User login
Top Dermatologic Procedures: ASDS Survey Results for 2014
Skin cancer treatments ranked as the most-performed procedures (3.08 million total procedures) for the fourth year in a row, according to survey results released by the American Society for Dermatologic Surgery (ASDS). Of them, 2.8 million procedures were for nonmelanoma skin cancers, and 206,000 were for melanomas. This finding confirms the growing incidence of skin cancer and the expertise of dermatologic surgeons in diagnosis and treatment.
Data were collected for the 2014 experience from 826 practicing members of the ASDS, with nearly 9.5 million medically necessary and cosmetic procedures performed.
Dermatologic surgeons performed 6.4 million cosmetic treatments in 2014. The top 5 cosmetic treatments were:
- Laser and light/energy-based devices: 2.06 million total procedures
- Wrinkle-relaxing injections (injectable neuromodulators): 1.74 million total procedures
- Soft-tissue fillers: 1.01 million total procedures
- Laser hair removal: 633,000 total procedures
- Chemical peels: 564,000 total procedures
Most laser and light/energy-based device treatments were reported for facial redness, followed by photorejuvenation, phototherapy, age spots, tissue tightening, laser resurfacing, acne scars, surgical scars, tattoo removal, and birthmarks.
Of the injectable neuromodulators used, nearly 1.2 million procedures were reported for onabotulinumtoxinA, followed by abobotulinumtoxinA (382,000) and incobotulinumtoxinA (175,000). The highest percentage of neuromodulator injections was reported in patients aged 46 to 50 years. Also, females (87%) received more injections than males (13%).
Soft-tissue fillers were performed the most in patients older than 55 years. Females (91%) received more treatments than males (9%).
The number of laser hair removal procedures performed in 2014 increased 27% from 2013 and 51% from 2012, emphasizing the role of dermatologists in providing safe and effective treatment.
Body sculpting procedures accounted for 208,000 total procedures, a 53% increase since 2012. The top treatments were cryolipolysis (79,000) and radiofrequency therapy (49,600).
View the full results of this survey on the ASDS Web site.
Skin cancer treatments ranked as the most-performed procedures (3.08 million total procedures) for the fourth year in a row, according to survey results released by the American Society for Dermatologic Surgery (ASDS). Of them, 2.8 million procedures were for nonmelanoma skin cancers, and 206,000 were for melanomas. This finding confirms the growing incidence of skin cancer and the expertise of dermatologic surgeons in diagnosis and treatment.
Data were collected for the 2014 experience from 826 practicing members of the ASDS, with nearly 9.5 million medically necessary and cosmetic procedures performed.
Dermatologic surgeons performed 6.4 million cosmetic treatments in 2014. The top 5 cosmetic treatments were:
- Laser and light/energy-based devices: 2.06 million total procedures
- Wrinkle-relaxing injections (injectable neuromodulators): 1.74 million total procedures
- Soft-tissue fillers: 1.01 million total procedures
- Laser hair removal: 633,000 total procedures
- Chemical peels: 564,000 total procedures
Most laser and light/energy-based device treatments were reported for facial redness, followed by photorejuvenation, phototherapy, age spots, tissue tightening, laser resurfacing, acne scars, surgical scars, tattoo removal, and birthmarks.
Of the injectable neuromodulators used, nearly 1.2 million procedures were reported for onabotulinumtoxinA, followed by abobotulinumtoxinA (382,000) and incobotulinumtoxinA (175,000). The highest percentage of neuromodulator injections was reported in patients aged 46 to 50 years. Also, females (87%) received more injections than males (13%).
Soft-tissue fillers were performed the most in patients older than 55 years. Females (91%) received more treatments than males (9%).
The number of laser hair removal procedures performed in 2014 increased 27% from 2013 and 51% from 2012, emphasizing the role of dermatologists in providing safe and effective treatment.
Body sculpting procedures accounted for 208,000 total procedures, a 53% increase since 2012. The top treatments were cryolipolysis (79,000) and radiofrequency therapy (49,600).
View the full results of this survey on the ASDS Web site.
Skin cancer treatments ranked as the most-performed procedures (3.08 million total procedures) for the fourth year in a row, according to survey results released by the American Society for Dermatologic Surgery (ASDS). Of them, 2.8 million procedures were for nonmelanoma skin cancers, and 206,000 were for melanomas. This finding confirms the growing incidence of skin cancer and the expertise of dermatologic surgeons in diagnosis and treatment.
Data were collected for the 2014 experience from 826 practicing members of the ASDS, with nearly 9.5 million medically necessary and cosmetic procedures performed.
Dermatologic surgeons performed 6.4 million cosmetic treatments in 2014. The top 5 cosmetic treatments were:
- Laser and light/energy-based devices: 2.06 million total procedures
- Wrinkle-relaxing injections (injectable neuromodulators): 1.74 million total procedures
- Soft-tissue fillers: 1.01 million total procedures
- Laser hair removal: 633,000 total procedures
- Chemical peels: 564,000 total procedures
Most laser and light/energy-based device treatments were reported for facial redness, followed by photorejuvenation, phototherapy, age spots, tissue tightening, laser resurfacing, acne scars, surgical scars, tattoo removal, and birthmarks.
Of the injectable neuromodulators used, nearly 1.2 million procedures were reported for onabotulinumtoxinA, followed by abobotulinumtoxinA (382,000) and incobotulinumtoxinA (175,000). The highest percentage of neuromodulator injections was reported in patients aged 46 to 50 years. Also, females (87%) received more injections than males (13%).
Soft-tissue fillers were performed the most in patients older than 55 years. Females (91%) received more treatments than males (9%).
The number of laser hair removal procedures performed in 2014 increased 27% from 2013 and 51% from 2012, emphasizing the role of dermatologists in providing safe and effective treatment.
Body sculpting procedures accounted for 208,000 total procedures, a 53% increase since 2012. The top treatments were cryolipolysis (79,000) and radiofrequency therapy (49,600).
View the full results of this survey on the ASDS Web site.
Cosmetic Corner: Dermatologists Weigh in on OTC Cleansers for Rosacea Patients
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC cleansers for rosacea patients. Consideration must be given to:
- Avène Antirougeurs Redness Relief Dermo-Cleansing Milk
Pierre Fabre Dermo-Cosmétique USA
Recommended by Julie Woodward, MD, Durham, North Carolina
- Avène Extremely Gentle Cleanser Lotion
Pierre Fabre Dermo-Cosmétique USA
Recommended by Julie Woodward, MD, Durham, North Carolina
- Cetaphil Gentle Skin Cleanser
Galderma Laboratories, LP
“I always recommend for all of my rosacea patients a strict regimen of cleansing and sun protection with Cetaphil cleanser and moisturizing sunscreen.”—Wm. Philip Werschler, MD, Seattle, Washington
Recommended by Julie Woodward, MD, Durham, North Carolina
- Toleriane Dermo-Cleanser
La Roche-Posay Laboratoire Dermatologique
“Excellent for rosacea because it doesn’t contain any surfactants. This product has a very hydrated formula that helps repair the skin barrier.”—Whitney Bowe, MD, Brooklyn, New York
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Face washes and products for babies will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to cutis@frontlinemedcom.com.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC cleansers for rosacea patients. Consideration must be given to:
- Avène Antirougeurs Redness Relief Dermo-Cleansing Milk
Pierre Fabre Dermo-Cosmétique USA
Recommended by Julie Woodward, MD, Durham, North Carolina
- Avène Extremely Gentle Cleanser Lotion
Pierre Fabre Dermo-Cosmétique USA
Recommended by Julie Woodward, MD, Durham, North Carolina
- Cetaphil Gentle Skin Cleanser
Galderma Laboratories, LP
“I always recommend for all of my rosacea patients a strict regimen of cleansing and sun protection with Cetaphil cleanser and moisturizing sunscreen.”—Wm. Philip Werschler, MD, Seattle, Washington
Recommended by Julie Woodward, MD, Durham, North Carolina
- Toleriane Dermo-Cleanser
La Roche-Posay Laboratoire Dermatologique
“Excellent for rosacea because it doesn’t contain any surfactants. This product has a very hydrated formula that helps repair the skin barrier.”—Whitney Bowe, MD, Brooklyn, New York
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Face washes and products for babies will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to cutis@frontlinemedcom.com.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC cleansers for rosacea patients. Consideration must be given to:
- Avène Antirougeurs Redness Relief Dermo-Cleansing Milk
Pierre Fabre Dermo-Cosmétique USA
Recommended by Julie Woodward, MD, Durham, North Carolina
- Avène Extremely Gentle Cleanser Lotion
Pierre Fabre Dermo-Cosmétique USA
Recommended by Julie Woodward, MD, Durham, North Carolina
- Cetaphil Gentle Skin Cleanser
Galderma Laboratories, LP
“I always recommend for all of my rosacea patients a strict regimen of cleansing and sun protection with Cetaphil cleanser and moisturizing sunscreen.”—Wm. Philip Werschler, MD, Seattle, Washington
Recommended by Julie Woodward, MD, Durham, North Carolina
- Toleriane Dermo-Cleanser
La Roche-Posay Laboratoire Dermatologique
“Excellent for rosacea because it doesn’t contain any surfactants. This product has a very hydrated formula that helps repair the skin barrier.”—Whitney Bowe, MD, Brooklyn, New York
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Face washes and products for babies will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to cutis@frontlinemedcom.com.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Stroke, blindness are risks of unintended injection of fillers into blood vessels
Rare but serious side effects can result when soft tissue fillers are unintentionally injected into blood vessels in the face, according to a press release from the Food and Drug Administration.
Blood vessels can be blocked and blood flow restricted following unintentional soft tissue filler injection. The injection material can also migrate and embolization may cause vision impairment, blindness, stroke, and skin necrosis. Some injection sites result in blood vessel blockage more often, including the glabella and the periorbital region, though blockage can occur at any site on the face.
The FDA recommends that only people with appropriate training and knowledge of injection areas deliver injections, and that patients understand the risk beforehand and potential symptoms afterwards. A full list of recommendations can be found on the FDA website.
“FDA is working with manufacturers to update their labeling. The request asks that the labeling include additional warnings, precautions, and other statements about the risk of unintentional injection into blood vessels, consistent with the recommendations in this communication, so that both health care providers and patients would have a better understanding of the risks,” the FDA said.
Find the full press release on the FDA website.
Rare but serious side effects can result when soft tissue fillers are unintentionally injected into blood vessels in the face, according to a press release from the Food and Drug Administration.
Blood vessels can be blocked and blood flow restricted following unintentional soft tissue filler injection. The injection material can also migrate and embolization may cause vision impairment, blindness, stroke, and skin necrosis. Some injection sites result in blood vessel blockage more often, including the glabella and the periorbital region, though blockage can occur at any site on the face.
The FDA recommends that only people with appropriate training and knowledge of injection areas deliver injections, and that patients understand the risk beforehand and potential symptoms afterwards. A full list of recommendations can be found on the FDA website.
“FDA is working with manufacturers to update their labeling. The request asks that the labeling include additional warnings, precautions, and other statements about the risk of unintentional injection into blood vessels, consistent with the recommendations in this communication, so that both health care providers and patients would have a better understanding of the risks,” the FDA said.
Find the full press release on the FDA website.
Rare but serious side effects can result when soft tissue fillers are unintentionally injected into blood vessels in the face, according to a press release from the Food and Drug Administration.
Blood vessels can be blocked and blood flow restricted following unintentional soft tissue filler injection. The injection material can also migrate and embolization may cause vision impairment, blindness, stroke, and skin necrosis. Some injection sites result in blood vessel blockage more often, including the glabella and the periorbital region, though blockage can occur at any site on the face.
The FDA recommends that only people with appropriate training and knowledge of injection areas deliver injections, and that patients understand the risk beforehand and potential symptoms afterwards. A full list of recommendations can be found on the FDA website.
“FDA is working with manufacturers to update their labeling. The request asks that the labeling include additional warnings, precautions, and other statements about the risk of unintentional injection into blood vessels, consistent with the recommendations in this communication, so that both health care providers and patients would have a better understanding of the risks,” the FDA said.
Find the full press release on the FDA website.
Radiofrequency device significantly cut abdominal fat
KISSIMMEE, FLA. – Eight treatments with a noninvasive radiofrequency device reduced unwanted abdominal fat by an average of 428 cc in a prospective study.
“Can we consider this permanent fat loss? Yes, if a healthy lifestyle is maintained,” said Dr. Diane Duncan of Plastic Surgical Associates in Fort Collins, Colo. “I think the best candidates for these treatments are thin to modestly overweight patients, because while we did see significant fat reductions in obese patients, they want all their fat gone, and this won’t do that,” she said at the annual conference of the American Society for Laser Medicine and Surgery.

The study assessed the effects of the BodyFX device (Invasix, Yokneam, Israel) on 19 women aged 20-65 years who had localized abdominal adiposity, with body mass indices ranging from 18 to 30 kg/m2. Dr. Duncan used an energy setting of 42 watts until the target area reached 41° Celsius, which typically took 3-5 minutes, she said. Then she administered high-voltage pulses of oscillating radiofrequency waves in order to create holes in the cell walls of adipocytes, which triggered gradual cell death.
After adjusting for age and height, eight treatments with the device led to a 53% decrease in abdominal fat thickness at a 3-month follow-up visit, Dr. Duncan reported. “Visual results were similar to liposuction,” she added. “But generally, not much change was noted before the fourth treatment.”
The analysis included sequences of three-dimensional Vectra ultrasound measurements, which were taken at four sites around the abdomen at the moment when patients reached their maximum exhale, Dr. Duncan said. She excluded two patients from final analyses because they had gained or lost more than 5 pounds, compared with baseline.
“I think the mechanism of action of this device is what makes it so special,” said Dr. Duncan. Scanning electron microscope photographs showed that adipocytes treated with the radiofrequency device underwent pyroptosis, which combines programmed cell death with the proinflammatory features of necrosis. That process stimulates formation of new collagen, resulting in localized skin tightening, she noted. “These new SEM data show a different and more beneficial process is taking place,” she explained. “Apoptosis, by definition, would not stimulate neocollagenesis, so no tissue tightening would occur.”
Dr. Duncan reported no funding sources or relevant financial disclosures.
KISSIMMEE, FLA. – Eight treatments with a noninvasive radiofrequency device reduced unwanted abdominal fat by an average of 428 cc in a prospective study.
“Can we consider this permanent fat loss? Yes, if a healthy lifestyle is maintained,” said Dr. Diane Duncan of Plastic Surgical Associates in Fort Collins, Colo. “I think the best candidates for these treatments are thin to modestly overweight patients, because while we did see significant fat reductions in obese patients, they want all their fat gone, and this won’t do that,” she said at the annual conference of the American Society for Laser Medicine and Surgery.
The study assessed the effects of the BodyFX device (Invasix, Yokneam, Israel) on 19 women aged 20-65 years who had localized abdominal adiposity, with body mass indices ranging from 18 to 30 kg/m2. Dr. Duncan used an energy setting of 42 watts until the target area reached 41° Celsius, which typically took 3-5 minutes, she said. Then she administered high-voltage pulses of oscillating radiofrequency waves in order to create holes in the cell walls of adipocytes, which triggered gradual cell death.
