluids, but which of these signals will be best to serve as the basis of an MCED (multi-cancer detection test) that has clinical utility in a screening population has yet to be determined, he noted. “And it’s possible that no single test will be optimum for every clinical situation.”
“The results of this study appear promising, but it is not possible to claim superiority of one test over another based on individual case-control studies because of uncontrolled differences in the selected populations,” Dr. Klein continued. “The only scientifically accurate way to do this is to perform different tests on the same patient samples in a head-to-head comparison.”
There is only one study that he is aware of that has done this recently, in which multiple different assays looking at various signals in cell-free DNA were directly compared on the same samples (Cancer cell. 2022;40:1537-49.e12). “A targeted methylation assay that is the basis for Galleri was best for the lowest limit of detection and for predicting cancer site of origin,” said Dr. Klein.
Another expert agreed that a direct head-to-head study is needed to compare assays. “Based on this data, you cannot say that this method is better than the other one because that requires a comparative study,” said Fred Hirsch, MD, PhD, executive director of the Center for Thoracic Oncology, Tisch Cancer Institute at Mount Sinai, New York.
Metabolomics is interesting, and the data are encouraging, he continued. “But this is a multicancer early detection test and metabolism changes may vary from cancer type to cancer type. I’m not sure that the metabolism of lung cancer is the same as that of a gynecologic cancer.”
Dr. Hirsch also pointed out that there could also be confounding factors. “They have excluded inflammatory disease, but there can be other variables such as smoking,” he said. “Overall it gives some interesting perspectives but I would like to see more prospective validation and studies in specific disease groups, and eventually comparative studies with other methodologies.”
Study details
The authors evaluated if plasma and urine free GAGomes (free glycosaminoglycan profiles) deviated from baseline physiological levels in 14 cancer types and could serve as metabolic cancer biomarkers. They also then validated using free GAGomes for MCED in an external population with 2,064 samples obtained from 1,260 patients with cancer and healthy individuals.
In an in vivo cancer progression model, they observed widespread cancer-specific changes in biofluidic free GAGomes and then developed three machine-learning models based on urine (nurine = 220 cancer vs. 360 healthy) and plasma (nplasma = 517 cancer vs. 425 healthy) free GAGomes that were able to detect any cancer with an area under the receiver operating characteristic curve of 0.83-0.93 (with up to 62% sensitivity to stage I disease at 95% specificity).
To assess if altered GAGome features associated with cancer suggested more aggressive tumor biology, they correlated each score with overall survival. The median follow-up time was 17 months in the plasma cohort (n = 370 across 13 cancer types), 15 months in the urine cohort (n = 162 across 4 cancer types), and 15 months in the combined cohort (n = 152 across 4 cancer types).
They found that all three scores independently predicted overall survival in a multivariable analysis (hazard ratio, 1.29; P = .0009 for plasma; HR, 1.79; P = .0009 for urine; HR, 1.91; P = .0004 for combined) after adjusting for cancer type, age, sex, and stage IV or high-grade disease.
These findings showed an association of free GAGome alterations with aggressive cancer phenotypes and suggested that scores below the 95% specificity cutoff might have a better prognosis, the authors comment.
In addition, other analyses showed that free GAGomes predicted the putative cancer location with 89% accuracy. And finally, to confirm whether the free GAGome MCED scores could be used for screening, a validation analysis was conducted using a typical “screening population,” which requires at least 99% specificity. The combined free GAGomes were able to predict a poor prognosis of any cancer type within 18 months and with 43% sensitivity (21% in stage I; n = 121 and 49 cases).
Dr. Gatto believes that these results, as well as those from other studies looking at glycosaminoglycans as cancer biomarkers, will lead to the next steps of development. “But I speculate that this test could be most useful to assess in a cheap, practical, and noninvasive manner if a person at increased risk of cancer should be selected for cancer screening as part of established or emerging screening programs.”
The study was sponsored by Elypta. Dr. Gatto is listed as an inventor in patent applications related to the biomarkers described in this study and later assigned to Elypta, and is a shareholder and employed at Elypta. Dr. Hirsch reports no relevant financial relationships. Dr. Klein is a consultant for GRAIL and an investigator for CCGA and Pathfinder.
A version of this article first appeared on Medscape.com.
The leader in this field is the Galleri test (from GRAIL) which is already in clinical use in some health care networks across the United States. That test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating tumor (or cell-free) DNA (cfDNA) in a blood sample.
The new test, under development by Swedish biotechnology company Elypta AB, has a different premise. It can detect 14 cancer types based on the analysis of glycosaminoglycans, which are a diverse group of polysaccharides that are altered by the presence of tumors. Using plasma and urine samples, the method had a 41.6%-62.3% sensitivity for detecting stage I cancer at 95% specificity.
In comparison, say the authors, other assays have reported 39%-73% sensitivity to stage I cancers, but these estimates are usually limited to 12 cancer types that are considered “high-signal,” and the assays perform poorly in cancers that emit little cfDNA, such as genitourinary and brain malignancies.
“The main advantage of glycosaminoglycans appears to be that they change in the blood and urine at the earliest stages of cancer,” said study author Francesco Gatto, PhD, founder and chief scientific officer at Elypta. “Consequently, this method showed an impressive detection rate in stage I compared to other emerging methods.”
The study was published online in Proceedings of the National Academy of Sciences.
Combine tests?
Dr. Gatto commented that he “could envision that one day we may be able to combine these methods.”
“The same blood specimen could be used to test both glycosaminoglycans and genomic biomarkers,” said Dr. Gatto. “This strategy could hopefully detect even more cancers than with either method alone, and the resulting performance may well be sufficient as a one-stop-shop screening program.”
So how does the new test from Elypta compare with the Galleri test?
“Galleri and similar methods mostly focused on information coming from molecules of DNA naturally floating in the blood,” explained Dr. Gatto. “It makes sense to conduct research there because cancers typically start with events in the DNA.”
He noted that the current study explored a new layer of information, molecules called glycosaminoglycans, that participate in the metabolism of cancer.
“This method detected many cancers that the previous methods missed, and a substantial proportion of these were at stage I,” said Dr. Gatto. “Cancer is a complex disease, so the most layers of information we can probe noninvasively, say with a blood test, the more likely we can catch more cancers at its earliest stage.”
Other platforms typically rely on sequencing and detecting cancer-derived fractions of cfDNA, but these methods have challenges that can interfere with their usage. For example, some cancer types do not shed sufficient cfDNA and it cannot be accurately measured.
“An advantage on focusing on glycosaminoglycans is that the method does not require next-generation sequencing or similarly complex assays because glycosaminoglycans are informative with less than 10 simultaneous measurements as opposed to Galleri that looks at over 1 million DNA methylation sites,” he said.
“This makes the assay behind the test much cheaper and robust – we estimated a 5-10 times lower cost difference,” Dr. Gatto said.
Prospective and comparative data needed
In a comment, Eric Klein, MD, emeritus chair of the Glickman Urological and Kidney Institute at the Cleveland Clinic explained that the “only accurate way to know how a test will perform in an intended-use population is to actually test it in that population. It’s not possible to extrapolate results directly from a case-control study.”
Cancers shed many different biologic markers into body fluids, but which of these signals will be best to serve as the basis of an MCED (multi-cancer detection test) that has clinical utility in a screening population has yet to be determined, he noted. “And it’s possible that no single test will be optimum for every clinical situation.”
“The results of this study appear promising, but it is not possible to claim superiority of one test over another based on individual case-control studies because of uncontrolled differences in the selected populations,” Dr. Klein continued. “The only scientifically accurate way to do this is to perform different tests on the same patient samples in a head-to-head comparison.”
There is only one study that he is aware of that has done this recently, in which multiple different assays looking at various signals in cell-free DNA were directly compared on the same samples (Cancer cell. 2022;40:1537-49.e12). “A targeted methylation assay that is the basis for Galleri was best for the lowest limit of detection and for predicting cancer site of origin,” said Dr. Klein.
Another expert agreed that a direct head-to-head study is needed to compare assays. “Based on this data, you cannot say that this method is better than the other one because that requires a comparative study,” said Fred Hirsch, MD, PhD, executive director of the Center for Thoracic Oncology, Tisch Cancer Institute at Mount Sinai, New York.
