User login
A Novel Method of Skin Closure for Aging or Fragile Skin
Patients who have been on steroids, aspirin, or anticoagulants or who are elderly may have a fragile outer skin layer that is similar to parchment paper, which may be challenging for surgeons. In these patients, the epidermal layer is thin and translucent; when a surgeon cuts through this thin layer, the tissue beneath shows minimal dermis and poor-quality fat with weakened tissue support. When undergoing excisional surgery, there is no strong tissue to help the closure sutures remain intact. Surgeons may struggle with skin tears around the sutures and dehiscence on suture removal.
This article describes a novel approach to skin closure in patients with aging or thin skin using a polyethylene film with an acrylate adhesive in the excision area to aid in maintaining skin integrity throughout the healing process following surgery.
Closure Technique
First, the skin area is cleansed with a sterilizing soap preparation. A sterile marking pen then is used to outline the excision area. A 10×12-cm layer of polyethylene film is then attached to the excision site. Excision of the tumor is performed by cutting through the film in the marked area (Figure 1A), and closure is performed by suturing the wound edges through the polyethylene film while the area is still covered with the film (Figure 1B). The sutures can be left in for 2 weeks or longer if necessary. The patient should be instructed not to remove the film or perform any extensive cleansing of the treatment area. Antibiotics should be administered, as the polyethylene film maintains its sterile integrity for 7 days only. Because sutures are on the surface of the film, they are easily accessed for removal. Figure 1C shows the excision site after removal of the sutures and polyethylene film on the left tibia of a 95-year-old woman. Adhesive butterfly closures can be applied to strengthen the excision area after suture removal and prevent dehiscence.



|
Figure 1. The excision site was marked after polyethylene adhesive film was applied to a squamous cell carcinoma on the left tibia of 95-year-old woman (A). Closure was performed by suturing the wound edges through the polyethylene film (B). The excision site appeared to have no dehiscence or signs of infection after removal of the sutures and polyethylene film (C). |
Case Reports
Twelve procedures for skin cancer excision were conducted in 10 patients using polyethylene adhesive film as a surgical aid due to extremely poor quality of the epidermis. The tumors were all squamous cell carcinomas and were located on the arms and legs. Patients were aged 73 to 95 years. Figure 2 demonstrates an example of excision of a squamous cell carcinoma on the left tibia of an 82-year-old man with prior dehiscence and infection after leg surgeries. Good results were achieved using the closure technique described here, along with prophylactic antibiotics.


|
Figure 2. A squamous cell carcinoma excision site on the left tibia of an 82-year-old man that had been covered with polyethylene adhesive film prior to excision (A) and 17 days following removal of the sutures and film (B). |
One patient had complications from a Staphylococcus infection because antibiotics were not administered. The patient had prior infections with other surgeries. Antibiotics were given 4 days after surgery. The infection was cleared and the polyethylene film was retained for a total of 12 days.
Sutures were removed after 14 days for excision sites on the arms and 17 days for excision sites on the legs. All excision sites healed without dehiscence with a cosmetically acceptable scar. Figure 3A shows a completed excision on the left hand of a 92-year-old man, and Figure 3B is the result 5 weeks after excision.


|
Figure 3. A squamous cell carcinoma excision site on the left thumb of a 92-year-old man that had been covered with polyethylene adhesive film prior to exci- sion (A). No visible scarring or dehiscence was noted 5 weeks after excision, following removal of the sutures and film (B). |
None of the patients reported discomfort from the polyethylene film remaining on the skin following surgery, though postoperative care required extra caution when dressing so as not to disturb or compromise the film. Patients were advised about postoperative care and were instructed not to remove the dressing. They were all given antibiotics as a necessary adjunct to maintain a lessened bacteria burden imposed by an impervious layer of acrylate adhesive. Complications resulted from failure to immediately provide antibiotics to 1 patient. The polyethylene film did not hinder healing or postoperative results.
Comment
Various techniques for handling fragile skin during surgery have been described in the literature. Fomon et al1 discussed aging skin as it relates to plastic surgery. Foster and Chan2 described a skin support technique for closing elliptical incisions in patients with fragile skin. Mazzurco and Krach3 discussed the use of a hydrocolloid dressing to aid in the closure of surgical wounds in patients with fragile skin.
The closure method described here was found to be particularly helpful when used as an adjunct to surgery in patients with fragile skin that lacked a suitable dermis. The polyethylene adhesive film helped to hold the sutures more securely. This method is cost-effective and is associated with a high level of patient satisfaction. For the surgeon, this technique may aid in dealing with difficult surgical situations and helps prevent wound complications in elderly patients or those with fragile skin.
1. Fomon S, Bell JW, Schattner A. Aging skin, a surgical challenge. AMA Arch Otolaryngol. 1955;61:554-562.
2. Foster RS, Chan J. The Fixomull skin support method for wound closure in patients with fragile skin. Australas J Dermatol. 2011;52:209-211.
3. Mazzurco JD, Krach KJ. Use of a hydrocolloid dressing to aid in the closure of surgical wounds in patients with fragile skin. J Am Acad Dermatol. 2012;66:335-336.
Patients who have been on steroids, aspirin, or anticoagulants or who are elderly may have a fragile outer skin layer that is similar to parchment paper, which may be challenging for surgeons. In these patients, the epidermal layer is thin and translucent; when a surgeon cuts through this thin layer, the tissue beneath shows minimal dermis and poor-quality fat with weakened tissue support. When undergoing excisional surgery, there is no strong tissue to help the closure sutures remain intact. Surgeons may struggle with skin tears around the sutures and dehiscence on suture removal.
This article describes a novel approach to skin closure in patients with aging or thin skin using a polyethylene film with an acrylate adhesive in the excision area to aid in maintaining skin integrity throughout the healing process following surgery.
Closure Technique
First, the skin area is cleansed with a sterilizing soap preparation. A sterile marking pen then is used to outline the excision area. A 10×12-cm layer of polyethylene film is then attached to the excision site. Excision of the tumor is performed by cutting through the film in the marked area (Figure 1A), and closure is performed by suturing the wound edges through the polyethylene film while the area is still covered with the film (Figure 1B). The sutures can be left in for 2 weeks or longer if necessary. The patient should be instructed not to remove the film or perform any extensive cleansing of the treatment area. Antibiotics should be administered, as the polyethylene film maintains its sterile integrity for 7 days only. Because sutures are on the surface of the film, they are easily accessed for removal. Figure 1C shows the excision site after removal of the sutures and polyethylene film on the left tibia of a 95-year-old woman. Adhesive butterfly closures can be applied to strengthen the excision area after suture removal and prevent dehiscence.
|
|
Figure 1. The excision site was marked after polyethylene adhesive film was applied to a squamous cell carcinoma on the left tibia of 95-year-old woman (A). Closure was performed by suturing the wound edges through the polyethylene film (B). The excision site appeared to have no dehiscence or signs of infection after removal of the sutures and polyethylene film (C). |
Case Reports
Twelve procedures for skin cancer excision were conducted in 10 patients using polyethylene adhesive film as a surgical aid due to extremely poor quality of the epidermis. The tumors were all squamous cell carcinomas and were located on the arms and legs. Patients were aged 73 to 95 years. Figure 2 demonstrates an example of excision of a squamous cell carcinoma on the left tibia of an 82-year-old man with prior dehiscence and infection after leg surgeries. Good results were achieved using the closure technique described here, along with prophylactic antibiotics.
|
|
Figure 2. A squamous cell carcinoma excision site on the left tibia of an 82-year-old man that had been covered with polyethylene adhesive film prior to excision (A) and 17 days following removal of the sutures and film (B). |
One patient had complications from a Staphylococcus infection because antibiotics were not administered. The patient had prior infections with other surgeries. Antibiotics were given 4 days after surgery. The infection was cleared and the polyethylene film was retained for a total of 12 days.
Sutures were removed after 14 days for excision sites on the arms and 17 days for excision sites on the legs. All excision sites healed without dehiscence with a cosmetically acceptable scar. Figure 3A shows a completed excision on the left hand of a 92-year-old man, and Figure 3B is the result 5 weeks after excision.
|
|
Figure 3. A squamous cell carcinoma excision site on the left thumb of a 92-year-old man that had been covered with polyethylene adhesive film prior to exci- sion (A). No visible scarring or dehiscence was noted 5 weeks after excision, following removal of the sutures and film (B). |
None of the patients reported discomfort from the polyethylene film remaining on the skin following surgery, though postoperative care required extra caution when dressing so as not to disturb or compromise the film. Patients were advised about postoperative care and were instructed not to remove the dressing. They were all given antibiotics as a necessary adjunct to maintain a lessened bacteria burden imposed by an impervious layer of acrylate adhesive. Complications resulted from failure to immediately provide antibiotics to 1 patient. The polyethylene film did not hinder healing or postoperative results.
Comment
Various techniques for handling fragile skin during surgery have been described in the literature. Fomon et al1 discussed aging skin as it relates to plastic surgery. Foster and Chan2 described a skin support technique for closing elliptical incisions in patients with fragile skin. Mazzurco and Krach3 discussed the use of a hydrocolloid dressing to aid in the closure of surgical wounds in patients with fragile skin.
The closure method described here was found to be particularly helpful when used as an adjunct to surgery in patients with fragile skin that lacked a suitable dermis. The polyethylene adhesive film helped to hold the sutures more securely. This method is cost-effective and is associated with a high level of patient satisfaction. For the surgeon, this technique may aid in dealing with difficult surgical situations and helps prevent wound complications in elderly patients or those with fragile skin.
Patients who have been on steroids, aspirin, or anticoagulants or who are elderly may have a fragile outer skin layer that is similar to parchment paper, which may be challenging for surgeons. In these patients, the epidermal layer is thin and translucent; when a surgeon cuts through this thin layer, the tissue beneath shows minimal dermis and poor-quality fat with weakened tissue support. When undergoing excisional surgery, there is no strong tissue to help the closure sutures remain intact. Surgeons may struggle with skin tears around the sutures and dehiscence on suture removal.
This article describes a novel approach to skin closure in patients with aging or thin skin using a polyethylene film with an acrylate adhesive in the excision area to aid in maintaining skin integrity throughout the healing process following surgery.
Closure Technique
First, the skin area is cleansed with a sterilizing soap preparation. A sterile marking pen then is used to outline the excision area. A 10×12-cm layer of polyethylene film is then attached to the excision site. Excision of the tumor is performed by cutting through the film in the marked area (Figure 1A), and closure is performed by suturing the wound edges through the polyethylene film while the area is still covered with the film (Figure 1B). The sutures can be left in for 2 weeks or longer if necessary. The patient should be instructed not to remove the film or perform any extensive cleansing of the treatment area. Antibiotics should be administered, as the polyethylene film maintains its sterile integrity for 7 days only. Because sutures are on the surface of the film, they are easily accessed for removal. Figure 1C shows the excision site after removal of the sutures and polyethylene film on the left tibia of a 95-year-old woman. Adhesive butterfly closures can be applied to strengthen the excision area after suture removal and prevent dehiscence.
|
|
Figure 1. The excision site was marked after polyethylene adhesive film was applied to a squamous cell carcinoma on the left tibia of 95-year-old woman (A). Closure was performed by suturing the wound edges through the polyethylene film (B). The excision site appeared to have no dehiscence or signs of infection after removal of the sutures and polyethylene film (C). |
Case Reports
Twelve procedures for skin cancer excision were conducted in 10 patients using polyethylene adhesive film as a surgical aid due to extremely poor quality of the epidermis. The tumors were all squamous cell carcinomas and were located on the arms and legs. Patients were aged 73 to 95 years. Figure 2 demonstrates an example of excision of a squamous cell carcinoma on the left tibia of an 82-year-old man with prior dehiscence and infection after leg surgeries. Good results were achieved using the closure technique described here, along with prophylactic antibiotics.
|
|
Figure 2. A squamous cell carcinoma excision site on the left tibia of an 82-year-old man that had been covered with polyethylene adhesive film prior to excision (A) and 17 days following removal of the sutures and film (B). |
One patient had complications from a Staphylococcus infection because antibiotics were not administered. The patient had prior infections with other surgeries. Antibiotics were given 4 days after surgery. The infection was cleared and the polyethylene film was retained for a total of 12 days.
