User login
Kids’ self-reports of symptoms, side effects reliable

A small study of 20 children aged 8 to 18 years with incurable or refractory cancers indicates children are reliable reporters of their symptoms and side effects.
The investigators collected reports from the children, who were enrolled on phase 1/2 clinical trials at 4 cancer centers and undergoing their first courses of chemotherapy.
The team assessed the feasibility and acceptability of collecting symptom, function, and quality of life (QOL) reports from the study participants.
The investigators also evaluated the measurement tool and interview questions at 2 time points.
They contend the youths’ self-reports potentially could be a new trial endpoint.
According to the investigators, only rarely do patient-reported outcomes (PROs) get incorporated into pediatric phase 1 or phase 2 trials.
And because these trials contribute to drug indications and labeling, the researchers decided to assess whether it was feasible to enroll young people and retain them in a PRO endeavor.
The researchers also assessed the reliability, validity, responsiveness, and range of the pediatric measures employed. They used the Patient-Reported Outcomes Measurement Information System (PROMIS) to capture statistically significant and clinically meaningful changes or minimally important differences (MIDs) in PROs.
Pamela S. Hinds, PhD, RN, of George Washington University in Washington, DC, reported the findings on behalf of the Children's National Health System researchers in Cancer, the journal of the American Cancer Society.
"When experimental cancer drugs are studied, researchers collect details about how these promising therapies affect children's organs, but rarely do they ask the children themselves about symptoms they feel or the side effects they experience," Dr Hinds said.
"Without this crucial information, the full impact of the experimental treatment on the pediatric patient is likely underreported and clinicians are hobbled in their ability to effectively manage side effects," she added.
The team recruited children and adolescents enrolled in phase 1 safety or phase 2 efficacy trials at Children's National, Seattle Children's Hospital, Children's Hospital of Philadelphia, and Boston Children's Hospital.
Findings
Sixty percent of the participants were male and 70% were white.
Median age of the participants was 13.6 years: 7 (35%) were age 8 to 12, and 13 (65%) were 13 to 17.
Thirteen participants (65%) had solid tumors, 5 (25%) had brain tumors, and 2 (10%) had lymphoma.
A total of 29 patients were eligible to participate in the trial during 20 months of screening. Five parents and 2 patients declined to participate.
The remaining 22 patients who agreed to participate accounted for a 75.9% enrollment rate. Twenty of them (90.9%) participated at the first data time point, which was at the time of enrollment, and 77.3% participated 3 weeks later at time point 2.
The authors noted that refusals to enroll were more likely to come from parents (17.2%) than the eligible patients (8.3%).
And refusals only occurred when the self-report measures were not embedded in the clinical trial.
Of the 10 protocols represented, 7 patients were enrolled on the same protocol in which the PRO measures were embedded.
The researchers administered the 6-item short-form measures for the scales of Mobility, Pain, Fatigue, Depressive Symptoms, Anxiety, and Peer Relationships.
They asked the 4 open-ended questions—concerning QOL while receiving therapy and acceptability of the patient reporting—at time point 2.
At time point 1, 3 patients did not complete 3 PROMIS measures, for a person-missing rate of 15% and a measure-missing rate of 3.3%.
At the second time point, 2 patients did not complete 1 measure each, for a person-missing rate of 11.8% and a measure-missing rate of 2%.
All but one measure at time point 1 met the reliability criterion and all measures did so at time point 2.
The research team believes their findings support the feasibility and acceptability of completing quantitative and qualitative measures regarding symptom, function, and QOL experiences among children and adolescents with incurable cancer.
The researchers note the small study size and the number of parent refusals are limitations of the trial.
Nevertheless, they recommend embedding PROs in future pediatric oncology phase 1/2 trials. ![]()
A small study of 20 children aged 8 to 18 years with incurable or refractory cancers indicates children are reliable reporters of their symptoms and side effects.
The investigators collected reports from the children, who were enrolled on phase 1/2 clinical trials at 4 cancer centers and undergoing their first courses of chemotherapy.
The team assessed the feasibility and acceptability of collecting symptom, function, and quality of life (QOL) reports from the study participants.
The investigators also evaluated the measurement tool and interview questions at 2 time points.
They contend the youths’ self-reports potentially could be a new trial endpoint.
According to the investigators, only rarely do patient-reported outcomes (PROs) get incorporated into pediatric phase 1 or phase 2 trials.
And because these trials contribute to drug indications and labeling, the researchers decided to assess whether it was feasible to enroll young people and retain them in a PRO endeavor.
The researchers also assessed the reliability, validity, responsiveness, and range of the pediatric measures employed. They used the Patient-Reported Outcomes Measurement Information System (PROMIS) to capture statistically significant and clinically meaningful changes or minimally important differences (MIDs) in PROs.
Pamela S. Hinds, PhD, RN, of George Washington University in Washington, DC, reported the findings on behalf of the Children's National Health System researchers in Cancer, the journal of the American Cancer Society.
"When experimental cancer drugs are studied, researchers collect details about how these promising therapies affect children's organs, but rarely do they ask the children themselves about symptoms they feel or the side effects they experience," Dr Hinds said.
"Without this crucial information, the full impact of the experimental treatment on the pediatric patient is likely underreported and clinicians are hobbled in their ability to effectively manage side effects," she added.
The team recruited children and adolescents enrolled in phase 1 safety or phase 2 efficacy trials at Children's National, Seattle Children's Hospital, Children's Hospital of Philadelphia, and Boston Children's Hospital.
Findings
Sixty percent of the participants were male and 70% were white.
Median age of the participants was 13.6 years: 7 (35%) were age 8 to 12, and 13 (65%) were 13 to 17.
Thirteen participants (65%) had solid tumors, 5 (25%) had brain tumors, and 2 (10%) had lymphoma.
A total of 29 patients were eligible to participate in the trial during 20 months of screening. Five parents and 2 patients declined to participate.
The remaining 22 patients who agreed to participate accounted for a 75.9% enrollment rate. Twenty of them (90.9%) participated at the first data time point, which was at the time of enrollment, and 77.3% participated 3 weeks later at time point 2.
The authors noted that refusals to enroll were more likely to come from parents (17.2%) than the eligible patients (8.3%).
And refusals only occurred when the self-report measures were not embedded in the clinical trial.
Of the 10 protocols represented, 7 patients were enrolled on the same protocol in which the PRO measures were embedded.
The researchers administered the 6-item short-form measures for the scales of Mobility, Pain, Fatigue, Depressive Symptoms, Anxiety, and Peer Relationships.
They asked the 4 open-ended questions—concerning QOL while receiving therapy and acceptability of the patient reporting—at time point 2.
At time point 1, 3 patients did not complete 3 PROMIS measures, for a person-missing rate of 15% and a measure-missing rate of 3.3%.
At the second time point, 2 patients did not complete 1 measure each, for a person-missing rate of 11.8% and a measure-missing rate of 2%.
All but one measure at time point 1 met the reliability criterion and all measures did so at time point 2.
The research team believes their findings support the feasibility and acceptability of completing quantitative and qualitative measures regarding symptom, function, and QOL experiences among children and adolescents with incurable cancer.
The researchers note the small study size and the number of parent refusals are limitations of the trial.
Nevertheless, they recommend embedding PROs in future pediatric oncology phase 1/2 trials. ![]()
A small study of 20 children aged 8 to 18 years with incurable or refractory cancers indicates children are reliable reporters of their symptoms and side effects.
The investigators collected reports from the children, who were enrolled on phase 1/2 clinical trials at 4 cancer centers and undergoing their first courses of chemotherapy.
The team assessed the feasibility and acceptability of collecting symptom, function, and quality of life (QOL) reports from the study participants.
The investigators also evaluated the measurement tool and interview questions at 2 time points.
They contend the youths’ self-reports potentially could be a new trial endpoint.
According to the investigators, only rarely do patient-reported outcomes (PROs) get incorporated into pediatric phase 1 or phase 2 trials.
And because these trials contribute to drug indications and labeling, the researchers decided to assess whether it was feasible to enroll young people and retain them in a PRO endeavor.
The researchers also assessed the reliability, validity, responsiveness, and range of the pediatric measures employed. They used the Patient-Reported Outcomes Measurement Information System (PROMIS) to capture statistically significant and clinically meaningful changes or minimally important differences (MIDs) in PROs.
Pamela S. Hinds, PhD, RN, of George Washington University in Washington, DC, reported the findings on behalf of the Children's National Health System researchers in Cancer, the journal of the American Cancer Society.
"When experimental cancer drugs are studied, researchers collect details about how these promising therapies affect children's organs, but rarely do they ask the children themselves about symptoms they feel or the side effects they experience," Dr Hinds said.
"Without this crucial information, the full impact of the experimental treatment on the pediatric patient is likely underreported and clinicians are hobbled in their ability to effectively manage side effects," she added.
The team recruited children and adolescents enrolled in phase 1 safety or phase 2 efficacy trials at Children's National, Seattle Children's Hospital, Children's Hospital of Philadelphia, and Boston Children's Hospital.
Findings
Sixty percent of the participants were male and 70% were white.
Median age of the participants was 13.6 years: 7 (35%) were age 8 to 12, and 13 (65%) were 13 to 17.
Thirteen participants (65%) had solid tumors, 5 (25%) had brain tumors, and 2 (10%) had lymphoma.
A total of 29 patients were eligible to participate in the trial during 20 months of screening. Five parents and 2 patients declined to participate.
The remaining 22 patients who agreed to participate accounted for a 75.9% enrollment rate. Twenty of them (90.9%) participated at the first data time point, which was at the time of enrollment, and 77.3% participated 3 weeks later at time point 2.
The authors noted that refusals to enroll were more likely to come from parents (17.2%) than the eligible patients (8.3%).
And refusals only occurred when the self-report measures were not embedded in the clinical trial.
Of the 10 protocols represented, 7 patients were enrolled on the same protocol in which the PRO measures were embedded.
The researchers administered the 6-item short-form measures for the scales of Mobility, Pain, Fatigue, Depressive Symptoms, Anxiety, and Peer Relationships.
They asked the 4 open-ended questions—concerning QOL while receiving therapy and acceptability of the patient reporting—at time point 2.
At time point 1, 3 patients did not complete 3 PROMIS measures, for a person-missing rate of 15% and a measure-missing rate of 3.3%.
At the second time point, 2 patients did not complete 1 measure each, for a person-missing rate of 11.8% and a measure-missing rate of 2%.
All but one measure at time point 1 met the reliability criterion and all measures did so at time point 2.
The research team believes their findings support the feasibility and acceptability of completing quantitative and qualitative measures regarding symptom, function, and QOL experiences among children and adolescents with incurable cancer.
The researchers note the small study size and the number of parent refusals are limitations of the trial.
Nevertheless, they recommend embedding PROs in future pediatric oncology phase 1/2 trials. ![]()
Twofer drug blocks SYK/JAK pathways in advanced NHL
MADRID – Cerdulatinib, a single oral agent targeting two different pathways that lymphomas rely on for survival, produced rapid tumor responses in patients with relapsed or refractory non-Hodgkin lymphomas (NHL) in a phase II study.
The overall response rate among 47 patients enrolled in a phase II study was 50%, including responses among 67% of patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and 56% of patients with follicular lymphoma (FL), reported Paul A. Hamlin, MD, of the Memorial Sloan Kettering Cancer Center in New York.

“At a dose of 30 mg b.i.d., cerdulatinib inhibited pathways of interest, so both SYK and JAK are inhibited at maximum amounts at physiologically attained doses,” he said at a briefing at the annual congress of the European Hematology Association.
Certain B cell malignancies are “addicted” to B cell antigen-receptor (BCR) signaling. A combination of selective SYK and JAK inhibitors can syngergistically suppress this response in B cell malignancies, he said.
In a phase I dose escalation study of cerdulatinib in 43 patients with relapsed/refractory CLL and NHL reported by Dr. Hamlin and his colleagues at the 2016 EHA annual congress, inhibition with cerdulatinib of both the BCR/SYK and JAK/STAT pathways in peripheral blood assays was well tolerated.
In the current phase II, multicenter, open-label study, the investigators plan on enrolling up to 40 patients in each of three cohorts: relapsed refractory CLL/SLL, relapsed/refractory indolent NHL, and relapsed diffuse large B cell lymphoma (DLBCL), mantle cell lymphoma (MCL) and transformed FL. The investigators have also begun to enroll patients with peripheral T-cell lymphoma (PTCL) based on efficacy of the dual pathway inhibitor against this malignancy.
The patients received 30-mg cerdulatinib orally twice daily until disease progression or intolerable toxicity.
As noted, the overall response rate was 50% (47 patients), including partial responses (PR) in 12 of 18 (67%) of patients with CLL/SLL, in five of nine patients (56%) with FL, and in one of seven patients with relapsed refractory marginal zone lymphoma and Waldenstrom macroglobulinemia.
In addition, the investigators identified one complete response in the first enrolled patient with PTCL.
“I think this is a proof of principle that the biology suggesting that SYK is expressed in T-cell lymphomas and may have an important role in its pathogenesis holds true,” Dr. Hamlin said.
Responses have been detected in heavily pretreated patients, including one patient with FL who had a relapse on ibrutinib and a patient with SLL who had a relapse during treatment with venetoclax. Both patients remain on cerdulatinib after 10 months. At the time of the data presentation, 15 patients are continuing therapy with the dual inhibitor, including 4 who have been taking it for more than 300 days.
The responses occurred after a median of two cycles, Dr. Hamlin noted, and improved over time, as seen in seven of nine patients with increased reduction of nodal masses at the second or third rescan.
The most frequent adverse events with cerdulatinib at the target dose of 30 mg are fatigue, diarrhea, nausea, and cytopenias.
In the dose-escalation phase, three patients at a dose of 35 mg b.i.d. had higher than expected drug concentrations and experienced severe adverse events, including two fatal infections and one grade 3 pancreatitis. The investigators launched a pharmacokinetics monitoring strategy in hopes of avoiding this complication in the future.
Dr. Hamlin said the efficacy to date suggests the cerdulatinib could be used as a single agent but added that its generally favorable safety profile may make it a good partner in combination therapies.
The study is supported by Molecular Templates. Dr. Hamlin disclosed grant/research support and/or consultant role for Spectrum, GlaxoSmithKline, Pfizer, Seattle Genetics, Genentech, and Gilead.
MADRID – Cerdulatinib, a single oral agent targeting two different pathways that lymphomas rely on for survival, produced rapid tumor responses in patients with relapsed or refractory non-Hodgkin lymphomas (NHL) in a phase II study.
The overall response rate among 47 patients enrolled in a phase II study was 50%, including responses among 67% of patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and 56% of patients with follicular lymphoma (FL), reported Paul A. Hamlin, MD, of the Memorial Sloan Kettering Cancer Center in New York.
“At a dose of 30 mg b.i.d., cerdulatinib inhibited pathways of interest, so both SYK and JAK are inhibited at maximum amounts at physiologically attained doses,” he said at a briefing at the annual congress of the European Hematology Association.
Certain B cell malignancies are “addicted” to B cell antigen-receptor (BCR) signaling. A combination of selective SYK and JAK inhibitors can syngergistically suppress this response in B cell malignancies, he said.
In a phase I dose escalation study of cerdulatinib in 43 patients with relapsed/refractory CLL and NHL reported by Dr. Hamlin and his colleagues at the 2016 EHA annual congress, inhibition with cerdulatinib of both the BCR/SYK and JAK/STAT pathways in peripheral blood assays was well tolerated.
