User login
FDA releases updates on BIA-ALCL
The US Food and Drug Administration (FDA) has released new information on breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL).
The agency said it is now aware of 414 cases of BIA-ALCL, which includes 9 patients who died.
In addition, the medical literature suggests that patients with textured breast implants have a lifetime risk of developing BIA-ALCL that ranges from 1 in 3817 to 1 in 30,000.
“The FDA has been closely tracking the relationship between breast implants and a rare type of non-Hodgkin’s lymphoma since we first identified this possible association,” said Binita Ashar, MD, director of the division of surgical devices in the FDA’s Center for Devices and Radiological Health.
“We’ve been working to gather additional information to better characterize and quantify the risk so that patients and providers can have more informed discussions about breast implants. As part of that effort, we are working to update and enhance the information we have on this association, including updating the total number of known cases of BIA-ALCL and the lifetime risk of developing BIA-ALCL as reported in medical literature.”
Reports to FDA
Most of the BIA-ALCL cases reported to the FDA occurred in patients with textured implants (n=242), but 30 occurred in patients with smooth implants. In the remaining 173 cases, the implant surface was not specified.
There were more silicone implants (n=234) than saline implants (n=179), and there was 1 case in which the implant filling was not specified.
The patients’ median age was 53 (range, 24-90), and the median time from last implant to BIA-ALCL diagnosis was 8 years (range, 0-44).
Cases of BIA-ALCL were ALK-negative (n=124) or did not have ALK status specified (n=290). And they were CD30-positive (n=126) or did not have CD30 status specified (n=288).
The most common clinical presentation was seroma (n=203), followed by breast swelling/pain (n=101), peri-implant mass/lump (n=45), and capsular contracture (n=42). In some cases, more than one clinical presentation was listed, and there were 141 cases where clinical presentation was unspecified/uncertain.
Medical literature
The FDA said a “significant body of medical literature” on BIA-ALCL has been published since the agency’s 2011 report on this malignancy.
For the aforementioned lifetime risk estimates—1 case of BIA-ALCL in 3817 to 30,000 individuals with textured implants—the FDA cited 3 sources:
- BIA-ALCL Resources : By the numbers, and what they mean
- Breast Implant–Associated Anaplastic Large Cell Lymphoma in Australia and New Zealand: High-Surface-Area Textured Implants Are Associated with Increased Risk
- Breast Implants and the Risk of Anaplastic Large-Cell Lymphoma in the Breast.
Recommendations, more updates
The FDA said this updated information does not change its recommendations regarding breast implants. The agency said the decision to obtain breast implants should be made based on individual needs and with the most complete information about risks and benefits.
“We hope that this information prompts providers and patients to have important, informed conversations about breast implants and the risk of BIA-ALCL,” Dr Ashar said. “At the same time, we remain committed to working in partnership with all stakeholders to continue to study, understand, and provide updates about this important public health issue.”
The FDA is also updating the content and format of the webpage for the agency’s breast implant post-approval studies to make current information about these studies easier for patients to read and understand.
The US Food and Drug Administration (FDA) has released new information on breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL).
The agency said it is now aware of 414 cases of BIA-ALCL, which includes 9 patients who died.
In addition, the medical literature suggests that patients with textured breast implants have a lifetime risk of developing BIA-ALCL that ranges from 1 in 3817 to 1 in 30,000.
“The FDA has been closely tracking the relationship between breast implants and a rare type of non-Hodgkin’s lymphoma since we first identified this possible association,” said Binita Ashar, MD, director of the division of surgical devices in the FDA’s Center for Devices and Radiological Health.
“We’ve been working to gather additional information to better characterize and quantify the risk so that patients and providers can have more informed discussions about breast implants. As part of that effort, we are working to update and enhance the information we have on this association, including updating the total number of known cases of BIA-ALCL and the lifetime risk of developing BIA-ALCL as reported in medical literature.”
Reports to FDA
Most of the BIA-ALCL cases reported to the FDA occurred in patients with textured implants (n=242), but 30 occurred in patients with smooth implants. In the remaining 173 cases, the implant surface was not specified.
There were more silicone implants (n=234) than saline implants (n=179), and there was 1 case in which the implant filling was not specified.
The patients’ median age was 53 (range, 24-90), and the median time from last implant to BIA-ALCL diagnosis was 8 years (range, 0-44).
Cases of BIA-ALCL were ALK-negative (n=124) or did not have ALK status specified (n=290). And they were CD30-positive (n=126) or did not have CD30 status specified (n=288).
The most common clinical presentation was seroma (n=203), followed by breast swelling/pain (n=101), peri-implant mass/lump (n=45), and capsular contracture (n=42). In some cases, more than one clinical presentation was listed, and there were 141 cases where clinical presentation was unspecified/uncertain.
Medical literature
The FDA said a “significant body of medical literature” on BIA-ALCL has been published since the agency’s 2011 report on this malignancy.
For the aforementioned lifetime risk estimates—1 case of BIA-ALCL in 3817 to 30,000 individuals with textured implants—the FDA cited 3 sources:
- BIA-ALCL Resources : By the numbers, and what they mean
- Breast Implant–Associated Anaplastic Large Cell Lymphoma in Australia and New Zealand: High-Surface-Area Textured Implants Are Associated with Increased Risk
- Breast Implants and the Risk of Anaplastic Large-Cell Lymphoma in the Breast.
Recommendations, more updates
The FDA said this updated information does not change its recommendations regarding breast implants. The agency said the decision to obtain breast implants should be made based on individual needs and with the most complete information about risks and benefits.
“We hope that this information prompts providers and patients to have important, informed conversations about breast implants and the risk of BIA-ALCL,” Dr Ashar said. “At the same time, we remain committed to working in partnership with all stakeholders to continue to study, understand, and provide updates about this important public health issue.”
The FDA is also updating the content and format of the webpage for the agency’s breast implant post-approval studies to make current information about these studies easier for patients to read and understand.
The US Food and Drug Administration (FDA) has released new information on breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL).
The agency said it is now aware of 414 cases of BIA-ALCL, which includes 9 patients who died.
In addition, the medical literature suggests that patients with textured breast implants have a lifetime risk of developing BIA-ALCL that ranges from 1 in 3817 to 1 in 30,000.
“The FDA has been closely tracking the relationship between breast implants and a rare type of non-Hodgkin’s lymphoma since we first identified this possible association,” said Binita Ashar, MD, director of the division of surgical devices in the FDA’s Center for Devices and Radiological Health.
“We’ve been working to gather additional information to better characterize and quantify the risk so that patients and providers can have more informed discussions about breast implants. As part of that effort, we are working to update and enhance the information we have on this association, including updating the total number of known cases of BIA-ALCL and the lifetime risk of developing BIA-ALCL as reported in medical literature.”
Reports to FDA
Most of the BIA-ALCL cases reported to the FDA occurred in patients with textured implants (n=242), but 30 occurred in patients with smooth implants. In the remaining 173 cases, the implant surface was not specified.
There were more silicone implants (n=234) than saline implants (n=179), and there was 1 case in which the implant filling was not specified.
The patients’ median age was 53 (range, 24-90), and the median time from last implant to BIA-ALCL diagnosis was 8 years (range, 0-44).
Cases of BIA-ALCL were ALK-negative (n=124) or did not have ALK status specified (n=290). And they were CD30-positive (n=126) or did not have CD30 status specified (n=288).
The most common clinical presentation was seroma (n=203), followed by breast swelling/pain (n=101), peri-implant mass/lump (n=45), and capsular contracture (n=42). In some cases, more than one clinical presentation was listed, and there were 141 cases where clinical presentation was unspecified/uncertain.
Medical literature
The FDA said a “significant body of medical literature” on BIA-ALCL has been published since the agency’s 2011 report on this malignancy.
For the aforementioned lifetime risk estimates—1 case of BIA-ALCL in 3817 to 30,000 individuals with textured implants—the FDA cited 3 sources:
- BIA-ALCL Resources : By the numbers, and what they mean
- Breast Implant–Associated Anaplastic Large Cell Lymphoma in Australia and New Zealand: High-Surface-Area Textured Implants Are Associated with Increased Risk
- Breast Implants and the Risk of Anaplastic Large-Cell Lymphoma in the Breast.
Recommendations, more updates
The FDA said this updated information does not change its recommendations regarding breast implants. The agency said the decision to obtain breast implants should be made based on individual needs and with the most complete information about risks and benefits.
“We hope that this information prompts providers and patients to have important, informed conversations about breast implants and the risk of BIA-ALCL,” Dr Ashar said. “At the same time, we remain committed to working in partnership with all stakeholders to continue to study, understand, and provide updates about this important public health issue.”
The FDA is also updating the content and format of the webpage for the agency’s breast implant post-approval studies to make current information about these studies easier for patients to read and understand.
FDA approves BV plus chemo for untreated cHL

The US Food and Drug Administration (FDA) has approved brentuximab vedotin (ADCETRIS) in combination with chemotherapy for adults with previously untreated, stage III or IV classical Hodgkin lymphoma (cHL).
This is the fifth approved indication for BV in the US and the first regimen approved for frontline, stage III/IV cHL in the US in more than 40 years.
“The standard of care for treating newly diagnosed, advanced Hodgkin lymphoma has not changed in more than 4 decades,” said Joseph M. Connors, MD, of BC Cancer in Vancouver, British Columbia, Canada.
“For years, the physician community has been conducting clinical trials to identify improved regimens that are both less toxic and more effective—to no avail.”
The ECHELON-1 study changed that, according to Dr Connors.
“The ECHELON-1 study results demonstrated superior efficacy of the ADCETRIS plus chemotherapy regimen, when compared to the standard of care, while removing bleomycin—an agent that can cause unpredictable and sometimes fatal lung toxicity—completely from the regimen,” he said. “This represents a meaningful advance for this often younger patient population.”
In the phase 3 ECHELON-1 trial, researchers compared BV plus doxorubicin, vinblastine, and dacarbazine (A+AVD) to doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD).
In addition to supporting the new approval for BV in cHL, ECHELON-1 results also served to convert an accelerated approval of BV to standard approval. The drug now has standard FDA approval for the treatment of adults with systemic anaplastic large-cell lymphoma (ALCL) who have failed at least 1 prior multi-agent chemotherapy regimen.
BV also has standard FDA approval for:
- Adults with cHL who have failed autologous hematopoietic stem cell transplant (auto-HSCT) or, in those who are not auto-HSCT candidates, have failed at least 2 prior multi-agent chemotherapy regimens
- Post-auto-HSCT consolidation in adults with cHL at high risk of relapse or progression
- Adults with primary cutaneous ALCL or CD30-expressing mycosis fungoides who have received prior systemic therapy.
ECHELON-1
Result from ECHELON-1 were presented at the 2017 ASH Annual Meeting and simultaneously published in NEJM.
In this trial, researchers compared A+AVD to ABVD as frontline treatment for 1334 patients with advanced cHL. The primary endpoint was modified progression-free survival (PFS), which was defined as time to progression, death, or evidence of non-complete response after completion of frontline therapy followed by subsequent anticancer therapy.
According to an independent review facility, A+AVD provided a significant improvement in modified PFS compared to ABVD. The hazard ratio was 0.77 (P=0.035), which corresponds to a 23% reduction in the risk of progression, death, or the need for additional anticancer therapy.
The 2-year modified PFS rate was 82.1% in the A+AVD arm and 77.2% in the ABVD arm.
There was no significant difference between the treatment arms when it came to response rates or overall survival.
The objective response rate was 86% in the A+AVD arm and 83% in the ABVD arm (P=0.12). The complete response rate was 73% and 70%, respectively (P=0.22).
The interim 2-year overall survival rate was 97% in the A+AVD arm and 95% in the ABVD arm (hazard ratio=0.72; P=0.19).
The overall incidence of adverse events (AEs) was 99% in the A+AVD arm and 98% in the ABVD arm. The incidence of grade 3 or higher AEs was 83% and 66%, respectively, and the incidence of serious AEs was 43% and 27%, respectively.
Neutropenia, febrile neutropenia, and peripheral neuropathy were more common with A+AVD, while pulmonary toxicity was more common with ABVD.
The US Food and Drug Administration (FDA) has approved brentuximab vedotin (ADCETRIS) in combination with chemotherapy for adults with previously untreated, stage III or IV classical Hodgkin lymphoma (cHL).
This is the fifth approved indication for BV in the US and the first regimen approved for frontline, stage III/IV cHL in the US in more than 40 years.
“The standard of care for treating newly diagnosed, advanced Hodgkin lymphoma has not changed in more than 4 decades,” said Joseph M. Connors, MD, of BC Cancer in Vancouver, British Columbia, Canada.
“For years, the physician community has been conducting clinical trials to identify improved regimens that are both less toxic and more effective—to no avail.”
The ECHELON-1 study changed that, according to Dr Connors.
“The ECHELON-1 study results demonstrated superior efficacy of the ADCETRIS plus chemotherapy regimen, when compared to the standard of care, while removing bleomycin—an agent that can cause unpredictable and sometimes fatal lung toxicity—completely from the regimen,” he said. “This represents a meaningful advance for this often younger patient population.”
In the phase 3 ECHELON-1 trial, researchers compared BV plus doxorubicin, vinblastine, and dacarbazine (A+AVD) to doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD).
In addition to supporting the new approval for BV in cHL, ECHELON-1 results also served to convert an accelerated approval of BV to standard approval. The drug now has standard FDA approval for the treatment of adults with systemic anaplastic large-cell lymphoma (ALCL) who have failed at least 1 prior multi-agent chemotherapy regimen.