Sutures were removed after 14 days for excision sites on the arms and 17 days for excision sites on the legs. All excision sites healed without dehiscence with a cosmetically acceptable scar. Figure 3A shows a completed excision on the left hand of a 92-year-old man, and Figure 3B is the result 5 weeks after excision.
|
|
Figure 3. A squamous cell carcinoma excision site on the left thumb of a 92-year-old man that had been covered with polyethylene adhesive film prior to exci- sion (A). No visible scarring or dehiscence was noted 5 weeks after excision, following removal of the sutures and film (B). |
None of the patients reported discomfort from the polyethylene film remaining on the skin following surgery, though postoperative care required extra caution when dressing so as not to disturb or compromise the film. Patients were advised about postoperative care and were instructed not to remove the dressing. They were all given antibiotics as a necessary adjunct to maintain a lessened bacteria burden imposed by an impervious layer of acrylate adhesive. Complications resulted from failure to immediately provide antibiotics to 1 patient. The polyethylene film did not hinder healing or postoperative results.
Comment
Various techniques for handling fragile skin during surgery have been described in the literature. Fomon et al1 discussed aging skin as it relates to plastic surgery. Foster and Chan2 described a skin support technique for closing elliptical incisions in patients with fragile skin. Mazzurco and Krach3 discussed the use of a hydrocolloid dressing to aid in the closure of surgical wounds in patients with fragile skin.
The closure method described here was found to be particularly helpful when used as an adjunct to surgery in patients with fragile skin that lacked a suitable dermis. The polyethylene adhesive film helped to hold the sutures more securely. This method is cost-effective and is associated with a high level of patient satisfaction. For the surgeon, this technique may aid in dealing with difficult surgical situations and helps prevent wound complications in elderly patients or those with fragile skin.
1. Fomon S, Bell JW, Schattner A. Aging skin, a surgical challenge. AMA Arch Otolaryngol. 1955;61:554-562.
2. Foster RS, Chan J. The Fixomull skin support method for wound closure in patients with fragile skin. Australas J Dermatol. 2011;52:209-211.
3. Mazzurco JD, Krach KJ. Use of a hydrocolloid dressing to aid in the closure of surgical wounds in patients with fragile skin. J Am Acad Dermatol. 2012;66:335-336.
1. Fomon S, Bell JW, Schattner A. Aging skin, a surgical challenge. AMA Arch Otolaryngol. 1955;61:554-562.
2. Foster RS, Chan J. The Fixomull skin support method for wound closure in patients with fragile skin. Australas J Dermatol. 2011;52:209-211.
3. Mazzurco JD, Krach KJ. Use of a hydrocolloid dressing to aid in the closure of surgical wounds in patients with fragile skin. J Am Acad Dermatol. 2012;66:335-336.
Practice Points
- A novel method of skin closure using a polyethylene film with an acrylate adhesive can aid in strengthening suture integrity and preventing skin tears.
- Dehiscence of excision sites in patients with aging or fragile skin can be prevented.
- This closure technique promotes healing and efficient scar formation.

Merkel cell carcinoma responds to immunotherapy
VIENNA – High response rates to pembrolizumab and to intratumoral delivery of plasmid interleukin-12 (IL-12) were observed among patients with advanced Merkel cell carcinoma (MCC), based on studies presented at the 2015 European Cancer Congress.
There is strong rationale for immunotherapy in MCC. For one thing, the Merkel cell polyomavirus, which is expressed in 80% of tumors, serves as a powerful antigen for stimulating an immune response. Secondly, MCC tumors often express the ligand for the programmed death protein (PD-1), creating an opportunity for PD-1 pathway blockade with PD-1 inhibitors such as pembrolizumab, according to the investigators.
Responses in 10 of 14 given pembrolizumab
Dr. Paul Nghiem of the University of Washington in Seattle, led an open-label, single-arm, multicenter phase II trial of pembrolizumab, which is approved for metastatic melanoma and which could become the first systemic therapy for unresectable or metastatic MCC (Abstract 22LBA).

In the study, which opened in January 2015, there are 24 evaluable patients treated with pembrolizumab 2 mg/kg every 3 weeks for up to 2 years. Fourteen had at least one posttreatment scan; 10 of these 14 patients (71%) have responded, 2 had complete responses. One patient had stable disease and three progressed.
“Responses were rapid, and appear more durable than we see with chemotherapy,” Dr. Nghiem said.
The drug was generally well tolerated, with an adverse event profile similar to what has been seen in melanoma. One patient experienced grade 4 myocarditis after one dose and one developed grade 4 transaminase elevation after two doses. Both improved after discontinuing pembrolizumab and starting corticosteroids.
“Strikingly, despite receiving only one or two doses, both patients had profound and ongoing responses to pembrolizumab,” Dr. Nghiem observed.
Many subjects had “profound shrinkage of tumor that has not rebounded,” he noted. “Pembrolizumab looks to be very favorable in terms of durability of response. With chemotherapy, at 90 days half of our patients have gone off treatment.”
The researchers are considering expanding the study population, and may include a chemotherapy-relapsed cohort. They are also analyzing biomarkers, and hope to evaluate response according to virus-positive versus virus-negative status.

Dr. Caroline Robert of the Institut Gustave Roussy in Villejuif, France, commented on the findings, first noting the difficulty of treating patients for whom there are no approved therapies. Median overall survival is less than 10 months, she said, and clinicians have lacked clinical trials to enroll patients.
“MCC patients represent a high medical need,” she said. Although the results with pembrolizumab are early, “they are very promising.”
Intratumoral plasmid IL-12
Dr. Shailender Bhatia of the University of Washington in Seattle, described a different immunotherapeutic approach in an MCC population (Abstract 504).

IL-12, which regulates adaptive type-1 immunity, has demonstrated antitumor efficacy in MCC but is associated with severe toxicities when administered systemically. Local IL-12 delivery to the tumor microenvironment “may provide adequate cytokine concentration in the vicinity of tumor antigens, and therefore improve efficacy while sparing systemic toxicity,” he said.
Intratumoral IL-12 plasmid DNA (pIL-12) injection with electroporation (which uses pulsed electricity to open pores in cell membranes) has shown antitumor activity in melanoma, and might also work in MCC, Dr. Bhatia and his colleagues hypothesized. The concept is one of promoting tumor inflammation and thereby a systemic antitumor immune response. This would be reflected, and measured, by increased IL-12 protein expression in the tumor microenvironment, which became this study’s primary endpoint.
“To the best of our knowledge, this study represents the first prospective clinical trial of immunotherapy in advanced MCC,” Dr. Bhatia noted.
Beginning in January 2012, the study enrolled 15 patients with MCC and superficial injectable tumors. Patients received injections of pIL-12 on days 1, 5, and 8; 2 weeks later, on day 22, their lesions were biopsied. The 3-person cohort with localized MCC (stage IIIb) then underwent definitive surgery and/or radiation therapy starting in week 4, while the 12 with distant metastatic disease (stage IV) could receive additional treatment cycles (maximum of 4) at least 6 weeks apart.
The treatment was well tolerated, with most adverse events – primarily pain and local inflammatory reaction – being mild and transient. No patients discontinued because of toxicity.
The primary endpoint, sustained local expression of IL-12 protein on day 22, was observed in 79% of patients. In paired biopsy samples, comparing baseline to day 22 levels, IL-12 protein expression increased by almost 2-fold to more than 3,000-fold.
In addition, enrichment of Merkel cell polyomavirus-specific CD8-positive T cells were found in the tumor infiltrating lymphocytes (TILs) of treated and distant tumors in some patients.
“Additionally, the pIL-12/electroporation treatment led to objective clinical responses in metastatic MCC,” Dr. Bhatia reported.
Among the three patients with locally advanced disease, one had a pathologic complete response and remains free of recurrence more than 6 months later. Another patient has been recurrence free for more than 3 years. The third patient was recurrence free for 9 months before developing progressive disease.
Among the 12 patients with metastatic disease, 3 responded to treatment and 1 achieved stable disease, while 8 (52%) progressed.
The injections led to regression not only of treated lesions, but also of clearly distinct noninjected MCC tumors. The proportion of treated lesions with major (more than 30%) regression was 44%. Among 10 patients with at least one distant lesion, 30% of noninjected distant lesions regressed.
“We believe this approach warrants further exploration in MCC, perhaps in combination with emerging systemic therapies, such as anti-PD-1/PD-L1 agents,” Dr. Bhatia said.
Dr. Nghiem and Dr. Bhatia had no relevant disclosures. In the IL-12 study, some investigators have financial relationships with OncoSec Medical, which manufactures the study drug.
VIENNA – High response rates to pembrolizumab and to intratumoral delivery of plasmid interleukin-12 (IL-12) were observed among patients with advanced Merkel cell carcinoma (MCC), based on studies presented at the 2015 European Cancer Congress.
There is strong rationale for immunotherapy in MCC. For one thing, the Merkel cell polyomavirus, which is expressed in 80% of tumors, serves as a powerful antigen for stimulating an immune response. Secondly, MCC tumors often express the ligand for the programmed death protein (PD-1), creating an opportunity for PD-1 pathway blockade with PD-1 inhibitors such as pembrolizumab, according to the investigators.
Responses in 10 of 14 given pembrolizumab
Dr. Paul Nghiem of the University of Washington in Seattle, led an open-label, single-arm, multicenter phase II trial of pembrolizumab, which is approved for metastatic melanoma and which could become the first systemic therapy for unresectable or metastatic MCC (Abstract 22LBA).
In the study, which opened in January 2015, there are 24 evaluable patients treated with pembrolizumab 2 mg/kg every 3 weeks for up to 2 years. Fourteen had at least one posttreatment scan; 10 of these 14 patients (71%) have responded, 2 had complete responses. One patient had stable disease and three progressed.
“Responses were rapid, and appear more durable than we see with chemotherapy,” Dr. Nghiem said.
The drug was generally well tolerated, with an adverse event profile similar to what has been seen in melanoma. One patient experienced grade 4 myocarditis after one dose and one developed grade 4 transaminase elevation after two doses. Both improved after discontinuing pembrolizumab and starting corticosteroids.
“Strikingly, despite receiving only one or two doses, both patients had profound and ongoing responses to pembrolizumab,” Dr. Nghiem observed.
Many subjects had “profound shrinkage of tumor that has not rebounded,” he noted. “Pembrolizumab looks to be very favorable in terms of durability of response. With chemotherapy, at 90 days half of our patients have gone off treatment.”
The researchers are considering expanding the study population, and may include a chemotherapy-relapsed cohort. They are also analyzing biomarkers, and hope to evaluate response according to virus-positive versus virus-negative status.
Dr. Caroline Robert of the Institut Gustave Roussy in Villejuif, France, commented on the findings, first noting the difficulty of treating patients for whom there are no approved therapies. Median overall survival is less than 10 months, she said, and clinicians have lacked clinical trials to enroll patients.
“MCC patients represent a high medical need,” she said. Although the results with pembrolizumab are early, “they are very promising.”
Intratumoral plasmid IL-12
Dr. Shailender Bhatia of the University of Washington in Seattle, described a different immunotherapeutic approach in an MCC population (Abstract 504).
IL-12, which regulates adaptive type-1 immunity, has demonstrated antitumor efficacy in MCC but is associated with severe toxicities when administered systemically. Local IL-12 delivery to the tumor microenvironment “may provide adequate cytokine concentration in the vicinity of tumor antigens, and therefore improve efficacy while sparing systemic toxicity,” he said.
Intratumoral IL-12 plasmid DNA (pIL-12) injection with electroporation (which uses pulsed electricity to open pores in cell membranes) has shown antitumor activity in melanoma, and might also work in MCC, Dr. Bhatia and his colleagues hypothesized. The concept is one of promoting tumor inflammation and thereby a systemic antitumor immune response. This would be reflected, and measured, by increased IL-12 protein expression in the tumor microenvironment, which became this study’s primary endpoint.
“To the best of our knowledge, this study represents the first prospective clinical trial of immunotherapy in advanced MCC,” Dr. Bhatia noted.
Beginning in January 2012, the study enrolled 15 patients with MCC and superficial injectable tumors. Patients received injections of pIL-12 on days 1, 5, and 8; 2 weeks later, on day 22, their lesions were biopsied. The 3-person cohort with localized MCC (stage IIIb) then underwent definitive surgery and/or radiation therapy starting in week 4, while the 12 with distant metastatic disease (stage IV) could receive additional treatment cycles (maximum of 4) at least 6 weeks apart.
The treatment was well tolerated, with most adverse events – primarily pain and local inflammatory reaction – being mild and transient. No patients discontinued because of toxicity.
The primary endpoint, sustained local expression of IL-12 protein on day 22, was observed in 79% of patients. In paired biopsy samples, comparing baseline to day 22 levels, IL-12 protein expression increased by almost 2-fold to more than 3,000-fold.
In addition, enrichment of Merkel cell polyomavirus-specific CD8-positive T cells were found in the tumor infiltrating lymphocytes (TILs) of treated and distant tumors in some patients.