After adjusting for age and height, eight treatments with the device led to a 53% decrease in abdominal fat thickness at a 3-month follow-up visit, Dr. Duncan reported. “Visual results were similar to liposuction,” she added. “But generally, not much change was noted before the fourth treatment.”
The analysis included sequences of three-dimensional Vectra ultrasound measurements, which were taken at four sites around the abdomen at the moment when patients reached their maximum exhale, Dr. Duncan said. She excluded two patients from final analyses because they had gained or lost more than 5 pounds, compared with baseline.
“I think the mechanism of action of this device is what makes it so special,” said Dr. Duncan. Scanning electron microscope photographs showed that adipocytes treated with the radiofrequency device underwent pyroptosis, which combines programmed cell death with the proinflammatory features of necrosis. That process stimulates formation of new collagen, resulting in localized skin tightening, she noted. “These new SEM data show a different and more beneficial process is taking place,” she explained. “Apoptosis, by definition, would not stimulate neocollagenesis, so no tissue tightening would occur.”
Dr. Duncan reported no funding sources or relevant financial disclosures.
KISSIMMEE, FLA. – Eight treatments with a noninvasive radiofrequency device reduced unwanted abdominal fat by an average of 428 cc in a prospective study.
“Can we consider this permanent fat loss? Yes, if a healthy lifestyle is maintained,” said Dr. Diane Duncan of Plastic Surgical Associates in Fort Collins, Colo. “I think the best candidates for these treatments are thin to modestly overweight patients, because while we did see significant fat reductions in obese patients, they want all their fat gone, and this won’t do that,” she said at the annual conference of the American Society for Laser Medicine and Surgery.
The study assessed the effects of the BodyFX device (Invasix, Yokneam, Israel) on 19 women aged 20-65 years who had localized abdominal adiposity, with body mass indices ranging from 18 to 30 kg/m2. Dr. Duncan used an energy setting of 42 watts until the target area reached 41° Celsius, which typically took 3-5 minutes, she said. Then she administered high-voltage pulses of oscillating radiofrequency waves in order to create holes in the cell walls of adipocytes, which triggered gradual cell death.
After adjusting for age and height, eight treatments with the device led to a 53% decrease in abdominal fat thickness at a 3-month follow-up visit, Dr. Duncan reported. “Visual results were similar to liposuction,” she added. “But generally, not much change was noted before the fourth treatment.”
The analysis included sequences of three-dimensional Vectra ultrasound measurements, which were taken at four sites around the abdomen at the moment when patients reached their maximum exhale, Dr. Duncan said. She excluded two patients from final analyses because they had gained or lost more than 5 pounds, compared with baseline.
“I think the mechanism of action of this device is what makes it so special,” said Dr. Duncan. Scanning electron microscope photographs showed that adipocytes treated with the radiofrequency device underwent pyroptosis, which combines programmed cell death with the proinflammatory features of necrosis. That process stimulates formation of new collagen, resulting in localized skin tightening, she noted. “These new SEM data show a different and more beneficial process is taking place,” she explained. “Apoptosis, by definition, would not stimulate neocollagenesis, so no tissue tightening would occur.”
Dr. Duncan reported no funding sources or relevant financial disclosures.
AT LASER 2015
Key clinical point: A noninvasive radiofrequency device significantly reduced abdominal fat in adults.
Major finding: Eight treatments with the device reduced abdominal fat by an average of 428 cc.
Data source: Prospective, 5-month study of 17 patients with localized abdominal adiposity.
Disclosures: Dr. Duncan reported no funding sources or relevant financial disclosures.

Early combination laser treatment boosts scar healing
KISSIMMEE, FLA. – Early treatment with fractional carbon dioxide ablative laser and light-emitting diode phototherapy sped healing and improved texture, discoloration, and range of motion in hypertrophic burn scars in a controlled, blinded study of 20 patients.
“I think as long as we have intact epithelium, we’re going to have improvements if we can laser these patients as early as possible,” Dr. Jill Waibel said at the annual conference of the American Society for Laser Medicine and Surgery.

Approximately 100 million new scars occur annually in developed countries, almost a third of which result from trauma or burns, noted Dr. Waibel, a dermatologist specializing in treating burn scars at the Miami Dermatology and Laser Institute. Scarred areas begin to hypertrophy about 3-7 months after injury, when they undergo increased collagen production and slowed collagen breakdown, said Dr. Waibel. “Traditionally, reconstructive efforts have been delayed until a year after injury,” she emphasized. “But by this time, many patients have formed hypertrophic scars and have significant decreases in range of motion.”
To determine how early treatment with a combination of laser/LED therapy might interrupt hypertrophy and improve outcomes, Dr. Waibel and coinvestigator Ashley Rudnick treated 20 patients aged 21-55 years with moderate to severe burns on at least 5% of the body surface area that had occurred in the past 1-3 months. For each patient, they divided similarly scarred areas into four 5- by 5-cm squares, one of which served as an untreated control. They treated the other three areas with 120-micron spot fractional ablative carbon dioxide laser only, continuous wave LED phototherapy only, or fractional ablative laser followed by LED. They spaced the three laser sessions 2 months apart, and used eight 20-minute LED treatments per laser session. The fractional laser wavelength was 10,600 nm, energy was 80-120 mJ per pixel, and the frequency was up to 200 Hz, Dr. Waibel said. The LED wavelength was 830 nm, and energy intensity was 40-100 mW per cm2.
All treated areas improved more than the untreated control areas of scarring, but combining the modalities was associated with the fastest healing, according to blinded photographic reviews by physicians based on the visual analog Manchester scar scale, Dr. Waibel reported.
Phototherapy with LED can penetrate up to an inch of tissue and promotes selective ATP production and DNA and RNA activity, she added. “The positive effects occur only in injured cells,” she said. “LED has wound healing and anti-inflammatory effects that might benefit acutely wounded skin.”
Based on her experience, patients usually need from three to five sessions of fractional laser/LED sessions to see clear results, Dr. Waibel said in response to a question from an audience member. “We know that every time we treat a hypertrophic scar, it will get better,” she added. “When patients stop coming for treatment, you know they’re happy. If you can combine modalities softly and safely, you’ll need fewer treatments.”
Dr. Waibel disclosed financial and advisory relationships with ALMA, Cutera, DUSA, Harvest Technologies, L’Oreal/SkinCeuticals, Lumenis, Lutronics, Sebacia, Syneron-Candela, Valeant, and Zeltiq.
KISSIMMEE, FLA. – Early treatment with fractional carbon dioxide ablative laser and light-emitting diode phototherapy sped healing and improved texture, discoloration, and range of motion in hypertrophic burn scars in a controlled, blinded study of 20 patients.
“I think as long as we have intact epithelium, we’re going to have improvements if we can laser these patients as early as possible,” Dr. Jill Waibel said at the annual conference of the American Society for Laser Medicine and Surgery.
Approximately 100 million new scars occur annually in developed countries, almost a third of which result from trauma or burns, noted Dr. Waibel, a dermatologist specializing in treating burn scars at the Miami Dermatology and Laser Institute. Scarred areas begin to hypertrophy about 3-7 months after injury, when they undergo increased collagen production and slowed collagen breakdown, said Dr. Waibel. “Traditionally, reconstructive efforts have been delayed until a year after injury,” she emphasized. “But by this time, many patients have formed hypertrophic scars and have significant decreases in range of motion.”
To determine how early treatment with a combination of laser/LED therapy might interrupt hypertrophy and improve outcomes, Dr. Waibel and coinvestigator Ashley Rudnick treated 20 patients aged 21-55 years with moderate to severe burns on at least 5% of the body surface area that had occurred in the past 1-3 months. For each patient, they divided similarly scarred areas into four 5- by 5-cm squares, one of which served as an untreated control. They treated the other three areas with 120-micron spot fractional ablative carbon dioxide laser only, continuous wave LED phototherapy only, or fractional ablative laser followed by LED. They spaced the three laser sessions 2 months apart, and used eight 20-minute LED treatments per laser session. The fractional laser wavelength was 10,600 nm, energy was 80-120 mJ per pixel, and the frequency was up to 200 Hz, Dr. Waibel said. The LED wavelength was 830 nm, and energy intensity was 40-100 mW per cm2.
All treated areas improved more than the untreated control areas of scarring, but combining the modalities was associated with the fastest healing, according to blinded photographic reviews by physicians based on the visual analog Manchester scar scale, Dr. Waibel reported.
Phototherapy with LED can penetrate up to an inch of tissue and promotes selective ATP production and DNA and RNA activity, she added. “The positive effects occur only in injured cells,” she said. “LED has wound healing and anti-inflammatory effects that might benefit acutely wounded skin.”
Based on her experience, patients usually need from three to five sessions of fractional laser/LED sessions to see clear results, Dr. Waibel said in response to a question from an audience member. “We know that every time we treat a hypertrophic scar, it will get better,” she added. “When patients stop coming for treatment, you know they’re happy. If you can combine modalities softly and safely, you’ll need fewer treatments.”
Dr. Waibel disclosed financial and advisory relationships with ALMA, Cutera, DUSA, Harvest Technologies, L’Oreal/SkinCeuticals, Lumenis, Lutronics, Sebacia, Syneron-Candela, Valeant, and Zeltiq.
KISSIMMEE, FLA. – Early treatment with fractional carbon dioxide ablative laser and light-emitting diode phototherapy sped healing and improved texture, discoloration, and range of motion in hypertrophic burn scars in a controlled, blinded study of 20 patients.
“I think as long as we have intact epithelium, we’re going to have improvements if we can laser these patients as early as possible,” Dr. Jill Waibel said at the annual conference of the American Society for Laser Medicine and Surgery.
Approximately 100 million new scars occur annually in developed countries, almost a third of which result from trauma or burns, noted Dr. Waibel, a dermatologist specializing in treating burn scars at the Miami Dermatology and Laser Institute. Scarred areas begin to hypertrophy about 3-7 months after injury, when they undergo increased collagen production and slowed collagen breakdown, said Dr. Waibel. “Traditionally, reconstructive efforts have been delayed until a year after injury,” she emphasized. “But by this time, many patients have formed hypertrophic scars and have significant decreases in range of motion.”
To determine how early treatment with a combination of laser/LED therapy might interrupt hypertrophy and improve outcomes, Dr. Waibel and coinvestigator Ashley Rudnick treated 20 patients aged 21-55 years with moderate to severe burns on at least 5% of the body surface area that had occurred in the past 1-3 months. For each patient, they divided similarly scarred areas into four 5- by 5-cm squares, one of which served as an untreated control. They treated the other three areas with 120-micron spot fractional ablative carbon dioxide laser only, continuous wave LED phototherapy only, or fractional ablative laser followed by LED. They spaced the three laser sessions 2 months apart, and used eight 20-minute LED treatments per laser session. The fractional laser wavelength was 10,600 nm, energy was 80-120 mJ per pixel, and the frequency was up to 200 Hz, Dr. Waibel said. The LED wavelength was 830 nm, and energy intensity was 40-100 mW per cm2.
All treated areas improved more than the untreated control areas of scarring, but combining the modalities was associated with the fastest healing, according to blinded photographic reviews by physicians based on the visual analog Manchester scar scale, Dr. Waibel reported.
Phototherapy with LED can penetrate up to an inch of tissue and promotes selective ATP production and DNA and RNA activity, she added. “The positive effects occur only in injured cells,” she said. “LED has wound healing and anti-inflammatory effects that might benefit acutely wounded skin.”
Based on her experience, patients usually need from three to five sessions of fractional laser/LED sessions to see clear results, Dr. Waibel said in response to a question from an audience member. “We know that every time we treat a hypertrophic scar, it will get better,” she added. “When patients stop coming for treatment, you know they’re happy. If you can combine modalities softly and safely, you’ll need fewer treatments.”
Dr. Waibel disclosed financial and advisory relationships with ALMA, Cutera, DUSA, Harvest Technologies, L’Oreal/SkinCeuticals, Lumenis, Lutronics, Sebacia, Syneron-Candela, Valeant, and Zeltiq.
AT LASER 2015
Key clinical point: Fractional carbon dioxide ablative laser with light-emitting diode (LED) phototherapy sped healing and improved the appearance and function of burn scars.
Major finding: Both laser and LED alone improved scar healing, compared with untreated control scars, but combining the modalities led to the best outcomes. The fractional laser wavelength was 10,600 nm, and the LED wavelength was 830 nm.
Data source: Prospective, blinded, controlled study of 20 adults with acute moderate to severe burns.
Disclosures: Dr. Waibel disclosed financial and advisory relationships with ALMA, Cutera, DUSA, Harvest Technologies, L’Oreal/Skinceuticals, Lumenis, Lutronic, Sebacia, Syneron-Candela, Valeant, and Zeltiq.

Microwave system cuts axillary hair by 70%
KISSIMMEE, FLA. – A noninvasive microwave system reduced light and dark axillary hair by approximately 70%, with durable results 1 year after treatment, according to data from a prospective multicenter study of 44 patients.
The device is Food and Drug Administration–approved for thermal treatment of axillary sweat glands, and has been used for about 35,000 such procedures, Dr. Jeremy Brauer said at the annual meeting of the American Society for Laser Medicine and Surgery.
The system targets microwave energy at the interface between the dermis and the hypodermis, “and we hypothesized that heat at this level in the skin may also have an important effect on the hair bulb,” he said.
Hair reduction is the third most common cosmetic procedure that U.S. dermatologists perform, said Dr. Brauer, a dermatologist with the Laser & Skin Surgery Center of New York. Laser is the primary modality, but is not always effective and can cause serious tissue damage if melanin concentrations in the hair and skin are too similar, he said.
For the study, Dr. Bauer and his associates used the microwave device to treat the axillae of 44 patients during either one or two treatment sessions. Average age of the patients was 33 years (range, 18-61 years), 80% were female, and 62% had dark axillary hair. Most had Fitzpatrick skin type II (33%), III (27%), or I (23%), but about 18% had type IV or V. During follow-up visits at 3, 6, 9, and 12 months, three blinded assessors counted hairs within a 2 cm x 2 cm area in the center of each axilla, and also qualitatively compared follow-up and baseline photos.
The blinded assessors correctly chose the baseline photos for all the photographic series, Dr. Brauer said. At 12 months, mean hair reduction was 75% for all patients, 72% for light-haired patients, and 76% for dark-haired patients, he reported. Ranges of response within these subgroups were relatively narrow, but patients who were treated at higher energy levels (settings of 3 or 4) achieved significantly more hair reduction (P < .0001) at 12 months than did patients who were treated at a setting of 1, he said. He recommended that future studies examine dose response and optimal number of treatment sessions.
Dr. Brauer reported consulting fees from Miramar, maker of the device.
KISSIMMEE, FLA. – A noninvasive microwave system reduced light and dark axillary hair by approximately 70%, with durable results 1 year after treatment, according to data from a prospective multicenter study of 44 patients.