BV also has standard FDA approval for:
- Adults with cHL who have failed autologous hematopoietic stem cell transplant (auto-HSCT) or, in those who are not auto-HSCT candidates, have failed at least 2 prior multi-agent chemotherapy regimens
- Post-auto-HSCT consolidation in adults with cHL at high risk of relapse or progression
- Adults with primary cutaneous ALCL or CD30-expressing mycosis fungoides who have received prior systemic therapy.
ECHELON-1
Result from ECHELON-1 were presented at the 2017 ASH Annual Meeting and simultaneously published in NEJM.
In this trial, researchers compared A+AVD to ABVD as frontline treatment for 1334 patients with advanced cHL. The primary endpoint was modified progression-free survival (PFS), which was defined as time to progression, death, or evidence of non-complete response after completion of frontline therapy followed by subsequent anticancer therapy.
According to an independent review facility, A+AVD provided a significant improvement in modified PFS compared to ABVD. The hazard ratio was 0.77 (P=0.035), which corresponds to a 23% reduction in the risk of progression, death, or the need for additional anticancer therapy.
The 2-year modified PFS rate was 82.1% in the A+AVD arm and 77.2% in the ABVD arm.
There was no significant difference between the treatment arms when it came to response rates or overall survival.
The objective response rate was 86% in the A+AVD arm and 83% in the ABVD arm (P=0.12). The complete response rate was 73% and 70%, respectively (P=0.22).
The interim 2-year overall survival rate was 97% in the A+AVD arm and 95% in the ABVD arm (hazard ratio=0.72; P=0.19).
The overall incidence of adverse events (AEs) was 99% in the A+AVD arm and 98% in the ABVD arm. The incidence of grade 3 or higher AEs was 83% and 66%, respectively, and the incidence of serious AEs was 43% and 27%, respectively.
Neutropenia, febrile neutropenia, and peripheral neuropathy were more common with A+AVD, while pulmonary toxicity was more common with ABVD.
The US Food and Drug Administration (FDA) has approved brentuximab vedotin (ADCETRIS) in combination with chemotherapy for adults with previously untreated, stage III or IV classical Hodgkin lymphoma (cHL).
This is the fifth approved indication for BV in the US and the first regimen approved for frontline, stage III/IV cHL in the US in more than 40 years.
“The standard of care for treating newly diagnosed, advanced Hodgkin lymphoma has not changed in more than 4 decades,” said Joseph M. Connors, MD, of BC Cancer in Vancouver, British Columbia, Canada.
“For years, the physician community has been conducting clinical trials to identify improved regimens that are both less toxic and more effective—to no avail.”
The ECHELON-1 study changed that, according to Dr Connors.
“The ECHELON-1 study results demonstrated superior efficacy of the ADCETRIS plus chemotherapy regimen, when compared to the standard of care, while removing bleomycin—an agent that can cause unpredictable and sometimes fatal lung toxicity—completely from the regimen,” he said. “This represents a meaningful advance for this often younger patient population.”
In the phase 3 ECHELON-1 trial, researchers compared BV plus doxorubicin, vinblastine, and dacarbazine (A+AVD) to doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD).
In addition to supporting the new approval for BV in cHL, ECHELON-1 results also served to convert an accelerated approval of BV to standard approval. The drug now has standard FDA approval for the treatment of adults with systemic anaplastic large-cell lymphoma (ALCL) who have failed at least 1 prior multi-agent chemotherapy regimen.
BV also has standard FDA approval for:
- Adults with cHL who have failed autologous hematopoietic stem cell transplant (auto-HSCT) or, in those who are not auto-HSCT candidates, have failed at least 2 prior multi-agent chemotherapy regimens
- Post-auto-HSCT consolidation in adults with cHL at high risk of relapse or progression
- Adults with primary cutaneous ALCL or CD30-expressing mycosis fungoides who have received prior systemic therapy.
ECHELON-1
Result from ECHELON-1 were presented at the 2017 ASH Annual Meeting and simultaneously published in NEJM.
In this trial, researchers compared A+AVD to ABVD as frontline treatment for 1334 patients with advanced cHL. The primary endpoint was modified progression-free survival (PFS), which was defined as time to progression, death, or evidence of non-complete response after completion of frontline therapy followed by subsequent anticancer therapy.
According to an independent review facility, A+AVD provided a significant improvement in modified PFS compared to ABVD. The hazard ratio was 0.77 (P=0.035), which corresponds to a 23% reduction in the risk of progression, death, or the need for additional anticancer therapy.
The 2-year modified PFS rate was 82.1% in the A+AVD arm and 77.2% in the ABVD arm.
There was no significant difference between the treatment arms when it came to response rates or overall survival.
The objective response rate was 86% in the A+AVD arm and 83% in the ABVD arm (P=0.12). The complete response rate was 73% and 70%, respectively (P=0.22).
The interim 2-year overall survival rate was 97% in the A+AVD arm and 95% in the ABVD arm (hazard ratio=0.72; P=0.19).
The overall incidence of adverse events (AEs) was 99% in the A+AVD arm and 98% in the ABVD arm. The incidence of grade 3 or higher AEs was 83% and 66%, respectively, and the incidence of serious AEs was 43% and 27%, respectively.
Neutropenia, febrile neutropenia, and peripheral neuropathy were more common with A+AVD, while pulmonary toxicity was more common with ABVD.
Drug receives orphan designation for CTCL

The US Food and Drug Administration (FDA) has granted orphan drug designation to TTI-621 for the treatment of cutaneous T-cell lymphoma (CTCL).
TTI-621 is designed to activate the innate immune system by blocking the activity of CD47, a protein commonly found on the surface of cancer cells.
TTI-621 is a SIRPaFc fusion protein that consists of the CD47-binding domain of human SIRPa linked to the Fc region of a human immunoglobulin.
The drug is intended to act as a soluble decoy receptor, preventing CD47 from delivering its inhibitory signal, thereby enabling the activation of macrophage anti-tumor effects by pro-phagocytic signals.
TTI-621 is under investigation in a phase 1 trial of patients with relapsed/refractory solid tumors and CTCL (NCT02890368). Results from the dose-escalation portion of this study were presented at the 2017 ASH Annual Meeting (abstract 4076*).
The dose-escalation portion had a 3+3 design. TTI-621 was first given as a single intratumoral injection at 1 mg, 3 mg, or 10 mg. Then, it was given at 10 mg on Monday, Wednesday, and Friday for 1 week. Next, it was given on the same 3-day schedule for 2 weeks.
Results were reported for 18 patients, 56% of whom were male. They had a median age of 69 (range, 32-85) and a median number of 3 prior therapies (range, 1-16), including radiation (39%).
Eleven patients had CTCL, and 10 were evaluable. Researchers said they observed “rapid decreases in circulating Sézary cells and/or the size of mycosis fungoides tumors” after treatment with TTI-621.
Nine of the 10 patients had a reduction in CAILS score from baseline, and 3 had a reduction in circulating Sézary cells.
There were no dose-limiting toxicities, so the 10 mg dose given 3 times a week for 2 weeks was considered the optimal dose schedule.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
*Data in the abstract differ from the presentation.
The US Food and Drug Administration (FDA) has granted orphan drug designation to TTI-621 for the treatment of cutaneous T-cell lymphoma (CTCL).
TTI-621 is designed to activate the innate immune system by blocking the activity of CD47, a protein commonly found on the surface of cancer cells.
TTI-621 is a SIRPaFc fusion protein that consists of the CD47-binding domain of human SIRPa linked to the Fc region of a human immunoglobulin.
The drug is intended to act as a soluble decoy receptor, preventing CD47 from delivering its inhibitory signal, thereby enabling the activation of macrophage anti-tumor effects by pro-phagocytic signals.
TTI-621 is under investigation in a phase 1 trial of patients with relapsed/refractory solid tumors and CTCL (NCT02890368). Results from the dose-escalation portion of this study were presented at the 2017 ASH Annual Meeting (abstract 4076*).
The dose-escalation portion had a 3+3 design. TTI-621 was first given as a single intratumoral injection at 1 mg, 3 mg, or 10 mg. Then, it was given at 10 mg on Monday, Wednesday, and Friday for 1 week. Next, it was given on the same 3-day schedule for 2 weeks.
Results were reported for 18 patients, 56% of whom were male. They had a median age of 69 (range, 32-85) and a median number of 3 prior therapies (range, 1-16), including radiation (39%).
Eleven patients had CTCL, and 10 were evaluable. Researchers said they observed “rapid decreases in circulating Sézary cells and/or the size of mycosis fungoides tumors” after treatment with TTI-621.
Nine of the 10 patients had a reduction in CAILS score from baseline, and 3 had a reduction in circulating Sézary cells.
There were no dose-limiting toxicities, so the 10 mg dose given 3 times a week for 2 weeks was considered the optimal dose schedule.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
*Data in the abstract differ from the presentation.
The US Food and Drug Administration (FDA) has granted orphan drug designation to TTI-621 for the treatment of cutaneous T-cell lymphoma (CTCL).
TTI-621 is designed to activate the innate immune system by blocking the activity of CD47, a protein commonly found on the surface of cancer cells.
TTI-621 is a SIRPaFc fusion protein that consists of the CD47-binding domain of human SIRPa linked to the Fc region of a human immunoglobulin.
The drug is intended to act as a soluble decoy receptor, preventing CD47 from delivering its inhibitory signal, thereby enabling the activation of macrophage anti-tumor effects by pro-phagocytic signals.
TTI-621 is under investigation in a phase 1 trial of patients with relapsed/refractory solid tumors and CTCL (NCT02890368). Results from the dose-escalation portion of this study were presented at the 2017 ASH Annual Meeting (abstract 4076*).
The dose-escalation portion had a 3+3 design. TTI-621 was first given as a single intratumoral injection at 1 mg, 3 mg, or 10 mg. Then, it was given at 10 mg on Monday, Wednesday, and Friday for 1 week. Next, it was given on the same 3-day schedule for 2 weeks.
Results were reported for 18 patients, 56% of whom were male. They had a median age of 69 (range, 32-85) and a median number of 3 prior therapies (range, 1-16), including radiation (39%).
Eleven patients had CTCL, and 10 were evaluable. Researchers said they observed “rapid decreases in circulating Sézary cells and/or the size of mycosis fungoides tumors” after treatment with TTI-621.
Nine of the 10 patients had a reduction in CAILS score from baseline, and 3 had a reduction in circulating Sézary cells.
There were no dose-limiting toxicities, so the 10 mg dose given 3 times a week for 2 weeks was considered the optimal dose schedule.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
*Data in the abstract differ from the presentation.
FDA approves new option in Hodgkin lymphoma treatment
The Food and Drug Administration has approved brentuximab vedotin, in combination with chemotherapy, for previously untreated adults with stage III or IV classical Hodgkin lymphoma.
The drug, which is marketed by Seattle Genetics as Adcetris, is already approved in classical Hodgkin lymphoma after relapse and after stem cell transplant when the patient is at risk of relapse or progression. The drug is also approved to treat both systemic anaplastic large cell lymphoma (ALCL) and primary cutaneous ALCL after failure on other treatments.
The modified 2-year progression-free survival in the trial was 82.1% for patients receiving brentuximab plus AVD versus 77.2% for ABVD (P = .03), a 23% relative risk reduction (N Engl J Med. 2018;378:331-44).
Common side effects of brentuximab vedotin include neutropenia, anemia, peripheral neuropathy, nausea, fatigue, constipation, diarrhea, vomiting, and pyrexia. The drug carries a boxed warning highlighting the risk of John Cunningham virus infection resulting in progressive multifocal leukoencephalopathy.
The Food and Drug Administration has approved brentuximab vedotin, in combination with chemotherapy, for previously untreated adults with stage III or IV classical Hodgkin lymphoma.
The drug, which is marketed by Seattle Genetics as Adcetris, is already approved in classical Hodgkin lymphoma after relapse and after stem cell transplant when the patient is at risk of relapse or progression. The drug is also approved to treat both systemic anaplastic large cell lymphoma (ALCL) and primary cutaneous ALCL after failure on other treatments.
The modified 2-year progression-free survival in the trial was 82.1% for patients receiving brentuximab plus AVD versus 77.2% for ABVD (P = .03), a 23% relative risk reduction (N Engl J Med. 2018;378:331-44).
Common side effects of brentuximab vedotin include neutropenia, anemia, peripheral neuropathy, nausea, fatigue, constipation, diarrhea, vomiting, and pyrexia. The drug carries a boxed warning highlighting the risk of John Cunningham virus infection resulting in progressive multifocal leukoencephalopathy.
The Food and Drug Administration has approved brentuximab vedotin, in combination with chemotherapy, for previously untreated adults with stage III or IV classical Hodgkin lymphoma.
The drug, which is marketed by Seattle Genetics as Adcetris, is already approved in classical Hodgkin lymphoma after relapse and after stem cell transplant when the patient is at risk of relapse or progression. The drug is also approved to treat both systemic anaplastic large cell lymphoma (ALCL) and primary cutaneous ALCL after failure on other treatments.
The modified 2-year progression-free survival in the trial was 82.1% for patients receiving brentuximab plus AVD versus 77.2% for ABVD (P = .03), a 23% relative risk reduction (N Engl J Med. 2018;378:331-44).
Common side effects of brentuximab vedotin include neutropenia, anemia, peripheral neuropathy, nausea, fatigue, constipation, diarrhea, vomiting, and pyrexia. The drug carries a boxed warning highlighting the risk of John Cunningham virus infection resulting in progressive multifocal leukoencephalopathy.
