User login
Herbs reduce fatigue in cancer patients

Photo by Alexander Baxevanis
An herbal mixture used in traditional Chinese medicine can reduce fatigue in cancer patients, results of a phase 1/2 study suggest.
The mixture, Ren Shen Yangrong Tang (RSYRT), is a soup containing 12 herbs.
In the study, cancer patients suffering from moderate to severe fatigue reported significantly less fatigue after taking RSYRT for 2 to 3 weeks.
Researchers reported these results in the Journal of Alternative and Complementary Medicine.
Yichen Xu, MD, of Beijing Cancer Hospital & Institute in China, and colleagues evaluated RSYRT in 33 patients who had completed cancer treatment. The patients had stable disease and no anemia.
Eleven patients had moderate fatigue (a score of 4-6 on a 0-10 scale), and 22 had severe fatigue (a score of 7-10). All patients had experienced fatigue for at least 4 months.
Patients took RSYRT twice a day for 6 weeks and experienced a significant decrease in fatigue severity. The mean fatigue score decreased from 7.06 at baseline to 3.30 at the 6-week mark (P<0.001).
The fatigue category also changed significantly (P=0.024). Among the 22 patients who had severe fatigue before RSYRT, half had mild fatigue after therapy, and half had moderate fatigue.
Among the 11 patients who had moderate fatigue at baseline, only 1 still had moderate fatigue after receiving RSYRT. The rest had mild fatigue.
All of the patients said they felt better after taking RSYRT for 4 weeks.
There were no “uncomfortable events” related to RSYRT, such as gastrointestinal upset, insomnia, headache, or rash. None of the patients required a dose reduction or dose interruption.
None of the patients had blood chemistry abnormalities or abnormal liver/kidney function. Two patients who had a change in ST segment before RSYRT had normal electrocardiogram results after treatment. ![]()
Photo by Alexander Baxevanis
An herbal mixture used in traditional Chinese medicine can reduce fatigue in cancer patients, results of a phase 1/2 study suggest.
The mixture, Ren Shen Yangrong Tang (RSYRT), is a soup containing 12 herbs.
In the study, cancer patients suffering from moderate to severe fatigue reported significantly less fatigue after taking RSYRT for 2 to 3 weeks.
Researchers reported these results in the Journal of Alternative and Complementary Medicine.
Yichen Xu, MD, of Beijing Cancer Hospital & Institute in China, and colleagues evaluated RSYRT in 33 patients who had completed cancer treatment. The patients had stable disease and no anemia.
Eleven patients had moderate fatigue (a score of 4-6 on a 0-10 scale), and 22 had severe fatigue (a score of 7-10). All patients had experienced fatigue for at least 4 months.
Patients took RSYRT twice a day for 6 weeks and experienced a significant decrease in fatigue severity. The mean fatigue score decreased from 7.06 at baseline to 3.30 at the 6-week mark (P<0.001).
The fatigue category also changed significantly (P=0.024). Among the 22 patients who had severe fatigue before RSYRT, half had mild fatigue after therapy, and half had moderate fatigue.
Among the 11 patients who had moderate fatigue at baseline, only 1 still had moderate fatigue after receiving RSYRT. The rest had mild fatigue.
All of the patients said they felt better after taking RSYRT for 4 weeks.
There were no “uncomfortable events” related to RSYRT, such as gastrointestinal upset, insomnia, headache, or rash. None of the patients required a dose reduction or dose interruption.
None of the patients had blood chemistry abnormalities or abnormal liver/kidney function. Two patients who had a change in ST segment before RSYRT had normal electrocardiogram results after treatment. ![]()
Photo by Alexander Baxevanis
An herbal mixture used in traditional Chinese medicine can reduce fatigue in cancer patients, results of a phase 1/2 study suggest.
The mixture, Ren Shen Yangrong Tang (RSYRT), is a soup containing 12 herbs.
In the study, cancer patients suffering from moderate to severe fatigue reported significantly less fatigue after taking RSYRT for 2 to 3 weeks.
Researchers reported these results in the Journal of Alternative and Complementary Medicine.
Yichen Xu, MD, of Beijing Cancer Hospital & Institute in China, and colleagues evaluated RSYRT in 33 patients who had completed cancer treatment. The patients had stable disease and no anemia.
Eleven patients had moderate fatigue (a score of 4-6 on a 0-10 scale), and 22 had severe fatigue (a score of 7-10). All patients had experienced fatigue for at least 4 months.
Patients took RSYRT twice a day for 6 weeks and experienced a significant decrease in fatigue severity. The mean fatigue score decreased from 7.06 at baseline to 3.30 at the 6-week mark (P<0.001).
The fatigue category also changed significantly (P=0.024). Among the 22 patients who had severe fatigue before RSYRT, half had mild fatigue after therapy, and half had moderate fatigue.
Among the 11 patients who had moderate fatigue at baseline, only 1 still had moderate fatigue after receiving RSYRT. The rest had mild fatigue.
All of the patients said they felt better after taking RSYRT for 4 weeks.
There were no “uncomfortable events” related to RSYRT, such as gastrointestinal upset, insomnia, headache, or rash. None of the patients required a dose reduction or dose interruption.
None of the patients had blood chemistry abnormalities or abnormal liver/kidney function. Two patients who had a change in ST segment before RSYRT had normal electrocardiogram results after treatment. ![]()
Inhibitor promotes chemosensitization in CLL

PHILADELPHIA—A DNA-dependent protein kinase (DNA-PK) inhibitor can sensitize chronic lymphocytic leukemia (CLL) cells to chemotherapy, according to
preclinical research.
The inhibitor, NDD0004, sensitized CLL cells—even those from patients with high-risk cytogenetics—to treatment with mitoxantrone.
However, not all CLL samples were sensitive to treatment, so researchers are now trying to determine which patients might derive benefit from DNA-PK inhibitors.
Gesa Junge, a PhD student at Newcastle University in the UK, and her colleagues conducted this research and presented the results at the AACR Annual Meeting 2015 (abstract 3624*). The work was supported by AstraZeneca.
The researchers’ goal was to validate that DNA-PK inhibition is a valid approach to chemosensitization in CLL. So the team tested NU7441—a compound that inhibits DNA-PK and PI3 kinase—and NDD0004—a more selective DNA-PK inhibitor.
The team isolated CLL cells from patients’ peripheral blood, cultured the cells, and treated them with mitoxantrone and/or 1μM of NDD0004 or 1μM of NU7441.
Junge and her colleagues found that NDD0004 sensitized cells to mitoxantrone more effectively than NU7441. Sensitization was 202-fold higher with NDD004 plus mitoxantrone than with mitoxantrone alone and 69-fold higher with NU7441 plus mitoxantrone than with mitoxantrone alone (P=0.02).
However, sensitization varied between CLL samples, and the researchers have yet to determine why. Their experiments showed that variability was not a result of DNA-PK levels.
Still, the team found that CLL cells from patients with poor prognostic markers were sensitive to DNA-PK inhibition.
Sensitization with NU7441 plus mitoxantrone was 69-fold higher than mitoxantrone alone in CLL samples with del(13q), 25-fold higher in samples with del(11q), 12-fold higher in samples with TP53 mutation, and 16-fold higher in samples with ATM dysfunction.
Sensitization with NDD0004 plus mitoxantrone was 201-fold higher than mitoxantrone alone in CLL samples with del(13q), 314-fold higher in samples with del(11q), 27-fold higher in samples with TP53 mutation, and 18-fold higher in samples with ATM dysfunction.
To confirm that sensitization was a result of DNA-PK inhibition, Junge and her colleagues tested NDD0004 in an isogenic pair of DNA-PK-deficient and DNA-PK-proficient HCT116 cells. They found that HCT116 cells lacking DNA-PK were not sensitive to NDD0004, but cells with DNA-PK were sensitive.
The researchers also investigated the mechanism of NDD0004. Their results suggest the drug works by inhibiting the repair of DNA double-strand breaks.
“What we think is happening is that we are inducing DNA damage with mitoxantrone, and that gets repaired by 24 hours,” Junge said. “But if the DNA-PK inhibitor is there, the damage persists, and that seems to translate quite nicely into an apoptosis response.”
To further this research, Junge and her colleagues are hoping to identify biomarkers that can help them determine which CLL patients are likely to respond to DNA-PK inhibitors. ![]()
*Information in the abstract differs from that presented at the meeting.
PHILADELPHIA—A DNA-dependent protein kinase (DNA-PK) inhibitor can sensitize chronic lymphocytic leukemia (CLL) cells to chemotherapy, according to
preclinical research.
