User login
No hydroxychloroquine benefit in small, randomized COVID-19 trial
However, two experts caution that, because of confounding, the trial is unable to answer convincingly the question of whether HCQ can benefit COVID-19 patients.
Wei Tang, with the Departments of Pulmonology and Critical Care Medicine at Ruijin Hospital, in Shanghai, China, and colleagues enrolled patients with COVID-19 from 16 treatment centers in China in February. They posted their findings on the medRxiv preprint server, but their paper has not been peer reviewed. A coauthor told Medscape Medical News the work has been submitted to a journal.
The overall 28-day negative conversion rate of SARS-CoV-2, which was the primary endpoint, was similar in the two 75-patient treatment groups. The Kaplan-Meier estimate for negative conversion rate was 85.4% in the HCQ plus standard of care (SOC) arm, vs 81.3% in the SOC-only group (P = .341). Negative conversion rates for the two groups were similar at days 4, 7, 10, 14, and 21.
Adverse events were reported in 8.8% of patients in the control group compared with 30% in the HCQ group. Diarrhea was the most common side effect, occurring in 10% of patients in the HCQ group vs none in the control group. Two patients in the HCQ arm had serious adverse events; one experienced disease progression, and the other experienced upper respiratory tract infection.
Patients in the HCQ group received a high loading dose of 1200 mg daily for 3 days followed by a maintenance dose of 800 mg daily for the remaining days. Total duration was 2 weeks for patients with mild or moderate disease and 3 weeks for those with severe disease.
No Difference in Relief of Symptoms
The two arms were similar in alleviation of symptoms by day 28: 59.9% with HCQ plus SOC vs 66.6% with SOC alone.
However, the researchers said that in a post hoc analysis, they found a significant reduction of symptoms after adjusting for the confounding effects of antiviral agents (hazard ratio, 8.83; 95% confidence interval, 1.09 – 71.3).
In addition, Tang and colleagues report a significantly greater reduction of C-reactive protein (CRP), a biomarker for inflammation, from baseline to day 28 in the HCQ group in comparison with the control group (6.986 vs 2.723 mg/L).
The authors suggest the alleviation of symptoms may come from HCQ’s anti-inflammatory effects.
The mean age of the patients was 46 years, and 55% were male. Almost all patients had mild or moderate disease; two had severe disease.
Experts Say Study Arms May Not Have Been Comparable
J. Michelle Kahlenberg, MD, PhD, research professor of rheumatology at the University of Michigan in Ann Arbor, told Medscape Medical News that it’s important to note that in the post hoc analysis, 89% of the patients in this trial were receiving other therapy in addition to HCQ.
“When [the researchers] say they saw improvement in symptoms when they removed the confounders, what they actually did was remove the patients from the analysis that got antivirals, and that left 14 patients in each arm,” Kahlenberg said.
Moreover, Kahlenberg noted, 20% of patients who received HCQ had mild symptoms, whereas only 9% of those in the SOC group did.
“We don’t know how those patients played out in the post hoc analysis — whether it was the patients who were really mild that didn’t get the antivirals that were left in the hydroxychloroquine group and that’s why they had a slightly faster resolution of symptoms,” she said.
She said that in this study, the researchers calculated CRP in milligrams per liter, whereas in the United States, it is measured in milligrams per deciliter. The conversion highlights the fact that the reduction in CRP was not terribly noteworthy, she said.
“The patients with COVID who tend to tank and have cytokine storms ― their CRP is much higher,” she said. “So the small improvement in CRP wasn’t that exciting.
“I don’t think this gets us anywhere closer to an answer. It’s another muddy study,” she said.
Similarly, Christopher V. Plowe, MD, MPH, director of the Global Health Institute at Duke University in Durham, North Carolina, told Medscape Medical News he sees no convincing answers in this study.
Plowe, professor of medicine, molecular genetics, microbiology, and global health at Duke, also noted differences between the two groups at enrollment.
For example, the HCQ group had more than three times the number of patients with shortness of breath (22.1% vs 5.9%); more with sputum production (16.2 vs 5.9%); and more with cough (51.5% vs 38.2%). In addition, the average age was 4 years higher in the HCQ group.
“It makes me wonder whether the randomization was truly random,” Plowe said.
Plowe also questioned the authors’ statement that they didn’t see cardiac arrhythmia events, such as prolonged QT intervals. “I can’t see any evidence that they did an EKG on anybody,” he said.
“This study leaves the door open to the possibility that hydroxychloroquine may have a clinical benefit. If there is a benefit, it seems to be related to the drug’s anti-inflammatory properties. If that’s the case, I’m not sure this particular drug, as opposed to others, would be the way to go,” Plowe said.
Mixed Results in Other Studies
“Our negative results on the anti-viral efficacy of HCQ obtained in this trial are on the contrary to the encouraging in-vitro results and to the recently reported promising results from a non-randomized trial with 36 COVID-19 patients,” the authors write.
However, the 36-patient trial to which they refer has since been called into question, as previously reported by Retraction Watch.
Despite lack of clear evidence of benefit, HCQ is recommended off label for the treatment of COVID-19 by the Chinese National guideline, and the US Food and Drug Administration has issued an emergency-use authorization for the treatment of adult patients with COVID-19.
By contrast, the Infectious Diseases Society of America recently concluded that because of insufficient data, they could not recommend any particular treatment for patients with COVID-19.
The work was supported by the Emergent Projects of National Science and Technology; the National Natural Science Foundation of China; the National Key Research and Development Program of China; the Shanghai Municipal Key Clinical Specialty; the National Innovative Research Team of High-Level Local Universities in Shanghai; the Shanghai Key Discipline for Respiratory Diseases; the National Major Scientific and Technological Special Project for Significant New Drugs Development; and Key Projects in the National Science and Technology Pillar Program. The authors, Kahlenberg, and Plowe have disclosed no relevant financial relationships.
This story first appeared on Medscape.com.
However, two experts caution that, because of confounding, the trial is unable to answer convincingly the question of whether HCQ can benefit COVID-19 patients.
Wei Tang, with the Departments of Pulmonology and Critical Care Medicine at Ruijin Hospital, in Shanghai, China, and colleagues enrolled patients with COVID-19 from 16 treatment centers in China in February. They posted their findings on the medRxiv preprint server, but their paper has not been peer reviewed. A coauthor told Medscape Medical News the work has been submitted to a journal.
The overall 28-day negative conversion rate of SARS-CoV-2, which was the primary endpoint, was similar in the two 75-patient treatment groups. The Kaplan-Meier estimate for negative conversion rate was 85.4% in the HCQ plus standard of care (SOC) arm, vs 81.3% in the SOC-only group (P = .341). Negative conversion rates for the two groups were similar at days 4, 7, 10, 14, and 21.
Adverse events were reported in 8.8% of patients in the control group compared with 30% in the HCQ group. Diarrhea was the most common side effect, occurring in 10% of patients in the HCQ group vs none in the control group. Two patients in the HCQ arm had serious adverse events; one experienced disease progression, and the other experienced upper respiratory tract infection.
Patients in the HCQ group received a high loading dose of 1200 mg daily for 3 days followed by a maintenance dose of 800 mg daily for the remaining days. Total duration was 2 weeks for patients with mild or moderate disease and 3 weeks for those with severe disease.
No Difference in Relief of Symptoms
The two arms were similar in alleviation of symptoms by day 28: 59.9% with HCQ plus SOC vs 66.6% with SOC alone.
However, the researchers said that in a post hoc analysis, they found a significant reduction of symptoms after adjusting for the confounding effects of antiviral agents (hazard ratio, 8.83; 95% confidence interval, 1.09 – 71.3).
In addition, Tang and colleagues report a significantly greater reduction of C-reactive protein (CRP), a biomarker for inflammation, from baseline to day 28 in the HCQ group in comparison with the control group (6.986 vs 2.723 mg/L).
The authors suggest the alleviation of symptoms may come from HCQ’s anti-inflammatory effects.
The mean age of the patients was 46 years, and 55% were male. Almost all patients had mild or moderate disease; two had severe disease.
Experts Say Study Arms May Not Have Been Comparable
J. Michelle Kahlenberg, MD, PhD, research professor of rheumatology at the University of Michigan in Ann Arbor, told Medscape Medical News that it’s important to note that in the post hoc analysis, 89% of the patients in this trial were receiving other therapy in addition to HCQ.
“When [the researchers] say they saw improvement in symptoms when they removed the confounders, what they actually did was remove the patients from the analysis that got antivirals, and that left 14 patients in each arm,” Kahlenberg said.
Moreover, Kahlenberg noted, 20% of patients who received HCQ had mild symptoms, whereas only 9% of those in the SOC group did.
“We don’t know how those patients played out in the post hoc analysis — whether it was the patients who were really mild that didn’t get the antivirals that were left in the hydroxychloroquine group and that’s why they had a slightly faster resolution of symptoms,” she said.
She said that in this study, the researchers calculated CRP in milligrams per liter, whereas in the United States, it is measured in milligrams per deciliter. The conversion highlights the fact that the reduction in CRP was not terribly noteworthy, she said.
“The patients with COVID who tend to tank and have cytokine storms ― their CRP is much higher,” she said. “So the small improvement in CRP wasn’t that exciting.
“I don’t think this gets us anywhere closer to an answer. It’s another muddy study,” she said.
Similarly, Christopher V. Plowe, MD, MPH, director of the Global Health Institute at Duke University in Durham, North Carolina, told Medscape Medical News he sees no convincing answers in this study.
Plowe, professor of medicine, molecular genetics, microbiology, and global health at Duke, also noted differences between the two groups at enrollment.
For example, the HCQ group had more than three times the number of patients with shortness of breath (22.1% vs 5.9%); more with sputum production (16.2 vs 5.9%); and more with cough (51.5% vs 38.2%). In addition, the average age was 4 years higher in the HCQ group.
“It makes me wonder whether the randomization was truly random,” Plowe said.
Plowe also questioned the authors’ statement that they didn’t see cardiac arrhythmia events, such as prolonged QT intervals. “I can’t see any evidence that they did an EKG on anybody,” he said.
“This study leaves the door open to the possibility that hydroxychloroquine may have a clinical benefit. If there is a benefit, it seems to be related to the drug’s anti-inflammatory properties. If that’s the case, I’m not sure this particular drug, as opposed to others, would be the way to go,” Plowe said.
Mixed Results in Other Studies
“Our negative results on the anti-viral efficacy of HCQ obtained in this trial are on the contrary to the encouraging in-vitro results and to the recently reported promising results from a non-randomized trial with 36 COVID-19 patients,” the authors write.
However, the 36-patient trial to which they refer has since been called into question, as previously reported by Retraction Watch.
Despite lack of clear evidence of benefit, HCQ is recommended off label for the treatment of COVID-19 by the Chinese National guideline, and the US Food and Drug Administration has issued an emergency-use authorization for the treatment of adult patients with COVID-19.
By contrast, the Infectious Diseases Society of America recently concluded that because of insufficient data, they could not recommend any particular treatment for patients with COVID-19.
The work was supported by the Emergent Projects of National Science and Technology; the National Natural Science Foundation of China; the National Key Research and Development Program of China; the Shanghai Municipal Key Clinical Specialty; the National Innovative Research Team of High-Level Local Universities in Shanghai; the Shanghai Key Discipline for Respiratory Diseases; the National Major Scientific and Technological Special Project for Significant New Drugs Development; and Key Projects in the National Science and Technology Pillar Program. The authors, Kahlenberg, and Plowe have disclosed no relevant financial relationships.
This story first appeared on Medscape.com.
However, two experts caution that, because of confounding, the trial is unable to answer convincingly the question of whether HCQ can benefit COVID-19 patients.
Wei Tang, with the Departments of Pulmonology and Critical Care Medicine at Ruijin Hospital, in Shanghai, China, and colleagues enrolled patients with COVID-19 from 16 treatment centers in China in February. They posted their findings on the medRxiv preprint server, but their paper has not been peer reviewed. A coauthor told Medscape Medical News the work has been submitted to a journal.
The overall 28-day negative conversion rate of SARS-CoV-2, which was the primary endpoint, was similar in the two 75-patient treatment groups. The Kaplan-Meier estimate for negative conversion rate was 85.4% in the HCQ plus standard of care (SOC) arm, vs 81.3% in the SOC-only group (P = .341). Negative conversion rates for the two groups were similar at days 4, 7, 10, 14, and 21.
Adverse events were reported in 8.8% of patients in the control group compared with 30% in the HCQ group. Diarrhea was the most common side effect, occurring in 10% of patients in the HCQ group vs none in the control group. Two patients in the HCQ arm had serious adverse events; one experienced disease progression, and the other experienced upper respiratory tract infection.
Patients in the HCQ group received a high loading dose of 1200 mg daily for 3 days followed by a maintenance dose of 800 mg daily for the remaining days. Total duration was 2 weeks for patients with mild or moderate disease and 3 weeks for those with severe disease.
No Difference in Relief of Symptoms
The two arms were similar in alleviation of symptoms by day 28: 59.9% with HCQ plus SOC vs 66.6% with SOC alone.
However, the researchers said that in a post hoc analysis, they found a significant reduction of symptoms after adjusting for the confounding effects of antiviral agents (hazard ratio, 8.83; 95% confidence interval, 1.09 – 71.3).
In addition, Tang and colleagues report a significantly greater reduction of C-reactive protein (CRP), a biomarker for inflammation, from baseline to day 28 in the HCQ group in comparison with the control group (6.986 vs 2.723 mg/L).
The authors suggest the alleviation of symptoms may come from HCQ’s anti-inflammatory effects.
The mean age of the patients was 46 years, and 55% were male. Almost all patients had mild or moderate disease; two had severe disease.
Experts Say Study Arms May Not Have Been Comparable
J. Michelle Kahlenberg, MD, PhD, research professor of rheumatology at the University of Michigan in Ann Arbor, told Medscape Medical News that it’s important to note that in the post hoc analysis, 89% of the patients in this trial were receiving other therapy in addition to HCQ.
“When [the researchers] say they saw improvement in symptoms when they removed the confounders, what they actually did was remove the patients from the analysis that got antivirals, and that left 14 patients in each arm,” Kahlenberg said.
Moreover, Kahlenberg noted, 20% of patients who received HCQ had mild symptoms, whereas only 9% of those in the SOC group did.
“We don’t know how those patients played out in the post hoc analysis — whether it was the patients who were really mild that didn’t get the antivirals that were left in the hydroxychloroquine group and that’s why they had a slightly faster resolution of symptoms,” she said.
She said that in this study, the researchers calculated CRP in milligrams per liter, whereas in the United States, it is measured in milligrams per deciliter. The conversion highlights the fact that the reduction in CRP was not terribly noteworthy, she said.
“The patients with COVID who tend to tank and have cytokine storms ― their CRP is much higher,” she said. “So the small improvement in CRP wasn’t that exciting.
“I don’t think this gets us anywhere closer to an answer. It’s another muddy study,” she said.
Similarly, Christopher V. Plowe, MD, MPH, director of the Global Health Institute at Duke University in Durham, North Carolina, told Medscape Medical News he sees no convincing answers in this study.
Plowe, professor of medicine, molecular genetics, microbiology, and global health at Duke, also noted differences between the two groups at enrollment.
For example, the HCQ group had more than three times the number of patients with shortness of breath (22.1% vs 5.9%); more with sputum production (16.2 vs 5.9%); and more with cough (51.5% vs 38.2%). In addition, the average age was 4 years higher in the HCQ group.
“It makes me wonder whether the randomization was truly random,” Plowe said.
Plowe also questioned the authors’ statement that they didn’t see cardiac arrhythmia events, such as prolonged QT intervals. “I can’t see any evidence that they did an EKG on anybody,” he said.
“This study leaves the door open to the possibility that hydroxychloroquine may have a clinical benefit. If there is a benefit, it seems to be related to the drug’s anti-inflammatory properties. If that’s the case, I’m not sure this particular drug, as opposed to others, would be the way to go,” Plowe said.
Mixed Results in Other Studies
“Our negative results on the anti-viral efficacy of HCQ obtained in this trial are on the contrary to the encouraging in-vitro results and to the recently reported promising results from a non-randomized trial with 36 COVID-19 patients,” the authors write.
However, the 36-patient trial to which they refer has since been called into question, as previously reported by Retraction Watch.
Despite lack of clear evidence of benefit, HCQ is recommended off label for the treatment of COVID-19 by the Chinese National guideline, and the US Food and Drug Administration has issued an emergency-use authorization for the treatment of adult patients with COVID-19.
By contrast, the Infectious Diseases Society of America recently concluded that because of insufficient data, they could not recommend any particular treatment for patients with COVID-19.