The Long and Winding Road: PTCL 10 Years from Now

Release Date: March 20, 2018
Expiration Date: March 19, 2019
Note: This activity is no longer available for credit
Agenda
New targeted agents for PTCL
(Duration: 20 minutes)
Pier Luigi Zinzani, MD, PhD
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Recently approved therapies for PTCL in Asia:
What have we learned from the US experience?
(Duration: 18 minutes)
Won Seog Kim, MD, PhD
Samsung Medical Center
Seoul, Republic of Korea
Novel combination therapies:
Where are we now and where are we going?
(Duration: 23 minutes)
Owen A. O’Connor, MD, PhD
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Provided by:
![]()
Original activity supported by an educational grant from:
Spectrum Pharmaceuticals
Learning Objectives
At the conclusion of this educational activity, the healthcare team will be better able to:
- Discuss the treatment and management of peripheral T-cell lymphoma
- Appraise how U.S. T-cell lymphoma treatment experience can impact practice in Asia
- Summarize the importance of combination therapy in peripheral T-cell lymphoma
Target Audience
Hematologists, oncologists, and other clinicians and scientists with an interest in T-cell lymphoma
Statement of Need
Peripheral T-cell lymphomas (PTCL) are rare, heterogeneous and aggressive neoplasms that are associated with a poor prognosis. In addition, with current therapies, up to 70% of patients undergo relapse or develop refractory disease. Recent evidence has indicated an increase in the incidence of PTCLs and hence current challenges including pathobiology, clinical management, new drug testing as well as clinical trial accrual, need to be addressed. This activity will provide the healthcare team with the ideal foundation to facilitate progress in PTCL treatment and management.
Won Seog Kim, MD, PhD (Presenter)
Samsung Medical Center
Seoul, Republic of Korea
Disclosure: Consulting fees: Celltrion; Contracted research: Takeda; Kyowa-Kirin; J & J; Merck; Donga; Novartis; Celltrion
Owen A. O’Connor, MD, PhD (Presenter)
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Disclosure: Contracted research: Celgene; Merck; Spectrum; Agensys
Pier Luigi Zinzani, MD, PhD (Presenter)
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Disclosure: Speakers Bureau: Janssen; Merck; Servier; Gilead; Verastem; BMS; Sandoz; Mundipharma
Permissions
Won Seog Kim presentation
Slide 4: Frequency of T and NK-cell lymphomas in Asia
Park S, Ko YH. Peripheral T cell lymphoma in Asia. Int J Hematol 2014;99:227-239. Reprinted with permission of the Japanese Society of Hematology.
Slide 29: Off-label use: 100mg of pembrolizumab, HK, Singapore, Korea
Republished with permission of the American Society of Hematology, from Kwong YL, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing L-asparaginase. Blood. 2017;129(17):2437-2442; permission conveyed through Copyright Clearance Center, Inc.
Owen A. O’Connor presentation
Slide 12: Schematic of study design, patient disposition, and thrombocytopenia as a function of schedule & dose
Republished with permission of American Society of Hematology, from Amengual JE…O’Connor OA. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018;131:397-407; permission conveyed through Copyright Clearance Center, Inc.
Slide 13: Summary of response rates across study population for patients treated with romidepsin and pralatrexate
Same as slide above.
Slide 14: Pharmacokinetic parameters for pralatrexate and romidepsin in the study population
Same as slide above.
Slide 15: PFS and OS as a function of treatment in study population
Same as slide above.
Slide 19: The combination of HoME and HDAC inhibitor synergistically produces apoptosis across panel of T-cell lymphomas: tCTCL H9
Marchi E . . . O’Connor OA.The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol 2015; 171:215-226.
Slide 20: Supervised hierarchial clustering based on GEP
Same as slide above.
Slide 27: Panobinostat plus bortezomib in PTCL
Reprinted from Lancet Haematol, Tan D, et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: an open-label, multicentre phase 2 trial. 2015; 2(8):e326-e333, with permission from Elsevier.
Pier Luigi Zinzani presentation
Slides 4, 11: New agents in T-cell lymphomas (2), Belinostat (2)
O’Connor OA, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: Results of the pivotal phase II BELIEF (CLN-19) study. J Clin Oncol 2015; 33: 2492-2499. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
Slides 5, 8, 10, 12, 18, 20: Pralatrexate (1), Romidepsin (1), Belinostat (1), Brentuximab vedotin – Anaplastic large cell lymphoma (1), Brentuximab vedotin – CD30+ peripheral T-cell lymphoma (1), Off-label compounds in peripheral T-cell lymphomas
Reprinted from Cancer Treat Rev, volume 60, Broccoli A, Argnani L, Zinzani PL. Peripheral T-cell lymphomas: Focusing on novel agents in relapsed and refractory disease, pp 120-129, © 2017, with permission from Elsevier.
Slides 6, 7: Pralatrexate (2) and Pralatrexate (3)
O’Connor OA, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. J Clin Oncol, 2011; 29: 1182-1189. Reprinted with permission. © 2011 American Society of Clinical Oncology. All rights reserved.
Slide 9: Romidepsin (2)
Coiffier B, et al. J Clin Oncol 2012; 30: 631-636. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 13, 14: Brentuximab vedotin – Anaplastic large cell lymphoma (2), Brentulximab vedotin — Anaplastic large cell lymphoma (3)
Pro B, et al. J Clin Oncol 2012; 30: 2190-2196. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 16, 17: Brentuximab vedotin – Anaplastic large cell lymphoma (5), Brentuximab vedotin – Anaplastic large cell lymphoma (6)
Broccoli A, et al. Italian real-life experience with brentuximab vedotin: results of a large observational study of 40 cases of relapsed/refractory systemic anaplastic large cell lymphoma. Haematologica 2017; 102: 1931-1935. Obtained from the Haematologica Journal website http://www.haematologica.org
Slide 19: Brentuximab vedotin –CD30+ peripheral T-cell lymphomas (2)
Horwitz SM, et al. Blood 2014; 123: 3095-3100. Permission conveyed through Copyright Clearance Center, Inc.
Slide 21: Gemcitabine in peripheral T-cell lymphomas
Zinzani PL, et al. Ann Oncol 2010; 21: 860-863. European Society of Medical Oncology licensee.
Slide 23: Lenalidomide in T-cell lymphomas (2)
Reprinted from Morschhauser F, et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: the EXPECT trial. Eur J Cancer 2013, with permission from Elsevier.
Slides 24, 25: Bendamustine in T-cell lymphomas (1), Bendamustine in T-cell lymphomas (2)
Damaj G, et al. J Clin Oncol 2012; 31: 104-110. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Disclaimer
The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Hemedicus, the supporter, or Frontline Medical Communications. This material is prepared based upon a review of multiple sources of information, but it is not exhaustive of the subject matter. Therefore, healthcare professionals and other individuals should review and consider other publications and materials on the subject matter before relying solely upon the information contained within this educational activity.
Release Date: March 20, 2018
Expiration Date: March 19, 2019
Note: This activity is no longer available for credit
Agenda
New targeted agents for PTCL
(Duration: 20 minutes)
Pier Luigi Zinzani, MD, PhD
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Recently approved therapies for PTCL in Asia:
What have we learned from the US experience?
(Duration: 18 minutes)
Won Seog Kim, MD, PhD
Samsung Medical Center
Seoul, Republic of Korea
Novel combination therapies:
Where are we now and where are we going?
(Duration: 23 minutes)
Owen A. O’Connor, MD, PhD
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Provided by:
![]()
Original activity supported by an educational grant from:
Spectrum Pharmaceuticals
Learning Objectives
At the conclusion of this educational activity, the healthcare team will be better able to:
- Discuss the treatment and management of peripheral T-cell lymphoma
- Appraise how U.S. T-cell lymphoma treatment experience can impact practice in Asia
- Summarize the importance of combination therapy in peripheral T-cell lymphoma
Target Audience
Hematologists, oncologists, and other clinicians and scientists with an interest in T-cell lymphoma
Statement of Need
Peripheral T-cell lymphomas (PTCL) are rare, heterogeneous and aggressive neoplasms that are associated with a poor prognosis. In addition, with current therapies, up to 70% of patients undergo relapse or develop refractory disease. Recent evidence has indicated an increase in the incidence of PTCLs and hence current challenges including pathobiology, clinical management, new drug testing as well as clinical trial accrual, need to be addressed. This activity will provide the healthcare team with the ideal foundation to facilitate progress in PTCL treatment and management.
Won Seog Kim, MD, PhD (Presenter)
Samsung Medical Center
Seoul, Republic of Korea
Disclosure: Consulting fees: Celltrion; Contracted research: Takeda; Kyowa-Kirin; J & J; Merck; Donga; Novartis; Celltrion
Owen A. O’Connor, MD, PhD (Presenter)
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Disclosure: Contracted research: Celgene; Merck; Spectrum; Agensys
Pier Luigi Zinzani, MD, PhD (Presenter)
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Disclosure: Speakers Bureau: Janssen; Merck; Servier; Gilead; Verastem; BMS; Sandoz; Mundipharma
Permissions
Won Seog Kim presentation
Slide 4: Frequency of T and NK-cell lymphomas in Asia
Park S, Ko YH. Peripheral T cell lymphoma in Asia. Int J Hematol 2014;99:227-239. Reprinted with permission of the Japanese Society of Hematology.
Slide 29: Off-label use: 100mg of pembrolizumab, HK, Singapore, Korea
Republished with permission of the American Society of Hematology, from Kwong YL, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing L-asparaginase. Blood. 2017;129(17):2437-2442; permission conveyed through Copyright Clearance Center, Inc.
Owen A. O’Connor presentation
Slide 12: Schematic of study design, patient disposition, and thrombocytopenia as a function of schedule & dose
Republished with permission of American Society of Hematology, from Amengual JE…O’Connor OA. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018;131:397-407; permission conveyed through Copyright Clearance Center, Inc.
Slide 13: Summary of response rates across study population for patients treated with romidepsin and pralatrexate
Same as slide above.
Slide 14: Pharmacokinetic parameters for pralatrexate and romidepsin in the study population
Same as slide above.
Slide 15: PFS and OS as a function of treatment in study population
Same as slide above.
Slide 19: The combination of HoME and HDAC inhibitor synergistically produces apoptosis across panel of T-cell lymphomas: tCTCL H9
Marchi E . . . O’Connor OA.The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol 2015; 171:215-226.
Slide 20: Supervised hierarchial clustering based on GEP
Same as slide above.
Slide 27: Panobinostat plus bortezomib in PTCL
Reprinted from Lancet Haematol, Tan D, et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: an open-label, multicentre phase 2 trial. 2015; 2(8):e326-e333, with permission from Elsevier.
Pier Luigi Zinzani presentation
Slides 4, 11: New agents in T-cell lymphomas (2), Belinostat (2)
O’Connor OA, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: Results of the pivotal phase II BELIEF (CLN-19) study. J Clin Oncol 2015; 33: 2492-2499. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
Slides 5, 8, 10, 12, 18, 20: Pralatrexate (1), Romidepsin (1), Belinostat (1), Brentuximab vedotin – Anaplastic large cell lymphoma (1), Brentuximab vedotin – CD30+ peripheral T-cell lymphoma (1), Off-label compounds in peripheral T-cell lymphomas
Reprinted from Cancer Treat Rev, volume 60, Broccoli A, Argnani L, Zinzani PL. Peripheral T-cell lymphomas: Focusing on novel agents in relapsed and refractory disease, pp 120-129, © 2017, with permission from Elsevier.
Slides 6, 7: Pralatrexate (2) and Pralatrexate (3)
O’Connor OA, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. J Clin Oncol, 2011; 29: 1182-1189. Reprinted with permission. © 2011 American Society of Clinical Oncology. All rights reserved.
Slide 9: Romidepsin (2)
Coiffier B, et al. J Clin Oncol 2012; 30: 631-636. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 13, 14: Brentuximab vedotin – Anaplastic large cell lymphoma (2), Brentulximab vedotin — Anaplastic large cell lymphoma (3)
Pro B, et al. J Clin Oncol 2012; 30: 2190-2196. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 16, 17: Brentuximab vedotin – Anaplastic large cell lymphoma (5), Brentuximab vedotin – Anaplastic large cell lymphoma (6)
Broccoli A, et al. Italian real-life experience with brentuximab vedotin: results of a large observational study of 40 cases of relapsed/refractory systemic anaplastic large cell lymphoma. Haematologica 2017; 102: 1931-1935. Obtained from the Haematologica Journal website http://www.haematologica.org
Slide 19: Brentuximab vedotin –CD30+ peripheral T-cell lymphomas (2)
Horwitz SM, et al. Blood 2014; 123: 3095-3100. Permission conveyed through Copyright Clearance Center, Inc.
Slide 21: Gemcitabine in peripheral T-cell lymphomas
Zinzani PL, et al. Ann Oncol 2010; 21: 860-863. European Society of Medical Oncology licensee.
Slide 23: Lenalidomide in T-cell lymphomas (2)
Reprinted from Morschhauser F, et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: the EXPECT trial. Eur J Cancer 2013, with permission from Elsevier.
Slides 24, 25: Bendamustine in T-cell lymphomas (1), Bendamustine in T-cell lymphomas (2)
Damaj G, et al. J Clin Oncol 2012; 31: 104-110. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Disclaimer
The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Hemedicus, the supporter, or Frontline Medical Communications. This material is prepared based upon a review of multiple sources of information, but it is not exhaustive of the subject matter. Therefore, healthcare professionals and other individuals should review and consider other publications and materials on the subject matter before relying solely upon the information contained within this educational activity.