The inhibitor, NDD0004, sensitized CLL cells—even those from patients with high-risk cytogenetics—to treatment with mitoxantrone.
However, not all CLL samples were sensitive to treatment, so researchers are now trying to determine which patients might derive benefit from DNA-PK inhibitors.
Gesa Junge, a PhD student at Newcastle University in the UK, and her colleagues conducted this research and presented the results at the AACR Annual Meeting 2015 (abstract 3624*). The work was supported by AstraZeneca.
The researchers’ goal was to validate that DNA-PK inhibition is a valid approach to chemosensitization in CLL. So the team tested NU7441—a compound that inhibits DNA-PK and PI3 kinase—and NDD0004—a more selective DNA-PK inhibitor.
The team isolated CLL cells from patients’ peripheral blood, cultured the cells, and treated them with mitoxantrone and/or 1μM of NDD0004 or 1μM of NU7441.
Junge and her colleagues found that NDD0004 sensitized cells to mitoxantrone more effectively than NU7441. Sensitization was 202-fold higher with NDD004 plus mitoxantrone than with mitoxantrone alone and 69-fold higher with NU7441 plus mitoxantrone than with mitoxantrone alone (P=0.02).
However, sensitization varied between CLL samples, and the researchers have yet to determine why. Their experiments showed that variability was not a result of DNA-PK levels.
Still, the team found that CLL cells from patients with poor prognostic markers were sensitive to DNA-PK inhibition.
Sensitization with NU7441 plus mitoxantrone was 69-fold higher than mitoxantrone alone in CLL samples with del(13q), 25-fold higher in samples with del(11q), 12-fold higher in samples with TP53 mutation, and 16-fold higher in samples with ATM dysfunction.
Sensitization with NDD0004 plus mitoxantrone was 201-fold higher than mitoxantrone alone in CLL samples with del(13q), 314-fold higher in samples with del(11q), 27-fold higher in samples with TP53 mutation, and 18-fold higher in samples with ATM dysfunction.
To confirm that sensitization was a result of DNA-PK inhibition, Junge and her colleagues tested NDD0004 in an isogenic pair of DNA-PK-deficient and DNA-PK-proficient HCT116 cells. They found that HCT116 cells lacking DNA-PK were not sensitive to NDD0004, but cells with DNA-PK were sensitive.
The researchers also investigated the mechanism of NDD0004. Their results suggest the drug works by inhibiting the repair of DNA double-strand breaks.
“What we think is happening is that we are inducing DNA damage with mitoxantrone, and that gets repaired by 24 hours,” Junge said. “But if the DNA-PK inhibitor is there, the damage persists, and that seems to translate quite nicely into an apoptosis response.”
To further this research, Junge and her colleagues are hoping to identify biomarkers that can help them determine which CLL patients are likely to respond to DNA-PK inhibitors. ![]()
*Information in the abstract differs from that presented at the meeting.
PHILADELPHIA—A DNA-dependent protein kinase (DNA-PK) inhibitor can sensitize chronic lymphocytic leukemia (CLL) cells to chemotherapy, according to
preclinical research.
The inhibitor, NDD0004, sensitized CLL cells—even those from patients with high-risk cytogenetics—to treatment with mitoxantrone.
However, not all CLL samples were sensitive to treatment, so researchers are now trying to determine which patients might derive benefit from DNA-PK inhibitors.
Gesa Junge, a PhD student at Newcastle University in the UK, and her colleagues conducted this research and presented the results at the AACR Annual Meeting 2015 (abstract 3624*). The work was supported by AstraZeneca.
The researchers’ goal was to validate that DNA-PK inhibition is a valid approach to chemosensitization in CLL. So the team tested NU7441—a compound that inhibits DNA-PK and PI3 kinase—and NDD0004—a more selective DNA-PK inhibitor.
The team isolated CLL cells from patients’ peripheral blood, cultured the cells, and treated them with mitoxantrone and/or 1μM of NDD0004 or 1μM of NU7441.
Junge and her colleagues found that NDD0004 sensitized cells to mitoxantrone more effectively than NU7441. Sensitization was 202-fold higher with NDD004 plus mitoxantrone than with mitoxantrone alone and 69-fold higher with NU7441 plus mitoxantrone than with mitoxantrone alone (P=0.02).
However, sensitization varied between CLL samples, and the researchers have yet to determine why. Their experiments showed that variability was not a result of DNA-PK levels.
Still, the team found that CLL cells from patients with poor prognostic markers were sensitive to DNA-PK inhibition.
Sensitization with NU7441 plus mitoxantrone was 69-fold higher than mitoxantrone alone in CLL samples with del(13q), 25-fold higher in samples with del(11q), 12-fold higher in samples with TP53 mutation, and 16-fold higher in samples with ATM dysfunction.
Sensitization with NDD0004 plus mitoxantrone was 201-fold higher than mitoxantrone alone in CLL samples with del(13q), 314-fold higher in samples with del(11q), 27-fold higher in samples with TP53 mutation, and 18-fold higher in samples with ATM dysfunction.
To confirm that sensitization was a result of DNA-PK inhibition, Junge and her colleagues tested NDD0004 in an isogenic pair of DNA-PK-deficient and DNA-PK-proficient HCT116 cells. They found that HCT116 cells lacking DNA-PK were not sensitive to NDD0004, but cells with DNA-PK were sensitive.
The researchers also investigated the mechanism of NDD0004. Their results suggest the drug works by inhibiting the repair of DNA double-strand breaks.
“What we think is happening is that we are inducing DNA damage with mitoxantrone, and that gets repaired by 24 hours,” Junge said. “But if the DNA-PK inhibitor is there, the damage persists, and that seems to translate quite nicely into an apoptosis response.”
To further this research, Junge and her colleagues are hoping to identify biomarkers that can help them determine which CLL patients are likely to respond to DNA-PK inhibitors. ![]()
*Information in the abstract differs from that presented at the meeting.
Improving targeted therapy for leukemia, other diseases

Photo by Sam Ogden
A chemical strategy may allow researchers to target “undruggable” proteins and overcome resistance to current targeted therapies, according to a report published in Science.
The strategy uses tumor cells’ own protein-elimination system to break down and dispose of the proteins that drive cancer growth.
When tested in vitro and in vivo, the approach caused leukemia cells to die more quickly than they do with conventional targeted
therapies.
“One of the reasons [treatment] resistance occurs is that cancer-related proteins often have multiple functions within the cell, and conventional targeted therapies inhibit just one or a few of those functions,” said study author James Bradner, MD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“Conventional drugs allow the targeted protein to adapt to the drug, and the cell finds alternate routes for its growth signals. We began designing approaches that cause the target protein to disintegrate, rather than merely be inhibited. It would be very powerful if we could chemically convert an inhibitor drug into a degrader drug.”
With this in mind, Dr Bradner’s team designed a chemical adapter that attaches to a targeted drug molecule. The adapter enables the drug to tow the cell’s protein-degradation machinery directly to the protein of interest. Once bound to the protein, the combination drug-and-protein-degrader essentially demolishes it.
The investigators tested the technology in leukemia cells. They built an adapter out of phthalimide, a chemical derivative of the drug thalidomide, and attached it to the BRD4 inhibitor JQ1. The phthalimide was designed to “hijack” the cereblon E3 ubiquitin ligase complex.
When the researchers treated the leukemia cells with a JQ1-phthalimide conjugate called dBET1, the BRD4 protein within the cells was degraded in less than an hour. The team said such rapid and extensive degradation suggests conjugates may be able to prevent or hinder cancer cells from developing resistance to targeted therapies.
“The potency, selectivity, and rapidity of this approach—namely, the ability to home in specifically on BRD4—are unprecedented in clinical approaches to protein degradation,” Dr Bradner said.
To determine how selective dBET1 actually is, the investigators measured the levels of all proteins in leukemia cells at 1 hour and 2 hours after treatment.
“We were stunned to find that only 3 proteins of more than 7000 in the entire cell were degraded: BRD2, 3, and 4, an exceptional degree of selectivity guided by the intended targets of JQ1,” Dr Bradner said. “It’s as though dBET1 is laser-guided to deliver protein-degrading machinery to targeted proteins.”
The researchers then tested dBET1 in mice bearing leukemia. As in the cell samples, there was a rapid degradation of BRD4 in the tumor cells and a potent anti-leukemic effect, with few noticeable side effects.
To see if compounds other than JQ1 can be used as a guidance system for a conjugate, the investigators created a set of molecules that lock the protein-degradation machinery onto a compound called SLF, which targets the protein FKBP12.
When they treated cancer cells with SLF, the team found it degraded the vast majority of FKBP12 in the cells within a few hours.
