User login
Similar 10-year survival after CABG, PCI in heavy calcification
Patients with complex coronary artery disease (CAD) – either three-vessel disease and/or left main disease – who also had heavy coronary artery calcification (CAC) had greater all-cause mortality 10 years after revascularization, compared with those without such lesions.
However, perhaps unexpectedly, patients with heavily calcified lesions (HCLs) had similar 10-year survival whether they had undergone coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI).
These findings from a post hoc analysis of the SYNTAX Extended Survival (SYNTAXES) study led by Hideyuki Kawashima, MD, PhD, National University of Ireland, Galway, and the University of Amsterdam, were published online Dec. 29, 2021, in JACC: Cardiovascular Interventions.
“There was an apparent lack of benefit at very long-term with CABG versus PCI in the presence of HCL,” Dr. Kawashima and corresponding author Patrick W. Serruys, MD, PhD, National University of Ireland and Imperial College London, summarized in a joint email to this news organization.
“Since HCLs – the final status of atherosclerosis and inflammation – reflect the aging process, complexity, and extensiveness of CAD, and comorbidity, it is possible that the currently available revascularization methods do not provide benefit in the prevention of long-term [10-year] mortality,” they suggested.

In an accompanying editorial, Usman Baber, MD, commented that this study provides a “novel insight.”
Specifically, while patients without HCLs had significantly lower 10-year mortality with CABG versus PCI (18.8% vs. 26.0%; P = .003), an opposite trend was observed among those with HCLs (39.0% vs. 34.0%; P = .26; P int = .005).
The patients with HCLs had higher SYNTAX scores (30.8 vs. 22.4; P < .001) and more complex CAD, so their lack of 10-year mortality benefit with CABG “is somewhat unexpected and warrants further scrutiny,” added Dr. Baber, from the University of Oklahoma Health Sciences Center in Oklahoma City.
Dr. Serruys and Dr. Kawashima agreed that “this study highlights the need for further research on this topic focusing on this specific population with HCLs,” which were 30% of the patients with complex lesions who participated in SYNTAXES.
Consider factors beyond coronary anatomy
The current findings reinforce “the importance of considering not just coronary anatomy, but patient age and other comorbid factors when evaluating mode of revascularization,” said Dr. Baber.
“Coronary calcification is a strong factor in deciding between CABG versus PCI, as multiple studies have shown that CAC increases risk after PCI, even with contemporary safe stent platforms,” he explained in an email.
The current study suggests the adverse prognosis associated with CAC also persists for patients treated with CABG.
Dr. Baber said that, “for patients in whom PCI may not be feasible due to extensive and bulky coronary calcification, it is important to emphasize that the benefits of CABG (versus PCI) may not be as significant or durable.”
“The lack of benefit with CABG,” he added, “is likely due to comorbid factors that tend to increase in prevalence with vascular calcification (older age, peripheral arterial disease, renal impairment, etc).”
This study reinforces “the importance of not just considering coronary complexity, but also additional noncoronary factors that influence long-term prognosis in patients with advanced multivessel CAD,” Dr. Baber stressed.
More aggressive lipid-lowering or antithrombotic therapy may improve the prognosis for such patients, he suggested.
“In general,” Dr. Serruys and Dr. Kawashima similarly noted, “for short-/mid-term outcomes, CABG is preferred to PCI in patients with HCLs because of a higher rate of complete revascularization and less need for repeat revascularization.”
“Our findings at 10 years are in line with the general findings preferring CABG in mid and long term, whereas the benefit of very long-term follow-up might be more complex to capture and comprehend,” they concluded. “Whether HCLs require special consideration when deciding the mode of revascularization beyond their contribution to the SYNTAX score deserves further evaluation.
“Newer PCI technology or CABG methods may become a game-changer in the future,” they speculated.
Worse clinical outcomes
Heavy coronary calcification is associated with worse clinical outcomes after PCI or CABG, but to date, no trial has compared 10-year outcomes after PCI or CABG in patients with complex CAD with versus without HCLs.
To look at this, Dr. Kawashima and colleagues performed a subanalysis of patients in the SYNTAXES study. The original SYNTAX trial had randomized 1,800 patients with complex CAD who were eligible for either PCI or CABG 1:1 to these two treatments, with a 5-year follow-up, and SYNTAXES extended the follow-up to 10 years.
Of the 1,800 patients, 532 (29.6%) had at least one HCL and the rest (70.4%) did not.
The median follow-up in SYNTAXES was 11.2 years overall and 11.9 years in survivors.
At baseline, compared with other patients, those with HCLs were older and had a lower body mass index and higher rates of insulin-treated diabetes, hypertension, previous cerebrovascular disease, peripheral vascular disease, chronic obstructive pulmonary disease, chronic kidney disease, and heart failure.
After adjusting for multiple variables, having a HCL was an independent predictor of greater risk of 10-year mortality (hazard ratio, 1.36; 95% confidence interval, 1.09-1.69; P = .006).
In patients without HCLs, mortality was significantly higher after PCI than CABG (HR, 1.44; 95% CI, 1.14-1.83; P = .003), whereas in those with HCLs, there was no significant difference (HR, 0.85; 95% CI, 0.64-1.13; P = .264).
The location of the HCL did not have any impact on 10-year mortality regardless of the assigned treatment.
Among patients with at least one HCL who underwent CABG, those with at least two HCLs had greater 10-year all-cause mortality than those with one HCL; this difference was not seen among patients with at least one HCL who underwent PCI.
The researchers acknowledge study limitations include that it was a post hoc analysis, so it should be considered hypothesis generating.
In addition, SYNTAX was conducted between 2005 and 2007, when PCI mainly used first-generation paclitaxel drug-eluting stents, so the findings may not be generalizable to current practice.
SYNTAXES was supported by the German Foundation of Heart Research. SYNTAX, during 0- to 5-year follow-up, was funded by Boston Scientific. Dr. Serruys reported receiving personal fees from SMT, Philips/Volcano, Xeltis, Novartis, and Meril Life. Dr. Kawashima reported no relevant financial relationships. Dr. Baber reported receiving honoraria and speaker fees from AstraZeneca, Biotronik, and Amgen.
A version of this article first appeared on Medscape.com.
Patients with complex coronary artery disease (CAD) – either three-vessel disease and/or left main disease – who also had heavy coronary artery calcification (CAC) had greater all-cause mortality 10 years after revascularization, compared with those without such lesions.
However, perhaps unexpectedly, patients with heavily calcified lesions (HCLs) had similar 10-year survival whether they had undergone coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI).
These findings from a post hoc analysis of the SYNTAX Extended Survival (SYNTAXES) study led by Hideyuki Kawashima, MD, PhD, National University of Ireland, Galway, and the University of Amsterdam, were published online Dec. 29, 2021, in JACC: Cardiovascular Interventions.
“There was an apparent lack of benefit at very long-term with CABG versus PCI in the presence of HCL,” Dr. Kawashima and corresponding author Patrick W. Serruys, MD, PhD, National University of Ireland and Imperial College London, summarized in a joint email to this news organization.
“Since HCLs – the final status of atherosclerosis and inflammation – reflect the aging process, complexity, and extensiveness of CAD, and comorbidity, it is possible that the currently available revascularization methods do not provide benefit in the prevention of long-term [10-year] mortality,” they suggested.
In an accompanying editorial, Usman Baber, MD, commented that this study provides a “novel insight.”
Specifically, while patients without HCLs had significantly lower 10-year mortality with CABG versus PCI (18.8% vs. 26.0%; P = .003), an opposite trend was observed among those with HCLs (39.0% vs. 34.0%; P = .26; P int = .005).
The patients with HCLs had higher SYNTAX scores (30.8 vs. 22.4; P < .001) and more complex CAD, so their lack of 10-year mortality benefit with CABG “is somewhat unexpected and warrants further scrutiny,” added Dr. Baber, from the University of Oklahoma Health Sciences Center in Oklahoma City.
Dr. Serruys and Dr. Kawashima agreed that “this study highlights the need for further research on this topic focusing on this specific population with HCLs,” which were 30% of the patients with complex lesions who participated in SYNTAXES.
Consider factors beyond coronary anatomy
The current findings reinforce “the importance of considering not just coronary anatomy, but patient age and other comorbid factors when evaluating mode of revascularization,” said Dr. Baber.
“Coronary calcification is a strong factor in deciding between CABG versus PCI, as multiple studies have shown that CAC increases risk after PCI, even with contemporary safe stent platforms,” he explained in an email.
The current study suggests the adverse prognosis associated with CAC also persists for patients treated with CABG.
Dr. Baber said that, “for patients in whom PCI may not be feasible due to extensive and bulky coronary calcification, it is important to emphasize that the benefits of CABG (versus PCI) may not be as significant or durable.”
“The lack of benefit with CABG,” he added, “is likely due to comorbid factors that tend to increase in prevalence with vascular calcification (older age, peripheral arterial disease, renal impairment, etc).”
This study reinforces “the importance of not just considering coronary complexity, but also additional noncoronary factors that influence long-term prognosis in patients with advanced multivessel CAD,” Dr. Baber stressed.
More aggressive lipid-lowering or antithrombotic therapy may improve the prognosis for such patients, he suggested.
“In general,” Dr. Serruys and Dr. Kawashima similarly noted, “for short-/mid-term outcomes, CABG is preferred to PCI in patients with HCLs because of a higher rate of complete revascularization and less need for repeat revascularization.”
“Our findings at 10 years are in line with the general findings preferring CABG in mid and long term, whereas the benefit of very long-term follow-up might be more complex to capture and comprehend,” they concluded. “Whether HCLs require special consideration when deciding the mode of revascularization beyond their contribution to the SYNTAX score deserves further evaluation.
“Newer PCI technology or CABG methods may become a game-changer in the future,” they speculated.
Worse clinical outcomes
Heavy coronary calcification is associated with worse clinical outcomes after PCI or CABG, but to date, no trial has compared 10-year outcomes after PCI or CABG in patients with complex CAD with versus without HCLs.
To look at this, Dr. Kawashima and colleagues performed a subanalysis of patients in the SYNTAXES study. The original SYNTAX trial had randomized 1,800 patients with complex CAD who were eligible for either PCI or CABG 1:1 to these two treatments, with a 5-year follow-up, and SYNTAXES extended the follow-up to 10 years.
Of the 1,800 patients, 532 (29.6%) had at least one HCL and the rest (70.4%) did not.
The median follow-up in SYNTAXES was 11.2 years overall and 11.9 years in survivors.
At baseline, compared with other patients, those with HCLs were older and had a lower body mass index and higher rates of insulin-treated diabetes, hypertension, previous cerebrovascular disease, peripheral vascular disease, chronic obstructive pulmonary disease, chronic kidney disease, and heart failure.
After adjusting for multiple variables, having a HCL was an independent predictor of greater risk of 10-year mortality (hazard ratio, 1.36; 95% confidence interval, 1.09-1.69; P = .006).
In patients without HCLs, mortality was significantly higher after PCI than CABG (HR, 1.44; 95% CI, 1.14-1.83; P = .003), whereas in those with HCLs, there was no significant difference (HR, 0.85; 95% CI, 0.64-1.13; P = .264).
The location of the HCL did not have any impact on 10-year mortality regardless of the assigned treatment.
Among patients with at least one HCL who underwent CABG, those with at least two HCLs had greater 10-year all-cause mortality than those with one HCL; this difference was not seen among patients with at least one HCL who underwent PCI.
The researchers acknowledge study limitations include that it was a post hoc analysis, so it should be considered hypothesis generating.
In addition, SYNTAX was conducted between 2005 and 2007, when PCI mainly used first-generation paclitaxel drug-eluting stents, so the findings may not be generalizable to current practice.
SYNTAXES was supported by the German Foundation of Heart Research. SYNTAX, during 0- to 5-year follow-up, was funded by Boston Scientific. Dr. Serruys reported receiving personal fees from SMT, Philips/Volcano, Xeltis, Novartis, and Meril Life. Dr. Kawashima reported no relevant financial relationships. Dr. Baber reported receiving honoraria and speaker fees from AstraZeneca, Biotronik, and Amgen.
A version of this article first appeared on Medscape.com.
Patients with complex coronary artery disease (CAD) – either three-vessel disease and/or left main disease – who also had heavy coronary artery calcification (CAC) had greater all-cause mortality 10 years after revascularization, compared with those without such lesions.
However, perhaps unexpectedly, patients with heavily calcified lesions (HCLs) had similar 10-year survival whether they had undergone coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI).
These findings from a post hoc analysis of the SYNTAX Extended Survival (SYNTAXES) study led by Hideyuki Kawashima, MD, PhD, National University of Ireland, Galway, and the University of Amsterdam, were published online Dec. 29, 2021, in JACC: Cardiovascular Interventions.
“There was an apparent lack of benefit at very long-term with CABG versus PCI in the presence of HCL,” Dr. Kawashima and corresponding author Patrick W. Serruys, MD, PhD, National University of Ireland and Imperial College London, summarized in a joint email to this news organization.
“Since HCLs – the final status of atherosclerosis and inflammation – reflect the aging process, complexity, and extensiveness of CAD, and comorbidity, it is possible that the currently available revascularization methods do not provide benefit in the prevention of long-term [10-year] mortality,” they suggested.
In an accompanying editorial, Usman Baber, MD, commented that this study provides a “novel insight.”
Specifically, while patients without HCLs had significantly lower 10-year mortality with CABG versus PCI (18.8% vs. 26.0%; P = .003), an opposite trend was observed among those with HCLs (39.0% vs. 34.0%; P = .26; P int = .005).
The patients with HCLs had higher SYNTAX scores (30.8 vs. 22.4; P < .001) and more complex CAD, so their lack of 10-year mortality benefit with CABG “is somewhat unexpected and warrants further scrutiny,” added Dr. Baber, from the University of Oklahoma Health Sciences Center in Oklahoma City.
Dr. Serruys and Dr. Kawashima agreed that “this study highlights the need for further research on this topic focusing on this specific population with HCLs,” which were 30% of the patients with complex lesions who participated in SYNTAXES.
Consider factors beyond coronary anatomy
The current findings reinforce “the importance of considering not just coronary anatomy, but patient age and other comorbid factors when evaluating mode of revascularization,” said Dr. Baber.
“Coronary calcification is a strong factor in deciding between CABG versus PCI, as multiple studies have shown that CAC increases risk after PCI, even with contemporary safe stent platforms,” he explained in an email.
The current study suggests the adverse prognosis associated with CAC also persists for patients treated with CABG.
Dr. Baber said that, “for patients in whom PCI may not be feasible due to extensive and bulky coronary calcification, it is important to emphasize that the benefits of CABG (versus PCI) may not be as significant or durable.”
“The lack of benefit with CABG,” he added, “is likely due to comorbid factors that tend to increase in prevalence with vascular calcification (older age, peripheral arterial disease, renal impairment, etc).”
This study reinforces “the importance of not just considering coronary complexity, but also additional noncoronary factors that influence long-term prognosis in patients with advanced multivessel CAD,” Dr. Baber stressed.
More aggressive lipid-lowering or antithrombotic therapy may improve the prognosis for such patients, he suggested.
“In general,” Dr. Serruys and Dr. Kawashima similarly noted, “for short-/mid-term outcomes, CABG is preferred to PCI in patients with HCLs because of a higher rate of complete revascularization and less need for repeat revascularization.”
“Our findings at 10 years are in line with the general findings preferring CABG in mid and long term, whereas the benefit of very long-term follow-up might be more complex to capture and comprehend,” they concluded. “Whether HCLs require special consideration when deciding the mode of revascularization beyond their contribution to the SYNTAX score deserves further evaluation.
“Newer PCI technology or CABG methods may become a game-changer in the future,” they speculated.
Worse clinical outcomes
Heavy coronary calcification is associated with worse clinical outcomes after PCI or CABG, but to date, no trial has compared 10-year outcomes after PCI or CABG in patients with complex CAD with versus without HCLs.
To look at this, Dr. Kawashima and colleagues performed a subanalysis of patients in the SYNTAXES study. The original SYNTAX trial had randomized 1,800 patients with complex CAD who were eligible for either PCI or CABG 1:1 to these two treatments, with a 5-year follow-up, and SYNTAXES extended the follow-up to 10 years.
Of the 1,800 patients, 532 (29.6%) had at least one HCL and the rest (70.4%) did not.
The median follow-up in SYNTAXES was 11.2 years overall and 11.9 years in survivors.
At baseline, compared with other patients, those with HCLs were older and had a lower body mass index and higher rates of insulin-treated diabetes, hypertension, previous cerebrovascular disease, peripheral vascular disease, chronic obstructive pulmonary disease, chronic kidney disease, and heart failure.
After adjusting for multiple variables, having a HCL was an independent predictor of greater risk of 10-year mortality (hazard ratio, 1.36; 95% confidence interval, 1.09-1.69; P = .006).
In patients without HCLs, mortality was significantly higher after PCI than CABG (HR, 1.44; 95% CI, 1.14-1.83; P = .003), whereas in those with HCLs, there was no significant difference (HR, 0.85; 95% CI, 0.64-1.13; P = .264).
The location of the HCL did not have any impact on 10-year mortality regardless of the assigned treatment.
Among patients with at least one HCL who underwent CABG, those with at least two HCLs had greater 10-year all-cause mortality than those with one HCL; this difference was not seen among patients with at least one HCL who underwent PCI.
The researchers acknowledge study limitations include that it was a post hoc analysis, so it should be considered hypothesis generating.
In addition, SYNTAX was conducted between 2005 and 2007, when PCI mainly used first-generation paclitaxel drug-eluting stents, so the findings may not be generalizable to current practice.
SYNTAXES was supported by the German Foundation of Heart Research. SYNTAX, during 0- to 5-year follow-up, was funded by Boston Scientific. Dr. Serruys reported receiving personal fees from SMT, Philips/Volcano, Xeltis, Novartis, and Meril Life. Dr. Kawashima reported no relevant financial relationships. Dr. Baber reported receiving honoraria and speaker fees from AstraZeneca, Biotronik, and Amgen.
A version of this article first appeared on Medscape.com.
FROM JACC: CARDIOVASCULAR INTERVENTIONS
The child with hypertension: Diagnosis and management
This transcript has been edited for clarity. The transcript and an accompanying video first appeared on Medscape.com.
Justin L. Berk, MD, MPH, MBA: Welcome back to The Cribsiders, our video recap of our pediatric medicine podcast. We interview leading experts in the field to bring clinical pearls and practice-changing knowledge, and answer lingering questions about core topics in pediatric medicine. Chris, what is our topic today?
Christopher J. Chiu, MD: I was really happy to be able to talk about our recent episode with Dr. Carissa Baker-Smith, a pediatric cardiologist and director of the Nemours preventive cardiology program. She helped us review the pediatric screening guidelines for blood pressure, including initial workup and treatment.
Dr. Berk: This was a really great episode that a lot of people found really helpful. What were some of the key takeaway pearls that you think listeners would be interested in?
Dr. Chiu: We talked about when and how we should be checking blood pressures in children. Blood pressure should be checked at every well-child visit starting at age 3. But if they have other risk factors like kidney disease or a condition such as coarctation of the aorta, then blood pressure should be checked at every visit.
Dr. Berk: One thing she spoke about was how blood pressures should be measured. How should we be checking blood pressures in the clinic?
Dr. Chiu: Clinic blood pressures are usually checked with oscillometric devices. They can differ by manufacturer, but basically they find a mean arterial pressure and then each device has a method of calculating systolic and diastolic pressures. Now after that, if the child’s blood pressure is maybe abnormal, you want to double-check a manual blood pressure using Korotkoff sounds to confirm the blood pressure.
She reminded us that blood pressure should be measured with the child sitting with their back supported, feet flat on the floor, and arm at the level of the heart. Make sure you use the right size cuff. The bladder of the cuff should be 40% of the width of the arm, and about 80%-100% of the arm circumference. She recommends sizing up if you have to.
Dr. Berk: Accuracy of blood pressure management was a really important point, especially for diagnosis at this stage. Can you walk us through what we learned about diagnosis of hypertension?
Dr. Chiu: The definitions of hypertension come from the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Up until the age of 13, they define prehypertension as systolic and diastolic blood pressures between the 90th and 95th percentile, or if the blood pressure exceeds 120/80 mm Hg. Hypertension is defined when blood pressure reaches the 95th percentile. Now age 13 is when it gets a little hazy. Many changes in the guidelines happen at age 13, when hypertension starts being defined by adult guidelines. The 2017 adult hypertension guidelines define stage 1 hypertension as 130/89 to 139/89, and stage 2 hypertension as greater than 140/90.
Dr. Berk: How about workup of hypertension? The work of pediatric hypertension is always a little bit complex. What are some of the pearls you took away?
Dr. Chui: She talked about tailoring the workup to the child. So when we’re doing our workup, obviously physical exam should be the first thing we do. You have to assess and compare pulses, which is one of the most important parts of the initial evaluation. Obviously, looking at coarctation of the aorta, but also looking for things like a cushingoid appearance. If the child is less than 6 years of age, she recommends a referral to nephrology for more comprehensive renovascular workup, which probably will include renal ultrasound, urinalysis, metabolic panel, and thyroid studies.
We have to be cognizant of secondary causes of hypertension, such as endocrine tumors, hyperthyroidism, aortic disease, or even medication-induced hypertension. She told us that in the majority of these cases, especially with our obese older children, primary hypertension or essential hypertension is the most likely cause.
Dr. Berk: That was my big takeaway. If they’re really young, they need a big workup, but otherwise it is likely primary hypertension. What did we learn about treatment?
Dr. Chui: Just as we tailor our assessment to the child, we also have to tailor treatment. We know that lifestyle modification is usually the first line of treatment, especially for primary hypertension, and Dr. Baker-Smith tells us that we really need to perform counseling that meets the patient where they are. So if they like dancing to the newest TikTok trends or music videos, maybe we can encourage them to move more that way. Using our motivational interviewing skills is really key here.
If you want to start medication, Dr. Baker-Smith uses things like low-dose ACE inhibitors or calcium channel blockers, but obviously it’ll be tailored to the patient and any underlying conditions.
Dr. Berk: That’s great – a lot of wonderful pearls on the diagnosis and management of pediatric hypertension. Thank you for joining us for another video recap of The Cribsiders pediatric podcast. You can download the full podcast, Off the Cuff: Managing Pediatric Hypertension in Your Primary Care Clinic, on any podcast player, or check out our website at www.theCribsiders.com.
