User login
Certain skin cancers respond to nonsurgical treatments
BOSTON – Surgery is the standard of care for most skin cancers, but nonsurgical and adjuvant treatments can be good options for certain skin cancers when surgery would be neither curative nor feasible, according to Anthony Rossi, MD.
“Whether you’re treating a superficial basal cell or superficial squamous cell carcinoma, I think first and foremost, if you’re going to use nonsurgical treatment options, it’s important to have a good biopsy diagnosis,” Dr. Rossi said at the American Academy of Dermatology summer meeting. He also advised that the biopsy capture the entire lesion or a good portion of it to get a good representation. “You don’t want to be surprised by any hiding, high-risk subtypes,” said Dr. Rossi, of the Memorial Sloan Kettering Cancer Center in New York.

Deciding on a nonsurgical treatment option should be based on knowing the patient. For example, know the patient’s concerns about cosmetic deformities, willingness to undergo surgery or not, and ability and willingness to do follow-up self-care.
For superficial basal cell or squamous cell carcinomas in situ and even lentigo maligna in situ not amenable to surgery, imiquimod may be an appropriate treatment. Dr. Rossi said his practice is to use it in an incremental fashion, starting with application five times per week, going to every day if there is no response after 1 to 2 weeks. If the response remains inadequate, he recommended adding a topical retinoid, such as tazarotene, in an effort to increase penetration.
For basal cell carcinomas and squamous cell carcinoma in situ, he uses imiquimod for a total of 6 to 8 weeks, starting from the time of the first reaction. For melanoma in situ, he uses it for more than 60 applications (12 weeks).
To show patients where they should be applying any topical treatment, Dr. Rossi marks the skin, photographs it, and prints out a picture for the patient. Sometimes he uses the patient’s phone to take the picture. For a basal cell or squamous cell carcinoma in situ, he indicates an area at least 5 to 10 mm beyond the margin of the tumor. The area is even larger for melanomas.
Dr. Rossi studies confocal microscopy to detect skin cancers. He uses it before treating a lesion to define the clinical boundaries of the lesion and the boundaries for the nonsurgical treatments, and then he uses it on follow up to look for any recurrences.
New anti-tumor agents
Two oral inhibitors of the sonic hedgehog pathway have been approved within the past 5 years for locally advanced or metastatic basal cell carcinomas. “In the right person, they can be quite beneficial if surgery would leave them with a very large cosmetic deformity or if surgery would be not curative,” Dr. Rossi said. “We’re seeing good results” with acceptable adverse events, specifically taste disturbances, muscle cramps, and hair loss. The first such drug, vismodegib (Erivedge), was approved in 2012, and sonidegib (Odomzo) came on the market about 1 year ago.
Besides oral agents, photodynamic therapy (PDT) with photosensitizers are another option for certain skin tumors. Dr. Rossi said his practice is to keep the treatment room fairly warm to assure good blood flow to the skin and thus good penetration of the drug. Because PDT acts by generating singlet oxygen to kill tumors, good blood flow to the tumor is necessary. To minimize discomfort, he uses pretreatment acetaminophen if patients can take it. After a skin reaction occurs, cool compresses are used, along with dilute acetic acid soaks on crusted or scaling lesions in an effort to prevent infection.
And while these treatments can produce quite angry-looking lesions in the short term, very good healing usually occurs if patients are diligent about wound care. However, Dr. Rossi cautioned that they may need “more hand holding with these nonsurgical treatments, because it is a longer duration of treatment.”
In general for counseling patients on nonsurgical treatments, Dr. Rossi said it is advisable to have good pretreatment and post-treatment plans. “They have to know that they will need to be following up to make sure that there is no recurrence,” he said. “We don’t have clear surgical margins if we’re using these topical treatments, so we have to make sure that they have good, constant follow-up.”
Dr. Rossi reported consulting relationships with Merz, DynaMed, and Novartis.
BOSTON – Surgery is the standard of care for most skin cancers, but nonsurgical and adjuvant treatments can be good options for certain skin cancers when surgery would be neither curative nor feasible, according to Anthony Rossi, MD.
“Whether you’re treating a superficial basal cell or superficial squamous cell carcinoma, I think first and foremost, if you’re going to use nonsurgical treatment options, it’s important to have a good biopsy diagnosis,” Dr. Rossi said at the American Academy of Dermatology summer meeting. He also advised that the biopsy capture the entire lesion or a good portion of it to get a good representation. “You don’t want to be surprised by any hiding, high-risk subtypes,” said Dr. Rossi, of the Memorial Sloan Kettering Cancer Center in New York.
Deciding on a nonsurgical treatment option should be based on knowing the patient. For example, know the patient’s concerns about cosmetic deformities, willingness to undergo surgery or not, and ability and willingness to do follow-up self-care.
For superficial basal cell or squamous cell carcinomas in situ and even lentigo maligna in situ not amenable to surgery, imiquimod may be an appropriate treatment. Dr. Rossi said his practice is to use it in an incremental fashion, starting with application five times per week, going to every day if there is no response after 1 to 2 weeks. If the response remains inadequate, he recommended adding a topical retinoid, such as tazarotene, in an effort to increase penetration.
For basal cell carcinomas and squamous cell carcinoma in situ, he uses imiquimod for a total of 6 to 8 weeks, starting from the time of the first reaction. For melanoma in situ, he uses it for more than 60 applications (12 weeks).
To show patients where they should be applying any topical treatment, Dr. Rossi marks the skin, photographs it, and prints out a picture for the patient. Sometimes he uses the patient’s phone to take the picture. For a basal cell or squamous cell carcinoma in situ, he indicates an area at least 5 to 10 mm beyond the margin of the tumor. The area is even larger for melanomas.
Dr. Rossi studies confocal microscopy to detect skin cancers. He uses it before treating a lesion to define the clinical boundaries of the lesion and the boundaries for the nonsurgical treatments, and then he uses it on follow up to look for any recurrences.
New anti-tumor agents
Two oral inhibitors of the sonic hedgehog pathway have been approved within the past 5 years for locally advanced or metastatic basal cell carcinomas. “In the right person, they can be quite beneficial if surgery would leave them with a very large cosmetic deformity or if surgery would be not curative,” Dr. Rossi said. “We’re seeing good results” with acceptable adverse events, specifically taste disturbances, muscle cramps, and hair loss. The first such drug, vismodegib (Erivedge), was approved in 2012, and sonidegib (Odomzo) came on the market about 1 year ago.
Besides oral agents, photodynamic therapy (PDT) with photosensitizers are another option for certain skin tumors. Dr. Rossi said his practice is to keep the treatment room fairly warm to assure good blood flow to the skin and thus good penetration of the drug. Because PDT acts by generating singlet oxygen to kill tumors, good blood flow to the tumor is necessary. To minimize discomfort, he uses pretreatment acetaminophen if patients can take it. After a skin reaction occurs, cool compresses are used, along with dilute acetic acid soaks on crusted or scaling lesions in an effort to prevent infection.
And while these treatments can produce quite angry-looking lesions in the short term, very good healing usually occurs if patients are diligent about wound care. However, Dr. Rossi cautioned that they may need “more hand holding with these nonsurgical treatments, because it is a longer duration of treatment.”
In general for counseling patients on nonsurgical treatments, Dr. Rossi said it is advisable to have good pretreatment and post-treatment plans. “They have to know that they will need to be following up to make sure that there is no recurrence,” he said. “We don’t have clear surgical margins if we’re using these topical treatments, so we have to make sure that they have good, constant follow-up.”
Dr. Rossi reported consulting relationships with Merz, DynaMed, and Novartis.
BOSTON – Surgery is the standard of care for most skin cancers, but nonsurgical and adjuvant treatments can be good options for certain skin cancers when surgery would be neither curative nor feasible, according to Anthony Rossi, MD.
“Whether you’re treating a superficial basal cell or superficial squamous cell carcinoma, I think first and foremost, if you’re going to use nonsurgical treatment options, it’s important to have a good biopsy diagnosis,” Dr. Rossi said at the American Academy of Dermatology summer meeting. He also advised that the biopsy capture the entire lesion or a good portion of it to get a good representation. “You don’t want to be surprised by any hiding, high-risk subtypes,” said Dr. Rossi, of the Memorial Sloan Kettering Cancer Center in New York.
Deciding on a nonsurgical treatment option should be based on knowing the patient. For example, know the patient’s concerns about cosmetic deformities, willingness to undergo surgery or not, and ability and willingness to do follow-up self-care.
For superficial basal cell or squamous cell carcinomas in situ and even lentigo maligna in situ not amenable to surgery, imiquimod may be an appropriate treatment. Dr. Rossi said his practice is to use it in an incremental fashion, starting with application five times per week, going to every day if there is no response after 1 to 2 weeks. If the response remains inadequate, he recommended adding a topical retinoid, such as tazarotene, in an effort to increase penetration.
For basal cell carcinomas and squamous cell carcinoma in situ, he uses imiquimod for a total of 6 to 8 weeks, starting from the time of the first reaction. For melanoma in situ, he uses it for more than 60 applications (12 weeks).
To show patients where they should be applying any topical treatment, Dr. Rossi marks the skin, photographs it, and prints out a picture for the patient. Sometimes he uses the patient’s phone to take the picture. For a basal cell or squamous cell carcinoma in situ, he indicates an area at least 5 to 10 mm beyond the margin of the tumor. The area is even larger for melanomas.
Dr. Rossi studies confocal microscopy to detect skin cancers. He uses it before treating a lesion to define the clinical boundaries of the lesion and the boundaries for the nonsurgical treatments, and then he uses it on follow up to look for any recurrences.
New anti-tumor agents
Two oral inhibitors of the sonic hedgehog pathway have been approved within the past 5 years for locally advanced or metastatic basal cell carcinomas. “In the right person, they can be quite beneficial if surgery would leave them with a very large cosmetic deformity or if surgery would be not curative,” Dr. Rossi said. “We’re seeing good results” with acceptable adverse events, specifically taste disturbances, muscle cramps, and hair loss. The first such drug, vismodegib (Erivedge), was approved in 2012, and sonidegib (Odomzo) came on the market about 1 year ago.
Besides oral agents, photodynamic therapy (PDT) with photosensitizers are another option for certain skin tumors. Dr. Rossi said his practice is to keep the treatment room fairly warm to assure good blood flow to the skin and thus good penetration of the drug. Because PDT acts by generating singlet oxygen to kill tumors, good blood flow to the tumor is necessary. To minimize discomfort, he uses pretreatment acetaminophen if patients can take it. After a skin reaction occurs, cool compresses are used, along with dilute acetic acid soaks on crusted or scaling lesions in an effort to prevent infection.
And while these treatments can produce quite angry-looking lesions in the short term, very good healing usually occurs if patients are diligent about wound care. However, Dr. Rossi cautioned that they may need “more hand holding with these nonsurgical treatments, because it is a longer duration of treatment.”
In general for counseling patients on nonsurgical treatments, Dr. Rossi said it is advisable to have good pretreatment and post-treatment plans. “They have to know that they will need to be following up to make sure that there is no recurrence,” he said. “We don’t have clear surgical margins if we’re using these topical treatments, so we have to make sure that they have good, constant follow-up.”
Dr. Rossi reported consulting relationships with Merz, DynaMed, and Novartis.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2016

Skin Examinations for Early Melanoma Detection


USPSTF: Visual skin cancer screening lacks supporting evidence
The benefits and harms of visual screen cancer screening exams for asymptomatic adults can’t be adequately assessed with current evidence, according to a new recommendation from the U.S. Preventive Services Task Force.
“Evidence is inadequate to reliably conclude that early detection of skin cancer through visual skin examination by a clinician reduces morbidity or mortality,” according to the statement published online July 26 in JAMA (2016;316[4]:429-435. doi:10.1001/jama.2016.8465).