The device is Food and Drug Administration–approved for thermal treatment of axillary sweat glands, and has been used for about 35,000 such procedures, Dr. Jeremy Brauer said at the annual meeting of the American Society for Laser Medicine and Surgery.
The system targets microwave energy at the interface between the dermis and the hypodermis, “and we hypothesized that heat at this level in the skin may also have an important effect on the hair bulb,” he said.
Hair reduction is the third most common cosmetic procedure that U.S. dermatologists perform, said Dr. Brauer, a dermatologist with the Laser & Skin Surgery Center of New York. Laser is the primary modality, but is not always effective and can cause serious tissue damage if melanin concentrations in the hair and skin are too similar, he said.
For the study, Dr. Bauer and his associates used the microwave device to treat the axillae of 44 patients during either one or two treatment sessions. Average age of the patients was 33 years (range, 18-61 years), 80% were female, and 62% had dark axillary hair. Most had Fitzpatrick skin type II (33%), III (27%), or I (23%), but about 18% had type IV or V. During follow-up visits at 3, 6, 9, and 12 months, three blinded assessors counted hairs within a 2 cm x 2 cm area in the center of each axilla, and also qualitatively compared follow-up and baseline photos.
The blinded assessors correctly chose the baseline photos for all the photographic series, Dr. Brauer said. At 12 months, mean hair reduction was 75% for all patients, 72% for light-haired patients, and 76% for dark-haired patients, he reported. Ranges of response within these subgroups were relatively narrow, but patients who were treated at higher energy levels (settings of 3 or 4) achieved significantly more hair reduction (P < .0001) at 12 months than did patients who were treated at a setting of 1, he said. He recommended that future studies examine dose response and optimal number of treatment sessions.
Dr. Brauer reported consulting fees from Miramar, maker of the device.
KISSIMMEE, FLA. – A noninvasive microwave system reduced light and dark axillary hair by approximately 70%, with durable results 1 year after treatment, according to data from a prospective multicenter study of 44 patients.
The device is Food and Drug Administration–approved for thermal treatment of axillary sweat glands, and has been used for about 35,000 such procedures, Dr. Jeremy Brauer said at the annual meeting of the American Society for Laser Medicine and Surgery.
The system targets microwave energy at the interface between the dermis and the hypodermis, “and we hypothesized that heat at this level in the skin may also have an important effect on the hair bulb,” he said.
Hair reduction is the third most common cosmetic procedure that U.S. dermatologists perform, said Dr. Brauer, a dermatologist with the Laser & Skin Surgery Center of New York. Laser is the primary modality, but is not always effective and can cause serious tissue damage if melanin concentrations in the hair and skin are too similar, he said.
For the study, Dr. Bauer and his associates used the microwave device to treat the axillae of 44 patients during either one or two treatment sessions. Average age of the patients was 33 years (range, 18-61 years), 80% were female, and 62% had dark axillary hair. Most had Fitzpatrick skin type II (33%), III (27%), or I (23%), but about 18% had type IV or V. During follow-up visits at 3, 6, 9, and 12 months, three blinded assessors counted hairs within a 2 cm x 2 cm area in the center of each axilla, and also qualitatively compared follow-up and baseline photos.
The blinded assessors correctly chose the baseline photos for all the photographic series, Dr. Brauer said. At 12 months, mean hair reduction was 75% for all patients, 72% for light-haired patients, and 76% for dark-haired patients, he reported. Ranges of response within these subgroups were relatively narrow, but patients who were treated at higher energy levels (settings of 3 or 4) achieved significantly more hair reduction (P < .0001) at 12 months than did patients who were treated at a setting of 1, he said. He recommended that future studies examine dose response and optimal number of treatment sessions.
Dr. Brauer reported consulting fees from Miramar, maker of the device.
AT LASER 2015
Key clinical point: A noninvasive microwave device reduced axillary hair by about 70%, with stable results 1 year later.
Major finding: Mean reduction in both light and dark axillary hair was about 70%, 12 months after one to two treatment sessions.
Data source: Prospective multicenter study of 44 patients with blinded assessments.
Disclosures: Dr. Brauer reported consulting fees from Miramar, maker of the device.
Up the anesthesia when treating axillary hyperhidrosis
KISSIMMEE, FLA. – Patients who received more local anesthesia before undergoing microwave-based treatment for axillary hyperhidrosis were happier with results and achieved the same objective improvements as patients who received less anesthesia, a follow-up study found.
“Patient satisfaction with the procedure was extremely high,” said Dr. Carolyn Jacob, a dermatologist and founding director of Chicago Cosmetic Surgery and Dermatology. “You can’t regenerate sweat glands – once they’re gone, they’re gone, and these patients have sustained results.”
The microwave system has been used commercially for more than 30,000 treatment sessions over 3 years and achieved high rates of efficacy and patient satisfaction in two pivotal trials, Dr. Jacob noted (Dermatol. Surg. 2012;38:185-91; Dermatol. Surg. 2012;38:728-35).
But clinicians often have kept to the relatively low volumes of local anesthesia used in the trials because they were concerned that higher volumes would interact with microwave energy and diminish efficacy, she said at the annual meeting of the American Society for Laser Medicine and Surgery.
To investigate that concern and assess overall longer-term treatment outcomes, Dr. Jacob and her associates compared 110 patients who received 10-25 cc of local lidocaine/epinephrine solution per axilla (the amount used in the clinical trials) with 30 patients who received 60-275 cc per axilla before undergoing microwave-based treatment of hyperhidrosis. At baseline, the two groups scored similarly on the 4-point measure of hyperhidrosis severity and on 10-point measures of sweat and odor severity (average scores of 3.4, 8.5, and 5.2, respectively, for the group that received less anesthesia and 3.3, 8.7, and 5.8, respectively, for the group that received more anesthesia), said Dr. Jacob. Patients were treated at energy levels of 3-5, and most were female. The researchers followed the lower anesthesia group and the higher anesthesia group for an average of 6 and 9 months, respectively.
At follow-up, 88% of patients in the lower-volume anesthesia group scored 1 or 2 on the 4-point measure of hyperhidrosis, as did 93% of patients in the higher-volume group, said Dr. Jacob. The groups also had very similar efficacy results on the 10-point measures of sweat and odor severity, she said (respective average scores, 3.0 and 3.2 on the sweat measure, and 1.9 and 2.0 on the odor measure). In all, 85% of patients who received less anesthesia said they were satisfied with results, as did 93% of patients in the higher-volume group.
Patients usually needed two treatment sessions that lasted 60-75 minutes each, depending on the size of the treatment area, Dr. Jacob noted. A few needed only one session. “There’s a high efficacy that’s consistent with the previous publications we have,” she concluded. “The high volumes of anesthesia seem to work just as well as the lower volumes.”
KISSIMMEE, FLA. – Patients who received more local anesthesia before undergoing microwave-based treatment for axillary hyperhidrosis were happier with results and achieved the same objective improvements as patients who received less anesthesia, a follow-up study found.
“Patient satisfaction with the procedure was extremely high,” said Dr. Carolyn Jacob, a dermatologist and founding director of Chicago Cosmetic Surgery and Dermatology. “You can’t regenerate sweat glands – once they’re gone, they’re gone, and these patients have sustained results.”
The microwave system has been used commercially for more than 30,000 treatment sessions over 3 years and achieved high rates of efficacy and patient satisfaction in two pivotal trials, Dr. Jacob noted (Dermatol. Surg. 2012;38:185-91; Dermatol. Surg. 2012;38:728-35).
But clinicians often have kept to the relatively low volumes of local anesthesia used in the trials because they were concerned that higher volumes would interact with microwave energy and diminish efficacy, she said at the annual meeting of the American Society for Laser Medicine and Surgery.
To investigate that concern and assess overall longer-term treatment outcomes, Dr. Jacob and her associates compared 110 patients who received 10-25 cc of local lidocaine/epinephrine solution per axilla (the amount used in the clinical trials) with 30 patients who received 60-275 cc per axilla before undergoing microwave-based treatment of hyperhidrosis. At baseline, the two groups scored similarly on the 4-point measure of hyperhidrosis severity and on 10-point measures of sweat and odor severity (average scores of 3.4, 8.5, and 5.2, respectively, for the group that received less anesthesia and 3.3, 8.7, and 5.8, respectively, for the group that received more anesthesia), said Dr. Jacob. Patients were treated at energy levels of 3-5, and most were female. The researchers followed the lower anesthesia group and the higher anesthesia group for an average of 6 and 9 months, respectively.
At follow-up, 88% of patients in the lower-volume anesthesia group scored 1 or 2 on the 4-point measure of hyperhidrosis, as did 93% of patients in the higher-volume group, said Dr. Jacob. The groups also had very similar efficacy results on the 10-point measures of sweat and odor severity, she said (respective average scores, 3.0 and 3.2 on the sweat measure, and 1.9 and 2.0 on the odor measure). In all, 85% of patients who received less anesthesia said they were satisfied with results, as did 93% of patients in the higher-volume group.
Patients usually needed two treatment sessions that lasted 60-75 minutes each, depending on the size of the treatment area, Dr. Jacob noted. A few needed only one session. “There’s a high efficacy that’s consistent with the previous publications we have,” she concluded. “The high volumes of anesthesia seem to work just as well as the lower volumes.”
KISSIMMEE, FLA. – Patients who received more local anesthesia before undergoing microwave-based treatment for axillary hyperhidrosis were happier with results and achieved the same objective improvements as patients who received less anesthesia, a follow-up study found.
“Patient satisfaction with the procedure was extremely high,” said Dr. Carolyn Jacob, a dermatologist and founding director of Chicago Cosmetic Surgery and Dermatology. “You can’t regenerate sweat glands – once they’re gone, they’re gone, and these patients have sustained results.”
The microwave system has been used commercially for more than 30,000 treatment sessions over 3 years and achieved high rates of efficacy and patient satisfaction in two pivotal trials, Dr. Jacob noted (Dermatol. Surg. 2012;38:185-91; Dermatol. Surg. 2012;38:728-35).
But clinicians often have kept to the relatively low volumes of local anesthesia used in the trials because they were concerned that higher volumes would interact with microwave energy and diminish efficacy, she said at the annual meeting of the American Society for Laser Medicine and Surgery.
To investigate that concern and assess overall longer-term treatment outcomes, Dr. Jacob and her associates compared 110 patients who received 10-25 cc of local lidocaine/epinephrine solution per axilla (the amount used in the clinical trials) with 30 patients who received 60-275 cc per axilla before undergoing microwave-based treatment of hyperhidrosis. At baseline, the two groups scored similarly on the 4-point measure of hyperhidrosis severity and on 10-point measures of sweat and odor severity (average scores of 3.4, 8.5, and 5.2, respectively, for the group that received less anesthesia and 3.3, 8.7, and 5.8, respectively, for the group that received more anesthesia), said Dr. Jacob. Patients were treated at energy levels of 3-5, and most were female. The researchers followed the lower anesthesia group and the higher anesthesia group for an average of 6 and 9 months, respectively.
At follow-up, 88% of patients in the lower-volume anesthesia group scored 1 or 2 on the 4-point measure of hyperhidrosis, as did 93% of patients in the higher-volume group, said Dr. Jacob. The groups also had very similar efficacy results on the 10-point measures of sweat and odor severity, she said (respective average scores, 3.0 and 3.2 on the sweat measure, and 1.9 and 2.0 on the odor measure). In all, 85% of patients who received less anesthesia said they were satisfied with results, as did 93% of patients in the higher-volume group.
Patients usually needed two treatment sessions that lasted 60-75 minutes each, depending on the size of the treatment area, Dr. Jacob noted. A few needed only one session. “There’s a high efficacy that’s consistent with the previous publications we have,” she concluded. “The high volumes of anesthesia seem to work just as well as the lower volumes.”
AT LASER 2015
Key clinical point: Higher volumes of local anesthesia did not adversely affect the efficacy of microwave-based treatment of axillary hyperhidrosis.
Major finding: At follow-up, 88% of the lower-volume group and 93% of the higher-volume group<b/>scored 1 or 2 on the 4-point measure of hyperhidrosis.
Data source: Multicenter follow-up study of 110 patients who received the standard low amount of local anesthesia and 30 who received higher volumes.
Disclosures: Dr. Jacob reported financial relationships with Miramar, Abbvie, Allergan, Galderma, and Medicis/Valeant.
LASER: How to succeed in perioperative ablative laser resurfacing
KISSIMMEE, FLA. – Ablative laser resurfacing may be the most effective cosmetic treatment for the periorbital area, excluding blepharoplasty, according to Dr. Suzanne L. Kilmer, a dermatologist specializing in laser and skin surgery in Sacramento, Calif.
“It gives you definite tightening and has the most predictable results,” Dr. Kilmer said at the annual meeting of the American Society for Laser Medicine and Surgery. “It also has the worst down time and side effects, but not for the upper lid – I’ve never had any scarring on the upper eyelid.”

In addition to its cosmetic potential, ablative laser resurfacing can remove epidermal lesions that might otherwise become actinic keratoses or basal cell carcinomas, and can smooth out syringomas, nevi, and seborrheic keratoses, Dr. Kilmer said. She shared some of her top tips for successful use of this technique.
Technique, safety, and analgesia
When treating patients with perioperative ablative laser resurfacing, Dr. Kilmer said she performs the first pass with a carbon dioxide laser at computerized pattern-generator (CPG) settings of pattern 3, size 9, density 6. She follows that with erbium laser resurfacing at a depth of 75-100 microns. “The first pass removes the epidermis,” she said. “Be sure to feather peripherally, and wipe everywhere you will do a second pass.”
The skin usually tightens visibly with the second pass, which can include the upper eyelids if patients have lax skin in this area, Dr. Kilmer noted. “You can be aggressive, like 3-9-5 [CPG settings],” she added. She then performs a “very light” second pass to the lower lids, with lower CPG settings of 3-7-3 or 3-6-2. She again follows with erbium ablation, including to the areas of the central face and midcheek.
The third pass includes the glabella and perioral area, as well as the upper eyelids if they are especially lax, Dr. Kilmer said. She ends with a sculpting pass with erbium laser.
Dr. Kilmer explained that she always treats the upper eyelids with ablative laser therapy in combination with fractional carbon dioxide laser treatment. “I also will include any area I think looks safe to do ablative on an individual patient,” she added. She noted that she sometimes combines ablative and fractional therapies with botulinum toxin treatment.
Patients should always wear eye shields during laser treatment sessions, Dr. Kilmer emphasized. Acceptable options include David-Baker lid clamps, Jaeger lid plates, and individual steel eye shields, but plastic corneal protectors should be avoided because they can sustain thermal damage with laser exposure, she said.
Options for analgesia during treatment include codeine, hydrocodone, hydromorphone, or nonsteroidal anti-inflammatory agents such as Toradol (ketorolac), which Dr. Kilmer gives intramuscularly at a dose of 30-60 mg. Furthermore, EMLA (lidocaine/prilocaine) cream enhances comfort, even if patients are also receiving conscious sedation or blocks, she said. The cream helps prevent several adverse effects, including superficial coagulative thermal damage, prolonged erythema, and delayed hypopigmentation, and does not seem to decrease efficacy, she added.
