User login
What are the most prescribed medications for type 2 diabetes?
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
new research shows.
The findings, from U.S.-based administrative claims data, were published online in Diabetes Care by Chintan V. Dave, PharmD, PhD, and colleagues.
Among patients initiating oral sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors) over the 5-year period, empagliflozin (Jardiance, Boehringer Ingelheim/Lilly) became the most commonly prescribed glucose-lowering drug, primarily driven by an increasing proportion of patients with diabetes who had a diagnosis of myocardial infarction, stroke, or heart failure (collectively called cardiovascular disease-heart failure [CVD-HF]).
And within the subcutaneous injectable glucagonlike peptide–1 receptor (GLP-1) agonist class, initiations of dulaglutide (Trulicity, Lilly) surpassed liraglutide in 2013-2018, although patients starting liraglutide (Victoza, Novo Nordisk) were more likely to have a CVD-HF diagnosis.
“This study shows that by preferring empagliflozin, prescribers have largely reacted in accordance with the available evidence and drug labels, while other factors such as lower price, frequency of administration [dulaglutide is given weekly and liraglutide is given daily], or prior authorizations may have led prescribers to select dulaglutide over liraglutide,” Dr. Dave, of the Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, and colleagues wrote.
Internists and endocrinologists were the most frequent prescribers of both drug classes, but cardiologists rarely prescribed them, even for patients with established CVD-HF. “As patients with co-occurring diabetes and CVD are likely to see their cardiologist, these encounters may provide an additional opportunity to optimize their treatment,” the authors emphasized.
SGLT2 inhibitors and label changes
Over the study period, the proportion of patients who had CVD-HF and who received SGLT2 inhibitors rose by 3.4 percentage points, from 8.8% to 12.2% (P trend < .001).
The proportion of overall prescriptions for SGLT2 inhibitors written by endocrinologists dropped by 12.0%, although the absolute number of SGLT2-inhibitor prescriptions written by endocrinologists increased (P < .001).
The proportion written by internists did not change (P = .58), whereas it increased slightly among cardiologists but still barely exceeded 1% (P < .001). The findings were similar for the subgroup of patients with CVD-HF who initiated SGLT2 inhibitors.
By individual agents, canagliflozin (Invokana, Janssen) prescriptions dropped by 75.1 percentage points over the study period, from 100% in 2013 to just 24.9% by 2018 (P < .001), whereas empagliflozin initiation rose by 51.7 percentage points, from 13.9% to 65.6% of all SGLT2 inhibitor initiations (P < .001).
Among those initiating empagliflozin, the proportion with CVD-HF rose by 5.3 percentage points, from 8.8% to 14.1% (P < .001), mostly after the additional indication for reducing CV events and death was added to the U.S. label in December 2016.
In contrast, there were no significant changes in the proportions of those with CVD-HF who initiated canagliflozin (P = 065), dapagliflozin (P = .87), or other medications (P = .060).
“Changes in the drug label for canagliflozin (boxed warning for amputation) and empagliflozin (for reduction in CV events and death) in 2016 likely contributed to a rapid change in prescribing preference for empagliflozin,” Dr. Dave and colleagues wrote.
GLP-1 agonists and frequency
Among the patients starting GLP-1 agonists, the proportion with CVD-HF increased by 3.9 percentage points, from 10.5% to 14.4% (P < .001) during the study period.
Prescriptions by endocrinologists declined as a proportion, but rose in absolute numbers (P < .001), and remained consistent for internists (> 55%; P = .12).
Prescribing of GLP-1 agonists by cardiologists remained low (< 0.5%) and was not higher for individuals with CVD-HF.
By individual GLP-1 agonist, liraglutide initiation declined by 32.1 percentage points, from 72.4% to 40.3% of GLP-1 agonist initiations (P < .001), whereas dulaglutide initiation rose by 43.8 percentage points, from 5.0% to 48.8% (P < .001). Again, these trends were similar in the subgroup of patients with CVD-HF.
The proportion of patients with CVD-HF in liraglutide initiators increased by 5.1 percentage points, from 10.5% to 15.6% (P = .018), and in exenatide initiators by 2.1 percentage points, from 10.3% to 13.8% (P = .77).
“Due to the reduced frequency of administration and possible formulary preferences, dulaglutide initiations surpassed liraglutide, the only GLP-1 agonist with evidence of CV benefit at the time,” Dr. Dave and colleagues noted.
Dulaglutide has just been granted an additional approval by the Food and Drug Administration for reducing the risk of major adverse cardiovascular events in adults with type 2 diabetes with and without established CVD or multiple CV risk factors. That makes it the first and only type 2 diabetes medicine approved to reduce the risk of CV events for both primary and secondary prevention populations.
The study was funded by the Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. Dr. Dave has reported receiving support from the New Jersey Alliance for Clinical and Translational Science.
This article first appeared on Medscape.com.
Beginning estrogen soon after menopause slows atherosclerosis progression
PHOENIX – Oral estrogen therapy taken within 6 years after the onset of menopause significantly reduced progression of lipid deposition in the carotid arterial wall, compared with placebo. However, starting oral estrogen 10 years after menopause did not confer a similar benefit.

“The clinical practice of estradiol therapy has been nothing short of a roller coaster ride,” lead study author Roksana Karim, PhD, MBBS, said in an interview at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting sponsored by the American Heart Association. “Clinicians have been sort of conservative in terms of prescribing estradiol therapy. But over the last 2 decades things have changed, and eventually the timing hypothesis evolved based on the final analysis of the Women’s Health Initiative results as well.”
The findings come from a secondary analysis of the Early Versus Late Intervention Trial With Estradiol (ELITE), which examined the effects of oral 17-beta-estradiol (estrogen) on the progression of early atherosclerosis and cognitive decline in healthy postmenopausal women.
In the original trial, 643 healthy postmenopausal women were randomized to receive 1 mg/day of estradiol or a placebo pill either within 6 years after the onset of menopause or more than a decade after menopause (N Engl J Med 2016;374[13]:1221-31). All study participants took estradiol or placebo daily for an average of 5 years. The study’s initial findings showed that the mean carotid intima-media thickness progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
For the current analysis, researchers led by Dr. Karim looked further into estradiol’s impact on heart health by using echogenicity to analyze lipids in the arterial wall among the ELITE participants. The main outcome of interest was gray-scale median (GSM, unitless), a qualitative measure of atherosclerosis based on echogenicity obtained by high-resolution ultrasonography of the common carotid arterial wall. Whereas higher GSM values result with plaques rich in calcium and fibrous tissue, lower GSM values indicate more lipid deposition.
Dr. Karim, an associate professor of clinical preventive medicine at the University of Southern California, Los Angeles, and colleagues assessed GSM and serum concentrations of estradiol every 6 months over a median 5-year trial period, and used linear mixed effects regression models to compare the rate of GSM progression between the randomized groups within time-since-menopause strata.
The researchers found that effect of estradiol on the annual rate of GSM progression significantly differed between women in the early and late postmenopause groups (P for interaction = .006). Specifically, the annual GSM progression rate among women in early postmenopause fell by 0.30 per year in women taking estradiol, compared with 1.41 per year in those in the placebo group (P less than .0001), indicating significantly more atherosclerosis in the placebo group. On the other hand, the annual GSM progression rate was not significantly different between the estradiol and placebo groups among the late postmenopausal women (P = .37).
“I think this should comfort clinicians in terms of prescribing estradiol therapy to women who don’t have any contraindications and who are within 6 years of menopause,” Dr. Karim said. “Accumulation of lipids is the key event for atherosclerosis progression.” She and her colleagues also observed that the positive association between mean on-trial serum estradiol levels and GSM progression rate was stronger and significant among early postmenopausal women (P = .008), compared with women in the late postmenopausal group (P = .003). However, this differential association between estradiol level and GSM progression rate was not statistically significant (P for interaction = .33).
“This study is important and raises a critical question: Is there a time period where getting hormone therapy would be most beneficial for the heart?” Nieca Goldberg, MD, medical director of the New York University women’s heart program and senior advisor for women’s health strategy at NYU Langone Health, said in an interview. “I think more studies and more analyses are needed, but we haven’t changed the indications for estradiol. We’re not giving estradiol to prevent progression of heart disease. We use estradiol hormone therapy as indicated for women who are having menopausal symptoms.”
Dr. Karim and colleagues plan to conduct a follow-up analysis from the same cohort of ELITE study participants to validate the findings by assessing lipid particles and markers of inflammation.
She reported having no financial disclosures. The study was funded by the National Institute on Aging.
SOURCE: Karim R et al. Epi/Lifestyle 2020, Abstract MP09.
PHOENIX – Oral estrogen therapy taken within 6 years after the onset of menopause significantly reduced progression of lipid deposition in the carotid arterial wall, compared with placebo. However, starting oral estrogen 10 years after menopause did not confer a similar benefit.
“The clinical practice of estradiol therapy has been nothing short of a roller coaster ride,” lead study author Roksana Karim, PhD, MBBS, said in an interview at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting sponsored by the American Heart Association. “Clinicians have been sort of conservative in terms of prescribing estradiol therapy. But over the last 2 decades things have changed, and eventually the timing hypothesis evolved based on the final analysis of the Women’s Health Initiative results as well.”
The findings come from a secondary analysis of the Early Versus Late Intervention Trial With Estradiol (ELITE), which examined the effects of oral 17-beta-estradiol (estrogen) on the progression of early atherosclerosis and cognitive decline in healthy postmenopausal women.
In the original trial, 643 healthy postmenopausal women were randomized to receive 1 mg/day of estradiol or a placebo pill either within 6 years after the onset of menopause or more than a decade after menopause (N Engl J Med 2016;374[13]:1221-31). All study participants took estradiol or placebo daily for an average of 5 years. The study’s initial findings showed that the mean carotid intima-media thickness progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
For the current analysis, researchers led by Dr. Karim looked further into estradiol’s impact on heart health by using echogenicity to analyze lipids in the arterial wall among the ELITE participants. The main outcome of interest was gray-scale median (GSM, unitless), a qualitative measure of atherosclerosis based on echogenicity obtained by high-resolution ultrasonography of the common carotid arterial wall. Whereas higher GSM values result with plaques rich in calcium and fibrous tissue, lower GSM values indicate more lipid deposition.
Dr. Karim, an associate professor of clinical preventive medicine at the University of Southern California, Los Angeles, and colleagues assessed GSM and serum concentrations of estradiol every 6 months over a median 5-year trial period, and used linear mixed effects regression models to compare the rate of GSM progression between the randomized groups within time-since-menopause strata.
The researchers found that effect of estradiol on the annual rate of GSM progression significantly differed between women in the early and late postmenopause groups (P for interaction = .006). Specifically, the annual GSM progression rate among women in early postmenopause fell by 0.30 per year in women taking estradiol, compared with 1.41 per year in those in the placebo group (P less than .0001), indicating significantly more atherosclerosis in the placebo group. On the other hand, the annual GSM progression rate was not significantly different between the estradiol and placebo groups among the late postmenopausal women (P = .37).
“I think this should comfort clinicians in terms of prescribing estradiol therapy to women who don’t have any contraindications and who are within 6 years of menopause,” Dr. Karim said. “Accumulation of lipids is the key event for atherosclerosis progression.” She and her colleagues also observed that the positive association between mean on-trial serum estradiol levels and GSM progression rate was stronger and significant among early postmenopausal women (P = .008), compared with women in the late postmenopausal group (P = .003). However, this differential association between estradiol level and GSM progression rate was not statistically significant (P for interaction = .33).
“This study is important and raises a critical question: Is there a time period where getting hormone therapy would be most beneficial for the heart?” Nieca Goldberg, MD, medical director of the New York University women’s heart program and senior advisor for women’s health strategy at NYU Langone Health, said in an interview. “I think more studies and more analyses are needed, but we haven’t changed the indications for estradiol. We’re not giving estradiol to prevent progression of heart disease. We use estradiol hormone therapy as indicated for women who are having menopausal symptoms.”
Dr. Karim and colleagues plan to conduct a follow-up analysis from the same cohort of ELITE study participants to validate the findings by assessing lipid particles and markers of inflammation.
She reported having no financial disclosures. The study was funded by the National Institute on Aging.
SOURCE: Karim R et al. Epi/Lifestyle 2020, Abstract MP09.
PHOENIX – Oral estrogen therapy taken within 6 years after the onset of menopause significantly reduced progression of lipid deposition in the carotid arterial wall, compared with placebo. However, starting oral estrogen 10 years after menopause did not confer a similar benefit.
“The clinical practice of estradiol therapy has been nothing short of a roller coaster ride,” lead study author Roksana Karim, PhD, MBBS, said in an interview at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting sponsored by the American Heart Association. “Clinicians have been sort of conservative in terms of prescribing estradiol therapy. But over the last 2 decades things have changed, and eventually the timing hypothesis evolved based on the final analysis of the Women’s Health Initiative results as well.”
The findings come from a secondary analysis of the Early Versus Late Intervention Trial With Estradiol (ELITE), which examined the effects of oral 17-beta-estradiol (estrogen) on the progression of early atherosclerosis and cognitive decline in healthy postmenopausal women.
In the original trial, 643 healthy postmenopausal women were randomized to receive 1 mg/day of estradiol or a placebo pill either within 6 years after the onset of menopause or more than a decade after menopause (N Engl J Med 2016;374[13]:1221-31). All study participants took estradiol or placebo daily for an average of 5 years. The study’s initial findings showed that the mean carotid intima-media thickness progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
For the current analysis, researchers led by Dr. Karim looked further into estradiol’s impact on heart health by using echogenicity to analyze lipids in the arterial wall among the ELITE participants. The main outcome of interest was gray-scale median (GSM, unitless), a qualitative measure of atherosclerosis based on echogenicity obtained by high-resolution ultrasonography of the common carotid arterial wall. Whereas higher GSM values result with plaques rich in calcium and fibrous tissue, lower GSM values indicate more lipid deposition.
Dr. Karim, an associate professor of clinical preventive medicine at the University of Southern California, Los Angeles, and colleagues assessed GSM and serum concentrations of estradiol every 6 months over a median 5-year trial period, and used linear mixed effects regression models to compare the rate of GSM progression between the randomized groups within time-since-menopause strata.
The researchers found that effect of estradiol on the annual rate of GSM progression significantly differed between women in the early and late postmenopause groups (P for interaction = .006). Specifically, the annual GSM progression rate among women in early postmenopause fell by 0.30 per year in women taking estradiol, compared with 1.41 per year in those in the placebo group (P less than .0001), indicating significantly more atherosclerosis in the placebo group. On the other hand, the annual GSM progression rate was not significantly different between the estradiol and placebo groups among the late postmenopausal women (P = .37).
“I think this should comfort clinicians in terms of prescribing estradiol therapy to women who don’t have any contraindications and who are within 6 years of menopause,” Dr. Karim said. “Accumulation of lipids is the key event for atherosclerosis progression.” She and her colleagues also observed that the positive association between mean on-trial serum estradiol levels and GSM progression rate was stronger and significant among early postmenopausal women (P = .008), compared with women in the late postmenopausal group (P = .003). However, this differential association between estradiol level and GSM progression rate was not statistically significant (P for interaction = .33).
“This study is important and raises a critical question: Is there a time period where getting hormone therapy would be most beneficial for the heart?” Nieca Goldberg, MD, medical director of the New York University women’s heart program and senior advisor for women’s health strategy at NYU Langone Health, said in an interview. “I think more studies and more analyses are needed, but we haven’t changed the indications for estradiol. We’re not giving estradiol to prevent progression of heart disease. We use estradiol hormone therapy as indicated for women who are having menopausal symptoms.”
Dr. Karim and colleagues plan to conduct a follow-up analysis from the same cohort of ELITE study participants to validate the findings by assessing lipid particles and markers of inflammation.
She reported having no financial disclosures. The study was funded by the National Institute on Aging.
SOURCE: Karim R et al. Epi/Lifestyle 2020, Abstract MP09.
REPORTING FROM EPI/LIFESTYLE 2020
AFib patients do best on a DOAC started 7-10 days post stroke
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.

The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.

A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
LOS ANGELES – When a patient with atrial fibrillation (AFib) has a cardioembolic stroke, the best blood thinner to start may be a direct-acting oral anticoagulant (DOAC), possibly beginning 7-10 days after the index stroke, according to an analysis of 90-day, observational outcomes data from nearly 1,300 patients.
The analysis also suggested that the use of “bridging” anticoagulant treatment by injection before a patient with atrial fibrillation (AFib) starts a daily oral anticoagulant regimen following a cardioembolic stroke is not a good idea. Patients who received bridging anticoagulation had a nearly threefold higher rate of symptomatic intracranial hemorrhage than did patients who did not, and their bridging treatment failed to protect them from recurrent ischemic events, Shadi Yaghi, MD, said at the International Stroke Conference, sponsored by the American Heart Association. The bridging regimens delivered either heparin or low-molecular-weight heparin.
Based on the findings, “it seems reasonable to avoid bridging unless absolutely necessary, to initiate a DOAC unless it’s contraindicated, and to start the DOAC on day 7-10 following the stroke in most patients,” said Dr. Yaghi, a vascular neurologist and director of stroke research at NYU Langone Health in New York.
“It’s been hard to develop a broad guideline on when to start oral anticoagulation” after a cardioembolic stroke in AFib patients. The best time “depends on a lot of variables and how the patient responded to acute treatment,” commented Alexis Simpkins, MD, a vascular and stroke neurologist at the University of Florida in Gainesville. “You want to start treatment before the patient has another stroke, but not so soon that the treatment causes symptomatic hemorrhagic transformation.”
Dr. Yaghi’s suggestion, based on his findings, to start treatment for most patients with a DOAC 7-10 days after their index stroke “shows consistency” with the prevailing guideline recommendation from the AHA/American Stroke Association to start oral anticoagulation in this patient population 4-14 days after the index stroke (Stroke. 2018 March;49[3]:e46-e99), she noted.
A recent article reviewed the uncertainty about the best time to start oral anticoagulation in AFib patients after a cardioembolic stroke and the subtle differences that distinguish various international medical groups that, like the ASA, have made recommendations (Lancet Neurol. 2019 Jan 1;18[1]:117-26). According to this review, a major limitation of these various recommendations has been the lack of actual evidence collected from AFib patients who began receiving a DOAC shortly after a cardioembolic stroke, although the article added that several studies in progress are collecting these data.