Approximately 76,400 adults in the United States will develop melanoma, and more than 10,000 will die from it, according to the USPSTF. However, more than 98% of skin cancer cases in the United States are basal and squamous cell carcinoma, which have much lower morbidity and mortality rates, noted the USPSTF researchers, led by Kirsten Bibbins-Domingo, MD, PhD, of the University of California, San Francisco.
The current statement updates the USPSTF’s 2009 recommendation, which also found insufficient evidence to assess the harms and benefits of visual skin cancer screening in asymptomatic adults with no history of premalignant or malignant skin lesions. However, the current recommendation eliminates a statement about patients’ skin self-exams.
According to the USPSTF, evidence is “adequate” that a clinician’s visual skin exam has “modest sensitivity and specificity for detecting melanoma,” but evidence is inconsistent to support the ability of a visual skin exam to detect nonmelanoma skin cancer.
The USPSTF commissioned an evidence review that included 11 studies previously reviewed and 2 additional studies conducted since 2009. The two new studies included one that evaluated skin cancer screening performed by dermatologists or plastic surgeons and one that evaluated skin cancer screening performed by primary care physicians. Sensitivity and specificity in the two studies ranged from 40% to 70% and from 86% to 98%, respectively.
“None of the studies could draw reliable conclusions as to whether screening performed by any of the clinical specialties differed in diagnostic accuracy,” the researchers noted. In addition, “no [randomized controlled trial] has directly evaluated the effectiveness of the clinical visual skin examination for reducing skin cancer morbidity and mortality,” they wrote.
The recommendation was accompanied by several editorials published online July 26 in JAMA journals.
In JAMA, Hensin Tsao, MD, PhD, of Massachusetts General Hospital, Boston, and Martin Weinstock, MD, PhD, of Brown University, Providence, R.I., noted that the USPSTF considered the possibility of including information from high-quality case-control studies in lieu of randomized controlled trials, which have been difficult to conduct in skin cancer screening. “The evidentiary standard needs to be further refined to be appropriate to the modest magnitude of potential harms of a properly performed skin cancer screening,” they wrote (JAMA. 2016;316:398-400). Dr. Tsao disclosed an honorarium from Lubax.
In JAMA Dermatology, Susan Swetter, MD, of the Veterans Affairs Palo Alto (Calif.) Health Care System; Alan C. Geller, MPH, of Harvard School of Public Health, Boston; and Allan C. Halpern, MD, of Memorial Sloan Kettering Cancer Center, New York, wrote about ways to promote broader uptake of skin cancer screening. “Alternative models should be explored to bundle skin screening with other preventive services (e.g., blood pressure measurements or flu shots) and to engage advanced practice providers (e.g., nurse practitioners and physician assistants) to promote screening among individuals with less access to dermatologists,” they wrote (JAMA Dermatol. 2016. doi: 10.1001/jamadermatol.2016.2606).
In JAMA Oncology, Vinayak K. Nahar, MD, of the University of Mississippi Medical Center, Jackson; Jonathan E. Mayer, MD, of Johns Hopkins University, Baltimore; and Jane M. Grant-Kels, MD, of the University of Connecticut, Farmington, addressed concerns over performing more biopsies. “The USPSTF also raises concern over the number needed to biopsy to detect 1 case of melanoma. In weighing these data, one must also consider that many of the nonmelanomas biopsied were likely severely atypical nevi that have their own risk of malignant transformation. Although difficult to quantify, there is some benefit to removing a severely atypical nevus, both for risk of transformation and for a patient’s peace of mind,” they wrote (JAMA Oncol. 2016. doi: 10.1001/jamaoncol.2016.2440).
In JAMA Internal Medicine, Eleni Linos, MD, of the University of California, San Francisco; Kenneth A. Katz, MD, of Kaiser Permanente, San Francisco; and Graham A. Colditz, MD, of Washington University, St. Louis, cautioned that the USPSTF recommendations shouldn’t be interpreted as minimizing the importance of skin cancer. “Instead, the report should motivate us to improve the evidence base for identifying groups of people in whom the benefits of screening might outweigh risks,” they wrote. “Meanwhile, we should also fully implement skin cancer primary prevention by eliminating indoor tanning exposure, especially among youths, and increasing the use of sun-protection strategies that work” (JAMA Intern. Med. 2016. doi: 10.1001/jamaintermed.2016.5008).
The recommendations are not an official position of the U.S. Department of Health and Human Services or the Agency for Healthcare Research and Quality.
“The American Academy of Dermatology is disappointed with this recommendation, as dermatologists know that skin cancer screenings can save lives, yet we acknowledge the need for additional research on the benefits and harms of skin cancer screening in the primary care setting,” Dr. Abel Torres, president of the American Academy of Dermatology, said in a statement responding to the USPSTF skin cancer screening recommendations.
“It is important for the public to understand that the USPSTF is not recommending against skin cancer screenings; it means the group did not find conclusive evidence to make a recommendation one way or another,” Dr. Torres said. “The public should know that this recommendation does not apply to individuals with suspicious skin lesions and those with an increased skin cancer risk, and it does not address the practice of skin self-exams.”
“The AAD encourages everyone to serve as their own health advocate by regularly conducting skin self-exams. Individuals who notice any unusual spots on their skin, including those that are changing, itching, or bleeding, should make an appointment with a board-certified dermatologist. In addition, individuals with an increased risk of melanoma – including men older than 50; people with more than 50 moles, or large or unusual moles; individuals with fair skin; and those with a history of skin cancer – should talk to a dermatologist about how often they should receive a skin exam from a doctor.”
Dr. Abel Torres is president of the American Academy of Dermatology. The comments are taken from his AAD statement on USPSTF Recommendation on Skin Cancer Screening issued on July 26, 2016.
“The American Academy of Dermatology is disappointed with this recommendation, as dermatologists know that skin cancer screenings can save lives, yet we acknowledge the need for additional research on the benefits and harms of skin cancer screening in the primary care setting,” Dr. Abel Torres, president of the American Academy of Dermatology, said in a statement responding to the USPSTF skin cancer screening recommendations.
“It is important for the public to understand that the USPSTF is not recommending against skin cancer screenings; it means the group did not find conclusive evidence to make a recommendation one way or another,” Dr. Torres said. “The public should know that this recommendation does not apply to individuals with suspicious skin lesions and those with an increased skin cancer risk, and it does not address the practice of skin self-exams.”
“The AAD encourages everyone to serve as their own health advocate by regularly conducting skin self-exams. Individuals who notice any unusual spots on their skin, including those that are changing, itching, or bleeding, should make an appointment with a board-certified dermatologist. In addition, individuals with an increased risk of melanoma – including men older than 50; people with more than 50 moles, or large or unusual moles; individuals with fair skin; and those with a history of skin cancer – should talk to a dermatologist about how often they should receive a skin exam from a doctor.”
Dr. Abel Torres is president of the American Academy of Dermatology. The comments are taken from his AAD statement on USPSTF Recommendation on Skin Cancer Screening issued on July 26, 2016.
“The American Academy of Dermatology is disappointed with this recommendation, as dermatologists know that skin cancer screenings can save lives, yet we acknowledge the need for additional research on the benefits and harms of skin cancer screening in the primary care setting,” Dr. Abel Torres, president of the American Academy of Dermatology, said in a statement responding to the USPSTF skin cancer screening recommendations.
“It is important for the public to understand that the USPSTF is not recommending against skin cancer screenings; it means the group did not find conclusive evidence to make a recommendation one way or another,” Dr. Torres said. “The public should know that this recommendation does not apply to individuals with suspicious skin lesions and those with an increased skin cancer risk, and it does not address the practice of skin self-exams.”
“The AAD encourages everyone to serve as their own health advocate by regularly conducting skin self-exams. Individuals who notice any unusual spots on their skin, including those that are changing, itching, or bleeding, should make an appointment with a board-certified dermatologist. In addition, individuals with an increased risk of melanoma – including men older than 50; people with more than 50 moles, or large or unusual moles; individuals with fair skin; and those with a history of skin cancer – should talk to a dermatologist about how often they should receive a skin exam from a doctor.”
Dr. Abel Torres is president of the American Academy of Dermatology. The comments are taken from his AAD statement on USPSTF Recommendation on Skin Cancer Screening issued on July 26, 2016.
The benefits and harms of visual screen cancer screening exams for asymptomatic adults can’t be adequately assessed with current evidence, according to a new recommendation from the U.S. Preventive Services Task Force.
“Evidence is inadequate to reliably conclude that early detection of skin cancer through visual skin examination by a clinician reduces morbidity or mortality,” according to the statement published online July 26 in JAMA (2016;316[4]:429-435. doi:10.1001/jama.2016.8465).
Approximately 76,400 adults in the United States will develop melanoma, and more than 10,000 will die from it, according to the USPSTF. However, more than 98% of skin cancer cases in the United States are basal and squamous cell carcinoma, which have much lower morbidity and mortality rates, noted the USPSTF researchers, led by Kirsten Bibbins-Domingo, MD, PhD, of the University of California, San Francisco.
The current statement updates the USPSTF’s 2009 recommendation, which also found insufficient evidence to assess the harms and benefits of visual skin cancer screening in asymptomatic adults with no history of premalignant or malignant skin lesions. However, the current recommendation eliminates a statement about patients’ skin self-exams.
According to the USPSTF, evidence is “adequate” that a clinician’s visual skin exam has “modest sensitivity and specificity for detecting melanoma,” but evidence is inconsistent to support the ability of a visual skin exam to detect nonmelanoma skin cancer.
The USPSTF commissioned an evidence review that included 11 studies previously reviewed and 2 additional studies conducted since 2009. The two new studies included one that evaluated skin cancer screening performed by dermatologists or plastic surgeons and one that evaluated skin cancer screening performed by primary care physicians. Sensitivity and specificity in the two studies ranged from 40% to 70% and from 86% to 98%, respectively.
“None of the studies could draw reliable conclusions as to whether screening performed by any of the clinical specialties differed in diagnostic accuracy,” the researchers noted. In addition, “no [randomized controlled trial] has directly evaluated the effectiveness of the clinical visual skin examination for reducing skin cancer morbidity and mortality,” they wrote.
The recommendation was accompanied by several editorials published online July 26 in JAMA journals.
In JAMA, Hensin Tsao, MD, PhD, of Massachusetts General Hospital, Boston, and Martin Weinstock, MD, PhD, of Brown University, Providence, R.I., noted that the USPSTF considered the possibility of including information from high-quality case-control studies in lieu of randomized controlled trials, which have been difficult to conduct in skin cancer screening. “The evidentiary standard needs to be further refined to be appropriate to the modest magnitude of potential harms of a properly performed skin cancer screening,” they wrote (JAMA. 2016;316:398-400). Dr. Tsao disclosed an honorarium from Lubax.
In JAMA Dermatology, Susan Swetter, MD, of the Veterans Affairs Palo Alto (Calif.) Health Care System; Alan C. Geller, MPH, of Harvard School of Public Health, Boston; and Allan C. Halpern, MD, of Memorial Sloan Kettering Cancer Center, New York, wrote about ways to promote broader uptake of skin cancer screening. “Alternative models should be explored to bundle skin screening with other preventive services (e.g., blood pressure measurements or flu shots) and to engage advanced practice providers (e.g., nurse practitioners and physician assistants) to promote screening among individuals with less access to dermatologists,” they wrote (JAMA Dermatol. 2016. doi: 10.1001/jamadermatol.2016.2606).