The work was supported by the Emergent Projects of National Science and Technology; the National Natural Science Foundation of China; the National Key Research and Development Program of China; the Shanghai Municipal Key Clinical Specialty; the National Innovative Research Team of High-Level Local Universities in Shanghai; the Shanghai Key Discipline for Respiratory Diseases; the National Major Scientific and Technological Special Project for Significant New Drugs Development; and Key Projects in the National Science and Technology Pillar Program. The authors, Kahlenberg, and Plowe have disclosed no relevant financial relationships.
This story first appeared on Medscape.com.
COVID-19 mythconceptions

Let’s start with a case:
A 37-year-old woman is seen in clinic for a 5-day history of cough, fever, chest tightness, and onset of dyspnea on the day of her office visit.
An exam reveals her blood pressure is 100/60 mm Hg, her pulse is 100 beats per minute, her temperature is 38.7° C, her oxygen saturation is 93%, and her respiratory rate is 20 breaths per minute.
Auscultation of the chest revealed bilateral wheezing and rhonchi. A nasopharyngeal swab is sent for COVID-19 and is negative; she also tests negative for influenza.
Her hemoglobin level is 13 g/dL, hematocrit was 39%, platelet count was 155,000 per mcL of blood, and D-dimer level was 8.4 mcg/mL (normal is less than 0.4 mcg/mL.) Her white blood cell count was 6,000 per mcL of blood (neutrophils, 4,900; lymphocytes, 800; basophils, 200). Her chest x-ray showed bilateral lower lobe infiltrates.
What do you recommend?
A. Begin azithromycin plus ceftriaxone
B. Begin azithromycin
C. Begin oseltamivir
D. Obtain chest CT
E. Repeat COVID-19 test
With the massive amount of information coming out every day on COVID-19, it is hard to keep up with all of it, and sort out accurate, reviewed studies. We are in a position where we need to take in what we can and assess the best data available.
In the case above, I think choices D or E would make sense. This patient very likely has COVID-19 based on clinical symptoms and lab parameters. The negative COVID-19 test gives us pause, but several studies show that false negative tests are not uncommon.
Long et al. reported on 36 patients who had received both chest CT and real-time reverse transcription polymerase chain reaction (rRT-PCR) for COVID-19.1 All were eventually diagnosed with COVID-19 pneumonia. The CT scan had a very high sensitivity (35/36) of 97.2%, whereas the rRT-PCR had a lower sensitivity (30/36) of 83%. All six of the patients with a negative COVID-19 test initially were positive on repeat testing (three on the second test, three on the third test).
There are concerns about what the sensitivity of the rRT-PCR tests being run in the United States are. At this point, I think that, when the pretest probability of COVID-19 infection is very high based on local epidemiology and clinical symptoms, a negative COVID rRT-PCR does not eliminate the diagnosis. In many cases, COVID-19 may still be the most likely diagnosis.
Early in the pandemic, the symptoms that were emphasized were fever, cough, and dyspnea. Those were all crucial symptoms for a disease that causes pneumonia. GI symptoms were initially deemphasized. In an early study released from Wuhan, China, only about 5% of COVID-19 patients had nausea or diarrhea.2 In a study of 305 patients focused on gastrointestinal symptoms, half of the patients had diarrhea, half had anorexia and 30% had nausea.3 In a small series of nine patients who presented with only GI symptoms, four of these patients never developed fever or pulmonary symptoms.3
On March 14, the French health minister, Olivier Véran, tweeted that “taking anti-inflammatory drugs (ibuprofen, cortisone ...) could be an aggravating factor for the infection. If you have a fever, take paracetamol.” This was picked up by many news services, and soon became standard recommendations, despite no data.
There is reason for concern for NSAIDs, as regular NSAID use has been tied to more complications in patients with respiratory tract infections.4 I have never been a proponent of regular NSAID use in patients who are infected, because the likelihood of toxicity is elevated in patients who are volume depleted or under physiologic stress. But at this time, there is no evidence on problems with episodic NSAID use in patients with COVID-19.
Another widely disseminated decree was that patients with COVID-19 should not use ACE inhibitors and angiotensin II receptor blockers (ARBs). COVID-19 binds to their target cells through ACE2, which is expressed by epithelial cells of the lung, intestine and kidney. Patients who are treated with ACE inhibitors and ARBs have been shown to have more ACE2 expression.
In a letter to the editor by Fang et al. published in Lancet Respiratory Medicine, the authors raised the question of whether patients might be better served to be switched from ACE inhibitors and ARBs to calcium-channel blockers for the treatment of hypertension.5 A small study by Meng et al. looked at outcomes of patients on these drugs who had COVID-19 infection.6 They looked at 417 patients admitted to a hospital in China with COVID-19 infection. A total of 42 patients were on medications for hypertension. Group 1 were patients on ACE inhibitors/ARBs (17 patients) and group 2 were patients on other antihypertensives (25 patients). During hospitalization 12 patients (48%) in group 2 were categorized as having severe disease and 1 patient died. In group 1 (the ACE inhibitor/ARB–treated patients) only four (23%) were categorized as having severe disease, and no patients in this group died.
Vaduganathan et al. published a special report in the New England Journal of Medicine strongly arguing the point that “[u]ntil further data are available, we think that [renin-angiotensin-aldosterone system] inhibitors should be continued in patients in otherwise stable condition who are at risk for, being evaluated for, or with COVID-19”.7 This position is supported by the American Heart Association, the American College of Cardiology, the American College of Physicians, and 11 other medical organizations.
Take-home messages
- Testing isn’t perfect – if you have strong suspicion for COVID-19 disease, retest.
- GI symptoms appear to be common, and rarely may be the only symptoms initially.
- NSAIDs are always risky in really sick patients, but data specific to COVID-19 is lacking.
- ACE inhibitors/ARBs should not be avoided in patients with COVID-19.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact Dr. Paauw at imnews@mdedge.com.
References
1. Long C et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. 2020 Mar 25;126:108961.
2. Zhou F et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054-62.
3. Tian Y et al. Review article: Gastrointestinal features in COVID-19 and the possibility of faecal transmission. Aliment Pharmacol Ther. 2020;00:1–9.
4. Voiriot G et al. Risks related to the use of nonsteroidal anti-inflammatory drugs in community-acquired pneumonia in adult and pediatric patients. J Clin Med. 2019;8:E786.
5. Fang L et al. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020 Mar 11. doi:10.1016/S2213-2600(20)30116-8.
6. Meng J et al. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg Microbes Infect. 2020 Dec;9(1):757-60.
7. Vaduganathan M et al. Renin-angiotensin-aldosterone system inhibitors in patients with COVID-19. N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760.
Let’s start with a case:
A 37-year-old woman is seen in clinic for a 5-day history of cough, fever, chest tightness, and onset of dyspnea on the day of her office visit.
An exam reveals her blood pressure is 100/60 mm Hg, her pulse is 100 beats per minute, her temperature is 38.7° C, her oxygen saturation is 93%, and her respiratory rate is 20 breaths per minute.
Auscultation of the chest revealed bilateral wheezing and rhonchi. A nasopharyngeal swab is sent for COVID-19 and is negative; she also tests negative for influenza.
Her hemoglobin level is 13 g/dL, hematocrit was 39%, platelet count was 155,000 per mcL of blood, and D-dimer level was 8.4 mcg/mL (normal is less than 0.4 mcg/mL.) Her white blood cell count was 6,000 per mcL of blood (neutrophils, 4,900; lymphocytes, 800; basophils, 200). Her chest x-ray showed bilateral lower lobe infiltrates.
What do you recommend?
A. Begin azithromycin plus ceftriaxone
B. Begin azithromycin
C. Begin oseltamivir
D. Obtain chest CT
E. Repeat COVID-19 test
With the massive amount of information coming out every day on COVID-19, it is hard to keep up with all of it, and sort out accurate, reviewed studies. We are in a position where we need to take in what we can and assess the best data available.
In the case above, I think choices D or E would make sense. This patient very likely has COVID-19 based on clinical symptoms and lab parameters. The negative COVID-19 test gives us pause, but several studies show that false negative tests are not uncommon.
Long et al. reported on 36 patients who had received both chest CT and real-time reverse transcription polymerase chain reaction (rRT-PCR) for COVID-19.1 All were eventually diagnosed with COVID-19 pneumonia. The CT scan had a very high sensitivity (35/36) of 97.2%, whereas the rRT-PCR had a lower sensitivity (30/36) of 83%. All six of the patients with a negative COVID-19 test initially were positive on repeat testing (three on the second test, three on the third test).
There are concerns about what the sensitivity of the rRT-PCR tests being run in the United States are. At this point, I think that, when the pretest probability of COVID-19 infection is very high based on local epidemiology and clinical symptoms, a negative COVID rRT-PCR does not eliminate the diagnosis. In many cases, COVID-19 may still be the most likely diagnosis.
Early in the pandemic, the symptoms that were emphasized were fever, cough, and dyspnea. Those were all crucial symptoms for a disease that causes pneumonia. GI symptoms were initially deemphasized. In an early study released from Wuhan, China, only about 5% of COVID-19 patients had nausea or diarrhea.2 In a study of 305 patients focused on gastrointestinal symptoms, half of the patients had diarrhea, half had anorexia and 30% had nausea.3 In a small series of nine patients who presented with only GI symptoms, four of these patients never developed fever or pulmonary symptoms.3
On March 14, the French health minister, Olivier Véran, tweeted that “taking anti-inflammatory drugs (ibuprofen, cortisone ...) could be an aggravating factor for the infection. If you have a fever, take paracetamol.” This was picked up by many news services, and soon became standard recommendations, despite no data.
There is reason for concern for NSAIDs, as regular NSAID use has been tied to more complications in patients with respiratory tract infections.4 I have never been a proponent of regular NSAID use in patients who are infected, because the likelihood of toxicity is elevated in patients who are volume depleted or under physiologic stress. But at this time, there is no evidence on problems with episodic NSAID use in patients with COVID-19.
Another widely disseminated decree was that patients with COVID-19 should not use ACE inhibitors and angiotensin II receptor blockers (ARBs). COVID-19 binds to their target cells through ACE2, which is expressed by epithelial cells of the lung, intestine and kidney. Patients who are treated with ACE inhibitors and ARBs have been shown to have more ACE2 expression.
In a letter to the editor by Fang et al. published in Lancet Respiratory Medicine, the authors raised the question of whether patients might be better served to be switched from ACE inhibitors and ARBs to calcium-channel blockers for the treatment of hypertension.5 A small study by Meng et al. looked at outcomes of patients on these drugs who had COVID-19 infection.6 They looked at 417 patients admitted to a hospital in China with COVID-19 infection. A total of 42 patients were on medications for hypertension. Group 1 were patients on ACE inhibitors/ARBs (17 patients) and group 2 were patients on other antihypertensives (25 patients). During hospitalization 12 patients (48%) in group 2 were categorized as having severe disease and 1 patient died. In group 1 (the ACE inhibitor/ARB–treated patients) only four (23%) were categorized as having severe disease, and no patients in this group died.
Vaduganathan et al. published a special report in the New England Journal of Medicine strongly arguing the point that “[u]ntil further data are available, we think that [renin-angiotensin-aldosterone system] inhibitors should be continued in patients in otherwise stable condition who are at risk for, being evaluated for, or with COVID-19”.7 This position is supported by the American Heart Association, the American College of Cardiology, the American College of Physicians, and 11 other medical organizations.
Take-home messages
- Testing isn’t perfect – if you have strong suspicion for COVID-19 disease, retest.
- GI symptoms appear to be common, and rarely may be the only symptoms initially.
- NSAIDs are always risky in really sick patients, but data specific to COVID-19 is lacking.
- ACE inhibitors/ARBs should not be avoided in patients with COVID-19.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact Dr. Paauw at imnews@mdedge.com.
References
1. Long C et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. 2020 Mar 25;126:108961.
2. Zhou F et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054-62.
3. Tian Y et al. Review article: Gastrointestinal features in COVID-19 and the possibility of faecal transmission. Aliment Pharmacol Ther. 2020;00:1–9.
4. Voiriot G et al. Risks related to the use of nonsteroidal anti-inflammatory drugs in community-acquired pneumonia in adult and pediatric patients. J Clin Med. 2019;8:E786.
5. Fang L et al. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020 Mar 11. doi:10.1016/S2213-2600(20)30116-8.
6. Meng J et al. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg Microbes Infect. 2020 Dec;9(1):757-60.
7. Vaduganathan M et al. Renin-angiotensin-aldosterone system inhibitors in patients with COVID-19. N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760.
Let’s start with a case:
A 37-year-old woman is seen in clinic for a 5-day history of cough, fever, chest tightness, and onset of dyspnea on the day of her office visit.
An exam reveals her blood pressure is 100/60 mm Hg, her pulse is 100 beats per minute, her temperature is 38.7° C, her oxygen saturation is 93%, and her respiratory rate is 20 breaths per minute.
Auscultation of the chest revealed bilateral wheezing and rhonchi. A nasopharyngeal swab is sent for COVID-19 and is negative; she also tests negative for influenza.
Her hemoglobin level is 13 g/dL, hematocrit was 39%, platelet count was 155,000 per mcL of blood, and D-dimer level was 8.4 mcg/mL (normal is less than 0.4 mcg/mL.) Her white blood cell count was 6,000 per mcL of blood (neutrophils, 4,900; lymphocytes, 800; basophils, 200). Her chest x-ray showed bilateral lower lobe infiltrates.
What do you recommend?
A. Begin azithromycin plus ceftriaxone
B. Begin azithromycin
C. Begin oseltamivir
D. Obtain chest CT
E. Repeat COVID-19 test
With the massive amount of information coming out every day on COVID-19, it is hard to keep up with all of it, and sort out accurate, reviewed studies. We are in a position where we need to take in what we can and assess the best data available.
In the case above, I think choices D or E would make sense. This patient very likely has COVID-19 based on clinical symptoms and lab parameters. The negative COVID-19 test gives us pause, but several studies show that false negative tests are not uncommon.
Long et al. reported on 36 patients who had received both chest CT and real-time reverse transcription polymerase chain reaction (rRT-PCR) for COVID-19.1 All were eventually diagnosed with COVID-19 pneumonia. The CT scan had a very high sensitivity (35/36) of 97.2%, whereas the rRT-PCR had a lower sensitivity (30/36) of 83%. All six of the patients with a negative COVID-19 test initially were positive on repeat testing (three on the second test, three on the third test).
There are concerns about what the sensitivity of the rRT-PCR tests being run in the United States are. At this point, I think that, when the pretest probability of COVID-19 infection is very high based on local epidemiology and clinical symptoms, a negative COVID rRT-PCR does not eliminate the diagnosis. In many cases, COVID-19 may still be the most likely diagnosis.
Early in the pandemic, the symptoms that were emphasized were fever, cough, and dyspnea. Those were all crucial symptoms for a disease that causes pneumonia. GI symptoms were initially deemphasized. In an early study released from Wuhan, China, only about 5% of COVID-19 patients had nausea or diarrhea.2 In a study of 305 patients focused on gastrointestinal symptoms, half of the patients had diarrhea, half had anorexia and 30% had nausea.3 In a small series of nine patients who presented with only GI symptoms, four of these patients never developed fever or pulmonary symptoms.3
On March 14, the French health minister, Olivier Véran, tweeted that “taking anti-inflammatory drugs (ibuprofen, cortisone ...) could be an aggravating factor for the infection. If you have a fever, take paracetamol.” This was picked up by many news services, and soon became standard recommendations, despite no data.
There is reason for concern for NSAIDs, as regular NSAID use has been tied to more complications in patients with respiratory tract infections.4 I have never been a proponent of regular NSAID use in patients who are infected, because the likelihood of toxicity is elevated in patients who are volume depleted or under physiologic stress. But at this time, there is no evidence on problems with episodic NSAID use in patients with COVID-19.
Another widely disseminated decree was that patients with COVID-19 should not use ACE inhibitors and angiotensin II receptor blockers (ARBs). COVID-19 binds to their target cells through ACE2, which is expressed by epithelial cells of the lung, intestine and kidney. Patients who are treated with ACE inhibitors and ARBs have been shown to have more ACE2 expression.
In a letter to the editor by Fang et al. published in Lancet Respiratory Medicine, the authors raised the question of whether patients might be better served to be switched from ACE inhibitors and ARBs to calcium-channel blockers for the treatment of hypertension.5 A small study by Meng et al. looked at outcomes of patients on these drugs who had COVID-19 infection.6 They looked at 417 patients admitted to a hospital in China with COVID-19 infection. A total of 42 patients were on medications for hypertension. Group 1 were patients on ACE inhibitors/ARBs (17 patients) and group 2 were patients on other antihypertensives (25 patients). During hospitalization 12 patients (48%) in group 2 were categorized as having severe disease and 1 patient died. In group 1 (the ACE inhibitor/ARB–treated patients) only four (23%) were categorized as having severe disease, and no patients in this group died.