Release Date: March 20, 2018
Expiration Date: March 19, 2019
Note: This activity is no longer available for credit
Agenda
New targeted agents for PTCL
(Duration: 20 minutes)
Pier Luigi Zinzani, MD, PhD
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Recently approved therapies for PTCL in Asia:
What have we learned from the US experience?
(Duration: 18 minutes)
Won Seog Kim, MD, PhD
Samsung Medical Center
Seoul, Republic of Korea
Novel combination therapies:
Where are we now and where are we going?
(Duration: 23 minutes)
Owen A. O’Connor, MD, PhD
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Provided by:
![]()
Original activity supported by an educational grant from:
Spectrum Pharmaceuticals
Learning Objectives
At the conclusion of this educational activity, the healthcare team will be better able to:
- Discuss the treatment and management of peripheral T-cell lymphoma
- Appraise how U.S. T-cell lymphoma treatment experience can impact practice in Asia
- Summarize the importance of combination therapy in peripheral T-cell lymphoma
Target Audience
Hematologists, oncologists, and other clinicians and scientists with an interest in T-cell lymphoma
Statement of Need
Peripheral T-cell lymphomas (PTCL) are rare, heterogeneous and aggressive neoplasms that are associated with a poor prognosis. In addition, with current therapies, up to 70% of patients undergo relapse or develop refractory disease. Recent evidence has indicated an increase in the incidence of PTCLs and hence current challenges including pathobiology, clinical management, new drug testing as well as clinical trial accrual, need to be addressed. This activity will provide the healthcare team with the ideal foundation to facilitate progress in PTCL treatment and management.
Won Seog Kim, MD, PhD (Presenter)
Samsung Medical Center
Seoul, Republic of Korea
Disclosure: Consulting fees: Celltrion; Contracted research: Takeda; Kyowa-Kirin; J & J; Merck; Donga; Novartis; Celltrion
Owen A. O’Connor, MD, PhD (Presenter)
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Disclosure: Contracted research: Celgene; Merck; Spectrum; Agensys
Pier Luigi Zinzani, MD, PhD (Presenter)
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Disclosure: Speakers Bureau: Janssen; Merck; Servier; Gilead; Verastem; BMS; Sandoz; Mundipharma
Permissions
Won Seog Kim presentation
Slide 4: Frequency of T and NK-cell lymphomas in Asia
Park S, Ko YH. Peripheral T cell lymphoma in Asia. Int J Hematol 2014;99:227-239. Reprinted with permission of the Japanese Society of Hematology.
Slide 29: Off-label use: 100mg of pembrolizumab, HK, Singapore, Korea
Republished with permission of the American Society of Hematology, from Kwong YL, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing L-asparaginase. Blood. 2017;129(17):2437-2442; permission conveyed through Copyright Clearance Center, Inc.
Owen A. O’Connor presentation
Slide 12: Schematic of study design, patient disposition, and thrombocytopenia as a function of schedule & dose
Republished with permission of American Society of Hematology, from Amengual JE…O’Connor OA. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018;131:397-407; permission conveyed through Copyright Clearance Center, Inc.
Slide 13: Summary of response rates across study population for patients treated with romidepsin and pralatrexate
Same as slide above.
Slide 14: Pharmacokinetic parameters for pralatrexate and romidepsin in the study population
Same as slide above.
Slide 15: PFS and OS as a function of treatment in study population
Same as slide above.
Slide 19: The combination of HoME and HDAC inhibitor synergistically produces apoptosis across panel of T-cell lymphomas: tCTCL H9
Marchi E . . . O’Connor OA.The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol 2015; 171:215-226.
Slide 20: Supervised hierarchial clustering based on GEP
Same as slide above.
Slide 27: Panobinostat plus bortezomib in PTCL
Reprinted from Lancet Haematol, Tan D, et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: an open-label, multicentre phase 2 trial. 2015; 2(8):e326-e333, with permission from Elsevier.
Pier Luigi Zinzani presentation
Slides 4, 11: New agents in T-cell lymphomas (2), Belinostat (2)
O’Connor OA, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: Results of the pivotal phase II BELIEF (CLN-19) study. J Clin Oncol 2015; 33: 2492-2499. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
Slides 5, 8, 10, 12, 18, 20: Pralatrexate (1), Romidepsin (1), Belinostat (1), Brentuximab vedotin – Anaplastic large cell lymphoma (1), Brentuximab vedotin – CD30+ peripheral T-cell lymphoma (1), Off-label compounds in peripheral T-cell lymphomas
Reprinted from Cancer Treat Rev, volume 60, Broccoli A, Argnani L, Zinzani PL. Peripheral T-cell lymphomas: Focusing on novel agents in relapsed and refractory disease, pp 120-129, © 2017, with permission from Elsevier.
Slides 6, 7: Pralatrexate (2) and Pralatrexate (3)
O’Connor OA, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. J Clin Oncol, 2011; 29: 1182-1189. Reprinted with permission. © 2011 American Society of Clinical Oncology. All rights reserved.
Slide 9: Romidepsin (2)
Coiffier B, et al. J Clin Oncol 2012; 30: 631-636. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 13, 14: Brentuximab vedotin – Anaplastic large cell lymphoma (2), Brentulximab vedotin — Anaplastic large cell lymphoma (3)
Pro B, et al. J Clin Oncol 2012; 30: 2190-2196. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 16, 17: Brentuximab vedotin – Anaplastic large cell lymphoma (5), Brentuximab vedotin – Anaplastic large cell lymphoma (6)
Broccoli A, et al. Italian real-life experience with brentuximab vedotin: results of a large observational study of 40 cases of relapsed/refractory systemic anaplastic large cell lymphoma. Haematologica 2017; 102: 1931-1935. Obtained from the Haematologica Journal website http://www.haematologica.org
Slide 19: Brentuximab vedotin –CD30+ peripheral T-cell lymphomas (2)
Horwitz SM, et al. Blood 2014; 123: 3095-3100. Permission conveyed through Copyright Clearance Center, Inc.
Slide 21: Gemcitabine in peripheral T-cell lymphomas
Zinzani PL, et al. Ann Oncol 2010; 21: 860-863. European Society of Medical Oncology licensee.
Slide 23: Lenalidomide in T-cell lymphomas (2)
Reprinted from Morschhauser F, et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: the EXPECT trial. Eur J Cancer 2013, with permission from Elsevier.
Slides 24, 25: Bendamustine in T-cell lymphomas (1), Bendamustine in T-cell lymphomas (2)
Damaj G, et al. J Clin Oncol 2012; 31: 104-110. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Disclaimer
The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Hemedicus, the supporter, or Frontline Medical Communications. This material is prepared based upon a review of multiple sources of information, but it is not exhaustive of the subject matter. Therefore, healthcare professionals and other individuals should review and consider other publications and materials on the subject matter before relying solely upon the information contained within this educational activity.
Metabolic changes in T cells may limit CAR potential in kids

Researchers analyzed peripheral blood T cells from 157 pediatric cancer patients at diagnosis and after chemotherapy and found the potential to produce effective chimeric antigen receptor (CAR) T cells declined with each cycle of chemotherapy.
This was also true for acute lymphoblastic leukemia (ALL) and Wilms’ tumor, which had high CAR T-cell manufacturing potential in the pre-chemotherapy samples.
Children younger than 3 years particularly showed a significant decline in CAR T-cell potential with cumulative cycles of chemotherapy.
“Everybody knows that chemotherapy is really bad for your T cells, and the more chemo you get, the less likely you are to have healthy T cells,” David M. Barrett, MD, PhD, of Children’s Hospital of Philadelphia in Pennsylvania, said at a press preview of research to be presented at the AACR Annual Meeting 2018.
“We know a lot about what a highly active, highly successful CAR T cell looks like right before it goes back into the patient after it’s finished manufacturing,” Dr Barrett added.
But he and his colleagues wanted to determine what goes into producing high-quality cells from a patient and the difference between cells that were good starting material and cells that weren’t.
The investigators analyzed blood samples from pediatric patients with ALL, non-Hodgkin lymphoma, neuroblastoma, osteosarcoma, rhabdomyosarcoma, Wilms’ tumor, Hodgkin lymphoma, chronic myeloid leukemia, and Ewing sarcoma. The team collected samples at diagnosis and after every cycle of chemotherapy.
Using flow cytometry, they quantified the CD3+ cell population and expanded the T cells using CD3 and CD28 stimulatory beads, “the backbone of pretty much every center’s way to make CAR T cells in the lab,” Dr Barrett said.
And the researchers found poor CAR T-cell manufacturing potential in all tumor types at diagnosis except for ALL and Wilms’ tumor. In standard-risk and high-risk ALL, more than 90% of patients had high-quality T cells at diagnosis.
The team report the findings in abstract 1631, which is scheduled to be presented at the AACR Annual Meeting on April 15.
“This may have played into why pediatric ALL is one of the great successes with CAR T-cell therapy,” Dr Barrett explained. “We may have actually been working with uniquely well-suited, good starting material to build a CAR T cell.”
T cells from lymphoma patients—Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal B-cell lymphoma, and Hodgkin lymphoma—were actually quite poor in their potential to become good CAR T cells, Dr Barrett noted.
“This may be reflected clinically in pediatrics at Children’s Hospital of Philadelphia,” he said. “We’ve only been able to successfully treat 3 children with lymphoma, as opposed to more than 200 children with leukemia.”
The only other type of tumor that seemed to have good CAR T potential was Wilms’ tumor.
“I don’t have a CAR T cell for Wilms’ tumor yet,” Dr Barrett said, “but, if I wanted to make one, I would at least have a degree of confidence that the cells gotten from a patient would at least be able to be successfully made into a highly functional T cell that can go back into a patient.”
The investigators also observed that cumulative chemotherapy alters the metabolic profile in T cells, “gradually turning them by cycle 6 into something that doesn’t work anymore,” Dr Barrett said.
The researchers then looked into what differences there were in the quality of collected T cells and found that metabolic changes varied with tumor and treatment.
T cells with poor CAR T-cell potential were biased toward using glycolysis as their energy source instead of using fatty acids.
“Normal, healthy donor T cells cluster together in terms of metabolic pathways that are active or inactive,” Dr Barrett explained.
“[P]atients who had leukemia and the Wilms’ tumor patients could make successful CAR T cells from those samples. On the other hand, solid tumors and a Hodgkin disease patient look like they have a very different metabolic profile. And that is associated with failure to make a good CAR T cell.”
The investigators were able to get the T cells to shift metabolic pathways by “essentially force-feeding T cells things like fatty acids so they don’t use as much glucose,” Dr Barrett said.
“We’ve had some success in force-feeding them essentially neutral amino acids and others like arginine. And so you can actually potentially provide a T cell with an attractive alternative fuel source.”
Dr Barrett noted that the findings have already altered practice for children at his institution.
They now collect T cells early even if the patient is not eligible for a CAR trial, “simply because we know that cumulative chemotherapy is going to progressively deteriorate the likelihood that those cells will make a functional CAR product, and we’ve been recommending that to other centers,” Dr Barrett said.
“We’re trying to understand what goes into making the best starting material so that we can alter our approaches to make sure that we make a highly functional CAR T-cell product not only for kids with leukemia and CART19, but also potentially for solid tumor CARs as we try to develop those in the future.”
Researchers analyzed peripheral blood T cells from 157 pediatric cancer patients at diagnosis and after chemotherapy and found the potential to produce effective chimeric antigen receptor (CAR) T cells declined with each cycle of chemotherapy.
This was also true for acute lymphoblastic leukemia (ALL) and Wilms’ tumor, which had high CAR T-cell manufacturing potential in the pre-chemotherapy samples.
Children younger than 3 years particularly showed a significant decline in CAR T-cell potential with cumulative cycles of chemotherapy.
“Everybody knows that chemotherapy is really bad for your T cells, and the more chemo you get, the less likely you are to have healthy T cells,” David M. Barrett, MD, PhD, of Children’s Hospital of Philadelphia in Pennsylvania, said at a press preview of research to be presented at the AACR Annual Meeting 2018.
“We know a lot about what a highly active, highly successful CAR T cell looks like right before it goes back into the patient after it’s finished manufacturing,” Dr Barrett added.
But he and his colleagues wanted to determine what goes into producing high-quality cells from a patient and the difference between cells that were good starting material and cells that weren’t.
The investigators analyzed blood samples from pediatric patients with ALL, non-Hodgkin lymphoma, neuroblastoma, osteosarcoma, rhabdomyosarcoma, Wilms’ tumor, Hodgkin lymphoma, chronic myeloid leukemia, and Ewing sarcoma. The team collected samples at diagnosis and after every cycle of chemotherapy.
Using flow cytometry, they quantified the CD3+ cell population and expanded the T cells using CD3 and CD28 stimulatory beads, “the backbone of pretty much every center’s way to make CAR T cells in the lab,” Dr Barrett said.
And the researchers found poor CAR T-cell manufacturing potential in all tumor types at diagnosis except for ALL and Wilms’ tumor. In standard-risk and high-risk ALL, more than 90% of patients had high-quality T cells at diagnosis.
The team report the findings in abstract 1631, which is scheduled to be presented at the AACR Annual Meeting on April 15.
“This may have played into why pediatric ALL is one of the great successes with CAR T-cell therapy,” Dr Barrett explained. “We may have actually been working with uniquely well-suited, good starting material to build a CAR T cell.”
T cells from lymphoma patients—Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal B-cell lymphoma, and Hodgkin lymphoma—were actually quite poor in their potential to become good CAR T cells, Dr Barrett noted.