In the current phase II, multicenter, open-label study, the investigators plan on enrolling up to 40 patients in each of three cohorts: relapsed refractory CLL/SLL, relapsed/refractory indolent NHL, and relapsed diffuse large B cell lymphoma (DLBCL), mantle cell lymphoma (MCL) and transformed FL. The investigators have also begun to enroll patients with peripheral T-cell lymphoma (PTCL) based on efficacy of the dual pathway inhibitor against this malignancy.
The patients received 30-mg cerdulatinib orally twice daily until disease progression or intolerable toxicity.
As noted, the overall response rate was 50% (47 patients), including partial responses (PR) in 12 of 18 (67%) of patients with CLL/SLL, in five of nine patients (56%) with FL, and in one of seven patients with relapsed refractory marginal zone lymphoma and Waldenstrom macroglobulinemia.
In addition, the investigators identified one complete response in the first enrolled patient with PTCL.
“I think this is a proof of principle that the biology suggesting that SYK is expressed in T-cell lymphomas and may have an important role in its pathogenesis holds true,” Dr. Hamlin said.
Responses have been detected in heavily pretreated patients, including one patient with FL who had a relapse on ibrutinib and a patient with SLL who had a relapse during treatment with venetoclax. Both patients remain on cerdulatinib after 10 months. At the time of the data presentation, 15 patients are continuing therapy with the dual inhibitor, including 4 who have been taking it for more than 300 days.
The responses occurred after a median of two cycles, Dr. Hamlin noted, and improved over time, as seen in seven of nine patients with increased reduction of nodal masses at the second or third rescan.
The most frequent adverse events with cerdulatinib at the target dose of 30 mg are fatigue, diarrhea, nausea, and cytopenias.
In the dose-escalation phase, three patients at a dose of 35 mg b.i.d. had higher than expected drug concentrations and experienced severe adverse events, including two fatal infections and one grade 3 pancreatitis. The investigators launched a pharmacokinetics monitoring strategy in hopes of avoiding this complication in the future.
Dr. Hamlin said the efficacy to date suggests the cerdulatinib could be used as a single agent but added that its generally favorable safety profile may make it a good partner in combination therapies.
The study is supported by Molecular Templates. Dr. Hamlin disclosed grant/research support and/or consultant role for Spectrum, GlaxoSmithKline, Pfizer, Seattle Genetics, Genentech, and Gilead.
MADRID – Cerdulatinib, a single oral agent targeting two different pathways that lymphomas rely on for survival, produced rapid tumor responses in patients with relapsed or refractory non-Hodgkin lymphomas (NHL) in a phase II study.
The overall response rate among 47 patients enrolled in a phase II study was 50%, including responses among 67% of patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and 56% of patients with follicular lymphoma (FL), reported Paul A. Hamlin, MD, of the Memorial Sloan Kettering Cancer Center in New York.
“At a dose of 30 mg b.i.d., cerdulatinib inhibited pathways of interest, so both SYK and JAK are inhibited at maximum amounts at physiologically attained doses,” he said at a briefing at the annual congress of the European Hematology Association.
Certain B cell malignancies are “addicted” to B cell antigen-receptor (BCR) signaling. A combination of selective SYK and JAK inhibitors can syngergistically suppress this response in B cell malignancies, he said.
In a phase I dose escalation study of cerdulatinib in 43 patients with relapsed/refractory CLL and NHL reported by Dr. Hamlin and his colleagues at the 2016 EHA annual congress, inhibition with cerdulatinib of both the BCR/SYK and JAK/STAT pathways in peripheral blood assays was well tolerated.
In the current phase II, multicenter, open-label study, the investigators plan on enrolling up to 40 patients in each of three cohorts: relapsed refractory CLL/SLL, relapsed/refractory indolent NHL, and relapsed diffuse large B cell lymphoma (DLBCL), mantle cell lymphoma (MCL) and transformed FL. The investigators have also begun to enroll patients with peripheral T-cell lymphoma (PTCL) based on efficacy of the dual pathway inhibitor against this malignancy.
The patients received 30-mg cerdulatinib orally twice daily until disease progression or intolerable toxicity.
As noted, the overall response rate was 50% (47 patients), including partial responses (PR) in 12 of 18 (67%) of patients with CLL/SLL, in five of nine patients (56%) with FL, and in one of seven patients with relapsed refractory marginal zone lymphoma and Waldenstrom macroglobulinemia.
In addition, the investigators identified one complete response in the first enrolled patient with PTCL.
“I think this is a proof of principle that the biology suggesting that SYK is expressed in T-cell lymphomas and may have an important role in its pathogenesis holds true,” Dr. Hamlin said.
Responses have been detected in heavily pretreated patients, including one patient with FL who had a relapse on ibrutinib and a patient with SLL who had a relapse during treatment with venetoclax. Both patients remain on cerdulatinib after 10 months. At the time of the data presentation, 15 patients are continuing therapy with the dual inhibitor, including 4 who have been taking it for more than 300 days.
The responses occurred after a median of two cycles, Dr. Hamlin noted, and improved over time, as seen in seven of nine patients with increased reduction of nodal masses at the second or third rescan.
The most frequent adverse events with cerdulatinib at the target dose of 30 mg are fatigue, diarrhea, nausea, and cytopenias.
In the dose-escalation phase, three patients at a dose of 35 mg b.i.d. had higher than expected drug concentrations and experienced severe adverse events, including two fatal infections and one grade 3 pancreatitis. The investigators launched a pharmacokinetics monitoring strategy in hopes of avoiding this complication in the future.
Dr. Hamlin said the efficacy to date suggests the cerdulatinib could be used as a single agent but added that its generally favorable safety profile may make it a good partner in combination therapies.
The study is supported by Molecular Templates. Dr. Hamlin disclosed grant/research support and/or consultant role for Spectrum, GlaxoSmithKline, Pfizer, Seattle Genetics, Genentech, and Gilead.
AT EHA 2017
Key clinical point: Cerdulatinib, an inhibitor of the SYK and JAK pathways, has shown efficacy against relapsed/refractory non-Hodgkin lymphomas.
Major finding: The overall response rate was 50%, including one complete response in a patient with peripheral T-cell lymphoma.
Data source: An open label, phase II study in 47 patients with non-Hodgkin lymphoma or peripheral T-cell lymphoma.
Disclosures: The study is supported by Molecular Templates. Dr. Hamlin disclosed grant/research support and/or consultant roles for Spectrum, GlaxoSmithKline, Pfizer, Seattle Genetics, Genentech, and Gilead.
Chemo-free induction in MCL keeps getting better
Lugano, Switzerland – It’s not the end of chemotherapy for young patients with newly diagnosed mantle cell lymphoma (MCL), but it’s a start.
For these patients, induction with a combination of ibrutinib and rituximab, followed by shorter cycles of chemoimmunotherapy, was associated in an early study with an objective response rate of 100%, including 90% complete responses (CR), reported Michael Wang, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“This is the first time for a chemo-free therapy – ibrutinib/rituximab – to achieve an overall response rate of 100%. This has an unprecedented efficacy in the frontline in young patients with mantle-cell lymphoma,” he said at the 14th International Congress on Malignant Lymphoma.
In patients with relapsed or refractory MCL, the combination of ibrutinib and rituximab has been associated with durable responses in 88% of patients. The success of the combination suggests that fit patients younger than age 65 years with newly diagnosed MCL might benefit from a chemotherapy-free induction regimen with ibrutinib and rituximab, followed by consolidation with a short but intense course of chemoimmunotherapy, Dr. Wang said.
He presented updated results from the phase II Window I study, first results of which were reported at the 2016 meeting of the American Society of Hematology.
“Frontline therapy is the most important therapy for mantle cell lymphoma, because mantle cell lymphoma cells are most vulnerable to frontline attack. If the frontline therapy is good enough, it could kill all the mantle cell lymphoma cells, therefore leaving no chance for secondary resistance, and thereby (resulting in) long-term survival. And it is really my belief that if we ideally optimized the frontline therapy, that would be a shortcut to a cure,” he said.
To test this idea, Dr. Wang and MD Anderson colleagues initiated a phase II trial at their institution with 50 patients age 65 years or under with newly diagnosed, CD20-positive and Cyclin D1-positive MCL.
A total of 50 patients age 65 years or younger (median age 54) with newly diagnosed, untreated MCL underwent induction with continuous daily ibrutinib 560 mg, plus rituximab 375 mg/m2 administered weekly for 4 weeks during cycle 1 and on day 1 of cycles 3-12. Consolidation consisted of rituximab plus hyper-CVAD (hyper-fractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone), alternating every 28 days with rituximab plus high-dose methotrexate–cytarabine.
Patients who had complete responses to induction received four cycles of chemoimmunotherapy, while those who experienced disease progression and those who had partial responses received chemoimmunotherapy for two cycles beyond the point of complete remissions.
At the time of the presentation, all 50 patients were evaluable for the induction phase (part 2), and 47 were evaluable for both induction and consolidation (part 2) .Of the evaluable patients, the overall response rate (ORR) to chemotherapy-free induction therapy alone (Part 1 ) was 100% (50), with CR in 90% of patients and partial responses (PR) in 10%. Of the 47 patients evaluable for part 2 (chemoimmunotherapy), all had CRs, for an ORR of 100%.
Dr. Wang noted that one patient had a dramatic radiographic reduction in spleen size following just two cycles of chemotherapy-free induction, and two other patients had similar reductions after four and six cycles, respectively.
After a median follow-up of 15.9 months, neither the median duration of response, progression-free survival, nor overall survival have been reached. There have been no deaths and only one case of disease progression after one year of therapy.
The patients generally tolerated the regimen very well, Dr. Wang said. There were no cases of lymphocytosis, bleeding, or atrial fibrillation after 332 combined cycles.
Nonhematological adverse events were primarily grade 1 or 2. Grade 3 fatigue was reported in approximately 10% of patients. There were no grade 4 adverse events.
“This study may provide a window of opportunity to reduce the frontline therapies and reduce the long-term toxicities such as secondary malignancies.” Dr. Wang said.
He acknowledged that four cycles of intensive chemotherapy is still toxic and that further efforts to reduce these toxicities are needed. The investigators are currently planning the Window II study, in which a fraction of patients will be treated with no chemotherapy at all, he said.
The study was supported by Pharmacyclics and Janssen. Dr. Wang disclosed receiving research grants and honoraria and serving as a consultant for the companies.
Lugano, Switzerland – It’s not the end of chemotherapy for young patients with newly diagnosed mantle cell lymphoma (MCL), but it’s a start.
For these patients, induction with a combination of ibrutinib and rituximab, followed by shorter cycles of chemoimmunotherapy, was associated in an early study with an objective response rate of 100%, including 90% complete responses (CR), reported Michael Wang, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“This is the first time for a chemo-free therapy – ibrutinib/rituximab – to achieve an overall response rate of 100%. This has an unprecedented efficacy in the frontline in young patients with mantle-cell lymphoma,” he said at the 14th International Congress on Malignant Lymphoma.
In patients with relapsed or refractory MCL, the combination of ibrutinib and rituximab has been associated with durable responses in 88% of patients. The success of the combination suggests that fit patients younger than age 65 years with newly diagnosed MCL might benefit from a chemotherapy-free induction regimen with ibrutinib and rituximab, followed by consolidation with a short but intense course of chemoimmunotherapy, Dr. Wang said.
He presented updated results from the phase II Window I study, first results of which were reported at the 2016 meeting of the American Society of Hematology.
“Frontline therapy is the most important therapy for mantle cell lymphoma, because mantle cell lymphoma cells are most vulnerable to frontline attack. If the frontline therapy is good enough, it could kill all the mantle cell lymphoma cells, therefore leaving no chance for secondary resistance, and thereby (resulting in) long-term survival. And it is really my belief that if we ideally optimized the frontline therapy, that would be a shortcut to a cure,” he said.
To test this idea, Dr. Wang and MD Anderson colleagues initiated a phase II trial at their institution with 50 patients age 65 years or under with newly diagnosed, CD20-positive and Cyclin D1-positive MCL.
A total of 50 patients age 65 years or younger (median age 54) with newly diagnosed, untreated MCL underwent induction with continuous daily ibrutinib 560 mg, plus rituximab 375 mg/m2 administered weekly for 4 weeks during cycle 1 and on day 1 of cycles 3-12. Consolidation consisted of rituximab plus hyper-CVAD (hyper-fractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone), alternating every 28 days with rituximab plus high-dose methotrexate–cytarabine.
Patients who had complete responses to induction received four cycles of chemoimmunotherapy, while those who experienced disease progression and those who had partial responses received chemoimmunotherapy for two cycles beyond the point of complete remissions.
At the time of the presentation, all 50 patients were evaluable for the induction phase (part 2), and 47 were evaluable for both induction and consolidation (part 2) .Of the evaluable patients, the overall response rate (ORR) to chemotherapy-free induction therapy alone (Part 1 ) was 100% (50), with CR in 90% of patients and partial responses (PR) in 10%. Of the 47 patients evaluable for part 2 (chemoimmunotherapy), all had CRs, for an ORR of 100%.
Dr. Wang noted that one patient had a dramatic radiographic reduction in spleen size following just two cycles of chemotherapy-free induction, and two other patients had similar reductions after four and six cycles, respectively.
After a median follow-up of 15.9 months, neither the median duration of response, progression-free survival, nor overall survival have been reached. There have been no deaths and only one case of disease progression after one year of therapy.
The patients generally tolerated the regimen very well, Dr. Wang said. There were no cases of lymphocytosis, bleeding, or atrial fibrillation after 332 combined cycles.
Nonhematological adverse events were primarily grade 1 or 2. Grade 3 fatigue was reported in approximately 10% of patients. There were no grade 4 adverse events.
“This study may provide a window of opportunity to reduce the frontline therapies and reduce the long-term toxicities such as secondary malignancies.” Dr. Wang said.
He acknowledged that four cycles of intensive chemotherapy is still toxic and that further efforts to reduce these toxicities are needed. The investigators are currently planning the Window II study, in which a fraction of patients will be treated with no chemotherapy at all, he said.
The study was supported by Pharmacyclics and Janssen. Dr. Wang disclosed receiving research grants and honoraria and serving as a consultant for the companies.
Lugano, Switzerland – It’s not the end of chemotherapy for young patients with newly diagnosed mantle cell lymphoma (MCL), but it’s a start.
For these patients, induction with a combination of ibrutinib and rituximab, followed by shorter cycles of chemoimmunotherapy, was associated in an early study with an objective response rate of 100%, including 90% complete responses (CR), reported Michael Wang, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“This is the first time for a chemo-free therapy – ibrutinib/rituximab – to achieve an overall response rate of 100%. This has an unprecedented efficacy in the frontline in young patients with mantle-cell lymphoma,” he said at the 14th International Congress on Malignant Lymphoma.
In patients with relapsed or refractory MCL, the combination of ibrutinib and rituximab has been associated with durable responses in 88% of patients. The success of the combination suggests that fit patients younger than age 65 years with newly diagnosed MCL might benefit from a chemotherapy-free induction regimen with ibrutinib and rituximab, followed by consolidation with a short but intense course of chemoimmunotherapy, Dr. Wang said.
He presented updated results from the phase II Window I study, first results of which were reported at the 2016 meeting of the American Society of Hematology.