“Additionally, the pIL-12/electroporation treatment led to objective clinical responses in metastatic MCC,” Dr. Bhatia reported.
Among the three patients with locally advanced disease, one had a pathologic complete response and remains free of recurrence more than 6 months later. Another patient has been recurrence free for more than 3 years. The third patient was recurrence free for 9 months before developing progressive disease.
Among the 12 patients with metastatic disease, 3 responded to treatment and 1 achieved stable disease, while 8 (52%) progressed.
The injections led to regression not only of treated lesions, but also of clearly distinct noninjected MCC tumors. The proportion of treated lesions with major (more than 30%) regression was 44%. Among 10 patients with at least one distant lesion, 30% of noninjected distant lesions regressed.
“We believe this approach warrants further exploration in MCC, perhaps in combination with emerging systemic therapies, such as anti-PD-1/PD-L1 agents,” Dr. Bhatia said.
Dr. Nghiem and Dr. Bhatia had no relevant disclosures. In the IL-12 study, some investigators have financial relationships with OncoSec Medical, which manufactures the study drug.
VIENNA – High response rates to pembrolizumab and to intratumoral delivery of plasmid interleukin-12 (IL-12) were observed among patients with advanced Merkel cell carcinoma (MCC), based on studies presented at the 2015 European Cancer Congress.
There is strong rationale for immunotherapy in MCC. For one thing, the Merkel cell polyomavirus, which is expressed in 80% of tumors, serves as a powerful antigen for stimulating an immune response. Secondly, MCC tumors often express the ligand for the programmed death protein (PD-1), creating an opportunity for PD-1 pathway blockade with PD-1 inhibitors such as pembrolizumab, according to the investigators.
Responses in 10 of 14 given pembrolizumab
Dr. Paul Nghiem of the University of Washington in Seattle, led an open-label, single-arm, multicenter phase II trial of pembrolizumab, which is approved for metastatic melanoma and which could become the first systemic therapy for unresectable or metastatic MCC (Abstract 22LBA).
In the study, which opened in January 2015, there are 24 evaluable patients treated with pembrolizumab 2 mg/kg every 3 weeks for up to 2 years. Fourteen had at least one posttreatment scan; 10 of these 14 patients (71%) have responded, 2 had complete responses. One patient had stable disease and three progressed.
“Responses were rapid, and appear more durable than we see with chemotherapy,” Dr. Nghiem said.
The drug was generally well tolerated, with an adverse event profile similar to what has been seen in melanoma. One patient experienced grade 4 myocarditis after one dose and one developed grade 4 transaminase elevation after two doses. Both improved after discontinuing pembrolizumab and starting corticosteroids.
“Strikingly, despite receiving only one or two doses, both patients had profound and ongoing responses to pembrolizumab,” Dr. Nghiem observed.
Many subjects had “profound shrinkage of tumor that has not rebounded,” he noted. “Pembrolizumab looks to be very favorable in terms of durability of response. With chemotherapy, at 90 days half of our patients have gone off treatment.”
The researchers are considering expanding the study population, and may include a chemotherapy-relapsed cohort. They are also analyzing biomarkers, and hope to evaluate response according to virus-positive versus virus-negative status.
Dr. Caroline Robert of the Institut Gustave Roussy in Villejuif, France, commented on the findings, first noting the difficulty of treating patients for whom there are no approved therapies. Median overall survival is less than 10 months, she said, and clinicians have lacked clinical trials to enroll patients.
“MCC patients represent a high medical need,” she said. Although the results with pembrolizumab are early, “they are very promising.”
Intratumoral plasmid IL-12
Dr. Shailender Bhatia of the University of Washington in Seattle, described a different immunotherapeutic approach in an MCC population (Abstract 504).
IL-12, which regulates adaptive type-1 immunity, has demonstrated antitumor efficacy in MCC but is associated with severe toxicities when administered systemically. Local IL-12 delivery to the tumor microenvironment “may provide adequate cytokine concentration in the vicinity of tumor antigens, and therefore improve efficacy while sparing systemic toxicity,” he said.
Intratumoral IL-12 plasmid DNA (pIL-12) injection with electroporation (which uses pulsed electricity to open pores in cell membranes) has shown antitumor activity in melanoma, and might also work in MCC, Dr. Bhatia and his colleagues hypothesized. The concept is one of promoting tumor inflammation and thereby a systemic antitumor immune response. This would be reflected, and measured, by increased IL-12 protein expression in the tumor microenvironment, which became this study’s primary endpoint.
“To the best of our knowledge, this study represents the first prospective clinical trial of immunotherapy in advanced MCC,” Dr. Bhatia noted.
Beginning in January 2012, the study enrolled 15 patients with MCC and superficial injectable tumors. Patients received injections of pIL-12 on days 1, 5, and 8; 2 weeks later, on day 22, their lesions were biopsied. The 3-person cohort with localized MCC (stage IIIb) then underwent definitive surgery and/or radiation therapy starting in week 4, while the 12 with distant metastatic disease (stage IV) could receive additional treatment cycles (maximum of 4) at least 6 weeks apart.
The treatment was well tolerated, with most adverse events – primarily pain and local inflammatory reaction – being mild and transient. No patients discontinued because of toxicity.
The primary endpoint, sustained local expression of IL-12 protein on day 22, was observed in 79% of patients. In paired biopsy samples, comparing baseline to day 22 levels, IL-12 protein expression increased by almost 2-fold to more than 3,000-fold.
In addition, enrichment of Merkel cell polyomavirus-specific CD8-positive T cells were found in the tumor infiltrating lymphocytes (TILs) of treated and distant tumors in some patients.
“Additionally, the pIL-12/electroporation treatment led to objective clinical responses in metastatic MCC,” Dr. Bhatia reported.
Among the three patients with locally advanced disease, one had a pathologic complete response and remains free of recurrence more than 6 months later. Another patient has been recurrence free for more than 3 years. The third patient was recurrence free for 9 months before developing progressive disease.
Among the 12 patients with metastatic disease, 3 responded to treatment and 1 achieved stable disease, while 8 (52%) progressed.
The injections led to regression not only of treated lesions, but also of clearly distinct noninjected MCC tumors. The proportion of treated lesions with major (more than 30%) regression was 44%. Among 10 patients with at least one distant lesion, 30% of noninjected distant lesions regressed.
“We believe this approach warrants further exploration in MCC, perhaps in combination with emerging systemic therapies, such as anti-PD-1/PD-L1 agents,” Dr. Bhatia said.
Dr. Nghiem and Dr. Bhatia had no relevant disclosures. In the IL-12 study, some investigators have financial relationships with OncoSec Medical, which manufactures the study drug.
AT THE EUROPEAN CANCER CONGRESS 2015
Key clinical point: Merkel cell carcinoma may respond well to immunotherapeutic approaches.
Major finding: Patients had robust and durable responses to the PD-1 inhibitor pembrolizumab and to intratumoral IL-12 injections.
Data source: Single-arm open label studies; pembrolizumab study included 24 patients. IL-2 study included 15 patients.
Disclosures: Dr. Nghiem reported no conflicts of interest. In the IL-12 study, some investigators have financial relationships with OncoSec Medical, which manufactures the study drug. Dr. Bhatia had no relevant disclosures.

Nab-paclitaxel marginally superior to dacarbazine for metastatic melanoma
In chemotherapy-naive patients with metastatic melanoma, progression-free survival (PFS) was significantly longer with nab-paclitaxel, compared with dacarbazine, according to results from a phase III trial.
Median PFS for the nab-paclitaxel arm vs. the dacarbazine arm was 4.8 vs. 2.5 months, respectively (hazard ratio, 0.792; 95% confidence interval, 0.631-0.992; P = .044). Overall survival was similar in the two arms: 12.6 months for nab-paclitaxel vs. 10.5 months for dacarbazine (P = .27). The nab-paclitaxel group had an increased, but not significant, overall response rate (15% vs. 11%) and a significantly improved disease control rate (P = .004). The disease control rate reflects the number of complete responses plus partial responses plus stable disease for 16 or more weeks.
Nab-paclitaxel benefited patients regardless of BRAF mutation status, noted Dr. Evan Hersh, professor of medicine at the University of Arizona, Tucson, and colleagues.
“Additionally, in a post hoc analysis of this trial, nab-paclitaxel was shown to benefit a subgroup of patients with low or absent TILs [tumor-infiltrating lymphocytes], a poor prognostic factor in melanoma,” they wrote (Ann Oncol 2015 Sep 26. doi: 10.1093/annonc/mdv324).
The most common treatment-related adverse events of grade 3 or greater were neuropathy (25% vs. 0%), neutropenia (20% vs. 10%), and leukopenia (12% vs. 7%) for the nab-paclitaxel and dacarbazine arms, respectively. The median onset of grade 3 or greater peripheral neuropathy was 101 days after treatment began.
Between April 2009 and June 2011, the multicenter, phase III, randomized, controlled trial enrolled 529 adults with stage IV malignant melanoma who had no prior cytotoxic therapy.
A majority of participants from both treatment arms underwent post-study therapy, including newer agents such as BRAF inhibitors and ipilimumab. This may account for the diminished treatment affect of nab-paclitaxel on overall survival, compared with the more significant benefit in PFS observed early in the study.
A biomarker analysis found no correlation between tumor expression of the albumin-binding protein SPARC and PFS with nab-paclitaxel treatment. SPARC was hypothesized to enrich nab-paclitaxel in the tumor microenvironment thereby increasing its efficacy.
The study by Hersh et al. was conceived prior to the success of immune checkpoint inhibitors and targeted therapies for melanoma. The treatment landscape has changed rapidly, and the current role of chemotherapy, and nab-paclitaxel specifically, is uncertain.
In the last 5 years, four classes of therapies have significantly improved overall survival over dacarbazine: ipilimumab (HR, 0.72; P less than .001), vemurafenib (HR, 0.37; P less than .001), trametinib (HR, 0.54; P = .01), and nivolumab (HR, 0.42; P less than .001).
For the large majority of patients, chemotherapy would not be considered for the first line of therapy. Patients typically considered for chemotherapy would have failed or would have been intolerant to ipilimumab and an anti-PD1 agent, as well as BRAF/MEK inhibitors if the tumors were BRAF-mutation positive. In these heavily pretreated patients, however, toxicities associated with chemotherapy may outweigh benefits.
In patients with a history of autoimmune disease, some have suggested checkpoint inhibitors may exacerbate these conditions. However, recent retrospective studies suggest that ipilimumab is safe for patients with autoimmune disorders such as inflammatory bowel disease and rheumatoid arthritis.
The current study did not include quality of life data, and given the lack of improvement in overall survival, the superiority of nab-paclitaxel over dacarbazine has not been shown definitively.
Chemotherapy may have a role in combination with targeted or immunotherapeutic agents. Checkpoint inhibitors may be more active in patients with baseline tumor-infiltrating lymphocytes (TILs) and tumor PDL1 expression. Chemotherapy may induce TILs in tumors where the cells are low or absent, and nab-paclitaxel may be a good candidate to explore such combinations.
It remains to be determined if chemotherapy offers greater benefit than the many other strategies under consideration. This brings to the forefront the urgent need for preclinical models to enable comparisons of combination strategies.
Dr. Matteo Carlino is a clinical senior lecturer at the Sydney Medical School, University of Sydney and a medical oncologist at Westmead Hospital and Blacktown Hospital, Australia. Dr. Georgina Long is an associate professor and medical oncologist at Melanoma Institute Australia, University of Sydney. These remarks were part of an editorial accompanying the report (Ann Oncol. 2015 Sep 15. doi: 10.1093/annonc/mdv361). Dr. Carlino and Dr. Long reported having no disclosures.
The study by Hersh et al. was conceived prior to the success of immune checkpoint inhibitors and targeted therapies for melanoma. The treatment landscape has changed rapidly, and the current role of chemotherapy, and nab-paclitaxel specifically, is uncertain.
In the last 5 years, four classes of therapies have significantly improved overall survival over dacarbazine: ipilimumab (HR, 0.72; P less than .001), vemurafenib (HR, 0.37; P less than .001), trametinib (HR, 0.54; P = .01), and nivolumab (HR, 0.42; P less than .001).
For the large majority of patients, chemotherapy would not be considered for the first line of therapy. Patients typically considered for chemotherapy would have failed or would have been intolerant to ipilimumab and an anti-PD1 agent, as well as BRAF/MEK inhibitors if the tumors were BRAF-mutation positive. In these heavily pretreated patients, however, toxicities associated with chemotherapy may outweigh benefits.