Metabolomics is interesting, and the data are encouraging, he continued. “But this is a multicancer early detection test and metabolism changes may vary from cancer type to cancer type. I’m not sure that the metabolism of lung cancer is the same as that of a gynecologic cancer.”
Dr. Hirsch also pointed out that there could also be confounding factors. “They have excluded inflammatory disease, but there can be other variables such as smoking,” he said. “Overall it gives some interesting perspectives but I would like to see more prospective validation and studies in specific disease groups, and eventually comparative studies with other methodologies.”
Study details
The authors evaluated if plasma and urine free GAGomes (free glycosaminoglycan profiles) deviated from baseline physiological levels in 14 cancer types and could serve as metabolic cancer biomarkers. They also then validated using free GAGomes for MCED in an external population with 2,064 samples obtained from 1,260 patients with cancer and healthy individuals.
In an in vivo cancer progression model, they observed widespread cancer-specific changes in biofluidic free GAGomes and then developed three machine-learning models based on urine (nurine = 220 cancer vs. 360 healthy) and plasma (nplasma = 517 cancer vs. 425 healthy) free GAGomes that were able to detect any cancer with an area under the receiver operating characteristic curve of 0.83-0.93 (with up to 62% sensitivity to stage I disease at 95% specificity).
To assess if altered GAGome features associated with cancer suggested more aggressive tumor biology, they correlated each score with overall survival. The median follow-up time was 17 months in the plasma cohort (n = 370 across 13 cancer types), 15 months in the urine cohort (n = 162 across 4 cancer types), and 15 months in the combined cohort (n = 152 across 4 cancer types).
They found that all three scores independently predicted overall survival in a multivariable analysis (hazard ratio, 1.29; P = .0009 for plasma; HR, 1.79; P = .0009 for urine; HR, 1.91; P = .0004 for combined) after adjusting for cancer type, age, sex, and stage IV or high-grade disease.
These findings showed an association of free GAGome alterations with aggressive cancer phenotypes and suggested that scores below the 95% specificity cutoff might have a better prognosis, the authors comment.
In addition, other analyses showed that free GAGomes predicted the putative cancer location with 89% accuracy. And finally, to confirm whether the free GAGome MCED scores could be used for screening, a validation analysis was conducted using a typical “screening population,” which requires at least 99% specificity. The combined free GAGomes were able to predict a poor prognosis of any cancer type within 18 months and with 43% sensitivity (21% in stage I; n = 121 and 49 cases).
Dr. Gatto believes that these results, as well as those from other studies looking at glycosaminoglycans as cancer biomarkers, will lead to the next steps of development. “But I speculate that this test could be most useful to assess in a cheap, practical, and noninvasive manner if a person at increased risk of cancer should be selected for cancer screening as part of established or emerging screening programs.”
The study was sponsored by Elypta. Dr. Gatto is listed as an inventor in patent applications related to the biomarkers described in this study and later assigned to Elypta, and is a shareholder and employed at Elypta. Dr. Hirsch reports no relevant financial relationships. Dr. Klein is a consultant for GRAIL and an investigator for CCGA and Pathfinder.
A version of this article first appeared on Medscape.com.
The leader in this field is the Galleri test (from GRAIL) which is already in clinical use in some health care networks across the United States. That test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating tumor (or cell-free) DNA (cfDNA) in a blood sample.
The new test, under development by Swedish biotechnology company Elypta AB, has a different premise. It can detect 14 cancer types based on the analysis of glycosaminoglycans, which are a diverse group of polysaccharides that are altered by the presence of tumors. Using plasma and urine samples, the method had a 41.6%-62.3% sensitivity for detecting stage I cancer at 95% specificity.
In comparison, say the authors, other assays have reported 39%-73% sensitivity to stage I cancers, but these estimates are usually limited to 12 cancer types that are considered “high-signal,” and the assays perform poorly in cancers that emit little cfDNA, such as genitourinary and brain malignancies.
“The main advantage of glycosaminoglycans appears to be that they change in the blood and urine at the earliest stages of cancer,” said study author Francesco Gatto, PhD, founder and chief scientific officer at Elypta. “Consequently, this method showed an impressive detection rate in stage I compared to other emerging methods.”
The study was published online in Proceedings of the National Academy of Sciences.
Combine tests?
Dr. Gatto commented that he “could envision that one day we may be able to combine these methods.”
“The same blood specimen could be used to test both glycosaminoglycans and genomic biomarkers,” said Dr. Gatto. “This strategy could hopefully detect even more cancers than with either method alone, and the resulting performance may well be sufficient as a one-stop-shop screening program.”
So how does the new test from Elypta compare with the Galleri test?
“Galleri and similar methods mostly focused on information coming from molecules of DNA naturally floating in the blood,” explained Dr. Gatto. “It makes sense to conduct research there because cancers typically start with events in the DNA.”
He noted that the current study explored a new layer of information, molecules called glycosaminoglycans, that participate in the metabolism of cancer.
“This method detected many cancers that the previous methods missed, and a substantial proportion of these were at stage I,” said Dr. Gatto. “Cancer is a complex disease, so the most layers of information we can probe noninvasively, say with a blood test, the more likely we can catch more cancers at its earliest stage.”
Other platforms typically rely on sequencing and detecting cancer-derived fractions of cfDNA, but these methods have challenges that can interfere with their usage. For example, some cancer types do not shed sufficient cfDNA and it cannot be accurately measured.
“An advantage on focusing on glycosaminoglycans is that the method does not require next-generation sequencing or similarly complex assays because glycosaminoglycans are informative with less than 10 simultaneous measurements as opposed to Galleri that looks at over 1 million DNA methylation sites,” he said.
“This makes the assay behind the test much cheaper and robust – we estimated a 5-10 times lower cost difference,” Dr. Gatto said.
Prospective and comparative data needed
In a comment, Eric Klein, MD, emeritus chair of the Glickman Urological and Kidney Institute at the Cleveland Clinic explained that the “only accurate way to know how a test will perform in an intended-use population is to actually test it in that population. It’s not possible to extrapolate results directly from a case-control study.”
Cancers shed many different biologic markers into body fluids, but which of these signals will be best to serve as the basis of an MCED (multi-cancer detection test) that has clinical utility in a screening population has yet to be determined, he noted. “And it’s possible that no single test will be optimum for every clinical situation.”
“The results of this study appear promising, but it is not possible to claim superiority of one test over another based on individual case-control studies because of uncontrolled differences in the selected populations,” Dr. Klein continued. “The only scientifically accurate way to do this is to perform different tests on the same patient samples in a head-to-head comparison.”
There is only one study that he is aware of that has done this recently, in which multiple different assays looking at various signals in cell-free DNA were directly compared on the same samples (Cancer cell. 2022;40:1537-49.e12). “A targeted methylation assay that is the basis for Galleri was best for the lowest limit of detection and for predicting cancer site of origin,” said Dr. Klein.
Another expert agreed that a direct head-to-head study is needed to compare assays. “Based on this data, you cannot say that this method is better than the other one because that requires a comparative study,” said Fred Hirsch, MD, PhD, executive director of the Center for Thoracic Oncology, Tisch Cancer Institute at Mount Sinai, New York.
Metabolomics is interesting, and the data are encouraging, he continued. “But this is a multicancer early detection test and metabolism changes may vary from cancer type to cancer type. I’m not sure that the metabolism of lung cancer is the same as that of a gynecologic cancer.”
Dr. Hirsch also pointed out that there could also be confounding factors. “They have excluded inflammatory disease, but there can be other variables such as smoking,” he said. “Overall it gives some interesting perspectives but I would like to see more prospective validation and studies in specific disease groups, and eventually comparative studies with other methodologies.”
Study details
The authors evaluated if plasma and urine free GAGomes (free glycosaminoglycan profiles) deviated from baseline physiological levels in 14 cancer types and could serve as metabolic cancer biomarkers. They also then validated using free GAGomes for MCED in an external population with 2,064 samples obtained from 1,260 patients with cancer and healthy individuals.