The study reported by Dr. Yaghi pooled data collected from 2,084 recent AFib patients with a cardioembolic stroke treated at any of eight comprehensive U.S. stroke centers. They excluded patients who died from causes unrelated to the primary endpoint, those who did not receive an anticoagulant or had incomplete data, and patients lost to follow-up, leaving 1,289 evaluable patients. During their 90-day follow-up, 10% of the patients had an ischemic event, a symptomatic intracranial hemorrhage, or an extracranial hemorrhage.
The study’s primary analysis showed no statistically significant difference in the incidence of recurrent ischemic events, symptomatic intracranial hemorrhage, or both based on when oral anticoagulant treatment began: 0-3 days, 4-14 days, or more than 14 days after the index stroke.
The investigators then subdivided patients into the subgroup that started treatment with a DOAC and the subgroup that started treatment with warfarin and also further subdivided the 4-14 day time window for starting treatment. Results of this analysis showed that patients who received a DOAC and began this treatment 7-10 days after their stroke had a 50% cut in their 90-day events compared with other patients, a difference that fell just short of statistical significance at P = .07. All the other combinations of oral anticoagulant and time of treatment initiation analyzed showed neutral effects that never came near statistical significance.
Secondary data analyses also showed that both patients with a history of a stroke prior to their index stroke and patients with ipsilateral atherosclerosis came close to having a statistically significant increased rate of a subsequent ischemic event during 90-day follow-up. Furthermore, women, patients with a history of hyperlipidemia, and patients who developed hemorrhagic transformation of their index stroke all had significantly increased rates of developing a symptomatic intracranial hemorrhage during 90-day follow-up. When the endpoint was limited to recurrent ischemic events only, patients who received a DOAC were 50% less likely to have an event than were patients treated with warfarin, a statistically significant difference.
Although starting a DOAC 7-10 days after the index stroke seems reasonable based on this analysis, the question needs a prospective, randomized study to create an appropriate evidence base, Dr. Yaghi said.
Dr. Yaghi disclosed a financial relationship with Medtronic. Dr. Simpkins had no disclosures.
SOURCE: Yaghi S et al. Stroke. 2020 Feb;51(suppl 1):A119.
REPORTING FROM ISC 2020
MACE benefits with dapagliflozin improve with disease duration
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
Treatment with the sodium-glucose transporter 2 inhibitor dapagliflozin reduced the risk for cardiovascular disease or hospitalization for heart failure (CVD/HHF) in patients with diabetes, regardless of the duration of the disease, but had a greater protective benefit against major adverse cardiovascular events (MACE) and renal events in patients with longer disease duration, according to new findings from a post hoc analysis of the DECLARE-TIMI 58 trial.
The positive effect of dapagliflozin in patients with MACE – which includes myocardial infarction (MI), CVD, and ischemic stroke – may have been driven by lower rates of MI and ischemic stroke with the drug, compared with placebo, in patients with longer disease duration, wrote Harpreet S. Bajaj, MD, and colleagues. Their report is in Diabetes, Obesity and Metabolism (2020 Feb 23. doi: 10.1111/dom.14011).
It has been previously reported that the risk for complications in diabetes increases with increasing duration of the disease. Recent studies with SGLT-2 inhibitors have shown that the drugs improve cardiovascular and renal outcomes in diabetes, and they are recommended by the American Diabetes Association as second-line therapy in patients with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure. The European Society of Cardiology and the European Association for the Study of Diabetes recommend that patients with diabetes patients who have three or more risk factors, or those with a disease duration of more than 20 years, should be deemed very high risk and be considered for early treatment with SGLT2 inhibitors.
“The MACE benefit observed with dapagliflozin in this study in patients with diabetes duration of [more than] 20 years, clearly supports that notion,” the authors wrote.
In DECLARE-TIMI 58, 17,160 patients with type 2 diabetes received dapagliflozin or placebo and were followed for a median of 4.2 years. Of those patients, 22.4% had a disease duration of fewer than 5 years; 27.6%, a duration of 5-10 years; 23.0%, 10-15 years; 14.2%, 10-15 years; and 12.9%, more than 20 years. The median duration of disease was 11 years.
Patients in all the age groups had similar reductions in CVD/HHF, compared with placebo, with hazard ratios of 0.79 (disease duration of 5 or fewer years), 0.86, 0.92, 0.81, and 0.75 (duration of 20 years), respectively (interaction trend P = .760).
Treatment with dapagliflozin reduced the incidence of MACE, but the benefit was more apparent in patients with longer-term disease: HR, 1.08; 1.02; 0.94; 0.92; and 0.67, respectively (interaction trend P = .004). Similar trends were seen with MI (interaction trend P = .019) and ischemic stroke (interaction trend P = .015).
The researchers also reported improved benefits in renal-specific outcome with increasing disease duration, with HRs ranging from 0.79 in patients with diabetes duration of fewer than 5 years, to 0.42 in those with a duration of more than 20 years (interaction trend P = .084).
Limitations of the study include the fact that the information about diabetes duration relied on patient reports, and that the original trial was not powered for all subgroup interactions. This authors emphasized that this was a post hoc analysis and as such, should be considered hypothesis generating.
All but two of the authors reported relationships with Astra Zeneca, which funded the study, and other drug companies.
SOURCE: Bajaj HS et al. Diabetes Obes Metab. 2020 Feb 23. doi: 10.1111/dom.14011.
FROM DIABETES, OBESITY AND METABOLISM
Prescription cascade more likely after CCBs than other hypertension meds
Elderly adults with hypertension who are newly prescribed a calcium-channel blocker (CCB), compared to other antihypertensive agents, are at least twice as likely to be given a loop diuretic over the following months, a large cohort study suggests.
The likelihood remained elevated for as long as a year after the start of a CCB and was more pronounced when comparing CCBs to any other kind of medication.
“Our findings suggest that many older adults who begin taking a CCB may subsequently experience a prescribing cascade” when loop diuretics are prescribed for peripheral edema, a known CCB adverse effect, that is misinterpreted as a new medical condition, Rachel D. Savage, PhD, Women’s College Hospital, Toronto, Canada, told theheart.org/Medscape Cardiology.
Edema caused by CCBs is caused by fluid redistribution, not overload, and “treating euvolemic individuals with a diuretic places them at increased risk of overdiuresis, leading to falls, urinary incontinence, acute kidney injury, electrolyte imbalances, and a cascade of other downstream consequences to which older adults are especially vulnerable,” explain Savage and coauthors of the analysis published online February 24 in JAMA Internal Medicine.
However, 1.4% of the cohort had been prescribed a loop diuretic, and 4.5% had been given any diuretic within 90 days after the start of CCBs. The corresponding rates were 0.7% and 3.4%, respectively, for patients who had started on ACE inhibitors or angiotensin receptor blocker (ARB) rather than a CCB.
Also, Savage observed, “the likelihood of being prescribed a loop diuretic following initiation of a CCB changed over time and was greatest 61 to 90 days postinitiation.” At that point, it was increased 2.4 times compared with initiation of an ACE inhibitor or an ARB in an adjusted analysis and increased almost 4 times compared with starting on any non-CCB agent.
Importantly, the actual prevalence of peripheral edema among those started on CCBs, ACE inhibitors, ARBs, or any non-CCB medication was not available in the data sets.
However, “the main message for clinicians is to consider medication side effects as a potential cause for new symptoms when patients present. We also encourage patients to ask prescribers about whether new symptoms could be caused by a medication,” senior author Lisa M. McCarthy, PharmD, told theheart.org/Medscape Cardiology.
“If a patient experiences peripheral edema while taking a CCB, we would encourage clinicians to consider whether the calcium-channel blocker is still necessary, whether it could be discontinued or the dose reduced, or whether the patient can be switched to another therapy,” she said.
Based on the current analysis, if the rate of CCB-induced peripheral edema is assumed to be 10%, which is consistent with the literature, then “potentially 7% to 14% of people who develop edema while taking a calcium channel blocker may then receive a loop diuretic,” an accompanying editorial notes.
“Patients with polypharmacy are at heightened risk of being exposed to [a] series of prescribing cascades if their current use of medications is not carefully discussed before the decision to add a new antihypertensive,” observe Timothy S. Anderson, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, and Michael A. Steinman, MD, San Francisco Veterans Affairs Medical Center and University of California, San Francisco.
“The initial prescribing cascade can set off many other negative consequences, including adverse drug events, potentially avoidable diagnostic testing, and hospitalizations,” the editorialists caution.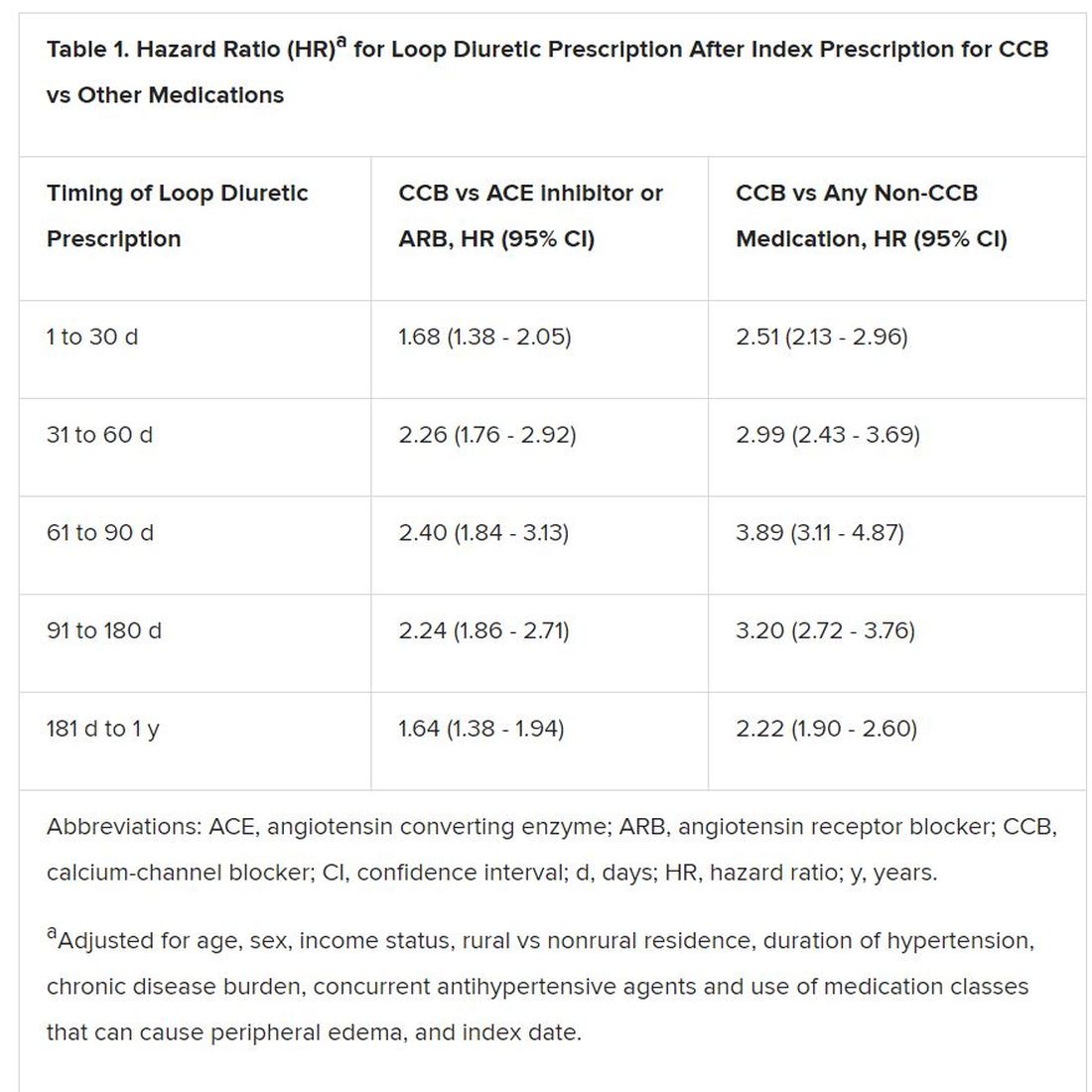
“Identifying prescribing cascades and their consequences is an important step to stem the tide of polypharmacy and inform deprescribing efforts.”
The analysis was based on administrative data from almost 340,000 adults in the community aged 66 years or older with hypertension and new drug prescriptions over 5 years ending in September 2016, the report notes. Their mean age was 74.5 years and 56.5% were women.
The data set included 41,086 patients who were newly prescribed a CCB; 66,494 who were newly prescribed an ACE inhibitor or ARB; and 231,439 newly prescribed any medication other than a CCB. The prescribed CCB was amlodipine in 79.6% of patients.
Although loop diuretics could possibly have been prescribed sometimes as a second-tier antihypertensive in the absence of peripheral edema, “we made efforts, through the design of our study, to limit this where possible,” Savage said in an interview.
For example, the focus was on loop diuretics, which aren’t generally recommended for blood-pressure lowering. Also, patients with heart failure and those with a recent history of diuretic or other antihypertensive medication use had been excluded, she said.
“As such, our cohort comprised individuals with new-onset or milder hypertension for whom diuretics would unlikely to be prescribed as part of guideline-based hypertension management.”
Although amlodipine was the most commonly prescribed CCB, the potential for a prescribing cascade seemed to be a class effect and to apply at a range of dosages.
That was unexpected, McCarthy observed, because “peripheral edema occurs more commonly in people taking dihydropyridine CCBs, like amlodipine, compared to non–dihydropyridine CCBs, such as verapamil and diltiazem.”
Savage, McCarthy, their coauthors, and the editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Elderly adults with hypertension who are newly prescribed a calcium-channel blocker (CCB), compared to other antihypertensive agents, are at least twice as likely to be given a loop diuretic over the following months, a large cohort study suggests.
The likelihood remained elevated for as long as a year after the start of a CCB and was more pronounced when comparing CCBs to any other kind of medication.
“Our findings suggest that many older adults who begin taking a CCB may subsequently experience a prescribing cascade” when loop diuretics are prescribed for peripheral edema, a known CCB adverse effect, that is misinterpreted as a new medical condition, Rachel D. Savage, PhD, Women’s College Hospital, Toronto, Canada, told theheart.org/Medscape Cardiology.
Edema caused by CCBs is caused by fluid redistribution, not overload, and “treating euvolemic individuals with a diuretic places them at increased risk of overdiuresis, leading to falls, urinary incontinence, acute kidney injury, electrolyte imbalances, and a cascade of other downstream consequences to which older adults are especially vulnerable,” explain Savage and coauthors of the analysis published online February 24 in JAMA Internal Medicine.
However, 1.4% of the cohort had been prescribed a loop diuretic, and 4.5% had been given any diuretic within 90 days after the start of CCBs. The corresponding rates were 0.7% and 3.4%, respectively, for patients who had started on ACE inhibitors or angiotensin receptor blocker (ARB) rather than a CCB.
Also, Savage observed, “the likelihood of being prescribed a loop diuretic following initiation of a CCB changed over time and was greatest 61 to 90 days postinitiation.” At that point, it was increased 2.4 times compared with initiation of an ACE inhibitor or an ARB in an adjusted analysis and increased almost 4 times compared with starting on any non-CCB agent.
Importantly, the actual prevalence of peripheral edema among those started on CCBs, ACE inhibitors, ARBs, or any non-CCB medication was not available in the data sets.
However, “the main message for clinicians is to consider medication side effects as a potential cause for new symptoms when patients present. We also encourage patients to ask prescribers about whether new symptoms could be caused by a medication,” senior author Lisa M. McCarthy, PharmD, told theheart.org/Medscape Cardiology.
“If a patient experiences peripheral edema while taking a CCB, we would encourage clinicians to consider whether the calcium-channel blocker is still necessary, whether it could be discontinued or the dose reduced, or whether the patient can be switched to another therapy,” she said.
Based on the current analysis, if the rate of CCB-induced peripheral edema is assumed to be 10%, which is consistent with the literature, then “potentially 7% to 14% of people who develop edema while taking a calcium channel blocker may then receive a loop diuretic,” an accompanying editorial notes.
“Patients with polypharmacy are at heightened risk of being exposed to [a] series of prescribing cascades if their current use of medications is not carefully discussed before the decision to add a new antihypertensive,” observe Timothy S. Anderson, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, and Michael A. Steinman, MD, San Francisco Veterans Affairs Medical Center and University of California, San Francisco.
“The initial prescribing cascade can set off many other negative consequences, including adverse drug events, potentially avoidable diagnostic testing, and hospitalizations,” the editorialists caution.
“Identifying prescribing cascades and their consequences is an important step to stem the tide of polypharmacy and inform deprescribing efforts.”
The analysis was based on administrative data from almost 340,000 adults in the community aged 66 years or older with hypertension and new drug prescriptions over 5 years ending in September 2016, the report notes. Their mean age was 74.5 years and 56.5% were women.
The data set included 41,086 patients who were newly prescribed a CCB; 66,494 who were newly prescribed an ACE inhibitor or ARB; and 231,439 newly prescribed any medication other than a CCB. The prescribed CCB was amlodipine in 79.6% of patients.
Although loop diuretics could possibly have been prescribed sometimes as a second-tier antihypertensive in the absence of peripheral edema, “we made efforts, through the design of our study, to limit this where possible,” Savage said in an interview.
For example, the focus was on loop diuretics, which aren’t generally recommended for blood-pressure lowering. Also, patients with heart failure and those with a recent history of diuretic or other antihypertensive medication use had been excluded, she said.
“As such, our cohort comprised individuals with new-onset or milder hypertension for whom diuretics would unlikely to be prescribed as part of guideline-based hypertension management.”
Although amlodipine was the most commonly prescribed CCB, the potential for a prescribing cascade seemed to be a class effect and to apply at a range of dosages.
That was unexpected, McCarthy observed, because “peripheral edema occurs more commonly in people taking dihydropyridine CCBs, like amlodipine, compared to non–dihydropyridine CCBs, such as verapamil and diltiazem.”
Savage, McCarthy, their coauthors, and the editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Elderly adults with hypertension who are newly prescribed a calcium-channel blocker (CCB), compared to other antihypertensive agents, are at least twice as likely to be given a loop diuretic over the following months, a large cohort study suggests.
The likelihood remained elevated for as long as a year after the start of a CCB and was more pronounced when comparing CCBs to any other kind of medication.