Christopher J. Chiu, MD, is assistant professor, department of internal medicine, division of general internal medicine, Ohio State University, Columbus; lead physician, general internal medicine, OSU Outpatient Care East; department of internal medicine, division of general internal medicine, Ohio State University Wexner Medical Center. Dr. Chiu has disclosed no relevant financial relationships. Justin L. Berk, MD, MPH, MBA, is assistant professor, department of medicine; assistant professor, department of pediatrics, Brown University, Providence, R.I.
This transcript has been edited for clarity. The transcript and an accompanying video first appeared on Medscape.com.
Justin L. Berk, MD, MPH, MBA: Welcome back to The Cribsiders, our video recap of our pediatric medicine podcast. We interview leading experts in the field to bring clinical pearls and practice-changing knowledge, and answer lingering questions about core topics in pediatric medicine. Chris, what is our topic today?
Christopher J. Chiu, MD: I was really happy to be able to talk about our recent episode with Dr. Carissa Baker-Smith, a pediatric cardiologist and director of the Nemours preventive cardiology program. She helped us review the pediatric screening guidelines for blood pressure, including initial workup and treatment.
Dr. Berk: This was a really great episode that a lot of people found really helpful. What were some of the key takeaway pearls that you think listeners would be interested in?
Dr. Chiu: We talked about when and how we should be checking blood pressures in children. Blood pressure should be checked at every well-child visit starting at age 3. But if they have other risk factors like kidney disease or a condition such as coarctation of the aorta, then blood pressure should be checked at every visit.
Dr. Berk: One thing she spoke about was how blood pressures should be measured. How should we be checking blood pressures in the clinic?
Dr. Chiu: Clinic blood pressures are usually checked with oscillometric devices. They can differ by manufacturer, but basically they find a mean arterial pressure and then each device has a method of calculating systolic and diastolic pressures. Now after that, if the child’s blood pressure is maybe abnormal, you want to double-check a manual blood pressure using Korotkoff sounds to confirm the blood pressure.
She reminded us that blood pressure should be measured with the child sitting with their back supported, feet flat on the floor, and arm at the level of the heart. Make sure you use the right size cuff. The bladder of the cuff should be 40% of the width of the arm, and about 80%-100% of the arm circumference. She recommends sizing up if you have to.
Dr. Berk: Accuracy of blood pressure management was a really important point, especially for diagnosis at this stage. Can you walk us through what we learned about diagnosis of hypertension?
Dr. Chiu: The definitions of hypertension come from the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Up until the age of 13, they define prehypertension as systolic and diastolic blood pressures between the 90th and 95th percentile, or if the blood pressure exceeds 120/80 mm Hg. Hypertension is defined when blood pressure reaches the 95th percentile. Now age 13 is when it gets a little hazy. Many changes in the guidelines happen at age 13, when hypertension starts being defined by adult guidelines. The 2017 adult hypertension guidelines define stage 1 hypertension as 130/89 to 139/89, and stage 2 hypertension as greater than 140/90.
Dr. Berk: How about workup of hypertension? The work of pediatric hypertension is always a little bit complex. What are some of the pearls you took away?
Dr. Chui: She talked about tailoring the workup to the child. So when we’re doing our workup, obviously physical exam should be the first thing we do. You have to assess and compare pulses, which is one of the most important parts of the initial evaluation. Obviously, looking at coarctation of the aorta, but also looking for things like a cushingoid appearance. If the child is less than 6 years of age, she recommends a referral to nephrology for more comprehensive renovascular workup, which probably will include renal ultrasound, urinalysis, metabolic panel, and thyroid studies.
We have to be cognizant of secondary causes of hypertension, such as endocrine tumors, hyperthyroidism, aortic disease, or even medication-induced hypertension. She told us that in the majority of these cases, especially with our obese older children, primary hypertension or essential hypertension is the most likely cause.
Dr. Berk: That was my big takeaway. If they’re really young, they need a big workup, but otherwise it is likely primary hypertension. What did we learn about treatment?
Dr. Chui: Just as we tailor our assessment to the child, we also have to tailor treatment. We know that lifestyle modification is usually the first line of treatment, especially for primary hypertension, and Dr. Baker-Smith tells us that we really need to perform counseling that meets the patient where they are. So if they like dancing to the newest TikTok trends or music videos, maybe we can encourage them to move more that way. Using our motivational interviewing skills is really key here.
If you want to start medication, Dr. Baker-Smith uses things like low-dose ACE inhibitors or calcium channel blockers, but obviously it’ll be tailored to the patient and any underlying conditions.
Dr. Berk: That’s great – a lot of wonderful pearls on the diagnosis and management of pediatric hypertension. Thank you for joining us for another video recap of The Cribsiders pediatric podcast. You can download the full podcast, Off the Cuff: Managing Pediatric Hypertension in Your Primary Care Clinic, on any podcast player, or check out our website at www.theCribsiders.com.
Christopher J. Chiu, MD, is assistant professor, department of internal medicine, division of general internal medicine, Ohio State University, Columbus; lead physician, general internal medicine, OSU Outpatient Care East; department of internal medicine, division of general internal medicine, Ohio State University Wexner Medical Center. Dr. Chiu has disclosed no relevant financial relationships. Justin L. Berk, MD, MPH, MBA, is assistant professor, department of medicine; assistant professor, department of pediatrics, Brown University, Providence, R.I.
This transcript has been edited for clarity. The transcript and an accompanying video first appeared on Medscape.com.
Justin L. Berk, MD, MPH, MBA: Welcome back to The Cribsiders, our video recap of our pediatric medicine podcast. We interview leading experts in the field to bring clinical pearls and practice-changing knowledge, and answer lingering questions about core topics in pediatric medicine. Chris, what is our topic today?
Christopher J. Chiu, MD: I was really happy to be able to talk about our recent episode with Dr. Carissa Baker-Smith, a pediatric cardiologist and director of the Nemours preventive cardiology program. She helped us review the pediatric screening guidelines for blood pressure, including initial workup and treatment.
Dr. Berk: This was a really great episode that a lot of people found really helpful. What were some of the key takeaway pearls that you think listeners would be interested in?
Dr. Chiu: We talked about when and how we should be checking blood pressures in children. Blood pressure should be checked at every well-child visit starting at age 3. But if they have other risk factors like kidney disease or a condition such as coarctation of the aorta, then blood pressure should be checked at every visit.
Dr. Berk: One thing she spoke about was how blood pressures should be measured. How should we be checking blood pressures in the clinic?
Dr. Chiu: Clinic blood pressures are usually checked with oscillometric devices. They can differ by manufacturer, but basically they find a mean arterial pressure and then each device has a method of calculating systolic and diastolic pressures. Now after that, if the child’s blood pressure is maybe abnormal, you want to double-check a manual blood pressure using Korotkoff sounds to confirm the blood pressure.
She reminded us that blood pressure should be measured with the child sitting with their back supported, feet flat on the floor, and arm at the level of the heart. Make sure you use the right size cuff. The bladder of the cuff should be 40% of the width of the arm, and about 80%-100% of the arm circumference. She recommends sizing up if you have to.
Dr. Berk: Accuracy of blood pressure management was a really important point, especially for diagnosis at this stage. Can you walk us through what we learned about diagnosis of hypertension?
Dr. Chiu: The definitions of hypertension come from the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Up until the age of 13, they define prehypertension as systolic and diastolic blood pressures between the 90th and 95th percentile, or if the blood pressure exceeds 120/80 mm Hg. Hypertension is defined when blood pressure reaches the 95th percentile. Now age 13 is when it gets a little hazy. Many changes in the guidelines happen at age 13, when hypertension starts being defined by adult guidelines. The 2017 adult hypertension guidelines define stage 1 hypertension as 130/89 to 139/89, and stage 2 hypertension as greater than 140/90.
Dr. Berk: How about workup of hypertension? The work of pediatric hypertension is always a little bit complex. What are some of the pearls you took away?
Dr. Chui: She talked about tailoring the workup to the child. So when we’re doing our workup, obviously physical exam should be the first thing we do. You have to assess and compare pulses, which is one of the most important parts of the initial evaluation. Obviously, looking at coarctation of the aorta, but also looking for things like a cushingoid appearance. If the child is less than 6 years of age, she recommends a referral to nephrology for more comprehensive renovascular workup, which probably will include renal ultrasound, urinalysis, metabolic panel, and thyroid studies.
We have to be cognizant of secondary causes of hypertension, such as endocrine tumors, hyperthyroidism, aortic disease, or even medication-induced hypertension. She told us that in the majority of these cases, especially with our obese older children, primary hypertension or essential hypertension is the most likely cause.
Dr. Berk: That was my big takeaway. If they’re really young, they need a big workup, but otherwise it is likely primary hypertension. What did we learn about treatment?
Dr. Chui: Just as we tailor our assessment to the child, we also have to tailor treatment. We know that lifestyle modification is usually the first line of treatment, especially for primary hypertension, and Dr. Baker-Smith tells us that we really need to perform counseling that meets the patient where they are. So if they like dancing to the newest TikTok trends or music videos, maybe we can encourage them to move more that way. Using our motivational interviewing skills is really key here.
If you want to start medication, Dr. Baker-Smith uses things like low-dose ACE inhibitors or calcium channel blockers, but obviously it’ll be tailored to the patient and any underlying conditions.
Dr. Berk: That’s great – a lot of wonderful pearls on the diagnosis and management of pediatric hypertension. Thank you for joining us for another video recap of The Cribsiders pediatric podcast. You can download the full podcast, Off the Cuff: Managing Pediatric Hypertension in Your Primary Care Clinic, on any podcast player, or check out our website at www.theCribsiders.com.
Christopher J. Chiu, MD, is assistant professor, department of internal medicine, division of general internal medicine, Ohio State University, Columbus; lead physician, general internal medicine, OSU Outpatient Care East; department of internal medicine, division of general internal medicine, Ohio State University Wexner Medical Center. Dr. Chiu has disclosed no relevant financial relationships. Justin L. Berk, MD, MPH, MBA, is assistant professor, department of medicine; assistant professor, department of pediatrics, Brown University, Providence, R.I.
Nicotine and Nicotine Replacement Therapy Use During Myocardial Perfusion Imaging
Chest pain is one of the most common concerns in patients presenting to the emergency department in the United States, accounting for approximately 7.6 million visits annually.1 Given the high mortality rate associated with acute coronary syndromes, prompt evaluation of chest pain is essential.2 Even in mild cases, recognition of newly onset or worsening coronary artery disease (CAD) is crucial to ensure that patients receive optimal medication therapy.
In symptomatic patients with risk factors for CAD, such as advanced age, hypertension, hyperlipidemia, obesity, and diabetes mellitus, myocardial perfusion imaging (MPI) is frequently used as a modality to assess the presence, location, and severity of ischemic or infarcted myocardium.2 MPI requires administration of a radiopharmaceutical before and after the patient undergoes a form of stress.2 This radiopharmaceutical is then detected in the myocardium with a nuclear camera, and images are obtained of the heart to assess myocardial blood flow.2
MPI can be performed using exercise-induced stress via a treadmill, or medication-induced stress (Table 1). In both strategies, healthy coronary arteries dilate to provide the myocardium with more blood flow to meet the increasing myocardial oxygen demand during this period of stress. While healthy vessels are able to dilate appropriately, coronary arteries with flow-limiting stenoses are unable to dilate to the same extent in response to stress.2 Because radioactive isotope uptake by the myocardium is directly related to arterial blood flow, MPI is able to demonstrate a mismatch in coronary blood flow between healthy and diseased coronary arteries indicated by differences in radioisotope uptake.2 The presence of such a mismatch, in conjunction with clinical history, potentially suggests the presence of CAD.
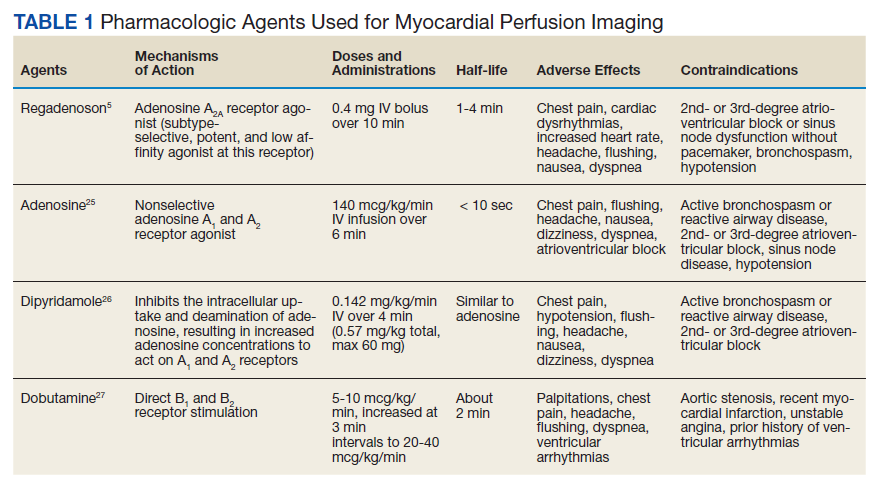
Prior to conducting MPI with a medication, certain substances should be avoided. For instance, methylxanthines, such as caffeine, aminophylline, and theophylline, antagonize adenosine receptors and can have major drug interactions with regadenoson, adenosine, and dipyridamole. Therefore, it is advised that these substances be stopped for at least 12 hours before testing.3 In some cases, other medications that can affect coronary blood flow, such as long-acting nitrates, β-blockers, and calcium channel blockers, are recommended to be avoided for 12 to 48 hours in order to obtain the most accurate depiction of underlying coronary disease.4
Because nicotine and nicotine replacement therapy (NRT) may have substantial effects on coronary circulation, a current area of controversy is whether these should be stopped prior to the use of a stress-inducing medication during MPI. To date, no formal drug interaction studies have been conducted between nicotine and regadenoson.5 Similarly, the ADVANCE MPI 2 Trial, which led to the US Food and Drug Administration approval of regadenoson, did not specify restrictions on the use of nicotine prior to stress testing in the protocol.6 However, as this trial was multicenter, investigators admit that individual study sites could have had their own restrictions on the use of nicotine prior to stress testing with regadenoson, but this information was not collected.6 The current review focuses on how the simultaneous use of nicotine or NRT during MPI with pharmacologic agents, such as regadenoson, may affect the accuracy of imaging results and the clinical impact of this interaction.
Nicotine Coronary Artery Effect
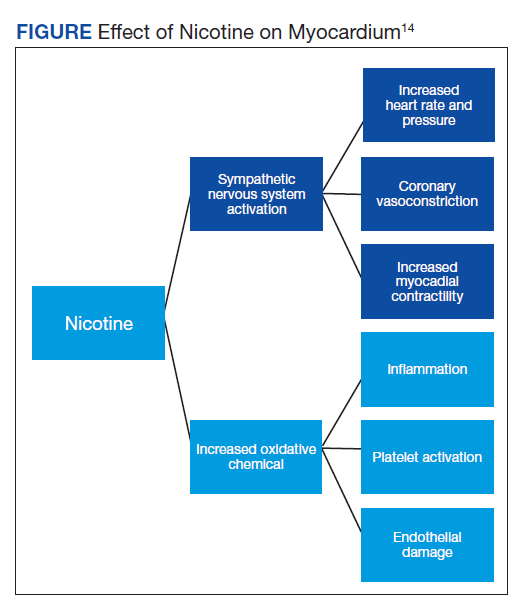
It is well documented that long-term cigarette smoking is a major risk factor for CAD.7 Compared with nonsmokers, cigarette smokers experience 2 times greater risk of morbidity and mortality from ischemic heart disease.7 There are several mechanisms by which nicotine induces damage to the myocardium (Figure). Nicotine has direct effects on both the sympathetic nervous system (SNS) and myocardial endothelium.8 Together, these factors result in reduced coronary blood flow, leading to less oxygen supply to meet an increased oxygen demand, resulting in myocardial ischemia.
Nicotine’s effect on coronary vasomotor tone occurs primarily through noradrenergic stimulation of α and β receptors associated with coronary vasoconstriction or vasodilation, respectively.9,10 These competing influences on coronary blood flow appear to manifest differently based on whether patients are at rest or in a stressed state. A study by Czerin and colleagues demonstrated that in healthy patients with relatively short smoking histories and in a healthy nonsmoker control group, coronary blood flow increased by 25% and 40%, respectively, with nicotine use at rest.9 However, when these patients were stressed with dipyramidole and while smoking during the examination, myocardial blood flow was reduced by 11% in the study group and 14% in the control group.9 This is likely because the patients studied had relatively healthy coronary arteries that were able to maximally dilate when stressed. In this scenario, nicotine’s dilatory effects are offset by nicotine’s α-receptor–mediated vasoconstriction effects.9 Of note, patients in the study group experienced a somewhat diminished increase in coronary blood flow at rest with nicotine use, suggesting that even a short smoking history may damage the myocardial endothelium, rendering it less responsive to nicotine’s vasodilatory effects.9
These principles similarly apply to patients with underlying moderate-to-severe cardiovascular disease (CVD). With nicotine use at rest, patients with significant CAD do not experience as dramatic of an increase in coronary blood flow, which typically decreases or remains the same despite increased myocardial work.10 This may be because patients with moderate-to-severe CAD often have flow-limiting stenoses and damaged endothelium that do not allow vessels to respond as efficiently to increased myocardial demand or to nicotine’s β-receptor–mediated vasodilatory effects.10,11 Moreover, when stressed, diseased coronary arteries are not able to further dilate and nicotine’s α-receptor–mediated vasoconstriction effects dominate.10,11
In a study by Quillen and colleagues of patients with moderate-to-severe CAD, the mean diameter of proximal coronary artery segments decreased by 5%, the distal coronary diameter decreased 8%, and the coronary vascular resistance increased by 21% while smoking at rest.12 The investigators did not analyze how parameters changed when these diseased coronary arteries were stressed using a medication during MPI. However, it can be predicted that coronary arteries would have constricted to a similar or greater degree than observed in Czerin and colleagues’ study, given that the underlying myocardium was diseased and more susceptible to nicotine’s vasoconstriction effects.9 Importantly, these studies have several limitations, most notably that they are older and have small sample sizes. Additionally, while statistically significant differences were found in the degree of changes in coronary circulation with nicotine use at rest and during stress, it is unclear whether this translates to a clinically significant and impactful finding.9-12
Nicotine Replacement Therapy and Stress Testing
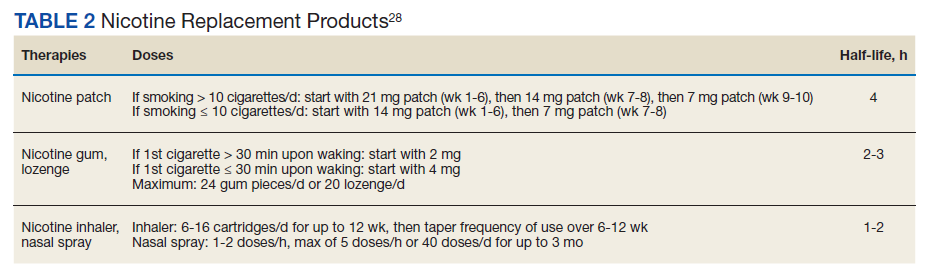
Given the association between cigarette smoking and CAD, medical practitioners strongly encourage patients to quit smoking to reduce their risk of adverse cardiovascular outcomes. Various smoking cessation treatments are available for patients. Common, readily accessible forms of therapy include nicotine replacement products (Table 2).
Early studies of NRT in patients with underlying CVD found an increased risk of cardiovascular events, such as myocardial infarction, presumably due to the nicotine content of these products.13,14 However, the concentration of nicotine in NRT is substantially lower than that found in cigarettes and in some formulations, such as transdermal patches, nicotine is delivered over a prolonged period of time.15 For this reason, NRT is thought to be safe in patients with underlying CVD and stable ischemic heart disease. A recent systematic review and meta-analysis found that while NRT may be associated with tachycardia, it did not increase the risk of more serious cardiovascular adverse effects (AEs).16,17
Given the lower nicotine concentration in NRT products, the associated hemodynamic effect of nicotine also is thought to be less pronounced. In a study conducted by Tzivoni and colleagues in patients with CAD using transdermal nicotine patches, no differences in blood pressure, heart rate, ischemia, or arrhythmias were found from baseline to 2 weeks.18 These findings were further confirmed in a small study by Lucini and colleagues, which found that nicotine patches produced slight hemodynamic effects, but to a lesser extent than cigarette smoking.19 For the NRT gum formulation, while a small study found that 4 mg produced coronary vasoconstriction in patients with underlying CAD, a study by Nitenberg and Antony demonstrated that healthy and diseased coronary arteries did not significantly constrict while patients were using nicotine gum both before and after a cold pressor test, suggesting a lesser degree of coronary vasoconstriction than nicotine from cigarette smoking.20,21 Similar findings have been described with the nicotine intranasal spray in a study by Keeley and colleagues, which showed no additional AEs on myocardial demand or vasoconstriction when an intranasal nicotine spray was added to cigarette smoking.22 Importantly, a review of the transdermal and gum formulations found that these less pronounced hemodynamic effects were observed across different doses of NRT; however, further studies are needed to clarify the relationship between NRT dose and cardiovascular effects.23
Overall, NRT does not seem to activate the SNS to the same degree as nicotine obtained via cigarette smoking and likely does not increase the myocardial oxygen demand as much. Additionally, by containing a lower concentration of nicotine, NRT may not impair the myocardium’s ability to supply oxygen to coronary arteries to the same extent as nicotine from cigarette smoking. Therefore, the effects of NRT on MPI using a stress-inducing medication may not be as pronounced. However, due to study limitations, results should be interpreted cautiously.18-23
Conclusions
Because of the close relationship between cigarette smoking and CAD, many patients with underlying CVD are either current smokers or may be using NRT for smoking cessation. Therefore, the question of whether to refrain from nicotine use prior to MPI is clinically relevant. Currently, there is a lack of high-quality studies demonstrating the effects of nicotine and NRT on coronary perfusion. Because of this, the impact of nicotine and NRT use on the accuracy of MPI using stress-inducing medications remains uncertain. Nevertheless, given that nicotine and NRT may largely affect the accuracy of imaging results, several institutions have adopted protocols that prohibit patients from using these drugs on the day of nuclear stress testing.