Buoyed by these results, the researchers are working to create a derivative of dBET1 that can be used as a drug in humans and to extend the conjugate strategy for the treatment of other diseases.
“The dBET1 and the dFKBP12 compounds are presently in a late stage of lead optimization for therapeutic development in both cancer and non-malignant diseases,” said Prem Das, PhD, chief research business development officer at Dana-Farber.
“Composition-of-matter and method-of-use patent applications have been filed on these and other additional targeted agents, as well as on the chemistry platform. They will be licensed for commercialization to an appropriate company according to standard Dana-Farber practice.” ![]()
Photo by Sam Ogden
A chemical strategy may allow researchers to target “undruggable” proteins and overcome resistance to current targeted therapies, according to a report published in Science.
The strategy uses tumor cells’ own protein-elimination system to break down and dispose of the proteins that drive cancer growth.
When tested in vitro and in vivo, the approach caused leukemia cells to die more quickly than they do with conventional targeted
therapies.
“One of the reasons [treatment] resistance occurs is that cancer-related proteins often have multiple functions within the cell, and conventional targeted therapies inhibit just one or a few of those functions,” said study author James Bradner, MD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“Conventional drugs allow the targeted protein to adapt to the drug, and the cell finds alternate routes for its growth signals. We began designing approaches that cause the target protein to disintegrate, rather than merely be inhibited. It would be very powerful if we could chemically convert an inhibitor drug into a degrader drug.”
With this in mind, Dr Bradner’s team designed a chemical adapter that attaches to a targeted drug molecule. The adapter enables the drug to tow the cell’s protein-degradation machinery directly to the protein of interest. Once bound to the protein, the combination drug-and-protein-degrader essentially demolishes it.
The investigators tested the technology in leukemia cells. They built an adapter out of phthalimide, a chemical derivative of the drug thalidomide, and attached it to the BRD4 inhibitor JQ1. The phthalimide was designed to “hijack” the cereblon E3 ubiquitin ligase complex.
When the researchers treated the leukemia cells with a JQ1-phthalimide conjugate called dBET1, the BRD4 protein within the cells was degraded in less than an hour. The team said such rapid and extensive degradation suggests conjugates may be able to prevent or hinder cancer cells from developing resistance to targeted therapies.
“The potency, selectivity, and rapidity of this approach—namely, the ability to home in specifically on BRD4—are unprecedented in clinical approaches to protein degradation,” Dr Bradner said.
To determine how selective dBET1 actually is, the investigators measured the levels of all proteins in leukemia cells at 1 hour and 2 hours after treatment.
“We were stunned to find that only 3 proteins of more than 7000 in the entire cell were degraded: BRD2, 3, and 4, an exceptional degree of selectivity guided by the intended targets of JQ1,” Dr Bradner said. “It’s as though dBET1 is laser-guided to deliver protein-degrading machinery to targeted proteins.”
The researchers then tested dBET1 in mice bearing leukemia. As in the cell samples, there was a rapid degradation of BRD4 in the tumor cells and a potent anti-leukemic effect, with few noticeable side effects.
To see if compounds other than JQ1 can be used as a guidance system for a conjugate, the investigators created a set of molecules that lock the protein-degradation machinery onto a compound called SLF, which targets the protein FKBP12.
When they treated cancer cells with SLF, the team found it degraded the vast majority of FKBP12 in the cells within a few hours.
Buoyed by these results, the researchers are working to create a derivative of dBET1 that can be used as a drug in humans and to extend the conjugate strategy for the treatment of other diseases.
“The dBET1 and the dFKBP12 compounds are presently in a late stage of lead optimization for therapeutic development in both cancer and non-malignant diseases,” said Prem Das, PhD, chief research business development officer at Dana-Farber.
“Composition-of-matter and method-of-use patent applications have been filed on these and other additional targeted agents, as well as on the chemistry platform. They will be licensed for commercialization to an appropriate company according to standard Dana-Farber practice.” ![]()
Photo by Sam Ogden
A chemical strategy may allow researchers to target “undruggable” proteins and overcome resistance to current targeted therapies, according to a report published in Science.
The strategy uses tumor cells’ own protein-elimination system to break down and dispose of the proteins that drive cancer growth.
When tested in vitro and in vivo, the approach caused leukemia cells to die more quickly than they do with conventional targeted
therapies.
“One of the reasons [treatment] resistance occurs is that cancer-related proteins often have multiple functions within the cell, and conventional targeted therapies inhibit just one or a few of those functions,” said study author James Bradner, MD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“Conventional drugs allow the targeted protein to adapt to the drug, and the cell finds alternate routes for its growth signals. We began designing approaches that cause the target protein to disintegrate, rather than merely be inhibited. It would be very powerful if we could chemically convert an inhibitor drug into a degrader drug.”
With this in mind, Dr Bradner’s team designed a chemical adapter that attaches to a targeted drug molecule. The adapter enables the drug to tow the cell’s protein-degradation machinery directly to the protein of interest. Once bound to the protein, the combination drug-and-protein-degrader essentially demolishes it.
The investigators tested the technology in leukemia cells. They built an adapter out of phthalimide, a chemical derivative of the drug thalidomide, and attached it to the BRD4 inhibitor JQ1. The phthalimide was designed to “hijack” the cereblon E3 ubiquitin ligase complex.
When the researchers treated the leukemia cells with a JQ1-phthalimide conjugate called dBET1, the BRD4 protein within the cells was degraded in less than an hour. The team said such rapid and extensive degradation suggests conjugates may be able to prevent or hinder cancer cells from developing resistance to targeted therapies.
“The potency, selectivity, and rapidity of this approach—namely, the ability to home in specifically on BRD4—are unprecedented in clinical approaches to protein degradation,” Dr Bradner said.
To determine how selective dBET1 actually is, the investigators measured the levels of all proteins in leukemia cells at 1 hour and 2 hours after treatment.
“We were stunned to find that only 3 proteins of more than 7000 in the entire cell were degraded: BRD2, 3, and 4, an exceptional degree of selectivity guided by the intended targets of JQ1,” Dr Bradner said. “It’s as though dBET1 is laser-guided to deliver protein-degrading machinery to targeted proteins.”
The researchers then tested dBET1 in mice bearing leukemia. As in the cell samples, there was a rapid degradation of BRD4 in the tumor cells and a potent anti-leukemic effect, with few noticeable side effects.
To see if compounds other than JQ1 can be used as a guidance system for a conjugate, the investigators created a set of molecules that lock the protein-degradation machinery onto a compound called SLF, which targets the protein FKBP12.
When they treated cancer cells with SLF, the team found it degraded the vast majority of FKBP12 in the cells within a few hours.
Buoyed by these results, the researchers are working to create a derivative of dBET1 that can be used as a drug in humans and to extend the conjugate strategy for the treatment of other diseases.
“The dBET1 and the dFKBP12 compounds are presently in a late stage of lead optimization for therapeutic development in both cancer and non-malignant diseases,” said Prem Das, PhD, chief research business development officer at Dana-Farber.
“Composition-of-matter and method-of-use patent applications have been filed on these and other additional targeted agents, as well as on the chemistry platform. They will be licensed for commercialization to an appropriate company according to standard Dana-Farber practice.” ![]()
Team reports new method to identify immune cells

Photo by Graham Colm
A new method for identifying immune cells could pave the way for rapid detection of hematologic malignancies from a small blood sample, according to researchers.
The team found they could use wavelength modulated Raman spectroscopy (WMRS) to identify subsets of T cells, natural killer cells, and dendritic cells.
Traditional methods of identifying these cells usually involve labeling them with fluorescent or magnetically labeled antibodies.
Using WMRS, the researchers were able to identify immune cells with no labeling at all, thus permitting rapid identification and further analysis to take place with no potential alteration to the cells.
Simon Powis, PhD, of the University of St Andrews in Fife, Scotland, and his colleagues described this work in PLOS ONE.
Raman scattering refers to light scattering from molecules in a sample where the light energy can be shifted up or down and recorded as a “molecular fingerprint” that can be used for identification. Normally, this process is very weak and further hampered by other background light (eg, fluorescence).
WMRS subtly changes the incident laser light that, in turn, results in a modulation of the Raman signal, allowing it to be extracted from any (stationary) interfering signal.
Using WMRS, Dr Powis and his colleagues found they could identify CD4+ T cells, CD8+ T cells, CD56+ natural killer cells, CD303+ lymphoid/plasmacytoid dendritic cells, and CD1c+ myeloid dendritic cells.
“Under a normal light microscope, these immune cells essentially all look identical,” Dr Powis said. “With this new method, we can identify key cell types without any labeling.”