Vaduganathan et al. published a special report in the New England Journal of Medicine strongly arguing the point that “[u]ntil further data are available, we think that [renin-angiotensin-aldosterone system] inhibitors should be continued in patients in otherwise stable condition who are at risk for, being evaluated for, or with COVID-19”.7 This position is supported by the American Heart Association, the American College of Cardiology, the American College of Physicians, and 11 other medical organizations.
Take-home messages
- Testing isn’t perfect – if you have strong suspicion for COVID-19 disease, retest.
- GI symptoms appear to be common, and rarely may be the only symptoms initially.
- NSAIDs are always risky in really sick patients, but data specific to COVID-19 is lacking.
- ACE inhibitors/ARBs should not be avoided in patients with COVID-19.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact Dr. Paauw at imnews@mdedge.com.
References
1. Long C et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. 2020 Mar 25;126:108961.
2. Zhou F et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054-62.
3. Tian Y et al. Review article: Gastrointestinal features in COVID-19 and the possibility of faecal transmission. Aliment Pharmacol Ther. 2020;00:1–9.
4. Voiriot G et al. Risks related to the use of nonsteroidal anti-inflammatory drugs in community-acquired pneumonia in adult and pediatric patients. J Clin Med. 2019;8:E786.
5. Fang L et al. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020 Mar 11. doi:10.1016/S2213-2600(20)30116-8.
6. Meng J et al. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg Microbes Infect. 2020 Dec;9(1):757-60.
7. Vaduganathan M et al. Renin-angiotensin-aldosterone system inhibitors in patients with COVID-19. N Engl J Med. 2020 Mar 30. doi: 10.1056/NEJMsr2005760.
Sodium nitrite disappoints in cardiac arrest
Among patients who had an out-of-hospital cardiac arrest, intravenous sodium nitrite given by paramedics during resuscitation did not significantly improve their chances of being admitted to or discharged from the hospital alive.

The study was presented at the recent “virtual” American College of Cardiology 2020 Scientific Session (ACC.20)/World Congress of Cardiology (WCC).
Lead investigator Francis Kim, MD, professor of medicine at the University of Washington, Seattle, explained that sodium nitrate is an antioxidant; animal studies have suggested that under conditions of hypoxia, it is converted into the vasodilator nitric oxide, which can increase blood flow to the brain and heart tissues.
In animal models of cardiac arrest, the use of sodium nitrite during resuscitation increased survival by almost 50%.
For the current study, 1,502 patients who had an out-of-hospital cardiac arrest were randomly assigned to receive either a low dose (45 mg) or a high dose (60 mg) of sodium nitrite or a placebo. The average age of the patients who were included in the study was 64 years, and 66% were male; 22% had ventricular fibrillation, 43% had asystole, and 29% had pulseless electrical activity.
Results showed no statistically significant differences between the groups who received placebo, low-dose sodium nitrite, or high-dose sodium nitrite on survival to hospital admission (the primary endpoint) or on hospital discharge (the secondary endpoint). There was also no difference in either endpoint in the subgroup with ventricular fibrillation.
“Our results are disappointing, especially after the promising findings in animal studies, but we feel this trial shuts the door on using this drug in this indication,” Kim said.
Discussing the study at an ACC press conference, Dhanunjaya Lakkireddy, MD, University of Kansas Hospital and Medical Center and ACC Electrophysiology Council chair, said this was “an excellent trial in the unending quest to try to improve survival in out-of-hospital cardiac arrest.
“As we all aware, if we don’t get blood circulation to the brain for more than 5 seconds, we pass out, and if don’t get blood circulation to the brain for more than 5 minutes, brain death occurs. When people suffer out-of-hospital cardiac arrest, the rate of survival is therefore dramatically lower when the ability to resuscitate goes beyond 5 minutes,” Lakkireddy noted.
He questioned why the current trial showed no effect when there had been significant early promise in animal studies. He suggested factors that could have been relevant included the time to intervention ― which was an average of 22 minutes from call to randomization ― perfusion of the brain, whether the drug cleared the blood-brain barrier, whether nitric oxide levels in the brain were sufficient, and the patient population that was included in the study.
“A large percentage of patients had asystole or pulseless electrical activity ― these are known to have worse outcomes ― and 60% of patients in the study did not have a witnessed arrest and could have been down for much longer and therefore could have had a significantly higher level of irreversible brain damage,” Lakkireddy pointed out.
“If we can understand some of the issues, we may be able to do another trial in a different subset of patients in whom the duration of arrest is significantly lower,” he commented.
The study was funded by the National Heart, Lung, and Blood Institute. Kim has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Among patients who had an out-of-hospital cardiac arrest, intravenous sodium nitrite given by paramedics during resuscitation did not significantly improve their chances of being admitted to or discharged from the hospital alive.
The study was presented at the recent “virtual” American College of Cardiology 2020 Scientific Session (ACC.20)/World Congress of Cardiology (WCC).
Lead investigator Francis Kim, MD, professor of medicine at the University of Washington, Seattle, explained that sodium nitrate is an antioxidant; animal studies have suggested that under conditions of hypoxia, it is converted into the vasodilator nitric oxide, which can increase blood flow to the brain and heart tissues.
In animal models of cardiac arrest, the use of sodium nitrite during resuscitation increased survival by almost 50%.
For the current study, 1,502 patients who had an out-of-hospital cardiac arrest were randomly assigned to receive either a low dose (45 mg) or a high dose (60 mg) of sodium nitrite or a placebo. The average age of the patients who were included in the study was 64 years, and 66% were male; 22% had ventricular fibrillation, 43% had asystole, and 29% had pulseless electrical activity.
Results showed no statistically significant differences between the groups who received placebo, low-dose sodium nitrite, or high-dose sodium nitrite on survival to hospital admission (the primary endpoint) or on hospital discharge (the secondary endpoint). There was also no difference in either endpoint in the subgroup with ventricular fibrillation.
“Our results are disappointing, especially after the promising findings in animal studies, but we feel this trial shuts the door on using this drug in this indication,” Kim said.
Discussing the study at an ACC press conference, Dhanunjaya Lakkireddy, MD, University of Kansas Hospital and Medical Center and ACC Electrophysiology Council chair, said this was “an excellent trial in the unending quest to try to improve survival in out-of-hospital cardiac arrest.
“As we all aware, if we don’t get blood circulation to the brain for more than 5 seconds, we pass out, and if don’t get blood circulation to the brain for more than 5 minutes, brain death occurs. When people suffer out-of-hospital cardiac arrest, the rate of survival is therefore dramatically lower when the ability to resuscitate goes beyond 5 minutes,” Lakkireddy noted.
He questioned why the current trial showed no effect when there had been significant early promise in animal studies. He suggested factors that could have been relevant included the time to intervention ― which was an average of 22 minutes from call to randomization ― perfusion of the brain, whether the drug cleared the blood-brain barrier, whether nitric oxide levels in the brain were sufficient, and the patient population that was included in the study.
“A large percentage of patients had asystole or pulseless electrical activity ― these are known to have worse outcomes ― and 60% of patients in the study did not have a witnessed arrest and could have been down for much longer and therefore could have had a significantly higher level of irreversible brain damage,” Lakkireddy pointed out.
“If we can understand some of the issues, we may be able to do another trial in a different subset of patients in whom the duration of arrest is significantly lower,” he commented.
The study was funded by the National Heart, Lung, and Blood Institute. Kim has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Among patients who had an out-of-hospital cardiac arrest, intravenous sodium nitrite given by paramedics during resuscitation did not significantly improve their chances of being admitted to or discharged from the hospital alive.
The study was presented at the recent “virtual” American College of Cardiology 2020 Scientific Session (ACC.20)/World Congress of Cardiology (WCC).
Lead investigator Francis Kim, MD, professor of medicine at the University of Washington, Seattle, explained that sodium nitrate is an antioxidant; animal studies have suggested that under conditions of hypoxia, it is converted into the vasodilator nitric oxide, which can increase blood flow to the brain and heart tissues.
In animal models of cardiac arrest, the use of sodium nitrite during resuscitation increased survival by almost 50%.
For the current study, 1,502 patients who had an out-of-hospital cardiac arrest were randomly assigned to receive either a low dose (45 mg) or a high dose (60 mg) of sodium nitrite or a placebo. The average age of the patients who were included in the study was 64 years, and 66% were male; 22% had ventricular fibrillation, 43% had asystole, and 29% had pulseless electrical activity.
Results showed no statistically significant differences between the groups who received placebo, low-dose sodium nitrite, or high-dose sodium nitrite on survival to hospital admission (the primary endpoint) or on hospital discharge (the secondary endpoint). There was also no difference in either endpoint in the subgroup with ventricular fibrillation.
“Our results are disappointing, especially after the promising findings in animal studies, but we feel this trial shuts the door on using this drug in this indication,” Kim said.
Discussing the study at an ACC press conference, Dhanunjaya Lakkireddy, MD, University of Kansas Hospital and Medical Center and ACC Electrophysiology Council chair, said this was “an excellent trial in the unending quest to try to improve survival in out-of-hospital cardiac arrest.
“As we all aware, if we don’t get blood circulation to the brain for more than 5 seconds, we pass out, and if don’t get blood circulation to the brain for more than 5 minutes, brain death occurs. When people suffer out-of-hospital cardiac arrest, the rate of survival is therefore dramatically lower when the ability to resuscitate goes beyond 5 minutes,” Lakkireddy noted.
He questioned why the current trial showed no effect when there had been significant early promise in animal studies. He suggested factors that could have been relevant included the time to intervention ― which was an average of 22 minutes from call to randomization ― perfusion of the brain, whether the drug cleared the blood-brain barrier, whether nitric oxide levels in the brain were sufficient, and the patient population that was included in the study.
“A large percentage of patients had asystole or pulseless electrical activity ― these are known to have worse outcomes ― and 60% of patients in the study did not have a witnessed arrest and could have been down for much longer and therefore could have had a significantly higher level of irreversible brain damage,” Lakkireddy pointed out.
“If we can understand some of the issues, we may be able to do another trial in a different subset of patients in whom the duration of arrest is significantly lower,” he commented.
The study was funded by the National Heart, Lung, and Blood Institute. Kim has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
COVID-19 cases highlight longstanding racial disparities in health care
African Americans are overrepresented among patients who have died as a result of the COVID-19 pandemic, but the current crisis puts a spotlight on long-standing racial disparities in health care and health access in the United States, according to David R. Williams, PhD, a professor of public health at the Harvard T.H. Chan School of Public Health in Boston.

Dr. Williams, a social scientist specializing in the link between race and health, is a professor of African and African American Studies and of Sociology at Harvard. He spoke on the topic of racial disparities amid the COVID-19 pandemic in a teleconference sponsored by the Robert Wood Johnson Foundation.
“Many Americans are shocked” by the higher mortality rates among African American COVID-19 patients, said Dr. Williams. However, data from decades of research show that “black people in America live sicker and shorter lives,” he said.
Keys to the increased mortality among African Americans include an increased prevalence of risk factors, increased risk for exposure to the virus because of socioeconomic factors, and less access to health care if they do become ill, he said.
Many minority individuals work outside the home in areas deemed essential during the pandemic, such as transit, delivery, maintenance, cleaning, and in businesses such as grocery stores, although in general “race continues to matter for health at every level of income and education,” Dr. Williams said.
In addition, social distance guidelines are not realistic for many people in high-density, low-income areas, who often live in shared, multigenerational housing, he said.
Data show that individuals with chronic conditions such as diabetes and cardiovascular disease are more likely to die as a result of COVID-19, and minority populations are more likely to develop these conditions at younger ages, Dr. Williams noted. Access to health care also plays a role. Many minority individuals of lower socioeconomic status are less likely to have health insurance, or if they do, may have Medicaid, which is not consistently accepted, he said. Also, some low-income neighborhoods lack convenient access to primary care and thus to screening services, he noted.
Dr. Williams said the COVID-19 pandemic could serve as an opportunity to examine and improve health care services for underserved communities. In the short term, “we need to collect data so we can see patterns” and address pressing needs, he said, but long-term goals should “prioritize investments that would create healthy homes and communities,” he emphasized.
A recent study from the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report cited COVID-NET (the COVID-19 Associated Hospitalization Surveillance Network) as showing that, in their catchment population, “approximately 59% of residents are white, 18% are black, and 14% are Hispanic; however, among 580 hospitalized COVID-19 patients with race/ethnicity data, approximately 45% were white, 33% were black, and 8% were Hispanic, suggesting that black populations might be disproportionately affected by COVID-19,” the researchers said.
“These findings, including the potential impact of both sex and race on COVID-19–associated hospitalization rates, need to be confirmed with additional data,” according to the report.
Collecting racial/ethnic information is not always feasible on the front lines, and many areas still face shortages of ventilators and protective equipment, said Dr. Williams.
“I want to salute the providers on the front lines of this pandemic, many putting their own lives at risk, I want to acknowledge the good that they are doing,” Dr. Williams emphasized. He noted that all of us, himself included, may have conscious or unconscious stereotypes, but the key is to acknowledge the potential for these thoughts and feelings and continue to provide the best care.

Clyde W. Yancy, MD, of Northwestern University in Chicago, expressed similar concerns about disparity in COVID-19 cases in an editorial published on April 15 in JAMA.
“Researchers have emphasized older age, male sex, hypertension, diabetes, obesity, concomitant cardiovascular diseases (including coronary artery disease and heart failure), and myocardial injury as important risk factors associated with worse outcomes,” wrote Dr. Yancy. However, evidence also suggests that “persons who are African American or black are contracting SARS-CoV-2 at higher rates and are more likely to die,” he said.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
“Even though these data are preliminary and further study is warranted, the pattern is irrefutable: Underrepresented minorities are developing COVID-19 infection more frequently and dying disproportionately,” said Dr. Yancy.
Dr. Williams’ and Dr. Yancy’s comments were supported by an analysis of COVID-19 patient data from several areas of the country conducted by the Washington Post. In that analysis, data showed that several counties with a majority black population showed three times the rate of COVID-19 infections and approximately six times as many deaths compared with counties with a majority of white residents.
“The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event,” said Dr. Yancy. “Certainly, within the broad and powerful economic and legislative engines of the US, there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain,” he said.
Dr. Williams had no financial conflicts to disclose. Dr. Yancy had no financial conflicts to disclose.
SOURCES: Yancy CW. JAMA 2020 Apr 15. doi: 10.1001/jama.2020.6548Garg S et al. MMWR Morb Mortal Wkly Rep 2020 Apr 8;69:458-64.
Thebault R et al. The coronavirus is infecting and killing black Americans at an alarmingly high rate. Washington Post. 2020 Apr 7.
African Americans are overrepresented among patients who have died as a result of the COVID-19 pandemic, but the current crisis puts a spotlight on long-standing racial disparities in health care and health access in the United States, according to David R. Williams, PhD, a professor of public health at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Williams, a social scientist specializing in the link between race and health, is a professor of African and African American Studies and of Sociology at Harvard. He spoke on the topic of racial disparities amid the COVID-19 pandemic in a teleconference sponsored by the Robert Wood Johnson Foundation.
“Many Americans are shocked” by the higher mortality rates among African American COVID-19 patients, said Dr. Williams. However, data from decades of research show that “black people in America live sicker and shorter lives,” he said.
Keys to the increased mortality among African Americans include an increased prevalence of risk factors, increased risk for exposure to the virus because of socioeconomic factors, and less access to health care if they do become ill, he said.
Many minority individuals work outside the home in areas deemed essential during the pandemic, such as transit, delivery, maintenance, cleaning, and in businesses such as grocery stores, although in general “race continues to matter for health at every level of income and education,” Dr. Williams said.
In addition, social distance guidelines are not realistic for many people in high-density, low-income areas, who often live in shared, multigenerational housing, he said.
Data show that individuals with chronic conditions such as diabetes and cardiovascular disease are more likely to die as a result of COVID-19, and minority populations are more likely to develop these conditions at younger ages, Dr. Williams noted. Access to health care also plays a role. Many minority individuals of lower socioeconomic status are less likely to have health insurance, or if they do, may have Medicaid, which is not consistently accepted, he said. Also, some low-income neighborhoods lack convenient access to primary care and thus to screening services, he noted.
Dr. Williams said the COVID-19 pandemic could serve as an opportunity to examine and improve health care services for underserved communities. In the short term, “we need to collect data so we can see patterns” and address pressing needs, he said, but long-term goals should “prioritize investments that would create healthy homes and communities,” he emphasized.
A recent study from the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report cited COVID-NET (the COVID-19 Associated Hospitalization Surveillance Network) as showing that, in their catchment population, “approximately 59% of residents are white, 18% are black, and 14% are Hispanic; however, among 580 hospitalized COVID-19 patients with race/ethnicity data, approximately 45% were white, 33% were black, and 8% were Hispanic, suggesting that black populations might be disproportionately affected by COVID-19,” the researchers said.
“These findings, including the potential impact of both sex and race on COVID-19–associated hospitalization rates, need to be confirmed with additional data,” according to the report.
Collecting racial/ethnic information is not always feasible on the front lines, and many areas still face shortages of ventilators and protective equipment, said Dr. Williams.
“I want to salute the providers on the front lines of this pandemic, many putting their own lives at risk, I want to acknowledge the good that they are doing,” Dr. Williams emphasized. He noted that all of us, himself included, may have conscious or unconscious stereotypes, but the key is to acknowledge the potential for these thoughts and feelings and continue to provide the best care.
Clyde W. Yancy, MD, of Northwestern University in Chicago, expressed similar concerns about disparity in COVID-19 cases in an editorial published on April 15 in JAMA.
“Researchers have emphasized older age, male sex, hypertension, diabetes, obesity, concomitant cardiovascular diseases (including coronary artery disease and heart failure), and myocardial injury as important risk factors associated with worse outcomes,” wrote Dr. Yancy. However, evidence also suggests that “persons who are African American or black are contracting SARS-CoV-2 at higher rates and are more likely to die,” he said.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
“Even though these data are preliminary and further study is warranted, the pattern is irrefutable: Underrepresented minorities are developing COVID-19 infection more frequently and dying disproportionately,” said Dr. Yancy.
Dr. Williams’ and Dr. Yancy’s comments were supported by an analysis of COVID-19 patient data from several areas of the country conducted by the Washington Post. In that analysis, data showed that several counties with a majority black population showed three times the rate of COVID-19 infections and approximately six times as many deaths compared with counties with a majority of white residents.
“The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event,” said Dr. Yancy. “Certainly, within the broad and powerful economic and legislative engines of the US, there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain,” he said.
Dr. Williams had no financial conflicts to disclose. Dr. Yancy had no financial conflicts to disclose.
SOURCES: Yancy CW. JAMA 2020 Apr 15. doi: 10.1001/jama.2020.6548Garg S et al. MMWR Morb Mortal Wkly Rep 2020 Apr 8;69:458-64.
Thebault R et al. The coronavirus is infecting and killing black Americans at an alarmingly high rate. Washington Post. 2020 Apr 7.
African Americans are overrepresented among patients who have died as a result of the COVID-19 pandemic, but the current crisis puts a spotlight on long-standing racial disparities in health care and health access in the United States, according to David R. Williams, PhD, a professor of public health at the Harvard T.H. Chan School of Public Health in Boston.
Dr. Williams, a social scientist specializing in the link between race and health, is a professor of African and African American Studies and of Sociology at Harvard. He spoke on the topic of racial disparities amid the COVID-19 pandemic in a teleconference sponsored by the Robert Wood Johnson Foundation.
“Many Americans are shocked” by the higher mortality rates among African American COVID-19 patients, said Dr. Williams. However, data from decades of research show that “black people in America live sicker and shorter lives,” he said.
Keys to the increased mortality among African Americans include an increased prevalence of risk factors, increased risk for exposure to the virus because of socioeconomic factors, and less access to health care if they do become ill, he said.
Many minority individuals work outside the home in areas deemed essential during the pandemic, such as transit, delivery, maintenance, cleaning, and in businesses such as grocery stores, although in general “race continues to matter for health at every level of income and education,” Dr. Williams said.
In addition, social distance guidelines are not realistic for many people in high-density, low-income areas, who often live in shared, multigenerational housing, he said.
Data show that individuals with chronic conditions such as diabetes and cardiovascular disease are more likely to die as a result of COVID-19, and minority populations are more likely to develop these conditions at younger ages, Dr. Williams noted. Access to health care also plays a role. Many minority individuals of lower socioeconomic status are less likely to have health insurance, or if they do, may have Medicaid, which is not consistently accepted, he said. Also, some low-income neighborhoods lack convenient access to primary care and thus to screening services, he noted.
Dr. Williams said the COVID-19 pandemic could serve as an opportunity to examine and improve health care services for underserved communities. In the short term, “we need to collect data so we can see patterns” and address pressing needs, he said, but long-term goals should “prioritize investments that would create healthy homes and communities,” he emphasized.
A recent study from the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report cited COVID-NET (the COVID-19 Associated Hospitalization Surveillance Network) as showing that, in their catchment population, “approximately 59% of residents are white, 18% are black, and 14% are Hispanic; however, among 580 hospitalized COVID-19 patients with race/ethnicity data, approximately 45% were white, 33% were black, and 8% were Hispanic, suggesting that black populations might be disproportionately affected by COVID-19,” the researchers said.
“These findings, including the potential impact of both sex and race on COVID-19–associated hospitalization rates, need to be confirmed with additional data,” according to the report.
Collecting racial/ethnic information is not always feasible on the front lines, and many areas still face shortages of ventilators and protective equipment, said Dr. Williams.
“I want to salute the providers on the front lines of this pandemic, many putting their own lives at risk, I want to acknowledge the good that they are doing,” Dr. Williams emphasized. He noted that all of us, himself included, may have conscious or unconscious stereotypes, but the key is to acknowledge the potential for these thoughts and feelings and continue to provide the best care.
Clyde W. Yancy, MD, of Northwestern University in Chicago, expressed similar concerns about disparity in COVID-19 cases in an editorial published on April 15 in JAMA.
“Researchers have emphasized older age, male sex, hypertension, diabetes, obesity, concomitant cardiovascular diseases (including coronary artery disease and heart failure), and myocardial injury as important risk factors associated with worse outcomes,” wrote Dr. Yancy. However, evidence also suggests that “persons who are African American or black are contracting SARS-CoV-2 at higher rates and are more likely to die,” he said.
“Why is this uniquely important to me? I am an academic cardiologist; I study health care disparities; and I am a black man,” he wrote.
“Even though these data are preliminary and further study is warranted, the pattern is irrefutable: Underrepresented minorities are developing COVID-19 infection more frequently and dying disproportionately,” said Dr. Yancy.
Dr. Williams’ and Dr. Yancy’s comments were supported by an analysis of COVID-19 patient data from several areas of the country conducted by the Washington Post. In that analysis, data showed that several counties with a majority black population showed three times the rate of COVID-19 infections and approximately six times as many deaths compared with counties with a majority of white residents.
“The U.S. has needed a trigger to fully address health care disparities; COVID-19 may be that bellwether event,” said Dr. Yancy. “Certainly, within the broad and powerful economic and legislative engines of the US, there is room to definitively address a scourge even worse than COVID-19: health care disparities. It only takes will. It is time to end the refrain,” he said.
Dr. Williams had no financial conflicts to disclose. Dr. Yancy had no financial conflicts to disclose.
SOURCES: Yancy CW. JAMA 2020 Apr 15. doi: 10.1001/jama.2020.6548Garg S et al. MMWR Morb Mortal Wkly Rep 2020 Apr 8;69:458-64.
Thebault R et al. The coronavirus is infecting and killing black Americans at an alarmingly high rate. Washington Post. 2020 Apr 7.
FROM A TELECONFERENCE SPONSORED BY THE ROBERT WOOD JOHNSON FOUNDATION
Troponins touted as ‘ally’ in COVID-19 triage, but message is nuanced
, cardiologists in the United Kingdom advise in a recently published viewpoint.
The tests can be used to “inform the triage of patients to critical care, guide the use of supportive treatments, and facilitate targeted cardiac investigations in those most likely to benefit,” Nicholas Mills, MD, PhD, University of Edinburgh, United Kingdom, told theheart.org | Medscape Cardiology. He is senior author on the viewpoint published online April 6 in the journal Circulation.
Older adults and those with a history of underlying cardiovascular disease appear to be at greatest risk of dying from COVID-19. “From early reports it is clear that elevated cardiac troponin concentrations predict in-hospital mortality,” said Mills.
In a recent report on hospitalized patients with COVID-19 in Wuhan, China, for example, cardiac injury (hs-cTn above the 99th-percentile upper reference limit) was seen in 1 in 5 patients and was an independent predictor of dying in the hospital. Mortality was 10-fold higher in those with cardiac injury on presentation.
Elevated cardiac troponin in the setting of COVID-19, Mills said, “may reflect illness severity with myocardial injury arising due to myocardial oxygen supply–demand imbalance. Or it may be due to direct cardiac involvement through viral myocarditis or stress cardiomyopathy, or where the prothrombotic and proinflammatory state is precipitating acute coronary syndromes.”
In their viewpoint, the authors note that circulating cTn is a marker of myocardial injury, “including but not limited to myocardial infarction or myocarditis, and the clinical relevance of this distinction has never been so clear.”
Therefore, the consequence of not measuring cardiac troponin may be to “ignore the plethora of ischemic and nonischemic causes” of myocardial injury related to COVID-19. “Clinicians who have used troponin measurement as a binary test for myocardial infarction independent of clinical context and those who consider an elevated cardiac troponin concentration to be a mandate for invasive coronary angiography must recalibrate,” they write.
“Rather than encouraging avoidance of troponin testing, we must harness the unheralded engagement from the cardiovascular community due to COVID-19 to better understand the utility of this essential biomarker and to educate clinicians on its interpretation and implications for prognosis and clinical decision making.”
Based on “same logic” as recent ACC guidance
The viewpoint was to some extent a response to a recent informal guidance from the American College of Cardiology (ACC) that advised caution in use of troponin and natriuretic peptide tests in patients with COVID-19.
Even so, that ACC guidance and the new viewpoint in Circulation are based on the “same logic,” James Januzzi Jr, MD, Massachusetts General Hospital, Boston, told theheart.org | Medscape Cardiology. Both documents:
- Point out that troponins are frequently abnormal in patients with severe cases of COVID-19
- Caution that clinicians should not equate an abnormal hs-cTn with acute myocardial infarction
- Note that, in most cases, hs-cTn elevations are a result of noncoronary mechanisms
- Recognize the potential risk to caregivers and the continued unchecked spread of SARS-CoV-2 related to downstream testing that might not be needed
“The Circulation opinion piece states that clinicians often use troponin as a binary test for myocardial infarction and a mandate for downstream testing, suggesting clinicians will need to recalibrate that approach, something I agree with and which is the central message of the ACC position,” Januzzi said.
Probably the biggest difference between the two documents, he said, is in the Circulation authors’ apparent enthusiasm to use hs-cTn as a tool to judge disease severity in patients with COVID-19.
It’s been known for more than a decade that myocardial injury is “an important risk predictor” in critical illness, Januzzi explained. “So the link between cardiac injury and outcomes in critical illness is nothing new. The difference is the fact we are seeing so many patients with COVID-19 all at once, and the authors suggest that using troponin might help in triage decision making.”
“There may be [such] a role here, but the data have not been systematically collected, and whether troponin truly adds something beyond information already available at the bedside — for example, does it add anything not already obvious at the bedside? — has not yet been conclusively proven,” Januzzi cautioned.
“As well, there are no prospective data supporting troponin as a trigger for ICU triage or for deciding on specific treatments.”
Positive cTn status “common” in COVID-19 patients
In his experience, Barry Cohen, MD, Morristown Medical Center, New Jersey, told theheart.org | Medscape Cardiology, that positive cTn status is “common in COVID-19 patients and appears to have prognostic value, not only in type 1 MI due to atherothrombotic disease (related to a proinflammatory and prothrombotic state), but more frequently type 2 MI (supply–demand mismatch), viral myocarditis, coronary microvascular ischemia, stress cardiomyopathy or tachyarrhythmias.”
Moreover, Cohen said, hs-cTn “has identified patients at increased risk for ventilation support (invasive and noninvasive), acute respiratory distress syndrome, acute kidney injury, and mortality.”
Echoing both the ACC document and the Circulation report, Cohen also said hs-cTn measurements “appear to help risk stratify COVID-19 patients, but clearly do not mean that a troponin-positive patient needs to go to the cath lab and be treated as having acute coronary syndrome. Only a minority of these patients require this intervention.”
Mills discloses receiving honoraria from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. Januzzi has previously disclosed receiving personal fees from the American College of Cardiology, Pfizer, Merck, AbbVie, Amgen, Boehringer Ingelheim, and Takeda; grants and personal fees from Novartis, Roche, Abbott, and Janssen; and grants from Singulex and Prevencio. Cohen has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
, cardiologists in the United Kingdom advise in a recently published viewpoint.
The tests can be used to “inform the triage of patients to critical care, guide the use of supportive treatments, and facilitate targeted cardiac investigations in those most likely to benefit,” Nicholas Mills, MD, PhD, University of Edinburgh, United Kingdom, told theheart.org | Medscape Cardiology. He is senior author on the viewpoint published online April 6 in the journal Circulation.
Older adults and those with a history of underlying cardiovascular disease appear to be at greatest risk of dying from COVID-19. “From early reports it is clear that elevated cardiac troponin concentrations predict in-hospital mortality,” said Mills.
In a recent report on hospitalized patients with COVID-19 in Wuhan, China, for example, cardiac injury (hs-cTn above the 99th-percentile upper reference limit) was seen in 1 in 5 patients and was an independent predictor of dying in the hospital. Mortality was 10-fold higher in those with cardiac injury on presentation.
Elevated cardiac troponin in the setting of COVID-19, Mills said, “may reflect illness severity with myocardial injury arising due to myocardial oxygen supply–demand imbalance. Or it may be due to direct cardiac involvement through viral myocarditis or stress cardiomyopathy, or where the prothrombotic and proinflammatory state is precipitating acute coronary syndromes.”
In their viewpoint, the authors note that circulating cTn is a marker of myocardial injury, “including but not limited to myocardial infarction or myocarditis, and the clinical relevance of this distinction has never been so clear.”
Therefore, the consequence of not measuring cardiac troponin may be to “ignore the plethora of ischemic and nonischemic causes” of myocardial injury related to COVID-19. “Clinicians who have used troponin measurement as a binary test for myocardial infarction independent of clinical context and those who consider an elevated cardiac troponin concentration to be a mandate for invasive coronary angiography must recalibrate,” they write.
“Rather than encouraging avoidance of troponin testing, we must harness the unheralded engagement from the cardiovascular community due to COVID-19 to better understand the utility of this essential biomarker and to educate clinicians on its interpretation and implications for prognosis and clinical decision making.”
Based on “same logic” as recent ACC guidance
The viewpoint was to some extent a response to a recent informal guidance from the American College of Cardiology (ACC) that advised caution in use of troponin and natriuretic peptide tests in patients with COVID-19.
Even so, that ACC guidance and the new viewpoint in Circulation are based on the “same logic,” James Januzzi Jr, MD, Massachusetts General Hospital, Boston, told theheart.org | Medscape Cardiology. Both documents:
- Point out that troponins are frequently abnormal in patients with severe cases of COVID-19
- Caution that clinicians should not equate an abnormal hs-cTn with acute myocardial infarction
- Note that, in most cases, hs-cTn elevations are a result of noncoronary mechanisms
- Recognize the potential risk to caregivers and the continued unchecked spread of SARS-CoV-2 related to downstream testing that might not be needed
“The Circulation opinion piece states that clinicians often use troponin as a binary test for myocardial infarction and a mandate for downstream testing, suggesting clinicians will need to recalibrate that approach, something I agree with and which is the central message of the ACC position,” Januzzi said.
Probably the biggest difference between the two documents, he said, is in the Circulation authors’ apparent enthusiasm to use hs-cTn as a tool to judge disease severity in patients with COVID-19.
It’s been known for more than a decade that myocardial injury is “an important risk predictor” in critical illness, Januzzi explained. “So the link between cardiac injury and outcomes in critical illness is nothing new. The difference is the fact we are seeing so many patients with COVID-19 all at once, and the authors suggest that using troponin might help in triage decision making.”
“There may be [such] a role here, but the data have not been systematically collected, and whether troponin truly adds something beyond information already available at the bedside — for example, does it add anything not already obvious at the bedside? — has not yet been conclusively proven,” Januzzi cautioned.
“As well, there are no prospective data supporting troponin as a trigger for ICU triage or for deciding on specific treatments.”