In an in vivo cancer progression model, they observed widespread cancer-specific changes in biofluidic free GAGomes and then developed three machine-learning models based on urine (nurine = 220 cancer vs. 360 healthy) and plasma (nplasma = 517 cancer vs. 425 healthy) free GAGomes that were able to detect any cancer with an area under the receiver operating characteristic curve of 0.83-0.93 (with up to 62% sensitivity to stage I disease at 95% specificity).
To assess if altered GAGome features associated with cancer suggested more aggressive tumor biology, they correlated each score with overall survival. The median follow-up time was 17 months in the plasma cohort (n = 370 across 13 cancer types), 15 months in the urine cohort (n = 162 across 4 cancer types), and 15 months in the combined cohort (n = 152 across 4 cancer types).
They found that all three scores independently predicted overall survival in a multivariable analysis (hazard ratio, 1.29; P = .0009 for plasma; HR, 1.79; P = .0009 for urine; HR, 1.91; P = .0004 for combined) after adjusting for cancer type, age, sex, and stage IV or high-grade disease.
These findings showed an association of free GAGome alterations with aggressive cancer phenotypes and suggested that scores below the 95% specificity cutoff might have a better prognosis, the authors comment.
In addition, other analyses showed that free GAGomes predicted the putative cancer location with 89% accuracy. And finally, to confirm whether the free GAGome MCED scores could be used for screening, a validation analysis was conducted using a typical “screening population,” which requires at least 99% specificity. The combined free GAGomes were able to predict a poor prognosis of any cancer type within 18 months and with 43% sensitivity (21% in stage I; n = 121 and 49 cases).
Dr. Gatto believes that these results, as well as those from other studies looking at glycosaminoglycans as cancer biomarkers, will lead to the next steps of development. “But I speculate that this test could be most useful to assess in a cheap, practical, and noninvasive manner if a person at increased risk of cancer should be selected for cancer screening as part of established or emerging screening programs.”
The study was sponsored by Elypta. Dr. Gatto is listed as an inventor in patent applications related to the biomarkers described in this study and later assigned to Elypta, and is a shareholder and employed at Elypta. Dr. Hirsch reports no relevant financial relationships. Dr. Klein is a consultant for GRAIL and an investigator for CCGA and Pathfinder.
A version of this article first appeared on Medscape.com.
FROM PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCES
Overturning Roe: Exacerbating inequities in abortion care and ObGyn training
On a recent overnight shift, our ObGyn on-call team was urgently paged to the emergency room for a patient who was brought in hemorrhaging after having passed out mid-flight from Texas to Boston. She was 12-weeks pregnant. We rushed her to the operating room for surgical removal of the pregnancy by dilation and curettage to stop her bleeding. Landing in Massachusetts had saved her life.
The significance of this patient’s case was not lost on the multidisciplinary teams caring for her, as the—at the time—impending Roe v Wade decision weighed heavily on our minds. One of many, her story foreshadows the harrowing experiences that we anticipate in the coming months and highlights the danger that the Supreme Court has inflicted on pregnant people nationally.
The Supreme Court decision on Dobbs v Jackson condemns us as a nation in which abortion rights are no longer federally protected under Roe v Wade.1 Twenty-six states have been poised to ban abortion, and in at least 12 states, abortion is now illegal.2,3 Political decision making will soon deny pregnant people the right to bodily autonomy, and the United States will lag behind other nations in abortion access.4 As ObGyn resident physicians who practice in tertiary referral hospitals in Massachusetts, where the ROE Act protects abortion beyond 24 weeks’ gestational age, we affirm abortion as essential health care that saves lives.5
Collectively as physician residents, we have provided an abortion for the patient at 22 weeks with a desired pregnancy who would have otherwise died from high blood pressures, the patient who ended her pregnancy to expedite breast cancer treatment, and the 16-year-old who feared for her life after suffering an assault by her partner for disclosing her pregnancy. With the overturn of Roe v Wade, patients like these will suffer dramatically divergent fates as race, class, and, now more than ever, geography will impact who is able to access abortion care.
Ramifications of the overturn of Roe
History foreshadows the grim impact of repealing Roe. Ohio’s 2011 law that requires the use of the restrictive protocol approved by the US Food and Drug Administration for mifepristone administration deepened existing inequities in abortion access.6 Patients with private insurance, higher income, higher level of education, and those who were White were more likely to obtain abortion care.7 In Texas, after the implementation of SB8 and other restrictive laws, Hispanic women whose travel distance increased more than 100 miles had the greatest reduction in abortion rates.8,9 A recent study regarding banning abortion in the United States estimated a 7% increase in pregnancy-related deaths in 1 year, with a 21% increase in subsequent years.10
Inequities in abortion access subsequently will disparately increase deaths of pregnant individuals in certain populations.11,12 Communities with the highest rates of unintended pregnancy, medical comorbidities, and lack of access to abortion, as well as historically marginalized populations—including non-Hispanic Black people, LGBTQIA people, those with limited English proficiency, and undocumented persons—will experience the greatest increase in pregnancy-related deaths due to a total abortion ban.13-15
The US maternal mortality rate is already the highest among developed nations, and it will only climb if ObGyns are not appropriately trained to operate within our full scope of practice and, thus, are unable to provide the highest quality of care.16,17
Continue: Abortion is a medical treatment that requires resident training...
Abortion is a medical treatment that requires resident training
Abortion care must be protected. Uterine evacuation by medical management, suction curettage, or dilation and evacuation is indicated for undesired pregnancy, regardless of reasoning or life circumstance. Pregnancy carries inherent risks that can at times be deadly.18 Abortion serves as first-line treatment for certain life-threatening pregnancy risks, including septic miscarriage, maternal hemorrhage, early-onset severe preeclampsia, and certain health conditions.19 Surgical skills and medical management of abortion are therefore fundamental components of ObGyn care and residency training.20
In choosing to become ObGyns,and particularly in selecting our training program, the ability to provide safe abortion care was a calculated priority. A recent study on the implications of overturning Roe predicted that nearly half of ObGyn residents will likely or certainly lose access to in-state abortion training.21 As demonstrated already in states with restrictive abortion laws, we will lose an entire generation of medical professionals skilled in performing this lifesaving procedure.9,22 While privileged patients may travel across state borders to access care, ObGyn and other medical trainees who are contract bound to residency programs do not have such flexibility to seek out abortion training. Although we hope the reversal of Roe will be fleeting, the consequences of this lost generation are irreparable.23,24 For physicians like ourselves, who fortunately are trained in surgical abortions and safe management of medical terminations, the discrepancy between evidence-based guidelines and impending political restrictions is distressing. We are forced to imagine refusing patients necessary health care—or face incarceration to save their lives.
The idea of watching a patient die, whether by hemorrhage, sepsis, or suicide, while armed with the tools of safe abortion technique is horrific. As authors with roots in Texas, Michigan, and Georgia, where abortion has or will almost certainly become illegal now that Roe v Wade is overturned, this scene is personal. It affects our future patients, our families, our colleagues, and our ability to return to our home states to live and practice.