“Our findings suggest that many older adults who begin taking a CCB may subsequently experience a prescribing cascade” when loop diuretics are prescribed for peripheral edema, a known CCB adverse effect, that is misinterpreted as a new medical condition, Rachel D. Savage, PhD, Women’s College Hospital, Toronto, Canada, told theheart.org/Medscape Cardiology.
Edema caused by CCBs is caused by fluid redistribution, not overload, and “treating euvolemic individuals with a diuretic places them at increased risk of overdiuresis, leading to falls, urinary incontinence, acute kidney injury, electrolyte imbalances, and a cascade of other downstream consequences to which older adults are especially vulnerable,” explain Savage and coauthors of the analysis published online February 24 in JAMA Internal Medicine.
However, 1.4% of the cohort had been prescribed a loop diuretic, and 4.5% had been given any diuretic within 90 days after the start of CCBs. The corresponding rates were 0.7% and 3.4%, respectively, for patients who had started on ACE inhibitors or angiotensin receptor blocker (ARB) rather than a CCB.
Also, Savage observed, “the likelihood of being prescribed a loop diuretic following initiation of a CCB changed over time and was greatest 61 to 90 days postinitiation.” At that point, it was increased 2.4 times compared with initiation of an ACE inhibitor or an ARB in an adjusted analysis and increased almost 4 times compared with starting on any non-CCB agent.
Importantly, the actual prevalence of peripheral edema among those started on CCBs, ACE inhibitors, ARBs, or any non-CCB medication was not available in the data sets.
However, “the main message for clinicians is to consider medication side effects as a potential cause for new symptoms when patients present. We also encourage patients to ask prescribers about whether new symptoms could be caused by a medication,” senior author Lisa M. McCarthy, PharmD, told theheart.org/Medscape Cardiology.
“If a patient experiences peripheral edema while taking a CCB, we would encourage clinicians to consider whether the calcium-channel blocker is still necessary, whether it could be discontinued or the dose reduced, or whether the patient can be switched to another therapy,” she said.
Based on the current analysis, if the rate of CCB-induced peripheral edema is assumed to be 10%, which is consistent with the literature, then “potentially 7% to 14% of people who develop edema while taking a calcium channel blocker may then receive a loop diuretic,” an accompanying editorial notes.
“Patients with polypharmacy are at heightened risk of being exposed to [a] series of prescribing cascades if their current use of medications is not carefully discussed before the decision to add a new antihypertensive,” observe Timothy S. Anderson, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, and Michael A. Steinman, MD, San Francisco Veterans Affairs Medical Center and University of California, San Francisco.
“The initial prescribing cascade can set off many other negative consequences, including adverse drug events, potentially avoidable diagnostic testing, and hospitalizations,” the editorialists caution.
“Identifying prescribing cascades and their consequences is an important step to stem the tide of polypharmacy and inform deprescribing efforts.”
The analysis was based on administrative data from almost 340,000 adults in the community aged 66 years or older with hypertension and new drug prescriptions over 5 years ending in September 2016, the report notes. Their mean age was 74.5 years and 56.5% were women.
The data set included 41,086 patients who were newly prescribed a CCB; 66,494 who were newly prescribed an ACE inhibitor or ARB; and 231,439 newly prescribed any medication other than a CCB. The prescribed CCB was amlodipine in 79.6% of patients.
Although loop diuretics could possibly have been prescribed sometimes as a second-tier antihypertensive in the absence of peripheral edema, “we made efforts, through the design of our study, to limit this where possible,” Savage said in an interview.
For example, the focus was on loop diuretics, which aren’t generally recommended for blood-pressure lowering. Also, patients with heart failure and those with a recent history of diuretic or other antihypertensive medication use had been excluded, she said.
“As such, our cohort comprised individuals with new-onset or milder hypertension for whom diuretics would unlikely to be prescribed as part of guideline-based hypertension management.”
Although amlodipine was the most commonly prescribed CCB, the potential for a prescribing cascade seemed to be a class effect and to apply at a range of dosages.
That was unexpected, McCarthy observed, because “peripheral edema occurs more commonly in people taking dihydropyridine CCBs, like amlodipine, compared to non–dihydropyridine CCBs, such as verapamil and diltiazem.”
Savage, McCarthy, their coauthors, and the editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Varied nightly bedtime, sleep duration linked to CVD risk
People who frequently alter the amount of sleep and time they go to bed each night are twofold more likely to develop cardiovascular disease, independent of traditional CVD risk factors, new research suggests.
Prior studies have focused on shift workers because night shift work will influence circadian rhythm and increase CVD risk. But it is increasingly recognized that circadian disruption may occur outside of shift work and accumulate over time, particularly given modern lifestyle factors such as increased use of mobile devices and television at night, said study coauthor Tianyi Huang, ScD, MSc, of Brigham and Women’s Hospital and Harvard Medical School in Boston, Massachusetts.
“Even if they tend to go to sleep at certain times, by following that lifestyle or behavior, it can interfere with their planned sleep timing,” he said.
“One thing that surprised me in this sample is that about one third of participants have irregular sleep patterns that can put them at increased risk of cardiovascular disease. So I think the prevalence is higher than expected,” Huang added.
As reported today in the Journal of the American College of Cardiology, the investigators used data from 7-day wrist actigraphy, 1 night of at-home polysomnography, and sleep questionnaires to assess sleep duration and sleep-onset timing among 1,992 Multi-Ethnic Study of Atherosclerosis () participants, aged 45 to 84 years, who were free of CVD and prospectively followed for a me MESA dian of 4.9 years.
A total of 786 patients (39.5%) had sleep duration standard deviation (SD) > 90 minutes and 510 (25.6%) had sleep-onset timing SD > 90 minutes.
During follow-up, there were 111 incident CVD events, including myocardial infarction, coronary heart disease death, stroke, and other coronary events.
Compared with people who had less than 1 hour of variation in sleep duration, the risk for incident CVD was 9% higher for people whose sleep duration varied 61 to 90 minutes (hazard ratio [HR], 1.09; 95% confidence interval [CI], 0.62 - 1.92), even after controlling for a variety of cardiovascular and sleep-related risk factors such as body mass index, systolic blood pressure, smoking status, total cholesterol, average sleep duration, insomnia symptoms, and sleep apnea.
Moreover, the adjusted CVD risk was substantially increased with 91 to 120 minutes of variation (HR, 1.59; 95% CI, 0.91 - 2.76) and more than 120 minutes of variation in sleep duration (HR, 2.14; 95% CI, 1.24 - 3.68).
Every 1-hour increase in sleep duration SD was associated with 36% higher CVD risk (95% CI; 1.07 - 1.73).
Compared with people with no more than a half hour of variation in nightly bedtimes, the adjusted hazard ratios for CVD were 1.16 (95% CI, 0.64 - 2.13), 1.52 (95% CI, 0.81 - 2.88), and 2.11 (95% CI, 1.13 - 3.91) when bedtimes varied by 31 to 60 minutes, 61 to 90 minutes, and more than 90 minutes.
For every 1-hour increase in sleep-onset timing SD, the risk of CVD was 18% higher (95% CI; 1.06 - 1.31).
“The results are similar for the regularity of sleep timing and the regularity of sleep duration, which means that both can contribute to circadian disruption and then lead to development of cardiovascular disease,” Huang said.
This is an important article and signals how sleep is an important marker and possibly a mediator of cardiovascular risk, said Harlan Krumholz, MD, of Yale School of Medicine in New Haven, Connecticut, who was not involved with the study.
“What I like about this is it’s a nice longitudinal, epidemiologic study with not just self-report, but sensor-detected sleep, that has been correlated with well-curated and adjudicated outcomes to give us a strong sense of this association,” he told theheart.org/Medscape Cardiology. “And also, that it goes beyond just the duration — they combine the duration and timing in order to give a fuller picture of sleep.”
Nevertheless, Krumholz said researchers are only at the beginning of being able to quantify the various dimensions of sleep and the degree to which sleep is a reflection of underlying physiologic issues, or whether patients are having erratic sleep patterns that are having a toxic effect on their overall health.
Questions also remain about the mechanism behind the association, whether the increased risk is universal or more harmful for some people, and the best way to measure factors during sleep that can most comprehensively and precisely predict risk.
“As we get more information flowing in from sensors, I think we will begin to develop more sophisticated approaches toward understanding risk, and it will be accompanied by other studies that will help us understand whether, again, this is a reflection of other processes that we should be paying attention to or whether it is a cause of disease and risk,” Krumholz said.
Subgroup analyses suggested positive associations between irregular sleep and CVD in African Americans, Hispanics, and Chinese Americans but not in whites. This could be because sleep irregularity, both timing and duration, was substantially higher in minorities, especially African Americans, but may also be as a result of chance because the study sample is relatively small, Huang explained.
The authors note that the overall findings are biologically plausible because of their previous work linking sleep irregularity with metabolic risk factors that predispose to atherosclerosis, such as obesity, diabetes, and hypertension. Participants with irregular sleep tended to have worse baseline cardiometabolic profiles, but this only explained a small portion of the associations between sleep irregularity and CVD, they note.
Other possible explanations include circadian clock genes, such as clock, per2 and bmal1, which have been shown experimentally to control a broad range of cardiovascular functions, from blood pressure and endothelial functions to vascular thrombosis and cardiac remodeling.
Irregular sleep may also influence the rhythms of the autonomic nervous system, and behavioral rhythms with regard to timing and/or amount of eating or exercise.
Further research is needed to understand the mechanisms driving the associations, the impact of sleep irregularity on individual CVD outcomes, and to determine whether a 7-day SD of more than 90 minutes for either sleep duration or sleep-onset timing can be used clinically as a threshold target for promoting cardiometabolically healthy sleep, Huang said.
“When providers communicate with their patients regarding strategies for CVD prevention, usually they focus on healthy diet and physical activity; and even when they talk about sleep, they talk about whether they have good sleep quality or sufficient sleep,” he said. “But one thing they should provide is advice regarding sleep regularity and [they should] recommend their patients follow a regular sleep pattern for the purpose of cardiovascular prevention.”
In a related editorial, Olaf Oldenburg, MD, Luderus-Kliniken Münster, Clemenshospital, Münster, Germany, and Jens Spiesshoefer, MD, Institute of Life Sciences, Scuola Superiore Sant’Anna, Pisa, Italy, write that the observed independent association between sleep irregularity and CVD “is a particularly striking finding given that impaired circadian rhythm is likely to be much more prevalent than the extreme example of shift work.”
They call on researchers to utilize big data to facilitate understanding of the association and say it is essential to test whether experimental data support the hypothesis that altered circadian rhythms would translate into unfavorable changes in 24-hour sympathovagal and neurohormonal balance, and ultimately CVD.
The present study “will, and should, stimulate much needed additional research on the association between sleep and CVD that may offer novel approaches to help improve the prognosis and daily symptom burden of patients with CVD, and might make sleep itself a therapeutic target in CVD,” the editorialists conclude.
This research was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI), and by grants from the National Center for Advancing Translational Sciences. The MESA Sleep Study was supported by an NHLBI grant. Huang was supported by a career development grant from the National Institutes of Health.
Krumholz and Oldenburg have disclosed no relevant financial relationships. Spiesshoefer is supported by grants from the Else-Kröner-Fresenius Stiftung, the Innovative Medical Research program at the University of Münster, and Deutsche Herzstiftung; and by young investigator research support from Scuola Superiore Sant’Anna Pisa. He also has received travel grants and lecture honoraria from Boehringer Ingelheim and Chiesi.
Source: J Am Coll Cardiol. 2020 Mar 2. doi: 10.1016/j.jacc.2019.12.054.
This article first appeared on Medscape.com.
People who frequently alter the amount of sleep and time they go to bed each night are twofold more likely to develop cardiovascular disease, independent of traditional CVD risk factors, new research suggests.
Prior studies have focused on shift workers because night shift work will influence circadian rhythm and increase CVD risk. But it is increasingly recognized that circadian disruption may occur outside of shift work and accumulate over time, particularly given modern lifestyle factors such as increased use of mobile devices and television at night, said study coauthor Tianyi Huang, ScD, MSc, of Brigham and Women’s Hospital and Harvard Medical School in Boston, Massachusetts.
“Even if they tend to go to sleep at certain times, by following that lifestyle or behavior, it can interfere with their planned sleep timing,” he said.
“One thing that surprised me in this sample is that about one third of participants have irregular sleep patterns that can put them at increased risk of cardiovascular disease. So I think the prevalence is higher than expected,” Huang added.
As reported today in the Journal of the American College of Cardiology, the investigators used data from 7-day wrist actigraphy, 1 night of at-home polysomnography, and sleep questionnaires to assess sleep duration and sleep-onset timing among 1,992 Multi-Ethnic Study of Atherosclerosis () participants, aged 45 to 84 years, who were free of CVD and prospectively followed for a me MESA dian of 4.9 years.
A total of 786 patients (39.5%) had sleep duration standard deviation (SD) > 90 minutes and 510 (25.6%) had sleep-onset timing SD > 90 minutes.
During follow-up, there were 111 incident CVD events, including myocardial infarction, coronary heart disease death, stroke, and other coronary events.
Compared with people who had less than 1 hour of variation in sleep duration, the risk for incident CVD was 9% higher for people whose sleep duration varied 61 to 90 minutes (hazard ratio [HR], 1.09; 95% confidence interval [CI], 0.62 - 1.92), even after controlling for a variety of cardiovascular and sleep-related risk factors such as body mass index, systolic blood pressure, smoking status, total cholesterol, average sleep duration, insomnia symptoms, and sleep apnea.
Moreover, the adjusted CVD risk was substantially increased with 91 to 120 minutes of variation (HR, 1.59; 95% CI, 0.91 - 2.76) and more than 120 minutes of variation in sleep duration (HR, 2.14; 95% CI, 1.24 - 3.68).
Every 1-hour increase in sleep duration SD was associated with 36% higher CVD risk (95% CI; 1.07 - 1.73).
Compared with people with no more than a half hour of variation in nightly bedtimes, the adjusted hazard ratios for CVD were 1.16 (95% CI, 0.64 - 2.13), 1.52 (95% CI, 0.81 - 2.88), and 2.11 (95% CI, 1.13 - 3.91) when bedtimes varied by 31 to 60 minutes, 61 to 90 minutes, and more than 90 minutes.
For every 1-hour increase in sleep-onset timing SD, the risk of CVD was 18% higher (95% CI; 1.06 - 1.31).
“The results are similar for the regularity of sleep timing and the regularity of sleep duration, which means that both can contribute to circadian disruption and then lead to development of cardiovascular disease,” Huang said.
This is an important article and signals how sleep is an important marker and possibly a mediator of cardiovascular risk, said Harlan Krumholz, MD, of Yale School of Medicine in New Haven, Connecticut, who was not involved with the study.
“What I like about this is it’s a nice longitudinal, epidemiologic study with not just self-report, but sensor-detected sleep, that has been correlated with well-curated and adjudicated outcomes to give us a strong sense of this association,” he told theheart.org/Medscape Cardiology. “And also, that it goes beyond just the duration — they combine the duration and timing in order to give a fuller picture of sleep.”
Nevertheless, Krumholz said researchers are only at the beginning of being able to quantify the various dimensions of sleep and the degree to which sleep is a reflection of underlying physiologic issues, or whether patients are having erratic sleep patterns that are having a toxic effect on their overall health.
Questions also remain about the mechanism behind the association, whether the increased risk is universal or more harmful for some people, and the best way to measure factors during sleep that can most comprehensively and precisely predict risk.
“As we get more information flowing in from sensors, I think we will begin to develop more sophisticated approaches toward understanding risk, and it will be accompanied by other studies that will help us understand whether, again, this is a reflection of other processes that we should be paying attention to or whether it is a cause of disease and risk,” Krumholz said.
Subgroup analyses suggested positive associations between irregular sleep and CVD in African Americans, Hispanics, and Chinese Americans but not in whites. This could be because sleep irregularity, both timing and duration, was substantially higher in minorities, especially African Americans, but may also be as a result of chance because the study sample is relatively small, Huang explained.
The authors note that the overall findings are biologically plausible because of their previous work linking sleep irregularity with metabolic risk factors that predispose to atherosclerosis, such as obesity, diabetes, and hypertension. Participants with irregular sleep tended to have worse baseline cardiometabolic profiles, but this only explained a small portion of the associations between sleep irregularity and CVD, they note.
Other possible explanations include circadian clock genes, such as clock, per2 and bmal1, which have been shown experimentally to control a broad range of cardiovascular functions, from blood pressure and endothelial functions to vascular thrombosis and cardiac remodeling.
Irregular sleep may also influence the rhythms of the autonomic nervous system, and behavioral rhythms with regard to timing and/or amount of eating or exercise.
Further research is needed to understand the mechanisms driving the associations, the impact of sleep irregularity on individual CVD outcomes, and to determine whether a 7-day SD of more than 90 minutes for either sleep duration or sleep-onset timing can be used clinically as a threshold target for promoting cardiometabolically healthy sleep, Huang said.
“When providers communicate with their patients regarding strategies for CVD prevention, usually they focus on healthy diet and physical activity; and even when they talk about sleep, they talk about whether they have good sleep quality or sufficient sleep,” he said. “But one thing they should provide is advice regarding sleep regularity and [they should] recommend their patients follow a regular sleep pattern for the purpose of cardiovascular prevention.”
In a related editorial, Olaf Oldenburg, MD, Luderus-Kliniken Münster, Clemenshospital, Münster, Germany, and Jens Spiesshoefer, MD, Institute of Life Sciences, Scuola Superiore Sant’Anna, Pisa, Italy, write that the observed independent association between sleep irregularity and CVD “is a particularly striking finding given that impaired circadian rhythm is likely to be much more prevalent than the extreme example of shift work.”
They call on researchers to utilize big data to facilitate understanding of the association and say it is essential to test whether experimental data support the hypothesis that altered circadian rhythms would translate into unfavorable changes in 24-hour sympathovagal and neurohormonal balance, and ultimately CVD.
The present study “will, and should, stimulate much needed additional research on the association between sleep and CVD that may offer novel approaches to help improve the prognosis and daily symptom burden of patients with CVD, and might make sleep itself a therapeutic target in CVD,” the editorialists conclude.
This research was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI), and by grants from the National Center for Advancing Translational Sciences. The MESA Sleep Study was supported by an NHLBI grant. Huang was supported by a career development grant from the National Institutes of Health.