In patients with a history of autoimmune disease, some have suggested checkpoint inhibitors may exacerbate these conditions. However, recent retrospective studies suggest that ipilimumab is safe for patients with autoimmune disorders such as inflammatory bowel disease and rheumatoid arthritis.
The current study did not include quality of life data, and given the lack of improvement in overall survival, the superiority of nab-paclitaxel over dacarbazine has not been shown definitively.
Chemotherapy may have a role in combination with targeted or immunotherapeutic agents. Checkpoint inhibitors may be more active in patients with baseline tumor-infiltrating lymphocytes (TILs) and tumor PDL1 expression. Chemotherapy may induce TILs in tumors where the cells are low or absent, and nab-paclitaxel may be a good candidate to explore such combinations.
It remains to be determined if chemotherapy offers greater benefit than the many other strategies under consideration. This brings to the forefront the urgent need for preclinical models to enable comparisons of combination strategies.
Dr. Matteo Carlino is a clinical senior lecturer at the Sydney Medical School, University of Sydney and a medical oncologist at Westmead Hospital and Blacktown Hospital, Australia. Dr. Georgina Long is an associate professor and medical oncologist at Melanoma Institute Australia, University of Sydney. These remarks were part of an editorial accompanying the report (Ann Oncol. 2015 Sep 15. doi: 10.1093/annonc/mdv361). Dr. Carlino and Dr. Long reported having no disclosures.
The study by Hersh et al. was conceived prior to the success of immune checkpoint inhibitors and targeted therapies for melanoma. The treatment landscape has changed rapidly, and the current role of chemotherapy, and nab-paclitaxel specifically, is uncertain.
In the last 5 years, four classes of therapies have significantly improved overall survival over dacarbazine: ipilimumab (HR, 0.72; P less than .001), vemurafenib (HR, 0.37; P less than .001), trametinib (HR, 0.54; P = .01), and nivolumab (HR, 0.42; P less than .001).
For the large majority of patients, chemotherapy would not be considered for the first line of therapy. Patients typically considered for chemotherapy would have failed or would have been intolerant to ipilimumab and an anti-PD1 agent, as well as BRAF/MEK inhibitors if the tumors were BRAF-mutation positive. In these heavily pretreated patients, however, toxicities associated with chemotherapy may outweigh benefits.
In patients with a history of autoimmune disease, some have suggested checkpoint inhibitors may exacerbate these conditions. However, recent retrospective studies suggest that ipilimumab is safe for patients with autoimmune disorders such as inflammatory bowel disease and rheumatoid arthritis.
The current study did not include quality of life data, and given the lack of improvement in overall survival, the superiority of nab-paclitaxel over dacarbazine has not been shown definitively.
Chemotherapy may have a role in combination with targeted or immunotherapeutic agents. Checkpoint inhibitors may be more active in patients with baseline tumor-infiltrating lymphocytes (TILs) and tumor PDL1 expression. Chemotherapy may induce TILs in tumors where the cells are low or absent, and nab-paclitaxel may be a good candidate to explore such combinations.
It remains to be determined if chemotherapy offers greater benefit than the many other strategies under consideration. This brings to the forefront the urgent need for preclinical models to enable comparisons of combination strategies.
Dr. Matteo Carlino is a clinical senior lecturer at the Sydney Medical School, University of Sydney and a medical oncologist at Westmead Hospital and Blacktown Hospital, Australia. Dr. Georgina Long is an associate professor and medical oncologist at Melanoma Institute Australia, University of Sydney. These remarks were part of an editorial accompanying the report (Ann Oncol. 2015 Sep 15. doi: 10.1093/annonc/mdv361). Dr. Carlino and Dr. Long reported having no disclosures.
In chemotherapy-naive patients with metastatic melanoma, progression-free survival (PFS) was significantly longer with nab-paclitaxel, compared with dacarbazine, according to results from a phase III trial.
Median PFS for the nab-paclitaxel arm vs. the dacarbazine arm was 4.8 vs. 2.5 months, respectively (hazard ratio, 0.792; 95% confidence interval, 0.631-0.992; P = .044). Overall survival was similar in the two arms: 12.6 months for nab-paclitaxel vs. 10.5 months for dacarbazine (P = .27). The nab-paclitaxel group had an increased, but not significant, overall response rate (15% vs. 11%) and a significantly improved disease control rate (P = .004). The disease control rate reflects the number of complete responses plus partial responses plus stable disease for 16 or more weeks.
Nab-paclitaxel benefited patients regardless of BRAF mutation status, noted Dr. Evan Hersh, professor of medicine at the University of Arizona, Tucson, and colleagues.
“Additionally, in a post hoc analysis of this trial, nab-paclitaxel was shown to benefit a subgroup of patients with low or absent TILs [tumor-infiltrating lymphocytes], a poor prognostic factor in melanoma,” they wrote (Ann Oncol 2015 Sep 26. doi: 10.1093/annonc/mdv324).
The most common treatment-related adverse events of grade 3 or greater were neuropathy (25% vs. 0%), neutropenia (20% vs. 10%), and leukopenia (12% vs. 7%) for the nab-paclitaxel and dacarbazine arms, respectively. The median onset of grade 3 or greater peripheral neuropathy was 101 days after treatment began.
Between April 2009 and June 2011, the multicenter, phase III, randomized, controlled trial enrolled 529 adults with stage IV malignant melanoma who had no prior cytotoxic therapy.
A majority of participants from both treatment arms underwent post-study therapy, including newer agents such as BRAF inhibitors and ipilimumab. This may account for the diminished treatment affect of nab-paclitaxel on overall survival, compared with the more significant benefit in PFS observed early in the study.
A biomarker analysis found no correlation between tumor expression of the albumin-binding protein SPARC and PFS with nab-paclitaxel treatment. SPARC was hypothesized to enrich nab-paclitaxel in the tumor microenvironment thereby increasing its efficacy.
In chemotherapy-naive patients with metastatic melanoma, progression-free survival (PFS) was significantly longer with nab-paclitaxel, compared with dacarbazine, according to results from a phase III trial.
Median PFS for the nab-paclitaxel arm vs. the dacarbazine arm was 4.8 vs. 2.5 months, respectively (hazard ratio, 0.792; 95% confidence interval, 0.631-0.992; P = .044). Overall survival was similar in the two arms: 12.6 months for nab-paclitaxel vs. 10.5 months for dacarbazine (P = .27). The nab-paclitaxel group had an increased, but not significant, overall response rate (15% vs. 11%) and a significantly improved disease control rate (P = .004). The disease control rate reflects the number of complete responses plus partial responses plus stable disease for 16 or more weeks.
Nab-paclitaxel benefited patients regardless of BRAF mutation status, noted Dr. Evan Hersh, professor of medicine at the University of Arizona, Tucson, and colleagues.
“Additionally, in a post hoc analysis of this trial, nab-paclitaxel was shown to benefit a subgroup of patients with low or absent TILs [tumor-infiltrating lymphocytes], a poor prognostic factor in melanoma,” they wrote (Ann Oncol 2015 Sep 26. doi: 10.1093/annonc/mdv324).
The most common treatment-related adverse events of grade 3 or greater were neuropathy (25% vs. 0%), neutropenia (20% vs. 10%), and leukopenia (12% vs. 7%) for the nab-paclitaxel and dacarbazine arms, respectively. The median onset of grade 3 or greater peripheral neuropathy was 101 days after treatment began.
Between April 2009 and June 2011, the multicenter, phase III, randomized, controlled trial enrolled 529 adults with stage IV malignant melanoma who had no prior cytotoxic therapy.
A majority of participants from both treatment arms underwent post-study therapy, including newer agents such as BRAF inhibitors and ipilimumab. This may account for the diminished treatment affect of nab-paclitaxel on overall survival, compared with the more significant benefit in PFS observed early in the study.
A biomarker analysis found no correlation between tumor expression of the albumin-binding protein SPARC and PFS with nab-paclitaxel treatment. SPARC was hypothesized to enrich nab-paclitaxel in the tumor microenvironment thereby increasing its efficacy.
FROM ANNALS OF ONCOLOGY
Key clinical point: Nab-pacilitaxel had significantly longer PFS than dacarbazine in chemotherapy-naive patients with metastatic melanoma.
Major finding: Median PFS in the nab-paclitaxel vs. dacarbazine arms was 4.8 vs. 2.5 months, respectively (HR, 0.792; 95% CI, 0.631-0.992; P = .044).
Data source: The phase III, randomized, controlled trial enrolled 529 patients between April 2009 and June 2011.
Disclosures: Dr. Hersh reported research funding from Celgene. His coauthors reported financial ties to several industry sources.
Erythematous Scaly Patch on the Jawline
The Diagnosis: Amelanotic Melanoma In Situ
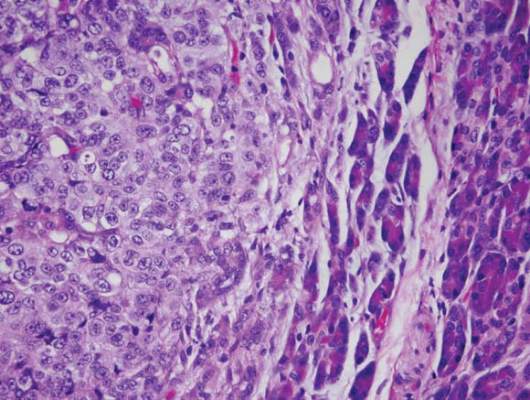
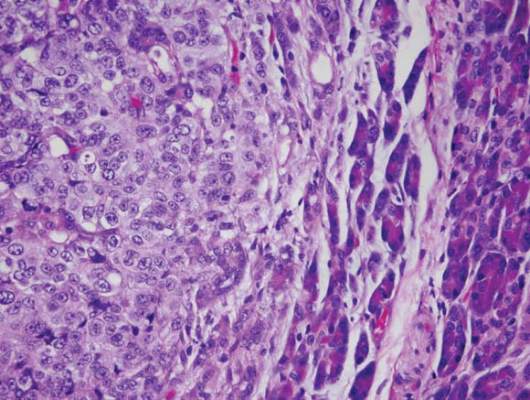
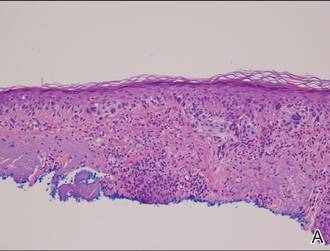
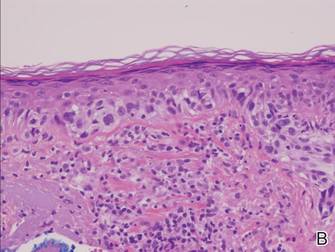
Histopathology revealed a broad asymmetric melanocytic proliferation at the dermoepidermal junction, consisting both of singly dispersed cells as well as randomly positioned nests (Figure 1). The single cells demonstrated junctional confluence and extension along adnexal structures highlighted by melan-A stain (Figure 2). The melanocytes were markedly atypical with enlarged and hyperchromatic nuclei containing multiple nucleoli. No dermal involvement was seen. There was papillary dermal fibrosis and an active host lymphocytic response. Based on these findings, a diagnosis of amelanotic melanoma in situ was made.
|
Figure 1. Histopathology revealed confluence of atypical melanocytes at the dermoepidermal junction and pagetoid scatter of melanocytes to the spinous layer (A)(H&E, original magnification ×4). Higher-power magnification highlighted the atypia of the individual melanocytes (B)(H&E, original magnification ×10). |
Subsequent scouting punch biopsies at the superior, anterior, and posterior aspects of the lesion were performed (Figure 3). All 3 revealed a similar nested and single cell proliferation at the dermoepidermal junction, confirming residual amelanotic melanoma in situ. The patient was referred to the otolaryngology department and underwent wide local excision with 5-mm margins and reconstructive repair.