“This may be reflected clinically in pediatrics at Children’s Hospital of Philadelphia,” he said. “We’ve only been able to successfully treat 3 children with lymphoma, as opposed to more than 200 children with leukemia.”
The only other type of tumor that seemed to have good CAR T potential was Wilms’ tumor.
“I don’t have a CAR T cell for Wilms’ tumor yet,” Dr Barrett said, “but, if I wanted to make one, I would at least have a degree of confidence that the cells gotten from a patient would at least be able to be successfully made into a highly functional T cell that can go back into a patient.”
The investigators also observed that cumulative chemotherapy alters the metabolic profile in T cells, “gradually turning them by cycle 6 into something that doesn’t work anymore,” Dr Barrett said.
The researchers then looked into what differences there were in the quality of collected T cells and found that metabolic changes varied with tumor and treatment.
T cells with poor CAR T-cell potential were biased toward using glycolysis as their energy source instead of using fatty acids.
“Normal, healthy donor T cells cluster together in terms of metabolic pathways that are active or inactive,” Dr Barrett explained.
“[P]atients who had leukemia and the Wilms’ tumor patients could make successful CAR T cells from those samples. On the other hand, solid tumors and a Hodgkin disease patient look like they have a very different metabolic profile. And that is associated with failure to make a good CAR T cell.”
The investigators were able to get the T cells to shift metabolic pathways by “essentially force-feeding T cells things like fatty acids so they don’t use as much glucose,” Dr Barrett said.
“We’ve had some success in force-feeding them essentially neutral amino acids and others like arginine. And so you can actually potentially provide a T cell with an attractive alternative fuel source.”
Dr Barrett noted that the findings have already altered practice for children at his institution.
They now collect T cells early even if the patient is not eligible for a CAR trial, “simply because we know that cumulative chemotherapy is going to progressively deteriorate the likelihood that those cells will make a functional CAR product, and we’ve been recommending that to other centers,” Dr Barrett said.
“We’re trying to understand what goes into making the best starting material so that we can alter our approaches to make sure that we make a highly functional CAR T-cell product not only for kids with leukemia and CART19, but also potentially for solid tumor CARs as we try to develop those in the future.”
Researchers analyzed peripheral blood T cells from 157 pediatric cancer patients at diagnosis and after chemotherapy and found the potential to produce effective chimeric antigen receptor (CAR) T cells declined with each cycle of chemotherapy.
This was also true for acute lymphoblastic leukemia (ALL) and Wilms’ tumor, which had high CAR T-cell manufacturing potential in the pre-chemotherapy samples.
Children younger than 3 years particularly showed a significant decline in CAR T-cell potential with cumulative cycles of chemotherapy.
“Everybody knows that chemotherapy is really bad for your T cells, and the more chemo you get, the less likely you are to have healthy T cells,” David M. Barrett, MD, PhD, of Children’s Hospital of Philadelphia in Pennsylvania, said at a press preview of research to be presented at the AACR Annual Meeting 2018.
“We know a lot about what a highly active, highly successful CAR T cell looks like right before it goes back into the patient after it’s finished manufacturing,” Dr Barrett added.
But he and his colleagues wanted to determine what goes into producing high-quality cells from a patient and the difference between cells that were good starting material and cells that weren’t.
The investigators analyzed blood samples from pediatric patients with ALL, non-Hodgkin lymphoma, neuroblastoma, osteosarcoma, rhabdomyosarcoma, Wilms’ tumor, Hodgkin lymphoma, chronic myeloid leukemia, and Ewing sarcoma. The team collected samples at diagnosis and after every cycle of chemotherapy.
Using flow cytometry, they quantified the CD3+ cell population and expanded the T cells using CD3 and CD28 stimulatory beads, “the backbone of pretty much every center’s way to make CAR T cells in the lab,” Dr Barrett said.
And the researchers found poor CAR T-cell manufacturing potential in all tumor types at diagnosis except for ALL and Wilms’ tumor. In standard-risk and high-risk ALL, more than 90% of patients had high-quality T cells at diagnosis.
The team report the findings in abstract 1631, which is scheduled to be presented at the AACR Annual Meeting on April 15.
“This may have played into why pediatric ALL is one of the great successes with CAR T-cell therapy,” Dr Barrett explained. “We may have actually been working with uniquely well-suited, good starting material to build a CAR T cell.”
T cells from lymphoma patients—Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal B-cell lymphoma, and Hodgkin lymphoma—were actually quite poor in their potential to become good CAR T cells, Dr Barrett noted.
“This may be reflected clinically in pediatrics at Children’s Hospital of Philadelphia,” he said. “We’ve only been able to successfully treat 3 children with lymphoma, as opposed to more than 200 children with leukemia.”
The only other type of tumor that seemed to have good CAR T potential was Wilms’ tumor.
“I don’t have a CAR T cell for Wilms’ tumor yet,” Dr Barrett said, “but, if I wanted to make one, I would at least have a degree of confidence that the cells gotten from a patient would at least be able to be successfully made into a highly functional T cell that can go back into a patient.”
The investigators also observed that cumulative chemotherapy alters the metabolic profile in T cells, “gradually turning them by cycle 6 into something that doesn’t work anymore,” Dr Barrett said.
The researchers then looked into what differences there were in the quality of collected T cells and found that metabolic changes varied with tumor and treatment.
T cells with poor CAR T-cell potential were biased toward using glycolysis as their energy source instead of using fatty acids.
“Normal, healthy donor T cells cluster together in terms of metabolic pathways that are active or inactive,” Dr Barrett explained.
“[P]atients who had leukemia and the Wilms’ tumor patients could make successful CAR T cells from those samples. On the other hand, solid tumors and a Hodgkin disease patient look like they have a very different metabolic profile. And that is associated with failure to make a good CAR T cell.”
The investigators were able to get the T cells to shift metabolic pathways by “essentially force-feeding T cells things like fatty acids so they don’t use as much glucose,” Dr Barrett said.
“We’ve had some success in force-feeding them essentially neutral amino acids and others like arginine. And so you can actually potentially provide a T cell with an attractive alternative fuel source.”
Dr Barrett noted that the findings have already altered practice for children at his institution.
They now collect T cells early even if the patient is not eligible for a CAR trial, “simply because we know that cumulative chemotherapy is going to progressively deteriorate the likelihood that those cells will make a functional CAR product, and we’ve been recommending that to other centers,” Dr Barrett said.
“We’re trying to understand what goes into making the best starting material so that we can alter our approaches to make sure that we make a highly functional CAR T-cell product not only for kids with leukemia and CART19, but also potentially for solid tumor CARs as we try to develop those in the future.”
In myeloma, third ASCT is a viable option
A third autologous stem cell transplantation (ASCT) is feasible and provides clinical benefit to patients with relapsed multiple myeloma, according to findings from a retrospective study.
The benefits appear to be most pronounced in patients who had a long duration of response to the previous ASCT, the researchers wrote in Biology of Blood and Marrow Transplantation.
“A salvage third ASCT is of value for patients with relapsed multiple myeloma,” Laurent Garderet, MD, of the department of hematology, Hôpital Saint Antoine, Paris, and coauthors wrote in the report.
A third transplantation is most commonly used in patients who relapse following tandem ASCT. Less often, it is done in patients who receive upfront ASCT, relapse, undergo a second ASCT, and relapse again.
“The first scenario gives much better results, due in part to a better remission status at the third ASCT with no signs of increased [second primary malignancy],” the researchers wrote.
In that group, median overall survival was greater than 5 years if the relapse occurred 3 years or more after the initial tandem ASCT, study results show.
The retrospective analysis, based on European Society for Blood and Marrow Transplantation data, included 570 patients who had undergone a third ASCT between 1997 and 2010. Of that group, 482 patients (81%) received the third transplantation after tandem ASCT and subsequent relapse, and 88 (15%) received it after second relapse.
After third ASCT, overall survival was 33 months in the larger tandem transplant group with 61 months of follow-up, and 15 months in the smaller group of patients who received two salvage ASCTs after 48 months of follow-up.
Median progression-free survival was 13 and 8 months for the tandem ASCT and two-salvage–ASCT groups, respectively, while 100-day nonrelapse mortality was 4% and 7%, respectively.
For both groups, better outcomes were associated with longer duration of remission after the second ASCT, the researchers reported.
Moreover, the time from second ASCT to relapse was the only favorable prognostic factor associated with survival after third ASCT in a multivariate analysis of the patients who relapsed following tandem transplant. The hazard ratio for relapse occurring between 18 and 36 months vs. within 18 months was 0.62 (95% confidence interval, 0.47-0.82; P = .01); for relapse after 36 months, the HR was 0.35 (95% CI, 0.25-0.49; P less than .001).
The researchers acknowledged that, beyond transplant, treatment of myeloma has changed substantially in recent years and could change the clinical picture for patients undergoing a third ASCT.
“The availability of novel agents may further improve the response to a third ASCT, rather than impairing its usefulness in the salvage setting, by enhancing the depth of response before ASCT, which could result in improved durability of the outcome,” they wrote.
The researchers reported having no financial disclosures related to this study.
SOURCE: Garderet L et al. Biol Blood Marrow Transplant. 2018 Feb 3. doi: 10.1016/j.bbmt.2018.01.035.
A third autologous stem cell transplantation (ASCT) is feasible and provides clinical benefit to patients with relapsed multiple myeloma, according to findings from a retrospective study.
The benefits appear to be most pronounced in patients who had a long duration of response to the previous ASCT, the researchers wrote in Biology of Blood and Marrow Transplantation.
“A salvage third ASCT is of value for patients with relapsed multiple myeloma,” Laurent Garderet, MD, of the department of hematology, Hôpital Saint Antoine, Paris, and coauthors wrote in the report.
A third transplantation is most commonly used in patients who relapse following tandem ASCT. Less often, it is done in patients who receive upfront ASCT, relapse, undergo a second ASCT, and relapse again.
“The first scenario gives much better results, due in part to a better remission status at the third ASCT with no signs of increased [second primary malignancy],” the researchers wrote.
In that group, median overall survival was greater than 5 years if the relapse occurred 3 years or more after the initial tandem ASCT, study results show.
The retrospective analysis, based on European Society for Blood and Marrow Transplantation data, included 570 patients who had undergone a third ASCT between 1997 and 2010. Of that group, 482 patients (81%) received the third transplantation after tandem ASCT and subsequent relapse, and 88 (15%) received it after second relapse.
After third ASCT, overall survival was 33 months in the larger tandem transplant group with 61 months of follow-up, and 15 months in the smaller group of patients who received two salvage ASCTs after 48 months of follow-up.
Median progression-free survival was 13 and 8 months for the tandem ASCT and two-salvage–ASCT groups, respectively, while 100-day nonrelapse mortality was 4% and 7%, respectively.
For both groups, better outcomes were associated with longer duration of remission after the second ASCT, the researchers reported.
Moreover, the time from second ASCT to relapse was the only favorable prognostic factor associated with survival after third ASCT in a multivariate analysis of the patients who relapsed following tandem transplant. The hazard ratio for relapse occurring between 18 and 36 months vs. within 18 months was 0.62 (95% confidence interval, 0.47-0.82; P = .01); for relapse after 36 months, the HR was 0.35 (95% CI, 0.25-0.49; P less than .001).
The researchers acknowledged that, beyond transplant, treatment of myeloma has changed substantially in recent years and could change the clinical picture for patients undergoing a third ASCT.
“The availability of novel agents may further improve the response to a third ASCT, rather than impairing its usefulness in the salvage setting, by enhancing the depth of response before ASCT, which could result in improved durability of the outcome,” they wrote.
The researchers reported having no financial disclosures related to this study.
SOURCE: Garderet L et al. Biol Blood Marrow Transplant. 2018 Feb 3. doi: 10.1016/j.bbmt.2018.01.035.
A third autologous stem cell transplantation (ASCT) is feasible and provides clinical benefit to patients with relapsed multiple myeloma, according to findings from a retrospective study.
The benefits appear to be most pronounced in patients who had a long duration of response to the previous ASCT, the researchers wrote in Biology of Blood and Marrow Transplantation.
“A salvage third ASCT is of value for patients with relapsed multiple myeloma,” Laurent Garderet, MD, of the department of hematology, Hôpital Saint Antoine, Paris, and coauthors wrote in the report.
A third transplantation is most commonly used in patients who relapse following tandem ASCT. Less often, it is done in patients who receive upfront ASCT, relapse, undergo a second ASCT, and relapse again.
“The first scenario gives much better results, due in part to a better remission status at the third ASCT with no signs of increased [second primary malignancy],” the researchers wrote.
In that group, median overall survival was greater than 5 years if the relapse occurred 3 years or more after the initial tandem ASCT, study results show.
The retrospective analysis, based on European Society for Blood and Marrow Transplantation data, included 570 patients who had undergone a third ASCT between 1997 and 2010. Of that group, 482 patients (81%) received the third transplantation after tandem ASCT and subsequent relapse, and 88 (15%) received it after second relapse.
After third ASCT, overall survival was 33 months in the larger tandem transplant group with 61 months of follow-up, and 15 months in the smaller group of patients who received two salvage ASCTs after 48 months of follow-up.
Median progression-free survival was 13 and 8 months for the tandem ASCT and two-salvage–ASCT groups, respectively, while 100-day nonrelapse mortality was 4% and 7%, respectively.
For both groups, better outcomes were associated with longer duration of remission after the second ASCT, the researchers reported.