Political organizing is critical to protect and restore abortion rights and defend against conservative coercive politics.25 Nearly half of pregnancies in the United States are unintended, and more than half of these end in abortion.26,27 Threats to abortion access require action from every one of the 59% of Americans who believe abortion should remain legal.28 This is especially important from a social and racial justice perspective as abortion bans will disproportionately affect marginalized groups and further exacerbate inequities in maternal mortality.13
Call to action
Now is the time for community action for reproductive justice and human rights. We urge everyone to donate to abortion funds, vote for leaders who support reproductive justice, and petition your state legislators to codify Roe into law. Now is the time to expand legislation to protect abortion providers and our patients. To ObGyns, family medicine physicians, internists, and other reproductive health clinicians, now is the time to maximize your abortion training. Now is the time to act; otherwise, pregnant individuals will die and future generations of physicians will not have the training to save their lives. ●
- de Vogue A, Sneed T, Duster C, et al. Supreme Court overturns Roe v Wade. CNN Politics. June 24, 2022. Accessed July 19, 2022. https://www.cnn.com/2022/06/24/politics/dobbs-missis sippi-supreme-court-abortion-roe-wade/index.html
- Nash E, Cross L. 26 States are certain or likely to ban abortion without Roe: here’s which ones and why. Guttmacher Institute. October 28, 2021. Updated April 19, 2022. Accessed July 19, 2022. https://www.guttmacher.org/article/2021/10/26-states-are-certain-or-likely-ban-abortion-without-roe-heres-which-ones-and-why
- Messerly M. Abortion laws by state: where abortions are illegal after Roe v Wade overturned. Politico. June 24, 2022. Accessed July 19, 2022. https://www.politico.com/news/2022/06/24/abortion-laws-by-state-roe-v-wade-00037695
- Archie A. US would lag behind global abortion access if Roe v Wade is undone, advocates say. NPR. May 5, 2022. Accessed July 19, 2022. https://www.npr.org/2022/05/05/1096805490/abortion-access-supreme-court-roe-v-wade-united-nations
- Romo V. Massachusetts senate overrides veto, passes law expanding abortion access. NPR. December 29, 2020. Accessed July 19, 2022. https://www.npr.org/2020/12/29/951259506/massachusetts-senate-overrides-veto-passes-law-expanding-abortion-access
- Upadhyay UD, Johns NE, Combellick SL, et al. Comparison of outcomes before and after Ohio’s law mandating use of the FDA-approved protocol for medication abortion: a retrospective cohort study. PLoS Med. 2016;13:e1002110.
- Upadhyay UD, Johns NE, Cartwright AF, et al. Sociodemographic characteristics of women able to obtain medication abortion before and after Ohio’s law requiring use of the Food and Drug Administration protocol. Health Equity. 2018;2:122-130.
- Goyal V, Brooks IHM, Powers DA. Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law. Contraception. 2020;102:109-114.
- Noyes E Holder BH, Evans ML. Texas SB8 and the future of abortion care. OBG Manag. 2021;33. doi:12788/obgm.0151.
- Vilda D, Wallace ME, Daniel C, et al. State abortion policies and maternal death in the United States, 2015‒2018. Am J Public Health. 2021;111:1696-1704.
- The Lancet. Why Roe v Wade must be defended. Lancet. 2022;399:1845.
- Nambiar A, Patel S, Santiago-Munoz P, et al. Maternal morbidity and fetal outcomes among pregnant women at 22 weeks’ gestation or less with complications in two Texas hospitals after legislation on abortion. Am J Obstet Gynecol. 2022;227:648-650.e1.
- Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. 2021;58:20192028.
- Medley S. Gutting abortion rights would be devastating for LGBTQ+ people. Them. September 17, 2021. Accessed July 20, 2022. https://www.them.us/story/gutting-abortion-rights-devastating-lgbtq-people
- Holter L. Detained immigrant women are facing a grueling abortion struggle. National Latina Institute for Reproductive Justice. May 10, 2017. Accessed July 20, 2022. https://www.latinainsti tute.org/es/node/4620
- Haddad LB, Nour NM. Unsafe abortion: unnecessary maternal mortality. Rev Obstet Gynecol. 2009;2:122-126.
- Tikkanen R, Gunja MZ, FitzGerald M, et al. Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund. November 18, 2020. Accessed November 17, 2022. https://www .commonwealthfund.org/publications/issue -briefs/2020/nov/maternal-mortality-maternity -care-us-compared-10-countries
- Collier A-RY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561-e574.
- ACOG practice bulletin no. 135: Second-trimester abortion. Obstet Gynecol. 2013;121:1394-1406.
- Committee on Health Care for Underserved Women. ACOG Committee opinion no. 612: Abortion training and education. Obstet Gynecol. 2014;124:1055-1059.
- Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in US obstetrics and gynecology residency programs. Obstet Gynecol. 2022;140:146-149.
- Horvath S, Turk J, Steinauer J, et al. Increase in obstetrics and gynecology resident self-assessed competence in early pregnancy loss management with routine abortion care training. Obstet Gynecol. 2022;139:116-119.
- Anderson N. The fall of Roe scrambles abortion training in university hospitals. The Washington Post. June 30, 2022. Accessed July 20, 2022. https://www.washingtonpost.com/educa tion/2022/06/30/abortion-training-upheaval-dobbs/
- Weiner S. How the repeal of Roe v Wade will affect training in abortion and reproductive health. AAMC. June 24, 2022. Accessed July 20, 2022. https://www.aamc.org/news-insights/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health
- Dreweke J. Coercion is at the heart of social conservatives’ reproductive health agenda. Guttmacher Institute. February 7, 2018. Accessed July 20, 2022. https://www.guttmacher.org/gpr/2018/02/coercion-heart-social-conservatives-reproduc tive-health-agenda
- Unintended pregnancy and abortion worldwide. Guttmacher Institute. March 2022. Accessed July 20, 2022. https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide
- Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374:843-852.
- Hartig H. About six-in-ten Americans say abortion should be legal in all or most cases. Pew Research Center. June 13, 2022. Accessed July 20, 2022. https://www.pewresearch.org/fact-tank/2022/06/13/about-six-in-ten-americans-say-abortion-should-be-legal-in-all-or-most-cases-2/

Samantha Truong, MD
Dr. Truong is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, Massachusetts.

Emily R. Burdette, MD, MPH
Dr. Burdette is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.

Ellen C. Murphy, MD
Dr. Murphy is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
The authors report no financial relationships relevant to this article.
Samantha Truong, MD
Dr. Truong is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, Massachusetts.
Emily R. Burdette, MD, MPH
Dr. Burdette is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
Ellen C. Murphy, MD
Dr. Murphy is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
The authors report no financial relationships relevant to this article.
Samantha Truong, MD
Dr. Truong is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, Massachusetts.
Emily R. Burdette, MD, MPH
Dr. Burdette is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
Ellen C. Murphy, MD
Dr. Murphy is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
The authors report no financial relationships relevant to this article.
On a recent overnight shift, our ObGyn on-call team was urgently paged to the emergency room for a patient who was brought in hemorrhaging after having passed out mid-flight from Texas to Boston. She was 12-weeks pregnant. We rushed her to the operating room for surgical removal of the pregnancy by dilation and curettage to stop her bleeding. Landing in Massachusetts had saved her life.
The significance of this patient’s case was not lost on the multidisciplinary teams caring for her, as the—at the time—impending Roe v Wade decision weighed heavily on our minds. One of many, her story foreshadows the harrowing experiences that we anticipate in the coming months and highlights the danger that the Supreme Court has inflicted on pregnant people nationally.
The Supreme Court decision on Dobbs v Jackson condemns us as a nation in which abortion rights are no longer federally protected under Roe v Wade.1 Twenty-six states have been poised to ban abortion, and in at least 12 states, abortion is now illegal.2,3 Political decision making will soon deny pregnant people the right to bodily autonomy, and the United States will lag behind other nations in abortion access.4 As ObGyn resident physicians who practice in tertiary referral hospitals in Massachusetts, where the ROE Act protects abortion beyond 24 weeks’ gestational age, we affirm abortion as essential health care that saves lives.5
Collectively as physician residents, we have provided an abortion for the patient at 22 weeks with a desired pregnancy who would have otherwise died from high blood pressures, the patient who ended her pregnancy to expedite breast cancer treatment, and the 16-year-old who feared for her life after suffering an assault by her partner for disclosing her pregnancy. With the overturn of Roe v Wade, patients like these will suffer dramatically divergent fates as race, class, and, now more than ever, geography will impact who is able to access abortion care.
Ramifications of the overturn of Roe
History foreshadows the grim impact of repealing Roe. Ohio’s 2011 law that requires the use of the restrictive protocol approved by the US Food and Drug Administration for mifepristone administration deepened existing inequities in abortion access.6 Patients with private insurance, higher income, higher level of education, and those who were White were more likely to obtain abortion care.7 In Texas, after the implementation of SB8 and other restrictive laws, Hispanic women whose travel distance increased more than 100 miles had the greatest reduction in abortion rates.8,9 A recent study regarding banning abortion in the United States estimated a 7% increase in pregnancy-related deaths in 1 year, with a 21% increase in subsequent years.10
Inequities in abortion access subsequently will disparately increase deaths of pregnant individuals in certain populations.11,12 Communities with the highest rates of unintended pregnancy, medical comorbidities, and lack of access to abortion, as well as historically marginalized populations—including non-Hispanic Black people, LGBTQIA people, those with limited English proficiency, and undocumented persons—will experience the greatest increase in pregnancy-related deaths due to a total abortion ban.13-15
The US maternal mortality rate is already the highest among developed nations, and it will only climb if ObGyns are not appropriately trained to operate within our full scope of practice and, thus, are unable to provide the highest quality of care.16,17
Continue: Abortion is a medical treatment that requires resident training...