Before treatment
Clinicians should consider how a patient’s unique characteristics might affect treatment outcomes, Dr. Kilmer said. For example, ablation is more likely to cause hypopigmentation in patients with lighter skin types, and is unlikely to sufficiently resolve wrinkles that involve the facial muscles. “Always discuss Botox [botulinum toxin],” added Dr Kilmer. “If you’re tightening up the skin, and the area underneath is moving a lot, you’re not going to get as much tightening.” Clinicians also should discuss a face lift as an option for patients with substantial excess facial skin, she said.
The overall treatment plan should address existing skin lesions, too. Larger syringomas, trichoepitheliomas, and hyperplastic sebaceous glands should be “drilled out” with erbium ablation, but small tumors usually need only multiple or fractional laser treatment, said Dr. Kilmer.
For antimicrobial prophylaxis, patients should receive acyclovir, valcyclovir, or famvir starting 1 day before the procedure and continuing for 10-14 days, Dr. Kilmer said. “If I’m just treating around the eyes, I don’t worry as much about antivirals. I think about them more if I’m doing the full face,” she noted. Likewise, preoperative antibiotics such as doxycycline, cephalexin, azithromycin, or ciprofloxacin are especially important for full face or perioral ablative resurfacing, she said. To help prevent yeast infections, she gives patients a dose of fluconazole on day 3 after the procedure. “If they have a history of multiple yeast infections, I give it four times a day,” she said.
After the procedure
Postoperative diligence is key to good outcomes, Dr. Kilmer emphasized. During the first 10-14 days after the procedure, patients and clinicians should watch for signs of complications such as pain, purulence, itching, and worsening redness. If patients develop pain accompanied by purulence and redness, clinicians should perform bacterial cultures and switch patients to a quinolone, Dr. Kilmer said. Patients who develop pain consistent with herpes simplex virus infection should receive valcyclovir, she added. “If they’re itchy and red, think about yeast [infection] or contact dermatitis, and treat for both if you’re unsure,” she said.
Dr. Kilmer disclosed advisory relationships with Candela-Syneron, Living Proof, Lumeis, Miramar, Ulthera, and Zeltiq. She reported having received research funding from the same companies, and also from Allergan, CoolTouch, Cutera, Cynosure, Palomar, Sciton, and Solta.
KISSIMMEE, FLA. – Ablative laser resurfacing may be the most effective cosmetic treatment for the periorbital area, excluding blepharoplasty, according to Dr. Suzanne L. Kilmer, a dermatologist specializing in laser and skin surgery in Sacramento, Calif.
“It gives you definite tightening and has the most predictable results,” Dr. Kilmer said at the annual meeting of the American Society for Laser Medicine and Surgery. “It also has the worst down time and side effects, but not for the upper lid – I’ve never had any scarring on the upper eyelid.”
In addition to its cosmetic potential, ablative laser resurfacing can remove epidermal lesions that might otherwise become actinic keratoses or basal cell carcinomas, and can smooth out syringomas, nevi, and seborrheic keratoses, Dr. Kilmer said. She shared some of her top tips for successful use of this technique.
Technique, safety, and analgesia
When treating patients with perioperative ablative laser resurfacing, Dr. Kilmer said she performs the first pass with a carbon dioxide laser at computerized pattern-generator (CPG) settings of pattern 3, size 9, density 6. She follows that with erbium laser resurfacing at a depth of 75-100 microns. “The first pass removes the epidermis,” she said. “Be sure to feather peripherally, and wipe everywhere you will do a second pass.”
The skin usually tightens visibly with the second pass, which can include the upper eyelids if patients have lax skin in this area, Dr. Kilmer noted. “You can be aggressive, like 3-9-5 [CPG settings],” she added. She then performs a “very light” second pass to the lower lids, with lower CPG settings of 3-7-3 or 3-6-2. She again follows with erbium ablation, including to the areas of the central face and midcheek.
The third pass includes the glabella and perioral area, as well as the upper eyelids if they are especially lax, Dr. Kilmer said. She ends with a sculpting pass with erbium laser.
Dr. Kilmer explained that she always treats the upper eyelids with ablative laser therapy in combination with fractional carbon dioxide laser treatment. “I also will include any area I think looks safe to do ablative on an individual patient,” she added. She noted that she sometimes combines ablative and fractional therapies with botulinum toxin treatment.
Patients should always wear eye shields during laser treatment sessions, Dr. Kilmer emphasized. Acceptable options include David-Baker lid clamps, Jaeger lid plates, and individual steel eye shields, but plastic corneal protectors should be avoided because they can sustain thermal damage with laser exposure, she said.
Options for analgesia during treatment include codeine, hydrocodone, hydromorphone, or nonsteroidal anti-inflammatory agents such as Toradol (ketorolac), which Dr. Kilmer gives intramuscularly at a dose of 30-60 mg. Furthermore, EMLA (lidocaine/prilocaine) cream enhances comfort, even if patients are also receiving conscious sedation or blocks, she said. The cream helps prevent several adverse effects, including superficial coagulative thermal damage, prolonged erythema, and delayed hypopigmentation, and does not seem to decrease efficacy, she added.
Before treatment
Clinicians should consider how a patient’s unique characteristics might affect treatment outcomes, Dr. Kilmer said. For example, ablation is more likely to cause hypopigmentation in patients with lighter skin types, and is unlikely to sufficiently resolve wrinkles that involve the facial muscles. “Always discuss Botox [botulinum toxin],” added Dr Kilmer. “If you’re tightening up the skin, and the area underneath is moving a lot, you’re not going to get as much tightening.” Clinicians also should discuss a face lift as an option for patients with substantial excess facial skin, she said.
The overall treatment plan should address existing skin lesions, too. Larger syringomas, trichoepitheliomas, and hyperplastic sebaceous glands should be “drilled out” with erbium ablation, but small tumors usually need only multiple or fractional laser treatment, said Dr. Kilmer.
For antimicrobial prophylaxis, patients should receive acyclovir, valcyclovir, or famvir starting 1 day before the procedure and continuing for 10-14 days, Dr. Kilmer said. “If I’m just treating around the eyes, I don’t worry as much about antivirals. I think about them more if I’m doing the full face,” she noted. Likewise, preoperative antibiotics such as doxycycline, cephalexin, azithromycin, or ciprofloxacin are especially important for full face or perioral ablative resurfacing, she said. To help prevent yeast infections, she gives patients a dose of fluconazole on day 3 after the procedure. “If they have a history of multiple yeast infections, I give it four times a day,” she said.
After the procedure
Postoperative diligence is key to good outcomes, Dr. Kilmer emphasized. During the first 10-14 days after the procedure, patients and clinicians should watch for signs of complications such as pain, purulence, itching, and worsening redness. If patients develop pain accompanied by purulence and redness, clinicians should perform bacterial cultures and switch patients to a quinolone, Dr. Kilmer said. Patients who develop pain consistent with herpes simplex virus infection should receive valcyclovir, she added. “If they’re itchy and red, think about yeast [infection] or contact dermatitis, and treat for both if you’re unsure,” she said.
Dr. Kilmer disclosed advisory relationships with Candela-Syneron, Living Proof, Lumeis, Miramar, Ulthera, and Zeltiq. She reported having received research funding from the same companies, and also from Allergan, CoolTouch, Cutera, Cynosure, Palomar, Sciton, and Solta.
KISSIMMEE, FLA. – Ablative laser resurfacing may be the most effective cosmetic treatment for the periorbital area, excluding blepharoplasty, according to Dr. Suzanne L. Kilmer, a dermatologist specializing in laser and skin surgery in Sacramento, Calif.
“It gives you definite tightening and has the most predictable results,” Dr. Kilmer said at the annual meeting of the American Society for Laser Medicine and Surgery. “It also has the worst down time and side effects, but not for the upper lid – I’ve never had any scarring on the upper eyelid.”
In addition to its cosmetic potential, ablative laser resurfacing can remove epidermal lesions that might otherwise become actinic keratoses or basal cell carcinomas, and can smooth out syringomas, nevi, and seborrheic keratoses, Dr. Kilmer said. She shared some of her top tips for successful use of this technique.
Technique, safety, and analgesia
When treating patients with perioperative ablative laser resurfacing, Dr. Kilmer said she performs the first pass with a carbon dioxide laser at computerized pattern-generator (CPG) settings of pattern 3, size 9, density 6. She follows that with erbium laser resurfacing at a depth of 75-100 microns. “The first pass removes the epidermis,” she said. “Be sure to feather peripherally, and wipe everywhere you will do a second pass.”
The skin usually tightens visibly with the second pass, which can include the upper eyelids if patients have lax skin in this area, Dr. Kilmer noted. “You can be aggressive, like 3-9-5 [CPG settings],” she added. She then performs a “very light” second pass to the lower lids, with lower CPG settings of 3-7-3 or 3-6-2. She again follows with erbium ablation, including to the areas of the central face and midcheek.
The third pass includes the glabella and perioral area, as well as the upper eyelids if they are especially lax, Dr. Kilmer said. She ends with a sculpting pass with erbium laser.
Dr. Kilmer explained that she always treats the upper eyelids with ablative laser therapy in combination with fractional carbon dioxide laser treatment. “I also will include any area I think looks safe to do ablative on an individual patient,” she added. She noted that she sometimes combines ablative and fractional therapies with botulinum toxin treatment.
Patients should always wear eye shields during laser treatment sessions, Dr. Kilmer emphasized. Acceptable options include David-Baker lid clamps, Jaeger lid plates, and individual steel eye shields, but plastic corneal protectors should be avoided because they can sustain thermal damage with laser exposure, she said.
Options for analgesia during treatment include codeine, hydrocodone, hydromorphone, or nonsteroidal anti-inflammatory agents such as Toradol (ketorolac), which Dr. Kilmer gives intramuscularly at a dose of 30-60 mg. Furthermore, EMLA (lidocaine/prilocaine) cream enhances comfort, even if patients are also receiving conscious sedation or blocks, she said. The cream helps prevent several adverse effects, including superficial coagulative thermal damage, prolonged erythema, and delayed hypopigmentation, and does not seem to decrease efficacy, she added.
Before treatment
Clinicians should consider how a patient’s unique characteristics might affect treatment outcomes, Dr. Kilmer said. For example, ablation is more likely to cause hypopigmentation in patients with lighter skin types, and is unlikely to sufficiently resolve wrinkles that involve the facial muscles. “Always discuss Botox [botulinum toxin],” added Dr Kilmer. “If you’re tightening up the skin, and the area underneath is moving a lot, you’re not going to get as much tightening.” Clinicians also should discuss a face lift as an option for patients with substantial excess facial skin, she said.
The overall treatment plan should address existing skin lesions, too. Larger syringomas, trichoepitheliomas, and hyperplastic sebaceous glands should be “drilled out” with erbium ablation, but small tumors usually need only multiple or fractional laser treatment, said Dr. Kilmer.
For antimicrobial prophylaxis, patients should receive acyclovir, valcyclovir, or famvir starting 1 day before the procedure and continuing for 10-14 days, Dr. Kilmer said. “If I’m just treating around the eyes, I don’t worry as much about antivirals. I think about them more if I’m doing the full face,” she noted. Likewise, preoperative antibiotics such as doxycycline, cephalexin, azithromycin, or ciprofloxacin are especially important for full face or perioral ablative resurfacing, she said. To help prevent yeast infections, she gives patients a dose of fluconazole on day 3 after the procedure. “If they have a history of multiple yeast infections, I give it four times a day,” she said.
After the procedure
Postoperative diligence is key to good outcomes, Dr. Kilmer emphasized. During the first 10-14 days after the procedure, patients and clinicians should watch for signs of complications such as pain, purulence, itching, and worsening redness. If patients develop pain accompanied by purulence and redness, clinicians should perform bacterial cultures and switch patients to a quinolone, Dr. Kilmer said. Patients who develop pain consistent with herpes simplex virus infection should receive valcyclovir, she added. “If they’re itchy and red, think about yeast [infection] or contact dermatitis, and treat for both if you’re unsure,” she said.
Dr. Kilmer disclosed advisory relationships with Candela-Syneron, Living Proof, Lumeis, Miramar, Ulthera, and Zeltiq. She reported having received research funding from the same companies, and also from Allergan, CoolTouch, Cutera, Cynosure, Palomar, Sciton, and Solta.
EXPERT ANALYSIS FROM LASER 2015

Laser treatment cut the fat on flank and abs
KISSIMMEE, FLA. – Single noninvasive treatments with a prototype 1,060-nm diode laser led to statistically significant, visually discernible reductions of adipose tissue covering the abdomen and flanks in two prospective multicenter studies.
“The treatment is well tolerated, with only mild and transient side effects,” said Dr. Bruce Katz of Mount Sinai School of Medicine in New York, who presented the results of the flank study at the annual meeting of the American Society for Laser Medicine and Surgery.
Most patients were “satisfied” or “very satisfied” with the results, added Dr. Sean Doherty, a plastic surgeon in group practice in Boston, who presented the results of the abdominal study.
Noninvasive fat reduction procedures rose 43% in the past year, said Dr. Doherty. The 1,060-nm diode laser damages adipocytes in targeted areas, eventually resulting in apoptosis, he added. Sessions in both studies lasted 25 minutes, with irradiance at 0.9-1.4 W/cm2 and treatment areas of 48-144 cm2 for the flanks and 192-288 cm2 for the abdomen, the investigators said.
The abdominal study included 34 patients, and the flank study included 42 patients. Investigators treated only one side for each patient in the flank study, reserving the other as a “sham” or control, Dr. Katz said. A blinded review of photographs taken before and 12 weeks after the procedures served as the primary endpoint in both studies. Assessors correctly identified an average of 95% of “before” photographs of the abdomen and 90.3% of those of the flank, Dr. Doherty and Dr. Katz reported.
The secondary endpoint was change in thickness of the adipose layer at 12 weeks post procedure, as measured by ultrasound. The average reduction was 3.1 mm for the abdomen (standard deviation, 1.7 mm) and 2.6 mm for the flank (standard deviation not reported; P < .001 for both), the researchers said. In the abdominal study, 85% of patients said they were “satisfied” or “extremely satisfied” with the results, while 6% were “slightly satisfied,” Dr. Doherty said. In the flank study, 86% of patients said they were “satisfied” or “extremely satisfied,” while 10% were “slightly satisfied.”
Mean pain scores were 3.7 out of 10 for the abdominal procedure and 4.0 out of 10 for the flank procedure. The most common side effect was mild to moderate tenderness that usually subsided within about 2 weeks of treatment. Other side effects included localized firmness, edema, and ecchymosis. No patients had serious adverse effects, the researchers said.
Most of the patients were approximately 45-49 years of age. Those in the abdominal study had an average body mass index of 25.5 kg/m2, while those in the flank study averaged 26.4 kg/m2, the researchers reported. Most of the patients in both studies were women (94% of abdominal patients and 86% of flank patients).