Krumholz and Oldenburg have disclosed no relevant financial relationships. Spiesshoefer is supported by grants from the Else-Kröner-Fresenius Stiftung, the Innovative Medical Research program at the University of Münster, and Deutsche Herzstiftung; and by young investigator research support from Scuola Superiore Sant’Anna Pisa. He also has received travel grants and lecture honoraria from Boehringer Ingelheim and Chiesi.
Source: J Am Coll Cardiol. 2020 Mar 2. doi: 10.1016/j.jacc.2019.12.054.
This article first appeared on Medscape.com.
People who frequently alter the amount of sleep and time they go to bed each night are twofold more likely to develop cardiovascular disease, independent of traditional CVD risk factors, new research suggests.
Prior studies have focused on shift workers because night shift work will influence circadian rhythm and increase CVD risk. But it is increasingly recognized that circadian disruption may occur outside of shift work and accumulate over time, particularly given modern lifestyle factors such as increased use of mobile devices and television at night, said study coauthor Tianyi Huang, ScD, MSc, of Brigham and Women’s Hospital and Harvard Medical School in Boston, Massachusetts.
“Even if they tend to go to sleep at certain times, by following that lifestyle or behavior, it can interfere with their planned sleep timing,” he said.
“One thing that surprised me in this sample is that about one third of participants have irregular sleep patterns that can put them at increased risk of cardiovascular disease. So I think the prevalence is higher than expected,” Huang added.
As reported today in the Journal of the American College of Cardiology, the investigators used data from 7-day wrist actigraphy, 1 night of at-home polysomnography, and sleep questionnaires to assess sleep duration and sleep-onset timing among 1,992 Multi-Ethnic Study of Atherosclerosis () participants, aged 45 to 84 years, who were free of CVD and prospectively followed for a me MESA dian of 4.9 years.
A total of 786 patients (39.5%) had sleep duration standard deviation (SD) > 90 minutes and 510 (25.6%) had sleep-onset timing SD > 90 minutes.
During follow-up, there were 111 incident CVD events, including myocardial infarction, coronary heart disease death, stroke, and other coronary events.
Compared with people who had less than 1 hour of variation in sleep duration, the risk for incident CVD was 9% higher for people whose sleep duration varied 61 to 90 minutes (hazard ratio [HR], 1.09; 95% confidence interval [CI], 0.62 - 1.92), even after controlling for a variety of cardiovascular and sleep-related risk factors such as body mass index, systolic blood pressure, smoking status, total cholesterol, average sleep duration, insomnia symptoms, and sleep apnea.
Moreover, the adjusted CVD risk was substantially increased with 91 to 120 minutes of variation (HR, 1.59; 95% CI, 0.91 - 2.76) and more than 120 minutes of variation in sleep duration (HR, 2.14; 95% CI, 1.24 - 3.68).
Every 1-hour increase in sleep duration SD was associated with 36% higher CVD risk (95% CI; 1.07 - 1.73).
Compared with people with no more than a half hour of variation in nightly bedtimes, the adjusted hazard ratios for CVD were 1.16 (95% CI, 0.64 - 2.13), 1.52 (95% CI, 0.81 - 2.88), and 2.11 (95% CI, 1.13 - 3.91) when bedtimes varied by 31 to 60 minutes, 61 to 90 minutes, and more than 90 minutes.
For every 1-hour increase in sleep-onset timing SD, the risk of CVD was 18% higher (95% CI; 1.06 - 1.31).
“The results are similar for the regularity of sleep timing and the regularity of sleep duration, which means that both can contribute to circadian disruption and then lead to development of cardiovascular disease,” Huang said.
This is an important article and signals how sleep is an important marker and possibly a mediator of cardiovascular risk, said Harlan Krumholz, MD, of Yale School of Medicine in New Haven, Connecticut, who was not involved with the study.
“What I like about this is it’s a nice longitudinal, epidemiologic study with not just self-report, but sensor-detected sleep, that has been correlated with well-curated and adjudicated outcomes to give us a strong sense of this association,” he told theheart.org/Medscape Cardiology. “And also, that it goes beyond just the duration — they combine the duration and timing in order to give a fuller picture of sleep.”
Nevertheless, Krumholz said researchers are only at the beginning of being able to quantify the various dimensions of sleep and the degree to which sleep is a reflection of underlying physiologic issues, or whether patients are having erratic sleep patterns that are having a toxic effect on their overall health.
Questions also remain about the mechanism behind the association, whether the increased risk is universal or more harmful for some people, and the best way to measure factors during sleep that can most comprehensively and precisely predict risk.
“As we get more information flowing in from sensors, I think we will begin to develop more sophisticated approaches toward understanding risk, and it will be accompanied by other studies that will help us understand whether, again, this is a reflection of other processes that we should be paying attention to or whether it is a cause of disease and risk,” Krumholz said.
Subgroup analyses suggested positive associations between irregular sleep and CVD in African Americans, Hispanics, and Chinese Americans but not in whites. This could be because sleep irregularity, both timing and duration, was substantially higher in minorities, especially African Americans, but may also be as a result of chance because the study sample is relatively small, Huang explained.
The authors note that the overall findings are biologically plausible because of their previous work linking sleep irregularity with metabolic risk factors that predispose to atherosclerosis, such as obesity, diabetes, and hypertension. Participants with irregular sleep tended to have worse baseline cardiometabolic profiles, but this only explained a small portion of the associations between sleep irregularity and CVD, they note.
Other possible explanations include circadian clock genes, such as clock, per2 and bmal1, which have been shown experimentally to control a broad range of cardiovascular functions, from blood pressure and endothelial functions to vascular thrombosis and cardiac remodeling.
Irregular sleep may also influence the rhythms of the autonomic nervous system, and behavioral rhythms with regard to timing and/or amount of eating or exercise.
Further research is needed to understand the mechanisms driving the associations, the impact of sleep irregularity on individual CVD outcomes, and to determine whether a 7-day SD of more than 90 minutes for either sleep duration or sleep-onset timing can be used clinically as a threshold target for promoting cardiometabolically healthy sleep, Huang said.
“When providers communicate with their patients regarding strategies for CVD prevention, usually they focus on healthy diet and physical activity; and even when they talk about sleep, they talk about whether they have good sleep quality or sufficient sleep,” he said. “But one thing they should provide is advice regarding sleep regularity and [they should] recommend their patients follow a regular sleep pattern for the purpose of cardiovascular prevention.”
In a related editorial, Olaf Oldenburg, MD, Luderus-Kliniken Münster, Clemenshospital, Münster, Germany, and Jens Spiesshoefer, MD, Institute of Life Sciences, Scuola Superiore Sant’Anna, Pisa, Italy, write that the observed independent association between sleep irregularity and CVD “is a particularly striking finding given that impaired circadian rhythm is likely to be much more prevalent than the extreme example of shift work.”
They call on researchers to utilize big data to facilitate understanding of the association and say it is essential to test whether experimental data support the hypothesis that altered circadian rhythms would translate into unfavorable changes in 24-hour sympathovagal and neurohormonal balance, and ultimately CVD.
The present study “will, and should, stimulate much needed additional research on the association between sleep and CVD that may offer novel approaches to help improve the prognosis and daily symptom burden of patients with CVD, and might make sleep itself a therapeutic target in CVD,” the editorialists conclude.
This research was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI), and by grants from the National Center for Advancing Translational Sciences. The MESA Sleep Study was supported by an NHLBI grant. Huang was supported by a career development grant from the National Institutes of Health.
Krumholz and Oldenburg have disclosed no relevant financial relationships. Spiesshoefer is supported by grants from the Else-Kröner-Fresenius Stiftung, the Innovative Medical Research program at the University of Münster, and Deutsche Herzstiftung; and by young investigator research support from Scuola Superiore Sant’Anna Pisa. He also has received travel grants and lecture honoraria from Boehringer Ingelheim and Chiesi.
Source: J Am Coll Cardiol. 2020 Mar 2. doi: 10.1016/j.jacc.2019.12.054.
This article first appeared on Medscape.com.
New strategies cut esophageal damage from AFib catheter ablation
NATIONAL HARBOR, MD. – Thermal injury of a patient’s esophagus during radiofrequency catheter ablation of atrial fibrillation is notorious as a relatively common and problematic complication of the procedure, but two new approaches showed promise for substantially cutting the risk of esophageal thermal injury and the potential for the most severe damage: perforation.

One of these innovations is intensive esophageal cooling with a commercially marketed, fluid-chilled catheter placed in a patient’s esophagus during radiofrequency catheter ablation that keeps the inner surface of the esophagus at 4°C. This approach cut the incidence of periprocedural episodes of endoscopically detected esophageal thermal injury from 20% among controls to 3% in patients who had esophageal cooling in a randomized study with 120 patients, Mark M. Gallagher, MD, said at the annual International AF Symposium. The same device can also maintain a temperature on the inner surface of the esophagus of 42 ° C in patients undergoing cryoablation of atrial fibrillation, noted Dr. Gallagher, a cardiac electrophysiologist at St. George’s University Hospitals in London.
A second approach to cutting esophageal damage focuses on modifying the energy delivery with a radiofrequency ablation method known as high-power short-duration (HPSD). As the name says, this strategy uses a relatively high level of radiofrequency energy, 50 watts in the reported experience, for the brief interval of about 7 seconds, ideally delivering an overall Ablation Index of at least 350 but below 360, said Thomas Deneke, MD, an electrophysiologist, professor, and cochief of cardiology at the Heart Center in Bad Neustadt, Germany.
Dr. Deneke and his associates in Bad Neustadt began using this HPSD approach in mid-2019, and by early 2020 they had data from 179 patients who underwent first-time catheter ablation of atrial fibrillation (AFib), all of whom had undergone routine esophageal endoscopy 1-3 days after their treatment. Eight patients (4%) showed evidence of endoscopically detected esophageal lesions (EDEL), including three patients (2%) with an actual esophageal ulcer, and one (0.6%) who developed a perforation that healed after 52 days, Dr. Deneke reported. An additional 55 patients underwent a redo catheter ablation procedure using the HPSD method during this period, and in that group follow-up endoscopy in all patients showed EDEL in two patients (4%). In contrast, during Jan. 2012–May 2019, the same German center treated 2,102 patients who had a first radiofrequency catheter ablation using convention energy levels and treatment times, which resulted in 291 patients having an EDEL (14%), including 94 (4%) with an ulcer, and six patients (0.3%) with an esophageal perforation, he said.

His center’s recent safety experience with HPSD radiofrequncy ablation, compared with the historical controls, suggests that this technique can produce a substantial reduction in esophageal thermal injury, but HPSD has not completely eliminated the risk and hence there is need for continued alertness for this potential complication Dr. Deneke concluded. The HPSD method is also limited by having “a very narrow window” between efficacy at an Ablation Index of 350 and safety when the index remains below 360, he added.
The randomized study that Dr. Gallagher ran at St. George’s followed an analysis he and his associates recently published that suggested efficacy using esophageal cooling in prior reports when the data combined in a meta-analysis (J Interv Card Electrophysiol. 2019 Nov 22. doi: 10.1007/s10840-019-00661-5). They also concluded that the clinical setting required a temperature control device with an enhanced capacity for rapid cooling, which prior studies had lacked. So they turned to a Food and Drug Administration–approved catheter designed for placement in the esophagus for the purpose of either whole-body cooling or warming.
The study randomized a total of 187 patients, but collected follow-up endoscopy at 5-7 days after the ablation procedure on 120 patients, of whom 60 received esophageal cooling and 60 did not. The types of ablations performed on patients in the two study arms were similar, and use of esophageal cooling had no impact on treatment duration or efficacy, either acute and longer term, Dr. Gallagher reported.
Cooling had a marked and statistically significant impact on endoscopically detected thermal injury. Although two patients in the group that underwent cooling had injuries, in one of these cases the injury involved a protocol violation: Radiofrequency ablation mistakenly occurred after the cooling device shut off, and it was during this period when the injury happened. In the second case of thermal injury, blinded scoring judged the injury as grade 2 in severity – an erosion of less than 5 mm – on a nine-item scale that ranged from zero to grade 6, the most severe level denoting a fistula. By contrast, among the 12 patients with thermal injury in the nonprotected subgroup, one patient had a grade 5a lesion denoting a deep ulcer, one had a 4b denoting a superficial ulcer with a clot, and four had a 4a lesion defined as a clean superficial ulcer.
“This is really effective. It’s the first study to show reduced damage without affecting ablation efficacy,” Dr. Gallagher said. He plans to now use this method of esophageal protection routinely for his AFib ablation patients who pay privately, and for patients insured under the national U.K. system once this coverage is approved. Dr. Deneke expressed his interest in also using this approach to esophageal protection, but noted that currently he did not have access to the cooling catheter that Dr. Gallagher used because of regulatory constraints.
The esophageal cooling study was sponsored by Attune Medical, which markets the cooling device. Dr. Gallagher has received research funding from Attune Medical, and has received honoraria as a speaker on behalf of Biosense Webster and Medtronic. Dr. Deneke has been a speaker on behalf of Abbott, Biosense Webster, Biotronik, and Boston Scientific, and his institution has received research funding from Biosense Webster and Securus/Boston Scientific.
NATIONAL HARBOR, MD. – Thermal injury of a patient’s esophagus during radiofrequency catheter ablation of atrial fibrillation is notorious as a relatively common and problematic complication of the procedure, but two new approaches showed promise for substantially cutting the risk of esophageal thermal injury and the potential for the most severe damage: perforation.
One of these innovations is intensive esophageal cooling with a commercially marketed, fluid-chilled catheter placed in a patient’s esophagus during radiofrequency catheter ablation that keeps the inner surface of the esophagus at 4°C. This approach cut the incidence of periprocedural episodes of endoscopically detected esophageal thermal injury from 20% among controls to 3% in patients who had esophageal cooling in a randomized study with 120 patients, Mark M. Gallagher, MD, said at the annual International AF Symposium. The same device can also maintain a temperature on the inner surface of the esophagus of 42 ° C in patients undergoing cryoablation of atrial fibrillation, noted Dr. Gallagher, a cardiac electrophysiologist at St. George’s University Hospitals in London.
A second approach to cutting esophageal damage focuses on modifying the energy delivery with a radiofrequency ablation method known as high-power short-duration (HPSD). As the name says, this strategy uses a relatively high level of radiofrequency energy, 50 watts in the reported experience, for the brief interval of about 7 seconds, ideally delivering an overall Ablation Index of at least 350 but below 360, said Thomas Deneke, MD, an electrophysiologist, professor, and cochief of cardiology at the Heart Center in Bad Neustadt, Germany.
Dr. Deneke and his associates in Bad Neustadt began using this HPSD approach in mid-2019, and by early 2020 they had data from 179 patients who underwent first-time catheter ablation of atrial fibrillation (AFib), all of whom had undergone routine esophageal endoscopy 1-3 days after their treatment. Eight patients (4%) showed evidence of endoscopically detected esophageal lesions (EDEL), including three patients (2%) with an actual esophageal ulcer, and one (0.6%) who developed a perforation that healed after 52 days, Dr. Deneke reported. An additional 55 patients underwent a redo catheter ablation procedure using the HPSD method during this period, and in that group follow-up endoscopy in all patients showed EDEL in two patients (4%). In contrast, during Jan. 2012–May 2019, the same German center treated 2,102 patients who had a first radiofrequency catheter ablation using convention energy levels and treatment times, which resulted in 291 patients having an EDEL (14%), including 94 (4%) with an ulcer, and six patients (0.3%) with an esophageal perforation, he said.
His center’s recent safety experience with HPSD radiofrequncy ablation, compared with the historical controls, suggests that this technique can produce a substantial reduction in esophageal thermal injury, but HPSD has not completely eliminated the risk and hence there is need for continued alertness for this potential complication Dr. Deneke concluded. The HPSD method is also limited by having “a very narrow window” between efficacy at an Ablation Index of 350 and safety when the index remains below 360, he added.
The randomized study that Dr. Gallagher ran at St. George’s followed an analysis he and his associates recently published that suggested efficacy using esophageal cooling in prior reports when the data combined in a meta-analysis (J Interv Card Electrophysiol. 2019 Nov 22. doi: 10.1007/s10840-019-00661-5). They also concluded that the clinical setting required a temperature control device with an enhanced capacity for rapid cooling, which prior studies had lacked. So they turned to a Food and Drug Administration–approved catheter designed for placement in the esophagus for the purpose of either whole-body cooling or warming.
The study randomized a total of 187 patients, but collected follow-up endoscopy at 5-7 days after the ablation procedure on 120 patients, of whom 60 received esophageal cooling and 60 did not. The types of ablations performed on patients in the two study arms were similar, and use of esophageal cooling had no impact on treatment duration or efficacy, either acute and longer term, Dr. Gallagher reported.
Cooling had a marked and statistically significant impact on endoscopically detected thermal injury. Although two patients in the group that underwent cooling had injuries, in one of these cases the injury involved a protocol violation: Radiofrequency ablation mistakenly occurred after the cooling device shut off, and it was during this period when the injury happened. In the second case of thermal injury, blinded scoring judged the injury as grade 2 in severity – an erosion of less than 5 mm – on a nine-item scale that ranged from zero to grade 6, the most severe level denoting a fistula. By contrast, among the 12 patients with thermal injury in the nonprotected subgroup, one patient had a grade 5a lesion denoting a deep ulcer, one had a 4b denoting a superficial ulcer with a clot, and four had a 4a lesion defined as a clean superficial ulcer.
“This is really effective. It’s the first study to show reduced damage without affecting ablation efficacy,” Dr. Gallagher said. He plans to now use this method of esophageal protection routinely for his AFib ablation patients who pay privately, and for patients insured under the national U.K. system once this coverage is approved. Dr. Deneke expressed his interest in also using this approach to esophageal protection, but noted that currently he did not have access to the cooling catheter that Dr. Gallagher used because of regulatory constraints.
The esophageal cooling study was sponsored by Attune Medical, which markets the cooling device. Dr. Gallagher has received research funding from Attune Medical, and has received honoraria as a speaker on behalf of Biosense Webster and Medtronic. Dr. Deneke has been a speaker on behalf of Abbott, Biosense Webster, Biotronik, and Boston Scientific, and his institution has received research funding from Biosense Webster and Securus/Boston Scientific.
NATIONAL HARBOR, MD. – Thermal injury of a patient’s esophagus during radiofrequency catheter ablation of atrial fibrillation is notorious as a relatively common and problematic complication of the procedure, but two new approaches showed promise for substantially cutting the risk of esophageal thermal injury and the potential for the most severe damage: perforation.