There are currently no data specifying the number of hours to hold nicotine products prior to cardiac stress testing. It is generally recommended that other medications that affect coronary blood flow be held for 5 half-lives before conducting MPI.4 Following the same guidance for nicotine and NRT may present a reasonable approach to ensure accurate imaging results. Based on the discussed literature, patients should be instructed to refrain from cigarette smoking for at least 5 to 10 hours prior to MPI, given nicotine’s half-life of about 1 to 2 hours.24
The data for NRT are less clear. While use of NRT may not be an absolute contraindication to conducting MPI, it is important to consider that this may affect the accuracy of results. Given this uncertainty, it is likely ideal to hold NRT prior to MPI, based on the specific formulation of NRT and that product's half-life. Further robust studies are needed to analyze the impact of nicotine and NRT on the accuracy of nuclear stress testing using a medication.
1. Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf
2. Lange RA. Cardiovascular testing. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. McGraw Hill; 2017.
3. Mace S. Observation Medicine: Principles and Protocols. Cambridge University Press; 2017.
4. Currie GM. Pharmacology, part 4: nuclear cardiology. J Nucl Med Technol. 2019;47(2):97-110. doi:10.2967/jnmt.118.219675
5. Regadenoson; Package insert. Astellas Pharma US Inc; 2008.
6. Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14(5):645-658. doi:10.1016/j.nuclcard.2007.06.114
7. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109-114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
8. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends Cardiovasc Med. 2016;26(6):515-523. doi:10.1016/j.tcm.2016.03.001
9. Czernin J, Sun K, Brunken R, Böttcher M, Phelps M, Schelbert H. Effect of acute and long-term smoking on myocardial blood flow and flow reserve. Circulation. 1995;91:2891-2897. doi:10.1161/01.CIR.91.12.2891
10. Winniford MD, Wheelan KR, Kremers MS, et al. Smoking-induced coronary vasoconstriction in patients with atherosclerotic coronary artery disease: evidence for adrenergically mediated alterations in coronary artery tone. Circulation. 1986;73(4):662-667. doi:10.1161/01.cir.73.4.662
11. Klein LW, Ambrose J, Pichard A, Holt J, Gorlin R, Teichholz LE. Acute coronary hemodynamic response to cigarette smoking in patients with coronary artery disease. J Am Coll Cardiol. 1984;3(4):879-886. doi:10.1016/s0735-1097(84)80344-7
12. Quillen JE, Rossen JD, Oskarsson HJ, Minor RL Jr, Lopez AG, Winniford MD. Acute effect of cigarette smoking on the coronary circulation: constriction of epicardial and resistance vessels. J Am Coll Cardiol. 1993;22(3):642-647. doi:10.1016/0735-1097(93)90170-6
13. Dacosta A, Guy JM, Tardy B, et al. Myocardial infarction and nicotine patch: a contributing or causative factor?. Eur Heart J. 1993;14(12):1709-1711. doi:10.1093/eurheartj/14.12.1709
14. Ottervanger JP, Festen JM, de Vries AG, Stricker BH. Acute myocardial infarction while using the nicotine patch. Chest. 1995;107(6):1765-1766. doi:10.1378/chest.107.6.1765
15. Dollerup J, Vestbo J, Murray-Thomas T, et al. Cardiovascular risks in smokers treated with nicotine replacement therapy: a historical cohort study. Clin Epidemiol. 2017;9:231-243. Published 2017 Apr 26. doi:10.2147/CLEP.S127775
16. Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis. 2010;8(1):8. Published 2010 Jul 13. doi:10.1186/1617-9625-8-8
17. Mills EJ, Thorlund K, Eapen S, Wu P, Prochaska JJ. Cardiovascular events associated with smoking cessation pharmacotherapies: a network meta-analysis. Circulation. 2014;129(1):28-41. doi:10.1161/CIRCULATIONAHA.113.003961
18. Tzivoni D, Keren A, Meyler S, Khoury Z, Lerer T, Brunel P. Cardiovascular safety of transdermal nicotine patches in patients with coronary artery disease who try to quit smoking. Cardiovasc Drugs Ther. 1998;12(3):239-244. doi:10.1023/a:1007757530765
19. Lucini D, Bertocchi F, Malliani A, Pagani M. Autonomic effects of nicotine patch administration in habitual cigarette smokers: a double-blind, placebo-controlled study using spectral analysis of RR interval and systolic arterial pressure variabilities. J Cardiovasc Pharmacol. 1998;31(5):714-720. doi:10.1097/00005344-199805000-00010
20. Kaijser L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985;5(6):541-552. doi:10.1111/j.1475-097x.1985.tb00767.x
21. Nitenberg A, Antony I. Effects of nicotine gum on coronary vasomotor responses during sympathetic stimulation in patients with coronary artery stenosis. J Cardiovasc Pharmacol. 1999;34(5):694-699. doi:10.1097/00005344-199911000-00011
22. Keeley EC, Pirwitz MJ, Landau C, et al. Intranasal nicotine spray does not augment the adverse effects of cigarette smoking on myocardial oxygen demand or coronary arterial dimensions. Am J Med. 1996;101(4):357-363. doi:10.1016/s0002-9343(96)00237-9
23. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422-1431. doi:10.1016/s0735-1097(97)00079-x
24. Flowers L. Nicotine replacement therapy. Amer J Psych. 2017;11(6):4-7.
25. Adenosine; Package insert. Astellas Pharma US Inc; 1989.
26. Dipyridamole; Package insert. Boehringer Ingelheim Pharmaceuticals Inc; 2019.
27. Dobutamine; Package insert. Baxter Healthcare Corporation; 2012.
Chest pain is one of the most common concerns in patients presenting to the emergency department in the United States, accounting for approximately 7.6 million visits annually.1 Given the high mortality rate associated with acute coronary syndromes, prompt evaluation of chest pain is essential.2 Even in mild cases, recognition of newly onset or worsening coronary artery disease (CAD) is crucial to ensure that patients receive optimal medication therapy.
In symptomatic patients with risk factors for CAD, such as advanced age, hypertension, hyperlipidemia, obesity, and diabetes mellitus, myocardial perfusion imaging (MPI) is frequently used as a modality to assess the presence, location, and severity of ischemic or infarcted myocardium.2 MPI requires administration of a radiopharmaceutical before and after the patient undergoes a form of stress.2 This radiopharmaceutical is then detected in the myocardium with a nuclear camera, and images are obtained of the heart to assess myocardial blood flow.2
MPI can be performed using exercise-induced stress via a treadmill, or medication-induced stress (Table 1). In both strategies, healthy coronary arteries dilate to provide the myocardium with more blood flow to meet the increasing myocardial oxygen demand during this period of stress. While healthy vessels are able to dilate appropriately, coronary arteries with flow-limiting stenoses are unable to dilate to the same extent in response to stress.2 Because radioactive isotope uptake by the myocardium is directly related to arterial blood flow, MPI is able to demonstrate a mismatch in coronary blood flow between healthy and diseased coronary arteries indicated by differences in radioisotope uptake.2 The presence of such a mismatch, in conjunction with clinical history, potentially suggests the presence of CAD.
Prior to conducting MPI with a medication, certain substances should be avoided. For instance, methylxanthines, such as caffeine, aminophylline, and theophylline, antagonize adenosine receptors and can have major drug interactions with regadenoson, adenosine, and dipyridamole. Therefore, it is advised that these substances be stopped for at least 12 hours before testing.3 In some cases, other medications that can affect coronary blood flow, such as long-acting nitrates, β-blockers, and calcium channel blockers, are recommended to be avoided for 12 to 48 hours in order to obtain the most accurate depiction of underlying coronary disease.4
Because nicotine and nicotine replacement therapy (NRT) may have substantial effects on coronary circulation, a current area of controversy is whether these should be stopped prior to the use of a stress-inducing medication during MPI. To date, no formal drug interaction studies have been conducted between nicotine and regadenoson.5 Similarly, the ADVANCE MPI 2 Trial, which led to the US Food and Drug Administration approval of regadenoson, did not specify restrictions on the use of nicotine prior to stress testing in the protocol.6 However, as this trial was multicenter, investigators admit that individual study sites could have had their own restrictions on the use of nicotine prior to stress testing with regadenoson, but this information was not collected.6 The current review focuses on how the simultaneous use of nicotine or NRT during MPI with pharmacologic agents, such as regadenoson, may affect the accuracy of imaging results and the clinical impact of this interaction.
Nicotine Coronary Artery Effect
It is well documented that long-term cigarette smoking is a major risk factor for CAD.7 Compared with nonsmokers, cigarette smokers experience 2 times greater risk of morbidity and mortality from ischemic heart disease.7 There are several mechanisms by which nicotine induces damage to the myocardium (Figure). Nicotine has direct effects on both the sympathetic nervous system (SNS) and myocardial endothelium.8 Together, these factors result in reduced coronary blood flow, leading to less oxygen supply to meet an increased oxygen demand, resulting in myocardial ischemia.
Nicotine’s effect on coronary vasomotor tone occurs primarily through noradrenergic stimulation of α and β receptors associated with coronary vasoconstriction or vasodilation, respectively.9,10 These competing influences on coronary blood flow appear to manifest differently based on whether patients are at rest or in a stressed state. A study by Czerin and colleagues demonstrated that in healthy patients with relatively short smoking histories and in a healthy nonsmoker control group, coronary blood flow increased by 25% and 40%, respectively, with nicotine use at rest.9 However, when these patients were stressed with dipyramidole and while smoking during the examination, myocardial blood flow was reduced by 11% in the study group and 14% in the control group.9 This is likely because the patients studied had relatively healthy coronary arteries that were able to maximally dilate when stressed. In this scenario, nicotine’s dilatory effects are offset by nicotine’s α-receptor–mediated vasoconstriction effects.9 Of note, patients in the study group experienced a somewhat diminished increase in coronary blood flow at rest with nicotine use, suggesting that even a short smoking history may damage the myocardial endothelium, rendering it less responsive to nicotine’s vasodilatory effects.9
These principles similarly apply to patients with underlying moderate-to-severe cardiovascular disease (CVD). With nicotine use at rest, patients with significant CAD do not experience as dramatic of an increase in coronary blood flow, which typically decreases or remains the same despite increased myocardial work.10 This may be because patients with moderate-to-severe CAD often have flow-limiting stenoses and damaged endothelium that do not allow vessels to respond as efficiently to increased myocardial demand or to nicotine’s β-receptor–mediated vasodilatory effects.10,11 Moreover, when stressed, diseased coronary arteries are not able to further dilate and nicotine’s α-receptor–mediated vasoconstriction effects dominate.10,11
In a study by Quillen and colleagues of patients with moderate-to-severe CAD, the mean diameter of proximal coronary artery segments decreased by 5%, the distal coronary diameter decreased 8%, and the coronary vascular resistance increased by 21% while smoking at rest.12 The investigators did not analyze how parameters changed when these diseased coronary arteries were stressed using a medication during MPI. However, it can be predicted that coronary arteries would have constricted to a similar or greater degree than observed in Czerin and colleagues’ study, given that the underlying myocardium was diseased and more susceptible to nicotine’s vasoconstriction effects.9 Importantly, these studies have several limitations, most notably that they are older and have small sample sizes. Additionally, while statistically significant differences were found in the degree of changes in coronary circulation with nicotine use at rest and during stress, it is unclear whether this translates to a clinically significant and impactful finding.9-12
Nicotine Replacement Therapy and Stress Testing
Given the association between cigarette smoking and CAD, medical practitioners strongly encourage patients to quit smoking to reduce their risk of adverse cardiovascular outcomes. Various smoking cessation treatments are available for patients. Common, readily accessible forms of therapy include nicotine replacement products (Table 2).
Early studies of NRT in patients with underlying CVD found an increased risk of cardiovascular events, such as myocardial infarction, presumably due to the nicotine content of these products.13,14 However, the concentration of nicotine in NRT is substantially lower than that found in cigarettes and in some formulations, such as transdermal patches, nicotine is delivered over a prolonged period of time.15 For this reason, NRT is thought to be safe in patients with underlying CVD and stable ischemic heart disease. A recent systematic review and meta-analysis found that while NRT may be associated with tachycardia, it did not increase the risk of more serious cardiovascular adverse effects (AEs).16,17
Given the lower nicotine concentration in NRT products, the associated hemodynamic effect of nicotine also is thought to be less pronounced. In a study conducted by Tzivoni and colleagues in patients with CAD using transdermal nicotine patches, no differences in blood pressure, heart rate, ischemia, or arrhythmias were found from baseline to 2 weeks.18 These findings were further confirmed in a small study by Lucini and colleagues, which found that nicotine patches produced slight hemodynamic effects, but to a lesser extent than cigarette smoking.19 For the NRT gum formulation, while a small study found that 4 mg produced coronary vasoconstriction in patients with underlying CAD, a study by Nitenberg and Antony demonstrated that healthy and diseased coronary arteries did not significantly constrict while patients were using nicotine gum both before and after a cold pressor test, suggesting a lesser degree of coronary vasoconstriction than nicotine from cigarette smoking.20,21 Similar findings have been described with the nicotine intranasal spray in a study by Keeley and colleagues, which showed no additional AEs on myocardial demand or vasoconstriction when an intranasal nicotine spray was added to cigarette smoking.22 Importantly, a review of the transdermal and gum formulations found that these less pronounced hemodynamic effects were observed across different doses of NRT; however, further studies are needed to clarify the relationship between NRT dose and cardiovascular effects.23
Overall, NRT does not seem to activate the SNS to the same degree as nicotine obtained via cigarette smoking and likely does not increase the myocardial oxygen demand as much. Additionally, by containing a lower concentration of nicotine, NRT may not impair the myocardium’s ability to supply oxygen to coronary arteries to the same extent as nicotine from cigarette smoking. Therefore, the effects of NRT on MPI using a stress-inducing medication may not be as pronounced. However, due to study limitations, results should be interpreted cautiously.18-23
Conclusions
Because of the close relationship between cigarette smoking and CAD, many patients with underlying CVD are either current smokers or may be using NRT for smoking cessation. Therefore, the question of whether to refrain from nicotine use prior to MPI is clinically relevant. Currently, there is a lack of high-quality studies demonstrating the effects of nicotine and NRT on coronary perfusion. Because of this, the impact of nicotine and NRT use on the accuracy of MPI using stress-inducing medications remains uncertain. Nevertheless, given that nicotine and NRT may largely affect the accuracy of imaging results, several institutions have adopted protocols that prohibit patients from using these drugs on the day of nuclear stress testing.
There are currently no data specifying the number of hours to hold nicotine products prior to cardiac stress testing. It is generally recommended that other medications that affect coronary blood flow be held for 5 half-lives before conducting MPI.4 Following the same guidance for nicotine and NRT may present a reasonable approach to ensure accurate imaging results. Based on the discussed literature, patients should be instructed to refrain from cigarette smoking for at least 5 to 10 hours prior to MPI, given nicotine’s half-life of about 1 to 2 hours.24
The data for NRT are less clear. While use of NRT may not be an absolute contraindication to conducting MPI, it is important to consider that this may affect the accuracy of results. Given this uncertainty, it is likely ideal to hold NRT prior to MPI, based on the specific formulation of NRT and that product's half-life. Further robust studies are needed to analyze the impact of nicotine and NRT on the accuracy of nuclear stress testing using a medication.
Chest pain is one of the most common concerns in patients presenting to the emergency department in the United States, accounting for approximately 7.6 million visits annually.1 Given the high mortality rate associated with acute coronary syndromes, prompt evaluation of chest pain is essential.2 Even in mild cases, recognition of newly onset or worsening coronary artery disease (CAD) is crucial to ensure that patients receive optimal medication therapy.
In symptomatic patients with risk factors for CAD, such as advanced age, hypertension, hyperlipidemia, obesity, and diabetes mellitus, myocardial perfusion imaging (MPI) is frequently used as a modality to assess the presence, location, and severity of ischemic or infarcted myocardium.2 MPI requires administration of a radiopharmaceutical before and after the patient undergoes a form of stress.2 This radiopharmaceutical is then detected in the myocardium with a nuclear camera, and images are obtained of the heart to assess myocardial blood flow.2
MPI can be performed using exercise-induced stress via a treadmill, or medication-induced stress (Table 1). In both strategies, healthy coronary arteries dilate to provide the myocardium with more blood flow to meet the increasing myocardial oxygen demand during this period of stress. While healthy vessels are able to dilate appropriately, coronary arteries with flow-limiting stenoses are unable to dilate to the same extent in response to stress.2 Because radioactive isotope uptake by the myocardium is directly related to arterial blood flow, MPI is able to demonstrate a mismatch in coronary blood flow between healthy and diseased coronary arteries indicated by differences in radioisotope uptake.2 The presence of such a mismatch, in conjunction with clinical history, potentially suggests the presence of CAD.
Prior to conducting MPI with a medication, certain substances should be avoided. For instance, methylxanthines, such as caffeine, aminophylline, and theophylline, antagonize adenosine receptors and can have major drug interactions with regadenoson, adenosine, and dipyridamole. Therefore, it is advised that these substances be stopped for at least 12 hours before testing.3 In some cases, other medications that can affect coronary blood flow, such as long-acting nitrates, β-blockers, and calcium channel blockers, are recommended to be avoided for 12 to 48 hours in order to obtain the most accurate depiction of underlying coronary disease.4
Because nicotine and nicotine replacement therapy (NRT) may have substantial effects on coronary circulation, a current area of controversy is whether these should be stopped prior to the use of a stress-inducing medication during MPI. To date, no formal drug interaction studies have been conducted between nicotine and regadenoson.5 Similarly, the ADVANCE MPI 2 Trial, which led to the US Food and Drug Administration approval of regadenoson, did not specify restrictions on the use of nicotine prior to stress testing in the protocol.6 However, as this trial was multicenter, investigators admit that individual study sites could have had their own restrictions on the use of nicotine prior to stress testing with regadenoson, but this information was not collected.6 The current review focuses on how the simultaneous use of nicotine or NRT during MPI with pharmacologic agents, such as regadenoson, may affect the accuracy of imaging results and the clinical impact of this interaction.
Nicotine Coronary Artery Effect
It is well documented that long-term cigarette smoking is a major risk factor for CAD.7 Compared with nonsmokers, cigarette smokers experience 2 times greater risk of morbidity and mortality from ischemic heart disease.7 There are several mechanisms by which nicotine induces damage to the myocardium (Figure). Nicotine has direct effects on both the sympathetic nervous system (SNS) and myocardial endothelium.8 Together, these factors result in reduced coronary blood flow, leading to less oxygen supply to meet an increased oxygen demand, resulting in myocardial ischemia.
Nicotine’s effect on coronary vasomotor tone occurs primarily through noradrenergic stimulation of α and β receptors associated with coronary vasoconstriction or vasodilation, respectively.9,10 These competing influences on coronary blood flow appear to manifest differently based on whether patients are at rest or in a stressed state. A study by Czerin and colleagues demonstrated that in healthy patients with relatively short smoking histories and in a healthy nonsmoker control group, coronary blood flow increased by 25% and 40%, respectively, with nicotine use at rest.9 However, when these patients were stressed with dipyramidole and while smoking during the examination, myocardial blood flow was reduced by 11% in the study group and 14% in the control group.9 This is likely because the patients studied had relatively healthy coronary arteries that were able to maximally dilate when stressed. In this scenario, nicotine’s dilatory effects are offset by nicotine’s α-receptor–mediated vasoconstriction effects.9 Of note, patients in the study group experienced a somewhat diminished increase in coronary blood flow at rest with nicotine use, suggesting that even a short smoking history may damage the myocardial endothelium, rendering it less responsive to nicotine’s vasodilatory effects.9
These principles similarly apply to patients with underlying moderate-to-severe cardiovascular disease (CVD). With nicotine use at rest, patients with significant CAD do not experience as dramatic of an increase in coronary blood flow, which typically decreases or remains the same despite increased myocardial work.10 This may be because patients with moderate-to-severe CAD often have flow-limiting stenoses and damaged endothelium that do not allow vessels to respond as efficiently to increased myocardial demand or to nicotine’s β-receptor–mediated vasodilatory effects.10,11 Moreover, when stressed, diseased coronary arteries are not able to further dilate and nicotine’s α-receptor–mediated vasoconstriction effects dominate.10,11
In a study by Quillen and colleagues of patients with moderate-to-severe CAD, the mean diameter of proximal coronary artery segments decreased by 5%, the distal coronary diameter decreased 8%, and the coronary vascular resistance increased by 21% while smoking at rest.12 The investigators did not analyze how parameters changed when these diseased coronary arteries were stressed using a medication during MPI. However, it can be predicted that coronary arteries would have constricted to a similar or greater degree than observed in Czerin and colleagues’ study, given that the underlying myocardium was diseased and more susceptible to nicotine’s vasoconstriction effects.9 Importantly, these studies have several limitations, most notably that they are older and have small sample sizes. Additionally, while statistically significant differences were found in the degree of changes in coronary circulation with nicotine use at rest and during stress, it is unclear whether this translates to a clinically significant and impactful finding.9-12
Nicotine Replacement Therapy and Stress Testing
Given the association between cigarette smoking and CAD, medical practitioners strongly encourage patients to quit smoking to reduce their risk of adverse cardiovascular outcomes. Various smoking cessation treatments are available for patients. Common, readily accessible forms of therapy include nicotine replacement products (Table 2).