In JAMA Oncology, Vinayak K. Nahar, MD, of the University of Mississippi Medical Center, Jackson; Jonathan E. Mayer, MD, of Johns Hopkins University, Baltimore; and Jane M. Grant-Kels, MD, of the University of Connecticut, Farmington, addressed concerns over performing more biopsies. “The USPSTF also raises concern over the number needed to biopsy to detect 1 case of melanoma. In weighing these data, one must also consider that many of the nonmelanomas biopsied were likely severely atypical nevi that have their own risk of malignant transformation. Although difficult to quantify, there is some benefit to removing a severely atypical nevus, both for risk of transformation and for a patient’s peace of mind,” they wrote (JAMA Oncol. 2016. doi: 10.1001/jamaoncol.2016.2440).
In JAMA Internal Medicine, Eleni Linos, MD, of the University of California, San Francisco; Kenneth A. Katz, MD, of Kaiser Permanente, San Francisco; and Graham A. Colditz, MD, of Washington University, St. Louis, cautioned that the USPSTF recommendations shouldn’t be interpreted as minimizing the importance of skin cancer. “Instead, the report should motivate us to improve the evidence base for identifying groups of people in whom the benefits of screening might outweigh risks,” they wrote. “Meanwhile, we should also fully implement skin cancer primary prevention by eliminating indoor tanning exposure, especially among youths, and increasing the use of sun-protection strategies that work” (JAMA Intern. Med. 2016. doi: 10.1001/jamaintermed.2016.5008).
The recommendations are not an official position of the U.S. Department of Health and Human Services or the Agency for Healthcare Research and Quality.
The benefits and harms of visual screen cancer screening exams for asymptomatic adults can’t be adequately assessed with current evidence, according to a new recommendation from the U.S. Preventive Services Task Force.
“Evidence is inadequate to reliably conclude that early detection of skin cancer through visual skin examination by a clinician reduces morbidity or mortality,” according to the statement published online July 26 in JAMA (2016;316[4]:429-435. doi:10.1001/jama.2016.8465).
Approximately 76,400 adults in the United States will develop melanoma, and more than 10,000 will die from it, according to the USPSTF. However, more than 98% of skin cancer cases in the United States are basal and squamous cell carcinoma, which have much lower morbidity and mortality rates, noted the USPSTF researchers, led by Kirsten Bibbins-Domingo, MD, PhD, of the University of California, San Francisco.
The current statement updates the USPSTF’s 2009 recommendation, which also found insufficient evidence to assess the harms and benefits of visual skin cancer screening in asymptomatic adults with no history of premalignant or malignant skin lesions. However, the current recommendation eliminates a statement about patients’ skin self-exams.
According to the USPSTF, evidence is “adequate” that a clinician’s visual skin exam has “modest sensitivity and specificity for detecting melanoma,” but evidence is inconsistent to support the ability of a visual skin exam to detect nonmelanoma skin cancer.
The USPSTF commissioned an evidence review that included 11 studies previously reviewed and 2 additional studies conducted since 2009. The two new studies included one that evaluated skin cancer screening performed by dermatologists or plastic surgeons and one that evaluated skin cancer screening performed by primary care physicians. Sensitivity and specificity in the two studies ranged from 40% to 70% and from 86% to 98%, respectively.
“None of the studies could draw reliable conclusions as to whether screening performed by any of the clinical specialties differed in diagnostic accuracy,” the researchers noted. In addition, “no [randomized controlled trial] has directly evaluated the effectiveness of the clinical visual skin examination for reducing skin cancer morbidity and mortality,” they wrote.
The recommendation was accompanied by several editorials published online July 26 in JAMA journals.
In JAMA, Hensin Tsao, MD, PhD, of Massachusetts General Hospital, Boston, and Martin Weinstock, MD, PhD, of Brown University, Providence, R.I., noted that the USPSTF considered the possibility of including information from high-quality case-control studies in lieu of randomized controlled trials, which have been difficult to conduct in skin cancer screening. “The evidentiary standard needs to be further refined to be appropriate to the modest magnitude of potential harms of a properly performed skin cancer screening,” they wrote (JAMA. 2016;316:398-400). Dr. Tsao disclosed an honorarium from Lubax.
In JAMA Dermatology, Susan Swetter, MD, of the Veterans Affairs Palo Alto (Calif.) Health Care System; Alan C. Geller, MPH, of Harvard School of Public Health, Boston; and Allan C. Halpern, MD, of Memorial Sloan Kettering Cancer Center, New York, wrote about ways to promote broader uptake of skin cancer screening. “Alternative models should be explored to bundle skin screening with other preventive services (e.g., blood pressure measurements or flu shots) and to engage advanced practice providers (e.g., nurse practitioners and physician assistants) to promote screening among individuals with less access to dermatologists,” they wrote (JAMA Dermatol. 2016. doi: 10.1001/jamadermatol.2016.2606).
In JAMA Oncology, Vinayak K. Nahar, MD, of the University of Mississippi Medical Center, Jackson; Jonathan E. Mayer, MD, of Johns Hopkins University, Baltimore; and Jane M. Grant-Kels, MD, of the University of Connecticut, Farmington, addressed concerns over performing more biopsies. “The USPSTF also raises concern over the number needed to biopsy to detect 1 case of melanoma. In weighing these data, one must also consider that many of the nonmelanomas biopsied were likely severely atypical nevi that have their own risk of malignant transformation. Although difficult to quantify, there is some benefit to removing a severely atypical nevus, both for risk of transformation and for a patient’s peace of mind,” they wrote (JAMA Oncol. 2016. doi: 10.1001/jamaoncol.2016.2440).
In JAMA Internal Medicine, Eleni Linos, MD, of the University of California, San Francisco; Kenneth A. Katz, MD, of Kaiser Permanente, San Francisco; and Graham A. Colditz, MD, of Washington University, St. Louis, cautioned that the USPSTF recommendations shouldn’t be interpreted as minimizing the importance of skin cancer. “Instead, the report should motivate us to improve the evidence base for identifying groups of people in whom the benefits of screening might outweigh risks,” they wrote. “Meanwhile, we should also fully implement skin cancer primary prevention by eliminating indoor tanning exposure, especially among youths, and increasing the use of sun-protection strategies that work” (JAMA Intern. Med. 2016. doi: 10.1001/jamaintermed.2016.5008).
The recommendations are not an official position of the U.S. Department of Health and Human Services or the Agency for Healthcare Research and Quality.
FROM JAMA

Here’s how to tackle teenage tanning
MINNEAPOLIS, MINN. – Indoor tanning is a significant contributor to the U.S. skin cancer epidemic and represents a 100% preventable source of exposure to these cancers. Understanding exactly who is using indoor tanning – and why – can provide insight and leverage to help change behavior, according to Cindy Firkins Smith, MD, adjunct professor of dermatology at the University of Minnesota, Minneapolis.
Dr. Smith noted that the typical indoor tanning bed user is female and between 17 and 30 years old. Other aspects of her lifestyle may be unhealthy; for example, she may smoke cigarettes, have an unhealthy pattern of alcohol consumption, and make unhealthy food choices (Cancer Causes Control 2006 June. doi:10.1007/s10552-005-0453-9). She also is likely to watch beauty-focused reality TV shows (J Am Acad Dermatol 2013 May. doi:10.1016/j.jaad.2012.09.055) and is likely to objectify her own body, seeing it as something to be viewed and judged (Arch Dermatol 2009 Sep 1. doi:10.1001/archdermatol.2009.190).

Tanning is a behavior that provides relaxation and positive emotions, and she receives support for this behavior from family and friends. “Tanning often starts with mom, which is one reason that parental permission legislation doesn’t work,” she said at the annual meeting of the Society for Pediatric Dermatology.
Dr. Smith said that up to 30 million people tan indoors every year. Rates of tanning for teenage girls are very high: up to 40% of American teenagers use indoor tanning, and 20%-30% of all 18- to 29-year-olds have used a tanning bed in the previous year (Jama Dermatol 2014 April doi: 10.1001/jamadermatol.2013.6896).
The ubiquity of tanning salons contributes to the problem, said Dr. Smith. “More is not better; in the largest U.S. cities, tanning salons outnumber [both] Starbucks and McDonald’s,” she said, noting that studies have shown that both proximity to tanning salons and the low cost of tanning encourage their use (Am J Prev Med. 2009 Mar 36[3]:243-6).
A 2015 study surveyed 125 colleges, finding that 48% had indoor tanning facilities in their campus or off-campus housing. College cash cards were acceptable payment at 14.4% of colleges, and 96% of off-campus housing facilities that offered tanning provided it as a free “perk” to residents (JAMA Dermatol 2015 Jan. doi: 10.1001/jamadermatol.2014.3590).
Further, some data suggest that tanning really can be addictive for some patients. Ultraviolet light exposure has been shown to “light up” pleasure centers in PET-CT studies, and some frequent tanners report relaxation and pleasure from tanning as well as craving and feelings of withdrawal when they miss sessions. Dr. Smith said she does not hesitate to refer teen patients to mental health providers if there are concerns about mood and depression.
Having an understanding of patient motivations to tan can help in getting patients to take steps toward change, said Dr. Smith. “What can we do? We can actually do a lot. We have a lot more influence than we think we do.”
At the level of the individual patient, just opening up a conversation can make a big difference. “We assume we know why teenagers go to a tanning booth. But do we? When you notice a young woman who’s been to a tanning booth, ask why,” using a nonjudgmental approach to begin a dialogue about the near-term and long-term dangers of tanning. A positive approach is key, noted Dr. Smith. “Focusing on the benefits of avoiding UV tanning is more effective than a heavy reliance on scare tactics,” she said. Also, “multiple interventions work better.”
Before-and-after photos of celebrities whose appearance has been affected by photoaging can be effective. Another tactic with a more positive spin is to share images of celebrities who have chosen not to tan and who celebrate their fair skin. These conversations are particularly important at prom time, peak tanning season for many young women, said Dr. Smith. She has a portfolio of photos showing fair-skinned women wearing high-contrast gowns, which she says are more flattering for pale skin than white or nude colors.
For patients who still want that tan look, “Tanning for reasons of appearance can be satisfied with sunless tanners,” said Dr. Smith. The most common ingredient in sunless tanners is dihydroxyacetone (DHA), which was approved in the 1970s for topical use. However, the Food and Drug Administration issued a warning in 2011 about spray tanning, noting that the “industry has not provided safety data to FDA in order for the agency to consider approving it for … ‘misting’ from tanning booths.” The FDA’s specific concern had to do with the unknown safety of ingestion, inhalation, and mucous membrane exposure that can result from spray tanning.
Moving to the legislative and policy level, change can be achieved when stakeholders band together to “ban the tan,” said Dr. Smith. “The best way to do it is with a village. It really takes a lot of people to do this.”
There are solid epidemiologic and economic reasons to focus on the skin cancer epidemic, said Dr. Smith. Skin cancer is now the most common cancer in the United States, and more new cases “are diagnosed each year than breast, prostate, lung, and colon cancers combined,” she said. Of nonmelanoma skin cancers, 90% are thought to be UV-related, and “the vast majority of mutations found in melanoma are caused by UV radiation.”
Skin cancers cost the United States over $8 billion annually, and although promising new immunotherapies are extending the lives of those with melanoma, these treatments cost hundreds of thousands of dollars a year. “This type of treatment is unaffordable for our system,” said Dr. Smith.
Progress is being made, she said, despite industry opposition. Individual states have regulated or banned tanning for minors, and at the federal level, tanning beds are now considered by the FDA to be Class II (moderate-risk) medical devices, a step up from their previous classification as the lowest-risk Class I devices, “The same as a tongue blade,” she said.
Dr. Smith had no relevant financial disclosures.
On Twitter @karioakes
MINNEAPOLIS, MINN. – Indoor tanning is a significant contributor to the U.S. skin cancer epidemic and represents a 100% preventable source of exposure to these cancers. Understanding exactly who is using indoor tanning – and why – can provide insight and leverage to help change behavior, according to Cindy Firkins Smith, MD, adjunct professor of dermatology at the University of Minnesota, Minneapolis.