Moreover, the time from second ASCT to relapse was the only favorable prognostic factor associated with survival after third ASCT in a multivariate analysis of the patients who relapsed following tandem transplant. The hazard ratio for relapse occurring between 18 and 36 months vs. within 18 months was 0.62 (95% confidence interval, 0.47-0.82; P = .01); for relapse after 36 months, the HR was 0.35 (95% CI, 0.25-0.49; P less than .001).
The researchers acknowledged that, beyond transplant, treatment of myeloma has changed substantially in recent years and could change the clinical picture for patients undergoing a third ASCT.
“The availability of novel agents may further improve the response to a third ASCT, rather than impairing its usefulness in the salvage setting, by enhancing the depth of response before ASCT, which could result in improved durability of the outcome,” they wrote.
The researchers reported having no financial disclosures related to this study.
SOURCE: Garderet L et al. Biol Blood Marrow Transplant. 2018 Feb 3. doi: 10.1016/j.bbmt.2018.01.035.
FROM BIOLOGY OF BLOOD AND MARROW TRANSPLANTATION
Key clinical point:
Major finding: Relapse-free interval was a favorable prognostic factor and significantly correlated with overall survival (P less than .001) in patients who underwent a third ASCT.
Study details: A retrospective analysis of European Society for Blood and Marrow Transplantation data including 570 patients who had undergone a third ASCT between 1997 and 2010.
Disclosures: The study authors reported having no financial disclosures related to the study.
Source: Garderet L et al. Biol Blood Marrow Transplant. 2018 Feb 3. doi: 10.1016/j.bbmt.2018.01.035.
A global snapshot of leukemia incidence
, according to an analysis of World Health Organization cancer databases.
Incidence also is generally higher in males, with a global male to female ratio of 1.4. For men, the highest regional leukemia rate – estimated at 11.3 per 100,000 population for 2012 – was found in Australia and New Zealand, with northern America (the United States and Canada) next at 10.5 per 100,000. Australia/New Zealand and northern America had the highest rate for women at 7.2 per 100,000, followed by western Europe and northern Europe at 6.0 per 100,000, reported Adalberto Miranda-Filho, PhD, of the WHO’s International Agency for Research on Cancer in Lyon, France, and his associates.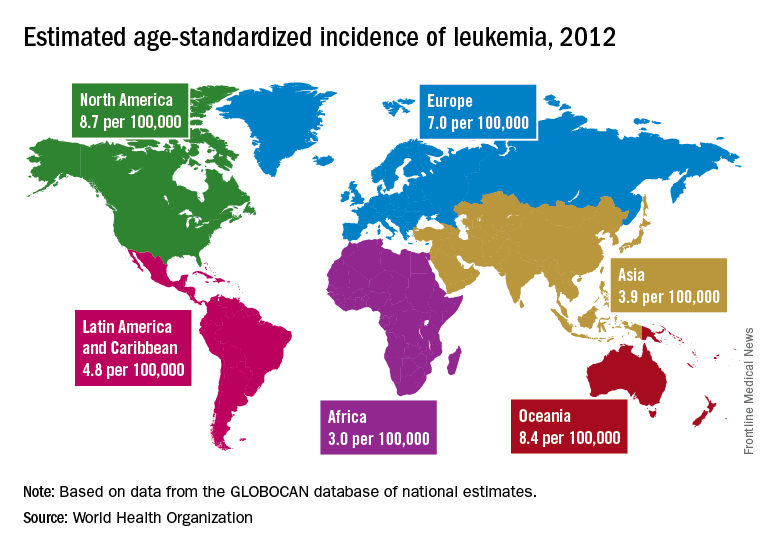
The lowest regional rates for women were found in western Africa (1.2 per 100,000), middle Africa (1.8), and Micronesia/Polynesia (2.1). For men, leukemia incidence was lowest in western Africa (1.4 per 100,000), middle Africa (2.6), and south-central Asia (3.4), according to data from the WHO’s GLOBOCAN database. The report was published in The Lancet Haematology.
Estimates for leukemia subtypes in 2003-2007 – calculated for 54 countries, not regions – also showed a great deal of variation. For acute lymphoblastic leukemia, Ecuador had the highest rates for both males (2.8 per 100,000) and females (3.3), with high rates seen in Costa Rica, Columbia, and Cyprus. Rates in the United States were near the top: 2.1 for males and 1.6 for females. Rates were lowest for men in Jamaica (0.4) and Serbia (0.6) and for women in India (0.5) and Serbia and Cuba (0.6), Dr. Miranda-Filho and his associates said.
Incidence rates for acute myeloid leukemia were highest in Australia for men (2.8 per 100,000) and Austria for women (2.2), with the United States near the top for both men (2.6) and women (1.9). The lowest rates occurred in Cuba and Egypt for men (0.9 per 100,000) and Cuba for women (0.4), data from the WHO’s Cancer Incidence in Five Continents Volume X show.
Chronic lymphocytic leukemia incidence was highest for men in Canada (4.5 per 100,000), Ireland and Lithuania (4.4), and Slovakia (4.3). The incidence was highest for women in Lithuania (2.5), Canada (2.3), and Slovakia and Denmark (2.1). Incidence in the United States was 3.5 for men and 1.8 for women. At the other end of the scale, the lowest rates for both men and women were in Japan and Malaysia (0.1), the investigators’ analysis showed.
Chronic myeloid leukemia rates were the lowest of the subtypes, and Tunisia was the lowest for men at 0.4 per 100,000 and tied for lowest with Serbia, Slovenia, and Puerto Rico for women at 0.3. Incidence was highest for men in Australia at 1.8 per 100,000 and highest for women in Uruguay at 1.1. Rates in the United States were 1.3 for men and 0.8 for women, Dr. Miranda-Filho and his associates said.
“The higher incidence of acute lymphoblastic leukaemia in parts of South America, as well as of chronic lymphocytic leukaemia in populations across North America and Oceania, alongside a lower incidence in Asia, might be important markers for further epidemiological study, and a means to better understand the underlying factors to support future cancer prevention strategies,” the investigators wrote.
SOURCE: Miranda-Filho A et al. Lancet Haematol. 2018;5:e14-24.
, according to an analysis of World Health Organization cancer databases.
Incidence also is generally higher in males, with a global male to female ratio of 1.4. For men, the highest regional leukemia rate – estimated at 11.3 per 100,000 population for 2012 – was found in Australia and New Zealand, with northern America (the United States and Canada) next at 10.5 per 100,000. Australia/New Zealand and northern America had the highest rate for women at 7.2 per 100,000, followed by western Europe and northern Europe at 6.0 per 100,000, reported Adalberto Miranda-Filho, PhD, of the WHO’s International Agency for Research on Cancer in Lyon, France, and his associates.
The lowest regional rates for women were found in western Africa (1.2 per 100,000), middle Africa (1.8), and Micronesia/Polynesia (2.1). For men, leukemia incidence was lowest in western Africa (1.4 per 100,000), middle Africa (2.6), and south-central Asia (3.4), according to data from the WHO’s GLOBOCAN database. The report was published in The Lancet Haematology.
Estimates for leukemia subtypes in 2003-2007 – calculated for 54 countries, not regions – also showed a great deal of variation. For acute lymphoblastic leukemia, Ecuador had the highest rates for both males (2.8 per 100,000) and females (3.3), with high rates seen in Costa Rica, Columbia, and Cyprus. Rates in the United States were near the top: 2.1 for males and 1.6 for females. Rates were lowest for men in Jamaica (0.4) and Serbia (0.6) and for women in India (0.5) and Serbia and Cuba (0.6), Dr. Miranda-Filho and his associates said.
Incidence rates for acute myeloid leukemia were highest in Australia for men (2.8 per 100,000) and Austria for women (2.2), with the United States near the top for both men (2.6) and women (1.9). The lowest rates occurred in Cuba and Egypt for men (0.9 per 100,000) and Cuba for women (0.4), data from the WHO’s Cancer Incidence in Five Continents Volume X show.
Chronic lymphocytic leukemia incidence was highest for men in Canada (4.5 per 100,000), Ireland and Lithuania (4.4), and Slovakia (4.3). The incidence was highest for women in Lithuania (2.5), Canada (2.3), and Slovakia and Denmark (2.1). Incidence in the United States was 3.5 for men and 1.8 for women. At the other end of the scale, the lowest rates for both men and women were in Japan and Malaysia (0.1), the investigators’ analysis showed.
Chronic myeloid leukemia rates were the lowest of the subtypes, and Tunisia was the lowest for men at 0.4 per 100,000 and tied for lowest with Serbia, Slovenia, and Puerto Rico for women at 0.3. Incidence was highest for men in Australia at 1.8 per 100,000 and highest for women in Uruguay at 1.1. Rates in the United States were 1.3 for men and 0.8 for women, Dr. Miranda-Filho and his associates said.
“The higher incidence of acute lymphoblastic leukaemia in parts of South America, as well as of chronic lymphocytic leukaemia in populations across North America and Oceania, alongside a lower incidence in Asia, might be important markers for further epidemiological study, and a means to better understand the underlying factors to support future cancer prevention strategies,” the investigators wrote.
SOURCE: Miranda-Filho A et al. Lancet Haematol. 2018;5:e14-24.
, according to an analysis of World Health Organization cancer databases.
Incidence also is generally higher in males, with a global male to female ratio of 1.4. For men, the highest regional leukemia rate – estimated at 11.3 per 100,000 population for 2012 – was found in Australia and New Zealand, with northern America (the United States and Canada) next at 10.5 per 100,000. Australia/New Zealand and northern America had the highest rate for women at 7.2 per 100,000, followed by western Europe and northern Europe at 6.0 per 100,000, reported Adalberto Miranda-Filho, PhD, of the WHO’s International Agency for Research on Cancer in Lyon, France, and his associates.
The lowest regional rates for women were found in western Africa (1.2 per 100,000), middle Africa (1.8), and Micronesia/Polynesia (2.1). For men, leukemia incidence was lowest in western Africa (1.4 per 100,000), middle Africa (2.6), and south-central Asia (3.4), according to data from the WHO’s GLOBOCAN database. The report was published in The Lancet Haematology.
Estimates for leukemia subtypes in 2003-2007 – calculated for 54 countries, not regions – also showed a great deal of variation. For acute lymphoblastic leukemia, Ecuador had the highest rates for both males (2.8 per 100,000) and females (3.3), with high rates seen in Costa Rica, Columbia, and Cyprus. Rates in the United States were near the top: 2.1 for males and 1.6 for females. Rates were lowest for men in Jamaica (0.4) and Serbia (0.6) and for women in India (0.5) and Serbia and Cuba (0.6), Dr. Miranda-Filho and his associates said.
Incidence rates for acute myeloid leukemia were highest in Australia for men (2.8 per 100,000) and Austria for women (2.2), with the United States near the top for both men (2.6) and women (1.9). The lowest rates occurred in Cuba and Egypt for men (0.9 per 100,000) and Cuba for women (0.4), data from the WHO’s Cancer Incidence in Five Continents Volume X show.
Chronic lymphocytic leukemia incidence was highest for men in Canada (4.5 per 100,000), Ireland and Lithuania (4.4), and Slovakia (4.3). The incidence was highest for women in Lithuania (2.5), Canada (2.3), and Slovakia and Denmark (2.1). Incidence in the United States was 3.5 for men and 1.8 for women. At the other end of the scale, the lowest rates for both men and women were in Japan and Malaysia (0.1), the investigators’ analysis showed.
Chronic myeloid leukemia rates were the lowest of the subtypes, and Tunisia was the lowest for men at 0.4 per 100,000 and tied for lowest with Serbia, Slovenia, and Puerto Rico for women at 0.3. Incidence was highest for men in Australia at 1.8 per 100,000 and highest for women in Uruguay at 1.1. Rates in the United States were 1.3 for men and 0.8 for women, Dr. Miranda-Filho and his associates said.
“The higher incidence of acute lymphoblastic leukaemia in parts of South America, as well as of chronic lymphocytic leukaemia in populations across North America and Oceania, alongside a lower incidence in Asia, might be important markers for further epidemiological study, and a means to better understand the underlying factors to support future cancer prevention strategies,” the investigators wrote.
SOURCE: Miranda-Filho A et al. Lancet Haematol. 2018;5:e14-24.
FROM THE LANCET HAEMATOLOGY
Lymphoma, breast cancer survivors have greater risk of CHF

ORLANDO—Results of a retrospective study showed that survivors of lymphoma or breast cancer had a significantly greater risk of congestive heart failure (CHF) than patients who did not have cancer.
This increased risk was observed as early as a year after cancer diagnosis but was still present 20 years after diagnosis.
Overall, 1 in 10 cancer patients had CHF at the 20-year mark.
“The majority of patients do not develop heart failure, but our research helps us recognize the factors associated with it and the importance of appropriate heart care following cancer treatment,” said Carolyn Larsen, MD, of the Mayo Clinic in Rochester, Minnesota.
“Our research suggests that periodic cardiac imaging to monitor for heart damage may be needed for some cancer patients, even if they have no signs of heart damage initially after chemotherapy. Additionally, it emphasizes that working to live a heart-healthy lifestyle is important for cancer patients and survivors to reduce the overall risk of heart disease.”
Dr Larsen and her colleagues presented this research as a poster (abstract 1105-066) at the American College of Cardiology’s 67th Annual Scientific Session & Expo (ACC.18).
Patients
Using data from the Rochester Epidemiology Project, the researchers retrospectively tracked CHF cases in 900 cancer patients and 1550 non-cancer patients. Patients were treated in Olmsted County in Minnesota from 1985 to 2010.
For both patient groups, the median age at baseline was about 53, a little more than 90% of each group was white, and nearly 80% of each group was female.