Early studies of NRT in patients with underlying CVD found an increased risk of cardiovascular events, such as myocardial infarction, presumably due to the nicotine content of these products.13,14 However, the concentration of nicotine in NRT is substantially lower than that found in cigarettes and in some formulations, such as transdermal patches, nicotine is delivered over a prolonged period of time.15 For this reason, NRT is thought to be safe in patients with underlying CVD and stable ischemic heart disease. A recent systematic review and meta-analysis found that while NRT may be associated with tachycardia, it did not increase the risk of more serious cardiovascular adverse effects (AEs).16,17
Given the lower nicotine concentration in NRT products, the associated hemodynamic effect of nicotine also is thought to be less pronounced. In a study conducted by Tzivoni and colleagues in patients with CAD using transdermal nicotine patches, no differences in blood pressure, heart rate, ischemia, or arrhythmias were found from baseline to 2 weeks.18 These findings were further confirmed in a small study by Lucini and colleagues, which found that nicotine patches produced slight hemodynamic effects, but to a lesser extent than cigarette smoking.19 For the NRT gum formulation, while a small study found that 4 mg produced coronary vasoconstriction in patients with underlying CAD, a study by Nitenberg and Antony demonstrated that healthy and diseased coronary arteries did not significantly constrict while patients were using nicotine gum both before and after a cold pressor test, suggesting a lesser degree of coronary vasoconstriction than nicotine from cigarette smoking.20,21 Similar findings have been described with the nicotine intranasal spray in a study by Keeley and colleagues, which showed no additional AEs on myocardial demand or vasoconstriction when an intranasal nicotine spray was added to cigarette smoking.22 Importantly, a review of the transdermal and gum formulations found that these less pronounced hemodynamic effects were observed across different doses of NRT; however, further studies are needed to clarify the relationship between NRT dose and cardiovascular effects.23
Overall, NRT does not seem to activate the SNS to the same degree as nicotine obtained via cigarette smoking and likely does not increase the myocardial oxygen demand as much. Additionally, by containing a lower concentration of nicotine, NRT may not impair the myocardium’s ability to supply oxygen to coronary arteries to the same extent as nicotine from cigarette smoking. Therefore, the effects of NRT on MPI using a stress-inducing medication may not be as pronounced. However, due to study limitations, results should be interpreted cautiously.18-23
Conclusions
Because of the close relationship between cigarette smoking and CAD, many patients with underlying CVD are either current smokers or may be using NRT for smoking cessation. Therefore, the question of whether to refrain from nicotine use prior to MPI is clinically relevant. Currently, there is a lack of high-quality studies demonstrating the effects of nicotine and NRT on coronary perfusion. Because of this, the impact of nicotine and NRT use on the accuracy of MPI using stress-inducing medications remains uncertain. Nevertheless, given that nicotine and NRT may largely affect the accuracy of imaging results, several institutions have adopted protocols that prohibit patients from using these drugs on the day of nuclear stress testing.
There are currently no data specifying the number of hours to hold nicotine products prior to cardiac stress testing. It is generally recommended that other medications that affect coronary blood flow be held for 5 half-lives before conducting MPI.4 Following the same guidance for nicotine and NRT may present a reasonable approach to ensure accurate imaging results. Based on the discussed literature, patients should be instructed to refrain from cigarette smoking for at least 5 to 10 hours prior to MPI, given nicotine’s half-life of about 1 to 2 hours.24
The data for NRT are less clear. While use of NRT may not be an absolute contraindication to conducting MPI, it is important to consider that this may affect the accuracy of results. Given this uncertainty, it is likely ideal to hold NRT prior to MPI, based on the specific formulation of NRT and that product's half-life. Further robust studies are needed to analyze the impact of nicotine and NRT on the accuracy of nuclear stress testing using a medication.
1. Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf
2. Lange RA. Cardiovascular testing. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. McGraw Hill; 2017.
3. Mace S. Observation Medicine: Principles and Protocols. Cambridge University Press; 2017.
4. Currie GM. Pharmacology, part 4: nuclear cardiology. J Nucl Med Technol. 2019;47(2):97-110. doi:10.2967/jnmt.118.219675
5. Regadenoson; Package insert. Astellas Pharma US Inc; 2008.
6. Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14(5):645-658. doi:10.1016/j.nuclcard.2007.06.114
7. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109-114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
8. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends Cardiovasc Med. 2016;26(6):515-523. doi:10.1016/j.tcm.2016.03.001
9. Czernin J, Sun K, Brunken R, Böttcher M, Phelps M, Schelbert H. Effect of acute and long-term smoking on myocardial blood flow and flow reserve. Circulation. 1995;91:2891-2897. doi:10.1161/01.CIR.91.12.2891
10. Winniford MD, Wheelan KR, Kremers MS, et al. Smoking-induced coronary vasoconstriction in patients with atherosclerotic coronary artery disease: evidence for adrenergically mediated alterations in coronary artery tone. Circulation. 1986;73(4):662-667. doi:10.1161/01.cir.73.4.662
11. Klein LW, Ambrose J, Pichard A, Holt J, Gorlin R, Teichholz LE. Acute coronary hemodynamic response to cigarette smoking in patients with coronary artery disease. J Am Coll Cardiol. 1984;3(4):879-886. doi:10.1016/s0735-1097(84)80344-7
12. Quillen JE, Rossen JD, Oskarsson HJ, Minor RL Jr, Lopez AG, Winniford MD. Acute effect of cigarette smoking on the coronary circulation: constriction of epicardial and resistance vessels. J Am Coll Cardiol. 1993;22(3):642-647. doi:10.1016/0735-1097(93)90170-6
13. Dacosta A, Guy JM, Tardy B, et al. Myocardial infarction and nicotine patch: a contributing or causative factor?. Eur Heart J. 1993;14(12):1709-1711. doi:10.1093/eurheartj/14.12.1709
14. Ottervanger JP, Festen JM, de Vries AG, Stricker BH. Acute myocardial infarction while using the nicotine patch. Chest. 1995;107(6):1765-1766. doi:10.1378/chest.107.6.1765
15. Dollerup J, Vestbo J, Murray-Thomas T, et al. Cardiovascular risks in smokers treated with nicotine replacement therapy: a historical cohort study. Clin Epidemiol. 2017;9:231-243. Published 2017 Apr 26. doi:10.2147/CLEP.S127775
16. Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis. 2010;8(1):8. Published 2010 Jul 13. doi:10.1186/1617-9625-8-8
17. Mills EJ, Thorlund K, Eapen S, Wu P, Prochaska JJ. Cardiovascular events associated with smoking cessation pharmacotherapies: a network meta-analysis. Circulation. 2014;129(1):28-41. doi:10.1161/CIRCULATIONAHA.113.003961
18. Tzivoni D, Keren A, Meyler S, Khoury Z, Lerer T, Brunel P. Cardiovascular safety of transdermal nicotine patches in patients with coronary artery disease who try to quit smoking. Cardiovasc Drugs Ther. 1998;12(3):239-244. doi:10.1023/a:1007757530765
19. Lucini D, Bertocchi F, Malliani A, Pagani M. Autonomic effects of nicotine patch administration in habitual cigarette smokers: a double-blind, placebo-controlled study using spectral analysis of RR interval and systolic arterial pressure variabilities. J Cardiovasc Pharmacol. 1998;31(5):714-720. doi:10.1097/00005344-199805000-00010
20. Kaijser L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985;5(6):541-552. doi:10.1111/j.1475-097x.1985.tb00767.x
21. Nitenberg A, Antony I. Effects of nicotine gum on coronary vasomotor responses during sympathetic stimulation in patients with coronary artery stenosis. J Cardiovasc Pharmacol. 1999;34(5):694-699. doi:10.1097/00005344-199911000-00011
22. Keeley EC, Pirwitz MJ, Landau C, et al. Intranasal nicotine spray does not augment the adverse effects of cigarette smoking on myocardial oxygen demand or coronary arterial dimensions. Am J Med. 1996;101(4):357-363. doi:10.1016/s0002-9343(96)00237-9
23. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422-1431. doi:10.1016/s0735-1097(97)00079-x
24. Flowers L. Nicotine replacement therapy. Amer J Psych. 2017;11(6):4-7.
25. Adenosine; Package insert. Astellas Pharma US Inc; 1989.
26. Dipyridamole; Package insert. Boehringer Ingelheim Pharmaceuticals Inc; 2019.
27. Dobutamine; Package insert. Baxter Healthcare Corporation; 2012.
1. Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed March 30, 2020. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf
2. Lange RA. Cardiovascular testing. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. McGraw Hill; 2017.
3. Mace S. Observation Medicine: Principles and Protocols. Cambridge University Press; 2017.
4. Currie GM. Pharmacology, part 4: nuclear cardiology. J Nucl Med Technol. 2019;47(2):97-110. doi:10.2967/jnmt.118.219675
5. Regadenoson; Package insert. Astellas Pharma US Inc; 2008.
6. Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14(5):645-658. doi:10.1016/j.nuclcard.2007.06.114
7. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109-114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
8. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trends Cardiovasc Med. 2016;26(6):515-523. doi:10.1016/j.tcm.2016.03.001
9. Czernin J, Sun K, Brunken R, Böttcher M, Phelps M, Schelbert H. Effect of acute and long-term smoking on myocardial blood flow and flow reserve. Circulation. 1995;91:2891-2897. doi:10.1161/01.CIR.91.12.2891
10. Winniford MD, Wheelan KR, Kremers MS, et al. Smoking-induced coronary vasoconstriction in patients with atherosclerotic coronary artery disease: evidence for adrenergically mediated alterations in coronary artery tone. Circulation. 1986;73(4):662-667. doi:10.1161/01.cir.73.4.662
11. Klein LW, Ambrose J, Pichard A, Holt J, Gorlin R, Teichholz LE. Acute coronary hemodynamic response to cigarette smoking in patients with coronary artery disease. J Am Coll Cardiol. 1984;3(4):879-886. doi:10.1016/s0735-1097(84)80344-7
12. Quillen JE, Rossen JD, Oskarsson HJ, Minor RL Jr, Lopez AG, Winniford MD. Acute effect of cigarette smoking on the coronary circulation: constriction of epicardial and resistance vessels. J Am Coll Cardiol. 1993;22(3):642-647. doi:10.1016/0735-1097(93)90170-6
13. Dacosta A, Guy JM, Tardy B, et al. Myocardial infarction and nicotine patch: a contributing or causative factor?. Eur Heart J. 1993;14(12):1709-1711. doi:10.1093/eurheartj/14.12.1709
14. Ottervanger JP, Festen JM, de Vries AG, Stricker BH. Acute myocardial infarction while using the nicotine patch. Chest. 1995;107(6):1765-1766. doi:10.1378/chest.107.6.1765
15. Dollerup J, Vestbo J, Murray-Thomas T, et al. Cardiovascular risks in smokers treated with nicotine replacement therapy: a historical cohort study. Clin Epidemiol. 2017;9:231-243. Published 2017 Apr 26. doi:10.2147/CLEP.S127775
16. Mills EJ, Wu P, Lockhart I, Wilson K, Ebbert JO. Adverse events associated with nicotine replacement therapy (NRT) for smoking cessation. A systematic review and meta-analysis of one hundred and twenty studies involving 177,390 individuals. Tob Induc Dis. 2010;8(1):8. Published 2010 Jul 13. doi:10.1186/1617-9625-8-8
17. Mills EJ, Thorlund K, Eapen S, Wu P, Prochaska JJ. Cardiovascular events associated with smoking cessation pharmacotherapies: a network meta-analysis. Circulation. 2014;129(1):28-41. doi:10.1161/CIRCULATIONAHA.113.003961
18. Tzivoni D, Keren A, Meyler S, Khoury Z, Lerer T, Brunel P. Cardiovascular safety of transdermal nicotine patches in patients with coronary artery disease who try to quit smoking. Cardiovasc Drugs Ther. 1998;12(3):239-244. doi:10.1023/a:1007757530765
19. Lucini D, Bertocchi F, Malliani A, Pagani M. Autonomic effects of nicotine patch administration in habitual cigarette smokers: a double-blind, placebo-controlled study using spectral analysis of RR interval and systolic arterial pressure variabilities. J Cardiovasc Pharmacol. 1998;31(5):714-720. doi:10.1097/00005344-199805000-00010
20. Kaijser L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985;5(6):541-552. doi:10.1111/j.1475-097x.1985.tb00767.x
21. Nitenberg A, Antony I. Effects of nicotine gum on coronary vasomotor responses during sympathetic stimulation in patients with coronary artery stenosis. J Cardiovasc Pharmacol. 1999;34(5):694-699. doi:10.1097/00005344-199911000-00011
22. Keeley EC, Pirwitz MJ, Landau C, et al. Intranasal nicotine spray does not augment the adverse effects of cigarette smoking on myocardial oxygen demand or coronary arterial dimensions. Am J Med. 1996;101(4):357-363. doi:10.1016/s0002-9343(96)00237-9
23. Benowitz NL, Gourlay SG. Cardiovascular toxicity of nicotine: implications for nicotine replacement therapy. J Am Coll Cardiol. 1997;29(7):1422-1431. doi:10.1016/s0735-1097(97)00079-x
24. Flowers L. Nicotine replacement therapy. Amer J Psych. 2017;11(6):4-7.
25. Adenosine; Package insert. Astellas Pharma US Inc; 1989.
26. Dipyridamole; Package insert. Boehringer Ingelheim Pharmaceuticals Inc; 2019.
27. Dobutamine; Package insert. Baxter Healthcare Corporation; 2012.
Surgical groups push back against new revascularization guidelines
The new 2021 coronary revascularization guidelines are spurring controversy, as surgical associations raise concerns about the interpretation of the evidence behind key recommendations and the makeup of the writing committee.
The guideline was published in December by the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions (ACC/AHA/SCAI), and replaces the 2011 coronary artery bypass surgery (CABG) and the 2011 and 2015 percutaneous coronary intervention (PCI) guidelines.
The American Association for Thoracic Surgery (AATS) and Society of Thoracic Surgeons (STS) were part of the development of the document but have withdrawn their support, citing three areas of concern in a recent editorial in Annals of Thoracic Surgery.
“I do have to emphasize this is not just the AATS and STS – the European societies, Latin American societies, Asian societies, and even cardiologists are all coming out against these guidelines,” Joseph F. Sabik III, MD, University Hospitals Cleveland Medical Center, lead author of the editorial, said in an interview. “So, I think that tells us that something didn’t go right here.”
The main objection is the downgrading of CABG surgery from a class 1 to weak 2b recommendation to improve survival in patients with three-vessel coronary artery disease (CAD) and normal left ventricular function.
The ISCHEMIA trial was used to support this two-level downgrade and a class 1 to 2a downgrade for CABG in three-vessel CAD with mild to moderate left ventricular dysfunction. But the trial wasn’t powered for survival, only 20% of patients underwent CABG as the initial invasive strategy, and patients were followed for less than 5 years, the editorialists observed.
At the same time, there’s plenty of observational and randomized studies such as SYNTAX, EXCEL, and FAME 3 showing a clear survival benefit of CABG over PCI, Dr. Sabik said. “The criticism is that these are old studies and aren’t applicable today, but we don’t understand downgrading without any evidence suggesting it [CABG] isn’t effective anymore.”
CABG and PCI treated as equal
AATS and STS also object to the new guidelines treating PCI and CABG as equivalent revascularization strategies in decreasing ischemic events. Both were given a 2b recommendation for survival with triple-vessel disease, but randomized trials have demonstrated not only lower mortality with surgery but fewer reinterventions and myocardial infarctions.
“None of that gets acknowledged in the guidelines; they are treated equally,” Dr. Sabik said. “So if you’re going to say that CABG isn’t any better than medical therapy, in our mind, you have to say that PCI is worse than medical therapy. And we don’t believe that, I want you to know. We just think that the logic doesn’t make any sense. The committee used what it wanted to but didn’t use many things that committees have used in the past to give CABG a level 1 recommendation.”
The downgrade is also at odds with the 2018 European Society of Cardiology (ESC)/ European Association for Cardio-Thoracic Surgery (EACTS) guidelines, which give CABG a class 1 recommendation in three-vessel CAD as well as one- or two-vessel CAD with proximal left atrial descending artery stenosis.
In a Dec. 14 letter to the ACC/AHA Joint Committee, the Latin American Association of Cardiac and Endovascular Surgery (LACES) also called out the guideline committee for the 2b class of recommendation (COR) for PCI and CABG, saying it contradicts the text, which “clearly considers” the need to give a weaker endorsement for PCI than for CABG in patients with multivessel CAD.
“Considering that this section has the most significant impact due to the prevalence of stable ischemic heart disease in patients with multivessel CAD, such a contradiction may affect the lives and survival of millions of patients worldwide and have a major socioeconomic impact,” the letter states.
“Therefore, LACES respectfully but vehemently believes the Task Force should seriously reconsider the wording and recommendations in this specific large group of patients.”
Class I for radial conduit
AATS and STS also express concern about the new class 1 recommendation for the radial artery as a conduit in CABG. They note this is higher than bilateral internal mammary artery grafting and based on a meta-analysis of six relatively small studies with very strict inclusion criteria favorable for radial artery usage and patency.
“There’s a lot of studies that showed if you use the radial artery incorrectly, you have worse outcomes, and that’s what scares us a bit,” Dr. Sabik said. “If they’re giving it a class 1 recommendation, does that mean that becomes standard of care and could that cause patient harm? We think that level 1 is too high and that a [class] 2a with qualifications would be appropriate.”
Unequal footing
In a Dec. 23 letter, EACTS said it is “extremely concerned” about downgrading the COR for CABG without new randomized controlled trials to support the decision or to reject previously held evidence.
“The downgrading of CABG, and placing PCI at the same COR, does not meet our interpretation of the evidence, and may lead to avoidable loss of life,” EACTS officials said. “These guidelines also have implications on patient care: A COR IIb entails that CABG may not be reimbursable in some countries.”
EACTS called on AHA, ACC, and SCAI to review the evidence and called out the makeup of the guideline writing committee. “It is astonishing that no surgical association was involved, coauthored, or endorsed these guidelines.”
The AATS and STS each had a single representative on the guidelines’ writing committee but note that the six remaining surgeons were chosen by the ACC and AHA. Surgeons were also in the minority and only a majority was needed to approve the guidelines, highlighting the need to revisit the guideline development process to ensure equal representation by multidisciplinary experts across specialties.
“I hope the cardiology and surgical societies can come together and figure out how we do this better in the future, and we take a look again at these guidelines and come up with what we think is appropriate, especially since this is not just AATS and STS,” Dr. Sabik said.
In an emailed statement, the ACC/AHA said the AATS and STS representatives “actively participated throughout the writing process the past 3 years” and that the AATS and STS were involved in the “extensive peer review process” for the document with a reviewer from each organization. Nevertheless, AATS and STS both elected not to endorse the guidelines when at the organizational approval stage.
“Consequently, the AATS representative chose to stay with the committee and be recognized as having been appointed on behalf of the ACC and the AHA,” according to the statement. “The STS representative chose to withdraw from the committee and is not listed as a writing committee member on the final guideline. The final guideline reflects the latest evidence-based recommendations for coronary artery revascularization, as agreed by the ACC, AHA, SCAI, and the full writing committee.”
Despite pleas from the surgical groups to reconsider the evidence, “there is no further review process for the revascularization guideline,” the ACC/AHA spokesperson noted.
Jennifer S. Lawton, MD, chief of cardiac surgery at Johns Hopkins University, Baltimore, and guideline writing committee chair, did not respond to numerous requests for comment.
A version of this article first appeared on Medscape.com.
The new 2021 coronary revascularization guidelines are spurring controversy, as surgical associations raise concerns about the interpretation of the evidence behind key recommendations and the makeup of the writing committee.
The guideline was published in December by the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions (ACC/AHA/SCAI), and replaces the 2011 coronary artery bypass surgery (CABG) and the 2011 and 2015 percutaneous coronary intervention (PCI) guidelines.
The American Association for Thoracic Surgery (AATS) and Society of Thoracic Surgeons (STS) were part of the development of the document but have withdrawn their support, citing three areas of concern in a recent editorial in Annals of Thoracic Surgery.
“I do have to emphasize this is not just the AATS and STS – the European societies, Latin American societies, Asian societies, and even cardiologists are all coming out against these guidelines,” Joseph F. Sabik III, MD, University Hospitals Cleveland Medical Center, lead author of the editorial, said in an interview. “So, I think that tells us that something didn’t go right here.”
The main objection is the downgrading of CABG surgery from a class 1 to weak 2b recommendation to improve survival in patients with three-vessel coronary artery disease (CAD) and normal left ventricular function.
The ISCHEMIA trial was used to support this two-level downgrade and a class 1 to 2a downgrade for CABG in three-vessel CAD with mild to moderate left ventricular dysfunction. But the trial wasn’t powered for survival, only 20% of patients underwent CABG as the initial invasive strategy, and patients were followed for less than 5 years, the editorialists observed.
At the same time, there’s plenty of observational and randomized studies such as SYNTAX, EXCEL, and FAME 3 showing a clear survival benefit of CABG over PCI, Dr. Sabik said. “The criticism is that these are old studies and aren’t applicable today, but we don’t understand downgrading without any evidence suggesting it [CABG] isn’t effective anymore.”
CABG and PCI treated as equal
AATS and STS also object to the new guidelines treating PCI and CABG as equivalent revascularization strategies in decreasing ischemic events. Both were given a 2b recommendation for survival with triple-vessel disease, but randomized trials have demonstrated not only lower mortality with surgery but fewer reinterventions and myocardial infarctions.
“None of that gets acknowledged in the guidelines; they are treated equally,” Dr. Sabik said. “So if you’re going to say that CABG isn’t any better than medical therapy, in our mind, you have to say that PCI is worse than medical therapy. And we don’t believe that, I want you to know. We just think that the logic doesn’t make any sense. The committee used what it wanted to but didn’t use many things that committees have used in the past to give CABG a level 1 recommendation.”
The downgrade is also at odds with the 2018 European Society of Cardiology (ESC)/ European Association for Cardio-Thoracic Surgery (EACTS) guidelines, which give CABG a class 1 recommendation in three-vessel CAD as well as one- or two-vessel CAD with proximal left atrial descending artery stenosis.
In a Dec. 14 letter to the ACC/AHA Joint Committee, the Latin American Association of Cardiac and Endovascular Surgery (LACES) also called out the guideline committee for the 2b class of recommendation (COR) for PCI and CABG, saying it contradicts the text, which “clearly considers” the need to give a weaker endorsement for PCI than for CABG in patients with multivessel CAD.
“Considering that this section has the most significant impact due to the prevalence of stable ischemic heart disease in patients with multivessel CAD, such a contradiction may affect the lives and survival of millions of patients worldwide and have a major socioeconomic impact,” the letter states.
“Therefore, LACES respectfully but vehemently believes the Task Force should seriously reconsider the wording and recommendations in this specific large group of patients.”
Class I for radial conduit
AATS and STS also express concern about the new class 1 recommendation for the radial artery as a conduit in CABG. They note this is higher than bilateral internal mammary artery grafting and based on a meta-analysis of six relatively small studies with very strict inclusion criteria favorable for radial artery usage and patency.
“There’s a lot of studies that showed if you use the radial artery incorrectly, you have worse outcomes, and that’s what scares us a bit,” Dr. Sabik said. “If they’re giving it a class 1 recommendation, does that mean that becomes standard of care and could that cause patient harm? We think that level 1 is too high and that a [class] 2a with qualifications would be appropriate.”
Unequal footing
In a Dec. 23 letter, EACTS said it is “extremely concerned” about downgrading the COR for CABG without new randomized controlled trials to support the decision or to reject previously held evidence.