“Frontline therapy is the most important therapy for mantle cell lymphoma, because mantle cell lymphoma cells are most vulnerable to frontline attack. If the frontline therapy is good enough, it could kill all the mantle cell lymphoma cells, therefore leaving no chance for secondary resistance, and thereby (resulting in) long-term survival. And it is really my belief that if we ideally optimized the frontline therapy, that would be a shortcut to a cure,” he said.
To test this idea, Dr. Wang and MD Anderson colleagues initiated a phase II trial at their institution with 50 patients age 65 years or under with newly diagnosed, CD20-positive and Cyclin D1-positive MCL.
A total of 50 patients age 65 years or younger (median age 54) with newly diagnosed, untreated MCL underwent induction with continuous daily ibrutinib 560 mg, plus rituximab 375 mg/m2 administered weekly for 4 weeks during cycle 1 and on day 1 of cycles 3-12. Consolidation consisted of rituximab plus hyper-CVAD (hyper-fractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone), alternating every 28 days with rituximab plus high-dose methotrexate–cytarabine.
Patients who had complete responses to induction received four cycles of chemoimmunotherapy, while those who experienced disease progression and those who had partial responses received chemoimmunotherapy for two cycles beyond the point of complete remissions.
At the time of the presentation, all 50 patients were evaluable for the induction phase (part 2), and 47 were evaluable for both induction and consolidation (part 2) .Of the evaluable patients, the overall response rate (ORR) to chemotherapy-free induction therapy alone (Part 1 ) was 100% (50), with CR in 90% of patients and partial responses (PR) in 10%. Of the 47 patients evaluable for part 2 (chemoimmunotherapy), all had CRs, for an ORR of 100%.
Dr. Wang noted that one patient had a dramatic radiographic reduction in spleen size following just two cycles of chemotherapy-free induction, and two other patients had similar reductions after four and six cycles, respectively.
After a median follow-up of 15.9 months, neither the median duration of response, progression-free survival, nor overall survival have been reached. There have been no deaths and only one case of disease progression after one year of therapy.
The patients generally tolerated the regimen very well, Dr. Wang said. There were no cases of lymphocytosis, bleeding, or atrial fibrillation after 332 combined cycles.
Nonhematological adverse events were primarily grade 1 or 2. Grade 3 fatigue was reported in approximately 10% of patients. There were no grade 4 adverse events.
“This study may provide a window of opportunity to reduce the frontline therapies and reduce the long-term toxicities such as secondary malignancies.” Dr. Wang said.
He acknowledged that four cycles of intensive chemotherapy is still toxic and that further efforts to reduce these toxicities are needed. The investigators are currently planning the Window II study, in which a fraction of patients will be treated with no chemotherapy at all, he said.
The study was supported by Pharmacyclics and Janssen. Dr. Wang disclosed receiving research grants and honoraria and serving as a consultant for the companies.
AT14-ICML
Key clinical point: A chemotherapy-free induction regimen with ibrutinib and rituximab was associated with high response rates in patients with newly diagnosed mantle cell lymphoma (MCL).
Major finding: The overall response rate after induction was 100%, including 90% complete responses.
Data source: Update results from phase II investigator-initiated study in 50 patients aged 65 years and younger with MCL.
Disclosures: The study was supported by Pharmacyclics and Janssen. Dr. Wang disclosed receiving research grants and honoraria and serving as a consultant for the companies.
Chemo-free triplet produces ‘favorable’ results in advanced disease

LUGANO, SWITZERLAND—A chemotherapy-free combination regimen has demonstrated “favorable” safety and efficacy in patients with advanced chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and non-Hodgkin lymphoma (NHL), according to researchers.
They found that treatment with ublituximab, umbralisib, and ibrutinib produced responses in patients with CLL/SLL, marginal zone lymphoma (MZL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B-cell lymphoma (DLBCL).
Many of these patients are still receiving the combination, some of them beyond 1 year, said Lorretta Nastoupil, MD, of MD Anderson Cancer Center in Houston, Texas.
She presented results with the treatment at the 14th International Conference on Malignant Lymphoma (ICML).
The research was sponsored by TG Therapeutics, the company developing ublituximab (TG-1101) and umbralisib (TGR-1202).
Patients and treatment
Dr Nastoupil presented data on 38 patients—20 with CLL/SLL, and 18 with NHL. Three of the CLL/SLL patients were treatment-naïve. The rest had relapsed/refractory disease.
All NHL patients had relapsed/refractory disease—6 with DLBCL, 6 with FL, 4 with MCL, and 2 with MZL.
For the entire cohort, the median age was 65 (range, 32-85), and most patients (n=29) were male. They had received a median of 3 prior treatment regimens (range, 0-6).
In this trial, the patients received:
- Ublituximab at 900 mg
- Ibrutinib at 420 mg (CLL/SLL) or 560 mg (NHL)
- Umbralisib at 400 mg, 600 mg, or 800 mg.
Eighty-one percent of patients have been on study for more than 6 months. The median time on study is 11.1 months (range, 0.4 to 30+ months).
Safety
There was 1 dose-limiting toxicity in the CLL cohort (umbralisib at 400 mg)—reactivated varicella zoster. And 2 patients discontinued treatment due to an adverse event (AE)—1 due to sepsis and 1 due to pneumonia.
Neutropenia (18%) and pneumonia (11%) were the only grade 3/4 AEs that occurred in more than 10% of patients. Other grade 3/4 AEs included thrombocytopenia (8%), diarrhea (3%), dizziness (3%), pyrexia (3%), rash (3%), anemia (3%), dyspnea (3%), and stomatitis (3%).
The most common AEs of any grade were diarrhea (47%), fatigue (47%), dizziness (37%), insomnia (34%), nausea (34%), neutropenia (32%), cough (32%), and infusion-related reactions (32%).
Efficacy
Thirty-six patients were evaluable for efficacy—19 with CLL/SLL and 17 with NHL patients. Two patients discontinued treatment before the first efficacy assessment—1 due to pneumonia and 1 at investigator discretion.
For the entire cohort, the overall response rate (ORR) was 83%.
In the CLL/SLL cohort, the ORR was 100% (19/19), and the complete response (CR) rate was 32% (n=6). However, 4 of the 6 CRs are pending bone marrow confirmation.
Dr Nastoupil noted that 8 of the CLL patients had a 17p and/or 11q deletion, and 3 had previously received treatment with a BTK and/or PI3Kδ inhibitor.
One patient who was refractory to both idelalisib and ibrutinib achieved a CR with the triplet regimen, and this response has been ongoing for more than 1.5 years.
Among patients with NHL, the ORR was 100% in patients with MZL (2/2) and MCL (4/4). The ORR was 80% (4/5) in FL patients, and 17% (1/6) in DLBCL patients.
The CR rate was 50% in patients with MZL (1/2) and MCL (2/4) and 20% in patients with FL (1/5).
Dr Nastoupil pointed out that the FL patients were heavily pretreated. Two of them had received an autologous stem cell transplant, 1 was refractory to prior ibrutinib treatment, and 1 had received 5 prior lines of rituximab-based therapy.
She also noted that the DLBCL patients had a median of 4 prior therapies, and 4 of these patients had non-GCB DLBCL, including the only patient who responded to the triplet.
“[T]he combination of ublituximab, umbralisib, and ibrutinib in advanced CLL and NHL demonstrated a favorable toxicity profile as well as favorable efficacy,” Dr Nastoupil said in closing.
“[This] suggests umbralisib may be safely combined with other targeted agents to overcome mechanisms of resistance.” ![]()
LUGANO, SWITZERLAND—A chemotherapy-free combination regimen has demonstrated “favorable” safety and efficacy in patients with advanced chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and non-Hodgkin lymphoma (NHL), according to researchers.
They found that treatment with ublituximab, umbralisib, and ibrutinib produced responses in patients with CLL/SLL, marginal zone lymphoma (MZL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B-cell lymphoma (DLBCL).
Many of these patients are still receiving the combination, some of them beyond 1 year, said Lorretta Nastoupil, MD, of MD Anderson Cancer Center in Houston, Texas.
She presented results with the treatment at the 14th International Conference on Malignant Lymphoma (ICML).
The research was sponsored by TG Therapeutics, the company developing ublituximab (TG-1101) and umbralisib (TGR-1202).
Patients and treatment
Dr Nastoupil presented data on 38 patients—20 with CLL/SLL, and 18 with NHL. Three of the CLL/SLL patients were treatment-naïve. The rest had relapsed/refractory disease.
All NHL patients had relapsed/refractory disease—6 with DLBCL, 6 with FL, 4 with MCL, and 2 with MZL.
For the entire cohort, the median age was 65 (range, 32-85), and most patients (n=29) were male. They had received a median of 3 prior treatment regimens (range, 0-6).
In this trial, the patients received:
- Ublituximab at 900 mg
- Ibrutinib at 420 mg (CLL/SLL) or 560 mg (NHL)
- Umbralisib at 400 mg, 600 mg, or 800 mg.
Eighty-one percent of patients have been on study for more than 6 months. The median time on study is 11.1 months (range, 0.4 to 30+ months).
Safety
There was 1 dose-limiting toxicity in the CLL cohort (umbralisib at 400 mg)—reactivated varicella zoster. And 2 patients discontinued treatment due to an adverse event (AE)—1 due to sepsis and 1 due to pneumonia.
Neutropenia (18%) and pneumonia (11%) were the only grade 3/4 AEs that occurred in more than 10% of patients. Other grade 3/4 AEs included thrombocytopenia (8%), diarrhea (3%), dizziness (3%), pyrexia (3%), rash (3%), anemia (3%), dyspnea (3%), and stomatitis (3%).
The most common AEs of any grade were diarrhea (47%), fatigue (47%), dizziness (37%), insomnia (34%), nausea (34%), neutropenia (32%), cough (32%), and infusion-related reactions (32%).
Efficacy
Thirty-six patients were evaluable for efficacy—19 with CLL/SLL and 17 with NHL patients. Two patients discontinued treatment before the first efficacy assessment—1 due to pneumonia and 1 at investigator discretion.
For the entire cohort, the overall response rate (ORR) was 83%.
In the CLL/SLL cohort, the ORR was 100% (19/19), and the complete response (CR) rate was 32% (n=6). However, 4 of the 6 CRs are pending bone marrow confirmation.
Dr Nastoupil noted that 8 of the CLL patients had a 17p and/or 11q deletion, and 3 had previously received treatment with a BTK and/or PI3Kδ inhibitor.
One patient who was refractory to both idelalisib and ibrutinib achieved a CR with the triplet regimen, and this response has been ongoing for more than 1.5 years.
Among patients with NHL, the ORR was 100% in patients with MZL (2/2) and MCL (4/4). The ORR was 80% (4/5) in FL patients, and 17% (1/6) in DLBCL patients.
The CR rate was 50% in patients with MZL (1/2) and MCL (2/4) and 20% in patients with FL (1/5).
Dr Nastoupil pointed out that the FL patients were heavily pretreated. Two of them had received an autologous stem cell transplant, 1 was refractory to prior ibrutinib treatment, and 1 had received 5 prior lines of rituximab-based therapy.
She also noted that the DLBCL patients had a median of 4 prior therapies, and 4 of these patients had non-GCB DLBCL, including the only patient who responded to the triplet.
“[T]he combination of ublituximab, umbralisib, and ibrutinib in advanced CLL and NHL demonstrated a favorable toxicity profile as well as favorable efficacy,” Dr Nastoupil said in closing.
“[This] suggests umbralisib may be safely combined with other targeted agents to overcome mechanisms of resistance.” ![]()
LUGANO, SWITZERLAND—A chemotherapy-free combination regimen has demonstrated “favorable” safety and efficacy in patients with advanced chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and non-Hodgkin lymphoma (NHL), according to researchers.
They found that treatment with ublituximab, umbralisib, and ibrutinib produced responses in patients with CLL/SLL, marginal zone lymphoma (MZL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B-cell lymphoma (DLBCL).
Many of these patients are still receiving the combination, some of them beyond 1 year, said Lorretta Nastoupil, MD, of MD Anderson Cancer Center in Houston, Texas.
She presented results with the treatment at the 14th International Conference on Malignant Lymphoma (ICML).
The research was sponsored by TG Therapeutics, the company developing ublituximab (TG-1101) and umbralisib (TGR-1202).
Patients and treatment
Dr Nastoupil presented data on 38 patients—20 with CLL/SLL, and 18 with NHL. Three of the CLL/SLL patients were treatment-naïve. The rest had relapsed/refractory disease.
All NHL patients had relapsed/refractory disease—6 with DLBCL, 6 with FL, 4 with MCL, and 2 with MZL.
For the entire cohort, the median age was 65 (range, 32-85), and most patients (n=29) were male. They had received a median of 3 prior treatment regimens (range, 0-6).
In this trial, the patients received:
- Ublituximab at 900 mg
- Ibrutinib at 420 mg (CLL/SLL) or 560 mg (NHL)
- Umbralisib at 400 mg, 600 mg, or 800 mg.
Eighty-one percent of patients have been on study for more than 6 months. The median time on study is 11.1 months (range, 0.4 to 30+ months).
Safety
There was 1 dose-limiting toxicity in the CLL cohort (umbralisib at 400 mg)—reactivated varicella zoster. And 2 patients discontinued treatment due to an adverse event (AE)—1 due to sepsis and 1 due to pneumonia.
Neutropenia (18%) and pneumonia (11%) were the only grade 3/4 AEs that occurred in more than 10% of patients. Other grade 3/4 AEs included thrombocytopenia (8%), diarrhea (3%), dizziness (3%), pyrexia (3%), rash (3%), anemia (3%), dyspnea (3%), and stomatitis (3%).
The most common AEs of any grade were diarrhea (47%), fatigue (47%), dizziness (37%), insomnia (34%), nausea (34%), neutropenia (32%), cough (32%), and infusion-related reactions (32%).
Efficacy
Thirty-six patients were evaluable for efficacy—19 with CLL/SLL and 17 with NHL patients. Two patients discontinued treatment before the first efficacy assessment—1 due to pneumonia and 1 at investigator discretion.
For the entire cohort, the overall response rate (ORR) was 83%.
In the CLL/SLL cohort, the ORR was 100% (19/19), and the complete response (CR) rate was 32% (n=6). However, 4 of the 6 CRs are pending bone marrow confirmation.
Dr Nastoupil noted that 8 of the CLL patients had a 17p and/or 11q deletion, and 3 had previously received treatment with a BTK and/or PI3Kδ inhibitor.
One patient who was refractory to both idelalisib and ibrutinib achieved a CR with the triplet regimen, and this response has been ongoing for more than 1.5 years.
Among patients with NHL, the ORR was 100% in patients with MZL (2/2) and MCL (4/4). The ORR was 80% (4/5) in FL patients, and 17% (1/6) in DLBCL patients.
The CR rate was 50% in patients with MZL (1/2) and MCL (2/4) and 20% in patients with FL (1/5).
Dr Nastoupil pointed out that the FL patients were heavily pretreated. Two of them had received an autologous stem cell transplant, 1 was refractory to prior ibrutinib treatment, and 1 had received 5 prior lines of rituximab-based therapy.
She also noted that the DLBCL patients had a median of 4 prior therapies, and 4 of these patients had non-GCB DLBCL, including the only patient who responded to the triplet.
“[T]he combination of ublituximab, umbralisib, and ibrutinib in advanced CLL and NHL demonstrated a favorable toxicity profile as well as favorable efficacy,” Dr Nastoupil said in closing.