Six to 7% of patients had diabetes, and about 30% of each group had hypertension. Thirty-eight percent of each group had hyperlipidemia, and 31% were obese.
Five percent of cancer patients and 2% of controls had coronary artery disease (P<0.001). This was the only significant difference in baseline characteristics.
Cancer patients had been diagnosed with non-Hodgkin lymphoma (28%), Hodgkin lymphoma (9%), or breast cancer (64%). Forty-seven percent had received radiation, including right chest (21%), left chest (23%), and mediastinal (4%).
Eighty-four percent of patients had received anthracycline therapy. The median doxorubicin isotoxic dose was 240 mg/m2.
At baseline, 12% of cancer patients were on beta-blockers, 8% were on angiotensin converting enzyme inhibitors, 4% were on angiotensin receptor blockers, and 11% were on statins.
Results
Cancer patients were more than 3 times as likely as controls to develop CHF. The hazard ratio (HR) was 3.6 (P<0.01) in an analysis adjusted for age, gender, diabetes, hypertension, coronary artery disease, dyslipidemia, and obesity at baseline.
The increased CHF risk among cancer patients was evident after the first year from cancer diagnosis and persisted at 20 years of follow-up.
“The risk of heart failure doesn’t go away after a couple of years,” Dr Larsen said. “It’s a long-term issue that patients need to discuss with their doctors and use as motivation to stay heart healthy.”
The incidence of CHF—in cancer patients and controls, respectively—was as follows:
- 1 year—1.5% vs 0.1%
- 5 years—3.1% vs 0.9%
- 10 years—5.0% vs 2%
- 20 years—10.1% vs 5.8%.
A multivariable analysis in the cancer patients revealed a few independent risk factors for CHF, including:
- Doxorubicin isotoxic dose ≥ 300 mg/m2 (HR=2.34, P=0.003)
- Age at diagnosis (HR=3.06 for age ≥ 80 vs 60-69, P=0.01)
- Coronary artery disease at diagnosis (HR=2.27, P=0.04)
- Diabetes mellitus at diagnosis (HR=2.39, P<0.01).
Dr Larsen said additional research is needed to determine why diabetes carries a greater risk than other traditional risk factors, such as high blood pressure, in this group.
Mitigating risk
These findings raise important questions about what the appropriate surveillance should be for heart problems post-cancer treatment, Dr Larsen said. She believes more frequent cardiac imaging may be warranted in some patients to detect signs of CHF earlier.
“It’s an area that needs to be better defined,” Dr Larsen said. “An echocardiogram is usually done 6 to 12 months after cancer treatment with an anthracycline, but how often should it be done after that? We need to be more vigilant in making sure we try to prevent or control heart issues post-cancer care, especially in light of the growing appreciation of the connection between some cancer treatments and heart disease.”
Dr Larsen also noted that patients themselves can play a role in decreasing their risk of CHF, even if they are starting at a disadvantage.
A heart-healthy lifestyle—maintaining a normal body weight, regular exercise, and controlling other risk factors such as high blood pressure, diabetes, and high cholesterol—can help lower the risk of heart disease and CHF.
“If patients know they have received a drug treatment that might increase their risk of heart failure, it’s even more important to take care of the aspects of their life that they can control to reduce their risk as much as possible and to work with their medical care team to detect issues as early as possible,” Dr Larsen said.
ORLANDO—Results of a retrospective study showed that survivors of lymphoma or breast cancer had a significantly greater risk of congestive heart failure (CHF) than patients who did not have cancer.
This increased risk was observed as early as a year after cancer diagnosis but was still present 20 years after diagnosis.
Overall, 1 in 10 cancer patients had CHF at the 20-year mark.
“The majority of patients do not develop heart failure, but our research helps us recognize the factors associated with it and the importance of appropriate heart care following cancer treatment,” said Carolyn Larsen, MD, of the Mayo Clinic in Rochester, Minnesota.
“Our research suggests that periodic cardiac imaging to monitor for heart damage may be needed for some cancer patients, even if they have no signs of heart damage initially after chemotherapy. Additionally, it emphasizes that working to live a heart-healthy lifestyle is important for cancer patients and survivors to reduce the overall risk of heart disease.”
Dr Larsen and her colleagues presented this research as a poster (abstract 1105-066) at the American College of Cardiology’s 67th Annual Scientific Session & Expo (ACC.18).
Patients
Using data from the Rochester Epidemiology Project, the researchers retrospectively tracked CHF cases in 900 cancer patients and 1550 non-cancer patients. Patients were treated in Olmsted County in Minnesota from 1985 to 2010.
For both patient groups, the median age at baseline was about 53, a little more than 90% of each group was white, and nearly 80% of each group was female.
Six to 7% of patients had diabetes, and about 30% of each group had hypertension. Thirty-eight percent of each group had hyperlipidemia, and 31% were obese.
Five percent of cancer patients and 2% of controls had coronary artery disease (P<0.001). This was the only significant difference in baseline characteristics.
Cancer patients had been diagnosed with non-Hodgkin lymphoma (28%), Hodgkin lymphoma (9%), or breast cancer (64%). Forty-seven percent had received radiation, including right chest (21%), left chest (23%), and mediastinal (4%).
Eighty-four percent of patients had received anthracycline therapy. The median doxorubicin isotoxic dose was 240 mg/m2.
At baseline, 12% of cancer patients were on beta-blockers, 8% were on angiotensin converting enzyme inhibitors, 4% were on angiotensin receptor blockers, and 11% were on statins.
Results
Cancer patients were more than 3 times as likely as controls to develop CHF. The hazard ratio (HR) was 3.6 (P<0.01) in an analysis adjusted for age, gender, diabetes, hypertension, coronary artery disease, dyslipidemia, and obesity at baseline.
The increased CHF risk among cancer patients was evident after the first year from cancer diagnosis and persisted at 20 years of follow-up.
“The risk of heart failure doesn’t go away after a couple of years,” Dr Larsen said. “It’s a long-term issue that patients need to discuss with their doctors and use as motivation to stay heart healthy.”
The incidence of CHF—in cancer patients and controls, respectively—was as follows:
- 1 year—1.5% vs 0.1%
- 5 years—3.1% vs 0.9%
- 10 years—5.0% vs 2%
- 20 years—10.1% vs 5.8%.
A multivariable analysis in the cancer patients revealed a few independent risk factors for CHF, including:
- Doxorubicin isotoxic dose ≥ 300 mg/m2 (HR=2.34, P=0.003)
- Age at diagnosis (HR=3.06 for age ≥ 80 vs 60-69, P=0.01)
- Coronary artery disease at diagnosis (HR=2.27, P=0.04)
- Diabetes mellitus at diagnosis (HR=2.39, P<0.01).
Dr Larsen said additional research is needed to determine why diabetes carries a greater risk than other traditional risk factors, such as high blood pressure, in this group.
Mitigating risk
These findings raise important questions about what the appropriate surveillance should be for heart problems post-cancer treatment, Dr Larsen said. She believes more frequent cardiac imaging may be warranted in some patients to detect signs of CHF earlier.
“It’s an area that needs to be better defined,” Dr Larsen said. “An echocardiogram is usually done 6 to 12 months after cancer treatment with an anthracycline, but how often should it be done after that? We need to be more vigilant in making sure we try to prevent or control heart issues post-cancer care, especially in light of the growing appreciation of the connection between some cancer treatments and heart disease.”
Dr Larsen also noted that patients themselves can play a role in decreasing their risk of CHF, even if they are starting at a disadvantage.
A heart-healthy lifestyle—maintaining a normal body weight, regular exercise, and controlling other risk factors such as high blood pressure, diabetes, and high cholesterol—can help lower the risk of heart disease and CHF.
“If patients know they have received a drug treatment that might increase their risk of heart failure, it’s even more important to take care of the aspects of their life that they can control to reduce their risk as much as possible and to work with their medical care team to detect issues as early as possible,” Dr Larsen said.
ORLANDO—Results of a retrospective study showed that survivors of lymphoma or breast cancer had a significantly greater risk of congestive heart failure (CHF) than patients who did not have cancer.
This increased risk was observed as early as a year after cancer diagnosis but was still present 20 years after diagnosis.
Overall, 1 in 10 cancer patients had CHF at the 20-year mark.
“The majority of patients do not develop heart failure, but our research helps us recognize the factors associated with it and the importance of appropriate heart care following cancer treatment,” said Carolyn Larsen, MD, of the Mayo Clinic in Rochester, Minnesota.
“Our research suggests that periodic cardiac imaging to monitor for heart damage may be needed for some cancer patients, even if they have no signs of heart damage initially after chemotherapy. Additionally, it emphasizes that working to live a heart-healthy lifestyle is important for cancer patients and survivors to reduce the overall risk of heart disease.”
Dr Larsen and her colleagues presented this research as a poster (abstract 1105-066) at the American College of Cardiology’s 67th Annual Scientific Session & Expo (ACC.18).
Patients
Using data from the Rochester Epidemiology Project, the researchers retrospectively tracked CHF cases in 900 cancer patients and 1550 non-cancer patients. Patients were treated in Olmsted County in Minnesota from 1985 to 2010.
For both patient groups, the median age at baseline was about 53, a little more than 90% of each group was white, and nearly 80% of each group was female.
Six to 7% of patients had diabetes, and about 30% of each group had hypertension. Thirty-eight percent of each group had hyperlipidemia, and 31% were obese.
Five percent of cancer patients and 2% of controls had coronary artery disease (P<0.001). This was the only significant difference in baseline characteristics.
Cancer patients had been diagnosed with non-Hodgkin lymphoma (28%), Hodgkin lymphoma (9%), or breast cancer (64%). Forty-seven percent had received radiation, including right chest (21%), left chest (23%), and mediastinal (4%).
Eighty-four percent of patients had received anthracycline therapy. The median doxorubicin isotoxic dose was 240 mg/m2.
At baseline, 12% of cancer patients were on beta-blockers, 8% were on angiotensin converting enzyme inhibitors, 4% were on angiotensin receptor blockers, and 11% were on statins.
Results
Cancer patients were more than 3 times as likely as controls to develop CHF. The hazard ratio (HR) was 3.6 (P<0.01) in an analysis adjusted for age, gender, diabetes, hypertension, coronary artery disease, dyslipidemia, and obesity at baseline.
The increased CHF risk among cancer patients was evident after the first year from cancer diagnosis and persisted at 20 years of follow-up.
“The risk of heart failure doesn’t go away after a couple of years,” Dr Larsen said. “It’s a long-term issue that patients need to discuss with their doctors and use as motivation to stay heart healthy.”
The incidence of CHF—in cancer patients and controls, respectively—was as follows:
- 1 year—1.5% vs 0.1%
- 5 years—3.1% vs 0.9%
- 10 years—5.0% vs 2%
- 20 years—10.1% vs 5.8%.
A multivariable analysis in the cancer patients revealed a few independent risk factors for CHF, including:
- Doxorubicin isotoxic dose ≥ 300 mg/m2 (HR=2.34, P=0.003)
- Age at diagnosis (HR=3.06 for age ≥ 80 vs 60-69, P=0.01)
- Coronary artery disease at diagnosis (HR=2.27, P=0.04)
- Diabetes mellitus at diagnosis (HR=2.39, P<0.01).
Dr Larsen said additional research is needed to determine why diabetes carries a greater risk than other traditional risk factors, such as high blood pressure, in this group.
Mitigating risk
These findings raise important questions about what the appropriate surveillance should be for heart problems post-cancer treatment, Dr Larsen said. She believes more frequent cardiac imaging may be warranted in some patients to detect signs of CHF earlier.
“It’s an area that needs to be better defined,” Dr Larsen said. “An echocardiogram is usually done 6 to 12 months after cancer treatment with an anthracycline, but how often should it be done after that? We need to be more vigilant in making sure we try to prevent or control heart issues post-cancer care, especially in light of the growing appreciation of the connection between some cancer treatments and heart disease.”
Dr Larsen also noted that patients themselves can play a role in decreasing their risk of CHF, even if they are starting at a disadvantage.
A heart-healthy lifestyle—maintaining a normal body weight, regular exercise, and controlling other risk factors such as high blood pressure, diabetes, and high cholesterol—can help lower the risk of heart disease and CHF.
“If patients know they have received a drug treatment that might increase their risk of heart failure, it’s even more important to take care of the aspects of their life that they can control to reduce their risk as much as possible and to work with their medical care team to detect issues as early as possible,” Dr Larsen said.
Outpatient CAR T infusions feasible using liso-cel
SALT LAKE CITY – A CD19-directed 4-1BB chimeric antigen receptor (CAR) T cell product showed efficacy and a low rate of cytokine release syndrome and neurotoxicity in patients with aggressive lymphomas and poor prognoses, raising the possibility of outpatient administration and fewer hospitalization days in this high-risk group.
A total of 86 patients who received inpatient infusions of lisocabtagene maraleucel (liso-cel, also known as JCAR017) had a mean 15.6 days of hospitalization, compared with 9.3 days for 8 outpatient recipients, said Jeremy Abramson, MD, speaking at a top abstracts session of the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.

As of October 2017, eight patients had received liso-cel infusion as outpatients with at least 28 days of postinfusion data, Dr. Abramson said.
Although all but one required hospital admission, at a median of 5 days postinfusion (range, 4-22 days), there had been no intensive care unit admissions, and no outpatient recipients had experienced severe cytokine release syndrome (CRS) or neurotoxicity. All admitted patients presented with fever.