Amelanotic melanoma comprises 2% to 8% of cutaneous melanomas. It is more common in fair-skinned elderly women with an average age of diagnosis of 61.8 years. Because features typically associated with melanoma such as asymmetry, border irregularity, and color variegation often are absent, amelanotic melanoma represents a notable diagnostic challenge for clinicians. Lesions can present nonspecifically as erythematous macules, papules, patches, or plaques and can have associated pruritus and scale.1,2

Clinical misdiagnoses for amelanotic melanoma include Bowen disease, basal cell carcinoma, actinic keratosis, lichenoid keratosis, intradermal nevus, dermatofibroma, inflamed seborrheic keratosis, nummular dermatitis, pyogenic granuloma, and granuloma annulare.1-6 There have been few case reports of amelanotic melanoma in situ, with most being the lentigo maligna variant that were initially clinically diagnosed as superficial basal cell carcinoma, Bowen disease, or dermatitis.7,8 In one case report, an amelanotic lentigo maligna was incidentally discovered after performing a mapping shave biopsy on what was normal-appearing skin.9
Dermoscopic evidence of vascular structures in lesions, including the presence of dotted vessels, milky red areas, and/or serpentine (linear irregular) vessels, may be the only clues to suggest amelanotic melanoma before biopsy. However, these findings are nonspecific and can be seen in other benign and malignant skin conditions.2
Complete surgical excision is the standard treatment of amelanotic melanoma in situ given its potential for invasion. However, the lack of pigment can make margins difficult to define. Because of its ability to detect disease beyond visual margins, Mohs micrographic surgery may have better cure rates than conventional excision.4 Prognosis for amelanotic melanoma is the same as other melanomas of equal thickness and location, though delay in diagnosis can adversely affect outcomes. Furthermore, amelanotic melanoma in situ can rapidly progress to invasive melanoma.3,5 Thus it is important to maintain clinical suspicion for amelanotic melanoma in fair-skinned elderly women presenting with a persistent or recurring erythematous scaly lesion on sun-exposed skin.
- Rahbari H, Nabai H, Mehregan AH, et al. Amelanotic lentigo maligna melanoma: a diagnostic conundrum— presentation of four new cases. Cancer. 1996;77:2052-2057.
- Jaimes N, Braun RP, Thomas L, et al. Clinical and dermoscopic characteristics of amelanotic melanomas that are not of the nodular subtype. J Eur Acad Dermatol Venereol. 2012;26:591-596.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000;42:731-734.
- Conrad N, Jackson B, Goldberg L. Amelanotic lentigo maligna melanoma: a unique case presentation. Dermatol Surg. 1999;25:408-411.
- Cliff S, Otter M, Holden CA. Amelanotic lentigo maligna melanoma of the face: a case report and review of the literature. Clin Exp Dermatol. 1997;22:177-179.
- Dalton SR, Fillman EP, Altman CE, et al. Atypical junctional melanocytic proliferations in benign lichenoid keratosis. Hum Pathol. 2003;34:706-709.
- Paver K, Stewart M, Kossard S, et al. Amelanotic lentigo maligna. Australas J Dermatol. 1981;22:106-108.
- Lewis JE. Lentigo maligna presenting as an eczematous lesion. Cutis. 1987;40:357-359.
- Perera E, Mellick N, Teng P, et al. A clinically invisible melanoma. Australas J Dermatol. 2014;55:e58-e59.
The Diagnosis: Amelanotic Melanoma In Situ
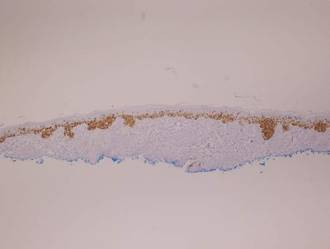
Histopathology revealed a broad asymmetric melanocytic proliferation at the dermoepidermal junction, consisting both of singly dispersed cells as well as randomly positioned nests (Figure 1). The single cells demonstrated junctional confluence and extension along adnexal structures highlighted by melan-A stain (Figure 2). The melanocytes were markedly atypical with enlarged and hyperchromatic nuclei containing multiple nucleoli. No dermal involvement was seen. There was papillary dermal fibrosis and an active host lymphocytic response. Based on these findings, a diagnosis of amelanotic melanoma in situ was made.
|
|
Figure 1. Histopathology revealed confluence of atypical melanocytes at the dermoepidermal junction and pagetoid scatter of melanocytes to the spinous layer (A)(H&E, original magnification ×4). Higher-power magnification highlighted the atypia of the individual melanocytes (B)(H&E, original magnification ×10). |
Subsequent scouting punch biopsies at the superior, anterior, and posterior aspects of the lesion were performed (Figure 3). All 3 revealed a similar nested and single cell proliferation at the dermoepidermal junction, confirming residual amelanotic melanoma in situ. The patient was referred to the otolaryngology department and underwent wide local excision with 5-mm margins and reconstructive repair.
Amelanotic melanoma comprises 2% to 8% of cutaneous melanomas. It is more common in fair-skinned elderly women with an average age of diagnosis of 61.8 years. Because features typically associated with melanoma such as asymmetry, border irregularity, and color variegation often are absent, amelanotic melanoma represents a notable diagnostic challenge for clinicians. Lesions can present nonspecifically as erythematous macules, papules, patches, or plaques and can have associated pruritus and scale.1,2
Clinical misdiagnoses for amelanotic melanoma include Bowen disease, basal cell carcinoma, actinic keratosis, lichenoid keratosis, intradermal nevus, dermatofibroma, inflamed seborrheic keratosis, nummular dermatitis, pyogenic granuloma, and granuloma annulare.1-6 There have been few case reports of amelanotic melanoma in situ, with most being the lentigo maligna variant that were initially clinically diagnosed as superficial basal cell carcinoma, Bowen disease, or dermatitis.7,8 In one case report, an amelanotic lentigo maligna was incidentally discovered after performing a mapping shave biopsy on what was normal-appearing skin.9
Dermoscopic evidence of vascular structures in lesions, including the presence of dotted vessels, milky red areas, and/or serpentine (linear irregular) vessels, may be the only clues to suggest amelanotic melanoma before biopsy. However, these findings are nonspecific and can be seen in other benign and malignant skin conditions.2
Complete surgical excision is the standard treatment of amelanotic melanoma in situ given its potential for invasion. However, the lack of pigment can make margins difficult to define. Because of its ability to detect disease beyond visual margins, Mohs micrographic surgery may have better cure rates than conventional excision.4 Prognosis for amelanotic melanoma is the same as other melanomas of equal thickness and location, though delay in diagnosis can adversely affect outcomes. Furthermore, amelanotic melanoma in situ can rapidly progress to invasive melanoma.3,5 Thus it is important to maintain clinical suspicion for amelanotic melanoma in fair-skinned elderly women presenting with a persistent or recurring erythematous scaly lesion on sun-exposed skin.
The Diagnosis: Amelanotic Melanoma In Situ
Histopathology revealed a broad asymmetric melanocytic proliferation at the dermoepidermal junction, consisting both of singly dispersed cells as well as randomly positioned nests (Figure 1). The single cells demonstrated junctional confluence and extension along adnexal structures highlighted by melan-A stain (Figure 2). The melanocytes were markedly atypical with enlarged and hyperchromatic nuclei containing multiple nucleoli. No dermal involvement was seen. There was papillary dermal fibrosis and an active host lymphocytic response. Based on these findings, a diagnosis of amelanotic melanoma in situ was made.
|
|
Figure 1. Histopathology revealed confluence of atypical melanocytes at the dermoepidermal junction and pagetoid scatter of melanocytes to the spinous layer (A)(H&E, original magnification ×4). Higher-power magnification highlighted the atypia of the individual melanocytes (B)(H&E, original magnification ×10). |
Subsequent scouting punch biopsies at the superior, anterior, and posterior aspects of the lesion were performed (Figure 3). All 3 revealed a similar nested and single cell proliferation at the dermoepidermal junction, confirming residual amelanotic melanoma in situ. The patient was referred to the otolaryngology department and underwent wide local excision with 5-mm margins and reconstructive repair.
Amelanotic melanoma comprises 2% to 8% of cutaneous melanomas. It is more common in fair-skinned elderly women with an average age of diagnosis of 61.8 years. Because features typically associated with melanoma such as asymmetry, border irregularity, and color variegation often are absent, amelanotic melanoma represents a notable diagnostic challenge for clinicians. Lesions can present nonspecifically as erythematous macules, papules, patches, or plaques and can have associated pruritus and scale.1,2
Clinical misdiagnoses for amelanotic melanoma include Bowen disease, basal cell carcinoma, actinic keratosis, lichenoid keratosis, intradermal nevus, dermatofibroma, inflamed seborrheic keratosis, nummular dermatitis, pyogenic granuloma, and granuloma annulare.1-6 There have been few case reports of amelanotic melanoma in situ, with most being the lentigo maligna variant that were initially clinically diagnosed as superficial basal cell carcinoma, Bowen disease, or dermatitis.7,8 In one case report, an amelanotic lentigo maligna was incidentally discovered after performing a mapping shave biopsy on what was normal-appearing skin.9
Dermoscopic evidence of vascular structures in lesions, including the presence of dotted vessels, milky red areas, and/or serpentine (linear irregular) vessels, may be the only clues to suggest amelanotic melanoma before biopsy. However, these findings are nonspecific and can be seen in other benign and malignant skin conditions.2
Complete surgical excision is the standard treatment of amelanotic melanoma in situ given its potential for invasion. However, the lack of pigment can make margins difficult to define. Because of its ability to detect disease beyond visual margins, Mohs micrographic surgery may have better cure rates than conventional excision.4 Prognosis for amelanotic melanoma is the same as other melanomas of equal thickness and location, though delay in diagnosis can adversely affect outcomes. Furthermore, amelanotic melanoma in situ can rapidly progress to invasive melanoma.3,5 Thus it is important to maintain clinical suspicion for amelanotic melanoma in fair-skinned elderly women presenting with a persistent or recurring erythematous scaly lesion on sun-exposed skin.
- Rahbari H, Nabai H, Mehregan AH, et al. Amelanotic lentigo maligna melanoma: a diagnostic conundrum— presentation of four new cases. Cancer. 1996;77:2052-2057.
- Jaimes N, Braun RP, Thomas L, et al. Clinical and dermoscopic characteristics of amelanotic melanomas that are not of the nodular subtype. J Eur Acad Dermatol Venereol. 2012;26:591-596.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000;42:731-734.
- Conrad N, Jackson B, Goldberg L. Amelanotic lentigo maligna melanoma: a unique case presentation. Dermatol Surg. 1999;25:408-411.
- Cliff S, Otter M, Holden CA. Amelanotic lentigo maligna melanoma of the face: a case report and review of the literature. Clin Exp Dermatol. 1997;22:177-179.
- Dalton SR, Fillman EP, Altman CE, et al. Atypical junctional melanocytic proliferations in benign lichenoid keratosis. Hum Pathol. 2003;34:706-709.
- Paver K, Stewart M, Kossard S, et al. Amelanotic lentigo maligna. Australas J Dermatol. 1981;22:106-108.
- Lewis JE. Lentigo maligna presenting as an eczematous lesion. Cutis. 1987;40:357-359.
- Perera E, Mellick N, Teng P, et al. A clinically invisible melanoma. Australas J Dermatol. 2014;55:e58-e59.
- Rahbari H, Nabai H, Mehregan AH, et al. Amelanotic lentigo maligna melanoma: a diagnostic conundrum— presentation of four new cases. Cancer. 1996;77:2052-2057.
- Jaimes N, Braun RP, Thomas L, et al. Clinical and dermoscopic characteristics of amelanotic melanomas that are not of the nodular subtype. J Eur Acad Dermatol Venereol. 2012;26:591-596.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000;42:731-734.
- Conrad N, Jackson B, Goldberg L. Amelanotic lentigo maligna melanoma: a unique case presentation. Dermatol Surg. 1999;25:408-411.
- Cliff S, Otter M, Holden CA. Amelanotic lentigo maligna melanoma of the face: a case report and review of the literature. Clin Exp Dermatol. 1997;22:177-179.
- Dalton SR, Fillman EP, Altman CE, et al. Atypical junctional melanocytic proliferations in benign lichenoid keratosis. Hum Pathol. 2003;34:706-709.
- Paver K, Stewart M, Kossard S, et al. Amelanotic lentigo maligna. Australas J Dermatol. 1981;22:106-108.
- Lewis JE. Lentigo maligna presenting as an eczematous lesion. Cutis. 1987;40:357-359.
- Perera E, Mellick N, Teng P, et al. A clinically invisible melanoma. Australas J Dermatol. 2014;55:e58-e59.

Atypia of the individual melanocytes.
Melan-A stain highlighted the density and confluence of melanocytes within the epidermis.
Three scouting punch biopsies were performed along the periphery of the lesion.
A 70-year-old white woman with a history of basal cell carcinoma presented with a 2.7×1.9-cm ill-defined, erythematous, scaly patch along the left side of the jawline. Ten months prior to presentation, the lesion appeared as a grayish macule that was clinically diagnosed as a pigmented actinic keratosis and was treated with cryotherapy with resolution noted at 6-month follow-up. Differential diagnosis of the current lesion included actinic keratosis, lichenoid keratosis, and superficial basal cell carcinoma. A shave biopsy was performed.