“Our next goal is to make a full catalogue of all the normal cell types of the immune system that can be detected in the bloodstream. Once we have this completed, we can then collaborate with our clinical colleagues to start identifying when these immune cells are altered, in conditions such as leukemia and lymphoma, potentially providing a rapid detection system from just a small blood sample.” ![]()
Photo by Graham Colm
A new method for identifying immune cells could pave the way for rapid detection of hematologic malignancies from a small blood sample, according to researchers.
The team found they could use wavelength modulated Raman spectroscopy (WMRS) to identify subsets of T cells, natural killer cells, and dendritic cells.
Traditional methods of identifying these cells usually involve labeling them with fluorescent or magnetically labeled antibodies.
Using WMRS, the researchers were able to identify immune cells with no labeling at all, thus permitting rapid identification and further analysis to take place with no potential alteration to the cells.
Simon Powis, PhD, of the University of St Andrews in Fife, Scotland, and his colleagues described this work in PLOS ONE.
Raman scattering refers to light scattering from molecules in a sample where the light energy can be shifted up or down and recorded as a “molecular fingerprint” that can be used for identification. Normally, this process is very weak and further hampered by other background light (eg, fluorescence).
WMRS subtly changes the incident laser light that, in turn, results in a modulation of the Raman signal, allowing it to be extracted from any (stationary) interfering signal.
Using WMRS, Dr Powis and his colleagues found they could identify CD4+ T cells, CD8+ T cells, CD56+ natural killer cells, CD303+ lymphoid/plasmacytoid dendritic cells, and CD1c+ myeloid dendritic cells.
“Under a normal light microscope, these immune cells essentially all look identical,” Dr Powis said. “With this new method, we can identify key cell types without any labeling.”
“Our next goal is to make a full catalogue of all the normal cell types of the immune system that can be detected in the bloodstream. Once we have this completed, we can then collaborate with our clinical colleagues to start identifying when these immune cells are altered, in conditions such as leukemia and lymphoma, potentially providing a rapid detection system from just a small blood sample.” ![]()
Photo by Graham Colm
A new method for identifying immune cells could pave the way for rapid detection of hematologic malignancies from a small blood sample, according to researchers.
The team found they could use wavelength modulated Raman spectroscopy (WMRS) to identify subsets of T cells, natural killer cells, and dendritic cells.
Traditional methods of identifying these cells usually involve labeling them with fluorescent or magnetically labeled antibodies.
Using WMRS, the researchers were able to identify immune cells with no labeling at all, thus permitting rapid identification and further analysis to take place with no potential alteration to the cells.
Simon Powis, PhD, of the University of St Andrews in Fife, Scotland, and his colleagues described this work in PLOS ONE.
Raman scattering refers to light scattering from molecules in a sample where the light energy can be shifted up or down and recorded as a “molecular fingerprint” that can be used for identification. Normally, this process is very weak and further hampered by other background light (eg, fluorescence).
WMRS subtly changes the incident laser light that, in turn, results in a modulation of the Raman signal, allowing it to be extracted from any (stationary) interfering signal.
Using WMRS, Dr Powis and his colleagues found they could identify CD4+ T cells, CD8+ T cells, CD56+ natural killer cells, CD303+ lymphoid/plasmacytoid dendritic cells, and CD1c+ myeloid dendritic cells.
“Under a normal light microscope, these immune cells essentially all look identical,” Dr Powis said. “With this new method, we can identify key cell types without any labeling.”
“Our next goal is to make a full catalogue of all the normal cell types of the immune system that can be detected in the bloodstream. Once we have this completed, we can then collaborate with our clinical colleagues to start identifying when these immune cells are altered, in conditions such as leukemia and lymphoma, potentially providing a rapid detection system from just a small blood sample.” ![]()
IL-2 variant proves active against ATL, GVHD

Photo by Rhoda Baer
Researchers say they have created interleukin-2 (IL-2) variants that function as IL-2-receptor signaling “clamps” and allow for “fine tuning” of the signaling amplitude.
One variant, known as H9-RETR, was able to inhibit the actions of endogenous IL-2 and IL-15, prolong survival in a mouse model of graft-vs-host disease (GVHD), and inhibit the proliferation of cells derived from a patient with smoldering adult T-cell
leukemia (ATL).
The researchers reported these results in Immunity.
Warren J. Leonard, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues developed IL-2 variants in which activity can be tuned to either boost or block immune responses, depending on the desired therapeutic application.
The researchers said these variants had high affinity for IL-2Rβ and inhibited binding of endogenous IL-2, but their interaction with γc was weakened, thereby weakening IL-2Rβ-γc heterodimerization.
The team found that IL-2 signaling strength was inversely correlated with the degree of mutation at the γc interface. And differential effects on cell proliferation were dependent upon the cells’ state of activation.
One of the IL-2 variants, H9-RETR, inhibited IL-2- and IL-15-mediated proliferation and cytotoxicity. H9-RETR inhibited cytokine signaling and natural killer cell activity as well or better than blocking antibodies to IL-2Rα and IL-2Rβ.
In experiments with cells isolated from a patient with smoldering ATL, H9-RETR blocked IL-2 signaling and inhibited the spontaneous proliferation of ATL cells. In this regard, H9-RETR was at least as effective as the anti-IL-2Rα antibody daclizumab and much more effective than the anti-IL-2Rβ antibody Mikβ1.
In a mouse model of GVHD, animals that received a stabilized, Fc-fusion version of H9-RETR (H9-RETR-Fc4) had significantly longer survival than control mice (which received only Fc4 protein).
All of the control mice had died by 40 days post-injection, but it took 60 days for all of the H9-RETR-Fc4-treated mice to die (P=0.0001).
The researchers believe their receptor-clamping approach could potentially be used to engineer other immune-system cytokines with therapeutic potential. ![]()
Photo by Rhoda Baer
Researchers say they have created interleukin-2 (IL-2) variants that function as IL-2-receptor signaling “clamps” and allow for “fine tuning” of the signaling amplitude.
One variant, known as H9-RETR, was able to inhibit the actions of endogenous IL-2 and IL-15, prolong survival in a mouse model of graft-vs-host disease (GVHD), and inhibit the proliferation of cells derived from a patient with smoldering adult T-cell
leukemia (ATL).
The researchers reported these results in Immunity.
Warren J. Leonard, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues developed IL-2 variants in which activity can be tuned to either boost or block immune responses, depending on the desired therapeutic application.
The researchers said these variants had high affinity for IL-2Rβ and inhibited binding of endogenous IL-2, but their interaction with γc was weakened, thereby weakening IL-2Rβ-γc heterodimerization.
The team found that IL-2 signaling strength was inversely correlated with the degree of mutation at the γc interface. And differential effects on cell proliferation were dependent upon the cells’ state of activation.
One of the IL-2 variants, H9-RETR, inhibited IL-2- and IL-15-mediated proliferation and cytotoxicity. H9-RETR inhibited cytokine signaling and natural killer cell activity as well or better than blocking antibodies to IL-2Rα and IL-2Rβ.
In experiments with cells isolated from a patient with smoldering ATL, H9-RETR blocked IL-2 signaling and inhibited the spontaneous proliferation of ATL cells. In this regard, H9-RETR was at least as effective as the anti-IL-2Rα antibody daclizumab and much more effective than the anti-IL-2Rβ antibody Mikβ1.
In a mouse model of GVHD, animals that received a stabilized, Fc-fusion version of H9-RETR (H9-RETR-Fc4) had significantly longer survival than control mice (which received only Fc4 protein).
All of the control mice had died by 40 days post-injection, but it took 60 days for all of the H9-RETR-Fc4-treated mice to die (P=0.0001).
The researchers believe their receptor-clamping approach could potentially be used to engineer other immune-system cytokines with therapeutic potential. ![]()
Photo by Rhoda Baer
Researchers say they have created interleukin-2 (IL-2) variants that function as IL-2-receptor signaling “clamps” and allow for “fine tuning” of the signaling amplitude.
One variant, known as H9-RETR, was able to inhibit the actions of endogenous IL-2 and IL-15, prolong survival in a mouse model of graft-vs-host disease (GVHD), and inhibit the proliferation of cells derived from a patient with smoldering adult T-cell
leukemia (ATL).
The researchers reported these results in Immunity.
Warren J. Leonard, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues developed IL-2 variants in which activity can be tuned to either boost or block immune responses, depending on the desired therapeutic application.
The researchers said these variants had high affinity for IL-2Rβ and inhibited binding of endogenous IL-2, but their interaction with γc was weakened, thereby weakening IL-2Rβ-γc heterodimerization.