Dr. Smith noted that the typical indoor tanning bed user is female and between 17 and 30 years old. Other aspects of her lifestyle may be unhealthy; for example, she may smoke cigarettes, have an unhealthy pattern of alcohol consumption, and make unhealthy food choices (Cancer Causes Control 2006 June. doi:10.1007/s10552-005-0453-9). She also is likely to watch beauty-focused reality TV shows (J Am Acad Dermatol 2013 May. doi:10.1016/j.jaad.2012.09.055) and is likely to objectify her own body, seeing it as something to be viewed and judged (Arch Dermatol 2009 Sep 1. doi:10.1001/archdermatol.2009.190).
Tanning is a behavior that provides relaxation and positive emotions, and she receives support for this behavior from family and friends. “Tanning often starts with mom, which is one reason that parental permission legislation doesn’t work,” she said at the annual meeting of the Society for Pediatric Dermatology.
Dr. Smith said that up to 30 million people tan indoors every year. Rates of tanning for teenage girls are very high: up to 40% of American teenagers use indoor tanning, and 20%-30% of all 18- to 29-year-olds have used a tanning bed in the previous year (Jama Dermatol 2014 April doi: 10.1001/jamadermatol.2013.6896).
The ubiquity of tanning salons contributes to the problem, said Dr. Smith. “More is not better; in the largest U.S. cities, tanning salons outnumber [both] Starbucks and McDonald’s,” she said, noting that studies have shown that both proximity to tanning salons and the low cost of tanning encourage their use (Am J Prev Med. 2009 Mar 36[3]:243-6).
A 2015 study surveyed 125 colleges, finding that 48% had indoor tanning facilities in their campus or off-campus housing. College cash cards were acceptable payment at 14.4% of colleges, and 96% of off-campus housing facilities that offered tanning provided it as a free “perk” to residents (JAMA Dermatol 2015 Jan. doi: 10.1001/jamadermatol.2014.3590).
Further, some data suggest that tanning really can be addictive for some patients. Ultraviolet light exposure has been shown to “light up” pleasure centers in PET-CT studies, and some frequent tanners report relaxation and pleasure from tanning as well as craving and feelings of withdrawal when they miss sessions. Dr. Smith said she does not hesitate to refer teen patients to mental health providers if there are concerns about mood and depression.
Having an understanding of patient motivations to tan can help in getting patients to take steps toward change, said Dr. Smith. “What can we do? We can actually do a lot. We have a lot more influence than we think we do.”
At the level of the individual patient, just opening up a conversation can make a big difference. “We assume we know why teenagers go to a tanning booth. But do we? When you notice a young woman who’s been to a tanning booth, ask why,” using a nonjudgmental approach to begin a dialogue about the near-term and long-term dangers of tanning. A positive approach is key, noted Dr. Smith. “Focusing on the benefits of avoiding UV tanning is more effective than a heavy reliance on scare tactics,” she said. Also, “multiple interventions work better.”
Before-and-after photos of celebrities whose appearance has been affected by photoaging can be effective. Another tactic with a more positive spin is to share images of celebrities who have chosen not to tan and who celebrate their fair skin. These conversations are particularly important at prom time, peak tanning season for many young women, said Dr. Smith. She has a portfolio of photos showing fair-skinned women wearing high-contrast gowns, which she says are more flattering for pale skin than white or nude colors.
For patients who still want that tan look, “Tanning for reasons of appearance can be satisfied with sunless tanners,” said Dr. Smith. The most common ingredient in sunless tanners is dihydroxyacetone (DHA), which was approved in the 1970s for topical use. However, the Food and Drug Administration issued a warning in 2011 about spray tanning, noting that the “industry has not provided safety data to FDA in order for the agency to consider approving it for … ‘misting’ from tanning booths.” The FDA’s specific concern had to do with the unknown safety of ingestion, inhalation, and mucous membrane exposure that can result from spray tanning.
Moving to the legislative and policy level, change can be achieved when stakeholders band together to “ban the tan,” said Dr. Smith. “The best way to do it is with a village. It really takes a lot of people to do this.”
There are solid epidemiologic and economic reasons to focus on the skin cancer epidemic, said Dr. Smith. Skin cancer is now the most common cancer in the United States, and more new cases “are diagnosed each year than breast, prostate, lung, and colon cancers combined,” she said. Of nonmelanoma skin cancers, 90% are thought to be UV-related, and “the vast majority of mutations found in melanoma are caused by UV radiation.”
Skin cancers cost the United States over $8 billion annually, and although promising new immunotherapies are extending the lives of those with melanoma, these treatments cost hundreds of thousands of dollars a year. “This type of treatment is unaffordable for our system,” said Dr. Smith.
Progress is being made, she said, despite industry opposition. Individual states have regulated or banned tanning for minors, and at the federal level, tanning beds are now considered by the FDA to be Class II (moderate-risk) medical devices, a step up from their previous classification as the lowest-risk Class I devices, “The same as a tongue blade,” she said.
Dr. Smith had no relevant financial disclosures.
On Twitter @karioakes
MINNEAPOLIS, MINN. – Indoor tanning is a significant contributor to the U.S. skin cancer epidemic and represents a 100% preventable source of exposure to these cancers. Understanding exactly who is using indoor tanning – and why – can provide insight and leverage to help change behavior, according to Cindy Firkins Smith, MD, adjunct professor of dermatology at the University of Minnesota, Minneapolis.
Dr. Smith noted that the typical indoor tanning bed user is female and between 17 and 30 years old. Other aspects of her lifestyle may be unhealthy; for example, she may smoke cigarettes, have an unhealthy pattern of alcohol consumption, and make unhealthy food choices (Cancer Causes Control 2006 June. doi:10.1007/s10552-005-0453-9). She also is likely to watch beauty-focused reality TV shows (J Am Acad Dermatol 2013 May. doi:10.1016/j.jaad.2012.09.055) and is likely to objectify her own body, seeing it as something to be viewed and judged (Arch Dermatol 2009 Sep 1. doi:10.1001/archdermatol.2009.190).
Tanning is a behavior that provides relaxation and positive emotions, and she receives support for this behavior from family and friends. “Tanning often starts with mom, which is one reason that parental permission legislation doesn’t work,” she said at the annual meeting of the Society for Pediatric Dermatology.
Dr. Smith said that up to 30 million people tan indoors every year. Rates of tanning for teenage girls are very high: up to 40% of American teenagers use indoor tanning, and 20%-30% of all 18- to 29-year-olds have used a tanning bed in the previous year (Jama Dermatol 2014 April doi: 10.1001/jamadermatol.2013.6896).
The ubiquity of tanning salons contributes to the problem, said Dr. Smith. “More is not better; in the largest U.S. cities, tanning salons outnumber [both] Starbucks and McDonald’s,” she said, noting that studies have shown that both proximity to tanning salons and the low cost of tanning encourage their use (Am J Prev Med. 2009 Mar 36[3]:243-6).
A 2015 study surveyed 125 colleges, finding that 48% had indoor tanning facilities in their campus or off-campus housing. College cash cards were acceptable payment at 14.4% of colleges, and 96% of off-campus housing facilities that offered tanning provided it as a free “perk” to residents (JAMA Dermatol 2015 Jan. doi: 10.1001/jamadermatol.2014.3590).
Further, some data suggest that tanning really can be addictive for some patients. Ultraviolet light exposure has been shown to “light up” pleasure centers in PET-CT studies, and some frequent tanners report relaxation and pleasure from tanning as well as craving and feelings of withdrawal when they miss sessions. Dr. Smith said she does not hesitate to refer teen patients to mental health providers if there are concerns about mood and depression.
Having an understanding of patient motivations to tan can help in getting patients to take steps toward change, said Dr. Smith. “What can we do? We can actually do a lot. We have a lot more influence than we think we do.”
At the level of the individual patient, just opening up a conversation can make a big difference. “We assume we know why teenagers go to a tanning booth. But do we? When you notice a young woman who’s been to a tanning booth, ask why,” using a nonjudgmental approach to begin a dialogue about the near-term and long-term dangers of tanning. A positive approach is key, noted Dr. Smith. “Focusing on the benefits of avoiding UV tanning is more effective than a heavy reliance on scare tactics,” she said. Also, “multiple interventions work better.”
Before-and-after photos of celebrities whose appearance has been affected by photoaging can be effective. Another tactic with a more positive spin is to share images of celebrities who have chosen not to tan and who celebrate their fair skin. These conversations are particularly important at prom time, peak tanning season for many young women, said Dr. Smith. She has a portfolio of photos showing fair-skinned women wearing high-contrast gowns, which she says are more flattering for pale skin than white or nude colors.
For patients who still want that tan look, “Tanning for reasons of appearance can be satisfied with sunless tanners,” said Dr. Smith. The most common ingredient in sunless tanners is dihydroxyacetone (DHA), which was approved in the 1970s for topical use. However, the Food and Drug Administration issued a warning in 2011 about spray tanning, noting that the “industry has not provided safety data to FDA in order for the agency to consider approving it for … ‘misting’ from tanning booths.” The FDA’s specific concern had to do with the unknown safety of ingestion, inhalation, and mucous membrane exposure that can result from spray tanning.
Moving to the legislative and policy level, change can be achieved when stakeholders band together to “ban the tan,” said Dr. Smith. “The best way to do it is with a village. It really takes a lot of people to do this.”
There are solid epidemiologic and economic reasons to focus on the skin cancer epidemic, said Dr. Smith. Skin cancer is now the most common cancer in the United States, and more new cases “are diagnosed each year than breast, prostate, lung, and colon cancers combined,” she said. Of nonmelanoma skin cancers, 90% are thought to be UV-related, and “the vast majority of mutations found in melanoma are caused by UV radiation.”
Skin cancers cost the United States over $8 billion annually, and although promising new immunotherapies are extending the lives of those with melanoma, these treatments cost hundreds of thousands of dollars a year. “This type of treatment is unaffordable for our system,” said Dr. Smith.
Progress is being made, she said, despite industry opposition. Individual states have regulated or banned tanning for minors, and at the federal level, tanning beds are now considered by the FDA to be Class II (moderate-risk) medical devices, a step up from their previous classification as the lowest-risk Class I devices, “The same as a tongue blade,” she said.
Dr. Smith had no relevant financial disclosures.
On Twitter @karioakes
EXPERT ANALYSIS FROM THE SPD ANNUAL MEETING

Pembrolizumab-ipilimumab combo is highly active in advanced melanoma
CHICAGO – The combination of pembrolizumab, an antibody to the human cell surface receptor programmed death-1 (PD-1), and ipilimumab, an antibody to the human T-cell receptor cytotoxic T-lymphocyte-associated antigen 4 (CTLA4), is highly active against advanced melanoma and has acceptable safety, finds the KEYNOTE 029 trial’s expansion cohort.
The 153 patients in the cohort received a standard dose of pembrolizumab (2 mg/kg every 3 weeks) with a reduced dose of ipilimumab (1 mg/kg every 3 weeks for four doses) on the basis of earlier data showing substantial toxicity when a standard dose of ipilimumab was combined with other immune checkpoint inhibitors.
Results reported at the annual meeting of the American Society of Clinical Oncology showed that the overall response rate was 57%, and the disease control rate was 78%. Although 42% of patients experienced grade 3 or 4 treatment-related adverse events, most of these events resolved, and there were no treatment-related deaths.
“Pembrolizumab 2 mg/kg in combination with four doses of ipilimumab 1 mg/kg has a manageable toxicity profile and provides robust antitumor activity in patients with advanced melanoma,” concluded the investigators, who were led by Georgina Long, PhD, MBBS, chair of Melanoma Medical Oncology and Translational Research at the Melanoma Institute Australia and Royal North Shore Hospital, University of Sydney.