The average weight gain at 12 weeks for the abdominal study was 0.1 pounds (range, –5.2 to 5.6 pounds), while patients in the flank study gained an average of 0.8 pounds (range, –0.7 to 13 pounds), the researchers noted. Six patients in the flank study gained more than 5 pounds, and one gained more than 37 pounds and was therefore excluded from the efficacy analysis, Dr. Katz noted.
The researchers did not report funding sources for the studies. They disclosed advisory and financial relationships with Allergan, Merz Pharmaceuticals, Cynosure, Valeant, Syneron, and several other pharmaceutical companies.
KISSIMMEE, FLA. – Single noninvasive treatments with a prototype 1,060-nm diode laser led to statistically significant, visually discernible reductions of adipose tissue covering the abdomen and flanks in two prospective multicenter studies.
“The treatment is well tolerated, with only mild and transient side effects,” said Dr. Bruce Katz of Mount Sinai School of Medicine in New York, who presented the results of the flank study at the annual meeting of the American Society for Laser Medicine and Surgery.
Most patients were “satisfied” or “very satisfied” with the results, added Dr. Sean Doherty, a plastic surgeon in group practice in Boston, who presented the results of the abdominal study.
Noninvasive fat reduction procedures rose 43% in the past year, said Dr. Doherty. The 1,060-nm diode laser damages adipocytes in targeted areas, eventually resulting in apoptosis, he added. Sessions in both studies lasted 25 minutes, with irradiance at 0.9-1.4 W/cm2 and treatment areas of 48-144 cm2 for the flanks and 192-288 cm2 for the abdomen, the investigators said.
The abdominal study included 34 patients, and the flank study included 42 patients. Investigators treated only one side for each patient in the flank study, reserving the other as a “sham” or control, Dr. Katz said. A blinded review of photographs taken before and 12 weeks after the procedures served as the primary endpoint in both studies. Assessors correctly identified an average of 95% of “before” photographs of the abdomen and 90.3% of those of the flank, Dr. Doherty and Dr. Katz reported.
The secondary endpoint was change in thickness of the adipose layer at 12 weeks post procedure, as measured by ultrasound. The average reduction was 3.1 mm for the abdomen (standard deviation, 1.7 mm) and 2.6 mm for the flank (standard deviation not reported; P < .001 for both), the researchers said. In the abdominal study, 85% of patients said they were “satisfied” or “extremely satisfied” with the results, while 6% were “slightly satisfied,” Dr. Doherty said. In the flank study, 86% of patients said they were “satisfied” or “extremely satisfied,” while 10% were “slightly satisfied.”
Mean pain scores were 3.7 out of 10 for the abdominal procedure and 4.0 out of 10 for the flank procedure. The most common side effect was mild to moderate tenderness that usually subsided within about 2 weeks of treatment. Other side effects included localized firmness, edema, and ecchymosis. No patients had serious adverse effects, the researchers said.
Most of the patients were approximately 45-49 years of age. Those in the abdominal study had an average body mass index of 25.5 kg/m2, while those in the flank study averaged 26.4 kg/m2, the researchers reported. Most of the patients in both studies were women (94% of abdominal patients and 86% of flank patients).
The average weight gain at 12 weeks for the abdominal study was 0.1 pounds (range, –5.2 to 5.6 pounds), while patients in the flank study gained an average of 0.8 pounds (range, –0.7 to 13 pounds), the researchers noted. Six patients in the flank study gained more than 5 pounds, and one gained more than 37 pounds and was therefore excluded from the efficacy analysis, Dr. Katz noted.
The researchers did not report funding sources for the studies. They disclosed advisory and financial relationships with Allergan, Merz Pharmaceuticals, Cynosure, Valeant, Syneron, and several other pharmaceutical companies.
KISSIMMEE, FLA. – Single noninvasive treatments with a prototype 1,060-nm diode laser led to statistically significant, visually discernible reductions of adipose tissue covering the abdomen and flanks in two prospective multicenter studies.
“The treatment is well tolerated, with only mild and transient side effects,” said Dr. Bruce Katz of Mount Sinai School of Medicine in New York, who presented the results of the flank study at the annual meeting of the American Society for Laser Medicine and Surgery.
Most patients were “satisfied” or “very satisfied” with the results, added Dr. Sean Doherty, a plastic surgeon in group practice in Boston, who presented the results of the abdominal study.
Noninvasive fat reduction procedures rose 43% in the past year, said Dr. Doherty. The 1,060-nm diode laser damages adipocytes in targeted areas, eventually resulting in apoptosis, he added. Sessions in both studies lasted 25 minutes, with irradiance at 0.9-1.4 W/cm2 and treatment areas of 48-144 cm2 for the flanks and 192-288 cm2 for the abdomen, the investigators said.
The abdominal study included 34 patients, and the flank study included 42 patients. Investigators treated only one side for each patient in the flank study, reserving the other as a “sham” or control, Dr. Katz said. A blinded review of photographs taken before and 12 weeks after the procedures served as the primary endpoint in both studies. Assessors correctly identified an average of 95% of “before” photographs of the abdomen and 90.3% of those of the flank, Dr. Doherty and Dr. Katz reported.
The secondary endpoint was change in thickness of the adipose layer at 12 weeks post procedure, as measured by ultrasound. The average reduction was 3.1 mm for the abdomen (standard deviation, 1.7 mm) and 2.6 mm for the flank (standard deviation not reported; P < .001 for both), the researchers said. In the abdominal study, 85% of patients said they were “satisfied” or “extremely satisfied” with the results, while 6% were “slightly satisfied,” Dr. Doherty said. In the flank study, 86% of patients said they were “satisfied” or “extremely satisfied,” while 10% were “slightly satisfied.”
Mean pain scores were 3.7 out of 10 for the abdominal procedure and 4.0 out of 10 for the flank procedure. The most common side effect was mild to moderate tenderness that usually subsided within about 2 weeks of treatment. Other side effects included localized firmness, edema, and ecchymosis. No patients had serious adverse effects, the researchers said.
Most of the patients were approximately 45-49 years of age. Those in the abdominal study had an average body mass index of 25.5 kg/m2, while those in the flank study averaged 26.4 kg/m2, the researchers reported. Most of the patients in both studies were women (94% of abdominal patients and 86% of flank patients).
The average weight gain at 12 weeks for the abdominal study was 0.1 pounds (range, –5.2 to 5.6 pounds), while patients in the flank study gained an average of 0.8 pounds (range, –0.7 to 13 pounds), the researchers noted. Six patients in the flank study gained more than 5 pounds, and one gained more than 37 pounds and was therefore excluded from the efficacy analysis, Dr. Katz noted.
The researchers did not report funding sources for the studies. They disclosed advisory and financial relationships with Allergan, Merz Pharmaceuticals, Cynosure, Valeant, Syneron, and several other pharmaceutical companies.
AT LASER 2015
Key clinical point: One 25-minute noninvasive treatment with a 1,060-nm laser significantly reduced abdominal and flank fat.
Major finding: At 12 weeks, blinded assessors correctly chose 95% and 90.3% of “before” (compared with “after”) photographs of the abdomen and flank, respectively.
Data source: Two prospective multicenter studies of 34 patients who underwent abdominal treatment and 42 patients who underwent flank treatment.
Disclosures: Dr. Katz and Dr. Doherty did not report funding sources for the studies. They disclosed advisory and financial relationships with Allergan, Merz Pharmaceuticals, Cynosure, Valeant, Syneron, and several other pharmaceutical companies.
Acne Scarring: A Review of Cosmetic Therapies
Acne vulgaris is one of the most common inflammatory dermatoses affecting nearly all adolescents and a large proportion of adults.1 Incidence rates trend downward with age, but prevalence has been reported to be as high as 51% in individuals aged 20 to 29 years.2 Notably, recent evidence suggests there is an increasing incidence rate of acne among postadolescent women, with the severity associated with the menstrual cycle.3,4 Scarring is a common result of acne and may even occur in the setting of appropriate medical therapy. In particular, some form of facial scarring has been reported to occur in up to 95% of acne patients, with severe scarring in 30% of these patients.5 The detrimental effects of acne scarring are not only limited to impaired cosmetic appearance, as it also has been associated with depression symptoms, suicidal ideation, mental health problems, and general social impairment.6 Given the negative impact of acne scarring on overall health and well-being as well as its permanent nature, early and effective treatment is essential to maximize cosmetic outcomes and minimize long-term deleterious effects.
Acne scarring can be broadly divided into 2 major categories: atrophic and hypertrophic. Atrophic scarring is more common and is characterized by an overall localized reduction in collagen content. Clinically, atrophic scars present as depressions in the skin secondary to inflammatory fibrous contractions induced by acne. This type of scarring can be further divided into various subtypes based on morphologic criteria (eg, size, depth), such as boxcar, ice pick, and rolling scars.7 Conversely, hypertrophic scarring is characterized by an overall increase in collagen content and presents as firm raised lesions. Hypertrophic scars should be distinguished from keloid scars, as the former will not outgrow the margins of the original wound while the latter will.8 Treatment of acne scarring is based on scar type and can be accomplished through a variety of medical and surgical modalities (Table). In this article, we review some of the most commonly utilized therapies for both atrophic and hypertrophic acne scarring with a focus on cosmetic outcomes. It is important to keep in mind, however, that the best treatment is to prevent the occurrence of acne scarring through early and proactive treatment of acne.9
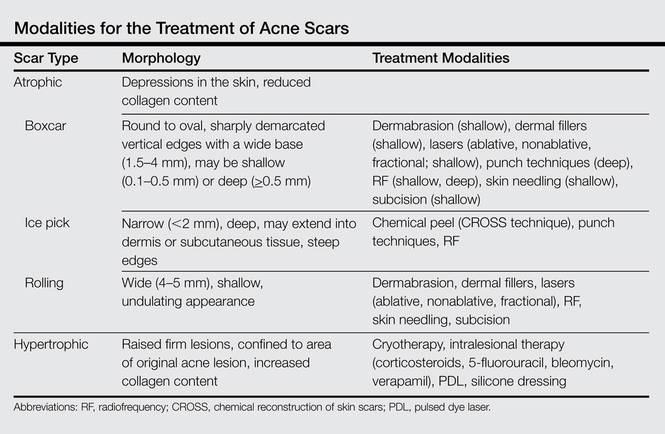
Dermabrasion
Dermabrasion is a decades-old technique that employs the use of a motorized device equipped with an abrasive material to physically remove the superficial layers of the skin, thus inducing the wound-healing process with subsequent formation of new collagen.10 In the same vein, microdermabrasion utilizes aluminum oxide crystals ejected from a nozzle to induce superficial microlacerations.11 This technique is most successful when used to soften scar edges in superficial atrophic scars of the rolling or boxcar subtypes.12 Dermabrasion has been shown to be equally as effective as laser therapy in the treatment of facial scars but is reported to have a much greater risk for adverse effects (AEs)(eg, erythema, edema) that may last for several weeks posttherapy.13,14 Dermabrasion is a particularly operator-dependent technique for which outcomes may vary depending on operator experience. As such, it is not generally recommended as a first-line therapy given its risks and relatively modest results; however, dermabrasion can be a useful adjunct when performed in the right setting. This technique, in addition to laser resurfacing, should be used with caution in patients who have recently taken or currently are taking isotretinoin, as several case series have reported postprocedural development of hypertrophic or keloid scars,15-17 but these findings subsequently were questioned in the literature.18
Laser Therapy
Laser technology has advanced tremendously over the last few decades and there are now a multitude of available lasers that are capable of variable depth penetration and energy delivery patterns. Common to all, however, is the ability to induce localized thermal damage with eventual collagen remodeling. Lasers can be divided into 2 major categories: ablative and nonablative. Ablative lasers cause epidermal destruction, while nonablative lasers are able to selectively target dermal layers without disrupting the overlying epithelium. Generally speaking, ablative lasers are more effective than nonablative lasers in the treatment of atrophic scars, with reported mean improvements of up to 81%.19 This increased efficacy comes with an increased risk for AEs such as postinflammatory hyperpigmentation, prolonged posttreatment erythema, and formation of additional scarring.20 Both ablative and nonablative lasers can be applied in the more recently developed technology of fractional photothermolysis. With this method, noncontiguous microscopic columns of thermal injury surrounded by zones of viable tissue are created, which is in contrast to the traditional manner of inducing broad thermal injury. Fractional ablative lasers can achieve efficacy rates similar to traditional ablative lasers with a reduced risk for permanent scarring or dispigmentation.21 Notably, recent studies have shown promising results for the use of fractional ablative lasers as a mechanism to enhance drug delivery of topically applied medications such as poly-L-lactic acid and triamcinolone acetonide in the treatment of atrophic and hypertrophic scars, respectively.22,23
Lasers also play a role in the treatment of hypertrophic acne scars with the use of nonablative pulsed dye lasers. These lasers cause selective thermolysis of dermal vasculature, and average clinical improvements in hypertrophic scars of 67.5% after a single treatment have been reported.24 Temporary postoperative purpura and long-term hyperpigmentation are reported outcomes of this therapy.20
Radiofrequency
Nonablative radiofrequency (RF) is a relatively novel technique that creates an electric current in the dermis at preset depths to induce thermal damage and eventual collagen synthesis. There are a variety of modalities for which RF can be applied, but microneedle bipolar RF and fractional bipolar RF treatments offer the best results for atrophic acne scars. Improvements in scar appearance of 25% to 75% have been reported after several treatment sessions.25 Better results have been reported in the treatment of ice pick scars as compared to more superficial scars,26 but additional studies will be necessary to validate this claim. Adverse effects are largely limited to temporary erythema and posttreatment scabbing.27
Subcision
Subcision is a more physically intensive technique useful for treatment of superficial atrophic acne scars. This method involves the use of a small needle that is inserted into the periphery of a scar before being moved in a back-and-forth manner underneath the base of the scar to loosen the fibrotic adhesions that result in the depressed appearance of the scar. Additionally, loosening of the tissue and resultant bleeding creates a potential space for future collagen deposition during the subsequent wound-healing phase. Subcision has a reported success rate of 50% to 60% in the treatment of rolling scars, and prospective, randomized, split-face trials have indicated that the short-term outcomes of subcision are superior to dermal fillers while being equally effective long-term.28,29 Of note, a small percentage of patients may develop a localized nodule at the site of treatment, which can be resolved with intralesional steroids.11
Skin Needling
Skin needling, also referred to as collagen induction therapy, utilizes vertical needle punctures rather than the horizontally directed punctures that are used in subcision and can be used to treat rolling and boxcar scars. Traditionally, a small roller equipped with rows of small needles typically ranging in size from 0.5 to 3.0 mm in length is passed over the skin using gentle pressure, puncturing the superficial layers of the skin to loosen fibrotic adhesions and induce collagen synthesis. This procedure may be repeated several times within a single session or over multiple sessions depending on the depth and quality of the scars. This technique has been reported to reduce scar depth up to 25% after 2 sessions.30
Punch Techniques
Punch techniques are useful for treatment of deeper atrophic acne scarring, for which most other treatment modalities are not particularly effective. A punch excision approximately equal to the scar size is first performed, which may then be followed by either removal of the scar tissue with subsequent suturing, graft replacement of the removed tissue, or elevation of the already established scar tissue to the level of surrounding skin where it is then held in place by sutures or adhesive skin closure material. Success rates with this method are largely limited to case series, but punch techniques are reported to be efficacious, especially for treatment of ice pick scars. Risks for this method include graft failure, graft depression, and formation of sinus tracts.31
Chemical Peels
Chemicals peels traditionally employ the use of acidic compounds to strip away the outer layers of skin to variable depths depending on the concentration of the agent being applied. Chemical peels are not generally recommended for application in a nonspecific manner in the treatment of acne scars given the relatively mild cosmetic improvements seen and the high rate of AEs such as pigmentary alterations and additional scar formation.12 Rather, clinicians should employ the CROSS (chemical reconstruction of skin scars) technique, in which peel agents such as trichloroacetic acid are applied in high concentrations only to areas of atrophic scarring. Use of this method can minimize AEs while simultaneously achieving high success rates, with excellent results in 100% (32/32) of patients after 5 to 6 treatment sessions.32 This method has been successful for hard-to-treat ice pick scars.33
Soft-Tissue Augmentation
Soft-tissue augmentation is another effective treatment of superficial atrophic acne scarring that utilizes injections of collagen fillers such as hyaluronic acid, calcium hydroxylapatite, poly-L-lactic acid, silicone, and even autologous fat to replace lost tissue volume while simultaneously inducing collagen production via stretching of dermal fibroblasts.34 These treatments may require multiple sessions for cosmetic improvement but have shown considerable efficacy in the treatment of atrophic acne scars. Hyaluronic acid has been reported to be particularly effective for rolling scars.12 However, these compounds only provide temporary results, thus requiring repeated treatments to maintain cosmetic outcomes. Permanent options include the recently US Food and Drug Administration–approved polymethylmethacrylate microspheres suspended in bovine collagen as well as the novel technique of autologous fibroblast transfer. These options are relatively new, but initial double-blind, randomized, controlled trials have shown minimal AEs with substantial improvements in 64% to 100% of atrophic scars treated.35,36
Intralesional Therapy
Intralesional corticosteroid injections are a mainstay treatment of hypertrophic acne scarring and are believed to exert their effects by decreasing fibroblast proliferation and promoting collagen degradation.37 Treatment with steroids generally is effective, with reported improvement in 75% (6/8) of patients and complete flattening in 50% (4/8) of lesions according to one study.38 Development of hypopigmentation, dermal atrophy, and telangiectasia are potential sequelae of this treatment.37
5-Fluorouracil, bleomycin, and verapamil also have been used with good results as intralesional treatments of hypertrophic scars, but these agents typically are reserved for cases of corticosteroid failure. Such compounds are thought to mediate their effects through inhibition of dermal fibroblast proliferation.39 Results with these therapies are varied, but greater than 75% improvement is seen in most cases. Adverse effects include injection-site ulceration and hyperpigmentation.39
Cryotherapy
Contact cryotherapy has been studied as treatment of hypertrophic acne scars. The exact mechanism through which scars are reduced is unclear, but it is hypothesized that the physical damage caused by freezing and thrombosis lead to collagen restructuring. According to one study, cryotherapy was reported to achieve good or excellent results in 76% (29/38) of cases.40 Permanent pigmentary alterations are a possible AE.