The team found that IL-2 signaling strength was inversely correlated with the degree of mutation at the γc interface. And differential effects on cell proliferation were dependent upon the cells’ state of activation.
One of the IL-2 variants, H9-RETR, inhibited IL-2- and IL-15-mediated proliferation and cytotoxicity. H9-RETR inhibited cytokine signaling and natural killer cell activity as well or better than blocking antibodies to IL-2Rα and IL-2Rβ.
In experiments with cells isolated from a patient with smoldering ATL, H9-RETR blocked IL-2 signaling and inhibited the spontaneous proliferation of ATL cells. In this regard, H9-RETR was at least as effective as the anti-IL-2Rα antibody daclizumab and much more effective than the anti-IL-2Rβ antibody Mikβ1.
In a mouse model of GVHD, animals that received a stabilized, Fc-fusion version of H9-RETR (H9-RETR-Fc4) had significantly longer survival than control mice (which received only Fc4 protein).
All of the control mice had died by 40 days post-injection, but it took 60 days for all of the H9-RETR-Fc4-treated mice to die (P=0.0001).
The researchers believe their receptor-clamping approach could potentially be used to engineer other immune-system cytokines with therapeutic potential. ![]()
CTLs captured on video destroying cancer cells
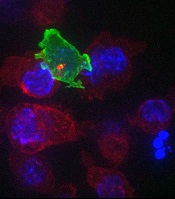
cancer cells (blue)
Image courtesy of Gillian
Griffiths and Jonny Settle
New research has illuminated the behavior of cytotoxic T cells (CTLs) as they hunt down and eliminate cancer cells.
Investigators used novel imaging techniques to capture the process on film and described their findings in an article published in Immunity.
The team captured the footage through high-resolution, 3D, time-lapse, multi-color imaging, making use of both spinning disk confocal microscopy and lattice light sheet microscopy.
These techniques involve capturing “slices” of an object and “stitching” them together to provide the final 3D images across the whole cell.
These approaches allowed the investigators to determine the order of events leading to the lethal “hit” CTLs deliver to cancer cells.
“Inside all of us lurks an army of ‘serial killers’ whose primary function is to kill again and again,” said study author Gillian Griffiths, PhD, of the Cambridge Institute for Medical Research in the UK.
“These [CTLs] patrol our bodies, identifying and destroying virally infected and cancer cells, and they do so with remarkable precision and efficiency.”
The CTLs, seen in the video as orange or green amorphous “blobs,” move around rapidly, investigating their environment as they travel.
When a CTL finds a cancer cell (blue), membrane protrusions rapidly explore the surface of the cell, checking for tell-tale signs that this is an uninvited guest.
The CTL binds to the cancer cell and injects cytotoxins (red) down microtubules to the interface between the T cell and the cancer cell, before puncturing the surface of the cancer cell and delivering its deadly cargo.
“In our bodies, where cells are packed together, it’s essential that the T cell focuses the lethal hit on its target,” Dr Griffiths explained. “Otherwise, it will cause collateral damage to neighboring, healthy cells.”
“Once the cytotoxins are injected into the cancer cell, its fate is sealed, and we can watch as it withers and dies. The T cell then moves on, hungry to find another victim.”
The investigators’ video is available on YouTube. ![]()
cancer cells (blue)
Image courtesy of Gillian
Griffiths and Jonny Settle
New research has illuminated the behavior of cytotoxic T cells (CTLs) as they hunt down and eliminate cancer cells.
Investigators used novel imaging techniques to capture the process on film and described their findings in an article published in Immunity.
The team captured the footage through high-resolution, 3D, time-lapse, multi-color imaging, making use of both spinning disk confocal microscopy and lattice light sheet microscopy.
These techniques involve capturing “slices” of an object and “stitching” them together to provide the final 3D images across the whole cell.
These approaches allowed the investigators to determine the order of events leading to the lethal “hit” CTLs deliver to cancer cells.
“Inside all of us lurks an army of ‘serial killers’ whose primary function is to kill again and again,” said study author Gillian Griffiths, PhD, of the Cambridge Institute for Medical Research in the UK.
“These [CTLs] patrol our bodies, identifying and destroying virally infected and cancer cells, and they do so with remarkable precision and efficiency.”
The CTLs, seen in the video as orange or green amorphous “blobs,” move around rapidly, investigating their environment as they travel.
When a CTL finds a cancer cell (blue), membrane protrusions rapidly explore the surface of the cell, checking for tell-tale signs that this is an uninvited guest.
The CTL binds to the cancer cell and injects cytotoxins (red) down microtubules to the interface between the T cell and the cancer cell, before puncturing the surface of the cancer cell and delivering its deadly cargo.
“In our bodies, where cells are packed together, it’s essential that the T cell focuses the lethal hit on its target,” Dr Griffiths explained. “Otherwise, it will cause collateral damage to neighboring, healthy cells.”
“Once the cytotoxins are injected into the cancer cell, its fate is sealed, and we can watch as it withers and dies. The T cell then moves on, hungry to find another victim.”
The investigators’ video is available on YouTube. ![]()
cancer cells (blue)
Image courtesy of Gillian
Griffiths and Jonny Settle
New research has illuminated the behavior of cytotoxic T cells (CTLs) as they hunt down and eliminate cancer cells.
Investigators used novel imaging techniques to capture the process on film and described their findings in an article published in Immunity.
The team captured the footage through high-resolution, 3D, time-lapse, multi-color imaging, making use of both spinning disk confocal microscopy and lattice light sheet microscopy.
These techniques involve capturing “slices” of an object and “stitching” them together to provide the final 3D images across the whole cell.
These approaches allowed the investigators to determine the order of events leading to the lethal “hit” CTLs deliver to cancer cells.
“Inside all of us lurks an army of ‘serial killers’ whose primary function is to kill again and again,” said study author Gillian Griffiths, PhD, of the Cambridge Institute for Medical Research in the UK.
“These [CTLs] patrol our bodies, identifying and destroying virally infected and cancer cells, and they do so with remarkable precision and efficiency.”
The CTLs, seen in the video as orange or green amorphous “blobs,” move around rapidly, investigating their environment as they travel.
When a CTL finds a cancer cell (blue), membrane protrusions rapidly explore the surface of the cell, checking for tell-tale signs that this is an uninvited guest.
The CTL binds to the cancer cell and injects cytotoxins (red) down microtubules to the interface between the T cell and the cancer cell, before puncturing the surface of the cancer cell and delivering its deadly cargo.
“In our bodies, where cells are packed together, it’s essential that the T cell focuses the lethal hit on its target,” Dr Griffiths explained. “Otherwise, it will cause collateral damage to neighboring, healthy cells.”
“Once the cytotoxins are injected into the cancer cell, its fate is sealed, and we can watch as it withers and dies. The T cell then moves on, hungry to find another victim.”
The investigators’ video is available on YouTube. ![]()
How a vaccine may reduce the risk of ALL

Photo by Petr Kratochvil
Researchers believe they have discovered how a commonly administered vaccine protects children from developing acute lymphoblastic leukemia (ALL).
The Haemophilus influenzae Type b (Hib) vaccine is part of the standard vaccination schedule recommended for children by the US Centers for Disease Control and Prevention. The vaccine is routinely given in 4 doses before children reach 15 months of age.
The Hib vaccine prevents ear infections and meningitis caused by the Hib bacterium, but it may also protect against ALL.
This protection has been suggested in previous studies, but it is not well-known among the public at large, and the mechanism underlying this effect has been poorly understood.
Now, researchers have shown that recurrent Hib infections can shift certain genes into overdrive, converting pre-leukemic cells into full-blown cancer. The team described this work in Nature Immunology.
“These experiments help explain why the incidence of leukemia has been dramatically reduced since the advent of regular vaccinations during infancy,” said study author Markus Müschen, MD, PhD, of the University of California San Francisco.
“Hib and other childhood infections can cause recurrent and vehement immune responses, which we have found could lead to leukemia, but infants that have received vaccines are largely protected and acquire long-term immunity through very mild immune reactions.”
For this study, Dr Müschen and his colleagues tested the idea that chronic inflammation caused by recurrent infections might cause additional genetic lesions in blood cells already carrying an oncogene, promoting their transformation to overt disease.
The team conducted experiments in mice and discovered that the enzymes AID and RAG1-RAG2 drive this process. AID and RAG1-RAG2 introduce mutations in DNA that allow immune cells to adapt to infectious challenges, and these enzymes are necessary for a normal and efficient immune response.