One of these innovations is intensive esophageal cooling with a commercially marketed, fluid-chilled catheter placed in a patient’s esophagus during radiofrequency catheter ablation that keeps the inner surface of the esophagus at 4°C. This approach cut the incidence of periprocedural episodes of endoscopically detected esophageal thermal injury from 20% among controls to 3% in patients who had esophageal cooling in a randomized study with 120 patients, Mark M. Gallagher, MD, said at the annual International AF Symposium. The same device can also maintain a temperature on the inner surface of the esophagus of 42 ° C in patients undergoing cryoablation of atrial fibrillation, noted Dr. Gallagher, a cardiac electrophysiologist at St. George’s University Hospitals in London.
A second approach to cutting esophageal damage focuses on modifying the energy delivery with a radiofrequency ablation method known as high-power short-duration (HPSD). As the name says, this strategy uses a relatively high level of radiofrequency energy, 50 watts in the reported experience, for the brief interval of about 7 seconds, ideally delivering an overall Ablation Index of at least 350 but below 360, said Thomas Deneke, MD, an electrophysiologist, professor, and cochief of cardiology at the Heart Center in Bad Neustadt, Germany.
Dr. Deneke and his associates in Bad Neustadt began using this HPSD approach in mid-2019, and by early 2020 they had data from 179 patients who underwent first-time catheter ablation of atrial fibrillation (AFib), all of whom had undergone routine esophageal endoscopy 1-3 days after their treatment. Eight patients (4%) showed evidence of endoscopically detected esophageal lesions (EDEL), including three patients (2%) with an actual esophageal ulcer, and one (0.6%) who developed a perforation that healed after 52 days, Dr. Deneke reported. An additional 55 patients underwent a redo catheter ablation procedure using the HPSD method during this period, and in that group follow-up endoscopy in all patients showed EDEL in two patients (4%). In contrast, during Jan. 2012–May 2019, the same German center treated 2,102 patients who had a first radiofrequency catheter ablation using convention energy levels and treatment times, which resulted in 291 patients having an EDEL (14%), including 94 (4%) with an ulcer, and six patients (0.3%) with an esophageal perforation, he said.
His center’s recent safety experience with HPSD radiofrequncy ablation, compared with the historical controls, suggests that this technique can produce a substantial reduction in esophageal thermal injury, but HPSD has not completely eliminated the risk and hence there is need for continued alertness for this potential complication Dr. Deneke concluded. The HPSD method is also limited by having “a very narrow window” between efficacy at an Ablation Index of 350 and safety when the index remains below 360, he added.
The randomized study that Dr. Gallagher ran at St. George’s followed an analysis he and his associates recently published that suggested efficacy using esophageal cooling in prior reports when the data combined in a meta-analysis (J Interv Card Electrophysiol. 2019 Nov 22. doi: 10.1007/s10840-019-00661-5). They also concluded that the clinical setting required a temperature control device with an enhanced capacity for rapid cooling, which prior studies had lacked. So they turned to a Food and Drug Administration–approved catheter designed for placement in the esophagus for the purpose of either whole-body cooling or warming.
The study randomized a total of 187 patients, but collected follow-up endoscopy at 5-7 days after the ablation procedure on 120 patients, of whom 60 received esophageal cooling and 60 did not. The types of ablations performed on patients in the two study arms were similar, and use of esophageal cooling had no impact on treatment duration or efficacy, either acute and longer term, Dr. Gallagher reported.
Cooling had a marked and statistically significant impact on endoscopically detected thermal injury. Although two patients in the group that underwent cooling had injuries, in one of these cases the injury involved a protocol violation: Radiofrequency ablation mistakenly occurred after the cooling device shut off, and it was during this period when the injury happened. In the second case of thermal injury, blinded scoring judged the injury as grade 2 in severity – an erosion of less than 5 mm – on a nine-item scale that ranged from zero to grade 6, the most severe level denoting a fistula. By contrast, among the 12 patients with thermal injury in the nonprotected subgroup, one patient had a grade 5a lesion denoting a deep ulcer, one had a 4b denoting a superficial ulcer with a clot, and four had a 4a lesion defined as a clean superficial ulcer.
“This is really effective. It’s the first study to show reduced damage without affecting ablation efficacy,” Dr. Gallagher said. He plans to now use this method of esophageal protection routinely for his AFib ablation patients who pay privately, and for patients insured under the national U.K. system once this coverage is approved. Dr. Deneke expressed his interest in also using this approach to esophageal protection, but noted that currently he did not have access to the cooling catheter that Dr. Gallagher used because of regulatory constraints.
The esophageal cooling study was sponsored by Attune Medical, which markets the cooling device. Dr. Gallagher has received research funding from Attune Medical, and has received honoraria as a speaker on behalf of Biosense Webster and Medtronic. Dr. Deneke has been a speaker on behalf of Abbott, Biosense Webster, Biotronik, and Boston Scientific, and his institution has received research funding from Biosense Webster and Securus/Boston Scientific.
THE AF SYMPOSIUM 2020
Bad behavior by medical trainees target of new proposal
Some instances of unprofessional behavior by medical trainees are universally deemed egregious and worthy of discipline — for example, looking up a friend’s medical data after HIPAA training.
Conversely, some professionalism lapses may be widely thought of as a teaching and consoling moment, such as the human error involved in forgetting a scheduled repositioning of a patient.
But between the extremes is a vast gray area. To deal with those cases appropriately, Jason Wasserman, PhD, and colleagues propose a new framework by which to judge each infraction.
The framework draws from “just culture” concepts used to evaluate medical errors, Wasserman, associate professor of biomedical science at Oakland University William Beaumont School of Medicine in Rochester, Michigan, told Medscape Medical News. Such an approach takes into account the environment in which the error was made, the knowledge and intent of the person making the error, and the severity and consequences of the infraction so that trainees and institutions can learn from mistakes.
“Trainees by definition are not going to fully get it,” he explained. “By definition they’re not going to fully achieve professional expectations. So how can we respond to the things we need to respond to, but do it in a way that’s educational?”
Wasserman and coauthors’ framework for remediation, which they published February 20 in The New England Journal of Medicine, takes into account several questions: Was the expectation clear? Were there factors beyond the trainees› control? What were the trainees› intentions and did they understand the consequences? Did the person genuinely believe the action was inconsequential?
An example requiring discipline, the authors say, would be using a crib sheet during an exam. In that case the intent is clear, there is no defensible belief that the action is inconsequential, and there is a clear understanding the action is wrong.
But a response of “affirm, support, and advise” is more appropriate, for example, when a student’s alarm doesn’t go off after a power outage and they miss a mandatory meeting.
Wasserman points out that this framework won’t cover all situations.
“This is not an algorithm for answering your questions about what to do,” he said. “It’s an architecture for clarifying the discussion about that. It can really tease out all the threads that need to be considered to best respond to and correct the professionalism lapse, but do it in a way that is developmentally appropriate.”
A Core Competency
For two decades, professionalism has been considered a core competency of medical education. In 1999, the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties formalized it as such. In 2013, the Association of American Medical Colleges formally required related professionalism competencies.
However, identifying lapses has operated largely on an “I-know-it-when-I-see-it” basis, leading to widely varying remediation practices judged by a small number of faculty members or administrators.
The ideas outlined by Wasserman and colleagues are “a terrific application of the ‘just-culture’ framework,” according to Nicole Treadway, MD, a first-year primary care resident at Emory School of Medicine in Atlanta, Georgia.
At Emory, discussions of professionalism start from day 1 of medical school and the subject is revisited throughout training in small groups, Treadway told Medscape Medical News.
But, she said, as the authors point out, definitions of unprofessionalism are not always clear and the examples the authors put forward help put lapses in context.
The framework also allows for looking at mistakes in light of the stress trainees encounter and the greater chance of making a professionalism error in those situations, she noted.
In her own work, she says, because she is juggling both inpatient and outpatient care, she is finding it is easy to get behind on correspondence or communicating lab results or having follow-up conversations.
Those delays could be seen as lapses in professionalism, but under this framework, there may be system solutions or training opportunities to consider.
“We do need this organizational architecture, and I think it could serve us well in really helping us identify and appropriately respond to what we see regarding professionalism,” she said.
Framework Helps Standardize Thinking
She said having a universal framework also helps because while standards of professionalism are easier to monitor in a single medical school, when students scatter to other hospitals for clinical training, those hospitals may have different professionalism standards.
Wasserman agrees, saying, “This could be easily adopted in any environment where people deal with professionalism lapses. I don’t even think it’s necessarily relegated to trainees. It’s a great way to think about any kind of lapses, just as hospitals think about medical errors.”
He said the next step is presenting the framework at various medical schools for feedback and research to see whether the framework improves processes.
Potential criticism, he said, might come from those who say such a construct avoids punishing students who make errors.
“There will always be people who say we’re pandering to medical students whenever we worry about the learning environment,” he said. “There are old-school purists who say when people screw up you should punish them.”
But he adds healthcare broadly has moved past that thinking.
“People recognized 20 years ago or more from the standpoint of improving healthcare systems and safety that is a bad strategy. You’ll never get error-free humans working in your system, and what you have to do is consider how the system is functioning and think about ways to optimize the system so people can be their best within it.”
Wasserman and Treadway have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Some instances of unprofessional behavior by medical trainees are universally deemed egregious and worthy of discipline — for example, looking up a friend’s medical data after HIPAA training.
Conversely, some professionalism lapses may be widely thought of as a teaching and consoling moment, such as the human error involved in forgetting a scheduled repositioning of a patient.
But between the extremes is a vast gray area. To deal with those cases appropriately, Jason Wasserman, PhD, and colleagues propose a new framework by which to judge each infraction.
The framework draws from “just culture” concepts used to evaluate medical errors, Wasserman, associate professor of biomedical science at Oakland University William Beaumont School of Medicine in Rochester, Michigan, told Medscape Medical News. Such an approach takes into account the environment in which the error was made, the knowledge and intent of the person making the error, and the severity and consequences of the infraction so that trainees and institutions can learn from mistakes.
“Trainees by definition are not going to fully get it,” he explained. “By definition they’re not going to fully achieve professional expectations. So how can we respond to the things we need to respond to, but do it in a way that’s educational?”
Wasserman and coauthors’ framework for remediation, which they published February 20 in The New England Journal of Medicine, takes into account several questions: Was the expectation clear? Were there factors beyond the trainees› control? What were the trainees› intentions and did they understand the consequences? Did the person genuinely believe the action was inconsequential?
An example requiring discipline, the authors say, would be using a crib sheet during an exam. In that case the intent is clear, there is no defensible belief that the action is inconsequential, and there is a clear understanding the action is wrong.
But a response of “affirm, support, and advise” is more appropriate, for example, when a student’s alarm doesn’t go off after a power outage and they miss a mandatory meeting.
Wasserman points out that this framework won’t cover all situations.
“This is not an algorithm for answering your questions about what to do,” he said. “It’s an architecture for clarifying the discussion about that. It can really tease out all the threads that need to be considered to best respond to and correct the professionalism lapse, but do it in a way that is developmentally appropriate.”
A Core Competency
For two decades, professionalism has been considered a core competency of medical education. In 1999, the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties formalized it as such. In 2013, the Association of American Medical Colleges formally required related professionalism competencies.
However, identifying lapses has operated largely on an “I-know-it-when-I-see-it” basis, leading to widely varying remediation practices judged by a small number of faculty members or administrators.
The ideas outlined by Wasserman and colleagues are “a terrific application of the ‘just-culture’ framework,” according to Nicole Treadway, MD, a first-year primary care resident at Emory School of Medicine in Atlanta, Georgia.
At Emory, discussions of professionalism start from day 1 of medical school and the subject is revisited throughout training in small groups, Treadway told Medscape Medical News.
But, she said, as the authors point out, definitions of unprofessionalism are not always clear and the examples the authors put forward help put lapses in context.
The framework also allows for looking at mistakes in light of the stress trainees encounter and the greater chance of making a professionalism error in those situations, she noted.
In her own work, she says, because she is juggling both inpatient and outpatient care, she is finding it is easy to get behind on correspondence or communicating lab results or having follow-up conversations.
Those delays could be seen as lapses in professionalism, but under this framework, there may be system solutions or training opportunities to consider.
“We do need this organizational architecture, and I think it could serve us well in really helping us identify and appropriately respond to what we see regarding professionalism,” she said.
Framework Helps Standardize Thinking
She said having a universal framework also helps because while standards of professionalism are easier to monitor in a single medical school, when students scatter to other hospitals for clinical training, those hospitals may have different professionalism standards.
Wasserman agrees, saying, “This could be easily adopted in any environment where people deal with professionalism lapses. I don’t even think it’s necessarily relegated to trainees. It’s a great way to think about any kind of lapses, just as hospitals think about medical errors.”
He said the next step is presenting the framework at various medical schools for feedback and research to see whether the framework improves processes.
Potential criticism, he said, might come from those who say such a construct avoids punishing students who make errors.
“There will always be people who say we’re pandering to medical students whenever we worry about the learning environment,” he said. “There are old-school purists who say when people screw up you should punish them.”
But he adds healthcare broadly has moved past that thinking.
“People recognized 20 years ago or more from the standpoint of improving healthcare systems and safety that is a bad strategy. You’ll never get error-free humans working in your system, and what you have to do is consider how the system is functioning and think about ways to optimize the system so people can be their best within it.”
Wasserman and Treadway have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Some instances of unprofessional behavior by medical trainees are universally deemed egregious and worthy of discipline — for example, looking up a friend’s medical data after HIPAA training.
Conversely, some professionalism lapses may be widely thought of as a teaching and consoling moment, such as the human error involved in forgetting a scheduled repositioning of a patient.
But between the extremes is a vast gray area. To deal with those cases appropriately, Jason Wasserman, PhD, and colleagues propose a new framework by which to judge each infraction.
The framework draws from “just culture” concepts used to evaluate medical errors, Wasserman, associate professor of biomedical science at Oakland University William Beaumont School of Medicine in Rochester, Michigan, told Medscape Medical News. Such an approach takes into account the environment in which the error was made, the knowledge and intent of the person making the error, and the severity and consequences of the infraction so that trainees and institutions can learn from mistakes.
“Trainees by definition are not going to fully get it,” he explained. “By definition they’re not going to fully achieve professional expectations. So how can we respond to the things we need to respond to, but do it in a way that’s educational?”
Wasserman and coauthors’ framework for remediation, which they published February 20 in The New England Journal of Medicine, takes into account several questions: Was the expectation clear? Were there factors beyond the trainees› control? What were the trainees› intentions and did they understand the consequences? Did the person genuinely believe the action was inconsequential?
An example requiring discipline, the authors say, would be using a crib sheet during an exam. In that case the intent is clear, there is no defensible belief that the action is inconsequential, and there is a clear understanding the action is wrong.
But a response of “affirm, support, and advise” is more appropriate, for example, when a student’s alarm doesn’t go off after a power outage and they miss a mandatory meeting.
Wasserman points out that this framework won’t cover all situations.
“This is not an algorithm for answering your questions about what to do,” he said. “It’s an architecture for clarifying the discussion about that. It can really tease out all the threads that need to be considered to best respond to and correct the professionalism lapse, but do it in a way that is developmentally appropriate.”
A Core Competency
For two decades, professionalism has been considered a core competency of medical education. In 1999, the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties formalized it as such. In 2013, the Association of American Medical Colleges formally required related professionalism competencies.
However, identifying lapses has operated largely on an “I-know-it-when-I-see-it” basis, leading to widely varying remediation practices judged by a small number of faculty members or administrators.
The ideas outlined by Wasserman and colleagues are “a terrific application of the ‘just-culture’ framework,” according to Nicole Treadway, MD, a first-year primary care resident at Emory School of Medicine in Atlanta, Georgia.
At Emory, discussions of professionalism start from day 1 of medical school and the subject is revisited throughout training in small groups, Treadway told Medscape Medical News.
But, she said, as the authors point out, definitions of unprofessionalism are not always clear and the examples the authors put forward help put lapses in context.
The framework also allows for looking at mistakes in light of the stress trainees encounter and the greater chance of making a professionalism error in those situations, she noted.
In her own work, she says, because she is juggling both inpatient and outpatient care, she is finding it is easy to get behind on correspondence or communicating lab results or having follow-up conversations.
Those delays could be seen as lapses in professionalism, but under this framework, there may be system solutions or training opportunities to consider.
“We do need this organizational architecture, and I think it could serve us well in really helping us identify and appropriately respond to what we see regarding professionalism,” she said.
Framework Helps Standardize Thinking
She said having a universal framework also helps because while standards of professionalism are easier to monitor in a single medical school, when students scatter to other hospitals for clinical training, those hospitals may have different professionalism standards.
Wasserman agrees, saying, “This could be easily adopted in any environment where people deal with professionalism lapses. I don’t even think it’s necessarily relegated to trainees. It’s a great way to think about any kind of lapses, just as hospitals think about medical errors.”
He said the next step is presenting the framework at various medical schools for feedback and research to see whether the framework improves processes.
Potential criticism, he said, might come from those who say such a construct avoids punishing students who make errors.
“There will always be people who say we’re pandering to medical students whenever we worry about the learning environment,” he said. “There are old-school purists who say when people screw up you should punish them.”
But he adds healthcare broadly has moved past that thinking.
“People recognized 20 years ago or more from the standpoint of improving healthcare systems and safety that is a bad strategy. You’ll never get error-free humans working in your system, and what you have to do is consider how the system is functioning and think about ways to optimize the system so people can be their best within it.”
Wasserman and Treadway have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Mortality sevenfold higher post TAVR with severe kidney injury
NATIONAL HARBOR, MD. – Acute kidney injury (AKI), a potentially modifiable risk factor in some cases, predicts increased mortality within the first year after transcatheter aortic valve transplantation (TAVR), according to an analysis of a U.S. registry presented at CRT 2020 sponsored by MedStar Heart & Vascular Institute.
“After adjustment, there are higher rates of all-cause mortality regardless of the severity of AKI,” reported Howard M. Julien, MD, of the University of Pennsylvania, Philadelphia.
Relative to the absence of AKI (stage 0), the hazard ratio for death at 1 year was more than threefold greater (HR, 3.26), even for those with stage 1 AKI. When unadjusted for covariates, it remained more than twice as high (HR, 2.67; P less than .001), Dr. Julien reported.