Silicone Dressings
Silicone dressings are a reasonable treatment option for hypertrophic acne scarring given their proven efficacy and minimal risk for AEs. Thin sheets of silicone gels or membranes are applied daily in a topical manner to acne scars and are believed to be therapeutic through a combination of pressure and hydration, which subsequently inhibits fibroblast production of collagen. Notable reductions in scar appearance and size are seen in 60% to 80% of individuals using this method.41 Adverse effects are limited to pruritus and local skin maceration. Patient noncompliance may be an issue, as the silicone dressings may be applied on highly visible areas such as the face. Patients may apply the dressings at night, but efficacy may be reduced.
Conclusion
When determining which treatment options to use in a patient with acne scarring, it is important to first determine the patient’s treatment goals while simultaneously establishing realistic expectations. Important factors to consider are the patient’s preferences regarding treatment risk, duration, and permanence, as well as budget and social or work requirements. As such, treatment plans for each patient should be determined on a case-by-case basis. It also is important to note that a combination of different treatment modalities often is necessary and superior to monotherapy in achieving satisfactory cosmetic outcomes.
1. Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity, and severity risk factors of acne in high school pupils: a community-based study. J Invest Dermatol. 2009;129:2136-2141.
2. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59.
3. Kim GK, Michaels BB. Post-adolescent acne in women: more common and more clinical considerations. J Drugs Dermatol. 2012;11:708-713.
4. Geller L, Rosen J, Frankel A, et al. Perimenstrual flare of adult acne. J Clin Aesthet Dermatol. 2014;7:30-34.
5. Layton AM, Henderson CA, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303-308.
6. Halvorsen JA, Stern RS, Dalgard F, et al. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2011;131:363-370.
7. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109-117.
8. Rivera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol. 2008;59:659-676.
9. Goodman GJ. Acne and acne scarring: why should we treat? Med J Aust. 1999;171:62-63.
10. Frank W. Therapeutic dermabrasion. back to the future. Arch Dermatol. 1994;130:1187-1189.
11. Goodman GJ. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857-871.
12. Hession MT, Graber EM. Atrophic acne scarring: a review of treatment options. J Clin Aesthet Dermatol. 2015;8:50-58.
13. Levy LL, Zeichner JA. Management of acne scarring, part II: a comparative review of non-laser-based, minimally invasive approaches. Am J Clin Dermatol. 2012;13:331-340.
14. Christophel JJ, Elm C, Endrizzi BT, et al. A randomized controlled trial of fractional laser therapy and dermabrasion for scar resurfacing. Dermatol Surg. 2012;38:595-602.
15. Katz BE, McFarlane DF. Atypical facial scarring after isotretinoin therapy in a patient with previous dermabrasion. J Am Acad Dermatol. 1994;30:852-853.
16. Bernestein LJ, Geronemus RG. Keloid formation with the 585-nm pulsed dye laser during isotretinoin treatment. Arch Dermatol. 1997;133:111-112.
17. Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118:703-706.
18. Wootton CI, Cartwright RP, Manning P, et al. Should isotretinoin be stopped prior to surgery? a critically appraised topic. Br J Dermatol. 2014;170:239-244.
19. Alster TS, West TB. Resurfacing of atrophic facial acne scars with a high-energy, pulsed carbon dioxide laser. Dermatol Surg. 1996;22:151-155.
20. Sobanko JF, Alster TS. Management of acne scarring, part I: a comparative review of laser surgical approaches. Am J Clin Dermatol. 2012;13:319-330.
21. Cho SB, Lee SJ, Oh SH, et al. Non-ablative 1550nm erbium-glass and ablative 10,600nm carbon dioxide fractional lasers for acne scar: a randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24:921-925.
22. Rkein A, Ozog D, Waibel JS. Treatment of atrophic scars with fractionated CO2 laser facilitating delivery of topically applied poly-L-lactic acid. Dermatol Surg. 2014;40:624-631.
23. Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med. 2013;45:135-140.
24. Alster TS, McMeekin TO. Improvement of facial acne scars by the 585-nm flashlamp-pumped pulsed dye laser. J Am Acad Dermatol. 1996;35:79-81.
25. Simmons BJ, Griffith RD, Falto-Aizpurua LA, et al. Use of radiofrequency in cosmetic dermatology: focus on nonablative treatment of acne scars. Clin Cosmet Investig Dermatol. 2014;7:335-339.
26. Ramesh M, Gopal M, Kumar S, et al. Novel technology in the treatment of acne scars: the matrix-tunable radiofrequency technology. J Cutan Aesthet Surg. 2010;3:97-101.
27. Johnson WC. Treatment of pitted scars; punch transplant technique. J Dermatol Surg Oncol. 1986;12:260-265.
28. Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005;31:310-317.
29. Sage R, Lopiccolo M, Liu A, et al. Subcuticular incision versus naturally sourced porcine collagen filler for acne scars: a randomized split-face comparison. Dermatol Surg. 2011;37:426-431.
30. Fabbrocini G, Annunziata MC, D’arco V, et al. Acne scars: pathogenesis, classification and treatment [published online ahead of print October 14, 2010]. Dermatol Res Pract. 2010;2010:893080.
31. Johnson WC. Treatment of pitted scars: punch transplant technique. J Dermatol Surg Oncol. 1986;12:260-265.
32. Lee JB, Chung WG, Kwahck H, et al. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg. 2002;28:1017-1021.
33. Bhardwaj D, Khunger N. An assessment of the efficacy and safety of CROSS technique with 100% TCA in the management of ice pick acne scars. J Cutan Aesthet Surg. 2010;3:93-96.
34. Wang F, Garza LA, Kang S, et al. In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143:155-163.
35. Karnik J, Baumann L, Bruce S, et al. A double-blind, randomized, multicenter, controlled trial of suspended polymethylmethacrylate microspheres for the correction of atrophic facial acne scars. J Am Acad Dermatol. 2014;71:77-83.
36. Munavalli GS, Smith S, Maslowski JM, et al. Successful treatment of depressed, distensible acne scars using autologous fibroblasts: a multi-site, prospective, double blind, placebo-controlled clinical trial. Dermatol Surg. 2013;39:1226-1236.
37. Leventhal D, Furr M, Reiter D. Treatment of keloids and hypertrophic scars: a meta-analysis and review of the literature. Arch Facial Plast Surg. 2006;8:362-368.
38. Darzi MA, Chowdri NA, Kaul SK, et al. Evaluation of various methods of treating keloids and hypertrophic scars: a 10-year follow-up study. Br J Plast Surg. 1992;45:374-379.
39. Ledon JA, Savas J, Franca K, et al. Intralesional treatment for keloids and hypertrophic scars: a review. Dermatol Surg. 2013;39:1745-1757.
40. Zouboulis CC, Blume U, Büttner P, et al. Outcomes of cryosurgery in keloids and hypertrophic scars. a prospective consecutive trial of case series. Arch Dermatol. 1993;129:1146-1151.
41. Puri N, Talwar A. The efficacy of silicone gel for the treatment of hypertrophic scars and keloids. J Cutan Aesthet Surg. 2009;2:104-106.
Acne vulgaris is one of the most common inflammatory dermatoses affecting nearly all adolescents and a large proportion of adults.1 Incidence rates trend downward with age, but prevalence has been reported to be as high as 51% in individuals aged 20 to 29 years.2 Notably, recent evidence suggests there is an increasing incidence rate of acne among postadolescent women, with the severity associated with the menstrual cycle.3,4 Scarring is a common result of acne and may even occur in the setting of appropriate medical therapy. In particular, some form of facial scarring has been reported to occur in up to 95% of acne patients, with severe scarring in 30% of these patients.5 The detrimental effects of acne scarring are not only limited to impaired cosmetic appearance, as it also has been associated with depression symptoms, suicidal ideation, mental health problems, and general social impairment.6 Given the negative impact of acne scarring on overall health and well-being as well as its permanent nature, early and effective treatment is essential to maximize cosmetic outcomes and minimize long-term deleterious effects.