The researchers found that, in the presence of chronic infection, AID and RAG1-RAG2 were hyperactivated, randomly cutting and mutating genes.
Additional experiments revealed that AID and RAG1-RAG2 working together is critical to introduce the additional lesions that result in ALL.
Though the researchers focused on a bacterial infection in this study, they believe the same mechanisms may be at work in viral infections.
The team is currently conducting experiments to determine if protection against leukemia is provided by vaccines against viral infections, such as the measles-mumps-rubella vaccine. ![]()
Photo by Petr Kratochvil
Researchers believe they have discovered how a commonly administered vaccine protects children from developing acute lymphoblastic leukemia (ALL).
The Haemophilus influenzae Type b (Hib) vaccine is part of the standard vaccination schedule recommended for children by the US Centers for Disease Control and Prevention. The vaccine is routinely given in 4 doses before children reach 15 months of age.
The Hib vaccine prevents ear infections and meningitis caused by the Hib bacterium, but it may also protect against ALL.
This protection has been suggested in previous studies, but it is not well-known among the public at large, and the mechanism underlying this effect has been poorly understood.
Now, researchers have shown that recurrent Hib infections can shift certain genes into overdrive, converting pre-leukemic cells into full-blown cancer. The team described this work in Nature Immunology.
“These experiments help explain why the incidence of leukemia has been dramatically reduced since the advent of regular vaccinations during infancy,” said study author Markus Müschen, MD, PhD, of the University of California San Francisco.
“Hib and other childhood infections can cause recurrent and vehement immune responses, which we have found could lead to leukemia, but infants that have received vaccines are largely protected and acquire long-term immunity through very mild immune reactions.”
For this study, Dr Müschen and his colleagues tested the idea that chronic inflammation caused by recurrent infections might cause additional genetic lesions in blood cells already carrying an oncogene, promoting their transformation to overt disease.
The team conducted experiments in mice and discovered that the enzymes AID and RAG1-RAG2 drive this process. AID and RAG1-RAG2 introduce mutations in DNA that allow immune cells to adapt to infectious challenges, and these enzymes are necessary for a normal and efficient immune response.
The researchers found that, in the presence of chronic infection, AID and RAG1-RAG2 were hyperactivated, randomly cutting and mutating genes.
Additional experiments revealed that AID and RAG1-RAG2 working together is critical to introduce the additional lesions that result in ALL.
Though the researchers focused on a bacterial infection in this study, they believe the same mechanisms may be at work in viral infections.
The team is currently conducting experiments to determine if protection against leukemia is provided by vaccines against viral infections, such as the measles-mumps-rubella vaccine. ![]()
Photo by Petr Kratochvil
Researchers believe they have discovered how a commonly administered vaccine protects children from developing acute lymphoblastic leukemia (ALL).
The Haemophilus influenzae Type b (Hib) vaccine is part of the standard vaccination schedule recommended for children by the US Centers for Disease Control and Prevention. The vaccine is routinely given in 4 doses before children reach 15 months of age.
The Hib vaccine prevents ear infections and meningitis caused by the Hib bacterium, but it may also protect against ALL.
This protection has been suggested in previous studies, but it is not well-known among the public at large, and the mechanism underlying this effect has been poorly understood.
Now, researchers have shown that recurrent Hib infections can shift certain genes into overdrive, converting pre-leukemic cells into full-blown cancer. The team described this work in Nature Immunology.
“These experiments help explain why the incidence of leukemia has been dramatically reduced since the advent of regular vaccinations during infancy,” said study author Markus Müschen, MD, PhD, of the University of California San Francisco.
“Hib and other childhood infections can cause recurrent and vehement immune responses, which we have found could lead to leukemia, but infants that have received vaccines are largely protected and acquire long-term immunity through very mild immune reactions.”
For this study, Dr Müschen and his colleagues tested the idea that chronic inflammation caused by recurrent infections might cause additional genetic lesions in blood cells already carrying an oncogene, promoting their transformation to overt disease.
The team conducted experiments in mice and discovered that the enzymes AID and RAG1-RAG2 drive this process. AID and RAG1-RAG2 introduce mutations in DNA that allow immune cells to adapt to infectious challenges, and these enzymes are necessary for a normal and efficient immune response.
The researchers found that, in the presence of chronic infection, AID and RAG1-RAG2 were hyperactivated, randomly cutting and mutating genes.
Additional experiments revealed that AID and RAG1-RAG2 working together is critical to introduce the additional lesions that result in ALL.
Though the researchers focused on a bacterial infection in this study, they believe the same mechanisms may be at work in viral infections.
The team is currently conducting experiments to determine if protection against leukemia is provided by vaccines against viral infections, such as the measles-mumps-rubella vaccine.
FDA grants inhibitor fast track designation for AML

The US Food and Drug Administration (FDA) has granted fast track designation to AG-120 for the treatment of patients with acute myelogenous leukemia (AML) who harbor an isocitrate dehydrogenase-1 (IDH1) mutation.
AG-120 is an oral, selective inhibitor of the mutated IDH1 protein that is under investigation in two phase 1 clinical trials, one in hematologic malignancies and one in advanced solid tumors.
Data from the phase 1 trial in hematologic malignancies were previously presented at the 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics in November 2014.
Updated data from this trial are scheduled to be presented at the 20th Annual Congress of the European Hematology Association (EHA) next month.
About fast track designation
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
“We are pleased that now both AG-120 and AG-221 have been granted fast track designation, demonstrating the FDA’s commitment to facilitate the development and expedite the review of our lead IDH programs as important new therapies for people with AML who carry these mutations,” said Chris Bowden, MD, chief medical officer of Agios Pharmaceuticals, Inc., the company developing AG-120 in cooperation with Celgene Corporation.
Phase 1 results
At the EORTC-NCI-AACR symposium, researchers presented results from the ongoing phase 1 trial of AG-120 in hematologic malignancies. The data included 17 patients with relapsed and/or refractory AML who had received a median of 2 prior treatments.
The patients were scheduled to receive AG-120 in 1 of 4 dose groups: 100 mg twice a day, 300 mg once a day, 500 mg once a day, and 800 mg once a day over continuous, 28-day cycles.
Of the 14 patients evaluable for response, 7 responded. Four patients achieved a complete response, 2 had a complete response in the marrow, and 1 had a partial response.
Responses occurred at all the dose levels tested. The maximum-tolerated dose was not reached. All responding patients were still on AG-120 at the time of presentation, and 1 patient with stable disease remained on the drug.
Researchers said AG-120 was generally well-tolerated. The majority of adverse events were grade 1 and 2. The most common of these were nausea, fatigue, and dyspnea.
Eight patients experienced serious adverse events, but these were primarily related to disease progression.
One patient experienced a dose-limiting toxicity of asymptomatic grade 3 QT prolongation at the highest dose tested, which improved to grade 1 with dose reduction. The patient was in complete remission and remained on AG-120 at the time of presentation.
There were 6 patient deaths, all unrelated to AG-120. Five deaths occurred after patients discontinued treatment due to progressive disease, and 1 patient died due to disease-related intracranial hemorrhage while on treatment.
“We look forward to presenting new data from the ongoing phase 1 study at the EHA Annual Congress next month,” Dr Bowden said, “and remain on track to initiate a global, registration-enabling, phase 3 study in collaboration with Celgene in AML patients who harbor an IDH1 mutation in the first half of 2016.”
The US Food and Drug Administration (FDA) has granted fast track designation to AG-120 for the treatment of patients with acute myelogenous leukemia (AML) who harbor an isocitrate dehydrogenase-1 (IDH1) mutation.
AG-120 is an oral, selective inhibitor of the mutated IDH1 protein that is under investigation in two phase 1 clinical trials, one in hematologic malignancies and one in advanced solid tumors.
Data from the phase 1 trial in hematologic malignancies were previously presented at the 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics in November 2014.
Updated data from this trial are scheduled to be presented at the 20th Annual Congress of the European Hematology Association (EHA) next month.
About fast track designation
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
“We are pleased that now both AG-120 and AG-221 have been granted fast track designation, demonstrating the FDA’s commitment to facilitate the development and expedite the review of our lead IDH programs as important new therapies for people with AML who carry these mutations,” said Chris Bowden, MD, chief medical officer of Agios Pharmaceuticals, Inc., the company developing AG-120 in cooperation with Celgene Corporation.
Phase 1 results
At the EORTC-NCI-AACR symposium, researchers presented results from the ongoing phase 1 trial of AG-120 in hematologic malignancies. The data included 17 patients with relapsed and/or refractory AML who had received a median of 2 prior treatments.