Positive cTn status “common” in COVID-19 patients
In his experience, Barry Cohen, MD, Morristown Medical Center, New Jersey, told theheart.org | Medscape Cardiology, that positive cTn status is “common in COVID-19 patients and appears to have prognostic value, not only in type 1 MI due to atherothrombotic disease (related to a proinflammatory and prothrombotic state), but more frequently type 2 MI (supply–demand mismatch), viral myocarditis, coronary microvascular ischemia, stress cardiomyopathy or tachyarrhythmias.”
Moreover, Cohen said, hs-cTn “has identified patients at increased risk for ventilation support (invasive and noninvasive), acute respiratory distress syndrome, acute kidney injury, and mortality.”
Echoing both the ACC document and the Circulation report, Cohen also said hs-cTn measurements “appear to help risk stratify COVID-19 patients, but clearly do not mean that a troponin-positive patient needs to go to the cath lab and be treated as having acute coronary syndrome. Only a minority of these patients require this intervention.”
Mills discloses receiving honoraria from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. Januzzi has previously disclosed receiving personal fees from the American College of Cardiology, Pfizer, Merck, AbbVie, Amgen, Boehringer Ingelheim, and Takeda; grants and personal fees from Novartis, Roche, Abbott, and Janssen; and grants from Singulex and Prevencio. Cohen has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
, cardiologists in the United Kingdom advise in a recently published viewpoint.
The tests can be used to “inform the triage of patients to critical care, guide the use of supportive treatments, and facilitate targeted cardiac investigations in those most likely to benefit,” Nicholas Mills, MD, PhD, University of Edinburgh, United Kingdom, told theheart.org | Medscape Cardiology. He is senior author on the viewpoint published online April 6 in the journal Circulation.
Older adults and those with a history of underlying cardiovascular disease appear to be at greatest risk of dying from COVID-19. “From early reports it is clear that elevated cardiac troponin concentrations predict in-hospital mortality,” said Mills.
In a recent report on hospitalized patients with COVID-19 in Wuhan, China, for example, cardiac injury (hs-cTn above the 99th-percentile upper reference limit) was seen in 1 in 5 patients and was an independent predictor of dying in the hospital. Mortality was 10-fold higher in those with cardiac injury on presentation.
Elevated cardiac troponin in the setting of COVID-19, Mills said, “may reflect illness severity with myocardial injury arising due to myocardial oxygen supply–demand imbalance. Or it may be due to direct cardiac involvement through viral myocarditis or stress cardiomyopathy, or where the prothrombotic and proinflammatory state is precipitating acute coronary syndromes.”
In their viewpoint, the authors note that circulating cTn is a marker of myocardial injury, “including but not limited to myocardial infarction or myocarditis, and the clinical relevance of this distinction has never been so clear.”
Therefore, the consequence of not measuring cardiac troponin may be to “ignore the plethora of ischemic and nonischemic causes” of myocardial injury related to COVID-19. “Clinicians who have used troponin measurement as a binary test for myocardial infarction independent of clinical context and those who consider an elevated cardiac troponin concentration to be a mandate for invasive coronary angiography must recalibrate,” they write.
“Rather than encouraging avoidance of troponin testing, we must harness the unheralded engagement from the cardiovascular community due to COVID-19 to better understand the utility of this essential biomarker and to educate clinicians on its interpretation and implications for prognosis and clinical decision making.”
Based on “same logic” as recent ACC guidance
The viewpoint was to some extent a response to a recent informal guidance from the American College of Cardiology (ACC) that advised caution in use of troponin and natriuretic peptide tests in patients with COVID-19.
Even so, that ACC guidance and the new viewpoint in Circulation are based on the “same logic,” James Januzzi Jr, MD, Massachusetts General Hospital, Boston, told theheart.org | Medscape Cardiology. Both documents:
- Point out that troponins are frequently abnormal in patients with severe cases of COVID-19
- Caution that clinicians should not equate an abnormal hs-cTn with acute myocardial infarction
- Note that, in most cases, hs-cTn elevations are a result of noncoronary mechanisms
- Recognize the potential risk to caregivers and the continued unchecked spread of SARS-CoV-2 related to downstream testing that might not be needed
“The Circulation opinion piece states that clinicians often use troponin as a binary test for myocardial infarction and a mandate for downstream testing, suggesting clinicians will need to recalibrate that approach, something I agree with and which is the central message of the ACC position,” Januzzi said.
Probably the biggest difference between the two documents, he said, is in the Circulation authors’ apparent enthusiasm to use hs-cTn as a tool to judge disease severity in patients with COVID-19.
It’s been known for more than a decade that myocardial injury is “an important risk predictor” in critical illness, Januzzi explained. “So the link between cardiac injury and outcomes in critical illness is nothing new. The difference is the fact we are seeing so many patients with COVID-19 all at once, and the authors suggest that using troponin might help in triage decision making.”
“There may be [such] a role here, but the data have not been systematically collected, and whether troponin truly adds something beyond information already available at the bedside — for example, does it add anything not already obvious at the bedside? — has not yet been conclusively proven,” Januzzi cautioned.
“As well, there are no prospective data supporting troponin as a trigger for ICU triage or for deciding on specific treatments.”
Positive cTn status “common” in COVID-19 patients
In his experience, Barry Cohen, MD, Morristown Medical Center, New Jersey, told theheart.org | Medscape Cardiology, that positive cTn status is “common in COVID-19 patients and appears to have prognostic value, not only in type 1 MI due to atherothrombotic disease (related to a proinflammatory and prothrombotic state), but more frequently type 2 MI (supply–demand mismatch), viral myocarditis, coronary microvascular ischemia, stress cardiomyopathy or tachyarrhythmias.”
Moreover, Cohen said, hs-cTn “has identified patients at increased risk for ventilation support (invasive and noninvasive), acute respiratory distress syndrome, acute kidney injury, and mortality.”
Echoing both the ACC document and the Circulation report, Cohen also said hs-cTn measurements “appear to help risk stratify COVID-19 patients, but clearly do not mean that a troponin-positive patient needs to go to the cath lab and be treated as having acute coronary syndrome. Only a minority of these patients require this intervention.”
Mills discloses receiving honoraria from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. Januzzi has previously disclosed receiving personal fees from the American College of Cardiology, Pfizer, Merck, AbbVie, Amgen, Boehringer Ingelheim, and Takeda; grants and personal fees from Novartis, Roche, Abbott, and Janssen; and grants from Singulex and Prevencio. Cohen has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
TWILIGHT-COMPLEX: Tap ticagrelor monotherapy early after complex PCI
Patients who underwent complex PCI for acute coronary syndrome followed by 3 months of dual-antiplatelet therapy (DAPT) with ticagrelor plus aspirin fared significantly better by dropping aspirin at that point in favor of long-term ticagrelor monotherapy than with continued dual-antiplatelet therapy in the TWILIGHT-COMPLEX study.

The rate of clinically relevant bleeding was significantly lower at 12 months of follow-up in the ticagrelor monotherapy group than it was in patients randomized to continued DAPT. Moreover, this major benefit came at no cost in terms of ischemic events, which were actually numerically less frequent in the ticagrelor plus placebo group, George D. Dangas, MD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. ACC organizers chose to present parts of the meeting virtually after COVID-19 concerns caused them to cancel the meeting.
“We found that the aspirin just doesn’t add that much, even in complex patients – just bleeding complications, for the most part,” explained Dr. Dangas, professor of medicine and of surgery at the Icahn School of Medicine at Mount Sinai, New York.
The TWILIGHT-COMPLEX study was a secondary post hoc analysis of outcomes in 2,342 participants in the previously reported larger parent TWILIGHT randomized trial who underwent complex PCI. The main TWILIGHT trial included 7,119 patients in 11 countries who underwent PCI for acute coronary syndrome, successfully completed 3 months of DAPT with ticagrelor plus aspirin without incident, and were then randomized double blind to 12 months of ticagrelor plus placebo or to another 12 months of ticagrelor and aspirin.
In the overall TWILIGHT trial, ticagrelor alone resulted in a significantly lower clinically relevant bleeding rate than did long-term ticagrelor plus aspirin, with no increase in the risk of death, MI, or stroke (N Engl J Med 2019; 381:2032-42). But the results left many interventional cardiologists wondering if a ticagrelor monotherapy strategy was really applicable to their more challenging patients undergoing complex PCI given that the risk of ischemic events is known to climb with PCI complexity. The TWILIGHT-COMPLEX study was specifically designed to address that concern.
To be eligible for TWILIGHT-COMPLEX, patients had to meet one or more prespecified angiographic or procedural criteria for complex PCI, such as a total stent length in excess of 60 mm, three or more treated lesions, use of an atherectomy device, or PCI of a left main lesion, a chronic total occlusion, or a bifurcation lesion with two stents. These complex PCI patients accounted for one-third of the total study population in TWILIGHT; 36% of them met more than one criteria for complex PCI.
TWILIGHT-COMPLEX findings
In the 12 months after randomization, patients who received ticagrelor plus placebo had a 4.2% incidence of clinically significant Bleeding Academic Research Consortium (BARC) type 2, 3, or 5 bleeding, which was significantly lower than the 7.7% rate in the group on long-term DAPT and represented a 46% relative risk reduction. Severe or fatal bleeding – that is, BARC type 3 or 5 – occurred in 1.1% of those on ticagrelor monotherapy and 2.6% of the DAPT group, for a significant 59% relative risk reduction.
The composite ischemic endpoint comprising cardiovascular death, MI, or ischemic stroke occurred in 3.6% of the ticagrelor monotherapy group and 4.8% of patients on long-term DAPT, a trend that didn’t achieve statistical significance. The all-cause mortality rate was 0.9% in the ticagrelor monotherapy group and 1.5% with extended DAPT, again a nonsignificant difference. Similarly, the rate of definite or probable stent thrombosis was numerically lower with ticagrelor monotherapy, by a margin of 0.4% versus 0.8%, a nonsignificant difference.
The results were consistent regardless of which specific criteria for complex PCI a patient had or how many of them.
Results are ‘reassuring’
At a press conference where Dr. Dangas presented the TWILIGHT-COMPLEX results, discussant Claire S. Duvernoy, MD, said she was “very impressed” with just how complex the PCIs were in the study participants.
“Really, these are the patients that in my own practice we’ve always been the most cautious about, the most worried about thrombotic risk, and the ones where we get down on our house staff when they drop an antiplatelet agent. So this study is very reassuring,” said Dr. Duvernoy, professor of medicine at the University of Michigan, Ann Arbor.
She identified two key differences between TWILIGHT-COMPLEX and earlier studies that showed a benefit for extended DAPT in higher-risk patients. In the earlier studies, it was the P2Y12 inhibitor that was dropped; TWILIGHT was the first major randomized trial to discontinue the aspirin instead. And patients in the TWILIGHT study received second-generation drug-eluting stents.
“That makes a huge difference,” Dr. Duvernoy said. “We have stents now that are much safer than the old ones were, and that’s what allows us to gain this incredible benefit of reduced bleeding.”
Dr. Dangas cautioned that since this was a secondary post hoc analysis, the TWILIGHT-COMPLEX study must be viewed as hypothesis-generating.
The TWILIGHT trial was funded by AstraZeneca. Dr. Dangas reported receiving institutional research grants from that company as well as Bayer and Daichi-Sankyo. He also served as a paid consultant to Abbott Vascular, Boston Scientific, and Biosensors.
Simultaneous with his presentation at ACC 2020, the TWILIGHT-COMPLEX results were published online (J Am Coll Cardiol. 2020 Mar 13. doi: 10.1016/j.jacc.2020.03.011).
SOURCE: Dangas GD. ACC 20, Abstract 410-09.
Patients who underwent complex PCI for acute coronary syndrome followed by 3 months of dual-antiplatelet therapy (DAPT) with ticagrelor plus aspirin fared significantly better by dropping aspirin at that point in favor of long-term ticagrelor monotherapy than with continued dual-antiplatelet therapy in the TWILIGHT-COMPLEX study.
The rate of clinically relevant bleeding was significantly lower at 12 months of follow-up in the ticagrelor monotherapy group than it was in patients randomized to continued DAPT. Moreover, this major benefit came at no cost in terms of ischemic events, which were actually numerically less frequent in the ticagrelor plus placebo group, George D. Dangas, MD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. ACC organizers chose to present parts of the meeting virtually after COVID-19 concerns caused them to cancel the meeting.
“We found that the aspirin just doesn’t add that much, even in complex patients – just bleeding complications, for the most part,” explained Dr. Dangas, professor of medicine and of surgery at the Icahn School of Medicine at Mount Sinai, New York.
The TWILIGHT-COMPLEX study was a secondary post hoc analysis of outcomes in 2,342 participants in the previously reported larger parent TWILIGHT randomized trial who underwent complex PCI. The main TWILIGHT trial included 7,119 patients in 11 countries who underwent PCI for acute coronary syndrome, successfully completed 3 months of DAPT with ticagrelor plus aspirin without incident, and were then randomized double blind to 12 months of ticagrelor plus placebo or to another 12 months of ticagrelor and aspirin.
In the overall TWILIGHT trial, ticagrelor alone resulted in a significantly lower clinically relevant bleeding rate than did long-term ticagrelor plus aspirin, with no increase in the risk of death, MI, or stroke (N Engl J Med 2019; 381:2032-42). But the results left many interventional cardiologists wondering if a ticagrelor monotherapy strategy was really applicable to their more challenging patients undergoing complex PCI given that the risk of ischemic events is known to climb with PCI complexity. The TWILIGHT-COMPLEX study was specifically designed to address that concern.
To be eligible for TWILIGHT-COMPLEX, patients had to meet one or more prespecified angiographic or procedural criteria for complex PCI, such as a total stent length in excess of 60 mm, three or more treated lesions, use of an atherectomy device, or PCI of a left main lesion, a chronic total occlusion, or a bifurcation lesion with two stents. These complex PCI patients accounted for one-third of the total study population in TWILIGHT; 36% of them met more than one criteria for complex PCI.
TWILIGHT-COMPLEX findings
In the 12 months after randomization, patients who received ticagrelor plus placebo had a 4.2% incidence of clinically significant Bleeding Academic Research Consortium (BARC) type 2, 3, or 5 bleeding, which was significantly lower than the 7.7% rate in the group on long-term DAPT and represented a 46% relative risk reduction. Severe or fatal bleeding – that is, BARC type 3 or 5 – occurred in 1.1% of those on ticagrelor monotherapy and 2.6% of the DAPT group, for a significant 59% relative risk reduction.
The composite ischemic endpoint comprising cardiovascular death, MI, or ischemic stroke occurred in 3.6% of the ticagrelor monotherapy group and 4.8% of patients on long-term DAPT, a trend that didn’t achieve statistical significance. The all-cause mortality rate was 0.9% in the ticagrelor monotherapy group and 1.5% with extended DAPT, again a nonsignificant difference. Similarly, the rate of definite or probable stent thrombosis was numerically lower with ticagrelor monotherapy, by a margin of 0.4% versus 0.8%, a nonsignificant difference.
The results were consistent regardless of which specific criteria for complex PCI a patient had or how many of them.
Results are ‘reassuring’
At a press conference where Dr. Dangas presented the TWILIGHT-COMPLEX results, discussant Claire S. Duvernoy, MD, said she was “very impressed” with just how complex the PCIs were in the study participants.
“Really, these are the patients that in my own practice we’ve always been the most cautious about, the most worried about thrombotic risk, and the ones where we get down on our house staff when they drop an antiplatelet agent. So this study is very reassuring,” said Dr. Duvernoy, professor of medicine at the University of Michigan, Ann Arbor.
She identified two key differences between TWILIGHT-COMPLEX and earlier studies that showed a benefit for extended DAPT in higher-risk patients. In the earlier studies, it was the P2Y12 inhibitor that was dropped; TWILIGHT was the first major randomized trial to discontinue the aspirin instead. And patients in the TWILIGHT study received second-generation drug-eluting stents.
“That makes a huge difference,” Dr. Duvernoy said. “We have stents now that are much safer than the old ones were, and that’s what allows us to gain this incredible benefit of reduced bleeding.”
Dr. Dangas cautioned that since this was a secondary post hoc analysis, the TWILIGHT-COMPLEX study must be viewed as hypothesis-generating.
The TWILIGHT trial was funded by AstraZeneca. Dr. Dangas reported receiving institutional research grants from that company as well as Bayer and Daichi-Sankyo. He also served as a paid consultant to Abbott Vascular, Boston Scientific, and Biosensors.
Simultaneous with his presentation at ACC 2020, the TWILIGHT-COMPLEX results were published online (J Am Coll Cardiol. 2020 Mar 13. doi: 10.1016/j.jacc.2020.03.011).