For stage 3 AKI, the unadjusted risk was more than nine times higher and remained roughly seven times greater after adjustment (HR, 7.04; P less than .001). Stage 2 AKI was linked with an adjusted risk of about the same magnitude.
Drawn from the National Cardiovascular TAVR Registry, which is maintained jointly by the Society of Thoracic Surgeons and the American College of Cardiology, data were analyzed on more than 100,000 TAVRs performed during 2012-2018. A subset of TAVRs performed between January 2016 and June 2018 served as a source of trends in what Dr. Julien described as the “modern era” of this procedure.
The incidence of AKI overall was about 10%, but rates were higher at the earliest time point in the analysis and fell modestly over the study period for all three stages. In a logistic regression analysis, the factors associated with the greatest odds ratio of developing AKI in patients following TAVR were conversion to open heart surgery (OR, 10.84, P less than .001), nonfemoral access (OR, 2.33; P less than .001), anemia (OR, 1.90; P less than .001), general versus moderate sedation (OR, 1.62; P less than .001), diabetes (OR, 1.61; P less than .001), and cardiogenic shock within 24 hours (OR, 1.60; P less than .023).
Other factors with a significant but lower relative risk association with AKI included a high contrast volume (OR, 1.004; P less than .001), use of a self-expanding valve (HR, 1.22; P = .009), severe lung disease (OR, 1.21; P = .043) and prior peripheral artery disease (HR, 1.20; P = .043).
“The message from these data is that there appears to be a cluster of patients who are unstable at the time of their procedure and are more likely to develop the most severe forms of AKI,” Dr. Julien reported.
The higher rate of AKI in patients who have diabetes is “not surprising,” but several of the factors associated with AKI are potentially modifiable. This includes choices in regard to sedation and arterial access. The value of modifying the amount of contrast is less clear, because the volume of contrast was no longer significant after an adjustment with multivariate analysis.
In fact, all of these factors require validation. Dr. Julien warned that neither the cause of AKI nor its temporal relationship to TAVR could be consistently determined from the registry data. In addition, retrospective analyses always include the potential for unrecognized residual confounders.
Still, these data are useful for drawing attention to the fact that AKI is a common complication of TAVR and one that is associated with adverse outcomes, including reduced survival at 1 year.
“The factors taken from these data might be useful to help identify patients who are at risk of the most severe forms of AKI and, hopefully, lead to prevention strategies that take these characteristics into consideration,” Dr. Julien said.
Dr. Julien reported no potential financial conflicts of interest.
NATIONAL HARBOR, MD. – Acute kidney injury (AKI), a potentially modifiable risk factor in some cases, predicts increased mortality within the first year after transcatheter aortic valve transplantation (TAVR), according to an analysis of a U.S. registry presented at CRT 2020 sponsored by MedStar Heart & Vascular Institute.
“After adjustment, there are higher rates of all-cause mortality regardless of the severity of AKI,” reported Howard M. Julien, MD, of the University of Pennsylvania, Philadelphia.
Relative to the absence of AKI (stage 0), the hazard ratio for death at 1 year was more than threefold greater (HR, 3.26), even for those with stage 1 AKI. When unadjusted for covariates, it remained more than twice as high (HR, 2.67; P less than .001), Dr. Julien reported.
For stage 3 AKI, the unadjusted risk was more than nine times higher and remained roughly seven times greater after adjustment (HR, 7.04; P less than .001). Stage 2 AKI was linked with an adjusted risk of about the same magnitude.
Drawn from the National Cardiovascular TAVR Registry, which is maintained jointly by the Society of Thoracic Surgeons and the American College of Cardiology, data were analyzed on more than 100,000 TAVRs performed during 2012-2018. A subset of TAVRs performed between January 2016 and June 2018 served as a source of trends in what Dr. Julien described as the “modern era” of this procedure.
The incidence of AKI overall was about 10%, but rates were higher at the earliest time point in the analysis and fell modestly over the study period for all three stages. In a logistic regression analysis, the factors associated with the greatest odds ratio of developing AKI in patients following TAVR were conversion to open heart surgery (OR, 10.84, P less than .001), nonfemoral access (OR, 2.33; P less than .001), anemia (OR, 1.90; P less than .001), general versus moderate sedation (OR, 1.62; P less than .001), diabetes (OR, 1.61; P less than .001), and cardiogenic shock within 24 hours (OR, 1.60; P less than .023).
Other factors with a significant but lower relative risk association with AKI included a high contrast volume (OR, 1.004; P less than .001), use of a self-expanding valve (HR, 1.22; P = .009), severe lung disease (OR, 1.21; P = .043) and prior peripheral artery disease (HR, 1.20; P = .043).
“The message from these data is that there appears to be a cluster of patients who are unstable at the time of their procedure and are more likely to develop the most severe forms of AKI,” Dr. Julien reported.
The higher rate of AKI in patients who have diabetes is “not surprising,” but several of the factors associated with AKI are potentially modifiable. This includes choices in regard to sedation and arterial access. The value of modifying the amount of contrast is less clear, because the volume of contrast was no longer significant after an adjustment with multivariate analysis.
In fact, all of these factors require validation. Dr. Julien warned that neither the cause of AKI nor its temporal relationship to TAVR could be consistently determined from the registry data. In addition, retrospective analyses always include the potential for unrecognized residual confounders.
Still, these data are useful for drawing attention to the fact that AKI is a common complication of TAVR and one that is associated with adverse outcomes, including reduced survival at 1 year.
“The factors taken from these data might be useful to help identify patients who are at risk of the most severe forms of AKI and, hopefully, lead to prevention strategies that take these characteristics into consideration,” Dr. Julien said.
Dr. Julien reported no potential financial conflicts of interest.
NATIONAL HARBOR, MD. – Acute kidney injury (AKI), a potentially modifiable risk factor in some cases, predicts increased mortality within the first year after transcatheter aortic valve transplantation (TAVR), according to an analysis of a U.S. registry presented at CRT 2020 sponsored by MedStar Heart & Vascular Institute.
“After adjustment, there are higher rates of all-cause mortality regardless of the severity of AKI,” reported Howard M. Julien, MD, of the University of Pennsylvania, Philadelphia.
Relative to the absence of AKI (stage 0), the hazard ratio for death at 1 year was more than threefold greater (HR, 3.26), even for those with stage 1 AKI. When unadjusted for covariates, it remained more than twice as high (HR, 2.67; P less than .001), Dr. Julien reported.
For stage 3 AKI, the unadjusted risk was more than nine times higher and remained roughly seven times greater after adjustment (HR, 7.04; P less than .001). Stage 2 AKI was linked with an adjusted risk of about the same magnitude.
Drawn from the National Cardiovascular TAVR Registry, which is maintained jointly by the Society of Thoracic Surgeons and the American College of Cardiology, data were analyzed on more than 100,000 TAVRs performed during 2012-2018. A subset of TAVRs performed between January 2016 and June 2018 served as a source of trends in what Dr. Julien described as the “modern era” of this procedure.
The incidence of AKI overall was about 10%, but rates were higher at the earliest time point in the analysis and fell modestly over the study period for all three stages. In a logistic regression analysis, the factors associated with the greatest odds ratio of developing AKI in patients following TAVR were conversion to open heart surgery (OR, 10.84, P less than .001), nonfemoral access (OR, 2.33; P less than .001), anemia (OR, 1.90; P less than .001), general versus moderate sedation (OR, 1.62; P less than .001), diabetes (OR, 1.61; P less than .001), and cardiogenic shock within 24 hours (OR, 1.60; P less than .023).
Other factors with a significant but lower relative risk association with AKI included a high contrast volume (OR, 1.004; P less than .001), use of a self-expanding valve (HR, 1.22; P = .009), severe lung disease (OR, 1.21; P = .043) and prior peripheral artery disease (HR, 1.20; P = .043).
“The message from these data is that there appears to be a cluster of patients who are unstable at the time of their procedure and are more likely to develop the most severe forms of AKI,” Dr. Julien reported.
The higher rate of AKI in patients who have diabetes is “not surprising,” but several of the factors associated with AKI are potentially modifiable. This includes choices in regard to sedation and arterial access. The value of modifying the amount of contrast is less clear, because the volume of contrast was no longer significant after an adjustment with multivariate analysis.
In fact, all of these factors require validation. Dr. Julien warned that neither the cause of AKI nor its temporal relationship to TAVR could be consistently determined from the registry data. In addition, retrospective analyses always include the potential for unrecognized residual confounders.
Still, these data are useful for drawing attention to the fact that AKI is a common complication of TAVR and one that is associated with adverse outcomes, including reduced survival at 1 year.
“The factors taken from these data might be useful to help identify patients who are at risk of the most severe forms of AKI and, hopefully, lead to prevention strategies that take these characteristics into consideration,” Dr. Julien said.
Dr. Julien reported no potential financial conflicts of interest.
REPORTING FROM CRT 2020
Avoiding missteps in BP measurement
Blood pressure (BP) measurement is an essential component of the physical examination. The information gleaned through this simple but vitally important assessment provides a basis for critical decisions about diagnosis, prognosis, and therapy in a variety of health care settings. In the emergency department, it helps guide resuscitation efforts; in the intensive care unit, it helps to identify the deteriorating patient and guide vasopressor drug titration; in the ambulatory office setting, it helps to identify hypertension and the need for antihypertensive therapy.
In the office setting, inaccurate BP measurement can have profound effects. An overestimation by only 5 mm Hg would result in an erroneous diagnosis and unnecessary treatment of hypertension for about 27 million patients—entailing medication costs, potential adverse effects, and psychologic issues associated with this diagnosis. Conversely, underestimation by 5 mm Hg would miss about 21 million patients who actually have hypertension.1
Why accurate BP measurement matters so much
About 75 million adults in the United States have high BP,2 which costs the nation $46 billion annually in health care services, antihypertensive medications, and missed days of work.3 Among US adults ages 20 or older, the age-adjusted prevalence of hypertension is estimated to be 34%, equivalent to 85.7 million adults.4
Defining hypertension. For the general population, the Eighth Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-8) defines hypertension as a BP of 140/90 mm Hg or higher in adults younger than 60 and a BP of 150/90 mm Hg or higher in adults ages 60 or older. For patients with comorbid hypertension and diabetes, JNC-8 recommends pharmacologic treatment when BP is 140/90 mm Hg or higher, regardless of age.5
Accurate measurement of BP provides the rational basis for the management of hypertension, which in turn may decrease the risk for stroke, congestive heart failure, and other cardiovascular diseases. Several investigators6-8 have observed that differences in interarm systolic BP are associated with an increased risk for peripheral vascular disease, stroke, and other cardiovascular problems.
Multiple factors impact accuracy; some might surprise you
A number of factors may influence the accuracy of BP measurement in the office; these are generally classified as related to the patient, the observer, the technique or procedure, or the equipment used. A recent systematic review by Kallioinen et al9 empirically evaluated 29 potential sources of inaccuracy in the measurement of adult resting BP. Among them were
Patient-related: Recent meal or alcohol intake; recent caffeine or nicotine use; full bladder distention; cold exposure; white-coat effect. Given the simplicity of assessing for these influences, it is worthwhile for office staff to ask patients, prior to the recommended 3 to 5 minutes of rest before BP measurement, if they were rushing to make their appointment, need to void their bladder, or have consumed food or drink or used tobacco within the past 30 minutes.
Continue to: Observer-related...
Observer-related: Hearing deficit; terminal digit bias (ie, preference for rounding BP reading to a specific end digit, eg, 0); measurement of diastolic BP at Korotkoff phase IV rather than phase V.
Procedure-related: Patient’s body position (eg, standing vs supine; legs crossed at knee; unsupported back or arm; arm lower than heart level); incorrect size or placement of cuff; talking during measurement (the content of conversation may influence results); and reliance on a single BP measurement.
Equipment-related: Device model bias; device calibration error.
As reported by Kallioinen et al9, the magnitude of these potential errors ranges from small to large in both the positive and negative direction for both systolic and diastolic BP, and several sources of error are potentially bidirectional. For example, talking during BP measurement may result in an increase in systolic BP of 4 to 19 mm Hg and in diastolic BP of 5 to 14.3 mm Hg; measurement of diastolic BP at Korotkoff phase IV rather than phase V significantly increases diastolic BP by 12.5 mm Hg; and recent alcohol intake can affect systolic BP by –23.6 to +24 mm Hg and diastolic BP by –14 to +16 mm Hg. Overall, the researchers found significant directional effects for 27 of the 29 potential sources of error, ranging from a mean –24 mm Hg to +33 mm Hg error for estimating systolic BP and a mean –14 mm Hg to +23 mm Hg for estimating diastolic BP.9
Careful adherence to guidelines ensures accurate BP measurement
Adequate training and standardized procedures can target and mitigate many of the identified sources of error; accordingly, all clinical staff responsible for obtaining a patient’s BP measurement should be trained not only in the correct method for accurate measurement but also in the identification of factors that may introduce errors.
Continue to: The American Heart Association...
The American Heart Association (AHA) recommends that BP be measured in both arms at the initial evaluation, with the higher measurement used for monitoring BP. The AHA also recommends obtaining at least 2 readings at least 1 minute apart and averaging them as the patient’s BP.10 Other research recommends using a fully automated sphygmomanometer to take multiple readings with the patient resting quietly alone in either the exam room or the waiting room11 as an effective and efficient method for accurate BP averaging.
The 2 principal noninvasive methods of BP measurement are the manual auscultatory technique and the oscillatory technique. Because of its simplicity and relative degree of accuracy (when correctly performed), the auscultatory measurement remains common in everyday medical practice. Remarkably, it is one of only a few techniques for clinical examination of patients that has remained relatively unchanged since it was introduced by the Russian physician and scientist Nikolai Sergeevich Korotkoff in 1905.12 However, accurate performance of the auscultatory method requires adequate training and experience.
In contrast, automated oscillometric BP measurement is easily performed and requires minimal training. However, it is important to note that any condition altering oscillation amplitude or regularity (eg, arterial wall stiffness or cardiac arrhythmia) will produce erroneous results, and the reading must be confirmed by auscultatory measurement.13, 14
Auscultatory methods of BP measurement
The mainstay of clinical BP measurement has been auscultatory methods to detect the Korotkoff sounds, using a stethoscope and either mercury, aneroid, or “hybrid” sphygmomanometers. Traditionally, the mercury device was the “gold standard,” but the widespread ban of mercury in health care settings has now all but eliminated its use.
Aneroid gauge sphygmomanometers have a metallic spring and a metal membrane that flexes elastically to translate pressure signals from the cuff and operate a needle in the gauge. Owing to their complexity, these devices require regular recalibration, since inaccurate results may occur anytime the needle does not rest on 0 before use.
Contine to: The newer hybrid sphygmomanometers...
The newer hybrid sphygmomanometers have an electronic transducer in place of a mercury column; BP measurement is performed in the same fashion as with a mercury device, using a stethoscope and auscultation for the Korotkoff sounds.
Variations in technique for BP measurement can result in significantly different readings. In 2005, the AHA published recommendations for BP monitoring to increase the accuracy of in-clinic measurements.10 Recommendations for accurate BP measurement include:
Patient preparation. The patient should be seated in a chair with his or her back supported, legs uncrossed, and feet flat on the floor. The patient’s bare arm should be supported such that the midpoint of the upper arm is at heart level. An appropriately sized cuff (ie, bladder encircles 80% of the arm for an adult or 100% of the arm for a child younger than 13 years) should be secured around the bare upper arm and the bladder centered over the brachial artery, with the lower edge of the cuff about 2 cm above the antecubital fossa.10
Technique. The cuff is inflated while palpating the radial artery to the approximate systolic pressure (ie, the point at which the radial pulse is no longer palpated). The bell of the stethoscope is placed just proximal and medial to the antecubital fossa and the cuff is inflated another 20 to 30 mm Hg above the point at which the radial pulse is no longer felt. The cuff is deflated at a rate of about 2 mm Hg per second.10
BP recording. The systolic BP is recorded at the appearance of the Korotkoff sounds (phase I) for an auscultatory measurement. The diastolic BP is recorded at the disappearance of the Korotkoff sounds (phase V) in adults and at the muffling of sounds (phase IV) in children for an auscultatory measurement.10
Continue to: Oscillometric methods of BP measurement
Oscillometric methods of BP measurement
The auscultatory methods of BP measurement are gradually being replaced by oscillometric techniques that are better suited to automated methods of measurement. When oscillations of pressure in the gradually deflating bladder cuff are sensed and recorded, the point of maximal oscillation corresponds to the mean intra-arterial pressure.15 The oscillations sensed are vibrations in the arterial wall that are detected and transduced to an electric signal, producing a digital readout, and correspond approximately to the systolic pressure and continue below the diastolic pressure. The actual systolic and diastolic pressures are indirectly estimated according to a proprietary, empirically derived algorithm that differs from 1 manufacturer to another.
Validated oscillometric techniques have been successfully used in ambulatory BP monitors, which record pressure at regular intervals (typically 20 to 30 minutes) over a 24-hour period while patients perform normal daily activities, including sleep. The US Preventive Services Task Force16, the UK’s National Institute for Health and Clinical Excellence17, the European Society of Hypertension18, and the Canadian Hypertension Education Program19 collectively endorse ambulatory BP monitoring as the optimal method for BP measurement.
The oscillometric method has also been used for automated office BP measurement, which averages multiple BP readings recorded with a fully automated device while the patient rests alone in a quiet room in clinic. Compared with conventional auscultatory office BP measurement, this method has been promoted to provide a more standardized BP measurement by reducing observer error and the “white coat” effect.20-22
There are some limitations to oscillometric methods. The amplitude of oscillations is influenced by factors other than BP, notably, arterial wall stiffness. Therefore, in older patients13 or those with diabetes14 who have reduced arterial wall elasticity, oscillometric BP measurements overestimate systolic pressure and underestimate diastolic pressure. In contrast, acutely ill patients, particularly those with hypovolemia and more compliant arterial walls, may have significant underestimation of BP by oscillometric techniques.23 In patients with peripheral arterial disease, calcified leg vessels can affect the diagnostic accuracy of oscillometric measurement of the ankle-brachial index (ABI).24 A meta-analysis reported that in patients with atrial fibrillation, oscillometric measurement accurately assesses systolic BP but not diastolic BP, and therefore it may be inappropriate for office measurement of BP in these patients.25 Other studies have reported that atrial fibrillation does not significantly affect the accuracy of oscillometric BP measurement if 3 repeated measurements are performed.26,27
Moreover, the algorithms used in these devices are proprietary trade secrets that can be modified by the manufacturer at any time without notice. Therefore, different devices—and even different models from the same manufacturer—may function differently. Only devices calibrated using a validated protocol should be used.10,28 There are currently 4 unique protocols for validation of BP devices, although an international collaborative group recently published recommendations for a universal protocol for validation of BP measurement devices.29
Continue to: The takeaway
The takeaway
Accurate office BP measurement is essential for patient evaluation and provides the basis for critical decisions about diagnosis, prognosis, and treatment of hypertensive disease. It is imperative to control for factors that may introduce error in BP determination by using a standard protocol and calibrated BP measurement equipment.