“[This] suggests umbralisib may be safely combined with other targeted agents to overcome mechanisms of resistance.” ![]()
FDA approves rituximab + hyaluronidase human for FL, DLBCL, and CLL
The Food and Drug Administration has approved rituximab plus hyaluronidase human for adult patients with follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), and chronic lymphocytic leukemia (CLL).
The combination product, to be marketed as Rituxan Hycela, is administered subcutaneously, shortening administration time to 5 to 7 minutes as compared with the several hours needed for intravenous infusion, the FDA said in a statement.
Approval was based on noninferior rituximab trough concentrations for the subcutaneously administered combination, compared with intravenous rituximab, and comparable efficacy and safety results as shown in multiple randomized clinical trials.
The most common adverse events seen with the combination in patients with FL included infections, neutropenia, nausea, constipation, cough, and fatigue. In patients with DLBCL, the most common adverse events were infections, neutropenia, alopecia, nausea, and anemia; in CLL patients, infections, neutropenia, nausea, thrombocytopenia, pyrexia, vomiting, and injection site erythema occurred most commonly.
The combination is indicated for the following previously approved indications for rituximab:
- Relapsed or refractory FL as a single agent.
- Previously untreated FL in combination with first line chemotherapy and, in patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy.
- Nonprogressing (including stable disease) FL as a single agent after first-line cyclophosphamide, vincristine, and prednisone chemotherapy.
- Previously untreated DLBCL in combination with cyclophosphamide, doxorubicin, vincristine, prednisone or other anthracycline-based chemotherapy regimens.
- Previously untreated and previously treated CLL in combination with fludarabine and cyclophosphamide.
The recommended doses are 1,400 mg rituximab and 23,400 units hyaluronidase human for FL and DLBCL and 1,600 mg rituximab and 26,800 units hyaluronidase human for CLL. The combination treatment should be initiated only after patients have received at least one full dose of a rituximab product by intravenous infusion, according to the prescribing information.
Rituxan Hycela is marketed by Genentech.
The Food and Drug Administration has approved rituximab plus hyaluronidase human for adult patients with follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), and chronic lymphocytic leukemia (CLL).
The combination product, to be marketed as Rituxan Hycela, is administered subcutaneously, shortening administration time to 5 to 7 minutes as compared with the several hours needed for intravenous infusion, the FDA said in a statement.
Approval was based on noninferior rituximab trough concentrations for the subcutaneously administered combination, compared with intravenous rituximab, and comparable efficacy and safety results as shown in multiple randomized clinical trials.
The most common adverse events seen with the combination in patients with FL included infections, neutropenia, nausea, constipation, cough, and fatigue. In patients with DLBCL, the most common adverse events were infections, neutropenia, alopecia, nausea, and anemia; in CLL patients, infections, neutropenia, nausea, thrombocytopenia, pyrexia, vomiting, and injection site erythema occurred most commonly.
The combination is indicated for the following previously approved indications for rituximab:
- Relapsed or refractory FL as a single agent.
- Previously untreated FL in combination with first line chemotherapy and, in patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy.
- Nonprogressing (including stable disease) FL as a single agent after first-line cyclophosphamide, vincristine, and prednisone chemotherapy.
- Previously untreated DLBCL in combination with cyclophosphamide, doxorubicin, vincristine, prednisone or other anthracycline-based chemotherapy regimens.
- Previously untreated and previously treated CLL in combination with fludarabine and cyclophosphamide.
The recommended doses are 1,400 mg rituximab and 23,400 units hyaluronidase human for FL and DLBCL and 1,600 mg rituximab and 26,800 units hyaluronidase human for CLL. The combination treatment should be initiated only after patients have received at least one full dose of a rituximab product by intravenous infusion, according to the prescribing information.
Rituxan Hycela is marketed by Genentech.
The Food and Drug Administration has approved rituximab plus hyaluronidase human for adult patients with follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), and chronic lymphocytic leukemia (CLL).
The combination product, to be marketed as Rituxan Hycela, is administered subcutaneously, shortening administration time to 5 to 7 minutes as compared with the several hours needed for intravenous infusion, the FDA said in a statement.
Approval was based on noninferior rituximab trough concentrations for the subcutaneously administered combination, compared with intravenous rituximab, and comparable efficacy and safety results as shown in multiple randomized clinical trials.
The most common adverse events seen with the combination in patients with FL included infections, neutropenia, nausea, constipation, cough, and fatigue. In patients with DLBCL, the most common adverse events were infections, neutropenia, alopecia, nausea, and anemia; in CLL patients, infections, neutropenia, nausea, thrombocytopenia, pyrexia, vomiting, and injection site erythema occurred most commonly.
The combination is indicated for the following previously approved indications for rituximab:
- Relapsed or refractory FL as a single agent.
- Previously untreated FL in combination with first line chemotherapy and, in patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy.
- Nonprogressing (including stable disease) FL as a single agent after first-line cyclophosphamide, vincristine, and prednisone chemotherapy.
- Previously untreated DLBCL in combination with cyclophosphamide, doxorubicin, vincristine, prednisone or other anthracycline-based chemotherapy regimens.
- Previously untreated and previously treated CLL in combination with fludarabine and cyclophosphamide.
The recommended doses are 1,400 mg rituximab and 23,400 units hyaluronidase human for FL and DLBCL and 1,600 mg rituximab and 26,800 units hyaluronidase human for CLL. The combination treatment should be initiated only after patients have received at least one full dose of a rituximab product by intravenous infusion, according to the prescribing information.
Rituxan Hycela is marketed by Genentech.
Bendamustine plus rituximab may have edge for treating indolent NHL, MCL
CHICAGO – Overall survival was comparable at 5 years of follow up for three regimens in treatment-naive patients with indolent non-Hodgkin lymphoma (NHL) or mantle cell lymphoma (MCL), based on long-term results from the BRIGHT study.
While progression-free survival, event-free survival, and duration of response were significantly better with bendamustine plus rituximab (BR), overall survival at 5 years did not significantly differ in patients given this regimen and compared to patients given rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) or rituximab with cyclophosphamide, vincristine and prednisone (R-CVP), Ian Flinn, MD, of Tennessee Oncology, Nashville, reported at the annual meeting of the American Society of Clinical Oncology.

Quality of life was somewhat better for the patients given BR, but those patients were also at higher risk for secondary malignancies (42 vs. 24), most of which were squamous cell carcinomas, observed Dr. Kahl, professor of medicine at Washington University, St. Louis.
In BRIGHT, 224 treatment-naive patients with indolent NHL or MCL were randomized to receive BR and were compared to 223 similar patients who received either R-CHOP (104 patients) or R-CVP (119 patients). At least six cycles of therapy were completed by 203 patients in the BR group and by 196 in the R-CHOP/R-CVP group. Rituximab maintenance therapy was given to 43% of the BR group and to 45% of the R-CHOP/R-CVP group.

For BR and R-CHOP/R-CVP, the 5-year progression-free survival rate was 65.5% (95% CI, 58.5-71.6) and 55.8% (95% CI, 48.4-62.5), respectively. The overall survival rate for the entire patient group was 81.7% (75.7-86.3) and 85% (79.3-89.3) respectively. Comparing BR and R-CHOP/R-CVP, the hazard ratio (95% CI) for progression-free survival was 0.61 (0.45-0.85; P = .0025), the HR for event-free survival was 0.63 (0.46-0.84; P = .0020), the HR for duration of response was 0.66 (0.47-0.92; P = .0134), and the HR for overall survival was 1.15 (0.72-1.84; P = .5461).
Similar results were found in indolent NHL (progression-free survival 0.70 [0.49-1.01; P = .0582]) and MCL (progression-free survival 0.40 [0.21-0.75; P = .0035]), with the strongest effect in MCL, Dr. Flinn said.
Dr. Kahl noted that the advantages for the BR regimen include that it is not associated with alopecia, neuropathy, or steroid issues, and that it may extend progression-free survival and time to next treatment. On the other hand, R-CHOP is associated with less GI toxicity, rash, opportunistic infections, and prolonged cytopenia. Also, the BR regimen was associated with a higher risk of secondary cancers, primarily squamous cell carcinomas.
There were 42 secondary malignancies in the BR group and 24 in the R-CHOP/R-CVP group, Dr. Flinn reported.
It is theoretically possible that BR equals R-CHOP plus maintenance therapy from an efficacy perspective, Dr. Kahl said.
As virtually all excess adverse event fatalities occurred during maintenance therapy, it is possible that maintenance therapy after BR “does more harm than good.” This high priority issue “should be evaluated in the BRIGHT data set,” Dr. Kahl recommended.
Teva Branded Pharmaceutical Products R&D sponsored the study. Dr. Flinn had no relationships to disclose; two of his fellow researchers are Teva employees. Dr. Kahl disclosed serving as an adviser or consultant to Abbvie, Acerta Pharma, Celgene, Cell Therapeutics, Genentech/Roche, Incyte, Infinity Pharmaceuticals, Juno Therapeutics, Millennium, Pharmacyclics, Sandoz, and Seattle Genetics.
mdales@frontlinemedcom.com
On Twitter @maryjodales
CHICAGO – Overall survival was comparable at 5 years of follow up for three regimens in treatment-naive patients with indolent non-Hodgkin lymphoma (NHL) or mantle cell lymphoma (MCL), based on long-term results from the BRIGHT study.
While progression-free survival, event-free survival, and duration of response were significantly better with bendamustine plus rituximab (BR), overall survival at 5 years did not significantly differ in patients given this regimen and compared to patients given rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) or rituximab with cyclophosphamide, vincristine and prednisone (R-CVP), Ian Flinn, MD, of Tennessee Oncology, Nashville, reported at the annual meeting of the American Society of Clinical Oncology.
Quality of life was somewhat better for the patients given BR, but those patients were also at higher risk for secondary malignancies (42 vs. 24), most of which were squamous cell carcinomas, observed Dr. Kahl, professor of medicine at Washington University, St. Louis.
In BRIGHT, 224 treatment-naive patients with indolent NHL or MCL were randomized to receive BR and were compared to 223 similar patients who received either R-CHOP (104 patients) or R-CVP (119 patients). At least six cycles of therapy were completed by 203 patients in the BR group and by 196 in the R-CHOP/R-CVP group. Rituximab maintenance therapy was given to 43% of the BR group and to 45% of the R-CHOP/R-CVP group.
For BR and R-CHOP/R-CVP, the 5-year progression-free survival rate was 65.5% (95% CI, 58.5-71.6) and 55.8% (95% CI, 48.4-62.5), respectively. The overall survival rate for the entire patient group was 81.7% (75.7-86.3) and 85% (79.3-89.3) respectively. Comparing BR and R-CHOP/R-CVP, the hazard ratio (95% CI) for progression-free survival was 0.61 (0.45-0.85; P = .0025), the HR for event-free survival was 0.63 (0.46-0.84; P = .0020), the HR for duration of response was 0.66 (0.47-0.92; P = .0134), and the HR for overall survival was 1.15 (0.72-1.84; P = .5461).
Similar results were found in indolent NHL (progression-free survival 0.70 [0.49-1.01; P = .0582]) and MCL (progression-free survival 0.40 [0.21-0.75; P = .0035]), with the strongest effect in MCL, Dr. Flinn said.
Dr. Kahl noted that the advantages for the BR regimen include that it is not associated with alopecia, neuropathy, or steroid issues, and that it may extend progression-free survival and time to next treatment. On the other hand, R-CHOP is associated with less GI toxicity, rash, opportunistic infections, and prolonged cytopenia. Also, the BR regimen was associated with a higher risk of secondary cancers, primarily squamous cell carcinomas.
There were 42 secondary malignancies in the BR group and 24 in the R-CHOP/R-CVP group, Dr. Flinn reported.
It is theoretically possible that BR equals R-CHOP plus maintenance therapy from an efficacy perspective, Dr. Kahl said.
As virtually all excess adverse event fatalities occurred during maintenance therapy, it is possible that maintenance therapy after BR “does more harm than good.” This high priority issue “should be evaluated in the BRIGHT data set,” Dr. Kahl recommended.
Teva Branded Pharmaceutical Products R&D sponsored the study. Dr. Flinn had no relationships to disclose; two of his fellow researchers are Teva employees. Dr. Kahl disclosed serving as an adviser or consultant to Abbvie, Acerta Pharma, Celgene, Cell Therapeutics, Genentech/Roche, Incyte, Infinity Pharmaceuticals, Juno Therapeutics, Millennium, Pharmacyclics, Sandoz, and Seattle Genetics.
mdales@frontlinemedcom.com
On Twitter @maryjodales
CHICAGO – Overall survival was comparable at 5 years of follow up for three regimens in treatment-naive patients with indolent non-Hodgkin lymphoma (NHL) or mantle cell lymphoma (MCL), based on long-term results from the BRIGHT study.
While progression-free survival, event-free survival, and duration of response were significantly better with bendamustine plus rituximab (BR), overall survival at 5 years did not significantly differ in patients given this regimen and compared to patients given rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) or rituximab with cyclophosphamide, vincristine and prednisone (R-CVP), Ian Flinn, MD, of Tennessee Oncology, Nashville, reported at the annual meeting of the American Society of Clinical Oncology.
Quality of life was somewhat better for the patients given BR, but those patients were also at higher risk for secondary malignancies (42 vs. 24), most of which were squamous cell carcinomas, observed Dr. Kahl, professor of medicine at Washington University, St. Louis.
In BRIGHT, 224 treatment-naive patients with indolent NHL or MCL were randomized to receive BR and were compared to 223 similar patients who received either R-CHOP (104 patients) or R-CVP (119 patients). At least six cycles of therapy were completed by 203 patients in the BR group and by 196 in the R-CHOP/R-CVP group. Rituximab maintenance therapy was given to 43% of the BR group and to 45% of the R-CHOP/R-CVP group.
For BR and R-CHOP/R-CVP, the 5-year progression-free survival rate was 65.5% (95% CI, 58.5-71.6) and 55.8% (95% CI, 48.4-62.5), respectively. The overall survival rate for the entire patient group was 81.7% (75.7-86.3) and 85% (79.3-89.3) respectively. Comparing BR and R-CHOP/R-CVP, the hazard ratio (95% CI) for progression-free survival was 0.61 (0.45-0.85; P = .0025), the HR for event-free survival was 0.63 (0.46-0.84; P = .0020), the HR for duration of response was 0.66 (0.47-0.92; P = .0134), and the HR for overall survival was 1.15 (0.72-1.84; P = .5461).
Similar results were found in indolent NHL (progression-free survival 0.70 [0.49-1.01; P = .0582]) and MCL (progression-free survival 0.40 [0.21-0.75; P = .0035]), with the strongest effect in MCL, Dr. Flinn said.
Dr. Kahl noted that the advantages for the BR regimen include that it is not associated with alopecia, neuropathy, or steroid issues, and that it may extend progression-free survival and time to next treatment. On the other hand, R-CHOP is associated with less GI toxicity, rash, opportunistic infections, and prolonged cytopenia. Also, the BR regimen was associated with a higher risk of secondary cancers, primarily squamous cell carcinomas.
There were 42 secondary malignancies in the BR group and 24 in the R-CHOP/R-CVP group, Dr. Flinn reported.
It is theoretically possible that BR equals R-CHOP plus maintenance therapy from an efficacy perspective, Dr. Kahl said.
As virtually all excess adverse event fatalities occurred during maintenance therapy, it is possible that maintenance therapy after BR “does more harm than good.” This high priority issue “should be evaluated in the BRIGHT data set,” Dr. Kahl recommended.
Teva Branded Pharmaceutical Products R&D sponsored the study. Dr. Flinn had no relationships to disclose; two of his fellow researchers are Teva employees. Dr. Kahl disclosed serving as an adviser or consultant to Abbvie, Acerta Pharma, Celgene, Cell Therapeutics, Genentech/Roche, Incyte, Infinity Pharmaceuticals, Juno Therapeutics, Millennium, Pharmacyclics, Sandoz, and Seattle Genetics.
mdales@frontlinemedcom.com
On Twitter @maryjodales
AT ASCO 2017
Key clinical point:
Major finding: For BR and R-CHOP/R-CVP, the 5-year progression-free survival rate was 65.5% (95% CI, 58.5-71.6) and 55.8% (95% CI, 48.4-62.5), respectively.
Data source: In BRIGHT, 224 treatment-naive patients with indolent non-Hodgkin lymphoma or mantle cell lymphoma were randomized to receive BR and were compared to 223 similar patients who received either R-CHOP (104 patients) or R-CVP (119 patients).
Disclosures: Teva Branded Pharmaceutical Products R&D sponsored the study. Dr. Flinn had no relationships to disclose; two of his fellow researchers are Teva employees. Dr. Kahl disclosed serving as an adviser or consultant to Abbvie, Acerta Pharma, Celgene, Cell Therapeutics, Genentech/Roche, Incyte, Infinity Pharmaceuticals, Juno Therapeutics, Millennium, Pharmacyclics, Sandoz, and Seattle Genetics.
Inhibitor elicits responses in heavily pretreated FL, DLBCL

LUGANO, SWITZERLAND—Interim results of a phase 2 trial suggest tazemetostat can be effective in patients with heavily pretreated, relapsed or refractory non-Hodgkin lymphoma.
The EZH2 inhibitor produced the highest overall response rate in patients with EZH2-mutated follicular lymphoma (FL), followed by EZH2-mutated diffuse large B-cell lymphoma (DLBCL).
However, the drug also produced complete responses in FL and DLBCL patients with wild-type EZH2.
“If we had focused [only] on patients with EZH2 mutations, we would have missed those other complete responders in the wild-type setting,” said study investigator Franck Morschhauser, MD, PhD, of Centre Hospitalier Régional Universitaire de Lille in France.
He presented results of the trial* during the plenary session of the 14th International Conference on Malignant Lymphoma (ICML). The research was sponsored by Epizyme, the company developing tazemetostat.
The trial enrolled patients with relapsed or refractory DLBCL or FL who had received at least 2 prior therapies. The patients received tazemetostat at 800 mg twice daily until disease progression or study withdrawal.
Efficacy in FL
Dr Morschhauser presented efficacy data on 67 patients with FL. Thirteen had EZH2 mutations, and 54 had wild-type EZH2. The median age was 62 in the mutated group and 61 in the wild-type group.
Both groups had a median of 4 prior lines of therapy. Fifty-four percent of EZH2-mutated patients were refractory to their last treatment, as were 48% of wild-type patients.
The median time from diagnosis was 7.4 years in mutated patients and 4.9 years in wild-type patients. The median time from last therapy was 13 weeks and 41.3 weeks, respectively.
The overall response rate was 92% (12/13) in EZH2-mutated patients and 26% (14/54) in wild-type patients. The complete response rates were 8% (n=1) and 6% (n=3), respectively.
The median time to first response was 11.9 weeks and 15.2 weeks, respectively.
None of the EZH2-mutated patients have progressed, but 13 (24%) wild-type patients have.
Forty-eight percent of all FL patients remain on study. One EZH2-mutated patient with stable disease is still on study, as are 23 wild-type patients with stable disease.
Efficacy in DLBCL
Dr Morschhauser presented data on 137 patients with DLBCL, 17 with EZH2 mutations and 120 with wild-type EZH2. The median age was 61 in the mutated group and 69 in the wild-type group.
Both groups had a median of 3 prior lines of therapy. Eighty-two percent of EZH2-mutated patients were refractory to their last treatment, as were 63% of wild-type patients.
The median time from diagnosis was 1 year in mutated patients and 2 years in wild-type patients. The median time from last therapy was 8.6 weeks and 11.6 weeks, respectively.
The overall response rate was 29% (5/17) in EZH2-mutated patients and 15% (18/119) in wild-type patients. The complete response rates were 0% (n=0) and 8% (n=10), respectively.
The median time to first response was 8.3 weeks and 8.5 weeks, respectively.
Six (35%) of the EZH2-mutated patients have progressed, as have 60 (50%) wild-type patients.
Twelve percent of all DLBCL patients remain on study. One EZH2-mutated patient with stable disease is still on therapy, as are 4 wild-type patients with stable disease.
Predictors of response
Dr Morschhauser and his colleagues performed next-generation sequencing of samples from 92 patients in an attempt to identify predictors of response to tazemetostat.
The data suggested that EZH2 and MYD88 activating mutations are positive predictors of response, and negative predictors include MYC, TP53, and HIST1H1E.
Safety
Safety data were available for 210 patients. The overall rate of treatment-related adverse events (AEs) was 59%, the rate of grade 3 or higher treatment-related AEs was 18%, and the rate of serious treatment-related AEs was 10%.
There were treatment-related AEs leading to dose interruption (15%), dose reduction (3%), and discontinuation of tazemetostat (2%).
The most common treatment-related AEs were nausea (14%), thrombocytopenia (13%), anemia (10%), neutropenia (9%), diarrhea (8%), asthenia (8%), and fatigue (7%).
Dr Morschhauser said these results “confirm that tazemetostat is quite safe” in this patient population, and enrollment in this trial is ongoing. ![]()
*Data in the abstract differ from the presentation.
LUGANO, SWITZERLAND—Interim results of a phase 2 trial suggest tazemetostat can be effective in patients with heavily pretreated, relapsed or refractory non-Hodgkin lymphoma.
The EZH2 inhibitor produced the highest overall response rate in patients with EZH2-mutated follicular lymphoma (FL), followed by EZH2-mutated diffuse large B-cell lymphoma (DLBCL).
However, the drug also produced complete responses in FL and DLBCL patients with wild-type EZH2.
“If we had focused [only] on patients with EZH2 mutations, we would have missed those other complete responders in the wild-type setting,” said study investigator Franck Morschhauser, MD, PhD, of Centre Hospitalier Régional Universitaire de Lille in France.
He presented results of the trial* during the plenary session of the 14th International Conference on Malignant Lymphoma (ICML). The research was sponsored by Epizyme, the company developing tazemetostat.
The trial enrolled patients with relapsed or refractory DLBCL or FL who had received at least 2 prior therapies. The patients received tazemetostat at 800 mg twice daily until disease progression or study withdrawal.
Efficacy in FL
Dr Morschhauser presented efficacy data on 67 patients with FL. Thirteen had EZH2 mutations, and 54 had wild-type EZH2. The median age was 62 in the mutated group and 61 in the wild-type group.
Both groups had a median of 4 prior lines of therapy. Fifty-four percent of EZH2-mutated patients were refractory to their last treatment, as were 48% of wild-type patients.
The median time from diagnosis was 7.4 years in mutated patients and 4.9 years in wild-type patients. The median time from last therapy was 13 weeks and 41.3 weeks, respectively.
The overall response rate was 92% (12/13) in EZH2-mutated patients and 26% (14/54) in wild-type patients. The complete response rates were 8% (n=1) and 6% (n=3), respectively.
The median time to first response was 11.9 weeks and 15.2 weeks, respectively.
None of the EZH2-mutated patients have progressed, but 13 (24%) wild-type patients have.
Forty-eight percent of all FL patients remain on study. One EZH2-mutated patient with stable disease is still on study, as are 23 wild-type patients with stable disease.
Efficacy in DLBCL
Dr Morschhauser presented data on 137 patients with DLBCL, 17 with EZH2 mutations and 120 with wild-type EZH2. The median age was 61 in the mutated group and 69 in the wild-type group.
Both groups had a median of 3 prior lines of therapy. Eighty-two percent of EZH2-mutated patients were refractory to their last treatment, as were 63% of wild-type patients.
The median time from diagnosis was 1 year in mutated patients and 2 years in wild-type patients. The median time from last therapy was 8.6 weeks and 11.6 weeks, respectively.
The overall response rate was 29% (5/17) in EZH2-mutated patients and 15% (18/119) in wild-type patients. The complete response rates were 0% (n=0) and 8% (n=10), respectively.
The median time to first response was 8.3 weeks and 8.5 weeks, respectively.
Six (35%) of the EZH2-mutated patients have progressed, as have 60 (50%) wild-type patients.
Twelve percent of all DLBCL patients remain on study. One EZH2-mutated patient with stable disease is still on therapy, as are 4 wild-type patients with stable disease.
Predictors of response
Dr Morschhauser and his colleagues performed next-generation sequencing of samples from 92 patients in an attempt to identify predictors of response to tazemetostat.
The data suggested that EZH2 and MYD88 activating mutations are positive predictors of response, and negative predictors include MYC, TP53, and HIST1H1E.
Safety
Safety data were available for 210 patients. The overall rate of treatment-related adverse events (AEs) was 59%, the rate of grade 3 or higher treatment-related AEs was 18%, and the rate of serious treatment-related AEs was 10%.
There were treatment-related AEs leading to dose interruption (15%), dose reduction (3%), and discontinuation of tazemetostat (2%).
The most common treatment-related AEs were nausea (14%), thrombocytopenia (13%), anemia (10%), neutropenia (9%), diarrhea (8%), asthenia (8%), and fatigue (7%).
Dr Morschhauser said these results “confirm that tazemetostat is quite safe” in this patient population, and enrollment in this trial is ongoing. ![]()
*Data in the abstract differ from the presentation.
LUGANO, SWITZERLAND—Interim results of a phase 2 trial suggest tazemetostat can be effective in patients with heavily pretreated, relapsed or refractory non-Hodgkin lymphoma.
The EZH2 inhibitor produced the highest overall response rate in patients with EZH2-mutated follicular lymphoma (FL), followed by EZH2-mutated diffuse large B-cell lymphoma (DLBCL).
However, the drug also produced complete responses in FL and DLBCL patients with wild-type EZH2.
“If we had focused [only] on patients with EZH2 mutations, we would have missed those other complete responders in the wild-type setting,” said study investigator Franck Morschhauser, MD, PhD, of Centre Hospitalier Régional Universitaire de Lille in France.
He presented results of the trial* during the plenary session of the 14th International Conference on Malignant Lymphoma (ICML). The research was sponsored by Epizyme, the company developing tazemetostat.
The trial enrolled patients with relapsed or refractory DLBCL or FL who had received at least 2 prior therapies. The patients received tazemetostat at 800 mg twice daily until disease progression or study withdrawal.
Efficacy in FL
Dr Morschhauser presented efficacy data on 67 patients with FL. Thirteen had EZH2 mutations, and 54 had wild-type EZH2. The median age was 62 in the mutated group and 61 in the wild-type group.
Both groups had a median of 4 prior lines of therapy. Fifty-four percent of EZH2-mutated patients were refractory to their last treatment, as were 48% of wild-type patients.
The median time from diagnosis was 7.4 years in mutated patients and 4.9 years in wild-type patients. The median time from last therapy was 13 weeks and 41.3 weeks, respectively.
The overall response rate was 92% (12/13) in EZH2-mutated patients and 26% (14/54) in wild-type patients. The complete response rates were 8% (n=1) and 6% (n=3), respectively.
The median time to first response was 11.9 weeks and 15.2 weeks, respectively.
None of the EZH2-mutated patients have progressed, but 13 (24%) wild-type patients have.
Forty-eight percent of all FL patients remain on study. One EZH2-mutated patient with stable disease is still on study, as are 23 wild-type patients with stable disease.
Efficacy in DLBCL
Dr Morschhauser presented data on 137 patients with DLBCL, 17 with EZH2 mutations and 120 with wild-type EZH2. The median age was 61 in the mutated group and 69 in the wild-type group.
Both groups had a median of 3 prior lines of therapy. Eighty-two percent of EZH2-mutated patients were refractory to their last treatment, as were 63% of wild-type patients.
The median time from diagnosis was 1 year in mutated patients and 2 years in wild-type patients. The median time from last therapy was 8.6 weeks and 11.6 weeks, respectively.
The overall response rate was 29% (5/17) in EZH2-mutated patients and 15% (18/119) in wild-type patients. The complete response rates were 0% (n=0) and 8% (n=10), respectively.
The median time to first response was 8.3 weeks and 8.5 weeks, respectively.
Six (35%) of the EZH2-mutated patients have progressed, as have 60 (50%) wild-type patients.
Twelve percent of all DLBCL patients remain on study. One EZH2-mutated patient with stable disease is still on therapy, as are 4 wild-type patients with stable disease.
Predictors of response
Dr Morschhauser and his colleagues performed next-generation sequencing of samples from 92 patients in an attempt to identify predictors of response to tazemetostat.
The data suggested that EZH2 and MYD88 activating mutations are positive predictors of response, and negative predictors include MYC, TP53, and HIST1H1E.
Safety
Safety data were available for 210 patients. The overall rate of treatment-related adverse events (AEs) was 59%, the rate of grade 3 or higher treatment-related AEs was 18%, and the rate of serious treatment-related AEs was 10%.
There were treatment-related AEs leading to dose interruption (15%), dose reduction (3%), and discontinuation of tazemetostat (2%).
The most common treatment-related AEs were nausea (14%), thrombocytopenia (13%), anemia (10%), neutropenia (9%), diarrhea (8%), asthenia (8%), and fatigue (7%).
Dr Morschhauser said these results “confirm that tazemetostat is quite safe” in this patient population, and enrollment in this trial is ongoing. ![]()
*Data in the abstract differ from the presentation.
New frontline treatments needed for Hodgkin lymphoma

In this editorial, Anna Sureda, MD, PhD, details the need for new frontline treatments for patients with Hodgkin lymphoma, including those with advanced stage disease.
Dr Sureda is head of the Hematology Department and Hematopoietic Stem Cell Transplant Programme at the Institut Català d'Oncologia, Hospital Duran i Reynals, in Barcelona, Spain. She has received consultancy fees from Takeda/Millennium Pharmaceuticals, Merck Sharp & Dohme, and Bristol-Myers Squibb.
Hodgkin lymphoma has traditionally been known as a cancer with generally favorable outcomes. Yet, as with any cancer treatment, there is always room for improvement. For Hodgkin lymphoma specifically, there remains a significant unmet need in the frontline setting for patients with advanced disease (Stage III or Stage IV).
Hodgkin lymphoma most commonly affects young adults as well as adults over the age of 55.1 Both age at diagnosis and stage of the disease are significant factors that must be considered when determining treatment plans, as they can affect a patient’s success in achieving long-term remission.
Though early stage patients have demonstrated 5-year survival rates of approximately 90%, this number drops to 70% in patients with advanced stage disease,2-4 underlining the challenges of treating later stage Hodgkin lymphoma.
Additionally, only 50% of patients with relapsed or refractory disease will experience long-term remission with high-dose chemotherapy and an autologous stem cell transplant (ASCT)5-6— a historically and frequently used treatment regimen.
These facts support the importance of successful frontline treatment and highlight a gap with current treatment regimens.7-10
With current frontline Hodgkin lymphoma treatments, it can be a challenge for physicians to balance efficacy with safety. While allowing the patient to achieve long-term remission remains the goal, physicians are also considering the impact of treatment-related side effects including endocrine dysfunction, cardiac dysfunction, lung toxicity, infertility, and an increased risk of secondary cancers when determining the best possible treatment.8-15
Advanced stage vs early stage Hodgkin lymphoma
Stage of disease at diagnosis has a large influence on outcomes, with advanced stage patients having poorer outcomes than earlier stage patients.7,15-16 Advanced Hodgkin lymphoma patients are more likely to progress or relapse,7,15-16 with nearly one third remaining uncured following standard frontline therapy.7-10
As seen in Figure 1 below, there is a clear difference in progression-free survival for early versus advanced stage Hodgkin lymphoma.16
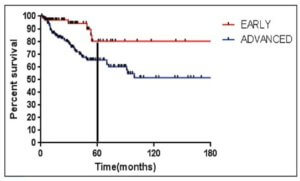
The difference between early stage and advanced stage patients treated with doxorubicin, bleomycin, vinblastine, dacarbazine (ABVD) demonstrates the heightened importance of successful frontline treatment for those with advanced stage disease.16
Unmet needs with current frontline Hodgkin lymphoma treatment
Though current treatments for frontline Hodgkin lymphoma, including ABVD and bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone (BEACOPP), have improved outcomes for patients, these standard regimens are more than 20 years old.
ABVD is generally regarded as the treatment of choice based on its efficacy, relative ease of administration, and side effect profile.17
Escalated BEACOPP, on the other hand, was developed to improve outcomes for advanced stage patients but is associated with increased toxicity.8-10,13,18
Positron emission tomography (PET) scans have also been identified as a pathway to help guide further treatment, but patients with advanced stage Hodgkin lymphoma may relapse more often, despite a negative interim PET scan, compared to stage II patients.19
Among current treatments, side effects including lung and cardiotoxicity as well as an increased risk of secondary cancers are a concern for both physicians and their patients.8-10,13-15
Similarly, radiation therapy, often used in conjunction with chemotherapy for patients who have a large tumor burden in one part of the body, usually the chest,20 is also associated with an increased risk of secondary cancers and cardiotoxicity.8-10,21
With these complications in mind, stabilizing the effects between improved efficacy and minimizing the toxicities associated with current frontline treatments needs to be a focus as new therapies are developed.
For young patients specifically, minimizing toxicities is crucial, as many will have a lifetime ahead of them after Hodgkin lymphoma and will want to avoid the risks associated with current treatments including lung disease, heart disease and infertility.8-10,12-15,22
Treating elderly patients can also be challenging due to their reduced ability to tolerate aggressive frontline treatment and multi-agent chemotherapy, which causes inferior survival outcomes when compared to younger patients.23-25 These secondary effects can affect a patient’s quality of life8-9,12,14-15,22,26-28 and exacerbate preexisting conditions commonly experienced by those undergoing treatment, including long-term fatigue, chronic medical and psychosocial complications, and general deterioration in physical well-being.22
Studies have shown that most relapses after ASCT typically occur within 2 years.29 After a relapse, the patient may endure a substantial physical and psychological burden due to the need for additional treatment, impacting quality of life for both the patient and their caregiver.22,26,30
Goals of clinical research
Despite its recognition as a highly treatable cancer, newly diagnosed Hodgkin lymphoma remains incurable in up to 30% of patients with advanced disease.7-10 Though current therapies seek to achieve remission and extend the lives of patients, it is often at the cost of treatment-related toxicities and side effects that can significantly reduce quality of life.
Moving forward, it is critical that these gaps in treatment are addressed in new frontline treatments that aim to benefit patients, including those with advanced stage disease, while reducing short-term and long-term toxicities. ![]()
Acknowledgements: The author would like to acknowledge the W2O Group for their writing support, which was funded by Millennium Pharmaceuticals Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.
______________________________________________________
1American Cancer Society. What Are the Key Statistics About Hodgkin Disease? https://www.cancer.org/cancer/hodgkin-lymphoma/about/key-statistics.html. Accessed February 16, 2017.
2Ries LAG, Young JL, Keel GE, Eisner MP, Lin YD, Horner M-J (editors). SEER Survival Monograph: Cancer Survival Among Adults: U.S. SEER Program, 1988-2001, Patient and Tumor Characteristics. National Cancer Institute, SEER Program, NIH Pub. No. 07-6215, Bethesda, MD, 2007.
3American Cancer Society. Survival Rates for Hodgkin Disease by Stage. https://www.cancer.org/cancer/hodgkin-lymphoma/detection-diagnosis-staging/survival-rates.html. Accessed February 16, 2017.
4Fermé C, et al. New Engl J Med, 2007.357:1916–27.
5Sureda A, et al. Ann Oncol, 2005;16: 625–633.
6Majhail NS, et al. Biol Blood Marrow Transplant, 2006;12:1065–1072.
7Gordon LI, et al. J Clin Oncol, 2013;31:684-691.
8Carde P, et al. J Clin Oncol, 2016;34(17):2028-2036.
9Engert A, et al. J Clin Oncol, 2009;27(27):4548-4554
10Viviani S, et al. New Engl J Med, 2011;365(3):203-212.
11Sklar C, et al. J Endocrinology & Metabolism, 2000;85(9):3227-3232
12Behringer K, et al. J Clin Oncol, 2013;31:231-239.
13Borchmann P, et al. J Clin Oncol, 2011;29(32):4234-4242.
14Duggan DB, et al. J Clin Oncol, 2003;21(4):607-614.
15Johnson P, McKenzie H. Blood, 2015;125(11):1717-1723.
16Maddi RN, et al. Indian J Medical and Paediatric Oncology, 2015;36(4):255-260
17Ansell SM. American Journal of Hematology, 2014;89: 771–779.
18Merli F, et al. J Clin Oncol, 34:1175-1181.
19Johnson P, et al. N Engl J Med. 2016;374:2419‑2429
20American Cancer Society. Treating Hodgkin Disease: Radiation Therapy for Hodgkin Disease. https://www.cancer.org/cancer/hodgkin-lymphoma/treating/radiation.html. Accessed January 30, 2017.
21Adams MJ, et al. J Clin Oncol, 2004; 22: 3139–48.
22Khimani N, et al. Ann Oncol, 2013;24(1):226-230.
23Engert A, et al. J Clin Oncol, 2005;23(22):5052-60.
24Evens AM, et al. Br J Haematol, 2013;161: 76–86.
25Janssen-Heijnen ML, et al. Br J Haematol, 2005;129:597-606.
26Ganz PA et al. J Clin Oncol, 2003;21(18):3512-3519.
27Daniels LA, et al. Br J Cancer 2014;110:868-874.
28Loge JH, et al. Ann Oncol. 1999;10:71-77.
29Brusamolino E, Carella AM. Haematologica, 2007;92:6-10
30Consolidation Therapy After ASCT in Hodgkin Lymphoma: Why and Who to Treat? Personalized Medicine in Oncology, 2016. http://www.personalizedmedonc.com/article/consolidation-therapy-after-asct-in-hodgkin-lymphoma-why-and-who-to-treat/. Accessed February 16, 2017.
In this editorial, Anna Sureda, MD, PhD, details the need for new frontline treatments for patients with Hodgkin lymphoma, including those with advanced stage disease.
Dr Sureda is head of the Hematology Department and Hematopoietic Stem Cell Transplant Programme at the Institut Català d'Oncologia, Hospital Duran i Reynals, in Barcelona, Spain. She has received consultancy fees from Takeda/Millennium Pharmaceuticals, Merck Sharp & Dohme, and Bristol-Myers Squibb.
Hodgkin lymphoma has traditionally been known as a cancer with generally favorable outcomes. Yet, as with any cancer treatment, there is always room for improvement. For Hodgkin lymphoma specifically, there remains a significant unmet need in the frontline setting for patients with advanced disease (Stage III or Stage IV).
Hodgkin lymphoma most commonly affects young adults as well as adults over the age of 55.1 Both age at diagnosis and stage of the disease are significant factors that must be considered when determining treatment plans, as they can affect a patient’s success in achieving long-term remission.
Though early stage patients have demonstrated 5-year survival rates of approximately 90%, this number drops to 70% in patients with advanced stage disease,2-4 underlining the challenges of treating later stage Hodgkin lymphoma.
Additionally, only 50% of patients with relapsed or refractory disease will experience long-term remission with high-dose chemotherapy and an autologous stem cell transplant (ASCT)5-6— a historically and frequently used treatment regimen.
These facts support the importance of successful frontline treatment and highlight a gap with current treatment regimens.7-10
With current frontline Hodgkin lymphoma treatments, it can be a challenge for physicians to balance efficacy with safety. While allowing the patient to achieve long-term remission remains the goal, physicians are also considering the impact of treatment-related side effects including endocrine dysfunction, cardiac dysfunction, lung toxicity, infertility, and an increased risk of secondary cancers when determining the best possible treatment.8-15
Advanced stage vs early stage Hodgkin lymphoma
Stage of disease at diagnosis has a large influence on outcomes, with advanced stage patients having poorer outcomes than earlier stage patients.7,15-16 Advanced Hodgkin lymphoma patients are more likely to progress or relapse,7,15-16 with nearly one third remaining uncured following standard frontline therapy.7-10
As seen in Figure 1 below, there is a clear difference in progression-free survival for early versus advanced stage Hodgkin lymphoma.16
The difference between early stage and advanced stage patients treated with doxorubicin, bleomycin, vinblastine, dacarbazine (ABVD) demonstrates the heightened importance of successful frontline treatment for those with advanced stage disease.16
Unmet needs with current frontline Hodgkin lymphoma treatment
Though current treatments for frontline Hodgkin lymphoma, including ABVD and bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone (BEACOPP), have improved outcomes for patients, these standard regimens are more than 20 years old.
ABVD is generally regarded as the treatment of choice based on its efficacy, relative ease of administration, and side effect profile.17
Escalated BEACOPP, on the other hand, was developed to improve outcomes for advanced stage patients but is associated with increased toxicity.8-10,13,18
Positron emission tomography (PET) scans have also been identified as a pathway to help guide further treatment, but patients with advanced stage Hodgkin lymphoma may relapse more often, despite a negative interim PET scan, compared to stage II patients.19
Among current treatments, side effects including lung and cardiotoxicity as well as an increased risk of secondary cancers are a concern for both physicians and their patients.8-10,13-15
Similarly, radiation therapy, often used in conjunction with chemotherapy for patients who have a large tumor burden in one part of the body, usually the chest,20 is also associated with an increased risk of secondary cancers and cardiotoxicity.8-10,21
With these complications in mind, stabilizing the effects between improved efficacy and minimizing the toxicities associated with current frontline treatments needs to be a focus as new therapies are developed.
For young patients specifically, minimizing toxicities is crucial, as many will have a lifetime ahead of them after Hodgkin lymphoma and will want to avoid the risks associated with current treatments including lung disease, heart disease and infertility.8-10,12-15,22
Treating elderly patients can also be challenging due to their reduced ability to tolerate aggressive frontline treatment and multi-agent chemotherapy, which causes inferior survival outcomes when compared to younger patients.23-25 These secondary effects can affect a patient’s quality of life8-9,12,14-15,22,26-28 and exacerbate preexisting conditions commonly experienced by those undergoing treatment, including long-term fatigue, chronic medical and psychosocial complications, and general deterioration in physical well-being.22
Studies have shown that most relapses after ASCT typically occur within 2 years.29 After a relapse, the patient may endure a substantial physical and psychological burden due to the need for additional treatment, impacting quality of life for both the patient and their caregiver.22,26,30
Goals of clinical research
Despite its recognition as a highly treatable cancer, newly diagnosed Hodgkin lymphoma remains incurable in up to 30% of patients with advanced disease.7-10 Though current therapies seek to achieve remission and extend the lives of patients, it is often at the cost of treatment-related toxicities and side effects that can significantly reduce quality of life.
Moving forward, it is critical that these gaps in treatment are addressed in new frontline treatments that aim to benefit patients, including those with advanced stage disease, while reducing short-term and long-term toxicities. ![]()
Acknowledgements: The author would like to acknowledge the W2O Group for their writing support, which was funded by Millennium Pharmaceuticals Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.
______________________________________________________
1American Cancer Society. What Are the Key Statistics About Hodgkin Disease? https://www.cancer.org/cancer/hodgkin-lymphoma/about/key-statistics.html. Accessed February 16, 2017.
2Ries LAG, Young JL, Keel GE, Eisner MP, Lin YD, Horner M-J (editors). SEER Survival Monograph: Cancer Survival Among Adults: U.S. SEER Program, 1988-2001, Patient and Tumor Characteristics. National Cancer Institute, SEER Program, NIH Pub. No. 07-6215, Bethesda, MD, 2007.
3American Cancer Society. Survival Rates for Hodgkin Disease by Stage. https://www.cancer.org/cancer/hodgkin-lymphoma/detection-diagnosis-staging/survival-rates.html. Accessed February 16, 2017.
4Fermé C, et al. New Engl J Med, 2007.357:1916–27.
5Sureda A, et al. Ann Oncol, 2005;16: 625–633.
6Majhail NS, et al. Biol Blood Marrow Transplant, 2006;12:1065–1072.
7Gordon LI, et al. J Clin Oncol, 2013;31:684-691.
8Carde P, et al. J Clin Oncol, 2016;34(17):2028-2036.
9Engert A, et al. J Clin Oncol, 2009;27(27):4548-4554
10Viviani S, et al. New Engl J Med, 2011;365(3):203-212.
11Sklar C, et al. J Endocrinology & Metabolism, 2000;85(9):3227-3232
12Behringer K, et al. J Clin Oncol, 2013;31:231-239.
13Borchmann P, et al. J Clin Oncol, 2011;29(32):4234-4242.
14Duggan DB, et al. J Clin Oncol, 2003;21(4):607-614.
15Johnson P, McKenzie H. Blood, 2015;125(11):1717-1723.
16Maddi RN, et al. Indian J Medical and Paediatric Oncology, 2015;36(4):255-260
17Ansell SM. American Journal of Hematology, 2014;89: 771–779.
18Merli F, et al. J Clin Oncol, 34:1175-1181.
19Johnson P, et al. N Engl J Med. 2016;374:2419‑2429
20American Cancer Society. Treating Hodgkin Disease: Radiation Therapy for Hodgkin Disease. https://www.cancer.org/cancer/hodgkin-lymphoma/treating/radiation.html. Accessed January 30, 2017.
21Adams MJ, et al. J Clin Oncol, 2004; 22: 3139–48.
22Khimani N, et al. Ann Oncol, 2013;24(1):226-230.
23Engert A, et al. J Clin Oncol, 2005;23(22):5052-60.
24Evens AM, et al. Br J Haematol, 2013;161: 76–86.
25Janssen-Heijnen ML, et al. Br J Haematol, 2005;129:597-606.
26Ganz PA et al. J Clin Oncol, 2003;21(18):3512-3519.
27Daniels LA, et al. Br J Cancer 2014;110:868-874.
28Loge JH, et al. Ann Oncol. 1999;10:71-77.
29Brusamolino E, Carella AM. Haematologica, 2007;92:6-10
30Consolidation Therapy After ASCT in Hodgkin Lymphoma: Why and Who to Treat? Personalized Medicine in Oncology, 2016. http://www.personalizedmedonc.com/article/consolidation-therapy-after-asct-in-hodgkin-lymphoma-why-and-who-to-treat/. Accessed February 16, 2017.
In this editorial, Anna Sureda, MD, PhD, details the need for new frontline treatments for patients with Hodgkin lymphoma, including those with advanced stage disease.
Dr Sureda is head of the Hematology Department and Hematopoietic Stem Cell Transplant Programme at the Institut Català d'Oncologia, Hospital Duran i Reynals, in Barcelona, Spain. She has received consultancy fees from Takeda/Millennium Pharmaceuticals, Merck Sharp & Dohme, and Bristol-Myers Squibb.
Hodgkin lymphoma has traditionally been known as a cancer with generally favorable outcomes. Yet, as with any cancer treatment, there is always room for improvement. For Hodgkin lymphoma specifically, there remains a significant unmet need in the frontline setting for patients with advanced disease (Stage III or Stage IV).
Hodgkin lymphoma most commonly affects young adults as well as adults over the age of 55.1 Both age at diagnosis and stage of the disease are significant factors that must be considered when determining treatment plans, as they can affect a patient’s success in achieving long-term remission.
Though early stage patients have demonstrated 5-year survival rates of approximately 90%, this number drops to 70% in patients with advanced stage disease,2-4 underlining the challenges of treating later stage Hodgkin lymphoma.
Additionally, only 50% of patients with relapsed or refractory disease will experience long-term remission with high-dose chemotherapy and an autologous stem cell transplant (ASCT)5-6— a historically and frequently used treatment regimen.
These facts support the importance of successful frontline treatment and highlight a gap with current treatment regimens.7-10
With current frontline Hodgkin lymphoma treatments, it can be a challenge for physicians to balance efficacy with safety. While allowing the patient to achieve long-term remission remains the goal, physicians are also considering the impact of treatment-related side effects including endocrine dysfunction, cardiac dysfunction, lung toxicity, infertility, and an increased risk of secondary cancers when determining the best possible treatment.8-15
Advanced stage vs early stage Hodgkin lymphoma
Stage of disease at diagnosis has a large influence on outcomes, with advanced stage patients having poorer outcomes than earlier stage patients.7,15-16 Advanced Hodgkin lymphoma patients are more likely to progress or relapse,7,15-16 with nearly one third remaining uncured following standard frontline therapy.7-10
As seen in Figure 1 below, there is a clear difference in progression-free survival for early versus advanced stage Hodgkin lymphoma.16
The difference between early stage and advanced stage patients treated with doxorubicin, bleomycin, vinblastine, dacarbazine (ABVD) demonstrates the heightened importance of successful frontline treatment for those with advanced stage disease.16
Unmet needs with current frontline Hodgkin lymphoma treatment
Though current treatments for frontline Hodgkin lymphoma, including ABVD and bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone (BEACOPP), have improved outcomes for patients, these standard regimens are more than 20 years old.
ABVD is generally regarded as the treatment of choice based on its efficacy, relative ease of administration, and side effect profile.17
Escalated BEACOPP, on the other hand, was developed to improve outcomes for advanced stage patients but is associated with increased toxicity.8-10,13,18
Positron emission tomography (PET) scans have also been identified as a pathway to help guide further treatment, but patients with advanced stage Hodgkin lymphoma may relapse more often, despite a negative interim PET scan, compared to stage II patients.19
Among current treatments, side effects including lung and cardiotoxicity as well as an increased risk of secondary cancers are a concern for both physicians and their patients.8-10,13-15
Similarly, radiation therapy, often used in conjunction with chemotherapy for patients who have a large tumor burden in one part of the body, usually the chest,20 is also associated with an increased risk of secondary cancers and cardiotoxicity.8-10,21
With these complications in mind, stabilizing the effects between improved efficacy and minimizing the toxicities associated with current frontline treatments needs to be a focus as new therapies are developed.
For young patients specifically, minimizing toxicities is crucial, as many will have a lifetime ahead of them after Hodgkin lymphoma and will want to avoid the risks associated with current treatments including lung disease, heart disease and infertility.8-10,12-15,22
Treating elderly patients can also be challenging due to their reduced ability to tolerate aggressive frontline treatment and multi-agent chemotherapy, which causes inferior survival outcomes when compared to younger patients.23-25 These secondary effects can affect a patient’s quality of life8-9,12,14-15,22,26-28 and exacerbate preexisting conditions commonly experienced by those undergoing treatment, including long-term fatigue, chronic medical and psychosocial complications, and general deterioration in physical well-being.22
Studies have shown that most relapses after ASCT typically occur within 2 years.29 After a relapse, the patient may endure a substantial physical and psychological burden due to the need for additional treatment, impacting quality of life for both the patient and their caregiver.22,26,30
Goals of clinical research
Despite its recognition as a highly treatable cancer, newly diagnosed Hodgkin lymphoma remains incurable in up to 30% of patients with advanced disease.7-10 Though current therapies seek to achieve remission and extend the lives of patients, it is often at the cost of treatment-related toxicities and side effects that can significantly reduce quality of life.
Moving forward, it is critical that these gaps in treatment are addressed in new frontline treatments that aim to benefit patients, including those with advanced stage disease, while reducing short-term and long-term toxicities. ![]()
Acknowledgements: The author would like to acknowledge the W2O Group for their writing support, which was funded by Millennium Pharmaceuticals Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited.
______________________________________________________
1American Cancer Society. What Are the Key Statistics About Hodgkin Disease? https://www.cancer.org/cancer/hodgkin-lymphoma/about/key-statistics.html. Accessed February 16, 2017.
2Ries LAG, Young JL, Keel GE, Eisner MP, Lin YD, Horner M-J (editors). SEER Survival Monograph: Cancer Survival Among Adults: U.S. SEER Program, 1988-2001, Patient and Tumor Characteristics. National Cancer Institute, SEER Program, NIH Pub. No. 07-6215, Bethesda, MD, 2007.
3American Cancer Society. Survival Rates for Hodgkin Disease by Stage. https://www.cancer.org/cancer/hodgkin-lymphoma/detection-diagnosis-staging/survival-rates.html. Accessed February 16, 2017.
4Fermé C, et al. New Engl J Med, 2007.357:1916–27.
5Sureda A, et al. Ann Oncol, 2005;16: 625–633.
6Majhail NS, et al. Biol Blood Marrow Transplant, 2006;12:1065–1072.
7Gordon LI, et al. J Clin Oncol, 2013;31:684-691.
8Carde P, et al. J Clin Oncol, 2016;34(17):2028-2036.
9Engert A, et al. J Clin Oncol, 2009;27(27):4548-4554
10Viviani S, et al. New Engl J Med, 2011;365(3):203-212.
11Sklar C, et al. J Endocrinology & Metabolism, 2000;85(9):3227-3232
12Behringer K, et al. J Clin Oncol, 2013;31:231-239.
13Borchmann P, et al. J Clin Oncol, 2011;29(32):4234-4242.
14Duggan DB, et al. J Clin Oncol, 2003;21(4):607-614.
15Johnson P, McKenzie H. Blood, 2015;125(11):1717-1723.
16Maddi RN, et al. Indian J Medical and Paediatric Oncology, 2015;36(4):255-260
17Ansell SM. American Journal of Hematology, 2014;89: 771–779.
18Merli F, et al. J Clin Oncol, 34:1175-1181.
19Johnson P, et al. N Engl J Med. 2016;374:2419‑2429
20American Cancer Society. Treating Hodgkin Disease: Radiation Therapy for Hodgkin Disease. https://www.cancer.org/cancer/hodgkin-lymphoma/treating/radiation.html. Accessed January 30, 2017.
21Adams MJ, et al. J Clin Oncol, 2004; 22: 3139–48.
22Khimani N, et al. Ann Oncol, 2013;24(1):226-230.
23Engert A, et al. J Clin Oncol, 2005;23(22):5052-60.
24Evens AM, et al. Br J Haematol, 2013;161: 76–86.
25Janssen-Heijnen ML, et al. Br J Haematol, 2005;129:597-606.
26Ganz PA et al. J Clin Oncol, 2003;21(18):3512-3519.
27Daniels LA, et al. Br J Cancer 2014;110:868-874.
28Loge JH, et al. Ann Oncol. 1999;10:71-77.
29Brusamolino E, Carella AM. Haematologica, 2007;92:6-10
30Consolidation Therapy After ASCT in Hodgkin Lymphoma: Why and Who to Treat? Personalized Medicine in Oncology, 2016. http://www.personalizedmedonc.com/article/consolidation-therapy-after-asct-in-hodgkin-lymphoma-why-and-who-to-treat/. Accessed February 16, 2017.
Lenalidomide-rituximab induces high CR rate in untreated follicular lymphoma
LUGANO, SWITZERLAND – The chemotherapy-free combination of lenalidomide (Revlimid) and rituximab was highly active as frontline therapy for patients with low- and intermediate-risk follicular lymphoma in a multicenter phase II trial.
Among 66 patients with previously untreated follicular lymphoma, the overall response rate to the combination was 95%, including complete responses in 72% of patients. The 5-year progression-free survival (PFS) rate was 70%, reported John P. Leonard, MD, of Weill Cornell Medicine, New York.
“I think this overall is a useful validation – confirmation of the single-center data that showed that this [combination] in a multicenter setting can be a highly effective and reasonably well-tolerated treatment approach for patients with untreated follicular lymphoma,” he said at the International Conference on Malignant Lymphoma, on behalf of colleagues in the National Cancer Institute Alliance for Clinical Trials in Oncology and Cancer and Leukemia Group B (CALGB) 50803 trial.
In the 50803 study, the investigators enrolled 66 treatment-naive patients. The median age was 53 years (range 32-79). Patients were eligible if they had grade 1-3a, stage 3-4 or bulky stage 2 untreated follicular lymphoma, with Follicular Lymphoma International Prognostic Index (FLIPI) scores of 0-2.
They received lenalidomide 20 mg/day on days 1 through 21 of each 28-day cycle for 12 cycles, plus rituximab administered once weekly for each week of cycle 1, and on the first day of cycles 4, 6, 8 and 10.
The investigators also evaluated polymorphisms in the Fc fragment of immunoglobulin G receptor IIa and IIIa (FcGR2A/FcGR3A).
One of the 66 patients never started treatment, leaving 65 for the response analysis.
As noted, the overall response rate was 95%, including 94% of 21 patients with FLIPI 0 or 1 disease, and 96% of 44 patients with FLIPI 2 or 3. There were no associations between FLIPI score and likelihood of achieving a complete response, and no associations between FcR polymorphism or change in angiogenic markers and either complete responses or PFS, Dr. Leonard said.
Complete responses, the primary endpoint, were seen in 15 of the 21 (71%) of patients with FLIPI 0-1, and in 32 of the 44 (73%) with FLIPI 2-3, for an overall complete response rate of 72%.
Partial responses occurred in 5 patients (23%) with FLIPI 0-1 and 10 patients (23%) with FLIPI 2-3, for an overall PR rate of 23%.
Respective rates of stable disease were 0, 2%, and 2%. One patient in each FLIPI group was not evaluated because of adverse events.
After a median follow-up of 5 years, the progression free survival rate was 70%.
The most common grade 3 or 4 adverse events were neutropenia, seen in 21% of patients, and infections, seen in 40% (including one grade 3 febrile neutropenia).
Grade 1-2 fatigue was reported by 51 patients, and grade 3 fatigue was reported by 4.
Other grade 3 or 4 events seen in more than 5% of patients included rash in 9%, and hyperglycemia, hypophosphatemia, or hypertension, each in 6% of patients.
Celgene and Genentech supported the study. Dr. Leonard has served as an adviser/consultant to Celgene and other companies.
LUGANO, SWITZERLAND – The chemotherapy-free combination of lenalidomide (Revlimid) and rituximab was highly active as frontline therapy for patients with low- and intermediate-risk follicular lymphoma in a multicenter phase II trial.
Among 66 patients with previously untreated follicular lymphoma, the overall response rate to the combination was 95%, including complete responses in 72% of patients. The 5-year progression-free survival (PFS) rate was 70%, reported John P. Leonard, MD, of Weill Cornell Medicine, New York.
“I think this overall is a useful validation – confirmation of the single-center data that showed that this [combination] in a multicenter setting can be a highly effective and reasonably well-tolerated treatment approach for patients with untreated follicular lymphoma,” he said at the International Conference on Malignant Lymphoma, on behalf of colleagues in the National Cancer Institute Alliance for Clinical Trials in Oncology and Cancer and Leukemia Group B (CALGB) 50803 trial.
In the 50803 study, the investigators enrolled 66 treatment-naive patients. The median age was 53 years (range 32-79). Patients were eligible if they had grade 1-3a, stage 3-4 or bulky stage 2 untreated follicular lymphoma, with Follicular Lymphoma International Prognostic Index (FLIPI) scores of 0-2.
They received lenalidomide 20 mg/day on days 1 through 21 of each 28-day cycle for 12 cycles, plus rituximab administered once weekly for each week of cycle 1, and on the first day of cycles 4, 6, 8 and 10.
The investigators also evaluated polymorphisms in the Fc fragment of immunoglobulin G receptor IIa and IIIa (FcGR2A/FcGR3A).
One of the 66 patients never started treatment, leaving 65 for the response analysis.
As noted, the overall response rate was 95%, including 94% of 21 patients with FLIPI 0 or 1 disease, and 96% of 44 patients with FLIPI 2 or 3. There were no associations between FLIPI score and likelihood of achieving a complete response, and no associations between FcR polymorphism or change in angiogenic markers and either complete responses or PFS, Dr. Leonard said.
Complete responses, the primary endpoint, were seen in 15 of the 21 (71%) of patients with FLIPI 0-1, and in 32 of the 44 (73%) with FLIPI 2-3, for an overall complete response rate of 72%.
Partial responses occurred in 5 patients (23%) with FLIPI 0-1 and 10 patients (23%) with FLIPI 2-3, for an overall PR rate of 23%.
Respective rates of stable disease were 0, 2%, and 2%. One patient in each FLIPI group was not evaluated because of adverse events.
After a median follow-up of 5 years, the progression free survival rate was 70%.
The most common grade 3 or 4 adverse events were neutropenia, seen in 21% of patients, and infections, seen in 40% (including one grade 3 febrile neutropenia).
Grade 1-2 fatigue was reported by 51 patients, and grade 3 fatigue was reported by 4.
Other grade 3 or 4 events seen in more than 5% of patients included rash in 9%, and hyperglycemia, hypophosphatemia, or hypertension, each in 6% of patients.
Celgene and Genentech supported the study. Dr. Leonard has served as an adviser/consultant to Celgene and other companies.
LUGANO, SWITZERLAND – The chemotherapy-free combination of lenalidomide (Revlimid) and rituximab was highly active as frontline therapy for patients with low- and intermediate-risk follicular lymphoma in a multicenter phase II trial.
Among 66 patients with previously untreated follicular lymphoma, the overall response rate to the combination was 95%, including complete responses in 72% of patients. The 5-year progression-free survival (PFS) rate was 70%, reported John P. Leonard, MD, of Weill Cornell Medicine, New York.
“I think this overall is a useful validation – confirmation of the single-center data that showed that this [combination] in a multicenter setting can be a highly effective and reasonably well-tolerated treatment approach for patients with untreated follicular lymphoma,” he said at the International Conference on Malignant Lymphoma, on behalf of colleagues in the National Cancer Institute Alliance for Clinical Trials in Oncology and Cancer and Leukemia Group B (CALGB) 50803 trial.
In the 50803 study, the investigators enrolled 66 treatment-naive patients. The median age was 53 years (range 32-79). Patients were eligible if they had grade 1-3a, stage 3-4 or bulky stage 2 untreated follicular lymphoma, with Follicular Lymphoma International Prognostic Index (FLIPI) scores of 0-2.
They received lenalidomide 20 mg/day on days 1 through 21 of each 28-day cycle for 12 cycles, plus rituximab administered once weekly for each week of cycle 1, and on the first day of cycles 4, 6, 8 and 10.
The investigators also evaluated polymorphisms in the Fc fragment of immunoglobulin G receptor IIa and IIIa (FcGR2A/FcGR3A).
One of the 66 patients never started treatment, leaving 65 for the response analysis.
As noted, the overall response rate was 95%, including 94% of 21 patients with FLIPI 0 or 1 disease, and 96% of 44 patients with FLIPI 2 or 3. There were no associations between FLIPI score and likelihood of achieving a complete response, and no associations between FcR polymorphism or change in angiogenic markers and either complete responses or PFS, Dr. Leonard said.
Complete responses, the primary endpoint, were seen in 15 of the 21 (71%) of patients with FLIPI 0-1, and in 32 of the 44 (73%) with FLIPI 2-3, for an overall complete response rate of 72%.
Partial responses occurred in 5 patients (23%) with FLIPI 0-1 and 10 patients (23%) with FLIPI 2-3, for an overall PR rate of 23%.
Respective rates of stable disease were 0, 2%, and 2%. One patient in each FLIPI group was not evaluated because of adverse events.
After a median follow-up of 5 years, the progression free survival rate was 70%.
The most common grade 3 or 4 adverse events were neutropenia, seen in 21% of patients, and infections, seen in 40% (including one grade 3 febrile neutropenia).
Grade 1-2 fatigue was reported by 51 patients, and grade 3 fatigue was reported by 4.
Other grade 3 or 4 events seen in more than 5% of patients included rash in 9%, and hyperglycemia, hypophosphatemia, or hypertension, each in 6% of patients.
Celgene and Genentech supported the study. Dr. Leonard has served as an adviser/consultant to Celgene and other companies.
AT 14-ICML
Key clinical point: The combination of lenalidomide and rituximab was highly active against previously untreated follicular lymphoma.
Major finding: The overall response rate was 95%; 5-year progression-free survival was 70%.
Data source: Open-label prospective study of lenalidomide-rituximab in 66 patients with previously untreated follicular lymphoma.
Disclosures: Celgene and Genentech supported the study. Dr. Leonard has served as an adviser/consultant to Celgene and other companies.
GALEN safe and effective in relapsed and refractory follicular lymphoma
LUGANO, SWITZERLAND – For patients with relapsed or refractory follicular lymphoma, a pairing of lenalidomide (Revlimid) and obinutuzumab (Gazyva) appeared to be especially useful among patients who had disease progression within 24 months, based on results from a Lymphoma Academic Research Organisation trial.
Among 86 patients who were enrolled in a phase II trial and were assessable for efficacy, overall response rates (ORR) with the combination therapy, nicknamed “GALEN,” were 80.2% by 1999 International Working Group criteria, and 74.4% according to the 2007 IWG criteria, reported Franck Morschhauser, MD, PhD, of the University of Lille, France.

The rationale for this combination is the known synergy between lenalidomide and rituximab in relapsed refractory non-Hodgkin lymphomas and in the frontline setting for patients with follicular lymphoma. Obinutuzumab, a follow-on to rituximab, is a unique type II glycoengineered monoclonal antibody directed against CD20, but with increased antibody-dependent cell-mediated cytotoxicity and increased direct cytotoxicity, compared with rituximab, he explained.
In the phase Ib part of the study, researchers settled on a dose of obinutuzumab 1000 mg and lenalidomide 20 mg. Obinutuzumab was administered on days 8, 15 and 22 and lenalidomide on days 1 to 21 of each 28 day cycle. Patients were evaluated for response after three cycles and at the end of induction (after completion of 4 to 6 cycles).
The maintenance phase consisted of obinutuzumab on day 1 of every other cycle beginning with cycle 1, and lenalidomide on days 1 through 22 for cycles 7 through 18. From cycles 19 through 24, obinutuzumab was given alone on the first day of every 56-day cycle.
The overall response rate (ORR) at the end of induction according to the IWG 1999 criteria, the primary endpoint, was 80.2%, including 39.5% complete or unconfirmed complete responses.
When the same patients were assessed according to 2007 IWG criteria, the ORR rate was slightly lower, at 74.4%, but the complete or unconfirmed complete response rate was slightly higher, at 44.2%.
An analysis of responses by time to relapse showed that the ORR among 24 patients with disease progression within 24 months was 70.8%, including 33.3% complete or unconfirmed complete responses by the 1999 criteria, and 66.7% with 54.2% complete or unconfirmed complete responses by the 2007 criteria.
ORR among the 64 patients with disease progression after more than 24 months was 83.9% with 41.9% complete or unconfirmed complete responses by 1999 criteria, and 77.4% with 40.3% complete or unconfirmed complete responses by 2007 criteria. The differences between the groups with disease progression within 24 months and later relapse groups were not significant.
A subanalysis by refractory status, however, showed that the 63 nonrefractory patients fared significantly better, with 87.3% ORR and 41.3% complete or unconfirmed complete responses by 1999 criteria, and 81.0% with 49.2% complete or unconfirmed complete response rate by 2007 determinations, compared with respective rates among 23 refractory patients of 60.9%/34.8% complete or unconfirmed complete response rate and 56.5% with 30.4% complete or unconfirmed complete responses (P = .0212 by 1999 criteria, and P = .022 by 2007 criteria).
After a median follow-up of 18 months, 1-year progression-free survival (PFS) among all patients was 75.5%, and 1-year overall survival (OS) was 88.8%.
There were no significant differences in either progression-free survival or overall survival by time to relapse. Although there appeared to be a nonsignificant trend toward worse outcomes among patients with refractory vs. nonrefractory disease, there was a significantly lower 1-year overall survival rate among refractory patients, at 71.5% compared with 95% for nonrefractory patients (censored logrank P = .0098).
Dr. Morschhauser said that the combination had no unexpected toxicities. Hematologic toxicities of grade 3 or greater included neutropenia in 28.4%, thrombocytopenia in 11.4%, and anemia and lymphopenia in 3.4% each.
The most common nonhematologic toxicities of all grades included infections in 62.5% of patients (grade 3 or greater in 6.8%), and asthenia in 52.3% of patients (grade 3 or greater in 2.3%). The only other grade 3 or greater toxicities were peripheral neuropathy in 1.1%, and infusion related rash in 3.4%.
Additional follow-up will be need for evaluation of the full impact of maintenance on outcomes, he added.
The study was funded by Celgene and Roche. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies.
LUGANO, SWITZERLAND – For patients with relapsed or refractory follicular lymphoma, a pairing of lenalidomide (Revlimid) and obinutuzumab (Gazyva) appeared to be especially useful among patients who had disease progression within 24 months, based on results from a Lymphoma Academic Research Organisation trial.
Among 86 patients who were enrolled in a phase II trial and were assessable for efficacy, overall response rates (ORR) with the combination therapy, nicknamed “GALEN,” were 80.2% by 1999 International Working Group criteria, and 74.4% according to the 2007 IWG criteria, reported Franck Morschhauser, MD, PhD, of the University of Lille, France.
The rationale for this combination is the known synergy between lenalidomide and rituximab in relapsed refractory non-Hodgkin lymphomas and in the frontline setting for patients with follicular lymphoma. Obinutuzumab, a follow-on to rituximab, is a unique type II glycoengineered monoclonal antibody directed against CD20, but with increased antibody-dependent cell-mediated cytotoxicity and increased direct cytotoxicity, compared with rituximab, he explained.
In the phase Ib part of the study, researchers settled on a dose of obinutuzumab 1000 mg and lenalidomide 20 mg. Obinutuzumab was administered on days 8, 15 and 22 and lenalidomide on days 1 to 21 of each 28 day cycle. Patients were evaluated for response after three cycles and at the end of induction (after completion of 4 to 6 cycles).
The maintenance phase consisted of obinutuzumab on day 1 of every other cycle beginning with cycle 1, and lenalidomide on days 1 through 22 for cycles 7 through 18. From cycles 19 through 24, obinutuzumab was given alone on the first day of every 56-day cycle.
The overall response rate (ORR) at the end of induction according to the IWG 1999 criteria, the primary endpoint, was 80.2%, including 39.5% complete or unconfirmed complete responses.
When the same patients were assessed according to 2007 IWG criteria, the ORR rate was slightly lower, at 74.4%, but the complete or unconfirmed complete response rate was slightly higher, at 44.2%.
An analysis of responses by time to relapse showed that the ORR among 24 patients with disease progression within 24 months was 70.8%, including 33.3% complete or unconfirmed complete responses by the 1999 criteria, and 66.7% with 54.2% complete or unconfirmed complete responses by the 2007 criteria.
ORR among the 64 patients with disease progression after more than 24 months was 83.9% with 41.9% complete or unconfirmed complete responses by 1999 criteria, and 77.4% with 40.3% complete or unconfirmed complete responses by 2007 criteria. The differences between the groups with disease progression within 24 months and later relapse groups were not significant.
A subanalysis by refractory status, however, showed that the 63 nonrefractory patients fared significantly better, with 87.3% ORR and 41.3% complete or unconfirmed complete responses by 1999 criteria, and 81.0% with 49.2% complete or unconfirmed complete response rate by 2007 determinations, compared with respective rates among 23 refractory patients of 60.9%/34.8% complete or unconfirmed complete response rate and 56.5% with 30.4% complete or unconfirmed complete responses (P = .0212 by 1999 criteria, and P = .022 by 2007 criteria).
After a median follow-up of 18 months, 1-year progression-free survival (PFS) among all patients was 75.5%, and 1-year overall survival (OS) was 88.8%.
There were no significant differences in either progression-free survival or overall survival by time to relapse. Although there appeared to be a nonsignificant trend toward worse outcomes among patients with refractory vs. nonrefractory disease, there was a significantly lower 1-year overall survival rate among refractory patients, at 71.5% compared with 95% for nonrefractory patients (censored logrank P = .0098).
Dr. Morschhauser said that the combination had no unexpected toxicities. Hematologic toxicities of grade 3 or greater included neutropenia in 28.4%, thrombocytopenia in 11.4%, and anemia and lymphopenia in 3.4% each.
The most common nonhematologic toxicities of all grades included infections in 62.5% of patients (grade 3 or greater in 6.8%), and asthenia in 52.3% of patients (grade 3 or greater in 2.3%). The only other grade 3 or greater toxicities were peripheral neuropathy in 1.1%, and infusion related rash in 3.4%.
Additional follow-up will be need for evaluation of the full impact of maintenance on outcomes, he added.
The study was funded by Celgene and Roche. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies.
LUGANO, SWITZERLAND – For patients with relapsed or refractory follicular lymphoma, a pairing of lenalidomide (Revlimid) and obinutuzumab (Gazyva) appeared to be especially useful among patients who had disease progression within 24 months, based on results from a Lymphoma Academic Research Organisation trial.
Among 86 patients who were enrolled in a phase II trial and were assessable for efficacy, overall response rates (ORR) with the combination therapy, nicknamed “GALEN,” were 80.2% by 1999 International Working Group criteria, and 74.4% according to the 2007 IWG criteria, reported Franck Morschhauser, MD, PhD, of the University of Lille, France.
The rationale for this combination is the known synergy between lenalidomide and rituximab in relapsed refractory non-Hodgkin lymphomas and in the frontline setting for patients with follicular lymphoma. Obinutuzumab, a follow-on to rituximab, is a unique type II glycoengineered monoclonal antibody directed against CD20, but with increased antibody-dependent cell-mediated cytotoxicity and increased direct cytotoxicity, compared with rituximab, he explained.
In the phase Ib part of the study, researchers settled on a dose of obinutuzumab 1000 mg and lenalidomide 20 mg. Obinutuzumab was administered on days 8, 15 and 22 and lenalidomide on days 1 to 21 of each 28 day cycle. Patients were evaluated for response after three cycles and at the end of induction (after completion of 4 to 6 cycles).
The maintenance phase consisted of obinutuzumab on day 1 of every other cycle beginning with cycle 1, and lenalidomide on days 1 through 22 for cycles 7 through 18. From cycles 19 through 24, obinutuzumab was given alone on the first day of every 56-day cycle.
The overall response rate (ORR) at the end of induction according to the IWG 1999 criteria, the primary endpoint, was 80.2%, including 39.5% complete or unconfirmed complete responses.
When the same patients were assessed according to 2007 IWG criteria, the ORR rate was slightly lower, at 74.4%, but the complete or unconfirmed complete response rate was slightly higher, at 44.2%.
An analysis of responses by time to relapse showed that the ORR among 24 patients with disease progression within 24 months was 70.8%, including 33.3% complete or unconfirmed complete responses by the 1999 criteria, and 66.7% with 54.2% complete or unconfirmed complete responses by the 2007 criteria.
ORR among the 64 patients with disease progression after more than 24 months was 83.9% with 41.9% complete or unconfirmed complete responses by 1999 criteria, and 77.4% with 40.3% complete or unconfirmed complete responses by 2007 criteria. The differences between the groups with disease progression within 24 months and later relapse groups were not significant.
A subanalysis by refractory status, however, showed that the 63 nonrefractory patients fared significantly better, with 87.3% ORR and 41.3% complete or unconfirmed complete responses by 1999 criteria, and 81.0% with 49.2% complete or unconfirmed complete response rate by 2007 determinations, compared with respective rates among 23 refractory patients of 60.9%/34.8% complete or unconfirmed complete response rate and 56.5% with 30.4% complete or unconfirmed complete responses (P = .0212 by 1999 criteria, and P = .022 by 2007 criteria).
After a median follow-up of 18 months, 1-year progression-free survival (PFS) among all patients was 75.5%, and 1-year overall survival (OS) was 88.8%.
There were no significant differences in either progression-free survival or overall survival by time to relapse. Although there appeared to be a nonsignificant trend toward worse outcomes among patients with refractory vs. nonrefractory disease, there was a significantly lower 1-year overall survival rate among refractory patients, at 71.5% compared with 95% for nonrefractory patients (censored logrank P = .0098).
Dr. Morschhauser said that the combination had no unexpected toxicities. Hematologic toxicities of grade 3 or greater included neutropenia in 28.4%, thrombocytopenia in 11.4%, and anemia and lymphopenia in 3.4% each.
The most common nonhematologic toxicities of all grades included infections in 62.5% of patients (grade 3 or greater in 6.8%), and asthenia in 52.3% of patients (grade 3 or greater in 2.3%). The only other grade 3 or greater toxicities were peripheral neuropathy in 1.1%, and infusion related rash in 3.4%.
Additional follow-up will be need for evaluation of the full impact of maintenance on outcomes, he added.
The study was funded by Celgene and Roche. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies.
AT 14-ICML
Key clinical point: A combination of lenalidomide and obinutuzumab was safe and effective in patients with relapsed/refractory follicular lymphoma.
Major finding: The overall response rate according to 1999 International Working Group criteria was 80.2%, including 39.5% CR/CRu.
Data source: Single-arm phase II study with 86 patients evaluable for efficacy and 88 evaluable for safety.
Disclosures: The study was funded by Celgene and Roche. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies.