Abortion is a medical treatment that requires resident training
Abortion care must be protected. Uterine evacuation by medical management, suction curettage, or dilation and evacuation is indicated for undesired pregnancy, regardless of reasoning or life circumstance. Pregnancy carries inherent risks that can at times be deadly.18 Abortion serves as first-line treatment for certain life-threatening pregnancy risks, including septic miscarriage, maternal hemorrhage, early-onset severe preeclampsia, and certain health conditions.19 Surgical skills and medical management of abortion are therefore fundamental components of ObGyn care and residency training.20
In choosing to become ObGyns,and particularly in selecting our training program, the ability to provide safe abortion care was a calculated priority. A recent study on the implications of overturning Roe predicted that nearly half of ObGyn residents will likely or certainly lose access to in-state abortion training.21 As demonstrated already in states with restrictive abortion laws, we will lose an entire generation of medical professionals skilled in performing this lifesaving procedure.9,22 While privileged patients may travel across state borders to access care, ObGyn and other medical trainees who are contract bound to residency programs do not have such flexibility to seek out abortion training. Although we hope the reversal of Roe will be fleeting, the consequences of this lost generation are irreparable.23,24 For physicians like ourselves, who fortunately are trained in surgical abortions and safe management of medical terminations, the discrepancy between evidence-based guidelines and impending political restrictions is distressing. We are forced to imagine refusing patients necessary health care—or face incarceration to save their lives.
The idea of watching a patient die, whether by hemorrhage, sepsis, or suicide, while armed with the tools of safe abortion technique is horrific. As authors with roots in Texas, Michigan, and Georgia, where abortion has or will almost certainly become illegal now that Roe v Wade is overturned, this scene is personal. It affects our future patients, our families, our colleagues, and our ability to return to our home states to live and practice.
Political organizing is critical to protect and restore abortion rights and defend against conservative coercive politics.25 Nearly half of pregnancies in the United States are unintended, and more than half of these end in abortion.26,27 Threats to abortion access require action from every one of the 59% of Americans who believe abortion should remain legal.28 This is especially important from a social and racial justice perspective as abortion bans will disproportionately affect marginalized groups and further exacerbate inequities in maternal mortality.13
Call to action
Now is the time for community action for reproductive justice and human rights. We urge everyone to donate to abortion funds, vote for leaders who support reproductive justice, and petition your state legislators to codify Roe into law. Now is the time to expand legislation to protect abortion providers and our patients. To ObGyns, family medicine physicians, internists, and other reproductive health clinicians, now is the time to maximize your abortion training. Now is the time to act; otherwise, pregnant individuals will die and future generations of physicians will not have the training to save their lives. ●
On a recent overnight shift, our ObGyn on-call team was urgently paged to the emergency room for a patient who was brought in hemorrhaging after having passed out mid-flight from Texas to Boston. She was 12-weeks pregnant. We rushed her to the operating room for surgical removal of the pregnancy by dilation and curettage to stop her bleeding. Landing in Massachusetts had saved her life.
The significance of this patient’s case was not lost on the multidisciplinary teams caring for her, as the—at the time—impending Roe v Wade decision weighed heavily on our minds. One of many, her story foreshadows the harrowing experiences that we anticipate in the coming months and highlights the danger that the Supreme Court has inflicted on pregnant people nationally.
The Supreme Court decision on Dobbs v Jackson condemns us as a nation in which abortion rights are no longer federally protected under Roe v Wade.1 Twenty-six states have been poised to ban abortion, and in at least 12 states, abortion is now illegal.2,3 Political decision making will soon deny pregnant people the right to bodily autonomy, and the United States will lag behind other nations in abortion access.4 As ObGyn resident physicians who practice in tertiary referral hospitals in Massachusetts, where the ROE Act protects abortion beyond 24 weeks’ gestational age, we affirm abortion as essential health care that saves lives.5
Collectively as physician residents, we have provided an abortion for the patient at 22 weeks with a desired pregnancy who would have otherwise died from high blood pressures, the patient who ended her pregnancy to expedite breast cancer treatment, and the 16-year-old who feared for her life after suffering an assault by her partner for disclosing her pregnancy. With the overturn of Roe v Wade, patients like these will suffer dramatically divergent fates as race, class, and, now more than ever, geography will impact who is able to access abortion care.
Ramifications of the overturn of Roe
History foreshadows the grim impact of repealing Roe. Ohio’s 2011 law that requires the use of the restrictive protocol approved by the US Food and Drug Administration for mifepristone administration deepened existing inequities in abortion access.6 Patients with private insurance, higher income, higher level of education, and those who were White were more likely to obtain abortion care.7 In Texas, after the implementation of SB8 and other restrictive laws, Hispanic women whose travel distance increased more than 100 miles had the greatest reduction in abortion rates.8,9 A recent study regarding banning abortion in the United States estimated a 7% increase in pregnancy-related deaths in 1 year, with a 21% increase in subsequent years.10
Inequities in abortion access subsequently will disparately increase deaths of pregnant individuals in certain populations.11,12 Communities with the highest rates of unintended pregnancy, medical comorbidities, and lack of access to abortion, as well as historically marginalized populations—including non-Hispanic Black people, LGBTQIA people, those with limited English proficiency, and undocumented persons—will experience the greatest increase in pregnancy-related deaths due to a total abortion ban.13-15
The US maternal mortality rate is already the highest among developed nations, and it will only climb if ObGyns are not appropriately trained to operate within our full scope of practice and, thus, are unable to provide the highest quality of care.16,17
Continue: Abortion is a medical treatment that requires resident training...
Abortion is a medical treatment that requires resident training
Abortion care must be protected. Uterine evacuation by medical management, suction curettage, or dilation and evacuation is indicated for undesired pregnancy, regardless of reasoning or life circumstance. Pregnancy carries inherent risks that can at times be deadly.18 Abortion serves as first-line treatment for certain life-threatening pregnancy risks, including septic miscarriage, maternal hemorrhage, early-onset severe preeclampsia, and certain health conditions.19 Surgical skills and medical management of abortion are therefore fundamental components of ObGyn care and residency training.20
In choosing to become ObGyns,and particularly in selecting our training program, the ability to provide safe abortion care was a calculated priority. A recent study on the implications of overturning Roe predicted that nearly half of ObGyn residents will likely or certainly lose access to in-state abortion training.21 As demonstrated already in states with restrictive abortion laws, we will lose an entire generation of medical professionals skilled in performing this lifesaving procedure.9,22 While privileged patients may travel across state borders to access care, ObGyn and other medical trainees who are contract bound to residency programs do not have such flexibility to seek out abortion training. Although we hope the reversal of Roe will be fleeting, the consequences of this lost generation are irreparable.23,24 For physicians like ourselves, who fortunately are trained in surgical abortions and safe management of medical terminations, the discrepancy between evidence-based guidelines and impending political restrictions is distressing. We are forced to imagine refusing patients necessary health care—or face incarceration to save their lives.
The idea of watching a patient die, whether by hemorrhage, sepsis, or suicide, while armed with the tools of safe abortion technique is horrific. As authors with roots in Texas, Michigan, and Georgia, where abortion has or will almost certainly become illegal now that Roe v Wade is overturned, this scene is personal. It affects our future patients, our families, our colleagues, and our ability to return to our home states to live and practice.
Political organizing is critical to protect and restore abortion rights and defend against conservative coercive politics.25 Nearly half of pregnancies in the United States are unintended, and more than half of these end in abortion.26,27 Threats to abortion access require action from every one of the 59% of Americans who believe abortion should remain legal.28 This is especially important from a social and racial justice perspective as abortion bans will disproportionately affect marginalized groups and further exacerbate inequities in maternal mortality.13
Call to action
Now is the time for community action for reproductive justice and human rights. We urge everyone to donate to abortion funds, vote for leaders who support reproductive justice, and petition your state legislators to codify Roe into law. Now is the time to expand legislation to protect abortion providers and our patients. To ObGyns, family medicine physicians, internists, and other reproductive health clinicians, now is the time to maximize your abortion training. Now is the time to act; otherwise, pregnant individuals will die and future generations of physicians will not have the training to save their lives. ●
- de Vogue A, Sneed T, Duster C, et al. Supreme Court overturns Roe v Wade. CNN Politics. June 24, 2022. Accessed July 19, 2022. https://www.cnn.com/2022/06/24/politics/dobbs-missis sippi-supreme-court-abortion-roe-wade/index.html
- Nash E, Cross L. 26 States are certain or likely to ban abortion without Roe: here’s which ones and why. Guttmacher Institute. October 28, 2021. Updated April 19, 2022. Accessed July 19, 2022. https://www.guttmacher.org/article/2021/10/26-states-are-certain-or-likely-ban-abortion-without-roe-heres-which-ones-and-why
- Messerly M. Abortion laws by state: where abortions are illegal after Roe v Wade overturned. Politico. June 24, 2022. Accessed July 19, 2022. https://www.politico.com/news/2022/06/24/abortion-laws-by-state-roe-v-wade-00037695
- Archie A. US would lag behind global abortion access if Roe v Wade is undone, advocates say. NPR. May 5, 2022. Accessed July 19, 2022. https://www.npr.org/2022/05/05/1096805490/abortion-access-supreme-court-roe-v-wade-united-nations
- Romo V. Massachusetts senate overrides veto, passes law expanding abortion access. NPR. December 29, 2020. Accessed July 19, 2022. https://www.npr.org/2020/12/29/951259506/massachusetts-senate-overrides-veto-passes-law-expanding-abortion-access
- Upadhyay UD, Johns NE, Combellick SL, et al. Comparison of outcomes before and after Ohio’s law mandating use of the FDA-approved protocol for medication abortion: a retrospective cohort study. PLoS Med. 2016;13:e1002110.
- Upadhyay UD, Johns NE, Cartwright AF, et al. Sociodemographic characteristics of women able to obtain medication abortion before and after Ohio’s law requiring use of the Food and Drug Administration protocol. Health Equity. 2018;2:122-130.
- Goyal V, Brooks IHM, Powers DA. Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law. Contraception. 2020;102:109-114.
- Noyes E Holder BH, Evans ML. Texas SB8 and the future of abortion care. OBG Manag. 2021;33. doi:12788/obgm.0151.
- Vilda D, Wallace ME, Daniel C, et al. State abortion policies and maternal death in the United States, 2015‒2018. Am J Public Health. 2021;111:1696-1704.
- The Lancet. Why Roe v Wade must be defended. Lancet. 2022;399:1845.
- Nambiar A, Patel S, Santiago-Munoz P, et al. Maternal morbidity and fetal outcomes among pregnant women at 22 weeks’ gestation or less with complications in two Texas hospitals after legislation on abortion. Am J Obstet Gynecol. 2022;227:648-650.e1.
- Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. 2021;58:20192028.
- Medley S. Gutting abortion rights would be devastating for LGBTQ+ people. Them. September 17, 2021. Accessed July 20, 2022. https://www.them.us/story/gutting-abortion-rights-devastating-lgbtq-people
- Holter L. Detained immigrant women are facing a grueling abortion struggle. National Latina Institute for Reproductive Justice. May 10, 2017. Accessed July 20, 2022. https://www.latinainsti tute.org/es/node/4620
- Haddad LB, Nour NM. Unsafe abortion: unnecessary maternal mortality. Rev Obstet Gynecol. 2009;2:122-126.
- Tikkanen R, Gunja MZ, FitzGerald M, et al. Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund. November 18, 2020. Accessed November 17, 2022. https://www .commonwealthfund.org/publications/issue -briefs/2020/nov/maternal-mortality-maternity -care-us-compared-10-countries
- Collier A-RY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561-e574.
- ACOG practice bulletin no. 135: Second-trimester abortion. Obstet Gynecol. 2013;121:1394-1406.
- Committee on Health Care for Underserved Women. ACOG Committee opinion no. 612: Abortion training and education. Obstet Gynecol. 2014;124:1055-1059.
- Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in US obstetrics and gynecology residency programs. Obstet Gynecol. 2022;140:146-149.
- Horvath S, Turk J, Steinauer J, et al. Increase in obstetrics and gynecology resident self-assessed competence in early pregnancy loss management with routine abortion care training. Obstet Gynecol. 2022;139:116-119.
- Anderson N. The fall of Roe scrambles abortion training in university hospitals. The Washington Post. June 30, 2022. Accessed July 20, 2022. https://www.washingtonpost.com/educa tion/2022/06/30/abortion-training-upheaval-dobbs/
- Weiner S. How the repeal of Roe v Wade will affect training in abortion and reproductive health. AAMC. June 24, 2022. Accessed July 20, 2022. https://www.aamc.org/news-insights/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health
- Dreweke J. Coercion is at the heart of social conservatives’ reproductive health agenda. Guttmacher Institute. February 7, 2018. Accessed July 20, 2022. https://www.guttmacher.org/gpr/2018/02/coercion-heart-social-conservatives-reproduc tive-health-agenda
- Unintended pregnancy and abortion worldwide. Guttmacher Institute. March 2022. Accessed July 20, 2022. https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide
- Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374:843-852.
- Hartig H. About six-in-ten Americans say abortion should be legal in all or most cases. Pew Research Center. June 13, 2022. Accessed July 20, 2022. https://www.pewresearch.org/fact-tank/2022/06/13/about-six-in-ten-americans-say-abortion-should-be-legal-in-all-or-most-cases-2/
- de Vogue A, Sneed T, Duster C, et al. Supreme Court overturns Roe v Wade. CNN Politics. June 24, 2022. Accessed July 19, 2022. https://www.cnn.com/2022/06/24/politics/dobbs-missis sippi-supreme-court-abortion-roe-wade/index.html
- Nash E, Cross L. 26 States are certain or likely to ban abortion without Roe: here’s which ones and why. Guttmacher Institute. October 28, 2021. Updated April 19, 2022. Accessed July 19, 2022. https://www.guttmacher.org/article/2021/10/26-states-are-certain-or-likely-ban-abortion-without-roe-heres-which-ones-and-why
- Messerly M. Abortion laws by state: where abortions are illegal after Roe v Wade overturned. Politico. June 24, 2022. Accessed July 19, 2022. https://www.politico.com/news/2022/06/24/abortion-laws-by-state-roe-v-wade-00037695
- Archie A. US would lag behind global abortion access if Roe v Wade is undone, advocates say. NPR. May 5, 2022. Accessed July 19, 2022. https://www.npr.org/2022/05/05/1096805490/abortion-access-supreme-court-roe-v-wade-united-nations
- Romo V. Massachusetts senate overrides veto, passes law expanding abortion access. NPR. December 29, 2020. Accessed July 19, 2022. https://www.npr.org/2020/12/29/951259506/massachusetts-senate-overrides-veto-passes-law-expanding-abortion-access
- Upadhyay UD, Johns NE, Combellick SL, et al. Comparison of outcomes before and after Ohio’s law mandating use of the FDA-approved protocol for medication abortion: a retrospective cohort study. PLoS Med. 2016;13:e1002110.
- Upadhyay UD, Johns NE, Cartwright AF, et al. Sociodemographic characteristics of women able to obtain medication abortion before and after Ohio’s law requiring use of the Food and Drug Administration protocol. Health Equity. 2018;2:122-130.
- Goyal V, Brooks IHM, Powers DA. Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law. Contraception. 2020;102:109-114.
- Noyes E Holder BH, Evans ML. Texas SB8 and the future of abortion care. OBG Manag. 2021;33. doi:12788/obgm.0151.