The response rate seen in KEYNOTE 029 was almost identical to that seen in the CheckMate 067 trial with the combination of nivolumab and standard-dose ipilimumab (3 mg/kg every 3 weeks for four doses), noted invited discussant Marc S. Ernstoff, MD, professor and chair of the department of medicine at the Roswell Park Cancer Institute in Buffalo, N.Y. It was also “remarkably comparable” to the 69% seen in the COMBI-d melanoma trial with the combination of dabrafenib (a BRAF inhibitor) and trametinib (an inhibitor of MEK MAPK/ERK kinase).
“There is a significant amount of grade 3 and 4 toxicity, but the dose of ipilimumab appeared to decrease this in the pembrolizumab-ipilimumab study compared to the nivolumab-ipilimumab study,” he noted. “There was a high percent of low-grade toxicities reported in all of these studies, and I would argue that as we are seeing patients survive longer, these low-grade toxicities are going to become more of an issue for us as oncologists to be able to deal with in terms of quality of life for patients surviving.”
There is good rationale for combining CTLA4 blockade and PD1 (or PD-L1) blockade in melanoma, Dr. Long maintained when introducing the research. “We know that CTLA inhibition at the priming phase in the periphery, at antigen presentation, is effective, as is PD-1 or PD-L1 [inhibition] at the effector phase down in the tumor bed,” she elaborated.
The patients with advanced melanoma enrolled in the expansion cohort could have received any number of prior therapies other than immune checkpoint inhibitors. However, in 87%, the study regimen was their first therapy.
At the time of data cutoff, 72% of patients had received all four planned doses of ipilimumab (Yervoy), and 56% were continuing on pembrolizumab (Keytruda).
The rates of any-grade and grade 3 or 4 treatment-related adverse events were 95% and 42%, respectively. The corresponding rates of immune-mediated adverse events were 58% and 25%.
The most common grade 3 or 4 treatment-related adverse events were lipase elevation (14%) and rash (3%). The former was asymptomatic and had no sequelae in the majority of cases, Dr. Long reported.
Hepatitis, colitis, and skin reactions were the most common grade 3 or 4 immune-mediated adverse events. The majority of immune-mediated adverse events were managed with systemic treatment, usually corticosteroids, and resolved.
When it came to efficacy, the overall response rate with the combination was similar across subgroups of patients stratified by PD-L1 status in the tumor and adjacent immune tissue, treatment history, baseline lactate dehydrogenase level, and BRAF mutational status.
Responses were ongoing in 98% of patients at data cutoff, with the duration of response ranging from about 6 weeks to 43 weeks, Dr. Long said. The disease control rate was 78%.
With a median follow-up of 10.0 months, median progression-free survival and overall survival were not yet reached. However, the 6-month rates of these outcomes were 70% and 93%, respectively.
Dr. Long disclosed that she is a consultant/adviser to Amgen, Bristol-Myers Squibb, Merck, Novartis, Provectus, and Roche, and that she has received honoraria from Bristol-Myers Squibb, Merck, and Novartis. The trial was supported by Merck.
CHICAGO – The combination of pembrolizumab, an antibody to the human cell surface receptor programmed death-1 (PD-1), and ipilimumab, an antibody to the human T-cell receptor cytotoxic T-lymphocyte-associated antigen 4 (CTLA4), is highly active against advanced melanoma and has acceptable safety, finds the KEYNOTE 029 trial’s expansion cohort.
The 153 patients in the cohort received a standard dose of pembrolizumab (2 mg/kg every 3 weeks) with a reduced dose of ipilimumab (1 mg/kg every 3 weeks for four doses) on the basis of earlier data showing substantial toxicity when a standard dose of ipilimumab was combined with other immune checkpoint inhibitors.
Results reported at the annual meeting of the American Society of Clinical Oncology showed that the overall response rate was 57%, and the disease control rate was 78%. Although 42% of patients experienced grade 3 or 4 treatment-related adverse events, most of these events resolved, and there were no treatment-related deaths.
“Pembrolizumab 2 mg/kg in combination with four doses of ipilimumab 1 mg/kg has a manageable toxicity profile and provides robust antitumor activity in patients with advanced melanoma,” concluded the investigators, who were led by Georgina Long, PhD, MBBS, chair of Melanoma Medical Oncology and Translational Research at the Melanoma Institute Australia and Royal North Shore Hospital, University of Sydney.
The response rate seen in KEYNOTE 029 was almost identical to that seen in the CheckMate 067 trial with the combination of nivolumab and standard-dose ipilimumab (3 mg/kg every 3 weeks for four doses), noted invited discussant Marc S. Ernstoff, MD, professor and chair of the department of medicine at the Roswell Park Cancer Institute in Buffalo, N.Y. It was also “remarkably comparable” to the 69% seen in the COMBI-d melanoma trial with the combination of dabrafenib (a BRAF inhibitor) and trametinib (an inhibitor of MEK MAPK/ERK kinase).
“There is a significant amount of grade 3 and 4 toxicity, but the dose of ipilimumab appeared to decrease this in the pembrolizumab-ipilimumab study compared to the nivolumab-ipilimumab study,” he noted. “There was a high percent of low-grade toxicities reported in all of these studies, and I would argue that as we are seeing patients survive longer, these low-grade toxicities are going to become more of an issue for us as oncologists to be able to deal with in terms of quality of life for patients surviving.”
There is good rationale for combining CTLA4 blockade and PD1 (or PD-L1) blockade in melanoma, Dr. Long maintained when introducing the research. “We know that CTLA inhibition at the priming phase in the periphery, at antigen presentation, is effective, as is PD-1 or PD-L1 [inhibition] at the effector phase down in the tumor bed,” she elaborated.
The patients with advanced melanoma enrolled in the expansion cohort could have received any number of prior therapies other than immune checkpoint inhibitors. However, in 87%, the study regimen was their first therapy.
At the time of data cutoff, 72% of patients had received all four planned doses of ipilimumab (Yervoy), and 56% were continuing on pembrolizumab (Keytruda).
The rates of any-grade and grade 3 or 4 treatment-related adverse events were 95% and 42%, respectively. The corresponding rates of immune-mediated adverse events were 58% and 25%.
The most common grade 3 or 4 treatment-related adverse events were lipase elevation (14%) and rash (3%). The former was asymptomatic and had no sequelae in the majority of cases, Dr. Long reported.
Hepatitis, colitis, and skin reactions were the most common grade 3 or 4 immune-mediated adverse events. The majority of immune-mediated adverse events were managed with systemic treatment, usually corticosteroids, and resolved.
When it came to efficacy, the overall response rate with the combination was similar across subgroups of patients stratified by PD-L1 status in the tumor and adjacent immune tissue, treatment history, baseline lactate dehydrogenase level, and BRAF mutational status.
Responses were ongoing in 98% of patients at data cutoff, with the duration of response ranging from about 6 weeks to 43 weeks, Dr. Long said. The disease control rate was 78%.
With a median follow-up of 10.0 months, median progression-free survival and overall survival were not yet reached. However, the 6-month rates of these outcomes were 70% and 93%, respectively.
Dr. Long disclosed that she is a consultant/adviser to Amgen, Bristol-Myers Squibb, Merck, Novartis, Provectus, and Roche, and that she has received honoraria from Bristol-Myers Squibb, Merck, and Novartis. The trial was supported by Merck.
CHICAGO – The combination of pembrolizumab, an antibody to the human cell surface receptor programmed death-1 (PD-1), and ipilimumab, an antibody to the human T-cell receptor cytotoxic T-lymphocyte-associated antigen 4 (CTLA4), is highly active against advanced melanoma and has acceptable safety, finds the KEYNOTE 029 trial’s expansion cohort.
The 153 patients in the cohort received a standard dose of pembrolizumab (2 mg/kg every 3 weeks) with a reduced dose of ipilimumab (1 mg/kg every 3 weeks for four doses) on the basis of earlier data showing substantial toxicity when a standard dose of ipilimumab was combined with other immune checkpoint inhibitors.
Results reported at the annual meeting of the American Society of Clinical Oncology showed that the overall response rate was 57%, and the disease control rate was 78%. Although 42% of patients experienced grade 3 or 4 treatment-related adverse events, most of these events resolved, and there were no treatment-related deaths.
“Pembrolizumab 2 mg/kg in combination with four doses of ipilimumab 1 mg/kg has a manageable toxicity profile and provides robust antitumor activity in patients with advanced melanoma,” concluded the investigators, who were led by Georgina Long, PhD, MBBS, chair of Melanoma Medical Oncology and Translational Research at the Melanoma Institute Australia and Royal North Shore Hospital, University of Sydney.
The response rate seen in KEYNOTE 029 was almost identical to that seen in the CheckMate 067 trial with the combination of nivolumab and standard-dose ipilimumab (3 mg/kg every 3 weeks for four doses), noted invited discussant Marc S. Ernstoff, MD, professor and chair of the department of medicine at the Roswell Park Cancer Institute in Buffalo, N.Y. It was also “remarkably comparable” to the 69% seen in the COMBI-d melanoma trial with the combination of dabrafenib (a BRAF inhibitor) and trametinib (an inhibitor of MEK MAPK/ERK kinase).
“There is a significant amount of grade 3 and 4 toxicity, but the dose of ipilimumab appeared to decrease this in the pembrolizumab-ipilimumab study compared to the nivolumab-ipilimumab study,” he noted. “There was a high percent of low-grade toxicities reported in all of these studies, and I would argue that as we are seeing patients survive longer, these low-grade toxicities are going to become more of an issue for us as oncologists to be able to deal with in terms of quality of life for patients surviving.”
There is good rationale for combining CTLA4 blockade and PD1 (or PD-L1) blockade in melanoma, Dr. Long maintained when introducing the research. “We know that CTLA inhibition at the priming phase in the periphery, at antigen presentation, is effective, as is PD-1 or PD-L1 [inhibition] at the effector phase down in the tumor bed,” she elaborated.
The patients with advanced melanoma enrolled in the expansion cohort could have received any number of prior therapies other than immune checkpoint inhibitors. However, in 87%, the study regimen was their first therapy.
At the time of data cutoff, 72% of patients had received all four planned doses of ipilimumab (Yervoy), and 56% were continuing on pembrolizumab (Keytruda).
The rates of any-grade and grade 3 or 4 treatment-related adverse events were 95% and 42%, respectively. The corresponding rates of immune-mediated adverse events were 58% and 25%.
The most common grade 3 or 4 treatment-related adverse events were lipase elevation (14%) and rash (3%). The former was asymptomatic and had no sequelae in the majority of cases, Dr. Long reported.
Hepatitis, colitis, and skin reactions were the most common grade 3 or 4 immune-mediated adverse events. The majority of immune-mediated adverse events were managed with systemic treatment, usually corticosteroids, and resolved.
When it came to efficacy, the overall response rate with the combination was similar across subgroups of patients stratified by PD-L1 status in the tumor and adjacent immune tissue, treatment history, baseline lactate dehydrogenase level, and BRAF mutational status.
Responses were ongoing in 98% of patients at data cutoff, with the duration of response ranging from about 6 weeks to 43 weeks, Dr. Long said. The disease control rate was 78%.
With a median follow-up of 10.0 months, median progression-free survival and overall survival were not yet reached. However, the 6-month rates of these outcomes were 70% and 93%, respectively.
Dr. Long disclosed that she is a consultant/adviser to Amgen, Bristol-Myers Squibb, Merck, Novartis, Provectus, and Roche, and that she has received honoraria from Bristol-Myers Squibb, Merck, and Novartis. The trial was supported by Merck.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Dual immune checkpoint blockade with pembrolizumab and ipilimumab is efficacious in advanced melanoma.
Major finding: The overall response rate was 57%, and the disease control rate was 78%.
Data source: An expansion cohort from a phase I/II trial among 153 patients with advanced melanoma (KEYNOTE 029).
Disclosures: Dr. Long disclosed that she is a consultant/advisor to Amgen, Bristol-Myers Squibb, Merck, Novartis, Provectus, and Roche, and that she has received honoraria from Bristol-Myers Squibb, Merck, and Novartis. The trial was supported by Merck.
SU2C announces researcher-industry collaboration on immunotherapy
Stand Up To Cancer is calling for proposals to investigate additional uses for nivolumab, ipilimumab, elotuzumab, and urelumab, as part of a new researcher-industry collaborative program.
As many as four projects will be funded by Bristol-Myers Squibb, maker of the four agents, in the range of $1 million to $3 million each, according to a written statement from the American Association for Cancer Research (AACR).
The company will provide access to the three drugs already approved for the treatement of various cancers –nivolumab, ipilimumab, and elotuzumab– and to urelumab, an investigational agent that is currently in early clinical trials.
Proposals can include the study of one or more of the products, alone or in combination with other treatments, and may include products from other companies, as well as explore potential new uses for the drug(s), AACR said in the statement.
Nivolumab (Opdivo) is currently approved to treat advanced melanoma, non-small cell lung cancer, renal cell carcinoma, and classical Hodgkin lymphoma; Ipilimumab (Yervoy) is approved to treat melanoma; and elotuzumab (Empliciti) is approved to treat multiple myeloma, in conjunction with other drugs. Urelumab is being evaluated as a treatment for a range of cancers, including some hematological cancers, advanced colorectal cancer, and head and neck cancers.
The Stand Up To Cancer (SU2C) Catalyst program was launched in April to “use funding and materials from the pharmaceutical, biotechnology, diagnostic, and medical devices industries to accelerate research on cancer prevention, detection, and treatment,” according to a written statement from SU2C. Founding collaborators in addition to Bristol-Myers Squibb include Merck and Genentech.
The Catalyst projects must follow the SU2C model be carried out by a collaborative team, and be designed to accelerate the clinical use of therapeutic agents within the 3-year term of the grant, and to deliver near-term patient benefit.
The Request for Proposal for the Bristol-Myers Squibb agents is available at proposalCENTRAL, with proposals due by noon ET Monday, Aug. 15.
lnikolaides@frontlinemedcom.com
On Twitter @NikolaidesLaura
Stand Up To Cancer is calling for proposals to investigate additional uses for nivolumab, ipilimumab, elotuzumab, and urelumab, as part of a new researcher-industry collaborative program.
As many as four projects will be funded by Bristol-Myers Squibb, maker of the four agents, in the range of $1 million to $3 million each, according to a written statement from the American Association for Cancer Research (AACR).
The company will provide access to the three drugs already approved for the treatement of various cancers –nivolumab, ipilimumab, and elotuzumab– and to urelumab, an investigational agent that is currently in early clinical trials.
Proposals can include the study of one or more of the products, alone or in combination with other treatments, and may include products from other companies, as well as explore potential new uses for the drug(s), AACR said in the statement.
Nivolumab (Opdivo) is currently approved to treat advanced melanoma, non-small cell lung cancer, renal cell carcinoma, and classical Hodgkin lymphoma; Ipilimumab (Yervoy) is approved to treat melanoma; and elotuzumab (Empliciti) is approved to treat multiple myeloma, in conjunction with other drugs. Urelumab is being evaluated as a treatment for a range of cancers, including some hematological cancers, advanced colorectal cancer, and head and neck cancers.
The Stand Up To Cancer (SU2C) Catalyst program was launched in April to “use funding and materials from the pharmaceutical, biotechnology, diagnostic, and medical devices industries to accelerate research on cancer prevention, detection, and treatment,” according to a written statement from SU2C. Founding collaborators in addition to Bristol-Myers Squibb include Merck and Genentech.
The Catalyst projects must follow the SU2C model be carried out by a collaborative team, and be designed to accelerate the clinical use of therapeutic agents within the 3-year term of the grant, and to deliver near-term patient benefit.
The Request for Proposal for the Bristol-Myers Squibb agents is available at proposalCENTRAL, with proposals due by noon ET Monday, Aug. 15.
lnikolaides@frontlinemedcom.com
On Twitter @NikolaidesLaura
Stand Up To Cancer is calling for proposals to investigate additional uses for nivolumab, ipilimumab, elotuzumab, and urelumab, as part of a new researcher-industry collaborative program.
As many as four projects will be funded by Bristol-Myers Squibb, maker of the four agents, in the range of $1 million to $3 million each, according to a written statement from the American Association for Cancer Research (AACR).
The company will provide access to the three drugs already approved for the treatement of various cancers –nivolumab, ipilimumab, and elotuzumab– and to urelumab, an investigational agent that is currently in early clinical trials.
Proposals can include the study of one or more of the products, alone or in combination with other treatments, and may include products from other companies, as well as explore potential new uses for the drug(s), AACR said in the statement.
Nivolumab (Opdivo) is currently approved to treat advanced melanoma, non-small cell lung cancer, renal cell carcinoma, and classical Hodgkin lymphoma; Ipilimumab (Yervoy) is approved to treat melanoma; and elotuzumab (Empliciti) is approved to treat multiple myeloma, in conjunction with other drugs. Urelumab is being evaluated as a treatment for a range of cancers, including some hematological cancers, advanced colorectal cancer, and head and neck cancers.
The Stand Up To Cancer (SU2C) Catalyst program was launched in April to “use funding and materials from the pharmaceutical, biotechnology, diagnostic, and medical devices industries to accelerate research on cancer prevention, detection, and treatment,” according to a written statement from SU2C. Founding collaborators in addition to Bristol-Myers Squibb include Merck and Genentech.
The Catalyst projects must follow the SU2C model be carried out by a collaborative team, and be designed to accelerate the clinical use of therapeutic agents within the 3-year term of the grant, and to deliver near-term patient benefit.
The Request for Proposal for the Bristol-Myers Squibb agents is available at proposalCENTRAL, with proposals due by noon ET Monday, Aug. 15.
lnikolaides@frontlinemedcom.com
On Twitter @NikolaidesLaura
Sunscreens May Fail to Meet SPF Claims on Product Labels
New data from Consumer Reports indicate that 48% of all sunscreens tested (N=104) over 4 years did not provide the sun protection factor (SPF) promised on product labels, leaving consumers with insufficient sun protection, which could lead to long-term sun damage including wrinkles or skin cancer. Furthermore, 42% of chemical sunscreens (n=85) and 74% of mineral sunscreens (n=19) did not meet their SPF claims.
The study also reveals that more than one-third (35%) of sunscreens registered below SPF 30, which is the minimum recommended by the American Academy of Dermatology (AAD). Although product labels featured claims of water resistance, nearly half of the sunscreens tested failed to meet their SPF claim following water immersion.
Dermatologists can educate patients about correct sunscreen use and product labels to ensure the highest level of protection against melanoma and other skin cancers. According to a 2016 AAD survey, only 32% of respondents knew that an SPF 30 sunscreen does not provide twice as much protection as an SPF 15 sunscreen. Furthermore, only 45% of respondents knew that a higher-SPF sunscreen does not protect skin from sun exposure longer than a lower-SPF sunscreen.
The AAD has issued a list of talking points highlighting key messages that dermatologists can share with patients and/or the media when asked about sun-protection techniques and the recent sunscreen data released by Consumer Reports.
New data from Consumer Reports indicate that 48% of all sunscreens tested (N=104) over 4 years did not provide the sun protection factor (SPF) promised on product labels, leaving consumers with insufficient sun protection, which could lead to long-term sun damage including wrinkles or skin cancer. Furthermore, 42% of chemical sunscreens (n=85) and 74% of mineral sunscreens (n=19) did not meet their SPF claims.
The study also reveals that more than one-third (35%) of sunscreens registered below SPF 30, which is the minimum recommended by the American Academy of Dermatology (AAD). Although product labels featured claims of water resistance, nearly half of the sunscreens tested failed to meet their SPF claim following water immersion.
Dermatologists can educate patients about correct sunscreen use and product labels to ensure the highest level of protection against melanoma and other skin cancers. According to a 2016 AAD survey, only 32% of respondents knew that an SPF 30 sunscreen does not provide twice as much protection as an SPF 15 sunscreen. Furthermore, only 45% of respondents knew that a higher-SPF sunscreen does not protect skin from sun exposure longer than a lower-SPF sunscreen.
The AAD has issued a list of talking points highlighting key messages that dermatologists can share with patients and/or the media when asked about sun-protection techniques and the recent sunscreen data released by Consumer Reports.
New data from Consumer Reports indicate that 48% of all sunscreens tested (N=104) over 4 years did not provide the sun protection factor (SPF) promised on product labels, leaving consumers with insufficient sun protection, which could lead to long-term sun damage including wrinkles or skin cancer. Furthermore, 42% of chemical sunscreens (n=85) and 74% of mineral sunscreens (n=19) did not meet their SPF claims.
The study also reveals that more than one-third (35%) of sunscreens registered below SPF 30, which is the minimum recommended by the American Academy of Dermatology (AAD). Although product labels featured claims of water resistance, nearly half of the sunscreens tested failed to meet their SPF claim following water immersion.
Dermatologists can educate patients about correct sunscreen use and product labels to ensure the highest level of protection against melanoma and other skin cancers. According to a 2016 AAD survey, only 32% of respondents knew that an SPF 30 sunscreen does not provide twice as much protection as an SPF 15 sunscreen. Furthermore, only 45% of respondents knew that a higher-SPF sunscreen does not protect skin from sun exposure longer than a lower-SPF sunscreen.
The AAD has issued a list of talking points highlighting key messages that dermatologists can share with patients and/or the media when asked about sun-protection techniques and the recent sunscreen data released by Consumer Reports.
40% of top-rated sunscreens fall short of AAD guidelines
Customer satisfaction ratings of sunscreens do not always reflect the products’ effectiveness, as 40% of the 65 top-rated sunscreens available on Amazon.com did not adhere to all three of the American Academy of Dermatology’s recommended criteria.
The AAD recommends the following for all sunscreens: sun protection factor (SPF) of 30 more, broad-spectrum protection, and water and/or sweat resistance. Of those criteria, water/sweat resistance was missing in 19 (29%), compared with SPF less than 30 in 7 (11%) products and lack of broad-spectrum protection in 4 (6%). Some products missed more than one criterion, said Shuai Xu, MD, of Northwestern University, Chicago, and his associates (JAMA Dermatolol. 2016 Jul 6. doi: 10.1001/jamadermatol.2016.2344).

Of the qualities besides performance that were analyzed, “cosmetic elegance,” which the investigators “defined as any feature associated with skin sensation on application, color, or scent,” was the positive feature most often mentioned in the customer reviews. On the other hand, they noted, “dermatologist recommendations were not a significantly cited positive feature.”
The sunscreens in the analysis represented the top 1 percentile by customer rating of the 6,500 products categorized as sunscreens on Amazon as of December 2015. The 65 products included in the study had more than 24,400 customer reviews and a median rating of 4.5 out of 5 stars, Dr. Xu and his associates said.
The investigators did not report any conflicts of interest.
Customer satisfaction ratings of sunscreens do not always reflect the products’ effectiveness, as 40% of the 65 top-rated sunscreens available on Amazon.com did not adhere to all three of the American Academy of Dermatology’s recommended criteria.
The AAD recommends the following for all sunscreens: sun protection factor (SPF) of 30 more, broad-spectrum protection, and water and/or sweat resistance. Of those criteria, water/sweat resistance was missing in 19 (29%), compared with SPF less than 30 in 7 (11%) products and lack of broad-spectrum protection in 4 (6%). Some products missed more than one criterion, said Shuai Xu, MD, of Northwestern University, Chicago, and his associates (JAMA Dermatolol. 2016 Jul 6. doi: 10.1001/jamadermatol.2016.2344).