Children with multiple congenital melanocytic nevi should have CNS MRI
For children born with multiple congenital melanocytic nevi, a single MRI of the central nervous system within the first year of life was an effective way to screen for future outcomes, according to Dr. Regula Waelchli of Great Ormond Street Hospital for Children, London, and her associates.
Of the 271 children screened, 21% had an abnormal CNS MRI. An abnormal MRI increased the odds of negative future outcomes significantly. The most likely outcome was requirement for neurosurgery with an odds ratio of 71, followed by seizure with an OR of 13.4, and neurodevelopmental problems with an OR of 3.
The most common abnormality was intraparenchymal melanosis, present in most of the children with abnormal MRIs. However, if the only abnormality present was intraparenchymal melanosis, as it was for more than half of the abnormal group, no routine follow-up MRI was necessary and neurosurgery wasn’t required.
In patients with normal MRIs, seizures were temporary and/or easy to control with a single medication, and neurodevelopmental issues were mild, the investigators found.
While only those patients with an abnormality other than intraparenchymal melanosis require repeat MRIs, “any change in neurological status at any age should always trigger a repeat MRI, independent of the initial MRI findings,” Dr. Waelchli and her associates concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.13898).
For children born with multiple congenital melanocytic nevi, a single MRI of the central nervous system within the first year of life was an effective way to screen for future outcomes, according to Dr. Regula Waelchli of Great Ormond Street Hospital for Children, London, and her associates.
Of the 271 children screened, 21% had an abnormal CNS MRI. An abnormal MRI increased the odds of negative future outcomes significantly. The most likely outcome was requirement for neurosurgery with an odds ratio of 71, followed by seizure with an OR of 13.4, and neurodevelopmental problems with an OR of 3.
The most common abnormality was intraparenchymal melanosis, present in most of the children with abnormal MRIs. However, if the only abnormality present was intraparenchymal melanosis, as it was for more than half of the abnormal group, no routine follow-up MRI was necessary and neurosurgery wasn’t required.
In patients with normal MRIs, seizures were temporary and/or easy to control with a single medication, and neurodevelopmental issues were mild, the investigators found.
While only those patients with an abnormality other than intraparenchymal melanosis require repeat MRIs, “any change in neurological status at any age should always trigger a repeat MRI, independent of the initial MRI findings,” Dr. Waelchli and her associates concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.13898).
For children born with multiple congenital melanocytic nevi, a single MRI of the central nervous system within the first year of life was an effective way to screen for future outcomes, according to Dr. Regula Waelchli of Great Ormond Street Hospital for Children, London, and her associates.
Of the 271 children screened, 21% had an abnormal CNS MRI. An abnormal MRI increased the odds of negative future outcomes significantly. The most likely outcome was requirement for neurosurgery with an odds ratio of 71, followed by seizure with an OR of 13.4, and neurodevelopmental problems with an OR of 3.
The most common abnormality was intraparenchymal melanosis, present in most of the children with abnormal MRIs. However, if the only abnormality present was intraparenchymal melanosis, as it was for more than half of the abnormal group, no routine follow-up MRI was necessary and neurosurgery wasn’t required.
In patients with normal MRIs, seizures were temporary and/or easy to control with a single medication, and neurodevelopmental issues were mild, the investigators found.
While only those patients with an abnormality other than intraparenchymal melanosis require repeat MRIs, “any change in neurological status at any age should always trigger a repeat MRI, independent of the initial MRI findings,” Dr. Waelchli and her associates concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.13898).
Children with multiple congenital melanocytic nevi should have CNS MRI
For children born with multiple congenital melanocytic nevi, a single MRI of the central nervous system within the first year of life was an effective way to screen for future outcomes, according to Dr. Regula Waelchli of Great Ormond Street Hospital for Children, London, and her associates.
Of the 271 children screened, 21% had an abnormal CNS MRI. An abnormal MRI increased the odds of negative future outcomes significantly. The most likely outcome was requirement for neurosurgery with an odds ratio of 71, followed by seizure with an OR of 13.4, and neurodevelopmental problems with an OR of 3.
The most common abnormality was intraparenchymal melanosis, present in most of the children with abnormal MRIs. However, if the only abnormality present was intraparenchymal melanosis, as it was for more than half of the abnormal group, no routine follow-up MRI was necessary and neurosurgery wasn’t required.
In patients with normal MRIs, seizures were temporary and/or easy to control with a single medication, and neurodevelopmental issues were mild, the investigators found.
While only those patients with an abnormality other than intraparenchymal melanosis require repeat MRIs, “any change in neurological status at any age should always trigger a repeat MRI, independent of the initial MRI findings,” Dr. Waelchli and her associates concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.13898).
For children born with multiple congenital melanocytic nevi, a single MRI of the central nervous system within the first year of life was an effective way to screen for future outcomes, according to Dr. Regula Waelchli of Great Ormond Street Hospital for Children, London, and her associates.
Of the 271 children screened, 21% had an abnormal CNS MRI. An abnormal MRI increased the odds of negative future outcomes significantly. The most likely outcome was requirement for neurosurgery with an odds ratio of 71, followed by seizure with an OR of 13.4, and neurodevelopmental problems with an OR of 3.
The most common abnormality was intraparenchymal melanosis, present in most of the children with abnormal MRIs. However, if the only abnormality present was intraparenchymal melanosis, as it was for more than half of the abnormal group, no routine follow-up MRI was necessary and neurosurgery wasn’t required.
In patients with normal MRIs, seizures were temporary and/or easy to control with a single medication, and neurodevelopmental issues were mild, the investigators found.
While only those patients with an abnormality other than intraparenchymal melanosis require repeat MRIs, “any change in neurological status at any age should always trigger a repeat MRI, independent of the initial MRI findings,” Dr. Waelchli and her associates concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.13898).
For children born with multiple congenital melanocytic nevi, a single MRI of the central nervous system within the first year of life was an effective way to screen for future outcomes, according to Dr. Regula Waelchli of Great Ormond Street Hospital for Children, London, and her associates.
Of the 271 children screened, 21% had an abnormal CNS MRI. An abnormal MRI increased the odds of negative future outcomes significantly. The most likely outcome was requirement for neurosurgery with an odds ratio of 71, followed by seizure with an OR of 13.4, and neurodevelopmental problems with an OR of 3.
The most common abnormality was intraparenchymal melanosis, present in most of the children with abnormal MRIs. However, if the only abnormality present was intraparenchymal melanosis, as it was for more than half of the abnormal group, no routine follow-up MRI was necessary and neurosurgery wasn’t required.
In patients with normal MRIs, seizures were temporary and/or easy to control with a single medication, and neurodevelopmental issues were mild, the investigators found.
While only those patients with an abnormality other than intraparenchymal melanosis require repeat MRIs, “any change in neurological status at any age should always trigger a repeat MRI, independent of the initial MRI findings,” Dr. Waelchli and her associates concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.13898).
FDA approves nivolumab-ipilimumab combination for melanoma
Nivolumab, a programmed death receptor-1 (PD-1)–blocking antibody, has been approved for use in combination with ipilimumab for treating people with BRAF V600 wild-type, unresectable or metastatic melanoma.
Approval was based on demonstration of an increase in the objective response rate, prolonged response durations, and improvement in progression-free survival (PFS) in an international, multicenter, double-blind, randomized, two-arm, active-controlled trial in patients who were previously untreated for unresectable or metastatic, BRAF V600 wild-type melanoma, according to a Sept. 30 statement issued by the Food and Drug Administration.
Nivolumab, marketed as Opdivo Injection by Bristol-Myers Squibb, was approved in 2014 for the treatment of patients with unresectable or metastatic melanoma and disease progression following ipilimumab therapy and, if BRAF V600 mutation positive, a BRAF inhibitor. Ipilimumab, approved in 2011 and marketed as Yervoy by BMS, is a human cytotoxic T-lymphocyte antigen 4 (CTLA-4)–blocking antibody indicated for treating unresectable or metastatic melanoma.
“Combined nivolumab (anti–PD-1) and ipilimumab (anti–CTLA-4) mediated inhibition results in enhanced T-cell function that is greater than the effects of either antibody alone, and results in improved antitumor responses in metastatic melanoma,” the updated nivolumab prescribing information states.
This is the first FDA approval of a cancer treatment regimen that includes two immuno-oncology agents, according to the company’s statement announcing the approval.
The phase II CheckMate 069 study enrolled 142 patients, including 109 patients with BRAF V600 wild-type melanoma, randomized in a 2:1 ratio to receive the combination or ipilimumab plus placebo; their median age was 66 years; 84% had an ECOG performance score of 0, and 15% had a score of 1. The overall response rate was 60% among those on the combination therapy vs. 11% among those on ipilimumab alone – a 49% improvement (P less than .001), according to the FDA.
Nine of the 43 patients with an objective response (ranging from 3 to 7 months) in the combination therapy group “have progressed after response, died, or received subsequent therapy,” the FDA said. Among the 34 patients who continued to have a response at the last analysis, 14 had responses that had lasted from at least 6 months to less than 9 months. The remaining 20 patients had responses that had lasted at least 9 months.
The estimated median PFS was 8.9 months in the combination group vs. 4.7 months in the ipilimumab-only arm, a 60% reduced risk (P less than .002)
Serious adverse reactions, adverse reactions resulting in permanent discontinuation or a delayed dose, and grade 3 or 4 adverse reaction were higher among those treated with the combination. Colitis, diarrhea, pyrexia, and pneumonitis were the most common serious adverse reactions among those on the combination.
The recommended dose and schedule is as follows, according to the FDA: 1 mg/kg of nivolumab administered as an IV infusion over 60 minutes, followed by ipilimumab on the same day, every 3 weeks for four doses. “The recommended subsequent dose of nivolumab, as a single agent, is 3 mg/kg as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity.”
Both indications for nivolumab were approved as accelerated approvals, based on the “tumor response rate and durability of response. Continued approval for these indications may be contingent upon verification and description of clinical benefit in the confirmatory trials,” according to the prescribing information.
Serious adverse events associated with this therapy should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch.
Nivolumab, a programmed death receptor-1 (PD-1)–blocking antibody, has been approved for use in combination with ipilimumab for treating people with BRAF V600 wild-type, unresectable or metastatic melanoma.
Approval was based on demonstration of an increase in the objective response rate, prolonged response durations, and improvement in progression-free survival (PFS) in an international, multicenter, double-blind, randomized, two-arm, active-controlled trial in patients who were previously untreated for unresectable or metastatic, BRAF V600 wild-type melanoma, according to a Sept. 30 statement issued by the Food and Drug Administration.
Nivolumab, marketed as Opdivo Injection by Bristol-Myers Squibb, was approved in 2014 for the treatment of patients with unresectable or metastatic melanoma and disease progression following ipilimumab therapy and, if BRAF V600 mutation positive, a BRAF inhibitor. Ipilimumab, approved in 2011 and marketed as Yervoy by BMS, is a human cytotoxic T-lymphocyte antigen 4 (CTLA-4)–blocking antibody indicated for treating unresectable or metastatic melanoma.
“Combined nivolumab (anti–PD-1) and ipilimumab (anti–CTLA-4) mediated inhibition results in enhanced T-cell function that is greater than the effects of either antibody alone, and results in improved antitumor responses in metastatic melanoma,” the updated nivolumab prescribing information states.
This is the first FDA approval of a cancer treatment regimen that includes two immuno-oncology agents, according to the company’s statement announcing the approval.
The phase II CheckMate 069 study enrolled 142 patients, including 109 patients with BRAF V600 wild-type melanoma, randomized in a 2:1 ratio to receive the combination or ipilimumab plus placebo; their median age was 66 years; 84% had an ECOG performance score of 0, and 15% had a score of 1. The overall response rate was 60% among those on the combination therapy vs. 11% among those on ipilimumab alone – a 49% improvement (P less than .001), according to the FDA.
Nine of the 43 patients with an objective response (ranging from 3 to 7 months) in the combination therapy group “have progressed after response, died, or received subsequent therapy,” the FDA said. Among the 34 patients who continued to have a response at the last analysis, 14 had responses that had lasted from at least 6 months to less than 9 months. The remaining 20 patients had responses that had lasted at least 9 months.
The estimated median PFS was 8.9 months in the combination group vs. 4.7 months in the ipilimumab-only arm, a 60% reduced risk (P less than .002)
Serious adverse reactions, adverse reactions resulting in permanent discontinuation or a delayed dose, and grade 3 or 4 adverse reaction were higher among those treated with the combination. Colitis, diarrhea, pyrexia, and pneumonitis were the most common serious adverse reactions among those on the combination.
The recommended dose and schedule is as follows, according to the FDA: 1 mg/kg of nivolumab administered as an IV infusion over 60 minutes, followed by ipilimumab on the same day, every 3 weeks for four doses. “The recommended subsequent dose of nivolumab, as a single agent, is 3 mg/kg as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity.”
Both indications for nivolumab were approved as accelerated approvals, based on the “tumor response rate and durability of response. Continued approval for these indications may be contingent upon verification and description of clinical benefit in the confirmatory trials,” according to the prescribing information.
Serious adverse events associated with this therapy should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch.
Nivolumab, a programmed death receptor-1 (PD-1)–blocking antibody, has been approved for use in combination with ipilimumab for treating people with BRAF V600 wild-type, unresectable or metastatic melanoma.
Approval was based on demonstration of an increase in the objective response rate, prolonged response durations, and improvement in progression-free survival (PFS) in an international, multicenter, double-blind, randomized, two-arm, active-controlled trial in patients who were previously untreated for unresectable or metastatic, BRAF V600 wild-type melanoma, according to a Sept. 30 statement issued by the Food and Drug Administration.
Nivolumab, marketed as Opdivo Injection by Bristol-Myers Squibb, was approved in 2014 for the treatment of patients with unresectable or metastatic melanoma and disease progression following ipilimumab therapy and, if BRAF V600 mutation positive, a BRAF inhibitor. Ipilimumab, approved in 2011 and marketed as Yervoy by BMS, is a human cytotoxic T-lymphocyte antigen 4 (CTLA-4)–blocking antibody indicated for treating unresectable or metastatic melanoma.
“Combined nivolumab (anti–PD-1) and ipilimumab (anti–CTLA-4) mediated inhibition results in enhanced T-cell function that is greater than the effects of either antibody alone, and results in improved antitumor responses in metastatic melanoma,” the updated nivolumab prescribing information states.
This is the first FDA approval of a cancer treatment regimen that includes two immuno-oncology agents, according to the company’s statement announcing the approval.
The phase II CheckMate 069 study enrolled 142 patients, including 109 patients with BRAF V600 wild-type melanoma, randomized in a 2:1 ratio to receive the combination or ipilimumab plus placebo; their median age was 66 years; 84% had an ECOG performance score of 0, and 15% had a score of 1. The overall response rate was 60% among those on the combination therapy vs. 11% among those on ipilimumab alone – a 49% improvement (P less than .001), according to the FDA.
Nine of the 43 patients with an objective response (ranging from 3 to 7 months) in the combination therapy group “have progressed after response, died, or received subsequent therapy,” the FDA said. Among the 34 patients who continued to have a response at the last analysis, 14 had responses that had lasted from at least 6 months to less than 9 months. The remaining 20 patients had responses that had lasted at least 9 months.
The estimated median PFS was 8.9 months in the combination group vs. 4.7 months in the ipilimumab-only arm, a 60% reduced risk (P less than .002)
Serious adverse reactions, adverse reactions resulting in permanent discontinuation or a delayed dose, and grade 3 or 4 adverse reaction were higher among those treated with the combination. Colitis, diarrhea, pyrexia, and pneumonitis were the most common serious adverse reactions among those on the combination.
The recommended dose and schedule is as follows, according to the FDA: 1 mg/kg of nivolumab administered as an IV infusion over 60 minutes, followed by ipilimumab on the same day, every 3 weeks for four doses. “The recommended subsequent dose of nivolumab, as a single agent, is 3 mg/kg as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity.”
Both indications for nivolumab were approved as accelerated approvals, based on the “tumor response rate and durability of response. Continued approval for these indications may be contingent upon verification and description of clinical benefit in the confirmatory trials,” according to the prescribing information.
Serious adverse events associated with this therapy should be reported to the FDA’s MedWatch program at 800-332-1088 or www.fda.gov/medwatch.
Topical fluorouracil shows long-term benefit for actinic keratoses
One course of topical fluorouracil cream reduced the need for localized treatments and the number of actinic keratoses (AK) over a mean follow-up of 2.6 years in the Veterans Affairs Keratinocyte Carcinoma Chemoprevention (VAKCC) trial.
These results “indicate that treating a patient with a single course of fluorouracil would reduce the subsequent number of spot treatments and benefit care of patients with multiple AKs for longer than 2 years,” concluded Dr. Hyemin Pomerantz of the department of dermatoepidemiology at the Providence (R.I.) VA Medical Center and his coauthors. Previous studies on treating AKs with topical fluorouracil have followed up participants for less than 6 months, they pointed out (JAMA Dermatol. 2015;9:952-60).

In the randomized, double-blinded, placebo-controlled study, conducted from 2009 to 2011 at 12 VA dermatology clinics, participants received topical fluorouracil cream, 5%, or a vehicle control cream, applied twice a day for 4 weeks, and were followed up for a mean of 2.6 years. There were no significant differences in the baseline characteristics of the 468 participants randomized to receive fluorouracil cream and the 464 participants randomized to receive the control cream.
The mean total AK count on the face and ears in both groups was about 11. At 6 months, the mean number of AKs per participant had dropped to 3 in the fluorouracil group (a 73% reduction from baseline) vs. a mean of 8.1 in the control group, a 24% reduction from baseline (P less than .001). Over the study period, those treated with fluorouracil had significantly fewer AKs. Over the entire study, there was not a significant difference in the number of hypertrophic AKs between the two groups, although the number of hypertrophic AKs was lower in the treatment group at 6 months.
During the study period, more participants treated with fluorouracil had complete clearance of AKs on the face and ears, compared with the control group (P less than .001). Finally, the fluorouracil group required 2 spot treatments per visit per participant vs. 3.9 in the control group (P less than .001).
“Our findings highlight the long-term efficacy of topical fluorouracil cream in treating and preventing AKs. A single course of topical fluorouracil cream, 5%, treatment led to a sustained reduction of the number of AKs and subsequent AK treatments,” in the population of patients at high risk for basal cell and squamous cell carcinomas, the authors wrote.
The study was supported by the Office of Research and Development Cooperative Studies Program at the Department of Veterans Affairs. Three of the authors reported several disclosures, including serving as a consultant to several pharmaceutical companies; the others, including the lead author, had no disclosures.
One course of topical fluorouracil cream reduced the need for localized treatments and the number of actinic keratoses (AK) over a mean follow-up of 2.6 years in the Veterans Affairs Keratinocyte Carcinoma Chemoprevention (VAKCC) trial.
These results “indicate that treating a patient with a single course of fluorouracil would reduce the subsequent number of spot treatments and benefit care of patients with multiple AKs for longer than 2 years,” concluded Dr. Hyemin Pomerantz of the department of dermatoepidemiology at the Providence (R.I.) VA Medical Center and his coauthors. Previous studies on treating AKs with topical fluorouracil have followed up participants for less than 6 months, they pointed out (JAMA Dermatol. 2015;9:952-60).
In the randomized, double-blinded, placebo-controlled study, conducted from 2009 to 2011 at 12 VA dermatology clinics, participants received topical fluorouracil cream, 5%, or a vehicle control cream, applied twice a day for 4 weeks, and were followed up for a mean of 2.6 years. There were no significant differences in the baseline characteristics of the 468 participants randomized to receive fluorouracil cream and the 464 participants randomized to receive the control cream.
The mean total AK count on the face and ears in both groups was about 11. At 6 months, the mean number of AKs per participant had dropped to 3 in the fluorouracil group (a 73% reduction from baseline) vs. a mean of 8.1 in the control group, a 24% reduction from baseline (P less than .001). Over the study period, those treated with fluorouracil had significantly fewer AKs. Over the entire study, there was not a significant difference in the number of hypertrophic AKs between the two groups, although the number of hypertrophic AKs was lower in the treatment group at 6 months.
During the study period, more participants treated with fluorouracil had complete clearance of AKs on the face and ears, compared with the control group (P less than .001). Finally, the fluorouracil group required 2 spot treatments per visit per participant vs. 3.9 in the control group (P less than .001).
“Our findings highlight the long-term efficacy of topical fluorouracil cream in treating and preventing AKs. A single course of topical fluorouracil cream, 5%, treatment led to a sustained reduction of the number of AKs and subsequent AK treatments,” in the population of patients at high risk for basal cell and squamous cell carcinomas, the authors wrote.
The study was supported by the Office of Research and Development Cooperative Studies Program at the Department of Veterans Affairs. Three of the authors reported several disclosures, including serving as a consultant to several pharmaceutical companies; the others, including the lead author, had no disclosures.
One course of topical fluorouracil cream reduced the need for localized treatments and the number of actinic keratoses (AK) over a mean follow-up of 2.6 years in the Veterans Affairs Keratinocyte Carcinoma Chemoprevention (VAKCC) trial.
These results “indicate that treating a patient with a single course of fluorouracil would reduce the subsequent number of spot treatments and benefit care of patients with multiple AKs for longer than 2 years,” concluded Dr. Hyemin Pomerantz of the department of dermatoepidemiology at the Providence (R.I.) VA Medical Center and his coauthors. Previous studies on treating AKs with topical fluorouracil have followed up participants for less than 6 months, they pointed out (JAMA Dermatol. 2015;9:952-60).
In the randomized, double-blinded, placebo-controlled study, conducted from 2009 to 2011 at 12 VA dermatology clinics, participants received topical fluorouracil cream, 5%, or a vehicle control cream, applied twice a day for 4 weeks, and were followed up for a mean of 2.6 years. There were no significant differences in the baseline characteristics of the 468 participants randomized to receive fluorouracil cream and the 464 participants randomized to receive the control cream.
The mean total AK count on the face and ears in both groups was about 11. At 6 months, the mean number of AKs per participant had dropped to 3 in the fluorouracil group (a 73% reduction from baseline) vs. a mean of 8.1 in the control group, a 24% reduction from baseline (P less than .001). Over the study period, those treated with fluorouracil had significantly fewer AKs. Over the entire study, there was not a significant difference in the number of hypertrophic AKs between the two groups, although the number of hypertrophic AKs was lower in the treatment group at 6 months.
During the study period, more participants treated with fluorouracil had complete clearance of AKs on the face and ears, compared with the control group (P less than .001). Finally, the fluorouracil group required 2 spot treatments per visit per participant vs. 3.9 in the control group (P less than .001).
“Our findings highlight the long-term efficacy of topical fluorouracil cream in treating and preventing AKs. A single course of topical fluorouracil cream, 5%, treatment led to a sustained reduction of the number of AKs and subsequent AK treatments,” in the population of patients at high risk for basal cell and squamous cell carcinomas, the authors wrote.
The study was supported by the Office of Research and Development Cooperative Studies Program at the Department of Veterans Affairs. Three of the authors reported several disclosures, including serving as a consultant to several pharmaceutical companies; the others, including the lead author, had no disclosures.
FROM JAMA DERMATOLOGY
Key clinical point:One course of topical fluorouracil cream, 5%, decreased the need for localized treatment and the number of actinic keratoses long term.
Major finding: Participants whose AKs were treated with a course of fluorouracil cream, 5%, had significantly fewer AKs and required fewer treatments, compared with the control group, for over 2 years.
Data source: The randomized, double-blind study compared the effect of a course of topical fluorouracil cream with a vehicle cream on the number of AKs and other measures, over a mean follow-up of 2.6 years, in 932 patients treated at 12 VA dermatology clinics.
Disclosures: The study was supported by the Office of Research and Development Cooperative Studies Program at the Department of Veterans Affairs. Three of the authors reported several disclosures, including serving as a consultant to several pharmaceutical companies; the others had no disclosures.

Topical resiquimod effective for early-stage cutaneous T-cell lymphoma
Topical resiquimod was effective and well tolerated in patients with early-stage cutaneous T-cell lymphoma (CTCL), in some cases inducing regression in both treated and untreated lesions, according to researchers.
The mean number of prior unsuccessful therapies among the patients was 6, yet the majority of patients (11 of 12) experienced significant improvement, and 2 patients had complete clinical responses with no evidence of disease after treatment. One patient, despite a 15-year history of disease and 11 unsuccessful treatments, experienced a complete resolution of both treated and untreated skin lesions.
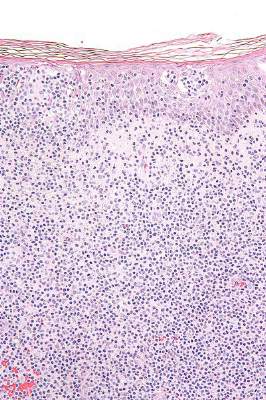
The open-label, phase I trial evaluated 12 patients with early-stage CTCL. Patients experienced minor adverse effects (all grade 1), which were primarily skin irritation. The trial evaluated 0.03% and 0.06% resiquimod, with complete and more rapid responses occurring at the higher dose. Both doses were equally well tolerated.