SOURCE: Dangas GD. ACC 20, Abstract 410-09.
Patients who underwent complex PCI for acute coronary syndrome followed by 3 months of dual-antiplatelet therapy (DAPT) with ticagrelor plus aspirin fared significantly better by dropping aspirin at that point in favor of long-term ticagrelor monotherapy than with continued dual-antiplatelet therapy in the TWILIGHT-COMPLEX study.
The rate of clinically relevant bleeding was significantly lower at 12 months of follow-up in the ticagrelor monotherapy group than it was in patients randomized to continued DAPT. Moreover, this major benefit came at no cost in terms of ischemic events, which were actually numerically less frequent in the ticagrelor plus placebo group, George D. Dangas, MD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. ACC organizers chose to present parts of the meeting virtually after COVID-19 concerns caused them to cancel the meeting.
“We found that the aspirin just doesn’t add that much, even in complex patients – just bleeding complications, for the most part,” explained Dr. Dangas, professor of medicine and of surgery at the Icahn School of Medicine at Mount Sinai, New York.
The TWILIGHT-COMPLEX study was a secondary post hoc analysis of outcomes in 2,342 participants in the previously reported larger parent TWILIGHT randomized trial who underwent complex PCI. The main TWILIGHT trial included 7,119 patients in 11 countries who underwent PCI for acute coronary syndrome, successfully completed 3 months of DAPT with ticagrelor plus aspirin without incident, and were then randomized double blind to 12 months of ticagrelor plus placebo or to another 12 months of ticagrelor and aspirin.
In the overall TWILIGHT trial, ticagrelor alone resulted in a significantly lower clinically relevant bleeding rate than did long-term ticagrelor plus aspirin, with no increase in the risk of death, MI, or stroke (N Engl J Med 2019; 381:2032-42). But the results left many interventional cardiologists wondering if a ticagrelor monotherapy strategy was really applicable to their more challenging patients undergoing complex PCI given that the risk of ischemic events is known to climb with PCI complexity. The TWILIGHT-COMPLEX study was specifically designed to address that concern.
To be eligible for TWILIGHT-COMPLEX, patients had to meet one or more prespecified angiographic or procedural criteria for complex PCI, such as a total stent length in excess of 60 mm, three or more treated lesions, use of an atherectomy device, or PCI of a left main lesion, a chronic total occlusion, or a bifurcation lesion with two stents. These complex PCI patients accounted for one-third of the total study population in TWILIGHT; 36% of them met more than one criteria for complex PCI.
TWILIGHT-COMPLEX findings
In the 12 months after randomization, patients who received ticagrelor plus placebo had a 4.2% incidence of clinically significant Bleeding Academic Research Consortium (BARC) type 2, 3, or 5 bleeding, which was significantly lower than the 7.7% rate in the group on long-term DAPT and represented a 46% relative risk reduction. Severe or fatal bleeding – that is, BARC type 3 or 5 – occurred in 1.1% of those on ticagrelor monotherapy and 2.6% of the DAPT group, for a significant 59% relative risk reduction.
The composite ischemic endpoint comprising cardiovascular death, MI, or ischemic stroke occurred in 3.6% of the ticagrelor monotherapy group and 4.8% of patients on long-term DAPT, a trend that didn’t achieve statistical significance. The all-cause mortality rate was 0.9% in the ticagrelor monotherapy group and 1.5% with extended DAPT, again a nonsignificant difference. Similarly, the rate of definite or probable stent thrombosis was numerically lower with ticagrelor monotherapy, by a margin of 0.4% versus 0.8%, a nonsignificant difference.
The results were consistent regardless of which specific criteria for complex PCI a patient had or how many of them.
Results are ‘reassuring’
At a press conference where Dr. Dangas presented the TWILIGHT-COMPLEX results, discussant Claire S. Duvernoy, MD, said she was “very impressed” with just how complex the PCIs were in the study participants.
“Really, these are the patients that in my own practice we’ve always been the most cautious about, the most worried about thrombotic risk, and the ones where we get down on our house staff when they drop an antiplatelet agent. So this study is very reassuring,” said Dr. Duvernoy, professor of medicine at the University of Michigan, Ann Arbor.
She identified two key differences between TWILIGHT-COMPLEX and earlier studies that showed a benefit for extended DAPT in higher-risk patients. In the earlier studies, it was the P2Y12 inhibitor that was dropped; TWILIGHT was the first major randomized trial to discontinue the aspirin instead. And patients in the TWILIGHT study received second-generation drug-eluting stents.
“That makes a huge difference,” Dr. Duvernoy said. “We have stents now that are much safer than the old ones were, and that’s what allows us to gain this incredible benefit of reduced bleeding.”
Dr. Dangas cautioned that since this was a secondary post hoc analysis, the TWILIGHT-COMPLEX study must be viewed as hypothesis-generating.
The TWILIGHT trial was funded by AstraZeneca. Dr. Dangas reported receiving institutional research grants from that company as well as Bayer and Daichi-Sankyo. He also served as a paid consultant to Abbott Vascular, Boston Scientific, and Biosensors.
Simultaneous with his presentation at ACC 2020, the TWILIGHT-COMPLEX results were published online (J Am Coll Cardiol. 2020 Mar 13. doi: 10.1016/j.jacc.2020.03.011).
SOURCE: Dangas GD. ACC 20, Abstract 410-09.
FROM ACC 2020

Hypertension goes unmedicated in 40% of adults
Roughly 30% of adults in the United States had hypertension in 2017, and just under 60% of those adults reported using antihypertensive medication, according to the Centers for Disease Control and Prevention.
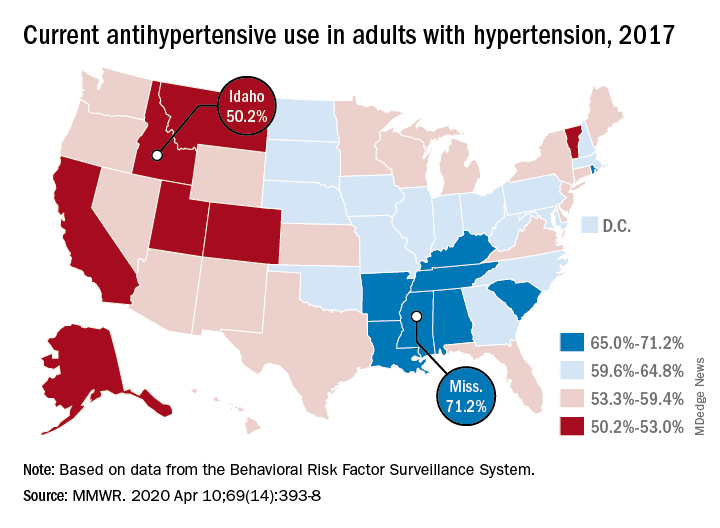
There is, however, quite a bit of variation from those age-standardized national figures when state-level data are considered.
In Alabama and West Virginia, the prevalence of hypertension in 2017 was 38.6%, the highest in the country, with Arkansas (38.5%) and Mississippi (38.2%) not far behind. Meanwhile, Minnesota came in with a lowest-in-the-nation rate of 24.3%, which was nearly matched by Colorado at 24.8%, Claudine M. Samanic, PhD, and associates wrote in the MMWR.
There was also a considerable gap between the states in hypertensive adults’ self-reported use of antihypertensive drugs, which was generally higher in the states with a greater prevalence of disease, they noted.
Adults in Mississippi were the most likely (71.2%) to be taking medication, along with those in Alabama (70.5%) and Arkansas (69.3%). Idaho occupied the other end of the scale with a rate of 50.2%, while Montana and Vermont were slightly better at 51.7%, based on survey data from the Behavioral Risk Factor Surveillance System.
“Prevalence of antihypertensive medication use was higher in older age groups, highest among blacks, and higher among women [64.0%] than men [56.7%]. This overall gender difference has been reported previously, but the reasons are unclear,” wrote Dr. Samanic and associates at the CDC’s National Center for Chronic Disease Prevention and Health Promotion.
The BRFSS data for 2017 are based on based on interviews with 450,016 adults. Respondents were asked, “Have you ever been told by a doctor, nurse, or other health professional that you have high blood pressure?” and were considered to have hypertension if they answered yes.
SOURCE: Samanic CM et al. MMWR. 2020 Apr 10;69(14):393-8.
Roughly 30% of adults in the United States had hypertension in 2017, and just under 60% of those adults reported using antihypertensive medication, according to the Centers for Disease Control and Prevention.
There is, however, quite a bit of variation from those age-standardized national figures when state-level data are considered.
In Alabama and West Virginia, the prevalence of hypertension in 2017 was 38.6%, the highest in the country, with Arkansas (38.5%) and Mississippi (38.2%) not far behind. Meanwhile, Minnesota came in with a lowest-in-the-nation rate of 24.3%, which was nearly matched by Colorado at 24.8%, Claudine M. Samanic, PhD, and associates wrote in the MMWR.
There was also a considerable gap between the states in hypertensive adults’ self-reported use of antihypertensive drugs, which was generally higher in the states with a greater prevalence of disease, they noted.
Adults in Mississippi were the most likely (71.2%) to be taking medication, along with those in Alabama (70.5%) and Arkansas (69.3%). Idaho occupied the other end of the scale with a rate of 50.2%, while Montana and Vermont were slightly better at 51.7%, based on survey data from the Behavioral Risk Factor Surveillance System.
“Prevalence of antihypertensive medication use was higher in older age groups, highest among blacks, and higher among women [64.0%] than men [56.7%]. This overall gender difference has been reported previously, but the reasons are unclear,” wrote Dr. Samanic and associates at the CDC’s National Center for Chronic Disease Prevention and Health Promotion.
The BRFSS data for 2017 are based on based on interviews with 450,016 adults. Respondents were asked, “Have you ever been told by a doctor, nurse, or other health professional that you have high blood pressure?” and were considered to have hypertension if they answered yes.
SOURCE: Samanic CM et al. MMWR. 2020 Apr 10;69(14):393-8.
Roughly 30% of adults in the United States had hypertension in 2017, and just under 60% of those adults reported using antihypertensive medication, according to the Centers for Disease Control and Prevention.
There is, however, quite a bit of variation from those age-standardized national figures when state-level data are considered.
In Alabama and West Virginia, the prevalence of hypertension in 2017 was 38.6%, the highest in the country, with Arkansas (38.5%) and Mississippi (38.2%) not far behind. Meanwhile, Minnesota came in with a lowest-in-the-nation rate of 24.3%, which was nearly matched by Colorado at 24.8%, Claudine M. Samanic, PhD, and associates wrote in the MMWR.
There was also a considerable gap between the states in hypertensive adults’ self-reported use of antihypertensive drugs, which was generally higher in the states with a greater prevalence of disease, they noted.
Adults in Mississippi were the most likely (71.2%) to be taking medication, along with those in Alabama (70.5%) and Arkansas (69.3%). Idaho occupied the other end of the scale with a rate of 50.2%, while Montana and Vermont were slightly better at 51.7%, based on survey data from the Behavioral Risk Factor Surveillance System.
“Prevalence of antihypertensive medication use was higher in older age groups, highest among blacks, and higher among women [64.0%] than men [56.7%]. This overall gender difference has been reported previously, but the reasons are unclear,” wrote Dr. Samanic and associates at the CDC’s National Center for Chronic Disease Prevention and Health Promotion.
The BRFSS data for 2017 are based on based on interviews with 450,016 adults. Respondents were asked, “Have you ever been told by a doctor, nurse, or other health professional that you have high blood pressure?” and were considered to have hypertension if they answered yes.
SOURCE: Samanic CM et al. MMWR. 2020 Apr 10;69(14):393-8.
FROM THE MMWR
AHA updates management when CAD and T2DM coincide
Patients with stable coronary artery disease and type 2 diabetes mellitus could benefit from a “plethora of newly available risk-reduction strategies,” but their “adoption into clinical practice has been slow” and inconsistent, prompting an expert panel organized by the American Heart Association to collate the range of treatment recommendations now applicable to this patient population in a scientific statement released on April 13.

“There are a number of things to consider when treating patients with stable coronary artery disease [CAD] and type 2 diabetes mellitus [T2DM], with new medications and trials and data emerging. It’s difficult to keep up with all of the complexities,” which was why the Association’s Councils on Lifestyle and Cardiometabolic Health and on Clinical Cardiology put together a writing group to summarize and prioritize the range of lifestyle, medical, and interventional options that now require consideration and potential use on patients managed in routine practice, explained Suzanne V. Arnold, MD, chair of the writing group, in an interview.
The new scientific statement (Circulation. 2020 Apr 13; doi: 10.1161/CIR.0000000000000766), aimed primarily at cardiologists but also intended to inform primary care physicians, endocrinologists, and all other clinicians who deal with these patients, pulls together “everything someone needs to think about if they care for patients with CAD and T2DM,” said Deepak L. Bhatt, MD, professor of medicine at Harvard Medical School in Boston and vice chair of the statement-writing panel in an interview. “There is a lot to know,” he added.
The statement covers antithrombotic therapies; blood pressure control, with a discussion of both the appropriate pressure goal and the best drug types used to reach it; lipid management; glycemic control; lifestyle modification; weight management, including the role of bariatric surgery; and approaches to managing stable angina, both medically and with revascularization.

“The goal was to give clinicians a good sense of what new treatments they should consider” for these patients, said Dr. Bhatt, who is also director of interventional cardiovascular programs at Brigham and Women’s Hospital, also in Boston. Because of the tight associations between T2DM and cardiovascular disease in general including CAD, “cardiologists are increasingly involved in managing patients with T2DM,” he noted. The statement gives a comprehensive overview and critical assessment of the management of these patients as of the end of 2019 as a consensus from a panel of 11 experts .
The statement also stressed that “substantial portions of patients with T2DM and CAD, including those after an acute coronary syndrome, do not receive therapies with proven cardiovascular benefit, such as high-intensity statins, dual-antiplatelet therapy, angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers, and glucose-lowering agents with proven cardiovascular benefits.
“These gaps in care highlight a critical opportunity for cardiovascular specialists to assume a more active role in the collaborative care of patients with T2DM and CAD,” the statement said. This includes “encouraging cardiologists to become more active in the selection of glucose-lowering medications” for these patients because it could “really move the needle,” said Dr. Arnold, a cardiologist with Saint Luke’s Health System in Kansas City, Mo. She was referring specifically to broader reliance on both the SGTL2 (sodium-glucose cotransporter 2) inhibitors and the GLP-1 (glucagonlike peptide-1) receptor agonists as top choices for controlling hyperglycemia. Based on recent evidence drugs in these two classes “could be considered first line for patients with T2DM and CAD, and would likely be preferred over metformin,” Dr. Arnold said in an interview. Although the statement identified the SGLT2 inhibitors as “the first drug class [for glycemic control] to show clear benefits on cardiovascular outcomes,” it does not explicitly label the class first-line and it also skirts that designation for the GLP-1 receptor agonist class, while noting that metformin “remains the drug most frequently recommended as first-line therapy in treatment guidelines.”
“I wouldn’t disagree with someone who said that SGLT2 inhibitors and GLP-1 receptor agonists are first line,” but prescribing patterns also depend on familiarity, cost, and access, noted Dr. Bhatt, which can all be issues with agents from these classes compared with metformin, a widely available generic with decades of use. “Metformin is safe and cheap, so we did not want to discount it,” said Dr. Arnold. Dr. Bhatt recently coauthored an editorial that gave an enthusiastic endorsement to using SGLT2 inhibitors in patients with diabetes (Cell Metab. 2019 Nov 5;30[5]:47-9).
Another notable feature of the statement is the potential it assigns to bariatric surgery as a management tool with documented safety and efficacy for improving cardiovascular risk factors. However, the statement also notes that randomized trials “have thus far been inadequately powered to assess cardiovascular events and mortality, although observational studies have consistently shown cardiovascular risk reduction with such procedures.” The statement continues that despite potential cardiovascular benefits “bariatric surgery remains underused among eligible patients,” and said that surgery performed as Roux-en-Y bypass or sleeve gastrectomy “may be another effective tool for cardiovascular risk reduction in the subset of patients with obesity,” particularly patients with a body mass index of at least 35 kg/m2.
“While the percentage of patients who are optimal for bariatric surgery is not known, the most recent NHANES [National Health and Nutrition Examination Study] study showed that less than 0.5% of eligible patients underwent bariatric surgery,” Dr. Arnold noted. Bariatric surgery is “certainly not a recommendation for everyone, or even a majority of patients, but bariatric surgery should be on our radar,” for patients with CAD and T2DM, she said.