Of the qualities besides performance that were analyzed, “cosmetic elegance,” which the investigators “defined as any feature associated with skin sensation on application, color, or scent,” was the positive feature most often mentioned in the customer reviews. On the other hand, they noted, “dermatologist recommendations were not a significantly cited positive feature.”
The sunscreens in the analysis represented the top 1 percentile by customer rating of the 6,500 products categorized as sunscreens on Amazon as of December 2015. The 65 products included in the study had more than 24,400 customer reviews and a median rating of 4.5 out of 5 stars, Dr. Xu and his associates said.
The investigators did not report any conflicts of interest.
Customer satisfaction ratings of sunscreens do not always reflect the products’ effectiveness, as 40% of the 65 top-rated sunscreens available on Amazon.com did not adhere to all three of the American Academy of Dermatology’s recommended criteria.
The AAD recommends the following for all sunscreens: sun protection factor (SPF) of 30 more, broad-spectrum protection, and water and/or sweat resistance. Of those criteria, water/sweat resistance was missing in 19 (29%), compared with SPF less than 30 in 7 (11%) products and lack of broad-spectrum protection in 4 (6%). Some products missed more than one criterion, said Shuai Xu, MD, of Northwestern University, Chicago, and his associates (JAMA Dermatolol. 2016 Jul 6. doi: 10.1001/jamadermatol.2016.2344).
Of the qualities besides performance that were analyzed, “cosmetic elegance,” which the investigators “defined as any feature associated with skin sensation on application, color, or scent,” was the positive feature most often mentioned in the customer reviews. On the other hand, they noted, “dermatologist recommendations were not a significantly cited positive feature.”
The sunscreens in the analysis represented the top 1 percentile by customer rating of the 6,500 products categorized as sunscreens on Amazon as of December 2015. The 65 products included in the study had more than 24,400 customer reviews and a median rating of 4.5 out of 5 stars, Dr. Xu and his associates said.
The investigators did not report any conflicts of interest.
FROM JAMA DERMATOLOGY
Study tracks distant metastatic patterns of Merkel cell carcinoma
SCOTTSDALE, ARIZ. – Distant metastatic sites of Merkel cell carcinoma most often involved the supraclavicular, retroperitoneal, and iliac lymph nodes, in a single center retrospective study of 305 patients.
Merkel cell carcinoma metastases “clearly favored distant nodes, but the distribution of other metastatic sites was distinct from other cancers, such as melanoma,” Jamiluddin Qazi, an undergraduate student at the University of Washington, Seattle, said at the annual meeting of the Society for Investigative Dermatology. The findings could help guide imaging and other surveillance of patients after they develop a primary Merkel cell tumor, he added.
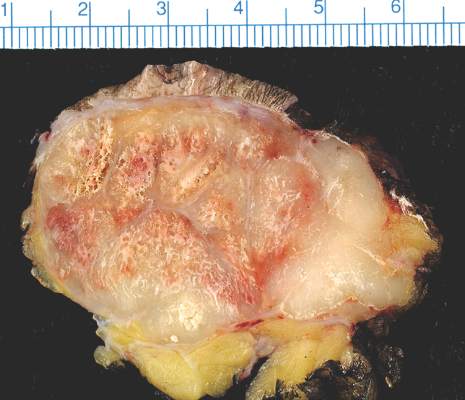
About 2,000 individuals in the United States are diagnosed with Merkel cell carcinoma every year. About 40% of these patients develop metastatic disease, which has a 5-year survival rate of less than 25%, Mr. Qazi noted. Indeed, median survival after diagnosis of metastatic Merkel cell carcinoma was only 9.5 months in one recent study (J Cutan Pathol. 2010;37:20-7). Programmed death 1 (PD-1) blockade with pembrolizumab (Keytruda) can potentially improve survival (N Engl J Med. 2016; 374:2542-52), “but there is no consensus regarding follow-up for Merkel cell carcinoma. The 2016 National Comprehensive Cancer Network (NCCN) guidelines recommend ‘follow up as clinically indicated,’ and a lack of data has led to ambiguity,” Mr. Qazi said.
Working with oncologists and radiologists at the Seattle Cancer Care Alliance, he analyzed a tissue and clinical database of 442 initial distant Merkel cell carcinoma metastases among 305 patients. Initial distant metastases were defined as the first lesions detected beyond the regional lymph nodes of the primary tumor. A total of 69% of patients had one initial distant metastasis, 19% had two concurrently identified lesions, 9% had three lesions, and 4% had at least four lesions, Mr. Qazi reported.
“Merkel cell carcinoma seemed to metastasize to unusual places, but clearly preferred the distant lymph nodes. In all, 26% of metastases localized there, most commonly to the supraclavicular, retroperitoneal, and iliac nodes,” he said. The next most common site of distant metastasis was the liver (15% of lesions), followed by the skin and bone (13% of lesions each), lung (6%), and pancreas (5%). Less common sites included the heart, spleen, abdominal muscle, brain, kidneys, adrenal glands, gonad, chest wall, and stomach.
Comparing these findings with a similar study in melanoma (J Oncol 2012. doi: 10.1155/2012/647684) showed that both cancers have about the same chances of metastasizing to the liver, bone, kidneys, adrenal glands, and stomach, Mr. Qazi said. However, Merkel cell carcinoma was less likely to metastasize to the brain (3% of lesions, vs. 12% for melanoma) and lung (6% vs. 14%), and was more likely to metastasize to the pancreas (5% vs. 1%).
Now the investigators are working to link metastatic sites with factors such as the location of the primary tumor, the presence or absence of lymphovascular invasion, and the status of the immune system and Merkel polyomavirus infection, said Mr. Qazi. They also are analyzing time from diagnosis or treatment to metastasis to help guide decisions about when to order follow-up imaging. Ultimately, they hope to create an online tool that enables clinicians to describe a primary Merkel cell carcinoma and rapidly receive automated information about the most likely timing and location of metastasis.
The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
SCOTTSDALE, ARIZ. – Distant metastatic sites of Merkel cell carcinoma most often involved the supraclavicular, retroperitoneal, and iliac lymph nodes, in a single center retrospective study of 305 patients.
Merkel cell carcinoma metastases “clearly favored distant nodes, but the distribution of other metastatic sites was distinct from other cancers, such as melanoma,” Jamiluddin Qazi, an undergraduate student at the University of Washington, Seattle, said at the annual meeting of the Society for Investigative Dermatology. The findings could help guide imaging and other surveillance of patients after they develop a primary Merkel cell tumor, he added.
About 2,000 individuals in the United States are diagnosed with Merkel cell carcinoma every year. About 40% of these patients develop metastatic disease, which has a 5-year survival rate of less than 25%, Mr. Qazi noted. Indeed, median survival after diagnosis of metastatic Merkel cell carcinoma was only 9.5 months in one recent study (J Cutan Pathol. 2010;37:20-7). Programmed death 1 (PD-1) blockade with pembrolizumab (Keytruda) can potentially improve survival (N Engl J Med. 2016; 374:2542-52), “but there is no consensus regarding follow-up for Merkel cell carcinoma. The 2016 National Comprehensive Cancer Network (NCCN) guidelines recommend ‘follow up as clinically indicated,’ and a lack of data has led to ambiguity,” Mr. Qazi said.
Working with oncologists and radiologists at the Seattle Cancer Care Alliance, he analyzed a tissue and clinical database of 442 initial distant Merkel cell carcinoma metastases among 305 patients. Initial distant metastases were defined as the first lesions detected beyond the regional lymph nodes of the primary tumor. A total of 69% of patients had one initial distant metastasis, 19% had two concurrently identified lesions, 9% had three lesions, and 4% had at least four lesions, Mr. Qazi reported.
“Merkel cell carcinoma seemed to metastasize to unusual places, but clearly preferred the distant lymph nodes. In all, 26% of metastases localized there, most commonly to the supraclavicular, retroperitoneal, and iliac nodes,” he said. The next most common site of distant metastasis was the liver (15% of lesions), followed by the skin and bone (13% of lesions each), lung (6%), and pancreas (5%). Less common sites included the heart, spleen, abdominal muscle, brain, kidneys, adrenal glands, gonad, chest wall, and stomach.
Comparing these findings with a similar study in melanoma (J Oncol 2012. doi: 10.1155/2012/647684) showed that both cancers have about the same chances of metastasizing to the liver, bone, kidneys, adrenal glands, and stomach, Mr. Qazi said. However, Merkel cell carcinoma was less likely to metastasize to the brain (3% of lesions, vs. 12% for melanoma) and lung (6% vs. 14%), and was more likely to metastasize to the pancreas (5% vs. 1%).
Now the investigators are working to link metastatic sites with factors such as the location of the primary tumor, the presence or absence of lymphovascular invasion, and the status of the immune system and Merkel polyomavirus infection, said Mr. Qazi. They also are analyzing time from diagnosis or treatment to metastasis to help guide decisions about when to order follow-up imaging. Ultimately, they hope to create an online tool that enables clinicians to describe a primary Merkel cell carcinoma and rapidly receive automated information about the most likely timing and location of metastasis.
The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
SCOTTSDALE, ARIZ. – Distant metastatic sites of Merkel cell carcinoma most often involved the supraclavicular, retroperitoneal, and iliac lymph nodes, in a single center retrospective study of 305 patients.
Merkel cell carcinoma metastases “clearly favored distant nodes, but the distribution of other metastatic sites was distinct from other cancers, such as melanoma,” Jamiluddin Qazi, an undergraduate student at the University of Washington, Seattle, said at the annual meeting of the Society for Investigative Dermatology. The findings could help guide imaging and other surveillance of patients after they develop a primary Merkel cell tumor, he added.
About 2,000 individuals in the United States are diagnosed with Merkel cell carcinoma every year. About 40% of these patients develop metastatic disease, which has a 5-year survival rate of less than 25%, Mr. Qazi noted. Indeed, median survival after diagnosis of metastatic Merkel cell carcinoma was only 9.5 months in one recent study (J Cutan Pathol. 2010;37:20-7). Programmed death 1 (PD-1) blockade with pembrolizumab (Keytruda) can potentially improve survival (N Engl J Med. 2016; 374:2542-52), “but there is no consensus regarding follow-up for Merkel cell carcinoma. The 2016 National Comprehensive Cancer Network (NCCN) guidelines recommend ‘follow up as clinically indicated,’ and a lack of data has led to ambiguity,” Mr. Qazi said.
Working with oncologists and radiologists at the Seattle Cancer Care Alliance, he analyzed a tissue and clinical database of 442 initial distant Merkel cell carcinoma metastases among 305 patients. Initial distant metastases were defined as the first lesions detected beyond the regional lymph nodes of the primary tumor. A total of 69% of patients had one initial distant metastasis, 19% had two concurrently identified lesions, 9% had three lesions, and 4% had at least four lesions, Mr. Qazi reported.
“Merkel cell carcinoma seemed to metastasize to unusual places, but clearly preferred the distant lymph nodes. In all, 26% of metastases localized there, most commonly to the supraclavicular, retroperitoneal, and iliac nodes,” he said. The next most common site of distant metastasis was the liver (15% of lesions), followed by the skin and bone (13% of lesions each), lung (6%), and pancreas (5%). Less common sites included the heart, spleen, abdominal muscle, brain, kidneys, adrenal glands, gonad, chest wall, and stomach.
Comparing these findings with a similar study in melanoma (J Oncol 2012. doi: 10.1155/2012/647684) showed that both cancers have about the same chances of metastasizing to the liver, bone, kidneys, adrenal glands, and stomach, Mr. Qazi said. However, Merkel cell carcinoma was less likely to metastasize to the brain (3% of lesions, vs. 12% for melanoma) and lung (6% vs. 14%), and was more likely to metastasize to the pancreas (5% vs. 1%).