The patients were scheduled to receive AG-120 in 1 of 4 dose groups: 100 mg twice a day, 300 mg once a day, 500 mg once a day, and 800 mg once a day over continuous, 28-day cycles.
Of the 14 patients evaluable for response, 7 responded. Four patients achieved a complete response, 2 had a complete response in the marrow, and 1 had a partial response.
Responses occurred at all the dose levels tested. The maximum-tolerated dose was not reached. All responding patients were still on AG-120 at the time of presentation, and 1 patient with stable disease remained on the drug.
Researchers said AG-120 was generally well-tolerated. The majority of adverse events were grade 1 and 2. The most common of these were nausea, fatigue, and dyspnea.
Eight patients experienced serious adverse events, but these were primarily related to disease progression.
One patient experienced a dose-limiting toxicity of asymptomatic grade 3 QT prolongation at the highest dose tested, which improved to grade 1 with dose reduction. The patient was in complete remission and remained on AG-120 at the time of presentation.
There were 6 patient deaths, all unrelated to AG-120. Five deaths occurred after patients discontinued treatment due to progressive disease, and 1 patient died due to disease-related intracranial hemorrhage while on treatment.
“We look forward to presenting new data from the ongoing phase 1 study at the EHA Annual Congress next month,” Dr Bowden said, “and remain on track to initiate a global, registration-enabling, phase 3 study in collaboration with Celgene in AML patients who harbor an IDH1 mutation in the first half of 2016.”
The US Food and Drug Administration (FDA) has granted fast track designation to AG-120 for the treatment of patients with acute myelogenous leukemia (AML) who harbor an isocitrate dehydrogenase-1 (IDH1) mutation.
AG-120 is an oral, selective inhibitor of the mutated IDH1 protein that is under investigation in two phase 1 clinical trials, one in hematologic malignancies and one in advanced solid tumors.
Data from the phase 1 trial in hematologic malignancies were previously presented at the 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics in November 2014.
Updated data from this trial are scheduled to be presented at the 20th Annual Congress of the European Hematology Association (EHA) next month.
About fast track designation
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
“We are pleased that now both AG-120 and AG-221 have been granted fast track designation, demonstrating the FDA’s commitment to facilitate the development and expedite the review of our lead IDH programs as important new therapies for people with AML who carry these mutations,” said Chris Bowden, MD, chief medical officer of Agios Pharmaceuticals, Inc., the company developing AG-120 in cooperation with Celgene Corporation.
Phase 1 results
At the EORTC-NCI-AACR symposium, researchers presented results from the ongoing phase 1 trial of AG-120 in hematologic malignancies. The data included 17 patients with relapsed and/or refractory AML who had received a median of 2 prior treatments.
The patients were scheduled to receive AG-120 in 1 of 4 dose groups: 100 mg twice a day, 300 mg once a day, 500 mg once a day, and 800 mg once a day over continuous, 28-day cycles.
Of the 14 patients evaluable for response, 7 responded. Four patients achieved a complete response, 2 had a complete response in the marrow, and 1 had a partial response.
Responses occurred at all the dose levels tested. The maximum-tolerated dose was not reached. All responding patients were still on AG-120 at the time of presentation, and 1 patient with stable disease remained on the drug.
Researchers said AG-120 was generally well-tolerated. The majority of adverse events were grade 1 and 2. The most common of these were nausea, fatigue, and dyspnea.
Eight patients experienced serious adverse events, but these were primarily related to disease progression.
One patient experienced a dose-limiting toxicity of asymptomatic grade 3 QT prolongation at the highest dose tested, which improved to grade 1 with dose reduction. The patient was in complete remission and remained on AG-120 at the time of presentation.
There were 6 patient deaths, all unrelated to AG-120. Five deaths occurred after patients discontinued treatment due to progressive disease, and 1 patient died due to disease-related intracranial hemorrhage while on treatment.
“We look forward to presenting new data from the ongoing phase 1 study at the EHA Annual Congress next month,” Dr Bowden said, “and remain on track to initiate a global, registration-enabling, phase 3 study in collaboration with Celgene in AML patients who harbor an IDH1 mutation in the first half of 2016.”
MRD doesn’t suggest need for more treatment
© Hind Medyouf, German
Cancer Research Center
A new study suggests that minimal residual disease (MRD) alone is not predictive of outcomes in children with T-cell acute lymphoblastic leukemia (T-ALL).
Study investigators analyzed a small group of T-ALL patients who received similar treatment regimens, comparing those with and without MRD after induction.
None of the MRD-positive patients relapsed within the follow-up period, despite not receiving intensified treatment to fully eradicate their disease.
These results, published in Pediatric Blood & Cancer, suggest T-ALL patients with MRD may not need intensified treatment and can therefore avoid additional toxicities.
“Until now, the dogma has been that, for patients with leukemia who have minimal residual disease at the end of induction, we need to intensify their treatment, which also increases side effects,” said study author Hisham Abdel-Azim, MD, of Children’s Hospital Los Angeles in California.
“We have found, for T-ALL, patients have excellent outcomes without therapy intensification and its associated toxicities.”
Dr Abdel-Azim and his colleagues studied 33 children (ages 1 to 21) with newly diagnosed T-ALL. Their treatment included induction, augmented consolidation, interim maintenance (high-dose [5 g/m2] or escalating-dose intravenous methotrexate), 1 delayed intensification, and maintenance. Twenty-one patients underwent cranial irradiation, and 1 received a transplant.
After induction, 19 of the 32 patients analyzed had MRD, which was defined as ≥ 0.01% residual leukemia cells. At the end of consolidation, 6 of the 11 patients tested were MRD-positive. And at the end of interim maintenance, 2 of the 4 patients tested were MRD-positive.
The 19 patients who were MRD-positive after induction were in continuous complete remission at a median follow-up of 4 years (range, 1.3-7.1 years). The same was true for 13 of the 14 MRD-negative patients. One of the MRD-negative patients relapsed 18 months after diagnosis but was still alive with refractory disease at last follow-up.
Dr Abdel-Azim and his colleagues noted that there were no significant differences in treatment variables between MRD-positive patients and MRD-negative patients. However, 1 patient did receive a transplant for rising MRD at 5.4 months after diagnosis.
The investigators also said they did not find any associations between MRD positivity after induction and patients’ age, sex, ethnicity, weight, white blood cell count at diagnosis, cytogenetics, immunophenotype, or the type of steroid they received during induction therapy.
The team said these results may be explained by the fact that clearance of leukemia cells from the blood is slower in patients with T-ALL than in those with B-cell ALL. However, the leukemia cells ultimately clear in T-ALL without changes in therapy.
© Hind Medyouf, German
Cancer Research Center
A new study suggests that minimal residual disease (MRD) alone is not predictive of outcomes in children with T-cell acute lymphoblastic leukemia (T-ALL).
Study investigators analyzed a small group of T-ALL patients who received similar treatment regimens, comparing those with and without MRD after induction.
None of the MRD-positive patients relapsed within the follow-up period, despite not receiving intensified treatment to fully eradicate their disease.
These results, published in Pediatric Blood & Cancer, suggest T-ALL patients with MRD may not need intensified treatment and can therefore avoid additional toxicities.
“Until now, the dogma has been that, for patients with leukemia who have minimal residual disease at the end of induction, we need to intensify their treatment, which also increases side effects,” said study author Hisham Abdel-Azim, MD, of Children’s Hospital Los Angeles in California.
“We have found, for T-ALL, patients have excellent outcomes without therapy intensification and its associated toxicities.”
Dr Abdel-Azim and his colleagues studied 33 children (ages 1 to 21) with newly diagnosed T-ALL. Their treatment included induction, augmented consolidation, interim maintenance (high-dose [5 g/m2] or escalating-dose intravenous methotrexate), 1 delayed intensification, and maintenance. Twenty-one patients underwent cranial irradiation, and 1 received a transplant.
After induction, 19 of the 32 patients analyzed had MRD, which was defined as ≥ 0.01% residual leukemia cells. At the end of consolidation, 6 of the 11 patients tested were MRD-positive. And at the end of interim maintenance, 2 of the 4 patients tested were MRD-positive.
The 19 patients who were MRD-positive after induction were in continuous complete remission at a median follow-up of 4 years (range, 1.3-7.1 years). The same was true for 13 of the 14 MRD-negative patients. One of the MRD-negative patients relapsed 18 months after diagnosis but was still alive with refractory disease at last follow-up.
Dr Abdel-Azim and his colleagues noted that there were no significant differences in treatment variables between MRD-positive patients and MRD-negative patients. However, 1 patient did receive a transplant for rising MRD at 5.4 months after diagnosis.