- Vilda D, Wallace ME, Daniel C, et al. State abortion policies and maternal death in the United States, 2015‒2018. Am J Public Health. 2021;111:1696-1704.
- The Lancet. Why Roe v Wade must be defended. Lancet. 2022;399:1845.
- Nambiar A, Patel S, Santiago-Munoz P, et al. Maternal morbidity and fetal outcomes among pregnant women at 22 weeks’ gestation or less with complications in two Texas hospitals after legislation on abortion. Am J Obstet Gynecol. 2022;227:648-650.e1.
- Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. 2021;58:20192028.
- Medley S. Gutting abortion rights would be devastating for LGBTQ+ people. Them. September 17, 2021. Accessed July 20, 2022. https://www.them.us/story/gutting-abortion-rights-devastating-lgbtq-people
- Holter L. Detained immigrant women are facing a grueling abortion struggle. National Latina Institute for Reproductive Justice. May 10, 2017. Accessed July 20, 2022. https://www.latinainsti tute.org/es/node/4620
- Haddad LB, Nour NM. Unsafe abortion: unnecessary maternal mortality. Rev Obstet Gynecol. 2009;2:122-126.
- Tikkanen R, Gunja MZ, FitzGerald M, et al. Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund. November 18, 2020. Accessed November 17, 2022. https://www .commonwealthfund.org/publications/issue -briefs/2020/nov/maternal-mortality-maternity -care-us-compared-10-countries
- Collier A-RY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561-e574.
- ACOG practice bulletin no. 135: Second-trimester abortion. Obstet Gynecol. 2013;121:1394-1406.
- Committee on Health Care for Underserved Women. ACOG Committee opinion no. 612: Abortion training and education. Obstet Gynecol. 2014;124:1055-1059.
- Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in US obstetrics and gynecology residency programs. Obstet Gynecol. 2022;140:146-149.
- Horvath S, Turk J, Steinauer J, et al. Increase in obstetrics and gynecology resident self-assessed competence in early pregnancy loss management with routine abortion care training. Obstet Gynecol. 2022;139:116-119.
- Anderson N. The fall of Roe scrambles abortion training in university hospitals. The Washington Post. June 30, 2022. Accessed July 20, 2022. https://www.washingtonpost.com/educa tion/2022/06/30/abortion-training-upheaval-dobbs/
- Weiner S. How the repeal of Roe v Wade will affect training in abortion and reproductive health. AAMC. June 24, 2022. Accessed July 20, 2022. https://www.aamc.org/news-insights/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health
- Dreweke J. Coercion is at the heart of social conservatives’ reproductive health agenda. Guttmacher Institute. February 7, 2018. Accessed July 20, 2022. https://www.guttmacher.org/gpr/2018/02/coercion-heart-social-conservatives-reproduc tive-health-agenda
- Unintended pregnancy and abortion worldwide. Guttmacher Institute. March 2022. Accessed July 20, 2022. https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide
- Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374:843-852.
- Hartig H. About six-in-ten Americans say abortion should be legal in all or most cases. Pew Research Center. June 13, 2022. Accessed July 20, 2022. https://www.pewresearch.org/fact-tank/2022/06/13/about-six-in-ten-americans-say-abortion-should-be-legal-in-all-or-most-cases-2/

Mindfulness, exercise strike out in memory trial
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
We are coming to the end of the year, which always makes me think about getting older. Much like the search for the fountain of youth, many promising leads have ultimately led to dead ends. And yet, I had high hopes for a trial that focused on two cornerstones of wellness – exercise and mindfulness – to address the subjective loss of memory that comes with aging. Alas, meditation and exercise do not appear to be the fountain of youth.
I’m talking about this study, appearing in JAMA, known as the MEDEX trial.
It’s a clever design: a 2 x 2 factorial randomized trial where participants could be randomized to a mindfulness intervention, an exercise intervention, both, or neither.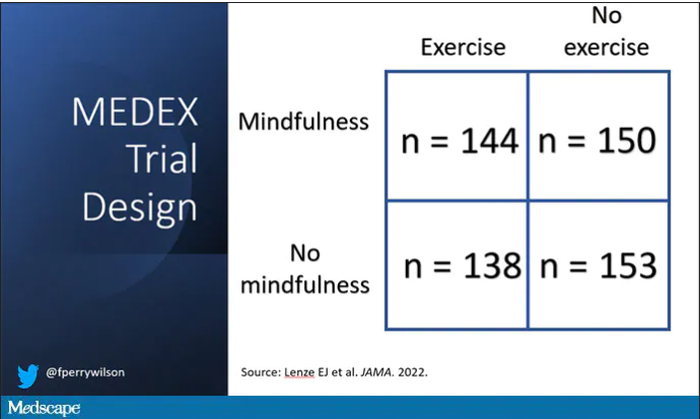
In this manner, you can test multiple hypotheses exploiting a shared control group. Or as a mentor of mine used to say, you get two trials for the price of one and a half.
The participants were older adults, aged 65-84, living in the community. They had to be relatively sedentary at baseline and not engaging in mindfulness practices. They had to subjectively report some memory or concentration issues but had to be cognitively intact, based on a standard dementia screening test. In other words, these are your average older people who are worried that they aren’t as sharp as they used to be.
The interventions themselves were fairly intense. The exercise group had instructor-led sessions for 90 minutes twice a week for the first 6 months of the study, once a week thereafter. And participants were encouraged to exercise at home such that they had a total of 300 minutes of weekly exercise.
The mindfulness program was characterized by eight weekly classes of 2.5 hours each as well as a half-day retreat to teach the tenets of mindfulness and meditation, with monthly refreshers thereafter. Participants were instructed to meditate for 60 minutes a day in addition to the classes.
For the 144 people who were randomized to both meditation and exercise, this trial amounted to something of a part-time job. So you might think that adherence to the interventions was low, but apparently that’s not the case. Attendance to the mindfulness classes was over 90%, and over 80% for the exercise classes. And diary-based reporting of home efforts was also pretty good.
The control group wasn’t left to their own devices. Recognizing that the community aspect of exercise or mindfulness classes might convey a benefit independent of the actual exercise or mindfulness, the control group met on a similar schedule to discuss health education, but no mention of exercise or mindfulness occurred in that setting.
The primary outcome was change in memory and executive function scores across a battery of neuropsychologic testing, but the story is told in just a few pictures.
Memory scores improved in all three groups – mindfulness, exercise, and health education – over time. Cognitive composite score improved in all three groups similarly. There was no synergistic effect of mindfulness and exercise either. Basically, everyone got a bit better.
But the study did way more than look at scores on tests. Researchers used MRI to measure brain anatomic outcomes as well. And the surprising thing is that virtually none of these outcomes were different between the groups either.
Hippocampal volume decreased a bit in all the groups. Dorsolateral prefrontal cortex volume was flat. There was no change in scores measuring tasks of daily living.
When you see negative results like this, right away you worry that the intervention wasn’t properly delivered. Were these people really exercising and meditating? Well, the authors showed that individuals randomized to exercise, at least, had less sleep latency, greater aerobic fitness, and greater strength. So we know something was happening.
They then asked, would the people in the exercise group with the greatest changes in those physiologic parameters show some improvement in cognitive parameters? In other words, we know you were exercising because you got stronger and are sleeping better; is your memory better? The answer? Surprisingly, still no. Even in that honestly somewhat cherry-picked group, the interventions had no effect.
Could it be that the control was inappropriate, that the “health education” intervention was actually so helpful that it obscured the benefits of exercise and meditation? After all, cognitive scores did improve in all groups. The authors doubt it. They say they think the improvement in cognitive scores reflects the fact that patients had learned a bit about how to take the tests. This is pretty common in the neuropsychiatric literature.
So here we are and I just want to say, well, shoot. This is not the result I wanted. And I think the reason I’m so disappointed is because aging and the loss of cognitive faculties that comes with aging are just sort of scary. We are all looking for some control over that fear, and how nice it would be to be able to tell ourselves not to worry – that we won’t have those problems as we get older because we exercise, or meditate, or drink red wine, or don’t drink wine, or whatever. And while I have no doubt that staying healthier physically will keep you healthier mentally, it may take more than one simple thing to move the needle.