Acne scarring can be broadly divided into 2 major categories: atrophic and hypertrophic. Atrophic scarring is more common and is characterized by an overall localized reduction in collagen content. Clinically, atrophic scars present as depressions in the skin secondary to inflammatory fibrous contractions induced by acne. This type of scarring can be further divided into various subtypes based on morphologic criteria (eg, size, depth), such as boxcar, ice pick, and rolling scars.7 Conversely, hypertrophic scarring is characterized by an overall increase in collagen content and presents as firm raised lesions. Hypertrophic scars should be distinguished from keloid scars, as the former will not outgrow the margins of the original wound while the latter will.8 Treatment of acne scarring is based on scar type and can be accomplished through a variety of medical and surgical modalities (Table). In this article, we review some of the most commonly utilized therapies for both atrophic and hypertrophic acne scarring with a focus on cosmetic outcomes. It is important to keep in mind, however, that the best treatment is to prevent the occurrence of acne scarring through early and proactive treatment of acne.9
Dermabrasion
Dermabrasion is a decades-old technique that employs the use of a motorized device equipped with an abrasive material to physically remove the superficial layers of the skin, thus inducing the wound-healing process with subsequent formation of new collagen.10 In the same vein, microdermabrasion utilizes aluminum oxide crystals ejected from a nozzle to induce superficial microlacerations.11 This technique is most successful when used to soften scar edges in superficial atrophic scars of the rolling or boxcar subtypes.12 Dermabrasion has been shown to be equally as effective as laser therapy in the treatment of facial scars but is reported to have a much greater risk for adverse effects (AEs)(eg, erythema, edema) that may last for several weeks posttherapy.13,14 Dermabrasion is a particularly operator-dependent technique for which outcomes may vary depending on operator experience. As such, it is not generally recommended as a first-line therapy given its risks and relatively modest results; however, dermabrasion can be a useful adjunct when performed in the right setting. This technique, in addition to laser resurfacing, should be used with caution in patients who have recently taken or currently are taking isotretinoin, as several case series have reported postprocedural development of hypertrophic or keloid scars,15-17 but these findings subsequently were questioned in the literature.18
Laser Therapy
Laser technology has advanced tremendously over the last few decades and there are now a multitude of available lasers that are capable of variable depth penetration and energy delivery patterns. Common to all, however, is the ability to induce localized thermal damage with eventual collagen remodeling. Lasers can be divided into 2 major categories: ablative and nonablative. Ablative lasers cause epidermal destruction, while nonablative lasers are able to selectively target dermal layers without disrupting the overlying epithelium. Generally speaking, ablative lasers are more effective than nonablative lasers in the treatment of atrophic scars, with reported mean improvements of up to 81%.19 This increased efficacy comes with an increased risk for AEs such as postinflammatory hyperpigmentation, prolonged posttreatment erythema, and formation of additional scarring.20 Both ablative and nonablative lasers can be applied in the more recently developed technology of fractional photothermolysis. With this method, noncontiguous microscopic columns of thermal injury surrounded by zones of viable tissue are created, which is in contrast to the traditional manner of inducing broad thermal injury. Fractional ablative lasers can achieve efficacy rates similar to traditional ablative lasers with a reduced risk for permanent scarring or dispigmentation.21 Notably, recent studies have shown promising results for the use of fractional ablative lasers as a mechanism to enhance drug delivery of topically applied medications such as poly-L-lactic acid and triamcinolone acetonide in the treatment of atrophic and hypertrophic scars, respectively.22,23
Lasers also play a role in the treatment of hypertrophic acne scars with the use of nonablative pulsed dye lasers. These lasers cause selective thermolysis of dermal vasculature, and average clinical improvements in hypertrophic scars of 67.5% after a single treatment have been reported.24 Temporary postoperative purpura and long-term hyperpigmentation are reported outcomes of this therapy.20
Radiofrequency
Nonablative radiofrequency (RF) is a relatively novel technique that creates an electric current in the dermis at preset depths to induce thermal damage and eventual collagen synthesis. There are a variety of modalities for which RF can be applied, but microneedle bipolar RF and fractional bipolar RF treatments offer the best results for atrophic acne scars. Improvements in scar appearance of 25% to 75% have been reported after several treatment sessions.25 Better results have been reported in the treatment of ice pick scars as compared to more superficial scars,26 but additional studies will be necessary to validate this claim. Adverse effects are largely limited to temporary erythema and posttreatment scabbing.27
Subcision
Subcision is a more physically intensive technique useful for treatment of superficial atrophic acne scars. This method involves the use of a small needle that is inserted into the periphery of a scar before being moved in a back-and-forth manner underneath the base of the scar to loosen the fibrotic adhesions that result in the depressed appearance of the scar. Additionally, loosening of the tissue and resultant bleeding creates a potential space for future collagen deposition during the subsequent wound-healing phase. Subcision has a reported success rate of 50% to 60% in the treatment of rolling scars, and prospective, randomized, split-face trials have indicated that the short-term outcomes of subcision are superior to dermal fillers while being equally effective long-term.28,29 Of note, a small percentage of patients may develop a localized nodule at the site of treatment, which can be resolved with intralesional steroids.11
Skin Needling
Skin needling, also referred to as collagen induction therapy, utilizes vertical needle punctures rather than the horizontally directed punctures that are used in subcision and can be used to treat rolling and boxcar scars. Traditionally, a small roller equipped with rows of small needles typically ranging in size from 0.5 to 3.0 mm in length is passed over the skin using gentle pressure, puncturing the superficial layers of the skin to loosen fibrotic adhesions and induce collagen synthesis. This procedure may be repeated several times within a single session or over multiple sessions depending on the depth and quality of the scars. This technique has been reported to reduce scar depth up to 25% after 2 sessions.30
Punch Techniques
Punch techniques are useful for treatment of deeper atrophic acne scarring, for which most other treatment modalities are not particularly effective. A punch excision approximately equal to the scar size is first performed, which may then be followed by either removal of the scar tissue with subsequent suturing, graft replacement of the removed tissue, or elevation of the already established scar tissue to the level of surrounding skin where it is then held in place by sutures or adhesive skin closure material. Success rates with this method are largely limited to case series, but punch techniques are reported to be efficacious, especially for treatment of ice pick scars. Risks for this method include graft failure, graft depression, and formation of sinus tracts.31
Chemical Peels
Chemicals peels traditionally employ the use of acidic compounds to strip away the outer layers of skin to variable depths depending on the concentration of the agent being applied. Chemical peels are not generally recommended for application in a nonspecific manner in the treatment of acne scars given the relatively mild cosmetic improvements seen and the high rate of AEs such as pigmentary alterations and additional scar formation.12 Rather, clinicians should employ the CROSS (chemical reconstruction of skin scars) technique, in which peel agents such as trichloroacetic acid are applied in high concentrations only to areas of atrophic scarring. Use of this method can minimize AEs while simultaneously achieving high success rates, with excellent results in 100% (32/32) of patients after 5 to 6 treatment sessions.32 This method has been successful for hard-to-treat ice pick scars.33
Soft-Tissue Augmentation
Soft-tissue augmentation is another effective treatment of superficial atrophic acne scarring that utilizes injections of collagen fillers such as hyaluronic acid, calcium hydroxylapatite, poly-L-lactic acid, silicone, and even autologous fat to replace lost tissue volume while simultaneously inducing collagen production via stretching of dermal fibroblasts.34 These treatments may require multiple sessions for cosmetic improvement but have shown considerable efficacy in the treatment of atrophic acne scars. Hyaluronic acid has been reported to be particularly effective for rolling scars.12 However, these compounds only provide temporary results, thus requiring repeated treatments to maintain cosmetic outcomes. Permanent options include the recently US Food and Drug Administration–approved polymethylmethacrylate microspheres suspended in bovine collagen as well as the novel technique of autologous fibroblast transfer. These options are relatively new, but initial double-blind, randomized, controlled trials have shown minimal AEs with substantial improvements in 64% to 100% of atrophic scars treated.35,36
Intralesional Therapy
Intralesional corticosteroid injections are a mainstay treatment of hypertrophic acne scarring and are believed to exert their effects by decreasing fibroblast proliferation and promoting collagen degradation.37 Treatment with steroids generally is effective, with reported improvement in 75% (6/8) of patients and complete flattening in 50% (4/8) of lesions according to one study.38 Development of hypopigmentation, dermal atrophy, and telangiectasia are potential sequelae of this treatment.37
5-Fluorouracil, bleomycin, and verapamil also have been used with good results as intralesional treatments of hypertrophic scars, but these agents typically are reserved for cases of corticosteroid failure. Such compounds are thought to mediate their effects through inhibition of dermal fibroblast proliferation.39 Results with these therapies are varied, but greater than 75% improvement is seen in most cases. Adverse effects include injection-site ulceration and hyperpigmentation.39
Cryotherapy
Contact cryotherapy has been studied as treatment of hypertrophic acne scars. The exact mechanism through which scars are reduced is unclear, but it is hypothesized that the physical damage caused by freezing and thrombosis lead to collagen restructuring. According to one study, cryotherapy was reported to achieve good or excellent results in 76% (29/38) of cases.40 Permanent pigmentary alterations are a possible AE.
Silicone Dressings
Silicone dressings are a reasonable treatment option for hypertrophic acne scarring given their proven efficacy and minimal risk for AEs. Thin sheets of silicone gels or membranes are applied daily in a topical manner to acne scars and are believed to be therapeutic through a combination of pressure and hydration, which subsequently inhibits fibroblast production of collagen. Notable reductions in scar appearance and size are seen in 60% to 80% of individuals using this method.41 Adverse effects are limited to pruritus and local skin maceration. Patient noncompliance may be an issue, as the silicone dressings may be applied on highly visible areas such as the face. Patients may apply the dressings at night, but efficacy may be reduced.
Conclusion
When determining which treatment options to use in a patient with acne scarring, it is important to first determine the patient’s treatment goals while simultaneously establishing realistic expectations. Important factors to consider are the patient’s preferences regarding treatment risk, duration, and permanence, as well as budget and social or work requirements. As such, treatment plans for each patient should be determined on a case-by-case basis. It also is important to note that a combination of different treatment modalities often is necessary and superior to monotherapy in achieving satisfactory cosmetic outcomes.
Acne vulgaris is one of the most common inflammatory dermatoses affecting nearly all adolescents and a large proportion of adults.1 Incidence rates trend downward with age, but prevalence has been reported to be as high as 51% in individuals aged 20 to 29 years.2 Notably, recent evidence suggests there is an increasing incidence rate of acne among postadolescent women, with the severity associated with the menstrual cycle.3,4 Scarring is a common result of acne and may even occur in the setting of appropriate medical therapy. In particular, some form of facial scarring has been reported to occur in up to 95% of acne patients, with severe scarring in 30% of these patients.5 The detrimental effects of acne scarring are not only limited to impaired cosmetic appearance, as it also has been associated with depression symptoms, suicidal ideation, mental health problems, and general social impairment.6 Given the negative impact of acne scarring on overall health and well-being as well as its permanent nature, early and effective treatment is essential to maximize cosmetic outcomes and minimize long-term deleterious effects.
Acne scarring can be broadly divided into 2 major categories: atrophic and hypertrophic. Atrophic scarring is more common and is characterized by an overall localized reduction in collagen content. Clinically, atrophic scars present as depressions in the skin secondary to inflammatory fibrous contractions induced by acne. This type of scarring can be further divided into various subtypes based on morphologic criteria (eg, size, depth), such as boxcar, ice pick, and rolling scars.7 Conversely, hypertrophic scarring is characterized by an overall increase in collagen content and presents as firm raised lesions. Hypertrophic scars should be distinguished from keloid scars, as the former will not outgrow the margins of the original wound while the latter will.8 Treatment of acne scarring is based on scar type and can be accomplished through a variety of medical and surgical modalities (Table). In this article, we review some of the most commonly utilized therapies for both atrophic and hypertrophic acne scarring with a focus on cosmetic outcomes. It is important to keep in mind, however, that the best treatment is to prevent the occurrence of acne scarring through early and proactive treatment of acne.9
Dermabrasion
Dermabrasion is a decades-old technique that employs the use of a motorized device equipped with an abrasive material to physically remove the superficial layers of the skin, thus inducing the wound-healing process with subsequent formation of new collagen.10 In the same vein, microdermabrasion utilizes aluminum oxide crystals ejected from a nozzle to induce superficial microlacerations.11 This technique is most successful when used to soften scar edges in superficial atrophic scars of the rolling or boxcar subtypes.12 Dermabrasion has been shown to be equally as effective as laser therapy in the treatment of facial scars but is reported to have a much greater risk for adverse effects (AEs)(eg, erythema, edema) that may last for several weeks posttherapy.13,14 Dermabrasion is a particularly operator-dependent technique for which outcomes may vary depending on operator experience. As such, it is not generally recommended as a first-line therapy given its risks and relatively modest results; however, dermabrasion can be a useful adjunct when performed in the right setting. This technique, in addition to laser resurfacing, should be used with caution in patients who have recently taken or currently are taking isotretinoin, as several case series have reported postprocedural development of hypertrophic or keloid scars,15-17 but these findings subsequently were questioned in the literature.18
Laser Therapy
Laser technology has advanced tremendously over the last few decades and there are now a multitude of available lasers that are capable of variable depth penetration and energy delivery patterns. Common to all, however, is the ability to induce localized thermal damage with eventual collagen remodeling. Lasers can be divided into 2 major categories: ablative and nonablative. Ablative lasers cause epidermal destruction, while nonablative lasers are able to selectively target dermal layers without disrupting the overlying epithelium. Generally speaking, ablative lasers are more effective than nonablative lasers in the treatment of atrophic scars, with reported mean improvements of up to 81%.19 This increased efficacy comes with an increased risk for AEs such as postinflammatory hyperpigmentation, prolonged posttreatment erythema, and formation of additional scarring.20 Both ablative and nonablative lasers can be applied in the more recently developed technology of fractional photothermolysis. With this method, noncontiguous microscopic columns of thermal injury surrounded by zones of viable tissue are created, which is in contrast to the traditional manner of inducing broad thermal injury. Fractional ablative lasers can achieve efficacy rates similar to traditional ablative lasers with a reduced risk for permanent scarring or dispigmentation.21 Notably, recent studies have shown promising results for the use of fractional ablative lasers as a mechanism to enhance drug delivery of topically applied medications such as poly-L-lactic acid and triamcinolone acetonide in the treatment of atrophic and hypertrophic scars, respectively.22,23
Lasers also play a role in the treatment of hypertrophic acne scars with the use of nonablative pulsed dye lasers. These lasers cause selective thermolysis of dermal vasculature, and average clinical improvements in hypertrophic scars of 67.5% after a single treatment have been reported.24 Temporary postoperative purpura and long-term hyperpigmentation are reported outcomes of this therapy.20
Radiofrequency
Nonablative radiofrequency (RF) is a relatively novel technique that creates an electric current in the dermis at preset depths to induce thermal damage and eventual collagen synthesis. There are a variety of modalities for which RF can be applied, but microneedle bipolar RF and fractional bipolar RF treatments offer the best results for atrophic acne scars. Improvements in scar appearance of 25% to 75% have been reported after several treatment sessions.25 Better results have been reported in the treatment of ice pick scars as compared to more superficial scars,26 but additional studies will be necessary to validate this claim. Adverse effects are largely limited to temporary erythema and posttreatment scabbing.27
Subcision
Subcision is a more physically intensive technique useful for treatment of superficial atrophic acne scars. This method involves the use of a small needle that is inserted into the periphery of a scar before being moved in a back-and-forth manner underneath the base of the scar to loosen the fibrotic adhesions that result in the depressed appearance of the scar. Additionally, loosening of the tissue and resultant bleeding creates a potential space for future collagen deposition during the subsequent wound-healing phase. Subcision has a reported success rate of 50% to 60% in the treatment of rolling scars, and prospective, randomized, split-face trials have indicated that the short-term outcomes of subcision are superior to dermal fillers while being equally effective long-term.28,29 Of note, a small percentage of patients may develop a localized nodule at the site of treatment, which can be resolved with intralesional steroids.11
Skin Needling
Skin needling, also referred to as collagen induction therapy, utilizes vertical needle punctures rather than the horizontally directed punctures that are used in subcision and can be used to treat rolling and boxcar scars. Traditionally, a small roller equipped with rows of small needles typically ranging in size from 0.5 to 3.0 mm in length is passed over the skin using gentle pressure, puncturing the superficial layers of the skin to loosen fibrotic adhesions and induce collagen synthesis. This procedure may be repeated several times within a single session or over multiple sessions depending on the depth and quality of the scars. This technique has been reported to reduce scar depth up to 25% after 2 sessions.30
Punch Techniques
Punch techniques are useful for treatment of deeper atrophic acne scarring, for which most other treatment modalities are not particularly effective. A punch excision approximately equal to the scar size is first performed, which may then be followed by either removal of the scar tissue with subsequent suturing, graft replacement of the removed tissue, or elevation of the already established scar tissue to the level of surrounding skin where it is then held in place by sutures or adhesive skin closure material. Success rates with this method are largely limited to case series, but punch techniques are reported to be efficacious, especially for treatment of ice pick scars. Risks for this method include graft failure, graft depression, and formation of sinus tracts.31
Chemical Peels
Chemicals peels traditionally employ the use of acidic compounds to strip away the outer layers of skin to variable depths depending on the concentration of the agent being applied. Chemical peels are not generally recommended for application in a nonspecific manner in the treatment of acne scars given the relatively mild cosmetic improvements seen and the high rate of AEs such as pigmentary alterations and additional scar formation.12 Rather, clinicians should employ the CROSS (chemical reconstruction of skin scars) technique, in which peel agents such as trichloroacetic acid are applied in high concentrations only to areas of atrophic scarring. Use of this method can minimize AEs while simultaneously achieving high success rates, with excellent results in 100% (32/32) of patients after 5 to 6 treatment sessions.32 This method has been successful for hard-to-treat ice pick scars.33
Soft-Tissue Augmentation
Soft-tissue augmentation is another effective treatment of superficial atrophic acne scarring that utilizes injections of collagen fillers such as hyaluronic acid, calcium hydroxylapatite, poly-L-lactic acid, silicone, and even autologous fat to replace lost tissue volume while simultaneously inducing collagen production via stretching of dermal fibroblasts.34 These treatments may require multiple sessions for cosmetic improvement but have shown considerable efficacy in the treatment of atrophic acne scars. Hyaluronic acid has been reported to be particularly effective for rolling scars.12 However, these compounds only provide temporary results, thus requiring repeated treatments to maintain cosmetic outcomes. Permanent options include the recently US Food and Drug Administration–approved polymethylmethacrylate microspheres suspended in bovine collagen as well as the novel technique of autologous fibroblast transfer. These options are relatively new, but initial double-blind, randomized, controlled trials have shown minimal AEs with substantial improvements in 64% to 100% of atrophic scars treated.35,36
Intralesional Therapy
Intralesional corticosteroid injections are a mainstay treatment of hypertrophic acne scarring and are believed to exert their effects by decreasing fibroblast proliferation and promoting collagen degradation.37 Treatment with steroids generally is effective, with reported improvement in 75% (6/8) of patients and complete flattening in 50% (4/8) of lesions according to one study.38 Development of hypopigmentation, dermal atrophy, and telangiectasia are potential sequelae of this treatment.37
5-Fluorouracil, bleomycin, and verapamil also have been used with good results as intralesional treatments of hypertrophic scars, but these agents typically are reserved for cases of corticosteroid failure. Such compounds are thought to mediate their effects through inhibition of dermal fibroblast proliferation.39 Results with these therapies are varied, but greater than 75% improvement is seen in most cases. Adverse effects include injection-site ulceration and hyperpigmentation.39
Cryotherapy
Contact cryotherapy has been studied as treatment of hypertrophic acne scars. The exact mechanism through which scars are reduced is unclear, but it is hypothesized that the physical damage caused by freezing and thrombosis lead to collagen restructuring. According to one study, cryotherapy was reported to achieve good or excellent results in 76% (29/38) of cases.40 Permanent pigmentary alterations are a possible AE.