Right now, “few cardiologists think about bariatric surgery,” as a treatment option, but study results have shown that “in carefully selected patients treated by skilled surgeons at high-volume centers, patients will do better with bariatric surgery than with best medical therapy for improvements in multiple risk factors, including glycemic control,” Dr. Bhatt said in the interview. “It’s not first-line treatment, but it’s an option to consider,” he added, while also noting that bariatric surgery is most beneficial to patients relatively early in the course of T2DM, when its been in place for just a few years rather than a couple of decades.
The statement also notably included a “first-line” call out for icosapent ethyl (Vascepa), a novel agent approved in December 2019 for routine use in U.S. patients, including those with CAD and T2DM as long as their blood triglyceride level was at least 150 mg/dL. Dr. Bhatt, who led the REDUCE-IT study that was pivotal for proving the safety and efficacy of icosapent ethyl (N Engl J Med. 2019 Jan 3;380[1]:11-22), estimated that anywhere from 15% to as many as half the patients with CAD and T2DM might have a triglyceride level that would allow them to receive icosapent ethyl. One population-based study in Canada of nearly 200,000 people with atherosclerotic cardiovascular disease found a 25% prevalence of the triglyceride level needed to qualify to receive icosapent ethyl under current labeling, he noted (Eur Heart J. 2020 Jan 1;41[1]:86-94). However, the FDA label does not specify that triglycerides be measured when fasting, and a nonfasting level of about 150 mg/dL will likely appear for patients with fasting levels that fall as low as about 100 mg/dL, Dr. Bhatt said. He hoped that future studies will assess the efficacy of icosapent ethyl in patients with even lower triglyceride levels.
Other sections of the statement also recommend that clinicians: Target long-term dual-antiplatelet therapy to CAD and T2DM patients with additional high-risk markers such as prior MI, younger age, and tobacco use; prescribe a low-dose oral anticoagulant along with an antiplatelet drug such as aspirin for secondary-prevention patients; promote a blood pressure target of less than 140/90 mm Hg for all CAD and T2DM patients and apply a goal of less than 130/80 mm Hg in higher-risk patients such as blacks, Asians, and those with cerebrovascular disease; and reassure patients that “despite a modest increase in blood sugars, the risk-benefit ratio is clearly in favor of administering statins to people with T2DM and CAD.”
Dr. Arnold had no disclosures. Dr. Bhatt has been an adviser to Cardax, Cereno Scientific, Medscape Cardiology, PhaseBio; PLx Pharma, and Regado Biosciences, and he has received research funding from numerous companies including Amarin, the company that markets icosapent ethyl.
Patients with stable coronary artery disease and type 2 diabetes mellitus could benefit from a “plethora of newly available risk-reduction strategies,” but their “adoption into clinical practice has been slow” and inconsistent, prompting an expert panel organized by the American Heart Association to collate the range of treatment recommendations now applicable to this patient population in a scientific statement released on April 13.
“There are a number of things to consider when treating patients with stable coronary artery disease [CAD] and type 2 diabetes mellitus [T2DM], with new medications and trials and data emerging. It’s difficult to keep up with all of the complexities,” which was why the Association’s Councils on Lifestyle and Cardiometabolic Health and on Clinical Cardiology put together a writing group to summarize and prioritize the range of lifestyle, medical, and interventional options that now require consideration and potential use on patients managed in routine practice, explained Suzanne V. Arnold, MD, chair of the writing group, in an interview.
The new scientific statement (Circulation. 2020 Apr 13; doi: 10.1161/CIR.0000000000000766), aimed primarily at cardiologists but also intended to inform primary care physicians, endocrinologists, and all other clinicians who deal with these patients, pulls together “everything someone needs to think about if they care for patients with CAD and T2DM,” said Deepak L. Bhatt, MD, professor of medicine at Harvard Medical School in Boston and vice chair of the statement-writing panel in an interview. “There is a lot to know,” he added.
The statement covers antithrombotic therapies; blood pressure control, with a discussion of both the appropriate pressure goal and the best drug types used to reach it; lipid management; glycemic control; lifestyle modification; weight management, including the role of bariatric surgery; and approaches to managing stable angina, both medically and with revascularization.
“The goal was to give clinicians a good sense of what new treatments they should consider” for these patients, said Dr. Bhatt, who is also director of interventional cardiovascular programs at Brigham and Women’s Hospital, also in Boston. Because of the tight associations between T2DM and cardiovascular disease in general including CAD, “cardiologists are increasingly involved in managing patients with T2DM,” he noted. The statement gives a comprehensive overview and critical assessment of the management of these patients as of the end of 2019 as a consensus from a panel of 11 experts .
The statement also stressed that “substantial portions of patients with T2DM and CAD, including those after an acute coronary syndrome, do not receive therapies with proven cardiovascular benefit, such as high-intensity statins, dual-antiplatelet therapy, angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers, and glucose-lowering agents with proven cardiovascular benefits.
“These gaps in care highlight a critical opportunity for cardiovascular specialists to assume a more active role in the collaborative care of patients with T2DM and CAD,” the statement said. This includes “encouraging cardiologists to become more active in the selection of glucose-lowering medications” for these patients because it could “really move the needle,” said Dr. Arnold, a cardiologist with Saint Luke’s Health System in Kansas City, Mo. She was referring specifically to broader reliance on both the SGTL2 (sodium-glucose cotransporter 2) inhibitors and the GLP-1 (glucagonlike peptide-1) receptor agonists as top choices for controlling hyperglycemia. Based on recent evidence drugs in these two classes “could be considered first line for patients with T2DM and CAD, and would likely be preferred over metformin,” Dr. Arnold said in an interview. Although the statement identified the SGLT2 inhibitors as “the first drug class [for glycemic control] to show clear benefits on cardiovascular outcomes,” it does not explicitly label the class first-line and it also skirts that designation for the GLP-1 receptor agonist class, while noting that metformin “remains the drug most frequently recommended as first-line therapy in treatment guidelines.”
“I wouldn’t disagree with someone who said that SGLT2 inhibitors and GLP-1 receptor agonists are first line,” but prescribing patterns also depend on familiarity, cost, and access, noted Dr. Bhatt, which can all be issues with agents from these classes compared with metformin, a widely available generic with decades of use. “Metformin is safe and cheap, so we did not want to discount it,” said Dr. Arnold. Dr. Bhatt recently coauthored an editorial that gave an enthusiastic endorsement to using SGLT2 inhibitors in patients with diabetes (Cell Metab. 2019 Nov 5;30[5]:47-9).
Another notable feature of the statement is the potential it assigns to bariatric surgery as a management tool with documented safety and efficacy for improving cardiovascular risk factors. However, the statement also notes that randomized trials “have thus far been inadequately powered to assess cardiovascular events and mortality, although observational studies have consistently shown cardiovascular risk reduction with such procedures.” The statement continues that despite potential cardiovascular benefits “bariatric surgery remains underused among eligible patients,” and said that surgery performed as Roux-en-Y bypass or sleeve gastrectomy “may be another effective tool for cardiovascular risk reduction in the subset of patients with obesity,” particularly patients with a body mass index of at least 35 kg/m2.
“While the percentage of patients who are optimal for bariatric surgery is not known, the most recent NHANES [National Health and Nutrition Examination Study] study showed that less than 0.5% of eligible patients underwent bariatric surgery,” Dr. Arnold noted. Bariatric surgery is “certainly not a recommendation for everyone, or even a majority of patients, but bariatric surgery should be on our radar,” for patients with CAD and T2DM, she said.
Right now, “few cardiologists think about bariatric surgery,” as a treatment option, but study results have shown that “in carefully selected patients treated by skilled surgeons at high-volume centers, patients will do better with bariatric surgery than with best medical therapy for improvements in multiple risk factors, including glycemic control,” Dr. Bhatt said in the interview. “It’s not first-line treatment, but it’s an option to consider,” he added, while also noting that bariatric surgery is most beneficial to patients relatively early in the course of T2DM, when its been in place for just a few years rather than a couple of decades.
The statement also notably included a “first-line” call out for icosapent ethyl (Vascepa), a novel agent approved in December 2019 for routine use in U.S. patients, including those with CAD and T2DM as long as their blood triglyceride level was at least 150 mg/dL. Dr. Bhatt, who led the REDUCE-IT study that was pivotal for proving the safety and efficacy of icosapent ethyl (N Engl J Med. 2019 Jan 3;380[1]:11-22), estimated that anywhere from 15% to as many as half the patients with CAD and T2DM might have a triglyceride level that would allow them to receive icosapent ethyl. One population-based study in Canada of nearly 200,000 people with atherosclerotic cardiovascular disease found a 25% prevalence of the triglyceride level needed to qualify to receive icosapent ethyl under current labeling, he noted (Eur Heart J. 2020 Jan 1;41[1]:86-94). However, the FDA label does not specify that triglycerides be measured when fasting, and a nonfasting level of about 150 mg/dL will likely appear for patients with fasting levels that fall as low as about 100 mg/dL, Dr. Bhatt said. He hoped that future studies will assess the efficacy of icosapent ethyl in patients with even lower triglyceride levels.
Other sections of the statement also recommend that clinicians: Target long-term dual-antiplatelet therapy to CAD and T2DM patients with additional high-risk markers such as prior MI, younger age, and tobacco use; prescribe a low-dose oral anticoagulant along with an antiplatelet drug such as aspirin for secondary-prevention patients; promote a blood pressure target of less than 140/90 mm Hg for all CAD and T2DM patients and apply a goal of less than 130/80 mm Hg in higher-risk patients such as blacks, Asians, and those with cerebrovascular disease; and reassure patients that “despite a modest increase in blood sugars, the risk-benefit ratio is clearly in favor of administering statins to people with T2DM and CAD.”
Dr. Arnold had no disclosures. Dr. Bhatt has been an adviser to Cardax, Cereno Scientific, Medscape Cardiology, PhaseBio; PLx Pharma, and Regado Biosciences, and he has received research funding from numerous companies including Amarin, the company that markets icosapent ethyl.
Patients with stable coronary artery disease and type 2 diabetes mellitus could benefit from a “plethora of newly available risk-reduction strategies,” but their “adoption into clinical practice has been slow” and inconsistent, prompting an expert panel organized by the American Heart Association to collate the range of treatment recommendations now applicable to this patient population in a scientific statement released on April 13.
“There are a number of things to consider when treating patients with stable coronary artery disease [CAD] and type 2 diabetes mellitus [T2DM], with new medications and trials and data emerging. It’s difficult to keep up with all of the complexities,” which was why the Association’s Councils on Lifestyle and Cardiometabolic Health and on Clinical Cardiology put together a writing group to summarize and prioritize the range of lifestyle, medical, and interventional options that now require consideration and potential use on patients managed in routine practice, explained Suzanne V. Arnold, MD, chair of the writing group, in an interview.
The new scientific statement (Circulation. 2020 Apr 13; doi: 10.1161/CIR.0000000000000766), aimed primarily at cardiologists but also intended to inform primary care physicians, endocrinologists, and all other clinicians who deal with these patients, pulls together “everything someone needs to think about if they care for patients with CAD and T2DM,” said Deepak L. Bhatt, MD, professor of medicine at Harvard Medical School in Boston and vice chair of the statement-writing panel in an interview. “There is a lot to know,” he added.
The statement covers antithrombotic therapies; blood pressure control, with a discussion of both the appropriate pressure goal and the best drug types used to reach it; lipid management; glycemic control; lifestyle modification; weight management, including the role of bariatric surgery; and approaches to managing stable angina, both medically and with revascularization.
“The goal was to give clinicians a good sense of what new treatments they should consider” for these patients, said Dr. Bhatt, who is also director of interventional cardiovascular programs at Brigham and Women’s Hospital, also in Boston. Because of the tight associations between T2DM and cardiovascular disease in general including CAD, “cardiologists are increasingly involved in managing patients with T2DM,” he noted. The statement gives a comprehensive overview and critical assessment of the management of these patients as of the end of 2019 as a consensus from a panel of 11 experts .
The statement also stressed that “substantial portions of patients with T2DM and CAD, including those after an acute coronary syndrome, do not receive therapies with proven cardiovascular benefit, such as high-intensity statins, dual-antiplatelet therapy, angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers, and glucose-lowering agents with proven cardiovascular benefits.
“These gaps in care highlight a critical opportunity for cardiovascular specialists to assume a more active role in the collaborative care of patients with T2DM and CAD,” the statement said. This includes “encouraging cardiologists to become more active in the selection of glucose-lowering medications” for these patients because it could “really move the needle,” said Dr. Arnold, a cardiologist with Saint Luke’s Health System in Kansas City, Mo. She was referring specifically to broader reliance on both the SGTL2 (sodium-glucose cotransporter 2) inhibitors and the GLP-1 (glucagonlike peptide-1) receptor agonists as top choices for controlling hyperglycemia. Based on recent evidence drugs in these two classes “could be considered first line for patients with T2DM and CAD, and would likely be preferred over metformin,” Dr. Arnold said in an interview. Although the statement identified the SGLT2 inhibitors as “the first drug class [for glycemic control] to show clear benefits on cardiovascular outcomes,” it does not explicitly label the class first-line and it also skirts that designation for the GLP-1 receptor agonist class, while noting that metformin “remains the drug most frequently recommended as first-line therapy in treatment guidelines.”
“I wouldn’t disagree with someone who said that SGLT2 inhibitors and GLP-1 receptor agonists are first line,” but prescribing patterns also depend on familiarity, cost, and access, noted Dr. Bhatt, which can all be issues with agents from these classes compared with metformin, a widely available generic with decades of use. “Metformin is safe and cheap, so we did not want to discount it,” said Dr. Arnold. Dr. Bhatt recently coauthored an editorial that gave an enthusiastic endorsement to using SGLT2 inhibitors in patients with diabetes (Cell Metab. 2019 Nov 5;30[5]:47-9).
Another notable feature of the statement is the potential it assigns to bariatric surgery as a management tool with documented safety and efficacy for improving cardiovascular risk factors. However, the statement also notes that randomized trials “have thus far been inadequately powered to assess cardiovascular events and mortality, although observational studies have consistently shown cardiovascular risk reduction with such procedures.” The statement continues that despite potential cardiovascular benefits “bariatric surgery remains underused among eligible patients,” and said that surgery performed as Roux-en-Y bypass or sleeve gastrectomy “may be another effective tool for cardiovascular risk reduction in the subset of patients with obesity,” particularly patients with a body mass index of at least 35 kg/m2.
“While the percentage of patients who are optimal for bariatric surgery is not known, the most recent NHANES [National Health and Nutrition Examination Study] study showed that less than 0.5% of eligible patients underwent bariatric surgery,” Dr. Arnold noted. Bariatric surgery is “certainly not a recommendation for everyone, or even a majority of patients, but bariatric surgery should be on our radar,” for patients with CAD and T2DM, she said.
Right now, “few cardiologists think about bariatric surgery,” as a treatment option, but study results have shown that “in carefully selected patients treated by skilled surgeons at high-volume centers, patients will do better with bariatric surgery than with best medical therapy for improvements in multiple risk factors, including glycemic control,” Dr. Bhatt said in the interview. “It’s not first-line treatment, but it’s an option to consider,” he added, while also noting that bariatric surgery is most beneficial to patients relatively early in the course of T2DM, when its been in place for just a few years rather than a couple of decades.
The statement also notably included a “first-line” call out for icosapent ethyl (Vascepa), a novel agent approved in December 2019 for routine use in U.S. patients, including those with CAD and T2DM as long as their blood triglyceride level was at least 150 mg/dL. Dr. Bhatt, who led the REDUCE-IT study that was pivotal for proving the safety and efficacy of icosapent ethyl (N Engl J Med. 2019 Jan 3;380[1]:11-22), estimated that anywhere from 15% to as many as half the patients with CAD and T2DM might have a triglyceride level that would allow them to receive icosapent ethyl. One population-based study in Canada of nearly 200,000 people with atherosclerotic cardiovascular disease found a 25% prevalence of the triglyceride level needed to qualify to receive icosapent ethyl under current labeling, he noted (Eur Heart J. 2020 Jan 1;41[1]:86-94). However, the FDA label does not specify that triglycerides be measured when fasting, and a nonfasting level of about 150 mg/dL will likely appear for patients with fasting levels that fall as low as about 100 mg/dL, Dr. Bhatt said. He hoped that future studies will assess the efficacy of icosapent ethyl in patients with even lower triglyceride levels.