Both manual auscultatory and oscillometric methods of measurement are appropriate for office assessment, but oscillometric evaluation is inappropriate for patients with severe atherosclerotic disease, peripheral arterial disease (for ABI), or small arm circumference. If oscillometric BP measurement is performed in patients with atrial fibrillation, at least 3 repeated measurements should be done to improve accuracy. Automated oscillometric BP assessment that records multiple measurements in the quietly resting patient has been promoted to provide a more standardized BP measurement by reducing observer error and the “white coat” effect. Ambulatory oscillometric BP monitoring has been widely endorsed as the optimal method for BP measurement.
CORRESPONDENCE
Darrell R. Over, MD, MSc, FAAFP, 1601 West 40th Street, Pine Bluff, AR 71603; OverDarrellR@uams.edu
1. Jones DW, Appel LJ, Sheps SG, et al. Measuring blood pressure accurately: new and persistent challenges. JAMA. 2003;289:1027-1030.
2. Meral R, Rakotz M, Bausch P, et al. CDC Grand Rounds: a public health approach to detect and control hypertension. Morb Mortal Wkly Rep. 2016;18:65:1261-1264.
3. Mozzafarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29-e322.
4. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135:e146-e603.
5. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
6. Weinberg I, Gona P, O’Donnell CJ, et al. The systolic blood pressure difference between arms and cardiovascular disease in the Framingham study. Am J Med. 2014;127:209-215.
7. Lane D, Beevers M, Barnes N, et al. Interarm differences in blood pressure: when are they clinically significant? J Hypertens. 2002;20:1089-1095.
8. Clark CE, Taylor RS, Shore AC, et al. The difference in blood pressure readings between arms and survival: primary cohort study. BMJ. 2012;344:e1327. [Erratum in BMJ. 2012;344:e2714.]
9. Kallioinen N, Hill A, Horswill MS, et al. Sources of inaccuracy in measurement of adult patients’ resting blood pressure in clinical settings: a systematic review. J Hyertens. 2017;35:421-441.
10. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals. Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension. 2005;45:142-161.
11. Armstrong D, Matangi M, Brouillard D, et al. Automated office blood pressure—being alone and not location is what matters most. Blood Pressure Monit. 2015;20:204-208.
12. Shevchenko YL, Tsitlik JE. 90th anniversary of the development by Nikolai S. Korotkoff of the auscultatory method of measuring blood pressure. Circulation. 1996;94:116-118.
13. Van Montfrans GA. Oscillometric blood pressure measurement: progress and problems. Blood Press Monit. 2001;6:287-290.
14. Van Popele NM, Bos WJ, de Beer NA, et al. Arterial stiffness as underlying mechanism of disagreement between an oscillometric blood pressure monitor and a sphygmomanometer. Hypertension. 2000;36:484-488.
15. Mauck GW, Smith CR, Geddes LA, et al. The meaning of the point of maximum oscillations in cuff pressure in the indirect measurement of blood pressure—part ii. J Biomech Eng. 1980;102:28-33.
16. Siu AL; US Preventive Services Task Force. Screening for high blood pressure in adults: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163:778-786.
17. National Institute for Health and Clinical Excellence (NICE). Hypertension: the clinical management of hypertension in adults. London: Royal College of Physicians (UK); 2011.
18. O’Brien E, Parati G, Stergiou G, et al; European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31:1731-1768.
19. Leung AA, Nerenberg K, Daskalopoulou SS, et al; CHEP Guidelines Task Force. Hypertension Canada’s 2016 Canadian Hypertension Education Program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2016;32:569-588.
20. Myers MG. Eliminating the human factor in office blood pressure measurement. J Clin Hypertens. 2014;16:83-86.
21. Myers MG, Godwin M, Dawes M, et al. Measurement of blood pressure in the office: recognizing the problem and proposing the solution. J Clin Hypertens. 2010;55:195-200.
22. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce the white coat response. J Hypertens. 2009;27:280-286.
23. Bur A, Herkner H, Vlcek M, et al. Factors influencing the accuracy of oscillometric blood pressure measurements in critically ill patients. Crit Care Med. 2003;31:793-799.
24. Herrálz-Adillo Á, Martínez-Vizcaíno V, Cavero-Redondo I, et al. Diagnostic accuracy of an oscillometric ankle-brachial index in peripheral arterial disease: the influence of oscillometric errors and calcified legs. PLoS One. 2016;11:e0167408.
25. Stergiou GS, Kollias A, Destounis A, et al. Automated blood pressure measurement in atrial fibrillation: a systematic review and meta-analysis. J Hypertens. 2012;30:2074-2082.
26. Pagonas N, Schmidt S, Eysel J, et al. Impact of atrial fibrillation on the accuracy of oscillometric blood pressure monitoring. Hypertension. 2013;62:579-584.
27. Myers MG, Stergiou GS. Should oscillometric blood pressure monitors be used in patients with atrial fibrillation? J Clin Hypertens. 2015;17:565-566.
28. Munter P, Shimbo D, Carey RM, et al. Measurement of blood pressure in humans. a scientific statement from the American Heart Association. Hypertension. 2019;73:e35-e66.
29. Stergiou GS, Alpert B, Mieke S, et al. A universal standard for validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. Hypertension. 2018;71:368-374.
Blood pressure (BP) measurement is an essential component of the physical examination. The information gleaned through this simple but vitally important assessment provides a basis for critical decisions about diagnosis, prognosis, and therapy in a variety of health care settings. In the emergency department, it helps guide resuscitation efforts; in the intensive care unit, it helps to identify the deteriorating patient and guide vasopressor drug titration; in the ambulatory office setting, it helps to identify hypertension and the need for antihypertensive therapy.
In the office setting, inaccurate BP measurement can have profound effects. An overestimation by only 5 mm Hg would result in an erroneous diagnosis and unnecessary treatment of hypertension for about 27 million patients—entailing medication costs, potential adverse effects, and psychologic issues associated with this diagnosis. Conversely, underestimation by 5 mm Hg would miss about 21 million patients who actually have hypertension.1
Why accurate BP measurement matters so much
About 75 million adults in the United States have high BP,2 which costs the nation $46 billion annually in health care services, antihypertensive medications, and missed days of work.3 Among US adults ages 20 or older, the age-adjusted prevalence of hypertension is estimated to be 34%, equivalent to 85.7 million adults.4
Defining hypertension. For the general population, the Eighth Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-8) defines hypertension as a BP of 140/90 mm Hg or higher in adults younger than 60 and a BP of 150/90 mm Hg or higher in adults ages 60 or older. For patients with comorbid hypertension and diabetes, JNC-8 recommends pharmacologic treatment when BP is 140/90 mm Hg or higher, regardless of age.5
Accurate measurement of BP provides the rational basis for the management of hypertension, which in turn may decrease the risk for stroke, congestive heart failure, and other cardiovascular diseases. Several investigators6-8 have observed that differences in interarm systolic BP are associated with an increased risk for peripheral vascular disease, stroke, and other cardiovascular problems.
Multiple factors impact accuracy; some might surprise you
A number of factors may influence the accuracy of BP measurement in the office; these are generally classified as related to the patient, the observer, the technique or procedure, or the equipment used. A recent systematic review by Kallioinen et al9 empirically evaluated 29 potential sources of inaccuracy in the measurement of adult resting BP. Among them were
Patient-related: Recent meal or alcohol intake; recent caffeine or nicotine use; full bladder distention; cold exposure; white-coat effect. Given the simplicity of assessing for these influences, it is worthwhile for office staff to ask patients, prior to the recommended 3 to 5 minutes of rest before BP measurement, if they were rushing to make their appointment, need to void their bladder, or have consumed food or drink or used tobacco within the past 30 minutes.
Continue to: Observer-related...
Observer-related: Hearing deficit; terminal digit bias (ie, preference for rounding BP reading to a specific end digit, eg, 0); measurement of diastolic BP at Korotkoff phase IV rather than phase V.
Procedure-related: Patient’s body position (eg, standing vs supine; legs crossed at knee; unsupported back or arm; arm lower than heart level); incorrect size or placement of cuff; talking during measurement (the content of conversation may influence results); and reliance on a single BP measurement.
Equipment-related: Device model bias; device calibration error.
As reported by Kallioinen et al9, the magnitude of these potential errors ranges from small to large in both the positive and negative direction for both systolic and diastolic BP, and several sources of error are potentially bidirectional. For example, talking during BP measurement may result in an increase in systolic BP of 4 to 19 mm Hg and in diastolic BP of 5 to 14.3 mm Hg; measurement of diastolic BP at Korotkoff phase IV rather than phase V significantly increases diastolic BP by 12.5 mm Hg; and recent alcohol intake can affect systolic BP by –23.6 to +24 mm Hg and diastolic BP by –14 to +16 mm Hg. Overall, the researchers found significant directional effects for 27 of the 29 potential sources of error, ranging from a mean –24 mm Hg to +33 mm Hg error for estimating systolic BP and a mean –14 mm Hg to +23 mm Hg for estimating diastolic BP.9
Careful adherence to guidelines ensures accurate BP measurement
Adequate training and standardized procedures can target and mitigate many of the identified sources of error; accordingly, all clinical staff responsible for obtaining a patient’s BP measurement should be trained not only in the correct method for accurate measurement but also in the identification of factors that may introduce errors.
Continue to: The American Heart Association...
The American Heart Association (AHA) recommends that BP be measured in both arms at the initial evaluation, with the higher measurement used for monitoring BP. The AHA also recommends obtaining at least 2 readings at least 1 minute apart and averaging them as the patient’s BP.10 Other research recommends using a fully automated sphygmomanometer to take multiple readings with the patient resting quietly alone in either the exam room or the waiting room11 as an effective and efficient method for accurate BP averaging.
The 2 principal noninvasive methods of BP measurement are the manual auscultatory technique and the oscillatory technique. Because of its simplicity and relative degree of accuracy (when correctly performed), the auscultatory measurement remains common in everyday medical practice. Remarkably, it is one of only a few techniques for clinical examination of patients that has remained relatively unchanged since it was introduced by the Russian physician and scientist Nikolai Sergeevich Korotkoff in 1905.12 However, accurate performance of the auscultatory method requires adequate training and experience.
In contrast, automated oscillometric BP measurement is easily performed and requires minimal training. However, it is important to note that any condition altering oscillation amplitude or regularity (eg, arterial wall stiffness or cardiac arrhythmia) will produce erroneous results, and the reading must be confirmed by auscultatory measurement.13, 14
Auscultatory methods of BP measurement
The mainstay of clinical BP measurement has been auscultatory methods to detect the Korotkoff sounds, using a stethoscope and either mercury, aneroid, or “hybrid” sphygmomanometers. Traditionally, the mercury device was the “gold standard,” but the widespread ban of mercury in health care settings has now all but eliminated its use.
Aneroid gauge sphygmomanometers have a metallic spring and a metal membrane that flexes elastically to translate pressure signals from the cuff and operate a needle in the gauge. Owing to their complexity, these devices require regular recalibration, since inaccurate results may occur anytime the needle does not rest on 0 before use.
Contine to: The newer hybrid sphygmomanometers...
The newer hybrid sphygmomanometers have an electronic transducer in place of a mercury column; BP measurement is performed in the same fashion as with a mercury device, using a stethoscope and auscultation for the Korotkoff sounds.
Variations in technique for BP measurement can result in significantly different readings. In 2005, the AHA published recommendations for BP monitoring to increase the accuracy of in-clinic measurements.10 Recommendations for accurate BP measurement include:
Patient preparation. The patient should be seated in a chair with his or her back supported, legs uncrossed, and feet flat on the floor. The patient’s bare arm should be supported such that the midpoint of the upper arm is at heart level. An appropriately sized cuff (ie, bladder encircles 80% of the arm for an adult or 100% of the arm for a child younger than 13 years) should be secured around the bare upper arm and the bladder centered over the brachial artery, with the lower edge of the cuff about 2 cm above the antecubital fossa.10
Technique. The cuff is inflated while palpating the radial artery to the approximate systolic pressure (ie, the point at which the radial pulse is no longer palpated). The bell of the stethoscope is placed just proximal and medial to the antecubital fossa and the cuff is inflated another 20 to 30 mm Hg above the point at which the radial pulse is no longer felt. The cuff is deflated at a rate of about 2 mm Hg per second.10
BP recording. The systolic BP is recorded at the appearance of the Korotkoff sounds (phase I) for an auscultatory measurement. The diastolic BP is recorded at the disappearance of the Korotkoff sounds (phase V) in adults and at the muffling of sounds (phase IV) in children for an auscultatory measurement.10
Continue to: Oscillometric methods of BP measurement
Oscillometric methods of BP measurement
The auscultatory methods of BP measurement are gradually being replaced by oscillometric techniques that are better suited to automated methods of measurement. When oscillations of pressure in the gradually deflating bladder cuff are sensed and recorded, the point of maximal oscillation corresponds to the mean intra-arterial pressure.15 The oscillations sensed are vibrations in the arterial wall that are detected and transduced to an electric signal, producing a digital readout, and correspond approximately to the systolic pressure and continue below the diastolic pressure. The actual systolic and diastolic pressures are indirectly estimated according to a proprietary, empirically derived algorithm that differs from 1 manufacturer to another.
Validated oscillometric techniques have been successfully used in ambulatory BP monitors, which record pressure at regular intervals (typically 20 to 30 minutes) over a 24-hour period while patients perform normal daily activities, including sleep. The US Preventive Services Task Force16, the UK’s National Institute for Health and Clinical Excellence17, the European Society of Hypertension18, and the Canadian Hypertension Education Program19 collectively endorse ambulatory BP monitoring as the optimal method for BP measurement.
The oscillometric method has also been used for automated office BP measurement, which averages multiple BP readings recorded with a fully automated device while the patient rests alone in a quiet room in clinic. Compared with conventional auscultatory office BP measurement, this method has been promoted to provide a more standardized BP measurement by reducing observer error and the “white coat” effect.20-22
There are some limitations to oscillometric methods. The amplitude of oscillations is influenced by factors other than BP, notably, arterial wall stiffness. Therefore, in older patients13 or those with diabetes14 who have reduced arterial wall elasticity, oscillometric BP measurements overestimate systolic pressure and underestimate diastolic pressure. In contrast, acutely ill patients, particularly those with hypovolemia and more compliant arterial walls, may have significant underestimation of BP by oscillometric techniques.23 In patients with peripheral arterial disease, calcified leg vessels can affect the diagnostic accuracy of oscillometric measurement of the ankle-brachial index (ABI).24 A meta-analysis reported that in patients with atrial fibrillation, oscillometric measurement accurately assesses systolic BP but not diastolic BP, and therefore it may be inappropriate for office measurement of BP in these patients.25 Other studies have reported that atrial fibrillation does not significantly affect the accuracy of oscillometric BP measurement if 3 repeated measurements are performed.26,27
Moreover, the algorithms used in these devices are proprietary trade secrets that can be modified by the manufacturer at any time without notice. Therefore, different devices—and even different models from the same manufacturer—may function differently. Only devices calibrated using a validated protocol should be used.10,28 There are currently 4 unique protocols for validation of BP devices, although an international collaborative group recently published recommendations for a universal protocol for validation of BP measurement devices.29
Continue to: The takeaway
The takeaway
Accurate office BP measurement is essential for patient evaluation and provides the basis for critical decisions about diagnosis, prognosis, and treatment of hypertensive disease. It is imperative to control for factors that may introduce error in BP determination by using a standard protocol and calibrated BP measurement equipment.
Both manual auscultatory and oscillometric methods of measurement are appropriate for office assessment, but oscillometric evaluation is inappropriate for patients with severe atherosclerotic disease, peripheral arterial disease (for ABI), or small arm circumference. If oscillometric BP measurement is performed in patients with atrial fibrillation, at least 3 repeated measurements should be done to improve accuracy. Automated oscillometric BP assessment that records multiple measurements in the quietly resting patient has been promoted to provide a more standardized BP measurement by reducing observer error and the “white coat” effect. Ambulatory oscillometric BP monitoring has been widely endorsed as the optimal method for BP measurement.
CORRESPONDENCE
Darrell R. Over, MD, MSc, FAAFP, 1601 West 40th Street, Pine Bluff, AR 71603; OverDarrellR@uams.edu
Blood pressure (BP) measurement is an essential component of the physical examination. The information gleaned through this simple but vitally important assessment provides a basis for critical decisions about diagnosis, prognosis, and therapy in a variety of health care settings. In the emergency department, it helps guide resuscitation efforts; in the intensive care unit, it helps to identify the deteriorating patient and guide vasopressor drug titration; in the ambulatory office setting, it helps to identify hypertension and the need for antihypertensive therapy.
In the office setting, inaccurate BP measurement can have profound effects. An overestimation by only 5 mm Hg would result in an erroneous diagnosis and unnecessary treatment of hypertension for about 27 million patients—entailing medication costs, potential adverse effects, and psychologic issues associated with this diagnosis. Conversely, underestimation by 5 mm Hg would miss about 21 million patients who actually have hypertension.1
Why accurate BP measurement matters so much
About 75 million adults in the United States have high BP,2 which costs the nation $46 billion annually in health care services, antihypertensive medications, and missed days of work.3 Among US adults ages 20 or older, the age-adjusted prevalence of hypertension is estimated to be 34%, equivalent to 85.7 million adults.4
Defining hypertension. For the general population, the Eighth Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-8) defines hypertension as a BP of 140/90 mm Hg or higher in adults younger than 60 and a BP of 150/90 mm Hg or higher in adults ages 60 or older. For patients with comorbid hypertension and diabetes, JNC-8 recommends pharmacologic treatment when BP is 140/90 mm Hg or higher, regardless of age.5
Accurate measurement of BP provides the rational basis for the management of hypertension, which in turn may decrease the risk for stroke, congestive heart failure, and other cardiovascular diseases. Several investigators6-8 have observed that differences in interarm systolic BP are associated with an increased risk for peripheral vascular disease, stroke, and other cardiovascular problems.