Silicone Dressings
Silicone dressings are a reasonable treatment option for hypertrophic acne scarring given their proven efficacy and minimal risk for AEs. Thin sheets of silicone gels or membranes are applied daily in a topical manner to acne scars and are believed to be therapeutic through a combination of pressure and hydration, which subsequently inhibits fibroblast production of collagen. Notable reductions in scar appearance and size are seen in 60% to 80% of individuals using this method.41 Adverse effects are limited to pruritus and local skin maceration. Patient noncompliance may be an issue, as the silicone dressings may be applied on highly visible areas such as the face. Patients may apply the dressings at night, but efficacy may be reduced.
Conclusion
When determining which treatment options to use in a patient with acne scarring, it is important to first determine the patient’s treatment goals while simultaneously establishing realistic expectations. Important factors to consider are the patient’s preferences regarding treatment risk, duration, and permanence, as well as budget and social or work requirements. As such, treatment plans for each patient should be determined on a case-by-case basis. It also is important to note that a combination of different treatment modalities often is necessary and superior to monotherapy in achieving satisfactory cosmetic outcomes.
1. Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity, and severity risk factors of acne in high school pupils: a community-based study. J Invest Dermatol. 2009;129:2136-2141.
2. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59.
3. Kim GK, Michaels BB. Post-adolescent acne in women: more common and more clinical considerations. J Drugs Dermatol. 2012;11:708-713.
4. Geller L, Rosen J, Frankel A, et al. Perimenstrual flare of adult acne. J Clin Aesthet Dermatol. 2014;7:30-34.
5. Layton AM, Henderson CA, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303-308.
6. Halvorsen JA, Stern RS, Dalgard F, et al. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2011;131:363-370.
7. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109-117.
8. Rivera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol. 2008;59:659-676.
9. Goodman GJ. Acne and acne scarring: why should we treat? Med J Aust. 1999;171:62-63.
10. Frank W. Therapeutic dermabrasion. back to the future. Arch Dermatol. 1994;130:1187-1189.
11. Goodman GJ. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857-871.
12. Hession MT, Graber EM. Atrophic acne scarring: a review of treatment options. J Clin Aesthet Dermatol. 2015;8:50-58.
13. Levy LL, Zeichner JA. Management of acne scarring, part II: a comparative review of non-laser-based, minimally invasive approaches. Am J Clin Dermatol. 2012;13:331-340.
14. Christophel JJ, Elm C, Endrizzi BT, et al. A randomized controlled trial of fractional laser therapy and dermabrasion for scar resurfacing. Dermatol Surg. 2012;38:595-602.
15. Katz BE, McFarlane DF. Atypical facial scarring after isotretinoin therapy in a patient with previous dermabrasion. J Am Acad Dermatol. 1994;30:852-853.
16. Bernestein LJ, Geronemus RG. Keloid formation with the 585-nm pulsed dye laser during isotretinoin treatment. Arch Dermatol. 1997;133:111-112.
17. Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118:703-706.
18. Wootton CI, Cartwright RP, Manning P, et al. Should isotretinoin be stopped prior to surgery? a critically appraised topic. Br J Dermatol. 2014;170:239-244.
19. Alster TS, West TB. Resurfacing of atrophic facial acne scars with a high-energy, pulsed carbon dioxide laser. Dermatol Surg. 1996;22:151-155.
20. Sobanko JF, Alster TS. Management of acne scarring, part I: a comparative review of laser surgical approaches. Am J Clin Dermatol. 2012;13:319-330.
21. Cho SB, Lee SJ, Oh SH, et al. Non-ablative 1550nm erbium-glass and ablative 10,600nm carbon dioxide fractional lasers for acne scar: a randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24:921-925.
22. Rkein A, Ozog D, Waibel JS. Treatment of atrophic scars with fractionated CO2 laser facilitating delivery of topically applied poly-L-lactic acid. Dermatol Surg. 2014;40:624-631.
23. Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med. 2013;45:135-140.
24. Alster TS, McMeekin TO. Improvement of facial acne scars by the 585-nm flashlamp-pumped pulsed dye laser. J Am Acad Dermatol. 1996;35:79-81.
25. Simmons BJ, Griffith RD, Falto-Aizpurua LA, et al. Use of radiofrequency in cosmetic dermatology: focus on nonablative treatment of acne scars. Clin Cosmet Investig Dermatol. 2014;7:335-339.
26. Ramesh M, Gopal M, Kumar S, et al. Novel technology in the treatment of acne scars: the matrix-tunable radiofrequency technology. J Cutan Aesthet Surg. 2010;3:97-101.
27. Johnson WC. Treatment of pitted scars; punch transplant technique. J Dermatol Surg Oncol. 1986;12:260-265.
28. Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005;31:310-317.
29. Sage R, Lopiccolo M, Liu A, et al. Subcuticular incision versus naturally sourced porcine collagen filler for acne scars: a randomized split-face comparison. Dermatol Surg. 2011;37:426-431.
30. Fabbrocini G, Annunziata MC, D’arco V, et al. Acne scars: pathogenesis, classification and treatment [published online ahead of print October 14, 2010]. Dermatol Res Pract. 2010;2010:893080.
31. Johnson WC. Treatment of pitted scars: punch transplant technique. J Dermatol Surg Oncol. 1986;12:260-265.
32. Lee JB, Chung WG, Kwahck H, et al. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg. 2002;28:1017-1021.
33. Bhardwaj D, Khunger N. An assessment of the efficacy and safety of CROSS technique with 100% TCA in the management of ice pick acne scars. J Cutan Aesthet Surg. 2010;3:93-96.
34. Wang F, Garza LA, Kang S, et al. In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143:155-163.
35. Karnik J, Baumann L, Bruce S, et al. A double-blind, randomized, multicenter, controlled trial of suspended polymethylmethacrylate microspheres for the correction of atrophic facial acne scars. J Am Acad Dermatol. 2014;71:77-83.
36. Munavalli GS, Smith S, Maslowski JM, et al. Successful treatment of depressed, distensible acne scars using autologous fibroblasts: a multi-site, prospective, double blind, placebo-controlled clinical trial. Dermatol Surg. 2013;39:1226-1236.
37. Leventhal D, Furr M, Reiter D. Treatment of keloids and hypertrophic scars: a meta-analysis and review of the literature. Arch Facial Plast Surg. 2006;8:362-368.
38. Darzi MA, Chowdri NA, Kaul SK, et al. Evaluation of various methods of treating keloids and hypertrophic scars: a 10-year follow-up study. Br J Plast Surg. 1992;45:374-379.
39. Ledon JA, Savas J, Franca K, et al. Intralesional treatment for keloids and hypertrophic scars: a review. Dermatol Surg. 2013;39:1745-1757.
40. Zouboulis CC, Blume U, Büttner P, et al. Outcomes of cryosurgery in keloids and hypertrophic scars. a prospective consecutive trial of case series. Arch Dermatol. 1993;129:1146-1151.
41. Puri N, Talwar A. The efficacy of silicone gel for the treatment of hypertrophic scars and keloids. J Cutan Aesthet Surg. 2009;2:104-106.
1. Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity, and severity risk factors of acne in high school pupils: a community-based study. J Invest Dermatol. 2009;129:2136-2141.
2. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59.
3. Kim GK, Michaels BB. Post-adolescent acne in women: more common and more clinical considerations. J Drugs Dermatol. 2012;11:708-713.
4. Geller L, Rosen J, Frankel A, et al. Perimenstrual flare of adult acne. J Clin Aesthet Dermatol. 2014;7:30-34.
5. Layton AM, Henderson CA, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303-308.
6. Halvorsen JA, Stern RS, Dalgard F, et al. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2011;131:363-370.
7. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109-117.
8. Rivera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol. 2008;59:659-676.
9. Goodman GJ. Acne and acne scarring: why should we treat? Med J Aust. 1999;171:62-63.
10. Frank W. Therapeutic dermabrasion. back to the future. Arch Dermatol. 1994;130:1187-1189.
11. Goodman GJ. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857-871.
12. Hession MT, Graber EM. Atrophic acne scarring: a review of treatment options. J Clin Aesthet Dermatol. 2015;8:50-58.
13. Levy LL, Zeichner JA. Management of acne scarring, part II: a comparative review of non-laser-based, minimally invasive approaches. Am J Clin Dermatol. 2012;13:331-340.
14. Christophel JJ, Elm C, Endrizzi BT, et al. A randomized controlled trial of fractional laser therapy and dermabrasion for scar resurfacing. Dermatol Surg. 2012;38:595-602.
15. Katz BE, McFarlane DF. Atypical facial scarring after isotretinoin therapy in a patient with previous dermabrasion. J Am Acad Dermatol. 1994;30:852-853.
16. Bernestein LJ, Geronemus RG. Keloid formation with the 585-nm pulsed dye laser during isotretinoin treatment. Arch Dermatol. 1997;133:111-112.
17. Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118:703-706.
18. Wootton CI, Cartwright RP, Manning P, et al. Should isotretinoin be stopped prior to surgery? a critically appraised topic. Br J Dermatol. 2014;170:239-244.
19. Alster TS, West TB. Resurfacing of atrophic facial acne scars with a high-energy, pulsed carbon dioxide laser. Dermatol Surg. 1996;22:151-155.
20. Sobanko JF, Alster TS. Management of acne scarring, part I: a comparative review of laser surgical approaches. Am J Clin Dermatol. 2012;13:319-330.
21. Cho SB, Lee SJ, Oh SH, et al. Non-ablative 1550nm erbium-glass and ablative 10,600nm carbon dioxide fractional lasers for acne scar: a randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24:921-925.
22. Rkein A, Ozog D, Waibel JS. Treatment of atrophic scars with fractionated CO2 laser facilitating delivery of topically applied poly-L-lactic acid. Dermatol Surg. 2014;40:624-631.
23. Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med. 2013;45:135-140.
24. Alster TS, McMeekin TO. Improvement of facial acne scars by the 585-nm flashlamp-pumped pulsed dye laser. J Am Acad Dermatol. 1996;35:79-81.
25. Simmons BJ, Griffith RD, Falto-Aizpurua LA, et al. Use of radiofrequency in cosmetic dermatology: focus on nonablative treatment of acne scars. Clin Cosmet Investig Dermatol. 2014;7:335-339.
26. Ramesh M, Gopal M, Kumar S, et al. Novel technology in the treatment of acne scars: the matrix-tunable radiofrequency technology. J Cutan Aesthet Surg. 2010;3:97-101.
27. Johnson WC. Treatment of pitted scars; punch transplant technique. J Dermatol Surg Oncol. 1986;12:260-265.
28. Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005;31:310-317.
29. Sage R, Lopiccolo M, Liu A, et al. Subcuticular incision versus naturally sourced porcine collagen filler for acne scars: a randomized split-face comparison. Dermatol Surg. 2011;37:426-431.
30. Fabbrocini G, Annunziata MC, D’arco V, et al. Acne scars: pathogenesis, classification and treatment [published online ahead of print October 14, 2010]. Dermatol Res Pract. 2010;2010:893080.
31. Johnson WC. Treatment of pitted scars: punch transplant technique. J Dermatol Surg Oncol. 1986;12:260-265.
32. Lee JB, Chung WG, Kwahck H, et al. Focal treatment of acne scars with trichloroacetic acid: chemical reconstruction of skin scars method. Dermatol Surg. 2002;28:1017-1021.
33. Bhardwaj D, Khunger N. An assessment of the efficacy and safety of CROSS technique with 100% TCA in the management of ice pick acne scars. J Cutan Aesthet Surg. 2010;3:93-96.
34. Wang F, Garza LA, Kang S, et al. In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143:155-163.
35. Karnik J, Baumann L, Bruce S, et al. A double-blind, randomized, multicenter, controlled trial of suspended polymethylmethacrylate microspheres for the correction of atrophic facial acne scars. J Am Acad Dermatol. 2014;71:77-83.
36. Munavalli GS, Smith S, Maslowski JM, et al. Successful treatment of depressed, distensible acne scars using autologous fibroblasts: a multi-site, prospective, double blind, placebo-controlled clinical trial. Dermatol Surg. 2013;39:1226-1236.
37. Leventhal D, Furr M, Reiter D. Treatment of keloids and hypertrophic scars: a meta-analysis and review of the literature. Arch Facial Plast Surg. 2006;8:362-368.
38. Darzi MA, Chowdri NA, Kaul SK, et al. Evaluation of various methods of treating keloids and hypertrophic scars: a 10-year follow-up study. Br J Plast Surg. 1992;45:374-379.
39. Ledon JA, Savas J, Franca K, et al. Intralesional treatment for keloids and hypertrophic scars: a review. Dermatol Surg. 2013;39:1745-1757.
40. Zouboulis CC, Blume U, Büttner P, et al. Outcomes of cryosurgery in keloids and hypertrophic scars. a prospective consecutive trial of case series. Arch Dermatol. 1993;129:1146-1151.
41. Puri N, Talwar A. The efficacy of silicone gel for the treatment of hypertrophic scars and keloids. J Cutan Aesthet Surg. 2009;2:104-106.
Practice Points
- Scarring is a common and undesirable outcome of acne vulgaris that can occur even in the setting of appropriate medical management.
- Acne scars can be classified into several different types based on scar quality and appearance. The choice of treatment with medical or surgical measures should be made with respect to the type of scar present.
- A combination of therapeutic modalities often is necessary to achieve optimal cosmetic outcomes in the treatment of both atrophic and hypertrophic acne scars.