“The downgrading of CABG, and placing PCI at the same COR, does not meet our interpretation of the evidence, and may lead to avoidable loss of life,” EACTS officials said. “These guidelines also have implications on patient care: A COR IIb entails that CABG may not be reimbursable in some countries.”
EACTS called on AHA, ACC, and SCAI to review the evidence and called out the makeup of the guideline writing committee. “It is astonishing that no surgical association was involved, coauthored, or endorsed these guidelines.”
The AATS and STS each had a single representative on the guidelines’ writing committee but note that the six remaining surgeons were chosen by the ACC and AHA. Surgeons were also in the minority and only a majority was needed to approve the guidelines, highlighting the need to revisit the guideline development process to ensure equal representation by multidisciplinary experts across specialties.
“I hope the cardiology and surgical societies can come together and figure out how we do this better in the future, and we take a look again at these guidelines and come up with what we think is appropriate, especially since this is not just AATS and STS,” Dr. Sabik said.
In an emailed statement, the ACC/AHA said the AATS and STS representatives “actively participated throughout the writing process the past 3 years” and that the AATS and STS were involved in the “extensive peer review process” for the document with a reviewer from each organization. Nevertheless, AATS and STS both elected not to endorse the guidelines when at the organizational approval stage.
“Consequently, the AATS representative chose to stay with the committee and be recognized as having been appointed on behalf of the ACC and the AHA,” according to the statement. “The STS representative chose to withdraw from the committee and is not listed as a writing committee member on the final guideline. The final guideline reflects the latest evidence-based recommendations for coronary artery revascularization, as agreed by the ACC, AHA, SCAI, and the full writing committee.”
Despite pleas from the surgical groups to reconsider the evidence, “there is no further review process for the revascularization guideline,” the ACC/AHA spokesperson noted.
Jennifer S. Lawton, MD, chief of cardiac surgery at Johns Hopkins University, Baltimore, and guideline writing committee chair, did not respond to numerous requests for comment.
A version of this article first appeared on Medscape.com.
The new 2021 coronary revascularization guidelines are spurring controversy, as surgical associations raise concerns about the interpretation of the evidence behind key recommendations and the makeup of the writing committee.
The guideline was published in December by the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions (ACC/AHA/SCAI), and replaces the 2011 coronary artery bypass surgery (CABG) and the 2011 and 2015 percutaneous coronary intervention (PCI) guidelines.
The American Association for Thoracic Surgery (AATS) and Society of Thoracic Surgeons (STS) were part of the development of the document but have withdrawn their support, citing three areas of concern in a recent editorial in Annals of Thoracic Surgery.
“I do have to emphasize this is not just the AATS and STS – the European societies, Latin American societies, Asian societies, and even cardiologists are all coming out against these guidelines,” Joseph F. Sabik III, MD, University Hospitals Cleveland Medical Center, lead author of the editorial, said in an interview. “So, I think that tells us that something didn’t go right here.”
The main objection is the downgrading of CABG surgery from a class 1 to weak 2b recommendation to improve survival in patients with three-vessel coronary artery disease (CAD) and normal left ventricular function.
The ISCHEMIA trial was used to support this two-level downgrade and a class 1 to 2a downgrade for CABG in three-vessel CAD with mild to moderate left ventricular dysfunction. But the trial wasn’t powered for survival, only 20% of patients underwent CABG as the initial invasive strategy, and patients were followed for less than 5 years, the editorialists observed.
At the same time, there’s plenty of observational and randomized studies such as SYNTAX, EXCEL, and FAME 3 showing a clear survival benefit of CABG over PCI, Dr. Sabik said. “The criticism is that these are old studies and aren’t applicable today, but we don’t understand downgrading without any evidence suggesting it [CABG] isn’t effective anymore.”
CABG and PCI treated as equal
AATS and STS also object to the new guidelines treating PCI and CABG as equivalent revascularization strategies in decreasing ischemic events. Both were given a 2b recommendation for survival with triple-vessel disease, but randomized trials have demonstrated not only lower mortality with surgery but fewer reinterventions and myocardial infarctions.
“None of that gets acknowledged in the guidelines; they are treated equally,” Dr. Sabik said. “So if you’re going to say that CABG isn’t any better than medical therapy, in our mind, you have to say that PCI is worse than medical therapy. And we don’t believe that, I want you to know. We just think that the logic doesn’t make any sense. The committee used what it wanted to but didn’t use many things that committees have used in the past to give CABG a level 1 recommendation.”
The downgrade is also at odds with the 2018 European Society of Cardiology (ESC)/ European Association for Cardio-Thoracic Surgery (EACTS) guidelines, which give CABG a class 1 recommendation in three-vessel CAD as well as one- or two-vessel CAD with proximal left atrial descending artery stenosis.
In a Dec. 14 letter to the ACC/AHA Joint Committee, the Latin American Association of Cardiac and Endovascular Surgery (LACES) also called out the guideline committee for the 2b class of recommendation (COR) for PCI and CABG, saying it contradicts the text, which “clearly considers” the need to give a weaker endorsement for PCI than for CABG in patients with multivessel CAD.
“Considering that this section has the most significant impact due to the prevalence of stable ischemic heart disease in patients with multivessel CAD, such a contradiction may affect the lives and survival of millions of patients worldwide and have a major socioeconomic impact,” the letter states.
“Therefore, LACES respectfully but vehemently believes the Task Force should seriously reconsider the wording and recommendations in this specific large group of patients.”
Class I for radial conduit
AATS and STS also express concern about the new class 1 recommendation for the radial artery as a conduit in CABG. They note this is higher than bilateral internal mammary artery grafting and based on a meta-analysis of six relatively small studies with very strict inclusion criteria favorable for radial artery usage and patency.
“There’s a lot of studies that showed if you use the radial artery incorrectly, you have worse outcomes, and that’s what scares us a bit,” Dr. Sabik said. “If they’re giving it a class 1 recommendation, does that mean that becomes standard of care and could that cause patient harm? We think that level 1 is too high and that a [class] 2a with qualifications would be appropriate.”
Unequal footing
In a Dec. 23 letter, EACTS said it is “extremely concerned” about downgrading the COR for CABG without new randomized controlled trials to support the decision or to reject previously held evidence.
“The downgrading of CABG, and placing PCI at the same COR, does not meet our interpretation of the evidence, and may lead to avoidable loss of life,” EACTS officials said. “These guidelines also have implications on patient care: A COR IIb entails that CABG may not be reimbursable in some countries.”
EACTS called on AHA, ACC, and SCAI to review the evidence and called out the makeup of the guideline writing committee. “It is astonishing that no surgical association was involved, coauthored, or endorsed these guidelines.”
The AATS and STS each had a single representative on the guidelines’ writing committee but note that the six remaining surgeons were chosen by the ACC and AHA. Surgeons were also in the minority and only a majority was needed to approve the guidelines, highlighting the need to revisit the guideline development process to ensure equal representation by multidisciplinary experts across specialties.
“I hope the cardiology and surgical societies can come together and figure out how we do this better in the future, and we take a look again at these guidelines and come up with what we think is appropriate, especially since this is not just AATS and STS,” Dr. Sabik said.
In an emailed statement, the ACC/AHA said the AATS and STS representatives “actively participated throughout the writing process the past 3 years” and that the AATS and STS were involved in the “extensive peer review process” for the document with a reviewer from each organization. Nevertheless, AATS and STS both elected not to endorse the guidelines when at the organizational approval stage.
“Consequently, the AATS representative chose to stay with the committee and be recognized as having been appointed on behalf of the ACC and the AHA,” according to the statement. “The STS representative chose to withdraw from the committee and is not listed as a writing committee member on the final guideline. The final guideline reflects the latest evidence-based recommendations for coronary artery revascularization, as agreed by the ACC, AHA, SCAI, and the full writing committee.”
Despite pleas from the surgical groups to reconsider the evidence, “there is no further review process for the revascularization guideline,” the ACC/AHA spokesperson noted.
Jennifer S. Lawton, MD, chief of cardiac surgery at Johns Hopkins University, Baltimore, and guideline writing committee chair, did not respond to numerous requests for comment.
A version of this article first appeared on Medscape.com.
Midlife cardiovascular conditions tied to greater cognitive decline in women
Even though men in midlife have more cardiovascular (CV) conditions and risk factors than women of the same age, women are more affected by these conditions in terms of cognitive decline, new research suggests.
Analyses of almost 1,400 participants in the population-based Mayo Clinic Study of Aging showed that diabetes, dyslipidemia, and coronary heart disease (CHD) all had stronger associations with global cognitive decline in women than in men.
“All men and women should be treated for cardiovascular risk factors and conditions, but this study really highlights the importance of very early and perhaps more aggressive treatment in women with these conditions,” co-investigator Michelle M. Mielke, PhD, professor of epidemiology and neurology, Mayo Clinic, Rochester, Minn., told this news organization.
The findings were published online Jan. 5 in Neurology.
Assessing sex differences
Most previous studies in this area have focused on CV risk factors in midlife in relation to late-life dementia (after age 75) or on late-life vascular risk factors and late-life dementia, Dr. Mielke noted.
However, a few recent studies have suggested vascular risk factors can affect cognition even in midlife. The current investigators sought to determine whether there are sex differences in these associations.
They assessed 1,857 nondemented participants aged 50 to 69 years from the Mayo Clinic Study on Aging. The mean education level was 14.9 years, and the mean body mass index (BMI) was 29.7.
Among the participants, 78.9% had at least one CV condition or risk factor, and the proportion was higher in men than women (83.4% vs. 74.5%; P < .0001).
Frequency of each individual CV condition or risk factor was also higher in men than women, and they had more years of education and higher BMI but took fewer medications.
Every 15 months, participants had an in-person interview and physical examination that included a neurologic assessment and short test of memory.
The neuropsychological battery included nine tests across four domains: memory, language, executive function, and visuospatial skills. Researchers calculated z-scores for these domains and for global cognition.
Multiple cognitive domains
Whereas this study evaluated multiple cognitive domains, most previous research has focused on global cognitive decline and/or decline in only one or two cognitive domains, the investigators note.
They collected information from medical records on CV conditions such as CHD, arrhythmias, congestive heart failure, peripheral vascular disease (PVD), and stroke; and CV risk factors such as hypertension, diabetes, dyslipidemia, smoking status, and BMI.
Because of the small number of patients with stroke and PVD, these were classified as “other cardiovascular conditions” in the statistical analysis.
Researchers adjusted for sex, age, years of education, depressive symptoms, comorbidities, medications, and apolipoprotein E (APOE) genotyping. The mean follow-up was 3 years and did not differ by sex.
As some participants didn’t have a follow-up visit, the current analysis included 1,394 individuals. Those without follow-up visits were younger, had less education and more comorbidities, and took more medications compared with those with a follow-up.
Results showed most CV conditions were more strongly associated with cognitive function among women than men. For example, CHD was associated with global decline only in women (P < .05).
CHD, diabetes, and dyslipidemia were associated with language decline in women only (all, P < .05), but congestive heart failure was significantly associated with language decline in men only.
Dr. Mielke cautioned about reading too much into the language results for women.
“It’s an intriguing finding and definitely we need to follow up on it,” she said. However, “more studies are needed to examine sex differences before we start saying it only has an effect on language.”
‘Treat aggressively and right away’
The researchers were somewhat surprised by the study findings. Because there is a higher prevalence of CV conditions and risk factors in men, they presumed men would be more affected by these conditions, said Dr. Mielke.
“But that’s not what we saw; we saw the reverse. It was actually the women who were affected more by these cardiovascular risk factors and conditions,” she said.
As midlife is when women enter menopause, fluctuating estrogen levels may help explain the differential impact on cognition among women. But Dr. Mielke said she wants to “move beyond” just looking at hormones.
She pointed out there are a variety of psychosocial factors that may also contribute to an imbalance in the cognitive impact of CV conditions on women.
“Midlife is when many women are still taking care of their children at home, are also taking care of their adult parents, and may be undergoing more stress while continuing to do a job,” Dr. Miekle said.
Structural brain development and genetics may also contribute to the greater effect on cognition in women, the investigators note.
Dr. Mielke stressed that the current study only identifies associations. “The next steps are to understand what some of the underlying mechanisms for this are,” she said.
In the meantime, these new results suggest middle-aged women with high blood pressure, cholesterol, or glucose measures “should be treated aggressively and right away” said Dr. Mielke.
“For example, for women who are just starting to become hypertensive, clinicians should treat them right away and not watch and wait.”
Study limitations cited include that its sample was limited to Olmsted County, Minnesota – so results may not be generalized to other populations. Also, as researchers combined PVD and stroke into one group, larger sample sizes are needed, especially for stroke. Another limitation was the study did not have information on duration of all CV conditions or risk factors.
Helpful for tailoring interventions?
Commenting on the study, Glen R. Finney, MD, director, Memory and Cognition Program, Geisinger Health Clinic, Wilkes-Barre, Pennsylvania, said the results are important.
“The more we understand about risk factors for the development of Alzheimer’s disease and related dementias, the better we understand how we can reduce the risks,” said Dr. Finney, who was not involved with the research.
Awareness that CV conditions are major risk factors in midlife has been “definitely rising,” said Dr. Finney. “Many studies originally were looking at late life and are now looking more at earlier in the disease process, and I think that’s important.”
Understanding how sex, ethnicity, and other demographic variables affect risks can help to “tailor interventions” for individual patients, he said.
The study was supported by the National Institutes of Health, the GHR Foundation, and the Rochester Epidemiology Project. Dr. Mielke is a consultant for Biogen and Brain Protection Company and is on the editorial boards of Neurology and Alzheimer’s and Dementia. Dr. Finney has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Even though men in midlife have more cardiovascular (CV) conditions and risk factors than women of the same age, women are more affected by these conditions in terms of cognitive decline, new research suggests.
Analyses of almost 1,400 participants in the population-based Mayo Clinic Study of Aging showed that diabetes, dyslipidemia, and coronary heart disease (CHD) all had stronger associations with global cognitive decline in women than in men.
“All men and women should be treated for cardiovascular risk factors and conditions, but this study really highlights the importance of very early and perhaps more aggressive treatment in women with these conditions,” co-investigator Michelle M. Mielke, PhD, professor of epidemiology and neurology, Mayo Clinic, Rochester, Minn., told this news organization.
The findings were published online Jan. 5 in Neurology.
Assessing sex differences
Most previous studies in this area have focused on CV risk factors in midlife in relation to late-life dementia (after age 75) or on late-life vascular risk factors and late-life dementia, Dr. Mielke noted.
However, a few recent studies have suggested vascular risk factors can affect cognition even in midlife. The current investigators sought to determine whether there are sex differences in these associations.
They assessed 1,857 nondemented participants aged 50 to 69 years from the Mayo Clinic Study on Aging. The mean education level was 14.9 years, and the mean body mass index (BMI) was 29.7.
Among the participants, 78.9% had at least one CV condition or risk factor, and the proportion was higher in men than women (83.4% vs. 74.5%; P < .0001).
Frequency of each individual CV condition or risk factor was also higher in men than women, and they had more years of education and higher BMI but took fewer medications.
Every 15 months, participants had an in-person interview and physical examination that included a neurologic assessment and short test of memory.
The neuropsychological battery included nine tests across four domains: memory, language, executive function, and visuospatial skills. Researchers calculated z-scores for these domains and for global cognition.
Multiple cognitive domains
Whereas this study evaluated multiple cognitive domains, most previous research has focused on global cognitive decline and/or decline in only one or two cognitive domains, the investigators note.
They collected information from medical records on CV conditions such as CHD, arrhythmias, congestive heart failure, peripheral vascular disease (PVD), and stroke; and CV risk factors such as hypertension, diabetes, dyslipidemia, smoking status, and BMI.
Because of the small number of patients with stroke and PVD, these were classified as “other cardiovascular conditions” in the statistical analysis.
Researchers adjusted for sex, age, years of education, depressive symptoms, comorbidities, medications, and apolipoprotein E (APOE) genotyping. The mean follow-up was 3 years and did not differ by sex.
As some participants didn’t have a follow-up visit, the current analysis included 1,394 individuals. Those without follow-up visits were younger, had less education and more comorbidities, and took more medications compared with those with a follow-up.
Results showed most CV conditions were more strongly associated with cognitive function among women than men. For example, CHD was associated with global decline only in women (P < .05).
CHD, diabetes, and dyslipidemia were associated with language decline in women only (all, P < .05), but congestive heart failure was significantly associated with language decline in men only.
Dr. Mielke cautioned about reading too much into the language results for women.
“It’s an intriguing finding and definitely we need to follow up on it,” she said. However, “more studies are needed to examine sex differences before we start saying it only has an effect on language.”
‘Treat aggressively and right away’
The researchers were somewhat surprised by the study findings. Because there is a higher prevalence of CV conditions and risk factors in men, they presumed men would be more affected by these conditions, said Dr. Mielke.
“But that’s not what we saw; we saw the reverse. It was actually the women who were affected more by these cardiovascular risk factors and conditions,” she said.
As midlife is when women enter menopause, fluctuating estrogen levels may help explain the differential impact on cognition among women. But Dr. Mielke said she wants to “move beyond” just looking at hormones.
She pointed out there are a variety of psychosocial factors that may also contribute to an imbalance in the cognitive impact of CV conditions on women.
“Midlife is when many women are still taking care of their children at home, are also taking care of their adult parents, and may be undergoing more stress while continuing to do a job,” Dr. Miekle said.
Structural brain development and genetics may also contribute to the greater effect on cognition in women, the investigators note.
Dr. Mielke stressed that the current study only identifies associations. “The next steps are to understand what some of the underlying mechanisms for this are,” she said.
In the meantime, these new results suggest middle-aged women with high blood pressure, cholesterol, or glucose measures “should be treated aggressively and right away” said Dr. Mielke.
“For example, for women who are just starting to become hypertensive, clinicians should treat them right away and not watch and wait.”
Study limitations cited include that its sample was limited to Olmsted County, Minnesota – so results may not be generalized to other populations. Also, as researchers combined PVD and stroke into one group, larger sample sizes are needed, especially for stroke. Another limitation was the study did not have information on duration of all CV conditions or risk factors.
Helpful for tailoring interventions?
Commenting on the study, Glen R. Finney, MD, director, Memory and Cognition Program, Geisinger Health Clinic, Wilkes-Barre, Pennsylvania, said the results are important.
“The more we understand about risk factors for the development of Alzheimer’s disease and related dementias, the better we understand how we can reduce the risks,” said Dr. Finney, who was not involved with the research.
Awareness that CV conditions are major risk factors in midlife has been “definitely rising,” said Dr. Finney. “Many studies originally were looking at late life and are now looking more at earlier in the disease process, and I think that’s important.”
Understanding how sex, ethnicity, and other demographic variables affect risks can help to “tailor interventions” for individual patients, he said.
The study was supported by the National Institutes of Health, the GHR Foundation, and the Rochester Epidemiology Project. Dr. Mielke is a consultant for Biogen and Brain Protection Company and is on the editorial boards of Neurology and Alzheimer’s and Dementia. Dr. Finney has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Even though men in midlife have more cardiovascular (CV) conditions and risk factors than women of the same age, women are more affected by these conditions in terms of cognitive decline, new research suggests.
Analyses of almost 1,400 participants in the population-based Mayo Clinic Study of Aging showed that diabetes, dyslipidemia, and coronary heart disease (CHD) all had stronger associations with global cognitive decline in women than in men.
“All men and women should be treated for cardiovascular risk factors and conditions, but this study really highlights the importance of very early and perhaps more aggressive treatment in women with these conditions,” co-investigator Michelle M. Mielke, PhD, professor of epidemiology and neurology, Mayo Clinic, Rochester, Minn., told this news organization.
The findings were published online Jan. 5 in Neurology.
Assessing sex differences
Most previous studies in this area have focused on CV risk factors in midlife in relation to late-life dementia (after age 75) or on late-life vascular risk factors and late-life dementia, Dr. Mielke noted.
However, a few recent studies have suggested vascular risk factors can affect cognition even in midlife. The current investigators sought to determine whether there are sex differences in these associations.
They assessed 1,857 nondemented participants aged 50 to 69 years from the Mayo Clinic Study on Aging. The mean education level was 14.9 years, and the mean body mass index (BMI) was 29.7.
Among the participants, 78.9% had at least one CV condition or risk factor, and the proportion was higher in men than women (83.4% vs. 74.5%; P < .0001).
Frequency of each individual CV condition or risk factor was also higher in men than women, and they had more years of education and higher BMI but took fewer medications.
Every 15 months, participants had an in-person interview and physical examination that included a neurologic assessment and short test of memory.
The neuropsychological battery included nine tests across four domains: memory, language, executive function, and visuospatial skills. Researchers calculated z-scores for these domains and for global cognition.
Multiple cognitive domains
Whereas this study evaluated multiple cognitive domains, most previous research has focused on global cognitive decline and/or decline in only one or two cognitive domains, the investigators note.
They collected information from medical records on CV conditions such as CHD, arrhythmias, congestive heart failure, peripheral vascular disease (PVD), and stroke; and CV risk factors such as hypertension, diabetes, dyslipidemia, smoking status, and BMI.
Because of the small number of patients with stroke and PVD, these were classified as “other cardiovascular conditions” in the statistical analysis.
Researchers adjusted for sex, age, years of education, depressive symptoms, comorbidities, medications, and apolipoprotein E (APOE) genotyping. The mean follow-up was 3 years and did not differ by sex.
As some participants didn’t have a follow-up visit, the current analysis included 1,394 individuals. Those without follow-up visits were younger, had less education and more comorbidities, and took more medications compared with those with a follow-up.
Results showed most CV conditions were more strongly associated with cognitive function among women than men. For example, CHD was associated with global decline only in women (P < .05).
CHD, diabetes, and dyslipidemia were associated with language decline in women only (all, P < .05), but congestive heart failure was significantly associated with language decline in men only.
Dr. Mielke cautioned about reading too much into the language results for women.
“It’s an intriguing finding and definitely we need to follow up on it,” she said. However, “more studies are needed to examine sex differences before we start saying it only has an effect on language.”
‘Treat aggressively and right away’
The researchers were somewhat surprised by the study findings. Because there is a higher prevalence of CV conditions and risk factors in men, they presumed men would be more affected by these conditions, said Dr. Mielke.
“But that’s not what we saw; we saw the reverse. It was actually the women who were affected more by these cardiovascular risk factors and conditions,” she said.
As midlife is when women enter menopause, fluctuating estrogen levels may help explain the differential impact on cognition among women. But Dr. Mielke said she wants to “move beyond” just looking at hormones.