Now the investigators are working to link metastatic sites with factors such as the location of the primary tumor, the presence or absence of lymphovascular invasion, and the status of the immune system and Merkel polyomavirus infection, said Mr. Qazi. They also are analyzing time from diagnosis or treatment to metastasis to help guide decisions about when to order follow-up imaging. Ultimately, they hope to create an online tool that enables clinicians to describe a primary Merkel cell carcinoma and rapidly receive automated information about the most likely timing and location of metastasis.
The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: Distant metastases of Merkel cell carcinoma most often involve the lymph nodes, followed by the liver, skin, and bone.
Major finding: Distant lymph node metastases comprised 26% of lesions, the liver comprised 15%, and skin and bone made up 13% each.
Data source: A single-center retrospective study of 442 initial distant metastases of Merkel cell carcinoma among 305 patients.
Disclosures: The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
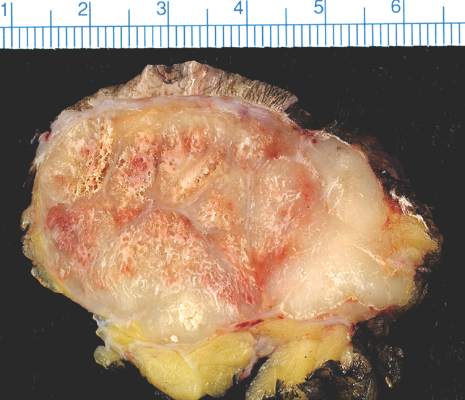
Study tracks distant metastatic patterns of Merkel cell carcinoma
SCOTTSDALE, ARIZ. – Distant metastatic sites of Merkel cell carcinoma most often involved the supraclavicular, retroperitoneal, and iliac lymph nodes, in a single center retrospective study of 305 patients.
Merkel cell carcinoma metastases “clearly favored distant nodes, but the distribution of other metastatic sites was distinct from other cancers, such as melanoma,” Jamiluddin Qazi, an undergraduate student at the University of Washington, Seattle, said at the annual meeting of the Society for Investigative Dermatology. The findings could help guide imaging and other surveillance of patients after they develop a primary Merkel cell tumor, he added.
About 2,000 individuals in the United States are diagnosed with Merkel cell carcinoma every year. About 40% of these patients develop metastatic disease, which has a 5-year survival rate of less than 25%, Mr. Qazi noted. Indeed, median survival after diagnosis of metastatic Merkel cell carcinoma was only 9.5 months in one recent study (J Cutan Pathol. 2010;37:20-7). Programmed death 1 (PD-1) blockade with pembrolizumab (Keytruda) can potentially improve survival (N Engl J Med. 2016; 374:2542-52), “but there is no consensus regarding follow-up for Merkel cell carcinoma. The 2016 National Comprehensive Cancer Network (NCCN) guidelines recommend ‘follow up as clinically indicated,’ and a lack of data has led to ambiguity,” Mr. Qazi said.
Working with oncologists and radiologists at the Seattle Cancer Care Alliance, he analyzed a tissue and clinical database of 442 initial distant Merkel cell carcinoma metastases among 305 patients. Initial distant metastases were defined as the first lesions detected beyond the regional lymph nodes of the primary tumor. A total of 69% of patients had one initial distant metastasis, 19% had two concurrently identified lesions, 9% had three lesions, and 4% had at least four lesions, Mr. Qazi reported.
“Merkel cell carcinoma seemed to metastasize to unusual places, but clearly preferred the distant lymph nodes. In all, 26% of metastases localized there, most commonly to the supraclavicular, retroperitoneal, and iliac nodes,” he said. The next most common site of distant metastasis was the liver (15% of lesions), followed by the skin and bone (13% of lesions each), lung (6%), and pancreas (5%). Less common sites included the heart, spleen, abdominal muscle, brain, kidneys, adrenal glands, gonad, chest wall, and stomach.
Comparing these findings with a similar study in melanoma (J Oncol 2012. doi: 10.1155/2012/647684) showed that both cancers have about the same chances of metastasizing to the liver, bone, kidneys, adrenal glands, and stomach, Mr. Qazi said. However, Merkel cell carcinoma was less likely to metastasize to the brain (3% of lesions, vs. 12% for melanoma) and lung (6% vs. 14%), and was more likely to metastasize to the pancreas (5% vs. 1%).
Now the investigators are working to link metastatic sites with factors such as the location of the primary tumor, the presence or absence of lymphovascular invasion, and the status of the immune system and Merkel polyomavirus infection, said Mr. Qazi. They also are analyzing time from diagnosis or treatment to metastasis to help guide decisions about when to order follow-up imaging. Ultimately, they hope to create an online tool that enables clinicians to describe a primary Merkel cell carcinoma and rapidly receive automated information about the most likely timing and location of metastasis.
The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
SCOTTSDALE, ARIZ. – Distant metastatic sites of Merkel cell carcinoma most often involved the supraclavicular, retroperitoneal, and iliac lymph nodes, in a single center retrospective study of 305 patients.
Merkel cell carcinoma metastases “clearly favored distant nodes, but the distribution of other metastatic sites was distinct from other cancers, such as melanoma,” Jamiluddin Qazi, an undergraduate student at the University of Washington, Seattle, said at the annual meeting of the Society for Investigative Dermatology. The findings could help guide imaging and other surveillance of patients after they develop a primary Merkel cell tumor, he added.
About 2,000 individuals in the United States are diagnosed with Merkel cell carcinoma every year. About 40% of these patients develop metastatic disease, which has a 5-year survival rate of less than 25%, Mr. Qazi noted. Indeed, median survival after diagnosis of metastatic Merkel cell carcinoma was only 9.5 months in one recent study (J Cutan Pathol. 2010;37:20-7). Programmed death 1 (PD-1) blockade with pembrolizumab (Keytruda) can potentially improve survival (N Engl J Med. 2016; 374:2542-52), “but there is no consensus regarding follow-up for Merkel cell carcinoma. The 2016 National Comprehensive Cancer Network (NCCN) guidelines recommend ‘follow up as clinically indicated,’ and a lack of data has led to ambiguity,” Mr. Qazi said.
Working with oncologists and radiologists at the Seattle Cancer Care Alliance, he analyzed a tissue and clinical database of 442 initial distant Merkel cell carcinoma metastases among 305 patients. Initial distant metastases were defined as the first lesions detected beyond the regional lymph nodes of the primary tumor. A total of 69% of patients had one initial distant metastasis, 19% had two concurrently identified lesions, 9% had three lesions, and 4% had at least four lesions, Mr. Qazi reported.
“Merkel cell carcinoma seemed to metastasize to unusual places, but clearly preferred the distant lymph nodes. In all, 26% of metastases localized there, most commonly to the supraclavicular, retroperitoneal, and iliac nodes,” he said. The next most common site of distant metastasis was the liver (15% of lesions), followed by the skin and bone (13% of lesions each), lung (6%), and pancreas (5%). Less common sites included the heart, spleen, abdominal muscle, brain, kidneys, adrenal glands, gonad, chest wall, and stomach.
Comparing these findings with a similar study in melanoma (J Oncol 2012. doi: 10.1155/2012/647684) showed that both cancers have about the same chances of metastasizing to the liver, bone, kidneys, adrenal glands, and stomach, Mr. Qazi said. However, Merkel cell carcinoma was less likely to metastasize to the brain (3% of lesions, vs. 12% for melanoma) and lung (6% vs. 14%), and was more likely to metastasize to the pancreas (5% vs. 1%).
Now the investigators are working to link metastatic sites with factors such as the location of the primary tumor, the presence or absence of lymphovascular invasion, and the status of the immune system and Merkel polyomavirus infection, said Mr. Qazi. They also are analyzing time from diagnosis or treatment to metastasis to help guide decisions about when to order follow-up imaging. Ultimately, they hope to create an online tool that enables clinicians to describe a primary Merkel cell carcinoma and rapidly receive automated information about the most likely timing and location of metastasis.
The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
SCOTTSDALE, ARIZ. – Distant metastatic sites of Merkel cell carcinoma most often involved the supraclavicular, retroperitoneal, and iliac lymph nodes, in a single center retrospective study of 305 patients.
Merkel cell carcinoma metastases “clearly favored distant nodes, but the distribution of other metastatic sites was distinct from other cancers, such as melanoma,” Jamiluddin Qazi, an undergraduate student at the University of Washington, Seattle, said at the annual meeting of the Society for Investigative Dermatology. The findings could help guide imaging and other surveillance of patients after they develop a primary Merkel cell tumor, he added.
About 2,000 individuals in the United States are diagnosed with Merkel cell carcinoma every year. About 40% of these patients develop metastatic disease, which has a 5-year survival rate of less than 25%, Mr. Qazi noted. Indeed, median survival after diagnosis of metastatic Merkel cell carcinoma was only 9.5 months in one recent study (J Cutan Pathol. 2010;37:20-7). Programmed death 1 (PD-1) blockade with pembrolizumab (Keytruda) can potentially improve survival (N Engl J Med. 2016; 374:2542-52), “but there is no consensus regarding follow-up for Merkel cell carcinoma. The 2016 National Comprehensive Cancer Network (NCCN) guidelines recommend ‘follow up as clinically indicated,’ and a lack of data has led to ambiguity,” Mr. Qazi said.
Working with oncologists and radiologists at the Seattle Cancer Care Alliance, he analyzed a tissue and clinical database of 442 initial distant Merkel cell carcinoma metastases among 305 patients. Initial distant metastases were defined as the first lesions detected beyond the regional lymph nodes of the primary tumor. A total of 69% of patients had one initial distant metastasis, 19% had two concurrently identified lesions, 9% had three lesions, and 4% had at least four lesions, Mr. Qazi reported.
“Merkel cell carcinoma seemed to metastasize to unusual places, but clearly preferred the distant lymph nodes. In all, 26% of metastases localized there, most commonly to the supraclavicular, retroperitoneal, and iliac nodes,” he said. The next most common site of distant metastasis was the liver (15% of lesions), followed by the skin and bone (13% of lesions each), lung (6%), and pancreas (5%). Less common sites included the heart, spleen, abdominal muscle, brain, kidneys, adrenal glands, gonad, chest wall, and stomach.
Comparing these findings with a similar study in melanoma (J Oncol 2012. doi: 10.1155/2012/647684) showed that both cancers have about the same chances of metastasizing to the liver, bone, kidneys, adrenal glands, and stomach, Mr. Qazi said. However, Merkel cell carcinoma was less likely to metastasize to the brain (3% of lesions, vs. 12% for melanoma) and lung (6% vs. 14%), and was more likely to metastasize to the pancreas (5% vs. 1%).
Now the investigators are working to link metastatic sites with factors such as the location of the primary tumor, the presence or absence of lymphovascular invasion, and the status of the immune system and Merkel polyomavirus infection, said Mr. Qazi. They also are analyzing time from diagnosis or treatment to metastasis to help guide decisions about when to order follow-up imaging. Ultimately, they hope to create an online tool that enables clinicians to describe a primary Merkel cell carcinoma and rapidly receive automated information about the most likely timing and location of metastasis.
The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: Distant metastases of Merkel cell carcinoma most often involve the lymph nodes, followed by the liver, skin, and bone.
Major finding: Distant lymph node metastases comprised 26% of lesions, the liver comprised 15%, and skin and bone made up 13% each.
Data source: A single-center retrospective study of 442 initial distant metastases of Merkel cell carcinoma among 305 patients.
Disclosures: The National Institutes of Health supported the study. Mr. Qazi had no conflicts of interest.