Dr. Wilson is associate professor, department of medicine, and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
We are coming to the end of the year, which always makes me think about getting older. Much like the search for the fountain of youth, many promising leads have ultimately led to dead ends. And yet, I had high hopes for a trial that focused on two cornerstones of wellness – exercise and mindfulness – to address the subjective loss of memory that comes with aging. Alas, meditation and exercise do not appear to be the fountain of youth.
I’m talking about this study, appearing in JAMA, known as the MEDEX trial.
It’s a clever design: a 2 x 2 factorial randomized trial where participants could be randomized to a mindfulness intervention, an exercise intervention, both, or neither.
In this manner, you can test multiple hypotheses exploiting a shared control group. Or as a mentor of mine used to say, you get two trials for the price of one and a half.
The participants were older adults, aged 65-84, living in the community. They had to be relatively sedentary at baseline and not engaging in mindfulness practices. They had to subjectively report some memory or concentration issues but had to be cognitively intact, based on a standard dementia screening test. In other words, these are your average older people who are worried that they aren’t as sharp as they used to be.
The interventions themselves were fairly intense. The exercise group had instructor-led sessions for 90 minutes twice a week for the first 6 months of the study, once a week thereafter. And participants were encouraged to exercise at home such that they had a total of 300 minutes of weekly exercise.
The mindfulness program was characterized by eight weekly classes of 2.5 hours each as well as a half-day retreat to teach the tenets of mindfulness and meditation, with monthly refreshers thereafter. Participants were instructed to meditate for 60 minutes a day in addition to the classes.
For the 144 people who were randomized to both meditation and exercise, this trial amounted to something of a part-time job. So you might think that adherence to the interventions was low, but apparently that’s not the case. Attendance to the mindfulness classes was over 90%, and over 80% for the exercise classes. And diary-based reporting of home efforts was also pretty good.
The control group wasn’t left to their own devices. Recognizing that the community aspect of exercise or mindfulness classes might convey a benefit independent of the actual exercise or mindfulness, the control group met on a similar schedule to discuss health education, but no mention of exercise or mindfulness occurred in that setting.
The primary outcome was change in memory and executive function scores across a battery of neuropsychologic testing, but the story is told in just a few pictures.
Memory scores improved in all three groups – mindfulness, exercise, and health education – over time. Cognitive composite score improved in all three groups similarly. There was no synergistic effect of mindfulness and exercise either. Basically, everyone got a bit better.
But the study did way more than look at scores on tests. Researchers used MRI to measure brain anatomic outcomes as well. And the surprising thing is that virtually none of these outcomes were different between the groups either.
Hippocampal volume decreased a bit in all the groups. Dorsolateral prefrontal cortex volume was flat. There was no change in scores measuring tasks of daily living.
When you see negative results like this, right away you worry that the intervention wasn’t properly delivered. Were these people really exercising and meditating? Well, the authors showed that individuals randomized to exercise, at least, had less sleep latency, greater aerobic fitness, and greater strength. So we know something was happening.
They then asked, would the people in the exercise group with the greatest changes in those physiologic parameters show some improvement in cognitive parameters? In other words, we know you were exercising because you got stronger and are sleeping better; is your memory better? The answer? Surprisingly, still no. Even in that honestly somewhat cherry-picked group, the interventions had no effect.
Could it be that the control was inappropriate, that the “health education” intervention was actually so helpful that it obscured the benefits of exercise and meditation? After all, cognitive scores did improve in all groups. The authors doubt it. They say they think the improvement in cognitive scores reflects the fact that patients had learned a bit about how to take the tests. This is pretty common in the neuropsychiatric literature.
So here we are and I just want to say, well, shoot. This is not the result I wanted. And I think the reason I’m so disappointed is because aging and the loss of cognitive faculties that comes with aging are just sort of scary. We are all looking for some control over that fear, and how nice it would be to be able to tell ourselves not to worry – that we won’t have those problems as we get older because we exercise, or meditate, or drink red wine, or don’t drink wine, or whatever. And while I have no doubt that staying healthier physically will keep you healthier mentally, it may take more than one simple thing to move the needle.
Dr. Wilson is associate professor, department of medicine, and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
We are coming to the end of the year, which always makes me think about getting older. Much like the search for the fountain of youth, many promising leads have ultimately led to dead ends. And yet, I had high hopes for a trial that focused on two cornerstones of wellness – exercise and mindfulness – to address the subjective loss of memory that comes with aging. Alas, meditation and exercise do not appear to be the fountain of youth.
I’m talking about this study, appearing in JAMA, known as the MEDEX trial.
It’s a clever design: a 2 x 2 factorial randomized trial where participants could be randomized to a mindfulness intervention, an exercise intervention, both, or neither.
In this manner, you can test multiple hypotheses exploiting a shared control group. Or as a mentor of mine used to say, you get two trials for the price of one and a half.
The participants were older adults, aged 65-84, living in the community. They had to be relatively sedentary at baseline and not engaging in mindfulness practices. They had to subjectively report some memory or concentration issues but had to be cognitively intact, based on a standard dementia screening test. In other words, these are your average older people who are worried that they aren’t as sharp as they used to be.
The interventions themselves were fairly intense. The exercise group had instructor-led sessions for 90 minutes twice a week for the first 6 months of the study, once a week thereafter. And participants were encouraged to exercise at home such that they had a total of 300 minutes of weekly exercise.
The mindfulness program was characterized by eight weekly classes of 2.5 hours each as well as a half-day retreat to teach the tenets of mindfulness and meditation, with monthly refreshers thereafter. Participants were instructed to meditate for 60 minutes a day in addition to the classes.
For the 144 people who were randomized to both meditation and exercise, this trial amounted to something of a part-time job. So you might think that adherence to the interventions was low, but apparently that’s not the case. Attendance to the mindfulness classes was over 90%, and over 80% for the exercise classes. And diary-based reporting of home efforts was also pretty good.
The control group wasn’t left to their own devices. Recognizing that the community aspect of exercise or mindfulness classes might convey a benefit independent of the actual exercise or mindfulness, the control group met on a similar schedule to discuss health education, but no mention of exercise or mindfulness occurred in that setting.
The primary outcome was change in memory and executive function scores across a battery of neuropsychologic testing, but the story is told in just a few pictures.
Memory scores improved in all three groups – mindfulness, exercise, and health education – over time. Cognitive composite score improved in all three groups similarly. There was no synergistic effect of mindfulness and exercise either. Basically, everyone got a bit better.
But the study did way more than look at scores on tests. Researchers used MRI to measure brain anatomic outcomes as well. And the surprising thing is that virtually none of these outcomes were different between the groups either.
Hippocampal volume decreased a bit in all the groups. Dorsolateral prefrontal cortex volume was flat. There was no change in scores measuring tasks of daily living.
When you see negative results like this, right away you worry that the intervention wasn’t properly delivered. Were these people really exercising and meditating? Well, the authors showed that individuals randomized to exercise, at least, had less sleep latency, greater aerobic fitness, and greater strength. So we know something was happening.
They then asked, would the people in the exercise group with the greatest changes in those physiologic parameters show some improvement in cognitive parameters? In other words, we know you were exercising because you got stronger and are sleeping better; is your memory better? The answer? Surprisingly, still no. Even in that honestly somewhat cherry-picked group, the interventions had no effect.
Could it be that the control was inappropriate, that the “health education” intervention was actually so helpful that it obscured the benefits of exercise and meditation? After all, cognitive scores did improve in all groups. The authors doubt it. They say they think the improvement in cognitive scores reflects the fact that patients had learned a bit about how to take the tests. This is pretty common in the neuropsychiatric literature.
So here we are and I just want to say, well, shoot. This is not the result I wanted. And I think the reason I’m so disappointed is because aging and the loss of cognitive faculties that comes with aging are just sort of scary. We are all looking for some control over that fear, and how nice it would be to be able to tell ourselves not to worry – that we won’t have those problems as we get older because we exercise, or meditate, or drink red wine, or don’t drink wine, or whatever. And while I have no doubt that staying healthier physically will keep you healthier mentally, it may take more than one simple thing to move the needle.
Dr. Wilson is associate professor, department of medicine, and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.