She pointed out there are a variety of psychosocial factors that may also contribute to an imbalance in the cognitive impact of CV conditions on women.
“Midlife is when many women are still taking care of their children at home, are also taking care of their adult parents, and may be undergoing more stress while continuing to do a job,” Dr. Miekle said.
Structural brain development and genetics may also contribute to the greater effect on cognition in women, the investigators note.
Dr. Mielke stressed that the current study only identifies associations. “The next steps are to understand what some of the underlying mechanisms for this are,” she said.
In the meantime, these new results suggest middle-aged women with high blood pressure, cholesterol, or glucose measures “should be treated aggressively and right away” said Dr. Mielke.
“For example, for women who are just starting to become hypertensive, clinicians should treat them right away and not watch and wait.”
Study limitations cited include that its sample was limited to Olmsted County, Minnesota – so results may not be generalized to other populations. Also, as researchers combined PVD and stroke into one group, larger sample sizes are needed, especially for stroke. Another limitation was the study did not have information on duration of all CV conditions or risk factors.
Helpful for tailoring interventions?
Commenting on the study, Glen R. Finney, MD, director, Memory and Cognition Program, Geisinger Health Clinic, Wilkes-Barre, Pennsylvania, said the results are important.
“The more we understand about risk factors for the development of Alzheimer’s disease and related dementias, the better we understand how we can reduce the risks,” said Dr. Finney, who was not involved with the research.
Awareness that CV conditions are major risk factors in midlife has been “definitely rising,” said Dr. Finney. “Many studies originally were looking at late life and are now looking more at earlier in the disease process, and I think that’s important.”
Understanding how sex, ethnicity, and other demographic variables affect risks can help to “tailor interventions” for individual patients, he said.
The study was supported by the National Institutes of Health, the GHR Foundation, and the Rochester Epidemiology Project. Dr. Mielke is a consultant for Biogen and Brain Protection Company and is on the editorial boards of Neurology and Alzheimer’s and Dementia. Dr. Finney has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SGLT2 inhibitors improve cardiovascular outcomes across groups
Sodium-glucose cotransporter 2 (SGLT2) inhibitors show “remarkable consistency of class benefit” for improving cardiovascular outcomes in high-risk people across age, sex, and race/ethnicity categories.
The findings, from a meta-analysis of 10 major randomized clinical trials, were published online Jan. 5, 2021, in JAMA Network Open by Mukul Bhattarai, MD, a cardiology fellow at Southern Illinois University, Springfield, and colleagues.
“Our meta-analysis evaluated a wide spectrum of efficacy outcomes, further characterizing the primary outcome in different subgroups from several well-designed large clinical trials. It supports that SGLT2 inhibitors have emerged as an effective class of drugs for improving cardiovascular morbidity and mortality, including the prevention of [hospitalization for heart failure] and reducing all-cause mortality in selected patients,” Dr. Bhattarai and colleagues wrote.
The cardiovascular outcomes of SGLT2 inhibitor therapy, they noted, “can be compared across all trials, and it demonstrates remarkable consistency of class benefit, despite the variations in populations enrolled.”
However, they also noted that SGLT inhibitors did not reduce the risk of acute MIn overall, and that most of the trials were short term, with a mean follow-up of just 2.3 years.
Ten trials, consistent cardiovascular benefits
Dr. Bhattarai and colleagues searched the literature through Jan. 10, 2021, as well as meeting presentations and other sources. They identified 10 placebo-controlled, randomized clinical trials in which participants had atherosclerotic cardiovascular disease or ASCVD risk factors, diabetes, or heart failure. Among a total of 71,553 high-risk patients, 39,053 received an SGLT2 inhibitor and 32,500 received a placebo.
The primary outcome of cardiovascular death or hospitalization for heart failure occurred in 8.10% randomized to SGLT2 inhibitors, compared with 11.56% in the placebo group, a significant difference with odds ratio 0.67 (P < .001). Both individual outcomes were lower in the SGLT2-inhibitor group, with a number needed to treat of 5.7 (P < .001).
Patients receiving SGLT2 inhibitors also had significantly lower rates of major adverse cardiovascular events, defined as death due to cardiovascular causes, nonfatal MI, or nonfatal stroke. Those events occurred in 9.82% versus 10.22%(OR, 0.90; P = .03).
Hospitalizations and ED visits with heart failure were also reduced with SGLT2 inhibitors (4.37% vs. 6.81%; OR, 0.67; P < .001), as was cardiovascular death (4.65% vs. 5.14%; OR, 0.87; P = .009). The reduction in heart failure is likely caused by a combination of a natriuretic effect and reduced interstitial fluid, along with inhibition of cardiac fibrosis, the authors said.
On the other hand, no reductions were seen in acute MI, evaluated in five of the studies. That event occurred in 4.66% taking SGLT2 inhibitors, compared with 4.70% of the placebo group, a nonsignificant difference with an OR of 0.95 (P = 0.22). This is likely because of the fact that SGLT2 inhibitors don’t have known antianginal properties or vasodilatory effects, they don’t reduce myocardial oxygen consumption, and they don’t prevent cardiac muscle remodeling, they noted.
All-cause mortality was significantly lower with SGLT2 inhibitors, though, at 7.09% versus 7.86% (odds ratio, 0.87; P = .004).
Benefits seen across age, sex, and race/ethnicity subgroups
While no differences in benefit were found between men and women when compared with placebo groups, the rates of cardiovascular death or heart failure hospitalizations were slightly higher in men than in women (9.01% [OR, 0.75; P < .001] vs. 5.34% [OR, 0.78; P = .002]).
By age, SGLT2 inhibitors benefited people both those younger than 65 years and those aged 65 years and older, although the primary outcome was slightly lower in the younger group (6.94% [OR, 0.79; P < 0.001] vs. 10.47% [OR, 0.78; P < .001]).
And by race, similar benefits from SGLT2 inhibitors were seen among individuals who were White, compared with those who were Asian, Black, or of other race/ethnicity, with event rates of 8.77% (OR, 0.82; P < .001) and 8.75% (OR, 0.66; P = .06), respectively.
“Owing to the short-term trial durations, future long-term prospective studies and postmarketing surveillance studies are warranted to discover the rate of cardiovascular outcomes,” Dr. Bhattarai and colleagues concluded.
The authors have no disclosures.
A version of this article first appeared on Medscape.com.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors show “remarkable consistency of class benefit” for improving cardiovascular outcomes in high-risk people across age, sex, and race/ethnicity categories.
The findings, from a meta-analysis of 10 major randomized clinical trials, were published online Jan. 5, 2021, in JAMA Network Open by Mukul Bhattarai, MD, a cardiology fellow at Southern Illinois University, Springfield, and colleagues.
“Our meta-analysis evaluated a wide spectrum of efficacy outcomes, further characterizing the primary outcome in different subgroups from several well-designed large clinical trials. It supports that SGLT2 inhibitors have emerged as an effective class of drugs for improving cardiovascular morbidity and mortality, including the prevention of [hospitalization for heart failure] and reducing all-cause mortality in selected patients,” Dr. Bhattarai and colleagues wrote.
The cardiovascular outcomes of SGLT2 inhibitor therapy, they noted, “can be compared across all trials, and it demonstrates remarkable consistency of class benefit, despite the variations in populations enrolled.”
However, they also noted that SGLT inhibitors did not reduce the risk of acute MIn overall, and that most of the trials were short term, with a mean follow-up of just 2.3 years.
Ten trials, consistent cardiovascular benefits
Dr. Bhattarai and colleagues searched the literature through Jan. 10, 2021, as well as meeting presentations and other sources. They identified 10 placebo-controlled, randomized clinical trials in which participants had atherosclerotic cardiovascular disease or ASCVD risk factors, diabetes, or heart failure. Among a total of 71,553 high-risk patients, 39,053 received an SGLT2 inhibitor and 32,500 received a placebo.
The primary outcome of cardiovascular death or hospitalization for heart failure occurred in 8.10% randomized to SGLT2 inhibitors, compared with 11.56% in the placebo group, a significant difference with odds ratio 0.67 (P < .001). Both individual outcomes were lower in the SGLT2-inhibitor group, with a number needed to treat of 5.7 (P < .001).
Patients receiving SGLT2 inhibitors also had significantly lower rates of major adverse cardiovascular events, defined as death due to cardiovascular causes, nonfatal MI, or nonfatal stroke. Those events occurred in 9.82% versus 10.22%(OR, 0.90; P = .03).
Hospitalizations and ED visits with heart failure were also reduced with SGLT2 inhibitors (4.37% vs. 6.81%; OR, 0.67; P < .001), as was cardiovascular death (4.65% vs. 5.14%; OR, 0.87; P = .009). The reduction in heart failure is likely caused by a combination of a natriuretic effect and reduced interstitial fluid, along with inhibition of cardiac fibrosis, the authors said.
On the other hand, no reductions were seen in acute MI, evaluated in five of the studies. That event occurred in 4.66% taking SGLT2 inhibitors, compared with 4.70% of the placebo group, a nonsignificant difference with an OR of 0.95 (P = 0.22). This is likely because of the fact that SGLT2 inhibitors don’t have known antianginal properties or vasodilatory effects, they don’t reduce myocardial oxygen consumption, and they don’t prevent cardiac muscle remodeling, they noted.
All-cause mortality was significantly lower with SGLT2 inhibitors, though, at 7.09% versus 7.86% (odds ratio, 0.87; P = .004).
Benefits seen across age, sex, and race/ethnicity subgroups
While no differences in benefit were found between men and women when compared with placebo groups, the rates of cardiovascular death or heart failure hospitalizations were slightly higher in men than in women (9.01% [OR, 0.75; P < .001] vs. 5.34% [OR, 0.78; P = .002]).
By age, SGLT2 inhibitors benefited people both those younger than 65 years and those aged 65 years and older, although the primary outcome was slightly lower in the younger group (6.94% [OR, 0.79; P < 0.001] vs. 10.47% [OR, 0.78; P < .001]).
And by race, similar benefits from SGLT2 inhibitors were seen among individuals who were White, compared with those who were Asian, Black, or of other race/ethnicity, with event rates of 8.77% (OR, 0.82; P < .001) and 8.75% (OR, 0.66; P = .06), respectively.
“Owing to the short-term trial durations, future long-term prospective studies and postmarketing surveillance studies are warranted to discover the rate of cardiovascular outcomes,” Dr. Bhattarai and colleagues concluded.
The authors have no disclosures.
A version of this article first appeared on Medscape.com.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors show “remarkable consistency of class benefit” for improving cardiovascular outcomes in high-risk people across age, sex, and race/ethnicity categories.
The findings, from a meta-analysis of 10 major randomized clinical trials, were published online Jan. 5, 2021, in JAMA Network Open by Mukul Bhattarai, MD, a cardiology fellow at Southern Illinois University, Springfield, and colleagues.
“Our meta-analysis evaluated a wide spectrum of efficacy outcomes, further characterizing the primary outcome in different subgroups from several well-designed large clinical trials. It supports that SGLT2 inhibitors have emerged as an effective class of drugs for improving cardiovascular morbidity and mortality, including the prevention of [hospitalization for heart failure] and reducing all-cause mortality in selected patients,” Dr. Bhattarai and colleagues wrote.
The cardiovascular outcomes of SGLT2 inhibitor therapy, they noted, “can be compared across all trials, and it demonstrates remarkable consistency of class benefit, despite the variations in populations enrolled.”
However, they also noted that SGLT inhibitors did not reduce the risk of acute MIn overall, and that most of the trials were short term, with a mean follow-up of just 2.3 years.
Ten trials, consistent cardiovascular benefits
Dr. Bhattarai and colleagues searched the literature through Jan. 10, 2021, as well as meeting presentations and other sources. They identified 10 placebo-controlled, randomized clinical trials in which participants had atherosclerotic cardiovascular disease or ASCVD risk factors, diabetes, or heart failure. Among a total of 71,553 high-risk patients, 39,053 received an SGLT2 inhibitor and 32,500 received a placebo.
The primary outcome of cardiovascular death or hospitalization for heart failure occurred in 8.10% randomized to SGLT2 inhibitors, compared with 11.56% in the placebo group, a significant difference with odds ratio 0.67 (P < .001). Both individual outcomes were lower in the SGLT2-inhibitor group, with a number needed to treat of 5.7 (P < .001).
Patients receiving SGLT2 inhibitors also had significantly lower rates of major adverse cardiovascular events, defined as death due to cardiovascular causes, nonfatal MI, or nonfatal stroke. Those events occurred in 9.82% versus 10.22%(OR, 0.90; P = .03).
Hospitalizations and ED visits with heart failure were also reduced with SGLT2 inhibitors (4.37% vs. 6.81%; OR, 0.67; P < .001), as was cardiovascular death (4.65% vs. 5.14%; OR, 0.87; P = .009). The reduction in heart failure is likely caused by a combination of a natriuretic effect and reduced interstitial fluid, along with inhibition of cardiac fibrosis, the authors said.
On the other hand, no reductions were seen in acute MI, evaluated in five of the studies. That event occurred in 4.66% taking SGLT2 inhibitors, compared with 4.70% of the placebo group, a nonsignificant difference with an OR of 0.95 (P = 0.22). This is likely because of the fact that SGLT2 inhibitors don’t have known antianginal properties or vasodilatory effects, they don’t reduce myocardial oxygen consumption, and they don’t prevent cardiac muscle remodeling, they noted.
All-cause mortality was significantly lower with SGLT2 inhibitors, though, at 7.09% versus 7.86% (odds ratio, 0.87; P = .004).
Benefits seen across age, sex, and race/ethnicity subgroups
While no differences in benefit were found between men and women when compared with placebo groups, the rates of cardiovascular death or heart failure hospitalizations were slightly higher in men than in women (9.01% [OR, 0.75; P < .001] vs. 5.34% [OR, 0.78; P = .002]).
By age, SGLT2 inhibitors benefited people both those younger than 65 years and those aged 65 years and older, although the primary outcome was slightly lower in the younger group (6.94% [OR, 0.79; P < 0.001] vs. 10.47% [OR, 0.78; P < .001]).
And by race, similar benefits from SGLT2 inhibitors were seen among individuals who were White, compared with those who were Asian, Black, or of other race/ethnicity, with event rates of 8.77% (OR, 0.82; P < .001) and 8.75% (OR, 0.66; P = .06), respectively.
“Owing to the short-term trial durations, future long-term prospective studies and postmarketing surveillance studies are warranted to discover the rate of cardiovascular outcomes,” Dr. Bhattarai and colleagues concluded.
The authors have no disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Statin therapy seems safe in pregnancy
Statins may be safe when used during pregnancy, with no increase in risk for fetal anomalies, although there may be a higher risk for low birth weight and preterm labor, results of a large study from Taiwan suggest.
The Food and Drug Administration relaxed its warning on statins in July 2021, removing the drug’s blanket contraindication in all pregnant women.
Removal of the broadly worded contraindication should “enable health care professionals and patients to make individual decisions about benefit and risk, especially for those at very high risk of heart attack or stroke,” the FDA said in their announcement.
“Our findings suggested that statins may be used during pregnancy with no increase in the rate of congenital anomalies,” wrote Jui-Chun Chang, MD, from Taichung Veterans General Hospital, Taiwan, and colleagues in the new study, published online Dec. 30, 2021, in JAMA Network Open.
“For pregnant women at low risk, statins should be used carefully after assessing the risks of low birth weight and preterm birth,” they said. “For women with dyslipidemia or high-risk cardiovascular disease, as well as those who use statins before conception, statins may be continuously used with no increased risks of neonatal adverse effects.”
The study included more than 1.4 million pregnant women aged 18 years and older who gave birth to their first child between 2004 and 2014.
A total of 469 women (mean age, 32.6 years; mean gestational age, 38.4 weeks) who used statins during pregnancy were compared with 4,690 matched controls who had no statin exposure during pregnancy.
After controlling for maternal comorbidities and age, women who used statins during pregnancy were more apt to have low-birth-weight babies weighing less than 2,500 g (risk ratio, 1.51; 95% confidence interval, 1.05-2.16) and to deliver preterm (RR, 1.99; 95% CI, 1.46-2.71).
The statin-exposed babies were also more likely to have a lower 1-minute Apgar score (RR, 1.83; 95% CI, 1.04-3.20). Importantly, however, there was no increase in risk for fetal anomalies in the statin-exposed infants, the researchers said.
In addition, for women who used statins for more than 3 months prior to pregnancy, maintaining statin use during pregnancy did not increase the risk for adverse neonatal outcomes, including congenital anomalies, low birth weight, preterm birth, very low birth weight, low Apgar scores, and fetal distress.
The researchers called for further studies to confirm their observations.
Funding for the study was provided by Taichung Veterans General Hospital. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Statins may be safe when used during pregnancy, with no increase in risk for fetal anomalies, although there may be a higher risk for low birth weight and preterm labor, results of a large study from Taiwan suggest.
The Food and Drug Administration relaxed its warning on statins in July 2021, removing the drug’s blanket contraindication in all pregnant women.
Removal of the broadly worded contraindication should “enable health care professionals and patients to make individual decisions about benefit and risk, especially for those at very high risk of heart attack or stroke,” the FDA said in their announcement.
“Our findings suggested that statins may be used during pregnancy with no increase in the rate of congenital anomalies,” wrote Jui-Chun Chang, MD, from Taichung Veterans General Hospital, Taiwan, and colleagues in the new study, published online Dec. 30, 2021, in JAMA Network Open.
“For pregnant women at low risk, statins should be used carefully after assessing the risks of low birth weight and preterm birth,” they said. “For women with dyslipidemia or high-risk cardiovascular disease, as well as those who use statins before conception, statins may be continuously used with no increased risks of neonatal adverse effects.”
The study included more than 1.4 million pregnant women aged 18 years and older who gave birth to their first child between 2004 and 2014.
A total of 469 women (mean age, 32.6 years; mean gestational age, 38.4 weeks) who used statins during pregnancy were compared with 4,690 matched controls who had no statin exposure during pregnancy.
After controlling for maternal comorbidities and age, women who used statins during pregnancy were more apt to have low-birth-weight babies weighing less than 2,500 g (risk ratio, 1.51; 95% confidence interval, 1.05-2.16) and to deliver preterm (RR, 1.99; 95% CI, 1.46-2.71).
The statin-exposed babies were also more likely to have a lower 1-minute Apgar score (RR, 1.83; 95% CI, 1.04-3.20). Importantly, however, there was no increase in risk for fetal anomalies in the statin-exposed infants, the researchers said.
In addition, for women who used statins for more than 3 months prior to pregnancy, maintaining statin use during pregnancy did not increase the risk for adverse neonatal outcomes, including congenital anomalies, low birth weight, preterm birth, very low birth weight, low Apgar scores, and fetal distress.
The researchers called for further studies to confirm their observations.
Funding for the study was provided by Taichung Veterans General Hospital. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Statins may be safe when used during pregnancy, with no increase in risk for fetal anomalies, although there may be a higher risk for low birth weight and preterm labor, results of a large study from Taiwan suggest.
The Food and Drug Administration relaxed its warning on statins in July 2021, removing the drug’s blanket contraindication in all pregnant women.
Removal of the broadly worded contraindication should “enable health care professionals and patients to make individual decisions about benefit and risk, especially for those at very high risk of heart attack or stroke,” the FDA said in their announcement.
“Our findings suggested that statins may be used during pregnancy with no increase in the rate of congenital anomalies,” wrote Jui-Chun Chang, MD, from Taichung Veterans General Hospital, Taiwan, and colleagues in the new study, published online Dec. 30, 2021, in JAMA Network Open.
“For pregnant women at low risk, statins should be used carefully after assessing the risks of low birth weight and preterm birth,” they said. “For women with dyslipidemia or high-risk cardiovascular disease, as well as those who use statins before conception, statins may be continuously used with no increased risks of neonatal adverse effects.”
The study included more than 1.4 million pregnant women aged 18 years and older who gave birth to their first child between 2004 and 2014.
A total of 469 women (mean age, 32.6 years; mean gestational age, 38.4 weeks) who used statins during pregnancy were compared with 4,690 matched controls who had no statin exposure during pregnancy.
After controlling for maternal comorbidities and age, women who used statins during pregnancy were more apt to have low-birth-weight babies weighing less than 2,500 g (risk ratio, 1.51; 95% confidence interval, 1.05-2.16) and to deliver preterm (RR, 1.99; 95% CI, 1.46-2.71).
The statin-exposed babies were also more likely to have a lower 1-minute Apgar score (RR, 1.83; 95% CI, 1.04-3.20). Importantly, however, there was no increase in risk for fetal anomalies in the statin-exposed infants, the researchers said.
In addition, for women who used statins for more than 3 months prior to pregnancy, maintaining statin use during pregnancy did not increase the risk for adverse neonatal outcomes, including congenital anomalies, low birth weight, preterm birth, very low birth weight, low Apgar scores, and fetal distress.
The researchers called for further studies to confirm their observations.
Funding for the study was provided by Taichung Veterans General Hospital. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
My favorite physical exam pearls
I would like to start the new year off by returning to the past – when the physical exam was emphasized and utilized in decision making. I think a big reason that its use has diminished in recent years is due to the physical exam not having been emphasized in training.
For those seeking to increase their comfort with conducting the physical exam, below are several methods I have found helpful to use in practice.
Examining the pharynx
We were usually taught to ask the patient to say ahhh, with or without a nasty tongue depressor.

When I was on my pediatrics rotation, I was taught to ask the patients to roar like a lion, which always gave a nice look at their posterior pharynx. The kids also really liked doing this, but it might seem a little strange to ask adults to do this.
A technique I have found that works well with adults is to ask them to yawn. I have found that this get me a great look at the pharynx for about half of my patients.
Auscultatory percussion for pleural effusions
Guarino and colleagues described a technique that is easily mastered and very effective for determining the presence of pleural effusions.1 It involves placing the stethoscope 3 cm below the last rib in the mid clavicular line and tapping from the apex down to the last rib.
For patients without effusion, a sharp change to a loud percussion note will occur at the last rib.
If the patient has an effusion, the loud percussion note will start at the top of the effusion.
This method was remarkably successful at finding pleural effusions. In the study, Dr. Guarino found a sensitivity of 96% and a specificity of 100%.
Physical exam for anemia
Look at the nails and see if they look pale. How can we do this?
The first step is to know what your own hematocrit is. You can then compare the color of your nail to that of the patient.