Among the study population, “Cytokine release syndrome was only seen in 35% of our entire dataset,” with neurologic toxicity seen in 19% of participants, Dr. Abramson said. “The majority of subjects had no CRS and no toxicity,” he said. Severe CRS occurred in 1% of the study population, and severe neurotoxicity in 12%. There were no deaths related to either complication.
Dr. Abramson reported these results from the TRANSCEND NHL 001 trial, a seamless design phase 1 pivotal trial of liso-cel enrolling patients with relapsed and refractory aggressive B cell non-Hodgkin lymphoma (NHL). Liso-cel delivers CD19-directed CD4 and CD8 CAR T cells in a 1:1 ratio, said Dr. Abramson, director of the lymphoma program at the Massachusetts General Hospital Cancer Center, Boston.
A total of 91 patients were randomized to one of the three dose-finding cohorts of the multicenter trial of liso-cel. One cohort received 5 x 107 cells in a single dose; a second cohort received the same number of cells but in two doses administered 14 days apart; the third cohort received a single dose of 1 x 108 cells.
The seamless trial design then moved to dose expansion, using the two single doses established in the dose-finding phase of the study. Ultimately, Dr. Abramson said, the third and pivotal diffuse large B-cell lymphoma (DLBCL) cohort received the higher single dose, since a dose-response relationship was seen in the earlier cohorts. No increase in cytokine release syndrome or neurotoxicity has been seen with the higher dose in patients evaluated to date.
Patients (median age, 61 years) were eligible to participate in the trial if they had relapsed or refractory DLBCL, primary mediastinal B-cell lymphoma, grade 3B follicular lymphoma, or mantle cell lymphoma. Patients with a failed prior allogeneic stem cell transplant or secondary central nervous system involvement were eligible, but all patients had to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0-2.
As the trial moved to the core pivotal phase, eligibility requirements shifted slightly to include patients with ECOG status 0 or 1, and lymphoma diagnoses narrowed to include only DLBCL not otherwise specified (NOS), transformed follicular lymphoma, and high-grade B-cell lymphoma with double- and triple-hit cytogenetics. The core group was nearing completion of accrual at the time of the presentation, which presented preliminary results from this phase of the trial.
Among the 88 evaluable patients in the initial population with DLBCL receiving any of three dose levels, the best overall response rate (ORR) was 74% (95% confidence interval, 63%-83%); 52% of these patients achieved complete response (CR; 95% CI, 41%-63%).
For patients receiving the higher dose of liso-cel, the ORR was 81% (95% CI, 62%-94%), with a 63% CR rate (95% CI, 42%-81%), bearing out the dose-response rate that had been seen earlier in the trial, Dr. Abramson said.
The median duration of response in all TRANSCEND patients was 9.2 months; the median duration of remission has not been reached, he said. “We see evidence of durable response at 3 months in all our high-risk subsets, and that includes double- and triple-hit lymphomas, double-expresser lymphomas, patients who’ve never achieved prior complete remission, and patients with refractory disease.”
“The overall results are similarly encouraging,” Dr. Abramson said, with 86% of all patients alive at 6 months. Among the complete responders, 94% are alive at the 6-month mark. “The median duration of complete responders has not been reached in this cohort,” he said.
These results are notable, Dr. Abramson said, since about 90% of study participants have at least one disease risk factor that would predict median overall survival of 3-6 months.
During the period after leukapheresis while the CAR T cells were in production, patients could have ongoing treatment, but received PET scans to confirm disease before continuing enrollment in the trial and receiving liso-cel. The time from apheresis to product release for the pivotal cohort is now under 21 days, he said.
The study was supported by Juno Therapeutics, which plans to market liso-cel. Dr. Abramson reported ties with Celgene, Gilead, Seattle Genetics, Novartis, and Genentech.
SOURCE: Abramson J et al. Abstract 5.
SALT LAKE CITY – A CD19-directed 4-1BB chimeric antigen receptor (CAR) T cell product showed efficacy and a low rate of cytokine release syndrome and neurotoxicity in patients with aggressive lymphomas and poor prognoses, raising the possibility of outpatient administration and fewer hospitalization days in this high-risk group.
A total of 86 patients who received inpatient infusions of lisocabtagene maraleucel (liso-cel, also known as JCAR017) had a mean 15.6 days of hospitalization, compared with 9.3 days for 8 outpatient recipients, said Jeremy Abramson, MD, speaking at a top abstracts session of the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
As of October 2017, eight patients had received liso-cel infusion as outpatients with at least 28 days of postinfusion data, Dr. Abramson said.
Although all but one required hospital admission, at a median of 5 days postinfusion (range, 4-22 days), there had been no intensive care unit admissions, and no outpatient recipients had experienced severe cytokine release syndrome (CRS) or neurotoxicity. All admitted patients presented with fever.
Among the study population, “Cytokine release syndrome was only seen in 35% of our entire dataset,” with neurologic toxicity seen in 19% of participants, Dr. Abramson said. “The majority of subjects had no CRS and no toxicity,” he said. Severe CRS occurred in 1% of the study population, and severe neurotoxicity in 12%. There were no deaths related to either complication.
Dr. Abramson reported these results from the TRANSCEND NHL 001 trial, a seamless design phase 1 pivotal trial of liso-cel enrolling patients with relapsed and refractory aggressive B cell non-Hodgkin lymphoma (NHL). Liso-cel delivers CD19-directed CD4 and CD8 CAR T cells in a 1:1 ratio, said Dr. Abramson, director of the lymphoma program at the Massachusetts General Hospital Cancer Center, Boston.
A total of 91 patients were randomized to one of the three dose-finding cohorts of the multicenter trial of liso-cel. One cohort received 5 x 107 cells in a single dose; a second cohort received the same number of cells but in two doses administered 14 days apart; the third cohort received a single dose of 1 x 108 cells.
The seamless trial design then moved to dose expansion, using the two single doses established in the dose-finding phase of the study. Ultimately, Dr. Abramson said, the third and pivotal diffuse large B-cell lymphoma (DLBCL) cohort received the higher single dose, since a dose-response relationship was seen in the earlier cohorts. No increase in cytokine release syndrome or neurotoxicity has been seen with the higher dose in patients evaluated to date.
Patients (median age, 61 years) were eligible to participate in the trial if they had relapsed or refractory DLBCL, primary mediastinal B-cell lymphoma, grade 3B follicular lymphoma, or mantle cell lymphoma. Patients with a failed prior allogeneic stem cell transplant or secondary central nervous system involvement were eligible, but all patients had to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0-2.
As the trial moved to the core pivotal phase, eligibility requirements shifted slightly to include patients with ECOG status 0 or 1, and lymphoma diagnoses narrowed to include only DLBCL not otherwise specified (NOS), transformed follicular lymphoma, and high-grade B-cell lymphoma with double- and triple-hit cytogenetics. The core group was nearing completion of accrual at the time of the presentation, which presented preliminary results from this phase of the trial.
Among the 88 evaluable patients in the initial population with DLBCL receiving any of three dose levels, the best overall response rate (ORR) was 74% (95% confidence interval, 63%-83%); 52% of these patients achieved complete response (CR; 95% CI, 41%-63%).
For patients receiving the higher dose of liso-cel, the ORR was 81% (95% CI, 62%-94%), with a 63% CR rate (95% CI, 42%-81%), bearing out the dose-response rate that had been seen earlier in the trial, Dr. Abramson said.
The median duration of response in all TRANSCEND patients was 9.2 months; the median duration of remission has not been reached, he said. “We see evidence of durable response at 3 months in all our high-risk subsets, and that includes double- and triple-hit lymphomas, double-expresser lymphomas, patients who’ve never achieved prior complete remission, and patients with refractory disease.”
“The overall results are similarly encouraging,” Dr. Abramson said, with 86% of all patients alive at 6 months. Among the complete responders, 94% are alive at the 6-month mark. “The median duration of complete responders has not been reached in this cohort,” he said.
These results are notable, Dr. Abramson said, since about 90% of study participants have at least one disease risk factor that would predict median overall survival of 3-6 months.
During the period after leukapheresis while the CAR T cells were in production, patients could have ongoing treatment, but received PET scans to confirm disease before continuing enrollment in the trial and receiving liso-cel. The time from apheresis to product release for the pivotal cohort is now under 21 days, he said.
The study was supported by Juno Therapeutics, which plans to market liso-cel. Dr. Abramson reported ties with Celgene, Gilead, Seattle Genetics, Novartis, and Genentech.
SOURCE: Abramson J et al. Abstract 5.
SALT LAKE CITY – A CD19-directed 4-1BB chimeric antigen receptor (CAR) T cell product showed efficacy and a low rate of cytokine release syndrome and neurotoxicity in patients with aggressive lymphomas and poor prognoses, raising the possibility of outpatient administration and fewer hospitalization days in this high-risk group.
A total of 86 patients who received inpatient infusions of lisocabtagene maraleucel (liso-cel, also known as JCAR017) had a mean 15.6 days of hospitalization, compared with 9.3 days for 8 outpatient recipients, said Jeremy Abramson, MD, speaking at a top abstracts session of the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
As of October 2017, eight patients had received liso-cel infusion as outpatients with at least 28 days of postinfusion data, Dr. Abramson said.
Although all but one required hospital admission, at a median of 5 days postinfusion (range, 4-22 days), there had been no intensive care unit admissions, and no outpatient recipients had experienced severe cytokine release syndrome (CRS) or neurotoxicity. All admitted patients presented with fever.
Among the study population, “Cytokine release syndrome was only seen in 35% of our entire dataset,” with neurologic toxicity seen in 19% of participants, Dr. Abramson said. “The majority of subjects had no CRS and no toxicity,” he said. Severe CRS occurred in 1% of the study population, and severe neurotoxicity in 12%. There were no deaths related to either complication.
Dr. Abramson reported these results from the TRANSCEND NHL 001 trial, a seamless design phase 1 pivotal trial of liso-cel enrolling patients with relapsed and refractory aggressive B cell non-Hodgkin lymphoma (NHL). Liso-cel delivers CD19-directed CD4 and CD8 CAR T cells in a 1:1 ratio, said Dr. Abramson, director of the lymphoma program at the Massachusetts General Hospital Cancer Center, Boston.
A total of 91 patients were randomized to one of the three dose-finding cohorts of the multicenter trial of liso-cel. One cohort received 5 x 107 cells in a single dose; a second cohort received the same number of cells but in two doses administered 14 days apart; the third cohort received a single dose of 1 x 108 cells.
The seamless trial design then moved to dose expansion, using the two single doses established in the dose-finding phase of the study. Ultimately, Dr. Abramson said, the third and pivotal diffuse large B-cell lymphoma (DLBCL) cohort received the higher single dose, since a dose-response relationship was seen in the earlier cohorts. No increase in cytokine release syndrome or neurotoxicity has been seen with the higher dose in patients evaluated to date.
Patients (median age, 61 years) were eligible to participate in the trial if they had relapsed or refractory DLBCL, primary mediastinal B-cell lymphoma, grade 3B follicular lymphoma, or mantle cell lymphoma. Patients with a failed prior allogeneic stem cell transplant or secondary central nervous system involvement were eligible, but all patients had to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0-2.
As the trial moved to the core pivotal phase, eligibility requirements shifted slightly to include patients with ECOG status 0 or 1, and lymphoma diagnoses narrowed to include only DLBCL not otherwise specified (NOS), transformed follicular lymphoma, and high-grade B-cell lymphoma with double- and triple-hit cytogenetics. The core group was nearing completion of accrual at the time of the presentation, which presented preliminary results from this phase of the trial.
Among the 88 evaluable patients in the initial population with DLBCL receiving any of three dose levels, the best overall response rate (ORR) was 74% (95% confidence interval, 63%-83%); 52% of these patients achieved complete response (CR; 95% CI, 41%-63%).
For patients receiving the higher dose of liso-cel, the ORR was 81% (95% CI, 62%-94%), with a 63% CR rate (95% CI, 42%-81%), bearing out the dose-response rate that had been seen earlier in the trial, Dr. Abramson said.
The median duration of response in all TRANSCEND patients was 9.2 months; the median duration of remission has not been reached, he said. “We see evidence of durable response at 3 months in all our high-risk subsets, and that includes double- and triple-hit lymphomas, double-expresser lymphomas, patients who’ve never achieved prior complete remission, and patients with refractory disease.”
“The overall results are similarly encouraging,” Dr. Abramson said, with 86% of all patients alive at 6 months. Among the complete responders, 94% are alive at the 6-month mark. “The median duration of complete responders has not been reached in this cohort,” he said.
These results are notable, Dr. Abramson said, since about 90% of study participants have at least one disease risk factor that would predict median overall survival of 3-6 months.
During the period after leukapheresis while the CAR T cells were in production, patients could have ongoing treatment, but received PET scans to confirm disease before continuing enrollment in the trial and receiving liso-cel. The time from apheresis to product release for the pivotal cohort is now under 21 days, he said.
The study was supported by Juno Therapeutics, which plans to market liso-cel. Dr. Abramson reported ties with Celgene, Gilead, Seattle Genetics, Novartis, and Genentech.
SOURCE: Abramson J et al. Abstract 5.
REPORTING FROM THE 2018 BMT TANDEM MEETINGS
Key clinical point:
Major finding: High-risk lymphoma patients had more than 6 fewer inpatient days with outpatient CAR T infusion.
Study details: Seamless phase 1 trial initially evaluating 91 patients with relapsed/refractory diffuse large B cell lymphoma.
Disclosures: Juno Therapeutics sponsored the study. Dr. Abramson reported ties with Celgene, Gilead, Seattle Genetics, Novartis, and Genentech.
Source: Abramson J et al. Abstract 5.