Multiple factors impact accuracy; some might surprise you
A number of factors may influence the accuracy of BP measurement in the office; these are generally classified as related to the patient, the observer, the technique or procedure, or the equipment used. A recent systematic review by Kallioinen et al9 empirically evaluated 29 potential sources of inaccuracy in the measurement of adult resting BP. Among them were
Patient-related: Recent meal or alcohol intake; recent caffeine or nicotine use; full bladder distention; cold exposure; white-coat effect. Given the simplicity of assessing for these influences, it is worthwhile for office staff to ask patients, prior to the recommended 3 to 5 minutes of rest before BP measurement, if they were rushing to make their appointment, need to void their bladder, or have consumed food or drink or used tobacco within the past 30 minutes.
Continue to: Observer-related...
Observer-related: Hearing deficit; terminal digit bias (ie, preference for rounding BP reading to a specific end digit, eg, 0); measurement of diastolic BP at Korotkoff phase IV rather than phase V.
Procedure-related: Patient’s body position (eg, standing vs supine; legs crossed at knee; unsupported back or arm; arm lower than heart level); incorrect size or placement of cuff; talking during measurement (the content of conversation may influence results); and reliance on a single BP measurement.
Equipment-related: Device model bias; device calibration error.
As reported by Kallioinen et al9, the magnitude of these potential errors ranges from small to large in both the positive and negative direction for both systolic and diastolic BP, and several sources of error are potentially bidirectional. For example, talking during BP measurement may result in an increase in systolic BP of 4 to 19 mm Hg and in diastolic BP of 5 to 14.3 mm Hg; measurement of diastolic BP at Korotkoff phase IV rather than phase V significantly increases diastolic BP by 12.5 mm Hg; and recent alcohol intake can affect systolic BP by –23.6 to +24 mm Hg and diastolic BP by –14 to +16 mm Hg. Overall, the researchers found significant directional effects for 27 of the 29 potential sources of error, ranging from a mean –24 mm Hg to +33 mm Hg error for estimating systolic BP and a mean –14 mm Hg to +23 mm Hg for estimating diastolic BP.9
Careful adherence to guidelines ensures accurate BP measurement
Adequate training and standardized procedures can target and mitigate many of the identified sources of error; accordingly, all clinical staff responsible for obtaining a patient’s BP measurement should be trained not only in the correct method for accurate measurement but also in the identification of factors that may introduce errors.
Continue to: The American Heart Association...
The American Heart Association (AHA) recommends that BP be measured in both arms at the initial evaluation, with the higher measurement used for monitoring BP. The AHA also recommends obtaining at least 2 readings at least 1 minute apart and averaging them as the patient’s BP.10 Other research recommends using a fully automated sphygmomanometer to take multiple readings with the patient resting quietly alone in either the exam room or the waiting room11 as an effective and efficient method for accurate BP averaging.
The 2 principal noninvasive methods of BP measurement are the manual auscultatory technique and the oscillatory technique. Because of its simplicity and relative degree of accuracy (when correctly performed), the auscultatory measurement remains common in everyday medical practice. Remarkably, it is one of only a few techniques for clinical examination of patients that has remained relatively unchanged since it was introduced by the Russian physician and scientist Nikolai Sergeevich Korotkoff in 1905.12 However, accurate performance of the auscultatory method requires adequate training and experience.
In contrast, automated oscillometric BP measurement is easily performed and requires minimal training. However, it is important to note that any condition altering oscillation amplitude or regularity (eg, arterial wall stiffness or cardiac arrhythmia) will produce erroneous results, and the reading must be confirmed by auscultatory measurement.13, 14
Auscultatory methods of BP measurement
The mainstay of clinical BP measurement has been auscultatory methods to detect the Korotkoff sounds, using a stethoscope and either mercury, aneroid, or “hybrid” sphygmomanometers. Traditionally, the mercury device was the “gold standard,” but the widespread ban of mercury in health care settings has now all but eliminated its use.
Aneroid gauge sphygmomanometers have a metallic spring and a metal membrane that flexes elastically to translate pressure signals from the cuff and operate a needle in the gauge. Owing to their complexity, these devices require regular recalibration, since inaccurate results may occur anytime the needle does not rest on 0 before use.
Contine to: The newer hybrid sphygmomanometers...
The newer hybrid sphygmomanometers have an electronic transducer in place of a mercury column; BP measurement is performed in the same fashion as with a mercury device, using a stethoscope and auscultation for the Korotkoff sounds.
Variations in technique for BP measurement can result in significantly different readings. In 2005, the AHA published recommendations for BP monitoring to increase the accuracy of in-clinic measurements.10 Recommendations for accurate BP measurement include:
Patient preparation. The patient should be seated in a chair with his or her back supported, legs uncrossed, and feet flat on the floor. The patient’s bare arm should be supported such that the midpoint of the upper arm is at heart level. An appropriately sized cuff (ie, bladder encircles 80% of the arm for an adult or 100% of the arm for a child younger than 13 years) should be secured around the bare upper arm and the bladder centered over the brachial artery, with the lower edge of the cuff about 2 cm above the antecubital fossa.10
Technique. The cuff is inflated while palpating the radial artery to the approximate systolic pressure (ie, the point at which the radial pulse is no longer palpated). The bell of the stethoscope is placed just proximal and medial to the antecubital fossa and the cuff is inflated another 20 to 30 mm Hg above the point at which the radial pulse is no longer felt. The cuff is deflated at a rate of about 2 mm Hg per second.10
BP recording. The systolic BP is recorded at the appearance of the Korotkoff sounds (phase I) for an auscultatory measurement. The diastolic BP is recorded at the disappearance of the Korotkoff sounds (phase V) in adults and at the muffling of sounds (phase IV) in children for an auscultatory measurement.10
Continue to: Oscillometric methods of BP measurement
Oscillometric methods of BP measurement
The auscultatory methods of BP measurement are gradually being replaced by oscillometric techniques that are better suited to automated methods of measurement. When oscillations of pressure in the gradually deflating bladder cuff are sensed and recorded, the point of maximal oscillation corresponds to the mean intra-arterial pressure.15 The oscillations sensed are vibrations in the arterial wall that are detected and transduced to an electric signal, producing a digital readout, and correspond approximately to the systolic pressure and continue below the diastolic pressure. The actual systolic and diastolic pressures are indirectly estimated according to a proprietary, empirically derived algorithm that differs from 1 manufacturer to another.
Validated oscillometric techniques have been successfully used in ambulatory BP monitors, which record pressure at regular intervals (typically 20 to 30 minutes) over a 24-hour period while patients perform normal daily activities, including sleep. The US Preventive Services Task Force16, the UK’s National Institute for Health and Clinical Excellence17, the European Society of Hypertension18, and the Canadian Hypertension Education Program19 collectively endorse ambulatory BP monitoring as the optimal method for BP measurement.
The oscillometric method has also been used for automated office BP measurement, which averages multiple BP readings recorded with a fully automated device while the patient rests alone in a quiet room in clinic. Compared with conventional auscultatory office BP measurement, this method has been promoted to provide a more standardized BP measurement by reducing observer error and the “white coat” effect.20-22
There are some limitations to oscillometric methods. The amplitude of oscillations is influenced by factors other than BP, notably, arterial wall stiffness. Therefore, in older patients13 or those with diabetes14 who have reduced arterial wall elasticity, oscillometric BP measurements overestimate systolic pressure and underestimate diastolic pressure. In contrast, acutely ill patients, particularly those with hypovolemia and more compliant arterial walls, may have significant underestimation of BP by oscillometric techniques.23 In patients with peripheral arterial disease, calcified leg vessels can affect the diagnostic accuracy of oscillometric measurement of the ankle-brachial index (ABI).24 A meta-analysis reported that in patients with atrial fibrillation, oscillometric measurement accurately assesses systolic BP but not diastolic BP, and therefore it may be inappropriate for office measurement of BP in these patients.25 Other studies have reported that atrial fibrillation does not significantly affect the accuracy of oscillometric BP measurement if 3 repeated measurements are performed.26,27
Moreover, the algorithms used in these devices are proprietary trade secrets that can be modified by the manufacturer at any time without notice. Therefore, different devices—and even different models from the same manufacturer—may function differently. Only devices calibrated using a validated protocol should be used.10,28 There are currently 4 unique protocols for validation of BP devices, although an international collaborative group recently published recommendations for a universal protocol for validation of BP measurement devices.29
Continue to: The takeaway
The takeaway
Accurate office BP measurement is essential for patient evaluation and provides the basis for critical decisions about diagnosis, prognosis, and treatment of hypertensive disease. It is imperative to control for factors that may introduce error in BP determination by using a standard protocol and calibrated BP measurement equipment.
Both manual auscultatory and oscillometric methods of measurement are appropriate for office assessment, but oscillometric evaluation is inappropriate for patients with severe atherosclerotic disease, peripheral arterial disease (for ABI), or small arm circumference. If oscillometric BP measurement is performed in patients with atrial fibrillation, at least 3 repeated measurements should be done to improve accuracy. Automated oscillometric BP assessment that records multiple measurements in the quietly resting patient has been promoted to provide a more standardized BP measurement by reducing observer error and the “white coat” effect. Ambulatory oscillometric BP monitoring has been widely endorsed as the optimal method for BP measurement.
CORRESPONDENCE
Darrell R. Over, MD, MSc, FAAFP, 1601 West 40th Street, Pine Bluff, AR 71603; OverDarrellR@uams.edu
1. Jones DW, Appel LJ, Sheps SG, et al. Measuring blood pressure accurately: new and persistent challenges. JAMA. 2003;289:1027-1030.
2. Meral R, Rakotz M, Bausch P, et al. CDC Grand Rounds: a public health approach to detect and control hypertension. Morb Mortal Wkly Rep. 2016;18:65:1261-1264.
3. Mozzafarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29-e322.
4. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135:e146-e603.
5. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
6. Weinberg I, Gona P, O’Donnell CJ, et al. The systolic blood pressure difference between arms and cardiovascular disease in the Framingham study. Am J Med. 2014;127:209-215.
7. Lane D, Beevers M, Barnes N, et al. Interarm differences in blood pressure: when are they clinically significant? J Hypertens. 2002;20:1089-1095.
8. Clark CE, Taylor RS, Shore AC, et al. The difference in blood pressure readings between arms and survival: primary cohort study. BMJ. 2012;344:e1327. [Erratum in BMJ. 2012;344:e2714.]
9. Kallioinen N, Hill A, Horswill MS, et al. Sources of inaccuracy in measurement of adult patients’ resting blood pressure in clinical settings: a systematic review. J Hyertens. 2017;35:421-441.
10. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals. Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension. 2005;45:142-161.
11. Armstrong D, Matangi M, Brouillard D, et al. Automated office blood pressure—being alone and not location is what matters most. Blood Pressure Monit. 2015;20:204-208.
12. Shevchenko YL, Tsitlik JE. 90th anniversary of the development by Nikolai S. Korotkoff of the auscultatory method of measuring blood pressure. Circulation. 1996;94:116-118.
13. Van Montfrans GA. Oscillometric blood pressure measurement: progress and problems. Blood Press Monit. 2001;6:287-290.
14. Van Popele NM, Bos WJ, de Beer NA, et al. Arterial stiffness as underlying mechanism of disagreement between an oscillometric blood pressure monitor and a sphygmomanometer. Hypertension. 2000;36:484-488.
15. Mauck GW, Smith CR, Geddes LA, et al. The meaning of the point of maximum oscillations in cuff pressure in the indirect measurement of blood pressure—part ii. J Biomech Eng. 1980;102:28-33.
16. Siu AL; US Preventive Services Task Force. Screening for high blood pressure in adults: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163:778-786.
17. National Institute for Health and Clinical Excellence (NICE). Hypertension: the clinical management of hypertension in adults. London: Royal College of Physicians (UK); 2011.
18. O’Brien E, Parati G, Stergiou G, et al; European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31:1731-1768.
19. Leung AA, Nerenberg K, Daskalopoulou SS, et al; CHEP Guidelines Task Force. Hypertension Canada’s 2016 Canadian Hypertension Education Program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2016;32:569-588.
20. Myers MG. Eliminating the human factor in office blood pressure measurement. J Clin Hypertens. 2014;16:83-86.
21. Myers MG, Godwin M, Dawes M, et al. Measurement of blood pressure in the office: recognizing the problem and proposing the solution. J Clin Hypertens. 2010;55:195-200.
22. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce the white coat response. J Hypertens. 2009;27:280-286.
23. Bur A, Herkner H, Vlcek M, et al. Factors influencing the accuracy of oscillometric blood pressure measurements in critically ill patients. Crit Care Med. 2003;31:793-799.
24. Herrálz-Adillo Á, Martínez-Vizcaíno V, Cavero-Redondo I, et al. Diagnostic accuracy of an oscillometric ankle-brachial index in peripheral arterial disease: the influence of oscillometric errors and calcified legs. PLoS One. 2016;11:e0167408.
25. Stergiou GS, Kollias A, Destounis A, et al. Automated blood pressure measurement in atrial fibrillation: a systematic review and meta-analysis. J Hypertens. 2012;30:2074-2082.
26. Pagonas N, Schmidt S, Eysel J, et al. Impact of atrial fibrillation on the accuracy of oscillometric blood pressure monitoring. Hypertension. 2013;62:579-584.
27. Myers MG, Stergiou GS. Should oscillometric blood pressure monitors be used in patients with atrial fibrillation? J Clin Hypertens. 2015;17:565-566.
28. Munter P, Shimbo D, Carey RM, et al. Measurement of blood pressure in humans. a scientific statement from the American Heart Association. Hypertension. 2019;73:e35-e66.
29. Stergiou GS, Alpert B, Mieke S, et al. A universal standard for validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. Hypertension. 2018;71:368-374.
1. Jones DW, Appel LJ, Sheps SG, et al. Measuring blood pressure accurately: new and persistent challenges. JAMA. 2003;289:1027-1030.
2. Meral R, Rakotz M, Bausch P, et al. CDC Grand Rounds: a public health approach to detect and control hypertension. Morb Mortal Wkly Rep. 2016;18:65:1261-1264.
3. Mozzafarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29-e322.
4. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135:e146-e603.
5. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
6. Weinberg I, Gona P, O’Donnell CJ, et al. The systolic blood pressure difference between arms and cardiovascular disease in the Framingham study. Am J Med. 2014;127:209-215.
7. Lane D, Beevers M, Barnes N, et al. Interarm differences in blood pressure: when are they clinically significant? J Hypertens. 2002;20:1089-1095.
8. Clark CE, Taylor RS, Shore AC, et al. The difference in blood pressure readings between arms and survival: primary cohort study. BMJ. 2012;344:e1327. [Erratum in BMJ. 2012;344:e2714.]
9. Kallioinen N, Hill A, Horswill MS, et al. Sources of inaccuracy in measurement of adult patients’ resting blood pressure in clinical settings: a systematic review. J Hyertens. 2017;35:421-441.
10. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals. Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension. 2005;45:142-161.
11. Armstrong D, Matangi M, Brouillard D, et al. Automated office blood pressure—being alone and not location is what matters most. Blood Pressure Monit. 2015;20:204-208.
12. Shevchenko YL, Tsitlik JE. 90th anniversary of the development by Nikolai S. Korotkoff of the auscultatory method of measuring blood pressure. Circulation. 1996;94:116-118.
13. Van Montfrans GA. Oscillometric blood pressure measurement: progress and problems. Blood Press Monit. 2001;6:287-290.
14. Van Popele NM, Bos WJ, de Beer NA, et al. Arterial stiffness as underlying mechanism of disagreement between an oscillometric blood pressure monitor and a sphygmomanometer. Hypertension. 2000;36:484-488.
15. Mauck GW, Smith CR, Geddes LA, et al. The meaning of the point of maximum oscillations in cuff pressure in the indirect measurement of blood pressure—part ii. J Biomech Eng. 1980;102:28-33.
16. Siu AL; US Preventive Services Task Force. Screening for high blood pressure in adults: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163:778-786.
17. National Institute for Health and Clinical Excellence (NICE). Hypertension: the clinical management of hypertension in adults. London: Royal College of Physicians (UK); 2011.
18. O’Brien E, Parati G, Stergiou G, et al; European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31:1731-1768.
19. Leung AA, Nerenberg K, Daskalopoulou SS, et al; CHEP Guidelines Task Force. Hypertension Canada’s 2016 Canadian Hypertension Education Program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2016;32:569-588.
20. Myers MG. Eliminating the human factor in office blood pressure measurement. J Clin Hypertens. 2014;16:83-86.
21. Myers MG, Godwin M, Dawes M, et al. Measurement of blood pressure in the office: recognizing the problem and proposing the solution. J Clin Hypertens. 2010;55:195-200.
22. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce the white coat response. J Hypertens. 2009;27:280-286.
23. Bur A, Herkner H, Vlcek M, et al. Factors influencing the accuracy of oscillometric blood pressure measurements in critically ill patients. Crit Care Med. 2003;31:793-799.
24. Herrálz-Adillo Á, Martínez-Vizcaíno V, Cavero-Redondo I, et al. Diagnostic accuracy of an oscillometric ankle-brachial index in peripheral arterial disease: the influence of oscillometric errors and calcified legs. PLoS One. 2016;11:e0167408.
25. Stergiou GS, Kollias A, Destounis A, et al. Automated blood pressure measurement in atrial fibrillation: a systematic review and meta-analysis. J Hypertens. 2012;30:2074-2082.
26. Pagonas N, Schmidt S, Eysel J, et al. Impact of atrial fibrillation on the accuracy of oscillometric blood pressure monitoring. Hypertension. 2013;62:579-584.
27. Myers MG, Stergiou GS. Should oscillometric blood pressure monitors be used in patients with atrial fibrillation? J Clin Hypertens. 2015;17:565-566.
28. Munter P, Shimbo D, Carey RM, et al. Measurement of blood pressure in humans. a scientific statement from the American Heart Association. Hypertension. 2019;73:e35-e66.
29. Stergiou GS, Alpert B, Mieke S, et al. A universal standard for validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. Hypertension. 2018;71:368-374.