“These studies support further trials of this medication in early-stage, skin-limited CTCL and suggest resiquimod might also be useful as an adjuvant therapy in the treatment of more advanced CTCL,” wrote Dr. Alain Rook of the Department of Dermatology and the Center for Clinical Biostatistics and Epidemiology, Perelman School of Medicine, Philadelphia, and colleagues.
Arising from T cells that traffic to the skin, CTCLs are non-Hodgkin lymphomas whose only potential cure is stem cell transplantation. Studies suggest that host antitumor immunity plays an important role in the disease, and in this study, high responders showed recruitment and expansion of benign T-cell clones and activation of T cells and natural killer cells in the skin.
In the absence of cell-surface markers to distinguish malignant from benign T cells in the lesion, the team used high throughput screening of the T-cell receptor–beta gene to quantify malignant cells and monitor response to therapy. Of the 10 patients with identified malignant cells, biopsied lesions showed that most had reduction of malignant T-cell clones and 3 had complete eradication. The results may not reflect responses in nonbiopsied lesions.
Resiquimod recruits T cells and other immune cells to the skin, causing inflammation that the researchers observed persisted after complete or nearly complete malignant T-cell eradication. Study results suggested that activation of CD4+ cells and expansion of tumor-specific T cells is critical for effectiveness of resiquimod.
Topical resiquimod was effective and well tolerated in patients with early-stage cutaneous T-cell lymphoma (CTCL), in some cases inducing regression in both treated and untreated lesions, according to researchers.
The mean number of prior unsuccessful therapies among the patients was 6, yet the majority of patients (11 of 12) experienced significant improvement, and 2 patients had complete clinical responses with no evidence of disease after treatment. One patient, despite a 15-year history of disease and 11 unsuccessful treatments, experienced a complete resolution of both treated and untreated skin lesions.
The open-label, phase I trial evaluated 12 patients with early-stage CTCL. Patients experienced minor adverse effects (all grade 1), which were primarily skin irritation. The trial evaluated 0.03% and 0.06% resiquimod, with complete and more rapid responses occurring at the higher dose. Both doses were equally well tolerated.
“These studies support further trials of this medication in early-stage, skin-limited CTCL and suggest resiquimod might also be useful as an adjuvant therapy in the treatment of more advanced CTCL,” wrote Dr. Alain Rook of the Department of Dermatology and the Center for Clinical Biostatistics and Epidemiology, Perelman School of Medicine, Philadelphia, and colleagues.
Arising from T cells that traffic to the skin, CTCLs are non-Hodgkin lymphomas whose only potential cure is stem cell transplantation. Studies suggest that host antitumor immunity plays an important role in the disease, and in this study, high responders showed recruitment and expansion of benign T-cell clones and activation of T cells and natural killer cells in the skin.
In the absence of cell-surface markers to distinguish malignant from benign T cells in the lesion, the team used high throughput screening of the T-cell receptor–beta gene to quantify malignant cells and monitor response to therapy. Of the 10 patients with identified malignant cells, biopsied lesions showed that most had reduction of malignant T-cell clones and 3 had complete eradication. The results may not reflect responses in nonbiopsied lesions.
Resiquimod recruits T cells and other immune cells to the skin, causing inflammation that the researchers observed persisted after complete or nearly complete malignant T-cell eradication. Study results suggested that activation of CD4+ cells and expansion of tumor-specific T cells is critical for effectiveness of resiquimod.
Topical resiquimod was effective and well tolerated in patients with early-stage cutaneous T-cell lymphoma (CTCL), in some cases inducing regression in both treated and untreated lesions, according to researchers.
The mean number of prior unsuccessful therapies among the patients was 6, yet the majority of patients (11 of 12) experienced significant improvement, and 2 patients had complete clinical responses with no evidence of disease after treatment. One patient, despite a 15-year history of disease and 11 unsuccessful treatments, experienced a complete resolution of both treated and untreated skin lesions.
The open-label, phase I trial evaluated 12 patients with early-stage CTCL. Patients experienced minor adverse effects (all grade 1), which were primarily skin irritation. The trial evaluated 0.03% and 0.06% resiquimod, with complete and more rapid responses occurring at the higher dose. Both doses were equally well tolerated.
“These studies support further trials of this medication in early-stage, skin-limited CTCL and suggest resiquimod might also be useful as an adjuvant therapy in the treatment of more advanced CTCL,” wrote Dr. Alain Rook of the Department of Dermatology and the Center for Clinical Biostatistics and Epidemiology, Perelman School of Medicine, Philadelphia, and colleagues.
Arising from T cells that traffic to the skin, CTCLs are non-Hodgkin lymphomas whose only potential cure is stem cell transplantation. Studies suggest that host antitumor immunity plays an important role in the disease, and in this study, high responders showed recruitment and expansion of benign T-cell clones and activation of T cells and natural killer cells in the skin.
In the absence of cell-surface markers to distinguish malignant from benign T cells in the lesion, the team used high throughput screening of the T-cell receptor–beta gene to quantify malignant cells and monitor response to therapy. Of the 10 patients with identified malignant cells, biopsied lesions showed that most had reduction of malignant T-cell clones and 3 had complete eradication. The results may not reflect responses in nonbiopsied lesions.
Resiquimod recruits T cells and other immune cells to the skin, causing inflammation that the researchers observed persisted after complete or nearly complete malignant T-cell eradication. Study results suggested that activation of CD4+ cells and expansion of tumor-specific T cells is critical for effectiveness of resiquimod.
FROM BLOOD
Key clinical point: Topical resiquimod was effective and well tolerated in patients with early-stage cutaneous T-cell lymphoma (CTCL).
Major finding: In total, 11 of 12 patients had significant improvement: 2 had resolution of all evidence of disease, and 9 experienced improvement greater than or equal to 50%.
Data source: The open-label, phase I trial evaluated 12 patients with early stage CTCL.
Disclosures: Dr. Rook and one coauthor have patents pending on HTS in cutaneous lymphoma. His coauthor is employed by Adaptive Biotechnologies.
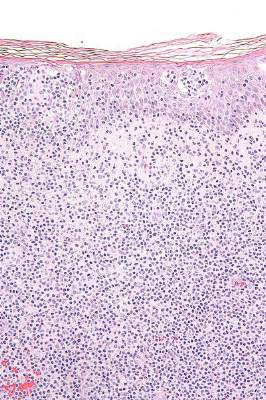
Natalizumab-Associated Melanoma: A Report of 139 Cases From the Southern Network on Adverse Reactions (SONAR)
Background: Natalizumab is an effective immunosuppressive therapy for multiple sclerosis (MS) that received its initial FDA approval in 2004. Its most notable toxicity is progressive multifocal leukoencephalopathy (PML), an opportunistic infection that is the focus of an FDA-mandated registry, TOUCH. The Southern Network on Adverse Reactions identified a fatal case of natalizumab-associated urethral melanoma and undertook an extensive evaluation of all cases of natalizumab-associated melanoma included in the FDA’s Adverse Event Reporting System (FAERS) (between 2005 and 2014).
Methods: Patient characteristics were determined from the FAERS reports and put into a comprehensive dataset. The quality of these reports was assessed based on a 15-point scale of various clinical, demographic, and pharmacy components. Cases were identified as being reported through the TOUCH system, using TOUCH information but reporting outside the system, not using TOUCH at all in the U.S. or not U.S. Quality scores and their components within the 4 Touch groups were statistically compared across all attributes using the mathematical programming-based statistical methodology univariate optimal discriminant analysis.
Results: The mean patient age at the time of diagnosis of melanoma was 46 years (SD 11). Seventeen patients were diagnosed with cutaneous melanoma developing in nonsun-exposed areas. We found that cases reported through the TOUCH registry were of lower quality (mean score 7.7) compared with others that reported outside of the U.S. (mean score 8.5, P < .008). Those cases reported through the TOUCH system were less likely to report the site of melanoma (P < .019) and have overall lower clinical scores (P < .04) compared with reports using TOUCH information but reporting outside of the system.
Conclusions: Our findings suggest that in the U.S., the TOUCH Registry should be expanded to require clinicians to report details of natalizumab-associated melanoma, an opportunistic illness that frequently develops in immunocompromised persons. Also, the FDA-approved product label for natalizumab should be revised to include information on occurrences of melanoma among natalizumab-treated MS patients, particularly those who have cutaneous nevi prior to natalizumab initiation. Natalizumab-treated MS patients and their physicians should be vigilant for changes in nevi appearances and development of new cutaneous lesions (particularly in nonsun-exposed cutaneous areas).
Background: Natalizumab is an effective immunosuppressive therapy for multiple sclerosis (MS) that received its initial FDA approval in 2004. Its most notable toxicity is progressive multifocal leukoencephalopathy (PML), an opportunistic infection that is the focus of an FDA-mandated registry, TOUCH. The Southern Network on Adverse Reactions identified a fatal case of natalizumab-associated urethral melanoma and undertook an extensive evaluation of all cases of natalizumab-associated melanoma included in the FDA’s Adverse Event Reporting System (FAERS) (between 2005 and 2014).
Methods: Patient characteristics were determined from the FAERS reports and put into a comprehensive dataset. The quality of these reports was assessed based on a 15-point scale of various clinical, demographic, and pharmacy components. Cases were identified as being reported through the TOUCH system, using TOUCH information but reporting outside the system, not using TOUCH at all in the U.S. or not U.S. Quality scores and their components within the 4 Touch groups were statistically compared across all attributes using the mathematical programming-based statistical methodology univariate optimal discriminant analysis.
Results: The mean patient age at the time of diagnosis of melanoma was 46 years (SD 11). Seventeen patients were diagnosed with cutaneous melanoma developing in nonsun-exposed areas. We found that cases reported through the TOUCH registry were of lower quality (mean score 7.7) compared with others that reported outside of the U.S. (mean score 8.5, P < .008). Those cases reported through the TOUCH system were less likely to report the site of melanoma (P < .019) and have overall lower clinical scores (P < .04) compared with reports using TOUCH information but reporting outside of the system.
Conclusions: Our findings suggest that in the U.S., the TOUCH Registry should be expanded to require clinicians to report details of natalizumab-associated melanoma, an opportunistic illness that frequently develops in immunocompromised persons. Also, the FDA-approved product label for natalizumab should be revised to include information on occurrences of melanoma among natalizumab-treated MS patients, particularly those who have cutaneous nevi prior to natalizumab initiation. Natalizumab-treated MS patients and their physicians should be vigilant for changes in nevi appearances and development of new cutaneous lesions (particularly in nonsun-exposed cutaneous areas).
Background: Natalizumab is an effective immunosuppressive therapy for multiple sclerosis (MS) that received its initial FDA approval in 2004. Its most notable toxicity is progressive multifocal leukoencephalopathy (PML), an opportunistic infection that is the focus of an FDA-mandated registry, TOUCH. The Southern Network on Adverse Reactions identified a fatal case of natalizumab-associated urethral melanoma and undertook an extensive evaluation of all cases of natalizumab-associated melanoma included in the FDA’s Adverse Event Reporting System (FAERS) (between 2005 and 2014).
Methods: Patient characteristics were determined from the FAERS reports and put into a comprehensive dataset. The quality of these reports was assessed based on a 15-point scale of various clinical, demographic, and pharmacy components. Cases were identified as being reported through the TOUCH system, using TOUCH information but reporting outside the system, not using TOUCH at all in the U.S. or not U.S. Quality scores and their components within the 4 Touch groups were statistically compared across all attributes using the mathematical programming-based statistical methodology univariate optimal discriminant analysis.
Results: The mean patient age at the time of diagnosis of melanoma was 46 years (SD 11). Seventeen patients were diagnosed with cutaneous melanoma developing in nonsun-exposed areas. We found that cases reported through the TOUCH registry were of lower quality (mean score 7.7) compared with others that reported outside of the U.S. (mean score 8.5, P < .008). Those cases reported through the TOUCH system were less likely to report the site of melanoma (P < .019) and have overall lower clinical scores (P < .04) compared with reports using TOUCH information but reporting outside of the system.
Conclusions: Our findings suggest that in the U.S., the TOUCH Registry should be expanded to require clinicians to report details of natalizumab-associated melanoma, an opportunistic illness that frequently develops in immunocompromised persons. Also, the FDA-approved product label for natalizumab should be revised to include information on occurrences of melanoma among natalizumab-treated MS patients, particularly those who have cutaneous nevi prior to natalizumab initiation. Natalizumab-treated MS patients and their physicians should be vigilant for changes in nevi appearances and development of new cutaneous lesions (particularly in nonsun-exposed cutaneous areas).