If you have a normal hematocrit and the patient’s nail bed color is lighter than yours, the patient likely has anemia. If you do this frequently, you will get good at estimating hematocrit. This is especially important if you do not have labs readily available.
Another way to assess for anemia is to look at the color tint of the lower conjunctiva. The best way to look for this is to look at whether there is a generous amount of visible capillaries in the lower conjunctiva. Patients without anemia have a darker red color because of these vessels, whereas patients with anemia are a lighter pink.
Strobach and colleagues2 looked at both nail bed rubor and color tint of the lower conjunctiva and found that both reliably predicted presence and degree of anemia.
Determining if clubbing is present
Most physicians are aware of Shamroth sign, and use it to evaluate for clubbing. Shamroth sign is the loss of the diamond that is created by placing the back surfaces of opposite terminal phalanges together.
I have found that it’s easier to diagnose mild clubbing by looking at the finger in profile. If the ratio of the distal phalangeal depth compared to the depth across the distal interphalangeal joint is greater than 1:1, then clubbing is present.3
Pearls
1. Have the patient try yawning to better see the pharynx without using a tongue blade.
2. Try the technique of auscultatory percussion to be more accurate at picking up pleural effusions.
3. Know your hematocrit, so you can better use color shade to assess for anemia.
4. Try looking at fingers in profile to pick up clubbing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Guarino JR and Guarino JC. Auscultatory percussion: A simple method to detect pleural effusion. J Gen Intern Med. 1994 Feb;9(2):71-4.
2. Strobach RS et al. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2.
3. Spicknall KE et al. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. 2005 Jun;52(6):1020-8.
I would like to start the new year off by returning to the past – when the physical exam was emphasized and utilized in decision making. I think a big reason that its use has diminished in recent years is due to the physical exam not having been emphasized in training.
For those seeking to increase their comfort with conducting the physical exam, below are several methods I have found helpful to use in practice.
Examining the pharynx
We were usually taught to ask the patient to say ahhh, with or without a nasty tongue depressor.
When I was on my pediatrics rotation, I was taught to ask the patients to roar like a lion, which always gave a nice look at their posterior pharynx. The kids also really liked doing this, but it might seem a little strange to ask adults to do this.
A technique I have found that works well with adults is to ask them to yawn. I have found that this get me a great look at the pharynx for about half of my patients.
Auscultatory percussion for pleural effusions
Guarino and colleagues described a technique that is easily mastered and very effective for determining the presence of pleural effusions.1 It involves placing the stethoscope 3 cm below the last rib in the mid clavicular line and tapping from the apex down to the last rib.
For patients without effusion, a sharp change to a loud percussion note will occur at the last rib.
If the patient has an effusion, the loud percussion note will start at the top of the effusion.
This method was remarkably successful at finding pleural effusions. In the study, Dr. Guarino found a sensitivity of 96% and a specificity of 100%.
Physical exam for anemia
Look at the nails and see if they look pale. How can we do this?
The first step is to know what your own hematocrit is. You can then compare the color of your nail to that of the patient.
If you have a normal hematocrit and the patient’s nail bed color is lighter than yours, the patient likely has anemia. If you do this frequently, you will get good at estimating hematocrit. This is especially important if you do not have labs readily available.
Another way to assess for anemia is to look at the color tint of the lower conjunctiva. The best way to look for this is to look at whether there is a generous amount of visible capillaries in the lower conjunctiva. Patients without anemia have a darker red color because of these vessels, whereas patients with anemia are a lighter pink.
Strobach and colleagues2 looked at both nail bed rubor and color tint of the lower conjunctiva and found that both reliably predicted presence and degree of anemia.
Determining if clubbing is present
Most physicians are aware of Shamroth sign, and use it to evaluate for clubbing. Shamroth sign is the loss of the diamond that is created by placing the back surfaces of opposite terminal phalanges together.
I have found that it’s easier to diagnose mild clubbing by looking at the finger in profile. If the ratio of the distal phalangeal depth compared to the depth across the distal interphalangeal joint is greater than 1:1, then clubbing is present.3
Pearls
1. Have the patient try yawning to better see the pharynx without using a tongue blade.
2. Try the technique of auscultatory percussion to be more accurate at picking up pleural effusions.
3. Know your hematocrit, so you can better use color shade to assess for anemia.
4. Try looking at fingers in profile to pick up clubbing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Guarino JR and Guarino JC. Auscultatory percussion: A simple method to detect pleural effusion. J Gen Intern Med. 1994 Feb;9(2):71-4.
2. Strobach RS et al. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2.
3. Spicknall KE et al. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. 2005 Jun;52(6):1020-8.
I would like to start the new year off by returning to the past – when the physical exam was emphasized and utilized in decision making. I think a big reason that its use has diminished in recent years is due to the physical exam not having been emphasized in training.
For those seeking to increase their comfort with conducting the physical exam, below are several methods I have found helpful to use in practice.
Examining the pharynx
We were usually taught to ask the patient to say ahhh, with or without a nasty tongue depressor.
When I was on my pediatrics rotation, I was taught to ask the patients to roar like a lion, which always gave a nice look at their posterior pharynx. The kids also really liked doing this, but it might seem a little strange to ask adults to do this.
A technique I have found that works well with adults is to ask them to yawn. I have found that this get me a great look at the pharynx for about half of my patients.
Auscultatory percussion for pleural effusions
Guarino and colleagues described a technique that is easily mastered and very effective for determining the presence of pleural effusions.1 It involves placing the stethoscope 3 cm below the last rib in the mid clavicular line and tapping from the apex down to the last rib.
For patients without effusion, a sharp change to a loud percussion note will occur at the last rib.
If the patient has an effusion, the loud percussion note will start at the top of the effusion.
This method was remarkably successful at finding pleural effusions. In the study, Dr. Guarino found a sensitivity of 96% and a specificity of 100%.
Physical exam for anemia
Look at the nails and see if they look pale. How can we do this?
The first step is to know what your own hematocrit is. You can then compare the color of your nail to that of the patient.
If you have a normal hematocrit and the patient’s nail bed color is lighter than yours, the patient likely has anemia. If you do this frequently, you will get good at estimating hematocrit. This is especially important if you do not have labs readily available.
Another way to assess for anemia is to look at the color tint of the lower conjunctiva. The best way to look for this is to look at whether there is a generous amount of visible capillaries in the lower conjunctiva. Patients without anemia have a darker red color because of these vessels, whereas patients with anemia are a lighter pink.
Strobach and colleagues2 looked at both nail bed rubor and color tint of the lower conjunctiva and found that both reliably predicted presence and degree of anemia.
Determining if clubbing is present
Most physicians are aware of Shamroth sign, and use it to evaluate for clubbing. Shamroth sign is the loss of the diamond that is created by placing the back surfaces of opposite terminal phalanges together.
I have found that it’s easier to diagnose mild clubbing by looking at the finger in profile. If the ratio of the distal phalangeal depth compared to the depth across the distal interphalangeal joint is greater than 1:1, then clubbing is present.3
Pearls
1. Have the patient try yawning to better see the pharynx without using a tongue blade.
2. Try the technique of auscultatory percussion to be more accurate at picking up pleural effusions.
3. Know your hematocrit, so you can better use color shade to assess for anemia.
4. Try looking at fingers in profile to pick up clubbing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Guarino JR and Guarino JC. Auscultatory percussion: A simple method to detect pleural effusion. J Gen Intern Med. 1994 Feb;9(2):71-4.
2. Strobach RS et al. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2.
3. Spicknall KE et al. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. 2005 Jun;52(6):1020-8.
At-home geriatric assessment offers cost-effective alternative to hospital
The comprehensive geriatric assessment (CGA) is an established strategy for guiding care of older adults in a hospital setting, but its use in other settings has not been well studied, Surya Singh, PhD, of the University of Oxford (England), and colleagues wrote in their paper published in Age and Ageing. Hospital at home is active treatment by health care professionals in the patient’s home for a condition that otherwise would require acute hospital inpatient care, for a limited time period.
Interest in providing health care in the home as an alternative to hospitalization is on the rise as a way to improve patient outcomes and reduce costs, but actual cost-effectiveness data on HAH interventions are limited, the authors said. “Wide scale implementation of such services has also been constrained by the practical difficulties of designing and delivering services that cut across primary and secondary care, might involve social care and require different workforce and funding arrangements.”
In this study, the researchers conducted a cost-effectiveness analysis alongside a randomized trial of an admission avoidance CGA hospital at home (CGAHAH) service as an alternative to hospital admission. They identified individuals aged 65 years and older who were living in the community but being considered for an unplanned hospital admission in the United Kingdom. A total of 700 individuals were randomized to CGAHAH and 355 to hospital care using a 2:1 ratio. Patients were assessed at baseline in the community or in an acute care setting before being transferred to CGAHAH service. These services included access to social workers, home care, district nursing, community rehabilitation, community mental health services and acute hospital services, such as diagnostic tests and transfer to hospital. The core workforce usually included consultant geriatricians, junior doctors, nurse practitioners, health care assistants or support workers, physiotherapists, occupational therapists, and community pharmacists. There were at least daily virtual ward rounds
Comparison between HAH and in-hospital groups
Patients in the CGAHAH group had a mean of 7.17 days of care, and those in hospital had a mean of 4.92 hospital days. At 6 months’ follow-up, the mean number of care days was 9.47 in the CGAHAH group and 10.58 in the hospital group, which was a nonsignificant difference.
“For complete cases, we found that allocation to CGAHAH resulted in 3 fewer days in hospital, a difference that was reduced to 1 day at 6 months follow-up,” the researchers wrote.
Overall, after adjusting for baseline variables, the health and social care costs after 6 months were less for CGAHAH than admission to hospital. The average cost differences between the two were approximately $3,000 or 2,265 pounds. The cost difference remained and increased to a mean difference of 2,840 pounds in favor of HAH after adding informal care/societal costs.
In addition, patients randomized to CGAHAH were less likely to have been admitted to long-term residential care at 6 months follow-up, compared with the hospital group; the mean days in residential care at 6 months were 3.43 and 6.14, respectively.
Both groups showed an approximate 15% decrease in measures of quality of life from baseline to 6 months, and no differences were noted in quality-adjusted survival between the groups.
Pandemic ‘has accelerated interest’ in HAH
“Health systems around the world are exploring alternatives to hospital admission, such as hospital at home, to act as a buffer to the increasing demand for hospital care,” corresponding author Sasha Shepperd, MSc, DPhil, said in an interview. “This is partly due to a growing older population with increased health needs, but also an emphasis on providing health care that limits a decline in capacity for the older population. Inevitably, the COVID-19 pandemic has accelerated interest in hospital at home to create additional acute health care capacity.”

The take home-message supports the home service option. “If you can access a hospital-at-home service, consider this as an option for older people who would otherwise be admitted to hospital and are eligible for hospital at home care. However, is important that the provision of hospital at home is adequately resourced, and that families and caregivers are supported,” she said.
“Barriers include delivering a different type of service that requires easy access to hospital services, including admission if required; a trained workforce to provide multidisciplinary care in a patient’s home; and ensuring a good fit with existing health and social care services,” Dr. Shepperd said.
Future research areas include the demands placed on caregivers from hospital-at-home services, and how the provision of hospital at home impacts hospital and community services, she added.
Findings support use of HAH
The data from the current study support the use of a hospital at home concept, especially in the geriatric age population, for acute health conditions that could be managed at home rather than acutely in a hospital-based environment,” Noel Deep, MD, emphasized in an interview.
Dr. Deep, who is a general internist in group practice in Antigo, Wisc., said he was not surprised by the study findings.
“I am a big proponent of the hospital at home approach to taking care of patients who can be safely and appropriately managed in the familiarity and comfort of their own home environment with help from physicians, nurses, and other home health care services,” he said. “It is a valuable option for appropriately screened and selected patients to be provided this approach to management of their acute health care situations.”
Primary care physicians should explore using HAH when faced with the decision of admitting an elderly individual to the hospital for management of an acute worsening of a chronic medical condition or a reversible acute illness, said Dr. Deep, who serves on the editorial advisory board of Internal Medicine News.
The current study reinforces previous studies and data showing the benefits of managing acute health problems of elderly individuals in their home environment. These benefits include “an opportunity to free up the emergency rooms and hospitals for providing care to those individuals who truly would be best served by being admitted to the hospital,” Dr. Deep explained. Home care for the elderly “would also lead to decreased utilization of the personal protective equipment and limit exposure of the vulnerable elderly individuals to the coronavirus. Primary care physicians should always explore this possibility of providing care to the patients in their homes if it is a viable option.
“While our practice environment [in the United States] is slightly different than that referenced in this article, many, if not almost all, of our primary care physicians provide care to the geriatric age population and provide assessment and management which would be comparable to this comprehensive geriatric assessment that is discussed in the article,” and many primary care physicians have seen similar results in outcomes that the study shows, said Dr. Deep. The available research and expert opinions are quite similar and agree upon the positive outcomes in terms of providing the CGAHAH approach.
Study is important but raises questions
The study is important because patient-centered, effective care should be the goal of any health system, William Golden, MD, of the University of Arkansas for Medical Sciences, Little Rock, said in an interview.
Dr. Golden also noted that the study raised a number of questions. How each patient entered the treatment protocol was not clear. “Similarly, it is not clear whether admission criteria and resource costs in England cross to the United States experience.”
“Having close follow up of patients at home as opposed to an ‘observation status’ could be a nice innovation, but more details are needed to consider implementation in a specific community setting,” he emphasized.
As for the clinical value of the study for primary care, “primary care professionals should welcome well-staffed alternatives to inpatient care for select patient presentations,” said Dr. Golden, who is also a member of the editorial advisory board of Internal Medicine News.
The current study does not identify the conditions that were treated at home and the logistics of delivering such services, which limits comparison with what experts have seen in practice in terms of outcomes using the CGAHAH, he said. “Interested practitioners would benefit from literature detailing the staffing and decision support tools that form the core framework of this innovation.”
Limitations and strengths of study, according to authors
The study findings were limited by several factors including the calculation of CGAHAH based on service budgets, rather than from collecting information on the actual resources used; potential errors in patients’ estimation of their informal care; and lack of data on a differential impact of CGAHAH for underserved communities, the researchers noted.
However, the results were strengthened by the large study population and randomized design, and support the value of CGAHAH, which addresses the need for management of multiple long-term conditions and the potential decline in functional and cognitive ability in older adults, they said. Providing CGAHAH as an alternative to admission to hospital for older people, with a focus on multidimensional assessment, is one option that might reduce reliance on hospitalization and residential care and at a lower cost.
The study was supported by the National Institute for Health Research, and several coauthors received individual grants from the NIHR, with no other financial conflicts to disclose. Dr. Golden and Dr. Deep had no financial conflicts to disclose.
The comprehensive geriatric assessment (CGA) is an established strategy for guiding care of older adults in a hospital setting, but its use in other settings has not been well studied, Surya Singh, PhD, of the University of Oxford (England), and colleagues wrote in their paper published in Age and Ageing. Hospital at home is active treatment by health care professionals in the patient’s home for a condition that otherwise would require acute hospital inpatient care, for a limited time period.
Interest in providing health care in the home as an alternative to hospitalization is on the rise as a way to improve patient outcomes and reduce costs, but actual cost-effectiveness data on HAH interventions are limited, the authors said. “Wide scale implementation of such services has also been constrained by the practical difficulties of designing and delivering services that cut across primary and secondary care, might involve social care and require different workforce and funding arrangements.”
In this study, the researchers conducted a cost-effectiveness analysis alongside a randomized trial of an admission avoidance CGA hospital at home (CGAHAH) service as an alternative to hospital admission. They identified individuals aged 65 years and older who were living in the community but being considered for an unplanned hospital admission in the United Kingdom. A total of 700 individuals were randomized to CGAHAH and 355 to hospital care using a 2:1 ratio. Patients were assessed at baseline in the community or in an acute care setting before being transferred to CGAHAH service. These services included access to social workers, home care, district nursing, community rehabilitation, community mental health services and acute hospital services, such as diagnostic tests and transfer to hospital. The core workforce usually included consultant geriatricians, junior doctors, nurse practitioners, health care assistants or support workers, physiotherapists, occupational therapists, and community pharmacists. There were at least daily virtual ward rounds
Comparison between HAH and in-hospital groups
Patients in the CGAHAH group had a mean of 7.17 days of care, and those in hospital had a mean of 4.92 hospital days. At 6 months’ follow-up, the mean number of care days was 9.47 in the CGAHAH group and 10.58 in the hospital group, which was a nonsignificant difference.
“For complete cases, we found that allocation to CGAHAH resulted in 3 fewer days in hospital, a difference that was reduced to 1 day at 6 months follow-up,” the researchers wrote.
Overall, after adjusting for baseline variables, the health and social care costs after 6 months were less for CGAHAH than admission to hospital. The average cost differences between the two were approximately $3,000 or 2,265 pounds. The cost difference remained and increased to a mean difference of 2,840 pounds in favor of HAH after adding informal care/societal costs.
In addition, patients randomized to CGAHAH were less likely to have been admitted to long-term residential care at 6 months follow-up, compared with the hospital group; the mean days in residential care at 6 months were 3.43 and 6.14, respectively.
Both groups showed an approximate 15% decrease in measures of quality of life from baseline to 6 months, and no differences were noted in quality-adjusted survival between the groups.
Pandemic ‘has accelerated interest’ in HAH
“Health systems around the world are exploring alternatives to hospital admission, such as hospital at home, to act as a buffer to the increasing demand for hospital care,” corresponding author Sasha Shepperd, MSc, DPhil, said in an interview. “This is partly due to a growing older population with increased health needs, but also an emphasis on providing health care that limits a decline in capacity for the older population. Inevitably, the COVID-19 pandemic has accelerated interest in hospital at home to create additional acute health care capacity.”
The take home-message supports the home service option. “If you can access a hospital-at-home service, consider this as an option for older people who would otherwise be admitted to hospital and are eligible for hospital at home care. However, is important that the provision of hospital at home is adequately resourced, and that families and caregivers are supported,” she said.
“Barriers include delivering a different type of service that requires easy access to hospital services, including admission if required; a trained workforce to provide multidisciplinary care in a patient’s home; and ensuring a good fit with existing health and social care services,” Dr. Shepperd said.
Future research areas include the demands placed on caregivers from hospital-at-home services, and how the provision of hospital at home impacts hospital and community services, she added.
Findings support use of HAH
The data from the current study support the use of a hospital at home concept, especially in the geriatric age population, for acute health conditions that could be managed at home rather than acutely in a hospital-based environment,” Noel Deep, MD, emphasized in an interview.
Dr. Deep, who is a general internist in group practice in Antigo, Wisc., said he was not surprised by the study findings.
“I am a big proponent of the hospital at home approach to taking care of patients who can be safely and appropriately managed in the familiarity and comfort of their own home environment with help from physicians, nurses, and other home health care services,” he said. “It is a valuable option for appropriately screened and selected patients to be provided this approach to management of their acute health care situations.”
Primary care physicians should explore using HAH when faced with the decision of admitting an elderly individual to the hospital for management of an acute worsening of a chronic medical condition or a reversible acute illness, said Dr. Deep, who serves on the editorial advisory board of Internal Medicine News.
The current study reinforces previous studies and data showing the benefits of managing acute health problems of elderly individuals in their home environment. These benefits include “an opportunity to free up the emergency rooms and hospitals for providing care to those individuals who truly would be best served by being admitted to the hospital,” Dr. Deep explained. Home care for the elderly “would also lead to decreased utilization of the personal protective equipment and limit exposure of the vulnerable elderly individuals to the coronavirus. Primary care physicians should always explore this possibility of providing care to the patients in their homes if it is a viable option.
“While our practice environment [in the United States] is slightly different than that referenced in this article, many, if not almost all, of our primary care physicians provide care to the geriatric age population and provide assessment and management which would be comparable to this comprehensive geriatric assessment that is discussed in the article,” and many primary care physicians have seen similar results in outcomes that the study shows, said Dr. Deep. The available research and expert opinions are quite similar and agree upon the positive outcomes in terms of providing the CGAHAH approach.
Study is important but raises questions
The study is important because patient-centered, effective care should be the goal of any health system, William Golden, MD, of the University of Arkansas for Medical Sciences, Little Rock, said in an interview.
Dr. Golden also noted that the study raised a number of questions. How each patient entered the treatment protocol was not clear. “Similarly, it is not clear whether admission criteria and resource costs in England cross to the United States experience.”
“Having close follow up of patients at home as opposed to an ‘observation status’ could be a nice innovation, but more details are needed to consider implementation in a specific community setting,” he emphasized.
As for the clinical value of the study for primary care, “primary care professionals should welcome well-staffed alternatives to inpatient care for select patient presentations,” said Dr. Golden, who is also a member of the editorial advisory board of Internal Medicine News.
The current study does not identify the conditions that were treated at home and the logistics of delivering such services, which limits comparison with what experts have seen in practice in terms of outcomes using the CGAHAH, he said. “Interested practitioners would benefit from literature detailing the staffing and decision support tools that form the core framework of this innovation.”
Limitations and strengths of study, according to authors
The study findings were limited by several factors including the calculation of CGAHAH based on service budgets, rather than from collecting information on the actual resources used; potential errors in patients’ estimation of their informal care; and lack of data on a differential impact of CGAHAH for underserved communities, the researchers noted.
However, the results were strengthened by the large study population and randomized design, and support the value of CGAHAH, which addresses the need for management of multiple long-term conditions and the potential decline in functional and cognitive ability in older adults, they said. Providing CGAHAH as an alternative to admission to hospital for older people, with a focus on multidimensional assessment, is one option that might reduce reliance on hospitalization and residential care and at a lower cost.
The study was supported by the National Institute for Health Research, and several coauthors received individual grants from the NIHR, with no other financial conflicts to disclose. Dr. Golden and Dr. Deep had no financial conflicts to disclose.
The comprehensive geriatric assessment (CGA) is an established strategy for guiding care of older adults in a hospital setting, but its use in other settings has not been well studied, Surya Singh, PhD, of the University of Oxford (England), and colleagues wrote in their paper published in Age and Ageing. Hospital at home is active treatment by health care professionals in the patient’s home for a condition that otherwise would require acute hospital inpatient care, for a limited time period.
Interest in providing health care in the home as an alternative to hospitalization is on the rise as a way to improve patient outcomes and reduce costs, but actual cost-effectiveness data on HAH interventions are limited, the authors said. “Wide scale implementation of such services has also been constrained by the practical difficulties of designing and delivering services that cut across primary and secondary care, might involve social care and require different workforce and funding arrangements.”