Other sections of the statement also recommend that clinicians: Target long-term dual-antiplatelet therapy to CAD and T2DM patients with additional high-risk markers such as prior MI, younger age, and tobacco use; prescribe a low-dose oral anticoagulant along with an antiplatelet drug such as aspirin for secondary-prevention patients; promote a blood pressure target of less than 140/90 mm Hg for all CAD and T2DM patients and apply a goal of less than 130/80 mm Hg in higher-risk patients such as blacks, Asians, and those with cerebrovascular disease; and reassure patients that “despite a modest increase in blood sugars, the risk-benefit ratio is clearly in favor of administering statins to people with T2DM and CAD.”
Dr. Arnold had no disclosures. Dr. Bhatt has been an adviser to Cardax, Cereno Scientific, Medscape Cardiology, PhaseBio; PLx Pharma, and Regado Biosciences, and he has received research funding from numerous companies including Amarin, the company that markets icosapent ethyl.
FROM CIRCULATION
Cardiology groups push back on hydroxychloroquine, azithromycin for COVID-19
The .

“Hydroxychloroquine and azithromycin have been touted for potential prophylaxis or treatment for COVID-19; both drugs are listed as definite causes of torsade de pointes” and increase in the risk of other arrhythmias and sudden death, the American Heart Association, the American College of Cardiology, and the Heart Rhythm Society said in a joint statement April 8 in Circulation.
The statement came amid ongoing promotion by the Trump administration of hydroxychloroquine, in particular, for COVID-19 despite lack of strong data.
In addition to underlying cardiovascular disease, “seriously ill patients often have comorbidities that can increase risk of serious arrhythmias,” including hypokalemia, hypomagnesemia, fever, and systemic inflammation, the groups said.
They recommended withholding the drugs in patients with baseline QT prolongation (e.g., QTc of at least 500 msec) or with known congenital long QT syndrome; monitoring cardiac rhythm and QT interval and withdrawing hydroxychloroquine and azithromycin if QTc exceeds 500 msec; correcting hypokalemia to levels greater than 4 mEq/L and hypomagnesemia to more than 2 mg/dL; and avoiding other QTc-prolonging agents when possible.
The groups noted that, “in patients critically ill with COVID-19 infection, frequent caregiver contact may need to be minimized, so optimal electrocardiographic interval and rhythm monitoring may not be possible.” There is also a possible compounding arrhythmic effect when hydroxychloroquine and azithromycin are used together, but that has not been studied.
There’s a known risk of torsade de pointes with chloroquine and a possible risk with the antiviral HIV combination drug lopinavir-ritonavir, two other candidates for COVID-19 treatment. Hydroxychloroquine and chloroquine, both antimalarials, might help prevent or treat infection by interfering with angiotensin-converting enzyme 2 receptors, which the COVID-19 virus uses for cell entry, the groups said.
“The urgency of COVID-19 must not diminish the scientific rigor with which we approach COVID-19 treatment. While these medications may work against COVID-19 individually or in combination, we recommend caution with these medications for patients with existing cardiovascular disease,” Robert A. Harrington, MD, AHA president and chair of the department of medicine at Stanford (Calif.) University, emphasized in a press release.
SOURCE: Roden DM et al. Circulation. 2020 Apr 8. doi:10.1161/CIRCULATIONAHA.120.047521.
The .
“Hydroxychloroquine and azithromycin have been touted for potential prophylaxis or treatment for COVID-19; both drugs are listed as definite causes of torsade de pointes” and increase in the risk of other arrhythmias and sudden death, the American Heart Association, the American College of Cardiology, and the Heart Rhythm Society said in a joint statement April 8 in Circulation.
The statement came amid ongoing promotion by the Trump administration of hydroxychloroquine, in particular, for COVID-19 despite lack of strong data.
In addition to underlying cardiovascular disease, “seriously ill patients often have comorbidities that can increase risk of serious arrhythmias,” including hypokalemia, hypomagnesemia, fever, and systemic inflammation, the groups said.
They recommended withholding the drugs in patients with baseline QT prolongation (e.g., QTc of at least 500 msec) or with known congenital long QT syndrome; monitoring cardiac rhythm and QT interval and withdrawing hydroxychloroquine and azithromycin if QTc exceeds 500 msec; correcting hypokalemia to levels greater than 4 mEq/L and hypomagnesemia to more than 2 mg/dL; and avoiding other QTc-prolonging agents when possible.
The groups noted that, “in patients critically ill with COVID-19 infection, frequent caregiver contact may need to be minimized, so optimal electrocardiographic interval and rhythm monitoring may not be possible.” There is also a possible compounding arrhythmic effect when hydroxychloroquine and azithromycin are used together, but that has not been studied.
There’s a known risk of torsade de pointes with chloroquine and a possible risk with the antiviral HIV combination drug lopinavir-ritonavir, two other candidates for COVID-19 treatment. Hydroxychloroquine and chloroquine, both antimalarials, might help prevent or treat infection by interfering with angiotensin-converting enzyme 2 receptors, which the COVID-19 virus uses for cell entry, the groups said.
“The urgency of COVID-19 must not diminish the scientific rigor with which we approach COVID-19 treatment. While these medications may work against COVID-19 individually or in combination, we recommend caution with these medications for patients with existing cardiovascular disease,” Robert A. Harrington, MD, AHA president and chair of the department of medicine at Stanford (Calif.) University, emphasized in a press release.
SOURCE: Roden DM et al. Circulation. 2020 Apr 8. doi:10.1161/CIRCULATIONAHA.120.047521.
The .
“Hydroxychloroquine and azithromycin have been touted for potential prophylaxis or treatment for COVID-19; both drugs are listed as definite causes of torsade de pointes” and increase in the risk of other arrhythmias and sudden death, the American Heart Association, the American College of Cardiology, and the Heart Rhythm Society said in a joint statement April 8 in Circulation.
The statement came amid ongoing promotion by the Trump administration of hydroxychloroquine, in particular, for COVID-19 despite lack of strong data.
In addition to underlying cardiovascular disease, “seriously ill patients often have comorbidities that can increase risk of serious arrhythmias,” including hypokalemia, hypomagnesemia, fever, and systemic inflammation, the groups said.
They recommended withholding the drugs in patients with baseline QT prolongation (e.g., QTc of at least 500 msec) or with known congenital long QT syndrome; monitoring cardiac rhythm and QT interval and withdrawing hydroxychloroquine and azithromycin if QTc exceeds 500 msec; correcting hypokalemia to levels greater than 4 mEq/L and hypomagnesemia to more than 2 mg/dL; and avoiding other QTc-prolonging agents when possible.
The groups noted that, “in patients critically ill with COVID-19 infection, frequent caregiver contact may need to be minimized, so optimal electrocardiographic interval and rhythm monitoring may not be possible.” There is also a possible compounding arrhythmic effect when hydroxychloroquine and azithromycin are used together, but that has not been studied.
There’s a known risk of torsade de pointes with chloroquine and a possible risk with the antiviral HIV combination drug lopinavir-ritonavir, two other candidates for COVID-19 treatment. Hydroxychloroquine and chloroquine, both antimalarials, might help prevent or treat infection by interfering with angiotensin-converting enzyme 2 receptors, which the COVID-19 virus uses for cell entry, the groups said.
“The urgency of COVID-19 must not diminish the scientific rigor with which we approach COVID-19 treatment. While these medications may work against COVID-19 individually or in combination, we recommend caution with these medications for patients with existing cardiovascular disease,” Robert A. Harrington, MD, AHA president and chair of the department of medicine at Stanford (Calif.) University, emphasized in a press release.
SOURCE: Roden DM et al. Circulation. 2020 Apr 8. doi:10.1161/CIRCULATIONAHA.120.047521.
COVID-19 linked to multiple cardiovascular presentations
It’s becoming clear that COVID-19 infection can involve the cardiovascular system in many different ways, and this has “evolving” potential implications for treatment, say a team of cardiologists on the frontlines of the COVID-19 battle in New York City.
In an article published online April 3 in Circulation, Justin Fried, MD, Division of Cardiology, Columbia University, New York City, and colleagues present four case studies of COVID-19 patients with various cardiovascular presentations.
Case 1 is a 64-year-old woman whose predominant symptoms on admission were cardiac in nature, including chest pain and ST elevation, but without fever, cough, or other symptoms suggestive of COVID-19.
“In patients presenting with what appears to be a typical cardiac syndrome, COVID-19 infection should be in the differential during the current pandemic, even in the absence of fever or cough,” the clinicians advise.
Case 2 is a 38-year-old man with cardiogenic shock and acute respiratory distress with profound hypoxia who was rescued with veno-arterial-venous extracorporeal membrane oxygenation (VV ECMO).
The initial presentation of this patient was more characteristic of severe COVID-19 disease, and cardiac involvement only became apparent after the initiation of ECMO, Fried and colleagues report.
Based on this case, they advise a “low threshold” to assess for cardiogenic shock in patients with acute systolic heart failure related to COVID-19. If inotropic support fails in these patients, intra-aortic balloon pump should be considered first for mechanical circulatory support because it requires the least maintenance from medical support staff.
In addition, in their experience, when a patient on VV ECMO develops superimposed cardiogenic shock, adding an arterial conduit at a relatively low blood flow rate may provide the necessary circulatory support without inducing left ventricular distension, they note.
“Our experience confirms that rescue of patients even with profound cardiogenic or mixed shock may be possible with temporary hemodynamic support at centers with availability of such devices,” Fried and colleagues report.
Case 3 is a 64-year-old woman with underlying cardiac disease who developed profound decompensation with COVID-19 infection.
This case demonstrates that the infection can cause decompensation of underlying heart failure and may lead to mixed shock, the clinicians say.
“Invasive hemodynamic monitoring, if feasible, may be helpful to manage the cardiac component of shock in such cases. Medications that prolong the QT interval are being considered for COVID-19 patients and may require closer monitoring in patients with underlying structural heart disease,” they note.
Case 4 is a 51-year-old man who underwent a heart transplant in 2007 and a kidney transplant in 2010. He had COVID-19 symptoms akin to those seen in nonimmunosuppressed patients with COVID-19.
The COVID-19 pandemic presents a “unique challenge” for solid organ transplant recipients, with only “limited” data on how to adjust immunosuppression during COVID-19 infection, Fried and colleagues say.
The pandemic also creates a challenge for the management of heart failure patients on the heart transplant wait list; the risks of delaying a transplant need to be balanced against the risks of donor infection and uncertainty regarding the impact of post-transplant immunosuppression protocols, they note.
As reported by Medscape Medical News, the American Heart Association has developed a COVID-19 patient registry to collect data on cardiovascular conditions and outcomes related to COVID-19 infection.
To participate in the registry, contact qualityresearch@heart.org.
This article first appeared on Medscape.com.
It’s becoming clear that COVID-19 infection can involve the cardiovascular system in many different ways, and this has “evolving” potential implications for treatment, say a team of cardiologists on the frontlines of the COVID-19 battle in New York City.
In an article published online April 3 in Circulation, Justin Fried, MD, Division of Cardiology, Columbia University, New York City, and colleagues present four case studies of COVID-19 patients with various cardiovascular presentations.
Case 1 is a 64-year-old woman whose predominant symptoms on admission were cardiac in nature, including chest pain and ST elevation, but without fever, cough, or other symptoms suggestive of COVID-19.
“In patients presenting with what appears to be a typical cardiac syndrome, COVID-19 infection should be in the differential during the current pandemic, even in the absence of fever or cough,” the clinicians advise.
Case 2 is a 38-year-old man with cardiogenic shock and acute respiratory distress with profound hypoxia who was rescued with veno-arterial-venous extracorporeal membrane oxygenation (VV ECMO).
The initial presentation of this patient was more characteristic of severe COVID-19 disease, and cardiac involvement only became apparent after the initiation of ECMO, Fried and colleagues report.
Based on this case, they advise a “low threshold” to assess for cardiogenic shock in patients with acute systolic heart failure related to COVID-19. If inotropic support fails in these patients, intra-aortic balloon pump should be considered first for mechanical circulatory support because it requires the least maintenance from medical support staff.
In addition, in their experience, when a patient on VV ECMO develops superimposed cardiogenic shock, adding an arterial conduit at a relatively low blood flow rate may provide the necessary circulatory support without inducing left ventricular distension, they note.
“Our experience confirms that rescue of patients even with profound cardiogenic or mixed shock may be possible with temporary hemodynamic support at centers with availability of such devices,” Fried and colleagues report.
Case 3 is a 64-year-old woman with underlying cardiac disease who developed profound decompensation with COVID-19 infection.
This case demonstrates that the infection can cause decompensation of underlying heart failure and may lead to mixed shock, the clinicians say.
“Invasive hemodynamic monitoring, if feasible, may be helpful to manage the cardiac component of shock in such cases. Medications that prolong the QT interval are being considered for COVID-19 patients and may require closer monitoring in patients with underlying structural heart disease,” they note.
Case 4 is a 51-year-old man who underwent a heart transplant in 2007 and a kidney transplant in 2010. He had COVID-19 symptoms akin to those seen in nonimmunosuppressed patients with COVID-19.
The COVID-19 pandemic presents a “unique challenge” for solid organ transplant recipients, with only “limited” data on how to adjust immunosuppression during COVID-19 infection, Fried and colleagues say.
The pandemic also creates a challenge for the management of heart failure patients on the heart transplant wait list; the risks of delaying a transplant need to be balanced against the risks of donor infection and uncertainty regarding the impact of post-transplant immunosuppression protocols, they note.
As reported by Medscape Medical News, the American Heart Association has developed a COVID-19 patient registry to collect data on cardiovascular conditions and outcomes related to COVID-19 infection.
To participate in the registry, contact qualityresearch@heart.org.
This article first appeared on Medscape.com.
It’s becoming clear that COVID-19 infection can involve the cardiovascular system in many different ways, and this has “evolving” potential implications for treatment, say a team of cardiologists on the frontlines of the COVID-19 battle in New York City.
In an article published online April 3 in Circulation, Justin Fried, MD, Division of Cardiology, Columbia University, New York City, and colleagues present four case studies of COVID-19 patients with various cardiovascular presentations.
Case 1 is a 64-year-old woman whose predominant symptoms on admission were cardiac in nature, including chest pain and ST elevation, but without fever, cough, or other symptoms suggestive of COVID-19.
“In patients presenting with what appears to be a typical cardiac syndrome, COVID-19 infection should be in the differential during the current pandemic, even in the absence of fever or cough,” the clinicians advise.
Case 2 is a 38-year-old man with cardiogenic shock and acute respiratory distress with profound hypoxia who was rescued with veno-arterial-venous extracorporeal membrane oxygenation (VV ECMO).
The initial presentation of this patient was more characteristic of severe COVID-19 disease, and cardiac involvement only became apparent after the initiation of ECMO, Fried and colleagues report.
Based on this case, they advise a “low threshold” to assess for cardiogenic shock in patients with acute systolic heart failure related to COVID-19. If inotropic support fails in these patients, intra-aortic balloon pump should be considered first for mechanical circulatory support because it requires the least maintenance from medical support staff.
In addition, in their experience, when a patient on VV ECMO develops superimposed cardiogenic shock, adding an arterial conduit at a relatively low blood flow rate may provide the necessary circulatory support without inducing left ventricular distension, they note.
“Our experience confirms that rescue of patients even with profound cardiogenic or mixed shock may be possible with temporary hemodynamic support at centers with availability of such devices,” Fried and colleagues report.
Case 3 is a 64-year-old woman with underlying cardiac disease who developed profound decompensation with COVID-19 infection.
This case demonstrates that the infection can cause decompensation of underlying heart failure and may lead to mixed shock, the clinicians say.
“Invasive hemodynamic monitoring, if feasible, may be helpful to manage the cardiac component of shock in such cases. Medications that prolong the QT interval are being considered for COVID-19 patients and may require closer monitoring in patients with underlying structural heart disease,” they note.
Case 4 is a 51-year-old man who underwent a heart transplant in 2007 and a kidney transplant in 2010. He had COVID-19 symptoms akin to those seen in nonimmunosuppressed patients with COVID-19.
The COVID-19 pandemic presents a “unique challenge” for solid organ transplant recipients, with only “limited” data on how to adjust immunosuppression during COVID-19 infection, Fried and colleagues say.
The pandemic also creates a challenge for the management of heart failure patients on the heart transplant wait list; the risks of delaying a transplant need to be balanced against the risks of donor infection and uncertainty regarding the impact of post-transplant immunosuppression protocols, they note.
As reported by Medscape Medical News, the American Heart Association has developed a COVID-19 patient registry to collect data on cardiovascular conditions and outcomes related to COVID-19 infection.
To participate in the registry, contact qualityresearch@heart.org.
This article first appeared on Medscape.com.