The investigators also said they did not find any associations between MRD positivity after induction and patients’ age, sex, ethnicity, weight, white blood cell count at diagnosis, cytogenetics, immunophenotype, or the type of steroid they received during induction therapy.
The team said these results may be explained by the fact that clearance of leukemia cells from the blood is slower in patients with T-ALL than in those with B-cell ALL. However, the leukemia cells ultimately clear in T-ALL without changes in therapy.
© Hind Medyouf, German
Cancer Research Center
A new study suggests that minimal residual disease (MRD) alone is not predictive of outcomes in children with T-cell acute lymphoblastic leukemia (T-ALL).
Study investigators analyzed a small group of T-ALL patients who received similar treatment regimens, comparing those with and without MRD after induction.
None of the MRD-positive patients relapsed within the follow-up period, despite not receiving intensified treatment to fully eradicate their disease.
These results, published in Pediatric Blood & Cancer, suggest T-ALL patients with MRD may not need intensified treatment and can therefore avoid additional toxicities.
“Until now, the dogma has been that, for patients with leukemia who have minimal residual disease at the end of induction, we need to intensify their treatment, which also increases side effects,” said study author Hisham Abdel-Azim, MD, of Children’s Hospital Los Angeles in California.
“We have found, for T-ALL, patients have excellent outcomes without therapy intensification and its associated toxicities.”
Dr Abdel-Azim and his colleagues studied 33 children (ages 1 to 21) with newly diagnosed T-ALL. Their treatment included induction, augmented consolidation, interim maintenance (high-dose [5 g/m2] or escalating-dose intravenous methotrexate), 1 delayed intensification, and maintenance. Twenty-one patients underwent cranial irradiation, and 1 received a transplant.
After induction, 19 of the 32 patients analyzed had MRD, which was defined as ≥ 0.01% residual leukemia cells. At the end of consolidation, 6 of the 11 patients tested were MRD-positive. And at the end of interim maintenance, 2 of the 4 patients tested were MRD-positive.
The 19 patients who were MRD-positive after induction were in continuous complete remission at a median follow-up of 4 years (range, 1.3-7.1 years). The same was true for 13 of the 14 MRD-negative patients. One of the MRD-negative patients relapsed 18 months after diagnosis but was still alive with refractory disease at last follow-up.
Dr Abdel-Azim and his colleagues noted that there were no significant differences in treatment variables between MRD-positive patients and MRD-negative patients. However, 1 patient did receive a transplant for rising MRD at 5.4 months after diagnosis.
The investigators also said they did not find any associations between MRD positivity after induction and patients’ age, sex, ethnicity, weight, white blood cell count at diagnosis, cytogenetics, immunophenotype, or the type of steroid they received during induction therapy.
The team said these results may be explained by the fact that clearance of leukemia cells from the blood is slower in patients with T-ALL than in those with B-cell ALL. However, the leukemia cells ultimately clear in T-ALL without changes in therapy.
Combo targets AML, BL in the same way

Image by Ed Uthman
Combining a cholesterol-lowering drug and a contraceptive steroid could be a safe, effective treatment for leukemias, lymphomas, and other malignancies, according to researchers.
Their work helps explain how this combination treatment, bezafibrate and medroxyprogesterone acetate (BaP), kills cancer cells.
The team discovered that BaP’s mechanism of action is the same in acute myeloid leukemia (AML) and Burkitt lymphoma (BL) cells.
The findings have been published in Cancer Research.
BaP has been shown to prolong survival in early stage trials of elderly AML patients, when compared to standard palliative care. BaP has also been used alongside chemotherapy to successfully treat children with BL.
However, it was unclear whether BaP’s activity against these 2 very different malignancies was mediated by a common mechanism or by different effects in each cancer.
To gain some insight, Andrew Southam, PhD, of the University of Birmingham in the UK, and his colleagues investigated the drugs’ effects on the metabolism and chemical make-up of AML and BL cells.
They found that, in both cell types, BaP blocks stearoyl CoA desaturase, an enzyme crucial to the production of fatty acids, which cancer cells need to grow and multiply. The team also showed that BaP’s ability to deactivate stearoyl CoA desaturase was what prompted the cancer cells to die.
“Developing drugs to target the fatty-acid building blocks of cancer cells has been a promising area of research in recent years,” Dr Southam said. “It is very exciting we have identified these non-toxic drugs already sitting on pharmacy shelves.”
He and his colleagues believe these findings also open up the possibility that BaP could be used to treat other cancers that rely on high levels of stearoyl CoA desaturase to grow, including chronic lymphocytic leukemia and some types of non-Hodgkin lymphoma, as well as prostate, colon, and esophageal cancers.
“This drug combination shows real promise,” said Chris Bunce, PhD, also of the University of Birmingham.
“Affordable, effective, non-toxic treatments that extend survival, while offering a good quality of life, are in demand for almost all types of cancer.”
Image by Ed Uthman
Combining a cholesterol-lowering drug and a contraceptive steroid could be a safe, effective treatment for leukemias, lymphomas, and other malignancies, according to researchers.
Their work helps explain how this combination treatment, bezafibrate and medroxyprogesterone acetate (BaP), kills cancer cells.
The team discovered that BaP’s mechanism of action is the same in acute myeloid leukemia (AML) and Burkitt lymphoma (BL) cells.
The findings have been published in Cancer Research.
BaP has been shown to prolong survival in early stage trials of elderly AML patients, when compared to standard palliative care. BaP has also been used alongside chemotherapy to successfully treat children with BL.
However, it was unclear whether BaP’s activity against these 2 very different malignancies was mediated by a common mechanism or by different effects in each cancer.
To gain some insight, Andrew Southam, PhD, of the University of Birmingham in the UK, and his colleagues investigated the drugs’ effects on the metabolism and chemical make-up of AML and BL cells.
They found that, in both cell types, BaP blocks stearoyl CoA desaturase, an enzyme crucial to the production of fatty acids, which cancer cells need to grow and multiply. The team also showed that BaP’s ability to deactivate stearoyl CoA desaturase was what prompted the cancer cells to die.
“Developing drugs to target the fatty-acid building blocks of cancer cells has been a promising area of research in recent years,” Dr Southam said. “It is very exciting we have identified these non-toxic drugs already sitting on pharmacy shelves.”
He and his colleagues believe these findings also open up the possibility that BaP could be used to treat other cancers that rely on high levels of stearoyl CoA desaturase to grow, including chronic lymphocytic leukemia and some types of non-Hodgkin lymphoma, as well as prostate, colon, and esophageal cancers.
“This drug combination shows real promise,” said Chris Bunce, PhD, also of the University of Birmingham.
“Affordable, effective, non-toxic treatments that extend survival, while offering a good quality of life, are in demand for almost all types of cancer.”
Image by Ed Uthman
Combining a cholesterol-lowering drug and a contraceptive steroid could be a safe, effective treatment for leukemias, lymphomas, and other malignancies, according to researchers.
Their work helps explain how this combination treatment, bezafibrate and medroxyprogesterone acetate (BaP), kills cancer cells.
The team discovered that BaP’s mechanism of action is the same in acute myeloid leukemia (AML) and Burkitt lymphoma (BL) cells.
The findings have been published in Cancer Research.
BaP has been shown to prolong survival in early stage trials of elderly AML patients, when compared to standard palliative care. BaP has also been used alongside chemotherapy to successfully treat children with BL.
However, it was unclear whether BaP’s activity against these 2 very different malignancies was mediated by a common mechanism or by different effects in each cancer.
To gain some insight, Andrew Southam, PhD, of the University of Birmingham in the UK, and his colleagues investigated the drugs’ effects on the metabolism and chemical make-up of AML and BL cells.
They found that, in both cell types, BaP blocks stearoyl CoA desaturase, an enzyme crucial to the production of fatty acids, which cancer cells need to grow and multiply. The team also showed that BaP’s ability to deactivate stearoyl CoA desaturase was what prompted the cancer cells to die.
“Developing drugs to target the fatty-acid building blocks of cancer cells has been a promising area of research in recent years,” Dr Southam said. “It is very exciting we have identified these non-toxic drugs already sitting on pharmacy shelves.”
He and his colleagues believe these findings also open up the possibility that BaP could be used to treat other cancers that rely on high levels of stearoyl CoA desaturase to grow, including chronic lymphocytic leukemia and some types of non-Hodgkin lymphoma, as well as prostate, colon, and esophageal cancers.
“This drug combination shows real promise,” said Chris Bunce, PhD, also of the University of Birmingham.
“Affordable, effective, non-toxic treatments that extend survival, while offering a good quality of life, are in demand for almost all types of cancer.”