In this study, the researchers conducted a cost-effectiveness analysis alongside a randomized trial of an admission avoidance CGA hospital at home (CGAHAH) service as an alternative to hospital admission. They identified individuals aged 65 years and older who were living in the community but being considered for an unplanned hospital admission in the United Kingdom. A total of 700 individuals were randomized to CGAHAH and 355 to hospital care using a 2:1 ratio. Patients were assessed at baseline in the community or in an acute care setting before being transferred to CGAHAH service. These services included access to social workers, home care, district nursing, community rehabilitation, community mental health services and acute hospital services, such as diagnostic tests and transfer to hospital. The core workforce usually included consultant geriatricians, junior doctors, nurse practitioners, health care assistants or support workers, physiotherapists, occupational therapists, and community pharmacists. There were at least daily virtual ward rounds
Comparison between HAH and in-hospital groups
Patients in the CGAHAH group had a mean of 7.17 days of care, and those in hospital had a mean of 4.92 hospital days. At 6 months’ follow-up, the mean number of care days was 9.47 in the CGAHAH group and 10.58 in the hospital group, which was a nonsignificant difference.
“For complete cases, we found that allocation to CGAHAH resulted in 3 fewer days in hospital, a difference that was reduced to 1 day at 6 months follow-up,” the researchers wrote.
Overall, after adjusting for baseline variables, the health and social care costs after 6 months were less for CGAHAH than admission to hospital. The average cost differences between the two were approximately $3,000 or 2,265 pounds. The cost difference remained and increased to a mean difference of 2,840 pounds in favor of HAH after adding informal care/societal costs.
In addition, patients randomized to CGAHAH were less likely to have been admitted to long-term residential care at 6 months follow-up, compared with the hospital group; the mean days in residential care at 6 months were 3.43 and 6.14, respectively.
Both groups showed an approximate 15% decrease in measures of quality of life from baseline to 6 months, and no differences were noted in quality-adjusted survival between the groups.
Pandemic ‘has accelerated interest’ in HAH
“Health systems around the world are exploring alternatives to hospital admission, such as hospital at home, to act as a buffer to the increasing demand for hospital care,” corresponding author Sasha Shepperd, MSc, DPhil, said in an interview. “This is partly due to a growing older population with increased health needs, but also an emphasis on providing health care that limits a decline in capacity for the older population. Inevitably, the COVID-19 pandemic has accelerated interest in hospital at home to create additional acute health care capacity.”
The take home-message supports the home service option. “If you can access a hospital-at-home service, consider this as an option for older people who would otherwise be admitted to hospital and are eligible for hospital at home care. However, is important that the provision of hospital at home is adequately resourced, and that families and caregivers are supported,” she said.
“Barriers include delivering a different type of service that requires easy access to hospital services, including admission if required; a trained workforce to provide multidisciplinary care in a patient’s home; and ensuring a good fit with existing health and social care services,” Dr. Shepperd said.
Future research areas include the demands placed on caregivers from hospital-at-home services, and how the provision of hospital at home impacts hospital and community services, she added.
Findings support use of HAH
The data from the current study support the use of a hospital at home concept, especially in the geriatric age population, for acute health conditions that could be managed at home rather than acutely in a hospital-based environment,” Noel Deep, MD, emphasized in an interview.
Dr. Deep, who is a general internist in group practice in Antigo, Wisc., said he was not surprised by the study findings.
“I am a big proponent of the hospital at home approach to taking care of patients who can be safely and appropriately managed in the familiarity and comfort of their own home environment with help from physicians, nurses, and other home health care services,” he said. “It is a valuable option for appropriately screened and selected patients to be provided this approach to management of their acute health care situations.”
Primary care physicians should explore using HAH when faced with the decision of admitting an elderly individual to the hospital for management of an acute worsening of a chronic medical condition or a reversible acute illness, said Dr. Deep, who serves on the editorial advisory board of Internal Medicine News.
The current study reinforces previous studies and data showing the benefits of managing acute health problems of elderly individuals in their home environment. These benefits include “an opportunity to free up the emergency rooms and hospitals for providing care to those individuals who truly would be best served by being admitted to the hospital,” Dr. Deep explained. Home care for the elderly “would also lead to decreased utilization of the personal protective equipment and limit exposure of the vulnerable elderly individuals to the coronavirus. Primary care physicians should always explore this possibility of providing care to the patients in their homes if it is a viable option.
“While our practice environment [in the United States] is slightly different than that referenced in this article, many, if not almost all, of our primary care physicians provide care to the geriatric age population and provide assessment and management which would be comparable to this comprehensive geriatric assessment that is discussed in the article,” and many primary care physicians have seen similar results in outcomes that the study shows, said Dr. Deep. The available research and expert opinions are quite similar and agree upon the positive outcomes in terms of providing the CGAHAH approach.
Study is important but raises questions
The study is important because patient-centered, effective care should be the goal of any health system, William Golden, MD, of the University of Arkansas for Medical Sciences, Little Rock, said in an interview.
Dr. Golden also noted that the study raised a number of questions. How each patient entered the treatment protocol was not clear. “Similarly, it is not clear whether admission criteria and resource costs in England cross to the United States experience.”
“Having close follow up of patients at home as opposed to an ‘observation status’ could be a nice innovation, but more details are needed to consider implementation in a specific community setting,” he emphasized.
As for the clinical value of the study for primary care, “primary care professionals should welcome well-staffed alternatives to inpatient care for select patient presentations,” said Dr. Golden, who is also a member of the editorial advisory board of Internal Medicine News.
The current study does not identify the conditions that were treated at home and the logistics of delivering such services, which limits comparison with what experts have seen in practice in terms of outcomes using the CGAHAH, he said. “Interested practitioners would benefit from literature detailing the staffing and decision support tools that form the core framework of this innovation.”
Limitations and strengths of study, according to authors
The study findings were limited by several factors including the calculation of CGAHAH based on service budgets, rather than from collecting information on the actual resources used; potential errors in patients’ estimation of their informal care; and lack of data on a differential impact of CGAHAH for underserved communities, the researchers noted.
However, the results were strengthened by the large study population and randomized design, and support the value of CGAHAH, which addresses the need for management of multiple long-term conditions and the potential decline in functional and cognitive ability in older adults, they said. Providing CGAHAH as an alternative to admission to hospital for older people, with a focus on multidimensional assessment, is one option that might reduce reliance on hospitalization and residential care and at a lower cost.
The study was supported by the National Institute for Health Research, and several coauthors received individual grants from the NIHR, with no other financial conflicts to disclose. Dr. Golden and Dr. Deep had no financial conflicts to disclose.
FROM AGE AND AGEING
Benign adrenal tumors linked to hypertension, type 2 diabetes
In more than 15% of people with benign adrenal tumors, the growths produce clinically relevant levels of serum cortisol that are significantly linked with an increased prevalence of hypertension and, in 5% of those with Cushing syndrome (CS), an increased prevalence of type 2 diabetes, based on data from more than 1,300 people with benign adrenal tumors, the largest reported prospective study of the disorder.
The study results showed that mild autonomous cortisol secretion (MACS) from benign adrenal tumors “is very frequent and is an important risk condition for high blood pressure and type 2 diabetes, especially in older women,” said Alessandro Prete, MD, lead author of the study which was published online Jan. 3, 2022, in Annals of Internal Medicine.
“The impact of MACS on high blood pressure and risk for type 2 diabetes has been underestimated until now,” said Dr. Prete, an endocrinologist at the University of Birmingham (England), in a written statement.
Results from previous studies “suggested that MACS is associated with poor health. Our study is the largest to establish conclusively the extent of the risk and severity of high blood pressure and type 2 diabetes in patients with MACS,” said Wiebke Arlt, MD, DSc, senior author and director of the Institute of Metabolism & Systems Research at the University of Birmingham.
All patients found to have a benign adrenal tumor should undergo testing for MACS and have their blood pressure and glucose levels measured regularly, Dr. Arlt advised in the statement released by the University of Birmingham.
MACS more common than previously thought
The new findings show that MACS “is more common and may have a more negative impact on health than previously thought, including increasing the risk for type 2 diabetes,” commented Lucy Chambers, PhD, head of research communications at Diabetes UK. “The findings suggest that screening for MACS could help identify people – particularly women, in whom the condition was found to be more common – who may benefit from support to reduce their risk of type 2 diabetes.”
The study included 1,305 people with newly diagnosed, benign adrenal tumors greater than 1 cm, a subset of patients prospectively enrolled in a study with the primary purpose of validating a novel way to diagnose adrenocortical carcinomas. Patients underwent treatment in 2011-2016 at any of 14 tertiary centers in 11 countries.
Researchers used a MACS definition of failure to suppress morning serum cortisol concentration to less than 50 nmol/L after treatment with 1 mg oral dexamethasone at 11 p.m. the previous evening in those with no clinical features of CS.
Roughly half of patients (n = 649) showed normal cortisol suppression with dexamethasone, identifying them as having nonfunctioning adrenal tumors, and about 35% showed possible MACS based on having moderate levels of excess cortisol.
Nearly 11% (n = 140) showed definitive MACS with more robust cortisol levels, and 5% (n = 65) received a diagnosis of clinically overt CS despite selection criteria meant to exclude people with clinical signs of CS.
There was a clear relationship between patient sex and severity of autonomous cortisol production. Among those with nonfunctioning adrenal tumors, 64% were women, which rose to 74% women in those with definitive MACS and 86% women among those with CS. The median age of participants was 60 years old.
Increasing cortisol levels linked with cardiometabolic disease
Analysis of the prevalence of hypertension and type 2 diabetes after adjustment for age, sex, and body mass index showed that, compared with people with nonfunctioning adrenal tumors, those with definitive MACS had a significant 15% higher rate of hypertension and those with overt CS had a 37% higher rate.
Higher levels of excess cortisol were also directly linked with an increased need for treatment with three or more antihypertensive agents to control blood pressure. Those with definitive MACS had a significant 31% higher rate of being on three or more drugs, and those with overt CS had a greater than twofold higher rate.
People with overt CS also had a significant 62% higher rate of type 2 diabetes, compared with those with a nonfunctioning tumor, but in those with definitive MACS the association was not significant. However, people with definitive MACS or overt CS who had type 2 diabetes and also had significantly increased rates of requiring insulin treatment.
The findings show that “people with definitive MACS carry an increased cardiometabolic burden similar to that seen in CS even if they do not display typical features of clinically overt cortisol excess,” the authors wrote in the report.
Even among those with apparently nonfunctioning tumors, each 10 nmol/L rise in cortisol level during a dexamethasone-suppression test was associated with a higher cardiometabolic disease burden. This observation suggests that current diagnostic cutoffs for the suppression test may miss some people with clinically relevant autonomous cortisol secretion, the report said. The study findings also suggest that people with benign adrenal tumors show a progressive continuum of excess cortisol with clinical consequences that increase as levels increase.
Determine the consequences of cortisol secretion
“These data clearly support the European Society of Endocrinology guideline recommendations that clinicians should determine precisely the cardiometabolic consequences of mild cortisol secretion in patients with adrenal lesions,” André Lacroix, MD, wrote in an accompanying editorial.
But Dr. Lacroix included some caveats. He noted the “potential pitfalls in relying on a single total serum cortisol value after the 1-mg dexamethasone test.” He also wondered whether the analysis used optimal cortisol values to distinguish patient subgroups.
Plus, “even in patients with nonfunctioning adrenal tumors the prevalence of diabetes and hypertension is higher than in the general population, raising concerns about the cardiometabolic consequences of barely detectable cortisol excess,” wrote Dr. Lacroix, an endocrinologist at the CHUM Research Center and professor of medicine at the University of Montreal.
The study received no commercial funding. Dr. Prete, Dr. Chambers, and Dr. Lacroix have reported no relevant financial relationships. Dr. Arlt is listed as an inventor on a patent on the use of steroid profiling as a biomarker tool for the differential diagnosis of adrenal tumors.
A version of this article first appeared on Medscape.com.
In more than 15% of people with benign adrenal tumors, the growths produce clinically relevant levels of serum cortisol that are significantly linked with an increased prevalence of hypertension and, in 5% of those with Cushing syndrome (CS), an increased prevalence of type 2 diabetes, based on data from more than 1,300 people with benign adrenal tumors, the largest reported prospective study of the disorder.
The study results showed that mild autonomous cortisol secretion (MACS) from benign adrenal tumors “is very frequent and is an important risk condition for high blood pressure and type 2 diabetes, especially in older women,” said Alessandro Prete, MD, lead author of the study which was published online Jan. 3, 2022, in Annals of Internal Medicine.
“The impact of MACS on high blood pressure and risk for type 2 diabetes has been underestimated until now,” said Dr. Prete, an endocrinologist at the University of Birmingham (England), in a written statement.
Results from previous studies “suggested that MACS is associated with poor health. Our study is the largest to establish conclusively the extent of the risk and severity of high blood pressure and type 2 diabetes in patients with MACS,” said Wiebke Arlt, MD, DSc, senior author and director of the Institute of Metabolism & Systems Research at the University of Birmingham.
All patients found to have a benign adrenal tumor should undergo testing for MACS and have their blood pressure and glucose levels measured regularly, Dr. Arlt advised in the statement released by the University of Birmingham.
MACS more common than previously thought
The new findings show that MACS “is more common and may have a more negative impact on health than previously thought, including increasing the risk for type 2 diabetes,” commented Lucy Chambers, PhD, head of research communications at Diabetes UK. “The findings suggest that screening for MACS could help identify people – particularly women, in whom the condition was found to be more common – who may benefit from support to reduce their risk of type 2 diabetes.”
The study included 1,305 people with newly diagnosed, benign adrenal tumors greater than 1 cm, a subset of patients prospectively enrolled in a study with the primary purpose of validating a novel way to diagnose adrenocortical carcinomas. Patients underwent treatment in 2011-2016 at any of 14 tertiary centers in 11 countries.
Researchers used a MACS definition of failure to suppress morning serum cortisol concentration to less than 50 nmol/L after treatment with 1 mg oral dexamethasone at 11 p.m. the previous evening in those with no clinical features of CS.
Roughly half of patients (n = 649) showed normal cortisol suppression with dexamethasone, identifying them as having nonfunctioning adrenal tumors, and about 35% showed possible MACS based on having moderate levels of excess cortisol.
Nearly 11% (n = 140) showed definitive MACS with more robust cortisol levels, and 5% (n = 65) received a diagnosis of clinically overt CS despite selection criteria meant to exclude people with clinical signs of CS.
There was a clear relationship between patient sex and severity of autonomous cortisol production. Among those with nonfunctioning adrenal tumors, 64% were women, which rose to 74% women in those with definitive MACS and 86% women among those with CS. The median age of participants was 60 years old.
Increasing cortisol levels linked with cardiometabolic disease
Analysis of the prevalence of hypertension and type 2 diabetes after adjustment for age, sex, and body mass index showed that, compared with people with nonfunctioning adrenal tumors, those with definitive MACS had a significant 15% higher rate of hypertension and those with overt CS had a 37% higher rate.
Higher levels of excess cortisol were also directly linked with an increased need for treatment with three or more antihypertensive agents to control blood pressure. Those with definitive MACS had a significant 31% higher rate of being on three or more drugs, and those with overt CS had a greater than twofold higher rate.
People with overt CS also had a significant 62% higher rate of type 2 diabetes, compared with those with a nonfunctioning tumor, but in those with definitive MACS the association was not significant. However, people with definitive MACS or overt CS who had type 2 diabetes and also had significantly increased rates of requiring insulin treatment.
The findings show that “people with definitive MACS carry an increased cardiometabolic burden similar to that seen in CS even if they do not display typical features of clinically overt cortisol excess,” the authors wrote in the report.
Even among those with apparently nonfunctioning tumors, each 10 nmol/L rise in cortisol level during a dexamethasone-suppression test was associated with a higher cardiometabolic disease burden. This observation suggests that current diagnostic cutoffs for the suppression test may miss some people with clinically relevant autonomous cortisol secretion, the report said. The study findings also suggest that people with benign adrenal tumors show a progressive continuum of excess cortisol with clinical consequences that increase as levels increase.
Determine the consequences of cortisol secretion
“These data clearly support the European Society of Endocrinology guideline recommendations that clinicians should determine precisely the cardiometabolic consequences of mild cortisol secretion in patients with adrenal lesions,” André Lacroix, MD, wrote in an accompanying editorial.
But Dr. Lacroix included some caveats. He noted the “potential pitfalls in relying on a single total serum cortisol value after the 1-mg dexamethasone test.” He also wondered whether the analysis used optimal cortisol values to distinguish patient subgroups.
Plus, “even in patients with nonfunctioning adrenal tumors the prevalence of diabetes and hypertension is higher than in the general population, raising concerns about the cardiometabolic consequences of barely detectable cortisol excess,” wrote Dr. Lacroix, an endocrinologist at the CHUM Research Center and professor of medicine at the University of Montreal.
The study received no commercial funding. Dr. Prete, Dr. Chambers, and Dr. Lacroix have reported no relevant financial relationships. Dr. Arlt is listed as an inventor on a patent on the use of steroid profiling as a biomarker tool for the differential diagnosis of adrenal tumors.
A version of this article first appeared on Medscape.com.
In more than 15% of people with benign adrenal tumors, the growths produce clinically relevant levels of serum cortisol that are significantly linked with an increased prevalence of hypertension and, in 5% of those with Cushing syndrome (CS), an increased prevalence of type 2 diabetes, based on data from more than 1,300 people with benign adrenal tumors, the largest reported prospective study of the disorder.
The study results showed that mild autonomous cortisol secretion (MACS) from benign adrenal tumors “is very frequent and is an important risk condition for high blood pressure and type 2 diabetes, especially in older women,” said Alessandro Prete, MD, lead author of the study which was published online Jan. 3, 2022, in Annals of Internal Medicine.
“The impact of MACS on high blood pressure and risk for type 2 diabetes has been underestimated until now,” said Dr. Prete, an endocrinologist at the University of Birmingham (England), in a written statement.
Results from previous studies “suggested that MACS is associated with poor health. Our study is the largest to establish conclusively the extent of the risk and severity of high blood pressure and type 2 diabetes in patients with MACS,” said Wiebke Arlt, MD, DSc, senior author and director of the Institute of Metabolism & Systems Research at the University of Birmingham.
All patients found to have a benign adrenal tumor should undergo testing for MACS and have their blood pressure and glucose levels measured regularly, Dr. Arlt advised in the statement released by the University of Birmingham.
MACS more common than previously thought
The new findings show that MACS “is more common and may have a more negative impact on health than previously thought, including increasing the risk for type 2 diabetes,” commented Lucy Chambers, PhD, head of research communications at Diabetes UK. “The findings suggest that screening for MACS could help identify people – particularly women, in whom the condition was found to be more common – who may benefit from support to reduce their risk of type 2 diabetes.”
The study included 1,305 people with newly diagnosed, benign adrenal tumors greater than 1 cm, a subset of patients prospectively enrolled in a study with the primary purpose of validating a novel way to diagnose adrenocortical carcinomas. Patients underwent treatment in 2011-2016 at any of 14 tertiary centers in 11 countries.
Researchers used a MACS definition of failure to suppress morning serum cortisol concentration to less than 50 nmol/L after treatment with 1 mg oral dexamethasone at 11 p.m. the previous evening in those with no clinical features of CS.
Roughly half of patients (n = 649) showed normal cortisol suppression with dexamethasone, identifying them as having nonfunctioning adrenal tumors, and about 35% showed possible MACS based on having moderate levels of excess cortisol.
Nearly 11% (n = 140) showed definitive MACS with more robust cortisol levels, and 5% (n = 65) received a diagnosis of clinically overt CS despite selection criteria meant to exclude people with clinical signs of CS.
There was a clear relationship between patient sex and severity of autonomous cortisol production. Among those with nonfunctioning adrenal tumors, 64% were women, which rose to 74% women in those with definitive MACS and 86% women among those with CS. The median age of participants was 60 years old.
Increasing cortisol levels linked with cardiometabolic disease
Analysis of the prevalence of hypertension and type 2 diabetes after adjustment for age, sex, and body mass index showed that, compared with people with nonfunctioning adrenal tumors, those with definitive MACS had a significant 15% higher rate of hypertension and those with overt CS had a 37% higher rate.
Higher levels of excess cortisol were also directly linked with an increased need for treatment with three or more antihypertensive agents to control blood pressure. Those with definitive MACS had a significant 31% higher rate of being on three or more drugs, and those with overt CS had a greater than twofold higher rate.
People with overt CS also had a significant 62% higher rate of type 2 diabetes, compared with those with a nonfunctioning tumor, but in those with definitive MACS the association was not significant. However, people with definitive MACS or overt CS who had type 2 diabetes and also had significantly increased rates of requiring insulin treatment.
The findings show that “people with definitive MACS carry an increased cardiometabolic burden similar to that seen in CS even if they do not display typical features of clinically overt cortisol excess,” the authors wrote in the report.
Even among those with apparently nonfunctioning tumors, each 10 nmol/L rise in cortisol level during a dexamethasone-suppression test was associated with a higher cardiometabolic disease burden. This observation suggests that current diagnostic cutoffs for the suppression test may miss some people with clinically relevant autonomous cortisol secretion, the report said. The study findings also suggest that people with benign adrenal tumors show a progressive continuum of excess cortisol with clinical consequences that increase as levels increase.
Determine the consequences of cortisol secretion
“These data clearly support the European Society of Endocrinology guideline recommendations that clinicians should determine precisely the cardiometabolic consequences of mild cortisol secretion in patients with adrenal lesions,” André Lacroix, MD, wrote in an accompanying editorial.
But Dr. Lacroix included some caveats. He noted the “potential pitfalls in relying on a single total serum cortisol value after the 1-mg dexamethasone test.” He also wondered whether the analysis used optimal cortisol values to distinguish patient subgroups.
Plus, “even in patients with nonfunctioning adrenal tumors the prevalence of diabetes and hypertension is higher than in the general population, raising concerns about the cardiometabolic consequences of barely detectable cortisol excess,” wrote Dr. Lacroix, an endocrinologist at the CHUM Research Center and professor of medicine at the University of Montreal.
The study received no commercial funding. Dr. Prete, Dr. Chambers, and Dr. Lacroix have reported no relevant financial relationships. Dr. Arlt is listed as an inventor on a patent on the use of steroid profiling as a biomarker tool for the differential diagnosis of adrenal tumors.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE